War "4re, W(Ae ,Pu r 'y, and tize Casualty - DTIC
300
War "4re, W(Ae ,Pu r 'y, and tize Casualty A37 72 Volume 2 fir "'t BEST AVAILABLE CCPY oK\ 7fJý ,Nt~ t
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of War "4re, W(Ae ,Pu r 'y, and tize Casualty - DTIC
War "4re, W(Ae ,Pu r 'y, and tize CasualtyA37 72 Volume 2
fir "'t BEST AVAILABLE CCPY
oK\
7fJý
,Nt~ t

"DISCLAIMER NOTICE
THIS DOCUMENT IS BEST
QUALITY AVAILABLE. THE COPY
FURNISHED TO DTIC CONTAINED
A SIGNIFICANT NUMBER OF
COLOR PAGES WHICH DO NOT
REPRODUCE LEGIBLY ON BLACK
AND WHITE MICROFICHE.

MEDICAL CONSEQUENCES OF NUCLEAR WARFARE
DTc QUA•ITY ISPECD 3
94 4 26 035

The Coat of Arms1818
Medical Department of the Army
A 1976i etching by Vassil Ekirnov of ailoriginal color print that appeared in
Thc~ Mi/itarrY Siiyc'on, VOL. XLI, No. 2, 19-17

Textbook of Military Medicine
SERIES ON COMBAT CASUALTY CARE
Published bv the
Office of the Surgeon GeneralDepartment of the Armny, United States of America
Senior Editor
Colonel Russ Zajtchuk, MC, U.S. ArmyDeputy Commander,
Walter Reed Army Medical CenterFormer Deputy Director, Directorate of Professional Services,
Office of the Surgeon GeneralProfessor of Surgery, Uniformed Services University of the Health Sciences
Managing Editor
Donald P. Jenkins, Ph.D.Office of the Surgeon General
Associate Professor of Surgery, Georgetown UniversityVisiting Associate Professor (f Anatomy,
Uniformed Services University of the Health Sciences
Associate Editor
Colonel Ronald F. Bellamy, MC, U.S. ArmyThoracic Surgery Service. Walter Reed Army Medical Center
Associate Professor of Military Medicine and Surgery,Uniformed Services University of the Health Sciences
Production Editor
Virginia M. IngramTMM Publications, Office of the Surgeon General
and the American Registry of Pathology

The first line of medical defense in wartime is the combat medic.Although in ancient times medics carried the caduceus into battle tosignify the neutral, humanitarian nature of their tasks, they havenever been immune to the perils of war. They have made the high-est sacrifices to save the lives of others, and their dedication to thewounded soldier is the foundation of military medical care.
Aooesslon ForNTIS QRA&I
DTIC TAB 0Unannounced 0Just i fiat ion
By
Distr~butbioa/
"Availability SedusJIi Sinai.
Spinla

The TMM Series
Part I. Warfire, WeaponrY, and tith Casnaltl!
Vol u me
I HAITI FFII 0U, ENVIRO\NIENT
2 MIEDICAlL ONSFQUE\CES OF NL(CI FAR WARFARE
3 MEDIC..\L CONSEQL ENCES OF BIOI X;ICAL %%ARFARE
4 MEDICAL. CONSFQCE\C(FS OF CI IF\IICAL WARFARE
CONVENIIONAL WARFARE: BALLISTIC, BLAST, ANDBLRN INICRIES
t, COM BAT STRESS
Part II. Principles of Medical Command and Support
Volume
I MEDICAL COMMAND AND SL PINORT IN AIRLAND BATTLE
2 MEDICINE IN LOW-INTENSITN CONFLICT
Part II1. Military Preventive Medicine and the Environment
Volume
I DEPLOYMENT AND MOBILIZATION
2 OCCCPATIONAL IIEALTIH: THE SOLDIER IN THEINDUSTRIAL. BASE
3 PERSONAL AND PHYSICAL READINESS OF THE SOLDIER
4 THE NATURAL. ENVIRONMENT: ALTITUDE, COLD.AND HtEAT
Part IV. Suirgical Combat Casualty Care
Volume
I TIlE CASUALTY
2 MEDICAL IMAGING
I A\ESTIIESIA AND CRITICAL CARE
4 IHEAD AND NECK SURGERY
5OPIITHALMIC SLRGERY AND NEUROSURGERY
CARDIOTIIORACIC SURGERY
7 ABDO\IINAL AND UROGENITAL SURGERY
S ORTHOPEDIC SURGERY
The artist, Ken Nakagawa, witnessed rescue operations performedby japanese naval personnel along a riverbank in Hiroshima at 0840on 6 Au~gust 1945. Approximately 280,000 deaths occurred as aconsequence of this first atomnic bombing. The reactions of othersurvivors are explored in Chapter 8.
Reprinted, by permission, from the Japanese Broadcasting Corporation(N HKy nottn).ie ~j c aci 'iaoi oI zios1tAei
can ed., 90. New York: Pantheon Books, Random I louse, Inc., c1981.
MEDICAL CONSEQUENCESOF NUCLEAR WARFARE
Specialty Editors
RICHARD I. WALKERT. JAN CERVENY
Contributing Authors
LEONARD A. ALTVICTOR BOGO
ROBERT F. DONSNUSHIN K. FARZANEHC. DOUGLAS FORCINO
LEO I. GIAMBARRESILARRY W. LUCKETT
THOMAS J. MacVITTIEG. ANDREW MICKLEY
BRUCE E. VESPERTHOMAS L. WALIZrN, Jr.
BRUCE R. WESTROBERT W. YOUNG
Armed Forces Radiobiology Research InstituteBethesda, Maryland
Defense Nuclear AgencyAlexandria, Virginia

CERTAIN PARTI; OF Tt IIS I'L BFI(A rIO\, PERTAIN TO COP)•RI(ItT REiS RICTIONS.
Al I. RKIGItl RE•ERVED
NO Ct•p' RII ITIED 'ART OF TIIs PI'Lil.-I-TIO\ MAY BE REPRODLLC FD ORtRA\\SM\IrrED IN A\) FORM OR B) ANNY MEANS, ELECTRONICOR \.IF( IIANICAI.. INCI LD)IN(, P1 IOTOPOI'Y, RECORDINC;, ORAN) INFORMATION. STORAGE AND RETRIEVAL SYSTEM. WITHOUTI'ERMISSIO\ IN WRITINV FROM THE PUBLISHER.
(tIAPTERS I,2,3,5,,7 10, AND I1ARE L S. GO\ERNMFNT WORKS IN THIE PUBLIC DOMAIN.
Published by TMM Publications, Office of the Surgeon General,5111 Leesburg Pike, Falls Church, Virginia 22041-3258
Colleen Mathews Quick, Publications Specialist
Librarlt of Consress Cataloging in Publication Data
Medical Consequences of Nuclear Warfare
Includes index.1. Radiation-Physiological effect. 2. Nuclear weapons-
Physiological effect. (eds.) Zaitchuk, 1i'; Jenkins, D. P.; Bellamy, R. F.; Ingram, V. M.I. Walker, Richard I II. Cerveny, T. Jar,
PRINTED IN THE UNITED STATES OF AMERICA
96 95 94 93 92 91 90 89 5 4 3 2 1

Contents
Foreword bv the Surgeon General xiPreface xiii
1 Nuclear Events and Their Consequences 1
2 Acute Radiation Syndrome in Humans 15
3 Triage and Treatment of Radiation-Injured MassCasualties 37
4 Treatment of Internal Radionuclide Contamination 55
5 Infectious Complications of Radiation Injury 67
6 Biological Assessment of Radiation Damage 85
7 Behavioral and Neurophysiological Changeswith Exposure to Ionizing Radiation 105
8 Psychological Factors in Nuclear Warfare 153
9 Long-term and Low-level Effects of Ionizing Radiation 171
10 Radiological Considerations in Medical Operations 227
11 Prospects for Radioprotection 245
Addresses 275Index 276
ix

Foreword
The dramatic technological, social, and economic progress of thetwentieth century has yet to prevent the use of armed conflict to re-solve political differences among nations. As those of us in militarymedicine prepare to support our forces into the next century, wemust continually be ready for the many challenges presented bymodern warfare.
The Army Medical Department has embarked on an ambitiousreadiness initiative. This new doctrine focuses on far-foward surgi-cal care, increased intensive-care capabilities, a policy of returningsoldiers to duty as far foward as possible, improved ground and airevacuation capabilities, new medical logistics systems that incorpo-rate blood-distribution networks, and improved management ofcombat stress. Our goals are to maintain our momentum as weconserve fighting strength and to support our soldiers and theirfamilies both in peacetime and in time of war.
The military health-care system is the largest comprehensivehealth-care organization in the United States. Because the vast ma-jority of our patients are not active duty military personnel, it mayseem that our day-to-day activities are far removed from what wewould be required to do during time of war. The ability to deploy ahighly trained medical corps to any area of the world, however, isour highest priority. To be effective, we must not only maintain thehighest standards of technical competence, but must also be pre-pared to use our skills creatively and courageously in situationsthat may be primitive, dangerous, or unknown. Major GeneralJames H. Rumbaugh, the late commander of Walter Reed ArmyMedical Center (who aptly described his organization as "the larg-est live-fire range in the Army"), understood that everything we doin our daily practice hones our expertise. Our readiness initiativewill provide a clearer combat context in which to apply that exper-tise. Lessons of medical survival have been learned in previousconflicts at great cost. We cannot afford to forget them.
It is my hope that you will find the Textbook of Military Medicineseries a useful addition to your readiness training programs, andthat it will stimulate you to think about and plan for what will berequired of each of us should the need arise to make a transitionfrom peace to war.
Lieutenant General Frank F. Ledford, Jr.The Surgeon General
U.S. Army
April 1989Washington, D.C.
xi
PrefaceMedical Consequences of Nuclear Warfare is the second volume of Part I, Warfare,
Weaponry, and tire Casualty. It addresses the increasingly important medical challengesof the consequences and management of radiation injuries.
The presence of vast nuclear arsenals has had a paradoxical effect on our collectivehuman consciousness: because we are unavoidably aware of the potential destructionstored in those warheads, we are less likely to use them in a global thermonuclear war.However, maintaining this deterrent carries its own high price. The likelihood of acci-dental detonations, small-yield nuclear attacks in regional conflicts, and radiation inju-ries in reactors and weapons plants increases as familiarity with this powerful forcespreads. Arms limitations agreements among superpowers are important, but third-world nations now too have access to the materials and technology necessary to enterthe nuclear arena. The volatility of world politics may be moving beyond the ability ofany policy- or lawmaking group to control. Given the devastating medical conse-quences that would follow a nuclear detonation or accident, the training of the medicalcorps in treating radiation syndromes will be a crucial factor in the effective manage-ment of casualties.
The rapidly expanding science of medical radiobiology has greatly affected the pro-spective readiness of the military medical corps to deal with these injuries. The ArmedForces Radiobiology Research Institute has been a leader in the establishment of thebase of scientific and clinical knowledge from which the current concepts of medicalmanagement have evolved. In addition to research, the institute is involved in continu-ing medical education and in our nation's emergency response system. It is in a uniqueposition to understand the importance of converting vast amounts of laboratory datainto practical, efficient medical techniques and treatments. The authors have writtentheir chapters from a combined academic and military perspective in order to specifi-cally help the military physician.
Captain Richard I. Walker, MC, U.S. Navy, and Major T. Jan Cerveny, MC, U.S. AirForce, provided the expertise in the organization of this textbook. The first chapter isan overview of nuclear events and their consequences. The following chapters examinethe effects of radiation exposure on humans and the ways they will affect triage, diag-nosis, and treatment protocols as well as military logistics. A discussion of the latestprospects for radioprotection concludes the text.
It is possible that no amount of knowledge or training will help any medical unit todeal with the mass casualties that a large-scale radiation incident or accident would in-cur. However, data from accidental and therapeutic radiation exposures, together withongoing clinical research results, are all useful in determining the treatment of individ-ual victims of smaller incidents who are in a position to be saved.
The Textbook of Military Medicine series is a reality because of the vision and supportof the late Major General James H. Rumbaugh; Lieutenant General Frank F. Ledford,Jr., the Surgeon General of the Army; Lieutenant General (ret.) Quinn H. Becker, ourformer Surgeon General; and Major General Robert H. Buker, Deputy Surgeon Generalof the Army.
The editors gratefully acknowledge the assistance in the preparation of this volumeof Junith Van Deusen, Modeste E. Greenville, Sonia Jones, and Carolyn B. Wooden ofthe Publications Division of the Armed Forces Radiobiology Research Institute.
Colonel Russ ZajtchukU.S. Army
April 1989
xiii

Chapter 1
NUCLEAR EVENTSAND THEIR CONSEQUENCES
LEONARD A. ALT, M.S.,* C. DOUGLAS FORCINO, Ph.D.,** and RICHARD I. WALKER, Ph.D.***
INTRODUCTION
NUCLEAR AND PHYSICAL PROCESSES IN WEAPONS
Nuclear EnergyEnergy Release in Nuclear WeaponsProduction of Blast and Thermal Effects
BLAST, THERMAL, AND RADIATION EFFECTS
Blast EffectsThermal Effects
Burn InjuryEye Injury
Effects of Initial and Residual RadiationsFalloutCharacteristics of Fallout and the Prediction of Hazards
MEDICAL CONSEQUENCES OF NUCLEAR WEAPONS
The Chernobyl AccidentNature of Radiation InjuriesAcute Radiation Syndrome and Associated SubsyndromesCombined Injury
*Major, United States Army, Program Manager, Radiation Sources Department, Armed Forces Radiobiology Research Institute,Bethesda, Maryland 20814-5145-Lieutenant, United States Navy; Department of Military Medicine, Uniformed Services University of the Health Sciences,Bethesda, Maryland 20814-4799***Captain, United States Nazy; Director, Enteric Diseases Program, Naval Medical Research Institute,Bethesda, Maryland 20814-5055 and Armed Forces Radiobiology Research Institute, Bethesda, Maryland 20814-5145

Medical Coniset'qeices Of Nuchear Warfaire
INTRODUCTION
Radiation damage to human cells was first recog- these nuclear weapons in a confrontation would nul-nized just 4 months after the reported discovery of X lify an effective medical response. Rational mindsrays by Wilhelm Conrad Roentgen. In 1896, Dr. J. must continue to recognize this potentially devastat-Daniels found that the irradiation of his colleague's ing nuclear power and maintain a general peace, asskull resulted in loss of hair. Since then, many other they have for over 40 years.biomedical effects of radiation have been described. The deterrent effect of nuclear weapons does not
The understanding of atomic physics increased mean that military physicians can ignore the possi-rapidly in the early twentieth century and culmi- bility of their use. The most likely situations requir-nated in the Manhattan Project, which harnessed the ing a medical response are the use of weaponspower of the atom in a bomb. Thus began the nu- against a deployed naval force, a remote city, or aclear era in international relations and warfare, remote facility; a third-world conflict; a terroristbringing new challenges to the military physician. act; or an accident involving a nuclear weapon.
Today, more and more countries are developing Military medical preparedness can focus beyondnuclear weapons, with those in the United States nuclear weapon events. Today, nuclear material isand the Soviet Union achieving the greatest capabili- used in medicine, industry, and power generation,ties. One modern American or Soviet submarine bringing increased risk of occupational and acciden-carries nuclear weapons that can release energy tal exposures. New radiation hazards in space willequivalent to 500 bombs of the size used at Hiro- have to be overcome if successful peacetime andshima in 1945. This vast power is greater than the military uses of that frontier are to be realized. Mili-energy released from all weapons in all previous tary physicians trained to respond to weapons-re-wars combined. Of course, the extensive use of lated injuries can bring expertise to these situations.
NUCLEAR AND PHYSICAL PROCESSES IN WEAPONS
Weapons-related injuries can be best understood energy can, under suitable conditions, be trans-after examining the destructive forces-blast, ther- formed into kinetic energy, which is energy of mo-real, and radiation-that produce them. In compari- tion. When a conventional explosive such as TNT isson with a conventional explosive weapon, a nu- detonated, the relatively unstable chemical bondsclear weapon's effectiveness is due to its unequalled are converted into bonds that are more stable, pro-capacity to liberate a tremendous quantity of energy ducing kinetic energy in the form of blast and ther-in a very small space in an extremely short time. mal energies. This process of transforming a chemi-This section presents a simple description of the cal system's bonds from lesser to greater stability isphysical processes taking place within the first few exothermic (there is a net production of energy).thousandths of a second after a nuclear weapon Likewise, a nuclear detonation derives its energydetonation. from transformations of the powerful nuclear bonds
that hold the neutrons and protons together withinNuclear Energy the nucleus. The conversion of relatively less stable
nuclear bonds into bonds with greater stabilityEnergy may be broadly classified as potential or leads not only to the liberation of vast quantities of
kinetic. Potential energy is energy of configuration kinetic energy in blast and thermal forms, but alsoor position, or the capacity to perform work. For to the generation of ionizing radiations.example, the relatively unstable chemical bonds To discover where these energies come from,among the atoms that comprise trinitrotoluene consider the nucleus of the helium atom, which is(TNT) possess chemical potential energy. Potential composed of two neutrons and two protons bound
2

Nuclear Events and Their Consequences
z0tUw01
z FISSION4-J
CL.
z
z
NUMBER OF NUCLEONS(neutrons plus protons)
Fig. 1-1. Curve of binding energy per nucleon
tightly together by the strong (or specifically nu- has a large amount of binding energy. If the totalclear) force. If we compare the bound neutrons and binding energy for each element is calculated andprotons to those in the unbound state, we find that divided by its total number of nucleons (that is,the total mass of the separate neutrons and protons neutrons plus protons; for helium, two neutronsis greater than their mass when they bind together plus two protons equals four nucleons), a measureto form the helium nucleus. The mass that has been is obtained of how tightly the average nucleon islost in the process of forming the nuclear bonds is bound for that particular atom. A plot of this "aver-called the mass defect. Einstein's famous equation, age binding energy per nucleon" for each elementE = mc2 (energy equals mass multiplied by the gives the curve in Figure 1-1.speed of light squared), quantifies the conversion of It is significant that this curve has a broad maxi-this missing mass into the binding energy that holds mum. This means that there is a range of elementstogether the helium nucleus. This is the potential for which the neutrons and protons are most tightlyenergy stored in the bonds of the strong force. A bound and, thus, have the most stable nuclej.small amount of mass, when multiplied by the bonds. If nuclei having less stable nuclear bondspeed of light squared (an extremely large number), can be converted into nuclei having more stable

Medical Constq4ences of Niclear Wartart
bonds, the system will pass from a state of lesser to kiloton, or kt, equals the energy released by detona-greater stability, and energy will be released. This is tion of 1,000 tons of TNT, and 1 megaton, or MT,the energy source of nuclear weapons. The process equals 1,000,000 tons of TNT). The implosioncan occur in two ways: fission or fusion. Fission is weapon uses an extremely complex system of pre-the process of breaking less stable larger elements cisely formed, conventional chemical-explosive(such as uranium and plutonium) into two of the lenses to crush a mass of plutonium-239 to super-more stable midrange elements. Fusion is the pro- critical density. The first tested nuclear weapon (thecess of combining lighter nuclei (such as those of Trinity device) and the 21-kt-vield weapon used atdeuterium and tritium, which are isotopes of hydro- Nagasaki were implosion devices. From the view-gen) into heavier elements lying farther up the curve point of a weapon's accessibility, it is fortunate thatof binding energy per nucleon, the much more easily constructed gun-assembled
weapon cannot effectively use the more readily pro-Energy Release in Nuclear Weapons ducible plutonium-239. Instead, it must be fueled
with uranium-235, which is more difficult to obtain.A fission nuclear device is practical for only three The limit on a fission weapon's yield, from an
elements: uranium-233, uranium-235, and pluto- engineering viewpoint, is several hundred kilotons.nium-239. In order to construct an efficient weapon, Therefore, the multi-megaton weapons in theinstability is induced in one of these nuclei by strik- American and Soviet inventories are fusion weap-ing it with a neutron. The unstable nuclear bonds ons, deriving much of their power from the combi-are broken, the nucleus splits apart, and relatively nation of light isotopes of hydrogen (deuterium andmore stable nuclear bonds are reformed by each of tritium) into heavier nuclei lying farther up thethe two midrange fission fragments. This is accom- curve of binding energy per nucleon. Due to thepanied by the release of a large quantity of energy presence of powerful forces of electrostatic repul-and the prompt emission of gamma rays and neu- sion, initiation of the fusion of deuterium and tri-trons (initial nuclear radiation). It is important to note tium requires extremely high temperatures, aboutthat approximately 82% of the fission energy is re- 50,000,000°C. The only practical way to achieveleased as kinetic energy of the two large fission frag- those temperatures in a weapon on earth is to deto-ments. These fragments, being massive and highly nate a fission device inside the fusion materials.charged particles, interact readily with matter. They The deuterium and tritium then fuse and releasetransfer their energy quickly to the surrounding energy, partly in the form of highly energetic andweapon materials, which rapidly become heated. penetrating fusion neutrons, which have energiesThe fission fragments consist of over 300 different about ten times the typical energies of fission-gener-isotopes of thirty-eight separate chemical elements. ated neutrons. The fusion weapon then uses theseMost of the fragments are highly unstable radioac- high-energy fusion neutrons to cause secondary fis-tively and will later contribute to the radiologically sions. Thus, a fusion weapon actually generatesand chemically complex fallout field, power from both fission and fusion processes, usu-
One fission event alone does not make a weapon, ally in roughly equal proportions.which requires a self-perpetuating, exponentially es- An enhanced radiation weapon, or neutron bomb,calating chain reaction of fissions. This is achieved might be produced by altering the design of a stan-by the suitable physical arrangement of certain nu- dard small-yield fusion weapon to permit the high-clear materials. Also, since the weapon must not energy fusion neutrons to better escape the device.reach the proper, or critical, configuration until the This modification increases the initial production ofdesired time of detonation, some way must be found neutron radiation, reduces the proportion of theto make the transition on demand from a safe, or weapon's energy expressed in blast and t' "mreal ef-subcritical, condition to the critical state. In a func- fects, and reduces the amount of residual tailout ra-tioning fission device, this is done by altering the diation. Thus, a given total yield produces moremass, shape, or density of the nuclear materials, biologically damaging neutron radiation, less de-
The two basic classes of fission weapons are the struction of materiel from blast and thermal effects,gun-assembled device and the implosion device. The and less residual radiation fallout.gun-assembled weapon is a mechanically simple de-sign that uses a "gun tube" arrangement to blow Production of Blast and Thermal Effectstogether two small masses of uranium-235 to form asupercritical mass. The 15-kiloton-yield weapon The blast and thermal effects of detonation pro-used at Hiroshima was a gun-assembled device (1 duce by far the greatest number of immediate hu-
4

Nuclear Ezents and Their Consequiences
EnhancedStandard Fission/Fusion Radiation Weapon
Residual
Thermal (fallout)Therm25% Radiation35%
Blast Blast
10% Residual50% (fallout) 40% 30% Initial
% Radiation Radiation
InitialRadiation
Fig. 1-2. Energy partition of a nuclear weapon
man casualties in nuclear warfare. The nuclear re- is the source of the destructive blast wave and fur-actions within the weapon have died out after the ther thermal radiations. A unique interaction be-first one-millionth of a second, and the fission and tween the X-ray-heated air and the case-shock-fusion events have produced a vast quantity of en- heated air is responsible for the nuclear weapon'sergy, which has been rapidly and locally transferred characteristic double pulse of thermal output.to the bomb materials in the form of heat. The Added to these blast and thermal effects is the ini-weapon's materials (bomb casing, electronics, tial nuclear radiation (primarily neutrons andchemical explosive residues, and 80% of the original gamma rays) which is produced promptly by thenuclear fuels, which even in a relatively efficient fission and fusion processes, and the residual radia-device remain unreacted) now exist as a highly en- tion (primarily gamma rays and high-energy elec-ergetic plasma of positive ions and free electrons at trons) which are produced later by decay of the ra-high temperature and high pressure. Through a dioactive fission fragments composing the falloutprocess of electron-ion interaction known as field. Figure 1-2 depicts the typical energy partitionbremsstrahlung, the plasma becomes an intense for a standard fission or fusion device and the en-source of X rays. These X rays leave the vicinity of ergy partition expected from a typical enhanced-ra-the bomb materials at the speed of light, heat the diation weapon (neutron bomb).first several meters of air surrounding the weapon, The range of the blast, thermal, and radiation ef-and generate a fireball with an initial temperature of fects produced by the detonation of a nuclear1,000,000°C. The intensely hot fireball reradiates weapon depends on many factors, perhaps the mostthermal energy in the form of electromagnetic ra- significant of which, for the battlefield soldier, is to-diation at infrared, visible, and ultraviolet frequen- tal weapon yield. Figure 1-3 shows the range overcies. which the various effects are lethal, as a function of
At about the same time, the weapon's materials yield. It is noteworthy that initial radiation is thehave started to expand supersonically outward, dominant threat for only very small tactical devices,dramatically compressing and heating the sur- and thermal effects are dominant for large-yieldrounding air. This phenomenon, called case shock, strategic weapons.
5

MIedical Conse'que'nces of Nuhlear Warfare
BLAST, THERMAL, AND RADIATION EFFECTS
The destructive blast, thermal, and radiation ef- eardrum is about 5 psi. Although this injury is veryfects of a fission or fusion weapon all stem from the painful, it would not limit the accomplishment of adevice's capacity to transform the very strong nu- critical military mission. The 160-mph winds thatclear bonds of uranium, plutonium, deuterium, and accompany the passage of a 5-psi blast wave wouldtritium from a relatively unstable state to a more be sufficiently strong to cause displacement andstable one. The quantitative difference between the possible injuries. At the other end of the spectrum,effects of a nuclear weapon and the effects of a con- a pressure level of 15 psi will produce serious in-ventional explosive is the result of the dramatically trathoracic injuries, including alveolar and pulmo-greater strength of the nuclear bonds. A qualitative nary vascular rupture, interstitial hemorrhage,difference arises from the production of (a) initial edema, and air emboli. If the air emboli make theirnuclear radiations from the fission and fusion pro- way into the arterial circulation, cerebral and myo-cesses themselves and (b) delayed radioactivity cardial infarctions may ensue. The initial outwardfrom decay of the unstable fission fragment by- signs of such pulmonary damage are frothy bleed-products. ing through the nostrils, dyspnea, and coughing.
Victims may be in shock without any visibleBlast Effects wounds. In addition, serious abdominal injuries,
including hepatic and splenic rupture, may resultDuring the detonation of a standard fission or from a rapid and violent compression of the abdo-
fusion nuclear device, the rapidly expanding men.plasma gives rise to a shock or blast that is respon- The blast winds that accompany the blast wavesible for dissipating about 50% of the total energy of can also produce injuries. Debris carried by thethe weapon. This represents a tremendous amount wind may cause missile injuries ranging from lac-of energy, even in small, tactical-sized weapons of a erations and contusions to fractures and bluntfew kilotons. As the blast wave travels outward trauma, depending on the projectile's size, shape,from the site of the explosion, it is composed of and mass. Wind velocity of 100 mph will displacestatic and dynamic components that are capable of a person, resulting in lacerations, contusions, andproducing medical injuries and structural damage. fractures from tumbling across the terrain or fromThe static component of the blast wave is a wall of being thrown against stationary structures. Windscompressed air that exerts a crushing effect on ob- capable of causing displacement injuries or missilejects in its path. The dynamic component is the injuries would be produced by a blast wave with anmovement of air caused by and proportional to the overpressure of less than 5 psi. At this pressuredifference between the static overpressure and the level, the blast winds are more significant in pro-ambient pressure. In this discussion, the static and ducing injury than is the static component of thedynamic components will be called the blast wave blast wave. At high pressure levels, both the staticand blast wind, respectively, and dynamic components are capable of producing
In discussing the structural damage to buildings serious injuries.after a nuclear detonation, it is difficult to separate Although the LD, (lethal dose, or fatal injury, forthe effects of the static component from those of the 50% of cases) from tumbling occurs at about 50dynamic component. For example, the 5-psi mph, the LD•, from impact occurs at about 20-25(pounds per square inch) blast wave and 160-mph mph. The LD, from blast is estimated to occur at 6blast winds associated with the blast wave's pas- psi, due primarily to the force of blast winds. For asage would destroy a two-story brick house. small tactical weapon or terrorist device with a
However, the medical problems resulting from yield of 0.5 kt, the range for this level of overpres-exposure to the shock wave can be divided into sure would extend to slightly less than 0.5 km. Forthose that result from the static component and larger tactical or strategic weapons with yields of 50those that result from the dynamic component. In- and 500 kt, the range for LD,0 at 6 psi would ex-juries resulting from the blast waves will be caused pand to just under 2 km and just under 4 km, re-by exposure to high pressures with very short rise spectively.times, and will consist primarily of internal injuries. Protection from the effects of the blast wave isFor example, the threshold level for rupture of the difficult to achieve because it is an engulfing phe-
6

Nuclear E pitts and Their Conseiqpent's
nomenon. The best protection can be found in a netic energy of the thermal pulse travels in ablast-resistant shelter. However, protection from straight line, so any barrier placed in its path willthe effects of the blast winds can be achieved in any offer some protection. Even clothing will providelocation offering shielding from the wind. If ade- some protection from the deposition of thermal en-quate shelter is not found, the best defens- against ergy onto the skin. Since light colors tend to reflectblast effects is to lie face down on the ground with rather than absorb thermal energy, light-coloredfeet pointed toward ground zero. This reduces the clothing will offer more protection than dark-col-body's surface area that is exposed to wind-borne ored clothing.debris and offers less resistance to the force of the Figure 1-3 shows the range of LD, for burn in-blast wind. jury from weapons of different yields. Notice that
for weapons of very low yield, the range for burnThermal Effects injury LD•,, is about equal to the range for the LD,
from blast and radiation. As the weapon yield in-Following the detonation of a standard fission or creases, the range for burn injury increases much
fusion device, approximately 357 of the weapon's more rapidly than the range for blast injury or ra-energy is dissipated as thermal energy. The general diation injury. This means that burns will alwaystypes of injuries resulting from this energy are be present after the detonation of a nuclear device,burns, including flash burns and flame burns, and and for weapons with a yield above 10 kt, burnscertain eye injuries, including flash blindness and will be the predominant injury. Because of the largeretinal b71rns. number of burn casualties and the time- and labor-
The thermal output after a nuclear detonation intensive treatment that they require, burn injury isoccurs in two distinct pulses, as a result of the inter- the most difficult problem to be faced by the mili-action of the shock wave with the leading edge of tary medical community in a nuclear conflict.the fireball. The first pulse contains only about 1% Eye Injury. Thermal energy may also cause eyeof the total thermal energy output and is composed injury. The two types of eye injury that would oc-primarily of energy in the ultraviolet range. Be- cur would not burden a medical facility. Flashcause the first pulse is of very short duration and blindness is a temporary condition that results fromthe ultraviolet energy is rapidly absorbed by the a depletion of photopigment from the retinal recep-atmosphere, it does not contribute significantly to tors. This happens when a person indirectly ob-producing casualties. The second pulse is com- serves the brilliant flash of intense light energy fromposed primarily of energy in the infrared and vis- a fireball. The duration of flash blindness can be asible portions of the electromagnetic spectrum, con- short as several seconds during the day, followedtains about 99%4 of the thermal energy liberated by by a darkened afterimage for several minutes. Atthe nuclear detonation, and is responsible for subse- night, flash blindness can last three times longer,quent burns and vision problems. with a loss of dark adaptation for up to 30 minutes.
Burn Injury. The two types of burn injury, flash This could seriously compromise military opera-burn and flame burn, are caused by different events tions.and have different prognoses. Flash burn results Another eye injury is retinal burn, which resultsfrom the skin's exposure to a large quantity of ther- from looking directly at the fireball and focusing itsmal energy in a very brief time. This often leaves image on the retina. This intense light energy isthe affected area of the skin with a charred appear- strong enough to kill the retinal receptors and createance. However, since the heat pulse occurs rapidly a permanent blind spot. It is surprising that retinaland the thermal conductivity of the skin is low, the burn is no more detrimental to mission accomplish-burn is often superficial, killing only the outer der- ment than is flash blindness.mal layers and leaving the germinal layer essen- To protect against injury, the eyes can be closedtially undamaged. In contrast, flame burn results and shielded after the individual receives warningfrom contact with a conventional fire, such as cloth- of a detonation. Using one of the lead-lanthanum-ing or the remains of a building ignited by the fire- zirconium-titanium goggles that have been devel-ball's thermal pulse. In most cases, the healing of a oped may provide further protection.flame burn is abnormal because the germinal layerhas been damaged.
Since the heat pulse travels at the speed of light, Effects of Initial and Residual Radiationsprotection from burns is not possible unless warn-ing is given in time to find cover. The electromag- A detonating fission or fusion weapon produces
7

12 ~ PS/~(50% 96h.
and~~~~~t
e
dr Thfhd a e b a t r y
pro 8041deona e~ r d m gn )' c s~ bu O he ae a tia8
de on ti S pr du T a
f2g~~ 5 r
Fig th.ane ofTheffecsof atheafrs weain 10k WS 0 Mof inititl oftr
en r~ d by t e Oofrs nauto andea en eeraed
1 safe to the ins
the ra i~ a sti cthe of the fuIission rand ifusionprrn t reactios ga hbby
ti nsiclu dIe a : 9 athe r wth sle h rays id ray- iR esdad lx o
ndiha e ng e I n td laurtd'
n
ro gh in b s teouct io of d. r t rays, highl radionP o u eandr nul blst b Prtcles Praimatiyionta Paticls ganinar raia- Y~d Th e firs reba lllue
en sM ey eren~ Iqhcureboa ap aP r ics, thas upard
thet-s oantand residta
thia rand t neut ro Weca pon Ta h' io Whic initial d lon gerqd ia i J n' ec ani W iapnth e g- e T h ig t frn ansu f tc e rM t racti ated o n so n p osis , rs Mn, s 60h secas herad
the (ad) it tea
after an

N\ith'r [L nt. 100d Thor Coni't'(qt1ciC
strike the ground. A person on the ground would nium or plutonium account for most of the activitytherefore be safe from the initial radiations after I in the fallout field, the fusion process is relativelyminute. As the yield of the weapon is increased, the "clean" regarding the production of residual radia-fireball rises more quickly, but t , 60-second point tion.remains approximately the same. The main hazard Early fallout is radioactive material depositedfrom initial radiation is acute external whole-bodyv within the first day after detonation. This fallout isirradiation bv neutrons and gamma rays. Figure 1-3 the most significant for the military because it isshows that it is only for very small tactical weapons highly radioactive, geographically concentrated,that the initial radiation is potentially fatal at dis- and local. It tends to consist of larger particles (ap-tances where the blast and thermal effects are sur- proximately 0.01-1.0 cm in diameter) usually depos-v'iv'able. Therefore, significant initial radiation haz- ited within a few hundred miles of ground zero.ards are restricted to the first minute after detona- Because the material has had little time to decay, ittion and to several hundred meters surrounding a is radiologically very active. The biological hazardssmall-yield tactical weapon. Conversely, residual from early fallout are external whole-body gamma-fallout covers a wide geographic area and remains a ray irradiation from gamma emitters deposited onsignificant biological hazard long after detonation. the ground; external beta-particle irradiation from
Fallout. Our consideration of the origin of ra- beta emitters deposited on the skin; and internaldioactive debris begins with a review of the basic beta-particle irradiation from beta-emitting isotopesnuclear and physical processes that occur as the de- that are ingested, injected, or inhaled.vice detonates. As the fissile material splits, the Delayed fallout generally consists of the smallermassive and highly charged fragments carry away particles deposited after the first 24 hours. This ma-82'; of the fission energy, and release it as heat terial is less significant as an immediate hazard towithin the bomb components. This transforms the the military because it has a longer time to decaycomponents into an extremely hot plasma. and it is deposited over a wider area. Under certainBremsstrahlung interactions between the electrons circumstances, delayed fallout may be distributedand positive ions within this plasma generate an in- worldwide, presenting a long-term health hazard,tense source of low-energy X rays, which leave the primarily through internalized exposure.plasma and interact with the first several meters of The ultimate deposition of nuclear fallout on theair surrounding the weapon. The X rays heat this ground is influenced by the physical interactions ofair to an extremely high temperature and initiate the rising fireball with the atmosphere. For athe development of the fireball that is characteristic ground or near-surface burst, the interaction of theof nuclear explosions. The rapid outward expan- fireball with ground debris also affects the falloutsion of weapon material dramatically compresses deposition. As the hot gas bubble quickly risesand heats the air around the weapon (case shock), through the atmosphere, it creates and is followedfurther contributing to the generation of the fireball, by a strong vacuum directly from below. This gen-This hot bubble of gas, containing highly radioac- erates winds that rush radiallv inward towardtive fission fragments and activated weapon mate- ground zero and upward toward the ascending fire-rial, is the origin of the fallout radiation. ball. For a near-surface burst, these winds can pick
Sources of fallout include (a) highly unstable up large quantities of dirt and debris from thefragments produced by the fissioning of plutonium ground and inject them into the fireball (a processor uranium, (11) roughly 801 of the nuclear fuels called stem firination). This material, along with anythat remain unreacted after the weapon has blown other ground material directly vaporized by a sur-itself apart (uranium or plutonium for all weapons, face burst, then provides condensation centersas well as tritium for fusion devices), and (c) activa- within the fireball. The gaseous fission fragmentstion products (weapon components and ground ele- condense more quickly on these relatively larger de-ments made radioactive by exposure to the bris particles than they would have otherwise,weapon's intense neutron flux). Another contribu- greatly increasing early local fallout. This fallout istor to fallout is salting, the inclusion of materials in a deposited quickly in a concentrated area relativelyweapon that will activate when exposed to the ini- near ground zero. Thus, a ground or near-surfacetial neutron flux, thus increasing the amount of re- detonation is the most significant fallout hazard tosidual radioactive isotopes. Because of operational the military. The activation of surface materialslimitations in using a salted weapon, it is expected through irradiation of ground elements by the di-that this technique will be rarely used. Since the fis- rect neutron flux of a near-surface burst may alsosion fragments produced by the fissioning of ura- increase the local fallout hazard to troops traveling
9

through that area soon after detonation. • The meteorological conditions (windsIn the case of a pure airburst detonation with no and precipitation introduce by far
sNecondarv ground materials injected into the fireball, the greatest uncertainties in predict-tile cloud rises and cools, and the fission fragment ing where and when the tallout willvapors be-in to cool and condense at certain tern- be deposited)peratures (characteristic of their particular elements). The time after detonation (the moreTherefore, because the time for airburst fission-prod- time allowed for radiological decay.uct condensation is delayed and because fission the less the activitV of the falloutproducts do not condense on large particles of field)ground debris, the proportion of falhlut actiVitV e\- In terms of absolute quantity ot energy from fall-pressed as early local fallout is greatly reduced. out, appro\imatelV 10' 1 of the quoted energy yield
Chalracteristics of Fallout and the Prediction of of a typical fission weapon will be decay radiation;Hazards. The factors that determine the e\tent of for fusion weapons, it will be appro\imatelv 5'anticipated fallout hazard are: The elemental distribution of fission fragments is
"* The total fission yield (fission frag- almost independent of whether the fissile materialments are the largest contributor to is plutonium or uranium. In each case, approxi-fallout activity) matelv 38 different chemical elements are produced,
"* The ratio of energy produced in a consisting of about 30t) separate radionuclides.fusion weapon, by fission process Thus, the chemical and radiological characteristicsversus ftusion process (the higher the of the fallout field are e\tremely comple\ and, infission fract'on, the more fission practice, are amenable only to empirical analysis.products and consequently tile Tile fission fragments are highly unstable and decaygreater the radiological hazard) primarily by emitting gamma rays and beta par-
"* The specific design of the weapon (for tides. Activated weapon materials and ground ele-e\ample, an enhanced radiation ments, as well as unspent tritium from a fLsJiOnweapon will produce proportion- weapon, will decay by the same means. The un-atelv less fallout than an equivalent- spent uranium and plutonium from fission pro-vield standard nuclear weapon) cesses decay by emitting alpha particles, which are
"* The altitude of burst (a ground or a hazard primarily if they are inhaled. The immedi-near-surface detonation produces the ate detection of fallout radiation is not possible withgreatest earl, local hazard) the physical senses, so appropriate instruments
"* The composition of surface elements must be used. However, the heavv early, local fall-near ground zero in a near-surface out material is usuallv visible as a dust-like depositburst (accounting for the neutron that may look like a film on shiny surfaces. Theseflu\-induced activation potential of visible particles are the most hazardous componentsurface materials) of fallout.
MEDICAL CONSEQUENCES OF NUCLEAR WEAPONS
Military planners are concerned with the effect The Chernobyl Accidentof nuclear weapons on the human component of op-erational systems. It is futile to harden machineryto large amounts of radiation if the human operator Unlike controlled radiotherapy, radiation associ-is incapacitated by relatively small doses. Radiobi- ated with weapon detonations or accidents can re-ology research can help reduce the logistical drain suit in uncontrolled and usually unpredictable expo-on medical resources caused by large numbers of sures, which make radioprotective measures diffi-severely injured casualties. Targeting and contin- cult. As seen in the 1986 accident in Chernobyl,gency planning depend on knowing radiation ef- USSR, dsimetr '/ (measurement of radiation dose) isfects on military personnel, also difficult. Physical dosimeters, if available, may
10(

Nuclear Ezvi'its and Their Cozs'quwice•
TABLE 1-1
PERCENT DISTRIBUTION OF INJURIES SUSTAINED IN ANUCLEAR WAR
Type of Percent
Injury Distribution
Single Injuries (301; -4017)
Irradiation* 15-20
Burns 15-20
Wounds -5
Combined Injuries (65%-70%)
Burns + Irradiation 40
Bums + Wounds + Irradiation 20
Wounds + Irradiation 5
Wounds + Burns 5
*Including fallout
be lost during a nuclear event or may record cumu- tion injuries. The prognosis for these combined in-lative doses with no information on dose rate. Fur- juries is much graver than for radiation injuriesthermore, dosimeters provide point data rather than alone, so combined injuries must be carefully con-whole-body data. Biological dosimetry is also im- sidered during triage (sorting of casualties). It is es-perfect, and the time-consuming tests of lymphocyte timated that 65%-70% of weapon-related injuriesdepletion and cytogenetic damage (such as those will be combined injuries, with burns and radiationused for Chernobyl victims) give different results. being the most common combination (Table 1-1).Dosimetry with uncontrolled exposures is compli- Burns and radiation effects were the most com-cated by two other factors with which military phy- mon injuries seen in seriously injured victims of thesicians may have to cope. Chernobyl disaster. Thousands of medical and
One is the uneven distribution of exposures on a paramedical personnel were available for the rela-victim due to shielding. Thus, pockets of critical tively small number of patients at Chernobyl, butcells that are necessary to regenerate affected tissues this will not be the case in military situations. If amay survive, even if some parts of the body receive nuclear weapon is detonated, physicians will havevery high doses of radiation. Bone-marrow trans- to adapt to mass-casualty management techniques,plants were generally unsuccessful in Chernobyl which require simplified and standardized care.victims, partially because of the survival of some Today, scientists are exploiting the tremendoushost stem cells in the bone marrow; as surviving advances in biotechnology-the new knowledgemarrow was regenerated, it rejected the trans- and techniques in gene regulation, immunology,planted marrow cells. neurobiology, and related sciences-and will soon
Another complication of dosimetry in accidents develop significant protection for the human bodyor warfare is that other injuries, such as bums or from the consequences of radiation exposure andmechanical trauma, can be superimposed on radia- associated injuries.
HI

Alh'eial Con.cqucucS or Nudcar 1,%'d\hrc
INFECTION FLUID LOSS IRREVERSIBLE
Hematopoietic Gastrointestinal Neurovascular
PlueofRdatltio IjrE lesolt Make oboheetmanicrdtonsuha
Almost eeymejront syTherapy baf sComforbtabpriles,?wihaehg-pe lcf Infedcraitionepoueanmaaeetia trnonetos.Tienrydoiinrsls
Fig 1-4.lMajr devie rdiationated overo ame ajoer cin vto bonemarrily watestineform n reasctive spsecis(uha
wilNature oRaitiomndu Injuriers tru foratis bhdogen pelromide.gTeti elementsithn (schmbineday~ ~ ~ ~ ~ ~~~~~~rv afte gammoain,4,0 ed n 00in ihcluar components partiause lamg.the radiato
Almost every majore orga syrstema Moden beaf- (schasy tareta of amage~s wihic hecl are hihsedelecr-fecte woul radiation expoure, andmngernmbent in as tronscrleutrons).(whish eanberg atacepostion rsltsnultear accdeth oubr wafarersn willrequimmetecodiately reactive chemical products, incutasbydinfret radi-tntdueffotost and physiiasalljuied inhealtspoession cals (scha the radiation isf)ceulrandincal).Teeafrmem-the andmbealthphyicdvdas personnel ditnefo radicas, cand futernzym biewts.heias
Ah epicleatr dehvie deriousabte poverntmjoity pimrly wu- Teamuter tofor damactie susaiec is a(functio aswill ause intriemTerefore, numbnersofcsatanies. The thydraitogn peroxide). These, elementse rthend combndyatheer thures detontion, 4-mporteadand 9000 preerv wtheidvua cellula copoentsitivty cau e damghe. Thepijured were contd insuireothima sucesodeitrn operap- dosary thergreater ofdaae weoithion the clareadiatione-
atiens. Astenme fprosklemeitl ergytive raehemia prducsmutalso exetd.Qaiy d rete-etdamae to batndtherhmal njre boyboiincrass soadiao est ariuayes ofth radiation itef,(slla n uclear gmem-
vivabl injurised byTherdeforeition ufnderstnigy ofi the radiation' qrnualtron rditose, and dosei raelandive
12

N • ILI t -1 1: 'cutI It11 ThoIG Com I'Ii"'q l It t
TABLE 1-2
1MFDICAL CO\SFQLUENCES OF NUCLEAR WEAPONS
Performance Decrement Acute Effects Delayed Effects
ETI* / Hvpotension Infection Cancer
Motor Bleeding Life shortening
Cognitive Dehvdration
Emesis/ Diarrhea Delayed wound healing
*Early Transient Incapacitation
abilities to damage humans. Neutrons seem to be cal protective suit could be critically affected by amore effective in producing organism death, and symptom like emesis. Performance decrement maygamma rays appear to be more effective in inducing be due to lesions other than those associated withperformance decrement. In general, the more the lethal consequences of radiation injury to cells.quickly a dose of radiation is delivered to the body, This hypothesis might be significant in the develop-the more severe the consequences. The most sensi- ment of practical radioprotectants.tive cells are those that tend to divide rapidly, suchas the bone-marrow cells and the cells lining the Acute Radiation Syndromecrypts of the gastrointestinal tract. Less sensitivity and Associated Subsyndromesis exhibited by cells that divide more slowly or notat all, such as cells in the central nervous system With increasing doses of radiation, changes take(CNS). place in body tissues or organs, some of which are
The irradiation of cells has both acute and de- life threatening. The symptoms that appear soon af-laved effects (Table 1-2). Acute effects involve cell ter radiation exposure are called the acute radiationdeath, cell injury, and the release of disruptive me- syndromc (ARS). This large category may be brokendiators within the cell, which can lead to perform- down into the hiematopoie'tic,,, 'astroiittc;ti;Iml, and nciu-ance decrements. Other acute effects are infection rozascular subsy',:droines (Figure 1-4).and uncontrolled bleeding due to destruction of the The hematopoietic subsvndrome is seen withinbone marrow, dehvdration and electrolvte imbal- two weeks after biologically significant radiationance due to denudation of the epithelial lining of doses of 1.0-2.5 grays (Gy). This damage to thethe intestine, and slow healing of wounds. Delayed body's blood-forming organs, specifically to theeff cts include cancer and nonspecific life shorten- bone marrow, can lead to suppressed production ofing. Eventually, either the organism dies, or regen- white blood cells and platelets, which in turn leadseration and recovery occur. to increased susceptibility to infection and uncon-
Military attention is focused primarily on acute trolled bleeding. Treatment consists of administer-effects because they are of the most immediate con- ing platelets and preventing infection during thecern to the tactical military commander. Perform- time required for bone-marrow repair. Much re-ance decrement occurs within minutes or hours af- search is directed toward finding means to enhanceter relatively low exposures to radiation. It includes the repair or replacement of this tissue.a phenomenon called early transient incapacitation The gastrointestinal subsyndrome appears(ETI), a temporary inability to perform physically or within a week or two after exposure to highercognitively demanding tasks. This inability can be doses, which are sometimes survivable. After thisaccompanied by hypotension, emesis, or diarrhea. exposure, crypt cells in the epithelial lining of theA pilot or a soldier in a nuclear/biological/chemi- intestine are destroyed. This leads to excessive fluid
13

Mlcd(al C, l ) t NICleIr WarfI t(
100 U Burns
80•11 Irradiation (R)* Burns +60 ----- ------ •Irradiation
Lethality 60
(%) 40
20
0 0
100 250 500R R R
Fig. 1-3. Comnbined effects of simultaneous burns and ivhole-body irradiation onl rats
loss and imbalance of electrolytes within the body, the body from combined radiation and conven-which may result in loss of the intestinal wall. tional injuries is much more severe than it would beTreatment focuses on preventing tluid loss and on from a single injury.balancing electrolytes during the time required for In Figure 1-5, the percent of mortality in rats thatgastrointestinal repair. received an LD,,, burn is compared to the percent of
The neurovascular subsyndrome appears within mortality when this insult was combined with sub-a few days after much higher doses of radiation, lethal to minimally lethal doses of radiation. Rats re-an~d consists of irreversible damage to the CNS. ceiving 1.0 or 2.5 Gyv of radiation alone had no mor-There is no treatment, other than making the patient tality, while those receiving 5.0 Gv alone had aboutas comfortable as possible. 2017 mortality. Animals that received an LD~,, burn
and 1.0 Gy o f radiation (which by itself was not le-thal) had increased mortality tip to 70%1. Animals
Combined Injury that received 2.5 Cv of radiation in combinationwith an LD, burn had mortality approaching 95%ý(.
ARS and its medical effects are significantly Those that received an LID., burn and an LD, irra-complicated when radiation injury is combined diation with 5.0 Cv showed 10017 mortality. Thus,with conventional blast trauma or thlermal burn in- radiation combine's synergistically with either burnjuries. The following data show that the insult to or blast injuries to increase lethality. 1
REFERENCE
1. Alpen, E. L., and Sheline, C. E. 1954. The comibined effects of thermial burns and %vhole-body X-radiation oil survivaltime and mortality. Ann,. Stirg. 140-.113-118.
14

Chapter 2
ACUTE RADIATION SYNDROMEIN HUMANS
T. JAN CERVENY, Ph.D.,* THOMAS J. MacVITTIE, Ph.D.,** and ROBERT W. YOUNG, Ph.D.***
INTRODUCTION
PATHOPHYSIOLOGICAL SUBSYNDRON.
Hematopoietic SubsyndromeGastrointestinal SubsyndromeNeurovascular Subsyndrome
DETERMINANTS OF RADIATION EFFECTS ON HUMANS
Lethality CurveModification of Dose-Response CurveInfluence of Radiation Quality and Exposure Geometry on LD50Influence of Trauma on LD5Effect of Clinical-Support Therapy on LD50 Dose-Effect CurveExposure Geometry: Heterogeneous Partial-Body and Nonuniform ExposureConsiderations on Establishing the Human LD_
RadiotherapyRadiation Accidents
PRESENT VIEW OF RADIATION EFFECTS ON HUMANS
*Major, United States Air Force; Program Manager, Bioenvironmental Hazards, Air Force Office of Scientific Research,Boiling Air Force Base, Washington, D.C. 20332-6448-Chairman, Experimental Hematology, Armed Forces Radiobiology Research Institute,
Bethesda, Maryland 20814-5145***Human Response Program Manager, Radiation Policy Division, Defense Nuclear Agency,6801 Telegraph Road, Alexandria, Virginia 22310-3398
15

',,dical Contsequeices of Nuclear Warfare
INTRODUCTION
The importance of human sensitivity to ionizing effects. Several comprehensive analyses of humanradiation was recognized even before the detona- data and animal data have been conducted in an ef-tion of the first nuclear weapon. However, the ex- fort to derive a dose-response for humans.act relationship of dose to human mortality is still Information on humans and animals has made itnot precisely known because clear human data are possible to describe the symptomatology associatedlacking, and analyses of human mortality have with the acute radiation syndrome (ARS). In hu-been based primarily on data from radiation acci- mans, ARS is defined as the symptoms manifesteddents, radiation therapy patients, and atomic-bomb after exposure to ionizing radiation, and is oftenvictims. These studies have been faulted because of called radiation sickness. From a physiologicalthe small numbers of subjects, imprecise dosimetry, standpoint, ARS is a combination of subsyndromes.or patients' pre-existing health problems and treat- They appear in stages and are directly related to thements. Therefore, many studies with laboratory level of radiation received (Figure 2-1). These sub-animals have been undertaken in an effort to define syndromes begin to occur within hours after expo-the relationship between radiation exposures and sure and may last for several weeks.
PATHOPHYSIOLOGICAL SUBSYNDROMES
Radiation damage results from the sensitivity of the maximum state of immunoincompetence thatcells to radiation, and those that replicate most rap- the patient will suffer. If the patient survives theidly are the most sensitive to radiation exposure. In manifest illness stage, recovery is almost assured.descending order of sensitivity, these cell types are Therefore, treatment during the first 6 weeks to 2spermatogonia; lymphocytes; erythroblasts; other months after exposure is crucial to ensure recoveryhematopoietic cells; cells of the small intestine, from a rapidly received, high dose (less than 5 Gy)stomach, colon, epithelium, skin, CNS, muscle, and of ionizing radiation.bone; and the protein collagen. Mature cells thatare more highly differentiated appear to be the least Hematopoietic Subsyndromeaffected by radiation. This difference in cell sensi-tivity is the basis for the distinction among the The target cells of the hematopoietic tissue arethree subsyndromes of ARS. the stem cells. Their anatomical location in the
In order of their occurrence with increasing bone marrow distributes them throughout thedoses of radiation, ARS is divided into hematopo- body. Dorsal exposure would maximize damage toetic, gastrointestinal, and neurovascular subsyn- the hematopoietic system, because the greatest per-dromes. centage of active bone marrow lies in the spine and
Each subsyndrome can be further divided into dorsal regions of the ribs and pelvis. Vertical expo-four stages: prodromal, latent, manifest illness, and re- sure would be the least damaging per equivalentcovery. Prodromal symptoms begin a few hours to dose, due to absorption and consequent nonuni-4 days after exposure. The severity, time of onset, form dose distribution, thus sparing the dorsaland duration of symptoms relate directly to the ex- marrow. A dose-dependent suppression of boneposure dose received. The latent period is a brief marrow may lead to marrow atrophy and pancy-reprieve from symptoms, when the patient may topenia. Prompt radiation doses of about 1-8 Gyappear to have recovered. This reprieve may last cause significant damage to the bone marrow.up to 4 weeks, depending on the dose, and then is Doses of approximately 3 Gy may result in death tolikely to be followed by 2-3 weeks of manifest ill- 50% of exposed persons.' The biological responseness. The manifest illness stage is the most difficult of bone-marrow stem and progenitor cells to radia-to manage from a therapeutic standpoint, for this is tion exposure is exponential in nature. For ex-
16

INCREASINTESINA
AtA
k I
L . , I I-, ! 1 I 1 1". 1 11 I I I I I • I • , I I I I I I I
i ,k - Ill : I , I l ',lT 1 1r,,nl I I , I - tt1 t , ITII In II t, :I III ,t i It i, \ n I I I ITT j1 1 1i 1i1,1ii _ ",,i
I I II -,,, l I TIll, '\ . I iii I I IllT .T i I In I t.i IT " Ii y I I m . 1
I 'ii ,, I ,,-klliI1T -\i ll } {, ll il Hl ll• Vi ' lll l• < \ -'1 i ' r<. - l', I.i ... lIi < ItT I T't,, 2 I i' - k -TTi TTli th, • I-i
tll\-II=;p -ll• I TT ,l!. < Ti 21k,. l-I - T\ j''l ' k-ikr m.l TI'<\, Thu ,ll, ,'Al.:• .iTTTA,,I ht 'tlk, t' \ ii ii, .12i,,t 1
i i-<illl• i, TT''T! '• I ,i I ''--- ITT~! , l u t>< ll Iitu t\'-i{,tI,, ITT,,n! lt ,TTT l•,,t-ITIT li TT l.-• T ltl, lITl''
h Th\ ' l k t,' I lTi•, IT I•' hl'I2 •<t ,, i 'i' I•',l, t' l,,hril /k t 'lNT- II, l I/"i'l /';' rII, .lTiT~, hT < IT T lllI,
I I- I I - .Ik I I T , I I I I I \ t I
If' I,, -l~ llll, ; T~ • . il T \ < .il t!•'T It' tti' T TTT T ''t T 'T 'lt >-i I T111
1T I,l ! i I - , l i , l • ,T n T .I .< -,, - :1 l• lV l . t ,{ , ll •~ ,k i ' ill i<' l ' NI I T t '1, \ h i I i l -'T T , \, l ll ' (

M Cdih'Il Coal st'Ittt'Itt't' of Nt lhitr l'¥arhtarc
14
12- Gy
10 THROMBOC YTESD 1 HEMOGLOBIN1 300
12 6 2LOC T2008 [ NEUTROPHILS14o 0 8 r __ _ _ _ __ _ _ _
0~-~0L 0 10 20 30 40 50 60
X L14 1 T I IT 0
0:0 O0- 12 3 Gy -
Mw ,-i 10- THROMBOC YTES
8-0 L LYMPHOCYTES 100
010 10 20 30 40 50 60
TIME (days)
Fig. 2-2. Hematological response to whole-body exposure. Comparison of l-Gv and 3-Gy gamma-radiation effects onhematopoietic system.
bly severe infection. tion, followed by a much shorter asymptomatic la-Overall, the systemic effects that can occur from tent period of 5-7 days. Then the manifest illness
the hematopoietic subsyndrome include immuno- begins, with vomiting and severe diarrhea accom-dysfunction, increased infectious complications, panied by fever. At higher doses, bloody diarrhea,hemorrhage, anemia, and impaired wound healing, shock, and death may ensue.Impaired wound healing may be due in part to The intestinal mucosa suffers severe pathologicalendothelial damage, which significantly depresses damage following radiation exposure. The turn-the revascularization of injured tissue." over time of 3-5 days for intestinal mucosal epithe-
lial cells explains the shortened latent period. SinceGastrointestinal Subsyndrome severely damaged crypt stem cells do not divide,
the aging mucosal lining is shed and not replaced.The gastrointestinal subsvndrome overlaps the This results in loss of absorption and provides a
hematopoietic subsyndrome, but its consequences portal for intestinal flora to enter the systemic circu-are more immediate. At radiation doses above 12 lation. Figure 2-3 depicts vascular coalescence,Gy, this subsvndrome supersedes the hematopoi- which also significantly decreases intestinal absorp-etic subsyndrome in lethality. Its prodromal stage tion abilities. Severe mucosal hemorrhage has beenincludes severe nausea, vomiting, watery diarrhea, seen in experimental animal models (Figures 2-4and cramps occurring within hours after irradia- and 2-5). The overall intestinal pathology includes
18
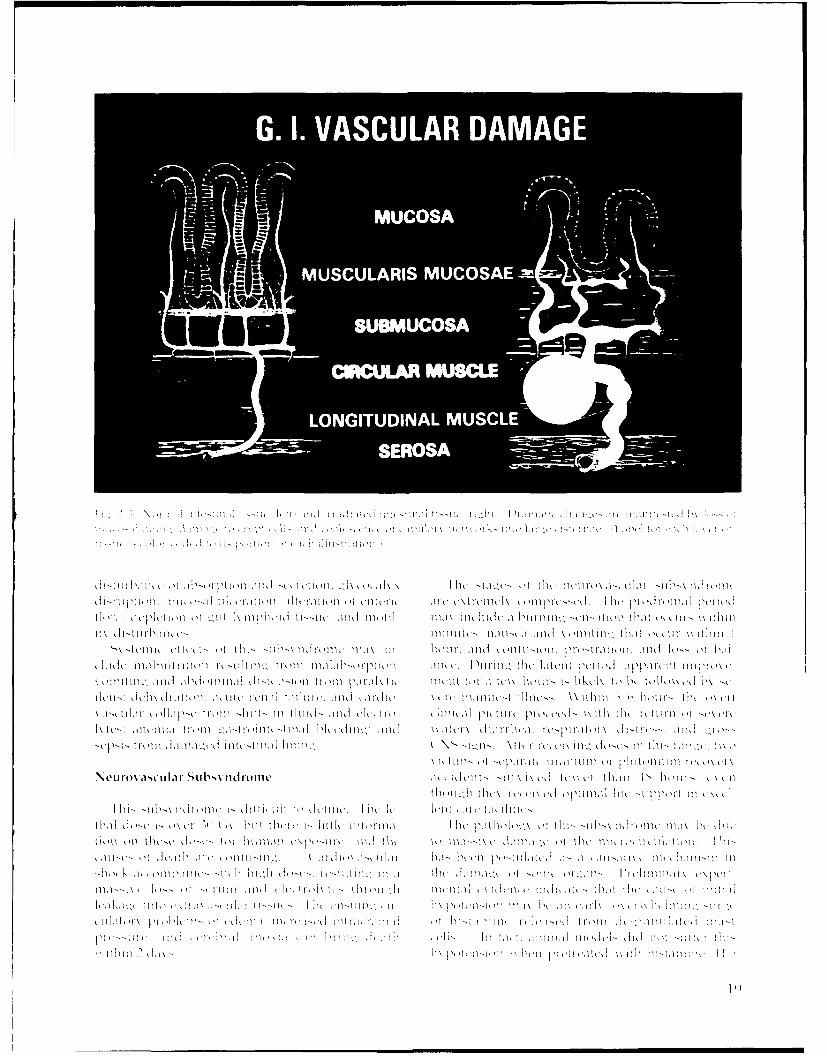
N< ci-ot a,ciji ilar... Su•~~ 1 i ,oI11cl ,~.`r l<, , 'll'l 2,}lt i"\{I.iti ll.. iii\ < ,Ul tV . 1'-< I ut ', I,, tl,'iii-.. xli,
,ltl~, l~ l iii il <'ti\--l~ l n~ Itl.. t'll ,Ii <''i i- 'It in 1. Ih,. ii 1 'nlt .t, 'r i,, t I-Il l I<n 1.,* ,\
Gn .l VASCULAR DAMAG,\
iL'u•=7 MlUlCrO SAl tt` .'l/ ~~ti, l/il~ i, \ti.ilill`- il <- \ t~ • + Iii t, ,<!
\ ~~ ~ ~ US U A I M1- U<CO,!St-AlEl Ill-Il!t!l tl~ ',,i, in<<l}i il' •i, `.'t t i/Ill'tinI-' '
Il ... :,il.'lhl Ik~l .t/- iil<'•IS U !l',<i M.U.<i C O S Atti tl ln. l`-"Ilt ,i- !' - ,~,] ;i..
J l i l O t A -I l il 'l 1tJllll) , \, I kI .h I lk l' t o f', 'l 1 't, Il,,} 0 \' 1"n < (1i , 11l , , , l I ,
J I h i- I tl-t I I i cit i, ,m ' i <t tli t1 1 1 I, t.1 I, In .I , I, C IIICI ,t .I,' k t~ I H ll 1 1 1 1 I tJ II k , t 11 ) 1 I k ! WIh t I t , , I - ,,\c ,n 1 , ' 1 11,\ Itltp! 1h ,1I ti- I lIl , l ld 11"in!l II I I I.II, I d ll I,.t 1,i tl i I-l, It I~ t'll nth ' nI t k ],,1 1 11h
ti 'I \ ,n t ( I I I , t I ,It 'k t ,, /t l /, II'\I I I I I I It • tI I, I lk ILI I j ,.' k III I I 1 1 ,1 1 rl, ' lI t l.I , I I./It] hIk I I i
SI t l,' 1 1 1 1 1t` , t , k, I, LI II I II I I II " I Ikt , \ , - } l / k! l I•` . , ,• l l t (. 11< I• . I ,Ill . t Ill , l l l - l t I
Ih ,, till I 11 "11 1 1 1 1 'tk I i• I• It,- I 'I I l l .I l 1l l 1Ilt' <~ll t t I 'C•' 1, L I, I I. , I k kl- '1\ k t k Ii i ~ l , \,I I k
Ill it'l \t k .. . .[ -I l l l l t I , I I I,, I , . II\ I}i u t t I , I IIi• '.\ -t I11nk, , \ I ý I, 111- l ,• I I• , . t t , i l I,
<~~~~~~~ ~~~ ki.l' ! t~,l~ , • k, ,'kll . \) •,- '. il .,1 11.i , f !. -~ i~ I, ,. - '. I II,,l ki ; l I i lI ,, ll-
t'It>- - Ill•' lil~~~~~~t , , I, }'l~~~ll k ,, iI t ki I'~ l : \i' l l , t,' I I~ ~ . l l ! l] t ,, t i- tl~ , ' - l ', l l '
eu ili oNl a ct~l I II a•,f rl-h i S\ 11'l b I I d ro I I c!k L I ti I I II, ;,,, I ' II '
1 1ljI Ilt I I I I Ilnl l il Inn d Inl l Iim i

DUODENUM JEJUNUM ILEUJM CECUM SPIRAL COLON DISTAL COLON
AFRRI CONTROLCENTIMETERS
Fig. 2-4. P'orcine hitct;tinal segments from normal aninial. Normal fissuc appears pink to gray.
DUODENUM JEJUNUM ILEUM CECUM SPIRAL COLON DISTAL COLON
AFRRI CONTROLCENTIMETERS
Fig. 2-;. Porcine fiiti'Stji1,i Segmewnt'. from 4- ~iriitdaia.Irradiated ti'tes fo alsemnt ho igsoýevvrc henmrrhage and ulIcerat ion.
20

Acidte Radiation Syndromne in Humtans
PERFORMANCEDECREMENT
NEUROVASCULAR
GASTRO-Radiation INTESTINAL
Dose HEMATOLOGICAL/
IMMUNOLOGICAL
DELAYED. .EFFECTS
0 2 4 6 8 10 12 14 16 18 20 22
(days) (years)TIME
Fig. 2-6. Occurrence of radiation effects in relation to dose and time. As radiation dose increases, time to manifestation ofeffect decreases.
blockers.s dose is 50 or 100 Gy is inconsequential; either is aThe radiation threshold for this dual subsyn- supralethal dose resulting in severe performance
drome is not as well defined as it is for the others. decrement. Figure 2-6 shows the occurrence of ra-Experimental evidence indicates that 50 Gv will diation effects in relation to dose and time. Table 2-elicit the neurovascular subsyndrome. Whether the I charts the pathophysiological events.
DETERMINANTS OF RADIATION EFFECTS ON HUMANS
Energy deposition, known as linear energy trans- exit from the body. In contrast, high-LET neutron,fer (LET), can be correlated to the severity of dam- exposure results in significant absorption of energyage to the tissue. Gamma and X rays, which are within the first few centimeters, with diminution ofprimarily responsible for ARS, pass through tissue dose at increasing tissue depth. In these cases, uni-almost unimpeded by the skin or protective cloth- lateral radiation results in more uniform exposureing. Thick shielding (such as lead, concrete, or dirt) with gamma than with neutron radiation. Bilateralis required to protect a person from these radia- or multilateral exposure increases the uniformity oftions. These rays are called low LET because they dose in all cases.do not leave a great deal of their energy behind. Alpha and most beta particles have low energyExposure to gamma emitters (such as cobalt-60) re- levels and cannot pass through skin (high-energysults in an accumulation of the dose within the tirt beta excepted) or clothing. Therefore, internaliza-few centimeters of tissue, folliwed by a gradual tion (ingestion, inhalation, or absorption through adecline of the dose level to 50'" at the radiation's wound) and systemic contamination with alpha or
21

M.It di~iI Lt~ i 'a L t' lt't" 4 N er ~VI Itarc
TABLE 2-1
PATHOPHYSIOLOGICAL EVENTS OF ACUTE RADIATION SYNDROME
Pathophysiological Events
Dose Range Prodromal Manifest-Illness Survival(Gv) Effects Effects
0.5-1.0 Mild Slight decrease in Almost certainblood cell count
1.0-2.0 Mild to Early symptoms of Probable (>90')Moderate bone-marrow damage
2.0-3.5 Moderate Moderate to severe Possible**bone-marrow damage
3.5-5.5 Severe Severe bone-marrow Death withindamage; slight 3.5-6.0 weekstintestinal damage
5.5-7.5 Severe Bone-marrow Death withinpancytopenia and 2-3 weeksmoderate intestinaldamage
7.5-10.0 Severe Combined Death withingastrointestinal 1.0-2.5 weeksand bone-marrowdamage; hypotension
10.0-20.0 Severe gastrointestinal damage; Death withinupper half of range: ETI;* 5-12 davsgastrointestinal death
Gastrointestinal and Death within
cardiov'ascular damage 2-5 days
*Earlv Transient Incapacitation
**Top third of range: LD-,,,....
Middle third: LD ,,,,Bottom third: LD,/,,,
t Top half: LD,•,,,,,
Bottom half: LD,4,,
Source: Data from reference I.
ACu te Radiatiow, Sqiliidrot' i hlt Hiiithis
100
80-Mortality
Rate 60(0)M LD 9 5
40 LD5
20-
0 L -
LD5 LD95
Radiation Dose -
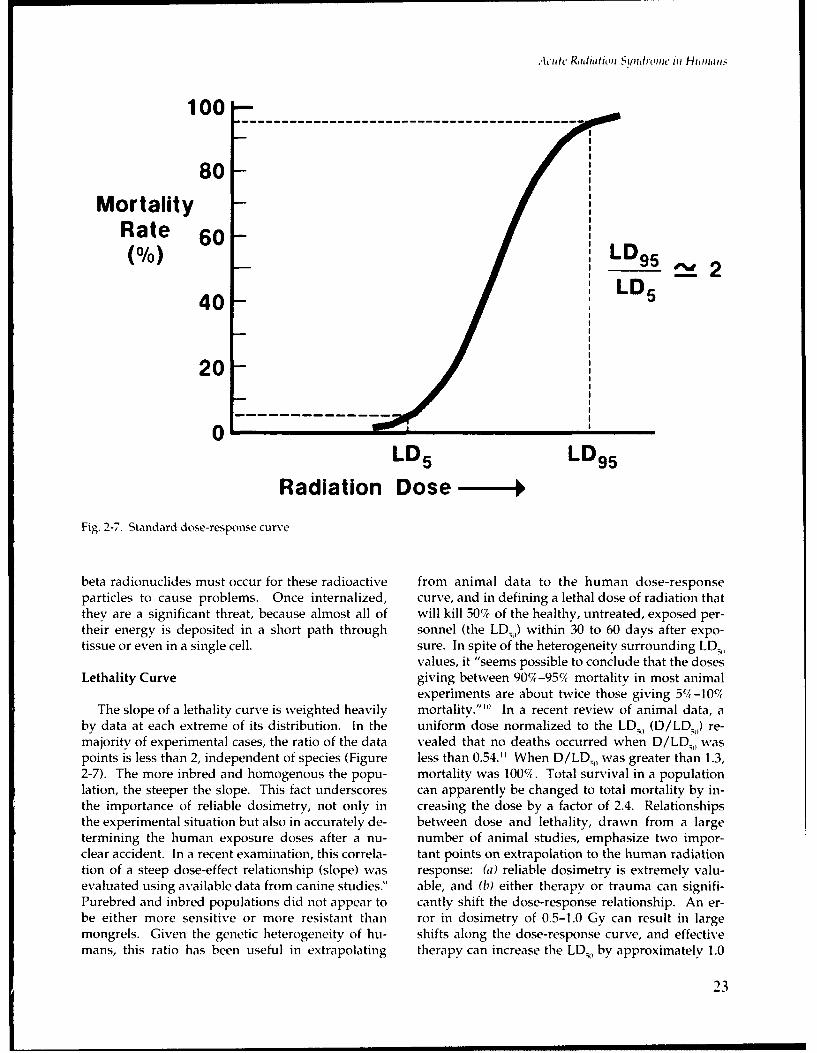
Fig. 2-7. Standard dose-response curve
beta radionuclides must occur for these radioactive from animal data to the human dose-responseparticles to cause problems. Once internalized, curve, and in defining a lethal dose of radiation thatthey are a significant threat, because almost all of will kill 50% of the healthy, untreated, exposed per-their energy is deposited in a short path through sonnel (the LD 5 ) within 30 to 60 days after expo-tissue or even in a single cell. sure. In spite of the heterogeneity surrounding LD,,
values, it "seems possible to conclude that the dosesLethality Curve giving between 907-95% mortality in most animal
experiments are about twice those giving 5%-10%c,The slope of a lethality curve is weighted heavily mortality.""' In a recent review of animal data, a
by data at each extreme of its distribution. In the uniform dose normalized to the LD., (D/LD;,) re-majority of experimental cases, the ratio of the data vealed that no deaths occurred when D/LDQ, waspoints is less than 2, independent of species (Figure less than 0.54." When D/LD,,, was greater than 1.3,2-7). The more inbred and homogenous the popu- mortality was 10014. Total survival in a populationlation, the steeper the slope. This fact underscores can apparently be changed to total mortalitv by in-the importance of reliable dosimetry, not only in creasing the dose by a factor of 2.4. Relationshipsthe experimental situation but also in accurately de- between dose and lethality, drawn from a largetermining the human exposure doses after a nu- number of animal studies, emphasize two impor-clear accident. In a recent examination, this correla- tant points on extrapolation to the human radiationtion of a steep dose-effect relationship (slope) was response: (a) reliable dosimetry is extremely .'alu-evaluated using available data from canine studies." able, and (17) either therapy or trauma can signifi-Purebred and inbred populations did not appear to cantly shift the dose-response relationship. An er-be either more sensitive or more resistant than ror in dosimetry of 0.5-1.0 Gy can result in largemongrels. Given the genetic heterogeneity of hu- shifts along the dose-response curve, and effectivemans, this ratio has been useful in extrapolating therapy can increase the LD•, by approximately 1.0
23

M tcd ConL ; tincqiwe, tot Nutihar OVi'rtaric
0 2 Depth (in) 61001 1
0 5" Depth
80 , 0 6" Depth
AbsorbedDose 6I% of
SurfaceDose) 4
40201 Ga m 0
08
0 5 10 15Depth (cm)
Fig. 2-8. Depth-dose relationship in phantoms. Effect of tissue depth on absorbed radiation dose from unilateral mixed-fission gamma and I-MeV neutron radiations. Low-LET, high-energy gamma radiation produces a more uniformexposure than does fission neutron radiation.
Gy. The degree of trauma depends on the duration trauma, poor nutritional status, and stress are inand intensity of the radiation exposure, and it can this category. Other factors that significantly mod-shift along the mortality curve. ifv the dose-effect curve are radiation quality, expo-
sure geometry (such as partial-body exposure orModification of Dose-Response Curve nonuniform exposure), and dose rate.
Radiation lethality may be a consequence of Influence of Radiation Quality and Exposurechanges in the cellular kinetics of renewal systems Geometry on LDs0critical for survival.'12 1
1 If this is correct, then modi-fication of the dose-response relationship is achie,- Distribution of radiation dose (energy deposi-able by replacement of the mature functional cells tion) throughout the target tissue varies signifi-or their essential factors, or by actual substitutions cantly with the energy and quality of radiation andin the damaged cell-renewal system. with the geometry of the exposure. Figure 2-8 illus-
Factors that compromise or damage the hemato- trates the effects of tissue depth on absorbed radia-poietic system or the immune system will also tion dose from unilateral cobalt-60 and 1 MeV (mil-negatively affect the dose-response curve. Severe lion electron-volts) of mixed neutron-gamma radia-
24

Acl-tw Radiatnion Siondromc ii, Ha nima.
tions. To reconstruct the effects of an accidental tered by most military and civilian physicians. Inexposure involving neutrons, we must consider the combined injury, two (or more) injuries that aretissue depth of a large-animal model (such as the sublethal or minimally lethal when occurring alonecanine) and that of humans, relative to the absorp- will act synergistically, resulting in much greatertion characteristics of these two different radiation mortality than the simple sum of both injuriestypes (gamma and neutron, I MeV). would have produced. The mechanisms respon-
Equivalent doses of different types of radiation, sible for combined-injury sequelae are unknown,or of the same type at different energy levels, do but they can significantly increase the consequencesnot produce equivalent biological effects. How- of radiation exposure across the entire dose-re-ever, the relative biological effectiveness (RBE) of two sponse curve. It must be emphasized that the sur-types of radiation can be compared. A significant vival of a patient following exposure in the hemato-number of studies establishes the LD•, for hemato- poietic dose range requires (a) a minimum criticalpoietic death in canines at approximately 2.60 Gy number of surviving stem cells to regenerate a corn-for 1,000 kVp (plate voltage in kiloelectron-volts) of petent host defense system, (1b) the functional corn-cobalt-60 radiation, or 2,000 kVp of X radiation. For petence of surviving cells composing the specificlower-energy X radiation (50-250 kVp), an average and nonspecific immune system, or (c) effective re-dose of 2.28 Gy would yield this LD•.'--' These placement or substitution therapy during the criti-values suggest an RBE of approximately 0.87 for cal postexposure cytopenic phase. Trauma alone,radiation higher than the standard 250 kVp of X- depending on its intensity, may effectively depressray energy. Canine exposure to mixed-fission neu- host resistance to infection. 2 "' When imposed on atron-gamma radiation yields an LD., value of 1.48 radiation-injured system, it can be lethal. In mostGy (compared to a derived value of 2.60 Gy for co- instances, trauma symptoms will either mask orbalt-60).` This results in an RBE of approximately exacerbate the first reliable signs of radiation in-1.7. Using a neutron spectrum of similar energy, an jury. This will cloud the situation if one is relyingLD,, of 2.03 Gy (compared to 2.80 Gy for I MVp of on biological dosimetry and prodromal symptomsX radiation) was determined to have an RBE value for estimation of dose. In addition, the choice ofof 1.38.22 An RBE value of approximately 2.0 has treatment in these cases should include considera-been reported for rhesus monkeys exposed to fis- tion of not only the patient's initial status but alsosion neutrons of I MeV energy (the LD,,, value was the condition that will exist 7-21 days later when2.60 Gy) and for X radiation of 300 kVp energy (the the radiation effects are seen.LDI, value was 5.25 Gy).23 A significant RBE has Relatively few animal models of combined in-been observed in the rhesus (LDv0) using gamma- jury are available for determining effective therapy.neutron exposure, compared to the RBE for 250 The few reported studies demonstrate the synergis-kVp of X radiation. 24,2i Several studies used mice tic effect of combined injuries. Sheep were exposedto establish RBE values for fission and high-energy to 4 Gy of mixed neutron-gamma radiation andneutrons pertaining to X radiation and cobalt-60 ra- then 1 hour later subjected to an abrupt overpres-diation.2;-28 sure; this resulted in increased mortality from 25%'c
A radiation dose delivered to hematopoeitic for irradiated-only animals to 50% for the com-stem cells in bone marrow is the most damaging to bined-injury animals."' A rat model showed a syn-the organism. Therefore, unilateral exposure with ergistic effect when a 250-kVp X-ray dose (LD•,)either gamma or neutron radiation will result in was followed in 7 days by a low-lethal (55/) level ofnonuniform dose distribution, whereas bilateral or air blast.3 7 Mortality increased from approximatelyrotational whole-body neutron exposure will have 46% for the irradiated-only animals to 767 for thea greater RBE. Unilateral exposure usually occurs combined-injury animals, and was related to radia-
in accidents or warfare. Exposure to any type of tion-induced thrombocytopenia, which compro-unilateral radiation can result in lower doses to mised normal coagulation and maintenance of thestem-cell populations that are distant from the capillary endothelium.source, with a consequent rise in the LD 5)value An open skin wound (combined injury) mark-(Table 2-2). edly increases the chances of infection. The imme-
diate closure of wounds has been recommended."Influence of Trauma on LDs0 Mortality in mice from exposure to 5.1 Gy of
gamma radiation alone rose from 25%7, to 90% whenThe combination of radiation exposure and combined with open dorsal skin wounds occurring
trauma produces a set of circumstances not encoun- 2 days after exposure. If wounds were immedi-
25

Medical Conls.'LlwePices tf Niaclear Wartare
TABLE 2-2
MODIFICATION OF LETHAL DOSE ACCORDING TO LATERALITY OF EXPOSURE*
Factor Dog Sheep Pig
Body Mass (kg) 7-13 32-57 62 (average)
Radiation X rays (1 MeV) X rays (1 MeV) X rays (2 MeV)
LD50 Mean ± SE (Roentgen at midplane of exposure volume in absenceof animal)
Unilateral 386 ± 10 303 ± 13 434 ± 13Exposure (UE)
Bilateral ± 9 252 ± 17 362 ± 13Exposure (BE)
Difference 65 51 72(UE - BE)
Ratio(UE 1.20 1.20 1.20(UE/13E)
*A unilateral exposure from any radiation type may result in the sparing of distant stem-cell populations, thereby raising the LD,.
ately closed, mortality decreased to 18%. Closing high as 2.5. The addition of trauma to radiationof the skin wound obviously affected the mecha- exposures also significantly reduced the LD,.. Thenism of pathogenesis. effect of combined injury on lethality was d,, mi-
In combined injuries, burns produce the most nated by radiation. The RBE did not change withsignificant synergistic increases in mortality. The the addition of trauma.dog, pig, rat, and guinea pig have been studied as Injuries to the abdomen may present significantanimal models.3 4.13 -4 ' Table 2-3 summarizes this problems to the irradiated subject. Blast overpres-synergistic effect on the lethality of combined ra- sure, blunt trauma, and penetrating trauma are alldiation and trauma. As little as 0.25 Gy, combined significant causes of abdominal injury. The impactwith a bum of 20% body surface area, increased of laparotomy or splenectomy in mice that had re-mortality in dogs from 12% to 20% .41 ceived whole-body radiation has been evaluatedc.-
In the early 1980s, investigators performed the Exposure to 5.1 Gy alone caused mortality of 27%,most comprehensive analysis to date of the effect of whereas laparotomy or splenectomy alone causedcombined injury (thermal and skin wound) on le- an approximate 5% mortality. Splenectomy at 2, 4,thality and on the suppression of host resistance to or 8 days after irradiation increased the mortality tosubsequent bacterial challenge. 44 ,45 In addition, 60%, 75%, and 85%, respectively. Laparotomythey used cobalt-60 gamma versus mixed-fission combined with radiation caused maximum mortal-neutron-gamma radiations in various ratios of LD•, ity when surgery was performed on day 8. Theon mice that 'ad either thermal injuries or skin role of the spleen in nonspecific resistance to bacte-wounds. The addition of fission-energy neutrons rial infection has recently been demonstrated.4'to gamma radiation significantly lowered the LD, The impact of combined injuries on the radiationin radiation-only experiments to give RBE values as dose-effect curve depends on the intensity and the
26

Acute R1diat1on nSndromte in Humans
nobyl victims also experienced medical complica-TABLE 2-3 tions associated with bone-marrow damage and
COMBINED EFFECTS OF WHOLE-BODY immunosuppression.
RADIATION AND BURNS ON VARIOUSANIMAL MODELS*
Effect of Clinical-Support Therapy on LD:;0Percent Dose-Effect Curve
Subjects LethalityModification of survival throughout the LD5 ,
Dog dose range is achievable using a simple regimen ofclinical support to replace or substitute the de-
20%, burns 12 pleted functional cells after stem-cell destruction.
100 R exposure 0 In the cases of large-animal models (monkey, ca-
20%7 burns + 100 R 73 nine, and swine) and the human, therapy is di-rected at replacing the functions of the granulocytes
Pig and platelets. Experimental work performed morethan 20 years ago showed the efficacy of supportive
10%-15% burns 0 care centered on systemic antibiotics and transfu-
400 R exposure 20 sions of fresh platelets. Several canine studies indi-
107-151c burns + 400 R 90 cated that antibiotics, singly or in combination,were successful in reducing mortality in the LDv
Rat range.1 41A Combination antibiotics, in conjunction
with fresh whole-blood transfusions and parenteral
31%-35% burns 50 fluids, have been effective in controlling dehydra-
250 R exposure 0 tion and thereby reducing mortality. Reports that
500 R exposure 20 hemorrhage is easier to control than infection may
15%-31 % burns + 100 R 65 be traced to the fact that several types of opportun-
31 /-35% burns + 250 R 95 istic pathogens are capable of overwhelming a com-
31c-35% burns + 500 R 100 promised host."8
In an attempt to determine the lowest dose at
Guinea Pig which spontaneous regeneration would not occur,the dose range was extended in a later animal
1.5% burns 9 study from 4.0 to 5.5 Gy, well into 100% lethality
250 R exposure 11 (LD10,). The dose of 4.2 Gy resulted in an LD,r,.
1.5% burns + 250 R 38 Survival was significantly increased with goodclinical support. This support consisted of (a) sev-
*Significant increases in mortality occur when eral antibiotics (penicillin G, dihydrostreptomycin,
radiation is superimposed on concomitant and tetracycline) administered at the onset of feverconventional trauma. (8-13 days after exposure) and continued until fe-
ver subsided for 3-4 days and white cell count wasgreater than 1,000/mm3 ; (b) the infusion of fresh
time of injury relative to radiation exposure. 47' 48 platelet-rich plasma from 50 ml of blood, givenThe biological consequences of these combined in- when blood platelet levels were below 5,000/mm'juries will significantly affect the patient's abilities (10-12 days after exposure); and (c) fluid therapyto survive and recover, and will markedly increase (isotonic saline or 5% dextrose) given during thethe casualty burden on medical personnel. Those period of anorexia. Soft food was usually givenpatients in Hiroshima and Nagasaki who suffered during this period to entice the animals to eat. Theconventional trauma along with radiation exposure success with these regimens supports the hypothe-developed significant complications 2-3 weeks sis that infection and hemorrhage are the main con-later, corresponding to the time of hematopoietic tributors to lethal consequences of radiation expo-depression. Until the 1986 reactor disaster in Cher- sure in the hematopoietic subsyndrome range.nobyl, the victims of Hiroshima and Nagasaki pro- Controlling infection during the critical granulocy-vided the only documentation on human radiation topenic and thrombocytopenic phase is the limitinginjuries and associated trauma. Hospitalized Cher- factor in successful treatment.49 ,5'
27

Medical Consequences of Nuclear Warfare
99 0
9795 LD7 0 2.60 (Gy) 5 L0 5 0 = 3.39 (Gy)
90 Nonsupport Support
% 70 0 0
Mortality /so/
30 "0
10-
5-3-
2.0 2.2 2.4 2.6 2.8 3.0 3.2 3.4 3.6 3.8 4.0 4.2
Dose (Gy)
Fig. 2-9. Effect of clinical support therapy on LD,0. Parenteral fluids, platelets, and antibiotics to control infection duringcritical nadirs in granulocyte and platelet counts provide the basis for successful treatment.
These studies have been extended over a dose spontaneous regeneration.range that is capable of determining the shift inLD0 that is due to treatment. Figure 2-9 shows the Exposure Geometry: Heterogeneous Partial-Bodyshift in the canine LD5 0 from 2.60 Gy to approxi- and Nonuniform Exposuremately 3.39 Gy measured as midline tissue dose.This results in a dose reduction factor of 1.3. The Partial-body exposure can result in deathtreatment regimen was essentially the same as through irradiation of specific target organs, suchabove, with the addition of the newer antibiotics, as the brain, lungs, and gastrointestinal structures.gentamicin and claforan (cephotaxime-S0 4)•5 However, significant variations in the hematopoi-These collective data indicate that modest clinical etic subsyndrome and related lethality can be seencare consisting of the infusion of fluids, antibiotics, when portions of the active marrow are eitherand fresh platelets is capable of shifting the LD., by shielded physically from exposure or receive aa factor of 1.5. A more intensive regimen of sup- smaller radiation dose due to nonuniform dose dis-port, including use of a sterile barrier and selective tribution through the body tissue. The earliest re-decontamination of intestinal bacteria, should al- port of a shielding effect on the hematopoietic sy;-low an even greater shift in the LD.. It must be tem was in 1963.52 Exteriorized spleens of miceemphasized that the practical application of these were shielded, which increased the LDs5 from 550concepts requires that the damage to the stem-cell to 975 R (roentgens). It was concluded that thesystem be reversible; that is, the surviving fraction shielded spleen contained competent and mobil-of hematopoietic stem cells must be capable of izable hematopoietic stem cells that were capable of
28

Acutiet Radiation Syndromet in Hiu mans
totally repopulating the depleted marrow space trauma can significantly modify the relationship ofand significantly modifying the hematopoietic sub- dose and response.syndrome's dose-effect relationship. Many later Several comprehensive analyses of human andexperiments supported this finding by shielding ei- animal data have been conducted over the years inther the hind limbs or tails of mice. A further com- an effort to derive a dose-response curve for hu-parison in mice has been made of the therapeutic mans. Some reports serve as landmarks, but noneefficacy of this autorepopulation versus the efficacy has been completely successful. The quest for anof autologous and/or syngeneic bone-marrow LD51 for humans began in the late 1940s and contin-transplantation. 2" In this study, one leg was ues today.icb5b.'7 The most recent activity on thisshielded from lethal total-body exposure, allowing subject has shifted from the United States to thestem cells of the shielded leg to reseed the irradi- United Kingdom, where interest from the Britishated marrow space. Another set of mice received a Home Office produced comprehensive analy-similar exposure with the shielded leg later ampu- ses."5 ,3*-s. The suggestion emerging from thesetated. The marrow contents were harvested by a analyses-that the LD. might be as high as 6 Gygrinding technique and then autotransplanted. (body surface, free-in-air dose)-was controversial(The grinding allowed greater efficiency in the in light of the long-held view that the value was 4.5stem-cell harvest.) Results indicated that autore- Gy or less. The 6-Gy free-in-air dose correspondspopulation of the marrow was more efficient than to an approximately 4.5-Gy bone-marrow dose, andmarrow transplant. the 4.5-Gy free-in-air dose corresponds to a 3.6-Gy
A series of experiments using canines further il- bone-marrow dose. The 1986 LD5 value of 1.54 Gylustrated the protective effects of partial-body to the bone marrow added to the controversy andshielding. .V4 Large-animal models can not only il- sparked new interest in resolving these discrepan-lustrate the relationships between tissue depth and cies.5.dose, but can also approximate the nonuniform ef- Available data on uncomplicated radiation expo-fects of exposure for more reliable extrapolation to sures to the human within the hematopoietic-sub-the human radiation response. Shielding the lower syndrome range are relatively limited. The evi-body indicated an approximately sevenfold in- dence to date (excluding the 1986 nuclear disastercrease in LD7.4 One report emphasized that con- in Chernobyl and the 1987 radiation isotope inci-siderable hematopoietic tissue may be spared by dent in Goiania, Brazil) is from three sources: (a)nonuniform exposures to cobalt-60 gamma radia- twenty cases of radiotherapy with whole-body, bi-tion.7 Results indicated that the greater the dose lateral exposure to gamma radiation; (b) two nu-gradient and the more nonuniform the exposure, clear criticality accidents involving mixed neutron-the greater the survival of stem cells that are ca- gamma exposure of nine persons, one of whompable of repopulation. died; and (c) the cases of thousands of persons ex-
These canine experiments illustrate the complex- posed to the nuclear detonations over Hiroshimaity of determining the dose received during an acci- and Nagasaki in 1945. The following descriptionsdental exposure. Accidental whole-body irradia- of the radiotherapy patients and nuclear criticalitytion will most likely not be strictly unilateral, due to patients illustrate the type of information that, untilbackscatter and reflection of the radiation. It is also recently, was used in determining the human LD,.possible that some body regions may be shielded. Radiotherapy. Twenty adolescent patientsThese factors, as well as the anatomical position of (nineteen with Ewing's sarcoma and one misdiag-the exposed subjects, can either increase or decrease nosed who actually had leukemia) were uniformlythe total dose received. Shielding and nonuniform exposed to 3.0 Gy of whole-body cobalt-60 gammadose distribution can therefore differ markedly in radiation as a midline tissue dose at a dose rate ofhow much hematopoietic tissue they spare. The 0.2 Gy/minute.!" All patients survived for at least 1biological response of marrow stem and progenitor year. It appears that this experience would set thecells to radiation is exponential in nature. lower limit for the lethal dose at a dose greater than
3.0 Gy. However, several modifying factors mustConsiderations on Establishing the Human LD 5 0 be considered. These patients were given excellent
supportive clinical care during their hospital stay.Similarly, it is difficult to calculate accurately the They received fluids, electrolytes, and blood re-
dose that a human has received after accidental ra- placement (platelets for some) as necessary, anddiation exposure. Radiation quality or type, dose simple antibiotic treatment while under barrierrate, shielding, exposure geometry, and coincident nursing. It has been recently revealed that many of
29

Medical Consetqences of Niclear Warfare
TABLE 2-4
ANIMAL-MODEL PREDICTIONS OF LETHAL RADIATION DOSESTO HUMANS*
Dose Rate (Gy/minute)
LethalDose 0.01 0.02 0.05 0.10 0.20 0.50
LDM 194 177 156 143 130 115
LD,, 210 192 171 157 144 128
LD! 275 257 234 218 204 186
LD•, 341 321 297 279 263 243
LD, 360 339 313 295 278 257
*The predictions from the model express the relationship between the dose
rate and the LD,.
these patients received local radiation to the sites of curred during maintenance operations at a fuel-re-the tumors before, and in some cases after, the processing plant. A uranyl nitrate solution was in-whole-body exposure. These prior exposures corn- advertently allowed to collect, and a fission chainplicate the picture because of possible abscopal ef- reaction began, followed by a second reaction andfects on distant hematopoietic tissue. It is difficult perhaps more. The first reaction probably gave theto determine the effect of hospital-based care and greatest part of the total dose to the workers. Sevensupport, but the Chernobyl experience and animal persons received 1.0 Gy or more, and of them, fourdata point to a significant decrease in lethal conse- are considered to have received the higher homoge-quences. neous doses, which are more relevant.
Radiation Accidents. Of many radiation acci- Nausea and vomiting occurred in three workersdents reviewed (Chernobyl excluded), two in- within 2 hours after exposure, and one vomited onvolved shielding, dose uniformity, and acute expo- the second day. Diarrhea was not evident. Somesure (estimated as 2-10 Gy) that were comparable complaints of soreness, fatigue, and weakness wereto LDs0 values in humans. Both accidents were registered. All showed hematological changes re-criticality accidents that involved fission neutrons, flecting severe marrow damage. Hospital treat-low-energy photons, and high-energy gamma rays. ment was conservative, and the patients were dis-Four of the seven male workers exposed in the 1958 charged 39 days after exposure.Y-12 Oak Ridge, Tennessee, accident and five of the At Vinca, the exposure of five persons rangedworkers exposed in the 1958 Vinca, Yugoslavia, ac- from a lower limit of 1.8-2.3 Gy to an upper limit ofcident are considered to have received relevant ra- 2.3-3.1 Gyi) occurring over several minutes whendiation doses. an unshielded research reactor temporarily ran out
Reconstruction of the Y-12 accident dose indi- of control.".1 2 This led to the emission of a "softer"cates a total marrow dose range of 3.25-4.40 Gy for neutron spectrum than that which occurred in theupper limits to 1.9-2.6 Gy for lower limits, assum- accident at Y-12. Low-energy neutrons are not verying lateral or anterior-posterior exposure."' These penetrating, but do give rise to a measurable tissueworkers most likely were exposed to two pulses gamma dose. Therefore, a calculation of marrowseparated by several seconds. The accident oc- dose had to be estimated. Although the dose levels
30

Acute Radiation Syndromne in Humans
at both accidents were similar, the clinical re- ened through the 3 weeks after exposure, and fivesponses of the victims differed significantly. patients were injected with donor-matched bone-
For the Vinca victims, severe nausea and vomit- marrow cells at 4-5 weeks after exposure. Theing occurred within the first hour. A larger dose to value of the marrow transplant is moot. It has beenthe superficial tissues was indicated by erythema, argued that the recipients were on their way to re-conjunctivitis, and loss of body hair. The most covery and that the benefits of these transplantshighly irradiated victim suffered severe diarrhea. were temporary at best. One man, who receivedVictims were nursed under sterile conditions, re- the highest dose of radiation, did not respond toceiving fluids, electrolytes, blood-cell transfusions, treatment; he died of gastrointestinal complicationsand antibiotics. The hematological picture wors- on day 32.
PRESENT VIEW OF RADIATION EFFECTS ON HUMANS
Several new studies relate to the establishment laboratory animals.',6 This dependence is particu-of an LD,, for a low-LET radiation dose to the bone larly important when attempting to use low-dose-marrow of healthy young adults. These studies in- rate studies as estimates of prompt LD,. Table 2-4clude several important observations that must be shows a model for the relationship between doseconsidered when estimating the radiation mortality rate and LD•Q. 1Iresponse of humans. First, in selecting data groups The third observation is that the LD,0 for thefor analysis, the influence of postirradiation clinical human cannot be modeled on a 70-kg animal. Thistreatment must be taken into account. Carefully is true even if the analysis is based on all animalcontrolled experiments clearly indicate that treat- studies to date, if the model is carefully controlledment will elevate the estimate of the LD5 0 by as for body weight, and if the dose rate is below 0.5much as 30%."3 The calculated LD:0 of approxi- Gy/minute. The LD.0 may be more species-inde-mately 6 Gy for the Chernobyl patients treated for pendent at prompt dose rates, where data from sev-ARS also indicates a benefit from intensive clinical eral large mammals, including humans, appear tosupport. This observation is reinforced by the fact converge.1'5that many of these patients had complicating burns, A fourth observation is that although the LD,which have been shown to lower the LD50 in the for the human may not be exactly like that of an-Nagasaki victims and in studies of laboratory ani- other 70-kg mammal, the slope derived from themals. These observations suggest that the British animal model is much more credible than the unac-value of 4.5 Gy overestimates the bone-marrow ceptably shallow slope observed in the HiroshimaLDv, since this value is derived entirely from per- and Nagasaki analyses. These differences in slopesons who received supportive therapy."( The data may be due to differences in (a) the accuracy offrom the Ewing's sarcoma patients in this study dose determination, (b) the homogeneity of theseem particularly compromised, because these pa- sample populations for humans and animals, or (c)tients received not only antibiotics and platelets but the postirradiation treatment. With no acceptablealso barrier nursing and possibly tumor pretreat- slope that can be empirically derived directly fromment with X rays before receiving the 3 Gy of total- human data, the recommendation is to use thebody radiation.') If this pretreatment with X rays slope obtained from the Oak Ridge National Labo-can be confirmed, we must assume that the sensi- ratory animal model (Figure 2-10). The LD, andtivity of the patients to subsequent radiation ther- LD1 0 should be taken as the values for the limits ofapy was reduced. These several factors suggest that the dose-response curve because the extrapolationsanchoring the low end of a dose-response curve are totally unreliable beyond that range. The slopewith these data is not justified. should be expressed as the ratio of the LD,0 to the
The second observation to emerge from these LDW(. This expression maintains linearity over thenew studies is the dependence of LD5 ,, on dose rate, entire curve and has a value of 1.9, which is in goodparticularly at rates of 0.6 Gy/hour or less, as seen agreement with other such values.?",'in data from human experience and studies with The final observation is the degree of agreement
31

MAedical Con.e'qiiences of Nuclear Warfare
90 LD9 o 4.0
(5.7 FIA)80 -
70 -
Mortality 60 - LD50 3.0Probability (4.3 FIA) "•(%/) 50 -
40
30 LD90 /LD 1 o = 4.0/2.0 "2
20ID1 o 2.0
/(2.85 FIA)
10 1 1 1 1 1
2.0 2.2 2.4 2.6 2.8 3.0 3.2 3.4 3.6 3.8 4.0Dose (Gy)
Fig. 2-10. Human mortality for high-dose-rate, low-LET radiation doses to bone marrow. Doses beyond LD,0 or belowLDW cannot be reliably extrapolated. Slope, calculated from this animal model, is expressed as ratio of LD., to LD,,.
that is emerging among the values for the LDO, es- tially the same model.6 Both of these values werepecially from the Hiroshima and Nagasaki data. skewed by the inclusion of data from deaths due toRecently, a value of 1.54 Gy for the midlethal bone- burns and blast effects. If one increases these val-marrow dose for Hiroshima was published.' This ues by 17.5% (the difference in LDO for radiationvalue was derived from survey data relating the only, and radiation combined with blast injuriesmortality of persons in wooden houses to their dis- and bums), the values increase to 2.75-3.0 Gy. An-tance from the hypocenter of the bomb. Using pre- other recent analysis of the data from Hiroshima es-liminary calculations of dose versus ground range, timates the LD. to be 2.72 Gy by correlating whitethe Hiroshima LD0 was determined to be 1.54 Gy-5' blood-cell counts to the percentage of mortality.However, if one uses the latest calculations, the Considering the diversity of these analyses and thevalue becomes 2.3 Gy to the bone marrow. This approaches by which they were derived, theirvalue is in general agreement with the reported agreement is remarkable. Even more remarkable isvalue of 2.24-2.50 Gy, based on doses and essen- the fact that these values agree with the human val-
32

Acute Radiation Syndrome in Hinitans
ues obtained 20 years ago for patients, when ad- Nagasaki) that the NATO human LC; should notjusted for bone-marrow dose and prompt dose be raised for healthy untreated persons. Based onrates. the range of values discussed, the recommended
There is good agreement among the data (par- value for the LD, is 3.0 Gy to bone marrow (4.3 Gyticularly the recent data from Hiroshima and free in air).
REFERENCES
1. Young, R. W. 1987. Acute radiation syndrome. In Military Radiobiology, edited by J. J. Conklin and R. I. Walker, 165-190. Orlando, FL: Academic Press.
2. Annex 7. 1986. Medical-biological problems from the USSR State Committee on the Utilization of Atomic Energy. InThe Accident at the Chernobiyl Nuclear Power Plant and Its Consequences. Vienna: International Atomic EnergyAgency Experts Meeting.
3. Bowers, G. J. The combined injury syndrome. In reference 1, 191-217.
4. Gunter-Smith, P. J. Effect of ionizing radiation on gastrointestinal physiology. In reference 1, 135-151.
5. Hawkins, R. N., and Cockerham, L. G. Postirradiation cardiovascular dysfunction. In reference 1, 153-163.
6. Cockerham, L. G.; Doyle, T. F.; Donlon, M. A.; and Helgeson, E. A. 1984. Canine postradiation histamine levels andsubsequent response to Compound 48/80. Aviat. Space Environ. Med. 55(11): 1041-1045.
7. Cockerham, L. G.; Pautler, E. L.; Carraway, R. E.; Cochrane, D. E.; and Hampton, J. D. Effect of disodium cromogly-cate (DSCG) and antihistamines on postirradiation cerebral blood flow and plasma levels of histamine andneurotensin. Fundain. Appl. Toxicol., in press.
8. Cockerham, L. G.; Prell, G. D.; Cerveny, T. J.; O'Brien, M.; and Hampton, J. D. Effects of aminoguanidine on pre- andpostirradiation regional cerebral blood flow and systemic blood pressure in the primate. In preparation.
9. Jones, T. D. 1981. Hematologic syndrome in man modelled from mammalian lethality. Health Phys. 41: 83-103.
10. Baverstock, K. F., and Ash, P. J. N. D. 1983. A review of radiation accidents involving whole body exposure and therelevance to the LD;,,,,., for man. Br. ]. Radiol. 56: 837.
11. Jones, T. D.; Morris, M. D.; Wells, S. M.; and Young, R. W. 1986. Animal mortality resulting from uniform exposures tophoton radiations: Calculated LD;,,s and a compilation of animal data [Publication 63381. Oak Ridge, TN: OakRidge National Laboratory.
12. Bond, V. P.; Fleidner, T. M.; and Archambeau, J. V. 1965. Mammalian radiation lethality. New York: Academic Press.
13. Bond, V. P., and Sugahara, T. 1969. Comparative cellular and species radiosensitivity. Baltimore: Williams and WilkinsCo.
14. Ainsworth, E. J.; Leong, G. F.; and Alpen, E. L. 1984. Early radiation mortality and recovery in large animals and
primates. In Response of Different Species to Total Body Irradiation, edited by J. J. Broerse, and T. J. MacVittie, 87-111. Dordrecht, The Netherlands: Martinus Nijhoff Publishers.
15. MacVittie, T. J.; Monroy, R. L.; Patchen, M. L.; and Darden, J. H. Acute lethality and radiosensitivity of the caninehematopoietic system to cobalt-60 gamma and mixed neutron-gamma irradiation. In reference 14, 113-129.
16. Krebs, J. S., and Jones, D. C. L. 1975. Radiobiology of large animals [Final report for contract DAHc2O-70-C-0219,Defense Civil Preparedness Agency work unit 24310, SRI Project PYU-81501. Washington, DC: DefenseTechnical Information Center.
33

Medical Consequences of Nuclear Warfare
17. Norris, W. P.; Fritz, T. E.; Rehfeld, C. E.; and Poole, C. M. 1968. The response of the beagle dog to cobalt-60 gammaradiation: Determination of the LRD , and description of associated changes. Radiat. Res. 35: 681.
18. Sorensen, D. K.; Bond, V. P.; Cronkite, E. P.; and Perman, V. 1960. An effective therapeutic regimen for the hemato-poietic phase of the acute radiation syndrome in dogs. Radiat. Res. 13: 669.
19. Alpen, E. L.; Jones, D. M.; Hechter, H. H.; and Bond, V. P. 1958. The comparative biological response of dogs to 250kVp X-rays and 100 kVp X-rays. Radiology 70: 541.
20. Shively, J. N.; Michaelson, S. M.; and Howland, J. W. 1958. The response of the dog to bilateral whole-bo~dv cobalt-60irradiation. i. Lethal dose determination. Radiat. Res. 9: 445.
21. Vriesendorp, H. M., and van Bekkum, D. W. Susceptibility to total body irradiation. In reference 14,43-57.
22. Ainsworth, E. J.; Leong, G. F.; Kendall, K.; and Alpen, E. L. 1965. Comparative lethality responses of neutron- and X-irradiated dogs: Influence of dose-rate and exposure aspect. Radiat. Res. 26: 32.
23. Broerse, J. J.; van Bekkum, D. W.; Hollander, C. V.; and Davids, J. A. G. 1978. Mortality of monkeys after exposure tofission neutrons and the effort of autologous bone marrow transplanation. Int. 1. Radiat. Biol. 34: 253.
24. Wise, D., and Turbyfill, C. L. 1968. The acute inortality response of inonkeys (Macaca mulatta) to pulsed mixed gamma-neutron radiations. [Scientific Report SR68-17]. Bethesda, MD: Armed Forces Radiobiology Research Institute.
25. Stanley, R. E.; Seigneur, L. J.; and Strike, 'i. A. 1966. The acute mortality responses of monkeys (Macaca mulatta) to mixedgamma-neutron radiations and 250 KVP rays [Special Report SP66-231. Bethesda, MD: Armed Forces Radiobiol-ogy Research Institute.
26. Carsten, A. L. Acute lethality-the hematopoietic syndrome in different species. In reference 14, 59-86.
27. Ainsworth, E. J.; Long, G. F.; Kendall, K.; and Alpen, L. 1964. The effects of pulsed neutron or gamma irradiation inmice. Radiat. Res. 21: 75-85.
28. Davis, J. A. G. 1966. Relative biological effectiveness of fission neutrons for production of the bone marrow syn-drome in mice. Int. 1. Radiat. Biol. 10: 299.
29. Duque, R. E.; Phan, S. H.; Hudson, J. L.; Till, G. D.; and Ward, P. A. 1985. Functional defects in phagocytic cellsfollowing thermal injury. Application of flow cytometric analysis. Am. ]. Pathol. 118:116.
30. Shires, G. T., and Dineen, P. 1982. Sepsis following bums, trauma, and intra-abdominal infections. Arch. Intern. Med.142: 2012-2022.
31. Munster, A. M. 1976. Post-traumatic immunosuppression is due to activation of suppressor T cells. Lancet 1: 1329-
1330.
32. Saba, J. M., and Scovill, W. A. 1975. Effects of surgical trauma on host defense. Ann. Surg. 7: 71-81.
33. Alexander, J. W., and Wixson, D. 1970. Neutrophil dysfunction and sepsis following burn injury. Surg. Gynecol.Obstet. 130: 431-438.
34. Korlof, B. 1956. Infection in bums. Acta. Chir. Scand. [Suppl.[ 209:117-139.
35. Balch, H. H. 1955. The effect of severe battle injury and of post traumatic renal failure on resistance to infection.Ann. Surg. 142: 45-153.
36. Jones, R. K.; Chiffelle, T. L.; and Richmond, D. R. 1968. A study of effects of combined blast and radiation injury insheep. In Intermedes Proceedings 1968: Combined Injuries and Shock, 57-66. Stockholm: ForsvaretsForskningsanstalt.
34

Acute Radiation Syndrome in Humans
37. Richmond, D. R.; Jones, R. K.; and White, C. S. The effects of blast and ionizing radiation in rats. In reference 36,67-74.
38. Messerschmidt, 0. 1966. Untersuchungen uber Kombinationsschaden. Uber die Lebenserwartung von Mausen, diemit Ganzkorperbestrahlungen in Kombination mit offenen oder geschlossenen Hautverletzungen, Bauchop-erationen oder Kompressionsschaden belastet wu rden. Strahlentherapie 131: 298-311.
39. Valeriote, F. A., and Baker, D. G. 1964. The combined effects of thermal trauma and x-irradiation on early mortality.Radiat. Res. 22: 693-703.
40. Vogel, C. E. H. 1961. Burns and other trauma associated with radiation exposure. Milit .led. 126: 688-692.
41. Alpen, E. L., and Sheline, G. E. 1954. The combined effects of thermal burns and whole body X-irradiation onsurvival time and mortality. Ann. Surg. 140: 113-118.
42 -r, H.; Drummond, J. A.; Stephens-Newsham, L. G.; and Randall. R. G. 1953. Reduction of mortality in swinefrom combined total body radiation and thermal burn- Iwy streptomycin. Ann. Surg. 137: 450-455.
43. ii,, J. W.; Evans, E. I.; Ham, W. T.; and Reid, R. D. 1952. The influence of external body radiation on mortalityfrom thermal burns. Ann. Surg. 136: 533-545.
44. Ledney, G. D.; Stewart, D. A.; and Exum, E. D. 1980. Proliferative responses of lymphomyelopoietic cells of miceafter wound trauma. J. Trauma 20:141-147.
45. Ledney, G. D.; Stewart, D. A.; Exum, E. D.; and Sheehy, P. A. 1981. Skin wound-enhanced survival and myelocyto-poieses in mice after whole-body irradiation. Acta Radiol. [Oncol.] 20: 29-38.
46. Singer, D. 1976. Postsplenectomy sepsis. Perspect. Pediatr. Pathol. 1: 285-311.
47. Schildt, B., and Thoren, L. 1968. Experimental and clinical aspects of combined injuries. In Combined Injuries andShock, edited by B. Schildt and L. Thoren, 3-15. Stockholm: Forsvarets Forskningsanstalt.
48. Schraibor, M. I., and Korchanov, L. S. Relevance of radiation injury in the combined injury syndrome. In reference36, 17-20.
49. Perman, V.; Sorensen, D. K.; Usenik, E. A.; Bond, V. P.; and Cronkite, E. P. 1962. Hematopoietic regeneration incontrol and recovered heavily irradiated dogs following severe hemorrhage. Blood 19: 738-742.
50. Perman, V.; Cronkite, E. P.; Bond, V. P.; and Sorensen, D. K. 1962. The regenerative ability of hematopoietic tissuefollowing lethal x-irradiation in dogs. Blood 19: 724-737.
51. Jackson, D. P.; Sorenson, D. K.; Cronkite, E. P.; Bond, V. P.; and Fliedner, T. M. 1959. Effectiveness of transfusions offresh and lyophilized platelets in controlling bleeding due to thrombocytopenia. J. Clin. Invest. 38:1689-1697.
52. Jacobson, L. 0.; Marks, E. K.; and Gaston, E. 0. 1963. Observations on the effect of spleen-shielding and the injectionof cell suspensions on survival following irradiation. Proc. Soc. Exp. Biol. Med. 119:122.
53. Maille, H. D.; Krasavage, W.; and Mermagen, H. 1966. On the partial-body irradiation of the dog. Health Phys. 12:883.
54. Hansen, C. L.; Michaelson, S. M.; and Howland, S. W. 1961. Lethality of upper body exposure in beagles. PublicHealth Rep. 76: 242.
55. Gozenbuk, V. L., and Keirim-Markus, T. B. 1977. Dosimetric criteria of canine mortality following total body non-uniform irradiation. Radiobiologiia 17(6): 936-938.
56. Lushbaugh, C. C., and Havier, 1. 1969. Reestimation of the human LD50 radiation levels at Hiroshima and Nagasaki.Radiat. Res. 39: 526.
35

Medical Cons,'qwences tit Nuclh•r Wa rart,
57. Martin, J. H. 1983. Human survival-Radiation exposure levels. 1. Soc. Radtiolog. Protection 3: 15-23.
58. Lushbaugh, C. C.; Comas, F.; and Hofstra, R. 1907. Clinical studies on the radition effects in man: A preliminaryreport of a retrospective search for dose relationships in the prodromal syndrome. Radiat. Res. 7: 398-412.
59. Rotblat, J. 198b. Acute radiation mortality in a nuclear war. In The Medical lInplications of Nuclear War, Institute ofMedicine, National Academy of Sciences, 233-250. Washington, DC: National Academy Press.
W0. Rider, W. D., and Hasselback, R. 1968. The symptomatic and haematological disturbance following total bodyirradiation of 300 rad gamma-ray irradiation. In Guidelines to Radiological Health [Public Health ServicePublication No. 999-RH-331, 139-144. Washington, DC: U.S. Department of Health, Education, and Welfare.
61. jammet, H. 1961. Treatment of victims of the zero energy research accident at Vinca. In Diagnosis and Treatment ofAcute Radiation Injury. Proceedings of WHO Scientific Meeting, Geneva, October 196), 85. Geneva: World
Health Organization.
62. Hurst, G. S.; Ritchie, R. H.; Sanders, F. W.; Reinhardt, P. W.; Auxier, J. A.; Wagner, E. B.; Callihan, A. D.; and Morgan,K. Z. 1961. Dosimetric investigation of the Yugoslav radiation accident. Health Phyvs. 5: 179-202.
63. MacVittie, T. 1. 1988. Unpublished information.
64. Jones, T. D. 1981. Hematologic syndrome in man modelled from mammalian lethality. Health Phiys. 41: 83-103.
65. Scott, B. R.; Seiler, F. A.; and Young, R. W. Predicted deaths from bone marrow dysfunction after protracted radiationin a fallout field. Abstract presented at 36th Annual Meeting of Radiation Research Society, Philadelphia,
April 1988.
66. Schull, W. J. Implications of the new dosimetry for risk estimates. In Ntew DositnetrY ,at Hiroshima and Nagasaki and ItsImplications for Risk Estimnates, Proceedings No. 9 of the 23rd Annual Meeting of National Council on RadiationProtection, Washington, DC, 1987. In press.
36

Chapter 3
TRIAGE AND TREATMENT OFRADIATION-INJUREDMASS CASUALTIES
ROBERT F DONS, M.D.,* and T. JAN CERv ENY, Ph.D.**
INTRODUCTION
PRINCIPLES OF TRIAGE
Operational Considerations for TriagePeacetime TriageMilitary Triage
Signs and Symptoms of Radiation InjuryCutaneous PhenomenaGastrointestinal PhenomenaCardiovascular, Respiratory, Metabolic, and Neurological PhenomenaHematological Phenomena
Triage of the Combined-Injury PatientBurn InjuryBlast InjuryEye Injury
MEDICAL MANAGEMENT OF THE COMBINED-INJURY CASUALTY
Concerns in the Treatment of the Combined-Injury PatientSpecific Treatment Concerns
SurgeryAnesthesia and Pain ControlControl of InfectionsAntiemetics and AntidiarrhealsFluids and ElectrolytesBlood Component TherapyChelation TherapyNutritional Support
SUMMARY
*Lieutenant Colonel, United States Air Force; Department of Experimental Hematology, Armed Forces Radiobiology Research Institute,Bethesda, Maryland 20814-5145**Major, United States Air Force; Program Manager, Bioenvironmental Hazards, Air Force Office of Scientific Research,Boiling Air Force Base, Washington, D.C. 20332-6448
37

MAedical Co's,'quences tf idulear Warfarc'
INTRODUCTION
The effective medical sorting of mass casualties However, if a nuclear event occurs, it is more(triage) and their subsequent treatment after a nu- likely to take place on a limited scale rather than asclear event have been considered extremely diffi- a strategic weapons exchange.' After a smaller-cult or even impossible.' In the case of a major ex- scale tactical detonation (0.1-2.0 kt) or a nuclearchange of strategic nuclear weapons (500-5,000 detonation by terrorists, hundreds or a few thou-MT), the triage of casualties using the remainiag re- sand casualties are more probable than millions2 orsources would certainly be futile and frustrating. billions. ' Considerable medical resources may beWithout transportation and tertiary medical-care intact and available for treating many of them. Thisfacilities, the only benefit would be to identify per- chapter presents plans for the management of largesons who are capable of combat. Even the mini- numbers of casualties suffering either radiation in-mally injured casualty may receive little (if any) jury alone or conventional trauma combined withmeaningful attention in such a situation. radiation injury.
PRINCIPLES OF TRIAGE
In conventional triage, patients are assigned to category (Table 3-1). A slower but more accurateone of the following priority categories, depending method of assessment is to expose the injured areaon the nature and extent of their injuries: (a) The directly and perform an abdominal examination.immediate treatment group includes patients who Even with a relatively small number of casualties,have a high chance of survival if they are given this exam might be prohibitively time consuming inimmediate life-saving treatment or surgery that is the critical moments shortly after a nuclear event.relatively quick and uncomplicated. (b) The delayed Rapid assessment based on physiological statustreatment group includes patients who may need will permit the gathering of useful information onmajor surgery, but who can be sustained on sup- respiratory rate and systolic blood pressure in aportive treatments until surgery is possible. (c) The large number of patients. In contrast, a determi-a-minimal treatment group includes patients with rela- tion of the Glasgow coma scale score 4 (althoughtively minor injuries who can care for themselves or fairly rapid in experienced hands) is less usefulwho can be helped by untrained personnel. (d) The than a brief neurological evaluation of the patient'sexpectant category includes patients with serious or degree of alertness, responsiveness to verbal andmultiple injuries requiring extensive treatment, as painful stimuli, and state of consciousness. Atten-well as patients with a poor chance of survival. tion to other relatively obvious factors, such as ex-This group should receive supportive treatments tremes of age (under 5 years or over 55 years) andthat are compatible with resources, including large preexisting or recently induced cardiovascular ordoses of analgesics. respiratory illness, will aid in establishing a pa-
The speed of assessing and categorizing the tient's status as expectant.status of patients is the key to effective triage. Anymethod is useful that gives the triage officer a Operational Considerations for Triagequick, accurate idea of the extent of injury. Whenmaking the assessment rapidly based on anatomi- Regardless of the findings from an anatomical orcal findings, the probability of injury is related to physiological assessment of the patient, the firstthe degree of estimated force on the body part. For priority of the military triage officer is to conserveexample, a patient close enough to a nuclear explo- the fighting force. Combatants in the expectantsion to be caught in the blast wind is assumed to category, however, should not receive aid or re-have internal and possibly occult traumatic injury, sources that might be of greater benefit to less se-Such a patient will most likely be in the expectant verely injured noncombatants, even if these re-
38

Triage and Treatment of Raidiation-lnij, red Mass Caslialties
TABLE 3-1
PRIORITIES IN COMBINED-INJURY TRIAGE WHENRADIATION DOSES ARE KNOWN*
Conventional Triage Changes in Expected TriageCategories if Injuries Category FollowingAre Only Trauma** Whole-Body Radiation Dose
(Gy)
No radiation ,xi't. <1.5 1.5-4.5 >4.5
TI T1 T1 T4
T2 T2 T4 T4
T3 T3 T4 T4
T4 T4 T4 T4
*Decision based on whole-body radiation dose, assuming all
casualties are wearing personal dosimeters.
"Conventional Triage Categories:TI: Immediate treatment, high survival groupT2: Delayed treatment, patient can be sustainedT3: Minimal treatment, minor injury groupT4: Expectant, seriously injured-poor survival
Source: Adaptation from data in NATO Handbook on the Concept of MedicalSupport in NBC Envirntments (reference 15).
sources seem to be in adequate supply. In rare cir- with the management of mass casualties under thecumstances, a terminally injured unit commander constraints of peacetime disaster triage.might receive resources to permit continued func- Peacetime Triage. In peacetime, a two-tieredtioning in a crucial command role. system of care for the critically ill is assumed.
This chapter pertains primarily to the manage- Based on the triage decision, the patient goes eitherment of acutely irradiated casualties following the to the emergency room of the nearest communitydetonation of a nuclear weapon. The military phy- hospital or to the regional trauma center. This sys-sician should recognize two essential facts in deal- tem depends on rapid, reliable transportation ining with mass casualties during military triage in a which trained attendants monitor the patient withdeclared war: (a) all medical resources fall under radio guidance from trauma staff at the hospital orthe jurisdiction of the military, and (b) peacetime center.'triage practices are of limited use. However, in In this scheme, the sorting of patients is basedmore limited events (such as a major nuclear reac- on a physiological trauma score in which the less-tor accident), the military may be asked to assist injured patient, with a score of 15-16, is in the de-
39

Medical Consequences ,,f Nuclear Wartiare
TABLE 3-2
ESTIMATION OF POSSIBLE RADIATION INJURY BASED ONSYMPTOMS
Symptoms Unlikely Probable Severe
Nausea (-) (++)
Vomiting (-) (+)
Diarrhea (-) (W) (+ to +++)
Hyperthermia (-) (W) (+ to +++)
Erythema (-) (-) (- to ++)
Hypotension (-) (-) (+ to ++)
CNS dysfunction (-) (-) (- to ++)
layed category, a third priority. Patients with a Extra effort will be needed to keep the patient mov-trauma score of 3 or less are considered expectant ing forward in the system to an appropriate level of(the fourth, or last, priority). Third- and fourth-pri- care. The greatest number of lives will be savedority patients would probably be sent to the local only by ensuring that time and materials are not al-hospital emergency room. All patients with trauma located to hopeless cases or to those whose injuriesscores of 4-10 (first priority) and some with scores are so minor or uncomplicated that definitive careof 11-12 (second priority) would go to the trauma can be postponed.center. In a nuclear disaster, triage decisions cannot be
Military Triage. Military triage contrasts made on the evidence or probability of conven-starkly with that used in peacetime, but the two do tional injury alone. When significant radiation ex-have some elements in common. For example, posure is combined with conventional injuries,military triage decisions would most likely be made there may be a dramatic shift of patients to the ex-at the level of the batallion aid or clearing station. pectant category (Table 3-1). In order to make anThe local community hospital might be equivalent appropriate decision, the triage officer must recog-to the second-echelon radiation decontamination nize the symptoms of ARS and understand the dif-center and field hospital. Only fixed medical-care ficulties in estimating radiation exposure fromfacilities or existing tertiary-care facilities that are clinical findings.able to perform surgery would suffice as traumacenters for handling combined-injury casualties. Signs and Symptoms of Radiation Injury
In wartime, it cannot be assumed that rapid andreliable transportation of wounded persons is pos- It will be difficult to assess the radiation doses ofsible, as it is in peacetime or might be in smaller, persons who have been injured in a mass-casualtylow-yield nuclear events. In the confusion of disaster. Thus, a system has been devised to iden-armed conflict, casualties with a wide variety of in- tify radiation exposure based on the symptoms ofjuries might be expected to arrive at the nearest "unlikely," "probable," or "severe" radiation injurymedical-care facility regardless of its capability. (Table 3-2).6 These symptoms are nonspecific, and
40

Triage and Treatment of Radiation-Injured Mass Casualties
ERYTHEMA 2
%pigment
%: *
L 16 24 hours
I I I1 5 10 lays
I I i i1 2 4 8 weeks
Fig. 3-1. Appearance of waves of erythema after irradiation of human skin. Dotted lines indicate tp'gmented lesions.Source: Redrawn from reference 6.
permit only the cursory screening of a large num- teristic transient erythema secondary to capillaryber of cases. dilation and the release of histamine-like sub-
Cutaneous Phenomena. Information about the stances. The initial erythema usually peaks withincutaneous changes after ionizing radiation expo- 24 hours, and then disappears for 1-3 weeks.sure comes mainly from accidental or therapeutic Thereafter, it may reappear with pain and edema.high-dose local radiation exposures and, to a lesser Severe pain may occur if more radioresistant nerveextent, from studies of the victims of the 1986 nu- tissue is surrounded by necrotizing tissues. Mela-clear reactor accident in Chernobyl, USSR, and the notic pigmentation (Figure 3-1) or ulceration may1987 cesium-137 accident in Goi~nia, Brazil. Skin develop.7 Pain from nerve compression may occurinjury in those events resulted from very intense as healing and atrophy take place. Hair loss overlocal irradiation or direct contact of the skin with the affected area occurs at the end of the second orradioactive material. Burns among casualties at Hi- third week. In contrast to erythema induced byroshima and Nagasaki in 1945 were caused by heat high-dose beta radiation, skin injury from gammarather than radiation exposure.' radiation occurs only at doses that damage the
When extremely high doses of whole-body ra- bone marrow. Thus, if sufficient marrow is ex-diation (100 Gy) are delivered acutely, skin may posed, thrombocytopenia with cutaneous pe-have the sensation of tingling or being on fire even techiae, purpura, and hemorrhage can be expected.though no lesion immediately appears. Within the In granulocytopenic patients, otherwise-noninva-first 24 hours, there is the appearance of a charac- sive surface bacteria may colonize areas of wet
41

Medical Consequences of Nuclear Warfare
desquamation and lead to suppurative lesions. combined chemical-nuclear warfare environments,The threshold dose for gamma-radiation-in- chemical agents may account for much of the nau-
duced erythema is about 3-5 Gv; for desquamation, sea and vomiting.it is about 10 Gy. Ulceration develops at doses of Cardiovascular, Respiratory, Metabolic, and20 Gy. At doses of more than 40 Gy, gangrenous Neurological Phenomena. If a casualty has no con-radionecrosis can be confidently predicted, if the ventional injuries or psychosomatic complaints,dose is well documented and can be confirmed on then cardiovascular, respiratory, metabolic, andreview of the evidence.' Different body areas may neurological symptoms usually indicate terminalhave different radiation sensitivities; a gradient high-dose radiation exposure. Radiation-relatedfrom greater to lower resistance is observed for hypotension, radiation pneumonitis, or ETI identifyscalp, face and neck, trunk, ears, groin, and ex- persons who may be expected to die within 2-3tremities. Exposure of the skin to temperatures days. This prognosis is certain, despite a variablegreater than 42°C may enhance cutaneous radio- period of transient' improvement that occurs shortlysensitivity and increase the probability of a more after the event.severe injury., Initial symptoms of high-dose exposure may not
Beta-emitting isotopes from smoke and fallout be distinct from those of lower-dose exposures.can cause desquamation from high-dose local ra- Nausea and vomiting may occur even without di-diation delivered to exposed skin surfaces, but only rect exposure to the gut in patients who receivedif these isotopes are in contact with the skin for high-dose local radiation to the head or chest.longer than 1 hour. Since beta radiation is not as Metabolic abnormalities can be expected afterpenetrating as gamma radiation, dry desquamating radiation of moderate to high doses, and includeskin lesions secondary to beta burns may not be as the consistent finding of nonbacteria-mediated hy-serious as wet desquamating lesions, which occur perthermia with marked fever and shaking chills.as the result of high-dose exposure and suggest that A 2 517c drop in plasma glucose may occur withinunderlying structures are involved. The wet le- the first day, but a neuroglycopenic state of confu-sions may be complicated by secondary infection, sion has not been observed. Hemorrhagic coagulo-and usually indicate a poor prognosis. pathies, associated with disseninated intravascular
Gastrointestinal Phenomena. A sense of fatigue coagulation and a reduction in noncellular clottingand malaise associated with nausea and loss of ap- factors, are possible. Liver injury probably ac-petite is characteristic even of relatively low-dose counts for hypoglycemia and the coagulation factorradiation exposure (1-2 Gy). The abrupt onset of deficiencies.1 .1 2 Cardiac arrhythmias associatednausea and vomiting occurs with acute high-dose with electrolyte imbalance (hyper- or hypokalemia)radiation in the range of 5-10 Gy. These initial may occur.symptoms may be followed by a short latent period In the later stages after lung exposure, the loudof 1-2 days. The severity of initial symptoms, in- crepitus of radiation pneumonitis, which has beencluding diarrhea, serves as a useful index of prob- likened to the "thundering of a rain storm on anable outcome, as does the rapidity of onset or a de- iron roof,""' is associated with tachypnea and se-lay in the appearance of symptoms. Following the vere hypoxemia.latent period, an increase in vomiting, diarrhea, ETI in primates (and its locomotor equivalent inand anorexia, as well as dehydration and signs of rodents) is characterized by the complete but tem-infection, can be expected.' porary cessation of motor function, and does not
An abrupt onset of bloody diarrhea after acute occur unless high-dose radiation is deliveredhigh-dose radiation indicates lethal exposure. If acutely."3 Transient loss of consciousness is notless-acute doses are received, diarrhea may not ap- typical of ETI. Unconsciousness is more suggestivepear for several days or a week after exposure. The of conventional head injury.onset of diarrhea within a week of exposure is usu- Hematological Phenomena. The most usefulally associated with death. However, patients have and rapid method of assessing the degree of radia-survived when the onset of radiation-related diar- tion exposure is to obtain serial total lymphocyterhea was delayed for more than I week after pro- counts. Optimally, this should be done every 6tracted radiation exposure." hours during the first 48 hours, or at least once ev-
Nausea and vomiting occur after exposure to ery 24 hours after exposure. This estimate and itsdoses greater than 2.5 Gy. Identification of the on- interpretation need to be standardized for the avail-set of these symptoms may be useful in the initial able laboratory methodology. To that end, a charttriage of a radiation-only casualty. However, in of blood cell morphology (Fig.ire 3-2) and a nomo-
42

Triage and Treatinent of Radiation-Inirred Mass Casualties
Monocyte Lymphocytes
Large Small
Granulocytes
Non-Segmented Forms
"VMature Form
Fig. 3-2. Appearance of hunan mononuclear cells (lvmphocvtes and monocytes) compared to human granulocytic cells(eosinophils, neutrophils, and basophils) in their nonsegmented and segmented (mature) forms. Erythrocytes are shown forcontrast in size.
gram of the acute radiation-induced change in lym- tion on the nuclear battlefield at a field hospital.phocvtes/mm ' (Figure 3-3) may be useful. A lami- A drawback of this method is that monocytesnated copy of this nomogram should be included in cannot be differentiated from lymphocytes unless athe field kit of every medical officer. Changes in separate Wright-stained slide is prepared and inter-peripheral blood granulocytes do not give as clear a preted. Such a determination done by hand wouldpicture of the severity of radiation injury because become prohibitively time consuming and labor in-their numbers are affected by stress and infection, tensive in a mass-casualty situation. However,fall more slowly, and vary widely. with the QBC II methodology, the determination of
Sophisticated methodology has become avail- the total granulocyte percentage and the mononu-able that permits the rapid and quantitative deter- clear cell percentage is automated (although it stillmination of the total and differential leukocyte requires data transcription by hand).counts at DEPMEDS (Deployable Medical Systems)field hospitals. Using the QBC II assay methodol- Triage of the Combined-Injury Patientogy,' a total lymphocyte count requires only a fin-gerstick blood sample (rather than a phlebotomy) Priorities ;n handling patients of convention'aland can be performed by relatively inexperienced trauma are modified in cases of concurrent radia-personnel. Effective suppression of electrical tion injury. Triage priority is based on the conven-power surges and adequate supplies of special tional injury as well as the degree of radiation suf-sample tubes would be needed to permit this op- fered by the combined-injury victim (Table 3-1).
43

Medical ConseIitences of Nutchar Warfare
3000
NormalRange
0 20 0 ---0@O00
C.
OQ O 0 0 0 0 0 00 4D0 0
E 0
_ 1000 Moderate
1•0000000000
0 Severeo500o Very
100 SevereLethal
0 1 2Time (days)
Fig. 3-3. To use a lymphocyte nomogram: (a) determine total lympho-cytes/mm'every 6 hours; (N because the absolute number of lympho-cytes (Y axis) depends on technique, use standardized laboratorymethodology; (c) because the ordinal scale (X axis) depends on acutenessof radiation exposure, do not use scale shown if exposure is protracted.
44

Triage and Treatnent of Radiation-Ihlu red Mass Casualties
TABLE 3-3
PRIORITIES IN COMBINED-INJURY TRIAGE WHEN RADIATION INJURY IS POSSIBLE
Conventional Triage Changes in Expected Triage Category FollowingCategories if Injuries Possibility of Radiation InjuryAre Only Trauma*
Unlikely Probable Confirmed
No radiation exists Minimum** Moderate Severe
T3 T3 T3 T3 T3 T3
T2 T2 T2/T4 T3 T4 T4
T1 T1 T3/T4 T3 T4 T4
T4 T4 T4 T4 T4 T4
*Conventional Triage Categories:TI: Immediate treatment, high survival groupT2: Delayed treatment, patient can be sustainedT3: Minimal treatment, minor injury groupT4: Expectant, seriously injured-poor survival
"**Acute radiation dose of approximately 0.5 Gy
All patients exposed to more than 4.5 Gy are in the giving the benefit of the doubt to such patients,expectant category, as are those with exposure of those with injuries treatable on an immediate basis1.5-4.5 Gy who cannot be given care immediately. should receive prompt attention. However, if ra-If exposure was less than 1.5 Gy, the nature of the diation exposure does account for the observedconventional injury will dictate the treatment prior- symptoms, the patient in the conventional catego-ity. Casualties who receive radiation exposure ries of immediate (Table 3-3) or delayed (Table 3-1)alone over a wide range of doses will need little if may actually be expectant. Even with severe symp-any treatment initially.15 toms of radiation exposure, patients with minimal
Since an estimate of the exposure dose in the traumatic injury may be capable of survival ifearly phases of radiation-casualty triage will be al- evacuated for observation and advanced medicalmost impossible, a more practical triage scheme, management. However, if transportation resourcesbased on symptoms of unlikely, probable, or severe are limited, disposition of the minimally injuredradiation exposure, will be useful (Table 3-2). In but heavily exposed patient should coincide withthe event of combined injuries, symptoms of prob- that of the casualty in the expectant category. Pa-able or severe exposure may be confused with tients in the delayed category with probable radia-symptoms associated with conventional injury. In tion symptoms are expectant, unless adequate terti-
45

Medicil Ctnsequences of Nuclear WaMrfM'
ary-care facilities are readily available. Regardless Eye Injury. Eye injuries from a thermonuclearof the triage scheme used, it is probable that a num- flash may be as minor as transient blindness (for aber of combined-injury patients in the expectant few seconds to minutes) or a permanent retinal scarcategory will receive treatment for more immediate in which peripheral vision is spared.'" These areand delayed conventional injuries, minimal injuries. However, permanent foveal
Conventional injuries that are particularly rele- damage with 20/200 visual acuity may occur if thevant following a nuclear detonation include burn, victim focuses directly on the nuclear fireball. Ablast, and eye trauma. variety of eye injuries resulting primarily from pro-
Burn Injury. The extent of a thermal burn may tracted high-dose radiation exposure was observedbe rapidly estimated according to the "rule of among firefighters at the Chernobyl reactor acci-nines."4 Conventional thermal burns are predicted dent. These injuries will most likely lead to perma-to be among the most frequent injuries to troops on nently impaired vision."' Clearly, if the correctedthe nuclear battlefield." A more severe hematopoi- visual acuity of a patient is 20/200 or less afteretic subsyndrome is likely if partial-thickness burns more than 1 hour from time of injury, the useful-involve more than 10'7, of the body surface."' ness of that person as a combatant will be limited,
Blast Injury. Dynamic overpressure from the and assignment to a category of delayed treatmentexplosion of a nuclear weapon will induce overt is appropriate. Gross eye injuries, most likely fromcrush injuries and occult internal bleeding." The flying objects after a nuclear blast, may have a dra-triage officer should suspect occult traumatic inju- matic appearance, but they are frequently minimalries, which will likely place the irradiated patient in and should not divert attention from more signifi-the expectant category. cant injuries.
MEDICAL MANAGEMENT OF THE COMBINED-INJURY CASUALTY
Patient management will focus on three issues. not hazardous. No conclusive evidence exists thatFirst, basic life-support concerns need to be quickly any attendant has ever been adversely affected byaddressed for casualties in the immediate category; brief contact with a radiation casualty. On thean airway, adequate ventilation, and circulatory other hand, in a nuclear attack that is combinedfunction should be assured for patients whose inju- with chemical or biological weapons (which may beries will permit them to survive. Concerns about more likely than a nuclear attack alone), the atten-internal or external contamination with radioactiv- dant will need to wear protective gloves, as well asity should be second priority. Finally, an effort a mask outfitted with an entire chemical ensemble,should be made to retrieve data from any dosime- to manage these casualties safely.ters carried bv the military combat unit. Currently, Wearing this chemical ensemble will pose spe-radiation dosimeters cannot be relied on to accu- cial problems in primary medical management.rately estimate the severity of an individual's radia- Even if the mask is equipped with a voice emitter,tion injury. Dosimeters do not account for partial verbal communication over more than a few yardsshielding and do not reflect the delivery rate of a will be hampered. In the early phases of identifica-radiation dose, and so make only a small contribu- tion and triage, familiarity with a brief dictionary oftion to the diagnostic picture. Any data from sign language will be useful. The signs for "radia-physical dosimeters must be interpreted by the tion casualty" and "chemical casualty" are illus-medical attendant in light of the observed physio- trated in Figure 3-4.logical changes.
Because most of the radiation exposure likely to Concerns in the Treatment of the Combined-be encountered on the battlefield has no immediate Injury Patientlife-threatening consequences, the medical atten-dant should first focus on conventional injuries. Once an airway, proper ventilation, and circula-Needless risks, such as prolonged contact with con- tory stability have been established, definitive caretaminated clothing or wash water, must be should be planned for the casualty who can sur-avoided, but in emergency medical treatment, di- vive. Treatment planning is based on the compe-rect contact with a contaminated patient is usually tent handling of conventional injury and the antici-
46

Triage and Treatment of Radiation-Injured Mass Casualties
(IO"
Chemicnl Nuclear
Fig. 3-4. To sign for "chemical," make a "C" with hands and move them in a circle away from lower thorax and towardshoulders. To sign for "nuclear," thrust second and third fingers toward open palm of opposite hand.
pation of predictable sequelae of radiation injury. vanced life-support measures will not be in the bestIn the following discussion, early placement of a interests of a patient who will most likely suffer aperipheral intravenous catheter for infusion of ade- protracted, terminal illness. Nor will less-injuredquate quantities of fluids and blood components is patients benefit if their access to hospital resourcesassumed. The use of central venous lines in pro- is limited because of the excessive allocation totected sites for long-term infusions is also dis- hopeless cases. On the other hand, the military or-cussed. ganization should attempt to assure that the psy-
The decision to apply any of these measures to chological support of casualties in the expectantthe combined-injury patient will be a difficult one, category are augmented as much as possible byand will have to be based on the availability of re- nonmedical personnel.sources and the projected number of casualties.The prognosis for combined injury is markedly Specific Treatment Concernsworse than for either traumatic or radiation injuryalone. Patients with moderate or severe conven- Surgery. Since exposure to doses of less than 5tional injuries who arrive at tertiary centers that are Gy is of no immediate threat to health, conven-capable of handling combined injuries will proba- tional injury that is surgically remediable deservesbly receive the maximum available care, unless priority treatment. Ideally, surgery should be initi-they have received obviously massive doses of ra- ated as soon as possible, or within 36 hours of ra-diation (over 8 or 9 Gy). It will be hard to justify diation exposure,3 and be completed before 48the decision to continue therapeutic interventions hours.17 Surgery after this time is contraindicatedin a trauma patient whose dose of radiation is even- for at least 6 weeks, or until there is evidence thattually determined to exceed 4 Gy. Continuing ad- immunocompetence has returned and that incised
47

Mtedical Coisteimcncts t Nuclear Vartare
tissue is able to revascularize. Clearly, the best can- nosocomial infectious agents in plumbing fixturesdidate for surgery is the patient who requires only and ice machines, and food must be free of gram-one procedure with no surgical revision. Patients negative bacteria (no raw fruit, vegetables, orwho have been exposed to more than 1.5 Gy, who salad). The best result that might be achieved byhave extensive injuries, and who need multiple these methods is a reduction in the appearance ofprocedures and reconstructive surgery are classi- new infections. Meanwhile, endogenous reinfec-fied as expectant. However, patients who have suf- tion would be little affected unless antibiotics tofered severe conventional injury, who have had eliminate opportunistic pathogens from the gut aresuccessful wound closure, and who then received effectively used. Although measures to control in-radiation may actually be more radioresistant and fection are prudent, their efficacy has not beenbetter able to survive.7̀ Decontamination of the ra- clearly shown. Life-threatening infections remain adiation casualty should include prompt surgical complication in the management of radiation casu-debridement, if needed, and washing of the surgi- alties.cal area with mild antiseptic soaps. The skin Maximum doses of two or three antibiotics ofshould be cleansed before surgery to adequately different classes should be infused empiricallyreduce any radioactivity in the area of the incision, when specific signs of bacterial infection occur.An important secondary concern is to cleanse crev- These signs include the appearance of a sudden fe-ice areas (nails, ears, and skinfolds) and orifices ver spike, usually in the presence of a depressed(particularly mouth and anogenital regions). To leukocyte count (that is, granulocytes fewer thanavoid abrading the skin, washing should be done 500/mm3 ). Prophylactic antibiotic treatment hasgently with mild soaps and hair should be clipper- given good results when used perioperatively incut instead of shaved. These procedures will elimi- patients who have penetrating abdominalnate at least 95ý.4 of a patient's surface contamina- wounds.' The use of poorly absorbed oral antibi-tion with isotopes. otics that selectively decontaminate the gut may be
Anesthesia and Pain Control. In controlled indicated as a preventive measure in patientstrials with animals, the induction and recovery known to have been exposed to moderate or highfrom anesthesia for irradiated subjects do not differ radiation doses. Even commonly used and widelyfrom those for nonirradiated subjects.'8 However, available antibiotics (penicillins, streptomycins, andanecdotal experience in humans has suggested that sulfas) may be useful with mass casualties, becausethe times of induction and recovery from anesthe- sensitive and otherwise-noninvasive organismssia may be prolonged." In irradiated animals and usually become prominent pathogens in immuno-humans, there is a clear resistance to the effects of suppressed radiation casualties."' Antifungal andanalgesics. However, care should be exercised to antiviral agents are indicated when specific signs ofavoid overtreatment with sedative narcotics and these infections occur.anesthetics. Antibiotics may rapidly become scarce in a
In a local high-dose radiation injury (over 40 Gy) mass-casualty radiation disaster and should be allo-to an extremity, prompt amputation gives the pa- cated to the victims most likely to survive. Such pa-tient the greatest pain relief and makes the most ef- tients include (a) those with minimal injuries andficient use of resources. The use of nonsteroidal evidence of localized infection, (b) those who re-anti-inflammatory drugs and thrombolytic agents, quire only one surgical procedure, and (c) thoseas well as topical corticosteroids, has been claimed with contaminated wounds who have receivedto delay the appearance of dermal necrosis and to lower doses of radiation.lessen the pain of local skin damage.2'" However, Antiemetics and Antidiarrheals. The phe-topical corticosteroids are contraindicated in ther- nothiazine class of antiemetics, when used in themal burn injuries, high doses needed to relieve a radiation victim's
Control of Infections. A variety of measures has nausea and vomiting, has an unacceptably high in-been advocated to reduce infections in the irradi- cidence of extrapyramidal neurological side effects.ated patient. These measures include meticulous Since the currently available antiemetic agents arehygiene of skin and orifices, aseptic skin punctures, of limited use, intense research efforts have beenreverse isolation, and prophylactic administration directed to finding new agents. Promising resultsof immunoglobulin G. Difficulties associated with have been obtained with the use of serotonin (5-the strict maintenance of reverse isolation proce- HT3) blocking agents. This class of drugs signifi-dures are obvious. Laminar airflow rooms are in cantly reduces radiation-induced emesis in the fer-limited supply, constant surveillance is required for ret, nonhuman primate, and human. However,
48

Triiige and Treatment of Radhition-Injured Mass Casualties
some of the drugs may result in nausea.22 Results tients who need them most. However, a long-termof clinical trials of these relatively nontoxic agents illness following serious radiation injury will dic-are pending, as is their approval as agents poten- tate that long-term venous access be maintained.tiallv useful in the field by NATO forces. The goal The probability of wound-healing disturbances andin the use of any effective antiemetic is threefold: the chronicity of phlebotoxic intravenous therapy(a) to enhance patient comfort without drug side involved in the care and treatment of any criticallyeffects, (b) to reduce the risk of aspiration pneumo- ill patient make central venous access preferable tonia, and (c) to conserve body fluid and electrolytes. peripheral intravenous access.It may be possible to prevent emesis by administer- Using peripheral lines in the radiation casualtying serotonin antagonists prophylactically or imme- has further disadvantages: (a) placement is difficultdiately after exposure. if hemostasis is compromised and local hemor-
Diarrhea from radiation damage to the gut may rhage develops, (b) placement is restricted to per-be controlled in part by a restricted-fiber diet and in cutaneous insertion after 36 hours, even if a venouspart by medication. Drugs such as diphenoxylate cutdown is otherwise desirable, (c) the lines are un-HCI, codeine, or atropine have been advocated. If suitable for infusion of hyperosmolar solutions, andthese are ineffective and the damage is localized to (d) the lines are at greater risk of becoming infectedthe large bowel, hydrocortisone enemas may help. at the catheter tip if used longer than 72 hours.The late complication of bowel stricture from local Long-term use of the percutaneous subclavian can-radiation damage is managed surgically.23 nula made of polyethylene or polyvinyl chloride is
Fluids and Electrolytes. While adequate sup- contraindicated because of the high rates of infec-plies of intravenous fluids are not likely to be avail- tion, vascular occlusion, and thrombogenicity asso-able in a situation involving mass radiation casual- ciated with these materials.ties, the survival of patients with milder cases of Blood Component Therapy. Impaired hemosta-fluid and electrolyte loss may be enhanced by re- sis after radiation injury is best related to the de-placement therapy. Careful measurement of the cline in platelet numbers that occurs several weeksvolume of losses will serve two purposes: (a) pa- after exposure. After protracted lower-dose irra-tients with severe degrees of fluid loss can be cate- diation, the decline in platelets may take more thangorized as expectant, and (b) the proper volume of 2 weeks. In the interim, autologous platelets can bereplacement can be given to patients who are ca- harvested, cryopreserved, and stored for later rein-pable of surviving. Measurement of the relative fusion. This procedure was used successfully to aidvolumes of vomitus and diarrhea will help guide the victims of the Chernobyl reactor accident. Ifthe fluid replacement. Those with more vomiting bleeding develops, patients with reduced numbersthan diarrhea will suffer the greater loss of chlo- of platelets secondary to marrow suppression bene-rides and may develop alkalosis, while those with fit from platelet transfusion even if the count issecretory, cholera-like diarrhea may develop hy- greater than 20,000/mm 3. However, prophylacticpokalemia and hyponatremia with total-body salt platelet transfusions are indicated on a regular ba-depletion. The collection and measurement of ex- sis if the count falls below 20,000/mm 3, even in thecretions, including urine, serve another purpose: absence of bleeding.with the proper collection of serial specimens and Platelets can be collected either by harvestingaccess to radioanalysis equipment, estimates of in- the platelet-enriched plasma obtained by centrifu-ternal radionuclide contamination can be made by gation of fresh units of whole blood, or by usingmeasuring the radioactivity of the samples. In the plateletpheresis. Although pheresis technology isevent of combined-burn injury involving more than complicated and expensive, each pheresis platelet10% of the body surface, crystalloid infusions are concentrate provides the equivalent of plateletsjust as satisfactory as colloid, but a higher volume from five to eight whole-blood donations. Thus, aof infusate may be necessary.2" single pheresis unit is the usual transfusion dose
Placement of central venous catheters made of and can be obtained in a single cost-effective proce-silicone elastomer (such as the Hickman or Broviac dure .2
type)2 ý should be considered a minor surgical pro- Anemia develops rapidly in the critically injuredcedure and be accomplished within the first 36 radiation casualty. Maintenance of perfusion pres-hours, if needed. Vascular obstructions and exotic sure and oxygen delivery to injured areas, betterinfections increasingly complicate the use of these wound healing, and an enhanced sense of well-lines in immunocompromised patients, 2b-2$ and so being will depend on preventing anemia throughthey should be limited to the critically injured pa- red-cell transfusions. As with patients suffering
49

Medical Consequenices of Nuclear Warfalre
thermal burns alone, patients with radiation skin Diethylenetriaminepentaacetic acid (DTPA) isburns and those with combined injuries require more effective than EDTA for the treatment ofmore red-cell transfusions."' A recall system is es- transuranic element contamination. This agent issential for the large number of healthy blood do- particularly useful for plutonium, curium, califor-nors needed to keep up with the demand for red nium, berkelium, and americium, which are corn-cells for mass casualties. monly involved in nuclear weapons accidents.
Erythrocytes may be stored for up to 10 years DTPA is administered intravenously or by externalusing modern cryopreservation techniques. Criti- lavage as a dilute solution of the calcium or zinc tri-cal government and military leaders should stock- sodium salt in physiological saline or glucose. Thepile autologous blood for use in case of wartime recommended intravenous dose is 1,000 mg/dayemergency. infused over 1 hour in 250 ml of solution for 4-5
In the fight against infections, fresh heterologous days. Used as a solution for the irrigation of radi-granulocyte infusions, bone-marrow transplants, onuclide-contaminated wounds, it will cause painand even the use of recombinant leukocyte stimula- unless a local anesthetic (such as 2% lidocaine) istory factors, such as granulocyte-macrophage col- added."ony-stimulating factor (GM-CSF), have been advo- Nutritional Support. In combined-injury pa-cated. Adequately controlled clinical investigations tients and in nonirradiated critically ill patients,are needed to demonstrate the effectiveness and heightened catabolic stress and impaired nutri-safety of these three therapies. Unfortunately, such tional status may play pivotal roles in morbiditya study was not performed during the clinical use and mortality. The incidence of wound infectionsof GM-CSF in the 1987 radiation disaster in Bra- and sepsis has been reduced by correcting the indi-zil.""' Further research is needed if the preserva- ces of malnutrition in postoperative patients."tion of granulocytes for autologous transfusion is to Malnutrition may also contribute to impairedbe made practical. A protocol has yet to be devel- wound healing, depressed immune response, pro-oped for the rational and balanced use of the many longed postoperative ileus, bowel atrophy, in-humoral hematopoietic stimulatory factors and the creased respiratory infections and insufficiency,timing of their administration. The disappointing impaired ventilatory responses to hypoxia and hy-results from attempts to use conventional bone- percarbia, delayed weaning time for patients onmarrow transplants in radiation victims have obvi- ventilators, and prolonged hospitalization. Sinceated the use of this procedure in the treatment of many of the above phenomena or characteristicsmass radiation casualties."' can be linked to radiation exposure alone, their ac-
Chelation Therapy. Chelator treatment of inter- centuation in the malnourished radiation victim isnal contamination is most effective when initiated highly probable.within the first 2 hours, before the radionuclide Simple and reliable methods of nutritional as-leaves the vascular space and enters the cell. Cur- sessment are not available, particularly in the irra-rently available chelating agents are not lipophilic diated patient, whose lymphocytes will be affectedand will not cross the cell membrane. Ethylenedi- independent of nutritional status. However, para-aminetetraacetic acid (EDTA) is widely available, meters that can be used to assess nutritional statusbut it is toxic regardless of the route of administra- in critically ill patients are serum albumin, transfer-tion. The calcium disodium salt of EDTA is used to rin, body weight, allergic skin reactions, thicknessavoid hypocalcemic tetany. To avoid nephrotoxic- of triceps skin fold, and direct assay or clinical evi-ity, the maximal total dose of intravenous EDTA dence of micronutrient deficiencies.should not exceed 550 mg/kg given as a dilute so- In selecting the route of administration of nutri-lution in divided doses over at least 4 days. Intra- ents in the radiation victim, the following consid-muscular EDTA (75 mg/kg three times daily) is erations are important. The oral route is the safest,very painful and should only be given with a local most economical, and most natural way to provideanesthetic. EDTA is contraindicated in renal and nutrients. However, some patients will be unablehepatic disease. EDTA is used to chelate lead, zinc, to consume sufficient quantities of nutrients be-copper, cadmium, chromium, manganese, and cause anorexia occurs over a wide range of radia-nickel; none of these metals is related to nuclear tion doses. If the alimentary tract has not been in-weapons or reactor accidents. Its use in radiation jured by radiation, and if inanition supervenes andaccidents is largely confined to the treatment of persists, then nutrients can be infused by nasogas-contamination with the transuranic elements, plu- tric, gastric, or intestinal feeding tubes. Fluid losstonium and americium. associated with the cholera-like diarrhea of the gas-
50

Triae and Treatment t t Raidiatton-hi nred Mass Cas,ýa!t:cs
trointestinal subsvndrome may require that nutri- usual daily replacement dosages of essential water-ents and fluids be administered by both the enteral and fat-soluble vitamins, with the exception of vita-and parenteral routes. With appropriate placement min K, are commercially supplied in a single vial. Inof an enteral feeding tube, the use of intravenous thermal-burn-injury patients, the requirements for B-fluids can be reduced, and transition to enteral complex vitamins and vitamin Care increased. Vita-therapy alone will be facilitated. min K is given as a 10-mg intramuscular injection
The catabolic critically ill radiation casualty will once a week. If renal impairment supervenes, therequire no less than 2,500-2,800 kcal/dav. This re- normal requirement for potassium (60-100 meq/quirement can be met by the infusion of a balanced day), magnesium (8-12 meq/day), and phosphorusmixtureof glucose, aminoacidsorprotein,and lipids. (30-60 meq/day) may need to be reduced. SinceBased on ideal body weight, total protein or amino sodium depletion may occurvwith diarrhea in the gas-acid infusion should approach (but not exceed) 2 g/ trointestinal subsyndrome, sodium infusion of overkg/day. Simple carbohydrates (3.5-6.0 g/kg/day) 150 meq/day may be needed. If chelation therapyadequately supply most of the 30-40 kcal/kg of non- with EDTA is undertaken, supplements of zinc (> 4protein nutrients needed. Usually, a maximum of mg/day), copper (> 1.5 mg/day), chromium (> 15301-, of the total caloric requirement can be supplied jig/day), manganese (> 0.8 mg/day), and iron (> 2as lipids. However, short-term peripheral infusion of mg/day) may be needed. The patient who receivesup to 80%- of total calories as lipids is acceptable if multiple blood transfusions will not need iron sup-central venous access is unavailable. plements until after the blood count has stabilized.
The infusion of micronutrients, including vita- Trace element supplements, including iodine and se-mins, minerals, and trace elements, may need to be lenium, should be considered if prolonged parenteraladjusted with long-term parenteral therapy. The feeding becomes necessary.
SUMMARY
Triage to within 36 hours and whose condition does not callfor multiple procedures should go to surgery.
The degree of injury of a radiation casualty can be Decontamination of surface radionuclides is nearlycategorized by the symptoms of exposure. Casualties always a second priority after the initial resuscitativecan be rapidly sorted on the basis of unlikely, prob- support, and can be effectively done with lavageable, or severe radiation symptoms. This rapid sort- before surgery. Chelation therapy for internal radi-ing of victims allows the conventional traumatic inju- onuclide contamination can be safely accomplishedries to receive appropriate attention. with the experimental agent DTPA, but the effective-
Lymphocyte counts are the most necessary labora- ness of this therapy with mass casualties remainstory procedure in the first hours and days after expo- uncertain.sure. Information from currently available physical The use of antiemetics and antidiarrheals maydosimeters is of limited value and cannot be relied on contribute significantly to patient comfort. Unfortu-entirely in making triage decisions. nately, in effective doses, the currently available agents
Triage is greatly complicated if the patient has have major side effects that impair the patient's per-suffered combined injuries. A shift in priority to the formance.expectant category is likely for a radiation casualty The prevention of infection and the appropriatewho requires more than one surgical procedure or use of antibiotics are important in the first few weekswho has received a surface burn of more than 1017(. after exposure. Within the first 7-10 days, selective
gut decontamination should be used before leuko-penia and sepsis occur. Two to 3 weeks later, if
Medical Management infection is indicated by fever and leukopenia, par-enteral antibiotics should be initiated. To help pre-
In the first hours after radiation injury, the priority vent infection with new organisms, environmentalwill be to treat the injuries that require immediate control measures should be instituted as soon asattention. Candidates for surgery must be carefully possible.chosen. Only radiation victims who can be attended Supportive therapy with blood components has
51

Medical Conus,',IIuces .t Nuclear Warfare
been shown to be extremely effective in combating Effective triage will permit the use of limited re-hemorrhage and anemia following combined injury, sources to improve the greatest number of radiationHowever, granulocyte transfusions and bone-mar- casualties. Survival after either radiation injury alonerow transplants as currently used appear to beof little or combined injury can be greatly enhanced by thehelp. A combination of simple supportive measures, application of currently available treatments. Re-including fluids, electrolytes, antibiotics, adequate search into new and experimental therapeutic agentsnutrition, and platelet transfusions, can significantly for the treatment of radiation injury may be expectedreduce mortality, as shown by studies of animal re- not only to benefit the civilian population, but also tosearch models. enhance the survival of the fighting force.
REFERENCES
1. Walker, R. I., and Conklin, J. J. 1987. Military radiobiology: A perspective. In Military Radiobiology, edited by J. J.Conklin and R. I. Walker, 1-8. Orlando, FL: Academic Press.
2. Leaning, J. 1986. Burn and blast casualties: Triage in nuclear war. In The Medical Implications of Nuclear War, editedbv F. Solomon and R. Q. Marston, 251-281. Washington, DC: National Academy Press.
3. Wiener, S. L., and Barret, J. 1986. Thermonuclear weapons. In Trauma Management for Civilian and Military Physicians,497-506. Philadelphia: W. B. Saunders.
4. American College of Surgeons Committee on Trauma (D. D. Trunkey, chairperson). 1984. AdZanced trauma lift' supportcourse for physicians. Chicago: American College of Surgeons.
5. Champion, H. R., and Sacco, W. J. 1986. Triage of trauma victims. In vol. 2, Current Therapy of Trauma, edited by D. D.Trunkey, 5-12. Toronto: B. C. Decker.
6. Conklin, J. J., and Walker, R. 1. 1986. Diagnosis, triage, and treatment of casualties. Medical Bulletin of the U.S. Army,Europe 43(7): 11-15.
7. Dutreix, J. 1986. Human skin: Early and late reactions in relation to dose and its time distribution. Br. 1. Radiol.(Suppl.) 19: 22-28.
8. Lushbaugh, C. C.; Fry, S. A.; Ricks, R. C.; Hubner, K. F.; and Burr, W. W. 1986. Historical update of past and recentskin damage radiation accidents. Br. ]. Radiol. (Suppl.) 19:12-17.
9. Milroy, W. C. 1984. Management of irradiated and contaminated casualty victims. Emerg. Med. Clin. North Am. 2:667-686.
10. Gus'kovava, A. K., ed. 1987. Early acute effects among the victims of the accident at the Chernobyl Nuclear Power Plant[USSR Ministry of Health Order No. 4851]. Translated by U.S. Defense Intelligence Agency ILN 818-871.Moscow: USSR Ministry of Health.
11. Murano, G.; MacVittie, T. J.; Conklin, J. J.; Casey L. C.; and Walker, R. 1. 1985. Hemostatic changes in a canine modelof combined injury. In Tht, Pathophysiology of Combined Injury and Trawna, edited by R. 1. Walker, D. F. Gruber,T. J. MacVittie, and J. J. Conklin, 105-110. Baltimore: University Park Press.
12. Cockerham, L. G.; Simpson, S. A.; Doyle, T. F.; and Gossett-Hagerman, C. J. 1984. Canine post-irradiation plasmaglucose variations. Life Sci. 34: 2641-2646.
13. Landauer, M. R.; Ledney, G. D.; and Davis, H. D. 1987. Locomotor behavior in mice following exposure to fission-neutron irradiation and trauma. Aviat. Space Environ. Med. 58: 1205-1210.
14. Wardlaw, S. C., and Levine, R. A. 1983. Buffvcoat analysis. JAMA 249: 617-620.
52

1"rials' and Try'rmutrnet of Rldiation-lniijrd M~ass C2alsualta's
15. North Atlantic Treaty Organization. 1978. NATO. hitill'k on the con'cept of medical siipjort in NBC et'wiiropipieints
lAMed P-7 (A)!. Brussels: North Atlantic Treaty Organization.
It. Giambarresi, L. 198t. Nuclear weapons: Medical eftects and operational considerations. Medical Biulletin of the U.S.Armi., I-ntropte 43(7): 7-10.
17. Streffer. C., and Messerschmidt, 0. 19(76. Untersuchungen uber Kombinationsschaden. Die Ausscheidung vonTaurin und I larnstoff im Ur in wei er Mau,,e bei einer Kombination von Strahtenbelastung und Hautwunde.Strahleth"'rirpie t 130:285.
18. I-Hunt, W. Personal communication.
14. Conklin, J. J.; Walker, R. I.; and I lirsch, E. F. 1483. Current concepts in the management of radiation injuries andassociated trauma. Strg. Gitwcol. t)b-stct. 156: 804-829.
20. Messerschmidt, 0. 1986. Treatment of subcutaneous radiation lesions. Br. I. Radio/. (Suppl.) 19: 122-137.
21. Fabian, T. C.; Hoefling, S. J.; and Strom, P. R. 1482. Use of antibiotic prophylaxis in penetrating abdominal trauma.Clin. Th•er. 5: 38-47.
22. King, G. Personal communication.
23. Spiro, H. M. 1970. Inflammatory disorders other than ulcerative colitis. In Clinical Gastroenterolosy, 570-574. Toronto:Macmillan Co.
24. Kaplan, J. Z. Care of thermally injured victims of a thermonuclear explosion. In reference 11, 41-45.
25. Cormed, Inc. is located in Medina, NY.
26. Venezio, F. R., and O'Keefe, P. 1986. Infections of intravascular devices. J. Nosocotn. lntect. 4:10-26.
27. Kaufman, .. L. 1987. Venous catheter-related thrombosis and infection. JAMA 257: 2594.
28. Allo, M. D.; Miller, J.; Townsend, T.; and Tan, C. 1987. Primary cutaneous aspergillosis associated with Hickmanintravenous catheters. N. Engl. 1. Med. 317: 1105-1108.
29. Warkentin, P. 1. 1987. Plateletapheresis: An invaluable blood resource. Cleve. Clin. 1. Med. 54: 381-383.
30. Roberts, L. 1987. Radiation accident grips Goilnia. Science 238: 1028-1031.
31. Butturini, A.; Gale, R. P.; Lopes, D. M.; Cunha, C. B.; Ho, W. G.; Sanpai, J. M.; De Souza, P. C.; Cordiero, J. M.; Neto,C.: De Souza, C. E.; Tabek, D. G.; Burla, A.; and the Navy Hospital Radiation Team. 1988. Use of recombinantgranulocyte-macrophage colony-stimulating-factor in the Brazil radiation accident. Laoicet 2 (August 271: 471-475.
32. Durakovic, A. Internal contamination with medically significant radionuclides. In reference 1,241-264.
33. Schmitz, J.-E.; Ahnefeld, F. W.; and Burri, C. 1983. Nutritional support of the multiple trauma patient. World I. SXrg.7: 132-142.
53

Medical ConseqluenIces of Nuclear Warfare
54

Chapter 4
TREATMENT OF INTERNALRADIONUCLIDE CONTAMINATION
T. JAN CERVENY, Ph.D.*
INTRODUCTION
INITIAL MANAGEMENT
Uptake and ClearanceSampling of RadioactivityOn-Site ManagementHospital Management
MEASUREMENT OF RADIOACTIVE CONTAMINATION
TREATMENT DECISIONS
THERAPEUTIC MANAGEMENT
TREATMENT OF INTERNAL CONTAMINATION
Clearance of the Gastrointestinal TractPrevention or Reversal of Radionuclide Interaction with Tissues
Blocking and Diluting AgentsMobilizing AgentsChelating AgentsLung Lavage
SUMMARY
*Major, United States Air Force; Pro'gram Manlager, Bioenvirononental Hazards, Air Force Office of Scientific Research,Boiling Air Force Ra~e, Washington, D.C. 2'332-6448
55

Medical Consequences of Niiclehar Warfare
INTRODUCTION
Military and civilian providers of medical care Many aspects of medical management are basedmust be prepared to deal with the medical after- on judgments and evaluations that are difficult tomath of a nuclear detonation or accident. With the instruct. Treatment information is sparse and oftenearth's increasing nuclear arsenal and the growing subjective. This chapter discusses difficult treat-use of nuclear energy systems, our biosphere is ment decisions, with the understanding that con-threatened by the production and release of large siderable latitude exists in medical evaluation.quantities of radioisotopes. The accidents at Cher- In a nuclear explosion, over 400 radioactive iso-nobyl, USSR, in 1986 and at GoiAnia, Brazil, in 1987 topes are released into the biosphere.) About fortyhave stressed the importance of knowing how to are considered to be potentially hazardous to hu-manage the radioactive contamination of persons in mans because of either their organospecificity ormilitary and civilian settings. Such management their long half-life. Both early and delayed radioac-requires knowledge of the metabolism of various tive fallout will be deposited in our external envi-radionuclides in humans and methods to increase ronment, which could result in internal contamina-their elimination from the body. tion with radionuclides.
INITIAL MANAGEMENT
The medical staff providing the initial manage- tal of entry, chemistry, solubility, metabolism, andment of radionuclide-contaminated patients will particle size.14 Of the three main routes, inhalationhave varying responsibilities, depending on the iso- poses the biggest threat, especially in a fallout envi-topes involved, radiation-monitoring capabilities, ronment), 3 ," The size of the radioactive particlelocation, and available facilities. Thorough evalu- determines if it will be deposited in the lungs, be-ation and estimates of internal contamination may cause particles greater than 10 microns in diametertake days or weeks, however, so these decisions cannot pass by the nasal hairs. Clearance tine (timemay have to be based only on historical informa- required for particles to be removed from thetion and superficial measurements. Medical per- lungs) depends on which respiratory compartmentsonnel must proceed quickly to obtain information receives the deposit,1 -3 and time will be an impor-and make treatment decisions based on available tant factor in treatment decisions. Times for respi-early estimates of possible exposure. Treatment ratory clearance into the next higher compartmentrisks must be weighed against the presumed risks are as follows: trachea, 0.1 hour; bronchi, 1 hour;of untreated exposure. Damage from the latter bronchioles, 4 hours; and alveoli, 100-1,500 or moremay not be manifested until 20-30 years after inter- days." Soluble particles that are deposited into thenalization. alveoli may be systemically absorbed at the alveo-
Initial management may be divided into four lar-blood interface, and may thereby become incor-applications: (a) uptake and clearance, (b) sampling porated into target organs. Insoluble particles alsoof radioactivity, (c) on-site management, and (d) pose a threat, especially if plutonium from unspenthospital management."- fuel or industrial accidents is present. Prolonged
exposure of the alveolar epithelium to high-LET al-Uptake and Clearance pha emitters, like plutonium, has been related to
increased incidence of malignancy.3"Internal contamination occurs by three main In 1955, the International Commission on Radio-
routes (listed in order of importance): inhalation, in- logical Protection adopted a model for evaluatingg•stion, and wound contamination. A fourth and in- the hazards of inhaled radioactive particles.' Ac-frequent route is percutaneous absorption, which ap- cording to this model, 25% of inhaled radioactiveplies almost exclusively to the radioisotope tritium particles are immediately exhaled, and the remain-and its association with water. The uptake and re- ing 757 are deposited along the respiratory tree.tention of a radionuclide are influenced by its por- About half of the particles are deposited in the up-
56

Treatmtent (q Initernal Radioi iiilide Contlliimaltiol
per bronchial tree, where they are moved by the washing. The nasal swab should be taken at theciliary epithelium to the nasopharynx. In the naso- site and sent in a sealed, clean container to higher-pharynx, they are propelled by the mucociliary care facilities along with the patient. Although skinswallowing reflex into the digestive tract, where decontamination should be done as quickly as pos-they enter the gastrointestinal path.' sible, the stability of an injured patient is vital, and
Ingestion is usually secondary to inhalation and first aid must be the primary concern.the mucociliary swallowing response. However, ina fallout environment, direct ingestion from con- On-Site Managementtaminated foodstuffs is also probable. The degreeof intraluminal gastrointestinal exposure depends Contamination of the skin with radionuclides ison transit time through the gut, which will vary usually not immediately life threatening to eitherwidely from person to person.'I The mean clear- the patient or medical personnel, unless the con-ance times of the human digestive tract are stom- tamination is from a gamma emitter and the doseach, 1 hour; small intestine, 4 hours; upper large in- rate is several Gys per hour. Partial or completetestine, 13-20 hours; and lower large intestine, 24 emergency decontamination should be done at thehours, resulting in a total mean emptying time of 42 site before a patient is transported to a higher-carehour,. The much slower rate of movement in the facility. Discarding contaminated clothing will re-large intestine places its luminal lining at higher move up to 85% of external contaminants; follow-risk for damage from nonabsorbable radionuclides. ing this with showering or washing will removeGastrointestinal transit time may be shortened by more than 95% of surface contamination.'.3-7' Ause of emetic and/or purgative agents. combined nuclear-chemical war may present many
Some relatively soluble radionuclides may not problems for decontamination procedures. A lightbe absorbed due to acidic or caustic properties that wash-down and vacuuming or brushing of protec-fix them to tissue proteins.1.2.7,8 Systemic absorption tive clothing may be all that can be done.through the intestine varies widely, depending onthe radioisotope and its chemical form. Clear dif- Hospital Managementferences exist between radioiodine, which is rap-idly and completely absorbed, and plutonium, Hospital emergency plans should provide forwhich is almost nonabsorbed (0.003%). Further- the proper management of incoming contaminatedmore, nonabsorbable alpha emitters apparently do casualties. The National Council on Radiation Pro-not cause gastrointestinal injury, even in large tection and Measurements provides a universalamounts. Nevertheless, the gastrointestinal tract is outline guide that can be adapted for most facili-the critical target organ for the many insoluble radi- ties.' A designated decontamination area should beonuclides that travel its length almost unabsorbed. prepared, and traffic in this area should be one-way
Wounds contaminated by fallout and shrapnel to prevent contaminating "clean" areas of the facil-may provide continuous irradiation of surrounding ity. Ideal decontamination facilities should havetissues and increase the likelihood of systemic in- equipment to wash ambulatory and injured pa-corporation.'.." This hazard remains until the tients, shielding to use with high-level beta-gammacontaminant is removed by cleansing, surgical de- contamination, and a floor plan that minimizesbridement, or radionuclide decay. The last process cross-contamination of clean areas. 1-3 Medical per-may take a few days or millions of years, depend- sonnel should be rotated through the decontamina-ing on the contaminant. tion area to ensure that their radiation exposure is
kept to a minimum. Clothing and other contami-Sampling of Radioactivity nated materials should be discarded at a contained
location away from the health-care facility. AtSince the identification of radionuclide contami- many hospitals, the morgue or autopsy room is an
nants is important for treatment, it may be neces- excellent decontamination area. It has containedsary to know whether beta-gamma or alpha emit- liquid systems, a table easily adapted to wash aters are present. Health-physics personnel should contaminated patient, and often a heavily linedbe able to provide this information even with lim- area that can be used to store contaminated materi-ited radiation-detecting equipment. Separate als. Other possibilities include physiotherapy areasswabs of the nares should be taken to determine and cast rooms. Table 4-1 lists the supplies that areradioactivity and possible inhalation contamination recommended for a decontamination room.'before decontaminating the skin by showering or The initial evaluation of a patient should include
57
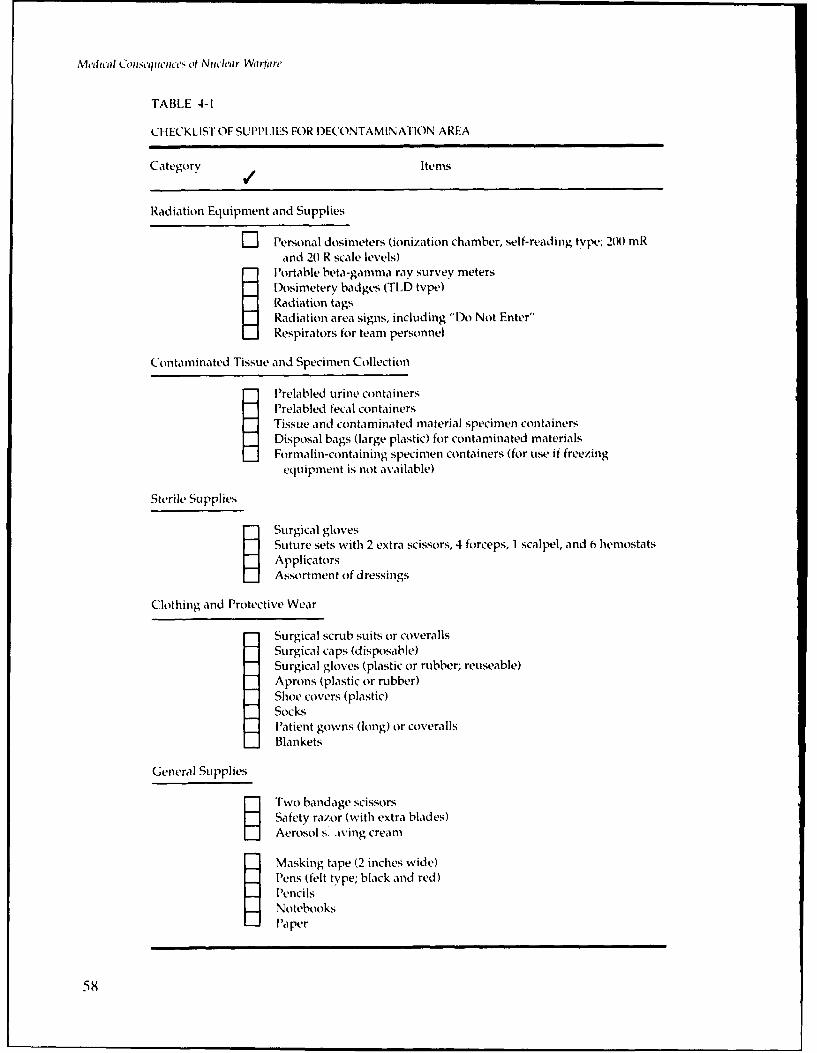
Metdod CoINsq',hC,'s Otf N iwh'ar Warfar'
TABLE 4-1
CHECKLIST OF SUPPLIES FOR DECONTAMINATION AREA
Category / Items
Radiation Equipment and Supplies
Z Personal dosimeters (ionization chamber, self-reading type; 200 mRand 20 R scale levels)
Portable beta-gamma ray survey metersDosirnetery badges (TLD type)Radiation tagsRadiation area signs, including "Do Not Enter"Respirators for team personnel
Contaminated Tissue and Specimen Collection
SPrelabled urine containersPrelabled fecal containers
Tissue and contaminated material specimen containersDisposal bags (large plastic) for contaminated materialsFormalin-containing specimen containers (for use if freezing
equipment is not available)
Sterile Supplies
SSurgical glovesSuture sets with 2 extra scissors, 4 forceps, 1 scalpel, and 6 hemostatsApplicatorsAssortment of dressings
Clothing and Protective Wear
Surgical scrub suits or coverallsSurgical caps (disposable)Surgical gloves (plastic or rubber; reuseable)Aprons (plastic or rubber)Shoe covers (plastic)SocksPatient gowns (long) or coverallsBlankets
General Supplies
STwo bandage scissors
Safety razor (with extra blades)Aerosol s. aving cream
- Masking tape (2 inches wide)Pens (felt type; black and red)PencilsNotebooks-Paper
58

Treatmient of Internal Radionuclhhd Contamination,
a complete history of the contamination incident, a internalization of radionuclides. The internaliza-physical examination to uncover conventional inju- tion may be from fallout; handling a damaged, un-ries (but which usually provides no evidence of ra- detonated nuclear weapon; accidental ingestion ofdionuclide contamination), and laboratory tests, in- (or external contamination by) a specific radioactivecluding a complete blood count with platelets and a substance; or radionuclide-contaminated wounds.routine urinalysis. The incident history should pro- The patient should then be placed into the emer-vide some background for predicting possible gency-plan triage system and treated accordingly.
MEASUREMENT OF RADIOACTIVE CONTAMINATION
Generally, health physicists at large medical fa- hazards. Instruments for measuring either type ofcilities will be responsible for radiation monitoring, radiation are similar, but the Geiger-Mueller (GM)However, all medical personnel should be aware of counter is the most common detection device. Un-the various monitoring techniques in order to un- fortunately, high radiation levels can saturate GMderstand their reliability, limitations, and sources of counters and give false or even zero readings. Ioni-possible error. The determination of surface con- zation chambers can measure higher dose rates.tamination will require monitoring for alpha and Both are sensitive to extremes of heat and humid-beta-gamma emissions, ity, and both may fail in a corrosive chemical envi-
Alpha particles have limited penetration, and a ronment. Shielding the probe of the detection de-patient will be protected by an intact epidermis. vice will provide a relatively pure reading of theAlpha contamination does not become hazardous gamma component, and the difference between theunless it is internalized through inhalation, inges- shielded and unshielded readings provides the betation, or wounds.I"-" Alpha particles are the most (and often soft gamma) component.difficult radiocontaminant to detect, and negative All medical personnel need to be alert to pos-monitoring results are not always reliable. Due to sible mixed external-internal contamination. A pa-the high absorption of alpha particles even in air, it tient may have inhaled contaminated steam or dustis important to keep the radiation monitor close to during the cleanup of an accident, as happened inthe measured surface. Direct contact readings are ;he 1986 nuclear reactor accident at Chernobyl- 2̀ 'preferred. Proportional counters are the most com- If the internalized materials are beta- or gamma-mon device for detecting alpha radiation in the emitting substances, they may provide radiationlaboratory, and they are capable of discriminating readings on the monitoring devices used for exter-between alpha and beta-gamma emitters. How- nal decontamination. Of course, internalized alphaever, the counters are not yet available for military particles will not register on monitoring devices,field use. Scintillation counters are currently used but their presence may be suggested by the inci-for determining radioactivity contamination while dent history or by the detection of external alphain the field, but they are less sensitive than propor- particles.tional counters. Surface monitoring with swipes If patients are few and there is a need to knowmay also be used to test for transferable alpha ma- (or closely estimate) the total internal radiationterial. Textured paper (such as filter paper) is dose, all body effluents must be collected for an ex-wiped across the test surface and then measured in tended time. Careful measurements of all excreteda laboratory scintillation counter. Results may radiation will provide data for calculating a closeidentify contamination with transferable alpha estimate of the total internal body burden.' De-(plutonium) or weak beta (tritium) radiation. The pending on the radioisotope involved and its phys-nose swipe is also used for alpha emitters. A cotton icochemical characteristics, the collections mayswab or narrow strip of filter paper moistened with have to be made for months.distilled water is gently wiped around the naris Many pitfalls exist in the interpretation of excre-opening (one per naris). After the swab or paper is tion data analyses. Variations in excretion ratesdry, the radioactivity is determined, from person to person will interfere, and the time
Beta and gamma radiations are often emitted si- of exposure, possible interim therapy with chela-multaneously by decaying radioisotopes. These tors, and data on the excretion of inhaled contami-types of radiation present internal and external nants may complicate the estimate.
59

Medical Consequences of Nluclear Warfare
A nuclear detonation or accident may result in to gamma, X, and neutron radiations include do-alpha, beta, gamma-ray, X-ray, and neutron emis- simeters, film badges, and thermoluminescent de-sions. Devices that are available to detect exposure tectors.
TREATMENT DECISIONS
Early information on the history of the expo- contaminant may determine its distribution withinsure incident may identify the major isotopes in- the body, or even its accessibility into the body. Asvolved and provide some dosimetry information, no material is completely insoluble, some small frac-Patients will likely present with no clinical symp- tion may rapidly become internalized from the lungtoms other than possible conventional trauma. or through a wound. In contrast, normally solubleTherefore, critical decisions on the initial treatment materials may be present in an insoluble form, ormay have to be based on knowledge of human may be made insoluble under systemic physiologi-physiology, the pharmacology of agents to be cal conditions. Therefore, treatment begun as earlyused, the metabolism of the radioisotopes, and the as possible after exposure will significantly increasehistorical information. Treatments for internal the probability of successful internal decontamina-contamination should begin within hours of expo- tion.135.:,7,10
sure.1 --:.4 Emergency planning will pay off by re- Medical personnel should be aware of the pos-ducing the time for dosimetric evaluations and sible presence of mixed-fission products (MFP), whichwill result in more informed initial decisions. Af- are groups of radionuclides likely to be found to-ter the initial treatment, there will generally be gether after nuclear reactor or detonation incidents.time to assess the situation as data from monitor- The appropriate treatment regimen is based on theing become available. Later, dose estimates will time of exposure after the nuclear event. Some MFPdetermine if further treatment and evaluation are groups are plutonium with associated americium,needed, or if the treatment involves risks, curium, and neptunium, and uranium with tho-
Usually no immediately life-threatening hazard rium, radium, and their decay products. Treatmentis associated with radiation contamination, espe- is determined by the particular radioisotopes.cially after the removal of clothing and washing. In a complete nuclear detonation, over 400 radio-The probability that a patient will incur radiation- nuclides are released. However, only about forty ofinduced health problems is low, and any incidence these are potentially hazardous to humans. 3 Themay be decades in the future. Risky decontamina- most significant radioisotopes from unspent nucleartion procedures (such as lung lavage or surgery) fuel are tritium, plutonium, and uranium. Of par-that could lead to internalization should be care- ticular interest are the radioisotopes whose organo-fully evaluated, and a decision may require assis- specificity and long half-lives may result in irrevers-tance by expert consultation."'3 ible damage or induction of malignant alterations.
Physicochemical properties of radiocontami- Radioisotopes of immediate medical significance arenants play a significant role in determining treat- listed in Table 4-2, with descriptions of properties,ment. The solubility of the material containing the target organs, and treatment.
THERAPEUTIC MANAGEMENT
Skin decontamination has two goals: (a) to re- The physician needs to understand the basic physi-move radiocontaminants and thereby reduce the cal and physiological principles involved. The con-total dose, and (b) to prevent possible internaliza- taminant's half-life, energy level, and dose rate musttion. If done appropriately, skin decontamination be weighed against continued and harsher decon-will also contribute to a more accurate determina- tamination procedures, which may abrade the intacttion of the internal contamination. If the radioac- skin or decrease the distance to the important der-tive contaminant is resistant to an initial washing mis basal layer. Because the skin regenerates everywith soap or detergent and water, further decon- 10-14 days, contamination would eventually betamination should be super.vised by a physician. shed naturally. Signs of excessive decontamination
60

Tr,,atnent of Internal Radioni4clide Contamination
TABLE 4-2
SIGNIFICANT RADIONUCLIDE INFORMATION
Radionuclide Radiation Critical Body Contamination TreatmentType Site Mode * Agent
trAmericium (X, y Bone I/W DTPA
Californium y, cX, n Bone I/W DTPA
Cerium •, y GI, lung I/GI DTPA
Cesium [, y Total body I/S/GI Prussian blue £
Curium a, y, n Bone I/GI DTPA
Iodine P, Y Thyroid I/Gl/S KI (sat.)
Plutonium c, y Bone I/W DTPA
Polonium (X Lung I Dimercaprolt
Strontium y Bone I/Gl AIPO4
Tritium Total body I/S/GI Forced H 2 0 §
Uranium Y, f, Y Bone I/S/W NaHCO 3
I: contamination by inhalation
GI: contamination by gastrointestinal absorptionS: contamination by skin absorptionW: contamination by wound absorption
•* The antacid aluminum phosphate in gel form used as a gastrointestinal adsorbentfor radiostrontium
• Sodium bicarbonate to maintain alkalinity of urine used in conjunction with diuretics
tiDiethylenetriaminepentaacetic acid used as a tissue chelation agent forming stable complexeswhich may be excreted by the kidney (approved by the FDA as an investigational new drug)
A mercury poisoning chelation agent (very toxic)
An agent blocking radioiodine absorption in tissues resulting in dilution of the
Simple forced intake of water, resulting in isotope dilution
£A dye used as an ion exchanger (not yet approved by the FDA)
61

M/edical C l lseiplc'•e•sc Nuclear Wartart'
efforts will be more evident 24 hours later, and two than conventional injuries require. This debride-or three less intensive decontamination efforts are ment involves a certain risk of translocation or ab-less traumatic to the skin than one major effort. If sorption (especially when working with possiblenecessary, further cleansing may include mild abra- alpha emitters, like americium or plutonium);sives, chelating agents, and bleach. Chemical tech- therefore, the chelating agent DTPA should beniques are rarely needed. given systemically and the wound should be irri-
After first aid to control hemorrhage and shock, gated with DTPA before debridement.the next steps are to determine if wounds are con- If limb wounds have high concentrations oftaminated and then to locate any other contamina- beta-gamma contaminants, medical personnel musttion.'• " Alpha emitters and possibly weak beta limit their exposure by frequently rotating shifts oremitters are difficult to locate around wounds. A by working with shields. Amputation of the limbsimple film of irrigation fluid, blood, or tissue fluid may have to be considered if (a) the wound iscan entirely mask this contamination, which then highly contaminated and decontamination at-may internalize via the circulatory or lymph sys- tempts cannot be made or are not successful, (b) thetems. Once the surface contaminant is located, irri- contamination is so intense that extensive radia-gation should be sufficient to remove it, although tion-induced necrosis is likely, or (c) the injury is sosome wounds may need debridement that is deeper severe that functional recovery is unlikely.
TREATMENT OF INTERNAL CONTAMINATION
The goals of internal decontamination are to re- selection of purgatives or laxatives should be basedduce absorption and to enhance elimination and on their speed of action (slowly acting drugs, likeexcretion. Treatment is most effective if it is started bulk-forming and wetting agents, are not appropri-as soon as possible after exposure. ate). These agents are contraindicated if the patient
has abdominal pain of unknown origin, or if sur-Clearance of the Gastrointestinal Tract is a possibility.
-ussian blue, an ion exchanger, was used toGastric absorption can be reduced by stomach . victims in the 1987 cesium-137 contamination
lavage, emetics, purgatives and laxatives, ion ex- incident in Goianial" and has been well tolerated inchangers, and aluminum antacids. Other less effec- humans (1 g given orally with water three timestive treatments are alginates, barium sulfate, and per day).1 2 It may be continued for 3 weeks orphytates, which currently are not recommended for longer, as indicated. However, Prussian blue is notinternal decontamination of radionuclides. approved by the Food and Drug Administration
Stomach lavage is useful only if the ingested (FDA), and emergency approval for an investiga-dose is known to be large, and if the intake is recent tional drug would have to be obtained. Ion-ex-and still in the stomach. Lavaged material must be change resins, like sodium polystyrene sulfonatemonitored for radioactivity and the patient must be (for adults, 15 g, 4 level teaspoons of resin suspen-kept in a head-low position to prevent aspiration. sion), have an assumed but untested usefulness for
The most common emetic agents are apomor- inhibiting the uptake of radionuclides in the gut.phine (5-10 mg, subcutaneous) and ipecac (1-2 g in Aluminum antacids are an effective treatmentcapsule or 15 ml in syrup), which should be given for reducing the uptake of radioactive strontium. Aconcomitantly with 200-300 ml of water. Caution dose of 100 ml of aluminum phosphate gel, givenshould be used not to induce emesis in an uncon- immediately after exposure, decreases the absorp-scious patient. tion of radioactive strontium in the gut by about
Laxatives or purgatives (such as castor oil) will 85'%. Aluminum hydroxide, given in a single dosestimulate intestinal motility, and saline cathartics of 60-100 ml, reduces uptake by about 5017. Bothwill increase water movement into the intestine and forms are nontoxic. This is the treatment of choiceinduce removal of contents within 3-6 hours. The for contamination with radiostrontium.1.2
62

Treatinent of Internal Radiotn iclide Contamination
within 48 hours. It is doubtful that DTPA will bePrevention or Reversal of Radionuclide available in combat.Interaction with Tissues DTPA is administered as an intravenous solu-
tion of 1 g dissolved in 250 ml of saline or 5% glu-Blocking and Diluting Agents. Blocking and di- cose, infused over 1 hour per day for up to 5
luting agents decrease the likelihood of absorption days."" As an irrigation solution, I g CaDTPA andby decreasing the availability of the radionuclide. 10 ml of 2% lidocaine are dissolved in 100 ml nor-A blocking agent, such as potassium iodide (300 mal saline for plutonium and americium contami-mg/day for 7-14 days) for radioiodine, blocks the nation.' If the contaminants have an atomic num-uptake of a radioisotope by significantly increasing ber greater than uranium's 92, the treatment isthe availability of the stable isotope. Diluting simple: DTPA is used for all contaminants exceptagents simply dilute the radioisotope, which statis- uranium. The use of DTPA is contraindicated fortically decreases the opportunity for absorption. treatment of uranium contamination because of theWater is a diluting agent in the treatment of tritium added risk of renal damage."' Uranium contamina-contamination. For maximum efficacy, the stable tion has been treated with oral sodium bicarbonate,isotopes that are used as the blocking or diluting regulated to maintain an alkaline urine pH, and ac-agents must be as rapidly absorbed or metabolized companied by diuretics.'as the radioisotopes are. Other chelating agents are dimercaprol, penicil-
Mobilizing Agents. Mobilizing agents are com- lamine, and deferoxamine (DFOA). Dimercaprol ispounds that enhance and increase the natural turn- a highly toxic chelator that has been effective inover processes and thereby induce the release of treating mercury poisoning. Penicillamine andradioisotopes from tissues. They are most effective CaEDTA are significantly less toxic and more effec-when given immediately, but they may retain some tive for mercury poisoning. (Radiomercury, how-effectiveness for up to 2 weeks after exposure. In- ever, is not a likely hazard of nuclear detonation.)cluded in this group are antithyroid drugs, ammo- Penicillamine is an amino acid derived from peni-nium chloride, diuretics, expectorants and inha- cillin, but it has no antibacterial properties. It haslants, parathyroid extract, and corticosteroids. been used to treat contamination with many met-These agents require experienced consultation, als, mainly copper, mercury, and lead. It does nottreatment, and management."M appear to be especially promising for the treatment
Chelating Agents. Chelators are substances that of internal radionuclide contamination. DFOA hasbind with some metals more strongly than others to been used to treat iron poisoning. In combinationform a stable complex that, when soluble, can be with DTPA, it has an increased affinity for iron.more readily excreted by the kidneys. The effec- DFOA appears to be more useful than DTPA intiveness of chelation therapy is influenced by many treating plutonium contamination, but until it isphysiological factors, including plasma proteins, approved by the FDA for this purpose its use can-blood pH, enzymes, and even nucleic acids. The not be recommended.most commonly known chelating agent is EDTA, Lung Lavage. Lung lavage has been successfulnormally given as the calcium salt. However, for in decreasing radiation-induced pneumonitis intreatment of the heavy-metal multivalent radionu- laboratory animals.' It has been used in humanclides expected from a nuclear yield, the powerful therapy for chronic obstructive lung diseases."chelator DTPA is generally more effective. DTPA- However, the procedure requires general anesthe-chelated complexes are more stable than EDTA sia, and a careful risk-benefit assessment must becomplexes, and are therefore less likely to release made before it is used for radionuclide decontami-the radionuclide before excretion. The calcium and nation. Endoscopy is the procedure most similar tozinc forms of DTPA have both been approved by lung lavage, and it has a mortality rate ofthe FDA as investigational new drugs (IND) for the 0.08%-0.85% in patients judged to be in good con-chelation of plutonium, berkelium, californium, dition. Considering that the risk from lung lavageamericium, and curium. Physicians finding a need is immediate and that the possible effects fromfor DTPA should contact the Radiation Emergency internal radionuclides are decades away, medicalAssistance Center/Training Site (REAC/TS) to be- personnel will have to weigh the benefit to the pa-come a coinvestigator (see address in reference tient carefully. Unless the lung burden is so greatnote).' 7 REAC/TS usually responds to nuclear acci- that it will result in acute radiation injury, lung lay-dents and incidents and will arrive at the site age is not recommended."3
63
Medical Consequences of Nuclear Warfare
SUMMARY
A plan for medical care must be available to deal inhalation, ingestion, and absorption throughwith the contingency of a nuclear event. The first wounds and skin. Treatment is determined by thepriority is basic first aid, followed by decontamina- particular radiation to which the patient has beention in a predesignated area. The level and type of exposed. Internal decontamination must be startedradiation exposure must be caculated as accurately in the first few hours after exposure if radionu-as possible. Contamination may be internalized via clides could have been internalized.
REFERENCES
1. National Council on Radiation Protection and Measurements. 1980. Management of persons accidentally contaminatedwith radionuclides INCRP Report 651. Washington, DC: National Council on Radiation Protection and Measure-ments.
2. Durakovic, A. 1987. Internal contamination with medically significant radionuclides. In Military Radiobiology, editedby J. J. Conklin and R. i. Walker, 241-264. Orlando, FL: Academic Press.
3. Cerveny, T. J., and Cockerham, L. G. 1986. Medical management of internal radionuclide contamination. MedicalBulletin of the U.S. Army, Europe 43(7): 24-27.
4. International Commission on Radiological Protection. 1955. Recommendations of International Commission on Ra-diological Protection. Br. ]. Radiol. (Suppl. 6).
5. Conklin, J. J.; Walker, R. I.; and Hirsch, E. F. 1983. Current concepts in the management of radiation injuries andassociated trauma. Surg. Gynecol. Obstet. 156: 809-829.
6. Biological effects of inhaled radionuclides. Ann. ICRP 31(1980): 4(1/2).
7. Moskalev, Y. I., ed. 1974. Distribution, biological effects and accelerated excretion of radioactive isotopes IAEC-TR-75901.Translated from the Russian by the U.S. Atomic Energy Commission. Springfield, VA: National TechnicalInformation Service.
8. Butler G. C. 1976. Metabolic excretion and retention patterns of incorporated radionuclides in reference mian [STI/PUB/411 ,3. Vienna: International Atomic Energy Agency.
9. Lushbaugh, C. C.; Andrews, G. A.; and Hubner, K. F. 1976. REACITS: A pragmatic approach for providing medical careand physician education for radiation emergencies ISTI/PUB/4111, 565. Vienna: International Atomic EnergyAgency.
10. Ohlenschlager, L. 1970. First aid measures in radiation accident with special reference to wounds contaminated withradioactivity. Atompraxis (Ger.) 16(4): 236.
11. Foreman, H. 1963. Medical management of radioactively contaminated wounds. In Proceedings of the Scientific Meet-ing on the Diagnosis and Treatment of Radioactive Poisoning. Vienna: International Atomic Energy Agency.
12. USSR State Committee on the Utilization of Atomic Energy. 1986. The accident at the Chernobyl Nuclear Power Plant and
its consequences. Part II, Annex 7. Vienna: International Atomic Energy Agency Experts' Meeting.
13. Gus'kovaya, A. K., ed. 1987. Early acute effects among the victims of the accident at the Chernobyl Nuclear Power Plant
[USSR Ministry of Health Order No. 48511. Translated by U.S. Defense Intelligence Agency [LN 818-871.Moscow: USSR Ministry of Health.
64

Treattnen t of hiternal Radionuclide Contamimation
14. Cosgriff, J. H., Jr. 1987. Guidelines for the emergency management of radiation injury. hiternal Medicine (for theSpecialist) 8: 170-180.
15. Program Update: DTPA chelation drugs. REACITS Neusletter (Winter/Spring, 1987).
16. Roberts, L. 1987. Radiation accident grips Goiinia. Science 238: 1028-1031.
17. Radiation Emergency Assistance Center/Training Site (REAC/TS) is located in Oak Ridge, TN. The telephonenumber is (615) 576-3086.
18. Update on chelation therapy: Chelators should not be used for uranium or neptunium. REACITS NMewsletter (April,1981)
19. Klvstra, J. A.; Rausch, D. C.; Hall, K. D.; and Spock, A. 1971. Volume controlled lung lavage in the treatment ofasthma, bronchiectasis, and mucoviscidosis. Ani. Rev. Respir. Dis. 103: 651.
65
aLa II

Medical Consequences of Nuclear Warfare
66

Chapter 5
INFECTIOUS COMPLICATIONSOF RADIATION INJURY
RICHARD I. WALKER, Ph.D.*
INTRODUCTION
INFECTIONS ASSOCIATED WITH CONVENTIONAL INJURIES
Incidence and Type of PathogensCauses of Opportunistic Infections
INFECTIONS ASSOCIATED WITH RADIATION INJURY
Importance of InfectionInfection and Combined Injury
FACTORS PREDISPOSING TO POSTIRRADIATION INFECTIONS
Impaired Inflammatory ResponseChanges in Resident Microbial Populations
MANAGEMENT OF INFECTIONS
AntibioticsSupportive TherapySurgery
SUMMARY
*Captain, United States Navy; Director, Enteric Diseases Program, Naval Medical Research Institute, Bethesda, Maryland 20814-5055 and ArmedForces Radiobiology Research Institute, Bethesda, Maryland 20814-5145
67
mA dioll cop I st'l'lft'ctts of Nut Ihar Warfartc
INTRODUCTION
Infection with normally harmless indigenous including disturbances of permeability in the intes-microorganisms is a major cause of morbidity and tine. Leakage of endotoxin from the intestinal lu-mortality when normal host defenses have been men can occur, and facultative anaerobic flora in-compromised. These opportunistic pathogens are crease in numbers in the gut. As this happens,responsible for hundreds of thousands of serious in- macrophages and other cells contribute to a suppres-fections in injured and immunosuppressed patients sion of the immune system. This early immunosup-in the United States annually, and the mortality rate pression may be beneficial and not pose a seriousfor these infections can range from 50"' to 70'> .'2 hazard because mucosal bacterial populations areAdvances in surgical and resuscitation techniques not excessive at this time.are increasing the immediate survival of victims of If the physiological and immunological deficien-severe trauma, but many die later from overwhelm- cies associated with trauma or radiation exposureing infections. In trauma victims who survive the are not resolved, then suppression of immunity per-first few days after the event, sepsis is the second sists. Subsequently, mucosal microorganisms, suchmajor cause of death (with head injury the first). as those in the intestine, multiply dramatically and
The nature of the postinjury events that are re- may translocate to other tissues. Many enteric florasponsible for infection is illustrated in Figure 5-1. find their way to wound surfaces, where they beginBoth radiation and trauma can cause damage to or to predominate. The best management of opportun-destruction of tissues. The insult triggers an inflam- istic infections is to use interventions that interruptmatorv response which, via mediators, activates sig- or compensate for these processes, thereby prevent-nificant physiological and immunological processes, ing overwhelming infection and shock.
INFECTIONS ASSOCIATED WITH CONVENTIONAL INJURIES
Incidence and Type of Pathogens tic pathogens are Streptococcus ft'calie and Staphithlococ-cus auretts as well as the Euterobacter and Bacteroides
The nature of the microbial agents responsible for species. However, many other microorganisms havemost opportunistic infections has changed since also been implicated in opportunistic infections.antibiotics were first used, but the incidence of infec- Because gram-negative bacteria can live in soil,tion has changed relatively little. For example, data they have evolved ways to adapt to the antibioticsfrom early World War 11 show a 617` incidence of in- produced naturally by other soil microorganisms,fections in soft-tissue wounds in 926 patients, a 14'7( and they maintain this ability to adaptively resist theincidence of serious infections with compound frac- antibiotic drugs that are used to fight infection.tures in 674 patients, and a 2215" incidence of burn in- Thus, gram-negative organisms are serious threatsfections in 591 patients." The incidence of infection in a hospital environment. Hospitals are contami-was not much different for soldiers injured in the nated with antibiotics, so only resistant organisms1973 Yom Kippur War in Israel (Table 5-1). The can colonize that environment. In studies of infec-overall incidence of infection was 2217( in 420 pa- tions among tornado casualties in Lubbock, Texas,tients.4 Of those, 49 burn patients had a 3517, inci- in 1970, seventy-eight isolates of gram-negative bac-dence of infection; 99 patients with fractures, 1817` teria were obtained from twenty-four hospitalizedincidence; 178 patients with soft-tissue injuries, 617; patients, versus eleven isolates in twenty-three vic-and 53 patients with penetrating abdominal wounds tims treated as outpatients. These results suggestand perforated colon, 3017,. that many of the organisms were acquired in the
With the increased use of antibiotics, organisms hospital.such as Clostridinm perfriungens (which causes gas A low incidence of infection was seen among Brit-gangrene) have become less important. Others have ish soldiers injured in the Falkland Islands War inbecome more troublesome, especially gram-negative 1982 ." One reason may have been that the patientsorganisms such as the Psettionioias or Klebsiella spe- were treated either on a makeshift hospital ship, thecies or Esclerichia coli. Other important opportunis- HMS LUganda, or in an abandoned icehouse at Ajax
68

lhfecht iý Coniplicatiol. o R() htiatioon InIjpi
Trauma 0 Target Cell Damage/Death -" IRadiationi
Primary Inflammatory, Response
Wound Surface IL-r1Colonization MMeia tor^s em
(G)GtE ffectsý Macrophage Downreguiation
Intest. Bacterial LPSPopulation•-•-•- - - - -- ----------.--.--- Early Immune
.C Pnhtoilogic * Trauma remains SuppressionI Physiologic ( _ ' " Marrow not '_
Facultative Dysfunction recovered TraumaBacterial > *Eliminated
Population -- Late Immune (i.e., closure)Increase Suppression I
L + Translocation IReoveryjEnterics0' and Spread
Colonize/'Wound I
L (G- Infection]
Fig. 5-1. Overview of postinjury events that contribute to development of infectious complications
Bay. Neither facility had been used previously as a 1-5 x 10" injected staphylococci caused a lesion inhospital and thus did not contain antibiotic-resistant humans, but if the organisms were introduced on abacteria. buried silk suture, as few as I x 102 bacteria pro-
duced spreading cellulitis.'Causes of Opportunistic Infections This effect of foreign material or damaged tissue
on the developmt.nt of infections demonstrates theImmunosuppression is a consequence of injury need for early surgical management and debride-
and is an underlying cause of many infectious corn- ment of wounds. Even the placement of originally,lications. Four other factors also contribute to post- sterile materials into the body of a patient can pro-trauma infections. In decreasing order of impor- vide a focus for infection. Inert biomaterials, such astance, they are (a) the presence of foreign bodies in catheters and other invasive devices, can becomewounds; (b) the time lag between injury and surgery; covered with biofilms in which indigenous bacteria(c) the number, location, and extent of wounds; and move onto the surface and become surrounded by(d) the virulence of the organism. exopolysaccharides and the host's accreted macro-
The influence of a foreign body on infection is moiecules.1 ' These biofilms also form on detritusseen in studies of the minimum dose of C. per frine•s and dead tissue. Bacteria in these colonics cannot bespores required to cause lethal infections in guinea cultured by usual means, and they are more resis-pigs.' The dose required when spores were injected tant to antibodies, phagocytes, and antibiotics. Foralone was 1 x 10". If the spores were inoculated into example, P. aeruginosa in a biofilm can withstandcrushed muscle, then only 1 x 103 spores were forty times the concentration of tobramycin that killsneeded. When sterile dirt was added to the spores floating cells. Therefore, the best intervention is theinjected into crushed muscle, then one spore instead early removal of material that can support the devel-of one million was required for lethality. Similarly, opment of biofilm. Because only living tissue resists
69

Me, fic, l Gmopsctieccs ot Niich', Wartire
TABLE 5-1
INCIDENCE OF WOUND INFECTION IN 1973 YOM KIPPUR WAR IN ISRAEL
Number of InfectionType of Injury Patients (L)
Overall 420 22
Soft tissue 178 6
Fracture 99 18
Involving femur 20 40Not involving femur 79 15
Penetrating abdomen 53 30
Colon perforated 19 58Colon not perforated 34 14
Burn 49 35
<25(7, 37 14>25% 12 100
the formation of a biofilm, debridement is an impor- opportunistic pathogens. Once these deficienciestant treatment. Artificial devices, such as catheters, develop, a variety of otherwise harmless microor-should be used carefully. ganisms can take over. Their uncontrolled multipli-
Resistant biofilms have a greater chance to de- cation in tissues of compromised hosts leads to thevelop on dead tissue and detritus if the time interval , ccumulation of both toxic microbial products andbetween injury and surgical resolution is prolonged, the products of host responses, which cai',es shockIn a study of gas gangrene, 511 patients (162 of and death.whom became infected) had a 1534 increased inci- Little is known about the lethal mechanisms ofdence of infection for each day between injury and most bacteria. Gram-positive organisms, such as S.debridement." These data from World War I are aI'urs, produce a variety of extracellular protein tox-relevant today because a similar situation could de- ins. Gram-negative organisms can produce extracel-velop with mass casualties in a modern conventional lular toins, but they also have a lipopolysaccharideor nuclear war. (LPS) cell wall component known as endotoxin
The incidence of infection is also influenced by which, if present in sufficient quantities, can inducethe nature of the wounds. Data from the 1973 Yom a variety of toxic hcut responses that mimic many ofKippur War in Israel (Table 5-1) show that burns of the responses associated with overwhelming bacte-less than 2517( of the body surface were rarelv com- rial infections. However, microbic' pathogenesis isplicated by infection, but all burns of more than than probably not due to a single factor. For example, al-25%7 of the body surface were associated with infec- though C3H/HeJ mice are low responders to en-tious complications.4 Perforation of the colon was dotoxin effects, they are easily infected with doses ofmore often associated with infection than was ab- gram-negative bacteria that cannot be established indominal penetration without perforation of the co- other mouse strains."2 The C3H/HeJ mice die withlon. Fractures involving tne femur were also fre- numbers of organisms in their tissues similar toquently associated with infection, numbers seen at death in other strains of mice chal-
In general, it is the failure of normal ho,;t barriers lenged with higher doses of bacteria. Other data il-and defense mechanisms that permits infection by lustrating the importance of multiple virulence fac-
"70

Infectious Coinphication& of Radiation Injury
tors can be taken from a survey of twenty-four Aero- (Table 5-2) not found among the low-virulenceinonas isolates that weie grouped according to high strains. The shock syndrome resulting from the ac-virulence and low virulence for mice challenged in- cumulation of lethal numbers of gram-positive bac-traperitoneally.' The high-virulence group of bac- teria in host tissues is similar to the syndrome in-teria was more often positive for a variety of factors volving gram-negative bacteria. 4
INFECTIONS ASSOCIATED WITH RADIATION INJURY
Importance of infection and wound injury.' 7 No mortality was seen in germ-
free rats exposed to 8.0 Gy of total-body radiationOpportunistic pathogens are not only a major compared to 55% mortality in conventional rats. If a
complication of conventional injuries, but also a ma- 3-cm wound was also inflicted, mortality was 17',jor cause of morbidity or mortality in radiation-asso- and 100% in germ-free and conventional animals, re-ciated injury. Histological specimens of spleen, spectively.liver, lymph node, intestinal wall, and other tissues As suggested in Figure 5-1, opportunistic infec-were taken from patients dying from the effects of tions do not occur until days or weeks after the in-the atomic blasts over Hiroshima and Nagasaki in jury. A chart from a Chernobyl victim (Figure 5-2)1945. Many specimens revealed microscopic bacte- shows that elevated temperature, indicating infec-rial colonies of both gram-positive and gram-nega- tion, was not recorded until more than 3 weeks aftertive bacteria growing freely in the tissues. There is a injury. In laboratory animals given lethal radiation,relationship in animals between infections and infections are detected at about 9 days after expo-deaths after whole-body radiation doses in the sure, and death occurs between days 11 and 15.'smidlethal range."; A curve based on mouse datadepicting increased incidence of infection can bedrawn parallel to but preceding the mortality curve.All mice that developed bacteremia after irradiation TABLE 5-2died, whereas those with no bacteremia survived.Studies such as these show that infection is an im- AEROMONAS INFECTION:portant cause of death during the hematopoieticsubsyndrome. ASSOCIATION OF VARIOUS CHARACTERISTICS
WITH VIRULENCE FOR MICEInfection and Combined Injury
Number of PositiveMore recently, data from severely injured victims Puleer Total
of the 1986 Chernobyl disaster also illustrate the seri- Viuence CulturesperTotal
ous threat of infections for radiation victims. Of Fact
twenty-nine deaths (not counting the two persons Factors High Low
killed by the explosion), most were caused by infec- Virulence Virulence
tions associated with burns and hematological injurydue to radiation exposure. This type of combinedinjury is predicted to be the most common trauma Cytotoxin 15/15 0/9
problem that will be seen in nuclear warfare. Insults Proteasethat are sublethal or minimally lethal when occur-
ring alone will act synergistically when occurring Lipase 13/15 1/9together. For example, almost 100I) mortality oc-
curred in rats given both 2.5 Gy of gamma radiation Elastase(no mortality when given alone) and a burn wound ]1/1 7/9
over 33'.11 of their body surface area (50(/c mortality Piliwhen given alone)." 9/13 2/8
A role for endogenous microorganisms in deaths Hemolysin 8/9 1/7following combined injury has been established bydetermining survival in germ-free rats and conven-tionil rats undergoing combined radiation exposure
71

Medical Constquiches ot NutIjcar Warfar'
PATIENT No. 21DAY AFTER EXPOSURE
m•.1. L -I . . . . 1 -- 7- - PLATE-LETS~~~~~~I -I... . .. TTFTTT7i'=,
r Fr I-f+• LEUKOCYTES
. . . .... .E.. . . U R E '- I f
S.....'-;o- GRANULOCYTES
I I II II I I I I IiI 2 3 "1 3 1 1 1 I I I I 1 [
I It l l I '• I H il 1 1 -R I I 1 1 2 2 1 1 1 1 1 !fi t I I1 1 1 1 •
1 . ... t a/ .. .. 1 440 26 Yin,~I1
S....... r . . ... iANTIBIO TIC i: I :: •
TREATM RT
Fig. 5-2. Medical chart of a victim of the Chernobyl reactor disaster, illustrating occurrence of infection associated withgranulocytopenia
FACTORS PREDISPOSING TO "OSTIRRADIATION INFECTIONS
Impaired Inflammatory Response help augment host defenses. Failure in systemichost defenses after trauma may be caused in part by
Postirradiation infections are associated with neu- a deficiency of circulating opsonic protein (plasmatropenia. In normal persons, inflammatory re- fibronectin). The infusion of this substance into per-sponses control many microorganisms that pene- sons depleted by trauma has been associated withtrate normally sterile tissues (Figure 5-3). Humoral enhanced RES activity." Since macrophages arecomponents of inflammation, such as complement, relatively long-lived, they can be used to augmentinteract with the microbial antigens and become ac- the host's resistance to infection after radiation expo-tivated to induce cellular responses, such as vaso- sure.constriction and exudation of polymorphonuclear In traumatized subjects, an adequate inflamma-leukocvtes. These cells phagocytose and kill many tory response is often not achieved because of im-microorganisms. Later, macrophages enter the in- munosuppressive factors and the loss of functionalflammatorv site where they contribute to the re- cells. For example, the mortality rate from infectionmoval of microorganisms and debris, and secrete varies directly with the degree of granulocytopenia.factors that promote tissue repair. Dogs given gentamicin plus granulocytes survived
Microorganisms are also removed from the circu- longer and cleared P. arciginosa better than dogslation bv the reticuloendothelial svstem (RES). In given the antibiotic alone.2" Although granulocytesthe presence of proper opsonins, RES macrophages, are undoubtedly important in controlling gram-such as those in the liver and spleen, sequester and negative sepsis, it is questionable whether transfu-kill microorganisms and also secrete mediators that sion with these cells is essential for effective therapy.
72

Infectiotis Comiplications of Radiation Injury
I Signals of InflammatonFibrogenesis Kinin System(Tissue Repair) Complement System
r! Clotting System
Macrophage Mediators A
Permeability~ Mircrcl r Chage Flow and Caliber
Debridement (By Macrophage PMN Exudation Fu xudation
(Phagocytosis) 2
(Tissue Damage
6 0 . ... Precursor Cell jjaLeu oports(Blood Monocyte) Factors
Marrow Reserve
Fig. 5-3. Overview of essential components of the inflammatory response
Antibiotics are available, and safer and more realis- sion or death than in nonirradiated animals.2tic agents are being developed for use in mass-casu- Postirradiation infections are often polymicrobial,alty situations. and it has recently been found that the complexity of
Other cells and humoral agents are also lost due infection in mice increases with increasing doses ofto trauma and radiation exposure. Fibronectin and radiation. 23 While S. aureus was more often recov-immunoglobulin G are depleted in trauma victims, ered at 9.0 Gy and below, E. coli and anaerobes wereand lymphocytes are directly injured by irradiation. isolated most frequently in mice receiving a dose ofIn addition, some injuries (such as burns) produce 10 Gy.immunosuppressive factors that may impair thefunction of macrophages or other surviving cells. 2'
There are several examples of increased suscepti- Changes in Resident Microbial Populationsbility to systemic infection after irradiation. Whenmice were challenged with K. pneunoniae, the LD, Various deficiencies in host defenses can increasewas I x 10". Radiation alone reduced the LD•, to I x the susceptibility to infection, but changes in the10', and radiation plus a 3-cm dermal wound re- microbial populations on body surfaces are also im-duced the LD•, still further to I x 10'. Similarly, the portant. Such population shifts can occur when pro-inoculation of E. coil, S. aureus, or S. pyogenes into tective coatings on epithelial cells are lost and whenmuscles of mice exposed to 6.5 Gy of gamma radia- indigenous flora, which resist colonization by ex-tion resulted in increased numbers of microorgan- ogenous pathogens, are reduced in number. Theseisms in their tissues 5 days later, compared to nor- events allow pathogens to colonize mucosal sur-mal mice. When S. aurmus was injected into the local faces, from which they may spread to ordinarilywounds of mice exposed to 7.0 Gy of gamma radia- sterile sites in the body.tion, fewer bacteria were required to produce a le- Recent evidence suggests that epithelial surfaces
73

oI II 11111k haiborier lver eplitheililm oit iflhlm'.e Iiinul ,ifter e\p)'.iri' to 10-( . colalt-6 r( i~iation. \oirnmi ileuiiihI m, nt~ikt IL nkct t Itnmuti. ti ktIi\ rilIlI th dlit'' ( AI. I'l hi' blanketit is ot tx' " IVs Mtt(Tir --a irr ltia t In. i'\p l'ing thli I I I I .
inll eirpar 0ge0 II011,1 1100 xi tvit\ ira tU ma Vidill nIs ca h&, iccu ~rred ill thiL' in"test i ni. '*VIwI't \-tOu r hou'. a M-
losi,( (e'! -snrtaie tjriin'lc~til Minnd beoi'cmi proni' to at- tiT'r 1u1b1et ha11 i\posti reV tO 7; i~ ot ammna rad ia tion,
tat-ih winit bv gra inl-nega tixi' bacteria, Nu1ch as, 1. SIAM\ diý,app~a rid from thi' rat ileumi. I lOXxevi'rL, VIVFl- 1% hi ma alsO occur alter u-iradiation dav 4, S1\1 populations were back to normal. Ini rat"
anld 111,1V in han11ci tlhi' po sihil1itv that paIthogens will xivvn a let hal rad iat h in di is (It W. G, ), SlAI did Ii otsIccM s CC l lkxc I n~' t-1II/ hi' hi 0st. return-1 at da\ 4 a ni wiTC'ritill ai't trom thi' ili'U mI
\ic~rOI _II irga iIms inl thi ilnti'st iln'lcra inl nu1 m- at da I VI I . ~'oti' til (ippOr'tunIItic rpathlO"i'n, mII'aN-bi'rs distlldl\ and proxMidi' a 10cus for abilirmal cobo- urif'd bV HLi' cu~ltiVationl Of dilUt ioN (ot in~testinlllnli/at ii , Which canI 1ald to .VT~ I'irhllmill, intectii lit hmiogenamtes, diclini'i inl numllbers shIortly aftir L'\-winCIý sx-ti'mclk hosýt i~tltesi' haxe a lkii be'n'l coin- postiri' to -It) ( Y..- At the lo we'r raidiat ion doisi'
pri ~ ~ ~ I -niii [hspeoio a i on nras tern b'sbgnt nrase atter thec return ot
"g-iensbehl or1[1111 letha rail, IIia t iOI ine1p11u0is. i SF\1 , buit they\ wI'\ri still subnormal at dav x1. Iniilciii (in Iiian nl rat ks coli 'iincd by. Iunusual haiti'- Ci n trast, rats ,iven 1 0 C v showed i ncr'asing nmin-
nia, known as I egm-inctetd ti Ianmen tiiu s inic ri 1ii ir bi'rs it tacuItat ivxi flora a ttir the first ti'w iiavs ti l-I ~ \ .w iiIi ai i t e ii t x td-Mit whs tuin- I10\6xi u irra-diation), aMil byV dax I I t hVi's orga,, sn
min i ro~ i'c px Ihe lit ir-anisi~nsa ri' in ti mati'l assi ci - ma I. li, is 'xint corri'la ti'i With sxsti'InIic in i'c~t ion
.Iti'iI 1x it h t hi' i'pithi'lciii infu tilti' iitest i ici. Fllei r pI'a- a1nil prici'di'i death.ki ri 'Ii'l inl th Iiitti ti'sticn is un1,1( k 1 iii vw ii ix'ir, be(- It is apparenit tHaM1t \ anei'nt asiiCiaii Wxith L'\ pi i
a u1se, t hex a ri assi i i ti'd w,\ith \\ cxll-bewi n", ~L\A 1cal 111i C ti) h IC ihrioisOt ra)iltiatl i kni ri'pons~ilf fiot r
lii tii'.i a'. ini(Mi~aor orgafinism, (Iimi'11ii1.rat in that abnormal1111k~ ll iin,atit'in prICk'ci'ilg in"ticLtiiin. I ittli' is
anl linjIirx whIi Ii Wi d alter- ba~kiI tirial poui s kon okmutilthe pathiiph\siiilogv ot this injurx.- Ini-
'74

Infectious Complications of Radiation Injury
testinal epithelial cells are almost as sensitive to ra- sive loss of this material was observed between irra-diation as are marrow cells, and even doses of radia- diation and day 3 (Figure 5-4). Prior to irradiation,tion below the gastrointestinal-subsyndrome level villi were not visible beneath the mucus, but by daycan cause injuries that affect bacterial colonization. 3, major sections of villi were completely uncovered.
Since most intestinal microorganisms are found in Loss of the mucous barrier and other ecologicalthe 450-micron mucin layer at the epithelial surface, and immunological changes in the intestine enableany injury that produces changes in this structure opportunistic pathogens to overgrow on the mu-can contribute to significant alterations in patterns of cosal surface and subsequently to translocate tomicrobial colonization in the intestine. Evidence for other tissues. Translocation from the intestine hasthe loss of the intestinal mucous barrier has been been well correlated with conventional disturbancesfound in mice that received 10 Gy of cobalt-60 radia- of mucosal ecology and also systemic trauma.2
7 Thistion.2 0 When procedures were used that stabilized process can lead to infections when defense mecha-the mucous gel for electron microscopy, a progres- nisms are also suppressed.
MANAGEMENT OF INFECTIONS
Opportunistic infections that are a consequence of cies and facultative gram-negative microorganismstrauma in conventional warfare have been difficult often occur together. One of these organisms mayto control. This will also be true in persons with ra- produce capsular material that protects the other or-diation injuries or combined injuries. In seriously ganism from phagocytosis, as well as beta-lactamaseinjured Chernobyl victims (Table 5-3), the number of for protection against antimicrobial therapy. Also,patients with radiation and thermal burns was one organism could create an anaerobic environ-greater with higher radiation doses, and mortality ment that is essential to the other organism, or couldrose with the severity of combined injuries. Of the produce nutritional growth factors. Many slowlytwenty-nine deaths, most were directly attributable growing and fastidious pathogens, which are impor-to infectious complications. It is clear from the Cher- tant in infections of severely compromised patients,nobyl experience that bone-marrow transplants in may still be unrecognized. Further studies of thesepersons who received uneven radiation exposures organisms will be necessary for better selection of(in whom stem cells may have survived) can be dan- antimicrobial therapy.gerous. It is important that initially avirulent bacterial
If bone-marrow transplantation is not practical in populations may become more virulent if allowed totreating radiation victims, the management options persist in mixed infections. Nonabscess-formingare those used in conventional injury: antibiotics, cultures, when inoculated into mice along with cap-surgery, and supportive therapy. sular material or other pathogens, may convert to
encapsulated populations that are capable of estab-Antibiotics lishing abscesses on their own. 28
Antibiotics can also be used to reduce the coloni-New antibiotics are continually being developed. zation of intestinal mucosa by opportunistic patho-
Figures 5-5 and 5-6 describe the different groups of gens. Total intestinal decontamination is difficult toantibiotic agents and indicate their usefulness achieve, and it creates further vulnerability to colo-against different kinds of infections. Some newer nization by antibiotic-resistant pathogens. How-antibiotics, such as ceftazidime or the quinolones, ever, selective decontamination with oral antibioticsmay be useful as monotherapy, but most antibiotics has already been tested clinically, and it offers prom-seem more effective when used in synergistic combi- ise for the management of mass casualties who havenations. Today, the effectiveness of some antibiotics been exposed to midlethal radiation. The oral ad-may be enhanced by the use of inhibitors of bacterial ministration of specific antibiotics eliminates oppor-enzymes (such as clavulanic acid) which inhibit tunistic pathogens but leaves intact the relativelybeta-lactamase activity and thereby preserve the benign intestinal flora .2.3° These benign flora in-function of penicillin derivatives, crease resistance to colonization by occupying bind-
Antibiotic effectiveness may also be enhanced by ing sites and creating an environment that is inhos-ensuring that therapy is directed against all compo- pitable to pathogens. This approach eliminates thenents of an infection. For example, Bacteroides spe- need for elaborate methods of isolation. In patients
75
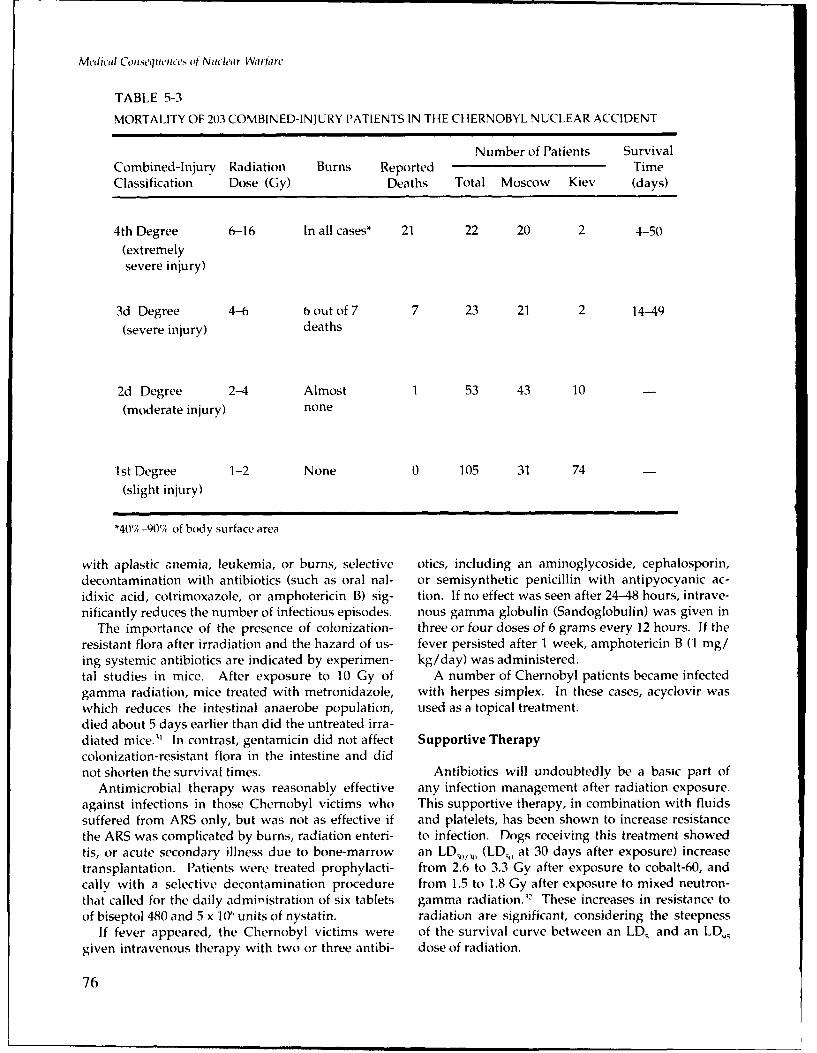
Medical Conisequetnces of Nuch'ar Warfare
TABLE 5-3
MORTALITY OF 203 COMBINED-INJURY PATIENTS IN THE CHERNOBYL NUCLEAR ACCIDENT
Number of Patients SurvivalCombined-Injury Radiation Burns Reported TimeClassification Dose (Gy) Deaths Total Moscow Kiev (days)
4th Degree 6-16 In all cases* 21 22 20 2 4-50
(extremelysevere injury)
3d Degree 4-6 b out of 7 7 23 21 2 14-49
(severe injury) deaths
2d Degree 2-4 Almost 1 53 43 10
(moderate injury) none
1st Degree 1-2 None 0 105 31 74
(slight injury)
"*4017,-90V7, of body surface area
with aplastic anemia, leukemia, or burns, selective otics, including an aminoglycoside, cephalosporin,decontamination with antibiotics (such as oral nal- or semisynthetic penicillin with antipyocyanic ac-idixic acid, cotrimoxazole, or amphotericin B) sig- tion. If no effect was seen after 24-48 hours, intrave-nificantly reduces the number of infectious episodes. nous gamma globulin (Sandoglobulin) was given in
The importance of the presence of colonization- three or four doses of 6 grams every 12 hours. If theresistant flora after irradiation and the hazard of us- fever persisted after 1 week, amphotericin B (1 mg/ing systemic antibiotics are indicated by experimen- kg/day) was administered.tal studies in mice. After exposure to 10 Gy of A number of Chernobyl patients became infectedgamma radiation, mice treated with metronidazole, with herpes simplex. In these cases, acyclovir waswhich reduces the intestinal anaerobe population, used as a topical treatment.died about 5 days earlier than did the untreated irra-diated mice." In contrast, gentamicin did not affect Supportive Therapycolonization-resistant flora in the intestine and didnot shorten the survival times. Antibiotics will undoubtedly be a basic part of
Antimicrobial therapy was reasonably effective any infection management after radiation exposure.against infections in those Chernobyl victims who This supportive therapy, in combination with fluidssuffered from ARS only, but was not as effective if and platelets, has been shown to increase resistancethe ARS was complicated by burns, radiation enteri- to infection. Dogs receiving this treatment showedtis, or acute secondary illness due to bone-marrow an LD,,/, (LD , at 30 days after exposure) increasetransplantation. Patients were treated prophylacti- from 2.6 to 3.3 Gy after exposure to cobalt-60, andcally with a selective decontamination procedure from 1.5 to 1.8 Gy after exposure to mixed neutron-that called for the daily administration of six tablets gamma radiation.)2 These increases in resistance toof biseptol 480 and 5 x 10" units of nystatin. radiation are significant, considering the steepness
If fever appeared, the Chernobyl victims were of the survival curve between an LD_ and an LD,4given intravenous therapy with two or three antibi- dose of radiation.
76

Infectious Coinplications of Radiation Injury
ANTIBIOTIC AGENTS
Third-generation 10Except for cettazidimeInfetvagis euo nsCephalosporins 1 fetv gis
Ce7_n7ami7 n
Amngyoie etilmicin Most effective against E Gram-negpative rodsAminolvcoidesTobramvcin
Aia in Effective, but less so than
Ureidopenicillhns licarcillin
aiolcsds gis
Carboxvpenicillins Piperacillin 0Are synergistic with Gram-negative entericsaminoglycosides against
Effective, to a lesser degree than aminoglycosides butSwithout their renal toxicity, against eaatmaerduigbcra(neoi,
Monobactams ealcaaepouigbcei(neri,
Combnaton Peicilin(amicilin r tcarilh) Efeciveaganstgram-positive, and gram-negative)
Agents Beta-lactamase inhibitor -- 0-Ineffective against Pseudomonas
(clavulanic acid or sulbactam) _P nfetv gis
Other organisms that resist penicilhins throughmechanisms other than beta-lactamase
Beta-lactam- Methicillinresistant Penicillins Dicloxicillin -- * Effective against Staphylococcus aureus
Vancomiqcin can be admninistered for the therapy, of niethicillin-resistant S. aureas)
Pseudomonas, Enterobacteriaceae ,Staphylococcusop Effective against
Quinolones Do Ineffective againstAneo s
(Quinolones are, effe'ctive for selective decontantination as well as for sys.temic thierapy~)
10 Only single effectiveImipenem agent against Aerobic gram-positive and gram-negative,
(combined with as well as anaerobic, bacteriacilastatin)
Fig. 5-5. Types of agents used in antibiotic therapy of irradiated host
77

Medical Conseiq'ences of Nuclear Warfare
ANTIBIOTIC THERAPYFUreidopenicillin, or 7nCarboxypenicillin, ori Cephalosporin, or
Monolactamj
Gram-negative Infection Ceftazidime (3d generation cephalosporin)
(Compares favorably with combination therapywith cephalosporin or carbenicillin and gentamicin)
Carbapenems and Quinolones (may be usefid mionotherapy)
Gram-positive Infection W Ainoglycoside + Fcombination of a beta-lactam- 1I resistant penicillin
j
Aminoglycoside + C oClindamycin, o
or Cefotoxin, orMixed aerobic- Quinolone + Metronidazoleanaerobic Infections 1
Imipenem (single agent therapy)
Norfloxacillin- (800 mg/day)
Trimethoprim-sulfamethoxazole -(six regular tablets/day)(Cotrimoxazole)
Selective Decontamination - Polymixin-(800 mg/day) + Cotrimoxazole-(six regular tablets/day)
(Oral treatmentfor colonizing- t Polymixin-(800 mg/day) + Nalidixic acid-(6 g/day)resistant flora)
Amphotericin B--(2 g/day)
Nystatin-(6 x 10 6 IU/day)
Fig. 5-6. Suggested therapies for specific infections
78

Inf'ctiouls Chnplications of Radhation hnur
Another supportive therapy that may be usefulagainst gram-negative infections in irradiated per-sons is immunoglobulin. Immunoglobulin will actagainst some portion of the LPS component of the TABLE 5-4cell wall of gram-negative bacteria. Most experiencewith anti-LPS antibody preparations has been in CONTRIBUTORS TO INFECTIONnonirradiated research models.""' Clinically, anti-serum prepared from the J5 mutant of E. coli hasbeen used to reduce deaths from 391 to 23Y in pa- e Colonization of oropharyngealtients with bacteremia, and from 77%,( to 44% in respiratory treethose with profound shock." Various immunoglob-ulin preparations have been used to protect experi- * Colonization of intestinal tractmental animals against infection."
The development of human monoclonal antibod- e Contamination of woundies opens new possibilities for passive immunizationagainst microbial infections. Passive antibody ther- 9 Profound immunosuppressionapy was widely used in the pre-antibiotic era to treatinfectious diseases. Although this therapy may be * Invasive treatment deviceseffective in specific instances, appropriate stocks ofspecific antibodies with high-affinity constants are * Environmental pathogensexpensive and difficult to prepare in large amountsby conventional methods. Further, since such anti-bodies are usually obtained from animals, particu-larly horses, humans often have immune reactionsto the injection of these immunoglobulins. This re-sults in serum sickness, which prevents further use As indicated in Figure 5-1, the closure of woundsof the specific therapy in that patient. The new tech- can eliminate late immunosuppression and othernique of producing antibodies in vitro by somatic synergistic effects of combined injury. This is illus-cell fusion (hybridoma technology) has the potential trated by experiments conducted in mice.' Expo-of generating the desired amounts of high concen- sure to 5.1 Gy of radiation resulted in 26% mortality,trations of pure human-specific antibody prepara- and the same exposure combined with an opentions, which can be used against opportunistic wound resulted in 90% mortality. When the woundpathogens in host tissues. was closed, the percentage of mortality dropped and
Active vaccination against specific antigens of was similar to that from radiation alone. This sug-gram-negative bacteria does not appear to be a good gests that a deleterious signal or mediator was inter-option for controlling infection. It is questionable rupted. Unfortunately, excision and closure are notwhether an immunosuppressed person can evoke or always easily achieved. Closure, if done prema-maintain an immune response. Moreover, the large turely, will promote the occurrence of systemic sep-number of potential opportunistic pathogens makes sis from microbial colonization of necrotic tissue orit unlikely that a sufficient number of different vac- detritus. Early debridement should be followed bycines can be developed in the near future. an inspection of the wound 48 hours later, and if the
wound seems free of infection or nonliving material,Surgery closure can be considered.
Although this approach has not been fully testedIn combined-injury victims, surgery is expected to for radiation victims, surgical experience suggests
be an important adjunct to supportive therapy, but that full-thickness burns should be primarily excisedwill be complicated by impairments in wound heal- and grafted, and partial-thickness burns shoulding that are manifested shortly after exposure to ra- probably be treated by aggressive topical therapydiation. In contrast to trauma without radiation, the and avoidance of nosocomial sepsis. Prophylacticperiod of opportunity for reparative surgery follow- topical management of bum wounds may be accom-ing irradiation is very short (1 to 2 days), followed plished with mafenide acetate (sulfamylon) or silverby a period of several weeks in which surgery sulfadiazine (silvadene).3 7 Antibiotics are used forshould not be attempted if it can possibly bc prophylaxis only in traumatic cutaneous wounds,avoided (Figure 5-7). selective decontamination, and early surgery.-"'
79

Medical Consequiences of Ntich'ar Warfarte
Routine TraumaInitial Reparative Reconstructive
Surgery Surgery Surgery
I I I t I I t I I1 2 5 10 50 100
Days after Injury
Radiation Plus TraumaInitial Reparative Reconstructive
Surgery Surgery SurgerySI•Surgery Precluded - ,p j p I i pil ,,p , 11.11
1 2 5 10 50 100Days after Injury
Fig. 5-7. Comparison of timing for surgical management of combined injuries in routine trauma victims and in those exposed
to radiation
SUMMARY
A number of conditions may allow opportunistic decreased host defenses, then uncontrolled multipli-infections to occur (Table 5-4). Changes in epithelial cation by opportunistic pathogens can quickly leadcell surfaces can enhance colonization of the oro- to shock and death.pharyngeal-respiratory tree. Frequently, wound It should 'Lte noted that more virulent organismscontamination, first by skin flora and later by gram- can also be a problem after a nuclear detonation.negative flora from the intestine, can also lead to Mild immunosuppression in nonhospitalized per-overwhelming infections. Antibiotic-resistant sonnel working in an environment with poor hy-pathogens in the environment can be particularly giene can lead to epidemics of respiratory and en-troublesome if they colonize wounds on vulnerable teric infections.mucosal surfaces. Artificial invasive devices also General principles of patient management (Tablesubject susceptible surfaces to colonization by patho- 5-5) and current technology can be used in treatinggens. Finally, if all these events are accompanied by postirradiation infections.
80

Infectious Complications of Radiation lnjurIr
TABLE 5-5
PRINCIPLES OF PATIENT MANAGEMENT
"* Treat conventional injuries first, since radiation injurieswill not be immediately life threatening.
"* Evaluate the extent of trauma and initiate resuscitationprocedures.
"• Begin corrective procedures, such as surgery and fluidadministration, based on the triage assessment ofconventional injuries.
"* Prevent infection until immunocompetence is regained.
"• Take steps to reduce the foci of infections fromcolonizing artificial devices or damaged tissues.
"* If infection is suspected, use empiric therapy withbroad-spectrum antibiotics to complement thesephysical interventions.
"* Take steps to improve immunocompetence andphysiological well-being of the patient.
REFERENCES
1. Zimmerman, J. J., and Dietrich, K. A. 1987. Current perspectives on septic shock. Ped. Clinics N. A. 34: 131-163.
2. Cavanagh, D.; Knuppel, R. A.; Shepherd, 1. H.; Anderson, R.; and Rao, P. S. 1982. Septic shock and the obstetrician,'gynecologist. South. Med. 1. 75: 804-810.
3. Meleney, F. L. 1945. A statistical analysis of a study of the prevention of infection in soft part wounds, compoundfractures and burns with special reference to sulfonamide. Surg. Gynecol. Obstet. 86: 263-296.
4. Klein, R. S.; Berger, S. A.; and Yekutiel, P. 1975. Wound infection during the Yom Kippur war: Observations concern-ing antibiotic prophylaxis and therapy. Ann. Surg. 182: 15-21.
5. Gilber, D. N.; Sanford, J. P.; Kutscher, E.; Sanders, C. V. J.; Luby, J. P.; and Barnett, J. A. 1973. Microbiologic study of
wound infections in tornado casualties. Arch. Environ. Health 26:125-130.
6. Beeley, M. 1983. Hospital ship HMS Uganda-At war in the South Atlantic. ]. R. Naval Med. Serv. 69: 21-25.
7. Jolly, R. T. 1983. Ajax Bay. J. R. Naval Med. Serv. 69: 35-39.
8. Altemeier, W. A., and Furste, W. L. 1949. Studies in virulence of Clostridium welchii. Surgery 25: 12-19.
9. Elek, S. D., and Cohen, P. E. 1957. The virulence of Staphylococcus pyogenes for man. A study of the problems ofwound infection. Br. /. Exp. Pathol. 38: 573-586.
81

Medical Consequences of Nuch'ar Warfare
10. Costerton, J. W.; Marrie, T. J.; Gristina, A. G.; and Moody, M. R. 1987. The role of bacterial biofilms in the etiology,persistence, and antibiotic resistance of wound infections. In The Pathophysiology of Combined Injuryt and Trauma:Managetnent of Infectious Coiplications in Mass Casualtiy Situations, edited by D. Gruber, R. 1. Walker, T. .MacVittie and J. J. Conklin, 165-190. New York: Academic Press.
11. Petit, R. T. 1919. Infections of wounds of war with special reference to gas gangrene. 1AMA 73: 494-496.
12. MacVittie, T. J.; O'Brien, A. D.; Walker, R. I.; and Weinberg, S. R. 1982. Inflammatory respoli, of LPS-hyporespon-sive and LPS-responsive mice to challenge with gram-negative bacteria Salmonella typhollurium and Klebsiellapneumoniae. In Macrophages and Natural Killer Culls: Regulation and Function, edited by S. J. Normann and E.Sorkin, 325-334. New York: Plenum Press.
13. Daily, 0. P.; Joseph. S.; Coolbaugh, J.; Walker, R. I.; Merrell, B. R.; Seidler, R.; Rollins, D.; Lissner, C.; Kaper, J.; andColwell, R. 1981. Association of Aeromonas sobria with human infection. 1. Clin. Microbiol. 13: 769-777.
14. Natanson, C.; Danner, R. L.; Elin, R. J.; Hosseini, J. M.; MacVittie, T. J.; Walker, R. I.; and Parrillo, J. E. 1989. The roleof endotoxemia in cardiovascular dysfunction and mortality: E. coli and S. aureus challenges in a canine modelof human septic shock. 1. Clin. Invest., in press.
15. Miller, C. P.; Hammond, C. W.; and Tompkins, M. 1950. The incidence of bacteria in mice subjected to whole-bodyX-radiation. Science 3: 540-551.
16. Alpen, E. L., and Sheline, G. E. 1954. The combined effects of thermal burns and whole-body X-radiation on survivaltime and mortality. Anit. Surg. 140:113-118.
17. Donati, R. M.; McLaughlin, M. M.; and Stromberg, L.-W. R. 1973. Combined surgical and radiation injury. VIII. Theeffect of the gnotobiotic state on wound closure. Experientia 29:1388-1390.
18. Walker, R. I.; Ledney, G. D.; and Galley, C. B. 1975. Aseptic endotoxemia in radiation injury and graft-versus-hostdisease. Radiat. Res. 62: 242-249.
19. Saba, T. M., and Jaffe, E. 1980. Plasma fibronectin (opsonic glycoprotein): Its synthesis by vascular endothelial celland role in cardiopulmonary integrity after trauma as related to reticuloendothelial function. Am. J. Med. 68:577-594.
20. Love, L. J.; Schimpf, S. C.; Schiffer, C. A.; and Wiernick, P. H. 1980. Improved prognosis for granulocytopenicpatients with gram-negative bacteremia. Am. 1. Med. 68: 643.
21. Ninnemann, J. L. 1983. Immune depression in burn and trauma patients: The role of circulating suppressors. InTraumatic Injury, Infection and Other hImunologic Sequelae, edited by J. L. Ninnemann, 33-35. 3altimore: Univer-sity Park Press.
22. Elliott, T. B., and Brook, I. 1986. Ionizing radiation and infected wounds. In Abstracts of 86th Annual Meeting ofAmerican Society for Microbiology [#B123], 44. Washington, DC: American Society for Microbiology.
23. Brook, I.; Walker, R. I.; and MacVittie, T. J. 1986. Effect of radiation dose on the recovery of aerobic and anaerobicbacteria from mice. Can. J. Microbiol. 32: 719-722.
24. Wood, E. E.; Straus, D. C.; Johanson, W. G., Jr.; and Bass, J. A. 1981. Role of fibronectin in the prevention of adher-ence of Pseudomonas aeruginosa to buccal cells. I. Infect. Dis. 143: 784-790.
25. Porvaznik, M.; Walker, R. I.; and Gillmore, J. D. 1979. Reduction of the indigenous filamentous microorganisms inthe rat ileum following radiation. Scan. Electron Microsc. 3:13-22.
26. Walker, R. I.; Brook, I.; Costerton, J. W.; MacVittie, T. J.; and Myhal, M. L. 1985. Possible association of mucousblanket integrity with postirradiation colonization resistance. Radiat. Res. 104: 346-357.
82

Infectious Comnplications of Radiation lnjurv
27. Deitch, E. A., and Bridges, R. 1987. Effect of stress and trauma on bacterial translocation from the gut. 1. Surg. Res.42: 53b-542.
28. Brook, I.; Gilmore, J. D.; Coolbaugh, J. C.; and Walker, R. 1. 1983. Pathogenicity of encapsulated Bacteroides melanino-genicus group, Bacteroides oralis and Bacteroides rulMicoll in abscesses in mice. ]. Infect. 7: 218-22t,.
29. Reeves, D. S. 1986. The effect of quinolone antibacterials on the gastrointestinal flora compared with that of otherantimicrobials. ]. Antimicrob. Chemotlher. (Suppl. D) 18: 89-102.
30. Mulder, N. H.; Nieweg, H. W.; Sleijfer, D. T.; de-Vries-Hospters, H. G.; van der Waaij, D.; Fidler, B.; and van Saene, H.K. F. 1979. Infection prevention in granulocytopenic patients by selective decontamination of the digestivetract. In New Criteria for Antimicrobial Therapiy: Maintenance of Digestive Tract Colonization Resistance, edited byD. van der Waaij and J. Verhoef, 113-117. Amsterdam: Exerpta Medica.
31. Brook I.; Walker, R. I.; and MacVittie, T. 1. 1988. Effect of antimicrobial therapy on the gut flora and bacterialinfection in irradiated mice. lut. J. Radiat. Biol. 53: 709-716.
32. MacVittie, T. J.; Monroy, R. L.; Vigneulle, R.; Nold, J.; Patchen, M.; Zeman, G. Treatment of the radiation inducedhemopoietic syndrome in canines. Paper presented at the NATO Research Study Group 11, Lyon-Bron, France,October 20-23, 1986.
33. Ziegler, E. J.; McCutchan, A.; Fierer, J.; Glauser, M. P.; Sadoff, J. C.; Douglas, H.; and Braude, A. 1. 1982. Treatment ofgram-negative bacteremia and shock with human antiserum to a mutant Escherichia coli. N. Engl. 1. Med. 307:1225-1230.
34. Pollack, M. 1983. Antibody activity against Pseudonionas aeruginosa in immune globulins prepared for intravenoususe in humans. J. Infect. Dis. 147: 1090-1098.
35. Braude, A. I.; Ziegler, E. J.; and Douglas, H. 1985. Treatment of gram-negative bacteremia, endotoxemia, and shockwith antibody to core glycolipid. In The Pat/lop!ihysiologl of Combined hIjury and Trauma: Radiation, Burn, andTrauma, edited by R. I. Walker, D. F. Gruber, T. J. MacVittie, and J. J. Conklin, 201-208. Baltimore: UniversityPark Press.
36. Messerschmidt, O. 1976. Kombinationsscheaden als Folge nuklearer explosion. In vol. 4 of Chirurgie der Gegenwert,edited by R. Zenker, M. Deucher, and W. Schink, 1-102. Munich: Urban und Schwarzenborg.
37. Pruitt, B. A., Jr. Opportunistic infections in the severely injured patient. In reference 10, 53-77.
38. Shack, R. B. 1987. Factors affecting the success of antibiotic treatment of traumatic cutaneous wounds. Internal. Med.8:154-170.
RECOMMENDED READING
Hathorn, J. W.; Rubin, M.; and Pizzo, P. A. 1987. Empiric antibiotic therapy in the febrile neutropenic cancer patient:Clinical efficacy and impact of monotherapy. Antinicrob. Agents Chemother. 31: 971-977.
Walker, R. L.; Gruber, D. F.; MacVittie, T. J.; and Conklin, J. J., eds. 1985. The pathophysiology of combined injuru and tran ma:Radiation, burn, and trauma. Baltimore: University Park Press.
Gruber, D.; Walker, R. I.; MacVittie, T. J.; and Conklin, J. J., eds. 1987. The pathophysiology of combined injury and trauma:Management of infectious complications in mass casualty situations. New York: Academic Press.
83

MeIdicall CLiSt•ivietceCs t4 Nof Mic r WVarfazre
84

Chapter 6
BIOLOGICAL ASSESSMENTOF RADIATION DAMAGE
THOMAS L. WALDEN, Jr., Ph.D.* AND NUSHIN K. FARZANEH, M.S.**
INTRODUCTION
PHYSICAL SYMPTOMATOLOGY AT THE PRODROMAL STAGE
HEMATOLOGICAL DOSIMETERS
BLOOD SERUM DOSIMETERS
URINARY DOSIMETERS
CHROMOSOMAL DOSIMETERS
Cultured Peripheral Blood Lymphocyte TechniquePremature Condensed Chromosome TechniqueMicronuclei Technique
OTHER DOSIMETERS
Fluorometric ImmunoassayDetermination of Whole-Body Radionuclides
PROBLEMS
SUMMARY
*Rdato Bi ologist, Radiation Biochenistrly Department , Armed Forces Radiobiology Research Institute, Bethesda, Mar.yland 20814-5145
-Radiation Biologist, Radiation Biochemistry Department, Armed Forces Radiobiology Research Institute, Bethesda, Maryland 20814-5145
85

Al-th'od Cot)?ls•'q 'tt'cs of Nt.icar Warta rt,
INTRODUCTION
Biological ,hosipietry involves measuring a given the local and systemic levels. Biological indicatorsphysiological response to a known or estimated are diverse and may include changes in levels ofexposure dose of a toxin (in this case, ionizing ra- tissue enzvmes,'H' metabolites,'4 and cell popu-diation). Reliable biological dosimeters of radia- lations (such as lymphocytes2 `2 ' or sperm-');tion injury are needed (a) to perform casualty changes in individual behavior;""22 and a generaltriage, (1) to determine probable exposures when onset of malaise. 2 Both early and late re-phyisical dosineters (external indicators of radiation sponses to radiation injury may be reflected. Ele-that are used in the field) are absent, (c) to confirm vations in serum amylase levels may occur withinphysical dosimetry, and (d) to monitor the prog- hours to days,"' and elevated levels of lactate de-ress of radiotherapy. This chapter deals with bio- hydrogenase",2 ' or zinc protoporphyrin2 " are ob-logical dosimetrv relating to accidental exposure served several weeks after irradiation. The idealor nuclear warfare, rather than the clinical moni- biological dosimeter should be reliable, able to de-toring of radiotherapeutic progress, although tect 0.1-10.0 Gy, linear in response regardless ofsimilarities exist. The armed forces presently is- dose or quality of radiation, simple to use, pref-sue physical radiation dosimeters to groups rather erablv noninvasive, sensitive to radiation occur-than to individuals; shielding differences -nay af- ring during the first hours or days after exposure,fect individual doses. Variations in age, gender, and preferably radiation specific.health, and genetic background may greatly affect A combination of five indicators (Table 6-1)the biological responses to a given radiation dose. may provide a reliable gauge of radiation expo-Careful monitoring through biological dosimetry sure: (a) the physical symptomatology of the pro-can provide more reliable indicators of exposure, dromal stage of ARS, (b) lymphocyte numbers, (c)which will be used in formulating prognoses on serum components (diamine oxidase and serumtreatment and survival. amylase), (if) urinary components, and (e) chromo-
Damage from ionizing radiation occurs at both somal aberrations.
PHYSICAL SYMPTOMATOLOGY AT THE PRODROMAL STAGE
The most reliable method of biological dosi- ciated with exposure to radiation doses in themetry is the physical symptomatology at the pro- high-lethality (greater than 5.5 Gy) range (Table 6-dromal stage of ARS, 2 -4 which occurs within min- 3). These symptoms usually reflect an unfavor-utes to 1 day after irradiation and includes nausea, able prognosis for survival without adequate hos-vomiting, anorexia, diarrhea, and general malaise. pitalization and extraordinary lifesaving meas-The severity, duration, and time of onset of these ures, such as bone-marrow transplantation. 21 .2 4-2-symptoms are related to the dose and quality of At still higher radiation doses, even these meas-the radiation received. A dose-dependent latent ures would not be effective.period occurs between the end of the prodromal Erythema and epilation are two other indica-symptoms and the onset of later hematopoietic or tors of clinically significant radiation exposure.gastrointestinal complications (Table 6-2). The Erythema has a threshold of 3-4 Gy, depending ononset and latency are inversely related to the dose, the area of irradiated skin, with a median dose es-whereas the duration and severity are directly re- timate of 6 Gy.2 ";- Erythema occurs in two phases:lated and vary for individuals. The median acute an early phase, appearing within several to 24gamma radiation doses have been estimated for hours after irradiation, and a later "mainanorexia (0.97 Gy), nausea (1.4 Gy), fatigue (1.5 erythema," reappearing 2-3 weeks after irradia-Gy), vomiting (1.8 Gy), and diarrhea (2.3 Gy).-;2.2 tion and persisting for several weeks." ErythemaProtraction of the dose over 1 to 7 days results in also depends on the type of radiation and the skindoubling the median doses. condition. Epilation occurs approximately 2
Several early physiological responses are asso- weeks after radiation doses larger than 2-3 Gy."
86

Biological Assessment of Radiation Damage
TABLE 6-1
BIOLOGICAL INDICATORS OF RADIATION INJURY
SERUM URINE
Acid phosphatase Amino acids, particularly metabolites of tryptophan
Acid deoxyribonuclease AmylaseAmylase Beta-aminoisobutaric acidA-T phosphatase Creatine and creatinine
Beta-glucuronidase DeoxyribonucleaseBeta-galactosidlase HistamineCatalase Indoxy sulfateCalcium Nucleic acids (pseudouridine)
Diamine oxidase Prostaglandins
Factor XXII Taurine
Fluorescence and/or chemiluminescenceFree amino acids: SALIVA
phenylalanineleucine Albuminprolinetyrosine CELL COUNTS AND MORPHOLOGY
GlucoseHistamine Peripheral blood: reticulocyte, granulocyteImmunoglobulins (chromosome aberration-micronuclei test)Iron incorporation into erythrocytes Sperm
Lactate dehydrogenase Sperm abnormality
Lipids:triglycerides PHYSICAL PARAMETERSphospholipids Early transient incapacitationcholesterol
Lipoproteins ErythemaLysylaminopeptidase Prodromal stage symptoms: nausea, vomiting,Nucleic acids diarrheaPlasma-free hemoglobinPlasma-free haptoglobin ANALYSIS OF ACTIVATED ELEMENTSProstaglandinsZinc protoporphyrin Neutron exposure and/or activation in body tissues
HEMATOLOGICAL DOSIMETERS
Peripheral blood lymphocytes are extremely sure as determined from the lymphocyte counts.sensitive to ionizing radiation. They may suc- A lymphocyte count of 1,200-1,500/mm3 at 24cumb to interphase death after exposure to a dose hours after irradiation is a reduction of 50%. Itof only 0.05-0.15 Gy.34 The decrease in the num- indicates a potentially lethal exposure, requiringber of blood lymphocytes at 24-48 hours after irra- immediate medical attention.23 Monitoring for thediation can be a useful indicator of radiation expo- onset of hematological problems at the end of thesure (Table b-4)." "ý24 The radiation doses listed in latency period (which may last several weeks) isTable 6-4 are based on exposure to gamma radia- advised for persons whose lymphocyte counts re-tion, but the lethality patterns should be similar flect a lower but potentially lethal level of expo-for a neutron or mixed-field pure radiation expo- sure. Lymphocyte counts drop to zero in persons
87

Medical Consequences tOf Nuclear Warfarte
TABLE 6-2
TIME OF PRODROMAL STAGE AS A FUNCTION OFRADIATION DOSE*
Dose Onset Duration Latency
(Gy) (hours) (hours)
0.5-2.0 Absent to 6 <24 Absent or 3 weeks
2.0-3.5 2-6 12-24 2-3 weeks
3.5-5.5 1-2 24 1.0-2.5 weeks
>5.5 Minutes to 1 48 2-4 days
*With larger radiation doses, prodromal stage may persist until death
TABLE 6-3
EARLY SYMPTOMS AFTER HIGH-LETHALITY EXPOSURE*
ComaFeverDizzinessConvulsionDisorientationSevere headacheMild to severe hypotensionLymphocyte count 0-300 /mm'Severe fluid loss and/or electrolyte imbalance
*0-24 hours after exposure
88

Biological Assessment of Radiation Damage
14
10 Abteeta
12 300
2 NuWhik Lymphocye10
0 10 20 30 40 50 60Time (days)
Fig. 6-1. Estimated changes in human blood-cell numbers after irradiation with 3 Gy of gamma raysSource: used by permission, reference 77.
TABLE 6-4
LYMPHOCYTE COUNT IN HUMANS AT 24-48 HOURSAFTER RADIATION
Lymphocyte Count Dose Range Lethality
(xl000/mm3 ) (Gy) (%)
3.0 0-0.25
1.2-2.0 1-2 <5
0.4-1.2 2.0-3.5 <50
0.1-0.4 3.5-5.5 50-99
0-0.1 >5.5 99-100
89

Medical Consequences ot Nuclear Warfare
400
300 V.
0 2o0
100
012345 789 15
Fig. 6-2. Elevation of serum amylase levels in humans receiving fractionated radiotherapy. Four different fractionationprotocols were used: patients receiving 2 Gy /day (9 --- e); three fractions per day of 2 Gy, each fraction separated by 3-4 hours(e ... -- ); three fractions per day of I Gy, each separated by 3--4 hours (0 -- ); and two fractions per day of 2 Gy (e...• o),separated by 7-8 hours. Control values are represented by shaded region.Source: redrawn; used by permission, reference 2.
who received doses greater than 5.5 Gy. ture differentiated cells may continue to developGranulocytes, platelets, reticulocytes, and without other precursor cells differentiating to
erythrocytes are also affected by radiation (Figure take their place. This same process may be ob-6-1). In particular, lymphocyte and granulocyte served in the irradiated testes, where radiationcounts proved to be valuable biological dosime- exposure is followed by temporary aspermia.2•ters after the 1986 reactor accident in Chernobyl, The length of the latency period between theUSSR. 12 Blood cell effects may be detectable in radiation exposure and the decrease in blood cellhumans after exposure to 0.5-1.0 Gy of gamma numbers depends on the degree of damage and onradiation. These responses reflect interphase cell the normal lifetime of that particular class ofdeath and also the mitotic delay or destruction of blood cells. Human platelets have a life span ofthe hematopoietic stem cells of the bone marrow .31 4-5 days, and because they decrease by attritionHematopoietic depression may result either di- without replacement, hemorrhage will occur. Ra-rectly from radiation damage to the hematopoietic diation-induced mortality after a dose of 2-12 Gystem cells, or indirectly from damage to the results from hemorrhage and other hematopoieticstromal stem cells that are responsible for main- problems. These symptoms are called the hemato-taining the microenvironment of the bone mar- poietic subsyndrome. Physical examination androw. Hematopoietic precursor cells in later stages blood cell counts are readily obtainable, althoughof development are less sensitive to radiation other technologies may be too time consuming ordamage than are the stem cells. In an abnormal otherwise not presently feasible for large-scaleprocess called maturation-depletion, these more ma- field use.
90
SilallI i ni nlniin iInu 0 i i

Biological Assessment of Radiation Dalmage
o 300
.0.
0
000
200-e*0
1 00 / sense=..............o0 0 ..... ........................
I I I I I I I I0 4 8 12 16
Radiation Dose (Gv)
Fig. 6-3. Plasma levels of diamine oxidase in mice as a function of radiation dose. Plasma levels of diamine oxidase weredetermined in mice on day 4 after irradiation with either cobalt-60 gamma (__ - or fission neutron (*-*) radiation.Source: used by permission, reference 1.
BLOOD SERUM DOSIMETERS
Although a number of serum factors may be salivary glands (levels of pancreatic serum amy-useful biological dosimeters, none has received lase are not altered in response to radiotherapy).'widespread verification or acceptance. However, Interestingly, the elevation of serum amylase intwo show potential: serum amylase 2-1 and di- response to radiation has been reported only inamine oxidase (DAO).1" 3 Serum amylase (Figure humans; it cannot be reproduced in rodent re-6-2) becomes elevated in humans who receive ra- search models. 7 The effect of neutron radiation ordiotherapy when the parotid gland is included in of combined injury on the elevations of serumthe field of exposure.2 4 This response is an early amylase has not been determined.indicator of damage, and elevation can be seen DAO is another serum enzyme that is a poten-within hours after irradiation. Amylase levels in- tial biological dosimeter of radiation injury.'' 3
crease almost tenfold, peaking at 24-36 hours after DAO is produced primarily by intestinal villi dur-exposure to 1 Gy.2 A linear correlation exists for ing cell proliferation and differentiation. In hu-the peak serum elevation and the radiation dose mans, DAO levels have been used to monitor thereceived; the peak response occurs slightly earlier effects of chemotherapy on the gut, but the re-with increasing doses. 2,4 Radiotherapeutic frac- sponse following irradiation has not been deter-tionated doses of 1-2 Gy/day result in the further mined.34 Plasma levels of DAO (Figure 6-3) in-destruction of the parotid gland and a reduction crease in a dose-dependent manner in mice onin serum amylase by the end of the first week. days 2-4 following exposure to cobalt-60 gammaThe response depends on exposure of only the or neutron radiation.' This initial increase may
91
A1tdical CtOscq(i'L oi lt Nuhr Warfare
not be associated with gut damage but may reflect humans receiving radiotherapy, but results area more systemic injury.' If the human response is sometimes difficult to interpret because of interac-consistent with the mouse model, patients who tions between the chemotherapy, cancer, and longreceive radiotherapy that does not involve the gut fractionation schedules. Changes in the levels andshould have changes in DAO levels related to the classes of immunoglobulins in association withradiation exposure. The mouse model also indi- immunosuppression after radiotherapy do not ap-cates that the DAO response may not be reliable in pear to be useful in biological dosimetry.' Serumcombined injuries involving radiation and burns.' lactate dehydrogenase increases during the first
Other changes in serum enzymes have been week of radiotherapy, with even higher levels atreported; however, they are not as indicative as weeks 4-5 in a majority of patients, but these in-those in serum amvlase and DAO. Serum alkaline creases may be influenced by other factors, includ-phosphatase in rats decreases after irradiation in a ing infection.'' Levels of plasma hemoglobin anddose-dependent manner."' The decrease occurs haptoglobin increase up to 40'14, but not untilprimarily in the intestinal and liver isozymes, and week 4 of radiotherapy in cancer patients." Hap-may be useful for dosimetry on days 2-4 after irra- toglobin is produced by the liver and hemoglobindiation. The intestinal isozyne decreases on dav 3 is produced by hematopoietic precursors. The ele-bv 77'-; after a 5-Gy radiation dose, and by 90%; af- vation of hemoglobin is probably associated withter an 8-Gv dose. The responses of these isozymes recoverv of the hematopoietic system, and thein humans have not been confirmed. dose dependency (not yet determined) will be as-
Other serum indicators have been examined in sociated with increased delay of elevation.
URINARY DOSIMETERS
Lacking metabolic enzymes, urine provides after irradiation.'o Elevated taurine levels haverelatively stable biological indicators. It can also been reported in exposed humans,"' and may bebe obtained noninvasively. After irradiation, attributed to altered excretion patterns from kid-urine contains more creatine,"'•'-. histamine, ney damage, altered synthesis, and increased re-taurine,"' amylase, and prostaglandins.' lease from damaged tissues (particularly lym-
Postirradiation elevation of creatine occurs phoid tissue).""during the first 3 days after exposure of rats to less Glvcine and hydroxyproline are also excretedthan 0.25 Gv of X radiation.'" The average urinary in increased amounts (up to ten times normal lev-creatine-creatinine ratio during this period is dose els) in the urine of humans during the first weekdependent for 0.25-6.5 Gy. Creatinuria occurs in after receiving 25-180 rem."' Elevations of prosta-humans after irradiation, but because it may also glandins have been detected in the plasma of pa-be affected by exercise, muscular atrophy, trauma, tients receiving radiotherapy' 4 and in the urine ofor starvation,2 ý " it cannot be considered specific laboratory mice receiving cobalt-60 gamma radia-to radiation injury, tion or neu.on radiation.'
Elevations of histamine occur in the blood of The development of biological dosimetry kitspatients receiving radiotherapy. 2" The maximal based on urinalvsis would be hindered by (a)elevation of histamine in the urine of rats occurred biphasic responses, such as occur withon the first day after exposure to 9 Gy of cobalt-60 prostaglandins' and taurine;! (17) diurnal vari-gamma radiation.'- ations, as with creatine;17 (c) reductions in urinary
Taurine is an amino acid that is excreted in volume following irradiation;' and (d) problemslarge concentrations from rats in the first 3 days with 24-hour urine collection.
CHROMOSOMAL DOSIMETERS
Although the most widely used biological do- mosomal aberrations in human blood lympho--imeter of radiation injury is prodromal sympto- cytes.4 ' Such chromosomal analysis has been usedmatology as revealed by physical examination, the to determine the radiation doses received aftermost precise method is the determination of chro- industrial accidents," -41 the occupational expo-
92

Biological Assessmnent of Rahiat io Damage
10rA B C D EFG
I6 F .,#0*: Zf
0 0
0 I4
CU2p
0 t -
0 1 2 3 4 5Dose (Gy)
Fig. 6-4. Dicentric chromosome yield as a function of radiation dose. Yields of dicentricchromosome formation per 100 lymphocytes in metaphase are shown for the following condi-tions: (A) alpha radiation, (B) neutron radiation, (C) high-dlose-rate X radiation, (D) low-dose-rate gamma radiation, (E) high-dose-rate gamma radiation, (F) high-dose-rate gamma radia-tion, and (G) low-dose-rate gamma radiation. Differences between laboratories are apparent incomparisons of curves D and G showing low-dose-rate gamma radiation and of curves E andF showing high-dose-rate gamma radiation.kiurce: redrawn; used by permission from references 57 and 59.
93

Medical CmtLicq rcncc, o Niwc Icar Wartlrft
TABLE 6•-
COMPARISON OF CttROMOSUOMAL ASSAY SYSTEMS
Volume of blood Assay timeAssay Type required (ml) (hours) Lowest radiation dose
Phytohemagglutinin- 5.0 48 4.0 rads (X rays)stimulated peripheral 20.0 rads (gamma rays)blood lymphocytes 0.2 rads (neutrons)
Premature chromosomal 0.5 2 6.0 rads (X rays)condensation method (PCC)
Micronuclei technique 5.0 48 Linear:0-400 R (gamma rays)0-80 R (neutrons)
sures received by uranium miners,44 and the radia- somes contains two centromeres. The formationtion exposure of the atomic-bomb survivors of Hi- of dicentric chromosomes is linearly related to theroshima and Nagasaki.4 A correlation of chromo- radiation dose (Figure 6-4), although the responsesomal damage with the radiation dose has been may vary with the type of radiation (and also be-confirmed with in vitro experiments and with pa- tween laboratories))"-; These differences can betients receiving radiotherapy.4 6 Response curves seen in curves D (curvilinear) and G (linear) ofhave been prepared for the various types of radia- Figure 6-4, which are low-dose-rate gamma radia-tion (Figure 6-4), and for the three assay methods tion exposures from two laboratories.in use (Table 6-5): (a) cultured peripheral blood him- In addition, Figure 6-4 shows a difference be-phoc*ite tech nique 4,''-7 (b) premature chromosomal Con- tween high-dose-rate X radiation (C) and high-denwed chromo)some (PCC) technique,4•"' and (c) mni- dose-rate gamma radiation (E and F), although thecronuclei technique with lymphocytes or erythroid RBE for gamma and X radiation is usually similar.precursors.' 4 Irradiation with high-LET alpha particles (curve
A) or medium-LET neutrons (curve B) is moreCultured Peripheral Blood Lymphocyte damaging than irradiation with low-LET radia-Technique tion, such as X rays and gamma rays (curves C-G).
To assess the dose accurately, the type of radiationTypically, blood lymphocytes are nondividing must be known. Beta radiation exposure may pro-
cells that have progressed to the G, stage of the duce skin damage of medical consequence, but itcell cycle. They may be stimulated into mitosis would not be accurately reflected in this assay.with phytohemagglutinin. This culturing process An average assay requires one workday for arequires about 48 hours to obtain a sufficient num- trained technician to count about 10,000 lympho-ber of lymphocytes in mitosis, at which time the cytes to obtain 200 cells in metaphaseY•-5' Lowerchromosomes have become condensed and the radiation doses produce lower aberration yields,damage is visible. 40" The number of dicentric ab- and require that even more cells be counted forerrations, ring structures, or total number of aber- statistical accuracy. Several problems are associ-rations per mitotic cell are tabulated and recorded. ated with the standardization of this technique, in-Dicentric (Figure 6-5) and ring chromosomes are cluding variations in tissue culture conditions be-formed from asymmetrical interchromosomal ex- tween laboratories, the percentage of cells in firstchanges, in which one of the resulting chromo- mitosis at 48 hours, variations in health and age of
94

Biological Assessmnent of Radiation Damage
Centromere
• ~Chromosome breaks and rejoins
A B RadiationChromosomes FrB
RejoinedChromosome" A A
Dicentric Duplication-I- Fragments for Mitosis
Fig. 6-5. Formation of dicentric chromosomes. Dicentric chromosomes are formed when two chromosomal fragments (A andB), each containing a centromere, rejoin to form a new chromosome containing two centromeres. During mitosis, whenchromosomes are separated by spindle fibers attached to the centromere, the new chromosome may be pulled from each pole(in a different direction) and may fail to separate properly, stopping the mitotic process. Additional chromosomal informationis lost at this time in the fragments that do not contain centromeres and are unable to migrate to either pole.
persons examined, whole-body versus partial- mosomal aberrations using parallel image proc-body exposure, and radiation effects resulting essing,bb but the preparation of samples still re-from different types of radiation (low versus high quires a specialized laboratory and is not feasibleLET) and dose rates.47,4. - The normal inci- for a military or civilian field hospital.dence of chromosomal aberrations increases withthe increasing age of the individual and previous Premature Condensed Chromosome Techniqueexposure to carcinogens.-2
, The time interval atwhich the sample was collected after irradiation The PCC technique eliminates many of the in-can also affect the results because the damage may herent problems of mitotic peripheral blood lym-have a chance to repair.47 A program coordinated phocyte cultures.8-5 0 In this method, human lym-by the International Atomic Energy Agency found phocytes are fused to mitotic Chinese hamstera 15%-36% difference in the scoring of a standard ovary (CHO) cells using polyethylene glycol. Thetest sample among fourteen test laboratories.' A mitotic CHO cells cause the individual lympho-previous study found an eightfold difference, cyte chromosomes to condense and become vis-which was attributed mainly to differences in cul- ible.612 ,
3 After staining, the human chromosomesture conditions and in the time of first mitosis.56 5 and those from CHO cells will be different col-When all laboratories examined the same slides, ors. 2", 3 The damage is assessed by determiningthe differences were greatly reduced. A computer the number of human chromosomal fragments insystem has been applied to the analysis of chro- excess of the normal forty-six. Samples for PCC
95

Medical Consequte'nct ot Nuclear Warfare
80 4C
N
60 3CO
o, 40 0 7" 2 --3
I 30
Co20
0, I I I 0
0 5 10 15 20 25 30Time Postirradiation (days)
Fig. 6-6. Radiation-induced elevation of zinc protoporphyrin (ZPP) in mouse erythrocytes. ZPP (---) becomes elevated inmice receiving 5.5 Gy of X radiation. ZPP is measured by fluorescent detection from a drop of whole blood. Its elevationoccurs after irradiation in association with recovery of hematopoiesis, as indicated by an increase in the hematocrit level (-)at the same time. It may be possible to develop dedicated spectrofluorometers for other fluorescent biological indicators inblood.Source: used by permission, reference 29.
analysis require less than 2 hours for preparation Micronuclei Techniquetime, eliminate variations due to culture condi-tions, and may be analyzed quickly because 200 Micronuclei are chromosomal fragments thatlymphocytes with visible chromosomes are easier lack centromeres. As a result, they are not incor-to locate and count.48 ;.,6 As with chromosomal porated into the new nucleus during mitosis butaberration analyses of cultured lymphocytes, as- form a smaller satellite structure. As with othersay-sampling time after irradiation remains a con- chromosomal aberrations, the rate of micronucleicern, because repair can reduce the aberration formation depends on the dose rate and the LET.yield.41-1 The effects of dose rate, radiation qual- Therefore, neutrons have an RBE of 4.4 in mouseity, and LET on the reliablity of this technique bone-marrow cells compared to a lower RBE of co-have not been investigated, nor have the possible balt-60 gamrnma radiation.-' Micronuclei are easieralterations from combined injury. Future research to detect in the bone-marrow normoblasts becausemay focus on the development of a nuclease-free the micronuclei remain after the main nucleus hashomogenate from mitotic cells that will induce the been eliminated. Control values for this assay arepremature condensation of chromosomes. This about 1-2 micronuclei /1,000 cells, based on anwould eliminate the requirement of specialized average screening of 2,000 cells) 4 The assay maytissue-culture laboratories for fresh mitotic cells also be performed on mitotically stimulated pe-and would permit the development of a standard- ripheral blood lymphocytes, extending the analy-ized assa.y kit. Even with computer analysis, the sis time by the standard 48-hour culture period, orassay may still be too time consuming for use with it may be performed on cells obtained from amass casualties. bone-marrow transplant.
96

B ýicidlll l t ot Radhlfti Di g
OTHER DOSIMETERS
Fluorometric Immunoassay one antigen; they do not reflect both colors as donormal cells. This assay has been used on blood
Fluorometric assavs or immunoassavs have samples from the atomic-bomb survivors in ja-been developed for specific biological indicators pan1' and the more recent victims of the nuclear-present in blood or urine. During the late 19 70s, reactor accident in Chernobyl.7' The change in theincreased emphasis was seen in the So% iet litera- MN blood-group antigen occurs in the stem cellsture on fluorescent and chemoluminescent of the bone marrow, and its earliest appearance inchanges in blood cell and serum components after the recovering marrow will be 2-3 weeks after ir-irradiation .,7-7,' Fluorescent techniques permit the radiation. It would not be useful as an early triagedevelopment of dedicated fluorometers for use in indicator during the first few days.screening blood samples rapidly for changes inspecific components. Dedicated field-portablefluorometers are currentlv used bv the U.S. Public Determination of Whole-Body RadionuclidesHealth Service for detection of zinc protoporphy-rin (ZPP) from a drop of blood.7' Elevation of ZPP The degree of internal contamination fromis a diagnostic indicator for lead poisoning and for most radionuclides can also be determined by theiron deficiency anemia.-2 ZPP also becomes ele- use of physical dosimeters, such as whole-bodyvated in the blood of mice following whole-body radiation scanners. Iodine-131, a radioactive iso-exposure to ionizing radiation (Figure 6-6).2" This tope with a half-life of 8 days, is usually releasedelevation is associated with the recovery of the he- in large quantities after a nuclear accident or ex-matopoietic svstem at 10-18 days after irradiation, plosion. It is usually either inhaled or ingested. Itand is not observed in animals dying from the he- enters the food chain when it is deposited onmatopoietic subsyndrome. The elevation of ZPP grass, which is eaten by dairy cows who, in turn,occurs too late to be useful in general screening or produce milk for human consumption. Oncetriage; however, it may be feasible to develop a internalized, iodine-131 collects in the thyroid,field-portable dedicated fluorometer for other bio- where sufficient concentrations may lead to hypo-logical dosimeters. thyroidism, organ ablatement, or increased inci-
Immunoassav offers another promising tech- dence of thyroid cancer. The levels of iodine-131nique for field-dosimeter assay kits. A fluorescent can be determined with an external thyroid scan.immunoassay has been developed at the Law- A neutron dose can be calculated either byrence Livermore National Laboratorv to detect measuring the presence and concentration of so-changes in the determinants of the MN antigens dium-24 in the plasma or by using a whole-bodylocated on the surface of red blood ceils.7 ,14 The scan. Exposure to neutrons results in the conver-M and N blood-group antigens are heterozygous sion (neutron activation) of sodium-23 (the nonra-forms of glycophorin A. Like those antigens of the dioactive, abundant isotopic form of sodium) toAB blood group, persons may be homozygous sodium-24. Sodium-24 is a radioactive isotopeMM or NN, heterozygous MN, or hemizygous NO with one more neutron than sodium-23. It has aand MO. The general population is predomi- half-life of 15 hours and decays to nonradioactivenantlv MN, and MN-antibodv-labeled human magnesium-24, releasing both beta and character-blood cells fluoresce red and green when exposed istic gamma radiation. Sodium-24 should be de-to laser light. Blood cells from MN-heterozygous termined from plasma samples rather than fromhumans exposed to ionizing radiation have a whole blood, because it appears mainly in plasmagreater variant frequency or proportional altera- rather than in red cells.7" The presence of sodium-tion in the MN blood antigen (MM, NN, MO, 24 above background levels indicates a neutronNO) .- These abnormal cells (nonheterozygous) exposure,7j and the radiation dose can be calcu-fluoresce red or green, reflecting the presence of lated from the levels of sodium-24 present.
PROBLEMS
Problems exist in the use of biological dosime- bined-injury situations.2 .47 4'""0 For example, theters, including their potential unreliability in com- value of a lymphocyte count becomes question-
97

Medaial Gseqeccs 'f Nof idhar War fare
able in a combined injury involving infection or RBE of 18 compared with X radia-burn. Additional problems include the following: tion for the production of dicentric
"* Collection, contamination, stability, chromosomal aberrations.r7 Theand reproducibility of the sample possibility exists for a significant
"* Variable changes in a biological re- error in measurement if the type ofsponse, according to the dose of radiation or proportion of mixed-radiation received and the time field radiation is not known.)elapsed between exposure and Many of these problems might be overcome byexamination using more than one biological indicator (for ex-
"• Length of time required for assay ample, using one as a screening agent and another(48-72 hours for some chromosomal as confirmation). Lymphocyte and granulocyteanalyses), which makes its feasibil- cell counts, combined with chromosomal aberra-ity for field use questionable tion assays, provided biological dosimetry for the
"* Lack of an appropriate research Chernobyl patients, in order to minimize the unre-model system (Some biological liability from burn indicators alone.)2 Biologicalchanges observed after radiation ex- indicators for use during different time periods af-posure in humans, such as serum ter irradiation need to be identified. For example,amylase, do not occur in laboratory one set would be used at 1-3 days and another setanimals.) at 1-2 weeks after exposure. Indicators from the
"* Radiation variables: dose, dose rate, different status groupings in Table 6-6 should bequality, type, and mixed-radiation used jointly to provide a more complete picture offields (Fission neutrons have an the damage and the biological response.
SUMMARY
The levels of a number of biological com- search needs to address the detection of immuno-pounds become altered in body tissues after radia- suppressive factors that are released in blood andtion exposure. These changes occur (a) as a direct tissue fluids after injury.result of the radiation damage, or (b) in response The most reliable indicator for mass casualtiesto mobilization for repair, regeneration, and cell is the characterization of early symptoms of theproliferation. In some cases, the degree of altera- prodromal stage of ARS: nausea, vomiting, andtion is proportional to the dose of radiation, and diarrhea. Greater accuracy may be obtained withthose degrees may serve as diagnostic aids in the a lymphocyte chromosomal analysis that can de-triage of casualties and in the monitoring of radio- tect radiation exposure as low as 0.03-0.06 Gy.therapy. With the exception of neutron activation However, this procedure must be performed by aof the elements in tissues, none of the biological tissue culture laboratory, and it is time consum-indicators is unique to radiation injury. ing. Table 6-6 shows biological indicators of post-
Several problems are associated with the use of irradiation damage in patients. For instance,most biological dosimeters, particularly in a mass- blood-cell counts may indicate the need for acasualty situation. Many biological indicators bone-marrow transplant, but indicators of guthave not been completely characterized in hu- status may show possible gastrointestinal cellmans. In addition, many indicators (including death, which would contraindicate the transplant.lymphocyte counts) may not be reliable with inju- Two serum enzymes, amylase and diamine oxi-ries involving radiation combined with burn or dase, show promise as biological dosimeters.infection. Combinations of nonlethal doses of ra- Each has drawbacks: the salivary glands must bediation, burn, or infection may result in mortal- in the field of exposure for elevations of serumity.2" Immunosuppression induced by radiation amylase to occur, and the response of DAO hasexposure may increase the likelihood of succumb- not been characterized in irradiated humans.ing to infection or neoplasm,7
7 and the degree of Portable fluorometers for specific biological com-immunosuppression is an important prognostic pounds and the development of specific immunol-indicator. At present, we have no reliable meas- ogical assays also hold promise for the future ofurement of that degree (Table 6-6). Future re- biological dosimetry.
98

Biological Assessment of Radiation Damage
TABLE 6-6
BIOLOGICAL INDICATORS OF POSTIRRADIATIONDAMAGE IN PATIENTS
DOSE-RESPONSIVE CLINICAL INDICATORSProstaglandins (?)
Diamine oxidase (?)
Serum amylase
STATUS OF BONE MARROWGranulocytes
PlateletsReticulocytopenia
INTESTINAL INJURYDiarrheaBloody stoolDiamine oxidase
DIRECT CELLULAR DAMAGELymphocytes
Cytogenetics
IMMUNOSUPPRESSIONUnknown
REFERENCES
1. DeBell, R. M.; Ledney, G. D.; and Snyder, S. L. Quantification of gut injury with diamine oxidase activity: Develop-ment of a fission neutron RBE and measurements with combined injury in mouse models. Radiat. Res., in press.
2. Becciolini, A.; Porciani, A.; Lanini, A.; Chiavacci, A.; and Cellai, E. 1987. Effects of irradiation with conventional and
multiple daily fractionation on serum amylase activity. Acta Oncologica 26:139-142.
3. Tomassi, I.; Balzi, M.; Cremonini, D.; Becciolini, A.; Giannardi, G.; and Pelu, G. 1979. Radiation effects on the parotidgland of mammals. Part 3. Behavior of enzyme activity after irradiation. Strahlentherapie 155: 570-573.
4. Becciolini, A.; Giannardi, G.; Cionini, L.; Porciani, S.; Fallai, C.; and Pirtoli, L. 1984. Plasma amylase activity asbiochemical indicator of radiation injury to salivary glands. Acta Radiol. [Oncol.] 23: 9-14.
5. Chen, W.; Kereiakes, J. G.; Silberstein, E. B.; Aron, B. S.; and Saenger, E. L. 1973. Radiation induces changes in serumand urinary amylase levels in man. Radiat. Res. 54:141-151.
6. Van Den Brenk, H. A. S.; Hurley, R. A.; Gomez, C.; and Richter, W. 1969. Serum amylase as a measure of salivarygland radiation damage: Hyperamylasaemia following fractionated exposure to 4 MV x-rays delivered in highpressure oxygen. Br. 1. Radiol. 42: 688-700.
99

Medical C on• qleicts of Niclh'ar Wartiare
7. Becciolini, A.; Balzi, M.; Cremonini, D.; Tomassi, 1.; Giannardi, G.; and Pelu, G. 1980. Radiation effects on the parotidgland of mammals. Part 4. Biochemical and morphological changes after local irradiation. Straldentherapie 156:bt-72.
8. Kashima, H. K.; Kirkham, W. R.; and Andrews, R. J. 19t)5. Postirradiation sialadenitis: A study of the clinical features,histopathologic changes and serum enzyme variations following irradiation of human salivary glands. Amer. ].RoenNen. 94: 271-291.
9. Vranovska, J.; Popisil, J.; and Dienstbier, Z. 1477. Changes of the activity of certain lysosomal enzymes in the bloodserum of whole-body irradiated rats. Strahdentherapie 153: 49t,-500.
10, Highman, B., and Hanks, A. R. 1470. Serum alkaline phosphatase in rats after 800 R whole-body or regional X-irradiation. Proc. Soc. Fxp. Biol. Med. 133: 1201-1206.
11. Horvath, M.; Rode, I. L.; Kralovanszkv, J.; and Volant, M. 1980. Investigation of a valuable biochemical indicator inradiotherapy. Ill. Serum lactate dehydrogenase enzyme level on irradiation of cancer patients. Strahlentherapie1 b: 244-247.
12. Stepan, J.; Havranek, T.; and Jojkova, K. 1977. Serum alkaline phosphatase as indicators of radiation damage in rats.Radiat. Res. 70: 406-414.
13. Ely, M. J.; Speicher, J. M.; Catravas, G. N.; and Snyder, S. L. 1985. Radiation effects on diamine oxidase activities inintestine and plasma of the rat. Radiat. Res. 103:158-162.
14. Tanner, N. S. B.; Stamford, 1. F.; and Bennett, A. 1981. Plasma prostaglandins in mucositis due to radiotherapy andchemotherapy for head and neck cancer. Br. 1. Cancer 43: 767-771.
15. Steel, L. K.; Rafferty, M. A.; Wolfe, W. W.; Egan, J. E.; Kennedy, D. A.; Catravas, G. N.; Jackson, W. E., Ill; and Dooley,M. A. 1986. Urinary excretion of cyclic nucleotides, creatinine, prostaglandin E,, and thromboxane B, frommice exposed to whole-body irradiation from an enhanced neutron field. Int. J. Radiat. Biol. 50: 695-71-5.
16. Abe, M.; Takahashi, M.; Takeuchi, K.; and Fukuda, M. 1968. Studies on the significance of taurine in radiation injury.Radiat. Res. 33: 563-573.
17. Donlon, M. A.; Helgeson, E. A.; Lambright, K. T.; and Catravas, G. N. 1981. Increased urinary excretion of histamineby rats following gamma radiation. Fed. Proc. 42: 1124.
18. Gerber, G. B.; Gertler, P.; Altman, K. I.; and Hemplemann, L. H. 1961. Dose dependency of radiation-inducedcreatine excretion in rat urine. Radiat. Res. 15: 307-313.
19. Gerber, G. B.; Gerber, G.; Kurohara, S.; Altman, K. I.; and Hemplemann, L. H. 1961. Urinary excretion of severalmetabolites in persons accidentally exposed to ionizing radiation. Radiat. Res. 15: 314-318.
20. Lasser, E. C., and Stenstrom, K. W. 1954. Elevation of circulating blood histamine in patients undergoing deeproentgen therapy. Amer. ]. Roentgen. 72: 985-988.
21. Young, R. W. 1987. Acute radiation syndrome. In Military RadiobioloýVj, edited by J. J. Conklin and R. I. Walker, 165-190. Orlando, FL: Academic Press.
22. Hunt, W.A. Effects of ionizing radiation on behavior and the brain. In reference 21, 321-330.
23. Conklin, J. J., and Walker, R. I. Diagnosis, triage, and treatment of casualties. In reference 21, 231-240.
24. Messerschmidt, 0. 1979. Medical procedures in a nuclear disaster. Munich: Verlag Karl Thiemig.
25. Nuclear Regulatory Commission. 1985. Health effects model for nuclear power plant accident consequences analysisINUREG/CR-4214, Sandia No. SAND85-7185). Washington, DC: U.S. Government Printing Office.
26. Clifton, D. K., and Bremner, W. J. 1983. The effect of testicular X-irradiation on spermatogenesis in man. ]. Androl. 4:387-392.
100

Biological Assessment of Radiation Damnage
27. Lushbaugh, C. C.; Hubner, K. F.; and Fry, S. A. 1982. The impact of estimates of human radiation tolerance uponradiation emergency management. In The Control of Exposure of the Public to Ionizing Radiation in the Event ofAccident or Attack. Proceedings of Symposium, April 1981, 46-57. Washington, DC: National Council onRadiation Protection and Measurements.
28. Altman, K. 1. 1971. Criteria for the evaluation and selection of radiation-induced metabolic changes as biochemicalindicators of radiation damage. In Biochemical Indicators of Radiation Injury in Man, edited by K. 1. Altman, 1-9.Vienna: International Atomic Energy Agency.
29. Walden, T. L., Jr.; Draganac, P. S.; and Farkas, W. R. 1984. The elevation of blood levels of zinc protoporphyrin inmice following whole body irradiation. Blood 63:1159-1167.
30. United Nations Scientific Committee on the Effects of Atomic Radiation. 1982. Ionizing radiation: Sources and biologicaleffects 11982 Report to the General Assembly]. New York: United Nations.
31. National Council on Radiation Protection and Measurements. 1974. Radiological factors affecting decision-making in aulclear attack [NCRP Report 421. Washington, DC: National Council on Radiation Protection and Measure-
ments.
32. Gale, R. P. 1987. Immediate medical consequences of nuclear accidents. Lessons from Chernobyl. JAMA 258: 625-628.
33. Department of Defense. 1962. Characteristics of acute whole body radiation injury. In The Effects of Nuclear Weapons,edited by S. Glasstone, 592-597. Washington, DC: U.S. Atomic Energy Commission.
34. Luk, G. D.; Vaughan, W. P.; Burke, P. J.; and Baylin, S. B. 1981. Diamine oxidase as a plasma marker of rat intestinalmucosal injury and regeneration after administration of 1-B-D-arabinofuranosylcytosine. Cancer Res. 41: 2334-2337.
35. Rode, I.; Horvath, M.; Petranyi, J.; and Kiss, B. 1979. Investigation of a valuable biochemical indicator in radiother-
apy. I. Immunological tests and reticulocyte number. Strahlentherapie 155: 387-391.
36. Horvath, M.; Geszti, 0.; Benedek, E.; Farkas, J.; and Reischi, G. 1979. Investigation of a valuable biochemical indica-tor in radiotherapy. I1. Plasma free hemoglobin and haptoglobin level changes. Strahlentherapie 155: 579-583.
37. Woo, J.; Treuting, J. J.; and Cannon, D. C. 1979. Metabolic intermediates and inorganic ions. In vol. 1, ClinicalDiagnosis and Management, edited by J. B. Henry, 262-264. Philadelphia: W. B. Saunders Co.
38. Katz, E. J., and Hasterlik, R. J. 1955. Aminoaciduria following total-body irradiation in the human. INCI 15:1085-1105.
39. Abe, M.; Takahashi, M.; Takeuchi, K.; and Fukuda, M. 1968. Studies on the significance of taurine in radiation injury.Radiat. Res. 33: 563-573.
40. Bender, M. A., and Gooch, P. C. 1962. Types and rates of X-ray-induced chromosome aberrations in human bloodirradiated in vitro. Proc. Nat!. Acad. Sci. USA 48: 522-532.
41. Popescu, H. L.; Pilat, L.; Hilt, M.; and Lancranjan, 1. 1972. Evolution of biological changes noticed in three cases ofaccidental mild gamma irradiation. I. Occup. Med. 14: 317-320.
42. EI-Alfi, 0. S.; Ragab, A. S.; and Eassa, E.-H. M. 1967. Detection of radiation damage in exposed personnel bychromosome study. Br. I. Radiol. 40: 760-764.
43. Dolphin, G. W.; Bolton, D.; Humphreys, 0. L. 0.; Speight, D. L.; and Stradling, G. N. 1970. Biological dosimetry andphysical dosimetry after a radiation accident. Nature 227:165.
44. Brandom, W. F.; Saccomanno, G.; Archer, V. E.; Archer, P. G.; and Bloom, A. D. 1978. Chromosome aberrations as abiological dose-response indicator of radiation exposure in uranium miners. Radiat. Res. 76:159-171.
101

Medical Conseqiiences of Nnclear Warfare
45. Randolph, M. L., and Brewen, J. G. 1980. Estimation of whole-body doses by means of chromosome aberrationsobserved in survivors of the Hiroshima A-bomb. Radiat. Res. 82: 393-407.
46. Schmid, E.; Bauchinger, M.; Bunde, E.; Ferbert, H. F.; and v. Lieven, H. 1974. Comparison of the chromosomedamage and its dose response after medical whole-body exposure to Co-60 gamma-rays and irradiation ofblood in vitro. Init. 1. Radiat. Biol. 26: 31-37.
47. Liniecki, J.; Bajerska, A.; and Wyszynska, K. 1983. Dose-response relationships for chromosome aberrations inperipheral blood lymphocytes after whole- and partial-body irradiations. II. Decline of aberration-carryingcells in blood with time post exposure. Mutat. Res. 110: 103-110.
48. Pantelias, G. E., and Maillie, H. D. 1985. Direct analysis of radiation-induced chromosome fragments and rings inunstimulated human blood lymphocytes by means of the premature chromosome condensation technique.Mutat. Res. 149: 67-72.
49. Cornforth, M. N., and Bedford, 1. S. 1983. X-ray-induced breakage and rejoining of human interphase chromosomes.Science 222: 1141-1143.
50. Waldren, C. A., and Johnson, R. T. 1974. Analysis of interphase chromosome damage by means of prematurechromosome condensation after X- and ultraviolet-irradiation. Proc. Natl. Acad. Sci. USA 71:.1137-1141.
51. Reddy, M. M.; Goh, K. 0.; and Hemplemann, L. H. 1980. Induction of micronuclei in PHA-stimulated humanlymphocyte cultures by therapeutic radiation. Experientia 36: 343-344.
52. Jessen, D., and Ramel, C. 1978. Factors affecting the induction of micronuclei at low doses of X-rays, MMS, and
dimethylnitrosamine in mouse erythroblasts. Mutat. Res. 58: 51-65.
53. Schmid, W. 1975. The micronuclei test. Mutat. Res. 31: 9-15.
54. Garriott, M. L., and Grahn, D. 1982. Neutron and gamma-ray effects measured by the micronucleus test. Mutat. Res.105:157-162.
55. Moorhead, P. S.; Nowell, P. C.; Mellman, W. J.; Battips, D. M.; and Hungerford, D. A. 1960. Chromosome prepara-tions of leukocytes cultured from human peripheral blood. Exp. Cell Res. 20: 613-616.
56. Bianchi, M.; Bianchi, N. 0.; Brewen, J. G.; Buckton, K. E.; Fabry, L.; Fischer, P.; Gooch, P. C.; Kucerova, M.; Leonard,A.; Mukherjee, R. N.; Mukherjee, U.; Nakai, S.; Natarajan, A. T.; Obe, G.; Palitti, F.; Pohl-Ruling, J.; Sch-warzacher, H. G.; Scott, D.; Sharma, T.; Takahashi, E.; Tanzarella, C.; and van Buul, P. P. W. 1982. Evaluationof radiation-induced chromosomal aberrations in human peripheral blood lymphocytes in vitro. Mutat. Res. 96:233-242.
57. Vulpis, N.; Tognacci, L.; and Scarpa, G. 1978. Chromosome aberrations as a dosimetric technique for fission neutronsover the dose-range 0.2-50 rad. Int. J. Radiat. Biol. 33: 301-306.
58. Dolphin, G. W., and Lloyd, D. C. 1974. The significance of radiation-induced chromosome abnormalities in radio-logical protection. J. Med. Genet. 11: 181-189.
59. Hacker, U.; Schumann, J.; and Gohde, W. 1982. Mammalian spermatogenesis as a new system for biologic dosimetryof ionizing irradiation. Acta Radiol. [Oncol.] 21: 349-351.
60. Takahashi, E.; Hirai, M.; Tobari, L.; Utsugi, T.; and Nakai, S. 1982. Radiation-induced chromosome aberrations inlymphocytes from man and crab-eating monkey. Mutat. Res. 94:115-123.
61. Das, B. C., and Sharma, T. 1983. Blood lymphocyte culture system: Quantitative analysis of X-ray-induced chromo-some aberrations in man, muntjac, and cattle. Mutat. Res. 110:111-139.
62. Maillie, H. D.; Baker, J. V.; Quinn, B. R.; and Fugo, E. D. 1986. Measuring damage to human lymphocytes in vitroafter low-level radiation exposure using prematurely condensed chromosomes. Health Phys. 51: 672-676.
102

Biological Assessment of Radiation Danuage
63. Pantelias, G. E., and Maillie, H. D. 1984. The use of peripheral blood mononuclear cell prematurely condensedchromosomes for biological dosimetry. Radiat. Res. 99:140-150.
64. Bloom, A. D. 1972. Induced chromosomal aberrations in man. In vol. 3, Advances in -lu man Genetics, edited by H.Harris and K. Hirschhorn, 99-173. New York: Plenum Press.
65. Van Buul, P. P. W., and Natarajan, A. T. 1980. Chromosomal radiosensitivity of human leukocytes in relation tosampling time. Mutat. Res. 70: 61-69.
66. Bille, J.; Scharfenberg, H.; and Manner, R. 1983. Biological dosimetry by chromosome aberration scoring withparallel image processing with the Heidelberg POLYP polyprocessor system. Comiput. Biol. Med. 13: 49-79.
67. Barkan, S., and Safronova, V. G. 1979. Investigation of intensity of ultraviolet fluorescence of leukocytes and bonemarrow cells during chronic exposure to radiation. Radiobiologiia 14: 275-278.
68. Baraboi, V. A.; Orel, V. Z.; Sribnaia, A. F.; and Tatsii, I. A. 1978. Mechanism of early postirradiation changes inintensity of spontaneous chemoluminescence of blood serum. Radiobiologiia 18: 305-309.
69. Serkiz, Y. I.; Ryabova, E. Z.; and Chebotarev, E. E. 1975. Spontaneous and induced luminescence of blood serum asan index of the degree of radiation damage to animals. Radiobiologiia 15: 716-721.
70. Serkiz, Y. A.; Kovtun, T. V.; Ryabova, E. Z.; and Chebotarev, E. E. 1977. Chemoluminescence of alpha- and beta-lipoproteins of blood plasma of rats exposed to fast neutrons. Radiobiologiia 17: 803-806.
71. Grunder, F. I., and Moffitt, A. E., Jr. 1979. Evaluation of zinc protoporphyrin in an occupational environment. Am.Ind. Hig. Assoc. 1. 40: 686-694.
72. Lamola, A. A., and Yamane, T. 1974. Zinc protoporphyrin in the erythrocytes of patients with lead intoxication andiron-deficiency anemia. Science 186: 936-938.
73. Edwards, M. 1987. Chernobyl: One year after. Natl. Geographic 171: 633-653.
74. Langlois, R. G.; Bigbee, W. L.; Kyoizumi, S.; Nakamura, N.; Bean, M. A.; Akiyama, M.; and Jensen, R. H. 1987.Evidence for increased somatic cell mutations at the glycophorin A locus in atomic bomb survivors. Science236: 445-448.
75. Mole, R. H. 1984. Sodium in man and the assessment of radiation dose after criticality accidents. Phys. Med. Biol. 29:1307-1327.
76. Conklin, J. J.; MacVittie, T. J.; and Walker, R. I. 1985. Pathophysiology of combined injury and trauma: An overview.In The Pathophysiology of Combined Injury and Trauma, edited by R. I. Walker, D. F. Gruber, T. J. MacVittie, and J.J. Conklin, 3-10. Baltimore: University Park Press.
77. Anderson, R. E., and Warner, N. L. 1976. Ionizing radiation and the immune response. Adv. Immunol. 24: 215-335.
103

Medltical Conspienttt"s of Nuclear Warfare
104

Chapter 7
BEHAVIORAL ANDNEUROPHYSIOLOGICAL CHANGESWITH EXPOSURE TOIONIZING RADIATIONG. ANDREW MICKLEY, Ph.D.,' VICTOR BOGO, M.A.," and BRUCE R. WEST, M.S.***
INTRODUCTION
BEHAVIORAL CHANGES IN IRRADIATED ANIMALS
Learning and MemoryCognitive Performance TasksMotor Performance TasksNaturalistic Behaviors
COMBINED INJURIES
EARLY TRANSIENT INCAPACITATION AND OTHER EARLY PERFORMANCE DEFICITS
Task ComplexityRadiation DoseRadiation Dose RateRadiation Quality
THE NEUROPHYSIOLOGICAL BASIS OF PERFORMANCE DECREMENTS
Sensory and Perceptual ChangesRadiation-Induced Changes in the Nervous SystemRadiogenic Pathology of the Nervous SystemAlterations in Nervous System Function
THE HUMAN EXPERIENCE WITH RADIATION
RADIATION-INDUCED CHANGES IN MILITARY PERFORMANCE
RADIOPROTECTION AND BEHAVIOR
Radioprotectants that Reduce MortalityEfficacy of AntiemeticsShieldingBone-Marrow FactorsRadiation in Space
SUMMARY
*Lieutenant Colonel, United States Air Force; Armed Forces Radiobiology Research Institute. Bethesda, Maryland 20814-5145**Armed Forces Radiobiology Research Institute, Bethesda, Mareland 20814-5145***Major, Uni!ed States Army; Human Response Officer, Radiation Policy Division, Defense Nuclear Agency, 6801 Telegraph Road, Alexandria,Virginia 22310-3398
105

Mediatl ConsteqIuetwts of Nuchlar Wirfaire
INTRODUCTION
The use of nuclear weapons in military conflicts rely on animal research.will significantly challenge the ability of the armed However, animal research brings with it prob-forces to function. The thermal and overpressure lems of extrapolation. While the relevance of animalstresses of conventional weapons will be signifi- models to human behavior has been frequentlycantly intensified during a nuclear battle. In addi- shown in the study of toxic effects of ionizing radia-tion, military personnel will have to contend with tion,-'- different species (even strains within species)the hazards of exposure to ionizing radiation, which may have different responses or sensitivities to ra-will be the main producer of casualties for nuclear diation exposure.4 It is important to understand theweapons of 50 kt or less. Present projections of nu- specific radiosensitivity of the animal model so thatclear combat operations suggest that between one- the radiation dose required to produce a similar ef-half and three-quarters of the infantry personnel tar- fect in humans can be reasonably estimated. For ex-geted by a tactical nuclear weapon would receive an ample, in humans the lethal dose for 50% of cases af-initial radiation dose of 1.5-30.0 Gy.' This acute ter 30 days (LD,,•) is 4.5 Gy, whereas in monkeysdose of ionizing radiation could dramatically affect a the LD,0/•, is 6.0 Gy. Similarly, the monkey is moresoldier's ability to complete combat tasks success- radiosensitive than the rat (LD 1,,,/, = 7.5 Gy) or thefully. This, in turn, may ultimately affect the out- mouse (LD,;,/ 3t = 9.0 Gy). ," Clearly, these classiccome of the armed conflict. LD:/3, values are estimates, because they will vary
Information about the consequences of ionizing with the animal strain, housing conditions, andradiation may be derived from the following: (a) the other factors. However, the values do give a sensenuclear detonations over Hiroshima and Nagasaki, of the relative radiosensitivity of the animal models(b) clinical irradiations, (c) nuclear accidents, and (d) most often used in radiation research, and will helplaboratory animal research. Each of these sources to put into context the radiation doses cited in thishas certain constraints. The Hiroshima and chapter.Nagasaki data are of limited value since there was Variations in radiosensitivity must also be con-no scientific assessment of behavior, and the reports sidered when measuring animal behavior. For in-were anecdotal, often conflicting, and not easily tied stance, at specific doses or dose rates, most animalto specific radiation doses. Clinical irradiations are models show a rapid, transient decrease in perform-also of questionable value because precise measures ance; however, this is not true for some dog orof behavior are not usually recorded, and patients mouse strains. 7-' Differences in CNS sensitivity toare behaviorally compromised by their illnesses or radiation have also been shown. The primate brainthe chemical therapy being used. Nuclear accidents may be more sensitive to radiation damage than thehave been few, and little behavioral information has rat brain." Although differing sensitivities of animalbeen obtained from those that have occurred. Al- strains can be enigmatic, they can be meaningful re-though information on human radiation exposure is search tools that reveal physiological substrates ofnormally preferred, the paucity of data forces us to natural radioresistance.'
BEHAVIORAL CHANGES IN IRRADIATED ANIMALS
Radiation has significant effects on a variety of plest form, learning is reflected by a linkage of abehavioral factors, including learning, performance, stimulus and a response. However, performanceand naturalistic and social behaviors. However, this also depends on the organism's capacity to make alist is not a complete taxonomy of behavior. For ex- response. Thus, postirradiation changes in behaviorample, performance can be somewhat arbitrarily may reflect deficits in either performance or learningseparated into tasks having a strong cognitive com- (or both). Psychologists consider these concepts toponent and tasks having a strong motor component. be distinct, but in some cases it is difficult to sepa-Also, an important distinction can sometimes be rate them, especially in animal studies. Whether themade between learning and performance. In its sim- mechanism of radiogenic behavioral change is based
106

Bchi,ioral and Neirophtysiological Ch/illt's with Ex sIiUrt' to Iot'iZing, Pi Radiatio
on deficits in learning, attention, retrieval, capacity memory, and the data agree with others suggestingto perform, or group disturbance, any of these dis- that radiogenic disruptions in behavior may notruptions can potentially determine an organism's merely reflect nonassociative factors."'ability to function in a nuclear environment. Human memory may also be impaired bv radia-
tion exposure. For instance, a few cases of acuteretrograde amnesia were reported by persons who
Learning and Memory survived the bombing of Hiroshima.'" Five years af-ter the attack, deficits in memory and intellectual
Pavlovian conditioning paradigms are especially capacity were noted in persons experiencing radia-useful in distinguishing between learning and per- tion sickness." These data seem consistent with theformance in animals. Studies suggest that learning Soviet studies reporting memory deficits in patientscan be altered by exposure to ionizing radiation. For who had undergone therapeutic irradiations."example, rabbits were conditioned to associate a However, although the human data corroborate thelight-and-tone stimulus with the respiratory reflex of animal studies, they suggest that memory impair-apnea that is produced by the inhalation of ammo- ments may have been strongly influenced by thenia vapor." Exposure to 15 Gy of cobalt-60 gamma other stressors of war or illness.radiation resulted in the absence or considerable re- Improved or unaltered learning capacity or per-duction of conditioned apnea. In contrast, the un- formance after exposure to radiation has been re-conditioned apnea (normal response to ammonia ported. For instance, although radiation caused ainhalation) was enhanced after irradiation, suggest- dose-dependent decrease in monkey activity anding that the animal's performance capacity was still appetite, animals showed no loss of ability to solveintact. These classical conditioning data suggest that "even the most complex learning problems" at doses(at least under the stated circumstances) radiation of 2-10 Gy of X radiation.2"' Task performance wasexposure can alter memory, and that this function is actually enhanced in some studies after 6.5 or 10 Gyseparate from the animal's performanrce. of X rays.2' This enhancement may have been due to
Experiments using operant techniques may also decreased general activity and lowered distractibil-be designed to allow some distinction between ity.22-2 In fact, performance and learning may havelearning and performance. If a task can be selected been better in the irradiated animals because the ra-in which a learning deficit is represented in a more diation exposure acted as a mild sedative, thus re-rapid or vigorous response, then it may be possible ducing anxiety and distractions.2 " After exposure toto rule out lethargy or reduced physical capacity as several types of radiation, some animals showed su-the primary mediator of a behavioral change. For perior learning when a premium was placed on pay-example, rats were trained to stay in a lighted area ing attention to the site of a food reward, althoughin order to avoid footshock in the adjacent dark area, their performance was worse on tasks requiring at-which they normally preferred."' The latency of the tention to peripheral stimuli.2- In a series of difficultsubject's movement from the safe, lighted area to the discrimination-learning problems, the performanceelectrified dark side was an indicator of learning, of monkeys exposed to 3.5 Gy of mixed neutron-Thus, a rapid move into the hazardous chamber sug- gamma radiation was superior to that of controlgested that the subject had a learning deficit. This monkeys.22 Finally, another series of studies withkind of learning appears to be extremely sensitive to monkeys indicated that radiation does not disruptdisruption by radiation exposure, since an electron performance on memory tasks.27
dose of only 0.001-0.1 Gy can produce significant Rodent studies yielded similar findings. For ex-retrograde aninesia. Retrograde amnesia is a short- ample, adult rats given 2-3 Gy of whole-body radia-term memory loss, or an inability to recall recent tion did not differ from control animals in learningevents, following trauma or a novel event. In this or remembering a water maze.2' The rat's ability tocase, the forgotten event (footshock) occurred only maintain a temporal discrimination was not alteredseconds before the novel event (irradiation). The following 3 Gy of X rays.2' Other maze-learningamnesia lasted for 4 seconds, was dependent on studies were done with rats using either food or wa-dose rate, and was produced by either electron or X ter rewards or escapes from aversive water orirradiation." The mechanism of radiogenic amnesia shock."' In these experiments, either no change inis still in question. However, sensory disruption, the rate of acquisition or improved acquisitionprimarily of the visual system, may explain the (faster running times and improved retention) wasmemory loss.i2,1.1 These data support the idea that found in rats exposed to 1-30 Gy of radiation.24.2S.31.32radiation affects some component of learning or Similarly, mice exposed to 8-72 Gy showed no re-
107

m a !
Mcdical Cou•,'qucm<• ,q ,•'t. h'm' V•,zrtan'
duction ill their ability to acquire an avoidance re- fi×ed-interval 2-minute sdledule of milk reinforcesponse.• u When mice were conditioned to shuttle merit. In the fixed-ratio task, anmlals made 50 ]ever
back and forth betwc,.m adiacent chambers while presses tor one reward; in the lixed-interval task, thebeing e×posed to (I.00l Gy/hour (total dose of l0 first lever press ,after 2 minutes \vas rewarded.Gy),"' no differences were found. Acute doses of 0.5-9.() Gv of gamma radiation were
Althou•,h some of the behavioral radiobiology lit- given at a dose rate of 2.5 Gv/minute. These studieserature suggests that learning and performance are indicated scheduled-controlled performancerather radioresistant, most studies have reported changes that were dose-dependent, reversible, andpostirradiation deficits. For instance, maze-learning beha\'ior-dept.ndent (that is, ratio responses werebehavior was reduced after X-ray exposure up to 10 more affected than interval responses). More impor-Gv." After it was suggested that more challenging tant, even at marginally lethal levels using positivetasks would be more radioser.sitive than easy ones, reinforcement, radiation disrupted the more physi-rats were found to ha\'e a temporary reduction in callv, demanding fixed-ratio performance. Thesetheir ability to reorganize previously learned mate- findings suggest that tasks with cognitive compo-rial after exposure to 4 Gv of gamma radiation.;- nents may be radiosensitive if the r•.,quirements are
sufficiently complex or demanding.•-"Experiments with monkeys hax'e simt, lated pilot
Cognitive Performance Tasks missions after a nuclear confrontation in order to as-
sess crew and aircraft \'ulnerabilitv and survivabil-Tht behavioral tasks in this category generally itv. Fhe\, involved moderate doses (11 Gv or less) of
require discrete physical movements and functional either neutron or gamma radiation delivered in dosecognitive processes, such as timing, decision mak- rates simulating either combat (rapid do,,•,s) or fall-ing, or concept formation. The tasks that require out (protracted doses). The first of this series was alearning in the laboratory are usually difficult to fallout study in which a dose of 3 Gv was deliveredteach to the animals, and significant time is required over 12 hours to monkeys performing a discrete re-to establish stable perfomlance before testing fo• ra- sponse task, which required pressing a lever after adiation effects, light came on. The task was performed for either
Generally, radiation-induced cognitix'e effects food reward or shock ax'oidance.•'' A loss of effi-have been reported in primates only after intermedi- ciencv occurred in two of eight negatively reinforct•.'late or high levels of radiation, and often these decre- monkeys and in two of seven food-reinforced mon-ments were still found if the animals were tested keys. Delayed reaction time was noted in threemonths or years later. For instance, a deficit in de- monkeys in each group. In addition, fimr food-rein-laved, response was noted in monkeys for a few days forced monkevs and one :;\'oidance monkey showedafter an 80-Gv irradiation. '* Cynomolgous monkeys emesis.tested 2.0-3.{ months after a 20-Gv head-only expo- In another pilot simulation study, monkeys \\'ere
sure to X or gamma rays showed a deficit on a dis- reqt, ired to maintain their chairs in a horizontal po-crimination problem series.•'' Their response was sition by compensating for pitch and roll to avoidsimilar to that of chimpanzees tested 2-5 years after shockr•" Three Gv of gamma radiation were deliv-expost, re to 4 Gv of whole-body gamma radiation, ered over 72 hours at dose rates from 0.014 Gy/min-In this case, the chimpanzees perfomaed an oddity- t, te to 0.01 Gy/hour. Monkey performance was rela-discrimination task in which an odd object was se- tivelv unimpaired, but all subjects demonstratedlected from a group of similar objects. In other classic prodromal symptoms, including productivemodels, delayed (2-week) deficits in pe,'formance ac- emesis. Given the common finding that behavioralcuracv occurred in dogs after 3 Gv of X rays?" while effects from low dose rates are usually less thandeficits were found in rats only after prolonged cu- those observed from high dose rates, it is not sur-mulative exposure." Thus, some cognitive deficits prising that the pilot simulation study revealedoccurred only following high radiation exposures, lesser radiation effects than the discrete responseand the deficits were often delayed or chronic.e task did.
A •'ecent lever-pressing study, examined dose-el- Other flight-simulation research was conductedfect relationships, time-course effects, reversibility of with monkeys trained to pc.J. ,rm a multiple avoid-behavioral decrements, and behavioral specificity?• ante task and exposed to pulsed doses of 5.0-8.8 Gvin this experiment, rats were maintained under re- of neutron-gamma radiation (5.5:1 ratio)2• The task
stricted feeding conditions and trained to press a required monkeys to respond on an appropriatelever under either a fixed-ratio (FR) 50 schedule or a lever below three randomly illuminated lights. On
108

KI zIo il an Io W/ I11J'I I1,I AI O l 1ýlX hI ý)III O1HI-I I 1| ,,dllit
I{,'huo,I loraI *\,Ifr pcrod~/wl~oh.<ica L/ia,im. a'otlt i• \pko. rC to Ii,ui:iI..• Rhilath',I
the exposure day, five subjects exhibited decreased cally demanding tasks. Miniature pigs that were re-efficiency, seven had increased reajtion time, and quired to shuttle between adjacent compartments insix experienced productive emesis within 3.5 hours order to avoid shock experienced transient behav-after t\posure. Follow-up measurements indicated ioral deficits after exposure to 15-150 Gv of gammathat as postirradiation time increased, the perform- or mixed neutron-gammna radiation." " Transientance of the subjects gradually decreased. Again, al- behavioral incapacitations were reported in ratsthough the behavioral degradation was not severe, it trained to move up to a safe shelf or stay on an accel-was greater than in the low-dose, low-dose-rate erating rotating rod in order to avoid shock.--";'studies. Further research used even higher doses, Rhesus monkeys showed a transient reduction inexposing monkeys to II Cv of neutron-gamma ra- performance in a running wheel task after exposurediation. On the exposure day, all eight subjects to 13-49 Gv of mixed neutron-gamma radiation."had significantly degraded response accuracy, seven Performance of a physically demanding task canhad increased reaction time, and seven experienced alter survival after irradiation. A rat's swimming toproductive emesis. While the onset of degradation exhaustion before and after irradiation will signifi-produced by I I Gv was not particularly rapid in the cantlv reduce performance and lower the LD,,, byanimals, either the emesis alone or similar direct be- about 2 Gv.'*' The increased mortality was propor-havioral effects in humans may be sufficient to pre- tional to the number of exercise trials during the ini-vent pilots from flying military missions. tial 3 weeks after radiation exposure"' and also to the
dose received.4 Some recent data support this gen-eral finding. Rats performing a strenuous, shock-
Motor Performance Tasks motivated motor task after irradiation had a lowerLD;,, than animals not required to perform this task
Many motor tasks require not only extensive (Figure 7-1)."` However, the finding of performance-training but also physical conditioning in order to stimulated mortality is not universal. No mortalityestablish baselines of behavior. In general, these are changes were noted in dogs and mice that ran in atasks that require physical exertion associated with motorized activity whee. and a motorized treadmill,the movement of large -triated muscles. respectively.v11"4
Several studies revealed chronic deterioration of The rat-swimming model also revealed a radio-
motor performance after doses oi radiation at or be- resistant benefit when the level of preirradiationlow the LD,,,. For example, long-term (42-week) pro- physical activity was adjusted. Rats that swam togressive deterioration of forced wheel-ru aning be- just short of exhaustion before irradiation showedhavior occurred in mice exposed to an LD., dose of increased radioresistance and a higher LD,." In aneutron radiation "' There was a significant reduc- follow-up study, rats recovered from radiation ef-tion in the motor capacity of rats that daily swam to fects sooner if they swain to just short of exhaustionexhaustion before and after exposure to 3-10 Gv of X before the radiation exposure.-" A positive correla-rays.' In this study, reduced swim times occurred 2 tion has been found between the initial preirradi.'-weeks after exposure, with maximum performance tion level of spontaneous activity and survival afterdeterioration by 4 weeks; the effects were dose re- X irradiation.`r It was speculated that the beneficiallated. However, when dogs exercised daily on a effects for rats of swimming to pre-exhaustion cametreadmill for 30 days after exposure to 1-3 Gy of X from radioprotective anoxia. Apparently, animalsrays, long-term deterioration was not confirmed." that reach exhaustion before or after irradiation willPerfot nance deteriorated only as dogs neared death show increased radiation effects, in contrast to ratsafter exposure to 3.0 Gv of radiation. The literature who became more radioresistant if their preirradia-on behavioral radiobiology contains frequent ex- tion exercise was stopped before exhaustion. Theamples of experiments in which postirradiation dog timing and stress o; the physical exercise may ex-performance does not confirm the behavioral decre- plain the differing results reported here.ments seen in the rat, the monkey, or even the hu- Sensitive measures of the strength and enduranceman; thus, the dog may not be a valid model for the of monkeys reveal that the force of pulling is not re-study of these effects. liably impaired after a 4-Gv radiation exposure."`
These early studies mav be contrasted with more Similarly, the postirradiati'on force of motor re-recent work identifying the transient changes in mo- sponse in rats is quite stable for days after a dose oftor performance after supralethal doses of ionizing 4.5 or 9.0 Gv."" A significant reduction in theseradiation. Significant deficits have been noted in a measures of strength is seen only when death is im-variety of animal species performing different physi- minent.
109

Medical Cons,',lteces of Nuiclear Warfare
99.9 1 1 1 1 .
99Performing
90 (LD5 0 / 3 0 = 8.18 Gy) 0400"
Mortality 70(%) 50
30 00
10 Nonperforming
1 (LD5 0 / 3 0 = 9.58 Gy)* P4 0.05
0.1 1 1 I6 7 8 9 10 11 12
Dose (Gy)
Fig. 7-1. LD,,•,, profiles after exposure to gamma radiation. Rats either rested or performed a motor task (acceleratedrod).
Naturalistic Behaviors even depressed in rats that were deprived of foodfor 6 weeks after irradiation and tested daily. 74
Naturalistic behaviors are a normal part of an (These data are significant because food deprivationanimal's response repertoire, and their performance normally increases activity.) This locomotor depres-requires no laboratory training. Naturalistic behav- sion lasted a few days, and was followed by partialiors often evaluated in the study of radiation effects recovery.71 At doses above 4 Gy, a second decreaseare spontaneous locomotion, social interaction (such in activity occurred after 1 week, suggesting thatas sexual and aggressive behaviors), consumption more than one response mechanism may be in-behaviors (eating and drinking), taste aversions and volved. This biphasic response' is similar to clinicalemesis. symptoms in humans.67
Locomotion. Spontaneous locomotion is a natu- In a recent study of the effects of sublethal dosesralistic behavior that is convenient to measure and of gamma rays on locomotion, mice were monitoredprovides a relatively powerful tool for studying per- for 30 days after exposure to 0.5-7.0 Gy of cobalt-60formance. Activity is of interest because radiation is radiation.76 Locomotion after the 7-Gy exposureknown to produce malaise, along with other pro- gradually dropped until it reached a significant lowdromal symptoms of general weakness, fatigue, 15 days later. Recovery of locomoti'rn occurred byheadache, nausea, anorexia, vomiting, hemorrhage, day 19. Thus, alterations in locomotion were de-and drowsiness or insomnia .7 tected at less than the LD•/30 (7.6 Gy).
An acute whole-body dose of 2-7 Gy of X radia- Curiosity and Investigative Behaviors. Curiositytion produced immediate depression in the rat's vo- and investigation are other naturalistic behaviorslitional activity-wheel performance. 71 These data that have been measured. Chimpanzees given 4 Gywere confirmed by others using guinea pigs, ham- of gamma radiation made fewer attempts to solve asters, rats, and primates.36'30,
72' 73 Locomotion was variety of puzzles.25 This deficit seemed to be inde-
110

Behia 1'ior-al iand Neurophysiolo~ical Changes zeith Exposure to lonizin Radiationi
pendent of changes in capacity, because measures of Changes in aggressiveness may reflect a moredexterity and strength were unchanged in the same general social phenomenon. Several investigatorsanimals. After monkeys were exposed to 4 Gv of X reported that mortality following irradiation will in-ravs, their manipulation of objects in the home cage crease if rats are kept in high-density housing."'--and their rapid expenditure of energy decreased; sit- Presumably, the combined stresses of maintainingting time lengthened; and chewing, scratching, territory and being exposed to radiation increasedgrooming, and number of cage movements de- the rat's mortality from the radiation. The mecha-creased." A systematic study of home-cage behav- nism of this aggregate toxicity is being studied.'ior was made with pairs of monkeys after 4 Gv of The effects of emotionalitv or dominance followingwhole-body exposure of both animals in each pair."' irradiation have been studied, but neither factorTen-minute structured observations were made seemed to alter postirradiation mortality., Finally,twice daily. To control for debilitation, the instances frequent sexual activity during the 30 days after ex-of each category of behavior were divided by the posure was found to increase the mortality rate ofnumber of times that the identifiable behavior oc- male mice."curred in that time period. The irradiated animals Consumption Behaviors. Exposure to ionizingshowed reliable deficits in curiosity, more inner- radiation is known to reduce food and water con-cage-directed movements to well-known stimuli, sumption and to produce nausea and vomiting. 1,o7and fewer instances of outer-directed movements or Intake will be decreased, at least initially, dependingattention to things outside the cage. Similarly, re- on the radiation dose and dose rate.2`- Instances ofduced curiosity or reduced visual exploration (look- radiation-induced anorexia and adipsia have beening around) has been observed in rats after receiving noted .7.S1 Subjects will not perform for food after 1050 Gv of X ravs.72 Since some of the procedures with Gy of radiation, but will continue to work to avoidthe monkeys tried to factor out general malaise, electric shock, suggesting that consumption behav-these findings suggest a specific change in curiosity iors are relatively radiosensitive.iand attention that developed after irradiation.- Changes in food preferences have also occurred
Social Behavior. Because military units are social after irradiation. Monkeys chose apples and carrotsstructures, the effect of radiation exposure on social more frequently and peanuts less often after expo-behavior is a military concern. The most commonly sure to 4 Gy of whole-body X radiation.'" 2 Thestudied social behaviors are aggression and fighting. changed preferences lasted 4 weeks and were dosePrimate studies showed that aggression in mon- dependent. Because the mouth, throat, and stomachkeys"' lo. 7S. -4 and the social interactions of chimpan- are highly sensitive to abrasion after irradiation, thezees' significantly decreased following irradiation. newly preferred foods may have been easier for theFighting among male mice (a very common group monkeys to swallow."'home-cage activity) decreased with an increasing Taste Aversions and Emesis. Animals readilydose of X radiation, but all signs of fighting were not learn to associate gastrointestinal upset and malaisetotally suppressed until shortly before death."s An with a novel taste and smell, and will avoid the newintruder mouse introduced into the home cage of substance when later exposed to it."3 Results indi-another mouse continued to be attacked for several cate that a conditioned taste aversion (CTA) can occurdays after the resident mouse had received 10 Gy of at doses as low as 0.25 Gy and can be reliablygamma radiation.' These behaviors persisted until achieved at 0.5 Gy. Because this may be the most re-the resident mouse showed radiogenic moribund liable and radiosensitive form of behavioral condi-behavior. tioning, CTA has been extensively used as a model
An extreme variant of aggression is muricide of radiation-induced gastrointestinal distress and(mouse killing), which some rats exhibit spontane- emesis.14ously. Muricide was frequently suppressed after The relationship of emesis and performance dec-radiation exposure.'2 Footshock can be used to in- rement is complex. When gamma radiation is used,duce aggression, however, and 7 Gv of gamma ra- the ED., (effective dose for 9097 of cases) for monkeydiation can stimulate this response." The increase in emesis is 8 Gy.'5 Emesis is more likely to be pro-this unnatural type of aggression may be related to duced after irradiation with neutrons than afterradiation-induced increased irritability.' This hy- gamma-ray exposure."' Up to 10 Gy, increasingpothesis is consistent with the report that head-irra- doses of radiation in the monkey correspond withdiated male rats were more "emotional" than were the enhanced likelihood of emesis.17 However,the sham-irradiated controls during the first 30 days above 10 Gy, the number of monkeys that vomit de-after exposurel,2 creases with increasing dose. The reason for this
111

MA,0 1ill U I'C,, it'.ClI t o 4if N,' li r .t'l ri.i OW
high-dose inhibition ot emesis is largely unknown, results were seen in monkeys pulsed with 22 Gv ofbut it may be that doses above 10 Gv interfere with radiation.4 "" Animals not incapacitated but receiv-the transmission or reception of afferent vagal im- ing the same dose as incapacitated animals willpulses from injured organs, which normally play a vomit as expected."' Although the data are reveal-pirt in this response. The report that no emesis oc- ing, the relationship between radiation-induced
r, l, during earl' behavioral incapacitations is fairlh emesis and behavioral deficits must be clarified.common. No relationship was found between eme- Despite some ambiguity in the animal data, eme-sis and early performance deficits in monkeys ex- sis will almost certainly interfere with the perform-posed to up to 50 Gv of mixed neutron-gamma ra- ance of some critical military tasks, such as thosediation and performing in a physical-activity that require the wearing of artificial breathing de-wheel."' Similar visual-discrimination performance v'ices.
COMBINED INJURIES
Nuclear war will produce few "pure" radiation ioral decrements. For example, a study in monkeysinjuries. It is more likely that victims will experience to test for synergy between radiation and motion ef-burns, w0ounds, and perhaps trauma from chemical fects reported an emesis ED-, of 4.5 Gv for radiationagents and environmental stresses combined with alone and 2.6 Gv for radiation plus motion.-' Radia-the damage from ionizing radiation. The physio- tion may reduce the tolerance of animals to thelogical effects and treatment of these combined inju- stress of G forces (acceleration) as measured by le-ries hav'e received significant attention.'''' Less thalitv and pathomorphological and cardiovascularclear are the behavioral consequences from com- end points." "'- But other experiments report that
bined traumas that include irradiation. an animal's resistance to critical acceleration in-Mice were exposed to 3 Gv of neutron-gamma creases for several days after irradiation (7-8.5
radiation and some of them were then exposed to Gy)."17 ,I OS The variables of timing and direction ofthe further trauma of a wound or burn."" The radia- acceleration combine with radiation dose factors totion exposure alone caused significantly depressed complicate the issue. However, to the best of ourmeasures of locomotion. In addition, the wound in- knowledge, only one behavioral experiment hasjury increased the harmful effects of radiation, while studied the combined effects of radiation and Gthe burn injury did not. forces. Rats were exposed to 9.5 Gv of X rays over a
In a study of the combined effects of radiation (7 24-hour period, followed 5-7 days later by 4 minutesGv) and an anticholinesterase agent (physostigmine, of positive 10 G of acceleration stress.""' Compared0.1 mg/kg), rats were evaluated on a behavioral test to animals that were only irradiated, the authors re-battery that included measuring their balance on a ported that rats that received both stresses exhibitedrotating rod and recording several components of a significant (about 25'(;) but transient decrease intheir locomotor activity."'" "' At 45 minutes after ir- the ability to learn new mazes. However, no changeradiation, a radiation-only group had a 30'1 deficit in the number of errors in an already-learned mazein performance, while a physostigmine-only group was observed in rats after combined treatment withhad a 40(/" deficit. A combined-treatment group positiveG forces and radiation.showed a 60'/; performance deficit on the rotating Other environmental stresses can alter the effec-rod task. In fact, all measures of performance indi- tiveness of radiation on behavior or lethality. Forcated that the effect of combined ionizing radiation instance, daily exhaustive exercise, continuous expo-and physostigmine was much greater than the effect sure to cold (W°0, or continuous exposure to high al-of either insult alone. In a follow-up dose-response titude (15,000 feet) considerably reduced the time tostudy, rats were required to balance on a rotating death and the incidence of death after irradiation."'rod.''" As in the above experiment, physostigmine Taken together, these data suggest that the behav-and radiation each produced a dose-dependent be- ioral effects of radiation mav summate or act svner-havioral decrement when presented alone. A syner- gistically with other stresses. Therefore, any esti-gistic behavioral effect was observed after combined mates of battlefield performance decrements that dotreatment with the chemical and radiation. not include these factors will probably be lower in
Environmental and combat stresses may also number and degree than the behavioral decrementscombine with radiation injuries to increase behav- actually observed in a military conflict.
112

Behaiioral and NeulIhyiohical Changes witzh EXIVSure to honizing Radiation
100
death
Correct 0Response
(%) 100
--EPD
d ihi death
1 1 hour hours-daysRadiationExposure
Fig. 7-2. Idealized performance time-course profiles for acute radiation-induced behavioral decrement. Soon after a suffi-ciently large dose of radiation, several animal species exhibit ETI (upper panel) or EPD (lower panel). Smaller transientdeficits may occur around 45 minutes and 4 hours later.
EARLY TRANSIENT INCAPACITATION AND OTHER EARLY PERFORMANCE DEFICITS
For the military, an abrupt inability to perform- may not be necessary to produce these effects.44,'1 Iaptly termed early transient incapacitation (ETI)-is Transient EPDs occur in monkeys, rats, and pigsa potentially devastating behavioral consequence of performing a variety of tasks, and the deficits are be-radiation exposure."" An idealized individual ETI lieved to occur in humans. However, this finding isprofile is shown in Figure 7-2. Prior to irradiation, not universal in animals, since EPD does not occurperformance is at maximum efficiency. But 5-10 in some strains of mice"'12 and dogs." 1.114
minutes after exposure to a large, rapidly delivereddose of ionizing radiation, performance falls rapidly Task Complexityto near zero, followed by partial or total recovery10-15 minutes later. Delayed ETIs may also occur at When ETI was first observed in monkeys in theabout 45 minutes and 4 hours after irradiation. In early 1950s, the dose levels reported to produce itvarious animal models, ETI is a strikingly short, in- were quite high, perhaps because the behaviorstense phenomenon. A less severe variant of ETI is tested were relatively undemanding and were there-early performance decrement (EPD), in which perform- fore radioresistant to disruption (Table 7-1).1",' ."'ance is significantly degraded rather than totally These early measurements involved either thesuppressed (Figure 7-2). Until recently, it was pre- simple observation of untrained monkeys or theirsumed that ETI and EPD would occur only at su- performance of a relatively easy continuous-avoid-pralethal radiation doses and that, after behavioral ance task (pressing a lever to avoid shock when arecovery, death would occur in hours or days. light came on in the operant chamber). In the con-However, more recent data reveal that high doses text of these minimal requirements, the effective
113

Medical Consequences of Nuclear Warfare
TABLE 7-1
RADIATION-INDUCED EARLY TRANSIENT INCAPACITATION (ETI) ASA FUNCTION OF TASK COMPLEXITY OR TASK DIFFICULTY
Rank Order Task or Dose toof Task Behavioral Produce ETIDifficulty* Criterion (Gy) Reference
1 Observation 50-300 110,115
2 Continuous avoidance** 50-100 116
3 Visual-discrimination 22 117,118task***
4 Speed-stress visual- 9 tt 44discrimination taskt
*Ranked from least to most difficult or complex
"**Presentation of light required monkey to press a lever every 20 seconds to
avoid shock***Circle and square randomly presented every 10 seconds on two backlit
press-plates. Subject had 5 seconds to touch the square to avoid shock.1 Subject had 0.7 seconds to avoid shock
"ttCalculated ED, = median effective dose. Other numbers in this column
were empirically observed instances of ETI and were not derivedfrom curve fitting.
ETI-producing radiation doses were found to be 50 complexity of the task that the animal is required toGy or more. When a more complex shock-avoid- perform; that is, complex or demanding tasks areance visual-discrimination task was later used, the more radiosensitive than easy tasks.median effective dose to produce ETi ,was reduced Another reason that the radiation dose requiredto approximately 22 Gy (Table 7-1)."'7' '. (_, this vis- to disrupt performance was presumed to be high isual-discrimination task, monkeys were required to that ETI is an all-or-none, relatively insensitive enddiscriminate (within 5 seconds) between a circle and point. When the ETI data are analyzed with a morea square (the square was always the correct choice) sensitive behavioral end point (that which measuresrandomly presented on backlit press-plates every 10 a significant change from a baseline response ratherseconds. Monkeys were trained later on a variant of than only a total cessation of response), the disrup-this visual-discrimination task, in which the tempo- tive dose is even lower (Table 7-2), approaching theral response criterion (set at 0.7 seconds) approached LD5 0 for the monkey.4 4 Furthermore, the ED50 forthe reaction time of the animal.41 Under these condi- transient behavioral deficits in monkeys may be astions (speed-stress visual discrimination), the me- low as 3 Gy if the animals are performing a moredian effective dose to produce ETI was approxi- difficult task requiring both visual discriminationmately 9 Gy (Figure 7-3). Thus, the dose of radiation and memory."' If these data can be generalized torequired to disrupt behavior is directly related to the the human, they suggest that under certain circum-
114

Belavioral and Neurophysiological Changes with Exposure to Ionizing Radiation
99.9 111 1 I I I , 1 , I , 11
99
90Subjects 70 Speed
Incapacitated So Stressed UnstressedM ~30 )
101 EDs0(GY) N
Stressed 9.0 201 Unstressed 18.0 141
0.1 I I 1 11 1 1 1 I 1 1 1 '1
2 s 10 50 100Dose (Gy)
Fig. 7-3. ETI as a function of radiation dose for monkeys performing a visual-discrimination task in which criterion ofminimum response time was either 5 seconds (unstressed) or 0.7 seconds (stressed). Incapacitation is defined as at least 1minute of nonresponding.
stances, relatively low doses of radiation may cause 20 minutes after irradiation (Figure 7-4). Wheel-run-rapid, transient disruptions in performance. ning performance was disrupted the most, and per-
The issues of task demands and task complexity formance returned to only about 50% of baseline atinfluencing the effective radiation level are common 60 minutes after irradiation. The above data suggestin the investigation of ETI. For instance, the dose of a hierarchy of behavioral effectiveness, with obviousradiation required to disrupt performance was com- implications for military missions."4,s6pared for three tasks: the visual-discrimination task(described above, with a 5-second response time), a Radiation Dosephysical activity task, and an equilibrium-mainte-nance task. In the physical activity task, monkeys A variety of radiation parameters, includingran at 1-5 mph in a nonmotorized, circular cage.39 In dose, can significantly influence EPD. Low doses ofthe equilibrium task, monkeys maintained horizon- radiation can sometimes produce behavioraltal alignment by compensating for the pitch and roll changes, such as locomotor activation,1'0 that are inof a platform on which they were seated."' Per- contrast to the locomotor depression observed afterformance on all three tasks was assessed in monkeys high doses."2' Beyond a certain threshold, more ra-exposed to a 25-Gy pulse of neutron-gamma radia- diation tends to produce increasingly depressedtion. Visual-discrimination performance with a 5- measures of performance.7 ,44,5' For example, in a re-second response time was disrupted the least, with cent study, 7.2 Gy was the EDR, for the speed-stressperformance returning to about 80% of baseline by visual-discrimination task.-" However, all monkeys
115

Medical Consequences of Nuclear Warfaire
TABLE 7-2
MEDIAN EFFECTIVE DOSES REQUIRED TO ACHIEVE DIFFERENTBEHAVIORAL END POINTS IN IRRADIATED MONKEYS
Task End Point ED(G Reference
(Gy) Reeec
Speed-stress Early transient 9 44visual-discrimination task* incapacitation
(ETI)**
Speed-stress Early performance 7 44visual-discrimination task decrement
(EPD)***
Delayed match-to- EPD+ 3-5 111sample task
*Response time 0.7 seconds or less
"**Defined as six consecutive ommissions or I minute of nonperformance
***EPD defined as 2 z-scores below baseline performance levels
exposed to 14.1 Gy of mixed neutron-gamma radia- behavior. For instance, monkeys performing a vis-tion showed transient EPD, while only one of five ual-discrimination task were exposed to a total dosesubjects showed this deficit at 6.8 Gy. Thus, at 7.3 of 50 Gy of gamma-neutron radiation delivered in aGy (Figure 7-3), the incidence of performance sup- reactor pulse.123" 24 One group of monkeys receivedpression ranged from 10% to 90%. These radiation the radiation treatment in one 50-Gy dose; the otherdose-response curves for measures of behavior in groups received 25 Gy at two intervals separated bysome ways parallel the curves observed for a num- zero time and intervals of 20, 30, and 40 minutes andber of end points, such as emesis and lethality.' 22 1, 3, 4.5, and 6 hours (Figure 7-6). Performance was
more severely disrupted for subjects who receivedthe whole dose at once than for subjects in the split-
Radiation Dose Rate dose conditions. In a recent study with rats, a singleacute exposure to 7.5 Gy of gamma radiation dis-
Another radiation factor that can influence be- rupted performance by reducing the rate of lever-havior is exposure dose rate. Monkeys trained to pressing under an FR 20 schedule (thus, 20 leverperform a delayed matching-to-sample task, involv- presses would be required to terminate electric foot-ing visual discrimination and short-term memory, shock).25 Behavioral disruption was characterizedwere exposed to 10 Gy of gamma radiation at dose by decreased response rates over the 40-day periodrates of 0.3-1.8 Gy/minute (Figure 7-5)."' Only 7% after exposure. However, when a different group ofof the subjects demonstrated transient EPD after a rats received a total dose of 7.5 Gy delivered at 1.5dose rate of 0.3 Gy/minute, while 81% showed be- Gy/day over 5 days, disruption in FR performancehavioral decrement after 1.8 Gy/minute. This in- was significantly less.'25 Although other behavioralcrease of 1.5 Gy/minute raised the incidence of early dose-rate effects have been reported,' 2
1-3' this find-
EPDs by 73%. ing is not universal and may depend on the behaviorFractionated (or split) doses have less impact on being measured.8"
116

Behavioral and Neorophysiological Changes with Exposure to Imizing Radiation
100
80 Visual Discrimeination
M a 60Maintenance65 TMean 60 75-T
Performance Man-lfc 75% ETI
S40 6- 100% ETI
20
00 20 40 60 80 100 120
Time Postirradlatlon (min)
Fig. 7-4. Comparison of monkey behavioral responses after a pulse of 25 Gy (neutron-gamma ratio: 0.4). Changes in per-formance after irradiation depend on task being performed. Physical activity task (wheel running) is more demandingand therefore more radiosensitive than other tasks illustrated. (See text for full descriptions of tasks.) Percentage of sub-jects experiencing ETI is listed for each task.
Radiation Quality accelerating rod for as long as possible. 3 -2 In thisstudy, bremsstrahlung, electron, gamma, and neu-
In addition to dose and dose rate, the type of ra- tron radiations were investigated, and a dose-re-diation can influence early behavior deficits. It is sponse relationship was found for all radiationsgenerally accepted that high-LET radiations (such as (Figure 7-7). A major finding of this research wasneutrons) are more effective in eliciting biological that electron radiation was the most effective in pro-responses and death than are low-LET radiations ducing EPD, and neutron radiation was the least ef-(such as gamma rays). However, research has fective. Gamma radiation was slightly more effec-shown that the opposite is true when the end point tive than neutrons. This is not the first time thatis performance. 7' 3 Neutron radiation was only electron radiation was found to be the most disrup-23% as effective as gamma radiation (based on ED,) tive to behavior. 21 Thus, substantial support is ac-in producing ETI in pigs performing a shuttlebox cumulating to suggest that radiations of differenttask, which required the subjects to move back and qualities are not equally effective in altering animalforth between adjacent chambers in order to avoid behavior. Furthermore, since electrons are more be-shock.5- In another study, the neutron-gamma RBE haviorally effective than high-LET radiation, thefor monkeys performing a visual-discrimination task quality factors derived from these data may be dif-was 0.68; that is, gamma radiation was more effec- ferent from those already established for damage totive than neutrons."4 Also, in a comparison of neu- biological systems.-"tron and bremsstrahlung (gamma-like) fields, it was Other factors that may affect behavioral disrup-reported that bremsstrahlung radiation was more ef- tion after irradiation include (but are not limited to)fective in producing ETI than was neutron radia- the physical well-being of the subject (sick ortion. 7 healthy, tired or rested), the presence or absence of
A recent comprehensive study of the behavioral physical shielding or pharmacological radioprotec-effects of various radiation qualities was done with tants, and the exposure or nonexposure of the sub-rats performing on an accelerating rotating rod. ject to radiation alone or to radiation and otherThis shock-motivated task required each subject to strcsses of the nuclear battlefield (such as blast, heat,maintain its position on a 2-inch-diameter gradually or flash).
117

Medical Conset'quences of Nuclear Warfare
80
w 60-
0"40-
20
000 50 100 150 200
Dose Rate (cGy/min)
Fig. 7-5. Effect of dose rate on monkey performance of a delayedmatching-to-sample visual-discrimination task. (Dose totaled 10Gy of gamma photons.)Source: Reference 111.
118

Beha'ioral and Neurophysiological Changes with Exposure to Ionizing Radiation
2636
Groups 4
7 d
81 I .I I I
0 25 50 75 100Mean Percent Correct
Fig. 7-6. Monkey performance decrements on a visual-discrimination task after either a single dose of 50 Gy (neutron-gamma ratio: 0.4) or two fractionated doses of 25 Gy at specified intervals. The tendency for dose fractionation to reduceradiogenic behavioral deficits is consistent except when the interval between fractions is either 40 minutes or 4.5 hours,when secondary and tertiary transient incapacitations are likely to occur (see Fig. 7-2).Source: References 122, 123
THE NEUROPHYSIOLOGICAL BASIS OF PERFORMANCE DECREMENTS
Sensory and Perceptual Changes vation can in fact occur at extremely low levels.13For instance, the olfactory response threshold to ra-
From the psychologist's viewpoint, sensory and diation is less than 10 mrad, and the visual system isperceptual processes are distinct, yet interrelated, sensitive to radiation levels below 0.5 mrad. Ioniz-The sensory process involves stimuli that impinge ing radiation is as efficient as light in producing reti-on the senses, such as vision, audition, olfaction, nal activity, as assessed by the electroretinogram.gustation, and skin sensation.133 The perceptual The visibility of ionizing radiation was reportedprocess involves the translation of these stimuli by shortly after the discovery of X rays and is nowthe CNS into appropriate overt or covert interpreta- firmly established.30tion and/or action. Ionizing radiation can be sensed Vision. Although the visual system can detect aand perceived, and radiation-induced sensory acti- low radiation dose, large doses are required to pro-
119

Mvedical Coipti'ntpncts of Nuclear Warfare
99.9I I I I IED50 (Gy) o
99 Neutron 98 -- 0Gamma 89 --.
Perfor- 90 Bremsstrahlung 81 --- do
mance Electron 61 ......mance 70 -o .... ,t+I .,Decrement 70Subjects 50 7
(%/) 30 _.... / _ -,'00 - 0
100
1 0
0.1 1 1 1, J40 50 60 70 80 90 100 160
Dose (Gy)
Fig. 7-7. Dose-response profiles and median effective doses (ED•,) for rats performing an accelerated-rod task after expo-sure to four radiation qualities. Performance decrement is defined as 2 z-scores below preirradiation baseline perform-ance. Electrons are significantly more effective in producing behavioral deficits than are other types of ionizing radiation.Neutron radiation is least effective.
duce pathological changes in the retina. This is es- in scotopic visual sensitivity 1 day after being ex-pecially true of the rods, which are involved in black posed to 0.3-1.0 Gy of X radiation.'-" Long-termand white vision."" Necrosis of rods has been re- (20-36 days) changes in dark adaptation were re-ported after doses of 150-200 Gy in rats and rabbits, ported in patients exposed to 4-62 Gy of X rays.:39
and after 600 Gy in monkeys. Cone (color vision) In terms of visual acuity, only long-term deficitsganglion cells are even more resistant. At these high were reported in monkeys at 1-3 years after expo-radiation doses, cataracts occur.') Monkey binocular sure to 3-60 Gy of radiation.-`-' However, compo-thresholds did not change during the 100 days after nents of attention may have caused some of this ef-35 Gy of X radiation."3 ' However, performance dete- fect. Since these exposures were not restricted to theriorated rapidly after this period, so that by day 210, visual pathways, brain damage (affecting the cogni-the animals were blind and no cortical photo-evoked tive aspects of learning and/or the motor compo-responses could be obtained. Similar findings were nent of visual-acuity tasks) probably also existed.reported in monkeys,"3 ' in rabbits,"• and in human These data are consistent with observations of irra-patients.13 7 diated chimpanzees that showed impaired visual
Pathological changes in the visual system occur acuity and accuracy on visual-discrimination tests.39
only at high doses, but this is not true of visual func- Audition and Vestibular Function. Few adversetion. Rats trained to a brightness-discrimination auditory changes have been noted after radiationtask were not able to differentiate between shades of exposure. Two Gy of X radiation to the head pro-gray after 3.6 Gy or to make sensitivity changes after duced no changes in cochlear microphonics in rats6 Gy of whole-body X rays. 3' In mice, low-rate examined up to 90 days after exposure.140 Likewise,whole-body irradiation adversely affected bright- 5 Gy delivered to the rear half of a rat's brain did notness discrimination tested 3-5 months after expo- affect intensity or frequency thresholds. However, asure. Humans experienced temporary decrements transient 5.5-decibel reduction in tone intensity
120

Behacvioral and Nearoph.tlsiologihal Chaniegw with Expsjire to oijtin a Raditioni
threshold that lasted 2-5 weeks did occur in dogs af- sory changes; however, transient alterations wereter as little as 0.39 Gy of X rays.2 • At larger doses of reported at doses of 1-5 Gy. High levels of radiation10-70 Gy, cochlear microphonics decreased in can cause longer-lasting sensory impairments. Fur-guinea pigs.Ii, thermore, high radiation doses that affect CNS mor-
The physiological substrate of hearing deficits phology will also impair perceptual function.has also been explored. Changes in the mouse earfollowing 20-30 Gy of whole-body X rays includedcellular necrosis in the organ of Corti and in the ep-ithelial cells of the ear canals." Rats exposed to a Radiation-Induced Changes in thewhole-body dose of 1-30 Gy of gamma or X radia- Nervous Systemtion demonstrated damage in the cochlea but not inthe cristae of the vestibular inner ear or the middle Although it is true that other organ systems mayear. Human patients who received 40-50 Gy of contribute to radiogenic lethargy and reduced re-therapeutic gamma radiation developed inflamma- sponsiveness, the nervous system's central role intion of the middle ear but only a temporary loss of behavior makes it the presumed primary mediatorauditory sensitivity and temporary tinnitus."' After of radiation-induced performance deficits. This pre-being exposed to 20-80 Gy of X radiation, the hear- sumpt.on is supported by the fact that electrical oring organs of guinea pigs were generally resistant to chemical stimulation of the brain can overcomeradiation."'4 some radiation-induced behavioral deficits. 12,4"4 In
Vestibular function may be more radiosensitive addition, experiments with partial-body shieldingthan audition. Depressed vestibular function was revealed the effectiveness of head-only irradiationsreported in dogs after exposure to 3.5-5.0 Gy of pro- in producing behavioral changes." In this regard,ton radiation or 2 Gy of gamma radiation.1 4
1 In an- severe long-term changes on a conditioned avoid-other study, 5 Gy of gamma radiation depressed the ance task (jumping a low barrier) and color visual-electromyogram of vestibular-tonic reflexes of rear discrimination learning were reported in monkeysextremity muscles in the guinea pig.14 4 At higher whose heads were irradiated with 20 Gy.) Thesedoses of 4-22 Gy, loss of the pinna reflex (ear twitch) data suggested functional derangement in the poste-was noted in the mouse, and disturbances in equilib- rior association areas. Also, monkeys whose headsrium and other vestibular functions were noted in received X radiation (frontal and posterior associa-the burro and hamster."' Thus, depression in yes- tion areas) 2 years earlier showed retarded learningtibular function may exist at doses close to the LD,,0, on a problem-solving task.,' Studies with rats, inand symptoms of vestibular disruption may last which 50 Gy was delivered directly to the frontallonger at higher than at lower doses. cerebrum " or 25 Gy to the whole cerebrum, revealed
Other Senses. Although the literature is sparse, a decreased ability to learn an alteration runningolfactory and gustatory changes have been reported pattern motivated by delayed reward.'" Decreasedin patients exposed to therapeutic radiation.' 45 Al- learning was observed in rats whose heads were ex-tered taste perceptions were also found in patients posed to up to 8 Gy of X radiation and who thenexposed to 36 Gy of X rays, with a metallic taste were required to learn a 14-unit maze."' Althoughbeing the most common report. Transient changes the importance of the brain in radiation-induced be-in taste and olfactory sensitivity were also reported havioral change is well established, the question stillin radiotherapy patients and in the rat."" remains: What specific changes in the CNS mediate
The effects of radiation on the skin senses have the performance deficits observed after exposure toalso not been fully assessed. In the work that does ionizing radiation? The answer is complex.exist, it is difficult to separate the direct receptor One hypothesis is that a sufficiently large radia-changes from the secondary changes arising from ef- tion dose causes permanent brain lesions, demyeli-fects on the vascular system."' However, radiation- nation, and necrosis, which in turn produce chronicinduced changes in pain perception have been ad- behavioral deficits. In addition, short-lived behav-dressed empirically. Gamma photons produced a ioral phenomena may be mediated by transient vas-dose-dependent analgesia in mice,14 6 but data sug- cular changes that induce edema or ischemia in thegest that X or gamma rays did not alter the analgesic CNS. A second hypothesis is that performanceeffects of morphine or the anesthetic effects of ha- changes are mediated by significant alterations inlothane in rats except under certain conditions.17,11 brain function due to changes in neurochemistry
In summary, whole-body radiation doses below and neurophysiology. As is often the case, there isthe LD5,, do not appear to produce permanent sen- some truth in both hypotheses.
121

Me, healCons•'qu N tis ot cer Wtirtilrct
accumulate and may become symptomatic. SinceRadiogenic Pathology of the Nervous System this pathology was observed at a dose of radiation
previously believed to be completely safe, confirma-Radiogenic damage to brain morphology may tion of these new data may profoundly influence our
occur after an exposure of less than 15 Gv and is a view of the radiosensitivity of brain tissue.well-accepted finding at higher doses. However, In an organ like the brain, different topographicalthese two conclusions have not always been re- regions may have varying susceptibility to ionizingported. A review of many standard radiobiology radiation. The most sensitive area is the braintextbooks reveals the common belief that the adult stem."• The brain cortex mav be less sensitive thannervous svstem, is relatively resistant to damage the subcortical structures,'- such as the hypothala-from ionizing radiation exposure."' This conclusion mus,"' the optic chiasm, and the dorsal medulla."-has been derived, in part, from early clinical reports Although radiation lesions tend to occur more fre-suggesting that radiation exposures, given to pro- quently in brain white matter,1 ,
7.1 the radiosensitiv-
duce some degree of tumor control, produced no itv of white matter also appears to vary from regionimmediate morphological effects on the nervous sys- to region.'
tem."" However, this view was eroded when it was In this regard, researchers have produced meas-later shown that the latency period for the appear- ures of the functional sensitivity of some brain areasance of radiation damage in the nervous system is and the insensitix it\j of others. 15',
1 ' The activation ofsimply longer than it is in other organ systems.'? behaviors through electrical stimulation of the lat-Subsequent interest in the pathogenesis of delayed eral hypothalamus (but not the septal nucleus orradiation necrosis in clinical medicine has produced substantia nigra) is still possible after 100 Gv.' 21 '1'
a significant body of literature. Recent studies of ra- However, years after clinical irradiations, dvsfunc-diation-induced brain damage in human patients tions of the hypothalamus are prominent even with-have used the technology of computed axial to- out evidence of hypothalamic necrosis.'12 Local sub-mography (CAT) to confirm CNS abnormalities that cortical changes may exist in the reticular formationare not associated with the tumor under treatment and account for radiation-induced convulsabilitv ofbut occur because of the radiotherapy."' the brain.1' ,7 4 Similarly, postirradiation spike dis-
General (although not universal) agreement ex- charges are more likely to be seen in the hippocam-ists that there is a threshold dose below which no pal electroencephalograph (EEG) than in the corticallate radiation-induced morphological sequelae in the EEG.7'7 This idea of selective neurosensitivity is fur-CNS occur. In laboratory animals, single doses of ther supported by experiments in which electricalradiation up to 10 Gy produced no late morphologi- recordings were made from individual nerve fiberscal changes in the brain or spinal cord.: Necrotic after irradiation.'" These data reveal a hierarchy oflesions were seen in the forebrain white matter from radiosensitivity in which gamma nerve fibers aredoses of 15 Gv but not 10 Gv."'"' In humans, the more sensitive than beta fibers, and alpha nerve f-"safe" dose has been a topic of considerable debate. bers are the least sensitive.Depending on the radiation field size, the threshold The functional radiosensitivity of specific brainfor CNS damage was estimated to be 30-40 Gy if the nuclei may in part explain the ability of a particularradiation is given in fractions,""' although spinal dose of ionizing radiation to disrupt one type of be-cord damage may occur with fractionated doses as havior but not another. For example, monkeys willlow as 25 Gy."" The difference between a safe and a continue to perform a visual-discrimination task butpathogenic radiation dose to the brain may be as not a more physically demanding task (wheel run-small as 4.3 Gv.•• 2 ning) after a similar dose of ionizing radiation."'
It is clear that the technique used to assess neuro- These data agree with the suggestion that classicallypathology can profoundly influence its detection. In conditioned reflexes are more radioresistant thana recent preliminary inspection of neutron-irradiated motor coordination, and that this selective disrup-brain tissue stained with silver to detect degenerat- tion of particular behaviors "indicate[s] that ionizinging neural elements, punctate brain lesions were radiation mainly affects the functions of the subcor-found within 3 days after a 2.57-Gy neutron expo- tico-Ibrain]stem formations of the brain."'-,"sure."'• This effect was transient, and no degenera- The phenomenon of latent CNS radiation damagetion was observed 30 days after irradiation. The le- with doses above threshold has been well docu-sions were not deth.ctable using standard H and E mented. I 2 '',7.S The long latent period has led tostains. These effects are similar to a multi-infarction considerable speculation on the likely pathogenesissyndrome in which the effects of small infarctions of late radiation lesions: (a) radiation may act pri-
122

Fchaa.iordal tdl Nc roht/iIoldn i 'hL CIhIaI cPs w'ith F.rposur t' htO lorl:m_ Radiation
marilv on the vascular system, with necrosis secon- ening of the nodes of Ranvier and segmental demve-darv to edema and ischmia, and (b) radiation may lination as earl%- as 2 weeks after a dose of 5-6Ohave a primary effect on cells of the neural paren- Gv.'" 4 Clinical evidence also suggests that radio-chvma, with vascular lesions exerting a minor influ- genic denvelination may occur. Several patientsence.J' experienced sensations like electric shock (refer-
The first evidence in support of a vascular hv- enced to sensory levels below the neck) after radio-pothesis was obtained when human brains that had therapy for head and neck cancers."' The syvmp-been exposed to X rays were examined.';' It was toms gradually abated and disappeared after 2-36suggested that delayed damage of capillary endo- weeks. Similarly, this transient radiation mvelopa-thelial cells may occur, leading to a breakdown of thy could be a result of tempo ary demnelination ofthe blood-brain barrier. This would result in sensorv neurons. In addition, mitotic activity in thevasogenic edema, the elevated pressure-impair,Žd subependymal plate (important in glia production)circulation of cerebral spinal fluid, and eventually did not recover after radiation doses producing ne-neuronal and myelin degeneration.'" Ir " I he finding crosis, but did recover after doses not producing ne-that hypertension accelerates the appearance of vas- ciosis. This supports the hypothesis that glia are acular lesions in the brain after irradiation with 10-30 primary target for radiogenic brain damage."Gy also supports a hypothesis of vascular patho- Both vascular and glial changes may be impor-genesis."'' The occlusive effects of radiation on arte- tant in the development of late radiation damage torial walls may cause a transient ce.ebral ischemia. 1"i the CNS." The preponderance of one type of cellSequential monkey-brain CAT scans revealed brain damage over another depends on the radiation doseedema and hydrocephalis that accompanied hypoac- used. "Vascular effects occur at lower dose levelstivitv and the animal's loss of alertness following 20 but after a longer latent period than effects mediatedGv of radiation.-" The exposure of forty-five rabbit through damage to the neuroglia.'"I Perhaps theheads to 4, 6, or 8 Gy of X radiation produced a dis- most important points for the present chapter areturbance of the permeability of the blood-brain bar- that (a) radiogenic brain damage is a well-acceptedrier that returned to normal only after 6 davs.'s The finding after high doses (greater than 15 Gy, and (11)transient nature of the vascular phenomena may it may occur after doses of less than 15 Gv under cer-partially explain some of the behavioral deficits ob- tain circumstances. The mechanisms of this damageserved after exposure to intermediate or large doses are still debatable.of ionizing radiation. 1s4. In addition to axonal demyelination, other direct
Evidence for the direct action of radiation on the neuronal damage may occur in the irradiated adultparenchymal cells of the nervous syst.m, rather than animal. Although mitotic neurons of the prenatal orthe indirect effect through the vascular bed, was first neonatal CNS are known to be extremely sensitive toprovided when brain tissue in irradiated human pa- radiation, the neurons of more mature animals aretients was examined."" None of the brain lesions thought to be quite resistant and less likely to resultcould be attributed to vascular damage because they in cell death.IWI 4
I7. However, as early as 1962,
were (a) predominantly in white matter and not co- neurogenesis was thought to take place in the cere-distributed with blood vessels, (1b) not morphologi- bral cortex of adult rats.'• Adult and juvenilecally typical of ischemic necrosis, and (c) often found neurogenesis was found to be especially prominentin the absence of any vascular effects. ,7-"1 Thus, it in the granule cell populations of the hippocampusappears that direct neuronal or glial mechanisms and the olfactory bulb. These newly formed cellscaused at least some of the observed radiogenic had the ultrastructural characteristics of neurons,"brain lesions. and the number of granule cells in the hippocampus
In the brain, hypertension accelerates the onset of increased in the adult rat. 2"'1",-' Although these find-radiogenic vascular damage but not white matter le- ings have not been confirmed in primates (thus re-sions."' These data help to separate vascular dam- ducing their ability to be generalized to the human),age from the pathogenesis of white-matter lesions, they suggest that certain neuron populations in themaking it difficult to support the view that ischemia adut. brain are radiosensitive due to their mitoticand edema are important in white-matter patho- state. 2"2 Neurogenesis was reported in the hip-genesis. It may be that selective necrosis of white pocampal subgranular cell layer of the adult rabbit,matter is due to the slow reproductive loss of glia or and these cells were quite radiosensitive (4.0-4.5their precursors. The radiosensitivity of certain Gv).2'0 2'" Therefore, it may be that certain popula-types of glial cells (beta astrocyte) is well recog- tions of proliferating neurons in the adult can benized."',"' The earliest sign of their damage is wid- damaged or destroyed by relatively low doses of
123

Medical Collst'(11401 tt Nucldear hiMrtifrc
ionizing radiation. behavioral incapacitation."" Exposures to 4-6 Gv ofRadiogenic changes in brain morphology are not gamma radiation seem to stimulate spontaneous ac-
limited to necrotic lesions or cell death. Subtle den- tivitv in the neocortex, whereas exposures of higherdritic alterations following X irradiation, including than 9 Gv inhibit all brain activities."'decreased dendritic intersections, branchings, and The hippocampus shows significant changes inlength, as well as reduced packing density of neu- physiological activities after gamma irradiation withronal elements in the irradiated cerebral cortex of even less than half of the 18-Gv threshold dosethe monkey, were reported.2'" needed to produce changes in cortical activities. ̀ 4
212
One of the most striking effects was hippocampalAlterations in Nervous System Function spike discharges, first identified in cats7' and later
confirmed in rabbits.2"' This spiking developed soonGiven the above data, we can say that (except for after irradiation (2-4 Gy) when no other clinical
the possibility of mitotic neurons in the CNS) the signs of neurological damage or radiation sicknessadult brain is indeed relatively resistant to radiation were present. The apparent radiosensitivity of thewhen the end point measured is cell death or change hippocampus and its importance in critical functionsin neuronal morphology. However, the point is that like learning, memory, and motor performance havethe CNS is quite sensitive to functional changes recently led others to investigate the electrophysiol-brought on by alterations in neurophysiology and ogy of this brain area. The firing of hippocampalneurochemistry. It is likely that these functional neurons was found to be altered by exposure to 4 Gychanges, brought about by low or intermediate of gamma radiation.""1 In addition, in vitro experi-doses (less than 15 Gy) of ionizing radiation, account ments suggest that spontaneous discharges of hip-for many of the behavioral changes observed. pocampal pacemaker-like neurons are induced by X
Supporting this view, changes in brain metabo- and gamma rays at a dose of 0.08 Gy.21- If con-lism were reported after very' low (0.11-0.24 Gv) firmed, these data suggest that hippocampal electro-doses of ionizing radiation.2"' In a more detailed physiology may be the most sensitive measure ofanalysis with the 14C-2-deoxyglucose method of functional brain changes after irradiation.measuring local cerebral glucose utilization, a dose Alterations in the thresholds and patterns forof 15 Gv of X radiation was administered to the rat audiogenic and electroconvulsive seizures have beenbrain.2 ',- Significantly lower rates of glucose use produced by exposing animals to ionizing radia-were found in sixteen different rat brain structures tions. Such effects are generally interpreted as re-at 4 days after irradiation and in twenty-five struc- flecting gross changes in CNS reactivity. Early worktures at 4 weeks. Although large radiogenic changes with dogs showed that spontaneous seizures some-exist in the metabolism of some brain nuclei, a times occurred following very large doses of radia-weighted average rate for the irradiated brains, as a tion." 4 Later experiments confirmed that seizureswhole, was approximately 157c below that for the can be induced by whole-body or head-only expo-controls. sures to 30-250 Gy in a variety of species. For ex-
Electrophysiologiy. Measures of electrophysiol- ample, rats were exposed to 5 Gy of X radiation andogy have been used to illustrate changes in brain the electroconvulsive shock (ECS) threshold was de-function after exposure to ionizing radiation. Sev- termined for 180 days after irradiation.-1 7 ECSeral studies were reviewed in which cortical EEG thresholds were reduced in irradiated rats over thechanges were observed in humans and in animals entire test period. In later studies,"'4 it was reportedfollowing doses of less than 0.05 Gy.-"' Typically, an that considerably lower doses (perhaps less thaninitial temporary increase in bioelectric amplitude 0.01 Gy) also reduced the thresholds for ECS sei-was followed, within minutes, by a depression. zures and audiogenic seizures.-"
Other investigations have frequently needed higher Unlike the CNS, peripheral nerves are quite resis-doses of radiation in order to observe changes in tant to the functional alterations produced by ioniz-EEG. For example, changes were not seen in EEGs ing radiation. Most data indicate that peripheralafter 0.03-0.04 Gy, but significant alterations were nerves do not show any changes in electrophysiol-observed after 2 Gy.2"' At a higher dose (15 Gy), ogy with X-ray exposures below 100 GV. 2 17 Aftermonkey cortical EEG abnormalities consisted of the higher doses, the action-potential amplitude and theslowing of activity, with an increase in amplitude."" conduction velocity temporarily increase but thenSpiking and patterns of grand mal seizure also oc- gradually decrease. -21-221 Also, alpha and beta par-curred. A rapid onset of high-amplitude slow ticles are more destructive to peripheral nerves thanwaves (delta waves) seemed to relate to periods of are gamma or X rays, and usually cause a monopha-
124

Bchaiworal and Newrophy /iohoical ChaLt)is with ' Y Erpsu re to Ionzitig tKalation
sic depression of function without the initial en- same cell were not significantly affected by a 12-Gvhancement of activity.-2 2 2--2 4 Perhaps the lowest dose exposure. -2" Similarly, polysynaptic EPSPs wereof ionizing radiation ever found to produce an al- significantly augmented as the dose increased,teration in the function of peripheral nerves was re- whereas the polysynaptic IPSPs were little influ-ported in a study in which T-shaped preparations of enced by even an exposure of 158 Gy. At higherisolated frog sciatic nerves were produced when the doses (50-200 Gy), ionizing radiation may damagenerves were partially divided longitudinally. 22- both synaptic and postsynaptic functioning, proba-Electrical stimulation was applied to the intact stem bly through different molecular mechanisms."of the T, and electrical recordings were made from These radiogenic changes in synaptic transmissionthe ends of the two branches. A small segment of may be important factors underlying the compli-one of the branches was irradiated with 0.04-0.06 Gy cated functional changes that occur in the CNS fol-of alpha particles, producing a definite decrease in lowing radiation exposures.action-potential amplitude and an increase in chro- Neurochemistry. One of the most importantnaxie. These results are remarkable, given the much mechanisms of postirradiation nervous transmissionhigher doses that have been required to affect these to be studied has been the ion flow across the neu-peripheral nerve functions in most other studies. ronal semipermeable membrane. In particular, the
Relatively little radiobiology research has been flow of sodium ions is believed to be involved in thedone using single isolated nerve fibers. However, control of neuronal excitability2- and apparently canthe results that do exist agree with those from ex- be disrupted after either a very high or very lowperiments with nerve trunks. In single fibers iso- dose of radiation. A study using the radioactive iso-lated from a frog sciatic nerve, effects on peripheral tope sodium-24 compared the sodium intake acrossnerve functions included the induction of an injury the membrane of the squid giant axon before and af-current in the irradiated segment and, with in- ter exposure to X rays.-17 A significant increase increased exposure, a sequence consisting of increased sodium intake was found to occur during the initialthreshold, reduced action potential, and finally a hyperactive period induced by a dose of 500 Gy.conduction block.2'-2 These observations were confirmed in a study of
It has been known for some time that paralysis of frog sciatic nerves that had been irradiated withthe hind limbs of animals can result from localized 1,500-2,000 Gy of alpha particles, although a simul-irradiation of the spinal cord. Rabbits developed taneous decrease in the rate of sodium extrusion alsothis paralysis at 4-33 weeks after exposure of the occurred..2 22 Peripheral nerves may be less radiosen-upper thoracic region to 30-110 Gy of X radiation at sitive than CNS neurons and perhaps differ in their2.5 Gy/day.-" The minimum single exposure found radiation response. In a study that used a differentto produce paralysis at 5 months was 20 Gy.-22 7 As in technique, the artificially stimulated uptake of so-other model systems, the time interval between irra- dium into brain synaptosomes was significantly re-diation and the appearance of neurological symp- duced by an ionizing radiation exposure (high-en-toms decreases as dose increases. For example, 50 ergy electrons) of 0.1-1,000.0 Gy.2-38 This CNS effectGy of X rays to the monkey midthoracic spinal cord was later confirmed for 1-100 Gy of gamma radia-produced immediate paraplegia, whereas 40 Gy was tion.23-
effective only after a latent period of about 5.5 The brain has been described as a radiosensitivemonths.22 " biochemical system,2 '" and in fact, many significant
Radiation effects on the electrophysiology of the changes in brain neurochemistry have been ob-synapse were first studied using the cat spinal re- served after irradiation. An early study revealedflex.-"--2 These studies showed that excitatory syn- that 1-2 days after an exposure to 3 Gy of X radia-aptic transmission is significantly increased by X-ray tion, neurosecretory granules in the hypophysial-exposures of 4-6 Gy. Synaptic transmission at the hypothalamic system showed a transient increase inupper cervical ganglion of the cat is also facilitated number over the controls. 24
" A leaking of brain15-20 minutes after exposure to 8 Gy of X rays.2
14 monoamines from the neuronal terminals of rats ir-
Both mono- and polysynaptic spinal reflexes are sig- radiated with 40 Gy of X rays has also been ob-nificantly augmented immediately after exposure to served.24' These changes in neuronal structure may5 Gv of X radiation. It is of interest that significant correlate with radiogenic alterations of neurotrans-augmentation of monosynaptic excitatory postsyn- mitter systems.aptic potentials (EPSP) was found immediately after Normal catecholamine functioning appears to beexposure to 6-12 Gy of X rays, whereas inhibitory damaged following exposure to intermediate orpostsynaptic potentials (IPSP) recorded from the high doses of ionizing radiation. After 100 Gy, a
125

Medical Cottsequeices otf Nuchar Warfan'
transient disruption in dopamine functioning (simi- smaller doses depress plasma acetylcholinesteraselar in some ways to dopamine-receptor blockade) by 30%.2ý2was demonstrated.242 This idea is further supported Cyclic nucleotides, such as cyclic AMP (adeno-by the finding that a 30-Gy radiation exposure in- sine-3,5'-cyclic monophosphate), act as second mes-creases the ability of haloperidol (a dopamine-recep- sengers in synaptic transmission. It is interestingtor-blocking drug) to produce cataleptic behavior.24
3 that after irradiation (50 Gy), concentrations of cyclicRadiation-induced effects on dopamine have been AMP are reduced in rats"" and monkeys.2 4 Thecorrelated in time with ETI, suggesting that changes transient nature of these changes also suggests theirin this neurotransmitter system may play a role in possible role in EPDs.behavioral disruptions. However, other neuro- Exposure to large doses of ionizing radiation re-modulators (such as prostaglandins) also seem to in- sults in postirradiation hypotension in mon-fluence dopaminergic systems to help produce some keys,"IL 25 2 •' with arterial blood pressure decreasingradiation-induced behavioral changes.243 A transient to less than 507 of normal.2 ý7 Postirradiation hypo-reduction in the norepinephrine content of a mon- tension also produces a decrease in cerebral bloodkey hypothalamus was also observed on the day of flow immediately after a single dose of either 25 orexposure to 6.6 Gy of gamma radiation. Levels of 100 Gy of cobalt-60 gamma radiation.272,2:;10 Thisthis neurotransmitter returned to normal 3 days hypotension may be responsible for the ETI ob-later."4' Similar effects have been reported,'2 4
; but served after a supralethal dose of ionizing radia-another study found no change in noradrenaline af- tion.ll 2' 2 bI In support of this hypothesis, the anti-ter 8.5 Gy of X rays.24" Monoamine oxidase (MAO), histamine chlorpheniramine maleate was effective inan enzyme which breaks down catecholamines, was reducing the monkeys' performance decrements andsignificantly reduced by a supralethal 200-Gy dose at the same time reducing postirradiation hypoten-of mixed neutron-gamma radiation. This enzymatic sion.2
;7 A study with untrained monkeys, whose
change occurred within 4 minutes of exposure and postirradiation blood pressures were maintained bylasted for at least 3 hours. In contrast, a very norepinephrine or other pressor drugs, showed thatmarked increase in MAO activity was observed as long as arterial pressure remained above a criticalwhen animals received the same dose of radiation level, the monkeys appeared to remain attentive andrich in gamma rays.-17 alert. 2 -,2 However, in a follow-up study on monkeys
Contradiction exists in the literature concerning trained to perform a task, norepinephrine main-radiation's effects on 5-hydroxytryptamine (5-HT). tained blood pressure but did not consistently im-Some investigators reported a radiogenic stimula- prove their performance during the first 30 minutestion of 5-HT release at approximately 10 Gy, while after irradiation. 2
(-l Other authors have not seen aothers observed a decrease or no change in the levels close association between blood pressure and behav-of this neurotransmitter. 24 " Although the physiologi- ioral changes.21 " Further contrary evidence was ob-cal mediators of transient functional deficits may not tained from experiments with the spontaneouslybe the mediators of radiation-induced mortality, it is hypertensive rat (SHR), in which exposure to ioniz-interesting that dopamine and 5-HT have been sug- ing radiation reduced the blood pressure of most ofgested as radioprotectants for prolonging the sur- them to near-normal levels. However, these irradi-vival of X-irradiated rats or mice.248.24- ated SHRs still showed a significant behavioral defi-
A variety of functions involving the neurotrans- cit after exposure to 100 Gy of high-energymitter acetylcholine (ACH) is significantly altered by electrons .2 4 Finally, a significant association wasexposure to ionizing radiation. ACH synthesis rap- found between the degree of hypotension and theidly increases in the hypothalamus of the rat after frequency of EPDs.H" Still, half the monkeys with aless than 0.02 Gy of beta radiation, but is inhibited at 50% drop in blood pressure did not show behavioralonly slightly higher radiation doses.21" A dose of 4 decrements. Thus, even though the relationship be-Gy of cobalt-60 gamma radiation produced a long- tween decreased blood pressure and impaired per-term increase in the rate of ACH synthesis in dogs. 25
4 formance is intriguing, simple changes in bloodAlso, high-affinity choline uptake (a correlate of pressure may not be sufficient to explain EPDs.ACH turnover and release) slowly increased to 24/ The massive release of histamine that is observedabove control levels 15 minutes after irradiation after exposure to a large dose of ionizing radiationwith 100 Gy. 242 Choline uptake was back to normal has been proposed as a mediator of radiogenicby 30 minutes after exposure. Massive doses of hypotension and EPDs. 2
b Histamine is a very activegamma or X rays (up to 600 Gy) are required to alter biogenic amine and putative neurotransmitter lo-brain acetylcholinesterase activity,2-' whereas much cated in neurons and mast cells throughout the
126

Bchiori)al and NwrphYsiWOyAgidl ChainllgCs with Extkpsuret to Imlizipg Radiation
body, especially around blood v'essels.-" Attempts analgesia of the rat was significantly enhanced 24to alter the development of behavioral deficits by hours after neutron (but not gamma) irradiation,treating animals with antihistamines before expo- suggesting some combined delayed effects of en-sure have been encouraging.-2 ý--2o' Monkeys pre- dogenous and exogenous analgesics that may be ra-treated with chlorpheniramine (H,-receptor blocker) diation-specific.'4 1 Ionizing radiation exposure canperformed better and survived longer after irradia- also attenuate the naloxone-precipitated abstinencetion than did controls.-'X Similar benefits were ob- syndrome in morphine-dependent rats.2"'served in irradiated rats."'"' Further, the use of Further supporting the hypothesis that endor-diphenhydramine (a histamine H,-receptor antago- phins are involved in radiation-induced behavioralnist) inhibited radiation-induced cardiovascular dys- change, C57BI/6J mice exhibited a stereotypic loco-function.2 "' Since these antagonists produced only motor hyperactivity similar to that observed afterpartial relief from radiation effects, it appears that morphine injection, after receiving 10-15 Gy of co-the histamine hypothesis explains only a portion of balt-60 gamma radiation.' This radiogenic behaviorthe behavioral and physiological deficits observed was reversed by administering naloxone or by pre-after radiation exposure.2 `'' exposing the mice to chronically stressful situations
When most animal species are exposed to a suffi- (a procedure that produces endorphin tolerance).2 1'
ciently large dose of ionizing radiation, they exhibit Further, opiate-experienced C57BI/6J mice reducedlethargy, hypokinesia, and deficits in perform- the self-administration of morphine after irradiation,ance."'.4.121 Because these behaviors seem similar to suggesting that the internal production of an endor-those observed after a large dose of morphine, a role phin reduced the requirement for an exogenousfor endogenous opioids (endorphins) has been pro- opioid compound.2
112 Biochemical assays also re-posed in the production of radiation-induced behav- vealed changes in mouse brain beta-endorphin afterioral changes.2-' 272 Endogenous morphine-like sub- exposure to ionizing radiation. 2"3 Rats and monkeysstances may be released as a reaction to some 27 -275 had enhanced blood levels of beta-endorphin afterbut not all' stressful situations. Like a sufficiently irradiation, 21. 2"' and morphine-tolerant rats showedlarge injection of morphine itself, endogenous less performance decrement after irradiation thanopioids can produce lethargy, somnolence, and re- nontolerant subjects .2"1 In addition, naloxone (1duction in behavioral responsiveness. 2:b, 2- mg/kg) given immediately before exposure to 100
Cross-tolerance between endorphins and mor- Gy of high-energy electrons significantly attenuatedphine has been demonstrated for a variety of behav- the ETI observed in rats.2"4 Conversely, rats eitherioral and physiological measures.- 7,27' Given the underwent no change&- or were made more sensitivesimilarity of radiation- and opiate-induced symp- to radiation effects after chronic treatment withtoms, it is not surprising that endorphins appear to naloxone on a schedule that increased the number ofbe involved in some aspects of radiogenic behavioral endorphin receptors.2"• However, the manipulationchange. Ionizing radiation can produce dose-de- of opioid systems did not produce total control overpendent analgesia in mice, and this radiogenic anal- postirradiation performance deficits. Thus, thesegesia can be reversed by the opiate antagonist nalox- data do not suggest an exclusive role for endorphinsone.14b In another experiment, morphine-induced in radiogenic behavioral change.
THE HUMAN EXPERIENCE WITH RADIATION
Humans have been exposed to radiation from least in a qualitative context, because they partiallyenvironmental and industrial sources, clinical ther- validate some work with animal models and alsoapy, accidents, wartime detonations at Hiroshima suggest new hypotheses for testing.and Nagasaki, and even experiments. Many of these Two radiation accidents are particularly instruc-exposures contribute little information about the be- tive. Both exposures occurred in the early days ofhavioral effects of ionizing radiation. In most of the the production of fissionable radiation material forcases, behavioral data were not collected. Many of nuclear weapons and involved radiation doses largethe data that were gathered are difficult to evaluate enough to produce an ETI. In spite of safety precau-because there is no information about the radiation tions to ensure that the plutonium-rich holdingdose received, the level of baseline performance, or tanks did not contain enough fissionable material toother circumstances. But the data are interesting, at permit the occurrence of a critical reaction, an acci-
127

Metdical C,•nst,11111CO, , \ýNCh'M arfare'iu
dental critical event took place in 19-58 at the Los duce EPDs. Both of the accident victims experiencedAlamos Scientific Laboratorv."' Mr. K. received an behavioral deficits to some degree soon after expo-average (and fatal) total body dose of 45 Gv and an sure. These deficits were transient and were mostupper abdominal dose estimated at 120 G- of mixed prominent in Mr. K. The data agree with generalneutron-gamma radiation. During the event, Mr. K. conclusions reached in a review of several radiationeither fell or was knocked to the floor. For a short accidents, in which a remission of early symptomsperiod, he was apparently dazed and turned his plu- occurred before the onset of the manifest illnesstonium-mixing apparatus off and on again. He was phase was recorded. 2') In comparison with theseable to run to another room but soon became ataxic high-dose accidents, lower radiation doses or par-and disoriented. Because he kept repeating, "I'm tial-body exposures may produce milder but moreburning up, I'm burning up," his co-workers helped persistent behavioral changes characterized byhim to a shower, but bv this time he could not stand weakness and fatigability. An accident victim ex-unaided. He was incapacitated and drifted in and posed to ionizing radiation from an unshieldedout of consciousness for over a half hour before he klystron tube received as much as 10 Gy to portionswas rushed to a local hospital. Before his death at 35 of his upper torso and experienced fatigability thathours after irradiation, Mr. K. regained conscious- lasted for more than 210 days after exposure.2
11
ness and a degree of coherence. From approxi- The 1986 Chernobyl nuclear reactor accident alsomatelv 2 to 30 hours after the accident, he showed produced behavioral deficits in persons attemptingsignificant behavioral recovery and at some points to perform their duties in high-radiation environ-actuallv experienced euphoria, although his clinical ments. A Soviet fireman who fought the blaze of thesigns were grave. The last few hours before Mr. K.'s burning reactor core suffered performance deficitsdeath were characterized by irritability, uncoopera- and eventually had to withdraw because of his ex-tiveness, mania, and eventually coma.2 i" posure to radiation.2 ' 2 Similarly, a Soviet physician
The 1964 case of Mr. P., an employee of a ura- who had received significant radiation exposuresnium-235 recovery plant, closely parallels that of Mr. while treating patients could not perform his du-K. This accident took place in Providence, Rhode Is- ties."" Both persons eventually recovered from theirland, when Mr. P. wvas trying to extract fissionable behaviorally depressed states and are (at this writ-material from uranium scraps. A criticality oc- ing) still alive. These recent accident data add to thecurred, and Mr. P. was thrown backward" and growing literature suggesting that sublethal doses ofstunned for a period of time. He received a head radiation can induce human performance decre-dose of 140 Gv and an average body dose of 120 Gv. ments.Unlike Mr. K., however, Mr. P. did not lose con- A few attempts have been made to assess humansciousness. After a period of disorientation and con- performance after clinical irradiations. The Halstedfusion, he stood up and ran from the building to an test battery for frontal-lobe functional deficits wasemergency shack, a distance of over 200 yards. Mr. used in four patients exposed to 0.12-1.90 Gy ofP.'s awareness of his surroundings during this early mixed neutron-gamma radiations..2 1
4 Test scores atperiod has been questioned because he ran into a 4- days 1-4 and 1 year after exposure were within theinch-wide sapling even though it was quite visible. normal range. Patients with advanced neoplasticUnfortunately, Mr. P. rode in an ambulance for al- disease were whole-bodv irradiated with 0.15-2.0most 2 hours, during which time behavioral obser- Gy given as a single dose or in 2-5 fractions sep:vations were not made. When he arrived at Rhode rated by intervals of up to 1 hour.12 The subjectsIsland Hospital, he had transient difficulty enunciat- were pretrained and served as their own controls ining words. Significant behavioral recover' occurred performing tests designed to assess hand-eve coordi-from 8 to 10 hours after the accident. During this nation. Tests were performed immediately after ex-period, Mr. P. was alert, cooperative, and talked of posure and at later intervals, but at no time did afuture activities in a euphoric manner, inconsistent performance decrement exist that could be ascribedwith his terminal diagnosis. In the hours before his to these relatively low radiation doses. However,death at 49 hours after the accident, Mr. P.'s condi- because the behavioral design of these experimentstion deteriorated significantly, and he exhibited rest- was secondary to medical treatment, the results arelessness, anxiety, extreme fatigue, and disorienta- inconclusive. The paucity of radiobiological data ontion.21', human behavior and the need to predict military
These cases of radiation accidents involving hu- performance after ionizing radiation exposure havemans are consistent with the animal literature sug- led to an extensive Defense Nuclear Agency pro-gesting that a supralethal radiation dose can pro- gram on the estimation of human radiation effects.2';
128

BehaIioral aind NVuroPhY,4tisiologic Change,; with Exposure to Ionizmin Radiation
Intermediate Dose ProgramRadiation Sickness Representative CombatSymptomatology Crew Functions
"* Radiation Accident Victims * Military Operation Analysis"* Radio oy Research " Military Systems Analysis"* Japanese A-Bomb Victims Mi*itary Task Analysis"* Radiation Therapy" Chrnoyl Combat Crew ' ,
Questionnaire• 1 ~" Armor t
S•" ArtilleryS•" Anti-Tank
Field Manuals Effectiveness TrainingSTANAGS Modeling * Circulars
* Crew/Unit * Field Exercises
Fig. 7-8. Outline of empirical approach used by Defense Nuclear Agency to estimate performance deficits after an inter-mediate dose (0.75-45 Gv) of ionizing radiation
RADIATION-INDUCED CHANGES IN MILITARY PERFORMANCE
The U.S. Army has predicted certain distributions Gy) on combat troops.of effect for combat personnel exposed to ionizing To predict human radiation-induced perform-radiation. For every soldier who receives a radiation ance deficits, the Defense Nuclear Agency used adose of greater than 30 Gv (a supralethal and behav- survey method of first identifying the physicaliorally incapacitating dose), another will receive a le- symptoms expected after various radiation dosesthal (4.5 Gy) dose that may alter behavior. Two and then determining the soldiers' estimates of theirmore soldiers will receive doses that are sublethal own changes in performance while experiencingbut greater than the present maximum (0.5 Gv) al- these symptoms (Figure 7-8). Briefly, this involvedlowed for troop safety."" Given this wide range of (a) an extensive review of the literature on humanexpected doses and the ambiguity of the expected radiation (including radiation-therapy patients,outcomes for human behavior, the Defense Nuclear Japanese atomic-bomb victims, and radiation-acci-Agency established methods for estimating the be- dent victims) to identify the symptoms to be ex-havioral effects of acute radiation doses (0.75-45.0 pected after the radiation doses of interest; (b) the
129

M~edical Consequences of Nucleawr Wa~rfare'
4,500
-3.000
S2.000 %
1.000-3
0a 500
200 0
wU 100
LL. 10075
0.2 0.5 1 2 5 10 20 50 100 200 500 1,000
TIME (Hour)
Fig. 7-14. Expected changes in performance at various times after a gun-crew chief is exposed to a single radiation dose, as
specified. Contours represent a person'-, average performance in increments of capability (such as performing at 10% of
normal capacity).ISotrce: Data are derivt ed fromi the Humnan Respoinse Proggrami of the Defense Nuclear Agency
10,000
Dose ....- ---
1,000
* * *... * ** .... * *. ** ** ............. **..
3 10 100 1,000 10,000 100,000A A A
Ilhr I day I moTime After Exposure (min)
Fig. 7-10. Expected behavioral response to radiation exposure for persons performing a physically demanding task. Com-
bat effective: 75'ý -ItXW, normal capacity. Degraded: 251/,-7,511 Combat ineffective: 0-2517, 0 cGy = I rad)Source: Data arc derivedi fromn the Huiman Respoinse Programn of the Defense Nuclear Agency
130

10,000
Dose(cGy) ...
1000 Combat
3.10.10.1,000 10,000 100,00Ef f e i ..........
10,000s
3 10 100 1,000 10,000 100,000A k &
1lhr 1iday 1 moTime After Exposure (min)
Fill. 7-12L F\pected behavioral response to radiation e\POSUre for persons performing ta xskslk reuirdeofandn task.eioptrce.Combat effective: 77' ,1)0 normial capacitv . Degraded: 2 5'; 1-73" Combat ineffective: 0-23';'4ource: Data ire deLriX edk trom the H Lman Rc~pon~c Program of the i DOC II se \iclIca r Agncil\
109131

Mc'dital Cog ItcqlItct' of N*\ ct''ar Wairtart'
compilation of symptom complexes that reflect vari- degraded similarly. The capabilities of crew mem-ous combinations of the expected radiogenic symp- bers performing physically demanding tasks are de-toms, including gastrointestinal distress, fatigability, graded more than the capabilities of members per-weakness, hypotension, infection, bleeding, fever, forming physically undemanding tasks. This latterfluid loss, and electrolyte imbalance;"-, (c) the devel- observation agrees with the data from animal stud-opment of accurate descriptions of the severity of ies on physical effort after irradiation (Figure 7-4).each symptom category at each postirradiation time Figures 7-10, 7-11, and 7-12 illustrate the behavioralof interest; (d) an analysis of tasks performed by five changes that might be expected during a one-monthdifferent crews, including a field artillery gun (155- period after various doses of ionizing radiation. Formm SP Howitzer) crew, a manual-operations field example, if crew members performing a physicallyartillery fire-direction crew, a tank (M60A3) crew, a demanding task are exposed to 10 Gy (Figure 7-10),CH-47 (Chinook helicopter) crew, and an anti-tank they will be combat effective for only a little over Iguided missile crew in a TOW vehicle; (0) the devel- hour. This period will be followed by an extendedopment of questionnaires that require experienced time (roughly 1 month) of degraded performancecrewmembers (NCOs or warrant officers) to predict before they become combat ineffective before death.task degradation (slowing of performance) during The outlook for performance (but not ultimate prog-particular symptom complexes; and (9 the evalu- nosis) is a little better for a person performing aation of monkey performance data from a visual-dis- physically undemanding task after a 10-Gy irradia-crimination (physically undemanding) task or a tion (Figure 7-11). This soldier would remain com-wheel-running (physically demanding) task.2-' This bat effective for 1.7 hours after exposure. Followinganalysis of animal data was performed, in the ab- this initial period of coping, a transient performancesence of sufficient human data, in order to estimate degradation of 2.8 days would ensue before a shortthe rapid behavioral decrements that follow large recovery and then a gradual decline, ending in death(10-45 Gy) radiation doses. at I month after irradiation.
For each crew position, sophisticated statistical In order to obtain an independent check of thetechniques made possible the construction of min- performance degradations predicted for radiationute-by-minute performance estimates and also sickness by this study, results were comparedsmoothed the summary curves as a function of ra- (where possible) to actual performance decrementsdiation dose and time (Figure 7-9). The analysis in- measured in members of the U.S. Coast Guard. Thevolved grouping the results from individual crew decrements occurred during motion-sickness epi-members into two categories: physically demanding sodes with symptoms similar to those of radiationtasks and physically undemanding tasks (Figures 7- sickness. This comparison revealed that the esti-10 and 7-11). A separate analysis of helicopter tasks mates of radiogenic performance decrements madewas also made (Figure 7-12). The degree of perform- by responders to the questionnaire were similar toance deficit for each of the five crew positions was the actual declines in short-term task performancedescribed in terms of the following categories: (a) that were measured during motion sickness.performance capability 75%-1007l of normal is corn- Although these are the best estimates of humanbat effective, (1)) performance capability 25§/-75/c of radiation-induced behavioral deficits that are cur-normal is degraded, and (c) performance capability rently available, their limitations are recognized.0-25% of normal is combat ineffective. These predictions apply to the physiological effects
This scheme was then used to summarize the ex- of prompt whole-body irradiation. The data do notpected changes in the performance of combatants af- predict the behavioral effects of protracted radiationter various doses of radiation exposure. 2'; In gen- exposures that would occur with fallout, nor do theyeral, the data indicate that the capabilities of crew attempt to account for degradation from the psycho-members performing tasks of similar demand are logical effects that are unique to nuclear combat.
RADIOPROTECTION AND BEHAVIOR
Relatively few studies have addressed the prob- tion. Research suggests that antihistamines and opi-lem of normalizing the behavioral changes that are ate antagonists (such as naloxone) may offer behav-seen immediately (and up to 24 hours) after irradia- ioral radioprotection under certain circumstances.
132

b'haz'ioral and Nei trophlisioloy0iciIl Ohani with Exposurtre to hizing R~adiation
Some data suggest that estrogens (known to reduce and tasks analyzed, ethiofos was behaviorally toxiclethal effects of ionizing radiation) 2 ""' can reduce when given alone (it disrupted trained behavior or itthe intensity and duration of radiation-induced early reduced locomotor activity), and it increased rathertransient behavioral deficits in castrated rats trained than decreased the radiation-induced performanceto perform an avoidance task."" Amphetamines can decrements. Thus, although ethiofos protects fromcontinue to produce locomotor hyperactivity in rats the lethal effects of radiation, it has limited use whenafter irradiation with 100 Gy of electrons at a time the recipient must remain functional. This conceptwhen the animals would normally be hypoactive. of a behaviorally tolerated drug dose is very impor-Experiments have also been performed to evaluate tant in evaluating the radio-protectant candidatesthe behavioral toxicity of radioprotectants that have for military use.the ability to (a) reduce the lethal effects of radiationor (b) challenge the emesis that sometimes accompa- Efficacy of Antiemeticsnies intermediate doses of ionizing radiation.02
Although considerable research on antiemetics
Radioprotectants that Reduce Mortality exists, its focus has been mainly limited to drugsthat are effective in radiation therapy.•`. 7 -' In this
Traditionally, the development of radioprotec- regard, various anti-inflammatory drugs (such astants has meant searching for compounds to protect dexamethasone and steroids) have been useful infrom the lethal effects of ionizing radiation."" More managing the emesis of patients.3 ) 3.3"' However,recently, radioprotective compounds have been therapy makes few task demands on the recipients;evaluated for their ability not only to decrease mor- in the military, antiemetics that are effective againsttality but also to preserve behavioral capacities after radiation-induced vomiting must also not disruptirradiation."2 -3 02 Two early studies administered n- performance capabilities. These requirements sig-decylaminoethanethiosulfuric acid (WR-1607) (10 nificantly reduce the field of potentially useful anti-mg/kg, intravenous) to monkeys and reported some emetics. For example, metoclopramide, dazopride,behavioral benefits.i1'.3 In the first study, monkeys and zacopride (5-HT3-receptor blockers) were testedtrained to perform a continuous-avoidance task for antiemetic effects in monkeys exposed to 8 Gy ofwere exposed to 100-400 Gy of pulsed neutron- gamma radiation."x All three drugs were found togamma radiation"' Protection from ETI was ob- be effective antiemetics. However, only zacoprideserved up to 4 hours after irradiation, and WR-1607 had no readily observable behavioral effects; meto-extended the lives of the subjects for almost 5 hours clopramide disrupted motor performance, andbeyond that observed in control animals. In the sec- dazopride produced drowsiness.' Additional workond study, monkeys trained to perform a visual-dis- assessed the behavioral toxicity of zacopride in mon-crimination task were exposed to 25 or 40 Gy of keys performing the speed-stress visual-discrimina-mixed neutron-gamma radiation. 3 ETI was tion task 3" and in rats performing the accelerating-blocked during the first hour, but performance rod task.3'
2 No behavioral toxicity was observed instarted to fall 2 hours after exposure. Although either performance model. In the future, these morethese behavioral results were promising, WR-1607 refined behavioral measures will be used to assessproduced severe emesis. This side effect may ex- the military usefulness of these and other putativeplain the current shift of interest to another promis- antiemetics after radiation exposure.ing drug, WR-2721 (ethiofos)."'-
Many experiments have assessed the behavioral Shieldingtoxicity of drugs that are known to offer protectionfrom radiation mortality. Researchers have been In addition to pharmacological radioprotection,studying ethiofos extensively, hoping that it has the immediate effects of radiation may be mitigatedfewer side effects than WR-1607.13 Troops who are by shielding (placing material between the radiationincapacitated on the battlefield from a radioprotec- source and the subject). Studies have focused on ei-tant are as great a loss as troops incapacitated by ther head shielding (body exposed) or body shield-ionizing radiation. Ethiofos has been tested in mice, ing (head exposed). In one study of ETI, pigs wererats, and monkeys for its behavioral toxicity and its trained to traverse a shuttle-box on cue and thenpotential ability to block radiogenic performance were either body-exposed or head-exposed todecrements, using spontaneous locomotor activities 60-130 Gy of mixed neutron-gamma radiation.3"as well as accelerating-rod and visual-discrimination The investigators reported that head shielding of-performance tests.-',27 ,II-•43 )1 In all of the species fered significant protection from ETI. Other short-
133

Mcth'c•al Ctpoit cs qtwt• t Nith'ar Wat tarc'
term shielding experiments were conducted with It is more important here that the initial decreases inmonkeys trained to perform a visual-discrimination spontaneous locomotor activity were less severe intask.'""' The monkeys were exposed to mixed neu- the marrow-treated rats. Instead of showing a sec-tron-gamma radiation at doses of 25, 45, or 100 Gv. ond drop in activity 10 days after irradiation, theIn the 25- and 100-Gv-dose groups, ETI was about treated rats showed near-normal activity for the en-equally severe for all shielding conditions. How- tire 35 days of testing.- A similar outcome for be-ever, the incidence of ETI in the 45-Gy-dose group havior was observed in rats exposed to 7.5 Gv ofwas lowest in the head-shielded condition. The re- whole-body X rays except for shielded marrow-con-suits from several other shielding studies with mon- taining bones.keys do not clearly indicate that head or body Bone-marrow transplantation may be impracticalshielding offers any differing protection from in military situations. However, shielding may en-ETI.1272s.1I -,'],, These equivocal results also raise able stem cells to survive so that certain immuno-questions about the exclusive role of the CNS in the modulators of growth factors may promote regen-production of radiation-induced performance defi- eration and thereby enhance performance.cits. As with radiation-induced taste aversion, post-irradiation behaviors may be influenced by periph- Radiation in Spaceeral mechanisms that have not been fully explored.'
The behavioral scientist who is interested in theseBone-Marrow Factors issues is constantly challenged by a variety of mili-
tary-relevant tasks that require empirical analysis.Bone-marrow transplants have been used to chal- As military operations move to outer space, new ra-
lenge radiation-induced damage to the blood-form- diation hazards will challenge the human's abilitiesing systems. It is interesting that this manipulation to carry out missions.'""'• The behavioral effects ofseems also to provide some subchronic behavioral ionizing radiations (such as protons and high-Z par-benefits.~7 Measures of activity and lethality were tides) in space are beginning to be explored.•"'recorded in rats that were irradiated with 6.5 Gv of Preliminary indications are that radiations in spaceX rays. Twenty percent of the nontreated rats died, may be significantly more disruptive to behaviorwhereas 86'" of the marrow-treated group survived, than are the radiations in the earth's environments.
SUMMARY
The success or failure of military operations can than are other radiations, such as neutron radiation.be measured in terms of missions completed or tasks In addition, combined injuries will probably beperformed. Under many circumstances, exposure to prevalent in any future nuclear conflicts; presentionizing radiation can significantly impede perform- data suggest that trauma can act synergistically withance. In the case of low-to-intermediate doses of ra- radiation exposure to greatly increase the behavioraldiation (up to 10 Gy), performance deficits may be deficits.slow to develop, may be relatively long lasting, and Possible sensory and neurophysiological media-will usually abate before the onset of chronic radia- tors of radiation-induced behavioral deficits havetion effects, such as cancers. After large doses, the been identified. Long-term changes in performancebehavioral effects are often rapid (within minutes), may be mediated in part by radiogenic brain dam-and they usually abate before the onset of the debili- age from ischemia, edema, or direct damage to thetating chronic radiation sickness. These rapid effects parenchymal tissues themselves (such as dendritescan also occur after intermediate doses. But all tasks and glia). More transient cerebrovascular changesare not equally radiosensitive; tasks with complex, after radiation exposure may also produce short-demanding requirements are more easily disrupted lived behavioral deficits. Postirradiation alterationsthan simple tasks. The exceptions may be certain in brain metabolism and the disruption of the nor-naturalistic behaviors which are also quite radiosen- mal electrophysiology of the axon and synapse maysitive. Radiation parameters such as dose, dose rate, have important roles in certain performance deficits.fractionation, and quality can all influence the ob- In addition, a wide range of radiogenic neurochemi-served degree of performance decrements. Electron cal alterations have been characterized. These in-radiation is more able to produce behavioral deficits clude the reduced ability of synaptic sodium chan-
134

Bchaiw'oral and Netirophyisiologicol Chin iges with ExpOswre to Ionizing Radiation
nels to respond to stimulation. The nervous sys- tion from animal studies. Based on all data nowtem's radiosensitivity is revealed by the fact that al- available, the Human Response Program of the De-terations in the basic substrate of neural excitation fense Nuclear Agency has estimated the expectedhave been observed at doses of less than 1 Gy. Vari- performance changes in irradiated soldiers. Theseous levels of neurotransmitters (such as ace- projections depend on such factors as radiation dose,tylcholine and dopamine), putative neurotransmit- time after exposure, and task difficulty. Althoughters (such as endorphins), and other neurochemicals the topics are complex, the human and laboratoryand biogenic amines (such as histamine) undergo animal data should permit the description, predic-significant changes after radiation exposure. Like tion, and (eventually) amelioration of the behavioralthe modifications of morphology and electrophysiol- effects of ionizing radiation exposure. Thus far,ogy, many of these neurochemical changes may also however, many of the pharmacological compoundsbe capable of mediating the performance decre- that protect animals from the lethality of ionizingments observed after ionizing radiation exposure. radiation have been found to have severe behavioral
The literature on performance deficits in animals toxicity. We must further explore the potential foris quite extensive compared to that for humans. using behaviorally compatible antiemetics and selec-Human data are derived from radiation accidents or tive physical shielding to help maintain performancetherapeutic studies, and many confirm the informa- after radiation exposure.
REFERENCES
This chapter addresses most of the significant issues on behavioral and neurophysiological changes after ionizing radia-tion exposure, but is not exhaustive. For more detail and less military orientation, consult references 10, 20, 30, 67, 145,and 196. A number of U.S. and NATO military publications (including U.S. Army Field Circular 50-10, NATO STANAG2083, and NATO STANAG 2866) concern troop performance in a variety of combat situations.
1. Young, R. W., and Auton, D. L. 1984. The Defense Nuclear Agency Intermediate Dose Program: An overview. InProceedings of the Psychology in the Department of Defense, Ninth Symposium [Technical Report TR-84-2; NTIS AD-A141-043-O1, edited by G. E. Lee and T. E. Ulrich, 85-89. Colorado Springs: U.S. Air Force Academy.
2. Mickley, G. A. 1987. Psychological phenomena associated with nuclear warfare: Potential animal models. InProceedings of the DNA Symnposiur/Workshop on the Psychological Effects of Tactical Nuclear Warfare [TechnicalReport TR-87-209; NTIS AD-A194-754-8-XABI, edited by R. W. Young, 7.1-7.35. Washington, DC: DefenseNuclear Agency.
3. Bogo, V. 1988. Early behavioral toxicity produced by acute ionizing radiation. Comments on Toxicology 2: 265-276.
4. Kimeldorf, D. J.; Jones, D. C.; and Castanera, T. J. 1953. Effect of X-irradiation upon the performance of daily exhaus-tive exercise by the rat. Am. 1. Physiol. 174: 331-335.
5. Casarett, A. P. 1968. Radiation biology. Englewood Cliffs, NJ: Prentice-Hall, Inc.
6. Hall, E. J. 1973. Radiobiology for the radiologist. Hagerstown, MD: Harper and Row.
7. Bogo, V. 1984. Effects of bremsstrahlung and electron radiation on rat motor performance. Radiat. Res. 100: 313-320.
8. Casarett, A. P. 1973. Swim-tank measurement of radiation-induced behavioral incapacitation. Psychol. Rep. 33: 731-736.
9. Mickley, G. A.; Stevens, K. E.; White, G. A.; and Gibbs, G. L. 1983. Endogenous opiates mediate radiogenic behavioralchange. Science 220:1185-1187.
10. Davis, R. T. 1965. The radiation syndrome. In Behavior of Nonhwman Primates, edited by A. M. Schrier, H. F. Harlow,and F. Stollnitz, 495-524. New York: Academic Press.
11. Meyerson, F. G. 1958. Effect of damaging doses of gamma-radiation on unconditioned and conditioned respiratoryreflexes. In Works of the Institute of Higher Nervous Activity. Vol. 4 of the Pathophysiological Series [IsraelProgram Sci. Transl. OTS:61-31,021, 19621, 25-41. Moscow, USSR: Izd. Akad. Nauk.
135

Medical Consequitnc- of Nuchear IVarfare
12. Wheeler, T. G., and Hardy, K. A. 19S5. Retrograde amnesia produced by electron beam exposure: Causal parame-ters and duration of memory loss. Radiat. Res. 101: 74-80.
13. W'Aheeler, T. G., and Tilton, B. M. 1983. DwLation of meinornj loss die to electron Ibeamn exposure RTechnical Report TR-83-33; NTIS AD-A132-941-tfl. Brooks Air Force Base, TX: School of Aerospace Medicine.
14. Page, K. R., and Wheeler, T. G. 1485. Potent-' ot ofphotoflash-oroduced retrograde arnniesia in rats ITechnical Paper TP-85-1;NTIS AD-AI59-149-4-XABI. Brooks Air Force Base, TX: School of Aerospace Medicine.
15. Wheeler, T. G. 1982. Amnesia production, 'i/ visual stimulation ITechnical Report TR-82-45; NTIS AD-A124-822-81.Brooks Air Force Base, TX: School of Aerospace Medicine.
lt. Burt, D. II., and Ingersoll, E. H. 19h.5. Behavioral and neuropathological changes in the rat following X-irradiation ofthe frontal brain. 1. Comp. Ilihysiol. Psychol. 59: 90-93.
17. Janis, I. L. 1951. Air war and emotional stress. New York: McGraw-Hill.
18. Committee for the Compilation of Materials on Damage Caused by the Atomic Bombs in Hiroshima and Nagasaki.1481. Psychological tr 'nds among A-bomb victims. In Hiroshinma and Nagasaki: Philsica, dMental and SocialEffects of the Atomic Bombings, translated by E. Ishikawa, E. and D. Swain, 485-500. New York: Basic Books.
19. Jammet, H.; Mathe, U,.; Pendic, B.; Duplan, J. F.; Maupin, B.; Laterlet, R.; Kalic, D.; Schwarzenberg, L.; Djukic, Z.; andVigne, J. 1959. Study of six cases of accidental whole-bodv irradiation. Rev,. Franc. Etud. Chim. Biol. 4: 210-225.
20. Van Cleave. C. D. 1963. Irradiation and thit, nervouts stistem. New York: Rowman and Littlefield, Inc.
21. Harlow, H. F., and Moon, L. E. 1956. The effects of repeated doses of total-body X-irradiation on motivation andlearning in rhesus monkeys. 1. Comp. Phvsiol. Psychol. 49: 60-65.
22. Riopelle, A. I.; Gradsky, M. A.; and Ades, H. IV. 1956. Learned performance of monkeys after single and repeated X-irradiations. 1. Comp. Phyi/siol. Psyichol. 49: 521-524.
23. McDowell, A. A. 1958. Comparison,, of distractibility in irradiated and nonirradiated monkeys. 1. Genet. Psychol. 93:03-72.
24. Blair, W. C., and Arnold, W. J. 195t. The effects of cranial X-irradiation on retention of maze learning in rats. 1.Coalmp. Plnisiol. Psujchol. 49: 525-528.
25. Brown, W. L., and McDowell, A. A. 1962. Some effects of radiation on psychologic processes in rhesus monkeys. InResponse of the Nervous Sy1stemn to Ionizing Radiation, edited by T. I. Halev and R. S. Snider, 729-746. New York:Academic Press, Inc.
26. McDowell, A. A., and Brown, W. L. 1958. Facilitative effects of irradiation on performance of monkeys on discrimi-nation problems with reduced stimulus cues. ]. Genet. Psychol. 93: 73.
27. Kaplan, S. J., and Gentry, G. 1954. Some effects ofa lethal dose of X-radiation upon mnemnory. A case study iReport NP-53211. Randolph Air Force Base, TX: School of Aviation Medicine.
28. Furchtgott, E. 1951. Effects of total body X-irradiation on learning: An exploratory study. /. Comp. Physiol. Psychol.44: 197-203.
29. Jarrard, L. E. 1963. Effects of X-irradiation on operant behavior in the rat. 1. Comp. Physiol. Psychol. 56:608-611.
30. Kimeldorf, D. J., and Hunt, E. L. 1965. lonizing radiation: Neural function and behavior. New York and London:Academic Press.
31. Blair, W. C. 195N. The effects of cranial X-irradiation on maze acquisition in rats. I. Cornp. Physiol. Psychol. 51:175-177.
136

Beliji 'onda anid Nc~r'/i~tl~ lChange, withi Exposii te to lonizii,1in Radiationi
32. Scarborough, B. B.; Martin, J.; and McLaurin, W. A. 196t6. Ionizing radiation: Effects of repeated low dose exposure.Phipsiol. Beha;'. 1: 147-1:;0.
33. Ordv, J. M.; Barnes, It. W.; Sanioralski, T.; Curtis, IH. J.; Wolin, L.; and Zeman, W. 1964. Patholo~ic and behavioralstudies in mice after deuteron irradiation of the central nervous system. Radiat. Res. 18: 31-4-5.
34. Ordy, -1 .M.; Samorajski, T.; Zeman, W.; Collins, R. L.; and Curtis, H. J. 1963. Long-term pathologic and behavioralchanges in mice after local deuteron irradiation of the brain. Riadiat. Res. 20: 30-42.
35. Meier, G. W. 1902. Irradiation, genetics, and aging: Behavioral implications. In Effect,; of lonizinu Rod jation oI tiltNerz'oii; Sipste-i: Pr)ceedi pigs, 187-196. Vienna: International Atomic Energy Agency.
36. Fields, P. E. 195;7. The effect of whole-body X-radiation upon activity drum, straightaway, and maze pent rmances otwhite rats. 1. Coinp. Phillsiol. Pszwlchl. 50: 386-391.
37. Urmer, A. H., and Brown, VV. L. 1960. The cffect of gamma radiation on the reorganization of a complex maze habit.G.Cenet. Ps.ellcol. 97: 67-76.
38. McDowell, A. A., and Brown, W. L. 1960. Visual aculity performai'ce of normal and chronic focal-head irradiatedmonkeys. /. Genet. Psyehol. 93: 139-144.
39. Riopelle, A.)J. Chehavioral effects of ionizing radiation on primates. In reference 25, 719-728.
40. Dimascio, A.; Fuller, J. F.; Azrin, N. H.; and letter, W. 1956. The effect of total-body X-irradiation on delayed-response performance of dogs. /. Comp'. Plillsiol. Psiicliol. 49: 600-604.
41. Brown, W. L.; Overall, J. E.; Logie, L. C.; and Wicker, J. E. 1960. Lever-press .ng behavior of albino rats duringprolonged exposures to X-irradiation. Radiat. Res. 13: 617-631.
42. Payne, R. B. 1959. Effects of ionizing radiation exposure on human psychomotor skills. U.S. Artied Forces Med. J. 10:.1009-1021.
43. Mele, P. C.; Franz, C. G.; and Harrison, J. R. 1988. Effects of sublethal ionizing radiation on schedule-controlledperf .ormance in rats. Pliarinacol. Biochein. Be/wv. 30: 1007-1014.
44. Bogo, V.; Franz, C. F.; and Young, R. W. 1987. Effects of radiation on monkey discrimination performance. InProceeding,~s of flthe Eig'hth linternatiollal Cong~ress of R;adiation Research (Abstract), edited by E. M. Fielden, J. F.Fowler, J. H. H-endrv, and D. Scott, 259. Edinburgh, Scotland: International Congress of Radiation Research.
45. Brown, G. C. 1984. Behavioral uand pathological chang'es follozviu'ý a 1 l00-rad radiation exposure. Ann Arbor, Ml: Univer-sity Microfilms International.
46. Yochmowitz, M. C., and Brown, C. C. 1977. Performance in a 12-hour, 300-rad profile. Aviat. Space Environl. Med. 48:241-247.
47. Barnes, D. J.; Patrick, R. P.; Yochmowitz, M. C.; Yaeger, R. J.; Lof, N. E.; Hardy, K. A.; and Bastien, R. W. 11Q77.Protracted low-dose ion izing,, radiation effects upon primate perfonrmance [Technical Report TR-77-30; NTIS AD-A054-958-41. Brooks Air Force Base, TX: School of Aerospace Medicine.
48. Yochmow".z, M.; Patrick, R.; Jaeger, R.; and Barnes, D. 1977. Protracted radiation-stressed primate performance.Aviat. Space Eli'iron. Med. 48: 598-606.
49. Yochmowitz, M. G;Brown, C. C.; and Hardy, K. A. 1985. Performance following a 500-675 rad neutron pulse. Az'iat.Space Environ. Med. 56: 525-533.
50. Stapleton, C. E., and Curtis, H. J. 1946. The effects of fast neutrons onl the ability of inice to take forced exercise [U.S. AtomicEnergy Commission Report MDDC-6961. Oak Ridge, TN: Oak Ridge National Laboratory.
137

Medical Conse'qiuences ot Nuclear Warfare
51. Jetter, W. W.; Lindsley, 0. R.; and Wohlwill, F. J. "453. The effects of X-irradiation on phy sical exercise and behavior in thedog; relaited hlematological and pathological control studies IU.S. Atomic Energy Commission Report NYO-45481.New York: Atomic Energy Commission.
52. George, R. E.; Chaput, R. L.; Verrelli, D. M.; and Barron, E. L. 1971. The relative effectiveness of fission neutrons forminiature pig performance decrement. Radiat. Res. 48: 332-345.
53. Chaput, R. L., and Barron, E. L. 1973. Postradiation performance of miniature pigs modified by tasks. Radiat. Res. 53:392-401.
54. Chaput, R. L., and Wise, D. 1970. Miniature pig incapacitation and performance decrement after mixed gamma-neutron irradiation. Aerospace Med. 41: 290-293.
55. Casarett, A. P., and Comar, C. L. 1973. Incapacitation and performance decrement in rats following split dose offission spectrum radiation. Radiat. Res. 53: 455-461.
56. Mickley, G. A. 1980. Behavioral and physiological changes produced by a supralethal dose of ionizing radiation:Evidence for hormone-influenced sex differences in the rat. Radiat. Res. 81: 48-75.
57. Bogo, V. Comparative effects of bremsstrahlung, gamma, and electron radiation on rat motor performance. Inreference 1, 68-72.
58. Wheeler, T. G.; Hardy, K. A.; Anderson, L. B.; and Richards, S. 1984. Motor performance in irradiated rats as a function ofradiation source, dose, and time since exposure [Technical Report TR-84-8; NTIS AD-A141-209-71. Brooks Air ForceBase, TX: School of Aerospace Medicine.
59. Franz, C. G. 1985. Effects of mixed neutron-gamma total body irradiation on physical activity performance of rhesusmonkeys. Radiat. Res. 101: 434-441.
60. Kimeldorf, D. J., and Jones, D.C. 1951. The relationship of radiation dose to lethality among exercised animalsexposed to roentgen rays. Am. 1. Physiol. 167: 626-632.
61. Jones, D. C.; Kimeldorf, D. J.; Rubadeau, D. 0.; and Castanera, T. J. 1953. Relationships between volitional activityand age in the male rat. Am. J. Physiol. 172: 109-114.
62. Bogo, V. 1988. Behavioral radioprotection. Pharmacol. Ther. 39: 73-78.
63. Martin, B. A., and Michaelson, S. M. 1966. Exercise performance of upper-body x-irradiated ),gs. Am. J. Physiol. 211:457-461.
64. Smith, F., and Smith, W. W. 1951. Exercise effects on tolerance to radiation. Am. J. Physiol. 165: 662-666.
65. Brown, W. L., and White, R. K. 1958. Preirradiation fatigue as a factor in the prevention of irradiation deaths in rats.f. Genet. Psychol. 93: 287-290.
66. Brown, W. L., and White, R. K. 1960. A study of fatigue and mortality in irradiated rats. Radiat. Res. 13: 610-616.
67. Furchtgott, E. 1975. Ionizing radiations and the nervous system. In vol. 3, Biology of Brain Dysfunction, edited by G.E. Galli, 343-2-79. New York: Plenum Press.
68. Leary, R. W., and Ruch, T. C. 1955. Activity, manipulation drive, and strength in monkeys subjected to low-levelirradiation. J. Comp. Physiol. Psychol. 48: 336-342.
69. Alderks, C. E.; Mickley, G. A.; and Harris, A. H. 1987. Effects of ionizing irradiation on time and force measuresduring a shock avoidance task. Paper presented at 13th Convention of the Association for Behavior Analyses,Nashville, Tennessee.
70. Furchtgott, E. 1971. Behavioral effects of ionizing radiations. In Pharmacology and Biophysical Agents and Behavior,edited by E. Furchtgott, 1-64. New York: Academic Press.
138

Behavioral anid Neurophysiolo.gical Changes with Exposure to Ionizing Radiation
71. Jones, D. C.; Kimeldort, D. J.; Rubadeau, D. 0.; Osborn, G. K.; and Castanera, T. J. 1954. Effects of X-irradiation onperformance of volitional activity by the adult male rat. Am. ]. Physiol. 177: 243-250.
72. Arnold, W. J. Behavioral effects of cranial irradiation of rats. In reference 25, 669-682.
73. Castanera, T. J.; Jones, D. C.; and Kimeldorf, D. J. 1959. The effects of X irradiation on the diffuse activity perform-ance of rats, guinea pigs and hamsters. Br. ]. Radiol. 32: 386-389.
74. McDowell, A. A., and Brown, W. L. 1960. Comparisons of running wheel activity of normal and chronic radiatedrats under varying conditions of food deprivation. 1. Genet. Psychol. 96: 79-83.
75. Landauer, M. R.; Davis, H. D.; Dominitz, J. A.; and Weiss, J. F. 1988. Long-term effects of the radioprotector WR-2721on locomotor activity and body weight of mice following ionizing radiation. Toxicology 49: 315-323.
76. Landauer, M. R.; Davis, H. D.; Dominitz, J. A.; and Pierce, S. J. 1987. Effects of acute gamma radiation exposure onlocomotor activity in Swiss-Webster mice. The Toxicologist 7: 253.
77. McDowell, A. A.; Davis, R. T.; and Steele, J. P. 1956. Application of systematic direct observational methods toanalysis of the radiation syndrome in monkeys. Percept. Mot. Skills (Monograph Suppl. 3), 6:117-130.
78. Mattsson, J. L., and Yochmowitz, M. G. 1980. Radiation-induced emesis in monkeys. Radiat. Res. 82: 191-199.
79. McDowell, A. A. 1954. The immediate effects of single dose of whole body X radiation upon the social behavior andself-care of caged rhesus monkeys. Am. Psychol. 9: 423.
80. Vogel, H., Jr. 1950. The effect of X irradiation on fighting behavior in male mice. Anat. Rec. 108: 547.
81. Maier, D. M., and Landauer, M. R. 1987. Effects of gamma radiation on aggressive behavior in male swiss webstermice. Soc. Neurosci. Abstr. 13(2): 933.
82. O'Boyle, M. 1976. Suppresssion of mouse-killing in rats following irradiation. Percept. Mot. Skills 42: 511-514.
83. Burke, R. D.; Mattsson, J. L.; and Fischer, J. R. 1981. Effect of ionizing radiation on shock-elicited aggression of male rats
[Technical Report TR-81-18; NTIS AD-A103-329-91. Brooks Air Force Base, TX: School of Aerospace Medicine.
84. Ader, R., and Hahn, E. W. 1963. Effects of social environment on mortality to whole body x-irradiation in the rat.Psychol. Rep. 13: 211-215.
85. Ader, R. and Hahn, E. W. 1963. Dominance and emotionality in the rat and their effects on mortality after whole-body x-irradiation. Psychol. Rep. 13: 617-618.
86. Mickley, G. A.; Bogo, V.; Landauer, M. R.; and Mele, P. C. 1988. Current trends in behavioral radiobiology. In Terres-trial Space Radiation and Its Biological Effects, edited by C. E. Swenberg, 517-536. New York: Plenum Press.
87. Maier, D. M. Personal communication, 1987.
88. Rugh, R., and Grupp, E. 1960. X-irradiation lethality aggravated by sexual activity of male mice. Am. ]. Physiol. 198:1352-1354.
89. Morse, D. G., and Mickley, G. A. 1988. Dose-rate and sex effects on the suppression of appetitive behavior followingexposure to gamma-spectrum radiation. In Abstracts of 36th Annual Meeting of Radiation Research Society, 163.Philadelphia: Radiation Research Society.
90. Sharp, J. C.; Kelly, D. D.; and Brady, J. V. 1968. The radio-attenuating effects of n-decylaminoethanethiosulfuric acidin the rhesus monkey. In Use of Nonhuman Primtates in Drug Evaluation, edited by H. Vagtborg, 338-346. SanAntonio, TX: Southwest Foundation for Research and Education.
91. Leary, R. W. 1955. Food-preference changes of monkeys subjected to low-level irradiation. ]. Comp. Physiol. Psychol.
48: 343-346.
139

Medical Consequences of Nuclear Warfare
92. Davis, R. T. 1958. Latent changes in the food preferences of irradiated monkeys. /. Genet. Psychol. 92: 53-59.
93. Garcia, J.; Kimeldorf, D. ind Koelling, R. A. 1955. A conditioned aversion towards saccharin resulting fromexposure to gamma radiation. Science 122: 157-158.
94. Rabin, B. M., and Hunt, W. A. 1986. Mechanisms of radiation-induced conditioned taste aversion learning. Neurosci.Biobehav. Rev. 10: 55-65.
95. Dubois, A.; Fiala, N.; and Bogo, V. 1987. Treatment of radiation induced vomiting and gastric emptying suppressionwith zacopride. Part 2. Gastroenterology 92(5): 1376.
96. Young, R. W. 1986. Mechanisms and treatment of radiation-induced nausea and vomiting. In Nausea and Vomiting:Mechanisms and Treatment, edited by C. J. Davis, G. V. Lake-Bakaar, and G. V. Grahame-Smith, 94-109. NewYork: Springer-Verlag.
97. Middleton, G. R., and Young, R. W. 1975. Emesis in monkeys following exposure to ionizing radiation. Aviat. SpaceEnviron. Med. 46: 170-172.
98. Bogo, V.; Franz, C. G.; Jacobs, A. F.; Weiss, J. F.; and Young, R. W. 1988. WR-2721, radiation, and visual discrimina-tion performance. Pharmacol. Ther. 39: 93-95.
99. Walker, R. I.; Gruber, D. F.; MacVittie, T. J.; and Conklin, J. J., eds. 1985. The pathophysiology of combined inunry andtrauma: Radiation, burn, and trauma. Baltimore: University Park Press.
100. Gruber, D.; Walker, R. I.; MacVittie, T. J.; and Conklin, J. J., eds. 1987. The pathophysiology of combined injuril andtraumna: Management of infectious complications in mass casualtyt situations. Orlando, FL: Academic Press.
101. Landauer, M. R.; Ledney, G. D.; and Davis, H. D. 1987. Locomotor behavior in mice following exposure to fission-neutron irradiation and trauma. Aviat. Space Environ. Med. 58:1205-1210.
102. Wheeler, T. G., and Cordts, R. E. 1983. Combined effects of ionizing radiation and anticholinesterase exposure onl rodentmotor performance [Technical Report TR-83-30; NTIS AD-A131-847-61. Brooks Air Force Base, TX: School ofAerospace Medicine.
103. Bogo, V.; Hill, T. A.; and Young, R. W. 1981. Comparison of accelerod and rotarod sensitivity in detecting ethanol-and acrylamide-induced performance decrement in rats: Review of experimental considerations of rotatingrod systems. Neurotoxicology 2: 765-787.
104. Wheeler, T. G., and Cordts, R. E. 1984. Nonlinear performnance interaction upon exposure to anticholinesterase and ionizingradiation [Technical Report TR-84-5; NTIS AD-A139-909-61. Brooks Air Force Base, TX: School of Aerospace
Medicine.
105. Casey, H. W., Cordy, D. R., Goldman, M., and Smith, A. H. 1967. Influence of chronic acceleration on the effects ofwhole-body irradiation in rats. Aerospace Med. 38: 451-457.
106. Mattsson, J. L.; Cordts, R. E.; and Deyak, R. R. 1981. Radiation and G tolerance in rats. Aviat. Space Environ. Med. 52:404-407.
107. Antipov, V. V.; Davyov, B. I.; Verigo, V. V.; and Svirezhev, Y. M. 1975. Combined effect of flight factors. InEcological and Phiysiological Bases of Space Biology a; 'd Medicine, Vol. 2, Book 2 of Foundations of Space Biology andMedicine, edited by M. Calvin and 0. G. Gazenko, 639-667. Washington, DC: National Aeronautics and SpaceAdministration.
108. Zellmer, R. W.; Womack, G. W.; McNee, R. C.; and Allen, R. G. 1963. Significance of combined stresses of G-forcesand irradiation. Aerospace Med. 34: 626-629.
109. Livshits, N. N.; Apanasenko, Z. I.; Kuznetsova, M. A.; Meizerov, E. S.; and Zakirova, R. M. 1975. Effects of accelera-tion on the higher nervous activity of previously irradiated rats. Radiobiologiia 15: 92-99.
140
Behavioral and Nerop)thysiological Chaniges with Exposu re to Ion izitig Radiation
110. Seigneur, L. J., and Brennan, 1. T. 146. Incapacitation in the mnonkev (Macaca nuilatta) following exposure to a pulse ofreactor radiation IScientific Report SR6b-21. Bethesda, MD: Armed Forces Radiobiology Research Institute.
111. Bruner, A. 1977. Immediate dose-rate effects of "'Co on performance and blood pressure in monkeys. Radiat. Res.70: 378-390.
112. Blondal, H. 1958. Initial irradiation reaction in mice. Nature 182: 1026-1027.
113. Pitchford, T. L. 1968. Beagle incapacitation and survival time afer pulsed mixed gamma-neutron irradiation [ScientificReport SR68-24]. Bethesda, MD: Armed Forces Radiobiology Research Institute.
114. Thorp, 1. W. 1970. Beagle and miniature pig response to partial hody irradiation: Dose relationships [Technical Note TN70-5; NTIS AD-717-5911. Bethesda, MD: Armed Forces Radiobiology Research Institute.
115. Langham, W. R.; Kaplan, S. J.; Pickering, J. E.; Lushbaugh, C. C.; Haymaker, W.; Storer, J. B.; and Harris, P. S. 1952.The effects of rapid, massive doses of gamnimma radiation on the behavior of sub-human primates [Technical Report LA-1558; OCLC 136132091. Los Alamos, NM: Los Alamos National Laboratory.
I 1). Sharp, J. C., and Keller, B. K. 1965. A comparison between the effects of exposure to a mixed fission spectrum delivered iii asingle "pulse" and X-rays delivered at a slower rate upon conditioned avoidance behavior of the primate [TechnicalReport TR41. Washington, DC: Walter Reed Army Institute of Research.
117. Curran, C. R.; Conrad, D. W.; and Young, R. W. 1971. The effects of 2000 rads of pulsed gamma-neutron radiation uponthe performance of umfettered nmonkeis [Scientific Report SR71-3; NTIS AD-724-6531. Bethesda, MD: Armed ForcesRadiobiology Research Institute.
118. Thorp, j. W., and Young, R. W. 1971. Monkey performance after partial body irradiation. Aerospace Med. 42: 503-507.
119. Barnes, D.J. 1966. An initil investigation t tihe effects of pulsed ionizing radiation on the primate eluilibrium function[Technical Report TR-66-106; OCLC 1768649]. Brooks Air Force Base, TX: School of Aerospace Medicine.
120. Hunt, E. L., and Kimeldorf, D. J. 1964. Behavioral arousal and neural activation as radiosensitive reactors. Radiat.Res. 21: 91-110.
121. Mickley, G. A., and Teitelbaum, H. 1978. Persistence of lateral hypothalamic-mediated behaviors after a supralethaldose of ionizing radiation. Aviat. Space Eniviron. Med. 49: 863-873.
122. Young, R. W. 1979. Prediction of the relative toxicityl of enviromnental toxins as a function of behavioral and non-behavioralend points IOCLC 58972331. Washington, DC: The Catholic University of America.
123. Young, R. W., and McFarland, W. L. 1972. Performuance of the monketj (Macaca mulatta) after two 2500-rad pulses ofmixed gamma-neutron radiation [Scientific Report SR72-19; NTIS AD-759-0171. Bethesda, MD: Armed ForcesRadiobiology Research Institute.
124. Germas, J. E., and Shelton, Q. H. 1969. Performnance of the monkeey following multiple supralethal pulses of radiation[Scientific Report SR69-21; NTIS AD-698-4811. Bethesda, MD: Armed Forces Radiobiology Research Institute.
125. Mele, P. C.; Franz, C. G.; and Harrison, J. R. 1987. Effects of ionizing radiation on fix-ratio escape performance inrats. Soc. Neurosci. Abstr. 13(2): 998.
126. Davis, R. T., and Steele, J. P. 1963. Performance selections through radiation death in rhesus monkeys. 1. Psychol.56:119.
127. Chapman, P. H., and Young, R. J. 1968. Effect of cobalt-60 gamma irradiation on blood pressure and cerebral bloodflow in the Macaca mulatta. Radiat. Res. 35: 78-85.
128. Hunt, W. A. 1983. Comparative effects of exposure to high-energy electrons and gamma radiation on activeavoidance behaviour. Jit. I. Radiat. Biol. 44: 257-260.
141
X1CiIlil Cl~ii'ci/iicniitt of NJutIonear ~~iaip'
121). Chaput, R. L.; Herardo,1. PA.; and Barron, E. L. 1`473. Imrea~ietl l',ain raidioie'istatiiu sitter ;ultraletital irraid at ion 11xieitn-titic Report SR73-7; NTIS AD-76-4-885-0[. Bethesda, MD: Armned Forces Radiobiologv Research Institute.
130. Barnes, 1). 1.; B~row~n, G. C.; and Fractor, Z. Ni. 1471. lPitt'rential etth'ct4 ot 11nultiphe dilgt silughe irradiatiions upoil the/lritiiite equdliiirnuin tioictuiin liechinical Report TR-7 1-7; NTIS AD 722-0.581. Brovoks Air Force Base, TX: Sihool oftAeros~pace Medicine.
1,31 G (eorge, R. F.; Cha put, R. L.; anzd Ba rron, F. 1L. P-)72. Jh eei~ III if Miniatue/ln ' / p riý IImauc erenun'lt upjonz 'ý mtlai-a i' djost- ratt' IScientific Report SR72-20; NTIS AI)-7371-0391. Bethesda, MDl: Armed Forces RadiobiologvResearch Institutc.
[32. Bogo. V.; Z.eman, G. If.; and IDoolev, M. A. 1981). Radiation quality and rat motor performance.. bRadial. Res. 1 18:341-352.
133. Gk'itman, FH. 1483. Rasht ipsycwologzu. New York: WA. W. Norton and Co.
134. Graham, F. S.; Farrer, D). N.; Carsten, A. L.; and Roizin, L. 11971. Decrements in the visual acuitv of rhesus monkeysas a delayed effect of occipital irradiation. Radial. Res. 45: 373-383.
13;. Caveness, WV. F.; Tanaka, A.; I less, K. I1.; Kemper, T. L.; Tso, M. C).; and Zimmerman, L. E. 1974. Delayed brainswelling and functional derangement after X-irradiation oif thle right visual cortex in the A'acat-a Mnulatta. Radial.Re-ý. 57: 104-120.
1361. Minamisawa, T.; Sugivamna. I I.; Tsuchiva, T.; and Ito, 1-1. 1970. Effects of X-irradiation onl evoked potentials fromvisual systemns in rabbits. 1. Radial. Res. 11: 127-133.
[37. Minamisawa, T.; Tsuchiva, T.; and Ito, 1-. 1472. Changes in the averaged evoked potentials of thle rabbit during andafter fractionated X-irradiation. l.vreieiaor Chit. Neurophvsiol. 33: 591-N)!.
138. Kekchevev, K. 1941. Changes in the threshold vi achromatic vision of manl by the action of ultrashort, ultraviolet,and X-rays wav'es. PrObl. Fiziol. Opt. 1: 77-79.
139. Lenoir. A. 1944. Adaptation und roentgenbesstrahlukng. Radio. Cliii. 13: 2t4-27(-.
14(1. Murphyv, J. E., and Harris, J. D. 1961. Negligible effects of X-irradiation of the head upon hearing in thle rat. 1. Aud.Re"s. 1: 117-132.
14 1. Borsanvi, S. 1962. The effects of radiation therapy on thle ear: With particular reference to radiation otitis media.Soulti. Med. 1. 55: 740-743.
142. Tokimloto, T., and Kanagawa, K. 1985. Effects of X-ray irradiation on hearing in guinea pigs. Acta Otolan.111gol.(Stockhi.) 100: 266-272.
143. Moskovskaya, N. V. [959. Effect oif ionizing radiations onl the functions of the vestibular analyzer. Vestit. Olorino-lriliigiil. 21: 59-62.
144. A pa nase.n ko, Z. I. 1967. Comblined effect of doubile exposurie to vibration andu clhroinic irradiation oii the fiuncitionial State ofi'estiwh'ulr apparatuts I Technical Translation F-4 131, 212-228. Washington, DC: National Aeronautics and SpaceAd miniistration.
145. Furchtgott, E. 1963. Behavioral effects of ionizing radiation: 1955-61. PsYchol. Bull. 60: 157-199.
146. Teskey, G. C., and Kavaliers, M. 1984. Ionizing radiation induces opioid-mediated analgesia in male mice. Lift, Sdi.35: 1547-1552.
147. Doull, 1. 1967. Pharmacological responses in irradiated animals. Radial. Res. .30: 333-341.
148. Burghardt, W. F., and Hunt, W. A. The interactive effects of morphine and ionizing radiation onl the latency of tailwithdrawal from warm water in thle rat. In reference 1, 73-76.
142

BehavLioral and NenrophYsiological Clanit s uith Exposure to lonizing - idiation
149. Mickley, G. A., and Stevens, K. E. 1986. Stimulation of brain muscarinic acetylcholine receptors acutely reversesradiogenic hypodipsia. Aziat. Space Eniron. Med. 57: 250-255.
150. Ingersoll, E. H.; Carsten, A. L.; and Brownson, R. H. 1967. Behavioral and structural changes following X-irradia-tions of the forebrain in the rat. Proc. Soc. Exp. Biol. Med. 125: 382-385.
151. Arnold, W. J. 1952. Maze learning and retention after X-irradiation of the head. I. Cornp. Physiol. PsYchol. 45: 358-361.
152. Cassaret, G. W. 1980. Radiation histopathology. Vol. Il. Boca Raton, FL: CRC Press.
153. Hopewell, J. W. 1979. Late radiation damage to the central nervous system: A radiobiological interpretation.Neuropathol. Appli. Neurobiol. 5: 329-343.
154. Lyman, R. S., Kupalov, R. S., and Scholz, W. 1933. Effects of roentgen rays on the central nervous system. Resultsof large doses on the brains of adult dogs. AMA Arch. Nenrol. Psychiat. 29: 56-87.
155. Hohwieler, M. L.; Lo, T. C.; Silverman, M. L.; and Freiberg, S. R. 1986. Brain necrosis after radiotherapy for primaryintracerebral tumor. Neurosurieriy 18: 67-74.
156. Haymaker, W. Morphological changes ir he nervous system following exposure to ionizing radiation. In reference35, 309-358.
157. Lindgren, M. 1958. On tolerance of brain tissue and sensitivity of brain tumors to irradiation. Acta Radiol. lSuppl.I170: 5-75.
158. Kemper, T. L.; O'Neill, R.; and Caveness, W. F. 1977. Effects of single dose supervoltage whole brain radiation inMacaca inidatta. I. Neuropathol. Exp. Neurol. 36: 916-940.
159. Caveness, W. F. 1977. Pathology of radiation damage to the normal brain of the monkey. Nat!. Cancer Inst. Monogr.46: 57-76.
160. Pallis, C. A.; Louis, S.; and Morgan, R. L. 1961. Brain myelopathy. Brain 84: 460-479.
161. Dynes, J. B., and Smedal, M. J. 1960. Radiation myelitis. Am. J. Roentgenol. Rad. Ther. Nuc. Med. 83: 78-87.
162. Marks, J. E., and Wong, J. 1985. The risk of cerebral radionecrosis in relation to dose, time and fractionation. Prog.Exp. Tumtor Res. 29: 210-218.
163. Switzer, R. C. Personal communication, 1988.
164. Arnold, A.; Bailey, P.; and I larvey, R. A. 1954. Intolerance of primate brain stem and hypothalamus to conventionalhigh energy radiations. Neurology 4: 575-585.
165. Yoshii, Y.; Maki, Y.; Tsunemoto, H.; Koike, S.; and Kasuga, T. 1981. The effect of total-head irradiation on C3H/Hemice. Radiat. Res. 86: 152-170.
166. Ross, J. A. T.; Levitt, S. R.; Hoist, E. A.; and Clemente, C. D. 1954. Neurological and electroencephalographic effectsof X irradiation of the head in monkeys. AMA Arch. Neurol. Psychiat. 71: 238-249.
167. Roizin, L.; Akai, K.; Carsten, A.; Liu, J. C.; and Eisenberg-Gelber, B. 1976. Post-X-ray myelinopathy (pathogenicmechanisms). In International Siiiposium on the Aetiology and Pathogenesis of Demiyelinating Diseases [OCLC89431921, edited by T. Yonawa, 29-57. Neiho-Sha: Japan Press Co.
168. Ibrahim, M. Z. M.; Haymaker, W.; Miquel, J.; and Riopelle, A. J. 1967. Effects of radiation on the hypothalamus inmonkeys. Arch/ii. fur Psychiatrie und Zeitschrift f.d. ges. Neurologie 210: 1-15.
169. van der Kogel, A. J. 1986. Radiation-induced damage in the central nervous system: An interpretation of target cellresponses. Br. I. Cancer (Suppl. VII) 53: 207-217.
143

Medical Conse(Iiienco, of NIth'llear Warflare
170. Abdullin, G. Z. 1`42. Sit 'v of cnl•,iprative radioslnsitit ' ity/ at differetnt parts of brain in terms oa altercd futnction [AtomicEnergy Commission TR-5141 I. Washington, DC: OTS/Department of Commerce.
171. Christensen, H. D.; Flesher, A. M.; and Haley, T. J. 1964. Changes in brain self-stimulation rates after exposure to X-irradiation. 1. Pharin. Sci. 58: 128-129.
172. Mechanick, J. L.; Htochberg, F. I I.; and LaRocque, A. 198t. I ypothalamic dysfunction following whole brainirradiation. 1. Nearosurg. h5: 490-444.
173. Rosenthal, F., and Timiras, I'. S. 19I1. Changes in brain excitability after whole-body X-irradiation in the rat. Radiat.Res. 18: t48-657.
174. Rosenthal, F., and Timiras, P. S. 1461. Threshold and pattern of electroshock seizures after 250 R whole-body X-irradiation in rats. Proc. Soc. Exp. Biol. Med. 108: 2b7-270.
175. Gangloff, H. Acute effects of X-irradiation on brain electrical activity in cats and rabbits. In reference 35, 123-138.
176. Gerstner, 11. B. 1956. Effect of high-intensity X-irradiation on the A group fibers of the frog sciatic nerve. Ai. I.Physiol. 184: 333-337.
177. Russel, D. S.; Wilson, C. W.; and Tanslev, K. 1949. Experimental radionecrosis in the brains of rabbits. I. Neurol.Ncttrostirg. Psvtlchiat. 12: 187-195.
178. Berg, N. 0., and Lindgren, M. 1958. Time dose relationship and morphology of delayed radiation lesions of thebrain of the rabbit. Acta Radiol. I Suppl.I 167: 1-118.
179. Caveness, W. F. 1980. Experimental observations: Delayed necrosis in normal monkey brain. In Radia•ion Damageto the Nerz,ous System, edited bv H. A. Gilbert and A. R. Kagen, 1-38. New York: Raven Press.
180. Hopewell, J. W., and Wright, E. A. 1970. The nature of latent cerebral irradiation damage and its modification byhypertension. Br. I. Radiol. 43: 161-167.
181. Hirata, Y.; Matsukado, Y.; Mihara, Y.; and Kochi, M. 1985. Occlusion of the internal carotid artery after radiationtherapy for the chiasmal lesion. Acti Neurochem. 74:141-147.
182. Halpern, J.; Kishel, S. P.; Park, J.; Tsukada, Y.; Johnson, R. J. R.; and Ambrus, J. L. 1984. Radiation-induced brainedema in primates, studied with sequential brain CAT scanning and histopathology. Res. Coninun. Chein.Pathol. Pharinacol. 45: 463-470.
183. Winkler, H. 1957. Untersuchungen uber die Wirkung von Roentgensstrahlen auf die Bluthirnschranke mit hilfe vonP32. Zbl. allg. Pathol. Anat. 97: 301-307.
184. McMahon, T., and Vahora, S. 198(6. Radiation damage to the brain. Neuropsiychiatric Aspects 8: 437-441.
185. Sheline, G. E.; Wara, W. M.; and Smith, V. 1980. Therapeutic irradiation and brain injury. hIt. 1. Radialt. Oncol. Biol.Phys. h: 1215-1228.
186. O'Connel, J. F. A., and Brunschwig, A. 1937. Observations on the roentgen treatment of intracranial gliomata withspecial reference to the effects of irradiation upon the surrounding brain. Brain 60: 230-258.
187. Crompton, M. R., and Layton, D. D. 1961. Delayed radionecrosis of the brain following therapeutic x-irradiation ofthe pituitary. Brain 84: 85-101.
188. Innes, J. R., and Carsten, A. 1961. Demyelination or malacic myelopathy. Arch. Neurol. 4:190-199.
189. Zeman, W. 1963. Disturbances of nucleic acid metabolism preceeding delayed radionecrosis of nervous tissue.Proc. Natl. Acad. Sci. LISA 50: 626-630.
144

Beiavioral and Ncirophyisiological Changes with Exposure to Ionizing Radiation
190. Hopewell, J. W., and Wright, E. A. 1975. The effects of dose and field size on late radiation damage to the rat spinalcord. Int. J. Radiat. Biol. 28: 325-333.
191. Pourquier, H.; Baker, J. R.; Giaux, G.; and Benirschke, K. 1958. Localized roentgen-ray beam irradiation of thehypophysohypothalarnic region of the guinea pig with a 2 million volt van de Graaf generator. Am. I. Roent-genol. Rad. Ther. Niic. Med. 80: 840-850.
192. Reyners, H.; Gianfelici de Reyners, E.; and Maisin, J.-R. 1982. The beta-astrocyte: A newly recognized radiosensi-tive glial cell type in the cerebral cortex. 1. Neurocytol. 11: 967-983.
193. Reyners, H., Gianfelici de Revners, E., and Maisin, J.-R. 1986. Early cell regeneration processes after split-dose X-irradiation of the cerebral cortex of the rat. Br. /. Cancer (Suppl. VII) 53: 218-220.
194. Mastaglia, F. L.; McDonald, W. I.; Watson, J. V.; and Yogendran, K. 1976. Effects of X-irradiation on the spinal cord:An experimental study of the morphological changes in central nerve fibers. Brain 99: 101-122.
195. Jones, A. 1964. Transient radiation myelopathy (with reference to Lhermitte's sign of electrical paresthesia). Br. ].Radio!. 37: 727-744.
196. Cavanagh, J. B., and Hopewell, J. W. 1972. Mitotic activity in the subependymal plate of rats and the long-termconsequences of X-irradiation. ]. Neurol. Sci. 15: 471-482.
197. Furchtgott, E. 1956. Behavioral effects of ionizing radiation. Psychol. Bill. 53: 321-334.
198. Altman, J. 1962. Are new neurons formed in the brains of adult mammals? Science 135: 1127-1129.
199. Kaplan, M. S., and Hinds, J. W. 1977. Neurogenesis in the adult rat: Electron microscopic analysis of lightradioautographs. Science 197: 1092-1094.
200. Bayer, S. A., and Altman, J. 1975. Radiation-induced interference with postnatal hippocampal cytogenesis in ratsand its long-term effects on the acquisition of neurons and glia. J. Colinp. Neurol. 163: 1-20.
201. Bayer, S. A. 1985. Neuron production in the hippocampus and olfactory bulb of the adult rat brain: Addition orreplacement. In Hope for a New Neurology, edited by F. Nottebohm, 163-172. New York: N. Y. Acad. Sci.
202. Rakic, P. DNA synthesis and cell division in the adult primate brain. In reference 201,193-211.
203. Gueneau, G.; Drouet, J.; Privat, A.; and Court, L. 1979. Differential radiosensitivity of neurons and neuroglia of thehippocampus in the adult rabbit. Acta Neuropathol. (Berl.) 48:199-209.
204. Gueneau, G.; Baille, V.; and Court, L. 1986. Protracted postnatal neurogenesis and radiosensitivity in the rabbit'sdentate gyrus. In Radiation Risks to the Developing Nervous Systeni, edited by H. Kriegel, W. Schmahl, G. B.Gerber, and F.-E. Stieve, 133-140. Stuttgart: Gustav Fischer Verlag.
205. Schade, J. P., and Caveness, W. F. 1968. Alterations in dendritic organi7ation. Brain Res. 7: 59-86.
206. Egana, E. 1962. Some effects of ionizing radiations on the metabolism of the central nervous system. Int. 1. Neurol. 3:631-647.
207. Ito, M.; Patronas, N. J.; Di Chiro, G.; Mansi, L.; and Kennedy, C. 1986. Effect of moderate level X-radiation to brainon cerebral glucose utilization. 1. Cornput. Assist. Tomogr. 10: 584-588.
208. Lebedinsky, A. V.; Grigoryev, U. G.; and Demirchoglyan, G. G. 1958. On the biological effect of small doses ofionizing radiation. In Proceedings of Second United Nations International Conference on Peaceful Uses of AtomicEnergy. IOCLC 22166411. Vol. 22, 17-28. Geneva: United Nations.
209. Haley, T. J. Changes induced in brain activity by low doses of X-irradiation. In reference 35, 171-185.
210. McFarland, W. L, and Levin, S. G. 1974. Electroencephalographic responses to 2500 rads of whole-body gamma-neutron radiation in the monkey Macaca Ynulatta. Radiat. Res. 58: 60-73.
145

Medical Consequepices of Nchlear Warfare
211. Monnier, M., and Krupp, P. Action of gamma radiation on electrical brain activity. In reference 25, 607-617.
212. Gangloff, H., and Haley, T. J. 1960. Effects of E-irradiation on spontaneous and evoked brain electrical activity incats. Radiat. Res. 12: 694-704.
213. Bassant, M. H., and Court, L. 1978. Effects of whole-body gamma irradiation on the activity of rabbit hippocampalneurons. Radiat. Res. 75: 593-606.
214. Peimer, S. 1.; Dudkin, A. 0.; and Swerdlov, A. G. 1986. Response of hippocampal pacemaker-like neurons to lowdoses of ionizing radiation. Int. J. Radiat. Biol. 49: 597-600.
215. Pollack, M., and Timiras, P.S. 1964. X-ray dose and electroconvulsive responses in adult rats. Radiat. Res. 21: 111-119.
216. Miller, D. S. Effects of low level radiation on audiogenic convulsive seizures in mice. In reference 25, 513-531.
217. Sato, M. 1978. Electrophysiological studies on radiation-induced changes in the adult nervous system. In vol. 7,Advaances in Radiation Biology, edited by J. T. Lett, and H. Adler, 181-210. New York: Academic Press.
218. Bachofer, C. S. 1957. Enhancement of activity of nerves by X-rays. Science 125: 1140-1141.
219. Bachofer, C. S., and Gautereaux, M. E. 1959. X-ray effects on single nerve fibers. 1. Gen. Physiol. 42: 723-735.
220. Bachofer, C. S., and Gautereaux, M. E. 1960. Bioelectric activity of mammalian nerves during X-irradiation. Radial.Res. 12: 575-586.
221. Bachofer, C. S., and Gautereaux, M. E. 1960. Bioelectric response in situ of mammalian nerves exposed to X-rays.Ani. 1. Physiol. 198: 715-717.
222. Gaffey, C. T. Bioelectric effects of high energy irradiation on nerve. In reference 25, 277-296.
223. Gasteiger, E. L., and Campbell, B. Alteration of mammalian nerve compound action potentials by beta irradiation.In reference 25, 597-605.
224. Yamashita, H., and Miyasaka, T. 1952. Effects of beta rays upon a single nerve fiber. Proc. Soc. Exp. Biol. Med. 80:375-377.
225. Kroebel, W., and Kroem, G. 1959. Die wirkung geringer strahlungsdosen auf die signalerzeugungs und fortlei-tungs-eigenshaftens-eigenschaften in froschnerven. Atomkerneneriie 4: 280-286.
226. Scholz, W.; Ducho, E. G.; and Breit, A. 1959. Experimentelle Roentgenspatschaden am ruchenmark des erwachse-nen kaninchens. Ein weiterer beitrag zur wirkungsweise ionisierender strahlen auf das zentralnervose gewebe.Psychiat. Neurol. Japan 61: 417-442.
227. Scholz, W.; Schlote, W.; and Hirschberger, W. Morphological effect of repeated low dosage and single high dosageof X-irradiation to the central nervous system. In reference 25, 211-232.
228. Davidoff, L. M.; Dyke, C. G.; Elsberg, C. A.; and Tarlov, I. M. 1938. The effect of radiation applied directly to brainand spinal cord. I. Experimental investigations on Macaca rhesus monkeys. Radiology 31: 451-463.
229. Lott, J. R. Changes in ventral root potentials during X-irradiation of the spinal cord in the cat. In reference 35, 85-92.
230. Sato, M.; Austin, G. M.; and Stahl, W. The effects of ionizing radiation on spinal cord neurons. In reference 25, 561-671.
231. Sato, M.; Austin, G. M.; and Stahl, W. Delayed radiation effects on neuronal activity in the spinal cord of the cat. Inreference 35, 93-110.
146

Behavioral and NeLi rophysiological Chanyes with Exposure to Ionizing Radiation
232. Sato, M.; Stahl, W.; and Austin, G. M. 1963. Acute radiation effects on synaptic activity in the mammalian spinalcord. Radiat. Res. 18: 307-320.
233. Sato, M., and Austin, G. 1964. Acute radiation effects on mammalian synaptic activities. In Reslpose of the NervousSysteI to Ionizing Radiation, edited by T. J. Halev and R. S. Snider, 279-289. Boston: Little, Brown and Co.
234. Mtskhvetadze, A. V., and Kucherenko, T. M. 1968. Direct and indirect effect of irradiation on the transmission of thestimulus in the upper neck sympathetic ganglion of cats. Radiobiologiia 8: 624-627.
235. Tolliver, J. M., and Pellmar, T. C. 1987. Ionizing radiation alters neuronal excitability in hippocampal slices of theguinea pig. Radiat. Res. 112: 555-563.
236. Catterall, W. A. 1984. The molecular basis of neuronal excitability. Science 223: 653-661.
237. Rothenberg, M. A. 1950. Studies on permeability in relation to nerve function. 11. Ionic movements across axonalmembranes. Biochin. Biophl/s. Acta 4: 96-114.
238. Wixon, H. N., and Hunt, W. A. 1983. Ionizing radiation decreases veratridine stimulated uptake of sodium in ratbrain synaptosomes. Science 220: 1073-1074.
239. Mullin, M. J.; Hunt, W. A.; and Harris, R. A. 1986. Ionizing radiation alters the properties of sodium channels in ratbrain synaptosomes. /. Neuroclhein. 47: 489-495.
240. Tanimura, H . 1957. Changes of the neurosecretory granules in hypothalamo-hypophysical system of rats byirradiating their heads with X-rays. Acta Anat. Nippon. 32: 529-533.
241. Dahlstrom, A.; Haggendal, J.; and Rosengren, B. 1973. The effect of Roentgen irradiation on monoamine containingneurons of the rat brain. Acta Radiol. Ther. Phys. Biol. 12: 191-200.
242. Hunt, W. A.; Dalton, T. K.; and Darden, J. H. 1979. Transient alterations in neurotransmitter activity in the caudatenucleus of rat brain after a high dose of ionizing radiation. Radiat. Res. 80: 556-562.
243. Joseph, J. A.; Kandasamy, S. B.; Hunt, W. A.; Dalton, T. K.; and Stevens, S. 1988. Radiation-induced increases insensitivity of cataleptic behavior to haloperidol: Possible involvements of prostaglandins. Pharmnacol. Biochem.Behav. 29: 335-341.
244. Kulinski, V. I., and Semenov, L. F. 1965. Content of catecholamines in the tissues of macaques during the earlyperiods after total gamma irradiation. Radiobiologiia 5: 494-500.
245. Varagic, V.; Stepanovic, S.; Svecenski, N.; and Hajdukovic, S. 1967. The effect of X-irradiation on the amount ofcatecholamines in heart atria and hypothalamus of the rabbit and in brain and heart of the rat. Int. 1. Radiat.Biol. 12:113-119.
246. Johnsson, J. E.; Owman, C. H.; and Sjoberg, N.-O. 1970. Tissue content of noradrenaline and 5-hydroxytryptaminein the rat after ionizing radiation. hnt. J. Radiat. Biol. 18: 311-316.
247. Catravas, G. N., and McHale, C. G. 1973. Activity changes of brain enzynes in rats exposed to different qualities of ionizingradiation [Scientific Report SR73-19; NTIS AD-777-383-11. Bethesda, MD: Armed Forces Radiobiology ResearchInstitute.
248. Rixon, R. H., and Baird, K. M. 1968. The therapeutic effect of serotonin on the survival of X-irradiated rats. Radiat.Res. 33: 395-402.
249. Prasad, K. N., and Van Woert, M. H. 1967. Dopamine protects mice against whole-body irradiation. Science 155:470-472.
250. Davydov, B. I. 1961. Acetylcholine metabolism on the thalamic region of the brain of dogs after acute radiationsickness. Radiobiolog'ia 1: 550-554.
147

Medical Consequences of Nuclear Wartaire
251. Sabine, J. C. 1956. Inactivation of cholinesterases by gamma radiation. Am. ]. Physiol. 187: 280-282.
252. Lundin, J.; Clemedson, C. J.; and Nelson, A. 1957. Early effects of whole-body irradiation on cholinesterase activityin guinea pig's blood with special regard to radiation sickness. Acta Radiol. 48: 52-64.
253. Hunt, W. A., and Dalton, T. K. 1980. Reduction in cyclic nucleotide levels in the brain after a high dose of ionizingradiation. Radiat. Res. 83: 210-215.
254. Catravas, G. N.; Wright, S. J.; Trocha, P. J.; and Takenaga, J. 1981. Radiation effects on cyclic AMP, cyclic GMP, andamino acid levels in the CSF of the primate. Radiat. Res. 87:198-203.
255. Hawkins, R., and Forcino, D. 1988. Postradiation cardiovascular dysfunction. Comments on Toxicology 2: 243-252.
256. Cockerham, L. G.; Pautler, E. L.; and Hampton, J. D. 1984. Postradiation blood flow in the visual cortex of primates.The Toxicologist 5: 82.
257. Doyle, T. F.; Curran, C. R.; and Turns, J. E. 1974. The prevention of radiation-induced early transient incapacitationof monkeys by an antihistamine. Proc. Soc. Exp. Biol. Med. 145:1018-1024.
258. Chapman, P. H., and Young, R. J. 1968. Effect of head versus trunk fission-spectrwn radiation on learned behavior in themonkey [Technical Report TR-68-801. Brooks Air Force Base, TX: School of Aerospace Medicine.
259. Cockerham, L. G.; Doyle, T. F.; Paulter, E. L.; and Hampton, J. D. 1986. Disodium cromoglycate, a mast-cellstabilizer, alters postradiation regional cerebral blood flow in primates. J. Toxicol. Environ. Health 18: 91-101.
260. Chapman, P. H., and Young, R. J. 1968. Effect of high energy x-irradiation of the head on cerebral blood flow andblood pressure in the Macaca mulatta. Aerospace Med. 3: 1316-1321.
261. Turbyfill, C. L.; Roudon, R. M.; and Kieffer, V. A. 1972. Behavior and physiology of the monkey (Macaca mulatta)following 2500 rads of pulse mixed gamma-neutron radiation. Aerospace Med. 7: 41-45.
262. Miletich, D. J., and Strike, T. A. 1970. Alteration of postirradiation hypotension and incapacitation in the monkei byadministration of vasopressor drugs [Scientific Report SR70-1; NTIS AD-702-723]. Bethesda, MD: Armed ForcesRadiobiology Research Institute.
263. Turns, J. E.; Doyle, T. F.; and Curran, C. R. 1971. Norepinephrine effects on early post-irradiation performance decrementin the inonke, [Scientific Report SR71-16; NTIS AD-737-2131. Bethesda, MD: Armed Forces RadiobiologyResearch Institute.
264. Mickley, G. A.; Teitelbaum, H.; Parker, G. A.; Vieras, F.; Dennison, B. A.; and Bonney, C. H. 1982. Radiogenicchanges in the behavior and physiology of the spontaneously hypertensive rat: Evidence for a dissociationbetween acute hypotension and incapacitation. Aviat. Space Environ. Med. 53: 633-638.
265. Doyle, T. F., and Strike, T. A. 1977. Radiation-released histamine in the rhesus monkey as modified by mast celldepletion and antihistamine. Experientia 33: 1047-1049.
266. Douglas, W. W. 1985. Histamine and 5-hydroxytryptamine (serotonin) and their antagonists. In Goodman andGilnan's The Pharmacological Basis of Therapeutics. 7th ed., 605-615. New York: Macmillan Publishing Co.
267. Doyle, T. F., Turns, J. E., and Strike, T. A. 1971. Effect of antihistamine on early transient incapacitation of monkeyssubjected to 4000 rads of mixed gamma-neutron radiation. Aerospace Med. 42: 400-403.
268. Mickley, G. A. 1981. Antihistamine provides sex-specific radiation protection. Aviat. Space Environ. Med. 52: 247-250.
269. Alter, W. A.; Catravas, G. N.; Hawkins, R. N.; and Lake, C. R. 1984. Effect of ionizing radiation on physiologicalfunction in the anesthetized rat. Radiat. Res. 99: 394-409.
148

Beita'ioral and Nenrophysiohogical Changes with Exposure to Ionizing Radiation
270. Carpenter, D. O. 1979. Early transient incapacitation: A review withi considerations of Inderlying mechanisms[Scientific Report SR79-1; NTIS AD-A071-803-1 1. Bethesda, MD: Armed Forces Radiobiology ResearchInstitute.
271. Iverson, S. D., and lver-,on, L. L. 1981. Behavioral pharmacolo•gy. New York: Oxford University Press.
272. DeRyck, M.; Schallert, T.; and Teitelbaum, P. 1980. Morphine versus haloperidol catalepsy in the rat: A behavioralanalysis of postural support mechanisms. Brain Res. 201: 143-172.
273. Grevert, D., and Goldstein, A. 1977. Some effects of naloxone on behavior in the mouse. Psychipharniacology 53: 111-113.
274. Herman, B. H., and Panksepp, 1. 1978. Effects of morphine and naloxone on separation distress and approachattachment: Evidence for opiate mediation of social effect. Pharmacol. Biochem. Behav. 9: 213-220.
275. Akil, H.; Madden, J.; Patrick, R. L., 1II; and Barchas, J. D. 1976. Stress-induced increase in endogenous opioidpeptides: Concurrent analgesia and its reversal by naloxone. In Opiates and Endogenous Opiate Peptides, editedby H. W. Kosterlitz, 63. Amsterdam: Elsevier North-Holland.
276. Margules, D. L. 1979. Beta-endorphin and endoloxone: Hormones of the autonomic nervous system for theconservation of expenditure of bodily resources and energy in anticipation of famine or feast. Neurosci.Biobehav. Rev. 3:155-162.
277. Katz, R. J.; Carroll, B. J.; and Baldrighi, G. 1978. Behavioral activation by enkephalins in mice. Pharmacol. Biochen.Behav. 8: 493-496.
278. Szekely, J. E., Ronai, A. Z., Dunai-Kovacs, Z., Bajusz, S., and Graf, L. 1977. Cross tolerance between morphine andbeta-endorphin in vivo. Life Sci. 20: 1259-1264.
279. Brown, R. G., and Segal, D. S. 1980. Alterations in beta-endorphin-induced locomotor hyperactivity in morphinetolerant rats. Neuropharmacology 19: 619-621.
280. Dafny, N., and Pellis, N. R. 1986. Evidence that opiate addiction is in part an immune respose: Immune systemdestruction by irradiation altered opiate withdrawal. Neuropharntacology 25: 815-818.
281. Mickley, G. A.; Sessions, G. R.; Bogo, V.; and Chantry, K. H. 1983. Evidence for endorphin-mediated cross-tolerancebetween chronic stress and the behavioral effects of ionizing radiation. Life Sci. 33: 749-754.
282. Mickley, G. A.; Stevens, K. E.; White, G. A.; and Gibbs, G. L. 1983. Changes in morphine self-administration afterexposure to ionizing radiation: Evidence for the involvement of endorphins. Life Sci. 33: 711-718.
283. Mickley, G. A. 1983. Ionizing radiation alters beta-endorphin-like immunoreactivity in brain but not blood. Pharnta-col. Bioch/em. Behav. 19: 979-983.
284. Alter, W.; Mickley, G. A.; Catravas, G.; Mueller, G.; Keiffer, V.; Doyle, T.; and Kovski, A. Role of histamine and beta-endorphin in radiation-induced hypotension and acute performance decrement in the rat. Paper presented atthe 1980 Annual Scientific Meeting of Aerospace Medical Association, Los Angeles, 225-226.
285. Danquechin-Dorval, E.; Mueller, G. P.; Eng, R. R.; Durakovic, A.; Conklin, J. J.; and Dubois, A. 1985. Effect ofionizing radiation on gastric secretion and gastric motility in monkeys. Gastroenterology 89: 374-380.
286. Mickley, G. A.; Stevens, K. E.; Burrows, J. M.; White, G. A.; and Gibbs, G. L. 1983. Morphine tolerance offersprotection from radiogenic performance decrements. Radiat. Res. 93: 381-387.
287. Morse, D. E., and Mickley, G. A. 1988. Interaction of the endogenous opioid system and radiation in the suppres-sion of appetite behavior. Society for Neuroscience Abstracts 14(2): 1106.
149

Medical Consequences of Nuclear War fare
288. Shipman, T. L.; Lushbaugh, C. C.; Peterson, D. F.; Langham, W. H.; Harris, P. S.; and Lawrence, J. N. P. 1961. Acuteradiation death resulting from an accidental nuclear critical excursion. 1. Occup. Med. 3:146-192.
289. Karas, J. S., and Stanburv, J. B. 1965. Fatal radiation syndrome from an accidental nuclear excursion. N. Engl. 1.Med. 272: 755-761.
290. Wald, N., and Thoma, G. E. 1961. Radiation accidents: Medical aspects of neutron and gamma ray exposure IU.S. AtomicEnergy Commission Report ORNL-2748, Part B; OCLC 127796421. Oak Ridge, TN: Oak Ridge NationalLaboratory.
291. Howland, J. W.; Ingram, M.; Mermagen, H.; and Hansen, C. L. 1961. The Lockport incident: Accidental exposure ofhumans to large doses of X-irradiation. In Diagnosis and Treatinent of Acute Radiation Injury, 11-26. Geneva:World Health Organization.
292. Telyatnikov, L. 1987. The top story of 1987. Paper presented at the Great American Firehouse Exposition andMuster, Baltimore, Maryland, 1987 IOCLC 185953711.
293. Young, R. Personal communication, 1987.
294. Hasterlik, R. J., and Marinelli, L. D. 1956. Physical dosimetry and clinical observations on four human beingsinvolved in an accidental critical assembly excursion. In vol. 11, Proceedings of the International Conference onPeaceful Uses of Atomic Energy [OCLC 5140571, 25-34. Geneva: International Atomic Energy Commission.
295. Anno, G. H.; Wilson, D. B.; and Dore, M. A. 1985. Nuclear weapon effect research at PSR-1983: Acute radiation effectson individual crewmeinber performance [Technical Report TR-85-52; NTIS AD-A166-282-4-XABI. Washington, DC:Defense Nuclear Agency.
296. Young, R. W., and Myers, P. H. 1986. The human response to nuclear radiation. Medical Bulletin 43, No. 7: 20-23.
297. Baum, S. J.; Anno, G. H.; Young, R. W.; and Withers, H. R. 1985. Nuclear weapon effect research at PSR-1983. In vol.10, Symptomatology of Acute Radiation Effects in Humans After Exposure to Doses of 75 to 4500 Rads (cGy) Free-in-air[Technical Report TR-85-50; NTIS AD-Al 66-280-8-XABi. Washington, DC: Defense Nuclear Agency.
298. Franz, C. G.; Young, R. W.; and Mitchell, W. E. 1981. Behavioral studies following ionizing radiation exposures: A database ITechnical Report TR81-4; NTIS AD-Al 15-825-2]. Bethesda, MD: Armed Forces Radiobiology ResearchInstitute.
299. Shapiro, N. I.; Nuzhdin, N. I.; and Kuzin, A. M. 1955. The action of estrogens on the radiation reaction in mice. InCollected Works on Radiobiology, edited by N. I. Nuzhdin [Atomic Energy Commission TR-3740; OCLC146220951, 13-29. Moscow: USSR Academy of Science.
300. Thompson, J. S.; Reilly, R. W.; Crawford, M.; and Russe, H. P. 1965. The effect of estradiol and estriol on thesurvival of sublethally and lethally irradiated mice. Radiat. Res. 26: 567-583.
301. Giambarresi, L., and Jacobs, A. J. 1987. Radioprotectants. In Military Radiobiology, edited by J. J. Conklin and R. I.Walker, 265-301. Orlando FL: Academic Press, Inc.
302. Bogo, V.; Jacobs, A. J.; and Weiss, J. F 1985. Behavioral toxicity and efficacy of WR-2721 as a radioprotectant.Radiat. Res. 104:182-190.
303. Turbyfill, C. L; Roudon, R. M.; Young, R. W.; and Kieffer, V. A. 1972. Alteration of radiation effects by 2-(n-decylamino)ethanethiolsulfuric acid (WR1607) in the monkely [Scientific Report SR72-3; NTIS AD-745-2841. Bethesda, MD:Armed Forces Radiobiology Research Institute.
304. Williams, C. D.; Weiss, J. F.; and Bogo, V. 1987. Motor performance evaluation of behavioral toxicity in mice: Effectof radiation and radioprotective agents. Proc. of Society of Armed Forces Medical Laboratory Scientists 16: 25.
305. Bogo, V., and Weiss, J. F. 1987. Ability of selenium and WR-2721 to mitigate radiation-induced performancedecrement in rats. Proceedings of the Ist International Neurotoxicology Association Meeting IOCLC 184215141, 148.Lunteren, Netherlands: International Neurotoxicology Association.
150

BehtaLioral and Neurophysiological Changes with Exposure to Ionizing Radiation
306. Landauer, M. R.; Davis, H. D.; Dominitz, J. A.; and Weiss, J. F. 1987. Dose and time relationships of the radioprotec-tor WR-2721 on locomotor activity in mice. Pharmacol. Biochem. Be/hav. 27: 573-576.
307. Young, R. W. Acute radiation syndrome. In reference 301, 165-190.
308. Dubois, A. 1988. Effect of ionizing radiation on the gastrointestinal tract. Comments on Toxicology 2: 233-242.
309. Salazer, 0. M.; Rubin, P.; Keller, B.; and Scarantino, C. 1978. Systemic (half body) radiation therapy: Response totoxicity. Int. 1. Radhat. Oncol. Biol. Phys. 4: 937-950.
310. Barrett, A.; Barrett, A. J.; and Powles, R. L. 1979. Total bodv irradiation and marrow transplantation for acuteleuk, mia. The Royal Marsden Hospital experience. Patiol. Biol. 27: 357-359.
311. Bugo, V.; Boward, C.; Fiala, N.; and Dubois, A. 1988. Zacopride: A promising radiation antiemetic. The Toxicologist8(0): 77.
312. Dubois, A.; Fiala, N.; Boward, C. A.; and Bogo, V. 1988. Prevention and treatment of the gastric symptoms ofradiation sickness. Radiat. Res. 115: 595-604.
313. Thorp, J. W.; Chaput, R. L.; and Kovacic, R. T. 1970. Performance of miniature pigs after partial body irradiation.Aerospace Med. 41: 379-382.
314. Thorp, J. W., and Germas, J. E. 1969. Performance of monkeys after partial body irradiation [Scientific Report SR69-18;NTIS AD-699-1271. Bethesda, MD: Armed Forces Radiobiology Research Institute.
315. Chapman, P. H. 1968. Behavioral and circulatorny responses to x-irradiation delivered at 200 rads per minute to whole bodyand trunk only [Technical Report TR-68-111 1. Brooks Air Force Base, TX: School of Aerospace V ýcine.
316. Chapman, P. H., and Hurst, C. M. 1968. Tihe effect of head versus trunk X-irradiation on avoidance behavior in the rhesusmonkey [Technical Report TR-68-37]. Brooks Air Force Base, TX: School of Aerospace Medicine.
317. Jones, D. C.; Kimeldorf, D. J.; Castanera, T. J.; Rubadeau, D. 0.; and Osborn, G. K. 1957. Effect of bone marrowtherapy on the volitional activity of whole-body X-irradiated rats. Am. 1. Physiol. 189: 21-23.
318. Bogo, V. 1988. Radiation: Behavioral implications for humans in space. Toxicology 49: 299-307.
319. Hunt, W. A.; Rabin, B. M.; Joseph, J. A.; Dalton, T. K.; Murray, W. E.; and Stevens, S. A. 1988. Effects of ion particleson behavior and brain function: Initial studies. In reference 86, 537-551.
320. Philpott, D. E.; Sapp, W.; Miquel, J.; Kato, K.; Corbett, R.; Stevenson, J.; Back, S.; Lindseth, K. 0.; and Benton, E. V.1985. The effect of high energy (HZE) particle radiation (40Ar) on aging parameter of mouse hippocampus andretina. In vol. 3, Scanning Electron Microscopy, edited by A. M. F. O'Hare, 1177-1182. Chicago: SEM, Inc.
151

Medical Conseque'nces of Nuclear Wa rfare
152

Chapter 8
PSYCHOLOGICAL FACTORS INNUCLEAR WARFAREG. ANDREW MICKLEY, Ph.D.*
INTRODUCTION
DETERMINANTS OF PSYCHOLOGICAL DYSFUNCTION INCONVENTIONAL WARFARE
Intensity of the BattleGroup CharacteristicsDuration of the BattlePhysical StrainConsequences of IncapacitationExpectations of the CultureCommunication
NUCLEAR WARFARE VERSUS CONVENTIONAL WARFARE
PSYCHOLOGY IN TODAY'S NUCLEAR MILIEU
LIMITATIONS ON THE CURRENT DISCUSSION
RADIOGENIC CNS CHANGES AND PSYCHOLOGICAL VARIABLES
Acute Psychological ChangesMotivationFear and TerrorSocial RelationsLearning and Memory
Chronic Psychological ReactionsPsychosesPost-Traumatic Stress DisorderAnxiety and PhobiasSurvivor Guilt
SUMMARY OF PSYCHOLOGICAL EFFECTS
PREDICTION OF NEUROPSYCHIATRIC CASUALTIES
CARE OF PSYCHOLOGICAL CASUALTIES
PREVENTION OF PSYCHOLOGICAL CASUALTIES
*Licute'nant Colonel, United States Air Force; Behavioral Sciences Department, Armed Forces Radiobiology Research Institute, Bethesda, Maryland20814-5145
153

Medicald .,+ Ift'lL'Stif Nllthlir VLrfti rt
INTRODUCTION
The psychological casualties of a nuclear conflict Israeli Yom Kippur War of 1973 lasted only 3 weeks,ma- seem to be insignificant compared to the casual- but its psychiatric casualties were 23,; of all nonfatalties from physical trauma, but they can dramatically casualties.' Even if neuropsychiatric trauma fromalter the outcome of a battle. The neuropsychiatric intense combat does not produce a casualty, it cancasualties of World War I1 were 1817--481 of all casu- degrade the performance of normal duties. Slightlyalties,'ý and they were the largest single cause of lost altered reaction times, attention, or motives may havemilitary personnel strength in that war." The Arab- important consequences in warfare.
DETERMINANTS OF PSYCHOLOGICAL DYSFUNCTIONIN CONVENTIONAL WARFARE
Much has been learned about the origins of psychi- difficulties with members of their units. In contrast,atric casualties of war. On the most basic level, even only 10- of the soldiers not suffering battle shockvisual representations of war evoke significant in- reported these unit problems.' Psychologically im-creases in sympathetic activity as indicated by in- paired persons were also more likely to have changedcreased electrodermal activity, decreased salivary teams in combat (63%) than were the control popula-function, and marked cardiac changes.? These changes tion who experienced no psychological difficultiesin physiology are correlated with higher scores on (157). These data suggest that strong, stable groupspsychological measures of stress. However, labora- play an important role in preserving the individual'story measurements significantly oversimplify the ar- psychological stability in combat.ray of variables that coproduce a particular behavioraland psychological outcome. These variables includethe intensity and duration of the battle, the leadership Duration of the Battleand cohesiveness of the group, the availability of infor-mation and ability or inability to communicate it, Expectations about the duration of hostilities affectphysical strain, individual expectations, experience, the psychiatric casualty rate. A decided decrease inand morale. neuropsychiatric casualties occurred in the European
theater of World War II toward the end of hostilities inIntensity of the Battle 1945. Conversely, the low psychiatric casualty rate of
the British soldiers has been attributed, in part, to theThe most important precipitating factor affecting British policy of long tours of duty. Believing there
the rate of neuropsychiatric casualties is the battle's was little chance of relief, the soldiers knew that theyintensity or the current degree of stress. 2,h Combat is would have to hold on.2
usually episodic, but the effect of combat stress is oftencumulative. An analysis of three infantry battalions in Physical Strainthe Sicilian campaign of World War II revealed that thenumber of casualties from physical wounds remained The terms "combat fatigue" and "combat exhaus-relatively constant over the 17 days studied, but the tion," widely used in the past, indicated that a lack ofnumber of psychiatric casualties steadily increased. 2 sleep, lack of food, and other fatiguing properties of
combat played an important role in psychiatric break-Group Characteristics down. This impression was supported when psycho-
logical symptoms were often partially relieved byMorale, group leadership, and cohesiveness are sleep and food. Although this suggested that physical
also good predictors of neuropsychiatric casualties.' fatigue precipitates psychiatric illness, it is now clearIn a study completed after the 1973 Yom Kippur War, that fatigue itself is not the primary cause of psychiat-the Israelis revealed that 40% of the soldiers with battle ric breakdown. Units advancing against slight enemyshock reported minimal group cohesion and unit id, .i- opposition may continue without sleep or food fortification, as well as a high incidence of interpers .al several days, and although the unit members may
154

Psychioh)ical Factors in Niclear Wartfare
suffer physical fatigue, they rarely show psychiatric and their officers were relatively untrained and new tosymptoms. A low incidence of psychiatric casualties is combat, it was expected that psychiatric casualtiesalso associated with long retreats. 2 Finally, typical would be high. However, this was not the case, be-psychiatric symptoms may appear early in combat or cause such behavior was not culturally acceptable.even prior to battle, before the occurrence of appre- Later in the war, when Korean soldiers were inte-ciable physical fatigue.-' grated into American units, they incurred psychiatric
breakdowns with the same frequency and symptomsConsequences of Incapacitation as their American comrades."'
Finally, anxiety states were far less common inNeuropsychiatric casualty rates in wartime tend to Indian soldiers than in British soldiers fighting side by
be low when the soldier perceives that becoming a side during the Arakan campaign in Burma incasualty either causes additional harm or produces no 1943-1944. The Indian soldiers may have felt as anx-important advantage. This was the case during the ious as their British comrades, but they could notGerman retreat at Stalingrad when the fleeing Ger- admit it; their culture dictated that they enjoy battle,mans feared capture by the Russians. Neuropsychia- and it was a point of honor to do so. The Indian soldiertriccasualties frequently occur after rather than during could deal with anxiety only by denying its existence,a battle, when the fate of an incapacitated person is by using a magical charm, orby self-inflicting a wounduncertain. 2 (which released him with honor intact). If these meth-
ods were not feasible, the Indian soldier might breakExpectations of the Culture into exuberant hysterical behavior similar to the ac-
cepted religious displays of his culture; this releasedExpectations of the group or the culture may also tension and entailed no social stigma.'
influence psychiatric casualty rates. The incidence ofpsychiatric casualties was low in both the American Communicationand South Vietnamese armies during the VietnamWar, but the total number of cases admitted (during a The way in which soldiers respond in any situation6-month period) to U.S. hospitals was almost double depends on how they perceive it; how they perceive itthe number admitted to South Vietnamese hospitals, depends on the information they have about it. Adespite the fact that the total population at risk was person who is uninformed in a complex, chaotic situ-considerably larger for the South Vietnamese. Some ation will be under great stress. Disruption of commu-authors have attributed this to the constraints on some nications during warfare may produce sufficient anxi-psychiatric diagnoses in the Vietnamese culture."I ety and fear to degrade performance. 2 Reduced com-
A similar situation occurred in the Korean War. munication can also impose significant psychologicalEarly in the war, when most Republic of Korea troops stress in a nuclear conflict. 12
NUCLEAR WARFARE VERSUS CONVEIL.ý FIONAL WARFARE
The debate continues over the expected differences Nuclear weapons have the power to produce suchbetween the psychological changes produced by con- devastation that the apparent unreality of the detona-ventional war and those produced by nuclear war. Ex- tion's aftermath may differentiate a nuclear battle fromperts at a recent symposium on the psychological a conventional battle. A modern warhead can produceeffects of tactical nuclear warfare agreed that differ- an explosion measured in megatons. Two megatons isences would exist, but there was considerable dis- roughly equal to the explosive output of all bombsagreement over whether the differences would be dropped during World War II.' A Japanese survivorquantitative, qualitative, or both. With a quantitative of the nuclear detonation at Hiroshima described adifference, more combatants would experience higher scene illustrative of the severity of the nuclear battle-levels of fear, stress, and confusion, resulting in a field:greater number of neuropsychiatric casualties. How- I had to cross the river to reach the station. Asever, if the differences are qualitative, the soldiers I came to the river and went down the bank to themight experience completely different psychological water, I found that the stream was filled with dead
symptoms, and a new and different response to the bodies. I started to cross by crawling over the
stress of war might emerge."' corpses, on my hands and knees. As I got about a
155

third of the wa acro, a dead bod began sk tinuclear war we will not be able to sacrifice ourselves soi under m\ weight d I went into thewater, wetting that our children, familv, or nation can survive. This
my burned skin. It pained a reverel. I could go no kSSOfassuranceota future for humanity may result inturther~a•therewa',a break inthebridgeolcorpev,, emotional changes that differ from those during aso I turned back to the shore, and started to walk conventional wvar.!"upstream,1 hoping to comet1 upon another wax' The psychological changes in persons exposed toacross.' nuclear weapons will partially coincide with those
seen in other disasters. But the magnitude and type ofBoth nuclear and con0ventional wveapons produce destruction from a nulclear weapon will probably (at
blast and thermal effects, but ionizing radiations are least) intensify most psychological reactions. By 1945,unique to nuclear weapons. Radiation effects may the people of Japan wvere accustomed to destructionhavCe caused as manv as I '; -210'f of the deaths at from conventional bombing. However, the atomicI liroshii,, and Nagasaki."' The insidious and lethal bomb effects were new and v'asth, more horrible, elic-nature of radiation makes it especially feared. In 1951, iting more extreme psychological reactions in the resi-Brigadier General James (.oonev worried about his dents of Hliroshima and Nagasaki who responded tosoldiers' ability to function in a nuclear battle, because the U.S. Strategic Bombing Survey several years later..'radiation associated with the atomic bomb was be- Still debatable is thequestion ofqualitativedifferenceslieved by many to "cause immediate and mvsterious in the psychological responses to different types ofinjury or death."'" Despite our current knowledge natural disasters and other stressful events. Psycho-about radiation effects, these beliefs are still perx'asive. logical symptom complexes may differ, depending onThe 1979 nuclear reactor accident at Three Mile Island the nature of the disaster.22 In some studies, the psv-produced almost no radiation exposure above nornmal chological morbidity is clearly defined by diagnosticbackground levels, but the public believed that a radia- criteria, such as those identified for post-traumatiction hazard was present, which evoked long-term stress disorder, anxiety, or depression. Other studiessigns of emotional, behavioral, and physiological address a more nonspecific psychological distressstress.'s reaction. Symptom clusters and perhaps specific
Thepsychological reactionsto nuclear warfarehaxve somatic complaints may be specifically related toan added dimension, namely, anxiety that the human particular types of disasters.2- It would not be surpris-species will be annihilated. People achieve symbolic ing if in-depth studies reveal that some components ofimmortality by identifying with their children, grand- stress reactions are more likely to be expressed duringchildren, and larger cultural units, such as their nation nuclear conflicts than during conventional warfare oror religion.'' Unlike all the past wars, in a strategic natural disasters.'
PSYCHOLOGY IN TODAY'S NUCLEAR MILIEU
When a person is faced with the horror of nuclear youngsters, particularly from white-collar families,warfare, the responses are fairly predictable: fear, are troubled by the prospect of nuclear war. They havedread, and finally denial. It has been suggested that fears about the future, and view their futures lessthe levels of fear and anxiety in the world's population hopefully than previous generations did.have been substantially increased I1v the prospect of Adults appear to be much more complacent aboutnuclear annihilation, in 1984, Gallup surveyed 514 the threat of nuclear war. "' Forexample, the movie Thenteenagers (ages 13-18), as a representative national Dat*, After, depicting a nuclear war and its aftermath,cross section, on the likelihood of the occurrence of was shown on network television in the United Statesnuclear confrontations in their lifetimes.' Fifty-one in November 1983. The film received extensive public-percent indicated that it was "somewhat likely" that a ity and a large audience viewed it. Mental-healthnuclear war would be started during their lifetimes, professionalsanticipated that the program would gen-and I5'; thought it was "very likely." Other survevs erate significant distress in viewers, so they publicizedby direct interview or questionnaire have been con- the crisis services that were 'o be available during andducted in the United States, theSoviet Union, and else- after the broadcast. The Massachusetts Psychologicalwhere. "' ̀ Alth( igh the methodology of some studies Association had 25 v'olunteers standing by telephoneshas been questioned,"their results indicate that many across the state. Not a single call was received.."
156

Psychological Factors in Nuclear Warfare
Much has been said and written about the apparent Since children worry about nuclear war and adultsapathy of the adult population to the prospect of generally do not, the process of active denial is sug-nuclear self-destruction. Psychic numbing, denial, gested. Furthermore, nuclear war is easy to deny. It isand other psychological techniques have been pro- an abstract concept, and we have no experience of it.posed as reasons. Despite the horrible possibilities of Many other urgent, immediate things compete for ourwar, remaining relatively unworried and inactive may attention. People seem less motivated by abstract fearsnot be irrational if people are correct in judging that than by immediate benefits (life insurance, for ex-their activities have no consequence. t For example, ample, is sold not on the basis of fear of the future, butthe citizens of the District of Columbia ("ground zero") rather on the basis of more security today)." Denial asdecided by referendum in 1982 that devising a civil a psychological defense may be comforting, but it hasdefense strategy would be a waste of time."2 its dangers. This trend, thought by some also to exist
It is often difficult to distinguish between a lack of in the U.S. military,24 could significantly affect the wayconcern about nuclear war and an active denial of it." one prepares for and functions in a nuclear conflict.' 7
LIMITATIONS TO THE CURRENT DISCUSSION
The circumstances of a tactical nuclear war will the reactions are similar to those observed after andramatically affect predictable psychological out- intense conventional battle or a natural disaster, suchcomes."4 A strategic exchange of nuclear weapons as a flood or earthquake. Although this approach haswould be expected to produce more devastation and merit, it also has a number of problems.3" In particular,cause more dramatic emotional changes in survivors the stress of ionizing radiation exposure is missing,than would a single local detonation. But the psycho- with its unique characteristics and implications tological changes from a tartical nuclear war are not those exposed. Persons exposed to radiation on aexpected to be simple, straightforward, or minor. One nuclear battlefield may have little or no initial knowl-study of predictable troop reactions to a tactical nu- edge of the severity of their radiogenic injuries. Thisclear battle identified specific psychological outcomes uncertainty, and each individual's interpretation of it,to be expected at different times (periods of shock, may affect the emotions and ability to perform. Theseinformal organization, formal organization, and reha- models also ignore the direct radiogenic changes in thebilitation) and distances (zones of destruction, heavy CNS, which may also alter the psychological variables.damage, light damage, and periphery) from the nu- The data derived from the atomic bombings ofclear weapon's detonation.' The study contains a de- Japan are flawed, in part, because the population wastailed hypothesis on the spectrum of possible psycho- predominately civilian. Civilians may or may not reactlogical changes in nuclear combatants. This chapter, to the use of nuclear weapons in the same way ahowever, is limited to a general overview of the acute military force might. Because this was the first use ofand chronic psychological symptoms that can be ex- an atomic bomb, the element of surprise was great.pected in soldiers actively involved in a tactical nu- Many of the Japanese citizens were unaware at firstclear battle. that radiation was present. In addition, the radiation
No definitive data speak directly to the issue of doses actually received by persons in Hiroshima andhuman psychological responses to radiation exposure Nagasaki were not well described.or use of nuclear weapons. Experiences of nuclear AlthoughtheJapanesedataarelimited, theyaretooaccident victims have usually been poorly documented important to ignore. The bombings of Hiroshima andregarding mental alterations. Patients who are ex- Nagasaki provide the only available data on the com-posed to ionizing radiation as part of cancer treatment bined results of blast, thermal, and radiation insults toalso frequently receive drugs to suppress the side a large human population. Some military personneleffects and enhance the effectiveness of the radiation. were present in both cities during the bombings, andThese patients are usually quite sick even before the provided a few examples of military actions in a nu-radiation therapy, so it is difficult to assess the psycho- clear environment.)7 Although data derived fromlogical effects of the radiation itself, other wars and disasters are not perf",' ýhev can also
A research model for psychological reactions to the give clues to the psychological fact, 'clear con-nuclear battle has been established by assuming that flict.
157

Me'dical Cots'qluctics of Nuclar WVrfart,
RADIOGENIC CNS CHANGES AND PSYCHOLOGICAL VARIABLES
One aspect of the psychological effects of nuclear being able to control the radiation dose and the testingweapons that has received little attention is the direct of behavior. The animal data apparently reinforceinteraction of nervous tissue and radiation. Since the much of the anecdotal human data from the Japanesebrain is the seat of emotion, ionizing radiation expo- experience.sure may be capable of directly influencing psycho- This section addresses the range of psychologicallogical changes. Especially relevant here are (a) data phenomena likely to be observed during the firstsuggesting that the CNS is sensitive to changes in- minutes and hours of a nuclear battle, based on bothduced by ionizing radiation exposure, and (b) data humanandexperimentalanimaldata. Thetimecoursesuggesting that radiation can change psychological of these acute changes is in question, and the changesvariables in nonhuman animals. may extend for days after the conflict.
Neurons were once thought to be relatively radio- Motivation. Motivation may be altered after ioniz-resistant, based on data from studies measuring cell ing radiation exposure. An animal's tendency to per-death rather than disruption of cell functioning.3' More form is governed by a number of factors, including thecurrent studies are revising these ideas. Developing physical capacity of the animal, rewards or punish-cells are particularly sensitive to the lethal effects of ments present, and the animal's perception of theseionizing radiation. The adult neurogenesis that takes reinforcements. If an experimental subject has theplace in some brain areas in certain animals suggests capacity to perform in the presence of previouslythat these nuclei may be damaged by much lower motivating stimuli but does not do so, then it may bedoses of ionizing radiation (less than 4 Gy) than previ- inferred that some change in the subject's motivationously expected." Changes in the amplitude and fre- has occurred. For example, after irradiation, rats willquency of EEG recordings occur after 1-4 Gy of X decrease the number of times they press a bar that,rays," and doses as low as 0.008 Gy can change the when struck, givesthemsomeinformationaboutwhenspontaneous electrical discharges of hippocampal shock will occur .4 However, they significantly in-pacemaker-like neurons." Metabolic alterations of the crease the number of times they press a bar to delayneurotransmitter dopamine have been reported in the footshock. These data suggest that the animal is fullybrain after 10 Gy of cobalt-60 radiation. 41 Levels of the capable of pressing the bar, but chooses to do so onlyputative neuromodulator beta-endorphin also change under certain conditions.in irradiated mice and monkeys at doses that do not Another study supports this concept. Rats willkill neurons.4' Neuronal sodium channels may lose work in order to receive electrical stimulation of par-their ability to respond properly to stimulation after ticulv, n areas."' In one rat, electrodes were im-only 1 Gy of high-energy electrons.43 Thus, a growing plar two brain areas (lateral hypothalamusbody of evidence suggests that ionizing radiation may and Before irradiation, the subject pressedalter neural physiology and function at doses substan- the bat ii the same rate to activate either site. Aftertially below those required to produce morphological irradiation, the animal worked to stimulate only thechanges and neuronal death. It would not be surpris- lateral hypothalamus. Clearly, the animal had theing if psychological changes correlate with these physical capacity to perform the task, but its motiva-changes in brain function. tion was altered after irradiation, producing a selective
decrease in responding to septal stimulation. TheseAcute Psychological Changes data suggest that motivation may, in some cases, be
more radiosensitive than physical capacity.Evidence suggests that emotional variables can be Some observations have been made about curiosity
influenced by radiation exposure. It may be possible to and investigative behaviors after radiation exposure.study this component of the psychological effects of Chimpanzees given 3.75-4.0 Gy of gamma radiationirradiation by reviewing some of the work done in made fewer attempts tosolvea variety of puzzles. Thislaboratory animals. The validity of using animals in deficit seems to be independent of changes in capacity,this kind of work has been detailed elsewhere." This because measures of dexterity and strength wereapproach has the disadvantage of ignoring (for the unchanged in these same animals.', In another experi-moment) some of the psychogenic aspects of a reaction ment, pairs of monkeys were irradiated with 4 Gy ofto a nuclear confrontation, but it has the advantage of whole-body X radiation.' Twice daily, continuous ob-
158

Psych)oh1'icaI Factors in Nuch'ar Warfhre
servations of home-cage behavior were made during a behavioral and psychological changes may have a10-minute period in accordance with a checklist. In psychogenic component, which may compound theorder to control for any debilitation factor, the number radiation-induced alterations described above in labo-of instances of each category of behavior was divided ratorv animals.by the total number of times that any identifiable Despite the emotional deadening and "mentalbehavior occurred in that same period. In these ani- weakness" reported by almost everyone influenced bymals, a reliable deficit in curiosity was measured by the the bombing of Hiroshima, it is remarkable how muchreduced relative frequency of manipulating inanimate physical activity was exhibited by some of the survi-objects. The monkeys exhibited relatively more cage- v'ors. Some of this activity seemed ill directed:directed movements (toward well-known stimuli) andless attention and orienting to incidental novel noises. There was no organized activity. The peopleThey selected food in their central line of sight, rarely seemed stunned by the catastrophe and rushedchosing food from the periphery. Furthermore, when about as jungle animals suddenly released from aattempts were made to distract them, they were less cage. Some few apparently attempted to help oth-likely to orient to the stimuli than were the controls. ers from the wreckage, particularly members ofBecause this procedure attempted to factor out general their family.... However, many injured were leftmalaise, the results suggested reduced levels of curios- trapped beneath collapsed buildings as people fleditv and attention in the animals. 4"' These observations by them in the streets.2
agree with others in which irradiated monkeys showedincreased performance of tasks that placed a premium This account of frantic activity raises the issue ofon attention to a known site of food reward. Con- panic. Was there mass panic after the dropping of theversely, the monkeys showed reduced performance of atomic bomb? Probably not. Although several iso-tasks that required attention to stimuli in the periphery lated instances of aimless and hysterical activity haveof vision." been reported, these did not seem to be typical behav-
The data from Hiroshima and Nagasaki suggest iors. Disaster victims are extremely concerned aboutthat a similar change in motivation may occur in how the disaster will affect the things and persons theyhumans exposed to the trauma of a nuclear detonation. value. They want to know what has happened to thoseThe defensive mechanism of "psychic numbing" or they hold dear, and they want to help them if neces-"psychic closing off" was observed in the atomic bomb sary. This concern often leads to a great deal of activity,victims. " One writer described this scene: which may appear to an observer as irrational and dis-
organized. Thus, the very rational and deliberateThose who were able walked silently toward flight of people from an area of danger (a highly adap-
the suburbs in the distant hills, their spirits broken, tive behavior) is often mistakenly described as panic.'5
their initiative gone. When asked whence they Reports from the U.S. Army (which interviewed thecame, they pointed toward the city and said "that survivors of the bombing)21 did not support the claimway;" and when asked where they were going, omin o notsor te caipointed away from the city and said, "this wav." that a sizable portion of the population behaved in anThev were so'broken and confused that thev moved ineffective, nonsocial, or nonrational way.;- The re-and behaved like automatons. port also clearly indicated that many people felt terri-
Their reactions astonished outsiders who re- fied or fearful, even though they did not exhibit panicported with amazement the spectacle of long files reactions. In only a few cases can one surmise fromof people holding stolidly to a narrow, rough path interviews that individuals might have exhibitedwhen close by was a smooth, easy road going in the uncontrolled emotional behavior. Instead, compliant,same direction. The outsiders could not grasp the subdued behaviors were more prominent, perhapsfact that they were witnessing the exodus of a mediated in part by some radiogenic CNS effects orpeople who walked in the realm of dreams." other injuries:
These data are consistent with others from Hiro- Many, although injured themselves, supportedshima reporting "fatigue," "mental weakness," "spiri- relatives who were worse off. Almost all had theirtual desolation," or "closing off."'1 7 Certainly, in the heads bowed, looked straight ahead, were silent,
case of these atomic-bomb survivors, this change in and showed no expression whatsoever. ý2
motivation cannot be solely attributed to a dose ofradiation. These people had just witnessed the devas- It seems that a depressed motivational state, rathertation of their homes and, in many cases, the deaths of than panic, was a typical reaction to the disaster.family members. Thus, it is very likely that these Obviously, eitherachaoticoranapatheticresponse
159

Medi'cal C•Ise'qient' c. of Nuth' lr Wtarfaire
to a bombing wvould not be adaptive in a military Fear and Terror. The main reaction of the Japaneseenvironment. Some evidence exists that inhabitants of populace in the atonlic-bomb target areas was "un-Hiroshima who had a specific job to perform or a goal qualified terror," fed by the horror of the destructionto meet tried valiantly to do so after the bombing. A and suffering either witnessed or experienced by thegroup of wounded soldiers was observed gamely at- survivors.'' Sixty-three percent of all respondents totemptingtostruggleoutof thedisasterarea in militarv the U.S. Strategic Bombing Survey reported eitherformation: generalized terror or fear for one's own life. Some
experiences cannot be described by cold figures:
At Misasa Bridge, the%, encountered a long lineof soldiers making a bizarre forced march away People were running toward our place withfrom the Chugoktu Regional Army I leadquarters terrible burns. That night they slept on the roadin the center of the town. All were grotesquely everywhere. Some collapsed during the day due toburned,and theysupported themselves withstaves the effects of burns. People would stop by and askor leaned on one another. for water, which was the most urgent need of these
people. They were so upset that they coulId n't thinkof food. It was a horrible sight---crving and scream-
One account orf a youngJapanese soldier is particu- ing. I can't describe the burns that were on theselarlv relevant here: people, and theodorof burning flesh was in the air,
and it was soawful you have to see it before you canWe were under military order to return to our actually describe it oreven talk about it. It's hard to
unit immediatelv in case of any attack or emer- comprehend. Some father with his entire familygency, so I returned almost without thinking .... At dead would be yelling to die, so that he would notfirst I couldn't get through . .. so in thie evening I have to live alone.2'started out again. This time I didn't try to helpany-one but just walked through them0. 1 was worried Social Relations. It is of psychological and socialabout the Army canmp because according to what importance that, in the extreme trauma after the atomicpeople told me, it had simply gone up in flames and explosions in Japan, most people behaved in a mannerdisappeared. I wasalsoa bit ashamed about having explo in eapan, stceo l badnm etaken such a long time to return. But when I finally compatible with established social norms.got back to camp, just about everyone was dead-so there was no one to scold me.... Next thing I did To Father Kleinsorge, an Occidental, the silencewas to look for theashes of the military code book- in the grove by a river, where hundreds of grue-since we had a military order to look for this book somely wounded suffered together, was one of theeven if it were burned, as it was a secret code which most dreadful and awesome events of his wholehad to be protected. Finally I located the ashes of experience: The hurt ones were quiet; no one wept,the book, and wrapped them in a furoshiki and car- much less screamed in pain; no one complained;ried this around with me. I wanted to take it to the none of the many who died did so noisily; not evenmilitary headqu artersas soon as possible, but when the children cried; very few people even spoke.I finally did take it there in the morning, the officer And when Father Kleinsorge gave water to somescolded me for doing such a stupid thing... I was whose faces had been almost blotted out by flashfresh from the Military Academy and my head was burns, they took their share and then raised them-full of such regulations. selves a little and bowed to him in thanks.7
hSome of these phenomena may be explained by With thedisruption of individual motivation, people
att'tional focusing, a behavior similar to that which seemed most likely to pursue the goals established bywas exhibited by irradiated laboratory animals. These others. Attention to leaders did not seem to be jeopard-people tended to focus on a particular aspect of their ized after the detonation. For example, a victim ofenvironment and to pursue it, sometimes to an illogi- Hiroshima recounted:cal or inappropriate end. The soldier above pursuedhis assigned task, ignoring the fact that the nuclear All the people were going in that direction anddetonation had totally changed his world (a behavior so I suppose I was taken into this movement andthat would not necessarily be discouraged by military went with them. . . . I couldn't make anv clearcommanders). Thus, although a generalized decrease decision in a specific way... so I followed the otherin motivation may have occurred in much of the Hiro- people.... I lost myself and was carried away.
shima population, some behaviors directed toward awell-defined goal apparently persisted after the catas- Various cultures may differ on the issue of confor-trophe. mity. But if we can generalize from these data, we can
160

Psiyciioh'ical Factors in Nuclhar Wartare
expect the social structure to be maintained after a ous civil disasters (such as hurricane, tornado, or fire).`nuclear conflict. It appears that psychoses are not the result of external
Learning and Memory. The results of animal stud- danger. When units new to combat are exposed toies are consistent with the hypothesis that functions of severe battle stress, they frequently exhibit severelearning and memory may be altered by some doses of behavioral disorganization and disorientation, hallu-radiation. For example, rabbits learned to associate a cinations, and even mute, catatonia-like states. Thesetone and a light with apnea produced by inhaling conditions are transient and usuallv subside in 1-3ammonia vapor." Once this classically conditioned days to become typical cases of neurosis.response was established, the tone and light alone Neuroses. Neurotic reactions to the traumas ofproduced apnea. However, after irradiation (15 Gy), nuclear combat are to be expected. Among 7,297the conditioned response was absent or considerably patientsexposed toionizing radiationduring theatomicreduced in duration. In contrast, the apnea produced bombings of Japan, 533 patients had neurosis-likeby the ammonia itself was enhanced after radiation symptoms.-" The patients were divided into twoexposure (confirming that the animal was still capable groups: those with symptoms of atomic-bomb radia-of this response). Retrograde-amnesia has also been tion illness and those without. Neurosis-like symp-reported in rats exposed to rapid, low doses (0.1 Gy) of toms were twice as common in the former group as inelectrons?' the latter. The Japanese researchers pointed out that
Interviews with people exposed to radiation at some of these cases were recognizable as "pure neuro-Hiroshima indicated few cases of acute retrograde ses" caused by psychogenic factors (other than theamnesia in the population.-2 However, 5 years after bombings), but that others could be caused by func-the detonation, deficits in memory and intellectual tional disorders of brain or body due to radiation. Notcapacity were noted in persons who had experienced surprisingly, the more severe the symptoms of atomic-radiation sickness." Acute radiogenic impairments of bomb radiation illness, the stronger the neuropsychia-memory in the human have also been reported in the tric aftereffects. The common symptoms includedSoviet literature. 7 weariness, lack of spirit, a tendency toward introver-
sion, and poor memory.
Chronic Psychological Reactions Post-Traumatic Stress Disorder. Seeing largenumbers of burned, cut, and maimed bodies was a
The initial reactions to a nuclear weapon detona- majorsourceof emotional trauma after the bombing oftion may be quite different from reactions that occur Hiroshima. Many survivors located a short distanceafter weeks, months, or years. Psychogenic changes in from the center of the explosion received two emo-emotionality, personality, and somatic effects usually tional shocks: the first from the physical impact of thetake a period of time to be expressed fully. Studies of explosion, and the second after they ran out into thepsychological symptoms in various cultures after the streets and saw so many casualties. Among those atdeath of a loved one reveal that reactions to grief are the periphery who escaped the full physical violenceseldom completed in less than I or 2 years. The more of the explosion, the first emotional impact seems tosevere or complicated the loss or injury in a disaster, have occurred when they saw the streams of injuredthe more extended the reaction time may be.3, These victims pouring out of the destroyed areas. Appar-data suggest that significant chronic psychological ently, it was not only the large number of casualties butdysfunctions may occur in nuclear combatants. also the specific character of the injuries (particularly
Psychoses. Serious psychological derangements the grossly altered physical appearance of personsinvolving distorted perceptions of reality and thought with severe burns) that produced emotional distur-were rare after the atomic-bomb detonations, just as bances in the people who saw them.-4 For example,they were after the large-scale conventional bombingsof WVorld War II;" The incidence of psychosis (mainly I walked past Hiroshima station ... and sawschizophrenia) in military populations is similar in people with their bowels and brains coming out...peace and war."' This is confirmed by evidence that a I saw an old lady badly burned and carrying a
variety of traumatic situations are not associated with suckling infant in her arms... I saw many childrenan increased rate of psychosis. For example, massive words the horror I felt utaerial bombardment of population centers in England,Germany, and Japan during World War II did not Post-traumatic stress disorders (PTSD) are seen afterproduce an increased number of psychoses, as indi- a variety of natural disasters"' and should be expectedcated by mental-hospital admission records. Simi- after the shock of a nuclear conflict."2 The full PTSDlarly, psychoses do not usually result from spontane- syndrome is a cluster of symptoms occurring after
161

Medical Ctonsequcnce!s t# Nucl'ar Warta rc
exposure to unpredictable life-threatening environ- ported to circulate during the postdisaster period.:"mental trauma.6' Sufferers of chronic PTSD continue For example, one woman reported:to live in the emotional environment of the traumaticevent, with prolonged vigilance for and sensitivity to i heard that people who had not been wound.edexternal threat. The five principal features of PTSD are and seemed to be all right would begin feeling out(a) persistence of startle responses and irritability, U') of sorts afld all of a sudden drop dead. It made meproclivity to react explosively, (c) fixation on the panicky. Here I was bustling around now, but Itrauma, (if) constriction of the general level of person- might go off myself.-ality functioning, and (e) an atypical dream life.
A numbing of responsiveness, reduced involve- Most of the survivors had never heard of radiationment with the external world, and constricted affect sickness and were unprepared for its manifestation.are part of the diagnostic criteria established for PTSD.' During the weeks following the atomic explosions,Long-term depressive reactions with these character- many survivors began to exhibit signs of organic pa-istics have been reported to occur after catastrophic thology: loss of hair, high fever, excessive fatigue,natural disasters, such as floods.' Depression is one of hemorrhagic spots under the skin, and other severethe prominent symptoms observed in soldiers during symptoms of what we now recognize as ARS. Wit-the extreme stresses of combat.' Although acute de- nessing the agonizing deaths of children and relativespression (evidenced by weakness and lethargy) char- probably touched off or reinforced rumors and sus-acterized much of the Hiroshima population for a few tained the fear reactions created by the disaster."days after the bombing, it is difficult to say if signifi- Rumors may play a significant part in any futurecant numbers of people experienced chronic depres- nuclear combat. Communication on the nuclear bat-sion. Although individual questionnaire responses tlefield will be disturbed by electronic warfare tacticsfrom Hiroshima residents seemed to describe a de- and by the spreading of deliberate misinformation bypressive reaction in many cases, statistical analyses the enemy. Negative rumors can be expected in anyrevealed no greater incidence of depression there than population if radiation is a perceived threat.-in other Japanese cities. 2 This may be misleading, Survivor Guilt. Although the adherence to socialhowever, because postwar apathy seemed to charac- customs seemed to be strong after the atomic bomb-terize most of the population of Japan. Chronic de- ings, not everyone acted in a completely altruisticpressive reactions havebeen known to follow a variety fashion. It was impossible to do so, given the sheerof traumas, so they are not exclusive characteristics of number of casualties. Some people fought fires andnuclear disasters. fed the hungry, but most people (especially those who
Anxiety and Phobias. In view of the horrors of the did not work in the helping or service professions)nuclear detonations in Japan, it is not surprising that restricted their assistance, when they could give it, tosevere anxiety persisted formany daysand sometimes people they knew: "Under many houses, peoplefor weeks and months, according to various sources.2' screamed for help, but no one helped; in general,One of the most frequent types of sustained emotional survivors... assisted only their relatives or immediatedisturbance appears to have been a phobia-like fear of neighbors, for they could not comprehend or tolerateexposure to another traumatic disaster. This reaction a wider circle of misery." As one survivor summa-consisted of strong feelings of anxiety and exaggerated rized, "The idea of 'love thy neighbor as thyself' that Iefforts to ward off new threats. A physician in Hiro- always believed in, had disappeared some place. Ishima wrote: guess it was too much for any of us.""h Persistent
survivor guilt may be an inevitable consequence ofWhenever a plane was seen after that, people atomic bombing. People in the heart of the city were
would rush into their shelters. They went in and able to survive only bv running away from the firesout so much that they did not have time to eat. They without stopping to rescue others. who were inwithout sp nertous rescuy ot .oPeoplewere so nervous they could not work." a position to give aid could not simultaneously per-
form all the duties and obligations of rescuing theAnother author described the following: "It began wounded, rushing to their own families, assisting
to rain .... The drops grew abnormally large, and neighbors, carrying out their civil defenseassignments,someone [in the evacuation area I shouted, 'The Amer- saving valuable materials at the offices or factoriesicans are dropping gasoline. They're going to set fire where they worked, preserving treasured householdto us!' "'7 articles, and so on. Although independent observa-
Further indications of sustained apprehension in tions indicate that some survivors experienced tempo-Hiroshima came from the anxiety-laden rumors re- rary guilt reactions following the atomic bombings, no
162

Psy1choh0,ica Factors in Nuclear Warfare
satisfactory evidence supports the claim that suchreactions persisted in large numbers of survivors or for mark of wounds-as if I were a cripple.... It is notverya matter of lacking something externally, but rather
vey Syoftime. S something like a handicap-something mental thatPsychosomatic Symptoms. Some patients may does not show-the feeling that I am mentally
have had a psychosomatic "atomic bomb neurosis," in different from ordinary people... so when I hearwhich the survivor's identification with the dead and about people who die from atomic bomb disease ormaimed initiates a vicious psychosomatic circle.' Such who have operations because of this illness, then Ia survivor is likely to associate the mildest everyday feel that I am the same kind of person as they....injury or sickness with possible radiation effects, andanything that could relate to radiation effects becomesassociated with death: Thus, combatants involved in a nuclear battle may
"share" physical symptoms of radiation sickness. ThisFrankly speaking, even now I have fear.... Even adoption of symptoms may be due, in part, to not
today people die in the hospitals from A-bomb understanding theirdisordersandalsotoanxietyaboutdisease, and lwhen I hear about this) I worry that I the lethal effects of radiation exposure. Physicianstoo might sooner or later have the same thing hap- may be caught in a conflict between the humanitarianpen to me.... I have a special feeling that I am provision of medical care and the danger of encourag-different from ordinary people.., that I have a ing the development in survivors of hypochondria,
general weakness, and dependency.
SUMMARY OF PSYCHOLOGICAL EFFECTS
Although the atomic bomb experience in Japan is still be able to take direction, but the capacities to learnthe best model available, it is difficult to determine and remember may be changed. The horrible wound-how much information this model and correlated ing and destruction produced by a nuclear weaponanimal data can provide on the psychological changes could be expected to have immediate psychologicalin a military nuclear confrontation. All psychological effects on the military personnel who observe them. Ifeffects (like all physiological effects) are dependent on they react like the citizens of Hiroshima, they will bethe dose of radiation received; the distance from ground fearful and anxious, perhaps even more so than duringzero (and correlated blast and thermal effects); and the a conventional conflict. These symptoms may beindefinable personal, psychological, and social back- heightened by rumor and by any misinformation aboutground of the potential nuclear victim. However, if we the threat. Group cohesion will contribute to the like-can assume a certain degree of congruity between the lihood of altruistic behaviors, but self-preservationpsychological response of the Japanese and the ex- may be a more compelling need for many. Social orderpected response of military personnel, the following (military protocol) will probably remain intact in manysummary may apply. cases. Longer-term psychological reactions may in-
With ionizing radiation exposure will come altera- clude phobias, PTSD, depression, and various psycho-tion of CNS physiology, which in turn may bring about somatic symptoms. Guilt concerning questions of per-acute behavioral and psychological changes, such as a sonal survival and inadequacies in performance couldgeneralized reduction of motivation. There may also contribute to the development of neurotic symptoms,be symptoms of lethargy and fatigue, which will in- as will the severity of physical wounding. Psychotichibit the likelihood of generalized panic. Persons will reactions are probably less likely to occur.
PREDICTION OF NEUROPSYCHIATRIC CASUALTIES
It is important to know how severely these psycho- may be consistent with a normal curve." Here, as inlogical changes will affect the performance of military other disasters, most survivors (about 75%) wouldunits or the outcome of a nuclear battle.1,2."- The distri- manifest a few of the symptoms described above.bution of the psychological effects of a nuclear disaster About half of the remaining survivors would be al-
163

Mtodical )ibo*Ci iCihtv ot Nuit lar Wi rtarti
most totally unaffected, and the others would show pected in a conventional conflict. Since the psycho-many or a high degree of acute and chronic psycho- logical casualties of high-intensity conventional wal-logical changes. If tactical nuclear weaponsareused in fare may be 18';-48'1 of the total casualties undercombination with the extensive conventional arsenals certain circumstances, it can be expected that psycho-that are available, then the predicted neuropsychiatric logical factors will play a substantial role in determin-casualties in a nuclear battle would exceed those ex- ing the outcome of a nuclear battle.
CARE OF PSYCHOLOGICAL CASUALTIES
Some of those with minor emotional symptoms recently as the Israeli war experiences of 1973 andwill never be seen clinically. However, the literature 1982, in which a few aggressive teams returned '45'j• ofsuggests that those who do find their way to psycho- battle-shock cases to duty with their units.'logical treatment should be handled in conventional This conventional approach to treatment is effec-ways. These techniques involve the principles of tive, but a nuclear conflict will present special prob-proiximity, IjjrT1i'llt', and i'.Vpctaniy. Individuals respond lems to medical personnel. One problem is the uncer-better if they recei ,'e therapy as soon as possibleand as tainty of personal injury. Most people now realize thatnear as possible to the scene of the battle. Medical radiation exposure can be lethal even though initialpersonnel should calmly accept the person's problems effects may be minimal. This uncertainty about one'sand regard them as a temporary incapacity, with re- health after irradiation will increase the medical treat-covery expected after a brief rest. The condition of ment load. It has been shown in previous studies ofpersons with situationally induced, acute psychologi- disasters that threats or dangers that cannot be reliablycal disorders will worsen or improve, depending on perceived by the senses can cause considerable psy-what is expected from them by the providers.' In chological disturbance. For example, a mass poison-World War I, military psychiatrists came to recognize ing of bootleg whiskey in Georgia resulted in a largethat the "shell shock" syndrome was fostered by pro- number of people seeking emergency medical treat-longed hospitalization and then evacuation to thezone ment. When tested, about 40'/, were unaffected byof the interior.' However, some British officers noticed lethal alcohol; some confessed that they did not knowthat if the shell-shocked soldiers were treated quickly if they were affected, but they wanted to be checked.7-
and near the front line, 70'/' -80'/, soon returned to full Under a current military plan, each soldier will beduty.'"' When soldiers are evacuated from the combat provided a dosimeter the size of a wristwatch before aarea, a vicious circle may be set in motion.7 ' Remloval nuclear battle, but it will be possible to read the dosefrom the front and admission to a hospital confirm only by using a heavy, bulky device at the unit's head-their belief in the seriousness of their condition. Then quarters.-" After a nuclear attack, many soldiers willthey discover (unconsciously orconsciously) that their wish to be reassured that they have not been exposedillness is an asset that keeps them out of combat. Under to appreciable levels of radiation.' The situation maytheseconditions, symptoms may become fixed and the be similar to one in World War I in which mustard andsoldiers may become incapacitated for further combat phosgene bombardments (both of which havedelayedduty. The practice of forward therapy was developed effects) were first used. For every true case of gasfrom these observations. If combat soldiers who be- exposure evacuated to the field hospitals, two soldierscome neuropsychiatric casualties are not long sepa- were evacuated who only believed they had beenrated from their groups and are quickly treated in the gassed."4 Without information, combatants are morevicinity of the fighting, they can frequently rejoin their likely to overestimate the danger and to succumb to
units in a few hours or days. The treatment includes rumor and hysteria. This could add to the chaos thatsome simple therapy with an interview, rest, perhaps may already exist at the treatment centers.sedation, and individual or group psychotherapy, Knowing that medical care is available has alwaysfollowed by a return to duty accompanied by friends, provided comfort to combatants, but the JapaneseThis is combined with assurances from the medical experience 7" as well as current estimates 217r suggestpersonnel that their symptoms are natural ones that that medical facilities will be stressed, if not over-may break out in almost any soldier under enemy whelmed, after a nuclear conflict. For example, burnfire.'' Although some of these techniques have been cases place a great strain on medical personnel. Usingrecently questioned,7 2 they were proven to be useful as evidence from the English experiences of World War I,
164

Pstc/hoho'('ica1 i L, tOrs in Mnchear Wartart'
the British Army Operational Research Group esti- Removal from the conventional battle allows psycho-mated an average time of 52 minutes for three persons logical and physical healing. However, in some cases,to simply dress a burned hand., Extrapolations from the progrt- ;sive physical radiation effects may con-their data suggest that the requirement for treating tinuallv erode the individual's ability to perform a task1,000 serious burn cases would be 5,000 health profes- that is necessary for the success of a military mission.sionals and 235 tons of supplies. Based on a case in The efficacy of removing psychologically impaired ir-which a 38-yuar-old man was accidentally exposed to radiated soldiers from the battlefield with any expec-2 Gv of cobalt-bO radiation, others have conservatively tation of their return is questionable.estimated that the cost of treating such a person would An ethical dilemma may present itself with soldiersbe $22,000 (in 1982 dollars). It is doubtrul that such who are believed to have received intermediate dosesextensive care could beguaranteed to large numbers of of radiation that may kill them, but whocan almost cer-battlefield casualties. If the medical load becomes too tainly be saved by treatment in a secure hospital set-extensive and reasonable care cannot be given to casu- ting.24 A researcher writes,alties, morale will suffer. The detrimental effect of in-adequate medical care on morale was noted in the Hi- Should he be evacuated, and Ithe unitl lose a
roshima experience, in which many medical facilities potentially effective soldierduring the latent phase?were destroyed. The care was so limited that it wav Or should he be returned to duty, knowing that he
have been a .factor in some acute depressive r, :ctlios has a greatly increased risk of death from disease orhand feelngs afactorlessness s ome acute depresiv tng. injury, even if not killed bv enemy action, due toand feelings of helplessness following the bombing.- impaired blood clotting, wound healing, and resis-
In addition, the concept of removing combatants tance to infection?"'from the field for psychological treatment and thenreturning them betterprepared todeal with the stresses These are difficult issues. Thev deserve our atten-of combat may be less useful in a nuclear conflict. tion now, before a nuclear weapon is used again.
PREVENTION OF PSYCHOLOGICAL CASUALTIES
Steps are available to reduce psychological prob- self-preservation.2 Recent recommendations havelemsaftera nuclearconfrontatioln. Proper training and called for the use of a nuclear simulator in order topreparedness apparently provide some degree of pro- desensitize soldiers to the unique destructiveness of atection. The benefits of training are confirmed by the nuclear battle."4 The following training may help toremarkable experiences of nine persons who survived prevent psychological casualties in a nuclear war:the Hiroshima bombing and then fled to Nagasaki intime for the second atomic bomb." They remembered First, every soldier should be trained in meth-very well what they had done that allowed them to ods of individual protectior against atomic attack,live, and they quickly instructed others in Nagasaki: for both the actual protection and the self-confi-
dence which such knowledge will give....
Y -naguchi's lecture on A-bomb precautions, Second, individual soldiers should be given
he pointed out later, was not lost upon his col- training designed to enable them to reorient them-
leagues. With the voting designer's words still selves after atomic attack. This should include
fresh in their minds lat the time of the second training in methods of determining whether the
bombingl they leaped for the cover of desks andi attack involved an air or ground burst, in methods
tables. "As a result." said Yamaguchi, "my section of estimating their own location with reference to
staff suffered the least in that building. 'In other the center of the disaster area, and in the use of in-
sections there was a hieavy toll of serious injuries struments for the measurement of radioactivity.
from ntving glass."a Third, individuals should be taught that thevare not defenseless against atomic attack, but thatthev should not expect to survive such an attack
In the most beneficial type of training, emphasis without suffering severe shock effects and seeingshould be on (a) realism, in order to reduce the psycho- manv of their own forces killed or wounded.logical shock of a nuclear confrontation, (11) accurate Fourth, individuals of all ranks should be im-information about the threat, and (c) information that pressed with the importance of offering all the
not only can be readily comprehended and assimilated resistance of which they are capable to ground
by the average person but also can be directed toward
165

Medical Couscquencc5 ot Nuclear Wartf•e
surrender than another member of the group who is inassault following an atomic attack, no matter how the same tactically hopeless situation but is still boundhopekss and ineffective it may seem. by the continuous ties of fighting, eating, and sleeping
Fifth, indoctrination should teach soldiers that next to fellow soldiers.' Also, a significant relationshipthe role of troops subjected to atomic bombing will exists between a group's cohesion, its confidence invery likelv be that of delaying the enemy ground combat 3kills, and measures of its actual performance.assault at all costs until relatively unharmed re- The Israelis reported almost no psychiatric casualtiesserves can establish ain effective defense or launchserves crdinantes h auntefcte din their elite (and cohesive) airborne forces, regardlessa coordinated counterattack. fteitniyo obti h 93YmKpu
Sixth, all personnel should be impressed with of the intensity of combat in the 1973 Yom Kippurthe importance of giving absolute priority to traffic War.' The ability of the primary group to resist disin-moving towards the front following an atomic at- tegration will greatly affect the capacity of its memberstack, no matter what their own reasons for moving to withstand the stress of a nuclear confrontation.toward the rear may be." However, we should recognize that disruption of the
primary group by loss of personnel and leadership,The forces of social cohesion will also influence the breaks in communication, and deterioration of supply
psychological and performance variables after a nu- and medical care are more likely to occur in nuclearclear weapon detonation. The single most important combat than in conventional confrontations.'factor that sustains soldiers in combat is the powerful Much of the current training promotes hopeless-psychological support of their fellows-th, ;quad, ness in our military forces and drives them further intoplatoon, company, and so on.2 Isolation increases avoidance and denial.24 More work needs to be donestress and also reduces the soldier's capacity to resist to meet the training needs outlined above and to pre-the effects of that stress. Various historical acLounts pare for the expected psychological reactions to the usehave suggested that an isolated soldier is more likely to of nuclear weapons.
REFERENCES
1. Marlowe, D. H. 1982. Cohesion, anticipated breakdown, and endurance in battle: Considerations for severe and highintensity combat. Paper prepared at Walter Reed Army Institute of Research, Washington, DC.
2. Vineberg, R. 1965. Human fictors in tactical nuclear combat ITR65-2 (Contract DA 44-188-ARO-2)]. Alexandria, VA:Human Resources Research Office, George Washington University.
3. Mandelbaum, D.G. 1954. Psychiatry in military socie tv. Human Organiz. 13: 5-15.
4. Belenky, G. L.; Tyner, C. F.; and Sodetz, F. J. 1983. Israeli battle shock casualties: 1973 and 1982 [WRAIR Report Num-ber NP-83-003; NTIS AD-A133-359-01. Washington, DC: Walter Reed Army Institute of Research.
5. Steele, K., and Cox, T. 1986. Psychological and physiological reactions to visual representations of war. Int. 1. Psy-chophisiol. 3: 237-252.
6. Vineberg, R. 1987. A preliminary model for predicting probable effects of stress on performance on the tactical nuclearbattlefield. In Proceedings of the Defense Nuclear Agenccy Siyinposiumi/Workshop on the Psychological Effects of TacticalNuclear Warifare IDNA-TR-87-209; NTIS AD-A194-754-8-XABI, edited by R. W. Young, 3.1-3.12. Washington,DC: Defense Nuclear Agency.
7. Cal, R. Yesterday's conventional warfare-tomorrow's nuclear warfare? Lessons from the Israeli experience. Inreference 6, 6.1-6.66.
8. Glass, A. J. 1951. Combat exhaustion. U.S. Armed Forces Med. 1. 2:1471-1478.
9. Glass, A. J. 1956. Psychological considerations in atomic warfare. U.S. Arined Forces Med. 1. 7: 625-639.
10. Glass, A. J. 1957. Observations upon the epidemiology of mental illness in troops during warfare. In Proceedings ofthe Sytniposiulin on Pre'enta tize a pid Social Psyjclhloghv 185-189. Waslngton, DC: Walter Reed Army Institute ofResearch, 185-198.
166

Ps.ychological Factors in Nuclear Warfare
11. Bourne, P.G. 1970. Men, stress and Vietnam. Boston: Little, Brown and Co.
12. Green, T. E. A description of the nuclear battlefield. In reference 6, 1.1-1.21.
13. Young, R. W., ed. 1987. Proceedings of the Defense Nuclear Agencyi Symposium/Workshop on the Psychological Effects ofTactical Nuclear Warfare IDNA-TR-87-209; NTIS AD-A194-754-8-XABI. Washington, DC: Defense NuclearAgency.
14. Sagan, C. 1983. The nuclear winter. Parade, 30 October: 4-7.
15. Trumbull, R. 1957. Nine who survived Hiroshima and Nagasaki. New York: E. P. Dutton and Co.
16. U.S. Strategic Bombing Survey. 1946. The effects of atomic bombs on Hiroshima and Nagasaki. Washington, DC: U.S.Government Printing Office.
17. Coonev, J. P. 1951. Psychological factors in atomic warfare. Can. Ariny] . (January): 19-22.
18. Baum, A.; Gatchel, R. J.; and Schaeffer, M. A. 1983. Emotional, behavioral, and physiological effects of chronic stressat Three Mile Island. J. Consult. Clin. Psychol. 51: 565-572.
19. Lifton, R. J. 1982. Beyond psychic numbing-a call to awareness. Am. 1. Orthopsychiatry 54: 619-629.
20. Lotto, D. 1986. The analytic response to the threat of nuclear war. Am. ]. Psychoanal. 46:191-202.
21. U.S. Strategic Bombing Survey. 1947. The effects of strategic bombing on Japanese morale. Washington, DC: U.S. Govern-ment Printing Office.
22. Raphael, B. 1985. Mental and physical health consequences of disasters. Med. !. Aust. 143: 180-181.
23. Black, S. Psychological effects on the nuclear battlefield. In reference 6, 5.1-5.9.
24. Stokes, J. W. Psychological aspects of nuclear defense. In reference 6, 2.1-2.51.
25. Gallup, G. 1984. The Gallup youth survey. Associated Press, 17 October.
26. Beardslee, W. R., and Mack, J. E. 1983. Adolescents and the threat of nuclear war: The evolution of the perspective.Yale J. Biol. Med. 56: 79-91.
27. Chivian, E.; Mack, J. E.; and Waletsky, J. P. Soviet children and the threat of nuclear war: A preliminary study. Am. !.Orthopsychiatry, in press.
28. Mack, J. E. 1984. Resistance to knowing in the nuclear age. Harvard Educ. Rev. 54: 260-270.
29. Gold, P. 1987. Psyche watching in the atomic age. Insight, 4 May, 48-50.
30. Leaning, J., and Leaf, A. 1986. Public health aspects of nuclear war. Anno. Rev. Public Health 7: 411-439.
31. Fiske, S. T. 1986. Adults' beliefs, images, feelings, and actions regarding nuclear war: Evidence from surveys andexperiments. In Proceedings of the Institute of Medicine, U.S. National Acadenmy of Science, Symposium on MedicalImplications of Nuclear War, 444-466. Washington, DC: National Academy Press.
32. Marshall, E. 1987. Armageddon revisited. Science236: 1421-1422.
33. Breznitz, S. Hope and denial of stress in the nuclear age. In reference 31, 467-473.
34. Marlowe, D. H. Human endurance on the nuclear battlefield: Thoughts on prediction and prophecy. In reference 6,10.1-10.23.
35. Logan, L., and Killian, L. K. 1953. Troop reactions to atomic attack: A preview [Technical Memorandum ORO-T-2051.
Chevy Chase, MD: Operations Research Office, Johns Hopkins University.
167

Medical Cosom~c tneqn it ~ Nucle a V'arfare,
31-. Litton, R. J. 14S2. P-svchological effects ot thle atomic bombings. IIn lAst Aid, edited by E. Chivian, S. (ihivian, R. ILitton, and J. F. Mack, 4S-08. New~ York: W. 11. Freeman and Co.
37. 1 lersey, 1. 11981. 1 lir-o~iinia. New York: Alfred A. Knopf Co.
38. K inmeld ort, 1). J., and I I1.111t, F. L.. I %5. hnit:izing.n r ai iato: Neu ral fuinction and ii blica uior. New York: Academic P ress.
31). (;ue'rau, G.; IDrouet, I.; I'rivat, A.; and Court, 1.. 198.1. Neurogenesis and reactivity in the SUbgranular zone of thlerabbit dentate gyrus as seen with 31 I-thy midine rad ioautography and gamima-irradiation. InI Proccoliiigs of theSept-cii il Intehrnationi al Co nn.ýN'Ss oif Radiatioitcni Researchi, D2-017. Amsterdam: Mart inus- Nijhot I.
44). l'eimer, S. L.; IDudkin, A. 0.; and Swerdlov, A. G. I198h. Response of hippocampal pacemaker-like neurons to lowdoses of ioni/ing radiation. hit. /. Radicit. Biol. 44: 59)7-h600.
41. 1 Itint, W. 1487. [Personal comnmunication at Armed Forces Radiobiology Research Institute,, Bethesda, MD 20814-5 145.
42. M ickl'vw, G. A.; Stevens, K. F:.; Moore, (C. I I.; Deere, W.; White, G. A.; Gibbs, G. L.; and Mueller, G. L. 1983. Ioniz~ingradiation alters beta-endorphin-like immunoreactiv'itv in brain but not blood. Pliarinacol. Hioclieii. Be/un'. 19:979-983.
43. Wixon, 11. N., and I lunt, W. A. 1983. Ionizing radiation decreases veratridine-stimulated uptake of sodium in ratbrain syna ptosomies. Scuinti' 220): 10)73-10)74.
44. Mickley, G. A. P'svchological phietrnoena associated wvith nuclear warfare: Potential animal models. InI reference 6,7. 1-7.35.
45. BUrghardt, W. F., and I lunt, W. A. 1985. Characterization of radiation-induced performance decrement using a two-lever shock-avoidance task. Radial. Res. 10)3: 149-1-57.
46. Mickley, G. A., and Teitelbaum, II. 1978. Persistence of lateral hypothalamiic-miediated behaviors after a su~pra-lethialdose of ioni/ing radiation. Al'iat. Spine Environ. Medl. 49: 868-873.
47. Davis, R. T. 1965. The radiation synldrome. In vol. 2, Behavior of Nooi,-lhimian P'rimactes, edited by A. M. Schrier, Hi. F.I larlow\, and F. Stollnitz, 495-524. New York: Academic Press.
48. Brown, W. I..,and McDowell, A. A. 1-)62. Some effects of radiation on psychologic processes in rhesus mionkeys. InRe-spioiiSe of thei Nerv' ms Silisten, to loiiizing Radiatioii, edited by T. J. H-aley and R. S. Snider, 729-746. New York:iAcademnic Press.
49. Davis, R. T.; Elami, C. B.; and McDowell, A. A. 1958. Laiteint effects of chroiiic wh'lroh-bodr irraiaitioii ofminoikeis wlitli iixc~d1orc0rdiatioii I Report No. 57-591. Brooks Air Force Base, TX School of Aerospace Medicine.
54). McDowell, A. A.; Davis, R. T.; and Steel, f. P'. [956. Application of systemnatic direct observational methods toanalysis of the radiation syndrome in mionkeys. Percept. Mot. Skills (Monograph Suppl. 3) 6: 117-1340.
51. I Iachiya, M. 1455. H iroshiiiau ciarrY, translated by W. Well. Chapel Hill: University of North Carolina Press.
52. Janis, 1. L. 1951. Air waraimid emotional stress. New York: McGraw-Hill Book Co.
;3. Quarentelli, F. L. 1954. The nature and conditions of panic. Ami. 1. Sociol. 60: 267-275.
54. 1.ifton. R. 1. I1967. l0eatli in life: Sm-iiriiors of I liroshiina. New York: Random flouse.
5.Wheeler, T. ., and I lardy,. K. A. 1985. Retrograde amnesia produced by electron beam exposure: Causal parametersand duration of memory loss. Radlial. Re's. 14)1: 74-80).
;fi. Nishikawa. T., and Tsuiki, S. 1961l. P1sychiatric investigations of atomnic bomib survivors. Nagasaki: Medical Journarl 36:717-7;2.
168

Psychological Factors in Nuclear Wartare
57. Furchtgott, E. 1963. Behavioral effects of ionizing radiations: 1955-61. Psychol. Bull. 60: 157-199.
58. Horowitz, M. J. 1985. Disasters and psychological responses to stress. Psychiat. Ann. 15: 161-167.
59. Von Greverz, W. 1902. Psiychoogy of survival. New York: Elsevier Publishing Co.
60. Sessions, G. R. Human emotional responses in tactical nuclear warfare: Literature review and current considerations.In reference 6, 9.1-9.44.
61. Madakasira, S., and O'Brien, K. F. 1987. Acute postraumatic stress disorder in victims of a natural disaster. I. Nerv.Ment. Dis. 175: 286-290.
62. Ross, W. D. 1952. The emotional effects of an atomic incident. Cincinnati I. Med. 33: 39-41.
63. Kardiner, A. 1941. The traumnatic neuroses of war. New York: P. Hoeber.
64. American Psychiatric Association. 1980. Diagnostic and statistical manual of mental disorders. 3d ed. Washington, DC:American Psychiatric Association.
65. Gleser, G. C.; Green, B. L.; and Winget, C. 1981. Prolonged psychosocial effects of disaster. New York: Academic Press.
66. Donnelly, C. 1982. The Soviet attitude to stress in battle. J. Royial Armjy Med. Corps. 128 (2): 72-78.
67. Nagai, T. 1958. We of Nagasaki. New York: Meredith Press.
68. Levin, S. G. Prediction of neuropsychiatric casualties in the nuclear battlefield. In reference 6, 8.1-8.37.
69. Gillespie, R. D. 1942. Psychological effects of war on citizen and soldier. New York: W. W. Norton and Co.
70. Appel, J. W., and Beebe, G. W, 1946. Preventative psychiatry. JAMA 131: 1469-1475.
71. Ranson, S. W. 1949. The normal battle reaction: Its relation to the pathologic battle reaction. Bull. U.S. Armny Med.Dept. (Suppl) 9: 3-l1.
72. Palinkas, L. A., and Coben, P. 1987. Psychiatric disorders among U.S. Marines wounded in action in Vietnam. ].Nerv. Merit. Dis. 175: 291-300.
73. British Medical Association, Board of Science and Education. 1983. The medical effects of muclear war. Chichester: JohnWiley and Sons.
74. Abrams, H. L. 1984. Medical resources after nuclear war: Availability vs. need. JAMA 252: 653-658.
75. Gellhorn, A. The immediate medical response. In reference 36, 181-201.
76. Thomas, L. 1983. Late niight thoughts on listening to Mahler's Ninth Synmphony. New York: Viking Press.
169

Medical Conscip.i'ites of Nt'hlar Warfare
170

Chapter 9
LONG-TERM ANDLOW-LEVEL EFFECTS OF IONIZINGRADIATION
THOMAS L. WALDEN, Jr., Ph.D.*
INTRODUCTION
BACKGROUND RADIATION
SOMATIC EFFECTSCataract FormationSterilityRadiation Effects on Skin and HairCancer
HUMAN DATA BASELeukemiaThyroid CancerBreast CancerOther Systemic CancersCancers of Negligible Risk
GENETIC EFFECTSGene MutationsChromosomal DamageFactors Affecting MutationRadiation-Induced Damage in HumansEstimating Genetic Risks
RADIATION EFFECTS IN UTEROStages of DevelopmentPreimplantationMajor OrganogenesisThe Fetal StageHumans Irradiated In UteroIncreased Incidence of Cancer with In Utero Exposure
RELATIVE BIOLOGICAL EFFECTIVENESS OF NEUTRONS
REGULATORY GUIDES FOR EXPOSURE
SUMMARY
"Radwtiort Biologist, Radiation Riot iheistr.t Departwenit. Armed Forces Radiobiology Research Institute, Bethesda, Marvland 20814-5145
171

Mcl'dical (Ci, fuflt,•q.u of Nm'a WVrtferc
INTRODUCTION
Ionizing radiation damages biological tissues by joule per kilogram, or by the si'evrt (Sv), which is anexcitingorionizing their atomsand molecules.' Addi- international unit equaling 0X) rem. The Sv allowstional indirect damage is caused by the formation of effects from radiations with differing LET values to befree radicals in water, which makes up 75'4 -80';; of the compared, since I Sv of neutron radiation has the samemass of living systems. The primary products of water biological effects as I Sv of low-LET gamma or Xradiolysis are the hydroxyl radical, hydrogen radical radiation. Comparisons cannot be made among ab-(hydrogen atom), and hydrated electron; hydroper- sorbed-dose measures of different kinds of radiationoxv radicals and hydrogen peroxide are also formed in (for example, 1 Gy of neutron radiation will not havethe presence of oxygen. The production of lysosomal the same effect as I Gy of gamma or X radiation).envzmes ,,:id biological mediators, such as histamine Low-level radiation exposure is generally consid-and prostaglandins, is another biological response to ered to be less than the dose that produces immediateradiation exposure.-' Depending on the radiation or short-term observable biological effects. In thedose and the biochemical processes altered, damage human, low-LET gamma or X radiation doses of lessmay be Prompt (expressed minutes to weeks after than 0.5 Gy do not produce any prodromal symptomsexposure) or delayed (expressed several months to or the hematopoietic subsyndrome;4." however, low-years later) (Figure '9-1). Some radiation-induced inju- level radiation exposure does increase the probabilityries may not become apparent until they are passed on that delayed effects will occur." ' Three primary de-to succeeding generations. layed effects-somatic, genetic, and teratogenic""-
Radiation doses to biological tissues are measured can be observed and are already present in the popu-in three ways. (a) The exposure dose of gamma or X lation and in the gene pool.",- Irradiation enhances therays in air is expressed in roenitgens (R). (17) The dose of naturally occurring frequency of the effect, and inany type of radiation absorbed by the tissues was, at some cases produces the observable end point by aone time, expressed by the rad, which is equivalent to processdifferent from thoseof natural selection. Certain100ergsof energy pergram of tissue. The international biological responses have such low thresholds thatmeasure of absorbed dose is now the gray (Gy), which they are statistically indistinguishable, in many cases,is equal to 100 rads (conversely, I rad equals I cGy). (c) from normal incidence. 7.1,' Even so, current radiopro-Finally, because the biological responses to radiation tection guidelines state that all exposures to radiationexposure may vary with the type of radiation, dose should beavoided if possibleand thatexposureshouldequivalents are expressed by the rein, which equals 1 be kept as low as is reasonably achievable."
BACKGROUND RADIATION
Living organisms are continually exposed to ioniz- duced from the natural decay of radium and tho-ing radiation in nature as well as from nuclear weap- rium. " High concentrations of radon gas escape fromons testing, occupations, consumer products, and soil and are released from marble and granite, accu-medical procedures.>. The radiation from all of these mulating in buildings with poor air circulation "'Radonsources together is called background radiation, and is exposure is a health concern because its solid daughterestimated to measure 180-200 mremr/person/year. products, polonium-214 and -218, decay by alpha-Medical procedures contribute most whole-body back- particle emission in the human body near the lungground radiation (Figure 9-2).7,, In addition, large tissue and may increase the incidence of lung cancer."dosesof partial-body radiationmaybedelivered tothe Extraterrestrial radiation includes solar-flare andlung by radon gas (radon-222 and radon-220), pro- cosmic radiation. Most cosmic radiation is absorbed
172

Lto)ni-r•,rni and L.o,-Leiv/ E cfst)ts f nii . :l ' Radiatiton
INDIRECT ACTION DIRECT ACTION
1'i4%RADIATION RADIATION
H20 -- ,,-He•
Ionization -H'T• •and Excitation
H2 02 % Amplification b
Biological Mediators
Free Radicals and 9 0Hydrogen Peroxide
DEATH SOMATICTERATOGENIC
10-17 to 1O- 5 seconds -- j 14 minutes to years 110
Fig. 9-1. Physical and biological responses to ionizing radiation. Ionizing radiation causes damage either directly bydamaging the molecular target or indirectly by generating free radicals, which attack the molecular target. Physical stepsleading to energy deposition and free radical formation occur within femtoseconds to microseconds, while the manifestationof actual biological damage may require seconds to years.
by the dense atmosphere before it reaches the earth's average of 275 mrem over 19.5 days.'surface. A person's exposure to cosmic radiation in- On earth, naturally occurring radioactive elementscreases at higher latitudes or altitudes, as the atmos- contribute to background radiation.7 ' External expo-phere becomes less dense.7,' A resident of the higher- sure sources include potassium-40, which may bealtitude city of Denver receives approximately 100 concentrated in concrete, and radon gas. Internalmrem more radiation exposure than does a resident of radiation comes primarily from radioactive isotopes ofWashington, D.C. A cross-country airplane flight naturallv occurring elements in biological systems,increases individual exposure by 0.2 mrem/l ,ur such as potassium-40 and sodium-24. In some areas ofbecause the level of cosmic radiation is greater at Brazil and India, large concentrations of monazite, a36,000 feet than at sea level.7 As humans venture mineral containing thorium, are present in the soil orfarther from the protective atmosphere, either in su- sand. Background-radiation exposures there rangepersonic air carriers or in spaceflight, their background from 0.008 to 0.17 Gy/year.'occupational exposures to cosmic radiation will in- Fallout from nuclear weapons testing peaked increase. The British Concorde supersonic transport 1964, after seventy-seven atmospheric detonationsmaintains radiation-monitoring equipment so that it occurred in 1962. Of the total fallout, 69%7c was frommay drop to lower-altitude flight routes if increases in carbon-1 4,4%7- was from cesium-137, and 3% was fromsolar or cosmic radiation are detected.' Spaceflight strontium-90. The remaining 24/c% was from radioac-increases exposure to solar and cosmic radiations; tive isotopes of plutonium, rubidium, barium, iodine,Apollo astronauts traveling to the moon received an iron, manganese, krypton, americium, tritium, and
173

Medical Consequences of Nnulear Wartare
ElNuclear Power Internal1.64 mrem 24 mrem
* Research Cosmic3.00 mrem 28 mrem
SiWeapons Testing Terrestrial4.50 mrem 26 mrem
Consumer and (not including radon)Air Travel • Medical
4.50 mrem 92.40 mrem
Fig. 9-2. Major contributors to average background radiation in the United States
zinc." Carbon-14 will be a long-term contributor to hour of use), video terminals, smoke detectors (which
background radiation because it has a half-life of 5,700 contain an alpha emitter, usually americium-241), and
years. Nuclear fallout has decreased because of the dinnerware that uses uranium for an orange color.7 '.
total ban on atmospheric testing by the United States, Ophthalmic glass, used in prescription lenses, con-
Great Britain, and the Soviet Union, although several tains trace impurities of thorium-232, and uranium is
other countries continue atmospheric testing. added to dental porcelain to give dentures a natural
Radiation is also emitted from consumer products, fluorescent quality."' The latter may result in an alpha
such as color television sets (averaging 0.3-1.0 rem/ radiation dose of 60 rem/year to the gums. 5
174

Louig-Tcrtn and Low-Level Effects of lontizin'g Radiation
SOMATIC EFFECTS
Delayed somatic effects of ionizing radiation result sure period."' The latency period for cataract forma-from somatic mutations and accumulated damage, tion in humans has been estimated to be 6 months to 35and include impaired circulation, necrosis, fibrosis of years; however, fractionation or protracted exposureskin and muscle tissue, loss of hair, loss of taste, lowers the incidence and prolongs the latency.9impaired bone growth, susceptibility to disease, im- Small radiation doses may increase the opacity, butmunodeficiency, aplastic anemia, cataracts, and in- visually impairing cataract formation results from ancreased incidence of cancer. "-,12 accumulation of dead or injured cells, and therefore
Some organs are more radioresistant than others. has a threshold. For low-LET radiation, this thresholdRadiation doses exceeding 15-50 Gy must be received is 2 Gy.7,• High-LET neutrons have thresholds of lessbefore damage to the liver or heart is detected.",' Other than 0.2 Gy.tissues, such as the lens and the sperm, show some Other parts of the eye are not as radiosensitive as isdetriment from doses as low as 0.15-0.30 Gy.7"''7 the lens. The threshold for corneal edema is 10 Gy ofDelayed somatic effects of intermediate- or high-level low-LET radiation; for atrophy of the lacrimal gland, itexposures include cataract formation, skin abnormali- is 20 Gy."'0 Doses of less than 0.1 Sv/year are notties, and sterility, thought to present appreciable risk for detectable vis-
ual impairment. The International Commission onCataract Formation Radiological Protection (ICRP) has recommended an
occupational exposure limit of 0.15 Sv for the eye.2"The lens tissue of the eye is particularly radiosensi-
tive, and radiation exposure can result in its increasedopacity. 5 .1.1- 22 Radiation cataractogenesis is the most Sterilitycommon delayed radiation injury,21 and is thought toresult from damage to the anterior equatorial cells of Males. Germ cells of the human testes are verythe lens's epithelial tissueY.2 These cells normally di- radiosensitive. 7,8 25 Temporary sterility may occur af-vide and migrate to the posterior portion of the lens, ter 0.1-Gy whole-body or local irradiation, with 50%where they gradually lose their nuclei and become lens incidence following 0.7 Gy.7S,811 Sperm cells becomefibers.5, 23 The lens tissue, like that of the testes and the more resistant as they develop; spermatogonia arebrain, is separated from the rest of the body bya barrier more radiosensitive than spermatocytes, which are insystem.' As a result, it has no direct blood supply, no turn more radiosensitive than spermatids. 2" The re-macrophages for phagocytosis, and no way to remove generating spermatogonial stem cell (As) is more radi-accum'."ated damage. In a study of 446 survivors of oresistant than the developing spermatogonia (B). Thethe Nagasaki atomic bomb, 45% of the 395 persons ED;, for damage to sperrnatogonia is 0.11 Gy of low-who were 0.1-2.0 km from the hypocenter of the bomb LET radiation.27 The spermatid is also fairly radio-developed cataracts by 1959 (whereas only 0.5%, or 2 resistant, requiring X-ray doses of 6 Gy to show visibleout of 395, had severe visual impairment).'- 2
1 Four of damage.2"the remaining fifty-one persons (7.8%) who were 2-4 Radiogenic aspermia is caused by a maturation-km from the bomb hypocenter developed mild cata- depletion process similar to that observed for hemato-ract impairment. Even survivors exposed to small poietic cells after irradiation. Radiation kills stem cellsdoses of radiation were at increased risk for cataract or delays mitosis, so that differentiating cells continueformation. By 1964, the incidence of cataract formation to divide without being replaced. The latency periodamong atomic-bomb survivors who received 0.01-0.99 for aspermia after radiation exposure is approximatelyGy of radiation was 1.5% in Hiroshima compared to 2 months, 2" and the time for recovery is several months1.0% in the control population, and 2.0% in Nagasaki to years. Chronic and protracted exposures producecompared to 0.9% in controls (Figure 9-3).22 Higher greater testicular damage than do acute large expo-doses tend to increase the degree of opacity and shorten sures. This damage is reflected in the duration ofthe latency period.--' There is a 10% risk of developing aspermia,8.25 and is thought to result from cycling ofa severely impairing cataract following a single expo- the radioresistant Asspermatogonia to the more radio-sure to 2.4 Gy of low-LET radiation, and a 50% risk for sensitive B spermatogonia. 7.5 25 A dose of about 0.35 Gya dose of 3.1 Gy." The estimated dose for 50% inci- produces a 50% incidence of aspermia after a pro-dence of cataract formation increases from 3.1 Gy to 9.3 tracted exposure of 1-10 days."' At low dose rates, theGy by lowering the dose rate or extending the expo- recovery period depends on the total dose received:
175

Medical Contsquenites of Nuclear Wartare
40
_ N•
3 0 ---
-- - - - - -- - - - - -- - - - - - - - - - - -
U 20 _--
0 AO V
(Cc
CO ql
10) ---------- ----- in" ---- "
""U (, V_ -
C nn M i
EU _
L• S
o LN L
Control 0.01-0.99 1.00-1.99 2.00-3.99 4.00-5.99 6.00+Dose (Gy)
Fig. 9-3. Incidence of severe cataracts in atomic-bomb survivors, according to radiation dose received. Cataracts weredetected by examinations in 1963-1964 for populations of Nagasaki and Hiroshima. Numbers in parentheses are the actualnumbers of cataracts observed per number of persons examined who received that dose of radiation. Radiation doses arebased on Oak Ridge National Laboratory (ORNL) calculations, which contain a lower neutron dose estimation in theHiroshima population than originally estimated. Based on the 1965 tentative dose relationship (T65D) estimate, the averagetotal dose for the 600+ Hiroshima group is 7.783 Gy, including 2.343 Gy of neutrons. Using ORNL dosimetry, the average dosefor this group is 8.514 Gy, with 0.74 Gy of neutrons. Dosimetry was recently revised based on new information on explosioncharacteristics. Risks will be revised by scientific advisory boards when these new estimates (DR86) become available.Source: References 107 and 108
approximately I year following a 1-Gy exposure, 3 irradiation .2' Following the onset of aspermia, there isyears for 2-3 Gy, and up to 5 years for 6 Gy.2"1 A a three- to fourfold increase in urinary gonadotropin,fractionated dose of 2-3 Gy may require up to 14 years plasma FSH, and luteinizing hormone. Elevated levelsfor recovery."• Doses of 0.08 Gy do not significantly return to normal when spermatogenesis resumes.26affect sperm count or alter plasma follicle stimulating Permanent male sterilityrmay occur after 2 Gy (localhormone (FSH) levels .21' Radiation doses of up to 6 Gy or whole-body exposure) but generally requires dosesdo not alter plasma levels of testosterone, but do between 5 and 9.5 Gy.' These doses are within thedecrease the levels of urinary hormone. Decreased lethal range for whole-body exposure.'production of testosterone by the Leydig cells has been Females. The ovary is not as sensitive to radiation-observed in humans receiving 6 Gy of X rays. Plasma induced temporary sterility as is the testis, but it islevels are not affected because there will be a compen- more sensitive to permanent sterility."',"2• These dis-sating increased number of Leydig cells 3months after tinctions are based on differences in the stages of
176

ltg-Terni mid Low-Level Effects oPf ht)tijnmg Radiation
development of the two germ cell groups. Shortly symptom) 3 hours after irradiation. Following abefore birth, the oogonia stop multiplying and pro- second exposure lasting 1.5 hours, the patient devel-ceed to prophase I of meiosis. 2" After puberty, meiosis oped a radiation sequela leading to ulcer formation atresumes for individual cells by ovulation. Oocytes the site of exposure, which was not responsive to skinlose the ability to renew after birth and are unable to grafting.replace stem cells that have been damaged or killed by An 1897 case study initiated the popularity of X-radiation. The oocyte is most radiosensitive as a pro- radiation treatment for dermatological ailments. Aliferative stem cell during the fetal stage of gestation, Viennese doctor administered X radiation in two hour-prior to ceasing mitosis and entering meiosis.--' long treatments per day for 10 days to depilate a nevus
Temporary sterility may be induced in females by pilosis birthmark covering the back of a 5-year-oldacute radiation doses of 1.5-6.4 Gy.... Permanent girl.' Epilation occurred 11 days after the initiation ofsterility results from doses of 2-10 Gy, and depends on treatment.the woman's age at the time of irradiation.'", 2
5 Older Before the introduction of the roentgen in 1928 as awomen, particularly those close to menopause, are unit to measure exposure dose, the skin erythema doseparticularly radiosensitive for sterilization. Two Gy of (SED) was commonly used." The SED is the radiationlow-LET radiation may result in permanent sterility of dose required to produce a given degree of erythema.50% of the exposed female population over 40 years of It depends on the quality, energy, and exposure time ofage, compared to an estimated 3.5 Gy for women the radiation. For X radiation, the SED is about 8.5 Gy.under 40."' This is simply due to the numbers of In 1925, it was proposed that the exposure of radiolo-oocytes present at the time of irradiation.7,2 .5 Women gists and X-ray machine operators not exceed 1 /100thhave about one-half million oocytes at puberty, which of the SED in a 30-day period."are almost depleted through atresia at menopause.29 During a radiation incident, skin may be exposed
Higher radiation doses of 3.6-20.0 Gy are required either by direct blast'irradiation or by beta burn fromfor sterilization when the exposures are prolonged or the direct deposition of particulate fallouti3 9 Thefractionated."' From the 1920s through the 1950s, degree of radiation-induced skin damage depends onradiation exposure was occasionally prescribed to treat a number of factors, including the type of radiation; theinfertility and sterility."" One-third of the women dose and dose rate; the area of skin irradiated; andreferred for this treatment had amenorrhea. Each skin-quality characteristics, such as texture, age, color,woman received a total dose of 0.65 Gy to the ovaries thickness, and location.7-,S,10.4- The neck is the mostand 0.75 Gy to the pituitary gland, divided in three radiosensitive area because its skin is thin and usuallyfractions over 2 weeks. In one study, this technique not protected by clothing.46,47 Additional traumahad a 55•'• success rate: 351 of 644 patients treated were through burn, abrasion, exposure to ultraviolet light,able to conceive."" The treatment has been discontin- or extreme temperature variations will increase theued because of the concern for associated risks of damage.43
,11,4b Environmental factors or inadequate
genetic and somatic damage. Higher doses of low-LET clothing may contribute to hyperthermia, and wool orradiation (1.25 Gy) can result in a delay of the men- other coarse fabrics may further abrade the damagedstrual cycle."' skin. An illness like diabetes 43 or a genetic disease like
ataxia telangiectasia',41,-" may also make the skin moreRadiation Effects on Skin and Hair radiosensitive. Alpha radiation is of little concern for
skin damage because the average penetrated dose isSoon after Roentgen's discovery of X rays,3' re- usually absorbed by the dead corneocytes of the stra-
searchers and radiologists became aware of the skin's tum corneum. However, it may present a problem atsensitivity to radiation damage.3 -2 ' Eight months after sites where the skin is thinner and the radiation canthe discovery of X rays in 1896, a German scientist re- penetrate to the basal level.4 1
ported a case of dermatitis and alopecia on the face and Beta particulates in fallout may contain extremelyback of a 17-year-old man who had been exposed to high radiation dose rates (tens of Gy per hour). Whenthese rays for 10-20 minutes a day for 4 weeks during they land on the skin, their energy may penetrate to thean investigation." Interestingly, the accompanying germinal basal cells.;39 41 49 This radiation damageerythema, which resembled a burn, was painless, (beta burn) was observed in the atomic-bomb survi-whereas chronic radiation dermatitis following re- vors and the Marshall Islanders (Figure 9-4) who hadpeated exposure is usually extremely painful.•• 7 been exposed to nuclear fallout.-C3 ,3 --'9 1 The threshold
In another 1896 case, a man received an hour-long dose of beta radiation for skin damage depends on theX-ray exposure during an examination for a kidney average energy of the beta particle, the total absorbedstone."7 The patient experienced nausea (a prodromal dose, and the dose rate. 49 The average penetrating
177

A t, /ith a/ C-01,C11HOI C,' t It \'11t lyre I \V troIty
44,
1 7-
Fig. 9-4. Beta burn on neck ot Mlarshall Islad ndwoman I month after exposure to fallout radiation from a nuclear weapon. Notediscoloration of skin on left and right sides.
range of a beta particle is proportional to its energy; (occurring earlier with higher doses), and (1) the mainthus, higher-energy beta emitters, such as strontium- erythema, appearing at 2-3 weeks and persisting for90 (0.61 MeV average), require lower surface doses to longer periods."'-4"'" In some cases, a third erythemaproduce wet desquamation than do lower-energy beta may occur at 6 weeks.4 Radiation-induced erythemaparticles, such as those from cobalt-60 (0.31 MeV aver- is a threshold phenomenon.'-"-; A dose of 6 Gv of low-age)." The surface threshold doses for transepidermal LET radiation received in less than 1 day, or 10 Gv in 10injury in the skin of pigs is 15 Gy for strontium-90, 40 days, will induce ervthema in 50%7 of exposed per-Gy for cobalt-60, and 200 Gy for sulfur-35.4 ' The sons.s"' The threshold for neutron radiation is 2 Gv.'exposure from each of these radioisotopes delivers Because of these variables, and the fact that the thresh-approximately the same tissue dose to the basal germ old dose decreases with an increase in the surface areacells. Lower-energy beta particles like sulfur-35 (0.17 exposed, erythema is iot a good biological dosime-MeV energy) are not capable of penetrating to the ter.'s 4 4 •4 Early erythema arises from the release ofdermis and cannot induce chronic radiation dermati- mediators and from increased capillary dilation andtis.4" Beta injuries from fallout can be minimized by permeability.4" It is equivalent to a first-degree burn ordecontamination and washing. mild sunburn, subsiding within 2 or 3 davs. 4ý.ý4 Al-
Radiation damage to the dermis has a threshold though indomethacin or other prostaglandin-synthe-dose of about 20 Gv, ' with 5017( incidence at 60 Gy.; sis inhibitors have been used topically to prevent orFive progressive categories of radiation damage are reduce erythema caused by sunburn or ultravioletobserved in skin: ervthema, transepithelial injury light,"2 they have not been widely used to treat radia-(moist desquamation), ulceration, necrosis, and skin tion-induced erythema. (One study suggested thatcancer.'2 , 414; systemic and topical applications of prostaglandin in-
Radiation-induced ervthema occurs in two stages: hibitors may be useful in minimizing late damage and(a) mild initial erythema, appearing usually within necrosis from large radiation doses.)" When earlyminutes or hours on the first day after irradiation erythema subsides, it will be latent for 2-3 weeks,
178

LomNi-Terip aind Low-Level Eftects of hottiziig lzduiation
depending on the dose. the fingernails in persons of dark-skinned races." TheThe second onset of erythema is attributed to im- threshold dose has not been determined. Fingernail
paired circulation in the arterioles and capillaries, pigmentation was observed in the Marshall Islanders,producing inflammation and edema.,' and accom- who received an average estimated whole-bodypanied by dry desquarnation of the epidermal corneo- gamma-radiation dose of 61 rem. The bluish-browncvtes. Low radiation doses induce mitotic delay, 4;•. pigment was slowly eliminated by normal fingernailwithsubsequentsloughingofepidermallayers. Higher growth over the first 6 months after irradiation."radiation doses extend the duration of mitotic delay Cracking or shedding of the nails may occasionallybut do not alter the rate of cell sloughing at the skin occur.4surface. Upper cells are sloughed or abraded off, The first report of epilation caused by X rays wasexposing cells that are not completely keratinized. written in 1896. 7 As a way to test the machine's abilitvCell death and moist desquamation ensue. to make a photograph of the skull (in preparation for
Both dry and wet desquamation occur about 1-4 locating a bullet in the head of a child who had beenweeks after irradiation." 4ý-•4 Regeneration of the stra- accidentally shot), the author exposed the head of aturn corneum requires 2 months to 4 years,-" and this colleague to X radiation for I hour. The photographregenerated tissue will be more sensitive to other skin- did not turn out, and 3 weeks later, the colleague devel-damaging agents. 4 '.4" The new skin may be thinner oped a 2-inch bald spot on his scalp.3-than the original, with greater sensitivity to touch and Generally, epilation occurs about 2 weeks afterpain.4 ,4"' Reduction or loss of the dermal ridges mak- irradiation with doses greater than 2-3 Gy." ,
4 2' 4 Thising up the fingerprint has occurred from large or loss is temporary, with regrowth occurring in 2-6chronic exposures." months. The returning hair may be thinner, with
Epidermal basal cells are thought to be the targets either different pigmentation or loss of pigmentation.of early radiation damage,4
;-;4 and further damagc to Permanent epilation occurs with doses greater than 6the surrounding vasculature is an important factor in Gy." Epilation results from a combination of mitoticlate radiation injury and necrosis.'-i' 2 .4';," The blood delay, interphase death, and reproductive death of thevessel damage may lead to telangiectasia, and fibrosis hair cell.and alterations in connective tissue may appears.842
.:.41
Hyper- or hypopigmentation may occur after radia- Cancertion exposure: low doses activate melanocytes andproduce hyperpigmentation, and higher doses may Two months after their discovery, X rays wereresult in death of melanocytes and hypopigmenta- being used to treat cancer."," The earliest radiother-tionY<;" apy was performed in 1896 for breast carcinoma." and
Dermal necrosis from radiation results from cell stomach tumors.'," However, with the increasing usedeath in the dermis, and is equivalent to third-degree of radiotherapy came reports that radiation actuallythermal burns.""'- Ulceration is seen with doses induces cancer.';] .-,S'2.3 One of the earliest radiation-greater than 20 Gy;"4 some muscular atrophy may induced cancers occurred in the laboratory of Thomasoccur with highly penetrating radiation.44
1,4 When the Edison, whose assistant died in 1904 from skin cancerproliferation rate of basal cells is depressed for long contracted while working on the development of aperiods, fibrotic repair may surpas:- the basal cell fluorescent light using an X-ray tube." By 1907, elevenrepair, 'eading to reduced tonicity and resiliency and mortalities were attributed to cancer induced by Xthe formation of scar tissue. 4'4 • Figure 9-5 shows the radiation.12 The first investigator to demonstrate thatgeneral pattern of skin damage of a patient who re- X radiation causes cancers in laboratory animals usedceived large doses of radiotherapy. Ulceration with a fractionated radiation schedule to induce spindle-scar-tissue formation occurs after 30 Gy," and severe cell carcinomas in rats."4 Many early radiologists,fibrosis after 55 Gy." Ulcerations may require correc- researchers, and workers experienced chronic radio-tive surgery, because the underlying tissue may main- dermatitis, increased incidence of cancers, and othertain the ulcer and the recovery of the immediate sur- damage before the dangers of radiation were clarifiedrounding tissue may be slow.4'- Chronic radiation and protective measures were initiated.7 , 1•3" Now, theexposure (chronic radiodermatitis) can also lead to National Academy of Sciences considers cancer induc-increased fibrosis and to ulceration.4 2,4 Skin cancers tion to be the most important somatic effect of low-may be evident after months or years.42,4;,41,= They may dose ionizing radiation.7result from either acute or chronic exposure, but are Cancer Induction. Cancer development is thoughtnot generally associated with increased mortality.78 ,45 to be a multistep process, in which the initial damage
Radiation induces a bluish-brown pigmentation of leads to a preneoplastic stage, followed by selection
179

Fi,, C linical con r'e of radia1tionl danmage to thle !,kill of a radiotherapy patient: (A:) erx-thenia, (13) erosion, (C) uilcer, (ID)
anid proliferation of the nevoplastic cell.- """' Chronio- wh-Iichlea,,ds to thedeveclopmient ofa neoplasm.i Damage
so1m1arl ad en/yrratic analyses indicate that all Of the can be initiated by various agents, including e\posure
cancer cells of a tumor and its mretastases are deriva- to radiation or another environmental or chemical
tives or clonies of a single cell."" ` A neoplasm is carcinogen.
characteri/ed by,\ unrestrained growth, irregular mi- [During the promotion stage, thle preneoplastic cell
gration, tra nsformation, and genetic d iversi tv.'- is stimulated to divide or is given Preferential selec-
-Fil three ',tagcs in cancer forimation are iiuitiatiti, tion. A ;'iomotcr is an agent that by itself does not cause
p'rofioto;i, and IatCUL I/ (Figure kbi' During initia- cancer, but once the initiating carcinogenic event has
tion, ti\a tionl of thle som~latic mu11tational even1t occurs, occurred, it promotes or stinmulates thle cell containing
]ISO

Long-Terin and Low-Level Effects of Ionizing Radiation
C), A J"l•- • O 0Tumor '
(a) Radiation YFixed
(C) Retrovirus ' t --
(d) ChromosimBreakage Syndrome
Initiation Promotion Latency
Gene Mutation: 0 Radiation-Induced 9 Genetic Diversity
"* Amplification Hyperplasia * Selection
"* Deregulation * Hormone I Proliferation"* Activation * Chemical 9 Immune
"* Inactivation Incompete , :e
* Altered Product Environmental
Fig. 9-6. Sequential steps in the development of cancer. Cancer originates from a single cell (clone) through a multistepprocess. Initiation by one of four methods (a-d) leads to repair of damage, or cell death, or fixation of DNA damage, whichmay predispose the cell to transition into a neoplastic state. Chromosome-breakage syndromes (also called geneticsyndromes, such as xeroderma pigmentosum and ataxia telangiectasia) are associated with deficiencies in DNA repair andgenetic instability. Environmental or host factors may play roles in cancer promotion and latency. End products of these stepsare the tumor and its potential metastases.
the original damage."" The National Toxicology Pro- breast cancer, and thyroid-stimulating hormone (TSH)gram lists 148 chemical agents and groups known tobe may act as a promoter of thyroid cancer. Conjugatedcarcinogenic in humans, including asbestos, benzene, and unconjugated estrogens have been identified as"vinyl chloride, nickel, soots, tars, formaldehyde, DDT, carcinogenic in human populations.72
saccharin, and urethane.7 2 Unlike most carcinogens, Radiation may also affect latency, which is the thirdradiation may act both as an initiator by inducing (and last) stage of cancer development. During la-somatic mutation, and as a promoter by stimulating tency, the transformed cell produces a number ofcell division as a result of recovery and repair proc- different phenotypic clones through continued ge-esses." Some chemotherapeutic alkylating agents netic diversity, although not all clones will be neoplas-(including cyclophosphamide and nitrogen mustard) tic.6"5. 7 ' Eventually, one phenotype acquires the selec-initiate biochemical damage similar to that caused by tive advantage of evading the host's defense systemsradiation, and are called radiomimetic agents. Like and metastasizing (Figure 9-6). The primary contribu-ionizing radiation, they are useful for chemotherapy tions of radiation in latency are the immunosuppres-but are also carcinogenic. Some hormones may act as sion and alteration of biological mediators released inpromoters by stimulating the growth of target tissues.7 the surrounding tumor microenvironment.For example, estrogen may function as a promoter of Environmental and host factors have roles in cancer
181

Mledical Copitiqeiitt of Nuclear Warfare
TABLE 9-1
LOWEST CANCER INCIDENCE RATES FROM SELECTED WORLD REGISTRIES*
Type or Site Connecticut Lowest Incidence Location ofof Cancer Registry Worldwide Incidence
Lung 325.8 9.0 Rural Norway
Colon 137.2 13.7 Ibada, Nigeria
Prostate 92.3 5.3 Miyagi, Japan
Stomach 66.2 28.0 New Mexico, United States
Leukemia 57.9 40.8 Miyagi, Japan
Myeloma 15.1 1.8 Miyagi, Japan
Thyroid 12.4 3.6 Southern metro region,United Kingdom
*Per million males younger than 65 years
Source: Condensed from reference 73
promotion.'-- The contribution of environmental agents virus selectively attacks and destroys a subclass of T-can be estimated by comparing high and low cancer cells (T-4 lymphocytes) that is responsible for monitor-incidences in different populations of the world.73 As ing the immunity of the spontaneously developingmany as 80/ of cancer deaths in the United States may neoplastic cells. Impairment of the immune systembe linked to environmental factors that could have may, therefore, promote cancer growth.been avoided.71 The incidence of lung cancer in males The differing incidences of cancer for males andinthestateofConnecticutin1968-1972was325.8cases females (Table 9-2) may be the result of hormonal,per million males under 65 years old, compared to nine environmental, or behavioral factors. Leukemias andcases per million in rural Norway (Table 9-1).71 Simi- lung cancer are more prevalent in men. Their higherlar differences occur for the incidences of prostate incidence of lung cancer may be due to the greatercancer and myeloma in the populations of Connecticut percentage of males who smoke. Thyroid cancers areand Miyagi, Japan. Environmental factors that may more prevalent in women. 3 Genetic studies havepromote cancer are the use of tobacco, alcohol, and shown that family tendencies for developing certainfood additives; other dietary factors; sexual behavior; canceri are associated with several genetic syndromes,occupation; air pollution; industrial products; medi- including xeroderma pigmentosum, ataxia telangiec-cines and medical procedures; bacterial and viral in- tasia, Fanconi's anemia, Bloom's syndrome, Gardner'sfections; and geophysical factors.73 Tumor registry syndrome, and Li-Fraumeni's syndrome."-'1.b7b Thesestudies have shown higher incidences of colon cancer diseases are associated with increased cellular muta-in the United States than in Japan, while higher inci- tion rates, sensitivity to environmental and chemicaldences of stomach cancer occur in Japan. 74 Japanese mutagens, and exposure to ionizing radiation. Chro-immigrants in the United States have a higher inci- mosomal translocations are observed more frequentlydence of colon cancer than those living in Japan, indi- in cells from persons with these diseases, and specificcating that environmental factors and dietary changes defects in the repair of deoxyribonucleic acid (DNA)may influence its development. One environmental have been identified for most of these syndromes.agent of increasing importance is the human immu- These hereditary syndromes may increase susceptibil-nodeficiency virus (HIV), implicated in the cause of ity to cancer by providing the genetic diversity that isacquired immune deficiency syndrome (AIDS).75 This necessary for its development.b9 ,7b
182

Long-Term and Low-level Effects of hmizing Radiation
TABLE 9-2
UNITED STATES CANCER MORTALITY RATESIN 1968-1972*
Type or Site Number of Number ofof Cancer Males Females
Lung 288.0 71.3
Colon 85.2 74.9
Prostate 25.5 -
Leukemia 43.4 3.0
Stomach 37.5 18.2
Thyroid 1.8 2.1
Breast 1.3 174.0
*Per million males or females younger than 65 years
Source: Condensed from reference 73
Specific gene mutations and chromosomal aberra- ing Burkitt's lymphoma in humans."9''•,•,s2 Anothertions are associated with particular cancers. 6s"7'69.77 oncogene (ras) codes for a G-protein that regulates cellResearch in this area has been stimulated by the dis- receptor activity by controlling adenyl cyclase activ-covery in recent years of oncogenes, proto-oncogenes, ity." Up to 40% of the surgically removed humanand antioncogenes.t,67.78,71 colon cancers contain an activated ras oncogene.84
Oncogenes are genes that induce the transforma- Radiation-induced skin tumors in rats and mice havetion of cells in culture when incorporated into the DNA been found to have activated forms of the c-myc, k-ras,of otherwise normal cells.b7 These genes have been and ras oncogenes as well as amplification of the c-mycfound to have structural similarity to normally occur- gene. 8
1-7 A mouse lymphoma induced by radiation
ring genes that are present in nontransformed, non- was shown to have an activated c-k-ras oncogene thatcancerous cells.,7 80 About forty different oncogenes differed from the normal gene by a single point muta-have been identified.' Their functions are diverse; tion, resulting in incorporation of aspartic acid insteadhowever, many of their gene products bind to DNA or of glycine into the corresponding protein.87
promote cellular proliferation.67 79, Oncogenic activation by itself is not necessarily a
The normally occurring counterpart of the onco- carcinogenic event because these genes have impor-gene is the proto-oncogene. Very few natural func- tant normal cell functionsY.67 6 They are thought totions of the proto-oncogenes are known, although participate in initiating a neoplasm state by eithersimilarity exists between the v-sis oncogene and the quantitative or qualitative changes in their specifiedgene coding for the platelet-derived growth factor-2 gene product as a result of amplification, mutation, orpeptide."'," deregulation.Y69n Some antioncogenes help repress
Most oncogenes were first isolated from avian leu- cancer induction.68,88 The deletion, inactivation, orkemia retroviruses, and later research identified onco- presence of that gene in a homozygous recessive stategenic and normal counterparts in laboratory animals may predispose or permit cancer development.6 98
and in humans.78 The viral oncogene is referred to as Hybridization experiments using normal cells andv-onc. One of the most commonly studied v-onc genes cancerous cells show that the cancerous actions ofis v-myc.Y'1'89 Its homologous cellular gene (c-myc) is some oncogenes are repressed by the presence of theamplified in several different forms of cancer, includ- normal chromosome in the new hybrid.6 ,9' An acti-
183
,hdt/COn4s11110CINtC Ot \!UJ011d N1 tll Cr
vated rat-oncogene has been implicated in the radi- less radiosensitive for stomach cancer and leukemia.oresistance of a human laryngeal cancer cell line"' and The minimum latency periods are 2-3 years for leuke-also in radioresistant benign skin fibroblasts from a mia and 5-4t0 years for solid tumors.patient with Li-Fraumeni's svnd rome.-" The probabilities of developing cancer as a result of
Radiation is known to induce chromosomalaberra- exposure to high doses of either low- or high-LETtions, and specific chromosomal aberrations are shown radiation are fairly well established, but the risks ofby many cancers. The most common translocations low-level exposure are not."-' Insufficient data exist toand trisomic conditions observed in human cancer accurately determine the risks to humans.-' 2 Theinv'olve chromosomes 1, 8, and 14."" The c-mvcand c- risk forlow-level exposureisextremely smalland maymos genes are located on chromosome 8." .. Translo- be nonexistent.- Epidemiological analyses for deter-cation of chromosome 8 to 14 is present in 80'; of mining the role of radiation exposure in carcinogene-patients with Burkitt's lymphonma and is associated sis are made difficult by the small numbers of irradi-with amplification of the c-rnc gene.-` A similar ated populations and the even smaller chance that atranslocation occurs in 10'; -20C( of patients with acute specific cancer resulting from a specific radiationT-cell leukemia.- The Philadelphia chromosome that exposure can be detected in a population.' ""01is present in )0' -' of patients with chronic my- Epidemiology is also clouded by the contributions ofeloid leukemia is a translocation of a portion of chro- other carcinogens, differences in health factors, inap-mosome 9 to chromosome 22,"1"" and it is thought to propriate control populations, and (in retrospectiveinvolve the c-abl proto-oncogene.--'•"7 A transforma- studies) possible death certificate inaccuracies, miss-tion is thought to arise by random selection in the ing data in the records, and poor or biased memo-tumor cell due to its greater genetic diversity. Once ries.'''1"-'.14 The most recent estimates for the inci-present, thetransformationprovidesaselectivegrowth dences of cancers resulting from I cGy of low-LETadvantage that allows the cell possessing that modifi- radiation are shown in Table 9-3.''cation to predominate.' ...... Within the limitations described above, the scien-
Models for Predicting Cancer Incidence. With few tific community has attempted to derive risk estimatesexceptions, radiation may induce cancer in any organ for low-level radiation exposures that may be used byof the bodV. 7 ' Radiation-induced cancers cannot be legislative bodies to prescribe occupational and publicdistinguished from spontaneous cancers.",'-" The safety standards. Four research models are used:possibility of radiation induction is based on a per- linear, line'ar-quadraitic, quadratic, and pure quadratic w'ithson's history of exposure to large doses, and is influ- cCII killing."-"8 '3 '""; Each model mav exist with orenced by a number of variables, including total dose, without thresholds. Two of these models, linear anddose rate, and radiation quality.7- As with other quadratic (nonlinear), are shown in Figure 9-7. Asomatic effects, genetic changes, and in uttro effects, linear model is more likely to overestimate the inci-high-LET radiation and high dose rates have a greater dence of cancer for lower doses. If the initial rate ofprobability of initiating or promoting cancer than does increase is shallow for the lower doses, then a thresh-low-LET radiation. Most leukemias and cancers of the old essentially exists for the lower doses of a nonlinearthyroid, breast, lung, liver, and bone are induced at model (Figure 9-7) because the incidence is extremelyhigher rates by high-LET radiation, but the incidence low in proportion to the dose. Different cancers may fitis not large enough to allow accurate determination of one model better than another. For some cancers, thethe RBE in human populations. Low dose rates permit confidence limits of the curve fit may not permit thepartial or complete cell repair of the radiation damage. selection of one model over another with any degree ofIn contrast, with high dose rates, the rate of cell dam- accuracy. Figure 9-8 shows the degree of fit to theage may be faster than the repair rate, resulting in incidence of leukemia in the Nagasaki atomic-bombdamage accumulation. Fractionation of the dose per- survivors."2 The data are best predicted by a linear-mits repair of a potential neoplasm and decreases the quadratic model,"-" although either model is appli-incidence of carcinogenesis for leukemia, but does not cable. The radiation-induced incidencesof breast cancerappear to be as important in reducing the incidence of and thyroid cancer are best described bv linear mod-breast and thyroid cancers. The latency and total risks els."1 Tihe cell-killing component of thie pure-quad-for breast, lung, intestinal, stomach, and thyroid can- ratic-with-cell-killing model refers to the fact thatsomecers vary with the age at exposure. In general, persons incidence curves decrease at the higher radiation doses.who are younger at the time of exposure are at in- Lower radiation doses increase the incidence of cancercreased risk for most cancers. For breast and thyroid cell induction, whereas the accumulated damage fromcancers, persons younger than 20 years at the time of higher doses is more likely to kill the cell, thus elimi-exposure are more radiosensitive, whereas they are nating potential neoplasms.
184

Long-Termn and Low-Level Effects of Ionizing Radhition
TABLE 9-3
RISK ESTIMATES FOR RADIATION-INDUCED INCIDENCE OFCANCER PER MILLION PERSONS EXPOSED PER cGy (rad) OFLOW-LET RADIATION
Type or Site Age at Years at Risk Absolute Riskof Cancer Exposure After Irradiation Male Female
Leukemia* 0-9 5-26 1.73 1.1010-19 5-26 0.85 0.5420-34 5-26 0.85 0.5435-49 5-26 1.05 0.67
50+ 5-26 1.56 0.99
Lung 10-19 10-33 0.30 0.3020-34 10-33 0.56 0.5635-49 10-33 0.86 0.86
50+ 10-33 1.20 1.20
Breast 0-9 10-35 - 3.8010-19 10-35 - 7.6020-29 10-35 - 4.9030-39 10-35 - 4.9040-49 10-35 - 1.30
50+ 10-35 - 0.80
Thyroid 0-9 10-34 1.50 5.0010-19 10-34 1.50 5.00
20+ 10-34 0.50 0.50
Colon 20-34 10-30 0.21 0.2135-49 10-30 0.34 0.34
50+ 10-30 0.89 0.89
Stomach 10-19 10-30 0.16 0.1620-34 10-30 0.31 0.3135-49 10-30 0.51 0.51
50+ 10-30 1.34 1.34
Liver 20+ 10-30 0.28 0.28
*Except chronic lymphocytic leukemia
Source: Condensed from reference 11, Table VI-l-A
185

Medical Conseltqetces, ot Niclear Warfare
o Linear Model
C. Nonlinear ModelC
-Probable Threshold Region
Radiation Dose -
Fig. 9-7. Mathematical models for radiation dose and incidence of cancer. Fourmodels estimate the effects of low-level radiation on incidence of cancer: linearmodel with threshold, linear model without threshold, nonlinear model withthreshold, and nonlinear model without threshold. A "quasi" or probablethreshold may exist in the nonlinear model (shaded area), where an increase inincidence within that region is so low that a threshold essentially exists.
186

Long-Terin and Low-Level Effects of Ionizing Radiatin
12 0.8
S0.6-;•100"4
S0.4-/
"(0 80 0.05 0.1 0.15 0.20
0 2I0
0 "[ I I
0 0.5 1.0 1.5 2.0 2.5 3.0
Bone Marrow Dose (Gy)
Fig. 9-8. Incidence of leukemia in Nagasaki atomic-bomb survivors through 1972.Bone-marrow doses have been adjusted for differences in age at time of exposure,and 50% confidence intervals are provided. Relative fits of four different mathe-matical models to data are shown: pure quadratic with cell killing (-.----), purequadratic (, - ), linear-quadratic ( ........ ), and linear (-). Insert isenlargement of the dose range (< 0.2 Gy).
Source: Redrawn from reference 102
187
Mtedical Conseces of Nuclear Warfare
HUMAN DATA BASE
Data from the human population on the effects of fessions; and victims of radiation accidents. In thelow-level radiation come from four sources (Table 9- early 1900s, workers in a number of occupations re-4): atomic-bomb survivors, medical exposures, occu- ceived large or chronic exposures to ionizing radiationpational exposures, and epidemiological comparisons because of inadequate safety standards and ignoranceof geographic areas containing high background ra- of its long-term biological effects. Three groups with adiation.-' high incidence of radiation-induced cancer were the
The 92,231 survivors of the atomic detonations in early radiologists, the radium-dial painters of theHiroshima and Nagasaki are being monitored by the 1920s,7' and uranium miners.-'"411
Radiation Research Foundation for possible radiation-induced health effects."' Of the 24,000 deaths in this Leukemiapopulation through 1982, 6,720 were attributable toradiogenic and nonradiogenic cancers. The founda- Leukemia is one of the most frequently observedtion is also following 27,000 children of the survivors radiation-induced cancers.`", It accounts for one-who were conceived after the detonations to deter- sixth of the mortality associated with radiocarcino-mine if genetic damage was induced in their parents genesis, with equal numbers of cancers of the lung,and passed on to them."'• Radiation doses received by breast, and gastrointestinal tract..A' Leukemia may
a majority of the survivors were first determined in be acute or chronic, and may take a lymphocytic or1965,"' and were recalculated in 1986 after more infor- myeloid form. With the exception of chronic lympho-mation on the explosions became available.I"' Earlier cytic leukemia, increases in all forms of leukemia havedifferences in the biological responses of the Hiro- been detected in humans exposed to radiation and inshima and Nagasaki populations were thought to be irradiated laboratory animals."- 5 ' More acute thanattributable to the larger neutron exposure and, hence, chronic leukemias are induced, although the latenciesthe greater RBE in the Hiroshima explosion;-' how- are roughly equal." Characteristic chromosomalever, reestimation of the radiation doses indicates less aberrations induced by radiation have been identifiedcontribution from neutrons and a greater influence in patients with either acute lymphocytic leukemia"'from gamma radiation in the Hiroshima bomb."•' This or chronic myelogenous leukemia." - The most com-necessitates revising the risk estimates for low-LET mon aberration is the Philadelphia chromosome, foundradiation exposure and may increase the potential risk in approximately 95% of patients with chronic myelo-estimates by 50c• ."'1 genous leukemia.," 4-'
The largest medically irradiated population for Leukemia first appeared in the atomic-bomb survi-which dosimetrv ik available comprises the 14,111 vors 2-3 years after the nuclear detonations, andpatients in the United Kingdom who received spinal reached a peak incidence 10-15 years after irradia-irradiation for treatment of ankylosing spondyti- tion.7.s,. The data for the Nagasaki atomic-bomb sur-tis."II"I I-I Ankylosing spondylitis is a rheumatoid vivors best fit a linear-quadratic model (Figure 9-8),disease primarily affecting the spine and characterized although the number of observations is so small that,by destruction of the cartilage and ossification of the statistically, either model fits well."'2 The averagevertebral joints. The patients received their radiation latency period for leukemia is thought to be 2-20treatments sometime between 1935 and 1954. In the years. ". ' The mean time from exposure to death wasmost recent study, they were monitored through 1970.' "' 6 years in the ankylosing spondylitis patients ","' andAn increased incidence of leukemia has been observed 13.7 years in the atomic-bomb casualties (Table 9-5)."1in this population. Other medically irradiated groups The difference between the two groups may reflect thewith increased cancer incidence are children who re- larger radiation dose (averaging 3.21 Gy) received by
ceived head radiation for treatment of tinea capitis,"1- the bone marrow of the ankylosing spondylitis pa-and patients who received routine fluoroscopy exami- tients, compared to an average dose of 0.27 Gy in thenations for postpartum mastitis" or during treatment atomic-bomb survivors. Table 9-5 shows the largeof tuberculosis. .11; numbers of observed leukemias in five irradiated
The third category includes occupational groups populations compared to the predicted numbers.with very low radiation doses (averaging less than 1 Between 1950 and 1972, sixty-three excess leukemiarem/year); the medical, scientific, and industrial pro- deaths occurred among the 92,000 survivors of the
188

Lo•ig,,-Term iand Loaw-L.•,el Ef•ects of homizmg Judiatiop
TABLE 9-4
SOURCES OF DATA ON RADIATION EXPOSURE TO HUMANS
Atomic-Bomb Detonation Exposures
SurvivorsOffspring of survivors
Medical Exposures
Treatment of tinea capitisX-ray treatment of ankylosing spondylitisPrenatal diagnostic X raysX-ray therapy for enlarged thymus glandsFluoroscopy (treatment for tuberculosis)Thorotrast treatment
Occupational Exposures
Radium dial painters (1920s)Uranium miners and millersNuclear dockyard workersNuclear-materials enrichment and processing workersParticipants in nuclear weapons testsConstruction workersIndustrial photography workersRadioisotope production workersReactor personnelCivil aviation and astronautic personnelPhosphate fertilizer industry workersScientific researchersDiagnostic and therapeutic radiation medical personnel
Epidemiological Comparisons of Areaswith High-Background Radiation
atomic bombs.5 1 •2•'0 Results from a group of women tion from Thorotrast is 32 persons per million, com-in Scotland treated for metropathia hemorrhagica with pared with 11.4 per million in the ankylosing spondy-pelvic X radiation are also shown in Table 9-5.'2I These litis patients, who received 1 cGy of low-LET X radia-patients received an average radiation dose of 1.34 Gy tion.5 The alpha particle releases so much energy intoto the bone marrow, and have experienced increased a small area that most of the local tissue is destroyedincidences of leukemia and cancers at the site of irra- before neoplasia occurs, thereby reducing the RBE fordiation (intestines, rectum, and uterus). neoplasia. Although the risk of inducing cancer in-
Thorotrast is a contrast medium that contains tho- creases with an increasing dose, the accumulatedrium-22 and decays by alpha emission (Table 9-5). It damage results in the death of the cell before it canwas used in diagnostic radiological procedures be- express its cancer potential. The RBE for leukemiatween 1928 and 1955.7,,'"1 An increased incidence of induction by neutron radiation is estimated to be 1-25,leukemia and liver cancer was observed in patients in according to data from the atomic-bomb survivors 122
whom thorium had concentrated in the liver and bone. The incidence of leukemia is influenced by age atThe mean radiation dose to the bone marrow from the time of exposure (Figure 9-9). The younger theThorotrast ingestion was 3.5 GyP' The estimated inci- person at the time of exposure, the shorter the latencydence of leukemia from 1 cGy of internal alpha radia- and the risk period for developing leukemia.781 The
189

Medical CmDI~t'i/110?htN t~f Nn c/tar Va rtarc
TABLE 9-3
LEUKEMI1A STATISTICS FOR IP)PULATIONS EXIPOED TO RADIATION
Average Follow-up Mean Latency Number of LeukemiaExposure Period to Death Persons Cases
opulation (Gy) (years) (vears) Exposed Observed*
Atomic-bomb 0.27 27 13.7 82,000) 84 (21)Survivors
Ankylosing 3.21 20 6.6 14,109 31(6.5)SpondylitisPatients
Pelvic 1.34 19 12.4 2,068 7(2.3)IrradiationPatients
Marshall 0.60 28 - 240 1 (-)IslandResidents
Thorotrast 3.50 27 - 4,594 60 (6)Patients(26 ml average)
*Nurnbers in parentheses are predicted cases of leukemia
incidence of leukemia decreases with increasing age at Nuclear Regulatory Commission regulations permitthe time of exposure; however, this individual is at persons in occupations with radiation exposures toincreased risk for a greater period of time (Figure 9-9). receive 3 rem in any calendar quarter or 5 rem perConversely, as the leukemia risk decreases, the risk of year.' 2' At the request of the Department of Defense,developing a solid tumor increases. For radiation the National Research Council conducted a study ofdoses of less than 0.2 Gy, there appears to be a thresh- mortalityamong participantsof nuclearweapons tests.old region in which increasing radiation doses carry Thestudy included 46,000of the approximately 200,000slightly increased risks for leukemia induction."2 This test participants and, of these, 5,100 deaths occurredmay simply be due to the sigmoid shape of the curve from all causes."' No increased incidence of leukemiain the low-dose region, but the result is a quasi-thresh- was observed. Significantly fewer circulatory deathsold effect. Apparently no difference exists in the occurred than expected (1,723 versus 2,541) as well asincidencesof leukemia in femalesand malesatanyage fewer cancer deaths (1,046 versus 1,243). The studyor at any dose.-" concluded that "there is no consistent or statistically
Over 200,000 U.S. military and civilian personnel significant evidence for an increase in leukemia orhave been involved in the testing of nuclear weapons other malignant disease in nuclear test participants."since 1945.'" This number includes military personnel However, a person who was present at the 1957who were permitted to viewa nucleardetonation from nuclear test shot (code-named SMOKY) developeda safe distance. Later U.S. weapons testing occurred at leukemia 19 years later.'` A follow-up study found athe Nevada test site and at the Pacific Proving Ground statistically significant increase of 8-10 cases of leuke-in the Marshall Islands. The average doses received by mia in the SMOKY test participants, compared withthe participants in those tests were 0.5 rem of gamma 3.5 leukemia cases expected in a general population ofradiation and 0.005 rem of neutron radiation. "" These that size."2 ' 2 The increase could be due to chancedoses were then and are now considered to be safe; alone because of the small population size or because
190

L.ong-Teri and Lowe-Level Eftects 4t Ioiizm,, Radiation
Age <1515-29
0
0 5 10 15 20 25
Time After Exposure (years)
Fig. 9-9. Effect of age at time of radiation exposure on incidence of leukemia in atomic-bomb survivors. Radiation-inducedrisks are shown for all forms of leukemia (combined) relative to age at time of atomic-bomb explosions, based on 1977 data.Chronic lymphocytic leukemia is not included because increased incidence has not been observed in any exposed humanpopulation.
-ource: Reference 118
of statistical fluctuation resultingfrom thehealthy worker incidence of leukemia increased, the total incidence ofeffect. The healthy worker effect states that in a small cancers did not.employed population, some change in mortality willoccur if there is better health care, and this factorstatistically sets that population apart from the general Thyroid Cancerpopulation. If mortality in one category decreases,then incidences in the other categories also shift. In- Thyroid cancer is also a concern for low-level expo-depth investigations by the Center for Disease Control sure and late radiation effects (Figure 9-10), possiblyand the National Research Council show that a healthy accounting for 6%-12% of the mortality attributed toworker effect is present in the SMOKY test partici- radiation-induced cancers.7,'`1pants."""'2 b Fewer circulatory-related deaths occurred Radiation-induced thyroid cancer is 2.0-3.5 timesin the SMOKY participants (103 versus 139 expected in more prevalent in women than in men (Figure 9-10 andthe general population) as well as fewer respiratory- Table 9-3).7.,1,127-32 Female atomic-bomb survivorsrelated deaths (9 versus 17 expected).'2" Although the had 3.5 times more thyroid cancer than male survi-
191

Medical Consequences ,tf Nuclear Warfimre
A B__
r - - - - - - - - - - - -- - - - - - - - ---- -- - -- - -- - -
0
0.1. -- - --- - - - - - - - -- - -- - - - -- --- - - - - - -
to|
00
Doe Gy os (y
EM-------- -&- - al -------------
0 4-------------------- ---------
z
00
0-0.49 0.-1.9 >2.0 0 2 4 6 8 1
Dose (Gy) Dose (Gy)
Fig. 9-10. Incidence of thyroid cancer in atomic-bomb survivors. (A) Incidence of thyroid cancer as a function of dose andgender (male C3, female 0). Data were obtained in a 1964 study of thyroid neoplasms. (B) Incidence of benign (0) andmalignant (U) thyroid neoplasms in persons who had received therapeutic radiation for tinea capitis.
Source: (A) redrawn from reference 130; (B) redrawn from reference 128
vors,"1 29 and as much as 5 times more cancer in one women studied, the risk was 48 per million. 12
' Theirclinical study.'21 The difference in thyroid tumor in- risk was16.5-fold greater than that for men in the sameductions in males and females is most likely due to study. Persons of North African ancestory may also behormonal influences on thyroid function."133 Depress- at increased risk.1 35
ing TSH levels in irradiated rats by supplementing A study on the atomic-bomb survivors,)29two stud-their diet with thyroxine reduces the incidence of ies of 11,000 Israelis irradiated for tinea capitis1 27,135
thyroid cancer."3' In the Marshall Islanders, the inci- and a study of patients treated by X-ray epilation fordence of hypothyroidism is associated with elevated tinea capitis1 2 indicate that the incidence of thyroidlevels of TSH and closely matches the incidence of nodules is affected by the age at exposure. The risk isbenign thyroid nodules.-1 '-4 greater during the first two decades of life (Table 9-
Variations also exist for ethnic groups. One study 3).127,135 Within this age range, children in the Israeliexamined thyroid neoplasms in Jewish and gentile study who were younger than 6 years at the time ofwomen who received radiotherapy during infancy for radiation treatment had a 1.6-2.3 times greater riskenlarged thymus glands.1 28 The thyroid was in the than their older counterparts.' 35 The average doseexposure field during treatment and received a mean received during treatment was less than 0.09 Gy.'-'dose of 3.99 Gy. The risk of thyroid cancer in women Fourteen thyroid tumors occurred in 3,762 personsof Jewish background was 163 per million women ex- younger than 6 years at the time of exposure, com-posed to 1 cGy of low-LET radiation; in the gentile pared with fifteen tumors per 7,080 persons 6-15 years
192

l.pig-Term and Low-LcivI Efc'tt, of lonizing Radia ttoi
old.'"' However, not all studies supportan ageeffect.)' cer is almost nonexistent in men.1>,4 !4' Because ofThyroid neoplasms induced by radiation are the their increased incidences of thyroid and breast can-
papillary (89(,) and follicular (1I' ) forms., These cer, women are also at greater risk of developing theseforms are usually benign and slow growing, with an cancers as a result of radiation.7,8
associated mortality rate of 53¼; (Figure 9-10).7 In a 20- The risk of breast cancer associated with radiationyear follow-up of patients who received X radiation exposure is age dependent (Table 9-3)."h 11-11;.11S.140,142
during infancy to shrink an enlarged thymus gland, Theabsoluterisk for women 10-19vearsold atthetime68"; of the thyroid neoplasms were benign."' Of the of exposure is 7.6 cases per million women per cGy ofsurgically removed thyroid nodules that developed in low-LET radiation; for persons over 40 years old, thethe Marshall Islanders as a result of their fallout expo- risk is 0.8-1.3 cases per million." In female adoles-sure, thirty-six out of forty-five (801,") were benign cents, cancer does not become manifest until afteradenomas, and nine were malignant tumors consist- puberty. Studies indicate increased incidence of breasting of seven occult papillary carcinomas and two cancer in atomic-bomb survivors who were youngerpapillary carcinomas."' Doses for these persons were than 10 years at the time of exposure.''I' 4 Previous1-8 Gy. Malignant thyroid nodules tended to develop studies detected no increase in numbers of females ofor to be detected earlier than the benign."' -2IS1
4 The that age group.'" Increases in breast cancer have beenlatency period for benign thyroid nodules is 5-34 observed in women who received radiotherapy dur-years; for thvroid malignancies, 10-34 years.-' In a ing infancy for treatment of enlarged thymus glands.follow-up investigation, an increase in thyroid neo- The latency period for breast cancer is 5-40plasms was observed in persons receiving X radiation years.7"l•'.4!!4 Women younger than 25 years havein childhood for treatment of tinea capitis. The thyroid longer latencies than do older women, and in general,doses were 0.043-0.113 Gv with a mean of 0.09 Gy.'" an increased incidence manifests itself in a woman'sThe dose response for thyroid cancer fits a linear thirties and forties.-,' ,13S, 4,'144 The mean latency pe-pattern.'' External radiation hasa higher incidence of riod varies from 18 years in the atomic-bomb survi-thyroid cancers than internal radiation.'37 vors1.1.14
1' to 27 years in one medical study." 4 Estro-Irradiation of the thyroid may produce other re- gen may promote breast cancer because a woman's age
sponses, including hypothyroidism and thyroiditis. at exposure is associated with increased risk, and be-Hypothyroidism may occur in individuals receiving cause few breast cancers occur until age 30.7,•"'40 Thislarge sublethal radiation doses from external expo- is supported by the fact that incidence of breast cancersures. Threshold estimates for hypothyroidism in does not increase in men following irradiation.l!!Oi!humans may vary by a factor of 25, from 2 Gy to 50 Gy, Several investigators have proposed that the actualdepending on whether the exposure source is external period in which estrogen is present as a promoter is theor internal.''' I7 Higher thresholds exist for internal important factor in determining cancer incidence andirradiation (50 Gy), where the concentration of radio- latencV. 7
.';.I4 Women irradiated after menopause areactive iodine by the thyroid may pose a problem.'17 less likely to incur radiation-induced breast can-Lower thresholds exist forchildren: 0.2 GC for internal cer:.• 7x.1. 2 A decreased incidence of breast canceriodine-131 exposureand 1 Gy forexternalexposure. In was seen in women who received X-radiotherapy tothe younger Marshall Island population exposed to 9 the ovaries for metropathia hemorrhagica, althoughGy, a high incidence of hypothyroidism occurred, the incidence of radiation-induced leukemia did in-characterized by elevated TSH levels. Above this dose, crease, as expected.' 2' The radiotherapy induced anincreasing incidence of hypofunction was associated artificial menopause, with a corresponding decreasewith decreased carcinoma. Ten percent of persons in estrogen production.with internal exposures of 200-300 Gv to the thyroid Breast cancer appears to fit a linear model. 7"''"•' Iffrom radioactive iodine in fallout will develop symp- a threshold exists, it is in the range of 1 cGy, althoughtoms of thyroiditis. At the upper end of that range a small increase in breast cancer occurred in atomic-estimate, thyroid ablation is likely.'' bomb survivors who received exposures of less than
0.5 Gy. 7,'' The estimated dose of radiation required toBreast Cancer double the naturally occurring incidence of breast
cancer is 0.8 Gy.` A 1950-1977 study of 23,318 Cana-Breast cancer is the major concern for women ex- dian women who received less than I Gy from fluoros-
posed to low-level radiation because of its high inci- copy during treatment of tuberculosis 20 years earlierdence (Table 9-3) and 40'( mortality rate .7,.,1.11 In the showed no significant increase in risk of breast can-United States, one in eleven women will get breast cer,' but in another study, increases in breast cancercancer.'"" The incidence of mortality from breast can- wereobserved in women who received multiplefluoro-
193

Mic(j1al Co)lScquINO Csc of 'It 1h0ar M01 rthr
scopic examinations during tuberculosis treatment."'4 vors."' Recent estimates by the National Institutes ofIn anothergroup of multiple fluoroscopy patients who Health indicate that stomach, colon, and esophagealreceived average doses of 0.66 Gv, no increase in cancers occur with greatest incidence in persons overcancer incidence was found.'17 These differences might 50 years old at the time of exposure (Table 9-3). Thebe attributed to lower radiation doses and older age at combined estimates in persons between 20 and 34exposure in the negative group. years old at the time of exposure for these three cancers
Dose fractionation does not appear to reduce the is 1.068 excess cancers per million persons per year forincidence of breast cancer ..- ` Damage in breast each cGv of radiation. They will incuran increased risktissue tends to accumulate rather than to be repaired, for at least 20 years, beginning about 10 years afterso the risk from acute exposure (such as the atomic exposure, producing a total excess of 21 cancers. Al-detonations) is the same as the risk from chronic expo- though an estimate for 1 cGy was used, there is nosure (such as small dailv doses from fluoroscopy or statistical evidence demonstrating that these cancerstreatment for postpartum mastitis) (Figure 9-11).''" can be induced by a dose this low. EnvironmentalThe data from medical studies and atomic-bomb sur- contributions from dietary and other sources may alsovivors are very similar in their dose responses." influence the development of cancers of the digestive
tract (Table 9-1).-174Other Systemic Cancers Tumors of the parotid gland have been observed
13-25 years after medical irradiation with doses as lowCancers of the stomach, colon, liver, pancreas, sali- as 0.9 Gy, and they may be either benign or malignant.
vary glands, lungs, and kidneys are also induced by In radiotherapy patients, large doses of radiation to theradiation."-'" The incidences of these neoplasms fit a parotid and other salivary glands may result in atro-linear-quadratic response model. Like most solid phy, with subsequent difficulty in chewing food andtumors, they have a latencv of 10-30 years, and no swallowing due to loss of lubrication fromsaliva secre-difference exists in the absolute risks for males and tions.females." With the exception of liver cancer, the Data on radiosensitivity of the liver are conflict-radiation-associated risks depend on the age at expo- ing.7' ""' Several updated studies of the atomic-bombsure and increase with age0-Pt".' The greatest risks are survivors have failed to demonstrate a radiation dose-for induction of lung or stomach cancer in persons over related increase in liver cancer." 5.2". 5 Increased inci-age 50 at the time of exposure.--" An association dence of liver cancer is observed in patients treatedbetween radiation exposure and induction of brain with Thorotrast, although doubt exists about the ori-tumors has been reported in two studies of children gin of the disease in these patients.7 ,
5' There are threewho received 1.4 Gv of X radiation as treatment for possibilities for cancer induction by Thorotrast: (a)tinea capitis.14s.4 In the combined studies totaling alpha radiation exposure, (b) chemical toxicity from13,100 children, twenty-four tumors were observed, thorium dioxide, and (c) metal toxicity from severalcompared to three of 17,800 in the control population. grams of thorium estimated to accumulate in the liver."
In the 1920s, workers who hand-painted the fluor- It is not likely that liver cancer is induced by alphaescent dials on wristwatches with radium-based paint radiation from internal contamination with plutoniumachieved the necessary fine detail by moistening the from fallout.7 Estimates for liver cancer range from 5.6tip of the brush into a point with their tongues; in so to 15 deaths per million persons per cGy of externaldoing, they ingested small amounts of the radium, low-LET radiation.7". Radiation hepatitis and cirrho-Because radium is a bone-seeking element with a half- sis of the liver may occur after large doses; may belife of 1,600 years, these workers had a higher inci- acute, intermediate, or chronic; and may appear indenceofbonesarcomas. Increased incidencesof breast some radiotherapy patients at 1-3 months aftercancer were also observed. 7. '-1. 140 irradiation.' 2," Sclerosis and blood-vessel narrow-
Digestive System Cancers. Significant increases in ing appear to be primary factors in its development.cancers of the digestive tract, including the esophagus, Hepatitis has been observed following doses as low asstomach, and colon, have been observed in the atomic- 4 Gy, although most clinical cases occur after 40-67bomb survivors"' and in patients following therapeu- Gy.' 3 Chronic radiation hepatitis is characterized bytic irradiation.'"'• These cancers are ranked in order of atrophy of the liver. Postnecrotic cirrhosis of the liverdescending radiation-induced cancer mortality as is two times greater in atomic-bomb survivors who re-follows: (a) stomach, (M) colon, (c) pancreas, (d) esopha- ceived doses of less than 0.5 Gy, compared with thegus, and (e) rectum." This order reflects an averaging control population. 25-of the data; dose responses for rectal and pancreatic Respiratory System Cancers. The induction ofcancer are not significant in the atomic-bomb survi- cancers may be affected by environmental factors,
194

Long-Term and Low-Level Effects of Ionizing Radiation
600
C
E0
S400-
I...CL
0..C
S)200 / /a)
4)4Cl) Ij i ,
(U
0 2 4 6Breast Dose (Gy)
Fig. 9-11. Incidence of breast cancer as a function of fractionated versus acute radiation exposure. The incidence of diseaseappears to be similar (within statistical limits) whether women received a single acute exposure, as in atomic-bomb survivors(a), or a fractionated series of smaller doses, as in mastitis patients (e) and fluoroscopy patients (A).
Source: Redrawn from reference 142
195

Medical Const'quet'ces of NI'uiar Warfaire
0.3
0.20
4-I
0
0.1
0 - -- - -
0 5-10 20
Number of Cigarettes/Day
Fig. 9-12. Mortality rate from lung cancer related to cigarette smoking in atomic-bomb survivors. Mortality in 1965-1978
is for persons exposed to 0-0.09 Gy (I3) and >1 Gy (0).
Source: Redrawn from reference 120
including occupational risks and personal habits, such rounding tissue, which 1, Is to a higher incidence ofas smoking (Figure 9-12) .7,11'7'1,151 lung cancer in this populaIion.1Y In some areas, high
Workers in uranium mines and mills receive con- radon concentrations in homes and buildings appearcentrated, high-LET alpha radiation from breathing to contribute to lung cancer."'uranium dust and concentrations of radon gas that In miners and atomic-bomb survivors, smokingseep into the mines from the surrounding rock .7 .. 2 .1 2 1 has been shown to be an important contributing factorOre dust becomes trapped in the bronchi and alveoli in lung cancer (Figure 9-12).,1•1417 Risk estimates forand releases large amounts of radiation to the sur- radiation-induced lung cancer are four times higher
196

Long- Term and loaw-Level Effects of lomi:imy, Radialtion
tor persons who smoke 1-10 cigarettes per day and nitis is usuallv followed within 6-12 months by persis-twenty-four times higher for persons who smoke 40 tent pulmonary fibrosis.'O'cigarettes.'' Increased cancer in smokers may result Reproductive System Cancers. A significant in-from the inhalation of volatile polonium-210, which is crease in malignant and benign tumors of the ovariesconcentrated in the lungs and circulatory system. II occurred in the atomic-bomb surrivors between 1965Contributing factors are complicated, because the and 1980.`- The latency period was 15 years, and aincidence of lung cancers induced by polonium-210 greater frequency was observed in women who wereexposure can be enhanced in laboratory animals by the younger than 20 years at the time of exposure.co-administration of saline."' Hamsters receiving 40nCi of polonium-210 by intratracheal administration Cancers of Negligible Riskfollowed by saline had a 35:; incidence of lung tumors,compared with 0':; for hamsters receiving polonium- Several types of cancer have a low or negligible risk210 alone. In addition, cigarette smoke contains other of induction from radiation exposure. No increase incarcinogens that may be important contributors to chronic lymphocytic leukemia has been observed tocancer development."''-,' date in irradiated populations,7 and increases in hairy
Radiation pneumonitis will occur 1-7 months after cell leukemia are low or nonexistent. '" Cancers of theirradiation in persons who survive large whole-body uterus, cervix, testis, mesenterv, prostate, and meso-or upper-body exposures."" Studies of patients receiv- thelium also have a low or nonexistent risk.7 .'4* Someing single exposures for radiotherapy indicate that the cancers are thought to be relatively insensitive to in-threshold for this response is 7.5 Gy to the lung.""' duction by radiation yet still have a small probabilitySince this dose is in the lethal range for the hematopoi- of occurrence, such as cancers of the larynx, nasal si-etic subsyndrome from whole-body exposure, the nuses, parathyroid, nervous tissue, and connectiveoccurrence of pneumonitis will be limited, but it may tissue.7.1:
be important as a late effect in patients receiving a In the most recent mortality study of the atomic-bone-marrow transplant because of the larger radia- bomb survivors, the frequency of cancer of the rectum,tion doses. A 5%" incidence of radiation-induced pneu- gallbladder, pancreas, uterus, lymph glands, and nerv-monitis is expected after a dose of 8.2 Gy, and a 5017 ous system was not statistically increased.""; Cancersincidence is expected at 9.3 Gv.1"" Characteristic syrup- with a low probability of induction are not observedtoms include dyspnea, tachypnea, and coughing. following low-level radiation because of the apparentSevere cases may result in death. Radiation pneumo- long latencies.7 "'•
GENETIC EFFECTS
In 1927, radiation was conclusively shown to population. Radiationcausesgeneticdamagebyeitherdamage cells."" Drosophila mtelanogaster (fruit fly) sperm gene miutations or chromosoinal damage .7,8,164-
were irradiated, and radiation-induced increases wereseen in (a) mutations leading to mortality and (17) Gene Mutationsmutations of characteristic morphological and pheno-typic traits, such as wing shape and eye color. Since Gene mutations are alterations in a single genethen, radiation-induced genetic damage has been con- locus, which is the smallest amount of genetic informa-sistently demonstrated in plant and animal species, tion that can code for a single protein. The gene isleading to the conclusions that (a) radiation is a potent composed of DNA (Figure 9-13), which is made up ofmutagenic agent, (b) most radiation-induced muta- four bases: adenine, guanine, cytosine, and thymine.tions are considered to be detrimental, and (c) radia- A group of three bases on a single strand of DNAtion-induced genetic damage is thought to have no represents a codon, coding for the insertion of one ofthreshold, so even very small doses of radiation carry twenty different amino acids into the protein to bepotential risk.7""'•"1-1, The natural incidence of genetic synthesized. A change in one of the three bases withindisorders is one in ten for live births and five in ten for a codon changes the blueprint for the amino acid to bespontaneous abortions. Background radiation (200 incorporated into the protein at that position.mrem per person per year) may account for up to 5% Radiation may cause point mutations, deletions,of the spontaneous genetic damage in the general insertions, and inversions.7."',' W. 1
7 The mutation may
197

tVot'iitd Copiseq UeUOUTS ()f Nticlear Warfare
PYRIMIDINE N UASC NG
DIMER 1
STRANDBREAK
A DO BL STRAu N Dn
BREAKBREAKAGE OF
HYDROGENBOND
Fig.9-13. General structures of the fourbases of DNA. Three hydrogen bonds occurbetween cytosine (C) and guanine (G), and two between adenine (A) and thymine(T). Several types of radiation damage to DNA are shown.
Source: Redrawn from reference 247
198

Long-Termi anud Low-Level Effects of lonizing Radiation
NORMAL BASE BASE BASESTRAND CHANGE INSERTION DELETION
AMINO AMINO AMINO AMINOACID ACID ACID ACID
10 1 1 I I1 0 1 G 1 G
A GLUTAMIC 2 A GLUTAMIC 2 A GLUTAMIC 2 A GLUTAMICI ACID ACID ACID ACID
3A 3 A 3 A 3 A1 1
5AA LYSINE *05 ARGININE 5 A ASPARAGINE 7 G ARGININEI I
0 A 70 AA @ A1 1
SOJ GLYCINE 8 0 GLYCINE 7 G ARGININE 10 C THREONINE
9I BA I IG I I
Fig. 9-14. Types of mutations in the gene. One normal strand of DNA (illustrating nine bases within the strand) is shownon the left. These nine bases code for three amino acids within a longer peptide chain. A base change at position 5 fromadenine to guanine changes the code for the second amino acid from lysine to arginine. The intercalation of cytosine betweenpositions 5 and 6 changes the codes for the second and third amino acids and for every amino acid in the chain coming afterthem. Deleting bases 5 and 6 and closing the gap between positions 4 and 7 change the coding for the second and third aminoacids and for each amino acid coming after them. Mutations may also occur by inversions (not shown).
occur in either the DNA sequence coding for the pro- mutagenic agent, radiation may induce mutation intein itself or in one of the regions regulating gene any gene. There are no radiation-specific mutations;transcription. Mutations in the regulatory region of radiation simply increases the incidence of those thatthe gene may modify or shut off a transcription. Some occur naturally.7,' The examples in this section shouldoncogenes, such as the myc-c oncogene, may induce a not be regarded as those of radiation-specific muta-precancerous state and increased cell proliferation by tions occurring after radiation exposure, but rather as(a) mutation in the promotor region, or (b) a transloca- particular classes of mutations (dominant or reces-tion that places the gene in a constant state of activation sive). Of particular concern is the induction of genesand transcription.h6,S29,9 A point mutation occurs that do not become expressed until after the individualthrough a change in a single base within the gene has reached reproductive age.7,8 ,165
,168,169 An example of
(Figure 9-14). By changing one base, the codon is such a genetic disease occurring in the natural popula-altered to represent a different amino acid and may tion is Huntington's chorea, a neurological degenera-affect the function of the protein. Sickle cell anemia, for tive disease that does not become symptomatic untilexample, is a disease resulting from a single point individuals reach their twenties or thirties.mutation. One form of the ras oncogene has been Recessive radiogenic gene mutations are of lessfound to differ from the normal by a point mutation, concern since they require homozygosity in order to beand this change in one base now codes for a protein expressed. Recessive genes are of more concern whenthat transforms cells in culture to a neoplastic state.98 they are located on the X chromosome. Since only one
A major concern for radiation genetics is the induc- copy of the genes on the X chromosome exists in males,tion of a dominant gene carrying a trait that results in those genes are dominant in their expression. Hemo-increased mortality or severe impairment. 7S.8,10165,6l8,1H9 philia, for example, is a recessive trait on the X chro-Examples of autosomal dominant genes are shown in mosome in the natural gene pool that may be ex-Table 9-6, although many more exist.' As a random pressed as a dominant condition in males (Table 9-6).
199

i ctdital l fcqt 0', N( t X Itar 4,1rtaric
TABLE 4-0 than be lost as an isolated fragment.II DECE OF SELECTED GE ETIC DISORDERS Chromosomal aberrations can be produced in both
somatic and germ cells, and their frequency is propor-tional to the dose of radiation received.' 1-1 Acentric
Incidence and dicentric fragments are the most lethal because
Disorder per 10,I00 they mav not properly separate at meiosis or mitosisLive Births and thus mav halt those cellular processes. As a
somatic mutation, the percentage of chromosomal
Autosomal Dominant aberrations in the lymphocytes of irradiated humanshas been used to estimate the dose received. Such
Huntington's chorea 5.0 damage persisted in the lyrmphocytes of the atomic-Osteogenesis imperfecta 0.4 bomb surviv'ors 23 years after their exposure.'-Marfan's svndrome 0.4 The gain or loss of an entire chromosome throughFamilial hypercholesterolemia 20.0 nondisjunction occurs less frequently and is more
Autosomal Recessive likely to result in mortality. 7I Mammalian studies
hav'e been unable to demonstrate increased incidenceCystic fibrosis T.0 of trisomies in the offspring of irradiated animals.PhenvIketonuria I.t0Neurogenic muscular distrophy 1.0 Factors Affecting Mutation
Sex-Linked Recessive A number of factors affect the ability of radiation toinduce mutations, including rate of biological repair,
Duchenne'snmusculardystrophy 2.0 dose rate, shielding, and number of expo-Hemophilia 1.0 sures._ ,, 1,,-, m, ,," 171 Several enzyme svstems constantly
monitor and repair the DNA, recognizing specific
Chromosomal Disorders kinds of base damage and initiating repair.`74 Duringexcision repair, for example, enzymes recognize the
Down's syndrome (trisomv 21) 12.0 damaged part and split the DNA strand to remove it.Edward's syndrome (trisomv 18) 1.0 The other strand then serves as a template to reincor-Klinefelter's swndrome (XXY) 5.0 porate the proper bases in the excised site, followed by
action of a DNA ligase that reseals the strand. Breaksin the DNA strands may also be reconnected, althoughproper rejoining (if it occurs at all) becomes moredifficult if a break has occurred in both DNA
Chromosomal Damage strands.'7, 17, Other enzymes repair specific basedamage, such as alkylations. Fractionation of the
Radiation mavalsoinducegenetic damagebvychronmo- radiation dose can reduce the damage by allowingsomal changes.,- The expression ofa number of genes repair to occur between exposures. If the rate ofmay be altered by damaging a portion of or a whole damage exceeds the rate of repair, then the mutationchromosome. Chromosomal changes may arise either rate will increase. Experiments in mice show thatas chUroMosoMWa abeCrrations or by noMndisjunction, mutation rates do not further decrease at dose ratesresulting in an unequal number of chromosomes.7.s below 8 mGv/minute.'-' Dose rates in this range areChromosomal aberrations are changes in the size, about one-third aseffectiv'eas high dose ratesof gammamorphology, or number of chromosomes, and include radiation in producing specific locus mutations indicentrics, acentrics, fragments, translocations, inver- mice. High-LET radiations, such as neutrons, impartsions, insertions, and deletions (Figure 9-15).-.s ` '"''" more energy per unit distance traveled through aThe most common chromosomal damage induced by biological material than do low-LET radiations. Moreradiation is reciprocal translocation.5 In this process, two energy deposited in the area of the DNA is more likelydifferent chromosomes experience double-stranded to produce more damage, increasing the likelihood ofDNA breaks, and the two fragments rejoin to different breaking both strands of the DNA.chromosomes rather than those to which they were Some DNA bases undergo spontaneous deamina-originally attached. By rejoining to a chromosome tion. Deaminationofcytosineproduces uridine, whichcontaining acentromere, thetranslocatedpiecenmaybe occurs in ribonucleic acid (RNA) but not in DNA.transferred into the new gamete during division rather Unless the deamination product is enzymatically cor-
200

Loti%-Termn and Lo.'-Lev'' Eftects of honizing Radiation
Radiation
Kk
Chrom at n (a) RestitutionS(b)
Acentric
A BNormal
chromosomes
Break withfragment
Dicent ric (c, d) Translocation
Translocationdicentric
Fig. 9-15. Radiation-induced chromosomal aberrations in two typical chro-mosomes (A and B). When a chromosome breaks, one of four events occurs:(a) the chromosome is restored to its original state (restitution), or the breakis rejoined, with no apparent damage; (b) the fragment is not replaced andmay be lost in subsequent divisions; (c) the fragment rejoins the original freeend, but in an inverted position; and (d) the fragment may be translocated ontoa nonhomologous chromosome.
201

Ahlt'1,1l )L". C ' t N li lcar ý\arrflp,
rected before replication, it can be mispaired, produc- children of atomic-bomb survivors, only two childrening a base substitution in the newly replicated strand. presented mutations that might be related to the radia-Spontaneous deamination can be accelerated by in- tion exposure of the parents."'creases in temperature. Earh, studies on the survivors' children examined
Six genetic syndromes.are known to be more sensi- whether radiation exposure caused an increase in sex-tiVe to ultraviolet light or X-radiation damage to cells linked lethal genes that would result in increasedin culture, and the\, are associated with increased prenatal death of males or alteration of the genderincidence of cancer.-""' These include xeroderma birth ratio. "' Data did not support that hyxpothesis.pigmentosurn, Down's syndrome, ata\ia telangiecta- Twelve studies have examined a possible increase insia, Fanconi's anemia, Bloom's syndrome, and theincidenceof Down'ssvndromeasa resultof mater-Cockawne's sx-ndrome." Most have associated defects nal irradiation, "'but onIv four of the studies showedin DNA-repair capability and increases in chromoso- statistical significance,'I 1`4 and the hypothesis has notmalaberrations. Age and gender are important secon- received widespread acceptance. Irradiation of thedarv determinants for mutagenesis; for instance, stud- human testes has been shown to produce an increase inies show that the mother's age at the time of conception the incidence of translocations,' ' although no addi-is an important factor in the incidence of Down's tional chromosomal aberrations have been detected insyndrome. The natural rate of chromosomal abnor- children of the atomic-bomb survivors.'realities is eight times higher in children whose moth-ers were 40 \'ears old at the time of conception than in Estimating Genetic Riskschildren whose mothers were 20 years old.'-' Paternalageat timeof conception isalsooficoncern, because the The geneticaflyv significant dose (GSD) is the dose ofrisk for a dominant gene mutation in the germ cells of ionizing radiation to the gonads that may result inmen 30 years old and older is at least eleven times increased incidenceof genetic mutations ingermicells.-'greater than in men who are younger than 30 years at Estimation of the GSD takes into account the numberthe time of conception.'-- of persons of reproductive age in a particular group in
Internalized radionuclides of hydrogen, carbon, determining a collective dose. In the United States, theand phosphorus may present special genetic damage, GSD from background and generated radiation sourcesbecause these elements are the basic elements found in is 122 mrem per person (Table 9-7) .7 The GSD fromDNA.'-' The radionuclides may damage the DNA occupational exposure in the military service is lesswhenthe\,releasetheirenergythroughbetadecavand than 0.04 mrem per person, which is less than thatas the' undergo transmutation, resulting in structural received in a national research laboratory (< 0.2 mrem/damage at the molecular site of incorporation. 7'-'- year) or a nuclear power plant (< 0.15 mrem/year)Carbon-14 located in a sugar or base of the DNA Most occupational exposures are less than those re-decays to nitrogen-I 4. Tritium (hydrogen-3) decays to ceived from consumer products over the same period.helium-3, and phosphorus-32 decays to sulfur-32. Another method of estimating radiation-inducedTransmutation of the phosphorous-32 in the sugar genetic damage is the calculation of the doubling dose,phosphate DNA chain can produce a strand break. or radiation dose required to double the spontaneous
Plutonium-239, an alpha emitter, has induced ge- mutation rate.7 s The spontaneous mutation rate innetic damage in mice following internalization.7:. Other humans is 5 x 10- per locus, and 6.7-15.1 x 104 peralpha and beta emitters from internalized fallout will gamete for chromosomal anomalies. 7 The doublingpresent similar problems. The RBE in mice following dose is 0.5-2.5 Gv of low-LET gamma or X radiation,injection of plutonium-239 citrate ranges from four for and I Gv is commonly used for calculation purposes.'specific locus mutations to fifty for translocations.7 The doubling dose for specific locus mutations in mice
with low dose rates (< 8 mGy/minute) of low-LETRadiation-Induced Damage in Humans gamma radiation is about 1.1 Gy.'s8
The effects of radiation exposure on the humanEvidence is lacking for radiation-induced genetic population have been examined by several national
mutation in humans, although mutations of human and international scientific committees, including thecells in culture have been shown.7. Based on current National Academy of Sciences Committee on Biologi-riskestimates, theexpected increaseofgeneticdamage cal Effects of Ionizing Radiation;7 the United Nationsin the atomic-bomb survivors is so low that it would Scientific Committee on Effects of Atomic Radiation;"-'not be detectable within the larger normal spontane- and the International Commission on Radiologicalous incidence., ' "' In screening twenty-eight different Protection (ICRP).•' 7 These groups arrived at similarprotein loci (498,000 loci tested) in the blood of 27,000 estimates for the effects of low-level exposure to ioniz-
202

Long-Terni and L&nc-Let'el Ef•ects of Itnuizig Radiation
TABLE 9-7
CONTRIBUTORS TO GENETICALLY SIGNIFICANT DOSES
Source Mremper Year
Natural 82.0
Man-made 40.0
Selected Man-made Contributors
Medical 20.0Nuclear power < 1.0Consumer products 4.5Weapons testing or fallout 4.5Military occupational applications < 0.004
Total 122.0
Source: Data from reference 7
ing radiation (Table 9-8, Table 9-9). geometric mean for its 60-1,100 range of additionalThe National Academy of Sciences estimates that genetic disorders in the next generation per million
for an exposure of I cGy to the present generation, births.7 . 0
there will be 5-65 additional genetic disorders per The ICRP estimates that for every million individu-million births in the succeeding generation resulting als receiving 1 cGy of radiation in the present genera-from increases in autosomal dominant mutations and tion, 125 additional cases of serious genetic disorderssex-linked dominant mutations. If a population is will occur over the next two generations."' Approxi-continually exposed to an increased radiation dose of mately half will come from dominant, sex-linked, andI cGy for each generation, an equilibrium will be irregularly inherited mutations. Of the 125 cases, 89reached between the induction of new genetic disor- will occur in the first generation. If a doubling doseders and the loss of the earlier induced disorders. In method is used, then (assuming a doubling dose of 1this equilibrium, an additional 60-1,100 genetic disor- Gy) 1,500 autosomal dominant and gender-linkedders would be expected in the population, with the diseases per million live births would be observed inmajority contributed by autosomal dominant and sex- the first generation, and 10,000 (approximately thelinked recessive mutations and a large contribution normal incidence) would be observed in succeedingfrom irregularly inherited genes. Irregularly inherited generations exposed to I Gy at equilibrium. The totalgenes make up family tendencies for diseases and incidence of genetic disorders, one in ten live births,situations of incomplete dominance (where pheno- would not be reached in equilibrium with a 1-Gytypic expression is neither the recessive trait nor the doubling dose, since the doubling dose cannot ap-dominant trait, but a blend of the two). Chromosomal proximate the irregularly inherited component.8 "0
damage and recessive mutations are thought to make Table 9-8 does not contain an estimated contributionminor contributions to the equilibrium rate. Chromo- for the irregularly inherited disorders in the first gen-somal damage and loss are generally either lethal or eration. The large variation within the equilibriumselected out, while recessives are expressed only in the category is responsible for the large range (60-1,100) ofhomozygous condition. The National Academy of total disorders expected in theequilibrium generation.Sciences does not provide a confidence interval or a Using the doubling-dose method, the U.N. com-
203

.\hI:n iil .',-q 'm - , \i. h,' t\,u '.iu,
TABLE. •)-S"
tWIR IF I :,TIM..\r1FS O: IM"LDI \(. 0I D[\I:Il D.\AMA.-\
lncrea'.0d Incidence in
Current Incidence in Liveborn Offspring*
Genetic Liveborn Ottspring (per million)
Disorder (per million) First Generation Equilibrium
Autosomal dominant and \-linked I0, )01) 0-00 40-200
Irregularly inherited 0•0,000) 5-05 2()-40
Recessive' 1, 100 <10
Chromosomal aberrations t-1,00t0 <10 <10
Total 107,100 ;-.1-,I
*Cominittee on Biological FItect, ot Ioniming Radiation ot the National Acadenw ot -Science',
**-W'hen ever\ individual in preceeding generation receives I e\tra rem
"1ourc- |),ita tromn rtcre ctw 7
TABLE L)_A)
FSTIM..VFEI) EFFFCT OF I Gv 1h DOIUBI IV; [)OSE METI 1O1) OF UNSCFAR*
Increased Incidence in
Lix'eborn Offspring;enetic Current Incidence miloGenetic Liveborn Offspring (per million)
Disorder (per million) First Generation Equilibrium
Autosomal dominant and X-linked I0,00(1 1,5000 I,0M00
Irregularlyv inherited 40,000 450 4,500
Recessive 2,500 slight slow
Chromosomal Diseases
Structural 400 240 400Numerical 3,000 small small
Total 1 (5,);9W 2,11)0 14,9M
*United Nations Scientific Committee on Effects of Atomic RadiationSurce: Data from reterence ,
204

n aii1++m td ! 'cI o 'tk-l Lczvl I .ict ot hom ipi,ý Radiat•, oi
FABLE 9-10
ESTIMATED lNCIDENCE OF I IL %1A\ GE\ETIC DAMAGE PER G%-
Genetic Spermatogonia OocvtesDamage
Dominant mutations 16--400 0-180
Balanced reciprocal translocations 220-8,750 0-875
Unbalanced translocations 440-17,500 0-5,250
X-chromosome loss negligible 0-500
*Lnbalainced tranislocations of chronmosome fragments5.'Urcv: Data tronm rectrcnce S
mittee predicts that after exposure to I Gv, a total of stroving the population. A dose of 1 Gv to each2,190 additional genetic disorders and an equilibrium generation would produce an equilibrium of 14,900of 14,900 will occur per million live births in the first genetic disorders per million live births, compared togeneration after exposure (Table 9-9). Assuming a a normal incidence of one in ten. This is an increase oflinear response, the U.N. committee estimates a mean only 1.5%.of 22 disorders per million live births compared to the The immature human oocvte is thought to be only5-h5 disorders per million live births predicted by the 44(' as radiosensitve for mutation incduction as theNational Acadenw' of Sciences for a population e\- male spermatocyte .7" The U.N. committee has esti-posed to I cGv. The U.N. committee extended its mated that most of the genetic damage induced byestimates to the detrimental effects of radiation expo- low-LET radiation will be unbalanced translocations,sureon thegeneralpopulation. Theaveragedominant and that a l-Gy low-LET exposure would inducemutation in children of parents receiving a 1-Gv radia- 440-17,500 unbalanced translocations per milliontion dose would result in 25 years of impaired life, with spermatogonia but only 0-5,250 in human oocvtesdeath occurring 13 years prematurely. Overall, a l-Gy (Table 9-10). These estimates were based on data forexposure to parents would result in a total of 53,800 spermatocytes from rhesus monkeys, marmosets, andyears of impaired life per million births from all causes humans. Using the direct method, I,()0-2,(KX) domi-of radiation-induced genetic damage, and a loss of nant mutations per million births wil! be expected in47,200 vears of life in the succeeding generation. the first generation following paternal irradiation of IThrough natural selection, the gene pool has the capac- Gy, but only 0-900 tollowing maternal irradiation withity to absorb large amounts of damage without de- the same dose.
RADIATION EFFECTS IN UTERO
The developing embryo is extremely sensitive to Stages of Developmentionizing radiation, and the public has shown increasedawareness and concern for exposure of the fetus to The gestation period can be divided into threelow-level radiation. Human and laboratory animal stages of embryo development: preinmplahtation, majordata indicate that doses as low as 0.05 or 0.1 Gv may organogenesis, and f'tal. In humans, the preimplanta-induce effects7.-. Thresholds are thought to exist for tion stagebegins with theunion of sperm and egg,andthe induction of in utiro responses because most occur continues through day 9 when the zygote becomesafter damage to more than one cell.7 embedded in the intrauterine wall. During this time,
205

MNdwtid CO/tistquc tc's of NMicdar Wartirc
the two pronuclei fuse, cleave, and form the morula In laboratory animals, the incidence of prenataland blastula. death can vary with the dose of radiation and the time
Major organogenesis begins on day 9-11 in hu- of exposure.' s''s" 41 The most sensitive times of expo-mansIxs'" and continues through day 45." "1 The sure in humans are at 12 hours after conception, whenorgan systems undergo differentiation and develop- the two pronuclei fuse to the one-cell stage, and againment. Neural cells are the first to differentiate, starting at 30 and 60 hours, when the first two divisions oc-on day 17-20.'""'" Neural development continues cur."' 7 "', At periods just preceding the cleavages, therethroughout the major organogenesis period and into would be insufficient time for repair of damage. Inthe fetal period. The fetal stage covers weeks 7-38, or animals, 30%7( of the prenatal death at this time isterm."" because of radiation damage to the mother and a
Four general responses may occur after radiation subsequent termination of pregnancy, rather thanexposure in utero, depending on the stage of gestation because of direct radiation damage to the embryo."'at the time of exposure. These responses range from no Chromosomal aberrations from radiation exposuredetectable effect to prenatal death, neonatal death, or at theone-cell stagecould resultin thelossofa chromo-induction of congenital anomalies."4 some in subsequent divisions that would be uniform
throughout the embryo.,--"` Most chromosomal losseslead to prenatal death, although the loss of a sex
Preimplantation chromosome in females may instead produce Turner'ssyndrome."'" Such individuals are phenotypicallyfemale. Although this might indicate that a slightly
The embryo is extremely radiosensitive during the higher proportion of phenotypic females will resultpreimplantation stage, and radiation can cause in- from radiation exposure during this period, an alteredcreased prenatal death and reabsorption of the embry- gender ratio was not found in the children of theonic tissue.'."""4 In humans, reabsorption does not atomic-bomb survivors"' or in laboratory mice irradi-occur, but there is an increase in prenatal death. In ated during precleavage."' In mice, a dose of 1 Gy onanimals, the incidence of prenatal death decreases as day 0 (preimplantation) resulted in 50% prenatal deathdevelopment proceeds into the major organogenesis and produced loss of a sex chromosome in 4% ofstage, and it varies with the dose and time of expo- survivors. A prenatal mortality of 25% and a sex-sure.'. 7'5,1,81 4 During this period, the incidence of con- chromosome loss in 0.5% of survivors occurred whengenital anomalies is low but not absent. Surviving the same dose was given 7 hours later."'"embryos show an all-or-none response that is essen-tially normal with no visible anomalies, even thoughradiation may have killed many cells. "I"I4 During Major Organogenesisorganogenesis, similar radiation doses might produce1007 incidence of a particular anomaly and probablegrowth retardation.5';'","4 Embryo malformation occurs most frequently with
Several factors, including repair capability,"'' un- radiation exposure during the organogenesis stage,differentiation, and a possible hypoxic state,' are and the resulting incidences of abnormalities andthought to account for the decreased ability of radia- prenatal death will peak during this time.:-°'"' 4
tion to induce anomalies during the preimplantation However, the incidence of prenatal death decreasesperiod. During the first few divisions, the cells are rapidly with increasing embryo development, andundifferentiated and lack predetermination for par- becomes equal to that of the control group when three-ticular organ systems. If cell death were to occur fourths of this stage has been completed.following radiation exposure at this stage, the remain- The produced effects depend on the stage of devel-ing cells could continue the embryonic development opment in which irradiation occurs. the dose, and thewithout gross malformation because they are still dose rate.>-S,-1, 4 Most anomalies have a critical periodindeterminant. However, chromosomal damage at during which the radiation exposure will result in thethis point may be passed on to appear in later stages. highest incidence of that anomaly (Figure 9-16).""""'".*When cells are no longer indeterminant, loss may lead Critical period is sometimes misinterpreted to meanto anomalies, growth retardation, or death. In mice, that the particular organ tissue is in its most sensitivelow incidences of exencephaly"' and skeletal anoma- or major developmental period. This, however, maylies""' have been observed following high-dose irradia- not necessarily be the case. Increased incidence duringtion during preimplantation. At a critical period, 0.5 this time may be the result of indirect effects arisingGy may cause polydactyly."' from damage to the adjacent tissue or from an inducer
206

Long-Term and Low-Level Eftf, ts of Ionizing Radiation
Mouse Gestation (days)Effect 0 2 4 6 8 10 12 14 16 18 20
Cataracts -
Cleavage death .....ExhaustibilityMandibleMicrocephaly- - -Microphthanlma .-- '-
Radiation neurosis - ---
Skeleton T I ISpina bitfida - -
Stunting
0 2 6 12 20 37 45 70Human Gestation (days)
Fig. 9-16. Critical periods (solid lines) for radiation-induced birth defects in mice. Studies were performed with 1-2Gy of acuteX radiation during gestation. Corresponding days for human gestation are shown at bottom.
Source: Redrawn from reference 190
material of that organ.' 144 tion exposures to rats from either X rays (1 cGy/day)Each organ system is not at identical risk during the or tritiated water (0.3-3.0 cGy/day) throughout their
entire major organogenesis period because each organ pregnancies produced decreases in brain weight.7°05206is not developing at the same rate. Some organs may Low doses of X radiation have also produced growthrequire the development of another organ or induce- retardation 20 1 and behavioral defects.20 7," Protractedment before undergoing development themselves, low doses commonly affect the nervous system andSome anomalies may have more than one critical pe- the germ cells (ovaries and testes). The long, continu-riod. As a congenital anomaly in mice, cataract forma- ous development of the nervous system makes it sen-tion has three critical periods: 0-4 days, 8-9 days, and sitive to damage by even these low doses.192
,193
209-2 11
14-17 days. These periods are due to the critical The range of a particular critical period may be ex-periods of several different systems that may in turn tended by increasing the dose of radiation. Radiationinfluence cataract formation. A slight but significant does not incrtase the length of pregnancy in laboratoryincreased incidence may be observed with lower doses animals.'9 4 Fractionation of the radiation dose mayof radiation during the critical period.'-1" 4 A dose as produce either an increase or a decrease in the inci-low as 0.05 Gy may cause polydactylyY7 skeletal dence of anomalies, depending on the time betweenmalformation, decreased litter weight, and reduced exposures. If the critical period has a narrow timetail length in mice.20 Similar low doses have produced window, then fractionation over short periods of timeanomalies in the human,201 monkey,2 02 rabbit,2 03 and may increase the damage by placing more radiation inrat.2" In utero exposure to doses of less than 0.05 Gy the critical period and producing more mitotic death.from the Hiroshima atomic bomb resulted in an 11% Exposures at an early stage will increase the sensitivityincrease in microcephaly.7.2(M Small continuous radia- to radiation exposure in a later critical period.
207

Medical CotseqUInces t'f NMuticar Nolarna
Variations in natural background radiation have cause there would be no maternal reduction of thenot produced significant differences in the incidence dose. The high energy levels are released within theof anomalies, although environmental factors maY local area of the biological target. Neutrons have anplay a role in their induction.7
_1-,12 It The incidence of RBE of 4.5 for inducing prenatal mortality in mice.""congenital malformations in mammals may be af- Animal studies in which either the mother or thefected bv seasonal differences, with greater sensitivity embrwo was shielded indicate that the induction ofin winter.214 21; In the human, 70'" of trisomv 18 malformations is due mainly to direct damage to the(Edward's svndrome) and trisomy 13-15 (Patau's embrvo.2' 22
1 It is difficult to assign an overall riskswndrome) live births are conceived in the winter.2 "" In estimate to the 119 different anomalies described in thelaboratory animals, anomalies such as those for the literature because, like cancers, certain malformationsrear appendages and eves have a greater incidence on are more inducible than others, and accounting for thethe right side of the body than on the left."",2," variables becomes difficult.,
Anomalies may arise in several ways. Radiationmay damage the primordial tissue of a particularorgan or limb by direct or indirect damage to the The Fetal Stagechromosome or gene."4 This in turn may result eitherin the failure to produce a functional gene product or The fetal stage is the final stage of development,in the production of an altered functional product. lasting from the end of major organogenesis untilRadiation may cause nondisjunction during mitosis, birth. In mice, this covers days 14-20 of gestation;'11,114
resulting in a trisomic cell and a monosomic cell. in humans, days 45-266.1" Radiation-induced prena-Development would be affected to the extent that tal death and anomalies are, for the most part, negli-either cell predominates in an organ system. gible during this stage. Anomalies of the nervous
Aberrations or other damage culminating in cell system and senseorgansare the primary typesthat aredeath could result in a reduction in the number of stem inducible during the fetal stage because these svstemscells available for differentiation, which affects future are still developing. A radiation dose of 0.2-0.4 Gyorgan systems. Growth reduction may result in the given to rats on days 16, 18, or 22 of gestation causeddeath of differentiated cells, leaving the embryo with delayed development, irregular arrangement, and lossa cell population too small to form the proper-sized of neurons in the brain cortex."2 Irradiation on day 18organ.2•17 A reduction in the size of one organ may resulted in a 251/( loss of neurons in the outer cortex,cause changes in the surrounding tissues, such as but no decrease in brain volume because there was anmicrocephaly and mental retardation in humans irra- associated increase in glial cells. Much of the damagediated in utter. The development of organs requires present during the fetal stage may not be manifested ascell cooperation, mediated by chemical messengers behavior alteration or mental retardation until later insuch as hormones, organizers, and inducers. Destruc- life. The incidence of neonatal-induced death alsotion or damage to cells that contain organizers or decreases with increased development during the fe-chemical inducers may result in prenatal death or tal stage. The LD;,v,' for neonatal death given on dayanomalies."' For example, the gray crescent material 10 of gestation to mouse embryos is about 1.15 Gy. BYis an inducer that guides formation of the dorsal lip of day 18 of gestation, the LD;,,.,, is 6 Gy and rapidly ap-the blastula, and eventually (throughanarea called the proaches that of the adult animal."'chordamesoderm) guides the development of the Stunting (retardation of growth) that is inducednervous system itself. Loss of the gray crescent or during this stage is a threshold phenomenon resultingother inducer would modify or terminate subsequent from the killing of many cells. Since differentiateddevelopment. Alterations in tissue contacts or areas of tissues (such as muscles and nerves) do not divide, cellgrowth also may cause abnormal organ development, death will lead to stunting that will still be evident in
The response of each organ to the induction of mal- the adult. This has been demonstrated in children bornformations is unique, based on dose, gestational age, soon after the atomic-bomb detonation who had re-type of radiation, RBE, oxygen tension, cell types ceived radiation exposures in utero.2 2 ' Stunting has notundergoing differentiation, relationships to surround- been observed in laboratory animals that received lessing organs, and other factors.--' Neutrons and beta thanO.05Gvorinhumansexposed todosesoflessthanparticles are more effective at inducing congenital 0.3 Gy',2 4 except in some of the Hiroshima atomic-anomalies than is low-LET radiation. As an internal bomb survivors.:'-' 1' The sensitivitv of some survivorsemitter, a beta particle released from tritiated water (or who received lower radiation exposures may resultan alpha particle released from plutonium-239) would from the contributions of neutron exposure and envi-cause more damage because of its high LET and be- ronmental factors.
208

Long-Termn and Low-Level Effects of Ionizing Radiation
Effect
Cataracts ,,,
Childhood leukemia I I - -
Mental retardation
Microcephaly I--- U -- - -.-
Microphthalmia
Reduced growth
Skeletal defect
0 2 4 8 14 1820 25 30 38Gestation (weeks)
Fig. 9-17. Critical periods (solid lines) for radiation-induced birth defects in humans. Children were exposed in utero as a resultof medical radiation treatments received by their mothers. The average dose to the midline of the pelvic region ranged from2.5 to tens of Gy. Most children had more than one anomaly, and mental retardation was usually associated withmicrocephaly.
Source: Data are from reference 227
Humans Irradiated In Utero sure during the last two trimesters. In Nagasaki, fourof sixteen surviving infants who in utero were close to
Two groups of humans who havebeen irradiated in the epicenter of the explosion had speech impair-utero are children of the atomic-bomb survivors and ments. In another study of 153 of these children, 33 hadchildren whose mothers received medical irradiation a head circumference two standard deviations below(therapeutic or diagnostic) during pregnancy. The average. Mental and growth retardations were alsopredominant effects observed in humans are micro- associated with the increased incidence of microceph-cephaly, mental retardation, and growth reduction al),#2
-- and they remained evident in these survivors(Figure 9-17).7,51193,201,225229 Eye anomalies227' 22 18 2
10 and as adults. 22-'234 The highest incidence of microcephaly
genital and skeletal abnormalities 21 I are less frequently in Hiroshima occurred with radiation exposure inobserved. weeks 6-11 of gestation.2°1 No incidence of microceph-
Microcephaly observed in children exposed in utero aly was observed during the first week of gestationto the the atomic-bomb radiation was proportional to (the preimplantation period) and was negligible forthe dose of radiation received by the mothers (Figure exposure after the 17th week. In the Nagasaki data,9-18); even small doses carried increased incidence. microcephaly did not occur with doses below 2 Gy.Mothers with radiation sickness had higher fetal, Similar observations on radiation effects in uteroneonatal, and infant mortalities. 23' Fetal mortality was have been reported after medical irradiation.2271-2highest in the first two trimesters, and neonatal and Twenty of twenty-eight children irradiated in utero asinfant mortalities were highest in mothers who devel- a result of pelvic radium or X-ray therapy to the motheroped radiation sickness as a result of radiation expo- were mentally retarded, and sixteen were also micro-
209

Medical Consequences of Nuclear Warfazre
50
Ca
t-C
(D0C,.)
(D
1030 - -----------
0-)'1)10 l.
o
0 1-9 10-19 20-29 30-49 50-149 150+
Radiation Dose (cGy)
Fig. 9-18. Incidence of microcephaly in Hiroshima atomic-bomb survivors irradiated in utero. Data are based on T65D doseestimates.
Source: Redrawn from reference 232
cephalic.228 Other dei. rmities, including abnormal all had received radiation exposure some time in weeksappendages, hydrocephaly, spina bifida, or blindness 3-20, and most had been irradiated in weeks 3-11.were found in eight of the children, and some also had Another study of 1,000 children exposed in uterolanguage deficiencies. One child received a fraction- showed no increase in nervous or eye anomalies butated dose totaling 6.8 Gy in weeks 19, 22, and 27 of did show increased incidence of hemangioma (fifty-gestation and did not develop any obvious congenital six versus thirty-seven in controls)-'anomalies or mental retardation.235 Although each occurrence should be evaluated
Increased incidence of eye anomalies has been individually, the prevailing scientific opinion is thatobserved following irradiation in utero.227,230 In a re- there are thresholds for the induction of congenitalview of twenty-six case histories, three primary eye anomalies. Doses in the range of 0.10-0.15 Gy areanomalies were identified.227 Three of twelve persons thought to carry negligible risk.7" 2 Denmark'sirradiated in weeks 3-8 developed cataracts; of fifteen medical profession automatically recommends thera-irradiated in weeks 3-11, six had pigmentary degen- peuticabortion foranyfetusexposed to 10rem ormoreeration of the retina and thirteen had microphthalmia. of radiation."1 ° At one time, radiation was widely usedIn the same patients, twenty-one were microcephalic; to induce therapeutic abortion in cases in which sur-
210

Long-Terni and Low-Le'zel Effects of hoiizjing Radiation
gery was deemed inadvisable. The standard treat- tions have subsequently derived risk estimates forment involved 3.6-5.1 Gygivenover2days,-23-
21which carcinogenesis that results from in utero irradiation.
was effective in 93% of cases.2 17 Abortion usually Neoplasms were three times more frequent for in utero
occurred about 1 month after radiation treatment, in exposures occurring during the first trimester than insome cases inducing live birth..2 17 the second or third trimesters. 7,2 42 The peak incidence
of childhood leukemia occurred between ages 2 and 4Increased Incidence of Cancer with and was higher in males.24" The higher risk for devel-In Utero Exposure oping one of the leukemias continues through the 10th
year of life. Children may be at increased risk forIncreased incidence of leukemia and solid cancers developing solid tumors for at least 14 years,-.'many of
may occur in children who received in utero exposure which will be neoplasms of the nervous system." Allfrom diagnostic X-irradiation.7 ",, 23
9-24 3 This observa- estimates of childhood cancer induced by radiation
tion was first reported in 1956 in a retrospective study exposure in utero are based on the earlier mortalityof childhood cancer ir, Great Britain. 2
1 It has been data and do not reflect the advances in modern treat-confirmed by a sinii ar study of 1.4 million children ment. In studies performed in the late 1940s and earlyborn in the northea-tern United States,243 but was not 1950s, leukemia was a rapid, always-fatal disease withobserved in the ato- ic-bomb survivors.7." The lack of a 3-year survival rate of 2%.71 By the early 1970s, 3-yearincreased frequency in the bomb survivors has been survival rates were 20%, and today's cure rates areattributed to the smaller sample size, where only one 40%-60%.71 By today's standards, the estimates areor two extra cases of childhood leukemia might be likely to overestimate the present mortality risks, be-expected on the basis of the other studies.' Most of the cause mortality is a different end point from incidence.animal studies do not demonstrate elevated rates of Current estimates predict two to three leukemia deathsneoplasms following in utero exposure.5' Criticisms of for each 10,000 children receiving 1 Gy of low-LETthese studies are based on objections that as-yet-unde- radiation in utero. Solid tumors will account for antermined factors may have affected the results. One additional 2.0-2.8 deaths in the same 10,000 children.postulate is that the mothers of children who devel- The combined increased mortality from childhoodoped cancer may have had complicated pregnancies cancer as a result of in utero exposure is 4.0-5.8 perrequiring X-ray examination, and that the cause for the 10,000 children per Gy. The natural total risk of mor-examination (and not the examination itself) was asso- tality from malignancy through age 10 is one in 1,200.ciated with the increased frequency. One study pointed If an average chest X ray delivers 250 mGy to the fetus,out that a primary reason for prenatal X-ray examina- the probability of that fetus developing a fatal cancertions was to confirm a diagnosis of twins.' The inci- during childhood is one in a million. The NCRPdence of childhood cancers in twins irradiated in utero recommends that fetal exposure be limited to 0.5 mSvwas higher than in twins not irradiated in utero. (0.05 rem) per total gestation period or 0.05 Sv/month.24
The human data have been evaluated by several The increased risk for mortality in children receivingscientific bodies, including the National Academy of the limit of 0.05 Sv/month in a single exposure wouldSciences 7 and the United Nations.5' These organiza- be two to three per 100,000 children.
RELATIVE BIOLOGICAL EFFECTIVENESS OF NEUTRONS
Some doubt exists regarding the RBE of neutrons tion increases with decreasing dose rate, because theand other high-LET radiation for producing biological effectiveness of low-LET gamma or X radiation de-effects at low dose rates and doses. In general, high- creases with decreasing dose rate. At low dose rates,LET radiation is more effective in producing biological the RBE for neutrons may range from 3 to 200 for tumordamage. The biological effects observed in the atomic- induction, from 10 to 45 for genetic end points, andbomb survivors are, for the most part, in agreement from 25 to 200 for lens opacification.2
4 These rangeswith human data from medical exposures. The RBE of are based on laboratory animal studies because noneutrons for leukemia and breast cancer appears to be human populations have been exposed to pure neu-I in persons receiving acute or very rapid exposures.' 22 tron radiation.As previously mentioned, the RBE of high-LET radia-
211

Meditl Conseqiiences of Nuclear Warfare
REGULATORY GUIDES FOR EXPOSURE
Based on the scientific evidence, the United States would result in temporary aspermia. 24' Lower doses ofgovernment (through the Environmental Protection 0.01-0.02 Gy would result in 0.12-0.24 additional can-Agency and the Nuclear Regulatory Commission) has cer deaths in the same battalion, assuming that noset regulatory guides for the occupational exposure of threshold for cancer exists.workers and for the general public.'12 The permissible The NCRP established a penalty table (Table 9-12)concentrations for the occupational exposure to radia- for making health-risk judgments in situations involv-tion workers (Table 9-11) are ten times higher than ex- ing the exchange of nuclear weapons. 4 Based on theposure levels for the general public. It is thought that information for protracted exposures, no medical carethe presumed detrimental effects on health from expo- should be required for low-LET radiation doses up tosures at these limits are negligible. Scientific bodies 1.5 Gy received over 1 week, or 2.0 Gy received over Icontinually reevaluate these risk estimates as addi- month, or 3 Gy received over 4 months. For dailytional information becomes available on radiation exposure of personnel over these same periods, theeffects in human populations. acceptable dose rates would be 0.21, 0.066, and 0.025
Modification of normal protection standards may Gy/day, respectively. Animal studies have shownbe required in civil defense and military operations. that the threshold dose is 0.05 Gy/day on a continuousTwo limits for radiation exposure are recommended basis, above which the stem cells are unable to competeby NCRP for occupational radiation workers and for with cell loss through maturation and depletion."' Therescue personnel during radiation emergencies.-25,2-6 immediate health concern is not cancer induction,The first limit is a one-time whole-body exposure of although increased incidence will occur. Some per-250 mSv, equivalent to a dose of 0.25 Gy of low-LET sons exceeding these doses will require medical care,radiation.2?" This limit was later reduced to 100 mSv(0.1 Gy)..24 Doses of 100-250 mSv are generally asymp-tomatic, do not require medical treatment, and wouldresult in three additional radiation-induced cancer TABLE 9-11mortalities over the lifetime of a battalion-sized groupof 1,000 men.7 The normal cancer incidence for this UNITED STATES NUCLEAR REGULATORYgroup is 250 cancers, with 200 cancer-related mortali- COMMISSION GUIDE FOR PERMISSIBLE
ties. It is unlikely that other somatic effects would be OCCUPATIONAL EXPOSURE TO RADIATION
observed in this group. The earlier acute-exposuredose limit of 250 mSv (25 rem) is also the lower dose Exposure
range estimate for inducing long-term fatigue in 10% Body Part (rem per calendar quarter)
of the individuals. Long-term fatigue occurs withdoses of 250-650 mSv, with 50% incidence after a Whole body 1.25150-mSv radiation dose received in 1 day.") For acute Skin of whole body 7.50exposure in a single day, doses higher than 250 mSv Head and trunk 1.25may result in increased incidence of fatigue that mayimpair performance and alertness. Hands and forearm 18.75
The second health limit for an acute exposure is a Feet and ankles 18.75one-time exposure of 1 Gy of low-LET radiation insituations requiring lifesaving actions.2
1" It also states Bone marrow and spleen 1.25that persons receiving doses greater than 1 Gy should Lens 1.25understand the risks for somatic injury.2" A dose of 1 Gonads 1.25Gy approaches the lower threshold limits for initiatingthe prodromal symptoms of nausea and vomiting andfor hematological depression. At this dose level, Source: Data modified from reference 123
approximately twelve extra cancer deaths would oc-cur in a battalion-sized group of 1,000 men over theirlifetimes. Minor visual opacities may occur in some ofthem. Both limits, 0.25 Gy (250 mSv) and 1 Gy (1 Sv),
212

Long-Terin and low-Lev'l Effects of honizzing Radaton
TABLE 9-12
PENALTY TABLE OF RISK ESTIMATES FOR CONTINUOUS RADIATION EXPOSURE
Accumulated Radiation Dose*(Sv) in any period of
MaximumPersons Requiring Cancer One Week One Month Four MonthsMedical Treatment Deaths**
Total Daily Total Daily Total Daily
None 18.0 1.5 0.21 2.0 0.066 3.0 0.025
Some (57 deaths) 28.5*** 2.5 0.35 3.5 0.12 5.0 0.16
Most (50%7 deaths) 27.0t 4.5 0.64 6.0 0.20 - -
*RBE of neutrons increases with decreasing dose rate
"**Per batallion (1,000 soldiers) over a lifetime:
WZ , -20% leukemia (minimal latency 3-5 yearslRemainder will be solid tumors (minimal latency 10 years)
***Based on calculations of 95% survivors using BEIR III estimatest Based on calculations of 507 survivors using BEIR III estimates
Source: Based on NCRP Penalty Table, reference 54
and some (5% or greater) may die from the hematopoi- increased risk of cancer. The average coffee drinkeretic subsyndrome. may lose 6 days because of the increased risk of blad-
It is sometimes difficult for the public to place der cancer, and the average unmarried male may loseradiation risks in the proper perspective, perhaps 9.6 years from his lifespan. For military personnel, thebecause of their association with nuclear weapons, the average loss of lifespan from a tour of duty in Vietnamdocumented effects from exposure, and the perception was 1.1 years.24'that radiation cannot be seen or controlled. Four- The NCRP has defined a dose of 0.01 mSv per year,tenths of a minute of life are lost for each mile driven in equivalent to 10 Gy or 1 mrad of low-LET radiation, asa car due to the risk of a fatal accident, and the average the negligible individual risk level.244 This implies thatsmoker loses 10 minutes of life for each cigarette almost every dose of radiation carries potential risk. Insmoked. In comparison, an estimated a1verage of 1.5 some cases, the risk is extremely small and difficult tominutes of life are lost for each 0.0015-mSv (1.5-mrem) identify, as illustrated by the comparison to smokingexposure to ionizing radiation."' It is expected that one cigarette. The goal is to keep exposures as low asdoubling the natural background radiation would is reasonably achievable in daily life and in emergencyresult in an average loss of 8 days of life from the situations.
213

Medical Conisequences of Nuchlar Wartare
SUMMARY
The late effects of ionizing radiation can be divided of gamma or low-LET radiation. These disorders willinto three major groups: somatic, genetic, and terato- be mainly autosomal dominant and gender-linkedgenic effects. Somatic damage ranges from fibrosis disorders. If each succeeding generation were to re-and necrosis of individual organs to cataracts, epila- ceive an additional 0.01 Gy of radiation, equilibriumtion, and cancer. would be reached in the gene pool, and an average
Most somatic effects require high-threshold doses increase of 60-1,100 genetic disorders per millionof radiation; cancer is the main health concern after persons would be observed in the population. Thisexposure to low-level radiation. The three most com- would result in a 1.5% increase in the overall incidencemon radiation-induced malignancies are leukemia, of genetic disorders. The normal incidence of geneticbreast cancer, and thyroid cancer. The latency periods disorders in the population is one in ten.for the detection of cancer after radiation exposure The third category of late radiation damage is therange from 2 years for leukemia to 30-40 years for teratogenic effects. The primary somatic effects seen insome solid tumors. humans exposed in utero are microcephaly, mental
Mathematical models predicting cancer risks based retardation, and growth retardation. These effectson observations from high radiation exposures imply have been observed with an increased incidence in thethat 120-180 additional cancer deaths will occur for atomic-bomb survivors exposed in utero to doses ofevery million persons receiving I cGy of radiation. less than 0.10 Gy, although a neutron component mayThis estimate range includes the incidence of all can- have enhanced the radiation effectiveness. In general,cers and presumes that no thresholds for induction thresholds exist for the induction of birth defects by ra-exist. Some evidence indicates that thresholds for diation, and effects below 0.10 Gy are negligible. Theradiation-induced cancer do exist, ranging from 0.01 normal incidence of birth defects is one in ten liveGy for breast cancer to 0.2 Gy for leukemia. births. One concern for low-level exposure to ionizing
Genetic effects are the second category of low-level radiation in utero is the increased incidence of cancer inor late effects of radiation. It is estimated that 5-65 childhood. An estimated twenty-five additional can-additional genetic disorders will occur in the next cer deaths are predicted for every million childrengeneration for every million persons receiving 0.01 Gy receiving I cGy of radiation in utero.
REFERENCES
1. Bacg, Z. M., and Alexander, P. 1966. Fundamentals of radiobiology. 2d ed., 45-62, 122-156. Oxford: Pergamon Press.
2. Snyder, S. L. 1977. Radiation-induced alterations in serum and splenic lysosomal hydrolases of the rat. Radiat. Res. 69:306-316.
3. Donlon, M. A., and Walden, T. L., Jr. 1988. The release of biological mediators in response to acute radiation injury.Comments on Toxicology 2: 205-216.
4. Young, R. W. 1987. Acute radiation syndrome. In Military Radiobiology, edited by J. J. Conklin and R. I. Walker, 165-190. New York: Academic Press.
5. Glasstone, S. 1964. The effects of nuclear weapons. Rev. ed. Washington, DC: United States Atomic Energy Commis-sion.
6. Upton, A. C. 1987. Cancer induction and non-stochastic effects. Br. 1. Radiol. 60:1-16.
7. Committee on the Biological Effects of Ionizing Radiation. 1980. The effects on populations of exposure to low levels ofionizing radiation. Washington, DC: National Academy Press.
214
Lon,-Terin and Low-Level Effects of lonizing Radiation
8. United Nations Scientific Committee on the Effects of Atomic Radiation. 1982. Ioniz:ing radiation: Sources and bilogicaleffects. New York: United Nations, New York.
9. Mole, R. H. 1987. Irradiation of the embryo and fetus. Br. 1. Radiol. 60: 17-31.
10. Nuclear Regulatory Commission. 1985. Health effects model for nuclear power plant accident cov.e, 1i,1cs a,,ahis [U.S.Nuclear Regulatory Commission Contractor Report NUREG/CR-4214 (Sandia No. SAND85-7185)]. Washing-ton, DC: U.S. Government Printing Office.
11. National Institutes of Health. 1985. Report of the National Institutes of Health Ad Hoc Working Group to Develop Radioepi-deniological Tables [NIH Publication No. 85-27481. Washington, DC: Department of Health and HumanServices.
12. Upton, A. C. 1982. The biological effects of low-level ionizing radiation. Sci. Am. 246: 41-49.
13. Webster, E. W. 1981. On the question of cancer induction by small X-ra,. :,ses. Ant. 1. Radiol. 137: 647-666.
14. Auxier, J. A., and Dickson, H. W. 1983. Guest editorial: Concern over recent use of the ALARA philosophy. HealthPhys. 44: 595-600.
15. National Council on Radiation Protection and Measurements. 1977. Radiation exposure from consumer products andmiscellaneous sources INCRP Report No. 561. Washington, DC: National Council on Radiation Protection andMeasurements.
16. Harley, J. H. 1981. Radioactive emissions and radon. Bull. NY Acad. Med. 57: 883-896.
17. Upton, A. C.; Christenberry, K. W.; Melville, G. S.; Furth, J.; and Hurst, G. S. 1956. The relative biological effective-ness of neutrons, X-rays, and gamma rays for the production of lens opacities: Observation,; on mice, rats,guinea pigs, and rabbits. Radiology 67: 686-696.
18. Burch, P. R., and Chesters, M. S. 1985. Natural and radiation-induced cataracts in man and mouse, and naturalmacular degeneration in man: Proposed mechanisms. Phys. Med. Biol. 30: 879-896.
19. Toda, S.; Hosokawa, Y.; Choshi, K.; Nakano, A.; and Takahashi, M. 1964. Occular changes in A-bomb survivorsexposed during infancy. Folia Ophthahnol. lap. 15: 96-103.
20. Hirose, K. 1956. Occular lesions development after exposure to atomic bomb in Nagasaki city. In Research in theeffects and influences of the nuclear bomb test explosions, compiled by the Committee for Compilation of Report onResearch in the Effects of Radioactivity, 1655. Ueno, Japan: Japan Society for the Promotion of Science.
21. Messerschmidt, 0. 1979. Medical procedures in a nuclear disaster: Pathogenesis and therapy, for nuclear-weapons injuries,187-190. Munich: Verlag Karl Theimig.
22. Otake, M., and Schull, W. J. 1982. The relationship of gamma and neutron radiation to posterior lenticular opacitiesamong atomic bomb survivors in Hiroshima and Nagasaki. Radiat. Res. 92: 574-595.
23. Ham, W. T., Jr. 1953. Radiation cataract. Arch. Oplithahnol. 50: 618-643.
24. International Commission on Radiological Protection. 1984. Non-stochastic effects of ionizing radiation. In vol. 14,Ann. ICRP [ICRP Publication 411. Oxford: Pergamon Press.
25. Ash, P. 1980. The influence of radiation on fertility in man. Br. 1. Radiol. 53: 271-278.
26. Rowley, M. J.; Leach, D. R.; Warner, G. A.; and Heller. C. G. 1974. Effect of graded doses of ionizing radiation on thehuman testis. Radiat. Res. 59: 665-678.
27. Sandeman, T. F. 1966. The effects of X-irradiation on male human fertility. Br. 1. Radiol. 39: 901-907.
28. Clifton, D. K., and Bremmer, W. J. 1983. The effect of testicular X-irradiation on spermatogenesis in man: A compari-son with the mouse. J. Androl. 4: 387-392.
215

Medical Consequpences of Nuclear Warfare
29. Carr, B. R., and Wilson, j. D. 1983. Disorders of the ovary and female reproductive tract. In Harrison's Principles ofInternal Medicine. 10th ed., edited by P. G. Petersdorf, R. D. Adams, E. Braunwald, K. J. Isselbacher, J. B. Martin,and J. D. Wilson, 700-720. New York: McGraw-Hill.
30. Kaplan, 1. 1. 1959. Genetic effects in children and grandchildren of women treated for infertility and sterility byRoentgen therapy. Report of a study of thirty-three years. Radiology 72: 518-521.
31. Roentgen, W. C. 1895. Uber eine neue Art von Strahlen. Sitzunsb. d. phyls.-ined. Gesellsch. zu Wurzb. : 132-141.
32. Malkinson, F. D., and Keane, J. T. 1981. Radiobiology of the skin: Review of some effects on epidermis and hair. I.Invest. Dermatol. 77:133-138.
33. Marcuse, W. 1896. Nactrag zu dem Fall von Dermatitis und Alopecie nach Durchleuchtungsversuchen mitRoentgenstrahlen. Delt. red. Wochschr. 22: 681-686.
34. Freund, L. 1897. Ein mit Roentgen-Strahlen behandelter Fall von Naevus pigmentosus piliferus. Wien. Med.Wochschr. 47: 428-434.
35. Hall-Edwards, J. 1904. On chronic X-ray dermatitis. Br. I. Med. 2: 993-995.
36. Harris, L. H. 1Q06. Treatment of chronic X-ray dermatitis. Br. ]. Med. 2: 695.
37. Drury, H. C. 1896. Dermatitis caused by Roentgen X-rays. Br. ]. Med. 2:1377.
38. Mutscheller, A. 1925. Physical standards of protection against Roentgen-ray dangers. Am. J. of Roentgenol. andRaditint Tlier. 13: 65-70.
39. Cronkite, E. P.; Bond, V. P.; Conard, R. A.; Durham, C. L.; Farr, R. S.; Schulman, N. R.; Sondhaus, C. A.; Cohn, S. H.;Hechter, H. H.; Sharp, R.; Alpen, E. L.; Browning, L. E.; Wood, D. A.; Rinehart, R. W.; Cong, J. K.; Robertson, J.S.; and Milne, W.L. 1956. Soine effects of ioni:ing radiation ol huinan beings: A report oln the Marshallese.andAmericans accidentally exposed to radiation fallout and at discussion of radiation injury in the hunlan being [U.S. AtomicEnergy Commission Publication AEC-TID 53851. Washington, DC: U.S. Government Printing Office.
40. Arlett, C., and Harcourt, S. 1980. Survey of radiosensitivity in a variety of human cell strains. Cancer Res. 40: 926-932.
41. Charles, M. W. 1986. Recent developments in the dosimetry of superficial tissues, 1.1. Br. 1. Radiol. (Suppl.) 19:1-7.
42. Archambeau, J. 0. 1987. Relative sensitivity of the integumentary system: Dose response of the epidermal, mi-crovasculature, and dermal populations. Adv. Radiat. Biol. 12:147-204.
43. Ernst, K., and Ehring, F. 1986. Unavoidable sequelae and accidental damage to the skin following irradiation. Br. 1.Radiol. (Suppl.) 19:15-18.
44. Dutreix, J. 1986. Human skin: Early and late reactions in relation to dose and its time distribution, 11.1. Br. !. Radiol.(Suppl.) 19: 22-27.
45. Malkinson, F. D., and Wiskemann. A. 1987. Some principles of radiobiology and the effects of ionizing radiation onthe skin. In Dermatology in General Medicine. 3d ed., 1431-1440. New York: McGraw-Hill.
46. Trott, K.-R. 1986. What can the experience of radiation therapy teach us about accidents? Br. ]. Radio)L. (Suppl.) 19: 28-30.
47. Kalz, F. 1941. Theoretical considerations and clinical use of Grenz rays in dermatology. Arch. Dermat. Syph. 43: 447-
472.
48. Stieve, F.-E. 1986. Experiences with accidents and consequences for treatment. Br. J. Radiol. (Suppl.) 19:18-21.
49. Moritz, A. R., and Henriques, F. W., Jr. 1952. Effect of beta rays on the skin as a function of the energy, intensity andduration of radiation. II. Animal experiments. Lab. Invest. 1: 167-185.
216

Long-Term and Low-Level Eftects of Ionizing Radiation
"10. Conard, R. A. 1484. Late radiation effects in Marshall Islanders exposed to fallout 28 years ago. In Radiation Carcino-gen'sis: Epidetniologi! and Biological Significance, edited by J. D. Boice and ]. F. Fraumeni, 57-71. New York:Raven Press.
51. United Nations Scientific Committee on the Effects of Atomic Radiation. 1977. Soiirces and effects of ioni:ing radiation.New York: United Nations.
52. Snvder, D. S. 1976. Effect of topical indomethacin on UVR-induced redness and PGE levels in sunburned guinea pigskin. Prostaglandlits II: 631-643.
53. Lushbaugh, C C.; Fry, S. A.; Ricks, R. C.; Hubner, K. F.; and Burr, W. W. 1986. Historical update of past and recentskin damage radiation accidents. Br. 1. Radiol. (Suppl.) 19: 7-12.
54. National Council on Radiation Protection and Measurements. 1974. Radiological factors affecting decision-making in anuclear attack INCRP Report 421. Washington, DC: National Council on Radiation Protection and Measure-ments.
55. Potten, C. S. 1986. Biological dosimetry of local radiation accidents of skin: Possible cytological and biochemicalmethods. Br. 1. Radiol. (Suppl.) 19- 82-85.
56. Ruben, P., and Cassaret, G. W. 1968. Clinical radiation pathology. Philadelphia: Saunders.
57. Daniel, J. 1896. The X-ravs. Science 3: 562-563.
58. Brown, P. 1936. American niartzrs to science through the Roentgen rays, 6-13, 32-42. Springfield, IL: Charles C. Thomas.
59. Upton, A. C. 1964. Cancer research 1964: Thoughts on the contributions of radiobiology. Cancer Res. 24: 1860-1868.
60. Grubbe, E. H. 1902. X-ravs in the treatment of cancer and other malignant diseases. Medical Record 62: 692-695.
61. Despeignes, V. 1896. Nouvelle observation de cancer traite par les rayons de Roentgen. Lyon Med. 83: 550.
62. Porter, C. A., and White, C. J. 1907. Multiple carcinomata following chronic X-ray dermatitis. Anti. Surg. 46: 649-671.
63. Furth, J. A., and Lorenz, E. 1954. Carcinogenesis by ionizing radiations. In vol. 1, Radiation Biology, edited by A.Hollaender, 145-201. New York: McGraw-Hill.
64. Marie, P.; Clunet, J.; and Raoulet-Lapointe, G. 1910. Contribution a l'etude du developement des tumeurs malignessur les ulceres de roentgen. Bill. de I'Assoc. Franc. pour I'Etude du Cancer 3: 404-426.
65. Weinstein, I. B.; Gattoni-Celli, S.; Kirschmeir, P.; Lambert, M.; Hsiao, W.; Backer, J.; and Jeffrey, A. 1984. Multistagecarcinogenesis involves multiple genes and multiple mechanisms. 1. Cell. Physiol. (Suppl.) 3:127-137.
66. Chaganti, R. S. K., and Jhanwar, S. C. 1983. Oncogenes, chromosome mutation, and the development of neoplasia.In Chromosome Mutation and Neoplasia, 397-412. New York: Alan R. Liss, Inc.
67. Temin, H. M. 1984. Do we understand the genetic mechanisms of oncogenesis. 1. Cell. Physiol. (Suppl.) 3: 1-il.
68. Ford, C. E., and Clarke, C. M. 1963. Cytogenetic evidence of clonal proliferation in primary reticular neoplasms.Can. Cancer Conf. 5:129-146.
69. Chaganti, R. S. K. The significance of chromosome change to neoplastic development. In reference 66, 359-396.
70. Fialkow, P. J. 1977. Clonal origin and stem cell evolution of human tumors. In Genetics of Human Cancer, edited by J.J. Mulvihill, R. W. Miller, and J. F. Fraumeni, Jr., 439-453. New York: Raven Press.
71. Fialkow, P. J.; Gartler, S. M.; and Yoshida, A. 1967. Clonal origin of chronic myelocytic leukemia in man. Proc. Nati.Acad. Sci. USA 58: 1468-1471.
217

Medical Co0is1qcILncT'; of Nuclear VVar farc
72. National Toxicology Program. 1985. Fourth annual report on carcinogens. Summary 19835 1NTP 854)02). Washington,DC: Department of Health and Human Services.
73. Doll, R., and Peto, A. 1981. Avoidable risks of cancer in the U.S. INCI 66: 1 1t-1308.
74. Waterhouse, J.; Muir C.; Correa, P.; and Powell, J., eds. 1976. Cancer incidence in fivc continents IIARC Sci Publications#151, vol. 3, 1-584. Lyon, France: International Agency for Research on Cancer.
75. Lavton, J.; Warzvnski, M.; and Idiris, A. 1986. Acquired immunodeficiency syndrome in the United States: Aselected review. Crit. Care Med. 14: 819-827.
7t). Chang, E. H.; Pirollo, K. F.; Zou, Z. Q.; Cheung, H.-Y.; Lawler, E. L.; Garner, R.; White, E.; Bernstein, W. B.; Fraumeni,J. W., Jr.; and Blattner, W. A. 1987. Oncogenes in radioresistant, noncancerous skin fibroblasts from a cancer-prone family. Science 237: 1036-1038.
77. Croce, C. M. 1987. Role of chromosome translocations in human neoplasia. Cell 49: 155-156.
78. Marshall, C.J. 1987. Oncogenes and growth control: 1987. Cell 49: 723-725.
79. Weinberg, R. A. 1985. The action of oncogenes in the cytoplasm and nucleus. Science 230: 770-776.
80. Bister, K., and Jansen, H. W. 1986. Oncogenes in retroviruses and cells: Biochemistry and molecular genetics.Advances in Cancer Res. 47: 99-188.
81. Antoniodeso H. N.; Pantazis, P.; and Owen, A. J. 1987. Human platelet-derived factor and the sis-PDGF-2 gene InOncogenes, Genes, and Growth Factors, edited by G. Guroff, 1-40. New York: John Wiley and Sons.
82. Klein, G., and Klein, E. 1987. Myc/ig juxtaposition by chromosomal translocations: Some new insights, puzzles, andparadoxes. In Oncogenes and Growth Factors, edited by R. A. Bradshaw and S. Prentis, 33-46. New York:Elsevier Science Publishers.
83. Gilman, A. G. 1984. G proteins and dual control of adenylate cyclase. Cell 36: 577-579.
84. Forrester, K.; Almoguera, C.; Han, K.; Grizzle, W. E.; and Perucho, M. 1987. Detection )f high incidence of K-rasoncogenes during human colon tumorigenesis. Nature 327: 298-303.
85. Jaffe, D. R., and Bowden, G. T. 1987. Enhanced malignant progression of mouse skin tumors by ionizing radiationand activation of oncogenes in radiation induced tumors. In vol. 1, Proceedings of 8th International Congress ofRadiation Research, edited by E. M. Fielden, J. F. Fowler, J. H. Hendry, and D. Scott, 188. London: Taylor andFrancis.
86. Sawev, M. J.; Burns, F. J.; and Garte, S. J. Activation of multiple oncogenes in radiation-induced rat skin carcinomas.In reference 85, 188.
87. Guerrero, I.; Villasante, A.; Corces, V.; and Pellicer, A. 1984. Activation of a c-k-ras oncogene by somatic mutation in
mouse lymphomas induced by gamma radiation. Science 225:1159-1162.
88. Kudson, A. G., Jr. 1985. Hereditary cancer, oncogenes, and antioncogenes. Cancer Res. 45: 1437-1443.
89. Sager, A. 1986. Genetic suppression of tumor formation: A new frontier in cancer research. Cancer Res. 46:1573-1580.
90. Harris, H. 1979. Some thoughts about genetics, differentiation, and malignancy. Somatic Cell Mol. Genet. 5: 923-930.
91. Kasid, U.; Pfeifer, A.; Weischelbaum, R. R.; Dritschilo, A.; and Mark, G. E. 1987. The raf oncogene is associated witha radiation-resistant human laryngeal cancer. Science 237:1039-1041.
92. Dalla-Favera, R.; Bregni, M.; Erikson, J.; Patterson, D.; Gallo, R. C.; and Croce, C. M. 1982. Human c-myc oncogene islocated on the region of chromosome 8 that is translocated in Burkitt's lymphoma cells. Proc. Nat!. Acad. Sci.USA 79: 7824-7827.
218

L.ong,- Terrn and Low-Level mtcits ot lonlziZ IjRdiation
93. Prakash, K.; McBride, 0. W.; Swan, D. C.; Devare, S. G.; Tronick, S. R.; and Aaronson, S. A. 1982. Molecular cloningand chromosomal mapping of a human locus related to the transtorming gene of Molonev murine sarcomavirus. Proc. Natl. Acad. SCi. USA 79: 5210-5214.
44. Nowell, P. C., and [lungerford, D. A. 1940). A minute chromosome in chronic granulocytic leukemia. Science 132:1497.
95. de Klein, A.; Geurts van Kessel, D. A.; Grosveld, G.; Bartrum, C. R.; Hagemeirer, A.; Bootsma, D.; Spurr, N. K.,Heisterkamp, N.; Groffen, J.; and Stephenson, J. R. 1982. A cellular oncogene is translocated to the Philadel-phia chromosome in chronic mvelocvtic leukemia. Nature 300: 765-767.
9%. Goffen, J.; Stephenson, J. K.; Heisterkamp, N.; de Klein, A.; Bartrum, C. R.; and Grosveld, G. 1984. Philadelphiachromosomal breakpoints are clustered within a limited region, bcr, on chromosome 22. Cell 3b: 93-99.
97. Konopka, J. B.; Watanabe, S. M.; and White, 0. N. 1984. An alteration of the human c-abl protein in K562 leukemiacells unmasks associated tvrosine kinase activity. Cell 37: 1035-1042.
98. Bishop, J. M. 1987. The molecular genetics of cancer. Science 235: 305-311.
99N. Cairns, J. 1975. Mutational selection and the natural history of cancer. Nature 255: 197-200.
100. Mossman, K. V. 1984. Ionizing radiation and cancer. Cancer Invest. 2(4): 301-310.
101. Upton, A.C. 1983. Environmental standards for ionizing radiation: Theoretical basis for dose-response curves.Environ. Health Perspect. 52: 31-39.
102. Land, C. E. 1980. Estimating cancer risks from low doses of ionizing radiation. Science 209: 1197-1203.
103. Jablon, S. Epidemiologic perspectives in radiation carcinogenesis. In reference 50, 1-8.
104. Robinette, C. D.; Jablon, S.; and Preston, T. L. 1985. Mortality of niclear weapons test participants. Washington, DC:National Research Council.
105. Preston, D. L.; Kato, H.; Kopeckv, K. J.; and Fujita, S. 1987. Studies of mortality of A-bomb survivors. 8. Cancermortality, 1950-1982. Radhit. Res. 111: 151-178.
106. Neel, J. V.; Satoh, C.; Hamilton, H. B.; Otake, M.; Goriki, K.; Kageoka, T.; Fujita, M.; Neriishi, S.; and Asakawa, J.1980. Search for mutations affecting protein structure in children of atomic bomb survivors: Preliminaryreport. Proc. Naitl. Acad. Sci. USA 77: 4221-4225.
107. Auxier, J. A. 1977. Ichiban, radiation dosimetry' ifor the survivors of the blombings of Hiroshima and Nagasaki [ERDA CriticalReview Series, TID-270801. Sprirvield, VA: National Technical Information Service.
108. U.S.-Japan Joint Reassessment of Atomic Bomb Radiation Dosimetry in Hiroshima and Nagasaki. 1987. In vol. 1,Final report [DS86, Dosimetry System 19861, edited by W. C. Roesch. Hiroshima: Radiation Effects ResearchFoundation.
109. Court Brown, W. M., and Doll, R 1965. Mortality from cancer and other causes after radiotherapy for ankylosingspondilitis. Br. 1. Med. 2: 1327-1332.
110. Smith, P. G. Late effects of X-ray treatment of ankylosing spondilitis. In reference 50, 107-118.
111. Smith, P. G., and Doll, R. 1982. Mortality among patients with ankylosing spondilitis after a single treatment coursewith X-ravs. Br. Med. 1. 284: 449-460.
112. Shore, R. E.; Albert, R. E.; and Pasternack, B. S. 1976. Follow-up study of patients treated by X-ray epilation for tineacapitis. Arch. Environ. Health 31: 17-28.
113. Shore, R. E.; Hemplemann, L. H.; Kowaluk, E.; Mansur, P. S.; Pasternack, B. S.; Albert, R. E.; and Haughie, G. E.1977. Breast neoplasms in women treated with X-rays for acute postpartum mastitis. JNCI 59: 813-822.
219

Medical Consequences of Nuclear Warfire
114. Boice, J. D., and Monson, R. R. 1977. Breast cancer in women after repeated fluoroscopic examinations of the chest.INCI 59: 823-832.
115. Boice, J. D., Jr.; Rosenstein, M.; and Trout, E. D. 1978. Estimation of breast doses and breast cancer risks associatedwith repeated fluoroscopic chest examinations of women with tuberculosis. Radiat. Res. 73: 373-390.
.116. Waxweiler, R. J.; Roscoe, R. J.; Archer, V. E.; Thun, M. J.; Wagoner, J. K.; and Lundin, F. E., Jr. 1981. Mortalityfollow-up through 1977 of the white underground uranium miners cohort examined by the United StatesPublic Health Service. In Radiation Hazards in Mining, 823-830. New York: Society of Mining Engineers.
117. Kunz, E.; Sevc, J.; Placek, V.; and Horacek, J. 1979. Lung cancer in man in relation to different time distribution ofradiation exposure. Health Phys. 36: 699-706.
118. lchimaru, M.; lshimaru, I.; Belsky, J. L.; Tomivasu, T.; Sadamori, N.; Hoshino, T.; Tomonaga, M.; Shimizu, N.; andOkada, H. 1976. Incidence of leukemia in atomic bonib survivors, Hiroshima and Nagasaki 1950-71, bhy radiation dose,
years after exposure, age, and type of leukemia [Technical Report RERF 10-76]. Hiroshima: Radiation EffectsResearch Foundation.
119. Clark, S. S.; McLaughlin, J.; Crist, W. M.; Champion, R.; and White, 0. N. 1987. Unique forms of the abl tyrosinekinase distinguish Phi-positive CML from Phi-positive ALL. Science 235: 85-88.
120. Kato, H., and Schull, W. J. 1982. Studies of the mortality of A-bomb survivors. Report 7. Mortality, 1950-1978: PartI. Cancer mortality. Radiat. Res. 90: 395-432.
121. Smith, P. G., and Doll, R. 1976. Late effects of X irradiation in patients treated for metropathia haemorrhagica. Br. J.Radial. 49: 224-232.
122. Straume, T., and Dobson, R. L. 1981. Implications of new Hiroshima and Nagasaki dose estimates: Cancer risksand neutron RBE. Health Phys. 41: 066-671.
123. Nuclear Regulatory Commission. 1983. Radiation dose standards for individuals in restricted areas [Code of FederalRegulations. Energy. Title 10, Part 20.101], 235. Washington, DC: Office of the Federal Register.
124. Center for Disease Control. 1979. Leukemia among persons present at an atmospheric nuclear test (SMOKY).MMWR 28: 361-362.
125. Caldwell, G. G.; Kelley, D. B.; and Heath, C. W. 1980. Leukemia among participants in military maneuvers at anuclear bomb test. A preliminary report. JAMA 244:1575-1578.
126. Caldwell, G. G.; Kelley, D. B.; Zack, M.; Falk, H.; and Heath, C. 1983. Mortality and cancer frequency amongmilitary nuclear test (SMOKY) participants, 1957 through 1979. JAMA 250: 620-624.
127. Ron, E., and Modan, B. 1980. Benign and malignant thyroid neoplasms after childhood irradiation for tinea capitis.INCI 65: 7-11.
128. Hemplemann, L. H.; Hall, W. J.; Phillips, M.; Cooper, R. A.; and Ames, W. R. 1975. Neoplasms in persons treatedwith X-rays in infancy: Fourth survey in 20 years. INC[ 55: 519-530.
129. Prentice, R. L.; Kato, H.; Yoshimoto, K.; and Mason, M. 1982. Radiation exposures and thyroid cancer incidenceamong Hiroshima and Nagasaki residents. In Third Symnposiumn on Epidemiology and Cancer Registries in thePacific Basin [National Cancer Institute Monograph 62], 207-212. Washington, DC: Government PrintingOffice.
130. Wood, J. W.; Tamagaki, H.; Neriishi, S.; Sato, T.; Sheldon, W. F.; Archer, P. G.; Hamilton, H1. B.; and Johnson, K. G.1969. Thyroid carcinoma in atomic bomb survivors, Hiroshima and Nagasaki. Am. J. E,,idemiol. 89: 4-14.
131. McTierman, M. M.; Weiss, N. S.; and Daling, J. R. 1984. Incidence of thyroid cancer in women in relation to previ-ous exposure to radiation therapy and history of thyroid disease. INCI 73: 575-581.
220

Long-Ternt and Low-Level Effects of Ionizing Radiation
132. Shore, R. E.; Woodard, E.; Hildreth, N.; Dvoretsky, P.; Hemplemann, L.; and Pasternack, B. 1985. Thyroid tumorsfollowing thymus irradiation. INCI 74:1117-1184.
133. Doniach, I. 1974. Carcinogenic effect of 100, 250, and 500 rad X-rays on the rat thyroid gland. Br. 1. Cancer 30: 487-495.
134. Conard, R. A.; Paglia, D. E.; Narsen, P. R.; Sutlow, W. W.; Dobyns, B. M.; Robins, J.; Krotsky, W. A.; Field, J. B.; Rail,J. E.; and Wolff, J. 1980. Rev'iew' of medical findings in a Marshallesc tpopulation twenty-six years after accideentalexposure to radioactive fallout jBrookhaven National Laboratory Report BNL 512611. Springfield, VA: NationalTechnical Information Service.
135. Ron, E., and Modan, B. Thyroid and other neoplasms following childhood scalp irradiation. In reference 50, 139-
151.
136. Modan, B.; Ron, E.; and Werner, A. 1977. Thyroid cancer following scalp irradiation. Radiology 123: 741-744.
137. National Council on Radiation Protection and Measurements. 1977. Protection of the thy*roid gland in the event ofreleases of radioiodi'e INCRP Report 551. Washington, DC: National Council on Radiation Protection andMeasurement.
138. Howe, G. R. Epidemiology of radiogenic breast cancer. In reference 50, 119-129.
139. Seidman, H., and Mushinski, M. H. 1983. Breast cancer: Incidence, mortality, survival, and prognosis. In BreastCarcinoma. Current Diagnosis and Treatment, edited by S. A. Feig and R. McLelland, 9-46. New York: MassonPublishing USA, Inc.
140. Tokunaga, M.; Land, C. E.; Yamamoto, T.; Masahide, A.; Tokuoka, S.; Ezaki, H.; Nishimori, L; and Fujikura, T.Breast cancer among atomic bomb survivors. In reference 50, 45-55.
141. Orine, S. K.; Chambers, R. W.; and Johnson, R. H. 1967. Postirradiation carcinoma of the male breast bilaterally.JAMA 201: 707.
142. Boice, J. D., Jr.; Land, C. E.; Shore, R. E.; Norman, J. E.; and Tokunaga, M. 1979. Risk of breast cancer following low-dose exposure. Radiology 131: 589-597.
143. Tokunaga, M.; Land, C. E.; Yamamoto, T.; Asano, M.; Tokuoka, S.; Ezaki, H.; and Nishimori, 1. 1982. Breast cancerin Japanese A-bomb survivors. Lancet 2: 924.
144. Tokunaga, M.; Norman, N. E., Jr.; Asano, M.; Tokuoka, S.; Ezaki, H.; Nishimori, I.; and Tsuju, Y. 1979. Malignantbreast tumors among atomic bomb survivors, Hiroshima and Nagasaki, 1950-1974. INC1 62: 13471359.
145. Hildreth, N. G.; Shore, R. E.; and Hemplemann, L. H. 1983. Risk of breast cancer among women receiving radiationtreatment in infancy for thymic enlargement. Lancet 2: 273.
146. Land, C. E.; Boice, J. D., Jr.; Shore, R. E.; Norman, J. E.; and Tokunaga, M. 1980. Breast cancer risks from low-doseexposures to ionizing radiation: Results of parallel analysis of three exposed populations of women. INC1 65:353-376.
147. Davis, F. G.; Boice, J. D., Jr.; Kelsey, J. L.; and Monson, R. R. 1987. Cancer mortality after multiple fluoroscopicexaminations of the chest. INCI 78: 645-652.
148. Rowland, R. E., and Lucas, H. F. Radium-dial workers. In reference 50,231-240.
149. Adams, E. E., and Brues, A. M. 1980. Breast canier in female radium dial workers first employed before 1930. 1.Occup. Med. 22: 583-587.
150. Modan, B.; Baidatz, D.; Mart, H.; Steintz, R.; and Levin, S. 1969. Radiation-induced intracranial meningiomas. Clin.Radiol. 20: 90-94.
221

Medical Consequences of Nuclear Warfare
151. Shore, R. E.; Albert, R. E.; and Pasternack, B. S. 1976. Followup study of patientb treated by x-ray epilation for tineacapitis. Resurvey of post-treatment illness and mortality experience. Arch. Environ. Health 31: 17-28.
152. Asano, M.; Kato, H.; Yoshimoto, K.; Seyama, S.; Itakura, H.; Hamada, T.; and lijima, S. 1982. Primary liver carci-noma and liver cirrhosis in atomic bomb survivors, Hiroshima and Nagasaki, 1961-75, with special reference tohepatitis B surface antigen. JNCI 69: 1221-1227.
153. Lewin, K., and Millis, R. R. 1973. Radiation hepatitis: A morphologic study with emphasis on the late changes.Arch. Pathol. 96: 21-26.
154. Prentice, R. L.; Yoshimoto, Y.; and Mason, W. W. 1983. Relationship of cigarette smoking and radiation exposure tocancer mortality in Hiroshima and Nagasaki. JNCI 70: 611-622.
155. Little, J. B.; Radford, E. P.; McCombs, H. L.; and Hunt, V. R. 1965. Distribution of polonium-210 in pulmonarytissues of cigarette smokers. N. Eng. ]. Med. 273:1343-1351.
156. Winters, T. H., and Di Franza, J. R. 1982. Radioactivity in cigarette smoke. N. Eng. 1. Med. 306: 364-365.
157. Radford, E. P., and Hunt, V. R. 1964. Polonium-210: A volatile radioactive element in cigarettes. Science 143: 247-249.
158. Little, J. B.; McGandy, R. B.; and Kennedy, A. R. 1978. Interactions between polonium-210, alpha-radiation,benzo(a)pyrene, and 0.9%: NaCI solution instillations in the induction of experimental lung cancer. Cancer Res.38: 1929-1935.
159. Wynder, E. L., and Hoffman, D. 1979. Tobacco and health: A societal challenge. N. Eng. 1. Med. 300: 894-903.
160. Van Dyk, J.; Keane, T. J.; Kan, S.; Rider, W. D.; and Fryer, C. J. H. 1981. Radiation pneumonitis following largesingle dose irradiation: A re-evaluation based on absolute dose to lung. Int. ]. Radiat. Oncol. Biol. Phys. 7: 461-467.
161. Gross, N.J. 1977. Pulmonary effects of radiation therapy. Ann. Intern. Med. 86: 81-92.
162. Tokuoka, S.; Kawai, K.; Shimizu, Y.; Inai, K.; Ohe, K.; Fujikura, T.; and Kato, H. 1987. Malignant and benign ovarianneoplasms among bomb survivors, Hiroshima and Nagasaki, 1950-80. ]NCI 79:47-57.
163. Muller, H. J. 1927. Artificial transmutation of the gene. Science 66: 84-87.
164. Muller, H. J. The nature of the genetic effects produced by radiation. In reference 63, 351-474.
165. Denniston, C. 1982. Low level radiation and genetic risk estimation in man. Annu. Rev'. Genet. 16: 329-355.
166. Russell, W. L., and Kelly, E. M. 1982. Mutational frequencies in male mice and the estimation of genetic hazards ofradiation in men. Proc. Nail. Acad. Sci. USA 79: 542-544.
167. Selby, P. B., and Selby, P. R. 1977. Gamma-ray-induced dominant mutations that cause skeletal abnormalities in
mice. Mutat. Res. 43: 907-975.
168. Searle, T. 1987. Radiation-the genetic risk. Trends Genet. 3: 152-157.
169. Abrahamson, S. 1979. Genetic effects of low level radiation. In Proceedings of a Conference: Known Effects of Low-LevelRadiation Exposure. Health Implications of the TMI Accident [NIH Publication 80-2087], 46-60. Washington, DC:U.S. Department of Health, Education, and Welfare.
170. Popescu, H. L.; Pilat, L.; Hilt, M.; and Lancranjan, I. 1972. Evolution of biological changes noticed in three cases ofaccidental mild gamma irradiation. ]. Occup. Med. 14: 317-320.
171. Dolphin, G. W.; Bolton, D.; Humphreys, D. L. 0.; Speight, D. L.; and Stradling, G. N. 1970. Biological dosimetry andphysical dosimetry after a radiation accident. Nature 227: 165.
222

Long-Term and Louw-l~ewl Effects of Ionizing Radiation
172. Randolph, M. L., and Brewen, J. G. 1980. Estimation of whole-body doses by means of chromosome aberrationsobserved in survivors of the Hiroshima A-bomb. Radiat. Res. 82: 393-407.
173. Cohen, B. L. 1984. Perspective on genetic effects of radiation. Health Phys. 46: 1113-1121.
174. Strauss, B. S. 1985. Cellular aspects of DNA repair. Adz,. Cancer Res. 45: 45-105.
175. Ward, J. F. 1975. Molecular mechanisms of radiation-induced damage to nucleic acids. Adt. Radiat. Biol. 5:181-239.
176. Hook, E. B. 1981. Rates of chromosome abnormalities in different maternal ages. Obstet. Gynecol. 58: 282-285.
177. Freidman, j. M. 1981. Genetic disease in the offspring of older fathers. Obstet. Gvnecol. 57: 745-749.
178. National Council on Radiation Protection and Measurements. 1979. Tritium and other radionuclide labeled organicconipounds incorporated in genetic material [NCRP Report 631. Washington, DC: National Council on RadiationProtection and Measurements.
179. National Council on Radiation Protection and Measurements. 1987. Genetic effects from internally deposited radionu-clides INCRD Report 891. Washington, DC: National Council on Radiation Protection and Measurement.
180. Jablon, S., and Kato, H. 1971. Sex ratio in offspring survivors exposed prenatally to the atomic bombs in Hiroshimaand Hagasaki. Am. 1. Epidemiol. 93: 253-258.
181. Sigler, A. T.; Lilienfield, A. M.; Cohen, B. H.; and Westlake, J. E. 1965. Radiation exposure in parents of childrenwith mongolism (Down's syndrome). Bull. Hopkins Hosp. 117: 374-399.
182. Uchida, 1. A., and Curtis, E. J. 1961. A possible association between maternal irradiation and mongolism. Lancet 2:845-850.
183. Uchida, I. A.; Holunga, R.; and Lawler, C. 1968. Maternal radiation and chromosomal aberrations. Lancet 2: 1045-1049.
184. Alberman, E.; Polani, P. E.; Roberts, J. A. F.; Spicer, C. C.; Elliot, M.; and Armstrong, E. 1972. Paternal exposure toX-irradiation and Down's syndrome. Ann. Hum. Genet. 36:195-208.
185. Schull, W. J.; Otake, M.; and Neel, J. V. 1981. Genetic effects of the atomic bomb: A reappraisal. Science 213: 1220-1227.
186. Brewen, J. G.; Preston, R. J.; and Gengozian, N. 1975. Analysis of X-ray induced translocations in human andmarmoset spermatogonial stem cells. Nature 253: 468-470.
187. Oftedal, P., and Searle, A. G. 1980. An overall genetic risk assessment for radiological protection purposes. J. Med.Genet. 17:15-20.
188. Russell, L. B. 1950. X-ray induced development abnormalities in the mouse and their use in the analysis of embryo-logical patterns. 1. External and gross visceral changes. 1. Exp. Zool. 114: 545-602.
189. Rugh, R. 1962. Ionizing radiations and congenital anomalies of the nervous system. Mil. Med. 127: 883-907.
190. Rugh, R. 1964. Why radiobiology? Radiology 82: 917-920.
191. Russell, L. B., and Russell, W. L. 1952. Radiation hazards to the embryo and fetus. Radiology 58: 369-376.
192. Rugh, R. 1971. X-ray induced teratogenesis in the mouse and its possible significance to man. Radiology 99: 433-443.
193. Yamazaki, J. 1966. A review of the literature on the radiation dosage required to cause manifest central nervoussystem disturbances from in utero and postnatal exposure. Pediatrics 37: 977-1003.
194. Russell, L. B., and Russell, W. L. 1954. An analysis of the changing radiation response of the developing mouseembryo. /. Cell Comp. Physiol. 43: 103-149.
223

Medical Conseqiuences ot Nuclear Warfare
195. Rugh, R., and Grupp, E. 1959. Response of the very early mouse embryo to low levels of ionizing radiations. 1. Exp.Zool. 141: 571-587.
196. Russell, L. B. 1956. X-ray induced developmental abnormalities in the mouse, and their use in analysis of embryo-logical patterns. II. Abnormalities of the vertebral column and thorax. 1. Exp. Zool. 131: 329-395.
197. Ohzu, E. 1965. Effects of low dose X-irradiation on early mouse embryos. Radiat. Res. 26: 107-113.
198. Rugh, R. 1969. Low dose X-ray effects on the precleavage mammalian zygote. Radiat. Res. 37: 401-414.
199. Russell, L. B., and Montgomery, C. S. 1966. Radiation-sensitivity differences within cell-division cycles duringmouse cleavage. Int. 1. Radiat. Biol. 10: 151-164.
200. Jacobson, L. 1968. Low-dose X-irradiation and teratogenesis: A quantitative experimnental study with reference to seasonali fluence on dose effects. Copenhagen: Munksgaard.
201. Miller, R. W., and Mulvihill, J. J. 1976. Small head size after atomic irradiation. Teratology 14: 355-358.
202. Dobson, R. L.; Koehler, C. G.; Felton, J. S.; Kwan, T. C.; Wuebbles, B. J.; and Jones, D. C. L. 1978. Vulnerability offemale germ cells in developing mice and monkeys to tritium, gamma rays, and polycyclic hydrocarbons. InDevelopment Toxicology of Energy-Related Pollutants. Proceedings of 17th Annual Hanford Biology Symposium[CONF-771017], 1-14. Washington, DC: U.S. Department of Energy Symposium Series.
203. Lebedinsky, A. V.; Grigoryev, U. G.; and Demirchoglyan, G. G. 1958. The biological effects of small doses ofionizing radiation. IThe cited work was done by V. V. Yokolev.] In Proceedings of Second United NationsInternational Conference on the Peaceful Uses of Atomic Energy. Vol. 22, Biological Effects of Radiation, 26. NewYork: United Nations Publications.
204. Brent, R. L. 1960. The effect of irradiation on the mammalian fetus. Clin. Obst. Cynecol. 3: 928-950.
205. Semagin, V .N. 1964. Higher nervous activity of adult rats irradiated daily with X-rays during the embryonicperiod. In Effects of Ionizing Radiation on the Functions of Higher Nervous System of Progeny, edited by I. A.Pintsovskoyo and translated by the U.S. Atomic Energy Commission [AEC-TR-5553], 77-103. Oak Ridge, TN:U.S. Atomic Energy Commission.
206. Cahill, D. F., and Yuile, C. L. 1970. Tritium. Some effects of continuous exposure in utero on mammaliandevelopment. Radiat. Res. 44: 727-737.
207. Bursian, S. J.; Cahill, D. F.; and Laskey, J. W. 1975. Some aspects of brain neurochemistry after intrauterine exposureto tritium. Int. 1. Radiat. Biol. 27: 455-461.
208. Kaplan, S. 1962. Behavioral manifestations of the deleterious effects of prenatal X-irradiation. in Effects of IonizingRadiation on the Nervous System, 225-243. Vienna: International Atomic Energy Agency.
209. Rugh, R., and Grupp, E. 1960. Fractionated X-irradiation of the mammalian embryo and congenital anomalies. Am.J. Roentgenol. 84:125-144.
210. Russell, L. B.; Badgett, S. K.; and Saylors, C. L. 1960. Comparison of the effects of acute continuous and fractionatedirradiation during embryonic development. In hImediate and Low-Level Effects of Ionizing Radiation, proceedingsof a conference held in Venice [Special Supplement to Int. J. Radiat. Biol.], 343-359. London: Taylor and Francis.
211. Krigel, H., and Reihart, S. 1969. Effect of a fractionated X-irradiation of the development of the mammalian fetus.In Radiation Biology of the Fetal and Juvenile Mammnal, edited by M. R. Sikov and D. D. Mahlum, 251-262. Wash-ington, DC: U.S. Atomic Energy Commission, Division of Technical Information.
212. Grahn, D., and Kratchman, J. 1963. Variation in neonatal death rate and birth weight in the United States andpossible relations to environmental radiation, geology and altitude. Ain. ]. Hum. Genet. 15: 329-352.
213. Hickey, R. J.; Bowers, E. J.; Spence, D. E.; Zemel, B. S.; Clelland, A. B.; and Clelland, R. C. 1981. Low level ionizing
radiation and human mortality: Multi-regional studies. A preliminary report. Health Phys. 40: 625-641.
224

Long-Terin and Lou,-Level Effects of lonizing Radiation
214. Jacobsen, L. Radiation-induced teratogenesis in relation to season and some features of reproductive biology. Inreference 211, 229-242.
215. Taylor, A. 1. 1968. Autosomal trisomy syndromes: A detailed study of 27 cases of E, i., ard's Syndrome and 27 casesof Patau's Syndrome. I. Med. Genet. 5: 227-252.
216. Murphree, R. L., and Graves, R. B. Effect of dose rate on prenatally irradiated lambs. In reference 211, 243-250.
217. Rugh, R. Chairman's remarks. In reference 211, 381-391.
218. Friedberg, W.; Hanneman, G. D.; Faulkner, D. N.; Darden, E. B., Jr.; and Deal, R. B., Jr. 1973. Prenatal survival ofmice irradiated with fission neutrons or 300 kVp X-rays during the pro-nuclear-zygote stage: Survival curves,effects of dose fractionation. Int. 1. Roddiat. Biol. 24: 549-560.
219. Brent, R. L., and Bolden, B. T. 1968. Indirect effect of X-irradiation on embryonic development: Utilization of highdoses of maternal irradiation on the first day of gestation. Radiat. Res. 36: 563-570.
220. Brent, R. L., and Bolden, B. T. 1967. The indirect effect of irradiation on embryonic development. I11. The contribu-tion of ovarian irradiation, uterine irradiation, oviduct irradiation, and zygote irradiation to fetal mortality andgrowth retardation in the rat. Radial. Res. 30: 759-773.
221. Brent, R. L., and McLaughlin, M. M. 1960. The indirect effect of irradiation on embryonic development. I. Irradia-tion of the mother while shielding the embryonic site. Am. 1. Dis. Child 100: 94-102.
222. Hicks, S. P., and D'Amatio, C. J. 1963. Low dose radiation of the developing brain. Science 141: 903-905.
223. Wood, J. W.; Johnson, K. G.; and Omori, Y. 1967. Int utero exposure to the Hiroshima atomic bomb. An evaluationof head size and mental retardation: 20 years later. Pediatrics 39: 385-392.
224. Brent, R. Radiation effects on the developing embryo. In reference 169, 61-75.
225. National Council on Radiation Protection and Measurement. 1977. Medical radiation exposure of pregnant andpotentialliv pregnant zomen [NCRP Report 541. Washington, DC: National Council on Radiation Protection andMeasurement.
226. National Council on Radiation Protection and Measurement. 1977. Review, of NCRP radiation dose limit for embrio andfetus in occupationallly-exposed women [NCRP Report 531. Was aington, DC: National Council on RadiationProtection and Measurement.
227. Dekaban, A. S. 1968. Abnormalities in children exposed to X-irradiation during various stages of gestation:Tentative timetable of radiation injury to human fetus. 1. Nuci. Med. 9: 471-477.
228. Goldstein, L., and Murphy, D. P. 1929. Etiology of ill-health in children born after postconceptional maternalirradiation. Am. 1. Roentgenol. 22: 322-331.
229. Goldstein, L., and Murphy, D. P. 1929. Microcephalic idiocy following radium therapy for uterine cancer duringpregnancy. Amer. I. Obstet. Giynecol. 18: 189-195, 281-283.
230. Jacobsen, L., and Mellemgaard, L. 1968. Anomalies of the eyes in descendants of women irradiated with small X-ray doses during the age of fertility. Acta Ophlihalmnol. 46: 352-354.
231. Yamazaki, J.; Wright, S.; and Wright, P. 1954. Outcome of pregnancy in women exposed to the atomic bomb inNagasaki. Am. 1. Dis. Child 82: 448-463.
232. Blot, W. J. 1975. Growth and develcpment following prenatal exposure and childhood exposure to atomicradiation. Radiat. Res. (Suppl.) 16: 82-88.
233. Blot, W. J., and Miller, R. J. 1973. Mental retardation following inm utero exposure to the atomic bombs of Hiroshimaand Nagasaki. Radiology 106: 617-619.
225

Medical Cosetiuences o(f Nutclear Warfare
234. lshimaru, T.; Nakashima, E.; and Kawamoto, S. 1985. Relationship of height, bkty Viuvight, head circuinference, and chestcirciol nference at ag' 18, to •alninia and nWeitron doses alnonl' inl tiero exjk)s.'ed children, Hiroshima and Nagasaki
[Technical Report RERF TR 14-841. Hiroshima: Radiation Effects Research Foundation.
235. Kallinger, W., and Granniger, W. 1979. The effect of a high gamma dose on a human fetus. Health Phys. 36: 1-6.
236. Griem, M. L.; Mewissen, D. J.; Meier, P.; and Dobben, G. D. Analvsis of the morbidity and mortalitv of childrenirradiated in fetal life. In reference 211, 651-659.
237. Harris, W. 1932. Therapeutic abortion produced by the roentgen ray. Am. 1. Roentgenol. 27: 415-419.
238. Mayer, M. D.; Harris, W.; and Wimptheimer, S. 1936. Therapeutic abortion by means of X-ray. Am. 1. Obstet.Gynecol. 32: 945-957.
239. Stewart, A. M.; Webb, J. W.; Giles, B. D.; and Hewitt, D. 1956. Malignant disease in childhood and diagnostic
irradiation in utero. Lancet 2: 447, 1956.
240. Stewart, A. M.; Webb, J. W.; and Hewitt, D. 1958. A survey of childhood malignancies. Br. Med. 1. 1: 1495-1508.
241. Stewart, A. M., and Kneale, G. W. 1970. Radiation dose effects in relation to obstetric X-rays and childhood cancers.Lancet 1: 1185-1188.
242. Kneale, G. W., and Stewart, A. M. 1976. Mantel-Haenszel analysis of Oxford data. II. Independent effects of fetalirradiation subfactors. INCI 57:1009-1014.
243. Monson, R. R., and MacMahon, B. Prenatal X-ray exposure and cancer in children. In reference 50, 97-105.
244. National Council on Radiation Protection and Measurement. 1987. Recommendations on linits for exposure to ionizing
radiation INCRP Report 911. Washington, DC: National Council on Radiation Protection and Measurement.
245. Cohen, B. L., and Lee, 1.-S. 1979. A catalog of risks. Health Phys. 36: 707-722.
246. National Council on Radiation Protection and Measurement. 1971. Basic radiation protection criteria [NCRP Report391. Washington, DC: National Council on Radiation Protection and Measurement.
247. Holahan, E. V., Jr. Cellular radiation biology. In reference 4, 87-110.
226

Chapter 10
RADIOLOGICAL CONSIDERATIONSIN MEDICAL OPERATIONS
LARRY W. LUCKETT, C.H.P.* AND BRUCE E. VESPER, M.S.**
INTRODUCTION
RADIATION INTERACTION AND DETECTION
InteractionRadiation Detection
STAFF-LEVEL MEDICAL PLANNING
Handling Mass CasualtiesRadiological Concerns of Medical PersonnelUnit Operations in Fallout
MEDICAL RESPONSE IN PEACETIME RADIATION ACCIDENTS
Peacetime ConstraintsHistorical PerspectiveNuclear Accident and Incident Response and Assistance OrganizationGuidelines for Medical AdvisorsRescue and Evacuation of Injured Persons at a Nuclear Accident SiteInitial Care, Resuscitation, and Admission of Contaminated PatientsOperating-Room Care of Contaminated Patients
SUMMARY
NUCLEAR WEAPONS ACCIDENT CHECKLISTS
PredeploymentField Deployment
*Lieutenant Colonel, United States Army; Health Physicist, Office of the Director, Armed Forces Radiobiology Research Institute, Bethesda,Maryland 20814-5145-Lieutenant Commander, United States Navy; Health Physics Advisor, Defense Nuclear Agency, Nuclear Weapons Accident AdvisoryCommittee; Military Applications Coordinator, Armed Forces Radiobiology Research Institute, Bethesda, Maryland 20814-5145
227

M'lctkiI ConIseqc e~d'ILs of NJ ILChI r War~tiirC
INTRODUCTION
The success of medical support operations in a order to ensure continued effective medical opera-nuclear war will depend to a great extent on the ade- tions in a nuclear environment.quacy of planning, training, and preparation before In many instances, the experience gained duringhostilities occur. Nuclear warfare will produce a conventional wars and peacetime nuclear incidentshuge disparity between the number of patients re- will be applicable to the casualties of a nuclear bat-quiring treatment and the available medical re- tlefield. A rigorous training and implementationsources. This problem will be further complicated program must be instituted at all levels of medicalby "he disruption of lines of communication; the iso- service for professional and nonprofessional medicallation of medical units; and shortages of transporta- personnel. Emphasis must be placed on practical,tion, supplies, and equipment. problem-related training rather than on theoretical
Preparation problems facing medical planners principles.and commanders can be divided into two distinct The information in this chapter on tactical opera-categories: (a) staff-level planning, including actions tions is extracted from current NATO doctrine forthat must be taken before the start of a nuclear war medical operations in a tactical nuclear environ-to minimize the prompt effects of enemy nuclear at- ment.' The information on peacetime operations istacks, and (b) unit preparations to minimize the im- from current Department of Defense doctrine frommediate and delayed effects of nuclear attacks, in the Defense Nuclear Agency2 and the U.S. Army.'
RADIATION INTERACTION AND DETECTION
The ability to recognize the potential for radio- for one-half of the excited material to convert (or de-logical damage is based on a knowledge of the basic cay) to stable, nonradioactive material. Dependinginteractions of radiation particles with biological on the material, the half-life can vary from less thanmolecules, and on the ability to detect the presence seconds to many thousands of years. The shorterof radiation or radioactive materials. The need to the half-life, the more probable it is that radiationmeasure or quantify a substance that dramatically will be emitted; the longer the half-life, the less likelyaffects the human system but cannot be detected are the atoms to decay. The amount of materialwith the senses has led to the development of radia- present can be termed the activity, measured by thetion detectors and dosimeters based on the physical number of nuclear transformations per seconds (nts)principles of radiation interactions. An understand- or disintegrations per minute (dpm). The activity ofing of the nature of radiation hazards and the char- a radioactive sample is a measure of its intensity.acteristics of various radiation types will help in the Units which measure activity are the btecquerel ( Bqselection of a specific radiation detector for a given equals one disintegration per second) and the curiesituation. (1 Ci equals 3.7 x 101 disintegrations per second).
The excess energy carried away from the radioac-tive material comprises the radiation (Table 10-1).
Interaction This energy may be carried away by particles ofmatter as they leave the nucleus (alpha, beta, or neu-
Radiation arises when excited or overly energetic tron radiation), or it may be emitted from the nu-atomic nuclei give off excess energy as their particles cleus independently of any nuclear particlesconvert to a more stable arrangement. The excited (gamma radiation). Either way, the radiation travelsatoms comprise the radioactive material-a physical from the radioactive material until it interacts withsubstance that, when present in sufficient quantity, the surrounding medium. The excess energy of thecan be weighed, measured, seen, or chemically sepa- radiation rapidly dissipates through multiple suc-rated. This radioactive material can be characterized cessive interactions, until the particles recombineby a half-life, the amount of time it takes, on average, with the atoms in the medium. The amount of dissi-
228

Padtiolo.ical Considerationis in Medical Oli'rationis
TABLE 10-1
CHARACTERISTICS OF NUCLEAR RADIATIONS
Relative Electric Emitted Range in Tissue RadiationName Mass Charge by Air Penetration stopped by
Alpha 7,300 +2 Unfissioned 5 cm First layer Clothinguranium and of skin Paperplutonium
Beta 1 -1 Fission 12 m Several layers Clothingproducts of skin
Gamma 0 0 Fission 100 m Total body Several feetproducts of concrete
or earth
Neutron 1,830 0 Emitted only 100 m Total body Several feetduring fission of concrete
or earth
pated energy absorbed in the exposed medium is the In order to increase the probability of interactionabIsorbed dose. Units of absorbed dose are the gray (1 with and absorption of the radiation, gamma-rayGy equals 1 Joule/kg) and the rad (1 rad equals 100 shields are made of high-density concrete or lead.ergs/g). Beta Radiation. Beta-particle radiation occurs
The interaction between radiations and any ab- when excess nuclear energy is emitted in conjunc-sorbing medium is ionization. In this process, the tion with a high-speed nuclear electron. Because ofenergy from the incoming radiation is transferred to its small mass and its one electric negative charge,an atom of the medium, exciting that atom and dis- the beta particle interacts more readily than does thelodging one of its orbital electrons. Each ionization uncharged gamma ray, traveling only several metersevent produces one ion pair, consisting of a free elec- through air and penetrating only several layers oftron and the positively charged remainder of the skin. The hazard from beta radiation is to the exter-atom. These free electrons, broken atomic bonds, nal skin surfaces; beta radiation cannot penetrate toand the resulting disrupted and distorted molecular internal organs unless it is inhaled or ingested. Beta-arrangements are the basis of biological damage. particle radiation shields may consist of lightweight
Gamma Radiation. Gamma radiation is a pure materials, such as a layer of clothing.energy packet (called a photon), unaccompanied by Alpha Radiation. The heaviest particle given offany nuclear particle. Without mass or electric in nuclear decay is the alpha particle. It is 7,300charge, the gamma rays have very little probability times heavier than the beta particle, and is positivelyof interacting and will travel great distances through charged with twice the beta particle's electric charge.sparse media, such as air or biological tissues. This Its mass and charge make the alpha particle a highlyability to penetrate and irradiate sensitive organs interactive form of radiation; it will travel only 5 cmwithin the body makes gamma radiation hazardous. in air and can be stopped by a sheet of paper. Alpha
229

Metdhil C nseLwuetc ot Itc'ar Wlfarirc
particles will not penetrate the external laver of dead chamber containing two electrodes, one of which is askin and thus are no direct hazard as long as they quartz fiber loop that is free to move on its mount-remain outside the body. Alpha-particle-emitting ing. Radiation entering the chamber causes ioniza-materials are a hazard when they can be inhaled or tion within the sensitive volume. The distance theingested, and are then able to irradiate sensitive or- fiber moves is proportional to the dose received ingans or tissues from within, the chamber. Instruments of this type are sensitive
Neutron Radiation. Neutron particle radiation is to severe shock and humidity, but are small enoughemitted only during the instant of fission by the to be worn comfortably. The advantage of this in-weapon material. A neutron particle has no electric strument is that it can be read at any time (withoutcharge but does have an intermediate nuclear mass the aid of a supplementary charger-reader) bv sim-(1,830 times the mass of the beta particle but only ply holding it up to the light and looking into it.one-fourth that of the alpha particle). Like a gamma Geiger-Mueller Counters. Geiger-Mueller count-rav, the neutron can travel great distances through ers are normally used for detecting single ionizingsparse media and can penetrate biological tissues. events that take place within the sensitive volume ofUnlike other radiations that interact with orbital the counter. The counters are rugged and sensitiveelectrons, neutrons are more likelv to interact di- to low levels of radiation. They are usuallyrectlv with the nuclei of atoms, particularly those equipped with audible indicators of radiation detec-having low atomic numbers. Thus, effective neutron tion that sound like clicks. Geiger-Mueller countersshields are composed of materials %ith a high detect gamma photons or beta particles, but the de-hydrogen content, such as water or paraffin. tection of the former is less efficient. A discriminat-
ing shield is usually provided with Geiger-Muellerinstruments; when it is opened, it admits both beta
Radiation Detection and gamma radiation. When the shield is closed,only gamma rays pass. Use of the shield may per-
No single instrument at present has all the char- mit qualitative differentiation between the ioniza-acteristics necessary to detect all types of radiation. tion caused by beta particles and that caused byAccordingly, different types of instruments must be gamma photons.used, depending on the nature of the radiation haz- Proportional Counters. Proportional countersard. For any type of instrument used, the time are used to detect one type of radiation in the pres-frame over which it operates can be instantaneous or ence of other types of radiation, or to obtain outputcontinuous. A ratemeter indicates the instantaneous signals greater than those obtainable with ionizationrate at which radiation is being detected, and an inte- chambers of equivalent size. Proportional countersgrating neter gives a reading of the total radiation mav be used either to detect events or to measureobserved since the meter was turned on or restarted absorbed energy (dose), bec',use the output pulse is(zeroed). directly proportional to the energy released in the
Radiation-detecting instruments are based on the sensitive volume of the counter. Proportional count-principles of the radiation interaction being ob- ers are used for the detection of alpha particles, neu-served. A detector that merely counts the incoming trons, and beta particles. They are often used inradiation particles is called a radiation coniter. An shielded laboratory facilities for sensitive low-levelinstrument designed to collect and measure the analysis.number of ion pairs produced is termed an exposure Scintillation Counters. A scintillation countermeter; because the unit of exposure is the roentgen combines a photomultiplier tube with a scintillating(R), it is also called an R-met'r. An instrument that material, which may be a crystal or other phosphormeasures the total energy absorbed in a detecting (solid, liquid, or gas). Light pulses, produced in themedium is an absorbed d&se meter; if the detector uses scintillator bv radiation, release electrons in thea tissue-equivalent absorbing medium, the detector photomultiplier tube, and this tube then amplifiesis called a remi-meter. The characteristics of some of the electrons to pulses of current that can bethe more commonly used detectors are summarized counted. Various scintillation counters can detectbelow. alpha and beta particles, gamma rays, neutrons, pro-
Ionization Chambers. Ionization chambers tons, and electrons. The most common dosimetersmeasure dose and dose rate from gamma and X ra- for field use are alpha counters or gamma-ray detec-diations. A typical ionization chamber that meas- tors. Although energy dependent, scintillationures total dose is the pocket dosimeter, which is the counters are more efficient at detecting low-energy,size of a large fountain pen (Figure 10-1). It has a low-level gamma-ray backgrounds than are Geiger-
230

Radiological Considerations in Medical Ot1rations
Cap with Window
Supporting Insulator
Wire Element
Quartz Fiber
Elcrode C
Pocket Clip
Electroscope
Lenses
Dosage Scale
Eyepiece Lens
Fig. 10-1. Pocket dosimeter
Mueller counters. Radiophotoluminescent Dosimeters. Radiopho-Thermoluminescent Dosimeters. A thermolu- toluminescent (RPL) glass is a dosimeter material
minescent dosimeter (TLD) responds to ionizing ra- that will luminesce following an excitation pulse ofdiation by trapping excited electrons in metastable ultraviolet light if it has been exposed to ionizingstates within the detector's crystalline structures. radiation. This effect is caused by radiation-inducedWhen the TLD is heated, the electrons escape these changes in the crystalline electronic structure of thetraps, releasing light as they return to their lower glass. As with TLDs, the response is proportional toenergy state. The amount of light is proportional to the radiation dose. The RPL dosimeter sensitivitythe absorbed radiation dose. The TLD is an integrat- depends on the type and manufacturer, and rangesing dosimeter and requires an elaborate electronic from 0.01 to several million cGy. This type of inte-readout device to interpret the absorbed-dose data. grating dosimeter will not be zeroed by the readoutThe readout instrument will zero the TLD so that it device; it gives a total cumulative dose reading thatmay be used again, fades very slowly with time.
231

Me4dioal CtmnstqiU01c, s ,, .hur Wla rfzrt'
STAFF-LEVEL MEDICAL PLANNING
As is the case with operations planning through- less fear and prompter, more effective action. Be-out the medical support system, the staff medical of- cause action relieves tension, the fear response is lessficer's planning is keyed to the functions of the likely to become severe or incapacitating. Prevent-forces supported by the medical unit. While the ing or treating stress reactions in nuclear warfareproblems confronted by medical units on the nuclear may determine the continuing effectiveness of abattlefield will be similar in some respects to those unit's combat performance.associated with conventional warfare, there are Public Health Concerns For centuries, the con-some dramatic differences. These include the vastlv duct and outcome of military operations have beenincreased numbers of casualties requiring care, the profoundly affected by a small number of infectiousneed to operate in fallout, and the requirements to diseases. Massive destruction from nuclear weap-treat and decontaminate combined-injury patients. ons could result in epidemics that would present se-
rious problems for a military medical service, par-Handling Mass Casualties ticularly when the effectiveness of civilian medical
facilities and personnel has been diminished. In pastEffective techniques of evacuation, medical man- wars, military medical forces have cared for civilian
agement, and triage become increasingly important populations and have helped to rebuild nations ray-with very large numbers of patients. The problem of aged by war. On the nuclear battlefield, the impacthandling mass casualties is not limited to hospitals. of classic diseases of disaster (such as dysentery, tv-It exists throughout the chain of medical evacuation, phus, typhoid fever, cholera, and plague) may seri-so the basic principles of triage must be understood ously affect the ability of the medical unit to treatby all medical personnel. Flexibility in applying battlefield casualties.these principles must be an established part of medi- Logistical Support System. The success of medi-cal guidance and training. cal support depends on the adequacy of prewar lo-
Effects of Combined Injuries. Analyses of the ex- gistical preparation. Planning should provide notpected battlefield situations in a tactical nuclear en- only for medical supplies and equipment, but alsovironment have concluded that a high proportion of for general supplies, food, clothing, water purifica-the casualties will have combined injuries, most of tion apparatus, radiation-detecting and -measuringwhich will be from thermal burns and radiation ex- instruments, communications equipment, andposure. Burn injuries provide portals for infection, modes of transportation.and both burns and radiation exposure decrease the The location of medical resources is crucial. Re-casualty's immunity to infectious microorganisms. sources must be close to the area of probable great-Medical planners at all levels must anticipate (a) per- est need, without being concentrated in areas likelysonnel with low-level exposures from nuclear weap- to become targets for enemy attack. This means thatons, who may need immediate medical attention be- medical planners must compromise between disper-cause of combined injuries, and (11) personnel with sal and the capability of the logistical system tootherwise recoverable conventional injuries, but move supplies and patients. Medical plannerswhose radiation exposures make their chances for should take advantage of the stages of military pre-survival poor. paredness that may precede the actual outbreak of
Effects of Psychological Stress. It is possible to hostilities. Because of the problems associated withestimate the number of personnel who would be in- long-term maintenance of medical equipment andjured or killed by the thermal, blast, and radiation medications in storage, extensive pre-positioningeffects of a nuclear explosion, but it is much more during peacetime is not practical.difficult to predict the numbers and types of psychi- Command Radiation Guidance. Line command-atric casualties. The types of acute psychological ers at all levels will need advice from medical advi-problems that would occur would probably be simi- sors about the effects of accumulated doses of radia-lar to those in other combat situations, and the treat- tion on the health of their personnel, as well as thement methods developed during past wars would hazards of potential exposures when operationsbe appropriate, must be conducted in areas contaminated with fall-
The most important factor in preventing stress out. This advice must be practical and be based onreactions is intensive training, which will result in an understanding of the requirements of the mission
232

Raidjhotgical Ctmsidieratiom1 in Medical Opt'rati, is
TABLE 10-2
RADIATION EXPOSURE STATUS IRES) CATEGORY SYSTEM
NuisanceDose Casualties symptoms
RES (cGv) (V) (11") Risk
0 0 0 0 None
1 0-70 1.0 2.5 Negligible
2 70-150 2.5 5.0 Moderate
3 150+ 5.0 - Severe
,well as on knowledge of the diverse human re- bat-ineffective personnel will be capable of perform-sponses to radiation. The effects of radiation must ing their tasks at 251c7 (at best) of their preexposurenot be either minimized or exaggerated, and the performance level.proper place of radiation effects relative to other Given an average dose of 400 cGy to a tacticalhazards of combat must be understood. unit required to perform a physically demanding
NATO Standardization Agreement (STANAG) task, the unit will become performance degraded2083 has established a Radiation Exposure Status about 2 hours after exposure and will remain so for(RES) category system (Table 10-2), incorporating longer than I month (Figure 10-2). However, if thethe most recent guidance on the operational effects required task is not physically demanding at thatof radiation exposures.4 This system will help mili- same radiation dose, performance degradation willtarv commanders maintain the fighting capability of occur at about 3 hours after exposure, and effectivethe tactical forces despite the troops' exposure to combat performance will recur 2 days to 2 weeksionizing radiation. When personnel have accumu- later, followed by a second performance degradationlated sufficient exposure to be placed in a particular (Figure 10-3).RES category, then commanders must restrict those Of course, these predictions assume that expo-units to activities in which additional radiation ex- sure to ionizing radiation will be the combatants'posure is not expected, unless they are willing to ac- only stress. The prediction of the performance ca-cept the next higher risk to those units. pacity of irradiated persons will have to be consid-
When exposures can be maintained below 150 ered with other stresses, such as conventional injury,cGy, the STANAG doctrine indicates that the overall endemic disease, continuous duty without sleep,eftectiveness of combat units will not be significantly and time in combat.degraded. However, if the exposures become rela-tive'-v large, tactical commanders must be advised of Radiological Concerns of Medical Personneltheir forces' capability to continue operations. Gen-erally, an effective military individual is one capable When fallout occurs, insufficiently sheltered per-of carrying out assigned missions, some of which sonnel will become contaminated. If these personnelrequire a high degree of physical and mental effec- are not wounded or sick, decontamination is not ativeness. Thus, in any attempt to relate radiation medical responsibility; it will be done at the unitdose to this effectiveness, the complexity or physical level under command supervision. If wounded per-demand of the task must be considered. sonnel become contaminated, their hospitalization is
Combat-effective personnel will suffer from ra- more complicated. Fallout contamination can bediation sickness, but will be able to maintain at least hazardous to the patient and to attending medical75(ý, of their preexposure performance level. Per- personnel, although in contrast to contaminationformance-degraded personnel will be operating at with chemical agents (in which the mere presence of259'-75'7 of their preexposure performance. Coin- the agent is life threatening), no immediate life-
233

10,000 7
Dose(cGy)
19000
3 10 100 1,000 10,000 100,000lhl iay lm~o
Time After Exposure (mi)iij~ M i. - i
i-, 10-2. E\pccted reponse to radiation for phyically demanding tasks
threatening radiation hazard e\ists. Thus, the de- diation associated with a nuclear detonation is verycontamination of patients and contamination-control rapid. The whole-body gamma-radiation hazard toprocedures within the medical facility (although im- persons handling the patient will be several ordersportant) are lower priorities than the lifesaving treat- of magnitude less than that to the patient, because ofment of conventional injuries, distance and elapsed time.
Radiation Hazards in Patient Treatment. Radi- The beta-contact hazard is a significant problemologically contaminated patients are those who have to the patient. If fallout residue remains on the skinbeen contaminated with fallout, which adheres for an extended time (several hours to days), betalooses, to clothing and skin in the form of dust, burns mav occur. These resemble first- and second-ashes, dirt, or mud. Once these residues have been degree thermal burns. Because the-% affect onlyremoved, the patient does not present a radiation those skin surfaces directly in contact with the radio-hazard. Patient decontamination should not pre- logical contamination, gently brushing or washingcede or interfere with either lifesaving procedures or the dust from the skin will eliminate the hazard tosurgical preparation, but rather should be an inte- the patient. Wearing rubber gloves and surgicalgral part of these procedures. Furthermore, care masks, as well as practicing good hygiene, willmust be taken to avoid accidentally forming a real eliminate the hazard to medical personnel.hazard by accumulating contaminated waste in the Under conditions of nuclear war, the minutedecontamination area. Effective procedures for de- quantities of radioactive material that might be in-cont,)mination, followed by monitoring and prop- gested, inhaled, or absorbed through wounds are aerlv d:.posing of contaminated waste, must be de- relatively minor radiation hazard. Extensive decon-velopcd and used. tamination therapy is unlikely to be used because of
Three distinct hazards are associated with radiol- the large number of patients and the limited time,ogicallv contaminated patients. These are the wholt- personnel, and available logistical resources./bod, I/a 01o1a-Iadiatioll hazard, the bcta-contact hazard, Patient Decontamination. Patients can easily beand the viternal hazard from inhalation and ingestion decontaminated without interfering with requiredof contaminated material, medical care. Simply removing the patient's outer
Whole-body gamma radiation is the most impor- clothing and shoes before admission xwill removetant hazard because gamma radiation has a long 00' -95f' of the contamination. Once removed, con-range in air. This danger should be considerably re- taminated clothing can be placed in bags, tagged,duced by the time the patient reaches a medical fa- and taken to a remote section of the medical facility.cilitY, however, because the loosely adhering Hllout The clothing can be decontaminated or disposed ofresidue will drop or brush off as the patient is by qualified personnel, as time permits.moved. In addition, the initial decay of residual ra- The second phase of decontamination consists of
234

RLh011'1110, dhIMcrtw - M Alc hI I t I A pr¢h
10,000
Dose
1,000 .....
390 10 001,00 0,00 0000
yiEffectiveo
T A r pe (mm )ITime~ee Afe Exosr (min
rig. Ii-3\pected rVýponI!e to radiation for phx 'iwaliv undemanding taský'
ashingl or wiping the patient's face, hands, and any\, The commander will need to know:skin surfaces not previously cov'ered by clothing. e Whether the unit wvill be inl a fallout areaThis Should leave thle patient 98" decontamlinated, 9 Thle expected timie of fallout arrival (oraind canl be done before or after admission. how long before most of it will be onl the
Thle third phase of decontamination consists of ei- ground and the dose rates wvili begýin tother washing or clipping thle hiair and washing the decline)scalp, and is required only if the patient arrives e The mlaximumlii dose rates expectedwVithoult hecadgear or if monitoring indicates that thle * Thle adequacy of existing facilities as fall-hair is contaminated, out shelters
Decisions about operations inl fa~lOlot areasUnit Operations in Fallout should be based onl actual survey data. However.
because it will be not be possible or desirable to ex-Whienever large areas are contaminated by fall- pose monitoring personnel when dlose rates are very
out, thle operations of all units will be hampered to high, a reliable miethod Of estimlatinlg fallout decay isvarying degrees, depending onl the level of contamii- required (Table 10-3). Note that these calculationsnation. When a serious radiation hazard exists, the are accurate only after all fallout is onl the groundmedical unit commander will be faced with the and the diose rate is beginning to decrease.question of whether to continue operations and ac- By eva]luatinlg these data along with the opera-cept hazardous exposures to unit personnel, or to tional situation, the commandier will be better able totake shlcter-an action that mnax seriously reduce make the proper decisions about moving the unit,thle unit's ability to care for patients. To make the diverting patients to other treatment units, moving'correct decision, the commander requires the follow- into fallout shelters, or remaining inl place and conl-ing capabilities: tinuing normial operations.
"* Ani effective radiation-mionitoring capabil- Medical unlits that are required to remain ir areasitv to correctly mecasure the fallout ra- of high dose rates canl survive and continue their pa-diation hazard tient-care activities if adequate shelter is available to
"* The ability to make rapid estimates ot anl- shield against radiation. Many materials that areticipated dose and dose rates available onl thle battlefield will afford substantial
"* Satisfactory linies Of commun1~lication Wvith shielding (Table 10-4), althoui lh somec of them, suchother units and headquarters to report as concrete, require engineering support and priorthe fallout situation and to receive fall- construction. Howvever, earth atfords excellent pro-out warnings, information, guidance, tection and Canl be used with a miiinimum of engi-and Order, neering effort.
• • •• • • • e• •o •e• )e• ••• 235

Medical Ct stiuenrts of Nit(,car Warfare
TABLE 10-3 trenches, and they require considerably more engi-THE 7:10 RULE FOR RESIDUAL RADIATION DECAY neering effort.TE_7:10_RULEFORRESIDUALRADIATIONDECAY Vehicle-Earth Shelter. A very effective shelter
can be constructed combining unit vehicles and dirt.Time after Amount of Dose Rate Two large tents can be joined end-to-end. A shallowDetonation Radiation Decay trench for the vehicles can be dug around them, with(in hours) Remaining (cGy/hour) the dirt piled carefully on the outside of the trench.
Another 15-cm trench should be dug for the outer
1 - 1,000 wheels of the vehicles. This shelter can give as muchas 807 protection if fallout contamination is re-
7 1/10 100 moved from inside the rectangle thus created. Tentliners and ponchos can be used for this purpose.
49 1/100 10 This shelter requires about 2 hours to build and canbe occupied or evacuated in minutes. As with other
343 1/1,000 1 expedient shelters, it could be constructed when themedical unit occupies the position.
Regardless of the type of shelter used, a systemmust be developed for its efficient operation. In thecase of medical units involved in the care of patients,
In some cases, construction will be unnecessary; it is usually advisable to separate the shelter man-terrain and structures that will afford excellent pro- agement functions from those of patient care. Shel-tection from radioactive fallout (such as tunnels, ter management personnel must provide essential
caves, culverts, overpasses, ditches, ravines, and services, such as radiological monitoring; monitor-heavily constructed buildings) may be available. In ing of water-storage facilities to prevent leaks andexisting buildings, below-ground basements give contamination; control of fire hazards; enforcementthe best protection. Windows and overhead floors of health and sanitation rules; waste disposal; andcan be sandbagged or covered with dirt to provide provision of safe food, water, and sleeping facilities.additional protection with a minimum of effort. Shelter management plans must be developed be-
As a matter of policy, mobile medical units fore the shelters are occupied, and the plans must beshould locate in or near existing shelter. When this familiar to all assigned personnel.is impossible, adequate shelter must be constructed.These shelters need not be elaborate; they have to becontinuously occupied only during the period of TABLE 10-4high radiation dose rates. SHIELDING PROPERTIES OF COMMON MATERIAL
Three common field-expedient fallout shelters FROM FALLOUT GAMMA RADIATIONcan be constructed quickly and without extraordi-nary engineering support.
Dozer Trench. For this type of shelter, a trench Half-value Layer Thickness*2.7 meters wide and 1.2 meters deep is dug with abulldozer. It is estimated that one bulldozer can cutsix 30-meter trenches in about 5 hours. About 0.6meters of trench would be required for each person Steel 2
to be sheltered; thus, in 5 hours, si-elters can be con-structed for about 300 people. Protection and com-fort can be improved later by digging the trenchdeeper, undercutting the walls, and erecting tentsover some portions of the trench. These trenchesshould provide adequate shelter for most fallout Water 12situations.
Dug-In Tents of a Mobile Hospital. The tents of Wood 22a mobile hospital can be dug to a depth of 1.2 metersand would be more comfortable than the dozer *Thickness required to reduce the incident dose or
trench. However, dug-in tents have two drawbacks: dose rate by one halfthey offer far less radiation protection than dozer
236

Riitilogicai Coisideratiots in Medical Operations
MEDICAL RESPONSE IN PEACETIME RADIATION ACCIDENTS
A medical response to a peacetime radiation acci- casualties, critical aspects of the response effort, anddent is similar, on a reduced scale, to the response of its consequences. Medical-response personnel mustmedical units on a tactical nuclear battlefield, al- be prepared to safeguard medical information in athough some of the radiological concerns differ. In a manner that would be unnecessary during tacticaltactical nuclear environment (as in a large-scale nu- operations.clear reactor accident), gamma- and beta-emittingfission products become airborne fallout, exposing Historical Perspectivepeople to hazardous levels of external radiation. Ina peacetime nuclear accident, the localized dispersal The U.S. military services have experiencedof alpha-emitting radioactive material is the govern- thirty-two accidents involving nuclear weaponsing concern. Alpha particles are not an external haz- through 1987.7 The complexity of the accidents hasard, but when inhaled or ingested they can expose ranged from (a) the simple dropping or dislocationinternal tissues to significant radiation doses. Due of a weapon, resulting in physical damage but noto the various levels of radiation and the different bodily injury or dispersal of radioactive materials, toradioactive particles in tactical situations, the radia- (b) the detonation of conventional explosives,tion-detecting equipment will be different from that spreading radioactive materials over hundreds ofused in peacetime. acres, contaminating private property, and requiring
Nuclear accidents may involve the military on restoration efforts costing millions of dollars. Theshort notice. Because the public will expect the re- medical functions performed in these nuclear acci-sponse team to be knowledgeable, especially regard- dents illustrate the potential roles of military medi-ing medical care and public health, a review of past cal units that respond to future accidents.experiences and the current doctrine for handling Palomares. In January 1966, two U.S. aircraft (anuclear accidents is essential. KC-135 tanker and a B-52 bomber) attempted a mid-
air refueling at 31,000 feet over the southeasternPeacetime Constraints coast of Spain, but collided in the final stages of
hookup. Wreckage of the two aircraft, including the
In a peacetime nuclear accident, the medical unit four nuclear weapons aboard the B-52, rained downis freed of some serious military concerns, such as on the seaside farming village of Palomares, thehostile fire. Because nuclear weapons are designed nearby Spanish countryside, and the Mediterraneanso that a nuclear yield is virtually impossible with- Sea. Four of the seven B-52 crew members survivedout a complete sequence of deliberate actions, the the accident, but none of the four crew members ofmajor concern at a weapon-accident site is the dis- the KC-135 survived. Evacuation and treatment ofpersal of radioactive materials by either fire or the the survivors were first provided by local Spanishdetonation of the conventional explosive. Thus, the authorities and hospitals. The first U.S. responseconsequences of a nuclear-weapon accident in personnel arrived at the remote site 12 hours afterpeacetime are greatly reduced, and the medical re- notification.'sponse is concentrated on a few patients rather than Three of the fallen nuclear weapons came downdirected toward mass casualties. on land; the fourth splashed down in the Mediterra-
In peacetime, the concern about exposing person- nean Sea and was not located for 81 days. The firstnel and the environment to radioactivity will have a weapon was found undamaged about 900 feet frommuch higher priority. Minute traces of material that the beach. The second was located the next day. Itwould be inconsequential in wartime will assume had suffered a partial high-explosive detonation,great importance. Medical procedures must be per- which made a crater about 20 feet wide and 6 feetformed to contain the contamination according to deep. The third weapon was found an hour later,strict regulatory limits, where it had landed within the limits of Palomares.
In managing a radiation incident, the response It had also undergone high-explosive detonation,team will face pressure to provide details on the and nuclear material had spread up to 500 yardsevent. News media, public officials, and private citi- from the impact point. Luckily, no one on thezens will demand information about the accident, ground was injured.
237

Medical Cotisetqictiits of Nucihar WVrfartr
A contingent of American military and civilian would melt in the approaching summer season, re-personnel went to the Palomares area to work on re- leasing the nuclear material into the environment.covery and the restoration of the accident site. The The aircraft and weapons had been almost totallypopulation rapidly increased to 747 (excluding off- destroyed, but fortunately most of the radioactiveshore naval forces), which required establishing an material had been immobilized when it froze intoon-site medical support facility to provide emer- the snow and ice cover. Discoloration of the snowgency medical treatment, supervise on-site field pack from the fire was an important clue in distin-sanitation, and assist workers who might be exposed guishing contaminated from uncontaminated snow.to radiation. As the population increased, the re- Innovation overcame some of the difficulties.sponsibility for obtaining routine bioassay samples The alpha detection instruments performed poorlyfrom those potentially exposed was given to the in the severe cold. At first, batteries lasted only 10camp medical facility. No cases of hazardous radia- minutes, and the detectors were even more fragiletion exposure occurred. Medical cases requiring than usual, so the operator wore the battery pack in-treatment beyond emergency care were evacuated, side his parka to warm it with body heat. After site
Within days after the accident, U.S. Air Force cleanup, the contaminated ice and snow were storedmedical officers (specialists in aviation medicine) in old petroleum tanks and later transferred to spe-and enlisted personnel were at the site in a field dis- cially modified containers for shipment to thepensary. The initial task was to identify supplies of United States.potable water. Most medical problems involved Chernobyl. In 1986, an accident at the Chernobylupper respiratory infections in personnel who were Nuclear Power Station in the Soviet Union initiatedexposed to high winds and cool temperatures. a sequence of events that mobilized civilian andMembers of search parties who walked in the fields military medical response forces worldwide."' Al-and hills suffered pulled muscles, cuts, -cratches, though the immediate fatalities and damage wereblisters, and sprains. On-site medical support localized, the extensive atmospheric fallout causedceased when the base camp was closed in April concern and action in health-care systems far from1966, after 84 days of searching, decontaminating, the accident site.and restoring the remote site. Following early reports of the accident, the U.S.
Thule. In January 1968, a B-52 aircraft on an air- European Command (EUCOM) established a Cher-borne alert mission near Thule Air Force Base, nobyl Task Force to evaluate the accident's radio-Greenland, developed a fire. The pilot was unable logical effects on the health of American personnelto extinguish it and began an emergency descent to in Europe. Directed by a medical corps officer, thethe airbase. Shortly after the descent began, the air- task force was composed of representatives of publiccraft lost all electrical power, and the order to bail affairs and safety, and medical consultants in publicout was given and executed. The aircraft struck the health, preventive medicine, radiological hygiene,sea ice several miles west of the base, and disinte- veterinary medicine/food sanitation, nuclear medi-grated from impact, explosion, and fire. Four nu- cine, medical logistics, and medical operations.clear weapons were on board the aircraft. Of the The task force's initial mission was to provideseven crew members who ejected, six survived. The medical screenings of U.S. military family membersseventh person died of a head injury, probably sus- who were touring Leningrad and Kiev at the time oftained when he ejected from the aircraft._ the reactor accident. The screening operations exe-
Response forces sped to the scene, and a tempo- cuted by army and air force medical units involvedrary camp was erected on the sea ice. Because the segregating planeloads of personnel, monitoring in-accident was close to the base, medical operations dividuals and their baggage for external contamina-were mounted from the regular base facilities. Only tion, obtaining individual histories, performing thy-camp sanitation was required in addition to normal roid counts and bioassay samples to assess internalmedical services. As at Palomares, the medical clinic contamination, and incorporating all analyses andwas responsible for collecting bioassay samples interpretations into the individual's medical record.throughout the recovery period. At the request of the U.S. State Department, EU-
Because of the arctic location, the next sunrise oc- COM deployed a radiation advisory medical team tocurred 24 days later. The darkness and severe cold assist the U.S. Ambassador in the USSR in definingaffected recovery operations, requiring intense cold- and managing the immediate consequences of theweather training, frequent rest breaks, and time-con- accident. Composed of military health physicists, asuming preventive maintenance, physician, and a food service veterinarian, the team
Time was a crucial factor because the sea ice went to the U.S. missions in Leningrad and Moscow,
238

Radiologictil Considerations in Medical Operations
evaluated the radiological environment, and advised commander will supervise all emergency forces andthe ambassador on potential hazards to the interna- direct all operations at the scene, including, but nottional community from the uncertain conditions. limited to, the following:
Veterinary service personnel in EUCOM ensured 9 Securing, safeguarding, and disposing ofthe safety of local food supplies for consumption by all classified materialAmerican personnel. Food inspectors with radiation * Treating casualtiesdetectors traveled to wholesale markets, bulk issue 9 Determining actual and potential hazardspoints, and commissary distribution warehouses to o Minimizing further hazardsmonitor the supplies. Inspectors also obtained rep- * Requesting required assistanceresentative food and dairy-product samples for labo- 9 Providing control and logistical supportratory analysis. They determined that all foods met of on-site personnelU.S. and host-nation contamination guidelines. * Handling claims, public information, and
Although fallout data were available from State relations with local civilian groupsDepartment and host-nation authorities, the infor- e Establishing communications between themation was sometimes delayed or unavailable for accident site and higher headquarterssome geographical areas in which Americans were Service Response Force. The capabilities of thestationed. The task force established an environ- IRF are limited. Total control of the accident re-mental monitoring program for U.S. communities, sponse will be the responsibility of the SRF, whichand obtained measurements of external fallout expo- should arrive within 24 hours after the accident oc-sure rates. Samples of air, soil, rainfall, and drinking curs. The SRF will consist of an aggregate of person-water were collected from U.S. facilities throughout nel, with a military staff as the nucleus. Members ofthe command and analyzed by medical personnel, the IRF will be integrated into the SRF and will con-using preventive medicine units and medical treat- tinue to play a major role in the response. The re-ment facilities. sponse force will be augmented by DOE scientific
and technical advisers and by specialized teamsNuclear Accident and Incident Response and from other services, as required. The SRF com-Assistance Organizat' n mander will be a general officer, designated as the
On-Scene Commander (OSC).2 Responsibilities ofThe Department of Defense (DOD) has estab- the OSC include, but are not limited to, the follow-
lished a policy for coordinating the response to a ing:nuclear-weapon accident which (a) identifies the re- o Safeguarding national-security materialssponsibilities for command at the scene, and (b) and informationclarifies the coordination among DOD and other 9 Coordinating with federal, state, and localfederal agencies, such as the Department of Energy authorities (a liaison officer should be(DOE) and the Federal Emergency Management provided to local, state, or host-nationAgency (FEMA).231 2 authorities and to the senior FEMA
All U.S. Army installations with custody of nu- official by the OSC as soon as possible)2
clear weapons will have a dedicated response force * Ensuring that a public-health hazardthat is prepared to respond to any nuclear incident, assessment is madeInitial response and service response procedures * Notifying civil authorities of the precau-will be included in the standard operating proce- tions and other measures required fordures for the installation's Nuclear Accident and In- protecting public health and safetycident Response and Assistance organization. 9 Establishing the priorities for response,
Initial Response Force. The Initial Response recovery, and restoration effortsForce (IRF) is the nearest military installation, re- * Coordinating, reviewing, and approvinggardless of size, to respond to an accident, to take public information and news releasesimmediate emergency lifesaving measures, to pro- - Communicating all required informationvide security, to reduce exposures, and to provide a and situation reports to the Nationalfederal presence and humanitarian support. IRF Military Command Center and servicemembers will coordinate on-scene hazard contain- operations centerment activities with civil authorities, and Will re- * Coordinating with the senior FEMAmain in charge until arrival of the Service Response official (in the continental United States)Force (SRF). The IRF unit should be trained and and state or host-nation authorities toequipped to provide 24-hour capability.' The IRF restore the accident site
239

tldical Conselquit1nces of Nitch'ar Warfare
"* Coordinating with the accident investiga- help medical authorities to make definitive treat-tion board ment decisions for individual casualties. The MRAT
"* Obtaining assets required to support maintains treatment protocols that are relevant toresponse operations the handling of radiation-accident injuries, based on
state-of-the-art radiobiology research and humanGuidelines for Medical Advisors radiobiology data from previous accident victims.
Department of Energy Assistance. Major DOE
The Installation Medical Authority (for the IRF) installations have medical support capabilities thatand the Medical Staff Advisor (for the SRF) are re- can be called on for assistance, if needed. Also, DOEsponsible for planning the medical support required facilities that routinely handle radioactive materialfor their respective portions of the nuclear-accident are equipped to give medical treatment to radiologi-response. They should maintain up-to-date plans cal casualties. The Radiation Emergency Assistanceand be prepared to train and supervise other medi- Center Training Site (REAC/TS) in Oak Ridge, Ten-cal personnel. Procedural guides should be pre- nessee, is prepared to deal with all types of radiationpared and distributed to any medical facility that exposure and can provide expert advice and assis-may become involved in the support of such a re- tance.2
sponse.These medical advisors must be prepared to deal Rescue and Evacuation of Injured Persons at a
with the question of how much long-term radiation Nuclear Accident Sitehazard exists for the local population in the contami-nated area. Another concern is the development of An accident involving a nuclear weapon willdefinitive treatment regimens for individual radia- probably result in casualties. The injuries may betion casualties and combined-injury casualties. Sev- severe and numerous, like those from a seriouseral army, DOD, and DOE advisory teams will assist multi-vehicle accident. Emergency personnel sent tothe medical advisors in determining appropriate an accident site must be well trained in trauma firstmedical guidance. Although these teams will re- aid. By the time medical personnel arrive at thespond to the accident site or treatment facility on re- scene, initial rescue may have been effected andquest, prior coordination between the IRF and SRF some first aid given. The medical personnel shouldmedical advisors and the special teams is recom- assist in further rescue operations and begin evacu-mended. ating casualties to the closest medical facility as soon
Radiological Advisory Medical Team. The army as possible. They should notify the receiving facilityhas established the Radiological Advisory Medical of the nature of the accident and the number andTeam (RAMT), which is staffed with health physi- type of patients involved.cists, physicians, and technicians trained to evaluate The weapons materials give off short-range alpharadiological health hazards and manage radiation radiation, which is not a hazard to attending person-casualties.13 At the accident scene and at the medi- nel unless the actual radioactive material itself is in-cal facility, the RAMT will assist with the following: haled. Standard military protective masks provide
"* Potential health hazards from radioactive excellent protection. They should be worn by per-contamination sonnel inside ambulances until the patients are
"• Medical treatment and decontamination brought to the medical facility. Hospital personnelof casualties can safely wear a standard surgical mask.
"* Decontamination procedures for person- After the patients have been brought to the hospi-nel, facilities, and equipment tal, the ambulance personnel and their vehicles
"* Control methods for radiation exposure should be decontaminated as soon as possible, evenduring on-site recovery and restoration if monitoring facilities are not available. They mustoperations not be released until monitoring indicates that they
"* Medical surveillance or bioassay proce- are no longer contaminated. This requires specialdures during site-restoring operations alpha-sensitive radiation equipment, which is gener-
Medical Radiobiology Advisory Team. The De- ally not available at hospitals, and will have to befense Nuclear Agency has established a Medical Ra- obtained from teams at the accident site.diobiology Advisory Team (MRAT) located at the The place for decontaminating ambulance per-Armed Forces Radiobiology Research Institute in Be- sonnel can be the same place used by other hospitalthesda, Maryland. 2 This team is trained in the bio- personnel (such as the emergency room staff), pref-medical consequences of radiation exposure. It will erably away from the emergency room. The place
240

Radiolt)gical Con.sidehrat ios hi Medical Operations
should have two entrances and a shower. A number plies to the physician but should not touch the pa-of laundry bags should be set up and tagged. The tient or the equipment. These personnel should notpersonnel should strip off all clothing and put it into leave the room. There should be other circulatingappropriate bags. If necessary, large tags should be personnel who would bring supplies to the roomattached to the clothing. Personal items, such as but who should not enter the room.watches and jewelry, should be put into plastic bags. The treatment priorities for a contaminated pa-Protective masks should also be put into a special tient will vary with the seriousness and nature of thebag. A complete set of clean clothing should be basic injuries. As lifesaving resuscitative measuresavailable to personnel. If this is not possible, clean are progressing, certain decontamination proceduresscrub suits should be provided until fresh clothing can be performed without compromising the care ofcan be obtained. Complete monitoring is essential the patient. The patient's clothing should be re-after showering, moved carefully and put into a tagged bag for later
decontamination or disposal. Valuables should beput into a tagged bag (preferably plastic) and held in
Initial Care, Resuscitation, and Admission of a designated place for monitoring and decontamina-Contaminated Patients tion; they should not be mixed with the valuables of
other patients. The patients should be thoroughlyEvery medical facility must have a plan for han- washed, especially their exposed surfaces. The rinse
dling contaminated patients, while still restricting water must be collected. Later disposal must be inany changes in basic operations to those that are ab- accordance with the limitations of the laws of the na-solutely essential. The most important objective is to tion in which the accident occurred. Consultationgive injured patients proper, efficient, and rapid care with expert personnel from among those at the acci-without spreading the contamination. Traffic dent site will be necessary to assure that this is doneshould be restricted, and a diagram of traffic properly. Normal surgical management of woundschanges should be posted in the emergency room will be more than adequate for removal of radioac-area. If possible, contaminated patients should be tive contamination. Special debridement procedurestreated in a room into which they can be brought are not required. Again, the rinse water or spongeswithout crossing main corridors in the building. should not be disposed of until expert advice has
If the hospital has been warned of possible con- been obtained. Material objects from the woundstamination, the route over which the patients are to must be saved. If they can be separated from thebe brought may be covered with paper. After the rest of the waste, they should be put into markedpatients enter the treatment room, this paper should bags. These fragments will be studied by expertsbe carefully rolled up by personnel wearing caps, and then disposed of through special procedures.gowns, masks, and gloves. The paper then should Patients should be admitted to designated wardsbe put into tagged bags. The process can be re- or rooms and kept in semi-isolation to limit thýpeated as often as necessary. If patients are brought spread of the contamination. All personnel shouldin over uncovered floors, the floors should be imme- put on gowns, gloves, caps, masks, and shoe coversdiately covered with paper. The paper must be left before entering the room and should remove themin place until personnel with the proper monitoring after each visit. All waste materials and linens mustequipment arrive to help evaluate the hazard. Traf- be marked and monitored. Frequent monitoring byfic over the paper must be limited to that which is trained health-physics personnel will be required toabsolutely essential. determine when it is proper to discontinue isolation
Several laundry hampers should be available in techniques.the treatment rooms and adjacent hallways. They The patient's urine should be saved to be ana-should be tagged so that all linens and clothing can lyzed for radiological contamination. Normal uri-be properly identified for later decontamination. nalyses can be done safely on portions of the sample,
A treatment team should be organized to func- but the laboratory should be notified that there is ation like an operating-room team, and will require a potential hazard of contamination with radioactivemoderate amount of prior training so that it will material. The laboratory must keep a record of thefunction smoothly and effectively. All members volumes of urine so that later calculations can beshould wear caps, gowns, masks, and gloves. The made of estimated body burdens of radioactive ma-physician and an assistant (if required) should be re- terials by appropriate laboratories. Fecal samplesstricted to the area immediately around the patient. should also be taken and retained, in addition toCirculating personnel in the room should bring sup- nose blows and swabs, when directed.
241

Meithol Conisepiuences of Nuclear War fir
the regular operating-room area. Alternative surgi-cal areas may be used, such as a plastic surgery
Operating-Room Care of Contaminated Patients clinic or an outpatient surgical facility.The actual surgery can be managed according to
Some of the patients from a nuclear accident may standard operating procedures for handling personsbe injured severely enough to require extensive sur- contaminated with infectious hazards, with the fol-gical care. These patients may be contaminated with lowing additions or exceptions:any of a variety of radioactive and nonradioactive * All waste material must be saved inmaterials. Most of the materials will not be a signifi- appropriate containers. Large plasticcant hazard to operating-room personnel if simple bags are the most suitable because theyprecautions are taken. The basic organization and do not leak, if properly handled. Theroutine of the operating room should not be containers must be tagged so that theychanged. can be identified later and examined by
Since the hazard from any contaminating mate- qualified personnel.rial will be respiratory, all personnel in the operating * Used surgical gowns, caps, and glovesroom should wear surgical masks at all times. Per- must also be considered contaminated.sonnel with monitoring equipment will be able to They must be removed carefully, andadvise the operating-room staff when it is safe to persons assisting in their removal mustunmask. be wearing caps, gowns, and gloves.
Once an operating room has been used for the The masks should be put in a markedsurgical care of nuclear-accident patients, decon- container.tamination and monitoring will be necessary before * All personnel should shower completelythe room can be used for normal surgical cases. The after working on such cases and mustsurgical service must be prepared to lose the use of not be released from the area until afterthe room for the time needed for these procedures. they are monitored. This monitoringIn some cases, it may be practical for a hospital to set must be done by qualified technical-up a temporary operating room close to but not in team personnel with special equipment.
SUMMARY
A nuclear event exposes people to a blast wave, more prompt, effective action. The experiencethermal pulse, and ionizing radiation. If medical gained through medical operations in peacetime ra-units are near the target area, injury and damage diation incidents provides skills that are directlymay disrupt their ability to perform. Thorough transferable to the medical support of the tacticalprior planning to adjust medical operations to the nuclear battlefield. Unless medical personnel recog-nuclear environment is essential. Intensive mission- nize and plan for the radiological effect on unit op-oriented training that addresses the concerns of erations, the health-care delivery system may be-medical personnel can reduce their stress and lead to come a casualty of the nuclear event.
242

Radiological Considerations in Medical Operations
NUCLEAR WEAPONS ACCIDENT CHECKLISTS
Predeployment
Publications. Establish necessary publications, including the Nuclear Weapons AccidentResponse Procedures Manual (Defense Nuclear Agency Manual 5100.1) and pertinent serviceand local directives.
Medical Matiriel. Establish necessary medical gear that can be immediately transferredto the accident site, ensuring that all shelf-life items are still effective. The gear will bebased on the expected number of casualties and the amount of medical materiel that can becarried by the initial response team(s).
Directory. Establish a directory of local radiological resources, including their locationsand telephone numbers. This should include military and civilian health-physics personneland equipment, as well as the nearest whole-body counters and persons trained to usethem. Also include the telephone numbers for REAC/TS as well as for local and state orregional coroners. Ensure that the lists include Autovon, FTS, and commercial numbers, asappropriate.
Training Plans. Establish regular and routine training for medical personnel in the han-dling of radiological hazards from a nuclear accident. This may be a part of nuclear/bio-logical/chemical training, but it should be emphasized that the hazards from a nuclearweapons accident differ from the hazards from most other radiation accidents. Ensure thatmedical team members from other units are also trained and aware of their roles.
Organization and Communications. Review the local organization chart for personsand groups to be notified in case of a nuclear weapons accident, and ensure that the lines ofcommunication and the duties of medical organization are clear and thoroughly under-stood. Review the communications assets to be used in the field, and ensure that personnelare aware of proper operational procedures.
Transportation. Review the transportation assets to ensure that equipment and person-nel can be quickly transported. Establish a priority list for personnel and equipment in casethe accident site is difficult to reach. Establish contingency plans for movement by four-wheel-drive vehicles and by helicopter.
Field Deployment
Casualty Treatment and Triage. The first medical personnel to arrive on the sceneshould begin immediately to treat casualties. If casualties have already been treated, con-tact the treatment facilities (in conjunction with radiological controls personnel) to followup on patient treatment and to perform radiological surveys of the facilities, as needed.Treatment should always be given in priority of medical condition. Radiation injury orcontamination should not upset the normal triage pattern.
Mortuary Affairs. Make arrangements with local coroners or civil officials for the re-moval of fatalities from the accident site, if necessary. This should be coordinated with thelegal and public affairs staffs.
243

Medical Consequences of Nuclear Warfare
REFERENCES
1. Department of the Army. 1973. NATO handbook on the medical aspects of NBC defensive operations IAMedP-6; FM 8-91.Washington, DC: Department of the Army (revision in press).
2. Defense Nuclear Agency. 1984. Nuclear weapons accident response procedures (NARP) manual [DNA Manual 5100.11.Washington, DC: Defense Nuclear Agency.
3. Department of the Army. 1988. Nuclear accident and incident response and assistance (NAIRA) ITC 3-151. Washington,DC: Department of the Army.
4. North Atlantic Treaty Organization. 1981. Commander's guide on nuclear radiation exposure of groups ISTANAG 20831.Brussels: North Atlantic Treaty Organization.
5. Reese, H. L. 1986. DOD nuclear mishaps fSpecial Report SP86-21. Bethesda, MD: Armed Forces Radiobiology Re-
search Institute.
6. Lewis, F. 1987. One of our H-bombs is missing. New York: Bantam Books.
7. Project Crested Ice. USAF nuclear safety [special ed., March 1970] 65(2).
8. Gus'kovava, A. K., ed. 1987. Earh! acute effects among the victims of the accident at the Chernobyl Nuclear Power Plant[USSR Ministry of Health Order Number 48511, translated by U.S. Defense Intelligence Agency ILN 818-871.Moscow: USSR Ministry of Health.
9. Linneman, R. E. 1987. Soviet medical response to the Chernobyl nuclear accident. JAMA 258(5): 637-643.
10. Parker, J. S. 1986. 7th MEDCOM Task Force monitors contamination. MEDCOM Examiner 17(6): 1.
11. Dickey, C. 1986. Chernobyl danger slight in EUCOM. The Stars and Stripes 45(63): 1.
12. Department of the Army. Nuclear surety [AR 50-51. 1986. Washington, DC: Department of the Army.
13. Department of the Army. 1985. Medical support-nuclear/chemical accidents and incidents [AR 40-13]. Washington, DC:Department of the Army.
RECOMMENDED READING
American Medical Association. 1984. A guide to the hospital mnanagemnent of injuries arising from exposure to or inwolvingionizing radiation. Chicago: American Medical Association.
Conklin, J. J., and Walker, R. I., eds. 1987. Military radiobiology. Orlando, FL: Academic Press.
Halperin, J. A.; Shleien, B.; Kahana, S. E.; and Bilstad, J. M. 1981. Background material for the development of the FDArecommendations on thyroid-blocking with potassium iodide [HHS Pub FDA81-81581. Washington, DC: Depart-ment of Health and Human Services.
Nishiyama, H.; Lukes, S. J.; and Saenger, E. L. 1984. Low-level internal radionuclide contamination: Use of gammacamera for detection. Radiology 150(1): 235-240.
Department of the Army. 1969. Nuclear Handbook for Medical Service Personnel [TM 8-2151. Washington, DC: Departmentof the Army.
Shleien, B. 1983. Preparedness and Response in Radiation Accidents IHHS Pub FDA83-82111. Washington, DC: Departmentof Health and Human Services.
Shleien, B.; Schmidt, G. D.; and Chiacchierini, R. P. 1982. Background for protective action recommendations: accidentalradioactive contamination of food and animal feeds [HHS Pub. FDA82-8196]. Washington, DC: Department ofHealth and Human Services.
244

Chapter 11
PROSPECTS FORRADIOPROTECTION
LEO I. GIAMBARRESI, Ph.D.* AND RICHARD 1. WALKER, Ph.D.**
INTRODUCTION
RADIATION INJURY
Ionizing RadiationBiological Damage
PROTECTION AGAINST RADIATION INJURY
MechanismsCandidate Agents
REPAIR OF RADIATION INJURY
Chemical Repair by Hydrogen TransferGenetic Repair
REGENERATION AFTER RADIATION INJURY
MechanismsCandidate Agents
COMBINATION AGENTS
RationaleExamples of Combination AgentsMitigation of Performance DecrementRadioprotectants and Supportive Therapy
DEVELOPMENT OF A RADIOPROTECTIVE REGIMEN
Level of ProtectionToxicityDeliverabilityOther Factors
SUMMARY
*Lieutenant, United States Navy; Armed Forces Radiobiology Research Institute, Bethesda, Mart/land 20814-5145-Captain, United States Nazy; Director, Enteric Disease Progran:, Naval Medical Research hlstitute, Bethesda, Maryland 20814-5055 andArmed Forces Radiobiolo, Research Institute, Bethesda, Marhland 20814-5145
245

Methdicl Coisequences orf Nichir Wartart
INTRODUCTION
One of the longest-sought and most elusive goals revolution, are providing exciting approaches forin radiobiology has been the development of a phar- developing specific and effective means to mitigatemacological agent that can mitigate the early dam- radiation injury.age produced in cells and tissues by ionizing radia- The primary objective is to develop an agent or
tion. The search for such an agent began in 1949 combination of agents that will substantially in-with the simultaneous demonstration by two differ- crease survival and enhance the postattack effective-ent laboratories of survival in rodents exposed to a ness of military personnel on a nuclear battlefield.leth,.l dose of radiation and treated with the sulfur- This radioprotective agent differs from the medicalcontaining compounds cysteine or glutathione.' 2 interventions discussed in previous chapters in thatSince that time, many diverse compounds have been it must be easily self-administered shortly before orshown to have protective activity (Table 11-1). after radiation exposure to reduce early molecular,
With new advances in immunology, biochemis- cellular, and tissue damage. This chapter briefly re-try, radiobiology, and pharmacology, the achieve- views the relevant radiobiological concepts, presentsment of that goal may be at hand. Over the longer the strategies and mechanisms for mitigating radia-term, newer concepts and techniques in molecular tion injury, and discusses some of the more promis-biology, arising from the so-called biotechnology ing agents being investigated.
RADIATION INJURY
To understand the various strategies being used Biological Damageto mitigate ionizing radiation injury, it is first neces-sary to define ionizing radiation and to consider the Death from radiation injury is the resuit of a se-events that occur in the development of ARS. quence of events that occurs over a period of less
than a billionth of a second to several weeks (FigureIG-aizing Radiation !1--l).>2" The first step in this sequence is the trans-
fer of radiation energy from the photon or particle toIonizing radiation can be defined as any type of atoms and molecules in its path. This results in the
electromagnetic radiation (such as X or gamma rays) production of the first discrete lesion in the se-or particulate radiation (such as neutrons or alpha quence: a chemical alteration in macromoleculesparticles) that has sufficient energy to ionize atoms that are critical for biological function. Although theor molecules; that is, to eject electrons from their importance of membrane damage is still beingouter orbits. evaluated, much of the evidence suggests that dam-
In considering the effects of radiation on biologi- age to DNA may be the most important factor in cellcal systems, it i, important to distinguish the differ- death. 2", This initial chemical injury can occur inent types of ionizing radiation according to their one of two ways. If a critical biological molecule isLET. This term describes the amount of energy de- in the radiation path, it becomes chemically alteredposited by a particular type of radiation per unit of by direct interaction with radiation energy. If thatpath length. Low-LET radiation (X and. gamma molecule is not in the radiation path, it can still be-rays) is sparsely ionizing because it causes few ioni- come chemically altered indirectly, via reactionszations per micron of path length, whereas high-LET with free radicals and reactive oxygen species pro-radiation (neutrons and alpha particles) is densely duced primarily from the radiolysis of water.ionizing because it produces many ionizations per These free radicals and oxygen species are impor-micron of path length. Generally, high-LET radia- tant in the overall scheme of radiation injury be-tion is much more efficient in producing biological cause their lifetime in solution is sufficiently long todamage than low-LET radiation." allow them to diffuse and extend the damage be-
246

Prospects for Radioprotection
TABLE 11-1
RADIOPROTECTIVE COMPOUNDS
Protective Probable MechanismCompounds Effectiveness* of Action References
Aminothiols Free-radical scavenging, hydrogen donationCysteine (+++) 3-6WR-2721 (+++) 3,6,7MPG (++) 3,8,9
Other Sulfur Compounds Free-radical scavengingDimethvlsulfoxide** (++) 4,10,11Thiourea (+) 10,12
Cyanide derivatives*** HypoxiaCyanide (++) 12-14Hydroxyacetonitrile (+++) 10,12, 14
Chelating Agent UncertainEDTA (+) 10,12
Metabolites Free-radical scavengingGlucoset (+) 12Fructoset (+) 12
Hypoxia inducers HypoxiaParaminopropiophenone (+++) Hemoglobin changes 6,12,14Carbon monoxide (++) 14Ethanol t (++) Respiratory-center depression 14Morphine (++) 14Serotonin (+++) Hemodvnamic alterations 14
Immunomodulators Hematopoietic system regenerationGlucan (++) 3,15Trehalose dimycolate (++) 16,17Endotoxin (++) 3,18-20
Cytokines Hematopoietic system regenerationlnterleukin-I (++) 21Tumor necrosis factor (+) 21
Antioxidants Free-radical scavengingVitamin E (+) 22,23Vitamin A (beta-carotene) (+) 24Superoxide dismutase (+++) Oxygen detoxification 25Selenium (+W 22
Eicosanoids UncertainDiPGE, (++) 26,27
*Data taken from studies using mice exposed to X or gamma radiation. Grading is according to following scale:(+) slight protection (DRF < 1.2); (++) moderate protection (DRF < 1.5); (+++ good protection (DRF > 5).
"**Provides protection when administered topically
'Highly toxic: Protective dose is very close to toxic dose
'Provides protection only at extremely high dose (glucose and fructose, 13,500 mg/kg; ethanol 6-7.5 ml/kg)
247

Medical Consettqiuences of Nuchear Warfizre
S+Direct --
on', ot"Damaged"-+ Cell Stem -+Organismmolecules death cell death
depletion
Indirect/.H0- Free .0 Superoxidest Idiec -2O+radicals PeroxidesX, -r
Fig. 11-1. Direct and indirect radiation effects on key biological molecules, which can lead to death of critical cells. Withoutthose cells, the organism cannot survive.
yond the primary path of radiation. In this way, the There are several strategies for reducing radiationeffects of ionizing radiation within the cell are injury and mortality. Pharmacological agents cangreatly amplified. Most radiation injury from low- protect against indirect damage, repair damage onceLET radiation is the result of this indirect damage, it occurs, or stimulate the regeneration of depletedwhile that from high-LET radiation is from direct cell populations (Figure 11-2). Spanning thesedamage." The net effect of direct and indirect dam- strategies are new genetic approaches that are justage is the disruption of molecular structure and beginning to be used in the development of ad-function, leading to altered cell metabolism. When vanced pharmacological agents. Combinations ofDNA is damaged, this is followed by altered cell di- agents that exploit the operative mechanisms in atvision, cell death, depletion of stem-cell pools, organ least two of these strategies may substantially im-system dysfunction, and, if the radiation dose is prove drug effectiveness.high enough, death of the organism.
PROTECTION AGAINST RADIATION INJURY
As indicated in Figure 11-2, almost nothing can LET radiation injury is more difficult to achieve.3
be done pharmacologically to protect against the ini- Protective agents would be most effective against atial transfer of radiation energy to either water or low-LET radiation hazard.critical biological molecules. The transfer occurs too The earliest point at which a protective effectrapidly (within 10-11 seconds after irradiation) and is from pharmacological agents can be detected isa purely physical process.2- around 10-12 seconds after irradiation.-9 At that time,
The failure of radioprotective agents to protect the pharmacological agents can begin to repairagainst direct damage to critical molecules indicates chemical damage produced in the critical biologicalan inherent upper limit to the degree of protection molecules and also react with the chemical interme-that can be achieved pharmacologically. Because in- diates that indirectly damage these molecules. Pro-jury from high-LET radiation is due primarily to di- tection depends on the ability of chemical agents torect damage, and because the relative yields of water reduce the intracellular concentration of free radicalsradiolytic products and reactive oxygen species de- and reactive oxygen species that are producedcrease with increasing LET, protection against high- within the first millisecond after irradiation.
248

Prospects for Rakiioprotectioii
, •,,,Direct am+on, ot
Sb: IOrganism
J. death
AA#InlrctAI- 20
TA
Repopulation
Increasedsurvival
Fig. 11-2. Strategies of protection, repair, and regeneration may prevent cell and organism death after radiation exposure
eral ways: induction of hemodynamic cardiovascu-lar alterations, interference with hemoglobin func-
Mechanisms tion, increased tissue oxygen utilization, and de-pressed respiratory-center function. At the cellular
The damage induced by the products of radiation and molecular levels, localized hypoxia can beinteractions with water can be reduced either by in- achieved by agents that take part in the chemicalhibiting the formation of these reactive radical inter- and biochemical reactions that use oxygen.mediates, or by eliminating them from the cellular Induction of hypoxia is a widespread protectiveenvironment. This can be accomplished by using mechanism that accounts, at least in part, for theagents that induce hypoxia or that scavenge toxic protective action of many different chemicals, drugs,products. and physiological mediators (Table 11-1). In spite of
Hypoxia. The formation of reactive oxygen spe- that, the usefulness of this mechanism must be con-cies can be inhibited by the induction of hypoxia. sidered with caution because of the potential effectsThe extent of radiation damage in a tissue is directly of hypoxia on normal physiological function. Thisrelated to the degree of oxygenation of that tissue; caution may apply more to agents that induce a svs-agents capable of reducing oxygenation will miti- temic hypoxic state than to those that create local-gate the injury.' 2 Many of these chemical agents are ized hypoxia.known to induce transient systemic or localized hy- Scavenging. Free-radical scavenging and enzy-poxia." Systemic hypoxia can be achieved in sev- matic detoxification refer to the ability of chemicals
249

Mcdi'ical C•'n•'S01tics tit Nm/car W•rrt,
and endogenous enzymes to remove products of WR-2721 also exerts differing protective effects forwater radiolvsis and highly reactive oxygen species normal tissue and at least some types of solid tu-before they can damage molecules of biological irn- mors." In addition, the drug significantly reducesportance.2-" In essence, these are competitive reac- the toxicity of the tumor chemotherapeutic agents,tions between protective agents and biological mole- cyclophosphamide and cisplatin," " without alteringcules. In aqueous solutions, protective agents and tl.eir chemotherapeutic effectiveness. For these rea-enzymes react with free radicils and oxygen species sons, WR-2721 is undergoing clinical trials as an ad-to form relatively stable, nontoxic end products, junct to tumor radiation and chemotherapy. Twothereby reducing the concentration of these reactive other potentially beneficial clinical side effects of thisspecies and sparing the biological target. Many pro- drug are that WR-2721 is a hvpocalcemic agent andtectants are very efficient scavengers of water-dce- inhibits parathyroid hormone secretion.4 'rived free radicals. WR-2721 is still not available as a field-useable
radioprotective agent because it induces nausea andvomiting." ` Although no cumulative or irrevers-
Candidate Agents ible toxicity has ever been observed in humans orexperimental animals that received this drug (even
Agents currently available as candidates for pro- at relatively high doses), the animals did show sig-tection against indirect damage fall into three main nificant performance degradation after its parenteralgroups: auinothiols, naturally occnrriunig, antioxidants, administration .4 .
4 Another problem that must beand eicosanoids (Tables 11-2 and 11-3). Research is overcome is the drug's poor oral bioavailability, duealso being conducted using various genetic ap- primarily to first-pass metabolism by the intestinalproaches. mucosa during absorption." In addition, the drug is
Aminothiols. The vast majority of agents that hydrolyzed in the acidic environment of the stom-have been developed and tested in laboratory mod- ach, a factor that is aggravated by its ability to slowels for their ability to increase survival after irradia- gastric emptying.4 "tion are the aminothiols." These compounds are Research is in progress to overcome these bio-chemical analogues of the sulfur-containing amino availability problems by using different formula-acid, cysteine. Like cysteine, they have a sulfhydryl tions and by developing prodrugs that are not sus-group separated by two or three carbon atoms from ceptible to first-pass metabolism. Researchers area strongly basic nitrogen group (Figure 11-3). also seeking to control or minimize the side effects
As a group, the aminothiols are very effective by combining WR-2721 with antiemetics, or by usingprotectants, and they must be present in the system subtoxic amounts of the drug in combination withduring irradiation. Optimal protection in laboratory other agents that act synergistically or additively. Aanimals is generally obtained by intravenous injec- DRF of about 1.2 has been obtained with WR-2721tion 15-30 minutes before irradiation. The amino- administered intraperitoneally to mice at a dose thatthiols function primarily through free-radical produced no observable side effects or performancescavengingý and hydrogen transfer.• Hypoxia in- degradation."4
duction may also play a part in their functioning.'" The side effects of WR-2721 and the pharmaco-One of the most significant events in the develop- logical problems associated with its administration
ment of radioprotective agents was the 1969 synthe- are serious obstacles that must be overcome before itsis of an aminothiol derivative known as WR-2721 can be fielded as a military radioprotective agent.(ethiofos)." This drug was developed through a However, a number of other compounds have beenprogram sponsored by the Walter Reed Army Insti- developed through the army's program that maytute of Research, and is the most thoroughly studied more readily satisfy the requirements of a militarilyof over 4,00( compounds developed and tested to useful agent (Table 11-4).date. WR-2721 has been reported to reduce the ef- To compare these compounds for their potentialfect of a radiation dose by a factor of 2.7 in mice military usefulness, it is necessary to consider a vari-given this drug intraperitoneally 30 minutes before ety of characteristics in addition to the DRF. Theseexposure to gamma radiation."",' This is the highest include the route of administration, effective drugdose reduction factor (DRF) a,:-,inst mouse lethality dose, and therapeutic index. 7 The therapeutic index,at 30 days reliably reported fi single injection of a as used here, refers to the ratio between the toxicconventional radioprotectant. Increased 30-day sur- LD;, and the protective dose used to produce a spe-vival is commonly interpreted as protection against cific DRF. Although it would also be advantageousdeath due to hematopoietic-system failure. to compare information on acute side effects pro-
250

Prospects for Radioprotection
TABLE 11-2
SUMMARY OF PROTECTIVE SCAVENGING AGENTS
Mechanism Level ot Side Effects andand Agent protection Therapeutic Index" Deliverability Advantages Diadvantag~eb
WR-2721 DRF > 2.0 Nausea, vomiting, Dose'* = 400 mg/kg Very high DRFs possible; Large doses ( > 2W0 mg/kg);Duration ot hypotension, Route:*** i.v. or i.p. DRF = 1.2 at behaviorlv ineffective p.o.;effect > 3 hr hypocalcemia, Time: _V minutes non-toxic dose in human high DRFs only at doses that
behavioral changes before irrdiation clinical trials produce serious side effectsTI = 1.4 tDRF = 2.7)TI = 35 (DRF = 1.2)
WR-15'243 DRF = 1.3 Unknown side effects Dose = 40 mg/kg Effective p.o.; UnknownTI = 7.5 Route; p.o. fairly ltW doset< mg/kg);
Time: 30 minutes large TI ( >5.0)
before irradiation
WR-76841 DRF= 1.19 Unknown side effects Dose = 175mg/kg Effective p.o.; Fairly largeddoses > 100 mg/kg);TI = 5.1 Route: p.o. large TI ( > 50.0) DRF < 1.2
Time: 30 minutes
before irradiation
WR-1551 DRF = 1.3 Unknown side effects Dose = 100 mg/kg Effective p.o. Unknown
TI = 3.0 Route: p.o.Time: 30 minutes
before irradiation
WR-3302 DRF = 1.3') Unknown side effects Dose = 5 mg/kg Low doses (5 20 mg/kg); Oral effectivenessTI = 6.0 Route: i.p. large TI ( > 5.0) not established
Time: 30 minutes
before irradiation
WR-2926 DRF = 1.7 Unknown side effects Dose = 50 mg/kiz DRF > 1.5 Oral effectivenessTI = 2.5 Route: i.p. not established;
Time: 30 minutes TI < 3.0
before irradiation
WR-1607 DRF = 1.4 Nausea, vomiting Dose = 5mg/kg Low doses ( > 20 mg/kg); Oral effectivenessTI = 3.4 Route: i.p. mitigates performance not established
Time: 3)) minutes decrementbefore irradiation
Mercapto- DRF = 1.4 Unknown side effects Dose = 20 mg/kg Low duses ( < 20 mg/kg); Oral effectivesspropionyl TI = 100.0 Route: i.p. or i.v. extremely highTl not established;glycine Time: .30 minutes in clinical use (Japan); protection at 20 mg/kg isMPG) before irradiation effective after irradiation difficult to reproduce
Vitamin E DRF = 1.1 Unknown side effects Dose = 3 x dietary Effective p.o.; Dietary regimen may berequirement naturally occurring impractical for field use;
Route: p.o. dietary component single dose effectivessFeeding Regimen: not established;
I week before irradiation DRF < 1.2;4 weeks after irradiation conflicting reports in
literature on effectiveness
Vitamin A DRF 1.2h Unknown side effects Dose = 28 x dietary Effective p.o.; Dietary regimen may berequirement naturally occurring impractical for field use;
Route: p.o. dietary component single dose effectivessFeeding Regimen: not established;
I week before irradiation large vitamin dose required(3 x dietary
requirement)
4 weeks after irradiation(28 x dietary
requirement)
*Therapeutic index (TI): ratio of toxic LD to the drug dose required to produce the DRF specified in the table
**Dose: dosage of drug required to produce the DRF indicated under "Level of Protection"***Routes of administration: i.v. (intravenous), i.p. (intraperitoneal), p.o. (oral), s.c. (subcutaneous)
251

Medical Consequences of Nuclear Warfare
TABLE 11-3
SUMMARY OF DETOXIFICATION AGENTS, REGENERATION AGENTS, AND OTHER AGENTS OF UNDEFINEDACTION
Mechanism Level of Side Effects andand Agent Protection Therapeutic Index* Deliverabilitv Advantages Disadv antages
DETOXIFICATION AGENTSSelenium DRE f f I Unknown Dos" 4 ppm i Effective p.o.; Oral regimen man be impractical
drinking water naturally occurring for field use;Route: - p.., dietary component single p.o. dose ettectiveness notRegimen: 2 months established;
before irradiation DRF < 1.2Dose =1.6 mg/kgRoute: i.p.Time: 24 hours
before irradiation
Superoxide DRF= 1.5t Unknown side effects Dose and Time = 20 mg/kg DRF > 1.5; Oral effectivess not established;dismutase (1 hour before irradiation) effective as single dcoses large molecular size
and given 1 hour before irradiation35 mg/kg (1 hour afterirradiation)
Route: i.e.REGENERATION AGENTS
Glucan F DRF < 1.2 Unknown side effects Dose = 250 mg/kg Effective after irradiation Oral effectiveness not established;Doses > 250 mg/kg provide DRF < 1.2;
no increased protection optimum protection at 20 hoursRoute: iv. after irradiation is impracticalTime: 24 hours before for field use
irradiation
Trehalose 70', survival Unknown side effects Dose -- 1.7mg/kg Effective after irradiation; Oral effectiveness not established;dimvcolate at LDIlt Route: i.p. low dose •520 mg/kg) DRF unknown(TDM) Time: 2 hours after irradiation
delivered as a squaleneemulsion
lnterleukin-1 DRF = 1.25 Unknown side effects Dose = 0.001 mg/kg Extremely low doses Oral effectiveness not established;(IL-I) Route: i.p. 45 0.01 mg/kg) optimum protection at 20 hours
Time: 20 hours after irradiation is impracticalbefore irradiation for field use;
effectiveness is strain dependent
Tumor-necrosis DRF 1.16 Unknown side effects Dose =_ 0.2 mg/kg Very low doses Oral effectiveness not established;factor (TNF) Route: i.p. ( < 0.5 mg/kg); effectiveness optimum protection at 20 hours
Time: 20 hours is not strain dependent before irradiation is impracticalbefore irradiation for field use
AGENTS OF UNDEFINED ACTION
16,16-Dimethvl DRF= 1.72 Diarrhea; Dose = 1.6 mg/kg Low doses ( < 20 mg/kg); Oral effectiveness not established;prostaglandin E2 decreased ambulation Route: s.c. DRF > 1.5 severe diarrhea at protective doses(DiI'E,) Time: 5-15 minutes
before irradiation
Leukotriene C 4 DRF= 1.9 Unknown side effects Dose= 0.4 mg/kg Very low doses ( <0.5 mg/kg); Oral effectiveness not established(LTC 4 ) Route: s.c. DRF > 1.5
Time: 5 minutesbefore irradiation
Platelet- DRF = 1.9 Unknown side effects Dose = 0.3 mg/kg Low doses ( < 20 mg/kg); Oral effectiveness not establishedactivating Route: s.c. DRF > 1.5factor (PAF) Time: 5-10 minutes
before irradiation
*Therapeutic index (TI): ratio of toxic LD5, to the drug dose required to produce the DRF specified in the table"**Dose: dosage of drug required to produce the DRF indicated under "Level of Protection"
***Routes of administration: i.v. (intravenous), i.p. (intraperitoneal), p.o. (oral), s.c. (subcutaneous)
252

Prospects for Radioprotection
Compound Structural Formula
SULFHYDRYLS COOH
Cysteine
MEA
WR-76841 OH 3
OH 3
MPG COOH O CH 3ICH,
PHOSPHOROTHIOATES
WR-2721 NH 2 CH2CH 2 CH 2 CH PO 3 H 2
WR-3689 CH 3 N H 2 CH 2 CH 2 CHPO 3 H2
NH
WR-159243 &-CH 2,PO 3 H
THIOSULFONATES
WR- 1607 CH 3 CH 2 CH2 CH 2 CH 2CH 2 CH 2 CH2 CH 2 CH2 SO 3 H
WR-3302 lO-CH 2 CH 2 CH 2 CH 2CCH 2' HSO 3 H
Fig. 11-3. Structural formulas for selected sulfur-containing radioprotectants. All compounds are chemical analogues ofcysteine and MEA.
duced by these agents at protective doses, the data dose (5 mg/kg) in protecting against radiation-in-are so limited that these factors cannot be included duced lethality, and (b) it is one of the few com-at this time. pounds available that not only enhance survival but
The compound that stands out as the most prom- also ameliorate ETI.•, 9 This latter effect may be re-ising candidate is the phosphorothioate WR-159243. lated to the drug's ability to minimize postirradia-Although its DRF is only 1.3, it is effective in mice tion hypotension.4when given orally, the protective dose is less than 50 WR-2721 has a therapeutic index of only 1.4 atmg/kg, and it has the highest safety margin or the dose required to produce a DRF of 2.7. How-therapeutic index (7.5) of all the compounds listed, ever, the therapeutic index increases dramatically toOther compounds with therapeutic indices greater 7.0 at a dose that produces minimal side effects (200than 2.5 that are being considered include (a) the mg/kg). The DRF obtained at this dose is 1.2.sulfhydryl WR-76841, because of its oral effective- WR-3689 is identical in structure to WR-2721, ex-ness and relatively high therapeutic index (5.1); and cept that WR-3689 possesses a terminal methyl(b) the thiosulfonates WR-1551, because of its oral ef- group (Figure 11-3). When given intraperitoneallyfectiveness; WR-3302, because of its very low effec- at a dose of 450 mg/kg, it provides a DRF of 1.7 withtive dose (5 mg/kg) and high therapeutic index a therapeutic ii' ')f 2.5. When given orally at a(6.0); and WR-2926, because of its relatively low ef- similar dose (' kg), WR-3689 is still capable offective dose (50 mg/kg) and relatively high DRF providing sign protection (DRF: 1.2). With(1.7). The thiosulfonate WR-1607 is particularly this regimen, the therapeutic index for WR-3689 in-interesting because (a) it has a very low effective creases to greater than 3.5 because the lethally toxic
253
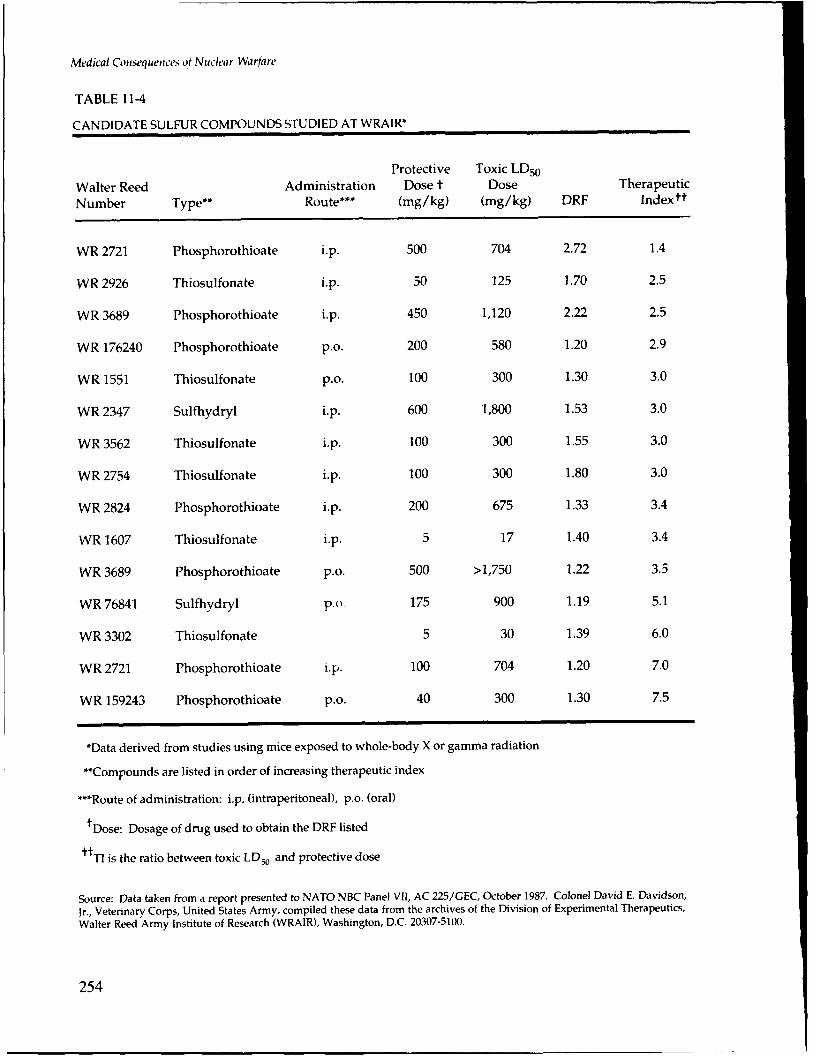
Medical Consequences of Nuch'ar Warfare
TABLE 11-4
CANDIDATE SULFUR COMPOUNDS STUDIED AT WRAIR*
Protective Toxic LD50Walter Reed Administration Dose t Dose Therapeutic
Number Type** Route*** (mg/kg) (mg/kg) DRF Indextt
WR 2721 Phosphorothioate i.p. 500 704 2.72 1.4
WR 2926 Thiosulfonate i.p. 50 125 1.70 2.5
WR 3689 Phosphorothioate i.p. 450 1,120 2.22 2.5
WR 176240 Phosphorothioate p.o. 200 580 1.20 2.9
WR 1551 Thiosulfonate p.o. 100 300 1.30 3.0
WR 2347 Sulfhydryl i.p. 600 1,800 1.53 3.0
WR 3562 Thiosulfonate i.p. 100 300 1.55 3.0
WR 2754 Thiosulfonate i.p. 100 300 1.80 3.0
WR 2824 Phosphorothioate i.p. 200 675 1.33 3.4
WR 1607 Thiosulfonate i.p. 5 17 1.40 3.4
WR 3689 Phosphorothioate p.o. 500 >1,750 1.22 3.5
WR 76841 Sulfhydryl po 175 900 1.19 5.1
WR 3302 Thiosulfonate 5 30 1.39 6.0
WR 2721 Phosphorothioate ip. 100 704 1.20 7.0
WR 159243 Phosphorothioate p.o. 40 300 1.30 7.5
*Data derived from studies using mice exposed to whole-body X or gamma radiation
"**Compounds are listed in order of increasing therapeutic index
***Route of administration: i.p. (intraperitoneal), p.o. (oral)
tDose: Dosage of drug used to obtain the DRF listed
tr TI is the ratio between toxic LD• and protective dose
Source: Data taken from a report presented to NATO NBC Panel VII, AC 225/GEC, October 1987. Colonel David E. Davidson,
Jr., Veterinary Corps, United States Army, compiled these data from the archives of the Division of Experimental Therapeutics,
Walter Reed Army Institute of Research (WRAIR), Washington, D.C. 20307-5100.
254

Prospects for Radioprotection
Radiation Metabolism Disease
Molecular Scavengingdamage Vitamin E
Enzymatic Detoxification AC
Catalase Glutathione
Superoxide02 dismutase L 02 + H 2 0 2 H 2 0 + 02
(Copper,Zinc) Glutathione
peroxidase
Glutathione Glutathione disulfide
Glutathionereductase
Fig. 11-4. Natural biochemical defense system of the cell, which scavenges free radicals and detoxifies reactive oxygen species
oral dose is much higher than that for the intraperi- cells against free radicals and reactive oxygen spe-toneal dose. cies arising from normal metabolic processes. This
Another potentially promising aminothiol com- defense can be divided into two components: com-pound is mercaptopropionylglycine (MPG). Under pounds of low molecular weight that scavenge freethe trade name Thiola, this drug has been available radicals, and enzymes that detoxify reactive oxygenin Japan since the 1970s. It has been used as a de- species (Figure 11-4).53
toxifying agent for heavy-metal poisoning, among The low-molecular-weight compounds that func-other clinical applications.' Evidence suggests that tion as free-radical scavengers in this defense systemMPG is also radioprotective. In the most promising include vitamins A and E, which are lipophilic, andstudies, it has provided a DRF of up to 1.4 when in- vitamin C, which is hydrophilic. The enzymatic armjected intraperitoneally at a dose (20 mg/kg) that is of this system includes superoxide dismutase, whichabout 100-fold lower than its toxic dose (2,100 mg/ catalyzes the conversion of superoxide anions to hy-kg).1' 52 drogen peroxide and molecular oxygen. The hydro-
Naturally Occurring Antioxidants. Naturally oc- gen peroxide produced by this reaction is removedcurring compounds that function as antioxidants, from the system by two other enzymes: catalase andsuch as certain vitamins, minerals, and enzymes, are glutathione peroxidase. Selenium contributes to thisalso being evaluated. These are part of a natural bio- scheme in that it is a cofactor for glutathione peroxi-chemical defense system that has evolved to protect dase.
255

Medical Ctuiset'quenC'S of Nuclear Warfrfe
Vitamin E has been shown to increase survival af- they are normal dietary components, and consider-ter irradiation.22 Groups of mice were fed either a able data on their toxicity, metabolism, and pharma-basal control diet or a diet supplemented with three cological action in the human are available. Theytimes the normal daily mouse requirement of vita- are also effective when given orally.min E (dl-alpha-tocopherol) for I week before an 8.5- The parenteral administration of superoxide dis-Gy dose of cobalt-60 gamma radiation and for 30 mutase has increased survival in mice exposed todays after exposure. All of the control animals suc- ionizing radiation. 2
5 Intravenous injection of thiscumbed by day 30, whereas 60% of the vitamin E- enzyme to mice at a dose of 200 mg/kg given 1 hourfed animals survived. At 7.5 Gy, 1017c of the controls before irradiation with X rays resulted in a DRF ofsurvived, while 100%7' of the vitamin E-fed animals 1.38. A single injection of only 35 mg/kg given 1survived. DRFs for vitamin E have not been deter- hour before irradiation with X rays was also able tomined experimentally. increase survival (DRF: 1.12). The highest DRF re-
Vitamin A is also able to increase postirradiation ported for this enzyme is 1.56, achieved in micesurvival when fed to mice as a dietary supplement.2 3 given two intravenous injections: one at a dose ofIn these experiments, mice were maintained on a ba- 200 mg/kg given 1 hour before irradiation with Xsal control diet containing three times the daily rays, and the other at a dose of 35 mg/kg given Imouse requirement of vitamin A for 1 week before hour after irradiation.2 •irradiation from a cesium-137 source. Immediately Eicosanoids. The eicosanoids are a large groupfollowing irradiation, they were maintained for the of potent inflammatory mediators derived from theremainder of the experiment on (a) the basal diet, (b) 20-carbon fatty-acid precursor, arachidonic acid.a diet supplemented with about twenty-eight times The compounds in this family that are being exam-the normal requirement of vitamin A, or (c) a diet ined for their ability to increase the survival of irra-supplemented with an amount of beta-carotene diated animals include 16,16-dimethyl prostaglandinequivalent to about ten times the normal require- E, (DiPGE_, a synthetic analogue of the naturally oc-ment of vitamin A. The vitamin A diet was able to curring prostaglandin GE), leukotriene C 4 (LTC 4),
produce DRFs of 1.12-1.25. The beta-carotene diet and platelet-activating factor (PAF). In one study,produced a DRF of 1.26. Significant mitigation of DiPGE, was given subcutaneously to mice at a doseradiation lethality was also provided by vitamin A of 1.6 mg/kg and was able to elicit a DRF of 1.72, al-when diet supplementation was delayed for up to 2 though severe diarrhea occurred at protectivedays after irradiation, although delaying the supple- doses.27 The optimal time for injection is 5-15 min-mentation for 6 days resulted in no increase in sur- utes before cobalt-60 gamma irradiation, but protec-vival over the basal-diet-fed animals. Vitamin A fed tion can still be achieved when the compound isto mice for 3 days before partial-body irradiation can given 1 hour before irradiation. LTC4 has just re-substantially reduce the effects of localized (hind cently been shown to be effective in increasing thelimb) X irradiation.4 survival of hematopoietic stem cells of mice exposed
In addition to its radioprotective ability, vitamin to cobalt-60 gamma radiation. 7 A DRF of 1.9, usingA or beta-carotene may also be able to promote re- 30-day lethality as the end point, has been achievedcovery from burn injury by reversing postburn with LTC4 in mice exposed to cobalt-60 gamma ra-immunosuppression.7 This point is significant be- diation."" Similarly, PAF is capable of producingcause burns are expected to be the most common fairly high DRFs (about 1.7)).type of injury on the nuclear battlefield. Genetic Approaches. Work is also under way, us-
Selenium is protective when administered either ing molecular biology techniques, to define se-orally or parenterally. When given orally as sodium quences in the DNA molecule that may be particu-selenite in drinking water (4 ppm) 2' or injected (1.6 larly sensitive to radiation. By precisely defining themg/kg) 24 hours before exposure to 900 Gy of co- mechanisms and sites of damage, it may be possiblebalt-60 radiation," selenium was able to provide to develop protective agents that can be targeted toslight but significant increases in survival. The real specific sensitive sites on the DNA molecule. Addi-potential for using selenium as a radioprotective tionally, because enzymes are part of the body'sagent lies in its ability to act synergistically with natural defense against reactive chemical intermedi-other agents. Selenium can also reduce the toxicity ates, it should be possible to identify the factors in-of the sulfur-containing radioprotective compound volved in regulating their synthesis and to define theWR-2721 .)` encoding gene sequences. This may provide a
Vitamins A and E and selenium are being consid- means by which the synthesis can be activated to in-ered as potential radioprotectant candidates because crease radioresistance.
256

Pro.s;'cts for Radioprotection
REPAIR OF RADIATION INJURY
The aim of this strategy is to restore the chemical that generate free radicals. In the case of DNA,structure and normal function of damaged biologi- mammalian cells have evolved an elaborate and re-cal molecules so that the injury or death of critical markably efficient system of enzymes that continu-cells is avoided, ally repair lesions in that critically important mole-
As with protection, the effectiveness of the repair cule. This system is complex, involving a number ofvaries with the LET. High-LET radiation is densely different enzymes and a variety of regulatory mole-ionizing and produces very intensive local chemical cules that control their synthesis and activity. Onedamage. As the density of damage increases, the of the potentially useful features of this system isabilitv of chemicals and enzymes to repair this dam- that it is inducible; that is, the synthesis of the repairage becomes overwhelmed. Therefore, repair strate- enzymes and regulatory factors is activated whengies are more effective for low-LET radiation. Re- the need arises.pair can be achieved either chemically (by hydrogen Strains of prokaryotic organisms exist that aretransfer) or enzymatically. capable of surviving very high doses of radiation.
One that has received attention is Deinococcus radi-
Chemical Repair by Hydrogen Transfer odurams, which is an extremely radioresistant strainof bacteria.'"t Although study of these relatively
Radiation damage to a critical biological molecule simple prokaryotic systems may provide some in-results in the transformation of that molecule into an sight into the genetic mechanisms involved in radia-organic free radical. In this form, the molecule can tion sensitivity, their lack of complexity compared tothen react with oxygen or other free radicals and be- mammalian cells is a limitation.come permanently altered chemically. However, if a About 25 years ago, a radiosensitive mammaliansuitable hydrogen donor is in the vicinity of the cell line was isolated in tissue culture from a rela-damaged molecule, it can compensate for the dam- tively radioresistant mouse lymphoma cell line.,
age by donating or transferring a hydrogen atom.'. 33 With the advent of new biotechnology techniques,Hydrogen atom transfer can be thought of as an in- this extensively characterized strain is just beginningstantaneous repair process, in which the original to be exploited to its full potential in uncovering ge-molecular structure is restored before the damaged netic mechanisms in radiosensitivity."- Recent evi-critical molecule becomes permanently altered by dence indicates that the radiosensitivity of this cellfurther chemical reaction. Many of the agents that line is due to a lower rate of DNA repair.03 Thefunction as free-radical scavengers also have the genomes of the resistant parental line can be com-ability to donate a hydrogen atom. pared with the sensitive daughter line by DNA hy-
No radioprotective agents that function primarily bridization techniques, making it possible (a) to de-or exclusively by chemical repair are available. termine if genes are induced by radiation to activateHowever, the aminothiols, which act as free-radical the repair process, (b) to identify the genes that arescavengers, are all capable of hydrogen transfer and so induced, and (c) to determine the proteins that aretherefore can function in the repair strategy.3 encoded.
It may be possible (as a long-term goal) to de-Genetic Repair velop agents that will function exclusively in genetic
repair. By increasing molecular repair capabilities,
Similar chemical alterations may also be induced these agents may prevent the effects of cellular dam-by natural biological processes and disease states age from overwhelming the organism.
REGENERATION AFTER RADIATION INJURY
The aim of this strategy is to increase survival by to radiation-induced cell death. Conceptually, thisstimulating the function and regeneration of stem- strategy can be applied to any organ system (such ascell populations that have decreased in number due the hematopoietic system and the gastrointestinal
257

Medical Conisequietces of Niclear Warfare
50
40
S30(I)
LLo 20LU Glucan-P
10
Glucan-F0-T - Radiation Control
6.5 7.0 7.5 8.0 8.5Radiation Dose (Gy)
Fig. 11-5. Hematopoietic stem-cell survival as a function of radiation dose treated or not treated with glucan, an agent usefulin promoting regeneration of stem cells. Glucan effectiveness decreases as increased numbers of stem cells are killed by higherdoses of radiation.
system) that relies on stem-cell proliferation to pro- cell death (greater than 8.5 Gy in Figure 11-5), regen-vide mature differentiated cells for proper function- eration becomes ineffective.ing. However, because hematopoietic stem cells are The utility of this strategy depends on the thresh-the most radiosensitive, only regeneration of the he- old point, a factor that can be influenced greatly bymatopoietic system is discussed here. partial shielding or by agents that operate in the pro-
Regeneration is a feasible strategy for mitigating tection or repair strategies. Because hematopoieticradiation injury at radiation doses below the thresh- stem cells are among the most radiosensitive in theold dose that would result in 100% death of hemato- body, this threshold occurs at a fairly low radiationpoietic stem cells. Figure 11-5 examines hematopoi- dose. For uniform whole-body radiation exposure,etic stem-cell survival as measured by the number of the threshold dose is approximately equal to thecolony-forming units found in the spleens (E-CFU/ LD1 , 01.• radiation dose. However, in battlefield orspleen) of irradiated mice. Some of the mice were accident situations, it is likely that the apparenttreated with the regenerating agent glucan. In the threshold will be substantially higher. Because theradiation control animals, which were not given inherent radiosensitivity of the hematopoietic stemglucan, the number of E-CFU/spleen decreased with cells would not change, other factors related to theincreasing radiation dose. Similarly, the effective- nature of radiation exposure contribute to this ap-ness of glucan in increasing the survival of these parent increase. In battlefield or accident situations,cells also decreased with increasing dose. This indi- some element of shielding, either deliberate or coin-cates that the effectiveness of these agents depends cidental, is likely to be present. This will provideon the number of surviving stem cells. Above the inhomogeneous exposures, so that high levels of ra-threshold radiation dose that results in 100% stem- diation reaching one part of the body may not reach
258

Prosjkcts tfr Ridwioprotectwn
TABLE 11-5
PRIMATE SURVIVAL FOLLOWING 8 Gv OF COBALT-t) IRRADIATION
Supportive Supportive TherapyNo Supportive Therapy (allogeneic bone- Partial
Category Therapy Only marrow transplant)* Shielding*"
Survivors 0 0 5 4
Total primates 4 4 5 4
Mean survival 12.5 16.3 >30.0 >30.0time in days
*Antibiotics, fluids, platelets"**Less than V1' surviving stem cells
others, thereby permitting increased stem-cell sur- proliferation and function of hematopoietic and im-vival. In these situations, it may also be possible to munopoietic stem cells. The precise biochemicalincrease stem-cell survival by minimizing the time mechanisms by which this stimulation occurs arespent in high-radiation fields and maintaining some complex and are as yet incompletely understood.distance from radiation sources. The contribution of Exactly which cell type becomes stimulated de-these protective measures was evident in the Cher- pends on the type of agent involved (Figure 11-6).nobyl accident victims, in whom bone-marrow Nonspecific immunomodulators are exogenousgrafts apparently failed. These failures were due, at agents that can bind to and stimulate a variety ofleast in part, to host-versus-graft reactions initiated different cell types, particularly macrophages. Theseby surviving stem cells, even in patients who were agents are thought to induce the stimulated cells toexposed to doses of radiation much greater than release a variety of peptides (cytokines) that act spe-those expected to completely deplete stem cells. cifically on immunopoietic and hematopoietic pro-
The effectiveness of minimal local shielding in genitor and stem cells to stimulate their growth andprotecting even small numbers of stem cells is dem- differentiation into mature, functional cells.,"onstrated in experiments done with monkeys (Table11-5)."1 Supportive therapy (fluid, platelets, and Candidate Agentsantibiotics) significantly increased the LD•,•, of irra-diated animals. In monkeys exposed to a lethal dose Agents that mitigate radiation injury via regen-(8 Gy) of whole-body cobalt-60 radiation, supportive eration can be grouped into two broad categories:therapy extended survival for a few days but had no ininumotodiulators and czytokines. Immunomodula-effect on 30-day survival rates because the radiation tors can be thought of as inducer molecules, and cv-dose completely depleted the stem-cell population. tokines as effector molecules.However, when the tibias of these animals were Figure 11-7 traces the development of early im-shielded so that less than 114 of their bone-marrow munomodulators to cytokines. Original immuno-stem cells survived, regeneration occurred and modulators were generally crude whole-cell micro-many of the animals survived. bial preparations (such as Bacillus Cahnette-Gucrin
[BCGI and Coryilnc'bacteriun parvum) that were usedMechanisms because they could nonspecifically stimulate host
immune responses. Later, the active components ofThe regeneration of depleted stem-cell popula- these cells (such as endotoxin and zvmosan) were
tions is brought about by agents that stimulate the identified and isolated from their cell walls. Further
259

Medical Consqiuences of Nuclear Warfare
IMMUNOMODULATORS
MACROPHAGEY
CVT OK INESIL- 1
PLASMA CELL ACTIVATED T CELLS
(HUMORAL STEM (• (CELLULARIMMUNITY) CELL\, IMMUNITY)
TMM6
Fig. 11-6. Relationship of immunomodulators with host-produced mediators (cytokines), which regulate immunological a 7hematological functions
work led to the purification, identification, and syn- be those that act primarily on the macrophage.thesis of the specific portions of the cell fragments Glucan and trehalose dimycolate (TDM) are two im-that were actually responsible for stimulating im- munomodulators that are currently being evaluatedmune responses (such as lipid A from endotoxin and as potential mitigating agents for radiation injury.glucan from zymosan). Stimulation of cells by im- Glucan is a beta-i,3-linked polysaccharide iso-munomodulators results in the release of cytokines, lated from the cell wall of the yeast Saccharomyceswhich act as specific stimulators of host immune re- cerevisiae. This agent is a potent immune modulatorsponses. Recent advances have seen the develop- that is capable of enhancing a variety of immunopoi-ment of biologically defined molecules and recombi- etic and hematopoietic responses.'"ýnantly produced cytokines (such as interleukin-1 The effect of glucan on preventing infection and[IL-1 I and granulocyte-macrophage colony-stimulat- enhancing the regeneration of bone-marrow cells af-ing factor [rGM-CSF]), which are relatively nontoxic ter irradiation is shown in Figure 11-8. In this ex-but allow specific manipulation of various compo- periment, mice were injected with either saline ornents of the immune and hematological systems. glucan 24 hours before exposure to 9 Gy of cobalt-60
Inmunomodulators. Immunomodulators are gamma radiation." The number of saline-treatedgenerally nonspecific immunostimulants that func- mice showing evidence of infection increased sub-tion as external stimuli for a broad range of cell stantially at 7-15 days following irradiation, and notypes in the hematopoietic system. To reduce radia- detectable marrow regeneration was evident. How-tion injury, the most effective compounds appear to ever, glucan was able to reduce infection signifi-
260

Prospects for Radioprotection
4 40na4 4IL-i, GM-CSF
Whole cells 4 Cell fragments Biochemically 4 Host mediatorsdefined
component
Yeast Zymosan 4 Glucan 4 Cytokines(Isolated (Synthesized) (Recombinant)
fr,- m yeast)
Fig. 11-7. Evolution of immunomodulators from crude cell preparations to biochemicaily defined molecules and host factorsproduced by recombinant DNA technology
cantly and to produce a substantial increase in mar- vival after irradiation. 16,1•
row regeneration. A temporal relationship was seen Cytokines. Cytokines are hormone-like peptidesbetween the two effects: the ability of glucan to con- that function as molecular signals between cells.trol infection occurred well before its demonstrable They are synthesized and released primarily byeffect on marrow regeneration. This suggests a dual macrophages and lymphocytes that have beenrole for glucan in enhancing postirradiation stimulated by inflammatory agents or immuno-survival: (a) this compound can stimulate the re- modulators. Included in this class of compounds aremaining mature, relatively radioresistant macro- the interleukins-1 through -6, tumor necrosis factorphages to control infection, and (b) it can also induce (TNF), a variety of hematopoietic growth factorsthe stimulation of stem and progenitor cells to pro- (such as granulocyte-macrophage colony-stimulat-liferate and repopulate the marrow. ing fa :tor, granulocyte colony-stimulating factor,
These data correlate with the ability of this com- and erythropoietin), and the alpha-, beta-, andpound to increase the survival of irradiated animals. gamma-interferons. All of these act in a variety ofAdministered intravenously to mice 24 hours before ways to stimulate proliferation, differentiation, or9 Gy of cobalt-60 gamma radiation, glucan increased function of cells in the hematopoietic system. Sev-the 30-day survival from 0% in the saline-injected eral have been examined for their ability to mitigatecontrol mice to 63% in the glucan-treated mice (DRF: radiation injury, and of these, IL-1 and TNF have1.2).67 In addition, glucan is capable of slightly en- been found to be the most effective.hancing survival (DRF: 1.08) in mice when it is ad- IL-A is released by activated macrophages. It hasministered 1 hour after an exposure to 9 Gy of co- a number of local immune effects, including the acti-balt-60 gamma radiation.' vation of resting T cells and the stimulation of cyto-
Trehalose dimycolate (TDM), also known as cord kine synthesis and release.69
factor, is a glycolipid consisting of 6,6'-diesters of the Although a significant increase in survival (43/sugar D-trehalose. It is isolated from the cell walls for treated versus 0% for control mice) is seen whenof Mycobacteria, Nocardia, and Corynebacteria, and is IL-1 is given 4 hours before irradiation, optimuman active component of Freund's complete adjuvant. survival (greater than 80% versus 0% in controls) isLike glucan, TDM is a potent immunostimulant that obtained when IL-1 is administered intraperitone-is capable of increasing host defense mechanisms ally 20 hours before exposure to 9.5 Gy of cobalt-60against a variety of organisms and of increasing sur- gamma radiation.70 Using that regimen, DRFs of up
261

Medical Cotnsequences tof Nuclear Wartart,
35 1 1.0
-_. 30 s'* 0.8--- Saline --
0 25 - o7 --- Glucan 0.6
- 2 0 -- : D
-0..= -"15 sS0.4 ¢
C))
03 -0.2 5'5 X
0 I I - 1L" 1 06 7 9 11 13 15 17 19
Days Postirradiation
Fig. 11-8. Effect of glucan on enhancement of nonspecific resistance to infection and marrow hematopoiesis in mice exposedto 9 Gy of radiation
to 1.25 have been achieved with IL-1 in C57BL/6 can be produced by -ecombinant DNA methodolo-mice. IL-1 is particularly attractive as a pharmaco- gies. One of these, a specific human recombinantlogical means of mitigating radiati, in injury because GM-CSF (rGM-CSF), accelerates marrow repair oronly very small doses are required. The DRF of 1.25 engraftment and may contribute to increased non-was achieved with a dose of only 0.1 pg of IL-1 per specific resistance. It functions by increasing themouse (approximately 0.004 mg/kg). The effective- number of circulating granulocytes and platelets inness of IL-1 in mice is strain dependent. While all normal animals and accelerating the recovery ofstrains of mice examined showed different degrees these cells after irradiation. This factor was used inof increased survival, optimum survival was ob- treating some victims of the radiation exposure acci-tained with the C57BL/6 strain.7 1 dent in Brazil.
TNF is also released by activated macrophages. The effectiveness of this factor in amelioratingIt was named for its ability to act as a direct cyto- radiation-induced cytopenia can be seen from datatoxin for some tumor cells. Like IL-I, it h's,, several obtained in the minimal-shielding experiment."' Inlocal immune effects, including the stimulation of that experiment, the survivai of partially shieldedcytokine synthesis and release." Unlike IL-I, how- monkeys that were given supportive therapy wasever, its effectiveness does not depend on the mouse enhanced. Unshielded animals rapidly became neu-strain. In most strains, TNF is less effective than is tropenic and died within 15 days. In the shieldedIL-1, and in others it is more effective due to the animals that survived beyond 30 days, peripheralvariability in effectiveness of IL-1. TNF is optimally granulocytes began to recover slowly between dayseffective (with DRFs of 1.08-1.16) when given in- 20 and 40. In contrast, shielded animals treated withtraperitoneally 20 hours before irradiation at a dose a growth factor showed evidence of granulocyte re-of 5-10 g per mouse (approximately 0.2 mg/kg).72 covery well before day 20, and granulocyte levels
Two other cytokines may be potentially useful quickly reached supranormal levels. Therefore, itagents: GM-CSF and interleukin-3 (IL-3). Several appears that this factor is a useful adjunct to radia-growth factors that are specific for different hemato- tion-injury therapy. However, its effectiveness as alogical cell populations have been discovered and regeneration agent in radioprotective regimens is
262

Pwspccts ftr Radioprott'ctihii
much lower than that for IL-I and TNF when it is scribed action of the cytokines (whose major targetgio en alone in the protocols described above for cells are primarily the more mature functional cellsthose cvtokines,.7 1 In spite of that, evidence suggests in the system), IL-3 is reported to act specifically inthat it may act synergistically when combined with stimulating the growth of pluripotent stem cells."other cvtokines.,-2 Because hematopoietic stem cells are among the
IL-3 has not yet been evaluated for its ability to most radiosensitive in the body, this cytokine mayincrease survival after irradiation. Unlike the de- be particularly effective as a regenerating agent.
COMBINATION AGENTS
Rationale would be able to mitigate radiation injury by allthree strategies. Two or more agents might be used
Agents that function in the three strategies (pro- either together or at intervals, but this is not desir-tection, repair, and regeneration) contribute in dif- able. The simplest dosing regimen (single dose) isferent ways t the mitigation of radiation injury. the most desirable for military personnel under bat-Each of the three strategies also has its limitations. tlefield conditions. Therefore, the goal is a singleNeither chemical nor enzymatic means of protection treatment consisting of a combination of two orare able to minimize direct damage. In addition, it is more agents that function in (a) either the protectionalmost impossible for any protective or repair agent or repair strategy, and (b) the regeneration strategy.either to completely eliminate all of the reactiveintermediates tormed or to repair all of the damaged Examples of Combination Agentsmolecules. Regardless of the efficiency of scaven-gers and repair agents and their concentration The concept of using combinations of agents thatwithin the cell at the time of irradiation, some mo- function by different mechanisms to achieve protec-lecular damage and cell death will occur. The effec- tion was developed and studied in the 1950s andtiveness of agents that function in the reg 'neration 1960s." In many of the combinations examined, syn-strategy is limited because the agents require a pool ergistic effects were seen. These results are particu-of surviving functional cells on which to work. That larly significant because increased protection withpool of highly radiosensitive hematopoietic stem the combinations was often achieved using substan-cells becomes depleted after fairly low radiation tially lower doses of individual drugs than those re-doses. quired for protection when each agent was given
It is reasonable to expect that optimal survival alone. For example, one study examined variouswould be provided by an agent or combination of combinations of five different radioprotectiveagents that would operate within two or more of agents: cysteine, beta-mercaptoethylamine (MEA),these strategies. Such a formulation would maxi- aminoethylisothiouronium (AET), glutathione, andmize the effectiveness of each strategy and minimize serotonin."7 AET, MEA, or serotonin used aloneits limitations. Protective and repair agents reduce provided similar protection (DRF: 1.7), cysteine wasthe concentration of reactive species that are pro- less effective (DRF: 1.12), and glutathione was mar-duced from the radiolysis of water and also repair ginally protective (DRF: 1.05). The most effectivethe damage to critical target molecules. In so doing, regimen was a combination of all five agents, whichthe agents increase the surviving fraction of stem produced a DRF of 2.8. In this combination, thecells, progenitor cells, and mature cells of the hema- doses were two-thirds that of the AET and one-halftopoietic svstem after irradiation. By allowing stem that of the MEA used when the drugs were given in-cells to survive higher radiation doses, the net effect dividually.is to increase the threshold radiation dose that limits More recently, additive and synergistic effectsthe effectiveness of regeneration agents. Regenera- were demonstrated with various combinations oftion agents further enhance the organism's survival aminothiols, antioxidant vitamins and minerals, im-by capitalizing on the advantages provided by pro- munomodulators, and cvtokines. It is likely that atective and repair agents; that is, they maximize the first-generation agent will be a combination of sub-proliferation and function of the extra cells pro- toxic doses of two or more of these agents. The ef-vided. fectiveness of several combinations is shown in
It would be difficult to produce one drug that Table 11-b.
263

Medical Consetquences of Nuclear Wafare'
TABLE 11-6
EFFECTIVENESS OF PHARMACOLOGICAL AGENT COMBINATIONS*
Agents and Agent Combinations Dose Reduction Factor (DRF)**
A B C A B C A+B A+B+C References
IL-I*** TNF*** - 1.19 1.12 - 1.38 - 64
Glucan Pt WR 2721± Seleniumt 1.22 1.33 1.01 1.51 1.64 67
Glucan F tt WR 2721tt - 1.07 1.32 - 1.53 - 68
Selenium$ WR 2721t - 1.10 2.20 - 2.50 - 54
DiPGEO WR 2721¥ - 1.40 1 .90 - 2.20 - 70
*Data obtained using mice exposed to gamma radiation from a cobalt-60 source
**DRF calculated as a ratio between radiation-treated group (LD,(/,,,) and radiation control group (LD5 ,/,)
***`-1 (150 ng/mouse) and TNF (5 pg/mouse) injected i.p., 20 hours after irradiation
t Glucan P (particulate) injected i.v., 75 mg/kg, 20 hours before irradiationWR-2721 (200 mg/kg) injected i.p., 30 minutes before irradiationSelenium (0.8 mg/kg) injected i.p., 20 hours before irradiation
t t Glucan F (soluble) injected i.v., 250 mg/kg, 1 hour after irradiation
WR-2721 (200 mg/kg) injected i.p., 30 minutes before irradiation
4: Selenium (1.6 mg/kg) injected i.p., 24 hours before irradiationWR-2721 (400 mg/kg) injected i.p., 30 minutes before irradiation
¥DiPGE, (0.4 mg/kg) injected s.c., 15 minutes before irradiationWR-2721 (200 mg/kg) injected i.p., 15 minutes before irradiation
Mitigation of Performance Decrement fact, except for a few notable exceptions, they usu-ally exacerbate radiation-induced performance dec-
Because a single, self-administrable agent is rements.4 344 Groups of drugs are being developed
sought as a radioprotectant, it might also be neces- that will, perhaps, stabilize performance by modu-sary to include moderators of performance decre- lating cellular permeability, altering regional bloodments in any regimen that is developed. While flow, and interrupting the release or action of vari-measures to enhance resistance to the lethal effects ous mediators. Drugs are being identified that canof radiation have been extensively studied, relatively modulate postirradiation emesis, ETI, and other per-little attention has been given to the application of formance decrements.pharmacological interventions to mitigate perform-ance and behavioral deficiencies, even though theseare of immediate military concern. Although it is Radioprotectants and Supportive Therapypossible for radioprotective agents to prevent someperformance decrements, drugs that increase sur- Radioprotectants will be most effective in person-vival generally have not enhanced performance. In nel exposed to radiation doses within the ranges re-
264

Prospects for Radioprotection
100 1 , I
80- Radiation
60- Alone
40-
-• 20-S 0 I I I. I I I
S100
80- Combined
60- Injury
40 o-oTDM2 - Saline
0 -
0 2 4 6 8 10 12 14 16 18 20Day Following Injury
Fig. 11-9. Comparative effects of trehalose dimycolate (TDM) on enhancement of survival in mice receiving either radiationalone or radiation and a 309 body-surface-area wound (combined injury)
quired to produce the hematopoietic subsyndrome mals). However, this protection was not seen in ani-(approximately 2.0-8.0 Gy) and mild gastrointestinal mals given a 1.0-by-1.5 inch skin wound and irradi-subsyndrome (approximately 8.0-10.0 Gy), and in ated with only 8.5 Gy. In the irradiated andwhom no associated injuries are present. In the wounded mice, death began to occur about 1 weekevent of more severe radiation injury, or if radiation earlier than in the irradiated-only animals, and allinjury is combined with traumatic or burn injuries (a mice died at the same rate regardless of treatmentlikely occurrence on the battlefield), then radiopro- with TDM.tective measures alone will be insufficient, and addi- This difference in protective response between ir-tional supportive therapy will be required. Al- radiated-only and combined-injury animals may bethough the effectiveness of radioprotectants may be due to a more profound immunosuppression (Fig-reduced in the face of more severe radiation injury ure 11-10) and/or physiological perturbations. Toor combined injury, their use at the time of irradia- avoid infection, the natural and artificial defensestion will likely increase the effectiveness of suppor- must be in balance so that host resistance is suffi-tive therapies provided days later. cient to control the number of microorganisms.
Traumatic injury can reduce the ability of phar- Therefore, as normal defenses are compromisedmacological agents to increase survival (Figure 11- (suppression), artificial interventions (enhancement)9)." Mice that were given TDM dissolved in are required to maintain the resistance above thesqualene within 2 hours after exposure to 10.25 Gy threshold for infection.of cobalt-60 gamma radiation were protected against The potential synergy between therapeuticthe infectious consequences of this exposure (70% agents, such as antibiotics, and substances that maysurvival versus 5% in vehicle-injected control ani- be used as radioprotectants is indicated by recent
265

Medical Conseiet lI ces of Niclear Wil tl
I!LIM
Lymphocytes * Cell growth factors
Macrophages Immunomodulators
PMN Antibiotics
Immunoglobulin Immunoglobulin
Tissue integrity Surgical restoration
Other defenses Supportive therapy
Suppression 9 Enhancement
Fig. 11 -10. Suppression of resistance to infection when normal defenses are lost. Various interventions to enhance resistancemay be used in combination to prevent infection in severely injured subjects.
data on the use of glucan and the antibiotic hour after irradiation, or incorporation of pefloxacinpefloxacin in the management of postirradiation in the animal's drinking water for 24 days after ex-mortality.74 In this experiment, only 30%9 of mice posure, had little or no effect on survival. However,given 7.9 Gy of whole-body cobalt-60 gamma radia- if the two treatments were combined, survival wastion survived. Treatment with glucan alone at I greater than 90%t.
DEVELOPMENT OF A RADIOPROTECTIVE REGIMEN
A variety of factors must be considered in evalu- not fully resolved. For many years, the goal wasating and developing candidate radioprotectant that pharmacological agents should have a DRF of atdrugs for military use, and a compromise must be least 2 against exposure to gamma radiation. Thisreached between the ideal and the achievable (Table goal may have caused promising drugs with lower11-7). DRFs to be overlooked. Protection at a DRF greater
than 2 is achievable in the laboratory, but the re-Level of Protection quired doses produce side effects that are unaccept-
able in type and severity for military use.The problem of defining a suitable minimum Although it may not be possible to field a first-
level of effectiveness in promoting survival is still generation drug with a DRF of 2, it is likely that one
266

Prospects for Radioprtectiowi
can be developed with a DRF of less than 2. A rea- are important. Oral administration is the most desir-sonably achievable lower limit would be a DRF of able route, but this may be difficult to achieve, atabout 1.4. Although this level of mitigation is gener- least for a first-generation agent. Transdermal ad-ally considered to be low to moderate, it is far from ministration (for example, via a dermal patch) is alsotrivial. First, because the animals used in research acceptable, but is limited by the fact that only micro-are immunologically naive, a laboratory-derived gram or smaller quantities of the drug can be deliv-DRF of 1.4 is likely to underestimate the degree of ered. Most of the agents under study are effective inprotection actually realized in the field by normal, milligram to gram quantities. The major exceptionshealthy persons. Second, as discussed previously, it are the cytokines, which are effective in very smallis likely that many cases of accidental exposure will dosages, and may be administrable by the transder-be accompanied by some degree of partial shielding. mal route. The transdermal route may have greaterIn light of evidence that even small amounts of par- applicability for second- and third-generation agentstial shielding are beneficial, shielding should aug-ment the effectiveness of pharmacological agents.Third, the difference between a dose of radiationthat is lethal to 95c7( of a population (LD,) and a TABLE 11-7dose lethal to 5t7 (LD;) is commonly less than 1.0-2.0 PHARMACOLOGICAL REQUIREMENTSGy. Therefore, the use of an agent with a DRF of 1.4for most species (including humans) can result in areduction of the LD,; to a value near the LD.. For Administration
persons exposed to doses greater than those result-ing in LD,,;, the use of an agent with a DRF of 1.4 Repeated administrationmay mean the difference between life and death, es- Easily self-administeredpecially if even minimal postirradiation therapy is Order of preference:available. Over a large population, the net effect is a Oral > transdermal >sublingual > intramuscular
substantial increase in survival. It is possible thatthis level of protection might be achieved with mini- Biological Action of Drugmal side effects. Adequate duration of effect
Toxicity Compatible with other drugs
Side effects are a major obstacle to the fielding of Chemical Characteristicsagents to mitigate radiation injury. Acute side ef-fects (such as nausea, vomiting, and hypotension) High chemical stability (long shelf-life)are common, especially with the sulfur compounds.For a fieldable drug, any acute side effects will have Doseto be reduced in severity so that military perform-ance is not impaired. If that is not possible, these ef- DRF > 1.4 (30-day lethality, gamma radiation)fects should be at least controllable by other conven- Single-dose regimeniently applied therapies. Manageable dose quantities (weight or volume)
In addition, these agents must not significantlyincrease the user's vulnerability to chemical or bio- Pharmacological Side Effectslogical agents or antidotes, exacerbate other battle-field injuries, negatively affect behavior, or interfere No chronic toxicitysignificantly with wound healing. The agent should Minimal behavioral toxicityhave a wide safety margin (therapeutic index) to Minimal or controllable acute side effects
compensate for the "if one is good, then two must be Minimal increased vulnerability to chemicalbetter" philosophy, or biological agents
"Minimal effect on wound healingDeliverability Wide safety margin
A prime requirement for an agent that will beused by many people under battlefield conditions isthat it be easily self-administered. The route of ad-ministration, drug dose, and simplicity of schedule
267

Medical Consoluoicts tft Nia-lear WitrPir"
developed via the genetic approaches described Other Factorsabove. The next most acceptable route of admini-stration is sublingual. The least acceptable practical Ease of administration, simplicity of dose sched-method is intramuscular injection. Intravenous and ule, minimal side effects, and a wide safety marginsubcutaneous injection and suppository administra- are particularly important because it may be neces-tion are unacceptable routes for a self-administered sary to take a radioprotective drug repeatedly forfield-deployed drug. several days. The agent should be compatible with
For oral, sublingual, or intramuscular administra- the other drugs and antidotes available to the soldiertion, the drug dose must be small enough to be dis- in the field, and it should have optimum effective-pensed as a reasonably sized tablet or capsule, or in ness for an adequate duration (up to b hours follow-a manageable volume. If taken as a liquid, either ing a single administration). Two hours of effective-orally or parenterally, the agent must also be soluble ness should be considered the minimum. Finally,and stable in a vehicle that is appropriate for ad- the agent should be formulated and packaged soministration. Finally, for simplicity of use in the that it has a shelf life of at least 5 years, to allowfield, the agent should be designed as a single treat- stockpiling. It should retain its potency under ament, rather than a regimen of two or more different wide variety of adverse conditions and, for an in-and sequentially spaced medications. jectable, should not deteriorate in solution.
SUMMARY
Historically, the development of radioprotective agents are administered along with a protectiveagents has been dominated by the study of sulfly- agent, additive and synergistic effects are seen.dryl compounds, particularly the aminothiols. Most important, these effects are often achieved us-These compounds function by a variety of mecha- ing subtoxic doses of the individual agents.nisms, almost all of which increase survival in the ir- Combining those agents that function in the pro-radiated organism by minimizing the radiation-in- tection or repair strategy with those that function induced damage to critical biological molecules. The the regeneration strategy offers the advantages of (a)ability of aminothiols to provide high levels of pro- circumventing the side effects of aminothiols, (b) en-tection has been demonstrated repeatedly. How- hancing the effectiveness of relatively nontoxicever, as a group, these compounds suffer from one agents that provide only mild protection when givenmajor drawback: high levels of protection have been alone, and (c) maximizing the therapeutic benefitachieved only at doses that are accompanied by un- provided by each agent.acceptable side effects. Therefore, it has been neces- The use of pharmacological agents to increasesary to look at less-toxic compounds in the search survival after irradiation will be most effective forfor a radioprotective agent. personnel exposed to low or intermediate doses of
Among the candidates being evaluated are natu- radiation who have minimal associated traumatic orrally occurring dietary components (selenium and burn injuries. Indeed, in a mass-casualty situation,vitamins E and A) and drugs of low toxicity that are these agents may be the only type of medical inter-being used clinically (such as MPG). The drawback vention that is available. On the other hand, withto these latter agents is that, generally, the protection smaller numbers of casualties, especially those withachieved is relatively low. combined injuries, it is likely that additional suppor-
The net effect of protective compounds, such as tive therapies will be available. When considered inthe aminothiols and dietary components, is an in- this context, radioprotection should be thought of ascrease in the number of stem cells and progenitor part of the holistic management of radiation injurycells that survive the initial radiation insult. To ex- (Figure 11-11) Here, in the face of increasing inju-ploit this early benefit, agents that stimulate the pro- ries, various dose-reducing events occur to minimizeliferation and differentiation of those cells would the effect of the injury. The early application of radi-help effect optimum repopulation of the organ sys- oprotector agents will minimize the need for subse-tems that were depleted by radiation-induced cell quent interventions and will enhance the effective-death. The use of such regeneration agents (such as ness of the interventions that are provided.immunomodulators and cytokines) alone has been Many factors must be considered in defining theshown to enhance survival after irradiation, al- desired properties of a potentially fieldable first-gen-though the effect is relatively low. But when these eration agent. Since the development of WR-2721,
268

Propects. tro Radioprotcctioi
Fig. 11-1i. A variety oft actors can act together to reduce lethality of increasing radiation doses
emphasis has been placed on studying agents that agent will probably be a combination of at least twoproduce DRFs greater than 2. This emphasis may of the candidate agents described above. Regardlessactually have hampered efforts to field a suitable of the number of candidates in this combination, it isagent. Some agents with lower DRFs can provide likely that at least one will be a protective agent andsignificant protection and may be more appropriate one will be a regeneration agent.for field use. Thus, the DRF used in evaluating a ra- Fielding a first-generation agent that satisfiesdioprotective drug need not be the maximum ob- most of the requirements discussed above is antainable. Rather, the DRF should be that obtainable achievable near-term goal that will satisfy, at least inat doses resulting in minimal acute side effects and part, a critical immediate need of the armed forces.behavioral toxicity. The agent should also have a Success will depend on making intelligent choiceshigh therapeutic index, because it will most likely be from the many available agents.self-administered. Whether or not the agent can be However, it is critical to note that fielding thistaken orally is an important consideration. first-generation agent is only an initial step. Much
Based on the strategies and candidate agents now work needs to be done to develop an agent that is ef-available, it should soon be possible to recommend fective against high-LET radiation. This need willseveral protective agents that sufficiently meet the become increasingly urgent as the human presencerequirements. After an agent has been recom- in space expands. Second- and third-generationmended, it will be evaluated as a first-generation agents will be developed only through intense stud-field-usable radioprotective drug (or drug combina- ies that are aimed at defining the mechanisms of ra-tion) in humans. The agent should have a DRF diation injury on the molecular and cellular levelsgreater than or equal to 1.4 and be effective when and determining how organisms can be stimulatedgiven as a single oral or intramuscular dose. The to protect themselves against this injury.
269

AMc'ti('i/ COPISC~lliLTS71C Of Nucela r Warfare,
REFERENCES
1. Patt, H. MW Tyree, E. B.; Straube, R. L.; and Smith, D. E. 1949. Cysteine protection against X-irradiation. Sciencte 110:213-214.
2. Chapman, W. H.; Cipte, C. R.: Elizholtz, D. C.; Cronkite, E. P.; and Chambers, F. W., Jr. 1949. Su/fli idr 'il-eontainingaegeii s 1110idflit, effectfs of ioniziiz g rad iatiouns. I. Belitficial effect of g/idafiif/iU),i iniject iopi on X-ra ' t induiced inortalifit rafteand ilvu'eiý/i los in nfice, INaval Medical Research Institute Project NMo(A)612.08.251. Bethesda, MD: NavalMedical Research Institute.
3. Giambarresi, L.,and Jacobs, A. A. 1987. Radioprotectants. In Militant~ Radiobliofogy, edited by J. J. Conklin and R. 1.Walker, 265-301. Orlando, FL: Academic Press, Inc.
4. Alper, T. 1979). Cellular ratliobiologyi. London and New York: Cambridge University Press.
5. Fabrikant, J. 1. 1972. Rauliobiologiy. Chicago: Year Book Medical Publications, Inc.
6. Carr, C. J.; Huff, J. E.; Fisher, K. D.; and Huber, T. E. 1970. Protective agents modifying biological effects of radiation.Arcli. Lnviron. Hoalfh 21: 88-98.
7. Yuhas, J. M.; Proctor, J. 0.; and Smith, L. H. 1973. Some pharmacologic effects of WR-2721: Their role in toxicity andradioprotection. Radiat. Re's. 54: 222-233.
8. Sugahara, T. 1974. 2-Mercaptopropionylglycine (MPG) and the recent development of chemical radioprotection. InPronceeding',s of flte Seconid hinternuifional Siypnposniniz on Thiohi, 17-22. Osaka: Santen Pharmaceutical Co., Ltd.
9. Avene, S. I., and Srivastava, P. N. 1985. Radioprotective effect of 2- mercaptopropionylglycine on radiation-inducedmicrosomal lipid peroxidation. lnf. 1. Radiaf . Biol. 48:197-205.
10. Fove, W. 0. 1969. Radiation-protective agents in mammals. 1. P/aia l. Sci. 58: 283-300.
11. Kim, S, E., and Moos, W. S. 1967. Radiation protection by topical DMS0 application. Hlealthi Phys. 13: 601-606.
12. Bacq, Z. M. 1965. Clwmnical lirofecf ion againstf ionizing radiat ion. Springfield, IL: Charles C. Thomas.
13. van der Meer, C.; Brocades Zaalberg, 0.; Vos, 0.; Vergroesen, A. J.; and v'an Bekkum, D. W. 1961. On the mecThanismof the radioprotective action of cyanide. tnt. 1. Rad. Biol. 4: 311-319.
14. Thomson, J. F. 1962. Radiaftion 1;rofect ion in ,,iannnals. New York: Reinhold Publishing Corporation.
V5. Patchen, M. L;D'Alesandro, M. M.; Brook, IL; Blakely, W. F.; and MacVittie, T. J. 1987. Glucan: Mechanisms in-volved in its radioprotective effect. /. xItekoci~te Biol. 42: 95-105.
16. Madonna, G. S.; Ledney, G. D.; Elliott, T. B.; Brook, L.; Ulrich, J. T.; Myers, K. R.; Patchen, M. L.; and Walker, R. I.Trehialose dimycolate enhances' resistance to infection in neutropenic animals. Infecf. bunn., in press.
17. Madonna, G. S_.; Ledney, G. D.; Funckes, D. C.; and Ribi, F. E. 1988. Monophosphoryl lipid A and trehalose dimvco-late therapy enhances survival in sublethally irradiated mice challenged with Kbeb1siel/a pneuinloniae. In bninmiuo-inodulators anid Nonspecific Hlost Defence, Mec/manisitis agzainst Microbia/ Infect ions, edited by K. N. Masihi and W.Lange, 351-356. Oxford: Pergamon Press.
18. Ainsworth, F. J.; Larsen, R. M.; Mitchell, F. A.; and Tavlor, J. F. 1970. Survival-promoting effects of endotoxin in mice,dogs, and sheep. In Radiation Proteef ion and Sensifizationm, edited by H. L. Moroson and M. Quintiliani, 381-388.London: Taylor and Francis.
19. Bertok, L. 1980. Radio-dletoxified endotoxin as a potent Stimulator oif nonspecific resistance. Perspecf. 13iot . Med. 24:6 1-66.
270

Prospects for Radioprotection
20. Snyder, S. L.; Walker, R. I.; MacVittie, T. J.; and Sheil, J. M. 1978. Biologic properties of bacterial lipopolysaccharidestreated with chromium chloride. Can. ]. Microbiol. 24: 495-501.
21. Neta, R. 1988. Role of cytokines in radioprotection. Pharinacol. Ther. 39: 261-266.
22. Jacobs, A. J.; Rankin, W. A.; Srinivasan, V.; and Weiss, J. F. 1983. Effects of vitamin E and selenium on glutathioneperoxidase activity and survival of irradiated mice. In Proceed ings of the 7th International Congress of RadiationResearch, edited by J. J. Broerse, G. W. Barendsen, H. B. Kal and A. J. van der Kogel, D5-D15. Amsterdam:Martinus Nijhoff Publishers.
23. Srinivasan, V.; Jacobs, A. J.; Simpson, S. A.; and Weiss, J. F. 1983. Radioprotection by vitamin E: Effects on hepaticenzymes, delayed type hypersensitivity, and postirradiation survival of mice. In Modulation and Mediation ofCancer 17y1 Vitamins, 119-131. Basel: Karger.
24. Seifter, E.; Rettura, G.; Padawar, J.; Stratford, F.; Weinzweig J.; Demetriou, A. A.; and Levenson, S. M. 1984. Mor-bidity and mortality reduction by supplemental vitamin A or beta-carotene in CBA mice given total-body-radiation. INCI 73: 1167-1177.
25. Petkau, A. 1978. Radiation protection by superoxide dismutase. Photochem. Photobiol. 28: 765-774.
26. Walden, T. L., Jr. 1987. Enhanced radiation survival in mice receiving a combined pretreatment of 16,16 dimethylprostaglandin E, and WR-2721. Abstracts of Papers for 35th Annual Meeting of Radiation Research Society, 120.Atlanta: Radiation Research Society.
27. Walden, T. L., Jr.; Patchen, M.; and Snyder, S. L. 1987. 16,16-Dimethyl prostaglandin E, increases survival in micefollowing irradiation. Radiat. Res. 109: 440-448.
28. Chapman, J. D., and Reuvers, A. P. 1977. The time-scale of radioprotection irn mammalian cells. Experientia (Suppl.)27: 9-18.
29. Singh, A., and Singh, H. 1982. Time-scale and nature of radiation-biological damage: Approaches to radiationprotection and post-irradiation therapy. Prog. Biophys. Mol. Biol. 39: 69-107.
30. Holahan, E. V. Cellular radiobiology. In reference 3, 87-110.
31. Greenstock, C. L. 1981. Redox processes in radiation biology and cancer. Radiat. Res. 86: 196-211.
32. Pizzarello, D. J., and Colombetti, L. G., eds. 1982. Radiation biology. Boca Raton, FL: CRC Press.
33. Copeland, E. S. 1978. Mechanisms of radioprotection-a review. Photochem. Photobiol. 28: 839-844.
34. Davidson, D. E.; Grenan, M. M.; and Sweeney, T. R. 1980. Biological characteristics of some improved radioprotec-tors. In Radiation Sensitizers: Their Use in the Clinical Management of Cancer, edited by L. W. Brady, 309-320.New York: Masson.
35. Piper, J. R.; Stringfellow, C. R., Jr.; Elliot, R. D.; and Johnston, T. P. 1969. S-2-(omega-aminoalkylamino)ethyl dihy-drogen phosphorothioates and related compounds as potential antiradiation agents. J. Med. Chem. 12: 236-243.
36. Yuhas, J. M. 1970. Biological factors affecting the radioprotective efficiency of S-2-(3-aminopropylamino)ethyl-phosphorothioic acid (WR-2721): LD1_3•(0 doses. Radiat. Res. 44: 621-628.
37. Yuhas, J. M., and Siorer, J. B. 1969. Differential chemoprotection of normal and malignant tissues. INC[ 42: 331-335.
38. Glover, D. J.; Glick, J. H.; Weiler, C.; Hurowitz, S.; and Kligerman, M. 1986. WR-2721 protects against the hematol-ogic toxicity of cyclophosphamide: A controlled phase 11 trial. 1. Clin. Oncol. 4: 584-588.
39. Glover, D. J.; Glick, J. H.; Weiler, C.; Fox, K.; and DuPont, G. 1987. WR-2721 and high dose cisplatin: An activecombination in the treatment of metastatic melanoma. J. Clin. Oncol. 5: 574-578.
271

Medical Consequences of Nuclear Warftre
40. Glover, D.; Riley, L.; Carmichael, K.; Spar, B.; Glick, J.; Kligerman, M. M.; Agus, Z. S.; Slatopolsky, E.; Attie, M.; andGoldfarb, S. 1983. Hypocalcemia and inhibition of parathyroid hormone secretion after administration of WR-2721 (a radioprotective and chemoprotective agent). N. Eng. /. Med. 309: 1137-1141.
41. Phillips, T. L. Rationale for initial clinical trials and future development of radioprotectors. In reference 33, 321-329.
42. Turrisi, A. T.; Glover, D. J.; Hurwitz, S.; Glick, J.; Norfleet, A. L.; Weiler, C.; Yuhas, J. M.; and Kligerman, M. M. 198b.Final report of the Phase I trial of single-dose WR-2721 lS-2-(3-aminopropylamino)ethylphosphorothioic acid].Cancer Treat. Rep. 70:1389-1393.
43. Bogo, V.; Jacobs, A. J.; and Weiss, J. F. 1985. Behavioral toxicity and efficacy of WR-2721 as a radioprotectant. Raiaht.Res. 104: 182-190.
44. Landauer, M. R.; Hirsch, D. D.; Dominitz, 1. A.; and Weiss, J. F. 1987. Dose and time relationships of the radioprotec-tor WR-2721 on locomotor activity in mice. Pharinacol. Biochein. Behav. 27: 573-576.
45. Fleckenstein, L.; Swynnerton, N.; Ludden, T. M.; and Mangold, D. Bioavailability and newer methods of delivery ofphosphorothioate radioprotectors. Pharniacol. Ther., in press.
46. Dubois, A.; Gueta, 0.; LaPorte, J. L.; and Conklin, J. J. 1986. Relation between gastric emptying and gastric motility inprimates. Gastroenterology 91: 1051A.
47. Katzung, B.G. 1984. Basicandclinicalpharnacolq. 2nd ed. Los Altos, CA: Lange Medical Publications.
48. Turbyfill, C. L.; Roudon, R. M.; Young, R. W.; and Kieffer, V. A. 1972. Alterition ofnradiation effcts by 2-(,g-decylaiino)ethanethiosulfuric acid (WRI607) in the ,nonkey1 [Scientific Report SR72-31. Bethesda, MD: Armed Forces Radiobi-ology Research Institute.
49. Sharp, J. C.; Kelly, D. D.; and Brady, J. V. 1968. The radio-attenuating effects of n-decylaminoethanethiosulfuric acidin the rhesus monkey. In Use of Nonhnuan Primnates in Drug Evaluation, edited by H. Vagtborg, 338-346. Austinand London: University of Texas Press.
50. Santen Pharmaceutical Co., Ltd. 1974. Proceedings of the Second International Syrnposiumn on Thiola. Osaka: SantenPharmaceutical Co., Ltd.
51. Sztanvik, L. B., and Santha, A. 1976. Synergistic effect of radioprotective substances having different mechanisms ofaction. In Modification of RadiosensitivitlY of Biological Systes, Proceedings of Advisorty Group, 47-59. Vienna:International Atomic Energy Agency.
52. Sugahara, T., and Srivastava, P. N. MPG (2-mercaptopropionylglycine): A review on its protective action againstionizing radiations. In reference 50, 77-87.
53. Freeman, B. A., and Crapo, J. D. 1982. Biology of disease: Free radicals and tissue injury. Lab. Invest. 47: 412-426.
54. Seifter, E.; Mendecki, J.; Holtzman, S.; Kanofsky, J. D.; Friedenthal, E.; Davis, L.; and Weinzweig, J. 1988. Role ofVitamin A and beta-carotene in radiation protection: Relation to antioxidant properties. Pharmacol. Ther. 39:357-365.
55. Fusi, S.; Kupper, T. S.; Green, D. G.; and Ariyan, S. 1984. Reversal of postburn immunosuppression by the admini-stration of vitamin A. Surgery 96: 330-335.
56. Weiss, J. F.; Hoover, R. L.; and Kumar, K. S. 1987. Selenium pretreatment enhances the radioprotective effect andreduces the lethal toxicity of WR-2721. Free Rad. Res. Conmns. 3: 33-38.
57. Walden, T. L., Jr.; Patchen, M. L.; and MacVittie, T. J. 1988. Leukotriene-induced radioprotection of hematopoieticstem cells in mice. Radiat. Res. 113: 388-395.
58. Walden, T. L., Jr. Personal communication.
272

Pros pectý for Radio protection
59. Hughes, H. Personal communication.
60. Serianni, R. W., and Bruce, A. K. 1908. Role of sulphur in radioprotective extracts ot Micrococciis radioifiiraiis. Nature218: 485-487.
61l. Alexander, P. 1961. Mouse lymphoma cells with different radiosensitivities. Nature 192: 572-573.
62. Beer, j. Z.; Budzicka, E.; Niepokojczycka, E.; Rosiek, 0.; Szumiel, I.; and Walicka, M/. 1983. Loss of tumorigenicitywith simultaneous changes in radiosensitivity and photosensitivity during in zitro growth of L5178Y murinelymphoma cells. Cancer Res. 43: 4736-4742.
63. Wlodek, D., and Hittelman, W. N. 1987. The repair of double-strand breaks correlates with radiosensitivity ofL5178Y-S and L5]78Y-R cells. Radiat. Res. 112: 146-155.
64. NMonrov. R. L.; Skellev, R. R.; Taylor, P.; Dubois, A.; Donahue, R. F.; and MacVittie, T. J. 1988. Recovery from severehematopoietic suppression using recombinant human granulocyte macrophage colony stimulating factor.Expt. Heniatologii 16: 344-348.
65. Cohen, S.; Pick, E.; and Oppenheim, J. J., eds. 1979. Biologii o tlie hIinpliokines. New York: Acajemic Press.
66. Patchen M. L. 1983. Immunomodulators and hemopoiesis. Siirv. Imninuol. Res. 2: 237-242.
67. Patchen, M. L.; D'Alesandro, M. NM.; Chirigos, M. J.; and Weiss, J. F. 1988. Radioprotection by biological responsemodifiers alone and in combination with WR-2721. Pizarniac. Titer. 39: 247-254.
68. Patchen, M. L.; MacVittie, T. J.; and Jackson, W. E. 1989. Postirradiation glucan administration enhances the radi-oprotective effects of WR-2721. Radiat. Res. 117: 59-69
69. Dinarello, C. A., and Mier, J. W. 1987. Lymphokines. N. Entgi. 1. Med. 317: 940-945.
70. Neta, R.; Vogel, S. N.; Oppenheim, J. 3.; and Douches, S. D. 'i986. Cytokines in radioprotection. Comparison of theradioprotective effects of IL-I to IL-2, GM-CSF and IFN. Lninpliokine Res. (Suppl.) 5: S105-S110.
71. Neta, R.; Oppenheim, J. J.; Douches, S. D.; Giclas, P. C.; Imbra, R. J.; and Karin, M. 1986. Radioprotection withInterleukin-1: Comparison with other cytokines. Progress in lImmunology 6: 900-908.
72. Neta, R.; Oppenheim, J. J.; and Douches, S. D. 1988. Interdependence of IL-I, TNF, and CSFs in radioprotection. Inuninunol. 140: 108-111.
73. Maisin, J. R.; Mattelin, G.; Fridman-Manduzio, A.; and van der Parren, J. 1968. Reduction of short- and long-termradiation lethality by mixtures of chemical protectors. Radiat. Res. 35: 26-44.
74. Brook, I. Personal communication.
273

M~edical CO~l~t'(jldt~lILCt of Nuclear Wairfart'
274

ADDRESSES
AFRRI NTISArmed Forces Radiobiology Research Institute National Technical Information ServiceOffice of the Director 5285 Port Royal ReadBethesda, MD 20814-5145 Springfield, VA 22161
301-295-1210 703-487-4600
OCLCDNA Online Computer Library CenterDefense Nuclear Agency 6565 Frantz Road6801 Telegraph Road Dublin, OH 43017Alexandria, VA 22310-3398 800-848-5800
701-325-7060
REAC/TSFEMA Radiation Emergency Assistance Center/Federal Emergency Management Agency Training Site, Oak Ridge Associated Universities500 C Street, SW PO Box 117Washington, DC 20472 Oak Ridge, TN 37831-0117
Eeiwrg'encyil hnfrmation Center: 202-646-2400 615-576-2210
IAEA RAMTInternational Atomic Energy Agency Radiological Advisory Medical TeamWagramerstrasse 5 Walter Reed Armv Medical CenterPO Box 100 Attention: HSHL-QHP/RAMTA 1400 Vienna, Austria Washington, DC 20307
For 1puiblications only: (AV) 291-5107UNIPUB 202-576-51074611-F Assembly DriveLanham, MD 20706-4391800-274-4888 EUCOM
U.S. European Command HeadquartersAttention: ECMD
ICRP APO New York 09128-4209International Commission on Radiological (AV) 430-7166
Protection Seventh Medical Command, HeidelbergScientific Secretary APO New York 09102-3304PO Box 35 (AV) 370-8816 andDidcot, Oxfordshire, OXII-ORJ United Kingdom (AV) 370-552-826
49-6211-572-55
MRATMedical Radiobiology Advisory Team WRAIRArmed Forces Radiobiology Research Institute Walter Reed Army Institute of ResearchOffice of the Director Office of the DihectorBethesda, MD 20814-5145 14th and Dahlia Streets, NW
24-hour energency number: 301-295-3909 Building 40, Room 1062Adininistrative offices: 301-295-0316 Washington, DC 20307-5100
202-576-3551Library: 202-576-3314
275
Methoidal LconsMjtCiitC's of N•h',lear Wrfar'e
INDEX
Absorbed dose, 229 see also Somatic radiation effects, sterility,Absorbed dose meter, 230 in malesAccidents. See Medical response in peacetime Ataxia telangiectasia, 182, 202nuclear accidents and its effect on skin radiosensitivity, 177
ACH. See Acetvlcholine Atmospheric testing, 173-174Acetvlcholine (ACH), 126 see also FalloutAcquired immune deficiency syndrome (AIDS), 182 Atom, 2-3Active vaccination Attentional focusing, 160
in the immunosuppressed, 79Acute radiation syndrome (ARS), 13, 15-33
pathophysiological subsyndromes of, 16-21 Bacillus Calmette-Gutrin (BCG), 259prodromal stage of (see Prodromal stage of ARS) Background radiation, 172-173
Adenine, 197 from consumer products, 174Addresses, 275 from extraterrestrial radiationAET. See Aminoethvlisothiouronium cosmic radiation, 172-173AFRRI (Armed Forces Radiobiology Research Institute) solar-flare radiation, 172-173
address, 275 from fallout, 173-174Age from medical procedures, 172
effect of, on cancer risk after radiation sourcesexposure, 184-185 potassium40, 173
AIDS. See Acquired immune deficiency syndrome sodium-24, 173Alginates, 62 thorium-232, 173, 174Alkalosis, 49 see also Radon gasAlopecia, 177 Barium sulfate, 62Alpha particles, 8, 21-23, 229-230, 246 BCG. See Bacillus Calmette-GutrinAlpha radiation, 229-230 Becquerel (Bq), 228Aminoethvlisothiouronium (AET), 263 Behavioral changes in irradiated animalsAminothiols, 250-255, 257 cognitive performance, 108-109
derivative of, 250-254 learning and memory, 107-108mercaptopropionylglycine (MPG), 251, 255 motor performance, 109
Amphetamines naturalistic behaviorsand locomotor hyperactivity after irradiation, 133 consumption, 111
Amylase, 86-87, 92 curiosity and investigatoryAnesthesia and pain control, 48 behaviors, 110-111Ankylosing spondylitis, 188 locomotion, 110Anorexia, 27 social behavior, 111
and gamma radiation, 86 taste aversions, 111-112Antibiotics, 27-28, 75-78 Beta burn, 177
broad-spectrum, 81 in atomic-bomb survivors and Marshallpotential synergy between, and Islanders, 177radioprotectants, 265-266 threshold radiation dose of various
Antidiarrheals. See Antiemetics and antidiarrheals isotopes, 177-178Antiemetics and antidiarrheals, 48-49, 133 see also Somatic radiation effects, on skin and hairAntihistamine Beta-carotene, 256
in radioprotection, and behavior, 132 Beta-mercaptoethylamine (MEA), 263Antioncogenes, 183 Beta particles, 8, 21-23, 229Antioxidants Beta radiation, 229
naturally occurring, as radioprotection, 250, 255-256 and lymphocytes, 94Arrhythmias, 42 shielding, 229ARS. See Acute radiation syndrome and skin injury, 42Aspermia, 90, 175 Biofilms, 69-70
duration, 175 Biological dosimetry, 86latency, 175 see also Blood serum dosimeters, Chromosomalrecovery, 175 dosimeters, Dosimeters, Hematological dosimeters,
276

and Urinarv Dosimeters liver, 184Biological mediators lung, 172, 182, 184, 194-197
as altered by radiation, 181 mveloid leukemia, chronic, 184Blast, 2 m\eloma, 182
LD-, of, prostate, 182Blast effects, 4-7 reproductive system, 197
blast wave, 6-7 and gender differences in incidence, 182blast wind, ti-7 stomach, 182, 184protection from, 6-7 T-cell leukemia, 184
Blast injuries, 6 sce also Breast cancer, Digestive system cancers, Genetictriage of, 4t syndromes associated with cancer susceptibility,
Blast wave. Sec Blast effects Leukemia, Ovarian cancer, Respiratory systemBlast wind. See Blast effects cancers, Thyroid cancerBlocking and diluting agents, 03 Cancer formation stagesBlood component therapy, 49-50 initiation, 180-181Blood serum dosimeters, 91-92 latency, 180-181
diamine oxidase (DAO), 91-42 promotion, 180-182animal response, 91 sec also Models for predicting cancer incidencewith combined injuries, 92 Cancer induction, 179-184
plasma haptoglobin, 92 and radiation dose, 184plasma hemoglobin, 92 Cancer promoters, 180-182serum alkaline phosphatase in rats, 92 environmental agents, 182serum amylase, 86, 90, 91 hormones, 181, 192
lack of animal model, 91 Carbon-14. Sec Fallout and Radioisotopesand parotid gland exposure, 91 Carboxypenicillin, 78
serum lactate dehydrogenase, 92 Carcinogenic agents and group,;. 181scc also Dosimeters as listed bv the National Toxicology Program, 181
Bloom's svndrome, 182, 202 Case shock, 5, 9Bone-marrow transplantation, 50, 75, 86 CAT. Sec Computed axial tomography
behavioral benefits of, 134 Catalase, 255in Chernobyl, USSR, 11, 259 Cataracts. See Somatic radiation effects, cataract formationmilitary practicality of, 134 Ceftazidime, 75versus autologous and/or syngeneic transplant, 29 Central venous catheterssce also Radioprotection for fluid and electrolyte therapy, 49
Bq. Sec Becquerel Cesium-137. See Fallout and RadioisotopesBreast cancer, 184, 193-195 Chelating agents, 63
latency, 193 deferoxamine (DFOA), 63and radiation induction, 193 diethylenetriaminepentaacetic acid (DTPA), 50, 62, 63
age dependence, 193 dose, 50, b3Bremsstrahlung, 5, 9, 117 as investigational new drug (IND), 63Burn injuries and renal damage, 63
flame burns, 7 dimercaprol, 63flash bums, 7 ethvlenediaminetetraacetic acid (EDTA), 50, 63full-thickness, 79 contraindications, 50LDQ,, for, 7 dose, 50partial-thickness, 79 penicillamine, 63prophylactic management of, 79 "Chemical casualtv" in sign language, 46-47protection from, 7 Chernobyl, USSR, nuclear plant accident at, 10-11, 27, 46,triage of, 46 71, 90, 128, 238-239, 259seecaiso Eve injuries, Thermal effects Chromosomal aberrations, 184, 188
with acute lymphocytic leukemia, 188with chronic mvelogenous leukemia, 188
Cancer, 179-197 radiation induced, 197, 200bone, 184 and X chromosome, 199Burkitt's lymphoma, 183, 184 sec also Antioncogenes, Genetic radiation effects,colon, 182 Oncogenes, Proto-oncogenesincidence of, 182 Chromosomal dosimetersintestinal, 184 cultured peripheral blood lymphocyte technique, 94-95laryngeal, 184 problems with, 94-95
277

,XMedioal Lou Sequetis t Nut\lea r Wartara.t'
and radiation dose and type, 94 Denial, 157micronuclei technique, 94, 96 Deoxyribonucleic acid (DNA), 12
and control values, 96 bass of, 197and bone-marrow transplant cells, 96 damage to, and cell death, 246, 248
premature condensed chromosome (PCC) set also Genetic syndromes associated withtechnique, 94, 9•5-96 susceptibility to cancer
and standardized kit, L6 Desquamating lesions, wet and dry, 42, 178-179and time required, 96 Determinants of psychological dysfunction in
seet also Dosimeters conventional warfareCi. Set Curie battle duration, 154Cisplatin for the British (World War I1), 154
and WR-2721, 250 in European theater (World War I1), 154Clavulanic acid, 75 battle intensity, 154Clearance time, 56 in Sicilian campaign (World War 11), 154Clinical-support therapy communication, 135
effect of, on LD,,, dose-effect curve, 27-28 consequences of incapacitation, 155Cobalt-t0 for Germans at Stalingrad (World War I1), 155
primate survival after irradiation, 259 cultural expectations, 155Cockayne's syndrome, 202 in Korean War, 155Codon, 197 in Vietnam War, 155Combined injuries, 14 in World War 11 (in Arakan campaign, Burma), 155
animal studies, 25-26, 27,112 group characteristics, 154and dosimetry problems, 97-98 among Israelis in Yomn Kippur War, 154in Japan, 27 physical strain, 154-1-55sec also Management of combined-injury casualties and Deuterium, 4Triage of patients with combined injuries Dexamethasone
.omputed axial tomography (CAT), 122 in managing emesis, 133Conditioned taste aversion (CTA), 11 DFOA. See DeferoxamineCord factor. Set, Trehalose dimycolate DiabetesCopit'nebiacterihon parulmn, 259 and its effect on skin radiosensitivity, 177Cosmic radiation. Set' Extraterrestrial radiation Diamine oxidase (DAO), 91-92Creatine, 92 set, also Radiation exposure, biological indicatorsCritical period Diethylenetriaminepentaacetic acid (DTPA), 50, 62, 63
for teratogenic radiation effects, 206 Digestive system cancers, 194CTA. See Conditioned taste aversion and Thorotrast induction, 194Cultured peripheral blood lymphocyte technique, 94-95 Diluting agents. Set, Blocking and diluting agentsCurie (Ci), 228 Disintegrations per minute (dpm), 228Cyclophosphamide, 181 District of Columbia, 157
and WR-2721, 250 di-alpha-tocopherol. See Vitamin ECysteine, 263 DNA (Defense Nuclear Agency)Cytokines, 259, 261-263, 267 address, 275
erythropoietin, 261 DNA. See Deoxyribonucleic acidgranulocyte-macrophage colony-stimulating factor Dose reduction factor (DRF), 250(GM-CSF), 50, 261-262 Dose-response curve, 23
interferons, 261 modification of, 24interleukin-1 through interleukin-6, 261-263 Dosimeters, 86-98, 164, 231tumor necrosis factor (TNF), 252, 261-263 fluorometric immunoassay, 97see also Recombinant leukocvte stimulatorv factors of MN antigens, 97
Cvtosine, 197 individual military, wristwatch-sized, 164problems with, 97-98radiophotoluminescent (RPL) dosimeters, 231
Daniels, J., 2 thermoluminescent dosimeters (TLD), 231DAO. See Blood serum dosimeters, diamine oxidase whole-body radionuclide determination, 97Dail After, The, 156 iodine-131, 97Dazopride (5-HT3-receptor blocker) sodium-24, 97
as an antiemetic, 133 see also Blood serum dosimeters, ChromosomalDebridement, 48, 57, 62, 69, 70, 79, 241 dosimeters, Hematological dosimeters, RadiationDeferoxamine (DFOA), 63 detection and measurement, and Urinary dosimetersDelayed fallout, 9 Dosimetry
278

Index
in Chernobyl, USSR, 10 Eve injuriesDouble pulse at Chernobyl, USSR, 46
of thermal output, 5, 7 and combatants, 46Doubling dose corneal edema, 175
of radiation, 202 flash blindness, 7Down's syndrome, 200, 202 foveal damage, 46dpm. See Disintegrations per minute lacrimal gland atrophy, 175DRF. See Dose reduction factor occupational radiation exposure limit, 175DTPA. See Diethylenetriaminepentaacetic acid protection from, 7
retinal burn, 7triage of, 46
E = m&c, defined, 3 see also Neurophysiology of performance decrementsEarly fallout, 9 and Somatic radiation effects, cataract formationEarly performance decrement (EPD), 113, 116, 117,
126, 128Early transient incapacitation (ETI), 13, 42, 113 Fallout, 4, 9-10, 173-174
ameliorated by WR-1607, 133, 253 from carbon-14, 173-174and shielding, 133-1-34 from cesium-137, 173
Edison, Thomas, 179 from strontium-90, 173EDTA. See Ethylenediaminetetraacetic acid see also Radiation hazards in patient treatmentEEG. See Radiogenic neuropathology, in and Radioisotopeselectroencephalograph (EEG) recordings Fallout decay
Eicosanoids, 250, 256 estimating, 235-236Electrolytes, 49 predicting hazards, 10Electrophysiology Fallout shelters
radiation-induced changes, 124-125 dozer trench, 236Emesis, 111-112 dug-in mobile hospital tents, 236
induced by WR-1607, 133 operation of, 236induced by WR-2721, 250 vehicle-earth shelter, 236
Emetics, 62 Fanconi's anemia, 182, 202Endorphins, 127 Federal Emergency Management Agency (FEMA), 239Endotoxin, 70, 259-260 address, 275Enhanced radiation weapon. See Neutron bomb FEMA. See Federal Emergency Management AgencyEnvironmental carcinogens. See Cancer promoters, Fibronectin, 72-73
environmental agents Fission, defined, 4Enzymatic detoxification, 249-250, 255-256 Fission fragments, 4Enzymes, 256 see also RadioisotopesEPD. See Early performance decrement Fission weaponsEpilation, 86, 177, 179 fuel, 4EPSP. See Excitatory postsynaptic potential plutonium-239, 4Ervthema, 41,86, 178-179 uranium-233, 4
set' also Radiation injury, cutaneous phenomena; Skin uranium-235, 4damage; and Skin erythema dose (SED), defined gun-assembled device, 4
Erythrocytes, 50, 90 implosion device, 4Erythropoietin, 261 Fluorometric immunoassay, 97Estrogens, 133 Follicle stimulating hormone (FSH), 176Ethiofos. See WR-2721 Forward therapy, 164Ethylenediaminetetraacetic acid (EDTA), 50, 63 Israeli experiences with, 164ETI. See Early transient incapacitation Free-radical scavenging, 249-251, 255-256, 257EUCOM. See U.S. European Command (EUCOM) Free radicals, 172, 246-248, 257Chernobyl Task Force FSH. See Follicle stimulating hormone
Excitatory postsynaptic potential (EPSP), 125 Fusion, 4Exothermic process, 2 see also RadioisotopesExposure geometry, 24-25, 26, 28-29 Fusion weapons, 4Exposure meter, 230 see also RadioisotopesExtraterres•tid radiation, 172-173
cosmic radiation, 172-173and radioprotection, 134 Gamma radiation, 59, 172, 229solar-flare radiation, 172-173 acute doses of, 86
279

AMedical Conset'q'Ices o( Niclear Wa rtare
and blood cell effects, •0 lymphocytes, 87-88, 89
and lymphocyte count, 87, 89, 94 platelets, 90
median doses of, for ARS symptoms, 86 reticulocytes, 90
shielding, 229, 236 see also Blood serum dosimeters, Dosimeters
and skin injury, 41-42 Hematopoielic depression, 27, 90
Gamma rays, 4, 8-9, 13, 21, 246 Hematopoietic precursor cells, 90
Gardner's syndrome, 182 sCC also Stem cells
Gastrointestinal subsvndrome, 13-14, 18-19 Hematopoietic subsyndrome, 13, 16-18, 90
and nutritional support, 50-51 and burn injury, 46
Geiger-Mueller (GM) counters, 59, 230 infection in, 71
Genetic approaches to radioprotection, 248, 250, 256, 257 Hematopoietic stem cells, 263
Genetic radiation ettects, 197-205 regeneration of, 257-263
estimating risks, 202-205 shielding of, 28
gene mutations, 197-200 Hemoglobin, 92
factors affecting mutation, 200-202 Hemorrhage, 90
Genetic svndromes associated with susceptibility to Hemorrhagic coagulopathies, 42
cancer, 182 High-LET radiation, 21, 246
ataxia telangiectasia, 182, 202 and radioprotection, 248
Bloom's syndrome, 182, 202 and teratogenic effects, 208
Fanconi's anemia, 182, 202 Histamine, 19, 41, 92, 126, 127, 135, 172
Gardner's syndrome, 182 HIV. See Human immunodeficiencv virus
Li-Fraumeni's syndrome, 182, 184 Human immunodeficiencv virus (HIV), 182
xeroderma pigmentosum, 182, 202 Huntington's chorea, 199
Genetically significant dose (GSD), 202 Hybridoma technology, 79
Glasgow coma scale, 38 Hydrocephaly, 210
Glucan, 252, 258, 260-261, 264, 266 Hydroxyproline, 92
Glutathione, 263 Hvperthermia, 42
Glutathione peroxidase, 255 Hvpocalcemia, induced by WR-2721, 250
Glvcine, 92 Hypoglycemia, 42
GM. Sete Geiger-Mueller (GM) counters I lypokalemia, 42, 49
GM-CSF. Set' Granulocyte-macrophage colonv- Hyponatremia, 49
stimulating factor Hypotension, 42
Goggles, lead-lanthanum-zirconium-titanium, 7 Hy-poxemia, 42
Goiinia, Brazil, radiation accident at, 29, 41, 56, 62 Hypoxia
Gonadotropin, 176 induction of, as radioprotection, 249, 250
Gram-negative organisms, 68, 70-72,74, 77-79Gram-positive organisms, 68, 70, 71, 77, 78 ICRP. See International Commission on Radiological
Granulocyte-macrophage colony-stimulating factor Protection
(GM-CSF), 50, 260, 262 IL-I. See Interleukin-I
Granulocvtes, 50, 90 IL-3. See Interleukin-3
Granulocytopenia, 72 Immunoglobulin, 48, 73, 79
Gray (Gv), defined, 172, 229 Immunomodulators, 259-261
"Ground zero," 157 Immunosuppression, 72-73
GSD. See Genetically significant dose and malnutrition, 50
Guanine, 197 in Chernobyl victims, 27
Guidelines for medical advisors, 240 by radiation in cancer latency, 181
Gun-assembled device, 4 Impaired inflammatory response, 72-73
Gv. See Gray (Gy), defined Implosion device, 4IND (investigational new drug), 63Infection, 67-81
Half-life, defined, 228 contributors to, 79
Haloperidol, 126 control of, 48
Haptoglobin, 92 with glucan, 260-261
Healthy worker effect, 191 as limiting factor in treatment, 27
Hematological dosimeters, 42-43, 87-90 in Chernobyl, 71
in Chernobyl, USSR, 90 in hematopoietic subsyndrome, 71
erythrocytes, 90 see also Infection management
granulocytes, 90 Infection management, 75-80
latency, 90 antibiotics, 75-78
280
Index
supportive therapy, 76-79 Laxatives and purgatives, 62surgery, 79-80 LD., (lethal dose, or fatal injury, for 50 percent ofsee also Antibiotics cases), 6, 23
Infections associated with radiation injury, 71-72 and dependence on dose rate, 31predisposing factors, 72-75 establishing, of radiation for humans, 29-30sCC also Opportunistic infections in air, 29
Infectious agents. See Pathogens to bone marrow, 29, 33Inhibitory postsynaptic potential (IPSP), 125 data sources for, 29-30Initial nuclear radiation, 4, 5 and exposure geometry, 24-25, 26
effects of, 7-10 in Hiroshima, 32Initial Response Force (IRF), 239 for humans, 31-33Integrating meter, 230 for low-LET radiation, 31-33Interferons, 261 and radiation quality, 24-25lnterleukin-1 (IL-I), 252, 260, 261-263, 264 and trauma, 25-27Interleukin-3 (IL-3), 262 Lead-lanthanum-zirconium-titanium goggles, 7Internal decontamination, 55-64 LET. See Linear energy transfer
clearing the gastrointestinal tract, 62 Lethality curve, 23-24alginates, 62 Leukemia, 182, 184, 188-191aluminum antacids, 62 Leukotriene C4 (LTC,), 252, 256barium sulfate, 62 Li-Fraumeni's syndrome, 182, 184emetics, 62 Linear energy transfer (LET), 21ion exchangers, 62 Lipopolysaccharide (LPS) cell-wall component, 70phytates, 62 see also Endotoxinpurgatives and laxatives, 62 Los Alamos, NM, radiation accident at, (Mr. K.), 127-128stomach lavage, 62 Low-LET radiation, 21, 177, 246
preventing or reversing radiobiological interaction, 63 and radioprotection, 248blocking and diluting agents, 63 LPS. See Lipopolysaccharide (LPS) cell-wall componentchelating agents, 63 LTC4. See Leukotriene C4lung lavage, 63 Lung cancer, 172, 182, 184, 194-197mobilizing agents, 63 Lung lavage, 63
see also Chelating agents Luteinizing hormone, 176Internal radionuclide contamination, 55-64 Lymphocytes, 87-90, 261
clearance time, 56 count as a biological dosimeter, 87-90ingestion, 56-57 nomogram, 42-43,inhalation, 56-57 Lymphoma
model for evaluating hazards of, 56 Burkitt's, 183, 184percutaneous absorption, 56wound contamination, 56-57
International Atomic Energy Agency (IAEA), 95 Macrophages, 72, 261, 262address, 275 Mafenide acetate (sulfamylon), 79
International Commission on Radiological Protection Management of combined-injury casualties, 46-52(ICRP), 56, 175, 202 anesthesia and pain control, 48
Ion exchangers, 62 antiemetics and antidiarrheals, 48-49Ionization, 229 atropine, 49Ionization chambers, 59, 230 diphenoxylate HCI, 49
pocket dosimeter, 230 codeine, 49Ionizing radiation, 246 hydrocortisone enemas, 49IPSP. See Inhibitory postsynaptic potential serotonin (5-HT3) blocking agents, 48-49IRF. Sec Initial Response Force blood component therapy, 49-50Irradiation anemia and, 49
synergy, with open wound, 79 and autologous platelets, 49and erythrocytes, 50and granulocytes, 50
Kiloton (kt), 4 chelation therapy, 50set' also Megaton fluids and electrolytes, 49
kt. See Kiloton. infection control, 48nutritional support, 50-51surgery, 47-48
Lactate dehydrogenase, 86, 87 see also Chelating agents
281
Medical Co)eq c tIe s (o! Nuctlear Wartare
Management of contaminated patients Initial Response Force (IRF), 239hospital management, 57-59 On-Scene Commander (050), 239-240initial care, resuscitation, and admission, 241 Service Response Force (SRF), 23)on-site management, 57 Mixed-fission products (MFP), W!
in combined nuclear-chemical war, 57 Mobilizing agents, 63operating-room care, 242 Models for predicting cancer incidence, 184-187
patient decontamination, ,(0-03, 234-235 and leukemia incidence among Nagasakirescue and evacuation in a nuclear accident, 240 survivors. 184-187sampling radioactivity, 57 linear, 184-187supply checklist, 58 linear-quadratic, 184, 187treatment decisions, WO pure quadratic with cell killing, 184, 187uptake and clearance, 36-57 quadratic, 184, 187
st, also Internal radionuclide contamination Monoamine oxidase (MAO), 126Management of mass casualties, 232-233 Monoclonal antibodie,;, 79
combined injuries, 232 Morphine, 127.oniinand radiation guidance, 232-233 Mortalitylogistical support, 232 radiation-induced, 90psychological stress, 232 reduced by radioprotectants, 133public health, 232 MPG. See Mercaptopropionylglycine
Manhattan Project, 2 MRAT. See Medical Radiobiology Advisory TeamMAO. Ste Monoamine oxidaseMarshall Islanders, effects of radiation on, 177-178, 179, n-decvlaminoethanethiosulfuric acid (WR-1 607), 133
192, 193 seC also WRAIR sulfur compoundsMass defect, 3 Naloxone, 127Maturation-depletion, 90 NATO Standardization Agreement (STANAG 2083), 233MEA. See Beta-mercaptoethylamine Nausea, 42Medical advisor guidelines, 240 gamma radiation dose for, 86Medical Radiobiology Advisory Team (MRAT), 240 induced by WR-2721, 250
address, 275 Necrosis, 41, 42, 48, 62, 1201, 121, 123, 175, 178, 179, 214, 26,1Medical response in peacetime nuclear accidents Neoplasm, 180
information demand, 237 see also Cancersee also NeurochemistrvChernobyl, USSR, nuclear power plant accident at; radiation-induced changes, 125-126Goiinia, Brazil, radiation accident at; Neurological changes induced by radiation, 105-135Los Alamos, NM, radiation accident at (Mr. K.); Neuropathological changes St', RadiogenicOak Ridge, TN, radiation accident at; neuropathologyPalomares, Spain, nuclear accident at; Neurophysiology of performance decrementsProvidence, RI, radiation accident at (Mr. P.); audition and vestibular function, 12(1-121Three Mile Island, nuclear power plant, accident at; olfactory function, 121Thule Air Force Base, Greenland, accident at; and gustatory function, 121Vinca, Yugoslavia, radiation accident at vision, 119-120
Megaton (MT), 4 Neuropsychiatric casualtiessee also Kiloton prediction of, 163-164
Menopause No irotransmitters, 126induced by radiation, 193 Neurovascular subsyndrome, 13, 14, 19-21
Menstrual cycle Neutron bomb, 4effect of radiation on, 177 Neutron particles, 3, 4, 8-9, 13, 229, 230, 246
Mercaptopropionvlglycine (MPG), 251, 255 Neutron radiation, 229, 230Metoclopramide (5-HT3-receptor blocker) and biological effects, 211
as antiemetic, 133 shielding, 230MFP. See Mixed fission products Nitrogen mustard, 181Microbes Nondisjunction, 200
population changes, 73-75 NTIS (National Technical Information Service)Microcephaly, 207, 209 address, 275Micronuclei technique, 94, 96 nts. See Nuclear transformations per secondMilitary operations in fallout, 235-236 "Nuclear casualty" in sign language, 46-47Military performance Nuclear energy, 2-5
radiation-induced changes, 129-132 kinetic energy, 2Military response to nuclear accident or incident potential energy, 2
282

Index
Nuclear transformations per second (nts), 228 Physiological mediators, 247, 249Nuclear weapons Phytates, 62
nuclear and physical processes, 2-5 PlasmaNuclear Weapons Accident Checklists, 243 of ions and electrons, 5, 6Nutritional support Platelet-activating factor (PAR, 252, 256
of combined-injury casualties, 50-51 Plateletpheresis, 49Nystatin, 78 Platelets, 49, 90
Plutonium. See Fission weapons, fuel, plutonium-239Pneumonitis, 42
Oak Ridge, TN, radiation accident at, 30 Polydactyly, 206OCLC (Online Computer Library Center) Post-traumatic stress disorder (PTSD), 161-162
address, 275 Postirradiation infections. Sete InfectionsOn-Scene Commander (OSC), 239-240 Premature condensed chromosome (PCC)Oncogenes, 183-184 technique, 94, 95-96Opiates Prodromal stage of ARS, 16, 17, 86
in radioprotection, and behavior, 132 dose-dependent latent stage of, 86Opportunistic infections, 68-71 duration and severity, 86, 88
pathogens, 79 onset and latency, 86, 88OSC. See On-Scene Commander symptoms, 86, 88Ovarian cancer, 197 Proportional counters, 59, 230Ovaries Prostaglandin inhibitors
radiosensitivity, 176-177 to minimize skin damage, 178see also Somatic radiation effects, sterility, in females Prostaglandins, 92, 172, 256
16,16-dimethyl prostaglandin E, (DiPGEJ), 252, 256, 264PAF. Set, Platelet-activating factor Proto-oncogenes, 183, 184Palomares, Spain, nuclear accident at, 327 Protons, 3Pathogens Providence, RI, radiation accident at (Mr. P.), 128
Bacteroides, 68 Prussian blue, 62Clostridiuin, 68, 69 Psychic numbing, 157, 159Enterobacter. 68 Psychological casualtiesEscherichia, 68, 73 care of, 164-165Klebsiella, 68, 73 and morale, 165Pseudoi,,onas, 68, 69 and uncertainty about personal injury, 164Staphylococcus, 68, 70, 73 differences in nuclear warfare versusStreptococcus, 68 conventional warfare, 155-156
Pathophysiological subsyndrome stages description by Hiroshima survivor, 155-156latent, 16 after Three Mile Island accident, 156manifest illness, 16 in U.S. Strategic Bombing Survey, 156prodromal, 16 prediction of, and military performance, 163-164recovery, 16 prevention of, 165-166
Patient management and self-preservation, 165principles of, 81 and social cohesion, 166
PCC. See Premature condensed chromosome (PCC) training recommendations, 165-166technique in World War II, 154
Peacetime radiation accidents. See Medical response in in Yom Kippur War, 154, 166peacetime nuclear accidents see also Determinants of psychological dysfunction in
Pefloxacin, 266 conventional warfarePerformance decrements, 113-118 Psychological changes (acute)
mitigating, through radioprotection, 132-134, 264 fear and terror, 160and radiation dose, 115-116 from U.S. Strategic Bombing Survey, 160and radiation dose rate, 116, 118 in learning and memory, 161and radiation quality, 117 absence of conditioned response in animals, 161role of CNS in, 133-134 in Hiroshima survivors, 161and task complexity, 113-115 retrograde amnesia in animals, 161
Philadelphia chromosome, 184, 188 from Soviet literature, 161see also Chromosomal aberrations in motivation, 158-160
Phosphorothioates, 253, 254 in animals, to receive brain stimulation, 158Photon, 229 in animals, of curiosity and attention, 158-159Physical dosimeters. See Dosimeters in Hiroshima and Nagasaki, 159-160
283

M011d0i11 C0tn1eS01nt'S tot Nich'lar Warftare
in social relations, Iio-1i1 data sources on, 189attention to leaders, I1i) regulatory guides, 212-213maintenance of social structure, 10-161 required to damage organs, 175-187
Psychological effects of nuclear warfare. Se' Psychological units of measure, 172 (see also Gray, Rad, Rem,changes (acute) antd Ps ' chological reactions (chronic) Roentgens, Sievert)
Psychological factors in nuclear warfare, 153-I 0 Radiation Exposure Status (RES) category system, 233Psychological reactions (chronic) Radiation hazards in patient treatment, 2.34
anxiety and phobias, 162 beta-contact, 234in Hiroshima, 1[2 internal, 234and rumors, 162 whole-body gamma radiation, 234
latency of, 161 set' also Management of contaminated patients aiimineuroses, 161 Medical advisor guidelines
in Japan, 161 Radiation injury, 12-13post-traumatic stress disorder (PTSD), 161-102 cardiovascular, respiratory, metabolic, and
after natural disasters, 161-162 neurological phenomena, 42depression in, 162 arrhvthmias, 42diagnostic criteria, 162 early transient incapacitation (ETI), 42principal features, 162 hemorrhagic coagulopathies, 42
psychoses, 161 hyperthermia, 42temporary, among new combat units, 161 hypoglycemia, 42
psychosomatic symptoms, 163 hypotension, 42survivor guilt, 162-163 pneumonitis, 42
PTSD. Set' Post-traumatic stress disorder cutaneous phenomena, 41-42Purgatives and laxatives, 62 erythema, 41
melanotic pigmentation, 41necrosis, 41
QBC II assay methodology, 43 skin sensations, 41Quinolones, 75 ulceration, 41
gastrointestinal phenomena, 42in combined chemical-nuclear
R. Sec Roentgens (R), defined environments, 42R-meter, 230 diarrhea, 42Rad, defined, 172, 229 nausea and vomiting, 42Radiation, 2, 228 hematological phenomena, 42-43"Radiation casualty" in sign language, 46 and blood cell morphology, 42-43Radiation counter, 230 and lymphocyte nomogram, 42-44Radiation detection and measurement, 59-60, 230-231 symptoms of, 40-41
Geiger-Mueller (GM) counters, 59, 230 see a1lso Beta burn, Skin damage, Somatic radiationfilm badges, 60 effects on skin and hairionization chambers, 59, 230 Radiation quality, 12, 24-25, 117proportional counters, 59, 230 and cancer induction, 184radiophotoluminescent (RPL) dosimeters, 231 and performance decrement, 117scintillation counters, 59, 230-231 Radioactive material, 228surface monitoring, 59 Radioactivity, 228thermoluminescent dosimeters (TLD), 60, 231 Radiogenic neuropat.,ology, 122-124, 157, 158-163set' also Dosimeters of beta-endorphin, 158
Radiation dose, 115-116, 230 cerebral ischemia, 123and cancer induction, 184 cortex, 122doubling, 202 data from Japan, 157and performance decrement, 115-116 demyelination, 121, 123
Radiation dose rate, 116, 184 of dopamine metabolism, 158and performance decrement, 116, 118 dorsal medulla, 122
Radiation Emergency Assistance Center/Training Site in electroencephalograph (EEG) recordings, 158(REAC/TS), Oak Ridge, TN, 63, 240 glial cells, 123
address, 275 hippocampus, 123Radiation exposure hypothalamus, 122
accidents, 30-31 morphology, 122biological indicators, 86, 87 necrosis, 121, 123case histories, 127-128 optic chiasm, 122
284

Index
Radioisotopes, 4, 173-174 Recombinant granulocyte-macrophage colony-stimulatingand chelation therapy, 50 factor, 2W0treatment of contamination by, W0-t1 Recombinant leukocvte stimulator, factors, 50set also Dosimeters, Whole-body radionuclide Relative biological effectiveness (RBE), 25
determination, and Management of contaminated Rem, 172patients Rem-meter, 230
Radiological Advisorv' Medical Team (RAMT), 240 RES. See Radiation Exposure Status (RES) category systemaddress, 275 RES. See Reticuloendothelial system
Radiolvsis Residual radiation, 5, 7-10, 23tproducts of, 172 effects of, 7- 10water, 250 estimating decay of, 236
Radiomimetic agents, 181 Respirator\, system cancers, 172, 182, 184, 194-197cvclophosphamide, 181 Reticulocytes, 90nitrogen mustard, 181 Reticuloendothelial system (RES), 72
Radionuclide contamination. See Internal radionuclide Retrograde amnesia, 107contamination Ribonucleic acid (RNA), 200
Radiophotoluminescent (RPL) dosimeters, 231 RNA. See Ribonucleic acidset also Dosimeters and Radiation detection and Roentgen, Wilhelm Conrad, 2, 177
measurement Roentgens (R), defined, 172Radioprotection, 245-206 RPL See Radiophotoluminescent (RPL) dosimeters
and behavior, 132-134in space, 134 Salting, 9and supportive therapy, 264-266 Scintillation counters, 59, 230-231see also Antiemetics and antidiarrheals, Radioprotective SED. See Skin erythema dose
agents, Radioprotective strategies, Shielding Segmented filamentous microflora (SFM), 74Radioprotective agents Selenium
aminothiols, 250-255, 257 as radioprotectant, 252, 255, 256, 264combination agents, 263-266 to reduce toxicity of WR-2721, 256cytokines, 259, 261-263 Serotoninof detoxification, 252, 255 as radioprotective agent, 263eicosanoids, 250, 256 Serum amylase, 86, 87, 90, 91genetic approaches, 250, 256 Service Response Force (SRF), 239naturally occurring antioxidants, 250, 255-256 SFM. See Segmented filamentous microfloraof regeneration, 252, 257-263 "Shell shock" syndrome, 164
Radioprotective regimen requirements, 266-268 Shielding, 28-29, 133-134, 235-236, 267deliverability, 267-268 set' also Radioprotectioneffectiveness, 266-267 Sievert (Sv), defined, 172toxicity, 267 Sign language
Radioprotective strategies for "chemical casualty," 46-47protection, 248-256 for "radiation casualty," 46-47
free radical scavenging, 249-250 Silvadene. See Silver sulfadiazinehypoxia, 249 Silver sulfadiazine (silvadene), 79
regeneration, 248, 257-263 Skin damage, 177-179repair, 248, 257 beta burn, 178
genetic, 257 cancer, 17>,-179hydrogen transfer, 257 epilation, 179
Radiotherapy, 29-30 erythema, 178-179Radon gas, 172 neutron radiation threshold, 178
daughter products fibrosis, 179polonium-214, 172 fingernail pigmentation, 179polonium-218, 172 in Marshall Islanders, 179
radon-220, 172 hyperpigmentation, 179radon-222, 172 hypopigmentation, 179
RAMT. See Radiological Advisory Medical Team necrosis, 178-179Ratemeter, 230 and radiation dose, 178RBE. See Relative biological effectiveness telangiectasia, 179REAC/TS. See Radiation Emergency Assistance Center/ transepithelial injury (moist desquamatio'.), 178-179Training Site (REAC/TS), Oak Ridge, TN ulceration, 178-179
Reciprocal translocation, 200 set' also Beta burn, Erythema
265

Metdital Constqu'i/tv'I )t N ii~har Wirtfarc
Skin decontamination, 48, -0-h2 Taurine, -2Skin ervthema dose (SED), defined, 177 TDM. See Trehalose dimncolate
expoi,,ure proposed tor radiologists, 177 Teenagersof X radiation, 177 survey of, on likelihood of nuclear war, 15-*
So•matic cell fusion (hvbridoma technology), 7') Telangiectasia, 179Somatic radiation ettects, 175-187 Television dramatization. See Dail After, The
cataract formation, 175 Teratogenic radiation effects, 205-211among Nagasaki survivors, 175 embryonic developmental stages, 203incidence, 179, 17t fetal, 205, 208latency, 179 major organogenesis, 205, 206-208radiation threshold, 179 preimplantation, 209, 206
on skin and hair, 177-179 humans irradiated in utero, 209-211as affected by disease, 177 and fetal mortality, 20')alopecia, 17/ and greater cancer incidence, 211from alpha radiation, 177 in Hiroshima, 207dermatitis, 177 Testesepilation, 177, 17'4 radiosensitivity, 175see l, o Beta burn, Skin damage see also Somatic radiation effects, sterility, in males
sterility, 175-177 Testosterone, 176in females, 176-177 Therapeutic index, defined, 250in males, 17;-176 Thermal effects, 7
see also Cancer induction production of, 4-5Spina bifida, 210 Thermal force, 2SRF. See Service Response Force Thermoluminescent dosimeters (TLr)), 60, 231STANAG. See NATO Standardization Agreement see also Dosimeters and Radiation detection and
(STANAG 2083) measurementStem cells Thiola. See Mercaptopropionylglycine
bone marrow, 25, 90 Thiosulfonates, 253, 254depletion of, 248 Thorotrast, 189hematopoictic, 25, 28, 90, 263 Three Mile Island, PA, nuclear power plant accident
mitotic delav or destruction of, 90 at, 156regeneration, capability of, 28 Thule Air Force Base, Greenland, accident at, 23Fstromal, 90 Thymine, 197survival of, increased, 263 Thvroid cancer, 182, 1R4, 185, 191-193
Stem formation, 9 and ethnic groups, 192Sterility, 175-177 prevalence in women, 191-193Steroids and thyroid irradiation, 193
and managing emesis, 133 TLD. See Thermoluminescent dosimetersStomach lavage, 62 TNF. See Tumor-necrosis factorStrong force, 3 Trauma, influence of,Strontium-90. See Fallout and Radioisotopes on LD;,,, 25-27Stunting, 208 Trehalose dimycolate (TDM), 252, 260-261, 265Sulfamylon. See Mafenide acetate Triage, 11, 37-46Sulfhydrvls, 253, 254 of blast injury, 46Superoxide dismutase, 252, 255, 256 of burn injury, 46Surgery, 47-48, 79 of eye injury, 46
and antibiotics, 79 military, 40timing of, after irradiation, 79 of patients with combined injuries, 43-46
Sv. Ste, Sievert and radiation dose, 40, 45Symptoms of irradiation, 88 in peacetime, 39-40
priority categories, 38-39delayed treatment, 38expectant, 38immediate treatment, 38
T-cell leukemia, 184 minimal treatment, 38T-cells Trinity device, 4
activation of, by interleukin-1, 261 Tritium, 4in AIDS, 182 Tumor-necrosis factor (TNF), 252, 261-263, 264T-4 lymphocytes, 182 Turner's syndrome, 206
286

Walter Reed Army Institute of Research (WRAIR', 250, 254address, 275
Ulceration, 41, 178-1794 Weapon yield, 5Uranium. See Fission weapons, fuel, uranium-233 and Whole-body radionuclide determination, 97uranium-235 Wound closure, 79
Urinarv dosimneters, 87, 92 And immunosuppression, 79amylase, 87, L92 and systemic sepsis, 79creatine, 87, 42 WR-2721 (ethiotos), 133, 250-254, 264glvcine, 92 WRAIR. See Walter Reed Army Institute of Researchhindrances to development, 42 WRAIR sulfur compounds, 133, 250-254histamine, 87, 92hydroxyproline, 92 X radiation, 172prostaglandins, 87, 92 and cancer induction, 179taurine, 879 2 and cancer treatment, 179see also Dosimeters exposure to, 177
U.S. European Command (EUCOM) Chernobyl I ask and lymphocytes, 94Force, 238-239 see also Radiotherapy
address, 275 X rays, 2, 246plasma as source of, 5
Vaccination. See Active vaccination Xeroderma pigmentosum, 182, 202Vinca, Yugoslavia, radiation accident at, 301-31Vitamin A, 251, 256 Yield. See Weapon yieldVitamin E, 25., 256
Zacopride (5-HT3-receptor blocker)as antiemetic, 133
Zinc protoporphyrin (ZPP), 86, 87, 97ZPP. See Zinc protoporphyrinZymosan, 259-260
* US GOVERNMENT PRINTING OFFICE 1989-223-543
PIN 902241-000 287