Waves-of-Change.pdf - CHETNA
52
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of Waves-of-Change.pdf - CHETNA

Acknowledgements
January-2013
The Participatory Communication Initiative for Improving Access to Public Health Care Services for Rural Communities’under NRHM has been a collective effort of several individuals, organisations and government departments at the state,district and block level.
We take this opportunity to acknowledge and extend our heartfelt gratitude to:
• The Communication for Health India Network (CHIN) partners – Child in Need Institute (CINI), Christian MedicalAssociation of India (CMAI) and Rural Unit for Health and Social Affairs (RUHSA) for contributing ideas, expertiseand inspiration to this initiative.
• The state, district and block officials of National Rural Health Mission (NRHM), Department of Health and FamilyWelfare, Department of Women and Child Development, Government of Gujarat and Government of Rajasthan whoprovided critical support in implementation of this project.
• The community members and representatives of women’s forums, Community based Organisations/Self HelpGroup representatives, Accredited Social Health Activists (ASHAs)/ Village Health, Sanitation and NutritionCommittee (VHSNC) members who willingly shared valuable experiences and information with us which motivatedus to document these stories of change.
• Representatives of our partner organisations from Gujarat and Rajasthan states, India, for their extensive and vitalrole throughout the project. In particular Mr. Mahesh Kumar, Mr. B.K Gupta, Mr. Vijendra Dosi, Mr. Mohammed IsmailKhan and Mr. Shishir Kumar from Rajasthan and Mr.Mahesh Ode, Mr.Lalsing Gamit, Mr.Wasim Chauhan and Ms.Bharti Khodiyar, Ms.Kanisha Chavda (both former colleagues), who collected information for the stories.
• Ms. Indu Capoor, Founder and Director of CHETNA who provided inspiration and guidance in the overall executionof this project. Her extensive discussions and insights have been very helpful at every stage.
• Ms.Ila Vakharia former Project Manager, CHETNA CHANGE 2008-2011 for her critical contribution in projectplanning and guiding the team in facilitating effective implementation of the project activities.
• Our colleagues at CHETNA for their critical insights and suggestions related to the content and design of thebooklet. Mr.Virendra Shekhawat, former team member and Ms. Kamal Popat drafted the stories. Mr. Anil Gajjardesigned the booklet and Ms. Arti Trivedi supported in the administrative tasks involved in the publication of booklet.
• We are extremely thankful to Ms.Rukmini Datta for building capacity of the team in documenting the stories and herinputs in editing the first draft of this booklet. We also acknowledge the editorial support of Ms.Aruna Mathur inmaking the publication print ready.
Last but not the least, we are extremely grateful to CMAI New Delhi, for recognizing the value of this work andproviding us technical and financial support for publishing this booklet.
Ms. Chitra Iyer Ms. Minaxi ShuklaProject Manager, CHETNA Deputy Director, CHETNA

1
Waves of Change
With Technical and Financial Support from
Christian Medical Association of India (CMAI),New Delhi.
Developed by

2
Our implementing partners
NarottamLalbhai RuralDevelopment
Fund(NLRDF)
Kutch MahilaVikas Sangathan
(KMVS)
ShroffsFoundation Trust
GramyaVikas Trust
Vedchhi PradeshSeva Samiti
Akhil Bhartiya GraminUtthan Samiti (ABGUS)
ALERTSansthan
ASSEFAShikshit Rojgar Kendra
Prabandhak Samiti
32
Index
Introduction ........................................................................................................................................... 4
Process ................................................................................................................................................ 5
Cable Network Brings Change ............................................................................................................. 7
Here Come the ASHAs... ...................................................................................................................... 8
Women’s Self-Help Group: A Guiding Force for the Village ................................................................ 11
From Confrontation to Cooperation .................................................................................................... 13
Advocacy for Change ......................................................................................................................... 15
Advocacy for Health Insurance ........................................................................................................... 17
Small Efforts, Big Results ................................................................................................................... 19
Community Monitoring: Making Health Functionaries Accountable to People ..................................... 21
Sustaining Commitment of Critical Health Workforce: The ASHAs ..................................................... 23
And the Roadshow came to them. ...................................................................................................... 24
Fighting Problems in Health Care Delivery...A Struggle....................................................................... 27
Overcoming the Obstacle of Ignorance. ............................................................................................. 29
A Toilet Brings in a Revolution! ........................................................................................................... 31
Ensuring Improved Access to Health Care Services ........................................................................... 33
The Story of an Inspirational Sarpanch ............................................................................................... 35
Making a Difference - The Power of One ............................................................................................ 37
Where there is a will, there is a way ................................................................................................... 39
A Little Handholding Goes a Long Way .............................................................................................. 41
Rhythmic Drum Beats for a Healthy Life ............................................................................................. 43
This Magic Works! .............................................................................................................................. 45
Listening to and Giving a Voice to the Marginalised ............................................................................ 46
Media Coverage ................................................................................................................................. 47
Communiction tools developed ........................................................................................................... 48
3

4
Introduction
The launch of the National Rural Health Mission (NRHM) in the year 2005 by the Government of India (GOI)is a welcome step towards improving the availability of and access to quality healthcare by people, especiallymarginalized communities like those residing in rural areas, the poor, women and children.
The Mission aims to carry out necessary architectural correction in the basic health care delivery system byincreasing public expenditure on health, reducing regional imbalances in health infrastructure, poolingresources, integration of organisational structures, optimization of health human-power, communityparticipation, etc.
To achieve the objectives of the Mission, the following core strategies have been included:
1. Enhance capacity of Panchayati Raj Institutions (PRIs) to own, control and manage public health services.
2. Promote access to improved healthcare at household level through appointment of Accredited SocialHealth Activist-ASHAs from amongst the local village women.
3. Health Plan for each village and community based monitoring of health services through Village HealthCommittees.
4. Strengthening facilities of Public Health Centres viz. Sub centres, Primary Health Centres and CommunityHealth Centres for improved curative care.
Enhancing Communities’ Access to Public Health Care Services
The NRHM recognizes the importance of improved communication for social change and increasedparticipation of community in the health movement to reach the un-reached population, however access topublic health services is a challenge for tribal and rural communities in remote villages. ParticipatoryCommunication conceives development as a transformative process at both individual and social levelsthrough which communities become empowered to initiate a process of change.
The concern with communication in implementation of NRHM is two-fold: communities are unable tocommunicate their needs to health workers, and health workers, in turn, are unable to communicateeffectively with the community. In an attempt to address this lacunae and building on the premise ofcommunication for social change, the Participatory Communication Initiative has been undertaken through apartnership based network called Communication for Health India Network (CHIN) since 2008 in 40 districtsof seven states of India.
As one of the CHIN partners, CHETNA implemented the project activities in five identified block of fivedistricts each in Gujarat and Rajasthan states, covering a total population of 18,89,798 in both the states toenhance community’s access to quality public health services as guaranteed under NRHM.

Process
5
In Gujarat state, the project was implemented in 461 villages in selected blocks of Jamnagar, Kutch,Sabarkantha, Tapi and Vadodara districts and in Rajasthan state, it was implemented in 794 villages inselected blocks of Alwar, Banswara, Churu, Karauli and Udaipur districts. The selection of the districts wasdone in consultation with the Department of Health and Family Welfare keeping in view the indicators such ashigh infant and maternal mortality, lower rate of immunisation, Antenatal Care (ANC) and institutional deliveries.
In about 10 percent of the total number of villages, a participatory needs assessment study was conductedto assess the knowledge level of community members regarding availability of health services, availablemeans of communication and training needs of service providers. The results of this study were shared withthe existing groups at the local level, as well as at the block and district level. Based on the findings of thestudy, discussions were held on developing communication strategies.
The project adapted a multi-pronged strategy and a range of processes for different geographical areas viz.tribal, arid and desert areas and rural areas to reach out to the community. Regular awareness meetings,forum meetings were facilitated in each of these identified blocks, local public fairs1/religious festivals likeJanmasthmi, Navratri in Gujarat were used as an opportunity to interact and inform the communities abouthealth entitlements. This enabled the communities in availing and demanding for health and nutritionservices. For dialogue with the service providers, spaces within the existing programmes of the governmentwere identified which proved useful for initiating a dialogue on community issues, better utilization ofresources and services for the benefit of the community.
During the project implementation, information regarding health and nutrition services as well theentitlements was disseminated among more than three lakh community members each in Gujarat andRajasthan states. For improving availability and accessibility of the services, training of more than 600service providers were conducted at the block and district level and more than 1500 ASHAs were trained sothat they could play their roles and responsibilities effectively.
Training of more than 3000 VHSNCs/CBO members was organised inorder to generate awareness regarding their roles and responsibilities.Training of youth groups, self help groups were also organised for enablingthem to take initiative for improving availability and accessibility of healthservices. After training they were provided guidance and support in theirmonthly meetings.
During the project, various participatory communication processes wereadopted. This booklet presents the impact of some of these processes inthe form of stories.1 Fairs in Rajasthan: Gangaur fair, Kailadevi fair, Swasthya Chetna YatraFairs in Gujarat: Bhadarvi Poonam fair, Urs fair, School Health Campaign
The traditional methods ofcommunication deal withbehavioural change in anindividual where asparticipatory communicationpromotes individual as wellas social change.
Social change signifiespositive change in the life ofpeople especially themarginalised group.
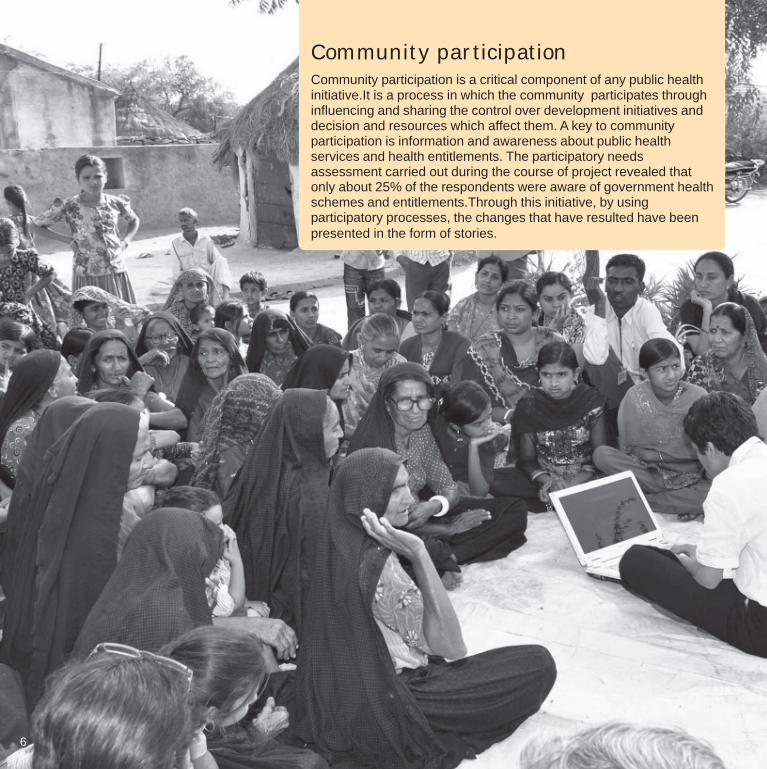
Community participationCommunity participation is a critical component of any public healthinitiative.It is a process in which the community participates throughinfluencing and sharing the control over development initiatives anddecision and resources which affect them. A key to communityparticipation is information and awareness about public healthservices and health entitlements. The participatory needsassessment carried out during the course of project revealed thatonly about 25% of the respondents were aware of government healthschemes and entitlements.Through this initiative, by usingparticipatory processes, the changes that have resulted have beenpresented in the form of stories.
6

Kutch, located on the western-most tip of India in thestate of Gujarat, is the largest district in the country.With more than 51% of its land covered by desertand with scant and irregular rains, it is underconstant threat of drought.
Abdasa is one of the remote coastal blocks of theKutch district. The area is arid and unproductive. It isinhabited by communities such as the BhanushalisKolis who are involved in fishing and wage labour,Maheshwaris who are primarily involved in farmlabour, Rabaris who are small cattle herders and,Muslims and Darbars, who own both land and cattle.
Lack of clean drinking water, food, fodder and greateconomic pressures have forced many people tomigrate to nearby towns. There is acute poverty andliteracy levels are also very poor. CHETNA’s partnerNGO in this project-Kutch Mahila Vikas Sangathan(KMVS) has been working in the region for over adecade with the overall aim of empowering womento increase their sustainable income. Theorganisation is also extensively involved in localradio broadcasting projects in tribal dialect to supportits community development work in the vastgeographic area. Localised research has been a keyapproach for developing radio programmes.
One of the major issues that arose during routinevillage visits in Abdasa was the low awareness of thecommunity about maternal and child healthentitlements under National Rural Health Mission(NRHM). In response, awareness activities werecarried out using posters, wall writings, streetmeetings and road shows. These were partlysuccessful in some villages.
During village level interactions, it was suggestedthat since most of the people in the block had
access to radio, televisions and local cable network,Compact Disc (CD) could be used forcommunicating health entitlements. This would alsohelp to reach out to a large audience at once.
KMVS picked up this idea, partnered with the localhealth department and produced an awarenesscapsule in the form of a audio CD, in local language(Kutchi). The aim was to educate the communityabout the importance of availing public healthservice, the interviews of Block Health Officials wereincluded to help community members identify andrecognise them.
The message in audio CD was given to the localcable operator for broadcasting repeatedly. It wasalso broadcast in the open: in village centres and inanganwadis. The health entitlements under NRHMwere also given in the form of jingles/advertisementsin Akashvani radio programme. The messages werereinforced with information given on the spot tomake learning interesting and memorable. In all, 100villages and four primary health centres werecovered with the broadcast, reaching out to close to26,000 people.
As a result, the demand for services at primaryhealth centres increased rapidly. Over a period ofnext eight months the usage of ‘108’ ambulanceservice and the number of institutional deliveries alsoincreased.
Community members are reported to have said thatthis was the first time they heard about the missionand entitlements related to maternal and child health.They expressed their gratitude for sharing informationin the local language.The format and content of theprogramme on the audio CD sold itself and asnowball effect brought about the desired result.
7
Cable Network Brings Change
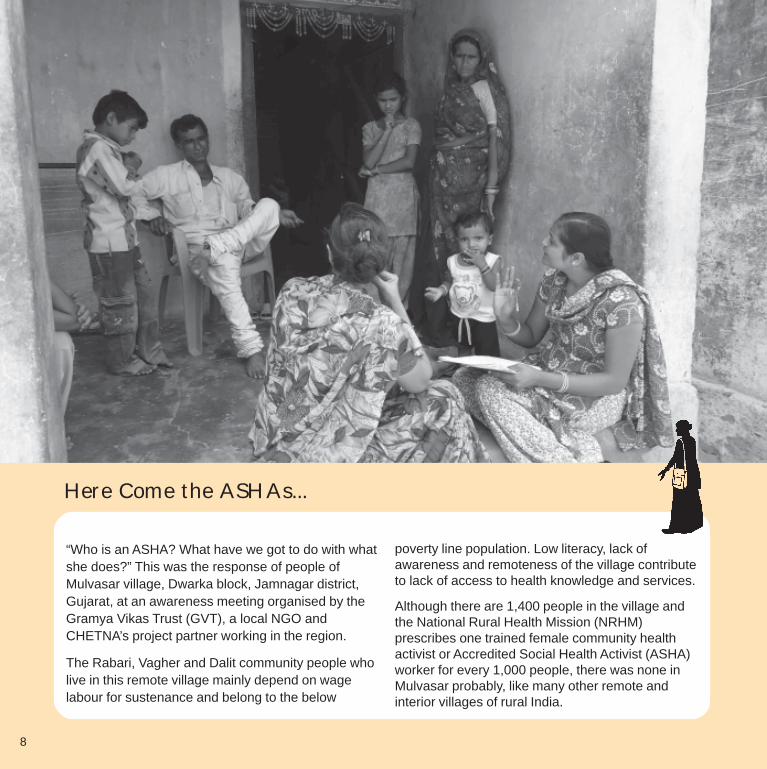
“Who is an ASHA? What have we got to do with whatshe does?” This was the response of people ofMulvasar village, Dwarka block, Jamnagar district,Gujarat, at an awareness meeting organised by theGramya Vikas Trust (GVT), a local NGO andCHETNA’s project partner working in the region.
The Rabari, Vagher and Dalit community people wholive in this remote village mainly depend on wagelabour for sustenance and belong to the below
poverty line population. Low literacy, lack ofawareness and remoteness of the village contributeto lack of access to health knowledge and services.
Although there are 1,400 people in the village andthe National Rural Health Mission (NRHM)prescribes one trained female community healthactivist or Accredited Social Health Activist (ASHA)worker for every 1,000 people, there was none inMulvasar probably, like many other remote andinterior villages of rural India.
Here Come the ASHAs...
8

9
Why have efforts to motivate local women to workas ASHA workers not been successful in thisvillage and many such villages in the country?Even when ASHAs are present, why are they notperforming their role efficiently? These questionsneed to be probed further. One possible reasoncould be that the key selection criteria for recruitingASHA worker is that she should be a literatewoman with formal education up to grade eight andpreferably a daughter-in-law (who is likely to livelonger in the village). Not many women venture outin this village due to lack of education and strictsocial and cultural norms for married women.
In 2011 as part of this project, the Gramya VikasTrust (GVT) team made the Block Health Officialaware that there was no ASHA in Mulvasar andthat local women needed to be motivated to workas ASHA workers. He agreed that some actionneeds to be taken and also suggested that foroptimal education in the community, instead ofholding a standardized training programme it wouldbe more appropriate to invite the existing ASHAsfrom other villages of the block to this village anddemonstrate how they play an important role inimplementing all MCH related schemes of NRHM.
In June 2011, in collaboration with the Block HealthAuthorities, GVT used the demonstration methodto introduce ASHA workers to the villagecommunity. For this, 21 existing ASHA workersfrom other villages were invited. They conductedhome visits and interacted with the community,assessed their knowledge on health entitlements,and gathered information on community concernsin accessing health services. The invitees also
shared their experiences of working as ASHAs withthe people in the village especially, women. Theymotivated them to register as ASHAs.
Open-ended questionnaires were provided to theASHA workers to gather information about theresidents’ level of knowledge and utilisation of healthservices. On the day of the demonstration, they wereable to reach close to 350 villagers from 64 families.
When the ASHA workers compiled and presentedtheir findings of the survey before the community andat the health sub-centre, it validated the fact thatresidents of Mulvasar had little information aboutmaternal and child health services.
After this initiative the community members realisedthat it was crucial to have an ASHA worker in theirvillage especially for maternal and child healthservices. Four women came forward to register asASHA. Similarly women from two other villages alsocame forward to register.
GVT motivated and supported the women andshared this information with the District HealthOfficials. They appreciated this innovative effort as itprovided an opportunity to see, hear, discuss andparticipate in the activity in the field and generatedinterest and enthusiasm among the communitywomen for practice.
One of the women was selected as ASHA worker forthe village. Needless to say, this methodology ofdemonstration and onsite mentoring will ensurebetter and efficient delivery of services by the ASHAswho represent the cornerstone of NRHM’sstrategies.

2010

11
Kataron ka Talaab is a small village in the Anandpuriblock of Banswara district, Rajasthan. It is populatedby the Bhil tribals who live here in nearly 600 housesscattered over a large terrain. More than half thepopulation here is illiterate with low awareness andutilisation of health and development services are low.
In spite of all the difficulties, the women of Kataronka Talaab have been running a Self-Help Group(SHG) named ‘Bhairavji’ through which they havebeen involved in various income generation activities.In March 2011, a local NGO, Association for AravaliSarva Seva Farms (ASSEFA), CHETNA’s projectpartner in the district, introduced health relatedactivities in the group. The organisation has beenmaking efforts to create health awareness amongthe members and mobilise them to access healthservices available from the government.
The ASSEFA team encouraged members of theBhairavji SHG to join the Village Health Sanitationand Nutrition Committee (VHSNC). They impartedtraining to the members and made them aware aboutthe community level health and nutrition servicesavailable to them under NRHM, and the role andresponsibilities of the VHSNC in ensuring theservices.
Kamla, a 50 year old homemaker and mother of four,was one of the participants at the ASSEFA training.She had studied up to grade two, many years ago.Inspired by the training, she started door-to-doormeetings with pregnant women and nursing mothersin her neighbourhood to spread awareness aboutmaternal and child health entitlements available to them.
Sulekha is one of the residents of the village and herstory exemplifies how Kamla’s small efforts areleading to big changes in the community.
Sulekha, a mother of a two year old girl waspregnant for the second time. On Kamla’s advice shediligently went for three antenatal check-ups and gottwo immunisation doses administered. The AuxiliaryNurse Midwife counselled her and ensured that shetook her Iron Folic Acid tablets as required. Close toher delivery date, Sulekha was also told about theimportance of institutional delivery and benefitsavailable to her under the Janani Suraksha Yojana.She received all the necessary services and help fora safe delivery.
Kamla shared that due to extreme poverty, most ofthe men migrate to nearby cities in search of work. Itis very difficult to contact and mobilise women andmotivate them to avail health services as they stay inscattered houses in this hilly region.
Kamla has been able to reach out to many womenlike Sulekha in the village. The process of involvingthe SHG members in mobilisation, action andbehaviour change on health related issues in additionto income-related activities has been tough. Butthere is hope because other SHG members arefollowing Kamla’s example and have taken theresponsibility of promoting health awareness in theirhutments.
For ASSEFA, this has been a lesson learnt. Alongwith a well organised primary and secondary healthsystem, community ownership is critical for healthawareness and utilisation of services.
Kamla rightly says, “Shuruat toh karo, karwan khudhba khudh jud jayega” meaning – take the first step inthe right direction and make a start; people willthemselves join in and make it a movement.
Women’s Self-Help Group: A GuidingForce for the Village

12
Late one night in February 2011, the mukhiya(village head) of Naal village, Gogunda, Udaipur,called “108”, the emergency medical referral service,so that a pregnant woman could be taken to thenearest community health centre for delivery. Thestaff who received the call informed that theambulance would reach the village only at 5 am thenext morning. The norms for the emergency referralservice prescribe immediate action; this delay ofabout four hours in accessing adequate medicalcare could have major health repercussions foranybody. Fortunately, the woman was transportedsafely when the ambulance arrived in the morning.
This incident came to light during a round table ofelected representatives, the mukhiya, ASHAworkers, Auxiliary Nurse Midwife and staff of a localNGO- Active for Literacy and EnvironmentalRenovation Task (ALERT Sansthan), which is alsoCHETNA’s partner and is working in 151 villages ofGogunda block. ALERT team helped the mukhiya toprobe the reasons for the delay in response from the108 service.
A conversation with the ambulance staff revealedthat the residents of Naal had pelted stones whenthe ambulance had entered the village on severaloccasions earlier. The staff had, therefore decided tostay away from the village during the late night hoursfor their own safety.
Naal is one of the remotest villages of the Gogundablock and is populated by the Bhil tribal community.Typically, the Bhils have a lower socio-economicstatus and they work on daily wages at nearby
construction sites. Traditionally they regard alcoholas “holy spirit” and many of them are involved inbrewing and consuming illicit liquor.
When the mukhiya questioned the villagers abouttheir strange behaviour towards the 108 ambulanceservice, they confessed that they were scared of theambulance’s siren. Some thought that the sirensignalled that the police was there to arrest thoseinvolved in brewing illicit liquor. Others thought theambulance would take their children away.
The ALERT representatives explained to the villagesarpanch (elected village head) about how using areferral transport was a health right and entitlementof the villagers. A meeting was called at the villagecentre. The panchayat members, the Auxiliary NurseMidwife, ASHA worker, school teachers, ALERTrepresentatives and local community-basedorganisations were invited. The idea was to explainto the villagers how their resistance could lead tomajor and negative health consequences.
After lengthy discussions, those present at themeeting were convinced and decided to takeresponsibility of ensuring safe passage of theambulance in their own hamlets on a 24/7 basis.The ambulance service staff was also informedabout this decision.
Ever since then, the ambulance has resumedservices in the Naal village. The story exemplifieshow the matter of ambulance service was simply,but quite effectively, addressed by building trustthrough open dialogue. This helped people realisehow the issue touched them personally and pavedthe way for their participation and ownership in theirlocal health service.
From Confrontation to Cooperation
13

Dialogic processThe Participatory Communication Initiative was built around debatesand negotiation to create linkages between different stakeholders ofNRHM, like panchayat. The Participatory Need Assessment (PNA)indicated to a lack of access of rural communities to forums fordialogue with service providers.
At the block and district level, meetings and consultations wereorganized with the health officials. The consultations focused onsharing the findings of the PNA, communication strategy and seekingtheir support in enhancing community’s awareness about the publichealth services. The health department and the service providersprovided support in organizing and implementing the activities. Theresults/outcomes achieved through the dialogue processes havebeen documented here in the form of stories.
14

The National Rural Health Mission (NRHM) is ahealth program for improving health care deliveryacross rural India. It aims at reduction of maternaland child mortality rates, universal access to publicservice with emphasis on woman and child health,prevention and control of communicable and non-communicable diseases, population stabilization,revitalization of local health traditions, genderbalance, etc.
Various factors are thought to be associated withmaternal mortality: factors that influence delays indeciding to seek medical care, in reaching a placewhere care is available and in receiving appropriatecare. The “108” free, ambulance service has beenintroduced mainly to transport pregnant women tothe nearest health centre, so that they receivetimely professional help. However, many questionsremain around the efficiency of the service and itsavailability for all rural communities.
The concerns related to operational issues of “108”were shared at a ‘Training of Trainers’ organised byCHETNA for its district partners, in February 2010.The findings from a participatory need assessmentconducted in five states indicated that the poorwere discouraged from using the “108” service
because further referrals (from the nearest healthcentre) were available for a fee. The possibility ofsuch a situation arising was discouraging womenfrom opting for institutional deliveries altogether.
When the Mission Director, who was also attendingthe session, learnt about this, she took up the issueseriously and after the training, held a meeting withthe concerned health officials. It was found that thiswas indeed a deterrent for poor, pregnant women allover the state. Within a week, a governmentresolution (RSD/Mission Director/D/10 dated March6, 2010) was passed stating that any pregnantwoman who is referred to the next health unit by aprimary or community health centre will receive freereferral transport support. In addition, the womancan avail of free transport service to return to hervillage from the health centre, after delivery.
Policy change rarely occurs quickly. But this strikingoutcome was a result of participatory andcollaborative processes among the network ofdistrict partner organisations who are working withthe common objective of improving the health statusof women and children in the rural areas of the stateas well as, the conviction and commitment of theMission Director towards reforming the healthservices in the country.
15
Advocacy for Change

16

17
For a person living below the poverty line, an illnessnot only represents a grave threat to her/his incomeearning capacity, it is often the reason why a familyfalls into a debt trap. Often, the need for treatment isoverlooked by the poor, not because of ignorancebut because of lack of resources and fearing loss ofwages. The Rashtriya Swasthya Bima Yojana(RSBY), a health insurance scheme, was launchedby the government under the National Rural HealthMission (NRHM) to address this lacuna, to help thepoor access services from hospitals.
In Valod, one of the tribal dominant blocks in Tapidistrict, issuance of RSBY schemes (and a card)had not been undertaken as envisaged underNRHM. Being a newly formed district, it had notbeen included in the RSBY information managementsystem yet.
Valod has a population of 87,127 and a literacy rateof 48 per cent. There is high incidence ofmalnutrition (close to 75 per cent) and Tuberculosis.The average lifespan of the population is 35 years,perhaps due to the high rate of liquor consumption.
In 2009, CHETNA’s project partner and a local NGO,Vedchhi Pradesh Seva Samiti (VPSS), conducted a
participatory needs assessment in the block. Itemerged from the assessment that due to lowawareness, NRHM services were not being availedof. With neither the RSBY card, nor the wherewithalto access private services, people were ignoringmost of their health needs until it was too late.
Looking to the organisation’s contribution in thedevelopment of the community in this area, theteam was invited to a high level meeting with all thesenior health officials of Tapi – the District Collector,the District Development Officer, Chief DistrictHealth Officer, and others. This was soon after theparticipatory need assessment in Valod. Apresentation by district health officials spoke aboutthe poor enrolment of RSBY in the district. TheVPSS team put forth its observations from Valod.The officials disclosed that Tapi, was recently movedout from the Surat district, and was yet to receive a‘district code’ from the central government, essentialfor issuing the RSBY cards.
The district development officer ordered the districtprogramme coordinator to visit New Delhi to followup on the district code. Within a week after themeeting, Tapi received its code and RSBY cardsbegan to be issued!
Advocacy for Health Insurance

18
‘Asha’ in Hindi means ‘hope’ and as the namesuggests, the ASHA worker is one, who inspiresconfidence of good health among the women andchildren of the deprived communities. She is the firstport of call for any health related demands of thepopulation, especially for women and children whofind it difficult to access health services.
She serves as an interface between the communityand public health system, creates awareness abouthealth and its social determinants among thecommunity and mobilises and facilitates them inaccessing the available services. But do all villageshave ASHAs?
Akhil Bharatiya Gramin Utthan Samiti (ABGUS) is aNGO and CHETNA’s partner organisation working inTijara block of Alwar district, Rajasthan. During acommunity meeting in the Fullavas village, it wasfound that people were not aware of the provision ofappointment of an “ASHA” worker in the area andthe health benefits that she could bring for thecommunity. This was perhaps because of the lack ofinterest of the sarpanch (elected village head) inhealth related issues.
In subsequent community awareness meetings, itwas found that there were many other villages wherean ASHA was not recruited at all.
The ABGUS team went to the primary health centreand gathered more information about the situation ofASHAs in other villages, the eligibility criteria for theirselection and the procedure for their appointment.
When this matter was discussed with the MedicalOfficer, he agreed that the health indicators invillages having ASHA workers were much better thanthose that did not have them and that this issueneeded to be taken up with block level authorities.
Over a period of four months, six meetings were heldwith the Block Chief Medical Officer, Block ProgramManager and Block ASHA facilitator to take action inthis matter. The problems in recruitment of ASHAs,awareness of the elected village heads, andperception of the community were discussed atlength. In the meantime ABGUS organised about100 awareness meetings in the Tijara block.
After this, when a meeting of sarpanchs was held atthe block level, the problems in the villages due toabsence of ASHAs were discussed. Everybodypresent, including the sarpanch of Fullavas assuredthat they would take on the responsibility ofidentifying and appointing ASHA workers. The ChiefMedical Officer of the block also sent out a writtennotice to this effect.
The collaborative effort of ABGUS team, BlockHealth Officials and Sarpanchs resulted in therecruitment of 25 ASHAs in the Tijara block in aperiod of four months. They are now spreading thelight of health information in the community. Goes toshow that small, simple actions can lead to bigresults provided enough of those small actions areput together in the same direction.
Small Efforts, Big Results
19
20
The Ribiya village lies 45 kilometres away fromChuru block in the Churu district of Rajasthan. Witha population of nearly 3,000 it has two anganwadicentres. One of CHETNA’s partner NGOs, theShikshit Rojgar Kendra Prabandhak Samiti(SRKPS), has been working in the Churu district.
In the last census survey it was found that thematernal and infant mortality rates here were higherthan the national average. Although SRKPS hasbeen creating awareness among the people aboutthe services available under National Rural HealthMission (NRHM), it was observed that when needed,these services were not available to the community.
In June 2011, during a community awarenessmeeting, the Block Link Worker of SRKPS, DhanpatSingh, shared details about the maternal and childhealth entitlements under NRHM. He also discussedthe health status of the village with the AuxiliaryNurse Midwife (ANM) and anganwadi workers.
When Singh visited Ribiya village for a communitymeeting the next month, he found that the ANM wasmissing. Community members informed him that theANM never opened the health sub-centre regularly.In fact the Maternal and Child Health Nutrition(MCHN) day was also not celebrated for the lastseven months. Because of this, nutrition and otherservices were not available in the village. Thecommunity members requested Singh to discuss
Community Monitoring: Making HealthFunctionaries Accountable to People
these irregularities with the higher authorities.However, he thought it would be better if thecommunity members take this issue up with thesarpanch. He encouraged them to do so.
In the next meeting in the following month, thecommunity members informed Singh that thesarpanch paid no heed to their complaints. Singh,along with some community members, went andmet the sarpanch and reminded him of hisresponsibility to ensure regular services at the sub-centre. The sarpanch was convinced that he shouldtake some action and, after repeated follow-ups bythe community, he sent a written complaint to theMedical Officer of the Primary Health Centre.
In response, the Medical Officer warned the ANM ofstrict action if services at the sub-centre were notregularised. Ever since then, the ANM has beenopening the sub-centre regularly. The MCHN day isalso being celebrated every month. The ANMcounsels the community members on health relatedissues and performs other duties as well.
People here have realised that they have a right tohealth services. They are now ready to takeresponsibility to bring about regularity in healthservices being provided at their village andcollectively solve any obstacles that come in the pathof realising their right to health.
21
Amplification of the voices of the vulnerableEvidently, an increased power and ability to communicate is what poorpeople wish for themselves as much as the more tangible developmentbenefits targeted by the Millennium Development Goals. When theWorld Bank asked 40,000 poor people in 1999 what they desired most,having ‘a voice’ was a very frequent reply, second only to improvedincome and basic necessities.
The Participatory Communication Initiative, not only assisted membersof the community to find a voice in appropriate forums, it also helpedservice providers address their concerns. advocacy issues emergedlike, non-receipt of remuneration on time, lack of proper training inputs,etc. Efforts were made to gather evidence and put them up at forumslike monthly meetings of primary health centres and ASHA sectormeetings among others. Some of these efforts have been documentedin the form of stories.22

Under the National Rural Health Mission (NRHM),the Accredited Social Health Activists (ASHAs) arecommunity based functionaries who have theresponsibility of acting as a change agent on healthat the village level. They are responsible formobilising the community towards local healthplanning and increased utilization of existing healthservices. Their success depends on their motivationlevel and the training and mentoring support theyreceive.
Most of them work in difficult circumstances and tryto deal with the community’s problems that arise ona day-to-day basis. But what happens when theythemselves face problems? Are they able to tacklethe problems on their own? This story is thoughtprovoking.
There were seven primary health centres inKhedbrahma block, Sabarkantha district, Gujarat,which is one of the most remote blocks, and ispopulated by the tribal communities. The healthstatus of the community is poor. GovernmentPrimary Health Centres are located at least 10 to 15kilometres apart and Community Health Centres areat a distance of about 40 to 50 kilometres from theinterior villages. In addition, every house is over akilometre away from the other making it difficult forthe community to access health services and healthworkers to reach the residents. But the ASHAworkers have been working tirelessly in all thevillages covered by these health centres.
In 2009, a local NGO, Narottam Lalbhai RuralDevelopment Fund (NLRDF) organised a trainingprogramme for these ASHA workers wherein theyshared that although they were working withcomplete dedication, they had not receivedincentives (amounting to Rs.700-1200 per month)for the past eight months. Understandably, they werefeeling demotivated. They did not, however, bringthis to the notice of government officials for fear ofannoying them and risking the renewal of ASHAcontracts the following year.
The NLRDF team convinced the ASHA workers thatthey should all raise the issue with governmenthealth officials in their Primary Health Centre (PHC)and with the block level health officials. They alsoassured them of complete support to ensure that therenewal of their contract would not be at risk.
The ASHA workers from Dantral, Lambadiya andDelwada gathered courage and spoke to the healthofficers at their PHC. As follow-up they also keptreminding the officers over the phone about theissue of pending dues.
After repeated reminders from the NLRDF team andthe Medical Officers, the BHO took up the issue atthe district level. The district authorities gave priorityto the issue and sanctioned the grants to therespective PHCs. Due to the collective efforts of theASHAs, NGO representatives and the HealthDepartment officials they received the incentives thatthey were entitled to within a period of 15 days.
23
Sustaining Commitment of CriticalHealth Workforce: The ASHAs

The Khedbrahma block of Sabarkantha district,Gujarat has a population of about 2.5 lakh people ofwhich over 60% comprises the Adivasis. In terms ofmaternal and child mortality, size of agriculturalholdings, access to water and electricity or literacylevels, the tribal communities lag far behind thegeneral population.
Remote location of villages, sparse, scatteredsettlements have resulted in poor acceptance andutilisation of health services. A Primary Health Centre(PHC) is located nearly 15 kilometres from thevillages and a Community Health Centre (CHC) is ata distance of about 50 kilometres. On an average, 19villages are serviced by one PHC. Over 80 villagesare severely inaccessible because of their location.Government and non-government health workers’outreach is restricted to houses in the proximity ofthe PHC. The issue is further compounded by low
levels of literacy (42 per cent among men and 32 percent among women) and associated myths andmisconceptions about medical treatments.
CHETNA’s partner organisation in this project,Narottam Lalbhai Rural Development Fund (NLRDF)is working along with the District Health and FamilyWelfare Department, Sabarkantha to promotecommunities’ access to quality health services in theKhedbrahma block.
In order to reach out to people in the interior villages,NLRDF proposed to use an innovative approach ofholding a two-week long “roadshow” in the month ofJune 2011.The idea was to go from village to village,share information about maternal and child healthentitlements, help the community to understand thepresent status of health services in the villages;provide a forum to share concerns related toaccessing health services; propose possible
24
And the Roadshow came to them...
25
solutions to address health concerns of communitiesand motivate them to access the services. This ideawas shared with the Block Health Officer whoencouraged and helped in charting out a route map ofvillages that could be covered by the roadshow.
The roadshow began on June 6, 2011, with jeepsdisplaying banners of health entitlements drivingthrough villages. Announcements were also made ona public address system attracting communitymembers to come and join the rally. Awarenessmeetings were organised; pamphlets and stickerswere disseminated as takeaways to reinforce the
messages. In the course of the road show, theNLRDF team spoke with ASHAs, pregnant womenand nursing mothers to assess their understandingof maternal and child health services, andexperiences of availing them.
As the roadshow travelled from one village toanother, volunteers, youth groups, members of self-help groups, health service providers and ASHAbegan to join in to help mobilise the community andto create awareness. Community members carriedout a signature campaign to highlight both concernsand possible solutions to health issues.
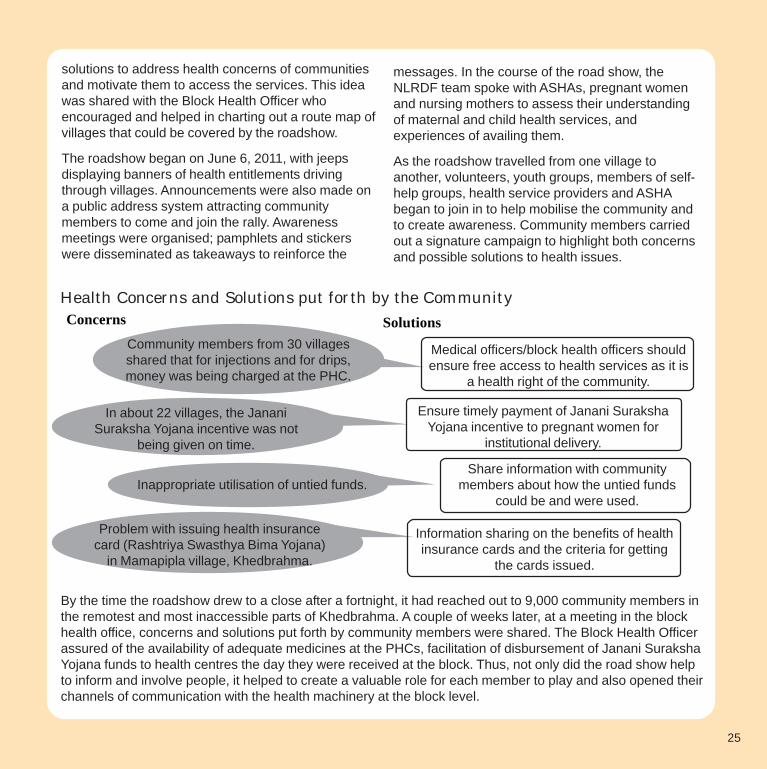
Health Concerns and Solutions put forth by the CommunityConcerns Solutions
Inappropriate utilisation of untied funds.
By the time the roadshow drew to a close after a fortnight, it had reached out to 9,000 community members inthe remotest and most inaccessible parts of Khedbrahma. A couple of weeks later, at a meeting in the blockhealth office, concerns and solutions put forth by community members were shared. The Block Health Officerassured of the availability of adequate medicines at the PHCs, facilitation of disbursement of Janani SurakshaYojana funds to health centres the day they were received at the block. Thus, not only did the road show helpto inform and involve people, it helped to create a valuable role for each member to play and also opened theirchannels of communication with the health machinery at the block level.
Community members from 30 villagesshared that for injections and for drips,money was being charged at the PHC.
In about 22 villages, the JananiSuraksha Yojana incentive was not
being given on time.
Problem with issuing health insurancecard (Rashtriya Swasthya Bima Yojana)
in Mamapipla village, Khedbrahma.
Information sharing on the benefits of healthinsurance cards and the criteria for getting
the cards issued.
Share information with communitymembers about how the untied funds
could be and were used.
Ensure timely payment of Janani SurakshaYojana incentive to pregnant women for
institutional delivery.
Medical officers/block health officers shouldensure free access to health services as it is
a health right of the community.

26
In January 2009, a disturbing trend was brought tolight at the monthly meeting of the Okha MandalShakti Sangathan, Dwarka (OSSD). The meetingwas organised by CHETNA’s partner NGO in thisproject, Gramya Vikas Trust (GVT), in the Dwarkablock of the Jamnagar District, to raise awareness ofmaternal and child health entitlements under theNational Rural Health Mission (NRHM) among thevillage community.
The OSSD self help group members shared that award boy had been employed in the CommunityHealth Centre (CHC) at Dwarka. Instead of thehealth worker, self-help group volunteers andtraditional birth attendants who were all women, andwere usually present in the health centre, he wouldbe present during labour in the labour room whichwas quite embarrassing for the women at the time ofdelivery. Further they complained that the ward boywould demand “tips” from the family members ofwomen after the delivery of the baby. He alsocharged more than the stipulated amount (Rs 60/-instead of Rs.16/-) for issuing age proof certificatesto senior citizens.
As decided in this meeting, the issue was raised withthe Superintendent of the CHC in February 2009.However, no action was taken against the ward boyin the next two months. In May 2009, OSSDmembers submitted a written complaint to theSuperintendent seeking necessary action. Thefollowing day, the Superintendent responded that thehealth worker and other women accompanying thepregnant lady are not allowed to enter the labourroom for hygiene purposes. Also, due to the non-
availability of appropriate woman staff, the boy hadbeen employed for cleaning the health centre. TheSuperintendent was open to considering womencandidates for cleaning staff (ward lady) if OSSDrecommended someone and agreed to pay her asalary of Rs 1,000 from the Rogi Kalyan Samiti’suntied fund. He urged the members to make thecommunity aware that there was no need to payanything more than the stipulated amount for ageproof certificates. He assured that stringent actionwould be taken against the errant ward boy and thatOSSD must not hesitate to bring up any such issuesin future too.
A ward lady was employed within a month. The wardboy’s job responsibility was altered so that heremained out of the labour room. Although theprocess took five months, the group felt it was worththe effort. However, despite efforts by thecommunity and members of the SHG, challengescontinue to loom large.
A follow up by OSSD, in August 2011, revealed thatthe ward boy had been reinstated because the wardlady left the job and no other qualified woman wasavailable.
Basic facilities and services at health centres aremany a time insensitive to women’s medical, socialand psychological needs. Simple issues such aslack of privacy could be a cause for acutediscomfort and embarrassment for womenrefraining them from accessing maternity care andother health care. Acts of corruption also impact thepoor heavily, affecting health outcomes. It is aconstant struggle to fill these loopholes.
27
Fighting Problems in Health CareDelivery...A Struggle

28

After going through two miscarriages will this 18 yearold pregnant woman be able to have a safe deliveryand give birth to a healthy child?
This story is about Munfida, who is a resident of theMilakpur Turk village, Tijara block, Alwar district,Rajasthan. She belongs to the “Meo” community, (aMuslim-Rajput community also called, Mewati),which is characterized by the practice of childmarriages.
Due to factors such as social insecurity, low financialstatus, illiteracy, and ignorance about theconsequences of early marriage, parents generallymarry their children off at a very early age. Munfidawas also married when she was 15 years of age andshe now lives with her husband in a joint family.
Even though this was the fifth month of her thirdpregnancy, Munfida had not been registered forantenatal and prenatal services, and had not takenimmunisation services due to lack of awareness.
During April 2011, Munfida happened to participatein an awareness meeting organised by CHETNA’sdistrict partner organisation- Akhil Bhartiya GraminUtthan Samiti (ABGUS). It is here that she learntabout the various maternal and child health servicesoffered by the government at the sub-centre, theimportance of institutional delivery, and the objectiveof celebration of Maternal and Child Health Nutrition(MCHN) day. She attentively listened to all the
information shared at this meeting and eagerlywaited for the next MCHN day celebration in hervillage.
When Munfida went to the sub-centre for the firsttime, she was very nervous. She hesitantly sharedher previous experiences of miscarriages with theAuxiliary Nurse Midwife (ANM). The nurse refused toregister her case saying that since she had not gonethrough the entire series of check-ups from thebeginning of her pregnancy she was not eligible toget registered at this late a stage. The ABGUS teammembers, who were present to support frontlinehealth workers on the MCHN day, overheard theconversation between Munfida and the ANM. Theyintervened and requested the ANM to registerMunfida since she had herself come forward to availthe available services now.
The ANM registered Munfida and gave her Iron Folictablets. Enthused by her new-found healthawareness, Munfida visited the health centre forregular check-ups and took the second vaccinationand the prescribed medicines. She continued toparticipate actively in all the awareness meetingsheld in her village.
A follow-up with the ANM revealed that Munfida gavebirth to a healthy baby and availed the benefitsunder the Janani Suraksha Yojana at the time ofdelivery. Munfida’s story shows that it is better latethan never.
Overcoming the Obstacle of Ignorance...
29

30

The toilet in the anganwadi centre of Sirsili village,Churu block, Churu district, Rajasthan, was in suchan appalling condition that it became a hugeproblem for the children who visited the centreeveryday as well as the women who visited thecentre on Maternal and Child Health Nutrition(MCHN) day every month. The communitymembers, ASHA worker and anganwadi workerrepeatedly raised the issue with the ward panch, thesarpanch, members of the Village Health Sanitationand Nutrition Committee (VHSNC), but no actionwas taken to repair it.
The toilet issue came up at one of the healthawareness meetings organised by Ms.Saroj, a BlockLink Worker of a local NGO and CHETNA’s partnerorganisation, Shikshit Rojgar Kendra PrabandhakSamiti (SRKPS). The Auxiliary Nurse Midwife (ANM)and ASHA worker shared that because of thedilapidated condition of the toilet the attendance ofchildren at the anganwadi had dropped. Womenwere also reluctant to visit the centre on the MCHNday for the same reason.
In February 2011, Ms.Saroj raised the issue at apanchayat meeting attended by all village levelhealth and panchayat functionaries. She alsodiscussed the importance of MCHN day, complete
immunisation and the availability of untied fund atthe disposal of the panchayat. She suggested to thesarpanch that some part of the fund could be usedto get the toilet at the anganwadi centre repaired.Other members at the meeting also supported heron the need to get the toilet repaired. Convincedabout the solution suggested, the sarpanch agreedto get the toilet repaired within a fortnight. As aconsequence, the toilet and other facilities at theAnganwadi centre which needed repair wererefurbished within a month.
Through this activity, the sarpanch realised theimportance of meeting the health needs of thevillage people. He shared the health relatedconcerns of the village in the monthly meeting of thepanchayat samiti at the block level. The BlockDevelopment Officer asked the appropriate officialsto ensure that all prescribed services were availableand facilities maintained well at anganwadi centresin each village of the block. All sarpanchs, andpanchayat samiti members as well as zilla parishadmembers were asked to participate in MCHN dayproceedings and to utilise the untied funds asrequired.
The results of all these efforts are now visible. Theutilisation of anganwadi services is reported to haveincreased dramatically by almost 80 percent.
A Toilet Brings in a Revolution!
31

Creating Ownership of and drivenby internal change agentsThe Participatory Communication Initiative has focused ondeveloping ownership of accessing NRHM entitlements fromwithin communities and community forums. In this view it hasinvested in building the capacity of village level functionariesand forums to play their part.
During the participatory need assessment, the members ofpanchayat and VHSNCs expressed the need for effectiveawareness programmes to be able to carry out theirresponsibilities better. Participatory communication initiativeemphasizes that communities should be the main protagonistsof process of social change rather than the passive beneficiariesmade by external players.
32
The Vadsar village in Abdasa block, Kutch district,has a predominantly illiterate and tribal population.In 2009, CHETNA’s partner NGO in this project,Kutch Mahila Vikas Sangathan (KMVS) carried outa participatory health needs assessment in theblock. It was found that there was ignoranceamong the villagers about health services,including maternal and child health schemes of thegovernment. The community members wereunaware of the entitlements under the NationalRural Health Mission (NHRM) and they wereconsistently paying for the services that areavailable free of cost at the government healthcentre under provisions of the Mission.
Although a Village Health Sanitation and NutritionCommittee (VHSNC) comprising 11 memberswere constituted in 2008, it was non-functional asneither the members themselves nor thecommunity were aware of their roles andresponsibilities. In one of the awareness meetingsit was found that the VHSNC members had noidea about the health issues in the village. Theywere not aware of the untied funds available in thebank and how they were to be utilised. Oninvestigation it turned out that the Auxiliary NurseMidwife (ANM) had just joined and the earlier ANMhad used some amount from the untied funds for
getting the village cleaned. An amount of Rs.6000/-was available in the bank.
KMVS organised a training programme for theVHSNC members to orient them and equip themto provide leadership as well as plan and monitorthe health activities in the village. They were madeaware of their role and responsibilities, providedclarity on untied fund and its use, and on thematernal and child health entitlements availableunder the NRHM. After this training, follow-upmeetings were held with the VHSNC membersregularly.
As a result the VHSNC members especially,women members, gained recognition in the villageand were successful in preventing doctors fromcharging for “free” services. They ensured thatcommunity members ask for receipt for all paidservices. They accompany pregnant women at thetime of their delivery and, wherever necessary,explain to doctors about the government normsunder NRHM. They have used the free, emergencyambulance service, gradually regularising its use inthe village.
In a period of more than two years, KMVS hasbeen successful in orienting the VHSNCs of theentire Abdasa block and this has improved thecommunity’s access to health services.
33
Ensuring Improved Access toHealth Care Services

34
Mohmadpura, on the banks of Mahi River, is oneof the most remote villages of Padra block inVadodara district. The population primarilycomprises the Madi, Chauhan and Darbarcommunities whose main livelihood is agriculture.
A local NGO and CHETNA’s partner in this project,the Shroffs Foundation Trust (SFT), has beenworking with the rural communities’ in the Padrablock to create awareness on maternal and childhealth issues and mobilise the community toaccess these services. During a training organisedby the NGO which was attended by frontline healthworkers of the block, members of Village HealthSanitation and Nutrition Committees (VHSNCs)and Sarpanchs, the representatives ofMohmadpura shared a concern that the monthly‘Mamta day’ (Maternal and Child Health Nutritionday celebrated once a month to provide essentialreproductive and child health services at theanganwadis under the National Rural HealthMission) was not being celebrated in the villageand this could be a cause for lack of awarenesson maternal and child health needs andentitlements. On follow-up, the SFT team learntthat the residents of the village were not aware ofNRHM and services and entitlements availableunder the mission.
In June 2010, seven meetings were facilitated bythe SFT team in the village. Cultural programmeswere organised in which health related informationwas shared in the form of “Bhavai” (popular folktheatre). Through the meetings, gradually, allmaternal and child health related issues werediscussed. The Sarpanch, Harman Padhyar,stayed in contact with the SFT team and acquiredmore detailed information about health servicesand entitlements. He initiated concerted effort toregularise Mamta day celebration. He would bepresent at every Mamta day celebration andadvise village health functionaries on how toconduct it. Anganwadi workers spread the wordabout Mamta day and its importance amongcommunity members when they visited theanganwadi and through home visits.
Over time, not only was Mamta day celebratedregularly, immunisation statistics went updrastically (to nearly 100 per cent). Nutritioncounselling was undertaken by frontline villagefunctionaries and followed by mothers. In all this,Sarpanch Padhyar played a key role. If one isclear about her/his aim and is determined to bringabout a change, then s/he is sure to find success.
35
The Story of an Inspirational Sarpanch

36

Madhuben, a traditional birth attendant inMohmadpura, is determined to promote institutionaldelivery of babies in her village. She knows thatinstitutional deliveries play a crucial role because ofthe availability of emergency obstetric care bytrained health professionals if required. Thematernal health components of National RuralHealth Mission (NRHM) are especially focused onenhancing women’s access to institutional deliveryat government health centres.
Notwithstanding provisions for services, poorawareness of entitlements and little control ondecision-making about their own health, force manywomen to opt for the private health care system. Ingeneral, there has not been much faith in publicsector healthcare.
Mohmadpura is the last village in Padra, locatednearly 25 kilometres from the block headquarter onthe banks of Mahi river. Most of the Chauhan, Madiand Darbar people in the village are farmers; somework in industries in Padra block, Vadodara districtin Gujarat. Low awareness led people to believe thatinstitutional delivery, use of government ambulanceservice, etc. would cost a lot of money.Consequently, home deliveries were rampant with itsattended dangers, a trend that came to light at acommunity awareness meeting organised by ShroffsFoundation Trust (SFT), a local NGO andCHETNA’s partner in this project.
The meeting was one of the many forums organisedto raise awareness levels about maternal and childhealth entitlements and services in villages. TheNGO approached Madhuben in June 2010, to helpthem in promoting safe deliveries. She is not only a
trained birth attendant, she is also a member of theVillage Health Sanitation and Nutrition Committeeand leader of a local women’s group. She has goodrapport with the community; they have faith in herand listen to her.
Although Madhuben has been working as a birthattendant for a long time, she realised her rolebeyond that of a TBA only when she participated inthe awareness meetings organised by the SFT overthe year. She learnt about how the risk of maternaland child mortality can be reduced throughinstitutional delivery and referrals to specialists.
She made it her mission to promote institutionaldeliveries in Mohmadpura. The shift was gradual butpeople’s faith in her helped to open their minds tounderstanding why it was necessary. She visitedAnganwadi centres, attended women’s forummeetings, ‘Mamta day’ celebrations and told mothersof children that shifting a new-born baby to a hospitalcan be dangerous. It is wise to have the delivery inthe hospital itself. Since decision makers in mostfamilies are mothers-in-law, she followed upmeetings with home visits.
Madhuben’s tireless efforts over eight monthsensured that 11 pregnant women registeredthemselves at the community health centre and thatall deliveries were conducted at health centres andhospitals during this period. She accompanied threewomen to the Centre for delivery. Pregnant womenthemselves used the free ambulance service to goto health centres. The staff of the community healthcentre and sarpanch acknowledged Madhuben’srole in enhancing the health status of women andthe new borns in Mohmadpura.
37
Making a Difference-The Power of One

38
Narayani Paliwal is 31 years of age and has beenworking as an ASHA in Parodi village, Gogundablock, Udaipur district, Rajasthan, for the past fouryears. She goes from door-to-door, mobilising thecommunity, encouraging and facilitating them toaccess health and nutrition related servicesavailable at the Anganwadi, sub-centre and theprimary health centre. This includes immunisation,Ante-Natal and Post-Natal check-up (ANC/PNC),supplementary nutrition, sanitation and otherservices being provided by the government. Shefulfils her responsibilities diligently.
What makes her case different from other ASHAsand is worth a special mention is that she does notlet her physical disability due to Polio come in theway of her work.
Narayani was married off at a very young age andshe lost her husband soon after giving birth to herthree children. Her youngest child was only threeyears old then. Since she had a family to fend for,she enquired about vacant positions for the post ofan Anganwadi worker in her village. There werenone. However, there were some vacant positionsfor ASHA workers.
In 2005 the sarpanch and other panchayat membersselected her for the post of ASHA and she tookcharge as an ASHA on 15th March 2005.
In 2010, a local NGO, ALERT Sansthan, which is apartner of CHETNA in this programme, organisedtraining for ASHA workers which helped her andothers gain clarity on their role and responsibilities.
The Pulse Polio Day is of special significance toNarayani. She goes door-to-door and administersPolio vaccine drops to children. She has vowed thatshe will not let any child in her work area suffer likeherself due to the negligence of her/his parentsregarding the available health services. Narayanisays in spite of being physically very demanding, thisjob gives her immense satisfaction and ALERT hassupported her at every step. Their trainingprogrammes have enabled her to understand herrole and responsibilities better. Regular discussionswith, and advice from ALERT staff has helped her toshare her concerns about field realities with peoplewith self-confidence.
Narayani’s tireless efforts have begun to showresults. There is more awareness about maternaland child health services among the community.With Narayani’s help, 11 women availed JananiSuraksha Yojana benefits in a period of six months.
Narayani brims with self confidence. She says“where there is a will, there is a way”. She is eagerto put in more efforts towards ensuring health anddevelopment of the community.
Where there is a will, there is a way...
39

40
Few years back, the dream of having healthy peoplein villages of Karauli district, Rajasthan, seemedfarfetched. In May 2009, CHETNA’s partner NGO inthis project, Society for Education ConscientisationAwareness and Training (ECAT), Bodhgram,conducted a participatory health needs assessmentexercise in 120 villages of the district. Strengtheningexisting Village Health Sanitation and NutritionCommittees (VHSNC) and enhancing universalaccess to public health services were highlighted ascrucial needs in the assessment.
It was evident that community members were notaware about the role and responsibility of VHSNCs.In fact, even the VHSNC members themselves wereunaware of their role and responsibility or about theprovisions of untied funds under the National RuralHealth Mission. Although the committees were inplace in 2008, VHSNC members had not undergoneany training until the assessment was done.
The ECAT team took on the challenge of revivingand strengthening the VHSNCs. The first step wasto make the members aware of the significance ofthe committee, and their role and responsibilities asmembers. Further, they had to be motivated toparticipate actively and contribute in the functioningof the committees.
As the first step, in July 2010, the ECAT team visitedKiratpura village and interacted with the VHSNCmembers. The idea was to ensure that the meetings
are held regularly and the members are motivated totake action. The team also met the auxiliary nursemidwife, anganwadi worker, ward panch and othermembers of the panchayat and spoke to them aboutthe importance of the VHSNC. Regular follow-upswere conducted throughout the year and this madesure that the VHSNC was working efficiently.
During a follow-up visit in February 2011, the ECATteam was informed that for the last two monthsnutritious food was not being supplied to theanganwadi. The VHSNC team was encouraged tobring up the matter during the next committeemeeting. The anganwadi helper shared this concernat the meeting and wrote a letter to the ChildDevelopment Project Officer (CDPO) of Karauliinforming about the situation on the field. The ECATteam also spoke to the CDPO over the phone. In aweek’s time, the anganwadi received the fresh,nutritious food supply.
Although this may seem like a small incident, it hasencouraged the VHSNC members to continueworking committedly towards creating a healthyvillage. VHSNC meetings are now held regularly inKiratpura and people are actively involved incommunity health care services. The ECAT teamhas helped in regularizing the functioning of 15VHSNCs in the Karauli block and the dream ofhaving healthy people and healthy villages in thisdistrict does not seem unachievable anymore.
A Little Handholding Goes a Long Way
41
42
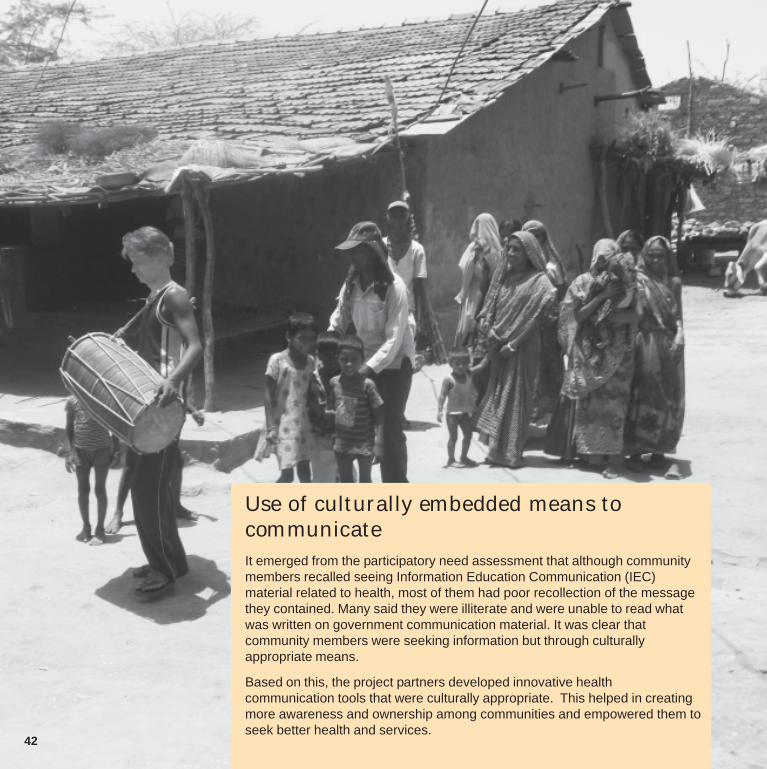
Use of culturally embedded means tocommunicateIt emerged from the participatory need assessment that although communitymembers recalled seeing Information Education Communication (IEC)material related to health, most of them had poor recollection of the messagethey contained. Many said they were illiterate and were unable to read whatwas written on government communication material. It was clear thatcommunity members were seeking information but through culturallyappropriate means.
Based on this, the project partners developed innovative healthcommunication tools that were culturally appropriate. This helped in creatingmore awareness and ownership among communities and empowered them toseek better health and services.

Rhythmic Drum Beats for a Healthy Life
Most villages in Anandpuri block of Banswaradistrict, Rajasthan, were performing poorly onmaternal and child health indicators – the level ofantenatal and postnatal check-ups, the extent ofimmunisation was worrisome. There was almost noawareness regarding the benefits of institutionaldelivery and entitlements under Janani SurakshaYojna among the local community. One wouldexpect the Maternal and Child Health Nutrition(MCHN) day celebrations to contribute in enhancingthe maternal and child health, but the attendanceduring this programme in these villages was alsodismal.
Under the National Rural Health Mission (NRHM)there is provision for the utilisation of untied funds ofRs 1,200 per year by the Village Health Sanitationand Nutrition Committee (VHSNC) for promotion ofMCHN day every month. But due to lack ofawareness, the untied funds were not being used forpromotion of MCHN day in Anandpuri. Theinformation about poor utilisation of the untied fundshere was published by a leading regionalnewspaper, Dainik Bhaskar.
This article caught the attention of one of the staffmembers of Association for Sarva Seva Farms(ASSEFA), CHETNA’s partner NGO in thisprogramme, working in Banswara district. Theorganisation held a series of meetings with thePanchayat (local self government) memberswherein the findings of an evaluation of the healthstatus of the region were discussed. Information onroles and responsibilities of the panchayat membersin implementation of NRHM, and the provision ofuntied funds was also shared.
Inspired by the discussions during these meetings,Devilal Masar, a member of the Navgaon panchayat,Anandpuri block, realised the importance of his roleand decided to do something to create healthawareness. He thought of using traditional folkmedia to promote the MCHN day. He used drums,which are a living tradition in the Indian socialsystem and are popularly used in ceremonial andreligious functions, to announce the MCHN day infour villages.
The initial response was slow. Women came out insmall numbers. Those who did, thought there was acelebration in the village. They were not interested inMCHN day services. It took a lot of convincing toensure that the initial curiosity generated by thebeating of drums was converted into utilisation ofservices. The panchayat members found it difficult togenerate and sustain the interest of the communitymembers in women and child health related issues.
Over time, the sarpanchs of six more villagesdecided to follow suit and utilise the untied fundsunder NRHM for MCHN day promotion using drumbeating. In these villages, the number of womenattending MCHN day celebrations and utilisingservices has begun to increase gradually from fouror five, to about 10 and 15. It is envisaged that thistrend will continue and all eligible women andchildren will be aware of the benefits of MCHN dayand they will actually utilise them. The story showshow Devilal harnessed the potential of traditionalmedia wisely and, gradually now a simplecommunication initiative seems to be converting intocommunity action.
43

44

The area under the Karauli block in the Karaulidistrict of Rajasthan is commonly known as ‘Daang’.The economy of this district mainly depends onmining activities. It is largely a rocky and forestcovered area and is inhabited by a scatteredpopulation comprising people working in the mines,or those engaged in agriculture or animal husbandry.Their literacy and education levels are dismal; as isthe awareness on maternal and child healthservices, especially, among the tribal community.
The Society for Education, Conscientisation,Awareness and Training (ECAT), Bodhgram -CHETNA’s project partner, adopted a novel way tocreate awareness on maternal and child healthservices and entitlements among the community.
They used magic shows as forums to share healthinformation. They felt it was an effective way ofbringing those people together who did not attendmeetings. It turned out to be effective in holding theirattention, making them think and act.
Since January 2011, the ECAT team has beenorganising magic shows in villages. For this, they gotin touch with a magician and discussed theinformation that was to be disseminated among thepeople. Team members visit the designated villagein the morning and inform residents about the show,individually and using public address systems. Closeto 300 people usually gather in the audience for themagic show, a majority among them are primarybeneficiaries of maternal and child healthentitlements.
The magician begins with items from his regularmagic shows. Once the crowd is engrossed in theshow, he begins sharing information about health
This Magic Works!
rights and entitlements typically in-between-items.He then speaks on various topics for example, theneed for Tetanus Toxoid injections and how they canbe accessed; the importance of completeimmunisation (BCG, DPT, Polio, and Hepatitis) andwhere one can get immunised; importance ofinstitutional delivery; the importance of nutritiousfood, etc. He sings songs to provide informationabout different diseases, precautions andtreatments. The magician also demonstrates how touse the ambulance service (‘108’) (what informationshould be provided once the call is made) and thebenefits of using the specialised service over otherprivate vehicle services.
Such magic shows were held eight times in a monthand were attended by nearly 2,000 people. At theend of each show, the ECAT team distributedleaflets containing information on maternal and childhealth and services.
A month after the magic shows, the Medical officerand staff of Kanchanpur Primary Health Centre inthe region validated that the number of calls for ‘108’ambulance service had indeed gone up. The turnoutat vaccinations had also increased.
The staff proposes that such magic shows should beorganised throughout the block for awarenessgeneration and utilisation of maternal and childhealth services.
This story shows how audience engagement wasused to communicate messages on maternal andchild health. It also goes to show that entertainment isprobably more powerful than delivering sermons andthat...this magic will surely work!
45

Listening to and Giving a Voice to the Marginalised
“It has been demonstrated that economic and technological inputs will go under-utilised without knowledge,and it is for the sharing of knowledge that communication is indispensable. For social change to occur theremust be opportunities for dialogue” says Silvia Balit, a noted Development Communication Consultant.The experience of implementing the “Participatory Communication Initiative for Improving Communities’Access to Health Services” project demonstrated that health communication is much more than providingone way information to people. It is a powerful medium for a two way dialogue among all the stakeholdersincluding the community, and can play a crucial role in empowering people to set their own agendas.Participatory health communication can be a means to develop local effort, local alliances, and to promote aspirit of self help in the community leading to a demand for better health standards.Stories in this booklet demonstrate that after the community members were empowered with healthinformation, over a period of time, a cadre of change agents was created who were able to communicate,discuss and take action on health related issues and concerns and achieve outreach and accountability.Learning: Participatory communication is a result-oriented process. It enhances the information, skills andself confidence of people and empowers them to gain control over the decision making on matters related totheir lives. It is difficult to implement it within the rigid time frames (of project and donor requirements) forquick results because for social change to occur it is important to pay attention to the needs and priorities ofthe community members and take them along.Interventions carried out under this project in 40 districts of seven states in India brought forth someimportant points which may be useful for the development of the other health programmes. They are:• Community members are the main actors in the process of social change and not merely passive
beneficiaries. They need to be involved from the programme planning stage itself.• The health of the community especially, the marginalised community is influenced by their social
environment which includes their personal behaviour. In view of this it is necessary that the campaign forsocial change is initiated by the community itself.
• Development should be seen as a transformative process (both at the individual and social levels)through which, communities become empowered to initiate a process of change.
On the basis of the experiences of the project, the following models were identified:• Integrating participatory communication in programmes: Principles and pillars of participatory
communication were used successfully at every stage of project implementation such as communityneeds assessment, capacity building, dialogue, as well as providing forums for advocacy.
• Communitisation of health care: Many a time, community participation in public health programmes islimited to them being passive beneficiaries. But in this project, the community members played an activerole in determining their own health needs and priorities, raised their voices and exercised their right tobetter health services and standards.
46
Media Coverage
47

Communication tools developed
48
CHETNA* meaning “awareness” in several Indian languages and anacronym for Centre for Health Education, Training and NutritionAwareness, is a non-government support organisation based inAhmedabad, Gujarat. Beginning its activities in 1980, CHETNAaddresses issues of women’s health and development in differentstages of her life from a “Rights” perspective.
CHETNA supports Government and Non-Government Organisations(GO and NGOs) through building the management capacities ofeducation/health practitioners/supervisors/ managers enabling them toimplement their programmes related to children, young people andwomen from a holistic and gender perspective and advocate forpeople centred policies and programmes.
CHETNA develops need-based training and education materials,which are widely disseminated at the State, National and Internationallevels.
CHETNA's Information and Documentation Centre (IDC) is a richsource of information for the needs of individuals, organisations,academicians, researchers and students.
CHETNA has been identified as a Regional Resource Centre (RRC)for Gujarat State and the Union Territories of Daman, Diu and DadraNagar Haveli to provide technical assistance to NGOs to improveReproductive and Child Health (RCH), facilitate GO-NGO partnership,document and disseminate successful approaches and provide inputsto Government of India (GoI) to ensure effective implementation ofpolicies.
*CHETNA is an activity of the Nehru Foundation for Development, which is a publiccharitable trust, registered under the Bombay Public Trust Act 1950.
Regarding Communication for Health India Network (CHIN):
CHIN was established in 1998 in partnership of four institutes.They are :
1 Child in Need Institute (CINI), Kolkata, West Bengal2 Christian Medical Association of India (CMAI), New Delhi3 Centre for Health Education, Training and Nutrition Awareness
(CHETNA), Ahmedabad4 Rural Unit for Health and Social Affairs (RUHSA), Vellore,
Tamilnadu
About CHETNA Partner OrganisationsKutch Mahila Vikas Sangathan (KMVS)Phone: 02832-223311/255125/222124Email: [email protected]
Gramya Vikas Trust (GVT)Phone: 02892-236551Email: [email protected]
Vedchhi Pradesh Seva Samiti (VPSS)Phone: 02625-222699/222064Email: [email protected]
Shroffs Foundation Trust (SFT)Phone: 0265-2680703/2680061Email: [email protected]
Narottam Lalbhai Rural DevelopmentFund (NLRDF)Phone: 079-22202999Email: [email protected]
Association for Sarva Seva Farms(ASSEFA)Phone: 02968-280758, 09468732198Email: [email protected]
Shikshit Rojgar Kendra PrabandhakSamiti (SRKPS)Phone: 01592-234664Email: [email protected]
Active for Literacy and EnvironmentalRenovation Task (ALERT) SansthanPhone: 0294-2420940Email: [email protected]
Society for Education, ConscientisationAwareness and Training (ECAT)BodhgramPhone: 01586-248919/248017Email: [email protected]
Akhil Bhartiya Gramin Utthan Samiti(ABGUS)Phone: 01493-243649, 513513Email: [email protected]