WHO indoor air quality guidelines on household fuel combustion: Strategy implications of new...
7
WHO indoor air quality guidelines on household fuel combustion: Strategy implications of new evidence on interventions and exposureerisk functions Nigel Bruce a, b, * , Dan Pope a , Eva Rehfuess c , Kalpana Balakrishnan d , Heather Adair-Rohani b , Carlos Dora b a Department of Public Health and Policy, University of Liverpool, UK b Department of Public Health, Environmental and Social Determinants of Health, World Health Organisation, Geneva, Switzerland c Institute for Medical Informatics, Biometry and Epidemiology, Ludwig-Maximilians-University, Munich, Germany d Department of Environmental Health Engineering, Sri Ramachandra University, Chennai, India highlights New WHO air quality guidelines will address household air pollution (HAP). Action on HAP could lower risk of multiple child and adult diseases by 20e50%. New evidence shows levels at or below 35 mg/m 3 PM 2.5 (WHO IT-1) are needed. Most improved solid fuel stoves result in PM 2.5 levels well above IT-1. Intervention strategy must shift towards accelerating access to clean fuels. article info Article history: Received 30 March 2014 Received in revised form 21 August 2014 Accepted 26 August 2014 Available online xxx Keywords: WHO guidelines Household air pollution Exposureeresponse Clean fuels Testing and standards abstract Background: 2.8 billion people use solid fuels as their primary cooking fuel; the resulting high levels of household air pollution (HAP) were estimated to cause more than 4 million premature deaths in 2012. The people most affected are among the world's poorest, and past experience has shown that securing adoption and sustained use of effective, low-emission stove technologies and fuels in such populations is not easy. Among the questions raised by these challenges are (i) to what levels does HAP exposure need to be reduced in order to ensure that substantial health benefits are achieved, and (ii) what intervention technologies and fuels can achieve the required levels of HAP in practice? New WHO air quality guidelines are being developed to address these issues. Aims: To address the above questions drawing on evidence from new evidence reviews conducted for the WHO guidelines. Methods: Discussion of key findings from reviews covering (i) systematic reviews of health risks from HAP exposure, (ii) newly developed exposureeresponse functions which combine combustion pollution risk evidence from ambient air pollution, second-hand smoke, HAP and active smoking, and (iii) a systematic review of the impacts of solid fuel and clean fuel interventions on kitchen levels of, and personal exposure to, PM 2.5 and carbon monoxide (CO). Findings: Evidence on health risks from HAP suggest that controlling this exposure could reduce the risk of multiple child and adult health outcomes by 20e50%. The new inte- grated exposureeresponse functions (IERs) indicate that in order to secure these benefits, HAP levels require to be reduced to the WHO IT-1 annual average level (35 mg/m 3 PM 2.5 ), or below. The second review found that, in practice, solid fuel ‘improved stoves’ led to large percentage and absolute re- ductions, but post-intervention kitchen levels were still very high, at several hundreds of mg/m 3 of PM 2.5, although most solid fuel stove types met the WHO 24-hr average guideline for CO of 7 mg/m 3 . Clean fuel user studies were few, but also did not meet IT-1 for PM 2.5 , likely due to a combination of continuing multiple stove and fuel use, other sources in the home (e.g. kerosene lamps), and pollution from neighbours and other outdoor sources. Conclusions: Together, this evidence implies there needs to be a strategic shift towards more rapid and widespread promotion of clean fuels, along with efforts to * Corresponding author. Department of Public Health and Policy, University of Liverpool, Whelan Building, Quadrangle, Liverpool L69 3GB, UK. E-mail address: [email protected] (N. Bruce). Contents lists available at ScienceDirect Atmospheric Environment journal homepage: www.elsevier.com/locate/atmosenv http://dx.doi.org/10.1016/j.atmosenv.2014.08.064 1352-2310/© 2014 Published by Elsevier Ltd. Atmospheric Environment xxx (2014) 1e7 Please cite this article in press as: Bruce, N., et al., WHO indoor air quality guidelines on household fuel combustion: Strategy implications of new evidence on interventions and exposureerisk functions, Atmospheric Environment (2014), http://dx.doi.org/10.1016/ j.atmosenv.2014.08.064
Transcript of WHO indoor air quality guidelines on household fuel combustion: Strategy implications of new...

lable at ScienceDirect
Atmospheric Environment xxx (2014) 1e7
Contents lists avai
Atmospheric Environment
journal homepage: www.elsevier .com/locate/atmosenv
WHO indoor air quality guidelines on household fuel combustion:Strategy implications of new evidence on interventions andexposureerisk functions
Nigel Bruce a, b, *, Dan Pope a, Eva Rehfuess c, Kalpana Balakrishnan d,Heather Adair-Rohani b, Carlos Dora b
a Department of Public Health and Policy, University of Liverpool, UKb Department of Public Health, Environmental and Social Determinants of Health, World Health Organisation, Geneva, Switzerlandc Institute for Medical Informatics, Biometry and Epidemiology, Ludwig-Maximilians-University, Munich, Germanyd Department of Environmental Health Engineering, Sri Ramachandra University, Chennai, India
h i g h l i g h t s
� New WHO air quality guidelines will address household air pollution (HAP).� Action on HAP could lower risk of multiple child and adult diseases by 20e50%.� New evidence shows levels at or below 35 mg/m3 PM2.5 (WHO IT-1) are needed.� Most improved solid fuel stoves result in PM2.5 levels well above IT-1.� Intervention strategy must shift towards accelerating access to clean fuels.
a r t i c l e i n f o
Article history:Received 30 March 2014Received in revised form21 August 2014Accepted 26 August 2014Available online xxx
Keywords:WHO guidelinesHousehold air pollutionExposureeresponseClean fuelsTesting and standards
* Corresponding author. Department of Public HeaLiverpool, Whelan Building, Quadrangle, Liverpool L6
E-mail address: [email protected] (N. Bruce).
http://dx.doi.org/10.1016/j.atmosenv.2014.08.0641352-2310/© 2014 Published by Elsevier Ltd.
Please cite this article in press as: Bruce, N.,new evidence on interventions andj.atmosenv.2014.08.064
a b s t r a c t
Background: 2.8 billion people use solid fuels as their primary cooking fuel; the resulting high levels ofhousehold air pollution (HAP) were estimated to cause more than 4 million premature deaths in 2012.The people most affected are among the world's poorest, and past experience has shown that securingadoption and sustained use of effective, low-emission stove technologies and fuels in such populations isnot easy. Among the questions raised by these challenges are (i) to what levels does HAP exposure needto be reduced in order to ensure that substantial health benefits are achieved, and (ii) what interventiontechnologies and fuels can achieve the required levels of HAP in practice? New WHO air qualityguidelines are being developed to address these issues. Aims: To address the above questions drawing onevidence from new evidence reviews conducted for the WHO guidelines. Methods: Discussion of keyfindings from reviews covering (i) systematic reviews of health risks from HAP exposure, (ii) newlydeveloped exposureeresponse functions which combine combustion pollution risk evidence fromambient air pollution, second-hand smoke, HAP and active smoking, and (iii) a systematic review of theimpacts of solid fuel and clean fuel interventions on kitchen levels of, and personal exposure to, PM2.5
and carbon monoxide (CO). Findings: Evidence on health risks from HAP suggest that controlling thisexposure could reduce the risk of multiple child and adult health outcomes by 20e50%. The new inte-grated exposureeresponse functions (IERs) indicate that in order to secure these benefits, HAP levelsrequire to be reduced to the WHO IT-1 annual average level (35 mg/m3 PM2.5), or below. The secondreview found that, in practice, solid fuel ‘improved stoves’ led to large percentage and absolute re-ductions, but post-intervention kitchen levels were still very high, at several hundreds of mg/m3 of PM2.5,
although most solid fuel stove types met the WHO 24-hr average guideline for CO of 7 mg/m3. Clean fueluser studies were few, but also did not meet IT-1 for PM2.5, likely due to a combination of continuingmultiple stove and fuel use, other sources in the home (e.g. kerosene lamps), and pollution fromneighbours and other outdoor sources. Conclusions: Together, this evidence implies there needs to be astrategic shift towards more rapid and widespread promotion of clean fuels, along with efforts to
lth and Policy, University of9 3GB, UK.
et al., WHO indoor air quality guidelines on household fuel combustion: Strategy implications ofexposureerisk functions, Atmospheric Environment (2014), http://dx.doi.org/10.1016/
N. Bruce et al. / Atmospheric Environment xxx (2014) 1e72
1 HAP: Household air pollution.2 LMIC: Low and middle income countries.3 UN: United Nations.4 AQG: Air quality guideline.
Please cite this article in press as: Bruce, N.,new evidence on interventions andj.atmosenv.2014.08.064
encourage more exclusive use and control other sources in and around the home. For householdscontinuing to rely on solid fuels, the best possible low-emission solid fuel stoves should be promoted,backed up by testing and in-field evaluation.
© 2014 Published by Elsevier Ltd.
1. Introduction
Household air pollution (HAP)1 from the combustion of solidand other polluting fuels, is responsible for a very substantial publichealth burden, impacting primarily on homes in low and middle-income countries (LMIC).2 In the 2010 Global Burden of Diseasestudy (GBD-2010), cooking with solid fuels (wood, dung, cropwastes, charcoal and coal), was estimated to cause 3.5 (uncertaintyinterval: 2.7, 4.5) million premature deaths in 2010, with a further0.5 million outdoor air pollution deaths being attributed to emis-sions from household cooking (Lim et al., 2012; Smith et al., 2014),and HAP was responsible for the largest global environmentalburden among the risk factors studied. New WHO estimates for2012 using similar methods but updated solid fuel use and mor-tality data, report 4.3 million premature deaths (WHO, 2014).
Recognising the extent of this problem, and in addition to effortswithin countries, a number of international initiatives haverecently been launched to accelerate access to cleaner householdenergy, including UN3 Sustainable energy for all (UN, 2014) and theUN Foundation Global Alliance for Clean Cookstoves (UNF, 2014).Whatever approach is taken by these various initiatives, planningmust take into account the fact that the 2.8 billion people relying onsolid fuels are also theworld's poorest people, and furthermore thatexperience has shown that securing adoption and lasting use ofclean and efficient stoves and fuels can be very challenging, forreasons that involve a wide range of factors (Rehfuess et al., 2014).In respect of this strategic challenge, two questions arise:
1. Towhat levels does HAP exposure need to be reduced in order toensure that substantial health benefits are achieved.
2. What intervention technologies and fuels can achieve therequired levels of HAP in practice?
New WHO indoor air quality guidelines (AQG)4 for householdfuel combustion are being developed to help address these ques-tions and thereby guide countries in effectively reducing this publichealth burden (Bruce et al., 2013a). The new guidelines build onexistingWHOAQGs for ambient air pollution (WHO, 2006), and the2010 volume of indoor AQG for selected pollutants (WHO, 2010).
Key to the new guidelines is a set of evidence reviews whichinform both the recommendations and plans for supportingimplementation in countries. The aim of this paper is to address thetwo questions set out above, drawing on key findings from two ofthese reviews, and to consider the implications for interventionstrategy.
2. Material and methods
The development of WHO guidelines follows well-definedprocedures (WHO, 2012), the application of which to the currentguidelines have been described (Bruce et al., 2013a), emphasizing
et al., WHO indoor air qualitexposureerisk functions,
the central role of thorough evaluation of evidence in formulatingrecommendations. The new guidelines include a wide range ofevidence relevant to the scientific and policy issues involved andcover: households fuel use, pollutant emissions, levels of HAP andexposure, health and safety (i.e. burns, poisoning) risks, interven-tion impacts, and factors relating to adoption, intervention costsand financing (Table 1). Two of the reviews (#5 and #7 in Table 1)are especially relevant to the questions set out in Section 1, andaddressed (i) health risks of exposure to HAP, and (ii) impacts ofinterventions on HAP and exposure. Themethods used for these arenow described.
2.1. Health risks of exposure to HAP
This review sought to answer two questions:
1. What child and adult disease outcomes are linked to solid fuelHAP exposure, and what are the estimated risks and strength ofcausal evidence?
2. What information is available on the relationships betweenexposure level and risk of important disease outcomes, andwhat are the shapes of these relationships?
For Question 1, the review draws on recently conducted sys-tematic reviews and meta-analyses, many of which were carriedout for the GBD-2010 study comparative risk assessment for HAP(Lim et al., 2012), the methods for which have been describedelsewhere (Smith et al., 2014). The strength of evidence for causa-tionwas assessed by reference to the Bradford Hill viewpoints (Hill,1965), and strength of evidence for intervention effect estimatesusing a revised version of GRADE (Balshem et al., 2011), which wasmodified to increase relevance to environmental health in-terventions (Bruce et al., 2013a, 2013b; Rehfuess et al., 2011;Schunemann et al., 2010).
For Question 2, the review first identified the very few epide-miologic studies which have reported exposure and risk data, andthen drew on ‘integrated exposure response functions’ (IERs)5
which were recently developed for the GBD-2010 study (Burnettet al., 2014). Drawing on prior work by Pope et al. (2009, 2011)and commentary on the relevance to HAP (Smith and Peel, 2010),these functions model risk estimates for PM2.5
6 from studies of foursources of combustion-derived pollution: outdoor air, second-handsmoke, HAP and active smoking (Burnett et al., 2014).
2.2. Impacts of interventions on HAP and exposure
The second review addressed the question of whether improvedsolid fuel stove and cleaner fuel interventions in everyday use areeffective in reducing average concentrations of, or exposure to,particulate matter (PM) and carbon monoxide (CO)7 amonghouseholds in LMIC. As this systematic review is currently beingprepared separately for publication in full, an overview of the
5 IER: Integrated exposureeresponse function.6 PM2.5: Particulate matter of aerodynamic diameter 2.5 microns and less.7 CO: Carbon monoxide.
y guidelines on household fuel combustion: Strategy implications ofAtmospheric Environment (2014), http://dx.doi.org/10.1016/

Table 1Evidence reviews included in the new WHO indoor air quality Guidelines for household fuel combustion.
Review topic Main issues addressed
1 Fuel use Fuels and technologies used for cooking, heating, lighting and other uses, for low and middle-income countries (LMIC), and for high incomecountries (HIC).
2 Emissions A systematic review of levels of emissions of health-damaging pollutants from a representative range of fuel and technology options, and thechallenges of field testing to capture real-life performance, which is found to differ (sometimes markedly) from laboratory performance.
3 Model Description and validation of an emissions model, developed to relate emission rates for PM2.5 and CO to WHO air quality guidelines levelsfor these two pollutants.
4 Population HAP levels A systematic review of household levels of PM2.5 and CO (kitchen, living area, and the local environment), and of personal exposure to thesesame pollutants.
5 Health risks from HAP A summary and synthesis of systematic reviews of health risks from solid fuel use in households for a wide range of health outcomes;summary of available exposure-risk evidence, including newly developed integrated exposure response (IER) functions; (Burnett et al.,2014) summary of evidence (including recent systematic reviews) of health risks with household use of gas and kerosene; summary ofspecific risks from household coal use, including toxic contaminants; summary of systematic review on impacts of interventions to reducesmoke levels on risk of vector-borne disease (mainly malaria).
6 Safety A systematic review of the risks of burns, scalds and poisoning from household fuels, and a summary of evidence from intervention studies toprevent these outcomes.
7 Intervention impacts A systematic review of the impacts of interventions (improved solid fuels stoves and clean fuels) on kitchen PM2.5 and CO, and of personalexposure to these pollutants, when in everyday use.
8 Adoption A systematic review of quantitative, qualitative and policy studies to identify key enabling and limiting factors for sustained adoption at scaleof improved solid fuel stoves and clean fuels.
9 Costs and financing A narrative review of intervention costs, economic evaluation studies, and financing options including climate finance.
N. Bruce et al. / Atmospheric Environment xxx (2014) 1e7 3
methods and key findings are provided here, with reference toanother recently published review of HAP exposure issues (Clark etal., 2013). This review includes several of the intervention studies ofsolid fuel stoves covered by the new systematic review, and theconclusions of the two reviews are consistent.
For the new systematic review, the focus was on intervention-based studies which reported average kitchen and/or personal(24 and/or 48-h) PM2.5 and/or carbon monoxide (CO) duringeveryday use in homes. Interventions covered were solid fuel(vented, unvented) ‘improved’ stoves, and clean fuels (all typeseligible). Data extracted included baseline and post-interventionlevels of PM2.5 and CO, and the percentage reduction in eachpollutant. For each type of intervention, random or fixed effectsmeta-analysis (depending on level of statistical heterogeneity) wasconducted to obtain a pooled estimate of the absolute reduction,and weighted averages for pre- and post-intervention values werecalculated. Investigation of publication bias was carried out, andsensitivity analysis conducted to determine whether the studydesign and approach to analysis influenced the findings.
3. Findings
3.1. Review 1 e Question 1
The findings of the systematic reviews on health risks aresummarized in Table 2. For those with strong evidence of causalassociations as assessed by reference to the Bradford Hill view-points, the odds ratios imply intervention effects of between 20%and 50% reduction in risk. This is based on a comparison of theexposed and unexposed (or exposed less) groups in the epidemi-ologic studies. Very few of such studies directly measured HAP orexposure, but relied on binary proxies emost commonly fuel type.In the circumstances of these studies, exposed groups can be ex-pected to experience high levels PM2.5 in the region of 200e300 mg/m3, but unexposed groups (e.g. those using clean fuels) are alsoexposed well above the WHO AQG annual average value for PM2.5of 10 mg/m3 (or even the IT-1 value of 35 mg/m3) Clark et al. (2013).As a consequence, while these risk estimates may be subject tosome bias away from the null due to their mainly observationaldesigns and hence likelihood of residual confounding, exposuremisclassification is also highly likely and would tend to bias effectestimates towards the null. The true exposure contrast for many of
Please cite this article in press as: Bruce, N., et al., WHO indoor air qualitnew evidence on interventions and exposureerisk functions,j.atmosenv.2014.08.064
these studies is estimated to be 200e300 mg/m3 of PM2.5 for‘exposed’ subjects vs. 35e80 mg/m3 of PM2.5 for ‘unexposed’ sub-jects (Smith et al., 2014) and reduction of exposure to levels at orbelow the WHO AQG of 10 mg/m3 PM2.5 may well lead to largereffects.
3.2. Review 1 e Question 2
Only two studies have reported exposureeresponse relation-ships for HAP exposure, one conducted in Kenya by Ezzati andKammen (2001) and the RESPIRE trial conducted in Guatemala(Smith et al., 2011). Due to differences in exposure and outcomeassessment methods, no attempt has been made to combine thefindings. Both are consistent in the sense of reporting statisticallysignificant exposureeresponse relationships, and that the shapes ofthese are non-linear, being steeper at lower exposures, and tendingto flatten-off at higher exposures.
Evidence from the new IER functions confirms these findings forchild ALRI (Burnett et al., 2014). This is in part to be expected as theHAP component of the model is derived solely from the RESPIREstudy results; the risk estimates from outdoor air pollution andsecond-hand smoking, however, are at considerably lower levels ofexposure and appear to fit the shape implied by the RESPIREfindings. The IER function for ALRI shows a steep slope at lowerlevels with relative risk (RR) reaching around 1.3 at 35 mg/m3 PM2.5,above which the slope continues to rise albeit becoming muchshallower: at around 200 mg/m3 PM2.5, the predicted RR is around2.6. The curve does not flatten off completely, but has a shallowgradient with the RR reaching around 3.1 at 600 mg/m3.
For the adult outcomes, for which the IER model additionallyincludes risk estimates for active smoking (AS), the shapes aresimilar (to ALRI) for IHD and stroke,with the steepest sections of thecurves at relatively low levels of exposure. The IER curve for IHDreaches a RR of 1.5 for high HAP exposure and a maximum of 2.5 forhigh AS exposure. The curve for stroke is also similar, but flattens offat levelswellwithin theHAP range at amaximumRRof just over 2.0.
By contrast, the IER model for lung cancer is much closer to alinear relationship: RRs in the range 1.5e2.5 are seen across theHAP range, but reach more than 40 at the highest levels of AS.Finally, the IER curve for COPD is somewhat intermediate in shape,but the HAP systematic review findings do not fit the model resultswell, being somewhat higher than predicted by the model. The
y guidelines on household fuel combustion: Strategy implications ofAtmospheric Environment (2014), http://dx.doi.org/10.1016/
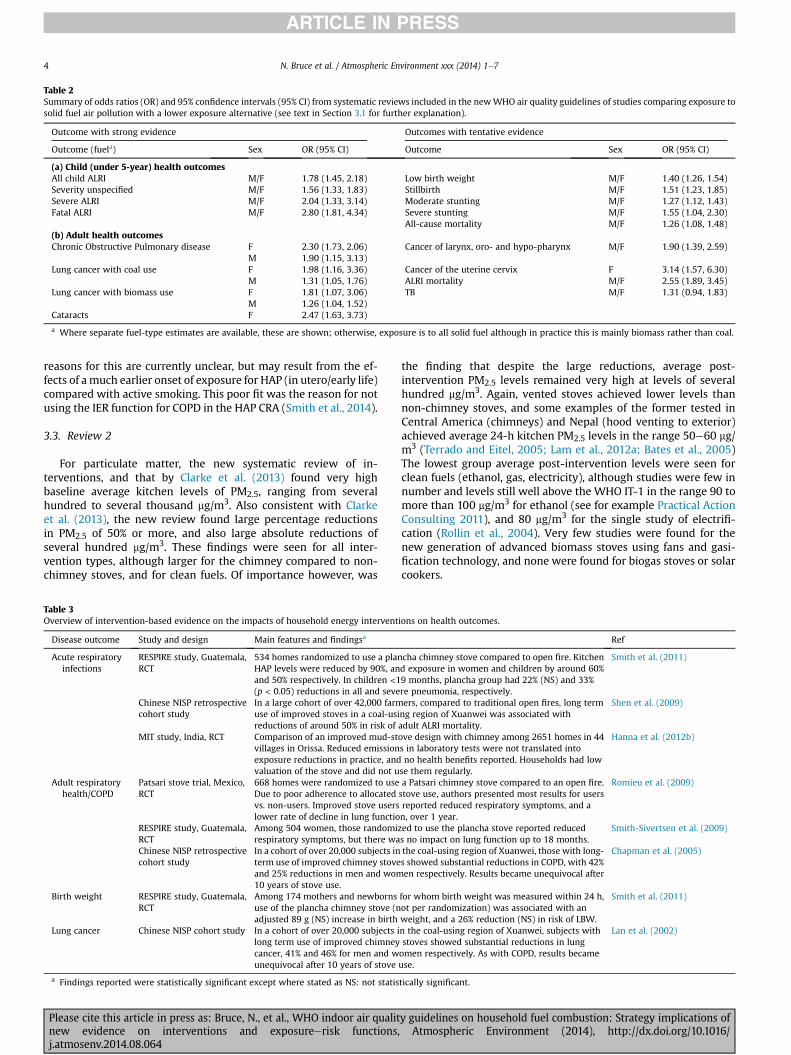
Table 2Summary of odds ratios (OR) and 95% confidence intervals (95% CI) from systematic reviews included in the newWHO air quality guidelines of studies comparing exposure tosolid fuel air pollution with a lower exposure alternative (see text in Section 3.1 for further explanation).
Outcome with strong evidence Outcomes with tentative evidence
Outcome (fuela) Sex OR (95% CI) Outcome Sex OR (95% CI)
(a) Child (under 5-year) health outcomesAll child ALRI M/F 1.78 (1.45, 2.18) Low birth weight M/F 1.40 (1.26, 1.54)Severity unspecified M/F 1.56 (1.33, 1.83) Stillbirth M/F 1.51 (1.23, 1.85)Severe ALRI M/F 2.04 (1.33, 3.14) Moderate stunting M/F 1.27 (1.12, 1.43)Fatal ALRI M/F 2.80 (1.81, 4.34) Severe stunting M/F 1.55 (1.04, 2.30)
All-cause mortality M/F 1.26 (1.08, 1.48)(b) Adult health outcomesChronic Obstructive Pulmonary disease F 2.30 (1.73, 2.06) Cancer of larynx, oro- and hypo-pharynx M/F 1.90 (1.39, 2.59)
M 1.90 (1.15, 3.13)Lung cancer with coal use F 1.98 (1.16, 3.36) Cancer of the uterine cervix F 3.14 (1.57, 6.30)
M 1.31 (1.05, 1.76) ALRI mortality M/F 2.55 (1.89, 3.45)Lung cancer with biomass use F 1.81 (1.07, 3.06) TB M/F 1.31 (0.94, 1.83)
M 1.26 (1.04, 1.52)Cataracts F 2.47 (1.63, 3.73)
a Where separate fuel-type estimates are available, these are shown; otherwise, exposure is to all solid fuel although in practice this is mainly biomass rather than coal.
N. Bruce et al. / Atmospheric Environment xxx (2014) 1e74
reasons for this are currently unclear, but may result from the ef-fects of a much earlier onset of exposure for HAP (in utero/early life)compared with active smoking. This poor fit was the reason for notusing the IER function for COPD in the HAP CRA (Smith et al., 2014).
3.3. Review 2
For particulate matter, the new systematic review of in-terventions, and that by Clarke et al. (2013) found very highbaseline average kitchen levels of PM2.5, ranging from severalhundred to several thousand mg/m3. Also consistent with Clarkeet al. (2013), the new review found large percentage reductionsin PM2.5 of 50% or more, and also large absolute reductions ofseveral hundred mg/m3. These findings were seen for all inter-vention types, although larger for the chimney compared to non-chimney stoves, and for clean fuels. Of importance however, was
Table 3Overview of intervention-based evidence on the impacts of household energy intervent
Disease outcome Study and design Main features and findingsa
Acute respiratoryinfections
RESPIRE study, Guatemala,RCT
534 homes randomized to use a planHAP levels were reduced by 90%, anand 50% respectively. In children <1(p < 0.05) reductions in all and seve
Chinese NISP retrospectivecohort study
In a large cohort of over 42,000 farmuse of improved stoves in a coal-usireductions of around 50% in risk of
MIT study, India, RCT Comparison of an improved mud-stvillages in Orissa. Reduced emissionexposure reductions in practice, andvaluation of the stove and did not u
Adult respiratoryhealth/COPD
Patsari stove trial, Mexico,RCT
668 homes were randomized to useDue to poor adherence to allocatedvs. non-users. Improved stove userslower rate of decline in lung functio
RESPIRE study, Guatemala,RCT
Among 504 women, those randomizrespiratory symptoms, but there wa
Chinese NISP retrospectivecohort study
In a cohort of over 20,000 subjects interm use of improved chimney stoveand 25% reductions in men and wom10 years of stove use.
Birth weight RESPIRE study, Guatemala,RCT
Among 174 mothers and newbornsuse of the plancha chimney stove (nadjusted 89 g (NS) increase in birth
Lung cancer Chinese NISP cohort study In a cohort of over 20,000 subjects ilong term use of improved chimneycancer, 41% and 46% for men and wunequivocal after 10 years of stove
a Findings reported were statistically significant except where stated as NS: not statis
Please cite this article in press as: Bruce, N., et al., WHO indoor air qualitnew evidence on interventions and exposureerisk functions,j.atmosenv.2014.08.064
the finding that despite the large reductions, average post-intervention PM2.5 levels remained very high at levels of severalhundred mg/m3. Again, vented stoves achieved lower levels thannon-chimney stoves, and some examples of the former tested inCentral America (chimneys) and Nepal (hood venting to exterior)achieved average 24-h kitchen PM2.5 levels in the range 50e60 mg/m3 (Terrado and Eitel, 2005; Lam et al., 2012a; Bates et al., 2005)The lowest group average post-intervention levels were seen forclean fuels (ethanol, gas, electricity), although studies were few innumber and levels still well above the WHO IT-1 in the range 90 tomore than 100 mg/m3 for ethanol (see for example Practical ActionConsulting 2011), and 80 mg/m3 for the single study of electrifi-cation (Rollin et al., 2004). Very few studies were found for thenew generation of advanced biomass stoves using fans and gasi-fication technology, and none were found for biogas stoves or solarcookers.
ions on health outcomes.
Ref
cha chimney stove compared to open fire. Kitchend exposure in women and children by around 60%9 months, plancha group had 22% (NS) and 33%re pneumonia, respectively.
Smith et al. (2011)
ers, compared to traditional open fires, long termng region of Xuanwei was associated withadult ALRI mortality.
Shen et al. (2009)
ove design with chimney among 2651 homes in 44s in laboratory tests were not translated intono health benefits reported. Households had low
se them regularly.
Hanna et al. (2012b)
a Patsari chimney stove compared to an open fire.stove use, authors presented most results for usersreported reduced respiratory symptoms, and an, over 1 year.
Romieu et al. (2009)
ed to use the plancha stove reported reduceds no impact on lung function up to 18 months.
Smith-Sivertsen et al. (2009)
the coal-using region of Xuanwei, those with long-s showed substantial reductions in COPD, with 42%en respectively. Results became unequivocal after
Chapman et al. (2005)
for whom birth weight was measured within 24 h,ot per randomization) was associated with anweight, and a 26% reduction (NS) in risk of LBW.
Smith et al. (2011)
n the coal-using region of Xuanwei, subjects withstoves showed substantial reductions in lungomen respectively. As with COPD, results becameuse.
Lan et al. (2002)
tically significant.
y guidelines on household fuel combustion: Strategy implications ofAtmospheric Environment (2014), http://dx.doi.org/10.1016/

N. Bruce et al. / Atmospheric Environment xxx (2014) 1e7 5
For carbon monoxide (CO) e not reviewed by Clarke et al. e theoverall pattern of intervention effects was found to be very similar,with the important difference being that post-intervention levelswere on average (for all stove/fuel type groups) at or below theWHO 24-h guideline level of 7 mg/m3. Thus, while baseline levelswere well above the guideline, it was encouraging to find that all ofthe technology and fuel groups studied could (on average) meet theguideline, with the exception of the unvented solid fuel stove groupwhich remained slightly above.
4. Discussion
The two reviews summarised here report evidence on healthrisks from HAP exposure, and on the everyday in-home perfor-mance of a variety of solid and clean fuel interventions. Beforeconsidering the implications of these findings for interventionstrategy, we will look at the quality of this evidence and assess theconfidence with which it can be used for this purpose.
4.1. Health risks
For the health risks review, the available studies are over-whelmingly observational designs; only three randomised trials(five reports) have been reported to date (Romieu et al., 2009;Smith et al., 2011; Hanna et al., 2012a; Smith-Sivertsen et al., 2009;Thompson et al., 2005), and other intervention-based designs withinformation on health outcomes are also few (Chapman et al.,2005; Lan et al., 2002; Shen et al., 2009), see Table 3. Some of theissues in attempting to define intervention impact estimates fromthe mainly observational evidence base have been discussed byBruce et al (2013a,b) for child survival outcomes, including expo-sure misclassification due to weak assessment methods, relativelyhigh exposure in control groups, and residual confounding (Bruceet al., 2013b). This was an important issue for the new WHOGuidelines, which adopted an approach that modified standardGRADE methodology for assessing strength of evidence by usingadditional criteria (Bruce et al., 2013a; Rehfuess et al., 2011), andassessing the consistency of different types of evidence using acausal chain framework.
The lack of exposure measurement in most studies led to reli-ance on the new IER functions for information on the shape ofexposureeresponse curves. The key assumptions are (i) equitox-icity of PM2.5 from different sources, (ii) that PM2.5 adequatelyrepresents risk from combustion mixtures, and (iii) that the healthoutcomes are sufficiently similar across exposure sources and set-tings. These points are discussed by Burnett et al. (2014). There wasreassuring consistency between the systematic review effect esti-mate for ALRI and the RR as predicted by the IER. Thus, the childALRI IER function predicts an increase in RR from approximately 1.6to 2.9 as exposure increases from 65 to 300 mg/m3 PM2.5; this isequivalent to a RR ratio of 1.8, and indicates a good level of con-sistency between the IER and the available epidemiologic evidenceon solid fuel use and ALRI risk for which the pooled estimate frommeta-analysis was 1.78 (Dherani et al., 2008).
In summary, although requiring further confirmation, the evi-dence compiled in the IERmodels do appear to provide an adequatestarting point for our understanding of relationships betweencombustion-related air pollution and disease risk.
4.2. Intervention impacts
For the interventions impacts reviews, it was found that anincreasing number of recent studies (over the past 5 years) hadused comparable pollution assessment methods, which contrib-uted to the overall quality of the available information, although
Please cite this article in press as: Bruce, N., et al., WHO indoor air qualitnew evidence on interventions and exposureerisk functions,j.atmosenv.2014.08.064
more rigorous study designs with a control group were rarelyemployed. On the other hand, very few studies were available forsome intervention categories, notably advanced solid fuels stoves,and all of the clean fuels. There were also relatively few studies forpersonal exposure, especially for PM2.5 reflecting the historic lack ofconvenient, lightweight technology for measuring personal PMexposure (Clark et al., 2013). Many of the studies also had shortfollow-up periods, some only a few weeks, so may not reflect truelonger term performance. Nevertheless, the post-intervention av-erages for PM2.5 make clear that the great majority of solid fuelstove interventions are not delivering results that are even close tothe levels needed, representing relatively reliable evidence. Resultsfor advanced solid fuel stoves and clean fuels can be expected to beless reliable due to the paucity of studies. Similar evidence qualityconsiderations apply to the findings for CO, and the more encour-aging conclusion that most interventions are meeting theWHO 24-h AQG level.
The reasons for these high post-intervention levels probably liewith a combination of factors, which have not been systematicallydocumented (or their impacts on emissions and pollutionmeasured). One important reason that has been reported inadoption studies is continued use of the traditional stove, so calledfuel or stove ‘stacking’ (Rehfuess et al., 2014). Other contributingsources of pollution within the home include kerosene lamps,which have been shown to emit high levels of particulate matter,for example Lam et al. (2012b). Outside the home under study,emissions from the solid fuel stoves in neighbouring houses, alongwith other sources of outdoor air pollution, can also be expected tocontribute in all but the most sparsely populated areas. Forexample, average ambient levels of PM2.5 in Indian villages havebeen found to be at or above 100 mg/m3 (Balakrishnan et al., 2013),in these circumstances, and even in the absence of any householdcombustion source, it would not be possible to achieve a level lowerthan this within the home.
4.3. Implications for intervention strategy
While the evidence for both health risks and intervention im-pacts has limitations, there is sufficient consistency in the formerand numbers of comparable studies for improved solid fuel stoves(at least) in the latter, to justify considering implications for inter-vention strategy. We begin this discussion by summarising themain findings from these two reviews:
� HAP is linked to multiple major disease outcomes, and effectestimates for putative interventions are likely to lie in range of20e50% risk reduction. These impacts are associated withachieving levels of HAP whiche although not directly measuredin most studies e are estimated to still exceed the annualaverage WHO IT-1 value for PM2.5 of 35 mg/m3.
� The IER models finds that levels at or below IT-1 for PM2.5 areneeded for substantial benefit for child ALRI, and probably alsofor IHD and stroke. For lung cancer, the relationship may bemore proportionate. That or COPD intermediate, but this is lesscertain due to a poorer fit between observed risks for HAP andmodel predictions at the relevant exposure levels.
� Field evaluation studies show that most solid fuel cookstoves, inpractice, achieve average kitchen concentrations of PM2.5 up toten (or more) times higher than IT-1. A few studies of chimneysstoves have reported levels just above IT-1, although the appli-cability of these findings to results that may be achieved at scaleis uncertain.
� There have been relatively few field evaluation studies of homesusing clean fuels. These have found average kitchen PM2.5 levelswell above IT-1 in these settings, implying that e since clean
y guidelines on household fuel combustion: Strategy implications ofAtmospheric Environment (2014), http://dx.doi.org/10.1016/

N. Bruce et al. / Atmospheric Environment xxx (2014) 1e76
fuels have very low emissions e other sources of PM2.5 in the airin and around homes are responsible, and need to be addressedin order to reach the desired levels.
In respect of clean fuels, since pollutant emission rates areknown to be low and adverse health risks also (at least whereadequately ventilated) (Lin et al., 2013; Vrijheid, 2013) e ourattention can be directedmore towards the challenges of increasingaccess across communities and ensuring more exclusive use.
One related issue in applying these findings to interventionstrategy is whether the key target is indoor area concentrations ofpollution (particularly PM2.5), or levels of personal exposure. Thus,while the IERs describe risk according to level of personal exposureto PM2.5, the air quality guidelines are area average concentrations.Personal exposure levels, wheremeasured, are almost always lowerthan kitchen concentrations, consistent with people not spending100% of their time in the presence of the lit stove. A review ofkitchen area to personal exposure ratios, carried out for the GDB-2010 study, found values of 0.742 for women, 0.628 for childrenunder 5 years of age, and 0.450 for men, or approximately half tothree-quarters of kitchen area concentrations (Smith et al., 2014).There is some evidence that as household energy sources becomecleaner, people spend more time in the vicinity or indoors, orperhaps spend less time avoiding uncomfortable pollution sources,culminating in the situation seen in developed countries where thegreat majority of time is spent indoors (WHO, 2010). Some popu-lation groups, including young children, the elderly and sick, mayalso spend more time indoors and close to the hearth or stove.Taken together, these considerations imply that, while exposure isimportant for epidemiological studies, the target for interventionemissions performance should be informed by area concentrations.
5. Conclusions
In light of the current evidence on health risks and in-fieldperformance of solid fuel stoves, there needs to be a muchgreater emphasis on rapidly increasing access to clean fuels,starting with those e for example living in urban/peri-urban areasand already paying for solid fuels e who can most easily make thistransition. In addition, it will be important to recognise that‘stacking’ is the norm, so efforts should be directed at encouraginghouseholds to move as quickly as is feasible towards more or lessexclusive use of clean fuels and technologies. Also important is theneed to secure adoption across communities, so that individualhomes are not affected by the pollution from neighbourscontinuing to use solid fuels.
Given the findings of these reviews, the role of improved solidfuel technologies in the mix is an important question for strategy.Decisions on what is most appropriate will undoubtedly varyacross communities and between countries, but it is clear thatthere are large numbers of lower income, mainly rural homes thatrely on mostly free (collected) biomass fuel, for whom the tran-sition to clean, commercially-based fuels can be expected to take5e10 years at least even in the presence of facilitative policy onmarket development, supply and financial support. During thistransition period, it is important that these households obtainmaximal health gains and other benefits including fuel and timesaving, improved safety, etc., through adoption of the mosteffective technologies that can meet their needs. The developmentof international standards for cookstoves and clean cooking solu-tions is an important step for implementing this strategy (ISO,2012; ISO, 2014).
Given that clean indoor air cannot be achieved in the presence ofelevated outdoor levels, whatever the source, there also needs to begreater coordination between agencies responsible for household
Please cite this article in press as: Bruce, N., et al., WHO indoor air qualitnew evidence on interventions and exposureerisk functions,j.atmosenv.2014.08.064
energy and pollution, and those dealingwith outdoor air. This inter-relationship between indoor and outdoor issue is not confined tocities, and recognition of this (including monitoring of ambient airin rural as well as urban areas as a basis for regulation) could makean important contribution.
Acknowledgements
We wish to acknowledge the contributions of members of theGuidelines development group for contributions to the reviews;funding for the guidelines project was received from DeutscheGesellschaft für Internationale Zusammenarbeit (GIZ), HealthCanada, the UN Foundation, and the UK Department of Interna-tional Development.
References
Balakrishnan, K., Ghosh, S., Ganguli, B., Sambandam, S., Bruce, N.G., Barnes, D.F.,et al., 2013. State and national household concentrations of PM2.5 from solidcookfuel use: results from measurements and modeling in India for estimationof the global burden of disease. Environ. Health 12, 77.
Balshem, H., Helfand, M., Schunemann, H.J., Oxmand, A.D., Kunz, R., Brozek, J., et al.,2011. GRADE guidelines: 3. Rating the quality of evidence. J. Clin. Epidemiol. 64(4), 401e406.
Bates, E., Pope, D., Bruce, N., 2005. Smoke, Health and Household Energy. Partici-patory Methods for Design, Installation, Monitoring and Assessment of SmokeAlleviation Technologies, vol. 1. Intermediate Technology Development Group,Rugby UK.
Bruce, N., Dora, C., Krzyzanowski, M., Adair-Rohani, H., Wangchuk, T., Morawska, L.,2013a. Tackling the health burden from household air pollution (HAP): devel-opment and implementation of new WHO Guidelines. Air Qual. Clim. Change47 (1), 32e38.
Bruce, N., Dherani, M., Das, J., Balakrishnan, K., Adair-Rohani, H., Bhutta, Z.A., et al.,2013b. Control of household air pollution for child survival: estimates forintervention impacts. BMC Public Health 13 (Suppl. 3).
Burnett, R.T., Pope, A.I., Ezzati, M., Olives, C., Lim, S.S., Mehta, S., et al., 2014. Anintegrated risk function for estimating the global burden of disease attributableto ambient fine particulate matter exposure. Environ. Health Perspect. 122 (4),397e403.
Chapman, R.S., He, X., Blair, A.E., Lan, Q., 2005. Improvement in household stovesand risk of chronic obstructive pulmonary disease in Xuanwei, China: retro-spective cohort study. Br. Med. J. 331, 1050e1055.
Clark, M.L., Peel, J.L., Balakrishnan, K., Breysse, P.N., Chillrud, S.N., Naeher, L.P., et al.,2013. Health and household air pollution from solid fuel use: the need forimproved exposure assessment. Environ. Health Perspect. 121, 1120e1128.
Dherani, M., Pope, D., Mascarenhas, M., Smith, K.R., Weber, M., Bruce, N.G., 2008.Indoor air pollution from unprocessed solid fuel use and pneumonia risk inunder-5 children: systematic review and meta-analysis. Bull. World HealthOrgan. 86 (5), 390e398.
Ezzati, M., Kammen, D.M., 2001. Quantifying the effects of exposure to indoor airpollution from biomass combustion on acute respiratory infections in devel-oping countries. Environ. Health Perspect. 109, 481e488.
Hanna, R., Duflo, E., Greenstone, M., 2012. Up in Smoke: the Influence of HouseholdBehavior on the Long-run Impact of Improved Cooking Stoves. Working Paper12-10. In: Social Science Research Network Paper Collection. MassachusettsInstitute of Technology Department of Economics Working Paper Series.
Hanna, R., Duflo, E., Greenstone, M., 2012. Up in Smoke: the Influence of HouseholdBehavior on the Long-run Impact of Improved Cooking Stoves. MassachusettsInstitute of Technology, Department of Economics. Contract No.: Working Paper12-10.
Hill, A.B., 1965. The environment and disease: association or causation? Proc. R. Soc.Med. 58, 295e300.
ISO, 2012. International Workshop Agreement 11:2012 Guidelines for EvaluatingCookstove Performance. International Organisation on Standardisation, Geneva.
ISO, 2014. ISO/TC 285 Clean Cookstoves and Clean Cooking Solutions. InternationalOrganization for Standardization 2014 [cited 2014 28 March], Geneva. Availablefrom: http://www.iso.org/iso/home/standards_development/list_of_iso_technical_committees/iso_technical_committee.htm?commid¼4857971.
Lam, N., Africano, S., Humphrey, S., Pennise, D., 2012a. Indoor air quality impact ofan improved chimney wood stove in peri-urban Honduras. personalcommunication.
Lam, N.L., Smith, K.R., Gauthier, A., Bates, M.N., 2012. Kerosene: a review ofhousehold uses and their hazards in low- and middle-income countries.J. Toxicol. Environ. Health Part B Crit. Rev. 15 (6), 396e432.
Lan, Q., Chapman, R.S., Schreinemachers, D.M., Tian, L., He, X., 2002. Householdstove improvement and risk of lung cancer in Xuanwei, China. J. Natl. CancerInst. 94, 826e835.
Lim, S.S., Vos, T., Flaxman, A.D., Danaei, G., Shibuya, K., Adair-Rohani, H., et al., 2012.A comparative risk assessment of burden of disease and injury attributable to67 risk factors and risk factor clusters in 21 regions, 1990e2010: a systematic
y guidelines on household fuel combustion: Strategy implications ofAtmospheric Environment (2014), http://dx.doi.org/10.1016/

N. Bruce et al. / Atmospheric Environment xxx (2014) 1e7 7
analysis for the Global Burden of Disease Study 2010. Lancet 380 (9859),2224e2260.
Lin, W., Brunekreef, B., Gehring, U., 2013. Meta-analysis of the effect of indoor ni-trogen dioxide and gas cooking on asthma and wheeze in children. Int. J. Epi-demiol. 42 (6), 1724e1737.
PAC. Practical Action Consulting, 2011. Ethanol as a Household Fuel in Madagascar:Health Benefits, Economic Assessment and Review of African Lessons forScaling up. In: Component A e Analysis of Household Air Pollution In-terventions in Madagascar.
Pope, C.A., Burnett, R.T., Krewski, D., Jerrett, M., Shi, Y., Calle, E.E., et al., 2009.Cardiovascular mortality and exposure to airborne fine particulate matter andcigarette smoke shape of the exposure-response relationship. Circulation 120,941e948.
Pope, C.A., Burnett, R.T., Turner, M.C., Cohen, A., Krewski, D., Jerrett, M., et al., 2011.Lung cancer and cardiovascular disease mortality associated with ambient airpollution and cigarette smoke: shape of the exposure-response relationships.Environ. Health Perspect. 119 (1), 1616e1621.
Rehfuess, E., Bruce, N., Pruss-Ustin, A., 2011. GRADE for the advancement of publichealth. J. Epidemiol. Community Health 65 (6), 559.
Rehfuess, E.A., Puzzolo, E., Stanistreet, D., Pope, D., Bruce, N.G., 2014. Enablers andbarriers to large-scale uptake of improved solid fuel stoves: a systematic review.Environ. Health Perspect. 122 (2), 120e130.
Rollin, H., Mathee, A., Bruce, N., Levin, J., von Schirnding, Y.E., 2004. Comparison ofindoor air quality in electrified and un-electrified dwellings in rural South Af-rican villages. Indoor Air 14, 208e216.
Romieu, I., Riojas-Rodríguez, H., Marr�on-Mares, A.T., Schilmann, A., Perez-Padilla, R.,Masera, O., 2009. Improved biomass stove intervention in rural Mexico: impacton the respiratory health of women. Am. J. Respir. Crit. Care Med. 180 (7),649e656.
Schunemann, H., Hill, S., Guyatt, G., Akl, E.A., Ahmed, F., 2010. The GRADE approachand Bradford Hill's criteria for causation. J. Epidemiol. Community Health 65(5), 392e395.
Shen, M., Chapman, R.S., Vermeulen, R., Tian, L., Zheng, T., Chen, B.E., et al., 2009.Coal use, stove improvement, and adult pneumonia mortality in Xuanwei,China: a retrospective cohort study. Environ. Health Perspect. 117 (2), 261e266.
Smith, K.R., Peel, J.L., 2010. Mind the Gap. Environ. Health Perspect. 118 (12),1643e1645. Epub 2010, Aug 20.
Please cite this article in press as: Bruce, N., et al., WHO indoor air qualitnew evidence on interventions and exposureerisk functions,j.atmosenv.2014.08.064
Smith, K.R., McCracken, J.P., Weber, M.W., Hubbard, A., Jenny, A., Thompson, L.M.,et al., 2011. Effect of reduction in household air pollution on childhood pneu-monia in Guatemala (RESPIRE): a randomised controlled trial. Lancet 378(9804), 1717e1726.
Smith, K.R., Bruce, N.G., Balakrishnan, K., Adair-Rohani, H., Balmes, J., Chafe, Z., et al.,2014. Millions dead: how do we know and what does it mean? Methods used inthe comparative risk assessment of household air pollution. Annu. Rev. PublicHealth 35, 185e206.
Smith-Sivertsen, T., Díaz, E., Pope, D., Lie, R.T., Díaz, A., McCracken, J.P., et al., 2009.Effect of reducing indoor air pollution on women's respiratory symptoms andlung function: the RESPIRE Randomized Trial. Guatem. Am. J. Epidemiol. 170 (2),211e220.
Terrado, E.N., Eitel, B., 2005. Pilot Commercialization of Improved Cookstoves inNicaragua. World Bank, Washington, DC. Available at. https://openknowledge.worldbank.org/handle/10986/18063 (accessed 16.07.14.).
Thompson, L., Bruce, N.G., Diaz, A., Arana, B., Klein, R., Jenny, A., et al., 2005. Lowbirth weight in rural Guatemala: indoor air pollution as a contributing factor.Epidemiology 16 (5), S100eS101.
UN, 2014. Sustainable Energy for All. United Nations. Available from: http://www.se4all.org/ (28.03.14.).
UNF, 2014. Global Alliance for Clean Cookstoves. Available from: http://cleancookstoves.org/ (cited 2014 March 28, 2014).
Vrijheid, M., 2013. Commentary: Gas cooking and child respiratory health e time toidentify the culprits? Int. J. Epidemiol. 42, 1737e1739.
WHO, 2006. WHO Air Quality Guidelines Global Update 2005: Particulate Matter,Ozone, Nitrogen Dioxide and Sulfur Dioxide. EUR/05/5046029. World HealthOrganization, Copenhagen. Available from: http://www.euro.who.int/__data/assets/pdf_file/0005/78638/E90038.pdf (accessed 17.07.14.).
WHO, 2010. WHO Guidelines for Indoor Air Quality: Selected Pollutants. WorldHealth Organization, Bonn. Available from: http://www.euro.who.int/__data/assets/pdf_file/0009/128169/e94535.pdf (accessed 17.07.14.).
WHO, 2012. WHO Handbook for Guideline Development. World Health Organisa-tion, Geneva.
WHO, 2014. Deaths from Household Air Pollution, 2012. World Health Organization,Geneva. Available from: http://apps.who.int/gho/data/node.main.140?lang¼en(accessed 17.07.14.).
y guidelines on household fuel combustion: Strategy implications ofAtmospheric Environment (2014), http://dx.doi.org/10.1016/