What's New, What's True & What's Poo - Alberta College of ...
181
Unpleasant Truths Comforting Lies Tina & Mike A (PEER) Department of Family Medicine, University of Alberta College of Family Physicians of Canada What’s New, What’s True & What’s Poo
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of What's New, What's True & What's Poo - Alberta College of ...

Unpleasant Truths
Comforting Lies
Tina & Mike A (PEER)Department of Family Medicine, University of Alberta
College of Family Physicians of Canada
What’s New, What’s True & What’s Poo

Faculty/Presenter Disclosures• Faculty: Mike, Tina• Salary: College of Family Physicians of Canada (MA), University of Alberta (TK) • Relationships with financial sponsors:
• Grants/Research Support: Alberta College of Family Physicians; Toward Optimized Practice, CIHR, PRIHS, Ontario LHIN grant,
• Speakers Bureau/Honoraria: All Non‐Profit ‐ Provincial chapters of the College of Family Physicians (Alberta, Ontario, NFLD, PEI, BC); Multiple University CPD depts, miscellaneous conferences
• Consulting Fees: N/A• Patents: N/A• Other: Bedmed, INR range (publicly funded research studies)

What’s new?
What’s new?
What’s True?
What’s new?
What’s True?
What’s Poo?

Roflumilast (cream) for Psoriasis
• RCT (331 pts) Roflumilast cream 0.3%, 0.15% and placebo OD x 12 weeks. • Mean age 54, 55% male, moderate psoriasis plaques on 6.4% (PASI score 8 on 0‐72 scale )
• Results: roflumilast 0.3% vs roflumilast 0.15% vs placebo• Almost clear or clear at 6 weeks: 28% of patients vs 23% vs 8% • Mean PASI score improvement vs baseline at 12 wks: 53% vs 55% vs 17%• PASI 75 at 12 weeks: 34% of patients vs 31% vs 16%• Adverse events: 39% vs 27% vs 30% ‐ none consistently higher.
• Bottom‐Line: Roflumilast appears to work relatively well for mild to moderate psoriasis over small areas.
N Engl J Med 2020;383:229-39.
TK
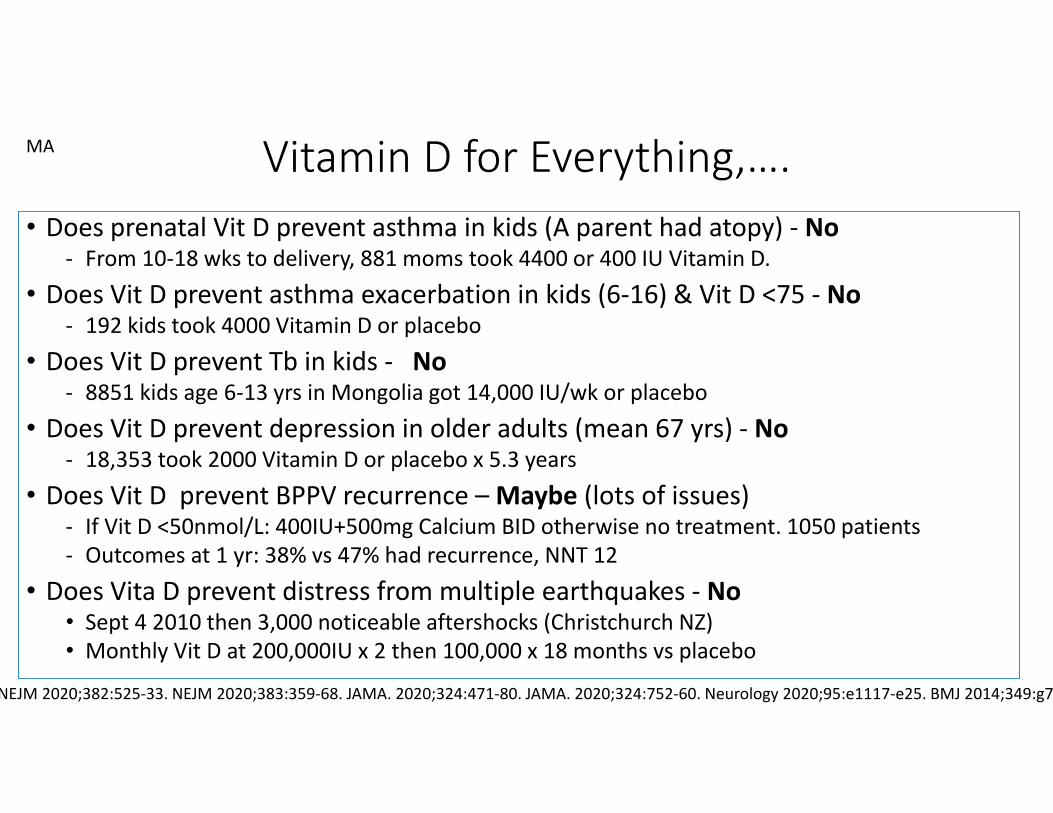
Vitamin D for Everything,….• Does prenatal Vit D prevent asthma in kids (A parent had atopy) ‐ No
‐ From 10‐18 wks to delivery, 881 moms took 4400 or 400 IU Vitamin D.• Does Vit D prevent asthma exacerbation in kids (6‐16) & Vit D <75 ‐ No
‐ 192 kids took 4000 Vitamin D or placebo• Does Vit D prevent Tb in kids ‐ No
‐ 8851 kids age 6‐13 yrs in Mongolia got 14,000 IU/wk or placebo• Does Vit D prevent depression in older adults (mean 67 yrs) ‐ No
‐ 18,353 took 2000 Vitamin D or placebo x 5.3 years• Does Vit D prevent BPPV recurrence –Maybe (lots of issues)
‐ If Vit D <50nmol/L: 400IU+500mg Calcium BID otherwise no treatment. 1050 patients‐ Outcomes at 1 yr: 38% vs 47% had recurrence, NNT 12
• Does Vita D prevent distress from multiple earthquakes ‐ No• Sept 4 2010 then 3,000 noticeable aftershocks (Christchurch NZ)• Monthly Vit D at 200,000IU x 2 then 100,000 x 18 months vs placebo
NEJM 2020;382:525‐33. NEJM 2020;383:359‐68. JAMA. 2020;324:471‐80. JAMA. 2020;324:752‐60. Neurology 2020;95:e1117‐e25. BMJ 2014;349:g7
MA
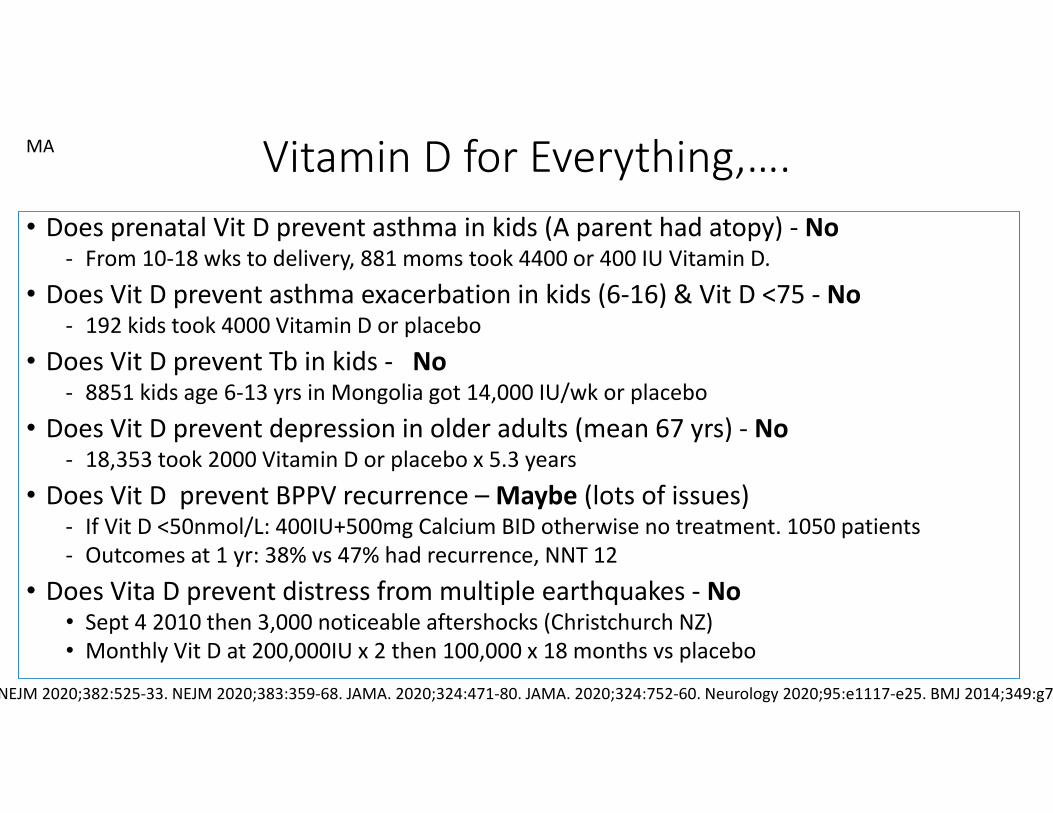
Vitamin D for Everything,….• Does prenatal Vit D prevent asthma in kids (A parent had atopy) ‐ No
‐ From 10‐18 wks to delivery, 881 moms took 4400 or 400 IU Vitamin D.• Does Vit D prevent asthma exacerbation in kids (6‐16) & Vit D <75 ‐ No
‐ 192 kids took 4000 Vitamin D or placebo• Does Vit D prevent Tb in kids ‐ No
‐ 8851 kids age 6‐13 yrs in Mongolia got 14,000 IU/wk or placebo• Does Vit D prevent depression in older adults (mean 67 yrs) ‐ No
‐ 18,353 took 2000 Vitamin D or placebo x 5.3 years• Does Vit D prevent BPPV recurrence –Maybe (lots of issues)
‐ If Vit D <50nmol/L: 400IU+500mg Calcium BID otherwise no treatment. 1050 patients‐ Outcomes at 1 yr: 38% vs 47% had recurrence, NNT 12
• Does Vita D prevent distress from multiple earthquakes ‐ No• Sept 4 2010 then 3,000 noticeable aftershocks (Christchurch NZ)• Monthly Vit D at 200,000IU x 2 then 100,000 x 18 months vs placebo
NEJM 2020;382:525‐33. NEJM 2020;383:359‐68. JAMA. 2020;324:471‐80. JAMA. 2020;324:752‐60. Neurology 2020;95:e1117‐e25. BMJ 2014;349:g7
MA

First your Toe, now your heart: What can’t Colchicine do?
• 5522 stable CAD patients on colchicine 0.5 mg OD vs placebo. ‐ Mean age 66, 85% male, 84% past Acute Coronary Syndrome
• After 29 months,…‐ CVD death, MI, stroke: 4.2% vs 5.7% (NNT=67), HR=0.72 (0.57–0.92)‐ Above + revascularization: 6.8% vs 9.6% (NNT=36), HR=0.69 (0.57‐0.83)‐ Death any cause: 0.9% vs 0.8% (no diff)‐ Harms: myalgia 21% vs 19% (NNH=37)
• Bottom‐Line: Something works! If there was just one more study,….• 2019 RCT of 4745 Post‐MI on colchicine 0.5mg or placebo x23 months
‐ CVD death, MI, stroke, revascularization: 5.5% vs 7.1% (NNT=63), HR=0.77 (0.61‐0.96)
NEJM: 10.1056/NEJMoa2021372. N Engl J Med 2019;381:2497‐505.
TK

Swollen Legs and recurrent cellulitis: Interrupting the inevitable.
• 84 compression stockings + education vs education alone. • Mean age 64, 51% male, obesity 63%, mostly below knee stockings
• At ~6 months• cellulitis in 15% compression vs 40% control (NNT=4), HR=0.23 (0.09‐0.59)• Leg volume down 6% (~240ml) vs control.• Quality of Life improved 8/100 vs control.
• Risk – cellulitis assessment unblinded. • Bottom‐Line: Compression stockings reduce leg volumes, improve quality of life and reduce cellulitis episodes (NNT=4 over 6 months).
N Engl J Med 2020;383:630-9.
MA

Gabapentin for Alcohol Use Disorder?• RCT of 90 heavy drinkers: 5/day x90 days & abstinent ≥3days
• Gabapentin titrated by 300mg/day x 4days to 300mg breakfast & lunch and 600mg hs(1200mg total) or placebo x 16 weeks. Mean age 50 and 77% male (drinks/day 11‐13).
• disialo Carbohydrate‐Deficient Transferrin to confirm abstinence (%dCDT >1.7% not)
• Outcome: At 12 weeks. • Confirmed no heavy drinking (27% vs 9%, NNT 6) & No drinking (18% vs 4%, NNT 8)• Prespecified subgroups: Group with lower AWS – Gabapentin had no effect• Higher AWS: No heavy drinking (46% vs 13%, NNT 4) & No drinking (41% vs 4%, NNT 3)• Adverse Events: Mild‐moderate dizziness – 57% vs 33% (NNH 5). Also more nervous & headache but less insomnia (numbers not given)
• Bottom‐Line: Gabapentin can help prevent return to drinking for Alcohol use disorder patients, particularly those who’ve had more withdrawal symptoms.
JAMA Intern Med. doi:10.1001/jamainternmed.2020.0249
TK
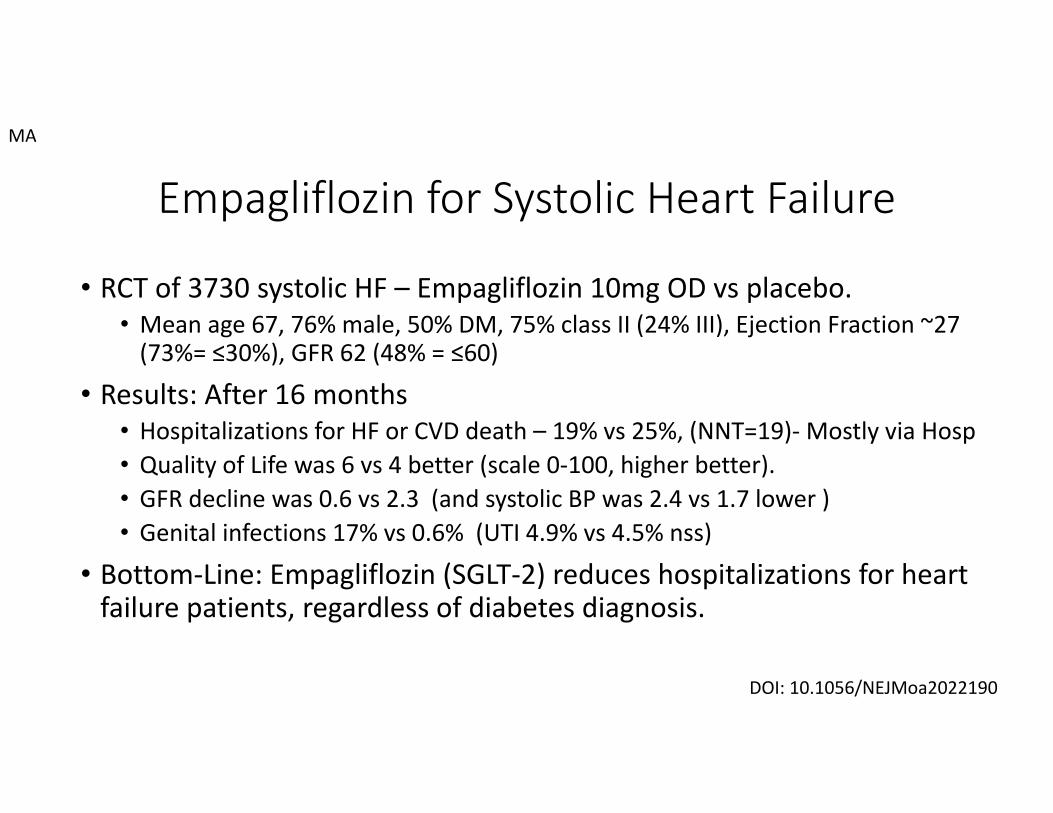
Empagliflozin for Systolic Heart Failure
• RCT of 3730 systolic HF – Empagliflozin 10mg OD vs placebo. • Mean age 67, 76% male, 50% DM, 75% class II (24% III), Ejection Fraction ~27 (73%= ≤30%), GFR 62 (48% = ≤60)
• Results: After 16 months• Hospitalizations for HF or CVD death – 19% vs 25%, (NNT=19)‐Mostly via Hosp• Quality of Life was 6 vs 4 better (scale 0‐100, higher better). • GFR decline was 0.6 vs 2.3 (and systolic BP was 2.4 vs 1.7 lower )• Genital infections 17% vs 0.6% (UTI 4.9% vs 4.5% nss)
• Bottom‐Line: Empagliflozin (SGLT‐2) reduces hospitalizations for heart failure patients, regardless of diabetes diagnosis.
DOI: 10.1056/NEJMoa2022190
MA

Risk of Prolonged Opioid use after MSK use. • Systematic Review: 13 cohort studies (13,263,393 patients, mostly USA)
• Follow‐up 3‐24 months (most 12), various MSK (or mostly MSK) injuries. • “prolonged definition varied: examples were ≥6 opioid scripts in year after first month; filled one opioid script >90 days after injury; many others.
• Results: Risk of Prolonged Opioid Use after MSK injury • low risk (general population) = 5.9% (4‐8.2%)• High risk (worker’s comp, veterans, high rates substance use disorder) =27% (18‐37%)• Risk Factors: Past SUD, longer scripts (>7days) and higher doses
• Slight with older age and more co‐morbidities)
• Bottom‐Line: Prolonger Opioid script risk ~6%. From 2019 TFP, risk of OUD ~ 3% (or <1% if no SUD Hx) and risk factors similar (longer scripts, higher doses and past SUD).
Ann Intern Med. doi:10.7326/M19-3600. Can Fam Phys 2019, 65 (10) 724
TK

Simplified meant we couldn’t handle complex medicine
MA
Simplified meant we couldn’t handle complex medicine
MA

Simplified meant we couldn’t handle complex medicine
MA

Management of Dyslipidemia for CVD Risk: Veterans & Dept of Defense Guideline
1. Do lipids q10 yrs and calculate risk every 2‐5 years (depending on risk)2. Continue to Treat to Target Dose, Not LDL‐C Level3. Don’t use of Additional Tests to Refine Risk Prediction4. Primary Prevention: Moderate‐Dose Statin Therapy;
• No to PCSK‐9 Inhibitors (or icosapent or other drugs)5. Secondary Prevention: Moderate Statin Doses Initially,
• Stepped Intensification in Higher‐Risk Patients6. Lab Testing: No Fasting or Monitoring Is Needed (once on statin, no testing)7. Physical Activity: Increased Aerobic Exercise for All
• Cardiac Rehabilitation After a Recent CVD Event8. Suggest Mediterranean Diet for High‐Risk Patients,
• Limit Icosapent Ethyl to Secondary Prevention, • Avoid Supplements. Niacin, and Fibrates
Ann Intern Med. doi:10.7326/M20-4648
MA
RESEARCH
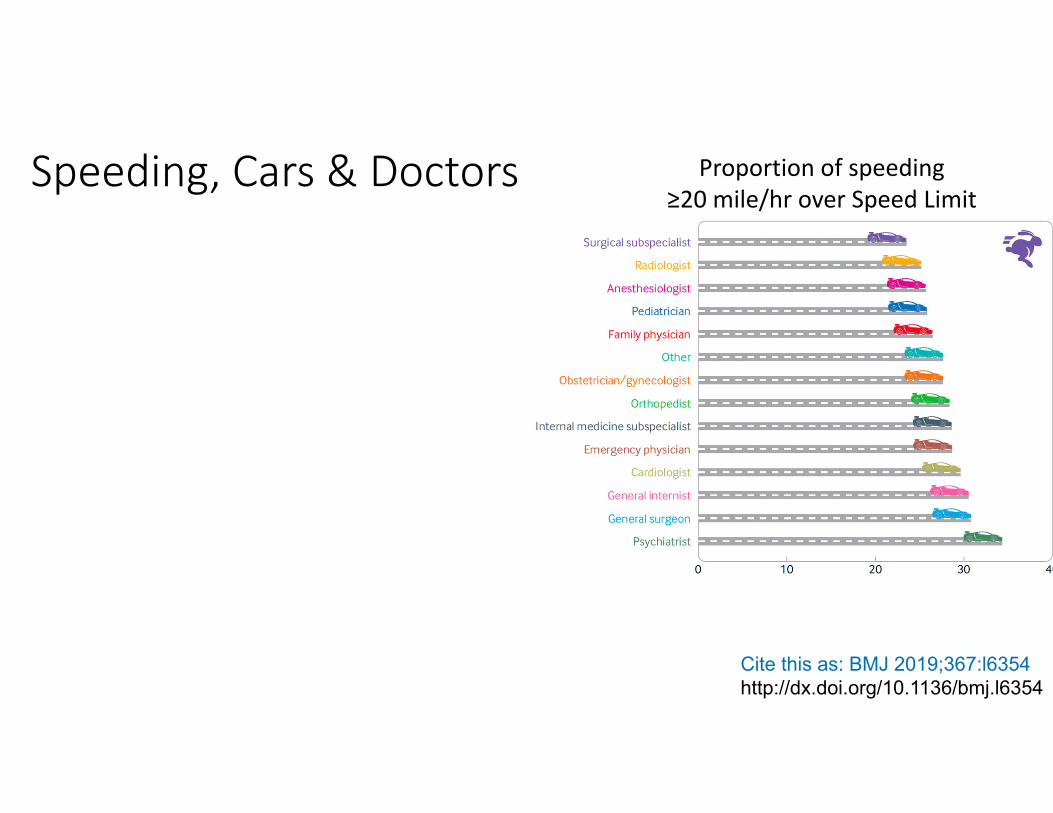
Speeding, Cars & Doctors Proportion of speeding ≥20 mile/hr over Speed Limit
Cite this as: BMJ 2019;367:l6354http://dx.doi.org/10.1136/bmj.l6354

Speeding, Cars & Doctors Proportion of speeding ≥20 mile/hr over Speed Limit
Cite this as: BMJ 2019;367:l6354http://dx.doi.org/10.1136/bmj.l6354
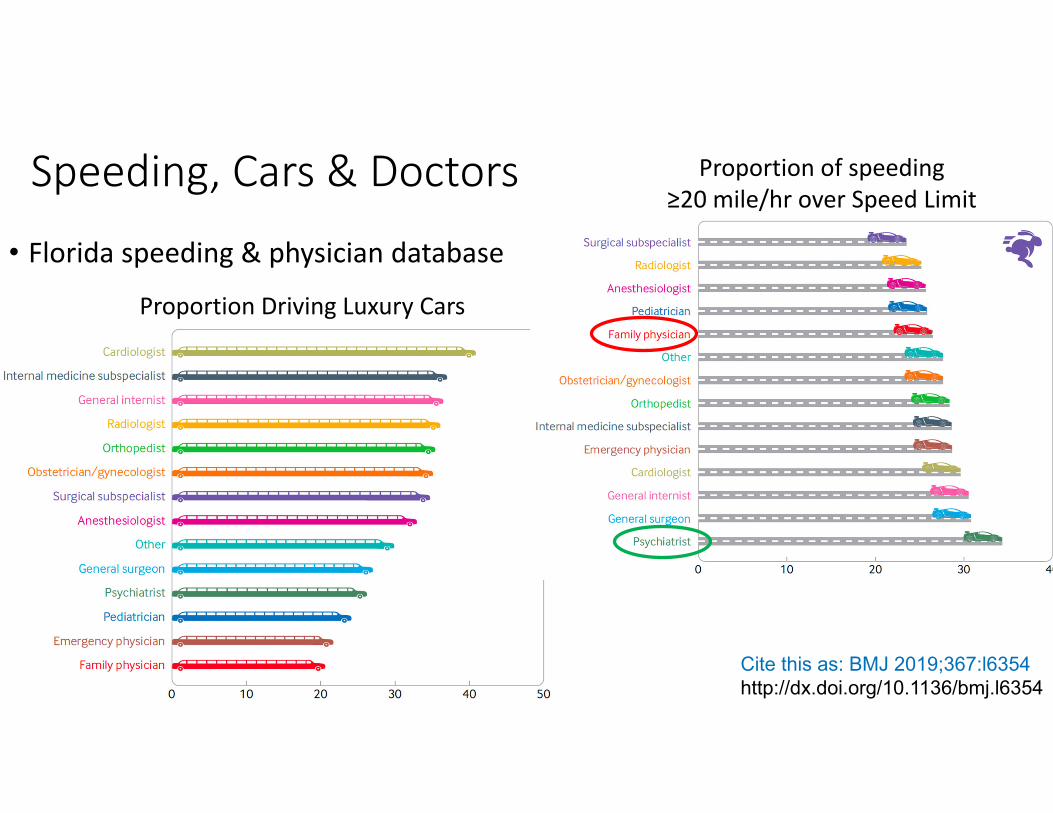
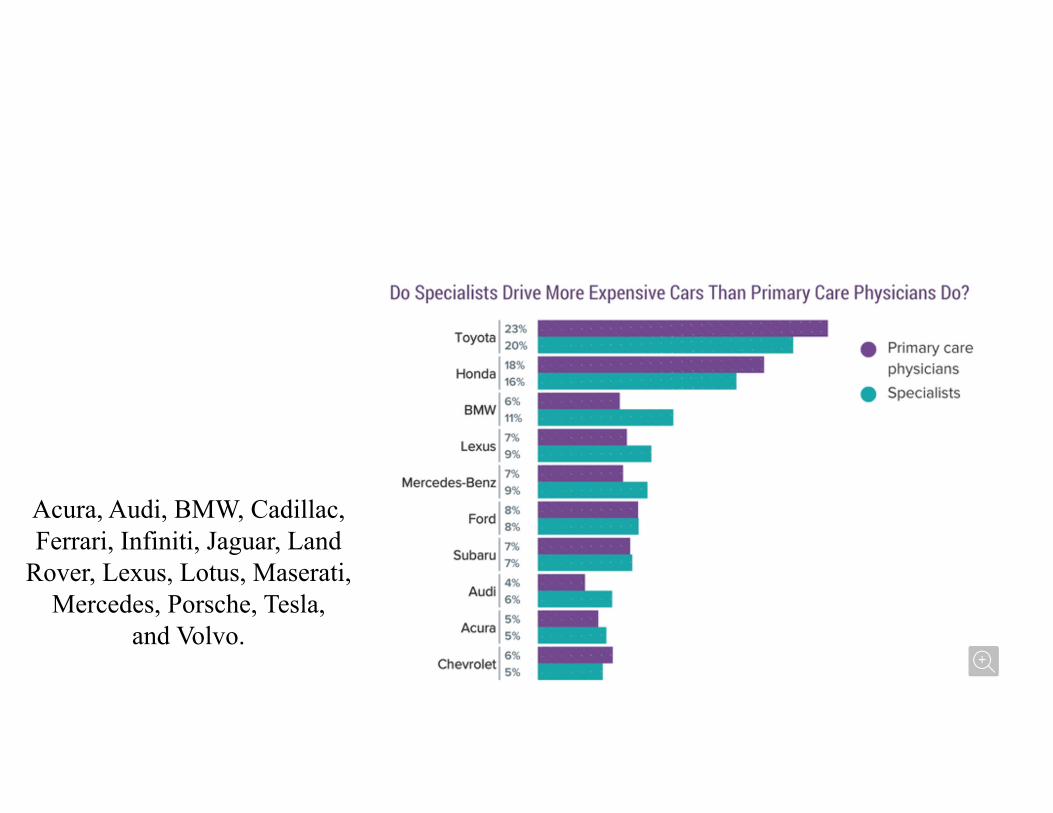
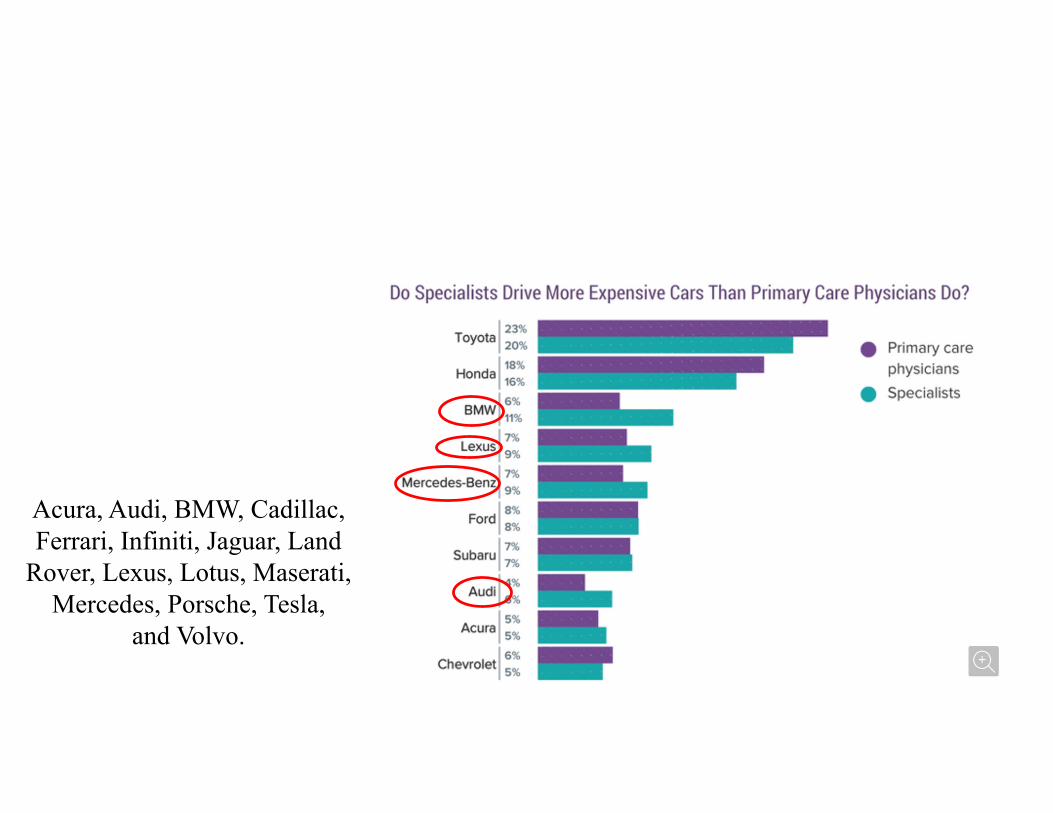
Speeding, Cars & Doctors
• Florida speeding & physician database
Proportion of speeding ≥20 mile/hr over Speed Limit
Proportion Driving Luxury Cars
Cite this as: BMJ 2019;367:l6354http://dx.doi.org/10.1136/bmj.l6354

Speeding, Cars & Doctors
• Florida speeding & physician database
Proportion of speeding ≥20 mile/hr over Speed Limit
Proportion Driving Luxury Cars
Cite this as: BMJ 2019;367:l6354http://dx.doi.org/10.1136/bmj.l6354
Acura, Audi, BMW, Cadillac, Ferrari, Infiniti, Jaguar, Land
Rover, Lexus, Lotus, Maserati, Mercedes, Porsche, Tesla,
and Volvo.
Acura, Audi, BMW, Cadillac, Ferrari, Infiniti, Jaguar, Land
Rover, Lexus, Lotus, Maserati, Mercedes, Porsche, Tesla,
and Volvo.
Acura, Audi, BMW, Cadillac, Ferrari, Infiniti, Jaguar, Land
Rover, Lexus, Lotus, Maserati, Mercedes, Porsche, Tesla,
and Volvo.

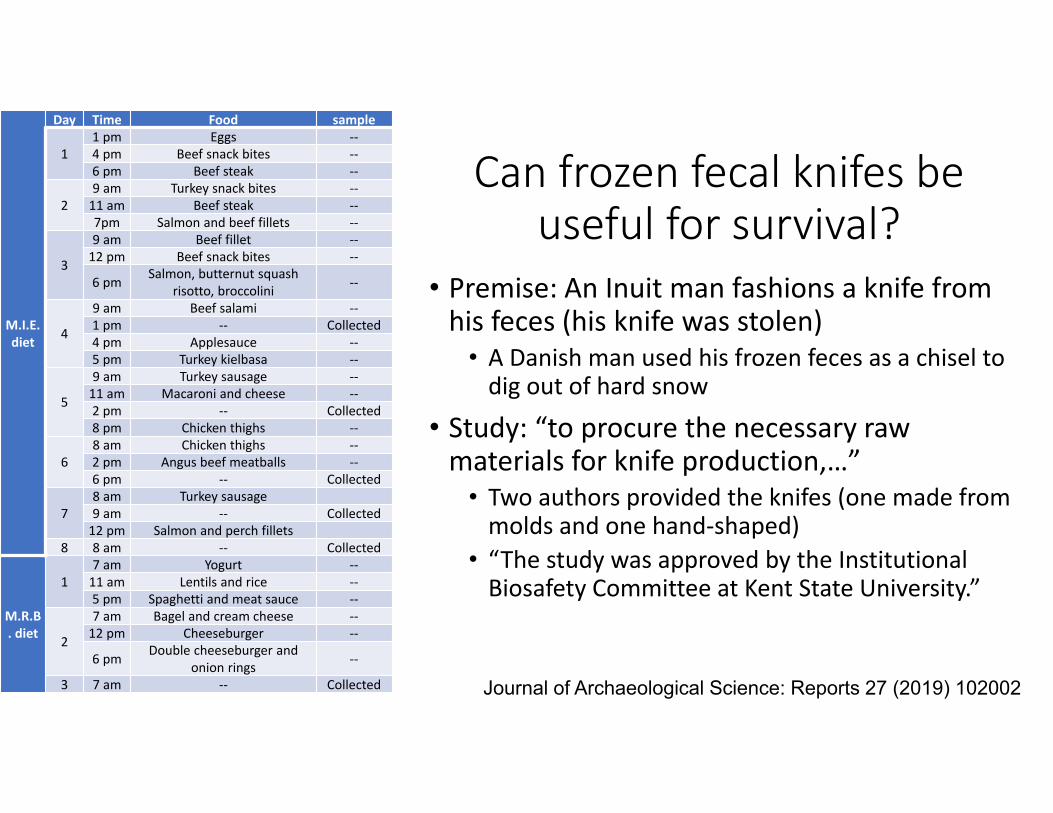
Can frozen fecal knifes be useful for survival?
• Premise: An Inuit man fashions a knife from his feces (his knife was stolen)
• A Danish man used his frozen feces as a chisel to dig out of hard snow
• Study: “to procure the necessary raw materials for knife production,…”
Journal of Archaeological Science: Reports 27 (2019) 102002
Can frozen fecal knifes be useful for survival?
• Premise: An Inuit man fashions a knife from his feces (his knife was stolen)
• A Danish man used his frozen feces as a chisel to dig out of hard snow
• Study: “to procure the necessary raw materials for knife production,…”
• Two authors provided the knifes (one made from molds and one hand‐shaped)
• “The study was approved by the Institutional Biosafety Committee at Kent State University.”
Journal of Archaeological Science: Reports 27 (2019) 102002
M.I.E. diet
Day Time Food sample
11 pm Eggs ‐‐4 pm Beef snack bites ‐‐6 pm Beef steak ‐‐
29 am Turkey snack bites ‐‐11 am Beef steak ‐‐7pm Salmon and beef fillets ‐‐
3
9 am Beef fillet ‐‐12 pm Beef snack bites ‐‐
6 pm Salmon, butternut squash risotto, broccolini ‐‐
4
9 am Beef salami ‐‐1 pm ‐‐ Collected4 pm Applesauce ‐‐5 pm Turkey kielbasa ‐‐
5
9 am Turkey sausage ‐‐11 am Macaroni and cheese ‐‐2 pm ‐‐ Collected8 pm Chicken thighs ‐‐
68 am Chicken thighs ‐‐2 pm Angus beef meatballs ‐‐6 pm ‐‐ Collected
78 am Turkey sausage9 am ‐‐ Collected12 pm Salmon and perch fillets
8 8 am ‐‐ Collected
M.R.B. diet
17 am Yogurt ‐‐11 am Lentils and rice ‐‐5 pm Spaghetti and meat sauce ‐‐
2
7 am Bagel and cream cheese ‐‐12 pm Cheeseburger ‐‐
6 pm Double cheeseburger and onion rings ‐‐
3 7 am ‐‐ Collected

Can frozen fecal knifes be useful for survival?
• Premise: An Inuit man fashions a knife from his feces (his knife was stolen)
• A Danish man used his frozen feces as a chisel to dig out of hard snow
• Study: “to procure the necessary raw materials for knife production,…”
• Two authors provided the knifes (one made from molds and one hand‐shaped)
• “The study was approved by the Institutional Biosafety Committee at Kent State University.”
Journal of Archaeological Science: Reports 27 (2019) 102002
M.I.E. diet
Day Time Food sample
11 pm Eggs ‐‐4 pm Beef snack bites ‐‐6 pm Beef steak ‐‐
29 am Turkey snack bites ‐‐11 am Beef steak ‐‐7pm Salmon and beef fillets ‐‐
3
9 am Beef fillet ‐‐12 pm Beef snack bites ‐‐
6 pm Salmon, butternut squash risotto, broccolini ‐‐
4
9 am Beef salami ‐‐1 pm ‐‐ Collected4 pm Applesauce ‐‐5 pm Turkey kielbasa ‐‐
5
9 am Turkey sausage ‐‐11 am Macaroni and cheese ‐‐2 pm ‐‐ Collected8 pm Chicken thighs ‐‐
68 am Chicken thighs ‐‐2 pm Angus beef meatballs ‐‐6 pm ‐‐ Collected
78 am Turkey sausage9 am ‐‐ Collected12 pm Salmon and perch fillets
8 8 am ‐‐ Collected
M.R.B. diet
17 am Yogurt ‐‐11 am Lentils and rice ‐‐5 pm Spaghetti and meat sauce ‐‐
2
7 am Bagel and cream cheese ‐‐12 pm Cheeseburger ‐‐
6 pm Double cheeseburger and onion rings ‐‐
3 7 am ‐‐ Collected

Yes, there are photos from the study
• Bottom‐Line: No matter what you hear or think, feces has very few household uses.
Yes, there are photos from the study
And now, the actual good PEIP speakers,….

Vitamin D for Everything,….• Does prenatal Vit D prevent asthma in kids (A parent had atopy)‐ From 10‐18 wks to delivery, 881 moms took 4400 or 400 IU Vitamin D.
‐ Recurrent wheeze or asthma at 6 yrs, 44% (Vit D) vs 46% (placebo), no diff.
‐ Eczema, rhinitis, pneumonias – no diff. ‐ Maternal Vit D level made no difference
• Does Vit D prevent Tb in kids ‐ 8851 kids age 6‐13 yrs in Mongolia got 14,000 IU/wk or placebo
‐ Start Vit D 30nmol/L to 75 vs 25 nmol/L‐ Any Tb Dx at 3 yrs, 0.5% (Vit D) vs 0.6%‐ No diff in confirmed Tb, RTI admission, any RTI, death, adverse events, etc.
NEJM 2020;382:525‐33. NEJM 2020;383:359‐68. JAMA. 2020;324(5):471‐480. JAMA. 2020;324(8):752‐760
• Does Vit D prevent depression in older adults (mean 67 yrs)‐ 18,353 took 2000 Vitamin D or placebo. ‐ Depression at 5.3 yrs, 6.6% (Vit D) vs 6.8% (placebo), no diff.
‐ New/recurrent, PHQ scores, etc – no diff‐ Adherence & baseline level – no diff
• Does Vit D prevent asthma exacerbation in kids (6‐16) & Vit D <75‐ 192 kids took 4000 Vitamin D or placebo. ‐ Severe exacerbation at ~1 yr, 38% (Vit D) vs 34% (placebo), no diff.
‐ Days to events, med use, etc– no diff
MA

Vitamin D,… for even more.
• RCT Vit D for BPPV recurrence• Tx group: If Vit D <50nmol/L then 400IU+500mg Calcium BID otherwise no treatment. Control was untreated.
• South Korea, 66 yrs old, 35% males• Outcomes at 1 yr,
• 38% vs 47% had recurrence, NNT 12• Incidence Rate Ratio 0.76 (0.66‐0.87).
• Unblinded, primary outcome unvalidated, imbalanced drop‐out (22% vs 8%).
• Bottom‐Line: Possible improved BPPV recurrence with Vitamin D/Calcium if low Vitamin D but very high risk of bias & no effect.
• RCT of Vitamin D preventing distress from multiple earthquakes.
• Sept 4 2010 then 3,000 noticeable aftershocks • Christchurch in trial of Vitamin D for URTI: mean age 47, 25% male
• Monthly Vit D at 200,000IU x 2 then 100,000 x 18 months vs placebo
• Outcomes: • Visits to healthcare etc – no difference• Scores on distress – no difference (except more with adverse family relationships in Vit D 22% vs 13% ‐ likely spurious).
• Bottom‐line: Vitamin D does not help manage distress related to earthquakes
BMJ 2014;349:g7260 doi: 10.1136/bmj.g7260Neurology 2020;95:e1117-e1125.
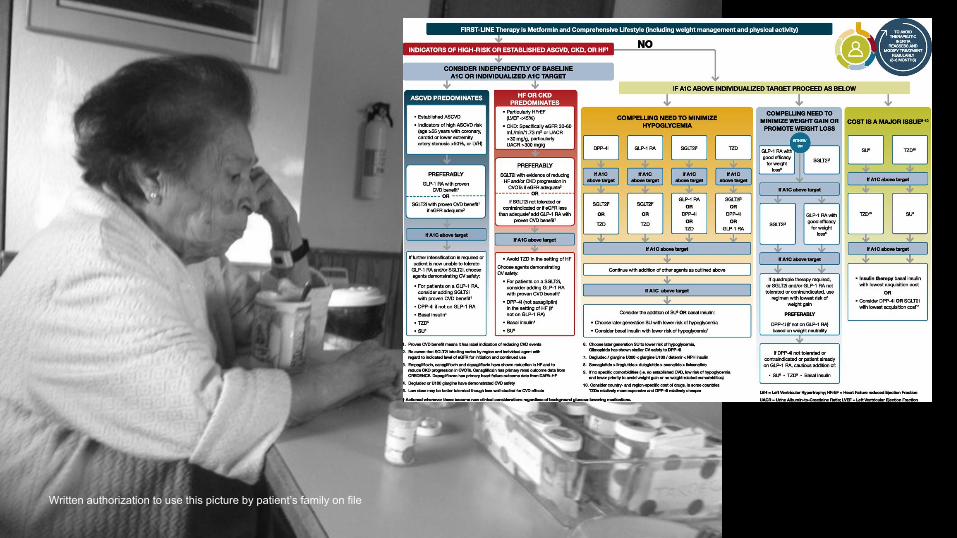
Caring forpatients with type 2 diabetes with
shared decision makingVictor M. Montori, MD, MSc
Professor of MedicineKER UNIT
Mayo Clinic
@vmontori
.org
Written authorization to use this picture by patient’s family on file
GUIDELINES
TARGETS
NEW DRUGS
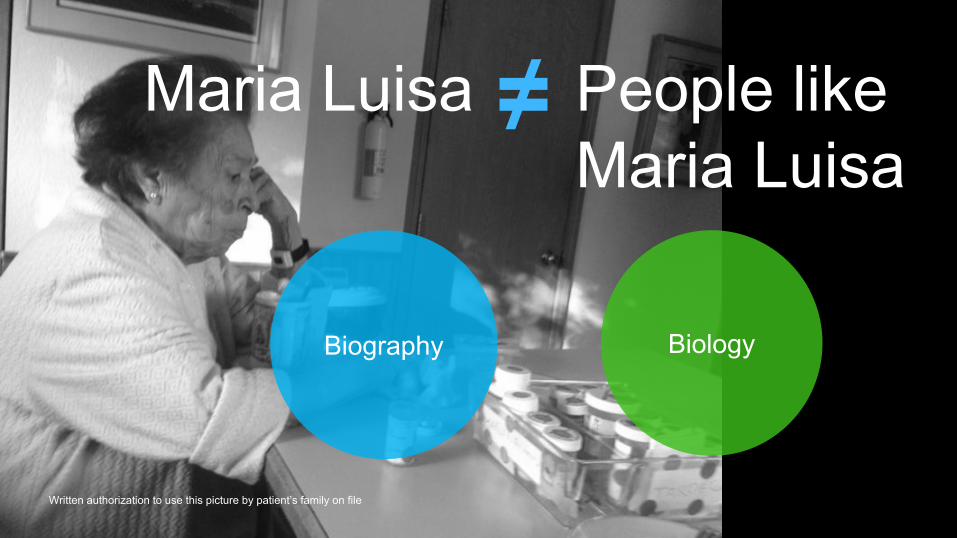
Written authorization to use this picture by patient’s family on file
People likeMaria Luisa
Maria Luisa ≠
Biology Biography

Shared decision making
BIOLOGY
BIOGRAPHY
CARE
is a method to care.

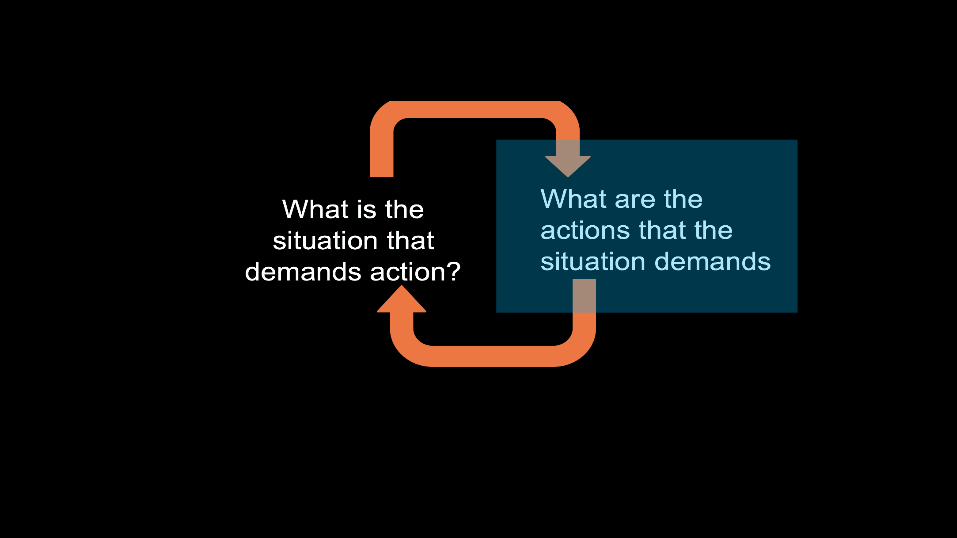
Relationship
Intentionto care
Noticing aproblem
Responding effectively
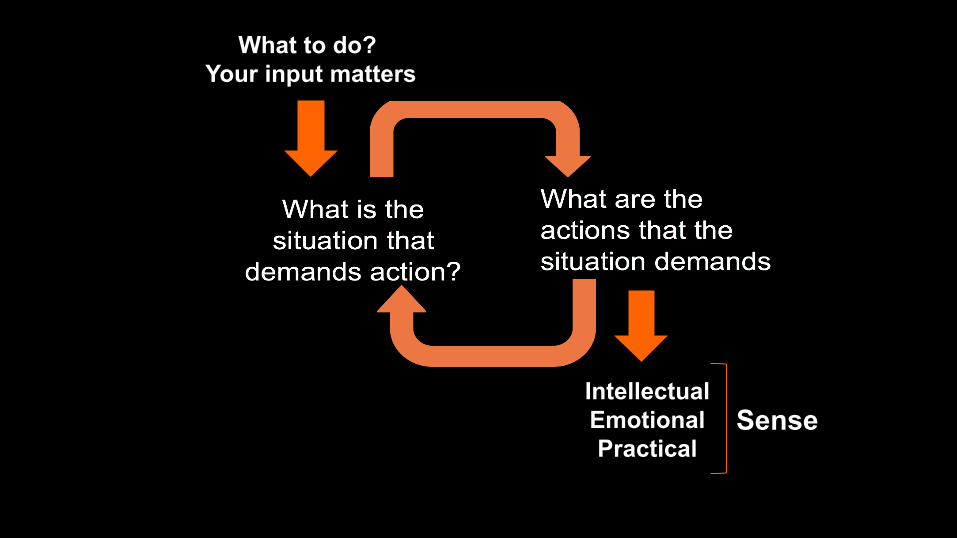
What to do? Your input matters
IntellectualEmotionalPractical
Sense

In trialsImprove knowledge about the options
More confident about decisionVariable effect on choice, cost, outcomes
In practiceImplementation?
Work for patients?SDM? Care?
Stacey D et al Cochrane 2017Montori VM et al JAMA 2017; 318, 617-618
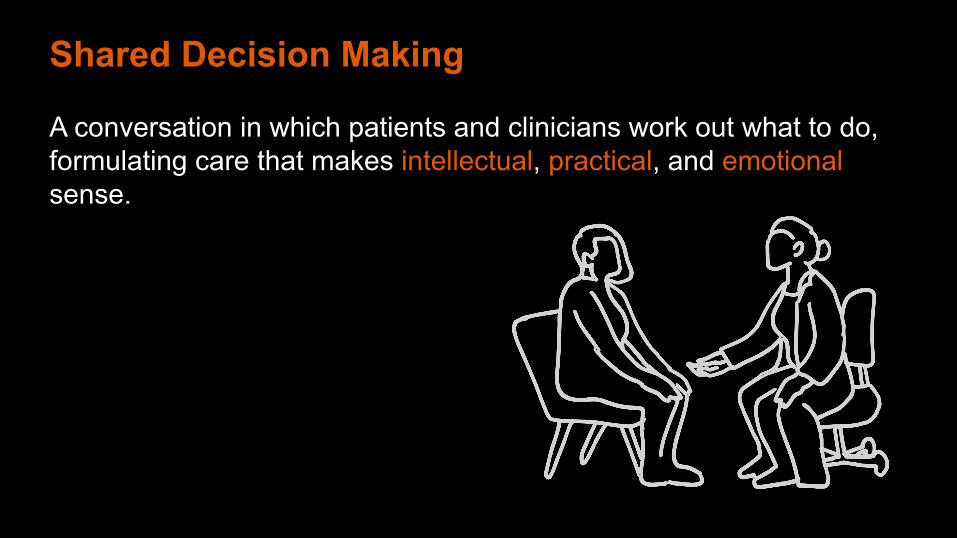
A conversation in which patients and clinicians work out what to do, formulating care that makes intellectual, practical, and emotionalsense.
Shared Decision Making


Statin Choicestatindecisionaid.mayoclinic.org
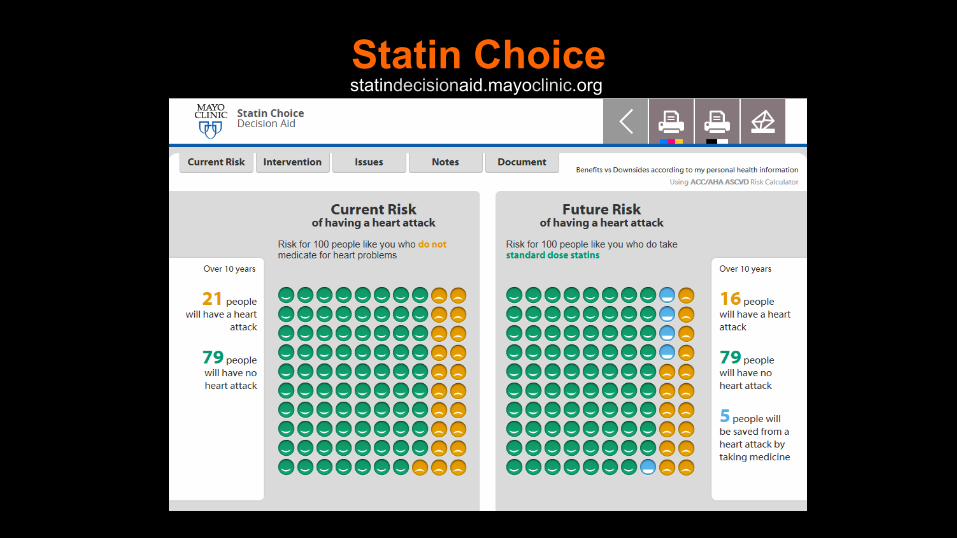
Statin Choicestatindecisionaid.mayoclinic.org
Mullan et al Arch Intern Med 2009
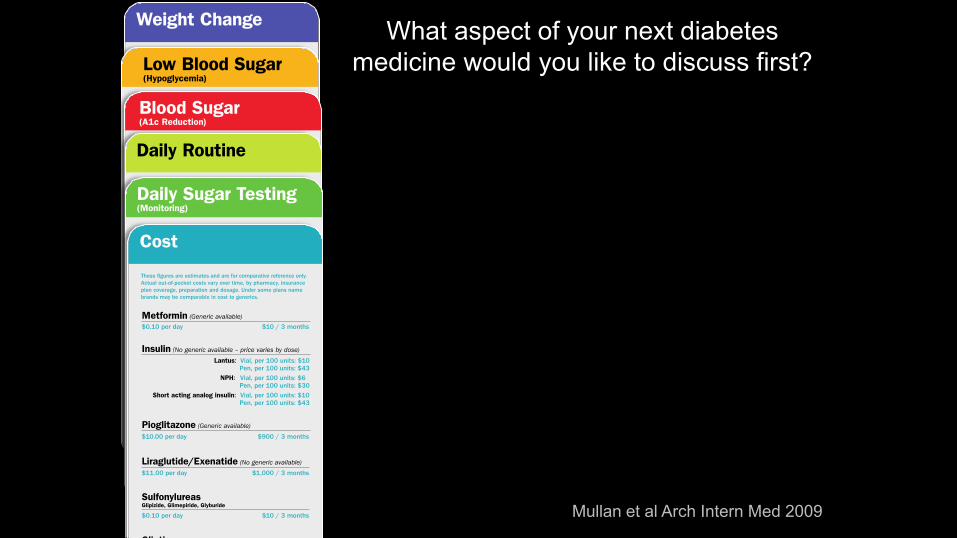
What aspect of your next diabetes medicine would you like to discuss first?

http://diabetesdecisionaid.mayoclinic.org
HbA1c?
*Rodriguez-Gutierrez and Montori; Circ Cardiovasc Qual Outcomes. 2016;9
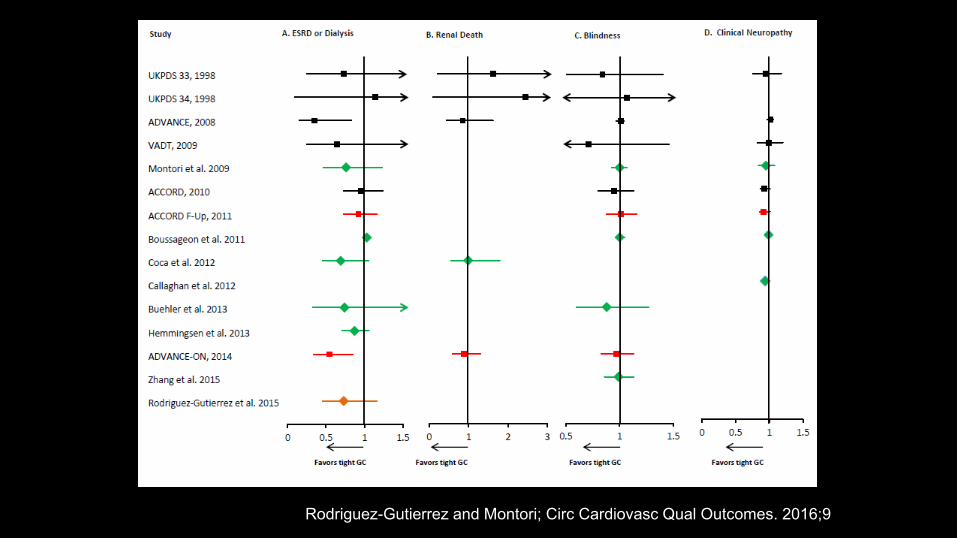
Rodriguez-Gutierrez and Montori; Circ Cardiovasc Qual Outcomes. 2016;9
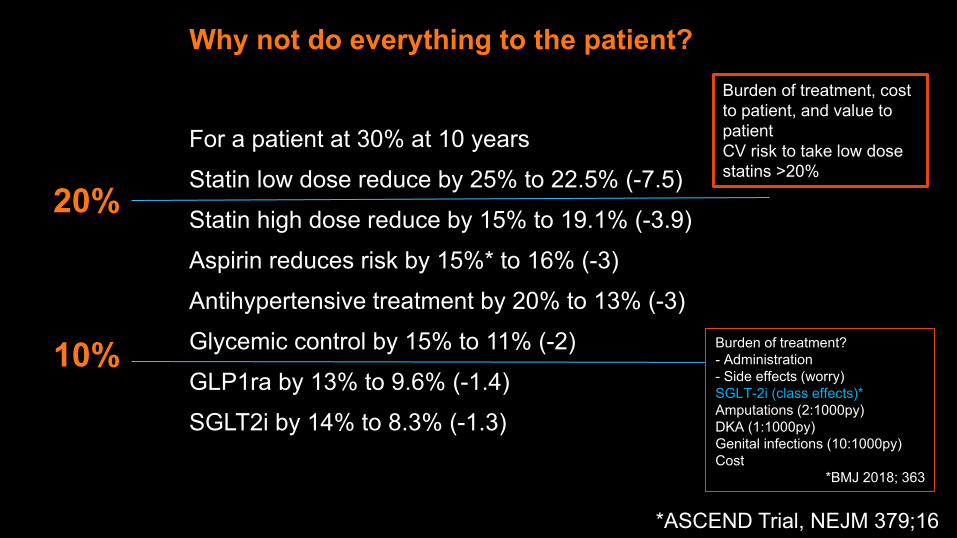
Why not do everything to the patient?
For a patient at 30% at 10 yearsStatin low dose reduce by 25% to 22.5% (-7.5)Statin high dose reduce by 15% to 19.1% (-3.9)Aspirin reduces risk by 15%* to 16% (-3)Antihypertensive treatment by 20% to 13% (-3)Glycemic control by 15% to 11% (-2)GLP1ra by 13% to 9.6% (-1.4)SGLT2i by 14% to 8.3% (-1.3)
20%
10%
Burden of treatment, cost to patient, and value to patientCV risk to take low dose statins >20%
*ASCEND Trial, NEJM 379;16
Burden of treatment?- Administration- Side effects (worry)SGLT-2i (class effects)*Amputations (2:1000py)DKA (1:1000py)Genital infections (10:1000py)Cost
*BMJ 2018; 363
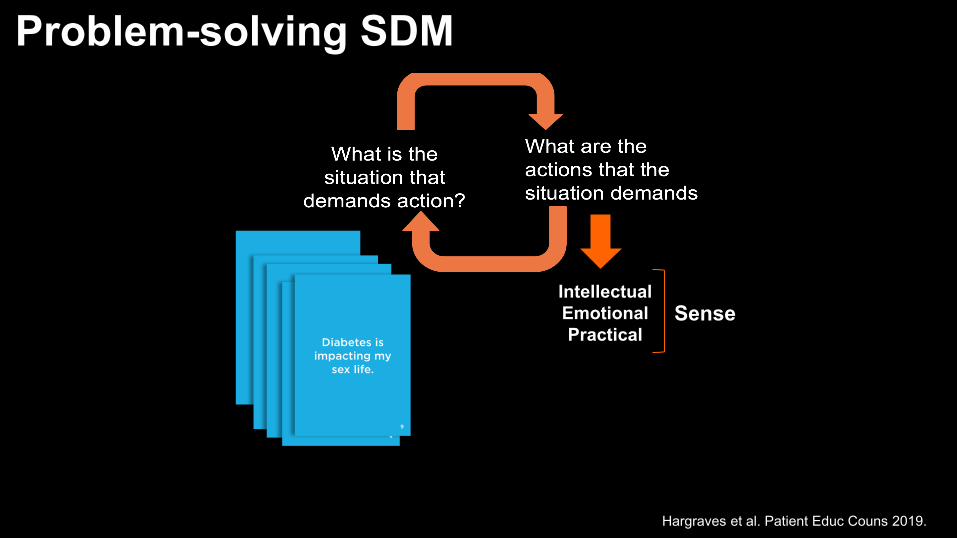
IntellectualEmotionalPractical
Sense
Problem-solving SDM
Hargraves et al. Patient Educ Couns 2019.

Key Learning Points1. SDM is a method to care via conversation2. Goal of SDM is not to get people to do what
YOU (or guidelines) think is right for them.3. Care that makes sense to this patient4. Tools can help but use doesn’t equal SDM

NoticeLife and lovesRisk for complicationsBurden of illness + treatment
RespondStressors, diet, activityPreventionMinimally disruptive careBMJ 2019;367:l5887

Last Call:Treatment Options for Alcohol Use DisorderJessica Kirkwood MD CCFP (AM)PEER TeamUniversity of Alberta
Faculty/Presenter Disclosure• Faculty/Presenter: Jessica Kirkwood
• Relationships with financial sponsors:• Any direct financial relationships
including receipt of honoraria: Alberta College of Family Physicians, Medical Panels Office
• Memberships on advisory boards of speakers bureau: N/A
• Patents for drugs or devices: N/A• Other: PEER Team member/University
of Alberta, Boyle McCauley Health Centre

Disclosure of Financial Support• This program does not receive financial support.
• This program is presented by the Alberta College of Family Physicians (ACFP) without financial support.
• The ACFP provides a speaker fee and expense support for presenting at the event.
• This program does not receive in‐kind support.• This program is presented by the ACFP without in‐kind support.
Background• 2018: 19.1% of Canadians age 12+ (~5.9 mil) reported alcohol consumption classified as
“heavy drinkers”1
• 2017: rates of hospital admissions2:– entirely caused by alcohol = 249 per 100,000– heart attacks = 243 per 100,000– 13X higher than opioid‐related admissions
• All about the Benjamins:‐ 2014: total cost of substance use in Canada = $38 billion3‐ Alcohol 38% ($14.6 billion)‐ Tobacco 31% ($12 billion)‐ All others 30.7% ($11.8 billion)
1) www150.statcan.gc.ca/n1/pub/82‐625‐x/2019001/article/00007‐eng.htm 2) www.ccsa.ca/sites/default/files/2019‐09/CCSA‐Canadian‐Drug‐Summary‐Alcohol‐2019‐en.pdf3) University of Victoria, Canadian Institute for Substance Use Research. British Columbia Alcohol and Other Drug Monitoring Project: per capita alcohol consumption

A Trip Down Memory Lane
A Trip Down Memory Lane
A Trip Down Memory Lane
Fast Forward• Prohibition/Temperance Movement• Alcoholics Anonymous• Treatment/Rehab/Detox
• But what about medications?

Screening
https://www.ccsa.ca/sites/default/files/2020‐07/2012‐Canada‐Low‐Risk‐Alcohol‐Drinking‐Guidelines‐Brochure‐en_0.pdf
Single Alcohol Screening Question (SASQ)
“In the past year, how often have you consumed more than 3 drinks (for adult women) or 4 drinks (for adult men) on any one occasion?”
Positive screen = Anything > “never/zero”
Sensitivity 60‐90% vs. reference standards1
1) O'Connor et al. JAMA. 2018;320(18):1910‐1928.
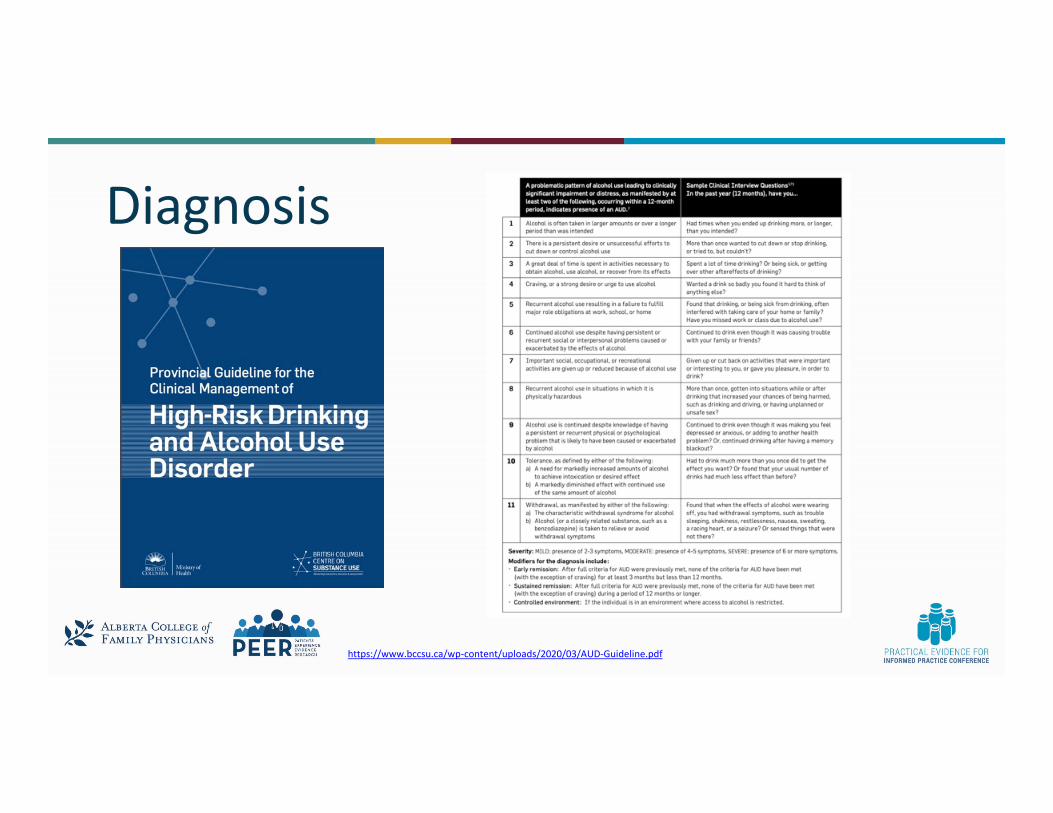
Diagnosis
https://www.bccsu.ca/wp‐content/uploads/2020/03/AUD‐Guideline.pdf

Treatment

Treatment Goals• Traditionally abstinence was the primary goal
• For some patients this is not desired or realistic
• More likely to achieve self‐identified goals:• Abstinence• Reduced overall• Less binges• No non‐beverage alcohol, limit hard alcohol vs. wine vs. beer• Sobriety for specific events (visits with kids, holidays)

The Neurobiology of AUD
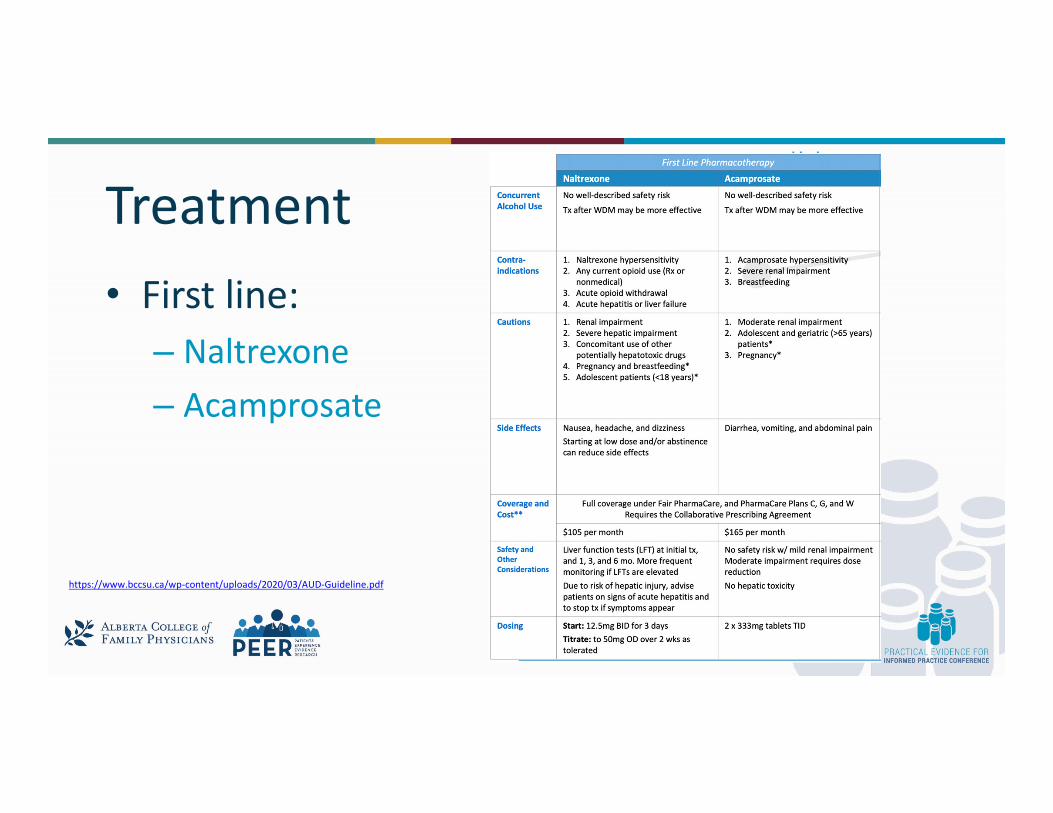
Treatment• First line:
– Naltrexone– Acamprosate
https://www.bccsu.ca/wp‐content/uploads/2020/03/AUD‐Guideline.pdf
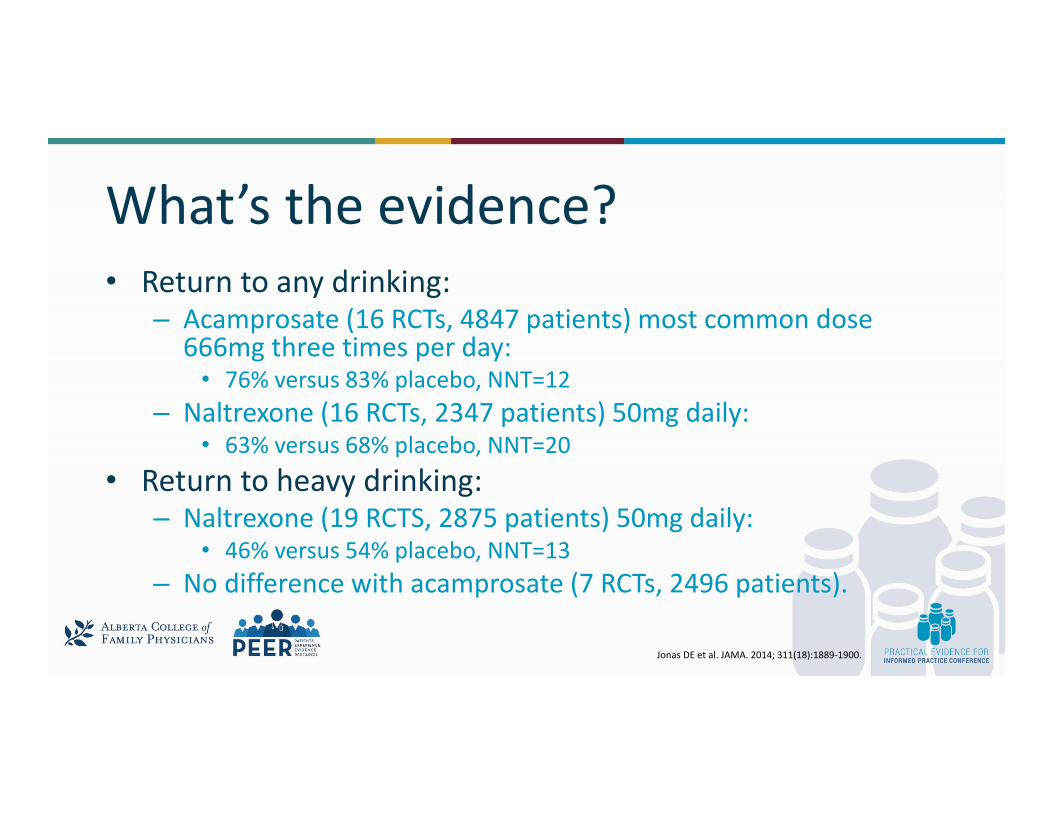
What’s the evidence?• Return to any drinking:
– Acamprosate (16 RCTs, 4847 patients) most common dose 666mg three times per day:
• 76% versus 83% placebo, NNT=12– Naltrexone (16 RCTs, 2347 patients) 50mg daily:
• 63% versus 68% placebo, NNT=20• Return to heavy drinking:
– Naltrexone (19 RCTS, 2875 patients) 50mg daily:• 46% versus 54% placebo, NNT=13
– No difference with acamprosate (7 RCTs, 2496 patients).
Jonas DE et al. JAMA. 2014; 311(18):1889‐1900.
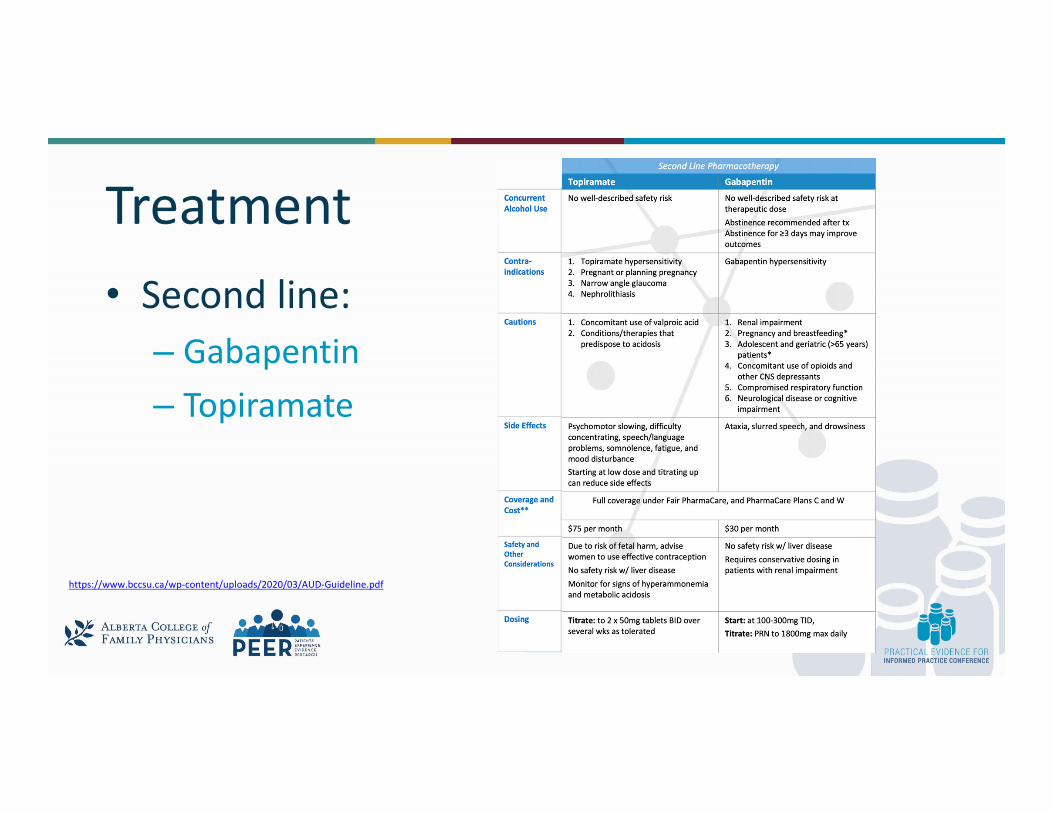
Treatment• Second line:
– Gabapentin– Topiramate
https://www.bccsu.ca/wp‐content/uploads/2020/03/AUD‐Guideline.pdf

What’s the evidence?• Gabapentin
• 2019 meta‐analysis (7 RCTs, ~750pts)1
• Appears effective for reducing heavy drinking days, overall no reported benefit for abstinence• Closer look at 2 largest RCTs within above MA
• No heavy drinking days ‐ 44.7% vs. 22.5%, NNT 5‐6• Total abstinence ‐ 17% vs. 4%, NNT = 8
• Why 2nd line? AEs (dizziness NNH = 4), safety (potential non‐medical use, dependence and withdrawal)
• Topiramate:• 2014 meta‐analysis (7 RCTs, ~1100 pts)2
• Possibly superior to naltrexone for heavy drinking and cravings• Possibly equal to naltrexone for abstinence
• Why 2nd line? Requires titration, more AEs
1) Kranzler HR et al. Addiction. 2019;114(9):1547‐15552) Blodgett et al. Alcohol Clin Exp Res. 2014; 38 (6): 1481‐1488
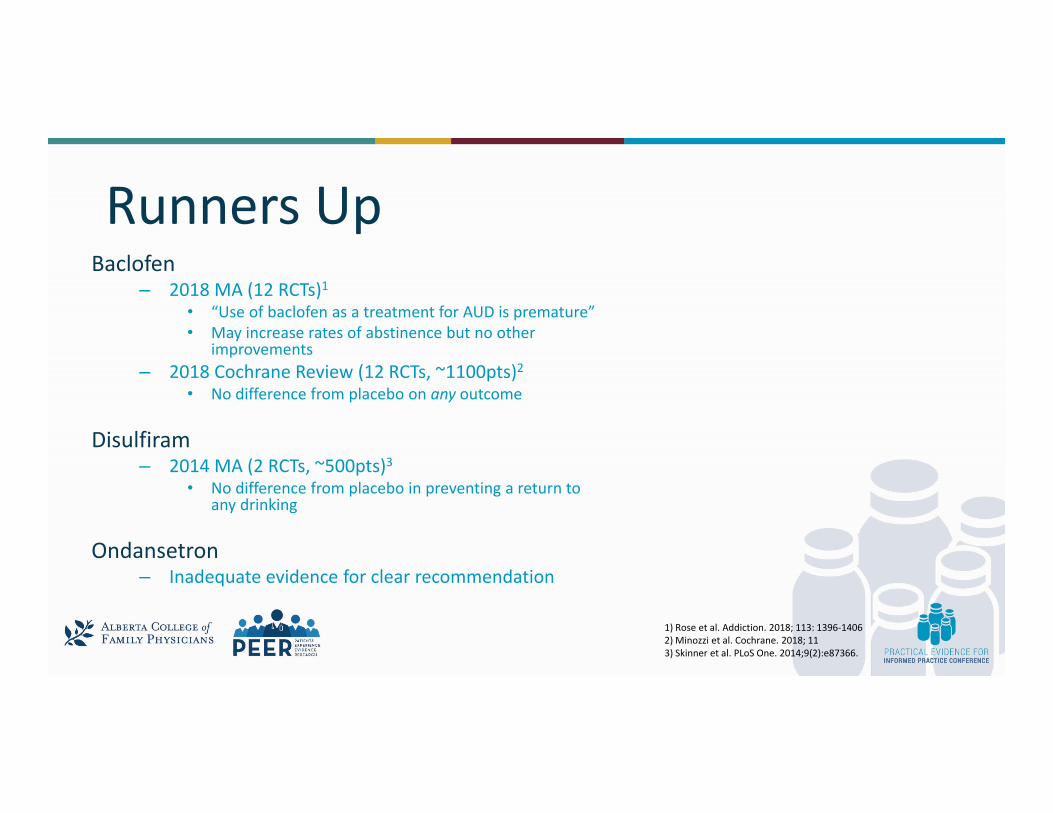
Runners UpBaclofen
– 2018 MA (12 RCTs)1• “Use of baclofen as a treatment for AUD is premature”• May increase rates of abstinence but no other
improvements– 2018 Cochrane Review (12 RCTs, ~1100pts)2
• No difference from placebo on any outcome
Disulfiram– 2014 MA (2 RCTs, ~500pts)3
• No difference from placebo in preventing a return to any drinking
Ondansetron– Inadequate evidence for clear recommendation
1) Rose et al. Addiction. 2018; 113: 1396‐14062) Minozzi et al. Cochrane. 2018; 113) Skinner et al. PLoS One. 2014;9(2):e87366.
How do I decide?• Availability• Patient preference• Co‐morbidities• Dosing regimen
Brief Intervention5‐min video on MI for AUDhttps://www.canada.ca/en/public‐health/services/chronic‐diseases/videos‐on‐supporting‐behaviour‐change/motivational‐interviewing‐alcohol.html
Resources
http://www.metaphi.ca/

Thank you!

Adil Virani, BSc (Pharm), Pharm D, FCSHPManager, Lower Mainland Pharmacy ServicesClinical Associate Professor, Faculty of Pharmaceutical Sciences, UBC
CAN I HAVE YOUR ‘ATTENTION’ PLEASE?
DIAGNOSIS & MANAGEMENT

My Disclosures• Relationships with financial sponsors:
• Any direct financial relationships including receipt of honoraria: None• Memberships on advisory boards of speakers bureau: None• Funded grants, research, or clinical trials: None• Patents for drugs or devices: None
• Honoraria received from:• 2019/20 Compendium of Therapeutics Choices: ADHD Chapter• Patented Medicine Price Review Board (PMPRB)• Canadian Agency for Drugs and Technologies (CADTH)
1. Describe five important considerations for diagnosing of ADHD in primary care
2. List some commonly used checklists for ADHD3. Compare and contrast the available treatment options for
ADHD with respect to efficacy and safety
Learning Objectives At the completion of this presentation, participants will be able to:
Overview• Case• Epidemiology• Diagnosis considerations• Treatment Options • Monitoring considerations
Epidemiology of ADHD• Among the most prevalent chronic health conditions affecting
children and adolescents– Most common psychiatric disorder in children in NA
• Prevalence: 5-9 % for children and adolescents1 & 3-5% for adults2
• Usual age of onset is 3 years old• Boys > girls 3:1 to 9:1• 30-70% of children have ADHD symptoms last into adulthood2
• 50-80% have at least one comorbid condition (70% in MTA study4)
1. Amer Acad Ped. Pediatr 2000; 2. Stubbe DE. Psych. Clin NA July 2000; 3. APA. DSM-IV-TR 2000 4. Wolraich et al. J Dev Behav Pediatr 1998; 5. Barbaresi et al. Acta Paediatr Suppl 2004; 6. Gaub, Carlson. JAACAP 1997
1. Polanczyk, GV et al. ADHD prevalence estimates across three decades: SR and MA. Int. J Epidemiology, 2014; 2. Wilens TE et al ADHD in Adults. JAMA 2004. 3. 4. Jensen PS et al. MTA study, JAACAP 2001.
7 7
Case: Oliver De Place• ID: 7 year old boy with combined type of ADHD • HPI: Oliver is easily distracted, constantly interrupts others
and talks excessively. • He consistently fidgets with his hands and runs around the
house often yelling and is difficult to settle down.• His grade 2 teacher has mentioned Oliver has difficulty
concentrating, following instructions and appears to be distracting other students.

8
What should you do next?A. Reassure the family that all boys are like that at this age and
not to worry about it.B. Start Oliver on a long-acting stimulant to see if it helps.C. Gather more information from Oliver’s family and teachers.D. Refer to a pediatrician or pediatric psychiatrist.E. All of the above.
Making a Diagnosis in Primary Care• Identify and assess ADHD symptoms (based on DSM 5)
o 6 of 9 Inattention subtype*, or o 6 of 9 Hyperactive-Impulsive subtype*, oro 12 of 18 Combinedo *Note: In adults it is only 5 of 9
• Onset of symptoms before 12 yrs of age?• Have symptoms have been present for at least 6 months?• Functional impairment in at least 2 places (e.g., home, school, work,
etc)?• Can the symptoms or impairment be explained by an alternate medical
or circumstantial condition?
APA. DSM-5. 5th ed. 2013.

Diagnostic and Statistical Manual (DSM-5) – ADHD Symptoms
Making a Diagnosis in Primary Care• No objective measure or blood test for ADHD• Collect childhood development history• Physical exam and review of medical history – (looking for other medical causes
that mimic ADHD)• Ask about triggers, psychosocial stressors (if there is trauma or loss) to
differentiate from longer term neurobiological ADHD • Focus on impairments and rating scales – not symptoms present in the clinic • Collect symptom inventory (e.g., through checklists from multiple sources; e.g.,
home, school, work)• Referral for psychoeducational assessment if learning disability or cognitive
deficits are expected. https://www.caddra.ca/canadian-adhd-practice-guidelines/https://www.nice.org.uk/guidance/ng87

Suggested Rating Scales for ADHD
PARENTS or CAREGIVERs• SNAP – IV, or • WFIRS-P (Weiss Functional
Impairment Rating Scale- Parent)
• ASRS (Adult ADHD Self Rating Scale)
TEACHERS • SNAP – IV • CADDRA Teachers
Assessment Form• Conners’ teaching rating
scale
There are >50 ADHD rating scales. Here are some I suggest you use.
https://www.caddra.ca/pdfs/caddraGuidelines2011SNAP.pdfHall CL et al. The validity of the SNAP-IV in children displaying ADHD symptoms. April 2019. https://journals.sagepub.com/doi/abs/10.1177/1073191119842255All forms available at CADDRA.ca
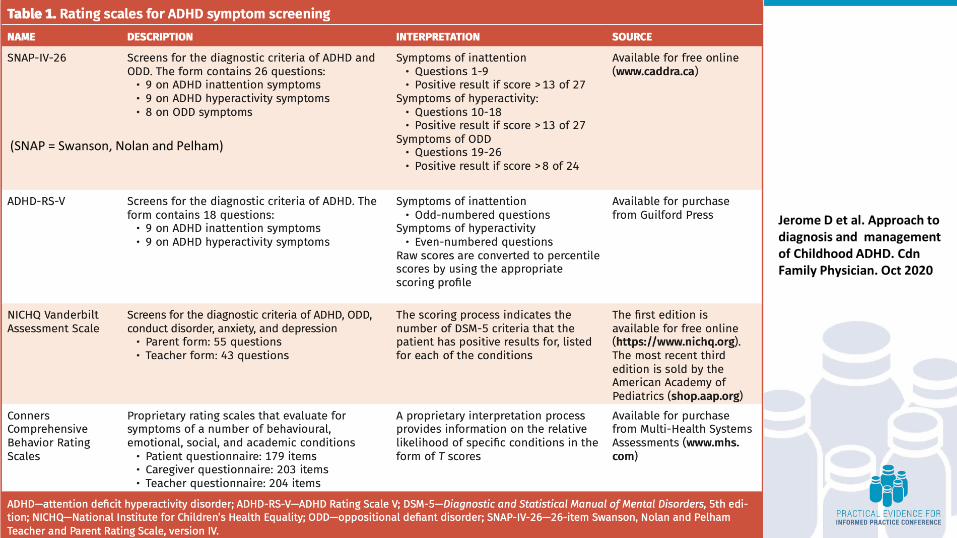
Jerome D et al. Approach to diagnosis and management of Childhood ADHD. CdnFamily Physician. Oct 2020
(SNAP = Swanson, Nolan and Pelham)

Other monitoring Rating Scales• ADHD-RS-V or ADHD-RS-IV• Connors RS (Parents, Teachers or Physician)• Child behaviour Checklist• Conners-Wells Adolescent Self-Report Scale• Brown Attention-Deficit Disorder Symptom Assessment Scale
(BADDS) for Adults
“Although rating scales alone are not sufficient to diagnose ADHD because of issues such as the variability of interpretation of questions by respondent, their use to enrich the process of evaluation is widely recommended”
CADRRA 2020 Guidelines
CADDRA 2020 Guidelines
https://www.caddra.ca/canadian-adhd-practice-guidelines/
• Good source of info for diagnostic strategies • CADDRA eToolkit (USB)• Diagnosis and treatment flowchart• Rating scales
• Treatment Guidelines – consensus based
Goals of Therapy• Eliminate or decrease symptoms• Shift in ‘focus’ from improving ADHD symptoms to
restoring normal functioning• Build self-esteem• Prevent the development of other psychiatric
disorders • Prevent/minimize side effects• Education
Treatment Options in ADHD• Behaviour Management• Stimulants:
• Methylphenidate (Ritalin®, Concerta®, Biphentin®, Foquest®, generics)• Amphetamines (Dexedrine, Dexedrine Spansule, Lisdexamfetamine
(Vyvanse®), Adderall XR®)• DexmethylphenidateX (Focalin®)
• Non-stimulants• Atomoxetine (Strattera®)*• Alpha-2 Agonists – Clonidine*, Guanfacine (Intuitiv)
• Antidepressants* - TCAs, Bupropion, Venlafaxine
• Other agents - Atypical antipsychotics*, modafinil, herbals, mood stabilizersX= not in Canada
Virani A. ADHD. CTC. CPhA 2019; CADDRA.CA

NMA for ADHD Medications
Cortese S et al. Lancet Psychiatry. 2018;5(9):727-38.
• 133 DB, RCTs (81 in C & A; 51 in adults) – includes unpublished• Includes: amphetamines, methylphenidate, atomoxetine,
bupropion, clonidine, guanfacine, and modafinil.• Duration: most data was 12 wks (~10-11,000 C & A; 5-8,000
Adults) – but searched for 24 and 52 wk data.• Primary Outcome:
• Efficacy – Change in rating scale• Tolerability- withdrawal due to AE
• Considerable heterogeneity limits drawing relevant conclusions for all the included medications.
• All agents considered superior to placebo (Clinician rating scale)
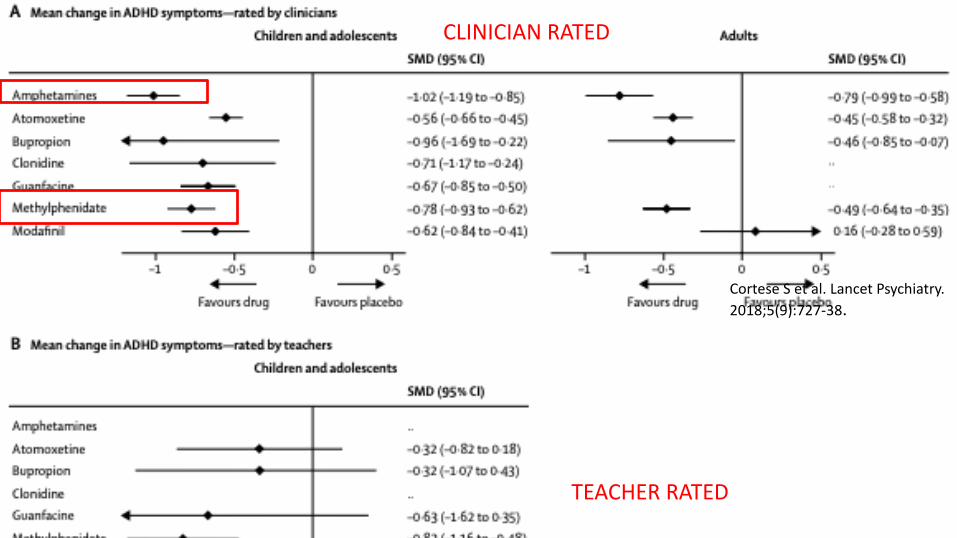
Cortese S et al. Lancet Psychiatry. 2018;5(9):727-38.
CLINICIAN RATED
TEACHER RATED
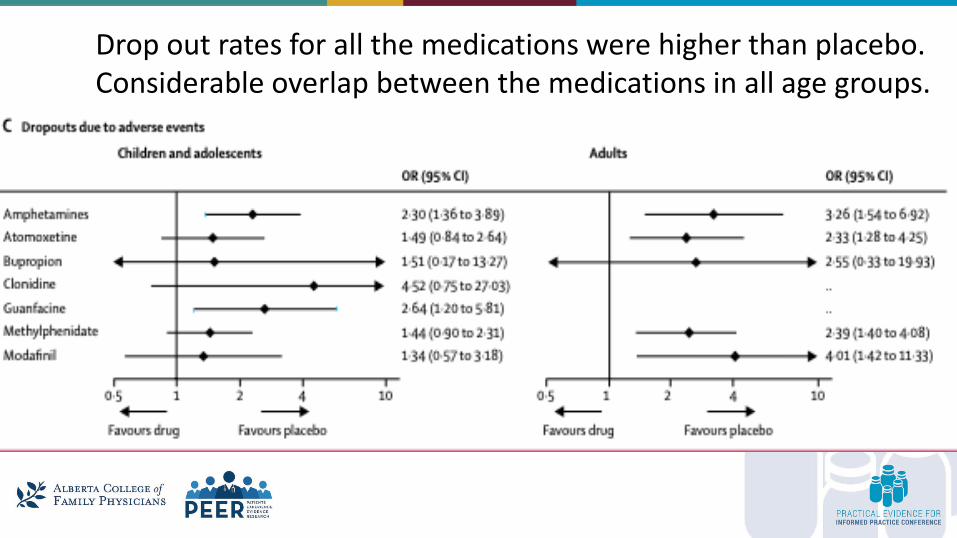
Drop out rates for all the medications were higher than placebo. Considerable overlap between the medications in all age groups.
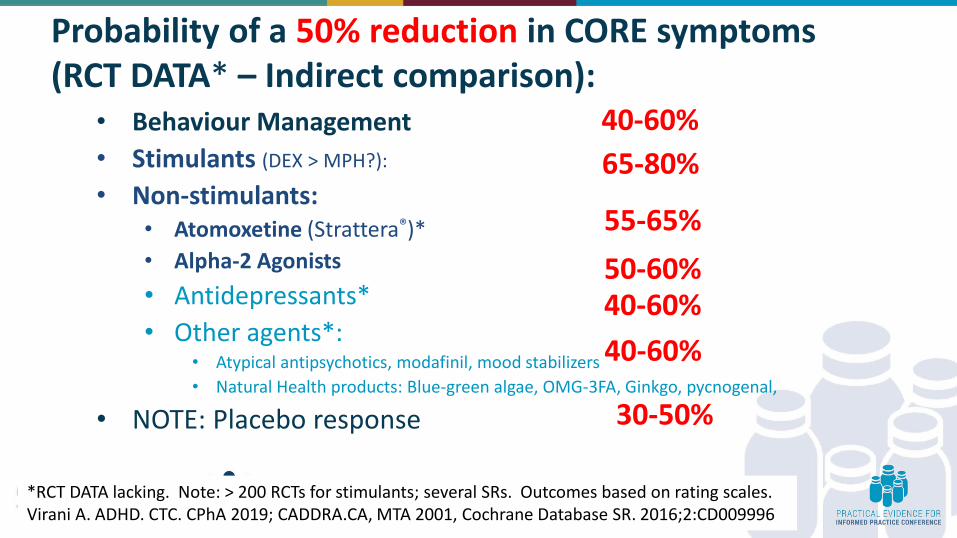
Probability of a 50% reduction in CORE symptoms (RCT DATA* – Indirect comparison):
• Behaviour Management• Stimulants (DEX > MPH?):
• Non-stimulants:• Atomoxetine (Strattera®)*• Alpha-2 Agonists• Antidepressants*• Other agents*:
• Atypical antipsychotics, modafinil, mood stabilizers• Natural Health products: Blue-green algae, OMG-3FA, Ginkgo, pycnogenal,
• NOTE: Placebo response
40-60%65-80%
55-65%50-60%40-60%40-60%
*RCT DATA lacking. Note: > 200 RCTs for stimulants; several SRs. Outcomes based on rating scales. Virani A. ADHD. CTC. CPhA 2019; CADDRA.CA, MTA 2001, Cochrane Database SR. 2016;2:CD009996
30-50%
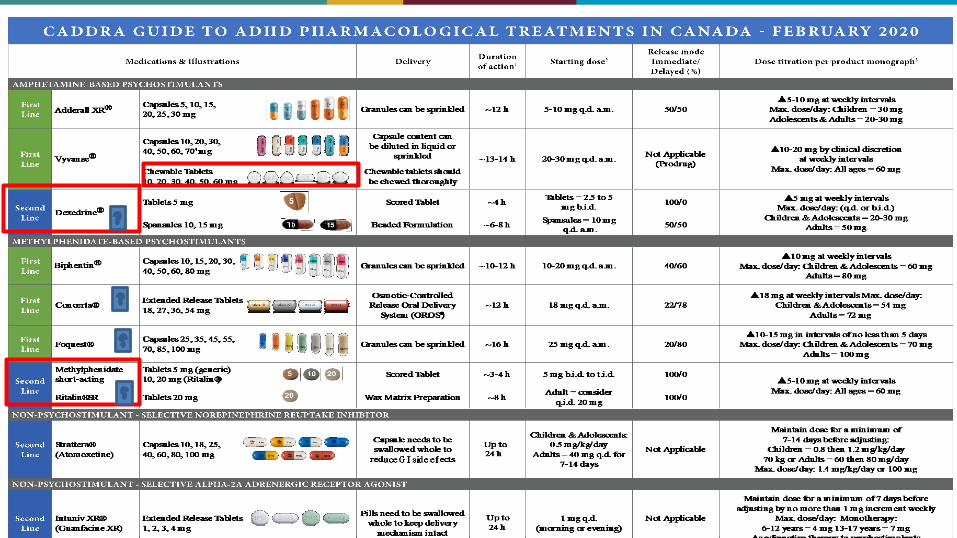
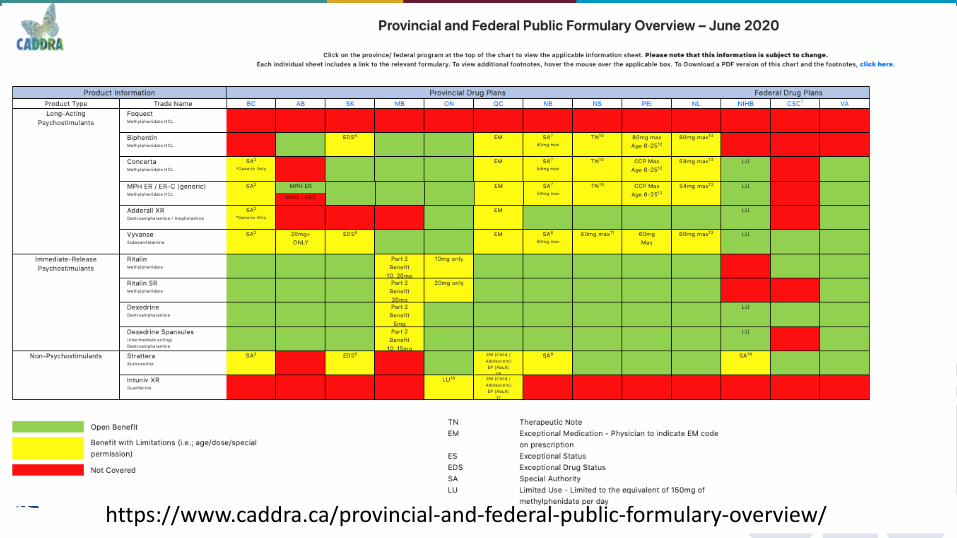
https://www.caddra.ca/provincial-and-federal-public-formulary-overview/
• Type of functional impairment (and timing)• Access to psychosocial assessments and interventions• Comorbid disorders• Implementation of behavioural management strategies• Patient preference• Potential adverse effects (e.g., insomnia, anorexia)• Risk of substance abuse• Cost of medications• Capacity for adherence• Urgency of response
Initial Considerations When Selecting Treatment
Canadian ADHD Resource Alliance (CADDRA): Canadian ADHD Practice Guidelines, 2011
Combination therapy is the best!
Consider :• Psychoeducation• Behavioural interventions• Social interventions• Psychotherapy• Educational / vocational accommodations
27
Combined therapy using medication plus psychosocial interventions is the most effective way to deal with the core symptoms of ADHD and the resulting impairments!
CADDRA.CA, MTA 2001,
Stimulants: What You Should Know…• Overall‘response’rate of ~ 75%. (NNT = 3 vs PLBO)• Limited large clinical head to head trials comparing stimulants• Amphetamines more effective than methylphenidate? • Effective on day 1 and continued benefits over several months• Immediate release preparation should be dosed 2-3 times /day• May offer the best benefit for the cost if tolerated• Side effects (sleep disruption, weight loss) are common• Height loss in children/adolescents ~3 cm at 3 yrs (MTA)• Consider N of 1 blister pack trial• Cardiac concerns
Cortese S et al. Lancet Psychiatry. 2018;5(9):727-38.
30
Stimulant Adverse Effects CNS: insomnia, anxiety, activation, irritability
(rebound), worsening tics, psychosis/mania HEENT: xerostomia, mydriasis CVS: ↑HR, ↑BP, palpitations, Sudden Cardiac Death RESP: URTI, sinusitis, cough GI: Anorexia, nausea, abdominal pain, wt loss GU: urinary retention, sexual dysfunction LAB/MSK/EXTR: growth delay (ht & wt),
rash, leukopenia, anemia
30
31 31
PsychostimulantsBenefits of stimulants include:• Decreased aggression, improved social interaction &
academic performance (parent & teacher rating)
Stimulants do not improve:• Anxiety, clinically significant academic performance
(testing), delinquency/substance abuse at 3 years
Not adequately studied:• QOL, school completion, employment, future health
Stimulants associated with ↓ ht/wt at 3 yrs
Therapeutics Initiative Newsletter 69. March-May 2008.
Atomoxetine: You Should Know
• “Selective” presynaptic NE reuptake inhibitor• Non-controlled substance• Metabolized by CYP2D6 (90% Extensive/10% Poor)• Half-life of 5 hrs, however duration of action is
significantly longer (18-21 hrs)• Role in inattentive type of ADHD? Comorbid
anxiety/depression?

Atomoxetine: Side Effects• Decreased Appetite• Nausea• Dyspepsia (7%)• Vomiting*• Somnolence(15%)*• Fatigue• Dizziness• Hepatic (2/3,400,000)
• Mood Swings• Transient Weight
Loss (0.5 kg)• Increased:
– HR (8 bpm)– SBP (3 mmHg) – DBP (2 mmHg)
• Sexual Dysfunction• Suicidal ideation?
33Wernicke JF, et al. J Clin Psychiatry. 2002;63 (suppl 12):50-5.; Kratochvil CJ, et al. JAACAP 2002;41:776-84.Kelsey DK et al. Pediatrics. 2004 Jul;114(1):e1-8.
*Occurred significantly more frequently in atomox. vs MPH patients
Summary• ADHD is the most common neuropsychiatric disorder in NA.• Use a systematic and comprehensive diagnostic approach based on the
DSM 5 diagnostic criteria and evidence of functional impairment.• Combination therapy is the best approach!• Stimulants are the most effective treatment options for reducing core
symptoms of ADHD (NNT ~3 vs placebo); limited data for other important outcomes.
• Rating scales can be used to aid in the diagnosis and monitoring of treatment effect.
• Important to monitor of adverse effects of treatment.

35
Thanks for your ‘Attention’!

A Painless Approach to Managing Chronic Pain
Danielle Perry & Joey Ton
PEERCollege of Family Physicians of Canada
Disclosure of Financial Support• This program does not receive financial support.
• This program is presented by the Alberta College of Family Physicians (ACFP) without financial support.
• The ACFP provides a speaker fee and expense support for presenting at the event.
• This program does not receive in‐kind support.• This program is presented by the ACFP without in‐kind support.

Faculty/Presenter Disclosure• Faculty/Presenter: Danielle Perry
• Relationships with financial sponsors:• Any direct financial relationships including receipt of honoraria:
Alberta College of Family Physicians• Memberships on advisory boards of speakers bureau: N/A• Funded grants, research, or clinical trials: BedMed Frail• Patents for drugs or devices: N/A• Other: Employee at College of Family Physicians of Canada,
Correctional Services of Canada
Faculty/Presenter Disclosure• Faculty/Presenter: Joey Ton
• Relationships with financial sponsors:• Any direct financial relationships including receipt of honoraria:
Alberta College of Family Physicians• Memberships on advisory boards of speakers bureau: N/A• Funded grants, research, or clinical trials: N/A• Patents for drugs or devices: N/A• Other: Employee at College of Family Physicians of Canada and Costco
Pharmacy

Chronic Pain

Chronic Pain
Chronic Pain

Deciding Treatment

Things that can complicate treatment decisions
• Conflicting Evidence• Individual unique Patient Factors• Cost of a treatment• Clinician’s beliefs• Confirmation Bias

Things that can complicate treatment decisions
• Patient beliefs and values• Patient’s parent's beliefs• Patient’s friend's uncle's beliefs.
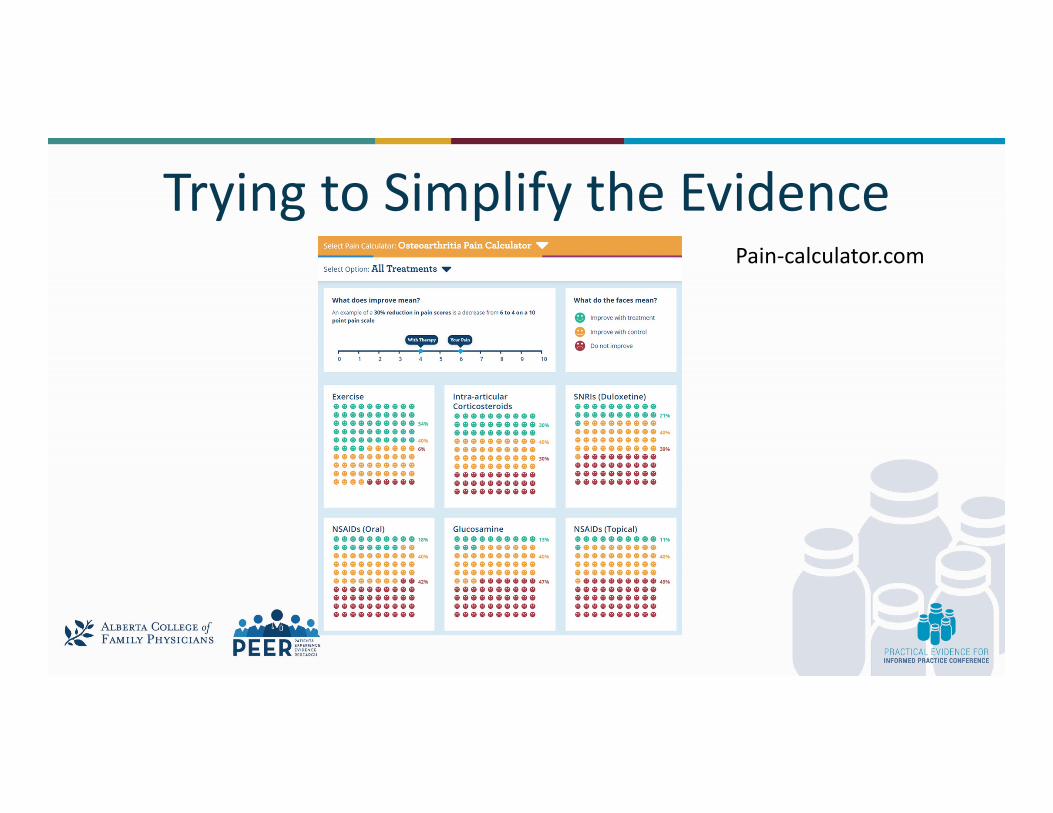
Trying to Simplify the EvidencePain‐calculator.com
What we’ve looked at…• Three Chronic Pain Conditions
1. Osteoarthritis Pain (Knee and Hip)2. Chronic Low Back Pain (Radicular and Non‐Radicular)
• A ton of studies on various interventions for each condition– 63,000+ RCTs titles/abstracts scanned.– 1400+ RCTs read in full. – 290 RCTs extracted and analyzed
Debate: Acupuncture Works Great • Evidence:
– Eight RCTs (4,618 patients) followed for 4‐24 weeks.– Patients: Chronic Low Back Pain– Interventions: Acupuncture between 10‐24 sessions compared to usual care
or sham acupuncture.
PEER Neuropathic Systematic Review not yet published

Debate: Acupuncture Works Great • Evidence:
– Eight RCTs (4,618 patients) followed for 4‐24 weeks.– Patients: Chronic Low Back Pain– Interventions: Acupuncture between 10‐24 sessions compared to usual care
or sham acupuncture.– Results:
• Patients benefitted: 54% in acupuncture versus 35% in control– RR 1.58 (95% CI 1.13, 2.21) NNT 6
– Conclusion: When compared to usual care or sham, acupuncture benefits 1 patient for every 6 treated.
PEER Neuropathic Systematic Review not yet published
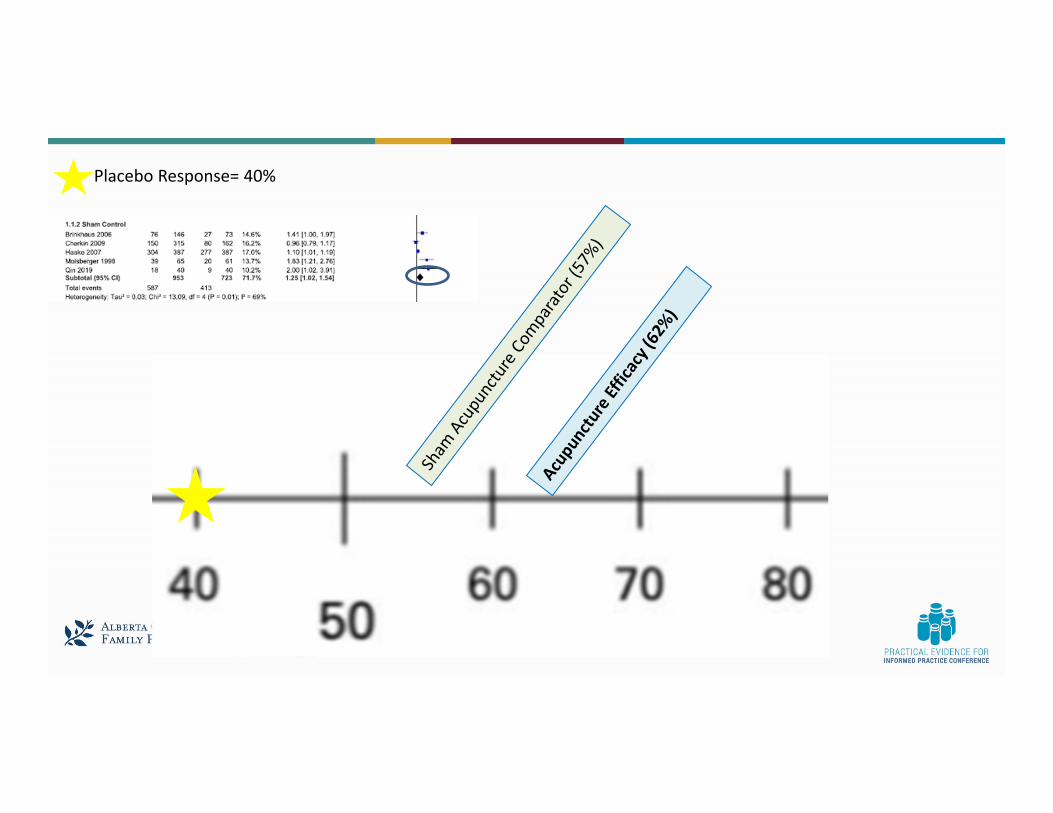
Debate: Acupuncture doesn’t work that well
• Evidence: – 5 RCTs (1,676 patients) followed for 4‐24 weeks.– Patients: Chronic Low Back Pain– Interventions: Acupuncture between 10‐24 sessions compared to sham
acupuncture.
PEER Neuropathic Systematic Review not yet published

Debate: Acupuncture doesn’t work that well
• Evidence: – 5 RCTs (1,676 patients) followed for 4‐24 weeks.– Patients: Chronic Low Back Pain– Interventions: Acupuncture between 10‐24 sessions compared to sham
acupuncture.– Results:
• Patients benefitted: 62% in acupuncture vs 57% in control– RR 1.25 (95% CI 1.02, 1.54) NNT 20
– Conclusion: When compared to sham, acupuncture benefits 1 patient for every 20 treated.
PEER Neuropathic Systematic Review not yet published

Who is right?

Debate: What’s going on?
Biden
Trump
PEER Neuropathic Systematic Review not yet published

Debate: What’s going on?• Sham Comparators vs Wait list or usual care
– The placebo effect is strong.• 1 study (270 patients)
– Sham acupuncture needle vs placebo pill for arm pain.
BMJ, doi:10.1136/bmj.38726.603310.55

Debate: What’s going on?• Sham Comparators vs Wait list or usual care
– The placebo effect is strong.• 1 study (270 patients)
– Sham acupuncture needle vs placebo pill for arm pain.– Results: 75% in sham group believed they were receiving an active treatment vs 48% with the placebo pill.
» Sham and Placebo pill effect was greater at the beginning of the trial. Effect was confined to subjective outcomes.
BMJ, doi:10.1136/bmj.38726.603310.55
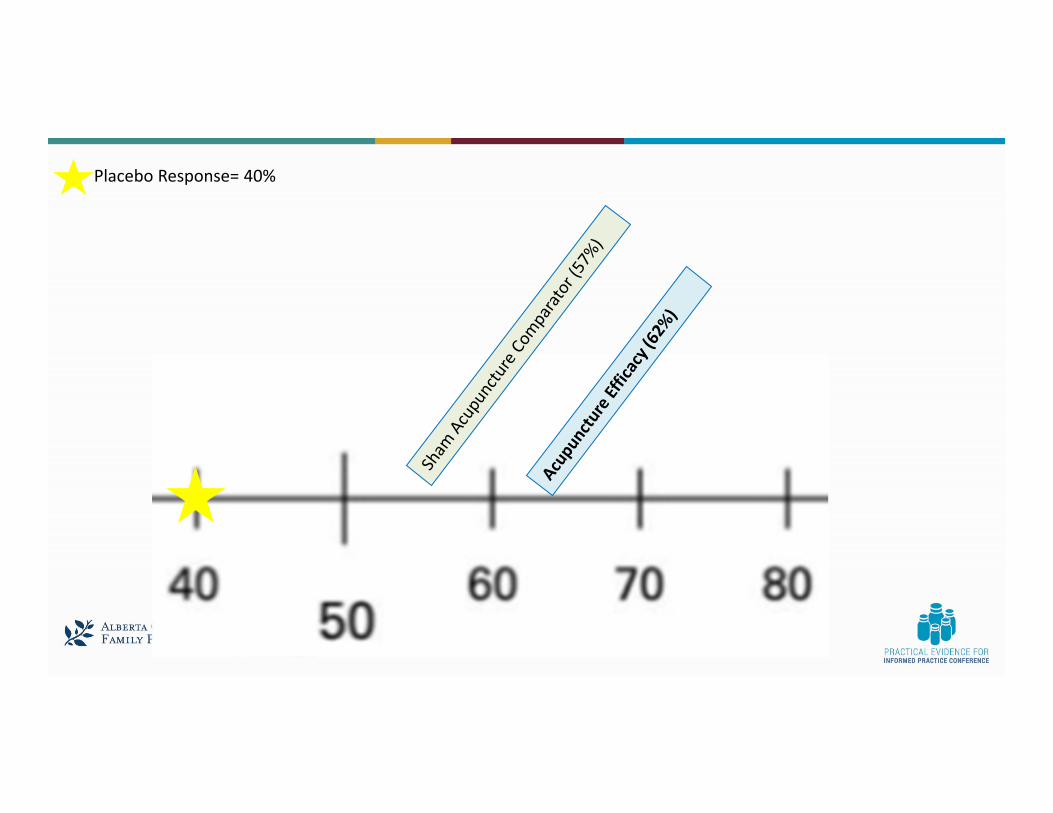
Placebo Response= 40%
Placebo Response= 40%

Debate: What’s going on?• Other high‐quality study markers
– Larger studies– Longer Studies– Publicly Funded Trials

Placebo Response (mostly placebo pill)= 40%
Debate: What’s going on?• Acupuncture might work, but the effectiveness varies depending on what factors you look at.
• It is even harder to determine which patients had a placebo effect vs a true effect in real life.
Acupuncture Cost and Harms• Cost:
– 60‐90min Appointments in AB: $80‐$150 • Can depend on provider, insurance, etc.
Acupuncture Cost and Harms• Cost:
– 60‐90min Appointments in AB: $80‐$150 • Can depend on provider, insurance, etc.
• Adverse Events: – Overall AEs, Serious AEs, and Withdrawals due to AEs were not
statistically significant.– Patients reported various adverse events such as hematoma and
bleeding in both intervention and comparator groups.

Bottom Line• Acupuncture for low back pain seems to work but “how well” is still up for
debate.
• Effect estimate is smaller when you look at sham‐controlled studies, however it still demonstrates benefit (62% vs 57%)
Bottom Line• Acupuncture for low back pain seems to work but “how well” is still up for
debate.
• Effect estimate is smaller when you look at sham‐controlled studies, however it still demonstrates benefit (62% vs 57%)
• Size of effect goes down when looking at higher quality study markers.
• Decision will depend on cost, patient and clinician values/experiences.
Answering whether acupuncture works

Easy Wins
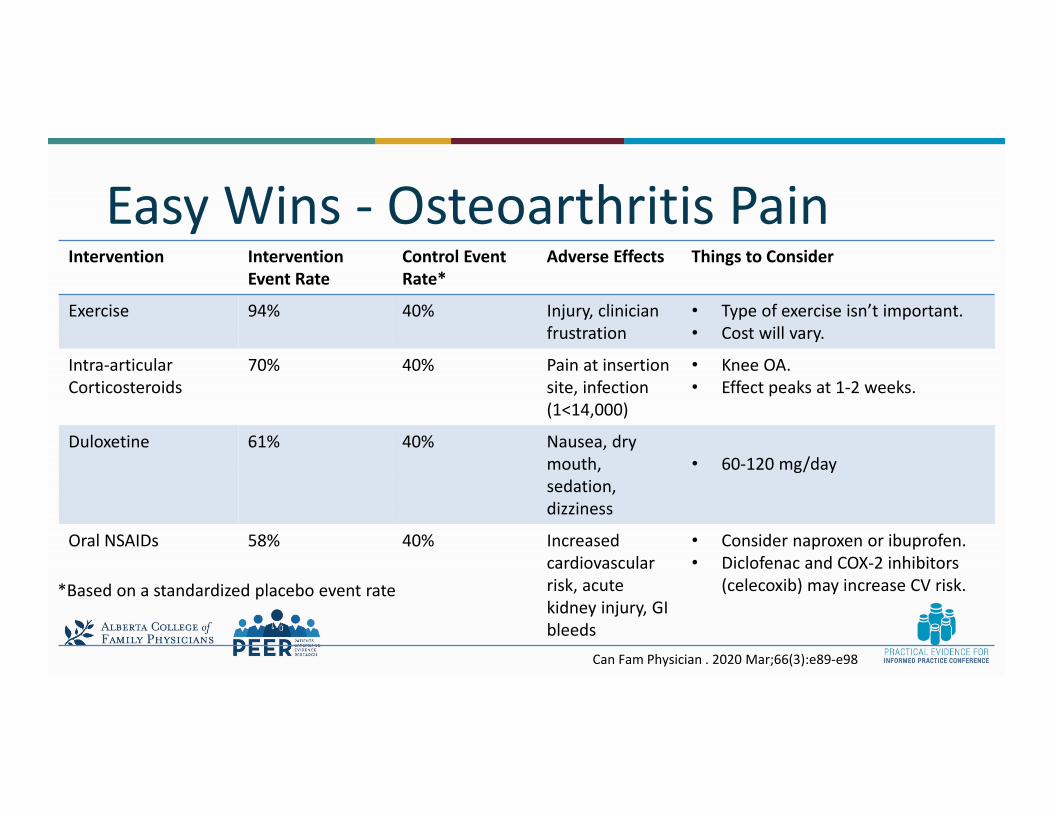
Easy Wins ‐ Osteoarthritis Pain Intervention Intervention
Event RateControl Event Rate*
Adverse Effects Things to Consider
Exercise 94% 40% Injury, clinician frustration
• Type of exercise isn’t important.• Cost will vary.
Intra‐articular Corticosteroids
70% 40% Pain at insertion site, infection (1<14,000)
• Knee OA.• Effect peaks at 1‐2 weeks.
Duloxetine 61% 40% Nausea, dry mouth, sedation, dizziness
• 60‐120 mg/day
Oral NSAIDs 58% 40% Increased cardiovascular risk, acute kidney injury, GI bleeds
• Consider naproxen or ibuprofen.• Diclofenac and COX‐2 inhibitors
(celecoxib) may increase CV risk.*Based on a standardized placebo event rate
Can Fam Physician . 2020 Mar;66(3):e89‐e98

Easy Wins ‐ Chronic Low Back Pain Intervention Intervention Event
RateControl Event Rate*
Adverse Effects Things to Consider
Exercise 63% 37% Injury, clinician frustration
• Type of exercise isn’t important.• Cost will vary.
Oral NSAIDs 53% 37% Increased cardiovascular risk, acute kidney injury, GI bleeds
• Consider naproxen or ibuprofen.• Diclofenac and COX‐2 inhibitors
(celecoxib) may increase CV risk.
Duloxetine 46% 37% Nausea, dry mouth, sedation, dizziness
• 60‐120 mg/day• Could be considered in patients
with comorbid depression
*Based on a standardized placebo event rate**Systematic Review not yet published
Easy Win‐ Avoid Opioids• No consistent benefit of opioids in the long‐term treatment of
osteoarthritis with many harms.• Benefit of opioids in chronic low back pain is present but many
harms have been reported..
Can Fam Physician . 2020 Mar;66(3):e89‐e98
Easy Win‐ Avoid Opioids• No consistent benefit of opioids in the long‐term treatment of
osteoarthritis with many harms.• Benefit of opioids in chronic low back pain is present but many
harms have been reported.. • Examples
– In Osteoarthritis (8 RCTs)• RCTs did not show improvement in function or pain in the long term (>12 weeks).
– In Chronic low back pain (6 RCTs)• Number needed to treat for meaningful pain improvement was 11• Number needed to harm of 5 for those who dropped out due to adverse effects.• Table full of other adverse events.
Can Fam Physician . 2020 Mar;66(3):e89‐e98
Summary• No one knows exactly how well treatments work. Research provides
an estimate of effect.
• If things are unclear, consider harms, costs, and patient values.
Summary• No one knows exactly how well treatments work. Research provides
an estimate of effect.
• If things are unclear, consider harms, costs, and patient values.
• High‐level evidence on chronic pain interventions may contradict itself and can do so for many years.
• Start with the easy wins
Summary• Easy Wins:
– Osteoarthritis: Exercise, Intra‐articular Corticosteroids, Duloxetine, Oral NSAIDs
– Chronic Low Back Pain: Exercise, Oral NSAIDs, Duloxetine

Thanks!

COVID:WHY IT’S NAMEDAFTER A BEER ANDOTHER ANSWERS
PRESENTED BY:MIKE ALLAN & TONY NICKONCHUK

Faculty/Presenter Disclosure• Faculty/Presenter: Tony Nickonchuk• Relationships with financial sponsors:
• Any direct financial relationships including receipt of honoraria: Alberta College of Family Physicians, Alberta Health Expert Committee for Drug Evaluation and Therapeutics, Alberta Health Services
• Funded grants, research, or clinical trials: N/A• Memberships on advisory boards of speakers bureau: N/A• Patents for drugs or devices: N/A• Other: N/A
Epidemiology 101: Risks • R0 estimated at ~3 [95% CI 2.8‐3.8]• Global case fatality rate ~3%• Infection fatality rate ~0.7% [0.4‐1.3%]
J Prev Med Public Health 2020 May; doi:10.3961/jpmph.20.076Worldometers Coronavirus. Accessed Sep 30/2020.Lancet Inf Dis 2020 Jun; doi:10.1016/S1473‐3099(20)30243‐7
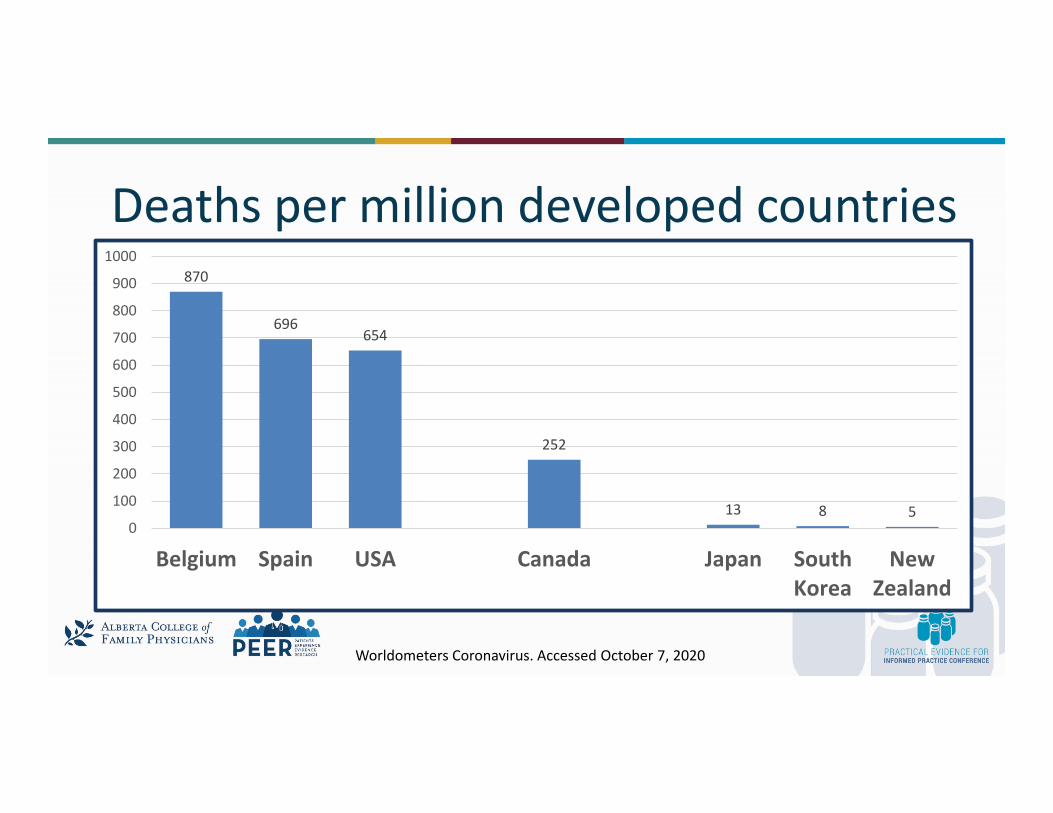
Deaths per million developed countries870
696654
252
13 8 50
100
200
300
400
500
600
700
800
900
1000
Belgium Spain USA Canada Japan SouthKorea
NewZealand
Worldometers Coronavirus. Accessed October 7, 2020
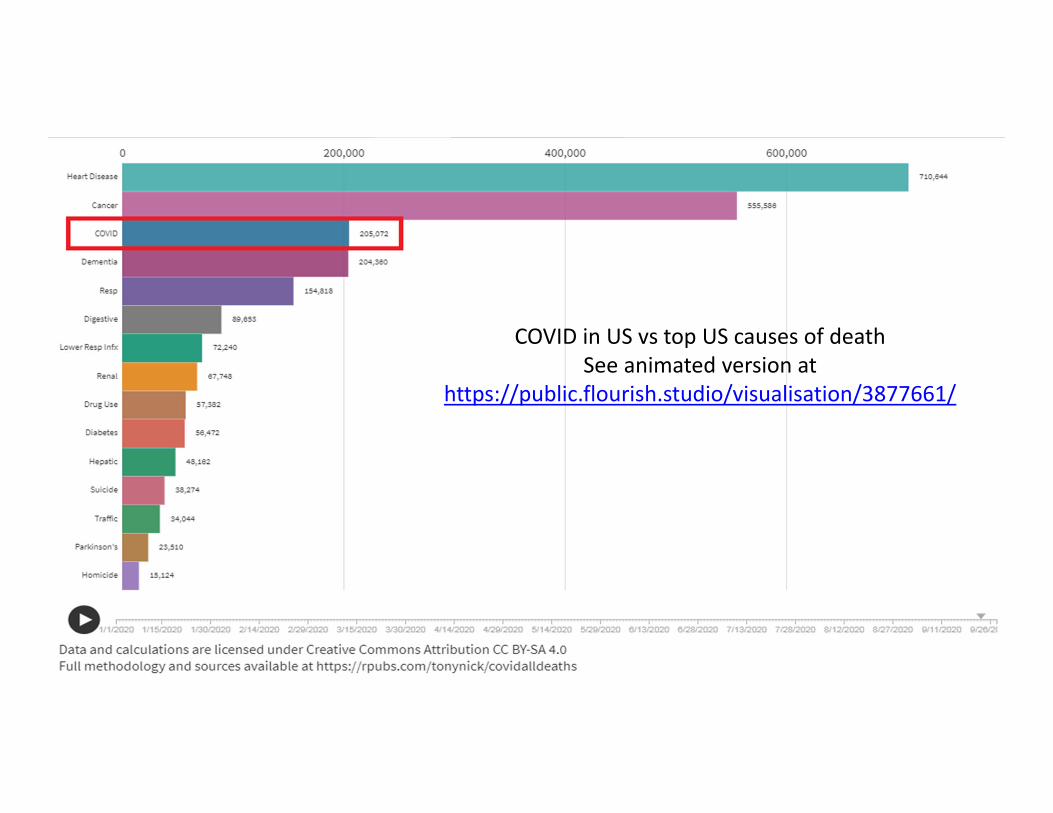
How Bad is This Thing?
COVID in US vs top US causes of deathSee animated version at
https://public.flourish.studio/visualisation/3877661/

PUBLIC HEALTH MEASURES

What Not To Do

Large time series analysis (149 countries): Public Health Measures
• Looked at: School closures*; Workplace closures*; Restrictions on mass gathering*; Public transit closure; Lockdown (restrictions on movement)– * strongest effect
• Implementing ANY measure:– 13% reduction in incidence rate after vs before
• No significant difference between four or five measures implemented• Lockdown had most significant connection to speed of implementation;
if late, did very little
BMJ 2020; 370 doi:10.1136/bmj.m2743
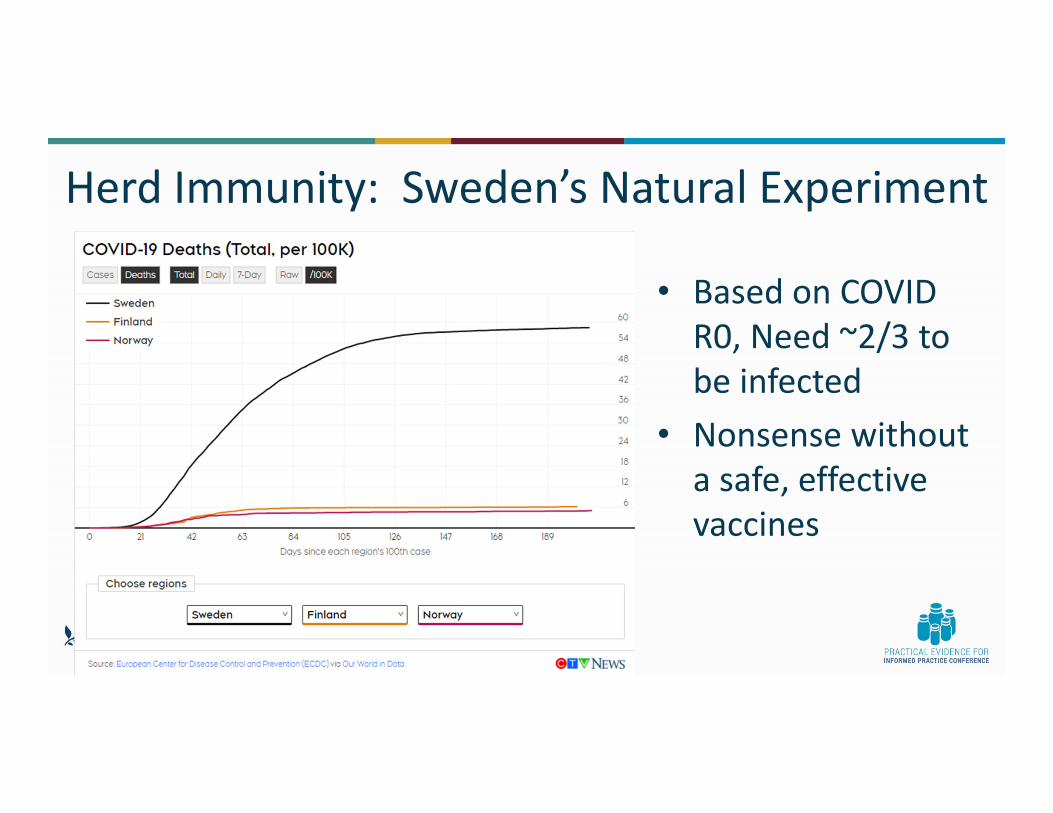
Herd Immunity: Sweden’s Natural Experiment
• Based on COVID R0, Need ~2/3 to be infected
• Nonsense without a safe, effective vaccines

Characteristics associated with adherence• Improved adherence to public health recommendations
– Trust in government/authority– Higher perceived threat from virus– Greater knowledge of the pandemic– Older age– Women
• If get information from – Traditional news media = more likely to adhere– Social media = less likely to adhere (& more likely to endorse conspiracy etc)
AHS COVID‐19 Scientific Advisory Group Rapid Evidence ReportAvailable at: https://www.albertahealthservices.ca/assets/info/ppih/if‐ppih‐covid‐19‐sag‐rapid‐evidence‐report‐attitudes‐and‐adherence‐to‐covid‐19‐guidelines.pdf
Characteristics associated with adherence• Improved adherence to public health recommendations
– Trust in government/authority– Higher perceived threat from virus– Greater knowledge of the pandemic– Older age– Women
• If get information from – Traditional news media = more likely to adhere– Social media = less likely to adhere (& more likely to endorse conspiracy etc)
AHS COVID‐19 Scientific Advisory Group Rapid Evidence ReportAvailable at: https://www.albertahealthservices.ca/assets/info/ppih/if‐ppih‐covid‐19‐sag‐rapid‐evidence‐report‐attitudes‐and‐adherence‐to‐covid‐19‐guidelines.pdf

Characteristics associated with adherence• Improved adherence to public health recommendations
– Trust in government/authority– Higher perceived threat from virus– Greater knowledge of the pandemic– Older age– Women
• If get information from – Traditional news media = more likely to adhere– Social media = less likely to adhere (& more likely to endorse conspiracy etc)
AHS COVID‐19 Scientific Advisory Group Rapid Evidence ReportAvailable at: https://www.albertahealthservices.ca/assets/info/ppih/if‐ppih‐covid‐19‐sag‐rapid‐evidence‐report‐attitudes‐and‐adherence‐to‐covid‐19‐guidelines.pdf

Faculty/Presenter Disclosure• Faculty/Presenter: G. Michael Allan• Relationships with financial sponsors:
• Any direct financial relationships including receipt of honoraria: College of Family Physicians of Canada and provincial chapters, University of Alberta
• Funded grants, research, or clinical trials: Towards Optimized Practice, CIHR, PRIHS, Alberta Health, ON LHIN, St. Paul's Hospital, Bedmed, INR range
• Memberships on advisory boards of speakers bureau: N/A• Patents for drugs or devices: N/A• Other: N/A

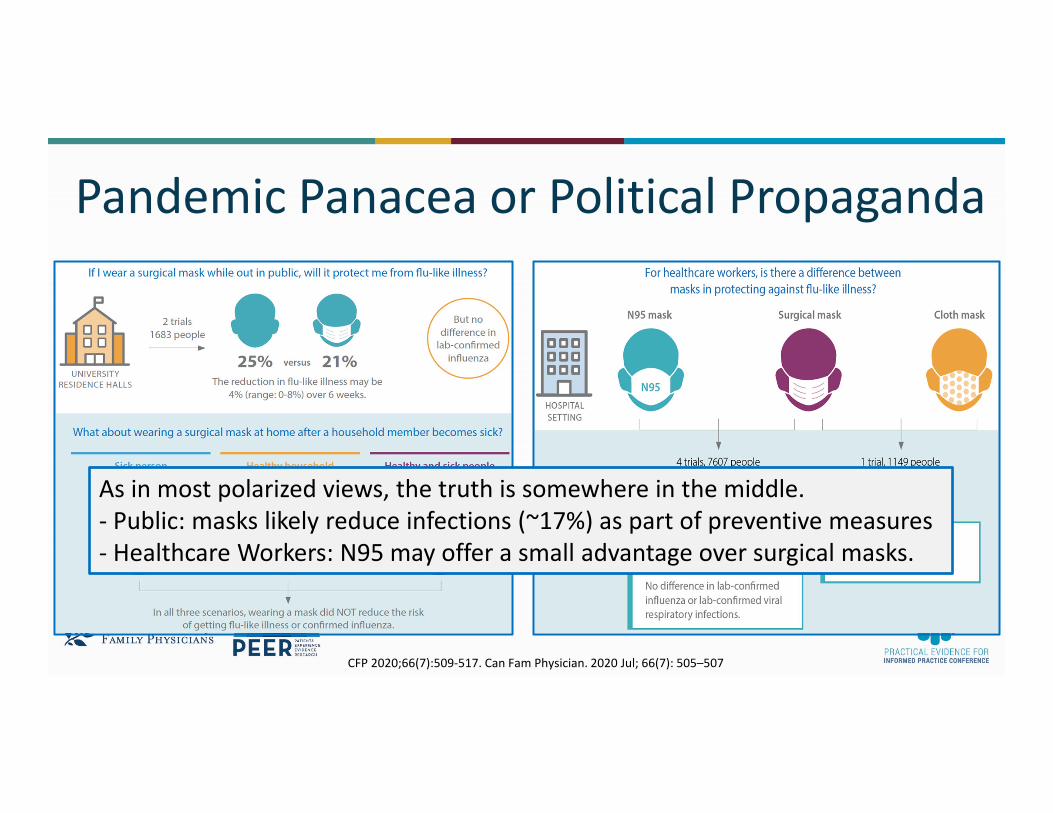
Pandemic Panacea or Political Propaganda
CFP 2020;66(7):509‐517. Can Fam Physician. 2020 Jul; 66(7): 505–507
Pandemic Panacea or Political Propaganda
CFP 2020;66(7):509‐517. Can Fam Physician. 2020 Jul; 66(7): 505–507
As in most polarized views, the truth is somewhere in the middle. ‐ Public: masks likely reduce infections (~17%) as part of preventive measures‐ Healthcare Workers: N95 may offer a small advantage over surgical masks.

WHAT SPREADS FASTER?A) COVID INFECTIONB) COVID MISINFORMATION
WHAT SPREADS FASTER?A) COVID INFECTIONB) COVID MISINFORMATION
WHAT SPREADS FASTER?A) COVID INFECTIONB) COVID MISINFORMATION

PCR (polymerase chain reaction) Test?• Specificity ~100%: Positive = COVID• Sensitivity ~80‐90%: (? ~50%). False Negatives
– If pretest probability ~5%, 0.5‐2.5% negatives are false– If pretest probability 80%, 8‐40% negatives are false.
• Missed diagnosis ‐ Collection technique, timing, etc.• Rapids tests – less consistent but Specificity similar while
sensitivity ~56% (30‐80%)Tools for Practice #263, May 21, 2020. BMJ Evidence‐Based Medicine doi:10.1136/bmjebm‐2020‐111511. CDSR:CD013705

Antibodies – here today,…• Multiple studies now show that antibodies persist ≥ 90 days
– 91% of 1215 icelanders ‐ DOI: 10.1056/NEJMoa2026116
– 496 Canadians https://doi.org/10.1101/2020.08.01.20166553.
Nature. 2020 Sep 16.Available at https://www.nature.com/articles/d41586‐020‐02661‐2
Asymptomatic Transmission• Case reports suggest asymptomatic transmission can occur in 6‐13%
• “Closed system” situations like cruise ships suggest as much as 50% of positive cases can be asymptomatic
• Aligns with experience in Iceland, where they did widespread random sample testing– At time of testing, 43% of positive cases reported no symptoms
TFP 258NEJM June 2020. doi:10.1056/NEJMoa2006100

Grab‐Bag of MedsACE inhibitors and ARB• No association with harm (>½
million)– Tools for Practice #264– Curr Hypertens Rep doi:10.1007/s11906‐020‐01101‐w– Hippisley‐Cox J, Young D, Coupland C, et al. Heart
doi:10.1136/ heartjnl‐2020‐317393
Hydroxychloroquine• Systematic Rev ‐ 3 RCTs (210 patients) no effect• 4716 Hospitalized: at 28 days more mech vent,
less discharge by 28 days, trend to ↑ mortality • 1853 hospital patients – trend to increase
mortality– J Gen Intern https://doi.org/10.1007/s11606‐020‐06146‐w– NEJM DOI: 10.1056/NEJMoa2022926 – NEW Solidarity (WHO trial) ‐https://doi.org/10.1101/2020.10.15.20209817.
Grab‐Bag of MedsACE inhibitors and ARB• No association with harm (>½
million)– Tools for Practice #264– Curr Hypertens Rep doi:10.1007/s11906‐020‐01101‐w– Hippisley‐Cox J, Young D, Coupland C, et al. Heart
doi:10.1136/ heartjnl‐2020‐317393
Hydroxychloroquine• Systematic Rev ‐ 3 RCTs (210 patients) no effect• 4716 Hospitalized: at 28 days more mech vent,
less discharge by 28 days, trend to ↑ mortality • 1853 hospital patients – trend to increase
mortality– J Gen Intern https://doi.org/10.1007/s11606‐020‐06146‐w– NEJM DOI: 10.1056/NEJMoa2022926 – NEW Solidarity (WHO trial) ‐https://doi.org/10.1101/2020.10.15.20209817.
Yes, can continue to useNo: Do not use for COVID.
Crazy

Grab‐Bag of MedsRemdesivir ‐ RCTs• Meta (2 RCTs‐992): 23% ↓ Serious AE• 584 (moderate): 5 d Tx recovery better vs
control (not 10 d) (NNT 10)• 1062 (hospital): recovery 10 v 15 day• 5421 (hospital): No mortality diff (maybe
better less ill) & and ? Delay recovery.– PLoS Med 17(9): E1003293– JAMA. 2020;324(11):1048‐1057.– NEJM: DOI: 10.1056/NEJMoa2007764– NEW Solidarity (WHO trial) https://doi.org/10.1101/2020.10.15.20209817.
Corticosteroid• Meta 7 RCTs (1703 severe), 5‐7 d• 28d mortality: ~30% steroid v 40%
– Tools for Practice #264– Curr Hypertens Rep doi:10.1007/s11906‐020‐
01101‐w– Hippisley‐Cox J, Young D, Coupland C, et al. Heart
doi:10.1136/ heartjnl‐2020‐317393
Grab‐Bag of MedsRemdesivir ‐ RCTs• Meta (2 RCTs‐992): 23% ↓ Serious AE• 584 (moderate): 5 d Tx recovery better vs
control (not 10 d) (NNT 10)• 1062 (hospital): recovery 10 v 15 day• 5421 (hospital): No mortality diff (maybe
better less ill) & and ? Delay recovery.– PLoS Med 17(9): E1003293– JAMA. 2020;324(11):1048‐1057.– NEJM: DOI: 10.1056/NEJMoa2007764– NEW Solidarity (WHO trial) https://doi.org/10.1101/2020.10.15.20209817.
Corticosteroid• Meta 7 RCTs (1703 severe), 5‐7 d• 28d mortality: ~30% steroid v 40%
– Tools for Practice #264– Curr Hypertens Rep doi:10.1007/s11906‐020‐
01101‐w– Hippisley‐Cox J, Young D, Coupland C, et al. Heart
doi:10.1136/ heartjnl‐2020‐317393
Yes: in hospital
Unclear: Maybe in less sick hospital pts

THANK YOU!

Resources• CFPC ‐ https://www.cfpc.ca/en/covid‐19‐information‐and‐resources• Government of Canada ‐ https://www.canada.ca/en/public‐
health/services/diseases/2019‐novel‐coronavirus‐infection/health‐professionals.html#a9
• Public health agency of Canada ‐ https://www.canada.ca/en/public‐health/services/diseases/2019‐novel‐coronavirus‐infection/clinical‐management‐covid‐19.html
• BMJ ‐ https://www.bmj.com/coronavirus• Living Systematic Reviews‐
https://journals.plos.org/plosmedicine/article?id=10.1371/journal.pmed.1003293
Vaccine – News • As of October 2, 170 vaccines in development currently being tracked by WHO
• 11 currently in Phase 3 trials• Sputnik V Russian vaccine registered and used, despite still recruiting Phase 3 subjects
• State owned Chinese subsidiary has given its vaccine to over 350,000 people despite no regulatory approval
https://www.theguardian.com/world/ng‐interactive/2020/oct/02/covid‐vaccine‐tracker‐when‐will‐a‐coronavirus‐vaccine‐be‐readyhttps://en.wikipedia.org/wiki/Gam‐COVID‐Vachttps://www.ctvnews.ca/world/china‐pushes‐emergency‐use‐of‐covid‐vaccine‐despite‐concerns‐1.5121404
Vaccines ‐ News• Moderna/NIAID and Pfizer/BioNTech likely furthest along
• AstraZeneca paused briefly over concerns with transverse myelitis
• Heavy military involvement in Operation Warp Speed, US government initiative to accelerate development– 60 military officials, including at least 4 generals, in leadership
https://www.bbc.com/news/uk‐54132066https://www.statnews.com/2020/09/28/operation‐warp‐speed‐vast‐military‐involvement/