Vaccines & Biologicals - WHO | World Health Organization
102
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Vaccines & Biologicals - WHO | World Health Organization



Vaccines & Biologicals Annual Report 1999
VACCINES AND BIOLOGICALS
-~ ~. . f ~ World Health Organization ~ ·1 ,# 2000 ---~
1 ~· r.(· 1
WHON&B/00.01 English only
Distr.: General

DEPARTMENT OF VACCINES AND BIOLOGICALS
The Department of Vaccines and Biologi,cals thanks. the donors whose unspecified financial support has made the production of this document possible.
Ordering code: WHON&B/00.01 Printed: April 2000
This document is available on the Internet at: www.vaccines.who.int/vaccines-documents/
Copies may be requested from: World Health Organization
Department of Vaccines and Biologicals CH-1211 Geneva 27, Switzerland
Fax: +22 791 4193/4192 E-mail: [email protected]
© World Health Organization 2000
This document is not a formal publication of the World Health Organization (WHO), and all rights are reserved by the Organization. The document may, however, be freely reviewed, abstracted, reproduced and translated, in part or in
whole, but .not for sale nor for use in conjunction with commercial purposes.
The views expressed in documents by named authors are solely the responsibility of those authors.
Maps: The designations employed and the presentation of material on maps included in this document do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any county, terrirtory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted
lines represent approximate border lines for which there may not yet be full agreement.
Design & Layout: 1:N Communications, Morges, Switzerland
ii

Contents
Glossary
Acknowledgements
1. Director's statement
2. Highlights of 1999 2.1 New look to departmental structure
ANNUAL REPORT 1999
[I]
2.2 The Global Alliance for Vaccines and Immunization 2.3 New vaccines 2.4 New culture of immunization safety 2.5 Polio eradication - nearly there! 2.6 Advice from the Strategic Advisory Group of Experts 2.7 AMRO and the World Bank 2.8 Funding vaccines in the Americas 2.9 On the move again
3. New structure of the Department
4. The Global Alliance for Vaccines and Immunization
5. Biological standardization 5.1 Recommendations for the production and control of oral polio vaccine 5.2 Harmonization of antigen content and potency measurement of diphtheria and
tetanus vaccines 5.3 Criteria for quality control of oral cholera vaccines 5.4 Standardization of serological assays for the evaluation of immune responses to
pneumococcal and meningococcal conjugate vaccines 5.5 Progress with interferon and cytokine standards 5.6 International standards
6. Innovation 6.1 Vaccine research 6.2 Introduction of new vaccines
7. Immunization systems 7.1 Introduction 7.2 Defining the elements of an immunization service 7.3 Supply and quality 7.4 Logistics and the cold chain 7.5 Surveillance 7.6 Immunization coverage 7.7 Target diseases 7.8 Communication and advocacy 7.9 Service delivery
iii
V
vii
ix
1 1 1 1 1 2 3 3 3 3
4
6
8 8
9 10
10 10 11
12 12 16
23 23 23 23 27 30 33 42 46 47

DEPARTMENT OF VACCINES AND BIOLOGICALS
7.10 Financing 7.11 Health sector reform 7.12 Immunization safety priority project
8. Accelerated disease control 8.1 Progress towards global polio eradication 8.2 Measles control 8.3 Neonatal tetanus 8.4 Vitamin A supplementation
Annex 1: Documents produced by the V&B Document Centre during 1999 Annex 2: Internet information
iv
49 51 53
59 59 71 80 82
85 89

Glossar ACHR ACIH AD AEFI AFP AMRO ATT AVI BASICS BBC BCT BCG CBER CDC CFC CFI CIDA CRS DANIDA DFID DTP ECBS ELISA EPI FDA GAVI GIS GMP GFCV GTN Hib HPIC HRS HSR HTP HVI ICC ISSS IFA IVR JICA MAPREC MECACAR MMR MNT MT NCC NCL NFP NID NORAD NPEV NRA
ANNUAL REPORT 1999
Advisory Committee on Health Research (SEARO) Agency for Cooperation in International Health auto-disable (syringes) adverse event following immunization acute flaccid paralysis Regional Office for the Americas (WHO/PAHO) Access To Technologies (Team) Accelerated Vaccine Introduction Basic Support for Institutionalizing Child Survival British Broadcasting Corporation Blood Safety and Clinical Technology Bacillus Calmette-Guerin (vaccine) Center for Biologics Evaluation and Research United States Centers for Disease Control and Prevention chlorofluorocarbon Canal France International Canadian International Development Agency congenital rubella syndrome Danish International Development Agency Department for International Development diphtheria-tetanus-pertussis (vaccine) Expert Committee on Biological Standardization enzyme-linked immunosorbent assay Expanded Programme on Immunization Federal Drug Administration (USA) Global Alliance for Vaccines and Immunization Graphic Information System good manufacturing practice Global Fund for Children's Vaccines Global Training Network Haemophilus influenzae type b Highly Indebted Poor Countries (initiative) Human Resources Services health sector reform Health Technology and Pharmaceuticals (cluster) HIV Vaccine Initiative lnteragency Coordinating Committee Immunization Safety Surveillance System Information for Action system lntercluster Vaccine Research (initiative) Japanese International Cooperation Agency mutant analysis by polymerase chain reaction and restriction enzyme cleavage Middle East, Central Asia and Caucasian Republics measles-mumps-rubella (combined vaccine) maternal and neonatal tetanus maternal tetanus national certification committee national control laboratory not-for-profit national immunization day Norwegian Agency for Development Cooperation non-polio enteroviruses national regulatory authority
V

NT OECD OPV PATH PMS RFI QSB SAGE SEDES SIGN SMO SNID sos SWOT TAG TB TCG TOR TECHNET TT TST UNICEF UNRWA USAID V&B VAD VAM VII VVM WWW
DEPARTMENT DF VACCINES AND BIOLOGICALS
neonatal tetanus Organization for Economic Cooperation and Development oral polio vaccine Program for Appropriate Technology in Health Post Marketing Surveillance Radio France Internationale Quality Assurance and Safety of Biologicals (Team) Strategic Advisory Group of Experts Departmental Health Services (Bolivia) Safe Injections Global Network surveillance medical officer subnational immunization day sustainable outreach services strengths, weaknesses, opportunities and threats Technical Advisory Group tuberculosis Technical Consultative Group Special Programme for Research and Training in Tropical Diseases Technical Network for Logistics in Health tetanus toxoid time-steam-temperature (indicator) United Nations Children's Fund United Nations Relief and Works Agency for Palestine Refugees in the Near East United States Agency for International Development Department of Vaccines and Biologicals Vaccine Development (Team) Vaccine Assessment and Monitoring (Team) Vaccine Independence Initiative vaccine vial monitor World Wide Web
vi

ANNUAL REPORT 1999
Acknowledg_em_e_nt_s _____ _
The World Health Organization would like to thank:
The Governments of: Australia Belgium Canada China (the People's Republic of) Denmark Finland France Germany Ireland Italy Japan Korea (the Republic of) Luxembourg Netherlands New Zealand Norway Spain Sweden United Kingdom of Great Britain and Northern Ireland United States of America
And: 3M, Denmark Agency for Cooperation in International Health, Japan American Association for World Health, USA Atlas Medical Resources Corporation, Canada Becton Dickinson and Co., USA Bill and Melinda Gates Children's Vaccine Program, USA Centre International de l'Enfance et de la Famille, France Children's Vaccine Initiative CIP Industries International, South Africa De Beers, UK Electrolux AB, Sweden Electrolux, Luxembourg International Development Research Centre, Canada International Federation of Pharmaceutical Manufacturers Associations International Foundation for the Millennium Fund, Switzerland Lifelines Technologies Inc., USA Ms Martina Hingis Micronutrient Initiative Organization of Petroleum Exporting Countries (Fund for International Development)
vii

DEPARTMENT OF VACCINES AND BIOLOGICALS
Pa Hu Oy, Finland Program for Appropriate Technology in Health, USA Rhein Biotech NV, Netherlands Rockefeller Foundation Rotary International Rotary. of Japan Saatchi and Saatchi, UK Shinnyo-en, Japan Smith Kline Biologicals, Belgium Task Force for Sight and Life, Switzerland The World Bank Joint United Nations Programme on HIV/AIDS (UNAIDS) United Nations Children's Fund (UNICEF) United Nations Development Programme (UNDP) United Nations Fund for International Partnerships (UNFIP) United States Agency for International Development United States Centers for Disease Control and Prevention Univec, USA Vestfrost, Denmark
Photography:
Page 53: All other photos:
Anthony Battersby, Feilden, Health System Analysts (FBA) UK WHON&B
viii

ANNUAL REPORT 1999
1. Director's statement
I n my last report I highlighted the profound changes that accompanied the creation of the
new Department with all the accompanying readjustments. Last year we were restructuring; in 1999 we have been getting down to business. The pace has been set by the Director-General, Dr Gro Harlem Brunddand. For the Department of Vaccines and Biologicals it has been a phase of consolidation in which staff have been adjusting to their new roles and activities. Some appointments still have to be made but, by and large, key staff have been appointed and are functioning well.
I am convinced that the cornerstones on which our work must be based are that immunization:
■ is the right of every child; ■ contributes to alleviating poverty; and ■ is a cost-effective investment in health.
These justifications are of particular relevance at a time when the international community is becoming increasingly concerned with human rights and when governments are striving to meet the O ECD target of halving poverty by 2015.
The bench-to-bush strategy of the Department is implemented by the Quality Assurance and Safety of Biologicals Team (QSB), the Vaccine Development Team (VAD), the Vaccine Assessment and Monitoring Team (VAM), the Access to
Technologies Team (ATT), and the Expanded Programme on Immunization (EPI).
The teams' efforts are aimed at achieving three major objectives: Innovation, i.e. facilitating the development of new vaccines, simplifying immunization and accelerating the introduction of new and improved vaccines; improving Immunization Systems, i.e. increasing overall immunization coverage to 90%, strengthening the system for
ix
epidemiological surveillance, assuring the safety of immunization, ensuring the functioning of cold chain and logistics systems and strengthening financial mechanisms; and Accelerated Disease Control by eradicating poliomyelitis by the end of the year 2000, reducing measles cases worldwide by 90%, eliminating neonatal tetanus and increasing the use of vitamin A supplements.
Each of our major objectives contains a time-limited priority project, the work of which cuts across the spectrum of activities undertaken by the Department and thus requires the expertise of each team. The Department, along with our partners, is justifiably proud of spearheading the polio eradication effort. This global priority for all our participating partners is being given the highest possible priority within WHO and UNICEF and is enjoying support from the top level in both organizations. Excitement mounts as we head towards the finishing line. Much more is written about this later in the report.
We are also concentrating our activities on Accelerated Vaccine Introduction (within the Innovation objective) and Immunization Safety (within the Immunization Systems objective). These projects are strongly supported by partners such as bilateral and multilateral development agencies and international organizations (e.g. UNICEF, the World Bank, PATH, the Bill and Melinda Gates Children's Vaccine Program and the Joint United Nations Programme on HIV/AIDS).
The aim of the Accelerated Vaccine Introduction project is to hasten the introduction of specific vaccines by developing the infrastructure, capacity and collaboration necessary to make new vaccine introduction an integral part of global immunization practice. The ultimate goal is the timely introduction of vaccines of public health importance into the developing world.

DEPARTMENT OF VACCINES AND BIOLOGICALS
I could not present this report without acknowledging the teamwork that supports our endeavours in every WHO Region and at country level. We enjoy the participation of excellent people operating at various levels throughout the health infrastructure in almost every country, making possible the task of reaching all target groups. I sincerely thank all of you. I am also delighted to acknowledge that V&B is just one of many partners and organizations participating in or supporting immunization efforts everywhere. What a privilege it is to be part of this family!
The teams have made a considerable effort over recent months in order to refine the strategic plan, our blueprint for the next biennium and beyond. I am confident that we will reap rich benefits from this plan, which underpins all our strategic activities, and I want to thank my team of professionals who have laboured to put it together.
One of the most important events during the year was the formation of the Global Alliance for Vaccines and Immunization (GAVI), the first board meeting of which was held on 28 October 1999 in New York. This followed a one-year review of immunization and vaccine development activities undertaken by major interested partners and the identification of three major gaps:
■ the 25 million children born every year in poor countries who still do not have access to routine immunization;
■ the growing disparity between industrialized and developing countries in the number of vaccines available to children;
■ the lack of investment in vaccine research and development for diseases prevalent in poorer countries, such as HIV/AIDS, malaria and tuberculosis.
X
GAVI is not a new organization but an alliance that will hold accountable each of the partners and the constituencies they represent. I believe that it will help to deliver more than the partners could have done acting independently. With Dr Brundtland chairing the Board of GAVI for the next two years, V&B will be the operating arm of WHO in the Alliance. We will collaborate closely with all partners to ensure that the objectives of GAVI become the immunization and vaccine development paradigm for the new decade.
It is worth reflecting on the lessons learned over the course of the last decades in the area of vaccines and immunization. Some of the world's most senior politicians are now focusing on vaccines, and this makes it clear to me that we are entering a new epoch where vaccines and immunization are being given an appropriate place in health care. It is therefore with a feeling of tremendous optimism that I look towards a future in which people from every country work together for a world in which all those at risk are protected against vaccinepreventable diseases.
B. Melgaard Director, Department of Vaccines and Biologicals

ANNUAL REPORT 1999
2. Highlights of 1999
2.1 New look to departmental structure
During 1999 the Department of Vaccines and
Biologicals consolidated its structure and matrix
management. The five teams work in support of
three objectives. For each objective, specific targets
have been set and one of them has been identified
as a priority project. The work of the Department
will be guided by the "2000-2003 Strategy for
Vaccines, Biologicals and Immunization" developed during the year and endorsed by the newly estab
lished V&B Strategic Advisory Group of Experts
(SAGE), which met in November.
2.2 The Global Alliance for Vaccines and Immunization
In October 1999 the Global Alliance for Vaccines and Immunization (GAVI) held its first Board
Meeting in New York. This was the last in a series of meetings that had been held throughout the
world since March 1998 with a view to redefining
and revitalizing the international coalition of public
and private partners supporting immunization and vaccine development. The meeting set the tone for
a new type of partnership and defined very ambi
tious objectives for the coming decade.
2.3 New vaccines
Along with the Polio Eradication Initiative and the
Safety of Immunization project, Accelerated Vaccine
Introduction has been chosen as a priority project by V&B. Over a number of years it has become appar
ent that new vaccines were being developed which
could be of tremendous value to the world commu
nity but were unlikely to reach those in greatest
1
need if market forces were left to control their intro
duction. These vaccines include hepatitis B, Haemophilus influenzae type b (Hib), and most
recently, the pneumococcal conjugate vaccines.
Several other vaccines that have been available for
longer periods are underutilized (such as rubella and yellow fever vaccines). New vaccines will soon
be available for other diseases as well. Creative ways
are being sought to overcome the many barriers to
the introduction of these vaccines.
2.4 New culture of immunization safety
Safety of Immunization has been chosen as a priori
ty project, in order to strengthen and optimize the impact of immunization services as part of health
delivery systems. The main target is to establish a
comprehensive system to ensure the safety of all
vaccines given in national immunization pro
grammes by the year 2003. To achieve this it is nec
essary to generate an overall culture of safety, enabling staff to prevent reactions, detect them
quickly, achieve rapid responses, and diminish the
negative impact of reactions on health and pro
grammes. Countries are the primary focus for this
project. The partner coalition already includes UNICEF, the World Bank, PATH, the Bill and Melinda Gates Children's Vaccines Program, the
industry, and national and imernational profession
al organizations. Several development and/or technical agencies, such as the Canadian International Development Agency (CIDA), the Japanese
International Cooperation Agency (JICA), the United States Agency for International
Development (USAID), and the United States
Centers for Disease Control and Prevention (CDC)
are also participating in this project.

DEPARTMENT OF VACCINES AND BIOLOGICALS
2.5 Polio eradication - nearly there!
Of the three priority projects, the Polio Eradication Initiative has the highest profile. The global initiative to eradicate polio by the end of 2000 has become the largest public health initiative in history. It is spearheaded by WHO, Rotary International, CDC and UNICEF. The number of countries in which polio was endemic declined from 50 in 1998 to 30 in 1999. Of the three types of poliovirus, type 2 reached the verge of extinction, the only known remaining foci being in northern India. Polio incidence declined to the lowest levels ever, although reported cases increased slightly to
2
6659 because of improvements in surveillance and because outbreaks occurred in Angola and Iraq. Existing challenges to the initiative included maintaining activities of high quality, gaining access to children in countries affected by conflict, and ensuring political and financial support until certification is achieved in 2005. The additional challenge of ensuring sufficient oral polio vaccine ( 0 PV) emerged as a result of a marked acceleration in immunization activities. The public-private sector partnership supporting the initiative expanded to include the Bill and Melinda Gates Foundation, Mr Ted Turner's United Nations Foundation, the World Bank, Aventis Pasteur and De Beers.

ANNUAL REPORT 1999
2.6 Advice from the Strategic Advisory Group of Experts
In the 1980s the Global Advisory Group advised
the Expanded Programme on Immunization (EPI),
and during the 1990s the Scientific Advisory Group of Experts advised the Global Programme for
Vaccines and Immunization. Because a number of
highly technical committees now advise WHO's
Department of Vaccines and Biologicals (V&B) on
specific issues such as polio eradication and immu
nization safety, a need was perceived for a committee that could take a broad view ofWHO's vaccine
related work. The Strategic Advisory Group of Experts (SAGE) was therefore established. The first
meeting of the group, whose members were select
ed for their expertise and geographical representa
tion, was convened on 1-3 November 1999 in
Geneva to advise V&B on the three main strategic
aspects of its programme.
2.7 AMRO and the World Bank
AMRO's partnership in immunization with the
World Bank grew to include two more countries.
Since 1998, AMRO has been working with the World Bank in Bolivia and more recently in Peru
and Paraguay in the immunization component of
the Bank's health sector reform projects. The
AMRO/World Bank collaboration in Bolivia is part
of a ten-year project seeking to improve the cover
age and quality of service networks, empower communities to improve their health status, and
3
strengthen local capabilities to respond to health
needs. Overall implementation of the World Bank project is being moniwred by the use of eight indi
cators, three of which are related to immunization.
2.8 Funding vaccines in the Americas
The AMRO Revolving Fund for Vaccine
Procurement is playing an instrumental role in the
rapid introduction of new and other vaccines in the Americas at affordable prices, such as Hib, measles
mumps-rubella (MMR), hepatitis B and yellow fever vaccines. The dramatic cuts seen in the prices
of these vaccines have resulted directly from
economies of scale derived from bulk purchasing
through the Revolving Fund.
2.9 On the move again
We hope that we have a reputation in V&B for per
petually looking for new ways of doing things. However, this year saw the majority of the Geneva Headquarters V&B staff on the move in another
way. Nearly everyone moved to a new office at least
once during 1999, although the telephone numbers
and e-mail addresses remained the same. By mid-2000 the entire Department will be housed on four
floors of the M building. There was general agreement that the move was a good opportunity to con
sign large quantities of paper to recycling and to dust off a few old files. D

DEPARTMENT DF VACCINES AND BIDLOGICALS
3. New structure of the Department
V B was established in July 1998 as a & successor to the Global Programme
for Vaccines and Immunization and the Biologicals Unit. It belongs to WHO's Health Technology and Pharmaceuticals cluster (HTP), and its mission is to create a situation in which all people at risk are protected against vaccine-preventable diseases.
During 1998 and 1999 an in-depth review of WHO's work in the area of vaccines and immunization was undertaken. This included a SWOT analysis of WHO activities in the field of immunization and vaccine development (i.e. a review of strengths, weaknesses, opportunities and threats), and there has been a definition of objectives and priorities with broad participation of the partners from within and outside WHO. This has resulted in the development of the "2000-2003 Strategy for Vaccines, Immunization and Biologicals". The Department is managed through a matrix structure whereby all teams work to support well-defined objectives, targets and priority projects (Fig. 1).
V&B teams
V&B comprises five teams, each of which is headed by a coordinator, has a mission statement and manages a work plan with identified products that contribute to the overall objectives of the Department (Fig. 1).
Quality Assurance and Safety of Biologicals Mission: To ensure the quality and safety of vaccines and other biological medicines through the development and establishment of global norms and standards.
Vaccine Development Mission: To coordinate and facilitate the development of new vaccines and immunization-related technologies.
4
Vaccine Assessment and Monitoring Mission: To assess the strategies and activities for reducing morbidity and mortality of vaccine-preventable diseases.
Access to Technologies Mission: To reduce financial and technical barriers to the introduction of new and existing vaccines and immunization-related technologies.
Expanded Programme on Immunization Mission: To develop policies and strategies for maximizing the use of vaccines of public health importance and their delivery, to help regions and countries to acquire the necessary skills, competence and infrastructure for implementing these policies and strategies, and to achieve disease control/elimination and eradication objectives.
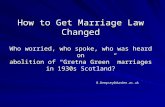
Figure 1: Structure and objectives of the Department of Vaccines and Biologicals
Objectives of the Department of Vaccines and Biologicals Some 130 million children are born every year, of whom 91 million live in the poorest countries and 30 million do not have access to routine

ANNUAL REPORT 1999
immunization services. Approximately three mil
lion children die every year from diseases that can
be prevented by available vaccines. Several million additional lives could be saved if effective vaccines
were developed against a range of maladies such as
AIDS, tuberculosis, acute respiratory infections and
diarrhoeal diseases.
This is why the Department of Vaccines and
Biologicals has organized its work to achieve the three objectives of Innovation, Immunization Systems and Accekrated Disease Control Progress made in each of these areas is critical to successfully
accomplishing the Department's mission and contributing to saving children's lives.
First of all, we need to make strides in Innovation. We must ensure that there is continued research
into and development of new vaccines against
diseases of public health importance, and that these
vaccines can be incorporated easily into existing immunization systems. We must also focus on new
vaccine delivery technologies and approaches, as
these advances are essential for improving the
performance of immunization services.
Immunization Systems have been established in all
countries. The services must now be strengthened. V&B will place more emphasis on improving the
quality of the services within the context of overall
health services and under the pressures of health
care reform.
5
The overall aim of immunization is to bring diseases under control and, in some cases, to eliminate
or even eradicate them. We have defined an objec
tive of Accekrated Disease Control whereby we concentrate our efforts on those diseases for which
routine immunization services are supplemented
with campaigns and special activities in order to
achieve control or an elimination/ eradication goal.
The present strategic plan is structured in three sec
tions, each covering the work to be accomplished
under the headings of Innovation, Immunization Systems andAccekrated Disease Control For each
of these objectives a time-limited priority project has been selected through broad consultation with
V&B partners inside and outside WHO. As defined
in the shaded areas of Fig. 1, the priority projects are Accelerated Vaccine Introduction, Safety of Immunization and Polio Eradication Initiative.
The priority projects are three of the main targets identified by V&B. Nine specific targets have been
delineated and each has been assigned a well
defined and measurable outcome or critical indica
tor. The targets encompass the expertise and contributions of all five teams and therefore require
collaborative activities.
For each target a limited number of "products" have
been defined in this document, representing the
areas that need to be tackled in order to achieve the
target and the measurable outcome of the teams'
work. D

DEPARTMENT OF VACCINES AND BIOLOGICALS
4. The Global Alliance for Vaccines and Immunization
I Global Aliance for I Yacdnes and Immunization
T he Global Alliance for Vaccines and Immunization (GAVI) was established after a
series of meetings (World Bank, Washington, March 1998; Bellagio, Italy, March 1999; Seattle, USA, July 1999) and a one-year, in-depth review of immunization-related activities. This was undertaken by major interested partners, including WHO, UNICEF, the World Bank, and the Bill and Melinda Gates Foundation's Children's Vaccine Program.
The underlying principle of the Alliance is that partners agree on a set of shared objectives to which they will all contribute through joint action.
The Alliance is not a new organization but a grouping that broadens the partnership for vaccines and immunization and enhances the synergy between the partners' contributions.
The strategic objectives of the Alliance are to: ■ improve access to sustainable immunization
services; ■ expand the use of all existing cost-effective vac
cines; ■ accelerate the development and introduction
of new vaccines; ■ accelerate research and development efforts on
vaccines and related products specifically needed by developing countries;
■ make immunization coverage an integral part of the design and assessment of health systems and international development efforts.
6
Milestones have been adopted for each target so as to assure, within a specific time frame, a reduction in the inequalities of access to vaccines, and to reduce the preventable disease burden, especially among the poor.
The Alliance will operate through the following mechanisms: ■ a governing Board, initially of 12 members,
expressing the highest political commitment of partners and providing a forum for decisionmaking on common objectives and strategies;
■ a coordinating secretariat accommodated in the Geneva premises of UNICEF, facilitating the work of the Board and helping to ensure the involvement and representation of all bodies involved in immunization activities;
■ a working group consisting of dedicated staff attached to each of the major partners, ensuring that the decisions of the Board are translated into operational actions appropriate to each lead agency;
■ task forces of limited duration, addressing specific issues (three task forces with agreed terms of reference are currently operating, on country coordination under WHO leadership, on advocacy led by UNICEF, and on financing led by the World Bank, and the Board has requested that an analysis of gaps in research and development be completed within a year);
■ a Global Fund for Children's Vaccines (GFCV), established in December 1999 with an initial grant of US$ 750 million from the Bill and Melinda Gates Foundation to facilitate the financing of underutilized and new vaccines, the strengthening of the immunization delivery infrastructure, and research into and development of priority vaccines for poor populations and countries;

ANNUAL REPORT 1999
■ an international meeting to be held approxi
mately every two years in order to bring togeth
er the broader immunization community.
The GAVI initiative provides a unique opportunity for the international community to make clear sus
tainable strides towards saving millions of children's
lives and protecting people's health against vaccine
preventable diseases. Greater equity and timeliness in protecting the children of the poorest countries
with vaccines is the most important challenge facing GAVI. The Fund will be one of the new and powerful tools intended to meet this challenge and devel
op a renewed global commitment to immunization.
Well in advance of the formal launch of GAVI at the World Economic Forum in Davos, Switzerland,
on 31 January 2000, intense work was under way in
the participating organizations in order to:
■ develop and substantiate key outcomes (reduc
tions in mortality and disease burden, development benefits, research and development);
■ outline a new strategy for immunization in
relation to health sector development;
■ develop a strategy for reaching those previous
ly unreached, in the light of experience of the
polio initiative;
■ establish research and development priorities.
The partners in GAVI will build on a comprehen
sive multi-year immunization plan within the health sector in each country, supported by a
national interagency coordinating committee. This
plan will be used to explore various tools for
7
strengthening the financing of national immuniza
tion services, including national resources, coordi
nated support by multilateral and bilateral partners,
the use of concessional development bank loans,
and debt relief funds. Where appropriate, there will
also be support from the Fund (which should be
both a means of applying leverage for additional financial resources for immunization and a catalyst
for improved performance at the country level).
The Fund is thus only one of a number of financing tools that should be used in support of a com
prehensive and well-coordinated plan.
The main challenges facing GAVI partners are to:
■ improve immunization coverage, building on
lessons of the polio initiative;
■ reduce the gap between the rich countries and the poor countries in the number of vaccines
used for children;
■ find new tools to secure research and develop
ment in relation to diseases prevalent in poor countries, such as malaria and HIV/AlDS.
Forging new partnerships for health and focusing on poor and marginalized populations, GAVI is
emblematic of the new way forward for WHO and
the HTP cluster. V&B is WHO's operating arm in
GAVI, fully contributing to the Alliance's objec
tives. V&B works in close collaboration with the
partners of the Alliance in order to ensure increased
synergy and optimum use of resources and thus to achieve GAVI's mission of fulfilling the right of
every child to be protected against vaccinepreventable diseases of public health concern. D

DEPARTMENT OF VACCINES AND BIOLOGICALS
5. Biological standardization
B iological medicines, which include vaccines, blood products and biological therapeutics,
have played a dominant role in improving health and are expected. to make an increasingly important contribution .to public health in the twenty-first century. Recent scientific and biotechnological developments have opened the way to novel products, new production methods and highly sensitive assay procedures. However, the nature of biologicals, especially new vaccines and therapeutics, raises particular questions regarding their standardization and quality control. These relate to both efficacy and safety, not only for the individual recipient but also for the population at large. Such advances highlight the complex issues that surround the standardization and control of biologicals.
A major international scientific review of the field was undertaken in 1996 by the National Biological Standards Board of the United Kingdom in collaboration with WHO. This review (Biological Standardization and Control. WHO/BLG/97.1) indicated a range of emerging products and technologies and clarified the need for new approaches to the evaluation and regulation of biological medicines. It was also a contributing factor in WHO's own external review of its arrangements for the standardization and control of biologicals (Review of the Remit and Activities of WHO in the Biologicals Field and of the Biologicals Unit: Report of the Review Team, October 1998). Both reviews emphasized the need for international collaboration and consensus on key issues related to the safety and quality of vaccines and other biologicals, and for continued support for regulatory research to protect public health.
WHO works closely in this area with its two International Laboratories for Biological Standards, namely the Central Laboratory of the Netherlands Red Cross Blood Transfusion Service, Amsterdam, and the National Institute for Biological Standards
8
and Control, Potters Bar, United Kingdom, as well as with its Collaborating Centre in Biological Standardization, the Center for Biologics Evaluation and Research (CBER/FDA), Bethesda. The responsibility for adopting WHO Recommendations for biological substances used in medicine and for establishing WHO International Standards and Reference Materials rests with the WHO Expert Committee on Biological Standardization (ECBS), established in 194 7, which held its fiftieth meeting in October 1999. Many of the items considered at this meeting reflected the increasing number and complexity of biological medicines.
5.1 Recommendations for the production and control of oral polio vaccine
Revised recommendations (formerly requirements) for the production and control of oral poliomyelitis vaccine (OPV) were developed in 1999 and adopted by ECBS. New quality control procedures have been introduced which have the potential to increase the stringency of control and lead to the production of even safer vaccines. This is an important consideration, given the considerable success of the polio eradication initiative. The new quality control procedures will also decrease the time taken to complete vaccine testing and will thus make vaccines available for use more quickly. As the demand for OPV is higher than ever, any procedure that shortens the supply time is welcome.
For the first time a test for the molecular consistency of production of a live virus vaccine is now available. Mutant analysis by polymerase chain reaction and restriction enzyme cleavage (MAPREC) quantifies the reversion of a key base, 472C, which correlates in type 3 poliovirus vaccine with the results of the WHO neurovirulence test. Studies of the

ANNUAL REPORT 1999
method coordinated by WHO have shown it to b.e
a standardized, robust and reliable procedure. The
results showed that MAPREC provided a very valuable additional test for consistency of production, and the method was endorsed as the in vitro test of
preference for the control of poliovirus type 3 vac
cine. Excellent progress is also being made with
MAPREC assays for poliovirus types I and 2 and
the possibility of introducing MAPREC for these
serotypes will be considered as soon as possible.
The discovery of the gene for the cellular receptor
for poliovirus led to the development of a transgenic mouse, TgPVR21, susceptible to poliovirus
infection. A neurovirulence test for poliovirus vac
cine has been developed in the T gPVR2 l transgenic
mouse line and the test in such mice was shown in studies coordinated by WHO to be a suitable alter
native to the neurovirulence assay in simians for
poliovirus type 3. It has therefore been introduced
into the new recommendations. The possibility of introducing the mouse neurovirulence test for
poliovirus types I and 2 is being pursued.
The entire cycle encompassing basic scientific
research, method development, standardization and
the application of MAPREC, and the transgenic
mouse model, were paradigms for regulatory
research. This work clearly illustrates the need for long-term commitment of resources if significant
advances are to be made in the control and stan
dardization of biologicals.
A period of international cooperation and consulta
tion is now being initiated under the auspices of
WHO to provide for a smooth and effective adoption of the new methodologies imo quality control
procedures. This will involve:
■ appropriate training for people using the methods and the provision of proficiency panels of samples to enable laboratories to validate
their performance with the new tests; ■ monitoring the consistency of the new meth
ods in different laboratories;
■ the identification and resolution of technical problems.
9
5.2 Harmonization of antigen content and potency measurement of diphtheria and tetanus vaccines
The diphtheria and tetanus vaccines are among the
most commonly used vaccines. Their use has result
ed in a tremendous decrease in disease in both
industrialized and developing countries.
Nevertheless, fundamental problems exist in stan
dardizing and controlling the potencies of these toxoids globally, even when the International Standards are used, and different approaches have
been adopted by different countries. Some follow
WHO and European Pharmacopoeia procedures,
while others take the USA approach. There has also
been much activity in recent years in simplifying
the tests and reducing the number of expensive ani
mals used in control testing.
Despite many attempts to harmonize requirements there is still no universally accepted potency assay.
This leads to problems in the international
exchange of these vaccines and in their licensing.
With the development of new combination vaccines and the internationalization of markets the
need for harmonization of diphtheria and tetanus
potency tests is heightened. It is considered that a
unique opportunity exists for resolving this long
standing issue. Agreement is also needed on the lev
els of diphtheria and tetanus antigens appropriate
for adult/adolescent formulations, bearing in mind
the safety implications.
With a view to resolving these difficulties a WHO
working group was established in 1999 to review data on current tests, evaluate progress with alterna
tive potency methods and develop a plan of action for harmonizing future approaches globally. It was
agreed to pursue the development of a simple,
robust and standardized assay for demonstrating the consistency of the immunologcal characteristics of vaccines, which could replace traditional assays in
lot release. This work is now in progress. Further
work ·will be needed to evaluate the value and
appropriateness of the specified limits of the current
WHO and European Pharmacopoeia potency

DEPARTMENT OF VACCINES AND BIOLOGICALS
assays. The working group emphasized that any proposed changes to current practice should not introduce difficulties similar to those experienced with the current approaches.
5.3 Criteria for quality control of oral cholera vaccines
Two oral cholera vaccines have recently been developed and licensed in a few countries. One is a live attenuated vaccine, the other a formaldehyde-inactivated whole cell vaccine consisting of Vibrio cholerae O l cells, and, in some formulations, including recombinant B subunit. WHO has a particular interest in the new cholera vaccines because of their potential to offer protection in emergency situations and because of the possibility of stockpiling vaccine for use at short notice.
A WHO working group met in 1999 to review current production and quality control procedures for these vaccines. It was concluded that two new sets of recommendations were required, one for each type of vaccine. The killed oral preparation was a new type of vaccine and there was no precedent for controlling it. It was agreed that control procedures should be scientifically relevant. This underscores the need to develop standardized methods and appropriate criteria for assessing quality, particularly in respect of safety and stability.
The current requirements for the parenteral whole cell cholera vaccine were considered inappropriate for the oral vaccines. This traditional vaccine is not recommended for use by WHO, and a recommendation was therefore made that the requirements be discontinued in order to avoid confusion and the possible use of inappropriate tests to control the new products. ECBS agreed to their discontinuation. Work is now required to develop more appropriate quality control procedures for the killed oral vaccines.
10
5.4 Standardization of serological assays for the evaluation of immune responses to pneumococcal and meningococcal conjugate vaccines
The development and introduction of pneumococcal conjugate vaccine is a priority for WHO. Trials are being organized in developing and industrialized countries. In these and future studies, serological assays will play a pivotal role in the licensing procedure. A working group on the standardization of serological assays for pneumococcal conjugate vaccines met in 1999 to consider progress in this difficult but crucial area. There are two types of serological assays: a functional assay based on opsonic activity and an immunoassay based on ELISA. In order to standardize the assays a panel of sera has been prepared and is under evaluation in a small collaborative study for suitability as run controls. The intention is to use these reagents to calibrate the assays. The possibility is also being considered of establishing a standard WHO cell line for opsonic assays.
Similar difficulties exist in relation to the standardization and validation of serological assays for the evaluation of immune responses to conjugate vaccines against Neisseria meningitidis serogroup NC. A working group is in place to coordinate activities in this area.
5.5 Progress with interferon and cytokine standards
A large and complex study has been undertaken in order to resolve longstanding problems with the calibration of the current International Standards for interferon alphas and to see if a single standard might be suitable for the whole of this family of therapeutically important proteins. Statistical analyses of the data indicated that a number of important distinctions existed between the bioassays used and confirmed discontinuities among the International Units of some of the current WHO standards. The data were extensively discussed by the manufacturers of interferons, the WHO Consultative Group on Cytokines and ECBS. Agreement was reached that separate International Standards were still required for the different molecular species of inter-

ANNUAL REPORT 1999
feron alphas. The issue of the discontinuity of the
International Units has also been resolved to the
general satisfaction of the interested parties. As a result, new International Standards for the interfer
on alphas were established by ECBS, minimizing as
far as possible any discontinuities with the units
most widely used in clinical practice and maintain
ing the continuity of interferon products used for
research and therapeutic purposes.
ECBS also considered progress in the standardiza
tion of other biological therapeutics and endorsed proposals to establish reference materials for a number of these molecules. Given the rapidly expanding
cytok.ine field and the limited resources available for
developing standards, ECBS considered a policy to prioritize work in this area. A decision tree, devel
oped by the WHO Consultative Group on
Cytok.ine Standards, was considered helpful and
was modified for use in setting priorities for work on all biological standards. There is increasing clin
ical concern about patients who develop neutraliz
ing antibodies to therepeutic proteins, including
cytok.ines, most of which are recombinant DNA
molecules. The measurement of immunogenicity
and the validation of methods for screening serum
and plasma samples remain controversial and this
area should be carefully monitored in the future.
Figure 2: WHO web pages on biological subtances
Biological Substances International Standards and Reference Reagents
Health TechnolQ!IY and Phamaceuticals homepage
11
5.6 International Biological Standards
In 1999, ECBS established 28 new or replacement
International Standards and Reference Materials
covering a wide range of products. Additionally, several International Standards and Reference
Materials that are no longer needed were discontin
ued following a public consultative process.
The review of"WHO International Standards and
Reference Materials, initiated two years ago, has
now been completed and the catalogue has been fully updated and made available on the Internet
(http:/ /www. who. int/technology/biological.html) Fig. 1. The entire list was made available as an
interactive web page allowing searches to be made
either alphabetically or by class of substance. This
database allows easy worldwide access to the list of
WHO International Standards and gives relevant
information about the contents and characteristics of the reference preparations. Future developments
will include linkages to the laboratories holding
the reference materials and to relevant WHO
documents and publications and to reports in the scientific literature. D
0 WHO International Biological Reference Preparations
0 Meeting Reports

DEPARTMENT OF VACCINES AND BIOLOGICALS
6. Innovation
6.1 Vaccine research
For many years, research and development activities in the field of vaccines against major infectious diseases prevailing in developing countries have been undertaken by two WHO programmes, V&B and the Special Programme for Research and Training in Tropical Diseases (TDR), while work on HIV/AIDS vaccines fell under the responsibility of UNAIDS. Today, the UNAIDS HIV/AIDS vaccine unit has joined the HTP cluster at WHO and is known as the WHO-UNAIDS HIV Vaccine Initiative (HVI). The work of all these groups has now been consolidated into a single, interactive, integrated and efficient effort, termed the Intercluster Vaccine Research Initiative (IVR). A common strategy is being developed for: (a) prioritization of objectives, (b) rationalization and simplification of management structures and review systems, and (c) a single resource mobilization strategy for the support of activities agreed to be necessary for the accomplishment ofIVR objectives.
IVR will be compatible with WHO's priorities in tackling the diseases that cause the highest burden in developing countries (AIDS, malaria and tuberculosis, these being among the highest priorities for WHO; and acute respiratory infections, diarrhoeal diseases and measles). This effort will be extended to areas often neglected by industry because of the lack of potential market return, for which WHO's role can be critical. These include dengue, leishmaniasis, shigellosis and schistosomiasis. IVR will also be concerned with new vaccination approaches to facilitate immunization.
IVR aims to make the best possible use of existing resources in a revamped, focused fashion. The current organizational and line management structures for V&B/VAD,TDR/CRD and HVI/HTP will remain the same, as IVR will operate on a functional matrix system. An IVR project leader is being
12
recruited and will be responsible for good functional 'management, maintaining the overview, ensuring that interfaces mesh, troubleshooting, collating plans and reports and mobilizing resources
In this way, WHO's core competences are being harnessed to the task of consolidating efforts in vaccine research ad development which will reduce the disease burden in developing countries. IVR is thus a good example of the new strategy of working across organizational boundaries within WHO and in external health organizations to deliver excellent results.
6.1.1 New tuberculosis vaccines
V&B provides support to tuberculosis vaccine development in the area of WHO's core competence, i.e. normative guidance, coordination of the global research agenda and definition of required vaccine profiles. However, this is not enough. A number of research bottlenecks must be cleared before a new TB vaccme 1s introduced. WHO/V&B, having global outreach to both the vaccine research and vaccine user communities, is best placed to address some of them. The scientific gaps include:
• the need for preclinical vaccine evaluation models and facilities;
• the need for immunological markers indicating that a vaccine provides protection from disease;
• the need to identify and develop clinical trial sites where the efficacy of new vaccines can be evaluated in human populations where TB is endemic.
In all these areas V&B has established research networks that are guided by a working group of highlevel international experts. The following progress was made over the last year:

ANNUAL REPORT 1999
Preclinical models and facilities: A network of laboratories was established together with a system for
validating laboratory facilities that can perform ani
mal testing of TB vaccines under standardized con
ditions. A vaccine-screening model was designed
with a view to limiting the use of primates to a
strictly necessary minimum.
Immunological markers: A trial was initiated in order
to detect immunological differences in response to
BCG vaccination between a population where the vaccine protects (United Kingdom) versus one
where it is completely ineffective (Malawi). Comparison of the results of the two arms of the
trial should allow the identification of immunolog
ical correlates of protection against TB.
Clinical trials: Guidelines for performing clinical
trials are being edited for publication. They include
very specific identification of potential geographical
sites and human populations that could be targeted for evaluation of a future TB vaccine.
6.1.2 A meningococcal serogroup A vaccine for Africa
The technology for producing a safe and effective
polysaccharide-protein conjugate vaccine for
serogroup A Neisseria meningitidis disease has been available for more than ten years, yet little progress
has been made towards achieving this goal. The dis
ease is largely limited to persons living in the poor
est countries of the world, and the potential returns
on investment are perceived by traditional manu
facturers to be too low. Several vaccine companies
are developing multivalent meningococcal conjugate vaccines that include a component for the pre
vention of serogroup A disease. However, it is
unlikely that rhese vaccines will be available for the
prevention of disease in Africa. They are intended
for sale in industrialized countries and will be
expensive. It therefore seems unlikely that the pri
vate sector will develop a meningococcal vaccine for use in Africa. Even if a commercial company
received funds from international donors its com
mitment would be compromised by competing projects with a higher return on investment.
An attractive alternative for developing a meningo
coccal A conjugate vaccine would be to establish a
not-for-profit (NFP) company funded by interna
tional donors. It would be dedicated to the licens
ing of a meningococcal A conjugate vaccine intend
ed for use in Africa, and would serve as a model for vaccine or drug development against diseases that
primarily occur in poor countries where traditional market forces are insufficient to stimulate private
investment. An advantage of the NFP approach
would be its ability to focus on the development of
a single product. Thus delays from work on com
peting projects of higher priority could be avoided.
Another advantage would be that the NFP compa
ny would be free to design the product specifically for use in Africa, rather than adapting a product
originally designed for an industrialized country.
For example, a meningococcal A conjugate vaccine
Figure 3: Cases of meningitis in the epidemic meningitis belt of Africa, 1950-1996
170000
140000
100000
80000
60000
40000
20000
13
88 939 80743

DEPARTMENT OF VACCINES AND BIOLOGICALS
for Africa would require consideration of special problems of maintaining vaccine stability where refrigeration may not be dependable or where the practice of reuse of needles poses a major health risk. This matter is currently at an exploratory stage: potential partners are being consulted and a business plan is being prepared.
6.1.3 Measles vaccine research
Important progress has been made towards the definition of a global research strategy for the elimination of measles. While obstacles to global measles eradication are perceived to be predominantly political and financial, there are also scientific and technical questions. These include: the refinement of measles elimination strategies in the light of recent outbreaks in the Americas; the implications of the HIV epidemic for measles elimination, issues around injection safety, and concerns about the possibility that secondary vaccine failures will contribute to sustaining transmission in highly vaccinated populations. The global priorities are to improve measles control in low-income countries, increase awareness of the importance of measles among industrialized countries, and conduct studies on technical aspects of measles elimination strategies.
An inventory has been prepared of all measles-related research activities. This represents a step towards ensuring that all the priority research issues are addressed in good time and that the results are widely distributed to support the development and implementation of strategies for measles control and elimination. Measles research studies have addressed the whole spectrum of priority issues for measles control and elimination, but in some key areas there are only a few studies or progress is slow. This is true for the areas of new safer vaccine delivery systems, vaccines for alternative routes, tests for differential diagnosis, rapid diagnostic field tests, and implications of HIV infection. Developing countries accounted for 88 of the 210 studies (42%) in the inventory, and only 20% of the principal researchers in the studies conducted in developing countries were actually from developing countries. The preparation of the inventory is a first step in a continuing process. We hope that it will encourage researchers all over the world to contact us.
14
6.1.4 Haemophilus influenzae type B and pneumococcal vaccines
VAD's work mostly relates to the planning and monitoring of l;uge field trials. In the Hib field, the Lombok Hib intervention study and - through support from the International Vaccine Institute - Hib disease burden studies got underway during 1999. In the area of pneumococcal conjugate vaccines, two trials are currently ongoing - the trial of a 7-valent vaccine among the Navajo and Apache populations in the USA, and the South African trial of a 9-valent vaccine being conducted in Soweto (South Africa). Other pneumococcal trials are being planned, e.g. in the Gambia (using the 9-valent vaccine) and the Philippines (using an 11-valent vaccine). The Gambian trial is due to start in April 2000 and it will be the only trial to study all cause mortality as the primary endpoint. VAD has been closely involved with the development of the Gambian study as well as in the development of the trial site for the study to be performed in The Philippines.
In addition to the above activities the work of the Pneumococcal Vaccine Trialists Group, which was set up by WHO in 1997, expanded during 1999. Standardization of procedures for radiological examination, image storage and image interpretation is now seen as a key outcome measure for pneumococcal vaccine trials and other international groups are now relying on this group to resolve the longstanding problems in this area. In this area VAD is working in partnership with BCT to develop agreed guidelines that will eventually form the basis for future pneumonia burden studies that can be linked in interpretation with the current vaccine trials. In addition to this activity, another working group has been formed to work towards agreed guidelines for the conduct of economic evaluation in the context of pneumococcal and Hib vaccine trials.
Other acnvmes relate to defining pneumococcal burden in early infancy, such as the recent completion and publication of a WHO sponsored multicentre study of serious infections in young infants. Furthermore, work is ongoing to plan the next round of Hib and pneumococcal studies.

ANNUAL REPORT 1999
6.1.5 Diarrhoeal disease vaccines
Rotavirus: There is only one licensed vaccine that
has 85-90% efficacy against severe disease and 55% efficacy against all rotaviral gastroenteritis.
However, following the identification of a possible
association between the vaccine and intussusception
in September 1999, VAD immediately terminated
all WHO-sponsored rotavirus trials in developing
countries ( Bangladesh, India). In October 1999 the
United States Advisory Committee on Immunization Practices revoked its recommendation for the use of this vaccine. However, there is an
urgent need for an effective vaccine in developing countries, where 650 000 children die each year
from rotaviral gastroenteritis. Data are needed on
the incidence and risk factors for intussusception in
developing countries, as well as on the attributable
risk of intussusception with the current vaccine. It
is also necessary to consider whether intussuscep
tion will be associated with all rotavirus vaccines
and whether alternative vaccine schedules might be used to minimize or eliminate the risk.
Shigel/a: A live oral vaccine candidate against
Shigella jlexneri 2a (SC602) has been tested in phase 1 and 2 studies in North American adult volun
teers. A single oral dose of the vaccine was shown to be safe and immunogenic. It conferred 100% pro
tection against severe shigellosis and 50% protec
tion against any diarrhoea after an experimental challenge with S. jlexneri 2a. An inpatient clinical
phase 1 study using the SC602 vaccine was com
pleted in 20 healthy Bangladeshi adults. They were randomized to receive a single oral dose of 1 x 104,
1 x 105 or 1 x 106 cfu of SC602 or placebo in a
double-blind controlled trial. There were no significant side-effects in any of the volunteers. None of
the volunteers had diarrhoea, fever or significant
abdominal pains.
Typhoid: An important development during the
last five years has been the transfer of the technology for production of typhoid (Vi) vaccine to China
and Viet Nam. China currently produces the vac
cine in six of its vaccine production institutes.
Several phase 2 trials and two phase 3 efficacy trials
of the locally produced vaccine were performed. Each randomized, placebo-controlled efficacy trial,
involved over 100 000 participants and demonstrated levels of protection of about 70% during
approximately two years of follow-up. This was
15
similar to the level of protection observed for the
Aventis Pasteur Vi vaccine tested in Nepal and South Africa. Promising newer-generation vaccines
under development include both injectable subunit
and genetically engineered live oral vaccines. A Vi
protein conjugate vaccine has yielded encouraging
results when given in two-dose regimens to United
States and Vietnamese volunteers. It has also been
safe and immunogenic when given as a single dose
to United States adults.
Cholera: Another line of development of killed oral cholera vaccine has been undertaken in Viet Nam by the National Institute of Hygiene and
Epidemiology, which, in collaboration with the
University of Gothenburg and SBL, has produced a killed oral whole cell vaccine similar to the Swedish
vaccine but lacking the cholera toxin B subunit. An
early generation version of this vaccine, which con
tained only O 1 serogroup cells, conferred ca. 60%
protection against El Tor cholera when tested as a
two-dose regimen in an open field trial in Hue during the early 1990s. Interestingly, young children
were as well protected as older persons, in contrast
to the findings in Bangladesh for the Swedish BS
WC vaccine, which did not protect young children
as well as older persons.
More recently, the Vietnamese killed oral whole cell
vaccine has been made bivalent (01 + 0139) by the
addition of formalinized 0139 killed whole cells.
This vaccine is similar to the first-generation
Vietnamese vaccine except that it is bivalent with respect to serogroups and that it contains twice the
content of El Tor 01 cells. Phase 2 studies of twodose regimens of this vaccine in Hanoi demonstrat
ed that the vaccine was safe and induced at least
fourfold vibriocidal seroconversions to the O 1 com
ponent in ca. 60% of adults and ca. 90% of children aged 1-10 years. Because these anti-01 responses
were similar in magnitude to those seen in volunteers concurrently given the monovalent SBL vac
cine, it seems that the 0139 component of the vaccine does not interfere with responses to the 01
component. Analyses of serum vibriocidal responses to the 0139 component have demonstrated sero
conversions in ca. 40% of adults and ca. 60% of
children receiving the vaccine. A randomized, placebo-controlled field trial of the effectiveness of a two
dose regimen of this vaccine was initiated in March
1997 in Viet Nam. In this trial the effectiveness of a
two-dose primary series followed by boosting at two

DEPARTMENT OF VACCINES AND BIOLOGICALS
years is being evaluated in ca. 300 000 persons aged 12 months or more in Nha Trang.
6.1.6 South-East Asia Region
The Twenty-fourth Session of South-East Asia Advisory Committee on Health Research (ACHR) recommended that: WHO/SEARO should (i) explore strategic ways of enhancing intercountry cooperation in areas of vaccine production, research and delivery, and (ii) set up a working group or task force of experts with the purpose of proposing a vaccine policy that would be comprehensive and specific to the region.
The guiding principles of developing a regional vaccine policy would be equity, self-reliance and regional solidarity. The policy should cover the areas of vaccination research, vaccine development, and vaccine mix as well as the sustainability of expanded programmes of immunization in Member States.
To this end, a core group was constituted and its first meeting was held in Bangkok on 11-12 October 1999. The group discussed various aspects of immunization programmes, · ranging from vaccine selection to delivery. Among the subjects covered were vaccine policy, the introduction of new available vaccines, disease burden of vaccine-preventable diseases, supply of vaccines in emergencies, and re-emerging diseases.
The core group concluded that each country in the Region needed to develop a national vaccine policy, which should then form the basis of a regional policy. The national policy could be best developed by promoting dialogue and constructive discussion with the major stakeholders in an immunization programme, namely the medical personnel involved with vaccine selection and use, the public health programme responsible for vaccine delivery, the National Regulatory Authority (NRA) responsible for vaccine quality, and those involved in vaccine supply, including procurement officers, agents and local producers.
The meeting agreed on the next steps in the development of national and regional policies. The members suggested a meeting of a small group of experts in early 2000 to discuss and select key priority areas. The expert group would have sufficient regional and external experts and would have the
16
flexibility to take responsibility for specific areas if necessary and to set the stage for consultations and activities at country level. The group would report to ACHR on status and progress.
• A review in the following key areas would be conducted on a country-by-country basis over a period of several months: • vaccine-preventable disease burden; • vaccine research and development initiatives
within the region; • vaccine clinical trials within the region; • vaccine production and supply sources; • vaccine regulation; • networking among vaccine regulatory
authorities.
• The review would include meetings with concerned individuals in three or four selected countries. Consultants with expertise in relevant areas would be contracted to conduct the studies.
• Dialogue and meetings at country level would be initiated to prioritize and prepare the ground for implementation.
A meeting at the regional level would be conducted in order to constitute the regional policy. It was expected that by this time there would be adequate acceptance of issues and emerging recommendations at the level of ministers of health, and that the policy would be discussed at the Regional Committee later in the year or early the following year.
6.2 Introduction of new vaccines
New vaccines that can prevent major causes of morbidity and mortality in the developing world are not being used widely in poorer countries. These include hepatitis B, Hib, and, most recently, the pneumococcal conjugate vaccines. Other underutilized vaccines have been available for a long time (rubella and yellow fever vaccines). Additional new vaccines will soon be available for other diseases. In order to take maximum advantage of these valuable prevention tools a number of barriers must be overcome. These include a lack of efficacy or impact data in developing country settings, a lack of burden and cost-effectiveness information, a lack of
technical assistance on introduction, issues related

ANNUAL REPORT 1999
to logistics, supply and quality control, and a lack of sustainable funding for vaccines.
Remarkable changes are taking place m national
routine immunization programmes in the Americas with the introduction of new vaccines of public
health importance. In 1999, over 90% of the chil
dren born in the Americas will benefit from Hib
and hepatitis B vaccines as part of their regular vac
cination schedule. MMR vaccine is now included in almost every country's routine programme. A
more aggressive yellow fever strategy is aiming to achieve prompt vaccination of the entire population in areas of endemicity and the incorporation the
vaccine into the routine immunization programme
for children under 1 year of age. The availability of
a new combination vaccine that includes the five
antigens of DTP, Hib and hepatitis B, has further facilitated the uptake of these new vaccines in
national immunization programmes. The AlvfRO
Revolving Fund for Vaccine Procurement has
played a fundamental role in the introduction of
these vaccines. Through its system of bulk purchas
ing the Fund has secured the supply of high-quality
vaccines for national immunization programmes at affordable prices.
Some of these vaccines, however, such as the MMR,
yellow fever and hepatitis B vaccines, have already
been on the international market for 15 years. Their
introduction in the Americas, as in other develop
ing countries, has been slow because of high prices
and the lack of additional resources to support the
expansion of surveillance systems for collecting
information on the burden of the diseases. MMR vaccine has been made available in response to
urgent requests from countries for vaccination
against rubella. The surveillance system established by AMRO with a view to measles eradication con
tinues showing widespread circulation of rubella virus in most countries in the Americas.
Reliable epidemiological data, for instance on burden of disease and cost-effectiveness in relation to
the use of specific vaccines, is recognized as the key
information required by decision-makers allocating
resources for vaccine introduction and guaranteeing
their sustainability. Many countries are now working to strengthen the capabilities of surveillance sys
tems and laboratories in monitoring vaccine-pre
ventable diseasesand the impact of vaccine intro
duction. These efforts will play a catalytic role in
17
the introduction of combined vaccines against
S. pneumoniae, N meningitidis A and C, and rotavirus, which are scheduled to be released short
ly and are also expected to have a substantial impact
on disease burden. The current surveillance systems for measles, polio and rubella could become the
basis for the surveillance of other viral diarrhoeal
(rotavirus) or respiratory diseases (respiratory syncytial virus , influenza), and the system in place for
H injluenzae and S. pneumoniae could be extended to include other bacterial pathogens (such as
Shigella and E. coli.)
6.2.1 The Accelerated Vaccine Introduction priority project
The Accelerated Vaccine Introduction (AVI) priori
ty project was developed by V&B in 1999 to address critical issues in new vaccine introduction.
The goal of the project is to implement a mecha
nism for accelerating the introduction of new and
underused vaccines of public health importance in
the developing world by 2003. This involves the
development of an infrastructure to complete a set of activities on vaccines at various stages of the
introduction process. The project focuses on critical
points in the vaccine evaluation and introduction continuum at which WHO could make a substan
tial difference and involves activities in each of V&B's teams.
The work of AVI during 1999 has been divided
into five activity areas, corresponding to V&B's five
teams:
• VAD has focused on efficacy evaluation. During 1999 this work included a series of
coordination meetings on methodological issues in the ongoing pneumococcal vaccine
trials, and initiation of the trial in the Gambia which will identify impact on mortality. Work
on rotavirus vaccine issues includes the evaluation of burden and serotype distribution.
• VM1 activities have been directed at the assess
ment of disease burden data for hepatitis B,
Hib, and other diseases of interest, and inte
grating the data with economic analysis tools
to facilitate decision-making at the country
level. A database on hepatitis B burden, and
collaboration with CDC to produce a
cost/benefit tool for developing countries, have

DEPARTMENT OF VACCINES AND BIOLOGICALS
been promoted in the last year. Studies on the burden of Hib disease in Russia were initiated. The collation of available data on Hib meningitis burden was undertaken.
• QSB has developed guidelines for the production and control of Hib vaccine and has initiated parallel work on pneumococcal conjugate vaccines.
• ATT activities in 1999 included provision of global guidance on financing mechanisms and vaccine demand, and country-level input into supply, financing and planning.
• EPI activities focused on technical assistance with new vaccine introduction. They included: the development of a set of guidelines for immunization programme reviews; convening, with VAD, an international group of experts to outline the next steps required for accelerating the development and introduction of Hib and pneumococcal vaccines; and supporting positions for persons devoted to new vaccine introduction in four of WHO's regions.
Major funding partners of the project include USAID and the Bill and Melinda Gates Children's Vaccine Program.
The priority project highlights the above activities and others for special focus but does not include all V&B activities in the field of new vaccines. WHO continues to publish position papers on new and underused vaccines. A total of eight such papers have been published, including, most recently, documents on pneumococcal and hepatitis A vaccines. These papers provide background information and guidance to policy-makers, national programme managers and others.
6.2.2 Hepatitis B
Three major obstacles must be overcome so that hepatitis B vaccine can be introduced into the poorest countries:
• lack of appreciation of the burden of disease associated with hepatitis B virus infection;
• weaknesses in the infrastructure of immunization programmes which limit coverage;
• insufficient financial support for countries to
Figure 4: Global status of routine hepatitis B vaccination implementation, September 1999
.. :~.
,J•. ~
',ii /
Routine Hepatitis B immunization status:
No routine immunization
■ Routine immunization
18

ANNUAL REPORT 1999
purchase a more expensive vaccine. Although the price of a dose of hepatitis B vaccine in
1999 was only US$ 0.58-0.99, compared to $8-12 ten years ago, the price for the three
dose series is more than that of all other routine EPI vaccines combined.
In the African Region the disease burden of hepati
tis B has been well established, as has the high to
very high (2-8%) chronic carrier rate throughout
the Region. In addition the efficacy of vaccines has
been demonstrated and the benefits have been made abundantly clear.
Six countries (Botswana, Gambia, Seychelles, South Africa, Swaziland, and Zimbabwe) have
introduced hepatitis B vaccination inro their
routine programmes.
A new goal of at least 75% coverage by 2005 was
recommended for the African Region. Countries
were classified to allow for prioritization according
to whether they had expressed interest in the vac
cine or had already included hepatitis B vaccine in
their programmes, had a DTP coverage higher than
50%, and had a per capita GNP below USS 1000.
The following actions were identified as increasing
the uptake of the hepatitis B vaccine:
• identification of the potential for financing vaccine purchase, including the development
of partnerships with the private sector, opti
mizing support from national ICCs, and assuring that ministries of finance considered the
high cost-benefit of hepatitis B vaccine during
their strategic planning;
• increased education on the efficacy/ safety of the vaccine;
• promotion of the inclusion of hepatitis B vaccine in vaccine supply agreements with partners;
• advocacy at all levels, including partnerships with professional associations and concerned
groups;
• use of evaluations conducted in countries that
have already introduced the vaccine, in order to demonstrate its impact to other countries.
In the South-East Asia Region, hepatitis B vaccine
is now routinely given in four countries: Bhutan (81 % coverage in 1998), Indonesia, Maldives (45%
coverage in 1998), and Thailand. V&B/SEARO
19
intends to fully integrate hepatitis B vaccine into
the routine immunization schedule in all countries
by 2003. In order to achieve this the following steps have been planned: 1) a technical visit to assess the
constraints on introducing hepatitis B vaccine in the national immunization programmes; 2) an
advocacy meeting on hepatitis B vaccine with high
level officials in the priority countries; 3) support
for an operational study of a new financing mecha
nism for hepatitis B vaccine; 4) use of the ICC
mechanism to make the vaccine available to the countries at an affordable price; 5) provision of
technical support for a review of the national
immunization programmes in Bangladesh, the Democratic People's Republic of Korea, India,
Myanmar, and Nepal; 6) follow-up and support of hepatitis B studies in countries.
India is conducting a pilot project for the introduc
tion of the vaccine on a limited scale. Bangladesh
and Myanmar are planning a similar study. Bhutan has planned to conduct a hepatitis B efficacy study.
Hepatitis B is being locally produced in Indonesia
and the Democratic People's Republic of Korea. A
feasibility study of Myanmar's capability to produce hepatitis B vaccine was concluded in 1999. A com
pany in India is planning to produce a combined DTP-HB vaccine by processing DTP manufac
tured in India with bulk hepatitis B vaccine pro
cured from abroad. These local productions will improve self-sufficiency in vaccine in the region and will help to reduce costs.
The most critical needs for hepatitis B control in the Western Pacific Region are to get the vaccine introduced in national immunization programmes
and to ensure an adequate uninterrupted, supply of
vaccine. All the countries in the region except for Cambodia and the Lao People's Democratic Republic, have introduced hepatitis B vaccines into
their national immunization programmes, and cov
erage in most countries is good. However, coverage remains less than optimal in China, Papua New
Guinea, the Philippines and Viet Nam, primarily
because of inadequate vaccine supply or difficulties
in accessing the vaccine. Most countries have
secured hepatitis B vaccines for the immediate
future but long-term sustainability remains prob
lematic, primarily because of the cost.
In nearly all countries of the Western Pacific
Region where comprehensive vaccine requirement

DEPARTMENT DF VACCINES AND BIOLDGICALS
Figure 5: Hepatitis B vaccine supply, Western Pacific Region, 1992-1997
calculations have been undertaken they have been
used to identify government and partner agency funds to meet vaccine requirements. The availabili
ty of vaccine throughout the region has improved (Fig. 5). In Cambodia and the Lao People's
Democratic Republic the calculations have been
incorporated into five-year immunization plans to
form the basis of government planning and to be
used in negotiations with partner agencies to ensure
adequate vaccine supplies in the medium term. It is likely that in both countries the introduction of hepatitis B vaccine will commence in 2000.
Many countries in the region .are now achieving high immunization coverage levels with hepatitis B
vaccine. In 1998, 26 countries reported over
50% coverage with three doses in infants, and 23
countries reported over 80% coverage Fig 6.
Figure 6: Hepatitis B coverage (% receiving three doses of hepatitis B vaccine), Western Pacific Region, 1992-1998
20
Although original estimates had suggested HbsAg
prevalence of2-8%, results ranged from 2% carriers
in Baltic and northern countries, 2-7% in Russia, and 5-10% in Bulgaria, Romania, Albania,
Moldova and some central Asian republics. Various
routes of transmission of HBV to patients have
been documented. The contribution of unsafe
injection practices to the burden of hepatitis B globally is unknown but likely to be substantial.
Implementation of hepatitis B vaccine in these
countries could be seen as a highly effective use of
health resources. A Viral Hepititis prevention Board (WHO/VHPB) meeting was conducted to review the allegation that hepatitis B vaccine might be
associated with demyelinating disorders. The claim was refuted and recommendations made to contin
ue to vaccinate target groups.
6.2.3 Haemophilus influenzae type b
Haemophilus influenzae type b (Hib) is the most common cause of bacterial meningitis and the
second commonest cause of bacterial pneumonia
among children. The vaccine was adopted in North
America and most of Western Europe by the early
1990s, primarily because of its ability to prevent meningitis. Uptake has been much slower in the
developing world, where its major impact is in the
prevention of pneumonia. By late 1999 more than
44 countries had adopted Hib vaccine for routine infant immunization, including South Africa, the
second African country to introduce the vaccine
and the first to support its introduction from its
own budget. Recent data from the Gambia confirmed a 90% decrease in meningitis caused by Hib
as a result of the introduction of the vaccine on a national scale. The current status of Hib vaccine
introduction is shown in Fig 7.
The following issues continue to affect the pattern of Hib vaccine use.
• The burden of disease is either unknown or
not appreciated in much of the world. This is
partly attributable to the difficulty in diagnos
ing the disease. Diagnosis of Hib meningitis requires laboratory material and the ability to
perform bacterial cultures on sick and febrile
children, which is lacking in many developing
countries. V&B results from five countries
should be available in 2000, and an additional study on Hib meningitis was initiated in

ANNUAL REPORT 1999
Figure 7: Countries that had introduced Hib into routine immunization schedules by July 1999
Routine HIB implementation status:
No policy
■ Routine policy
Russia in 1999. The main form of Hib disease in the developing world, pneumonia, is also caused by other bacteria; confirming that a specific case is caused by Hib is impossible in most situations, even with the best laboratory support. Our best information on the burden of Hib disease in the developing world has come from vaccine introduction studies in Chile and the Gambia. Additional information should be available soon from a study in Indonesia in which WHO is playing an advisory role. WHO has begun collaborating with CDC to develop a rapid assessment tool for use in countries wishing to estimate Hib disease burden on the basis of local data.
• Additional efforts are needed to emphasize and clarify the burden of pneumonia in the developing world. V&B is participating in a crosscluster effort to clarify this burden, a particularly critical matter because of the licensing of the pneumococcal conjugate vaccine in early 2000. We now have the tools to reduce most of the mortality from pneumonia in the developing world, but the case for disease burden and for the impact of these vaccines must be clear-
21
ly made to ensure rapid acceptance. • As with hepatitis B, sustainable financing for
Hib vaccines in the developing world is a major problem. New initiatives by the World Bank, the Bill and Melinda Gates Children's Vaccine Program and others have made it possible to introduce Hib vaccine into countries where this was financially impossible previously. Important issues remain, however, about the prioritization of funding for Hib vaccines and the gradual acquisition by national governments of financial responsibility for th~se vaccines.
In the Region of the Americas, 81 % of the countries have Hib vaccine in their national immunization programmes, reaching 90% of children born. There is a possibility that this level will go up to 96% by the end of year 2000, representing 90% of the countries in the region. This noteworthy achievement took place in less than ten years since the licensing and availability of Hib vaccines in the developed world.
A Regional surveillance system developed in order to monitor bacterial pneumonia and meningitis is

DEPARTMENT OF VACCINES AND BIOLOGICALS
Figure 8: Collaborative research projects on polysaccharide conjugated vaccine research in the Americas
H. influenzae type b
e S. pneumoniae
e QC of conjugated vaccines
providing feedback for monitoring the impact of Hib vaccination on meningitis. Case-control studies have been initiated to evaluate the impact of the vaccine on pneumonia in Brazil, Colombia, and Mexico. The results of these studies will be important in confirming the public health importance of Hib vaccine and promoting its use in other regions. Other surveillance systems are being formed to monitor vaccine-preventable diseases in relation to
vaccines to be released shortly and others still in development, namely pneumococcal, meningococcal and rotavirus vaccines. Data generated from the systems will be used for measuring disease burden and conducting cost-effectiveness studies.
The introduction of vaccines against Hib, which is responsible for many of the region's cases of bacterial pneumonia and meningitis, provides a useful example of the issues surrounding the sustainable introduction of a vaccine in a national immunization programme. Considering that the first conjugated vaccines against this pathogen were licensed in Canada, Europe, and the USA as recently as 1991, their introduction has been remarkably rapid. AMRO played a leading role in promoting
22
Brazil
the establishment of Hib surveillance in the region and in evaluating the introduction of Hib vaccine in routine immunization programmes. These initiatives were supported by recommendations of the Organization's Directing Council and the Technical Advisory Group on Vaccine-Preventable Diseases (TAG). The exchange of experiences among countries at meetings sponsored by AMRO has become an important catalyst stimulating the introduction ofHib vaccine into routine immunization schedules. Furthermore, the establishment of an epidemiological surveillance network to monitor invasive pneumococcal diseases in children aged under five years in six countries of the region has had a positive impact on Hib surveillance.
At the country level, decisive factors behind the speedy introduction of the Hib vaccine include: heightened awareness on meningitis diseases among parents; knowledge in the medical profession and health ministries of several clinical trials pointing to the vaccine's safety, efficacy and effectiveness; and previous experience with the vaccine in the private
sector. Having a well-structured surveillance system that provides the pertinent epidemiological information in advance about the disease is also a critical factor. Countries meeting these requirements have been able to analyse the cost-effectiveness of Hib vaccination quickly and obtain government commitment to finance the vaccine on a routine basis.
Reliable data are not available among the countries of the South-East Asia Region on the burden of invasive Hib disease. Nevertheless, a study of the effect of Hib vaccination on the incidence of pneumonia among children aged under five years is now progressing in Indonesia. Thailand is preparing a study on community surveillance for Hib meningitis with a view to ascertaining the burden of the disease among children aged under five years. India and Indonesia are conducting similar studies. V&B/SEARO aims to introduce Hib vaccine into the routine immunization schedules in Thailand and Indonesia during 2003. The remaining eight countries will have at least a plan of action on Hib introduction by the year 2003. The high cost of Hib vaccine is still a major constraint on its introduction in national immunization programmes. D

ANNUAL REPORT 1999
7. Immunization systems
7. 1 Introduction
As part of Immunization Services there have been
two overall foci of work. The first involves strengthening the infrastructure for immunization service
delivery. The second is the priority project on Safety
of Immunization. This infrastructure strengthening
process involves: • defining the elements of an immunization
service;
• determining the characteristics of an immunization service that is performing well;
• costing the elements of such a service;
• developing an assessment tool to assist countries in analysing their immunization services,
• identifying gaps and • developing plans for dealing with them.
Future activities will follow these six steps, focusing
on further assessments, the development of plans,
and collaboration with partners in immunization in
order to address the gaps through the provision of technical and financial resources. Finally, the
Immunization Systems priority project has been
developed in the area of safe immunization, thereby integrating with all the other work areas of the
Department.
7 .2 Defining the elements of an immunization service
In this analysis an immunization service is divided into five components: supply and quality, logistics,
surveillance, communication and advocacy, and service delivery. Two additional elements that are
part of the external environment, namely financing
and the overall health system, have also been defined. For each of these components, key indica
tors for identifying well-performing systems have
been defined in order to aid the assessment process.
The assessment tool is now being field-tested. This
23
division into concrete elements has been very use
ful to V&B in defining interventions. The activities pursued in each element throughout 1999 are
summarized below.
7 .3 Supply and quality
7.3.1 Global situation
Critical indicators: • proportion of countries using vaccmes of
assured quality;
• proportion of countries monitoring vaccines by means of vaccine vial monitors (VVMs) when
relevant;
• for OPV: ~ 175/190 countries using vaccines of assured quality, 82/164 with VVMs;
• for other vaccines: proportion of countries
using vaccines of assured quality varies with product, 0 to date with VVMs (to be imple
mented in 2000-2001).
One ofV&B's critical targets is to ensure that by the
year 2000 all countries have access to vaccines of
assured quality and that the quality is maintained
up to the time of administration in the target population. A vaccine of assured quality is one that is
produced in a country where an NRA exercises the six critical control functions identified by WHO,
with no unresolved problems reported.
A number of strategies have been developed to enable countries to obtain vaccines of assured qual
ity; Others are in place or under development in
order to help countries to implement the proce
dures ensuring that quality is maintained during the
storage, distribution, handling and administration
of vaccines:
(1) A centralized procurement system is offered by
UN procuring agencies. The UN procuring system

DEPARTMENT OF VACCINES AND BIOLOGICALS
uses the technical support of WHO/V&B to continuously monitor the quality of vaccines being purchased. The system covers not only the vaccines traditionally included in national immunization programmes but also new and underused vaccines and combinations. Fifteen new applications for vaccine assessment were received during 1999 and three have been completed. Twelve manufacturers' products were reassessed and one was removed from the pre-qualified list.
Critical indicators: .,. proportion of pre-qualified vaccines under con
tinuous surveillance and re-evaluation - 100%; .,. proportion of candidate vaccines evaluated -
20%.
(2) Appropriate regulatory functions must be in place to assure the quality, safety and efficacy of the products used in countries obtaining vaccines by direct procurement or by local production. WHO/V&B has defined these functions and developed indicators for assessing their effectiveness through an expert meeting held in 1999; Assessments against indicators were performed in eight countries during the year and the information obtained was added to a global database maintained in V&B.
Critical indicators: .,. percentage of vaccine doses of assured quality
- 56% for BCG, 73% for DTP, 69% for hepatitis B.
(3) WHO has identified 53 countries that are meeting at least some of their national vaccine needs by local production. A survey of the characteristics of these producers, usually belonging to the public sector, has revealed problems in the quality and reliability of the vaccines, as well as an inability to manage change, access new technologies and appropriately assess the cost of production. In the long term it is unlikely that many of these local producers will continue to be viable and relevant sources of national vaccine supply. In order to assess the reliability of suppliers, WHO has identified seven critical components of local manufacturer viability. To date, 37 local vaccine producers have been assessed and 13 (35%) were identified as viable, having attained a minimum viability score of 70% as measured by the critical functions. Progress is indicated in Fig. 9. Viability assessments were carried out in
24
four countries during 1999, and two papers (Donor Inputs to Local Vaccine Production, Motivations for Local Production) based on extensive global surveys were published.
Critical indicators: .,. percentage of local producers with a viability
rating of at least 70%: 35%.
Figure 9: Number of local vaccine manufacturers achieving 70% viability rating 1996-1999
(4) The Global Training Network (GTN) was developed in 1996 as a means of providing educational resources to vaccine regulatory and production staff throughout the world. To date, 387 staff of NRA.s and vaccine manufacturers have participated in GTN, 165 of them during 1999. The number of centres was increased by three to 17. Three of the standardized curriculum manuals already available in English were published in Spanish, one was published in French, and two new documents were published in Spanish and English. A new curriculum, specially designed for national regulatory staff in procuring countries, was developed, and three courses were held. An important part of GTN's work is continuing evaluation and follow-up to monitor the impact of training on vaccine quality. This was done in 1999 through two follow-up workshops, held in Egypt and Nigeria, and through a study of the proficiency of testing measles and pertussis vaccines. Recognizing the need for training in the management of adverse events at country level, GTN has provided a course

ANNUAL REPORT 1999
on the implementation of a system for monitoring
such events.
Critical indicators: • percentage of countries with independent, fully
functioning NRAs - 47/190 (25%).
(5) WHO is the focal point for reports of adverse
events following immunization (AEFI) wii:h vac
cines supplied through UNICEF and other UN
agencies. V&B staff give quick responses to the
considerable number of reports received each year. The majority of cases are attributable to programmatic errors putting at risk the quality of vaccines
at country level, usually at the time of reconstitution and administration. To improve the situation
in countries experiencing such problems. WHO
and UNICEF will perform country surveys on the
quality of vaccines at the point of use. A protocol
developed in 1999 includes a review of procedures in place at country level for the receipt, release,
storage, distribution and administration of vaccines. Furthermore, WHO and UNICEF devel
oped a vaccine arrival report for all vaccines, and
this was attached to the updated invii:ation-to-bid
documents.
Critical indicators: • proportion of field complaints received annual
ly that have been addressed and resolved -
100%;
• number of countries with effective monitoring
systems for AEFis - 71/190.
(6) The National Vaccine Supply Plan is a new tool
assisting countries to assure an adequate supply of vaccines of high quality through their planning
processes. It was tested in five countries before
being used in another four. A monitoring system for use of the plans is being developed with regional
offices.
Critical indicators: • percentage of countries regularly producing and
updating national vaccine supply plans; not yet measured, but systems are being developed and
regional offices are to perform monitoring.
7 .3.2 African Region
Vaccines for routine immunization are mostly
procured through UNICEF. Certain countries are
25
providing most or all of their vaccine needs from their own budgets. Some countries in the African
Region are actively involved in UNICEF's Vaccine
Independence Initiative (VII).
The status of vaccine production in the four pro
ducing countries of the region is as follows:
• South Africa has the capacity to produce
rei:anus toxiod (TT), DTP and BCG;
• as well as producing yellow fever vaccine for its
own use, Senegal supplies UN agencies;
• Cameroon will begin producing TT in 2000; • Nigeria stopped producing yellow fever
vaccine in 1997.
The number of countries contributing to their
national needs increased from seven in 1995 to 25
in 1998. This was achieved through established
budget lines and/or the adoption of financing
schemes proposed by partners in development e.g. VII of LTNICEF and the European Union in the Sahel countries of West Africa. However, there were
very strong limitations in the financing of new and
underutilized vaccines e.g. yellow fever, hepatitis B
and Hib vaccines, because of their relatively high
cost.
During the next five years, therefore, it will be nec
essary to consolidate the gains of financing routine
immunization and to accommodate the financing
of new and more expensive vaccines, through the
promotion of established budget lines, financing
schemes with partners in development, and the pro
posed global vaccine initiative.
7 .3.3 Region of the Americas
.AJ.\1RO collaboration with countries emphasizes
the need to strengthen activities related to the quality control and production of vaccines. Special emphasis ·was placed on vaccines used in national
and regional immunization programmes.
In the area of quality control, efforts were made to assisi: the national control laboratories (NCLs) of
Argentina, Brazil, Chile, Colombia, Cuba, Ecuador,
Mexico, and Venezuela in achieving the desired lev
els of proficiency and qualification. The support
was aimed at standardizing laboratory methodologies, the production and distribution of reference
reagents, training on the control of new vaccines,
validai:ion of alternative in vitro potency tests, and

DEPARTMENT OF VACCINES AND BIOLOGICALS
improving the communication and exchange of information between participating laboratories. A certification programme assessing the proficiency and performance of laboratories in the regional network was developed and initiated in order to guarantee access to vaccine testing at qualified laboratories, either by AMRO or by NRAs in the region. A database developed for the registration of all vaccine lots released and circulating in the Region was improved and is currently being evaluated by selected NRAs and laboratories.
In the area ofNRAs, AMRO is working towards the harmonization of regulatory activities for the licensing of vaccines in non-producing countries, specifically in Central America and the Dominican Republic. A generic document with harmonized procedures for vaccine licensing was developed and some countries are already using these recommendations for their licensing requirements. In order to strengthen the regulatory functions in these coun-
Figure 1 O: NRAs and NCLs of vaccine-producing countries in the Americas
Non producers
NCA/NCL complying with at least S of the 6 basic functions
■ NCA/NCL complying with less than 5 basic functions
I?"' Source:PAHO
26
tries, workshops were held on topics that included vaccine licensing processes, lot release and good manufacturing practice (GMP). Computers and access to the Internet were provided to improve communication and implement the database system for registering circulating vaccine lots.
In the area of vaccine production, AMRO continued to highlight the need for strong political commitment to improving local vaccine production and ensuring compliance with international requirements and GMP. This commitment will lead to the availability of resources for necessary improvements and investments, as well as for the implementation of managerial, administrative and organizational changes that are more in line with the productive processes. AMRO is promoting technical and economic feasibility studies of vaccine producers in the region in order to obtain information that can justify the continuation or termination of production activities. Mexico conducted such a study and
Brazil has requested assistance with a similar study. Peru is considering the possibility of producing yellow fever vaccine, and for this reason has also requested a study. Colombia, Ecuador, and Venezuela have been recommended to consider this kind of study.
Two countries in the Americas have initiated the WHO assessment for UN vaccine suppliers: CIGB in Cuba for hepatitis B vaccine and BioManguinhos/Fiocruz in Brazil for yellow fever vaccine.
7 .3.4 Eastern Mediterranean Region
Assessment of the vaccine NRAs in this region's countries continued in 1999. Furthermore, the first consultation on vaccine supply, quality and local production in the Eastern Mediterranean Region was held in September 1998 with the objective of reviewing the status of vaccine supply and production in the region and the development of country plans of action to ensure.vaccine quality. The consultation was attended by representatives from EPI programmes, the NRAs of Egypt, the

ANNUAL REPORT 1999
Islamic Republic of Iran, Jordan, Kuwait, Oman,
Pakistan, Saudi Arabia, the Syrian Arab Republic,
Sudan, and Tunisia, as well as representatives of local producers. Continued support was directed
towards the strengthening of the NRAs, with spe
cial emphasis on vaccine-producing countries. The
NRA in the Islamic Republic of Iran is performing
all six functions; that in Tunisia is performing four
(licensing, PMS, lot release and clinical evaluation);
that in Egypt is performing three (licensing, PMS and GMP inspection); and that in Pakistan is per
forming two (licensing and GMP inspection). Follow-up is maintained in the interest of further improvement.
7.3.5 South-East Asian Region
Achieving self-sufficiency means promoting the
ability to expand national efforts independently of outside donor support. By the countries in this
region had achieved rapid gains in self-sufficiency,
approximately 80% of funds being contributed by
the governments. India, Indonesia, and Thailand
are among the countries improving their NRAs'
capacity to perform regulatory functions assuring high-quality vaccine production. In order to
achieve self-sufficiency in supply, countries will need to be able to forecast their vaccine demand for
the near future.
7 .3.6 Western Pacific Region
The (NRAs of China, the Philippines, and Viet Nam have made progress in strengthening their vac
cine regulatory functions. Through participation in
GTN a loose network of NRAs has been formed
and specific vaccine regulatory needs have been identified for countries. The WHO guidelines on
establishing immunization safety surveillance have been adapted in the Philippines to form the frame
work for a national Immunization Safety
Surveillance System (ISSS).
7 .4 Logistics and the cold chain
The term "logistics" refers to the equipment and
management necessary for the safe and efficient
delivery of vaccines. It covers the cold chain and distribution systems, devices and policies which
affect the management of logistics systems, such as
VVMs, and the selection, use and disposal of
injection equipment.
27
Critical indicator: • The ratio of targeted countries implementing
satisfactory safe injection practices as defined by
a WHO standardized survey- currently 0/6.
7 .4.1 Cold chain and distribution systems
To assess the potential impact of the integration of
cold rooms for drugs and vaccines a study on the
integration of vaccine and drug storage and distribution was performed in two countries in Africa.
Another initiative to certify cold rooms is designed to prepare countries for stocking future vaccines.
The final draft protocol for cold room assessment
and certification was developed and preparations for field trials in selected countries were initiated.
A vaccine management study was completed in another African country. A WHO/UNICEF
document entitled "Quality of cold chain WHO
UNICEF" was printed.
A TECHNET consultation was held during 1999 in
Harare, Zimbabwe. There was a record number of
participants and all facets of logistics were considered. The recommendations included a call to for
malize TECHNET and to develop a strategic frame
work for its activities. This will be done in 2000.
7 .4.2 Vaccine vial monitors
VVMs are now on all OPV supplied by UNICEF
and also on OPV provided by a number of produc
ers not supplying vaccines to UNICEF, including all doses filled in India. Activities are now focused on
the assessment of impact, the completion of testing, and the translation and printing of information doc
uments entitled "Testing correlation between VVM
and vaccine potency'' and "Temperature monitors for vaccines and the cold chain''.
A study carried out in India in connection with a cold chain review confirmed the effectiveness of
VV1v1s in indicating vaccines that should not be used because of the possibility of reduced potency.
Critical indicators: • Percentage of OPV distributed through inter
national suppliers and fitted with VVMs - vir
tually 100% unless the purchaser requests that they should not be supplied.
• Percentage of OPV doses from local producers
which are fitted with VVMs - >50%

DEPARTMENT OF VACCINES AND BIOLOGICALS
7 .4.3 African Region
The presence of a logistics manager with the skills
necessary for carrying out increasingly complex tasks is essential for EPI operations. Only 23 of 46
countries (50%) have such managers, and only
about half of them have had the training and expe
rience needed to carry out the functions listed above
Another element essential to EPI operations is the
quality of the cold chain. As indicated by invento
ries made in several countries, much cold chain equipment currently in use was provided in con
nection with the Universal Childhood
Immunization Initiative lead by UNICEF in the late 1980s. Many units are nearing the end of their
useful life and should be replaced.
Studies of low-coverage areas frequently identify a lack of transport as the main barrier to the achieve
ment of targets for coverage and disease reduction.
Programme requirements for timely transportation
of heat-labile vaccines, outreach in rural areas, and
active surveillance mean that EPI is dependent on transport. Level-specific transport planning is there
fore essential for the effective implementation of
EPI tasks. As the effectiveness of outreach sessions
depends on the health system meeting its commitment to communities, reliance on vehicles that are
not always available is bad management.
The following proposals are being made with a view to establishing effective logistics and a reliable cold
chain:
• ministries of health should appoint adequate logistics managers and provide the resources
required, including those needed for transport
and cold chain management;
• training in logistics practices, planning and monitoring should be provided;
• aging cold chain equipment should be replaced entirely in most countries.
7 .4.4 Region of the Americas
AMRO's technical cooperation with countries dur
ing 1999 focused on improving the management of
the cold chain. Emphasis was also placed on
increasing the capacity of cold chain storage facili
ties at the central level, to accommodate new vac
cines, such as pentavalent vaccines (DTP/hepatitis
B/Hib), and increased volumes of other vaccines.
Population increase is overwhelming the capacity for safe storage, as many cold rooms in the Americas
were built more than a decade ago.
During national programme evaluations carried out in various countries, one of the major problems
identified was an ageing cold chain infrastructure and a lack of suitable plans for its renovation.
Several countries have not made the investments
needed to update cold chain equipment since the
late 1970s or early 1980s. There is also a need to focus more on strengthening the supervision of
management. In both cases, AMRO is working
Figure 11: Samples of oral polio vaccine vials showing vaccine vial monitors in place
28

ANNUAL REPORT 1999
with countries to begin the renovation of the cold
chain and to improve the training of supervisors. A few countries in Central America have already initi
ated this process by switching to the use of solar
powered refrigeration. In Brazil, on-the-job training
of health care workers was initiated in 1999 as part
of an overall effort to improve the management of
the cold chain. In support of these efforts, AMRO
will update its cold chain module in 2000.
In the area of vaccine stock management, At\1RO
continues to improve national management capabilities through the installation of a software
package (CLM) for vaccine inventory and manage
ment. Training on this package was given in Panama during 1999. Three more countries will
adopt the CLM software in 2000.
7 .4.5 South-East Asia Region
VVMs have been used with polio vaccme smce
1996. It has been found that in addition to assuring
vaccine potency they have significantly reduced vac
cine wastage. They make it possible to conduct
immunization campaign activities in areas where the cold chain infrastructure is weak or even non
existent.
During 1999 all polio vaccmes provided in the
Region had VVMs. Capitalizing on the training for
polio NIDs, V&B/SEAR assisted with the develop
ment of training materials on VVMs and supported
the mass training of health workers and vaccinators.
V&B was closely involved in the VVM impact study in the Kingdom of Bhutan. Lessons learnt from this
study have helped V&B in the development of fastchain strategy during NIDs. In 2000, V&B will 1)
participate in organizing a training workshop on VVM for mid-level EPI staff; 2) distribute VVM
manuals and guidelines to countries; 3) support
funding for training trainers at the central level; and
4) provide training modules for trainers.
7 .4.6 Western Pacific Region
WHO has facilitated the provision of partner
agency support for cold chain equipment and train
ing in China, the Pacific Island Countries and
Areas, and Papua New Guinea. In most countries in the Region, cold chain requirements are largely met
for the short term, although China and the
29
Philippines still have major needs. In Cambodia,
the Lao Peoples' Democratic Republic, and Viet Nam, injection practices during measles cam
paigns have been significantly improved through the introduction of auto-disable syringes and safety
boxes. This followed successful introductions in Papua New Guinea, the Pacific Island Countries
and Areas, and the Philippines (safety boxes only)
between 1997 and 1999. Major improvements in injection equipment have been made in several
provinces of China through projects supported by
partner agencies.
7 .5 Surveillance
7 .5.1 AFP/polio surveillance
Surveillance for polio eradication remains the prin
cipal priority. By 31 December 1999 all countries
where polio was endemic had established AFP / polio
surveillance. Many countries are now using experi
ence in this field to strengthen surveillance for other communicable diseases. (See also Section 8.1.)
7 .5.2 Estimation of burden associated with vaccine-preventable diseases
In order to ascertain the actual or potential impact
of immunization systems, to document the effec
tiveness of immunization services, and to provide a
tool for local decision-makers, V&B is working
with other WHO clusters, WHO Regional Offices
and other agencies and institutions to develop country-specific estimates of vaccine-preventable
diseases, recommendations for improving the esti
mates and methods and materials for making local
estimates of burden.
7 .5.3 Monitoring routine immunization systems
In collaboration with UNICEF, V&B has estab
lished a common standard reporting system that covers information on the occurrence of vaccine
preventable diseases, and immunization services
and policies. Included is information on the quality
of reported coverage data, on progress in the intro
duction of new vaccines, on the safety of immu
nization services, and on managerial, sustainability
and policy indicators.

DEPARTMENT OF VACCINES AND BIOLOGICALS
7 .5.4 Monitoring immunization safety
Establishing systems for ensuring and monitoring
immunization safety was a priority during 1999 and will continue in the coming years. Materials
have been developed for detecting problems with
immunization safety and for rapid investigation and
response to programmatic failure and vaccine safe
ty. Interventions involve working not only with
national officials responsible for vaccine safety and
immunization services but also with the media. Workshops were held for the countries of WHO's Eastern Mediterranean Region on the detection of
problems, response and working effectively with the
media.
7 .5.5 Monitoring supplemental immunization activities
Increasingly, immunization services include not
only the provision of routine immunization but also supplemental activities (usually time-limited, target
ed campaigns). While NIDs for polio are the dom
inant example, supplemental activities for measles and neonatal tetanus immunization as well as vita
min A distribution are becoming increasingly com
mon. In order to facilitate the forecasting of vaccine
needs, monitor the impact of immunization strate
gies and improve the estimation of disease burden,
V&B has begun routine and structured monitoring
of supplemental immunization activities.
7 .5.6 Improving the accuracy of data
On the basis of past analyses of the reliability, con
sistency and completeness of reported immunization coverage, V&B has begun a project to improve
the accuracy of these estimates. The project includes an active search for alternative data, the
documentation and review of methods used to derive reported coverage, the eliciting of expert
opinion, the cataloguing and promotion of various
interventions and recognized statistical methods for the improvement of coverage estimates, and the
development of tools for evaluating the accuracy of
coverage estimates at the national level.
7 .5. 7 Graphic Information System
In order to improve the analysis and presentation of
epidemiological and programmatic data related to the control of vaccine-preventable diseases, V&B
30
has been working with regional offices and other
WHO dusters to establish a library of base maps
formatted for use by popular GIS computer pro
grammes. The library now contains maps at the sec
ond subnational administrative level for the Western Pacific Region, the South-East Asia
Region, the Eastern Mediterranean Region and the
African Region. These data are currently being
fitted into a global standard.
7 .5.8 Building consensus and coordinating
During 1999, V&B continued to work closely with Regional Offices and UNICEF on issues related to
surveillance and monitoring. A meeting was held to
identify future needs and reach agreement on surveillance and monitoring activities. These activities
concern burden estimation, immunization safety
monitoring, and the accuracy of reported coverage
data.
7 .5.9 Pneumonia surveillance
A surveillance network initiated in.1993 to moni
tor the prevalence and antimicrobial resistance of
S. pneumoniae serotypes from invasive diseases in
children under 5 years of age in Argentina, Brazil, Chile, Colombia, Mexico, and Uruguay is serving
as the basis for a network of sentinel hospitals, pub
lic health laboratories and epidemiological surveil
lance units in these countries' Ministries of Health.
The objective is to monitor bacterial pneumonia
and meningitis caused by S. pneumoniae, H injluenzae and N meningitidis. The system will provide reliable national, subregional and regional
epidemiological information and will monitor sea
sonal and geographical changes in these infectious microorganisms and their antimicrobial resistance.
A regional quality control system, developed to assure the quality of the information, has the
National Center for Streptococcus in Alberta,
Canada, as its main reference centre, while three
laboratories in the region (in Brazil, Colombia, and Mexico) act as subregional centres. Meetings
were held at the centres with all the countries concerned, in order to define the basis of the surveil
lance and the standardized procedures, and to
identify needs for further training. To date, almost
all countries have established a surveillance system for meningitis and pneumonia with varying
degrees of complexity.

ANNUAL REPORT 1999
By-products of the initial surveillance have been
collaborative studies with Rockefeller University on
the genetic relatedness of pneumococcal penicillin
resistant clones in the region, and, in cojunction with the University of Alabama at Birmingham, a
study on the distribution of pneumococcal surface protein families among the isolates obtained so far.
This information will be valuable for the design of
alternative protein vaccines against pneumococcal
infections.
7 .5.1 D Measles surveillance
A sensitive epidemiological surveillance system for suspected cases of measles is critical for the success
ful conclusion of the measles eradication strategy. It
is also necessary to provide support for countries in their efforts to generate reliable official epidemio
logical data on measles, including detailed informa
tion on suspected measles cases with laboratory data
on each. AMRO is therefore working with countries to improve the quality and use of epidemiological
data. The objective is to establish and/or enhance
networks of communication that guarantee the con
tinuing and rapid flow of information between countries. The availability of data of high quality
will facilitate the preparation of national weekly bulletins on measles surveillance, which should be
distributed to health workers, including those in border areas. This information will enable policy
makers and other health staff to obtain surveillance
of high quality on measles outbreaks and other
vaccine-preventable diseases and to coordinate
public health responses.
As part of the measles eradication initiative, AMRO
and national health authorities are implementing:
• periodic and intensive active searches for cases
to find remaining chains of transmission, particularly in municipalities at high risk for measles outbreaks (including those where there
were cases during the preceding 12 weeks);
• intensive measles (mop-up) vaccination in municipalities with disease transmission and in
those that failed to reach 95% vaccination
coverage (estimated on the basis of either reported coverage or house-to-house monitor
ing of vaccination in high-risk areas).
Among other strategies being implemented by
AMRO is the thorough investigation of all out
breaks through:
31
• field investigation of the households, work
places and/or schools where cases occur, and
vaccination as appropriate;
• monitoring of vaccination in all these areas and performing mop-up vaccination if necessary;
• field investigation of places where cases have occurred 7-18 days prior to the onset of rash,
and of places visited by cases during the week
following the onset of rash.
In order to ensure the sustainability of the eradica
tion effort and the equity of vaccination, AMRO is stressing the importance of setting a target of high
(~95%) routine vaccination coverage for all vac
cines. This should be achieved through strengthening the routine vaccination services and education of
the community on the importance of vaccination.
Virological surveillance is a critical component of the measles surveillance system. To determine the
characteristics and probable origins of measles viruses are circulating in the Americas, enhanced
efforts are being made to collect appropriate clinical
specimens for measles virus isolation from every
chain of measles transmission that is detected by the
surveillance system. Surveillance personnel are
receiving special training on the collection of clini
cal samples. AMRO's efforts to strengthen laborato
ry diagnostic capabilities and the exchange of information under the measles eradication initiative will
serve as the foundation for establishing surveillance
for other emerging and re-emerging viral diseases in
the Region and elsewhere.
An active search for measles cases was conducted
during November and December 1999 in the eight largest cities in Colombia to determine whether the
measles virus was circulating. This action was taken
in response to laboratory-confirmed measles cases that occurred in isolation during 1998 and 1999 without any known source of infection. Following
the decentralization of health services there are many new health care providers who are not part of the formal national surveillance system and whose
measles surveillance work is still of unknown quality. Ai\1RO and Ministry of Health officials
reviewed all available cases and surveillance data for
both years and determined that only one depart
ment had a clustering of measles cases, especially in
an urban area, which suggested measles virus circu
lation. A review of case and laboratory data from
the other sporadic laboratory-confirmed measles

DEPARTMENT OF VACCINES AND BIOLOGICALS
cases with no source of infection indicated that the majority occurred after vaccination. No additional confirmed laboratory measles cases were found.
7 .5.11 Measuring the impact of Haemophilus influenzae vaccine
Following AMRO recommendations the Ministry of Health in Colombia initiated the use of a conjugated vaccine against Hib in May 1998, targeting children under 1 year of age. By December 1998, vaccination coverage had reached 50%. With the purpose of evaluating the impact of this intervention a trend analysis of the disease was carried out, utilizing data of the laboratory network for MBA. The number of MBA cases due to Hib (laboratoryconfirmed) in children under one year occurring between June 1994 and May 1999 was analysed. The quality of the surveillance system was evaluated by comparing the cases of MBA caused by Hib with those caused by S. pneumoniae in children under five years of age during the same period.
Between June 1994 and May 1999 the microbiology group confirmed 1166 bacterial isolations: 505 (43.3%) of H influenzae; 361 (31 %) of S. pneumo
niae; and 300 (25.7%) of Nei;seria meningitidis. Of the 464 H influenza.e isolations for which there was information on the patient's age, 286 (62%) corresponded to children under 1 year of age and 99% of them were of Hib.
Between June 1994 and May 1999 the annual numbers ofHib isolates were 45, 37, 61, 64 and 31. The trend analysis of the disease indicated that the expected number of cases in children under 1 year for this last period was 52; however, only 31 cases were observed (p < 0.0005). During the same years there were 25, 18, 33, 37 and 25 cases of MBA caused by S. pneumoniae in children under 1 year of age, and 32, 26, 43, 48 and 42 in children under 5 years of age. According to the trend analysis of the disease for the last period, 28 cases were expected in the under one age group, while 25 occurred (p < 0.74); and in the under 5 age group 37 were expected and 42 were observed (p < 0.22).
The results of this analysis showed a 40% reduction in the number of MBA cases caused by Hib in the under-1 age group during the period studied. This reduction was not attributable to changes in the surveillance system, as demonstrated by the isolations
32
of S. pneumonia.e, for which a slight increase occurred between the expected and observed numbers. It was concluded that the introduction of the conjugated vaccine had possibly led to a reduction of MBA cases caused by Hib.
7 .5.12 Eastern Mediterranean Region
Efforts to improve EPI disease .surveillance in Member States were sustained during 1999, and technical support for strengthening national surveillance systems for EPI target diseases continued. Issues and constraints facing the EPI target diseases surveillance activities and proposed solutions were discussed during various intercountry meetings. Country visits were made by regional office staff and short-term consultants to assess the surveillance systems and advise about methods for strengthening them. Support for the newly developed computerized national surveillance data management systems was continued. The surveillance systems are sufficiently sensitive in some Member States but remain weak elsewhere, and the timeliness and completeness of reporting require improvement.
7.5.13 Routine data collection in the South-East Asia Region
The Information for Action (IFA) system has been established in all Member States. Although it can be u.sed to, create databases for the other EPI target diseases, it is currently being employed for polio surveillance by all Member States. Every Member State sends a weekly data report on AFP and polio to SEARO; seven countries use electronic mail for this purpose and the others send faxes.
Indonesia, Myanmar, and Sri Lanka have linked measks and neonatal surveillance to AFP surveillance. This integration strategy requires evaluation.
Information on vaccination coverage, vaccine-preventable diseases and immunization systems is collected by means of the joint WHO/UNICEF data collection form and the reporting tables required for the regional TCG meeting each year.
Feedback to countries is provided in the region's Weekly Polio Bulletin. At the regional TCG meeting a forum is provided for the exchange of country-level information.

ANNUAL REPORT 1999
In 1999, V&B/SEARO conducted a workshop on mapping for disease surveillance based on GIS Arciew software.Efforts will be made in 2000 to provide a dynamic link ofIFA to GIS. Virologists of the region's Polio Laboratory Network will attend an IFA workshop organized by V&B/SEARO.
Table 1: Measles and yellow fever vacdne coverage, 1998
Yelfowfffer Mfas/es
WICcint ,accjne awerage (96) awerage (%)
Angola 36 65 Benin 82 Bolivia 80 Brazil 38 96 Burkina Faso 27 68 Burundi 44 Cameroon 47
.Cape Verde 66 Central African Republk 36 39 Chad 25 30 Colombia 75 Congo Cote d'Ivoire 57 66 Demoaatic Republk of Congo Ecuador Equatorial Guinea Eritrea Ethiopia .French Guiana Gabon
• Gambia 91 /Ghana 67 ~uinea 58 • Guinea-Bissau Guyana 7 93 Kenya 61 Liberia 31 Mali 10 58 Mauritania Niger 85 Nigeria 26 Panama 10 95 Peru 93 Rwanda Sao Tome & Principe 59 Senegal 50 6S Sierra Leone 68 Somalia 47 Sudan 63 Suriname 82 Togo 33 Trinidad & Tobago 91 90 Uganda 30 United Republic ofTanzania 72 Venezuela 79 94
33
7 .6 Immunization coverage
7 .6.1 Global immunization coverage
Reported immunization coverage trends remained stable except in the South-East Asia Region and the African Region (Fig. 12). Global coverage with DTP3 in 1998 was reported to be 7 4%, the Regional figures ranging from 47% to 93%.
The downward trend in the South-East Asia Region is explained primarily by the fact that three large countries (Bangladesh, India, and Indonesia) used survey data instead of administrative data. The discrepancies between survey and administrative coverage data reflect the problems encountered in many countries with regard to coverage data quality (Fig. 13).
In Africa, 13 countries experienced declining coverage, including two of the largest countries, namely Ethiopia and Nigeria, and this probably explains the slight overall downward trend (Fig. 14).
Of the 163 countries reporting to WHO in 1999 on DTP-3, 50 (30%) did not achieve 80% coverage. This means that 52% of the global birth cohort live in countries where immunization systems need strengthening. Most of these countries are in the African Region (Fig. 15).
WHO and UNICEF collected information during 1999 on key indicators of the sustainability, quality and safety of immunization systems in 1998. Fig. 16 shows countries reporting the proportion of vaccines financed by government, and Fig. 17 shows countries having injection safety as a component of their annual work plans.
Only six of the 31 countries at risk for yellow fever outbreaks in the African Region and neither of the two at such risk in the Eastern Mediterranean Region reported yellow fever immunization coverage figures. None of these countries achieved yellow fever coverage that was at least equal to measles coverage (Table 1), despite the fact that the vaccines were given during the same immunization visits. In the Americas, five of the ten countries considered at risk for yellow fever outbreaks reported coverage figures.

DEPARTMENT DF VACCINES AND BIDLDGICALS
Figure 12: Reported DTP3 coverage by WHO Region, 1989-1998
Figure 14: Reported DTP3 coverage in countries of South East Asia Region with the largest birth cohorts, 1980-1998
34

ANNUAL REPORT 1999
Figure 14: Countries in sub-Saharan Africa reporting decreasing DTP-3 coverage, 1996-1998
... ... ... ... -60 -50 -40 -30
Percentage (%) point decrease in DTP3 coverage
Figure 15: Reported DTP-3 global coverage in infants, 1998
>80%
■ 50-80%
■ <50%
No data
Data as of August 1999
---
... ... ... -20 -10 0
35
Ethiopia
Cote d'Ivoire
Gabon*
Zimbabwe
Central African Republic*
Uganda
Zambia*
Burundi*
Rwanda*
Mauritania*
Nigeria
Liberia*
Congo*

DEPARTMENT OF VACCINES AND BIOLOGICALS
Figure 16: Percentage of routine vaccines financed by governments
■ 0-49%
50-79%
>80%
No data
Sauret: Joint WH0/1/NICEF r,porting from 1999
Figure 17: Inclusion of a safe injections component to the national workplans
Sauret: Joint WH0/1/NICEF reporting from 1999
36
'.), ._1•:i,.
' ,,. ..... . )'

ANNUAL REPORT 1999
7.6.2 Immunization coverage in the African Region
Immunization coverage rates have generally been
stagnant or on a slight decline since 1995, although
there have been important variations between geo
graphical areas. For BCG, 22 of 46 countries
reported 280% coverage, six reported an increase and 22 reported a decline (Table 2). For DTP3,
eight of 46 countries reported 280% coverage, ten reported an increase and 21 reported a decline. For
measles, seven countries reported 280% coverage, 13 reported an increase and 23 reported a decline. For TT2+, three countries reported 280% coverage,
14 reported an increase and 19 reported a decline.
Table 2: Numbers of countries in the African Region reaching 280% reported routine coverage in 1998 and numbers of countries with a change in reported coverage (25%) from 1995 to 1998, by antigen
Antigen Reaching >80% Increase Decline No change
!!CG 22 18
~i:!1/ /.)··· 22 8 7
6 10 11 13 14
21 15 20 15 23 10 19 13
While there are specific local reasons for these
changes, several issues cut across many areas and may have had a large effect on coverage. These
issues should be considered when the strategies for re-energizing EPI in the region are being addressed.
• Civil unrest continues in many countries in Africa. The Organization of African Unity
estimated that in 1999 civil conflict was taking place in 22 countries and that 90% of the
victims were civilians.
• Health sector reform (HSR) occurred in many
countries during the previous four years, notably in the Eastern Block countries.
Decentralization has disrupted logistics, plan
ning and financial mechanisms. EPI was not well prepared for this transition. At the district
level, EPI now has to compete with other
district priorities for staff and funding. These
local priorities may legitimately be different
from national and global priorities, particular-
37
ly with regard to demands for curative care at the local level. Only in Ghana has HSR had a
positive effect on EPI coverage; this instance
should be studied further and the lessons learnt
should be used for guidance in other countries.
• Staff morale is very low in several countries ..
Peripheral and central level staff have been reduced in numbers. There are reports of staff
not being paid, of high staff turnover, and of
inadequate training.
• In some countries there may be fewer financial resources available for routine immunization
services, partly because of changes in donor
priorities and a lack of government resources
dedicated to EPI.
• It is unclear what the net effect of polio eradication has been on routine coverage: the intro
duction of activities such as polio NIDs,
together with other new priorities in EPI, may
have taken the focus away from achieving high
routine coverage.
7 .6.3 Region of the Americas
Provisional data for 1999 show an increase in vacci
nation coverage for all antigens in the Americas
(Fig. 18).
Overall regional DTP vaccine coverage in 1998 was
86%; 23 of 39 reporting countries (59%) had coverage of 2 90%. The following countries reported
DTP3 coverage below 80%: Bolivia (76%),
Colombia (70%), the Dominican Republic (74%), Haiti (39%), and Venezuela (39%).Overall region
al OPV3 vaccine coverage in 1998 was 89%; 25 of 38 reporting countries (66%) had coverage 2 90%
The following countries reported OPV3 coverage below 80%: Bolivia (75%), Colombia (72%), the
Dominican Republic (73%), Haiti (37%), and Venezuela (64%).
Overall regional BCG vaccine coverage in 1998 was
99%; 22 of 32 reporting countries (61 %) had coverage of at least 90%. Overall regional measles
vaccine coverage in 1998 was 86%; 22 of 39 report
ing countries (56%) had coverage of at least 90%.
Under 80% coverage was reported by Colombia
(75%i), Haiti (42%), and Paraguay (78%).

DEPARTMENT OF VACCINES AND BIOLOGICALS
7.6.4 Eastern Mediterranean Region
The improvement in regional immunization coverage observed since 1996 for all EPI antigens was maintained in 1998, mainly because of the sustained high coverage rates in most Member States. The reports received from Member States for 1998 indicate that the average regional coverage rates were 90% for BCG and 82% for OPV3/DTP3 and measles in children aged up to 1 year. Provisional data for 1999 indicate similar coverage rates.
Data for 1998 indicate that 17 countries were able to achieve an immunization coverage rate of90% or more for DT3/OPV3 (Bahrain, Cyprus, Egypt, Islamic Republic of Iran, Iraq, Jordan, Kuwait, Lebanon, Libyan Arab Jamahiriya,
fully integrated into national immunization programmes for children under one year of age in 16 Member States (Bahrain, Cyprus, Egypt, Islamic Republic of Iran, Iraq, Jordan, Kuwait, Libyan Arab Jamahiriya, Oman, Qatar, Saudi Arabia, Syrian Arab Republic, Tunisia, United Arab Emirates, Yemen and the Self-Ruled Areas in Palestine and the population served by UNRWA). These countries account for about 47% of the total infant population of the region. Coverage rates of90% or more were reported from nine of them, and the overall regional average was 88%. Member States that have not yet included hepatitis B vaccine in their EPI schedules were urged to give a high priority to doing so. Lebanon, Morocco, and Pakistan are planning to introduce hepatitis B vaccine into their routine programmes.
Morocco, Oman, Qatar, Saudi Arabia, Syrian Arab Republic, Tunisia, United Arab Emirates, and the Self-Ruled Areas in Palestine and the population served by UNRWA). Sixteen countries reported a measles coverage rate of 90% or more (Bahrain, Cyprus, Egypt, Islamic Republic of Iran, Iraq, Jordan, Kuwait, Libyan Arab Jamahiriya, Morocco, Oman, Saudi Arabia, Sudan, Syrian Arab Republic, Tunisia, the United Arab Emirates, and the Self-Ruled Areas in Palestine and the population served by UNRWA). Some improvement was observed for coverage rates in Pakistan and Yemen. However, low coverage rates were still reported from Afghanistan, Djibouti, and Somalia.
Figure 18: Immunization coverage of children underl year of age, Region of the Americas*, 1995-1999**
The average regional TT2+ coverage among pregnant women during 1998 was maintained at approximately 50%. However, it should be borne in mind that the proportion of immune women in the communities is higher than that calculated from TT2+ annual immunization coverage and that it could be estimated through monitoring the protection of children at birth.
Efforts are being made to expand the use of existing vaccines and to incorporate new ones into immunization programmes. Hepatitis B vaccine is now
38
Source: Country reports • Exduding Canada and USA
.. Provisional

ANNUAL REPORT 1999
Hib conjugate vaccines have been introduced into routine infant immunization schedules in four countries (Bahrain, Kuwait, Qatar, and the United Arab Emirates). Oman and Saudi Arabia have prepared plans for inclusion of the vaccine by 1999-2000. A pilot project was started in Syria for inclusion of the vaccine in routine immunization in a limit-
Figure 19: Immunization coverage, Eastern Mediterranean Region 1992-1998
lmmunllltioo roverage%
100
80
60
ed geographical area, which will be 40
expanded later. It was recommended that countries should implement infant 20
immunization in accordance with their capacities, national priorities and disease burdens. Rubella vaccine combined with measles and mumps vaccine is included in the routine immunization programmes of 12 countries in the Region.
In addition to routine immunization activities, other supplementary immunization activities were conducted, including polio NIDs and mopping-up operations and campaigns in areas at high risk for neonatal tetanus and measles.
0 '91
Immunization coverage%
100
80
60
40
20
0
'93 '94 '95 Ytor
BCG
'96 '97 '98
Measles
Immunization ·cowrage%
100
80
60
40
20
0 '91
Immunization coverage%
100
80
60
40
20
0
'93 '94 '95
Year
'.:' :,
'96 '97
During 1999 all Member States except Cyprus conducted supplemental immunization activities. NIDs were organized with high coverage in all Member States exceptthe Islamic Republic of Iran and Tunisia, where subnational immuniza-
'91 '93 '94 '95 '96 '97 '98 '91 '93 '94 '95 '96 '97•,.
tion activities were conducted in border and highrisk areas. Most significantly, immunization activities were accelerated in all remaining countries of endemicity. This included improving the quality of campaigns through better planning, increased resources and house-to-house vaccine delivery, and increasing the number of campaign rounds. Two NIDs were conducted in both Afghanistan and Egypt. In response to the outbreak that began during May 1999 in Iraq, two additional NID rounds were conducted. Pakistan, Sudan, and the Syrian Arab Republic conducted additional mop-up operations in high-risk and/or border areas. WHO provided technical assistance in all aspects ofNID planning, implementation and evaluation, particularly to countries where the virus was still circulating.
During 1999, coordinated immunization and surveillance activities continued under Operation
39
Year Year
MECACAR, involving countries of the European Region and the Eastern Mediterranean Region. Coordinated NIDs and mopping-up campaigns were conducted jointly by Afghanistan, the Islamic Republic of Iran, and Pakistan, and by the Islamic Republic of Iran, Iraq, the Syrian Arab Republic, and Turkey. Different Regional and inter-Regional epidemiological blocks coordinated immunization acrivities under the auspices of several organizations including the Gulf Cooperation Council, the Maghrebian Union and the South Asian Association for Regional Cooperation. Attention is currently focused on strengthening coordination between the countries of the Horn of Africa, especially Eritrea, Ethiopia, Djibouti, Somalia, and Sudan.
The high-risk approach to the elimination of neonatal tetanus, involving two rounds of immu-
;;
I! {9f •·
, ... I
I

DEPARTMENT DF VACCINES AND BIOLOGICALS
nization of all women of childbearing age in identified high-risk areas, was implemented in some Member States, including Egypt and Sudan. However, only limited areas were covered, and not all identified high-risk areas were covered. Plans of action for nationwide neonatal tetanus elimination, based on the high-risk approach, are available for all Member States needing them. District microplans were formulated with detailed costings for Egypt, Pakistan, Sudan, and Yemen.
Kuwait and Oman conducted national mass catchup campaigns during 1994. In Oman, the campaign included all children aged 9 months to 18 years and was followed by the administration of a second dose within the immunization schedule. Very low incidence was maintained in Oman and there was no indication of a need to conduct a follow-up campaign. In Kuwait the initial campaign included children aged 6 to 18 years; in response to an outbreak that began in 1998 a catch-up campaign including children aged 6 to 11 years was conducted. Bahrain and Jordan conducted the first phase of their campaigns in late 1997 and early 1998 respectively, targeting school-age children; the second phase, targeting preschool children, was conducted in both countries during May 1999. Catch-up campaigns were conducted during 1998 in Syria (targeting children aged 9 months to 15 years), Tunisia (targeting children aged 7 to 15 years), the United Arab Emirates (targeting children aged 9 months to 4 years), and Saudi Arabia (targeting children aged 12 to 15 years). During 1999 the second phase of the catch-up campaigns was completed in Saudi Arabia (targeting chi!-
Figure 20: Percent vaccination coverage by antigen, SEAR, 1995-1998
40
dren aged 6 to 12 years) and the United Arab Emirates (targeting children aged 4 to 15 years).
Countries were encouraged to deliver vitamin A supplementation in routine EPI schedules and supplementary immunization activities, including polio NIDs and anti-measles campaigns. Vitamin A was included in NIDs in Afghanistan, Pakistan, Somalia, and Yemen. Vitamin A was included in the routine immunization programmes in Egypt and Oman during 1999.
The question of unsafe lllJection practices was discussed during most intercountry meetings. Assessments of lllJection practices during immunization ~essions were conducted in Egypt, Sudan, and Yemen. Support is being provided for countries to develop plans for safe immunization.
7.6.5 South-East Asia Region
Coverage declined for OPV3, DTP3, BCG and measles vaccines from over 80% of children in their first year oflife during 1995-1997 to about 70% in 1998. Preliminary data for 1999 showed that 63% of districts in Bangladesh achieved routine coverage of more than 80 %. In India, coverage of more than 80% was reported for BCG by 47% of districts, for OPV3 by 44%, for DTP3 by 37 % and for measles by 9% only. Myanmar reported that 85% of districts achieved over 80% routine coverage. In Nepal, 80% of districts reported over 80% coverage for BCG but only 50% for OPV3 and DTP3. About 70% of districts reported over 80% coverage

ANNUAL REPORT 1999
Table 3: Immunization coverage by country,South-East Asia Region, 1997-1998
BCG DTP3 Country/Area 1997 1998 1997 1998
: Bangladesh 100 92 98 78 '.:Bhutan 92 94 87 86 : ·. DPR KKorea n.a. 64 n.a. 37 ( India 96 79 90 73 '.'Indonesia 99 85 90 65 ',,,,''
• Maldives 99 99 97 97 : Myanmar 94 91 90 87 '(Nepal 96 86 78 76
,.,,;,',,,
.. :~r!,La.nka 96 90 97 94 /:!:.TMiland 99 n.a. 98 n.a ::R~gion. 97 81 90 72
for measles. V&B/SEAR will attempt to increase and maintain high coverage in 2000.
7.6.6 Western Pacific Region
In 1998, reported routine immunization coverage
for all antigens remained high. Most countries reported routine coverage of infants with all anti
gens at over 80%. Some, however, including
Cambodia, the Lao People's Democratic Republic,
and Papua New Guinea, reported less than optimal coverage.
7. 7 Target diseases
In 1998, 2091 cases of diphtheria were reported in
the South-East Asia Region. This represented an increase in comparison with the fig-
ures for 1993-1996 but a decline
OPV3 Measles TT2 1997 1998 1997 1998 1997 1998
98 78 97 72 94 86 87 85 84 71 70 80
n.a. 77 n.a. 34 n.a. 5 91 73 81 66 80 87 77 93 76 78 97 97 96 98 96 91 90 88 88 85 83 78'· 78 70 85 73 19 65 98 94 94 91 89 95 n.a. n.a. n.a. 83 n.a:· 84 67 91 74 79 60
While these figures can easily be used to monitor a
trend, it is likely that the real incidence was higher.
The difficulty in diagnosing these diseases and the
poor quality of routine reporting are major reasons
for the production of inaccurate data. With regard
to pertussis, other sources have calculated that the
true incidence in the South-East Asia Region is
closer to 8.5 million cases and that 90 000 deaths are attributable to the disease.
7. 7 .1 Yellow fever
In 1998, reported routine immunization coverage
for all antigens remained high. Most countries reported routine coverage of infants with all anti
gens at over 80%. Some, however, including Cambodia, the Lao People's Democratic Republic,
from the 6549 cases reported in
1997. Countries in this Region reported 46 666 pertussis cases,
Figure 21: Reported cases of vaccine preventable diseases in SEAR
substantially more than in the pre
vious two years ( 41 940 cases in
1997 and 22 479 in 1996). The bulk of cases in 1998 were in India (31 199 cases) and Nepal (14 339
cases). In 1998 the numbers of
reported cases of measles, neonatal
tetanus and polio were 62 722,
3324 and 4777 respectively. A small
outbreak of pertussis was reported in Sri Lanka in 1997. However, no
outbreak of diphtheria was reported
during that year.
Cases
12000
10000
8000
6000
4000
2000
0 Pertussis*
41
■ 1995 ■ 1996 ■ 1997 1998 1999
Diphtheria Measles* NNT Polio
•numb,rofcas,s should be muttiplied by 10

DEPARTMENT DF VACCINES AND BIOLOGICALS
and Papua New Guinea, reported less than optimal coverage.
In 1988 the joint WHO/UNICEF Technical Group on Immunization in Africa recommended that yellow fever vaccination be integrated into EPI in countries considered to be at risk. Only 17 of these countries have given effect to the recommendation. In 1998 only eight countries reported immunization coverage, the estimated average being 40%.
The following strategies are proposed: • prevention of outbreaks by increasing routine
immunization coverage to at least 80%; • control of outbreaks through early detection
and laboratory analysis of blood specimens taken from suspected cases;
• emergency response to outbreaks through mass campaigns;
• prevention of outbreaks in high-risk areas through mass campaigns.
Yellow fever remains a major public health concern in Africa. Outbreaks occur periodically in the yel-
low fever belt, especially in the West African block. In general there has been poor surveillance and delayed response, sometimes resulting in catastrophic outbreaks. There has been marked underreporting of the disease. It is estimated that 200 000 cases and 30 000 deaths are attributable to yellow fever annually in sub-Saharan Africa.
The capacity for laboratory confirmation of epidemics has been strengthened in Africa. Of 31 countries at risk for yellow fever, 22 have benefited from training through the Regional Polio Laboratory Nerwork. Participants were provided with diagnostic reagents at the end of the course. There are 15 laboratories in the region with the facilities and expertise required for yellow fever serology. Polio laboratories in countries at risk for the disease are also capable of isolating the yellow fever virus. Sentinel surveillance systems have been created in some countries (e.g. Kenya, Senegal), allowing for constant monitoring of the yellow fever situation.
The lack of achievement in the control of yellow fever has been ascribed to the following factors:
Figure 22: Geographical distribution of yellow fever cases in South America, 1986-1999
1 dot = 1 case:
No case
■ With case
Source: Ministry of Htalth, data as of J 1 Dtcember 1999 (Bolivia, Colombia, Ewador, Ptru and Venezu,la)
1
Total: 204 cases !
42
1999 Yellow Fever Cases
Brazil 72 cases
Bolivia 68 cases

ANNUAL REPORT 1999
• a lack of motivation, commitment and politi
cal will, and of public and professional
awareness;
• competing priorities of other vaccines; • a lack of effective country plans of action, weak
surveillance and reliance on emergency vacci
nation;
• a lack of finance for the integration of yellow
fever vaccine into the routine EPI.
The risk of urbanization of yellow fever m the
Americas remains a concern because of the wide dissemination of Aedes aegypti in the 11 countries
located inside the enzootic area (Bolivia, Brazil,
Colombia, Ecuador, French Guiana, Guyana, Panama, Peru, Suriname, Trinidad and Tobago, and
Venezuela). Only Canada and Chile are free of
A. aegypti. The growing number of travellers by
road and air between countries in the region facilitates the introduction of yellow fever into urban
areas outside the traditional enzootic areas, where
there are heavy infestations of A. aegypti at present.
A more aggressive yellow fever strategy was recom
mended by AMRO's Technical Advisory Group on Vaccine-Preventable Diseases (TAG) with a view to
achieving prompt vaccination of the entire popula
tion in areas where yellow fever is endemic (Bolivia, Brazil, Colombia, Ecuador, Guyana, Peru, and
Venezuela). It was also recommended that the
vaccine be incorporated into the basic routine
Figure 23: Yellow fever cases per year in selected countries, 1985-1999"
Number of Cases
600
500
400
300
200
100
0
Source: HVP/PAHO
immunization schedule for children under one year
of age by administration with measles vaccine.
In 1999 there were reports of 204 cases and 97 deaths. Bolivia, Brazil, and Peru accounted for
96% of reported cases; Colombia and Ecuador also
reported cases. These numbers are close to the
averages reported during the last 10 years.
Underreporting is still a problem and the
differences between countries in disease incidence
have much to do with differences in the sensitivities
of surveillance systems.
AMRO is collaborating closely with national
authorities to enforce the TAG recommendations.
The following major obstacles exist: a lack of polit
ical commitment in some countries, partly attribut
able to a failure to recognize the severity of the current situation; financial difficulties in purchasing
yellow fever vaccine; and serious shortages of yellow
fever vaccine in the international market.
7. 7 .2 Rubella
AMRO's technical cooperation in the rubella field
focused on the introduction of rubella vaccine in
routine immunization programmes and on the inte
gration of measles and rubella surveillance. The objective of rubella surveillance is the detection of
circulating virus rather than of each case. Countries
were presented with options for either rapidly
*Data as of 10 December 1999 for Bolivia, Brazil, Colombia, Ecuado~ French Guyana, Peru and Venezuela
43

DEPARTMENT OF VACCINES AND BIOLOGICALS
controlling rubella or for preventing cases of con
genital rubella syndrome (CRS). AMRO has rec
ommended a one-time mass campaign with
measles- and rubella-containing vaccine aimed at
females aged 5-39 years in countries wishing to achieve rapid control of CRS. Countries wishing to
control both rubella and CRS should also conduct
mass campaigns with such vaccine for males and
females aged 5-39 years.
The majority of countries in the region now have MMR vaccine in their national immunization schedules. Bolivia, Guatemala, and Paraguay plan
to introduce MMR vaccine during 2000. Still
pending are Haiti and Peru.
Chile carried out a preventive vaccination campaign
for CRS, targeting females aged 10-29 years. The
campaign achieved 98% coverage with rubella vac
cine, thanks to the strength of the national immu
nization programme and a highly successful social
mobilization campaign. The Ministry of Health is
implementing a surveillance system in order to: provide information on the effectiveness of the
campaign and policies; measure its impact on the
occurrence of rubella and CRS; identify groups of
people or geographical areas in need of additional
control efforts to reduce disease incidence; and eval
uate vaccine effectiveness, duration of vaccine
induced immunity, and other aspects of the efficacy
and safety of the vaccine.
Costa Rica carried out an MMR campaign follow
ing a rubella outbreak during 1999 in which over 250 cases were reported. The campaign targeted
children aged 1-14 years. Selective adult vaccination
among risk groups (health workers, people working in educational establishments, tourist workers and
migrants) with MMR vaccine was also undertaken.
The rubella outbreak in Costa Rica highlighted the
need for all countries to adjust their surveillance
systems for suspected measles cases so as to include rubella. The outbreak in Costa Rica was accompanied by an increase in rubella activity in almost all
other Central American countries. The countries of
Central America are planning to move rapidly towards the integration of measles and rubella sur
veillance, creating a fever and rash surveillance sys
tem. AMRO is adapting the Measles Eradication
Surveillance System software and expects to provide
technical cooperation in the collection of proper
specimens for virus isolation and in the supply of lgm rubella kits to all laboratories.
The objectives of integrated measles and rubella surveillance are: to know where the virus is circulat
ing; to obtain timely detection of cases; to ensure
adequate outbreak control; to prevent CRS; to mea
sure the magnitude of the disease burden; and to
provide evidence of the impact of various interven-
Figure 24: Annual reported rubella cases, Latin America and the Caribbean, 1984-1998
Source: PAHO/MH
44

ANNUAL REPORT 1999
tions. Besides the Central American countries, other
F.gre2B: CaE3 cf dipJ. fur :iantreEurcpEmREgXJJ, 1991-19.'B
countries in the Region are
integrating measles and rubel-
la surveillance. AMRO
expects this integration to
have the added benefit of
greater reporting of suspected measles cases. For surveillance
purposes it has been decided
that any patient in whom a
health care worker suspects measles or rubella infection
should be considered to have
measles until the contrary has been proved. A blood speci
men should be obtained from
every patient who fits the case
definition of suspected rubella
25cm
:;n cm
JS cm
JO cm
or measles, unless the case is linked epidemiologi
cally. All sera from suspected measles cases that test
negative for measles IgM antibodies should be test
ed for rubella IgM antibodies and vice versa.
7. 7 .3 Diphtheria
Based on sound epidemiological projections, It 1s
estimated that the implementation of aggressive measures in the 15 diphtheria-epidemic countries
of the European Region has prevented more than 560,000 cases and more than 15,000 deaths. In
1999 there were 1,121 reported cases. All countries
have made significant efforts towards fully immu
nizing their child and adult populations. The European Laboratory Working Group on
Diphtheria, formed at the initiative of the \VHO
European Office in July 1993 is still very active in monitoring the microbiological surveillance of
diphtheria and typing the causative agent, leading to the establishment of a database of isolates of
C. diphtheriae.
The declining trend of epidemic diphtheria in the NIS reflects the resource mobilization and immu
nization activities undertaken by the affected coun
tries in close collaboration with the international
community. The situation in Armenia, Azerbaijan, Kazakhstan, Estonia, Lithuania, Moldova,
Turkmenistan and Uzbekistan shows that the epi
demic is clearly coming under control. During
1998/99, the situation greasdy improved in
Georgia. The trend in Russia is a clear decrease.
■ Rl!)crrtfrlcclffi PJg3!::tfrlcam
1932
45
However, an average of 100 cases are still being
reported every month, demonstrating gaps of
immunity, continuing circulation of C. diphtheriae and the potential for further spread. The situation
in Kyrgyzstan, Ukraine, and Tajikistan has also
improved. Epidemic control is still yet fully achieved, however. Concerns have been expressed
on the endemic status of Latvia. This country
showed an rising trend in 1998 and 1999, probably
due to the low acceptance of vaccination by hard
to-reach adulr populations. In December 1999, the
situation was reviewed and innovative ways were carefully considered of immunising the high risk
group 35-50 years of age.
7 .8 Communication and advocacy
WHO's Direcrnr-General declared war on polio
during the lvfarch 1999 Polio Management ;-.freeing. In Mar she met health ministers of coun
tries where the disease is endemic and of donor
countries at an extraordinary meeting during the \XTorld Health Assembly. Member States voted
unanimously to endorse acceleration of the initiative on the year 2000 target; India announced a
fast-track plan for NIDs to be held in four consec
utive months, followed by two monthly mop-ups in
eight high-risk states.
During the year the Director-General travelled to
Bangladesh and C6ce d'Ivoire in order to participate

DEPARTMENT DF VACCINES AND BIOLOGICALS
in NIDs, thus expressing her commitment to the initiative. In July a joint announcement by Mr Kofi Annan, Dr Gro Harlem Brundtland and Ms Carol Bellamy, issued by the UN Secretary-General's Office and UNICEF, called on belligerents to secure Days of Tranquillity in the Democratic Republic of Congo so that polio vaccination could be carried out. Dr Michael Scholtz travelled to this country to participate in the second round ofNIDs, while Dr Bjorn Melgaard performed the same function in India.
In July a press conference was held in London to introduce new partners in the initiative, namely the diamond mining and trading company De Beers and the world-renowned British photographer Lord Snowdon, who in May photographed polio sufferers in the Angola outbreak. In October a donation of 50 million doses of polio vaccine from a leading manufacturer, Aventis Pasteur, was announced. In the same month there was a public announcement of donations totalling US$ 78 million from the Bill and Melinda Gates Foundation and Mr Ted Turner's United Nations Foundation.
Effective implementation of immunization strategies has generally entailed strengthening the capacity of countries, making resources available, and reenforcement at global and regional levels. Achievements in 1999 included:
• the strengthening of national core teams from ministries of health, UNICEF and WHO through regional training and planning workshops;
• the strengthening of communication and social mobilization planning in countries by means of support for the development of research-based integrated plans for EPI/NIDs/surveillance which ensure that activities are organized throughout the year;
• high-level advocacy through regional leaders and bodies; heads of state and agencies were invited to preside over NID launches;
• advocacy through media relations and sports; WHO partnership with football became global when the Federation Internationale de Football Association (FIFA), the world governing body of football, decided to support the Kick Polio Out of Africa initiative. This unique contribution will dramatically boost the polio eradication campaign, ensuring that it will receive maximum attention and backing from
46
both the football world and millions of football fans.
Partnerships with media organizations have become stronger. Activities have been implemented with RPI, CFI, AITY, BBC and Africa No. 1, including educational programmes and tour visits to report on NIDs in some of the countries where there are particularly difficult conditions. Work with BBC has resulted in a project in Tanzania and may lead to one in Ethiopia, while work with RFI and Africa
No. I on the production of programmes could serve as a reference for future collaborative efforts.
The challenge for advocacy, social mobilization and communication in the coming years will be in expanding the gains made in political commitment and partnership relating to routine immunization.
7.9 Service delivery
7.9.1 Programme planning
After extensive deliberation and review during 1999, V&B developed a four-year Strategic Plan for 2000-2003, encompassing a broad range of activities linked to the objectives of Innovation, Immunization Systems and Accelerated Disease Control. Nine specific goals or targets were identified and each was assigned a well-defined and measurable outcome or critical indicator. The targets encompass the expertise and contributions of all five teams in V&B and therefore require the integration of activities. Three of these targets are timelimited priority projects, namely Accelerated Vaccine Introduction, Safety of Immunization and the Polio Eradication Initiative. For the purposes of the Strategic Plan a limited number of products were also defined, identifying the areas of work to be tackled in order to achieve the targets. These products represent the measurable outcome of the work of the V&B teams.
7.9.2 Programme assessment
The environment in which immunization systems operate is changing. Health sector structure, the location of authority and responsibility, and the mix of public and private participation are changing significantly in many countries.

ANNUAL REPORT 1999
As new vaccines, equipment and technologies
become available the need increases to determine the readiness of immunization systems to introduce
and sustain these innovations. New goals demand
new strategies. The capacity of existing services
must be assessed in order to determine whether they
can achieve new goals and implement new strategies (e.g. the need for stronger surveillance).
A common assessment tool is needed. Health sector
officials, managers of services, development part
ners and nongovernmental organizations have asked for a common assessment tool with a view to
identifying where improvements are needed and
planning individual and joint inputs.
A new methodology has been developed to examine the health systems and the external environments in
which immunization systems operate, as well as the
services themselves. Assessments carried out under
these guidelines should provide sufficient informa
tion to prepare or update long-term plans of action
or to prepare proposals for securing the support of
partners in order to:
• increase the accessibility and use of routine immunization services, especially for people
who are not reached at present;
• improve the efficacy of immunizations and the quality of immunization services;
• increase the availability of new vaccines and new technologies in countries that have the
capacity to integrate them;
• ensure adequate and reliable financing of national immunization activities;
• support the development of health systems.
The assessment methodology is based on a number
of concepts. First, the focus is on performance. Quantifiable information alone, for instance on the
number of vehicles assigned to a district office or on whether a national policy on safe injections exists,
does not provide evidence of service effectiveness
or safety.
The inquiry concentrates on the level at which ser
vices are provided, and problems are traced to the
level (service delivery, subnational or national) of
their origin. The assessment process involves the
people who know what the problems are and who
will participate in implementing the solutions. This methodology involves service providers, their
supervisors and other major stakeholders through
47
individual discussions and group work sessions at
every level.
Immunization operations, the health system and
the external environment are included in assessments. Immunizations are provided in a context
consisting of three components: the immunization
operations themselves, the health system and the
external environment. Because this context influ
ences who receives immunizations and how they are
provided, a comprehensive assessment must exam
ine all three. An assessment of immunization operations may include an examination of the costs of
services and financing.
On the basis of experience gained in an initial assessment the tool will be streamlined and simpli
fied for ease of use in guiding data collection and in
compiling reports.
7.9.3 Management
When EPI was launched, most countries were
introducing national immunization programmes. Their problems were mostly technical and mostly
the same because the countries were at similar stages
in controlling the target diseases. For example, it
was necessary to determine what strategies to use for providing routine immunization services and
how to ensure vaccine potency. Twenty years later,
managers are dealing with many of the same prob
lems but the environment in which they work is
more complex. They need to devise more effective
strategies for vaccinating against diseases at different
stages of control, the number of diseases covered by EPI is expanding, and government systems are
changing. All managers need more sophisticated
skills in forecasting, influencing and responding to,
for example: • changes in vaccines, equipment and procedures;
• problems, e.g. unsafe injection practices; • changes in the organization of health services,
e.g. increasing privatization;
• government reform, e.g. decentralization.
To meet these needs, managers must have access to
information that is accurate and up-to-date and
must have sharper skills in using information to plan
and execute strategies and meet programme goals.
A project to be implemented in eight African coun
tries will: 1) develop a comprehensive set of man-

DEPARTMENT OF VACCINES AND BIOLOGICALS
agement tools and materials enabling public health
personnel to strategically plan, manage and coordi
nate national immunization programmes; 2) con
duct extensive training of vaccine managers at the national and subnational levels, using the tools and
materials developed; and 3) establish an electronic
capacity that links vaccine managers at country level
with each other and with Headquarters in order to
provide immediate management support.
The goal of the proposed project incorporates three
major elements: • the collection and consolidation of informa
tion that can guide managers in decision-mak
ing and is presented in an accessible format;
• the promotion and dissemination of the information to all managers electronically and/or
via reference documents;
• keeping the information timely.
These elements require the development of three
products:
• a reference manual; • an electronic component; • a plan for updating information in the manual.
The reference manual will be the major product of
the proposed project.
7 .9.4 Sustainable outreach
Remote populations are exposed to specific health risks because of a combination of risk factors, such
as low coverage of health services. The aim of sus
tainable outreach services (SOS) is to bring immu
nization and a basket of minimum health interventions to populations physically beyond the reach of
the regular health system. The strategy was first proposed in 1998 and is now well developed. UNICEF
has adopted it as one of the strategies aimed at increasing immunization coverage, especially
among remote populations. The additional inter
ventions to be included in the basket may be determined by:
• the needs expressed by and/or found in the
community;
• the benefits, complications and conditions of including specific interventions;
• the operational constraints on bringing these interventions to the community.
48
The interventions may be of a non-medical nature,
including cattle immunization, sanitation or any
other service meeting community needs and complying with a defined set of operational constraints. SOS
is heavily based on community participation in:
• expressing specific needs; • facilitating the arrival of teams;
• appointing persons as focal points who can be trained to provide simple services on a more
continuous basis with the support of professional health staff making periodic visits.
SOS can be permanent if cost-benefit analyses show that a fixed health structure is not feasible
(e.g. periodic campaigns in Latin America), or tem
porary, exploring the possibilities of and leading to
a fixed structure. The approach is not completely new: lessons have been drawn from a number of
experiences, and SOS can be seen as their synthe
sis, to be applied and adapted in other Regions. All
the examples mentioned below are similar in that
several interventions have been brought to remote
populations:
• village health days in Tanzania; • periodic campaigns in the river area in Ghana;
• permanently rotating teams in Colombia; • periodic visits by health workers and midwives
in Benin, using the opportunity to train persons serving as dracunculiasis focal points;
• community health centres in Mali;
• certain vaccines beyond- the cold chain for Indonesian midwives working in remote
populations;
Figure 25: Diagrammatic representation of how SOS might work in different situations

ANNUAL REPORT 1999
• polio NIDs, based on flexible strategies and community participation, reaching cover
age figures far exceeding those of routine
immunization.
The elements of sustainability and system-building
vital to the development of SOS include strength
ening the capacity of the community to express and
demand needs and manage service delivery/imple
mentation, a sustainable transport management system, and capacity-building through the training
of staff.
SOS does not aim to bring global guidelines or prescriptions to countries, but rather to give support by
providing product specifications and experiences
from elsewhere, thus allowing countries to devise
health systems specifically for remote populations. In
1999, four countries were chosen to implement SOS
pilot projects jointly with UNICEF: Chad, Mali,
Mozambique, and Uganda. A WHO/UNICEF meeting was held in Nairobi to finalize the strategies
and to prepare for the project, which will last 30
months, beginning in 2000. SOS is a dialogue, open
to all suggestions aimed at the improvement of health among unreached populations.
7 .10 Financing
Critical indicators: • Number of countries having had at least one
ICC meeting to obtain financial support for routine immunization services. Current status
= 75/190.
1999 saw a major change in the focus on financing of immunization programmes and the promise of
more funds available, especially for the purchase of new vaccines. V&B financing activities were largely centred on activities for and with GAVI and its Task
Force on Financing. Attention was also paid to immunization costs in actual programmes and to
various financing mechanisms.
A paper on options for a global fund was published. The fund, called the Global Fund for Children's
Vaccines, was set up through GA\11. V&B staff
were involved in this process and helped to develop
a proposal to the Bill and Melinda Gates Foundation which resulted in substantial financial
support. V&B staff participated in the GA\11 Task
49
Force on Financing and collaborated in the devel
opment of a country assessment tool along with
critical indicators for its use.
Costing studies were conducted on immunization
programmes in conjunction with similar studies on
safe injections in several countries. The findings
provided important information about the sources
of funding for immunization, the proportions of
funding provided by countries and donors, and
breakdowns of costs in several types of immuniza
tion delivery situation. A preliminary analysis of costs for introducing new vaccines to countries that
might benefit from the Heavily Indebted Poor Countries initiative (HPIC) was completed and
used as the basis of a paper presented to the GAVI
Board.
Although the new Global Fund will be an impor
tant source of financing it is only one tool for
immunization funding. V&B is collaborating with other GA VI partners to definine the characteristics
of key financing methods for countries.
Typical of the efforts by Regions to fund immunization ,vas the annual intercountry meeting of
EPI managers held in Damascus in June 1999. The meeting was also attended by representatives from
UNICEF's Middle East and Northern Africa
Region and other collaborating agencies, including
Rotary International. Discussions were held on
progress in EPI activities relating to routine
and supplemental immunization, target disease
occurrence and the status of achievement of global goals in Member States. Recent advances and rec
ommendations for the improvement of EPI were
explained and discussed. The impressive progress
towards the eradication of poliomyelitis in the Eastern Mediterranean Region of WHO is a result of extensive efforts of national authorities and the
support provided by the consortium of partners for
polio eradication.
The largest share of human and financial resources
for eradication efforts in the Region has been committed br the ;-.,fember States. WHO/EMRO con
tinued to play a central coordination role and pro
Yided continuing technical and operational support
to all :'vfember Srates. During 1999, eight international staff and over 50 short-term consultants were
deployed in the priority countries that had not
achieved interruption of poliovirus transmission.

DEPARTMENT DF VACCINES AND BIOLOGICALS
About 100 national staff were recruited to support polio eradication activities, particularly AFP surveillance. WHO/EMRO further strengthened its partnership with international agencies and governments supporting polio eradication, particularly Rotary International, CDC, Mr Ted Turner's United Nations Foundation and the governments of Canada, Japan, and the United Kingdom. The central role of WHO/EMRO in polio eradication in the Region is highlighted by the fact that, during 1998 and 1999, voluntary funds amounting to nearly US$ 23 million were channelled through EMRO by partner agencies, mainly for Member States requiring external financial support. EMRO also played a key role in facilitating bilateral support to countries and in raising funds for the purchase of OPV through UNICEF in several Member States. It should be noted with special appreciation that the Council of Arab Ministers of the Gulf has agreed to provide US$ 1.5 million in support of polio eradication in the Region. It is hoped that this contribution will be followed by similar contributions from Regional organizations.
The meetings of the lnteragency Coordination Committee at both national and Regional levels have led to the identification and bridging of shortfalls in funding. Joint planning by national authorities, WHO and UNICEF has been instrumental in the identification of external support required to address national needs for polio eradication. The outcome of this dose collaboration was the development of a three-year plan for 2000-2002, representing a comprehensive budget for polio eradication in the priority countries and forming the basis of fund-raising for countries in need of external support.
7 .11 Health sector reform
Health reforms, taking place in most countries around the world, are changing the way health services are delivered. In 1998-99, EPI commissioned studies that were conducted in Kyrgyzstan, Uganda, and Zambia in collaboration with USAID/ BASICS. These studies aimed at drawing general lessons from the reform process, reviewing EPI in relation to the health reform process, and developing a reference guide for national immunization
programmes during health reforms.
50
No single model encapsulates health reform. It sometimes involves radical constitutional and structural changes in health services and other sectors. The reforms do not occur in a linear fashion; usually there are multiple streams of change. There are, however, similarities from which lessons can be drawn for strengthening immunization services. These lessons can be used to devise approaches ensuring that services of adequate quality are provided effectively, not only in reformed health systems but also during the process of change.
Health reform should be seen as an occasion and opportunity for reanalysing immunization priorities and policies. When this is done, due consideration must be given to financial and operational parameters.
A meeting entitled "Health Sector Reform and Priority Health Interventions: the Case of Immunization Services" was held in Washington DC on 15-16 November 1999. It was organized jointly by V&B/Health Technology and Pharmaceuticals, and the Cluster of Evidence and Information for Policy, both of WHO Headquarters, and the Division of Vaccines and Immunization and the Division of Health Systems and Services Development, both of PAHO.
The expected outcomes of the meeting included the identification of key issues in health sector development-reform, a review of the health sector development-reform perspectives from development partners, and a discussion on key steps and best practices whereby countries and regions can sustain effective immunization coverage and quality of services during the health reform process. Country case studies were presented which highlighted the key issues that immunization services are facing in a rapidly changing socioeconomic environment. Excerpts of the major recommendations are presented below.
• A posltlon paper should be prepared that includes information on best practices for priority health interventions using the case of immunization programmes as an example within the context of major health systems development issues (e.g. financing health sector reform, policy and advocacy).

ANNUAL REPORT 1999
• Fact sheets will be prepared to assist countries and their development partners to facilitate
and guide discussions and dialogue on health
systems development and priority health interventions.
• WHO and development partners should work with countries to ensure that the assessment of
priority health interventions incorporates
essential issues relating to health systems devel
opment.
• Countries should invite development partners
to participate in joint planning processes for the health sector, including priority health interventions and their financing. The latter
should include ensuring that the financial
envelope for immunization programmes is part of the overall financial framework. This should
be the first step in ensuring that national priorities are based on evidence and reflect peo
ple's health needs. Development partners
should ensure flexibility in financing priority health interventions and should avoid ear
marking.
• Countries and development partners should ensure that national immunization plans
become an integral part of national health sec
tor development plans and that the indicators
of performance of national immunization plans form a key part of the overall monitoring
system for the sector.
• Countries and development partners should
identify key indicators for monitoring the per
formance of the overall health system. Immunization indicators should be a part of
these indicators.
• Countries and development partners should work to ensure that the capacit:y for specific
technical skills and functions, planning and management are strengthened at all levels
so that they help all units to effectively and efficiently implement priority health interven
tions such as immunization.
• Countries should focus on developing managerial capacity at the district level, and this should
include integrated in-service training and the
development of performance incentives.
AMRO is monitoring the progress of health reform and decentralization in the Americas through its
evaluations of national immunization programmes.
In the past year, evaluations were performed in the
51
Dominican Republic, Ecuador, Paraguay, and Peru.
Extensive interviews conducted at the central and
local levels, as well as the political, managerial and beneficiary levels, allow AL\1RO to obtain a com
prehensive view of a country's national immuniza
tion programme within the context of ongoing
strucmral processes.
lessons learnt from these exercises point to changes
in some of the key instruments used by immuniza
tion programmes and to the addition of new instru
ments for planning, financing and delivering immunization programmes. National plans of action, for example, have been used as a template
for country planning, monitoring and evaluation of
national immunization programmes at the central
level. The plans, prepared for five-year periods, outline objectives and activities and provide estimates
of human and financial needs, investments and
sources of funding. The process of health sector
reform and decentralization is leading to changes in the development and implementation of these
plans, the make-up of partners and the funding
mechanisms used.
In Peru the Ministry of Health seeks to strengthen
the decentralization of basic health services through Committees of local Administration by
increasing the participation of communities,
municipalities and local health entities in the plan
ning, management and monitoring of health pro
grammes and services. The role of these commit
tees is to work with health providers to develop
local health plans, determine resources and monitor expenditures and the provision of health ser
vices. Ecuador is forming a system of decentralized health care networks to handle the delivery of
essential health services, especially maternal and
child health services. In Bolivia the Departmental Health SerYices are the main mechanism for
improving the coverage and quality of health services and developing health programmes that
respond better to the needs of the population at the local level. The results are measured by means of
specific indicators included in performance agree
ments, these being contracts signed between cen
tral health authorities and state governors as part of
the process of decentralization. The contracts are
being used in decision-making on resource allocation benveen the central and local levels.
DEPARTMENT DF VACCINES AND BIOLOGICALS
Table 4: Functions of immunization services and levels at which the responsibilities should be held
AMRO's collaboration with ministries of health has
been geared towards the clarification of roles, the
accountability of new partners, and assurance of the
delivery of immunization programmes that are effective and of high quality. Mexico, for example,
is showing positive results in the sharing of respon
sibility between vaccination and epidemiological
surveillance at the state level and planning, priority
setting and evaluation at the national level. Bolivia is also sharing roles and responsibilities at the sub
national level with departments and municipalities,
which, in turn, share roles and responsibilities
among themselves.
52
AMRO continued its dialogue with countries in order to ensure that clear mechanisms were in place
for transferring and managing financial and human
resources, and for managing the planning and implementation of the surveillance and delivery
components. Furthermore, advocacy will continue
to incorporate immunization indicators, especially
DTP3 coverage and drop-out rates, in performance
agreements. Bolivia and Nicaragua, for example, have included the indicator of DTP3 coverage in
their performance agreements.

ANNUAL REPORT 1999
7 .12 Immunization safety priority project
7.12.1 Global activities
Immunization programmes are among the most effective and safest of all health interventions. Yet
their implementation on a worldwide basis faces
many challenges. Immunization safety must be considered by those advocating the use of vaccines to
lessen the burden of vaccine-preventable diseases.
Adverse events following immunization (AEFis)
have been known to occur since the first vaccines
were administered. These events may be local (at the site of injection) or generalized. Common
adverse events are mild while certain rare events may be more serious. Some of them are caused by the vaccines themselves but many eYents reported as
being related to vaccines are actuallr coincidental,
occurring for other reasons. Countries are adminis
tering more doses of vaccine than ever before. Higher educational levels of parents and the greatly
increased speed and sophistication of communication have helped to produce a ne,v and sometimes
extremely hostile climate for vaccines.
53
Formerly, the first inclination after an adverse event
was to blame the quality of the vaccine that had
been administered. Because of the need to assure
and improve vaccine quality, WHO and the NRAs have devoted much energy and resources to work
ing with vaccine producers in order to enhance
their compliance with good manufacturing prac
tices, thus ensuring the highest possible quality of
vaccines. The availability of vaccines of good quality is, however, not enough. It has been reported that
up to a third of vaccine injections are not given in a
way that can guarantee sterility. Furthermore, there have been reports of mistakes in programmes.
The main target of the priority project is to estab
lish a comprehensive system ensuring the safety of all vaccines given in national immunization pro
grammes by the year 2003. To achieve this an over
all culture of safety has to be developed so as to
encourage prevention, early detection and quick
response ro adverse events related to immunization programmes and thereby to lessen their negative
impact on health and on the programmes.
To coordinate these activities, WHO has earmarked
human and financial resources and has established
strong collaboration between its Headquarters and
Regional Offices. An internal cross-cluster coordi
nation group meets regularly to share information
and monitor progress.
The principal areas of activity of the project are:
• ensuring vaccine safety at all stages from clinical trials to point of use;
• research into and development of safer and
simpler vaccine delivery systems; • expanded access to safe and effective delivery
technologies and their disposal;
• identification and management of risks related to immunization.
The first three areas are concerned with prevention, ,vhile the fourth involves the early management of events . .tvfuch effort is being dedicated to defining
proper methods and indicators for assessing all the
elements of immunization safety so as to monitor
progress. In themselves, immunization safety assess
ments will be critical for highlighting problems and paving the way ro intervention. The third of the
above areas of activity is also one of concerted
action within the common strategic framework of

DEPARTMENT DF VACCINES AND BIDLDGICALS
Figure 27: Participants in the "Partnership-building with the media" workshop, Islamabad, September 1999
the newly launched Safe Injections Global Network
(SIGN), the mission of which is to achieve safe and
appropriate use of all injections throughout the
world.
The project emphasizes the importance of advocating safety and building capacity at national level. It supports the implementation of a series of training activities, the development of a standard set of
information documents, and the fostering of collaboration between various interested parties at the global, national (particularly between immuniza
tion managers and NRAs) and subnational levels.
Two committees have been set up to guide the work
of V&B in this area: the external Steering
Committee on Immunization Safety has been creat
ed to provide technical and scientific advice on
strategies, activities, constraints and requirements of
the priority project, and the global Vaccine Safety
54
Advisory Committee has been established to
enhance WHO's ability to react to allegations of
adverse events related to immunization by provid
ing impartial scientific advice of high quality to WHO on specific issues related to vaccine safety as
they arise.
The Steering Committee on Immunization Safety
met for the first time on 25-26 October 1999. The importance of delivering safe vaccines of high quality was underlined, as was the need to concentrate
on prevention and safety assurance during all stages
of development and at the point of use. Also highlighted was the importance of prompt moni
toring and management of AEFis and of strength
ening NRAs and fostering proper collaboration
between vaccine NRAs and managers of immuniza
tion programmes. Among the recommendations
made were the following:

ANNUAL REPORT 1999
• The appropriate levels (e.g. ministers through the World Health Assembly and the Regional Committees) should be targeted as part of the
strategies for advocacy.
• All costs of safe delivery of vaccines, including
the disposal of residual waste, should be
encompassed in strategies for financing immu
nization services. It is important to promote
the concept of the cost of the safely immunized child.
• Immunization safety should be emphasized as a core function of immunization systems during the process of health services reform.
• Capacity for assessing and managing immunization safety should be enhanced at all levels.
• WHO, UNICEF and national immunization
programmes should expand access to training as a core element of immunization safety.
• A standard assessment tool of immunization safety should be developed for use by national
managers and other stakeholders.
• National immunization plans should include policies on waste management.
• Early detection, proper response and timely management of vaccine safety concerns, in particular the correction of programmatic errors,
should be implemented.
Because it was recognized that increased public
interest in immunization safety had altered the envi
ronment in which programme managers operated, specific media training workshops were held in the
Eastern Mediterranean Region. The holding of fur
ther workshops during the coming biennium is under consideration in all WHO Regions. Major
progress has been achieved in the area of training for
the monitoring and management of immunization safety, with the development of a curriculum on
immunization safety monitoring and management
as part of GTN. A course was held in Cape Town and training should be expanded during 2000.
Many activities were undertaken to improve the safety of injection devices. WHO's preferred syringe
for mass immunization campaigns is the auto-disable (AD) syringe. Overall, this syringe helps to
decrease the transmission of bloodborne pathogens
between patients by preventing reuse and resale,
both common practices in developing countries. However, AD syringes lack protection for the nee
dle and do not eliminate the hazards of sharp waste
in the environment. Furthermore, they are still
more expensive than other types of syringe,
55
although an effort is being made to reduce their cost
through technology transfer. WHO is contributing
to the process of technology transfer by means of manufacturer assessments, liaison between intellec
tual property owners and manufacturers, market
assessment in collaboration with health ministries,
the provision and modification of specifications,
and laboratory qualification testing. Studies to
assess the comparative (internal/external) costs of different injection strategies (disposable, sterilizable
and AD) have been performed in three African
countries. A joint WHO/UNICEF statement on the safety of all injections related to immunization
recommends that only AD syringes should be used in national immunization programmes.
Other strategies for improving immunization safety
that are under investigation as part of the project include:
• the use of monodose, prefilled vaccine presentations integrated with the injection device;
• the use of multidose injection systems, such as jet guns drawing vaccine from multidose vials
of vaccine;
• safe disposal of injection equipment.
7.12.2 African Region
Although a majority of past cases of reported AEFis
were mild and treated at the peripheral level, a few
serious cases necessitating vaccine withdrawal
and/or detailed investigation were also reported.
Examples are widespread BCG lymphadenitis in Uganda and Zimbabwe, and death after mass cam
paigns against measles in Zimbabwe.
The major needs for the monitoring and management of AEFis include:
• responding to field reports of inadequacies attributable to vaccines and/or immunization service delivery;
• reducing the heightened level of suspicion and rumours surrounding immunization during mass campaigns, and boosting confidence in
immunization in general;.
• establishing an effective post-marketing surveillance system that, in addition to meeting
safety concerns, facilitates the monitoring and
assessment of vaccine efficacy during field use.
An essential requirement of EPI is that every injec
tion be given safely with a sterile needle and syringe.
Although EPI injections are recognized as being

DEPARTMENT OF VACCINES AND BIOLOGICALS
among the safest, there are numerous studies docu
menting unsafe immunization injection practices in
Africa.
For countries where national data were available
(Table 8), 18-60% of health centres did not meet
sterility standards and 25-55% recorded abscesses.
Factors contributing to the failure to achieve 100%
compliance with requirements include a lack of
knowledge, the aging of sterilization equipment,
shortages of spare parts, equipment, needles and
syringes, and inadequate training and supervision.
AD syringes are recommended for all immunization
activities. The use of sterilizable syringes is a safe
and cost-effective strategy for ensuring safe injec
tion. However, time-steam-temperature (TST)
spots, which are very effective indicators of ade
quate sterilization, are not widely used in the
Region. The waste disposal problems associated with AD syringes are being addressed.
Current issues related to the quest for safe injections
include the following.
• Assuring safe injections appears not to be a priority in national programmes, despite the
availability of adequate technology and
resources for this purpose.
• Methods for the routine monitoring of injec
tion safety have not been implemented.
7.12.3 Region of the Americas
The Region of the Americas continues to work with
countries to improve safe injection practices. A
major impediment remains the lack of adequate safety boxes to collect properly used injection
equipment. AMRO is emphasizing to managers of national immunization programmes the dangers to
health workers of needle-stick injuries resulting
from the recapping of needles.
AMRO's Technical Advisory Group Meeting, held in Canada in April 1999, recommended the follow
ing actions to secure safe injection practices:
• single-use auto-destruct syringes should be used;
• all health care workers should be informed about the danger of recapping needles;
56
• funds should be provided for the procurement of sufficient syringes and safety boxes, for the
supervision and documenting of safe syringe
disposal, and for the proper disposal of used
equipment;
• support should be given for developmental studies on needle-free injection devices.
Countries are starting to purchase AD syringes but
the cost is still considered too high. AMRO is working to improve the advocacy of the use of AD
syringes and to stop the recapping of used needles by health workers. Much remains to be done to
make this advocacy campaign effective. AMRO will intensify its collaboration with countries in the
Region, especially in the area of supervision, with a
view to improving safe syringe practices, and will urge countries to allocate more resources in their
budgets for the introduction of products such as
safety boxes and small clinic incinerators.
7.12.4 Eastern Mediterranean Region
Notwithstanding the fact that vaccination is one of
the safest health interventions and that the risks of
vaccine-related adverse events are extremely rare
when set against the risk of complications arising
from natural disease in unprotected children, such
events, if not properly addressed, could seriously undermine public confidence in immunization.
The topic of adverse events was considered during
several intercountry meetings. Oman established a
surveillance system in 1996 and is reporting regularly to the Regional office. Egypt and Syria started
adverse events surveillance systems in mid-1998. A
series of intercountry workshops on AEFis were organized with a view to developing national plans
of action for the establishment/strengthening of adverse events surveillance. The first workshop was
held in December 1998 and the other two were
held in Cairo in February 1999 and in Oman in March 1999. National plans were developed for the
establishment/strengthening of adverse events surveillance systems in each Member State. Systems are functioning in Bahrain, Egypt, Kuwait, Oman,
Saudi Arabia, Syria, and Tunisia.

ANNUAL REPORT 1999
Late in 1998 reports about adverse events that were
considered to be related to vaccination activities
were received from Egypt and Jordan. These events were investigated and it was concluded that
although they were related to immunization there
was no direct association. It was also noted that
these events reflected negatively on immunization
activities and that the media mishandled the inci
dents. The national EPI managers faced numerous
difficulties in dealing with the events and the reac
tions of the media and the public. In response to
this situation,two workshops, each lasting two days, were conducted during 1999 with the aim of
strengthening the capabilities of the national EPI
managers in these areas.
7.12.5 European Region
There is an acknowledgement of the increasing
importance of the adverse events in the management
of national immunization programmes. In future
more opportunities for discussion of surveillance
techniques for detecting adverse events, analysis of data, and handling of risk communication in this
regard will be considered. The role of the media and
our relationships with them need to be included.
7 .12.6 South-East Asia Region
Injection safety and waste disposal are top priorities
for V&B/SEARO in terms of providing technical
support to Member States. Furthermore, this pre
sents an excellent opportunity to promote sustain
ability in systems development. A Regional plan of action is being developed to refocus attention on a
public health problem that requires the involvement of several curative and preventive disease
strategies. In the meantime, SEARO is promoting
the bundling of vaccines with equipment that helps to ensure safe injection and waste disposal. A prior
ity activity for 2000 will be an intercountry planning workshop to be held in collaboration with
WHO Headquarters. Other opportunities for sys
tems development include strengthening the man
agement and replacement of the cold chain. To this
end, SEARO has employed a full-time cold chain
consultant. A major challenge is that none of the countries has an adequate plan for converting to a
CFC-free cold chain.
57
The global movement for the strengthening of immunization activities has brought the issue of
cold chain management and equipment replacemem into focus. V&B/SEAR was actively involved
with the World Bank in formulating strategies for
strengthening immunization activities and the cold chain system in India. V&B also supported a num
ber of cold chain technician training courses using
a CFC-free system in Bangladesh and India.
Intensified NIDs in a number of countries called
for the strengthening of the cold chain system in areas of greatest need. While other agencies such as
UNICEF provided cold chain supplies and equip
ment to India, V&B/SEAR took the opportunity to conduct a rapid cold chain assessment in Uttar
Pradesh and Bihar, to ensure the timely installation
of the equipment, and to train local cold chain
technicians.
7.12.7 The Safe Injection Global Network
Because injection safety is essential to immuniza
tion programmes, efforts to achieve safe injections initially focused on the field of immunization.
Equipment developed for introduction in the field
included plastic sterilizable syringes (1982), steam
sterilizers (1984), AD syringes (1985), and TST indicators (1991). In addition, training materials
and injection survey materials were developed.
At the end of the 1990s, public health professionals
recognized that the safety of immunization injections could not be addressed in isolation. Efforts
had to reach beyond the field of immunization so as
to address therapeutic injections, these representing the majority of injections administered worldwide.
Simultaneously~ evidence became available suggesting that, in a number of countries where hepatitis B
virus or hepatitis C virus infections were highly endemic, the overuse of therapeutic injections com
bined with unsafe injection practices to account for
a large proportion of new cases of infection. Preparatory work in ATT resulted in public health
professionals from various backgrounds sharing a
common interest in a safe and appropriate use of
injections. On 4-5 October 1999 these groups
joined forces during the initial meeting of the Safe Injection Global Network (SIGN). A secretariat
based in the Blood Safety and Clinical Technology

DEPARTMENT OF VACCINES AND BIOLOGICALS
Department now coordinates this network because:
• 95% of injections administered each year are given for therapeutic purposes;
• injection safety fits well with blood transfusion safety in the prevention of infections from
blood-borne pathogens through all potential
percutaneous exposures.
WHO's Immunization Safety priority project sup
ports the initiative provided by SIGN for achieving safe immunization injections and is collaborating
closely with the SIGN secretariat. D
Figure 27: Disposable syringes and needles waiting to be re-used without sterilization in a container of tepid water
58

ANNUAL REPORT 1999
[I] 8. Accelerated disease control
8.1 Progress towards global polio eradication
The global effort to eradicate polio is the largest pubic health initiative in history. It was launched in 1988 by the World Health Assembly with the goal of eradicating polio while strengthening capacity to control other major childhood diseases. Extraordinary progress has been made towards achieving polio eradication by 2000 and global certification of eradication by 2005.
In 1988, polio existed in over 125 countries on five continents, and more than 350 000 children were paralysed that year. By the end of 1999 the number of polio-infected countries had fallen to 30
Figure 28: Polio eradication progress, 1988-1999
...
59
(Fig. 28), polio had been eliminated from three more continents, and the number of reported cases was 6659 (the estimated maximum number was 20 000). When polio is eradicated and polio immunization ceases the world will save US$ 1.5 billion per year.
Status of polio transmission
The number of countries in which polio was known or suspected to be endemic decreased from 50 in 1998 to 30 in 1999. Type 2 poliovirus (one of three types) is on the verge of extinction, the only known foci being in northern India. Polio incidence declined to the lowest levels ever in 1999, although reported cases increased slightly to 6 659 because of
• I
6 659 * cases *as of 21 February 2000

DEPARTMENT DF VACCINES AND BIOLOGICALS
improvements in surveillance and a large outbreak in Angola. Polio was eliminated from the fifth of the seven continents, more than a year having elapsed since the last case in Europe.
Polio-free Regions
Three of the six WHO Regions, representing 115 countries, have been polio-free for more than a year.
Region of the Americas: The last case of polio
occurred in 1991. During 1999 a polio outbreak in Angola appeared to threaten the polio-free status of the Americas when two suspected cases were reported in Brazil. Neither case was confirmed.
Western Pacific Region: The last case of endemic
polio was reported in 1997. A case in China in 1999 was associated with a poliovirus imported from India. The implications for Regional certification will be considered during 2000. No Region is safe from polio until all Regions are polio-free.
European Region: The last known case of polio
occurred in Turkey during November 1998.
Regions where polio is still endemic
African Region: Polio is endemic or probably
endemic in 20 of the 46 countries in the Region. In 1999, 2718 cases were reported and 218 of them were laboratory-confirmed (Table 5). Poliovirus circulation was confined largely to the Horn of Africa, West Africa and Central Africa. The most intense transmission occurred in Chad, the Democratic Republic of Congo, and Nigeria. Following is a summary of the situation in the
Region by countries in special circumstances and by epidemiological blocks.
Countries in special circumstances
Nigeria reported 951 cases during 1999, including 83 laboratory-confirmed cases. Intense polio transmission continues in nearly all parts of the country. Nigeria is a major reservoir of poliovirus and exports the virus to countries throughout West and Central Africa.
Angola reported 1103 cases and 89 deaths when a polio epidemic swept the country early in 1999. Displaced children who had never been vaccinated were at the highest risk during this outbreak.
The Democratic Republic of Congo, which reported 45 cases in 1999, is a major reservoir of poliovirus. The reported cases understated the actual incidence because surveillance was inadequate in most parts of the country. Poliovirus transmission in the Democratic Republic of Congo represents a continuing threat to the apparently polio-free status of neighbouring countries in East Africa.
Ethiopia reported 125 cases of polio in 1999 but none were laboratory-confirmed. Despite the lack of poliovirus isolates the real epidemiological situation remains unclear because surveillance sensitivity and laboratory capacity are inadequate.
Epidemiological blocks
Ail 14 countries of the southern Africa block appear. to be polio-free. The last confirmed case was reported from Madagascar in 1997. However, there
Table 5: Reported AFP cases, surveillance quality indicators and confirmed poliomyelitis cases 1998-1999, by WHO Region*
60

ANNUAL REPORT 1999
is a high risk of unrecognized low-level polio trans
mission in Madagascar, Malawi, and Mozambique in particular, because surveillance remains inade
quate. The cessation of NIDs in some southern
African countries coupled with poor routine OPV
coverage increases the risk that polio may become
re-established.
The East Africa block countries of Burundi,
Kenya, Rwanda, Tanzania, Uganda, and Zambia, appear to be polio-free. The last confirmed cases
occurred in Uganda in 1996 and in Tanzania and Zambia in 1995. Polio transmission continued to occur at low levels in Eritrea, which reported seven
cases in 1999. However, all seven countries in the
block are sat risk of importation and/or re-estab
lishment of polio because they border an area of
endemicity and have low coverage with the three childhood doses of O PV
The Central Africa block comprises six countries.
Intense polio transmission continued in Chad,
which reported 99 cases of which 34 were laborato
ry-confirmed; 66% of AFP cases for which specimens were collected proved positive for poliovirus
in that country. Cameroon and the Central African
Republic appeared to have low levels of polio transmission, but remained at risk because of their prox
imity to countries with high transmission levels.
Although Congo, Equatorial Guinea, and Gabon
had no virologically confirmed cases, surveillance
was extremely weak and there was a very high risk
of unrecognized transmission.
Polio transmission continues in the West Africa block, which comprises 16 countries. It is most intense in Benin, Liberia, Niger and, probably,
Sierra Leone. Ghana, Mali, Senegal, Sierra Leone,
and Togo reported low levels of transmission involving laboratory-confirmed cases. Because of to low
levels of poliovirus transmission and good AFP sur
veillance quality, six countries are poised to enter the mop-up phase of eradication (Cote d'Ivoire, Ghana, Guinea, Mali, Senegal, and Togo). Sub
optimal AFP surveillance quality limited the detec
tion of probable virus in Burkina Faso, Gambia,
and Guinea-Bissau.
Eastern Mediterranean Region: In 1999, 829
cases were reported in the Eastern Mediterranean
Region (Table 5), including 449 laboratory -con
firmed cases. Polio transmission continues to be
61
intense in Pakistan, which reported 466 cases and is
a major reservoir of poliovirus. There was widespread circulation in Afghanistan, where 141 cases
were reported and rhe virus had marked genotypic
similarity to that in Pakistan. Poliovirus from
Afghanistan was epidemiologically linked to the
three polio cases reported in Iran during 1999.
Although t\vo of these cases appear to have been
attributable to imported viruses, low-level endemic
transmission of poliovirus may be continuing. No
cases were reported from Iraq in 1998 but in 1999
there was a widespread outbreak in the country, involving 127 reported cases, including 72 labora
tory-confirmed cases.
Sudan reported 51 cases and Somalia reported 16
cases. Egypt has made substantial progress, report
ing irs lowest transmission ever, although focal transmission continued in Assiut and Minya in the
Upper Nile area.
South-East Asia Region: In 1999, 3111 polio cases
were reported, including 1072 laboratory-confirmed cases from four countries (Table 5). There
were 2628 reported cases in India, a 40% decline from 1998; intense transmission continues in the
states of Bihar and Uttar Pradesh, which are the
only known remaining foci of poliovirus type 2 transmission. Polio transmission has markedly
decreased in the southern part of India, which is
now entering the mop-up phase of eradication.
Bangladesh reported 335 cases in 1999. Despite this large number, genetic typing demonstrated that several poliovirus lineages were nearing extinction
and that rhe biodiversity of the virus had decreased substantially. Nepal reported only one laboratory
confirmed case in 1999 and appeared to have focal
transmission only along its border with India. In .i\1yanmar an imported case was detected and rapid mass vaccination was subsequently carried out. No
additional cases have been reported. The polio situ
ation in the Democratic People's Republic of Korea remains unclear because of a lack of surveillance
and laboratory data.
Status and quality of strategy implementation National immunization days
• Full NIDs or subnational immunization days
(SKIDs) were conducted in 83 countries,

DEPARTMENT OF VACCINES AND BIOLOGICALS
reaching more than 470 million children (Fig. 30). Full NIDS were conducted in 70 countries, often with SNID rounds in high-risk areas. In India alone, over a billion OPV doses were distributed during four NIDs and two SNIDs (October 1999 to March 2000). Thirteen mostly poliofree countries in the European Region and the Western Pacific Region conducted SNIDs only.
Figure 29: Accelerated polio immunization efforts, 1999-2000
• Vitamin A supplementation was given in 50 of the 83 countries conducting supplementary immunization activities during 1999.
1
,
• In order to accelerate polio eradication activities the number of NID rounds was increased in reservoir and other priority countries (Fig. 29). Afghanistan and India conducted four rounds of NIDs, and India conducted two addi-
Extra 'intensified' NIDs
II NIDs + SN IDs or 'Mop-ups'
tional SNID rounds early in 2000. Three rounds of NIDs were conducted in Angola and the Democratic Republic of Congo. However, many children were not immunized in Angola as a consequence of internal disturbances.
• The quality ofNIDs and SNIDs was improved by strengthened planning at provincial and district levels and by extensive use ofhouse-tohouse vaccination strategies. These intensified NIDs and SNIDs were held in Afghanistan, Nigeria, and Pakistan, with resulting increases of up to 50% in the number of children reached in some provinces.
• The quality ofNIDs was threatened by a global OPV shortfall that resulted from uncertainty of supply, cancelled shipments and rescheduling of major orders. Many countries were adversely effected by the uncertainty of the vaccine supply, including cancelled or delayed rounds in Chad and Ghana, inconsistent
62
presentations of the vaccine (e.g. Spanish labels in non-Spanish-speaking countries, vials with 10 instead of20 doses), and the postponement of routine orders.
• The evaluation of the quality of NIDs was improved by monitoring the number of children vaccinated for the first time (zero-dose monitoring), process evaluations, and limited use of coverage surveys. However, high-quality AFP surveillance remains the best means of evaluating the quality and effectiveness of NIDs and SNIDs.
Acute flaccid paralysis surveillance
AFP surveillance is used to detect polio cases. Certification standard is reached if the non-polio AFP rate is> 1/100 000 population aged< 15 years, if adequate specimens are collected from 80% or

ANNUAL REPORT 1999
more of AFP cases, and if the specimens are evaluated on a timely basis in accredited laboratories (Fig 31). High-quality surveillance was achieved in the Western Pacific Region, the European Region, the South-East Asia Region, and the Region of the Americas. At Regional and country levels, delay in achieving surveillance of certification standard can result in late detection of polio-infected areas. High priority must therefore be given to rapidly achieving this standard.
Regions where polio is endemic
• The African Region improved surveillance dramatically, the non-polio AFP rate more than doubling from 0.30 in 1998 to 0.70 in 1999. The increase in AFP surveillance was the result of extra funding for this purpose late in 1998, the initiation of active surveillance at the provincial level in some countries, the support of STOP teams in some countries, and the arrival of transport for active surveillance in 1999. However, adequate specimens were collected in respect of only 31 % of AFP cases. Priority countries for surveillance improvement include Burundi, Ethiopia, Madagascar, Malawi, Mozambique, and Rwanda. (Fig. 30).
• In the Eastern Mediterranean Region the non-polio AFP rate increased from 0.88 in 1998 to 1.13 in 1999. Among the six polioendemic countries, Egypt, Iraq, and Pakistan achieved a non-polio AFP rate > 1; for Afghanistan the figure was close at 0.95. Somalia and Sudan reported rates of 0.79 and 0.52 respectively. Over the Region as a whole the percentage of cases with adequate specimens rose slightly from 64% in 1998 to 69% in 1999. The continued surveillance achievements in Afghanistan, Somalia and Sudan demonstrate that high-quality surveillance can be implemented even in the most difficult circumstances.
• The South-East Asia Region increased its non-polio AFP rate from 1.25 in 1998 to 1.52 in 1999. Two of the four polio-endemic countries, India and Nepal, achieved the standard for reported non-polio AFP rates with values of 1.8 and 1.9 respectively. Nepal substantially improved surveillance, its non-polio AFP rate
increasing from 0.41 in 1998 to 1.91 in 1999.
63
Bangladesh also improved its AFP surveillance, from 0.33 in 1988 to 0.63 in 1999. AFP surveillance in the Democratic People's Republic of Korea remains inadequate. For the Region as a whole the percentage of cases with adequate specimens increased from 60% in 1998 to 71 % in 1999. During 2000 the priority countries for improving surveillance will be Bangladesh, the Democratic People's Republic of Korea, and Myanmar (Fig. 30).
Mop-up immunization campaigns
Mop-up is the final strategy for polio eradication where high-quality AFP surveillance information is used to identify remaining pockets of virus transmission. Intense house-to-house immunization activities are then targeted to eliminate the final chains of virus transmission. During early 1999, mop-up was conducted in south-east Turkey and neighbouring provinces of the Islamic Republic of Iran, Iraq, and Syria following a case reported in Turkey in late 1998. No additional cases have been reported since then in Iran, Syria, or Turkey.
NOTE: Although house-to-house immunization was conducted during NIDs or in response to a detected case in many countries during 1999, this was intended to improve the quality of activity and reach previously unreached children. It did not meet the criteria of classic mop-up to stop the final chains of poliovirus transmission.
Status of the Global Polio Laboratory Network
The Global Polio Laboratory Network was fully operational in all the WHO Regions, comprising a total of 148 laboratories, including 126 national or subnational laboratories, 16 Regional reference laboratories, and six global specialized laboratories (Fig. 32). By the end of 1999, 108 laboratories (73%) were fully accredited, 16 (11 %) were provisionally accredited, 14 (9%) had been reviewed but could not be accredited, and 10 (7%) remained to be reviewed. Only the Democratic People's Republic of Korea still lacks an accredited laboratory or access to an accredired laboratory outside the country.
Standard guidelines, procedures, cell lines and reagents have been introduced in laboratories at

DEPARTMENT OF VACCINES AND BIOLOGICALS
Figure 30: Endemic or recently endemic ciountry priorities for improving surveillance in the year 2000
■ Good quality surveillance or marked improvement*
Inadequate surveillance*
• Data as of February 1000, WHO/HQ
•
Figure 31: Global laboratory network for polio eradication, 2000
* Specialised reference laboratory e Regional reference laboratory A National/Sub-national laboratory
• Proposed National laboratory
64

ANNUAL REPORT 1999
each level of the network. During 1999, almost all
stool specimens from AFP cases were processed in
WHO-accredited laboratories. Over 50 000 speci
mens were processed for viral isolation, and over 3000 poliovirus isolates and over 10 000 non-polio
enterovirus isolates were obtained; serotyping and
intratypic differentiation were carried out on all
poliovirus isolates, and genomic sequencing infor
mation was provided on nearly all programmatical
ly important wild poliovirus isolates. There were marked increases in laboratory workloads between
1997 and 1999. Thus in India the number of specimens increased from 1570 in 1997 to 15 800 in 1999, a tenfold increase, and in Nigeria the corre
sponding numbers were 7land 923, a 13-fold
increase.
At the end of 1999, 123 (83%) laboratories had
international telephone or fax lines and/or access to e-mail, but 25 (17%) continued to have inadequate
communications. Arrangements are being made to
Figure 32: Polio-endemic countries and low OPV-3 coverage
The problem
D Known or probable poliovirus at end 1998
(millil Very high risk
65
ensure that wild-type poliovirus isolates are being
shipped promptly and frequently to specialized laboratories with the capacity to sequence isolates.
Routine immunization
Both reported and survey-confirmed routine
immunization coverage with OPV3 is low and
stagnating in the remaining priority countries. ImproYements in routine immunization are
urgemly needed. Efforts to accelerate polio eradi
cation proYide a useful opportunity to boost routine immunization, strengthen EPI target disease
surveillance together with AFP surveillance,
improve the cold chain, and train health workers
and middle-level programme managers. The
absence of reliable basic immunity to polio through routine immunization is one of the main
reasons underlying the need for additional nationwide immunization campaigns (Fig. 32).
The challenge
□ OPV3 <80% in large areas or nationwide

DEPARTMENT DF VACCINES AND BIOLOGICALS
Optimizing the impact of polio eradication on health systems
In 1998 the Forty-first World Health Assembly committed WHO to the goal of polio eradication by the year 2000 "in ways which strengthen national immunization programmes and health infrastructure". WHO and partner organizations, have continued working to ensure that polio eradication activities complement and support efforts to strengthen routine health services. In December 1999, WHO convened a meeting entitled The Impact of Targeted Programmes on Health Systems: a Case Study of the Polio Eradication Initiative, the key elements of which are outlined below.
• WHO, with support from USAID, DANIDA, NORAD and DFID, initiated a study in 1997 to develop a methodology and country case studies in the Lao People's Democratic Republic, Nepal, and Tanzania. These studies found both positive and negative impacts of polio eradication activities, and it was concluded that, with better planning and objectives, positive impacts could be increased and negative ones could be reduced.
• The evaluation of the Pulse Polio Immunization Programme by The All India Institute of Medical Sciences indicated that the polio eradication initiative had strengthened management capacity, improved social mobilization, and increased confidence in the health care system. It was recommended that there should be better planning in order to minimize the disruption caused by NIDs.
• A study funded by USAID found that the implementation of polio eradication activities was not associated with a decrease in funding for routine EPI in Bangladesh, Cote d'Ivoire, and Morocco. Indeed, overall funding for immunization activities increased.
• A report on lessons learnt in the development of the global polio eradication network concluded that the principles of quality assurance and laboratory accreditation used in the laboratory network could be used to improve the quality of other health programmes.
• A UNICEF study in Benin and Niger found no strong evidence on the impact of the polio eradication initiative on routine coverage, but recognized that opportunities to link polio
66
eradication with other programmes and to strengthen EPI had been missed.
• There was broad recognition that NIDs had served as a vehicle for Vitamin A supplementation. In the African Region, vitamin A supplementation had increased more than fivefold since NIDs were introduced in 1996.
Reported negative impacts of polio eradication activities include disruption of routine EPI work and of other health services, although there are few reliable quantifiable data on these matters. The effects could be reduced or avoided by better planning in which the focus on routine immunization was renewed, by linking AFP surveillance to surveillance for other diseases, and by using training and supervision for the polio eradication initiative as an opportunity for other health services. Other recommendations from the WHO meeting included the following.
• A matrix framework of indicators developed for the country case studies should be distributed as a simple planning and assessment tool for country managers.
• A state-of-the-art paper should be drafted, assembling documentation on the impact of polio eradication.
• Efforts should be initiated to document current gaps in knowledge of the impact of polio eradication.
Preparing for the post-eradication era
After 12 years the polio eradication initiative has reached every polio-endemic country, the burden of disease has been dramatically reduced, and wild poliovirus transmission has been restricted to a limited number of countries. The progress achieved makes it likely that polio will be eradicated throughout the world in the near future. V&B is therefore expanding its focus to deal with the issues of post-eradication: containment,certification and stopping immunization.
Containment
Since there is no animal or environmental reservoir for polioviruses the only sources of the virus after human transmission ceases will be laboratories. To prevent the possibility of an inadvertent escape of wild poliovirus, stocks must be stored in secure

ANNUAL REPORT 1999
laboratory facilities. A plan for the containment of
polioviruses was prepared in 1998 and circulated
widely for comment in the scientific and biosafety communities. A final plan of action has been pre
pared. It calls for national biosafety authorities to
inventory all stocks of poliovirus and potentially
infected materials. Poliovirus strains should no
longer be present in facilities where their use is not
essential. Strains of scientific value should be moved to secure repositories. One year after the last wild
poliovirus is identified all remaining stocks should
be placed in maximum containment laboratories where essential scientific work can continue. The procedures called for in the containment plan are
currently being field-tested in the Region of the
Americas, the European Region and the Western
Pacific Region.
Certification
The processes for certifying global polio eradication were defined in 1995 at the first meeting of the
Global Commission for the Certification of the
Eradication of Poliomyelitis. Certification requires
at least three years without polio cases under conditions of good surveillance. AFP surveillance is the
primary surveillance tool. The process calls for
national committees to prepare reports for review
by Regional Certification Commission, which, in
turn, will report to the Global Commission. By 1999 each Region had a certification commission
that had met to define Regional processes. The
Region of the Americas has been polio-free for eight years, and is increasingly focusing on the steps need to strengthen AFP surveillance at the country level
to meet certification criteria. The last indigenous
case in the Western Pacific Region having occurred
in March 1997, the Western Pacific Regional
Commission is preparing to receive reports from its Member States in the year 2000. The European
Regional Commission has begun reviewing prelim
inary reports from its Member States in anticipation of certifying freedom from polio in 2001, three years after the last case in Turkey. Although it has begun to receive preliminary reports from some
countries, the Eastern Mediterranean Region has
affirmed that this Region must be certified as a whole and has emphasized the need to achieve rapid
progress in the countries where polio is still endem
ic. The African Regional Commission and the
South-East Asia Regional Commission have met to
plan their work for the next years.
67
Stopping immunization
Stopping immunization against polio is the ulti
mate objective of the eradication initiative and,
along with averted health care costs, will yield
annual global savings of $1.5 billion. A meeting was held in March 1998 to review- scientific data con
cerning the stopping of immunization . A research
agenda was defined with a view to creating new data by means of modern techniques and to taking
advantage of opportunities presented by the
absence of circulating wild virus in developing countries. Three foci were outlined: the potential
for vaccine-derived viruses to continue circulating
after immunization is stopped; persistent shedding
of vaccine-derived polioviruses among some per
sons with certain immunodeficiency disorders; and
the need for new polio vaccines in the post-eradica
tion era. On this basis a number of research projects were initiated. A meeting was held in April 1999 to
review progress in these studies, and a meeting was
held in January 2000 to discuss new polio vaccines. Manufacturers will need a lead time of five to seven
years to ensure that sufficient quantities of any vac
cine other than the current OPV will be available
when needed. It is therefore anticipated that a meet
ing will be held later in 2000 to review new scien
tific data and recommend a strategy for stopping immunization.
Partnership support and advocacy
The success of the polio eradication initiative hinges
on the successful partnership between the public and private sectors. The partnership is spearheaded
by \'\THO, Rotary International, CDC and
UNICEF. The coalition is made up of national governments, private foundations (e.g. Mr Ted Turner's
United Nations Foundation, the Bill and Melinda Gates Foundation), development banks (e.g. the
World Bank), donor governments (e.g. those of Australia, Belgium, Canada, Denmark, Finland,
Germany, Ital), Japan, the United Kingdom, and the USA), and corporate partners (e.g. Aventis
Pasteur, De Beers).
Rotary International
Through its Polio Plus programme, Rotary
International has been a key player in stimulating,
developing and maintaining the global polio eradi
cation initiative. By the end of 2005, Rotary

DEPARTMENT DF VACCINES AND BIDLDGICALS
International estimates that its contribution to the initiative will total US$ 500 million, as well as millions of volunteer hours given to the promotion of and participation in polio eradication activities. During 1999, Rotary International awarded grants totalling $32 million.
New partnership support
• The Bill & Melinda Gates Foundation provided $50 million and Mr Ted Turner's United Nations Foundation granted $28 million to strengthen the vaccine delivery infrastructure and surveillance systems.
• De Beers made a multi-year donation of $2.7 million to fund six NIDs in Angola during 1999 and 2000, targeting 3.3 million children.
• Aventis Pasteur (formerly Pasteur Merieux Connaught) donated 50 million doses of vaccine (worth approximately $5 million) for NIDs to be conducted during 2000-2002 in five countries currently affected by war (Angola, Liberia, Sierra Leone, Somalia, and Sudan).
• The World Bank joined with India to support the huge acceleration in polio eradication activities in that country by reprogramming $48 million in health sector loans.
Increased support from existing partners
• India received increases in bilateral support from the United Kingdom (US$ 62 million), the European Union (US$ 6 million), Germany (US$ 7.5 million), and Italy (US$ 1 million). India has larger resource requirements than any other country, usually accounting for 35% of global external need in a given year.
• Canada pledged multi-year support to Nigeria in the amount of C$ 6 million (US$ 4.2 million). Nigeria is second to India in terms of resources required for polio eradication, usually accounting for 15% of annual global costs.
• In addition to the support targeted on India, the United Kingdom's Department for International Development pledged support for six of the ten priority countries on the African continent (Angola, the Democratic Republic of Congo, Ethiopia, Nigeria, Somalia, and Sudan) with a grant of £20 million (US$ 32 million).
68
• The USA, through CDC, responded to the joint UNICEF/WHO appeal for OPV with an additional commitment of $15 million for 2000. Japan is planning to increase its commitment for OPV in 2000.
Partnership advocates tor polio eradication
During 1999, many partners in civil society joined the advocacy for polio eradication led by Rotary International.
• Martina Hingis, one of the world's leading tennis stars, and Dikembe Mutombo, the Atlantic Hawks star basketball player, gave prominent support. Mr Mutombo lent support in his country, the Democratic Republic of Congo, by visiting a hospital to immunize babies and making public service announcements on the Voice of America.
• World-renowned British photographer Lord Snowdon, a victim of polio in the past, travelled to war-torn Angola in May with the support of De Beers to prepare photographic records of the 1999 polio outbreak and share them with the world.
• The Federation Internationale de Football Association committed players and resources to the Kick Polio out of Africa campaign. During 2000, messages recorded by players will be broadcast across the continent, billboard advertisements will be displayed and leaflets will be distributed at football matches.
• Ms Mia Farrow agreed to serve as UNICEF Special Representative for Polio Eradication. She participated with her son, Thaddeus, who contracted polio in the past, in the launch of UNICEF's annual Progress of Nations report, highlighting the eradication initiative during 1999.
Requirements for financial resources, 2000-2005
During January 1999 the first detailed financial resource estimates were compiled for the mop-up and certification phase in 2000-2005. The final mop-up phase will be the most expensive because of the intensity of activities, particularly the house-to-house immunization of large groups of children.

ANNUAL REPORT 1999
Figure 33: External resources: projected contributions by partner agencies and shortfall, 2000-2005
U.S.CDC
External resorce required= US$ 1,000 million Received/projected= USS 700 million Shortfall = US$ 300 million
It is projected that external resources amounting to US$ 1.0 billion will be needed for polio eradication activities from 2000 to 2005. Donor contributions until 2005 are projected at $700 million, leaving a shortfall of $300 million (Fig. 34). The external resources required by the ten global priority countries for polio eradication comprise approximately 70% of the global need of $300 million. Approximately two-thirds of the shortfall is required during the period 2000-2002. For every year that eradication is delayed, the total cost will increase by approximately $100 million.
Challenges and priorities during the "mopup and certification phase", 2000-2005
Challenges
Ensuring adequate supplies of OPV for NIDs and Mop-Ups During 1999, an OPV shortfall occurred due to rapid implementation of accelerated activities (especially the additional rounds of NIDs in large reservoir countries), interruption of production at one vaccine manufacturer, and rescheduling oflarge orders. To ensure the 2000 global OPV supply, UNICEF made available US$ 100 million to guarantee purchase of the total OPV amount offered in global tender for 2000. WHO, UNICEF, and manufacturers further streamlined information
United Kingdom
Gates and UN Foundations
69
*Italy, Finland, Germany,Aventis-Pasteur, DeBeers
exchange, and strengthened vaccine forecasting, planning, and coordination among UN agencies, vaccine manufacturers, and donor governments. However, ongoing problems with delivery dates and possibly insufficient total supply are major risks to timely completion of eradication activities in 2000 and 2001.
Maintaining Political Commitment Sustaining political commitment is a major challenge in the face of a disappearing disease, but is critical in polio endemic countries to support the acceleration of high-quality eradication activities, and to establish necessary multisectoral support. Some countries, particularly on the African continent, have stopped NIDs, despite surveillance sensitivity chat remains well below certification standards. Experience in other Regions has conclusively demonstrated that such actions may jeopardize progress because low-level polio transmission can continue undetected for more than 3 years in areas with sub-optimal surveillance. The longer that poliovirus transmission continues, the higher the risk of reinfecting polio-free areas.
Ensuring Access to All Children • In Conflict Countries: The success of the UN
Secretary-General and other partners in establishing "Days ofTranquillity'' for NIDs during 1999 in DR Congo demonstrated again the

DEPARTMENT OF VACCINES AND BIOLOGICALS
feasibility of working successfully in conflictaffected areas. These efforts must be expanded during 2000, drawing upon the strengths of the UN Secretary-General, many UN agencies, and other important partners to promote for peace and to support logistically operations during a cessation of hostilities, particularly in Afghanistan, Angola, DR Congo, Sierra Leona, Somalia, and Sudan.
• In All Polio-Endemic Countries: The slogan "Every Child Counts" was adopted for the final push for polio eradication, and to emphasize that all must be reached and vaccinated. To do so, all immunization campaigns must be of the highest quality, and many must include a house-to-house vaccination strategy to reach all children.
Ensuring Adequate Financial Resources The projected $300 million shortfall through 2005 must be rapidly met to ensure that the acceleration strategy is not delayed. Delay in achieving the target date will increase the total cost of eradication by as much as US$ 100 million per year. It will also be difficult to sustain current funding levels for more than 24-36 months, especially for polio-free countries that need to continue NIDs to protect against importations.
Country Priorities
Overcoming obstacles and ensuring the highest quality of activities in the 30 remaining polioendemic countries will be given highest priority. In particular, efforts will focus upon 17 of 30 countries. 10 are "global" priorities because they face particular challenges requiring multi-year intensified activities. These countries fall into two categories:
• "polio virus reservoirs" where transmission is particularly intense due to large dense populations, low routine immunization coverage, and poor sanitation. The countries in this category are India, Pakistan, DR Congo, Bangladesh, Nigeria, and Ethiopia.
• countries affected by conflict, where implementation of vaccination and surveillance activities is particularly challenging due to destroyed infrastructure. The countries in this category are DR Congo, Angola, Afghanistan, Somalia and Sudan. All have started accelerated immunization activities.
70
DR Congo is a special case. As both a global reservoir and a country affected by conflict, it faces challenges inherent to both groups.
Central to the success of polio eradication is ensuring that extra rounds of high-quality NIDs are conducted in 2000 and 2001, particularly in 9 of the 10 global priority countries: Afghanistan, Angola, Bangladesh, DR Congo, India, Nigeria, Pakistan, Somalia, and the Sudan. In the 10th priority country, Ethiopia, the critical priority 1s achieving certification standard surveillance.
Regional Priorities
In addition to the global priority countries, within each WHO region there are strategic priority countries that evolve as the polio eradication programme progresses. At beginning 2000, seven particular priorities are:
• AFRO: Chad, Congo, Liberia, Niger, Sierra Leone
• EMRO: Iraq • SEARO: DPR Korea
Programmatic Priorities
Ensuring High-Quality NID Strategy Implementation A multi-sectoral approach is needed in many countries to improve the quality of supplementary immunization activities to ensure that every child is reached. In PAHO countries, interruption of polio transmission required the collaborative efforts of all government agencies, including the armed forces, to reach and immunize all children. Although more children are now being vaccinated than ever before, some are still unreached due to poor microplanning, inadequate social mobilization, and lack of access due to conflict. During 2000, targeted efforts will seek to overcome these hurdles, including augmentation of country-level technical and administrative capacity.
High-quality AFP surveillance Late detection of polio-infected areas can be a consequence of non-certification standard surveillance. Particularly during the Mop-Up Phase of polio eradication, high-quality AFP surveillance is essential to identify the remaining pockets of polio and to target immunization activities to break the final chains of transmission.

ANNUAL REPORT 1999
Strengthening the Laboratory Network The laboratory network's workload will mcrease
dramatically once countries reach the standard level
of AFP performance, as demonstrated by Nigeria
and India. Laboratories in two important polio
endemic countries (i.e. Bangladesh and Ethiopia)
have not yet been accredited. While specimens from these countries do get processed in accredited labo
ratories elsewhere, it is important that these large
priority countries develop capacity to process stool
specimens. Laboratory accreditation in DPR Korea is critical.
8.2 Measles control
8.2.1 Global activities
Nearly a million deaths were attributed to measles
in 1998. The disease remains a major cause of vaccine-preventable illness and death, despite the wide
spread availability of an effective and safe vaccine for three decades. A failure to deliver at least one
dose of measles vaccine to all infants is the primary
reason for this preventable morbidity and mortality.
In 1989 the World Health Assembly adopted the
goal of reducing measles morbidity and mortality
by 90% and 95% respectively by 1995, relative to estimates of the disease burden in the pre-vaccine era. In 1990 the World Summit for Children adopt
ed a goal of vaccinating 90% of children against
measles by 2000. In 1994, WHO's Region of the Americas set itself the target of achieving elimina
tion by 2000; in 1997 the Eastern Mediterranean
Region decided on 2010 as its target date for elim
ination, and in 1998 the European Region chose 2007 for this purpose.
Global reported measles vaccination coverage
declined from 79% in 1997 to 72% in 1998. In 1998, 16 countries reported measles coYerage belo,v
50%, ten of them in rhe African Region (Burundi, Cameroon, Central African Republic, Chad,
Democratic Republic of Congo, Ethiopia, Liberia,
Nigeria, Togo, and uganda), one in the Region of
the Americas (Haiti), two in the Eastern
Mediterranean Region (Afghanistan, Somalia), and
one in the South-East Asia Region (Democratic People's Republic of Korea).
71
Figure 37: Estimated global measles morbidity and mortality
Millions
120
Morbidity
100
80
60
40
20
0 Pre-vaccine era 1998
WHO unpublished data
Millions
7
6
s
4
3
2
0
Mortality
Pre-vaccine ero 1998
The African Region reported the highest number of
measles cases and the highest incidence rate. Of all
the cases reported globally, more than half were reported from countries in this region. Of the
regions with measles elimination goals, the Region
of the Americas reported the lowest incidence rate
(1.6 per 100 000 in 1998).
Supplementary vaccination campaigns have been conducted in several countries, targeting either
measles elimination or reductions in mortality and
morbidity. In 1998 and 1999, 15 countries in the African Region (Angola, Benin, Burkina Faso,
Central African Republic, Chad, Congo,
Democratic Republic of Congo, Ethiopia, Madagascar, lv1ali, Mauritania, Mozambique, Sierra
Leone, Uganda, United Republic ofTanzania), two
in the Eastern Mediterranean Region (Egypt, Sudan), and two in the Western Pacific Region
(Lao People's Democratic Republic, Viet Nam) conducted mass vaccination campaigns in high-risk areas to reduce morbidity and mortality among
children who were nor vaccinated through routine . . . . 1mmun1zanon services.
Based on experience in the Region of the Americas,
\VHO's measles elimination strategy comprises
three parts, two of which involve supplemental
vaccination: catch-up is defined as a one-time,
nationwide vaccination campaign usually targeting
all children aged 9 months to 14 years, regardless of history of measles disease or vaccination status;

DEPARTMENT DF VACCINES AND BIDLDGICALS
Figure 35: Regions with established measles elimination goals
keep-up is defined as routine services aimed at
vaccinating at least 95% of each successive birth cohort; and follow-up is defined as subsequent
nationwide vaccination campaigns conducted every
two to five years, usually targeting all children born after the catch-up campaign. All countries in the
Region of the Americas except French Guiana, the
USA, and several Caribbean islands had completed
catch-up campaigns by 1996. Since then most
countries in this Region have been conducting
follow-up campaigns.
In 9 of 15 countries in the Eastern Mediterranean
Region where measles elimination activities are in
progress, 13 million children have been vaccinated during catch-up measles vaccination campaigns
conducted since 1994. In the European Region, Romania implemented a catch-up campaign during
1998-1999 and vaccinated more than 2 million
children aged 7-18 years (girls aged 15-18 years received measles and rubella vaccine).
Since 1995, 23 million children have been vacci
nated during catch-up campaigns in the six south
ern African nations where initiatives on measles
elimination initiatives have been launched. In 1998
72
and 1999, catch-up campaigns were conducted in Australia, China (Hong Kong), New Zealand, the
Philippines and other Pacific island nations.
The global measles laboratory network, which is in
the early stages of development, needs to be strengthened, especially in those countries with
elimination goals, by recruiting additional laborato
ries and compiling standard procedures for the
testing of samples. In 1998 and 1999, eight measles
laboratory workshops were conducted and 105 lab
oratory staff from 42 countries in five Regions were trained in basic methods for measles diagnosis.
In 1997 and 1998 the number of countries reporting vaccination coverage or measles cases decreased
in some regions. The European Region had the highest proportion of population from which data were not reported.
The strengthening of measles surveillance is
required in both developed and developing coun
tries so that progress towards achieving morbidity and mortality reduction or regional elimination
goals can be monitored. All countries should
improve routine reporting of measles cases by month of occurrence and geopolitical unit.

ANNUAL REPORT 1999
Countries should use outbreak investigations to
obtain data on the age and vaccination status of
measles cases and should estimate population-based
case-fatality ratios. Case-based epidemiological and
virological data are needed when the incidence of
measles decreases to low levels after measures have
been taken to eliminate the disease.
The priorities for countries pursuing accelerated
measles control include:
• improving routine vaccination coverage levels
to at least 80% in all districts;
• conducting supplementary vaccination cam
paigns together with the administration of vit
amin A in high-risk areas;
• improving the completeness and promptness
with which measles cases are reported at
district level.
The priorities for countries and reg10ns with a
measles elimination goal include:
• improving routine vaccination coverage levels
to at least 90% in all districts;
• achieving coverage of more than 90% in catch
up and follow-up campaigns or coverage of
more than 90% with a routine second dose of
measles vaccine;
• establishing case-based surveillance with labo
ratory confirmation of suspected cases and
virus isolation from all chains of transmission.
Adherence to these priorities should ensure that the
measles morbidity and mortality burden will rapid
ly decrease in 2000 and beyond, and that the
measles disease reduction targets will be reached.
8.2.2 African Region
Since the introduction of measles vaccine in Africa
there have been estimated reductions of 56% in
measles cases and of77% in deaths. WHO estimat
ed that in 1997 there were over 11 million cases and
500 000 deaths from measles in the African Region,
representing 37% and 57% respectively of the glob
al totals. In 1998 the region received reports of only
381 236 cases of measles, suggesting that routine
reporting underestimates disease incidence by at
least one order of magnitude.
The major burden of disease occurs in young chil
dren in countries of West and Central Africa, the
majority of which have vaccine coverage below
50%. However, this is steadily increasing.
Outbreaks continue to occur. Several countries have
implemented or are planning rotating measles cam
paigns covering most of their territory.
Countries in East Africa have a significant burden
of measles: Kenya, Tanzania, and Uganda each
report over 20 000 cases per year even though
reporting is known to be insensitive. Outbreaks are
Figure 36: Reported global measles cases and measles vaccine coverage, 1983-1998
■ Cases - Coverage
4 100
90
3 -;;,-,::
§ .§.
80 ~
70 i;l ~
:() 2 ~
s lil ...
8
60 ~ ol ~
~ ,ls 50
40
30 1983 1984 1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998
Reported at WHO Headquarters as of 8 August 1999
73

DEPARTMENT DF VACCINES AND BIOLOGICALS
Figure 37: Countries implementing strategies for measles elimination, 1999
j
Measles elimination
Figure 38: Global measles laboratory network training, 1998-2000
Laboratories with measle isolation
capabilities
74
o Reference Polio Lab 0 National Polio Lab J:i!j)Trained
Includes rubella training
II Training planned in 2000
'• -,a '
\ .... ~_Jo
-- G \,
Ill
~ )I

ANNUAL REPORT 1999
Table 6: Reported routine measles vaccination coverage among children aged 1 year by WHO Region and worldwide, 1997 and 1998
;•.",;',,!
fl !;~Jes elimination goal: ::; 'Afuericas i},f t:"lterranean
',,•·,,,•'''',:,,, '
·~;~~contrr,I goal: '. r11llippl11ti · :)~et .tfiinf .··•• • ·.
• Rtporttd to WHO as of August, 1999
1997
75%
80% 76%
56%
84% 93%
79%
Reported coverage
%change from
1997to 1998 1998
nro 2 78% -2 71% -5
49% -7
67% -17 93% 0
72'6 -7
.. 1998 estimates of surviving infanll by country (source: UN Population Dirision)
75
Completeness of reporting by countries
WHO Member States 96 of Region's infants""
Number of countries residing in countries that
have reported MCV coverage reporting to WHO
Total 1997 1998 1997 1998
47 40 38 74% 75%
24 23 30 97% 94%
53 35 30 64% 57%
48 41 36 92% 89% 10 8 9 96% 97% 35 34 30 100% 95%
217 181 163 91% 89%

DEPARTMENT DF VACCINES AND BIOLOGICALS
typically among children of preschool age,
although some districts, particularly in Tanzania, report that more than half their cases are in chil
dren aged over five years. These countries have
adopted a strategy for improving routine coverage,
implementing case-based surveillance, and con
ducting supplemental vaccination strategies.
Measles campaigns will be implemented over two
to three years in the age groups and districts where
measles cases are occurring.
The countries of southern Africa have embarked on a measles elimination programme, the first
stage of which has comprised mass campaigns to
immunize children aged 9 months to 14 years. Botswana, Malawi, Namibia, South Africa,
Swaziland, and Zimbabwe have implemented such
campaigns and have achieved coverage of at least
80%. The number of reported measles cases has
dropped from over 50 000 a year before the cam
paigns to less than 2000 in 1999. In Mozambique a strategy for vaccinating in high-risk urban areas
was adopted but initial results suggest that this has not had the desired result of decreasing the inci
dence of measles in either urban or surrounding
rural areas.
The following challenges for measles control in the
next five years have been identified.
• The 1995 goals for reducing measles mortality and morbidity have. not been achieved. However, there is a high
birth rates favour measles transm1ss10n, 1t 1s
necessary to have both high routine coverage and supplemental vaccination activities m
order to achieve high levels of control.
• Accelerated measles control requires improved surveillance. Data on age and vaccination status
are needed for nearly all reported measles cases.
• There is a crisis in the cold chain and in the quality of vaccination in many countries, par
ticularly the poorest ones in the region. This means that immunization safety may not be
guaranteed. Furthermore, logistical problems, including interruptions in supplies of vaccines,
have reduced coverage during campaigns in
some countries. The monitoring of adherence
to safe injection practices and of AEFls is not
routinely done or reported.
8.2.2 Region of the Americas
This region continues to make substantial progress towards the goal of eradicating indigenous measles
transmission by the end of 2000. During 1999 there were 2874 confirmed cases, a decline of 95% from the peak of 53 661 in 1997. They occurred in 11 countries, of which only Argentina, Bolivia,
Brazil, and the Dominican Republic experienced
indigenous transmission: Bolivia reported 1420 cases (49% of the total for the Region), Brazil
reported 762 (27%), Argentina reported 247 (9%),
demand for accelerated measles control actlvltles
throughout the region, and countries have reiterated their
commitment to the goals set at the World Summit for
Children. At least 25 coun
tries in the region have imple
ment.ed mass campaigns
against measles as a means of either eliminating the disease
(in the southern block) or
reducing the mortality attrib
utable to it.
Figure 43: Reported measles cases in 7 countries with measles elimination goals in Southern Africa, 1987-1999
• In areas where extremely high routine coverage has not been
achieved and where high pµpulation densities and high
76

ANNUAL REPORT 1999
and the Dominican Republic reported 206 (7%).
AMRO has emphasized the importance of heightened national and international coordination in
these priority countries in order to prevent the
spread of measles into other areas. The health
authorities have pledged their full support for the
goal set for measles eradication.
Attention is centred on progress achieved towards measles eradication in the four priority countries,
which are implementing a dual strategy involving intensive mop-up vaccination in municipalities that fail to reach 95% coverage, together with a
bimonthly active search for measles cases. Bolivia
has been the country most affected by measles, with
1420 confirmed cases during 1999, i.e. approximately 49% of those in the Region. Large areas of
under-immunized populations largely explain this
result. A majority of the confirmed cases occurred in children under 5 years of age; they were followed
by individuals aged 5 to 19 years and young adults
aged 20-29 years. The transmission of measles virus was initially clustered in urban centres, later moving
to certain forested areas. An aggressive plan of
action was launched by health authorities to stop
the outbreak and interrupt virus transmission, with
technical and financial support from AMRO and financial assistance from the World Bank, the Inter
American Development Bank, UNICEF and local nongovernmental organizations. The Ministry of Health issued a Ministerial Resolution supporting
the implementation of a comprehensive national
vaccination campaign, and this was held in
December 1999.
Figure 40: Immunization coverage and reported numbers of measles cases, Region of the Americas, 1980-2000* **
300000
250000
200000 el s ~ 1S0 000 ~ ;§
100000
soooo
Source: PAH0/WH0
■ Cases - Coverage
• Data as of 23 February- 52 confirmed cases •• 1999 provisional coverage data
Catch-upcampaigns
Priority activities for measles eradication in the Region of the Americas
100
follow-upcampaigns
■ Timely follow-up measles campaigns when the pool of susceptibles nears the number of children born in an average birth cohort. ■ Attainment of the goal of at least 95% vaccination coverage in all municipalities. ■ Proper investigation of all reported cases of suspected measles and obtainment of the appropriate blood and urine samples. ■ Avoidance of missed opportunities: when appropriate, contacts between children and health care workers should be used as
opportunities to vaccinate. ■ Assuring availability of the necessary vaccine supply at the central, regional and local level at all times. ■ -Identification of hard-to-reach population groups and implementation of social mobilization activities that will enhance compliance
with vaccination efforts. ■ Alerting health care workers about the Regional eradication initiative and stressing the importance of their cooperation in it.
77

DEPARTMENT OF VACCINES AND BIOLOGICALS
Figure 4S: Confirmed measles cases by state or province, Region of the Americas
.... -
Total Americas 2 826 cases
1 dot = 2 cases
Source: Country reports
A similar situation arose in the Dominican Republic. In conjunction with the country's health authorities, AMRO organized a task force to ensure the effective control of measles virus transmission. The outbreak began as a consequence of an importation to a tourist area from Argentina in 1997. Despite two vaccination efforts in 1998 the virus continued to circulate and subsequently spread throughout the country in 1999. Over 50% of the cases were reported from the Santo Domingo metropolitan area, where pockets of unimmunized children, overcrowding and low coverage rates from previous follow-up campaigns helped to spread the disease. As happened in Bolivia, a majority of cases were found in young children. In February 2000, a five-year plan of action for immunization, developed by the Ministry of Health with technical input from AMRO, received US$ 13 million from AMRO, the World Bank and the Japanese International Cooperation Agency.
In Brazil, most states are reporting a decrease in transmission, notwithstanding intense surveillance
by 27 additional epidemiologists engaged as part of the special task force. The remaining cases are primarily clustered in the north-east of the country, the
78
state of Pernambuco being the most affected. A follow-up campaign will be carried out in June 2000, targeting children aged from 5 to 15 years in some states. The government has undertaken to renew financing for the task force. Progress is also evident in Argentina, which reported a majority of the cases in 1998. A provisional total of762 measles cases has been confirmed in 1999, a decline from the 2930 confirmed cases in 1998. Unlike the 1997 outbreak in Sao Paulo, the age group most affected in 1999 was that of children aged under 1 year, , followed by children aged 1 year and children aged 2-5 years. An emergency plan was developed and four national epidemiologists were engaged to assist the country's health authorities with eradication efforts.
AMRO has intensified its collaboration with all countries to ensure that sufficient resources are allocated to maintain adequate stocks of measles vaccines and other vaccines, as well as supplies. These measures are critical for routine immunization services, mop-up vaccination activities, and the rapid execution of control measures in the event of an outbreak. Efforts are also being made to strengthen
surveillance systems and improve capabilities for case investigation.

ANNUAL REPORT 1999
8.2.4 Eastern Mediterranean Region
During 1998, 88 941 measles cases were reported, significantly more than the 22 941 reported in
1997. This was mainly attributable to an outbreak in Iraq in which more than 43 000 cases were
reported, and also to an improvement in measles
surveillance in other Member States. However, sur
veillance is weak in many countries, measles is
accepted as a natural event, and the great majority of mild cases do not present at health facilities.
Consequently, the reported cases represent only a small fraction of the total. Furthermore, reported
cases are usually severe ones that are admitted to
hospitals, while cases that are treated as outpatients
in basic health facilities, i.e. health units and health
centres, are not reported. In addition, few reports are received from the private sector, even though it is very active in most Member States.
8.2.5 European Region
The strategic plan for measles elimination in the
European Region was considered at the Thirteenth
European Advisory Group on Immunization (EAG). The EAG was convinced that the elimina
tion strategy, which is based on the identification of
susceptibility, was the most appropriate approach
for the region. It was agreed that the target date for elimination should be set at 2007.
To date, three intercountry workshops on measles
elimination have been conducted. The aim of these workshops was to review the epidemiological situa
tion in the participating countries. So far, 8 of the
CEE countries, the 5 Central Asian Republics and 10
of the Western countries have developed their
national plan based on the European strategy. One of
the greatest challenges is to get a strong political commitment and therefore every possible opportunity
should be sought to recruit the support of national and international agencies as soon as possible.
8.2.6 South East Asia Region
Measles continues to be a major cause of morbidity
and mortality in the region, 65 208 cases having
been reported in 1998. The true incidence, howev
er, is likely to be several million cases. In the absence
79
of a regional resolution calling for measles
elimination, countries are implementing strategies
aimed at disease control and at outbreak prevention. Improved surveillance is an essential prerequi
site for better-targeted immunization activities, and
countries are building on the experiences gained from AFP surveillance to establish NT and measles
surveillance. Indonesia, Sri Lanka, and Thailand
have established laboratory confirmation of measles
outbreaks.
The provision of technical support to Member States in relation to injection safety and waste dis
posal is a top priority for V&B/SEARO, and an excellent opportunity to promote sustainability in
systems development. To that end, a Regional plan
of action is being developed to revive interest in a
public health problem that requires inputs from several curative and preventive disease strategies. In the meantime, SEARO promotes the bundling of
vaccines with equipment that helps to ensure safe
injection and waste disposal. A priority activity for
2000 will be an intercountry planning workshop to
be held in collaboration with WHO Headquarters.
Other opportunities for systems development arise in connection with the strengthening of manage
ment and the replacement of the cold chain.
SEARO has employed a full-time cold chain con
sultant. None of the countries has an adequate plan for conversion to a CFC-free cold chain system, and
this presents a major challenge.
8.2. 7 Western Pacific Region
Pilot measles campaigns were conducted in Cambodia, the Lao People's Democratic Republic,
and Viet Nam,. In November and December 1999, Viet Nam conducted a campaign in Hai Phong
Province, targeting over 320 000 children aged from 9 months to 10 years, and reportedcoverage of
99.6%. In January and February 2000, Cambodia
conducted a campaign in six provinces and in March and April 2000 the Lao People's Democratic Republic conducted a campaign in Phongsaly and
Khammoune Provinces. A database for measles surveillance was installed in all three countries. Work
began on the establishment of a Regional laborato
ry network for measles, and Regional and national laboratories have been identified for most countries.

DEPARTMENT DF VACCINES AND BIDLDGICALS
8.3 Neonatal tetanus
8.3.1 Global activities
The goal of NT elimination has been achieved in
104 of 161 countries. However, in 1998 it was estimated that there were 289 000 cases of NT, resulting
in 215 000 deaths, and that there were 30 000 mater
nal tetanus (MT) deaths. Twenty-seven countries, 18
of them in the African Region, account for 90% of
the global burden of NT. The recommended strategy
for eliminating maternal and neonatal tetanus (MNT) focuses on the high-risk approach because NT and MT cases occur in areas with limited access
to antenatal care and clean delivery services.
The estimated cost over five years for eliminating MNT in the remaining countries is US$ 130 mil
lion., and it is estimated that the average contribu
tion from the targeted countries will amount to
approximately 25%. The requirement from external sources is thus $100 million, of which nearly
$45 million have already been raised. The US
Fund for UNICEF would like to secure funding commitments for all MNT activities by the year
2001.
Many issues still have to be addressed in order to
determine NT elimination accurately by district.
They include: the validity of methods in use; the
Figure 42: Neonatal tetanus in Latin America, 1985-1999*
Source: HVP/PAHO * Provisional data
80
improvement of information systems for district
level monitoring; the need to develop monitoring
standards and policies; and the need for consensus
on monitoring issues.
8.3.2 African Region
Neonatal tetanus remains an important public health problem in the African Region, causing
approximately 164 000 cases and llO 000 deaths a
year. Reported coverage with at least two doses of
tetanus toxoid (TT2+) has remained stable in the range of about 30-35% for the past five years
(35% in 1998). The reported numbers of NT cases
have not declined in the past seven years: there were
4517 cases in 1992 and 4838 in 1998.
Notwithstanding the lack of progress in NT control over the Region as a whole, several countries have
made progress. In Malawi, Mozambique (Maputo),
certain districts in Nigeria, and Tanzania, the sys
tematic vaccination of women of childbearing age has resulted in substantial reductions in the num
bers of cases. Case-based surveillance for MNT cases has been instituted in several West African
countries: Benin, Cote d'Ivoire, Liberia, Mali, and
Senegal.
Several issues associated with assessment, surveil
lance and certification are constraining NT control.

ANNUAL REPORT 1999
Underreporting of NT is estimated to amount to
96%, only 4838 cases having been reported in 1998.TT2+ coverage is not accurately reflecting the
immunity levels in women of childbearing age.
During the past five years, two studies indicated that immunity levels were underestimated by 20-
30% and one indicated an immunity level similar
to TT2+ coverage.
8.3.3 Region of the Americas
The number of NT cases continues to decline (Fig. 42), 157 having been reported during
1999.The strategy has been to vaccinate women in
areas and population groups at highest risk within the high-risk municipalities where there are still iso
lated cases. AMRO has therefore recommended that countries carry out national evaluations to
determine which municipalities remain in the
attack phase, requiring intensive vaccination, and
which have advanced to the maintenance phase,
involving vaccination through routine programmes.
Furthermore, countries should look into the epi
demiological and social conditions associated with
these cases, e.g. migration, lack of vaccination, and marginality, in order to target vaccination on those
groups or areas at highest risk within high-risk municipalities.
8.3.4 Eastern Mediterranean Region
The goal of less than one case of NT per 1000 live
births in each administrative district was achieved
in 15 of the 23 Member States, namely Bahrain,
Cyprus, Islamic Republic of Iran, Jordan, Kuwait, Lebanon, Libyan Arab Jamahiriya, Morocco,
Oman, the Self-Ruled Areas in Palestine and the
population served by UNRWA, Qatar, Saudi
Arabia, Syrian Arab Republic, Tunisia, and the United Arab Emirates. The elimination goal has not
yet been achieved in eight countries: Afghanistan,
Djibouti, Egypt, Iraq, Pakistan, Somalia, Sudan,
and Yemen. Among these countries, Djibouti, Egypt, and Iraq are very close to the goal, few
districts having higher rates than the target.
The total number of reported cases of NT in 1998
was 2955, which was similar to the numbers reported in previous years. However, NT is still seriously
underreported, the degree of under-reponing vary
ing between _Member States. In some countries,
such as Afghanistan and Somalia, the sun-eillance
81
Figure 43: Distribution of neonatal tetanus cases by country, 1999 Women of childbearing who live in districts classified as being at high risk for the disease.
system is extremely weak or almost non-existent.
Other countries, such as Egypt, have sensitive sur
veillance systems, whereby more than 70% of cases
are detected and reported. Because the disease occurs early in life its victims' deaths, and even their
births, may not be officially recorded. Moreover,
NT is most prevalent in poor rural areas with inef
ficient or non-existent health services, where it is
perceived by the people as having an inevitably
fatal outcome. Consequently, they tend not to seek medical advice and are inclined to delay the
regisuation of births.
8.3.5 South-East Asia Region
Five countries are considered as having eliminated
NT. In 1999, Myanmar implemented its elimina
tion plan based on the high-risk approach and has completed two of the three rounds of TT immunization in 54 targeted townships, administering
nvo doses rn 1.4 million women of childbearing
age. Bangladesh, India, Indonesia, Myanmar, and
~epal are developing plans to reach the target of less than one NT case per 1000 live births by 2000,
on i:he basis of the high-risk approach, whereby it is
intended to immunize all women of childbearing
age in high-risk areas ,vith at least three doses ofTT
vaccine. Bangladesh conducted an NT and measles

DEPARTMENT OF VACCINES ANO BIOLOGICALS
campaign in 1999, targeting approximately 10% of the population. Indonesia introduced school-based TT immunization. In Rajasthan (India) over 4 million women received two doses of TT during a UNICEF-sponsored campaign in 1998.
8.3.6 Western Pacific Region
Excluding China, reported coverage during 1998 with two doses ofTT in pregnant women was 71 %. China, the Philippines, and Viet Nam have achieved the elimination goal at the province/prefecture level and are progressing towards elimination at the district level. Cambodia, the Lao People's Democratic Republic, and Papua New Guinea have made progress but NT is still widespread in these countries.
8.4 Vitamin A supplementation
8.4.1 Global situation
In countries where vitamin A deficiency occurs the integration of vitamin A supplementation into
immunization services is increasingly common. The provision of a high dose of vitamin A every four to six months not only protects against blindness but also has a dramatic impact on the health of children aged 6-59 months, reducing the risks of all-cause, measles and diarrhoeal disease mortality by 23%, 50% and about 33% respectively.
Vitamin A deficiency is a public health problem in 118 countries, all of them in the developing world. The worst effects occur in Africa and Asia. Globally, between 100 million and 256 million children under 5 years of age are at risk. These children suffer a dramatically increased risk of death, blindness and illness, especially measles and diarrhoea. Annually, vitamin A deficiency causes blindness in 250 000 to 500 000 children and is a major factor contributing to between 1 million and 3 million child deaths. In 1990 the World Summit for Children set the goal of eliminating vitamin A deficiency by 2000.
Food fortification and dietary diversity are essential for the control of vitamin A deficiency, but are often difficult to achieve quickly or widely in those
Figure 48: Countries administering vitamin A supplementation during NIDs, 1999
lflj Vitamin A with NIDs (national or sub-national) (56 countries; indudes both polio and measles campaigns)
Vitamin A with routine EPI (26 countries; induding Samoa, Micronesia, Kirbati)
82

ANNUAL REPORT 1999
developing countries where the condition is most
severe. Consequently, supplementation has been
introduced as a low-cost, highly effective and
sustainable means of rapidly improving the vitamin
A status and health of children. Immunization ser
vices, particularly polio NIDs, provide a ready
made infrastructure for this purpose. Furthermore,
cost-effectiveness and impact can be increased by
combining these two interventions.
In 1999, 53 countries introduced vitamin A sup
plementation into their polio NIDs, and three additional countries introduced it into their measles
vaccination campaigns. Over 60 million children received vitamin A and benefited from its protective
effects. Moreover, 26 countries provided vitamin A
supplementation together with their routine immu
nization services. Fig. 44 is a summary of global vitamin A supplementation in conjunction with
immunization during 1999.
The integration of vitamin A with immunization
campaigns is building a platform for the longerterm strategy of adding vitamin A to routine immu
nization contacts (for postpartum mothers at the
first EPI contact and for children receiving measles
immunization at 9 months of age). For example,
NIDs with vitamin A supplementation have:
increased awareness and advocacy of vitamin A
deficiency among the highest levels of decisionmakers; strengthened the technical capacity of
health workers to administer vitamin A; and result
ed in an integrated reporting system. Furthermore, vitamin A supplementation is helping to increase
participation in NIDs and routine immunization
services because vitamins are highly valued by
mothers.
With continued funding from the Micronutrient
Initiative (Canada), during 1999, V&B has worked in dose partnership with WHO's Department of
Nutrition for Health and Development and
UNICEF to: • promote the policy of integrating vitamin A
supplementation into immunization services;
• develop guidelines and training materials (including a new CD-ROM Training and
Information Package on Immunization and
Vitamin A, produced jointly with Helen Keller
International);
• provide technical training and operational sup
port to countries;
83
• undertake research on simplifying the delivery method, confirming the seroconversion effect,
and assessing impact;
• adapt WHO's monitoring and surveillance
system to include linked vitamin A and EPI
activities and results.
Building on the momentum already generated,
efforts in 2000 will focus on promoting and strengthening the delivery of vitamin A with routine immunization services. This will include
expanding the opportunities to give vitamin A during early immunization contacts (i.e. DTP vaccina
tion), thereby making the most of the immuniza
tion-linked delivery schedule for children during
their first year of life.
8.4.2 Region of the Americas
The 12 countries in which subdinical vitamin A
deficiency is of severe to moderate public health significance (based on % prevalence of serum retinal
less than 20µg/ dl) are currently providing vitamin A
supplementation to targeted children, particularly through EPI contacts. Six of these countries
(Bolivia, Brazil, Dominican Republic, Ecuador,
Nicaragua and Peru) are participating in a two-year
project to provide vitamin A supplementation twice a year to children aged 6-24 months and once to
mothers up to six weeks postpartum. The purpose
of maternal supplementation is to increase the vitamin A content of breast milk so as to benefit lactat
ing infants aged under six months. This project,
coordinated by AMRO's Food and Nutrition
Programme and the Division of Vaccines and Immunization, is designed to review and imple
ment or reinforce vitamin A supplementation pro
grammes that are linked to immunization cam
paigns as well as to routine immunization and other maternal and child health contacts.
For children aged 6-11 months, coverage rates
are relatively high (>60%). However, they are somewhat lmver for children over 1 year of age and
even lower for the second dose per year. Attention is
being given to means of improving the level of vit
amin A supplementation through immunization
contacts, with particular reference to the management of the logistics of this intervention in the
field. Lines of coordination between EPI and nutri
tion programmes need to be dearly identified in the
areas of training, capsule distribution, data collec-

DEPARTMENT DF VACCINES AND BIOLOGICALS
tion, monitoring and supervision. In addition, supplies of vitamin A capsules could be handled together with vaccines for the purposes of stock checks, local transport and dissemination. These issues and others should be carefully dealt with in order to achieve an effective integrated programme.
8.4.3 South-East Asia Region
Vitamin A deficiency has been raised by WHO as a priority project at the Region's last three TCG meetings on immunization and polio eradication and at several meetings of the lnteragency Coordinating Committee at country level. Since immunization workers are likely to remain the most important means of getting vitamin A to children,
84
WHO will continue to encourage countries with adequate trained manpower to provide vitamin A during NIDs, on condition that there is a minimal risk of adversely affecting the performance of polio immunization. Bangladesh and the Democratic People's Republic of Korea aredistributing vitamin A during NIDs. Nepal distributes vitamin A during one round of its NIDs. Myanmar began the distribution of vitamin A during its NIDs in January 2000. In India's state of Orissa, vitamin A supplementation was introduced during an NID in October 1999 and an assessment and impact study, now in progress, is expected to influence the country's policy on vitamin A supplementation campaigns. D

ANNUAL REPORT 1999
[j] Annexes
Annex 1: Documents produced by the V&B Document Centre during 1999
Over the year the Document Centre produced 74 documents, 38 of them in English, 23 in French, 5 in Spanish and 4 in Russian. These documents are available on the Internet at: www.vaccines.who.int/vaccines-documents.
General V&B documents
WHO/V&B/99.01
WHO/V&B/99.02
WHO/V&B/99.03
WHO/V&B/99.04
WHO/V&B/99.05
WHO/V&B/99.06
WHO/V&B/99.07
WHO/V&B/99.08
WHO/V&B/99.09
V&B Annual Report, 1998 English only
V&B Catalogue '99 - Listing of materials currently available from V&B Document Centre English only
Informal consultation on the control of pertussis with whole cell and acellular vaccines, Geneva, 18-19 May 1998 English only
The current status of development of prohphylactic vaccines against human papillomavirus infection - Report of a technical meeting, Geneva, 16-18 February 1999 English only
Fourth informal consultation on the polio laboratory network, Geneva, 1-2 October 1998 English only
Informal meeting on issues of immunization data and monitoring/management of adverse events, Geneva, 17-20 November 1998 English only
Fourth annual meeting of the Advisory Committee on Training (ACT), Geneva, 23-24 February 1999 English onJ;,
Informal consultation of experts on national regulation of vaccines, Geneva, 21-22 January 1999 English only
Review of existing documents on planning, performance and assessment of clinical studies on vaccines English, French, Spanish
85

WHO/V&B/99.10
WHO/V&B/99.11
WHO/V&B/99.12
WHO/V&B/99.13
WHO/V&B/99.14
WHO/V&B/99.15
WHO/V&B/99.16
WHO/V&B/99.17
WHO/V&B/99.18
WHO/V&B/99.19
WHO/V&B/99.20
WHO/V&B/99.21
WHO/V&B/99.22
WHO/V&B/99.23
WHO/V&B/99.24
DEPARTMENT OF VACCINES AND BIOLOGICALS
Regulation of vaccines: Building on existing drug regulatory authorities English, French, Spanish
Testing the correlation between vaccine vial monitors and vaccine potency English, French
Procurement of vaccines for public-sector programmes. A reference manual English only
Options for a global fund for new vaccines English only
Field manual for neonatal tetanus elimination English, French
Temperature monitors for vaccines and the cold chain (Revises and replaces WHO/EPI/CCIS/85.02 Rev.5) English, French
Report of the first meeting of interested partners to the Health Technology and Pharmaceuticals Cluster, Geneva, 16-19 March 1999 English only
WHO vaccine-preventable diseases monitoring system, 1999 global summary (Revises and replaces WHO/EPI/GEN/98.10) English only
Quality of the cold chain - WHO/UNICEF policy statement on the use of vaccine vial monitors in immunization services English, French
Standardization and validation of serologic assays for the evaluation of immune responses to Neisseria meningitidis serogroup NC vaccines, Geneva, 8-9 March 1999 English only
Advocacy - A practical guide: with polio eradication as a case study English only
Study of donor inputs to vaccine production English only
Guidelines for surveillance of congenital rubella syndrome (CRS) and rubella - Field test version, May 1999 English (French in preparation)
Issues relating to the use of BCG in immunization programmes - A discussion document English (French in preparation)
Strategies, policies and practices for immunization of adolescents: A review English (French in preparation)
86

WHO/V&B/99 .25
WHO/V&B/99.26
WHO/V&B/99.27
WHO/V&B/99.28
WHO/V&B/99.29
WHO/V&B/99.30
WHO/V&B/99.31
WHO/V&B/99 .32
WHO/V&B/99.33
WHO/V&B/99.35
WHO/EPI/GEN/98.17
Newsletters
WHO/EPI/Measles/99.01
WHO/EPI/PN/99.01
WHO/EPI/PN/99 .02
ANNUAL REPORT 1999
Safety of injections - WHO/UNICEF joint statement on the use of auto-disable syringes in immunization services (Revises and replaces WHO/EPI/LHIS/98.04) English, Russian (French and Spanish in preparation)
Generic protocol to estimate the burden of Shigella diarrhoea and dysenteric mortality - Field resr version, May 1999 English only
Towards a CFC-free world - Training for refrigerator technicians. Module A: R12 - Recovery, recycling and repair English (French to follow)
Towards a CFC-free world - Training for refrigerator technicians. Module B: Working with R134a English (French to follow)
Towards a CFC-free world - Training for refrigerator technicians. Module C: Working with Lokring technology English (French to follow)
Towards a CFC-free world - Training for refrigerator technicians. Module D: Guidelines for the introduction of CFC-free equipment to national Expanded Programmes on Immunization English (French to follow)
Report of the fourth meeting of the Global Technical Consultative Group for poliomyelitis eradication, Geneva, 1-2 June 1999 English only
Global action plan for laboratory containment of wild poliovirus English (French and Spanish in preparation)
Immunization and health sector reform in the Kyrgyz Republic, March 1999 English (Russian in preparation)
Report on the overview of vaccine research in WHO and UNAIDS English on{y
Global eradication of poliomyelitis: Report of the third meeting of the Global Commission for the Certification of the Eradication of Polio, Geneva, 9 July 1998 English only
Measles Bulletin, Issue 1, September 1999 English, French
Polio News, Issue 3, March 1999 (English only)
Polio News, Issue 4, June 1999 (English only)
87

WHO/EPI/PN/99.03
WHO/EPI/PN/99.04
DEPARTMENT OF VACCINES AND BIOLOGICALS
Polio News, Issue 5, September 1999 (English only)
Polio News, Issue 6, December 1999 (English only)
Translations of previous years' documents
French WHO/EPI/GEN/98.08
WHO/EPI/GEN/98.09
WHO/EPI/GEN/98.11
WHO/EPI/TRAM/98.01 11
WHO/EPI/TRAM/98.12
WHO/EPI/TRAM/98.13
WHO/EPI/TRAM/97.06
WHO/EPI/TRAM/97.07
Russian WHO/EPI/GEN/97.03
Spanish WHO/VSQ/97.03
GAV/ documents
GAVl/99.01
GAVI/99.02
Fievre jaune - Reunion technique de consensus, Geneve, 2-3 Mars 1998
Fievre jaune - Surveillance de la fievre jaune: lignes directrices a l' echelon du district
Fievre jaune
Vaccination pratique: Modules 1-11
Vaccination pratique: Module d' activites pedagogiques
Vaccination pratique: Guide a !'usage du formateur
Cours a !'usage des agents de sante: Reperer et surmonter les obstacles a I' amelioration de la couverture vaccinale - Modules du stagiaire: Introduction au cours Module 1: Recueillir des informations dans la communaute et les exploiter Module 2: Communiquer avec les meres au sujet des vaccinations
Cours a !'usage des agents de same: Reperer et surmonter les obstacles a l' amelioration de la couverture vaccinale - Lignes directrices a l'usage de I' animateur: Introduction, Module 1, Module 2
Polio: The beginning of the end
Gufa para la inspecci6n de fabricantes de productos biol6gicos
Global Alliance for Vaccines and Immunization, Seattle, Washington, 12-15 July 1999 English, French
Global Alliance for Vaccines and Immunization - First Board Meeting, UNICEF House, New York, 28 October 1999 English, French
88

ANNUAL REPORT 1999
Annex 2: Internet information
The world wide web (www) pages of the Department of Vaccines and Biologicals (V&B) are part of the material on the web under the WHO home page and the HTP duster. The address for the home page for
vaccines and immunization is now ·www.vaccines.who.int. This is very easy to remember and to find via search
engines. A large amount of basic information about vaccines and immunization is posted on this site, together
with regularly revised data. Each unit is placing increasing emphasis on developing the site as a way of
disseminating technical information. Most publications are now posted on the V&B Document Centre web
site in pdf format as soon as they are sent to the printer. They are thus on the web before the printed material
is available.
Figure 45: Polio Eradication lnitiaitive web pages
ii :3 :;i ~ ~ iJt QJ r-' Iii :1 Forward Reload Home Search Guide Images Print Security Stop
ii L~cation:{ ht! ://www.olioeradication.org/ ·-- ~~--·"' " - --~-··- -.-•-
We,corne to the WHO official s;te cf \r·e /aroest ever disease eradical'on :r·JLative ...
Global
Polio Eradication lnHiatiYe
Find out the latest an:
PJdkt.lkWL Initiative. .. the latest news from the Global Polio Eradication
,· r. E,c}i:J,2,,;cr,--·:/c,/c5' f;_·se-c:,:r-d.~. -- Progress towards poliomyelitis eradic:ation.
Hor:1e ?age • Ba:i::kgri:iund • ·31':rba! ~:t2I1Js • N3!ional tmmunfa:ation Oay'S Oo~1.nb2:Js • Pdi,:i in th~ Ne:.1r.; • Phi::to Ga1le.f:/ • Partne.r.; ■ Ci:intact Us ■ Links
R°.JF ~I,:; and ~ pi,,a-sr, elk/,· i>s,,,, h g:, h oor ~ page or d,d,- i>s,,,, ;,, e--<mil u':S .
.ACROBAT Reader is needed to view many documents available in PDF format. ~:1ici: r.e,eto do unload from Afobe .com
World Health OC9ani,ation, Di>,ision for Vaooines and other Biologicals, E:apande.d Programme on Immunization, Geneva, Suitzer1and
89

DEPARTMENT DF VACCINES AND BIOLOGICALS
The Polio Eradication Initiative has an extensive site, much of the information on which is also available as a CD-Rom. Another priority project, Safety of Immunization, has a well-developed site entitled "Vaccines are safe". Large amounts of useful material are also posted under the ATT and VAM pages.
Figure 46: "Vaccines are safe''web pages
clot Topics 0 Vaccine safety current affairs of immediate interest to the public
90
• Rolavirus and intussusception (15 July 1999)
• Thiometsal (9 July 1999)
• SV40 virus and polio vaccine
• Hepatitis B vaccine and MS