What's New in Renal Medicine? - RCP London
88
How I Manage Advanced Renal Failure Dr Andrew Mooney GIM Trainees Day York February 2019
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of What's New in Renal Medicine? - RCP London
How I Manage Advanced
Renal Failure
Dr Andrew Mooney
GIM Trainees Day
York
February 2019

Learning objectives
1. How to be a good physician
Learning objectives
1. How to be a good physician
– Being a good enough mother is to be a good
mother, whereas the attempt to be the best
will guarantee that you won’t be (indeed, you
may be a highly damaging mother). Similarly,
you should aim to be a good enough medical
student and doctor (Smith R. Thoughts for new medical students at a
new medical school. BMJ. 2003;327(7429):1430–3)
Learning objectives
1. How to be a good physician
– Being a good enough mother is to be a good
mother, whereas the attempt to be the best
will guarantee that you won’t be (indeed, you
may be a highly damaging mother). Similarly,
you should aim to be a good enough medical
student and doctor(Smith R. Thoughts for new medical students at a new
medical school. BMJ. 2003;327(7429):1430–3)
2. How to be a great physician?
A Recent Case
A Recent Case
Mr HT
Born Autumn 1931
Admitted to Renal Unit in Leeds for further
management
– 27 August 2016
Mr HT
Presented to local DGH 23 August 2016
Presenting Complaint– Gradual deterioration over last 1 week
– Not been eating/drinking; some diarrhoea
– Breathless
History of Presenting Complaint– Worsening over last 1-2 weeks; maybe some
haemoptysis
– Wife concerned – brought to A&E
Mr HT
Previous Medical History
– NIDDM
– AF
– Myasthenia Gravis (2013)
Mr HT
Drug history
– Prednisolone (alendronate)
– Furosemide
– Simvastatin
– Apixaban
– Omeprazole
– Metformin
– Lisagliptin
– Gliclazide
– Cyanocobalamin
Mr HT
Social History
– Lives alone with wife in ground floor flat
– Walks short distances with stick
– Previous comedian/entertainer till 4-5 yrs ago
Family History
– 2 healthy adult sons aged ~55
– Parents died aged 70-80ish of uncertain
cause
Systems Review
– Possible haemoptysis (pink-staining sputum)
– No epistaxis, joint pains, rash, conjunctivitis
Mr HT
On examination
– Pulse 106 SR; BP112/65; Resp rate 23;
apyrexial; O2 Saturation 99%; GCS 15
– JVP ; Dry oral mucosa; reduced skin turgor
– HS 1+2+0; Bipedal oedema to mid-thigh
– Crackles left base
– Soft non-tender abdomen
– Catheterised 100mls clear urine
Mr HT
Blood Gases
– pH 7.33
– pCO2 2.9
– pO2 10.2
– Bicarbonate 9
– Na 128
– K 6.4
– Cl 100
– Lac 3.1
– BE -12.6
– Blood glucose 9.0
Mr HT
Blood Gases
– pH 7.33
– pCO2 2.9
– pO2 10.2
– Bicarbonate 9
– Na 128
– K 6.4
– Cl 100
– Lac 3.1
– BE -12.6
– Blood glucose 9.0
What is the acid base
disturbance?
Mr HT
Blood Gases
– pH 7.33
– pCO2 2.9
– pO2 10.2
– Bicarbonate 9
– Na 128
– K 6.4
– Cl 100
– Lac 3.1
– BE -12.6
– Blood glucose 9.0
What is the acid base
disturbance?
– Partially compensated
metabolic acidosis
Mr HT
Blood Gases
– pH 7.33
– pCO2 2.9
– pO2 10.2
– Bicarbonate 9
– Na 128
– K 6.4
– Cl 100
– Lac 3.1
– BE -12.6
– Blood glucose 9.0
What is the acid base
disturbance?
– Partially compensated
metabolic acidosis
What is the anion gap?
Mr HT
Blood Gases
– pH 7.33
– pCO2 2.9
– pO2 10.2
– Bicarbonate 9
– Na 128
– K 6.4
– Cl 100
– Lac 3.1
– BE -12.6
– Blood glucose 9.0
What is the acid base
disturbance?
– Partially compensated
metabolic acidosis
What is the anion gap?
– (Na + K) – (Cl + Bic) =
– (128 + 6) – (100 + 9) =
– 25 ie elevated

Mr HT
Blood Gases
– pH 7.33
– pCO2 2.9
– pO2 10.2
– Bicarbonate 9
– Na 128
– K 6.4
– Cl 100
– Lac 3.1
– BE -12.6
– Blood glucose 9.0
What is the acid base
disturbance?
– Partially compensated
metabolic acidosis
What is the anion gap?
– (Na + K) – (Cl + Bic) =
– (128 + 6) – (100 + 9) =
– 25 ie elevated
What is the differential?
Mr HT
Blood Gases
– pH 7.33
– pCO2 2.9
– pO2 10.2
– Bicarbonate 9
– Na 128
– K 6.4
– Cl 100
– Lac 3.1
– BE -12.6
– Blood glucose 9.0
What is the acid base
disturbance?
– Partially compensated
metabolic acidosis
What is the anion gap?
– (Na + K) – (Cl + Bic) =
– (128 + 6) – (100 + 9) =
– 25 ie elevated
What is the differential?
– Multiple mnemonics
Poisonings, DKA, Lactic
acidosis, Renal failure
Mr HT
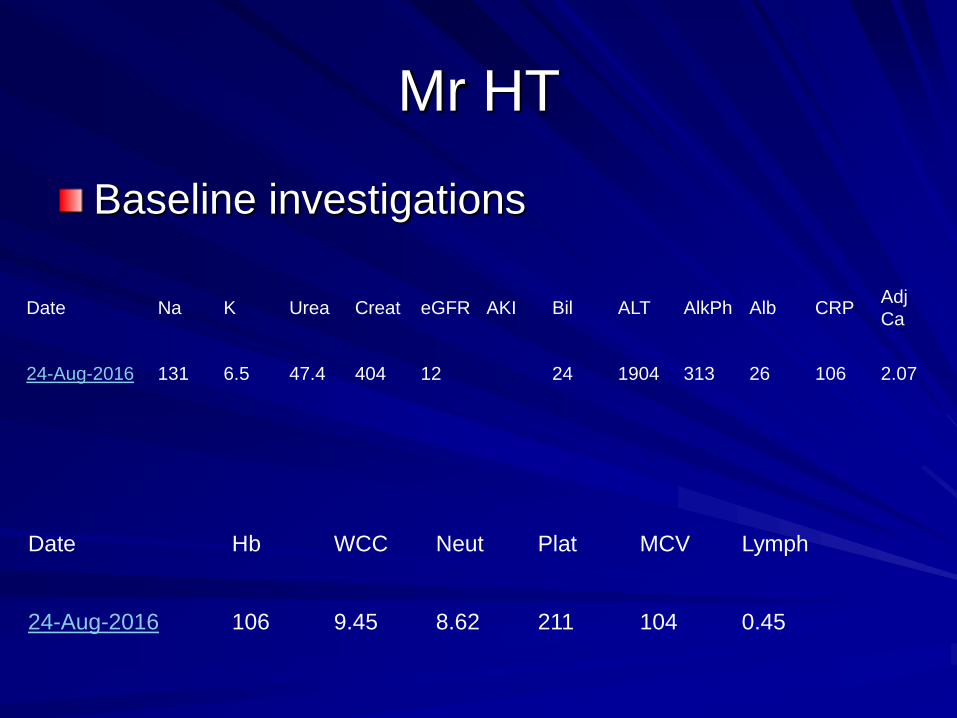
Baseline investigations
Date Na K Urea Creat eGFR AKI Bil ALT AlkPh Alb CRPAdj
Ca
24-Aug-2016 131 6.5 47.4 404 12 24 1904 313 26 106 2.07
Date Hb WCC Neut Plat MCV Lymph
24-Aug-2016 106 9.45 8.62 211 104 0.45

Mr HT
How would you proceed?
Mr HT
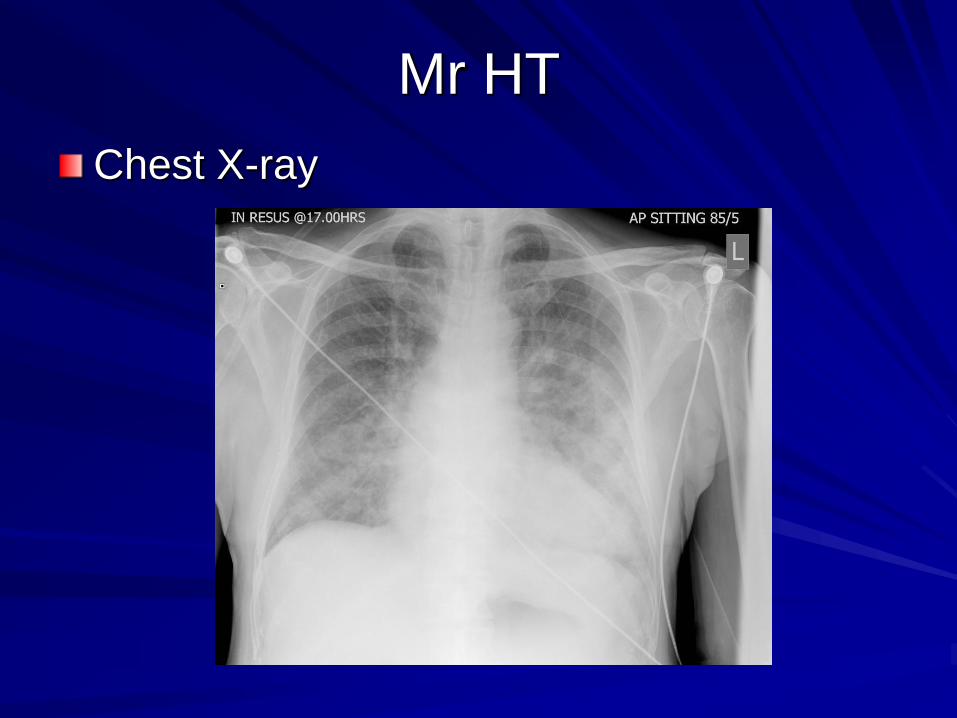
Chest X-ray
Mr HT
Ultrasound scan urinary tract
– “Normal size unobstructed kidneys;
catheterised bladder and ureters appear
normal; bladder indented by mildly enlarged
prostate”
Renal Screen
– Baseline assessment
Creatinine/eGFR/AKI score (plus historical results)
Urinalysis
BP
Nephrotoxins
Systemic symptoms
– ANCA
– ANA
– Complement
– Immunoglobulins and SEP (and BJP)
– Anti-GBM
How to be a good doctor
Very important to distinguish acute from
chronic renal failure
– Acute – try to reverse ASAP
– Chronic – prepare patient for long term RRT
Previous serum biochemistry
Ultrasound scan
– Renal size
Normal (10-12cm) – likely AKI (exceptions
amyloid, diabetes)
Small (up to 8cm) – likely CKD
Anything missing?

Mr HT
Progress and initial management
– Admitted
– Emergency K treatment
– Slow IVI
Contacted Critical Care Outreach and
Leeds Renal Unit

Mr HT
Progress
– No change in serum biochemistry
– Worsening respiratory distress pO2 5.4 (pO2
10.2 on admission; treated with oxygen)
Transferred Leeds Renal Unit

Mr HT
Arrived in Leeds 27 August 2016 (3-4 days
post admission)
Saturday of August Bank Holiday
Weekend
No additional tests available
Mr HTWhat should be done now?
– Observe until test results known?
– High Dose Prednisolone?
– Additional Cytotoxics/Biologics/Plasma
Exchange?
– Other care pathway?


Mr HT
At Leeds
Mr HT
At Leeds
Discovered
– DNACPR order in place
– ITU outreach had declined respiratory support
but had considered admission for CVVHF
Mr HT
At Leeds
Discovered
– DNACPR order in place
– ITU outreach had declined respiratory support
but had considered admission for CVVHF
– Echo had shown severe LVSD
Mr HT
At Leeds
Attempted dialysis
– Line inserted and attached to dialysis
machine
– Dropped BP and required saline resuscitation
– Whenever machine programmed to remove
fluid – same scenario
– After 2 hours dialysis ~ 100ml filtered
Mr HT
At Leeds
Further history now known to us
Further history taken (profoundly deaf)
Mr HT
At Leeds
Further history now known to us
Further history taken (profoundly deaf)
– Not left house for ~4-6 months
Mr HT
At Leeds
Further history now known to us
Further history taken (profoundly deaf)
– Not left house for ~4-6 months
– Needed help dressing & using bathroom for
same length of time
Mr HT
At Leeds
Further history now known to us
Further history taken (profoundly deaf)
– Not left house for ~4-6 months
– Needed help dressing & using bathroom for
same length of time
– 2-3 falls in house last few weeks
Mr HT
At Leeds
Further history now known to us
Further history taken (profoundly deaf)
– Not left house for ~4-6 months
– Needed help dressing & using bathroom for
same length of time
– 2-3 falls in house last few weeks
– Admission precipitated by wife unable to cope
and generally worried about him
Mr HT
At Leeds
Further history now known to us
Further history taken (profoundly deaf)
– Not left house for ~4-6 months
– Needed help dressing & using bathroom for
same length of time
– 2-3 falls in house last few weeks
– Admission precipitated by wife unable to cope
and generally worried about him
– eGFR 52, 39, 22 on GP bloods last 12 months
prior to presentation
Mr HT
At Leeds
No further dialysis attempted
Palliated and died in hospital 30 August
2016 (3 days later)
Mr HT
At Leeds
During discussions discovered
– Preferred place of care/death was home/local
hospice
– Wife unable to visit Leeds unaided, whereas
could attend local DGH or hospice within 15
minutes under own steam

Mr HT
Cause of death was Heart Failure
Probably every intervention following
hospital admission hastened his demise
and worsened his situation
How to be a good doctor

Anything missing?

Anything missing?

How to be a great doctor?
How to be a great doctor?
– …some new data!!
Dialysis and ITU
Dialysis and ITU
Unclear whether this was a case of
advanced CKD or AKI
For simplicity, let’s imagine AKI = ITU
admission and advanced CKD = chronic
dialysis programme
Dialysis and ITU
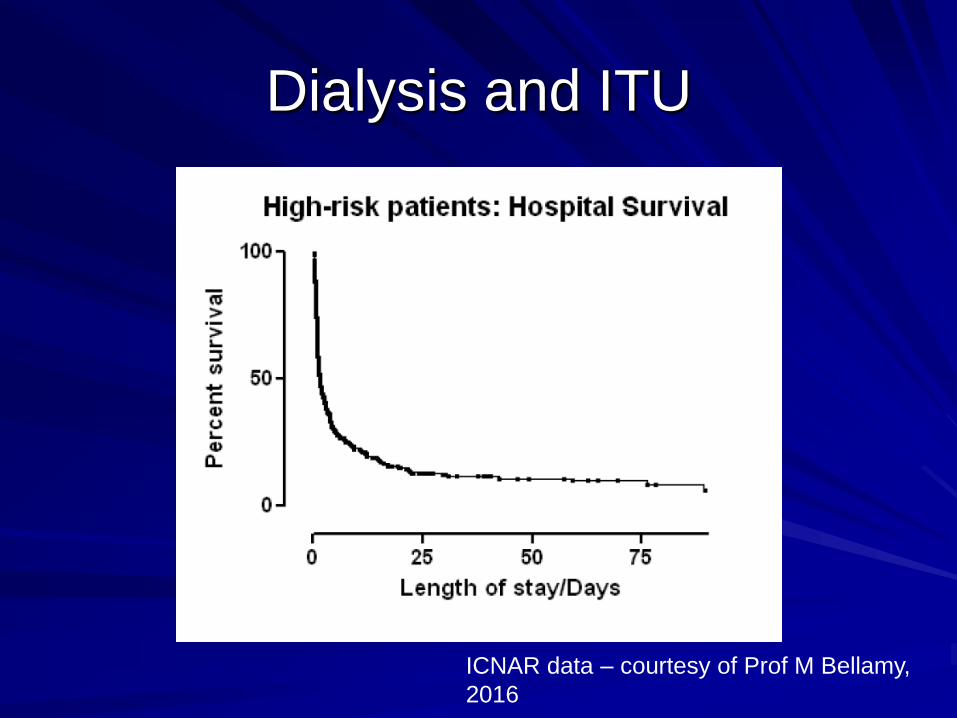
ICNAR data – courtesy of Prof M Bellamy,
2016
Dialysis and ITU
Dialysis and ITU
“Not for full ITU, but consideration of
CVVHF”

Dialysis and ITU
“Not for full ITU, but consideration of
CVVHF”
ITU is a bridging treatment; so is CVVHF
Dialysis and ITU
“Not for full ITU, but consideration of
CVVHF”
ITU is a bridging treatment; so is CVVHF
Something needs to improve for the
patient to move on to the next stage of
their treatment
Dialysis and ITU
What’s new in Renal Medicine?
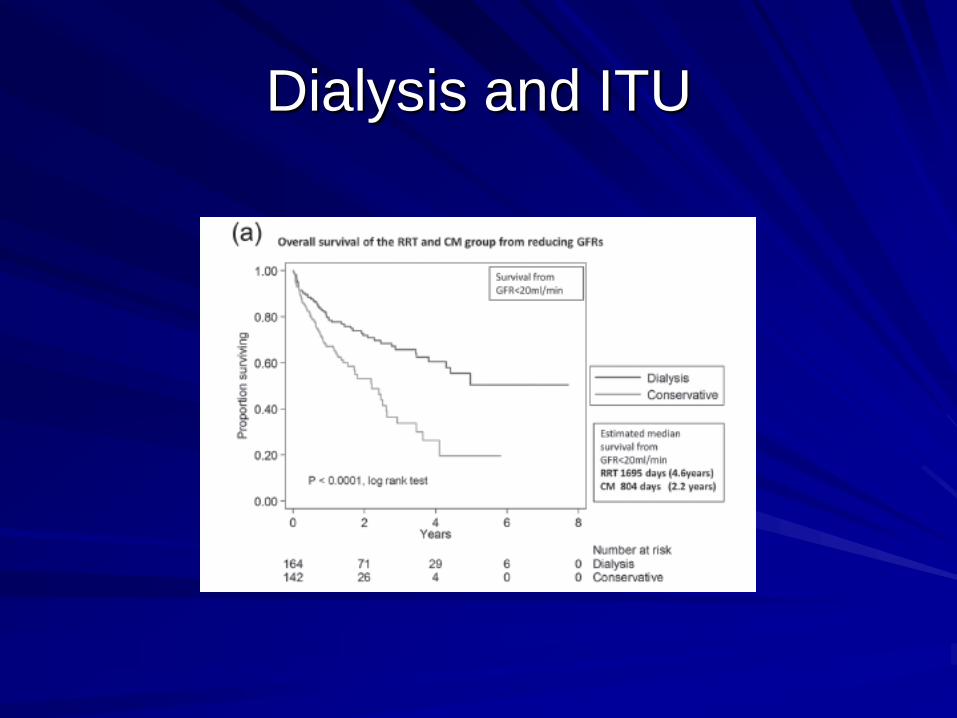
Dialysis and ITU
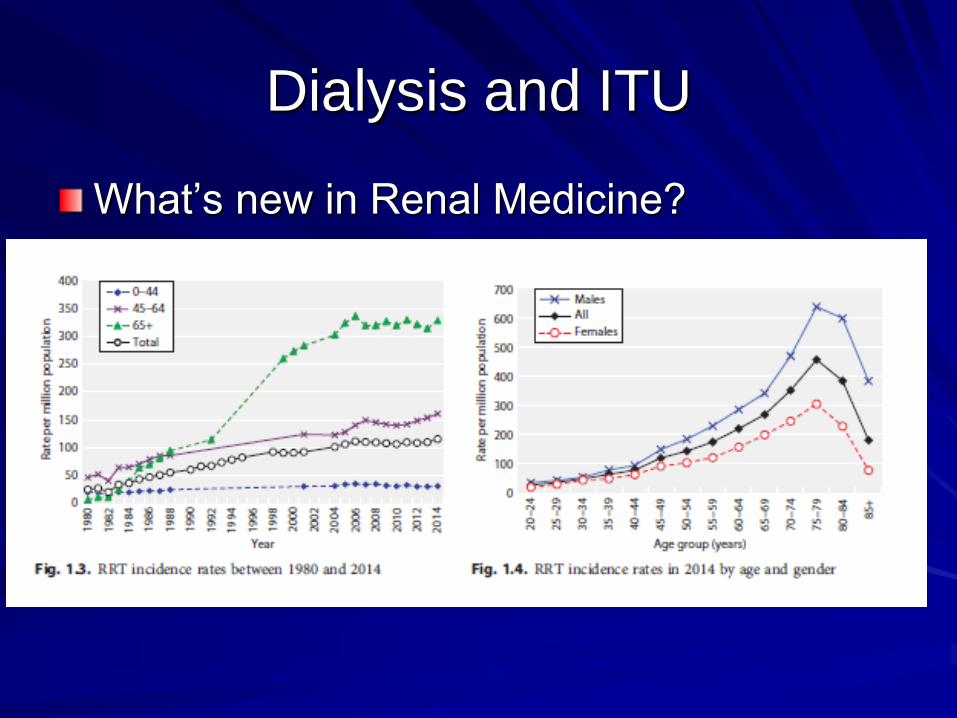
What’s new in Renal Medicine?
Dialysis and ITU
What’s new in Renal Medicine?
Dialysis and ITU
Dialysis and ITU
Dialysis and ITU
Dialysis and ITU
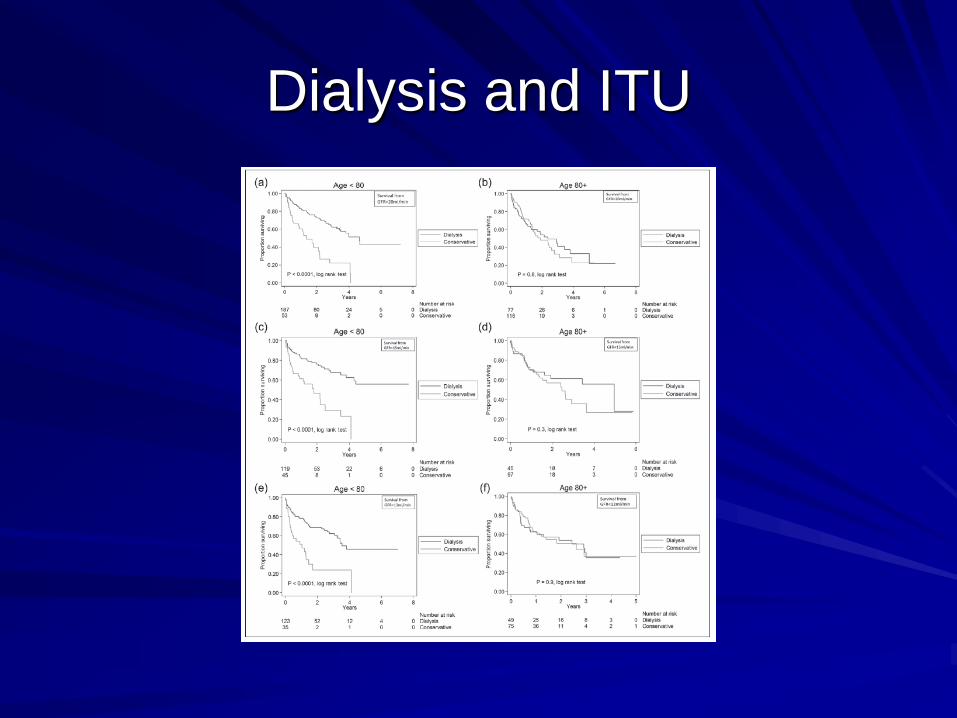
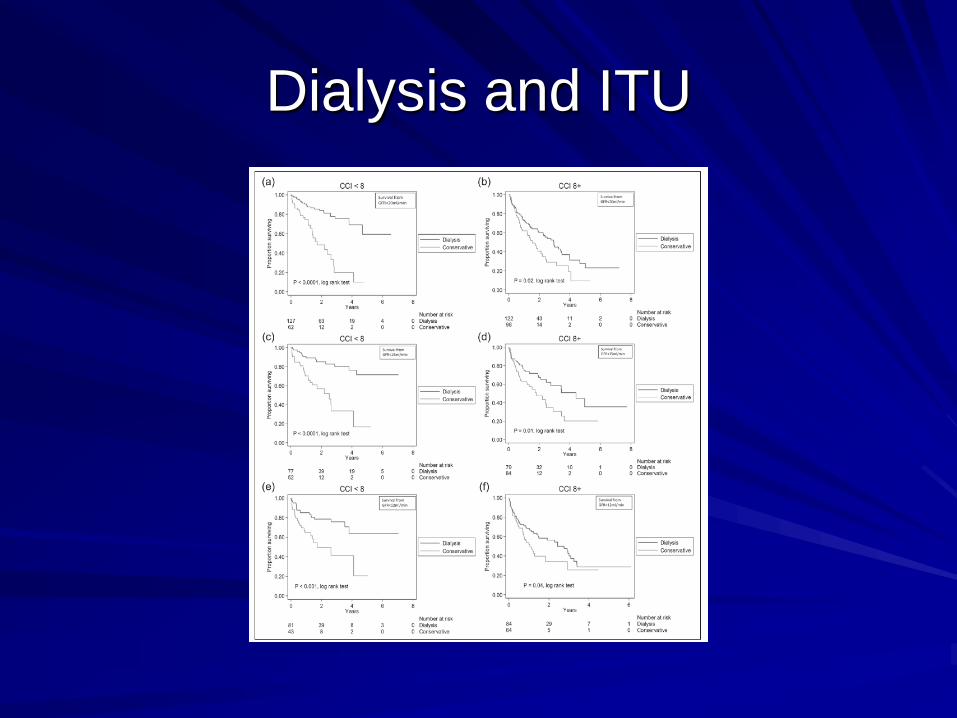
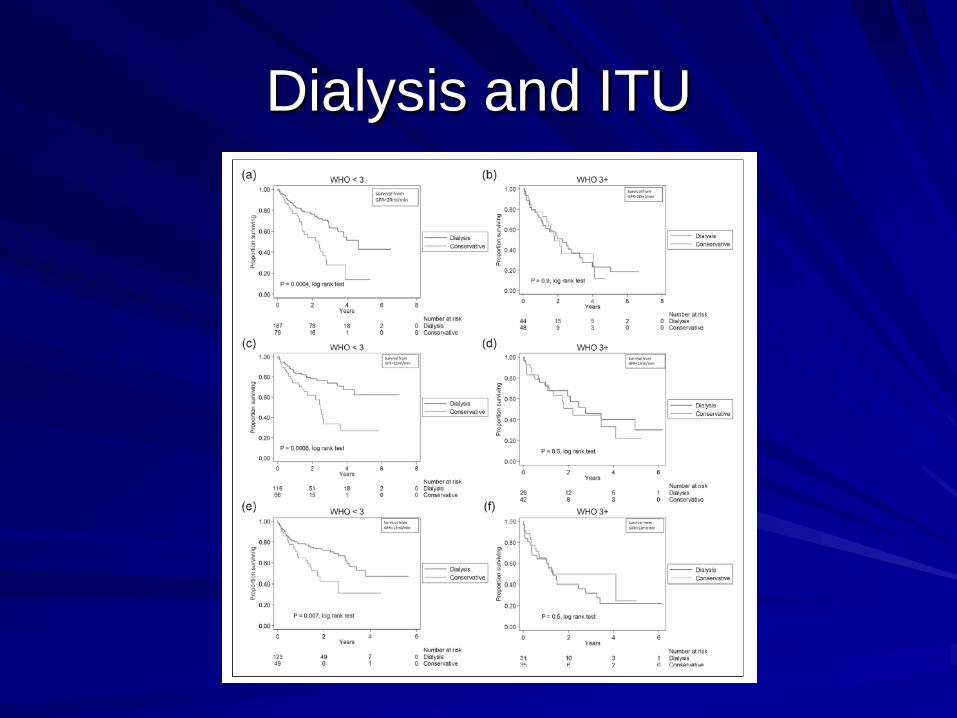
Assessing physical capacity to
withstand interventionsJust shown that choosing dialysis does not
necessarily provide increased survival if…
– Age>80
– Highly co-morbid (Charlson score ≥ 9)
– Dependent on others for ADL’s (WHO ≥ 3)
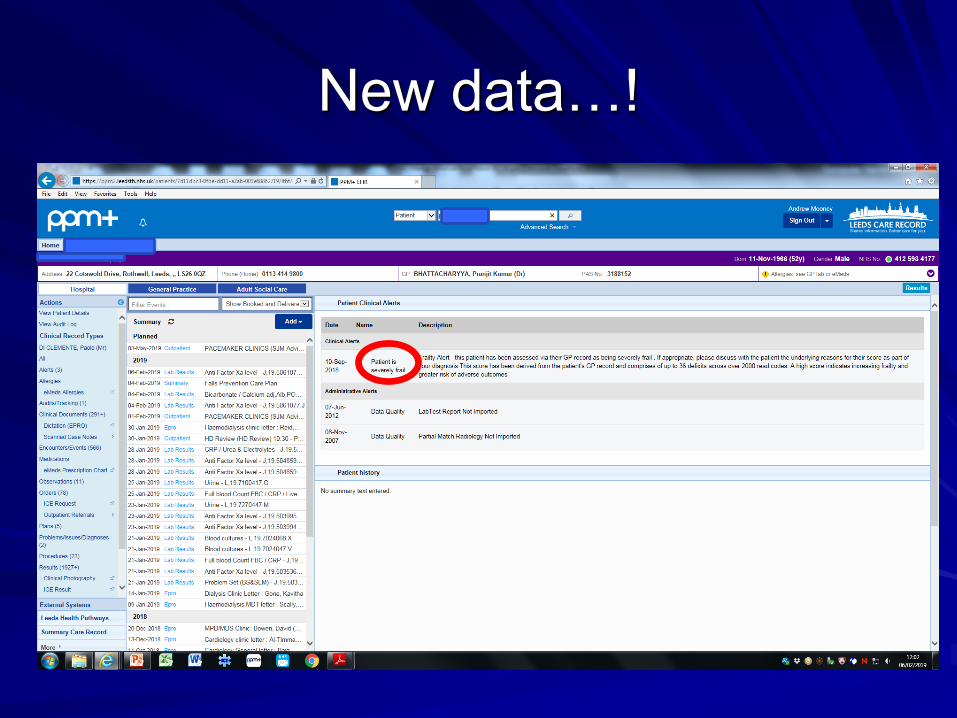
New data…!

New data…!
Frailty scores readily available by
calculation of number of deficits (maximum
36) calculated from >2000 GP read codes
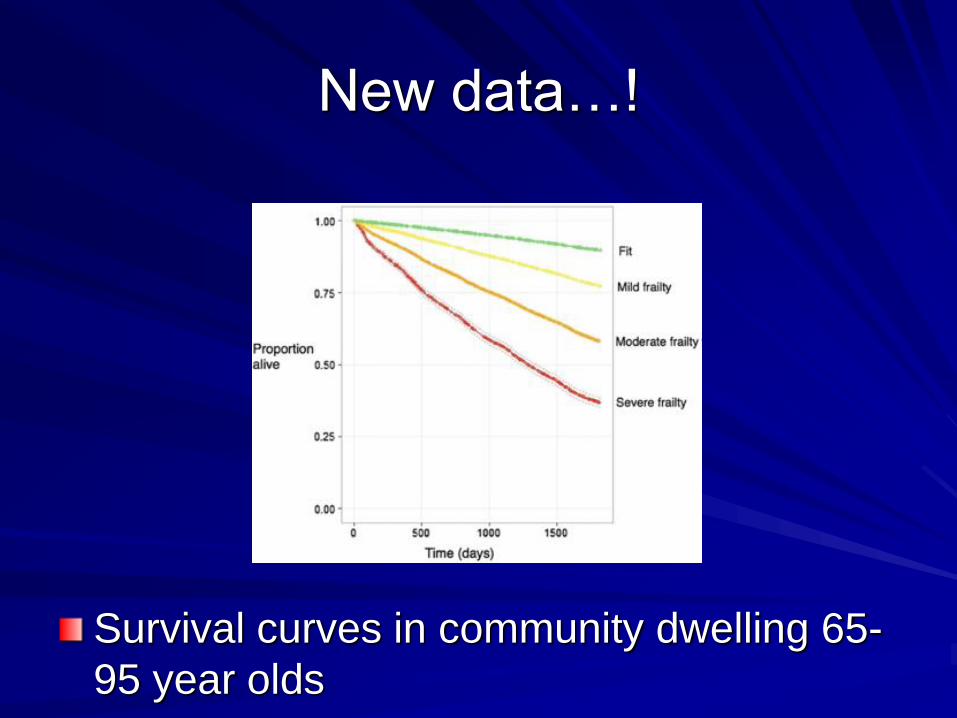
New data…!
Survival curves in community dwelling 65-
95 year olds
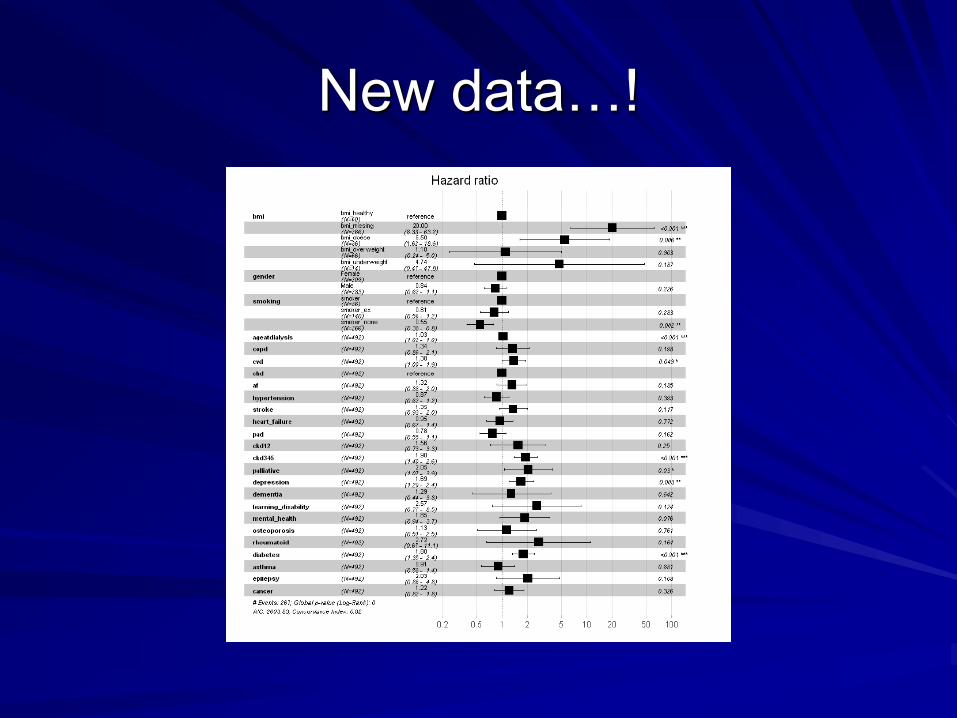
New data…!
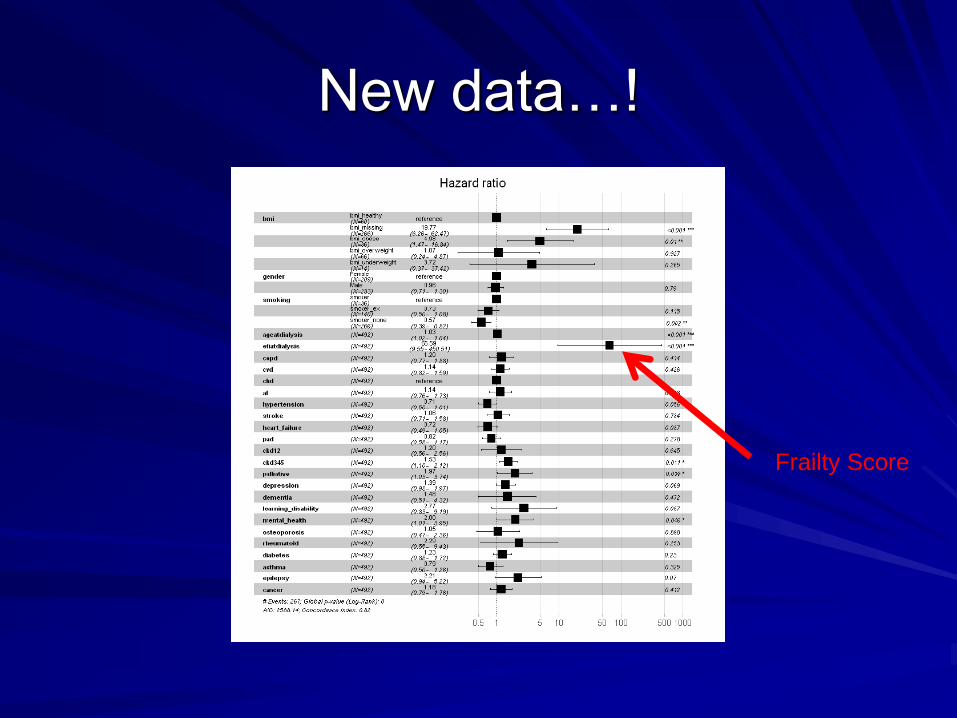
New data…!
Frailty Score
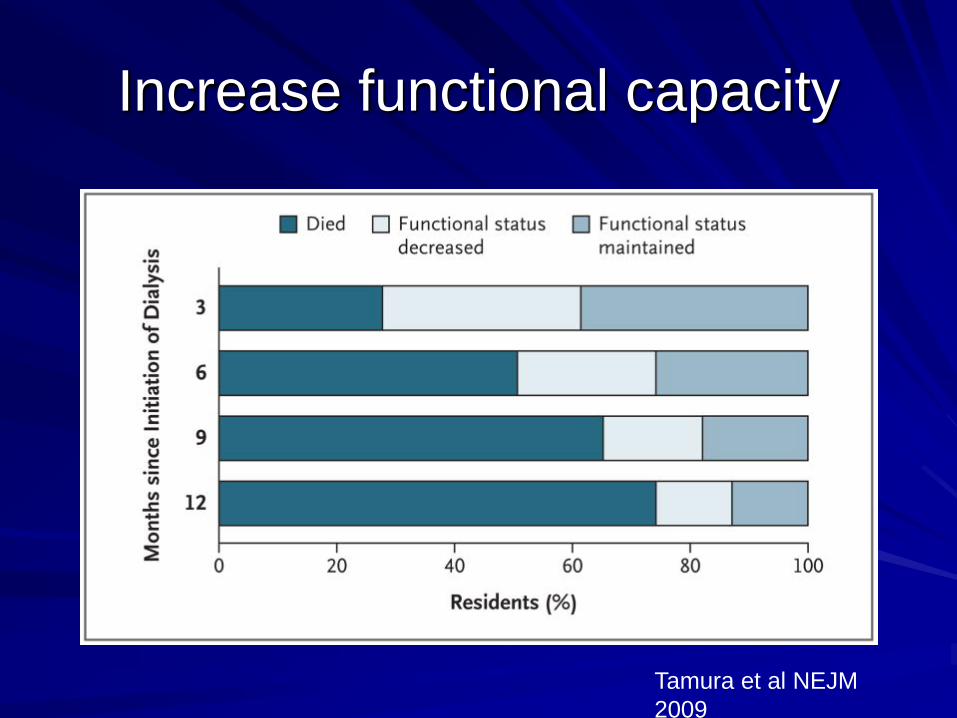
Increase functional capacity
Tamura et al NEJM
2009
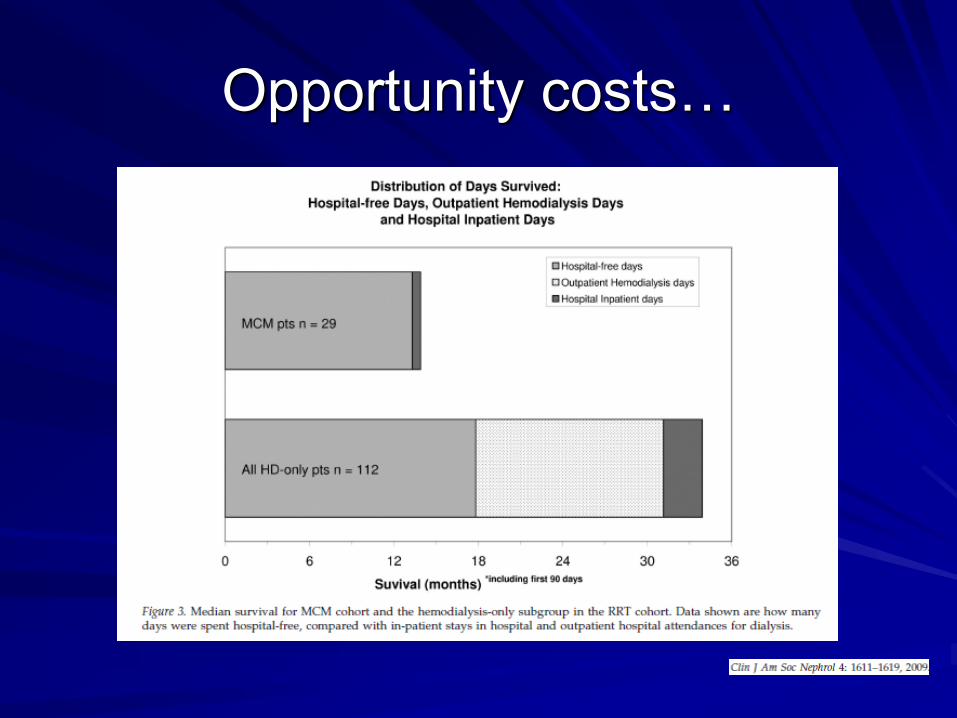
Opportunity costs…
Summary
Summary
AKI or Advanced CKD in young otherwise
completely healthy patients is generally
well recognised and well managed
Summary
AKI or Advanced CKD in young otherwise
completely healthy patients is generally
well recognised and well managed
AKI or advanced CKD in such
circumstances is rare…
Summary
Summary
AKI or advanced CKD is usually managed
in the setting of elderly, co-morbid, frail
patients of poor functional status
Summary
AKI or advanced CKD is usually managed
in the setting of elderly, co-morbid, frail
patients of poor functional status
Initiation of CVVHF, intensive care or
admission to the Chronic Dialysis
Programme should involve holistic
assessment of the patient
Summary
Intensive care support frequently fails to
lead to hospital discharge
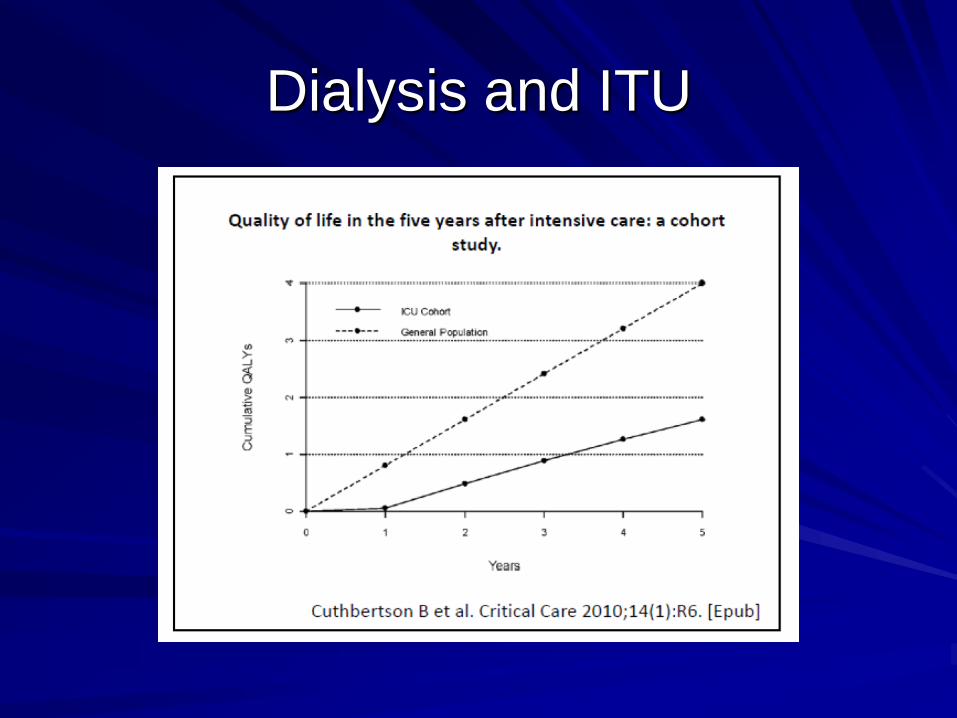
Even if discharged, it can take over 3
years to acquire 1 QALY
Summary
Intensive care support frequently fails to
lead to hospital discharge
Even if discharged, it can take over 3
years to acquire 1 QALY
It is unclear that dialysis enhances survival
if age>80, significant co-morbidity or
needing help with ADL’s (dressing,
cooking, going to the toilet, etc)

Learning points
Learning points
Mr HT was dying, but there were still
opportunities to make things better for him
Learning points
Mr HT was dying, but there were still
opportunities to make things better for him
All of us can put current results in context
and look up previous letters, test results
etc
Learning points
Mr HT was dying, but there were still
opportunities to make things better for him
All of us can put current results in context
and look up previous letters, test results
etc
All of us can ask whether patients can
dress/feed/toilet themselves
Learning points
This is not new
Learning points
William Osler FRCP (1849-1919)
– The good physician treats the disease – the
great physician treats the patient who has the
disease

Learning points
Maimonides (1135-1204)
– The physician should not treat the disease,
but the person suffering from it
Learning points
Hippocrates (~460-377 BC)
– It is more important to know what sort of
person has a disease than what sort of
disease a person has