Weekends influencing Process and Economic Results in a Swiss University Hospital in the Era of...
34
Weekends influencing Process and Economic Results in a Swiss University Hospital in the Era of SwissDRG Working Paper Christoph Napierala Address: 8320 Fehraltorf E-Mail: [email protected] Date: December 10, 2014
Transcript of Weekends influencing Process and Economic Results in a Swiss University Hospital in the Era of...
Weekends influencing Process andEconomic Results in a Swiss University
Hospital in the Era of SwissDRG
Working Paper
Christoph Napierala
Address: 8320 Fehraltorf
E-Mail: [email protected]
Date: December 10, 2014

Abstract
In current discussions hospital stakeholders seem to have a purely cost saving approach whentalking of result improvements in hospitals and generating saving at public health level.There is very little current evidence available on how diagnostics(Rechtzeitige Diagnosedank der Radiologie 2014) can influence hospital processes in order to be more efficient andthus also more profitable. One of the precariously researched areas is for example answersto how temporal aspects can influence the economic or clinical result dimension (Grootet al., 2012). One can encounter discussions on on how for example admission weekdayscan influence endpoint dimensions (e.g. mortality) for example in (Dismuke and Sena,1999) or (Aylin et al., 2013) but there is very little further evidence available. Howeverprior investigative research (Napierala and Koller, Stefan, 2014) provide indicative resultson how diagnostics might influence costs and benefits in hospitals. This working paperattempts to shed some light on these factors by driving findings ahead. The underlyinggeneral assumption remains that admission or intervention (i.e. in our case scan days)weekday influence a hospital’s economic results and largely drive average length of stay. Itthus is able to confirm the influence of radiology on both results through the analysis ofthe importance of weekdays and also how relevant it is (Woodcock, 2010).The evidence hereunder will, based on a large data sample a single university hospital,present on how single weekdays of either admittance or day of scanning patients withradiological modalities alter profitability of medical services in a hospital. The presentedresults will be developed in a threefold approach.
1. The case for action :The working paper which we will present deals with lingering assumptions that tempo-ral factors like weekdays have a significant influence on healthcare institutions successrate expressed by their profitability or their improvement in the average length ofstay.1 The latter is assuming that better ALOS ratios2 do also correspond to betterhospital management leading to improved results from a management’s and a finan-cial perspective. These assumptions are central to our approach. Other sources makeit clear that these questions have to be asked specially in Radiology practice. (ibid.).Implicitly this can mean that hospitals applying an active process management willhave to carry lower overall costs and be able to focus on improved health care deliveryquality. This last aspect is also relevant for the overall public health system.In order to proceed to the analysis our approach will start by describing the availabledata qualitatively. This will refine the research area and verify the validity of theunderlying hypothesis. Frequency tables and basic relational checks will lead to wayinto the deeper analysis in part two. We will be able to identify further potentialconfounding effects by our analysis which will be used in the model built within theparametric analysis. However we will mainly be able to display the need for deeperanalysis as there seems to prevail a relevant relationship between both admission daysand scan day (i.e. the diagnostic intervention day) on both the ALOS Ratio andthe economic benefit .3 This though is largely driven by the radiology departmentand confirms prior statements in that direction.(Dorio, 19, and 2011, 2014) Knowingthat alternative cost models(Klose and Bottcher, 2002) can potentially allow furtherinsights we have to restrain ourselves to a straightforward approach data availability
1From now on we will refer to the abbreviation ALOS or the full name without difference.2Our definition of the ALOS ratio corresponds to the referral ALOS (e.g. the SwissDRG catalog reference
value) divided by the effectively realized ALOS i.e. ALOSDRGiRatio = ALOSDRGCHi
/ALOSi3Within this context for simplicity of argument reasons and data availability we keep the profitability defini-
tion at a basic level by subtracting the total cost of a case of its DRG related revenue.
2

being the restricting factor. This relationship will be highlighted by graphical analysisas well as some contingency analysis. Furthermore it will be the initial part of analysisand validation for the model built in part two of the current paper.
2. Parametric Analysis :In this part of the work we will drive the parametric analysis further. Based on meancomparisons we then proceed to developing regression models that will focus on vari-ous approaches in estimating the influence of independent variables and highlightingpotential interdependencies amongst them. We will also present the issues with thedata and offer different approaches tackling them. Some of the work will be basedon the investigative first part of the document. A thorough estimation of factors andthe proof of their robustness as well as challenging the underlying assumption willrepresent the main part of this section of work. It will nonetheless provide a base forpolicy analysis in the closing section.
3

4

Contents
List of Tables 6
List of Figures 7
1 Introduction 8
2 Case for Action 82.1 Method . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
2.1.1 Data Description . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 92.1.2 Data Set Description . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
2.2 Intermediary Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
3 Parametric Analysis 183.1 Model Description . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 183.2 General Results on Outcome and Model . . . . . . . . . . . . . . . . . . . . . . 19
3.2.1 Model Results on Profitability . . . . . . . . . . . . . . . . . . . . . . . 203.2.2 Model Results on ALOS Ratio . . . . . . . . . . . . . . . . . . . . . . . 23
3.3 Issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 253.4 Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
Appendices 28
5

List of Tables
1 Distribution of Interventions (Scans) per Weekday and Modality . . . . . . . . 92 Gender Scanday of Week . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 103 Distribution of Interventions (Scans) per Weekday and Agegroup . . . . . . . . 104 Key Figures per Modality Group and Estimation of Degree of Complexity . . . 115 Age Ranges and Groups . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 126 Frequencies: ALOS Ratio Groups and Weekday of Admission . . . . . . . . . . 157 Weekday Scan, Weekday Admiss. and ALOR Ratio Group (Low vs. High) . . . 178 LR tests for hierachical log-linear model: Difference saturated and reduced model
- ALOS Ratio . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 179 Regression Results Positif vs. Negatif Profitability and Profitability in Percentage 2010 PseudoR2 - Profitability . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2111 Odds Ratios Saturated Model on Profitability . . . . . . . . . . . . . . . . . . . 2212 PseudoR2 - ALOS Ratio . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2413 Likelihood Comparison on Profitability: Saturated vs. Stripped Model . . . . . 2814 Chi Square - Profitability . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2815 Regression Results Larger than 1 vs. smaller than 1 ALOS Ratio in Percent . . 2916 Odds Ratios Saturated Model on LOS Compliance . . . . . . . . . . . . . . . . 3017 Likelihood Comparison on ALOS Ratio: Saturated vs. Stripped Model . . . . . 3018 Chi Square - ALOS Ratio . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3019 Regression Results Positif vs. Negatif Profitability and Profitability in Percent-
age MDC01 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3120 Odds Ratios Saturated Model on Profitability only MDC 01 . . . . . . . . . . . 3221 LR tests for hierachical log-linear model: Difference saturated and reduced model 32
6

List of Figures
1 Profitabiltiy and ALSO Ratio of Cases per Day of Week and Weekday - Admis-sion vs. Intervention (i.e. Scanday) . . . . . . . . . . . . . . . . . . . . . . . . 14
2 ALOS Groups per Day of Intervention (Scan) . . . . . . . . . . . . . . . . . . . 163 ALOS Groups per Day of Intervention (Scan) and per Weekday of Admission . 164 Profitabiltiy Group per Day of Intervention (Scan) and per Weekday of Admission 32
7

1 Introduction
In current discussions hospital stakeholders seem to have a purely cost saving approach whentalking of result improvements in hospitals and generating savings at public health level. Thereis very little current evidence available on how diagnostics(Rechtzeitige Diagnose dank derRadiologie 2014) can influence hospital processes in order to be more efficient and thus also moreprofitable. One of the precariously researched areas is for example answers to how temporalaspects can influence the economic or clinical result dimension (Groot et al., 2012). Onecan encounter discussions on on how for example admission weekdays can influence endpointdimensions (e.g. mortality) for example in (Dismuke and Sena, 1999) or (Aylin et al., 2013) butthere is very little further evidence available. However prior investigative research (Napieralaand Koller, Stefan, 2014) provide indicative results on how diagnostics might influence costsand benefits in hospitals.This working paper attempts to shed some light on these factors by driving findings ahead.The underlying general assumption remains that admission or intervention (i.e. in our casescan days) weekday influence a hospital’s economic results and largely drive average length ofstay. It thus is able to confirm the influence of radiology on both results through the analysisof the importance of weekdays and also how relevant it is (Woodcock, 2010).The evidence hereunder will, based on a large data sample a of a university hospital, presenton how single weekdays of either admittance or day of scanning patients with radiologicalmodalities alter profitability of medical services in a hospital and what the source of such adifference and leverage regarding hospital results can be.
2 Case for Action
The present article will increases the evidence base that admission and medical interventiondays of week largely influence economic and procedural outcomes in a modern led hospital (Jen,2012). The working paper compares radiology patients with regard to radiological assessmentand cost-effectiveness according to several influencing factors. A special focus has been laidupon their treatment (i.e. of the imaging procedure) and admission date and their influenceon economic results in a Swiss hospital. Our underlying assumption is that key factors (e.g.admission, scan days and their respective difference) have an substantial influence on hospitalresults. Furthermore, they can indicate that their active management improve the situationof such a healthcare provider. This would also help to support existing evidence (Sorenson,Drummond, and Bhuiyan-Khan, 2013) in clarifying reproaches that medical technology (e.g.imaging diagnostics) does not represent a cost driver for a health system overall. Even on thecontrary that they help saving resources and increasing clinical quality.We will see in the firstpart how the different factors potentially interact and what drives that influence. Above allwe will see that further investigations are required in order to add validity to the assumedrelationships.
8

2.1 Method
2.1.1 Data Description
The data used for this study contains on one hand the full so called ”BFS-Dataset”4 and on theother side more detailed Radiology Information System (RIS) data as well as cost accountingexcerpts. he have gathered case cost data and can therefore calculate results per case accordingto the overall cost or at any available cost dimension (i.e. per cost type). This data mergeallows a detailed analysis of intervention i.e. diagnostic data and cost and revenue data. Theavailable data all fall into the year 2013 and we can therefore assume only a minimal influenceby the DRG implementation of the prior year.The analyzed RIS data contained 38’198 examinations corresponding to 14’870 DRG casesoverall thus we do exclude all outpatients from our considerations. In order to eliminateobvious errors or cases that appeared to be implausible from a revenue and a cost perspectivewe eliminated cases where the difference between the admission day and the first scan daywas above 10 days. This assumption is sound as some mis-registration within the RIS systemseems plausible and also includes double registration due to process imprecisions. Furthermorewe excluded cases in which the scan sequence resulted in implausible or error cases. All thisdata sanitation leads to an overall number of cases in scope of 11’432. In table 1 we can alsosee the distribution of the interventions per modality i.e. per specific intervention room.5 Itis obvious that some modalities have an uneven weekly distribution. Weekends display theintuitively expected drops in interventions especially for Magnetic Resonance Imaging (MRI),Sonographie and conventional radiography services. This also stems from the fact that theelective interventions mainly take place during the working week i.e. weekdays (Mon-Fri).However we assume that the numbers are sufficiently well distributed for our further analysis.
Looking at the intensity of examinations per day during the week we however have to takeinto account the slow-down of examinations during the weekend (see table 1) in all modalitiesexcept for the Emgergency Intervention Modality (UNF) modality category (where we conven-tional radiography is predominant) where there is a steady patient flow all through the week.Generally we assume that examinations for MRI, Computer Tomography (CT), Sonographyand Ultrasound (SON) are more complex than Conventional Radiography (KR). This assump-tion entails that the latter is used in clinically more evident cases confirming diagnosis wherethe earlier ones are oftentimes used in a more investigative context. Thus we will categorizemodalities accordingly.
Scanday Mon Tue Wed Thu Fri Sat SunMRI 348 390 353 291 293 120 23SON 110 143 112 141 134 33 28
CT 424 475 465 440 448 220 207KR 866 827 723 713 632 93 71
UNF 343 323 352 314 315 347 315
Table 1: Distribution of Interventions (Scans) per Weekday and Modality4These data represent the full hospital case load that has to be delivered to the Swiss Casemix Of-
fice(SwissDRG AG). For further explanations refer to the respective publicly available information.5The abbreviation are indicated in the respective section of this paper.
9

The above assumption is validated looking for example at the distributions of interventionsfocusing on gender table 2 or at the age group in table 3. We do also have an evenly spreaddistribution of gender in our data despite a slightly larger number of men in our study popu-lation.
Scanday Mon Tue Wed Thu Fri Sat SunM 1098 1104 1056 1008 913 426 325F 993 1054 949 891 909 387 319
Table 2: Gender Scanday of Week
One can also see that there is a small number of interventions in the age group 11 to 20 this isdue to the clear patient group split as young patients are treated in the neighboring pediatrichospital.
Scanday Mon Tue Wed Thu Fri Sat Sun11-20yrs 23 27 27 21 23 13 1021-35yrs 142 140 147 139 127 61 4336-55yrs 391 407 361 368 356 142 9156-65yrs 370 358 339 319 292 129 7666-80yrs 725 763 692 653 613 241 23281+ yrs 440 463 439 399 411 227 192
Table 3: Distribution of Interventions (Scans) per Weekday and Agegroup
A really interesting perspective is provided when dividing the single modalities up into whatwe would call complexity groups. We grouped the investigation data pulled from the RIS intoan identifier which provides us with the sequence of diagnostic investigations. That means wecombine the respective modalities into groups. We have coded it in the following way:
1. Separation in Complex and Single: In a this step a simple categorization into cases ofassumed case complexity through modality use has been realized. All cases having hadmore than two conventional radiographies, more than one CT, or more than any otherintervention are considered to be complex (11090 cases). The remaining 3780 cases arebeing considered to be simple cases.
2. Category Build: In a next step, complexity categories were built. We have divided thecomplex cases into three types: LC Low Complexity; MC Medium Complexity; HC HighComplexity. LC are cases where only one scan has been applied. MC are cases up to twodifferent diagnostic interventions. The highly complex cases are the ones beyond threeinvestigations and beyond. The category also indicates the principal modality that hasbeen used. We can see that a majority of imaging activities is done in the Low Complexitycategory.
For more detail please refer to table 4 where the most important performance factors percategory are provided. Hence we can see apparent differences that hint at a worthy investigationwhich will follow in the chapters below.
10

cat
coun
tP
rof.
SDP
rof.
CM
IC
MI
SDA
LOSR
atio
SDA
LOSR
atio
ALO
SSD
ALO
SC
ost
per
Day
SDC
pDR
even
uepe
rD
aySD
RpD
HC
UK
R27
-0.4
70.
754.
072.
530.
810.
4021
.37
17.0
931
75.5
712
58.7
927
99.5
319
59.7
4LC
UK
RSi
ngle
1977
-0.0
20.
391.
471.
161.
571.
316.
444.
7137
53.6
243
02.1
141
74.7
047
78.5
1LC
MR
I17
48-0
.06
0.46
1.18
1.11
1.94
1.74
6.80
5.59
2742
.78
1915
.11
3019
.94
2406
.21
LCU
KR
1473
-0.0
90.
452.
041.
501.
250.
999.
355.
2230
04.9
921
84.6
131
70.3
225
77.6
1LC
SON
647
-0.1
40.
491.
090.
841.
681.
567.
706.
2622
74.5
018
02.5
222
88.4
618
77.7
7LC
UC
T24
12-0
.13
0.54
1.19
1.17
2.21
2.08
6.49
6.14
3114
.75
2534
.01
3214
.26
2851
.57
LCU
NFS
ingl
e12
26-0
.02
0.42
0.91
1.04
3.01
2.50
4.93
5.26
2742
.64
2481
.70
2984
.14
2882
.56
MC
UK
R42
9-0
.14
0.46
3.16
2.10
1.05
0.53
11.8
05.
9134
23.0
419
09.8
735
10.5
622
79.1
7LC
UN
F81
2-0
.15
0.52
1.43
1.63
2.35
2.28
7.16
6.48
3151
.54
3165
.34
3129
.70
3108
.91
MC
MR
I55
-0.2
30.
542.
291.
511.
110.
7713
.25
7.96
3343
.68
2576
.78
3304
.38
3016
.79
MC
SON
47-0
.36
0.63
2.62
2.40
1.29
0.99
12.4
78.
2742
77.3
254
22.3
936
55.1
447
68.6
0M
CU
CT
168
-0.2
60.
673.
152.
871.
441.
4012
.17
8.74
3913
.27
3026
.81
3827
.85
3234
.27
HC
MR
I5
-0.5
50.
436.
533.
380.
850.
4129
.40
10.6
035
39.4
210
96.4
724
78.7
611
70.3
3H
CU
CT
48-0
.27
0.65
6.39
3.54
1.03
0.64
22.4
012
.23
4538
.58
4127
.20
4403
.76
4805
.19
MC
UN
F20
9-0
.18
0.55
2.36
1.75
1.49
1.52
10.9
27.
1435
81.6
031
44.4
934
89.4
933
69.9
6LC
UC
TSi
ngle
12-0
.09
0.36
0.40
0.28
5.00
2.82
3.17
4.65
2500
.91
1277
.65
2439
.64
1056
.12
HC
UN
F30
-0.5
50.
774.
573.
361.
131.
5324
.93
18.8
337
74.5
134
42.4
835
24.4
741
36.3
5H
CSO
N4
-0.1
20.
274.
753.
150.
660.
4323
.25
7.41
3954
.58
3113
.04
3729
.26
3228
.51
Tabl
e4:
Key
Figu
res
per
Mod
ality
Gro
upan
dEs
timat
ion
ofD
egre
eof
Com
plex
ity
11

The most important used outcome indicators and variable definition shall be described herebelow in order to understand further analytical steps.
1. ALOS Ratio: This factor is used throughout our analysis as a measure of efficiencywithin a hospital. Altneratively Lenght of Stay (LOS) Compliance is being used toexplain this ratio. That links the effective length of stay per case to a benchmark value.Thus it indicates whether the institutions is better or worse off than the benchmark in ourcase the ALOS catalog value of the Case Mix Office (CMO). It is calculated as follows:ALOSDRGiRatio = ALOSDRGCHi
/ALOSi.ALOS Ratio groups have been implemented according to the following limits: 0.5, 0.75,1, 1.25, 1.5, 1.75, 2.Our basic assumption is that the higher the ratio the better it is from several perspectives.At first it is a sign of good process management within the hospital as they run theircases better than the national benchmark. On the other side it is relevant with respectto an overall health care production function. One can assume that the better the ratiois the more economical overall patients are being treated and thus enhancing the overallpublic health situation by being more efficient and spending less resources on the samehealth care service.
2. Profitability:def:prof In our analysis we use different perspectives of it. If not otherwisestated we use it as economic result per case indicated as percentage i.e. proportion ap-plying the formula Profitability(RentProz) = 1 −CostDRGi /RevenueDRGi . We hereassume a full cost approach. That means we have included all operative costs and de-preciation cost in it. Furthermore it needs to be underlined that the revenues are purelyDRG revenues thus additional income (e.g. privately insured patients additional fees orcomplexity fees acording to the DRG catalog) has not been taken into account. This leadsto the substantial part of negative profitabilities as no additional turnover like privatepatient fees or lump sum payments have been taken into account. For the sake of ouranalysis this is should not be of relevance. However it might distort the hospital’s generaleconomic overview should one not take this in consideration.Profitability categories have been introduced in order en ease the further analysis. Therespective thresholds have been set as follows: -0.75, -0.5, -0.25, -0.1, 0 , 0.1, 0.25, 0.5
3. Age groups: The following groups have been implemented in order to cluster age intoconvenient dimensions. It can be seen that the age distribution in the present data focuseson the expected age groups. We will in the further analysis enhance the argument andsee what influence on the various outcomes it has and at what degree.
Range Number0-9 Kids 010-20 Teenagers 14421-35 Young 79936-55 Adult 211656-65 Seniors 188366-80 Elderly 391981-139 Old 2571
Table 5: Age Ranges and Groups
12

4. Radiological Complexity Groups: In order to reflect the clinical complexity andin our case the sequence of radiological interventions we have divided these in threemajor groups. LC as reference dummy in regressions contains single use of a modalitywithout further investigation e.g. one conventional radiography. MC are more complexsequences of investigations involving one or two modalities e.g. one use of CT and oneor more subsequent use of further installations like conventional radiography, MRI, CTor US. The highest category(HC) contains all cases that had three or more radiologicalinvestigations.
5. Case Mix Index (CMI) This index indicates the average case weight per case andindicates the severity of the case. Multiplied by the prevailing baserate it provides therevenue per case.
6. Weekdays vs. Weekends: In our analysis we use weekday as being day Monday toFriday (i.e. day 1−5) 6) representing the working days of the week. Weekends are self-explanatory.
7. Day Difference: One of the factors that presumably influences all outcomes is theduration between the patient’s admission day and the intervention day (i.e. Scanday).The following categories with the respective thresholds have been set: ”0-2”, ”3-4”, ”5”,”6-7”, ”8-10”. Thus we assume that interventions that are have a bigger difference thanten days are not taken into consideration. As mentioned above there are no young patientspresent in the hospital as they are being treated in the pediatric ward of the childrenhospital nearby.
For more detail please refer to for example table ?? where the most important performancefactors per radiology category are provided. Hence we can see apparent differences that hintat a worthy investigation which will follow in the chapters below.
2.1.2 Data Set Description
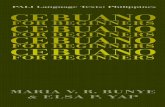
The base dataset comprised a total of 38’198 inpatient patients underwent radiological inter-ventions at a Swiss university hospital and remained at for at least one night thus were classifiedas inpatients being financed through DRG. Our dimensions of interest are the split of the in-terventions according to their occurrence. What we distinguish in first step are the weekdaysof admission and intervention. We then also introduce their differentiation into week-ends andweek-days i.e. working days. Figure 1 visually describes the difference in Profitability andALOS Ratio per daily dimension.In the top left corner the respective combination of day types is shown for the ALOS Ratio. Itappears to make a difference whether patients are being scanned on a working day and be ad-mitted on a week-end vice versa. It is also apparent that the spread of the combinations differsas well as the deviation to the mean. The dotted line highlights the mean of the ratio over allgroups. The figure in the top right corner follows the same idea simply splitting by single days.Here the image is not that clear any longer. There seems to exist a clear difference between
6using the variables WDScan (corresponding to the working day of the radiological intervention = scanday)or WDAdm for the working day where the admission has taken place
13

the beginning of the week for the admissions with a scan on a weekend (0.0 and 0.1) boththose categories lie above the mean. Hence these cases are being dealt with a higher efficacy astheir compliance to the benchmark seems to be better. This finding is quite intuitive. On thecontrary are the cases with the scan on a working day (1.0 and 1.1). The mean of both is belowthe average mean. The case where the scan and the admission both take place on a workingday (1.1) the mean goes in line with the average. But the (1.0) cases are quite below showingfactually a low ratio. This can be interpreted as a low process quality overall that leads to alower compliance ratio.The chart on the top right shows the same relationship simply display-ing the single admission days of the week and if the intervention has taken place on a workingday or not. Understanding these relationships appear to be paramount to improve, at least inparts, how processes are being run i.e. to improve such a ratio at least towards the benchmarkvalue. We have also to take care that the means of (1.1 and 0.1) only lie within the confidenceintervals depicted by the mean running through the notches of the boxplots. Nevertheless, ithas to be seen later on whether these differences are really significantly different.The lower pair of charts show the same relationships using profitability in percent instead.Yet the correlation is not as obvious. Profitability performs slightly better on day types (0.1and 1.1). Though only the mean of (1.1) is above the C.I. and thus indicating at a significantdifference. But generally we can only indicates that the admission on a working day is moreprofitable. The only cases below mean appear to be the (0.0) even so the general mean runningthrough the notch points at an insignificant relationship. So, in general the picture regardingprofitability is more blurred when the scan days are also taken into account. We have to seefurther what the parametric analysis will produce.Based on the described plots one can suspect certain interdependencies and correlations be-tween the working or week-end days of scans and admissions on both outcome factors. Therelation seems to be more distinct looking at the ALOS Ratio than at profitability.
0.0 1.0 0.1 1.1
01
23
4
ALOS Ratio Weekday Scan vs. Admiss.
WD Scan vs. WD Admiss.
ALOS
Rati
o
1.0 3.0 5.0 7.0 2.1 4.1 6.1
01
23
4
ALOS Ratio Weekday Admiss. vs. Scan(wo1
Admiss.Week.vs.WD Scan
ALOS
Rati
o
0.0 1.0 0.1 1.1
−0.4
−0.2
0.00.2
0.4
Prof. Weekday Scan vs. Admiss.
WD Scan vs. WD Admiss.
Prof
%
1.0 3.0 5.0 7.0 2.1 4.1 6.1
−0.4
−0.2
0.00.2
0.4
Prof. Weekday Admiss. vs. Scan
Admiss.Week.vs.WD Scan
Prof
%
Figure 1: Profitabiltiy and ALSO Ratio of Cases per Day of Week and Weekday - Admissionvs. Intervention (i.e. Scanday)
14

Interestingly we can further learn about the influencing or confounding factor applying a con-tingency tables to the same data and looking at the pairwise comparison of factor occurrence.
ALOS Ratio vs. ALOS Ratio Groups in Percentage RangesWeekday Admiss. 0-0.5 0.5-0.75 0.75-1 1-1.25 1.25-1.5 1.5-1.75 1.75-2 >2 Total
Mon 141 310 335 430 180 144 101 637 2278Tue 174 307 339 374 175 135 73 576 2153
Wed 129 302 294 356 175 121 55 479 1911Thu 137 255 252 285 161 99 68 447 1704
Fri 112 181 232 220 106 66 41 351 1309Sat 68 118 158 128 71 54 40 255 892Sun 66 150 203 166 87 60 38 312 1082
Total 827 1623 1813 1959 955 679 416 3057
Table 6: Frequencies: ALOS Ratio Groups and Weekday of Admission
The table shows the distribution of groups among admission days. So far the number donot show anything different to the findings described from the above figures. Although oneobservation needs take place and that is the large number of cases that are have a ratio above2. Meaning those cases are twice as good as the benchmark. What does drive such a numberof cases leading the distribution of the compliance ratios to be skewed to the right. Clinicallythose cases can make case and the concerned DRG groups distinct. But it can also be thatthe hospital manages these cases especially good. There are elective orthopedic examples (e.g.I75B, I77Z) that are being dealt with much more effectively than the benchmark assumes.That has two effects these cases overall lead to a more than satisfactory ALOS compliance butmost probably also on profitability. Only that it is not clear at what degree. We will look intothat at later stage of the investigation.The next step will further enhance the evidence for the significance of our hypothesis. We willprogress by highlighting the relevance of the intervention day on the result dimensions.
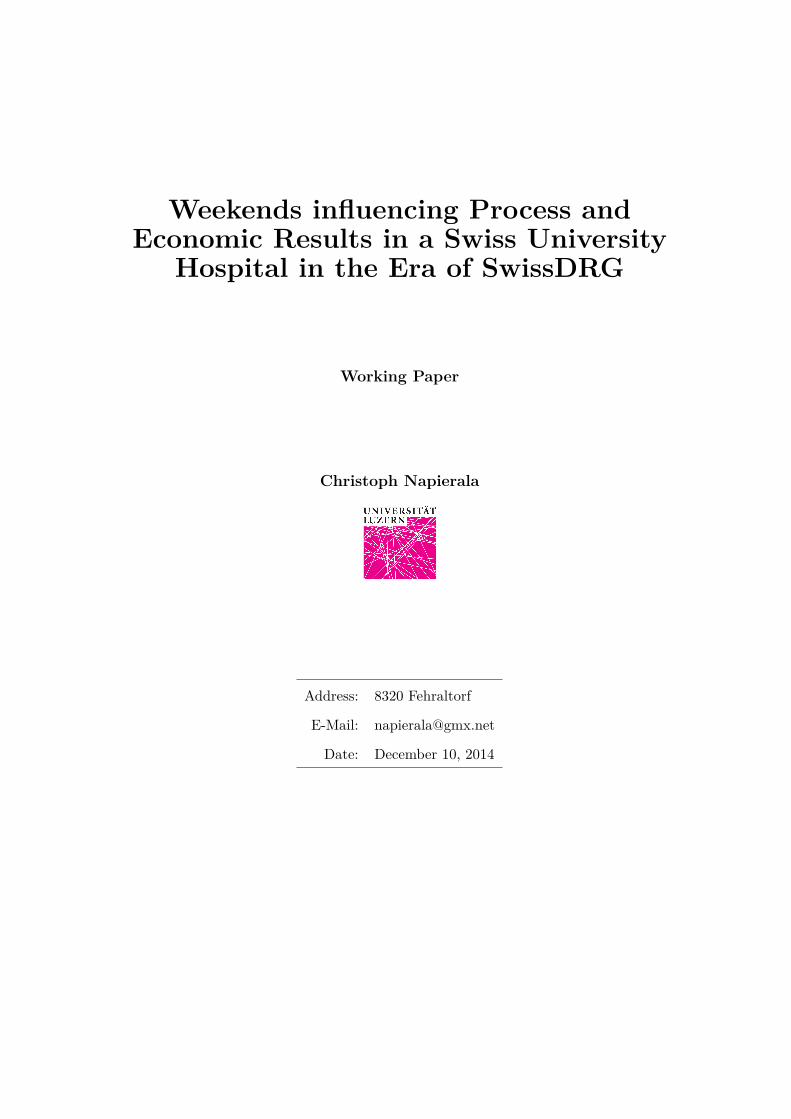
The hereunder mosaicplot in figure 2 shows that there is only little interaction on each weekdayand per ALOS Ratio group. This underlines the above findings and also indicates that aconfounding factor like the scan day can influence the relationship.
Only the lower groups seem to be positively correlated (blue colored) with Saturdays whereasthey seem to drive negatively the higher groups (red colored). But in general there seemsnot to be any strong influence on the ratio by the intervention day. However introducing theadmission day (split in week-end or week-days) appears to influence the results. Figure 3 putsthis into display and one can see a much different picture further explaining the commentsmade above using the boxplots describing the relationships.
6For further detail please refer to the R graphics package. Where need be the results are commented.
15

−2.1−2.0
0.0
2.0
2.3
Pearsonresiduals:
p−value =0.005
ALOS Ratio
Admis
s.Day
0−0.5
76
54
32
1
0.5−0.75 0.75−1 1−1.25 1.25−1.51.5−1.751.75−2 >2
Figure 2: ALOS Groups per Day of Intervention (Scan)
The graph shows the dependency of the admission and scan day. It furthermore also showsthat if the he admission and intervention day differ they influence the ALOS Ratio group theyfall in. There appears to be a strong relationship if the scanday falls onto a Saturday (day 6)or a Sunday (day 7) and the day of admission (either weekend or weekday) drives the ALOSRatio group.
−13
−4
−2
0
2
4
33
Pearsonresiduals:
p−value =<2e−16
VWDPos
Adm. Weekday
Scan
day
Low
7
0 1
65
43
21
High
0 1
Figure 3: ALOS Groups per Day of Intervention (Scan) and per Weekday of Admission
One of the advantages using the mosaicplot representation is that is allows for displaying theintersection of three categorical variables(see: Larson-Hall, 2009, p.146). The shading indicatesthat the trend in a specific box is large enough to expect statistical differences from the nullhypothesis that the variables are dependent.The above analysis can simply be represented in a loglinear model. Our model using threevariables can be denoted as follows in Field, 2012, p.835ff.:
outcomeijk = (b0 ++b1Ai + b2Bj + b3Ck + b4ABij + b5ACik + b6BCjk + b7ABCijk)+ εij) (1)
Where A corresponds to the ALOS Ratio group (ALOS Ratio), B to the intervention day
16

(WD Scan i.e. scanday), and C to the weekend or week-day of admission (WD Admiss.).The distribution of cases is give in the below contingency table 7 :
ALOS Ratio Weekend Admiss. Weekday Admiss.per Weekday Low High Low High
Mo 143 288 638 999Tu 130 125 679 1209We 91 77 679 1145Th 84 64 627 1113Fr 82 46 669 1012Sa 107 271 134 289Su 126 340 75 89
Table 7: Weekday Scan, Weekday Admiss. and ALOR Ratio Group (Low vs. High)
We have tested whether the interaction of the combination of all three variable and whetherthey play a significant role. Technically we compare the saturated model in a loglinear formand substract, by using ANOVA, the interaction term containing all three variables. We seethat the value p-value is less than 0.001 an thus is significant which made the model worse andtells that the three-fold interaction term makes the overall, saturated model a better fit. Beingaware of the downsides of such a more descriptive approach it still provides an indication thata parametric model should contain these factors in order to reflect reality.
Deviance df Delta(Dev) Delta(df) P(> Delta(Dev)Model 1 101.15 6 0Model 2 0 0 101.15 6 0
Saturated 0 0 0 0 1
Table 8: LR tests for hierachical log-linear model: Difference saturated and reduced model -ALOS Ratio
The resulting Chi-Squared test to validate the hypothesis that the respective weekdays influenceone another in the outcome measure, in our case the ALOS Ratio group, also shows significantresults underlining the above findings.
X − squared = 10176.23, df = 27, p− value < 2.2e− 16
The advantage of the chosen approach is that we can simply look at the model to verifywhether the likelihood ratio changes from one model to another which corresponds to thevisual comparisons and ideas represented in the above mosaicplots (see figures: 2 and 3).Thus it seems adequate to drive the analysis further using a more saturated model in order tovalidate our hypothesis.
2.2 Intermediary Conclusions
So far we have shown that the case for action appear in fact to be solid and can be shown bycategorical analysis measures. The finding indeed indicate a relationship between weekdays ofintervention and admission to hospital care. More specifically there seems to be an effect onboth the ALOS Ratio but also potentially on profitability. It also seems to be sensible to pursuethe analysis focusing on the binary outcomes as we are interested in the overall influence and
17

not in a determined range within the outcome. We will thus focus for our remaining analysison those aspects, especially on the latter, and discuss with parametric analysis measures.
3 Parametric Analysis
3.1 Model Description
In this part of the paper we will try to validate the below denoted null hypothesis that thereis indeed an effect of the weekday of either admission or radiological intervention on variousoutcome measures. We will use a generalized regression model using logistic outcome vari-able. In a first step we will investigate that the weekday influence the economic outcome i.e.profitability7. Simplified this can be denoted as:
H0 : yP rof = α+ β1 + β2 + β3 + β4 + β5 + ε = 0 (2)
Similarly to this we apply a similar hypothesis and logic for the ALOS Ratio or LOS Complianceoriented model. Here however we will eliminate the variable representing the ALOS Ratiobesides that the model remains the same.
H0 : yALOSRatio = α+ β1 + β2 + β3 + β4 + β5 + ε = 0 (3)
We have included several vectors grouped by subject in the analysis. Profitability is denotedas positive as soon as it is generating profit. The same logic applies to the ALOS Ratio wherewe use values >=1 as high and values < 1 as being low. They can be summarized for bothoutcomes as follows:
yP rof =
{1 if y∗
P rof ≥ 00 if y∗
P rof < 0
and accordingly
yALOSRatio =
{1 if y∗
ALOSRatio ≥ 10 if y∗
ALOSRatio < 1
The β1 vector contains basically variables that qualify the patient with an age and gendervariable. These are being used to enable exclusion of confounding of these basic patient char-acteristics.β2 and assembles variables that contain the relevant key performance indicators like AverageLength of Stay (ALOS) Ratio and the difference in Days between admission and intervention.These variables have been developed in order to measure efficacy in clinical treatment or inmanagement of patient pathways. It is those measures, besides CMI, that determines success
7The annexe contains all data for the LOS compliance as outcome as well
18

of hospitals in the age of DRG (e.g. Gocke, Debatin, and Doerselen, 2002).In β3 we have added the partition as factor variable, treated as dummy variable, which in-dicates whether the cases are clinically driven from a medical (M) or surgery(O) perspectivethe reference in this case are the mixed factors(A). The partition is defined by the SwissDRGcatalog. Here we should be able to distinguish complex cases from a internal medicine or moresurgical point of view. It can also indicate whether the clinical case in itself contains implicitlymore difficulty in treatment and therefor thus also bear more potential for influencing outcomein our terms.Another set of variables in the vector β4 integrates various cost factors like medical doctors,nursing, and infrastructure costs. The chosen cost dimensions do clearly impact on profitabil-ity. We would intuitively expect that they show solid significant results. On the complianceon length of stay the outcome is less predictable. As increasing costs can also have a beneficialeffect.The last block β5 contains our dummy variables of interest the day of week (working day)defined as binary variable 1 being the weekday vs. 0 being the weekend.
By validating the simplified hypothesis we will be able to validate the above working nullhypothesis. The estimated logarithmic regression model is based on the below general form(Fox, 2011, see p. 237 for detail).
loge
[µ(x)
1 − µ(x)
]= β0 + β1x1 + ... + bkxk (4)
In the below table 9 we firstly get an overview of the saturated regression model, secondlya stripped one in order to display the effect of leaving out our factors of interest (i.e. daysof week). Thus allowing for deviance analysis. The dependent variable is profitability andrepresented as a bivariable factor either benefit generating or not . Last, we show in thethird column last a linear model enabling to show the effect difference with a model having acontinuous dependent variable (i.e. profitability as a percentage) and how the single coefficientsdiffer none the last in significance.
3.2 General Results on Outcome and Model
Our main question though remains whether the weekday of either the intervention or theadmission day influence the profitability resulting from DRG cases. With respect to the logisticregression model we are testing the coefficients of interest are WD Scan (Weekday Scan) orWD Admiss. (Admission) and the interaction term regressed against either profitability orcompliance of LOS is only to be recognized at a low level as can be seen in table 9 for profitabilityand in table 15 for ALOS Ratio. Contrary to what we would have expected, from our abovecase for action loglinear analysis, the effect of the single coefficients is rather small or eveninsignificant. This at least indicates that our hypothesis finds some ground. But how robustis our analysis regarding loglikelihood? We will look into the two main dependent variables inthe following paragraphs.
19

Table 9: Regression Results Positif vs. Negatif Profitability and Profitability in Percentage
Dependent variable:Profitability Perc. Profitability
logistic normalGeneralised Model GLM w/o Days Lin.Mod. Perc.Prof.
(1) (2) (3)Gender −0.150∗∗∗ −0.150∗∗∗ −0.025∗∗∗
(−0.220, −0.081) (−0.220, −0.082) (−0.038, −0.011)Age 0.0001 0.00001 0.0003
(−0.002, 0.002) (−0.002, 0.002) (−0.0001, 0.001)Ins. Class HP 2.100∗∗∗ 2.100∗∗∗ 0.290∗∗∗
(2.000, 2.200) (2.000, 2.200) (0.270, 0.310)Ins. Class P 2.700∗∗∗ 2.700∗∗∗ 0.330∗∗∗
(2.500, 2.900) (2.500, 2.900) (0.310, 0.350)ALOS Ratio 0.065∗∗∗ 0.064∗∗∗ 0.019∗∗∗
(0.042, 0.087) (0.041, 0.087) (0.014, 0.023)Diff. Admiss. and Scan 0.037∗∗∗ 0.039∗∗∗ 0.003∗
(0.021, 0.053) (0.023, 0.055) (0.0001, 0.006)Partition M −0.910∗∗∗ −0.910∗∗∗ −0.160∗∗∗
(−1.100, −0.680) (−1.100, −0.670) (−0.210, −0.120)Partition O 0.190 0.200 0.064∗∗
(−0.047, 0.430) (−0.043, 0.430) (0.020, 0.110)MD Cost 0.0001∗∗∗ 0.0001∗∗∗ 0.00001∗∗∗
(0.0001, 0.0001) (0.0001, 0.0001) (0.00000, 0.00002)Treat. Cost −0.0001∗∗∗ −0.0001∗∗∗ −0.00002∗∗∗
(−0.0002, −0.0001) (−0.0002, −0.0001) (−0.00002, −0.00002)Infra.Cost −0.0004∗∗∗ −0.0004∗∗∗ −0.0001∗∗∗
(−0.0004, −0.0003) (−0.0004, −0.0003) (−0.0001, −0.0001)Scan Cat. MC 0.130 0.130 −0.002
(−0.010, 0.280) (−0.010, 0.280) (−0.028, 0.024)Scan Cat. HC 0.890∗∗∗ 0.880∗∗∗ 0.130∗∗∗
(0.460, 1.300) (0.450, 1.300) (0.061, 0.210)WD Scan 0.084 0.031
(−0.093, 0.260) (−0.003, 0.065)WD Admiss. 0.260∗∗ 0.047∗∗
(0.049, 0.460) (0.008, 0.086)WDSWEA −0.270∗ −0.051∗
(−0.510, −0.032) (−0.097, −0.006)Constant 0.950∗∗∗ 1.000∗∗∗ −0.007
(0.630, 1.300) (0.730, 1.300) (−0.067, 0.053)Observations 11,329 11,329 11,329Log Likelihood −6,299.000 −6,302.000 −6,594.000Akaike Inf. Crit. 12,633.000 12,631.000 13,221.000
Note: ∗p<0.1; ∗∗p<0.05; ∗∗∗p<0.01
3.2.1 Model Results on Profitability
3.2.1.1 Deviance
Looking at single factors appears to be important. The first model (table 9) shows no signifi-cance in the saturated GLM model for the WD Scan variable. But if the Admission Day fallsinto the week it the coefficient becomes significant at 5% and it clearly has a positive influencewith an odds ratio of 1.29 (compare table 11 in chapter 3.2.1.2). However the interesting factis that the interaction term is significant at a 10% significance level. The prediction assess-ment with chi2 which measures the difference between the saturated (1) and the stripped (2)model shows that the model seems not to influence considerably and thus do not improve thefit generally with a deviance of −4.54 and a of p− value = 0.2092 (compare table 14)and wecould reject the null hypothesis that the saturated model improves the evidence i.e. changingthe loglikelihood by adding the our variables of interest. The issue lies most probably with the
20

model in general as we have quite a high residual deviance (12600) and a χ2(1.702172e− 16)that is distinctively low.We have seen above the results of our parametric model but how reliable is it? We try in thefollowing assessment to validate the model and partially apply proposed dimensions in the liter-ature (Hosmer, Taber, and Lemeshow, 1991). In order to assess the goodness of fit have used theHosmer-Lemeshow (H-L) test and found a χ2 = 122.97, df = 12, p− value < 2.2e− 16 for thesaturated model and for the stripped model we got χ2 = 125.77, df = 12, p− value < 2.2e− 16.The high chi2 shows that we probably have a badly fitted model overall as we have to acceptthe H0 which is for the H-L model not what we want. We have also looked into the varyingp-value and found the same direction of values with 500 runs. However a big number of p = 0occurred which seems to be awkward and let’s us doubt whether H-L is the right mean forGoodness of Fit (GOF). We are here not sure whether we can really assess the goodness offit in our context using the H-L. Especially comparing the two AIC (12632.7 (saturated) vs.12631.3 (stripped))indicate that the models are quite close. But as the saturated one is slightlyhigher we would be inclined to say that based on AIC our model does not add any evidenceto our hypothesis. We have also approached the model with PseudoR2 as proposed in theliterature (Field, 2012, p. 316ff) . We find quite high values for both models and a slightlyhigher one for the saturated one. The values of both values for each model is acceptable forCox and Snell but rather low for Nagelkerke. All this leads us to say that the chosen modeldefinition is most probably not optimal. We will still assume that the significant result on theinteraction term is validating our H0 hypothesis.
Method R2 Saturated StrippedCox and Snell R2 0.231 0.23Nagelkerke R2 0.309 0.308
Table 10: PseudoR2 - Profitability
However the question remains what elements could be changed within the existing set of vari-ables in order to improve our model?Most probably a stratified view on the cases would enhance the predictive force of our model.We have therefor investigated into clustering the existing dataset into categories using prof-itability as outcome variable. However results were not substantially more conclusive either.Following our evaluation strategy we have solely used available dimensions. We have usedMajor Diagnostic Category (MDC), DRG complication levels, radiological categories (i.e. LC,MC, HC), single weekdays, and duration between admission and scan date. With the excep-tion MDC01 (Nervous System) and at some lesser degree MDC categories 08 (MusculoskeletalSystem And Connective Tissue) and 04(Respiratory System) findings were scarce. Looking atMDC 01 one gets its influence through the characteristics of the illnesses (e.g. myocardial in-farcts). Similarly to these groups other studies and proposals have hinted at these same groupsbeing interesting for further investigation (for example see A. Street et al., 2010, p. 15ff). Inour case the more restricted dataset show a more robust case on the interdependencies we arehypothesizing at least with respect to the significance level of the single coefficients (comparetable 19). Such a result indicates that there is potential for more evidence using more stratifieddata samples. However one cannot deny that at the level of profitability the H0-Hypothesis
21

has to looked at carefully but we would summarize saying that the day of week has indeed aninfluence on the profit per case.
3.2.1.2 Odds Ratios with Profitability as an Outcome
From the above model 4 we can derive odds ratios explaining the expected effect each coefficienthas on profitability. The below model equation 58 indicates the calculus that will lead to table 11containing the odds ratios of the above coefficients9
µ(x)
1 − µ(x)= exp(β0) ∗ exp(β1x1) ∗ ... ∗ exp(bkxk) (5)
Hence the odds ratios of a single case being profitable by having a scan or the admission ona weekday are 1.1 respectively 1.3 higher. However the confidence intervals display for thescanday a non-sustained relationship i.e. the C.I. passes one and thus the effect direction canchange and thus the result can as such not be evaluated. Furthermore we can see that thecomplexity of the radiological intervention indicated by the category HC increased the oddsof generating a positive economic result is 2.4. This result is somehow counter-intuitive aswe would expect those cases being less likely to be profitable. Another interesting factor isthe Partition where a clear cut-off between medical and surgical cases can be seen. Howeverthe latter is also not that evident as the C.I. runs through 1. As the calculus of C.I. in theGLM models is based on log-likelihoods opposite to the Wald statistics for linear models wecan assume that they are accurate10 and thus we have to be careful in the interpretationof the calculated and displayed effects. The more expected trends are that half-private and
Estimate 2.5 % 97.5 %(Intercept) 2.58 1.77 3.77
Gender 0.86 0.79 0.94Age 1.00 1.00 1.00
Ins. Class HP 8.24 7.15 9.53Ins. Class P 15.12 12.46 18.49ALOS Ratio 1.07 1.04 1.10
Diff. Admiss. and Scan 1.04 1.02 1.06Partition M 0.40 0.30 0.53Partition O 1.21 0.91 1.61
MD Cost 1.00 1.00 1.00Treat. Cost 1.00 1.00 1.00
Infra.Cost 1.00 1.00 1.00Scan Cat. MC 1.14 0.96 1.36Scan Cat. HC 2.44 1.45 4.08
WD Scan 1.09 0.88 1.34WD Admiss. 1.29 1.01 1.65
WDSWDA 0.76 0.57 1.01
Table 11: Odds Ratios Saturated Model on Profitability
private patients appear to have much higher odds ratios resulting in benefit generating casescompared to basic insured cases. That result is nonetheless quite surprising as one wouldnot expect having different results for treatments or diagnostic indications according to thetype of patient. We suspect that DRG driven costs and revenues are not fully separated fromadditional ones. Thus this result could be influenced by this imprecision. Finally we find thatthe magnitude of the odds on ALOS Ratio generating a positive result are not that distinctive.
8For the derivation of the function provided here below please refer to Fox, 2011.9We chose to interpret the coefficients using odds ratios instead of relative change in odds as both measures
are equally valid and can be adapted according to preference Winkelmann, 200910see Fox, 2011 p. 237 for more detail)
22

It seems that with 1.1 higher odds that the effect is not even lower than the weekdays one.But it touches 1, like the weekday of admission, and thus we are inclined to be careful ininterpreting the strength of that odds-ratio. The analysis of the interaction term between daysof week of scanning and admission of 0.76 has to be approached more carefully. The odds ratiowould mean that among weekday scans and weekday admissions are only 0.76 times more likelyto achieve a profitability bigger than 1. That result does not take the direction of effect wewould have expected. This result would indicate that if both types of day fall on a weekdaythe changes of being profitable would be lower.We can therefore finally conclude that according to our hypothesis the weekday has a someinfluence on profitability. The important factor though is the relevance of the interaction termwhich corresponds to what we have found in the loglinear analysis although not at the expectedscale and clarity.
3.2.2 Model Results on ALOS Ratio
3.2.2.1 Deviance
The second variable of interest is the LOS compliance the investigations bears other behaviorsof the single factors. Contrary to profitability as dependent variable we obtain a significancelevel of the scan day at a 1% level (table 15 on p. 29). This makes perfect sense as the patientpathway largely depends on the weekday. Astonishingly the logit is -0.32 that shows that theodds are lower generating a profit bearing case when the day of intervention falls on a weekday.The question why the intervention day drives the probability of being profitable or not. Withcurrent means at hand this point remains open and not fully understood. But more impor-tantly the interaction term looses in the bivariate model its significance. Why that is again notclear. The other model variable prove to be all significant with two notifiable exceptions. Thedummy variable Privat Patients (Ins. Class P) is not significant. This could mean that privatepatients are kept longer in hospital i.e. not respecting the CMO’s benchmark. Whether thatis done intentionally would remain to be seen. However that type of patient generate revenuebeyond the case related reimbursement. The other interesting variable that is not significantis the highly complex cases of modality use (Scan Cat. HC). This could be an indicator thatthose cases are indeed clinically more difficult to treat and have therefore a higher value thanthe benchmark and ceteris paribus have a lower ratio. A possible interpretation would be thatthese cases are difficult to manage and cannot follow a standard patient pathway.Opposite to this we can see that the comparative linear model which holds the dependentvariable continuous behaves differently. Although we generally doubt the model’s normal dis-tribution and that is why we applied the logistic regression for our investigations. We use theOLS model here solely as point of reference without further investigation.
Looking at the models goodness of fit we see that the AIC is for the full model (11907) isslightly smaller than the one without the days dimensions (11924) but the values are quiteclose. Thus we would estimate the saturated model the better one. The same direction ofeffects holds for the log-likelihood which is −5937 for model 1 and −5949 for model 2. The
23

chi2 measuring the difference between the saturated (1) and the stripped (2) model appearsto be significant with a good fit’s deviance of −23.14 and with a p− value = 3.767e− 05.(compare table 18 on p. 30)we can conclude that our saturated model adds to evidence.
The GOF has been started with the H-L test and found a χ2 = 600.6, df = 8, p− value <
2.2e− 16 for the saturated model (setting g11 to 0) and for the stripped model we got χ2 =
635.09, df = 8, p− value < 2.2e− 16. The high chi2 shows that we probably have a badlyfitted model overall and like with the profitability dimension we have to accept the H0 which isfor the H-L model not what we want. Validating the test with 500 runs provided a consistentp-value of 0. Like with the profitability outcom e we have also established the PseudoR2. Wefind quite good values for both models and a slightly higher one for the saturated one whichincrease evidence for the solidity of the model. The differences are small though. The valuesfor Cox and Snell are right above the thresshold of 0.20 but the Nagelkerke indicator is stillbelow 0.50. The results are not substantially different from our above findings.
Method R2 Saturated StrippedCox and Snell R2 0.241 0.24Nagelkerke R2 0.329 0.327
Table 12: PseudoR2 - ALOS Ratio
Below we will look into the effect size with odds ratios (table 16).
3.2.2.2 Odds Ratios on ALOS Ratio as Output Variable
Looking at the ALOS Ratio will yield some results that were expected from the case for ac-tion. (please refer to table 15 for further details). Effects do however have another order ofmagnitude or even take another direction. This is the case with the effect in the coefficientof duration of the difference between admission and scanday for example. Here the β valuechanges direction and the odds ratio is below 1. That means that the chances of generating agood ALOS ratio are 24% lower with an increase in the duration. That intuitively correspondsto what we would expect of the model contrary to the behavior with the profitability outcomewhere we obtain a converse effect. Also the patient class seems to have a less large influenceon results of the LOS compliance. The partition though reacts as expected with a 33% lowerchance to get a positive ratio when the class is a surgery one (Partition O). When it comesto the weekday argument we can observe that the scanday falling on a working day decreasethe chance of a positive resulting ratio by 28% that is not really intuitive and contradicts ourexpetancies. More imporantly table 16 shows for the values WD Admiss. and the interactionterm (WDSWDA) no significant effects nor seems the direction clear as both run through 1. Itseems that some of the expected results occur and other do move in an unexpected direction.This might require more investigation into the dependencies between factors.
11number of bins to use to calculate quantiles
24

3.3 Issues
• Heterogeneity of groups leads potentially to distorting results
• Preliminary investigations into clinical groups have shown clearer views but it is unclearto what extent
• How can the CfA show strong indications and why does the parametric model fail deliv-ering according results?
• Covariance between the day types has to be verified - as the sequence as well as thedifference might not be random? How to proceed to such a test?
• How can eventually a production function approach enhance the view? What wouldthe main indicators be? And can it be done without knowing the cost function of thehospital? What proxy?
The interesting fact though is that weekdays, for both admission and for scan day, significantlyinfluence both outcome variables. More analysis has been undertaken at single day level andresults have been confirmed(Aylin et al., 2013) at least in parts.
3.4 Conclusion
Management of patients going through a radiological analysis controls the latter induced costand influence average length of stay as well as the economic result. The gain from appropriatecase management can rely heavily on radiology expressed through an optimized radiology use.As it seems particular attention to weekdays both for admission and scan date pays off. Thisresult is underpinned by the relevance of these two key days being close to each other.
• Evidence that the interaction of weekdays influence economic and operative outcomesexists - but what happens to clinical outcome
• Investigate into omitted confounder in the actual dataset or make an attempt to enrichdata further
• Policy implications both at a hospital level and at a regional more public health orientedlevel benefit from such analysis and especially from its consequences to control theseprocesses better
• Further research including clinical factors could be redeeming
25

References
A. Street et al. (2010). Determinants of hospital costs and performance variation : Methods,models and variables for the EuroDRG project. Working Papers in Health Policy and Man-agement. 00000.
Aylin, P et al. (2013). “Day of week of procedure and 30 day mortality for elective surgery:retrospective analysis of hospital episode statistics”. In: BMJ : British Medical Journal 346.00028 PMID: 23716356. issn: 0959-8138. doi: 10.1136/bmj.f2424.
Dismuke, Clara Elizabeth and Vania Sena (1999). “Has DRG payment influenced the tech-nical efficiency and productivity of diagnostic technologies in Portuguese public hospitals?An empirical analysis using parametric and non parametric methods”. In: Health Care Man-agement Science 2.2. 00072, pp. 107–116. issn: 1386-9620, 1572-9389. doi: 10.1023/A:
1019027509833.Dorio, Paul, MD — Physician — October 19, and 2011 (2014). Why radiology is the cornerstone
of any hospital. KevinMD.com. 00000. url: http://www.kevinmd.com/blog/2011/10/
radiology-cornerstone-hospital.html (visited on 06/28/2014).Field, Andy (2012). Discovering statistics using R. In collab. with Jeremy Miles and Zoe Field.
00000. Los Angeles: SAGE Publications. 957 pp. isbn: 9781446200469.Fox, John (2011). An R companion to applied regression. In collab. with Sanford Weisberg. 2nd
ed. 00004. Thousand Oaks, Calif: SAGE Publications. 449 pp. isbn: 9781412975148.Gocke, P., J. F. Debatin, and L. F. J. Doerselen (2002). “Prozessmanagement und Controlling
in der Diagnostischen Radiologie im Krankenhaus”. In: Der Radiologe 42.5. 00012, pp. 332–343. issn: 0033-832X, 1432-2102. doi: 10.1007/s00117-002-0717-2.
Groot, N. L. de et al. (2012). “Admission time is associated with outcome of upper gastroin-testinal bleeding: results of a multicentre prospective cohort study”. In: Alimentary Phar-macology & Therapeutics 36.5. 00000, pp. 477–484. issn: 1365-2036. doi: 10.1111/j.1365-
2036.2012.05205.x.Hosmer, D W, S Taber, and S Lemeshow (1991). “The importance of assessing the fit of logistic
regression models: a case study.” In: American Journal of Public Health 81.12. 00397 PMID:1746660, pp. 1630–1635. issn: 0090-0036.
Jen, M. H. (2012). “PSU41 Day of Week of Procedure and 30-Day in-Hospital Mortality forElective Surgery”. In: Value in Health. ISPOR 17th Annual International Meeting ResearchAbstracts 15.4. 00000, A81. issn: 1098-3015. doi: 10.1016/j.jval.2012.03.444.
Klose, K. J. and J. Bottcher (2002). “”Activity based costing” in der Radiologie”. In: DerRadiologe 42.5. 00010, pp. 369–375. issn: 0033-832X, 1432-2102. doi: 10.1007/s00117-
002-0719-0.Larson-Hall, Jenifer (2009). A Guide to Doing Statistics in Second Language Research Using
SPSS. 00000. url: http://cw.routledge.com/textbooks/9780805861853/ (visited on09/15/2014).
Napierala, Christoph and Koller, Stefan (2014). “Kosten mit Diagnostik positiv beeinflussen :Diagnostik unter DRG”. In: Competence : hospital management forum 78.1. 00000, p. 26.issn: 1424-2168.
26

Rechtzeitige Diagnose dank der Radiologie (2014). Presseportal.ch. 00000. url: http://www.
presseportal.ch/de/pm/100056136/100756125/rechtzeitige-diagnose-dank-der-
radiologie (visited on 05/19/2014).Sorenson, Corinna, Drummond, and Bhuiyan-Khan (2013). “Medical technology as a key driver
of rising health expenditure: disentangling the relationship”. In: ClinicoEconomics and Out-comes Research. 00012, p. 223. issn: 1178-6981. doi: 10.2147/CEOR.S39634.
Winkelmann, Rainer (2009). Analysis of microdata. In collab. with Stefan Boes. 2nd ed. 00000.Berlin: Springer. 343 pp. isbn: 9783540927471.
Woodcock, Richard (2010). A clear understanding of your costs protects profits, eases planning— Diagnostic Imaging. 00000. url: http://www.diagnosticimaging.com/practice-
management/clear-understanding-your-costs-protects-profits-eases-planning
(visited on 06/28/2014).
27

Appendix
Data and Tables
Profitability Models
Likelihood and Anova Comparing Models
Table 13: Likelihood Comparison on Profitability: Saturated vs. Stripped Model
Statistic N Mean St. Dev. Min MaxResid. Df 2 11,314.000 2.100 11,312 11,315Resid. Dev 2 12,601.000 3.200 12,599.000 12,603.000Df 1 −3.000 −3 −3Deviance 1 −4.500 −4.500 −4.500Pr(>Chi) 1 0.210 0.210 0.210
Resid. Df Resid. Dev Df Deviance Pr(>Chi)1 11312 12598.762 11315 12603.30 -3 -4.54 0.2092
Table 14: Chi Square - Profitability
28

ALOS Ratio Models
Regression Models
Table 15: Regression Results Larger than 1 vs. smaller than 1 ALOS Ratio in Percent
Dependent variable:ALOS Ratio Perc. ALOS Ratio
logistic normalGeneralised Model GLM w/o Days Lin.Mod. Perc.ALOS Ratio
(1) (2) (3)Gender −0.190∗∗∗ −0.200∗∗∗ −0.044
(−0.270, −0.120) (−0.270, −0.120) (−0.093, 0.005)Age −0.0002 −0.0001 0.007∗∗∗
(−0.002, 0.002) (−0.002, 0.002) (0.006, 0.009)Ins. Class HP 0.190∗∗∗ 0.180∗∗∗ 0.072∗
(0.082, 0.290) (0.079, 0.290) (0.003, 0.140)Ins. Class P −0.017 −0.021 −0.050
(−0.130, 0.098) (−0.140, 0.094) (−0.130, 0.026)Diff. Admiss. and Scan −0.110∗∗∗ −0.120∗∗∗ −0.130∗∗∗
(−0.130, −0.098) (−0.140, −0.100) (−0.140, −0.120)Partition M 0.024 0.024 0.700∗∗∗
(−0.210, 0.260) (−0.210, 0.260) (0.540, 0.860)Partition O −0.400∗∗∗ −0.390∗∗∗ −0.150
(−0.640, −0.150) (−0.630, −0.140) (−0.310, 0.014)MD Cost −0.0001∗∗∗ −0.0001∗∗∗ −0.0002∗∗∗
(−0.0002, −0.0001) (−0.0002, −0.0001) (−0.0002, −0.0002)Treat. Cost −0.0003∗∗∗ −0.0003∗∗∗ −0.0001∗∗∗
(−0.0003, −0.0003) (−0.0004, −0.0003) (−0.0001, −0.0001)Infra.Cost 0.0004∗∗∗ 0.0004∗∗∗ 0.0003∗∗∗
(0.0003, 0.0004) (0.0003, 0.0004) (0.0002, 0.0003)Scan Cat. MC 0.450∗∗∗ 0.470∗∗∗ 0.079
(0.300, 0.600) (0.320, 0.620) (−0.018, 0.170)Scan Cat. HC −0.130 −0.130 0.470∗∗∗
(−0.610, 0.340) (−0.610, 0.340) (0.210, 0.740)WD Scan −0.320∗∗∗ −0.590∗∗∗
(−0.520, −0.140) (−0.710, −0.470)WD Admiss. 0.220 −0.290∗∗∗
(−0.009, 0.440) (−0.430, −0.150)WDSWDA 0.058 0.570∗∗∗
(−0.200, 0.320) (0.410, 0.740)Constant 2.300∗∗∗ 2.300∗∗∗ 2.300∗∗∗
(2.000, 2.700) (2.000, 2.600) (2.100, 2.500)Observations 11,329 11,329 11,329Log Likelihood −5,937.000 −5,949.000 −21,215.000Akaike Inf. Crit. 11,907.000 11,924.000 42,462.000
Note: ∗p<0.1; ∗∗p<0.05; ∗∗∗p<0.01
29

Odds Ratio with the Outcome variable ALOS Ratio
Estimate 2.5 % 97.5 %(Intercept) 10.32 6.94 15.41
Gender 0.82 0.75 0.90Age 1.00 1.00 1.00
Ins. Class HP 1.21 1.06 1.37Ins. Class P 0.98 0.86 1.13
Diff. Admiss. and Scan 0.89 0.88 0.91Partition M 1.02 0.77 1.36Partition O 0.67 0.50 0.90
MD Cost 1.00 1.00 1.00Treat. Cost 1.00 1.00 1.00
Infra.Cost 1.00 1.00 1.00Scan Cat. MC 1.57 1.32 1.87Scan Cat. HC 0.88 0.49 1.54
WD Scan 0.72 0.58 0.91WD Admiss. 1.24 0.95 1.63
WDSWDA 1.06 0.78 1.44
Table 16: Odds Ratios Saturated Model on LOS Compliance
Likelihood and Anova Comparing Models
Table 17: Likelihood Comparison on ALOS Ratio: Saturated vs. Stripped Model
Statistic N Mean St. Dev. Min MaxResid. Df 2 11,314.000 2.100 11,313 11,316Resid. Dev 2 11,886.000 16.000 11,875.000 11,898.000Df 1 −3.000 −3 −3Deviance 1 −23.000 −23.000 −23.000Pr(>Chi) 1 0.00004 0.00004 0.00004
Resid. Df Resid. Dev Df Deviance Pr(>Chi)1 11313 11874.692 11316 11897.83 -3 -23.14 0.0000
Table 18: Chi Square - ALOS Ratio
30

Profitability Stratified according to MDC 01
Regression Models
Table 19: Regression Results Positif vs. Negatif Profitability and Profitability in PercentageMDC01
Dependent variable:Profitability Perc. Profitability
logistic normalGeneralised Model GLM w/o Days Lin.Mod. Perc.Prof.
(1) (2) (3)Gender −0.180 −0.180∗ −0.020
(−0.360, 0.0004) (−0.360, −0.005) (−0.054, 0.014)Age −0.003 −0.003 0.0001
(−0.008, 0.002) (−0.008, 0.002) (−0.001, 0.001)Ins. Class HP 2.400∗∗∗ 2.400∗∗∗ 0.320∗∗∗
(2.000, 2.700) (2.000, 2.700) (0.270, 0.360)Ins. Class P 3.400∗∗∗ 3.300∗∗∗ 0.360∗∗∗
(2.900, 3.900) (2.800, 3.800) (0.310, 0.420)ALOS Ratio −0.140∗∗∗ −0.140∗∗∗ −0.031∗∗∗
(−0.190, −0.085) (−0.190, −0.086) (−0.042, −0.021)Diff. Admiss. and Scan 0.058∗∗ 0.065∗∗ 0.007
(0.009, 0.110) (0.018, 0.110) (−0.001, 0.016)Partition M −16.000 −16.000 −0.530
(−1,468.000, 1,436.000) (−1,468.000, 1,436.000) (−1.300, 0.210)Partition O −15.000 −15.000 −0.230
(−1,467.000, 1,437.000) (−1,467.000, 1,437.000) (−0.970, 0.510)MD Cost 0.0002∗∗∗ 0.0002∗∗∗ 0.00001
(0.0001, 0.0003) (0.0001, 0.0003) (−0.00001, 0.00003)Treat. Cost −0.0002∗∗∗ −0.0002∗∗∗ −0.00002∗∗∗
(−0.0002, −0.0002) (−0.0002, −0.0002) (−0.00003, −0.00002)Infra.Cost −0.001∗∗∗ −0.001∗∗∗ −0.0001∗∗∗
(−0.001, −0.001) (−0.001, −0.001) (−0.0001, −0.0001)Scan Cat. MC −0.320 −0.320 −0.110∗∗
(−0.720, 0.083) (−0.720, 0.088) (−0.180, −0.037)Scan Cat. HC −12.000 −12.000 −0.390∗∗
(−480.000, 456.000) (−483.000, 458.000) (−0.690, −0.080)WD Scan 0.440∗ 0.110∗∗
(0.038, 0.850) (0.036, 0.190)WD Admiss. 0.590∗∗ 0.130∗∗
(0.100, 1.100) (0.034, 0.220)WDSWEA −0.750∗∗ −0.170∗∗∗
(−1.300, −0.200) (−0.270, −0.061)Constant 17.000 18.000 0.540
(−1,435.000, 1,469.000) (−1,434.000, 1,470.000) (−0.210, 1.300)Observations 1,965 1,965 1,965Log Likelihood −1,016.000 −1,018.000 −1,202.000Akaike Inf. Crit. 2,065.000 2,064.000 2,437.000
Note: ∗p<0.1; ∗∗p<0.05; ∗∗∗p<0.01
31

OR MDC 01
Estimate 2.5 % 97.5 %(Intercept) 38468801.79 0.00
Gender 0.84 0.68 1.04Age 1.00 0.99 1.00
Ins. Class HP 10.81 7.35 16.27Ins. Class P 29.06 16.34 55.56ALOS Ratio 0.87 0.82 0.93
Diff. Admiss. and Scan 1.06 1.00 1.12Partition M 0.00Partition O 0.00
MD Cost 1.00 1.00 1.00Treat. Cost 1.00 1.00 1.00
Infra.Cost 1.00 1.00 1.00Scan Cat. MC 0.73 0.45 1.17Scan Cat. HC 0.00
WD Scan 1.56 0.96 2.53WD Admiss. 1.80 1.01 3.21
WDSWDA 0.47 0.24 0.91
Table 20: Odds Ratios Saturated Model on Profitability only MDC 01
Various
Moscaiplot on Profitability Groups and Working Day Admission
Figure 4: Profitabiltiy Group per Day of Intervention (Scan) and per Weekday of Admission
LR Tests
Deviance df Delta(Dev) Delta(df) P(¿ Delta(Dev)
Model 1 9029 26 0
Model 2 0 0 9029 26 0
Saturated 0 0 0 0 1
Table 21: LR tests for hierachical log-linear model: Difference saturated and reduced model
32
R Packages Used
Analysis has been done with the R version below and packages with the following versions:
• R version 3.1.0 (2014-04-10)
• Used packages:
– aod (vers. 1.3)
– BMA (vers. 3.17.1)
– boot (vers. 1.3-11)
– car (vers. 2.0-21)
– coin (vers. 1.0-23)
– colorspace (vers. 1.2-4)
– Deducer (vers. 0.7-7)
– doBy (vers. 4.5-10)
– dummies (vers. 1.5.6)
– epicalc (vers. 2.15.1.0)
– fmsb (vers. 0.5.0)
– foreign (vers. 0.8-61)
– Formula (vers. 1.1-2)
– ggplot2 (vers. 1.0.0)
– gnm (vers. 1.0-7)
– gvlma (vers. 1.0.0.2)
– Hmisc (vers. 3.14-4)
– iplots (vers. 1.1-7)
– JavaGD (vers. 0.6-1)
– JGR (vers. 1.7-16)
– lattice (vers. 0.20-29)
– latticeExtra (vers. 0.6-26)
– leaps (vers. 2.9)
– lme4 (vers. 1.1-7)
– lmtest (vers. 0.9-33)
– MASS (vers. 7.3-34)
33

– Matrix (vers. 1.1-4)
– memisc (vers. 0.96-9)
– multcomp (vers. 1.3-6)
– mvtnorm (vers. 1.0-0)
– nlme (vers. 3.1-117)
– nnet (vers. 7.3-8)
– papeR (vers. 0.4-0)
– partykit (vers. 0.8-1)
– pastecs (vers. 1.3-18)
– PerformanceAnalytics (vers. 1.1.0)
– psych (vers. 1.4.8.11)
– QuantPsyc (vers. 1.5)
– Rcmdr (vers. 2.1-1)
– RcmdrMisc (vers. 1.0-2)
– RcmdrPlugin.coin (vers. 1.0-21)
– RColorBrewer (vers. 1.0-5)
– Rcpp (vers. 0.11.2)
– regress (vers. 1.3-14)
– regtest (vers. 0.05)
– rJava (vers. 0.9-6)
– robustbase (vers. 0.91-1)
– sandwich (vers. 2.3-2)
– stargazer (vers. 5.1)
– survey (vers. 3.30-3)
– survival (vers. 2.37-7)
– TH.data (vers. 1.0-3)
– vcd (vers. 1.3-2)
– vcdExtra (vers. 0.6-1)
– xtable (vers. 1.7-3)
– xts (vers. 0.9-7)
– zoo (vers. 1.7-11)
34