Dermoscopy: what's new?
9
Dermoscopy: what's new? Ralph Peter Braun, MD a, ⁎ , Margaret Oliviero, AR b , Isabel Kolm, MD a , Lars E. French, MD a , Ashfaq A. Marghoob, MD c , Harold Rabinovitz, MD b a Department of Dermatology, University Hospital Zürich, Zürich 8091, Switzerland b Skin and Cancer Associates, Plantation, FL, USA c Dermatology Service, Memorial Sloan Kettering Cancer Center, New York, NY, USA Abstract Dermoscopy has been described as a useful tool for the early diagnosis of melanoma and the differential diagnosis of pigmented lesions of the skin. This has been proven by three independent meta analyses of the literature. Dermoscopy is a fast evolving field with a high number of new publications every year. Initially, the use of dermoscopy was limited to pigmented lesions, but it is used more and more in other situations. It has become an important tool for the diagnosis of nail pigmentations, hair and scalp disorders, and so forth. In this article we try to provide an update on recent trends and developments in dermoscopy. © 2009 Elsevier Inc. All rights reserved. Introduction Dermoscopy, also known as epiluminescence micro- scopy, dermatoscopy, or amplified surface microscopy, is an in vivo method that has been described as a useful tool for the early recognition of malignant melanoma. 1 The performance of dermoscopy has been investigated by many authors, and two meta analyses have confirmed the data. 2,3 Its use increases diagnostic accuracy by 5% to 30% compared with clinical visual inspection, depending on the type of skin lesion and experience of the physician. This was confirmed by two recent evidence-based publications and a meta-analysis of the literature. In recent years, many new ideas and concepts have been published. This chapter will provide an updated overview on what's new in dermoscopy. Equipment Important technologic improvements have occurred since the first description of dermatoscopes in the 1980s. 4 All second-generation devices have enhanced optics that use general light emitting diodes (LEDs) for illumination, and we therefore recommend the use of these dermatoscopes. Two types of dermatoscopes are available: those that use nonpolarized light with liquid immersion and those that use polarized light. A recent study investigated the differences between contact and noncontact polarized light dermoscopy and contact nonpolarized dermoscopy (standard dermoscopy). 5 The authors concluded that although the techniques did not provide equivalent images, they were complimentary. For example, milia like cysts can be easily identified under standard dermoscopy but are difficult to visualize using polarized light (Figure 1). Polarized light images seem to offer a better view of structures located deeper in the skin, whereas immersion-contact nonpolarized dermoscopy ⁎ Corresponding author. E-mail address: [email protected] (R.P. Braun). 0738-081X/$ – see front matter © 2009 Elsevier Inc. All rights reserved. doi:10.1016/j.clindermatol.2008.09.003 Clinics in Dermatology (2009) 27, 26–34
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Dermoscopy: what's new?

Clinics in Dermatology (2009) 27, 26–34
Dermoscopy: what's new?Ralph Peter Braun, MDa,⁎, Margaret Oliviero, ARb, Isabel Kolm, MDa,Lars E. French, MDa, Ashfaq A. Marghoob, MDc, Harold Rabinovitz, MDb
aDepartment of Dermatology, University Hospital Zürich, Zürich 8091, SwitzerlandbSkin and Cancer Associates, Plantation, FL, USAcDermatology Service, Memorial Sloan Kettering Cancer Center, New York, NY, USA
Abstract Dermoscopy has been described as a useful tool for the early diagnosis of melanoma and thedifferential diagnosis of pigmented lesions of the skin. This has been proven by three independent metaanalyses of the literature. Dermoscopy is a fast evolving field with a high number of new publicationsevery year. Initially, the use of dermoscopy was limited to pigmented lesions, but it is used more andmore in other situations. It has become an important tool for the diagnosis of nail pigmentations, hairand scalp disorders, and so forth. In this article we try to provide an update on recent trends anddevelopments in dermoscopy.© 2009 Elsevier Inc. All rights reserved.
Introduction
Dermoscopy, also known as epiluminescence micro-scopy, dermatoscopy, or amplified surface microscopy, isan in vivo method that has been described as a useful toolfor the early recognition of malignant melanoma.1 Theperformance of dermoscopy has been investigated by manyauthors, and two meta analyses have confirmed the data.2,3
Its use increases diagnostic accuracy by 5% to 30%compared with clinical visual inspection, depending onthe type of skin lesion and experience of the physician.This was confirmed by two recent evidence-basedpublications and a meta-analysis of the literature. In recentyears, many new ideas and concepts have been published.This chapter will provide an updated overview on what'snew in dermoscopy.
⁎ Corresponding author.E-mail address: [email protected] (R.P. Braun).
0738-081X/$ – see front matter © 2009 Elsevier Inc. All rights reserved.doi:10.1016/j.clindermatol.2008.09.003
Equipment
Important technologic improvements have occurred sincethe first description of dermatoscopes in the 1980s.4 Allsecond-generation devices have enhanced optics that usegeneral light emitting diodes (LEDs) for illumination, and wetherefore recommend the use of these dermatoscopes. Twotypes of dermatoscopes are available: those that usenonpolarized light with liquid immersion and those thatuse polarized light.
A recent study investigated the differences betweencontact and noncontact polarized light dermoscopy andcontact nonpolarized dermoscopy (standard dermoscopy).5
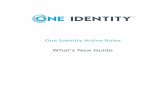
The authors concluded that although the techniques did notprovide equivalent images, they were complimentary. Forexample, milia like cysts can be easily identified understandard dermoscopy but are difficult to visualize usingpolarized light (Figure 1). Polarized light images seem tooffer a better view of structures located deeper in the skin,whereas immersion-contact nonpolarized dermoscopy

Fig. 1 A, Milia-like cysts can be easily identified with standardcontact nonpolarized dermoscopy. B, These cysts are difficult tovisualize using dermoscopy with polarized light.
ig. 2 A, Noncontact polarized dermoscopy allows betterisualization of blood vessels than (B) contact nonpolarized or) contact polarized dermoscopy.
27Dermoscopy: what's new?
allows for the visualization of more superficial structuressuch as milia like cysts. Noncontact polarized dermoscopyallows much better visualization of blood vessels (Figure 2).6
This can be useful for the diagnosis of nonmelanocyticlesions as well as for the diagnosis of hypomelanotic oramelanotic lesions.
Another important point is that granularity (peppering)was more clearly visualized with classic immersion dermo-scopy (Figure 3).5 This criterion is an important sign ofhistologic regression, which potentially creates a problembecause subtle cases of regression in early melanomas couldbe overlooked using dermoscopy with polarized light.
New dermoscopy criteria
Vascular structures have gained more importance indermoscopy in recent years. In the past too much pressurewas often applied on the lesion during the dermoscopic
Fv(C

Fig. 3 A, Granularity (peppering) is more clearly visualized withcontact nonpolarized dermoscopy. B, This feature is an importantsign of histologic regression, which potentially creates a problembecause subtle cases of regression in early melanomas could beoverlooked using dermoscopy with polarized light.
Table 1 Vascular pattern as seen by dermoscopy with themost likely diagnosis
Type of blood vessels Diagnoses
Arborizing vessels Basal cell carcinomaDotted vessels Spitz nevus or melanoma,
psoriasis, squamous cell carcinomaErythematous blush Melanoma, dysplastic nevusLinear irregular vessels Melanoma, dysplastic nevusComma vessels Compound or dermal nevusPolymorphous atypicalvessels
Melanoma
Hairpin vessels Regular seborrheic keratosis andkeratinizing tumors, irregularand thick melanoma, Spitz nevus
Glomerular vessels Bowen’s disease, melanoma, orstasis dermatitis
Milky red globules MelanomaCrown vessels Sebaceous gland hyperplasia
ig. 4 Arborizing vessels have a large diameter and branchregularly into smaller thinner vessels. The vessels within theeoplasm are bright red and in sharp focus.
28 R.P. Braun et al.
examination. Blood vessels were compressed and thereforewere not visible on examination. The best way to properlysee blood vessels is to use either noncontact polarizeddermoscopy or to use ultrasound gel for immersion.Ultrasound gel enables better visualization with lessapplication of pressure on the lesion. The following typesof blood vessels have been described (Table 1)6:
• Arborizing vessels have a large diameter and branchingirregularly into smaller thinner vessels. The vesselswithin the neoplasm are bright red and in sharp focus(Figure 4).
• Dotted vessels are tiny red dots that are densely alignednext to each other in an irregular fashion (Figure 5).
• Erythematous blush is a pinkish color usually seenwithin or in association with areas of regression at theborder of the lesion.
• Linear irregular vessels are linear and are irregular insize and shape.
• Comma vessels are coarse, slightly curved vessels.• Polymorphous atypical vessels are a combination oftwo or more different vascular structures. The mostfrequent is the combination of linear irregular anddotted vessels.
• Hairpin vessels are vascular loops that are sometimestwisted and bending. They are usually surrounded by awhitish halo when seen in keratinizing tumors(Figure 6).
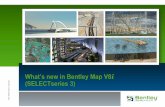
• Glomerular vessels are tortuous capillaries that areoften distributed in clusters mimicking the glomerularapparatus of the kidney (Figure 7).
• Milky red globules are globules in association withareas of a milky red color that usually correspond to anelevated part of the lesion.
Firn

Fig. 5 Dotted vessels are tiny red dots densely aligned next toeach other in an irregular fashion.
ig. 7 Glomerular vessels are tortuous capillaries often distrib-ted in clusters mimicking the glomerular apparatus of the kidney.
29Dermoscopy: what's new?
• Crown vessels are groups of orderly, bending, andsometimes branching vessels located along the borderof the lesion.
New algorithms
A new CASH algorithm for dermoscopy has recentlybeen described.7,8 This algorithm uses the criteria of color,architecture, symmetry, and homogeneity. For example, agiven lesion can have no architectural disorder, mildarchitectural disorder, moderate architectural disorder, ormarked architectural disorder. A summary of the CASHscore can be found in Table 2.
Fairy tales and dermoscopy
The “ugly duckling sign”9 comes from the Hans ChristianAndersen's tale. The ugly duckling was the one who was not
Fig. 6 Hairpin vessels are vascular loops. They sometimes twistand bend, are usually surrounded by a whitish halo, and are seen inkeratinizing tumors.
Fu
like his brothers and sisters. Nevi in a given individualusually resemble each other like brothers. The ugly ducklinglesion is the one that is different and does not resemble theother nevi. After a complete skin examination, a dermatol-ogist can generally identify a common profile of most nevi ina given patient. An ugly duckling lesion does not share thisprofile and can thus be easily detected. This ugly ducklinglesion deserves special attention even when the dermoscopyfeatures are suggestive of a benign neoplasm (Figure 8).
The “Little Red Riding Hood” sign10 comes from anotherfairy tale in which the wolf disguises himself as thegrandmother but can be still be recognized by his enormousteeth. Although this is described in the context for clinicallesions in high-risk patients, with dermoscopy, it is also usedto describe an individual lesion that at first glance looksbenign, but on closer inspection with dermoscopy showsfeatures of a melanoma (Figure 9).
The “Beauty and the Beast sign”11 of dermoscopy hasrecently been described. Benign melanocytic lesions areplaced in into nine categories. According to the premisethat melanocytic lesions will fit into one of the ninepatterns, a lesion that fits the definition of “beauty”demonstrates symmetry of pattern, structure, and color(Table 3). Experience has shown that one rarely, if ever,will encounter a melanoma that mimics one of these benignpatterns (Figure 10). Knowledge of these benign patternsmay be helpful in identifying those melanocytic lesions that
Table 2 The CASH algorithm
CASH Suspicion for melanoma
Colors 1–2 3–4 5–6Architectural disorder No/mild Moderate MarkedSymmetry Biaxial Monaxial NoneHomogeneity/heterogeneity
1structure
2structures
3+structures

Fig. 8 A, This melanoma clinically has the ugly duckling sign. B,Dermoscopically, it has a focal atypical network and the differentialdiagnosis (equivocal lesion) of an atypical nevus or a melanoma.Based on the ugly duckling sign it should be removed.
Fig. 9 A, This subtle melanoma in situ on first glance has thefeatures of a nevus. B, With the dermoscope, the nonuniformnetwork prominent at the periphery and the focal area of gray dots\granules (dermoscopy regression) are suggestive of a malignantneoplasm (the Little Red Riding Hood sign).
Table 3 Patterns of benign melanocytic nevi
30 R.P. Braun et al.
do not require further diagnostic evaluation. Melanomasymbolized by the “beast” is by definition a melanocyticlesion that derives from one of the malignant patterns.Melanomas almost invariably display at least some degreeof asymmetry of pattern, color, and structure and elicit asense of displeasure in the viewer. Most will also displayone or more of the following dermoscopy features: atypicalnetwork, atypical dots and globules streaks, asymmetricalblotches, blue white veil, negative pigment network,regression structures, or atypical vascular structures(Figure 11).
• Diffuse reticular pattern• Patchy reticular pattern• Peripheral reticular central homogeneous pattern• Structureless (homogeneous) pattern• Peripheral reticular and central globular pattern• Peripheral globular and central reticular pattern• Globular pattern• Symmetric multicomponent pattern
Computer-assisted dermoscopy
Commercially available instruments for digital dermo-scopy, which are designed to provide computer-assisteddiagnoses, have been tested in peer reviewed publicationsthat praised their diagnostic accuracy. Because many of thedata in these publications originate from the centers that have
an interest in these instruments, it is possible that the resultspresented in these publications are biased. This is primarilydue to selection bias of images (lesions) used for training andtesting the algorithms. A recent publication reported aninvestigation of the diagnostic performance of three com-mercially available instruments with those of an experienceddermoscopist.12 All of the instruments were able to identifyclinically obvious melanomas, but all three systems tended to

Fig. 10 This benign melanocytic lesion with a reticular patternfits the definition of “beauty” in the Beauty and the Beast signbecause it has symmetry of pattern, structure, and color.
31Dermoscopy: what's new?
over diagnose most seborrheic keratosis. Concerning suspectmelanocytic lesions, which are the group of lesions for whichthe dermatologist would welcome a second opinion, asignificant variability was found in diagnostic accuracy ofthe instruments tested. All three systems had a tendency toover diagnose benign melanocytic lesions as potentialmelanomas. Only one system had a higher specificity thanthe clinician because it had identified some lesions correctlyas benign that the clinician thought were malignant. Theauthors concluded that computer-assisted diagnostic imagingmachines currently provide only little added benefit for anexperienced dermatologist.
Fig. 11 This melanoma with a reticular disorganized pattern hasa nonuniform network with thin and thick lines and holes ofdifferent sizes and shapes. This lesion fits the definition of the“beast” in the Beauty and the Beast sign because there is asymmetryof pattern and structure.
The significance of multiple blue gray dots(granularity) for the diagnosis of melanoma
Because the presence of multiple blue-gray dots arewidely used by clinicians to decide if pigmented lesionsshould be removed, an evaluation was done on significanceof this criterion for dermoscopy diagnosis of melanoma.13
The authors found granularity in 26.5% of the benign lesionsand in 93.5% of all melanomas. Granularity at the periphery,irregularly distributed granularity, and granularity in associa-tion with red or white color was highly significantstatistically for the diagnosis of melanoma. Granularity wasmainly found in sun-damaged skin. In the prospective part oftheir study, the presence of granularity had 85% sensitivityfor the diagnosis of melanoma and 99% specificity. Theyconcluded that lesions with irregular granularity (peripheralor irregularly distributed) should be removed, especially ifthe granularity is associated with the colors red, blue, orwhite (Figure 12). Lesions with a benign dermoscopypattern, which have granularity with a uniform appearanceand involve only a small portion of the lesion, do not requiresurgical excision.
Dermoscopy in general dermatology
For many years the use of dermoscopy has been limited tothe diagnosis of melanoma and the differential diagnoses ofpigmented lesions. The use of dermoscopy in generaldermatology has recently been described.14 Conditionssuch as lichen planus (Figure 13), psoriasis (Figure 14),spongiotic dermatitis, urticaria, and urticarial vasculitis havebeen differentiated using dermoscopy. The dermatoscope canalso be used for the evaluation of scabies, where one canvisualize the presence of “a jet with a condensation trail.”This appears as a triangle of brown homogeneous pigmenta-tion at the anterior part, corresponding to the two pairs offront legs and the mouth part of the mite, followed by alinear, distal whitish trail. This is particularly useful for thediagnosis as well as for monitoring the treatment of scabies.
How to avoid missing melanoma
Seven management rules have been reported that allowthe clinician to avoid missing malignant melanoma withoutspecific dermoscopy criteria of melanoma15-17:
1. Dermoscopy should not be used only for suspiciousskin lesions.
2. Biopsy all lesions that lack a clinical dermoscopiccorrelation.
3. Biopsy lesions with a nonspecific pigment pattern.4. Biopsy lesions with spitzoid features.5. Biopsy lesions with extensive regression features.6. In patients with multiple nevi, biopsy lesions that
change during the short-term follow-up.7. Biopsy pink lesions with an atypical vascular pattern
(Figure 15).

Fig. 12 The appearance of lichen planus on dermoscopy oftenhas a central white scar like area.
ig. 14 This melanoma is characterized by scar like depigmenta-on and fine gray dots/granules irregularly distributed throughoute lesion. This regression pattern is commonly seen with earlyelanomas on sun-damaged skin.
32 R.P. Braun et al.
Nail dermoscopy
The use of dermoscopy for examination of nail pigmenta-tion was published in 2002.18 A recent review article on thediagnosis and management of nail pigmentation provides asimplified diagnostic algorithm.19 Similar to dermoscopy ofpigmented lesions, in the first step one has to determine if thenail pigmentation is of melanocytic or nonmelanocytic origin(blood or fungus). Melanonychia striata are tiny melaningranules (inclusions) of the nail plate visible with dermo-scopy. In nail pigmentation of nonmelanocytic origin (nailhyperchromia), the pigmentation is homogeneous, without
Fig. 13 The dermoscopy features of psoriasis are oftencharacterized by diffuse red dots/globules.
Ftithm
the granular aspect corresponding to melanin inclusions inthe nail plate.
Subungual hematoma appears as red to red-blackpigment, depending on when the insult to the nail occurred.With dermoscopy one is usually able to identify smallreddish to reddish-black globules along the proximal marginof the pigmentation. Streaks are often visible at the distaledge of the pigmentation. More importantly, a hematomawill progressively grow out distally as the nail plate grows. Itis key to remember that a subungual hematoma can eitheroccur because of a hemorrhage or neovascularization. Thus,the presence of subungual blood should not be used to ruleout the diagnosis of melanoma. Every subungual hemor-rhage that does not grow out with the nail, and that reappearsat the same place, requires special attention.
An x-ray study of the distal phalange should be performedto exclude exostosis. Infection of the nail with Trichophytonrubrum var nigricans can be pigmented. Although difficultto treat, the pigmentation will fade progressively aftersuccessful treatment of the fungal infection.
Once the lesion has been identified as melanocytic by thepresence of melanin inclusions in the nail plate, in thesecond step, one has to evaluate the color of the nailpigmentation. If dermoscopy shows the lesion is of agrayish color, the nail pigmentation is caused by epithelialhyperpigmentation, which might be due to ethnicity,induced by a drug, or by lentigo of the nail matrix. Nailpigmentation of a brownish color is a result of melanocyticproliferation (melanocytic hyperplasia). Once the lesion has

Fig. 15 A, This pink melanoma has an (B) atypical vasculardermoscopy pattern.
33Dermoscopy: what's new?
been identified to be a brownish color, one has to furtherevaluate if the brown band is regular or irregular. Regularbrown bands consist of narrow, brown lines with a regularpigmentation pattern, homogeneous in color, regular spa-cing, and thickness. A regular aspect of the pigmentationsuggests the presence of a benign lesion (nevus of the nailmatrix). Irregular brown bands tend to have an irregularpigmentation pattern with disruption of parallelism. Theyhave multiple colors and irregular spacing and thickness.The presence of the above criteria is suggestive of amalignant lesion (melanoma of nail matrix). One also mustconsider the following signs and symptoms:
1. Any isolated pigmentation of a single digit thatdevelops during the fourth to sixth decade of life.
2. Any nail pigmentation that develops abruptly in apreviously normal nail plate.
3. Any changing pigmentation that becomes larger orblurred.
4. Any subtle pigmentation of the thumb, index finger, orlarge toe.
5. Any pigmentation in association with a history ofdigital trauma.
6. Any new lesion in patients with a personal history ofmelanoma.
7. Any nail pigmentation in association with naildystrophy.
8. Any nail pigmentation with the presence of apigmentation of the periungual skin (Hutchinson sign).
Dermoscopy of the free edge of the nail plate
Nail dermoscopy is usually limited to the examinationof the nail plate. The use of a gel (ultrasound gel, cosmeticgel, or hand sanitizer) as an immersion fluid is recom-mended because the gel nicely fills out the space betweenthe curved nail plate and the dermoscopy contact plate.Before biopsy, it is important to know if the origin of thepigmentation is the proximal or distal nail matrix. Becausea biopsy of the proximal nail matrix is much more likely toresult in a permanent nail dystrophy, the patient should beinformed before the surgery. Nail clipping and histologicexamination is performed frequently, but dermoscopy ofthe free edge of the nail can provide the same informa-tion.20 Because of the anatomy of the nail apparatus,pigmentation of the proximal nail matrix will appear in theupper part of the free nail edge, whereas pigmentation ofthe distal nail matrix will appear as pigmentation of thelower part of the free nail edge.
Hair and scalp dermoscopy
The use of dermoscopy for the diagnosis of hair andscalp disorders has been recently published.21 Various hairand scalp disorders are evaluated and specific dermoscopicfindings are discussed. Three different vascular patternsare described:
1. Interfollicular simple red loops are rare, multiple,relatively evenly spaced, fine, red lasso-shaped loops.This entity was found in both normal and in diseasedscalps, with the exception of discoid lupus erythema-tosus, where loops were not seen due to atrophy ofthe epidermis.
2. Interfollicular twisted red loops are multiple, relativelyevenly spaced, twisted red loops. They were seen in allcases of psoriasis and folliculitis decalvans but lessfrequently in seborrheic dermatitis.
Simple and twisted loops seem to correspond to capillaryloops in the dermal papillae.

34 R.P. Braun et al.
“Yellow dots” are an important dermoscopic featurereported in the diagnosis of alopecia areata. The presence ofyellow dots allows differentiation of alopecia areata fromtrichotillomania or telogen effluvium. They are thought torepresent degenerated follicular keratinocytes and sebumwithin the affected follicles. Hair shaft anomalies found inalopecia areata such as “cadaverized” hairs, “exclamationmark” hairs, and dystrophic hairs can be easily seen with thehelp of dermoscopy.
Because the number of publications related to dermoscopyis steadily increasing and many new aspects of dermoscopyhave been published in recent years, we concluded that thatan update on dermoscopy would be useful.
References1. Braun RP, Rabinovitz HS, Oliviero M, Kopf AW, Saurat JH.
Dermoscopy of pigmented skin lesions. J Am Acad Dermatol 2005;52:109-21.
2. Bafounta ML, Beauchet A, Aegerter P, Saiag P. Is dermoscopy(epiluminescence microscopy) useful for the diagnosis of melanoma?Results of a meta-analysis using techniques adapted to the evaluation ofdiagnostic tests. Arch Dermatol 2001;137:1343-50.
3. Kittler H, Pehamberger H, Wolff K, Binder M. Diagnostic accuracy ofdermoscopy. Lancet Oncol 2002;3:159-65.
4. Marghoob AA, Swindle LD, Moricz CZ, et al. Instruments and newtechnologies for the in vivo diagnosis of melanoma. J Am AcadDermatol 2003;49:777-97.
5. Benvenuto-Andrade C, Dusza SW, Agero AL, et al. Differences betweenpolarized light dermoscopy and immersion contact dermoscopy for theevaluation of skin lesions. Arch Dermatol 2007;143:329-38.
6. Argenziano G, Zalaudek I, Corona R, et al. Vascular structures in skintumors: a dermoscopy study. Arch Dermatol 2004;140:1485-9.
7. Henning JS, Dusza SW, Wang SQ, et al. The CASH (color, architecture,symmetry, and homogeneity) algorithm for dermoscopy. J Am AcadDermatol 2007;56:45-52.
8. Henning JS, Stein JA, Yeung J, et al. CASH algorithm for dermoscopyrevisited. Arch Dermatol 2008;144:554-5.
9. Grob JJ, Bonerandi JJ. The ‘ugly duckling’ sign: identification of thecommon characteristics of nevi in an individual as a basis for melanomascreening. Arch Dermatol 1998;134:103-4.
10. Mascaro Jr JM, Mascaro JM. The dermatologist’s position concerningnevi: a vision ranging from “the ugly duckling” to “little red ridinghood.”. Arch Dermatol 1998;134:1484-5.
11. Marghoob AA, Korzenko AJ, Changchien L, Scope A, Braun RP,Rabinovitz H. The beauty and the beast sign in dermoscopy. DermatolSurg 2007;33:1388-91.
12. Perrinaud A, Gaide O, French LE, Saurat JH, Marghoob AA, Braun RP.Can automated dermoscopy image analysis instruments provide addedbenefit for the dermatologist? A study comparing the results of threesystems. Br J Dermatol 2007;157:926-33.
13. Braun RP, Gaide O, Oliviero M, et al. The significance of multiple blue-grey dots (granularity) for the dermoscopic diagnosis of melanoma. Br JDermatol 2007;157:907-13.
14. Zalaudek I, Argenziano G, Di Stefani A, et al. Dermoscopy ingeneral dermatology. Dermatology (Basel, Switzerland) 2006;212:7-18.
15. Argenziano G, Zalaudek I, Ferrara G, et al. Dermoscopy features ofmelanoma incognito: indications for biopsy. J Am Acad Dermatol2007;56:508-13.
16. Puig S, Argenziano G, Zalaudek I, et al. Melanomas that faileddermoscopic detection: a combined clinicodermoscopic approach fornot missing melanoma. Dermatol Surg 2007;33:1262-73.
17. Zalaudek I, Ferrara G, Di Stefani A, Argenziano G. Dermoscopy forchallenging melanoma; how to raise the ‘red flag’ when melanomaclinically looks benign. Br J Dermatol 2005;153:200-2.
18. Ronger S, Touzet S, Ligeron C, et al. Dermoscopic examination of nailpigmentation. Arch Dermatol 2002;138:1327-33.
19. Braun RP, Baran R, Le Gal FA, et al. Diagnosis and management of nailpigmentations. J Am Acad Dermatol 2007;56:835-47.
20. Braun RP, Baran R, Saurat JH, Thomas L. Surgical pearl: dermoscopyof the free edge of the nail to determine the level of nail platepigmentation and the location of its probable origin in the proximal ordistal nail matrix. J Am Acad Dermatol 2006;55:512-3.
21. Ross EK, Vincenzi C, Tosti A. Videodermoscopy in the evaluation ofhair and scalp disorders. J Am Acad Dermatol 2006;55:799-806.