Measuring the Glycemic Index of Foods: Interlaboratory Study

www.wjpps.com
1113
Sushanta et al. World Journal of Pharmacy and Pharmaceutical Sciences
ANTIOXIDANT EFFECT OF VITAMIN C ON TYPE 2 DIABETES
MELLITUS PATIENTS ALONG WITH TWO DIFFERENT ORAL
HYPOGLYCEMIC AGENTS FOR SMOOTH GLYCEMIC CONTROL
*Sushanta Kr. Das1, P.R. Anand Vijayakumar2, R. Senthil2, Jayesh Kumar Bhatt2, S.
Gupta2 1Department of Pharmacy Practice, RVS College of Pharmaceutical Sciences, 242B, Trichy
Road, Sulur, Coimbatore- 641402, Tamilnadu. India. 2Department of Pharmacy Practice & Pharmacology, JSS College of Pharmacy, Off Campus
JSS University, Post Box- 20, Rocklands, Ootacamund – 643001, Tamilnadu, India.
ABSTRACT
Background: Type 2 diabetes mellitus (T2DM) is a global epidemic
with major challenge to healthcare systems. T2DM patients have
increase the level of vitamin C’s primary oxidation product,
dehydroascorbate may be due to inadequate intracellular delivery of
vitamin C because it’s entry into cells depends on insulin. Chronic
vitamin C deficiency in T2DM patients can lead to a range of
complications. Supplementation with antioxidants as promising
complementary treatment can exert beneficial effects.
Objective: To investigate if antioxidant effect of vitamin C in
combination with two different oral hypoglycemic agents in T2DM
patients may produce smooth glycemic control or not.
Subject/Methods: 93 T2DM patients participated in this randomized
open label controlled study at out-patient department centre of
government headquarters hospital, Ootacamund, The Nilgiris, Tamil
Nadu, India. Enrolled patients were randomised in to six groups.
Control groups received glibanclamide, metformin and combination of these two drugs,
whereas in intervention groups viz; glibanclamide, metformin and combination of two drugs,
received vitamin C tablet (500mg/day) for a period of three months. Random blood sugar
WWOORRLLDD JJOOUURRNNAALL OOFF PPHHAARRMMAACCYY AANNDD PPHHAARRMMAACCEEUUTTIICCAALL SSCCIIEENNCCEESS
VVoolluummee 11,, IIssssuuee 33,, 11111133--11112222.. RReesseeaarrcchh AArrttiiccllee IISSSSNN 2278 – 4357
Article Received on 01 September 2012,
Revised on 14 September2 012, Accepted on 25 September2012
*Correspondence for
Author:
* Mr. Sushanta Kr. Das.
Assistant Professor
RVS College of
Pharmaceutical Sciences
242B, Trichy Road
Sulur, Coimbatore- 641402
Tamilnadu. India.

www.wjpps.com
1114
Sushanta et al. World Journal of Pharmacy and Pharmaceutical Sciences
were measured and simultaneously fasting blood samples were analysed for level of HbA1C,
ascorbic acid, TBAR, SOD, catalase, glutathione estimation by using specific assay methods.
Results: 93 T2DM patients participated in this randomized open label controlled study, were
randomized into two groups; control (n=47) and intervention (n=46). Control group received
glibenclamide/metformin/glibenclamide-metformin combination. Intervention group received
glibenclamide/metformin/glibenclamide-metformin combination along with vitamin C
(500mg/day) for three months. Blood samples were analyzed by using specific assay
methods. Mean serum levels of superoxide dismutase and ascorbic acid were significantly
increased with significant decrease of thiobarbituric acid reactive substances and HbA1C in
intervention group when compared to control group.
Conclusion: Our result shows that vitamin C supplementation with oral hypoglycemic agents
decreases oxidative stress & improves glycemic control, also has potential implications for
the prevention of further complications in T2DM patients.
Key words: T2DM, vitamin C, glibenclamide, metformin.
INTRODUCTION
Diabetes mellitus is a chronic and progressive disease state of worldwide significance. It can
affect children, young, and adults of all ages. Type 2 diabetes mellitus (T2DM) is a global
epidemic with an estimated worldwide prevalence is 285 million people in 2010, and set to be
increases to 438 million by 20301. The health, social, and economic burden is great
consequently, T2DM presents a major challenge to healthcare systems around the world 2, 3, 4.
Diabetes mellitus is primarily a metabolic disorder arising from a lack of or resistance to
insulin, which results in the impairment of uptake and storage of glucose and reduced glucose
utilization for energy purposes, that lead to the condition called hyperglycemia. Prolonged
exposure to elevated glucose induces repeated acute changes in intracellular metabolism as
well as cumulative long-term changes in the structure and function of macromolecules5.
The environment, stress factor and chain reaction - our own body metabolism generates free
radicals that are very reactive chemical species, can cause oxidative injury to the living
beings by attacking the macromolecules. There is a critical balance in the generation of
oxygen free radicals and antioxidant defense systems used by organisms to deactivate and
protect themselves against free radical toxicity under normal physiological conditions6, 7, 8.
Upset in the oxidant/antioxidant equilibrium lead to a condition called oxidative stress, which

www.wjpps.com
1115
Sushanta et al. World Journal of Pharmacy and Pharmaceutical Sciences
is known to be a component of molecular and cellular tissue damage mechanisms in a wide
range of human diseases including diabetes.
Patients with type 2 diabetes mellitus have 2 to 4 fold increase in the prevalence of
cardiovascular disease compared to non-diabetes mellitus patients9. It has been suggested that
free radical activity is increased in diabetes that contribute to increased oxidative stress
through, not only increased non-enzymatic glycosylation and auto oxidative glycosylation but
also metabolic stress resulting from changes in energy metabolism, alterations in sorbitol
pathway, changes in the level of inflammatory mediators. The status of antioxidant defense
systems and localized tissue damage results from hypoxia and ischemic reperfusion injury10.
People with type 2 diabetes have a relative vitamin C deficiency despite adequate dietary
intake, and increase the level of its primary oxidation product, dehydroascorbate that could be
due to inadequate intracellular delivery of vitamin C because vitamin C entry into cells
depends on insulin11. Chronic vitamin C deficiency in people with type 2 diabetes can lead to
a range of complications. Supplementation with antioxidants as a promising complementary
treatment can exert beneficial effects in diabetes. Although antioxidant has a beneficial effect
in type 2 diabetes mellitus, only limited studies have dealt with antioxidant supplement in
type 2 diabetes mellitus with Indian population. Hence, therefore, the present study was
designed to evaluate the role of antioxidant supplement (vitamin C) in patients with type 2
diabetes mellitus along with two different oral hypoglycemic drugs and their combination for
smooth glycemic control in south Indian population.
ETHICS
Written consent was obtained from all participants after debriefing session. The project
protocol was approved by Institutional Ethics Committee (IEC), JSS College of pharmacy,
Ootacamund, The Nilgiris, Tamil Nadu, India. All procedures followed were in accordance
with the ethical standards of the responsible committee on human experimentation.
MATERIALS & METHODS
A randomized open label controlled trial include 93 study patients divided into two groups
control (n=47) and intervention (n=46). Each group were subdivided in to three groups viz.
control-metformin CM (n=16), control-glibenclamide CG (n=16), control-combination CC
(n=15) and intervention-metformin IM (n=16), intervention-glibenclamide IG (n=15),
intervention-combination IC (n=15). The study was carried out at outpatient department
centre of Government headquarters hospital, Ootacamund, The Nilgiris, Tamil Nadu, India

www.wjpps.com
1116
Sushanta et al. World Journal of Pharmacy and Pharmaceutical Sciences
during the period of April 2005 to February 2006. Demographic data and general health
characteristics include height, body weight, body mass index, social habit, smoking status and
food habits were collected on standard structured data collection form by face to face
interview. Patients with type 2 diabetes mellitus aged between 35 to 65 years, duration of
disease ≥ 2 years, either sex with or without co-morbidities and on oral hypoglycemic agents
were included in the study, whereas exclusion criteria includes, type 1 diabetes, juvenile
diabetes, pregnant women and lactating mothers, voluntary withdrawal and significant
hepatic & renal dysfunction patients.
Patients were randomized by using computer assisted randomization procedure and assigned
to different treatment groups, control group (n=47) received, metformin (CM, n=16),
glibenclamide (CG, n=16), combination (CC, n=15), whereas in intervention group (n=46),
metformin (IM, n=16), glibenclamide (IG, n=15), combination (IC, n=15) received additional
vitamin C (500mg OD) tablet for a period of three months.
Random blood glucose level were measured at all visits including the day of enrolment and 5
ml of blood samples were collected from each patients at the day of enrolment and at the end
of 3 months trial.
Blood samples were collected in heparinized sample collection tubes and the plasma was
separated by centrifugation at 4000 rpm for 20 min. The isolated plasma was stored at -700 C
until biochemical analysis. Random blood glucose was measured by using Accu-chek Active
Blood Glucose Monitor® by Roche, Germany. HbA1C were determined by using semi-auto
analyzer (Micro lab 200 Merck). Ascorbic acid was estimated by the method of Roe and
Kuether12: this involves oxidation of ascorbic acid by copper followed by treatment with 2, 4-
dinitrophenylhydrazine that undergoes rearrangement to form a product with absorption
maximum at 520 nm. Superoxide dismutase (SOD) was determined using spectrophotometric
method by Kakkar13: based on inhibition of the formation of nicotine amide adenine
dinucleotide, phenazine methosulfate and amino blue tetrazolium formazan. Lipid peroxides
were estimated by measurement of thiobarbituric acid reactive substances (TBARs) in plasma
by the method of Yagi14: the pink chromogen produced by the reaction of thiobarbituric acid
with malondialdehyde, a secondary product of lipid peroxidation was estimated. The
absorbance of clear supernatant was measured against reference blank at 535 nm. Catalase
was assayed colorimetrically at 620 nm as described by Sinha15: the reaction mixture (1.5 ml,
vol) contained 1.0 ml of 0.01 M phosphate buffer (pH 7.0), 0.1 ml of erythrocyte lysate and

www.wjpps.com
1117
Sushanta et al. World Journal of Pharmacy and Pharmaceutical Sciences
0.4 ml of 2 M H2 O2 . The reaction was stopped by the addition of 2.0 ml of
dichromateacetic acid reagent (5% potassium dichromate and glacial acetic acid were mixed
in 1:3).
STATISTICS
The data obtained from the study were analyses by using one way of analysis of variance
(ANOVA) using the Graph Pad “Instat” and the “p” value of ≤ 0.05 were considered as
statistically significant. All the obtained data were plotted in the graph pad column and
comparison were done with different control group Vs different intervention group. Standard
deviation (SD), Mean, standard error mean (SEM) and p values were obtained from the graph
pad itself.
RESULTS
Table 1 shows the Demographic characteristic of the investigated study populations. The
mean age limit was 49.27±7.25 years in control diabetic patients and 48.07±6.25 years in
intervention group. In control group 35 patients had alone diabetes and 22 patients had co
morbidity with diabetes whereas in intervention group 21 patients had alone diabetes and 25
patients had co-morbidity along with diabetes mellitus. Body mass Index was slightly
elevated in both control and intervention patients with duration of disease 5.83±1.99 years in
control group and 6.56±1.91 years in intervention group.
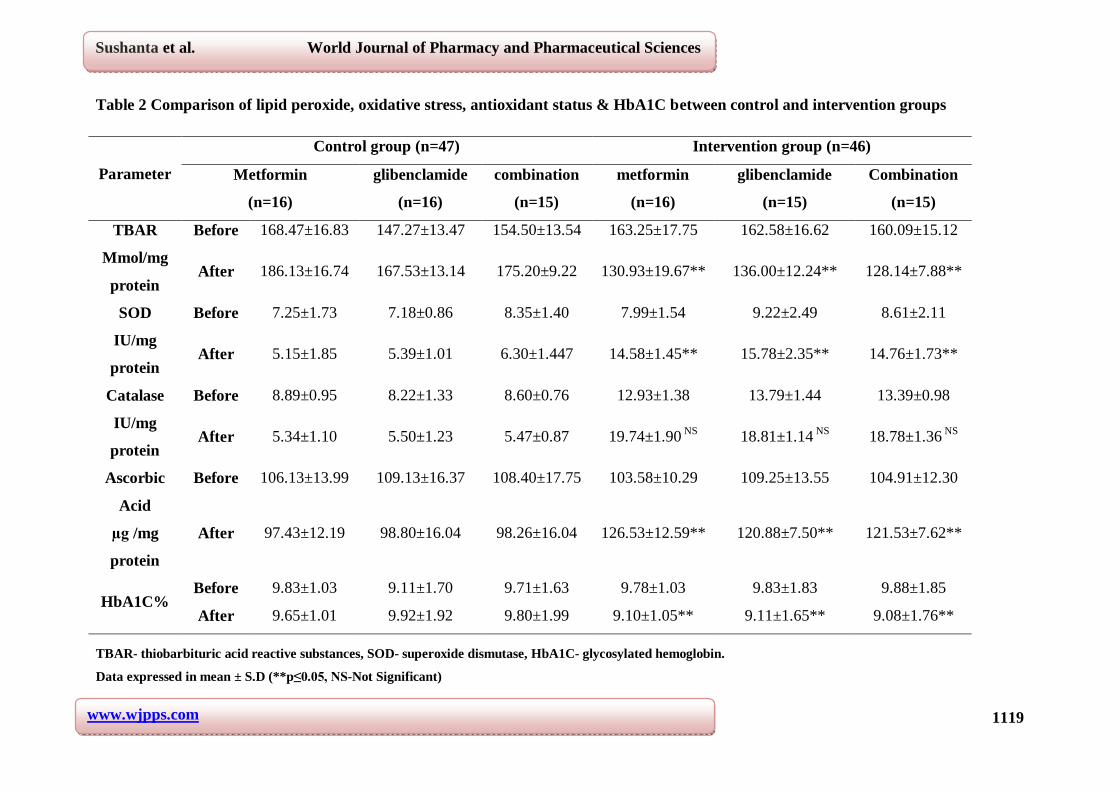
Table 2 shows the circulatory lipid peroxide, oxidative stress parameter, antioxidant status
and HbA1C level of control group and intervention group. The parameters include TBAR,
superoxide dismutase, Catalase, ascorbic acid and HbA1C. Mean serum levels of superoxide
dismutase and ascorbic acid were significantly increased with significant decrease of TBAR
and HbA1C level (vitamin C 500mg/day p≤0.05) in intervention group when compared to
control diabetic patients after three months of vitamin C supplementation. There were no
significant changes in the Catalase level in both the groups. Moreover in intervention group
there were no significant changes with respect to different drug regimen and their
combination.

www.wjpps.com
1118
Sushanta et al. World Journal of Pharmacy and Pharmaceutical Sciences
Table.1. Demographic comparison of control and Intervention group
Variables Control Group Intervention group
No. of Patients 47 46
Male/Female 12/35 17/29
Age (years) 49.27±7.25 48.07 ±6.25 NS
Smoker 3 4
Alcoholic 4 2
Non Vegetarian 32 33
Duration of disease 5.83±1.99 6.56±1.91 NS
Co-morbidty 22 25
Body Mass Index (kg/m2) 24.75 ±3.09 24.52±2.89 NS
Data expressed in mean ± S.D (NS-Not Significant)
DISCUSSION
In this study most of population was non-vegetarian and overweight, since the Nilgiris is
situated above 2400 meter, the climatic condition with the low atmospheric temperature
affects the life style of the residents. This is the important factor which may affects the basal
metabolic rate of the populations, forced to have the carbohydrate -rich non- vegetarian diet
and one of the epidemic cause for more diabetes7,8.
The extent of lipid peroxidation (TBAR) was decreased and superoxide dismutase (SOD) was
increased in intervention group when compared to control group. This clearly indicates the
antioxidant supplement really useful to minimize the oxidative stress and thereby reduce
related risks. The increased TBARs level observed in study patients as most of them were
coming under the age group of 41- 50 and above 50 years. This might be due to the
pathological condition, worsens with the age due to altered defense system and elevated free
radical production16.
In fast urban lifestyle, fast foods, changing diet pattern, lack of exercise, obesity, smoking
etc. are responsible for the diabetic epidemic17, these factors are greatly undermine the body’s
ability to remove toxic “free radicals “which are constantly being produced in the body”.
The role of oxidative stress in the causation of chronic tissue damage is being increasingly
recognized if antioxidant deficiency occurs. The low antioxidant level in diabetes may have
resulted from lower intake of antioxidant or increased oxidative stress. So, in this condition
the supplementation of antioxidants expected to be beneficial8.
www.wjpps.com
1119
Sushanta et al. World Journal of Pharmacy and Pharmaceutical Sciences
Table 2 Comparison of lipid peroxide, oxidative stress, antioxidant status & HbA1C between control and intervention groups
TBAR- thiobarbituric acid reactive substances, SOD- superoxide dismutase, HbA1C- glycosylated hemoglobin.
Data expressed in mean ± S.D (**p≤0.05, NS-Not Significant)
Parameter
Control group (n=47) Intervention group (n=46)
Metformin
(n=16)
glibenclamide
(n=16)
combination
(n=15)
metformin
(n=16)
glibenclamide
(n=15)
Combination
(n=15)
TBAR
Mmol/mg
protein
Before 168.47±16.83 147.27±13.47 154.50±13.54 163.25±17.75 162.58±16.62 160.09±15.12
After 186.13±16.74 167.53±13.14 175.20±9.22 130.93±19.67** 136.00±12.24** 128.14±7.88**
SOD
IU/mg
protein
Before 7.25±1.73 7.18±0.86 8.35±1.40 7.99±1.54 9.22±2.49 8.61±2.11
After 5.15±1.85 5.39±1.01 6.30±1.447 14.58±1.45** 15.78±2.35** 14.76±1.73**
Catalase
IU/mg
protein
Before 8.89±0.95 8.22±1.33 8.60±0.76 12.93±1.38 13.79±1.44 13.39±0.98
After 5.34±1.10 5.50±1.23 5.47±0.87 19.74±1.90 NS 18.81±1.14 NS 18.78±1.36 NS
Ascorbic
Acid
µg /mg
protein
Before 106.13±13.99 109.13±16.37 108.40±17.75 103.58±10.29 109.25±13.55 104.91±12.30
After 97.43±12.19 98.80±16.04 98.26±16.04 126.53±12.59** 120.88±7.50** 121.53±7.62**
HbA1C% Before 9.83±1.03 9.11±1.70 9.71±1.63 9.78±1.03 9.83±1.83 9.88±1.85
After 9.65±1.01 9.92±1.92 9.80±1.99 9.10±1.05** 9.11±1.65** 9.08±1.76**

www.wjpps.com
1120
Sushanta et al. World Journal of Pharmacy and Pharmaceutical Sciences
In our study most of the enrolled patients coming under economically deprived background.
Thus lower consumption of fruits and vegetables may have contributed to reduce the
consumption of vitamin C and carotenes among the patients with diabetes which may lead to
increase oxidative stress. These data are supported by the Enstrom study where consumption
of vitamin C decreases the risk of premature death18. There were no significant changes with
respect to different drug regimen and their combination.
Limitations of this study are as it was conducted at government hospital so turn out of the
patients were very irregular with a higher drop out, thus forced us to limit the number of
subject of the study. Different dose of vitamic C with more number of subjects will give a
much better result for clinical application. Use of different antioxidant other than vitamin C,
like vitamin E and alpha lipoic acid would have given a better comparison. More over a
placebo group would have been best used to measure the actual effect of vitamin C.
CONCLUSIONS
Although our results may have some clinical implications, measurement of antioxidants is not
routinely performed in clinical practice, reviewing the intake of food rich in antioxidants
particularly citrus fruits and green leafy vegetables and the appropriate antioxidant
supplements among patients with the metabolic syndrome may be instructive for the smooth
control of diabetes. If their dietary intake of vitamins A, C and E fails to meet the
recommended daily allowance, health care professionals should encourage people with the
metabolic syndrome to increase their intake of vitamins, preferably through the consumption
of healthy food sources rich in these vitamins or otherwise through the use of appropriate
vitamin supplements. The future studies may direct towards extended duration of treatment
and large number of patients.
ACKNOWLEDGEMENTS
The authors would like to acknowledge the support and co-operation received from the
medical and supporting staff of government headquarters hospital, Ootacamund, The Nilgiris,
Tamil Nadu, India and also all the participants who willingly enrolled themselves in the
study.
REFERENCES
1. IDF. The Diabetes Atlas 2010. [http://www.eatlas.idf.org/media]

www.wjpps.com
1121
Sushanta et al. World Journal of Pharmacy and Pharmaceutical Sciences
2. de Groot M., Anderson R., Freedland KE, Clouse RE, & Lustman PJ 2001. Association
of depression and diabetes complications: a meta-analysis. Psychosom Med 2001, 63:
619−630.
3. Derek Wanless. Securing our future health: taking a long-term view 2002.
[http://www.hmtreasury.gov.uk/consultations_and_legislation/wanless/consult_wanles
s_final.Cfm]
4. Jacobson AM. Impact of improved glycemic control on quality of life in patients with
diabetes. Endocr Pract 2004, 10:502−508.
5. Tiwari AK and Madhusudana Rao J. Diabetes mellitus and multiple therapeutic
approaches of phytochemicals: Present status and future prospects. Current Science 2002,
83:30-38.
6. Aragno M, Tamagno E, Gato V. Dehydroepiandrosterone protects tissues of
streptozotocin-treated rats againstoxidative stress. Free Radic Biol Med 1999, 26(11/12):
1467–1474.
7. Bonnefont RD, Bastard JP, Jaudon MC, Delattre J. Consequences of the diabetic status on
the oxidant/antioxidant balance. Diabetes Metab 2000, 26:163–176.
8. Moussa SA. Oxidative stress in diabetes mellitus. Romanian Journal of Biophys 2008,
18(3):225-236.
9. Malmberg K, Yusuf S, Gerstein HC. For the OASIS Registry Investigators. Impact of
diabetes on long-term prognosis in patients with unstable angina and non- Q-wave
myocardial infarction: results of the OASIS (Organization to Assess Strategies for
Ischemic Syndromes) Registry. Circulation 2000, 102:1014-1019.
10. Mullarkey CJ, Edelstein D, Brownlee L. Free radical generation by early glycation
products: a mechanism for accelerated atherogenesis in diabetes. Biochem Biophys Res
Comm 1990, 173:932–939.
11. Cunningham JJ. Reduced mononuclear leukocyte ascorbic acid content in adults with
IDDM consuming adequate vitamin C. Metabolism 1991, 40:146-149.
12. Roe HJ and Kuether CA. Detection of ascorbic acid in whole blood and urine through the
2, 4-dinitrophenyl-hydrazine derivative of dehydro ascorbic acid. J Biol Chem 1943,
147:399- 407.
13. Kakkar PS, Das B, Viswanathan PN. A modified spectrophotometric assay of superoxide
dismutase. Indian J. Biochem Biophys 1984, 21:130-132.
14. Yagi K. Lipid peroxides and human diseases. Chem. Phys. Lipids 1978, 45:337-351.
15. Sinha KA. Colorimetric assay of catalase. Anal Biochem 1972, 47:389-394.

www.wjpps.com
1122
Sushanta et al. World Journal of Pharmacy and Pharmaceutical Sciences
16. Nuttall SL, Dunne1 F, Kendall MJ and Martin U. Age-independent oxidative stress in
elderly patients with non-insulin-dependent diabetes mellitus. Q J Med 1999, 92:33-38.
17. Chowdhury TA, Grace C and Kopelman. Preventing diabetes in south Asians. BMJ PG
2003, 327:1059-1060.
18. Emstrom EJ. Vitamin C intake and mortality among a sample of the United States
population. Epidem 1992, 3:194-202.
Copyright © 2022 FDOKUMEN