Visual binding abilities in the initial and advanced stages of schizophrenia
10
Visual binding abilities in the initial and advanced stages of schizophrenia Parnas J, Vianin P, Sæbye D, Jansson L, Volmer-Larsen A, Bovet P. Visual binding abilities in the initial and advanced stages of schizophrenia. Acta Psychiatr Scand 2001: 103: 171–180. # Munksgaard 2001. Objective: The study tests the hypothesis that intramodal visual binding is disturbed in schizophrenia and should be detectable in all illness stages as a stable trait marker. Method: Three groups of patients (rehospitalized chronic schizophrenic, first admitted schizophrenic and schizotypal patients believed to be suffering from a pre-schizophrenic prodrome) and a group of normal control subjects were tested on three tasks targeting visual ‘binding’ abilities (Mu ¨ ller-Lyer’s illusion and two figure detection tasks) in addition to control parameters such as reaction time, visual selective attention, Raven’s test and two conventional cortical tasks of spatial working memory (SWM) and a global–local test. Results: Chronic patients had a decreased performance on the binding tests. Unexpectedly, the prodromal group exhibited an enhanced Gestalt extraction on these tests compared both to schizophrenic patients and to healthy subjects. Furthermore, chronic schizophrenia was associated with a poor performance on cortical tests of SWM, global–local and on Raven. This association appears to be mediated by or linked to the chronicity of the illness. Conclusion: The study confirms a variety of neurocognitive deficits in schizophrenia which, however, in this sample seem to be linked to chronicity of illness. However, certain aspects of visual processing concerned with Gestalt extraction deserve attention as potential vulnerability- or prodrome- indicators. The initial hypothesis of the study is rejected. J. Parnas 1,3 , P. Vianin 2 , D. Sæbye 3 , L. Jansson 1 , A. Volmer-Larsen 1 , P. Bovet 4 1 Copenhagen University Department of Psychiatry, Hvidovre Hospital, 2650 Hvidovre, Denmark, 2 Laboratory of Psychology of Perception, University of Geneva, Switzerland, 3 Institute of Preventive Medicine, Kommunehospitalet, Copenhagen, Denmark and 4 University Department of Adult Psychiatry, University of Lausanne, Switzerland Key words: schizophrenia; prodrome; Mu ¨ller-Lyer; ‘binding process’; schizotypy Dr Parnas, Institute of Preventive Medicine, Kommunehospitalet, 1399 Copenhagen K, Denmark Accepted for publication October 10, 2000 Introduction It is very well documented that schizophrenia is associated with multiple neuropsychological dys- functions, e.g. disturbances of attention, short-term memory, perceptual functioning, associative pro- cesses, concept-formation and planning–executive- monitoring processes. These dysfunctions are already observable in first admission cases (1, 2) but it is not yet resolved whether they are static or progress during the first years of manifest psychosis (3). Some of these dysfunctions have been observed in schizotypal personality disorder (4, 8), and in unaffected members of MZ twin pairs discordant for schizophrenia (9, 10). Partly because of the heterogeneity of dysfunctions, strictly modular pathogenetic views of schizophrenia are being progressively abandoned in favour of models pro- posing a generalized deficit or a widespread impreci- sion in the brain functioning (‘panmodal impre- cision’ (11) or ‘cognitive dysmetria’ (12)). The distinction between vulnerability-linked trait indica- tors and ‘state’ markers is still unclear (10, 13, 14). This latter group includes dysfunctions caused by a hypothetical neural processes implicated in the development of schizophrenic psychosis and poten- tial sequelae of certain symptoms (e.g. isolation) or of other adversities of a long-lasting illness. In practice, it is difficult or even impossible to compartmentalize neuropsychological test results into neatly defined ‘cause–effect’ segments, because of the complex Acta Psychiatr Scand 2001: 103: 171–180 Printed in UK. All rights reserved Copyright # Munksgaard 2001 ACTA PSYCHIATRICA SCANDINAVICA ISSN 0001-690X 171
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Visual binding abilities in the initial and advanced stages of schizophrenia
Visual binding abilities in the initial andadvanced stages of schizophrenia
Parnas J, Vianin P, Sñbye D, Jansson L, Volmer-Larsen A, Bovet P.Visual binding abilities in the initial and advanced stages ofschizophrenia.Acta Psychiatr Scand 2001: 103: 171±180. # Munksgaard 2001.
Objective: The study tests the hypothesis that intramodal visual bindingis disturbed in schizophrenia and should be detectable in all illness stagesas a stable trait marker.Method: Three groups of patients (rehospitalized chronic schizophrenic,®rst admitted schizophrenic and schizotypal patients believed to besuffering from a pre-schizophrenic prodrome) and a group of normalcontrol subjects were tested on three tasks targeting visual `binding'abilities (MuÈller-Lyer's illusion and two ®gure detection tasks) inaddition to control parameters such as reaction time, visual selectiveattention, Raven's test and two conventional cortical tasks of spatialworking memory (SWM) and a global±local test.Results: Chronic patients had a decreased performance on the bindingtests. Unexpectedly, the prodromal group exhibited an enhanced Gestaltextraction on these tests compared both to schizophrenic patients and tohealthy subjects. Furthermore, chronic schizophrenia was associatedwith a poor performance on cortical tests of SWM, global±local and onRaven. This association appears to be mediated by or linked to thechronicity of the illness.Conclusion: The study con®rms a variety of neurocognitive de®cits inschizophrenia which, however, in this sample seem to be linked tochronicity of illness. However, certain aspects of visual processingconcerned with Gestalt extraction deserve attention as potentialvulnerability- or prodrome- indicators. The initial hypothesis of thestudy is rejected.
J. Parnas1,3, P. Vianin2, D. Sñbye3,L. Jansson1, A. Volmer-Larsen1,P. Bovet4
1Copenhagen University Department of Psychiatry,
Hvidovre Hospital, 2650 Hvidovre, Denmark,2Laboratory of Psychology of Perception, University of
Geneva, Switzerland, 3Institute of Preventive
Medicine, Kommunehospitalet, Copenhagen, Denmark
and 4University Department of Adult Psychiatry,
University of Lausanne, Switzerland
Key words: schizophrenia; prodrome; MuÈller-Lyer;
`binding process'; schizotypy
Dr Parnas, Institute of Preventive Medicine,
Kommunehospitalet, 1399 Copenhagen K, Denmark
Accepted for publication October 10, 2000
Introduction
It is very well documented that schizophrenia isassociated with multiple neuropsychological dys-functions, e.g. disturbances of attention, short-termmemory, perceptual functioning, associative pro-cesses, concept-formation and planning±executive-monitoring processes. These dysfunctions arealready observable in ®rst admission cases (1, 2)but it is not yet resolved whether they are static orprogress during the ®rst years of manifest psychosis(3). Some of these dysfunctions have been observed inschizotypal personality disorder (4, 8), and inunaffected members of MZ twin pairs discordantfor schizophrenia (9, 10). Partly because of theheterogeneity of dysfunctions, strictly modular
pathogenetic views of schizophrenia are beingprogressively abandoned in favour of models pro-posing a generalized de®cit or a widespread impreci-sion in the brain functioning (`panmodal impre-cision' (11) or `cognitive dysmetria' (12)). Thedistinction between vulnerability-linked trait indica-tors and `state' markers is still unclear (10, 13, 14).This latter group includes dysfunctions caused by ahypothetical neural processes implicated in thedevelopment of schizophrenic psychosis and poten-tial sequelae of certain symptoms (e.g. isolation) or ofother adversities of a long-lasting illness. In practice,it is dif®cult or even impossible to compartmentalizeneuropsychological test results into neatly de®ned`cause±effect' segments, because of the complex
Acta Psychiatr Scand 2001: 103: 171±180Printed in UK. All rights reserved
Copyright # Munksgaard 2001
ACTA PSYCHIATRICASCANDINAVICAISSN 0001-690X
171

dependencies and correlations between the involvedvariables.
Our own approach originates in the long-itudinal prospective studies of phenotypic indica-tors of vulnerability to schizophrenia spectrumdisorders (15±17). We have proposed, guided by aphenomenological perspective, that typicality (oressence) of the clinical manifestations of theschizophrenia spectrum consists in a `de®cientpre-re¯ective attunement' or `crisis of commonsense' (18). Both expressions signify a de®ciencyin the automatic pre-re¯ective intentionality. Inclinical terms, such de®ciency manifests itself inunstable coherence of the perceptual world andfragile sense of self as the subject of experienceand action; both contributing to a weakeningof the intersubjective ties (19). Combiningpsychological and neurobiological developmentalapproaches, we have proposed a neurodevelop-mental hypothesis, suggesting that vulnerability toschizophrenia is linked to a faulty ontogenesis andfunctioning of intermodal sensory integration (20)caused by a malfunction in the physiological`binding' processes. Integration of sensory signalsfrom two or more channels is a basic step in theacquisition of an early sense of self (21) as well asof the sensorimotor mastery and intersubjectiveskills (22). Because the intra-modal perceptualprocessing involves integrative mechanisms on itsown level (23), we found it likely that thesemechanisms may also be affected in schizo-phrenia. Simply stated, intramodal bindingdemarcates objects from their surrounding back-ground ®eld. Thus, it is currently believed thatperceptual objects are recognized by a process inwhich consistent spatial and temporal relationsamong incoming signals (`features') are detectedand enacted by selective neuronal responses; objectperception is dependent on synchronized activity inthese neurones. Visual features to which speci®cneuronal responses have been demonstrated in themammalian brain comprise location, orientation,polarity of luminence gradients, their direction ofmotion, their spectral composition and interoculardisparity, indicating distance (23).
We decided to test aspects of intramodal visualprocessing in schizophrenia spectrum patients atdifferent stages of their illness, predicting thatdeviant performance in integration/binding tasksshould operate as a trait indicator, i.e. would notdiffer as a function of illness' stages. We includedfew other tasks as control parameters, because oftheir conventionally accepted relevance in theneuropsychological research on schizophrenia. Thechoice of control tasks was also dictated by ourdesire to keep the examination within reasonable
time limits, and to restrain it to visual tasks suitablefor easy computer manipulation.
Material and methods
Sampling
This study involves a series of ®rst-episode patientsadmitted to the Psychiatric University Departmentat Hvidovre Hospital in Copenhagen, with thediagnosis of schizophrenia or of a non-psychoticschizophrenia spectrum condition. The presentsample overlaps substantially the sample fromwhich prodromal phenomenological data havebeen reported (24).
The Department of Psychiatry at HvidovreHospital and its three out-patient sector-clinicsdeliver a comprehensive public psychiatric serviceto a de®ned geographical catchment area ofCopenhagen City with 130 000 inhabitants. Thereare no private psychiatric hospitals in Denmark,which eliminates the socioeconomic bias in patientselection. The majority of cases are referred fromthe primary health care system; some are self-referrals or referred by other agencies. Weattempted to consecutively test patients, admittedfor the ®rst time, who suffered from a schizophreniaspectrum condition. Nearly all ®rst admission casesof schizophrenia, other non-affective non-organicpsychosis (which are not severely ill or involuntarilyadmitted), non-psychotic schizophrenia spectrumdisorders, as well as diagnostically unclear cases, arehospitalized at one open specialized diagnostic unit(SDU), in which the present sample was recruitedfor testing during the period from September 1997to March 1998. Acute, severely ill and/or aggressive®rst-episode schizophrenic patients, initially hospi-talized in a closed ward, are later usually transferredto the SDU for a more detailed assessment, butsome may have been discharged quickly afteradmission or transferred elsewhere; such patientswere thus not available for the study. The SDU doesnot accept patients with serious acting-out problemsand signi®cant drug or alcohol abuse (which is asource of an ascertainment bias with few males). Inorder to compare ®rst-admitted patients to achronic, multiply re-admitted population, weincluded a random series of such patients, whowere all re-admitted (at least second admission).
None of the included patients was mentallyretarded or suffered from a clinically detectablecurrent or past organic brain syndrome or sig-ni®cant alcohol or drug abuse. Acutely and severelyill subjects were not included.
Patients were informed about the nature of thestudy and asked to participate. Two patients refused(one readmitted schizophrenic and one schizotype).
Parnas et al.
172
One patient, suffering from a ®rst-episode delu-sional disorder without schizotypal features, had tobe excluded from the analyses because he did not ®tinto any of the investigated diagnostic categories.
Diagnoses
All subjects were interviewed at different occasionsby two of us (J.P., L.J.; both consultant clinicians),in addition to the routine clinical evaluationsperformed by other clinicians. The interview wassemi-structured, of approximately 2±3 hours dura-tion, and covered all major areas of psychopathol-ogy, including the so-called `basic symptoms' and aphenomenologically guided exploration of thepatient's self-experience. The interviewer completeda SCAN-derived symptom checklist (25) supple-mented by an abridged version (section C and D) ofthe Danish translation of the BSABS (26).
All external information (e.g. records, dischargeletters) was reviewed by the interviewers. In the caseof ®rst admission cases, a separate interviewconcerning symptoms, illness evolution and pre-morbid pathology was performed by one of us(A.V.L., senior registrar) with a second informant,usually a biological relative or spouse.
An ICD-10 research diagnosis (27) was allocatedthrough a consensus agreement between all threeinterviewing clinicians at a case conference where allrelevant information on each subject was discussed.
The following diagnostic groups were delimited:
1) Chronic readmitted schizophrenia patients, i.e.cases ful®lling the ICD-10 criteria of schizo-phrenia for a period longer than 1 year, whowere at least second-episode patients (n=10).In that group, the median number of hospita-lizations is 4 (range 2±11), and the meanduration of illness (from the ®rst psychoticonset) of 4.3 years (SD 2.45).
2) First admitted schizophrenia patients, withlong illness duration, i.e. cases ful®lling theICD-10 criteria of schizophrenia for a periodlonger than 1 year prior to the ®rst hospitaliza-tion (n=4).
3) First admitted schizophrenia patients, butwhere the duration of psychosis was less than1 year (usually few months) (n=5).
4) Patients with a predominant picture of schizo-typal disorder and ful®lling at least four of itsICD-10 criteria, but where incipient (prodro-mal) schizophrenia was strongly suspected, dueto past or current micropsychotic episodes,increasing disintegration and experiences ofself-dissolution (n=10). We required that allpatients in this category exhibited signs offormal thought disorder and constricted or
inadequate emotionality and de®cient rapport.These patients were typically short of meetingthe criteria of schizophrenia, because theirmicropsychotic symptoms were too ¯eeting tosatisfy the criteria for delusions/hallucinationsand their expressive symptomatology wasbelow the severity level stipulated in theICD-10 Criterion 2.
5) A normal (unscreened) control group wasgenerated (n=14) from the paramedical staffof the hospital (secretaries, nurses, socialworkers and students).
In view of the small sample sizes we havedecided, for statistical purposes, to merge groups2 and 3 (henceforth called ®rst episode schizo-phrenia, FS) and operate with three groups inthe schizophrenia spectrum: 1) Chronic, read-mitted schizophrenia patients (CS), 2) ®rst admis-sion schizophrenia patients (FS), and 3) incipientor prodromal schizophrenia patients (PS).
We did not dichotomize the patients into para-noid±nonparanoid/positive±negative subgroups, asit is frequently done in neuropsychological research,because the sample sizes were too small. Allschizophrenia spectrum patients were stabilzed atthe time of neuropsychological testing, withoutpsychotic features nor negative symptomatologymarkedly in¯uencing their behaviour. All CS wereon antipsychotic treatment. Among FS, six were onneuroleptic treatment, and three had never beentreated with neuroleptics. Among PS, ®ve wereunder neuroleptic treatment and ®ve were not. Atthe time of examination, typical neuroleptics wereused, at low dosages.
Of the total patient sample, 25 were ethnic Danes,one was born in Eastern Europe, one was blackAfrican and two originated in North Africa. Noneof the ethnically non-Danish patients was an outlieron the test pro®les. All controls (CTR) were ethnicDanes. Educational level was scored on a six-pointscale from 0 (primary education not completed) to 5(university degree); for discretion reasons preciseeducational level of controls, who were members ofthe staff, was not asked; however, all controls had atleast achieved secondary school. Age, educationallevel and sex distributions appear in Table 1.
Apparatus and stimuli
The test battery was realized with the MacromediaAuthorware 4.0 software. The stimuli were preparedwith an IBM 32MB RAM Pentium Notebook andpresented on a 14" colour TFT screen.
The experiment consisted of three visual bindingtests. In addition, we tested visual reaction time,visual selective attention, Raven's coloured pro-
Visual binding abilities in schizophrenia
173
Tabl
e1.
Sam
ple
desc
ript
ion
and
resu
lts
Dia
gnos
isgr
oup
CS
FSPS
CTR
Bet
wee
n-gr
oup
com
pari
son
Age
28.7
25.1
27.5
31.9
(onl
ysi
gni®
cant
diff
eren
ces)
Educ
.le
vel
2.1
1.6
3.2
>3
No.
mal
es7
43
6
No.
fem
ales
35
78
Res
pons
eP-
valu
es1
Mea
nva
lues
that
are
com
pare
d(N
),S
Dw
hen
uneq
ual
vari
ance
and
norm
ally
dist
ribu
ted
resi
dual
s
Var
iabl
eEq
ual
mea
ns
Bin
ding
test
s
Con
tour
0.00
43**
6.6
6.8
10.6
8.1
CS<
PS3**
,FS<
PS*,
PS>
CTR
3*
Puls
0.03
72*
3.2
3.6
(8)
5.4
4.2
(13)
CS<
PS2**
ML5
000.
0083
**25
.221
.717
.3(9
)22
.3C
S>
PS3**
*,PS<
CTR
3*,
FS>
PS3*
Con
trol
test
s
RT
0.37
020.
374
0.38
3(8
)0.
359
0.34
5(1
3)
VS
A RT
0.36
630.
449
0.43
2(7
)0.
436
0.41
8
A'
0.17
620.
955
0.97
30.
985
0.97
6
Rav
en0.
0007
3**
*38
.6(8
)48
.0(6
)54
.4(8
)49
.8C
S<
PS3**
*,C
S<
CTR
3**
,C
S<
FS3*,
FS<
PS3*
Oth
erta
sks
SW
Mte
st0.
0253
*5.
464.
503.
323.
29C
S>
PS3**
,C
S>
CTR
3*
Glo
bal±
loca
l0.
0008
2**
*7.
99.
611
.411
.6C
S<
PS3**
,CS<
CTR
2**
*,FS<
CTR
2*
NC
GL
0.00
34**
15.2
SD
:3.
217
.3S
D:
2.8
19.1
SD
:1.
119
.5S
D:
0.9
CS<
PS3**
,CS<
CTR
2**
*,FS<
CTR
2*
1A
*in
dica
tes
that
the
effe
ctis
sign
i®ca
nton
5%le
vel,
**th
atth
eef
fect
issi
gni®
cant
on1%
leve
lan
d**
*th
atth
eef
fect
issi
gni®
cant
on0.
1%le
vel.
2Th
eP-
valu
est
ems
from
the
non-
para
met
ric
Kru
skal
±W
allis
test
(or
Man
n±W
hitn
eyte
st),
beca
use
mod
elre
sidu
als
are
not
norm
ally
dist
ribu
ted.
3Th
eP-
valu
est
ems
from
the
para
met
ric
anal
ysis
ofva
rian
ce,
AN
OV
A(o
rt-
test
).4
The
P-va
lue
stem
sfr
omth
epa
ram
etri
can
alys
isof
vari
ance
wit
hW
elch
corr
ecti
onbe
caus
eof
uneq
ual
vari
ance
give
nno
rmal
lydi
stri
bute
dre
sidu
als.
Occ
asio
nal
data
are
mis
sing
for
sing
lein
divi
dual
sin
sing
lete
sts;
inth
atca
se,
the
num
ber
ofte
sted
indi
vidu
als
isin
dica
ted
bew
een
brac
kets
(N).
Parnas et al.
174
gressive matrices as an index of IQ, spatial workingmemory (SWM), and performed a global±local test.Whereas SWM, Raven and VSA are known to beimpaired in schizophrenia, reaction time is an indexof global cognitive de®cit (28±30).
Visual binding tests
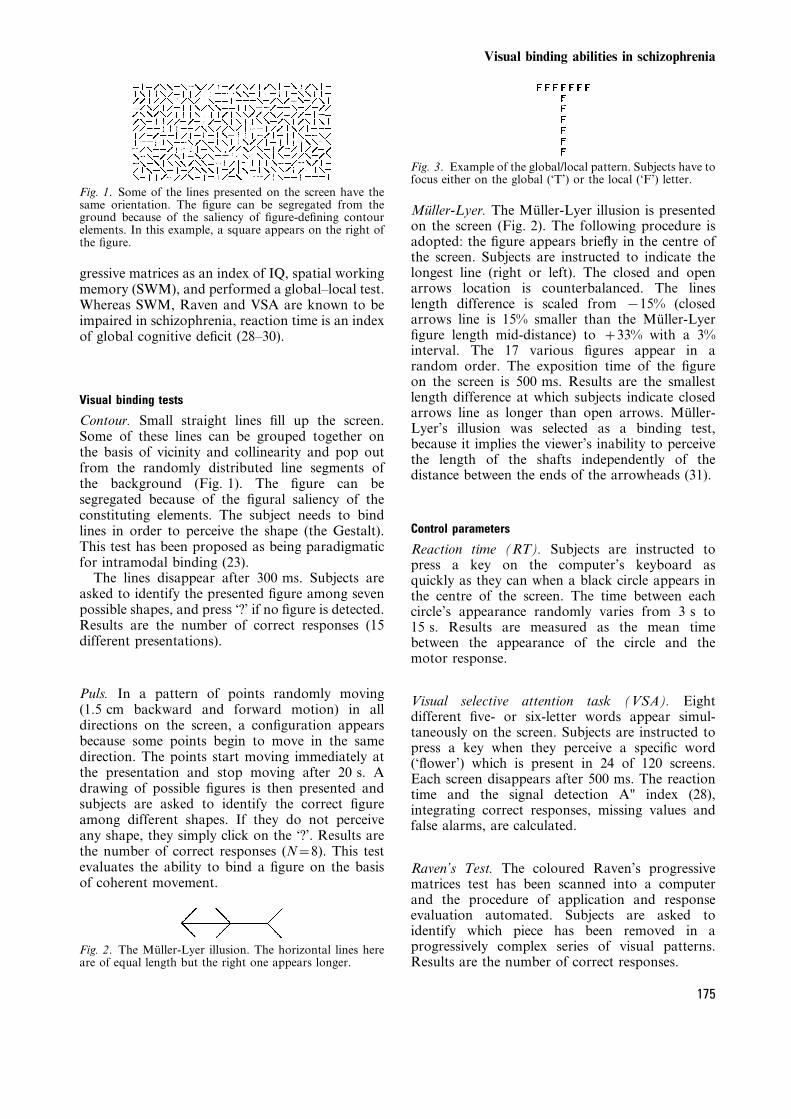
Contour. Small straight lines ®ll up the screen.Some of these lines can be grouped together onthe basis of vicinity and collinearity and pop outfrom the randomly distributed line segments ofthe background (Fig. 1). The ®gure can besegregated because of the ®gural saliency of theconstituting elements. The subject needs to bindlines in order to perceive the shape (the Gestalt).This test has been proposed as being paradigmaticfor intramodal binding (23).
The lines disappear after 300 ms. Subjects areasked to identify the presented ®gure among sevenpossible shapes, and press `?' if no ®gure is detected.Results are the number of correct responses (15different presentations).
Puls. In a pattern of points randomly moving(1.5 cm backward and forward motion) in alldirections on the screen, a con®guration appearsbecause some points begin to move in the samedirection. The points start moving immediately atthe presentation and stop moving after 20 s. Adrawing of possible ®gures is then presented andsubjects are asked to identify the correct ®gureamong different shapes. If they do not perceiveany shape, they simply click on the `?'. Results arethe number of correct responses (N=8). This testevaluates the ability to bind a ®gure on the basisof coherent movement.
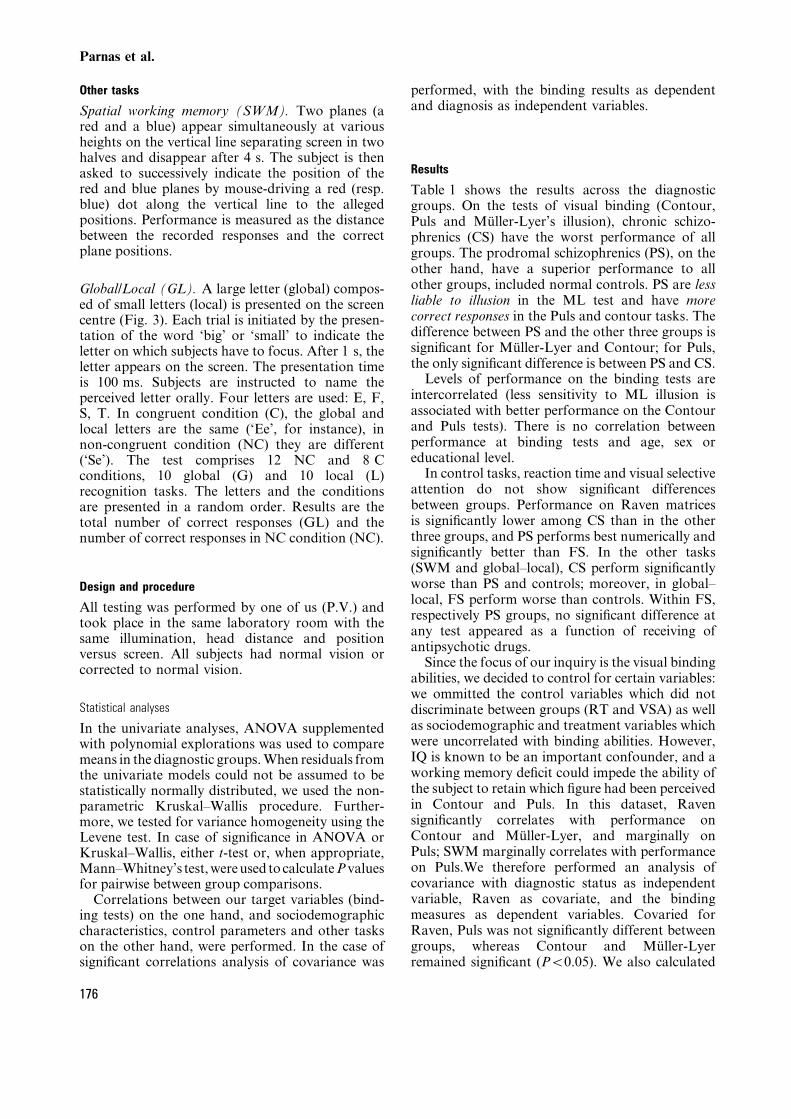
MuÈller-Lyer. The MuÈller-Lyer illusion is presentedon the screen (Fig. 2). The following procedure isadopted: the ®gure appears brie¯y in the centre ofthe screen. Subjects are instructed to indicate thelongest line (right or left). The closed and openarrows location is counterbalanced. The lineslength difference is scaled from x15% (closedarrows line is 15% smaller than the MuÈller-Lyer®gure length mid-distance) to +33% with a 3%interval. The 17 various ®gures appear in arandom order. The exposition time of the ®gureon the screen is 500 ms. Results are the smallestlength difference at which subjects indicate closedarrows line as longer than open arrows. MuÈller-Lyer's illusion was selected as a binding test,because it implies the viewer's inability to perceivethe length of the shafts independently of thedistance between the ends of the arrowheads (31).
Control parameters
Reaction time (RT). Subjects are instructed topress a key on the computer's keyboard asquickly as they can when a black circle appears inthe centre of the screen. The time between eachcircle's appearance randomly varies from 3 s to15 s. Results are measured as the mean timebetween the appearance of the circle and themotor response.
Visual selective attention task (VSA). Eightdifferent ®ve- or six-letter words appear simul-taneously on the screen. Subjects are instructed topress a key when they perceive a speci®c word(`¯ower') which is present in 24 of 120 screens.Each screen disappears after 500 ms. The reactiontime and the signal detection A" index (28),integrating correct responses, missing values andfalse alarms, are calculated.
Raven's Test. The coloured Raven's progressivematrices test has been scanned into a computerand the procedure of application and responseevaluation automated. Subjects are asked toidentify which piece has been removed in aprogressively complex series of visual patterns.Results are the number of correct responses.
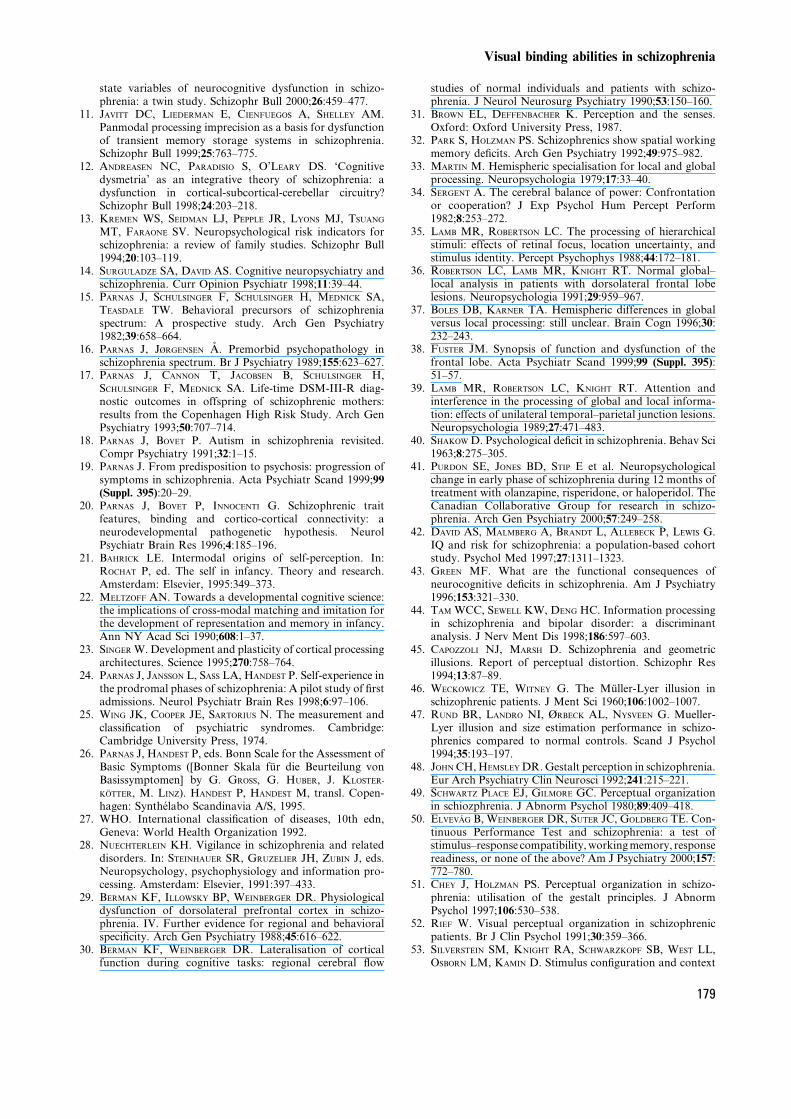
Fig. 3. Example of the global/local pattern. Subjects have tofocus either on the global (`T') or the local (`F') letter.
Fig. 1. Some of the lines presented on the screen have thesame orientation. The ®gure can be segregated from theground because of the saliency of ®gure-de®ning contourelements. In this example, a square appears on the right ofthe ®gure.
Fig. 2. The MuÈller-Lyer illusion. The horizontal lines hereare of equal length but the right one appears longer.
Visual binding abilities in schizophrenia
175
Other tasks
Spatial working memory (SWM). Two planes (ared and a blue) appear simultaneously at variousheights on the vertical line separating screen in twohalves and disappear after 4 s. The subject is thenasked to successively indicate the position of thered and blue planes by mouse-driving a red (resp.blue) dot along the vertical line to the allegedpositions. Performance is measured as the distancebetween the recorded responses and the correctplane positions.
Global/Local (GL). A large letter (global) compos-ed of small letters (local) is presented on the screencentre (Fig. 3). Each trial is initiated by the presen-tation of the word `big' or `small' to indicate theletter on which subjects have to focus. After 1 s, theletter appears on the screen. The presentation timeis 100 ms. Subjects are instructed to name theperceived letter orally. Four letters are used: E, F,S, T. In congruent condition (C), the global andlocal letters are the same (`Ee', for instance), innon-congruent condition (NC) they are different(`Se'). The test comprises 12 NC and 8 Cconditions, 10 global (G) and 10 local (L)recognition tasks. The letters and the conditionsare presented in a random order. Results are thetotal number of correct responses (GL) and thenumber of correct responses in NC condition (NC).
Design and procedure
All testing was performed by one of us (P.V.) andtook place in the same laboratory room with thesame illumination, head distance and positionversus screen. All subjects had normal vision orcorrected to normal vision.
Statistical analyses
In the univariate analyses, ANOVA supplementedwith polynomial explorations was used to comparemeans in the diagnostic groups. When residuals fromthe univariate models could not be assumed to bestatistically normally distributed, we used the non-parametric Kruskal±Wallis procedure. Further-more, we tested for variance homogeneity using theLevene test. In case of signi®cance in ANOVA orKruskal±Wallis, either t-test or, when appropriate,Mann±Whitney's test, were used to calculate P valuesfor pairwise between group comparisons.
Correlations between our target variables (bind-ing tests) on the one hand, and sociodemographiccharacteristics, control parameters and other taskson the other hand, were performed. In the case ofsigni®cant correlations analysis of covariance was
performed, with the binding results as dependentand diagnosis as independent variables.
Results
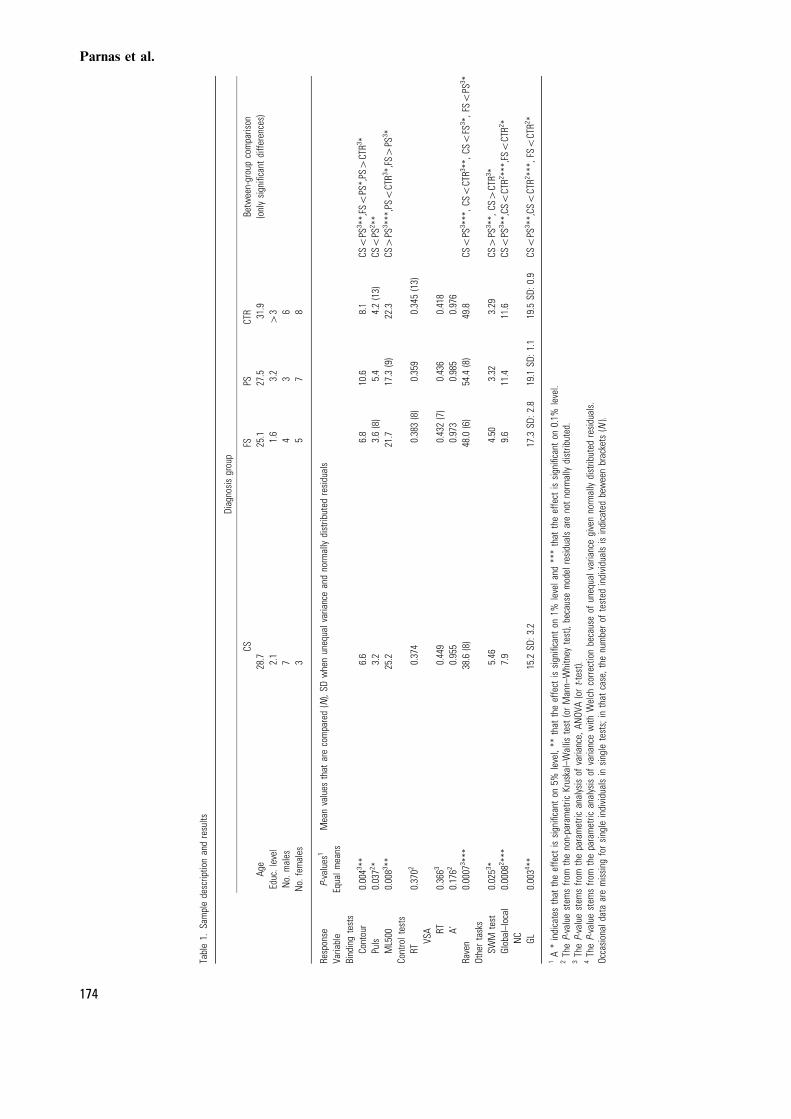
Table 1 shows the results across the diagnosticgroups. On the tests of visual binding (Contour,Puls and MuÈller-Lyer's illusion), chronic schizo-phrenics (CS) have the worst performance of allgroups. The prodromal schizophrenics (PS), on theother hand, have a superior performance to allother groups, included normal controls. PS are lessliable to illusion in the ML test and have morecorrect responses in the Puls and contour tasks. Thedifference between PS and the other three groups issigni®cant for MuÈller-Lyer and Contour; for Puls,the only signi®cant difference is between PS and CS.
Levels of performance on the binding tests areintercorrelated (less sensitivity to ML illusion isassociated with better performance on the Contourand Puls tests). There is no correlation betweenperformance at binding tests and age, sex oreducational level.
In control tasks, reaction time and visual selectiveattention do not show signi®cant differencesbetween groups. Performance on Raven matricesis signi®cantly lower among CS than in the otherthree groups, and PS performs best numerically andsigni®cantly better than FS. In the other tasks(SWM and global±local), CS perform signi®cantlyworse than PS and controls; moreover, in global±local, FS perform worse than controls. Within FS,respectively PS groups, no signi®cant difference atany test appeared as a function of receiving ofantipsychotic drugs.
Since the focus of our inquiry is the visual bindingabilities, we decided to control for certain variables:we ommitted the control variables which did notdiscriminate between groups (RT and VSA) as wellas sociodemographic and treatment variables whichwere uncorrelated with binding abilities. However,IQ is known to be an important confounder, and aworking memory de®cit could impede the ability ofthe subject to retain which ®gure had been perceivedin Contour and Puls. In this dataset, Ravensigni®cantly correlates with performance onContour and MuÈller-Lyer, and marginally onPuls; SWM marginally correlates with performanceon Puls.We therefore performed an analysis ofcovariance with diagnostic status as independentvariable, Raven as covariate, and the bindingmeasures as dependent variables. Covaried forRaven, Puls was not signi®cantly different betweengroups, whereas Contour and MuÈller-Lyerremained signi®cant (P<0.05). We also calculated
Parnas et al.
176

Puls with SWM as covariate: Puls remainedsigni®cant (P<0.05).
Discussion
Several methodological issues deserve attention.First, the sample size is small, but it is comparableto the samples reported in that type of studies.Moreover, potential inferences on the developmentof schizophrenia must be viewed with cautionbecause they are not based on the longitudinalobservations of the same people but on cross-sectional comparisons of patient groups. Here, theissue of diagnosis appears as crucial. Groupingcases of schizophrenia because of their status as®rst-admission (originally groups 2 and 3) mayobscure potential diversities in the nature of theillness, but such ®ne-grained aspects were in anycase outside the scope of this study. Whereas the CSgroup unproblematically re¯ects a standard sampleof chronic schizophrenic patients, the PS group is,to a certain extent, a product of our own particularpsychopathological interest. It is important toemphasize that the very existence of a specializedunit, shared by all departmental services, made adetection and sampling of such patients possible.Neither the ICD-10 or DSM-IV provide categoriesuseful for research on the prodromes or stagetransitions in schizophrenia. We have thereforemade a meticulous effort to elicit psychopathologyand to assign the diagnoses. From a clinical point ofview, the PS group is quite prototypical of earlyschizophrenia/severely decompensated schizotypy.
Before turning to the binding tests, we shallcomment brie¯y on the results from control andother tests. In general, they are in agreement withwhat is known from other studies: schizophrenicshave lower performance on Raven, SWM andglobal±local test. Raven's test demands complexvisuospatial, numerical and abstract logical opera-tions and is believed to implicate both frontal andmore rostral cortex (30). Spatial working memorytest re¯ects prefrontal cortical activity (32). In theglobal±local test, it was originally assumed that theright hemisphere had the advantage in recognizingglobal letters and the left hemisphere in recognizinglocal letters (33, 34). However, later studies havebeen less supportive of such lateralized effects(35±37). It is currently believed that the posteriorassociation cortex is strongly implicated in global±local recognition (36). The GL test implies a shift ofattention between levels and requires that subjectsinhibit one level by responding to the other (38, 39).In this sense, the dysfunction observed among theCS may be considered as being re¯ective of a
complex attentional de®cit and/or a dif®culty inchanging set (40).
Differences in performance on RT and VSA do notreach signi®cance, even though CS perform system-atically worse than controls; this lack of signi®cancemay evoke several, mutually not exclusive explana-tions: small sample size, ceiling effect due to easinessof the test tasks, and the fact that even chronicpatients in the present study have always been on lowneuroleptic dosage (it is known that typical neuro-leptics worsen cognitive performance [41]).
It is noteworthy that in all control and other tasks,PS performed better than CS, and in all but one(VSA-RT) better than FS; in fact, PS performed likethe CTR group. The polynomial analyses ofANOVAs reveal a highly signi®cant linear incrementof performance as a function of diagnosis from CS toCTR for SWM and GL. Such stepwise incrementmay indicate that the observed dysfunction is a statemarker linked to severity and duration of illness (infact, decreased level of performance at SWM and GLcorrelates signi®cantly with the number of hospita-lizations); it might be caused either by a hypotheticalprogressive degenerative process, or re¯ect biologicaland sociological sequelae of the illness, as well astreatment history. It is also possible that suchdysfunction may be a concomitant causal factor inschizophrenia, facilitating chronicity rather thanresulting from it. Such interpretation is consistentwith viewing cognitive impairments (e.g. low IQ) ascontributing causal factors, in¯uencing illness sever-ity and prognosis (42, 43).
As to the principal focus of the study: the resultsof the binding tests (ML, Contour, Puls) indicate anoverall decrease of performance in CS as comparedto CTR group. Several studies have reportedincreased liability to MuÈller-Lyer's illusion amongchronic schizophrenic patients (44±47). Perceptualdysfunction in schizophrenia is either seen as a top-down disturbance, due to insuf®cient attentionalresources and/or de®cient patterning in¯uences ofsedimented regularities (48), or as a bottom-upproblem, linked to peripheral dysfunctions in theearly stages of perceptual (sensory) processing (49,50). It has been shown that schizophrenics do notviolate conventional Gestalt principles in ®guredetection tasks (51), but that they may be lessin¯uenced by the global features of visual displays,indicative of a very early de®cit in visual informa-tion processing (49, 52). More recent studies showthat these de®cits are probably of a mixed, top-down/bottom up, origin and are more pronouncedin the chronic patients with poor premorbidadjustment (53). On the whole, impaired perceptualprocessing in schizophrenia is perhaps simply anaspect of a widespread de®cit (12).
Visual binding abilities in schizophrenia
177

Of considerable interest, therefore, is our ®ndingof a superior performance on the binding tests ofthe PS group, compared not only to CS and FS, butalso to CTR on the Contour and MuÈller-Lyer tests.The binding tests used in this study re¯ect `pre-attentive' Gestalt extraction. Enhanced extractionmay be due to a degraded in¯uence of backgroundon ®gure perception. Thus, for ML, the effect ofcontrast between the arrows (context) and the line(®gure) on the accuracy of the length estimation isvery well documented (54). There are three possibleinterpretations of our results. First, that it is achance ®nding linked to idiosyncratic samplecharacteristics, one of which is a high performanceon Raven. The nature of the link betweenperformance on Raven and binding tests shouldbe explored by using an independent, conventionalmeasure of IQ. Indeed, performance on Ravenmight be enhanced in the PS group independently ofIQ, due to Raven's and binding tests' shared visuo-spatial components. We must also point out the factthat the PS group is not uniformly better perform-ing: apart from Raven and binding tests, results onother cognitive measures are numerically inter-mediate between schizophrenics and controls.
Secondly, that the enhanced performance on thebinding tests is a marker of vulnerability toschizophrenia, but disappears with the progressionof the illness, and hence is detectable in the PSgroup only; this hypothesis should be tested onlongitudinal follow-up of schizotypes identi®ed infamily studies of schizophrenia.
Thirdly, that it is a prodrome marker, detectableonly in a particular temporal window of the illnessevolution. This last interpretation is supported bythe phenomenology of prodromes: in the lateprodromal phase and in the incipient psychosis,the patients frequently report perceptual distur-bances, especially in the visual modality (55±57).Many of these experiences are highly suggestive ofan enhanced Gestalt detection: the world may seemunusually clear, the objects captivate attention,appear obtrusive, conspicuous and salient in their`thinghood', as if unframed by normal embedednessin a context. There is an absence of normal sense ofauthenticity and functional meaning (57, 58). Theenhanced Gestalt extraction on the binding testsmight therefore be construed as a particularperceptual style, involving degraded in¯uence ofbackground on the ®gure perception. In phenom-enological terms there is a predominance ofre¯exive, thematic-focal intentionality and adegraded, faded sense of context.
In summary, the present study con®rms a varietyof de®cits in schizophrenia which, however, in thissample, seem to be linked to the chronicity of
illness. Certain aspects of visual processing con-cerned with Gestalt extraction deserve attention aspotential vulnerability- or prodrome-indicators.
Our original hypothesis that deviant performancein integration/binding tasks should operate as a traitindicator, i.e. would not differ as a function ofillness' stages is rejected because the poor perfor-mance on the binding tests is clearly mostpronounced in chronic schizophrenia. However,higher than normal performance in the PS groupmay be another type of deviation Ð in anunexpected direction. An excessive ®gure detectionmay be an ecological disadvantage because optimalperception relies on a balanced interplay betweensalient detail and its context.
Acknowledgements
This study was supported ®nancially by a grant from the SwissNational Research Foundation (Dr Bovet), a grant from theResearch Council of the Copenhagen Hospital Corporation (DrParnas) and a research grant from the Danish InsuranceAssociation (Dr Parnas).
References
1. RUBIN P, HOLM A, MéLLER-MADSEN S, et al. Neuropsycho-logical de®cit in newly diagnosed patients with schizo-phrenia or schizophreniform disorder. Acta PsychiatrScand 1995;92:35±43.
2. MOHAMED S, PAULSEN JS, O'LEARY D, ARNDT S, ANDREASEN
N. Generalized cognitive de®cits in schizophrenia. A studyof ®rst-episode patients. Arch Gen Psychiatry 1999;56:749±754.
3. WOODS BT. Is schizophrenia a progressive neurodevelop-mental disorder? Toward a unitary pathogenetic mechan-ism. Am J Psychiatry 1998;155:1661±1670.
4. CONDRAY R, STEINHAUER SR. Schizotypal personality dis-order in individuals with and without schizophrenicrelatives: similarities and contrasts in neurocognitive andclinical functioning. Schizophr Res 1992;7:33±41.
5. CADENHEAD KS, PERRY W, BRAFF DL. The relationship ofinformation-processing de®cits and clinical symptoms inschizotypal personality disorder. Biol Psychiatry 1996;40:853±858.
6. VOGLMAIER MM, SEIDMAN LJ, SALISBURY D, MCCARLEY RW.Neuropsychological dysfunction in schizotypal personalitydisorder: a pro®le analysis. Biol Psychiatry 1997;41:530±540.
7. FARMER CM, O'DONNELL BF, NIZNIKIEWICZ MA, VOGLMAIER
MM, MCCARLEY RW, SHENTON ME. Visual perception andworking memory in schizotypal personality disorder. Am JPsychiatry 2000;157:781±786.
8. VOGLMAIER MM, SEIDMAN LJ, NIZNIKIEWICZ MA, DICKEY
CC, SHENTON ME, MCCARLEY RW. Verbal and nonverbalneuropsychological test performance in subjects withschizotypal personality disorder. Am J Psychiatry 2000;157:787±793.
9. GOLDBERG TE, TORREY EF, GOLD JM et al. Genetic risk ofneuropsychological impairment in schizophrenia: a study ofmonozygotic twins discordant and concordant for thedisorder. Schizophr Res 1997;17:77±84.
10. PARDO PJ, KNESEVICH MA, VOGLER GP et al. Genetic and
Parnas et al.
178
state variables of neurocognitive dysfunction in schizo-phrenia: a twin study. Schizophr Bull 2000;26:459±477.
11. JAVITT DC, LIEDERMAN E, CIENFUEGOS A, SHELLEY AM.Panmodal processing imprecision as a basis for dysfunctionof transient memory storage systems in schizophrenia.Schizophr Bull 1999;25:763±775.
12. ANDREASEN NC, PARADISIO S, O'LEARY DS. `Cognitivedysmetria' as an integrative theory of schizophrenia: adysfunction in cortical-subcortical-cerebellar circuitry?Schizophr Bull 1998;24:203±218.
13. KREMEN WS, SEIDMAN LJ, PEPPLE JR, LYONS MJ, TSUANG
MT, FARAONE SV. Neuropsychological risk indicators forschizophrenia: a review of family studies. Schizophr Bull1994;20:103±119.
14. SURGULADZE SA, DAVID AS. Cognitive neuropsychiatry andschizophrenia. Curr Opinion Psychiatr 1998;11:39±44.
15. PARNAS J, SCHULSINGER F, SCHULSINGER H, MEDNICK SA,TEASDALE TW. Behavioral precursors of schizophreniaspectrum: A prospective study. Arch Gen Psychiatry1982;39:658±664.
16. PARNAS J, JéRGENSEN AÊ . Premorbid psychopathology inschizophrenia spectrum. Br J Psychiatry 1989;155:623±627.
17. PARNAS J, CANNON T, JACOBSEN B, SCHULSINGER H,SCHULSINGER F, MEDNICK SA. Life-time DSM-III-R diag-nostic outcomes in offspring of schizophrenic mothers:results from the Copenhagen High Risk Study. Arch GenPsychiatry 1993;50:707±714.
18. PARNAS J, BOVET P. Autism in schizophrenia revisited.Compr Psychiatry 1991;32:1±15.
19. PARNAS J. From predisposition to psychosis: progression ofsymptoms in schizophrenia. Acta Psychiatr Scand 1999;99(Suppl. 395):20±29.
20. PARNAS J, BOVET P, INNOCENTI G. Schizophrenic traitfeatures, binding and cortico-cortical connectivity: aneurodevelopmental pathogenetic hypothesis. NeurolPsychiatr Brain Res 1996;4:185±196.
21. BAHRICK LE. Intermodal origins of self-perception. In:ROCHAT P, ed. The self in infancy. Theory and research.Amsterdam: Elsevier, 1995:349±373.
22. MELTZOFF AN. Towards a developmental cognitive science:the implications of cross-modal matching and imitation forthe development of representation and memory in infancy.Ann NY Acad Sci 1990;608:1±37.
23. SINGER W. Development and plasticity of cortical processingarchitectures. Science 1995;270:758±764.
24. PARNAS J, JANSSON L, SASS LA, HANDEST P. Self-experience inthe prodromal phases of schizophrenia: A pilot study of ®rstadmissions. Neurol Psychiatr Brain Res 1998;6:97±106.
25. WING JK, COOPER JE, SARTORIUS N. The measurement andclassi®cation of psychiatric syndromes. Cambridge:Cambridge University Press, 1974.
26. PARNAS J, HANDEST P, eds. Bonn Scale for the Assessment ofBasic Symptoms ([Bonner Skala fuÈr die Beurteilung vonBasissymptomen] by G. GROSS, G. HUBER, J. KLOSTER-
KOÈ TTER, M. LINZ). HANDEST P, HANDEST M, transl. Copen-hagen: SyntheÂlabo Scandinavia A/S, 1995.
27. WHO. International classi®cation of diseases, 10th edn,Geneva: World Health Organization 1992.
28. NUECHTERLEIN KH. Vigilance in schizophrenia and relateddisorders. In: STEINHAUER SR, GRUZELIER JH, ZUBIN J, eds.Neuropsychology, psychophysiology and information pro-cessing. Amsterdam: Elsevier, 1991:397±433.
29. BERMAN KF, ILLOWSKY BP, WEINBERGER DR. Physiologicaldysfunction of dorsolateral prefrontal cortex in schizo-phrenia. IV. Further evidence for regional and behavioralspeci®city. Arch Gen Psychiatry 1988;45:616±622.
30. BERMAN KF, WEINBERGER DR. Lateralisation of corticalfunction during cognitive tasks: regional cerebral ¯ow
studies of normal individuals and patients with schizo-phrenia. J Neurol Neurosurg Psychiatry 1990;53:150±160.
31. BROWN EL, DEFFENBACHER K. Perception and the senses.Oxford: Oxford University Press, 1987.
32. PARK S, HOLZMAN PS. Schizophrenics show spatial workingmemory de®cits. Arch Gen Psychiatry 1992;49:975±982.
33. MARTIN M. Hemispheric specialisation for local and globalprocessing. Neuropsychologia 1979;17:33±40.
34. SERGENT A. The cerebral balance of power: Confrontationor cooperation? J Exp Psychol Hum Percept Perform1982;8:253±272.
35. LAMB MR, ROBERTSON LC. The processing of hierarchicalstimuli: effects of retinal focus, location uncertainty, andstimulus identity. Percept Psychophys 1988;44:172±181.
36. ROBERTSON LC, LAMB MR, KNIGHT RT. Normal global±local analysis in patients with dorsolateral frontal lobelesions. Neuropsychologia 1991;29:959±967.
37. BOLES DB, KARNER TA. Hemispheric differences in globalversus local processing: still unclear. Brain Cogn 1996;30:232±243.
38. FUSTER JM. Synopsis of function and dysfunction of thefrontal lobe. Acta Psychiatr Scand 1999;99 (Suppl. 395):51±57.
39. LAMB MR, ROBERTSON LC, KNIGHT RT. Attention andinterference in the processing of global and local informa-tion: effects of unilateral temporal±parietal junction lesions.Neuropsychologia 1989;27:471±483.
40. SHAKOW D. Psychological de®cit in schizophrenia. Behav Sci1963;8:275±305.
41. PURDON SE, JONES BD, STIP E et al. Neuropsychologicalchange in early phase of schizophrenia during 12 months oftreatment with olanzapine, risperidone, or haloperidol. TheCanadian Collaborative Group for research in schizo-phrenia. Arch Gen Psychiatry 2000;57:249±258.
42. DAVID AS, MALMBERG A, BRANDT L, ALLEBECK P, LEWIS G.IQ and risk for schizophrenia: a population-based cohortstudy. Psychol Med 1997;27:1311±1323.
43. GREEN MF. What are the functional consequences ofneurocognitive de®cits in schizophrenia. Am J Psychiatry1996;153:321±330.
44. TAM WCC, SEWELL KW, DENG HC. Information processingin schizophrenia and bipolar disorder: a discriminantanalysis. J Nerv Ment Dis 1998;186:597±603.
45. CAPOZZOLI NJ, MARSH D. Schizophrenia and geometricillusions. Report of perceptual distortion. Schizophr Res1994;13:87±89.
46. WECKOWICZ TE, WITNEY G. The MuÈller-Lyer illusion inschizophrenic patients. J Ment Sci 1960;106:1002±1007.
47. RUND BR, LANDRO NI, éRBECK AL, NYSVEEN G. Mueller-Lyer illusion and size estimation performance in schizo-phrenics compared to normal controls. Scand J Psychol1994;35:193±197.
48. JOHN CH, HEMSLEY DR. Gestalt perception in schizophrenia.Eur Arch Psychiatry Clin Neurosci 1992;241:215±221.
49. SCHWARTZ PLACE EJ, GILMORE GC. Perceptual organizationin schiozphrenia. J Abnorm Psychol 1980;89:409±418.
50. ELVEVAÊ G B, WEINBERGER DR, SUTER JC, GOLDBERG TE. Con-tinuous Performance Test and schizophrenia: a test ofstimulus±response compatibility, working memory, responsereadiness, or none of the above? Am J Psychiatry 2000;157:772±780.
51. CHEY J, HOLZMAN PS. Perceptual organization in schizo-phrenia: utilisation of the gestalt principles. J AbnormPsychol 1997;106:530±538.
52. RIEF W. Visual perceptual organization in schizophrenicpatients. Br J Clin Psychol 1991;30:359±366.
53. SILVERSTEIN SM, KNIGHT RA, SCHWARZKOPF SB, WEST LL,OSBORN LM, KAMIN D. Stimulus con®guration and context
Visual binding abilities in schizophrenia
179

effects in perceptual organization in schizophrenia. JAbnorm Psychol 1996;105:410±420.
54. DRAGOI V, LOCKHEAD G. Context-dependent changes invisual sensitivity induced by MuÈller-Lyer stimuli. VisionRes 1999;39:1657±1670.
55. MCGHIE A, CHAPMAN J. Disorders of attention andperception in early schizophrenia. Br J Med Psychol1961;34:103±115.
56. KLOSTERKOÈ TTER J, SCHULTZE-LUTTER F, GROSS G, HUBER G,
STEINMEYER EM. Early self-experienced neuropsychologicalde®cits and subsequent schizophrenic diseases: an 8-yearaverage follow-up prospective study. Acta Psychiatr Scand1997;95:396±404.
57. CUTTING J, DUNNE F. The nature of the abnormal perceptualexperiences at the onset of schizophrenia. Psychopathology1986;19:347±352.
58. SASS LA. Madness and modernism. New York: BasicBooks, 1992.
Parnas et al.
180