Where Am I? A new case of developmental topographical disorientation
18
Journal of Neuropsychology (2013) © 2013 The British Psychological Society www.wileyonlinelibrary.com Research paper Where Am I? A new case of developmental topographical disorientation Filippo Bianchini 1,2 , Liana Palermo 1,2 , Laura Piccardi 1,3 , Chiara Incoccia 1 , Federico Nemmi 1,2 , Umberto Sabatini 1 and Cecilia Guariglia 1,2 * 1 Dipartimento Psicologia 39, Sapienza Universit a di Roma, Italy 2 I.R.C.C.S. Fondazione Santa Lucia, Rome, Italy 3 Dipartimento di Scienze della Salute, Universit a degli Studi di L’Aquila, Coppito 2 (AQ), Italy Recently, developmental topographical disorientation (DTD) was described (Bianchini et al., 2010, J Clin Exp Neuropsychol, 20, 807–27; Iaria & Barton, 2010, Exp Brain Res, 206, 189–96; Iaria, Bogod, Fox, & Barton, 2009, Neuropsychologia, 47, 30–40) as a navigational deficit in the absence of neurological or psychiatric disorders. Here, we reported the case of a healthy subject who presented this disorder. Dr. WAI was a 29-year-old right-handed man with normal development and no clinical history of neurological or psychiatric diseases who was affected by a very pervasive topographical orientation and navigational disorder. A neuroradiological exam confirmed the absence of structural and anatomical alterations of the brain. Dr. WAI was submitted to an extensive neuropsychological examination and to a battery of tests specifically developed to assess developmental topographical disorder. Using this battery, we analysed Dr. WAI’s acquisition of navigational information and re- orientation processes. He showed severe DTD accompanied by deficits of different cognitive processes directly or indirectly involved in navigational skills. Dr. WAI showed a deficit in developing cognitive maps, already found in previous cases, plus difficulties in evaluating distances and computing metric environmental features. He represents a further confirmation of the existence of DTD suggesting dissociations within the disorder related to the level of development of the ability to build cognitive maps and the association of different imagery deficits. Dr. WAI can help in shedding some light on the mechanisms underlying lack of development of navigational skills. Human spatial navigation includes abilities such as wayfinding in complex environments, perceiving distances, and directional relationships, mentally transforming landmarks with respect to their position or orientation in space, planning routes to distant locations, *Correspondence should be addressed to Cecilia Guariglia, Dipartimento di Psicologia, Sapienza Universit a di Roma, Via dei Marsi, 78, Rome 00185, Italy (e-mail: [email protected]). DOI:10.1111/jnp.12007 1
Transcript of Where Am I? A new case of developmental topographical disorientation

Journal of Neuropsychology (2013)
© 2013 The British Psychological Society
www.wileyonlinelibrary.com
Research paper
Where Am I? A new case of developmentaltopographical disorientation
Filippo Bianchini1,2, Liana Palermo1,2, Laura Piccardi1,3,Chiara Incoccia1, Federico Nemmi1,2, Umberto Sabatini1 andCecilia Guariglia1,2*1Dipartimento Psicologia 39, Sapienza Universit�a di Roma, Italy2I.R.C.C.S. Fondazione Santa Lucia, Rome, Italy3Dipartimento di Scienze della Salute, Universit�a degli Studi di L’Aquila, Coppito 2
(AQ), Italy
Recently, developmental topographical disorientation (DTD) was described (Bianchini
et al., 2010, J Clin Exp Neuropsychol, 20, 807–27; Iaria & Barton, 2010, Exp Brain Res, 206,
189–96; Iaria, Bogod, Fox, & Barton, 2009, Neuropsychologia, 47, 30–40) as a navigationaldeficit in the absence of neurological or psychiatric disorders. Here, we reported the case
of a healthy subject who presented this disorder. Dr.WAI was a 29-year-old right-handed
manwith normal development andnoclinical historyof neurological or psychiatric diseases
whowas affected by a very pervasive topographical orientation andnavigational disorder.A
neuroradiological exam confirmed the absence of structural and anatomical alterations of
the brain.Dr.WAIwas submitted to an extensive neuropsychological examination and to a
battery of tests specifically developed to assess developmental topographical disorder.
Using this battery, we analysed Dr. WAI’s acquisition of navigational information and re-
orientation processes. He showed severe DTD accompanied by deficits of different
cognitive processes directly or indirectly involved in navigational skills. Dr.WAI showed a
deficit in developing cognitive maps, already found in previous cases, plus difficulties in
evaluating distances and computingmetric environmental features.He represents a further
confirmation of the existence of DTD suggesting dissociations within the disorder related
to the level of development of the ability to build cognitive maps and the association of
different imagery deficits. Dr. WAI can help in shedding some light on the mechanisms
underlying lack of development of navigational skills.
Human spatial navigation includes abilities such as wayfinding in complex environments,
perceiving distances, and directional relationships,mentally transforming landmarkswithrespect to their position or orientation in space, planning routes to distant locations,
*Correspondence should be addressed to Cecilia Guariglia, Dipartimento di Psicologia, Sapienza Universit�a di Roma, Via deiMarsi, 78, Rome 00185, Italy (e-mail: [email protected]).
DOI:10.1111/jnp.12007
1

returning to the starting point after a long walk in a novel environment (Lawton, 2010;
Wolbers & Hegarty, 2010). Humans present a large variability in navigational abilities,
concerning the precision with which spatial information is encoded from sensory
experiences, the ability to form spatial representations of external environments and theefficacy in using them to guide navigational behaviour. Levels of different navigational
skills are not independent and interact, contributing to obtain good performances in
navigational tasks (for a review see Wolbers & Hegarty, 2010).
Inhealthy children, navigational competencies develop gradually and at distinct points
in time (Siegel &White, 1975; Lehnung et al., 2003). By the age of 6–9 months, children
find their bearings in the environment using only egocentric strategies (see, Acredolo,
1978; Hermer & Spelke, 1994). At 11 months they use information about landmarks and
landmark arrays (Acredolo, 1978; Acredolo & Evans, 1980). Between 18 and 24 months,toddlers are able to find hidden objects by using both navigational strategies (Hermer and
Spelke, 1994; Hermer & Spelke, 1996; Newcombe et al., 1998). The cognitive mapping
knowledge develops later and it is not fully functioning until the age of 10 years (Lehnung
et al., 1998; 2003).
Wang and Spelke’s (2002) proposed a theoretical distinction among three cognitive
processes subserving topographical orientation, which humans share with other species
(1) path integration, which is a process that operates by dynamic updating subject’s
location according to her/his movements in the environment; (2) view-dependent placerecognition, a process based on place and landmark recognition that matches viewpoint-
dependent representations of landmarks; (3) re-orientation, which operates by congru-
ence-finding on representations of the shape of the environment. Some capabilities to rely
on these processes are already present in very young children (18–24 months old; Hermer
& Spelke, 1996) who are still unable to fully develop cognitive maps.
Siegel and White (1975) proposed a theoretical model of environmental knowledge
that considers three different levels in acquiring spatial information: landmark knowl-
edge, route knowledge, and survey knowledge. At level of landmark knowledge,
individuals possess the ability to perceptually discriminate and recognize landmarks, but
are unable to derive from them any directional information (where a landmark is, which is
its relation with the environment andwith other landmarks). At level of route knowledge
directional information based on egocentric representation are added to landmark
knowledge allowing individuals to navigate by following directional instructions linking
consecutive landmarks (turn left at this landmark to reach the next one). The survey
knowledge consists in a mental map representation of the environment, based on an
allocentric frame of reference.When a brain disease impairs navigational abilities, patients often experience
devastating effects on their everyday lives. Specifically, topographical disorientation is
generally considered a consequence of acquired focal brain damages, dementia, and
congenital brain malformations (Barrash, 1998; Iaria et al., 2005; Pai & Jacobs, 2004) and
is characterized by selective loss of the ability to navigate in new or well-known
environments (Maguire, Burke, Phillips, & Staunton, 1996). Recently, a developmental
type of topographical disorientation (DTD) has also been described (Bianchini et al.,
2010; Iaria et al., 2009). DTD is a selective disorder of topographical orientation andnavigation in people who have no cerebral damage or perinatal problems. Since, there is,
until now, an unknown factor that affects the brain’s ability to receive and process
navigational information causing DTD, authors placed this disorder in the category of
selective developmental disorders, which includes dyslexia, developmental prosopoagn-
osia and selective language delay. Also in these disorders as in DTD, patients showed a
2 Filippo Bianchini et al.
normal intelligence without brain damage or other clear factors that could explain the
disorder in itself. Patients with DTD normally developed other cognitive abilities, but
complained a specific topographical deficit pervasive throughout the lifespan (see
Bianchini et al., 2010 and Iaria et al., 2009). The first reported case (Iaria et al., 2009)wasa 43-year-old woman (Pt1) who had no brain injury or psychiatric disease, but showed
persistent difficulty in topographical orientation. Subsequently, Bianchini et al. (2010)
described a 22-year-old man (F.G.) who showed a more pervasive disorder including
almost all processes involved in topographical knowledge and environmental navigation.
Specifically, Pt1 had a severe deficit in the formation of the mental map of the
environment; however, once she had acquired such a map through overtraining, her
performance on the retrieval task was similar to that of a control group. According to Iaria
et al. (2009) these findings point to an impairment specific to the acquisition rather thanthe retrieval and use of amental representation of the environment. Furthermore, shewas
able to develop successfully verbal scripts that helped her in orienteering in route-based
navigation tasks. She has also developed the ability to segregate and identify landmarks in a
landscape. Differently, F.G., the case described by Bianchini et al. (2010), showed amore
pervasive and severe topographical disorientation. Indeed, he was unable to learn the
path shown by the examiner in the route-based navigation task as well as to follow a path
shown on amap, showing also a deficit in translating the visual–spatial information of the
maps into verbal scripts. F.G. used the verbal scripts only when someone else providesthem. He failed in segregating and identifying a landmark in a landscape, and even when
he recognized a landmark he did not know its location or the directional information he
could derive from it.
More recently, Iaria and Barton (2010) reported a consistent number of individuals
who showed deficits in navigation and the ability to orient themselves in the
environment in an online evaluation in which participants performed nine tests (object
recognition; face identity, and expression recognition; landmark recognition; heading
orientation; left/right orientation (no landmarks); path reversed (no landmarks;formation and use of a cognitive map) including recognition of face, objects, and
landmarks as well as navigation tasks in virtual environments. This study confirmed that
DTD is not rare and suggests that its incidence could be comparable to that of other
selective developmental disorders, such as developmental prosopagnosia. Although, the
online assessment did not permit a thorough analysis of the cognitive components of
DTD, the study provides a large sample in which many different orientation strategies are
affected. Specifically, they found that people affected by DTD differ from matched
healthy controls only in those skills confined to the orientation/navigation domain,among which the ability to form a cognitive map was the most significant factor
distinguishing a person with DTD from one without DTD.
Here, we present another case of DTD in a healthy subject who was submitted to an
extensive evaluation aimed at clarifying the nature of his disorder. To preserve the
subject’s anonymity, we call him Dr. WAI, which is an acronym derived from “Where Am
I?”. Dr.WAIwas a 29-year-old right-handedmanwith normal development and no clinical
history of neurological or psychiatric disorders. Hewas submitted to an extensive battery,
that is, the DDTDB (DiViNa Developmental Topographical Disorientation Battery)consisting of navigational tasks and neuropsychological tests to analyse the nature of his
topographical disorientation. Analysis of Dr. WAI’s performance confirmed the presence
of pervasive DTD, but with characteristics that differed somewhat from those of
previously described cases. Dr. WAI increases our knowledge of this recently described
disorder, throwing some light on the mechanisms underlying lack of development of
Developmental topographical disorientation 3

navigational skills. Indeed, this case adds to the literature the suggestion that not onlyDTD
exists, but different types of it might be observed depending on the level of development
of the ability to build cognitivemaps and the association of different imagery deficits. This
could represent the first step for reasoning about the need of a taxonomy for DTD thatcould be different from those existing for acquired topographical disorders.
Case Report
Dr.WAIwas a 29-year-old, right-handedman (Salmaso&Longoni, 1985). Hehad aMaster’s
degree and during the period of the DDTDB evaluation he was enrolled in a Ph.D.programme. Dr. WAI was normal at birth and had no perinatal complications;
furthermore, his clinical history showed no motor, neurological or cognitive develop-
mental delays or neurological or psychiatric diseases.
Dr. WAI contacted the Neuropsychological Unit of the IRCCS Fondazione Santa Lucia
in Rome after reading an announcement to recruit individuals with navigational disorders
at University, during the spring of 2009. At the first appointment, he had reported
difficulty in finding his way in familiar places and in learning new routes in the
environment. He said that he never knewwhich direction to take to arrive at his office andthat he always had doubts when he went towards the centre of town or in the opposite
direction. Furthermore, he only realized his errors when he reached the edge of the city
and the ring road (GRA in Rome) because hewas unable to calculate the distance between
one known landmark and another.
He reported that when he went out with friends they never wanted him to drive
because he often lost his way. He suffered because of this and felt under pressure to
choose the right route. But,when he came to an intersection hewas uncertainwhether he
should go left or right. When we interviewed his colleagues, they confirmed that Dr. WAIwas unable to orient himself in the environment. Indeed, for several months after he
started the Ph.D. programme, Dr. WAI was able to go from one wing of the institute
(where the Ph.D. courses were held) to another wing only if someone accompanied him
because he systematically had difficulty finding the correct route when he was alone. Dr.
WAI said that he used an external electronic aid (a GPS navigator) to orient himself,
especiallywhen hewas notwith his girlfriend.When hewaswith her, she gave him verbal
indications.
We decided to investigate Dr. WAI’s navigational abilities by assessing the differentcognitive processes and strategies involved in topographical orientation. For this
purpose, we submitted him to a neuroradiological examination (MRI), a neuropsycho-
logical assessment, which included tests of general cognitive functioning, memory, and
a comprehensive evaluation of his ability to navigate by means of DDTDB, which
was specifically developed to assess DTD (derived from Bianchini et al., 2010). We
obtained written informed consent from Dr. WAI and approval from the local ethics
committee.
Methods
Neuroradiological exam
Magnetic Resonance imaging (MRI) was performed on a scanner (Allegra; Siemens
Medical Solutions, Erlangen, Germany) operating at 3.0 T, with a maximum gradient
strength of 40 mT/m, using a standard quadrature birdcage head coil for both RF
4 Filippo Bianchini et al.
transmission and RF reception. The protocol included axial, coronal, and sagittal T2-
weighted turbo spin-echo sequences (TR = 3,500 ms, TE = 354 ms), axial fluid-attenu-
ated inversion recovery (FLAIR) sequences (TR = 8,500, TE = 109, inversion time = 200)
covering the whole brain. We obtained 22, 5 mm gapless sections and a 256 9 256matrix using all available MR imaging techniques. The axial and coronal sections ran,
respectively, parallel and perpendicular to a line joining the anterior and posterior
commissures (AC–PC line). Whole-brain T1-weighted images were also obtained in the
sagittal plane using a modified driven equilibrium Fourier transform sequence (TE/
TR = 2.4/7.92 ms, flip angle 15°, voxel-size 1 mm 9 1 mm 9 1 mm). Two neuroradi-
ologists assessed all of Dr. WAI’s images.
His MRI examinations revealed homogeneous signal intensity of the cerebral
parenchyma, with no focal abnormality in either grey or white matter. His cortex wasof normal thickness with regular sulcation and gyration. His corpus callosum was of
normal thickness and presented regular morphology and homogeneous signal intensity.
His ventricular system was normal in size and symmetrical at the midline. The sub-
arachnoid spaces were regular. Both hippocampi were normal in morphology and size,
with a regular profile and signal intensity. Overall, the MRI examination presented a
completely normal picture (see Figure 1).
Neuropsychological assessment
During the entire evaluation, Dr. WAI was motivated and cooperative. His language
production and comprehension were normal. Furthermore, his Intelligence Quotient,
evaluated by means of the WAIS-R (Italian Version; Laicardi & Orsini, 1997), was within
the normal range (Total IQ = 123) and with a significant 25-point difference between
Verbal IQ (132) and Performance IQ (107) (see Table 1). Dr. WAI’s short-term and long-
term memory abilities on visuospatial and verbal tests (Carlesimo et al., 1996, 1996;
Spinnler & Tognoni, 1987) were within the normal range (see Table 1).
Figure 1. Four axial (upper panel) and four coronal (lower panel) slices of Dr.WAI’s structural MP
RAGE showing medial temporal lobe structures. Two magnified images of the hippocampus proper in a
coronal view are shown. MTL structures and hippocampus, as confirmed by an experienced
neuroradiologist, show the absence of any acquired or congenital brain damage.
Developmental topographical disorientation 5
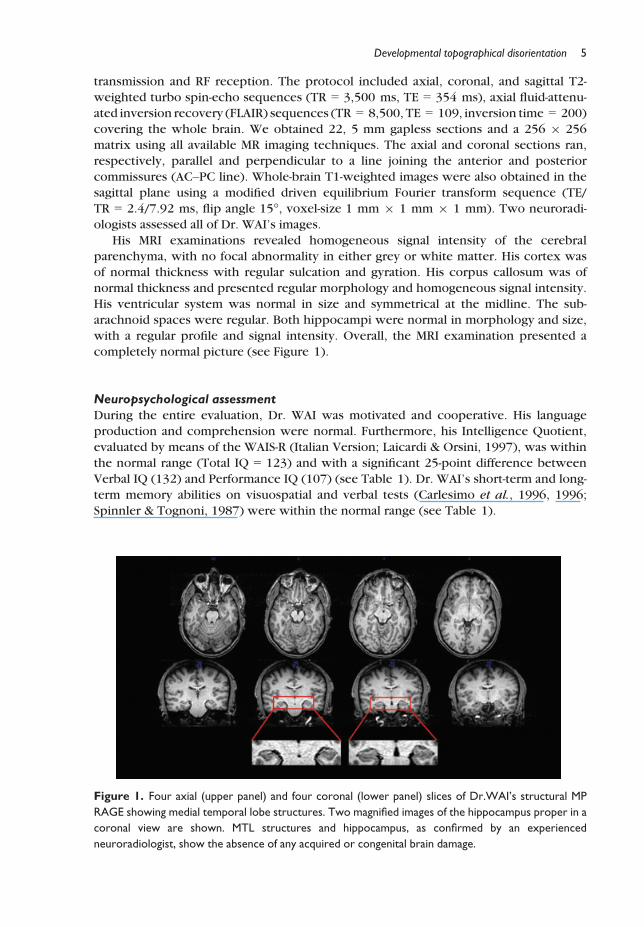
Table 1. Results of the neuropsychological assessment that included tests standardized for use with
Italian-speaking patients. For tests lacking standardization data (*) we recruited controls matched for age,
gender, and years of education. Performances below the cut-off are in bold
Test DR.WAI Score Cut-off
General intelligence
Wechsler adult intelligence Scale–Revised (Laicardi & Orsini, 1997)
Full scale IQ 123 <75Verbal IQ 132 <75Information 17 4
Digit span 9 4
Vocabulary 18 4
Arithmetic 14 4
Comprehension 17 4
Similarities 14 4
Performance IQ 107 <75Picture completion 10 4
Picture arrangement 10 4
Block design 12 4
Object assembly 12 4
Digit symbol 11 4
Memory
Verbal memory
Rey’s 15 word learning task (Carlesimo et al., 1996)
Immediate recall 65/75 40.12/75
15 min delayed recall 15/15 8.28/15
Spatial memory
Rey’s complex figure (Carlesimo et al., 2002)
Copy 36/36 27.36/36
30 s delayed recall 24/36 14.21/36
20 min delayed recall 22/36 14.33/36
Oblivion 2 >4.25Corsi Block Test (Spinnler & Tognoni, 1987)
Span 4/9 Mean = 5.28; SD = 0.88 (t = �1.437; p = n.s.)
*Supra-span (n.cubes) 130/144 Mean = 132.40; SD = 7.13 (t = 0.307; p = n.s.)
*Supra-span recall (n.cubes) 8/8 Mean = 8.00; SD = 0.00 (t = 0.00; p = n.s.)
Visual-perceptual abilities
VOSP (Warrington & James, 1991)
Object perception
Screening test 20/20 15/20
Incomplete letters 20/20 17/20
Silhouettes 22/30 16/30
Object decision 16/20 15/20
Progressive silhouettes 9/20 >14/20Space perception
Dot counting 10/10 8/10
Position discrimination 20/20 18/20
Number location 8/10 7/10
Cube analysis 11/10 6/10
Benton’s facial recognition
test (Benton et al., 1975)
47/54 40/54
6 Filippo Bianchini et al.
Navigational skills assessment
Processes of acquisition of navigational information and re-orientationwere assessedwith
the DDTDB, derived from tests used by Bianchini et al. (2010) in a previous study of DTD,
based on theoretical models of normal development and normal navigation stages (Siegel&White, 1975; Wang & Spelke, 2002). The battery included three different categories of
tasks. The first category assessed specific domains such as visual spatial perception,
visuospatial memory and visuospatial imagery (see Table 2). The second and third
categories of tests assessed specific navigational abilities, respectively, in an experimental
and an ecological environment (see Table 2).
Dr. WAI’s performance on tests lacking standardization data was compared with that
of male volunteers (C) matched for age and years; the number of C varied from 20 to 5 in
different tests. Dr.WAI’s and controls’ performanceswere compared bymeans of analysisdeveloped by Crawford and Howell (1998; CH), using the computer program
SINGLIMS.EXE. This analysis uses a modified t test described by Sokal and Rohlf (1995)
and is themore suitable analysis to estimate the abnormality of the individual scoreswhen
the normative sample is small (that is less than 50 subjects).
Results for each test (as well as size of C group) are described below and shown in
Table 2.
Visuospatial perception, memory, and imagery evaluation
Assessment of Dr. WAI’s basic visuospatial abilities included tests of visuospatial
perception (Visual Object Spatial Perception Battery, Benton’s Facial Recognition Test),
visuospatial memory (Corsi Block Tapping Test: Span and Supraspan), and visuospatial
imagery (Memory of buildings, Letter Inspection Test,Mental Rotation Test, Generation of
imagery from long-term memory as Map drawing of current home) (see Tables 1 and 2).
Only tests not commonly used in clinical practice are described below.
On the Corsi Block Tapping Test (CBT; Corsi, 1972), Dr. WAI had a normal span, aswell as normal Supra-span learning and delayed recallwhen comparedwith a group of five
controls. His performance in object and space perception (Visual Object Spatial
Perception Battery, Warrington & James, 1991) and face recognition (Benton’s Facial
Recognition Test, Benton, VanAllen, Hamsher, & Levin, 1975)waswellwithin the normal
range (see Table 1).
Topographical abilities involve some specific aspects of cognition, such as
recognizing landmarks and scenes and describing and drawing a map of a familiar
environment, which rely on visual imagery abilities (Farah, 1989; Riddoch & Humph-reys, 1989). As in Bianchini et al.’s (2010) study, we referred to Kosslyn’s model (2005)
in Dr. WAI’s assessment, to evaluate processes of generation, inspection, and
transformation of visual mental images. We used Buildings Task (a modified version of
Nori & Giusberti, 2006; described in Palermo, Piccardi, Nori, Giusberti, & Guariglia,
2010) for evaluating the ability to generate a visual mental image from short-term
memory. Dr. WAI was asked to close his eyes and generate the mental image of the
picture of a building he had inspected for 10 s.Whenhewas ready, he had to identify the
picture among three other pictures of similar buildings. The task included 20 items. Hecorrectly identified 19 of 20 stimuli (see Table 2). The ability to generate an image from
long-term memory was assessed by asking the subject to draw a map of his actual and
childhood home. Dr. WAI was able to draw a map of his present home; but, he was
unable to draw a map of his childhood home in which he lived for 15 years. Even after
Developmental topographical disorientation 7

Table 2. Dr WAI’s and average controls’ performances in the navigational skills assessment.
Performances below the cut-off or insufficient are in bold
Test DR.WAI Score Controls
Visual imagery testing
Buildings task
(Palermo et al., 2010)
19/20 Mean = 19.5 (SD = 0.89); t = �0.55; p = n.s.
Letter inspection test
(Nori et al., in press)
16/20 Mean = 19.6 (SD = 0.82); t = �4.28; p < .0005
Mental rotation test
(Palermo et al., 2010)
13/20 Mean = 18.1 (SD = 2.47); t = �2.01; p = .03
Generation of imagery from long-term memory
Map drawing of
actual home
Plausible
Map drawing of
childhood home
Implausible
(Three trials
before
achievement)
Navigational abilities in experimental environments
Walking Corsi test (Piccardi et al., 2008)
Span (n. squares) 4/9 Mean = 4.60 (SD = 0.55); CH: t = �0.996; p = n.s.
Supraspan (n. squares) 133/144 Mean = 134 (SD = 6.71); CH: t = 0.136; p = n.s.
Supraspan recall
(n. squares)
8/8 Mean = 8.00 (SD = 0.00); CH: t = 0.000; p = n.s.
Road map test
(Money et al., 1965)
30/32 Mean = 30.47 (SD = 2.58); CH: t = �0.18; p = n.s.
The human version of Morris test (Guariglia et al., 2005)
Searching 594 s Mean = 150.14 (SD = 183.00); CH: t = 2.372; p = 0.013
Immediate reaching
(A + B + C)
223 s Mean = 415.32 (SD = 217.51); CH: t = �0.865; p = n.s.
Delayed reaching 15 s Mean = 72.00 (SD = 139.61); CH: t = �0.399; p = n.s.
The human version of Morris test WL (Nico et al., 2008)
Searching 39 s Mean = 65.64 (SD = 54.33); CH: t = �0.481; p = n.s.
Immediate reaching
(A + B + C)
1,491 s Mean = 115.08 (SD = 77.98); CH: t = 17.302;
p < .0001
Delayed reaching 24 s Mean = 9.76 (SD = 3.61); CH: t = 3.868; p = .0001
Semmes test
(Semmes et al., 1955)
3/5 Mean = 4.30 (SD = 0.84); CH: t = �1.482 p = n.s
Navigational abilities in virtual environment
CMT (Iaria et al., 2007)
Learning task 540 s Mean = 575.29 (SD = 199.06); CH: t = �0.29; p = n.s.
Retrieval task 659 s Mean = 298.35 (SD = 112.58); CH: t = 2.25; p < .05
Navigational abilities in ecological environments
Real ambient drawing
(cognitive map)
7/20 Mean = 17.50 (SD = 2.64); CH: t = �3.79; p = .002
Landmark recognition 10/16 Mean = 12.38 (SD = 3.29); CH: t = 0.682; p = n.s.
Route strategy 4/6 Mean = 5.86 (SD = 0.38); CH: t = �4.579; p = .018
Map strategy 3/4 Mean = 3.75 (SD = 0.71); CH: t = �0.99; p = n.s.
Verbal strategy –
CH: Crawford and Howell (1998) analysis.
8 Filippo Bianchini et al.
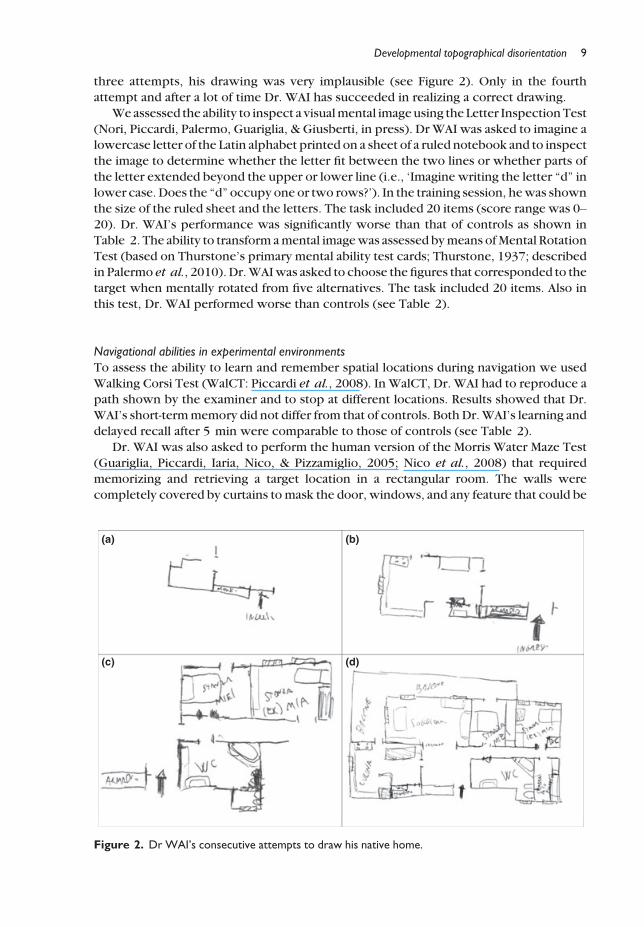
three attempts, his drawing was very implausible (see Figure 2). Only in the fourth
attempt and after a lot of time Dr. WAI has succeeded in realizing a correct drawing.
We assessed the ability to inspect a visualmental imageusing the Letter InspectionTest
(Nori, Piccardi, Palermo, Guariglia, & Giusberti, in press). Dr WAI was asked to imagine alowercase letter of the Latin alphabet printed on a sheet of a ruled notebook and to inspect
the image to determine whether the letter fit between the two lines or whether parts of
the letter extended beyond the upper or lower line (i.e., ‘Imagine writing the letter “d” in
lower case. Does the “d” occupy one or two rows?’). In the training session, hewas shown
the size of the ruled sheet and the letters. The task included 20 items (score range was 0–20). Dr. WAI’s performance was significantly worse than that of controls as shown in
Table 2. The ability to transform amental imagewas assessed bymeans ofMental Rotation
Test (based on Thurstone’s primary mental ability test cards; Thurstone, 1937; describedin Palermo et al., 2010). Dr.WAIwas asked to choose the figures that corresponded to the
target when mentally rotated from five alternatives. The task included 20 items. Also in
this test, Dr. WAI performed worse than controls (see Table 2).
Navigational abilities in experimental environments
To assess the ability to learn and remember spatial locations during navigation we used
Walking Corsi Test (WalCT: Piccardi et al., 2008). In WalCT, Dr. WAI had to reproduce apath shown by the examiner and to stop at different locations. Results showed that Dr.
WAI’s short-termmemory did not differ from that of controls. Both Dr.WAI’s learning and
delayed recall after 5 min were comparable to those of controls (see Table 2).
Dr. WAI was also asked to perform the human version of the Morris Water Maze Test
(Guariglia, Piccardi, Iaria, Nico, & Pizzamiglio, 2005; Nico et al., 2008) that required
memorizing and retrieving a target location in a rectangular room. The walls were
completely covered by curtains to mask the door, windows, and any feature that could be
(a) (b)
(c) (d)
Figure 2. Dr WAI’s consecutive attempts to draw his native home.
Developmental topographical disorientation 9

used as a reference point during navigation. Dr.WAI performed three tasks (1) searching:
starting from the centre of the room, he moved around until he reached the target point
signalled by awarning sound; (2) immediate reaching: he had to reach the target point by
following the shortest path and starting from the centre of the room in three differentpositions (0°, 90° and 270° of rotation with respect to the starting position during
searching); (3) delayed reaching: after a 30-min delay (spent in another room), he had to
reach the target point following the shortest path. Two different conditions were used,
each of which involved a different target location. In the first condition (without
landmark: Morris Test), no visual cue that could be used as a reference point or landmark
during navigation was present in the test room. In the second condition (with landmark:
Morris Test WL), two objects (a floor lamp and a hat stand) were placed at the centre of
two different walls opposite to the corner of the target location. In the condition withoutlandmarks, the immediate reaching task assessed the integrity of path integration when
Dr.WAI performed the task starting from a positionwith 0° of rotationwith respect of the
starting position of the searching task. Differently, the ability to reorient by means of
the geometric module was assessed when the same task was performed starting from the
positions with 90° and 270° of rotation. In the same condition, the delayed reaching task
evaluated the ability to develop simple cognitive maps representing only the shape of the
room and the target position. In the conditionwith landmarks, immediate reaching tested
the ability to use the configuration of the landmark, whereas delayed reaching assessedthe ability to develop more complex cognitive maps that included the position of the
landmarks in addition to the shape of the room and the position of the target location.
In both conditions, performance on the three tasks was video-recorded and the score
was the time spent on each task. In the searching condition of the Morris Test, Dr. WAI
needed more time than controls to reach the target point. A perusal of his video-recorded
performance showed that he searched for the target by following a concentric pattern that
started at the centre of the room and extended no more than 2 m from the walls; after
several attempts, however, he enlarged his searching area and found the target point. InImmediate Reaching, Dr. WAI’s performance was comparable to that of controls, that is,
with no difference in the use of path integration and re-orientation processes.
Analogously, in Delayed Reaching Dr. WAI’s performance did not differ from that of
controls (see Table 2 for Dr. WAI and CH analysis).
In the Morris Test, WL, the time Dr. WAI needed to reach the target point in the
Searching condition was comparable to that of controls. However, Dr. WAI was
significantly slower than controls in both Immediate Reaching and Delayed Reaching
after a 30-min delay (see Table 2 for Dr. WAI and CH analysis).Dr.WAIwas also asked to performRoadmap test (Money, Alexander, &Walzer, 1965)
in which he had to use a pen to track a path drawn on a map, while he imagined walking
along thepath. At each intersectionhehad to verbally indicatewhether hewas turning left
or right; the score was the number of correct indications. Again, as reported in Table 2,
Dr. WAI’s performance did not differ from that of controls. In the Map Reading test
(Semmes, Weinstein, Ghent, & Teuber, 1955), the task was to follow a path using a map,
but without rotating it. The map reproduced the 3 x 3 grid of red circles on the
grey carpet (1.5 x 1.5 m) on the floor. Five trials of increasing difficulty (number of turnsand rotations increase in successive trials) were administered. Dr. WAI was able
to reproduce the path by translating the allocentric coordinates into egocentric
coordinates (see Table 2).
Dr. WAI was also asked to perform Virtual reality test (CMT: Iaria, Chen, Guariglia,
Ptito, & Petrides, 2007), used also by Iaria et al. (2009) in Pt1. The CMT included two
10 Filippo Bianchini et al.
experimental tasks (1) a learning task, in whichDr.WAI had to explore a virtual city with
six landmarks and to create a mental representation of the city; and (2) a retrieval task in
which he had to use the mental representation of the city to reach a specific target
location. In the learning task,Dr.WAI took the same time as controls to generate themapof the city, but he needed more time to become oriented in the retrieval task (see
Table 2).
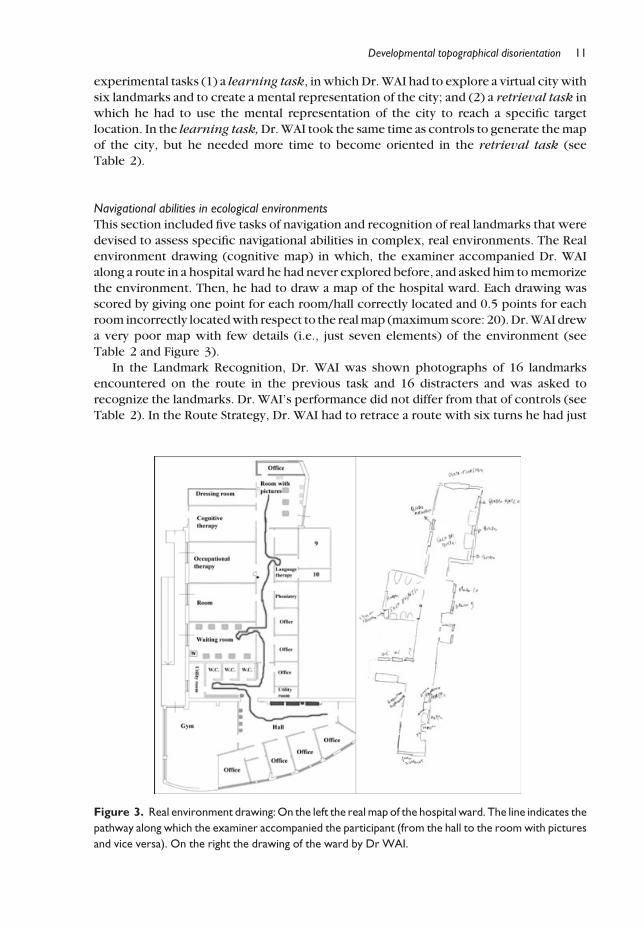
Navigational abilities in ecological environments
This section included five tasks of navigation and recognition of real landmarks that were
devised to assess specific navigational abilities in complex, real environments. The Real
environment drawing (cognitive map) in which, the examiner accompanied Dr. WAIalong a route in a hospital ward he had never explored before, and asked him tomemorize
the environment. Then, he had to draw a map of the hospital ward. Each drawing was
scored by giving one point for each room/hall correctly located and 0.5 points for each
room incorrectly locatedwith respect to the realmap (maximumscore: 20).Dr.WAI drew
a very poor map with few details (i.e., just seven elements) of the environment (see
Table 2 and Figure 3).
In the Landmark Recognition, Dr. WAI was shown photographs of 16 landmarks
encountered on the route in the previous task and 16 distracters and was asked torecognize the landmarks. Dr. WAI’s performance did not differ from that of controls (see
Table 2). In the Route Strategy, Dr. WAI had to retrace a route with six turns he had just
Figure 3. Real environment drawing:On the left the real map of the hospital ward. The line indicates the
pathway along which the examiner accompanied the participant (from the hall to the room with pictures
and vice versa). On the right the drawing of the ward by Dr WAI.
Developmental topographical disorientation 11
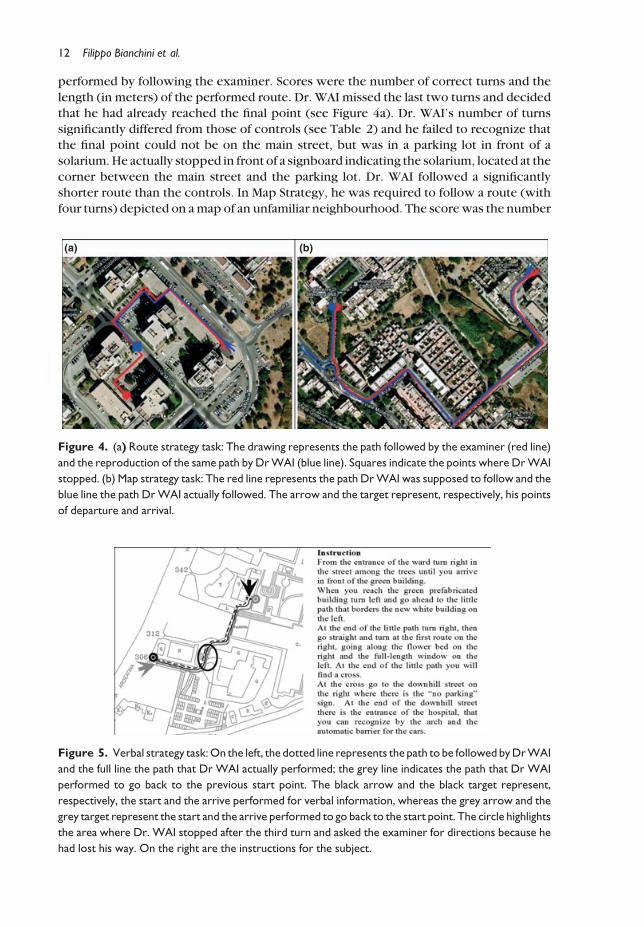
performed by following the examiner. Scores were the number of correct turns and the
length (in meters) of the performed route. Dr. WAI missed the last two turns and decided
that he had already reached the final point (see Figure 4a). Dr. WAI’s number of turns
significantly differed from those of controls (see Table 2) and he failed to recognize thatthe final point could not be on the main street, but was in a parking lot in front of a
solarium.He actually stopped in front of a signboard indicating the solarium, located at the
corner between the main street and the parking lot. Dr. WAI followed a significantly
shorter route than the controls. In Map Strategy, he was required to follow a route (with
four turns) depicted on amap of an unfamiliar neighbourhood. The scorewas the number
(a) (b)
Figure 4. (a) Route strategy task: The drawing represents the path followed by the examiner (red line)
and the reproduction of the same path by DrWAI (blue line). Squares indicate the points where DrWAI
stopped. (b) Map strategy task: The red line represents the path DrWAI was supposed to follow and the
blue line the path DrWAI actually followed. The arrow and the target represent, respectively, his points
of departure and arrival.
Figure 5. Verbal strategy task:On the left, the dotted line represents the path to be followed byDrWAI
and the full line the path that Dr WAI actually performed; the grey line indicates the path that Dr WAI
performed to go back to the previous start point. The black arrow and the black target represent,
respectively, the start and the arrive performed for verbal information, whereas the grey arrow and the
grey target represent the start and the arrive performed to go back to the start point. The circle highlights
the area where Dr. WAI stopped after the third turn and asked the examiner for directions because he
had lost his way. On the right are the instructions for the subject.
12 Filippo Bianchini et al.
of correct turns. When asked to perform the depicted pathway, Dr. WAI’s performance
(see Figure 4b) was not different from that of controls (see Table 2).
In the Verbal Strategy, Dr. WAI had to follow a new route in the hospital using written
instructions describing landmarks and direction (right/left) to take at each turning point.In this task, Dr. WAI stopped after the third turn and asked the examiner for directions
because he had lost his way (see Figure 5) stating he has already walked for a long time
without finding the next landmark. None of the 20 controls had any difficulty on this task.
In summary, Dr. WAI’s performance was clearly defective on some of the mental
imagery tests (i.e., Inspection Test, Mental Rotation Test, and Map drawing of childhood
home) that entailed retracing a previously travelled route and developing, storing, and
using cognitive maps of real environments (Real ambient drawing and Morris Test WL),
and in using cognitive maps of virtual environments.
Discussion
Dr. WAI showed a severe form of DTD in daily life. Unlike F.G. (Bianchini et al., 2010),
however, he had developed somenavigational skills (landmark strategy,map reading), but
had obvious difficulty in developing cognitive maps that extended beyond the generalgeometric features of the environment. He was able to use a map strategy only if he could
look at a paper map (map strategy, Semmes test), but was unable to develop a map based
on his own direct experience (Morris Test WL, Real environment drawing) or to
reproduce a route (Route strategy). Based on previously described cases, these
observations suggest that DTD is a complex syndrome involving different aspects of
navigational and topographical skills with different degrees of severity in different
subjects. Indeed, navigation being a complex ability subtended by several different skills,
it is very likely that a developmental disorder affects different individuals in different ways(e.g., involving different processes) andwith different degrees of severity. Caution should
be taken in describing DTD cases because individuals with low spatial skills and poor
sense of direction show significant low performances in forming a mental representation
of the environment (see, Thorndike & Golden, 1981; Kato & Takeuchi, 2003; Hegarty
et al., 2006; Nori & Giusberti, 2006; Pazzaglia & De Beni, 2001), suggesting that the
assessment of DTD has to be exhaustive in investigating navigational processes in the
environment. DTDbeing a developmental disorder, the possibilitymust also be taken into
account that different individuals develop different coping strategies to deal with theirorientation problems. Thus, it is theoretically possible that different behaviours we
observe are the results of differences in developed coping strategies, and not the results of
differences in the type of processes that are altered by DTD. For this reason, in studying
new cases of DTD it is very important to verify if they present differences in the
navigational processes involved in the disorder or just differences in the navigational
behaviour since the latter may be the result of compensatory strategies in individuals
affected by the same navigational alteration, even if at different degrees of severity.
One feature that might characterize different types of DTD is the presence ofnavigational memory deficits. Dr. WAI showed normal ability to learn and retrieve
sequential information in both peripersonal and navigational space. The presence of
normal long-termmemory in navigational space counters the results of our previous study
of F.G. who showed normal memory in peripersonal space and defective retrieval in
navigational space. This suggests that navigational memory deficits can differentiate
degree and characteristics of DTD in a future taxonomy also for developmental
topographical deficits. Furthermore, the existence of different types of DTD is also
Developmental topographical disorientation 13

supported by a direct comparison of Dr. WAI’s navigational behaviours with those of the
two previously described cases of DTD.
On the CMT, both F.G. and Pt1 had great difficulty in acquiring the map. By contrast,
Dr. WAI did not differ from controls in the learning phase, but was unable to use the maphe had learned for navigational purposes. Indeed, in real environments his test behaviour
differed from that of Pt1 and F.G. Specifically, like Pt1, but unlike F.G., Dr. WAI never
completely lost his way on tests assessing route strategy; but, unlike Pt1, he failed to reach
his goal. Like Pt1, but unlike F.G., Dr.WAIwas able to find hisway in themap strategy test,
and unlike both Pt1 and F.G., he lost his way when he had to follow verbal instructions.
Finally, like F.G., but unlike Pt1, Dr. WAI showed an abnormal difference between Verbal
IQ and Performance IQ, defective performance on themental rotation tests and omissions
and errors in locating items in the drawing of his own home, in addition to the scalingerrors also shown by Pt1.
Thus, it seems that the severity of Dr. WAI’s DTD fell between that of Pt1, who had
difficulty storing environmental information by transforming it into a cognitive map, and
that of F.G., who was completely unable to develop a cognitive map and was affected by
defective navigational memory. However, Dr. WAI’s DTD seemed to differ both
qualitatively and in terms of severity. Indeed, PT1 was reported to have ‘difficulty with
acquisition rather than retrieval of cognitive maps’ (Iaria et al., 2009 p. 39) and F.G. was
unable to developmaps. Thus, bothhaddeficits in the development of cognitivemaps.Dr.WAI seemed partially able to process cognitive maps because he learned the map of the
CMT normally and was able to develop a schematic map of the general shape of the
environment and the location of the target point in the Morris Water Maze without
landmarks. However, Dr. WAI was unable to develop a cognitive map when landmarks
were added to the Morris Maze or when the cognitive map had to be developed from real
navigation in a real environment. The apparent contradiction between performance on
the CMT and in real environments deserves to be discussed. In the learning task of the
CMT, a virtual city had to be explored and subjects had to place six landmarks in theircorrect positions on a paper map of the city. Thus, for at least two reasons learning in the
CMT is quite different from that in a real environment. First, when navigating in a virtual
environment subjects process only visual information (relative to optic flow, visuospatial
features, etc.), whereas in navigating in a real environment visual information has to be
integrated with vestibular information. Second, in the CMT the general features of the
environment (the shape of the city, streets and crossings, aswell as number, and shapes of
buildings) are already represented on the paper map on which subjects have to place the
six landmarks and do not need to be inferred during navigation. Thus, the development ofa cognitive map of the CMT city might be facilitated for both reasons.
Dr.WAI’s difficulty in developing complex cognitivemapswas similar to that observed
by Hermer and Spelke (1996) in young children. Children are able to develop schematic
cognitive maps in the real environment at 18 months of age (i.e., they are able to process
geometrical environmental features), but were unable to indicate the position of objects
and relevant visual cues on themaps. The ability to include landmarks in themaps appears
at around 4 1/2 years of age (Hermer & Spelke, 1996). On the basis of these data, we can
conclude that Dr. WAI’s ability to develop cognitive maps never developed beyond thelevel of an 18-month-old child.
In the light of Siegel andWhite’s (1975) model of human navigation development, we
can state that Dr.WAI never passed the route navigation level. Indeed, he recognized
landmarks, was able to describe their sequence along a route, and was able to direct his
navigation towards a visible landmark. But he had not completely acquired either the
14 Filippo Bianchini et al.
route phase or the survey phase and was able to navigate in familiar environments only
after over-learning the verbal directional labelling of landmarks. Failures could be ascribed
to errors in recalling directional labels (e.g., ‘at the post office turn right’ instead of ‘turn
left’) or to the inability to process metric information about the travelled route. Indeed,when giving or following verbal instructions to take a route, apart from the description of
the landmarks on turning points, information about the distance between landmarks has
an important role; indeed, it allows determining the correctness of the route, especially in
describing/estimating, and travelling distances between two landmarks (Denis, Pazzaglia,
Cornoldi, & Bertolo, 1999). In Dr. WAI’s case, a specific disorder in computing metric
environmental information was suggested from spontaneous descriptions of his difficulty
in the initial interview and from data derived from the neuropsychological assessment.
Indeed, his peculiar searching in the Morris Maze without landmarks suggested that Dr.WAI was unable to judge distances, indeed he failed to compute exact distance from the
walls failing in locating the target. Furthermore, he missed about 50 m in the Route Test
and in following the verbal instructions in the Verbal Strategy test he got lost after the
second turn because hewas unable to calculate the distanceheneeded to travel before the
next landmark and turning point. Difficulty in evaluating metric features was not limited
to environmental navigation, but also seemed to affect his performance on mental visual
imagery when hewas asked to judge whether a given letter of the alphabet would extend
beyond the lines of a ruled sheet of paper. Considering his difficulty in using metricproperties, it was evident that he never acquired the survey phase in which this kind of
ability is developed. According to Siegel and White’s model, F.G. was in the landmark
phase, Dr. WAI had only some rudimentary abilities in the route phase and Pt1 had only
some abilities in the survey phase. Taking into account all of the above results, we can
conclude that Dr. WAI’s DTD was characterized by two deficits, one in integrating visual
cues in a schematic cognitive map and one in computing metric environmental features
and walked distances.
Some final comments on Dr. WAI’s abilities are needed.Despite his inability to develop complex cognitive maps (i.e., maps not limited to the
general shape of the environment and a few target points) and in computing metric
distances, Dr. WAI showed normal ability on the Map reading Test (Semmes et al., 1955)
and on theMap-strategy test, suggesting that it is possible to learn how to translate graphic
allocentric representations into egocentric directions even when the ability to mentally
represent navigational information in an allocentric format is defective. This observation
suggests that it may be possible to train individuals with topographical disorientation and
DTD to use maps to compensate for their navigational difficulties, by teaching them totranslate the information on the map into verbal instructions.
In conclusion, this case of DTD not only increases our knowledge of this recently
described disorder but sheds some light on the mechanisms underlying lack of
development of navigational skills. Indeed, this case suggests that dissociations in
navigational abilities can be observed in the different cases affected by DTD related to the
level of development of the ability to build cognitive maps and the association of different
imagery deficits. In the first case of DTD (Pt1, Iaria et al., 2009), cognitive map
development was difficult and slow, but no mental imagery deficit was observed. In thesecond case (Bianchini et al., 2010), cognitive map development was impossible and a
deficit in transforming mental images and inability to process spatial relational
information severely affected the possibility of using route strategies. In this third case,
a deficit in placing landmarks on cognitive maps was present accompanied by a deficit in
processing the metric features of visuospatial stimuli that impedes the evaluation of
Developmental topographical disorientation 15
distances during navigation. This latter deficit severely affects the use of route strategies in
a subject who was able to recognize landmarks and know the sequence of landmarks
along familiar routes.
Concerning severity of the deficit, it is evident that the three individuals had differentlevels of difficulty in daily life: Pt1 showed the least severe deficit and F.G. themost severe
one. According to Iaria andBarton (2010) study, DTD seems to be a condition that affects a
significant number of people, who show clear impairments in a number of orientation
skills. Actually, it is still impossible to estimate the prevalence of DTD, but new evidence
can help to better define this condition as well as guideline for re-education.
Acknowledgements
We are thankful to NeuroLab (www.neurolab.ca) for providing CMT. The authors declare
they have no conflicts of interest or grants to declare.
References
Acredolo, L. P. (1978). Development of spatial orientation in infancy. Developmental Psychology,
14, 224–234. doi:10.1037/0012-1649.14.3.224Acredolo, L. P., & Evans, D. (1980). Developmental changes in the effects of landmarks on infant
spatial behavior. Developmental Psychology, 16, 312–318. doi:10.1037/0012-1649.16.4.312Barrash, J. A. (1998). Historical review of topographical disorientation and its neuroanatomical
correlates. Journal of Clinical and Experimental Neuropsychology, 20, 807–827. doi:10.1076/jcen.20.6.807.1114
Benton, A. L., Van Allen, M. W., Hamsher, K., & Levin, H. S. (1975). Test of facial recognition,
form SL. Iowa City, IA, USA: Benton Laboratory of Nauropsychology, University of Iowa
Hospital and Clinics.
Bianchini, F., Incoccia, C., Palermo, L., Piccardi, L., Zompanti, L., Sabatini, U.,…Guariglia, C. (2010).
Developmental topographical disorientation in a healthy subject.Neuropsychologia, 48, 1563–1573. doi:10.1016/j.neuropsychologia.2010.01.025
Carlesimo, G. A., Buccione, I., Fadda, L., Graceffa, A., Mauri, M., Lorusso, S., … & Caltagirone, C.
(2002). Standardizzazione di due test di memoria per uso clinico: Breve Racconto e Figura di
Rey.[Normative data of twomemory tasks: Short-Story recall andRey’s Figure].NuovaRivista di
Neurologia, 12, 1–3.Carlesimo, G. A., Caltagirone, C., Gainotti, G., Fadda, L., Gallassi, R., Lorusso, S.,… & Parnetti, L.
(1996). The mental deterioration battery: Normative data, diagnostic reliability and qualitative
analyses of cognitive impairment. European Neurology, 36, 378–384.Corsi, P. M. (1972). Human memory and the medial temporal region of the brain. Dissertation
Abstracts International, 34 (02), 891B (University micro-lms No. AA105-77717).
Crawford, J. R., & Howell, D. C. (1998). Comparing an individual’s test score against norms
derived from small samples. Clinical Neuropsychologist, 12, 482–486. doi:10.1076/
clin.12.4.482.7241
Denis, M., Pazzaglia, F., Cornoldi, C., & Bertolo, L. (1999). Spatial discourse and navigation: An
analysis of route directions in the city of Venice. Applied Cognitive Psychology, 13, 145–174.
Farah, M. J. (1989). The neuropsychology of mental imagery. In F. Boller & J. Grafman (Eds.), The
handbook of neuropsychology. Disorders of visual behavior (pp. 395–413). Amsterdam:
Elsevier.
Guariglia, C., Piccardi, L., Iaria, G., Nico, D., & Pizzamiglio, L. (2005). Representational neglect and
navigation in real space. Neuropsychologia, 43, 1138–1143. doi:10.1016/j.neuropsychologia.2004.11.021
16 Filippo Bianchini et al.
Hegarty, M.,Montello, D. R., Richardson, A. E., Ishikawa, T., & Lovelace, K. (2006). Spatial abilities at
different scales: individual differences in aptitude-test performance and spatial-layout learning.
Intelligence, 34, 151–176. doi:10.1016/j.intell.2005.09.005Hermer, L., & Spelke, E. S. (1994). A geometric process for spatial reorientation in young children.
Nature, 370, 57–59. doi:10.1038/370057a0Hermer, L., & Spelke, E. (1996). Modularity and development: The case of spatial reorientation.
Cognition, 61, 195–232. doi:10.1016/S0010-0277(96)00714-7Iaria, G., & Barton, J. J. (2010). Developmental topographical disorientation: A newly
discovered cognitive disorder. Experimental Brain Research, 206, 189–196. doi:10.1007/s00221-010-2256-9
Iaria, G., Bogod, N., Fox, C. J., & Barton, J. J. (2009). Developmental topographical
disorientation: Case one. Neuropsychologia, 47, 30–40. doi:10.1016/j.neuropsychologia.
2008.08.021
Iaria, G., Chen, J. K., Guariglia, C., Ptito, A., & Petrides, M. (2007). Retrosplenial and
hippocampal brain regions in human navigation: Complementary functional contributions to
the formation and use of cognitive maps. European Journal of Neuroscience, 25, 890–899.doi:10.1111/j.1460-9568.2007.05371.x
Iaria, G., Incoccia, C., Piccardi, L., Nico, D., Sabatini, U., & Guariglia, C. (2005). Lack of orientation
due to a congenital brain malformation: A case study. Neurocase, 11, 463–474. doi:10.1016/j.tics.2010.01.001
Kato, Y., & Takeuchi, Y. (2003). Individual differences in wayfinding strategies. Journal of
Environmental Psychology, 23, 171–188. doi:10.1016/S0272-4944(03)00011-2Kosslyn, S. M. (2005). Mental images and the brain. Cognitive Neuropsychology, 22, 333–347.
doi:10.1080/02643290442000130
Laicardi, C., & Orsini, A. (1997). WAIS-R: Wechsler adult intelligence scale revised. Traduzione e
adattamento italiano a cura di Caterina Laicardi e Arturo Orsini. Firenze: O. S. Giunti.
Lawton, C. A. (2010). Gender, spatial abilities, and wayfinding. In J. Chrisler & D. McCreary (Eds.),
Handbook of gender research in psychology (pp. 317–341). New York: Springer.
Lehnung, M., Leplow, B., Ekroll, V., Benz, B., Ritz, A., Mehdorn, M., & Ferstl, R. (2003). Recovery of
spatial memory and persistence of spatial orientation deficits after traumatic brain injury during
childhood. Brain injury, 17, 855–869. doi:10.1080/0269905031000089369Lehnung, M., Leplow, B., Friege, L., Ferstl, R., & Mehdorn, M. (1998). Development of spatial
memory and spatial orientation in preschoolers and primary school children. British Journal of
Psychology, 89, 463–480.Maguire, E. A., Burke, T., Phillips, J., & Staunton, H. (1996). Topographical disorientation following
unilateral temporal lobe lesions in humans. Neuropsychologia, 34, 993–1001. doi:10.1016/0028-3932(96)00022-X
Money, J., Alexander, D., &Walzer, H. T. (1965). A standardized road map test of direction sense.
Baltimore, MD: The Johns Hopkins Press.
Newcombe, N., Huttenlocher, J., Drummey, A. B., &Wiley, J. G. (1998). The development of spatial
location coding: Place learning and dead reckoning in the second and third years. Cognitive
Development, 13, 185–200.Nico, D., Piccardi, L., Iaria, G., Bianchini, F., Zompanti, L., & Guariglia, C. (2008). Landmark based
navigation in brain-damaged patients with neglect. Neuropsychologia, 46, 1898–1907.doi:10.1016/j.neuropsychologia.2008.01.013
Nori, R., & Giusberti, F. (2006). Predicting cognitive styles from spatial abilities. American
Journal of Psychology, 119, 67–86.Nori, R., Piccardi, L., Palermo, L., Guariglia, C., & Giusberti, F. (in press). Working memory
load elicits gender differences in mental imagery. In S. McGeown (Ed.), Psychology of gender
differences (pp. 161–173). New York: Nova Science Publishers.
Pai, M. C., & Jacobs,W. J. (2004). Topographical disorientation in community-residing patientswith
Alzheimer’s disease. International Journal of Geriatric Psychiatry, 19, 250–255. doi:10.1002/gps.1081
Developmental topographical disorientation 17

Palermo, L., Piccardi, L., Nori, R., Giusberti, F., &Guariglia, C. (2010). Does hemineglect affect visual
mental imagery? Imagery deficits in representational and perceptual neglect. Cognitive
Neuropsychology, 27, 115–133. doi:10.1080/02643294.2010.503478Pazzaglia, F., & De Beni, R. (2001). Strategies of processing spatial information in survey and
landmark-centred individuals. European Journal of Cognitive Psychology, 13, 493–508.Piccardi, L., Iaria, G., Ricci, M., Bianchini, F., Zompanti, L., & Guariglia, C. (2008). Walking in the
Corsi test: Which type of memory do you need? Neuroscience Letters, 432, 127–131.doi:10.1016/j.neulet.2007.12.044
Riddoch, M., & Humphreys, G. (1989). Finding the way around topographical impairments. In
J. W. Brown (Ed.), Neuropsychology of visual perception (pp. 79–103). New York: Lawrence
Erlbaum Associates.
Salmaso, D., & Longoni, A. M. (1985). Problems in the assessment of hand preference. Cortex, 21,
533–549.Semmes, J., Weinstein, S., Ghent, L., & Teuber, H. L. (1955). Spatial orientation inman after cerebral
injury: I. Analyses by locus of lesion. The Journal of Psychology, 39, 227–244.Siegel, A. W., & White, S. H. (1975). The development of spatial representations of large-scale
environments. In H. W. Reese (Ed.), Advances in child development & behavior (pp. 9–55).New York: Academic Press.
Sokal, R. R., & Rohlf, F. J. (1995). Biometry: The principles and practice of statistics in biological
research. New York: Freeman.
Spinnler, H., & Tognoni, G. (1987). Standardizzazione e taratura italiana di test neuropsicologici.
Italian Journal of Neurological Sciences, 6(suppl. 8), 1–120.Thurstone, L. L. (1937). Psychological tests for the study of mental abilities. Chicago: University of
Chicago Press.
Thorndyke, P. W., & Golden, S. E. (1981). Ability differences and cognitive mapping skill. Santa
Monica, CA: Rand Corp. (N-1667-ARMY).
Wang, R. F., & Spelke, E. S. (2002). Human spatial representation: Insight from animal. Trends in
cognitive sciences, 6, 376–381.Warrington, E. K., & James, M. (1991). The visual object and space perception battery (VOSP).
Bury St Edmunds: Thames Valley Test Company.
Wolbers, T., & Hegarty, M. (2010). What determines our navigational abilities? Trends in
Cognitive Sciences, 14, 138–146. doi:10.1016/j.tics.2010.01.001
Received 12 April 2012; revised version received 8 November 2012
18 Filippo Bianchini et al.