
Intolerance to piroxicam in patients with adverse reactions to nonsteroidal antiinflammatory drugs
Upload
independentCategory
view
0download
0
Practice Parameter
Adverse reactions to vaccinesChief Editors: John M. Kelso, MD and James T. Li, MD, PhD
Co-Editors: Richard A. Nicklas, MD; Joann Blessing-Moore, MD; Linda Cox, MD;David M. Lang, MD; John Oppenheimer, MD; Jay M. Portnoy, MD; Christopher Randolph, MD;Diane E. Schuller, MD; Sheldon L. Spector, MD; Stephen Tilles, MD; Dana Wallace, MD;Zuhair K. Ballas, MD; James R. Baker, MD; Joseph A. Bellanti, MD; Daniel Ein, MD; andLeslie C. Grammer, MD
TABLE OF CONTENTSI. Preface ................................................................................................................................................................................S2
II. Classification of Recommendations and Evidence ...........................................................................................................S3III. Summary Statements ..........................................................................................................................................................S3IV. Acknowledgments ............................................................................................................................................................S11V. References.........................................................................................................................................................................S12
those who served on the Joint Task Force, is authorized to provide anofficial AAAAI or ACAAI interpretation of these practice parameters. Anyrequest for information about or an interpretation of these practice param-eters by the AAAAI or ACAAI should be directed to the Executive Officesof the AAAAI, the ACAAI, and the Joint Council of Allergy, Asthma andImmunology. These parameters are not designed for use by pharmaceuticalcompanies in drug promotion.
Received for publication August 11, 2009; Accepted for publicationAugust 11, 2009.
These parameters were developed by the Joint Task Force on PracticeParameters, representing the American Academy of Allergy, Asthma andImmunology (AAAAI), the American College of Allergy, Asthma andImmunology (ACAAI), and the Joint Council of Allergy, Asthma andImmunology. The AAAAI and the ACAAI have jointly accepted re-sponsibility for establishing “Adverse Reactions to Vaccines.” This is acomplete and comprehensive document at the current time. The medicalenvironment is a changing environment, and not all recommenda-tions will be appropriate for all patients. Because this document incor-porated the efforts of many participants, no single individual, including
VOLUME 103, OCTOBER, 2009 S1
PREFACEThis practice parameter provides a practical, peer-reviewed,evidence-based guide for evaluation and management of pa-tients with suspected allergy to vaccines. This documentcontains detailed and specific guidelines not found in previ-ously published reviews.
The practice parameter offers both general and vaccine-spe-cific recommendations for skin testing to vaccines and compo-nents, serum specific IgE in vitro antibody testing, serologictesting for protective antibody responses to vaccines, vaccine
administration, and avoidance. The guidelines should prove use-ful for primary care physicians and specialists in allergy andimmunology. More importantly, most patients who avoid vac-cination because of allergy concerns will be able to receive theirappropriate vaccinations if this practice parameter is followed.
The 2 key points of the practice parameter are that (1)patients with suspected allergy to vaccines or vaccine com-ponents should be evaluated by an allergist/immunologist and(2) most patients with suspected allergy to vaccines canreceive vaccination safely. With the recent worldwide con-
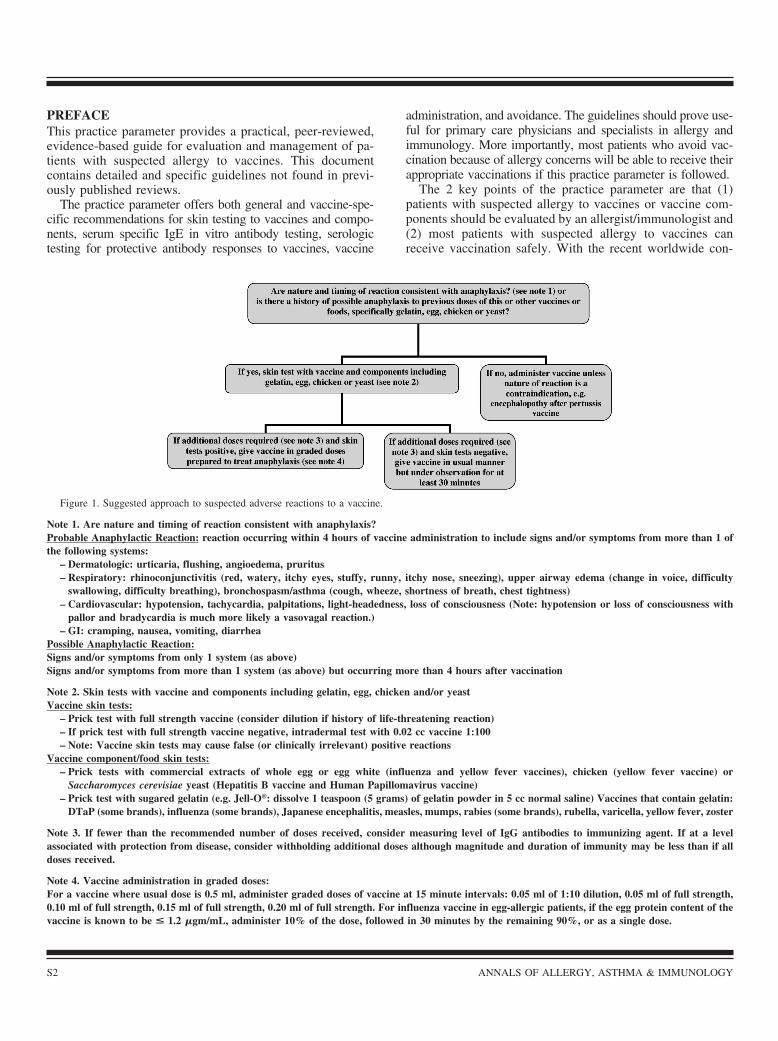
Figure 1. Suggested approach to suspected adverse reactions to a vaccine.
Note 1. Are nature and timing of reaction consistent with anaphylaxis?Probable Anaphylactic Reaction: reaction occurring within 4 hours of vaccine administration to include signs and/or symptoms from more than 1 ofthe following systems:
– Dermatologic: urticaria, flushing, angioedema, pruritus– Respiratory: rhinoconjunctivitis (red, watery, itchy eyes, stuffy, runny, itchy nose, sneezing), upper airway edema (change in voice, difficulty
swallowing, difficulty breathing), bronchospasm/asthma (cough, wheeze, shortness of breath, chest tightness)– Cardiovascular: hypotension, tachycardia, palpitations, light-headedness, loss of consciousness (Note: hypotension or loss of consciousness with
pallor and bradycardia is much more likely a vasovagal reaction.)– GI: cramping, nausea, vomiting, diarrhea
Possible Anaphylactic Reaction:Signs and/or symptoms from only 1 system (as above)Signs and/or symptoms from more than 1 system (as above) but occurring more than 4 hours after vaccination
Note 2. Skin tests with vaccine and components including gelatin, egg, chicken and/or yeastVaccine skin tests:
– Prick test with full strength vaccine (consider dilution if history of life-threatening reaction)– If prick test with full strength vaccine negative, intradermal test with 0.02 cc vaccine 1:100– Note: Vaccine skin tests may cause false (or clinically irrelevant) positive reactions
Vaccine component/food skin tests:– Prick tests with commercial extracts of whole egg or egg white (influenza and yellow fever vaccines), chicken (yellow fever vaccine) or
Saccharomyces cerevisiae yeast (Hepatitis B vaccine and Human Papillomavirus vaccine)– Prick test with sugared gelatin (e.g. Jell-O®: dissolve 1 teaspoon (5 grams) of gelatin powder in 5 cc normal saline) Vaccines that contain gelatin:
DTaP (some brands), influenza (some brands), Japanese encephalitis, measles, mumps, rabies (some brands), rubella, varicella, yellow fever, zoster
Note 3. If fewer than the recommended number of doses received, consider measuring level of IgG antibodies to immunizing agent. If at a levelassociated with protection from disease, consider withholding additional doses although magnitude and duration of immunity may be less than if alldoses received.
Note 4. Vaccine administration in graded doses:For a vaccine where usual dose is 0.5 ml, administer graded doses of vaccine at 15 minute intervals: 0.05 ml of 1:10 dilution, 0.05 ml of full strength,0.10 ml of full strength, 0.15 ml of full strength, 0.20 ml of full strength. For influenza vaccine in egg-allergic patients, if the egg protein content of thevaccine is known to be < 1.2 �gm/mL, administer 10% of the dose, followed in 30 minutes by the remaining 90%, or as a single dose.
S2 ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY

cerns about H1N1 influenza, interest in the health benefits ofvaccination is greater than ever. Our hope is that this publi-cation will result in safe vaccination for patients with sus-pected allergy to vaccines.
Immunization is perhaps the greatest public health achieve-ment of all time,1 having significantly reduced the morbidityand mortality of many infectious diseases.2 Routine immuni-zation of children, adolescents, and adults provides substan-tial protection from a large number of infectious diseases.The current vaccination schedules for children and adults areavailable at www.cdc.gov/vaccines/recs/schedules.3–5 Pa-tients who have experienced adverse reactions to vaccinesmay unnecessarily be advised to avoid subsequent immuni-zation, which may have important adverse personal and pop-ulation health consequences.6–10 Although there are someadverse reactions to vaccines that constitute absolute contra-indications to administration of future doses, most such re-actions do not preclude subsequent immunization.11 Patientswho have experienced some ill effect after receiving a vac-cine warrant evaluation by an allergist/immunologist. In mostcases, a risk-benefit analysis will favor subsequent immuni-zation (Figure 1).
CLASSIFICATION OF RECOMMENDATIONS ANDEVIDENCECategory of evidenceIa Evidence from meta-analysis of randomized controlled
trialsIb Evidence from at least one randomized controlled trialIIa Evidence from at least one controlled study without ran-
domizationIIb Evidence from at least one other type of quasiexperimen-
tal studyIII Evidence from nonexperimental descriptive studies, such
as comparative studiesIV Evidence from expert committee reports or opinions or
clinical experience of respected authorities or both
Strength of recommendationA Directly based on category I evidenceB Directly based on category II evidence or extrapolated
recommendation from category I evidenceC Directly based on category III evidence or extrapolated
recommendation from category I or II evidenceD Directly based on category IV evidence or extrapolated
recommendation from category I, II, or III evidence
SUMMARY STATEMENTSSummary Statement 1. Mild local reactions and constitutionalsymptoms, such as fever, after vaccinations are common anddo not contraindicate future doses. Rarely, delayed-type hy-persensitivity to a vaccine constituent may cause an injectionsite nodule, but this is not a contraindication to subsequentvaccination. (C)
Local, injection site reactions (swelling, redness, and/orsoreness) and constitutional symptoms, especially fever, are
common after the administration of most vaccines and are notcontraindications to subsequent vaccination.11 Neomycin iscontained in several vaccines.12 For those reporting a de-layed-type hypersensitivity contact dermatitis to neomycin,the only anticipated reaction is a small, temporary papule atthe injection site,13,14 and this is not a contraindication tosubsequent vaccination.11 Delayed-type hypersensitivity tothimerosal has also been reported.15 Although patients with a
Table 1. Levels of Antibody Associated With Protection FromVaccine-Preventable Diseases
VaccineProtective level of IgG
antibody >
Diphtheria 0.1 IU/mL11
Haemophilus influenzae type B 0.15 �g/mL29
Hepatitis A 10 mIU/mL30
Hepatitis B surface antibody 10 mIU/mL31
Measles (rubeola) 120 mIU/mL (PRN titer)32
Polio (inactivated) 1:8 neutralizing antibody titer33
Rabies 0.5 IU/mL (VNA titer)34
Rubella 10 IU/mL80
Tetanus 0.1 IU/mL11
Yellow fever 0.7 IU/mL29
Abbreviations: IU, international units; mIU, milli-international units;PRN, plaque reduction neutralization; VNA, virus-neutralizing anti-bodies.
Table 2. Gelatin Content of Vaccines 2008
Vaccine Gelatin content
DTaP (Tripedia/TriHIBit; SanofiPasteur, Swiftwater,Pennsylvania)
28 �g per 0.5-mL dosea
Influenza (Fluzone; SanofiPasteur)
250 �g per 0.5-mL doseb
Influenza (FluMist; MedimmuneVaccines, Gaithersburg,Maryland)
2000 �g per 0.2-mL doseb
Japanese Encephalitis (JE-VAX;Sanofi Pasteur)
500 �g per 1.0-mL doseb
Measles, Mumps, Rubella(ATTENUVAX, MERUVAXII,MMRII, MUMPSVAX; Merck,Whitehouse Station, NewJersey)
14,500 �g per 0.5-mL doseb
Measles, mumps, rubella,varicella (ProQuad; Merck)
11,000 �g per 0.5-mL doseb
Rabies (RabAvert; Novartis,Emeryville, California)
12,000 �g per 1.0-mL doseb
Typhoid Vaccine Live OralTy21a (VIVOTIF; Berna, CoralGables, Florida)
Capsuleb
Varicella (VARIVAX; Oka/Merck) 12,500 �g per 0.5-mL doseb
Yellow Fever (YF-VAX; SanofiPasteur)
7,500 �g per 0.5-mL dosea
Zoster (ZOSTAVAX; Oka/Merck) 15,580 �g per 0.65-mL doseb
a Sanofi Pasteur, oral communication, September 4, 2009.b Package inserts.
VOLUME 103, OCTOBER, 2009 S3

positive patch test result for thimerosal may have large localreactions to vaccination with thimerosal-containing vac-cines,16,17 most such patients do not.15,18–20 Neither a history ofsuch reactions nor a positive patch test result to thimerosal isa contraindication to future vaccination.11 There is a singlecase report of a generalized pruritic maculopapular rash at-tributed to thimerosal in an influenza vaccine.21 Aluminum-containing vaccines12 rarely cause persistent nodules at theinjection site, possibly because of delayed hypersensitivity orother immune responses to aluminum.22–24
Summary Statement 2. Anaphylactic reactions to vaccinesare estimated to occur at a rate of approximately 1 per milliondoses. There are approximately 235 million doses of vaccinesadministered in the United States each year. (B)
Anaphylaxis after vaccination is rare. The Vaccine SafetyDatalink reviewed the diagnosis codes from medical encoun-ters after the administration of more than 7.5 million doses ofvaccines and estimated the risk of anaphylaxis to be 0.65million to 1.53 per million doses.25 The Centers for DiseaseControl and Prevention (CDC) estimates that there were235,705,179 doses of all vaccines distributed in the UnitedStates in 2007 (Angela Calugar, CDC, written communica-tion, December 19, 2008). Thus, there are approximately 150to 350 cases of vaccine-induced anaphylaxis in the UnitedStates annually. Fatalities from vaccine-induced anaphylaxisare exceedingly rare.26
Summary Statement 3. All serious events occurring aftervaccine administration should be reported to the VaccineAdverse Event Reporting System, even if it is not certain thatthe vaccine was causal. (C)
In 1990, the Vaccine Adverse Event Reporting System(VAERS) was established by the CDC and Food and DrugAdministration (FDA).27 VAERS relies on reporting byhealth care professionals and parents or patients, and allserious events after vaccination should be reported.28 Thesereports of suspected associations between vaccine adminis-tration and adverse events can then be evaluated for strengthof potential causality.
Summary Statement 4. Measuring levels of IgG antibody tothe immunizing agent in a vaccine suspected of causing aserious adverse reaction to determine if they are at protectivelevels can help determine whether or not subsequent dosesare required. (B)
In a patient who has experienced an apparent adversereaction to vaccine yet has received fewer than the recom-mended number of doses, the level of IgG antibodies to theimmunizing agent can be measured to see if it is at a levelassociated with protection from disease. Such levels havebeen established for some, but not all, vaccines (Table1)11,29–34 and are available from many diagnostic laboratories.If so, consideration can be given to withholding additionaldoses, although the magnitude and duration of immunity maybe less than if all doses were received.35,36 Even if the rec-ommended number of doses has already been received or ifprotective antibody levels have already been achieved, eval-uation of the reaction, including skin testing if indicated,should be undertaken as discussed herein.
Summary Statement 5. All suspected anaphylactic reac-tions to vaccines should ideally be evaluated in an attempt todetermine the culprit allergen. (B)
When a patient experiences an apparently IgE-mediatedreaction after an immunization, the patient is often labeled asbeing “allergic” to the vaccine and advised against receivingfuture doses without further investigation. However, this ap-proach should be avoided because it may leave patientsinadequately immunized if they unnecessarily avoid vaccinesto which they are not allergic or if the vaccine could beadministered safely despite their allergy. In addition, notknowing the particular constituent of a vaccine to which thepatient is allergic may pose a risk with future vaccinationsthat contain the same ingredient.
Summary Statement 6. IgE-mediated reactions to vaccinesare more often caused by vaccine components, such as gelatinor egg protein, rather than the immunizing agent itself. (B)
Gelatin is added to many vaccines (Table 2) as a stabilizerand has been shown to be responsible for many anaphylacticreactions to MMR, varicella, and Japanese encephalitis vac-cines.37–40 Vaccine manufacturers in Japan and Germany re-moved gelatin or changed to a less allergenic gelatin with aresultant decrease in allergic reactions.41,42 A history of al-lergy to the ingestion of gelatin should be sought before theadministration of any gelatin-containing vaccine. A negativehistory, however, may not exclude an allergic reaction togelatin injected with the vaccine.38 Gelatin used in vaccines isof either bovine or porcine origin, which are extensively
Table 3. Egg Content of Vaccines
Vaccine Grown in Egg protein contentApproach in egg allergic
patient
Measles and mumps Chick embryo fibroblastcell cultures
Picograms to nanograms Administer in usual manner44–46
Purified chick embryo rabies Chick embryo fibroblastcell cultures
Picograms to nanograms Administer in usual manner109
Influenza (killed injected andlive attenuated nasal)
Chick extraembryonicallantoic fluid
Micrograms Skin test with egg and vaccinebefore administration48,110
Yellow fever Chick embryos Micrograms Skin test with egg and vaccinebefore administration67
S4 ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY

cross-reactive.37,38 There are no published reports of patientsallergic to both gelatin and beef or pork meat.
Measles and mumps vaccines and 1 type of rabies vaccineare grown in chick embryo fibroblast cultures and containnegligible or no egg protein (Table 3).43 Measles or MMRvaccines can be administered to egg allergic children withoutadverse reactions44,45 and can be given to such patients with-out skin testing.46 Egg protein is present in higher amounts inyellow fever and influenza vaccines12 (Table 3) and maycause reactions in egg allergic recipients. Administration ofinfluenza vaccine containing 1.2 �g/mL of egg protein hasbeen safely administered to egg allergic patients, initially in a2-dose protocol (10% of the dose followed in 30 minutes bythe remaining 90% of the dose) and later as a single dose.47
However, the influenza vaccine is newly made every year,and there are variable amounts of egg protein present in anygiven years’ vaccine (as high as 42 �g/mL of egg protein).48
Whether this is sufficient to cause a reaction in an egg allergicpatient is also not known but may pose a risk. Patients can beallergic to heat-labile egg proteins in raw egg and, becausethey tolerate the ingestion of cooked egg, do not think ofthemselves as being egg allergic.49 Thus, the clinical historymay not identify all persons allergic to egg proteins present ininfluenza or yellow fever vaccines. Chicken proteins otherthan those found in chicken egg may be present in yellowfever vaccine and may be responsible for reactions in chickenallergic recipients.50
Hepatitis B vaccines are grown in Saccharomyces cerevi-siae (baker’s yeast or brewer’s yeast) and contain residualyeast protein,12 but adverse reactions to these, if any, appearto be rare.51 Human papillomavirus vaccine may also containresidual yeast protein.52
The rubber in vaccine vial stoppers or syringe plungersmay be either dry natural rubber (DNR) latex or syntheticrubber. Those made with DNR pose a theoretical risk to thepatient who is latex allergic. There is 1 report of an anaphy-lactic reaction in a latex allergic patient after hepatitis Bvaccine attributed to rubber in the stopper.53 A review ofmore than 160,000 VAERS reports found only 28 cases ofpossible immediate-type allergic reactions after receiving aDNR-containing vaccine, and these may have been due toother components.54 The latex content of vaccine packagingis provided in Table 4 and is updated at www.cdc.gov/vaccines/pubs/pinkbook/pink-appendx.htm.55
There is a single report of an immediate-type allergicreaction to a vaccination that was attributed to neomycin.56
However, the patient had a maculopapular (not urticarial)rash to the topical application of neomycin, and no testing forIgE to neomycin was performed. There is a single case reportof an immediate-type reaction that may have been caused bythimerosal in a vaccine.57
However rare, if a patient gives a history of an immediate-type reaction to yeast, latex, neomycin, or thimerosal, it isappropriate to investigate with immediate-type skin testingbefore immunization with a vaccine containing these constit-uents.
Table 5 lists vaccine excipients by vaccine. Updated listsof vaccine excipients by vaccine and by excipient areavailable at www.cdc.gov/vaccines/pubs/pinkbook/pink-appendx.htm.12,58
Summary Statement 7. Patients who have had an apparentanaphylactic reaction after immunization should undergo im-mediate-type allergy skin testing to help confirm that thereaction was IgE mediated and determine the responsiblecomponent of the vaccine. (B)
To determine whether a vaccine was responsible for apatient’s apparent allergic reaction, skin testing with thevaccine should be performed.35,36 The vaccine should first betested by the prick method. Full-strength vaccine can be usedunless the history of the reaction was truly life-threatening, inwhich case beginning even the prick test with dilute vaccineis appropriate. If the full-strength prick test result is negative,with appropriate positive and negative controls, an intrader-mal test with the vaccine diluted 1:100 should be per-formed,59 again with appropriate controls.
As with any skin test reagent, and particularly with mate-rials not standardized for skin testing such as vaccines, false-positive (irritant) results and clinically irrelevant positiveresults may occur. Likewise, false-negative response mayalso be seen. Some patients known to have IgE antibodies tovarious vaccines by in vitro testing or skin testing havenonetheless received the vaccines in the usual manner with-out reaction.47,60–63 Although these findings complicate theinterpretation of vaccine skin tests, if the test result is positivein a patient with a history of an allergic reaction to thevaccine, the patient must be assumed to be allergic. Intrader-mal skin tests with some vaccines, such as tetanus toxoid, canalso induce delayed-type hypersensitivity responses.64
If the suspect vaccine contains gelatin (Table 2), egg(influenza and yellow fever), chicken (yellow fever), or yeast(hepatitis B vaccine and human papillomavirus vaccine), thepatient should also be skin tested for these allergens.35,36 Egg,chicken, and yeast extracts for skin testing are commerciallyavailable. Gelatin can be prepared by dissolving 1 teaspoon(5 g) of any sugared gelatin powder (for example, Jell-O) in5 mL of normal saline to create a prick skin test solution,recognizing that this is not a standardized, validated, FDA-approved method. In vitro assays for specific IgE antibodyare also commercially available for these foods, includinggelatin.
Summary Statement 8. If the intradermal skin test result isnegative, the chance that the patient has IgE antibody to anyvaccine constituent is negligible, and the vaccine can beadministered in the usual manner. It is prudent, nonetheless,in a patient with a history suggestive of an anaphylacticreaction to administer the vaccine under observation withepinephrine and other treatment available. (B)
Although there are no formal studies to evaluate the pos-itive and negative predictive values for intradermal skin testresults in patients who have had apparent allergic reactions tovaccines, the approach is almost certainly sufficiently sensi-tive to identify patients with IgE-mediated reactions to some
VOLUME 103, OCTOBER, 2009 S5

vaccine component. Intradermal skin tests are recommendedwhen increased sensitivity is required for the evaluation ofanaphylaxis.64 There are no reports of patients with negativeintradermal skin test results to a vaccine reacting to subse-quent administration of that vaccine. As with any diagnostictest, the increased sensitivity of intradermal testing likelycomes with some loss of specificity. Thus, although there arereports of patients being safely administered the vaccinesafter negative intradermal skin test results,47,65 there are alsoreports of patients with positive skin test results nonethelessreceiving the vaccines uneventfully.47,63 Dilutions of vaccinesof 1:100 have been demonstrated to be nonirritating.59 Thus,if the skin test results to the vaccine and its ingredients arenegative, particularly at the intradermal level (with the vac-cine diluted 1:100), then it is unlikely that the patient has IgEantibody to any component of the vaccine, and they can be
Table 4. Latex in Vaccine Packaginga
Vaccine Latex
Anthrax (BioThrax) Yes–vialComvax Yes–vialDTaP
Daptacel Yes–vialInfanrix Yes–syringe
No–vialTripedia Yes–vial
DT (generic) Yes–vialHib
HibTITER Yes–vialPedvaxHIB Yes–vialActHIB Yes–diluent vial
No–lyophilized vaccine vialHepatitis A
Havrix Yes–syringeNo–vial
Vaqta Yes–vialYes–syringe
Hepatitis BEngerix-B Yes–syringe
No–vialRecombivax HB Yes–vial
HPV (Gardasil) NoInfluenza
Fluarix Yes–syringeFluvirin NoFluzone NoFluLaval NoAfluria NoFluMist No
Japanese encephalitisJE-Vax NoIxiaro No
Kinrix Yes–syringeNo–vial
MMR (M-M-R II) NoMMRV (ProQuad) NoMeasles (Attenuvax) NoMumps (Mumpsvax) NoRubella (Meruvax II) NoMeningococcal
Menomune Yes–vialMenactra Yes–vial
No–syringePediarix Yes–syringe
No–vialPentacel NoPneumococcal
Pneumovax 23 NoPrevnar Yes–syringe, before lot D46873
No–syringe, lot D46873 andafter
Polio (IPOL) Yes–syringeNo–vial
RabiesImovax Rabies NoRabAvert No
Continued
Table 4. (Continued)
Vaccine Latex
RotavirusRotaTeq NoRotarix Yes–applicator
No–vial and transfer adapterTd
Decavac No–vialNo–syringe
Generic Yes–vialYes–syringe
TdapAdacel NoBoostrix Yes–syringe
No–vialTriHIBit Yes–vialTwinrix Yes–syringe
No–vialTyphoid
Typhim Vi NoVivotif Berna NA
Varicella (Varivax) NoVaccinia (smallpox) (ACAM2000) NoYellow fever (YF-Vax) Yes–vial
Abbreviations: DT, diphtheria and tetanus toxoids (pediatric formula-tion); DTaP, diphtheria and tetanus toxoids and acellular pertussis(pediatric formulation); Hib, Haemophilus influenzae type B; HPV,human papillomavirus; MMRV, measles, mumps, rubella and vari-cella; NA, not applicable; Td, tetanus and diphtheria toxoids (adult/adolescent formulation); Tdap, tetanus and diphtheria toxoids andacellular pertussis (adult/adolescent formulation).a “If a person reports a severe (anaphylactic) allergy to latex, vaccinessupplied in vials or syringes that contain natural rubber should not beadministered unless the benefit of vaccination outweighs the risk fora potential allergic reaction. For latex allergies other than anaphylacticallergies (e.g., a history of contact allergy to latex gloves), vaccinessupplied in vials or syringes that contain dry natural rubber or rubberlatex can be administered.” (Advisory Committee on ImmunizationPractices General Recommendations on Immunization, 2006). Thistable is accurate, to the best of our knowledge, as of June 2009. If indoubt, check the package insert for the vaccine in question.
S6 ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY

Table 5. Excipients Included in US Vaccines, by Vaccinea
Vaccine Contains
Anthrax (BioThrax) Aluminum hydroxide, amino acids, benzethonium chloride, formaldehyde or formalin, inorganic salts andsugars, vitamins
BCG (Tice) Asparagine, citric acid, lactose, glycerin, iron ammonium citrate, magnesium sulfate, potassium phosphateDTaP (Daptacel) Aluminum phosphate, ammonium sulfate, Casamino acid, dimethyl-�-cyclodextrin, formaldehyde or
formalin, glutaraldehyde, 2-phenoxyethanolDTaP (Infanrix) Aluminum hydroxide, bovine extract, formaldehyde or formalin, glutaraldehyde, 2-phenoxyethanol,
polysorbate 80DTaP (Tripedia) Aluminum potassium sulfate, ammonium sulfate, bovine extract, formaldehyde or formalin, gelatin,
polysorbate 80, sodium phosphate, thimerosalb
DTaP/Hib (TriHIBit) Aluminum potassium sulfate, ammonium sulfate, bovine extract, formaldehyde or formalin, gelatin,polysorbate 80, sucrose, thimerosalb
DTaP-IPV (Kinrix) Aluminum hydroxide, bovine extract, formaldehyde, lactalbumin hydrolysate, monkey kidney tissue,neomycin sulfate, polymyxin B, polysorbate 80
DTaP-Hep B-IPV (Pediarix) Aluminum hydroxide, aluminum phosphate, bovine protein, lactalbumin hydrolysate, formaldehyde orformalin, glutaraldehyde, monkey kidney tissue, neomycin, 2-phenoxyethanol, polymyxin B, polysorbate80, yeast protein
DtaP-IPV/Hib (Pentacel) Aluminum phosphate, bovine serum albumin, formaldehyde, glutaraldehyde, MRC-5 DNA and cellularprotein, neomycin, polymyxin B sulfate, polysorbate 80, 2-phenoxyethanol
DT (sanofi) Aluminum potassium sulfate, bovine extract, formaldehyde or formalin, thimerosal (multidose) orthimerosalb (single dose)
DT (Massachusetts) Aluminum hydroxide, formaldehyde or formalinHib (ACTHib) Ammonium sulfate, formaldehyde or formalin, sucroseHib (PedvaxHib) Aluminum hydroxyphosphate sulfateHib/Hep B (Comvax) Amino acids, aluminum hydroxyphosphate sulfate, dextrose, formaldehyde or formalin, mineral salts,
sodium borate, soy peptone, yeast proteinHep A (Havrix) Aluminum hydroxide, amino acids, formaldehyde or formalin, MRC-5 cellular protein, neomycin sulfate, 2-
phenoxyethanol, phosphate buffers, polysorbateHep A (Vaqta) Aluminum hydroxyphosphate sulfate, bovine albumin or serum, DNA, formaldehyde or formalin, MRC-5
cellular protein, sodium borateHep B (Engerix-B) Aluminum hydroxide, phosphate buffers, thimerosal,b yeast proteinHep B (Recombivax) Aluminum hydroxyphosphate sulfate, amino acids, dextrose, formaldehyde or formalin, mineral salts,
potassium aluminum sulfate, soy peptone, yeast proteinHep A/Hep B (Twinrix) Aluminum hydroxide, aluminum phosphate, amino acids, dextrose, formaldehyde or formalin, inorganic
salts, MRC-5 cellular protein, neomycin sulfate, 2-phenoxyethanol, phosphate buffers, polysorbate 20,thimerosal,b vitamins, yeast protein
HPV (Gardasil) Amino acids, amorphous aluminum hydroxyphosphate sulfate, carbohydrates, L-histidine, mineral salts,polysorbate 80, sodium borate, vitamins
Influenza (Afluria) �-Propiolactone, calcium chloride, neomycin, ovalbumin, Polymyxin B, potassium chloride, potassiumphosphate, sodium phosphate, sodium taurodeoxycholate.
Influenza (Fluarix) Egg albumin (ovalbumin), egg protein, formaldehyde or formalin, gentamicin, hydrocortisone, octoxynol-10,�-tocopheryl hydrogen succinate, polysorbate 80, sodium deoxycholate, sodium phosphate, thimerosalb
Influenza (Flulaval) Egg albumin (ovalbumin), egg protein, formaldehyde or formalin, sodium deoxycholate, phosphate buffers,thimerosal
Influenza (Fluvirin) �-Propiolactone, egg protein, neomycin, polymyxin B, polyoxyethylene 9–10 nonyl phenol (triton N-101,octoxynol 9), thimerosal (multidose containers), thimerosalb (single-dose syringes)
Influenza (Fluzone) Egg Protein, Formaldehyde or Formalin, Gelatin, Octoxinol-9 (Triton X-100), Thimerosal (multidosecontainers)
Influenza (FluMist) Chick kidney cells, egg protein, gentamicin sulfate, monosodium glutamate, sucrose phosphate glutamatebuffer
IPV (Ipol) Calf serum protein, formaldehyde or formalin, monkey kidney tissue, neomycin, 2-phenoxyethanol,polymyxin b, streptomycin
Japanese Encephalitis (JE-Vax) Formaldehyde or formalin, gelatin, mouse serum protein, polysorbate 80, thimerosalJapanese Encephalitis (Ixiaro) Aluminum hydroxide, bovine serum albumin, formaldehyde, protamine sulfate, sodium metabisulfiteMeningococcal (Menactra) Formaldehyde or formalin, phosphate buffersMeningococcal (Menomune) Lactose, thimerosal (10-dose vials only)MMR (MMR-II) Amino acid, bovine albumin or serum, chick embryo fibroblasts, human serum albumin, gelatin, glutamate,
neomycin, phosphate buffers, sorbitol, sucrose, vitamins
Continued
VOLUME 103, OCTOBER, 2009 S7

given the vaccine in the usual manner but observed for atleast 30 minutes afterward.35,36
Summary Statement 9. In patients with histories and skintests results consistent with an IgE-mediated reaction to avaccine, who require additional doses of the suspect vaccineor other vaccines with common ingredients, considerationcan be given to administering the vaccine in graded dosesunder observation. (C)
If vaccine or vaccine component skin test results are pos-itive, the vaccine may still be administered, if necessary, ingraded doses (Table 6).46,66,67 For a vaccine where the fullnormal dose volume is 0.5 mL, the patient is first given 0.05
mL of a 1:10 dilution and then given (at 15-minute intervals),0.05 mL of full-strength vaccine, with subsequent doses of0.1 mL, 0.15 mL, and finally 0.2 mL for a cumulative dose of0.5 mL. This or similar protocols have been used successfullyfor the administration of egg-containing vaccines to eggallergic recipients66 and with other vaccines as well.50,68
This procedure in a patient who is presumed to be allergicto the vaccine being administered needs to be performedunder direct medical supervision with emergency medica-tions and equipment to promptly treat an anaphylactic reac-tion should it occur.64 Whether such challenges are under-taken in the office vs hospital or with or without an
Table 5. (Continued)
Vaccine Contains
MMRV (ProQuad) Bovine albumin or serum, gelatin, human serum albumin, monosodium L-glutamate, MRC-5 CellularProtein, Neomycin, Sodium Phosphate Dibasic, Sodium Bicarbonate, Sorbitol, Sucrose, PotassiumPhosphate Monobasic, Potassium Chloride, Potassium Phosphate Dibasic
Pneumococcal (Pneumovax) Bovine protein, phenolPneumococcal (Prevnar) Aluminum phosphate, amino acid, soy peptone, yeast extractRabies (Imovax) Human serum albumin, �-propiolactone, MRC-5 cellular protein, neomycin, phenol red
(phenolsulfonphthalein), vitaminsRabies (RabAvert) Amphotericin B, �-propiolactone, bovine albumin or serum, chicken protein, chlortetracycline, egg
albumin (ovalbumin), EDTA, neomycin, potassium glutamateRotavirus (RotaTeq) Cell culture media, fetal bovine serum, sodium citrate, sodium phosphate monobasic monohydrate,
sodium hydroxide sucrose, polysorbate 80Rotavirus (Rotarix) Amino acids, calcium carbonate, calcium chloride, D-glucose, dextran, ferric (III) nitrate, L-cystine,
L-tyrosine, magnesium sulfate, phenol red, potassium chloride, sodium hydrogenocarbonate, sodiumphosphate, sodium L-glutamine, sodium pyruvate, sorbitol, sucrose, vitamins, xanthan
Td (Decavac) Aluminum potassium sulfate, bovine extract, formaldehyde or formalin, 2-phenoxyethanol, peptone,thimerosalb
Td (Massachusetts) Aluminum hydroxide, aluminum phosphate, formaldehyde or formalin, thimerosal (some multidosecontainers)
Tdap (Adacel) Aluminum phosphate, formaldehyde or formalin, glutaraldehyde, 2-phenoxyethanolTdap (Boostrix) Aluminum hydroxide, bovine extract, formaldehyde or formalin, glutaraldehyde, polysorbate 80Typhoid (inactivated - Typhim Vi) Disodium phosphate, monosodium phosphate, phenol, polydimethylsiloxane,
hexadecyltrimethylammonium bromideTyphoid (oral - Ty21a) Amino acids, ascorbic acid, bovine protein, casein, dextrose, galactose, gelatin, lactose, magnesium
stearate, sucrose, yeast extractVaccinia (ACAM2000) Glycerin, human serum albumin, mannitol, monkey kidney cells, neomycin, phenol, polymyxin BVaricella (Varivax) Bovine albumin or serum, EDTA, gelatin, monosodium L-glutamate, MRC-5 DNA and cellular protein,
neomycin, potassium chloride, potassium phosphate monobasic, sodium phosphate monobasic,sucrose
Yellow fever (YF-Vax) Egg protein, gelatin, sorbitolZoster (Zostavax) Bovine calf serum, hydrolyzed porcine gelatin, monosodium L-glutamate, MRC-5 DNA and cellular
protein, neomycin, potassium phosphate monobasic, potassium chloride, sodium phosphate dibasic,sucrose
Abbreviations: DT, diphtheria and tetanus toxoids (pediatric formulation); DTaP, diphtheria and tetanus toxoids and acellular pertussis (pediatricformulation); Hep A, hepatitis A; Hep B, hepatitis B; Hib, Haemophilus influenzae type B; HPV, human papillomavirus; IPV, inactivated poliovirus;MMRV, measles, mumps, rubella and varicella; Td, tetanus-diphtheria toxoids (adult/adolescent formulation); Tdap, tetanus and diphtheria toxoidsand acellular pertussis (adult/adolescent formulation).a Vaccine Excipient & Media Summary, Part 2. Includes vaccine ingredients (eg, adjuvants and preservatives) and substances used during themanufacturing process, including vaccine-production media, that are removed from the final product and present only in trace quantities. Inaddition to the substances listed, most vaccines contain sodium chloride (table salt). Adapted from Grabenstein JD. ImmunoFacts: Vaccines &Immunologic Drugs. St. Louis, MO: Wolters Kluwer Health; 2009 and individual product package inserts. All reasonable efforts have been madeto ensure the accuracy of this information, but manufacturers may change product contents before that information is reflected here.b The product should be considered equivalent to thimerosal-free products. This vaccine may contain trace amounts (�0.3 �g) of mercury left afterpostproduction thimerosal removal, but these amounts have no biological effect.
S8 ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY

intravenous line in place depends on the severity of theoriginal reaction to the vaccine and the patient’s medicalcondition.64
For influenza vaccine in egg allergic patients, if the eggprotein content of the vaccine is known to be 1.2 �g/mL orless, the vaccine can be administered in 2 doses (10% of thedose, followed in 30 minutes by the remaining 90%) or as asingle dose, without prior vaccine skin testing,47 althoughobservation for at least 30 minutes afterward seems prudent(Table 6). Unfortunately, the specific egg protein content ofany given year’s influenza vaccines is not readily available.47
Because of the lot to lot variability in the egg proteincontent of egg-containing vaccines,48 even if an egg allergicpatient has a negative vaccine skin test response and is giventhe vaccine in the usual manner or has a positive vaccine skintest response and is given the vaccine in graded doses, if thepatient needs to be given the vaccine again at a later time, thevaccine skin test, and graded challenge if necessary, wouldneed to be repeated.
Summary Statement 10. Some more serious, and less com-mon, reactions to vaccines require evaluation, but only a feware absolute contraindications to future doses. (B)
In addition to anaphylactic reactions (discussed herein),some vaccines are capable of causing other rare but seriousreactions that might contraindicate the administration of fu-ture doses.11
There was a particular type of influenza vaccine, namely,swine flu vaccine administered in 1976, which was associatedwith an increased risk for Guillain-Barre syndrome (GBS),estimated at 1 additional case per 100,000 vaccinations (overthe annual background rate of 10 to 20 cases per millionadults).69 In subsequent years, influenza vaccines have beencarefully monitored for this possible adverse effect and haveshown no consistent increased risk. If there is any increasedrisk, it is on the order of 1 per million.69,70 A low level of GBScases continues to be reported in temporal association withprevious influenza infection71 and with influenza and othervaccines.72,73 Previous GBS raises the risk of a recurrence ofGBS. Persons who developed GBS within 6 weeks of influ-enza vaccination should avoid subsequent immunization withinfluenza vaccines.69 However, individuals with a history ofGBS unrelated to influenza infection or vaccination whowould benefit from immunization can be vaccinated, partic-
ularly if the influenza infection risk is high or if the infectingstrain is resistant to antiviral therapy.69 The live attenuatedinfluenza vaccine is not recommended in persons with ahistory of GBS simply because it has not been studied forsafety in such persons.69
Measles, mumps, and rubella (MMR) vaccines can causeadverse reactions related to the live viruses they contain.Transient rashes appear in as many as 5% of recipients ofmeasles vaccine, and this probably represents vaccine-in-duced modified measles.32 There is a late-onset fever occur-ring 5 to 12 days after vaccine administration in as many as15% of recipients of the MMR vaccine.32,46,74 As with anyfever in young children, this increases the risk of febrileseizures; however, such seizures do not have any sort oflong-term sequelae.75,76 Recipients of the MMR vaccine canalso have thrombocytopenia, which is usually without anysignificant clinical consequence, but can rarely cause hemor-rhage.26,74,77,78 The rate of thrombocytopenia is much higherwith the disease itself.74 Rubella vaccine can cause acutearthritis in approximately 15% of adult women who receivedthe vaccine.79,80 This may represent a direct infection of thejoints by the vaccine virus but has a questionable associationwith chronic arthritis.79,80 None of these events are contrain-dications to the administration of subsequent doses of MMRvaccine.11
The most serious adverse effect related to pertussis vaccineis termed encephalopathy. This term describes a specific andsevere reaction characterized as an “acute, severe CNS [cen-tral nervous system] disorder occurring within 7 days follow-ing vaccination and generally consisting of major alterationsin consciousness, unresponsiveness, generalized or focal sei-zures that persist more than a few hours, with failure torecover within 24 hours.”26 This event happens with an inci-dence that may actually be 0, meaning that it is not actuallyincreased after vaccination, but to a maximum of 10 permillion doses of diphtheria and tetanus toxoids and whole-cell pertussis (DTP) vaccine.74 This can have permanentneurologic sequela and is an absolute contraindication tofurther pertussis vaccination.11 Pertussis vaccine can causeless severe apparent neurologic events, including febrile sei-zures,75 inconsolable crying,46 and hypotonic-hyporesponsiveepisodes.81 Although these are clearly concerning episodesfor parents to witness, none of them result in permanent
Table 6. Administration of Vaccines in Graded Doses
For a vaccine for which the full normal-dose volume is 0.5 mL,give the following doses at 15-minute intervals as tolerateda
For influenza vaccine in egg allergic patients, if the egg protein contentof the vaccine is known to be �1.2 �g/mL administer as followsb
0.05 mL, 1:10 dilution In 2 doses: 10% of the dose (0.025 mL or 0.05 mL) followed in 30minutes by the remaining 90% of the dose (0.225 mL or 0.45 mL) or0.05 mL, full strength
0.1 mL, full strength In a single dose (0.25 mL or 0.5 mL)0.15 mL, full strength0.2 mL, full strength
a Must be done under direct medical supervision with emergency medications and equipment to promptly treat an anaphylactic reaction shouldit occur.b Observe for at least 30 minutes afterward.
VOLUME 103, OCTOBER, 2009 S9

sequelae, and none of them are contraindications to furtherdoses of these vaccines.11,74,82 Of note is the fact that all theseserious and less serious neurologic events after pertussis-containing vaccines have been significantly reduced sincechanging from the diphtheria and tetanus toxoids and whole-cell pertussis vaccine (DTP) to the diphtheria and tetanustoxoids and acellular pertussis vaccine (DTaP).46,82–87
Tetanus toxoid often causes patients to develop a largelocal swelling.88 This probably represents an Arthus reactionin patients with preexisting antitetanus antibodies from priorimmunizations who then receive a large injection of antigenin the vaccine. These reactions may cause discomfort but arenot serious. Tetanus toxoid also has some potential associa-tion with Guillain-Barre syndrome and with a rare localneurologic event called brachial neuritis, which involvesshoulder pain followed by weakness.26
Varicella vaccine is another live virus immunization thatcan cause vaccine-induced illness, particularly the appear-ance of varicella lesions. These reactions occur at the injec-tion site in approximately 3% of recipients and in another 3%are more generalized.89 The disease due to coincident naturalexposure may be difficult to distinguish from vaccine-in-duced varicella. A zoster-type rash may rarely appear after avaricella vaccination and may contain either vaccine-strain orwild-type virus.90,91 Although varicella disease (chickenpox)itself can be more severe in children with atopic dermatitis,the varicella vaccine can be safely administered to childrenwith atopic dermatitis without an increased risk of complica-tions.92
A serious adverse effect of yellow fever vaccine is enceph-alitis.93 The risk for this complication is as high as 4 per 1000infants, and for this reason the vaccine is relatively contrain-dicated in this age group. It should not be given to any infantyounger than 4 months and to those younger than 9 monthsonly if their risk from the disease is very high.46 The yellowfever vaccine has recently been associated with a very severeillness in adults. There have been fatalities from multisystem
disease with features strikingly similar to the disease yellowfever itself.94–98 This has occurred in patients who are notknown to be immunocompromised. The cause of these reac-tions is still unknown, but this vaccine should not be given topatients unless they are at risk of acquiring yellow fever,typically by traveling to an area where the disease is endem-ic.99
Summary Statement 11. Pregnant women should not bevaccinated with live vaccines. However, pregnant womenshould be given inactivated influenza vaccine, as well astetanus and hepatitis B vaccine if otherwise indicated. (B)
Because of a theoretical risk of transmitting the live agentto the fetus, pregnant women should not receive live vaccinessuch as MMR, varicella, or live attenuated influenza vac-cine.100 There is an increased risk of hospitalization frominfluenza in pregnancy, and therefore (inactivated) influenzavaccine is specifically indicated in women who will be preg-nant during the influenza season.100 Hepatitis B vaccine andtetanus and diphtheria vaccines should also be administeredto pregnant women if they would otherwise be indicated.100
Summary Statement 12. In general, live vaccines shouldnot be given to persons who are immune compromised be-cause of a risk of generalized infection with the immunizingagent. (B)
Live vaccines (Table 7) are generally contraindicated inpatients with immune suppression, specifically those withsevere humoral or cellular immune deficiency.11,46,101 Thisincludes patients with X-linked agammaglobulinemia, com-mon variable immune deficiency, severe combined immunedeficiency, severe human immunodeficiency virus (HIV) in-fection, leukemia, lymphoma, other malignant neoplasms, orpatients requiring treatment for these or other conditions withtreatment modalities that impair immune responses, such ashigh-dose corticosteroids (2 weeks of daily treatment withprednisone, 20 mg or 2 mg/kg or equivalent per day). Thereare, however, exceptions even to this general rule that im-mune compromised patients should not receive live viralvaccines.11,46,101 For example, the MMR vaccine should begiven to HIV-infected children and adults if they have onlymild or moderate disease. Similarly varicella vaccine shouldbe given to mildly HIV-infected children.
Summary Statement 13. Specific vaccines or vaccination ingeneral have been purported to have long-term consequences,including atopy, autism, and multiple sclerosis. Epidemio-logic studies have not supported such associations. (B)
There are a number of controversies related to long-termconsequences of particular vaccines or of vaccination ingeneral. There have been claims that receiving childhoodvaccinations increases the likelihood of developing atopicdisease, autism, diabetes, or multiple sclerosis. The associa-tions have all been extensively evaluated using many appro-priate research methods and epidemiologic studies, and norelationship between vaccinations and any of these outcomeshas been demonstrated in these studies.102–106 There has beenparticular concern about thimerosal, which was previouslyused as a preservative in vaccines. Although studies have
Table 7. Live vs Killed Vaccines
Live vaccines Killed vaccines
Bacille Calmette-Guerin (BCG)Influenza (intranasal)
Diphtheria, tetanus and acellularpertussis (DTaP, Tdap)
Measles-mumps-rubella (MMR) Diphtheria-tetanus (DT, Td)Oral poliovirus (OPV Hepatitis ARotavirus Hepatitis BTyphoid (oral) Hib conjugatesVaccinia (smallpox) Human papillomavirus (HPV)Varicella Inactivated poliovirus (IPV)Yellow fever Influenza (injectable)Zoster Japanese encephalitis
MeningococcalMeningococcal conjugatePneumococcalPneumococcal conjugateRabiesTyphoid (injectable)
S10 ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY

failed to support any adverse effect from thimerosal exposurein vaccines,107,108 all routinely recommended vaccines forinfants and children in the United States are now availableonly as thimerosal-free formulations or contain only traceamounts of thimerosal, with the exception of some inacti-vated influenza vaccines. Inactivated influenza vaccine forpediatric use is available as a thimerosal preservative-con-taining formulation, a trace thimerosal-containing formula-tion, and a thimerosal-free formulation.46
ACKNOWLEDGMENTSPublished Practice Parameters of the Joint Task Force onPractice Parameters for Allergy & Immunology include thefollowing:
1. Practice parameters for the diagnosis and treatment ofasthma. J Allergy Clin Immunol. 1995;96(suppl):S707-S870.
2. Practice parameters for allergy diagnostic testing. AnnAllergy. 1995;75:543–625.
3. Practice parameters for the diagnosis and managementof immunodeficiency. Ann Allergy. 1996;76:282–294.
4. Practice parameters for allergen immunotherapy. J Al-lergy Clin Immunol. 1996;98:1001–1011.
5. Disease management of atopic dermatitis: a practiceparameter. Ann Allergy. 1997;79197–211.
6. The diagnosis and management of anaphylaxis. J Al-lergy Clin Immunol. 1998;101(suppl):S465-S528.
7. Algorithm for the diagnosis and management of asthma:a practice parameter update. Ann Allergy. 1998;81:415–420.
8. Diagnosis and management of rhinitis: parameter doc-uments of the Joint Task Force on Practice Parameters inAllergy, Asthma and Immunology. Ann Allergy. 1998;81(suppl):S463-S518.
9. Parameters for the diagnosis and management of sinus-itis. J Allergy Clin Immunol. 1998;102(suppl):S107-S144.
10. Stinging insect hypersensitivity: a practice parameter. JAllergy Clin Immunol. 1999;103:963–980.
11. Disease management of drug hypersensitivity: a prac-tice parameter. Ann Allergy. 1999;83(suppl):S665-S700.
12. Diagnosis and management of urticaria: a practiceparameter. Ann Allergy. 2000;85(suppl):S521-S544.
13. Allergen immunotherapy: a practice parameter. AnnAllergy. 2003;90(suppl):SI-S540.
14. Symptom severity assessment of allergic rhinitis: part I.Ann Allergy. 2003;91:105–114.
15. Disease management of atopic dermatitis: an updatedpractice parameter. Ann Allergy. 2004;93:S1-S21.
16. Stinging insect hypersensitivity: a practice parameterupdate. J Allergy Clin Immunol. 2004;114;:869–86.
17. The diagnosis and management of anaphylaxis: anupdated practice parameter. J Allergy Clin Immunol. 2005;115:S483-S523.
18. Practice parameter for the diagnosis and managementof primary immunodeficiency. Ann Allergy. 2005;94:S1-S63.
19. Attaining optimal asthma control: a practice parameter.J Allergy Clin Immunol. 2005;116:S3–11.
20. The diagnosis and management of sinusitis: a practiceparameter update. J Allergy Clin Immunol. 2005;116:S13–47.
21. Food allergy: a practice parameter. Ann Allergy. 2006;96:S1–68.
22. Contact dermatitis: a practice parameter. Ann Allergy.2006;97:S1-S38.
23. Allergen immunotherapy: a practice parameter secondupdate. J Allergy Clin Immunol. 2007;120:S25–85.
24. Bernstein IL, Li JT, Bernstein DI, et al. Allergy diag-nostic testing: an updated practice parameter. Ann Allergy.2008;100:S1-S147.
25. Wallace D, Dykewicz M, Bernstein DI, et al. Diagnosisand management of rhinitis: an updated practice parameter. JAllergy Clin Immunol. 2008;121:S1-S84.
These parameters are also available on the Internet athttp://www.jcaai.org
The Joint Task Force has made a concerted effort toacknowledge all contributors to this parameter. If any con-tributors have been excluded inadvertently, the Task Forcewill ensure that appropriate recognition of such contributionsis made subsequently.
These parameters were developed by the Joint Task Forceon Practice Parameters, representing the American Academyof Allergy, Asthma and Immunology; the American Collegeof Allergy, Asthma and Immunology; and the Joint Councilof Allergy, Asthma and Immunology.
Chief Editors, John M. Kelso, MD, Division of Allergy,Asthma and Immunology, Scripps Clinic, San Diego, Cali-fornia; and James T. Li, MD, PhD, Professor of Medicine,Mayo Clinic College of Medicine, Rochester, Minnesota;Task Force Reviewers, David I. Bernstein, MD, Departmentof Clinical Medicine, Division of Immunology, University ofCincinnati College of Medicine, Cincinnati, Ohio; JoannBlessing-Moore, MD, Department of Immunology, StanfordUniversity Medical Center, Palo Alto, California; Linda Cox,MD, Department of Medicine, Nova Southeastern University,Davie, Florida; David A. Khan, MD, Department of InternalMedicine, University of Texas Southwestern Medical Center,Dallas, Texas; David M. Lang, MD, Allergy/ImmunologySection, Division of Medicine, Cleveland Clinic Foundation,Cleveland, Ohio; Richard A. Nicklas, MD, Department ofMedicine, George Washington Medical Center, Washington,DC; John Oppenheimer, MD, Department of Internal Medi-cine, New Jersey Medical School, Morristown, New Jersey;Jay M. Portnoy, MD, Section of Allergy, Asthma & Immu-nology, The Children’s Mercy Hospital, University of Mis-souri-Kansas City School of Medicine, Kansas City, Mis-souri; Christopher Randolph, MD, Center for Allergy,Asthma and Immunology, Yale Affiliated Programs Water-bury Hospital, Waterbury, Connecticut; Diane E. Schuller,MD, Department of Pediatrics, Pennsylvania State Univer-sity, Milton S. Hershey Medical College, Hershey, Pennsyl-vania; Sheldon L. Spector, MD, Department of Medicine,UCLA School of Medicine, Los Angeles, California; StephenA. Tilles, MD, Department of Medicine, University of Wash-
VOLUME 103, OCTOBER, 2009 S11

ington School of Medicine, Redmond, Washington; DanaWallace, MD, Department of Medicine, Nova SoutheasternUniversity, Davie, Florida; Invited Reviewers, James Baker,MD, Professor of Medicine and Bioengineering, Director ofMichigan Nanotechnology Institute for Medicine and Biolog-ical Sciences, Chief Division of Allergy, Ann Arbor, Mich-igan; Zuhair K. Ballas, MD, Professor and Director Divisionof Allergy, Department of Internal Medicine, University ofIowa, Iowa City, Iowa; Joseph A. Bellanti, MD, Professor ofPediatrics, Microbiology and Immunology, Director of Inter-national Center for Interdisciplinary Studies of Immunology,Georgetown University Medical Center, Washington, DC;Daniel Ein, MD, Clinical Professor and Chief, Division ofAllergy, George Washington University School of Medicine,Washington, DC; Leslie C. Grammer, MD, Director BazleyAsthma and Allergy Center, Professor Feinberg School ofMedicine, Northwestern University, Chicago, Illinois.
REFERENCES1. Ten great public health achievements–United States, 1900 –1999.
MMWR Morb Mortal Wkly Rep. 1999;48:241–243. (IV)2. Roush SW, Murphy TV. Historical comparisons of morbidity and
mortality for vaccine-preventable diseases in the United States. JAMA.2007;298:2155–2163. (III)
3. Centers for Disease Control and Prevention. Recommended Immuni-zation Schedule for Persons Aged 0 Through 6 Years United States2009. http://www.cdc.gov/vaccines/recs/schedules/downloads/child/2009/09_0–6yrs_schedule_pr.pdf. 2009. Accessed September 4, 2009.(IB)
4. Centers for Disease Control and Prevention. Recommended Immuni-zation Schedule for Persons Aged 7 Through 18 Years United States2009. http://www.cdc.gov/vaccines/recs/schedules/downloads/child/2009/09_7–18yrs_schedule_pr.pdf. 2009. Accessed September 4,2009. (IB)
5. Centers for Disease Control and Prevention. Recommended AdultImmunization Schedule United States 2009. http://www.cdc.gov/vaccines/recs/schedules/downloads/adult/2009/adult-schedule.pdf.2009. Accessed September 4, 2009. (IB)
6. Salmon DA, Haber M, Gangarosa EJ, Phillips L, Smith NJ, Chen RT.Health consequences of religious and philosophical exemptions fromimmunization laws: individual and societal risk of measles. JAMA.1999;282:47–53. (IIB)
7. Danovaro-Holliday MC, LeBaron CW, Allensworth C, et al. A largerubella outbreak with spread from the workplace to the community.JAMA. 2000;284:2733–2739. (IIB)
8. Update: outbreak of poliomyelitis–Dominican Republic and Haiti,2000–2001. MMWR Morb Mortal Wkly Rep. 2001;50:855–856. (III)
9. Two fatal cases of adenovirus-related illness in previously healthyyoung adults–Illinois, 2000. MMWR Morb Mortal Wkly Rep. 2001;50:553–555. (III)
10. Jansen VA, Stollenwerk N, Jensen HJ, Ramsay ME, Edmunds WJ,Rhodes CJ. Measles outbreaks in a population with declining vaccineuptake. Science. 2003;301:804. (IIB)
11. Kroger AT, Atkinson WL, Marcuse EK, Pickering LK, AdvisoryCommittee on Immunization Practices Centers for Disease Control andPrevention. General recommendations on immunization: recommenda-tions of the Advisory Committee on Immunization Practices (ACIP).MMWR Morb Mortal Wkly Rep. 2006;55:1–48. (IV)
12. Vaccine Excipient and Media Summary, by Excipient. In: Atkinson W,Wolfe S, Hamborsky J, McIntyre L, eds. Centers for Disease Controland Prevention: Epidemiology and Prevention of Vaccine-PreventableDiseases. 11th ed. Washington, DC: Public Health Foundation; 2009.(III)
13. Rietschel RL, Bernier R. Neomycin sensitivity and the MMR vaccine.
JAMA. 1981;245:571. (IV)14. Elliman D, Dhanraj B. Safe MMR vaccination despite neomycin al-
lergy. Lancet. 1991;337:365. (IV)15. Cox NH, Forsyth A. Thiomersal allergy and vaccination reactions.
Contact Dermatitis. 1988;18:229–233. (III)16. Rietschel RL, Adams RM. Reactions to thimerosal in hepatitis B
vaccines. Dermatol Clin. 1990;8:161–164. (IV)17. Noel I, Galloway A, Ive FA. Hypersensitivity to thiomersal in hepatitis
B vaccine. Lancet. 1991;338:705. (IV)18. Aberer W. Vaccination despite thimerosal sensitivity. Contact Derma-
titis. 1991;24:6–10. (IIB)19. Audicana MT, Munoz D, del Pozo MD, Fernandez E, Gastaminza G,
Fernandez de Corres L. Allergic contact dermatitis from mercuryantiseptics and derivatives: study protocol of tolerance to intramuscularinjections of thimerosal. Am J Contact Dermatitis. 2002;13:3–9. (IIB)
20. Patrizi A, Rizzoli L, Vincenzi C, Trevisi P, Tosti A. Sensitization tothimerosal in atopic children. Contact Dermatitis. 1999;40:94–97. (IV)
21. Lee-Wong M, Resnick D, Chong K. A generalized reaction to thimer-osal from an influenza vaccine. Ann Allergy Asthma Immunol. 2005;94:90–94. (IV)
22. Kaaber K, Nielsen AO, Veien NK. Vaccination granulomas and alu-minium allergy: course and prognostic factors. Contact Dermatitis.1992;26:304–306. (III)
23. Bergfors E, Trollfors B, Inerot A. Unexpectedly high incidence ofpersistent itching nodules and delayed hypersensitivity to aluminium inchildren after the use of adsorbed vaccines from a single manufacturer.Vaccine. 2003;22:64–69. (III)
24. Lehman HK, Faden HS, Fang YV, Ballow M. A case of recurrentsterile abscesses following vaccination: delayed hypersensitivity toaluminum. J Pediatr. 2008;152:133–135. (IV)
25. Bohlke K, Davis RL, Marcy SM, et al. Risk of anaphylaxis aftervaccination of children and adolescents. Pediatrics. 2003;112:815–820. (IIB)
26. Stratton KH, Johnston RB. Adverse Events Associated With ChildhoodVaccines: Evidence Bearing on Causality. Washington, DC: NationalAcademy Press; 1994. (IIA)
27. Chen RT, Rastogi SC, Mullen JR, et al. The Vaccine Adverse EventReporting System (VAERS). Vaccine. 1994;12:542–550. (IV)
28. Vaccine Adverse Event Reporting System (VAERS). www.vaers.hhs.gov. Accessed September 4, 2009. (IV)
29. Plotkin SA. Immunologic correlates of protection induced by vaccina-tion. Pediatr Infect Dis J. 2001;20:63–75. (IIB)
30. Fiore AE, Feinstone SM, Bell BP. Hepatitis A vaccines. In: Plotkin SA,Orenstein WA, Offit PA, eds. Vaccines. Philadelphia, PA: Elsevier;2008. (IIB)
31. Centers for Disease Control and Prevention. Epidemiology and Pre-vention of Vaccine-Preventable Diseases. 11th ed. Washington, DC:Public Health Foundation; 2009. (IIB)
32. Strebel PM, Papania MJ, Dayan GH, Halsey NA. Measles vaccine. In:Plotkin SA, Orenstein WA, Offit PA, eds. Vaccines. Philadelphia, PA:Elsevier; 2008. (IIB)
33. Plotkin SA, Vidor E. Poliovirus vaccine-inactivated. In: Plotkin SA,Orenstein WA, Offit PA, eds. Vaccines. Philadelphia, PA: Elsevier;2008. (IIB)
34. Plotkin SA, Koprowski H, Rupprecht CE. Rabies vaccines. In: PlotkinSA, Orenstein WA, Offit PA, eds. Vaccines. Philadelphia, PA:Elsevier; 2008. (IIB)
35. Kelso JM. Adverse reactions to vaccines for infectious diseases. In:Adkinson NF, Bochner BS, Busse WW, Holgate ST, Lemanske RF,Simons FER, eds. Middleton’s Allergy: Principles & Practice. 7th ed.Philadelphia, PA: Mosby; 2008:1189–1204. (IIB)
36. Wood RA, Berger M, Dreskin SC, et al. An algorithm for treatment ofpatients with hypersensitivity reactions after vaccines. Pediatrics.2008;122:e771–7. (IIB)
37. Kelso JM, Jones RT, Yunginger JW. Anaphylaxis to measles, mumps,and rubella vaccine mediated by IgE to gelatin. J Allergy Clin Immunol.1993;91:867–872. (IV)
38. Sakaguchi M, Nakayama T, Inouye S. Food allergy to gelatin in
S12 ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY

children with systemic immediate-type reactions, including anaphy-laxis, to vaccines. J Allergy Clin Immunol. 1996;98:1058–1061. (IIA)
39. Sakaguchi M, Yamanaka T, Ikeda K, et al. IgE-mediated systemicreactions to gelatin included in the varicella vaccine. J Allergy ClinImmunol. 1997;99:263–264. (IIA)
40. Sakaguchi M, Miyazawa H, Inouye S. Specific IgE and IgG to gelatinin children with systemic cutaneous reactions to Japanese encephalitisvaccines. Allergy. 2001;56:536–539. (IIA)
41. Nakayama T, Aizawa C. Change in gelatin content of vaccines asso-ciated with reduction in reports of allergic reactions. J Allergy ClinImmunol. 2000;106:591–592. (III)
42. Zent O, Hennig R. Post-marketing surveillance of immediate allergicreactions: polygeline-based versus polygeline-free pediatric TBE vac-cine. Vaccine. 2004;23:579–584. (IIB)
43. O’Brien TC, Maloney CJ, Tauraso NM. Quantitation of residual hostprotein in chicken embryo-derived vaccines by radial immunodiffu-sion. Appl Microbiol. 1971;21:780–782. (III)
44. James JM, Burks AW, Roberson PK, Sampson HA. Safe administra-tion of the measles vaccine to children allergic to eggs. N Engl J Med.1995;332:1262–1266. (IIB)
45. Baxter DN. Measles immunization in children with a history of eggallergy. Vaccine. 1996;14:131–134. (IIB)
46. Red Book: Report of the Committee on Infectious Diseases. 28th ed.Elk Grove Village, IL: American Academy of Pediatrics; 2009. (IIA)
47. James JM, Zeiger RS, Lester MR, et al. Safe administration of influ-enza vaccine to patients with egg allergy. J Pediatr. 1998;133:624–628. (IIB)
48. Zeiger RS. Current issues with influenza vaccination in egg allergy. JAllergy Clin Immunol. 2002;110:834–840. (IIA)
49. Kelso JM. Raw egg allergy-a potential issue in vaccine allergy. JAllergy Clin Immunol. 2000;106:990. (IV)
50. Kelso JM, Cockrell GE, Helm RM, Burks AW. Common allergens inavian meats. J Allergy Clin Immunol. 1999;104:202–204. (IV)
51. DiMiceli L, Pool V, Kelso JM, Shadomy SV, Iskander J, TeamVAERS. Vaccination of yeast sensitive individuals: review of safetydata in the US vaccine adverse event reporting system (VAERS).Vaccine. 2006;24:703–707. (III)
52. GARDASIL: Human Papillomavirus Quadrivalent (Types 6, 11, 16,and 18) Vaccine, Recombinant [package insert]. 2008. (III)
53. Lear JT, English JS. Anaphylaxis after hepatitis B vaccination. Lancet.1995;345:1249. (IV)
54. Russell M, Pool V, Kelso JM, Tomazic-Jezic VJ. Vaccination ofpersons allergic to latex: a review of safety data in the Vaccine AdverseEvent Reporting System (VAERS). Vaccine. 2004;23:664–667. (III)
55. Latex in vaccine packaging In: Atkinson W, Wolfe S, Hamborsky J,McIntyre L, eds. Centers for Disease Control and Prevention: Epide-miology and Prevention of Vaccine-Preventable Diseases. 11th ed.Washington, DC: Public Health Foundation; 2009. (IIB)
56. Kwittken PL, Rosen S, Sweinberg SK. MMR vaccine and neomycinallergy. AJDC. 1993;147:128–129. (IV)
57. Zheng W, Dreskin SC. Thimerosal in influenza vaccine: an immediatehypersensitivity reaction. Ann Allergy Asthma Immunol. 2007;99:574–575. (IV)
58. Vaccine Excipient and Media Summary, by Vaccine. In: Atkinson W,Wolfe S, Hamborsky J, McIntyre L, eds. Centers for Disease Controland Prevention: Epidemiology and Prevention of Vaccine-PreventableDiseases. 11th ed. Washington, DC: Public Health Foundation; 2009.(IIB)
59. Wood RA, Setse R, Halsey N. Irritant skin test reactions to commonvaccines. J Allergy Clin Immunol. 2007;120:478–481. (III)
60. Nagel JE, White C, Lin MS, Fireman P. IgE synthesis in man, II:comparison of tetanus and diphtheria IgE antibody in allergic andnonallergic children. J Allergy Clin Immunol. 1979;63:308–314. (IIA)
61. Edelman K, Malmstrom K, He Q, Savolainen J, Terho EO, Mertsola J.Local reactions and IgE antibodies to pertussis toxin after acellulardiphtheria-tetanus-pertussis immunization. Eur J Pediatr. 1999;158:989–994. (IIB)
62. Aalberse RC, van Ree R, Danneman A, Wahn U. IgE antibodies to
tetanus toxoid in relation to atopy. Int Arch Allergy Immunol. 1995;107:169–171. (IIB)
63. Anolik R, Spiegel W, Posner M, Jakabovics E. Influenza vaccinetesting in egg sensitive patients. Ann Allergy Asthma Immunol. 1992;68:69. (III)
64. Bernstein IL, Li JT, Bernstein DI, et al. Allergy diagnostic testing: anupdated practice parameter. Ann Allergy Asthma Immunol. 2008;100:S1–148. (IIB)
65. Fasano MB, Wood RA, Cooke SK, Sampson HA. Egg hypersensitivityand adverse reactions to measles, mumps, and rubella vaccine. J Pe-diatr. 1992;120:878–881. (IIB)
66. Murphy KR, Strunk RC. Safe administration of influenza vaccine inasthmatic children hypersensitive to egg proteins. J Pediatr. 1985;106:931–933. (III)
67. YF-VAX (Sanofi Pasteur) [package insert]. In: Physicians’ Desk Ref-erence. Montvale, NJ: Medical Economics; 2008. (IV)
68. Carey AB, Meltzer EO. Diagnosis and “desensitization” in tetanusvaccine hypersensitivity. Ann Allergy. 1992;69:336–338. (IV)
69. Fiore AE, Shay DK, Broder K, et al. Prevention and control ofinfluenza: recommendations of the Advisory Committee on Immuni-zation Practices (ACIP), 2008. MMWR Recomm Rep. 2008;57:1–60.(IIA)
70. Lasky T, Terracciano GJ, Magder L, et al. The Guillain-Barre syn-drome and the 1992–1993 and 1993–1994 influenza vaccines. N EnglJ Med. 1998;339:1797–1802. (IIA)
71. Sivadon-Tardy V, Orlikowski D, Porcher R, et al. Guillain-Barresyndrome and influenza virus infection. Clin Infect Dis. 2009;48:48–56. (IIB)
72. Haber P, DeStefano F, Angulo FJ, et al. Guillain-Barre syndromefollowing influenza vaccination. JAMA. 2004;292:2478–2481. (III)
73. Souayah N, Nasar A, Suri MF, Qureshi AI. Guillain-Barre syndromeafter vaccination in United States a report from the CDC/FDA VaccineAdverse Event Reporting System. Vaccine. 2007;25:5253–5255. (III)
74. Centers for Disease Control and Prevention. Update: vaccine sideeffects, adverse reactions, contraindications, and precautions: recom-mendations of the Advisory Committee on Immunization Practices(ACIP). MMWR Morb Mortal Wkly Rep. 1996;45:1–35. (IIB)
75. Barlow WE, Davis RL, Glasser JW, et al. The risk of seizures afterreceipt of whole-cell pertussis or measles, mumps, and rubella vaccine.N Engl J Med. 2001;345:656–661. (IIB)
76. Vestergaard M, Hviid A, Madsen KM, et al. MMR vaccination andfebrile seizures: evaluation of susceptible subgroups and long-termprognosis. JAMA. 2004;292:351–357. (IIB)
77. Beeler J, Varricchio F, Wise R. Thrombocytopenia after immunizationwith measles vaccines: review of the vaccine adverse events reportingsystem (1990 to 1994). Pediatr Infect Dis J. 1996;15:88–90. (III)
78. Jadavji T, Scheifele D, Halperin S. Thrombocytopenia after immuni-zation of Canadian children, 1992 to 2001. Pediatr Infect Dis J.2003;22:119–122. (IIB)
79. Howson CP, Fineberg HV. Adverse events following pertussis andrubella vaccines: summary of a report of the Institute of Medicine.JAMA. 1992;267:392–396. (IIA)
80. Plotkin SA, Reef SE. Rubella vaccine. In: Plotkin SA, Orenstein WA,Offit PA, eds. Vaccines. Philadelphia, PA: Elsevier; 2008. (IIB)
81. Cody CL, Baraff LJ, Cherry JD, Marcy SM, Manclark CR. Nature andrates of adverse reactions associated with DTP and DT immunizationsin infants and children. Pediatrics. 1981;68:650–660. (IB)
82. DuVernoy TS, Braun MM. Hypotonic-hyporesponsive episodes re-ported to the Vaccine Adverse Event Reporting System (VAERS),1996–1998. Pediatrics. 2000;106:E52. (III)
83. Heijbel H, Ciofi degli Atti MC, Harzer E, et al. Hypotonic hypore-sponsive episodes in eight pertussis vaccine studies. Dev Biol Stan-dardization. 1997;89:101–103. (IIA)
84. Le Saux N, Barrowman NJ, Moore DL, et al. Decrease in hospitaladmissions for febrile seizures and reports of hypotonic-hyporespon-sive episodes presenting to hospital emergency departments sinceswitching to acellular pertussis vaccine in Canada: a report fromIMPACT. Pediatrics. 2003;112:e348. (IB)
VOLUME 103, OCTOBER, 2009 S13
85. Rosenthal S, Chen R, Hadler S. The safety of acellular pertussisvaccine vs whole-cell pertussis vaccine: a postmarketing assessment.Arch Pediatr Adolesc Med. 1996;150:457–460. (IIA)
86. Edwards KM, Decker MD. Pertussis vaccines. In: Plotkin SA, Oren-stein WA, Offit PA, eds. Vaccines. Philadelphia, PA: Elsevier; 2008.(IIB)
87. Zielinski A, Rosinska M. Comparison of adverse effects followingimmunization with vaccine containing whole-cell vs. acellular pertussiscomponents. Przegl Epidemiol. 2008;62:589–596. (IIA)
88. Wassilak SGF, Roper MH, Kretsinger K, Orenstein WA. Tetanustoxoid. In: Plotkin SA, Orenstein WA, Offit PA, eds. Vaccines. Phil-adelphia, PA: Elsevier; 2008. (IIB)
89. Gershon AA, Takahashi M, Seward JF. Varicella vaccine. In: PlotkinSA, Orenstein WA, Offit PA, eds. Vaccines. Philadelphia, PA:Elsevier; 2008. (IIB)
90. Wise RP, Salive ME, Braun MM, et al. Postlicensure safety surveil-lance for varicella vaccine. JAMA. 2000;284:1271–1279. (III)
91. Sharrar RG, LaRussa P, Galea SA, et al. The postmarketing safetyprofile of varicella vaccine. Vaccine. 2000;19:916–923. (III)
92. Kreth HW, Hoeger PH, Members of the VZVADsg. Safety, reactoge-nicity, and immunogenicity of live attenuated varicella vaccine inchildren between 1 and 9 years of age with atopic dermatitis. EurJ Pediatr. 2006;165:677–683. (IIB)
93. Monath TP, Cetron MS, Teuwen DE. Yellow fever vaccine. In: PlotkinSA, Orenstein WA, Offit PA, ed. Vaccines. Philadelphia, PA: Elsevier;2008. (IIB)
94. Vasconcelos PF, Luna EJ, Galler R, Silva LJ, Coimbra TL, Barros VLet al. Serious adverse events associated with yellow fever 17DD vac-cine in Brazil: a report of two cases. Lancet. 2001;358:91–97. (IV)
95. Chan RC, Penney DJ, Little D, Carter IW, Roberts JA, Rawlinson WD.Hepatitis and death following vaccination with 17D-204 yellow fevervaccine. Lancet. 2001;358:121–122. (IV)
96. Martin M, Tsai TF, Cropp B, et al. Fever and multisystem organ failureassociated with 17D-204 yellow fever vaccination: a report of fourcases. Lancet. 2001;358:98–104. (IV)
97. Centers for Disease Control and Prevention. Adverse events associatedwith 17D-derived yellow fever vaccination–United States, 2001–2002.MMWR Morb Mortal Wkly Rep. 2002;51:989–993. (IV)
98. Doblas A, Domingo C, Bae HG, et al. Yellow fever vaccine-associatedviscerotropic disease and death in Spain. J Clin Virol. 2006;36:156–158. (IV)
99. Lindsey NP, Schroeder BA, Miller ER, et al. Adverse event reportsfollowing yellow fever vaccination. Vaccine. 2008;26:6077–6082. (III)
100. Centers for Disease Control and Prevention. Guidelines for VaccinatingPregnant Women from Recommendations of the Advisory Committeeon Immunization Practices (ACIP). Atlanta, GA: Centers for DiseaseControl and Prevention; 2007. (IIB)
101. Moss WJ, Clements CJ, Halsey NA. Immunization of children at riskof infection with human immunodeficiency virus. Bull World HealthOrgan. 2003;81:61–70. (IV)
102. Koppen S, de Groot R, Neijens HJ, Nagelkerke N, van Eden W, RumkeHC. No epidemiological evidence for infant vaccinations to causeallergic disease. Vaccine. 2004;22:3375–3385. (IIA)
103. Stratton K, Gable A, Shetty P. Immunization Safety Review: Measles-Mumps-Rubella Vaccine and Autism. Washington, DC: National Acad-emy Press; 2001. (IIA)
104. Madsen KM, Hviid A, Vestergaard M, et al. A population-based studyof measles, mumps, and rubella vaccination and autism. N Engl J Med.2002;347:1477–1482. (IIB)
105. Confavreux C, Suissa S, Saddier P, Bourdes V, Vukusic S, Vaccines inMultiple Sclerosis Study Group. Vaccinations and the risk of relapse inmultiple sclerosis. N Engl J Med. 2001;344:319–326. (IIB)
106. DeStefano F, Verstraeten T, Jackson LA, et al. Vaccinations and risk ofcentral nervous system demyelinating diseases in adults. Arch Neurol.2003;60:504–509. (IIA)
107. Food and Drug Administration. Thimerosal in Vaccines. http://www.fda.gov/BiologicsBloodVaccines/SafetyAvailability/VaccineSafety/UCM096228.htm 2009. Accessed September 4, 2009. (IIB)
108. Parker SK, Schwartz B, Todd J, Pickering LK. Thimerosal-containingvaccines and autistic spectrum disorder: a critical review of publishedoriginal data. Pediatrics. 2004;114:793–804. (IIB)
109. RabAvert Rabies Vaccine (Chiron) [package insert]. 2004. (IV)110. Kelso JM, Yunginger JW. Immunization of egg-allergic individuals
with egg- or chicken-derived vaccines. Immunol Allergy Clin NorthAm. 2003;23:635–648. (IIB)
Requests for reprints should be addressed to:Joint Council of Allergy50 N Brockway St, #3–3Palatine, IL 60067
S14 ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY
Copyright © 2022 FDOKUMEN




















