Who do smokers feel ought to be responsible for informing people about the dangers associated with...
19
Int Public Health J 2015;7(3):301-319 ISSN: 1947-4989 © Nova Science Publishers, Inc. Who do smokers feel ought to be responsible for informing people about the dangers associated with smoking and regulating smoking behaviors? Claire E Sterk, PhD 1 , Hugh Klein, PhD 1,2 , and Kirk W Elifson, PhD 1 1 Rollins School of Public Health, Emory University, Atlanta, Georgia, USA 2 Kensington Research Institute, Silver Spring, Maryland, USA Abstract Purpose: The focus of this paper is to examine the extent to which a community-based sample of current cigarette smokers believes it to be the responsibility of outside persons and agencies to inform the public about the dangers of smoking and/or to regulate smoking behaviors (herein termed REGULATE). Also investigated is how REGULATE relates to smokers’ attitudes toward cigarette smoking and actual smoking practices, and whether REGULATE matters when the influence of other key variables is taken into account. Method: Questionnaire- based interviews were conducted with a community-based sample of 485 adult current cigarette smokers recruited from the Atlanta, Georgia metropolitan area. Active and passive recruiting approaches were used, along with a targeted sampling strategy. Results: Participants were divided in their beliefs pertaining to REGULATE. Their beliefs were related consistently to smoking-related attitudes but much less to actual smoking behaviors. Four factors (greater religiosity, older age of first purchasing a cigarette, lower levels of depression, and sexual abuse history) were found to underlie REGULATE. Structural equation analysis revealed that REGULATE is an influential measure to consider when trying to understand overall attitudes toward smoking and actual smoking behaviors. Conclusion: REGULATE is an important variable to consider when aiming to understand the factors associated with how people feel about their smoking practices, including actual cigarette use. It may be construed as a proxy measure for locus of control; and the implications of this are discussed. Keywords: Cigarette smoking, tobacco regulation, locus of control Introduction Locus of control is defined as the extent to which people perceive themselves as having the ability or “agency” to determine what happens to them versus
Transcript of Who do smokers feel ought to be responsible for informing people about the dangers associated with...

Int Public Health J 2015;7(3):301-319 ISSN: 1947-4989 © Nova Science Publishers, Inc.
Who do smokers feel ought to be responsible for informing people about the dangers associated with smoking
and regulating smoking behaviors?
Claire E Sterk, PhD1, Hugh Klein, PhD1,2, and Kirk W Elifson, PhD1 1Rollins School of Public Health, Emory University, Atlanta, Georgia, USA 2Kensington Research Institute, Silver Spring, Maryland, USA
Abstract
Purpose: The focus of this paper is to examine the extent to which a community-based sample of current cigarette smokers believes it to be the responsibility of outside persons and agencies to inform the public about the dangers of smoking and/or to regulate smoking behaviors (herein termed REGULATE). Also investigated is how REGULATE relates to smokers’ attitudes toward cigarette smoking and actual smoking practices, and whether REGULATE matters when the influence of other key variables is taken into account. Method: Questionnaire-based interviews were conducted with a community-based sample of 485 adult current cigarette smokers recruited from the Atlanta, Georgia metropolitan area. Active and passive recruiting approaches were used, along with a targeted sampling strategy. Results: Participants were divided in their beliefs pertaining to REGULATE. Their beliefs were related consistently to smoking-related attitudes but much less to actual smoking behaviors. Four factors (greater religiosity, older age of first purchasing a cigarette, lower levels of depression, and sexual abuse history) were found to underlie REGULATE. Structural equation analysis revealed that REGULATE is an influential measure to consider when trying to understand overall attitudes toward smoking and actual smoking behaviors. Conclusion: REGULATE is an important variable to consider when aiming to understand the factors associated with how people feel about their smoking practices, including actual cigarette use. It may be construed as a proxy measure for locus of control; and the implications of this are discussed. Keywords: Cigarette smoking, tobacco regulation, locus of control
Introduction
Locus of control is defined as the extent to which people perceive themselves as having the ability or “agency” to determine what happens to them versus

Claire E Sterk, Hugh Klein, and Kirk W Elifson 302
believing that outside forces and/or other persons are, to a greater extent, responsible for their experiences and actions. When discussing locus of control, researchers typically conceptualize people falling onto a continuum that is bounded, on one side, by those who are internally oriented (believing in their own ability to determine their own fate and experiences) and, on the other side, those who are externally oriented (believing that what happens to them is the result of outside forces that are beyond their personal control). Locus of control has been linked to a variety of health practices, such as cigarette smoking and tobacco cessation (1–3), smoking during pregnancy (4), substance use and abuse (5), healthy eating practices (1), and risky sexual behaviors (5), among others. This had led researchers to coin the term “health locus of control” to apply the underlying principles of locus of control to the scientific study and understanding of people’s health practices (6–8). Typically, research has found that people who are more internally oriented when it comes to locus of control tend to engage in lower rates of risky behaviors and higher rates of behavioral practices that can be considered to be beneficial or health protective in nature (2, 6, 9).
Closely related to the notions of locus of control and health locus of control is the construct of “powerful others” (10). Powerful others are people or institutions that are perceived as being dominant, persuasive, influential, and/or controlling in terms of determining how events in one’s life unfold. For persons who score higher on the external rather than the internal end of the locus of control continuum, powerful others are construed as being the principal source and the main underlying force of their experiences and actions, to the point where the individuals themselves believe that they have limited, if any, responsibility or agency for their life events. Research has demonstrated that people whose locus of control orientation supports the belief in powerful others are more apt to have adverse substance use/abuse outcomes than their peers who are not oriented toward believing in the importance of powerful others (1, 11).
In the present paper, the focus is on one specific measure that, conceptually, may be construed as a proxy for internal/external locus of control–namely, the extent to which people believe that outside
persons, organizations, and agencies (such as public health agencies and tobacco companies) ought to be responsible for informing the public about the potential health hazards of smoking and for regulating the public’s access to and usage of cigarettes. In this article, we examine the following research questions: 1) To what extent do adult smokers believe that it should be the responsibility of these “powerful others” to inform the public about the dangers of smoking and to regulate tobacco use in the United States? 2) How, if at all, does adhering to the external orientation locus of control-related belief in other persons and agencies being responsible for informing the public and regulating tobacco use relate to actual smoking practices and to smokers’ attitudes toward smoking? 3) What factors underlie greater versus lesser adherence to the belief that outside persons and agencies should be responsible for providing the public with information about the dangers of smoking and with regulating cigarette use/policy? 4) When we try to understand the factors that affect people’s smoking behaviors, does the extent to which they believe that outside persons and agencies should be responsible for providing the public with information about the dangers of smoking and with regulating cigarette use/policy matter when the effects of other relevant variables are taken into account?
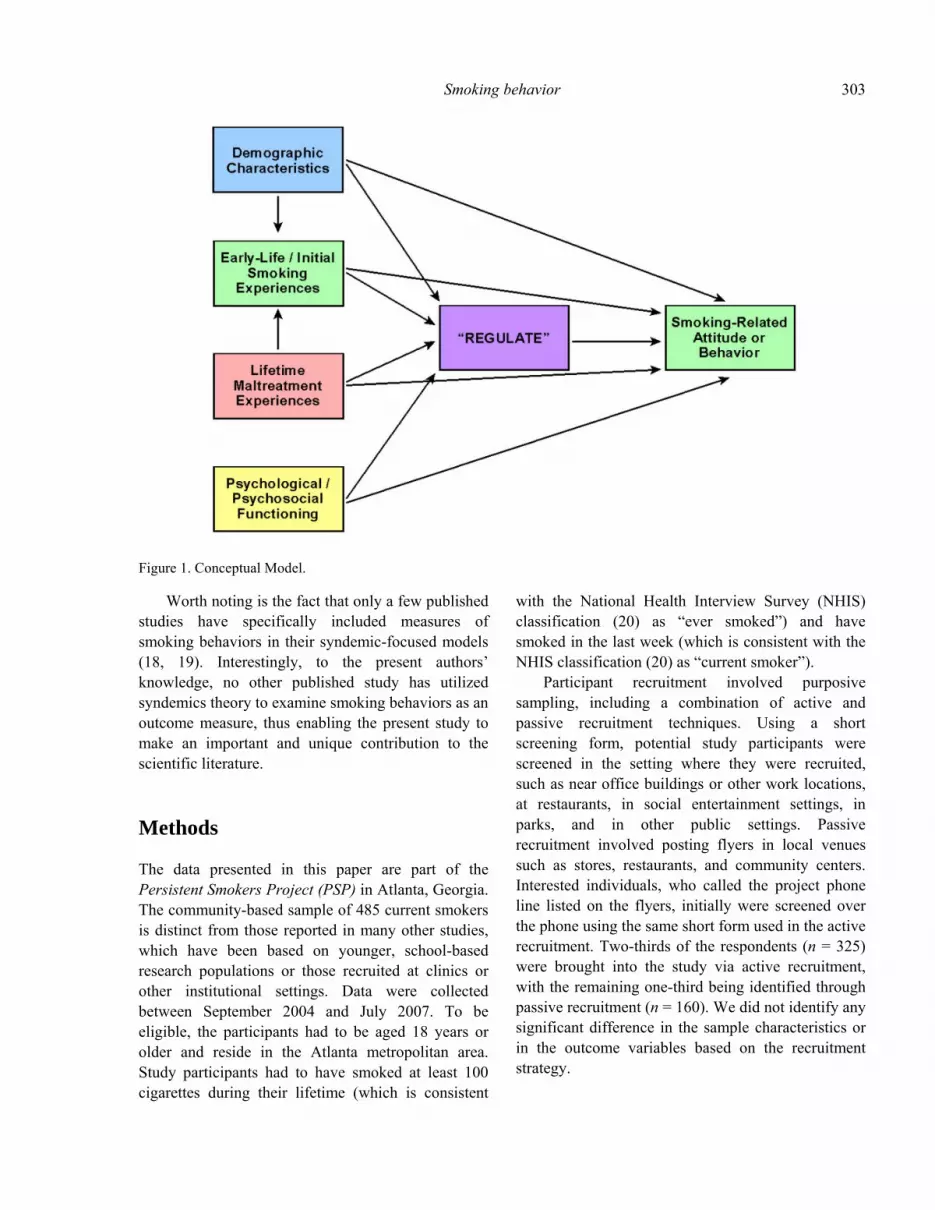
As part of addressing the latter three questions, we employ a conceptual model (see Figure 1) that owes its origins to syndemics theory (12). One of the principal tenets of syndemics theory is that certain types of influences may co-occur in such a manner so as to heighten the effects of one another and thereby make adverse health outcomes even more severe than they would have been had these measures not co-occurred. In the model used in the present research, four types of measures are hypothesized to interact syndemically with one another in the way that they influence one another, the main smoking-related outcome measure, and the REGULATE endogenous measure. These are 1) demographic characteristics, 2) lifetime maltreatment experiences, 3) early-life/initial smoking practices and 4) psychological/psychosocial functioning. In other published studies (13-17), syndemics theory has been used to study a wide array of populations and health behaviors, almost always including substance use/abuse measures as part of the analyses.
Smoking behavior 303
Figure 1. Conceptual Model.
Worth noting is the fact that only a few published studies have specifically included measures of smoking behaviors in their syndemic-focused models (18, 19). Interestingly, to the present authors’ knowledge, no other published study has utilized syndemics theory to examine smoking behaviors as an outcome measure, thus enabling the present study to make an important and unique contribution to the scientific literature.
Methods
The data presented in this paper are part of the Persistent Smokers Project (PSP) in Atlanta, Georgia. The community-based sample of 485 current smokers is distinct from those reported in many other studies, which have been based on younger, school-based research populations or those recruited at clinics or other institutional settings. Data were collected between September 2004 and July 2007. To be eligible, the participants had to be aged 18 years or older and reside in the Atlanta metropolitan area. Study participants had to have smoked at least 100 cigarettes during their lifetime (which is consistent
with the National Health Interview Survey (NHIS) classification (20) as “ever smoked”) and have smoked in the last week (which is consistent with the NHIS classification (20) as “current smoker”).
Participant recruitment involved purposive sampling, including a combination of active and passive recruitment techniques. Using a short screening form, potential study participants were screened in the setting where they were recruited, such as near office buildings or other work locations, at restaurants, in social entertainment settings, in parks, and in other public settings. Passive recruitment involved posting flyers in local venues such as stores, restaurants, and community centers. Interested individuals, who called the project phone line listed on the flyers, initially were screened over the phone using the same short form used in the active recruitment. Two-thirds of the respondents (n = 325) were brought into the study via active recruitment, with the remaining one-third being identified through passive recruitment (n = 160). We did not identify any significant difference in the sample characteristics or in the outcome variables based on the recruitment strategy.

Claire E Sterk, Hugh Klein, and Kirk W Elifson 304
Once a person was identified as eligible, the staff member described the study and time required to participate. The most common reason for ineligibility was having smoked an insufficient number of cigarettes to qualify, either during the person’s lifetime or during the preceding week. The interviews took place at a mutually-convenient location, such as one of the project offices, the respondent’s home, a local restaurant or coffee shop, or at community centers. Additional information was provided on the nature of the study, the time required, and the informed consent and other confidentiality procedures. The questionnaire contained items covering the respondent’s social background characteristics, smoking behaviors, attitudes, and opinions, as well as items about alcohol and other drugs, a health inventory, and self and identity items. The average length of the interview as 90 minutes and respondents received $20 as compensation for their time and participation. Prior to implementation in the field, all study protocols were reviewed and approved by the institutional review boards at Emory University and Georgia State University.
Measures used
The principal variable of interest in this paper is a 15-item scale (Cronbach’s alpha = 0.78) that was created specifically for use in this study, based on formative research conducted by the study’s investigators. Throughout the remainder of this paper, in an effort to keep verbiage to a minimum and to keep the writing simpler and easier to read/follow, this scale measure will be referred to as REGULATE. Taken as a group, the items comprising REGULATE assess the extent to which study participants believe that it ought to be the responsibility of outside persons and agencies to regulate smoking, to inform the public about the dangers associated with smoking, and to put into place various laws to regulate when and where smoking can occur legally. Table 1 shows the items comprising this scale measure. Individual items used in the construction of REGULATE were scored on a five-point Likert scale with responses ranging from “strongly disagree” to “strongly agree.” As appropriate, individual items have been recorded so that higher scores on the scale indicate a greater belief or perception that outside persons or agencies ought to be more responsible for informing the public and/or for regulating smoking behaviors.
Table 1. Perceptions of the Responsibilities of Outside Persons and Agencies to Inform the Public about the Potential
Dangers of Smoking and/or to Regulate Smoking Behaviors
REGULATE Measure % Agree % Disagree
Cigarette companies should be required to provide more information about how to stop smoking.
54.3 45.7
Cigarette companies should be required to provide more information about the health risks of smoking.
64.1 35.9
Cigarette companies should be required to provide more information about how to get screened for the diseases caused by smoking.
63.4 36.6
Cigarette companies should be required to provide more information about chemicals in cigarette smoke.
77.5 22.5
Public health agencies should be required to provide more information about how to stop smoking.
72.7 27.3
Public health agencies should be required to provide more information about the health risks of smoking.
73.8 26.2

Smoking behavior 305
REGULATE Measure % Agree % Disagree
Public health agencies should be required to provide more information about how to get screened for the diseases caused by smoking.
74.6 25.4
Public health agencies should be required to provide more information about chemicals in cigarette smoke.
76.7 23.3
Regulation of smoking in public spaces is a good thing. 69.2 19.8
Smoking should be permitted in bars. 11.6 79.6
Smoking on television or in movies should be prohibited. 25.0 64.1
Taxes on cigarettes should be increased. 14.7 76.9
Smoking should not be permitted in restaurants. 55.0 30.2
Smoking bans should be unconstitutional. 49.1 29.3
I have a right to smoke anywhere I want. 72.2 19.2
NOTE: In some instances, the percentages do not add up to 100% due to the exclusion of “neutral” or “don’t know: responses from this table.
To examine Research Question #2, 13 behavioral
and 11 attitudinal/psychosocial measures were used. Regarding the former, number of cigarettes smoked was assessed based on the number of cigarettes smoked per week (continuous measure). This was computed from the number of days respondents reported having smoked during the preceding month, the average number of cigarettes smoked on a typical weekday, and the average number of cigarettes smoked over the course of a typical weekend. Needing a cigarette to function was derived from the question “How often do you feel that you need a cigarette to help you function?” Response choices were: “never” (coded as 0), “less than once a month” (1), “about once a month” (2), “a few times a month” (3), “about once a week” (4), “several times a week” (5), “daily” (6), and “every 2-3 hours or more often” (7). Making a special trip to get cigarettes involved the question “How often do you make special trips to get cigarettes?” Chain smoking frequency was assessed by asking “How often do you chain-smoke, that is, smoke one cigarette right after another?” Smoking more than intended was derived from the question “How often do you smoke more cigarettes than you intend to smoke?” Response choices for these last three measures were “never” (coded as 0), “less than once a month” (1), “about once a month”
(2), “a few times a month” (3), “about once a week” (4), “several times a week” (5), and “daily” (6). Trying to get the most out of one’s smoking was an eight-item scale (all items coded yes/no) measuring the number of different things (e.g., smoking a cigarette to a shorter length, inhaling more deeply, removed a cigarette’s filter, holding cigarette smoke inside one’s lungs longer prior to exhaling) that smokers did in an effort to maximize the effects of their cigarette use (Kuder-Richardson20 = 0.68). The number of times trying to quit smoking and the number of times trying to cut down on smoking without actively trying to quit were both continuous measures. Twenty-one yes/no items were used to develop a scale to assess the number of different ways that the person tried to quit smoking (e.g., used medication to help stop smoking, stopped buying cigarettes from the store, used gum or candy to help stop smoking, used a nicotine lozenge). This scale assessed the variety of strategies that people employed to try to quit smoking (Kuder-Richardson20 = 0.78). Among persons who had previously tried to quit smoking, the final scale assessed the number of negative effects the person experienced the last time he/she tried to quit smoking. Sixteen yes/no items (e.g., became irritable, felt impatient, inability to think clearly, felt frustrated) comprised this scale (Kuder-

Claire E Sterk, Hugh Klein, and Kirk W Elifson 306
Richardson20 = 0.90). Smoking more cigarettes on weekends was assessed with a single yes/no item, as were lying to friends and relatives about one’s smoking practices and whether or not people had ever tried to quit smoking at any point in the past.
The perceived benefits of smoking (the first of the attitudinal/psychosocial measures) was assessed via 16 items scored in a five-point Likert fashion, with responses ranging from “strongly disagree” to “strongly agree” (Cronbach’s alpha = 0.81). Examples of items comprising this scale include “Smoking energizes me” and “Smoking calms me down when I feel nervous” and “Cigarettes can really make me feel good.” The perceived negative consequences of smoking was assessed via four items scored in similar fashion to the previous scale (Cronbach’s alpha = 0.82), with examples including such measures as “Smoking is hazardous to my health” and “By smoking, I risk heart disease and lung cancer.” The number of reasons for continuing to smoke was assessed via a nine-item scale (Cronbach’s alpha = 0.69), with all items again scored using a five-point Likert fashion, with responses ranging from “strongly disagree” to “strongly agree.” Constituent items included such measures as continuing to smoke due to physical dependence, as a form of weight control, to help in social situations, and coping with negative feelings. The perceived level of safety of light cigarettes is another scale (Cronbach’s alpha = 0.85), assessed by eight items scored on a five-point Likert scale with responses ranging from “definitely not true” to “definitely true.” It included statements such as “Light cigarettes are healthier” and “Light cigarettes give you less tar.” Perceived extent of cigarette industry efforts to make smoking safer is a scale measure comprised by six yes/no items, asking respondents whether they believed that Big Tobacco had been taking steps such as adding filters to make cigarettes less dangerous, reducing the amount of tar in cigarettes, and removing additives to cigarettes (Kuder-Richardson20 = 0.84). Having a negative self-view as a result of smoking is a 32-item scale measure (Cronbach’s alpha = 0.87), comprised by items scored on a five-point Likert scale with responses ranging from “strongly disagree” to “strongly agree.” It included such items as hating the way one smells after smoking, feeling looked down upon because of one’s smoking, and perceiving oneself to be viewed as a
criminal by others as a result of one’s smoking. Having friends and relatives complain about one’s smoking was a scale comprised by seven yes/no items (Kuder-Richardson20 = 0.74) that addressed such issues as friends complaining about the residual odor resulting from smoking, the amount of money that the person has spent on cigarettes, and how smoking has affected their health. Two separate scales assessed the number of reasons the person had for wanting to quit smoking (14 yes/no items; Kuder-Richardson20 = 0.81) and the number of reasons the person had for wanting to reduce his/her cigarette use without quitting (12 yes/no items; Kuder-Richardson20 = 0.84). People’s overall attitudes toward quitting smoking were assessed via an 18-item scale (Cronbach’s alpha = 0.71) comprised by five-point Likert-scored items with responses ranging from “strongly disagree” to “strongly agree.” Examples of items in this scale include: “I would quit if I knew I would not gain weight” and “I need to be ready before I will even try to quit smoking” and “I need to have a good reason to quit.” Higher scores on this scale indicate a greater overall willingness to consider quitting smoking. Perceived riskiness of smoking was another scale measure (Cronbach’s alpha = 0.71), assessed in a similar fashion, utilizing six items such as “Cigarettes still have not been proven to cause cancer” and “Lung cancer has more to do with genetics than with actual smoking” and “Pollution causes more lung cancer than does cigarette smoking.”
To examine Research Question #3, which examined the factors underlying higher/lower scores on REGULATE, items from four domains–demographic characteristics, earlier-life or initial smoking practices, lifetime maltreatment experiences, and psychological/psychosocial functioning–were used. Demographic characteristics included in this part of the analysis were: gender (male versus female), age (continuous measure), race (coded as African American versus all others), employment status (unemployed versus employed), educational attainment (continuous measure), marital/relationship status (“involved” versus not “involved”), and religiosity (a three-item scale measure; Cronbach’s alpha = 0.79). Two earlier-life or initial smoking practices measures were examined: age of first time smoking a cigarette (continuous measure) and age of

Smoking behavior 307
first time purchasing a cigarette (continuous measure). Lifetime maltreatment experiences were assessed with three measures asking people the number of times during their lifetime that they had experienced emotional abuse, physical abuse, or sexual abuse. For analytical purposes, in this paper, each item was dichotomized into “ever experienced” and “never experienced” each type of maltreatment. Six scales measuring various aspects of psychological or psychosocial functioning were utilized in this part of the analysis. They were: sociability (derived from Watson and Friend’s (21) Social Avoidance and Distress Scale) (11 items; Cronbach’s alpha = 0.89), social isolation (11 items; Cronbach’s alpha = 0.87), depression (the Center for Epidemiologic Studies Depression (CES-D) scale (22)) (20 items; Cronbach’s alpha = 0.90), perceived predictability/randomness of events in one’s life (derived from Schuessler’s (23) Doubt about Self-Determination Scale) (12 items; Cronbach’s alpha = 0.75), impulsiveness (derived from Zuckerman et al (24) Zuckerman-Kuhlman Personality Questionnaire) (12 items; Cronbach’s alpha = 0.81), and self-esteem (Rosenberg’s (25) Self-Esteem Scale) (10 items; Cronbach’s alpha = 0.86).
Analysis
Research Question #1–pertaining to how study participants feel about the prospect of having outside persons and agencies provide information about and regulate smoking practices–is analyzed with the use of descriptive statistics. In most instances, because the attitudinal and behavioral outcome measures in question are continuous variables (as is the REGULATE measure that serves as the focal point for this study), Research Question #2–examining how REGULATE relates to smoking-related attitudes and smoking practices–was analyzed via the computation of zero-order correlation coefficients (Pearson’s r). The only exceptions to this were the three yes/no behavioral outcomes items (smoking more on weekends, lying to friends/relatives about smoking, ever tried to quit smoking), for which logistic regression was deemed to be the more appropriate analytical approach.
For Research Question #3–identifying the factors
underlying higher/lower scores on REGULATE–the analysis was undertaken in two steps. Initially, bivariate analyses were conducted to learn which items were found to be related to REGULATE. Whenever the independent variable was dichotomous in nature (e.g., gender, race, any lifetime physical abuse), Student’s t tests were performed to ascertain whether the comparison groups differed from one another on the dimension in question. Whenever the independent variable was continuous in nature (e.g., religiosity, age, self-esteem), the bivariate analyses entailed the use of correlation coefficients. Subsequently, items found to be associated with REGULATE in the bivariate analyses either significantly (i.e., p<.05) or marginally (i.e., .10>p>.05) were entered into a multiple regression equation, to determine which ones contributed to the REGULATE scale scores when the effects of the other measures were taken into account. Items that were nonsignificant were removed from the equation in stepwise fashion, until a final “best fit” model containing only statistically-significant measures was derived.
For Research Question #4–determining whether REGULATE remains influential in the prediction of attitudes toward smoking and/or actual smoking behaviors when the effects of other relevant measures were taken into account–the analysis entailed a three-step process. The first two steps were similar to those described for Research Question #3, but using REGULATE as one of the independent variables instead of using it as the dependent variable in question. In these analyses, a smoking-related attitudinal measure or a smoking behavioral outcome measure served as the dependent variable; and separate multivariate analyses were performed for each outcome measure in question. The third step in this part of the analysis entailed subjecting the multivariate findings to structural equation analysis, to determine whether or not the relationships identified in the multivariate analyses “hold up” when considered as a totality. Separate structural equation analyses were undertaken for each of the different outcome measures. SAS’s PROC CALIS procedure was used to assess the overall fit of each model to the data. When we use this type of structural equation analysis, we look for several specific outcomes, including 1) an appropriate goodness-of-fit index, 2)

Claire E Sterk, Hugh Klein, and Kirk W Elifson 308
an acceptable Bentler-Bonett normed fit index value, 3) an overall chi-square value for the model that is statistically nonsignificant, and 4) a root mean square error approximation value close to zero. If these conditions are met, then the relationships depicted are considered to indicate a good fit with the data. Throughout the analyses, results are reported as statistically significant whenever p<.05.
Results
Slightly more than one-half of the study participants (56.8%) were male. Most respondents were either Caucasian (54.6%) or African American (39.0%). The median age was 34 (range = 18–70, mean = 36.4, s.d. = 12.3). This is a fairly well-educated sample, with 34.2% of the respondents having completed college and an additional 40.6% having attended college without completing it. Although most (55.1%) of the study participants were employed on a full-time basis, substantial proportions of them were working on a part-time basis (32.9%) or unemployed (12.0%). Respondents were relatively evenly split between those who were single (42.7%) or involved in a marital-type relationship (44.5%). Approximately one person in six (16.5%) self-identified as gay, lesbian, or bisexual.
Research Question #1 – How do people feel about the regulation of smoking-related behaviors?
Overall, summed across all items comprising the REGULATE scale, approximately one-half of the study participants (51.3%) scored in the moderate range in terms of their beliefs about the extent to which outside agencies ought to be responsible for informing the public about the potential dangers of smoking and/or to regulate cigarette smoking practices (see Table 1).
Very few people gave responses indicating that they did not feel that these duties were important and incumbent upon outside agencies and regulators (2.5%) or, alternatively, that they felt strongly that outside agencies and persons should be responsible for informing the public about the potential dangers of
smoking and/or to regulate cigarette smoking practices (1.0%). Respondents were about equally likely to score in the lower-moderate part of the range versus in the moderately-high part of the range on the REGULATE scale (25.4% versus 19.8%, respectively).
As Table 1 shows, there were large differences from item to item in terms of respondents’ likelihood of endorsing a particular measure. For example, approximately three-quarters of the study participants believed that cigarette companies and public health agencies should be required to provide more information about the chemicals in cigarette smoke (77.5% and 76.7%, respectively), public health agencies should be required to provide more information about how to get screened for the diseases caused by smoking (74.6%), public health agencies should be required to provide more information about the health risks of smoking (73.8%), and public health agencies should be required to provide more information about how people can stop smoking (72.7%). In contrast, most study participants believed that: smoking portrayals should not be prohibited on television or in movies (64.1%) or that taxes on cigarettes should not be increased (76.9%).
Table 1 shows that participants in this study believed that it was incumbent upon public health agencies (and to a slightly lesser extent, cigarette companies) to provide more information to the public about how to control smoking behaviors, while these same people were less inclined to agree with measures that would implement and enforce tobacco/smoking control policies.
Research Question #2 – How do people’s views regarding smoking regulation relate to their actual smoking behaviors and to their actual attitudes toward smoking?
Although not all measures demonstrated a relationship between REGULATE and people’s actual smoking-related perceptions and behaviors, most did (see Table 2). This was true for the perception and behavioral items alike.

Smoking behavior 309
Table 2. The Relationship between Perceptions Regarding the Regulation of Smoking and Actual Smoking Behaviors and Smoking-Related Attitudes
Smoking Behavior Correlation Coefficient
Statistical Significance
Number of cigarettes smoked per week –.18 <.001
Doing things to get the most out of smoking .02 n.s.
Perceived positive benefits experienced by smoking .19 <.001
Perceived negative consequences experienced by smoking .19 <.001
Number of reasons for continuing to smoke .17 <.001
Perceived level of safety of smoking light cigarettes –.11 .013
Perceived extent of cigarette industry’s efforts to make smoking safer over the years
–.08 .067
Extent of having negative self-view due to smoking .21 <.001
Extent to which nonsmoking friends/relatives have commented negatively or complained about one’s smoking
.06 n.s.
Number of times trying to cut down (but not quit) on smoking .05 n.s.
Number of times trying to quit smoking .10 .028
Number of reasons for wanting to quit smoking .27 <.001
Number of reasons for wanting to cut down (not quit) smoking .28 <.001
Number of different ways the person has tried to quit smoking .18 <.001
Overall attitude toward quitting smoking .12 .011
Number of negative effects experienced the last time the person attempted to quit smoking (among quit attempters only)
.05 n.s.
Extent to which person perceives smoking to be risky .31 <.001
Frequency of needing a cigarette in order to function properly –.11 .014
Frequency of making special trips in order to get cigarettes –.05 n.s.
Frequency of chain smoking –.14 .002
Frequency of smoking more than originally intended .06 n.s.
Regarding the former (i.e., smoking-related perceptions), as Table 2 demonstrates, endorsement of REGULATE was associated with: adhering to a
greater overall perception that smoking yields a variety of benefits for the smoker (r=.19, p<.001), adhering to a greater overall perception that smoking

Claire E Sterk, Hugh Klein, and Kirk W Elifson 310
causes a variety of adverse consequences for the smoker (r=.19, p<.001), having a larger number of reasons for continuing to smoke cigarettes (r=.17, p<.001), perceiving so-called light cigarettes not to be safer to smoke than regular cigarettes (r=–.11, p=.013), having a more negative self-view as a result of one’s smoking practices (r=.21, p<.001), adhering to a larger number of reasons for wanting to quit smoking (r=.27, p<.001), adhering to a larger number of reasons for wanting to cut down on one’s tobacco use rather than quitting smoking altogether (r=.28, p<.001), having more-favorable attitudes toward quitting smoking (r=.12, p=.011), and a greater perception that smoking carries with it a variety of risks (r=.31, p<.001). Regarding the latter (i.e., behavioral outcomes), endorsement of REGULATE was found to be related to: smoking fewer cigarettes per week (r=–.18, p<.001), a greater number of previous times having tried to quit smoking (r=.10, p=.028), a greater number of different methods for having tried to quit smoking in the past (r=.18, p<.001), less frequent experiences of needing a cigarette in order to function properly (r=–.11, p=.014), and chain smoking less frequently (r=–.14, p=.002).
In addition to the preceding, logistic regression analysis revealed that REGULATE was not related to whether or not study participants smoked more cigarettes on weekends (OR=0.997, CI95=0.67–1.48, n.s.) or to whether or not they lied to others about their smoking practices (OR=1.50, CI95=0.96–2.35, p=.074). Conversely, the more that people endorsed the items comprising the REGULATE scale, the more likely they were to report having tried to quit smoking at least once before (OR=2.10, CI95=1.25–3.53, p=.005).
Research Question #3 – What factors underlie people’s views regarding the regulation of smoking practices?
Bivariate analyses revealed several variables that were related either significantly or marginally to REGULATE. In terms of the demographic measures examined, African Americans scored somewhat higher on REGULATE than members of other racial groups did (2.32 versus 2.25; t=1.66, p=.097). There
was a slight tendency for REGULATE to be endorsed more with advancing age (r=.09, p=.060). People who were unemployed at the time of their interview were somewhat less inclined to support REGULATE than their employed counterparts were (2.18 versus 2.29; t=1.76, p=.078). The more religious people were, the more apt they were to endorse the REGULATE items (r=.09, p=.043).
Two earlier-life or initial smoking practices measures were examined, and were found to be related to people’s responses to the REGULATE scale items. The older people were the first time they smoked a cigarette, the more likely they tended to endorse the REGULATE items (r=.08, p=.093). Similarly, the older they were the first time they purchased a cigarette, the more supportive of REGULATE they were (r=.15, p=.001).
Some of the lifetime maltreatment experiences measures were found to be related to REGULATE as well. People who had experienced emotional abuse at some point during their lifetimes tended to endorse the REGULATE items more than their never-emotionally-abused counterparts (2.30 versus 2.17; t=2.41, p=.016). Persons who had been sexually abused were also more apt to support REGULATE than their counterparts who had not been subjected to such abuse (2.34 versus 2.25; t=1.86, p=.063). Such a relationship was not found for physical abuse, however.
Similarly, some but not all of the psychological /psychosocial functioning measures were found to be related to REGULATE. Higher scores on REGULATE were found to be associated with: lower levels of social isolation (r=–.11, p=.021), greater belief in the randomness or unpredictability of events (r=.09, p=.046), lower levels of depression (r=–.12, p=.011), and lower levels of impulsiveness (r=–.10, p=.036) but not with sociability (r=.05, p=.255) or self-esteem (r=.07, p=.132).
When the appropriate items were entered into a multivariate equation to determine which ones mattered when the effects of the others were taken into account, four items were found to contribute uniquely and significantly to the prediction of REGULATE. These were: level of religiosity (β=.09, p=.054), age of first purchasing cigarettes (β=.14, p=.002), level of depression (β=.14, p=.002), and whether or not the person had been sexually abused

Smoking behavior 311
during his/her lifetime (β=11, p=.012). Together, these items explained 5.5% of the total variance in REGULATE. It should be noted that the religiosity measure was retained in this equation despite narrowly failing to maintain statistical significance because its removal reduced the model’s overall explanatory power by a significant amount, therefore indicating the importance of its retention rather than its deletion.
Research Question #4 – When we try to understand the factors that affect people’s smoking behaviors, does REGULATE matter when the effects of other relevant variables are taken into account?
As a general rule, the answer to the question posed
here is “yes.” Figures 2, 3, and 4 present three specific examples from the data to support this contention. In each instance, REGULATE is a key endogenous variable in the overall determination of the smoking-related outcome measure in question. This was true when the outcome measure in question was the frequency of chain smoking (see Figure 2), the number of cigarettes smoked per week (see Figure 3), and the number of perceived risks associated with smoking (see Figure 4). In each model, the structural equation analysis revealed that REGULATE contributed significantly to the determination of the smoking-related dependent variable in question, and that it was one of several variables (different from model to model, based on the specific outcome measure being examined) influencing the smoking measure in question.
Figure 2. Beliefs about Regulating Smoking and the Frequency of Chain Smoking.

Claire E Sterk, Hugh Klein, and Kirk W Elifson 312
Figure 3. Beliefs about Regulating Smoking and the Number of Cigarettes Smoked per Week.
As the information presented in the encircled
portion of each figure shows, the structural equation analysis for all three of these models yielded strong statistical support for the applicability of each model. Further supporting its relevance and importance to the scientific understanding of smoking behaviors and smoking-related attitude/perception measures, we would like to point out that REGULATE was also retained as a multivariate predictor of several of the other smoking-related outcome measures that are listed in Table 2 but which, for brevity’s sake, are not depicted in the figures presented in the current paper.
Discussion
The analyses conducted in conjunction with this paper yielded several interesting and noteworthy findings with regard to REGULATE and its relevance to adult smokers’ smoking behaviors. First, as a group, the smokers who participated in this study were quite mixed in their overall feelings about the extent to which they believed that outside agencies and persons should be responsible for informing the public about the dangers of smoking and/or for regulating smoking behaviors.

Smoking behavior 313
Figure 4. Beliefs about Regulating Smoking and the Perceived Risks of Smoking.
By approximately a 3:1 margin, they advocated a position indicative of a desire to hold public health agencies responsible for informing the public about the dangers of smoking. Interestingly and, to us, intriguingly, respondents were noticeably less inclined to assign this same responsibility to the cigarette companies that make the cigarettes that cause the smoking-related dangers in question available to the public. When it came to assessing the REGULATE measures that pertained to individual liberties to smoke, our study participants were noticeably more divided in their responses, with many believing that it was acceptable to try to regulate or constrain smoking behaviors while many others adhered to beliefs standing in direct opposition to that mindset.
Our best professional judgment suggests that
these findings might be interpreted as follows: It appears that the smokers who participated in this research construe it as a central responsibility of public health agencies to uphold the principles of public safety, thereby leading those agencies to be held most accountable by smokers for informing the public about the dangers associated with smoking. In contrast, while smokers generally believe that the cigarette companies ought to be responsible for telling the public about the dangers associated with smoking, their adherence to this position may be tempered somewhat by their recognition of the existence of the competing interests of the business-related profit motive that these companies also have. That is, the smokers understand that these companies exist for the purpose of making money, and in order for them to do that, they must sell their product. At the same time,

Claire E Sterk, Hugh Klein, and Kirk W Elifson 314
however, there is a certain amount of responsibility to one’s customers that comes with selling them a product that has known dangers associated with its use; and with that responsibility comes a perceived duty of protecting one’s customers’ safety, at least to some extent. When it comes to affecting individual liberties, however, smokers are far more reluctant to want outsiders to be able to exert influence over their smoking behaviors. It appears to us that the smokers feared the potential impact of too much regulation of smoking practices, perhaps out of a concomitant concern that such regulation could affect their ability to afford the cigarettes they intended to smoke and their ability to smoke wherever they wanted. Thus, when the items comprising the REGULATE construct are combined into the scale measure, people’s scores are more disbursed, leaving them more mixed in their overall attitudes about the extent to which other persons and agencies ought to be responsible for informing the public about and for regulating smoking-related practices.
With respect to Research Question #2–whether or not REGULATE was related to people’s smoking-related attitudes and/or to their actual smoking behaviors–the findings obtained were somewhat more complicated. REGULATE was related inconsistently to cigarette smoking practices. It was not related to such measures as taking steps to get more from one’s smoking behaviors, the number of times people tried to cut down on (rather than quit) their smoking, the number of negative effects people experienced the last time they tried to quit smoking, smoking more than one intended, or making special trips to the store to ensure having cigarettes available. In contrast, greater endorsement of REGULATE was associated with smoking fewer cigarettes, a larger number of previous attempts to quit smoking, trying a larger number different ways to quit smoking, less frequent chain smoking, and experiencing less frequent urges to smoke in order to function properly. Overall, however, REGULATE was not found to be a strong, consistent predictor of the extent to which persistent adult smokers smoked cigarettes or of their smoking behavioral patterns. In contrast, however, REGULATE was related quite consistently with how people felt about their smoking behaviors. Generally speaking, the more that people believed that it ought to be the responsibility of other persons and agencies
to inform the public about the dangers associated with smoking and for regulating smoking behaviors: the more they wanted to quit smoking, the more they wanted to cut down on their cigarette use, the more favorably disposed they were toward the notion of quitting smoking, the more they perceived smoking to be risky, the more they tended to perceive smoking to cause them problems, and the more they tended to view themselves negatively as a result of their smoking behaviors.
The greatest relevance of REGULATE, therefore, appears to be in the psychosocial / attitudinal domain rather than in the behavioral domain. Thus, REGULATE has its greatest impact upon smoking behaviors indirectly rather than directly, through its “behind the scenes” influence on the attitudes that underlie people’s smoking practices rather than by impacting specifically and directly the smoking behaviors themselves. As the structural equation models presented in Figures 2, 3, and 4 clearly demonstrate, REGULATE matters greatly and centrally in the overall determination of a variety of smoking-related beliefs, attitudes, and behaviors; but it does so in the form of an endogenous variable.
As an endogenous variable, it becomes important to examine the findings obtained in conjunction with Research Question #3, which focused on identifying the factors associated with greater adherence to the belief that outside persons and/or agencies ought to be responsible for regulating smoking behaviors and/or informing the public about the dangers associated with smoking. Only by understanding more about the factors that underlie REGULATE can we determine which subgroups of smokers might be targeted for specific intervention and/or educational messages. In our analyses, four variables were identified as contributing uniquely and significantly to people’s scores on the REGULATE scale: level of religiosity, age of first purchasing cigarettes, level of depression, and sexual abuse history. Each of these merits a brief discussion.
Regarding level of religiosity, our analysis showed that the more religious people tended to be, the more likely they were to endorse REGULATE. A few previous, recent studies have examined the relationship between religiosity and smoking behaviors in the United States, and the present research contributes to that small but evolving

Smoking behavior 315
literature. Gillum (26), for example, reported that people who attended religious services more frequently were less likely to smoke cigarettes compared to their less-frequently-attending counterparts. Additionally, among current smokers, the frequency of religious service attendance was related inversely to the number of cigarettes that people smoked. In a study of older adult smokers in the American South (27), Roff and colleagues found that religiosity was related inversely to lifetime cigarette smoking. In their research on pregnant and post-partum women, Page, Ellison and Lee (28) found that the odds of smoking tobacco were significantly lower among people who attended worship services regularly or frequently when compared to their less-frequently-attending counterparts. Based on their study of Syracuse, New York residents, Masters and Knestel (29) found that religiosity was associated with whether or not people ever smoked cigarettes, being versus not being a current smoker, and the number of pack-years of cigarette use. Similar results were obtained by Hill and colleagues (30) based on their research on Texas adults, and by Salmoirago-Blotcher and colleagues (31) in their large study of post-menopausal women. As a result of the consistent nature of these studies’ findings, Aldwin and colleagues (32, p. 16) concluded that “Both cross-sectional and longitudinal studies have demonstrated relationships between religious service attendance and less cigarette smoking.” The current study’s finding for the REGULATE scale contributes to this body of literature by demonstrating a slightly different way in which smoking practices are influenced by religiosity–namely, in the form of people’s perceptions of the extent to which they believe that outside persons and/or agencies ought to be responsible for regulating smoking and informing the public about the dangers of cigarette use.
With respect to the age of first purchasing cigarettes, the older people were the first time they purchased a cigarette, the more likely they were to endorse REGULATE. A few studies have examined the age of onset of smoking behaviors, typically focusing on the age at which people begin using cigarettes regularly, and how age of onset relates to smoking practices later in life. In one study of early-onset cigarette smokers (defined as persons initiating use prior to age 12), about three-quarters of the young
people (77.0%) became regular smokers by mid-adolescence (33). In their research on smoking initiation during the college years, Clarkin, Tisch, and Glicksman (34) found that about one out of nine (11.7%) students had their first cigarette while in college years and 10.8% of college students began smoking regularly at some point during their college years. Having a positive experience (e.g., experiencing relaxation) when first smoking a cigarette has been associated with an increased risk of current smoking, daily smoking, nicotine dependence, and cue-induced cravings for a cigarette (35). The present study’s findings add to the literature on this subject by documenting one more way in which age of onset of smoking behaviors–in this specific instance, the age of making the decision to purchase one’s first cigarette–is relevant to later-life tobacco use.
Regarding people’s level of depression, the more depressed participants in the present study were, the less likely they were to endorse REGULATE. A substantial body of literature has been published on the topic of depression and smoking, with the large majority of studies reporting that depression tends to lead to increased cigarette smoking and/or that smokers have higher rates of depressive symptomatology when compared with their nonsmoking peers (36–38). The present study’s finding regarding the relationship between depression and REGULATE is generally consistent with these other research reports; yet it focuses on an aspect of smoking–namely, the belief in who should be responsible for protecting and informing the public about smoking, and to what extent such persons/agencies should be expected to perform such duties–that has not been addressed in any other published reports that the present authors have identified.
With respect to sexual abuse history, the tendency was for people who had experienced sexual abuse to be more likely to endorse REGULATE. As with the preceding measures, previous research has documented a link between early-life sexual abuse experiences and later-life smoking behaviors, with the former generally shown to be a risk factor for the latter (39–41). Once again, the present study’s findings are generally consistent with the scholarly literature and still able to extend this literature by

Claire E Sterk, Hugh Klein, and Kirk W Elifson 316
virtue of focusing on a somewhat different smoking-related measure, in the form of REGULATE.
Finally, we would like to switch our focus and revisit the findings obtained in the present study as they apply to the notions of locus of control, health locus of control, and powerful others, as introduced earlier in this paper. As we discussed earlier, one way of conceptualizing REGULATE is to think of it as a proxy for locus of control (or at least, as a proxy for one aspect of locus of control). More specifically, people who score high on REGULATE may be construed as being more externally-oriented than those who score low on this scale, because of their belief in the responsibility of other persons and other agencies to determine social and regulatory policies regarding smoking practices. To the extent that REGULATE may be used as a substitute measure for locus of control, the present study’s findings indicate that participants in the Persistent Smokers Project varied widely in their internal versus external locus of control when it came to their smoking behaviors. Previous researchers have found that people who are more internally oriented when it comes to locus of control tend to engage in lower rates of risky behaviors and higher rates of behavioral practices that can be considered to be beneficial or health protective in nature (2,4,6). In the present study, we found that people who scored higher on REGULATE–that is, those with a greater external locus of control orientation–generally had attitudes toward smoking that were aligned with a recognition of a need and/or a desire to stop smoking. This is the opposite of what we would have expected, based on the findings obtained by previous studies examining locus of control and health practices. It is possible that one reason for our finding is that REGULATE may not be a sufficiently precise measure of locus of control. It is also possible that locus of control operates differently with regard to attitudinal measures than it does with behavioral ones. Other interpretations of our finding may exist, too. Regardless of how one interprets our research findings, this is a subject worth exploring in future studies–namely, how, exactly, does locus of control affect smoking behaviors and the decision-making processes and attitudes that underlie smoking behaviors? This subject has been investigated only infrequently with regard to the behavioral outcomes in question and even less frequently with regard to the
attitudinal/psychosocial measures that also pertain to smoking practices.
With regard to the construct of “powerful others” (also discussed in this paper’s Introduction), the present study’s findings suggest that participants in the Persistent Smokers Project adhered to beliefs that indicated both a respect for and a simultaneous fear of what these so-called powerful others could do with regard to smoking behaviors and smoking-related public policies. When “powerful others” is operationalized in terms of public health agencies, the smokers who participated in this study believed that these were the very individuals/agencies who should be responsible for informing people about the dangers of smoking and how to minimize these dangers. Even when “powerful others” is operationalized in terms of cigarette companies, most of the study participants still believed that these companies should be duty-bound to inform the public about the dangers of smoking.
When “powerful others” is operationalized in terms of lawmakers and policymakers, though, our study participants appeared to be more leery. Nearly 1 respondent in 3 did not agree that it was a good idea to regulate smoking in public places. More than 1 respondent in 3 said that smoking should be banned from television programs and/or movies. Nearly one-half of the Persistent Smokers Project study participants believed that smoking should not be banned in restaurants, and a comparably-large proportion of the people who took part in this study believed that smoking bans should be unconstitutional. Thus, when faced with the prospect of having “powerful others” help the public with regard to smoking information, our study participants believed that this was well within the purview of their “proper” domain; but when faced with the prospect of having “powerful others” use their power for regulatory purposes, they seemed to be more conflicted about the extent to which they wanted these “powerful others” to avail themselves of their authority. Little, if any, research has been conducted with a focus or an emphasis on “powerful others” and the role that they can play in promoting healthier behaviors, particularly in the realm of cigarette smoking. About the closest analog has been the multitude of studies that have been done with a “community gatekeepers” or a “key informants”

Smoking behavior 317
approach; but those approaches typically have been used to gain access to difficult-to-find or difficult-to-recruit study participants rather than to help promote smoking cessation. Applying the construct of “powerful others” to the smoking cessation field might prove to be a fruitful endeavor for future intervention efforts, particularly (our findings suggest) if researchers/interventionists are able to tap into the respect-engendering aspects of what “powerful others” can do to bring about behavioral and attitudinal change while eschewing those other aspects of their powers and authority that are likely to instill fear into members of the target population.
Finally, we would like to touch upon the value of having used a syndemics theory approach to examining the topics at hand in this particular study. As the findings presented in Figures 2, 3, and 4 clearly demonstrate, elements from all of the domains that were included in the conceptual model shown in Figure 1 were relevant in these analyses. This indicates a strong level of support for the usefulness of syndemics theory for understanding the relationships amongst factors affecting smokers’ attitudes toward smoking and their actual smoking behaviors. Thus, one additional contribution made by the present research is its ability to demonstrate the applicability of this theoretical model to the study of yet another health behavior–namely, cigarette smoking–thereby expanding its importance and relevance beyond such behavioral domains as obesity (42), HIV risk taking (15,43,44), health disparities (45,46), criminal justice system involvement (47), and socioeconomic disadvantage (48) as other researchers have demonstrated in their own work.
Acknowledgments This research was supported by a grant from the
National Institute on Drug Abuse (R01 DA015707).
References
[1] Armitage CJ. The relationship between multidimensional health locus of control and perceived behavioural control: How are distal perceptions of control related to proximal perceptions of control? Psychol Health 2003;18:723-38.
[2] Sheffer C, MacKillop J, McGeary J, Landes R, Carter L, Yi R, et al. Delay discounting, locus of control, and cognitive impulsiveness independently predict tobacco dependence treatment outcomes in a highly dependent, lower socioeconomic group of smokers. Am J Addict 2012;21:221-32.
[3] Williams GC, McGregor HA, Sharp D, Levesque C, Kouides RW, Ryan RM, et al. Testing a self-determination theory intervention for motivating tobacco cessation: Supporting autonomy and competence in a clinical trial. Health Psychol 2006;25:91-101.
[4] Haslam C, Lawrence W. Health-related behavior and beliefs of pregnant smokers. Health Psychol 2004;23:486-91.
[5] Burnett AJ, Sabato TM, Walter KO, Kerr DL, Wagner L, Smith A. The influence of attributional style on substance use and risky sexual behavior among college students. Coll Stud J 2013;47:122-36.
[6] Reitzel LR, Lahoti S, Li Y, Cao Y, Wetter DW, Waters AJ, Vidrine JI. Neighborhood vigilance, health locus of control, and smoking abstinence. Am J Health Behav 2013;37:334-41.
[7] Wallston KA, Wallston BS, DeVellis R. Development of the Multidimensional Health Locus of Control (MHLC) scales. Health Educ Monogr 1978;6:160-70.
[8] Wallston BS, Wallston KA, Kaplan GD, Maides SA. The development and validation of the Health related Locus of Control (HLC) scale. J Consult Clin Psychol 1976;44:580-5.
[9] Haslam C, Lawrence W, Haefeli K. Intention to breastfeed and other important health-related behaviour and beliefs during pregnancy. Fam Pract 2003;20:1-5.
[10] Rotter JB. Some problems and misconceptions related to the construct of internal versus external control of reinforcement. J Consult Clin Psychol 1975;43:56-67.
[11] Dekel R, Benbenishty R, Amram Y. Therapeutic communities for drug addicts: Prediction of long-term outcomes. Addict Behav 2004;29:1833-7.
[12] Singer MC. Introduction to syndemics: A critical systems approach to public and community health. San Francisco, CA: John Wiley, 2009.
[13] Halkitis PN, Moeller RW, Siconolfi DE, Storholm ED, Solomon TM, Bub KL. Measurement model exploring a syndemic in emerging adult gay and bisexual men. AIDS Behav 2013;17:662-73.
[14] Illangasekare SL, Burke JG, McDonnell KA, Gielen AC. The impact of intimate partner violence, substance use, and HIV on depressive symptoms among abused low-income urban women. J Interpers Violence 2013;28:2831-48.
[15] Klein H. Using a syndemics theory approach to study HIV risk taking in a population of men who use the Internet to find partners for unprotected sex. Am J Men Health 2011;5:466-76.

Claire E Sterk, Hugh Klein, and Kirk W Elifson 318
[16] Meyer JP, Springer SA, Altice FL. Substance abuse, violence, and HIV in women: A literature review of the syndemic. J Women Health 2011:20:991-1006.
[17] Senn TE, Carey MP, Vanable PA. The intersection of violence, substance use, depression, and STDs: Testing of a syndemic pattern among patients attending an urban STD clinic. J Natl Med Assoc 2010;102:614-20.
[18] Greenwood GL, Paul JP, Pollack LM, Binson D, Catania JA, Chang J, et al. Tobacco use and cessation among a household-based sample of US urban men who have sex with men’: Greenwood et al respond. Am J Publ Health 2005;95:929-30.
[19] Yu F, Nehl EJ, Zheng T, He N, Berg CJ, Lemieux AF, et al. A syndemic including cigarette smoking and sexual risk behaviors among a sample of MSM in Shanghai, China. Drug Alcohol Depend 2013;132:265-70.
[20] Centers for Disease Control and Prevention. NHIS–Adult tobacco use information: Smoking status recodes. URL: www.cdc.gov/nchs/nhis/tobacco/tobacco_ recodes.htm
[21] Watson D, Friend R. Measurement of social-evaluative anxiety. J Consult Clin Psychol 1969;33:448-57.
[22] Radloff LS. The CES-D scale: A self-report depression scale for research in the general population. Appl Psychol Meas 1977;1:385-401.
[23] Schuessler K. Measuring social life feelings. San Francisco, CA: Jossey-Bass, 1982.
[24] Zuckerman M, Kuhlman DM, Joireman J, Teta P, Kraft M. A comparison of three strictiral models for personality: The Big Three, the Big Five, and the Alternative Five. J Pers Soc Psychol 1993;65:757-68.
[25] Rosenberg M. Society and the adolescent self-image. Princeton, NJ: Princeton University Press, 1965.
[26] Gillum RF. Frequency of attendance at religious services and cigarette smoking in American women and men: The Third National Health and Nutrition Examination Survey. Prev Med 2005;41:607-13.
[27] Roff LL, Klemmack DL, Parker M, Koenig HG, Sawyer-Baker P, Allman RM. Religiosity, smoking, exercise, and obesity among southern community-dwelling older adults. J Appl Gerontol 2005;24:337-54.
[28] Page RL, Ellison CG, Lee J. Does religiosity affect health risk behaviors in pregnant and postpartum women? Matern Child Health J 2009;13:621-32.
[29] Masters KS, Knestel A. Religious orientation among a random sample of community-dwelling adults: Relations with health status and health-relevant behaviors. Int J Psychol Relig 2011;21:63-76.
[30] Hill TD, Burdette AM, Ellison CG, Musick MA. Religious attendance and the health behaviors of Texas adults. Prev Med 2006;42:309-13.
[31] Salmoirago-Blotcher E, Fitchett G, Ockene JK, Schnall E, Crawford S, Granek I, et al. Religion and healthy lifestyle behaviors among postmenopausal women: The
Women’s Health Initiative. J Behav Med 2011;34:360-71.
[32] Aldwin CM, Park CL, Jeong YJ, Nath R. Differing pathways between religiousness, spirituality, and health: A self-regulation perspective. Psychol Relig Spiritual 2014;6:9-21.
[33] Vega WA, Gil AG. Revisiting drug progression: Long range effects of tobacco use. Addiction 2005;100:1358-69.
[34] Clarkin PF, Tisch LA, Glicksman AS. Socioeconomic correlates of current and regular smoking among college students in Rhode Island. J Am Coll Health 2008;57:183-90.
[35] Ursprung WWS, Savageau JA, DiFranza JR. What is the significance of experiencing relaxation in response to the first use of nicotine? Addict Res Theory 2011;19:14-21.
[36] Baek JH, Eisner LR, Nierenberg AA. Smoking and suicidality in subjects with major depressive disorder: Results from the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC). J Affect Disord 2013;150:1158-66.
[37] Kenney BA, Holahan CJ, North RJ, Holahan CK. Depressive symptoms and cigarette smoking in American workers. Am J Health Promot 2006;20:179-82.
[38] Payne TJ, Ma JZ, Crews KM, Li MD. Depressive symptoms among heavy cigarette smokers: The influence of daily rate, gender, and race. Nicotine Tob Res 2013;15:1714-21.
[39] Choudhary E, Coben JH, Bossarte RM. Gender and time differences in the associations between sexual violence victimization, health outcomes, and risk behaviors. Am J Men Health 2008;2:254-9.
[40] Nichols HB, Harlow BL. Child abuse and risk of smoking onset. J Epidemiol Commun Health 2004;58:402-6.
[41] Smith PH, Homish GG, Saddleson ML, Kozlowski LT, Giovino GA. Nicotine withdrawal and dependence among smokers with a history of childhood abuse. Nicotone Tob Res 2013;15:2016-21.
[42] Candib LM. Obesity and diabetes in vulnerable populations: Reflection on proximal and distal causes. Ann Fam Med 2007;5:547-56.
[43] Lyons T, Johnson AK, Garofalo R. What could have been different: A qualitative study of syndemic theory and HIV prevention among young men who have sex with men. J HIV/AIDS Soc Serv 2013;12:368-83.
[44] Talman A, Bolton S, Walson JL. Interactions between HIV/AIDS and the environment: Toward a syndemic framework. Am J Public Health 2013;103:253-61.
[45] Bruce D, Harper GW. Operating without a safety net: Gay male adolescents and emerging adults’ experiences of marginalization and migration, and implications for theory of syndemic production of health disparities. Health Educ Behav 2011;38:367-78.

Smoking behavior 319
[46] Egan JE, Frye V, Kurtz SP, Latkin C, Chen M, Tobin K, et al. Migration, neighborhoods, and networks: Approaches to understanding how urban environmental conditions affect syndemic adverse health outcomes among gay, bisexual and other men who have sex with men. AIDS Behav 2011;15:s35-s50.
[47] Kurtz SP. Arrest histories of high-risk gay and bisexual men in Miami: Unexpected additional evidence for syndemic theory. J Psychoactive Drugs 2008;40:513-21.
[48] Gonzalez-Guarda RM, McCabe BE, Florom-Smith A, Cianelli R, Peragallo N. Substance abuse, violence, HIV, and depression: An underlying syndemic factor among Latinas. Nurs Res 2011;60:182-9.
Submitted: June 02, 2014. Revised: July 15, 2014.
Accepted: July 31, 2014.