Which Domains of Thyroid-Related Quality of Life Are Most Relevant? Patients and Clinicians Provide...
107
FACULTY OF HEALTH SCIENCES UNIVERSITY OF COPENHAGEN PhD thesis Torquil Watt Development of a Danish thyroid-specific quality of life questionnaire Department of Endocrinology, Copenhagen University Hospital Rigshospitalet and Health Service Research, Institute of Public Health
Transcript of Which Domains of Thyroid-Related Quality of Life Are Most Relevant? Patients and Clinicians Provide...
F A C U L T Y O F H E A L T H S C I E N C E S U N I V E R S I T Y O F C O P E N H A G E N
PhD thesis Torquil Watt
Development of a Danish thyroid-specific quality of life questionnaire
Department of Endocrinology,
Copenhagen University Hospital Rigshospitalet
and Health Service Research,
Institute of Public Health
This thesis consists of four papers:
I Watt T, Groenvold M, Rasmussen AK, Bonnema SJ, Hegedüs L, Bjorner JB, Feldt-
Rasmussen U. Quality of life in patients with benign thyroid disorders. A review. Eur J Endo-crinol 2006; 154:501-510.
II Watt T, Hegedus L, Rasmussen AK, Groenvold M, Bonnema SJ, Bjorner JB, Feldt-Rasmussen U. Which domains of thyroid-related quality of life are most relevant? Patients and clinicians provide complementary perspectives. Thyroid 2007; 17(7):647-654.
III Watt T, Rasmussen AK, Groenvold M, Bjorner JB, Watt SH, Bonnema SJ, Hegedüs L, Feldt-Rasmussen U. Improving a newly developed patient-reported outcome for thyroid patients, us-ing cognitive interviewing. Qual Life Res 2008;(Online publication ahead of print)*.
IV Watt T, Bjorner JB, Groenvold M, Rasmussen AK, Bonnema SJ, Hegedüs L, Feldt-Rasmussen U. Establishing a reliable scale structure with convergent and discriminant validity for a new patient reported outcome measure for patients with thyroid disorders. Qual Life Res, submitted.**
*Subsequently printed: Qual Life Res 2008; 17(7):1009-1017
**Subsequently published as:
Watt T, Bjorner JB, Groenvold M, Rasmussen AK, Bonnema SJ, Hegedüs L, Feldt-Rasmussen U. Establishing construct validity for the thyroid-specific patient reported outcome measure (ThyPRO): an initial examination. Qual Life Res 2009; 18(4):483-496.
TABLE OF CONTENTS PREFACE ........................................................................................................................................... 4 List of abbreviations ....................................................................................................................... 6 INTRODUCTION ................................................................................................................................. 7 METHODS.......................................................................................................................................... 10 Phase I, issue generation ........................................................................................................ 11 Phase II, operationalization..................................................................................................... 13 Phase III, pretesting................................................................................................................. 17 Phase IV, quantitative scale validation.................................................................................... 19 RESULTS............................................................................................................................................ 22 Phase I, issue generation ........................................................................................................ 22 Phase II, operationalization..................................................................................................... 27 Phase III, pretesting ................................................................................................................ 27 Phase IV, quantitative scale validation ................................................................................... 31 DISCUSSION....................................................................................................................................... 37 Phase I, issue generation ........................................................................................................ 37 Phase III, pretesting ................................................................................................................ 40 Phase IV, quantitative scale validation ................................................................................... 43 CONCLUSIONS................................................................................................................................... 46 PERSPECTIVES .................................................................................................................................. 47 Summary ......................................................................................................................................... 48 Summary in Danish ........................................................................................................................ 49 REFERENCES..................................................................................................................................... 50 Appendix 1: Danish ThyPRO questionnaire ................................................................................... 55 Appendix 2: ThyPRO questionnaire, in English ............................................................................. 60 Appendix 3: Paper I, Quality of life in patients with benign thyroid disorders. A review ...................... 65 Appendix 4: Paper II, Which domains of thyroid-related quality of life are most relevant? Patients and clinicians provide complementary perspectives ......................................................... 75 Appendix 5: Paper III, Improving a newly developed patient-reported outcome for thyroid patients,
using cognitive interviewing ........................................................................................................ 83 Appendix 6: Paper IV, Establishing a reliable scale structure with convergent and discriminant
validity for a new patient reported outcome measure for patients with thyroid disorders ................. 92
PREFACE
This PhD thesis is the result of invaluable contributions by several persons. The project was initi-
ated by a question from my friend Professor Peder Charles: “If one should measure the quality of
life of thyroid patients, how would you do it?” I offered my help by looking into the literature, to
find out which disease-specific questionnaire would be the best. To my surprise, the only thyroid
patient group for whom such an instrument existed was patients with thyroid eye-disease (the GO-
QOL). From this brief literature review, I also got the notion, that quality of life measurement in
thyroid patients was indeed highly relevant. I was also inspired by a somewhat sensational study
demonstrating QoL-improvement in hypothyroid patients receiving T4/T3 combination treatment.
Peder therefore led me to Ulla Feldt-Rasmussen and Åse Krogh Rasmussen at Rigshospitalet. At
our first meeting, Åse politely pointed to the inherent contradiction between my intentions of per-
forming clinical QoL-studies and my conclusion that a valid QoL-tool for thyroid patients did not
exist, and suggested that I devoted an entire PhD-study on developing such a questionnaire. Ini-
tially, I was not tempted by the idea, but after a few days the reservation turned to eagerness. Luck-
ily, we were able to convince the two leading QoL-experts in the country, Jakob Bjørner and Mo-
gens Grønvold, to be QoL-supervisors, and the project started to take form. While writing protocols
and seeking finances, I worked as a registrar in internal medicine, where I met Steen Bonnema.
Knowing him from the thyroid literature, I had to brag about the project we were planning and it
turned out, that he and Laszlo Hegedüs in Odense were planning to develop a goitre-specific QoL-
instrument. The groups joined and a fruitful collaboration was born.
Without funding, this project would have been still-born. I wish to thank the Danish Medical Re-
search Council (Forskningsrådet for Sundhed og Sygdom), Agnes og Knut Mørks fond, Aase og
Ejnar Danielsens fond, Else og Mogens Wedell-Wedellsborgs fond, Genzyme Corporation and the
Danish Thyroid Foundation (Thyreoidea Landspatientforeningen). A special thank in this regards to
Mark Allyn from Genzyme for his enthusiasm, support and respect for the independent academic
research process.
Page 4 of 107
I wish to thank the colleagues at the Endocrine Departments at Rigshospitalet and Odense Univer-
sity Hospital, who were actively helping with the practical conduction of this study: Elisabeth
Mathiesen, Nils Knudsen, Tonny Jensen, Henrik Ullitz Andersen, Pernille Bach-Mortensen, Ane
Mette Zander Olsen, Heidi Storgaard, Tina Zimmermann-Belsing, Tina Elberling, Lone Larsen,
Helene Rosenørn, Viveque Egsgaard, Finn Bennedbæk and Thomas Brix. I also wish to thank the
staff and colleagues at the Endocrinological-/Nephrological Lab 2131; a special thank to my sister,
Sara Hope Watt, who was an invaluable research assistant and to Alexandra Hegedüs, likewise in
Odense, and to Peder Charles, who started it all. A special thank also to my colleagues at 2131,
Marianne, Vibeke, Peter, Lene and Mads, for discussions and laughter.
This thesis draws on methodology from two scientific traditions, quality of life research and thyroi-
dology. I have aimed to make it comprehensible to readers from both areas and apologize for being
banal when methodology from one area is attempted described in terms expected to be understand-
able to readers from the other area.
Finally, I wish to acknowledge and thank my supervisory team, Professor MD Jakob Bjørner, Na-
tional Research Centre for the Working Environment, MD PhD Steen Bonnema, Dept. of Endocri-
nology and Metabolism, Odense University Hospital, MD PhD Ulla Feldt-Rasmussen (main super-
visor), Dept. of Endocrinology, Copenhagen University Hospital Rigshospitalet, MD PhD Mogens
Grønvold (Project supervisor), Institute of Public Health, University of Copenhagen, Professor, MD
Laszlo Hegedüs, Dept. of Endocrinology and Metabolism, Odense University Hospital, and MD
PhD Åse Krogh Rasmussen, Dept. of Endocrinology, Copenhagen University Hospital Rigshospi-
talet, for their enthusiasm, engagement and support. In this regard, I have to express my grateful-
ness towards the unique, trustful atmosphere of academic freedom and room for creativity and yet
conscious care a young researcher receives under the leadership of my main supervisor, Ulla. Thank
you.
Page 5 of 107
List of abbreviations
CAS Clinical activity score
CASM Cognitive aspects of survey methodology
FDA US food and drug administration fT3 Non-proteinbound triiodothyronine
fT4 Non-proteinbound thyroxine
HRQL Health-related quality of life IRT Item response theory
MOS Medical outcomes study
NOSPECS A system for grading thyroid associated ophthalmopathy OUH Odense University Hospital
PRO Patient-reported outcome
QAS99 Questionnaire appraisal system QoL Quality of life
RH Copenhagen University Hospital Rigshospitalet
T3 Total triiodothyronine T4 Total thyroxine
TAO Thyroid associated ophthalmopathy
Tg-Ab thyroglobulin antibodies ThyPRO Thyroid-specific patient reported outcome
ThyQOL Thyroid-specific quality of life
TPO-Ab thyroid peroxidase antibodies TRAK TSH-receptor antibodies
TSH Thyroid stimulating hormone
Page 6 of 107
INTRODUCTION
Located in the junction between the head and the body, the thyroid gland may be envisioned as a
meeting point between psyche and soma. Somatic diseases within the thyroid have major impact on
the psyche of the patient and vice versa. Previously, a blunted response by thyroid stimulating hor-
mone (TSH) to externally administered TSH-releasing hormone was used in the diagnosis at that
time termed “endogenous depression” – the somatic function of the thyroid is affected in the de-
pressed patient1-3. In the recent quest within psychiatry for the biological correlates of psychiatric
diseases, the thyroid axis has gained renewed focus4. Another line of research has focused on the
consequences for the thyroid of psychological stress. The results from this methodologically chal-
lenging research indicate a possible relationship between psychological stress and subsequent onset
of autoimmune thyroid disease.5-8 Evidence regarding the opposite aetiological pathway, leading
from thyroid disease to psychological distress and psychiatric disease and ultimately reduced qual-
ity of life, is more readily obtained and more clinically relevant, and is indeed the focus for this the-
sis. A large amount of studies have found thyroid diseases to be a major risk factor for such im-
pairments.6, 9-60 Based on the well-documented high impact of psychological distress on quality of
life one might expect, that thyroid diseases pose substantial impact on quality of life.
Within health science, quality of life assessment is a vague and somewhat grandiloquent term cov-
ering measurement of subjective health, in terms of various aspects of physical, mental and social
well-being and function. Traditionally, quality of life has been regarded as a broader term than self-
rated health, the latter being more focused on physical function, symptoms and impact of illness
while the former place more emphasis on subjective aspects such as emotional and role function.
However, following the WHO 1948 definition of health, this seems to be an unnecessary distinc-
tion. In order to distinguish the term as it is applied within health science from other aspects of
quality of life, such as e.g. economy and freedom, the term health-related quality of life (HRQL)
Page 7 of 107
INTRODUCTION has gained wide acceptance. Recently, the broad, descriptive term patient-reported outcome (PRO)
is increasingly being applied, short-circuiting such theoretical discussions. In this thesis, PRO and
HRQL are considered synonymous. In practice, HRQL is assessed by self-completed question-
naires quantifying these various aspects of health (often termed domains), usually by one scale for
each domain. Each scale is usually based on several questions (within questionnaire-context termed
items), though broad, single items assessing overall health or HRQL is also applied. Sometimes,
higher-order domains, integrating several domains of HRQL, are constructed. For example, a
higher-order domain such as “physical health” may be constructed from single scales measuring
various aspects of physical health, e.g. physical function, bodily pain and physical fatigue.
Diseases related to the thyroid gland are very common, affecting individuals of all ages, mainly
women. Thyroid hormones target all cells/organs in the body, mainly as a promoter of metabolism,
and under- or overproduction of hormones therefore affects a broad range of human functions. Two
major disease mechanisms are involved in thyroid diseases, leading to a wide spectrum of clinical
manifestations: enlargement of the gland, termed goitre, and autoimmunity, where the immune sys-
tem falsely targets thyroid structures. Goitre without accompanying dysfunction (termed non-toxic
goitre) may cause neck discomfort and/or cosmetic concerns, but goitre may also be associated with
autonomous function, resulting in overproduction of hormones (hyperthyroidism, in this case
termed toxic nodular goitre). Autoimmunity can be associated with enlargement of the gland (dif-
fuse goitre), but most often leads to disturbed function, with either decreased secretion of thyroid
hormones (autoimmune hypothyroidism) or increased secretion (hyperthyroidism, termed Graves’
disease). A subgroup of patients with Graves’ disease has affection of the eyes, yielding a character-
istic protrusion and irritation of the eyes (termed thyroid associated ophthalmopathy (TAO) or
Graves’ orbitopathy (GO)). The classical symptoms of hypothyroidism are unspecific, but well-
described, with tiredness, slow cerebration, constipation, weight gain and depression as core ele-
Page 8 of 107
INTRODUCTION
ments. The typical symptoms of hyperthyroidism are rapid heart beats, tremor, weight loss, anxiety
and increased sweating.
The importance of involving HRQL-aspects in the evaluation of thyroid patients is increasingly
recognized. 61-63 This is well motivated, since benign thyroid disorders are common and rarely life-
threatening. Thus their treatment mainly deals with optimizing the quality of life of the patients who
can be treated by e.g. thyroid or antithyroid drugs, radioiodine, or surgery. The scientific documen-
tation about how these common, well-known diseases affect people’s lives is very limited, as is the
knowledge about how various treatments moderate these effects. Some questionnaires have been
developed for and have been used in specific thyroid sub-populations,20, 25, 26, 33, 42, 45, 46, 64, 65 but no
validated, thyroid specific patient-reported outcome instrument is available for use across different
thyroid diseases.66 The nature of thyroid diseases necessitates such an approach to HRQL-
measurement in these patients: these diseases are characterized by a substantial overlap between
various disease entities (e.g. coexistence of goitre and hyperthyroidism) and a shift between dis-
eases (e.g. hyperthyroid patients becoming hypothyroid through ablative therapy). If a HRQL-
questionnaire was confined to cover only one of these entities, the results of longitudinal studies
may be misleading, because important HRQL-aspects were not measured.
The purpose of this PhD was therefore to develop a questionnaire in Danish for measurement of
quality of life in patients with benign thyroid diseases.
Page 9 of 107
METHODS
The development followed four phases: phase I, issue generation, where HRQL-issues of possible
relevance for thyroid patients were identified, through a literature review (paper I Quality of life in
patients with benign thyroid disorders. A review. Eur J Endocrinol 2006; 154: 501-10, Appendix 3)
and interviews with clinicians and patients (paper II, Which domains of thyroid-related quality of
life are most relevant? Patients and clinicians provide complementary perspectives. Thyroid 2007;
17(7): 647-54, Appendix 4); phase II, operationalization, where selected, relevant issues were con-
verted to items in a draft questionnaire; phase III, pretesting, where the draft questionnaire was
tested and revised using cognitive interview techniques (paper III, Improving a newly developed
patient-reported outcome for thyroid patients, using cognitive interviewing. Quality of Life Re-
search, online publication ahead of print, Appendix 5); and finally phase IV, quantitative scale vali-
dation, where the reliability and scale validity of the constructed scales were tested in a large sam-
ple of patients(paper IV, Establishing a reliable scale structure with convergent and discriminant
validity for a new patient reported outcome measure for patients with thyroid disorders, Quality of
Life Research, submitted, Appendix 6).
The fact that thyroid diseases often change phenotype during time and treatment, can lead to several
ways of classifying patients. In previous studies, it is not always clear which patients a diagnosis
refers to. For example, many studies concerning “hypothyroid patients” included patients with both
autoimmune hypothyroidism, patients with previous toxic goitre and even with thyroid cancer, who
had been treated with surgery or radioactive iodine, and hence had become hypothyroid. In this the-
sis, the patients were consequently classified according to primary diagnosis, i.e. their initial diag-
nosis, prior to treatment. For example, patients with a non-toxic goitre, who had their thyroid re-
moved and thus have hypothyroidism and receive thyroid hormone replacement, are classified with
a diagnosis of non-toxic goitre. The only exception is patients with TAO, who may have a preced-
ing period of Graves’ disease without TAO.
Page 10 of 107
Phase I, Issue generation
During the quest for previously reported HRQL-issues of relevance for patients with thyroid dis-
eases, a systematic literature search on “thyroid diseases” AND “quality of life” (or related terms),
identified 2033 references. The abstracts were reviewed and possibly relevant articles reviewed in
full length. Further references were identified through the reference lists of these articles, ending up
in a total of 2094 references were screened. Seventy-five of the reviewed references were selected,
based on the following criteria: the study population should be thyroid patients, and the paper
should report on patient-experienced consequences of the thyroid disease. Consequences should be
documented either as a reported frequency or a higher score on a HRQL-scale compared to indi-
viduals without thyroid disease.
During the expert interviews, thirteen medical doctors and two nurses were interviewed. They rated
the relevance of each of the 138 issues identified in the literature review on a 5-point scale
(0=irrelevant to 4=very relevant), separately for each of the patient categories: non-toxic goitre,
toxic nodular goitre, Graves' hyperthyroidism, TAO and primary hypothyroidism. The experts were
instructed to include both frequency and importance of each issue in their considerations. Issues
considered relevant by an expert but absent from the list were recorded and rated as well.
Eighty thyroid patients without major non-thyroidal comorbidities from the endocrinological outpa-
tient clinics at Rigshospitalet and Odense University Hospital were interviewed. The interviews
lasted 1-1.5 hours and were carried out the day the patients were seen in the outpatient clinic. The
patients were selected by a non-random strategic sampling procedure, 67, 68 which aimed at maxi-
mizing the patient variation as regards diagnoses, treatment, disease duration and age (Table 1).
Clinical data were obtained from medical records.
Initially, a semi-structured interview with open-ended questions67 about the consequences of having
a thyroid disorder was conducted. Key issues mentioned spontaneously by the patient during this
part of the interview were registered by the interviewer, in order to discuss them with the patient
later. Subsequently, a structured interview evaluating the issue-list from the literature study was
Page 11 of 107
METHODS – phase I
conducted. Each issue on the issue-list was rated in a two-step procedure: First, the patient selected
the issues they had experienced at any time during their disease. Secondly, the importance, as re-
gards impact on quality of life, of each of the selected items was rated on a 0-4 point scale
(0=unimportant to 4=very important). After the structured interview, the key issues from the semi-
structured interview were discussed with the patient and added to the list of issues if not already on
it.
The relevance of each issue was quantified by three measures: an expert relevance rank for each
patient group, a patient relevance rank for each patient group and one overall relevance rank across
patient groups.
The expert relevance rank was derived by simply ranking the mean (0-4) relevance-ratings de-
scribed above, for each patient group. The issue having the highest mean relevance rating (most
relevant) was ascribed rank #1 and so on.
The patient relevance rank was derived as follows: The mean (0-4) patient importance-rating for
each issue in each patient-group was multiplied by the proportion of patients experiencing the issue
25, 69. For example: anxiety was experienced by 43% of patients with Graves' disease and the mean
importance rating of anxiety in patients with Graves' disease was 3.3; thus anxiety had a relevance
score of (0.43�3.3=) 1.4 in patients with Graves' disease. These calculated relevance scores were
ranked, with the most relevant (highest mean-score) ranked as #1.
The overall relevance rank for each issue was derived as the mean of the patient relevance scores
and the expert relevance ratings, across the five patient-groups. Again, these were ranked, with the
most relevant ranked as #1.
As a compromise between our wish to include as many issues as possible and the need to reduce the
number of items to a feasible amount in a future questionnaire, we selected the most relevant of the
identified issues. This selection was based on the above mentioned ranks: The 75 most relevant
overall (i.e. issues ranking 1-75) were included. In addition, to make sure that issues which were
very important in a single disease group were not missed, issues among the 15 most relevant in any
Page 12 of 107
METHODS – phase I
of the patient groups, according to either experts or patients, were included as well, even if not
among the 75 issues most relevant overall.
The identified issues were categorized using a qualitative, content-based analysis.70 The conceptual
frame-work for this analysis was a combination of a HRQL-model and a clinical, thyroidological
frame-work.11, 15 The HRQL-model was based on the model used in the Medical Outcomes Study
(MOS).71, 72 The MOS conceptualized HRQL as a multi-domain concept involving distinct domains
of physical, mental and social function and well-being and general health perception.73 According
to our literature study66 the HRQL-domains fatigue, social function, cognitive function and sex-life
were very relevant for thyroid patients. Therefore, our MOS-based theoretical frame-work was
elaborated further for these domains.74-78
Thus, each issue was analyzed to identify which domain (e.g. fatigue, social function, hyperthyroid-
ism, etc.) it was relating to, based on its content. Where issues could be classified according to both
frame-works, the HRQL-framework had the highest priority; i.e. impaired memory was not classi-
fied as a symptom of hypothyroidism, but as impaired cognitive function, under the HRQL-
framework. Issues not referable to any of the prespecified domains were analyzed and classified
according to the content.
Phase II, operationalization
The actual design of the questionnaire involved 1) transforming the identified issues into items,
consisting of a question with associated response options, 2) writing instructions and legends, 3)
choosing the order of items, 4) the character of the response options and 5) the graphical format of
the questionnaire79-84.
First, the issues excluded by the selection algorithm in phase I were evaluated through a delphi
round: re-entry of each of the excluded issues was considered by two endocrinologists and myself.
In case two of the participants found the issue too important to exclude at this point, it was retained.
This was the case for three issues: “feeling of being a burden to the family”, “getting into conflicts
Page 13 of 107
METHODS – phase II
with other people” and “difficulty finding the right words”. These were included because they rep-
resented important aspects of the higher-order concepts they were measuring (social function and
cognitive complaints).
Subsequently, the included issues were evaluated with regards to redundancy, primarily in terms of
issues about the same concept or symptom complex, which were adequately covered by other, typi-
cally less detailed wordings. For example, “dissatisfaction with weight” was considered covered by
“felt too thin” and “felt too fat”, “weaker voice” was considered covered by “hoarseness” and all
muscular-skeletal complaints were collapsed into one broad issue.
When deciding which issues to include in a disease-specific questionnaire, two tracks can be fol-
lowed: either to select the standard generic questionnaire that covers the identified issues the best
and then include only issues not captured by the generic questionnaire or to create a comprehensive
questionnaire covering them all. We chose the latter, because our intentions were to develop a new
“standard questionnaire” for use in multiple settings and studies, and we considered it a drawback in
this respect, that the questionnaire could not stand alone, but had to always be administered along
with the standard generic questionnaire, like SF36, to which it had been tied.
Most symptom issues were transformed to items in a one-to-one manner. However, other issues
represented well-established QoL-concepts (cognitive complaints, fatigue, anxiety, depression, so-
cial life, daily life, sex-life, cosmetic concern, overall quality of life) and one new higher-order con-
cept: emotional susceptibility. All of these had high relevance ratings, especially among patients,
and they were operationalized taking prior research and theory into account and aiming at arriving
at multi-item scales measuring these concepts. For each concept, key theoretical literature and exist-
ing measuring instruments were reviewed and a conceptual and measurement model was formu-
lated. The selected items were evaluated for coverage of this model and for expected performance
in a multi-item scale. In case important aspects within the conceptual and measurement model were
missing among the selected wordings from patients, such aspects were added. Also, additional items
were formulated in case the selected items did not cover the full range of impairment. Mainly, this
Page 14 of 107
METHODS – phase II
involved adding positively formulated items in order to cover also the mildest degree of impairment
and thus prevent ceiling effects (i.e., that respondents within the top range of impairment receive the
same score and thus cannot be differentiated, just as possible improvements in a longitudinal study
will not be captured within this group). In the end, the 92 issues were transformed into 99 items,
mostly in a one-to-one manner, but also with some issues converging into fewer items and some
issues diverging into several items.
When formulating disease targeted or specific questionnaires, two measurement principles can be
followed: questions can be asked with or without attribution, i.e. whether respondents are requested
to rate whether they experienced an impairment or problem as part of having a specified condition
(e.g. “Has your thyroid disorder caused you to feel tired?” vs. “Have you felt tired?”). Items with
attribution would be expected to be more specific. However, a precondition for such attributed
items to be valid is that the respondent recognizes the symptom or problem as being caused by her
thyroid disease. According to the frequent instances of “aha-experiences” among interview-patients
when presented to the list of issues identified in the literature in phase I, this precondition cannot
always be assumed to hold. For example, several patients were not aware that a change in attitude,
such as being irritable and emotionally unstable, could be caused by the thyroid disease.
Symptoms and physical and mental well-being and function which could be evaluated directly,
were therefore asked directly, without attribution to thyroid disease (i.e. physical symptoms, tired-
ness, cognitive function, anxiety, depression and emotional susceptibility). A drawback of non-
attributed items is that a given score cannot be interpreted in itself as representing impairment due
to thyroid disease, but must always be interpreted in relation to other groups, e.g. patients without
thyroid diseases or as pre-post treatment scores. Concepts which could be influenced by several
aspects of thyroid diseases in numerous ways, where asked with specific thyroid attribution (social
life impairment, daily life impairment, sexlife impairment and cosmetic concern).
Another decision we made was to ask about the symptoms, problems and states directly, rather than
asking about the bother it may inflict – e.g. asking about whether the respondent has had palpitation
Page 15 of 107
METHODS – phase II
rather than whether she has been bothered by palpitations. Some may argue, that the latter is more
in line with the HRQL-concept – why worry about a symptom if it does not bother the patient?
However, the measurement will thereby be affected by the coping ability of the patient. Instead, the
impact of a symptom on QoL may be evaluated by analyzing the regression of the symptom on
overall QoL-scales.
Given that this was becoming a long questionnaire, it was important to have as uniform response
options as possible, in order to ease completion. We chose a 5-point Likert-like scale asking to
“amount” of symptom/problem/impairment without distinguishing between frequency and severity.
The responses are thus considered evaluations integrating these two dimensions; the same response
from two respondents might thus reflect a mild degree of a symptom present all of the time or a
severe degree of the symptom, which is present a little of the time only. This may require more
cognitive effort from the patient when responding to an item; however, both dimensions are consid-
ered important and the alternative (to ask separately about frequency and intensity) would require
the double number of questions.
The order of items in a questionnaire is important and may influence the responses. For example, in
a study of a classical general self-rated health item, it was found that asking questions regarding
physical diseases prior to the general item, increased the association between the general item and a
scale measuring physical function, compared to when physical disease questions were placed after
the self-rated health item85. In order to take advantage of these context effects, we started the ques-
tionnaire with questions about simpler concepts, such as physical symptoms over physical and men-
tal well-being and function and saved the more complex items regarding impact of thyroid disease
on social life, daily life, etc. till the end of the questionnaire. Thus, when the respondent reached the
more complex items, we hoped to ease this cognitive task and to increase the probability, that all
relevant aspects of the thyroid disease were considered before a response was formulated, because
the respondent had been thinking about these aspects previously. We chose a reference period of 4
weeks, because of the long half lives of the most pervasive thyroid hormones and because there
Page 16 of 107
METHODS – phase II
often is a time lag of weeks or even months, between initiation of thyroid treatment and clinical
effect of the treatment. Also, the symptoms of thyroid dysfunction often fluctuate within weeks and
a longer reference period may give a better picture of the actual QoL-impairment under such cir-
cumstances. The graphical design was heavily influenced by the work by Paul Mullin and col-
leagues.86 They integrate cognitive theory and methods and knowledge about reading and graphics.
An important point is that the logic of the questionnaire should be compatible with the principles
guiding how people read a text. For example, check boxes for answers should come “downstream”
to the associated text; lines, which generally represent graphical stopping points, should not “block”
a path which should be visually followed, as is often the case in standard questionnaires, etc. They
recommend a set of features that characterize an effectively designed questionnaire; it should be
simple, consistent, organized, natural, clear, and attractive. The use of these principles has been
shown to reduce response time and number of items with non-responses, and increase patient un-
derstanding and overall completion rate.86
Phase III, pretesting
Cognitive interviewing is a methodology for questionnaire pretesting, based on theories and evi-
dence about the cognitive processes involved in survey responding. A basic model was formulated
by Tourangeau87 which divides the response process into four components:68 comprehension, re-
trieval, judgment and response.
In the approach of the methodology used here, the interviewer asks questions (probes) about the
processes going on during questionnaire completion. Such probes can be classified into concurrent
and retrospective probes. In concurrent probing, the verbal probes are asked immediately after the
question to be probed, and in retrospective probing, the probes are asked after the entire interview.
Concurrent probing minimizes the risk that respondents forget what was going on when answering a
question, but interrupts the response-process with risk of overlooking context effects, and such a
switching between tasks can be distracting. Furthermore, it may affect the response to subsequent
Page 17 of 107
METHODS – phase III
items. Retrospective probing allows the usual flow of an interview but carries a greater risk of recall
bias and hindsight effects.
Cognitive interview techniques were developed mainly for face-to-face interviews.83, 87 With self-
administered questionnaires, the administration of the questionnaire and the interview uses two dif-
ferent modes of communication, which makes the interruption of the survey logic by concurrent
probing even larger. In this study, we sought to adapt the cognitive interview methodology to better
fit patient self-assessment by developing a modified probing technique for self-administered ques-
tionnaires, immediate retrospective probing: we identified natural “breaking points” in the ques-
tionnaire (e.g. a change in topic, end of a page) where our verbal probes could be administered.
Thus, the respondent would self-complete a section of the questionnaire until reaching a “breaking
point”, where the interviewer would conduct a cognitive interview covering that section. The re-
spondent would then self-complete the next section and so on.
The interview consisted of 109 verbal probes, 57 specific and 52 non-specific.67 The non-specific
probes consisted of 5 probes administered after the completion of each of the 11 pages, covering the
4 cognitive processes in the four-stage model.68, 87 The specific probes were developed to cover
specific potential problems identified using the question appraisal system (QAS99) developed by
Willis et al.,67 which is a system aimed at identifying potential problems in questionnaires, includ-
ing problems within the Tourangeau model. Of the specific probes, 50 concerned comprehension,
four concerned retrieval, two judgment, three response and two was about acceptability. In addition,
the interviewer used emergent probing,67 when triggered by respondent behaviour (hesitation,
comments, sounds or gestures during questionnaire completion).
In order to evaluate the problems within the Tourangeau conceptual model, each problem was ana-
lyzed with regard to which of the four cognitive components involved in the survey responding
process was causing the problem. Problems not clearly related to any of the four components of the
Tourangeau model were content-analyzed and categorized accordingly. Data were analyzed after
Page 18 of 107
METHODS – phase III
approximately (depending on logistics) 5 interviews, and the questionnaire was revised, addressing
the problems raised. This process was repeated until only few significant new problems occurred.
Six rounds of interviews were conducted, each round including four to nine patients, yielding six
successively improved questionnaire versions and each interview lasted one hour on average (33
minutes to 1:23 hour). In total, 31 thyroid patients (Table 1), without major non-thyroidal comor-
bidity, sampled and described as in phase I, were interviewed.
Phase IV, quantitative scale validation
The draft questionnaire consisted of 98 items (two of the 99 item entering phase III were collapsed
into one during revisions, see Results) with a hypothesized structure of 14 domains: four symptom
domains covering the disease mechanisms in play within thyroid disorders (neck related goitre
symptoms, symptoms of hyperthyroidism, symptoms of hypothyroidism and eye symptoms), five
domains of physical and mental function and well-being and five impact domains concerning im-
pact of thyroid disease on central aspects of quality of life (Figure 2). In addition, there were two
physical symptoms not ascribable to any of the scales a priori: “Sleeping problems” and “Dizzi-
ness”. Each question (item) was rated on a five-point scale from 0=not at all to 4=very much, with a
4 weeks reference period. The multi-item scales were derived by averaging item scores within a
scale and linearly transforming them to a 0-100 scale with 0 being the best and 100 being the worst
possible score.
Also in this phase, the patients were recruited from the outpatient endocrine clinics at Rigshospitalet
and Odense University Hospital. At RH, the sampling strategy was cross-sectional: from February
June 2007, all thyroid patients born within the first 20 days of each month (to limit running sample
size) were invited by mail 3 weeks prior to their appointment in the clinic. A few days prior to the
appointment, participants came to a research laboratory for a study-specific visit where blood-
samples were drawn, a thyroid ultrasound scan performed and a written, signed informed consent
obtained by the medical staff. Questionnaires were either returned by mail or delivered by hand in
Page 19 of 107
METHODS – phase IV
the lab or at the clinic on the day of appointment. At OUH, all eligible patients referred to the thy-
roid unit of the endocrine outpatient clinic in the period May to November 2007 were recruited. The
questionnaire was sent about three weeks prior to the appointment, blood-samples were drawn the
week preceding their appointment, as part of the usual routine, and an ultrasound scan performed at
their visit to the clinic. Here, written signed informed consent was obtained by the endocrinologist.
At both sites, the patients were instructed to complete the questionnaire at the time when blood-
samples were drawn. Exclusion criteria were absence of any thyroid disorder, thyroid cancer, age
less than 15 and inability to complete a questionnaire due to communication problems (non-Danish
speaking, blindness, etc.). One reminder was sent after two weeks to non-responders.
Sociodemographic data and information about co-morbidity and non-thyroid medication were self-
reported. Paraclinical data, exact diagnosis, previous and current treatment and time of diagnosis
among respondents were obtained by chart review. Biochemical thyroid tests were thyroid stimulat-
ing hormone (TSH), total thyroxine (T4), total triiodothyronine (T3), non-proteinbound thyroxine
(fT4), non-proteinbound triiodothyronine (fT3), resin-T3-test (only OUH), thyroid peroxidase anti-
bodies (TPO-Ab), thyroglobulin antibodies (Tg-Ab, only in patients diagnosed with hypothyroidism
and negative TPO-Ab)) and TSH-receptor antibodies (TRAK, only in patients with a diagnosis of
hyperthyroidism). All analyses were performed using the standard methods at the laboratories of the
participating hospitals, except TRAK and TPO-Ab at RH, which were measured by duplicate-
measurements using BRAHMS TRAK-human and anti-TPOn radioimmunoassay. In patients with
thyroid eye-disease (thyroid-associated ophthalmopathy, TAO), NOSPECS88 classification was
performed by an ophthalmologist and Clinical Activity Scoring (CAS89) was performed by a physi-
cian. Thyroid volume was determined by ultrasound, using the ellipsoid method.90, 91 In the sub-
group analyses, the patients are aggregated in the previously described five major diagnostic catego-
ries: 1) non-toxic goitre comprising diffuse, uni- and multinodular non-toxic goitre as well as thy-
roid cysts. 2) toxic nodular goitre, comprising both uni- and multinodular disease. 3) Graves’ dis-
ease. 4) TAO. 5) autoimmune hypothyroidism. Subacute thyroiditis (De Quervain’s thyroiditis),
Page 20 of 107
METHODS – phase IV
postpartum thyroiditis and various other rare benign thyroid diseases (e.g. amiodarone- and lithium
induced thyroiditis, Riedel’s thyroiditis, thyroid agenesis, etc.) were not included in the diagnostic
subgroup analyses. Self-completed data were entered using optical scanning. All clinical data were
entered via SPSS Data Entry Builder 4.0 by medical staff. Data were converted to SAS datasets and
all analyses were performed with SAS 9.1. The project was approved by the local ethical committee
(KF01 2006-1579) and the Danish data protection agency and registered at ClinicalTrials.gov
(NCT00150033).
Multitrait scaling92-94 was used to evaluate whether all items in a scale appear to measure one unify-
ing concept (convergent validity), which is distinct from concepts measured by other scales (dis-
criminant validity). The analyses were performed on Pearson correlations between items and scales
and between scales. Item correlation with own scales were corrected for overlap. Item-own scale
correlations above 0.40 were considered indicative of appropriate convergent validity, and item-
other scale correlations lower than item-own scale correlations were identified as appropriate dis-
criminant validity. Reliability was estimated as internal consistency reliability, using Cronbach’s
alpha.95 Analyses were also performed using polychoric correlations,96-98 to allow for the skewness
often found in data like these.98
Initial analyses were performed on the total sample. Subgroup analyses were subsequently per-
formed with respect to recruiting hospital, gender, age-group (young (<40 years old), middle-aged
(40-60) and old (>60)) and primary thyroid diagnosis: non-toxic goitre, toxic nodular goitre,
Graves’ hyperthyroidism without signs of eye affection, TAO with or without hyperthyroidism and
autoimmune hypothyroidism with or without goitre. Based on these analyses, the scale structure
was revised and the analyses were repeated using the revised scale structure.
Page 21 of 107
RESULTS – phase I
RESULTS
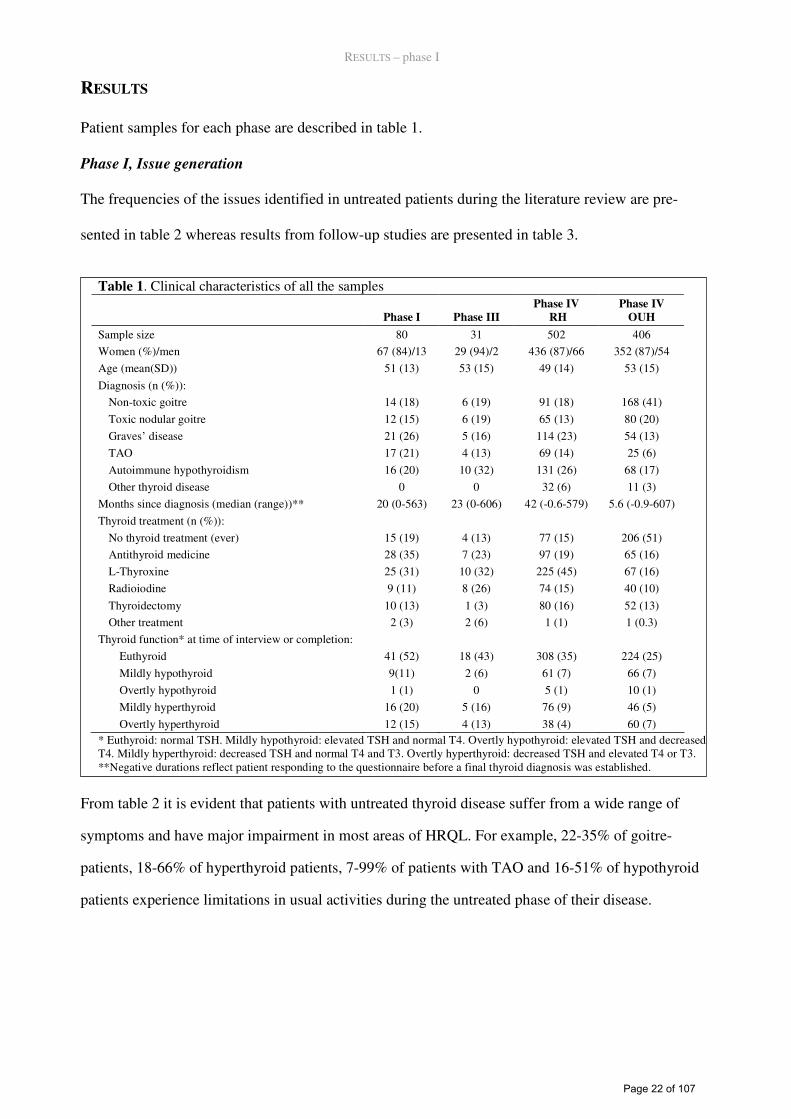
Patient samples for each phase are described in table 1.
Phase I, Issue generation
The frequencies of the issues identified in untreated patients during the literature review are pre-
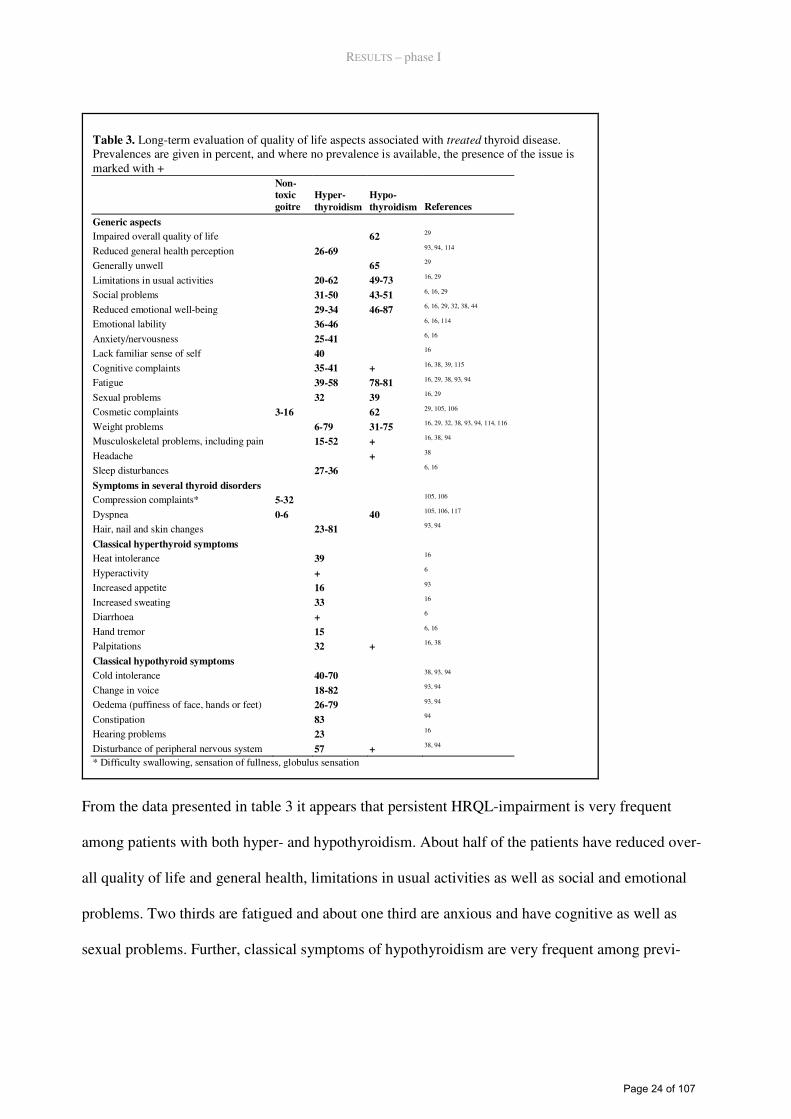
sented in table 2 whereas results from follow-up studies are presented in table 3.
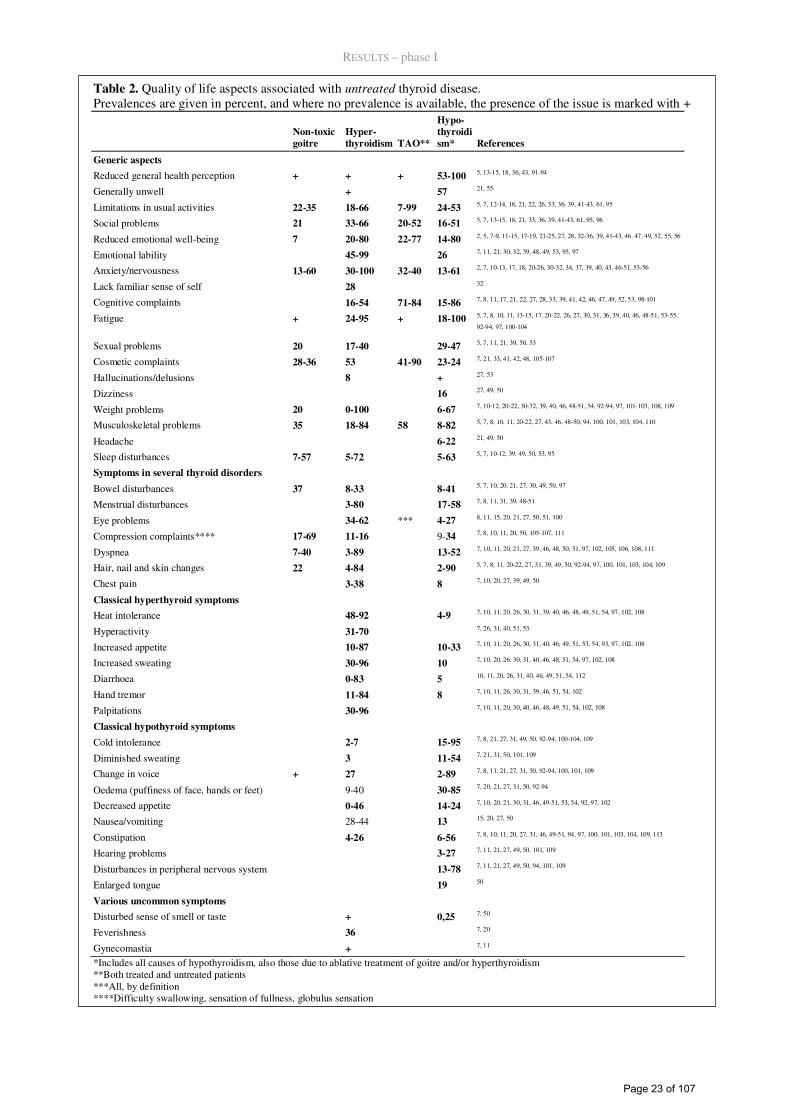
From table 2 it is evident that patients with untreated thyroid disease suffer from a wide range of
symptoms and have major impairment in most areas of HRQL. For example, 22-35% of goitre-
patients, 18-66% of hyperthyroid patients, 7-99% of patients with TAO and 16-51% of hypothyroid
patients experience limitations in usual activities during the untreated phase of their disease.
Table 1. Clinical characteristics of all the samples
Phase I Phase III
Phase IV
RH
Phase IV
OUH
Sample size 80 31 502 406
Women (%)/men 67 (84)/13 29 (94)/2 436 (87)/66 352 (87)/54
Age (mean(SD)) 51 (13) 53 (15) 49 (14) 53 (15)
Diagnosis (n (%)): Non-toxic goitre 14 (18) 6 (19) 91 (18) 168 (41)
Toxic nodular goitre 12 (15) 6 (19) 65 (13) 80 (20)
Graves’ disease 21 (26) 5 (16) 114 (23) 54 (13)
TAO 17 (21) 4 (13) 69 (14) 25 (6)
Autoimmune hypothyroidism 16 (20) 10 (32) 131 (26) 68 (17)
Other thyroid disease 0 0 32 (6) 11 (3)
Months since diagnosis (median (range))** 20 (0-563) 23 (0-606) 42 (-0.6-579) 5.6 (-0.9-607)
Thyroid treatment (n (%)):
No thyroid treatment (ever) 15 (19) 4 (13) 77 (15) 206 (51)
Antithyroid medicine 28 (35) 7 (23) 97 (19) 65 (16)
L-Thyroxine 25 (31) 10 (32) 225 (45) 67 (16)
Radioiodine 9 (11) 8 (26) 74 (15) 40 (10)
Thyroidectomy 10 (13) 1 (3) 80 (16) 52 (13)
Other treatment 2 (3) 2 (6) 1 (1) 1 (0.3)
Thyroid function* at time of interview or completion:
Euthyroid 41 (52) 18 (43) 308 (35) 224 (25)
Mildly hypothyroid 9(11) 2 (6) 61 (7) 66 (7)
Overtly hypothyroid 1 (1) 0 5 (1) 10 (1)
Mildly hyperthyroid 16 (20) 5 (16) 76 (9) 46 (5)
Overtly hyperthyroid 12 (15) 4 (13) 38 (4) 60 (7) * Euthyroid: normal TSH. Mildly hypothyroid: elevated TSH and normal T4. Overtly hypothyroid: elevated TSH and decreased T4. Mildly hyperthyroid: decreased TSH and normal T4 and T3. Overtly hyperthyroid: decreased TSH and elevated T4 or T3. **Negative durations reflect patient responding to the questionnaire before a final thyroid diagnosis was established.
Page 22 of 107
RESULTS – phase I
Table 2. Quality of life aspects associated with untreated thyroid disease. Prevalences are given in percent, and where no prevalence is available, the presence of the issue is marked with +
Non-toxic
goitre
Hyper-
thyroidism TAO**
Hypo-
thyroidi
sm* References
Generic aspects
Reduced general health perception + + + 53-100 5, 13-15, 18, 36, 43, 91-94
Generally unwell + 57 21, 55
Limitations in usual activities 22-35 18-66 7-99 24-53 5, 7, 12-14, 18, 21, 22, 26, 33, 36, 39, 41-43, 61, 95
Social problems 21 33-66 20-52 16-51 5, 7, 13-15, 18, 21, 33, 36, 39, 41-43, 61, 95, 96
Reduced emotional well-being 7 20-80 22-77 14-80 2, 5, 7-9, 11-15, 17-19, 21-25, 27, 28, 32-36, 39, 41-43, 46, 47, 49, 52, 55, 56
Emotional lability 45-99 26 7, 11, 21, 30, 32, 39, 48, 49, 53, 95, 97
Anxiety/nervousness 13-60
30-100 32-40 13-61 2, 7, 10-13, 17, 18, 20-26, 30-32, 34, 37, 39, 40, 43, 46-51, 53-56
Lack familiar sense of self 28 32
Cognitive complaints 16-54 71-84 15-86 7, 8, 11, 17, 21, 22, 27, 28, 33, 39, 41, 42, 46, 47, 49, 52, 53, 98-101
Fatigue + 24-95 + 18-100 5, 7, 8, 10, 11, 13-15, 17, 20-22, 26, 27, 30, 31, 36, 39, 40, 46, 48-51, 53-55,
92-94, 97, 100-104
Sexual problems 20 17-40 29-47 5, 7, 11, 21, 39, 50, 53
Cosmetic complaints 28-36 53 41-90 23-24 7, 21, 33, 41, 42, 48, 105-107
Hallucinations/delusions 8 + 27, 53
Dizziness 16 27, 49, 50
Weight problems 20 0-100 6-67 7, 10-12, 20-22, 30-32, 39, 40, 46, 48-51, 54, 92-94, 97, 101-103, 108, 109
Musculoskeletal problems 35 18-84 58 8-82 5, 7, 8, 10, 11, 20-22, 27, 43, 46, 48-50, 94, 100, 101, 103, 104, 110
Headache 6-22 21, 49, 50
Sleep disturbances 7-57 5-72 5-63 5, 7, 10-12, 39, 49, 50, 53, 95
Symptoms in several thyroid disorders
Bowel disturbances 37 8-33 8-41 5, 7, 10, 20, 21, 27, 30, 49, 50, 97
Menstrual disturbances 3-80 17-58 7, 8, 11, 31, 39, 48-51
Eye problems 34-62 *** 4-27 8, 11, 15, 20, 21, 27, 50, 51, 100
Compression complaints**** 17-69 11-16 9-34 7, 8, 10, 11, 20, 50, 105-107, 111
Dyspnea 7-40 3-89 13-52 7, 10, 11, 20, 21, 27, 39, 46, 48, 50, 51, 97, 102, 105, 106, 108, 111
Hair, nail and skin changes 22 4-84 2-90 5, 7, 8, 11, 20-22, 27, 31, 39, 49, 50, 92-94, 97, 100, 101, 103, 104, 109
Chest pain 3-38 8 7, 10, 20, 27, 39, 49, 50
Classical hyperthyroid symptoms
Heat intolerance 48-92 4-9 7, 10, 11, 20, 26, 30, 31, 39, 40, 46, 48, 49, 51, 54, 97, 102, 108
Hyperactivity 31-70 7, 26, 31, 40, 51, 53
Increased appetite 10-87 10-33 7, 10, 11, 20, 26, 30, 31, 40, 46, 49, 51, 53, 54, 93, 97, 102, 108
Increased sweating 30-96 10 7, 10, 20, 26, 30, 31, 40, 46, 48, 51, 54, 97, 102, 108
Diarrhoea 0-83 5 10, 11, 20, 26, 31, 40, 46, 49, 51, 54, 112
Hand tremor 11-84 8 7, 10, 11, 26, 30, 31, 39, 46, 51, 54, 102
Palpitations 30-96 7, 10, 11, 20, 30, 40, 46, 48, 49, 51, 54, 102, 108
Classical hypothyroid symptoms
Cold intolerance 2-7 15-95 7, 8, 21, 27, 31, 49, 50, 92-94, 100-104, 109
Diminished sweating 3 11-54 7, 21, 31, 50, 101, 109
Change in voice + 27 2-89 7, 8, 11, 21, 27, 31, 50, 92-94, 100, 101, 109
Oedema (puffiness of face, hands or feet) 9-40 30-85 7, 20, 21, 27, 31, 50, 92-94
Decreased appetite 0-46 14-24 7, 10, 20, 21, 30, 31, 46, 49-51, 53, 54, 92, 97, 102
Nausea/vomiting 28-44 13 15, 20, 27, 50
Constipation 4-26 6-56 7, 8, 10, 11, 20, 27, 31, 46, 49-51, 94, 97, 100, 101, 103, 104, 109, 113
Hearing problems 3-27 7, 11, 21, 27, 49, 50, 101, 109
Disturbances in peripheral nervous system 13-78 7, 11, 21, 27, 49, 50, 94, 101, 109
Enlarged tongue 19 50
Various uncommon symptoms
Disturbed sense of smell or taste + 0,25 7, 50
Feverishness 36 7, 20
Gynecomastia + 7, 11 *Includes all causes of hypothyroidism, also those due to ablative treatment of goitre and/or hyperthyroidism **Both treated and untreated patients ***All, by definition ****Difficulty swallowing, sensation of fullness, globulus sensation
Page 23 of 107
RESULTS – phase I
Table 3. Long-term evaluation of quality of life aspects associated with treated thyroid disease. Prevalences are given in percent, and where no prevalence is available, the presence of the issue is marked with + Non-
toxic
goitre
Hyper-
thyroidism
Hypo-
thyroidism References
Generic aspects Impaired overall quality of life 62 29
Reduced general health perception 26-69 93, 94, 114 Generally unwell 65 29
Limitations in usual activities 20-62 49-73 16, 29
Social problems 31-50 43-51 6, 16, 29
Reduced emotional well-being 29-34 46-87 6, 16, 29, 32, 38, 44
Emotional lability 36-46 6, 16, 114
Anxiety/nervousness 25-41 6, 16 Lack familiar sense of self 40 16
Cognitive complaints 35-41 + 16, 38, 39, 115
Fatigue 39-58 78-81 16, 29, 38, 93, 94
Sexual problems 32 39 16, 29
Cosmetic complaints 3-16 62 29, 105, 106
Weight problems 6-79 31-75 16, 29, 32, 38, 93, 94, 114, 116
Musculoskeletal problems, including pain 15-52 + 16, 38, 94
Headache + 38
Sleep disturbances 27-36 6, 16
Symptoms in several thyroid disorders Compression complaints* 5-32 105, 106
Dyspnea 0-6 40 105, 106, 117
Hair, nail and skin changes 23-81 93, 94
Classical hyperthyroid symptoms Heat intolerance 39 16
Hyperactivity + 6 Increased appetite 16 93
Increased sweating 33 16 Diarrhoea + 6
Hand tremor 15 6, 16 Palpitations 32 + 16, 38
Classical hypothyroid symptoms Cold intolerance 40-70 38, 93, 94
Change in voice 18-82 93, 94 Oedema (puffiness of face, hands or feet) 26-79 93, 94
Constipation 83 94 Hearing problems 23 16
Disturbance of peripheral nervous system 57 + 38, 94
* Difficulty swallowing, sensation of fullness, globulus sensation
From the data presented in table 3 it appears that persistent HRQL-impairment is very frequent
among patients with both hyper- and hypothyroidism. About half of the patients have reduced over-
all quality of life and general health, limitations in usual activities as well as social and emotional
problems. Two thirds are fatigued and about one third are anxious and have cognitive as well as
sexual problems. Further, classical symptoms of hypothyroidism are very frequent among previ-
Page 24 of 107
RESULTS – phase I
ously hyperthyroid patients and about a third has persistent hyperthyroid symptoms. In total, 138
issues were identified.
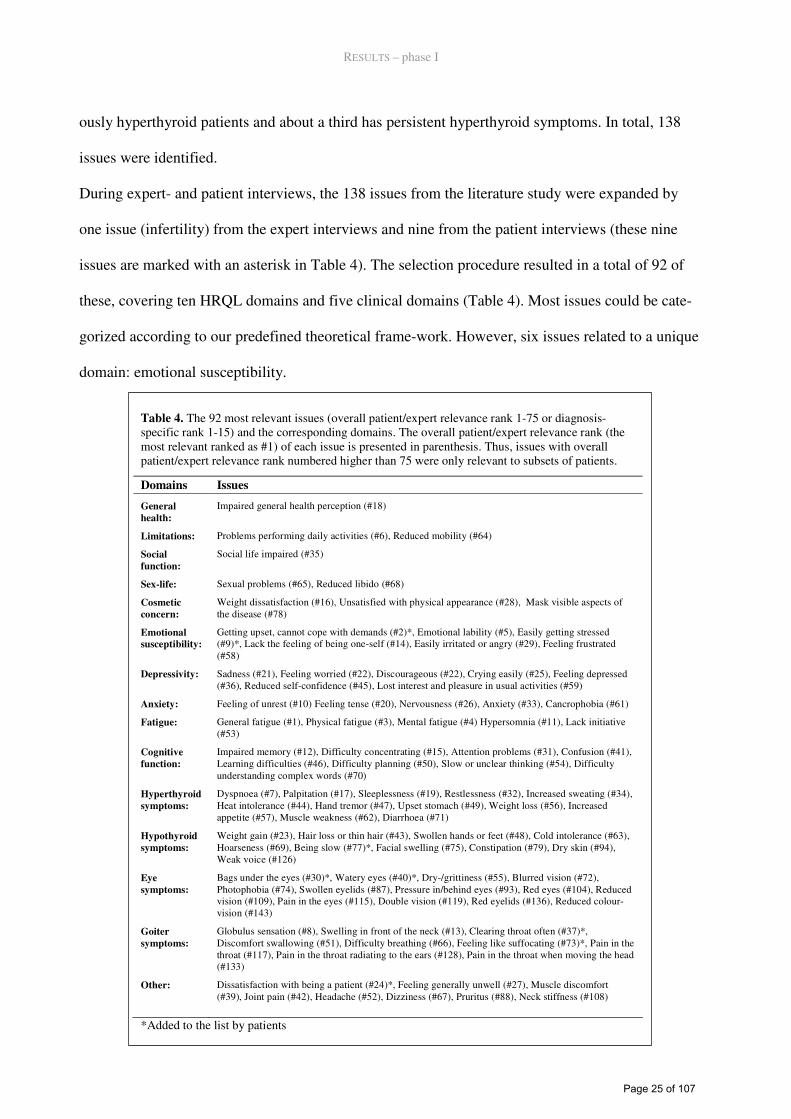
During expert- and patient interviews, the 138 issues from the literature study were expanded by
one issue (infertility) from the expert interviews and nine from the patient interviews (these nine
issues are marked with an asterisk in Table 4). The selection procedure resulted in a total of 92 of
these, covering ten HRQL domains and five clinical domains (Table 4). Most issues could be cate-
gorized according to our predefined theoretical frame-work. However, six issues related to a unique
domain: emotional susceptibility.
Table 4. The 92 most relevant issues (overall patient/expert relevance rank 1-75 or diagnosis-specific rank 1-15) and the corresponding domains. The overall patient/expert relevance rank (the most relevant ranked as #1) of each issue is presented in parenthesis. Thus, issues with overall patient/expert relevance rank numbered higher than 75 were only relevant to subsets of patients.
*Added to the list by patients
Domains Issues
General
health:
Impaired general health perception (#18)
Limitations: Problems performing daily activities (#6), Reduced mobility (#64)
Social
function:
Social life impaired (#35)
Sex-life: Sexual problems (#65), Reduced libido (#68)
Cosmetic
concern:
Weight dissatisfaction (#16), Unsatisfied with physical appearance (#28), Mask visible aspects of the disease (#78)
Emotional
susceptibility:
Getting upset, cannot cope with demands (#2)*, Emotional lability (#5), Easily getting stressed (#9)*, Lack the feeling of being one-self (#14), Easily irritated or angry (#29), Feeling frustrated (#58)
Depressivity: Sadness (#21), Feeling worried (#22), Discourageous (#22), Crying easily (#25), Feeling depressed (#36), Reduced self-confidence (#45), Lost interest and pleasure in usual activities (#59)
Anxiety: Feeling of unrest (#10) Feeling tense (#20), Nervousness (#26), Anxiety (#33), Cancrophobia (#61)
Fatigue: General fatigue (#1), Physical fatigue (#3), Mental fatigue (#4) Hypersomnia (#11), Lack initiative (#53)
Cognitive
function:
Impaired memory (#12), Difficulty concentrating (#15), Attention problems (#31), Confusion (#41), Learning difficulties (#46), Difficulty planning (#50), Slow or unclear thinking (#54), Difficulty understanding complex words (#70)
Hyperthyroid
symptoms:
Dyspnoea (#7), Palpitation (#17), Sleeplessness (#19), Restlessness (#32), Increased sweating (#34), Heat intolerance (#44), Hand tremor (#47), Upset stomach (#49), Weight loss (#56), Increased appetite (#57), Muscle weakness (#62), Diarrhoea (#71)
Hypothyroid
symptoms:
Weight gain (#23), Hair loss or thin hair (#43), Swollen hands or feet (#48), Cold intolerance (#63), Hoarseness (#69), Being slow (#77)*, Facial swelling (#75), Constipation (#79), Dry skin (#94), Weak voice (#126)
Eye
symptoms:
Bags under the eyes (#30)*, Watery eyes (#40)*, Dry-/grittiness (#55), Blurred vision (#72), Photophobia (#74), Swollen eyelids (#87), Pressure in/behind eyes (#93), Red eyes (#104), Reduced vision (#109), Pain in the eyes (#115), Double vision (#119), Red eyelids (#136), Reduced colour-vision (#143)
Goiter
symptoms:
Globulus sensation (#8), Swelling in front of the neck (#13), Clearing throat often (#37)*, Discomfort swallowing (#51), Difficulty breathing (#66), Feeling like suffocating (#73)*, Pain in the throat (#117), Pain in the throat radiating to the ears (#128), Pain in the throat when moving the head (#133)
Other: Dissatisfaction with being a patient (#24)*, Feeling generally unwell (#27), Muscle discomfort (#39), Joint pain (#42), Headache (#52), Dizziness (#67), Pruritus (#88), Neck stiffness (#108)
Page 25 of 107
RESULTS – phase I
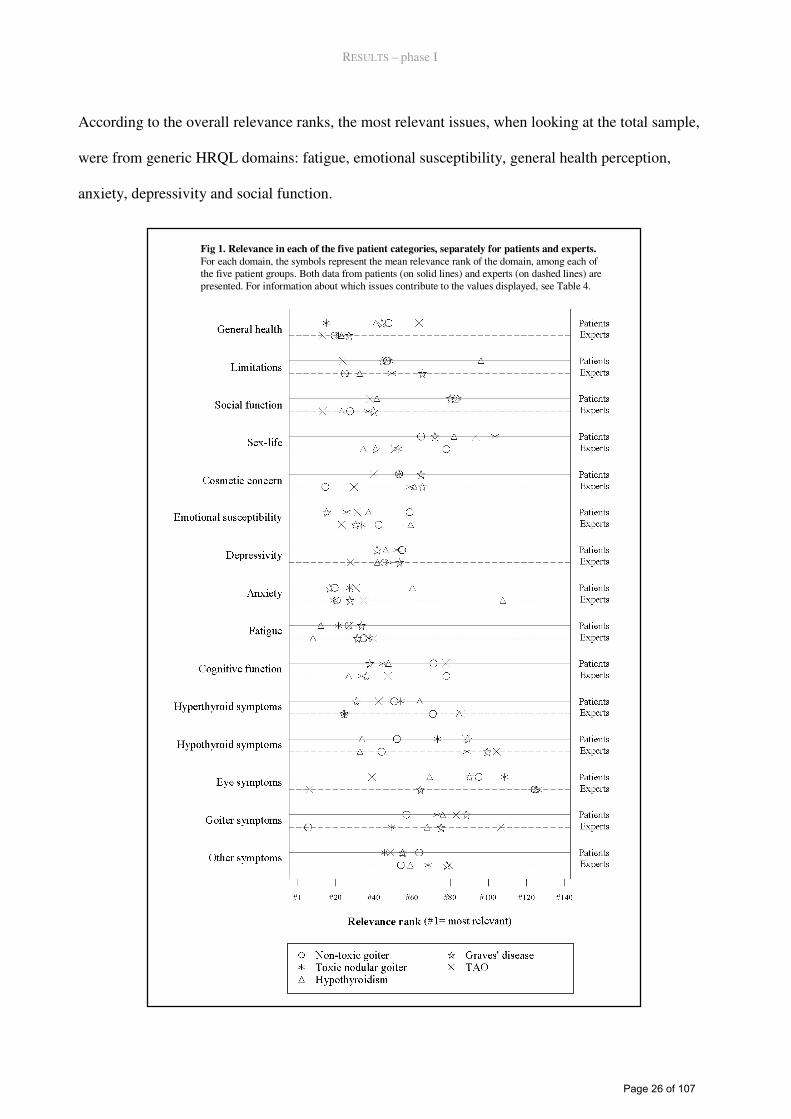
According to the overall relevance ranks, the most relevant issues, when looking at the total sample,
were from generic HRQL domains: fatigue, emotional susceptibility, general health perception,
anxiety, depressivity and social function.
Fig 1. Relevance in each of the five patient categories, separately for patients and experts.
For each domain, the symbols represent the mean relevance rank of the domain, among each of the five patient groups. Both data from patients (on solid lines) and experts (on dashed lines) are presented. For information about which issues contribute to the values displayed, see Table 4.
Page 26 of 107
RESULTS – phase I
In Figure 1, the mean relevance ranks of the 15 domains are displayed, separately for patients and
experts and for each diagnosis (for information about which issues contribute to the domain-score,
see table 4). Focusing thus on the individual patient groups, it is evident, that symptoms associated
with each diagnosis were very relevant for the patient groups with that particular diagnosis, in con-
trast to what was found regarding the overall relevance ranks in Table 4. Thus, compared to other
domains (comparisons cannot be validly made across diagnoses, because the relevance ratings have
been ranked according to relative relevance within each patient group) hypothyroid symptoms were
very relevant to patients with hypothyroidism, eye symptoms were very relevant to patients with
TAO, local pressure symptoms were very relevant to patients with non-toxic goitre and hyperthy-
roid symptoms were very relevant to patients with hyperthyroidism. An exception was toxic nodular
goitre-patients rating hyperthyroid symptoms as relatively less relevant than other domains.
Phase II, operationalization
The final Danish questionnaire is presented in Appendix 1, and an English version is found in Ap-
pendix 2.
Phase III, pretesting
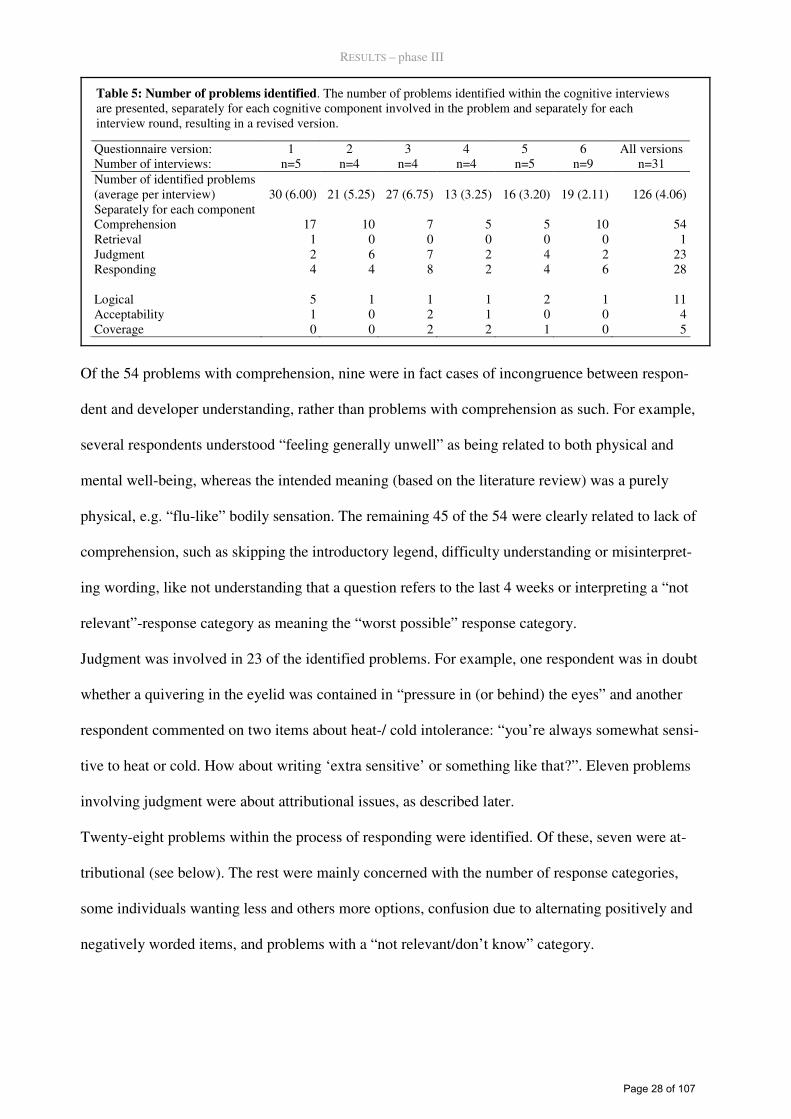
In total, problems in the questionnaire response process were identified 126 times during the 31
interviews (Table 5). Problems were identified in 43 of the 99 tested items, in 4 of the 15 introduc-
tions or legends and in 4 of the 5 various response categories. Fifty-four problems involved com-
prehension, one concerned retrieval, 23 related to judgment, 28 were with responding and 20 were
outside the four-stage model of cognitive processes involved in questionnaire completion.
Page 27 of 107
RESULTS – phase III
Table 5: Number of problems identified. The number of problems identified within the cognitive interviews are presented, separately for each cognitive component involved in the problem and separately for each interview round, resulting in a revised version.
Questionnaire version: 1 2 3 4 5 6 All versions Number of interviews: n=5 n=4 n=4 n=4 n=5 n=9 n=31 Number of identified problems (average per interview) 30 (6.00) 21 (5.25) 27 (6.75) 13 (3.25) 16 (3.20) 19 (2.11) 126 (4.06) Separately for each component Comprehension 17 10 7 5 5 10 54 Retrieval 1 0 0 0 0 0 1 Judgment 2 6 7 2 4 2 23 Responding 4 4 8 2 4 6 28 Logical 5 1 1 1 2 1 11 Acceptability 1 0 2 1 0 0 4 Coverage 0 0 2 2 1 0 5
Of the 54 problems with comprehension, nine were in fact cases of incongruence between respon-
dent and developer understanding, rather than problems with comprehension as such. For example,
several respondents understood “feeling generally unwell” as being related to both physical and
mental well-being, whereas the intended meaning (based on the literature review) was a purely
physical, e.g. “flu-like” bodily sensation. The remaining 45 of the 54 were clearly related to lack of
comprehension, such as skipping the introductory legend, difficulty understanding or misinterpret-
ing wording, like not understanding that a question refers to the last 4 weeks or interpreting a “not
relevant”-response category as meaning the “worst possible” response category.
Judgment was involved in 23 of the identified problems. For example, one respondent was in doubt
whether a quivering in the eyelid was contained in “pressure in (or behind) the eyes” and another
respondent commented on two items about heat-/ cold intolerance: “you’re always somewhat sensi-
tive to heat or cold. How about writing ‘extra sensitive’ or something like that?”. Eleven problems
involving judgment were about attributional issues, as described later.
Twenty-eight problems within the process of responding were identified. Of these, seven were at-
tributional (see below). The rest were mainly concerned with the number of response categories,
some individuals wanting less and others more options, confusion due to alternating positively and
negatively worded items, and problems with a “not relevant/don’t know” category.
Page 28 of 107
RESULTS – phase III
We also identified 20 problems outside the Tourangeau model. Eleven of these were problems in
the inherent logic or structure of the questionnaire,67 such as implicit assumptions (an item asking
about difficulty learning presupposed having faced a learning task) or unclear definitions of social
network. Four problems were about acceptability, of which two concerned the two items about sex-
life, one was about the wording “managing your feelings” and one found the introduction too per-
suasive. Finally, five problems were about whether the questionnaire lacked coverage of specific
issues experienced by the patients.
A particular kind of problem was identified among 11 of the problems within judgment and 7 prob-
lems within comprehension. These problems were categorized as “attributional problems”. They
concerned considerations about whether the content of the question was causally related to the thy-
roid disease or not and hence whether or not to report problems not considered being caused by the
thyroid disease. For example, one respondent said “I have a question: right now, I have other symp-
toms, which makes it difficult. Shall I answer according to the (thyroid) disease or an overall judg-
ment?” And another one: “If I was sitting at home, I would probably answer according to what has
to do with my thyroid; much of it has to do with my age”. Finally: “All of it is about a particular
disease, so you have that in the back of your head”. These comments concerned items that have
specific instructions to base the answers on an overall evaluation (as opposed to focusing on thyroid
disease).
Based on the problems identified in each round of interviews, the questionnaire was revised, reduc-
ing the number of problems per interview successively from initially six to two (Table 2). This was
due mainly to a reduction of the number of comprehension problems (from 3 to 1 per interview) and
logical problems (with version 1, 5 problems were identified in 5 interviews; with version 6, 1 prob-
lem was identified in 9 interviews), whereas the number of problems within judgment and respond-
ing (from 6 problems in 5 interviews to 8 problems in 9 interviews) were more constant. A total of
30 revisions were made in 22 of the 99 items (Table 6). Twelve revisions were made in version 1,
four in version 2, three in version 3, two in version 4 and nine in version 5. Within the 22 revised
Page 29 of 107
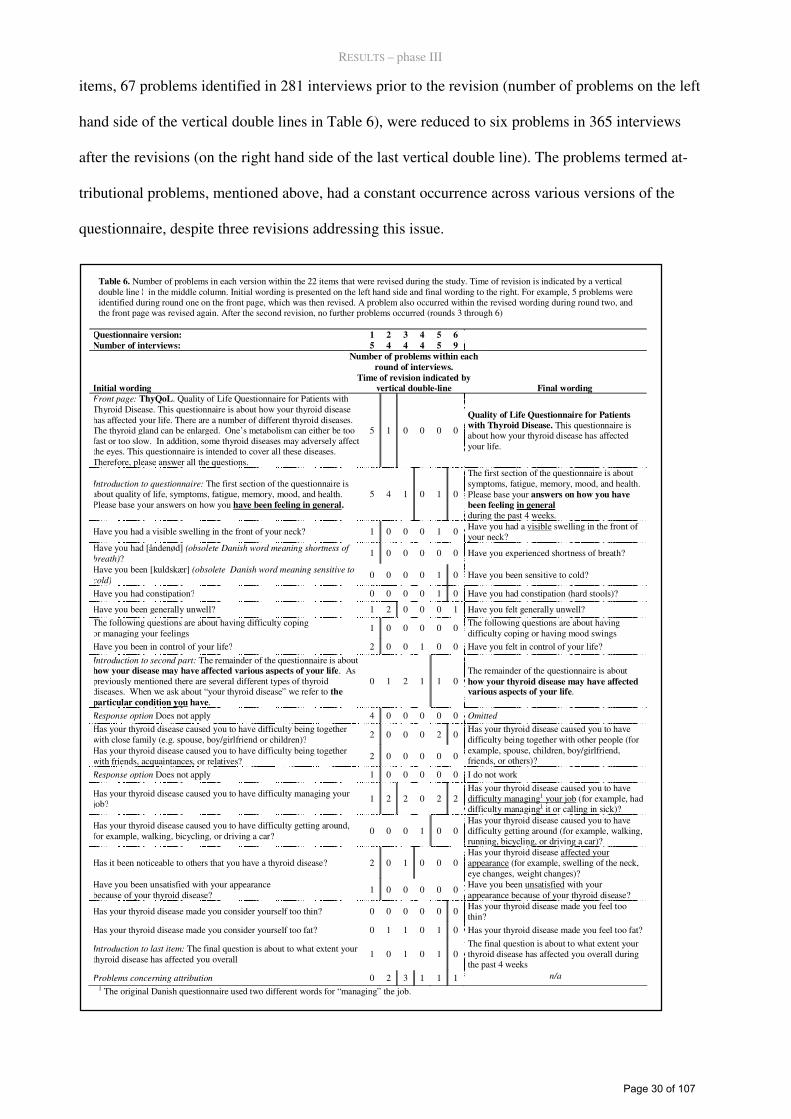
RESULTS – phase III
items, 67 problems identified in 281 interviews prior to the revision (number of problems on the left
hand side of the vertical double lines in Table 6), were reduced to six problems in 365 interviews
after the revisions (on the right hand side of the last vertical double line). The problems termed at-
tributional problems, mentioned above, had a constant occurrence across various versions of the
questionnaire, despite three revisions addressing this issue.
Table 6. Number of problems in each version within the 22 items that were revised during the study. Time of revision is indicated by a vertical double line ¦ in the middle column. Initial wording is presented on the left hand side and final wording to the right. For example, 5 problems were identified during round one on the front page, which was then revised. A problem also occurred within the revised wording during round two, and the front page was revised again. After the second revision, no further problems occurred (rounds 3 through 6)
Questionnaire version: 1 2 3 4 5 6 Number of interviews: 5 4 4 4 5 9
Initial wording
Number of problems within each
round of interviews.
Time of revision indicated by vertical double-line Final wording
Front page: ThyQoL. Quality of Life Questionnaire for Patients with Thyroid Disease. This questionnaire is about how your thyroid disease has affected your life. There are a number of different thyroid diseases. The thyroid gland can be enlarged. One’s metabolism can either be too fast or too slow. In addition, some thyroid diseases may adversely affect the eyes. This questionnaire is intended to cover all these diseases. Therefore, please answer all the questions.
5 1 0 0 0 0
Quality of Life Questionnaire for Patients with Thyroid Disease. This questionnaire is about how your thyroid disease has affected your life.
Introduction to questionnaire: The first section of the questionnaire is about quality of life, symptoms, fatigue, memory, mood, and health. Please base your answers on how you have been feeling in general.
5 4 1 0 1 0
The first section of the questionnaire is about symptoms, fatigue, memory, mood, and health. Please base your answers on how you have
been feeling in general during the past 4 weeks.
Have you had a visible swelling in the front of your neck? 1 0 0 0 1 0 Have you had a visible swelling in the front of your neck?
Have you had [åndenød] (obsolete Danish word meaning shortness of
breath)? 1 0 0 0 0 0 Have you experienced shortness of breath?
Have you been [kuldskær] (obsolete Danish word meaning sensitive to
cold) 0 0 0 0 1 0 Have you been sensitive to cold?
Have you had constipation? 0 0 0 0 1 0 Have you had constipation (hard stools)?
Have you been generally unwell? 1 2 0 0 0 1 Have you felt generally unwell?
The following questions are about having difficulty coping or managing your feelings
1 0 0 0 0 0 The following questions are about having difficulty coping or having mood swings
Have you been in control of your life? 2 0 0 1 0 0 Have you felt in control of your life?
Introduction to second part: The remainder of the questionnaire is about how your disease may have affected various aspects of your life. As previously mentioned there are several different types of thyroid diseases. When we ask about “your thyroid disease” we refer to the
particular condition you have.
0 1 2 1 1 0 The remainder of the questionnaire is about how your thyroid disease may have affected various aspects of your life.
Response option Does not apply 4 0 0 0 0 0 Omitted
Has your thyroid disease caused you to have difficulty being together with close family (e.g. spouse, boy/girlfriend or children)? 2 0 0 0 2 0
Has your thyroid disease caused you to have difficulty being together with friends, acquaintances, or relatives? 2 0 0 0 0 0
Has your thyroid disease caused you to have difficulty being together with other people (for example, spouse, children, boy/girlfriend, friends, or others)?
Response option Does not apply 1 0 0 0 0 0 I do not work
Has your thyroid disease caused you to have difficulty managing your job?
1 2 2 0 2 2 Has your thyroid disease caused you to have difficulty managing1 your job (for example, had difficulty managing1 it or calling in sick)?
Has your thyroid disease caused you to have difficulty getting around, for example, walking, bicycling, or driving a car?
0 0 0 1 0 0 Has your thyroid disease caused you to have difficulty getting around (for example, walking, running, bicycling, or driving a car)?
Has it been noticeable to others that you have a thyroid disease? 2 0 1 0 0 0 Has your thyroid disease affected your appearance (for example, swelling of the neck, eye changes, weight changes)?
Have you been unsatisfied with your appearance because of your thyroid disease?
1 0 0 0 0 0 Have you been unsatisfied with your appearance because of your thyroid disease?
Has your thyroid disease made you consider yourself too thin? 0 0 0 0 0 0 Has your thyroid disease made you feel too thin?
Has your thyroid disease made you consider yourself too fat? 0 1 1 0 1 0 Has your thyroid disease made you feel too fat?
Introduction to last item: The final question is about to what extent your thyroid disease has affected you overall
1 0 1 0 1 0 The final question is about to what extent your thyroid disease has affected you overall during the past 4 weeks
Problems concerning attribution 0 2 3 1 1 1 n/a
1 The original Danish questionnaire used two different words for “managing” the job.
Page 30 of 107
RESULTS – phase IV
Phase IV, quantitative scale validation
At Rigshospitalet, 878 patients were invited, of whom 41 were secondarily excluded. Five hundred
and two returned a completed questionnaire, yielding an overall response rate at RH of 60%. How-
ever, 92 patients cancelled their index appointment at the outpatient clinic for other reasons, thus
preventing them from participating, yielding a corrected response rate of 67%. At Odense Univer-
sity Hospital 632 were invited, 61 excluded, 404 responded, yielding a response rate at OUH of
71%; response rate for the total sample was thus 904/1408=64% (69% when corrected for appoint-
ment cancellations). Clinical characteristics are presented in Table 1 for the total sample.
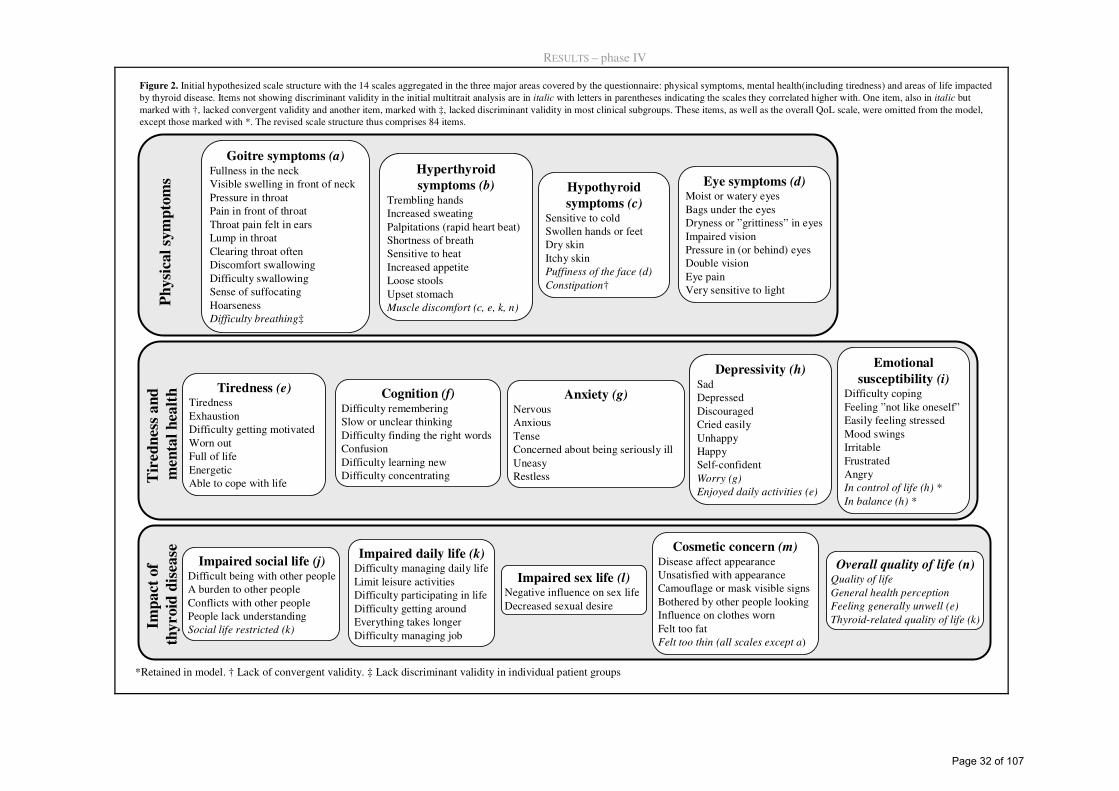
The initial multi-trait scaling analysis identified one instance of lack of convergent validity and 24
instances of lack of discriminant validity in 10 items (items in italic in Figure 2). Two of these
items belonged to the overall quality of life scale, which thus had scaling error in half its items. In
addition, analyses in the five patient-groups separately found lack of discriminant validity of “Diffi-
culty breathing” eight times across patient groups (data not shown).
On this background, the “Overall quality of life” scale was omitted, as were the items lacking dis-
criminant and convergent validity in the total sample and the “Difficulty breathing”-item. However,
the two positively worded items “In control of life” and “In balance” were retained due to high
relevance ratings and due to expected important scaling properties with respect to ceiling effect.
A multitrait scaling analysis of the remaining 84 scaled items in the total sample is presented in
Table 7. Now all items in all scales showed convergent validity with item-own scale correlations
above 0.40. One scaling error involving lack of discriminant validity occurred in the Emotional sus-
ceptibility scale (item “In control of life”). Inter-scale correlations were low to moderate, ranging
0.21-0.71, except for “Depressivity” and “Emotional susceptibility”, which had a high interscale
correlation of 0.83 (Table 8). Internal consistency reliability estimates (Cronbach’s α)
Page 31 of 107
RESULTS – phase IV
Goitre symptoms (a)Fullness in the neckVisible swelling in front of neckPressure in throatPain in front of throatThroat pain felt in earsLump in throatClearing throat oftenDiscomfort swallowingDifficulty swallowingSense of suffocatingHoarsenessDifficulty breathing‡
Hyperthyroid
symptoms (b)Trembling handsIncreased sweatingPalpitations (rapid heart beat)Shortness of breathSensitive to heatIncreased appetiteLoose stoolsUpset stomachMuscle discomfort (c, e, k, n)
Tiredness (e)TirednessExhaustionDifficulty getting motivatedWorn outFull of lifeEnergeticAble to cope with life
Impaired social life (j)Difficult being with other peopleA burden to other peopleConflicts with other peoplePeople lack understandingSocial life restricted (k)
Hypothyroid
symptoms (c)Sensitive to coldSwollen hands or feetDry skinItchy skinPuffiness of the face (d)
Constipation†
Eye symptoms (d)Moist or watery eyesBags under the eyes Dryness or ”grittiness” in eyesImpaired visionPressure in (or behind) eyesDouble visionEye painVery sensitive to light
Cognition (f)Difficulty rememberingSlow or unclear thinkingDifficulty finding the right wordsConfusionDifficulty learning newDifficulty concentrating
Anxiety (g)NervousAnxiousTenseConcerned about being seriously illUneasyRestless
Depressivity (h)SadDepressedDiscouragedCried easilyUnhappyHappySelf-confidentWorry (g)
Enjoyed daily activities (e)
Emotional
susceptibility (i)Difficulty copingFeeling ”not like oneself”Easily feeling stressedMood swingsIrritableFrustratedAngryIn control of life (h) *
In balance (h) *
Impaired daily life (k)Difficulty managing daily lifeLimit leisure activitiesDifficulty participating in lifeDifficulty getting aroundEverything takes longerDifficulty managing job
Impaired sex life (l)Negative influence on sex lifeDecreased sexual desire
Cosmetic concern (m)Disease affect appearanceUnsatisfied with appearanceCamouflage or mask visible signsBothered by other people lookingInfluence on clothes wornFelt too fatFelt too thin (all scales except a)
Ph
ysi
cal
sym
pto
ms
Tir
ed
nes
s a
nd
men
tal
hea
lth
Imp
act
of
thy
roid
dis
ease
Overall quality of life (n)Quality of life
General health perception
Feeling generally unwell (e)
Thyroid-related quality of life (k)
*Retained in model. † Lack of convergent validity. ‡ Lack discriminant validity in individual patient groups
Figure 2. Initial hypothesized scale structure with the 14 scales aggregated in the three major areas covered by the questionnaire: physical symptoms, mental health(including tiredness) and areas of life impacted by thyroid disease. Items not showing discriminant validity in the initial multitrait analysis are in italic with letters in parentheses indicating the scales they correlated higher with. One item, also in italic but marked with †, lacked convergent validity and another item, marked with ‡, lacked discriminant validity in most clinical subgroups. These items, as well as the overall QoL scale, were omitted from the model, except those marked with *. The revised scale structure thus comprises 84 items.
Page 32 of 107
RESULTS – phase IV
were very high, except for “Hypothyroid symptoms”, which just reached the limit of 0.70 (Table 8).
Repeating the analysis using polychoric correlations generally yielded higher correlation coeffi-
cients. No lack of convergent validity was found. Compared to Pearson correlations, only two dis-
similarities were found regarding discriminant validity: “In control of life” no longer had lack of
discriminant validity and “Cried easily” correlated higher with “Emotional susceptibility” (0.71)
than with its own “Depressivity” scale (0.70).
Performing analyses in separate subgroups (age, gender, hospitals) only showed minor deviations,
with preservation of convergent validity, except in a few cases among young patients (less than age
40), where the hypothyroid symptoms “sensitive to cold”, “swollen hands or feet” and “itchy skin”
correlated higher with other scales than with the ‘’Hypothyroid” scale, with which they correlated
less than 0.40. The same was the case for “double vision” from the “Eye symptoms” scale.
Performing the analyses separately in the five patient groups, convergent validity was preserved,
except for “itchy skin” among Graves’ patients, which correlated only 0.27 with the hypothyroid
symptom scale. In total, out of 5,040 correlations, 65 scaling errors involving lack of discriminant
validity was found, two thirds of which involved physical symptom items. Sixteen involved items
from the “Depressivity” and the “Emotional susceptibility” scale, five were from the “Social im-
pact” scale and two from the “Cosmetic concern” scale. Repeating the analyses using polychoric
correlations did not alter these results; in total, 4 fewer scaling errors occurred, compared to Pearson
correlations.
Page 33 of 107
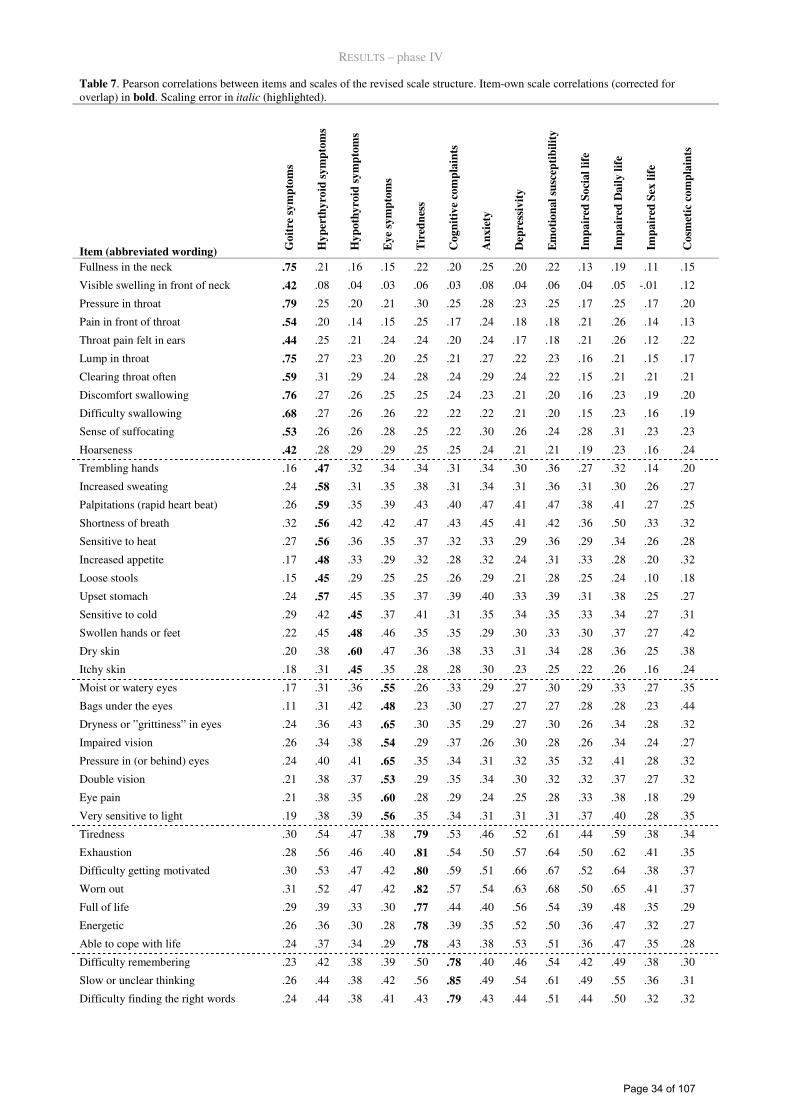
RESULTS – phase IV
Table 7. Pearson correlations between items and scales of the revised scale structure. Item-own scale correlations (corrected for overlap) in bold. Scaling error in italic (highlighted).
Item (abbreviated wording) Go
itre
sy
mp
tom
s
Hy
per
thy
roid
sy
mp
tom
s
Hy
po
thy
roid
sy
mp
tom
s
Ey
e sy
mp
tom
s
Tir
edn
ess
Co
gn
itiv
e co
mp
lain
ts
An
xie
ty
Dep
ress
ivit
y
Em
oti
on
al
susc
epti
bil
ity
Imp
air
ed S
oci
al
life
Imp
air
ed D
ail
y l
ife
Imp
air
ed S
ex l
ife
Co
smet
ic c
om
pla
ints
Fullness in the neck .75 .21 .16 .15 .22 .20 .25 .20 .22 .13 .19 .11 .15
Visible swelling in front of neck .42 .08 .04 .03 .06 .03 .08 .04 .06 .04 .05 -.01 .12
Pressure in throat .79 .25 .20 .21 .30 .25 .28 .23 .25 .17 .25 .17 .20
Pain in front of throat .54 .20 .14 .15 .25 .17 .24 .18 .18 .21 .26 .14 .13
Throat pain felt in ears .44 .25 .21 .24 .24 .20 .24 .17 .18 .21 .26 .12 .22
Lump in throat .75 .27 .23 .20 .25 .21 .27 .22 .23 .16 .21 .15 .17
Clearing throat often .59 .31 .29 .24 .28 .24 .29 .24 .22 .15 .21 .21 .21
Discomfort swallowing .76 .27 .26 .25 .25 .24 .23 .21 .20 .16 .23 .19 .20
Difficulty swallowing .68 .27 .26 .26 .22 .22 .22 .21 .20 .15 .23 .16 .19
Sense of suffocating .53 .26 .26 .28 .25 .22 .30 .26 .24 .28 .31 .23 .23
Hoarseness .42 .28 .29 .29 .25 .25 .24 .21 .21 .19 .23 .16 .24
Trembling hands .16 .47 .32 .34 .34 .31 .34 .30 .36 .27 .32 .14 .20
Increased sweating .24 .58 .31 .35 .38 .31 .34 .31 .36 .31 .30 .26 .27
Palpitations (rapid heart beat) .26 .59 .35 .39 .43 .40 .47 .41 .47 .38 .41 .27 .25
Shortness of breath .32 .56 .42 .42 .47 .43 .45 .41 .42 .36 .50 .33 .32
Sensitive to heat .27 .56 .36 .35 .37 .32 .33 .29 .36 .29 .34 .26 .28
Increased appetite .17 .48 .33 .29 .32 .28 .32 .24 .31 .33 .28 .20 .32
Loose stools .15 .45 .29 .25 .25 .26 .29 .21 .28 .25 .24 .10 .18
Upset stomach .24 .57 .45 .35 .37 .39 .40 .33 .39 .31 .38 .25 .27
Sensitive to cold .29 .42 .45 .37 .41 .31 .35 .34 .35 .33 .34 .27 .31
Swollen hands or feet .22 .45 .48 .46 .35 .35 .29 .30 .33 .30 .37 .27 .42
Dry skin .20 .38 .60 .47 .36 .38 .33 .31 .34 .28 .36 .25 .38
Itchy skin .18 .31 .45 .35 .28 .28 .30 .23 .25 .22 .26 .16 .24
Moist or watery eyes .17 .31 .36 .55 .26 .33 .29 .27 .30 .29 .33 .27 .35
Bags under the eyes .11 .31 .42 .48 .23 .30 .27 .27 .27 .28 .28 .23 .44
Dryness or ”grittiness” in eyes .24 .36 .43 .65 .30 .35 .29 .27 .30 .26 .34 .28 .32
Impaired vision .26 .34 .38 .54 .29 .37 .26 .30 .28 .26 .34 .24 .27
Pressure in (or behind) eyes .24 .40 .41 .65 .35 .34 .31 .32 .35 .32 .41 .28 .32
Double vision .21 .38 .37 .53 .29 .35 .34 .30 .32 .32 .37 .27 .32
Eye pain .21 .38 .35 .60 .28 .29 .24 .25 .28 .33 .38 .18 .29
Very sensitive to light .19 .38 .39 .56 .35 .34 .31 .31 .31 .37 .40 .28 .35
Tiredness .30 .54 .47 .38 .79 .53 .46 .52 .61 .44 .59 .38 .34
Exhaustion .28 .56 .46 .40 .81 .54 .50 .57 .64 .50 .62 .41 .35
Difficulty getting motivated .30 .53 .47 .42 .80 .59 .51 .66 .67 .52 .64 .38 .37
Worn out .31 .52 .47 .42 .82 .57 .54 .63 .68 .50 .65 .41 .37
Full of life .29 .39 .33 .30 .77 .44 .40 .56 .54 .39 .48 .35 .29
Energetic .26 .36 .30 .28 .78 .39 .35 .52 .50 .36 .47 .32 .27
Able to cope with life .24 .37 .34 .29 .78 .43 .38 .53 .51 .36 .47 .35 .28
Difficulty remembering .23 .42 .38 .39 .50 .78 .40 .46 .54 .42 .49 .38 .30
Slow or unclear thinking .26 .44 .38 .42 .56 .85 .49 .54 .61 .49 .55 .36 .31
Difficulty finding the right words .24 .44 .38 .41 .43 .79 .43 .44 .51 .44 .50 .32 .32
Page 34 of 107
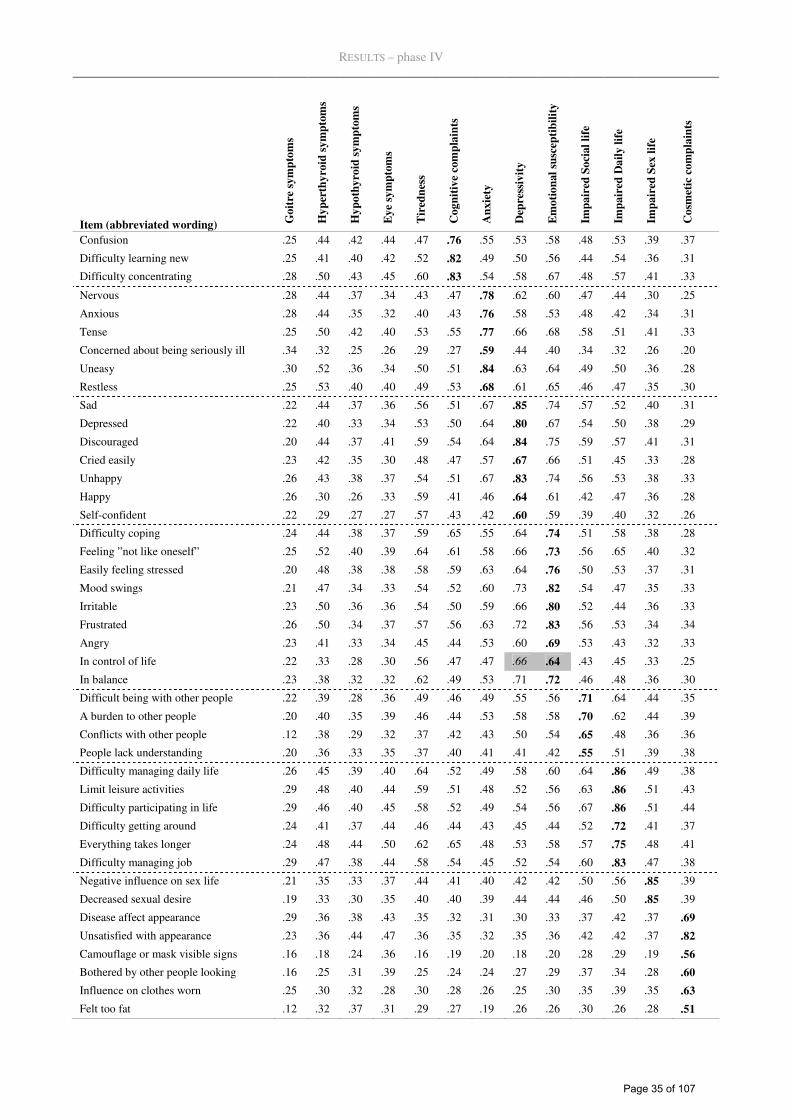
RESULTS – phase IV
Item (abbreviated wording) Go
itre
sy
mp
tom
s
Hy
per
thy
roid
sy
mp
tom
s
Hy
po
thy
roid
sy
mp
tom
s
Ey
e sy
mp
tom
s
Tir
edn
ess
Co
gn
itiv
e co
mp
lain
ts
An
xie
ty
Dep
ress
ivit
y
Em
oti
on
al
susc
epti
bil
ity
Imp
air
ed S
oci
al
life
Imp
air
ed D
ail
y l
ife
Imp
air
ed S
ex l
ife
Co
smet
ic c
om
pla
ints
Confusion .25 .44 .42 .44 .47 .76 .55 .53 .58 .48 .53 .39 .37
Difficulty learning new .25 .41 .40 .42 .52 .82 .49 .50 .56 .44 .54 .36 .31
Difficulty concentrating .28 .50 .43 .45 .60 .83 .54 .58 .67 .48 .57 .41 .33
Nervous .28 .44 .37 .34 .43 .47 .78 .62 .60 .47 .44 .30 .25
Anxious .28 .44 .35 .32 .40 .43 .76 .58 .53 .48 .42 .34 .31
Tense .25 .50 .42 .40 .53 .55 .77 .66 .68 .58 .51 .41 .33
Concerned about being seriously ill .34 .32 .25 .26 .29 .27 .59 .44 .40 .34 .32 .26 .20
Uneasy .30 .52 .36 .34 .50 .51 .84 .63 .64 .49 .50 .36 .28
Restless .25 .53 .40 .40 .49 .53 .68 .61 .65 .46 .47 .35 .30
Sad .22 .44 .37 .36 .56 .51 .67 .85 .74 .57 .52 .40 .31
Depressed .22 .40 .33 .34 .53 .50 .64 .80 .67 .54 .50 .38 .29
Discouraged .20 .44 .37 .41 .59 .54 .64 .84 .75 .59 .57 .41 .31
Cried easily .23 .42 .35 .30 .48 .47 .57 .67 .66 .51 .45 .33 .28
Unhappy .26 .43 .38 .37 .54 .51 .67 .83 .74 .56 .53 .38 .33
Happy .26 .30 .26 .33 .59 .41 .46 .64 .61 .42 .47 .36 .28
Self-confident .22 .29 .27 .27 .57 .43 .42 .60 .59 .39 .40 .32 .26
Difficulty coping .24 .44 .38 .37 .59 .65 .55 .64 .74 .51 .58 .38 .28
Feeling ”not like oneself” .25 .52 .40 .39 .64 .61 .58 .66 .73 .56 .65 .40 .32
Easily feeling stressed .20 .48 .38 .38 .58 .59 .63 .64 .76 .50 .53 .37 .31
Mood swings .21 .47 .34 .33 .54 .52 .60 .73 .82 .54 .47 .35 .33
Irritable .23 .50 .36 .36 .54 .50 .59 .66 .80 .52 .44 .36 .33
Frustrated .26 .50 .34 .37 .57 .56 .63 .72 .83 .56 .53 .34 .34
Angry .23 .41 .33 .34 .45 .44 .53 .60 .69 .53 .43 .32 .33
In control of life .22 .33 .28 .30 .56 .47 .47 .66 .64 .43 .45 .33 .25
In balance .23 .38 .32 .32 .62 .49 .53 .71 .72 .46 .48 .36 .30
Difficult being with other people .22 .39 .28 .36 .49 .46 .49 .55 .56 .71 .64 .44 .35
A burden to other people .20 .40 .35 .39 .46 .44 .53 .58 .58 .70 .62 .44 .39
Conflicts with other people .12 .38 .29 .32 .37 .42 .43 .50 .54 .65 .48 .36 .36
People lack understanding .20 .36 .33 .35 .37 .40 .41 .41 .42 .55 .51 .39 .38
Difficulty managing daily life .26 .45 .39 .40 .64 .52 .49 .58 .60 .64 .86 .49 .38
Limit leisure activities .29 .48 .40 .44 .59 .51 .48 .52 .56 .63 .86 .51 .43
Difficulty participating in life .29 .46 .40 .45 .58 .52 .49 .54 .56 .67 .86 .51 .44
Difficulty getting around .24 .41 .37 .44 .46 .44 .43 .45 .44 .52 .72 .41 .37
Everything takes longer .24 .48 .44 .50 .62 .65 .48 .53 .58 .57 .75 .48 .41
Difficulty managing job .29 .47 .38 .44 .58 .54 .45 .52 .54 .60 .83 .47 .38
Negative influence on sex life .21 .35 .33 .37 .44 .41 .40 .42 .42 .50 .56 .85 .39
Decreased sexual desire .19 .33 .30 .35 .40 .40 .39 .44 .44 .46 .50 .85 .39
Disease affect appearance .29 .36 .38 .43 .35 .32 .31 .30 .33 .37 .42 .37 .69
Unsatisfied with appearance .23 .36 .44 .47 .36 .35 .32 .35 .36 .42 .42 .37 .82
Camouflage or mask visible signs .16 .18 .24 .36 .16 .19 .20 .18 .20 .28 .29 .19 .56
Bothered by other people looking .16 .25 .31 .39 .25 .24 .24 .27 .29 .37 .34 .28 .60
Influence on clothes worn .25 .30 .32 .28 .30 .28 .26 .25 .30 .35 .39 .35 .63
Felt too fat .12 .32 .37 .31 .29 .27 .19 .26 .26 .30 .26 .28 .51
Page 35 of 107
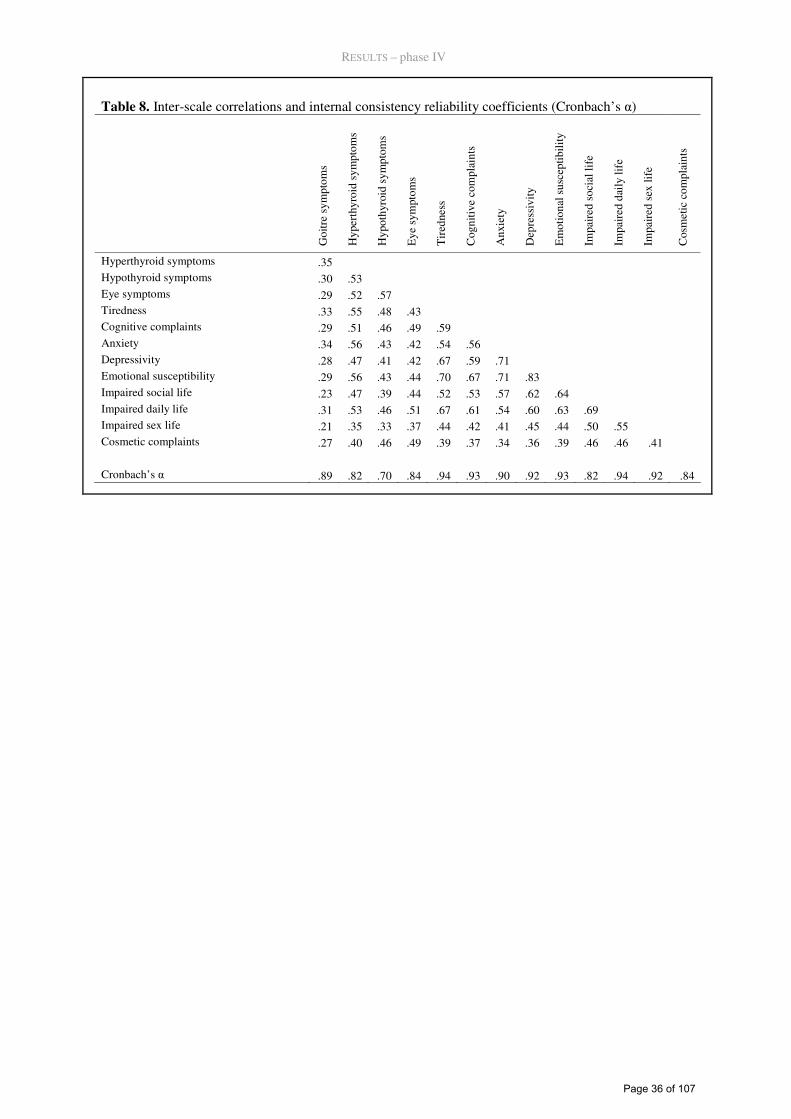
RESULTS – phase IV
Table 8. Inter-scale correlations and internal consistency reliability coefficients (Cronbach’s α)
Goi
tre
sym
ptom
s
Hyp
erth
yroi
d sy
mpt
oms
Hyp
othy
roid
sym
ptom
s
Eye
sym
ptom
s
Tir
edne
ss
Cog
nitiv
e co
mpl
aint
s
Anx
iety
Dep
ress
ivity
Em
otio
nal s
usce
ptib
ility
Impa
ired
soc
ial l
ife
Impa
ired
dai
ly li
fe
Impa
ired
sex
life
Cos
met
ic c
ompl
aint
s
Hyperthyroid symptoms .35 Hypothyroid symptoms .30 .53 Eye symptoms .29 .52 .57 Tiredness .33 .55 .48 .43 Cognitive complaints .29 .51 .46 .49 .59 Anxiety .34 .56 .43 .42 .54 .56 Depressivity .28 .47 .41 .42 .67 .59 .71 Emotional susceptibility .29 .56 .43 .44 .70 .67 .71 .83 Impaired social life .23 .47 .39 .44 .52 .53 .57 .62 .64 Impaired daily life .31 .53 .46 .51 .67 .61 .54 .60 .63 .69 Impaired sex life .21 .35 .33 .37 .44 .42 .41 .45 .44 .50 .55 Cosmetic complaints .27 .40 .46 .49 .39 .37 .34 .36 .39 .46 .46 .41 Cronbach’s α .89 .82 .70 .84 .94 .93 .90 .92 .93 .82 .94 .92 .84
Page 36 of 107
DISCUSSION – phase I
DISCUSSION
Phase I, Issue generation
According to the literature study, HRQL-impairment in patients with benign thyroid disorders is
prevalent, both in the untreated phase and in the long term. A wide range of problems have been
reported, covering both generic and specific aspects of HRQL. However, taken as evidence for im-
paired quality of life, the literature study suffers substantial limitations. Many of the studies are
small and use unvalidated measures. Most of them lack a thorough clinical description of the pa-
tients and include patients covering a wide range of phenotypes and etiological dissimilarities. The
aspects being evaluated are operationalized in numerous different ways, making the reported fre-
quencies difficult to interpret. However, they serve as an indication of QoL impairment among thy-
roid patients and provide a well-documented starting point for the expert- and patient interviews.
In the expert and patient interviews, we identified a wide range of relevant issues, covering 15
HRQL-domains ranging from general health perception and limitations of daily activities over men-
tal health, social function, fatigue and cognitive function to physical symptoms with varying de-
grees of thyroid specificity. Fatigue and emotional susceptibility were the most important issues
overall. When focusing on individual patient categories, the physical symptoms usually associated
with the disease in question were very important to patients belonging to that category, i.e. hyper-
thyroid symptoms were important to patients with a diagnosis of hyperthyroidism, etc. These data
offer novel and clinically very important insights into the perceived impact of a broad spectrum of
thyroid diseases on the quality of life of the patients. Based on patients describing the frequency as
well as the importance of encountered problems and experts rating relevance, a picture of potential
impairment in central aspects of quality of life, such as fatigue, mental health and social function as
well as a wide range of physical symptoms is drawn. Such data are fundamental to the development
of new HRQL-questionnaires for thyroid patients. Without empirical evidence about what is rele-
vant to the patients, content validity of a HRQL-instrument cannot be ensured. The results can also
Page 37 of 107
DISCUSSION – phase I
serve as a basis for the selection of the best suited of the available standard, generic measures of
HRQL, such as SF-36, EQ-5D or WHOQOL, when planning clinical studies involving thyroid pa-
tients.
A challenge for this project has been the intention to develop a comprehensive questionnaire appli-
cable to studies of several thyroid phenotypes. In this phase of the project we have presented and
applied a method for the selection of issues to ensure content validity across a number of patient
populations. Several aspects of this approach could be discussed. Firstly, we asked about problems
encountered during the whole disease period (which for some patients spanned over several dec-
ades) which may have imposed recall-bias on our results. However, this strategy was used in order
to increase effectiveness of the interviews - much more information could be provided by each pa-
tient- and to prevent that the timing of the interviews lead to omission of important problems ex-
perienced at an earlier point in time. Secondly, patient and expert relevance ranks took into account
both frequency and importance, in terms of impact on quality of life, of the issues. The experts were
specifically instructed to do so, whereas the patient relevance ranks were constructed by multiplying
the frequencies with the mean importance ratings. The reason for this difference was that an overall
judgement incorporating experiences from many patients was considered most meaningful for clini-
cians, whereas for patients it is obviously meaningless to evaluate the relevance of problems they do
not have, and therefore, separate assessment of presence and relevance was made. This approach
means that seldom but distressing issues may be selected at the expense of common but unimpor-
tant issues. For example, in patients with hypothyroidism, depression and coarse skin was experi-
ence by the same proportion of patients, but depression had a far higher relevance rank, due to its
much larger impact on QoL. Similarly, red eyelids had higher importance rating than fatigue, but a
much lower impact rank, because red eye-lids was only experienced by one patient, whereas fatigue
was present in the majority of patients. Thus, we consider the applied approach optimal for the
purpose of selecting the most relevant issues to be included in a future QoL-questionnaire. Thirdly,
we believe that the strategy with primary weight on the combined patient-expert rank in all patient
Page 38 of 107
DISCUSSION – phase I
groups, but non-exclusion of issues of very high importance to individual patient groups, was a ma-
jor advantage of our method. However, the cut-off values as regards definition of the most relevant
issues - the 75 most relevant overall or being rated among the 15 most relevant to individual groups
- were arbitrarily set. This procedure included around two thirds of the total number of issues (92
out of 148). This is a rather fine-meshed selection, but the purpose was to allow for a sufficient
number to be submitted to further selection procedures (based on analyses of large patient samples),
without imposing too large response-burdens on the patients of such future studies.
Another topic for discussion could be that we included only patients from two secondary and terti-
ary referral units. However, since the purpose of content validity studies is to ensure that potentially
relevant issues are not ignored, inclusion of patients from the presumably more diseased part of the
spectrum is preferable, since it is unlikely that less severely ill patients experience symptoms which
the more severely ill patients do not.
Compared to similar studies from other disease entities, our number of experts and patients is very
high; ten to fifteen are generally the rule.99, 100 However, in light of the heterogeneity of thyroid pa-
tients, we found that such a sample size was recommendable for these patients.
An advantage of the present study is that each patient was interviewed using both semi-structured
and structured techniques. This provided an initial, un-guided, un-probed narration of the way the
patients had been impacted by their disease, as well as a structured evaluation of all previously
identified possible problems associated with thyroid disorders. Moreover, the patients were clini-
cally well-described and we included both newly diagnosed and untreated patients as well as pa-
tients with long-standing illness treated in various ways. The latter increases the range of popula-
tions and application for which a HRQL-questionnaire developed on this ground has content valid-
ity. Additionally, combining input from both patients and experts yielded direct evidence from the
patients themselves but also cumulative information from all the patients seen during the many
years of experience by the participating endocrinologists.
Page 39 of 107
DISCUSSION – phase III
Phase III, pretesting
Measured by the number of problems identified in successive versions of the questionnaire cogni-
tive interviewing applying immediate retrospective probing proved useful for improving the ques-
tionnaire wording and format. This technique, in association with questionnaire revisions based on
cognitive methodology, was very efficient in reducing the number of problems occurring within
comprehension as well as the non-cognitive categories logical/structural problems and acceptability,
and moderately efficient in reducing problems within judgment and responding.
The four-stage model formulated by Tourangeau,87 covered most, but not all, of the problems iden-
tified during the cognitive interview testing. This was mainly due to problems not being cognitive
in nature, but rather being logical, or structural, as described by Willis.67 Most problems were
within comprehension, which was twice as frequent as problems with judgment and response. This
is very consistent with previous cognitive interviewing research that has used problem classification
systems.101-103
Cognitive interviewing was also efficient in identifying a particular aspect of judgment and re-
sponse problems, which we term attributional problems since they involve the attribution of symp-
toms and impairments to the disease under study. These problems concerned patients’ doubt about
whether to include an experienced problem (symptom, feeling, or impairment) in their judgment
and response, when they did not consider that problem as being caused by their thyroid disease.
These problems occurred mainly within the first half of the questionnaire where attribution was not
intended. In contrast, in the second half of the questionnaire respondents were explicitly instructed
to consider impact of their thyroid disorder. It was evident, that some respondents excluded prob-
lems considered unrelated to their thyroid. This is probably a mechanism affecting HRQL-
measurements in general, particularly when used in the context of the treatment of a specific dis-
ease.104
We have classified these problems within judgment and response (Tourangeau model), because the
respondents fully comprehended the question, but excluded some aspects when judging and formu-
Page 40 of 107
DISCUSSION – phase III
lating their response. It could be argued, though, that since the respondents were specifically in-
structed not to exclude problems of extrathyroidal origin, it is a problem within comprehension. It
would then be within the framing of the assessment, according to the theoretical model by Rapkin
and Schwartz 105. Within that model, respondents form a frame of reference, i.e. experiences they
deem relevant to their response. However, the fact that expansive probing revealed, that respondents
actually understood the instruction to respond without attribution, but ignored this information
when formulated their response, identified the problems as judgmental, rather than with comprehen-
sion. The conceptual framework offering the most salient explanation to the observed phenomenon
seems to be conversation-theory. As described by Tourangeau,87 the philosopher Paul Grice106 de-
scribed an implicit agreement between participants in a conversation that governed the conversation
which he called a cooperative principle. In order for a conversation to be meaningful, we rely on a
number of implicit assumptions or general rules of reasonable behaviour in conversations. For ex-
ample, we expect participants in a conversation to be as informative as is required (but not more)
for the purpose; to be truthful, to be relevant and clear. Viewing the questionnaire response process
as a piece of conversation, the investigator being one participant, speaking through the question-
naire and the respondent being the other part, the respondent expects the questions to be relevant
and interpret them with this perspective. For example, when a patient with a thyroid disorder and a
sore throat due to a recent viral infection is asked about pain in the throat as part of a study involv-
ing thyroid patients, she assumes that the investigator must refer to pain related to her thyroid, re-
gardless of the fact that this is not specified or even (as in our case) when it is explicitly specified
not to limit the considerations to problems of presumed thyroid causation. She therefore denies ex-
periencing pain in the throat, because she doesn’t consider it relevant according to the investigators
aims. Hence, the implicit assumptions are stronger than the introductory text in the questionnaire.
This phenomenon, that patients omit experiences from their considerations, when formulating a
response to a survey item, if they consider it not to be caused by the condition under investigation,
Page 41 of 107
DISCUSSION – phase III
has previously been described as selective reporting.104 It is distinct from the mechanisms underly-
ing response shifts,107 since it does not represent a “true” shift in HRQL-appraisal.
It is a strength of our study that it is fairly large for a cognitive interview study. Furthermore, it en-
compasses a range of clinical conditions in relation to thyroid morphology and function.
This phase of the project has several limitations. One limitation concerns the fact that the same
methods were used to revise the questionnaire and to evaluate its performance, this being based on
the number of problems identified, using cognitive interviews. In order to formally test the effect of
the revisions, an experimental study should be conducted. This could involve experimental cogni-
tive methods but also quantitative studies testing the measurement properties of the initial vs. the
final version. Further, the interviews were conducted in a hospital setting, which could affect the
response process, compared to patient response at home, for example by inspiring respondents to
focus more on disease compared to other domains of life. To investigate this, interviews could be
conducted at several locations within different subsets of participants. However, this was not logis-
tically possible in this study. Finally, the fact that the instrument developer is part of the research
team conducting this study could bias the results towards a more optimistic interpretation. The Eng-
lish version of the questionnaire is currently being cognitively tested by an independent team in US,
which, when completed, can be used to investigate this possible bias.
Page 42 of 107
Phase IV, quantitative scale validation
In phase IV, it was possible to revise the questionnaire to establish a scale structure with complete
convergent validity and almost complete discriminant validity in a large, heterogeneous sample of
patients comprising several benign thyroid diseases. During the revision, one scale was relinquished
and 8 items were omitted from the questionnaire. The remaining 13 scales are four specific symp-
tom scales, five non-specific scales measuring psychological states and tiredness and four thyroid
disease impact scales. The item lacking discriminant validity was related to both “Depressivity” and
“Emotional susceptibility” and these two scales also displayed high interscale correlation. All scales
had acceptable internal consistency reliability.
Generally, the instrument preserved this scale structure across sociodemographic and clinical sub-
groups. However, in individual diagnostic groups, lack of discriminant validity was found in a very
small proportion of cases (65 of 5,040 correlations), mainly among the physical symptoms. The
structure was also preserved using polychoric correlations.96, 97, 108, 109
The complete convergent and almost complete discriminant validity seen in the total sample pro-
vides strong support for the theoretically based (and slightly modified) scaling structure of the
ThyPRO. The fact that some scaling errors (0.8%) were found in certain subgroups (mainly be-
tween physical symptoms and scales measuring psychological states and impact of disease) does
not alter this overall result. There are a number of possible interpretations of the findings in sub-
groups. They may reflect that important thyroid symptoms impact the broader quality of life aspects
measured by these scales. Thus, using Fayers’ distinctions,110 this would be an expression of a
causal effect rather than reflecting that the physical symptom belongs to the quality of life dimen-
sion measured by that scale. Further exploration of such hypotheses could be done using structural
equations models111 in separate analyses of each clinical subgroup or in multigroup analyses.112
The “Depressivity” and “Emotional susceptibility” scales are closely related, judged by the one item
lacking discriminant validity, the scaling errors involving these scales in the patient-subgroup
Page 43 of 107
DISCUSSION – phase IV
analyses, and not least the high inter-scale correlation. Should the two scales be merged into one?
Emotional susceptibility was identified as an important unique concept emerging in the qualitative
analyses of 80 patient interviews. Further scale revision should therefore await additional, more
clinically oriented studies.
In general, we had a high threshold for omitting items in this study, because all items had been rated
as being important in patient and expert interviews and because important clinical data such as sen-
sitivity and responsiveness are not yet available. Also, valuable information regarding item charac-
teristics, such as information curves and severity-specific reliability, is only available through
analyses applying item response models and we prefer to take such results into account, before
omitting further items. Thus, our main purpose with this study was to establish a scale structure
allowing use and analysis of the questionnaire. This structure will serve as a framework for addi-
tional analyses to be conducted, which may lead to revisions.
It is a strength of our study that the sample is rather large and comprises several thyroid patient
groups with several thyroid diseases in multiple stages, as well as a broad spectrum of treatments.
The fact that a reliable and valid scale structure of the questionnaire was established in such a broad
sample indicates that it may be useful in longitudinal studies where disease stage, and even disease
entity, changes over time. However, additional longitudinal validation studies are warranted before
firm conclusions can be made. Further, analyses using item response theory models should be un-
dertaken to evaluate whether the simple summated scoring suggested here is adequate. They could
also evaluate and possibly ensure measurement precision over the full range of disease severity.
Multi-group structural equations models for ordinal data could be used to take causal relations be-
tween sub-domains into account, like the ones hypothesized to be in play between the symptom
items and the state/impact scales. The choice of statistical methodology could also be questioned,
particularly the choice of parametric statistics like the Pearson correlation. Likert-like response
scales like the ones used here are indisputably ordinal in nature and are often found to be skew.
However, these methods have been shown to be relatively robust to minor violations of these as-
sumptions98, 113 and it is reassuring that the use of polychoric correlations, which assumes that the
Page 44 of 107
DISCUSSION – phase IV
measured construct is normally distributed, but not necessarily measured continuously or even
equidistantly, did not alter the results.
The questionnaire is somewhat lengthy and future research could focus on item-reduction with
preservation of appropriate measurement properties, integrating additional information from item
response models and clinimetrical parameters.
Page 45 of 107
CONCLUSIONS
• According to the available literature, HRQL-impairment in patients with benign thyroid dis-
orders is prevalent, both in the untreated phase and in the long term. A wide range of prob-
lems have been reported, covering both generic and specific aspects of HRQL. However,
many of the studies are small and use unvalidated measures. Most of them lack a thorough
clinical description of the patients and include patients covering a wide range of phenotypes
and etiological dissimilarities.
• In the expert and patient interviews, we identified a wide range of relevant issues, covering
15 HRQL-domains ranging from general health perception and limitations of daily activities
over mental health, social function, fatigue and cognitive function to physical symptoms
with varying degrees of thyroid specificity. Fatigue and emotional susceptibility were the
most important issues overall. When focusing on individual patient categories, the physical
symptoms usually associated with the disease in question were very important to patients
belonging to that category.
• The modified cognitive interviewing technique for self-completed questionnaire, immediate
retrospective probing, was very efficient in improving the questionnaire. Problems within all
four cognitive stages of survey responding was identified. A particular subset of problems
related to the respondents’ attribution of their experiences to the condition under study, in-
volving selective reporting, which may be in play in many HRQL settings, especially where
a particular disease or condition is in focus.
• Excellent convergent and discriminant validity as well as satisfactory internal consistency
reliability of the 86-item, 13-scale ThyPRO questionnaire was found. The questionnaire al-
lows evaluation of the impact of the thyroid disease and existing and future treatments on
the quality of life of patients with benign thyroid diseases.
Page 46 of 107
FUTURE PERSPECTIVES
The availability to clinicians and researchers of this comprehensive HRQL-instrument opens a wide
range of possible applications. It may be used to fully document any HRQL-impairment associated
with thyroid diseases and thereby point at areas for potential improved intervention, as well as serve
as a basis for improved patient information. It may be used in clinical studies addressing clinically
important questions, such as whether there are any differences in health-related quality of life
among patients with hyperthyroidism being treated with antithyroid medicine, surgery or radioac-
tive iodine114; whether a block-replacement regimen with both antithyroid drug and thyroid hor-
mones give better health-related quality of life compared to antithyroid drugs alone62, and whether
treatment with a combination of the two forms of the thyroid hormones, T4 and T3, for hypothy-
roidism is an improvement over standard therapy with T4 alone.115, 116
An important and innovative future perspective would be to implement ThyPRO-measurements into
daily clinical practice and individual patient monitoring, but additional validation studies is required
before such use is recommendable. However, more than half of the scales already displayed reliabil-
ity coefficients above the level recommended for use in individual patients (>0.90).
Future validation studies should focus on clinical validation of the questionnaire, such as establish-
ment of minimal important differences to enhance interpretability of the measurements and evalua-
tion of responsiveness in longitudinal studies, on item-reduction to yield briefer questionnaire ver-
sions with preserved acceptable measurement properties, as well as on cross-cultural adaptation
enabling measurements and comparisons across different cultures and languages.
From an HRQL-methodological perspective, the presence and effect of attribution and selective
reporting in specific HRQL-measurements should be evaluated in further detail, possibly by a com-
bination of cognitive interviewing and structural equations modelling. Also, the effectiveness of
immediate retrospective probing could be further evaluated and tested, for example by quantitative
evaluations prior to and after revisions based on cognitive interviews.
Page 47 of 107

Summary
The purpose of this PhD was to develop a thyroid specific quality of life questionnaire. Four phases
were conducted: phase I, issue generation, identifying all quality of life issues relevant for thyroid
patients, phase II, operationalization, where identified issues were transformed into a questionnaire,
phase III, pretesting, where the drafted questionnaire was tested using qualitative interviews and
phase IV, quantitative scale validation, testing scale validity and reliability in large samples.
In phase I, a systematic literature review identified all previously reported problems associated with
thyroid diseases. In total, 138 issues were identified, during the screening of 2094 references, cover-
ing a broad spectrum of quality of life impairments in thyroid patients. Subsequently, the relevance
of each of these issues was rated in interviews with 15 clinicians and 31 patients. New issues ap-
pearing through these interviews were added to the list and rated too. The 92 most relevant were
selected, applying an algorithm integrating the relevance ratings from both clinicians and patients,
and transformed in into 99 items in a questionnaire, in phase II.
In phase III, cognitive interview technique was adapted to better fit self-completed questionnaires
and applied in 31 patient interviews, where problems with completions were identified and mini-
mized. Problems were identified 126 times within 43 items. The interview method proved effective
in identifying and reducing response errors.
In phase IV, multitrait scaling and internal consistency reliability (Cronbach’s α) testing were used
to evaluate and establish a scale structure with acceptable measurement properties, using data from
904 responses from thyroid patients. After one revision, an 84-item structure with complete conver-
gent and almost complete discriminant validity was established, comprising 13 scales: Goitre symp-
toms, hyperthyroid symptoms, hypothyroid symptoms, eye symptoms, tiredness, cognitive com-
plaints, anxiety, depressivity, emotional susceptibility, impaired social life, impaired daily life, im-
paired sex life and cosmetic complaints.
Future studies should now be able to address appropriately a number of important clinical quality of
life issues regarding thyroid diseases and their treatment. Clinimetric validity of the questionniare
should now be evaluated in longitudinal studies and shorter versions of the questionnaire could be
developed, optimally using item response models.
Page 48 of 107

Summary in Danish
Formålet med denne ph.d. var at udvikle et spørgeskema til måling af helbredsrelateret livskvalitet
hos patienter med thyroidea-sygdom. Projektet fulgte fire faser: fase I, indholds-generering, hvor
alle relevante problemstillinger søgtes identificeret, fase II, operationalisering, hvor de relevante
problemstillinger blev omarbejdet til et spørgeskema, fase III, prætestning, hvor skemaet blev testet
i kvalitative interviews, samt fase IV, skalavalidering, hvor skemaets målesikkerhed (reliabilitet) og
skala-struktur blev testet i en større kvantitativ undersøgelse.
I fase I blev først en systematisk litteraturgennemgang af alle tidligere rapporterede problemstillin-
ger hos thyreoidea-patienter gennemført. I alt 2094 artikler blev gennemgået, hvor 138 problemstil-
linger blev identificeret, dækkende et bredt spektrum af helbredsrelaterede livskvalitetsaspekter.
Dernæst blev relevansen af problemstillingerne evalueret gennem interviews med 15 klinikere og
80 patienter, hvor også listen over problemstillinger blev udvidet, i tilfælde af nye problemstillinger.
De 92 mest relevante problemstillinger blev udvalgt, via en selektionsalgoritme, der kombinerede
patient- og kliniker relevansvurderingerne, og omarbejdet i fase 2 til et spørgeskema på 99 spørgs-
mål.
I fase III anvendte vi en videreudvikling af kognitiv interview-teknik til selvudfyldte spørgeskemaer
i 31 patientinterviews, hvor problemer med forståelsen eller besvarelsen af skemaet blev undersøgt
og forsøgt elimineret. Der blev identificeret problemer 126 gange i 43 spørgsmål. Interviewmetoden
fandtes effektiv til at identificere og reducere forekomsten af fejl.
I fase 4 blev besvarelser fra 904 patienter anvendt til evaluering og etablering af en skalastruktur
med acceptable måleegenskaber, ved hjælp af ”multitrait scaling” og intern konsistens reliabili-
tetstestning (Cronbach’s α). Efter en revision, fandtes en 84-item struktur med komplet konvergent
validitet og næsten komplet diskriminant validitet samt acceptabel reliabilitet på 13 skalaer: struma
symptomer, hyperthyroide symptomer, hypothyroide symptomer, øjensymptomer, træthed, kogniti-
ve problemer, angst, depressivitet, følelsesmæssig sårbarhed, påvirket socialt liv, påvirket dagligliv,
påvirket sexliv og kosmetiske problemer.
Fremtidig anvendelse i kliniske studier bør nu kunne afklare væsentlige spørgsmål vedrørende livs-
kvalitet ved thyroideasygdomme og deres behandling. Klinimetrisk validitet bør belyses i forløbs-
studier og kortere versioner af skemaet kunne udvikles, optimalt ved brug af item response model-
ler.
Page 49 of 107
REFERENCES
1. Hein MD, Jackson IM. Review: thyroid func-tion in psychiatric illness. Gen Hosp Psychia-try 1990; 12(4):232-244.
2. Kirkegaard C, Faber J. Altered serum levels of thyroxine, triiodothyronines and diiodothyron-ines in endogenous depression. Acta Endocri-nol (Copenh) 1981; 96(2):199-207.
3. Kirkegaard C, Korner A, Faber J. Increased production of thyroxine and inappropriately elevated serum thyrotropin in levels in en-dogenous depression. Biol Psychiatry 1990; 27(5):472-476.
4. Rush AJ, Giles DE, Schlesser MA, Orsulak PJ, Weissenburger JE, Fulton CL, Fairchild CJ, Roffwarg HP. Dexamethasone response, thyrotropin-releasing hormone stimulation, rapid eye movement latency, and subtypes of depression. Biol Psychiatry 1997; 41(9):915-928.
5. Harris T, Creed F, Brugha TS. Stressful life events and Graves' disease. Br J Psychiatry 1992; 161:535-541.
6. Lee IT, Sheu WH, Liau YJ, Lin SY, Lee WJ, Lin CC. Relationship of stressful life events, anxiety and depression to hyperthyroidism in an asian population. Hormone Research 2003; 60(5):247-251.
7. Matos-Santos A, Nobre EL, Costa JG, No-gueira PJ, Macedo A, Galvao-Teles A, de Castro JJ. Relationship between the number and impact of stressful life events and the on-set of Graves' disease and toxic nodular goitre. Clin Endocrinol (Oxf) 2001; 55(1):15-19.
8. Sonino N, Girelli ME, Boscaro M, Fallo F, Busnardo B, Fava GA. Life events in the pathogenesis of Graves' disease. A controlled study. Acta Endocrinol (Copenh) 1993; 128(4):293-296.
9. Bianchi GP, Zaccheroni V, Solaroli E, Vescini F, Cerutti R, Zoli M, Marchesini G. Health-related quality of life in patients with thyroid disorders. Qual Life Res 2004; 13(1):45-54.
10. Bommer M, Eversmann T, Pickardt R, Leon-hardt A, Naber D. Psychopathological and neuropsychological symptoms in patients with subclinical and remitted hyperthyroidism. Klin Wochenschr 1990; 68(11):552-558.
11. Werner and Ingbars The Thyroid -a Funda-mental and Clinical Text. 9 ed. New York: Lippincott, Williams & Wilkins; 2005.
12. Canaris GJ, Steiner JF, Ridgway EC. Do tradi-tional symptoms of hypothyroidism correlate with biochemical disease? J Gen Int Med 1997; 12(9):544-550.
13. Cleare AJ, McGregor A, O'Keane V. Neuro-endocrine evidence for an association between hypothyroidism, reduced central 5-HT activity and depression. Clin Endocrinol (Oxf) 1995; 43(6):713-719.
14. Davis PJ, Davis FB. Hyperthyroidism in pa-tients over the age of 60 years. Clinical fea-tures in 85 patients. Medicine (Baltimore) 1974; 53(3):161-181.
15. Endocrinology. 5 ed. Philadelphia: Elsevier Saunders; 2006.
16. Demet MM, Ozmen B, Deveci A, Boyvada S, Adiguzel H, Aydemir O. Depression and anxiety in hyperthyroidism. Arch Med Res 2002; 33(6):552-556.
17. Egle UT, Kahaly GJ, Petrak F, Hardt J, Batke J, Best J, Rothenbacher M. The relevance of physical and psychosocial factors for the qual-ity of life in patients with thyroid-associated orbitopathy (TAO). Exp Clin Endocrinol Dia-betes 1999; 107 Suppl 5:S168-S171.
18. Elberling TV, Rasmussen AK, Feldt-Rasmussen U, Hording M, Perrild H, Walde-mar G. Impaired Health-Related Quality of Life in Graves' Disease. A Prospective Study. Eur J Endocrinol 2004; 151(5):549-555.
19. Escobar-Morreale HF, Botella-Carretero JI, Gomez-Bueno M, Galan JM, Barrios V, San-cho J. Thyroid hormone replacement therapy in primary hypothyroidism: a randomized trial comparing L-thyroxine plus liothyronine with L-thyroxine alone. Ann Intern Med 2005; 142(6):412-424.
20. Fahrenfort JJ, Wilterdink AM, van der Veen EA. Long-term residual complaints and psy-chosocial sequelae after remission of hyper-thyroidism. Psychoneuroendocrinology 2000; 25(2):201-211.
21. Farid M, Roch-Levecq AC, Levi L, Brody BL, Granet DB, Kikkawa DO. Psychological Disturbance in Graves Ophthalmopathy. Arch Ophthalmol 2005; 123(4):491-496.
22. Gerding MN, Terwee CB, Dekker FW, Koornneef L, Prummel MF, Wiersinga WM.
Page 50 of 107
Quality of life in patients with Graves' oph-thalmopathy is markedly decreased: meas-urement by the medical outcomes study in-strument. Thyroid 1997; 7(6):885-889.
23. Gunnarsson T, Sjoberg S, Eriksson M, Nordin C. Depressive symptoms in hypothyroid dis-order with some observations on biochemical correlates. Neuropsychobiology 2001; 43(2):70-74.
24. Harper MB. Vomiting, nausea, and abdominal pain: unrecognized symptoms of thyrotoxico-sis. J Fam Pract 1989; 29(4):382-386.
25. Jaeschke R, Guyatt G, Cook D, Harper S, Gerstein HC. Spectrum of quality of life im-pairment in hypothyroidism. Qual Life Res 1994; 3(5):323-327.
26. Jaeschke R, Guyatt G, Gerstein H, Patterson C, Molloy W, Cook D, Harper S, Griffith L, Carbotte R. Does treatment with L-thyroxine influence health status in middle-aged and older adults with subclinical hypothyroidism? J Gen Int Med 1996; 11(12):744-749.
27. Jain VK. Affective disturbance in hypothy-roidism. Br J Psychiatry 1971; 119(550):279-280.
28. Kahaly GJ, Hardt J, Petrak F, Egle UT. Psy-chosocial factors in subjects with thyroid-associated ophthalmopathy. Thyroid 2002; 12(3):237-239.
29. Kathol RG, Turner R, Delahunt J. Depression and anxiety associated with hyperthyroidism: response to antithyroid therapy. Psychoso-matics 1986; 27(7):501-505.
30. Klein I, Trzepacz PT, Roberts M, Levey GS. Symptom rating scale for assessing hyperthy-roidism. Arch Intern Med 1988; 148(2):387-390.
31. Laurberg P. Hypothyroidism. In: Greer MA, editor. The Thyroid Gland. 1 ed. New York: Raven Press; 1990 p. 497-535.
32. Maugeri D, Motta M, Salerno G, Rosso D, Mazzarella R, Salomone S, Russo MS, Elia G, Panebianco P. Cognitive and affective disor-ders in hyper- and hypothyreotic elderly pa-tients. Archives of Gerontology and Geriatrics 1998; Suppl. 6:305-312.
33. McMillan CV, Bradley C, Woodcock A, Razvi S, Weaver JU. Design of new question-naires to measure quality of life and treatment satisfaction in hypothyroidism. Thyroid 2004; 14(11):916-925.
34. Nordyke RA, Gilbert FI, Jr., Harada AS. Graves' disease. Influence of age on clinical findings. Arch Intern Med 1988; 148(3):626-631.
35. Oddie TH, Boyd CM, Fisher DA, Hales IB. Incidence of signs and symptoms in thyroid disease. Med J Austr 1972; 2(18):981-986.
36. O'Malley B, Hickey J, Nevens E. Thyroid dysfunction -- weight problems and the psy-che: the patients' perspective. Journal of Hu-man Nutrition and Dietetics 2000; 13(4):243-248.
37. Park JJ, Sullivan TJ, Mortimer RH, Wagenaar M, Perry-Keene DA. Assessing quality of life in Australian patients with Graves' ophthal-mopathy. Br J Ophtalmol 2004; 88(1):75-78.
38. Paschke R, Harsch I, Schlote B, Vardarli I, Schaaf L, Kaumeier S, Teuber J, Usadel KH. Sequential psychological testing during the course of autoimmune hyperthyroidism. Klin Wochenschr 1990; 68(19):942-950.
39. Radanovic-Grguric L, Filakovic P, Barkic J, Mandic N, Karner I, Smoje J. Depression in Patients with Thyroid Dysfunction. European Journal of Psychiatry 2003; 17(3):133-144.
40. Razvi S, Ingoe LE, McMillan CV, Weaver JU. Health status in patients with sub-clinical hypothyroidism. Eur J Endocrinol 2005; 152(5):713-717.
41. Sait Gonen M, Kisakol G, Savas Cilli A, Dik-bas O, Gungor K, Inal A, Kaya A. Assessment of anxiety in subclinical thyroid disorders. Endocr J 2004; 51(3):311-315.
42. Saravanan P, Chau WF, Roberts N, Vedhara K, Greenwood R, Dayan CM. Psychological well-being in patients on 'adequate' doses of l-thyroxine: results of a large, controlled com-munity-based questionnaire study. Clin Endo-crinol (Oxf) 2002; 57(5):577-585.
43. Stern RA, Robinson B, Thorner AR, Arruda JE, Prohaska ML, Prange AJ, Jr. A survey study of neuropsychiatric complaints in pa-tients with Graves' disease. J Neuropsychiatry Clin Neurosci 1996; 8(2):181-185.
44. Tak PP, Hermans J, Haak A. Symptomatology of Graves' disease and Plummer's disease in relation to age and thyroid hormone level. Neth J Med 1993; 42(5-6):157-162.
45. Terwee CB, Gerding MN, Dekker FW, Prummel MF, Wiersinga WM. Development of a disease specific quality of life question-naire for patients with Graves' ophthalmopa-
Page 51 of 107
thy: the GO-QOL. Br J Ophtalmol 1998; 82(7):773-779.
46. Terwee CB, Gerding MN, Dekker FW, Prummel MF, van der Pol JP, Wiersinga WM. Test-retest reliability of the GO-QOL: a dis-ease-specific quality of life questionnaire for patients with Graves' ophthalmopathy. J Clin Epidemiol 1999; 52(9):875-884.
47. Terwee C, Wakelkamp I, Tan S, Dekker F, Prummel MF, Wiersinga W. Long-term ef-fects of Graves' ophthalmopathy on health-related quality of life. Eur J Endocrinol 2002; 146(6):751-757.
48. Thomsen AF, Kvist TK, Andersen PK, Kes-sing LV. Increased risk of affective disorder following hospitalisation with hyperthyroid-ism - a register-based study. Eur J Endocrinol 2005; 152(4):535-543.
49. Thomsen AF, Kvist TK, Andersen PK, Kes-sing LV. Increased risk of developing affec-tive disorder in patients with hypothyroidism: a register-based study. Thyroid 2005; 15(7):700-707.
50. Trivalle C, Doucet J, Chassagne P, Landrin I, Kadri N, Menard JF, Bercoff E. Differences in the signs and symptoms of hyperthyroidism in older and younger patients. J Am Geriatr Soc 1996; 44(1):50-53.
51. Trzepacz PT, McCue M, Klein I, Levey GS, Greenhouse J. A psychiatric and neuropsy-chological study of patients with untreated Graves' disease. General Hospital Psychiatry 1988; 10(1):49-55.
52. Wallace JE, MacCrimmon DJ, Goldberg WM. Acute hyperthyroidism: cognitive and emo-tional correlates. J Abnorm Psychol 1980; 89(4):519-527.
53. Oxford textbook of endocrinology and diabe-tes. 1 ed. Oxford: Oxford University Press; 2002.
54. Watanakunakorn C, Hodges RE, Evans TC. Myxedema; a study of 400 cases. Arch Intern Med 1965; 116:183-190.
55. Wayne EJ. The diagnosis of thyrotoxicosis. BMJ 1954; 4859:411-419.
56. Whybrow PC, Prange AJ, Jr., Treadway CR. Mental changes accompanying thyroid gland dysfunction. A reappraisal using objective psychological measurement. Archives of Gen-eral Psychiatry 1969; 20(1):48-63.
57. Wilson WP, Johnson JE, Smith RB. Affective change in thyrotoxicosis and experimental hy-
permetabolism. Rec Adv Biol Psychiatry 1961; 4:234-243.
58. Yonem O, Dokmetas HS, Aslan SM, Erselcan T. Is antithyroid treatment really relevant for young patients with subclinical hyperthyroid-ism? Endocr J 2002; 49(3):307-314.
59. Zeitlhofer J, Saletu B, Stary J, Ahmadi R. Cerebral function in hyperthyroid patients. Psychopathology, psychometric variables, central arousal and time perception before and after thyreostatic therapy. Neuropsychobiol-ogy 1984; 11(2):89-93.
60. Zettinig G, Asenbaum S, Fueger BJ, Hofmann A, Diemling M, Mittlboeck M, Dudczak R. Increased prevalence of sublinical brain perfu-sion abnormalities in patients with autoim-mune thyroiditis: evidence of Hashimoto's en-cephalitis? Clin Endocrinol (Oxf) 2003; 59(5):637-643.
61. Ladenson PW. Psychological wellbeing in patients. Clin Endocrinol (Oxf) 2002; 57(5):575-576.
62. Abraham P, Avenell A, Watson WA, Park CM, Bevan JS. Antithyroid drug regimen for treating Graves' hyperthyroidism (Cochrane Review). The Cochrane Library, Issue 3. Chichester,UK: John Wiley & Sons, Ltd.; 2004.
63. Romijn JA, Smit JW, Lamberts SW. Intrinsic imperfections of endocrine replacement ther-apy. Eur J Endocrinol 2003; 149(2):91-97.
64. Terwee CB, Dekker FW, Mourits MP, Gerding MN, Baldeschi L, Kalmann R, Prummel MF, Wiersinga WM. Interpretation and validity of changes in scores on the Graves' ophthalmopathy quality of life ques-tionnaire (GO-QOL) after different treat-ments. Clin Endocrinol (Oxf) 2001; 54(3):391-398.
65. Tehrani M, Krummenauer F, Mann WJ, Pitz S, Dick HB, Kahaly GJ. Disease-specific as-sessment of quality of life after decompression surgery for Graves' ophthalmopathy. Eur J Ophtalmol 2004; 14(3):193-199.
66. Watt T, Groenvold M, Rasmussen AK, Bon-nema SJ, Hegedüs L, Bjorner JB, Feldt-Rasmussen U. Quality of life in patients with benign thyroid disorders. A review. Eur J En-docrinol 2006; 154:501-510.
67. Willis G. Cognitive interviewing. A tool for improving questionnaire design. California: Sage publications; 2005.
Page 52 of 107
68. Jobe JB. Cognitive psychology and self-reports: models and methods. Qual Life Res 2003; 12(3):219-227.
69. Groenvold M. Quality of life in breast cancer adjuvant therapy: validation and pilot testing of a combination of questionnaires. The Breast 1997; 6:97-107.
70. McColl E. Developing questionnaires. In: Fayers P, Hays RD, editors. Assessing quality of life in clinical trials. 2 ed. Oxford: Oxford University Press; 2005 p. 9-23.
71. Ware JE, Jr., Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Con-ceptual framework and item selection. Med Care 1992; 30:473-483.
72. Ware JE, Jr. Conceptualization and measure-ment of health-related quality of life: com-ments on an evolving field. Arch Phys Med Rehabil 2003; 84(4 Suppl 2):S43-S51.
73. Stewart AL, Ware JE, Jr. Measuring Func-tionning and Well-Being: The Medical Out-comes Study Approach. London: Duke Uni-versity Press; 1992.
74. Dalakas MC, Mock V, Hawkins MJ. Fatigue: definitions, mechanisms, and paradigms for study. Semin Oncol 1998; 25(1 Suppl 1):48-53.
75. Glaus A, Crow R, Hammond S. A qualitative study to explore the concept of fa-tigue/tiredness in cancer patients and in healthy individuals. Eur J Cancer Care (Engl) 1996; 5(2 Suppl):8-23.
76. Ream E, Richardson A. Fatigue: a concept analysis. Int J Nurs Stud 1996; 33(5):519-529.
77. Russell RD. Social health: an attempt to clar-ify this dimension of well-being. International Journal of Health Education 1973; 16:74-82.
78. McDowell I, Newell C. Social Health. In: McDowell I, Newell C, editors. Measuring Health. New York: Oxford University Press; 1996 p. 122-176.
79. Wärneryd B. At Fråga. Stockholm: Statistiska Centralbyrån; 1986.
80. Streiner DL, Norman GR. Health Measure-ment Scales. A Practical Guide to their Devel-opment and Use. 2 ed. Oxford: Oxford Uni-versity Press; 1995.
81. Münster K. Spørgeskemaundersøgelser. In: Koch L, Vallgårda S, editors. Forskningsme-toder i folkesundhedsvidenskab. 2 ed. Copen-hagen: Munksgaard; 2003 p. 179-198.
82. Bradburn NM, Sudman S, Wansink B. Asking questions. San Francisco: Jossey-Bass; 2004.
83. Sudman S, Bradburn NM, Schwarz N. Think-ing about answers. The application of cogni-tive processes to survey methodology. 1 ed. San Francisco: Jossey-Bass Publishers; 1996.
84. Fayers PM, Machin D. Quality of Life: As-sessment, Analysis and Interpretation. 2 ed. Chichester: John Wiley and Sons; 2007.
85. Bjorner JB, Ware JE, Jr., Kosinski M. The potential synergy between cognitive models and modern psychometric models. Qual Life Res 2003; 12(3):261-274.
86. Mullin PA, Lohr KN, Bresnahan BW, McNulty P. Applying cognitive design princi-ples to formatting HRQOL instruments. Qual Life Res 2000; 9(1):13-27.
87. Tourangeau R, Rips LJ, Rasinski K. The psy-chology of survey response. Cambridge,UK: Cambridge University Press; 2000.
88. Werner SC. Modification of the classification of the eye changes of Graves' disease: recom-mendations of the Ad Hoc Committee of the American Thyroid Association. J Clin Endo-crinol Metab 1977; 44(1):203-204.
89. Mourits MP, Prummel MF, Wiersinga WM, Koornneef L. Clinical activity score as a guide in the management of patients with Graves' ophthalmopathy. Clin Endocrinol (Oxf) 1997; 47(1):9-14.
90. Hegedus L. Thyroid ultrasound. Endocrinol Metab Clin North Am 2001; 30(2):339-3ix.
91. Knudsen N, Bols B, Bulow I, Jorgensen T, Perrild H, Ovesen L, Laurberg P. Validation of ultrasonography of the thyroid gland for epidemiological purposes. Thyroid 1999; 9(11):1069-1074.
92. Campbell DT, Fiske DW. Convergent and discriminant validation by the multitrait-multimethod matrix. Psychol Bull 1959; 56(2):81-105.
93. Hays RD, Hayashi T, Carson S, Ware JE, Jr. User's guide for the multitrait analysis pro-gram (MAP). Rand Corporation; 1988.
94. Ware JE, Jr., Harris WJ, Gandek B, Rogers BW, Reese PR. MAP-R for Windows: Multi-trait/multi-item analysis program - revised user's guide. Boston: Health Assessment Lab; 1997.
Page 53 of 107
95. Cronbach LJ. Coefficient alpha and the inter-nal structure of tests. Psychometrika 1951; 16:297-334.
96. Drasgow J. Polychoric and polyserial correla-tions. In: Kotz S, Johnson NL, Read CB, edi-tors. Encyclopedia of Statistical Sciences. New York: John Wiley and Sons; 1986 p. 68-74.
97. Muthen B. A General Structural Equation Model with Dichotomous, Ordered Categori-cal, and Continuous Latent Variable Indica-tors. Psychometrika 1984; 49(1):115-132.
98. Bjorner JB, Damsgaard MT, Watt T, Groen-vold M. Tests of data quality, scaling assump-tions, and reliability of the Danish SF-36. J Clin Epidemiol 1998; 51(11):1001-1011.
99. Sprangers MA, Cull A, Bjordal K, Groenvold M, Aaronson NK. The European Organization for Research and Treatment of Cancer. Ap-proach to quality of life assessment: guide-lines for developing questionnaire modules. EORTC Study Group on Quality of Life. Qual Life Res 1993; 2(4):287-295.
100. Webb SM, Prieto L, Badia X, Albareda M, Catala M, Gaztambide S, Lucas T, Paramo C, Pico A, Lucas A, Halperin I, Obiols G, As-torga R. Acromegaly Quality of Life Ques-tionnaire (ACROQOL) a new health-related quality of life questionnaire for patients with acromegaly: development and psychometric properties. Clin Endocrinol (Oxf) 2002; 57(2):251-258.
101. Presser S, Blair J. Survey pretesteing: do dif-ferent methods produce different results? So-ciological Methodology. American Sociologi-cal Association; 1994 p. 73-104.
102. Rothgeb J, Willis G, Forsyth B. Questionnaire pretesting methods: do different techniques and different organizations produce similar re-sults? Proceedings of the annual meeting of the American statistical association 2001.
103. May LA, Warren S. Measuring quality of life of persons with spinal cord injury: Substantive and structural validation. Qual Life Res 2001; 10:503-515.
104. Groenvold M, Klee MC, Sprangers MA, Aaronson NK. Validation of the EORTC QLQ-C30 quality of life questionnaire through combined qualitative and quantitative assessment of patient-observer agreement. J Clin Epidemiol 1997; 50(4):441-450.
105. Rapkin BD, Schwartz CE. Toward a theoreti-cal model of quality-of-life appraisal: Implica-tions of findings from studies of response shift. Health Qual Life Outcomes 2004; 2:14.
106. Grice P. Studies in the way of words. Cam-bridge, Mass.: Harvard University Press; 1989.
107. Sprangers MA, Schwartz CE. Integrating response shift into health-related quality of life research: a theoretical model. Soc Sci Med 1999; 48(11):1507-1515.
108. Olsson U. Maximum likelihood estimation of the polychoric correlation coefficient. Psy-chometrika 1979; 44(4):443-460.
109. van Nispen RM, Knol DL, Langelaan M, de Boer MR, Terwee CB, van Rens GH. Apply-ing multilevel item response theory to vision-related quality of life in Dutch visually im-paired elderly. Optom Vis Sci 2007; 84(8):710-720.
110. Fayers PM, Hand DJ, Bjordal K, Groenvold M. Causal indicators in quality of life re-search. Qual Life Res 1997; 6(5):393-406.
111. Fayers PM, Hand DJ. Factor analysis, causal indicators and quality of life. Qual Life Res 1997; 6(2):139-150.
112. Muthen B. Multiple-group structural model-ling with non-normal continuous variables. British Journal of Matemathical and Statistical Psychology 42, 55-62. 1989. Ref Type: Generic
113. Bollen KA, Barb KH. Pearson r and coarsely categorized measures. American Sociological Review 1981; 46:232-239.
114. Abraham-Nordling M, Torring O, Hamberger B, Lundell G, Tallstedt L, Calissendorff J, Wallin G. Graves' disease: a long-term qual-ity-of-life follow up of patients randomized to treatment with antithyroid drugs, radioiodine, or surgery. Thyroid 2005; 15(11):1279-1286.
115. Joffe RT, Brimacombe M, Levitt AJ, Stag-naro-Green A. Treatment of clinical hypothy-roidism with thyroxine and triiodothyronine: A literature review and metaanalysis. Psycho-somatics 2007; 48(5):379-384.
116. Watt T, Feldt-Rasmussen U, Rasmussen AK, Hegedus L, Bonnema SJ, Gronvold M, Bjor-ner JB. [Measurement of health-related quality of life in thyroid patients]. Ugeskr Laeger 2008; 170(10):850-852.
Page 54 of 107
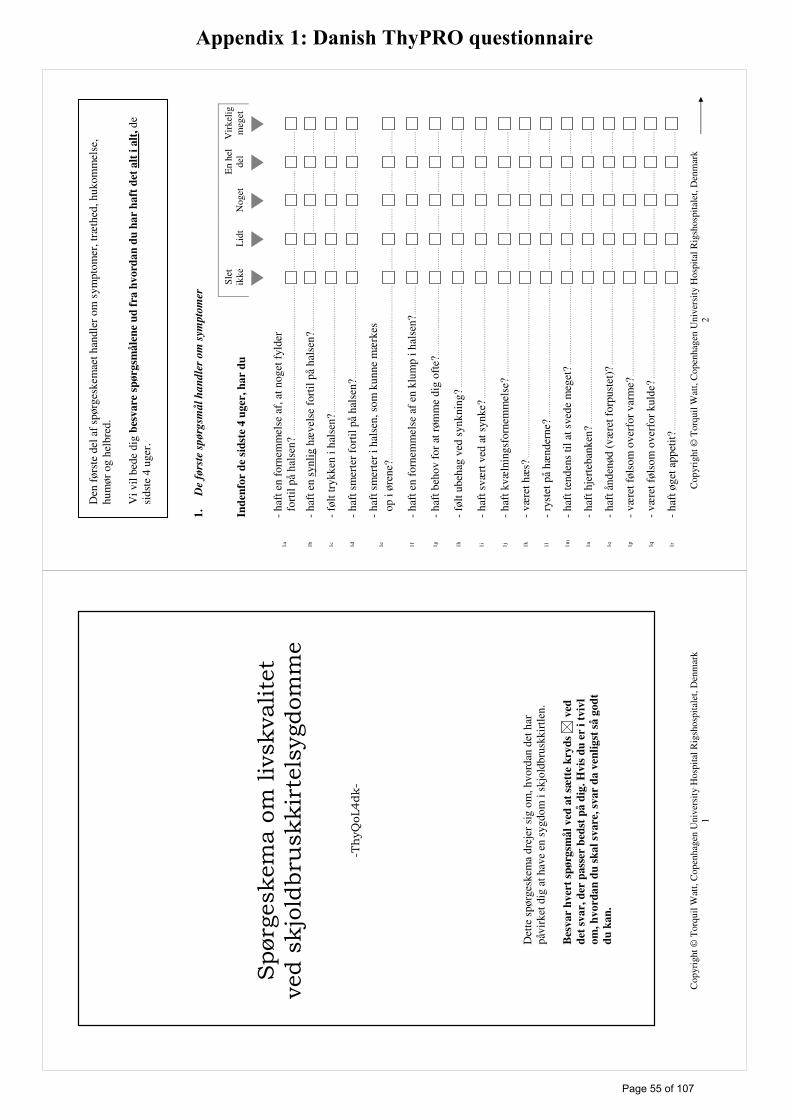
Cop
yrig
ht ©
Tor
quil
Wat
t, C
open
hage
n U
nive
rsit
y H
ospi
tal R
igsh
ospi
tale
t, D
enm
ark
1 Spørgeskema om livskvalitet
ved skjoldbruskkirtelsygdomme
-ThyQoL4dk-
Det
te s
pørg
eske
ma
drej
er s
ig o
m, h
vord
an d
et h
ar
påvi
rket
dig
at h
ave
en s
ygdo
m i
skjo
ldbr
uskk
irtle
n.
Bes
var
hv
ert
spø
rgsm
ål
ved
at
sætt
e k
ryd
s v
ed
det
sv
ar,
der
pass
er b
edst
på
dig
. H
vis
du
er
i tv
ivl
om
, h
vo
rda
n d
u s
ka
l sv
are
, sv
ar
da
ven
lig
st s
å g
od
t
du
ka
n.
Cop
yrig
ht ©
Tor
quil
Wat
t, C
open
hage
n U
nive
rsit
y H
ospi
tal R
igsh
ospi
tale
t, D
enm
ark
2
1.
De
førs
te s
pørg
smål
ha
nd
ler
om
sym
pto
mer
In
den
for
de
sid
ste
4 u
ger
, h
ar
du
Slet
ik
ke
Lid
t N
oget
E
n he
l de
l V
irke
lig
meg
et
�
� �
�
�
1a
- ha
ft e
n fo
rnem
mel
se a
f, a
t nog
et f
ylde
r
for
til p
å ha
lsen
?...
......
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
.
1b
- ha
ft e
n sy
nlig
hæ
vels
e fo
rtil
på h
alse
n?...
......
......
.....
......
....
......
....
......
....
......
....
1c
- fø
lt tr
ykke
n i h
alse
n?...
......
......
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
....
1d
- ha
ft s
mer
ter
fort
il på
hal
sen?
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
....
1e
- ha
ft s
mer
ter
i hal
sen,
som
kun
ne m
ærk
es
op
i øre
ne?.
......
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
....
1f
- ha
ft e
n fo
rnem
mel
se a
f en
klu
mp
i hal
sen?
......
......
....
......
....
......
....
......
....
......
.
1g
- ha
ft b
ehov
for
at r
ømm
e di
g of
te?.
......
......
......
......
......
......
....
......
....
......
....
......
....
1h
- fø
lt ub
ehag
ved
syn
knin
g?...
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
1i
- ha
ft s
vært
ved
at s
ynke
?....
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
....
1j
- ha
ft k
væln
ings
forn
emm
else
?...
......
......
......
......
......
......
....
......
....
......
....
......
....
......
.
1k
- væ
ret h
æs?
......
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
....
1l
- ry
stet
på
hænd
erne
?...
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
.
1m
- ha
ft te
nden
s til
at s
vede
meg
et?
......
......
......
......
......
.....
......
....
......
....
......
....
......
....
1n
- ha
ft h
jert
eban
ken?
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
.
1o
- ha
ft å
nden
ød (
være
t for
pust
et)?
......
......
......
......
......
.....
......
....
......
....
......
....
......
....
1p
- væ
ret f
ølso
m o
verf
or v
arm
e?...
......
......
......
......
......
......
....
......
....
......
....
......
....
......
.
1q
- væ
ret f
ølso
m o
verf
or k
ulde
?...
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
.
1r
- ha
ft ø
get a
ppet
it?...
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
.
Den
før
ste
del a
f sp
ørge
skem
aet h
andl
er o
m s
ympt
omer
, træ
thed
, huk
omm
else
, hu
mør
og
helb
red.
V
i vil
bede
dig
bes
vare
sp
ørg
små
len
e u
d f
ra h
vord
an
du
ha
r h
aft
det
alt
i a
lt, de
si
dste
4 u
ger.
Page 55 of 107
Appendix 1: Danish ThyPRO questionnaire
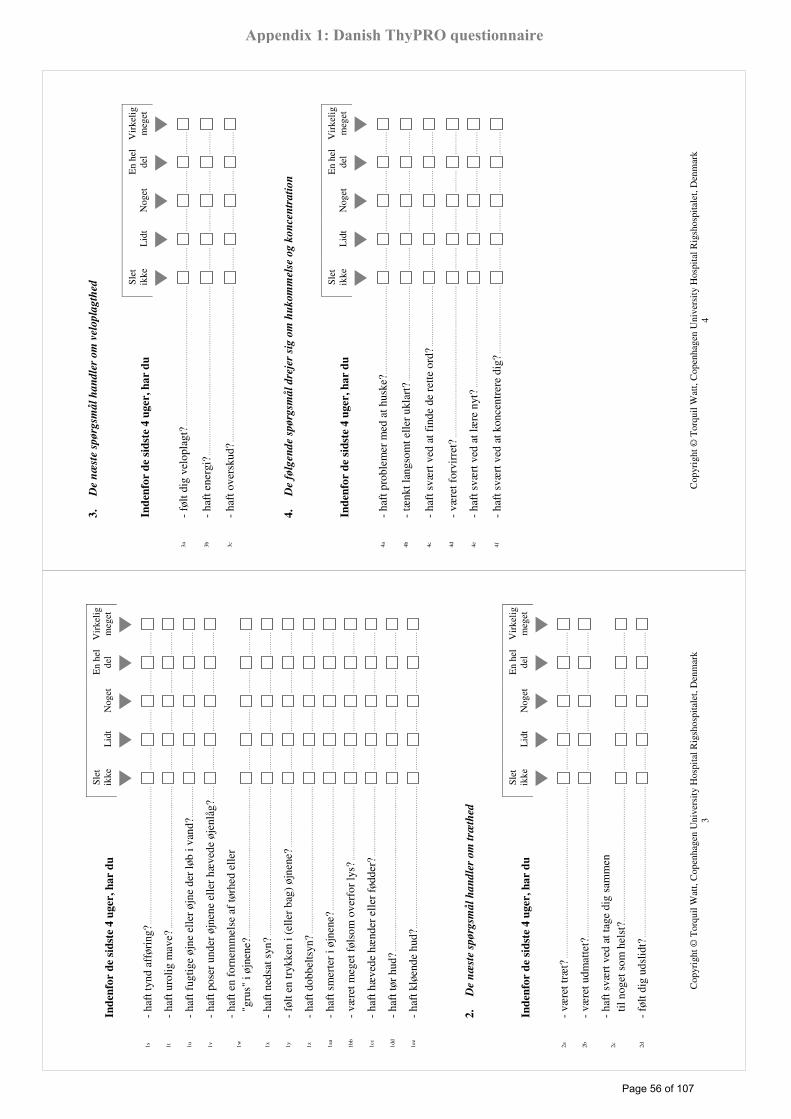
Cop
yrig
ht ©
Tor
quil
Wat
t, C
open
hage
n U
nive
rsit
y H
ospi
tal R
igsh
ospi
tale
t, D
enm
ark
3
Ind
enfo
r d
e si
dst
e 4
ug
er, h
ar
du
Slet
i k
ke
Lid
t N
oget
E
n he
l de
l V
irke
lig
meg
et
�
� �
�
�
1s
- ha
ft ty
nd a
ffør
ing?
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
.
1t
- ha
ft u
rolig
mav
e?...
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
1u
- ha
ft f
ugtig
e øj
ne e
ller
øjne
der
løb
i van
d?...
......
.....
......
....
......
....
......
....
......
....
1v
- ha
ft p
oser
und
er ø
jnen
e el
ler
hæve
de ø
jenl
åg?.
.....
......
....
......
....
......
....
......
....
1w
- ha
ft e
n fo
rnem
mel
se a
f tø
rhed
elle
r
"gr
us"
i øjn
ene?
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
.
1x
- ha
ft n
edsa
t syn
?...
......
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
.
1y
- fø
lt en
tryk
ken
i (el
ler
bag)
øjn
ene?
......
......
......
......
......
......
....
......
....
......
....
......
.
1z
- ha
ft d
obbe
ltsyn
?...
......
......
......
......
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
.
1aa
- ha
ft s
mer
ter
i øjn
ene?
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
.
1bb
- væ
ret m
eget
føl
som
ove
rfor
lys?
......
......
......
......
......
......
......
....
......
....
......
....
......
.
1cc
- ha
ft h
æve
de h
ænd
er e
ller
fødd
er?.
......
......
......
......
......
......
....
......
....
......
....
......
....
1dd
- ha
ft tø
r hu
d?...
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
....
1ee
- ha
ft k
løen
de h
ud?.
......
......
......
......
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
.
2.
De
næ
ste
spø
rgsm
ål
ha
nd
ler
om
træ
thed
In
den
for
de
sid
ste
4 u
ger
, h
ar
du
Slet
ik
ke
Lid
t N
oget
E
n he
l de
l V
irke
lig
meg
et
�
� �
�
�
2a
- væ
ret t
ræt?
......
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
....
2b
- væ
ret u
dmat
tet?
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
.
2c
- ha
ft s
vært
ved
at t
age
dig
sam
men
t
il no
get s
om h
elst
?....
......
......
......
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
.
2d
- fø
lt di
g ud
slid
t?...
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
....
Cop
yrig
ht ©
Tor
quil
Wat
t, C
open
hage
n U
nive
rsit
y H
ospi
tal R
igsh
ospi
tale
t, D
enm
ark
4
3.
De
næ
ste
spø
rgsm
ål
ha
nd
ler
om
vel
op
lag
thed
I n
den
for
de
sid
ste
4 u
ger
, h
ar
du
Slet
ik
ke
Lid
t N
oget
E
n he
l de
l V
irke
lig
meg
et
�
� �
�
�
3a
- fø
lt di
g ve
lopl
agt?
......
......
......
......
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
.
3b
- ha
ft e
nerg
i?...
......
......
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
3c
- ha
ft o
vers
kud?
......
......
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
.
4.
De
følg
end
e sp
ørg
små
l d
reje
r si
g o
m h
ukom
mel
se o
g k
on
cen
trati
on
Ind
enfo
r d
e si
dst
e 4
ug
er, h
ar
du
Slet
ik
ke
Lid
t N
oget
E
n he
l de
l V
irke
lig
meg
et
�
� �
�
�
4a
- ha
ft p
robl
emer
med
at h
uske
?....
......
......
......
......
......
.....
......
....
......
....
......
....
......
....
4b
- tæ
nkt l
angs
omt e
ller
ukla
rt?
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
4c
- ha
ft s
vært
ved
at f
inde
de
rette
ord
?....
......
......
......
.....
......
....
......
....
......
....
......
....
4d
- væ
ret f
orvi
rret
?...
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
....
4e
- ha
ft s
vært
ved
at l
ære
nyt
?...
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
4f
- ha
ft s
vært
ved
at k
once
ntre
re d
ig?
......
......
......
......
......
......
....
......
....
......
....
......
....
Page 56 of 107
Appendix 1: Danish ThyPRO questionnaire
Cop
yrig
ht ©
Tor
quil
Wat
t, C
open
hage
n U
nive
rsit
y H
ospi
tal R
igsh
ospi
tale
t, D
enm
ark
5
5.
De
næ
ste
spø
rgsm
ål
dre
jer
sig
om
ner
vøsi
tet
og
an
spæ
nd
thed
I n
den
for
de
sid
ste
4 u
ger
, h
ar
du
Slet
ik
ke
Lid
t N
oget
E
n he
l de
l V
irke
lig
meg
et
�
� �
�
�
5a
- væ
ret n
ervø
s?...
......
......
......
......
......
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
.
5b
- væ
ret b
ange
elle
r an
gst?
......
......
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
.
5c
- fø
lt di
g an
spæ
ndt?
......
......
......
......
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
.
5d
- væ
ret b
ange
for
at f
ejle
nog
et a
lvor
ligt?
......
......
......
....
......
....
......
....
......
....
......
.
5e
- fø
lt di
g ur
olig
?....
......
......
......
......
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
....
5f
- væ
ret r
astlø
s?...
......
......
......
......
......
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
.
6.
De
følg
end
e sp
ørg
små
l h
an
dle
r om
psy
kis
k v
elb
efin
den
de
Ind
enfo
r d
e si
dst
e 4
ug
er, h
ar
du
Slet
ik
ke
Lid
t N
oget
E
n he
l de
l V
irke
lig
meg
et
�
� �
�
�
6a
- væ
ret t
rist
?...
......
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
.
6b
- væ
ret d
epri
mer
et?
......
......
......
......
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
.
6c
- fø
lt di
g m
odlø
s?...
......
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
.
6d
- ha
ft le
t ved
at k
omm
e til
at g
ræde
?...
......
......
......
......
....
......
....
......
....
......
....
......
.
6e
- væ
ret k
ed a
f de
t?...
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
.
Ind
enfo
r d
e si
dst
e 4
ug
er, h
ar
du
Slet
ik
ke
Lid
t N
oget
E
n he
l de
l V
irke
lig
meg
et
�
� �
�
�
6f
- væ
ret g
lad?
......
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
....
6g
- ha
ft s
elvt
illid
?....
......
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
Cop
yrig
ht ©
Tor
quil
Wat
t, C
open
hage
n U
nive
rsit
y H
ospi
tal R
igsh
ospi
tale
t, D
enm
ark
6
7.
De
næ
ste
spø
rgsm
ål
ha
nd
ler
om
at
have
svæ
rt v
ed a
t o
vers
ku
e ti
ng
ene
elle
r at
v ære
føle
lses
mæ
ssig
t sv
ing
end
e
Ind
enfo
r d
e si
dst
e 4
ug
er, h
ar
du
Slet
ik
ke
Lid
t N
oget
E
n he
l de
l V
irke
lig
meg
et
�
� �
�
�
7a
- ha
ft s
vært
ved
at o
vers
kue
tinge
ne?
......
......
......
......
......
......
....
......
....
......
....
......
.
7b
- fø
lt, a
t du
"ikk
e va
r di
g se
lv"?
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
.
7c
- op
leve
t at d
u ne
mt b
lev
stre
sset
?....
......
......
......
......
.....
......
....
......
....
......
....
......
....
7d
- væ
ret f
ølel
sesm
æss
igt s
ving
ende
?...
......
......
......
......
......
......
....
......
....
......
....
......
.
7e
- væ
ret i
rrita
bel?
......
......
......
......
......
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
.
7f
- væ
ret f
rust
rere
t?...
......
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
.
7g
- væ
ret v
red?
......
......
......
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
.
Slet
ik
ke
Lid
t N
oget
I
høj
grad
Fu
ld-
stæ
ndig
�
� �
�
�
7h
- fø
lt at
du
havd
e ko
ntro
l ove
r di
t liv
?....
......
......
......
....
......
....
......
....
......
....
......
....
7i
- væ
ret i
bal
ance
med
dig
sel
v?...
......
......
......
......
......
......
......
....
......
....
......
....
......
....
Page 57 of 107
Appendix 1: Danish ThyPRO questionnaire
Cop
yrig
ht ©
Tor
quil
Wat
t, C
open
hage
n U
nive
rsit
y H
ospi
tal R
igsh
ospi
tale
t, D
enm
ark
7
8.
De
følg
end
e sp
ørg
små
l h
an
dle
r om
dit
sam
vær
med
an
dre
men
nes
ker
Slet
ik
ke
Lid
t N
oget
E
n he
l de
l V
irke
lig
meg
et
Ind
enfo
r d
e si
dst
e 4
ug
er, h
ar
din
sy
gd
om
i
skjo
ldb
rusk
kir
tlen
gjo
rt, at
du
� � �
�
�
8a
- ha
r ha
ft v
ansk
elig
t ved
at v
ære
sam
men
m
ed a
ndre
men
nesk
er (
for
ekse
mpe
l ægt
efæ
lle,
bør
n, k
ære
ste,
ven
ner
elle
r an
dre)
?....
......
.....
......
......
....
......
....
......
....
......
....
......
.
8b
- ha
r fø
lt di
g so
m e
n be
last
ning
f
or a
ndre
men
nesk
er?.
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
.
8c
- er
kom
met
i ko
nflik
t med
and
re m
enne
sker
?....
.....
......
....
......
....
......
....
......
....
Ind
enfo
r d
e si
dst
e 4
ug
er,
Slet
ik
ke
Lid
t N
oget
E
n he
l de
l V
irke
lig
meg
et
�
� �
�
�
8d
- ha
r du
føl
t, at
din
e om
give
lser
man
gled
e
for
ståe
lse
for
din
sygd
om i
skjo
ldbr
uskk
irtle
n?...
....
......
....
......
....
......
....
......
.
Res
ten
af s
pørg
eske
mae
t han
dler
om
hv
ord
an
din
sy
gd
om
i s
kjo
ldb
rusk
kir
tlen
ka
n h
av
e p
åv
irk
et f
ors
kel
lig
e fo
rhold
i d
in t
ilv
ære
lse.
Cop
yrig
ht ©
Tor
quil
Wat
t, C
open
hage
n U
nive
rsit
y H
ospi
tal R
igsh
ospi
tale
t, D
enm
ark
8
9.
De
følg
end
e sp
ørg
små
l d
reje
r si
g o
m d
ine
dagli
ge
akti
vite
ter
S let
ik
ke
Lid
t N
oget
E
n he
l de
l V
irke
lig
meg
et
Ind
enfo
r d
e si
dst
e 4
ug
er, h
ar
din
sy
gd
om
i
skjo
ldb
rusk
kir
tlen
gjo
rt, at
du
har
� � �
�
�
9a
- ha
ft v
ansk
elig
t ved
at k
lare
d
in d
aglig
dag?
......
......
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
.
9b
- væ
ret b
egræ
nset
i at
udf
øre
dine
f
ritid
sakt
ivite
ter
elle
r ho
bbie
s? ..
......
......
.....
......
......
....
......
....
......
....
......
....
......
....
9c
- væ
ret f
orhi
ndre
t i a
t del
tage
i
live
t om
krin
g di
g?...
......
......
......
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
.
9d
- ha
ft v
ansk
elig
t ved
at k
omm
e om
krin
g
(fo
r ek
sem
pel a
t gå,
løbe
, cyk
le e
ller
køre
i bi
l)?
....
......
....
......
....
......
....
......
.
9e
- ha
ft e
n fø
lels
e af
at v
ære
ble
vet
lan
gsom
mer
e til
alti
ng?
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
.
Har
ikke
ar
bejd
e Sl
et
ikke
L
idt
Nog
et
En
hel
del
Vir
kelig
m
eget
In
den
for
de
sid
ste
4 u
ger
, h
ar
din
syg
do
m i
sk
jold
bru
skk
irtl
en
gjo
rt, a
t d
u h
ar
� �
� �
�
�
9f
- ha
ft v
ansk
elig
t ved
at p
asse
dit
e
rhve
rvsa
rbej
de (
for
ekse
mpe
l h
aft s
vært
ved
at k
lare
det
e
ller
være
t syg
emel
dt)?
......
......
......
......
......
....
......
.....
......
....
......
....
......
....
......
....
Page 58 of 107
Appendix 1: Danish ThyPRO questionnaire
Cop
yrig
ht ©
Tor
quil
Wat
t, C
open
hage
n U
nive
rsit
y H
ospi
tal R
igsh
ospi
tale
t, D
enm
ark
9
10
. D
e n
æst
e sp
ørg
smål
ha
nd
ler
om
dit
sek
sua
lliv
.
I nd
enfo
r d
e si
dst
e 4
ug
er, h
ar
du
Slet
ik
ke
Lid
t N
oget
E
n he
l de
l V
irke
lig
meg
et
�
� �
�
�
10a
- fø
lt, a
t din
syg
dom
i sk
jold
brus
kkir
tlen
h
ar h
aft n
egat
iv in
dfly
dels
e
på
dit s
eksu
alliv
?....
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
10b
- ha
ft n
edsa
t sek
suel
lyst
?....
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
....
11
. S
ygd
om
me
i sk
jold
bru
skkir
tlen
(el
ler
beh
an
dli
ngen
af
dem
) ka
n p
åvi
rke
ud
seen
det
, fo
r ek
sem
pel
ved
at
giv
e h
æve
lse
på
ha
lsen
, væ
skea
nsa
mli
ng
er i
an
sig
tet,
på
hæ
nder
ell
er f
ødd
er, æ
ndre
de
øjn
e el
ler
vægtæ
ndri
ng
.
Ind
enfo
r d
e si
dst
e 4
ug
er,
Slet
ik
ke
Lid
t N
oget
E
n he
l de
l V
irke
lig
meg
et
�
� �
�
�
11a
- ha
r di
n sy
gdom
i sk
jold
brus
kkir
tlen
påv
irke
t d
it ud
seen
de (
for
ekse
mpe
l hæ
vels
e på
h
alse
n, f
oran
dred
e øj
ne, æ
ndre
t væ
gt)?
......
......
......
......
......
....
......
....
......
....
......
.
11b
- ha
r di
n sy
gdom
i sk
jold
brus
kkir
tlen
g
jort
, at d
u ha
r væ
ret u
tilfr
eds
med
dit
udse
ende
?...
......
....
......
....
......
....
......
.
11c
- ha
r du
for
søgt
at k
amuf
lere
elle
r m
aske
re s
ynlig
e t
egn
på s
ygdo
m i
skjo
ldbr
uskk
irtle
n (f
or e
ksem
pel
ved
at t
age
tørk
læde
elle
r so
lbri
ller
på)?
......
......
......
....
......
....
......
....
......
....
......
.
11d
- ha
r du
væ
ret g
ener
et a
f, a
t and
re k
igge
de p
å di
g?...
......
....
......
....
......
....
......
.
11e
- ha
r di
n sy
gdom
i sk
jold
brus
kkir
tlen
haft
i
ndfl
ydel
se p
å, h
vilk
et tø
j du
havd
e på
?...
......
......
....
......
....
......
....
......
....
......
....
11g
- ha
r du
føl
t dig
for
tyk?
......
......
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
....
Cop
yrig
ht ©
Tor
quil
Wat
t, C
open
hage
n U
nive
rsit
y H
ospi
tal R
igsh
ospi
tale
t, D
enm
ark
10
12
. D
et s
idst
e sp
ørg
smål
dre
jer
sig
om
, h
vor
meg
et d
in s
ygdom
i s
kjo
ldb
rusk
kir
tlen
ha
r på
virk
et d
ig a
lt i
alt
, d
e si
dst
e 4
ug
er
Ind
enfo
r d
e si
dst
e 4
ug
er,
Slet
ik
ke
Lid
t N
oget
E
n he
l de
l V
irke
lig
meg
et
�
� �
�
�
12
- ha
r di
n sy
gdom
i sk
jold
brus
kkir
tlen
haft
n
egat
iv in
dfly
dels
e på
din
livs
kval
itet?
......
......
......
.....
......
....
......
....
......
....
......
.
Kon
troll
ér v
enli
gst
, at
du
ha
r sv
are
t p
å a
lle
spørg
småle
ne.
Ma
ng
e ta
k f
or
din
hjæ
lp m
ed a
t b
esva
re d
ette
sp
ørg
esk
ema
!
Page 59 of 107
Appendix 1: Danish ThyPRO questionnaire
Cop
yrig
ht ©
Tor
quil
Wat
t, C
open
hage
n U
nive
rsit
y H
ospi
tal R
igsh
ospi
tale
t, D
enm
ark
1 Quality of Life Questionnaire
for Patients with Thyroid Disease
-ThyQoL4us-
Thi
s qu
estio
nnai
re is
abo
ut h
ow y
our
thyr
oid
dise
ase
has
affe
cted
you
r lif
e.
Ple
ase
an
swer
ea
ch q
ues
tion
by
ma
rkin
g
by
th
e
an
swer
th
at
bes
t fi
ts y
ou
. I
f yo
u a
re u
nsu
re a
bo
ut
how
yo
u w
an
t to
an
swer
, p
lease
giv
e th
e b
est
an
swer
yo
u c
an
.
Cop
yrig
ht ©
Tor
quil
Wat
t, C
open
hage
n U
nive
rsit
y H
ospi
tal R
igsh
ospi
tale
t, D
enm
ark
2
1.
Th
e fi
rst
qu
esti
on
s are
abo
ut
sym
pto
ms
D
uri
ng
th
e p
ast
4 w
eek
s h
av
e yo
u
Not
at
all
A li
ttle
Som
e Q
uite
a
bit
Ver
y m
uch
�
� �
�
�
1a
- ha
d th
e se
nsat
ion
of f
ulln
ess
in th
e ne
ck?.
......
......
......
......
....
......
....
......
....
......
.
1b
- ha
d a
visi
ble
swel
ling
in th
e fr
ont o
f yo
ur n
eck?
.....
......
....
......
....
......
....
......
.
1c
- fe
lt pr
essu
re in
you
r th
roat
?....
......
......
......
......
......
......
......
......
....
......
....
......
....
......
.
1d
- ha
d pa
in in
the
fron
t of
your
thro
at?
......
......
......
......
.....
......
....
......
....
......
....
......
.
1e
- ha
d pa
in in
you
r ne
ck th
at c
ould
be
felt
in
you
r ea
rs?
......
......
......
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
1f
- ha
d th
e se
nsat
ion
of a
lum
p in
you
r th
roat
?...
......
......
......
....
......
....
......
....
......
.
1g
- ha
d th
e ne
ed to
cle
ar y
our
thro
at f
requ
ently
?....
.....
......
....
......
....
......
....
......
....
1h
- fe
lt di
scom
fort
sw
allo
win
g?...
......
......
......
......
......
......
......
......
....
......
....
......
....
......
.
1i
- ha
d di
ffic
ulty
sw
allo
win
g?...
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
1j
- ha
d th
e se
nsat
ion
of s
uffo
catin
g?...
......
......
......
......
.....
......
....
......
....
......
....
......
....
1k
- be
en h
oars
e?...
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
....
1l
- ha
d tr
embl
ing
hand
s?...
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
....
1m
- ha
d a
tend
ency
to s
wea
t a lo
t?...
......
......
......
......
......
.....
......
....
......
....
......
....
......
....
1n
- ex
peri
ence
d pa
lpita
tions
(ra
pid
hear
t bea
t)?.
......
....
......
....
......
....
......
....
......
....
1o
- ex
peri
ence
d sh
ortn
ess
of b
reat
h?...
......
......
......
......
......
......
....
......
....
......
....
......
....
1p
- be
en s
ensi
tive
to h
eat?
......
......
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
....
1q
- be
en s
ensi
tive
to c
old?
......
......
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
....
1r
- ha
d an
incr
ease
d ap
petit
e?...
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
.
The
fir
st s
ectio
n of
the
ques
tionn
aire
is a
bout
sym
ptom
s, f
atig
ue, m
emor
y, m
ood,
an
d he
alth
. Pl
ease
bas
e yo
ur a
nsw
ers
on
how
yo
u h
av
e b
een
fee
lin
g i
n g
ener
al
duri
ng th
e pa
st 4
wee
ks.
Page 60 of 107
Appendix 2: ThyPRO questionnaire in English
Cop
yrig
ht ©
Tor
quil
Wat
t, C
open
hage
n U
nive
rsit
y H
ospi
tal R
igsh
ospi
tale
t, D
enm
ark
3
Du
rin
g t
he
past
4 w
eek
s h
av
e yo
u
Not
at
a ll
A li
ttle
Som
e Q
uite
a
bit
Ver
y m
uch
�
� �
�
�
1s
- ha
d lo
ose
stoo
ls?
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
....
1t
- ha
d an
ups
et s
tom
ach?
......
......
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
....
1u
- ha
d m
oist
or
wat
ery
eyes
?....
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
1v
- ha
d ba
gs u
nder
the
eyes
or
swol
len
eyel
ids?
......
....
......
....
......
....
......
....
......
....
1w
- ha
d th
e se
nsat
ion
of d
ryne
ss o
r “g
ritti
ness
”
in
the
eyes
?....
......
......
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
1x
- ha
d im
pair
ed v
isio
n?...
......
......
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
....
1y
- fe
lt pr
essu
re in
(or
beh
ind)
the
eyes
?....
......
......
......
......
......
....
......
....
......
....
......
.
1z
- ha
d do
uble
vis
ion?
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
.
1aa
- ha
d ey
e pa
in?.
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
....
1bb
- be
en v
ery
sens
itive
to li
ght?
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
1cc
- ha
d sw
olle
n ha
nds
or f
eet?
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
.
1dd
- ha
d dr
y sk
in?.
......
......
......
......
......
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
....
1ee
- ha
d itc
hy s
kin?
......
......
......
......
......
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
.
2.
Th
e fo
llo
win
g q
ues
tio
ns
are
ab
ou
t fa
tig
ue
D
uri
ng
th
e p
ast
4 w
eek
s h
av
e yo
u
Not
at
all
A li
ttle
Som
e Q
uite
a
bit
Ver
y m
uch
�
� �
�
�
2a
- be
en ti
red?
......
......
......
......
......
......
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
....
2b
- be
en e
xhau
sted
?....
......
......
......
......
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
.
2c
- ha
d di
ffic
ulty
get
ting
mot
ivat
ed to
do
a
nyth
ing
at a
ll...
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
.
2d
- fe
lt w
orn
out?
......
......
......
......
......
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
....
Cop
yrig
ht ©
Tor
quil
Wat
t, C
open
hage
n U
nive
rsit
y H
ospi
tal R
igsh
ospi
tale
t, D
enm
ark
4
3.
Th
e fo
llo
win
g q
ues
tio
ns
are
ab
ou
t yo
ur
vita
lity
D
uri
ng
th
e p
ast
4 w
eek
s h
av
e yo
u
Not
at
all
A li
ttle
Som
e Q
uite
a
bit
Ver
y m
uch
�
� �
�
�
3a
- fe
lt fu
ll of
life
?...
......
......
......
......
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
....
3b
- fe
lt en
erge
tic?
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
....
3c
- be
en a
ble
to c
ope
with
the
dem
ands
of
y
our
life?
......
......
......
......
......
......
......
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
.
4.
Th
e fo
llo
win
g q
ues
tio
ns
are
ab
ou
t m
emory
an
d c
on
cen
tra
tio
n
Du
rin
g t
he
past
4 w
eek
s h
av
e yo
u
Not
at
all
A li
ttle
Som
e Q
uite
a
bit
Ver
y m
uch
�
� �
�
�
4a
- ha
d di
ffic
ulty
rem
embe
ring
?....
......
......
......
......
......
......
....
......
....
......
....
......
....
......
.
4b
- ha
d sl
ow o
r un
clea
r th
inki
ng?.
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
.
4c
- ha
d di
ffic
ulty
fin
ding
the
righ
t wor
ds?
......
......
......
......
......
....
......
....
......
....
......
.
4d
- be
en c
onfu
sed?
......
......
......
......
......
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
.
4e
- ha
d di
ffic
ulty
lear
ning
som
ethi
ng n
ew?
......
......
......
....
......
....
......
....
......
....
......
.
4f
- ha
d di
ffic
ulty
con
cent
ratin
g?...
......
......
......
......
......
......
....
......
....
......
....
......
....
......
.
Page 61 of 107
Appendix 2: ThyPRO questionnaire in English
Cop
yrig
ht ©
Tor
quil
Wat
t, C
open
hage
n U
nive
rsit
y H
ospi
tal R
igsh
ospi
tale
t, D
enm
ark
5
5.
Th
e fo
llo
win
g q
ues
tio
ns
are
ab
ou
t n
ervo
usn
ess
an
d t
ensi
on
D
uri
ng
th
e p
ast
4 w
eek
s h
av
e yo
u
Not
at
all
A li
ttle
Som
e Q
uite
a
bit
Ver
y m
uch
�
� �
�
�
5a
- fe
lt ne
rvou
s?...
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
....
5b
- fe
lt af
raid
or
anxi
ous?
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
5c
- fe
lt te
nse?
......
......
......
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
5d
- be
en c
once
rned
abo
ut b
eing
ser
ious
ly il
l?...
......
......
......
....
......
....
......
....
......
....
5e
- fe
lt un
easy
?....
......
......
......
......
......
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
....
5f
- fe
lt re
stle
ss?.
......
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
.
6.
Th
e fo
llo
win
g q
ues
tio
ns
are
ab
ou
t p
sych
olo
gic
al
wel
l-b
ein
g
Du
rin
g t
he
past
4 w
eek
s h
av
e yo
u
Not
at
all
A li
ttle
Som
e Q
uite
a
bit
Ver
y m
uch
�
� �
�
�
6a
- fe
lt sa
d?...
......
......
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
.
6b
- fe
lt de
pres
sed?
......
......
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
.
6c
- fe
lt di
scou
rage
d?...
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
.
6d
- cr
ied
easi
ly?.
......
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
.
6e
- fe
lt un
happ
y?...
......
......
......
......
......
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
.
Du
rin
g t
he
past
4 w
eek
s h
av
e yo
u
Not
at
all
A li
ttle
Som
e Q
uite
a
bit
Ver
y m
uch
�
� �
�
�
6f
- fe
lt ha
ppy?
......
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
....
6g
- ha
d se
lf-c
onfi
denc
e?...
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
Cop
yrig
ht ©
Tor
quil
Wat
t, C
open
hage
n U
nive
rsit
y H
ospi
tal R
igsh
ospi
tale
t, D
enm
ark
6
7.
Th
e fo
llo
win
g q
ues
tio
ns
are
ab
ou
t h
avi
ng d
iffi
cult
y co
pin
g o
r h
avi
ng
mood
s win
gs
Du
rin
g t
he
past
4 w
eek
s h
av
e yo
u
Not
at
all
A li
ttle
Som
e Q
uite
a
bit
Ver
y m
uch
�
� �
�
�
7a
- ha
d di
ffic
ulty
cop
ing?
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
7b
- fe
lt “n
ot li
ke y
ours
elf”
?....
......
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
....
7c
- no
ticed
you
eas
ily f
elt s
tres
sed?
......
......
......
......
......
.....
......
....
......
....
......
....
......
....
7d
- ha
d m
ood
swin
gs?
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
.
7e
- fe
lt ir
rita
ble?
......
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
.
7f
- fe
lt fr
ustr
ated
?...
......
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
7g
- fe
lt an
gry?
......
......
......
......
......
......
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
....
Not
at
all
A li
ttle
So
me
Qui
te a
bi
t C
om-
plet
ely
�
� �
�
�
7h
- fe
lt in
con
trol
of
your
life
?....
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
....
7i
- fe
lt in
bal
ance
?....
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
....
Page 62 of 107
Appendix 2: ThyPRO questionnaire in English
Cop
yrig
ht ©
Tor
quil
Wat
t, C
open
hage
n U
nive
rsit
y H
ospi
tal R
igsh
ospi
tale
t, D
enm
ark
7
8.
Th
e fo
llo
win
g q
ues
tio
ns
are
ab
ou
t yo
ur
rela
tio
nsh
ips
wit
h o
ther
peo
ple
Not
at
all
A li
ttle
Som
e Q
uite
a
bit
Ver
y m
uch
Du
rin
g t
he
past
4 w
eek
s, h
as
yo
ur
thyro
id
dis
ease
ca
use
d y
ou
to
� � �
�
�
8a
- ha
ve d
iffi
culty
bei
ng to
geth
er w
ith o
ther
peo
ple
(fo
r ex
ampl
e, s
pous
e, c
hild
ren,
boy
/gir
lfri
end,
f
rien
ds, o
r ot
hers
)?..
......
......
......
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
....
8b
- fe
el y
ou w
ere
a bu
rden
to o
ther
peo
ple?
......
......
......
....
......
....
......
....
......
....
......
.
8c
- ha
ve c
onfl
icts
with
oth
er p
eopl
e?...
......
......
......
......
.....
......
....
......
....
......
....
......
....
Du
rin
g t
he
past
4 w
eek
s h
av
e yo
u
Not
at
all
A li
ttle
Som
e Q
uite
a
bit
Ver
y m
uch
�
� �
�
�
8d
- fe
lt th
at p
eopl
e in
you
r su
rrou
ndin
gs
hav
e la
cked
und
erst
andi
ng o
f yo
ur th
yroi
d
dis
ease
? ....
......
......
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
.
The
rem
aind
er o
f th
e qu
estio
nnai
re is
abo
ut h
ow
yo
ur
thy
roid
dis
ease
ma
y h
av
e
aff
ecte
d v
ari
ou
s a
spec
ts o
f yo
ur
life
Cop
yrig
ht ©
Tor
quil
Wat
t, C
open
hage
n U
nive
rsit
y H
ospi
tal R
igsh
ospi
tale
t, D
enm
ark
8
9.
Th
e fo
llo
win
g q
ues
tio
ns
are
ab
ou
t yo
ur
da
ily
act
ivit
ies
Not
at
all
A li
ttle
Som
e Q
uite
a
bit
Ver
y m
uch
Du
rin
g t
he
past
4 w
eek
s, h
as
yo
ur
thyro
id
dis
ease
ca
use
d y
ou
to
� � �
�
�
9a
- ha
ve d
iffi
culty
man
agin
g yo
ur d
aily
life
? ...
......
......
......
....
......
....
......
....
......
....
9b
- lim
it yo
ur le
isur
e ac
tiviti
es o
r ho
bbie
s?...
......
......
....
......
....
......
....
......
....
......
....
9c
- no
t be
able
to p
artic
ipat
e in
life
aro
und
you?
......
......
......
....
......
....
......
....
......
.
9d
- ha
ve d
iffi
culty
get
ting
arou
nd
(fo
r ex
ampl
e, w
alki
ng, r
unni
ng, b
icyc
ling,
o
r dr
ivin
g a
car)
?...
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
.
9e
- fe
el a
s if
eve
ryth
ing
take
s lo
nger
to d
o?...
......
......
....
......
....
......
....
......
....
......
....
I do
not
wor
k N
ot a
t al
l A
littl
e So
me
Qui
te a
bi
t V
ery
muc
h D
uri
ng
th
e p
ast
4 w
eek
s, h
as
yo
ur
thyro
id d
isea
se c
au
sed
yo
u
to
� �
� �
�
�
9f
- ha
ve d
iffi
culty
man
agin
g yo
ur
job
(fo
r ex
ampl
e, h
ad d
iffi
culty
m
anag
ing
it or
cal
ling
in s
ick)
?...
......
......
......
......
.....
......
....
......
....
......
....
......
.
Page 63 of 107
Appendix 2: ThyPRO questionnaire in English
Cop
yrig
ht ©
Tor
quil
Wat
t, C
open
hage
n U
nive
rsit
y H
ospi
tal R
igsh
ospi
tale
t, D
enm
ark
9
10
. T
he
foll
ow
ing
qu
esti
on
s a
re a
bou
t yo
ur
sex
lif
e
Du
rin
g t
he
past
4 w
eek
s h
av
e yo
u
Not
at
all
A li
ttle
Som
e Q
uite
a
bit
Ver
y m
uch
�
� �
�
�
10a
- fe
lt yo
ur th
yroi
d di
seas
e ha
d a
n
egat
ive
infl
uenc
e on
you
r se
x lif
e?...
......
......
......
......
......
....
......
....
......
....
......
....
10b
- ha
d a
decr
ease
d se
xual
des
ire?
......
......
......
......
......
......
....
......
....
......
....
......
....
......
.
11
. T
hyr
oid
dis
ease
s (o
r th
eir
trea
tmen
t) m
ay
aff
ect
you
r ap
pea
ran
ce. (
For
exam
ple
, b
y ca
usi
ng
sw
elli
ng
of
the
nec
k, sw
oll
en f
ace
, h
an
ds,
or
feet
, o
r
cha
ng
es i
n w
eig
ht
or
to t
he
eyes
.)
Du
rin
g t
he
past
4 w
eek
s,
Not
at
all
A li
ttle
Som
e Q
uite
a
bit
Ver
y m
uch
�
� �
�
�
11a
- ha
s yo
ur th
yroi
d di
seas
e af
fect
ed y
our
ap
pear
ance
(fo
r ex
ampl
e, s
wel
ling
of th
e ne
ck,
eye
chan
ges,
wei
ght c
hang
es)?
......
......
......
......
......
......
....
......
....
......
....
......
....
......
.
11b
- ha
ve y
ou b
een
unsa
tisfi
ed w
ith y
our
a
ppea
ranc
e be
caus
e of
you
r th
yroi
d di
seas
e?...
......
......
....
......
....
......
....
......
....
11c
- ha
ve y
ou tr
ied
to c
amou
flag
e or
mas
k vi
sibl
e s
igns
of
your
thyr
oid
dise
ase
(for
exa
mpl
e, b
y w
eari
ng a
sca
rf o
r su
ngla
sses
)?...
......
......
......
......
......
......
......
....
......
....
......
....
......
.
11d
- ha
ve y
ou b
een
both
ered
by
othe
r pe
ople
l
ooki
ng a
t you
? ....
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
......
....
11e
- ha
s yo
ur th
yroi
d di
seas
e in
flue
nced
whi
ch
clo
thes
you
wea
r?...
......
......
......
......
......
......
......
......
......
......
......
....
......
....
......
....
......
....
11g
- ha
s yo
ur th
yroi
d di
seas
e m
ade
you
feel
t
oo f
at? .
......
......
......
......
......
......
......
......
......
......
......
......
......
.....
......
....
......
....
......
....
......
....
Cop
yrig
ht ©
Tor
quil
Wat
t, C
open
hage
n U
nive
rsit
y H
ospi
tal R
igsh
ospi
tale
t, D
enm
ark
10
12
. T
he
fin
al
qu
esti
on
is
abo
ut
to w
ha
t ex
ten
t yo
ur
thyr
oid
dis
ease
ha
s a
ffec
ted
y ou
ove
rall
du
rin
g t
he
past
4 w
eeks
Du
rin
g t
he
past
4 w
eek
s,
Not
at
all
A li
ttle
Som
e Q
uite
a
bit
Ver
y m
uch
�
� �
�
�
12
- ha
s yo
ur th
yroi
d di
seas
e ha
d a
nega
tive
eff
ect o
n yo
ur q
ualit
y of
life
?....
......
......
......
......
......
......
......
....
......
....
......
....
......
....
Ple
ase
go
back
and
ch
eck
that
you
ha
ve a
nsw
ered
all
th
e qu
esti
on
s.
Th
an
k y
ou
ver
y m
uch
fo
r yo
ur
hel
p a
nsw
erin
g t
his
qu
esti
on
nair
e!
Page 64 of 107
Appendix 2: ThyPRO questionnaire in English

INVITED REVIEW
Quality of life in patients with benign thyroid disorders.A reviewTorquil Watt1,2, Mogens Groenvold2, Ase Krogh Rasmussen1, Steen Joop Bonnema3, Laszlo Hegedus3,Jakob Bue Bjorner4 and Ulla Feldt-Rasmussen1
1Department of Endocrinology, Copenhagen University Hospital, Rigshospitalet, Blegdamsvej 9, DK-2100, Copenhagen, Denmark, 2Institute of PublicHealth, University of Copenhagen, Denmark, 3Department of Endocrinology and Metabolism, Odense University Hospital, Odense, Denmark and4QualityMetric Inc., Lincoln, Rhode Island, USA
(Correspondence should be addressed to T Watt at Department of Endocrinology, Copenhagen University Hospital; Email: [email protected])
Abstract
The importance of patient-reported outcomes such as health-related quality of life (HRQL) in clinicalresearch is increasingly acknowledged. In order to yield valid results, the measurement properties ofHRQL questionnaires must be thoroughly investigated. One aspect of such a validation process is thedemonstration of content validity, i.e. that the questionnaire covers all relevant aspects. We reviewstudies reporting on consequences of thyroid disorders and present the frequency of identified aspects,both overall HRQL issues and classical thyroid symptoms, in order to evaluate which issues are rel-evant for patients with thyroid diseases. Furthermore, existing questionnaires for thyroid patientsare reviewed. A systematic search was performed in the Medline, Cinahl and Psycinfo databasesand the reference lists of the relevant articles were hand-searched. Seventy-five relevant studieswere identified. According to these studies, patients with untreated thyroid disease suffer from awide range of symptoms and have major impairment in most areas of HRQL. Furthermore, the studiesindicate that impairments in HRQL are also frequent in the long term. Six HRQL questionnaires forthyroid patients were identified. Generally, data supporting the validity of these questionnaireswere sparse. According to the available literature, the quality of life of thyroid patients is substantiallyimpaired over a wide range of aspects of HRQL in the untreated phase and continues to be so in manypatients also in the long term. Studies systematically exploring the relative importance of these var-ious aspects to thyroid patients are lacking, as is a comprehensive, validated thyroid-specific HRQLquestionnaire.
European Journal of Endocrinology 154 501–510
Background
The evaluation of health-related quality of life (HRQL)implies evaluations of the impact of a disease and itstreatment on all relevant dimensions of the patient’slife. HRQL measurements usually comprise aspects ofphysical, mental and social well-being and function.Generally, HRQL is best rated by the patients themselves,usually by means of standardized questionnaires. Thereare two main types of HRQL measures: disease-specificand generic. Disease-specific questionnaires concernissues of particular relevance for patients with a specificmedical condition, whereas generic instruments (e.g. SF-36 or EQ-5D) measure aspects common to mostpatients. Disease-specific measures often demonstrategreater sensitivity than generic measures, while thelatter allow for comparison across diseases and treat-ments and with scores obtained from the general
population. A combination of disease-specific and gen-eric measures is generally advocated because each pro-vides complementary information (1, 2). Theimportance of involving HRQL aspects in the evaluationof thyroid patients is increasingly recognized (3–5). Sev-eral features of thyroid diseases motivate this. First of all,benign thyroid disorders are rarely life threatening, andthus their treatment mainly deals with optimizing thequality of life of the patients. Furthermore, the diseasesare common and occur at all ages. Moreover, sincemany thyroid diseases can be treated in several ways(e.g. radioiodine, medical treatment or surgery), exactknowledge of the impact of each treatment modality onthe HRQL of the patients is important. To date, no trialhas compared validly the HRQL outcome of differenttreatments and there is still a well-documented lack ofconsensus regarding choice of treatment (6–15). Thedetrimental impact of acute thyroid disease on HRQL is
European Journal of Endocrinology (2006) 154 501–510 ISSN 0804-4643
q 2006 Society of the European Journal of Endocrinology DOI: 10.1530/eje.1.02124
Online version via www.eje-online.org
Page 65 of 107
Appendix 3: Paper I

obvious and has been documented in several studies(16–18). However, it is the clinical experience of manyendocrinologists that some patients have residual com-plaints despite adequate medical treatment. Applicationof valid HRQL measurements is crucial for proper clarifi-cation of a number of ongoing debates regarding man-agement of thyroid disorders. For example: do patientswith subclinical or mild thyroid dysfunction have symp-toms and are they fully alleviated by treatment? Is treat-ment of hypothyroidismwith a combination of thyroxine(T4) and triiodothyronine (T3) superior to T4 alone? Doesblock-replacement therapy as compared with titrationtherapy of hyperthyroidism result in improved HRQL?Some of the conflicting data regarding these and numer-ous other questions might be caused by lack of appropri-ate outcome measures. To ensure valid assessment of a
particular patient population, a number of requirementsin relation to HRQL instruments have to be documented(19–23) (Table 1 presents the terminology used).First, HRQL deals with the patients’ experience of the dis-ease and its impact on their lives, and is therefore bestassessed by the patients themselves. Secondly, the instru-ment should cover all aspects of HRQL that are relevantto the patients (content validity). Thirdly, empiricaltests should evaluate whether the questionnairemeasures what is intended (construct validity).For HRQL measures, where no external ‘gold standard’exists, several approaches to this subject havebeen implemented: qualitative, cognitive studies explor-ing patients’ understanding of the items or quantitativestudies investigating the underlying measurementmodel (Table 1). Finally, appropriate measurement
Table 1 Concepts concerning validation of HRQL questionnaires.
Concept Meaning Methods
Multi-item scale Multiple items measuring the same concept.The responses are combined to a singlescore to increase reliability and sensitivity.
Usually the responses to individual items are simply summatedtogether, but various other techniques, implying weightingsof items or standardizations to general population normscan be applied. The requirements of uni-dimensionality andlocal independence of individual items are important formulti-item scales and must be evaluated (see below).
Validity That an instrument measures what it wasintended to, i.e. lack of systematicmeasurement error.
Comprises content validity and construct validity (describedbelow).
Content validity Evidence supporting that a questionnairecovers all HRQL aspects relevant for theintended purpose.
Literature reviews and interviews or focus groups involvingprofessionals and patients. Qualitative methods are usuallyapplied when evaluating coverage and relevance,e.g. cognitive debriefing techniques.
Construct validity The extent to which a scale measures thehypothesized construct. Evaluation ofconstruct validity involves the formulationof a theoretical model, a measurementmodel, and testing hypotheses based onthat specified model.
Evaluation of response patterns. It involves testing thedimensionality of the measured scales by studying theresponse patterns of target populations. Items in a scaleshould be correlated with the other items in that scale andbe less correlated to dissimilar scales, just as scalesmeasuring related constructs should be more closelyrelated than scales measuring dissimilar constructs. Moresophisticated models involve the use of latent variablemodels, such as classical factor analyses or modernpsychometric methods including structural equation modelsand item response theory.
Dimensionality The number of concepts measured by a setof items. Most of the methods applied toHRQL data rely on the assumption thatone scale measures only one concept(or construct), i.e. that it is uni-dimensional.
Statistical analyses, see construct validity.
Sensitivity The ability of an instrument to differentiatebetween subjects differing in the measuredproperty.
Evaluate differences between groups assumed to differ in theevaluated scores.
Responsiveness The ability of an instrument to detect relevantchanges in HRQL over time, e.g. as theresult of a clinical intervention.
Longitudinal studies of patients undergoing change.
Reliability The extent to which a measure yields thesame score at independent assessments.Formally, it is calculated as a coefficient,which estimates the ratio of true variance tototal (i.e. true þ error) variance.
Three approaches are used:†Test-retest reliability - repeat the measurement and calculate
the degree of identity.For multi-item scales:†Split-half reliability - calculate the level of agreement between
two halves of the items in a multi-item scale.†Internal consistency reliability (Cronbach’s a) - theoretically
measures the mean of all possible split-half reliabilitycoefficients for a scale.
502 T Watt and others EUROPEAN JOURNAL OF ENDOCRINOLOGY (2006) 154
www.eje-online.org
Page 66 of 107
Appendix 3: Paper I

properties, including sensitivity and responsiveness,have to be demonstrated; that is, theremust be an accep-table ratio between true variance compared with var-iance due to random error (reliability), the measuremust be sensitive to clinically relevant differences andit must be responsive to relevant changes with time.Our review concerns content validity. We present a sys-tematic literature review the purpose of which is todescribe complaints and consequences of thyroid dis-orders found in previous studies.
The literature search
A Medline search on the Medline Subheadings (MeSH)thyroid diseases AND (quality of life OR questionnairesOR psychology OR health status OR psychiatric statusrating scales OR brief psychiatric rating scale OR severityof illness index OR patient satisfaction OR psychometricsOR depression ORanxiety OR symptoms [title]) NOT car-cinoma, identified 1015 references. The search wasrepeated in the Cinahl and Psycinfo databases, identify-ing a total of 2033 references. The abstracts werereviewed and possibly relevant articles reviewed in fulllength. Further references were identified through thereference lists of these articles. Thus, 2094 referenceswere screened. We also consulted leading thyroid text-books and included issues listed within these. Seventy-five of the reviewed references were selected, based onthe following criteria: the study population (indexpatients) should be thyroid patients, and the papershould report on patient-experienced consequences ofthe thyroid disease. Consequences should be documen-ted either as a reported frequency or a higher score onan HRQL scale compared with individuals without thyr-oid disease. This means that technical or ‘objective’measures like ‘digit span test’ and ‘ankle reflex relaxationtime’ without a subjective equivalent, or reported scale-scores without appropriate control groups were notincluded. In addition, all measures of symptoms andHRQL impact of thyroid disorders used in these studieswere identified.
Identified HRQL aspects and symptomsrelevant to thyroid patients
The frequencies of the identified issues in untreatedpatients are presented in Table 2 whereas results fromfollow-up studies are presented in Table 3.
From Table 2, it is evident that patients withuntreated thyroid disease suffer from a wide range ofsymptoms and have major impairment in most areasof HRQL. For example, 22–35% of goitre patients,18–66% of hyperthyroid patients, 7–99% of patientswith thyroid associated ophthalmopathy (TAO) and16–51% of hypothyroid patients experience limitationsin usual activities during the untreated phase of theirdisease. These rather wide ranges are due to different
ways of measuring the concepts in the studies, differ-ences in patient populations as well as our categoriz-ation of the issues; e.g. the term ‘limitations in usualactivities’ covers a wide range of different activitiesand includes scales from various questionnaires.There is evidence of impaired general health perceptionin all patient groups; for patients with goitre,hyperthyroidism and TAO this is evidenced by lowerscores on scales measuring general health perceptioncompared with scores in normal controls, and thusno percentage is available, whereas for hypothyroidpatients dichotomous variables document that 53–100% of patients conceive their health as impaired.Thus, a substantial proportion of thyroid patientsexperience limitations in their usual activities, perceivetheir general health as impaired and have social andemotional impairment. Cognitive problems are alsoprevalent, as is fatigue. Cosmetic concern is alsocommon for all thyroid patients. However, no studyhas reported on cognitive dysfunction in patients withgoitre and only one study has reported on fatigue inpatients with TAO. Generally, patients with goitre havebeen the least studied. All the classical symptoms ofhyperthyroidism appear to be consistently prevalent inhyperthyroid patients, whereas the classical symptomsof hypothyroidism are more variably present inhypothyroid patients. The latter may, in part, reflect thewide spectrum of clinical presentation of hypothyroid-ism, with a high frequency of subclinical dysfunction.
From the data presented in Table 3 it appears that per-sistent HRQL impairment is very frequent amongpatients with both hyper- and hypothyroidism. Abouthalf of the patients have reduced overall quality of lifeand general health, limitations in usual activities aswell as social and emotional problems. Two-thirds arefatigued and about one-third are anxious and have cog-nitive as well as sexual problems. Furthermore, classicalsymptoms of hypothyroidism are very frequent amongpreviously hyperthyroid patients and about one-thirdhave persistent hyperthyroid symptoms. However, theassociation with actual thyroid status has not beenaddressed in this study. Hypo- or hyperthyroid symptomshavenot been examined in long-term follow-up studies ofhypothyroid patients and no study has examined thelong-term HRQL outcome of goitre treatment. However,there is a general lack of detailed clinical description ofthe phenotypes of many of the patient populations inthese studies and therefore some of the patients classifiedas hypothyroid may, in fact, be treated goitre patients.
Available thyroid HRQL questionnaires
We have identified six thyroid HRQL questionnaires(24–29). In addition, various symptom indices(30–43), most of which were physician administered,and one satisfaction-questionnaire (29) have been pub-lished. The present review will focus on the six HRQL
Quality of life in thyroid patients 503EUROPEAN JOURNAL OF ENDOCRINOLOGY (2006) 154
www.eje-online.org
Page 67 of 107
Appendix 3: Paper I
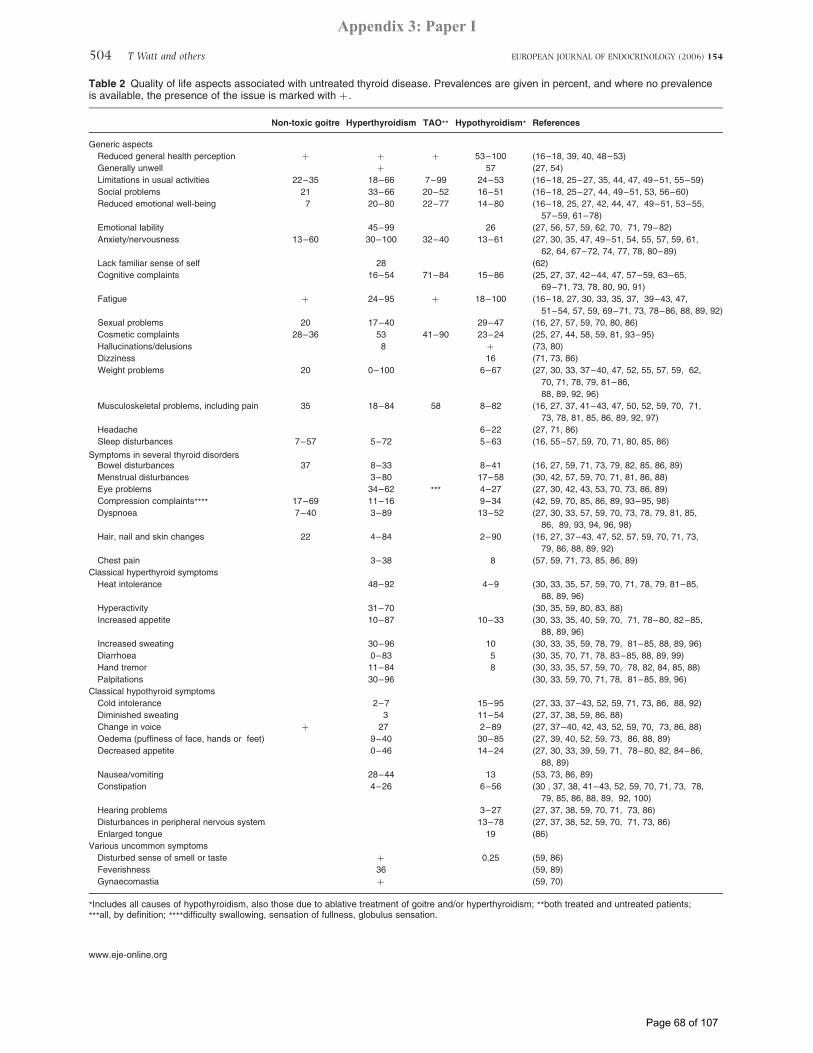
Table 2 Quality of life aspects associated with untreated thyroid disease. Prevalences are given in percent, and where no prevalenceis available, the presence of the issue is marked with þ .
Non-toxic goitre Hyperthyroidism TAO** Hypothyroidism* References
Generic aspects
Reduced general health perception þ þ þ 53–100 (16–18, 39, 40, 48–53)
Generally unwell þ 57 (27, 54)
Limitations in usual activities 22–35 18–66 7–99 24–53 (16–18, 25–27, 35, 44, 47, 49–51, 55–59)
Social problems 21 33–66 20–52 16–51 (16–18, 25–27, 44, 49–51, 53, 56–60)
Reduced emotional well-being 7 20–80 22–77 14–80 (16–18, 25, 27, 42, 44, 47, 49–51, 53–55,
57–59, 61–78)
Emotional lability 45–99 26 (27, 56, 57, 59, 62, 70, 71, 79–82)
Anxiety/nervousness 13–60 30–100 32–40 13–61 (27, 30, 35, 47, 49–51, 54, 55, 57, 59, 61,
62, 64, 67–72, 74, 77, 78, 80–89)
Lack familiar sense of self 28 (62)
Cognitive complaints 16–54 71–84 15–86 (25, 27, 37, 42–44, 47, 57–59, 63–65,
69–71, 73, 78, 80, 90, 91)
Fatigue þ 24–95 þ 18–100 (16–18, 27, 30, 33, 35, 37, 39–43, 47,
51–54, 57, 59, 69–71, 73, 78–86, 88, 89, 92)
Sexual problems 20 17–40 29–47 (16, 27, 57, 59, 70, 80, 86)
Cosmetic complaints 28–36 53 41–90 23–24 (25, 27, 44, 58, 59, 81, 93–95)
Hallucinations/delusions 8 þ (73, 80)
Dizziness 16 (71, 73, 86)
Weight problems 20 0–100 6–67 (27, 30, 33, 37–40, 47, 52, 55, 57, 59, 62,
70, 71, 78, 79, 81–86,
88, 89, 92, 96)
Musculoskeletal problems, including pain 35 18–84 58 8–82 (16, 27, 37, 41–43, 47, 50, 52, 59, 70, 71,
73, 78, 81, 85, 86, 89, 92, 97)
Headache 6–22 (27, 71, 86)
Sleep disturbances 7–57 5–72 5–63 (16, 55–57, 59, 70, 71, 80, 85, 86)
Symptoms in several thyroid disordersBowel disturbances 37 8–33 8–41 (16, 27, 59, 71, 73, 79, 82, 85, 86, 89)
Menstrual disturbances 3–80 17–58 (30, 42, 57, 59, 70, 71, 81, 86, 88)
Eye problems 34–62 *** 4–27 (27, 30, 42, 43, 53, 70, 73, 86, 89)
Compression complaints**** 17–69 11–16 9–34 (42, 59, 70, 85, 86, 89, 93–95, 98)
Dyspnoea 7–40 3–89 13–52 (27, 30, 33, 57, 59, 70, 73, 78, 79, 81, 85,
86, 89, 93, 94, 96, 98)
Hair, nail and skin changes 22 4–84 2–90 (16, 27, 37–43, 47, 52, 57, 59, 70, 71, 73,
79, 86, 88, 89, 92)
Chest pain 3–38 8 (57, 59, 71, 73, 85, 86, 89)
Classical hyperthyroid symptoms
Heat intolerance 48–92 4–9 (30, 33, 35, 57, 59, 70, 71, 78, 79, 81–85,
88, 89, 96)
Hyperactivity 31–70 (30, 35, 59, 80, 83, 88)
Increased appetite 10–87 10–33 (30, 33, 35, 40, 59, 70, 71, 78–80, 82–85,
88, 89, 96)
Increased sweating 30–96 10 (30, 33, 35, 59, 78, 79, 81–85, 88, 89, 96)
Diarrhoea 0–83 5 (30, 35, 70, 71, 78, 83–85, 88, 89, 99)
Hand tremor 11–84 8 (30, 33, 35, 57, 59, 70, 78, 82, 84, 85, 88)
Palpitations 30–96 (30, 33, 59, 70, 71, 78, 81–85, 89, 96)
Classical hypothyroid symptoms
Cold intolerance 2–7 15–95 (27, 33, 37–43, 52, 59, 71, 73, 86, 88, 92)
Diminished sweating 3 11–54 (27, 37, 38, 59, 86, 88)
Change in voice þ 27 2–89 (27, 37–40, 42, 43, 52, 59, 70, 73, 86, 88)
Oedema (puffiness of face, hands or feet) 9–40 30–85 (27, 39, 40, 52, 59, 73, 86, 88, 89)
Decreased appetite 0–46 14–24 (27, 30, 33, 39, 59, 71, 78–80, 82, 84–86,
88, 89)
Nausea/vomiting 28–44 13 (53, 73, 86, 89)
Constipation 4–26 6–56 (30 , 37, 38, 41–43, 52, 59, 70, 71, 73, 78,
79, 85, 86, 88, 89, 92, 100)
Hearing problems 3–27 (27, 37, 38, 59, 70, 71, 73, 86)
Disturbances in peripheral nervous system 13–78 (27, 37, 38, 52, 59, 70, 71, 73, 86)
Enlarged tongue 19 (86)
Various uncommon symptoms
Disturbed sense of smell or taste þ 0.25 (59, 86)
Feverishness 36 (59, 89)
Gynaecomastia þ (59, 70)
*Includes all causes of hypothyroidism, also those due to ablative treatment of goitre and/or hyperthyroidism; **both treated and untreated patients;
***all, by definition; ****difficulty swallowing, sensation of fullness, globulus sensation.
504 T Watt and others EUROPEAN JOURNAL OF ENDOCRINOLOGY (2006) 154
www.eje-online.org
Page 68 of 107
Appendix 3: Paper I
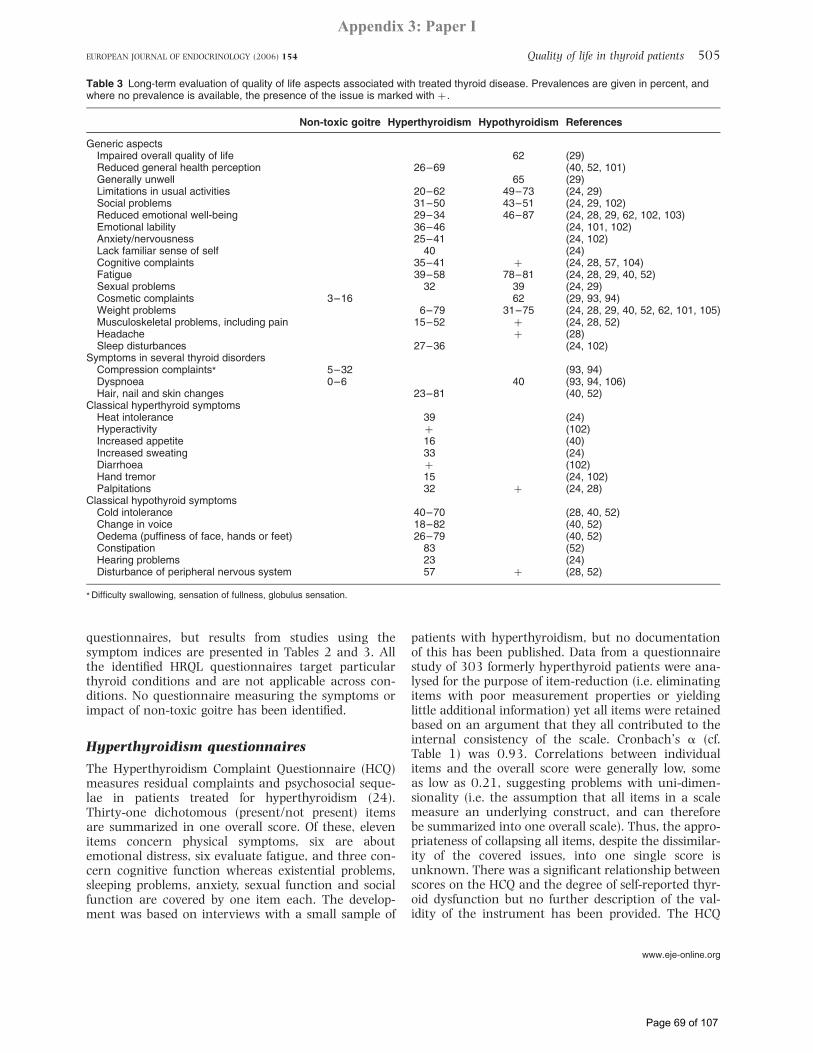
questionnaires, but results from studies using thesymptom indices are presented in Tables 2 and 3. Allthe identified HRQL questionnaires target particularthyroid conditions and are not applicable across con-ditions. No questionnaire measuring the symptoms orimpact of non-toxic goitre has been identified.
Hyperthyroidism questionnaires
The Hyperthyroidism Complaint Questionnaire (HCQ)measures residual complaints and psychosocial seque-lae in patients treated for hyperthyroidism (24).Thirty-one dichotomous (present/not present) itemsare summarized in one overall score. Of these, elevenitems concern physical symptoms, six are aboutemotional distress, six evaluate fatigue, and three con-cern cognitive function whereas existential problems,sleeping problems, anxiety, sexual function and socialfunction are covered by one item each. The develop-ment was based on interviews with a small sample of
patients with hyperthyroidism, but no documentationof this has been published. Data from a questionnairestudy of 303 formerly hyperthyroid patients were ana-lysed for the purpose of item-reduction (i.e. eliminatingitems with poor measurement properties or yieldinglittle additional information) yet all items were retainedbased on an argument that they all contributed to theinternal consistency of the scale. Cronbach’s a (cf.Table 1) was 0.93. Correlations between individualitems and the overall score were generally low, someas low as 0.21, suggesting problems with uni-dimen-sionality (i.e. the assumption that all items in a scalemeasure an underlying construct, and can thereforebe summarized into one overall scale). Thus, the appro-priateness of collapsing all items, despite the dissimilar-ity of the covered issues, into one single score isunknown. There was a significant relationship betweenscores on the HCQ and the degree of self-reported thyr-oid dysfunction but no further description of the val-idity of the instrument has been provided. The HCQ
Table 3 Long-term evaluation of quality of life aspects associated with treated thyroid disease. Prevalences are given in percent, andwhere no prevalence is available, the presence of the issue is marked with þ .
Non-toxic goitre Hyperthyroidism Hypothyroidism References
Generic aspectsImpaired overall quality of life 62 (29)Reduced general health perception 26–69 (40, 52, 101)Generally unwell 65 (29)Limitations in usual activities 20–62 49–73 (24, 29)Social problems 31–50 43–51 (24, 29, 102)Reduced emotional well-being 29–34 46–87 (24, 28, 29, 62, 102, 103)Emotional lability 36–46 (24, 101, 102)Anxiety/nervousness 25–41 (24, 102)Lack familiar sense of self 40 (24)Cognitive complaints 35–41 þ (24, 28, 57, 104)Fatigue 39–58 78–81 (24, 28, 29, 40, 52)Sexual problems 32 39 (24, 29)Cosmetic complaints 3–16 62 (29, 93, 94)Weight problems 6–79 31–75 (24, 28, 29, 40, 52, 62, 101, 105)Musculoskeletal problems, including pain 15–52 þ (24, 28, 52)Headache þ (28)Sleep disturbances 27–36 (24, 102)
Symptoms in several thyroid disordersCompression complaints* 5–32 (93, 94)Dyspnoea 0–6 40 (93, 94, 106)Hair, nail and skin changes 23–81 (40, 52)
Classical hyperthyroid symptomsHeat intolerance 39 (24)Hyperactivity þ (102)Increased appetite 16 (40)Increased sweating 33 (24)Diarrhoea þ (102)Hand tremor 15 (24, 102)Palpitations 32 þ (24, 28)
Classical hypothyroid symptomsCold intolerance 40–70 (28, 40, 52)Change in voice 18–82 (40, 52)Oedema (puffiness of face, hands or feet) 26–79 (40, 52)Constipation 83 (52)Hearing problems 23 (24)Disturbance of peripheral nervous system 57 þ (28, 52)
* Difficulty swallowing, sensation of fullness, globulus sensation.
Quality of life in thyroid patients 505EUROPEAN JOURNAL OF ENDOCRINOLOGY (2006) 154
www.eje-online.org
Page 69 of 107
Appendix 3: Paper I

has not been used in any subsequent study and appar-ently is available in Dutch only.
Questionnaires for patients with thyroid-associated ophthalmopathy
The Graves’ Ophthalmopathy Quality of Life Question-naire (GOQOL) is a disease-specific HRQL instrumentfor patients with TAO (25, 44, 45). The developmentwas based on a review of existing eye HRQL measures,as well as open-ended questionnaires from 24 patients.It has been pretested in 8 patients. A detailed descrip-tion of these content validity studies has not been pub-lished. The GOQOL consists of 16 items sub-divided intotwo scales: ‘visual functioning’ and ‘appearance’.Subsequent studies comprising 70–164 well-describedpatients have shown excellent reliability (25, 44), sup-ported its construct validity (25, 44, 45), and demon-strated good responsiveness (45). According to thedevelopers, the GOQOL is available in six languages(46). However, to our knowledge, the only publishedvalidation study regards the Dutch version.Tehrani and colleagues (26) have also developed a
90-item TAO-specific HRQL instrument in German. Itsdevelopment was based on contributions from clini-cians and was without any patient input. In a studyof 104 patients undergoing surgery, the developersfound Cronbach’s a as low as 0.63 for the 90-itemtotal score. Given the large number of items, this is alow reliability. No construct validation has been per-formed, but the low internal consistency reliabilitysuggests lack of uni-dimensionality. In validity analyses,the score did not correlate with clinical variables. Thus,these results do not lend strong support for thereliability and validity of this measure.
Hypothyroidism questionnaires
The Chronic Thyroid Questionnaire (CTQ) is ahypothyroidism and patient-specific HRQL question-naire. It consists of 104 items, each representing aspecific complaint, covering four domains: ‘physicalcomplaints’, ‘mood and emotions’, ‘energy and generalwell-being’, and ‘cognitive complaints’ (27, 47). Thedevelopment of the CTQ was quite thorough. Basedon a literature review, a list of symptoms or problemsrelated to hypothyroidism, potentially responsive totreatment and likely to influence the quality of life ofthe patients was generated (27). This list was expandedthrough interviews with endocrinologists and patients.The scoring of the CTQ is unusual: of the 104 com-plaints, each patient identifies applicable items andrates the degree of discomfort represented by theseitems. Thus, for a patient with two of the 104 com-plaints, the instrument consists of two items, whereasa patient with 22 complaints rates 22 items. Thisapproach increases the potential sensitivity of themeasure to improvements in the individual patient,
but it makes between-patient comparisons andinterpretations of what is actually measured difficultand new complaints arising from intervention areignored in longitudinal studies. We could not identifyany studies validating the resulting questionnaire.
The Thyroid Symptom Questionnaire (TSQ) consistsof twelve items: six items on cognitive complaints, fiveitems on physical symptoms and one item on fatigue,summarized in one overall score (28). The items wereselected on the basis of patient responses to a noticein the British Thyroid Foundation newsletter, invitingpatients to tell about persisting complaints despitereplacement therapy with L-thyroxine. Moderate corre-lations with the generic HRQL questionnaire GeneralHealth Questionnaire (GHQ-12) were found, but noother evidence of validity has been presented.
Recently, a new hypothyroidism-specific HRQLquestionnaire has been developed: the Underactive Thyr-oid-Dependent Quality of Life Questionnaire (ThyDQoL)(29). ThyDQoL is an 18-item questionnaire measuringthe impact of hypothyroidism on various domains ofHRQL: overall quality of life (two items), limitations inusual activities (six items), social function (four items),fatigue (two items), emotional well-being (two items),sexual function, cosmetic complaints, weight problems,and bodily discomfort (one item each). Items are scoredindividually in a two-step procedure: both impact andimportance of the items are rated, and the item score isderived by the multiplication of these two ratings. Nomulti-item scales are constructed. Problems with thisapproach are the reduced inter-individual comparabilityof themeasure and the sensitivity to a confounding effectof coping. Content validity was ensured by interviewswith 38 hypothyroid patients. However, a quarter ofthe patients had hypothyroidism secondary to treatmentof other thyroid disorders. No information regardingthe time since diagnosis or the present thyroid status ofthe interviewees is provided; all patients, except one,were undergoing treatment with L-thyroxine. Measure-ment properties (dimensionality, reliability, constructvalidity, sensitivity, and responsiveness) have not yetbeen evaluated.
Comparison of the questionnaires
The relationship between the identified issues and thethyroid questionnaires is presented in Table 4. TheCTQ includes items relating to a wide range ofthe identified issues. However, since these assessmentsare based on one single item, the reliability is probablylow for each issue. The well-documented GOQOL ques-tionnaire, which is concerned very specifically with thelimitations and social/cosmetic consequences of TAO,covers only three of the identified issues, but sinceeach issue is assessed by multiple items, reliability isprobably high. Questionnaires like the HCQ and TSQproduce an overall score, but if the set of issues coveredare multidimensional, one overall score might not be
506 T Watt and others EUROPEAN JOURNAL OF ENDOCRINOLOGY (2006) 154
www.eje-online.org
Page 70 of 107
Appendix 3: Paper I
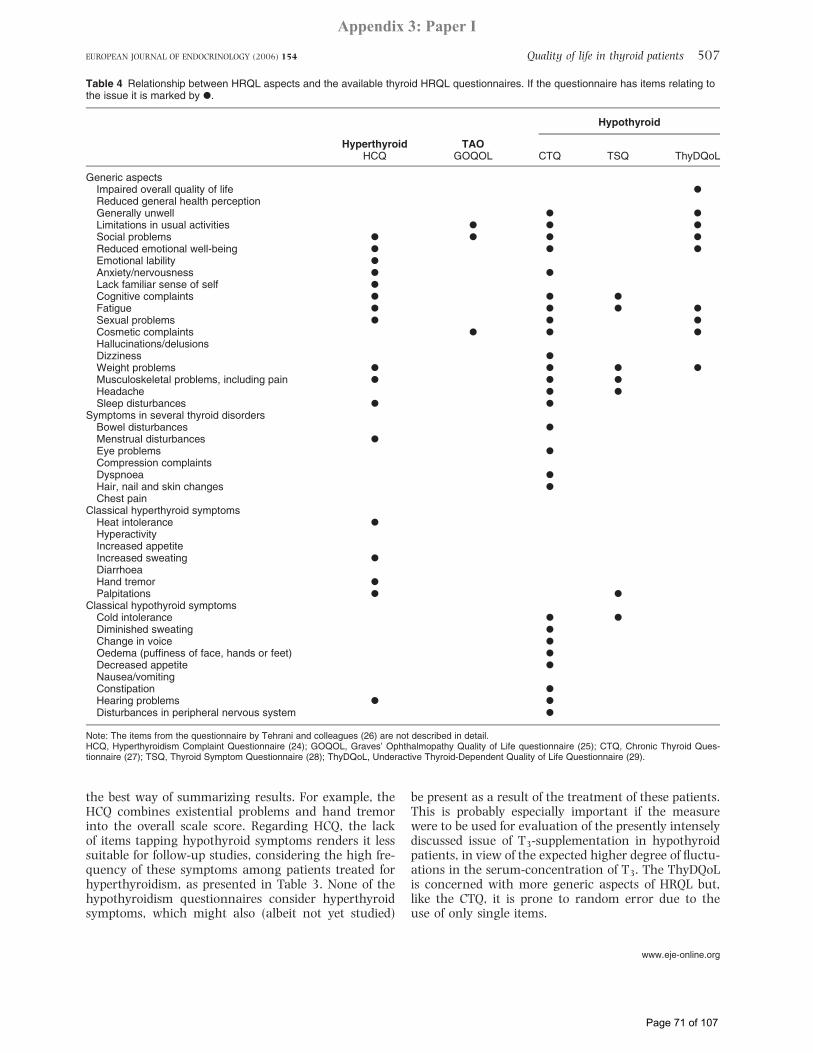
the best way of summarizing results. For example, theHCQ combines existential problems and hand tremorinto the overall scale score. Regarding HCQ, the lackof items tapping hypothyroid symptoms renders it lesssuitable for follow-up studies, considering the high fre-quency of these symptoms among patients treated forhyperthyroidism, as presented in Table 3. None of thehypothyroidism questionnaires consider hyperthyroidsymptoms, which might also (albeit not yet studied)
be present as a result of the treatment of these patients.This is probably especially important if the measurewere to be used for evaluation of the presently intenselydiscussed issue of T3-supplementation in hypothyroidpatients, in view of the expected higher degree of fluctu-ations in the serum-concentration of T3. The ThyDQoLis concerned with more generic aspects of HRQL but,like the CTQ, it is prone to random error due to theuse of only single items.
Table 4 Relationship between HRQL aspects and the available thyroid HRQL questionnaires. If the questionnaire has items relating tothe issue it is marked by X.
Hypothyroid
HyperthyroidHCQ
TAOGOQOL CTQ TSQ ThyDQoL
Generic aspectsImpaired overall quality of life XReduced general health perceptionGenerally unwell X XLimitations in usual activities X X XSocial problems X X X XReduced emotional well-being X X XEmotional lability XAnxiety/nervousness X XLack familiar sense of self XCognitive complaints X X XFatigue X X X XSexual problems X X XCosmetic complaints X X XHallucinations/delusionsDizziness XWeight problems X X X XMusculoskeletal problems, including pain X X XHeadache X XSleep disturbances X X
Symptoms in several thyroid disordersBowel disturbances XMenstrual disturbances XEye problems XCompression complaintsDyspnoea XHair, nail and skin changes XChest pain
Classical hyperthyroid symptomsHeat intolerance XHyperactivityIncreased appetiteIncreased sweating XDiarrhoeaHand tremor XPalpitations X X
Classical hypothyroid symptomsCold intolerance X XDiminished sweating XChange in voice XOedema (puffiness of face, hands or feet) XDecreased appetite XNausea/vomitingConstipation XHearing problems X XDisturbances in peripheral nervous system X
Note: The items from the questionnaire by Tehrani and colleagues (26) are not described in detail.HCQ, Hyperthyroidism Complaint Questionnaire (24); GOQOL, Graves’ Ophthalmopathy Quality of Life questionnaire (25); CTQ, Chronic Thyroid Ques-tionnaire (27); TSQ, Thyroid Symptom Questionnaire (28); ThyDQoL, Underactive Thyroid-Dependent Quality of Life Questionnaire (29).
Quality of life in thyroid patients 507EUROPEAN JOURNAL OF ENDOCRINOLOGY (2006) 154
www.eje-online.org
Page 71 of 107
Appendix 3: Paper I

Conclusion
According to the available literature, HRQL impairmentin patients with benign thyroid disorders is prevalent,both in the untreated phase and in the long term. Awide range of problems has been reported, coveringboth generic and specific aspects of HRQL. However,many of the studies are small and use unvalidatedmeasures. Most of them lack a thorough clinicaldescription of the patients and include patients coveringa wide range of phenotypes and aetiological dissimilari-ties. No available questionnaire has the potential tocover all aspects relevant to patients in longitudinalstudies, where individual patients may shift from onethyroid state to another as a result of natural historyor treatment. The available questionnaires lack docu-mented coverage of relevant HRQL issues and, apartfrom the GOQOL, they all lack a thorough validation.With this review, we have identified the possibly rel-evant issues reported in the literature. These data arevaluable as a basis for the development of HRQL ques-tionnaires possessing content validity. The next steptowards valid measures of disease-specific HRQL inthyroid patients would be to test the relevance of theissues presented here among samples of experts aswell as properly characterized thyroid patients.
Acknowledgements
We wish to express our gratitude to chief physician,Professor Peder Charles PhD for inspiration and toMarianne Klose MD for valuable discussions. This studyhas been supported by grants from the Danish MedicalResearch Council, the Agnes and Knut Mørk’s Foun-dation, the Aase and Ejnar Danielsen’s Foundation andthe Else and Mogens Wedell-Wedellsborg’s Foundation.
References
1 Guyatt GH, Feeny DH & Patrick DL. Measuring health-relatedquality of life. Annals of Internal Medicine 1993 118 622–629.
2 Hays RD. Generic versus disease-targeted instruments. In Asses-sing Quality of Life in Clinical Trials, pp 3–8. Eds P Fayers &RD Hays. Oxford: Oxford University Press, 2005.
3 Ladenson PW. Psychological well-being in patients. Clinical Endo-crinology 2002 57 575–576.
4 Abraham P, Avenell A, Watson WA, Park CM, Bevan JS. Antith-yroid Drug Regimen for Treating Graves’ Hyperthyroidism (CochraneReview), The Cochrane Library, issue 3. Chichester, UK: JohnWiley & Sons, Ltd., 2004.
5 Romijn JA, Smit JW & Lamberts SW. Intrinsic imperfections ofendocrine replacement therapy. European Journal of Endocrinology2003 149 91–97.
6 Bennedbaek FN, Perrild H & Hegedus L. Diagnosis and treatmentof the solitary thyroid nodule. Results of a European survey. Clini-cal Endocrinology 1999 50 357–363.
7 Bennedbaek FN & Hegedus L. Management of the solitary thyr-oid nodule: results of a North American survey. Journal of ClinicalEndocrinology and Metabolism 2000 85 2493–2498.
8 Bhagat MC, Dhaliwal SS, Bonnema SJ, Hegedus L & Walsh JP.Differences between endocrine surgeons and endocrinologists
in the management of non-toxic multinodular goitre. BritishJournal of Surgery 2003 90 1103–1112.
9 Bonnema SJ, Bennedbaek FN, Wiersinga WM & Hegedus L. Man-agement of the nontoxic multinodular goitre: a European ques-tionnaire study. Clinical Endocrinology 2000 53 5–12.
10 Bonnema SJ, Bennedbaek FN, Ladenson PW & Hegedus L. Man-agement of the nontoxic multinodular goiter: a North Americansurvey. Journal of Clinical Endocrinology and Metabolism 2002 87112–117.
11 Escobar-Jimenez F, Fernandez-Soto ML, Luna-Lopez V, Quesada-Charneco M & Glinoer D. Trends in diagnostic and therapeuticcriteria in Graves’ disease in the last 10 years. Postgraduate Medi-cal Journal 2000 76 340–344.
12 Geelhoed-Duyvestijn PH, Haak A, Hermans J & van der Heide D.Treatment of hypothyroidism in The Netherlands. Results of asurvey of Dutch internists. Netherlands Journal of Medicine1989 34 72–80.
13 Haak A, Geelhoed-Duyvestijn PH, Hermans J & van der Heide D.Diagnosis and treatment of Graves’ disease. Results of a survey ofDutch internists. Netherlands Journal of Medicine 1989 3464–71.
14 Solomon B, Glinoer D, Lagasse R & Wartofsky L. Current trendsin the management of Graves’ disease. Journal of Clinical Endo-crinology and Metabolism 1990 70 1518–1524.
15 Wartofsky L, Glinoer D, Solomon B, Nagataki S, Lagasse R,Nagayama Y & Izumi M. Differences and similarities in the diag-nosis and treatment of Graves’ disease in Europe, Japan, and theUnited States. Thyroid 1991 1 129–135.
16 Bianchi GP, Zaccheroni V, Solaroli E, Vescini F, Cerutti R, Zoli M &Marchesini G. Health-related quality of life in patients with thyr-oid disorders. Quality of Life Research 2004 13 45–54.
17 Elberling TV, Rasmussen AK, Feldt-Rasmussen U, Hording M,Perrild H & Waldemar G. Impaired health-related quality of lifein Graves’ disease. A prospective study. European Journal of Endo-crinology 2004 151 549–555.
18 Razvi S, Ingoe LE, McMillan CV & Weaver JU. Health status inpatients with sub-clinical hypothyroidism. European Journal ofEndocrinology 2005 152 713–717.
19 Fayers PM & Machin D. Quality of Life: Assessment, Analysis andInterpretation. Chichester: John Wiley and Sons, 2000.
20 Streiner DL & Norman GR. Health Measurement Scales. A PracticalGuide to their Development and Use, 2nd edn., Oxford: Oxford Uni-versity Press, 1995.
21 Sprangers MA, Cull A, Bjordal K, Groenvold M & Aaronson NK.The European Organization for Research and Treatment ofCancer. Approach to quality of life assessment: guidelines fordeveloping questionnaire modules. EORTC Study Group on Qual-ity of Life. Quality of Life Research 1993 2 287–295.
22 Testa MA & Simonson DC. Assessment of quality-of-life out-comes. New England Journal of Medicine 1996 334 835–840.
23 Assessing Quality of Life in Clinical Trials - Methods and Practice,2nd edn., Eds, PM Fayers & RD Hays. Oxford: Oxford UniversityPress, 2004.
24 Fahrenfort JJ, Wilterdink AM & van der Veen EA. Long-termresidual complaints and psychosocial sequelae after remission ofhyperthyroidism. Psychoneuroendocrinology 2000 25 201–211.
25 Terwee CB, Gerding MN, Dekker FW, Prummel MF &Wiersinga WM. Development of a disease-specific quality of lifequestionnaire for patients with Graves’ ophthalmopathy: theGO-QOL. British Journal of Ophthalmology 1998 82 773–779.
26 Tehrani M, Krummenauer F, Mann WJ, Pitz S, Dick HB &Kahaly GJ. Disease-specific assessment of quality of life afterdecompression surgery for Graves’ ophthalmopathy. EuropeanJournal of Ophthalmology 2004 14 193–199.
27 Jaeschke R, Guyatt G, Cook D, Harper S & Gerstein HC. Spectrumof quality of life impairment in hypothyroidism. Quality of LifeResearch 1994 3 323–327.
28 Saravanan P, Chau WF, Roberts N, Vedhara K, Greenwood R &Dayan CM. Psychological well-being in patients on‘adequate’ doses of L-thyroxine: results of a large, controlled
508 T Watt and others EUROPEAN JOURNAL OF ENDOCRINOLOGY (2006) 154
www.eje-online.org
Page 72 of 107
Appendix 3: Paper I

community-based questionnaire study. Clinical Endocrinology2002 57 577–585.
29 McMillan CV, Bradley C,WoodcockA, Razvi S &Weaver JU. Designof new questionnaires to measure quality of life and treatmentsatisfaction in hypothyroidism. Thyroid 2004 14 916–925.
30 Wayne EJ. The diagnosis of thyrotoxicosis. British Medical Journal1954 4859 411–419.
31 Crooks J, Murray IP & Wayne EJ. Statistical methods applied tothe clinical diagnosis of thyrotoxicosis. Quarterly Journal of Medi-cine 1959 28 211–234.
32 Murray IP. The clinical diagnosis of thyroid disease. Medical Jour-nal of Australia 1964 13 827–831.
33 Gurney C, Hall R, Harper M, Owen SG, Roth M & Smart GA.Newcastle thyrotoxicosis index. Lancet 1970 2 1275–1278.
34 Benvenga S, Ruggeri RM, Russo A, Lapa D, Campenni A &Trimarchi F. Usefulness of L-carnitine, a naturally occurring per-ipheral antagonist of thyroid hormone action, in iatrogenichyperthyroidism: a randomized, double-blind, placebo-controlledclinical trial. Journal of Clinical Endocrinology and Metabolism2001 86 3579–3594.
35 Klein I, Trzepacz PT, Roberts M & Levey GS. Symptom ratingscale for assessing hyperthyroidism. Archives of Internal Medicine1988 148 387–390.
36 Wayne E. The assessment of thyroid function. British Journal ofSurgery 1965 52 717–721.
37 Billewicz WZ, Chapman RS, Crooks J, Day ME, Gossage J,Wayne E & Young JA. Statistical methods applied to the diagno-sis of hypothyroidism. Quarterly Journal of Medicine 1969 38255–266.
38 Zulewski H, Muller B, Exer P, Miserez AR & Staub JJ. Estimationof tissue hypothyroidism by a new clinical score: evaluation ofpatients with various grades of hypothyroidism and controls.Journal of Clinical Endocrinology and Metabolism 1997 82771–776.
39 Barker DJ & Bishop JM. Computer-based screening system forpatients at risk of hypothyroidism. Lancet 1969 2 835–838.
40 Gardner MJ & Barker DJ. Diagnosis of hypothyroidism: a com-parison of statistical techniques. British Medical Journal 1975 2260–262.
41 Cooper DS, Halpern R, Wood LC, Levin AA & Ridgway EC.L-Thyroxine therapy in subclinical hypothyroidism. A double-blind, placebo-controlled trial. Annals of Internal Medicine 1984101 18–24.
42 Canaris GJ, Steiner JF & Ridgway EC. Do traditional symptoms ofhypothyroidism correlate with biochemical disease? Journal ofGeneral Internal Medicine 1997 12 544–550.
43 Canaris GJ, Manowitz NR, Mayor G & Ridgway EC. The Coloradothyroid disease prevalence study. Archives of Internal Medicine2000 160 526–534.
44 Terwee CB, Gerding MN, Dekker FW, Prummel MF, van der Pol JP& Wiersinga WM. Test-retest reliability of the GO-QOL: a disease-specific quality of life questionnaire for patients with Graves’ophthalmopathy. Journal of Clinical Epidemiology 1999 52875–884.
45 Terwee CB, Dekker FW, Mourits MP, Gerding MN, Baldeschi L,Kalmann R, Prummel MF & Wiersinga WM. Interpretationand validity of changes in scores on the Graves’ ophthalmopathyquality of life questionnaire (GO-QOL) after different treatments.Clinical Endocrinology 2001 54 391–398.
46 Wiersinga WM, Prummel MF & Terwee CB. Effects of Graves’ophthalmopathy on quality of life. Journal of EndocrinologicalInvestigation 2004 27 259–264.
47 Jaeschke R, Guyatt G, Gerstein H, Patterson C, Molloy W, Cook D,Harper S, Griffith L & Carbotte R. Does treatment with L-thyrox-ine influence health status in middle-aged and older adults withsubclinical hypothyroidism? Journal of General Internal Medicine1996 11 744–749.
48 Biondi B, Palmieri EA, Fazio S, Cosco C, Nocera M, Sacca L,Filetti S, Lombardi G & Perticone F. Endogenous subclinicalhyperthyroidism affects quality of life and cardiac morphology
and function in young and middle-aged patients. Journal of Clini-cal Endocrinology and Metabolism 2000 85 4701–4705.
49 Gerding MN, Terwee CB, Dekker FW, Koornneef L, Prummel MF& Wiersinga WM. Quality of life in patients with Graves’ophthalmopathy is markedly decreased: measurement by themedical outcomes study instrument. Thyroid 1997 7 885–889.
50 Terwee C, Wakelkamp I, Tan S, Dekker F, Prummel MF &Wiersinga W. Long-term effects of Graves’ ophthalmopathy onhealth-related quality of life. European Journal of Endocrinology2002 146 751–757.
51 Egle UT, Kahaly GJ, Petrak F, Hardt J, Batke J, Best J &Rothenbacher M. The relevance of physical and psychosocial fac-tors for the quality of life in patients with thyroid-associated orbi-topathy (TAO). Experimental and Clinical Endocrinology andDiabetes 1999 107 (Suppl 5) S168–S171.
52 Harrison LC, Buckley JD & Martin FI. Use of a computer-basedpostal questionnaire for the detection of hypothyroidism follow-ing radioiodine therapy for thyrotoxicosis. Australian and NewZealand Journal of Medicine 1977 7 27–32.
53 Escobar-Morreale HF, Botella-Carretero JI, Gomez-Bueno M,Galan JM, Barrios V & Sancho J. Thyroid hormone replacementtherapy in primary hypothyroidism: a randomized trial compar-ing L-thyroxine plus liothyronine with L-thyroxine alone. Annalsof Internal Medicine 2005 142 412–424.
54 Zeitlhofer J, Saletu B, Stary J & Ahmadi R. Cerebral function inhyperthyroid patients. Psychopathology, psychometric variables,central arousal and time perception before and after thyreostatictherapy. Neuropsychobiology 1984 11 89–93.
55 Demet MM, Ozmen B, Deveci A, Boyvada S, Adiguzel H &Aydemir O. Depression and anxiety in hyperthyroidism. Archivesof Medical Research 2002 33 552–556.
56 Rockey PH & Griep RJ. Behavioral dysfunction in hyperthyroid-ism. Improvement with treatment. Archives of Internal Medicine1980 140 1194–1197.
57 Stern RA, Robinson B, Thorner AR, Arruda JE, Prohaska ML &Prange AJ Jr. A survey study of neuropsychiatric complaints inpatients with Graves’ disease. Journal of Neuropsychiatry and Clini-cal Neurosciences 1996 8 181–185.
58 Park JJ, Sullivan TJ, Mortimer RH, Wagenaar M & Perry-Keene DA. Assessing quality of life in Australian patients withGraves’ ophthalmopathy. British Journal of Ophthalmology 200488 75–78.
59 Braverman LE & Utiger RD, Eds. Werner and Ingbars The Thyroid -a Fundamental and Clinical Text, 7th edn., New York: Lippincott-Raven, 1996.
60 Ljunggren JG, Torring O, Wallin G, Taube A, Tallstedt L,Hamberger B & Lundell G. Quality of life aspects and costs intreatment of Graves’ hyperthyroidism with antithyroid drugs,surgery, or radioiodine: results from a prospective, randomizedstudy. Thyroid 1998 8 653–659.
61 Kathol RG, Turner R & Delahunt J. Depression and anxietyassociated with hyperthyroidism: response to antithyroidtherapy. Psychosomatics 1986 27 501–505.
62 O’Malley B, Hickey J & Nevens E. Thyroid dysfunction - weightproblems and the psyche: the patients’ perspective. Journal ofHuman Nutrition and Dietetics 2000 13 243–248.
63 Maugeri D, Motta M, Salerno G, Rosso D, Mazzarella R,Salomone S, Russo MS, Elia G & Panebianco P. Cognitive andaffective disorders in hyper- and hypothyreotic elderly patients.Archives of Gerontology and Geriatrics 1998 Suppl. 6 305–312.
64 Trzepacz PT, McCue M, Klein I, Levey GS & Greenhouse J.A psychiatric and neuropsychological study of patients withuntreated Graves’ disease. General Hospital Psychiatry 1988 1049–55.
65 Whybrow PC, Prange AJ Jr & Treadway CR. Mental changesaccompanying thyroid gland dysfunction. A reappraisal usingobjective psychological measurement. Archives of General Psy-chiatry 1969 20 48–63.
Quality of life in thyroid patients 509EUROPEAN JOURNAL OF ENDOCRINOLOGY (2006) 154
www.eje-online.org
Page 73 of 107
Appendix 3: Paper I

66 Radanovic-Grguric L, Filakovic P, Barkic J, Mandic N, Karner I &Smoje J. Depression in patients with thyroid dysfunction. Euro-pean Journal of Psychiatry 2003 17 133–144.
67 Lee IT, Sheu WH, Liau YJ, Lin SY, Lee WJ & Lin CC. Relationshipof stressful life events, anxiety and depression tohyperthyroidism in an Asian population. Hormone Research2003 60 247–251.
68 Paschke R, Harsch I, Schlote B, Vardarli I, Schaaf L, Kaumeier S,Teuber J & Usadel KH. Sequential psychological testing duringthe course of autoimmune hyperthyroidism. Klinische Wochens-chrift 1990 68 942–950.
69 Farid M, Roch-Levecq AC, Levi L, Brody BL, Granet DB &Kikkawa DO. Psychological disturbance in Graves’ ophthalmopa-thy. Archives of Ophthalmology 2005 123 491–496.
70 DeGroot LJ & Jameson JL, Eds. Endocrinology, 4th edn., Philadel-phia: WB Saunders, 2001.
71 Wass JAH, Shalet SM, Gale E & Amiel SA, Eds. Oxford Textbook ofEndocrinology and Diabetes, 1st edn., Oxford: Oxford UniversityPress, 2002.
72 Kahaly GJ, Hardt J, Petrak F & Egle UT. Psychosocial factors insubjects with thyroid-associated ophthalmopathy. Thyroid 200212 237–239.
73 Laurberg P. Hypothyroidism. In The Thyroid Gland, pp 497–535.Ed. MA Greer. New York: Raven Press, 1990.
74 Jain VK. Affective disturbance in hypothyroidism. British Journalof Psychiatry 1971 119 279–280.
75 Gunnarsson T, Sjoberg S, Eriksson M & Nordin C. Depressivesymptoms in hypothyroid disorder with some observations onbiochemical correlates. Neuropsychobiology 2001 43 70–74.
76 Cleare AJ, McGregor A & O’Keane V. Neuroendocrine evidencefor an association between hypothyroidism, reduced central5-HT activity and depression. Clinical Endocrinology 1995 43713–719.
77 Zettinig G, Asenbaum S, Fueger BJ, Hofmann A, Diemling M,Mittlboeck M & Dudczak R. Increased prevalence of subclinicalbrain perfusion abnormalities in patients with autoimmune thy-roiditis: evidence of Hashimoto’s encephalitis? Clinical Endocrin-ology 2003 59 637–643.
78 Trivalle C, Doucet J, Chassagne P, Landrin I, Kadri N, Menard JF& Bercoff E. Differences in the signs and symptoms of hyperthyr-oidism in older and younger patients. Journal of the AmericanGeriatrics Society 1996 44 50–53.
79 Orgiazzi JJ & Mornex R. Hyperthyroidism. In The Thyroid Gland,pp 405–495. Ed. MA Greer. New York: Raven Press, 1990.
80 Wilson WP, Johnson JE & Smith RB. Affective change in thyro-toxicosis and experimental hypermetabolism. Recent Advancesin Biological Psychiatry 1961 4 234–243.
81 Wallace JE, MacCrimmon DJ & Goldberg WM. Acute hyperthyr-oidism: cognitive and emotional correlates. Journal of AbnormalPsychology 1980 89 519–527.
82 Nordyke RA, Gilbert FI Jr & Harada AS. Graves’ disease. Influ-ence of age on clinical findings. Archives of Internal Medicine1988 148 626–631.
83 Tak PP, Hermans J & Haak A. Symptomatology of Graves’ diseaseand Plummer’s disease in relation to age and thyroid hormonelevel. Netherlands Journal of Medicine 1993 42 157–162.
84 Yonem O, Dokmetas HS, Aslan SM & Erselcan T. Is antithyroidtreatment really relevant for young patients with subclinicalhyperthyroidism? Endocrine Journal 2002 49 307–314.
85 Davis PJ & Davis FB. Hyperthyroidism in patients over the age of60 years. Clinical features in 85 patients. Medicine 1974 53161–181.
86 Watanakunakorn C, Hodges RE & Evans TC. Myxedema: a studyof 400 cases. Archives of Internal Medicine 1965 116 183–190.
87 Sait Gonen M, Kisakol G, Savas Cilli A, Dikbas O, Gungor K,Inal A & Kaya A. Assessment of anxiety in subclinical thyroiddisorders. Endocrine Journal 2004 51 311–315.
88 Oddie TH, Boyd CM, Fisher DA & Hales IB. Incidence of signs andsymptoms in thyroid disease. Medical Journal of Australia 1972 2981–986.
89 Harper MB. Vomiting, nausea, and abdominal pain: unrecog-nized symptoms of thyrotoxicosis. Journal of Family Practice1989 29 382–386.
90 AlvarezMA,GomezA,Alavez E&NavarroD.Attentiondisturbancein Graves’ disease. Psychoneuroendocrinology 1983 8 451–454.
91 Monzani F, Del Guerra P, Caraccio N, Pruneti CA, Pucci E, Luisi M& Baschieri L. Subclinical hypothyroidism: neurobehavioral fea-tures and beneficial effect of L-thyroxine treatment. Clinical Inves-tigator 1993 71 367–371.
92 Eden S, Sundbeck G, Lindstedt G, Lundberg PA, Jagenburg R,Landahl S & Svanborg A. Screening for thyroid disease in theelderly. Serum concentrations of thyrotropin and 3,5,30-triio-dothyronine in a representative population of 79-year-oldwomen and men. Comprehensive Gerontology Section A, Clinicaland Laboratory Sciences 1988 2 40–45.
93 Wesche MF, Buul MM, Smits NJ & Wiersinga WM. Reduction ingoiter size by 131I therapy in patients with non-toxic multinod-ular goiter. European Journal of Endocrinology 1995 132 86–87.
94 Le Moli R, Wesche MF, Tiel-Van Buul MM & Wiersinga WM.Determinants of long-term outcome of radioiodine therapy ofsporadic non-toxic goitre. Clinical Endocrinology 1999 50783–789.
95 Bonnema SJ, Nielsen VE & Hegedus L. Long-term effects of radio-iodine on thyroid function, size and patient satisfaction in non-toxic diffuse goitre. European Journal of Endocrinology 2004 150439–445.
96 Schlote B, Nowotny B, Schaaf L, Kleinbohl D, Schmidt R,Teuber J, Paschke R, Vardarli I, Kaumeier S & Usadel KH. Subcli-nical hyperthyroidism: physical and mental state of patients.European Archives of Psychiatry and Clinical Neuroscience 1992241 357–364.
97 Monzani F, Caraccio N, Del GP, Casolaro A & Ferrannini E.Neuromuscular symptoms and dysfunction in subclinicalhypothyroid patients: beneficial effect of L-T4 replacementtherapy. Clinical Endocrinology 1999 51 237–242.
98 Armistead SH. Symptoms of non-toxic nodular goitre. UlsterMedical Journal 1976 45 178–180.
99 Papa A, Cammarota G, Tursi A, Certo M, Montalto M, Capelli G,de Rosa G, Cuoco L, Fedeli G &Gasbarrini G. Effects of propylthiour-acil on intestinal transit time and symptoms in hyperthyroidpatients. Hepatogastroenterology 1997 44 426–429.
100 Filteau SM, Sullivan KR, Anwar US, Anwar ZR & Tomkins AM.Iodine deficiency alone cannot account for goitre prevalenceamong pregnant women in Modhupur, Bangladesh. EuropeanJournal of Clinical Nutrition 1994 48 293–302.
101 Berg G, Michanek A, Holmberg E & Nystrom E. Clinical outcomeof radioiodine treatment of hyperthyroidism: a follow-up study.Journal of Internal Medicine 1996 239 165–171.
102 Bommer M, Eversmann T, Pickardt R, Leonhardt A & Naber D.Psychopathological and neuropsychological symptoms inpatients with subclinical and remitted hyperthyroidism. KlinischeWochenschrift 1990 68 552–558.
103 Thomsen AF, Kvist TK, Andersen PK & Kessing LV. Increased riskof affective disorder following hospitalisation with hyperthyroid-ism - a register-based study. European Journal of Endocrinology2005 152 535–543.
104 Perrild H, Hansen JM, Arnung K, Olsen PZ & Danielsen U. Intel-lectual impairment after hyperthyroidism. Acta Endocrinologica1986 112 185–191.
105 Jansson S, Berg G, Lindstedt G, Michanek A & Nystrom E. Over-weight - a common problemamongwomen treated for hyperthyr-oidism. Postgraduate Medical Journal 1993 69 107–111.
106 Birring SS, Morgan AJ, Prudon B, McKeever TM, Lewis SA,Falconer Smith JF, Robinson RJ, Britton JR & Pavord ID. Respir-atory symptoms in patients with treated hypothyroidism andinflammatory bowel disease. Thorax 2003 58 533–536.
Received 19 December 2005
Accepted 13 January 2006
510 T Watt and others EUROPEAN JOURNAL OF ENDOCRINOLOGY (2006) 154
www.eje-online.org
Page 74 of 107
Appendix 3: Paper I
Which Domains of Thyroid-Related Quality of LifeAre Most Relevant? Patients and Clinicians
Provide Complementary Perspectives
Torquil Watt,1,2 Laszlo Hegedus,3 Ase Krogh Rasmussen,1 Mogens Groenvold,2 Steen Joop Bonnema,3
Jakob Bue Bjorner,4 and Ulla Feldt-Rasmussen1
Objective: To identify how thyroid diseases impact the patients’ lives and to select the most relevant quality of life(QoL) issues for a thyroid-specific questionnaire.Design: Fifteen thyroid experts and 80 thyroid outpatients (14 withnontoxic goiter, 12 nodular toxic goiter, 21 Graves’ disease, 17 thyroid-associated ophthalmopathy, and 16 primaryhypothyroidism) were interviewed. Methods: The relevance of 138 thyroid disease–related issues was rated duringinterviews. For each issue, three relevance measures were obtained: a diagnosis-specific patient rating, a diagnosis-specific expert rating, and a combined overall patient=expert rating. The 75 most relevant issues overall and the 15most relevant issues in each patient category were selected. Results: Based on the above, 92 issues were selected,covering a broad range of clinical and QoL domains. Across patient groups, broader QoL domains were mostrelevant, especially fatigue and emotional susceptibility. However, when focusing on individual patient groups,diagnosis-related physical symptoms were very relevant too. Patients rated issues about psychosocial problemsand impact on daily life as more relevant, whereas clinicians focused on thyroid-characteristic issues.Conclusions: Abroad range of QoL issues and physical symptoms are relevant for thyroid patients, particularly fatigue andemotional susceptibility. Patients and clinicians offer complementary perspectives on relevance.
Introduction
The importance of including measurements of health-related quality of life (HRQL) in clinical studies of thyroid
patients is increasingly recognized (1–3), and evidence of re-duced quality of life (QoL) of thyroid patients is currently ac-cumulating (4–11). However, most of these studies have usedstandard generic HRQL questionnaires, for which the validityin the studied population has not been established. Otherstudies have used thyroid-specific HRQL questionnaires, forwhich the documentation of appropriate validity generally islimited (11).
In medical science, research on HRQL focuses on the use ofpatients’ self-ratings in clinical studies. During the last de-cades, a rapid development in the methodology concerningthe reliability and validity of such patient-reported outcomeshas resulted in marked improvements in their scientific qual-ity. Very recently, the U.S. Food and Drug Administration(FDA) published a guidance draft about how they evaluatesuch outcome measures, which probably will set the standardsfor the development and validation of new patient-reportedoutcome measures (12).
A basic and very important element of the validity of HRQLmeasurement is content validity: whether all issues relevant tothe patients and the question under study are covered by thechosen questionnaire (12,13). For example, the validity of ameasure that does not include items on fatigue is questionableif fatigue is a major problem for the population under study. Inorder to claim validity of a certain instrument, content validityfor the particular patients in focus must be demonstrated (14).For thyroid patients, as well as many other patient groups,content validity of HRQL instruments has not been convinc-ingly evaluated.
Benign thyroid diseases are characterized by a substantialoverlap between various disease entities (e.g., coexistence ofgoiter and hyperthyroidism) and a shift between diseases (e.g.,hyperthyroid patients becoming hypothyroid through abla-tive therapy). Therefore, optimally an HRQL outcome mea-sure for thyroid patients should encompass all thyroiddiseases in order to have content validity. If not, the results oflongitudinal studies may be misleading, because importantHRQL aspects are not measured.
In this study, we aim to (i) identify the full range of issuespertaining to the HRQL of thyroid patients and (ii) establish
1Department of Endocrinology, Copenhagen University Hospital Rigshospitalet, Copenhagen, Denmark.2Institute of Public Health, University of Copenhagen, Copenhagen, Denmark.3Department of Endocrinology and Metabolism, Odense University Hospital, Odense, Denmark.4QualityMetric Inc., Lincoln, Rhode Island.
THYROIDVolume 17, Number 7, 2007ª Mary Ann Liebert, Inc.DOI: 10.1089=thy.2007.0069
647
Page 75 of 107
Appendix 4: Paper II

a method for selecting the most relevant of these. We presenta method that integrates the input from experts (endocri-nologists and endocrine nurses) and patients. Due to theneed for a comprehensive thyroid questionnaire that can beused across all benign thyroid diagnoses, we balance theselection of the most important domains overall (i.e., acrosspatient groups) and the selection of domains with high im-portance to particular patient groups.
Methods
Identifying HRQL issues of potential relevancein thyroid disease
In accordance with standard methods for HRQL issuegeneration (15–17) and the FDA guidance (12), we tappedthree sources of possibly relevant HRQL issues: literature,experts, and patients. The purpose was to generate anexhaustive list of issues to include in a thyroid HRQL ques-tionnaire. In short, the list of possibly relevant issues wasgenerated as follows: 138 issues were identified through asystematic literature search, as described elsewhere (11). Thislist was presented to thyroid experts, and they rated the rel-evance of each issue; issues considered relevant by the ex-perts but absent in the list were also added by the experts.Subsequently, the list was evaluated and expanded in a sim-ilar way by thyroid patients. Each process is further describedbelow.
Expert interviews
Thirteen medical doctors were interviewed. They were ei-ther consultant physicians (n¼ 8) with 10–30 years of clinicaland scientific experience within thyroidology or registrars(n¼ 5) involved in thyroid research and having 4–8 years ofexperience with thyroid patients. In addition, two nurses re-sponsible for the care of the thyroid outpatients (4 and 6 yearsof experience with thyroid patients) were interviewed. Theyall rated the relevance of each of the 138 issues on a five-pointscale (0¼ irrelevant to 4¼very relevant), separately for each ofthe patient categories: nontoxic goiter, toxic nodular goiter,Graves’ hyperthyroidism, thyroid-associated ophthalmo-pathy (TAO), and primary hypothyroidism. Thus, they did notrate individual patients but evaluated the relevance for eachpatient category in general, based on their clinical experience.The experts were instructed to include both frequency andimportance of each issue in their considerations. Further, theywere instructed to exclude eye involvement while rating rel-evance for Graves’ hyperthyroidism and to exclude hyper-thyroid symptoms while rating relevance for TAO patients.Issues considered relevant by an expert but absent in the listwere recorded and rated as well.
Patient interviews
Eighty thyroid patients without major nonthyroidal co-morbidities in two Danish University hospital outpatientclinics (Copenhagen University Hospital Rigshospitalet andOdense University Hospital) were interviewed. The inter-views lasted 1–1.5 hours and were carried out by P.I. TorquilWatt on the day the patients were seen in the outpatient clinic,in order to have recent clinical data (e.g., thyroid functiontests) available. The patients were selected by a nonrandomstrategic sampling procedure (18,19), which aimed at maxi-
mizing the patient variation as regards diagnoses, treat-ment, disease duration (including both newly diagnosed,untreated patients and treated patients), and age (Table 1).Clinical data were obtained from medical records. The studywas approved by the local ethical committee (KF 01-100=04),and all patients gave written informed consent. Diagnoseswere based on clinical examination, thyroid function variables[thyroid-stimulating hormone (TSH), thyroxine (T4), and tri-iodothyronine (T3) (total and free)], thyroid autoantibodies,Tc-99m pertechnetate scintigraphy, and ultrasonography.Biochemical analyses were performed using standard meth-ods of the participating centers, and the reference ranges of thelocal laboratories were used. A diagnosis of mild thyroiddysfunction was defined as TSH level outside the normalrange of the laboratory and no history of abnormal peripheralthyroid hormone levels. The included patients comprised14 patients with nontoxic goiter (normal thyroid hor-mone levels and normal TSH and palpable goiter verified byTc-99m pertechnetate scan=ultrasonography), 12 with nodu-lar toxic goiter [nodular goiter on Tc-99m pertechnetate scan=ultrasonography, suppressed TSH with (overt) or without(mild) elevated thyroid hormones, and absence of TSH re-ceptor antibodies (TSHRAb)], 21 with Graves’ disease withouteye involvement [diffuse pattern on Tc-99m pertechnetatescan=ultrasonography, suppressed TSH with (overt) or with-out (mild) elevated thyroid hormone levels, and elevatedTSHRAb], 17 with TAO (Graves’ disease and ophthalmopathyverified by an ophthalmologist), and 16 with primary hypo-thyroidism [elevated serum TSH with (overt) or without(mild) decreased thyroid hormone levels and elevated levels ofserum TPO-Ab and=or TgAb]. All diagnostic definitions referto time of diagnosis.
Initially, a semistructured interview with open-endedquestions (18) about the consequences of having a thyroiddisorder was conducted. Key issues mentioned spontaneouslyby the patient during this part of the interview were registeredby the interviewer in order to discuss them with the patientlater. Subsequently, a structured interview evaluating the is-sue list described above was conducted. Each issue on theissue list was rated in a two-step procedure. First, the patientselected the issues they had experienced at any time duringtheir disease. Second, the importance, as regards impact onQoL, of each of the selected items was rated on a five-pointscale (0¼unimportant to 4¼very important). After the struc-tured interview, the key issues from the semistructured in-terview were discussed with the patient and added to the listof issues if not already present in it.
Issue selection procedure
The relevance of each issue was quantified by three mea-sures: an expert relevance rank for each patient group, a pa-tient relevance rank for each patient group, and an overallrelevance rank across patient groups.
The expert relevance rank was derived by simply rankingthe mean (0–4) relevance ratings described above, for eachpatient group. The issue having the highest mean relevancerating (most relevant) was ascribed rank #1 and so on.
The patient relevance rank was derived as follows: Themean (0–4) patient importance rating for each issue in eachpatient group was multiplied by the proportion of patientsexperiencing the issue (20,21). For example, anxiety was
648 WATT ET AL.
Page 76 of 107
Appendix 4: Paper II
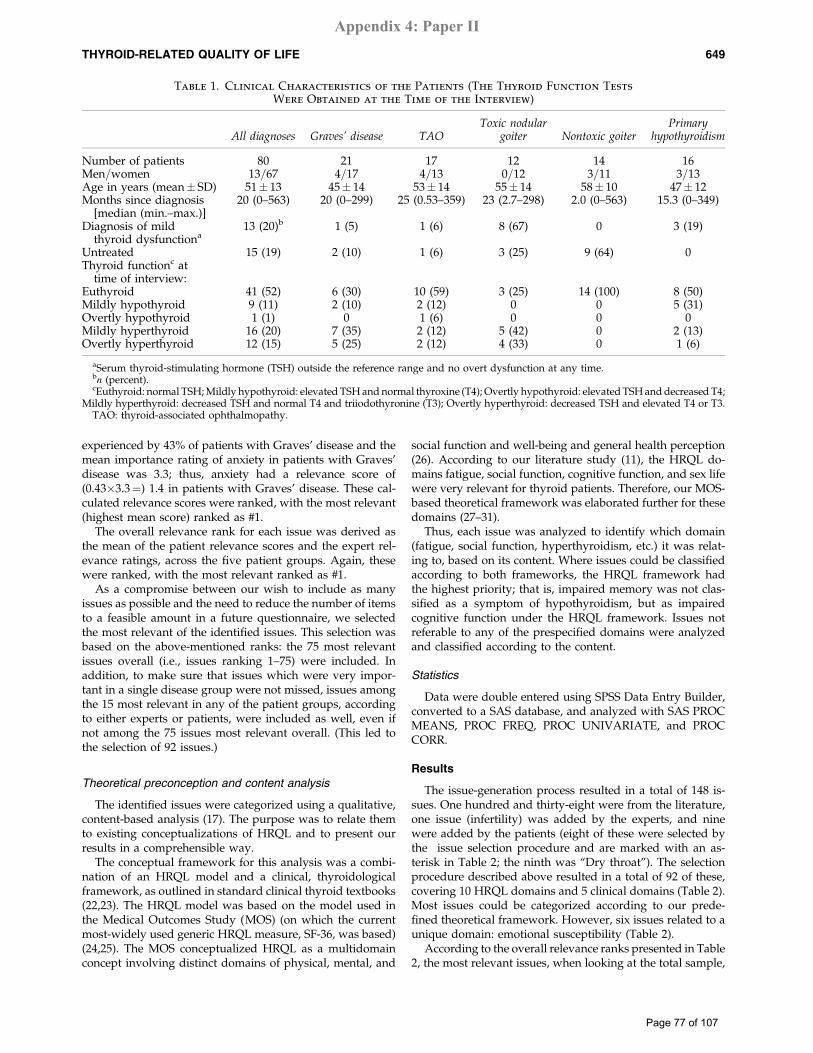
experienced by 43% of patients with Graves’ disease and themean importance rating of anxiety in patients with Graves’disease was 3.3; thus, anxiety had a relevance score of(0.43�3.3¼) 1.4 in patients with Graves’ disease. These cal-culated relevance scores were ranked, with the most relevant(highest mean score) ranked as #1.
The overall relevance rank for each issue was derived asthe mean of the patient relevance scores and the expert rel-evance ratings, across the five patient groups. Again, thesewere ranked, with the most relevant ranked as #1.
As a compromise between our wish to include as manyissues as possible and the need to reduce the number of itemsto a feasible amount in a future questionnaire, we selectedthe most relevant of the identified issues. This selection wasbased on the above-mentioned ranks: the 75 most relevantissues overall (i.e., issues ranking 1–75) were included. Inaddition, to make sure that issues which were very impor-tant in a single disease group were not missed, issues amongthe 15 most relevant in any of the patient groups, accordingto either experts or patients, were included as well, even ifnot among the 75 issues most relevant overall. (This led tothe selection of 92 issues.)
Theoretical preconception and content analysis
The identified issues were categorized using a qualitative,content-based analysis (17). The purpose was to relate themto existing conceptualizations of HRQL and to present ourresults in a comprehensible way.
The conceptual framework for this analysis was a combi-nation of an HRQL model and a clinical, thyroidologicalframework, as outlined in standard clinical thyroid textbooks(22,23). The HRQL model was based on the model used inthe Medical Outcomes Study (MOS) (on which the currentmost-widely used generic HRQL measure, SF-36, was based)(24,25). The MOS conceptualized HRQL as a multidomainconcept involving distinct domains of physical, mental, and
social function and well-being and general health perception(26). According to our literature study (11), the HRQL do-mains fatigue, social function, cognitive function, and sex lifewere very relevant for thyroid patients. Therefore, our MOS-based theoretical framework was elaborated further for thesedomains (27–31).
Thus, each issue was analyzed to identify which domain(fatigue, social function, hyperthyroidism, etc.) it was relat-ing to, based on its content. Where issues could be classifiedaccording to both frameworks, the HRQL framework hadthe highest priority; that is, impaired memory was not clas-sified as a symptom of hypothyroidism, but as impairedcognitive function under the HRQL framework. Issues notreferable to any of the prespecified domains were analyzedand classified according to the content.
Statistics
Data were double entered using SPSS Data Entry Builder,converted to a SAS database, and analyzed with SAS PROCMEANS, PROC FREQ, PROC UNIVARIATE, and PROCCORR.
Results
The issue-generation process resulted in a total of 148 is-sues. One hundred and thirty-eight were from the literature,one issue (infertility) was added by the experts, and ninewere added by the patients (eight of these were selected bythe issue selection procedure and are marked with an as-terisk in Table 2; the ninth was ‘‘Dry throat’’). The selectionprocedure described above resulted in a total of 92 of these,covering 10 HRQL domains and 5 clinical domains (Table 2).Most issues could be categorized according to our prede-fined theoretical framework. However, six issues related to aunique domain: emotional susceptibility (Table 2).
According to the overall relevance ranks presented in Table2, the most relevant issues, when looking at the total sample,
Table 1. Clinical Characteristics of the Patients (The Thyroid Function Tests
Were Obtained at the Time of the Interview)
All diagnoses Graves’ disease TAOToxic nodular
goiter Nontoxic goiterPrimary
hypothyroidism
Number of patients 80 21 17 12 14 16Men=women 13=67 4=17 4=13 0=12 3=11 3=13Age in years (mean� SD) 51� 13 45� 14 53� 14 55� 14 58� 10 47� 12Months since diagnosis
[median (min.–max.)]20 (0–563) 20 (0–299) 25 (0.53–359) 23 (2.7–298) 2.0 (0–563) 15.3 (0–349)
Diagnosis of mildthyroid dysfunctiona
13 (20)b 1 (5) 1 (6) 8 (67) 0 3 (19)
Untreated 15 (19) 2 (10) 1 (6) 3 (25) 9 (64) 0Thyroid functionc at
time of interview:Euthyroid 41 (52) 6 (30) 10 (59) 3 (25) 14 (100) 8 (50)Mildly hypothyroid 9 (11) 2 (10) 2 (12) 0 0 5 (31)Overtly hypothyroid 1 (1) 0 1 (6) 0 0 0Mildly hyperthyroid 16 (20) 7 (35) 2 (12) 5 (42) 0 2 (13)Overtly hyperthyroid 12 (15) 5 (25) 2 (12) 4 (33) 0 1 (6)
aSerum thyroid-stimulating hormone (TSH) outside the reference range and no overt dysfunction at any time.bn (percent).cEuthyroid: normal TSH; Mildly hypothyroid: elevated TSH and normal thyroxine (T4); Overtly hypothyroid: elevated TSH and decreased T4;
Mildly hyperthyroid: decreased TSH and normal T4 and triiodothyronine (T3); Overtly hyperthyroid: decreased TSH and elevated T4 or T3.TAO: thyroid-associated ophthalmopathy.
THYROID-RELATED QUALITY OF LIFE 649
Page 77 of 107
Appendix 4: Paper II

were from generic HRQL domains: fatigue, emotional sus-ceptibility, general health perception, anxiety, depressivity,and social function.
In Figure 1, the mean relevance ranks of the 15 domains aredisplayed, separately for patients and experts and for eachdiagnosis (for information about which issues contribute tothe domain score, see Table 2). While focusing thus on theindividual patient groups, it is evident that symptoms asso-ciated with each diagnosis were very relevant for the patientgroups with that particular diagnosis, in contrast to what wasfound regarding the overall relevance ranks in Table 2. Thus,compared to other domains (comparisons cannot be validlymade across diagnoses, because the relevance ratings havebeen ranked according to relative relevance within each pa-tient group), hypothyroid symptoms were very relevant topatients with hypothyroidism, eye symptoms were very rel-evant to patients with TAO, local pressure symptoms werevery relevant to patients with nontoxic goiter, and hyperthy-
roid symptoms were very relevant to patients with hyper-thyroidism. An exception was that patients with toxic nodulargoiter rated hyperthyroid symptoms as relatively less relevantthan other domains.
The 15 most relevant issues in each patient category ac-cording to patients and experts are presented in Table 3. Formost categories, less than half of the 15 issues were over-lapping between patients and experts (Graves’ disease 8, TAO4, toxic nodular goiter 6, nontoxic goiter 5, and primary hypo-thyroidism 8). Generally, issues among the 15 most relevantaccording to experts only were problems characteristic of thediagnosis in question (i.e., hyperthyroid symptoms forGraves’ and toxic nodular goiter, eye symptoms for TAO, andlocal pressure symptoms and cosmetic concern for patientswith nontoxic goiter). Issues among the 15 most relevant ac-cording to patients only were generally nonphysical aspects ofHRQL, such as emotional susceptibility and nervousness, aswell as noncharacteristic physical symptoms.
Table 2. The 92 Most Relevant Issues (Overall Patient=Expert Relevance Rank 1–75or Diagnosis-Specific Rank 1–15) and the Corresponding Domains
Domains Issues
General health Impaired general health perception (#18)
Limitations Problems performing daily activities (#6), reduced mobility (#64)
Social function Social life impaired (#35)
Sex life Sexual problems (#65), reduced libido (#68)
Cosmetic concern Weight dissatisfaction (#16), unsatisfied with physical appearance (#28), mask visibleaspects of the disease (#78)
Emotional susceptibility Getting upset, cannot cope with demands* (#2), emotional lability (#5), easily gettingstressed* (#9), lack the feeling of being oneself (#14), easily irritated or angry (#29),feeling frustrated (#58)
Depressivity Sadness (#21), feeling worried (#22), discouragement (#22), crying easily (#25), feelingdepressed (#36), reduced self-confidence (#45), lost interest and pleasure in usualactivities (#59)
Anxiety Feeling of unrest (#10), feeling tense (#20), nervousness (#26), anxiety (#33), cancro-phobia (#61)
Fatigue General fatigue (#1), physical fatigue (#3), mental fatigue (#4), hypersomnia (#11), lackinitiative (#53)
Cognitive function Impaired memory (#12), difficulty concentrating (#15), attention problems (#31),confusion (#41), learning difficulties (#46), difficulty planning (#50), slow or unclearthinking (#54), difficulty understanding complex words (#70)
Hyperthyroid symptoms Dyspnea (#7), palpitation (#17), sleeplessness (#19), restlessness (#32), increased sweating(#34), heat intolerance (#44), hand tremor (#47), upset stomach (#49), weight loss (#56),increased appetite (#57), muscle weakness (#62), diarrhea (#71)
Hypothyroid symptoms Weight gain (#23), hair loss or thin hair (#43), swollen hands or feet (#48), coldintolerance (#63), hoarseness (#69), being slow* (#77), facial swelling (#75), constipa-tion (#79), dry skin (#94), weak voice (#126)
Eye symptoms Bags under the eyes* (#30), watery eyes* (#40), dryness=grittiness (#55), blurred vision(#72), photophobia (#74), swollen eyelids (#87), pressure in=behind eyes (#93), red eyes(#104), reduced vision (#109), pain in the eyes (#115), double vision (#119), red eyelids(#136), reduced color vision (#143)
Goiter symptoms Globulus sensation (#8), swelling in front of the neck (#13), clearing throat often* (#37),discomfort swallowing (#51), difficulty breathing (#66), feeling like suffocating* (#73),pain in the throat (#117), pain in the throat radiating to the ears (#128), pain in thethroat when moving the head (#133)
Others Dissatisfaction with being a patient* (#24), feeling generally unwell (#27), musclediscomfort (#39), joint pain (#42), headache (#52), dizziness (#67), pruritus (#88), neckstiffness (#108)
The overall patient=expert relevance rank (the most relevant ranked as #1) of each issue is presented in parenthesis. Thus, issues withoverall patient=expert relevance rank numbered higher than 75 were only relevant to subsets of patients.
*Added to the list by patients.
650 WATT ET AL.
Page 78 of 107
Appendix 4: Paper II
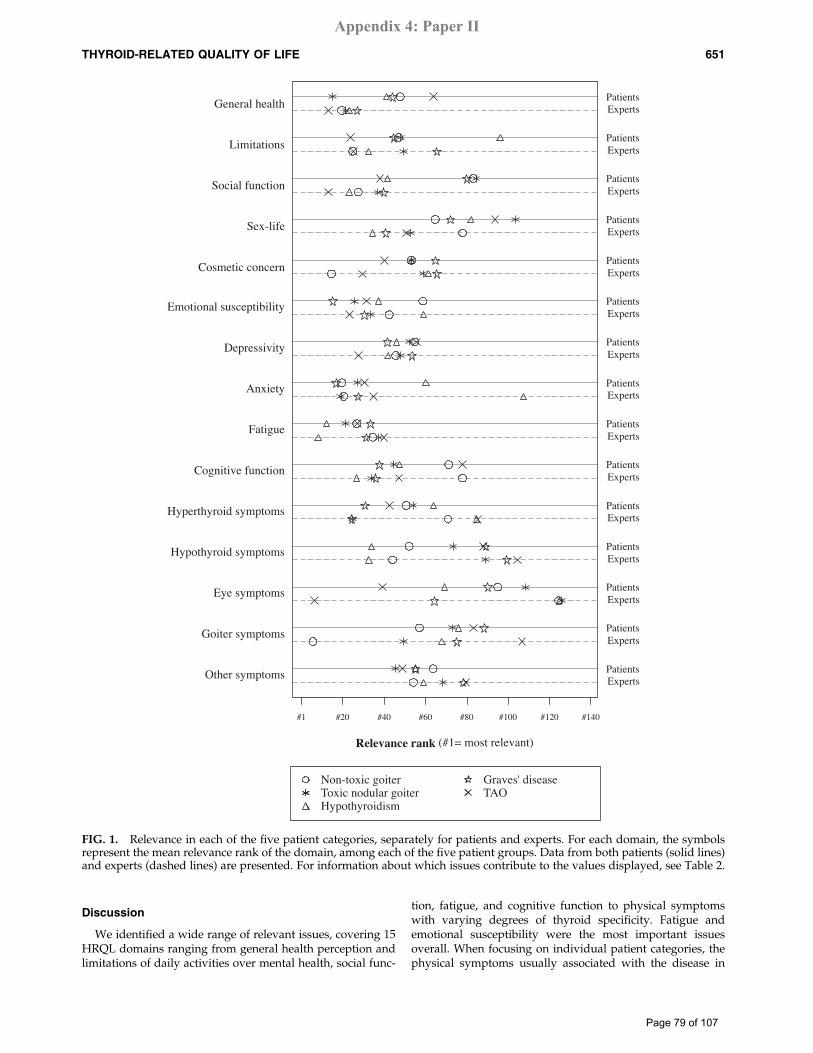
Discussion
We identified a wide range of relevant issues, covering 15HRQL domains ranging from general health perception andlimitations of daily activities over mental health, social func-
tion, fatigue, and cognitive function to physical symptomswith varying degrees of thyroid specificity. Fatigue andemotional susceptibility were the most important issuesoverall. When focusing on individual patient categories, thephysical symptoms usually associated with the disease in
Non-toxic goiter Graves' diseaseToxic nodular goiter TAOHypothyroidism
Other symptoms
Goiter symptoms
Eye symptoms
Hypothyroid symptoms
Hyperthyroid symptoms
Cognitive function
Fatigue
Anxiety
Depressivity
Emotional susceptibility
Cosmetic concern
Sex-life
Social function
Limitations
General health
Relevance rank (#1= most relevant)
#1 #20 #40 #60 #80 #100 #120 #140
ExpertsPatients
ExpertsPatients
ExpertsPatients
ExpertsPatients
ExpertsPatients
ExpertsPatients
ExpertsPatients
ExpertsPatients
ExpertsPatients
ExpertsPatients
ExpertsPatients
ExpertsPatients
ExpertsPatients
ExpertsPatients
ExpertsPatients
FIG. 1. Relevance in each of the five patient categories, separately for patients and experts. For each domain, the symbolsrepresent the mean relevance rank of the domain, among each of the five patient groups. Data from both patients (solid lines)and experts (dashed lines) are presented. For information about which issues contribute to the values displayed, see Table 2.
THYROID-RELATED QUALITY OF LIFE 651
Page 79 of 107
Appendix 4: Paper II
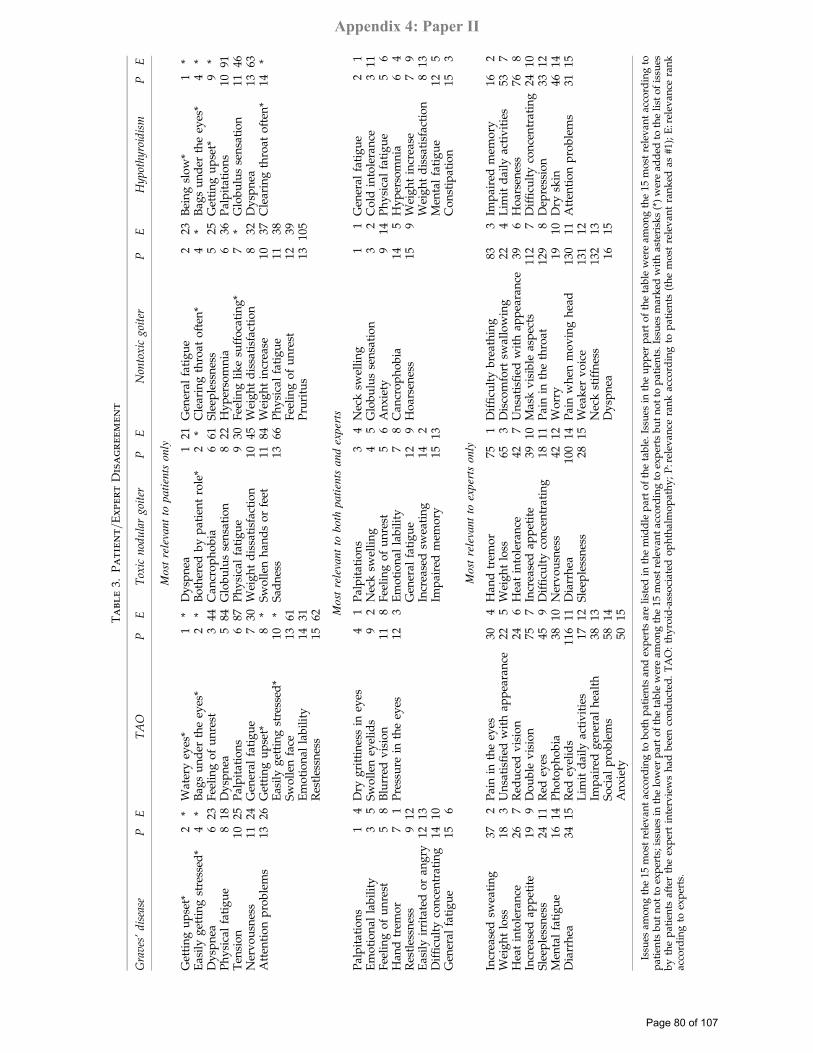
Ta
bl
e3.
Pa
tie
nt=
Exper
tD
isa
gr
eem
en
t
Graves’disease
PE
TAO
PE
Toxic
nodulargoiter
PE
Nontoxic
goiter
PE
Hypothyroidism
PE
Mostrelevantto
patients
only
Get
tin
gu
pse
t*2
*W
ater
yey
es*
1*
Dy
spn
ea1
21G
ener
alfa
tig
ue
223
Bei
ng
slo
w*
1*
Eas
ily
get
tin
gst
ress
ed*
4*
Bag
su
nd
erth
eey
es*
2*
Bo
ther
edb
yp
atie
nt
role
*2
*C
lear
ing
thro
ato
ften
*4
*B
ags
un
der
the
eyes
*4
*D
ysp
nea
623
Fee
lin
go
fu
nre
st3
44C
ancr
op
ho
bia
661
Sle
eple
ssn
ess
525
Get
tin
gu
pse
t*9
*P
hy
sica
lfa
tig
ue
818
Dy
spn
ea5
84G
lob
ulu
sse
nsa
tio
n8
22H
yp
erso
mn
ia6
36P
alp
itat
ion
s10
91T
ensi
on
1025
Pal
pit
atio
ns
687
Ph
ysi
cal
fati
gu
e9
30F
eeli
ng
lik
esu
ffo
cati
ng
*7
*G
lob
ulu
sse
nsa
tio
n11
46N
erv
ou
snes
s11
24G
ener
alfa
tig
ue
730
Wei
gh
td
issa
tisf
acti
on
1045
Wei
gh
td
issa
tisf
acti
on
832
Dy
spn
ea13
63A
tten
tio
np
rob
lem
s13
26G
etti
ng
up
set*
8*
Sw
oll
enh
and
so
rfe
et11
84W
eig
ht
incr
ease
1037
Cle
arin
gth
roat
oft
en*
14*
Eas
ily
get
tin
gst
ress
ed*
10*
Sad
nes
s13
66P
hy
sica
lfa
tig
ue
1138
Sw
oll
enfa
ce13
61F
eeli
ng
of
un
rest
1239
Em
oti
on
alla
bil
ity
1431
Pru
ritu
s13
105
Res
tles
snes
s15
62 Mostrelevantto
both
patients
andexperts
Pal
pit
atio
ns
14
Dry
gri
ttin
ess
iney
es4
1P
alp
itat
ion
s3
4N
eck
swel
lin
g1
1G
ener
alfa
tig
ue
21
Em
oti
on
alla
bil
ity
35
Sw
oll
eney
elid
s9
2N
eck
swel
lin
g4
5G
lob
ulu
sse
nsa
tio
n3
2C
old
into
lera
nce
311
Fee
lin
go
fu
nre
st5
8B
lurr
edv
isio
n11
8F
eeli
ng
of
un
rest
56
An
xie
ty9
14P
hy
sica
lfa
tig
ue
56
Han
dtr
emo
r7
1P
ress
ure
inth
eey
es12
3E
mo
tio
nal
lab
ilit
y7
8C
ancr
op
ho
bia
145
Hy
per
som
nia
64
Res
tles
snes
s9
12G
ener
alfa
tig
ue
129
Ho
arse
nes
s15
9W
eig
ht
incr
ease
79
Eas
ily
irri
tate
do
ran
gry
1213
Incr
ease
dsw
eati
ng
142
Wei
gh
td
issa
tisf
acti
on
813
Dif
ficu
lty
con
cen
trat
ing
1410
Imp
aire
dm
emo
ry15
13M
enta
lfa
tig
ue
125
Gen
eral
fati
gu
e15
6C
on
stip
atio
n15
3
Mostrelevantto
expertsonly
Incr
ease
dsw
eati
ng
372
Pai
nin
the
eyes
304
Han
dtr
emo
r75
1D
iffi
cult
yb
reat
hin
g83
3Im
pai
red
mem
ory
162
Wei
gh
tlo
ss18
3U
nsa
tisfi
edw
ith
app
eara
nce
225
Wei
gh
tlo
ss65
3D
isco
mfo
rtsw
allo
win
g22
4L
imit
dai
lyac
tiv
itie
s53
7H
eat
into
lera
nce
267
Red
uce
dv
isio
n24
6H
eat
into
lera
nce
427
Un
sati
sfied
wit
hap
pea
ran
ce39
6H
oar
sen
ess
768
Incr
ease
dap
pet
ite
199
Do
ub
lev
isio
n75
7In
crea
sed
app
etit
e39
10M
ask
vis
ible
asp
ects
112
7D
iffi
cult
yco
nce
ntr
atin
g24
10S
leep
less
nes
s24
11R
edey
es45
9D
iffi
cult
yco
nce
ntr
atin
g18
11P
ain
inth
eth
roat
129
8D
epre
ssio
n33
12M
enta
lfa
tig
ue
1614
Ph
oto
ph
ob
ia38
10N
erv
ou
snes
s42
12W
orr
y19
10D
rysk
in46
14D
iarr
hea
3415
Red
eyel
ids
116
11D
iarr
hea
100
14P
ain
wh
enm
ov
ing
hea
d13
011
Att
enti
on
pro
ble
ms
3115
Lim
itd
aily
acti
vit
ies
1712
Sle
eple
ssn
ess
2815
Wea
ker
vo
ice
131
12Im
pai
red
gen
eral
hea
lth
3813
Nec
kst
iffn
ess
132
13S
oci
alp
rob
lem
s58
14D
ysp
nea
1615
An
xie
ty50
15
Issu
esam
on
gth
e15
mo
stre
lev
ant
acco
rdin
gto
bo
thp
atie
nts
and
exp
erts
are
list
edin
the
mid
dle
par
to
fth
eta
ble
.Is
sues
inth
eu
pp
erp
art
of
the
tab
lew
ere
amo
ng
the
15m
ost
rele
van
tac
cord
ing
top
atie
nts
bu
tn
ot
toex
per
ts;
issu
esin
the
low
erp
art
of
the
tab
lew
ere
amo
ng
the
15m
ost
rele
van
tac
cord
ing
toex
per
tsb
ut
no
tto
pat
ien
ts.
Issu
esm
ark
edw
ith
aste
risk
s(*
)w
ere
add
edto
the
list
of
issu
esb
yth
ep
atie
nts
afte
rth
eex
per
tin
terv
iew
sh
adb
een
con
du
cted
.T
AO
:th
yro
id-a
sso
ciat
edo
ph
thal
mo
pat
hy
;P
:rel
evan
cera
nk
acco
rdin
gto
pat
ien
ts(t
he
mo
stre
lev
ant
ran
ked
as#1
);E
:rel
evan
cera
nk
acco
rdin
gto
exp
erts
.
Page 80 of 107
Appendix 4: Paper II

question were very important to patients belonging to thatcategory (e.g., hyperthyroid symptoms were important topatients with a diagnosis of hyperthyroidism). The data pre-sented here offer novel and clinically very important insightsinto the perceived impact of a broad spectrum of thyroid dis-eases on the QoL of the patients. Based on patients describingthe frequency as well as the importance of encountered prob-lems and experts rating relevance, a picture of potential im-pairment in central aspects of QoL, such as fatigue, mentalhealth, and social function, as well as a wide range of physicalsymptoms, is drawn. Such data are fundamental to the de-velopment of new HRQL questionnaires for thyroid patients.Without empirical evidence about what is relevant to the pa-tients, content validity of an HRQL instrument cannot be en-sured. The results can also serve as a basis for the selection ofthe best suited of the available standard, generic measures ofHRQL, such as SF-36, EQ-5D, or WHOQOL, when planningclinical studies involving thyroid patients.
Our comparison of the patient versus the expert perspectiveon relevance revealed a characteristic pattern. While the ex-perts focused on problems characteristic for the disease inquestion, the patients considered broader, nonspecific, psy-chological aspects of HRQL as more relevant. The differentperspectives held by patients and experts contribute comple-mentary information about which aspects are relevant, whenattempting to measure the QoL of thyroid patients. Thus,while patients reported on psychosocial issues and how theirdisease impacts their lives in general, experts seemed to bemore specifically concerned with what their thyroid patientsreport, in contrast to patients with other diseases. This stressesthe benefit of a ‘‘dual input’’ approach to content validitystudies when developing a disease-specific HRQL question-naire. The results might also caution that endocrinologists mayneed to broaden their view on the thyroid-related problemsfaced by their patients.
A challenge for this project has been the intention to de-velop a comprehensive questionnaire applicable to studies ofseveral thyroid phenotypes. Here, we have presented andapplied a method for the selection of issues to ensure contentvalidity across a number of patient populations. Several as-pects of this approach could be discussed. First, we askedabout problems encountered during the whole disease pe-riod (which for some patients spanned over several decades),which may have imposed recall bias on our results. How-ever, this strategy was used in order to increase effectivenessof the interviews—much more information could be pro-vided by each patient—and to prevent that the timing of theinterviews leads to omission of important problems experi-enced at an earlier point in time. Second, patient and expertrelevance ranks took into account both frequency and im-portance (in terms of impact on QoL) of the issues. The ex-perts were specifically instructed to do so, whereas thepatient relevance ranks were constructed by multiplying thefrequencies with the mean importance ratings. The reason forthis difference was that an overall judgment incorporatingexperiences from many patients was considered mostmeaningful for clinicians, whereas for patients it is obviouslymeaningless to evaluate the relevance of problems they donot have; therefore, separate assessment of presence andrelevance was made. This approach means that seldom butdistressing issues may be selected at the expense of commonbut unimportant issues. For example, in patients with hypo-
thyroidism, depression and coarse skin were experienced bythe same proportion of patients, but depression had a farhigher relevance rank due to its much larger impact on QoL.Similarly, red eyelids had higher importance rating than fa-tigue, but a much lower impact rank, because red eyelids wasonly experienced by one patient, whereas fatigue was presentin the majority of patients. Thus, we consider the applied ap-proach optimal for the purpose of selecting the most relevantissues to be included in a future QoL questionnaire. Third, webelieve that the strategy with primary weight on the combinedpatient–expert rank in all patient groups, but nonexclusion ofissues of very high importance to individual patient groups,was a major advantage of our method. However, the cutoffvalues as regards definition of the most relevant issues—the 75most relevant overall or being rated among the 15 most rele-vant to individual groups—were arbitrarily set. This proce-dure included around two thirds of the total number of issues(92 out of 148). This is a rather fine-meshed selection, but thepurpose was to allow for a sufficient number to be submittedto further selection procedures (based on analyses of largepatient samples), without imposing too large response bur-dens on the patients of such future studies.
Another topic for discussion could be that we includedonly patients from two secondary and tertiary referral units.However, since the purpose of content validity studies is toensure that potentially relevant issues are not ignored, in-clusion of patients from the presumably more diseased partof the spectrum is preferable, as it is unlikely that less se-verely ill patients experience symptoms which the more se-verely ill patients do not.
Compared to the recommendations in the HRQL field andto similar studies from other disease entities, our number ofexperts and patients is very high; 10 to 15 is generally the rule(15,32). However, in light of the heterogeneity of thyroid pa-tients, we found that this was recommendable for these pa-tients.
An advantage of the present study is that each patient wasinterviewed using both semistructured and structured tech-niques. This provided an initial, unguided, unprobed narra-tion of the way the patients had been impacted by theirdisease, as well as a structured evaluation of all previouslyidentified possible problems associated with thyroid disor-ders. Moreover, the patients were clinically well described,and we included both newly diagnosed, untreated patientsand patients with long-standing illness treated in variousways. The latter increases the range of populations and ap-plication for which a HRQL questionnaire developed on thisground has content validity. Additionally, combining inputfrom both patients and experts yielded direct evidence fromthe patients themselves and also cumulative information fromall the patients seen during the many years of experience by theparticipating endocrinologists.
One direction for future studies, as is indeed our intention, isto develop a questionnaire covering the aspects found in thisstudy and to validate it quantitatively using data from largerepresentative samples of clinically well-described thyroidpatients. This would involve construction of scales measuringthe domains identified in the present study, scale validation,evaluation of sensitivity and responsiveness to change, and toevaluate the relation between these scales and other clinicallyrelevant measures, such as thyroid function tests and thyroidimaging techniques.
THYROID-RELATED QUALITY OF LIFE 653
Page 81 of 107
Appendix 4: Paper II
Acknowledgments
We wish to express our gratitude to the patients and col-leagues, who took their time to participate in the interviews.This study was supported by grants from the Danish Med-ical Research Council, Agnes and Knut Mørk’s Foundation,Aase and Ejnar Danielsen’s Foundation, Else and MogensWedell-Wedellsborg’s Foundation, the Genzyme Corpora-tion, the Novo Nordisk Foundation, and the Danish ThyroidFoundation.
References
1. Ladenson PW 2002 Psychological well-being in patients.Clin Endocrinol (Oxf ) 57:575–576.
2. Abraham P, Avenell A, Watson WA, Park CM, Bevan JS2004 Antithyroid drug regimen for treating Graves’ hyper-thyroidism (Cochrane Review). The Cochrane Library, issue 3.John Wiley & Sons, Chichester, UK.
3. Romijn JA, Smit JW, Lamberts SW 2003 Intrinsic imperfectionsof endocrine replacement therapy. Eur J Endocrinol 149:91–97.
4. Terwee C, Wakelkamp I, Tan S, Dekker F, Prummel MF,Wiersinga W 2002 Long-term effects of Graves’ ophthalmo-pathy on health-related quality of life. Eur J Endocrinol146:751–757.
5. Elberling TV, Rasmussen AK, Feldt-Rasmussen U, HordingM, Perrild H, Waldemar G 2004 Impaired health-relatedquality of life in Graves’ disease. A prospective study. Eur JEndocrinol 151:549–555.
6. McMillan CV, Bradley C, Woodcock A, Razvi S, Weaver JU2004 Design of new questionnaires to measure quality of lifeand treatment satisfaction in hypothyroidism. Thyroid 14:
916–925.7. Bianchi GP, Zaccheroni V, Solaroli E, Vescini F, Cerutti R,
Zoli M, Marchesini G 2004 Health-related quality of life inpatients with thyroid disorders. Qual Life Res 13:45–54.
8. Abraham-Nordling M, Torring O, Hamberger B, Lundell G,Tallstedt L, Calissendorff J, Wallin G 2005 Graves’ disease: along-term quality-of-life follow up of patients randomized totreatment with antithyroid drugs, radioiodine, or surgery.Thyroid 15:1279–1286.
9. Kahaly GJ, Petrak F, Hardt J, Pitz S, Egle UT 2005 Psycho-social morbidity of Graves’ orbitopathy. Clin Endocrinol(Oxf ) 63:395–402.
10. Gulseren S, Gulseren L, Hekimsoy Z, Cetinay P, Ozen C,Tokatlioglu B 2006 Depression, anxiety, health-related qualityof life, and disability in patients with overt and subclinicalthyroid dysfunction. Arch Med Res 37:133–139.
11. Watt T, Groenvold M, Rasmussen AK, Bonnema SJ, Hege-dus L, Bjorner JB, Feldt-Rasmussen U 2006 Quality of life inpatients with benign thyroid disorders. A review. Eur JEndocrinol 154:501–510.
12. U.S. Food and Drug Administration 2006 Guidance for In-dustry. Patient-Reported Outcome Measures: Use in MedicalProduct Development to Support Labeling Claims. http://www.fda.gov/cder/guidance/5460dft.pdf
13. Fayers PM, Machin D 2000 Quality of Life: Assessment, Anal-ysis and Interpretation. John Wiley & Sons, Chichester, UK.
14. Terwee CB, Bot SD, de Boer MR, van der Windt DA, KnolDL, Dekker J, Bouter LM, de Vet HC 2007 Quality criteriawere proposed for measurement properties of health statusquestionnaires. J Clin Epidemiol 60:34–42.
15. Sprangers MA, Cull A, Bjordal K, Groenvold M, AaronsonNK 1993 The European Organization for Research and
Treatment of Cancer. Approach to quality of life assessment:guidelines for developing questionnaire modules. EORTCstudy group on quality of life. Qual Life Res 2:287–295.
16. Streiner DL, Norman GR 1995 Health Measurement Scales:A Practical Guide to Their Development and Use, 2nd edi-tion. Oxford University Press, Oxford.
17. McColl E 2005 Developing questionnaires. In: Fayers P,Hays RD (eds) Assessing Quality of Life in Clinical Trials,2nd edition. Oxford University Press, Oxford, pp 9–23.
18. Willis G 2005 Cognitive Interviewing: A Tool for ImprovingQuestionnaire Design. Sage publications, California.
19. Jobe JB 2003 Cognitive psychology and self-reports: modelsand methods. Qual Life Res 12:219–227.
20. Jaeschke R, Guyatt G, Cook D, Harper S, Gerstein HC 1994Spectrum of quality of life impairment in hypothyroidism.Qual Life Res 3:323–327.
21. Groenvold M 1997 Quality of life in breast cancer adjuvanttherapy: validation and pilot testing of a combination ofquestionnaires. Breast 6:97–107.
22. Braverman LE, Utiger RD (eds) 2005 Werner and Ingbar’sthe Thyroid: A Fundamental and Clinical Text, 9th edition.Lippincott Williams & Wilkins, New York.
23. DeGroot LJ, Jameson JL (eds) 2006 Endocrinology, 5th edi-tion. Elsevier Saunders, Philadelphia.
24. Ware JE Jr., Sherbourne CD 1992 The MOS 36-item short-form health survey (SF-36). I. Conceptual framework anditem selection. Med Care 30:473–483.
25. Ware JE Jr. 2003 Conceptualization and measurement ofhealth-related quality of life: comments on an evolving field.Arch Phys Med Rehabil 84:S43–S51.
26. Stewart AL, Ware JE Jr. 1992 Measuring Functionning andWell-Being: The Medical Outcomes Study Approach. DukeUniversity Press, London.
27. Dalakas MC, Mock V, Hawkins MJ 1998 Fatigue: definitions,mechanisms, and paradigms for study. Semin Oncol 25:
48–53.28. Glaus A, Crow R, Hammond S 1996 A qualitative study to
explore the concept of fatigue=tiredness in cancer patientsand in healthy individuals. Eur J Cancer Care (Engl) 5:8–23.
29. Ream E, Richardson A 1996 Fatigue: a concept analysis. Int JNurs Stud 33:519–529.
30. Russell RD 1973 Social health: an attempt to clarify this di-mension of well-being. Int J Health Educ 16:74–82.
31. McDowell I, Newell C 1996 Social health. In: McDowell I,Newell C (eds) Measuring Health. Oxford University Press,New York, pp 122–176.
32. Webb SM, Prieto L, Badia X, Albareda M, Catala M, Gaz-tambide S, Lucas T, Paramo C, Pico A, Lucas A, Halperin I,Obiols G, Astorga R 2002 Acromegaly Quality of Life Ques-tionnaire (ACROQOL) a new health-related quality of lifequestionnaire for patients with acromegaly: developmentand psychometric properties. Clin Endocrinol (Oxf ) 57:251–258.
Address reprint requests to:Torquil Watt, M.D.
Department of Endocrinology 2131RigshospitaletBlegdamsvej 9
DK-2100, Copenhagen ØDenmark
E-mail: [email protected]
654 WATT ET AL.
Page 82 of 107
Appendix 4: Paper II

Improving a newly developed patient-reported outcomefor thyroid patients, using cognitive interviewing
Torquil Watt Æ Ase Krogh Rasmussen Æ Mogens Groenvold Æ Jakob Bue Bjorner ÆSara Hope Watt Æ Steen Joop Bonnema Æ Laszlo Hegedus Æ Ulla Feldt-Rasmussen
Accepted: 22 May 2008
� Springer Science+Business Media B.V. 2008
Abstract Objective To improve a newly developed
patient-reported outcome measure for thyroid patients
using cognitive interviewing.
Methods Thirty-one interviews using immediate retro-
spective and expansive probing were conducted among
patients with non-toxic goiter (n = 4), nodular toxic goiter
(n = 5) Graves’ disease (n = 6), thyroid eye-disease
(n = 6), and primary hypothyroidism (n = 10). The ques-
tionnaire was revised successively. Six iterative rounds of
interviews were conducted. Identified problems were cate-
gorized according to Tourangeau’s four-stage model.
Results Problems were identified 126 times in 43 of the
99 tested items, four of the 15 introductions, and four of the
five response categories. Fifty-four problems involved
comprehension, one retrieval, 23 judgment, 28 response,
and 20 were not applicable to the four-stage model. Among
all problems identified, 18 concerned attribution, i.e.
whether or not to report only issues considered of thyroid
causality. Within each round of interviews, the number of
problems declined from an initial average of six per
interview to two, mainly due to a reduction in the number
of problems associated with comprehension. The least
amount of reduction was within the set of problems
involving attribution.
Conclusion The cognitive interview methodology was
effective in identifying and reducing problems within the
questionnaire responding process. Patients tended to selec-
tively report problems they considered to be caused by their
thyroid disease even when specifically instructed not to.
Keywords Cognitive interviews �Patient-reported outcomes � Quality of life �Questionnaire development � Thyroid disease
Introduction
Cognitive interviewing is a methodology based on the
interdisciplinary field termed cognitive aspects of survey
methodology (CASM), initiated in the 1980s, which
involves theories and results from studies on the cognitive
processes involved in survey responding. A basic model in
CASM was formulated by Tourangeau et al. [1] in which the
response process is divided into four components [2]: com-
prehension (attend to questions and instructions, represent
logical form of question, identify question focus, link key
terms to relevant concepts); retrieval (generate retrieval
strategy and cues, retrieve specific/generic memories, fill in
missing details); judgment (assess completeness and rele-
vance of memories, draw inferences based on accessibility,
T. Watt (&) � A. K. Rasmussen � S. H. Watt �U. Feldt-Rasmussen
Department of Endocrinology, Copenhagen University Hospital
Rigshospitalet, Blegdamsvej 9, 2100 Copenhagen Ø, Denmark
e-mail: [email protected]; [email protected]
T. Watt � M. Groenvold
Institute of Public Health, University of Copenhagen,
Copenhagen, Denmark
M. Groenvold
Department of Palliative Medicine, Bispebjerg Hospital,
Copenhagen, Denmark
J. B. Bjorner
National Research Centre for the Working Environment,
Copenhagen, Denmark
S. J. Bonnema � L. Hegedus
Department of Endocrinology and Metabolism, Odense
University Hospital, Odense, Denmark
123
Qual Life Res
DOI 10.1007/s11136-008-9364-z
Page 83 of 107
Appendix 5: Paper III

integrate material retrieved, estimate based on partial
retrieval); response (map judgment onto response category,
edit response)
By providing insight into various components of the
response process, cognitive interviewing has a potential for
improving the scientific quality of patient-reported out-
comes [3, 4]. Two different interview approaches can be
applied: think-aloud, where the respondents vocalize all
their thoughts while completing the questionnaire and the
interviewer listens, and verbal probing, where the inter-
viewer asks questions about the processes going on while
the respondents are completing the questionnaire. Think-
aloud is rather demanding for the interviewee, and analysis
and data presentation is time-consuming. Verbal probing
can be classified into concurrent and retrospective probing.
In concurrent probing, the verbal probes are asked imme-
diately after the question to be probed, and in retrospective
probing, the probes are asked after the entire interview.
Concurrent probing minimizes the risk that respondents
forget what was going on when answering a question, but it
has the disadvantage of interrupting the response-process,
with the risk of overlooking context effects; in addition,
such a switching between tasks can be distracting, and it
may affect the response to subsequent items. Retrospective
probing allows the usual flow of an interview but carries a
greater risk of recall bias and hindsight effects.
Cognitive interview techniques were developed mainly
for face-to-face interviews [1, 5]. With self-administered
questionnaires, the administration of the questionnaire and
the interview uses two different modes of communication,
which makes the interruption of the survey logic by con-
current probing even larger. A retrospective approach may
therefore be preferable [6].
Few studies applying this method have been published
within health-related quality of life research [7]. However,
the emphasis laid on these methods in the Food and Drug
Administration (FDA) draft guidance for industry regard-
ing their use of patient-reported outcomes will probably
lead to an increased focus on this methodology [8].
Thyroid diseases are common and occur among persons
of all ages, predominantly in women. They comprise thy-
roid swelling (goiter, nodules) and dysfunction of the gland
(hypo- or hyperthyroidism), often in conjunction. The
importance of involving HRQL-aspects in the evaluation of
thyroid patients is becoming increasingly recognized [9–
11]. The motivation behind such research is well placed
since benign thyroid disorders are common and rarely life-
threatening and, therefore, their treatment mainly deals
with optimizing the quality of life of the patients who can
be treated by drug therapies, such as thyroid or antithyroid
drugs, radioiodine, surgery, among other approaches. Sur-
prisingly, only few studies evaluating HRQL in thyroid
patients have been published [12–19], and a validated
disease-specific HRQL-measure is only available for
patients with thyroid eye-disease [20].
This absence of data in this area provided our group with
the motivation to develop a new, thyroid-specific HRQL-
measure in Danish and six other languages [21, 22]. The
study reported here concerns the original Danish version of
the questionnaire. Our aim was to improve the draft version
of this questionnaire by investigating patients’ responses to
it, using cognitive interviews. To do this, we sought to
adapt the cognitive interview methodology to better fit
patient self-assessment.
Material and methods
Patients
Thirty-one thyroid patients, without major non-thyroidal
comorbidity, in two Danish University hospital outpatient
clinics (Copenhagen University Hospital Rigshospitalet
and Odense University Hospital) were interviewed. The
interviews lasted 1–1.5 h and were carried out by two
research team members (one experienced and one exten-
sively trained within the project by receiving theoretical
and practical education, attending interviews, and direct
and subsequently indirect supervision) the day the patients
were seen in the outpatient clinic. The patients were
selected by a non-random strategic sampling procedure [2,
23], which aimed at maximizing the patient variation in
terms of diagnoses, treatment, disease duration (including
both newly diagnosed, treated, and untreated patients), and
age (Table 1). Clinical data were obtained from medical
records. Diagnoses were based on clinical examination,
thyroid function variables, thyroid autoantibodies, thyroid
scintigraphy, and ultrasonography. Biochemical analyses
were performed using the standard methods of the partic-
ipating centers, and the reference ranges of the local
laboratories were used. The patients included in the study
comprised four patients with non-toxic goiter, five with
nodular toxic goiter, six with Graves’ disease without eye
involvement, six with thyroid associated ophthalmopathy
(TAO), and ten patients with primary hypothyroidism.
ThyQoL questionnaire
The questionnaire being tested in this study, the ThyQoL
questionnaire, is aimed at patients with any benign thyroid
disorder, since thyroid disorders are linked together: some
diagnoses may co-exist (goiter and hyperthyroidism), and
the treatment of one disorder (e.g. hyperthyroidism) may
lead to another disorder (hypothyroidism). The question-
naire was constructed to cover thyroid-relevant HRQL-
issues identified through a literature review [21] as well as
Qual Life Res
123
Page 84 of 107
Appendix 5: Paper III

through expert- and patient interviews [22], using methods
for questionnaire wording and formatting developed within
a cognitive framework [24]. The draft questionnaire was
evaluated by a multidisciplinary panel of experts within the
fields of social science, medicine, linguistics, and
psychology. The version undergoing cognitive testing
consisted of 99 items covering 11 domains: symptoms (38
items), fatigue (seven items), cognition (six items), anxiety
(six items), mental well-being (nine items), emotional
susceptibility (nine items), social function (six items), daily
activities (six items), sex life (two items), appearance
(seven items), and overall quality of life (three items).
Six of the domains were physical and mental symptoms
or states (symptoms, fatigue, cognition, anxiety, mental
well-being, and emotional susceptibility) and were asked
non-attributed, i.e. respondents were requested to rate the
amount (the size of the problem), regardless of whether they
thought it was due to their thyroid disease or not. Five
domains dealt with the impact of the disease on various
aspects of life and were thus asked attributed, i.e. the
respondents were requested to rate the impact of their thy-
roid disease on that domain: social function, daily activities,
sex life, appearance, and overall quality of life. This was
specified in the questionnaire: the first part was asked non-
attributed (e.g. ‘‘During the past 4 weeks, have you been
tired?’’), and the last part was asked with attribution (e.g.
‘‘During the past 4 weeks, has your thyroid disease caused
you to have difficulty managing your daily life?’’).
Seven domains were thyroid-targeted: symptoms of
thyroid disease (subdivided into symptoms of goitre,
hyperthyroidism, hypothyroidism, and thyroid eye com-
plaints), emotional susceptibility (identified through
qualitative analysis of previous interviews [22]), social
function, daily activities, sex life, appearance, and overall
quality of life—the latter five by means of attribution. The
remaining domains (fatigue, cognition, anxiety, and mental
well-being) are not explicitly thyroid-targeted content but
were included in the questionnaire because they have been
rated as highly relevant to thyroid patients [22].
A 4-week recall period was chosen on clinical grounds,
because the symptomatology of thyroid diseases often
fluctuates over days or weeks, and thus the use of a shorter
recall period would risk not capturing a relevant impact on
the patients HRQL.
Interviews
We adopted a modified probing technique for self-admin-
istered questionnaires, denoted immediate retrospective
probing: we identified natural ‘‘breaking points’’ in the
questionnaire (e.g., a change in topic, end of a page) where
our verbal probes could be administered. Thus, the
respondent would self-complete a section of the question-
naire until he/she reached a ‘‘breaking point’’, where the
interviewer would conduct a cognitive interview covering
that section. The respondent would then self-complete the
next section until another ‘‘breaking point’’ was reached,
and the process would be continued until the questionnaire
was completed.
A detailed description of the intended content of each of
the 99 items was developed in order to provide a clear and
predefined basis for identifying misfits between the inten-
ded content and patient understanding revealed through
interviews.
The interview consisted of 109 verbal probes, 57 spe-
cific, and 52 non-specific [23]. The non-specific probes
consisted of five probes administered after the completion
of each of the 11 pages and covered the four cognitive
processes in the four-stage model [1, 2]: ‘‘Did you have
difficulty understanding anything on this page’’? ‘‘Were
there any questions you had difficulty answering’’? ‘‘Did
you wonder about anything’’?, and ‘‘Do you think the
response options fit the questions’’? The specific probes
were developed to cover specific potential problems iden-
tified using the question appraisal system (QAS99)
developed by Willis et al. (described in [23]), which is a
system aimed at identifying potential problems in ques-
tionnaires, including problems within the Tourangeau
Table 1 Clinical characteristics of the patients
Clinical characteristics Values
Number of patients 31
Men/women 2/29
Age, median in years (range) 53 (26–76)
Diagnosis, n (%)
Graves’ disease 6 (19)
Thyroid associated ophthalmopathy 6 (19)
Toxic nodular goiter 5 (16)
Non-toxic goiter 4 (13)
Autoimmune hypothyroidism 10 (32)
Months since diagnosis, median (range) 23 (0–606)
Diagnosis of mild thyroid dysfunctiona, n (%) 6 (19)
Untreated, n (%) 4 (13)
Thyroid functionb at time of interview, n (%)
Euthyroid 18 (43)
Mildly hypothyroid 2 (6)
Overtly hypothyroid 0
Mildly hyperthyroid 5 (16)
Overtly hyperthyroid 4 (13)
a Serum thyroid stimulating hormone (TSH) outside the reference
range and without overt thyroid dysfunction at any timeb Euthyroid, Normal TSH; mildly hypothyroid, elevated TSH and
normal T4; overtly hypothyroid, elevated TSH and decreased T4;
mildly hyperthyroid, decreased TSH and normal T4 and T3; overtly
hyperthyroid, decreased TSH and elevated T4 and/or T3
Qual Life Res
123
Page 85 of 107
Appendix 5: Paper III
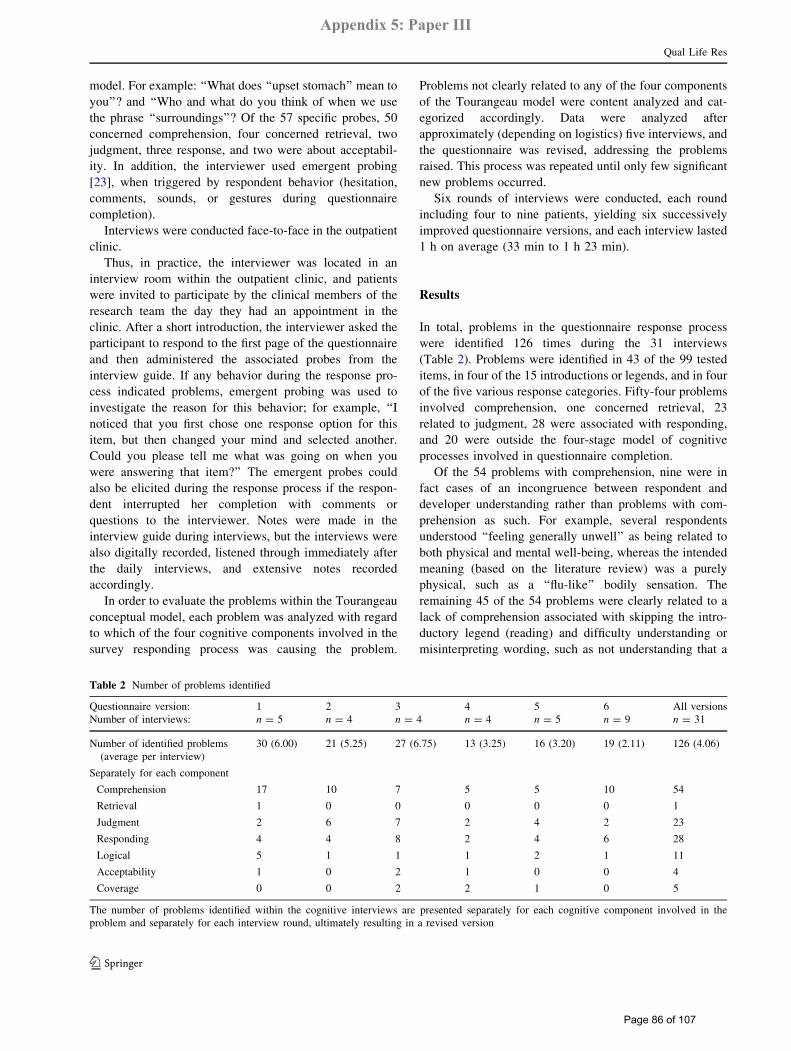
model. For example: ‘‘What does ‘‘upset stomach’’ mean to
you’’? and ‘‘Who and what do you think of when we use
the phrase ‘‘surroundings’’? Of the 57 specific probes, 50
concerned comprehension, four concerned retrieval, two
judgment, three response, and two were about acceptabil-
ity. In addition, the interviewer used emergent probing
[23], when triggered by respondent behavior (hesitation,
comments, sounds, or gestures during questionnaire
completion).
Interviews were conducted face-to-face in the outpatient
clinic.
Thus, in practice, the interviewer was located in an
interview room within the outpatient clinic, and patients
were invited to participate by the clinical members of the
research team the day they had an appointment in the
clinic. After a short introduction, the interviewer asked the
participant to respond to the first page of the questionnaire
and then administered the associated probes from the
interview guide. If any behavior during the response pro-
cess indicated problems, emergent probing was used to
investigate the reason for this behavior; for example, ‘‘I
noticed that you first chose one response option for this
item, but then changed your mind and selected another.
Could you please tell me what was going on when you
were answering that item?’’ The emergent probes could
also be elicited during the response process if the respon-
dent interrupted her completion with comments or
questions to the interviewer. Notes were made in the
interview guide during interviews, but the interviews were
also digitally recorded, listened through immediately after
the daily interviews, and extensive notes recorded
accordingly.
In order to evaluate the problems within the Tourangeau
conceptual model, each problem was analyzed with regard
to which of the four cognitive components involved in the
survey responding process was causing the problem.
Problems not clearly related to any of the four components
of the Tourangeau model were content analyzed and cat-
egorized accordingly. Data were analyzed after
approximately (depending on logistics) five interviews, and
the questionnaire was revised, addressing the problems
raised. This process was repeated until only few significant
new problems occurred.
Six rounds of interviews were conducted, each round
including four to nine patients, yielding six successively
improved questionnaire versions, and each interview lasted
1 h on average (33 min to 1 h 23 min).
Results
In total, problems in the questionnaire response process
were identified 126 times during the 31 interviews
(Table 2). Problems were identified in 43 of the 99 tested
items, in four of the 15 introductions or legends, and in four
of the five various response categories. Fifty-four problems
involved comprehension, one concerned retrieval, 23
related to judgment, 28 were associated with responding,
and 20 were outside the four-stage model of cognitive
processes involved in questionnaire completion.
Of the 54 problems with comprehension, nine were in
fact cases of an incongruence between respondent and
developer understanding rather than problems with com-
prehension as such. For example, several respondents
understood ‘‘feeling generally unwell’’ as being related to
both physical and mental well-being, whereas the intended
meaning (based on the literature review) was a purely
physical, such as a ‘‘flu-like’’ bodily sensation. The
remaining 45 of the 54 problems were clearly related to a
lack of comprehension associated with skipping the intro-
ductory legend (reading) and difficulty understanding or
misinterpreting wording, such as not understanding that a
Table 2 Number of problems identified
Questionnaire version: 1 2 3 4 5 6 All versions
Number of interviews: n = 5 n = 4 n = 4 n = 4 n = 5 n = 9 n = 31
Number of identified problems
(average per interview)
30 (6.00) 21 (5.25) 27 (6.75) 13 (3.25) 16 (3.20) 19 (2.11) 126 (4.06)
Separately for each component
Comprehension 17 10 7 5 5 10 54
Retrieval 1 0 0 0 0 0 1
Judgment 2 6 7 2 4 2 23
Responding 4 4 8 2 4 6 28
Logical 5 1 1 1 2 1 11
Acceptability 1 0 2 1 0 0 4
Coverage 0 0 2 2 1 0 5
The number of problems identified within the cognitive interviews are presented separately for each cognitive component involved in the
problem and separately for each interview round, ultimately resulting in a revised version
Qual Life Res
123
Page 86 of 107
Appendix 5: Paper III

question refers to the last 4 weeks or interpreting a ‘‘not
relevant’’-response category as meaning the ‘‘worst possi-
ble’’ response category.
One problem with retrieval was identified. This was a
patient with newly diagnosed hyperthyroidism who thought
that 4 weeks was a long time to relate to, given that the
symptoms were of a still unfamiliar disease. Most other
patients described no problems with this reference period,
and some would have preferred it to be even longer in order
to fully describe the impact of their disease.
Judgment was involved in 23 of the identified problems.
For example, one respondent was in doubt whether a
quivering in the eyelid was contained in ‘‘pressure in (or
behind) the eyes’’, and another respondent commented on
two items about heat- or cold-intolerance: ‘‘you’re always
somewhat sensitive to heat or cold. How about writing
‘‘extra sensitive’’ or something like that?’’. Eleven prob-
lems involving judgment were about attributional issues, as
described later.
Twenty-eight problems within the process of responding
were identified. Of these, seven were attributional (see
below). The rest were mainly concerned with the number
of response categories, with some individuals wanting
fewer options and others wanting more, confusion due to
alternating positively and negatively worded items, and
problems with a ‘‘not relevant/don’t know’’ category.
We also identified 20 problems outside the Tourangeau
model. Eleven of these were problems in the inherent logic
or structure of the questionnaire [23], such as implicit
assumptions (an item asking about difficulty learning pre-
supposed to having faced a learning task) or unclear
definitions of social network. Four problems were about
acceptability, of which two concerned the two items about
sex life: one was about the wording ‘‘managing your
feelings’’, and one found the introduction too persuasive.
Finally, five problems were about whether the question-
naire lacked coverage of specific issues experienced by the
patients.
A particular kind of problem was identified among 11 of
the problems within judgment and seven of the problems
within comprehension. These problems were categorized
as ‘‘attributional problems’’. They involved considerations
about whether the content of the question was causally
related to the thyroid disease or not and, consequently,
whether or not to report problems not considered being
caused by the thyroid disease. For example, one respondent
said ‘‘I have a question: right now, I have other symptoms,
which makes it difficult. Shall I answer according to the
(thyroid) disease or an overall judgment?’’ And another
one: ‘‘If I was sitting at home, I would probably answer
according to what has to do with my thyroid; much of it has
to do with my age’’. Finally: ‘‘All of it is about a particular
disease, so you have that in the back of your head’’. These
comments involved items that have specific instructions to
base the answers on an overall evaluation (as opposed to
focusing on thyroid disease).
Based on the problems identified in each round of
interviews, the questionnaire was revised, reducing the
number of problems per interview successively from ini-
tially six to two (Table 2). This was due mainly to a
reduction in the number of comprehension problems (from
three to one per interview) and logical problems (with
version 1, five problems were identified in five interviews;
with version 6, one problem was identified in nine inter-
views), whereas the number of problems within judgment
and responding (from six problems in five interviews to
eight problems in nine interviews) were more constant.
A total of 30 revisions were made in 22 of the 99 items
(Table 3). Twelve revisions were made in version 1, four in
version 2, three in version 3, two in version 4, and nine in
version 5. Within the 22 revised items, 67 problems iden-
tified in 281 interviews prior to the revision (number of
problems on the left hand side of the vertical double lines
in Table 3) were reduced to six problems in 365 interviews
after the revisions (on the right hand side of the last vertical
double line, Table 3). The problems termed attributional
problems, mentioned above, occurred consistently across
various versions of the questionnaire, despite three revi-
sions addressing this issue.
Discussion
Measured by the number of problems identified in succes-
sive versions of the questionnaire, cognitive interviewing
by applying immediate retrospective probing proved useful
for improving the wording and format of the questionnaire.
This technique, in association with questionnaire revisions
based on cognitive methodology, was very efficient in
reducing the number of problems occurring within the
comprehension and non-cognitive categories logical/struc-
tural problems and acceptability, and moderately efficient
in reducing problems within judgment and responding.
The four-stage model formulated by Tourangeau et al.
[1] covered most, but not all, of the problems identified
during the cognitive interview testing. This was mainly due
to the problems not being cognitive in nature, but rather
being logical or structural, as described by Willis et al. [6].
Most problems were within comprehension, which were
twice as frequent as problems with judgment and response.
This is very consistent with previous cognitive interview-
ing research that has used problem classification systems
[25–27]. In many instances, the patients were not aware of
their misunderstandings, which were only identified
through proactive probing and comparisons with the pre-
specified intended content of an item. These represent
Qual Life Res
123
Page 87 of 107
Appendix 5: Paper III
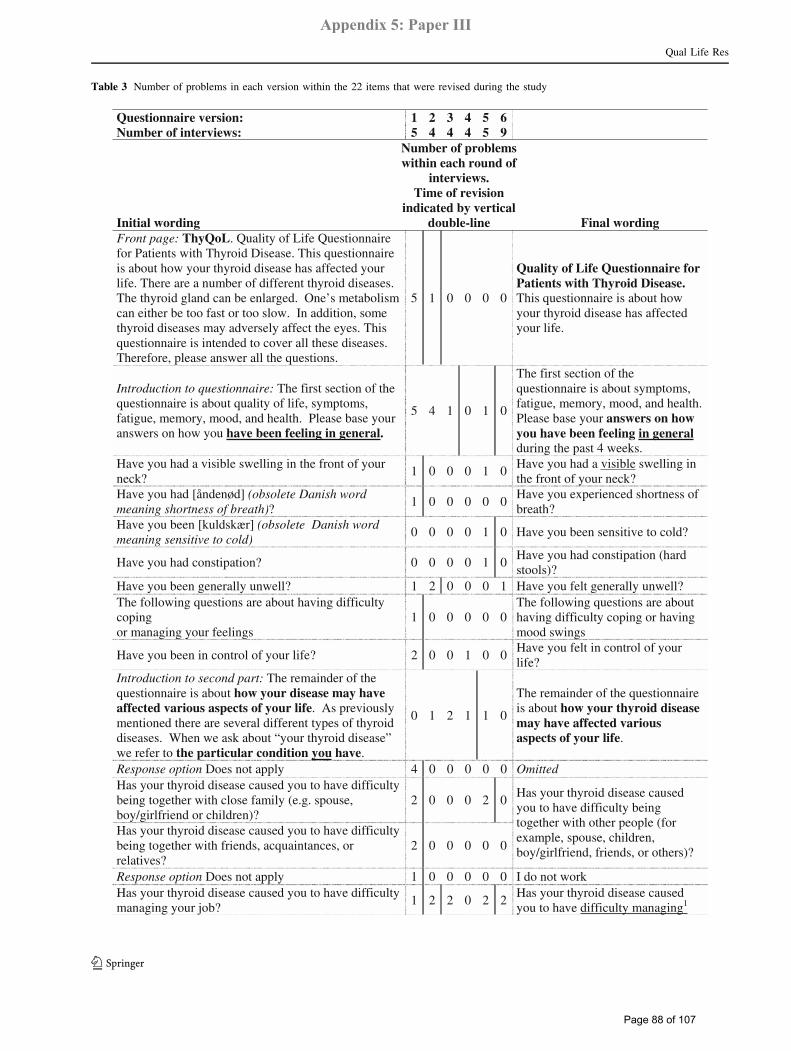
Table 3 Number of problems in each version within the 22 items that were revised during the study
65432 1 :noisrev eriannoitseuQ95444 5 :sweivretni fo rebmuN
Initial wording
Number of problems within each round of
interviews. Time of revision
indicated by vertical double-line Final wording
Front page: ThyQoL. Quality of Life Questionnaire for Patients with Thyroid Disease. This questionnaire is about how your thyroid disease has affected your life. There are a number of different thyroid diseases.The thyroid gland can be enlarged. One’s metabolism can either be too fast or too slow. In addition, some thyroid diseases may adversely affect the eyes. This questionnaire is intended to cover all these diseases. Therefore, please answer all the questions.
5 1 0 0 0 0
Quality of Life Questionnaire for Patients with Thyroid Disease. This questionnaire is about how your thyroid disease has affected your life.
Introduction to questionnaire: The first section of the questionnaire is about quality of life, symptoms, fatigue, memory, mood, and health. Please base your answers on how you have been feeling in general.
5 4 1 0 1 0
The first section of the questionnaire is about symptoms, fatigue, memory, mood, and health. Please base your answers on how you have been feeling in generalduring the past 4 weeks.
Have you had a visible swelling in the front of your neck?
1 0 0 0 1 0Have you had a visible swelling in the front of your neck?
Have you had [åndenød] (obsolete Danish word meaning shortness of breath)?
1 0 0 0 0 0Have you experienced shortness of breath?
Have you been [kuldskær] (obsolete Danish word meaning sensitive to cold)
0 0 0 0 1 0 Have you been sensitive to cold?
01000 0 ?noitapitsnoc dah uoy evaHHave you had constipation (hard stools)?
Have you been generally unwell? 1 2 0 0 0 1 Have you felt generally unwell? The following questions are about having difficulty coping or managing your feelings
1 0 0 0 0 0The following questions are about having difficulty coping or having mood swings
Have you been in control of your life? 2 0 0 1 0 0Have you felt in control of your life?
Introduction to second part: The remainder of the questionnaire is about how your disease may have affected various aspects of your life. As previously mentioned there are several different types of thyroid diseases. When we ask about “your thyroid disease” we refer to the particular condition you have.
0 1 2 1 1 0
The remainder of the questionnaire is about how your thyroid disease may have affected various aspects of your life.
Response option Does not apply 4 0 0 0 0 0 Omitted Has your thyroid disease caused you to have difficulty being together with close family (e.g. spouse, boy/girlfriend or children)?
2 0 0 0 2 0
Has your thyroid disease caused you to have difficulty being together with friends, acquaintances, or relatives?
2 0 0 0 0 0
Has your thyroid disease caused you to have difficulty being together with other people (for example, spouse, children, boy/girlfriend, friends, or others)?
Response option Does not apply 1 0 0 0 0 0 I do not work Has your thyroid disease caused you to have difficulty managing your job?
1 2 2 0 2 2Has your thyroid disease caused you to have difficulty managing1
Qual Life Res
123
Page 88 of 107
Appendix 5: Paper III

silent misinterpretations [28], which can only be identified
by prespecified (or proactive) probes, as opposed to
emergent (or reactive) probes [23]. In terms of the effec-
tiveness of each of these two probe types, the emergent
probes were more effective in the sense of identified
problem per probe administered, which is a consequence of
the nature of emergent probes. However, the total number
of problems would have been lower if they were not
actively sought for, as is the case when applying only
emergent probing.
One patient had experienced retrieval problems with the
4-week reference period. However, other patients would
have preferred a longer period—not due to retrieval prob-
lems, but because they would like to communicate
experiences farther back in time than 4 weeks.
Cognitive interviewing was also efficient in identifying
a particular aspect of judgment and response problems,
which we term attributional problems since they involve
the attribution of symptoms and impairments to the disease
under study. These problems concerned patients’ doubt
about whether to include an experienced problem (symp-
tom, feeling, or impairment) in their judgment and
response when they did not consider that problem as being
caused by their thyroid disease. These problems occurred
mainly within the first half of the questionnaire where
attribution was not intended. In contrast, in the second half
of the questionnaire, respondents were explicitly instructed
to consider the impact of their thyroid disorder. It was
evident that some respondents excluded problems that they
considered to be unrelated to their thyroid. This is probably
a mechanism affecting HRQL-measurements in general,
particularly when used in the context of the treatment of a
specific disease [29]. We have classified these problems
within judgment and response (Tourangeau model) because
the respondents fully comprehended the question, but they
excluded some aspects when judging and formulating their
response. It could be argued, though, that since the
respondents were specifically instructed not to exclude
problems of extrathyroidal origin, it is a problem within
comprehension. It would then be within the framing of the
assessment, according to the theoretical model by Rapkin
and Schwartz [30]. Within that model, respondents form a
frame of reference, i.e., experiences they deem relevant to
their response. However, the fact that expansive probing
Table 3 continued
your job (for example, had difficulty managing1 it or calling in sick)?
Has your thyroid disease caused you to have difficulty getting around, for example, walking, bicycling, or driving a car?
0 0 0 1 0 0
Has your thyroid disease caused you to have difficulty getting around (for example, walking, running, bicycling, or driving a car)?
Has it been noticeable to others that you have a thyroid disease?
2 0 1 0 0 0
Has your thyroid disease affected your appearance (for example, swelling of the neck, eye changes, weight changes)?
Have you been unsatisfied with your appearance because of your thyroid disease?
1 0 0 0 0 0Have you been unsatisfied with your appearance because of your thyroid disease?
Has your thyroid disease made you consider yourself too thin?
0 0 0 0 0 0Has your thyroid disease made you feel too thin?
Has your thyroid disease made you consider yourself too fat?
0 1 1 0 1 0Has your thyroid disease made you feel too fat?
Introduction to last item: The final question is about to what extent your thyroid disease has affected you overall
1 0 1 0 1 0
The final question is about to what extent your thyroid disease has affected you overall during the past 4 weeks
Problems concerning attribution 0 2 3 1 1 1 n/a1 The original Danish questionnaire used two different words for “managing” the job.
Time of revision is indicated by a vertical double line k in the middle column. Initial wording is presented on the left hand side, and final wording
on the right. For example, five problems were identified during round one on the front page, which was then revised. A problem also occurred
within the revised wording during round two, and the front page was revised again. After the second revision, no further problems occurred
(rounds 3 through 6)a The original Danish questionnaire used two different words for ‘‘managing’’ the job
Qual Life Res
123
Page 89 of 107
Appendix 5: Paper III

revealed that respondents actually understood the instruc-
tion to respond without attribution—but ignored this
information when formulating their response—identified
the problems as judgmental, rather than with comprehen-
sion. The conceptual framework offering the most salient
explanation to the observed phenomenon seems to be
conversation-theory. As described by Tourangeau et al. [1],
the philosopher Paul Grice [31] described an implicit
agreement between participants in a conversation that
governed the conversation which he called a cooperative
principle. In order for a conversation to be meaningful, we
rely on a number of implicit assumptions or general rules
of reasonable behavior in conversations. For example, we
expect participants in a conversation to be as informative as
is required (but not more) for the purpose; to be truthful, to
be relevant, and to be clear. Viewing the questionnaire
response process as a piece of conversation, the investi-
gator being one participant, speaking through the
questionnaire, and the respondent being the other part, the
respondent expects the questions to be relevant and inter-
pret them with this perspective. For example, when a
patient with a thyroid disorder and a sore throat due to a
recent viral infection is asked about pain in the throat as
part of a study involving thyroid patients, she assumes that
the investigator must refer to pain related to her thyroid,
regardless of the fact that this is not specified or even (as in
our case) when it is explicitly specified not to limit the
considerations to problems of presumed thyroid causation.
She therefore denies experiencing pain in the throat
because she does not consider it relevant according to the
investigator’s aims. Hence, the implicit assumptions are
stronger than the introductory text in the questionnaire.
This phenomenon, that patients omit experiences from their
considerations when formulating a response to a survey
item, if they consider it not to be caused by the condition
under investigation, has previously been described as
selective reporting [29]. It is distinct from the mechanisms
underlying response shifts [32], since it does not represent
a ‘‘true’’ shift in HRQL-appraisal.
It is a strength of our study that it is fairly large for a
cognitive interview study. Furthermore, it encompasses a
range of clinical conditions in relation to thyroid mor-
phology and function.
The study has several limitations. One limitation con-
cerns the fact that the same methods were used to revise the
questionnaire and to evaluate its performance, this being
based on the number of problems identified by means of
cognitive interviews. In order to formally test the effect of
the revisions, an experimental study should be conducted.
This could involve experimental cognitive methods but
also quantitative studies testing the measurement properties
of the initial versus the final version. Further, the inter-
views were conducted in a hospital setting, which could
affect the response process, compared to patient response at
home—for example, by inspiring respondents to focus
more on disease compared to other domains of life. To
investigate this, interviews could be conducted at several
locations within different subsets of participants. However,
this was not logistically possible in this study. Finally, the
fact that the instrument developer is part of the research
team conducting this study could bias the results towards a
more optimistic interpretation. The English version of the
questionnaire is currently being cognitively tested by an
independent team in the USA, which, when completed, can
be used to investigate this possible bias.
The quantitative measurement properties and clinical
applicability of this instrument are currently being evalu-
ated in an ongoing cross-sectional study of 900 thyroid
patients and in clinical, longitudinal studies, focusing on
responsiveness, minimal important differences, and refer-
ence periods.
In conclusion, we were able to improve a newly
developed questionnaire applying cognitive interview
techniques adapted to the self-administration mode. We
found problems across all four stages of the classical model
of cognitive processes involved in survey responses. We
identified a subset of problems related to the respondents’
attribution of their experiences to the condition under
study, involving selective reporting, and we postulate that
this may be in play in many HRQL settings, especially
where a particular disease or condition is the focus of the
study. Future research should explore this in greater detail.
Acknowledgements This study has been supported by grants from
the Danish Medical Research Council, Agnes and Kant Morle’s
Foundation, Aase and Ejnar Danielsen’s Foundation, Else and
Mogens Wedell-Wedells Gorg’s Foundation, the Genzyme Corpora-
tion, the Novo Nordish Foundation and the Danish Thyroid
Foundation.
References
1. Tourangeau, R., Rips, L. J., & Rasinski, K. (2000). The psy-chology of survey response. Cambridge, UK: Cambridge
University Press.
2. Jobe, J. B. (2003). Cognitive psychology and self-reports: Models
and methods. Quality of Life Research, 12(3), 219–227. doi:
10.1023/A:1023279029852.
3. Barofski, I. (1996). Cognitive aspects of quality of life assess-
ments. In B. Spilker (Ed.), Quality of life and pharmacoeconomicsin clinical trials (2nd ed.). Philadelphia: Lippincott-Raven.
4. Collins, D. (2003). Pretesting survey instruments: An overview of
cognitive methods. Quality of Life Research, 12(3), 229–238. doi:
10.1023/A:1023254226592.
5. Sudman, S., Bradburn, N. M., & Schwarz, N. (1996). Thinkingabout answers. The application of cognitive processes to surveymethodology (1st ed.). San Francisco: Jossey-Bass.
6. Willis, G., Reeve, B. B., & Barofsky, I. (2005). The use of
cognitive interviewing techniques in quality of life and patient-
reported outcomes assessment. In J. Lipscomb, C. C. Gotay, & C.
Qual Life Res
123
Page 90 of 107
Appendix 5: Paper III
Snyder (Eds.), Outcomes assessment in cancer: Measures,methods, and applications. Cambridge: Cambridge University
Press.
7. McColl, E., Meadows, K., & Barofsky, I. (2003). Cognitive aspects
of survey methodology and quality of life assessment. Quality ofLife Research, 12(3), 217–218. doi:10.1023/A:1023233432721.
8. US Food and Drug administration (2006). Guidance for Industry.
Patient-Reported Outcome Measures: Use in Medical Product
Development to Support Labeling Claims (Draft). Health andQuality of Life Outcomes, 4(79) (also available at www.fda.gov/
CDER/guidance/5460dft.pdf).
9. Ladenson, P. W. (2002). Psychological wellbeing in patients.
Clinical Endocrinology, 57(5), 575–576. doi:10.1046/j.1365-
2265.2002.01682.x.
10. Abraham, P., Avenell, A., Watson, W. A., et al. (2004). Anti-thyroid drug regimen for treating Graves’ hyperthyroidism(Cochrane Review). The Cochrane Library, Issue 3. Chichester,
UK: Wiley.
11. Romijn, J. A., Smit, J. W., & Lamberts, S. W. (2003). Intrinsic
imperfections of endocrine replacement therapy. European Jour-nal of Endocrinology, 149(2), 91–97. doi:10.1530/eje.0.1490091.
12. Gerding, M. N., Terwee, C. B., Dekker, F. W., Koornneef, L.,
Prummel, M. F., & Wiersinga, W. M. (1997). Quality of life in
patients with Graves’ ophthalmopathy is markedly decreased:
Measurement by the medical outcomes study instrument. Thyroid,7(6), 885–889.
13. Terwee, C., Wakelkamp, I., Tan, S., Dekker, F., Prummel, M. F.,
& Wiersinga, W. (2002). Long-term effects of Graves’ ophthal-
mopathy on health-related quality of life. European Journal ofEndocrinology, 146(6), 751–757. doi:10.1530/eje.0.1460751.
14. Bianchi, G. P., Zaccheroni, V., Solaroli, E., Vescini, F., Cerutti,
R., Zoli, M., et al. (2004). Health-related quality of life in patients
with thyroid disorders. Quality of Life Research, 13(1), 45–54.
doi:10.1023/B:QURE.0000015315.35184.66.
15. Elberling, T. V., Rasmussen, A. K., Feldt-Rasmussen, U.,
Hording, M., Perrild, H., & Waldemar, G. (2004). Impaired
health-related quality of life in Graves’ disease. A prospective
study. European Journal of Endocrinology, 151(5), 549–555. doi:
10.1530/eje.0.1510549.
16. Abraham-Nordling, M., Torring, O., Hamberger, B., Lundell, G.,
Tallstedt, L., Calissendorff, J., et al. (2005). Graves’ disease: A
long-term quality-of-life follow up of patients randomized to
treatment with antithyroid drugs, radioiodine, or surgery. Thy-roid, 15(11), 1279–1286. doi:10.1089/thy.2005.15.1279.
17. Samuels, M. H., Schuff, K. G., Carlson, N. E., Carello, P., &
Janowsky, J. S. (2007). Health status, psychological symptoms,
mood, and cognition in L-thyroxine-treated hypothyroid subjects.
Thyroid, 17(3), 249–258. doi:10.1089/thy.2006.0252.
18. Saravanan, P., Chau, W. F., Roberts, N., Vedhara, K., Greenwood,
R., & Dayan, C. M. (2002). Psychological well-being in patients
on ‘adequate’ doses of l-thyroxine: Results of a large, controlled
community-based questionnaire study. Clinical Endocrinology,57(5), 577–585. doi:10.1046/j.1365-2265.2002.01654.x.
19. Fahrenfort, J. J., Wilterdink, A. M., & van der Veen, E. A. (2000).
Long-term residual complaints and psychosocial sequelae after
remission of hyperthyroidism. Psychoneuroendocrinology, 25(2),
201–211. doi:10.1016/S0306-4530(99)00050-5.
20. Terwee, C. B., Gerding, M. N., Dekker, F. W., Prummel, M. F., &
Wiersinga, W. M. (1998). Development of a disease specific
quality of life questionnaire for patients with Graves’ Ophthal-
mopathy: The GO-QOL. British Journal of Ophthalmology,82(7), 773–779.
21. Watt, T., Groenvold, M., Rasmussen, A. K., Bonnema, S. J.,
Hegedus, L., Bjorner, J. B., et al. (2006). Quality of life in patients
with benign thyroid disorders. A review. European Journal ofEndocrinology, 154, 501–510. doi:10.1530/eje.1.02124.
22. Watt, T., Hegedus, L., Rasmussen, A. K., Groenvold, M., Bon-
nema, S. J., Bjorner, J. B., et al. (2007). Which domains of
thyroid-related quality of life are most relevant? Patients and
clinicians provide complementary perspectives. Thyroid, 17(7),
647–654. doi:10.1089/thy.2007.0069.
23. Willis, G. (2005). Cognitive interviewing. A tool for improvingquestionnaire design. London: Sage.
24. Mullin, P. A., Lohr, K. N., Bresnahan, B. W., & McNulty, P.
(2000). Applying cognitive design principles to formatting
HRQOL instruments. Quality of Life Research, 9(1), 13–27. doi:
10.1023/A:1008923301313.
25. Presser, S., & Blair, J. (1994). Survey pretesting: Do differentmethods produce different results? Sociological Methodology
American Sociological Association, Washington D.C.
26. Rothgeb, J., Willis, G., & Forsyth, B. (2001) Questionnairepretesting methods: Do different techniques and different orga-nizations produce similar results? Proceedings of the Annual
Meeting of the American Statistical Association
27. May, L. A., & Warren, S. (2001). Measuring quality of life of
persons with spinal cord injury: Substantive and structural vali-
dation. Quality of Life Research, 10, 503–515. doi:10.1023/
A:1013027520429.
28. DeMaio, T., & Rothgeb, J. (1996). Cognitive interviewing tech-
niques: In the lab and in the field. In N. Schwarz, & S. Sudman
(Eds.), Answering questions: Methodology for determining cog-nitive and communicative processes in survey research. San
Francisco: Jossey-Bass.
29. Groenvold, M., Klee, M. C., Sprangers, M. A., & Aaronson, N. K.
(1997). Validation of the EORTC QLQ-C30 quality of life ques-
tionnaire through combined qualitative and quantitative assessment
of patient-observer agreement. Journal of Clinical Epidemiology,50(4), 441–450. doi:10.1016/S0895-4356(96)00428-3.
30. Rapkin, B. D., & Schwartz, C. E. (2004). Toward a theoretical
model of quality-of-life appraisal: Implications of findings from
studies of response shift. Health and Quality of Life Outcomes, 2,
14. doi:10.1186/1477-7525-2-14.
31. Grice, P. (1989). Studies in the way of words. Cambridge: Harvard
University Press.
32. Sprangers, M. A., & Schwartz, C. E. (1999). Integrating response
shift into health-related quality of life research: A theoretical
model. Social Science & Medicine, 48(11), 1507–1515. doi:
10.1016/S0277-9536(99)00045-3.
Qual Life Res
123
Page 91 of 107
Appendix 5: Paper III

1
Establishing a reliable scale structure with convergent and
discriminant validity for a new patient reported outcome
measure for patients with thyroid disorders
Torquil Watt1,2, Jakob Bue Bjorner3, Mogens Groenvold2,4, Åse Krogh Rasmussen1, Steen Joop
Bonnema5, Laszlo Hegedüs5, Ulla Feldt-Rasmussen1.
1Dept. of Endocrinology, Copenhagen University Hospital Rigshospitalet, 2Institute of Public
Health, University of Copenhagen, Denmark, 3 National Research Centre for the Working
Environment, Copenhagen, Denmark, 4 Dept. of Palliative Medicine, Bispebjerg Hospital and 5Dept. of Endocrinology and Metabolism, Odense University Hospital, Denmark.
Address for correspondence and reprints: Torquil Watt, MD, Department of Endocrinology,
Rigshospitalet, Blegdamsvej 9, DK-2100, Copenhagen Ø, Denmark. Phone +45 3545 2537, Fax
+45 3545 2240, E-mail [email protected]
Running title: Reliability and scale validity of a new thyroid patient-reported outcome
Keywords: Patient-reported outcomes, quality of life, reliability, scale validation, questionnaire
development, thyroid disease.
Page 92 of 107
Appendix 6: Paper IV

2
Abstract
Objective: To establish a reliable scale structure of a
patient-reported outcome measuring thyroid-specific
quality of life.
Methods: The 98-item ThyPRO questionnaire was
administered to patients with benign thyroid diseases at
two university hospitals. Multi-trait scaling was
performed, evaluating lack of convergent validity
(item-own scale Pearson correlation <0.40) or lack of
discriminant validity (item-other scale correlation
higher than item-own scale correlation) of the
hypothesized scale structure. Analyses were repeated in
clinical and sociodemographic subgroups and with
polychoric correlations. Reliability was estimated by
Cronbach’s α.
Results: In total, 904 patients (64%) responded. Initial
multitrait scaling analysis identified 25 scaling errors.
Twelve items were omitted from the scale structure,
and a second analysis showed complete convergent
validity and only two instances of lack of discriminant
validity. Polychoric correlations yielded similar results.
Across all subgroups, convergent validity was
complete and discriminant validity was found in 99,2%
of tests. Lack of discriminant validity was mainly
between physical symptoms and psychological and
disease-impact scales. Cronbach’s α was acceptable
(>0.70) for all 13 scales.
Conclusion: A reliable scale structure displaying
complete convergent and almost complete discriminant
validity was established in general analyses and in
distinct clinical subgroups of patients with benign
thyroid diseases.
Page 93 of 107
Appendix 6: Paper IV

3
Introduction
Diseases related to the thyroid, which is an endocrine gland located in the front of the neck, are very common, affecting individuals of all ages, mainly women. Thyroid hormones target all cells/organs in the body, mainly as a promoter of metabolism, and under- or overproduction of hormones therefore affects a broad range of human functions. Two major disease mechanisms are involved in thyroid diseases, leading to a broad spectrum of clinical manifestations: enlargement of the gland, termed goiter, and autoimmunity, where the immune system falsely targets thyroid structures. Goiter without accompanying dysfunction (termed non-toxic goiter) may cause neck discomfort and/or cosmetic concerns, but may also be associated with autonomous function, resulting in overproduction of hormones (hyperthyroidism, in this case termed toxic nodular goiter). Autoimmunity can be associated with enlargement of the gland (diffuse goiter), but most often leads to disturbed function, with either decreased secretion of thyroid hormones (autoimmune hypothyroidism) or increased secretion (hyperthyroidism, termed Graves’ disease). A subgroup of patients with Graves’ disease has affection of the eyes, yielding a characteristic protrusion and irritation of the eyes (termed thyroid associated ophthalmopathy (TAO) or Graves’ orbitopathy (GO)). The classical symptoms of hypothyroidism are unspecific, but well-described, with tiredness, slow cerebration, constipation, weight gain and depression as core elements. The typical symptoms of hyperthyroidism are rapid heart beats, tremor, weight loss, anxiety and increased sweating. The scientific documentation about how these common, well-known diseases affect people’s lives is very limited, as is the knowledge about how various treatments moderate these effects. Some questionnaires have been developed for and have been used with specific thyroid sub-populations[1-9], but no validated, thyroid specific patient-reported outcome instrument is available for use across different thyroid diseases[10]. As part of a study concerning quality of life in thyroid patients, the ThyQoL project, we therefore developed a thyroid specific quality of life questionnaire, the ThyPRO (Thyroid Patient Reported Outcome), based on a literature review[10] and expert- and patient interviews[11,12]. The questionnaire is aimed at patients with any benign thyroid disorders, because the diseases overlap in their clinical presentation and as a consequence of treatment. During the questionnaire development, a broad range of relevant issues were identified and developed as items. The usefulness and reliability of an outcome instrument is increased if individual issues can be aggregated in broader domains and reported together. However, a precondition for such an approach is that the aggregated items truly measure a unifying meaningful concept, distinct from
other measurable concepts[13,14]. One way of evaluating it is by exploring the convergent and discriminant validity, i.e. that an item has strong correlation with other items measuring the same concept and less strong correlation with items not measuring that concept. We adopted the multitrait scaling approach[15,16], following the logic of the multitrait-multimethod analyses by Campbell and Fiske[17]. The purpose of the present study was to evaluate and modulate the scale structure and to test the reliability of the draft ThyPRO questionnaire. The primary aim of the analysis and scale revision was to establish a scale structure fitting the total sample. To test the stability of the scale structure, subgroup analyses were also performed. Material and methods
The draft ThyPRO questionnaire
The draft questionnaire consisted of 98 items with a hypothesized structure of 14 domains: four symptom domains covering the disease mechanisms in play within thyroid disorders (neck related goiter symptoms, symptoms of hyperthyroidism, symptoms of hypothyroidism and eye symptoms), five domains of physical and mental function and well-being and five impact domains concerning impact of thyroid disease on central aspects of quality of life (Figure 1). In addition, there were two physical symptoms not ascribable to any of the scales a priori: “Sleeping problems” and “Dizziness”. Each question (item) was rated on a five-point scale from 0=not at all to 4=very much, with a 4 weeks reference period. The multi-item scales were derived by averaging item scores within a scale and linearly transforming them to a 0-100 scale with 0 being the best and 100 being the worst possible score. Patients and study design
Patients were recruited from the endocrinological outpatient clinics at two university hospitals in Denmark: Copenhagen University Hospital Rigshospitalet (RH) and Odense University Hospital (OUH). At RH, the sampling strategy was cross-sectional: all thyroid patients born within the first 20 days of each month (to limit running sample size) were invited during February-June 2007 by mail 3 weeks prior to their appointment in the clinic. A few days prior to the appointment, participants came to a research laboratory for a study-specific visit where blood-samples were drawn, a thyroid ultrasound scan performed and a written, signed informed consent obtained by the medical staff. Questionnaires were either returned by mail or delivered by hand in the lab or at the clinic on the day of appointment. At OUH, all eligible patients referred to the thyroid unit of the endocrine outpatient clinic during May-November 2007 were recruited. The questionnaire was sent about
Page 94 of 107
Appendix 6: Paper IV
4
three weeks prior to the appointment, blood-samples were drawn the week preceding their appointment, as part of the usual routine, and an ultrasound scan performed at their visit to the clinic. Here, written signed informed consent was obtained by the endocrinologist. At both sites, the patients were instructed to complete the questionnaire at the time when blood-samples were drawn. Exclusion criteria were absence of any thyroid disorder, thyroid cancer, age less than 15 and inability to complete a questionnaire due to communication problems (non-Danish speaking, blindness, etc.). One reminder was sent after two weeks to non-responders. Sociodemographic data and information about co-morbidity and non-thyroid medication were self-reported. Paraclinical data, exact diagnosis, previous and current treatment and time of diagnosis among respondents were obtained by chart review. Biochemical thyroid tests were thyroid stimulating hormone (TSH), total thyroxine (T4), total triiodothyronine (T3), non-proteinbound thyroxine (fT4), non-proteinbound triiodothyronine (fT3), resin-T3-test (only OUH), thyroid peroxidase antibodies (TPO-Ab), thyroglobulin antibodies (Tg-Ab, only in patients diagnosed with hypothyroidism and negative TPO-Ab)) and TSH-receptor antibodies (TRAK, only in patients with a diagnosis of hyperthyroidism). All analyses were performed using the standard methods at the laboratories of the participating hospitals, except TRAK and TPO-Ab at Rigshospitalet, which were measured by double-measurements using BRAHMS TRAK-human and anti-TPOn radioimmunoassay. In patients with thyroid eye-disease (thyroid-associated ophthalmopathy, TAO), NOSPECS[18] classification was performed by an ophthalmologist and Clinical Activity Scoring (CAS[19]) was performed by a physician. Thyroid volume was determined by ultrasound, using the ellipsoid method.[20] The patients were classified according to primary diagnosis, i.e. their initial diagnosis, prior to treatment. For example, patients with a non-toxic goiter, who had their thyroid removed and thus have hypothyroidism and receive thyroid hormone replacement, are classified with a diagnosis of non-toxic goiter. In the subgroup analyses, the patients are aggregated in five major diagnostic categories:1) non-toxic goiter comprising diffuse, uni- and multinodular non-toxic goiter as well as thyroid cysts. 2) toxic nodular goiter, comprising both uni- and multinodular disease. 3) Graves’ disease. 4) TAO. 5) autoimmune hypothyroidism. Subacute thyroiditis (De Quervain’s thyroiditis), postpartum thyroiditis and various other rare benign thyroid diseases (e.g. amiodarone- and lithium induced thyroiditis, Riedel’s thyroiditis, thyroid agenesis, etc.) were not included in the diagnostic subgroup analyses. Self-completed data were entered using optical scanning. All clinical data were entered via SPSS Data Entry Builder 4.0 by medical staff. Data
were converted to SAS datasets and all analyses were performed with SAS 9.1. The project was approved by the local ethical committee (KF01 2006-1579) and the Danish data protection agency and registered at ClinicalTrials.gov (NCT00150033).
Statistical analyses
Multitrait scaling[15-17] is a psychometric technique that can be used when the researcher hypothesizes that the questionnaire measures several separate concepts, each measured by several items. Four criteria are evaluated by multitrait scaling: 1. Each item should have a substantial
correlation with the sum score computed from all the other items in the particular scale (convergent validity).
2. Each item should have a substantially higher correlation with the sum score of the rest of the items in its scale than with scales measuring other concepts (discriminant validity).
3. For items in the same scale, the correlation between one item and the sum of the other items should be of roughly the same magnitude for all items (equal item - own scale correlation).
4. Items in the same scale should have roughly equal variances.
The present analyses focus on criteria 1 and 2; these criteria are important for evaluating the grouping of items into scales. In classical psychometrics, criteria 3 and 4 are requirements for summating of items without weighting. However, for categorical items, item skewness may cause heterogenous item-total correlations and variances, even in situations where an unweighted sum score is the optimal scoring approach[21]. For this reason, this paper will not evaluate criteria 3 and 4. The analyses were performed using Pearson correlations between items and scales and between scales. Item correlation with own scales were corrected for overlap. Item-own scale correlations above 0.40 were considered indicative of appropriate convergent validity, and item-other scale correlations lower than item-own scale correlations were identified as appropriate discriminant validity. The symptom scales were not expected to show complete discriminant validity, since the symptoms themselves may directly influence the scores of the broader quality of life-scales and thus co-vary with them, without it being evidence of lack of discriminant validity. However, they were expected to show convergent validity, since they reflect clinically meaningful and etiologically distinct entities. Reliability was estimated as internal consistency reliability, using Cronbach’s alpha[22]. Analyses were also performed using polychoric correlations[21,23,24], to allow for the skewness often found in data like these[21].
Page 95 of 107
Appendix 6: Paper IV

5
Initial analyses were performed on the total sample. Subgroup analyses were subsequently performed with respect to recruiting hospital, gender, age-group (young (<40 years old), middle-aged (40-60) and old (>60)) and primary thyroid diagnosis: non-toxic goiter, toxic nodular goiter, Graves’ hyperthyroidism without signs of eye affection, TAO with or without hyperthyroidism and autoimmune hypothyroidism with or without goiter. Based on these analyses, the scale structure was revised and the analyses were repeated using the revised scale structure.
Results At Rigshospitalet, 878 patients were invited, of whom 41 were secondarily excluded. Five hundred and two returned a completed questionnaire, yielding an overall response rate at RH of 60%. However, 92 patients cancelled their index appointment at the outpatient clinic for other reasons, thus preventing them from participating, yielding a corrected response rate of 67%. At Odense University Hospital 632 were invited, 61 excluded, 404 responded, yielding a response rate at OUH of 71%; response rate for the total sample was thus 904/1408=64% (69% when corrected for appointment cancellations). Clinical characteristics are presented in Table 1 for the total sample and in Table 2 for the diagnostic subgroups used in the subgroup analyses. The initial multi-trait scaling analysis identified one instance of lack of convergent validity and 24 instances of lack of discriminant validity in 10 items (items in italic in Figure 1). Two of these items belonged to the overall quality of life scale, which thus had scaling error in half its items. In addition, analyses in the five patient-groups separately found lack of discriminant validity of “Difficulty breathing” eight times across patient groups (data not shown). On this background, the “Overall quality of life” scale was omitted, as were the items lacking discriminant and convergent validity in the total sample and the “Difficulty breathing”-item. However, the two positively worded items “In control of life” and “In balance” were retained due to high relevance ratings and due to expected important scaling properties with respect to ceiling effect. A multitrait scaling analysis of the remaining 84 scaled items in the total sample is presented in Table 3. Now all items in all scales showed convergent validity with item-own scale correlations above 0.40. One scaling error involving lack of discriminant validity occurred in the Emotional susceptibility scale (item “In control of life”). Inter-scale correlations were low to moderate, ranging 0.21-0.71, except for “Depressivity” and “Emotional susceptibility”, which had a high interscale correlation of 0.83 (Table 4). Internal consistency reliability estimates (Cronbach’s α) were very high, except for “Hypothyroid symptoms”, which just reached the limit of 0.70 (Table 4).
Repeating the analysis using polychoric correlations generally yielded higher correlation coefficients (data not shown). No lack of convergent validity was found. Compared to Pearson correlations, only two dissimilarities were found regarding discriminant validity: “In control of life” no longer had lack of discriminant validity and “Cried easily” correlated higher with “Emotional susceptibility” (0.71) than with its own “Depressivity” scale (0.70). Performing analyses in separate subgroups (age, gender, hospitals) only showed minor deviations, with preservation of convergent validity, except in a few cases among young patients (less than age 40), where the hypothyroid symptoms “sensitive to cold”, “swollen hands or feet” and “itchy skin” correlated higher with other scales than with the ‘’Hypothyroid” scale, with which they correlated less than 0.40. The same was the case for “double vision” from the “Eye symptoms” scale. Performing the analyses separately in the five patient groups, convergent validity was preserved, except for “itchy skin” among Graves’ patients, which correlated only 0.27 with the hypothyroid symptom scale. In total, out of 5,040 correlations, 65 scaling errors involving lack of discriminant validity was found, two thirds of which involved physical symptom items (Table 5). Sixteen involved items from the “Depressivity” and the “Emotional susceptibility” scale, five were from the “Social impact” scale and two from the “Cosmetic concern” scale. Repeating the analyses using polychoric correlations did not alter these results; in total, 4 fewer scaling errors occurred, compared to Pearson correlations (data not shown). Discussion
It was possible to revise the questionnaire to establish a scale structure with complete convergent validity and almost complete discriminant validity in a large, heterogeneous sample of patients comprising several benign thyroid diseases. During the revision, one scale was relinquished and 8 items were omitted from the questionnaire. The remaining 13 scales are four specific symptom scales, five non-specific scales measuring psychological states and tiredness and four thyroid disease impact scales. The item lacking discriminant validity was related to both “Depressivity” and “Emotional susceptibility” and these two scales also displayed high interscale correlation. All scales had acceptable internal consistency reliability. Generally, the instrument preserved this scale structure across sociodemographic and clinical subgroups. However, in individual diagnostic groups, lack of discriminant validity was found in a very small proportion of cases (65 of 5,040 correlations), mainly among the physical symptoms. The structure was also preserved using polychoric correlations, which
Page 96 of 107
Appendix 6: Paper IV

6
theoretically take into account the distributional properties of measurements like these[23-26]. The complete convergent and almost complete discriminant validity seen in the total sample provides strong support for the theoretically based (and slightly modified) scaling structure of the ThyPRO. The fact that some scaling errors (0.8%) were found in certain subgroups (mainly between physical symptoms and scales measuring psychological states and impact of disease) does not alter this overall result. There are a number of possible interpretations of the findings in subgroups. They may reflect that important thyroid symptoms impact the broader quality of life aspects measured by these scales. Thus, using Fayers’ distinctions[27], this would be an expression of a causal effect rather than reflecting that the physical symptom belongs to the quality of life dimension measured by that scale. Further exploration of such hypotheses could be done using structural equations models[28] in separate analyses of each clinical subgroup or in multigroup analyses[29]. The “Depressivity” and “Emotional susceptibility” scales are closely related, judged by the one item lacking discriminant validity, the scaling errors involving these scales in the patient-subgroup analyses, and not least the high inter-scale correlation. Should the two scales be merged into one? Emotional susceptibility was identified as an important unique concept emerging in the qualitative analyses of 80 patient interviews. Further scale revision should therefore await additional, more clinically oriented studies. In general, we had a high threshold for omitting items in this study, because all items had been rated as being important in patient and expert interviews and because important clinical data such as sensitivity and responsiveness are not yet available. Also, valuable information regarding item characteristics, such as information curves and severity-specific reliability, is only available through analyses applying item response models and we prefer to take such results into account, before omitting further items. Thus, our main purpose with this study was to establish a scale structure allowing use and analysis of the questionnaire. This structure will serve as a framework for additional analyses to be conducted, which may lead to revisions. It is a strength of our study that the sample is large and comprises several thyroid patient groups with several thyroid diseases in multiple stages, as well as a broad spectrum of treatments. The fact that a reliable and valid scale structure of the questionnaire was established in such a broad sample indicates that it may be useful in longitudinal studies where disease stage, and even disease entity, changes over time. However, additional longitudinal validation studies are warranted before firm conclusions can be made. Further, analyses using item response theory models should be undertaken to evaluate whether the simple summated
scoring suggested here is adequate. They could also evaluate and possibly ensure measurement precision over the full range of disease severity. Multi-group structural equations models for ordinal data could be used to take causal relations between sub-domains into account, like the ones hypothesized to be in play between the symptom items and the state/impact scales. The choice of statistical methodology could also be questioned, particularly the choice of parametric statistics like the Pearson correlation. Likert-like response scales like the ones used here are indisputably ordinal in nature and are often found to be skew. However, these methods have been shown to be relatively robust to minor violations of these assumptions[21,30] and it is reassuring that the use of polychoric correlations, which assumes that the measured construct is normally distributed, but not necessarily measured continuously or even equidistantly, did not alter the results. The questionnaire is somewhat lengthy and future research could focus on item-reduction with preservation of appropriate measurement properties, integrating additional information from item response models and clinimetrical parameters. Demonstration of responsiveness to clinical changes and establishment of minimal important differences warrant future longitudinal studies. Also, clinical studies should evaluate the relationship between the scale scores and relevant clinical variables, such as thyroid function tests, thyroid auto-antibodies, goiter size and eye symptoms.* In conclusion, we found evidence of excellent convergent and discriminant validity as well as satisfactory internal consistency reliability of a thirteen-scale version of the newly developed thyroid-specific ThyPRO questionnaire, when used in patients with benign thyroid diseases. The questionnaire allows evaluation of the impact of the thyroid disease and existing and future treatments on the quality of life of patients with benign thyroid diseases. Examples of important clinical questions to be answered in this respect are whether there are any differences in health-related quality of life among patients with hyperthyroidism being treated with antithyroid medicine, surgery or radioactive iodine[31]; whether a block-replacement regimen with both antithyroid drug and thyroid hormones gives better health-related quality of life compared to antithyroid drugs alone[32], and whether treatment with a combination of the two forms of the thyroid hormones, T4 and T3, for hypothyroidism is an improvement over standard therapy with T4 alone[33,34]. ACKNOWLEDGEMENTS We wish to express our gratitude to the staffs and colleagues at Rigshospitalet Endocrinological Department PE 2131 and 5201 and Odense University
Page 97 of 107
Appendix 6: Paper IV

7
Hospital, Department of Endocrinology and Metabolism M. A special thank to our research assistants Sara Hope Watt and Alexandra Hegedüs. This study has been supported by grants from the Danish Medical Research Council, Agnes and Knut Mørk's Foundation, Aase and Ejnar Danielsen's Foundation, Else and Mogens Wedell-Wedellsborg's Foundation, the Genzyme Corporation, the Novo Nordisk Foundation and the Danish Thyroid Foundation. *Researchers who want to use the ThyPRO may contact the first author ([email protected]). The ThyPRO is currently available in the following languages: Danish, English, German, French, Italian, Portuguese (Brazil) and Dutch.
Page 98 of 107
Appendix 6: Paper IV
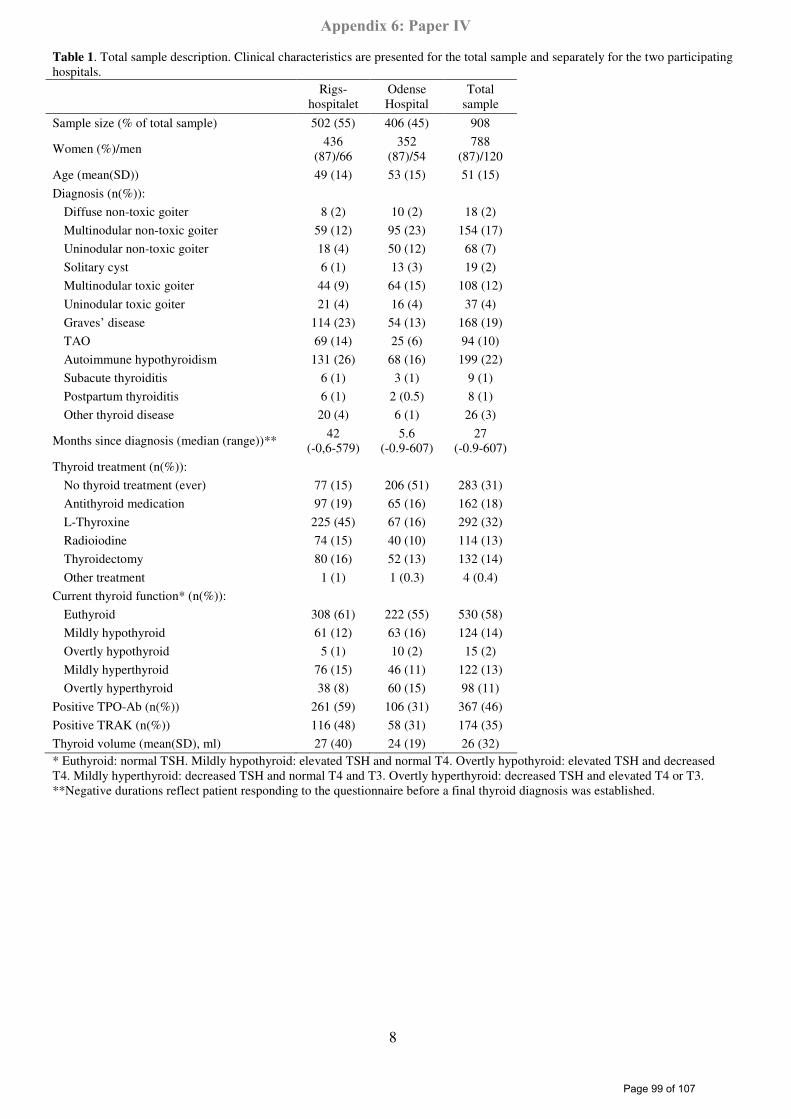
8
Table 1. Total sample description. Clinical characteristics are presented for the total sample and separately for the two participating hospitals. Rigs-
hospitalet Odense Hospital
Total sample
Sample size (% of total sample) 502 (55) 406 (45) 908
Women (%)/men 436 (87)/66
352 (87)/54
788 (87)/120
Age (mean(SD)) 49 (14) 53 (15) 51 (15)
Diagnosis (n(%)):
Diffuse non-toxic goiter 8 (2) 10 (2) 18 (2)
Multinodular non-toxic goiter 59 (12) 95 (23) 154 (17)
Uninodular non-toxic goiter 18 (4) 50 (12) 68 (7)
Solitary cyst 6 (1) 13 (3) 19 (2)
Multinodular toxic goiter 44 (9) 64 (15) 108 (12)
Uninodular toxic goiter 21 (4) 16 (4) 37 (4)
Graves’ disease 114 (23) 54 (13) 168 (19)
TAO 69 (14) 25 (6) 94 (10)
Autoimmune hypothyroidism 131 (26) 68 (16) 199 (22)
Subacute thyroiditis 6 (1) 3 (1) 9 (1)
Postpartum thyroiditis 6 (1) 2 (0.5) 8 (1)
Other thyroid disease 20 (4) 6 (1) 26 (3)
Months since diagnosis (median (range))** 42 (-0,6-579)
5.6 (-0.9-607)
27 (-0.9-607)
Thyroid treatment (n(%)):
No thyroid treatment (ever) 77 (15) 206 (51) 283 (31)
Antithyroid medication 97 (19) 65 (16) 162 (18)
L-Thyroxine 225 (45) 67 (16) 292 (32)
Radioiodine 74 (15) 40 (10) 114 (13)
Thyroidectomy 80 (16) 52 (13) 132 (14)
Other treatment 1 (1) 1 (0.3) 4 (0.4)
Current thyroid function* (n(%)):
Euthyroid 308 (61) 222 (55) 530 (58)
Mildly hypothyroid 61 (12) 63 (16) 124 (14)
Overtly hypothyroid 5 (1) 10 (2) 15 (2)
Mildly hyperthyroid 76 (15) 46 (11) 122 (13)
Overtly hyperthyroid 38 (8) 60 (15) 98 (11)
Positive TPO-Ab (n(%)) 261 (59) 106 (31) 367 (46)
Positive TRAK (n(%)) 116 (48) 58 (31) 174 (35)
Thyroid volume (mean(SD), ml) 27 (40) 24 (19) 26 (32) * Euthyroid: normal TSH. Mildly hypothyroid: elevated TSH and normal T4. Overtly hypothyroid: elevated TSH and decreased T4. Mildly hyperthyroid: decreased TSH and normal T4 and T3. Overtly hyperthyroid: decreased TSH and elevated T4 or T3. **Negative durations reflect patient responding to the questionnaire before a final thyroid diagnosis was established.
Page 99 of 107
Appendix 6: Paper IV
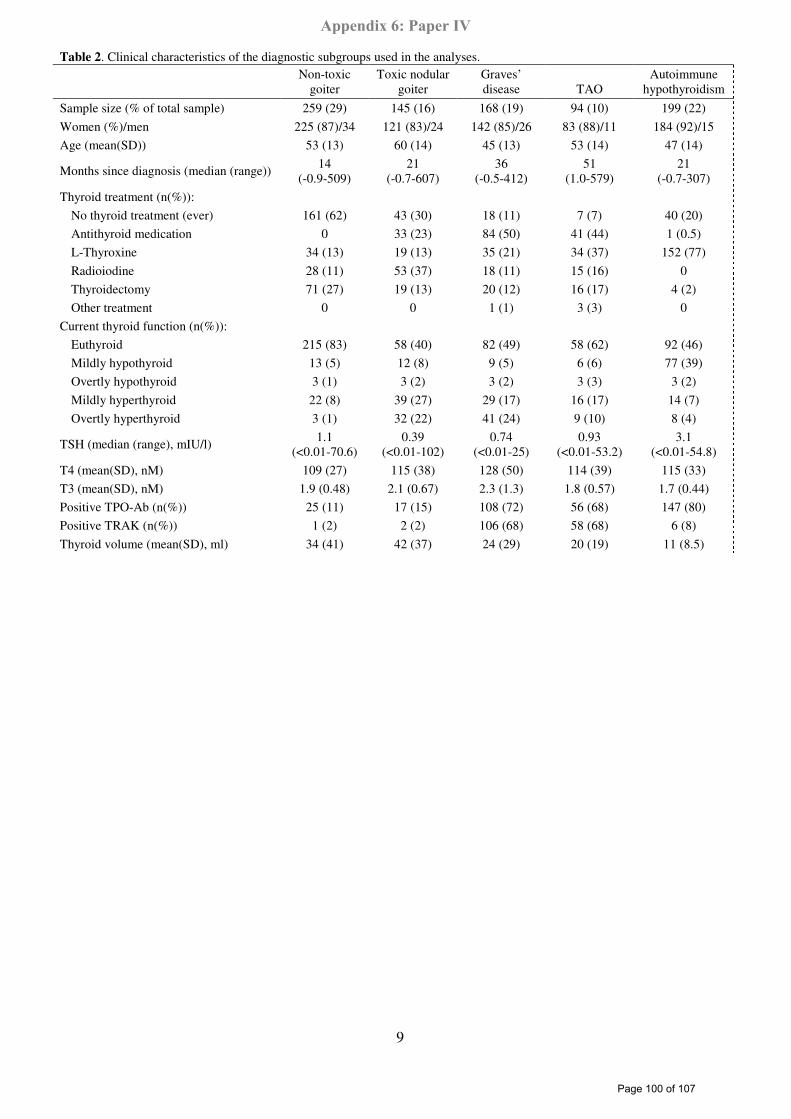
9
Table 2. Clinical characteristics of the diagnostic subgroups used in the analyses. Non-toxic
goiter Toxic nodular
goiter Graves’ disease TAO
Autoimmune hypothyroidism
Sample size (% of total sample) 259 (29) 145 (16) 168 (19) 94 (10) 199 (22)
Women (%)/men 225 (87)/34 121 (83)/24 142 (85)/26 83 (88)/11 184 (92)/15
Age (mean(SD)) 53 (13) 60 (14) 45 (13) 53 (14) 47 (14)
Months since diagnosis (median (range)) 14 (-0.9-509)
21 (-0.7-607)
36 (-0.5-412)
51 (1.0-579)
21 (-0.7-307)
Thyroid treatment (n(%)):
No thyroid treatment (ever) 161 (62) 43 (30) 18 (11) 7 (7) 40 (20)
Antithyroid medication 0 33 (23) 84 (50) 41 (44) 1 (0.5)
L-Thyroxine 34 (13) 19 (13) 35 (21) 34 (37) 152 (77)
Radioiodine 28 (11) 53 (37) 18 (11) 15 (16) 0
Thyroidectomy 71 (27) 19 (13) 20 (12) 16 (17) 4 (2)
Other treatment 0 0 1 (1) 3 (3) 0
Current thyroid function (n(%)):
Euthyroid 215 (83) 58 (40) 82 (49) 58 (62) 92 (46)
Mildly hypothyroid 13 (5) 12 (8) 9 (5) 6 (6) 77 (39)
Overtly hypothyroid 3 (1) 3 (2) 3 (2) 3 (3) 3 (2)
Mildly hyperthyroid 22 (8) 39 (27) 29 (17) 16 (17) 14 (7)
Overtly hyperthyroid 3 (1) 32 (22) 41 (24) 9 (10) 8 (4)
TSH (median (range), mIU/l) 1.1 (<0.01-70.6)
0.39 (<0.01-102)
0.74 (<0.01-25)
0.93 (<0.01-53.2)
3.1 (<0.01-54.8)
T4 (mean(SD), nM) 109 (27) 115 (38) 128 (50) 114 (39) 115 (33)
T3 (mean(SD), nM) 1.9 (0.48) 2.1 (0.67) 2.3 (1.3) 1.8 (0.57) 1.7 (0.44)
Positive TPO-Ab (n(%)) 25 (11) 17 (15) 108 (72) 56 (68) 147 (80)
Positive TRAK (n(%)) 1 (2) 2 (2) 106 (68) 58 (68) 6 (8)
Thyroid volume (mean(SD), ml) 34 (41) 42 (37) 24 (29) 20 (19) 11 (8.5)
Page 100 of 107
Appendix 6: Paper IV
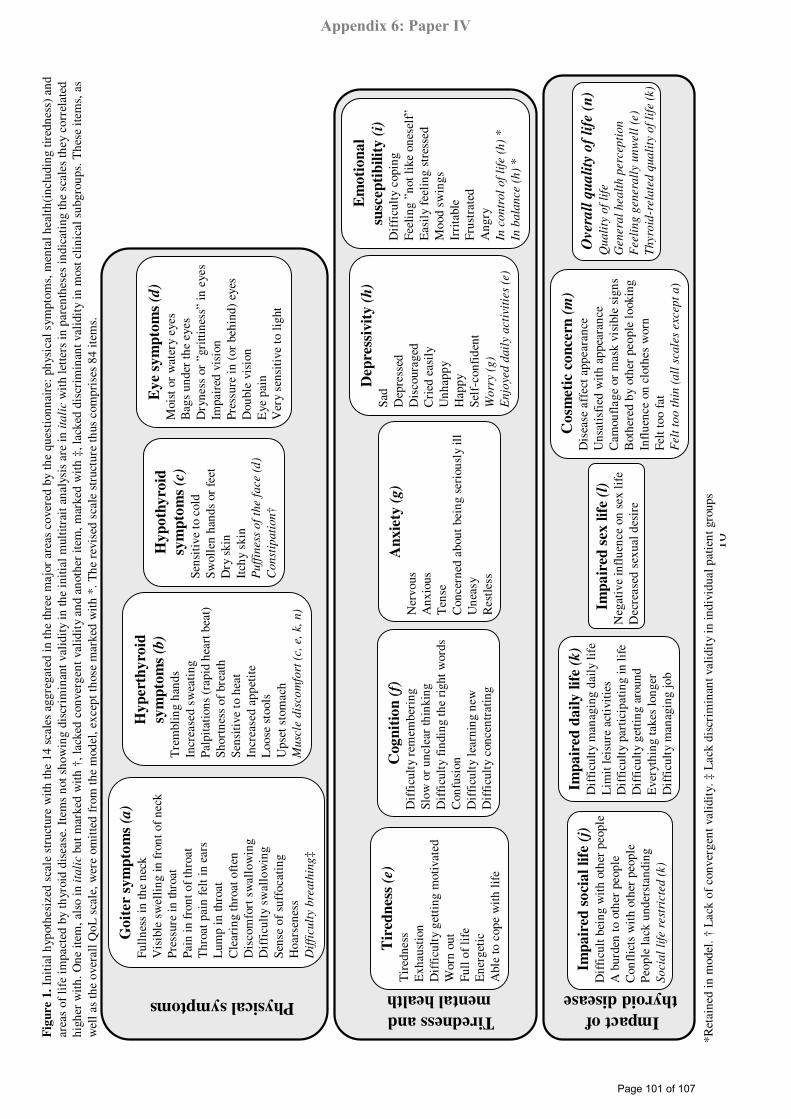
10
Go
iter
sym
pto
ms
(a)
Full
ness
in th
e ne
ckV
isib
le s
wel
ling
in f
ront
of
neck
Pres
sure
in th
roat
Pain
in f
ront
of
thro
atT
hroa
t pai
n fe
lt in
ear
sL
ump
in th
roat
Cle
arin
g th
roat
oft
enD
isco
mfo
rt s
wal
low
ing
Dif
ficu
lty
swal
low
ing
Sens
e of
suf
foca
ting
Hoa
rsen
ess
Dif
ficu
lty
bre
ath
ing
‡
Hy
pert
hy
roid
sym
pto
ms
(b)
Tre
mbl
ing
hand
sIn
crea
sed
swea
ting
Palp
itat
ions
(ra
pid
hear
t bea
t)Sh
ortn
ess
of b
reat
hSe
nsit
ive
to h
eat
Incr
ease
d ap
peti
teL
oose
sto
ols
Ups
et s
tom
ach
Mu
scle
dis
com
fort
(c,
e,
k,
n)
Tir
edn
ess
(e)
Tir
edne
ssE
xhau
stio
nD
iffi
cult
y ge
ttin
g m
otiv
ated
Wor
n ou
tFu
ll o
f li
feE
nerg
etic
Abl
e to
cop
e w
ith
life
Imp
air
ed s
oci
al
life
(j)
Dif
ficu
lt b
eing
wit
h ot
her
peop
leA
bur
den
to o
ther
peo
ple
Con
flic
ts w
ith
othe
r pe
ople
Peop
le la
ck u
nder
stan
ding
So
cia
l li
fe r
est
ricte
d (
k)
Hy
po
thy
roid
sym
pto
ms
(c)
Sens
itiv
e to
col
dS
wol
len
hand
s or
fee
tD
ry s
kin
Itch
y sk
inP
uff
iness
of
the f
ace
(d)
Con
stip
ati
on
†
Ey
e s
ym
pto
ms
(d)
Moi
st o
r w
ater
y ey
esB
ags
unde
r th
e ey
es
Dry
ness
or
”gri
ttine
ss”
in e
yes
Impa
ired
vis
ion
Pres
sure
in (
or b
ehin
d) e
yes
Dou
ble
visi
onE
ye p
ain
Ver
y se
nsit
ive
to li
ght
Cog
nit
ion
(f)
Dif
ficu
lty
rem
embe
ring
Slow
or
uncl
ear
thin
king
Dif
ficu
lty
find
ing
the
righ
t wor
dsC
onfu
sion
Dif
ficu
lty
lear
ning
new
Dif
ficu
lty
conc
entr
atin
g
An
xie
ty (
g)
Ner
vous
Anx
ious
Ten
seC
once
rned
abo
ut b
eing
ser
ious
ly il
lU
neas
yR
estl
ess
Dep
ress
ivit
y(h
)Sa
dD
epre
ssed
Dis
cour
aged
Cri
ed e
asil
yU
nhap
pyH
appy
Self
-con
fide
ntW
orr
y(g
)
En
joye
d d
ail
y a
cti
viti
es
(e)
Em
oti
on
al
susc
epti
bil
ity
(i)
Dif
ficu
lty
copi
ngFe
elin
g ”n
ot li
ke o
nese
lf”
Eas
ily
feel
ing
stre
ssed
Moo
d sw
ings
Irri
tabl
eFr
ustr
ated
Ang
ryIn
co
ntr
ol
of
life
(h
) *
In b
ala
nce (
h)
*
Imp
air
ed d
ail
yli
fe(k
)D
iffi
cult
y m
anag
ing
dail
y li
feL
imit
leis
ure
acti
viti
esD
iffi
cult
y pa
rtic
ipat
ing
in li
feD
iffi
cult
y ge
ttin
g ar
ound
Eve
ryth
ing
take
s lo
nger
Dif
ficu
lty
man
agin
g jo
b
Imp
air
ed s
exli
fe(l
)N
egat
ive
infl
uenc
e on
sex
life
Dec
reas
ed s
exua
l des
ire
Co
smeti
c co
nce
rn (
m)
Dis
ease
aff
ect a
ppea
ranc
eU
nsat
isfi
ed w
ith
appe
aran
ceC
amou
flag
e or
mas
k vi
sibl
e si
gns
Bot
here
d by
oth
er p
eopl
e lo
okin
gIn
flue
nce
on c
loth
es w
orn
Felt
too
fat
Felt
to
o t
hin
(a
ll s
cale
sexcep
t a
)
Physical symptomsTiredness and
mental health
Impact of
thyroid disease
Over
all
qu
ali
ty o
f li
fe(n
)Q
ua
lity
of
life
Gen
era
l h
ea
lth
perc
epti
on
Feeli
ng
gen
era
lly u
nw
ell
(e)
Th
yro
id-r
ela
ted
qu
ali
ty o
f li
fe(k
)
*Ret
aine
din
mod
el. †
Lac
kof
conv
erge
ntva
lidi
ty. ‡
Lac
kdi
scri
min
antv
alid
ity
in in
divi
dual
pati
ent g
roup
s
Fig
ure 1
.In
itia
l hyp
othe
size
d sc
ale
stru
ctur
e w
ith
the
14 s
cale
s ag
greg
ated
in th
e th
ree
maj
or a
reas
cov
ered
by
the
ques
tion
nair
e: p
hysi
cal s
ympt
oms,
men
tal h
ealt
h(in
clud
ing
tired
ness
) an
d ar
eas
of li
fe im
pact
ed b
y th
yroi
d di
seas
e. I
tem
s no
t sho
win
g di
scri
min
antv
alid
ity
in th
e in
itial
mul
titra
itan
alys
is a
re in
ita
lic
wit
h le
tter
s in
par
enth
eses
indi
cati
ng th
e sc
ales
they
cor
rela
ted
high
er w
ith.
One
item
, als
o in
itali
cbu
t mar
ked
wit
h †,
lack
ed c
onve
rgen
t val
idit
y an
d an
othe
r it
em, m
arke
d w
ith
‡, la
cked
dis
crim
inan
tval
idit
y in
mos
t cli
nica
l sub
grou
ps. T
hese
item
s, a
s w
ell a
s th
e ov
eral
l QoL
scal
e, w
ere
omit
ted
from
the
mod
el, e
xcep
t tho
se m
arke
d w
ith
*.T
he r
evis
ed s
cale
str
uctu
re th
us c
ompr
ises
84
item
s.
Page 101 of 107
Appendix 6: Paper IV
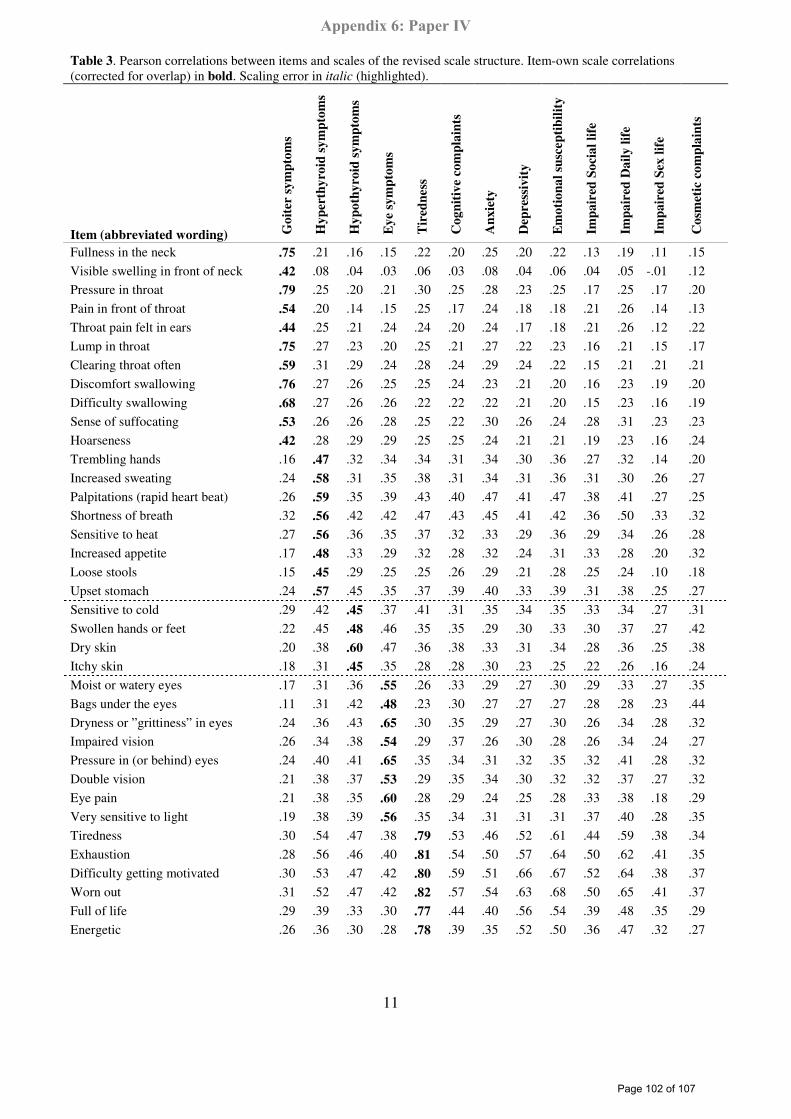
11
Table 3. Pearson correlations between items and scales of the revised scale structure. Item-own scale correlations (corrected for overlap) in bold. Scaling error in italic (highlighted).
Item (abbreviated wording) Go
iter
sy
mp
tom
s
Hy
per
thy
roid
sy
mp
tom
s
Hy
po
thy
roid
sy
mp
tom
s
Ey
e sy
mp
tom
s
Tir
edn
ess
Co
gn
itiv
e co
mp
lain
ts
An
xie
ty
Dep
ress
ivit
y
Em
oti
on
al
susc
ep
tib
ilit
y
Imp
air
ed S
oci
al
life
Imp
air
ed D
ail
y l
ife
Imp
air
ed S
ex l
ife
Co
smet
ic c
om
pla
ints
Fullness in the neck .75 .21 .16 .15 .22 .20 .25 .20 .22 .13 .19 .11 .15
Visible swelling in front of neck .42 .08 .04 .03 .06 .03 .08 .04 .06 .04 .05 -.01 .12 Pressure in throat .79 .25 .20 .21 .30 .25 .28 .23 .25 .17 .25 .17 .20
Pain in front of throat .54 .20 .14 .15 .25 .17 .24 .18 .18 .21 .26 .14 .13
Throat pain felt in ears .44 .25 .21 .24 .24 .20 .24 .17 .18 .21 .26 .12 .22
Lump in throat .75 .27 .23 .20 .25 .21 .27 .22 .23 .16 .21 .15 .17
Clearing throat often .59 .31 .29 .24 .28 .24 .29 .24 .22 .15 .21 .21 .21
Discomfort swallowing .76 .27 .26 .25 .25 .24 .23 .21 .20 .16 .23 .19 .20
Difficulty swallowing .68 .27 .26 .26 .22 .22 .22 .21 .20 .15 .23 .16 .19
Sense of suffocating .53 .26 .26 .28 .25 .22 .30 .26 .24 .28 .31 .23 .23
Hoarseness .42 .28 .29 .29 .25 .25 .24 .21 .21 .19 .23 .16 .24
Trembling hands .16 .47 .32 .34 .34 .31 .34 .30 .36 .27 .32 .14 .20
Increased sweating .24 .58 .31 .35 .38 .31 .34 .31 .36 .31 .30 .26 .27
Palpitations (rapid heart beat) .26 .59 .35 .39 .43 .40 .47 .41 .47 .38 .41 .27 .25 Shortness of breath .32 .56 .42 .42 .47 .43 .45 .41 .42 .36 .50 .33 .32
Sensitive to heat .27 .56 .36 .35 .37 .32 .33 .29 .36 .29 .34 .26 .28
Increased appetite .17 .48 .33 .29 .32 .28 .32 .24 .31 .33 .28 .20 .32
Loose stools .15 .45 .29 .25 .25 .26 .29 .21 .28 .25 .24 .10 .18
Upset stomach .24 .57 .45 .35 .37 .39 .40 .33 .39 .31 .38 .25 .27
Sensitive to cold .29 .42 .45 .37 .41 .31 .35 .34 .35 .33 .34 .27 .31
Swollen hands or feet .22 .45 .48 .46 .35 .35 .29 .30 .33 .30 .37 .27 .42
Dry skin .20 .38 .60 .47 .36 .38 .33 .31 .34 .28 .36 .25 .38
Itchy skin .18 .31 .45 .35 .28 .28 .30 .23 .25 .22 .26 .16 .24
Moist or watery eyes .17 .31 .36 .55 .26 .33 .29 .27 .30 .29 .33 .27 .35
Bags under the eyes .11 .31 .42 .48 .23 .30 .27 .27 .27 .28 .28 .23 .44
Dryness or ”grittiness” in eyes .24 .36 .43 .65 .30 .35 .29 .27 .30 .26 .34 .28 .32 Impaired vision .26 .34 .38 .54 .29 .37 .26 .30 .28 .26 .34 .24 .27
Pressure in (or behind) eyes .24 .40 .41 .65 .35 .34 .31 .32 .35 .32 .41 .28 .32
Double vision .21 .38 .37 .53 .29 .35 .34 .30 .32 .32 .37 .27 .32
Eye pain .21 .38 .35 .60 .28 .29 .24 .25 .28 .33 .38 .18 .29
Very sensitive to light .19 .38 .39 .56 .35 .34 .31 .31 .31 .37 .40 .28 .35
Tiredness .30 .54 .47 .38 .79 .53 .46 .52 .61 .44 .59 .38 .34
Exhaustion .28 .56 .46 .40 .81 .54 .50 .57 .64 .50 .62 .41 .35
Difficulty getting motivated .30 .53 .47 .42 .80 .59 .51 .66 .67 .52 .64 .38 .37
Worn out .31 .52 .47 .42 .82 .57 .54 .63 .68 .50 .65 .41 .37
Full of life .29 .39 .33 .30 .77 .44 .40 .56 .54 .39 .48 .35 .29
Energetic .26 .36 .30 .28 .78 .39 .35 .52 .50 .36 .47 .32 .27
Page 102 of 107
Appendix 6: Paper IV
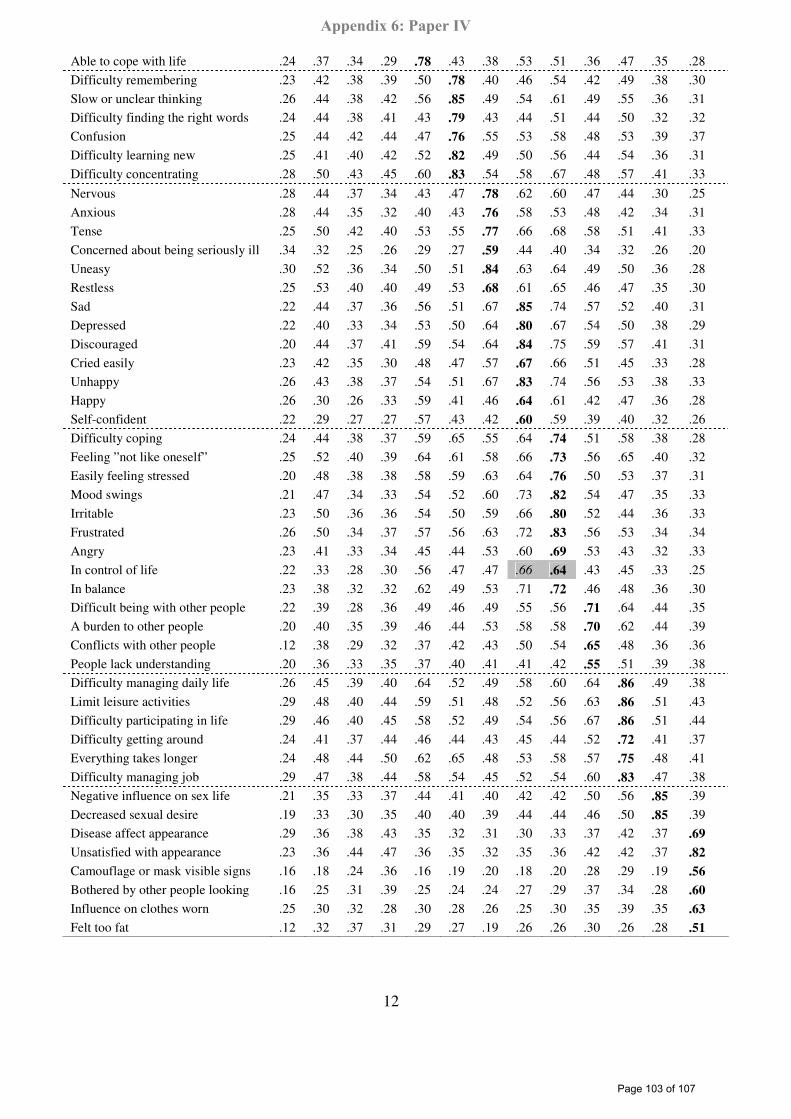
12
Able to cope with life .24 .37 .34 .29 .78 .43 .38 .53 .51 .36 .47 .35 .28
Difficulty remembering .23 .42 .38 .39 .50 .78 .40 .46 .54 .42 .49 .38 .30
Slow or unclear thinking .26 .44 .38 .42 .56 .85 .49 .54 .61 .49 .55 .36 .31 Difficulty finding the right words .24 .44 .38 .41 .43 .79 .43 .44 .51 .44 .50 .32 .32
Confusion .25 .44 .42 .44 .47 .76 .55 .53 .58 .48 .53 .39 .37
Difficulty learning new .25 .41 .40 .42 .52 .82 .49 .50 .56 .44 .54 .36 .31
Difficulty concentrating .28 .50 .43 .45 .60 .83 .54 .58 .67 .48 .57 .41 .33
Nervous .28 .44 .37 .34 .43 .47 .78 .62 .60 .47 .44 .30 .25
Anxious .28 .44 .35 .32 .40 .43 .76 .58 .53 .48 .42 .34 .31
Tense .25 .50 .42 .40 .53 .55 .77 .66 .68 .58 .51 .41 .33
Concerned about being seriously ill .34 .32 .25 .26 .29 .27 .59 .44 .40 .34 .32 .26 .20
Uneasy .30 .52 .36 .34 .50 .51 .84 .63 .64 .49 .50 .36 .28
Restless .25 .53 .40 .40 .49 .53 .68 .61 .65 .46 .47 .35 .30
Sad .22 .44 .37 .36 .56 .51 .67 .85 .74 .57 .52 .40 .31
Depressed .22 .40 .33 .34 .53 .50 .64 .80 .67 .54 .50 .38 .29
Discouraged .20 .44 .37 .41 .59 .54 .64 .84 .75 .59 .57 .41 .31
Cried easily .23 .42 .35 .30 .48 .47 .57 .67 .66 .51 .45 .33 .28 Unhappy .26 .43 .38 .37 .54 .51 .67 .83 .74 .56 .53 .38 .33
Happy .26 .30 .26 .33 .59 .41 .46 .64 .61 .42 .47 .36 .28
Self-confident .22 .29 .27 .27 .57 .43 .42 .60 .59 .39 .40 .32 .26
Difficulty coping .24 .44 .38 .37 .59 .65 .55 .64 .74 .51 .58 .38 .28
Feeling ”not like oneself” .25 .52 .40 .39 .64 .61 .58 .66 .73 .56 .65 .40 .32
Easily feeling stressed .20 .48 .38 .38 .58 .59 .63 .64 .76 .50 .53 .37 .31
Mood swings .21 .47 .34 .33 .54 .52 .60 .73 .82 .54 .47 .35 .33
Irritable .23 .50 .36 .36 .54 .50 .59 .66 .80 .52 .44 .36 .33
Frustrated .26 .50 .34 .37 .57 .56 .63 .72 .83 .56 .53 .34 .34
Angry .23 .41 .33 .34 .45 .44 .53 .60 .69 .53 .43 .32 .33
In control of life .22 .33 .28 .30 .56 .47 .47 .66 .64 .43 .45 .33 .25
In balance .23 .38 .32 .32 .62 .49 .53 .71 .72 .46 .48 .36 .30 Difficult being with other people .22 .39 .28 .36 .49 .46 .49 .55 .56 .71 .64 .44 .35
A burden to other people .20 .40 .35 .39 .46 .44 .53 .58 .58 .70 .62 .44 .39
Conflicts with other people .12 .38 .29 .32 .37 .42 .43 .50 .54 .65 .48 .36 .36
People lack understanding .20 .36 .33 .35 .37 .40 .41 .41 .42 .55 .51 .39 .38
Difficulty managing daily life .26 .45 .39 .40 .64 .52 .49 .58 .60 .64 .86 .49 .38
Limit leisure activities .29 .48 .40 .44 .59 .51 .48 .52 .56 .63 .86 .51 .43
Difficulty participating in life .29 .46 .40 .45 .58 .52 .49 .54 .56 .67 .86 .51 .44
Difficulty getting around .24 .41 .37 .44 .46 .44 .43 .45 .44 .52 .72 .41 .37
Everything takes longer .24 .48 .44 .50 .62 .65 .48 .53 .58 .57 .75 .48 .41
Difficulty managing job .29 .47 .38 .44 .58 .54 .45 .52 .54 .60 .83 .47 .38
Negative influence on sex life .21 .35 .33 .37 .44 .41 .40 .42 .42 .50 .56 .85 .39
Decreased sexual desire .19 .33 .30 .35 .40 .40 .39 .44 .44 .46 .50 .85 .39 Disease affect appearance .29 .36 .38 .43 .35 .32 .31 .30 .33 .37 .42 .37 .69
Unsatisfied with appearance .23 .36 .44 .47 .36 .35 .32 .35 .36 .42 .42 .37 .82
Camouflage or mask visible signs .16 .18 .24 .36 .16 .19 .20 .18 .20 .28 .29 .19 .56
Bothered by other people looking .16 .25 .31 .39 .25 .24 .24 .27 .29 .37 .34 .28 .60
Influence on clothes worn .25 .30 .32 .28 .30 .28 .26 .25 .30 .35 .39 .35 .63
Felt too fat .12 .32 .37 .31 .29 .27 .19 .26 .26 .30 .26 .28 .51
Page 103 of 107
Appendix 6: Paper IV
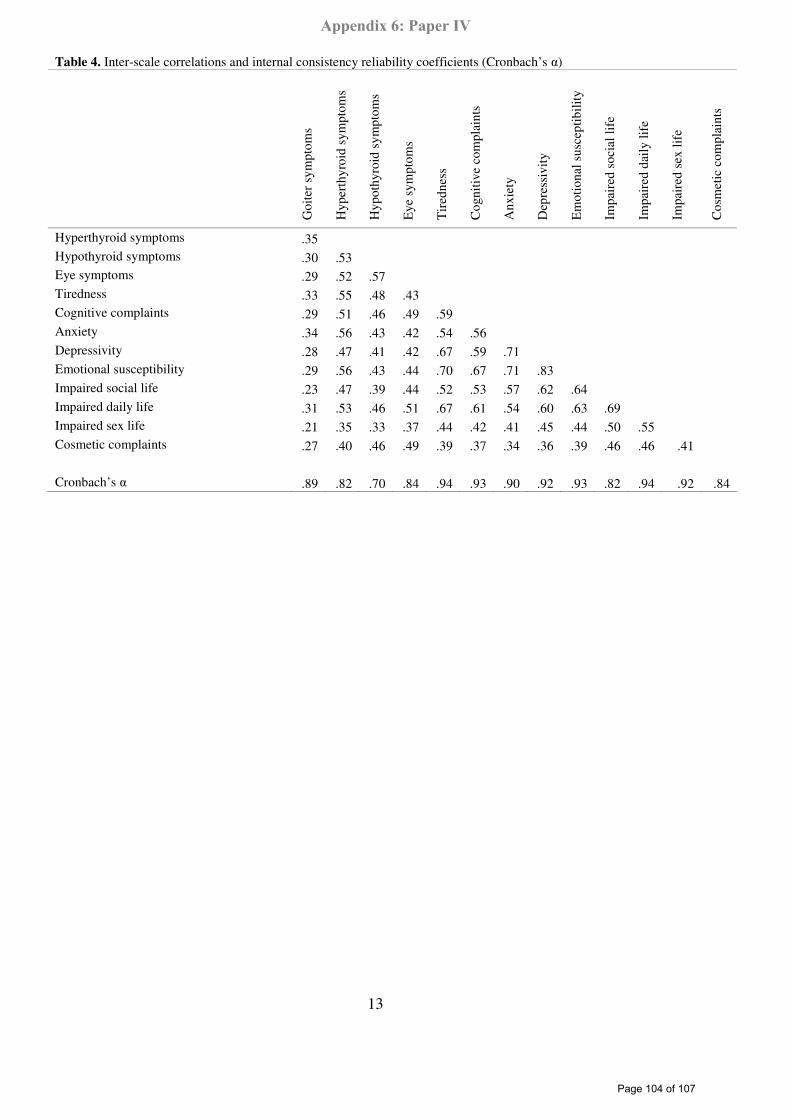
13
Table 4. Inter-scale correlations and internal consistency reliability coefficients (Cronbach’s α)
Goi
ter
sym
ptom
s
Hyp
erth
yroi
d sy
mpt
oms
Hyp
othy
roid
sym
ptom
s
Eye
sym
ptom
s
Tir
edne
ss
Cog
nitiv
e co
mpl
aint
s
Anx
iety
Dep
ress
ivity
Em
otio
nal s
usce
ptib
ility
Impa
ired
soc
ial l
ife
Impa
ired
dai
ly li
fe
Impa
ired
sex
life
Cos
met
ic c
ompl
aint
s
Hyperthyroid symptoms .35 Hypothyroid symptoms .30 .53 Eye symptoms .29 .52 .57 Tiredness .33 .55 .48 .43 Cognitive complaints .29 .51 .46 .49 .59 Anxiety .34 .56 .43 .42 .54 .56 Depressivity .28 .47 .41 .42 .67 .59 .71 Emotional susceptibility .29 .56 .43 .44 .70 .67 .71 .83 Impaired social life .23 .47 .39 .44 .52 .53 .57 .62 .64 Impaired daily life .31 .53 .46 .51 .67 .61 .54 .60 .63 .69 Impaired sex life .21 .35 .33 .37 .44 .42 .41 .45 .44 .50 .55 Cosmetic complaints .27 .40 .46 .49 .39 .37 .34 .36 .39 .46 .46 .41 Cronbach’s α .89 .82 .70 .84 .94 .93 .90 .92 .93 .82 .94 .92 .84
Page 104 of 107
Appendix 6: Paper IV
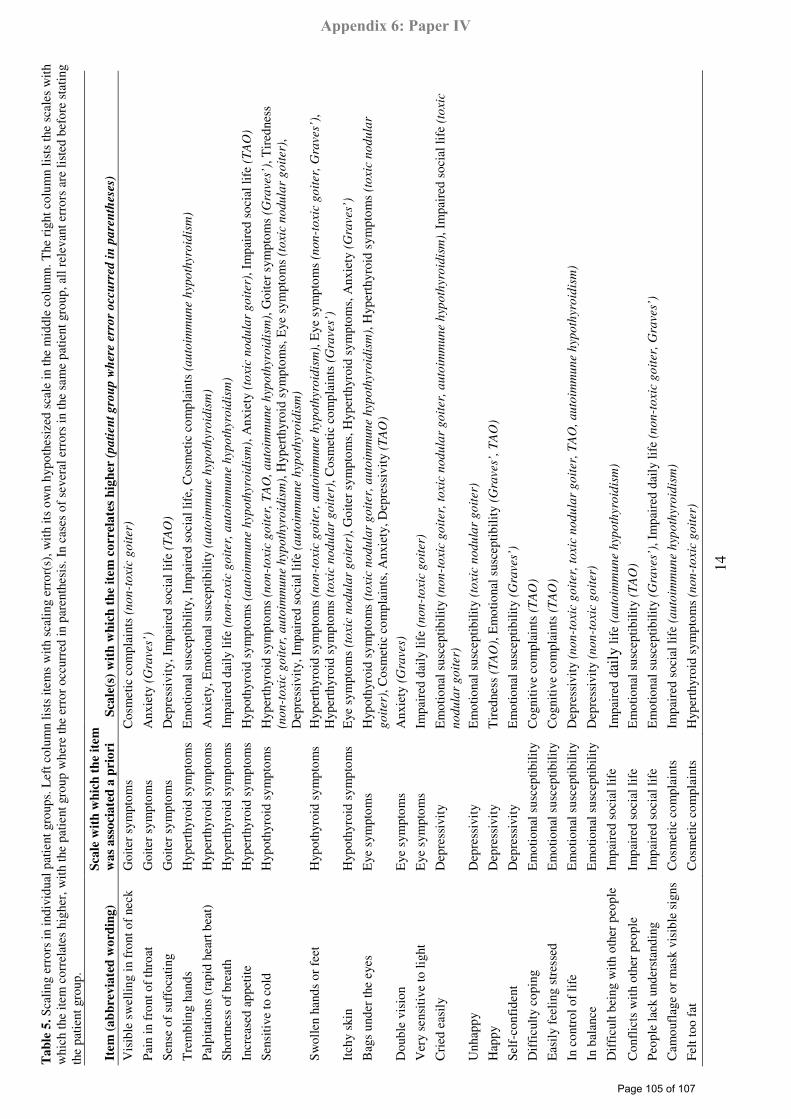
14
Ta
ble
5. S
calin
g er
rors
in in
divi
dual
pat
ient
gro
ups.
Lef
t col
umn
lists
item
s w
ith s
calin
g er
ror(
s), w
ith it
s ow
n hy
poth
esiz
ed s
cale
in th
e m
iddl
e co
lum
n. T
he r
ight
col
umn
lists
the
scal
es w
ith
whi
ch th
e ite
m c
orre
late
s hi
gher
, with
the
patie
nt g
roup
whe
re th
e er
ror
occu
rred
in p
aren
thes
is. I
n ca
ses
of s
ever
al e
rror
s in
the
sam
e pa
tient
gro
up, a
ll re
leva
nt e
rror
s ar
e lis
ted
befo
re s
tatin
g th
e pa
tient
gro
up.
Item
(a
bb
rev
iate
d w
ord
ing
)
Sca
le w
ith
wh
ich
th
e it
em
wa
s a
sso
cia
ted
a p
rio
ri
Sca
le(s
) w
ith
wh
ich
th
e it
em
co
rrel
ate
s h
igh
er (
pa
tien
t g
rou
p w
her
e er
ror
occ
urr
ed i
n p
are
nth
eses
)
Vis
ible
sw
ellin
g in
fro
nt o
f ne
ck
Goi
ter
sym
ptom
s C
osm
etic
com
plai
nts
(no
n-t
oxic
go
iter)
Pain
in f
ront
of
thro
at
Goi
ter
sym
ptom
s A
nxie
ty (
Gra
ves’
)
Sens
e of
suf
foca
ting
Goi
ter
sym
ptom
s D
epre
ssiv
ity,
Im
pair
ed s
ocia
l lif
e (T
AO
)
Tre
mbl
ing
hand
s H
yper
thyr
oid
sym
ptom
s E
mot
iona
l sus
cept
ibili
ty, I
mpa
ired
soc
ial l
ife,
Cos
met
ic c
ompl
aint
s (a
uto
imm
un
e h
ypo
thyro
idis
m)
Palp
itatio
ns (
rapi
d he
art b
eat)
H
yper
thyr
oid
sym
ptom
s A
nxie
ty, E
mot
iona
l sus
cept
ibili
ty (
au
toim
mu
ne h
yp
oth
yro
idis
m)
Shor
tnes
s of
bre
ath
Hyp
erth
yroi
d sy
mpt
oms
Impa
ired
dai
ly li
fe (
no
n-t
oxic
go
iter,
au
toim
mu
ne h
yp
oth
yro
idis
m)
Incr
ease
d ap
petit
e H
yper
thyr
oid
sym
ptom
s H
ypot
hyro
id s
ympt
oms
(au
toim
mu
ne h
yp
oth
yro
idis
m),
Anx
iety
(to
xic
no
du
lar
go
iter)
, Im
pair
ed s
ocia
l lif
e (T
AO
)
Sens
itive
to c
old
Hyp
othy
roid
sym
ptom
s H
yper
thyr
oid
sym
ptom
s (n
on
-to
xic
go
iter,
TA
O,
au
toim
mu
ne h
yp
oth
yro
idis
m),
Goi
ter
sym
ptom
s (G
raves’
), T
ired
ness
(n
on
-to
xic
go
iter,
au
toim
mu
ne
hyp
oth
yro
idis
m),
Hyp
erth
yroi
d sy
mpt
oms,
Eye
sym
ptom
s (t
oxic
no
du
lar
go
iter)
, D
epre
ssiv
ity,
Im
pair
ed s
ocia
l lif
e (a
uto
imm
un
e h
yp
oth
yro
idis
m)
Swol
len
hand
s or
fee
t H
ypot
hyro
id s
ympt
oms
Hyp
erth
yroi
d sy
mpt
oms
(no
n-t
oxic
go
iter,
au
toim
mu
ne
hypoth
yro
idis
m),
Eye
sym
ptom
s (n
on
-to
xic
go
iter,
Gra
ves’
),
Hyp
erth
yroi
d sy
mpt
oms
(to
xic
no
du
lar
go
iter)
, Cos
met
ic c
ompl
aint
s (G
raves’
) It
chy
skin
H
ypot
hyro
id s
ympt
oms
Eye
sym
ptom
s (t
oxic
no
du
lar
go
iter)
, Goi
ter
sym
ptom
s, H
yper
thyr
oid
sym
ptom
s, A
nxie
ty (
Gra
ves’
)
Bag
s un
der
the
eyes
E
ye s
ympt
oms
Hyp
othy
roid
sym
ptom
s (t
oxic
no
du
lar
go
iter,
au
toim
mu
ne
hyp
oth
yro
idis
m),
Hyp
erth
yroi
d sy
mpt
oms
(to
xic
no
du
lar
go
iter)
, Cos
met
ic c
ompl
aint
s, A
nxie
ty, D
epre
ssiv
ity (
TA
O)
Dou
ble
visi
on
Eye
sym
ptom
s A
nxie
ty (
Gra
ves)
Ver
y se
nsiti
ve to
ligh
t E
ye s
ympt
oms
Impa
ired
dai
ly li
fe (
no
n-t
oxic
go
iter)
Cri
ed e
asily
D
epre
ssiv
ity
Em
otio
nal s
usce
ptib
ility
(n
on
-to
xic
go
iter,
to
xic
nod
ula
r go
iter,
au
toim
mu
ne h
ypo
thyro
idis
m),
Im
pair
ed s
ocia
l lif
e (t
oxic
no
du
lar
go
iter)
U
nhap
py
Dep
ress
ivit
y E
mot
iona
l sus
cept
ibili
ty (
toxic
no
du
lar
go
iter)
Hap
py
Dep
ress
ivit
y T
ired
ness
(T
AO
), E
mot
iona
l sus
cept
ibili
ty (
Gra
ves’
, T
AO
)
Self
-con
fide
nt
Dep
ress
ivit
y E
mot
iona
l sus
cept
ibili
ty (
Gra
ves’
)
Dif
ficu
lty c
opin
g E
mot
iona
l sus
cept
ibili
ty
Cog
nitiv
e co
mpl
aint
s (T
AO
)
Eas
ily f
eelin
g st
ress
ed
Em
otio
nal s
usce
ptib
ility
C
ogni
tive
com
plai
nts
(TA
O)
In c
ontr
ol o
f lif
e E
mot
iona
l sus
cept
ibili
ty
Dep
ress
ivit
y (n
on
-to
xic
go
iter,
to
xic
nod
ula
r g
oit
er,
TA
O,
au
toim
mu
ne h
ypo
thyro
idis
m)
In b
alan
ce
Em
otio
nal s
usce
ptib
ility
D
epre
ssiv
ity
(no
n-t
oxic
go
iter)
Dif
ficu
lt be
ing
with
oth
er p
eopl
e Im
pair
ed s
ocia
l lif
e Im
pair
ed d
aily
life
(a
uto
imm
un
e h
ypo
thyro
idis
m)
Con
flic
ts w
ith o
ther
peo
ple
Impa
ired
soc
ial l
ife
Em
otio
nal s
usce
ptib
ility
(T
AO
)
Peop
le la
ck u
nder
stan
ding
Im
pair
ed s
ocia
l lif
e E
mot
iona
l sus
cept
ibili
ty (
Gra
ves’
), I
mpa
ired
dai
ly li
fe (
no
n-t
oxic
go
iter,
Gra
ves’
)
Cam
oufl
age
or m
ask
visi
ble
sign
s C
osm
etic
com
plai
nts
Impa
ired
soc
ial l
ife
(au
toim
mu
ne h
ypo
thyro
idis
m)
Felt
too
fat
Cos
met
ic c
ompl
aint
s H
yper
thyr
oid
sym
ptom
s (n
on
-to
xic
go
iter)
Page 105 of 107
Appendix 6: Paper IV
15
References 1. Fahrenfort JJ, Wilterdink AM, van der Veen EA.
Long-term residual complaints and psychosocial sequelae after remission of hyperthyroidism. Psychoneuroendocrinology 2000; 25(2): 201-11.
2. Terwee CB, Gerding MN, Dekker FW, Prummel MF, Wiersinga WM. Development of a disease specific quality of life questionnaire for patients with Graves' ophthalmopathy: the GO-QOL. Br J Ophtalmol 1998; 82(7): 773-9.
3. Terwee CB, Gerding MN, Dekker FW, Prummel MF, van der Pol JP, Wiersinga WM. Test-retest reliability of the GO-QOL: a disease-specific quality of life questionnaire for patients with Graves' ophthalmopathy. J Clin Epidemiol 1999; 52(9): 875-84.
4. Terwee CB, Dekker FW, Mourits MP, Gerding MN, Baldeschi L, Kalmann R, Prummel MF, Wiersinga WM. Interpretation and validity of changes in scores on the Graves' ophthalmopathy quality of life questionnaire (GO-QOL) after different treatments. Clin Endocrinol (Oxf) 2001; 54(3): 391-8.
5. Tehrani M, Krummenauer F, Mann WJ, Pitz S, Dick HB, Kahaly GJ. Disease-specific assessment of quality of life after decompression surgery for Graves' ophthalmopathy. Eur J Ophtalmol 2004; 14(3): 193-9.
6. Jaeschke R, Guyatt G, Gerstein H, Patterson C, Molloy W, Cook D, Harper S, Griffith L, Carbotte R. Does treatment with L-thyroxine influence health status in middle-aged and older adults with subclinical hypothyroidism? J Gen Int Med 1996; 11(12): 744-9.
7. Jaeschke R, Guyatt G, Cook D, Harper S, Gerstein HC. Spectrum of quality of life impairment in hypothyroidism. Qual Life Res 1994; 3(5): 323-7.
8. Saravanan P, Chau WF, Roberts N, Vedhara K, Greenwood R, Dayan CM. Psychological well-being in patients on 'adequate' doses of l-thyroxine: results of a large, controlled community-based questionnaire study. Clin Endocrinol (Oxf) 2002; 57(5): 577-85.
9. McMillan CV, Bradley C, Woodcock A, Razvi S, Weaver JU. Design of new questionnaires to measure quality of life and treatment satisfaction in hypothyroidism. Thyroid 2004; 14(11): 916-25.
10. Watt T, Groenvold M, Rasmussen AK, Bonnema SJ, Hegedüs L, Bjorner JB, Feldt-Rasmussen U. Quality of life in patients with benign thyroid disorders. A review. Eur J Endocrinol 2006; 154: 501-10.
11. Watt T, Hegedus L, Rasmussen AK, Groenvold M, Bonnema SJ, Bjorner JB, Feldt-Rasmussen U. Which domains of thyroid-related quality of life are most relevant? Patients and clinicians provide complementary perspectives. Thyroid 2007; 17(7): 647-54.
12. Watt T, Rasmussen AK, Groenvold M, Bjorner JB, Watt SH, Bonnema SJ, Hegedüs L, Feldt-Rasmussen U. Improving a newly developed patient-reported outcome for thyroid patients, using cognitive interviewing. Qual Life Res 2008; (Online publication ahead of print).
13. Nunnally JC, Bernstein I. Psychometric Theory., 3 Edn. New York: McGraw-Hill, 1994.
14. Fayers PM, Machin D. Quality of Life: Assessment, Analysis and Interpretation. Chichester: John Wiley and Sons, 2000.
15. Hays RD, Hayashi T, Carson S et al. User's guide for the multitrait analysis program (MAP). Rand Corporation, 1988.
16. Ware JE, Jr., Harris WJ, Gandek B et al. MAP-R for Windows: Multitrait/multi-item analysis program - revised user's guide. Boston: Health Assessment Lab, 1997.
17. Campbell DT, Fiske DW. Convergent and discriminant validation by the multitrait-multimethod matrix. Psychol Bull 1959; 56(2): 81-105.
18. Werner SC. Modification of the classification of the eye changes of Graves' disease: recommendations of the Ad Hoc Committee of the American Thyroid Association. J Clin Endocrinol Metab 1977; 44(1): 203-4.
19. Mourits MP, Prummel MF, Wiersinga WM, Koornneef L. Clinical activity score as a guide in the management of patients with Graves' ophthalmopathy. Clin Endocrinol (Oxf) 1997; 47(1): 9-14.
20. Hegedus L. Thyroid ultrasound. Endocrinol Metab Clin North Am 2001; 30(2): 339-ix.
Page 106 of 107
Appendix 6: Paper IV
16
21. Bjorner JB, Damsgaard MT, Watt T, Groenvold M. Tests of data quality, scaling assumptions, and reliability of the Danish SF-36. J Clin Epidemiol 1998; 51(11): 1001-11.
22. Cronbach LJ. Coefficient alpha and the internal structure of tests. Psychometrika 1951; 16: 297-334.
23. Drasgow J. Polychoric and polyserial correlations. In: Kotz S, Johnson NL, Read CB, editors. Encyclopedia of Statistical Sciences. New York: John Wiley and Sons, 1986.
24. Muthen B. A General Structural Equation Model with Dichotomous, Ordered Categorical, and Continuous Latent Variable Indicators. Psychometrika 1984; 49(1): 115-32.
25. Olsson U. Maximum likelihood estimation of the polychoric correlation coefficient. Psychometrika 1979; 44(4): 443-60.
26. van Nispen RM, Knol DL, Langelaan M, de Boer MR, Terwee CB, van Rens GH. Applying multilevel item response theory to vision-related quality of life in Dutch visually impaired elderly. Optom Vis Sci 2007; 84(8): 710-20.
27. Fayers PM, Hand DJ, Bjordal K, Groenvold M. Causal indicators in quality of life research. Qual Life Res 1997; 6(5): 393-406.
28. Fayers PM, Hand DJ. Factor analysis, causal indicators and quality of life. Qual Life Res 1997; 6(2): 139-50.
29. Muthen B. Multiple-group structural modelling with non-normal continuous variables. British Journal of Matemathical and Statistical Psychology 1989;42:55-62.
30. Bollen KA, Barb KH. Pearson r and coarsely categorized measures. American Sociological Review 1981; 46: 232-9.
31. Abraham-Nordling M, Torring O, Hamberger B, Lundell G, Tallstedt L, Calissendorff J, Wallin G. Graves' disease: a long-term quality-of-life follow up of patients randomized to treatment with antithyroid drugs, radioiodine, or surgery. Thyroid 2005; 15(11): 1279-86.
32. Abraham P, Avenell A, Watson WA et al. Antithyroid drug regimen for treating Graves' hyperthyroidism (Cochrane Review). The Cochrane Library, Issue 3. Chichester,UK: John Wiley & Sons, Ltd., 2004.
33. Joffe RT, Brimacombe M, Levitt AJ, Stagnaro-Green A. Treatment of clinical hypothyroidism with thyroxine and triiodothyronine: A literature review and metaanalysis. Psychosomatics 2007; 48(5): 379-84.
34. Watt T, Feldt-Rasmussen U, Rasmussen AK, Hegedus L, Bonnema SJ, Gronvold M, Bjorner JB. [Measurement of health-related quality of life in thyroid patients]. Ugeskr Laeger 2008; 170(10): 850-2.
Page 107 of 107
Appendix 6: Paper IV