Poultry as a Host for the Zoonotic Pathogen Campylobacter jejuni

REVIEW
Zoonotic viral diseases and the frontier of early diagnosis,
control and prevention
J . L . H E E N E YDepartment of Virology, BPRC, Rijswijk, and the Department of Medical Microbiology, University of Leiden, Leiden, The Netherlands
Abstract. Heeney JL. Zoonotic viral diseases and
the frontier of early diagnosis, control and
prevention (Review). J Intern Med 2006; 260:
399–408.
Public awareness of the human health risks of
zoonotic infections has grown in recent years.
Currently, concern of H5N1 flu transmission from
migratory bird populations has increased with foci of
fatal human cases. This comes on the heels of other
major zoonotic viral epidemics in the last decade.
These include other acute emerging or re-emerging
viral diseases such as severe acute respiratory
syndrome (SARS), West-Nile virus, Ebola virus,
monkeypox, as well as the more inapparent insidious
slow viral and prion diseases. Virus infections with
zoonotic potential can become serious killers once
they are able to establish the necessary adaptations
for efficient human-to-human transmission under
circumstances sufficient to reach epidemic
proportions. The monitoring and early diagnosis of
these potential risks are overlapping frontiers of
human and veterinary medicine. Here, current viral
zoonotics and evolving threats are reviewed.
Keywords: early diagnosis, Ebola, emerging
diseases, H5N1 flu, severe acute respiratory
syndrome, vaccines, West-Nile, Zoonosis, review.
Introduction
Of the >1400 documented human pathogens,
approximately 64% are zoonotic (from nonhuman
vertebrate hosts) [1–3]. Viruses and prions represent
just under 5% of the total list of human pathogens.
However, of the emerging or remerging diseases
there is a disproportionate number which are due to
RNA viruses (37%). The RNA viral families, Bun-
yviridae, Flaviviridae, Togaviridae and Reoviridae
contain viruses which represent more than half of
the currently defined viral zoonoses [2, 4].
Interestingly, a characteristic of most zoonotic
viral pathogens is that they are not readily trans-
missible from humans to humans. In the majority
of cases, humans are commonly dead-end hosts [5].
There are important exceptions but in most cases a
virus will require certain genetic adaptations (or
acquisition of genetic information from human
adapted viruses) for new variants within the new
human host to persist and to become successful in
human-to-human spread [6–8]. In extreme cases, it
is believed that certain animal viruses, following
transmission to humans, adapt to the new host so
effectively that they become almost exclusively
transmitted from humans to humans (i.e. measles
and influenza) [2, 8, 9]. Fortunately, these are
relatively infrequent events and it is estimated that
only about 25% of zoonotic pathogens are capable
of some person-to-person spread [1]. Most acute
viral zoonoses do not persist long in human
populations without repeated reintroductions from
a nonhuman reservoir (for instance Ebola virus)
[10–12].
Journal of Internal Medicine 2006; 260: 399–408 doi:10.1111/j.1365-2796.2006.01711.x
� 2006 Blackwell Publishing Ltd 399

Changes in behaviour, population dynamics and
imbalances in complex eco-systems are events often
associated with the emergence of zoonotic infections
[1, 13–15]. The clinical indications of zoonotic
infections are as diverse as the agents that cause
them [4, 16–18]. Early identification is dependent
on astute diagnostic prowess, recognition of the
unusual, an investigative history with a rapid and
comprehensive laboratory analysis [19–22]. Aetio-
logical identification and epidemiological assessment
requires effective communication and collaboration
[22–26]. Classically, identification of emerging zoo-
noses follows recognition of a health problem in the
human population, while generally only later is the
link made with an asymptomatic host reservoir or a
disease outbreak in a susceptible animal population
[12, 22, 25]. An important change in this trend has
developed based on scientific understanding of avian
flu, widespread media interest, and increased public
awareness coupled with international surveillance
and national intervention programmes [12, 27–31].
Avian flu and pandemic influenza
Clinical symptoms of Avian Influenza (Bird Flu,
influenza type A viruses) may vary from typical
human (influenza type B) influenza-like symptoms
characterized by fever, cough with pharyngitis and
muscle aches to conjunctivitis (for instance with
type A, H7), pneumonia or severe respiratory
distress and pleural effusion [19, 32–34]. Influenza
viruses are RNA viruses of the family Orthomyxov-
iridae, of which three types (A, B and C) are
recognized. The surface antigens haemaglutinin
(H) and neuraminidase (N) are of particular import-
ance and are used in the classification of the subtype
A viruses. Influenza subtypes A viruses naturally
infect the intestinal tract of wild birds and are
frequently asymptomatic in natural hosts. Shore-
birds and wildfowl are the most likely natural
reservoir [12, 14, 35, 36]. However, influenza A
can infect and cause disease in domestic birds, pigs,
horses, other animals as well as humans [36, 37].
The influenza A subtypes known to infect both birds
and people include H5, H7 and H9 [23, 38–40].
Influenza type B viruses, unlike A, are primarily
found only in humans and may cause epidemics
with morbidity and mortality (especially in the
elderly), but are not known to causes the pandemics
associated with influenza A [4, 32]. Strains of
influenza B appear regularly replacing older type B
strains by the process of amino acid selection called
antigenic drift. Thus, human influenza vaccines
require constant updating to keep up with strain
differences [29, 41, 42]. Influenza type C is relatively
stable compared with types A and B. It infects
humans, is less common, causes a very mild
respiratory illness or no symptoms and is not
reported to cause epidemics.
Antigenic drift and antigenic shift
In 2003, an outbreak of highly pathogenic influenza
A subtype H7N7 rapidly spread to 255 poultry
farms in the Netherlands. Causing high mortality in
chickens, this subtype was thought to be of low risk
of transmission [39]. The outbreak investigation
revealed a high incidence of conjunctivitis and flu
like symptoms in humans and one fatality in a
veterinarian directly involved in handling infected
poultry. Evidence of person-to-person transmission
was also documented [39].
The recent spread of A/H5N1 by migratory water
fowl in Asia which began in 2003 as large scale die-
offs in commercial poultry and duck farms in
Thailand, Vietnam, South Korea and Japan became
full scale outbreaks in 2004 [13, 14, 34, 35]. The
westward spread (Fig. 1) has continued on a yearly
basis since with the spread through Indonesia,
China, Kazakhstan, Mongolia, Russia, Iraq, Turkey,
Europe and Africa [13, 14, 34, 43]. Cases have not
been limited to domestic birds, but also included
domestic carnivores, captive tigers, leopards and
humans with >100 confirmed fatalities [13, 34, 43].
In contrast to A-H7N7, conjunctivitis is not
observed and upper respiratory tract symptoms are
more infrequent [9]. High fever with flu-like illness
with lower respiratory tract symptoms manifest
early. Diarrhoea, vomiting with abdominal and
pleuritic pain progress to respiratory distress. Almost
all patients have clinically apparent pneumonia.
Progression to respiratory or multi-organ failure is
common in hospitalised patients where the fatality
rate is high (on average 9–10 days after clinical
onset), although the overall rate is estimated to be
lower [19, 32, 33].
Diagnosis based on clinical presentation, history
of contact with sick or dying birds or contact with ill
individuals and who have had such contact, is
confirmed by laboratory virology, best performed by
� 2006 Blackwell Publishing Ltd Journal of Internal Medicine 260: 399–408
4 0 0 J . L . H E E N E Y

RT-PCR assays. Although PCR assays are often more
sensitive and more specific, they currently may not
be as quick to be performed in diagnostic laborat-
ories as commercial antigen capture tests [33].
The occurrence of human influenza A-H5N1 has
to date paralleled large outbreaks of avian influenza
A-H5N1 with exposure to poultry a week before
onset of illness [34, 43]. Human to human trans-
mission has so far been limited and infrequent, but it
is important that vigilance be maintained as the
avian epidemic with transmission to humans con-
tinues [1, 23, 34].
Unlike influenza types B and C, type A is notorious
for undergoing antigenic shift. Many RNA viruses
replicate their genomes imperfectly, giving rise to
amino acid changes which may ultimately be
selected for in a previously immune population. In
addition to this relatively slow seasonal evolution of
‘antigenic drift’, influenza subtype A viruses are able
to undergo genetic exchange (re-assortment) of one
or more of the eight segmented single stranded RNA
with other A subtype viruses [42]. One of the major
concerns is that the current pattern of limited person
to person spread could suddenly change, for
instance antigenic shift resulting in a highly patho-
genic new variant which is readily transmitted
between humans [8, 29, 42]. Since there is little or
no immunity to H5N1 in the human population, a
pandemic situation could arise with little or no ‘herd
immunity’ to slow widespread transmission in the
human population [23, 43]. Clearly, this situation
illustrates the need for careful collaboration between
human and veterinary medicine in closely monitor-
ing avian influenza and implementing outbreak
control measures as early as possible [10, 18, 21–
23, 25, 26, 38, 40, 41].
Severe acute respiratory syndrome
The clinical presentation and travel history of
persons with severe acute respiratory syndrome
(SARS) or influenza AH5N1 may overlap. Typically,
patients present with a nonspecific illness manifest-
ing fever, malaria, myalgia with chills, rigour or
diarrhoea in some cases [44]. While the clinical and
radiographic features of most viral pneumonias are
Fig. 1 The westward spread of Avian influenza H5N1. The seasonal North to South migratory routes ‘flyways’ correspond to overlapping
large shaded colour regions. The first cases of highly pathogenic avian influenza (HPAI) H5N1 in 1997 were identified in poultry farms and
markets in Hong Kong along with the first documented human fatality. HPAI H5N1 reappeared in 2002 in Hong Kong. In 2003 this
variant began spreading throughout the poultry industry in large areas of Southeast Asia and by March 2004 there were 23 confirmed
human cases of which 16 were fatal. By the first half of 2005 the virus had reached the north-west boarder of China (red dots), and by late
2005 (yellow dots) had reached central and south Western Russia, Turkey and had entered Europe in Romania and Croatia. In the first half
of 2006 many countries in Europe (purple dots) had reported cases including recent documentation of H5N1 in a dead swan in Scotland.
� 2006 Blackwell Publishing Ltd Journal of Internal Medicine 260: 399–408
R E V I E W : Z O O N O T I C V I R U S E S A N D E A R L Y D E T E C T I O N 4 0 1

not distinctive, SARS in contrast does not typically
have upper respiratory symptoms. A good clinical
history will be essential when considering exposure
and risk factors. Travel and contacts and contact
with specific types of animals, food handlers, farms
or markets will be important indications [45–48].
Before laboratory results, distinguishing clinical
features include a lack of upper respiratory tract
symptoms, a distinguishing feature from coughs and
dyspnoea observed in most SARS patients [6, 19,
20, 24].
In the differential diagnosis, influenza A should be
considered and laboratory sub-typing requested.
Both SARS and pandemic influenza are zoonotic in
origin, hence early veterinary detection and surveil-
lance of animals, coupled with human surveillance
and early detection will be key to preventing
epidemics [6, 19, 21, 22, 24, 40, 49].
There are important differences in the dynamics of
infection between SARS and influenza A/H5N1
which have had an impact on control. When SARS
was transmitted from animals it adapted to be able
to be efficiently transferred from human to human,
and within weeks had spread to other continents by
airline passengers [6]. Before the 2002/2003 epi-
demic, serological evidence suggested that transmis-
sion to wild animal market workers from animals
had already occurred. The interpretation is that the
earlier SARS–CoV variants were less adapted for
human infection, and human to human transmis-
sion of earlier variants was relatively inefficient.
Fortunately, as of April 2006, the current H5N1
avian flu is still inefficient at being transmitted from
humans to humans [32]. There are important risk
differences that are critical to consider with these
two zoonotic respiratory diseases. First, the popula-
tion dynamics and ecosystems of the two natural
host reservoirs are different. While the SARS–CoV
was probably transmitted to humans handling palm
civets, current data suggest that Horseshoe Bats are
the leading contenders as natural reservoirs [46, 47]
suggesting a complex and possibly localised ecosys-
tem. In comparison, the ecosystems of migratory
waterfowl currently distributing influenza A H5N1,
are vast (Fig. 1) and involve the interaction of many
susceptible species [14]. The closing of wildlife
markets in Guangdong province may certainly
reduce risks of SARS in humans, but with respect
to H5N1 the indoor confinement of domestic birds
along the vast migratory routes of wild fowl is a tall
order. Early diagnosis and rapid response pro-
grammes such as surveillance fever clinics supported
by a panel of rapid antigen tests and RT-PCR assays,
greatly increase speed and accuracy of clinical
laboratory reporting for both SARS–CoV and influ-
enza A and subtypes [24]. Fortunately, with SARS
the onset of symptoms in exposed infected individ-
uals precedes the period of high infectivity [20, 40].
Thus, fever surveillance, recognition and rapid
quarantine were effective in ultimately controlling
the 2003 SARS epidemic [24, 40]. Importantly,
however, in contrast with influenza A, a patient
may become infectious before clinical illness, mark-
edly reducing the effectiveness of quarantine in the
case of a human epidemic or pending pandemic
[40].
Flaviviruses and epidemics
These positive-stranded RNA viruses are commonly
transmitted by different species of mosquitoes. It is
the population dynamics and seasonal distribution of
the mosquito vectors and their potential hosts which
greatly influence the epidemiology of flavivirus
diseases. The genus Flavivirus includes West Nile
virus (WNV), Japanese encephalitis virus (JEV), St
Louis encephalitis (StLE), and Murray Valley enceph-
alitis, which belong to the JEV antigenic group, as
well as Dengue virus (DV) and Yellow Fever virus
(YFV) [4]. In general, flavivirus infections can
present as three clinical syndromes; 1) fever with
arthralgia and rash; 2) viral haemorrhagic fever
(VHF); and 3) neurological disease [50–53].
With respect to WNV infection, most are either
asymptomatic or may cause mild disease which may
go unreported [54, 55]. A mild clinical expression of
the infection ‘West Nile Fever’ is accompanied by
arthralgia and rash. Of persons with WNV infection,
roughly 50% develop a rash within a week with
lymphadenopathy which resolves. Less frequently,
but more importantly, dissemination to the central
nervous system may occur with clinical evidence of
spread developing approximately 2 days after peak
viraemia [56, 57]. Unlike with other arboviral
infections which cause encephalitis there is no
vasculitits, inflammatory infiltrates are minimal
and associated with neuronal proliferation and
microglial nodule formation [56, 57]. Fatalities are
often associated with inflammation in the brainstem
although other regions are involved [51, 53].
� 2006 Blackwell Publishing Ltd Journal of Internal Medicine 260: 399–408
4 0 2 J . L . H E E N E Y

In North America, the epidemic is associated with
disease in horses and birds, particularly related
members of the crow family which are highly
susceptible and whose mortality is unusually high
[50, 58, 59]. Seasonal cycles are associated with a
westward North America spread and following the
migratory routes of birds which are believed to be
amplification hosts as well as hosts of mosquitoes of
the Culex genus [15, 55, 59–61]. It is believed that
mammals do not sustain a viraemia sufficient for
further transmission [54, 55, 59, 60, 62].
Diagnosis can be confirmed by antigen specific
IgM in blood or CSF [62]. Clear effective treatment
has not been delineated. Other arboviral infections
should be ruled out. Prophylactic vaccine candidates
for humans are in clinical trials and at least two
WNV vaccines have been licensed for use in horses
[50]. While WNV is spreading seasonally in North
America, JEV is expanding in Australasia and is the
most important cause of arboviral induced enceph-
alitis worldwide [15, 63]. Again Culex sp. mosqui-
toes are the most important vector associated with
enzootics in the tropics. The cycle is maintained in
waterfowl and swine are believed to be the most
important amplifying hosts [63]. A formalin inacti-
vated vaccine is used prophylactically internation-
ally while a live attenuated vaccine strain is used
primarily in China [63, 64].
Dengue virus infection can be caused by four
distinct serotypes and in contrast to the encephalitic
disease potential of JEV and WNV, is best known for
its ability to cause fatal haemorrhagic disease [15,
52, 65]. Of all flaviviruses, DV causes the greatest
incidence of human illness, and is transmitted
primarily from person to person by Aedes aegypti
mosquitoes in endemic regions. Indeed, there has
been a global resurgence of Dengue and this has
been attributed to regional population growth
around large cities, increased transportation and
failing public health control measures [15, 58, 65,
66].
Yellow fever characteristically causes haemor-
rhagic fever with marked hepatic, renal and myo-
cardial injury with high mortality. Originally
endemic in Sub-Saharan Africa, it was believed to
be introduced into South America by the slave trade.
In urban areas, human-to-human transmission is
associated with Aedes aegypti mosquitoes, while as a
zoonosis it is transmitted by different Aedes species
from viremic nonhuman primate reservoirs in the
tropical forests of Africa and South America [15].
The live attenuated 17D vaccine developed in the
1930s, originally believed to be amongst the safest,
has recently been associated with a number of
fatalities [67].
Viral haemorrhagic fever
The clinical syndrome known as VHF can be caused
by a number of different RNA viruses belonging to
four diverse families. These include (i) the Flavivir-
idae, including dengue (DV) and YFV (mentioned in
the previous section); (ii) the Arenaviridae [for
example Lassa fever virus (LFV)], (iii); Bunyaviridae
[as represented by Rift Valley Fever (RVF)], and (iv);
the Filoviridae, the best known of which are the
Ebola related viruses [15–17, 31, 68–70].
These viral infections warrant special emphasis,
as they are associated with acute contagious
epidemics with high rates of life threatening illness
and high mortality. They represent infections that
must be reported and authorities mobilised for
containment and quarantine due to their potential
for rapid human-to-human dissemination. VHFs are
characterised by a febrile multi-systemic syndrome
with loss of micro vascular integrity, bleeding
diathesis, multi-organ failure and shock. Clinical
manifestations of VHF often overlap and vary
between individuals and aetiological agents making
an aetiological diagnosis based on clinical presenta-
tion unlikely in the absence of a revealing patient
history. The incubation period varies from 48 hours
up to 21 days with an apparent acute onset.
Typically, prodromal syndromes include fever, myal-
gia and anthralgias, headache with nausea, vomit-
ing or diarrhoea. Externally, there is often evidence
of a progressive diathesis manifested as conjunctival
and mucosal haemorrhage, haematuria, melina and
disseminated intravascular coagulation are observed
with hypotension, leukopenia and thrombocytope-
nia. As the syndrome progresses, neurological
manifestations such as delirium, seizures and coma
precede multiple system failure, shock and death
[16, 17, 31, 70, 71].
Generally, Arenavirus VHFs progress more slowly
and may have a lower mortality rate than Filovi-
ruses (i.e. Ebola-Zaire) [70]. While, in addition to
supportive care, therapeutic options may be limited,
rapid etiologic diagnosis may facilitate treatment
decisions such as intravenous Ribavirin therapy (not
� 2006 Blackwell Publishing Ltd Journal of Internal Medicine 260: 399–408
R E V I E W : Z O O N O T I C V I R U S E S A N D E A R L Y D E T E C T I O N 4 0 3

generally effective against Filoviruses and Flavivi-
ruses) [16, 17, 70]. Viral diagnostics are most
advisable by immediate contact with specialised
laboratories. Assays include PCR for multiple VHFs,
antigen capture and IgM ELISAs [71, 72]. As the
acute symptoms for VHFs are not usually indicative
of a specific aetiology, the speed of treatment and
quarantine are essential. An early aetiological diag-
nosis will guide treatment and containment of
others exposed but not yet symptomatic. The extent
of human-to-human spread depends on the nature
of the aetiological agent, and the nature of the
exposure (i.e. contact with body fluids or aerosol
from a vector such as rodents versus a bite from an
infected tick or mosquito).
The epidemiology of the agents which cause VHF
is generally variable and diverse. The Filoviruses
such as Ebola and Marburg are generally endemic in
certain regions of Africa [73, 74], and their natural
reservoirs still undefined, they are highly contagious
by contact and aerosol and recent international air
travel from a high-risk region must be considered in
any patient exhibiting unusual symptoms. Other
VHF viruses are transmitted to humans from ticks
[Congo–Crimean haemorrhagic fever (CCHFV)],
mosquitoes (Yellow fever and Dengue Fever Viruses)
or feces or urine from rodents [i.e. Arenaviruses
such as LFV, Argentinean haemorrhagic Fever
(Junin) and Bolivian haemorrhagic (Machupo) fever
viruses]. With the exception of Dengue, all of these
HFV are infectious by aerosol or fomites and human-
to-human transmission is frequently nosocomal
from viremic patients. The clinical diagnosis is
greatly facilitated by a detailed travel or contact
(i.e. nosocomial) history [16, 17, 31, 68, 70].
Contact with a rodent infested environment or bites
by ticks (e.g. CCHFV) or travel or stay in mosquito
prevalent regions where YFV or DV are known to
persist, provide time saving leads.
Emerging viral disease trends
Over the past decade, there has been an observed
increase in the number of zoonotic and vector-borne
viral diseases world wide, but particularly in South-
east Asia and the South Pacific ([75], WHO, CDC
databases). While SARS has come and gone, H5N1
continues its seasonal westward march from the
Western Pacific now eastwards over Europe to the
British Isles (Fig. 1). Seasonal migration habitats of
waterfowl that naturally asymptomatically carry
type A influenza is the main route of movement
between continents. Overlapping migration routes
and breeding grounds may in part explain how such
viruses are transmitted between migrating popula-
tions of birds [14]. In the case of vector-borne
diseases, the westward spread of WNV across North
America is a graphic example of a vector-ecosystem
shift causing seasonal spread and advance from the
Atlantic to the Pacific coasts of North America [76].
As WNV represents a new ‘emerging vector-borne’
viral disease in North America, it is a re-emerging
disease in Europe [77].
Dengue and Japanese encephalitis viruses repre-
sent the major vector-borne disease agents with
high numbers of human infections, but for which
accurate incidence markers remain difficult to
obtain (Table 1). Most emerging viruses have been
zoonotic, many of which are transmitted by bat
species (i.e. Nipah, Rabies and Hendra), but not
exclusively (as with Rabies). The cases of new
zoonotic infections can be incidental and disappear
Table 1 Estimated worldwide
morbidity and mortality figures of
selected viral zoonotic diseases,
2000–2005
Viral disease Estimated cases Estimated fatalities
H5/NI avian influenza 145 77
SARS corona virus 8102 774
West Nile disease (USA only) 19 525 771
Japanese encephalitis virus Approx. 30 000–50 000 Approx. 9000–15 000
Dengue virus Approx. 50 million Approx. 25 000 (DHF)
Ebola/Marburg 774/528 485/457
Lassa fever virus Approx. 100 000–300 000 5000
Nipahvirus 276 106
Hendravirus 3 2
Rabies NA 30 000
Prion diseases/TSE (vCSD) 188 182
� 2006 Blackwell Publishing Ltd Journal of Internal Medicine 260: 399–408
4 0 4 J . L . H E E N E Y
once the cause has been identified and preventative
measures taken (Nipah virus 1998–1999)
(Table 1).
Discussion
The early identification and diagnosis of viral
zoonoses are of great importance with respect to
treatment, containment and public health control.
The infectious disease dynamics of viral zoonoses are
very diverse and will have distinct prevention and
control strategies. Classical examples such as rabies
require careful monitoring of natural reservoirs, and
implementation of prophylactic vaccination of wild-
life in endemic regions. Cases in humans are limited
to exposed individuals and human-to-human spread
is highly unlikely. Early identification of the risk of
exposure and prophylactic immunotherapy are
effective in limiting the number of cases with fatal
consequences. At the other extreme are the highly
contagious viral pathogens which cause acute
diseases such as the respiratory, neurologic and
haemorrhagic fever diseases reviewed here. Each of
the viral agents which cause these diseases has an
unique aecology with their natural host, some of
which we are just beginning to understand, and
others where even the natural reservoir has yet to be
identified [74, 78]. New rapid diagnostic assays
based on PCR technology are potentially capable of
simultaneously identifying up to 10 different aetio-
logical agents which have the potential to cause
VHF syndrome [72].
There will undoubtedly be new zoonotic viruses
for which we must always be vigilant. There will not
always be acute symptoms and an epidemic may not
be initially apparent. Examples of this latter category
include the slow viral or prion diseases which may
be transmitted asymptomatically, potentially caus-
ing disease in humans a decade or more after
exposure has occurred [30]. The great BSE risk was
caused by the presence of potentially pathogenic
prions in the food chain and a potential asympto-
matic period as long as four to five decades. Similar,
in that it is transmitted between asymptomatic
individuals, HIV has had its origins from Zoonotic
cross-species transmissions from nonhuman pri-
mates [79, 80]. Having adapted to be efficiently
transmitted from humans-to-humans, HIV had
devastating effects early in the human epidemic
when it entered national blood supplies and was
widely transmitted unknowingly [5, 11].
The development of vaccines for the control of
potential zoonotic infections in wildlife (i.e. rabies
vaccines for foxes and raccoons) as well as the
prevention of spread and disease in humans is
ongoing. In some cases, there are good candidate
vaccines [81] but the risk of human disease may be
perceived to be too low to be economical [64], or
there may be insufficient supplies for the entire
population [29].
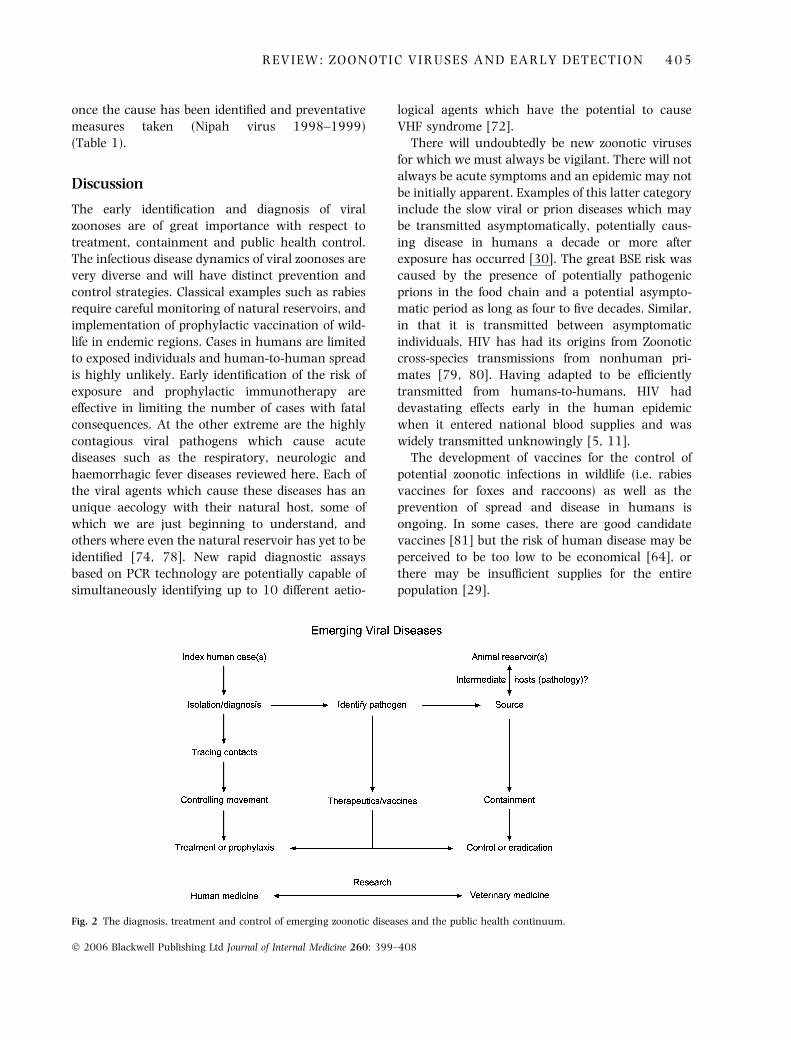
Fig. 2 The diagnosis, treatment and control of emerging zoonotic diseases and the public health continuum.
� 2006 Blackwell Publishing Ltd Journal of Internal Medicine 260: 399–408
R E V I E W : Z O O N O T I C V I R U S E S A N D E A R L Y D E T E C T I O N 4 0 5

Vaccines have been very successful at eradicating
devastating human diseases such as smallpox.
However, immunological niches for new emerging
diseases such as monkeypox may be created, and
for these possibilities we must remain vigilant
[74, 82].
The early identification, control and prevention of
re-emerging viral zoonotics lies not only with
clinicians and public health experts, but importantly
with veterinarians, animal scientists and wildlife
ecologists [10, 21]. The early identification of
perturbations in ecosystems, from die-offs of wildlife
or domestic animals (Fig. 2), especially those which
interface with wildlife (i.e. Nipha virus), is critical for
future prevention and control [83]. It is our aware-
ness and surveillance of the animal and human
health continuum which will facilitate early identi-
fication and control of new emerging and
re-emerging viral zoonotics [27].
Conflict of interest statement
No conflict of interest was declared.
Acknowledgements
For the assistance of Thea de Koning and H. van
Westbroek I am greatly indebted. I would especially
like to acknowledge the teamwork of H. Niphuis, N.
Beenhakker and D. Davis for the difficult task of
unravelling disease statistics and estimates from
various international databases.
References
1 Taylor LH, Latham SM, Woolhouse ME. Risk factors for hu-
man disease emergence. Philos Trans R Soc Lond B Biol Sci
2001; 356: 983–9.
2 Woolhouse ME, Gowtage-Sequeria S. Host range and emerging
and reemerging pathogens. Emerg Infect Dis 2005; 11: 1842–7.
3 Woolhouse ME, Taylor LH, Haydon DT. Population biology of
multihost pathogens. Science 2001; 292: 1109–12.
4 Acha P, Szyfres B, eds. Zoonoses and Communicable Diseases
Common to Man and Animals Volume II. Washington: Pan
American Health Organisation, 2003; 3–385.
5 Weiss RA, McMichael AJ. Social and environmental risk fac-
tors in the emergence of infectious diseases. Nat Med 2004;
10: S70–6.
6 Enserink M. Infectious diseases. One year after outbreak,
SARS virus yields some secrets. Science 2004; 304: 1097.
7 Martinez VP, Bellomo C, San Juan J, Pinna D, Forlenza R,
Elder M, Padula PJ. Person-to-person transmission of Andes
virus. Emerg Infect Dis 2005; 11: 1848–53.
8 Webby R, Hoffmann E, Webster R. Molecular constraints to
interspecies transmission of viral pathogens. Nat Med 2004;
10: S77–81.
9 van Riel D, Munster VJ, de Wit E, Rimmelzwaan GF, Fouchier
RA, Osterhaus AD, Kuiken T. H5N1 virus attachment to
lower respiratory tract. Science 2006; 312: 399.
10 Murphy FA. Emerging zoonoses. Emerg Infect Dis 1998; 4:
429–35.
11 Weiss RA. Cross-species infections. Curr Top Microbiol Immu-
nol 278: 47–71.
12 Elbers AR. 2002. Local and global impact of disease out-
breaks. Adv Pork Prod 2003; 13: 17–27.
13 Fergus R, Fry M, Karesh WB, Marra PP, Newman S, Paul E.
Migratory birds and avian flu. Science 2006; 312: 845–6.
14 Olsen B, Munster VJ, Wallensten A, Waldenstrom J, Oster-
haus AD, Fouchier RA. Global patterns of influenza a virus in
wild birds. Science 2006; 312: 384–8.
15 Petersen LR, Marfin AA. Shifting epidemiology of Flaviviridae.
J Travel Med 2005; 12 (Suppl. 1): S3–11.
16 CDC.Notice to Readers Update: Management of Patients with
Suspected Viral Hemorrhagic Fever – United States. MMWR
1995; 44: 475–9.
17 CDC. Brief Report: Outbreak of Marburg Virus Hemorrhagic
Fever — Angola, October 1, 2004–March 29, 2005. MMWR
2005; 54: 1–2.
18 Fenton A, Pedersen AB. Community epidemiology framework
for classifying disease threats. Emerg Infect Dis 2005; 11:
1815–21.
19 Agarwal SB, Karavadara N, Khakhkhar V. Bird flu: a diagnostic
dilemma in the present scenario. JIACM 2004; 5: 345–7.
20 Cauchemez S, Boelle PY, Donnelly DA et al. Real-time esti-
mates in early detection of SARS. Emerg Infect Dis 2006; 12:
110–3.
21 Chomel BB. Control and prevention of emerging zoonoses.
J Vet Med Educ 2003; 30: 145–7.
22 Vourc’h G, Bridges VE, Gibbens J, De Groot BD, McIntyre L,
Poland R, Barnouin J. Detecting emerging diseases in farm
animals through clinical observations. Emerg Infect Dis 2006;
12: 204–10.
23 Fauci AS. Pandemic influenza threat and preparedness. Emerg
Infect Dis 2006; 12: 73–77.
24 Ho MS, Su II. Preparing to prevent severe acute respiratory
syndrome and other respiratory infections. Lancet Infect Dis
2004; 4: 684–9.
25 Marano N, Arguin P, Pappaioanou M, King L. Role of
multisector partnerships in controlling emerging zoonotic
diseases. Emerg Infect Dis 2005; 11: 1813–4.
26 Mounier-Jack S, Coker RJ. How prepared is Europe for pan-
demic influenza? Analysis of national plans. Lancet 2006;
367: 1405–11.
27 Editorial. We have been warned. Nature 2003; 424: 113.
28 Arita I, Nakane M, Fenner F. Public health. Is polio eradica-
tion realistic? Science 2006; 312: 852–4.
29 Emanuel EJ, Wertheimer A. Public health. Who should get
influenza vaccine when not all can? Science 2006; 312: 854–5.
30 Glass RI. Perceived threats and real killers. Science 2004; 304:
927.
31 Pigott DC. Hemorrhagic fever viruses. Crit Care Clin 2005; 21:
765–83; vii.
32 Beigel JH, Farrar J, Han AM et al. Avian influenza A (H5N1)
infection in humans. N Engl J Med 2005; 353: 1374–85.
� 2006 Blackwell Publishing Ltd Journal of Internal Medicine 260: 399–408
4 0 6 J . L . H E E N E Y

33 Chotpitayasunondh T, Ungchusak K, Hanshaoworakul W
et al. Human disease from influenza A (H5N1), Thailand,
2004. Emerg Infect Dis 2005; 11: 201–9.
34 Tiensin T, Chaitaweesub P, Songserm T et al. Highly patho-
genic avian influenza H5N1, Thailand, 2004. Emerg Infect Dis
2005; 11: 1664–72.
35 Gilbert M, Chaitaweesub P, Parakamawongsa T et al. Free-
grazing ducks and highly pathogenic avian influenza, Thai-
land. Emerg Infect Dis 2006; 12: 227–34.
36 Neumann G. Host range restriction and pathogenicity in the
context of influenza pandemic. Emerg Infect Dis 2006; 12:
881–6.
37 Krause R. The swine flu episode and the fog of epidemics.
Emerg Infect Dis 2006; 12: 40–3.
38 Kilbourne ED. Influenza pandemics of the 20th century.
Emerg Infect Dis 2006; 12: 9–14.
39 Koopman M, Wilbrink B, Conyn M et al. Transmission of
H7N7 avian influenza A virus to human beings during a large
outbreak in commercial poultry farms in the Netherlands.
Lancet 2004; 363: 587–93.
40 Lipsitch M, Robins JM, Mills CE, Bergstrom CT. Multiple out-
breaks and flu containment plans. Science 2006; 312: 845.
41 Luke CJ, Subbarao K. Vaccines for pandemic influenza. Emerg
Infect Dis 2006; 12: 66–72.
42 Subbarao K, Murphy BR, Fauci AS. Development of effective
vaccines against pandemic influenza. Immunity 2006; 24: 5–
9.
43 Webster RG, Peiris M, Chen H, Guan Y. H5N1 outbreaks and
enzootic influenza. Emerg Infect Dis 2006; 12: 3–8.
44 Lo JY, Tsang TH, Leung YH, Yeung EY, Wu T, Lim WW.
Respiratory infections during SARS outbreak, Hong Kong,
2003. Emerg Infect Dis 2005; 11: 1738–41.
45 Bell D, Roberton S, Hunter PR. Animal origins of SARS cor-
onavirus: possible links with the international trade in small
carnivores. Philos Trans R Soc Lond B Biol Sci 2004; 359:
1107–14.
46 Lau SK, Woo PC, Li KS et al. Severe acute respiratory syn-
drome coronavirus-like virus in Chinese horseshoe bats. Proc
Natl Acad Sci U S A 2005; 102: 14040–5.
47 Li W, Shi Z, Yu M et al. Bats are natural reservoirs of SARS-
like coronaviruses. Science 2005; 310: 676–9.
48 Wang M, Yan M, Xu H et al. SARS–CoV infection in a
restaurant from palm civet. Emerg Infect Dis 2005; 11:
1860–5.
49 Chu CM, Cheng VC, Hung IF et al. Viral load distribution in
SARS outbreak. Emerg Infect Dis 2005; 11: 1882–6.
50 Hayes EB, Gubler DJ. West Nile virus: epidemiology and
clinical features of an emerging epidemic in the United States.
Annu Rev Med 2006; 57: 181–94.
51 Sampson BA, Armbrustmacher V. West Nile encephalitis: the
neuropathology of four fatalities. Ann N Y Acad Sci 2001;
951: 172–8.
52 Solomon T, Mallewa M. Dengue and other emerging flavivi-
ruses. J Infect 2001; 42: 104–15.
53 Madden K. West Nile virus infection and its neurological
manifestations. Clin Med Res 2003; 1: 145–50.
54 Green MS, Weinberger M, Ben-Ezer J et al. Long-term Death
Rates, West Nile virus epidemic, Israel, 2000. Emerg Infect Dis
2005; 11: 1754–7.
55 Mostashari F, Bunning ML, Kitsutani PT et al. Epidemic West
Nile encephalitis, New York, 1999: results of a household-
based seroepidemiological survey. Lancet 2001; 358: 261–4.
56 Hayes EB, Sejvar JJ, Zaki SR, Lanciotti RS, Bode AV, Campbell
GL. Virology, pathology, and clinical manifestations of West
Nile virus disease. Emerg Infect Dis 2005; 11: 1174–9.
57 Sejvar JJ, Bode AV, Marfin AA, Campbell GL, Papa J, Big-
gerstaff BJ, Petersen LR. West Nile virus-associated flaccid
paralysis outcome. Emerg Infect Dis 2006; 11: 514–6.
58 Stone WB, Therrien JE, Benson R, Kramer L, Kauffman EB,
Eldson M, Campbell S. Assays to detect West Nile virus in
dead birds. Emerg Infect Dis 2005; 11: 1770–3.
59 Molaei G, Andreadis G, Armstrong PM, Andersin JF, Vossbr-
inck CR. Host feeding patterns of Culex mosquitos and West
Nile virus transmission, northeastern United States. Emerg
Infect Dis 2006; 11: 468–74.
60 Hayes EB, Komar N, Nasci RS, Montgomery SP, O’Leary DR,
Campbell GL. Epidemiology and transmission dynamics of
West Nile virus disease. Emerg Infect Dis 2005; 11: 1167–73.
61 Mandalakas AM, Kippes C, Sedransk J et al. West Nile virus
epidemic, northeast Ohio, 2002. Emerg Infect Dis 2005; 11:
1774–7.
62 Komar N. West Nile viral encephalitis. Rev Sci Tech 19: 166–76.
63 Rosen L. The natural history of Japanese encephalitis virus.
Annu Rev Microbiol 1986; 40: 395–414.
64 Zohrabian A, Hayes EB, Petersen R. Cost-effectiveness of West-
Nile virus vaccination. Emerg Infect Dis 2006; 11: 375–80.
65 Gubler DJ. Epidemic dengue/dengue hemorrhagic fever as a
public health, social and economic problem in the 21st cen-
tury. Trends Microbiol 2002; 10: 100–3.
66 Ooi EE. Dengue prevention and 35 years of vector control in
singapore. Emerg Infect Dis 2006; 12: 887–93.
67 Chan RC, Penney DJ, Little D, Carter IW, Roberts JA, Raw-
linson WA. Hepatitis and death following vaccination with
17D-204 yellow fever vaccine. Lancet 2001; 358: 121–2.
68 Borio L, Inglesby T, Peters CJ et al. Hemorrhagic fever viruses
as biological weapons: medical and public health manage-
ment. Jama 2002; 287: 2391–405.
69 Chevalier V, Lancelot R, Thiongane Y, Sall B, Diaite A,
Mondet B. Rift Valley fever in small ruminants, Senegal,
2003. Emerg Infect Dis 11: 1693–700.
70 Jeffs B A clinical guide to viral haemorrhagic fevers: Ebola,
Marburg and Lassa. Trop Doct 2005; 36: 1–4.
71 Jahrling PB. Viral hemorrhagic fevers. In: Zajtchuk R, Bella-
my RF, eds. Medical Aspects of Chemical and Biological Warfare,
Textbook of Military Medicine. Washington, DC: Office of the
Surgeon General, U.S. Department of the Army, 1997: 591–
602.
72 Palacios G, Briese T, Kapoor V et al. MassTag polymerase
chain reaction for differential diagnosis of viral hemorrhagic
fever. Emerg Infect Dis 2006; 12: 692–5.
73 WHO. Marburg haemorrhagic fever in Angola – update 23. WHO
Factsheet 2005.
74 Wolfe ND. Bushmeat hunting, deforestation, and prediction of
zoonotic disease emergence. Emerg Infect Dis 2005; 11: 1822–7.
75 Mackenzie JS, Chua KB, Daniels PW et al. Emerging viral
diseases of Southeast Asia and the Western Pacific. Emerg
Infect Dis 2001; 7: 497–504.
76 Daszak P, Cunningham AA, Hyatt AD. Emerging infectious
diseases of wildlife–threats to biodiversity and human health.
Science 2000; 287: 443–9.
77 Hubalek Z, Lukacova L, Halouzka J, Sirucek P, Januska J,
Precechtelova J, Prochazka P. Import of West Nile virus
infection in the Czech Republic. Eur J Epidemiol 2006; 21:
323–4.
� 2006 Blackwell Publishing Ltd Journal of Internal Medicine 260: 399–408
R E V I E W : Z O O N O T I C V I R U S E S A N D E A R L Y D E T E C T I O N 4 0 7

78 Li TC, Chijiwa K, Sera N et al. Hepatitis E virus transmission
from wild boar meat. Emerg Infect Dis 2005; 11: 1958–60.
79 Hahn BH, Shaw GM, De Cock KM, Sharp PM. AIDS as a
zoonosis: scientific and public health implications. Science
2000; 287: 607–14.
80 Heeney JL, Dalgleish AG, Weiss RA. Origins of HIV and the
evolution of resistance to AIDS. Science 2006; 313: 462–6.
81 Daddario-DiCaprio KM, Geisbert TW, Stroher U et al. Postex-
posure protection against Marburg haemorrhagic fever with
recombinant vesicular stomatitis virus vectors in non-human
primates: an efficacy assessment. Lancet 2006; 367: 1399–404.
82 Frey SE, Belshe RB. Poxvirus zoonoses–putting pocks into
context. N Engl J Med 2004; 350: 324–7.
83 Chadha MS, Comer JA, Lowe L et al. Nipah virus-associated
encephalitis outbreak, Siliguri, India. Emerg Infect Dis 2006;
12: 235–40.
Correspondence: J. L. Heeney, Department of Virology, BPRC,
Rijswijk, and the Department of Medical Microbiology, University
of Leiden, Leiden, The Netherlands.
(fax: +31 15 284 2601; e-mail: [email protected]).
� 2006 Blackwell Publishing Ltd Journal of Internal Medicine 260: 399–408
4 0 8 J . L . H E E N E Y
Copyright © 2022 FDOKUMEN