
Xerox University Microfilms #Ann Arbor, Michigan 48106
206
76-9956 DERRICK, Sara Marian, 1918* INFANTS BORN TO NARCOTIC AND NONNARCOTIC ADDICTED WOMEN: A STUDY OF THEIR NEUROLOGICAL STATUS AT BIRTH AND RESPONSE TO AN INFANT STIMULATION PROGRAM IN THE FIRST THREE MONTHS OF LIFE. The Ohio State University, Ph.D., 1975 Education, psychology Xerox University Microfilms # Ann Arbor, Michigan 48106 THIS DISSERTATION HAS BEEN MICROFILMED EXACTLY AS RECEIVED. ©Copyright by Sara Marian Derrick 1975
-
Upload
khangminh22 -
Category
Documents
-
view
7 -
download
0
Transcript of Xerox University Microfilms #Ann Arbor, Michigan 48106

76-9956DERRICK, Sara Marian, 1918*
INFANTS BORN TO NARCOTIC AND NONNARCOTIC ADDICTED WOMEN: A STUDY OF THEIRNEUROLOGICAL STATUS AT BIRTH AND RESPONSE TO AN INFANT STIMULATION PROGRAM IN THE FIRST THREE MONTHS OF LIFE.The Ohio State University, Ph.D., 1975 Education, psychology
Xerox University Microfilms # Ann Arbor, Michigan 48106
THIS DISSERTATION HAS BEEN MICROFILMED EXACTLY AS RECEIVED.
©Copyright by Sara Marian Derrick
1975

INFANTS BORN TO NARCOTIC AND NONNARCOTIC ADDICTED WOMEN:
A STUDY OF THEIR NEUROLOGICAL STATUS AT BIRTH AND
RESPONSE TO AN INFANT STIMULATION PROGRAM
IN THE FIRST THREE MONTHS OF LIFE
DISSERTATION
Presented in Partial Fulfillment of the Requirements for
the Degree Doctor of Philosophy in the Graduate
School of The Ohio State University
BySara Marian Derrick, B.A., M. Ed
The Ohio State University
1975
Reading Committee: Approved By
Julia Dalrymple, Ph.D. William Dowling, Ph.D. Jean D. Powers, Ph.D.
Claribel Taylor, Ph.D. Ellen R. Hock, Ph.D. fa
School of Home Economics Department of Family Relations and Human Development

ACKNOWLEDGMENTS
Many persons have provided resources to make this study possible.
My first appreciation is extended to Dr. Ellen R, Hock, who first
brought to my awareness the exciting field of infant development and
who assisted in guiding my program through its entirety. Appreciation
is further extended to Dr. Claribel Taylor and to Dr. Julia Dalrymple
who patiently provided direction in formulating specifics in this study.
I wish also to thank my reading and examining committee who provided
much encouragement to me.
My most heartfelt thanks are extended to persons at The Ohio
State University Hospitals— Dr. Elizabeth Ruppert, Pediatrician, who
helped me develop facility in using medical data in this study,
administered neurological examinations, provided medical follow-up to
the infants and advice to their parents. Thanks to Mrs. Chris Harter,
Pediatric Nurse, who promptly alerted me to availability of subjects,
and who helped motivate the parents, to participate in the study and
to seek medical follow-up for their infants. Appreciation is also
extended to the other nurses at The Ohio State University for their
kindness in sharing their work areas with me in order that I might
have space for assessing the infants.
Thanks are also extended to Dr. Jean D. Powers and Ms. Linda C.
Rolfes, Department of Preventive Medicine, for providing statistical
sophistication for analysis of masses of data in this study, and to
Dr. Mary Anne Trause, of Rainbow Children’s Hospital, Case Western
Reserve University Hospital, Cleveland, Ohio, who guided me through
refinement of techniques for administering the Brazelton Scale.
The generosity and cooperation extended by staff of Vita Drug
Treatment Center, Project Lynden, and Traynor House, Columbus, Ohio
will never be forgotten.
Appreciation is extended to the typist, Mrs. Nancy V. Davidson,
for her thoroughness and diligence in completing the manuscript.
Special thanks are extended to the parents of the infants who
permitted me to enter their homes on so many occasions and work with
them. Without their cooperation this study would not have been possible.
Finally, sincere gratitude is extended to my husband, Bill, who
patiently made many sacrifices in order that this study might be
brought to fruition.
iii

VITA
January 4, 19 1 8............... .. Born - Cuthbert, Georgia
1956 .........................B.A., Howard UniversityWashington, D. C,
1957 - 1967 ............... Teacher, Sandusky Public Schools,Sandusky, Ohio
1959............................ M.Ed., Bowling Green State University,Bowling Green, Ohio
1963 - 1972.................... Director, Ebenezer Day Nursery,Sandusky, Ohio (Part-time)
1967 - 1968.................... Director, Remedial Reading,Sandusky Public Schools, Sandusky,Ohio
1968 - 1969 ................. Intern School Psychologist,Betty Jane Memorial Rehabilitation Center, Tiffin, Ohio
1969 - 1974 ................... Psychologist, Sandusky Public Schools,Sandusky, Ohio
1972 - 1973 . ........ . . . . . Graduate Research Associate,Department of Pediatrics,The Ohio State University Hospitals, Columbus, Ohio
1975 . . . . . . . . . . . . . . Instructor, Bowling Green StateUniversity, Bowling Green, Ohio
Major Fields of Study:
Family Studies and Child Development - Dr. Ellen HockDr. Claribel Taylor
Developmental Psychology - Dr. George Thompson
Early Childhood Education - Ms, Isabel Miller
iv

TABLE OF CONTENTS
page
ACKNOWLEDGMENTS......................................... U
V I T A ................................................... v
LIST OF T A B L E S ........................................ ix
LIST OF FIGURES ....................................... xii
Chapter
I INTRODUCTION ................................... 1
Background for the Study ..................... 1Significance of the Study ..................... 3Statement of the Problem ..................... 4Objectives............... 4Hypotheses ..................................... 7Limitations in the Study ....................... 9Relationship to a Larger Research Project . . . . 10Glossary....................................... 10Plan of S t u d y ................................. 13
II REVIEW OF LITERATURE............................. 15
Maternal Complications Associated withNarcotic Addiction ........................... 15Treatment Efforts for Narcotic Addiction . . . 18Neonatal Complications Associated withNarcotic Addiction ....................... 19
Onset of Infant Withdrawal Symptoms ........ 23Problems of Diagnosis . . . . . 24Prognosis of the Addicted Mother ............ 26Care of Infants of Addicted W o m e n .......... 27Prognosis of Infants of NarcoticAddicted Women ........................... 28
Developmental Outcome of Infants Bornto Narcotic Addicted Women............... 29
Theoretical Views of Family Functioning ........ 33Intervention Programs ......................... 36Studies of Infant Attention ................... 40
Studies of Attention to Auditory Stimuli . . . 41Studies of Attention to Visual Stimuli . . . . 42Studies of Attention to Stimuli that Move . . 46
v

page
Studies of Infant Responses to TactileExperiences......................... . • 48
Infant Assessment ........................... 50Apgar Procedure ................ . . . . . 50Neurological Evaluation ............... . 50Brazelton Neonatal Behavioral AssessmentScale . . . . . . . . . . . . . . . . . . 51
Bayley Scales of Infant Development . . . . 55Maternal Assessment . ..................... 57
The Caldwell et al. Inventory of HomeStimulation........................... 57
Ainsworth Maternal Care Scales........... 59Parent Counselor Home Visit Report ........ 61Infant Care Inventory................... 62Two Factor Index of Social Position . . . . 63
Summary..................................... 64
III METHOD......................................... 65
Research Design ............................. 65Subject Selection ....................... 65Case Histories of Addicted Women.......... 66
Marital Status ....................... 66Residential Characteristics . . . . . . 66Number of Children................... 69Extent of Child Care Provided for themby O t h e r s ......................... 69
Educational Level ................... 69Reason for Leaving School ............ 69Drug Experience..................... 69Receptivity to Intervention Program . . 70
Data Collection . . . . . . . . . . . . . . . . 71Intervention and Data Collection .......... 71
Phase I ............................. 71Phase I I ............................. 73Phase I I I ........................... 74
Intervention Materials . . . . . .......... 86Assessment Instruments ................... 87
Data Analysis . . . . . . . . . . . . . . . . . 87Amiel-Tison Neurological Evaluation of theMaturity of Newborn Infants ............ 88
Brazelton Neonatal Behavioral Assessment Scale 88 Bayley Scales of Infant Development . . . . 88Maternal Assessment ..................... 89Statistical Methods Employed .............. 89Usefulness of Instruments Utilized
in this S t u d y ......................... 91
vi

page
IV RESULTS.......................................... 93
Presentation of Results....................... . 93Intervention Results ........................... 129Feasibility of Planning and Implementinga Home-Based Intervention Program .............. 130
V SUMMARY AND IMPLICATIONS ......................... 131
Appendix
I Neurological Evaluation of the Maturity ofNewborn Infants ................................. 139
II Brazelton Neonatal Behavioral Assessment Scale . . . . 141
III Inventory of Home Stimulation...................... 152
IV Ainsworth Scale MA-1 Mother's Perceptionof B a b y ......................................... 162
V Ainsworth Scale MA-2 Mother's Delight in Baby . . . . 165
VI Ainsworth Scale MA-3 Mother's Acceptanceof B a b y ......................................... 168
VII Ainsworth Scale MC-1 Mother's Availabilityto B a b y ............•............................ 171
VIII Ainsworth Scale MC-3 Amount of InteractionOffered by M o t h e r ............................... 175
IX Ainsworth Scale MC-4 Appropriateness ofMother's Initiation of Interaction ............. 178
X Parent Counselor Home Visit Report ................... 182
XI Infant Care Inventory ...................... 187
XII Hollingshead Two Factor Index of Social Position . . . 196
XIII Parent Interview Report ............................ 210
XIV Help a Baby B o o k l e t............................... 214
XV Mother's Compliance with Medical Appointmentsand Suggestions................................. 223
XVI Tables 21 - 26 Summary of Results of Analyses ofVariance on Brazelton Items 3, 6, 7, 9, 20 and 26. . 227
vii

pageXVII Table 27a Summary of Significantly Different
Group Means on Those Items Where Time Was Significant as a Main Effect--No Interaction Significance..................................... . 235
Table 27b Summary of Significantly Different Time Means for Those Analyses of Variance on Items Where Group and Time Were Significantas Main Effects--No Interaction Significance ........ 235
BIBLIOGRAPHY ............................................... 236
viii I

LIST OF TABLES
Table page
1. Characteristics of the Sample..................... 67
2. Schedule of Data Collection....................... 72
3. Summary of Intervention........................... 85
4. Summary of Differences by Fisher ExactProbability Test in Gestational Ages of Newborn Infants of Addicted and Nonaddicted Mothers Determined by Items of the Amiel-Tison Neurological Evaluation of Maturity of Newborn 95Infants ...........................................
5. Summary of Results of Analysis of Variancefor Twenty-Seven Brazelton Behavioral Items ........ 97
6. Summary of Significance of Effects for GroupX Time for the Twenty-Seven Behavioral Items . . . . 98
7. Summary of Statistically Different Group Means for the Group X Time Analysis of Variance on Items Where Only Group Was Significant as aMain Effect.................................. 99
8. Summary of Results of Analysis of Variance with Brazelton Item l--Response Decrementto L i g h t ......................................... 100
9. Summary of Group Means for Those Items When Differences Were Significant With BrazeltonItem 14--Cuddliness . . . . ....................... 105
10. Summary of Analysis of Variance for BrazeltonItem 15--Pull To S i t ............................. 106
11, Summary of Results of Analysis of Variance For Brazelton Initial State and Predominant StateItems • 108
11a. Summary of Results of Group X Time Analysis ofVariance for Brazelton Initial State Items . . . . . 109
ix

page
112
113
114
115
117
118
120
122
123
123
228
229
230
Number or Infants in Each Group Receiving a Score of Two With Brazelton "Elicited Responses" at Four Age Periods (Three Days, T,; One Week, T2;Two Weeks, T^; Three Weeks, T^) Analyzed WithWilcoxon Signed Rank T e s t ..............................
Summary of Results of Analysis of Variance withBayley Scales of Infant Development--Mental Scale . . . . .
Summary of Results of Analysis of Variance of Visual Following Skills with Bayley Scales of Inf an t Development.......................................
Summary of Results of Analysis of Variance with Bayley Scales of Infant Development— Psychomotor Development............................................
Differences Between Scores of Addicted and Nonaddicted Women with Hock Infant CareInventory Analyzed with Mann Whitney U Test ..............
Differences Between Scores of Addicted and Nonaddicted Women with Ainsworth MaternalCare Scales Analyzed with Mann Whitney U Test ............
Differences Between Scores of Addicted and Nonaddicted Women with Caldwell et al.,Inventory of Home Stimulation Analyzed withMann Whitney U Test .....................................
Scores of Addicted and Nonaddicted Women withWright et al., Parent Counselor Home VisitReport--Analyzed with Mann Whitney U T est...............
Scores of Addicted and Nonaddicted Women withRespect to Compliance with Medical Appointments . . . . . .
Scores of Addicted and Nonaddicted Women withRespect to Compliance with Medical Suggestions ..........
Summary of Results of Analysis of Variance with Brazelton Item 3— Response Decrement to Bell ............
Summary of Results of Analysis of Variance with Brazelton Item 6— Orientation Response--Inanimate,Audxtory . . . . . . . . . . . . . . . . . . . . . . . . .
Summary of Results of Analysis of Variance with Brazelton Item 7--0rientation--Animate Visual ............
x

page
24. Summary of Results of Analysis of Variance with Brazelton Item 9-~0rientation Animate--Visualand Auditory......................... 231
25. Summary of Results of Analysis of Variance withBrazelton Item 20--Activity (Alert States) ............. 232
26. Summary of Results of Analysis of Variance withBrazelton Item 26--Hand to Mouth Facility ............. 233
27a. Summary of Significantly Different Group Means on Those Items Where Time was Significant as aMain Effect— No Interaction Significance ............... 235
27b. Summary of Significantly Different Time Means for Those Analyses of Variance on Items Where Group and Time Were Significant as Main Effects-- No Interaction Significance............. 235
xi

76
77
78
79
80
81
82
83
84
96
102
104
106
LIST OF FICURES
Materials Used as Auditory Stimuli .........
Materials Used as Visual Stimuli ...........
Materials Used as Visual Stimuli ...........
Materials Used as Visual Stimuli ...........
Materials Used as Visual Stimuli ...........
Materials Used as Visual-Movement Stimuli . ,
Materials Used as Visual-Movement Stimuli . ,
Materials Used as Visual-Movement Stimuli . .
Materials Used as Tactile Stimuli ..........
Summary of Means of Addicted and Nonaddicted Infants with 27 Brazelton Items ..........
Group Means of Brazelton Item 5, at Four Age Periods .................................
Group Means of Brazelton Item 14, at Four Age Periods .................................
Group Means of Brazelton Item 15, at Four Age Periods............... ................
xii

CHAPTER I
INTRODUCTION
Background for the Study
Case histories of infants born to narcotic addicted women have
been reported for nearly one hundred years (Coodfriend et al. 1956).
Lin-Fu (1969) noted that a review of the literature pertaining to
narcotic addicted women occurred approximately a decade ago and served
as impetus for further studies of infants born to narcotic addicted
women. Lin-Fu (1969) commented on findings from various studies.
All those (studies) indicated that narcotic addiction during pregnancy poses a dual problem: not only are the womenhigh-risk obstetrical patients, but most of their babies are born addicted and, unless diagnosed early and managed properly, suffer a formidable mortality and morbidity rate.
The extent of narcotic addiction may not bo fully known since
cany narcotic users fail to identify themselves as such (Trussell 1971
£i Zelson et al. 1973). Cobrinik et al. (1959) found that in the city
of New York alone during a one year period more than 800 pregnant
addicts registered with the Department of Narcotic Control and that
number would probably result in more than 800 potentially addicted
newborn infants. Zelson et al. (1973) estimated the number of narcotic
addicts in the United States between 100,000 and 200,000. That figure
represents an increase from 64,011 reported by Lin-Fu (1969) and a
greater increase from that reported by Hill and Desmond (1963).
1

The age distribution of narcotic addicts is noteworthy from the
standpoint of reproduction (Lin-Fu 1969), especially since several
physicians (Hill and Desmond 1963; Blinick et al. 1969; Reddy et al.
1971; Pierson et al. 1972; Wilson et al. 1973 and Zelson et al. 1971)
reported an age range of addicted women between twenty and forty years,
while Levy (1967) noted use of drugs by adolescents. Such an age
range may suggest that many infants may be born to narcotic addicted
women. The phenomenon of narcotic addiction and its impact on the
female addict are manifold.
Financial cost for maintaining a supply of narcotics may vary
within a range from two dollars to one hundred eighty dollars daily,
with the female addict engaging in prostitution and shoplifting to •
support her purchase of narcotics until advanced stages of pregnancy
occur (Statzer and Wardell 1972). Prostitution is noted to carry a
high risk of syphillis and other diseases. Finnegan and Macnew (1974)
noted that the addict's diet is poor and consists of that which she
can obtain in vending machines--candy bars, potato chips, pretzels,
an occasional sandwich and soft drinks. Her resulting malnutrition not
only affects her well-being but also that of her infant. Levy (1967)
noted that narcotic users may supplement their income by selling
narcotics to others. Blinick et al. (1967) commented regarding further
problems of narcotic addicts.
In addition to the influence on the psychological and social processes, narcotic addiction is known to have profound effects on the physiological processes as well. The narcotic addict spends most of her time unable to function. She experiences intermittent periods of normal alertness and well being, but for the bulk of her time the addict is "high" or "sick." The "high" or euphoric state finds the addict sedated, tranquilized, absorbed in herself and lost to responsibility. The "sick"

or abstinent state is characterized by craving for narcotics with malaise, nausea, perspiration, tremors and cramps.. . . The adict oscillates between "high" and being "sick" with little time to function.
Because of their life-styles and because of fear of calling
attention to their drug habits some pregnant addicts are reported to
maintain a low standard of self care and fail to seek prenatal inter
vention. Davis and Chappel (1974) reported that 75 percent of addicts
never visit a physician during their pregnancy periods and have a high
incidence of medical complications.
Sussman (1963) noted that the addict mother is often first seen
in labor and her addicted infant is frequently regarded as a diagnostic
problem until a history of maternal addiction is established. Krause
(1958) noted that only four of a group of 18 women received
prenatal care and that on admission to a hospital some of the women
experienced infected ulcerating veins. Perlmutter (1967) studied
22 heroin addicted women of whom four attended prenatal clinic
for a total of 14 visits; two registered but failed to maintain
their appointments. Untreated positive serologic tests for syphillis
ware found in five of the patients.
Significance of the Study
Evidence is available that Americans are becoming increasingly
cognizant of social problems that accompany narcotic addiction by some
members of American society. Much of that evidence is reflected in
efforts by persons in the medical profession for implementing procedures
designed to aid narcotic addicted persons. In the meantime newborn
infants of narcotic addicted women, because of reported neonatal

4characteristics, seem to represent a high-risk group and are cause
for concern upon their return in many instances to physically deprived
environments. Concern centers on whether or not infants born to
narcotic addicted women escape the environment that produced their
mothers and whether a short-term intervention program may make a
contribution toward motivating the mother to provide quality caretaking
skills to her infant. Effort that may be directed toward improving
the functioning of mothers of such infants, as well as providing
medical and cognitive intervention, may serve as contributions not only
toward helping an immediate need but toward improving the life-style
of addicts over that which was reported by Blinick et al. (1967).
Statement of the Problem
The purpose in this preliminary study was to compare the develop
ment of infants born to narcotic women to infants born to nonnarcotic
addicted women, as preliminary to a subsequent study, and to describe
family dynamics of addicted women in this study and their drug history.
In addition, the purpose in this study was to document whether
changes in infants' behavioral characteristics were evident after pre-
and post-tests of mother-infant pairs who participated in an interven
tion program which emphasized educational activities that involved
medical and cognitive approaches. A further purpose was to examine
the feasibility of a subsequent study.
Objectives
The objectives in this preliminary study were:
1. To determine if there is a difference between neurologic

maturity at birth, of infants born to narcotic addicted
women (as assessed by the Ameil-Tison Neurological Evaluation
of the Maturity of Newborn Infants), and neurological maturity
at birth, of infants born to nonnarcotic addicted women (as
assessed by the Ameil-Tison Neurological Evaluation of the
Maturity of Newborn Infants).
To determine if there is a difference between performance
with the behavioral items, state items and "Elicited
Responses" of infants born to narcotic addicted women (as
assessed by the Brazelton Neonatal Behavioral Assessment
Scale) and performance with the behavioral items, state items
and "Elicited Responses" of infants born to nonnarcotic
addicted women (as assessed by the Brazelton Neonatal Behavioral
Assessment Scale), at four age periods (three days, one, two
and three weeks).
To determine if there is a difference between Mental Develop
ment (as assessed with the Bayley Scales of Infant Development)
of infants born to narcotic addicted women and Mental Develop-
ment (as assessed with the Bayley Scales of Infant Development)
of infants born to nonnarcotic addicted women at two age
periods (one month 24 days, and three months).
To determine if there is a difference between Visual Following
skills (as assessed with the Bayley Scales of Infant Develop
ment) of infants born to narcotic addicted women, and Visual
Following skills (as assessed with the Bayley Scales of

o
Infant Development) of infants born to nonnarcotic addicted
women, at two age periods (one month 24 days, and three months).
6. To determine if there is a difference between narcotic
addicted women and nonnarcotic addicted women with respect
to their feelings of competency for providing infant caregiving
skills, as assessed with the Infant Care Inventory.
7. To determine if there is a difference between narcotic addicted
and nonnarcotic addicted women with respect to changes in
characteristics of mothering derived from pre- and post-tests
(assessed with Ainsworth Scales--perception of, delight in and
acceptance of baby; mother's availability to the baby, amount
of interaction offered by the mother and appropriateness of
the mother's interaction with the baby); also assessed with the
Caldwell et al. Inventory of Home Stimulation.
8. To determine if there is a difference between narcotic addicted
and nonnarcotic addicted women with respect to their acceptance
of home training provided by a parent counselor (assessed with
data from Wright et al. 1970).
9. To determine if there is a difference between narcotic
addicted and nonnarcotic addicted women with respect to their
compliance with medical appointments and instructions.
10. To provide case histories of maternal characteristics which
include the following:
a) Marital status
b) Residential characteristics
c) Number of children
7d) Extent of child care provided for them by others
e) Educational level
f) Reason for leaving school
g) Drug experience
h) Receptivity to intervention program
11. To make statements regarding the feasibility of planning and
implementing a home-based intervention program directed at
contributing to enhancing quality of mothering, helping mothers
become sensitive to infant needs and helping mothers develop
caregiving skills, as preliminary to a subsequent study.
12. To make statements regarding the usefulness of instruments
utilized in this study, as preliminary to a subsequent study.
Hypotheses
Hypothesis 1: There is no difference between neurological maturity at
birth, of infants born to narcotic addicted women (as
assessed with the Amiel-l'ison Neurological Evaluation
of the Maturity of Newborn Infants) and neurological
maturity at birth, of infants born to nonnarcotic
addicted women (as assessed with the Amiel-Tison
Neurological Evaluation of the Maturity of Nev/born
Infants).
Hypothesis 2: There is no difference between performance with the
behavioral items, state items and "Elicited Responses"
of infants born to narcotic addicted women (as assessed
with the Brazelton Neonatal Behavioral Assessment Scale)
and performance with the behavioral, state items and
Hypothesis 3
Hypothesis 4
Hypothesis 5
Hypothesis 6
"Elicited Responses" of infants born to nonnarcotic
addicted women (as assessed with the Brazelton Neonatal
Behavioral Assessment Scale) at four age periods (three
days, one, two, and thre^Veeks).
: There is no difference between Mental Development (as
assessed with the Bayley Scales of Infant Development)
of infants born to narcotic addicted women and Mental
Development (as assessed with the Bayley Scales of Infant
Development) of infants born to nonnarcotic addicted
women at two age periods (one month 24 days, and three
months).
: There is no difference between Visual Following skills
(as assessed with the Bayley Scales of Infant Develop
ment) of infants born to narcotic addicted women, and
Visual Following skills (as assessed with the Bayley
Scales of Infant Development) of infants born to non
narcotic addicted women at age three months.
: There is no difference between Motor Development (as
assessed with the Bayley Scales of Infant Development)
of infants born to narcotic addicted women and Motor
Development (as assessed with the Bayley Scales of
Infant Development) of infants born to nonnarcotic
addicted women, at two age periods (one month 24 days,
and three months)
There is no difference between narcotic addicted women
and nonnarcotic addicted women with respect to their

9
feelings of competency for providing infant care giving
skills, as assessed with the Infant Care Inventory.
Hypothesis 7: There is no difference between narcotic addicted women
and nonnarcotic addicted women with respect to changes
in characteristics of mothering, derived from pre- and
post-tests (assessed with Ainsworth Scales~~perception
of, delight in and acceptance of baby; mother's avail
ability to the baby, amount of interaction between
mother and infant and appropriateness of the mother's
interaction with the baby; and changes in indices of
behavior (assess with the Caldwell et al. Inventory of
Home Stimulation).
Hypothesis 8: There is no difference between narcotic addicted women
and nonnarcotic addicted women with respect to their
acceptance of home training provided by a parent
counselor (assessed with data from Wright et al. 1970).
Hypothesis 9: There is no difference between narcotic addicted women
and nonnarcotic addicted women with respect to their
compliance with medical appointments and medical
suggestions.
Limitations in the Study
Due to a limited number of eligible subjects within the city in
which this study was performed the sample size is small. Reports from
Drug Treatment Centers noted that some women who were referred to the
study experienced spontaneous abortion. Two women were lost to follow-up.
A further limitation related to the use of only one interviewer.

10It was not feasible to employ more than one person to collect data.
It would have been helpful to utilize naive evaluators who did not
become acquainted with the mothers who participated in this study. A
precaution in the study was directed toward the use of objective instru
ments in order that biases hopefully would not intrude.
Relationship to a Larger Research Project
This study represented the preliminary phase of a longitudinal
study planned for implementation within the Department of Pediatrics
at The Ohio State University Hospitals. The longitudinal study is
designed to develop interventional techniques for training mothers or
other primary caregivers of infants who are born to narcotic addicted
women, and to assess developmental status of infants throughout their
first year of life.
Glossary
Addiction is "the state of being given up to some habit, especially
strong dependence on a drug." (Dorland's, 1974).
Analgesic is "an agent to alleviate pain without causing loss of
consciousness." (Dorland's, 1974).
Bacterial Endocarditis is "a febrile (characterized by fever)
systemic disease (affecting the body as a whole), marked by bacterial
or fungal infection of the heart valves with formation of bacteria--
or fungus-laden vegetation." (Dorland's, 1974).
Cyanosis is "a bluish discoloration, applied especially to such
discoloration of skin and mucous membranes due to excessive concentra
tion of reduced hemoglobin (oxygen carrying pigment) in the blood."
(Dorland's, 1974).

11
Eclampsia is "associated with convulsion and coma," (Dorland's,
1974).
Endocarditis is "inflammation of the lining membrane of the heart
and the connective tissue bed on which it lies." (Dorland's, 1974).
Heroin (diacetylmorphine) is "a white, bitterish, crystalline
powder . . . formerly used as an analygesic and narcotic. Because it
is highly addictive, the importation of heroin and its salts in the
"nited States as well as its use in medicine is illegal." (Dorland's,
1974).
Lactose is "a constituent of milk (called milk sugar). It is not
colerated in many persons." (Dorland's, 1974).
Mongolism (Mongol, is "a member of one of the chief ethnological
divisions of Asiatic peoples"). Mongolism is "Down's syndrome--so-
called because of facial characteristics typical of this condition."
(Dorland's, 1974).
Morphine is "the principal and most active alkaloid (one of a large
group of substances found in plants) of opium . . . used as a narcotic
analygesic." (Dorland's, 1974).
Narcotic is "pertaining to or producing narcosis (a reversable
condition characterized by stupor and insensibility." (Dorland's, 1974).
Nasal Septem is "a dividing wall or partition separating the two
nasal cavities in the midplane, composed of cartilaginous, membranous
and bony parts." (Dorland's, 1974).
Nepenthe is "pertaining to or inducing peace and forgetfulness."
(Dorland's, 1974).
Opium is "an air-dried milky exudate obtained by incising the

12
unripe capsules of poppies. The unripe capsules yield a white latex
which when dried is known as crude opium." (Dorland's, 1974).
Phenylketonuria (PKU) is "an inborn error of metabolism." (Dor
land's, 1974).
Post Partum is "occurring after childbirth or after delivery, with
reference to the mother." (Dorland's, 1974).
Post Partum Psychosis is "a psychotic episode, usually schizo
phrenic in nature, occurring during the post partum period, which may
be precipitated by organic and/or toxic factors." (Dorland's, 1974).
Psychosis is "a general term for any-major mental disorder of
organic and/or emotional origin, characterized by derangement of the
personality and loss of contact with reality, often with delusions or
hallucinations." (Dorland's, 1974).
Pulmonary is "pertaining to the lungs." (Dorland's, 1974).
Staphylococcal Pneumonia is "caused by infection with staphyloccus,
many strains of which are antibiotic resistant; has a strong tendency
to extend beyond the original site of infection?** (Dorland's, 1974).
S taphylococcus is "a spiral bacterium occurring predominantly in
irregular masses of cells that are a common cause of pus forming
infections." (Dorland's, 1974),
Strabismus is "a squinting deviation of the eye which the patient
cannot overcome." (Dorland's, 1974).
Talc is "a hydrous silicate (salt), sometimes containing small
portions of aluminum silicate used as dusting powder." (Dorland's, 1974).
Tetanus is "an infectious disease in which muscle spasm and hyper-
ref lexia result in 'lock jaw1, generalized muscle spasm, arching of the back and seizures." (Dorland's, 1974).

13
Tetany is "a syndrome manifested by sharp flexion of the wrist and
ankle joints, muscle twitchings, cramps and convulsions," (Dorland's,
1974).
Toxemia is "a general intoxication sometimes due to absorption of
bacterial products formed at a local source of infection." (Dorland's,
1974).
Toxemia of Pregnancy is "a group of pathologic conditions occurring
in pregnant women, characterized by preeclampsia and fully developed
eclampsia, associated with edema (presence of abnormally large amounts
of fluid in the intercellular tissue spaces of the body.") (Dorland's,
1974).
Vasculature is "pertaining to blood vessels." (Dorland's, 1974).
Plan of Study
The purpose in this study was to compare the development of infants
born to narcotic addicted women to infants born to nonnarcotic addicted
women and discover family dynamics of addicted women in the study.
In addition, a purpose in this study was to document whether
changes in infant behavioral characteristics were evident, after pre-
and post-tests of mother-infant pairs who participated in an interven
tion program which emphasized educational activities and involved
medical and cognitive approaches. A further purpose was to examine the
feasibility of a subsequent study. Instructional materials were
developed and utilized in a home-based intervention program directed
toward strengthening quality of mothering, or helping mothers develop
caregiving skills to their* infants. The subjects in this study were
ten newborn infants who were born in The Ohio State University Hospitals
14and Grant Hospital, Columbus, Ohio. Mothers of those infants were also
included in the study. Infant development was assessed with three
instruments. They included: The Amiel-Tison Neurological Maturity of
Newborn Infants, Brazelton Neonatal Behavioral Assessment Scale and
Bayley Mental and Motor Scales of Infant Development.
Maternal behavior was assessed with eleven instruments. They
included: Infant Care Inventory, Six Ainsworth Maternal Care
Scales, Caldwell et al. Inventory of Home Stimulation and a Parent
Counselor Home Visit Report adapted from Wright et al. (1970). Maternal
compliance with medical directions and appointments were assessed with
an instrument designed for that purpose. Case histories were obtained
for addicted mothers in this study.
Sources of variation among the groups were analyzed with several
statistical procedures.
Subsequent sections of this study will include a review of
related literature, research design, results, summary and implications.

CHAPTER XI
REVIEW OF LITERATURE
The focus in this chapter will be on features of narcotic addiction
as they relate to women during pregnancy and the post partum period
and as they relate to newborn infants. Also, a theory will be pre
sented which might be useful when discussing infants of narcotic
addicted women. Views of Deutsch (1967), Cole and Bruner (1972),
Hess and Shipman (1965) and pavenstedt et al. (1967) will be presented
in support of theory.
Further, intervention programs and materials which have been
found to enhance infant attention will be described. In addition,
a description of some instruments which have been found useful for
infant and maternal assessment will be described.
Maternal Complications Associated with Narcotic Addiction
Several physicians have found that women who present histories of
narcotic addiction during pregnancy also manifest unfavorable symptoms
curing the period immediately following birth of their infants.
Among the symptoms reported are the presence of hepatitis (Stern,
1966; Schneck, 1958; Blinik, 1969) and syphillis (Stone, 1967 and Blinik,
1969). The complication of hepatitis is said to occur frequently in
addicts and is said to be related to common use of contaminated needle
and syringes. Blinik (1969) also found the presence of rheumatic fever,
15
16
anemia, epilepsy, diabetes and positive tests for syphillis among
narcotic addicted women.
In addition to the above complications Krause (1953) found women
who manifested withdrawal symptoms, retained placenta, hemorrhage and
also found one case of post partum psychosis. Few of the women had only
mild nervousness and insomnia, but most of them were reported to have
developed tremors and severe anxiety accompanied by episodes of crying.
Stern (1966) noted that chances of the presence of toxemia are
significantly greater among narcotic addicted women than among women
in the general population; placenta abnormalities are more frequent
and post partum hemorrhage is more likely to occur with narcotic
addicted women.
Stern (1966) studied obstetrical complications of sixty-six women
and found 15.1 percent of them to have experienced toxemia of pregnancy—
a figure which is reported to be highly significant when compared to
5.2 percent of all obstetric patients within the hospital in which the
study was made.
Other reported symptoms of narcotic addiction particularly with
heroin, are acute bacterial endocarditis, tetanus and malaria (Moser,
1974). He reported'that the medical problem is compounded by a total
lack of discrimination regarding what some people will pump into a
human vein. Virtually anything that is rumored to cause a "high" will
be reduced to an injectable sustrate. He reported that physicians may
encounter a person with a fever who may have an infected heart valve or
a patch of Staphylococcal pneumonia in relation to heroin addiction. He
further noted that physicians may anticipate a variety of non-infectuous

17
junk which is often injected into veins and may become lodged in the
lungs of a narcotic user.
Rosenow (1972) reported that heroin and other drugs are frequently
adulterated with quinine, lactose and talc as well as with baking soda.
In a pathetic effort to purify the mixture, it may be filtered through
cotton and as such, cotton fibres may become lodged in the pulmonary
vasculature. Other pulmonary complications may include abscesses of
the lungs.
Gottlieb and Boylen (1974) reported overdose coma and pneumonia.
Apton (1968) reported that a rare disease in heroin addicts is perfora
tion of the nasal septum which is said to result from sniffing heroin.
Other complications of heroin use have been reported as infectuous
arthritis and neurologic disorders (Light and Dunham, 1974 and Richter
et al., 1973) .
A dramatic statement was made by Moser (1974) in which he noted
that perhaps the most serious disease related to heroin use is the state
of emotional despair that causes one to elect the personal suffering
that accompanies narcotic addition. It is a disease of society that has
always been with us in one form or another. Whenever men find the
tedium or frustrations of living to be beyond endurance, some seek
escape with Nepenthe. Moser (1974) presented a negative prognosis for
drug addiction when he noted that "there is no indication that we are
close to a cure for this chronic despondency of the human spirit."
The aforementioned physicians have agreed that narcotic addiction
during pregnancy and the post partum period presents symptoms within
the drug user that are potentially harmful and damaging.

18
Treatment Efforts for Narcotic Addiction
Several physicians (Dole and Nyswander 1965; Maslanslcy 1971;
Blinick et al. 1969; Knowles et al. 1971; Kleber 1971; Hoozerbeth 1971
and Wallach et al. 1969) have reported efforts directed toward
penetrating the drug problem in the United States. Those efforts
include the employment of Methadone as an interim measure for use by
addicts who are being treated for drug use. Two types of Methadone
programs have been described and both involve the intake of Methadone
orally with a mixture of fruit juice.
The first program is that of detoxification (Blinick 1967).
Treatment within that program is designed to avoid severe symptoms of
withdrawal. Depending on the size of the "habit" a dose of 20-40
miligrams of Methadone is given initially to the patient while in a
hospital and thereafter the dose is gradually decreased over a period
of seven to ten days. When the patient is free from drugs and no
longer seems to desire continued intake3 he is asked to remain in the
hospital for an additional two to four weeks for rehabilitation.
Blinick (1967) reported that the detoxification type of program has
been unsuccessful; the addict invariably returns to heroin use after
discharge from the hospital.
The second program described by Wallach et al. (1369) is referred
to as the Methadone Maintenance Program. That program is aimed at
voluntary rehabilitation of the 1 hard-core" addict through gradual
intake of Methadone. Patients are given gradually increasing doses of
Methadone to induce a state of tolerance. They are initially given

small doses of five to ten miligrams daily and are continued at this
level for one to two weeks. Then the dose is increased by increments
of five to ten miligrams at intervals of four to seven days, until an
average daily dose of 80 to 100 miligrams is reached. At that stage
the dose is held constant with the belief that such large doses
induce narcotic blockage, so that heroin becomes neither necessary
nor desirable and the addict, hopefully can return to a normal useful
life. Wallach et al. (1969) noted that under one Methadone Mainte
nance Treatnent Program, with a comprehensive program of rehabili
tation, patients have shown marked improvement, have lost their
craving for heroin and none have become readdicted to heroin.
Several physicians (Knowles et al. 1971; Kleber 1971; Hoozerbeth
1971; Maslansky 1971 and Dole et al. 1968) seem to favor Methadone
maintenance programs. They noted that a high rate of social produc
tivity, as illustrated by stable employment and responsible behavior
on the part of persons who have participated in drug treatment programs,
has occurred with program participants.
Neonatal Complications Associated with Narcotic Addiction
Several unfavorable neonatal characteristics have been reported
for infants of narcotic addicted women. Prematurity of birth
(Gobrinik et al. 1956; Reddy et al. 1971), low birth weight among the
infants (Cobrinik et al. 1959; Slobody and Cobrinik 1959; Reddy et al.
1971), high mortality rates (Schneck 1958; Goodfriend et al.) and
periods of hospitalization ranging from four to twenty days are among
the conditions reported for infants of those women. Studies of

20
surviving permaturely born infants have found increased incidences
of mental and neurological deficit with increasing degrees of pre
maturity among the infants who have been studied (Caputo and Mandell
1970). Deprived environmental circumstances were noted to adversely
affect the course of development of prematurely born infants (Drillien
1965). Scott (1972) noted that a positive correlation exists between
"hard narcotic users" and lower gestational ages in their infants,
and also noted that some cases of low birth weight among infants may
have been due to anorexic effects of narcotic use and poor nutrition
by the mother.
Further unfavorable outcomes of infants born to narcotic addicted
women have been found. Pierson et al. (1972) found "sudden infant
death syndrome" among three infants who were born to women who partici
pated in Methadone Maintenance programs, but stated that the deaths
may or may not have been related to the use of Methadone.
Wilson et al. (1973) found behaviors of hyperactivity, brief atten
tion span and temper tantrums among 64 percent of the infants whom they
studied. In a ten-year follow-up study of infants born to narcotic ad
dicted women, Zelson et al. (1971) reported that maternal addiction seri
ously affects the fetus and has a damaging effect on the newborn infant.
Schneck (1958) found infants who developed respiratory symptoms accom
panied by the presence of mucous which necessitated use of oxygen therapy
for survival of the infants. He also found those infants to exhibit
irritability and restlessness, twitching and convulsive disorders

21
which he regarded as conditions that might lead one to suspect the
presence of tetany or central nervous system injury among the infants.
Lin-Fu (1969) noted that most infants born to narcotic addicted
women develop narcotic withdrawal symptoms and that approximately 83
to 91 percent of the infants are born addicted. There appears to be
general agreement among physicians regarding symptoms of withdrawal by
the infants: tremors, excessive and annoying high-pitched continuous
crying, generalized convulsions, vomiting, anorexia, weight loss, poor
feeding, diarrhea, tremulousness and excessive fist sucking (Kunstadter
et al. 1958; Cobrinik et al. 1956; Steg 1957; Schneck 1958; Stern
1966; Zelson 1971).
In addition, Schneck (1958) noted that as a result of restless
ness and irritability, severe excoriations of the infants' heels,
noses and other points of contact with mattresses occurred. He also
found increased perspiration severe enough to produce a rash and
temperature elevations slightly over 100 degrees Fahrenheit. Perlmutter
(1967) found one child who had a positive Phenylketonuria and presence
of cataracts. Krause (1958) reported one case of Mongolism, one
infant with an umbilical hernia and severe strabismus. Ho also
reported that 25 percent of the infants in his study expired. He
expressed concern regarding abnormal tremor of the arms and legs
observed in infants, which was believed to herald the advent of
vomiting and an inability of the infant to nurse. He also found many
of the infants to experience difficulty with swallowing which he
noted may contribute to occurrance of respiratory crisis and cyanosis.
Perlmutter (1967) grouped infant symptoms into several major

22
categories: those referrable to the central nervous system such as
marked irritability, excessive crying, sleeplessness, tremors and
convulsions; those referrable to the gastro-intestinal system such
as vomiting, diarrhea and poor feeding; those referrable to the
respiratory system such as yawning, sneezing, fever, perspiration and
pallor. He further noted that it is uncommon for the infant to experi
ence no clinical symptoms if the mother is taking drugs at the time of
delivery.
Physicians have attributed presence of withdrawal symptoms in the
infants to several factors. Goodfriend et al. (1956) and Statzer and
Wardell (1972) noted that the appearance or absence of withdrawal symp
toms in the newborn infant seems to be related to the duration of addic
tion by the mother, quantity of narcotics consumed by her and the time of
intake of her last dose.of narcotics immediately prior to the birth of her
infant. If the mother consumes large doses of narcotics until the very
end of her pregnancy there is the likelihood that the infant will be a
narcotic addict at birth. Zelson et al. (1973) attributed the degree
of illness of the infant to types of drugs consumed by the mother.
They noted that infants of addicted mothers who were using Methadone
alone or in combination with heroin appeared to exhibit a greater
degree of illness than those infants born to women who used heroin
alone. They found 12 percent of infants born to women who used
heroin required treatment as compared to 38 percent of infants born to
women who used Methadone and who were not treated. Those physicians
also found severity of withdrawal, frequency of withdrawal symptoms and
frequency of seizures to be greater in Methadone infants. Physicians

23
are nod in complete agreement regarding severity of withdrawal syndrome
in heroin and methadone addicted babies.
Blatman (1972) contended that Methadone babies are better off due
to the superior pre- and post-natal care available to mothers,
especially if they are treated in Methadone Maintenance Programs.
Harper et al. (1974) found that a low-dose Methadone program coupled
with intense psychological support appears to alleviate problems
associated with addiction in pregnancy, but fails to prevent withdrawal
in the newborn. Cohen et al. (1973) reported that acute symptoms may
occur more frequently, last longer and be more difficult to control in
infants born to women who receive methadone during pregnancy than
among those born to "street" heroin addicts. Rajegowda et al. (1972)
supported that notion. They noted that Methadone is not only
addictive to the fetus, but is associated with a higher incidence and
more prolonged duration of withdrawal symptoms that were observed
among newborn infants of heroin addicts. Weingold (1974) disagreed
with this position when he noted that there are no differences between
heroin effects and Methadone effects. Goodfriend et al. (1956) and
Steg (1957) noted that withdrawal symptoms do not occur in the newborn
infant unless the mother has been taking drugs consistently, with the
last dose being taken less than one week prior to birth of the infant.
Time of onset of symptoms may vary.
Onset of Infant Withdrawal Symptoms
Cobrinik et al. (1959) noted that the time of onset of clinical
findings in the infant depends on the duration of time the mother has
been consuming narcotics, type used and time of the last dose prior to
24
delivery. He noted that heroin is excreted more rapidly than morphine,
and therefore one would expect heroin to lead to earlier onset of
withdrawal symptoms. However, because of several factors no conclu
sions may be drawn from present data. In one study Glass et al. (1971)
found that the onset of withdrawal symptoms in the newborn infant
ranged from immediately after birth to 52 hours of life of the infants.
Sussman (1973) found symptoms to occur within 12 hours after birth.
He found several of the mothers to be without symptoms, however their
infants developed symptoms later and that factor suggests that
narcotic addiction by mothers may not be readily detected. Naeye (1973)
studied seven women who were in prison or other institutions during
the last trimester of pregnancy and who exhibited no clinical features
of withdrawal. There are several problems associated with diagnosing
withdrawal symptoms.
Problems of Diagnosis
Diagnosis of addiction is said to present no problems when a
history of maternal addiction is available. However, history of
narcotic addiction may be difficult to obtain and document. Rosenthal
et al. (1964) noted that unless the patient admits to being an addict
or begins to show withdrawal symptoms before delivery or shortly
thereafter, there is no easy way to make a diagnosis of addiction.
Certain signs, however may be utilised in raising the index of suspicion
by medical personnel. The signs include: tatoo-like scars over veins
on women's hands, arms and legs; superficial infections over veins;
burned fingers and burned holes in clothing; and drowsiness and lethargy,
at times accompanied by a desire to scratch the body. Rosenthal et al.

25(1964) noted that a more reliable indicator of maternal addiction is
the development of withdrawal symptoms. If the addict is deprived
of drugs for about 12 hours or more, symptoms usually begin. Informa
tion about the length and nature of the mother's addiction is usually
obtained from the mother with much difficulty and in most cases must
be considered unreliable, especially for several reasons.
The illegal nature of drug-taking activities hinders cooperative
effort between the addict and hospital personnel. In addition, drugs
available from criminal sources (primarily heroin) are subject to
widespread adultei'ation which makes assessment of actual doses nearly
impossible. Statzer and Wardell (1972) commented on strength of drugs.
The potency of pure heroin and quinine varies not only between
various areas of the country but within each city. Street heroin in
Detroit, for example, is said to contain approximately 10 percent
heroin, 10 percent quinine and 80 percent milk sugar. Lindsmith (1965)
noted that nearly all of the drugs used by American addicts are imported
into the United States from abroad. The drugs are said to arrive in
pure form and as they pass from the hands of one dealer to the next in
the long chain of distribution, which reaches from the importer to the
ultimate consumer, they are progressively diluted and broken up into
smaller and smaller units. Dilution at the lowest level is often in
excess of 90 percent and sometimes reaches 98 percent or more. Lind
smith (1965) further noted that smuggled drugs may pass through as
many as 50 or 100 hands before reaching the consumer. Given these
cynamics it appears that the problem of drug addiction is immense.
Douglas (1971) reported that no commercial standards of quality

26
exist for heroin, and no user knows, and no physician can guess what
is the actual level of drugs consumed.
Prognosis of the Addicted Mother
Douglas (1971) noted that Che addicted individual even after
withdrawal, detoxification or rehabilitation remains at high risk in
that subsequent intake, even years later, sets up an immediate urge
for more drugs in order for the user to maintain function. It is this
fact which poses a vicious problem in the pregnant woman. She carries
a potentially addicted fetus and while detoxification of the newborn
infant seems to be initially a successfully detoxified baby, he is
still an infant with a problem who is released into a disturbed environ
ment, in whom even a casual exposure to drugs later in life may induce
an addictive response.
Goodfriend et al. (1956) stressed the importance of an early
diagnosis in order that effective therapy may be instituted, without
delay. Stern (1966) noted that understanding the problems involved
with pregnant addicts, and knowledge concerning the behavior of the
drug addict is helpful.
Baer and Corrado (1974) noted that the most serious drug abuse
involves heroin and that some form of crisis intervention is necessary.
The investigators noted that long range solution to the problem must
regard the underlying causes and important influences which lead to
eventual drug use. Baer and Corrado (1974) attributed factors within
the family constellation during childhood, as contributing to drug
addiction during later life. They concluded that addicts more likely
led an unhappy childhood, experienced harsh physical punishment and

27
lacked parental concern in the areas of school, sexual conduct, friends
and career guidance. Stern (1966) noted that there are frequently no
goals, no plans, no responsibilities for the addict other than obtaining
enough money to pay for drugs. He further noted that the female addict
cares nothing about improving her condition as long as she can obtain
enough money to pay for drugs, and obtain enough of them to stave off
withdrawal symptoms and provide for her an occasional lift above the
condition in which she lives. Krause (1958) noted that although the
prognosis in heroin addiction is very poor he believes that with help
from Social Services and psychiatric assistance during the woman's post
partum convalescence some of the addicted women might be saved.
Care of Infants of Addicted Women
Several physicians expressed concern for infants of addicted women.
Lin-Fu (1969) noted that after an infant is cured of neonatal
narcotic addiction, his long-term care following discharge from the
hospital remains a problem. Because many addicts are not cured
permanently, and since some have been reported to deliberately induce
addiction in their children, early and perhaps permanent separation of
those infants from their mothers has been advocated by some physicians.
Cobrinik et al. (1956) and Slobody and Cobrinik (1959) advocated such
a procedure. Slobody and Cobrinik (1959) noted that since addiction
in a newborn is not based on conscious appetite with attendant
psychologic and sociologic problems, the infant can be cured permanently
of his addiction. However, if he is returned to his home, constant
follow-up is necessary to ensure him against environmental exposure to
addicts. He further noted that such a task is almost impossible since
28even their own mothers have been sometimes regarded as sources of
children's addiction at later dates. He concluded that if the
environment cannot be properly controlled, and he believes that it
rarely can, removing such an infant from his environment may be the
only hope for a permanent cure and a useful life.
Lin-Fu (1969) noted that such an action may not be desirable,
practical or possible in many situations. She proposed that careful
follow-up by health workers appears to represent an alternative, but
in many cases the unstable nature of the family setting precludes any
long-term supervision.
Schneck (1958) reported that since some babies are placed for
adoption one may wonder whether the infants are a good adoptive risk.
He posed the issue whether the mother's emotional instability, which
led her to resort to narcotics, foreshadows the neuro-hereditary
pattern of her offspring, or whether the infant's ultimate emotional
development is related to the environment. Resolution of these
crucial issues seems to pose problems that need solution as concern
continues to grow for the development of infants who are born to
narcotic-addicted women.
Prognosis of Infants of Narcotic Addicted Women
Blinick (1969) noted that the future of infants born to narcotic
addicted women, especially those infants of low birth weight, is
difficult to determine. Infants who are born with marked growth
retardation may have very different physical stamina and different
developmental capacities.
29
Developmental Outcome of Infants Born to Narcotic Addicted Women
Several investigators have devoted effort directed toward des
cribing the course of development of some infants who were born to
narcotic addicted women. Some of those studies have described behavior
of those infants during the early neonatal period only, while a limited
number of investigators have followed some infants through the first
year of life. The findings from some of those studies have revealed
that infants of narcotic addicted women differ from infants of non
narcotic addicted women on several behavioral dimensions. In some
instances those differences have been found with the use of the
Brazelton Neonatal Behavioral Assessment Scale (1973).
Soule et al, (1974) used the Brazelton Scale instrument for examin
ing 19 babies of women who had used Methadone. They were from several
races, with black predominating, while some babies appeared to be of
mixed racial backgrounds. The babies were compared with 41 babies who
were born at a military hospital, of white parents who represented
military personnel of all ranks. Infants of the narcotic addicted women
were found to be restive and in a neurologically irritable condition.
They cried more often, were more tremulous and manifested less motor
maturity than the comparison group of infants and responded more poorly
to visual stimuli.
The investigators noted that economic disparities between the two
groups precluded the study of methadone babies as an isolated clinical
problem of drug addiction.
Lessen-Firestone et al. (1974) also used the Brazelton (1973)
Scale and compared 22 infants of narcotic addicted women with 22 infants

30of non-narcotic addicted women. Results of the study are reported in
terms of clusters of items from the Brazelton Scale. The clusters
are: 1) an excitability cluster which contains items that describe
the infant's level of arousal, 2) a passive motor cluster, composed
of involuntary and reflexive motor responses, 3) an active motor
cluster which deals with the infant's self-initiated motor movements,
and A-) a cognitive sensory cluster which contains two types of items:
those that measure response decrement to visual and auditory stimuli
habituation item), and those that measure orientation to animate
and inanimate stimuli, and an alertness scale. The infants were
nested at two age periods (24 and 48 hours).
Relatively little change in behavior of the infants was found
ever the 24 hour period, however, some change was found with respect
to excitability of the infants and their responses to a cloth placed
ever their faces. There was also a reduction in tremulousness at
the 48 hour period. Several group effects were found.
With respect to the excitability cluster, addicted infants
responded irritably to more stimuli and their behavior states changed
nore often. The infants were more likely to be drowsy or active
awake and fussy than nonaddicted infants. Addicted and nonaddicted
infants did not differ in the peak of arousal often elicited by the
stimuli that are used with the Brazelton Scale.
There were differences in startles and tremulousness from the
passive motor cluster in favor of the nonaddicted infants. Both groups
exhibited appropriate degrees of muscle tone and did not differ
significantly.

31
Few differences were found for items in the active motor cluster.
However, addicted infants tended to manifest less mature motor
behavior; they were more jerky in their movements and less cuddly
than nonaddicted infants.
Differences in the cognitive-sensory cluster appeared with only
one habituation item. Addicted infants required more trials to habituate
to light than their controls. With respect to the orientation and
alertness portions of the cognitive-sensory cluster, the rate of missing
was significantly higher for addicted than nonaddicted infants.
Addicted infants were less often in alert states and were less available
to interaction with the examiner than nonaddicted infants.
Conclusions drawn from this study seem important with respect
to mother-infant interaction. Lessen-Firestone et al. (1974) concluded
that congenital addiction affects behavior of the infant; the infant's
behavior may have implication on the early development of maternal-
infant affectional bonds, and it is likely that addicted infants
differ most from nonaddicted infants with respect to effects on the
caregiver. The addicted infant is likely to elicit more caregiving
responses, yet he is less likely to mold and cuddle when held, and is
likely to tax the caregiver's adaptability to providing care for him.
Wilson et al. (1973) observed the course of development of 30
infants of heroin addicts in the setting of a Maternity and Infant Care
High Risk Clinic. Of that number 16 remained in the study for less
than a year while 14 were observed for one year or longer. Withdrawal
symptoms persisted with 82 percent of the infants for three to six
months. Behavioral disturbances of hyperactivity, brief attention span

32and temper tantrums predominated. Associated with those disturbances
was growth impairment; several of the infants had growth indexes below
the tenth percentile at one or two years.
After subsidence of withdrawal symptoms the infants demonstrated
age-appropriate behaviors except where hyperactivity and short atten
tion span interferred with adaptive performance.
During the course of developmental testing at 12 to 18 months
activity level of the children was decidedly abnormal. Although the
children completed age-specific tasks with swift precision, suggesting
normal potential, they lacked the persistence necessary to complete
the majority of tasks. One infant completed all required tasks, but
responded with constant motor activity which included climbing on
and creeping under the examination table.
Between one and two years, the emergence of impaired attention
span and hyperactivity were observed in half of the infants who were
enrolled in the clinic. Conclusion drawn was that the high incidence
of such problems in infants who previously experienced withdrawal
symptoms suggest that these findings may have a relationship to
intrauterin drug exposure.
The investigators expressed concern regarding the outcomes of
children of maternal drug addicts and suggested longitudinal study of
a larger group to confirm findings of the study.
Studies of infants born to narcotic addicted women have contained
information which suggests that many of those infants differ from
infants born to nonaddicted women along several dimensions. Theoretical
notions regarding functioning of some families will be presented.
33Theoretical Views of Family Functioning
Several writers have described the narcotic addicted population
on admission to hospitals for treatment (Knowles 1971; Lessen-Firestone
et al. 1974) and have found a group to emerge as being Negro with an
average age of 21 years or less who possessed less than high school
education, with no special vocational training and who emerged from
impoverished backgrounds with no employment. With such a profile
theoretical formulations may be viewed with the notion that certain
characteristics of disadvantaged persons may also be prevalent within
a population of narcotic addicted mothers of new born infants. The
populations described as disadvantaged relate to several ethnic groups
c£ persons (Deutsch 1967; Cole and Bruner 1972; Hess and Shipman 1965
and Pavenstedt et al. 1967).
Deutsch (1967) described the interaction of social and develop
mental factors and their impact on intellectual growth of the child.
He noted that many children who come from socially impoverished homes
tend to exhibit several problems. His thesis is that lower-class
children enter school situations so poorly prepared to produce that
vrhich the school demands, that initial failures are almost inevitable
and that school experiences become negatively reinforced. He further
noted that children from underprivileged environments tend to come to
school with a qualitatively different preparation for the demands of
the learning process and behavioral requirements of the academic setting
than the preparation of middle-class children. Deutsch (1967) described
several characteristics of homes of disadvantaged children.
Deutsch found that in a disadvantaged child's home there is a limited

number of objects especially of books, toys, puzzles, pencils and
scribbling paper. He noted that presence of and use of such items would
increase the child's functioning with the tools that will confront him
when he arrives at school. Vicually the urban home of the disadvantaged
child was said to offer the child a minimal range of stimuli. Sparsity
of objects and lack of diversity of home artifacts which are available
and meaningful to the child in addition to the unavailability of
individualized training, provides the child few opportunities to
manipulate and organize the visual properties of his environment.
Those would Include figure ground relationships and spatial organiza
tion of the visual field. Sparsity of objects to manipulate is said
to hamper development of functions in the tactile area. Children from
disadvantaged homes are said to lack perception of different shapes,
colors and sizes which middle class children have in the form of blocks
that are purchased for the children and also in the form of a variety
of cooking utensils which might be available to the child as playthings.
Homes of children from disadvantaged backgrounds are reported as
being void of verbally enriched interaction, but are regarded as noisy
homes which are for.the most part void of meaningful stimuli for the
child.
Deutsch (1967) believed that due to noise level within some homes
of disadvantaged persons the child under-develops the ability to wall
himself away from his surroundings and fails to develop the ability to
distinguish between relevant and irrelevant sounds and to screen out
the irrelevant. Further notions of poverty have been described.
Cole and Bruner (1972) proposed a notion that rests on the

35
assumption that a community of poverty is reflected in various forms
and deficits. The child of poverty is assumed to lack parental
attention on the basis that some homes are characterized by absence of
a father model, while the mother is said to be away at work or is less
involved in rearing her children than she would be according to middle
class standards. There is said to exist deficits in interaction and
less goal seeking behavior from the parents (Hess and Shipman 1965).
Pavenstadt et al. (1967) described families who were regarded as
disadvantaged and with "multiple problems." The families were noted
co be chronically on and off public relief, if not steady clients on
one or another public assistance program. The families were noted to
show minimal ability to plan ahead, while living largely in an un
comfortable present, with backgrounds of shifting denigrated past.
Cther characteristics of the families were minimal capability of
:oanaging their own affairs or of utilizing those facilities that
society has to offer to the greatest advantage.
Pavenstedt et al. (1967) further noted that families with multiple
problems are those who have never been able to or have never been
allowed to develop a consistent sense of self or identity, and who
have developed inconsistent identities. Caution is presented from
the study that children from such families will no doubt develop a
pattern of relying on public assistance for their survival unless the
vicious circle of the living patterns in which they are reared is some
how broken. Further theoretical efforts may be viewed in terms of
interventive involvement within the homes of infants or children.

Intervention Programs
The idea that providing intervention programs containing
stimulating activities would enhance the development of young children
from disadvantaged environments, was begun more than 30 years ago.
Skeels and Dye (1939) sought to determine effects on mental growth of
a radical shift in institutional environment of children who had been
regarded as mentally retarded. Thirteen children with ages ranging
between 7.1 and 35.9 months and IQ scores ranging from 35 to 89 com
prised the experimental group. All were from homes of low social,
economic and occupational levels. The children were transferred from
the Iowa Soldiers' Orphans' Home to the Iowa Institution for Feeble
minded Children and were placed in wards with older girls. Special
attention, play materials, language stimulation and outdoor play were
provided for the children. Each child had available to him one person
with whom he identified and who was especially interested in him.
The study was continued for two years. At the end of that period the
results were that an average gain of 27.5 IQ points was made, with
each child in the experimental group making a gain. Several conclu
sions from that study are available.
A change from mental retardation to normal intelligence in children
of preschool age is possible in the absence of organic involvement, by
providing a more adequate psychological prescription; conversely,
children of normal intelligence may become mentally retarded under a
continued adverse influence of a relatively nonstimulating environment.
Further, an intimate and close relationship between the child and an
interested adult seems to be a factor of importance in the mental

37development of young children. Approximately twenty-five years after
the Skeels and Dye (1939) study, other intervention programs emerged
on the American scene.
Karnes et al. (1970) described a program in which mothers in
disadvantaged families were provided, during weekly sessions, an
educational program to use at home for stimulating cognitive develop
ment of their children. Twenty mothers (including two grandmothers
who were responsible for care of their grandchildren), with infants
between the ages 12 and 24 months participated in the training
program, and fifteen of those mothers completed the program. They
were provided with transportation to a central meeting place and were
paid $1.50 an hour for attendance in order to pay for baby-sitting
services. The mothers met in two groups of ten persons each for
seven months during the first year, with weekly meetings being devoted
to child and mother-centered activities. Staff members made monthly
visits within the homes of the participants to help the mothers
establish a positive relationship with the baby and to reinforce
teaching strategies discussed at the meetings. During the second
year the program was conducted for eight months using the same format
as the previous year. The children were evaluated at the end of the
training program with the Stanford-Binet Intelligence Scale and the
Illinois Test of Psycholinguistic Abilities. On both measures the
children in the experimental group scored significantly higher than
those in the comparison group.
Wright et al. (1970) described a home visit program that pro
vided cognitive, nutritional and health information to mothers in

38
disadvantaged homes, during pregnancy and until the infants reached
18 months of age. Initial weekly home visits were made in order to
aid expectant mothers in understanding their own nutritional needs
and to prepare for the arrival of their infants. During the last
weeks prior to the infants' birth the expectant mothers were shown
sensory experiences and vocalizing games in preparation for play with
the infants. From birth to six months of age the mothers were supplied
with information which dealt with emotional, cognitive and medical
needs of the baby. When the infants were between six and eighteen
months of age inexpensive educational toys were made by the mother and
project staff during some home visits and left with the mother for use
with the infant. The children were enrolled in nursery school which
was a part of the program.
Visits at that time were scheduled aroung the children's attendance
in school. Library books were taken into the homes on a weekly basis
and exchanged for those that were left during the previous week.
Several types of information were obtained from this home based
intervention program.
Mothers' reactions to staff personnel and to the instructions
were noted. Also noted were whether other persons were present within
the homes during the sessions, extent of interruptions that occurred
during visits and whether books and other educational materials were
present within the homes.
The findings were that initially five of the mothers seemed merely
to tolerate the staff, but changes in their attitudes in a positive
direction were observed as the program continued. The majority of
39
mothers were found to perform the activities with the children when
asked to do so. Due to the presence of as many as seven other child
ren in some homes, specific activities were planned for older children
for the purpose of reducing the extent of interruptions during the
training sessions. Several families had books and other educational
materials within the homes; others had none initially but obtained
them as the program progressed.
Williams and Scarr (1971) provided early educational intervention
to a group of low birth weight children whose risks of both neurologi
cal and social impairment were regarded as being high. Thirty children
of four age groups "birth to one year, one to two years, two to three
years, three to four years" were chosen for the study. Ten children
within each of the four age groups were assigned to each of three
groups. The three and four year old children were assigned to the
primary experimental group on the basis of their residential proximity
to the university at which the study was performed. Others were
randomly assigned to the second experimental and control groups.
Intervention efforts were different for the three groups of children.
Children in the primary experimental group received both educa
tional toys and tutoring on a regular basis. Children in the second
experimental group received toys but no tutoring, while those in
control group received neither. Children were tutored for four months
by university students except the infants who were less than one year
old. Instead, the tutors talked with the mothers concerning the impor
tance of stimulation and suggested play activities for the children.
Also the mothers were encouraged to bring the infants out of their

40
usually dark bedrooms and place them into lighted and partially decorated
living areas; to place the infants on firm surfaces such as floors in
order to aid locomotion; to provide materials for the infants to look at
and to listen to. Mothers were also encouraged to talk with their
infants. Older children were provided with an assortment of toys.
Several findings emerged from the study.
Motor task performance was not influenced by treatment in either
group for any of the children. Motor performance was found, however to
be strongly related to neurological status of the particular child. The
neurologically intact children who received tutoring earned scores, after
intervention, which were equivalent to those of other lower class, full-
term children. The strength of treatment was influenced by neurological
impairment. Children with no neurological damage and who received tutor
ing and toys showed greater gains in verbal performance than the children
of the other groups. One interesting finding was that intervention with
provision of toys alone had no treatment effect on the children. Gains
seem to be related to instructional use of the toys as well as provision
of them.
Studies of Infant Attention
An intervention program for infants may include the use of several
types of stimuli. Many human newborns have exhibited the capacity to
various forms of stimuli. Evidence of such capacity has come from a va
riety of studies of infant attention. Those studies indicate that infant
attention appears to be a function of presenting stimuli affecting various
sensory modalities. Significant studies have included at least four
types of stimuli used to elicit infant responsivity.

41
Studies of Attention to Auditory Stimuli
Wertheimer (1961) studied responses to auditory stimulus on a
single neonate. He reported that his newborn daughter at age ten
minutes turned her eyes in the direction of a soft click made near
the infant’s ear. He replicated the study with another newborn infant.
At three minutes after birth a series of trials was begun with the
use of a click in systematic order, with a toy "cricket" near either
of the infant's ears. Two observers independently recorded whether
the infant exhibited eye movements.
As soon as the first click was sounded the neonate who had been
crying with eyes closed, opened them and oriented in the direction of
the sound. After* 52 trials at eight trials per minute the
infant ceased responding. Movement was observed during 22
of the trials, 18 were in the direction of the sound and four
were in a direction opposite the sound. On the basis of information
from the two studies Wortheimer (1961) concluded that within ten
minutes after birth, rudimentary directional response is possible with
a human neonate.
Birns (1965) applied two auditory stimuli to 30 babies during
the first four to five days of life. In consideration of a soft tune
and a loud tune he wanted to know whether there are individual differ
ences in the neonate's intensity of responses to several stimuli. He
found that neonates could be differentiated within the first 15
days of life in terms of constancy of their responsivity to external
stimuli. Types of infant responses included toe or finger flicker,
gross movement of extremities— flexion or extension, startle and crying.

42He found that some neonates consistently responded vigorously to all
stimuli; others responded moderately. Babies who responded vigorously
to one stimuli usually responded vigorously to all stimuli with
consistency. There appears to be general agreement among writers
regarding types of overt responses of infants when presented auditory
stimuli.
Field (1967) studied infants between the ages birth to 26 days
and found responses to include movements of the facial area, movements
of the arms, legs and feet, as well as cessation of movements and
changes in infant state. Daugherty and Cohen (1961) found similar
responses among infants who were between the ages four and 28 weeks,
lisenberg et al. (1964) found movements of the whole body, various
forms of arousal, such as increase in activity level on sudden onset of
r.ew activity and quiet orienting such as a significant decrease in
activity or complete cessation of on-going activity. Various forms
cf stimuli were used to elicit responses from the infants. Rattles,
china cups with metal spoons, human voice, xylophones (Daugherty and
Cohen 1961), soft and loud tones (Birns 1965), crumpling of fresh
sheets of onion skin paper, the striking together of wooden sticks,
root of a small plastic whistle and the beat of a drum (Eisenberg
at al. 1964), are among the stimuli used. In addition to responsivity
to auditory stimuli, infants have been found to respond to varying
types of visual stimuli.
Studies of Attention to Visual Stimuli
Darwin (1877) is said to have demonstrated interest in visual
attention of infants as he noted his infant son first began to visually

43
track a candle and other moving objects at the age of eight days. Since
Darwin's observations other studies have appeared. Recently, studies
by Berlyne (1958) and Fantz (1958) have been reported as having served
as a beginning of many other studies to appear in the literature.
Berlyne (1958) used four series of patterns constructed on
rectangular cards, with three different designs in each series. One
series contained black, gray and white rectangles; the other series
contained figures constructed of equal areas of black and white,
among which was a checkerboard design. One design consisted of black
and white dots randomly distributed on the background. Each pattern
had a one-half inch margin on each side. He presented the designs
to the infants and found that the black and white dots, together
with the checkerboard pattern were more likely to attract first
visual fixation by the infants.
Fantz (1958) sought to determine which pattern, among four pairs,
infants would prefer as measured by total fixation time on the pattern.
One pair of patterns consisted of a circle and a square equated in
area; another consisted of two identical triangles, while a third
consisted of a five-inch checkerboard that was paired on half the time
with a square of the same size and paired the remaining time with a
smaller square. The fourth pair of patterns consisted of a five-inch
square with alternating red and gray horizontal stripes and another
pattern that Fantz (1958) referred to as a "Bull's Eye." That pattern
consisted of a five-inch square on which was placed alternating circles
of gray and red with decreasing circumferences from the outer edges to
the central portion of the square.
44
While the infants were placed in supine position each pair of
patterned objects was presented to the infants for thirty seconds
twice in succession during weekly test sessions until ten records on
each infant were obtained. Several findings emerged from that study.
The pair of triangles and the cross and circle pair failed to
elicit consistent visual preferences among the infants. Two patterns
that presented variations in type and degree of patterns produced
significant results. Nineteen of the 22 infants fixated the checker
board more than the square and 20 infants showed higher time scores
for the "Bull's Eye." On the basis of their results Fantz (1958)
concluded that visual patterns were discriminated by the infants in
his study during the first six months of life as evidenced by differ
ences in fixation time.
Hershenson (1964) studied visual fixation in the human infant and
used,for a portion of his study, patterns that he classified as having
three levels of complexity. Least complex stimuli were constructed by
dividing stimulum area into quadrants and blackening in the first and
third quadrants. The intermediate stimulus was constructed by dividing
the stimulus area into 16 equal squares of checkerboard design,
while the most complex design was a checkerboard divided into 144
equal squares of one-half inch. He found that the least complex
pattern was significantly preferred over the most complex designs.
Mirando (1970) verified and extended the studies of Fantz (1958)
and Hershenson (1964). However, llirando studied prematurely born
infants and found that prematurely born infants showed preference for
patterned over plain stimuli. He concluded that infant preference was

45
so strong and consistent that such finding is potentially useful for
establishing presence or absence of pattern vision in newborn infants
and for revealing abnormalities in neural structures or function.
Salapatek (1968) utilized black and white solid and outline
circles and triangles of various sizes for eliciting visual fixation
and presented his figures on stimulus panels of 21 inches in diameter,
with the centers of all figures coinciding with the center of the panel.
He found that circles and triangles of any size that are centrally
placed in the infant's visual field attracted his gaze. He also
found that more time was spent looking at larger than at smaller
figures, while explaining that such a finding may be due to larger
figures occupying more of the infant's visual field. This study
verifies the Hershenson study in which infants fixated for longer
periods of time on figures of larger dimensions than of smaller.
Korner et al. (1971) utilized a different approach to the study
of infant visual attention than did Fantz (1958), Berlyne (1958),
Hershenson (1964), Mirando (1970) and Salapatek (1968). Korner et al.
(1971) investigated infant exploration within the context of maternal
care of the infant. She found that a high level of alertness was
evoked in the infants by holding the infant in an upright position to
the caregiver's shoulder. Such an intervention was said to involve
several simultaneous stimuli--contact, vestibular stimulation and
upright positioning. The finding was that in three out of four
trials, the process of holding the infant at the shoulder predictably
evoked alert scanning of the visual surroundings of a crying infant.
The conclusion was that vestibular stimulation has a powerful effect

46on evoking visual alertness. Also when a mother attempts to soothe
her infant by picking him up she will inadvertently provide him with
visual experiences which he could not receive were he not picked up
for soothing. Further, at least during the neonatal period, vestibular
stimulation is likely to be an important vehicle for stimulation of
certain types of developmental acquisitions. Assuming that visual
exploration is one of the most important pathways at the neonate's
disposal for early learning and for becoming acquainted with the
environment, vestibular stimulation and the upright position of the
infants attendant with maternal care, appear to be highly effective
vehicles for providing such opportunities.
Studies of Attention to Stimuli That Move
Studies have revealed that many human newborn infants have the
capacity to fixate on specific targets when presented within the
visual field. Other studies have shown that infants not only fixate
visually, in addition they are able to follow stimuli that are moved
across the visual field.
Carpenter (1974) studied visual following skills of infants who
were between two and seven weeks old. She was interested in determining
the effect of stimulus movement on the visual behavior of infants,
and in observing changes in visual responses to stimulus movement
over the early weeks of life. The infants were placed in a room
directly in front of a door on which blinking lights were mounted on
a white and black "bull's eye" pattern. The door was opened for
stimulus presentation parallel to the infant's face. Stimuli consisted
of three types of faces--tlie infant's mother's face and one of each,

47
a Caucasian and Negroid manakin head. The faces were presented in
stationary position and also while moving across the horizontal
plane of the infant's vision. Visual behavior was recorded in terms
of seconds. Four findings were in evidence from this study.
All faces received more visual regard from the infants when
moving than when stationary; infant attention increased with age for
both moving and stationary stimuli; manakin faces attracted more
attention than the mothers' faces. The conclusions drawn from this study
is that by at least two weeks of age stimulus movement is associated
with high fixation scores of infants.
Dayton et al. (1964) studied visual following behavior of 45
newborn infants whose ages ranged between eight hours and ten days.
To obtain results the investigators placed the infants on a bed-like
structure and suspended a semi-cylindrical plexiglass canopy, 30
inches in diameter over the infant's head. The target, which consisted
of a series of black dots four inches in diameter, and placed four
feet apart on a flat white surface was propelled by a motor over the
canopy in a left to right direction.
Fifteen of the infants fell asleep during the testing, 13 followed
less than two consecutive dots, while 17 of the infants were found to
demonstrate visual following of the stimuli for two or more presenta
tions. The infants were noted to have located a moving target in the
visual field and follow the target as it moved across the arched
canopy. During the process of visual pursuit each eye moved simultane
ously in the direction of the target. Some infants were found to pursue
two consecutive dots, then showed random movements as when no target was
presented and then again fixated on the target.
48Studies of Infant Responses to Tactile Experiences
Frank (1957) placed great significance on tactile experiences in
the newborn infant as a means of communication and as involvement in
interpersonal relations, extending from the period during gestation.
His notion is that infants need to be cuddled and patted. Such needs
are said to derive partially from uterine life, during which the fetus
is said to continually receive rhythmic impact of the maternal heart
beat. At birth the infant is said to emerge from a rhythmically
pulsating environment into a world where he has to learn to orient
himself to several modes of communication. The infant is said to
possess a repertory of processes that permit recognition of signals
and certain responses to those signals. He responds to the signals
given by the nipple and the tactile contacts during the nursing
process. His responses represent a message to the mother and she in
turn relieves his pain of hunger as she responds by lactation. She
further responds when she speaks or sings to him and he learns to
recognize his mother's voice as a partial substitute for her touch.
Frank (1957) noted that the child's later reception of verbal messages
is predicated to a great extent on his prior tactile experiences.
Tactile experiences, according to Frank (1957) are of such
importance that denial of them may compromise the infant's future
learning and capacity for more mature tactile communication. The
infant's communication with himself is said to provide a base on which
other experiences are built.
The infant is said to begin communication with himself by feeling
his own body, by exploring its shape and textures and as such he

49establishes his body image. Later such cues as focusing his eyes on
his hands and feet help him develop a visual image that may supplement
his tactile experiences. Frank (1957) talked about involvement of
tactile experiences in interpersonal relations. He noted:
Through the earliest bodily contacts and other tactile experiences, the baby communicates in a reciprocal way, mother to baby, and baby to mother, one evoking from the other what will in turn evoke his or her response in a tactile dialect. These experiences establish the individual's early pattern of intimacy and affection.. . . The baby develops confidence in the world, trust in people, through these early tactile relations which establish the meaning of the world for him and also his expectations and feelings toward that world. Thus, how the baby is treated, what tactual experiences he has while being bathed, clothed, tucked in bed, how he is mothered and handled by others govern his initial responses and by so much guides his subsequent learning and relationships.
Frank (1957) notes further:
If the baby is limited in his tactile experiences,denied much opportunity to send or receive tactilecommunications, he presumably must wait until his capacity for visual and auditory recognition have developed sufficiently to permit him to enter into communication with others. Such a child will not only have little of the primary tactile experiences upon which to develop his sign and symbolic communication, but will be expected to rely on visual and auditory symbols and to accept their meanings, not as experientially learned, but as prescribed by others.
Frank contends that tactual stimulation is largely responsible for the
individual's eventual verbal abilities and all the baby's perceptions
and interactions with the world.
Support of the importance of tactile experiences comes from
Provence and Lipton (1962) who compared 75 infants reared in an
institution with infants reared in homes with their families. Upon
the finding that institutionalized infants failed to adapt to adult

50
holding, the investigators concluded that poverty of the infant being
lifted, touched, moved and cuddled began early in life to influence
the infant's adaptation to the environment.
Infant Assessment
In order to obtain data for this study there was a necessity to
select assessment procedures that would describe infant status along
several dimensions over several time periods from the first few days
of life until three or four months. Four instruments are described.
Apgar Procedure
The Apgar (1953) procedure is based on five types of infant
behaviors: heart rate, respiratory effort, muscle tone, reflex irrita
bility and color, initially judged by physicians 60 seconds after
delivery of the infant. Each of those behaviors is assigned a rating
of 0, 1 or 2. A total score of 10 is said to be optimal and a score
of 3 or below represents an infant who is in poor physical condition
(Drage and Berendes 1966).
Neurological Evaluation
According to Amiel-Tison (1968) constant modification of muscle
tone and reflexes are affected by maturation of cerebral processes
during the last three months of fetal life. Procedures have been
devised for assessing neurological maturity of infants. A team of
French physicians (Andre-Thomas, Chesni and Saint Anne Dargassies, 1960)
described a procedure for neurological assessment of infants which
includes observations of spontaneous activity of the infant, elicitation
of reflex capacities and estimation of the extent to which latent

51
reaction might be present. Amiel-Tison (1968) described a neurological
examination procedure that is said to be based on the principles applied
by the French team (See Appendix I). The examination includes proce
dures whereby the physician applies certain movements to the infant
during resting posture while the amplitude of passive movements of
joints is measured. In contrast, active tone is studied with the
infant in an active situation such as while being held in an upright
position. Gestational age of the infant is assessed from these manipu
lations by the attending physician. Amiel-Tison (1968) presented no
evidence with respect to validity or reliability of the instrument.
Brazelton Neonatal Behavioral Assessment Scale
The Brazelton (1973) scale covers a wide range of infant behaviors.
It assesses some neurological items as well as social variables. The
behavioral items, of which are 27, are scored on a nine-point scale,
while the reflex items are scores on a three-point scale. A manual is
available for recording infant performance (See Appendix II). Four
pieces of materials are necessary for administration of the scale— a
standard flashlight, a bright colored ball, a rattle and a bell. The
examination requires between 20 and 30 minutes, and begins with a two-
minute observation prior to attempting to elicit infant responses. The
baby's initial state score is recorded at the end of the observation
period.
After the observation period stimuli which can be offered dis
cretely (i.e., auditory and visual) are presented. While the infant
is still in the wrapped, quiet state (state 1, 2 or 3) the flashlight
is flashed across his eyes until he awakens or ceases responding for at
52
least three times. After the infant becomes quiet again the rattle and
bell are presented for a maximum of nine trials each. The infant is
then uncovered and any reactions to that change are recorded (such as
skin color, rapidity of buildup from quiet to agitated state).
While the infant is still in quiet state the sole of one foot
receives a light pin-prick (without penetrating the skin). Notation
is made with respect to how rapidly the infant is able to shut down
response to subsequent pricks. Assessment is also made of the infant's
state change as he moves to a wide-awake state. While the infant is
still dressed muscle tone as well as several reflexes are assessed,
including the Babinski, plantar and palmar grasp and ankle clonus.
The examiner is free to vary the order of administration of items
after the infant has reached an awake-alert state. While orientation
items appear near the end of the test, the examiner may try some of
those as soon as the infant is awake, alert and not crying (before
testing pull to sit or prone behavior). Constraints on test flexibility
necessitate that stimuli regarded as aversive (uncovering, undressing,
being pulled to sit, being placed in prone) be administered when the
infant is not in a crying state. Stimuli regarded as strongly aversive
are pin-prick, elicitation of the tonic neck reflex, elicitation of the
Moro reflex and elicitation of defensive reactions (cloth on face).
The infant may be undressed as he moves from sleep to wide-awake
alertness. Again, he should be observed for state change, lability of
skin color in response to disturbing maneuvers by the examiner. Tone
is assessed when the infant is handled and when he is first undressed.
Passive movements are evaluated at this point and followed by testing

53
for orientation response to visual and auditory stimuli (items 5 and
6 on the scale).
If he remains in the awake state he can be pulled to sit. The
next sequence includes assessment of standing, walking and placing
reflexes, incurvation, body tone while being held prone across the
examiner's hands. The infant is then picked up, held, and spun around
slowly for vestibular responses and nystagmus. Testing for orientation
responses to animate stimuli (items 7, 8 and 9 of the scale), is followed
by response to a cloth placed on his face, the tonic neck reflex and
Moro reflex. These manipulations are disturbing to the infant and
provide an opportunity for observing the infant's self-quieting be
havior.
Measures such as hand-to-mouth facility, tremulousness, startle,
activity and alertness are continually assessed. A major emphasis on
the Brazelton Scale is to elicit the infant's best behavior. If the
infant has not responded to a particular stimulation, the examiner should
make every effort to verify that the infant is not capable of making a
better response, and should be aware of opportunities for repeating
tests later during the examination.
Another emphasis on the Brazelton scale is that the scale is to be
administered only during specified states. For example, infant response
to flashlight, bell, rattle and pin-prick are to be administered only
x̂ hile the infant is in states 1, 2 or 3. It is possible to utilize six
different states of the infant while administering the Brazelton Scale.
Brazelton (1973) noted that criteria for determining state are based on
personal experience as well as that of others. He defined them as

54
follows:
Sleep States
(1) Deep sleep with regular breathing, eyes closed, no spontaneous activity except atartles or jerky movements at regular intervals, no eye movements.
(2) Light sleep with eyes closed; rapid eye movements may be observed under closed lids; low activity level, with random movements and startles . . . respirations irregular, sucking movements occur on and off.
Awake States
(3) Drowsy or senii-dozing; eyes may be open or closed, eyelids fluttering; activity level variable, with mild startles from time to time. Movements are usually smooth.
(4) Alert with bright look; seems to focus attention on source of stimulation; impinging stimuli may breat through, but with some delay in response. Motor activity is at a minimum.
(5) Eyes open; considerable motor activity, with thrusting movements of the extremities; reactive to external stimulation; discrete reactions difficult to distinguish because of general high activity level.
(6) Crying; characterized by intense crying which is difficult to break through with stimulation.
The Brazelton Neonatal Behavioral Assessment Scale (1973), de
veloped by T. Berry Brazelton, M.D., has formerly existed as The
Cambridge Newborn Scales (Mimeographed). The Scale has been revised and
is now available from publishers. Self (1971) examined test-retest
reliability of the scale on the third and fourth days of life and again
at one month of age of infants. Mean Test-retest reliability for all
items within one agreement was 0.592; with agreement scores within
two points on the scale; it was 0.783 (Self, 1971).
The scale has been used to assess infants who have participated
in .several research projects. Scarr and Williams (1971) studied low

55
birth weight infants and examined the ability of the scale (the earlier
version) to predict developmental status of low birth infants at one
year of age. Assessment was performed at about seven days of age when
the infants' bodily temperature could be maintained outside an isolette
during the examining period, and again at four to six weeks of age,
when the infants were of nearly full-term weight. The findings were
twofold: 1) assessment at seven days of age was far more predictive
of later status than later assessments and 2) The Cambridge Newborn
Scales at one week proved much more useful than a standard neurological
examination given to prematurely born infants.
Freedman and Freedman (1969) used the Scale to study behavioral
differences between Chinese-American and European-Anerican newborn
infants. In that study the Caucasian infants showed greater lability
of state while Oriental infants tended to show more calmness in response
to aversive stimulation. Oriental infants also tended to show greater
habituation to presentation of a flashlight, and to show greater self-
quieting ability than Caucasian infants. In other areas (motor
development and social responsibity) the two groups were essentially
equal.
Brazelton (1975) noted that the scale may more accurately diagnose
"at risk" infants than the more commonly used neurological examination.
He reported that the standard neurological examination has been known
to produce 80 percent false alarm rate, while the Brazelton scale
produced only 24 percent false alarm.
Bayley Scales of Infant Development
The Bayley Scales of Infant Development are designed to provide

56
a basis for evaluating a child's developmental status in the first two
and one-half years of life (Bayley 1969). The Mental Scale is designed
to assess sensory-perceptual activities, discriminations and ability
to respond to these; the early acquisition of "object constancy" memory,
learning and problem solving ability; vocalizations and the beginnings
of verbal communications. Results from administration of the Mental
Scale are expressed as the Mental Development Index (MDI).
The Motor Scale is designed to provide a measure of the degree of
control of the body, coordination of the large muscles and finer
manipulatory skills of the hands and fingers. Results of the administra
tion of the Motor Scale are expressed as the Psychomotor Development
Index (PDI).
The Bayley scales were standardized on the sample of 1,262 children
from various social-economic backgrounds and geographical regions. Norms
are available for infants between one month, 24 days and 30 months.
Tester-observer reliability on the 1958-1960 version of the Bayley
Mental and Motor Scales is 89.4 agreement with the Mental Scale and
93.4 with the Motor Scale (Werner and Bayley, 1966, reported by Bayley,
1969).
In an earlier study Bayley and Jones (1937) used the Bayley Scales
to assess relationship between Socioeconomic status and Mental develop
ment. The finding was that for the first 18 months of life correlations
were close to zero or tended to be negative. After 18 months some
environmental factors develop positive correlations to mental scores.
By 72 months of age the total Socioeconomic scores showed .41. After

57the relationship became positive, the highest correlations were with
the mother's education (.58 and .59).
Cameron, Livson and Bayley (1967) extracted several clusters of
items from the California First Year Mental Scale (the scale from which
the Bayley Scales were derived). One of those clusters involved early
vocalization behavior of infants. The researchers found that vocaliza
tion items appeared to be related to girls' intelligence (but not
boys') as measured at years six through twenty-six.
The age range covered by the Bayley Scales, the high reliability
and continued use of the scales contribute to the usefulness as an
instrument for assessing infant behavior.
Maternal Assessment
In recent years studies of human development have included
descriptions of environments within homes of infants and children in
order to try and determine to what extent human behavior may be
explained in terms of situations within homes which may be observed by
home visitors. Three instruments ai'e presented which have been used
in the context of studying the home environment.
The Caldwell et al. Inventory of Home Stimulation
Caldwell et al. (1966) developed an inventory of person-person and
person-object qualities which was regarded as collectively comprising
the infant's learning environment within the home, and to determine
which specific features of the environment were most likely to influence
development. It was noted that data from such an inventory might some
how warn of developmental risk before age three years, and that such

58
data might help to pinpoint areas in which intervention may be needed.
A current inventory is now available which includes environment
characteristics believed to foster early development (See Appendix III),
The Inventory contains 45 items within six subscales: (1) Emotional
and Verbal Responsivity of the Mother, (2) Avoidance of Restriction of
Punishment, (3) Organization of Physical and Temporal Environment,
(4) Provision of Appropriate Play Materials, (5) Maternal Involvement
with the Child, and (6) Opportunities for Variety of Daily Stimulation.
Scoring of the Inventory is based on observation and partly on answers
to a semi-structured interview, administered in the home at a time
when the child is awake and when he may be observed in interaction
with the mother or primary caregiver.
Elardo et al. (1975) noted that extensive standardization data do
not exist for the inventory, however data from 176 families in Central
Arkansas indicate that the instrument is sensitive enough to register
a wide range of scores for families in identical social class designa
tions, and there is a moderate degree of stability across the 18-month
life span. Internal consistency coefficients based on 176 cases range
from .44 for subscale six to .89 for subscale three. The internal
consistency coefficient for the total scale was .89.
Elardo, Bradley and Caldwell (1975) used the Inventory in a
study of 77 mothers and infants to determine which aspects of the early
home environment were associated with the infants' mental test performance
at age three years. Results were reported which were based on assess
ment with the Inventory at three age periods (six months, twelve months
and twenty-four months).

59
High correlations were found between the Inventory at six months
of age and the infants' Stanford-Binet scores at age three years (.54).
High correlations were also found between the scores at 12 months
and 24 months, and the Binet scores at age three years.
The investigators concluded that the findings suggested that the
Inventory of Home Stimulation measures a complex of environmental
forces which may be prerequisites for later performance on cognitive
tasks. They further noted that the Inventory has the potential for use
in differential diagnosis of strengths and weaknesses which may be
present in an infant's environment and may assist those who are con
cerned with designing intervention strategies.
Ainsworth Maternal Care Scales
Ainsworth studied attachment behavior to describe mother-infant
relationships. Ainsworth and Bell (1970) defined attachment as:
an affectional tie that one person or animal forms between himself and another specific one--a tie that binds them together in space and endures over time. The behavioral hallmark of attachment is seeking to gain and to maintain a certain degree of proximity to the object of attachment, which ranges from close physical contact under some circumstances to interaction or communication across some distance under other circumstances.
Attachment behaviors are defined as behaviors which promote proximity
or contact. In the context of attachment behavior, Ainsworth (1973)
devised several scales for rating maternal behavior, during the first
quarter of the first year, of the infant's life.
Three of those scales are regarded as descriptions of subunits of
the general attitude of the mother towards baby, and her role. They
are: (1) Mother's Perception of Baby (Appendix IV), (2) Mother's

60Delight in Baby (Appendix V), (3) Mother's Acceptance of Baby (Appendix
VI). Three other scales are regarded as subunits of the mother's
availability and interaction. They are: (1) Mother's Availability to
Baby (Appendix VII), (2) Amount of Interaction Offered by Mother
(Appendix VIII), (3) Appropriateness of Mother's Initiation of Inter
action (Appendix IX).
In order to administer the scales, ratings are performed on the
basis of narrative reports of observations of mothers and infants within
the home setting. Ainsworth (1973) reported inter-rater reliability
coefficients of .80-i-, based on ratings of two judges of each mother.
First quarter scales were reported to intercorrelate on the
average, quite highly. Ainsworth (1973) stated that high intercorre
lations suggest that not all scales may be necessary to characterize
the first quarter of mother and infant interaction.
In the context of feeding behavior Ainsworth (1969) used four
scales which were utilized in this study of addicted infants: (1) Mother's
Perception of Baby, (2) Mother's Delight in Baby, (3) Mother's Acceptance
of Baby and (4) Appropriateness of Mother's Interaction with Baby. The
findings were that highest ratings earned by mothers were associated
with four types of feeding patterns: (1) a demand schedule (characterized
by consistent and demand feeding, (2) a flexible type of feeding
schedule (a schedule flexibly regulated by mothers who were highly
sensitive to infant signals), (3) a demand schedule (characterized by
overfeeding to gratify the infant) and (4) a scheduled type of feeding
(overfeeding to gratify the baby). Sensitivity to the baby's signals
and desire to gratify him were found to be prominent with mothers who

61
exhibited those feeding patterns. The mothers tended to respond promptly
and appropriately to the baby's crying and were found to be sensitive
to the baby's state and wishes.
Parent Counselor Home Visit Report
Wright et al. (1970) described a program which used home visitors
as disseminators of information designed to be helpful for growth and
development of the fetus and young children. Home visits were made to
families whose incomes were less than $5,000,00 a year, and were made
during the prenatal period and until the infants reached 18 months of
age. Emphasis was placed on nutritional needs of pregnancy and
lactation during the prenatal period. From birth of the infant until
six months emphasis was placed upon medical, emotional, cognitive and
material needs of the mother and the newborn infant.
Information from each home visit was summarized to provide several
types of data; (1) to note whether the parents or a caregiver were
available for the visit, (2) to determine how the caregiver reacted to
the home visitor on a personal level, (3) to note the extent of
activity and interruptions within the home during the visit, (4) to
note how the caregiver seemed to cope with the instructions provided
(whether or not she could or would do the exercises), (5) to note the
presence of educational materials within the home, and (6) to report
the way the caregiver seemed to feel about the program and her role in
it. Several findings emerged from the study.
During 90 percent of the visits, the mothers greeted the home
visitors warmly, were receptive and cooperative with their conversations.

62
Only five mothers continued to be disinterested. However, those mothers
changed their attitudes as the visitors made repeated visits.
Most of the visits were conducted at times when only the mother and
child were present. There were some cases in which from four to seven
adults were present in the room where the visit was taking place. One
visitor listed as many as seven children present in the room at the time
of the visit. Children would often interfere with the mother and baby,
and would attempt to take the materials which the home visitor had
brought for the mother's work with the infant. It was often necessary
for the home visitor to plan specific play activities for the other
children.
The majority of the mothers would perform the exercises when asked
to do so. Only three were reported as having refused. However, one
mother was reported to have refused consistently for the first seven
visits, but began to perform them when she discovered that her child
responded to the exercises which were provided.
Nineteen mothers appeared to have books or educational materials
available on the first visit and continued to have them. Ten mothers
had no books, but obtained them later. Eleven mothers had no educational
materials available when first visited, but obtained them later. The
majority of caregivers reported that the project was great for helping
them understand some of their infants' needs. Data with reference to
validity and reliability of the instrument were not available.
Infant Care Inventory
The Infant Care Inventory was developed by Hock (1972) for use
with mothers of infants who participated in a research study. In this

63
inventory mothers are asked to make a decision regarding whether they
or other persons could best perform various infant care skills. The
skills are the act of showing affection to the baby, preparing the
child and putting him to bed, calming the child, diapering the child,
understanding the baby's wants, teaching the baby games, feeding and
providing visual and verbal stimulation. Pairs of titles of persons
are presented for the mother to make her choice. The inventory is
presented in Appendix XI. Data which indicate validity and reliability
of the instrument were not available.
Two Factor Index of Social Position
The Two Factor Index of Social Position was said to have been
developed to meet the need for an objective, easily applicable procedure
to estimate the positions individuals occupy in the status structure
of American society (Hollingshead 1957). Its development was dependent
both upon detailed knowledge of the social structure and procedures
social scientists have used to delineate class position. It is premised
upon three assumptions: (1) the existence of a status structure in
the society; (2) positions in this structure are determined mainly by
a few commonly accepted symbolic characteristics; and (3) the char
acteristics symbolic of status may be scaled and combined by the use
of statistical procedures so that a researcher may quickly, reliably
and meaningfully stratify the population under study.
Occupation and education are the two factors utilized to determine
social position. Occupation is presumed to reflect the skill and power
individuals possess as they perform the many maintenance functions in
the society. Education is believed to reflect not only knowledge, but

also cultural tastes. The combination of these factors by the use of
statistical techniques enables a researcher to determine within
approximate limits the social position an individual occupies in the
status structure of American society.
To determine the social position of an individual or of a household
two items are essential: (1) the precise occupational role the head
of the household performs in the economy; and (2) the amount of formal
education he has received. Each of these factors is then scaled
according to a definite system of scores. See Appendix XII for the
occupational and educational scales.
Summary
This review of literature included discussions of features of
narcotic addiction as experienced by some women during pregnancy and
during the post partum period, and also as experienced by their newborn
infants. Also, views of several writers were presented as they relate
to disadvantaged persons.
In addition, descriptions of intervention programs and of materials
used for enhancing infant attention were presented. Some instruments
which have been utilized for infant and maternal assessment were described.
CHAPTER III
METHOD
In this study the variates of neonatal assessment and criterion
variables of infant development, maternal care, program acceptance and
maternal compliance with medical appointments and suggestions were
compared between addicted and nonaddicted mothers and their infants,
in order to determine whether differences were found between the two
groups. Feasibility of a subsequent study was assessed.
Research Design
Subject Selection
The mothers and their infants who comprised this study were
selected upon referral from three sources. Three pregnant women were
referred from Vita Drug Treatment Center, two from The Ohio State
University Obstetric Clinic and another was referred by Pediatricians
while the mother was a maternity patient at The Ohio State University
Hospitals. Each of those women reported having consumed heroin while
pregnant, and two of them were participating in a Methadone Maintenance
Program during their pregnancy periods. Another woman who had a
"suspicious" drug history was referred by Pediatricians after the'
woman was discharged from the hospital and while her infant was
retained in the hospital due to his exhibiting withdrawal symptoms.
All seven of those women consented to participate in the study. Two
65

66
of them were lost to follow-up and five remained in the study. They
are referred to as narcotic addicted women.
Five other women who had no known history of drug addiction were
contacted for participation in the study while they were maternity
patients at The Ohio State University Hospitals. Those women are
referred in this study as nonaddicted women. Addicted women and their
infants were selected one at a time and matched with nonaddicted women
and their infants on the basis of Social Class Position (Hollingshead,
1957), ages of the mothers, gestational ages, birth weights and Apgar
scores (Apgar 1963) of the infants.
The mean age of addicted women was 24 years, four months. The
mean age of nonaddicted women was 24 years, eight months. The women
were from low socioeconomic position with eight of them receiving
public welfare support. The mean birth weight of addicted infants
was 3,115 grams. Mean birth weight of nonaddicted infants was 2,918
grams. (Table 1).
Case Histories of Addicted Women
Marital Status
Of the sample of five addicted women, three were single, one was
widowed, but shared living quarters frequently with her infant's
father. One woman was married and lived with her husband.
Residential Characteristics
All of the addicted women in this study resided in predominantly
Black neighborhoods. Their home environments differed with respect
to quality of housekeeping and extent of living space that appeared

TABLE I
CHARACTERISTICS OF T1IE SAMPLE
Study Group n = 5 Comparison Group n = 5
Family Data: Welfare Supported 4 4Father Present In Home 2
Ages of Mothers: X number of years 24 years, 4 months 24 years, 8 months
Social Class Position 61* 63*
Black Women 5 4White Women 0 1
Infant Data: Gestational Ages X 38.8 weeks 39 weeks
Birth Weight (grams) X 3115 2918
Apgar Scores (1 minute) 8.6 8.4
*Hollingshead (1957)
68
available. One woman resided in a two-floor house with her two
children and a sixteen year old brother, next door to the home of her
parents. Her furnishings were deteriorated but seemed moderately clean.
Case 2 shared one bedroom with her husband and infant, A drawer from
a chest and a wicker basket were used for the infant's sleeping
facilities. This family lived with the paternal grandmother and
appeared to have no furnishings of their own. However, the family
owned a new model Buick automobile.
Case 3 lived with her infant and two other children in the home of
her parents, together with a teen-aged brother. The interior of the
home was always dimly lighted with the draperies closed. Poor
housekeeping standards were evident; roaches were frequently seen
crawling on furniture and floors. Exterior of the home was badly
deteriorated; steps were difficult to climb due to broken sections.
Case 4 lived in..a second-floor apartment which was situated in a
commercial neighborhood. The halls of the building were unclean and
dimly lighted. Interior of the apartment was free from debris, but
the furniture was worn and soiled. The apartment was dimly lighted,
while on one occasion a table lamp containing a red bulb was lighted.
Draperies were always closed.
Case 5 lived in a "Halfway House" for women until her baby was
born. At that time, through aid from the local Welfare Department,
she was placed in a first floor portion of a duplex house. The interior
was clean and neatly furnished with worn furniture.

Number oC Children
The women varied with respect to their number of children. Cases
1, 2 and 4 each had two children; cases 3 and 5 had three.
Extent of Child Care Provided for Them by Others
Case 3 relied to a great extent upon her 14 year old daughter
for providing caregiving responsibilities to the infant as well as to
another child. Case 4 had a nine year old son who resided with his
maternal grandparents in another city. Case 5 reported one child who
lived in a foster home and another who lived with a maternal aunt.
In that respect, addicted women in this study were regarded as
"high risk" women with respect to their returning to illegal drug use.
Rothstein and Gould (1974) noted that addicted women who received
child care help from others may return to drug use, and may be regarded
as "high risk" women.
Educational Level
All addicted women in this study except one were high school
graduates, while two of them had received additional technical training.
Reason for Leaving School
Each mother noted that she left school due to graduation. The
one who did not graduate said she left because she became bored with
school.
Drug Experience
Case 1 denied her drug experience, but reported that her brother
had used drugs illegally. She was included in the study on the basis

70
of her infant's condition at birth. Physicians were hesitant and
deliberated for a long time and made the assumption that the infant's
condition could have been drug related, as they found no other basis
for his condition.
Case 2 used heroin until her pregnancy reached the third month.
She reported that she ceased use at that time in order to prevent
harming her unborn infant. She reported that use of heroin was related
to feelings of depression, associated with her husband's difficulty with
military involvement of an unexplained nature.
Case 3 reported heroin as the first drug used and as her present
drug and let it be known that she was persuaded to use drugs by a
friend. She reported use of heroin for five years and reported her
participating in a Methadone Maintenance program during the past two
years.
Case 4 used heroin as her first drug. She was participating in a
Methadone Maintenance program at the time of enrollment in the study.
She discontinued with Methadone while in the hospital, and failed to
return to the program. Subjective evidence seemed to support the
notion that she had returned to illegal use of drugs.
Case 5 reported the use of Codeine, and other drugs prior to
using heroin. She provided information which included her incarceration
for drug use and other unexplained offenses. At the time of enrollment
in the study she was on parole from a woman's reformatory for drug
use and other reasons.
Receptivity to Intervention Program
All women in this study were receptive to the intervention program

71
which was directed at contributing to enhancing quality of mothering or
helping -others become sensitive to infant needs and helping mothers
develop caro : ivin e skills. However, two of the women were inconsistent
in adhering to scheduled appointments. They eagerly scheduled appoint
ments but failed to be available at designated times. All of the women
appeared to make some effort at attracting attention of their infants,
especially during presence of the visitor. A common occurrence among
the women was the act of presenting some form of auditory or visual
stimuli within the sensory range of the infants. Response of such
maneuvers was noted with the infants.
Data Collection
Intervention and Data Collection
Data collection for this study was interwoven with intervention
and was performed before delivery, during hospitalization following
delivery of infants and during home and Pediatric Clinic visits through
out the first three months of the infants' lives. Data collection
occurred during three major time periods: during Phases I, II and III,
(See Table 2).
Phase I--3efore Delivery. The investigator visited pregnant women
at two drug treatment centers, described the study to them,
obtained demographic data and drug history from them with a »
Parent Counselor Interview form which was adapted from Bloom and
Sudderth (See Appendix XIII). Social position of the women was
obtained with the Hollingshead (1957) Two Factor Index of Social
Position, Appendix XII.

TABLE 2
SCHEDULE OF DATA COLLECTION
Phase I--Before Delivery
•Phase II--After Delivery
Maternity Room Contact
Phase III--Out Patient Status Throughout the First Three Months
DATA COLLECTION:
1. Hollingshead Two Factor Index of Social Position
2. Parent Interview Report
1. Amiel-Tison Neurological Evaluation of the Maturity of Newborn Infants
2. Developmental Examination (Brazelton Neonatal Assessment Scale)
Home and Clinic Visits
Ages of the Infants (Weeks)
Clinic Clinic ClinicH om e H om e H o m e and H om e and H om e and
H o m e H om e H om e
1 2 3 4 6 8 1 0 1 2
U M H ro i—* ro t—1 to t-> to l-» to r-1 1—1 f - W N H
CD OS p> i t w s£ os ■rr1 r->•-C S SS os a n os >fo rj H- H i-i r-c i-t CD i-t p n cd n O so so r 1*H-> 3 3 H* (a H* 3 H< Co H- •< H. Co i->- (5 3P j N OS 00 N 00 N 00 H- 00 t-- 00 H- CjO ^ Br 1-1 K3 CD 3 3* CD 3" CD ST O ST CD ~ o S O Sro i-* o r t i-1 r t t—1 r t fts r t s j r t 3 rr ro '< ot—* r+ •-* r t rr I-* i-1 r-* rji—• O r t CD o to O CD CD CD CD r-> rr
3 3* r t 3 r t to r t H rt r t M rr 3*CD 3 3ti P> to 3 r t « So rr 3
t-“ 1—1 CD t-» t—‘ tD r-1ro • • rj • rj •i—1 < <» CD CD
3 3r t rrUs -p- H* US .p-Vw/ O O V '-Z
(P 5 s 3 3CD 2 H S
r t ft C r t I-t 3 CDH- O H- r r Oi
so oq 3 00 CD H-t-> ST H 3 rj O• f t • rr < 3CD 1—13rrh>-O3
-otO
73
rhase II--After Delivery and Maternity Room Contact. Visitation
was performed with five women who comprised the comparison group
and two other women in the study group, after delivery of their
infants. The qame information was obtained from them as in Phase
Infant data were obtained at varying time periods.
Apgar (1953) scores of the infants were obtained by physicians
at age one minute and were recorded on the infants' records. The
Amiel-Tison (1963) Neurological Evaluation of the Maturity of
Newborn Infants was performed by the Pediatrician who supervised
the medical aspects of the study. In addition, the Brazelton
<1973) Neonatal Assessment Scale was administered by the investi
gator when the infants reached approximately three days of age.
Hospital procedure was followed regarding clothing worn by staff
in the nursery areas.
Assessment of the infants was performed in a small room
adjoining the newborn nursery, after each infant was brought to
that area by staff nurses. Beginning the assessment with the
infant asleep as recommended by Brazelton (1973) often was not
possible. Administration of the scale provides for some flexi
bility and when necessary such flexibility was utilized. When,
for example, an infant was crying, directions were followed for
consoling the infant. An observation period was engaged in prior
to attempting to comfort him, thus allowing an opportunity for him
to engage in self-quieting behavior. When the infant did not quiet
himself, comforting was provided according to directions in the
Manual which included presenting the Examiner's face to the infant,

74
prostint ini’; the face and voice to the infant, placing the Examiner's
hand on the infant's stomach, restraining one arm, then both arms,
holding him, holding and rocking and finally holding, rocking
and talking to the baby. Often comforting procedures were
accompanied by state changes, which were recorded with the use
of a mechanical counter. When infants were asleep the scale was
administered according to standard procedure. Upon completion
of assessment the infant was returned to the nursery by a hospital
nurse.
Phase IIT.--Out-Patient Status Throughout the First Three Months.
Medical surveillance was performed by the Pediatrician who
supervised the medical aspects of the study until there no
longer existed concern about infant withdrawal. At that time
and until the infants reached three months of age they were seen
according to regular schedules as needed by each infant, for
pediatric and routine well-baby care. In addition, the writer
made regular weekly visits to the homes of the infants until
they reached one month of age. After that time home visits
were made on a bi-weekly basis until the infants reached three
months of age.
When the infants reached one, two and three weeks of age the
Brazelton (1973) Scale was administered within the infants' home.
The same procedure for assessment was followed as when assess
ments were performed in the hospital. A sofa, bassinett or infant
crib, when available, was utilized for handling the infant. A
booklet that contained suggestions for enjoying the infants was

75
l eft wiLli each mother at the end o I: Che first visit (Appendix
XIV). Maternal data were also gathered during the first home
visit (Table 2).
Each mother completed the Infant Care Inventory (Appendix
XI). The writer took notes in narrative form, of observations
of maternal care of the infant. On the basis of data derived
from those notes each mother was rated on six Ainsworth (1973)
scales. Ratings on those scales were recorded after having left
the infants' homes. Observations were also made concerning
social, emotional and cognitive support available within the
homes. Ratings of those indices were scored on the basis of the
Caldwell et al. (1966) Inventory of Home Stimulation (Appendix
III). Scores from Ainsworth (1973), Infant Care Inventory (1972)
and Caldwell et al. (1966) were used as pre-test data.
During the first three weeks of the infants' lives emphasis
was placed on talking to, playing with the infants and conversing
with the mothers regarding their concerns as well as needs of the
infants. When the infants reached four weeks of age materials
constructed from scraps of paper were used to enhance infant
attention (Figures 1-9). Use of those materials was continued
on a bi-weekly basis until the infants reached three months of
age. See Table 3 for schedule of intervention.
At the end of the three month period maternal behavior was
again derived from the Ainsworth, Caldwell et al. and other
instruments, and was used in the study as post-test data. Maternal
compliance with medical appointments and suggestions were rated on

Figure 1. Materials Used as Auditory Stimuli

77
Figure 2. Materials Used as Visual Stimuli

78
Figure 3. Materials Used as Visual Stimuli
Figure 4. Materials Used as Visual Stimuli

80
Figure 5. Materials Used as Visual Stimuli

81
Figure 6. Materials Used as Visual-movement Stimuli
82
Figure 7* Materials Used as Visual-movement Stimuli

83
Figure 8. Materials Used as Visual-movement Stimuli
84
Figure 9. Materials Used as Tactile Stimuli

SCHEDULE OF
INTERVENTION
fJJ■UrJw'4-te /-NM (A4-t a)o cu
e<D& (Ao 4Jw dcda> U-l
d4J Ha <4-1•w O4J CA•r4 0)W)<fiu•H<A•H>
CM
cc
vO
COI
85
1) Repeat use of Auditory Stimuli2) Repeat use of Visual Movement Stimuli3) Repeat use of Tactile Stimuli4) Repeat use of Stimuli with Marked
Contrast
1) Repeat use of Auditory Stimuli2) Repeat use of Visual Movement Stimuli3) Repeat use of Tactile Stimuli4) Present Visual Stimuli with Marked
Contrast
1) Repeat use of Auditory Stimuli2) Repeat use of Visual Movement Stimuli3) Present Tactile Stimuli
1) Repeat use of Auditory Stimuli
2) Present Visual Movement Stimuli
1) Utilize Auditory Stimuli with Infants
1) Play games with infants which require no materials
2) Talk with mothers regarding their concerns

86
a nonstandardized rating form designed for that purpose (Appendix
XV) which was based on the Ainsworth (1973) scoring criteria.
Case histories were prepared that described several charac
teristics of the families in the study, which included marital
status, residential characteristics, number of children, extent
of child care provided for them by other persons, educational
level, reasons for leaving school, drug experience and receptivity
to the intervention program that was provided during the study.
In addition, acceptance of the intervention program and maternal
attitudes toward the program were recorded at the end of each
home visit on a report adapted from Wright et al. (1970). See
Appendix X.
Intervention Materials
Materials focused on stimulation of three sensory modalities and
included auditory, visual, visual-movement and tactile stimuli. See
Figures 1-9. Rationale for using the specific materials was based on
findings from several studies. Those researchers have reported that
the use of auditory stimuli (Wortheimer, 1961; Birns, 1965; Field,
1967; Daugherty & Cohen, 1961; Eisenberg et al., 1964), visual stimuli
(Darwin, 1877; Berlyne, 1958; Fantz, 1958; Hershenson, 1964; Mirando,
1970; Salapetek, 1968 and Korner et al., 1971), moving stimuli (Carpen
ter, 1957; and Provence & Lipton, 1962) do enhance infant attention,
and evidence is found in various forms of infant responsivity, when
presented the stimulus materials. Activities for use with infants were
derived from Gordon and Lally (1968), Gordon (1970), Forrester et al.
(1971) and Cooper (1973).

87
A ssessment 1 ns trumonts
Thruu instruments were utilized to obtain infant data: 1) The
Amiol-Tison Neurological evaluation of the Maturity of Newborn
Infants (.1.968) was performed by the pediatrician while the infants
were in the hospital (See Appendix I). The neurological evaluation
was performed in order to assess gestational ages of the infants.
2) The brazelton Neonatal Behavioral Assessment Scale was administered
to the infants while they were in the hospital and again at ages one,
two and three weeks within the infants' homes according to directions
and scoring criteria which are found in Chapter II and in Appendix II.
3) The Bayley Scales of Infant Development provided a basis for
assessment of Mental and Motor Development and of Visual-Following
skills of the infants. Administration and scoring were performed
according to Bayley (1969).
Maternal data were assessed with eleven instruments; 1) Infant
Care Inventory, 2) six Scales from Ainsworth, 3) Caldwell et al.
Inventory of Home Stimulation, 4) A Parent Counselor Home Visit Report,
Wright et al,, 5) Mother's Compliance with Medical Appointments and
6) Mother's Compliance with Medical Suggestions. That instrument was
developed for use with this study. Scoring criteria were adapted from
Ainsworth (1973). No data with respect to validity and reliability
of the instrument were gathered.
Data Analysis
Data gathered for this study wore analyzed through the services
of the Department of Preventive Medicine and Veterinary Physiology
and Pharmacology. Dr. Jean Powers served as Consultant with
88
Ms. Linda Rolfes as Supervisor. Several scores were obtained Cor each
infant with the use of three instruments and for each mother with the
use of eleven instruments.
Amiel-Tison Neurological Evaluation of the Maturity of Newborn Infants
Differences between the groups of infants were obtained by means
of Fisher's Exact Probability Test. One hypothesis was tested
with the Amiel-Tison Neurological Evaluation of Maturity of Newborn
Infants.
Brazelton Neonatal Behavioral Assessment Scale
Three sources of data were derived from the Brazelton Scale:
1) infant response to 27 behavioral items, 2) response to the "Elicited
Responses" and 3) response to the state items. Sources of variation
of the items between groups and across four age periods were analyzed
through the use of Mixed Model Analyses of Variance. The statistical
technique Analysis of Variance allows for several items to be inves
tigated at one time (Weiner, 1973). Through the Analysis of Variance
one hypothesis (Hypothesis 2) with three subparts was examined.
Bayley Scales of Infant Development
Infant response to each item on this test is recorded as Pass or
Fail. The total raw score representing a sum of the total items an
infant passes, is converted to a standard score, representing a
Mental Development Index for the Mental Scale, and a Psychomotor
Development Index for the Motor Scale. With use of that instrument
three hypotheses were tested. Sources of variations between the

89
groups of infants were analyzed with the use of a mixed model and a
one-way Analysis of Variance.
Maternal Assessment
Maternal assessment was performed with the Hock Inventory (1972),
Ainsworth Scales (1973), Caldwell et al. (1966) Inventory of Home
Stimulation, Parent Counselor Home Visit Report (Wright et al. 1970)
and with two forms which were designed by the investigator to assign
ratings for maternal compliance with medical appointments and sugges
tions. Data received from maternal assessments were analyzed with
Mann Whitney U Tests.
Case studies were compiled for each mother who participated in
the study.
Statistical Methods Employed in this Study
Selection of statistical procedures to analyze data collected
was based on several considerations. In general, for the data yielded
by each assessment instrument, that procedure was chosen which
facilitated answering the maximum number of questions about the data
with maximum power. When an underlying normal distribution of the
data could bo assumed as with the 27 Brazelton behavioral items,
the State items, the Visual Following items from the Bayley Scales,
parametric procedures were used. For the Brazelton behavioral items
and state items, mixed model Analyses of Variance with repeated measures
and associated a posterori test such as Newman Keuls were employed.
For the Visual Following, a simple one-way Analysis of Variance was
the method of choice.

90
While the design of the investigation using the Brazelton "Elicited
Responses'' was identical to that of the behavioral and state items,
V.- no means couLd the data collected be considered normally distributed.
It was therefore, necessary to rely on a non-parametric technique.
Unfortunately, no nonparametric technique is said to exist that allows
one to explore three factors and their interactions. Wilcoxon Signed
Rank Test permitted evaluating differences between groups across the
"Elicited Responses" items at each of the four time periods, but could
not be used to test for differences among times or among the
"Elicited Responses" items.
Similarly, data collected with the Hock, Caldwell et al., the
Wright and the Compliance instruments fit into an experimental design
similar to that of the Bayley Visual Following. Once again, it was
not possible to treat the data as though it were normally distributed
and therefore, the Mann Whitney U Test was selected as the most power
ful available technique, the required assumptions for which could all
be satisfied.
The experimental design implied by the data collected with
Ainsworth Scales imposed somewhat more of a problem. As in the case
of the "Elicited Responses" data it was not found to be possible to
analyze possible differences on one Scale. Mann Whitney U Tests for
differences between groups for each Scale were selected because of
their relative power to detect group differences within each Scale.
Choice of an analysis technique was difficult to analyze data
collected with the Amiel-Tison. Several techniques were considered
and discarded because of the data's failure to satisfy important

91
assumptions. Final Ly ten Fisher's F.xact Tests, one for eaeh item
were performed. It is unfortunate that the power of the Fisher
tosts to detect differences where real differences occur is relatively
1 .
Usefulness of Instruments Utilized in this Study
The Amiel-Tison Neurological Evaluation of the Maturity of New
born Infants (1968) is a measure of infant postural indices. It is
useful by physicians for estimating gestational ages of infants.
Amiel-Tison (1968) reported no evidence of validity or reliability
of the instrument.
The Brazelton Neonatal Behavioral Assessment Scale (1973) provided
a means for assessing a comprehensive range of infant behaviors during
the neonatal period. Due to a narrow range of possible scores with
the "Elicited Responses" the possibility of determining significant
differences between groups of infants on the "Elicited Responses" is
1imited.Bayley Scales of Infant Development (1969) were useful for the
ai-e period which they are designed to assess. In addition to providing
a quantitative description of Mental and Motor development of infants,
the Scales are arranged such that an intra-test analysis may be made
and used for planning individual intervention strategies for infants.
The Ainsworth Scales (1973) failed to distinguish between changes
found in the groups of women in this study at pre- and post-test
periods. The lack of significant changes may have been related to
the hypotheses established in the study rather than to the instrument.
Significant differences may have been found had the research design
92
incorporated a provision for comparing prc-Lests of addicted women
with pre-tests of nonaddictcd women, as well as comparing post-test
scores of the two groups of women.
The Caldwell et al. (1966) Inventory of Home Stimulation was
useful for providing categories of indices which may be used by
home visitors. However, the Inventory comtains some items which are
of limited use with infants who are less than three months of age.
The Parent Counselor Home Visit Report was adapted from Wright
et al. (1970). The major divisions of the instrument contains unequal
numbers of subunits which create problems with respect to assigning
weights to each category of items in the instrument.
The Hollingshead Two Factor Index of Social Position (1957)
provides for ease in scoring. Some of the occupations listed in the
instrument may fail to appear with great frequency in the present
economy, especially those which pertain to rail road occupations.
The Parent Interview Report adapted from Bloom and Sudderth (1971)
appeared adequate for obtaining demographic data.
The instrument, Mother's Compliance with Medical Appointments and
Suggestions provided no data regarding validity and reliability of
the instrument.
The Infant Care Inventory (1972) failed to discriminate between
the groups of women in this study. Most women in the study earned
maximum scores with the instrument. It therefore appears that a
ceiling effect may have limited the power of the instrument to detect
group differences.
CHAPTER IV
RESULTS
The purpose in this study was to determine whether a difference
was found between development of infants born to narcotic addicted
women, and development of infants born to nonnarcotic addicted women.
Specifically, the purpose was twofold: 1) to test differences between
groups of infants and their mothers and 2) to describe the potential value of an intervention program for narcotic addicted and nonnarcotic
addicted women and their infants perliminary to a subsequent study.
In this study the variates of neurological maturity at birth of
the infants and neonatal status of the infants were examined in order
to determine whether significant differences were found between the two
groups of infants. With the use of several statistical procedures
thirteen criterion variables were examined to test the null hypotheses
of no difference between the groups.
Presentation of Results
Findings in this study with respect to each hypothesis are presented
sequentially.
No differences were found in neurological maturity (as assessed by
the Amiel-Tison Neurological Evaluation of the Maturity of Newborn
Infants), between infants of narcotic addicted women and infants of
nonnarcotic addicted women.93

94
Hypothesis 1: There is no difference between neurologicalmaturity at birth, of infants born to narcotic addicted women (as assess with the Amiel-Tison Neurological Evaluation of the Maturity of Newborn Infants) and neurological maturity at birth of infants born to nonnarcotic addicted women (as assessed by the Amiel-Tison Neurological Evaluation of the Maturity of Newborn Infants),
Alternative Hypothesis: Differences do exist between neurological maturity at birth, of infants born to narcotic addicted women (as assessed with the Amiel-Tison Neurological Evaluation of the Maturity of Newborn Infants) and neurological maturity at birth of infants born to nonnarcotic addicted women (as assessed by the Amiel-Tison Neurological Evaluation of the Maturity of Newborn Infants. Infants of narcotic addicted women earn lower scores than infants of nonnarcotic addicted women.
Each item of the Amiel-Tison Neurological Evaluation was tested
for differences between groups by Fisher's Exact Probability Test.
The number of infants who received gestational age of 38 weeks or 40
weeks for the addicted group of infants was not significantly different
from the number of nonaddicted infants who received gestational ages
of 38 or 40 weeks, as shown in Table 4. Therefore, Hypothesis 1 was
accepted. There is no significant difference in neurological maturity
at birth of infants in this study who were born to addicted mothers
as compared to those born to nonaddicted mothers.
However, it cannot be concluded that narcotic addiction in the
mother has no effect on the neurological maturity and gestational ages
of the newborn infant. Since the physical condition (as assessed by
the Apgar) of the infants in the addicted group was matched to that of
nonaddicted infants by Apgar scores, birthweight and gestational ages,
the matching process may thus have obscured such differences if they
existed.

TABLE 4
ITEMS
SUMMARY OF DIFFERENCES BY FISHER EXACT PROBABILITY TEST IN GESTATIONAL AGES OF NEWBORN INFANTS OF ADDICTED AND NONADDICTED MOTHERS DETERMINED BY ITEMS OF T1IE AMIEL-TISON NEUROLOGICAL EVALUATION OF MATURITY OF NEWBORN INFANTS
ADDICTED INFANTS N
Gestational Ages 38 40
1 0 5 5
2 1 4 5
3 5 0 5
4 0 5 5
5 0 5 5
6 0 5 5
7 0 5 5
8 0 5 5
9 0 5 5
10 0 5 5
NONADDICTED INFANTS N SIGNIFICANCE
38 40
1 4 5 N.S.
1 4 5 N.S.
2 3 5 N.S.
0 5 5 N.S.
0 5 5 N.S.
0 5 5 N.S.
0 5 5 N.S.
1 4 5 N.S.
1 4 5 N.S.
1 4 5 N.S.

ME
AN
SC
ORES
9•o A d d i c t e d G r o u p
K o n - A d d i c i e d G r o u p8
7
6
5
4
3
2
1
01 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
I T E M N U M B E R S
Figure 10. Summary of Means of Addicted and Nonaddicted Infants with Twenty-Seven Brazelton Behavioral Items VOO'

96
Hypothesis 2a: There is no difference between performance withthe 27 behavioral items (as assessed with the Brazelton Neonatal Behavioral Assessment Scale) of infants born to narcotic addicted women and performance with the 27 behavioral items (as assessed with the Brazelton Neonatal Behavioral Assessment Scale) of infants born to nonnarcotic addicted women at four age periods (three days, one, two and three weeks).
Alternative Hypothesis: Differences do exist between performancewith 27 behavioral items (as assessed with the Brazelton Neonatal Behavioral Assessment Scale) of infants born to narcotic addicted women and performance with the 27 behavioral items (as assessed with the Brazelton Neonatal Behavioral Assessment Scale) of infants born to nonnarcotic addicted women at four age periods (three days, one, two and three weeks). Infants of narcotic addicted women exhibit less complex behavior with the 27 behavioral items.
Ages of the infants in this study are referenced with four
symbols: T^ refers to age three days; T2, Tg and T^ refer to agesone, two and three weeks respectively.
Inspection of Figure 10 reveals that responses averaged over ages
of the groups of infants were different for some items. When the
responses of the infants were examined by the 2 (Group) X 4 (Time)
X 27 (Item) mixed model Analysis of Variance with repeated measures,
several differences were found. In addition, significant main effects
of Group, Time and Item, significant Group X Item, and Time X Item
interactions were found as shown in Table 5. The null Hypothesis was
therefore rejected, and the Alternative Hypothesis was accepted. The
initial analysis was followed by 2 (Group) X 4 (Time) mixed model
Analysis of Variance for each of the 27 items. A summary of the
significance of effects of Group, Time and Group X Time for the 27
behavioral items appears in Table 6.As seen in Table 6, seven items had only significant Group Main
Effects, that is, the infants scores differed only with respect to

97
TABLE 5
SUMMARY OF RESULTS OF ANALYSIS OF VARIANCE FOR TWENTY-SEVENBRAZELTON BEHAVIORAL ITEMS
Source of Variation df MS F Significance
Group 1 161.08 10,78(1,8) P < .05
Subjects Within Groups 8 14.94 N.S.
Time 3 20.63 5-48(3,24) P<.01
Group X Time 3 2.50 0.66 N.S.
Time X Subjects Within Groups 24 3.77 N.S.
Item 26 43.11 9.02 P <.001
Group X Item 26 19.82 4.15 p < .001Item X Subjects Within Groups 208 4.78 N.S.
Time X Item 78 1.75 1.59 p <.01Group X Time X Item 78 0.87 .80 N.S.
Time X Item X Subjects Within Groups 624 1.10 N.S.
I
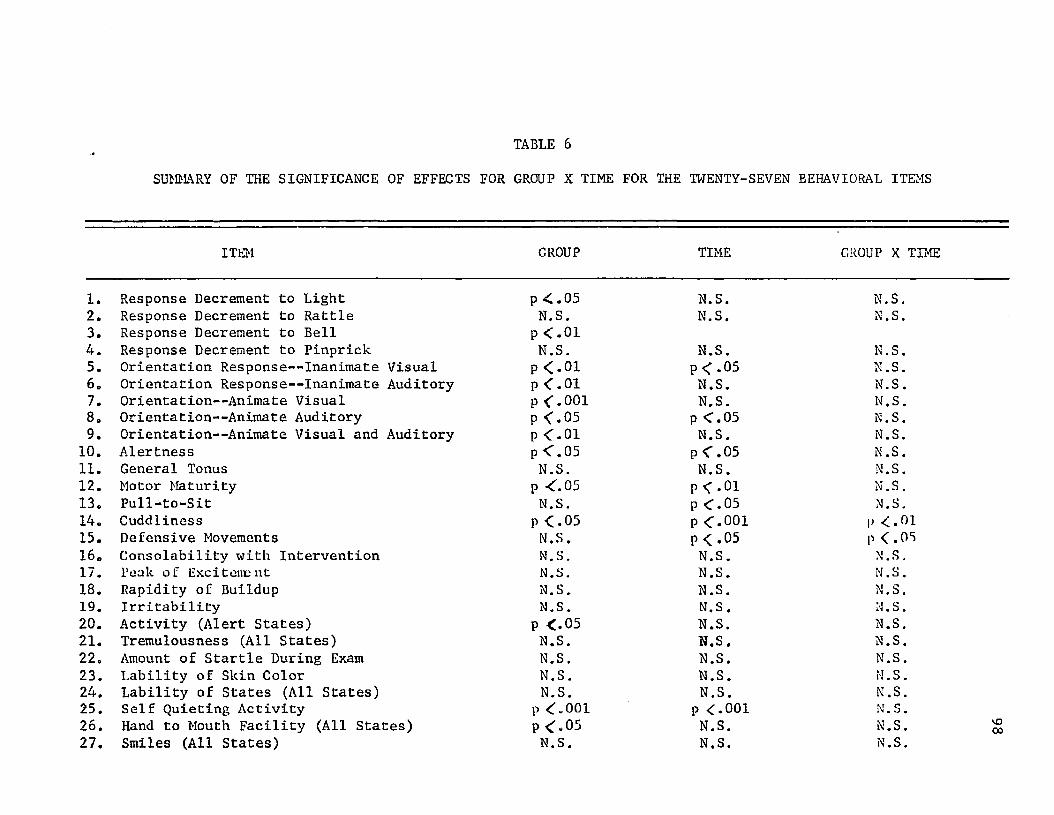
TABLE 6
SUMMARY OF THE SIGNIFICANCE OF EFFECTS FOR GROUP X TIME FOR THE TWENTY-SEVEN BEHAVIORAL ITEMS
ITEM GROUP TIME GROUP X TIME
1. Response Decrement to Light p < .05 N.S. N.S.2. Response Decrement to Rattle N.S. N.S. N.S.3.4.
Response Decrement to Bell Response Decrement to Pinprick
P <.01N.S. N.S. N.S.
5. Orientation Response— Inanimate Visual p <.01 p < .05 N.S.6. Orientation Response— Inanimate Auditory P<.01 N.S. N.S.7. Orientation— Animate Visual p <.001 N.S. N.S.8. Orientation— Animate Auditory P <.05 p <.05 N.S.9. Orientation— Animate Visual and Auditory P <.oi N.S. N.S.10. Alertness p <.05 P < .05 N.S.11. General Tonus N.S. N.S. N.S.12. Motor Maturity P <.05 p <.01 N.S.13. Pull-to-Sit N.S. P <.05 N.S.14. Cuddliness p <.05 p <.001 p <.0115. Defensive Movements N.S. P < *05 p <.0516. Consolability with Intervention N.S. N.S. N.S.17. Peak of Excitement N.S. N.S. N.S.18. Rapidity of Buildup N.S. N.S. N.S.19. Irritability N.S. N.S. N.S.20. Activity (Alert States) P <.05 N.S. N.S.21. Tremulousness (All States) N.S. N.S. N.S.22. Amount of Startle During Exam N.S. N.S. N.S.23. Lability of Skin Color N.S. N.S. M.S.24. Lability of States (All States) N.S. N.S. N.S.25. Self Quieting Activity p <„001 p <.001 N.S.26. Hand to Mouth Facility (All States) P <«05 N.S. N.S.27. Smiles (All States) N.S. N.S. N.S.
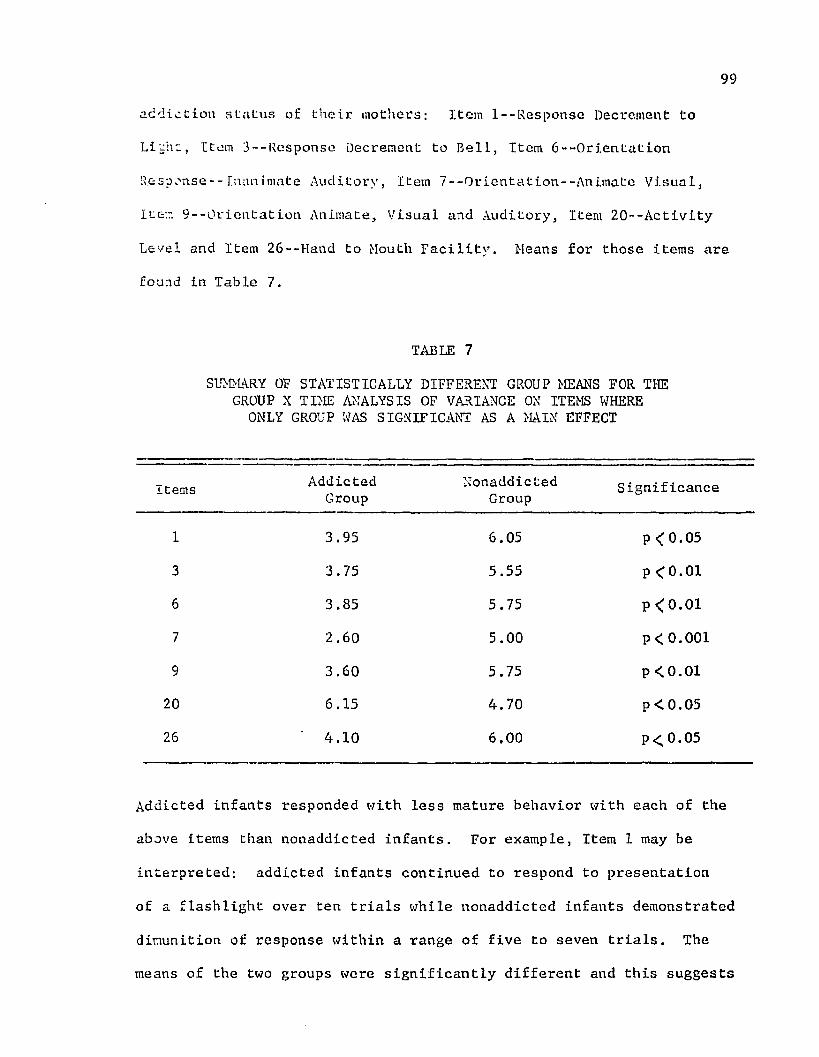
99
addiction status of their mothers; Item l--Response Decrement to
Li'cht, Item 3--Response Decrement to Bell, Item 6--0rientation
Response--Inanimate Auditory, Item 7--0rientation--Anj.mate Visual,
Iter. S--Orientation Animate, Visual and Auditory, Item 20--Activity
Level and Item 26--Hand to Mouth Facility. Means for those items are
found in Table 7.
TABLE 7
SUMMARY OF STATISTICALLY DIFFERENT GROUP MEANS FOR THE GROUP X TIME ANALYSIS OF VARIANCE ON ITEMS WHERE ONLY GROUP WAS SIGNIFICANT AS A MAIN EFFECT
Items AddictedGroup
NonaddictedGroup Significance
1 3.95 6.05 p < 0.05
3 3.75 5.55 p < 0.016 3.85 5.75 p < 0.017 2.60 5.00 P < 0.001
9 3.60 5.75 p < 0.0120 6.15 4.70 p < 0.05
26 ' 4.10 6.00 p<0.05
Addicted infants responded with less mature behavior with each of the
above items than nonaddicted infants. For example, Item 1 may be
interpreted: addicted infants continued to respond to presentation
of a flashlight over ten trials while nonaddicted infants demonstrated
dimunition of response within a range of five to seven trials. The
means of the two groups were significantly different and this suggests
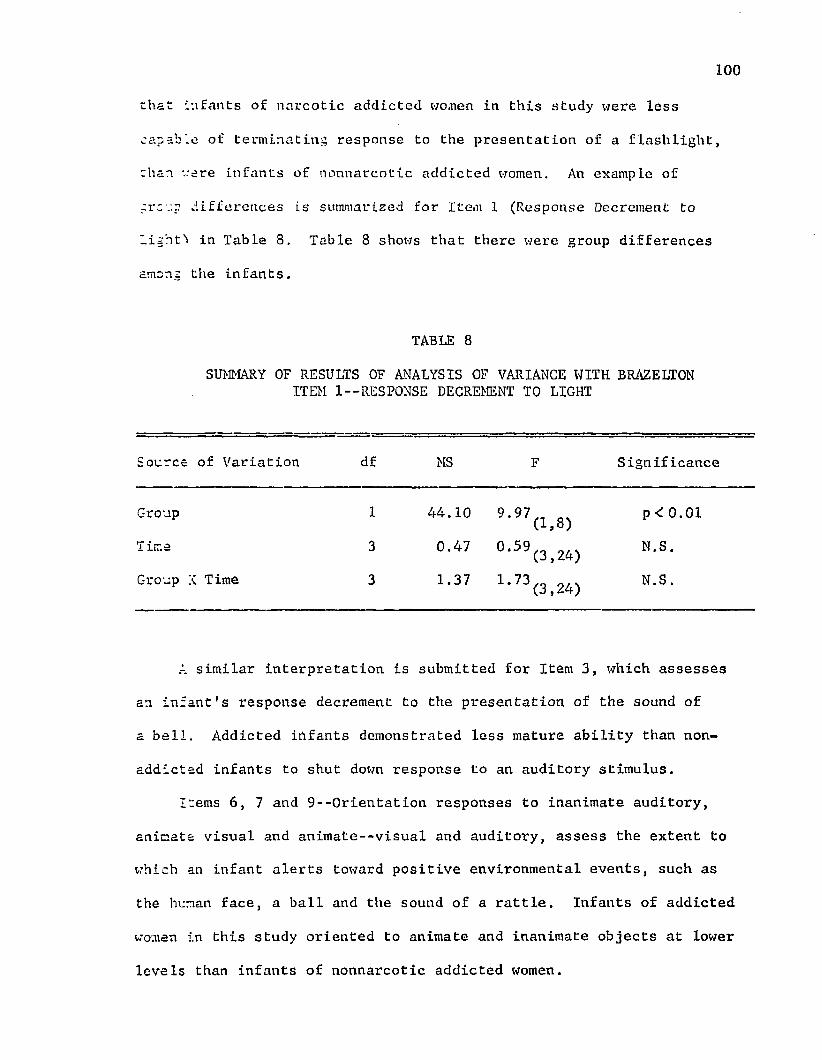
100
chat infants of narcotic addicted women in this study were less
capable of terminating response to the presentation of a flashlight,
than -cere infants of nonnarcotic addicted women. An example of
creep differences is summarized for Item 1 (Response Decrement to
Light'* in Table 8. Table 8 shows that there were group differences among the infants.
TABLE 8SUMMARY OF RESULTS OF ANALYSIS OF VARIANCE WITH BRAZELTON
ITEM 1— RESPONSE DECREMENT TO LIGHT
Source of Variation df MS F Significance
Group 1 44.10 9,97(1,8) pCO.Ol
I ima 3 0.47 °*59(3,24) N.S.
Group X Time 3 1.37 1,73 (3,24) N.S.
A similar interpretation is submitted for Item 3, which assesses
an infant's response decrement to the presentation of the sound of
a bell. Addicted infants demonstrated less mature ability than non
addicted infants to shut down response to an auditory stimulus.
Items 6, 7 and 9--0rientation responses to inanimate auditory, animate visual and animate--visual and auditory, assess the extent to
which an infant alerts toward positive environmental events, such as
the human face, a ball and the sound of a rattle. Infants of addicted
women in this study oriented to animate and inanimate objects at lower
levels than infants of nonnarcotic addicted women.

101
With Item 20--Activitv, infants of narcotic addicted women
exhibited more activity during the examining periods and demonstrated
less hand to mouth activity (Item 26> than infants of nonnarcotic
addicted women. Summaries of Items 3, 6, 7, 9, 20, and 26 are found in Tables 21-26 (Appendix XVI). With each of those items addicted infants
performed with less mature behavior than nonaddicted infants. Item
20--Activity (Table 8) reveals a higher score for addicted infants than for nonaddicted infants. A high score with activity represents a
less mature type of behavior on the Brazelton Scale than a lower score.
This indicates that addicted infants were more active during the
examining period than nonaddicted infants. After stimulation, which
triggered activity of the infants, addicted infants exhibited much
activity which tended to perpetrate itself during the examining period.
Group and Time differences as Main Effects were found with
respect to five items: Item 5--Orientation Response--Inanimate Visual,
Item 8--0rientation--Animate, Auditory, Item 10--Alertness, Item 12—
Motor Maturity and Item 25--Self-Quieting Activity. With Item 5 for
example, (Orientation Response— Inanimate Visual), the group means
across all four age periods of the infants were: Addicted--2.5;
Nonaddicted--5.5. This means that as the examiner moved a bright red
ball across the infant's field of vision, addicted infants stilled,
brightened their eyes and made brief following, while nonaddicted
infants focused on and followed the stimulus horizontally for at least
a 30° arc, thus exhibiting more mature behavior than addicted infants.
An example of Group and Time differences is presented for Item 5
(Figure 11). As seen in Figure 11, both groups of infants performed better over time.
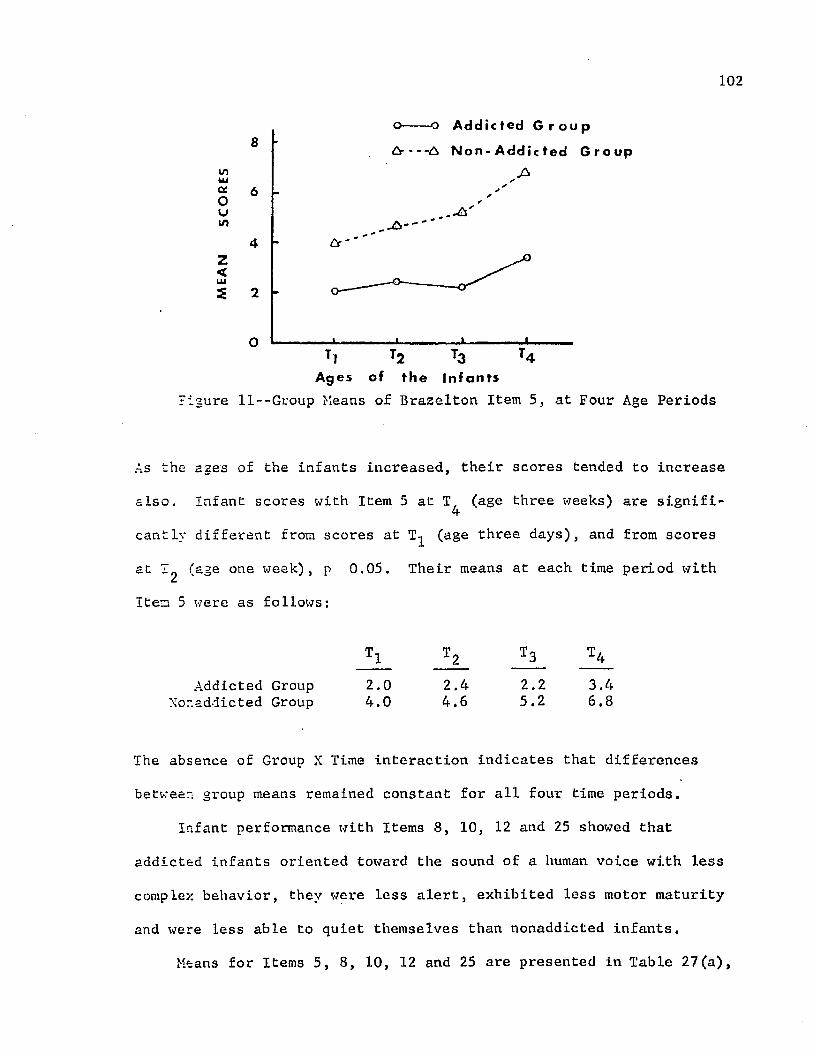
102
wUJa.Oum
Z<
o o A d d i c t e d G r o u p
Ar— A N o n - Add i c ted G r o u p8
6
4
2
OT4Tl
Ages of t h e I n f a n t s
^gure ll--Group Means of Brazelton Item 5, at Four Age Periods
As the ages of the infants increased, their scores tended to increase
also. Infant scores with Item 5 at T, (age three weeks) are signifi-4cantly different from scores at (age three days), and from scores
at I (age one week), p 0.05. Their means at each time period with
Item 5 were as follows:
Addicted Group 2.0 2.4 2.2 3.4Xor.adiicted Group 4.0 4.6 5.2 6.8
The absence of Group X Time interaction indicates that differences
between group means remained constant for all four time periods.
Infant performance with Items 8, 10, 12 and 25 showed that addicted infants oriented toward the sound of a human voice with less
complex behavior, they were less alert, exhibited less motor maturity
and were less able to quiet themselves than nonaddicted infants.
Means for Items 5, 8, 10, 12 and 25 are presented in Table 27(a),

103
Appendix XVII. Inspection of Table 27 (a) shows that significant
differences were found between the groups of infants with each of the
five items. Differences were in favor of nonaddicted infants. A
summary of significantly different Group and Time means is presented
in Table 27 (b), Appendix XVII. Pairs of means bracketed and flagged
with a single asterisk were found to be different at the significance
level, p 0.05, Those pairs of means bracketed and flazzed with a
double asterisk were found to be different at the significance level
p 0.01.With respect to Item 13 (Pull to Sit--a measure of the extent to
which the infant is able to right his head upon being pulled into a
sitting position), there were only time effects. The following means
at each time, across the two groups were found;
4.5 5.1 5.7 5.7
These means order themselves over time. T^ mean is the lowest; T^ is
next; T^ and T^ are alike numerically. Since T3 and T^ were alike, they were pooled for a collection of three means, rather than four,
upon which a Student's Newman Keuls test for all possible differences
was performed. Mean at T^ was found significantly different from means
at T3 and T^, (p 0.05). This indicates that changes occurred between
age three days and ages three and four weeks with both groups of infants.
At age three days when pulled to sitting position the infants1 shoulders and arm tone increased (Mean = 4.5); while in sitting position
they lifted their heads. Although they were unable to maintain a

104righting position, the infants made efforts to right the head. By
the time they reached age three weeks, they were able to bring their
head? to the midline of their bodies and maintain that position for one
or twc seconds (Mean - 5,7). No significant group differences were
found but both groups of infants made progressive gains with the Pull
to Sit item, as their ages increased.
Item 14 (Cuddliness) assesses the extent to which the infant
cuddles in the examiner's arms when held. Significant effects o f
Group. Time and the interaction of Group and Time were found. The
group means at each time follow:
Addicted Group
Nonaddicted Group
4.60
5.40
4.80
5.40
4.80
6.40
4.80
6.60
Inspection of Figure 12 shows that addicted infants remained relatively
constant in their cuddling and nestling behavior with the examiner,
while nonaddicted infants increased their level of cuddling behavior.
V)IUa0U)
Z<Uls
o— o A d d i c t e d G r o u p
a A N o n - A d d i c t e d G r o u p8
6
4
2
OU
Ages of t h e i n f a n t s
Figure 12--Group Means of Brazelton Item 14, at Four Age Periods

105
At T^, and tlie groups were different (p<0.05); at 1’2 there was no difference. Table 9 shows the means for each group at those times
where group differences were significant. In general, addicted infants
demonstrated less cuddling behavior than nonaddicted infants.
TABLE 9
SUMMARY OF GROUP MEANS FOR THOSE TIMES WHEN DIFFERENCES WERE SIGNIFICANT WITH BRAZELTON ITEM 14--CUDDLINESS
Ages Addicted Infants Nonaddicted Infants Significance
3 days (T^ 4.60 5.40 p < 0.05
2 weeks (T3) 4.80 6.40 p < 0.05
3 weeks (T,) 4 4.80 6.60 p < 0.05
With further respect to Item 14 (Cuddliness), at age three days
addicted infants were able to mold in the examiner's arms, but only
after a great deal of cuddling and nestling by the examiner. Nonaddicted
infants, on the other hand usually molded and relaxed when initially
held. They nestled the head in the elbow of the examiner; when placed
in vertical position at the shoulder they appeared to lean forward.
Little change was made over time in the cuddling behavior of addicted
infants.
Item 15 is a measure of the extent of defensive behavior exhibited
by the infant in removing a cloth held on the upper portion of his
face. Results of the Analysis of Variance shown in Table 10 indicate

106
that significant differences between infant groups with respect to
that behavior were not consistent over time.
TABLE 10
SUMMARY OF ANALYSIS OF VARIANCE FOR BRAZELTON ITEM 15--PULL TO SIT
Source of Variation df MS F Significance
Group 1 0.40 0,17(1,8) N.S.
Group X Time 3 2.83 3 91(3,24) p < 0.05
Figure 13 indicates that the direction of group differences is not
the same at T^ where the addicted group seems to be superior, as at T^
and T^, at. which the nonaddicted group is manifesting greater defensive
behavior. Although differences between groups are not significant at
any time, the cross-over of directions of difference probably accounts
for the significant Time interaction.
V)UJocOuVI
Z < uj2
o Ad d i e t e d G r o u p
Csr A N o n - A d d i c t e d G8
6
4
2
OT■ * o
Ages of the i n f a n t s
Figure 13--Group Means of Brazelton Item 15, at Four Age Periods

107
On the basis of findings of significant differences on behavioral
items in the Brazelton Scale (Table 6), Hypothesis 2a is thereforerejected, with consequent acceptance of the Alternative Hypothesis that
differences do exist between infants born to narcotic addicted women
and infants born to nonnarcotic addicted women.
Differences were found with respect to the infants' state which
was observed at each time period prior to administering the assessment
items. Within two minutes before the examination is begun with the
Brazelton Scale, an assessment of the infant's state is made by observing
his spontaneous behavior, respirations, eye movements, startles and
concurrent spontaneous events in the environment.
Hypothesis 2b: There is no difference between performancewith the Brazelton State items of infants born to narcotic addicted women and performance with the Brazelton State items of infants born to nonnarcotic addicted women at four age periods (three days, one, two and three weeks).
Alternative Hypothesis: Differences do exist betweenperformance with the Brazelton State items, of infantsborn to narcotic addicted women and performance with the Brazelton State items of infants born to nonnarcotic addicted women at four age periods (three days, one, two, and three weeks). Infants of narcotic addicted women demonstrate higher scores with State items than infants of nonnarcotic addicted women.
A 2 (Group) X 4 (Time) X 2 (State) mixed model Analysis of Variance
with repeated measures on Brazelton State scores was done, the results
of which appear in Table 11. Since the Group X Time X State interaction
was significant, this was followed by a 2 (Group) X 4 (Time) mixed
model Analysis with Repeated Measures for each state (Initial State and
Predominant states of the infants). Results of the analysis for
State 1, shown in Table 11a reveal that the groups of infants differed
at some point in time.

108
TABLE 11
SUMMARY OF RESULTS OF ANALYSIS OF VARIANCE FOR BRAZELTONINITIAL STATE AND PREDOMINANT STATE ITEMS
Source of Variation d£ MS F Significance
Group 1 5.00 2.82 (1,8) N.S.
Subjects Within Groups 8 1.78
Time 3 2.00 N.S.
Group X Time 3 4.60 3*91(3,24) p <*.05
Time X Subjects WithinGroups 3 1.18
State 1 140.45 158.25 (1,8) p <.001Group X State 1 2.45 2* 76 (1,8) N.S.
State X Subjects WithinState 1 0.89
Time X State 3 0.45 *58(3,24) N.S.
Group X Time X State 3 2.72 3*52(3,24) p <.05
Time X State X SubjectsWithin Group 3 0.77
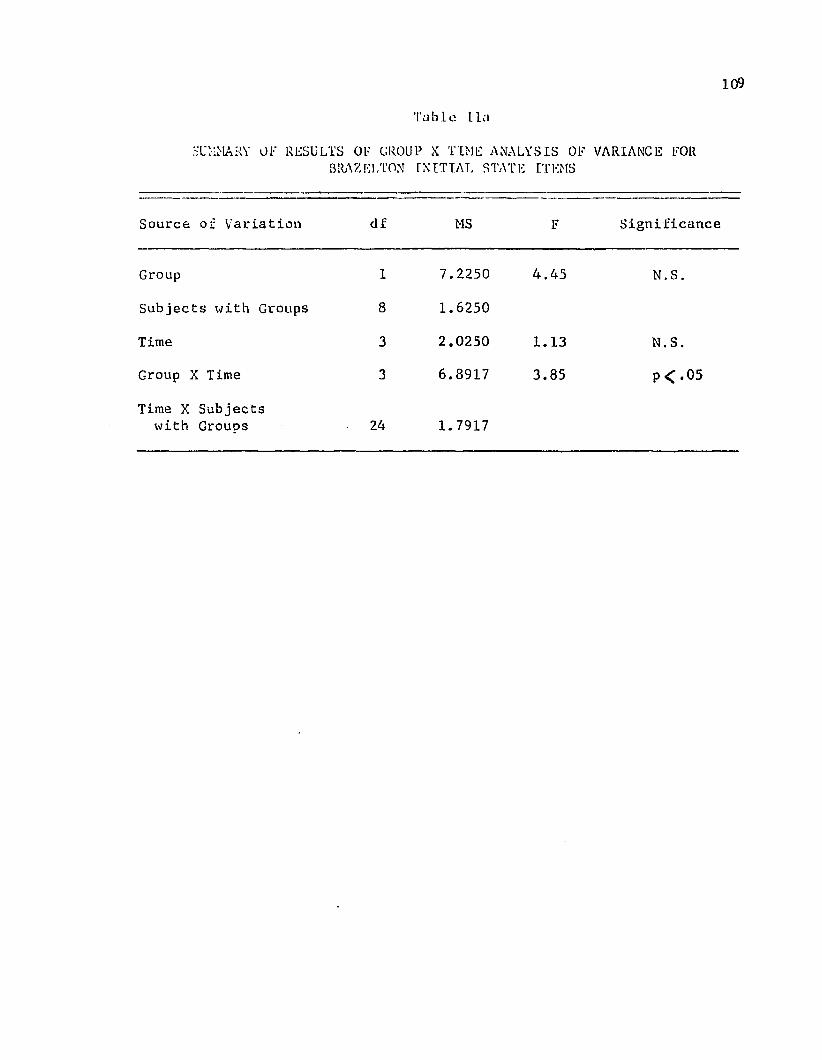
109Table I la
SUMMARY OF RESULTS OF GROUP X TIME ANALYSIS OF VARIANCE FOR BRAZELTON INITIAL STATE ITEMS
Source of Variation df MS F Significance
Group 1 7.2250 4.45 N.S.
Subjects with Groups 8 1.6250
Time 3 2.0250 1.13 N.S.
Group X Time 3 6.8917 3.85 P < • 05
Time X Subjects with Grouos 24 1.7917
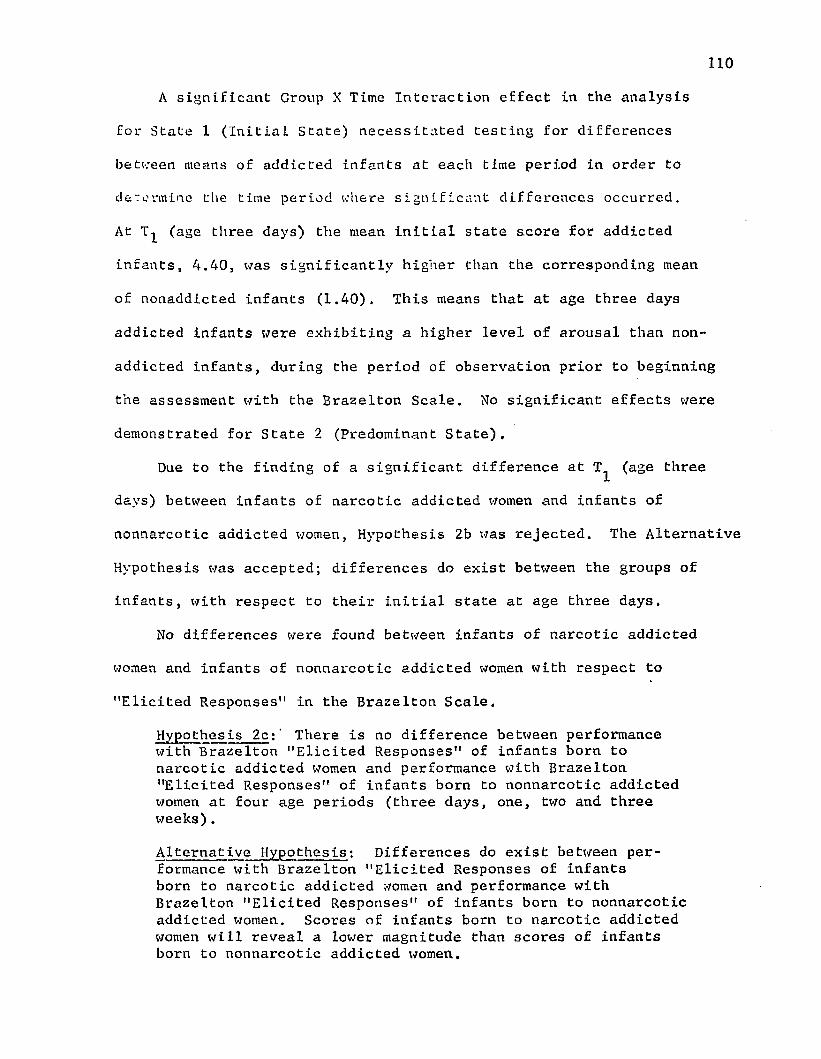
1 1 0
A significant Group X Time Interaction effect in the analysis
for State 1 (Initial State) necessitated testing for differences
between means of addicted infants at each time period in order to
determine the time period where significant differences occurred.
At (age three days) the mean initial state score for addicted
infants, 4.40, was significantly higher than the corresponding mean
of nonaddicted infants (1.40). This means that at age three days
addicted infants were exhibiting a higher level of arousal than non
addicted infants, during the period of observation prior to beginning
the assessment with the Brazelton Scale. No significant effects were
demonstrated for State 2 (Predominant State).
Due to the finding of a significant difference at T^ (age three
days) between infants of narcotic addicted women and infants of
nonnarcotic addicted women, Hypothesis 2b was rejected. The Alternative
Hypothesis was accepted; differences do exist between the groups of
infants, with respect to their initial state at age three days.
No differences were found between infants of narcotic addicted
women and infants of nonnarcotic addicted women with respect to
"Elicited Responses" in the Brazelton Scale.
Hypothesis 2c:' There is no difference between performance with Brazelton "Elicited Responses" of infants born to narcotic addicted women and performance with Brazelton "Elicited Responses" of infants born to nonnarcotic addicted women at four age periods (three days, one, two and three weeks).
Alternative Hypothesis: Differences do exist between performance with Brazelton "Elicited Responses of infants born to narcotic addicted women and performance with Brazelton "Elicited Responses" of infants born to nonnarcotic addicted women. Scores of infants born to narcotic addicted women will reveal a lower magnitude than scores of infants born to nonnarcotic addicted women.

Ill
""lie iced Weaponsos” arc reflex behaviors which are elicited by the
examiner on various regions of the infant's bory. No statistical
:es: •..■as done because by visually comparing the number of babies in
each group responding with a value of two on the Brazelton "Elicited
Responses" items, it is clear that both groups of babies were reacting
in a similar manner for each of the twenty items at each of the four
time periods. Results which show the number of infants who earned
scores of two, are summarized in Table 12. Hence, Hypothesis 2c
failed to be rejected.
No significant differences were found between Mental Development
(as assessed with the Bayley Scales of Infant Development) of the two
croups of infants.
Hypothesis 3: There is no difference between MentalDevelopment (as assessed with the Bayley Scales of Infant Development) of infants born to narcotic addicted women and Mental Development (as assessed with the Bayley Scales of Infant Development) of infants born to nonnarcotic addicted women at two age periods (one month, 24 days and three months).
Alternative Hypothesis: Differences do exist betweenthe two groups of infants. Infants of narcotic addicted women obtain lower scores with Mental Development (as assessed with the Bayley Scales of Infant Development) than infants of nonnarcotic addicted women (as assessed with the Bayley Scales of Infant Development) at two age periods (one month, 24 days and three months).
When results of infant performance were analyzed through a 2 (Group) X
2 (Time) mixed model Analysis of Variance, no differences were found
between the two groups. Therefore, Hypothesis 3 failed to be rejected.
Differences were found, however, between scores at one month, 24 days
and at three months of age (Table 13).

TABLE 12
Nil MB UR OF INFANT’S IN EACH GROUP RECEIVING A SCORE OF TWO WITH BRAZE LTON "ELICITED RET IMiCKS" AT FOUR AGE PERIODS (THREE DAYS, Tx; ONE WEEK, T2; TWO WEEKS, T3; THREE WEEKS, T/,)
ANALYZED WITH WILCOXON SIGNED RANK TEST
TIME PERIOD AND GROUP 1 2 3 4 5 6ELICITED 7 8 9
RESPONSE 10 11
ITEMS12 13 14 15 16 17 18 19 20
Addicted Infants •5 5 5 4 4 5 5 4 5 4 5 5 2 4 5 5 1 1 2 2T1
Nonaddicted Infants Addicted Minus
5 3 5 5 4 4 5 4 4 5 5 5 1 5 5 5 2 2 2 2
NonaddictedT" = 21.5; N = 9
0 +2 0 -1 0 +1 0 0 +1 -1 0 0 +1 -1 0 0 -1 -] 0 0
Addicted Infants 5 5 5 5 5 5 5 4 4 4 4 5 2 5 4 4 2 2 3 3
T2Nonaddicted Infants Addicted Minus
5 3 5 5 4 5 5 3 3 4 4 5 2 4 5 5 3 2 •> 2
NonaddictedT“ = 15; N = 10
0 +2 0 0 +1 0 0 +1 +1 0 0 0 0 +1 -1 -] -1 0 + 1 +1
Addicted Infants 5 5 5 4 5 5 5 4 5 4 5 5 1 3 5 5 3 3 3 3
T3Nonaddicted Infants Addicted Minus
5 5 5 5 4 4 4 5 5 5 5 5 2 5 5 5 4 4 4 4
NonaddictedT+ = 18; N = 12, N.S
0•
0 0 -1 +1 +1 +1 -1 0 -1 0 0 -1 -2 0 0 -1 -1 -1 -1
Addicted Infants 5 5 5 5 5 5 5 4 5 4 4 4 1 4 5 5 /, 4 4 4
T4Nonaddicted Infants Addicted Minus
5 5 5 5 5 4 5 5 5 5 5 4 1 5 5 5 2 2 2 2
NonaddictedT" = 12, N = 9, N.S.
0 0 0 0 0 +1 0 -1 0 -1 -1 0 0 -1 0 0 +2 +2 +2 +2H-1-N
112

113
TABLE 13
SUMMARY OF RESULTS OF ANALYSIS OF VARIANCE WITH BAYLEY SCALES OF INFANT DEVELOPMENT— MENTAL SCALE
Source of Variation df MS F Significance
Group 1 378.45 1,03(1,8) N.S.
lime 1 432.45 16.20(i,a) p < 0.01Group X Time 1 14.45 0,54(1,8) N.S.
Fhe mean score across groups at one month, 24 days was 85.1, while the
mean score at age three months was 94.4 (p<0.0l), thus indicating
increased performance of 9.3 points over the two time periods with both
groups of infants.
Differences ware found between Visual Following skills of the two
groups of infants as assessed, with the Bayley Scales of Infant Develop
ment .
Hypothesis 4: There is no difference between VisualFollowing skills (as assessed with the Bayley Scales of Infant Development) of infants born to narcotic addicted women, and Visual Following skills (as assessed with the Bayley Scales of Infant Development) of infants born to nonnarcotic addicted women at age three months.
Alternative Hypothesis; Differences do exist between infants of narcotic addicted women and infants of nonnarcotic addicted women with respect to Visual Following skills (as assessed with the Bayley Scales of Infant Development) at age three months. Infants of narcotic addicted women earn lower scores than infants of nonnarcotic addicted women.
With the use of a one-way Analysis of Variance, differences were found
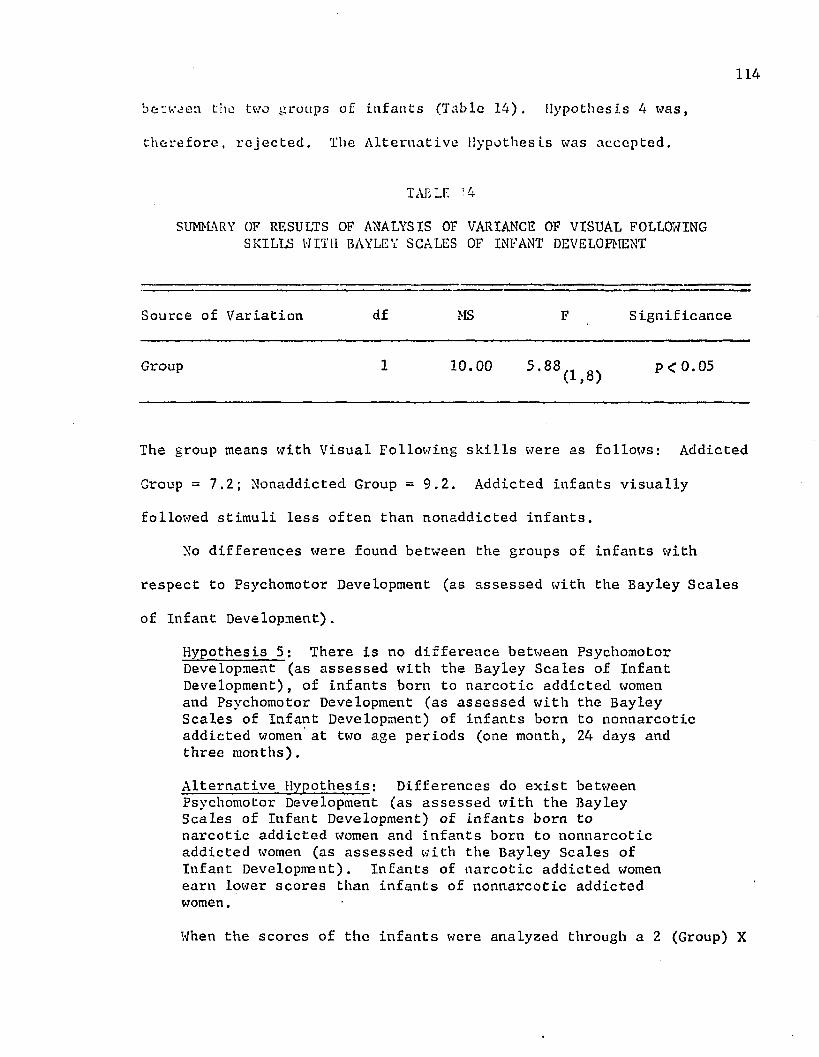
114between the two groups of infants (Table 14). Hypothesis 4 was,
therefore, rejected. The Alternative Hypothesis was accepted.
TAB If • 4
SUMMARY OF RESULTS OF ANALYSIS OF VARIANCE OF VISUAL FOLLOWING SKILLS WITH BAYLEY SCALES OF INFANT DEVELOPMENT
Source of Variation df MS F Significance
Group 1 10.00 5-88(l,8) P < °-05
The group means with Visual Following skills were as follows: Addicted
Group = 7.2; Nonaddicted Group = 9.2. Addicted infants visually
followed stimuli less often than nonaddicted infants.
No differences were found between the groups of infants with
respect to Psychomotor Development (as assessed with the Bayley Scales
of Infant Development).
Hypothesis 5: There is no difference between PsychomotorDevelopment (as assessed with the Bayley Scales of Infant Development), of infants born to narcotic addicted women and Psychomotor Development (as assessed with the Bayley Scales of Infant Development) of infants born to nonnarcotic addicted women at two age periods (one month, 24 days and three months).
Alternative Hypothesis: Differences do exist betweenPsychomotor Development (as assessed with the Bayley Scales of Infant Development) of infants born to narcotic addicted women and infants born to nonnarcotic addicted women (as assessed with the Bayley Scales of Infant Development). Infants of narcotic addicted women earn lower scores than infants of nonnarcotic addicted women.
When the scores of the infants were analyzed through a 2 (Group) X

115
2 (Time) mixed model Analysis of Variance, no differences were found
between the tvo groups of infants (Table 15). Hypothesis 5 failed to
be rejected. inspection of Table 15 reveals that significant differences
did occur between scores at age one month, 24 days and at age three
months of the infants. Both groups of infants demonstrated gains in
their scores ever the two time periods.
TABLE 15
SUMMARY 07 RESULTS OF ANALYSIS OF VARIANCE WITH BAYLEY SCALES 07 INFANT DEVELOPMENT— PSYCHOMOTOR DEVELOPMENT
Source of Variation df MS F Significance
Group 1 51.20 0 *38(1,8) N.S.
Time 1 1513.80 25'18(1,8) p < 0.01Group X Time 1 359.20 4-31(l,8) N.S.
No significant differences were found between narcotic addicted
women and nonnarcotic addicted women with respect to their feelings of
competency for providing caregiving skills to their infants.
Hypothesis 6; There is no difference between narcotic addicted women and nonnarcotic addicted women with respect to their feelings of competency for providing caregiving skills, as assessed with the Hock Infant Care Inventory.
Alternative Hypothesis: Differences do exist betweennarcotic addicted women and nonnarcotic addicted women with respect to their feelings of competency for providing caregiving skills to their infants.Narcotic addicted women exhibit less feelings of competency (as assessed with the Ilock Infant Care Inventory), than nonnarcotic addicted women.

116
When the scores of the groups of women were compared by means of the
Mann Whitney U Test, no differences were found (Table 16), Hypothesis
6 failed to be rejected,
No differences were found between addicted women and nonaddicted
women with respect to changes in characteristics of mothering between
pre- and post-test periods.
Hypothesis 7a: There is no difference between narcoticaddicted women and nonnarcotic addicted women with respect to amount of change in characteristics of mothering, derived from pre- and post-tests (as assessed with Ainsworth Maternal Care Scales: Perception of Baby, Delightin Baby, Availability to Baby, Acceptance of Baby, Amount of Interaction with Baby and Appropriateness of Initiation of Interaction with Baby).
Alternative Hypothesis: Differences do exist betweenaddicted and nonaddicted women, with respect to changes in characteristics of mothering derived from pre- and post-tests (as assessed with Ainsworth Maternal Care Scales) Perception of Baby, Delight in Baby, Availability to Baby, Acceptance of Baby, Amount of Interaction with Baby and Appropriateness of Initiation of Interaction with Baby), Narcotic addicted women earn lower scores with Ainsworth Maternal Care Scales than nonnarcotic addicted women.
Scores were obtained from both groups of women with respect to the
six Ainsworth Scales at two time periods; 1) at pre-test period
(during the first home visit) and 2) at post-test period (during the final home visit). When scores which reflected changes between pre-
and post-test values were compared by means of Mann Whitney U Tests,
no differences were found (Table 17). Therefore Hypothesis 7a failed
to be rejected.
No differences were found between narcotic addicted women and
nonnarcotic addicted women with respect to amount of ahcnge in charac
teristics of mothering assessed with the Caldwell et al. Inventory of Home Stimulation.

117
TABLE 16
DIFFERENCES BETWEEN SCORES OF ADDICTED AND NONADDICTED WOMEN WITH HOCK INFANT CARE INVENTORY ANALYZED WITH MANN WHITNEY U TEST
Groups Pre-Test Post-Test Differences Between Pre-and Post-Tests
Addicted Women 40 40 039 40 +139 40 +140 40 039 40 +1
Nonaddicted Women 34 39 4*540 38 -240 40 039 40 +140 40 0
U = 7 N.S.

1 1 8
TABLE 17
DIFFERENCES BETWEEN SCORES OF ADDICTED AND NONADDICTED WOMEN WITH AINSWORTH MATERNAL CARE SCALES ANALYZED WITH MANN WHITNEY U TESTS
Scale MA-1 Mother's Perception of Baby Scale MA-2 Mother's Delight in Baby
Addicted Women Nonaddicted Women Addicted Women Nonaddicted Women
Pre- Post- Pre- Post-Test Test D iff . Test Test D iff.
3 5 2 7 9 25 7 2 7 9 25 5 0 5 7 25 5 0 5 9 43 9 6 3 9 6
U = 12, cXl=1.00
Scale MA-3 Mother 's Acceptance of Baby
Addicted Women Nonaddicted Women
Pre- Post- Pre- Post-Test Test D if f . Test Test D iff .
5 5 0 7 9 25 7 2 9 9 05 7 2 7 9 27 7 0 5 9 43 9 6 9 9 0
U = 8, ot. = .420N.S.
Scale MC-3 Amount of InteractionOffered by Mother
Addicted Women Nonaddicted Women
Pre- Post- Pre- Post-Test Test Diff. Test Test Diff.
1 1 0 9 9 03 5 2 9 9 05 7 2 7 7 05 5 0 5 9 41 9 8 9 9 0
U = 8, oC =.420 N.S.
Pre- Post- Pre- Post-Test Test D iff . Test Test D iff.
3 5 2 7 9 21 5 4 9 9 05 3 -2 7 9 27 7 0 5 9 41 9 8 9 9 0
U = 9 <x = .588
Scale MC-1 Mother's A va ilab ility toBaby
Addicted Women Nonaddicted Women
Pre- Post- Pre- Post-Test Test D iff. Test Test D iff.
3 1 2 9 9 05 5 0 7 7 05 7 2 7 9 25 5 0 7 9 21 9 8 9 9 0
U = 9, OC = .588N.S.
Scale MC-4 Appropriateness of Mother'sIn it ia t io n of Interaction with Baby
Addicted Women Nonaddicted Women
Pre- Post- Pre- Post-Test Test D iff. Test Teat D iff.
1 1 0 9 9 05 5 0 7 9 25 7 2 5 7 25 5 0 5 9 41 9 8 9 9 0
U = 10, C < = .69 N.S.

119
Hypothesis 7b; There is no difference between narcotic addicted women and nonnarcotic addicted women with respect to changes in characteristics of mothering assessed with the Inventory of Home Stimulation.
Alternative Hypothesis: Differences do exist betweennarcotic addicted women and nonnarcotic addicted women with respect to changes in characteristics of mothering assessed with the Inventory of Home Stimulation. Narcotic addicted women earn lower scores with respect to changes in characteristics of mothering (assessed with the Inventory of Home Stimulation), than nonnarcotic addicted women.
Scores were obtained from both groups of women with respect to the
Inventory of Home Stimulation at two time periods: 1) at pre-test
period (during the first home visit), and 2) at post-test period (during the final home visit). When scores which reflected changes between pre-
and post-test values were compared by means of Mann Whitney U Test, no
significant differences were found between the groups (Table 18).
Therefore, Hypothesis 7b failed to be rejected.
No differences were found between addicted and nonaddicted women
with respect to their acceptance of home training probided by a home
visitor.
Hypothesis 8: There is no difference between narcoticaddicted women and nonnarcotic addicted women with respect to their acceptance of home training provided by a home visitor (as assessed with a Parent Interview Report--Wright et al.).
Alternative Hypothesis: Differences do exist betweennarcotic addicted women and nonnarcotic addicted women with respect to their acceptance of home training (assessed by a Parent Counselor Home Visit Report-- Wright et al.). Narcotic addicted women accept training by a home visitor less often than do nonnarcotic addicted women.
When scores of the two groups of women were analyzed by means of

120TABLE 18
DIFFERENCES BETWEEN SCORES OF ADDICTED AND NONADDICTED WOMEN WITH CALDWELL ET AL., INVENTORY OF HOME STIMULATION ANALYZED WITH MANN WHITNEY U TEST
Category I--Emotional and Verbal Responsivlty
Addicted Women
Category I I —Avoidance of Restriction of Punishment
Nonaddicted Women Addicted Women Nonaddicted Women
Prerest
Post-Test D iff.
Pre-Test
Post-Test D iff.
Pre-Test
Post-Test D iff .
Pre-Test
Post-Test D iff.
5 4 -1 7 8 1 6 6 0 6 6 04 5 1 9 9 0 5 6 1 6 6 09 9 0 7 8 1 5 5 0 6 6 09 7 -2 8 9 1 5 5 0 6 6 05 9 4 8 11 3 6 6 0 6 6 0
U « 8, < X = .420 N.S . U = 12.5, 04 = 1.00 N.S.
Category III--O rganization of Physical and Temporal Environment
Addicted Women Nonaddicted Women
Pre- Post- Pre- Post-Test Test D iff. Test Test D iff.
2 4 2 3 3 02 5 3 3 5 24 4 0 2 4 23 4 1 3 4 13 5 2 4 6 2
U = 11, OC- = .821 N.S.
Category V--Maternal Involvement with Child
Addicted Women Nonaddicted Women
Pre- Post- Test Test D iff.
Pre-Test
Post-Test D iff.
1 1 0 1 1 00 2 2 5 6 11 5 4 2 5 32 4 2 3 5 21 6 5 5 6 1
U = 7.5 04 = ,,31 N.S •
Category IV—Provision of Appropriate Play Materials
Addicted Women Nonaddicted Women
Pre- Post- Prer Post-Test Test D iff. Test Test D iff.
0 0 0 0 1 10 1 1 4 6 20 3 3 1 5 40 2 2 0 6 60 5 5 5 6 1
U = 11.5 r * =* .821 N.S.
Category VI—Opportunities for Varietyof Daily Stimulation
Addicted Women Nonaddicted Women
Pre- Post- Pre- Post-Test Test D iff. Test Test D iff.
3 3 0 1 3 20 3 3 4 4 02 2 0 2 2 02 0 -2 2 2 00 0 0 3 3 0
U = 11 6* = .842 N.S.
121
Mann Whitney U Test, (Table 19), no significant differences were found.
Therefore, Hypothesis 8 failed to be rejected.
No differences were found with respect to the mothers' compliance
with medical appointments and suggestions.
Hypothesis 9: There is no difference between narcoticaddicted women and nonnarcotic addicted women with respect to their compliance with medical appointments and suggestions.
Alternative Hypothesis: Differences do exist betweennarcotic addicted women and nonnarcotic addicted women with respect to their compliance with medical appointments and suggestions. Narcotic addicted women comply less than nonnarcotic addicted women.
When scores of the two groups of women were analyzed by means of Mann
Whitney U Test, (Tables 20a and 20b), Hypothesis 9 failed to be rejected.
Therefore, there is no difference between narcotic addicted women and
nonnarcotic addicted women with respect to their compliance with
medical appointments and suggestions.
Differences between narcotic addicted infants and nonnarcotic
addicted infants were not found in all of the items, (Hypothesis 2a),
with some items differences were only found at specific ages of the
infants. On those items where Group effects were significant and
Group X Time effect was not significant, the general interpretation was
that infants of narcotic addicted women differed from infants of non
narcotic addicted women at all ages or time periods. Significant
differences were found in favor of nonaddicted infants with respect to
the extent to which infants habituated to the presentation of aversive
stimuli (Items 1 and 3). Addicted infants demonstrated less mature
behavior than nonaddicted infants as they oriented toward animate and
inanimate visual and auditory stimuli (Items 6, 7 and 9). Addicted

122
TABLE 19
SCORES OF ADDICTED AND NONADDICTED NOMEN WITH WRIGHT ET AL. PARENT COUNSELOR HOME VISIT REPORT--ANALYZED
WITH MANN WHITNEY U TEST
Addicted NonaddictedWomen W omen
27 2727 2830 1426 2429 23
U = 5 <X.= .15, N.S.

123
TABLE 20a
SCORES OF ADDICTED AND NONADDICTED WOMEN WITH RESPECT TO COMPLIANCE WITH MEDICAL APPOINTMENTS
Addicted NonaddictedWomen Women
1 37 91 93 99 9
U = 4.5, Oi = .09, N.S.
TABLE 20b
SCORES OF ADDICTED AND NONADDICTED WOMEN WITH RESPECTTO COMPLIANCE WITH MEDICAL SUGGESTIONS
Addicted NonaddictedWomen Women
3- 59 95 95 99 9
U = 7, CX = .310, N.S.

124
infants exhibited more activity (Item 20) during the examining sessions
and were less able to utilize hand-to-mouth maneuvers for consoling
themselves than nonaddicted infants (Item 26).
Significant Group X Time interactions, whether or not in the
presence of significance for group, are somewhat more difficult to
explain. One interpretation might be that infants of narcotic addicted
women differed from infants of nonnarcotic addicted women, but not
necessarily at all ages. Alternatively, one could conclude that there
were differences due to the age of the infant (time period at which
measurements were obtained), but that this difference either did not
occur or was of a different magnitude for one or another of the groups.
Significant differences were found between the two groups in favor
of nonaddicted infants'as the ages of the infants increased. Between
age three days and three weeks both groups of infants increased their
level of performance in orienting toward the sound of the human voice
(Item 8), in alertness (Item 10), in Motor Maturity (Item 12) and in
self-quieting behavior (Item 25). With items 5, 8, 10, 12 and 25 both
groups of infants appeared to demonstrate similar configurations of
behavior (Figure 11, for example). Levels of differences however were
evident on the basis of addiction status of their mothers, with
nonaddicted infants demonstrating higher levels of performance than
addicted infants.
Both groups of infants were able to right their heads upon being
pulled into a sitting position (Item 13). Addicted infants cuddled in
the arms of the examiner less readily than nonaddicted infants (Item 14),
and little change in that behavior was demonstrated over time (Figure 12).

125
Direction of differences were found to increase in defensive behaviors
exhibited by both groups of infants (Item 15).
Analysis of results indicated that addicted infants exhibited a
higher level of arousal at age three days than nonaddicted infants
(Initial State, Hypothesis 2b). At age three days the infants' scores
were different in favor of nonaddicted infants. This means that
addicted infants were initially in an awake state, and engaged in
behaviors which ranged from exhibiting motor activity with thrusting
arm and leg movements to intense crying behavior. Cuddling by the
examiner was often necessary to aid in moving the infant into a sleep
state prior to beginning the assessment. Nonaddicted infants exhibited
behaviors which ranged from deep sleep to light sleep with eyes closed
at initial assessment.
It is noteworthy that initial state scores differed only at age
three days between the groups of infants. Higher state scores by the
addicted infants suggest that they were exhibiting a higher level of
arousal than nonaddicted infants within three days after birth and while
still in the hospital. It is possible that addicted infants may have
been experiencing transient effects of withdrawal. Their higher
initial state scores tend to suggest that they were exhibiting some
evidence of sleeplessness, a factor which has been found in other
studies of infants of narcotic addicted women.
With reference to Hypothesis 3, no differences were found between
Mental Development of the infants, on the basis of Bayley Scales of
Infant Development at either one month, 24 days or at three months.
Although Hypothesis 3 failed to be rejected, differences were found

126
between the two time periods. Part of the basis for this gain may
have been related to what appeared to represent an improved condition
of one of the infants in the addicted group. One of the infants
exhibited tremulousness that extended into the time period when the
initial Bayley Scale was administered (after one month of age), thus
lowering the scores at the first test period. Further, one infant
in the nonaddicted group failed to respond to several of the test
items at the first testing period, but made some changes with respect
to time. It is ultimately possible that the infants may have responded
to the activities provided by their mothers and thus showed some
changes with respect to the intervention program which was provided
for the infants and which may have been used by the mothers.
Results of analysis of Psychomotor Development, assessed with the
Bayley Scales were similar to results found on the Mental Scales of
the test. There were no differences between scores of groups of
infants, but there were significant differences with respect to time.
Infants in both groups earned higher scores at age three months (Mean =
125.4) than they did at one month, 24 days (Mean = 108). Time as well
as intervention appears to have made a difference with respect to
motor development as well as to mental development of the infants.
Infants were played with, handled, cuddled and talked with during the
three month period. Mothers were often observed imitating activities
of the home visitor with respect to working with their infants. It
therefore appears that some of such activities may have helped the
infants in some manner, as well as having provided ideas for the mothers
to imitate. It is realized that effects of maturation were expected

Ill
to be manifest; yet it also appears possible that the combined effects
of maturation and learning may have contributed to changes in the
infants' behavior.
There were no significant differences found with either of the
measures of maternal behavior as tested in Hypotheses 6, 7, 8 and 9. Inspection of Tables 16, 17, 18, 19, 20a and 20b shows that there were
some changes in scores between pre- and post-test periods, however,
they did not vary between the groups. It appears that addiction status
of the women in this study may not have discriminated finely between
the groups with respect to data derived from the instruments chosen.
However, inspection of Table 18, Category I--Emotional and Verbal
Responsivity, reveals that two addicted women received negative changes.
Circumstances in their lives were operating at the end of the study.
One mother who received a difference of -1, had contacted pulmonary
tuberculosis at the end of the study. During the last visit to her
home she appeared depressed and primarily involved with her own personal
problems and showed little concern for her infant. Another women, who
earned a difference of -2 with the same category appeared to have returned to drug use and appeared only minimally involved with her
infant. She had placed the baby with an older woman and appeared to
have removed herself from involvement with the infant. These two cases
seemed different from the others, and perhaps study of a larger sample
of women may have made a difference between the mothers.
A further explanation for lack of differences inchanges may be
related to selection of the sample. At the outset of the study efforts
were directed toward selecting women who would be similar along several

128
dimensions. Inspection of Table 1 shows that many women in the study
were supported by Public Welfare. When visiting homes one could easily
observe presence in the study of people from a low socioeconomic
strata with small resources available to them.
Finally, differences may have been found between the women had
the study included provisions for testing differences between the groups
at pre-test and post-test periods. For example, inspection of Table 17,
Ainsworth Scale MA-2 Mother's Delight in Baby, reveals that a pre-test
addicted women received scores which were of a lower magnitude that
nonaddicted women. Further study may include provision for determining
whether statistical differences are found.
Infants in this study differed along several dimensions on the
basis of addiction status of their mothers. Addicted infants demon
strated less mature behavior than nonaddicted infants as they habituated
to the presentation of aversive stimuli and when they oriented toward
animate and inanimate visual and auditory stimuli. Addicted infants
were more active during examining sessions and were less able to
utilize hand-to-mouth movements to aid in consoling themselves than
nonaddicted infants. Addicted infants cuddled in the arms of the
examiner less readily than nonaddicted infants. Also, addicted infants
exhibited a higher level of arousal (higher initial state score) at age
three days than nonaddicted infants. Higher scores with the initial
state item may have been related to effects of narcotic withdrawal.
No differences were found between the groups of women with respect
to their feelings of competency for providing caregiving skills to their
infants, with respect to maternal care behaviors with respect to the

129
arr.ount oC cognitive and emotional support available within their homes,
the extent to which they accepted an intervention program or the extent
tc which they exhibited compliance with Medical appointments and
sugges tions.
Although only one examiner performed all assessments in this study,
rigid adherence to administration and scoring guidelines was maintained
throughout the study. Such strict compliance served to minimize biases
which may have arisen and had their effect on the findings of this study.
Intervention Results
There were changes in infant behavior at the completion of the
intervention program. Both groups of infants increased their levels
of performance over the four age periods with respect to orienting
toward the sound of a human voice. The infants became more alert and
exhibited more mature motor maturity, more selfquieting behavior and
were better able to bring their heads to the midline of their bodies
as their ages increased. Also, both groups of infants increased in
their use of defensive movements for removing a cloth from their faces.
The infants demonstrated improved behavior with the Bayley Mental
and Motor Scales. The combined initial scores for both groups of
infants with the Mental Scales was 85.1. After intervention their
scores had risen to 94.4, thus, an increase of 9.3 points was evident
after completion of the project.
Initially the combined mean score with the Motor Scales was 108.
Their mean score rose to 125.4 at the end of intervention, thus showing
a gain of 7.4 points.
While it is difficult to separate changes which may have occurred

130
as a result of maturation, nevertheless it appeared important to have
observed spontaneous activity by some mothers as they Imitated many
activities which were performed by the investigator when working with
their infants. It therefore, seems reasonable that some maternal
behaviors may have aided in contributing to changes which were demon
strated in infant performance, and reflected in increased score values.
Feasibility of Planning and Implementing a Home-Based Intervention Program
In consideration of effort devoted by mothers with regard to
working with their infants, and in cooperating with the investigator
during this preliminary study, there were periods of anxiety associated
with the question of potential harm, observed especially by persons
who appeared to be visitors in some of the homes, and by some family
members, especially those who were lost to follow-up. Therefore some
benefit may be derived from considering the provision of a team of at
least two persons to visit homes of drug addicts during subsequent
studies, especially if those addicts are young adults.
Also, the provision of transportation of the women and their
infants to and from hospital based baby clinics may aid in assuring
that the infants receive recommended medical evaluations and treatments
at designated age periods.

CHAPTER V
a n d i m p l i c a t i o n s
The purpose in this study was to determine whether a difference
was found between development of infants born to narcotic addicted
women and infants born to nonnarcotic addicted women. The purpose
was also to determine whether changes were evident after pre- and
post-tests of mothers and their infants after they participated in an
intervention program. A third purpose was to examine the feasibility
of a subsequent study.
Instructional materials were developed and utilized in a home
based program directed toward strengthening mothering or helping
mothers become sensitive to infant needs, and helping mothers develop
caregiving skills to their infants. The subjects were ten infants and
their mothers. Five of the infants were born to narcotic addicted
women and five were born to women who presented no known history of
narcotic addiction. Nine of the families in this study were Black and
one was Caucasian, who were from low social position as defined in this
study by Hollingshead (1957).
Data were gathered during three phases. Phase I included the
pregnancy period of the mothers; Phase II included the hospital maternity
room contact with the mothers after delivery of their infants; and
Phase III which began in the homes of the infants at age one week,
131
132
after the mothers and infants were discharged from the hospital and
continued throughout the first three months of the infants' lives.
Three instruments were used for collecting infant data. They
were: 1) Amiel-Tison Neurological Maturity of Newborn Infants;
2) The Brazelton Neonatal Assessment Scale and 3) The Bayley Scales of
Infant Development— Mental and Motor Scales. Eleven instruments were
used to gather maternal data. The instruments were: 1) Hock Infant
Care Inventory; 2) Six Ainsworth Maternal Care Scales, a) Scale MA-1
Mother's Perception of Baby, b) MA-2 Mother's Delight in Baby, c) MA-3
Mother's Acceptance of Baby, d) MC-1 Mother's Availability to Baby,
e) MC-3 Amount of Interaction Offered by Mother, and f) MC-4 Appro
priateness of Mother's Initiation of Interaction; 3) The Caldwell et al.
Inventory of Home Stimulation; 4) A Parent Counselor Home Visit Report,
adapted from Wright et al. (1970); and 5) Mother's Compliance with
Medical Appointments and Compliance with Medical Suggestions.
Data from ten infants and their mothers were analyzed through
several statistical techniques. Significant differences were found
between infants of narcotic addicted women and infants of nonnarcotic
women with respect to functioning with several items in the Brazelton
Neonatal Behavioral Scale. All differences were found to be in favor
of nonaddicted infants. Addicted infants habituated to the presentation
of aversive stimuli less often than nonaddicted infants, Addicted
infants were more active during the examining sessions and utilized
less applicability of consoling techniques than nonaddicted infants.
Both groups of infants progressively improved their capability of

133
orienting toward the sound of the examiner's voice, became more alert
and demonstrated improved motor movements during the intervention
period.
Although addicted infants cuddled in the examiner's arms less
readily and demonstrated higher levels of arousal than nonaddicted
infants, addicted infants were similar to nonaddicted infants in their
increased capability to remove a cloth from their faces as a defensive
maneuver.
No differences were found with respect to groups of infants when
assessed with the Bayley Mental and Motor Scales. However, there were
differences across time periods with both of the Bayley Scales. Both
groups of infants demonstrated higher scores across time. Group
differences were found with respect to the Visual Following skills from
the Bayley Scales of Infant Development. Addicted infants visually
followed objects less often than nonaddicted infants.
Hypotheses 2a, 2b and 4 were rejected because differences were
found with respect to infant behavior.
Hypothesis 2a: There is no difference between performancewith the 27 behavioral items (as assessed with the Brazelton Neonatal Behavioral Assessment Scale) of infants born to narcotic addicted women and performance with the 27 behavioral items (as assessed with the Brazelton Neonatal Behavioral Assessment Scale) of infants born to nonnarcotic addicted women at four age periods (three days, one, two and three weeks).
Hypothesis 2b; There is no difference between performance with the Brazelton State items of infants born to narcotic addicted women and performance with the Brazelton State items of infants born to nonnarcotic addicted women at four age periods (three days, one, two and three weeks).

134
Hypothesis 4: There is no difference between VisualFollowiny skills (as assessed with the Bayley Scales of Infant Development) of infants born to narcotic addicted women, and Visual Following skills (as assessed with the Bayley Scales of Infant Development) of infants born to nonnarcotic addicted women at age three months.
No differences were found with respect to neurological maturity at
birth between the two groups of infants. Nor were differences found
with respect to Mental and Motor Development between the groups of
infants. Therefore, Hypothesis 1, 2c, 3 and 5 failed to be rejected.
Hypothesis 1: There is no difference between neurologicalmaturity at birth, of infants born to narcotic addicted women (as assessed with the Amiel-Tison Neurological Evaluation of the Maturity of Newborn Infants) and neurological maturity at birth of infants born to nonnarcotic addicted women (as assessed with the Amiel- Tison Neurological Evaluation of the Maturity of Newborn Infants).
Hypothesis 2c: There is no difference between performancewith Brazelton "Elicited Responses" of infants born to narcotic addicted women and performance with Brazelton "Elicited Responses" of infants born to nonnarcotic addicted women at four age periods (three days, one, two and three weeks).
Hypothesis 3: There is no difference between MentalDevelopment (as assessed v;ith the Bayley Scales of Infant Development) of infants born to narcotic addicted women and Mental Development (as assessed with the Bayley Scales of Infant Development) of infants born to nonnarcotic addicted women at two age periods (one month, 24 days and three months).
Hypothesis 5: There is no difference between PsychomotorDevelopment (as assessed wTith the Bayley Scales of Infant Development), of infants born to narcotic addicted women and Psychomotor Development (as assessed with the Bayley Scales of Infant Development), of infants born to nonnarcotic addicted women at two age periods (one month,24 days and three months).
No significant differences were found between narcotic addicted
women and nonnarcotic addicted women with respect to their feelings of

135
competency as measured with the Hock Infant Care Inventory, with
respect to their maternal care behaviors as measured with six Ainsworth
Scales, with respect to their home environments, as measured with the
Inventory of Home Stimulation, with regard to their acceptance of an
intervention program, assessed with a Parent Counselor Home Visit
Report from Wright et al., or with respect to their compliance with
medical appointments and suggestions. Hence, Hypotheses 6, 7, 8 and 9failed to be rejected.
Hypothesis 6: There is no difference between narcoticaddicted women and nonnarcotic addicted women with respect to their feelings of competency for providing caregiving skills, as assessed with the Hock Infant Care Inventory.
Hypothesis 7a: There is no difference between narcoticaddicted women and nonnarcotic addicted women with respect to amount of change in charcteristics of mothering, derived from pre- and post-tests (as assessed with Ainsworth Maternal Care Scales: Perception of Baby, Delight in Baby, Availabilityto Baby, Acceptance of Baby, Amount of Interaction with Baby, and Appropriateness of Mother's Initiation of Interaction with Baby).
Hypothesis 7b; There is no difference between narcotic addicted women and nonnarcotic addicted women with respect to changes in characteristics of mothering assessed with the Caldwell et al. Inventory of Home Stimulation.
Hypothesis 8: There is no difference between narcoticaddicted women and nonnarcotic addicted women with respect to their acceptance of home training (as assessed with a Parent Counselor Home Visit Report-- Wright et al.)
Hypothesis 9: There is no difference between narcoticaddicted women and nonnarcotic addicted women with respect to their compliance with medical appointments and suggestions.
Implications
Some of the results of this preliminary study may contribute to
subsequent studies of narcotic addicted women and their infants. The

oIlowing recommendations are offered;
1) Perform a replication of this study with a period of interven
tion to extend beyond three mouths. Opportunities for helping
mothers with their infants beyond that age level are needed.
At the end of the present study some of the infants had
reached a developmental level where they had begun to respond
to adult intervention with vocalizations and appeared ready
to benefit from further intervention. A longer period of
involvement may have increased impact on the development of
the infants, since infants may be more responsive at older ages.
In addition, a larger sample of infants seems desirable.
While conservative statistical tests were employed whenever
possible in order to minimize alpha error, finding differences
where none in fact exist, if cannot be gainsaid that a very
large number of tests were performed on only ten infants. Beta
error, failing to find differences that in fact exist, could
not be minimized simultaneously with alpha error and may be
quite large. The only way to reduce both types of error is
to increase the number of infants studied.
2) Another direction for future research might include directing
data analysis to determine whether a relationship is found
between availability of emotional and cognitive support
available within the infant's home (as assessed with the
Inventory of Home Stimulation), and infant performance at pre
school age. Such a finding might aid in devising strategies
for encouraging mothers toward manipulating their home environ
ments for the benefit of their infants.

137
3) Analysis of daLa might also include determining whether a
relationship is found between mother responses to Ainsworth
ScaLes and infant development at preschool age.
4) Analysis of mothers' feelings of competency with the Hock
Inventory may include obtaining separate scores for each of
the caregiving skills. That information might provide some
knowledge concerning whether mothers feel more competent with
respect to some caregiving skills than with others found on
that Inventory.
5) Perhaps a more basic need may exist with respect to extending
social action which would provide help in motivating addicted
women to develop productive life styles. Although some help
seems available through drug treatment centers as evidenced
by those centers which provided help with this study, it
appears that the question of how to best serve the needs of
addicted women may remain unanswered.
6) A further direction for research, if ethical, might attempt to study whether infants of narcotic addicted women should be
removed from their mothers and placed in foster homes, as has
been suggested by some writers, or whether or not infants should
remain with their mothers.
7) The administration of neurological examinations at a later
age of the infants may be of some value.
8) Extended knowledge concerning behavior of addicted infants may be gained from a similar study as the present but which would
include the use of a second control group. That group might

138
be studied without a component of intervention strategies.
Results of such a study might aid in determining possible
effects of an intervention program on addicted infants,
further research may attempt to provide answers to the following
questions:
1) Are there significant differences in behavior of infants whose
mothers have consumed drugs other than heroin during pregnancy?
2) Do addicted mothers who have only one child, differ significantly
from addicted mothers who have multiple children, with respect
to behaviors assessed by means of:
a) The Infant Care Inventory?
b) Six Ainsworth Scales utilized in this study?
c) The Caldwell et al. Inventory of Home Stimulation?
d) The Parent Counselor Home Interview Report (Wright et al.)?
e) Mother's Compliance with Medical Appointments and Suggestions?

APPENDIX I
NEUROLOGICAL EVALUATION OF THE MATURITY OF NEWBORN INFANTS
139

NEUROLOGICAL EVALUATION OF ’ THE •\ATURITY OF NEWBORN INFANTS
omo m a t e uiiivlk;>iiy clinic456 C l in ic Drive ^Columbus, O hio 43210
APPENDIX IIINAME:M0T| 1 LRi ‘BIRTHDATE: _ ______________
DATE OF EXAM
v #* f ̂,l_ r
celc Q
O r.O:
ccJ iiM̂I
. '.rr sJ^| fwll »•'*\orJ'
» 1« |l«"Ol' H'f „ Nt.O* *■'«*i»» 4»4 !•»' JO »«C|l> o*1 •••| r ' l « *•1
Pn.'Jsive Tone
4 »'WM
titi • *.« •*i ir-*M» iCft ®* V.*!!
III*1t*c*<* ,•« • % * f' • » «* • I*o • -w k I,.L̂ ,* * H« I \\m h» »«**<♦•* II '• w<*4 •'*mi4 Vm m M
.1
\u i»f Cil11 ’ i»j* ,lliCi li l̂
Active Tone
S P 8 9 5From: Amici-Tison, C . . Iteiiroloyicnl Evaluation of the
Maturity o£ Newborn Infants. Arch. Dir;', chiIdh .’( 43 :09,1960.

APPENDIX II
BRAZELTON NEONATAL BEHAVIORAL ASSESSMENT SCALE AND SCORE SHEET
141

PLEASE NOTE:
Pages 142-151, "Brazelton Neonatal Behavioral Assessment Scale", pages 152-161, "Inventory of Home Stimulation, pages 162-181, "Ainsworth Scales" and pages 197-209, "Hollingshead Two Factor Index of Social Position" all previously copyrighted, not microfilmed at request of author. Available for consultation at the Ohio State University Library.
UNIVERSITY MICROFILMS.

APPENDIX X
PARENT COUNSELOR HOME V i!SIT REPORT
182

183
Mother's Name
PAM 1:1 NT COUNSELOR HOME VISIT HE PORT
____________________C h i l d ' s Name _
D a t e o f Vi . s i t
Col. ____ The visit was
______ 1. Successfully made; mother was at home.
2. Mother was not at home but visited with someone else.
3. No one was at home; visit was not made.
______ 4. Someone was at home, but no visit made.
Col. ____ The mothering one
______ 1, Was warm, receptive, cooperative
2. Worked with (tolerated parent counselor)
______ 3. Showed little concern
______ 4. Made fun of parent counselor's ideas
_____ 5. Was openly hostile to parent counselor's ideas.
Col. The visit was
______ 1. Not delayed
______ 2. Delayed due to care of the children
______ 3. Delayed due to housework
______ 4. Delayed due to talking with friends or relatives
______ 5. Delayed due to getting dressed
6. Delayed due to other reasons

184
Today's visit was with
A mother who normally cares tor child most of the time.
A mother who docs not normally care lev the child.
Someone else who normally cares for the child most of the time.
Temporary baby sitter--probably paid.
How much activity was in the room in which you presented the exercises?
Nothing was going on beside the training.
Other activities were going on but did not distract attention of the baby.
Other activities in the room often pulled the baby's attention away from the training.
There was such a great deal of activity in the room that presenting the exercises was difficult.
How many interruptions were there during the task training period?
None
One or two
Three or four
There was almost always distraction in the home.
What was the most frequent or longest interruption?
There were no interruptions.
Mothering one had to care for another child.
An adult wanted something.
The phone rang.
Visitors came.
The child had to be fed.

185
The child went: lo sleep.
A d i stracu Lnc TV show, roc :nv. player or radio.
'.X iri.n ,: Che is i L , t iie m o t h e r : a i one was
Present all of the time.
Present most of the time.
Present part of the time.
Mot present.
During the visit, the father was
Present all of the time.
Present most of the time.
Present part of the time.
Mot present.
During the visit the father was
Interested in the training and wanted to help.
Interested but did not take an active part.
Mot interested but did not interrupt the training.
Not interested and interrupted the training for something trivial,
Openly hostile against the training and tried to disrupt and/or distract it.
Thought the training was foolish but did not interfere with it.
Mot applicable, no father present.
How did the mothering one react to instruction?
Was attentive while you were talking and asked questions, or made comments (favorable).

1.86
Did other th Logs while parent counse lor was demonstrnt ini; materials (straightened child's cLothers, looked around the room, did housework), Listened without comment,
Walked out of the room during a demonstration suss ton.
Refused to perform the task.
Laughed at instructions.
Asked the mothering one how the child responded to last visit demonstrations.
Showed evidence of response.
Showed no evidence of response.
Not applicable-new child in the project.
When the mothering one uses materials from the previous visit she
Becomes discouraged if the child does not respond during the first presentation.
Is satisfied, even though the child did not respond as well as she thought desirable.
Tries several times until she observes some type of response.
Continues to work with the task even after the child performs well.
What is the mothering one's verbalized attitudes toward the project?
Believes the project is great.
Believes it is OK.
Appears only moderately interested in the project.
Does not comment regarding the project.

APPENDIX XI
INFANT CARE INVENTORY
187

1S8
IMFANT CARE INVENTORY
Select: the one person in each pair that you feel could SHOW AFFECTIONTO YOUR RASY better:
YOURSELF ( ) OR ( ) BABY'S GRANDMOTHER
BABY'S GRANDMOTHER ( ) OR ( ) DAY CARE TEACHER
EXPERIENCED BABY SITTER ( ) OR ( ) FATHER
DAY CARE TEACHER ( ) OR ( ) YOURSELF
PEDIATRIC NURSE ( ) OR ( ) EXPERIENCED BABY SITTER
BABY'S GRANDMOTHER ( ) OR ( ) FATHER
DAY CARE TEACHER ( ) OR ( ) FATHER
EXPERIENCED BABY SITTER ( ) OR ( ) BABY'S GRANDMOTHER
FATHER ( ) OR ( ) YOURSELF
PEDIATRIC NURSE ( ) OR ( ) BABY'S GRANDMOTHER
FATHER ( ) OR ( ) PEDIATRIC NURSE
EXPERIENCED BABY SITTER ( ) OR ( ) DAY CARE TEACHER
YOURSELF ( ) OR ( ) PEDIATRIC NURSE

S9
Select the one person in eacli pair that you feel, could PREPARE YOURCHILD AND PUT IITM/HER TO BED better:
YOURSELF
FATHER
PEDIATRIC NURSE
YOURSELF
PEDIATRIC NURSE
BABY'S GRANDMOTHER
EXPERIENCED BABY SITTER
DAY CARE TEACHER
DAY CARE TEACHER
YOURSELF
FATHER
EXPERIENCED BABY SITTER
PEDIATRIC NURSE
BABY'S GRANDMOTHER
EXPERIENCED BABY SITTER
OR
OR
OR
OR
OR
OR
OR
OR
OR
OR
OR
OR
OR
OR
OR
BABY'S GRANDMOTHER
PEDIATRIC NURSE
EXPERIENCED BABY SITTER
PEDIATRIC NURSE
BABY'S GRANDMOTHER
FATHER
DAY CARE TEACHER
YOURSELF
FATHER
EXPERIENCED BABY SITTER
YOURSELF
BABY'S GRANDMOTHER
DAY CARE TEACHER
DAY CARE TEACHER
FATHER

190
Sc l a d the one person in each pair that you reel could CALM YOUR BAPbe tier:
FAT! IKK
EXPERIENCED BABY SITTER
BABY'S GRANDMOTHER
PEDIATRIC NURSE
YOURSELF
PEDIATRIC NURSE
EXPERIENCED BABY SITTER
YOURSELF
BABY'S GRANDMOTHER
PEDIATRIC NURSE
YOURSELF
FATHER
DAY CARE TEACHER
EXPERIENCED BABY SITTER
DAY CARE TEACHER
OR
OR
OR
OR
OR
OR
OR
OR
OR
OR
OR
OR
OR
OR
OR
FATHER
DAY CARE TEACHER
EXPERIENCED BABY SITTER
PEDIATRIC NURSE
DAY CARE TEACHER
DAY CARE TEACHER
BABY'S GRANDMOTHER
FATHER
BABY'S GRANDMOTHER
EXPERIENCED BABY SITTER
PEDIATRIC NURSE
YOURSELF
BABY'S GRANDMOTHER
FATHER

191
Select the one person in each pair that you feel could DIAPER YOUR BABYbetter:
YOURSELF ( ) o? ( ) EXPERIENCED BABY SITTER
FATHER ( ) OR ( ) PEDIATRIC NURSE
EXPERIENCED BABY SITTER ( ) OR ( ) BABY'S GRANDMOTHER
FATHER ( ) OR ( ) YOURSELF
YOURSELF ( ) OR ( ) BABY'S GRANDMOTHER
EXPERIENCED BABY SITTER ( ) OR ( ) DAY CARE TEACHER
YOURSELF ( ) OR ( ) PEDIATRIC NURSE
PEDIATRIC NURSE ( ) OR ( ) BABY'S GRANDMOTHER
DAY CARE TEACHER ( ) OR ( ) YOURSELF
DAY CARE TEACHER ( ) OR ( ) FATHER
PEDIATRIC NURSE ( ) OR ( ) DAY CARE TEACHER
EXPERIENCED BABY SITTER ( ) OR ( ) FATHER
BABY'S GRANDMOTHER ( ) OR ( ) DAY CARE TEACHER
BABY'S GRANDMOTHER ( ) OR ( ) FATHER
PEDIATRIC NURSE ( ) OR ( ) EXPERIENCED BABY SITTER

192
i 1".: o.io por.s...-i in cacli )L i\ i\.iiS oct c-ju ;
pair Liint: you fuel couLd UNDERSTAND '
nub ( ) ox ( ) BABY'S GHANDMiU'ilER
FATHER ( ) OR ( ) PEDIATRIC NURSE
EXPERIENCED BABY SITTER ( ) OR ( ) BABY'S GRANDMOTHER
FATHER ( ) OR ( ) YOURSELF
BABY'S GRANDMOTHER ( ) OR ( ) FATHER
YOURSELF ( ) OR ( ) EXPERIENCED BABY SITTER
PEDIATRIC NURSE ( ) OR ( ) BABY'S GRANDMOTHER
DAY CARE TEACHER ( ) OR ( ) YOURSELF
DAY CARE TEACHER ( ) OR ( ) FATHER
YOURSELF ( ) OR ( ) PEDIATRIC NURSE
EXPERIENCED BABY SITTER ( ) OR ( ) FATHER
PEDIATRIC NURSE ( ) OR ( ) DAY CARE TEACHER
BABY'S GRANDMOTHER ( ) OR ( ) DAY CARE TEACHER
PEDIATRIC NURSE ( ) OR ( ) EXPERIENCED BABY SITTER
EXPERIENCED BABY SITTER ( ) OR ( ) DAY CARE TEACHER

yourse! j- ( ) om
EXPERIENCED BABY SITTER ( ) OR
YOURSELF ( ) OR
PEDIATRIC NURSE ( ) OR
BABY'S GRANDMOTHER ( ) OR
PEDIATRIC NURSE ( ) OR
FATHER ( ) OR
YOURSELF ( ) OR
PEDIATRIC NURSE ( ) OR
DAY CARE TEACHER ( ) OR
EXPERIENCED BABY SITTER ( ) OR
DAY CARE TEACHER ( ) OR
FATHER ( ) OR
EXPERIENCED BABY SITTER ( ) OR
BABY'S GRANDMOTHER ( ) OR
FATHER
BABY 1S C-RANDMOT HER
EXPERIENCED BABY SITTER
DAY CARE TEACHER
BABY'S GRANDMOTHER
YOURSELF
EXPERIENCED BABY SITTER
DAY CARE TEACHER
BABY'S GRANDMOTHER
BABY'S C-RAXDMOTHER
YOURSELF
PEDIATRIC NURSE
DAY CARE TEACHER
FATHER

) 01;
PEDIATRIC NURSE ( ) OR
EXPERIENCED BABY SITTER ( ) OR
DAY CARE TEACHER ( ) OR
YOURSELF ( ) OR
DAY CARE TEACHER ( ) OR
PEDIATRIC NURSE ( ) OR
BABY'S GRANDMOTHER ( ) OR
YOURSELF ( ) OR
BABY'S GRANDMOTHER ( ) OR
YOURSELF ( ) OR
EXPERIENCED BABY SITTER ( ) OR
PEDIATRIC NURSE ( ) OR
FATHER ( ) OR
EXPERIENCED BABY SITTER ( ) OR
DAY CARE TEACHER
BABY’S GRANDMOTHER
FATHER
BABY'S GRANDMOTHER
YOURSELF
EXPERIENCED BABY SITTER
DAY CARE TEACHER
PEDIATRIC NURSE
FATHER
EXPERIENCED BABY SITTER
FATHER
BABY'S GRANDMOTHER
PEDIATRIC NURSE
DAY CARE TEACHER

195
p a i r t h a t you 1'oeL c o u ld P! U] VMF_APP!!0- BABY b e t t o r :
S e l e c t th e one p e rs o n i.n each PH I. ATE VISUAL AND VERBAL SIIMLL,-
pi: n la th i t : nurse i
DAY CARE TEACHER (
BABY'S GRANDMOTHER (
day care TEACHER (
BABY'S GRANDMOTHER (
EXPERIENCED BABY SITTER (
FATHER (
YOURSELF (
PEDIATRIC NURSE (
YOURSELF (
PEDIATRIC NURSE (
EXPERIENCED BABY SITTER (
YOURSELF (
OR ( ̂ DAY CASE TEACHER
OR ( ) FATHER
OR ( ) DAY CARE TEACHER
OR ( ) YOURSELF
OR ( ) FATHER
OR ( ) FATHER
OR. ( ) YOURSELF
OR ( ) BABY'S GRANDMOTHER
OR ( ) EXPERIENCED BABY SITTER
OR ( ) EXPERIENCED BABY SITTER
OR ( ) BABY'S GRANDMOTHER
OR ( ) DAY CARE TEACHER
OR ( ) PEDIATRIC NURSE
)

APPENDIX XII
HOLLINGSHEAD W O FACTOR INDEX OF SOCIAL POSITION
196

APPENDIX XIII
PARENT INTERVIEW REPORT
210

211
PARENT INTERVIEW REPORT
Name o£ Parent _______ ___________Name of Infant
Date of Birth_____________________ Date of Birth
Place of Interview Sex of Infant
( ) 1. FAMILY INFORMATION (Mother's parents)
Father:
a) living at homeb) deceasedc) not living at home; whereabouts knownd) whereabouts unknowne) other
( ) Mother:
a) living at homeb) deceasedc) not living at home; whereabouts knownd) whereabouts unknowne) other
( ) Birth Order:
a) oldestb)c) youngest
( ) 2. MARITAL STATUS (Infant's parents)
a) singleb) married, living with first spousec) married, not living with first spoused) married, living with second spousee) divorcedf) widow
( ) 3. NUMBER OF CHILDREN
4. Have any of your children living with persons other than yourself for any length of time? ______________________If so, with whom and for how long?

212
( )
( )
( )
5. C PI/C AT [OX
a) less than 3 yearsb) A-8 yearse) some high school or technical schoold) hi ah school graduatee) some college or technical school after high schoolf) graduate school or some graduate credit
6. REASON FOR LEAVING SCHOOL
a) still in schoolb) graduatedc) expelledd) dropped oute) other------------ specify
7. OCCUPATION -- Are you employed? Yes Mo
a) Is husband employed? Yes No
Place of Employment _____________________
Title of Position
8. DRUG EXPERIENCE
a) Age of first experienceb) First drug used by you
11. JUST PRIOR TO DELIVERY OF YOUR BABY, WHEN DID YOU RECEIVE YOUR LAST DRUG INTAKE?
a) the same dayb) one day before that timec) two days before that timed) other ___________________________________
c)9. OCCASION OF FIRST EXPERIENCE
a) curiosityb) enticed by friendc) in hospitald) for sleep
e) depressionf) for "kicks"g) dare
( ) 10. WHICH WAS THE SECOND DRUG USED BY YOU?
a) no change in drug use after first

213
( ) 12.
( ) 13.
( ) 14.
HOW DID YOU MANAGE TO STOP TAKING DRUGS?
a) participated in drug programb'l other______________________________o') If you participated in a drug program how did you
decide to do so?1) self imposed2) other ___________________________
WHILE PARTICIPATING IN THE PROGRAM DID YOU USE DRUGS?
a) Yesb) No
WITH WHOM DO YOU NOW LIVE?
a) Husband and children (or child)b) Parents (specify which)____________c) Other persons (specify) ____________
Adapted from: Bloom, William A., Jr., and Sudderth, E. Ward, "Methadonein New Orleans," in Stanley Einstein, Methadone Maintenance. New York; Marcel Dekker, Inc., 1971.

APPENDIX XIV
BOOKLET FOR MOTHERS
214
H H E L P t t A
D S I D
B O O K L E T

216
ACTIVITIES WITH INFANTS
This booklet is planned for parents of infants and very youngchi Ldren. T'.'.e ideas chat are Lnc Luded have come from experiences ofr.a-.y people who have been studying Infants and children for many years.Ihe activities in this booklet provide games that are fun for parents and their infants and at the same time provide learning as well.
The games are intended to help your baby develop some basic skills such as focusing his eyes on objects and coordinating his eyes with his hands. You will discover that baby learning is enjoyable and you will note that the child may seem to develop confidence in himself in knowing that he can do certain things in a skillful manner.
We suggest the following ideas:
Make learning a fun time. When your infant seems no longer interested, try another activity or stop playing completely. Your baby may be interested for only five minutes.
BABIES NEED LOVE
A baby's great need in life is love, affection and good physical care. Being loved and cuddled helps a baby learn to live with the world. Your baby will learn about love from the attention that is given him, from the way you respond to him when he says he needs you by crying.
IMITATION
Your baby will not be able to imitate you when he is very young. You may imitate some of the things that he does. Imitate his smile and the sounds that he makes, and also his movements.
A caretaker's response to the infant's needs will help the infant if the responses are satisfactory to him. A smile, a pleasant voice or a hug are positive responses to the infant. Praising your infant is a satisfactory response to him.
YOUR BABY MAY PROVIDE SIGNALS FOR YOU
There are several situations about the management of your baby in which you may be interested, and those situations may have serious meaning for his development. Some of those situations are related to the special feelings that your infant may have. You will be able to judge some of his feelings by the act of crying.

217
Cry ini: Ls the infant's way of ceiling you that lie needs you for something. If he cries with low -.-.loans and sighs he may be sleepy.1: he cries and sucks his fists or fingers he may be hungry. He may be uncomforLable--he may be wet and cold and his diaper may need to be changed. His clothes may need to be straightened. lie may be crying because he wants some kind of attention from you. Talking to dim for a .few minutes may stop his crying. At an early age he is too young to tell you why he is crying.
When your baby was only a few days old he probably had a set schedule for feeding. If he was born in a hospital he may have been fed every three or four hours on a regular schedule. As he grows older he may need fewer feedings, especially at night. You may help your baby by handling his feeding in a way that seems satisfactory to him. He may be less fussy if you don't let him cry from hunger, just because it may not be time for his feeding. A check with your physician will help you with your feeding plans.
Your baby may cry because he may want you to hold and cuddle him. You may be helped in knowing that he wants you to cuddle him if he scops crying when he sees you.
Babies also cry when they don't have anything else to do. Pick dim up, hold him and talk to him. You need not feel a concern for spoiling him. Sometimes you may be able to comfort your baby by:
--placing your hand slightly on his stomach,
--holding his hands or
--talking to him.
Your baby will enjoy feeling warm and cuddled. As you cuddle him talk to him. He will soon smile at you when you talk to him.
The way you talk to your baby, the way you treat him and the way he gets along with other people in the family are very important to him.
The things you say to the baby will influence how he feels about himself.
r
lie will learn to like himself better if you talk to him in a soothing voice that lets him know that he is a part of a loving and secure home.
Hold him close to you and show him that you enjoy being with him. Teach him that you and your family are fun to be with. Help him to learn to like other people.
218
s rn c i 'S T io x s fo r s t im u l a t io n
To S I iinu late Fee lino.
Sni:i ■; c V-by ’ a pos it ion From stomach to back.
As you diaper him gently massage him.
Cuddle and hold him firmly; talk and sing to him while doing so.
Move his arms over his head and then back.
To Stimulate His Vision
Shift him to different places in his crib to allow light to be available to both of his eyes.
Remove his crib bumpers often to allow him to see objects near him.
Place a patterned sheet on his bed if available. (Such a sheet may be made by sewing scraps of colored materials on his sheet--a red shape, or any color that may be available with the home.
To Stimulate His Hearing
Sing to him as you do different things for him, such as diapering.
Say a nursery rhyme to him.
Say his name while talking to him.
Let your baby hear different sounds and develop listening skills.
Place a clock that ticks quietly beside his bed.
To Enjoy Your Baby
Be friendly with him and enjoy how he feels as you hold him.
Enjoy giving him his bath.
Shift his crib to different places in the room.
Take him outdoors (when your doctor says he is old enough); go for a walk with him.
Place him nearby while the family is eating (if he is awake).
Place him in the kitchen occasionally while you are preparing meals.

219
Take him w i t h you when v i s i t i n g • . •e la t i . ves.
Change and f e e d him f ro m a l t e r n a t e s i d e s .
EASY J.-Y'YS
While you are changing diapers, feeding or just playing with your baby, play a couching and talking game.
Put your infant's hand on your ear and say "Ear." Repeat this by putting his hand on his ear and repeating the word. Do the same for other bodily parts.
The caretaker's face is something that the child sees and learns to recognize. As you do simple touching and talking games he will be able to recugnize the parts of your face and notice that they feel different and their names sound different.
While he is placed on his back, move a colorful rattle, ball or other toy slowly in the head-to-foot direction; then from right- to-left. Do these movements several times. After he follows for a while move the object in a circular direction around the baby's head so that he will have to turn his head in order to see it. While moving the object talk gently to him even though he obviously may not understand the words.
As the baby becomes older he may enjoy the same activity over and over again. Adults may find this boring, but the child may continually learn from repetition.
After the baby has learned to reach, make him "work" by placing an attractive toy beyond his reach. Provide small blocks (too large for him to swallow) for him to grasp.
Allow him to look at his image in the mirror.
Stand behind the infant and ring a bell, shake a rattle, a bunch of keys or any other noise maker. Let him find the direction of the sound by turning his body toward the sound. He will learn that his body may be used to find objects.
BABIES LEARN TO TALK
Babies know how to cry and make sounds. Babies may be encouraged to talk by parents and other caretakers. If you talk to your baby he will learn to make sounds.
When you are diapering, bathing and holding your baby, or just watching him lie in his crib making cooing sounds, respond to him by

220
s t r o k in .v h i s s tom ach , suit l i n y and m a k in g s i m i l a r sounds . l ie may r e p e a t h i s c o o i n : and you w i L l have a " c o n v e r s a t i o n " g o i n g . T h i s i s an easy a c t i v i t y and may be r e p e a t e d a t odd moments.
HASTES l e a k:: t h r o u g h t o u c h
A mother may help her newborn baby develop when she holds him close to her body. She helps him when she strokes his cheeks and rubs his hands and his body.
Babies learn through their skin. They learn by touching and feeling, linen they are held, stroked and cuddled they develop fast and feel safe.
Stroke his cheeks; rub his body when you bathe him. Babies will put toys in their mouths; give babies toys that are safe.
Keep things away from baby that he might swallow and that might make him sick.
Praise the child's effort; laugh and look proud when he does the movements that you want him to do. Try not to scold if he does not want to play.
PLAN ON REGULAR VISITS TO YOUR BABY’S DOCTOR
Although your baby is well, it is important that you take him to his doctor on regularly planned visits.
Your doctor will observe the baby's growth and development and will inform you about changes in care and feeding to fit your baby's particular needs.
Regular visits to the doctor will provide opportunities for your to discuss problems and will help you gain confidence in caring for your baby.

THIS BOOKLET HAS PREPARED
3Y
STAFF MEMBERS IN
TILE HELP-A-BA3Y-PROJECT
For more information call 422-3152


APPENDIX XV
MOTHER'S compliance with medical appointments and suggestions
223

224
MrmiKR'S VOMPLIANCE WITH MEDICAL APPOINTMENTS
The v a r i a b l e b e i n c c o n s i d e r e d h e re i s the e x t e n t t o w h ic h th e m o th e r ( p c i . m a r i . l v ) , o r a c a r e t a k e r h r i n as t h e baby to the or. t - o a t i o u t c l i n i c a t The Oh io S t a t e U n i v e r s i t y H o s p i t a l s a c c o r d i n g to a p la n n e d s c h e d u le ,Tor the purpose of routine or non-routine medicaL examinations and other medical problems. During the first three months of the infants' lives two routine visits are scheduled by the Pediatrician with the mother's consent. Other visits are scheduled when the need arises and are determined when a request is made by the parent, or when in the opinion of the Pediatrician, a need exists for the infant to be scheduled prior to his routine visit.
A mother may agree to a scheduled visit but fail to effect the appointment due to many reasons. She may telephone and notify hospital personnel regarding her inability to keep the appointment, while on the other hand she may complete no effort regarding her reasons for failure to return the baby as scheduled.
It seems reasonable to assume that a difference in effort exists between the mother who is unable to make the visit, but notifies hospital personnel to that effect, and the mother who is unable to make the visit and who makes no contact with hospital personnel.
1. Very Low Effort; This rating will be given to a mother whofails to keep any of her scheduled appointments, does notnotify hospital personnel, but will offer a reason if initiative is assumed by hospital personnel for contacting her to reschedule another appointment.
3. Low Effort: This rating will be given to a mother who does notkeep her appointment, but will telephone the hospital within a few days after the scheduled visit, ask for another appointment, provide no reason for failure to keep the previous appointment, or makes the statement that she forgot the appointment.
5. Moderate Effort; This rating will be given to a mother whoarrives on the scheduled date, but within one-half to one hour after her scheduled time, and provides no reason for her tardiness.
7. High Effort; This rating will be given to a mother who arrives on the scheduled date within one-half and one hour late, provides a reason for her tardiness and is willing to wait until other patients are served, if necessary.
9. Very High Effort: This rating will be given to a mother whoarrives promptLy and is willing to wait even though the Pediatrician may be unavailable immediately on the scheduled time.
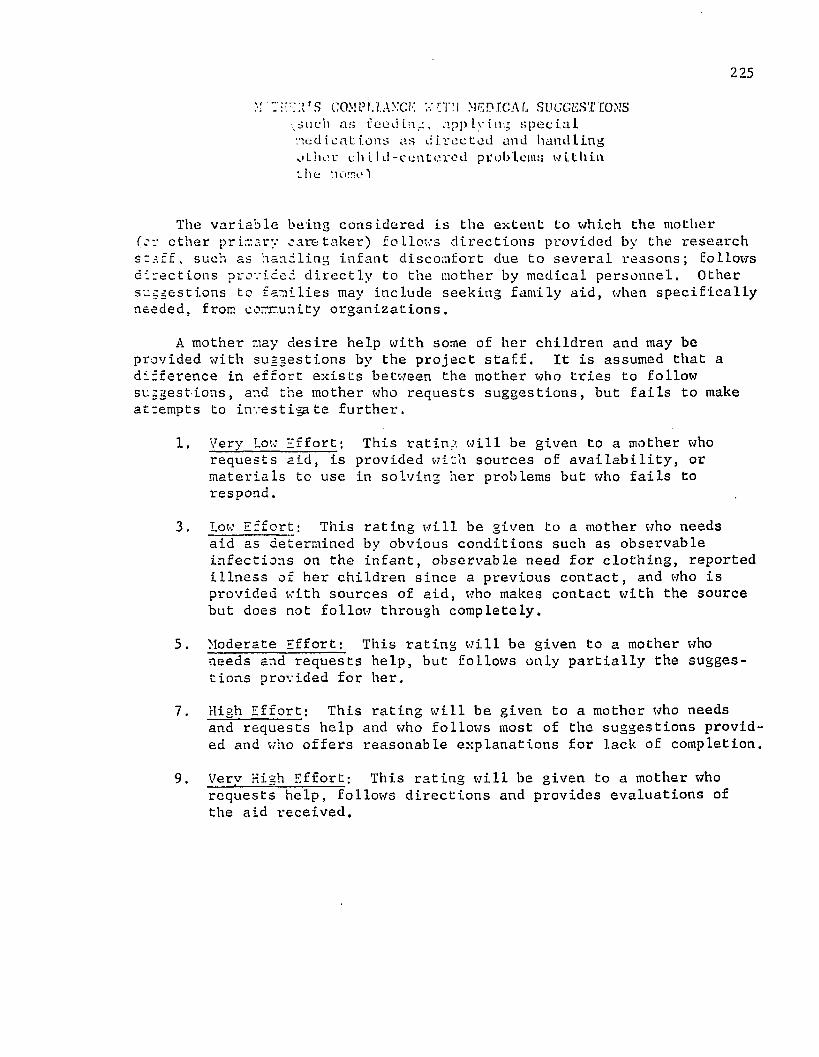
225
m c o m p u .axck medical suggestions;riuch as feeding, applying special medicat tons as directed and handling other child-centered problems within t h e hornel
The variable being considered is the extent to which the mother Tor other primary caretaker) follows directions provided by the research staff, such as handling infant discomfort due to several reasons; follows directions provided directly to the mother by medical personnel. Other suggestions to families may include seeking family aid, when specifically needed, from community organizations.
A mother may desire help with some of her children and may be provided with suggestions by the project staff. It is assumed that a difference in effort exists between the mother who tries to follow suggestions, and the mother who requests suggestions, but fails to make attempts to investigate further.
1. Very Low Iffort; This rating will be given to a mother whorequests aid, is provided with sources of availability, or materials to use in solving her problems but who fails to respond.
3* Low Effort; This rating will be given to a mother who needs aid as determined by obvious conditions such as observable infections on the infant, observable need for clothing, reported illness of her children since a previous contact, and who is provided with sources of aid, who makes contact with the source but does not follow through completely.
5. Moderate Effort; This rating will be given to a mother whoneeds and requests help, but follows only partially the suggestions provided for her.
7. High Effort; This rating will be given to a mother who needsand requests help and who follows most of the suggestions provided and who offers reasonable explanations for lack of completion.
9. Very High Effort; This rating will be given to a mother whorequests help, follows directions and provides evaluations of the aid i-eceived.
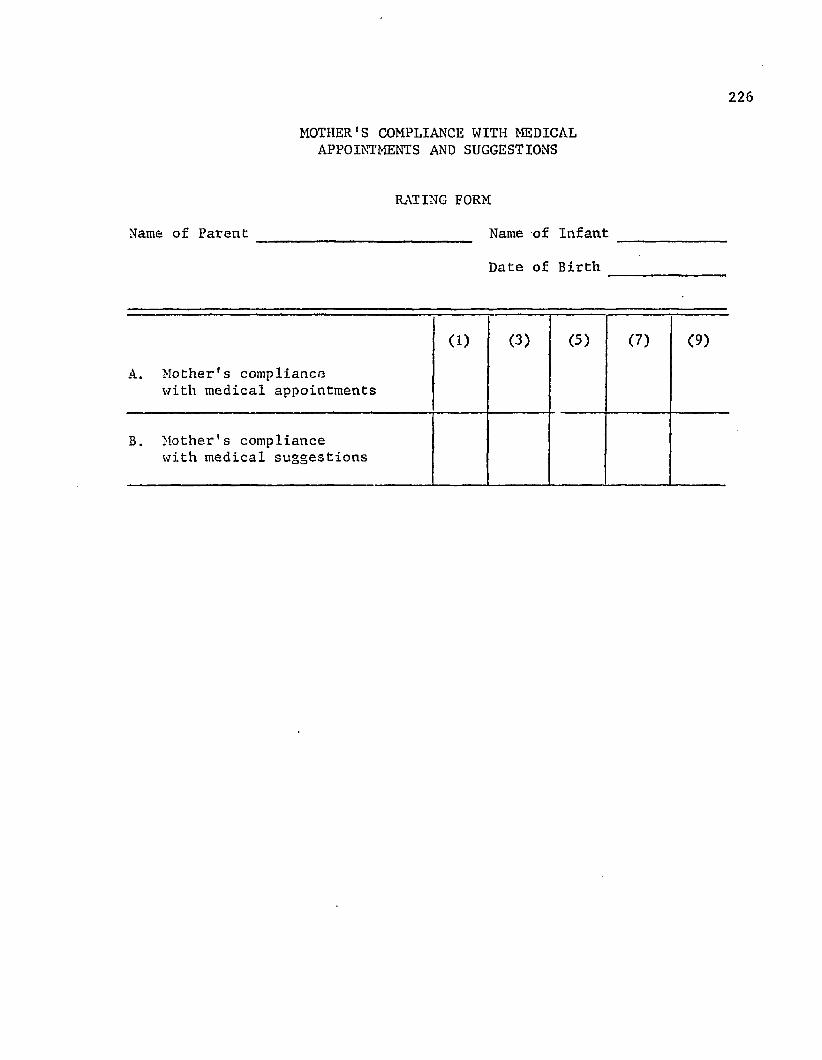
226
MOTHER'S COMPLIANCE WITH MEDICAL APPOINTMENTS AND SUGGESTIONS
RATING FORM
Name of Parent ________________________ Name of Infant
Date of Birth
A. Mother's compliancewith medical appointments
(1) (3) (5) (7) (9)
B. Mother's compliancewith medical suggestions

APPENDIX XVI
TABLES 21-26 SUMMARY OF RESULTS OF ANALYSES OF VARIANCE ON BRAZELTON ITEMS 3, 6, 7, 9, 20 AND 26
227

With respect to Item 3, Response Decrement to Bell, addicted
infants (X = 3.75) were less able to shut down responses than were
nonaddicted infants (X = 5.55). When addicted infants were presented
the sound of a bell their responses were the same within the ten
trials, whereas nonaddicted infants shut down body movements within a
range between seven to ten presentations of the bell. See Table 21 for a summary of those results. ,
TABLE 21
SUMMARY OF RESULTS OF ANALYSIS OF VARIANCE WITH BRAZELTON ITEM 3— RESPONSE DECREMENT TO BELL
i
Source of Variation df MS F Significance
Group 1 32.40 13*16(8) p <.01
Time 3 .90 *89(3,24) N.S.Group X Time 3 .67 *66(3,24) N.S.

229Item 6 - Orientation Response-Inanimate Auditory
This item is a measure of the extent to which an infant orients toward the sound of an inanimate auditory stimulus— the sound of a rattle. Addicted infants (X = 3.85) stilled, brightened their eyes but made no attempt to locate the sound; nonaddicted infants (X - 5.75)
shifted their eyes to the sound as well as turned their heads. The
results are presented in Table 22.
TABLE 22SUMMARY OF RESULTS OF ANALYSIS OF VARIANCE WITH BRAZELTON
ITEM 6— ORIENTATION RESPONSE— INANIMATE, AUDITORY
Source of Variation df MS F Significance
Group 1 36.10 24.47(8) p<.01Time 3 1.73 1,59<3,24) N.S.
Group X Time 3 3.03 2-78(3,24) N.S.

230Item 7 - Orientation— Animate Visual
This item assesses the infant's orienting toward an animate
object— a person's face. Addicted infants (X *= 2.60) responded by
stilling and brightening the eyes upon the presentation of examiner's
face within the line of the infant's vision; nonaddicted infants (X = 5.00) shifted their eyes to the sound as well as stilled and brightened their eyes. See Table 23 for a summary of results.
TABLE 23SUMMARY OF RESULTS OF ANALYSIS OF VARIANCE WITH BRAZELTON ITEM 7— ORIENTATION— ANIMATE VISUAL
Source of Variation df MS F Significance
Group 1 57.60 34.65(g) p <.001Time 3 3.87 2*74(3,24) N.S.
Group X Time 3 .67 ,4?(3,24) N.S.

231Item 9 - Orientation Animate— Visual and Auditory
This item assesses the infant's response to the presentation of examiner's face together with his face. Addicted infants (X - 3.60) stilled, focused on the stimulus when presented and made brief follow
ing; nonaddicted infants (X = 5.75) focused and followed for more than
a 30° arc, made smooth movements; they occasionally lost the stimulus,
but were able to find it again. See Table 24 for a summary of these
data.
TABLE 24SUMMARY OF RESULTS OF ANALYSIS OF VARIANCE WITH BRAZELTON ITEM 9—
ORIENTATION ANIMATE— VISUAL AND AUDITORY
Source of Variation df MS F Significance
Group 1 46.22 12.62 (8) p<.01
Time 3 3.23 1,92(3,24) P <.01Group X Time 3 .43 *25(3,24) p<.01

232Item 20 - Activity (Alert States)
This is a summary score of spontaneous and elicited activity of the infant, scored on a scale of 0-3 and converted to scores 1 through 9. A score of 0 indicates that the infant engaged in no activity; a
score of 3 indicates that the infant engaged in much activity. The
sums assigned to spontaneous and elicited activities are summed. For example, a total score of 2 receives a Brazelton score point of 3.
Addicted infants (X = 6.13) earned scores that summed to 5, which means
they engaged in activity within a range between moderate and much
activity; nonaddicted infants (X ® 4.10) earned scores that summed to 3, which means that they were less active during the examining periods. See Table 25 for a summary.
TABLE 25
SUMMARY OF RESULTS OF ANALYSIS OF VARIANCE WITH BRAZELTON ITEM 20— ACTIVITY (ALERT STATES)
Source of Variation df MS F Significance
Group 1 21.02 COw00• p<.05
Time 3 49.17 ,41<3,24) N.S.Group X Time 3 .69 ■58<3,24) N.S.

233Item 26 - Hand to Mouth Facility (All States)
This item represents the extent to which an infant brings his
hands to his mouth in order to aid in self-quieting behavior. Addicted
infants (X ® 4.10) typically brought their hands to the mouth area«•twice, but made no insertion; nonaddicted infants (X « 6.00) made one
brief insertion but were unable to maintain it. Table 26 contains the summary of results.
TABLE 26
SUMMARY OF RESULTS OF ANALYSIS OF VARIANCE WITH BRAZELTON ITEM 26— HAND TO MOUTH FACILITY
Source of Variation df MS F Significance
Group 1 36.10 9.53 P <.05Time 3 6.10 2.43 N.S.
Group X Time 3 .70 .28 N.S.

APPENDIX XVIITABLE 27 a) SUMMARY OF SIGNIFICANTLY DIFFERENT GROUP MEANS
ON THOSE ITEMS WHERE TIME WAS SIGNIFICANT AS A MAIN EFFECT— NO INTERACTION SIGNIFICANCE
TABLE 27 b) SUMMARY OF SIGNIFICANTLY DIFFERENT TIME MEANS FOR THOSE ANALYSES OF VARIANCE WHERE GROUP AND TIME
WERE SIGNIFICANT AS MAIN EFFECTS— NO INTERACTION SIGNIFICANCE
234

235
TABLE 27aSUMMARY OF SIGNIFICANTLY DIFFERENT GROUP MEANS ON THOSE ITEMS WHERE
TIME WAS SIGNIFICANT AS A MAIN EFFECT— NO INTERACTION SIGNIFICANCE
Items Addicted Infants Nonaddicted Infants Significance
5 2.50 5.15 p<.018 3.90 5.80 p<.0510 3.25 5.25 P < *0512 3.45 4.85 p < .0525 4.05 6.70 p<.001
TABLE 27b
SUMMARY OF SIGNIFICANTLY DIFFERENT TIME MEANS FOR THOSE ANALYSES OF VARIANCE ON ITEMS WHERE GROUP AND TIME WERE SIGNIFICANT AS
MAIN EFFECTS— NO INTERACTION SIGNIFICANCE
Item 5
13.0
23.5
33.7
*4
5.1
Item 25
* p <.05** p <.01
4.7 4.8 5.3 6.7|
. *
BIBLIOGRAPHY
Ainsworth, Mary D. Salter, "System for Rating Maternal Care Behaviors,11 In Boyer, E. Gil; Simon, Anita and Karafin, Gail R., Measures of Maturation: An Anthology of Early Childhood Observation Instruments . Vol. I, Philadelphia, Pennsylvania: Research for Better Schools, Inc., 1973.)
Ainsworth, Mary D. Salter and Bell, Sylvia M., "Some ContemporaryPatterns of Mother-Infant Interaction in the Feeding Situation."In Ambrose, J. A. (Ed.) Stimulation in Early Infancy. (London, England: Academic Press, 1969.)
Amiel-Tison, Claudine, "Neurological Evaluation of the Maturity of Newborn Infants." Archives of Diseases of Childhood, 43: 89, (1968).
Andre-Thomas, Chesni, Y.? Saint-Anne Dargassies, S., The Neurological Examination of the Infant. (London: Medical Advisory Committee, National Spasties Society, 1960.)
Apgar, Virginia, "A Proposal for a New Method of Evaluation of theNewborn Infant." Current Research in Anesth. and Analg., 32: 260, (1953).
Baer, Daniel J., and Corrado, James J., S. J., "Heroin Addict Relationships with Parents During Childhood and Early Adolescent Years." The Journal of Genetic Psychology, 124: 99-103, (1974).
Bayley, Nancy, Bayley Scales of Infant Development. (New York: Psychological Corporation, 1969).
Berlyne, David, "The Influence of the Albedo and Complexity of Stimuli • on Visual Fusion in the Human Infant." British Journal of Psychology, 49: 315-318, (1958).
Blatman, Saul, "Babies Seem Better Off When the Mothers are oh Methadone." Medical World News, 13: 16-18, (July 21, 1972).
Blinick, George, M.D., "Fertility of Narcotic Addicts and Effects of Addiction on the Offspring." Social Biology, 18: Supplement, (September, 1967).
, "Menstrual Function and Pregnancy in Narcotics Addicts Treated with Methadone." Nature, 219: (July 3, 1968).
236

237Blinick, George, M.D.; Wallach, Robert G., M.D.; and Jerez, Eulogio,
M.D., "Pregnancy in Narcotics Addicts Treated by Medical Withdrawal: The Methadone Detoxification Program." AmericanJournal of Obstetrics and Gynecology, 105: (1969).
Bloom, William and Sudderth, Ward, "Methadone in New Orleans." Cited in Einstein, Stanley, Methadone Maintenance. (New York:Marcel Dekker, Inc., 1971).
Brazelton, T. Berry, M.D., Neonatal Behavioral Assessment Scale. (Philadelphia, Pennsylvania: Lippincott & Company, 1973).
Caldwell, Bettye; Heider, J.; and Kaplan B., "The Inventory of Home Stimulation", (1966), cited in Caldwell, Betty et al., "The Relation of Infants’ Home Environments to Mental Test Performance from Six to Thirty-Six Months: A Longitudinal Analysis." ChildDevelopment, 46,1, 71-78, 0.975).
Caputo, Daniel and Mandel, Wallace, "Consequences of Low Birth Weight." Developmental Psychology, 3: (1970).
Carpenter, Genevieve C., "Visual Regard of Moving and Stationary Faces in Early Infancy." Merrill Palmer Quarterly, 20, 3, 181-194, (1974).
Cobrinik, Ralph W., M.D.j Hood, Thornton, M.D.j and Chusid, Emanual, M.D.; Slobody, Lawrence G., "The Effects of Maternal Narcotic Addiction on the Newborn Infant." American Medical Association Journal of Diseases of Children, 92: 504, (November, 1956),
Cobrinik, Ralph W., M.D.; Hood, Thornton, M.D.; and Chusid, Emanual,M.D., "The Effects of Maternal Narcotic Addiction on the Newborn Infant." Pediatrics, 24: 288, (1959).
Cohen, Sanford N., M.D., "Methadone Maintenance During Pregnancy."American Journal of Diseases of Childhood, 126: 445-446, October, (1973).
Cole, Michael and Bruner, Jerome S., "Preliminaries to a Theory of Cultural Differences." Cited in Gordon, Ira J., Ed., The Seventy-first Yearbook of the Study of Education. (Chicago:The University of Chicago Press, 1972).
Cooper, Grace C., Student Booklet— Book 1, "Child Development: Gettingto Know Your Baby and Yourself." (Washington, D.C.: Consortium on Early Childbearing and Childrearing, Child Welfare League of America, 1973)
__________ , Student Booklet— Book 3, "Child Development: Learning Aboutthe World." (Washington, D. C.: Consortium on Early Childbearing and Childrearing, Child Welfare League of America, 1973).

238, Student Booklet— Book 4, "Child Development: Your Baby
Grows." (Washington, D.C.: Consortium on Early Childbearingand Childrearing, Child Welfare League of America, 1973).
__________ , Student Booklet— Book 5, "Child Development: Learning MoreEach Day." (Washington, D. C.: Consortium on Early Childbearing and Childrearing, Child Welfare League of America, 1973).
__________ , Student Booklet— Book 6, "Child Development: The End ofthe First Year." (Washington, D. C.: Consortium on EarlyChildbearing and Childrearing, Child Welfare League of America,1973).
Darwin, Charles, "Biographical Sketch of an Infant." Mind, 7: 285-294, (July, 1877).
Daugherty, Ann L., and Cohen, Judity L., "Auditory Screening for Infants and Preschoolers." Nursing Outlook, 9, 5, 310, (May, 1961).
Davis, R. C. and Chappel, J. N., "Pregnancy in the Context of Narcotics Addiction and Methadone Maintenance." In Proceedings of the 5th Methadone Conference, held at Washington, D. C., March 17-19,1973, New York, National Association for the Prevention of Addiction to Narcotics, 1973, pp. 1146-1152, cited in Fennegan, Loretta p., and Macnew, Bonnie, "Care of the Addicted Infant." American Journal of Nursing, 74: 4, 685-693, (April, 1974).
Dayton, G. 0.; Jones, M.H.; Steele, B.; and Rose, M., "Developmental Study of Coordinated Eye Movements in the Human Neonate."Archives of Ophthalmology, 71: 871-875, (L964).
Deutsch, Martin, The Disadvantaged Child. (New York: Basic Books, 1967).Dole, Vincent P., M.D., and Nyswander, Marie, M.D., "A Medical Treatment
for Diacetylmorphine (Heroin) Addiction." Journal of American Medical Association, 193: 646, (1965).
Dorland's Illustrated Medical Dictionary, (Philadelphia, Pennsylvania:W. B. Saunders, 19741
Drage, J. S., M.D., and Berendes, H., M.D., "Apgar Scores and Outcomeof the Newborn." Pediatric Clinics of North America, 13: 635-643, (August, 1966).
Drillien, Cecil M., M.D., The Growth and Development of the Prematurely Born Infant. (Edinburgh and London: E. & S. Livingstone, Ltd.,1964).
Eisenberg, Rita B.; Griffin, Elizabeth J.j Coursin, David Vaird; andHunter, Mary Alice, "Auditory Behavior in the Human Neonate: APreliminary Report." Journal of Speech and Hearing Research.7: 245-269, (1964).

239Einstein, Stanley, Methadone Maintenance. (New York: Marcel Dekker,
Inc., 1971).
Elardo, Richard; Bradley, Robert; and Caldwell, Bettye M., "TheRelation of Infants' Home Environments to Mental Test Performance from Six to Thirty-Six Months: A Longitudinal Analysis."Child Development, 46: 71-76, (1975).
Fantz, Robert, "Pattern Vision in Young Infants." The Psychological Record. 8: 43-47, (1958).
Field, H.; Copack, P.; Derbyshire, A. J.; Driessen, G. J.*, and Marcus,R. E., "Response of Newborns to Auditory Stimulation." Journal of Auditory Research, 7: 271-285, (1967).
Finnegan, Loretta and Macnew, Bonnie A., "Care of the Addicted Infant." American Journal of Nursing, 74, 4, 685-693, (April, 1974).
Forrester, Bettye J.; Brooks, Geraldine; Mardge, Beulah.; and Outlaw, Doris D., Materials for Infant Development. (Nashville,Tennessee: John F. Kennedy Center for Research on Education andHuman Development, George Peabody College for Teachers, 1971).
Frank, Lawrence K., "Tactile Communication," Genetic Psychology Monograph, 66: 209-225, (1957).
Goodfriend, Milton J., M.D.; Shey, Irving, A., M.D.; and Klein, Milton D., "The Effects of Maternal Narcotic Addiction on the Newborn." American Journal of Obstetrics and Gynecology, 71, 1, 29-36, (1956).
Gordon, Ita J., and Guinah, Barry J., "A Home Learning Center Approach to Early Stimulation." (Gainesville, Florida: Institute for Development of Human Resources, College of Education, University of Florida, 1969).
Gordon, Ira J., Baby Learning Through Baby Play. (New York: St.Martin's Press, 1970).
Gordon, Ira J., and Lally, Ronald, Intellectual Stimulation for Infants and Toddlers. (Gainesville, Florida, The Institute for the Development of Human Resources, College of Education, University of Florida, 1968).
Gray, Susan, "The Child's First Teacher." Childhood Education (December, 1971).
Harper, Rita, M.D.; George I. Solish, M.D., Ph.D. ; Henry M. Purow, M.D.; Edward Sand, M.D.; and William C. Panepinto, M.S.W., "The Effect of a Methadone Treatment Program Upon Pregnant Heroin Addicts and Their Newborn Infants." Pediatrics. 54, 3, 300-305, (September,1974).

240Hess, R. D., and Shipman, Virginia C., "Early Experience and the
Socialization of Cognitive Modes in Children." Child Development . 36: 869-886, (1965).
Hill, Reba Michels, M.D., and Desmond, Murdina M., "Management of theNarcotic Withdrawal Syndrome in the Neonate." Pediatric Clinics of North America, 10; 67, (1963).
Hock, E., Ph.D., "Alternative Approaches to Child Rearing and Their Effects on the Mother-Infant Relationship." (Columbus, Ohio:The Ohio State University, 1972, unpublished).
Hollingshead, August B., Two Factor Index of Social Position. (1965 Yale Station, New Haven, Connecticut) (1957).
Hoozerbeth, Jacob, M.D., "Methadone in Miami." In Einstein, Stanley, Methadone Maintenance. (New York: Marcel Dekker, Inc., 1971).
Kaplan, Stuart I., M.D.; Kron, Reuben E., M.D.; Mitchell, Litt, M.D.;and Finnegan, Loretta, M.D., "Correlations Between Scores on the Brazelton Neonatal Assessment Scale, Measures of Newborn Sucking Behavior and Birthweight in Infants Born to Narcotic Addicted Mothers." (Philadelphia: Philadelphia General Hospital,undated, unpublished).
Karnes, Merle B.; Teska, James; Hodgins, Audry A.*, and Badger, Earladeen D., "Educational Intervention at Home by Mothers of Diadvantaged Infants." Child Development, 41, 4, 925-935, (1968).
Kleber, Herbert D., M.D., "The New Haven Methadone Maintenance Program." _ In Einstein, Stanley, Methadone Maintenance. (New York: Marcel Dekker, Inc., 1971).
Knowles, Roy, M.D.; Lahiri, S.; and Anderson G,, "Methadone Maintenance in St. Louis." In Einstein, Stanley, Methadone Maintenance.(New York: Marcel Dekker, Inc., 1971).
Korner, Anneliese and Thomas, Evelyn B., "Visual Alertness in Neonates as Evoked by Maternal Care." Journal of Experimental Child Psychology, 10: 67-78, (L970).
Krause, S., M.D., "Heroin Addiction Among Pregnant Women and TheirNewborn Babies." American Journal of Obstetrics and Gynecology.75: 754, (1958).
Kunstadter, Ralph H., M.D.; Klein, Reubin I., M.D.; Lundeen, Evelyn C., R.N.; and Witz, Winifred, R.N., "Narcotic Withdrawal Symptoms in Newborn Infants." Journal of American Medical Association, 168: 1008-1010, (1968).

241Lessen-Firestone, Joan K.; Strauss, Milton E.; Starr, Raymond H.; and
Ostrea, Enrique M., Jr., "Behavioral Characteristics of Methadone Addicted Neonates." (Wayne State University, Detroit, Michigan, 1974, unpublished).
Levy, Norman, "The Use of Drugs by Teenagers: For Sanctuary andIllustion." American Journal of Psychoanalysis, 28: 48, (1967).
Light, R. W., and Dunham, T. R., In Moser, Robert H., "Heroin Addiction." Journal of American Medical Association, 230, 5, 728-729, (1974).
Lindensmith, A.R., The Addict and the -Law. (Bloomington, Indiana, Indiana University Press, 1965).
Lin-Fu, Jane S., "Neonatal Narcotic Addiction." United States Department of Health Education and Welfare, Public Health Services,Maternal and Child Health, (1969).
Maslansky, Robert, "Methadone Maintenance Programs in Minneapolis."In Einstein, Stanley, Methadone Maintenance. (New York: Marcel Dekker, Inc., 1971).
Mirando, Simon B,, "Visual Abilities and Pattern Preferences of Premature Infants and Full Term Neonates." Journal of Experimental Child Psychology, 10: 189-205, (1970).
Moser, Robert H., M.D., "Heroin Addiction." Journal of American Medical Association, 230, 5, 728-729, (1974).
Naeye, Rochard L., M.D.; Blanc, William, M.D.; Werner, Leblanc, M.D.; Khatamee, Masood A., M.D., "Fetal Complications of Maternal Heroin Addiction: Abnormal Growth, Infections and Episodes ofStress." The Journal of Pediatrics, 83, 6, 1055-1061, (December, 1973).
Pavenstedt, Eleanor, M.D., Ed., The Drifters. (Boston: Little, Brownand Company, 1967).
Painter, Genevieve, Teach Your Baby. (New York: Simon and Schuster,1973).
Perlmutter, Johanna F., M.D., "Drug Addiction in Pregnant Women."American Journal of Obstetrics and Gynecology, 99, 4, 569-572, (October 15, 1967).
Pierson, Paul S., M.D.; Kleper, Herbert, M.D.; and Howard, Patricia,R.N., "Sudden Death in Infants Born to Methadone Maintained Addicts." Journal of American Medical Association, 220: 13, 1733-1734, (1972).

242Provence, Sally, M.D. and Lipton, Rose C., Infants in Institutions.
(New York: International Universities Press, 1962).
Rajegowda, B. K., M.D.; Blass, Leonard, M.D.; Evans, Hugh E., M.D.;Maso, Graciella; Swartz, Donald P., M.D.; and Leblanc, Wiener, "Methadone Withdrawal in Newborn Infants." Pediatrics. 81, 3, 532, (1972).
Reddy, A. Mahender; Harper, Rita G., M.D.; and Stern, Gertrude, M.D., "Observations in Heroin and Methadone Withdrawal in the Newborn." Pediatrics, 48, 3, 353-358, (1971).
Richter, R. W., et al., "Neurological Complications of Addiction toHeroin." In Moser, Robert H., "Heroin Addiction." Journal of American Medical Association. 230, 5, 728-729, (1974).
Rosenow, E. C., "The Spectrum of Drug-Induced Pulmonary Disease." In Moser, Robert H., "Heroin Addiction." Journal of American Medical Association, 230, 5, 728-729, (1974).
Rosenthal, Theodore, "Congenital Neonatal Narcotic Addiction: ANatural History." American Journal of Public Health, 54: 1252- 1262, (August, 1964).
Rothstein, Peter, M.D., and Gould, Jeffrey B., M.D., "Born With aHabit: Infants of Drug Addicted Mothers." Pediatrics Clinicsof North America, 21, 2, 307-319, (May 1974).
Salapatek, Phillip, "Visual Scanning of Geometric Figures By the Human Newborn." Journal of Comparative and Physiological Psychology, 66, 2, 247-258, (1968).
Scott, Joseph C., Jr., M.D., Discussant In Statzer, Darrell E., M.D., and Wardell, James N., "Heroin Addiction During Pregnancy." American Journal of Obstetrics and Gynecology, (May 15, 1972).
Schneck, Herman, M.D., "Narcotic Withdrawal Symptoms in Newborn Infants Resulting from Maternal Addiction." Journal of Pediatrics, 52: 584-587, (1958).
Self, Patricia, Ph.D., "Individual Differences in Auditory and Visual Responsiveness in Infants." Ann Arbor, Michigan, University Microfilms.
Skeels, Harold M., and Dye, Harold B., M.D., "A Study of the Effects of Differential Stimulation on Mentally Retarded Children."American Association on Mental Deficiency. Proceedings and Addresses of the 63rd Annual Session, held at Chicago, Illinois, May 3-6, 1939.
243Slobody, Lawrence and Cobrinik, Ralph, "Neonatal Narcotic Addiction."
Quarterly Review of Pediatrics, (July-September, 1959).
Soule, A. Bradley III, M.D.; Standley, Kay, M.D.; Copans, Stuart,M.D.; and Davis, Myriam, M.D., "Clinical Uses of the Brazelton Neonatal Scale." Paper Presented at the Biennial Meeting of the Society for Research in Child Development, Philadelphia, March 29 - April 1, 1973.
Statzer, Darrell E., M.D., and Wardell, James N., M.D., "Heroin Addiction During Pregnancy." American Journal of Obstetrics and Gynecology. (May 15, 1972).
Steg, Nina, M.D., "Narcotic Withdrawal Reactions in the Newborn."American Journal of Diseases in Children. 94: 286-288, (1957).
Stern, Roy, M.D., "The Pregnant Addict." American Journal of Obstetrics and Gynecology. 94, 2, 253-257, (January 15, 1966).
Sussman, Sidney, M.D., "Narcotic and Methamphetamine Use During Pregnancy", American Journal of Diseases of Children. 106: 325-330, (September, 1963).
Tronick, Edward and Greenfield, Patricia, Infant Curriculum. (New York: Media Products, Inc., 1973).
Trussell, Ray E., M.E., "Treatment of Narcotic Addicts in New YorkCity." In Einstein, Stanley, Methadone Maintenance. (New York: Marcel Dekker, Inc., 1971).
Wallach, Robert C., M.D.; Eulogio, Jerez, M.D.; and Blinick, George,M.D., "Pregnancy and Menstral Function in Narcotics Addicts Treated with Methadone." American Journal of Obstetrics and Gynecology. 105, 8, 1226-1228, (December 15, 1969).
Weingold, Allan B., "Fetal-Growth Effects of Heroin, Methadone Appear to be Direct." Pediatric News. (May, 1974).
Williams, Margaret and Scarr, Sandra, "Effects of Short Term Intervention on Performance in Low Birth Weight, Disadvantaged Children." Pediatrics, 47, 1, 289-298, (January, 1971).
Wilson, Geraldine, M.D., Desmond, Murdine M., M.D., and Verinaud, Willie M., "Early Development of Infants of Heroin-Addicted Mothers." American Journal of Diseases of Children, 126: 457-462, (October, 1973).
Winer, B. J., Statistical Principles and Experimental Design. (New York: McGraw Hill Book Co., 1962).
244Wright, Charlene; Lally, J. Ronald; Dibble, Marjorie, "Prenatal,
Postnatal Intervention: A Description and Discussion ofPreliminary Findings of a Home Visit Program Supplying Cognitive, Nutritional and Health Information to Disadvantaged Homes."Paper presented at the Miami, Florida, Annual Meeting of American Psychological Association, (September, 1970).
Zelson, Carl, M.D.j Estrellita, Rubio, M.D.; and Wasserman, Edward, M.D., "Neonatal Narcotic Addiction: Ten Year Observation." Pediatrics.48, 2, 178-189, (August, 1971).
Zelson, Carl, M.D., and Sook, Ja Lee, "Neonatal Narcotic Addiction— Exposure to Heroin and Methadone." Pediatric Research, 7: 61, (1973).




















