When patients portray their conduct as normal and healthy: An interactional challenge for thorough...
10
When patients portray their conduct as normal and healthy: An interactional challenge for thorough substance use history taking Paul M. Denvir Albany College of Pharmacy & Health Sciences, 106 New Scotland Avenue, Albany, NY 12208-3492, USA article info Article history: Available online 17 July 2012 Keywords: USA Physicianepatient interaction Lifestyle Substance use Conversation analysis (CA) abstract Researchers and medical practitioners have argued that routine substance use histories are performed less frequently and less thoroughly than they should be. Previous research has identified a range of structural, attitudinal, and socio-cultural barriers that help to explain this pattern. Using conversation analytic (CA) methods, this paper complements previous work by exploring a potential interactional barrier to thorough substance use history taking in the USA. In response to routine substance use queries (e.g. “Do you drink alcohol?”), patients often do more than just providing information. They also convey normative stances toward their conduct, essentially making a case for how it should be understood by the physician. One stance that patients may take is that their conduct is normal and healthy. This paper describes three interactional practices that patients used to enact such a stance: 1) employing marked lexical, intonational, or interactional features when indicating no use of a substance; 2) volunteering normalizing details about the type, quantity, frequency, or circumstances of substance use; 3) providing minimizing characterizations of substance use. The paper explores some reasons why physicians treated these as appropriate and sufficient responses and did not seek additional details even when the infor- mation provided was quite superficial. Two social functions of patients’“normal/healthy” stances are discussed: 1) redirecting the physician’s history taking to other topics and 2) presenting oneself as a health-conscious patient. “Normal/healthy” stances can represent an expression of patient agency, but can also present a dilemma for physicians, who must balance a concern for thoroughness with a concern for rapport. Recommendations for navigating this dilemma are discussed. Ó 2012 Elsevier Ltd. All rights reserved. Introduction and research problem During initial office visits and annual checkups, primary care physicians routinely perform comprehensive medical histories with their patients. A comprehensive medical history is designed for efficiently gathering, recording, and evaluating basic informa- tion about all aspects of a patient’s health (e.g. current and past medical conditions, medications, surgeries, hospitalizations, aller- gies, family history). Some aspects of health may be more difficult to discuss than others. Research has shown that “lifestyle” topics tend to be comparatively challenging for physicians and patients (Johanson, Larsson, Saljo, & Svardsudd, 1998; Larsson, Saljo, & Aronsson, 1987; Sorjonen, Raevaara, Haakana, Tammi, & Perakyla, 2006). In a primary care context, “lifestyle” generally refers to patients’ everyday circumstances, routines, and choices. Usage may vary by physician or medical practice, but the term generally includes such topics as dietary patterns, physical exercise, substance use, and sexual activities/relationships. This analysis focuses solely on one aspect of patient lifestyle: substance use conduct. Research conducted in Western medical settings has shown that physicians and patients do not address substance use as routinely or as thoroughly as the medical education literature recommends (Bertakis & Azari, 2007; Friedmann, McCullough, Chin, & Saitz, 2000; Maheux, Haley, Rivard, & Gervais, 1995; Mignon, 1996). Clark (1995) provides a fitting analogy: “Just as blood pressure should be routinely checked, so should alcohol problems be routinely screened for, as they are both highly prevalent and usually covert” (p. 28). Even if a patient does not present with substance use/abuse issues, it is still important for a primary care physician to conduct a reasonably detailed history. For example, when prescribing medications, a detailed history can help physicians to avoid possible chemical interactions and maximize the effectiveness of selected treatments. A thorough history can also be useful for making screening deci- sions; intravenous drug use in the past may prompt physicians to screen for associated health problems, such as hepatitis. In short, there are reasons for a thorough substance use history that have nothing to do with substance abuse. E-mail address: [email protected]. Contents lists available at SciVerse ScienceDirect Social Science & Medicine journal homepage: www.elsevier.com/locate/socscimed 0277-9536/$ e see front matter Ó 2012 Elsevier Ltd. All rights reserved. http://dx.doi.org/10.1016/j.socscimed.2012.06.021 Social Science & Medicine 75 (2012) 1650e1659
Transcript of When patients portray their conduct as normal and healthy: An interactional challenge for thorough...

at SciVerse ScienceDirect
Social Science & Medicine 75 (2012) 1650e1659
Contents lists available
Social Science & Medicine
journal homepage: www.elsevier .com/locate/socscimed
When patients portray their conduct as normal and healthy: An interactionalchallenge for thorough substance use history taking
Paul M. DenvirAlbany College of Pharmacy & Health Sciences, 106 New Scotland Avenue, Albany, NY 12208-3492, USA
a r t i c l e i n f o
Article history:Available online 17 July 2012
Keywords:USAPhysicianepatient interactionLifestyleSubstance useConversation analysis (CA)
E-mail address: [email protected].
0277-9536/$ e see front matter � 2012 Elsevier Ltd.http://dx.doi.org/10.1016/j.socscimed.2012.06.021
a b s t r a c t
Researchers and medical practitioners have argued that routine substance use histories are performedless frequently and less thoroughly than they should be. Previous research has identified a range ofstructural, attitudinal, and socio-cultural barriers that help to explain this pattern. Using conversationanalytic (CA) methods, this paper complements previous work by exploring a potential interactionalbarrier to thorough substance use history taking in the USA. In response to routine substance use queries(e.g. “Do you drink alcohol?”), patients often do more than just providing information. They also conveynormative stances toward their conduct, essentially making a case for how it should be understood bythe physician. One stance that patients may take is that their conduct is normal and healthy. This paperdescribes three interactional practices that patients used to enact such a stance: 1) employing markedlexical, intonational, or interactional features when indicating no use of a substance; 2) volunteeringnormalizing details about the type, quantity, frequency, or circumstances of substance use; 3) providingminimizing characterizations of substance use. The paper explores some reasons why physicians treatedthese as appropriate and sufficient responses and did not seek additional details even when the infor-mation provided was quite superficial. Two social functions of patients’ “normal/healthy” stances arediscussed: 1) redirecting the physician’s history taking to other topics and 2) presenting oneself asa health-conscious patient. “Normal/healthy” stances can represent an expression of patient agency, butcan also present a dilemma for physicians, who must balance a concern for thoroughness with a concernfor rapport. Recommendations for navigating this dilemma are discussed.
� 2012 Elsevier Ltd. All rights reserved.
Introduction and research problem
During initial office visits and annual checkups, primary carephysicians routinely perform comprehensive medical historieswith their patients. A comprehensive medical history is designedfor efficiently gathering, recording, and evaluating basic informa-tion about all aspects of a patient’s health (e.g. current and pastmedical conditions, medications, surgeries, hospitalizations, aller-gies, family history). Some aspects of health may be more difficultto discuss than others. Research has shown that “lifestyle” topicstend to be comparatively challenging for physicians and patients(Johanson, Larsson, Saljo, & Svardsudd, 1998; Larsson, Saljo, &Aronsson, 1987; Sorjonen, Raevaara, Haakana, Tammi, & Perakyla,2006). In a primary care context, “lifestyle” generally refers topatients’ everyday circumstances, routines, and choices. Usage mayvary by physician or medical practice, but the term generallyincludes such topics as dietary patterns, physical exercise,substance use, and sexual activities/relationships. This analysis
All rights reserved.
focuses solely on one aspect of patient lifestyle: substance useconduct.
Research conducted in Western medical settings has shown thatphysicians and patients do not address substance use as routinely oras thoroughly as the medical education literature recommends(Bertakis & Azari, 2007; Friedmann,McCullough, Chin, & Saitz, 2000;Maheux, Haley, Rivard, & Gervais, 1995; Mignon, 1996). Clark (1995)provides a fitting analogy: “Just as blood pressure should beroutinely checked, so should alcohol problems be routinely screenedfor, as they are both highly prevalent and usually covert” (p. 28). Evenif a patient does not present with substance use/abuse issues, it isstill important for a primary care physician to conduct a reasonablydetailed history. For example, when prescribing medications,a detailed history can help physicians to avoid possible chemicalinteractions and maximize the effectiveness of selected treatments.A thorough history can also be useful for making screening deci-sions; intravenous drug use in the past may prompt physicians toscreen for associated health problems, such as hepatitis. In short,there are reasons for a thorough substance use history that havenothing to do with substance abuse.

P.M. Denvir / Social Science & Medicine 75 (2012) 1650e1659 1651
Both physicians and patients have reported that substance use isan appropriate topic to address in primary care contexts (Graham,Zyzanski, Reeb, Sedlacek, & Emmitt-Myers, 1994), but these atti-tudes have not consistently translated into action during theconsultation. Even when a routine substance use history is per-formed, it may be so superficial that it does not effectively unearththose “covert” problems that warrant some form of medical inter-vention. Friedmann et al. (2000) report that 88% of physiciansusually or always asked new patients whether they drank alcohol,but fewer than half asked about maximum consumption on anysingle occasion and only 13% used formal multi-item alcoholscreening tools such as theMichigan Alcohol Screening Test (MAST)or CAGE (Have you ever felt you should cut down on your drinking?Have people annoyed you by criticizing your drinking? Have youever felt bad or guilty about your drinking? Eye opener: Have youever had a drink first thing in the morning to steady your nerves orto get rid of a hangover?). These types of screening instruments aregenerally effective in identifying substance issues, but do requiresome initiative and time investment from the participants (seeCherpitel (1997) for a review of several screening instruments,including CAGE and MAST).
Researchers have identified a range of structural challenges tomore consistent and thorough substance use history taking.These include: educational issues, such as a lack of physicianand/or patient training in this area; economic issues, such asa perceived lack of financial incentives for treating substanceproblems; and practical issues, such as the time constraints of anaverage office visit (Cotter & Callahan, 1987; Fleming, 2004/2005;Rapley, May, & Kaner, 2006; Thom & Tellez, 1986). Researchershave also identified a range of attitudinal challenges. Physicianstend to find patients with substance use issues professionallyunrewarding, perceiving them as interpersonally difficult andnon-compliant with medical recommendations (Najman, Klein, &Munro, 1982; Rapley et al., 2006; Thom & Tellez, 1986). Physi-cians may not be fully committed to unearthing health issuesthat they perceive to be frustrating or intractable. Socio-culturalissues also play an important role, particularly the normative andmoral understandings that surround substance use conduct(Cotter & Callahan, 1987; Fleming, Barry, Manwell, Johnson, &London, 1997; Maisto et al., 2001). Some patterns of substanceuse are regarded culturally as normatively problematic, evenstigmatized. Although primary care physicians have a role-basedobligation to evaluate the medical implications of patients’substance use conduct, the moral implications can also bea matter of concern for either party. Previous research has shownthat health providers and consumers do orient to moral concernswhen interacting in medical contexts (Bergmann, 1992; Heritage& Lindstrom, 1998; Silverman, 1994). Physicians have expressedconcern that querying and/or advising patients about theirsubstance use could seem invasive, insensitive, judgmental, oraccusatory, thereby threatening rapport (Clark, 1995; Friedmannet al., 2000; Mignon, 1993e1994, 1995). Patients report comple-mentary concerns about being embarrassed, judged, or con-fronted by their physicians, which is consistent with thewidespread belief that patients withhold information or under-report when it comes to their substance use.
Drawing on video recordings of primary care office visits in theNortheastern United States, this analysis complements previouswork on structural, attitudinal, and socio-cultural challenges byexamining an interactional challenge that may emerge duringroutine substance use histories. In their responses to physicians’initial substance use queries (e.g. “Do you drink?” or “Do you usedrugs?”), patients did not simply submit information for thephysician’s expert consideration. Frequently, they took evaluativestances toward their conduct, essentially making a case for how it
should be understood. These stances tacitly invoked shared culturalknowledge and normative expectations about substance use. In mydata, I found evidence of two broad types of stances: (1) those thatimplied that the patient’s substance use conduct has been normaland/or healthy and (2) those that implied that the patient’ssubstance use conduct has been potentially problematic. Thisanalysis focuses on the first type of stance; the second is addressedmore fully in a separate paper.
Both stances are worthy of investigation because they appearto influence physicians’ approaches to the remainder of thesubstance use history. In my data, when patients initially enacteda “potentially problematic” stance toward their substance use,physicians understandably asked additional questions andgenerally produced a more thorough history. However, whenpatients initially enacted a “normal/healthy” stance, physiciansrarely probed for additional specific information and generallyproduced a more superficial history. This pattern suggests thatphysicians are responsive to patients’ initial presentations of theirsubstance use conduct and may adapt their history taking prac-tices based on these cues. While patient-centered adaptation ofhistory taking is desirable in someways (Boyd & Heritage, 2006), itcan be problematic if physicians simply accept patients’ self-evaluations without gathering specific information or makingtheir own expert medical evaluations. This is especially true in“lifestyle” domains, where normative and moral concerns mayprompt patients to create a favorable impression. In this sense,patients’ “normal/healthy” stances, and the responses they tend toengender from physicians, represent something of a challenge tothorough substance use history taking.
This analysis addresses three primary research questions:
RQ1: What interactional resources did patients use to enact“normal/healthy” stances?
RQ2: How did physicians respond to patients’ “normal/healthy”stances?
RQ3: What are some potential social functions of patients’“normal/healthy” stances?
In the discussion section, I offer recommendations for providersto navigate some of the challenges posed by patients’ initial“normal/healthy” stances.
Methods
Setting
The data for this analysis consist of 24 video recordings ofphysicianepatient consultations during primary care office visits.They were recorded from 2006 to 2007 at a family practice groupassociatedwith a large teaching hospital in the northeastern UnitedStates. The research was IRB approved and a certificate of confi-dentiality, which protects the data from subpoena, was obtainedfrom the National Institutes of Health.
Participants
Six physicians voluntarily self selected to participate in thestudy. Three of the physicians are female. Five of the physicians areCaucasian; the sixth is Middle Eastern. At the time of data collec-tion, the physicians ranged in age from about 30 to 60. Althoughthere were medical residents at the practice, only attendingphysicians were asked to participate.
Twenty four patients participated in the study. Only thosepatients who were scheduled for a comprehensive history and

P.M. Denvir / Social Science & Medicine 75 (2012) 1650e16591652
physical with one of the six participating physicians were eligible toparticipate. A total of 55 patients were solicited, resulting ina participation rate of 44%. This included seven new patients and 17returning patients; the returning patients had been scheduled forannual checkups. Fourteen of the patients are female. Fifteen of thepatients are Caucasian; seven are African American; one is NativeAmerican; one is Asian American. Patients ranged in age from 25 to87, with a mean age of 52. All participants were aware they werebeing recorded, but were not informed about the focus on lifestylematters.
Data
Of the 24 cases in this collection, 16 cases (66%) included at leastsome reference to alcohol or drug use. Two cases included onlya brief mention by the patient, with no actual history taking by thephysician. For example, during a discussion of caffeine use andincontinence, one returning patient referred to drinking coffee ather Alcoholics Anonymous meetings. Of the 14 cases in which thephysician actually performed a substance use history, there were 7cases (50%) inwhich the patient enacted a “normal/healthy” stance.These 7 cases form the basis of this analysis, though one case is notpresented due to length restrictions.
Analysis
This analysis employs conversation analytic (CA) methodology,a discipline that shares some conceptual roots with ethnometh-odology (Garfinkel, 1967). Conversation analysts work with audio/video recordings and highly detailed transcriptions of naturallyoccurring interaction. The broad goal of CA is to describe theculturally shared knowledge, reasoning procedures, and interac-tional resources that people use in carrying out their everydayactivities. CA views interaction as the primordial site of socialorganization and the basis on which larger social structures arecreated and sustained. For additional reference on CAmethodology,see Pomerantz and Fehr (1997), Hopper (1989), and Clayman andGill (2004). A glossary of the specialized notation system used inconversation analytic transcripts can be found in Jefferson (1974).The typographic symbols of this system are meant to capture notjust spoken words, but all manner of speech sounds (e.g. “uh” or“mm”), phonological contours (i.e. pitch, speed, emphasis, etc.),pauses, overlapping speech, and many other features of naturallyoccurring speech.
Analysis
RQ1: what interactional resources did patients use to enact “normal/healthy” stances?
The notion that speakers can present information in ways thatconvey a stance toward that information is not a new one.Drawing on Sacks’s (1974) work on storytelling in everydayconversation, Stivers (2008) has shown how storytellers takestances toward the characters or events in the story, invitingrecipients to align with the stance taken. In that analysis, Stiversuses stance to refer to “the teller’s affective treatment of theevents he or she is describing” (p. 37), meaning the sense inwhichthe events are portrayed as right/wrong, appropriate/inappro-priate, desirable/undesirable, etc. In the medical context,Halkowski (2011) has shown how patients take epistemic stanceswhen assessing their own symptoms and experiences, essentiallyspeaking in ways that are sensitive to their non-expert status.Halkowski (1998) has also shown how patients display stancestoward their reported smoking habits, which providers can use to
make inferences about patients’motivation, readiness to quit, andsense of self-efficacy. The notion of stance I employ in this paperbuilds on these treatments and is primarily concerned with thenormative interpretations that patients build into their descrip-tions of substance use conduct, such that their conduct is recog-nizable as normal or healthy.
I identified three communicative practices that patients used toenact “normal/healthy” stances. They are: (1) employing markedlexical, intonational, or interactional features when indicating nouse of a substance; (2) volunteering normalizing details about thetype, quantity, frequency, or circumstances of substance use; (3)providing minimizing characterizations of substance use. In thissection, I describe each practice and analyze a few examples of thepractice in action.
1. Employing marked lexical, intonational, or interactionalfeatures when indicating no use of a substance.
In describing patients’ responses as “marked,” I mean that theydeparted in someways fromwhat would be considered the routine,expected, or default version of that response (Hopper, 1992). Whenspeakers use marking, they tacitly invite recipients to consider thespecial work their marking may have been designed to accomplish.For example, when someone asks a yes/no question, the response“Uhh.maybe?” could be seen as marked, in that is departs fromthe expected response types. This invites recipients to considerwhat the speaker may be doing, such as expressing ambivalence orresisting the question. To better appreciate how marking isconsequential here, it will be useful to briefly discuss the role ofroutine (i.e. unmarked) responses in history taking.
The interactional structure of routine history taking is generallyorganized around closed-ended queries from the physician andminimal responses from the patient (e.g. “yes” or “no”) (Boyd &Heritage, 2006; Heritage & Stivers, 2001). Many of the physician’sclosed-ended queries are designed to establish the presence orabsence of specific symptoms, conditions, or behaviors. This isparticularly prevalent in physicians’ initial queries within a topicaldomain, where the subsequent interactional trajectory oftendepends onwhether the symptom or condition is present or absent.When patients report the absence of a symptom, condition, orbehavior, they typically do so by providing a simple, straightforward(i.e. unmarked) “no.” In terms of information provision, patients andphysicians treat this as sufficient and appropriate. The following caseillustrates this pattern:
The patient’s “No.” in line 2 was minimal and intonationallyunmarked. The terminal intonation conveyed that the responsewascomplete. In making an entry in the patient’s electronic medicalrecord (EMR), the physician displayed receipt, thereby treating“No.” as a sufficient and appropriately informative response to thequery. This routine case serves as a backdrop against which toappreciate the special marking that patients used when reportingno use of a substance.
Like the unmarked “no” in case (1), patients’ marked responseswere also functional and appropriate for the history takingpurposes at hand; they answered the physician’s question. But inthe details of their formulations, patients also tacitly implied that

P.M. Denvir / Social Science & Medicine 75 (2012) 1650e1659 1653
the substance is not just absent, but “out of the question” for them,totally inapposite to their identity or life circumstances. Patientsused three types of marking: lexical, intonational, and interactional.By lexical marking, I am referring to words or phrases that are moreelaborate than a simple “no.” By intonational marking, I am refer-ring to the sound quality of the response, its pitch, volume,emphasis, and other phonological contours. By interactionalmarking, I am essentially referring to patients’ producing theirresponses in overlapwith physicians’ queries, an issue of sequentialpositioning.
Most of the instances of this practice involved patients’reporting not using drugs, meaning illicit or recreational “street”drugs. Use of such drugs is illegal, normatively problematic and, insome cases, medically problematic. In comparison with cigaretteuse or alcohol use, drug use is regarded culturally as more deviant.When patients employedmarked denials of drug use, their conductwas rendered sensible by reference to these shared culturalunderstandings about the relative deviance of drug use.
One instance did not involve drug use. In that case, a pregnantpatient provided a marked denial of alcohol use. Because alcoholuse can lead to various birth defects, including fetal alcoholsyndrome, there is a greater sense of deviance associated withdrinking while pregnant (Baxter, Hirokawa, Lowe, Nathan, &Pearce, 2004). According to Baxter et al., the moral implicationsof responsible motherhood were frequently implicated in infor-mants’ perspectives on drinking while pregnant. This may partlyexplain why the patient employed a marked response. That case ispresented last in this section.
In line 6, the physician queried the patient about drug use.She listed a few common street drugs, perhaps to help clarify thequery. In line 7, the patient responded in the negative, but notwith the same type of routine, unmarked “No.” that she had justused to indicate that she does not smoke cigarettes (line 4). Sheshifted to “�Na::h�,” which in this context had a somewhat flip-pant or dismissive quality, especially given its marked intona-tional contours. The patient elongated the vowel soundsignificantly and reduced her volume and timbre to a huskywhisper. With this marked prosody, “�Na::h�” implied that druguse was not just absent, but virtually irrelevant to her medicalhistory. She also responded in overlap with the physician’srecognizably incomplete list of street drugs, effectively cutting offher full query format. Through these features, the patient treatedthe physician’s querying her about drug use as unnecessary,a technical formality to be quickly dispensed with. She cast druguse as a “non-topic” for her, utterly inapposite to her lifecircumstances.
In line 8, the physician displayed receipt of the patient’s“�Na::h�” by typing in the EMR. The physician showed that she hadsufficiently heard the patient’s response despite the overlap.Nonetheless, the patient reproduced the same response in the clearin line 9 with virtually identical intonational features. This wasredundant on informational grounds. However, it further bolsteredthe sense of strenuous denial.
In the next case, the patient employed many of these samefeatures, but also employed a phenomenon known as “oh-pref-acing.” Heritage (1984, 1998, 2002) describes “oh” as a “change-of-state marker,” a way for speakers to display various kinds ofcognitive shifts (e.g. surprise or realization). These cognitive shiftscan also register different stances toward the actions or utter-ances to which they are responsive. For example, in prefacinga response with “oh,” a speaker can mark that prior action orutterance as unexpected or ill fitted (Heritage, 1998). This isessentially how the patient appeared to be using “oh-prefacing”in case (3), treating the physician’s query and/or its subjectmatter as inapposite to her life circumstances. I stress that I donot view this patient as taking exception with the physician’shistory taking activities. Rather, I argue that her “oh-preface”was a resource for communicating that drug use is unthinkablefor her.
In line 4, the physician queried the patient about drug use(“An’ did you ever do drugs in yer whole lif:e,¼”). The patientwas 87 years old at the time of the consultation, which mayaccount for the physician’s use of heavily past-oriented temporalmarkers like “did,” “ever,” and “in yer whole lif:e,.” The patientemployed “oh-prefacing” in reporting that she has not useddrugs (“¼O:h not dru:gs.” in line 6), treating the question asunexpected, even slightly outrageous. Other features of herformulation enhanced this hearing. The patient stressed andelongated portions of her utterance, performing it as a strenuousdenial of drug use. Also, the patient formulated her response asa clausal fragment, a simple negation of the word drugs (“notdru:gs”). The coherence of this formulation appears to rely onher having just reported some alcohol use in the past (line 3). Inthis sequential position, the heavily marked negation of drugs(the next category of substances to be inquired about) proposeda sharp contrast between these activities. The meaningfulness ofthis contrast relied upon shared cultural understandings aboutthe differences between alcohol and drugs as categories ofsubstances. Whereas some alcohol use is normatively appro-priate, drug use is both illegal and more normatively deviant. Indenouncing drug use, the patient framed her not using drugs asnormatively desirable.
The next case involves the aforementioned pregnant patientproviding an intonationally marked report of not using alcohol. Thephysician was well aware that the patient was pregnant fromprevious interactional context.

P.M. Denvir / Social Science & Medicine 75 (2012) 1650e16591654
In response to the physician’s cigarette use query in line 1, thepatient provided a routine, unmarked “no.” In line 5, the physicianqueried the patient about caffeine use, another substance that somephysicians ask about during a substance use history. The patientreported that she does not use caffeine, again in a fairly unmarkedfashion (“U:m no:.”). Although the patient had already answered, inline 8 the physician displayed his expectation that the patient waslikely limiting her caffeine use (“Prob’ly not much right no:wright,”). By emphasizing “right no:w,” the physician implied that thepatient’s pregnancy was a reason for limiting caffeine use. He alsoincluded the tag, “right,” which further displayed his expectationthat the patient was limiting her caffeine use for this reason. Thisutterance appeared to have a knowing and slightly playful quality.While this could help build rapport, it could also be potentiallyproblematic from an information gathering standpoint. By display-ing the favorable expectation that the patient was already limitingher use of caffeine, the physicianmay havemade it more difficult forthe patient to subsequently report alcohol or drug use. Patients maybe reticent to shatter their physicians’ favorable expectations.
In lines 9e10, the patient confirmed the physician’s expectation,even upgrading from “not much” to “not at a(h)ll-.” The patientlaughed during and after this utterance, displaying recognition ofthe slightly playful quality of the physician’s prior turn. Nonethe-less, she cast herself as knowledgeable and fully committed to thehealth of her pregnancy insofar as “everyday” substances are con-cerned. Up to this point, the patient had reported not using ciga-rettes or caffeine and confirmed that her pregnancy was at leastpart of the reason.
In line 11, the physician receipted this report (“A:right.”) andimmediately latched an alcohol use query (“¼Alcoho:l,”). At thispoint, the physician had every reason to assume that the patientwasnot using alcohol, but queried her anyway. This is a potentially riskymove in terms of patient rapport, but most medical training litera-ture would suggest that physicians should try to be this thorough(Clark, 1995). By providing an elliptical query format (droppingeverything but the word “alcohol”) the physician may have beenworking to frame the query as a standardized checklist item,something to be asked as a formality. This framing could possiblysoften the appearance that the physicianwas being insensitive to thepatient’s emerging depiction of her pregnant lifestyle.
In line 12, the patient provided an intonationallymarked “YN(ay)o:.” It is difficult to fully capture the intonational contours of herresponse, even using conversation analytic transcription symbols.
Impressionistically, her tone was emphatic and serious. It wasparticularly striking in its contrast from thehigher pitched, laughter-tinged quality of what came before. Her previous responses (lines 2and 7) served as a resource for appreciating the special work sheemployed in her marked response. Her emphatic “YN(ay)o:.” castalcohol use as not just absent, but out of the question for her.
2. Volunteering normalizing details about the type, quantity,frequency, or circumstances of substance use.
In this section, I describe some of the details that patients vol-unteered when reporting on their alcohol use. They described theiruse in ways that invited the inference that they are moderate, self-disciplined, and health conscious in their use. This work traded onshared cultural knowledge about the type, quantity, frequency, andcircumstances of alcohol use, as well as the colloquial languageavailable for describing these things.
This analysis supports and expands upon some aspects ofHalkowski’s (1998) work on patients’ quantification of smokingbehavior. For example, Halkowski found that patients used fourreporting formats, including “unmitigated quantification” (e.g. “Twopacks a day”) and “quantification with pre or post self-assessment”(e.g. “Not very much, three of four cigarettes a day”). The currentanalysis shows how culturally commonsensical formulations suchas “a couple” or “every now and then” can simultaneously accom-plish both quantification and self-assessment. It also shows howpatients’ references to circumstances of use can be a resource forcontextualizing the strictly quantitative aspects of substance use.
In line 3, the patient began his response with the term, “Social,”ostensibly a shortened formof social drinking. The patient relied uponthe physician to understand social drinking as implying drinking ina group setting or at gatherings where it would be appropriate to usealcohol (clubs, bars, parties, etc.). This stands in contrast to drinkingalone,which iswidely understoodas a risk factor for problemdrinking(Clark, 1995). The very notion of social drinking implies a kind oflocalized normative consensus; it is a context for drinking in which“everyone else is doing it.” In beginning his responsewith “Social,” thepatient provided for his subsequent report on the quantity/frequencyof use to be understood as occurring within this normatively appro-priate circumstance. Thepatientemployed thequantity term “couple,”which can be heard as exactly two drinks or an idiomatic gloss fora small amount. Under either interpretation, this is a quantity that isrecognizably unproblematic, particularly when considered withina frequency of one week. Based on these amounts, the patient wouldrarely, if ever, become intoxicated. The patient also specified that hedrinks beer, among the most culturally accepted forms of alcohol.
P.M. Denvir / Social Science & Medicine 75 (2012) 1650e1659 1655
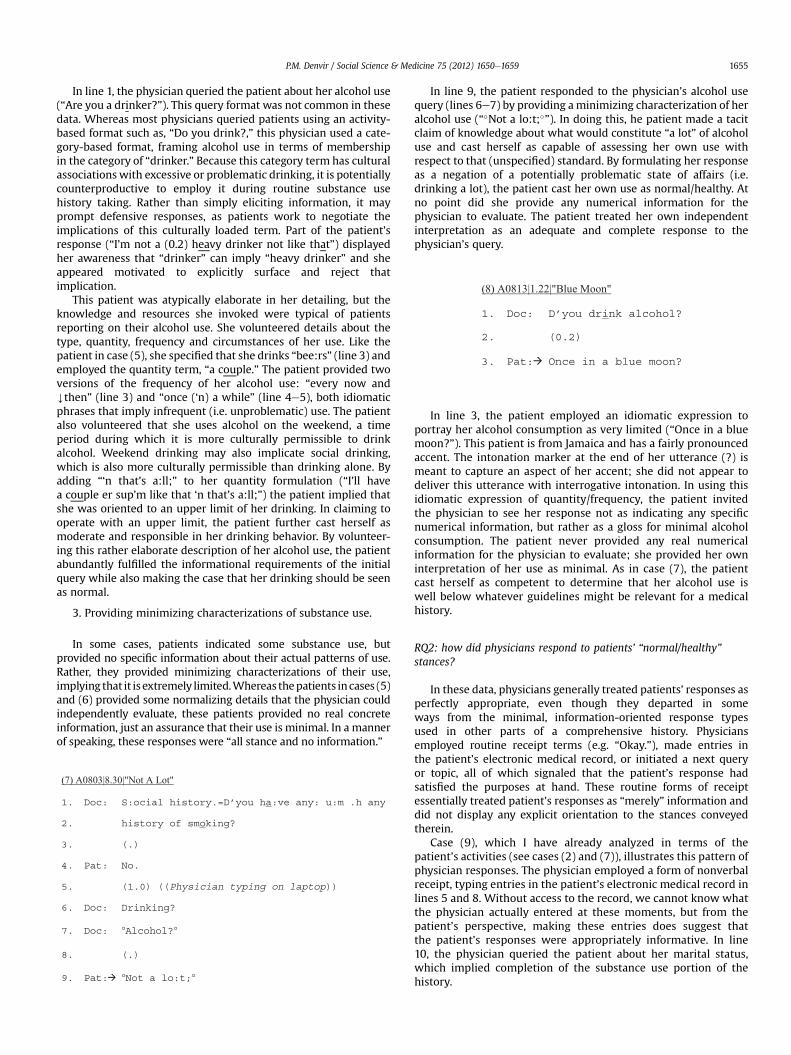
In line 1, the physician queried the patient about her alcohol use(“Are you a drinker?”). This query format was not common in thesedata. Whereas most physicians queried patients using an activity-based format such as, “Do you drink?,” this physician used a cate-gory-based format, framing alcohol use in terms of membershipin the category of “drinker.” Because this category term has culturalassociations with excessive or problematic drinking, it is potentiallycounterproductive to employ it during routine substance usehistory taking. Rather than simply eliciting information, it mayprompt defensive responses, as patients work to negotiate theimplications of this culturally loaded term. Part of the patient’sresponse (“I’m not a (0.2) heavy drinker not like that”) displayedher awareness that “drinker” can imply “heavy drinker” and sheappeared motivated to explicitly surface and reject thatimplication.
This patient was atypically elaborate in her detailing, but theknowledge and resources she invoked were typical of patientsreporting on their alcohol use. She volunteered details about thetype, quantity, frequency and circumstances of her use. Like thepatient in case (5), she specified that she drinks “bee:rs” (line 3) andemployed the quantity term, “a couple.” The patient provided twoversions of the frequency of her alcohol use: “every now andYthen” (line 3) and “once (‘n) a while” (line 4e5), both idiomaticphrases that imply infrequent (i.e. unproblematic) use. The patientalso volunteered that she uses alcohol on the weekend, a timeperiod during which it is more culturally permissible to drinkalcohol. Weekend drinking may also implicate social drinking,which is also more culturally permissible than drinking alone. Byadding “‘n that’s a:ll;” to her quantity formulation (“I’ll havea couple er sup’m like that ‘n that’s a:ll;”) the patient implied thatshe was oriented to an upper limit of her drinking. In claiming tooperate with an upper limit, the patient further cast herself asmoderate and responsible in her drinking behavior. By volunteer-ing this rather elaborate description of her alcohol use, the patientabundantly fulfilled the informational requirements of the initialquery while also making the case that her drinking should be seenas normal.
3. Providing minimizing characterizations of substance use.
In some cases, patients indicated some substance use, butprovided no specific information about their actual patterns of use.Rather, they provided minimizing characterizations of their use,implying that it is extremely limited.Whereas thepatients incases (5)and (6) provided some normalizing details that the physician couldindependently evaluate, these patients provided no real concreteinformation, just an assurance that their use is minimal. In a mannerof speaking, these responses were “all stance and no information.”
In line 9, the patient responded to the physician’s alcohol usequery (lines 6e7) by providing aminimizing characterization of heralcohol use (“�Not a lo:t;�”). In doing this, he patient made a tacitclaim of knowledge about what would constitute “a lot” of alcoholuse and cast herself as capable of assessing her own use withrespect to that (unspecified) standard. By formulating her responseas a negation of a potentially problematic state of affairs (i.e.drinking a lot), the patient cast her own use as normal/healthy. Atno point did she provide any numerical information for thephysician to evaluate. The patient treated her own independentinterpretation as an adequate and complete response to thephysician’s query.
In line 3, the patient employed an idiomatic expression toportray her alcohol consumption as very limited (“Once in a bluemoon?”). This patient is from Jamaica and has a fairly pronouncedaccent. The intonation marker at the end of her utterance (?) ismeant to capture an aspect of her accent; she did not appear todeliver this utterance with interrogative intonation. In using thisidiomatic expression of quantity/frequency, the patient invitedthe physician to see her response not as indicating any specificnumerical information, but rather as a gloss for minimal alcoholconsumption. The patient never provided any real numericalinformation for the physician to evaluate; she provided her owninterpretation of her use as minimal. As in case (7), the patientcast herself as competent to determine that her alcohol use iswell below whatever guidelines might be relevant for a medicalhistory.
RQ2: how did physicians respond to patients’ “normal/healthy”stances?
In these data, physicians generally treated patients’ responses asperfectly appropriate, even though they departed in someways from the minimal, information-oriented response typesused in other parts of a comprehensive history. Physiciansemployed routine receipt terms (e.g. “Okay.”), made entries inthe patient’s electronic medical record, or initiated a next queryor topic, all of which signaled that the patient’s response hadsatisfied the purposes at hand. These routine forms of receiptessentially treated patient’s responses as “merely” information anddid not display any explicit orientation to the stances conveyedtherein.
Case (9), which I have already analyzed in terms of thepatient’s activities (see cases (2) and (7)), illustrates this pattern ofphysician responses. The physician employed a form of nonverbalreceipt, typing entries in the patient’s electronic medical record inlines 5 and 8. Without access to the record, we cannot know whatthe physician actually entered at these moments, but from thepatient’s perspective, making these entries does suggest thatthe patient’s responses were appropriately informative. In line10, the physician queried the patient about her marital status,which implied completion of the substance use portion of thehistory.

P.M. Denvir / Social Science & Medicine 75 (2012) 1650e16591656
I offer two contrasting observations about these types ofresponses from physicians. On the one hand, by treating “normal/healthy” stances as appropriate and sufficient for advancing thehistory to other matters, physicians tacitly legitimized patients’entitlement to evaluate their own substance use conduct and topresent it to a physician in this way. This demonstrates ameasure ofrespect for what Mishler (1984) has termed a patient’s “lifeworld”perspective, referring to the everyday experiences, knowledge, andreasoning that patients draw upon to make sense of their ownhealth and health behaviors. This dynamic of legitimization feltmost pronounced when patients provided only a characterizationwithout any specific information (see line 4 of case (9) above). Bypassing on the opportunity to elicit the specific information theywould need to formulate their own assessments, physicians dis-played trust and confidence in patients’ everyday interpretations.This could enhance rapport and even lead to greater comfort indiscussing substance use in the future.
On the other hand, it may be medically problematic for physi-cians to rely only on patients’ subjective impressions and not probefor objective details. The medical education and training literaturegenerally recommends more thorough and detailed substance usehistories than were in evidence in these data. For example, physi-cians are encouraged to query patients specifically about drug usein the past, as patients may assume that only their current conductis relevant to report. Other research (Taj, 1998) has shown thata single query about binge drinking within the last year (diplo-matically designed) is a reasonably efficient and reliable way toidentify problem drinking. Given patients’ well-documentedreluctance to acknowledge substance issues, there is good reasonfor physicians to provide multiple opportunities for issues tosurface, a kind of gentle interrogative persistence. However, inthese data, when patients initially portrayed their substance useconduct as normal, appropriate, or desirable, physicians neverprovided any additional probes. Given previous research onphysicians’ reluctance to probe about substance use (e.g. Rapleyet al., 2006), it may be the case that patients’ initial “normal/healthy” stances simply give physicians a warrant (and tacitpermission) to conduct a cursory history.
As noted earlier, this pattern has generally been attributed tophysicians’ discomfort, inexperience, lack of training, lack of time,etc. Without diminishing the role that these practical and attitu-dinal factors almost certainly play, this analysis suggests thatinteractional factors can also constitute a barrier. When patients
initially enact “normal/healthy” stances toward their substance useconduct, they create a rather inhospitable interactional environ-ment for physicians to persist with additional questions about thatconduct. In the context of a comprehensive medical history,a “normal/healthy” report strongly projects completion andprogression to a next topic. Set against this expectation, additionalprobes could seem inattentive or even insensitive to the patient’sportrayal of his/her conduct. Worse yet, it could be heard asregistering skepticism that the patient has been fully forthcoming,warranting additional “digging” by the physician. It also might callinto question the patient’s knowledge or competence to make theassessments embodied by their stances. Just as Stivers (2008)argued that storytellers’ stances invite agreement/alignment fromstory recipients, patients’ “normal/healthy” stances appear to invitephysician acceptance.
By contrast, when a patient provides informationwithout takinga discernible stance toward it, follow-up queries from the physiciancould be understood simply as filling out additional details. In thisway, patients’ stances can create an interactional dilemma forphysicians: how can they pursue the specific details needed tomake an informed medical assessment without appearing to resistthe patients’ own assessment? I return to this question in theDiscussion section.
RQ3: what are some potential social functions of patients’ “normal/healthy” stances?
I begin with the premise that speakers can design their talk toattend to multiple social or interactional concerns; a single utter-ance can serve more than one purpose. In these cases, patientsclearly designed their utterances to provide information and toanswer physicians’ questions. These functions strike me asstraightforward requirements for participating as a patient ina medical history. But in taking stances toward their information,patients did something rather “special,” at least in the context ofa routine medical history. For what social and/or interactionalpurposes might patients choose to report in this way?
1. Redirecting the physician’s history taking to other topics.
Earlier research on physicianepatient communication (Frankel& Beckman, 1989; Mishler, 1984; Treichler, Frankel, Kramarae,Zoppi, & Beckman, 1984) tended to emphasize physicians’behavior, in part to expose and challenge the ways in which thestructures of traditional medical interviewing tended to minimizepatient involvement. Perhaps inadvertently, this emphasis tendedto cast patients as passive and reactive, not as fully engaged co-participants. More recent research has shown how patients canactively influence medical interactions and outcomes (Costello &Roberts, 2001; Gill, Pomerantz, & Denvir, 2010; Pomerantz, Gill, &Denvir, 2007; Stivers, 2002). A common theme in this research isthat when patients do assert their agency, they still do so in waysthat respect the physician’s activities and responsibilities.
In applying this perspective here, one potential social functionof “normal/healthy” stances is to subtly redirect the physician’sattention during a comprehensive medical history. This stanceimplies that there is nothing medically consequential to report,which provides somewarrant for performing amore circumscribedsubstance use history. Patients are aware that medical visits involvesome time constraints and may wish to reserve time for aspects ofhealth that they see as more immediately pressing. In light of this,“normal/healthy” stances can be understood as a patient’s resourcefor progressing quickly through certain topics. Without overtlychallenging the physician’s history taking agenda or initiative,a stance can shape what becomes a necessary, reasonable, orrelevant next action by the physician. In these data, physicians

P.M. Denvir / Social Science & Medicine 75 (2012) 1650e1659 1657
appeared to infer that additional follow-up or probing queries wereunnecessary after “normal/healthy” portrayals of substance use.These portrayals essentially served as the culturally commonsen-sical “raw materials” from which to make such an inference.Consistent with the patient-focused research cited above, thisstrategy for shaping medical interactions allows patients to expresssome control over the encounter while also respecting theauthority and expertise of the physician to ultimately decide howdetailed the history needs to be.
2. Presenting oneself as a health-conscious patient.
In Presentation of Self in Everyday Life (1959), sociologist ErvingGoffman employs a theatrical metaphor (dramaturgy) to describethe organization of social interaction. From this perspective,interaction is a collaborative “performance” among actors whocoordinate their activities to achieve a coherent “scene.” Thenature and details of these performances are context-sensitive;they are shaped by the actors’ ongoing analyses of the socialscenes in which they are participating and the “parts” they areplaying within those scenes. Goffman’s perspective emphasizesthe ways in which a person’s interactional conduct can project his/her incumbency in a specific situated role identity, such as spouse,restaurant patron, or patient. For example, the action of “placing anorder” projects incumbency in the role of restaurant patron.Essentially, we must “act” the part to be understood in that part byother social actors.
The notion of self-presentation implies that we are able to adaptour behavior around the expectations associated with the role(s)we are currently playing. Role performances are normative in thesense that claiming incumbency in a role obligates an actor to fulfillsome basic expectations of that role (e.g. a waiter should take thecustomer’s order). However, these normative parameters do notpreclude the possibility of more nuanced, idiosyncratic, or strategicrole performances. All performances are evaluable by all partici-pants in a scene, including the performer him/herself. Differentversions of a role performance may be deemed more or lessappropriate, desirable, or artful in a given situation.
From a dramaturgical perspective, when individuals interactwith health care professionals, they do so in and through theirperformance of the patient role. Patients project their incumbencyin this role in various ways: by describing medical complaints, byasking and answering health-related questions, by allowing theirbodies to be physically examined, etc. During the routine substanceuse histories that I examined, patients certainly fulfilled these basicperformance expectations; loosely speaking, they “acted likepatients.” But in enacting “normal/healthy” stances, they may havealso been working to project a more specific version of the patientrole: the health-conscious patient. By treating substance use asunthinkable for them or by describing their use as moderate andlimited, these patients portrayed themselves as mindful of the risksassociated with these substances. In their formulations, theyrevealed not just a pattern of low risk behavior, but also a norma-tively and/or medically informed commitment to that behavior.Given that wellness is the broad goal of the physicianepatientrelationship, health consciousness is a desirable aspect of “self”for patients to present in this context.
Such displays of health consciousness could be understood asa rapport-building resource for patients. As the professionalmember of the physicianepatient dyad, physicians are often heldresponsible for establishing rapport with patients, but this canobscure attention to some of the ways that patients can work tobuild rapport. By presenting themselves as actively and compe-tently managing their own everyday health risks, patients canencourage greater investment from physicians and ultimatelya more successful and satisfying therapeutic partnership.
Discussion and recommendations
It should be noted that some features of this sample may limitthe generalizability of these findings to other populations. Alldata were collected from a single medical setting, so the findingscould be reflective of the culture and practices of this particularsetting. The physician and patient participants were also fairlyhomogeneous from a racial/ethnic standpoint; most wereCaucasian. In addition, the mean patient age of 52 may haveinfluenced some of the physicians’ communicative choices.Physicians may be more committed to investigating substanceuse with younger patients, who they may expect to be usingsubstances socially and recreationally. Practitioners should exer-cise judgment when applying this work to other medical contextsor patient populations. That said, this analysis does provideimportant insights into the interactional challenges of patient-centered lifestyle history taking and the role of patient agencyin that process.
While patients may defer to physicians’ expertise when it comesto highly technical, biomedical aspects of health, this analysissuggests that they may be more assertive when talking aboutsubstance use. Patients spoke with a commonsensical authority inthis domain, drawing upon broadly shared cultural and normativepremises to propose that their conduct was not problematic. Froma patient-centered perspective, this kind of assertiveness is bothfunctional and, in some ways, desirable. The patients in these datafulfilled their basic reporting obligations (i.e. they answered ques-tions), while also streamlining the history and presenting them-selves as engaged and mindful agents in their own health.Proponents of patient-centered interviewing practices would likelyappreciate the trust and evaluative license that physiciansextended to patients in these data.
At the same time, “normal/healthy” stances can present some-thing of a dilemma for physicians who would otherwise becommitted to eliciting a detailed history. This dilemma can beexpressed in terms of countervailing precepts within thephysicianepatient therapeutic relationship. On one hand, physi-cians may be guided by the precept, “be thorough” and on the otherhand, “be respectful.” I would argue that additional probing after aninitial “normal/healthy” response would satisfy the thoroughnessprecept, but potentially at the expense of the respect precept. Icannot know for certain that this dilemma was present or salientfor the physicians in these data, but if so, it would appear that theyelected to respect patients’ interpretations of their own conduct atthe expense of being thorough. In some cases, physicians elicitedremarkably superficial substance use histories. From a practicalstandpoint, what might be done about this dilemma? I offer onepotential solution.
Physicians could begin the substance use history with a briefdisclaimer (Hewitt & Stokes, 1975). In interactional terms,disclaimers are prefatory utterances or actions designed to antic-ipate and attend to inferences that might be made about subse-quent utterances or actions. For example, when a person says, “Ihate to be the one to tell you this, but.” s/he forecasts that thenext action/utterance may be unwelcome and also displays someapprehension about having to provide it. “Disclaimers areprospective, defining the future in the present, creating interpre-tations of potentially problematic events intended to make themunproblematic when they occur” (Hewitt & Stokes, 1975, p. 2).Applied to the present context, physicians could use disclaimers tocontextualize the meaning and purpose of forthcoming substanceuse questions. Below, I suggest two elements that might beincluded in such disclaimers. In practice, physicians could adaptthese elements in ways that seem most appropriate or useful forthe situation at hand.

P.M. Denvir / Social Science & Medicine 75 (2012) 1650e16591658
1. Minimize the professional relevance of moral judgment.
Patients who are concerned about being morally judged(rather than medically evaluated) by their health providers mayemploy “normal/healthy” stances in order to invite favorablejudgments or resist unfavorable judgments. They may even usesuch stances to withhold potentially important health informa-tion that they view as morally or normatively problematic (e.g.current or past intravenous drug use). Physicians may be able topreempt or at least minimize that concern by stressing that theyare not interested in the moral implications of patients’ substanceuse, only the medical implications. They could frame morality asessentially outside of their professional interests or expertise. Forexample, physicians might say something like, “Substance use cansometimes feel like a sensitive or embarrassing topic, but I wantto assure you that there is no judgment here. That’s really notmy job. My job is to provide medical care for you and I can dothat better when I have a clear picture of your day-to-daylifestyle.”
2. Forecast a series of routine questions, regardless of what thepatient may report along the way.
I have argued that, if a physician continues probing foradditional information after an initial “normal/healthy”response, the patient may see the physician as not fully acceptingor trusting that initial account, which could diminish rapport.Physicians may be able to preempt or minimize that concern byindicating up front that they are going to ask a series of routinequestions, perhaps even indicating an approximate number ofquestions. This would provide patients with a different way tointerpret additional probing by the physician; rather thanattributing this to physicians’ suspicion or mistrust, patientswould be more able to view them simply as standardized“checklist” items for all patients. By depersonalizing (or gener-alizing) the basis for these questions, physicians can subtly invitepatients to see that they are not being singled out as needing anespecially thorough substance use history. For example, physi-cians might say something like, “I like to ask all of my patientsthe same four or five questions about substance use. It’s impor-tant to be thorough, so I tend to ask all of these questions everytime, even if what you tell me sounds pretty low risk froma health standpoint.”
This analysis sheds light on some of the challenges andcomplexities involved in lifestyle history taking. Substance use,diet, and exercise are all evaluable in medical terms, but they arealso evaluable in more culturally commonsensical ways. Whenpatients employed “normal/healthy” stances, they drew uponthese understandings to speak with a kind of everyday exper-tise. While this is encouraging in terms of patient engagementand assertiveness, it may create difficulties for physicians whoneed to pursue more detailed accounts without underminingrapport.
Additional research should examine the stances that patientsmay employ when reporting on other lifestyle domains. It wouldalso be useful to examine cases in which physicians did probe foradditional details after an initial “normal/healthy” report. That datamay yield additional strategies for being thorough withoutappearing inattentive or skeptical.
Acknowledgments
I wish to acknowledge Anita Pomerantz for her superbmentorship throughout this project.
References
Baxter, L. A., Hirokawa, R., Lowe, J. B., Nathan, P., & Pearce, L. (2004). Dialogic voicesin talk about drinking and pregnancy. Journal of Applied CommunicationResearch, 32(3), 224e248.
Bergmann, J. R. (1992). Veiled morality: notes on discretion in psychiatry. In P. Drew,& J. Heritage (Eds.), Talk at work: Interaction in institutional settings (pp.137e162). Cambridge: Cambridge University Press.
Bertakis, K., & Azari, R. (2007). Determinants of physician discussion regardingtobacco and alcohol abuse. Journal of Health Communication, 12, 513e525.
Boyd, E. A., & Heritage, J. (2006). Taking the history: questioning during compre-hensive history taking. In J. Heritage, & D. Maynard (Eds.), Communication inmedical care: Interaction between primary care physicians and patients. Cam-bridge: Cambridge University Press.
Cherpitel, C. (1997). Brief screening instruments for alcoholism. Alcohol Health &Research World, 21(4), 348e351.
Clark, W. (1995). Effective interviewing and intervention for alcohol problems. InM. Lipkin, Jr., S. Putnam, & A. Lazare (Eds.), The medical interview: Clinical care,education, and research (pp. 284e293). New York: Springer.
Clayman, S. E., & Gill, V. T. (2004). Conversation analysis. In M. Hardy, & A. Bryman(Eds.), Handbook of data analysis (pp. 589e606). London: Sage Publications.
Costello, B. A., & Roberts, F. (2001). Medical recommendations as joint socialpractice. Health Communication, 13(3), 241e260.
Cotter, F., & Callahan, C. (1987). Training primary care physicians to identify andtreat substance abuse. Alcohol Health & Research World, 11, 70e73.
Fleming, M. F. (2004/2005). Screening and brief intervention in primary caresettings. Alcohol Research and Health, 28, 57e62.
Fleming, M. F., Barry, K. L., Manwell, L. B., Johnson, K., & London, R. (1997). Briefphysician advice for problem alcohol drinkers: a randomized controlled trial incommunity-based primary care practices. Journal of the American MedicalAssociation, 277, 1039e1045.
Frankel, R., & Beckman, H. (1989). Evaluating the patient’s primary problem(s). InM. Stewart, & D. Roter (Eds.), Communicating with medical patients (pp. 86e98).Newbury Park, London: Sage Publications.
Friedmann, P. D., McCullough, D., Chin, M. H., & Saitz, R. (2000). Screening andintervention for alcohol problems: a national survey of primary care physiciansand psychiatrists. Journal of General Internal Medicine, 15, 84e91.
Garfinkel, H. (1967). Studies in ethnomethodology. Englewood Cliffs, NJ: Prentice-Hall.Gill, V. T., Pomerantz, A., & Denvir, P. (2010). Preemptive resistance: patients’
participation in diagnostic sense-making activities. Sociology of Health andIllness, 32, 1e20.
Graham, A. V., Zyzanski, S., Reeb, K., Sedlacek, D., & Emmitt-Myers, S. (1994).Physician documentation of family alcohol problems. Journal of Substance Abuse,6, 95e103.
Halkowski, T. R. (1998). Patients’ smoking counts: implications of quantificationpractices. Journal of General Internal Medicine, 13, 107.
Halkowski, T. (2011). Medical discourse. In K. Hyland, & B. Paltridge (Eds.),Companion to discourse analysis (pp. 321e331). London: The Continuum Inter-national Publishing Group Ltd.
Heritage, J. (1984). Garfinkel and ethnomethodology. Cambridge: Polity Press.Heritage, J. (1998). Oh-prefaced responses to inquiry. Language in Society, 27(3),
291e334.Heritage, J. (2002). Oh-prefaced responses to assessments: a method of modifying
agreement/disagreement. In C. E. Ford, B. A. Fox, & S. A. Thompson (Eds.), Thelanguage of turn and sequence (pp. 196e225). Oxford: Oxford University Press.
Heritage, J., & Lindstrom, A. (1998). Motherhood, medicine, and morality: scenesfrom a medical encounter. Research on Language & Social Interaction, 31(3&4),397e438.
Hewitt, J. P., & Stokes, R. (1975). Disclaimers. American Sociological Review, 40(1),1e11.
Hopper, R. (1989). Conversation analysis and social psychology as descriptions ofinterpersonal communication. In D. Roger, & P. Bull (Eds.), Conversation: Aninterdisciplinary perspective (pp. 48e65). Philadelphia: Multilingual Matters.
Hopper, R. (1992). Telephone conversation. Bloomington: Indiana University Press.Jefferson, G. (1974). Error correction as an interactional resource. Language in
Society, 2, 181e199.Johanson, M., Larsson, U. S., Saljo, R., & Svardsudd, K. (1998). Lifestyle discussion in
the provision of health care: an empirical study of patient-physician interac-tion. Social Science & Medicine, 47(1), 103e112.
Larsson, U. S., Saljo, R., & Aronsson, K. (1987). Patient-doctor communication onsmoking and drinking: lifestyle in medical consultations. Social Science &Medicine, 25, 1129e1137.
Maheux, B., Haley, N., Rivard, M., & Gervais, A. (1995). STD risk assessment and risk-reduction counseling by recently trained family physicians. Academic Medicine,70, 726e728.
Maisto, S. A., Conigliaro, J., McNeil, M., Kraemer, K., Conigliaro, R. L., & Kelley, M. E.(2001). Effects of two types of brief intervention and readiness to change onalcohol use in hazardous drinkers. Journal of Studies on Alcohol, 62, 605e614.
Mignon, S. I. (1993e1994). Physicians’ treatment of elderly alcoholics. SociologicalPractice, 11, 197e211.
Mignon, S. I. (1995). The discovery of patients’ alcoholism by physicians. Research inthe Sociology of Health Care, 12, 175e187.
Mignon, S. I. (1996). Physicians’ perceptions of alcoholics: the disease conceptreconsidered. Alcoholism Treatment Quarterly, 14, 33e45.

P.M. Denvir / Social Science & Medicine 75 (2012) 1650e1659 1659
Mishler, E. G. (1984). The discourse of medicine. Norwood, New Jersey: AblexPublishing Corporation.
Najman, J. M., Klein, D., & Munro, C. (1982). Patient characteristics negativelystereotyped by doctors. Social Science & Medicine, 16, 1781e1789.
Pomerantz, A., & Fehr, B. J. (1997). Conversation analysis: an approach to the studyof social action as sense making practices. In T. A. van Dijk (Ed.), Discourse associal interaction (pp. 64e91). London: Sage Publications.
Pomerantz, A., Gill, V., & Denvir, P. (2007). When patients present serious healthconditions as unlikely. In A. Hepburn, & S. Wiggins (Eds.), Discursive research inpractice: New approaches to psychology and interaction. Cambridge: CambridgeUniversity Press.
Rapley, T., May, C., & Kaner, E. F. (2006). Still a difficult business? Negotiatingalcohol-related problems in general practice consultations. Social Science &Medicine, 63, 2418e2428.
Sacks, H. (1974). An analysis of the course of a joke’s telling in conversation. InR. Bauman, & J. Sherzer (Eds.), Explorations in the ethnography of speaking (pp.337e353). Cambridge, England: Cambridge University Press.
Silverman, D. (1994). Describing sexual activities in HIV counseling: the cooperativemanagement of the moral order. Text, 14, 427e453.
Sorjonen, M., Raevaara, L., Haakana, M., Tammi, T., & Perakyla, A. (2006). Lifestylediscussions in medical interviews. In J. Heritage, & D. Maynard (Eds.),Communication in medical care: Interaction between primary care physicians andpatients (pp. 340e378). Cambridge: Cambridge University Press.
Stivers, T. (2002). Presenting the problem in pediatric encounters: “symptoms only”versus “candidate diagnosis” presentations. Health Communication, 14(3),299e338.
Stivers, T. (2008). Stance, alignment, and affiliation during storytelling: when noddingis a token of affiliation. Research on Language & Social Interaction, 41, 31e57.
Stivers, T., & Heritage, J. (2001). Breaking the sequential mold: answering ‘morethan the question’ during comprehensive history taking. Text, 21, 151e185.
Taj, N. (1998). Screening for problem drinking: does a single question work? Journalof Family Practice, 46, 328e335.
Thom, B., & Tellez, C. (1986). A difficult business: detecting and managing alcoholproblems in general practice. British Journal of Addiction, 81, 405e418.
Treichler, P., Frankel, R., Kramarae, C., Zoppi, K., & Beckman, H. (1984). Problems andproblems: power relationships in a medical encounter. In C. Kramarae,M. Schulz, & W. O’Barr (Eds.), Language and power (pp. 62e88). Beverly Hills,California: Sage Publishers.