Vacancy, turnover rates stable in face of staffing ... - OR Manager
36
September 2004 Vol 20, No 9 The monthly publication for OR decision makers In this issue JCAHO issues 2005 Patient Safety Goals . . . . . . . .5 Building a cross- generational workforce . . . .11 SALARY/CAREER SURVEY. Fewer staffing challenges for ASCs . . . . . . . . . . . . . . . .17 RECRUITMENT & RETENTION. Perioperative Education Pipeline gives Mayo staff a career path . . . . . . . . . . . . .21 RECRUITMENT & RETENTION. Hardy nurses less likely to burn out . . . . . . . . . . . . . .22 PATIENT SAFETY. Smart wristbands tested for patient ID . . . . . . . . . . . .24 AMBULATORY SURGERY CENTERS. What to know about ASC benchmarking . . . . . . .29 AT A GLANCE . . . . . . . . . . .36 ASC section on page 29 W hen it comes to staffing, OR managers may feel theyre running faster to stay in the same place. Managers say recruitment and reten- tion are their greatest challenges. Efforts they are making to prepare their own OR staff may be a major reason vacancy rates and turnover rates have remained fairly steady over the past 4 years. Just over half of managers51% are faced with a nursing shortage in their ORs. A little less than half46% have a shortage of anesthesia providers. Managers cover for shortages primari- ly with overtime and extended hours for surgery. A few have had to close ORs. In all, 57% have vacancies for RNs, and 48% have vacancies for surgical technologists (STs), roughly the same as last year. The average vacancy rate for those with openings is 8.6%, on a par with the 8.4% average for all RNs reported by the American Hospital Association. The findings are from OR Managers 2004 Salary/Career Survey. Results on the staffing portion of the survey are reported in this issue. This is the fourth year staffing questions have been asked. The rest of the survey results will be in the October issue. The survey was mailed in May to 1,229 OR Manager subscribers and had a return rate of 34%. A separate survey Vacancy, turnover rates stable in face of staffing challenges T he staff are volunteering for com- mittees, seeking out education, and stepping up to mentor new staff. They willingly sign up to give in- services and join in performance im- provement committees. When they have time, they ask if there are patient charts that need auditing. What made the difference? Managers attribute the enthusiasm to their clinical ladders for RNs and surgical technolo- gists (STs). The staff tend to be much more involved, volunteer more, and take responsibility for things, says Karen Dumond, RN, MSN, CNOR, nursing director of the Bramhall Campus OR at Maine Medical Center (MMC) in Port- land, Maine. A community hospital system in cen- tral California also finds participation is up among RNs in its clinical ladder pro- gram. The staff will say, Sure, Ill float to that unit. I can get clinical ladder points for that, says Marilyn Harris, RN, MSN, CNOR, director of surgical ser- vices for Hanford Community Medical Center and Central Valley General Hospital in Hanford, Calif. You hope it also is because they want to help their fellow nurses, but it adds an extra incen- tive. Though the hospitals dont have data linking the ladders to improved recruit- ment and retention, both ORs are fully staffed. Clinical ladders ramp up staff’s enthusiasm and participation Continued on page 19 Salary/Career Survey Continued on page 13 Recruitment & retention
-
Upload
khangminh22 -
Category
Documents
-
view
9 -
download
0
Transcript of Vacancy, turnover rates stable in face of staffing ... - OR Manager

September 2004 Vol 20, No 9
The monthly publication for OR decision makers
In this issue
JCAHO issues 2005 Patient Safety Goals . . . . . . . .5
Building a cross-generational workforce . . . .11
SALARY/CAREER SURVEY.Fewer staffing challenges for ASCs . . . . . . . . . . . . . . . .17
RECRUITMENT & RETENTION.Perioperative Education Pipeline gives Mayo staff a career path . . . . . . . . . . . . .21
RECRUITMENT & RETENTION.�Hardy nurses� less likely to burn out . . . . . . . . . . . . . .22
PATIENT SAFETY.�Smart� wristbands tested for patient ID . . . . . . . . . . . .24
AMBULATORYSURGERY CENTERS.What to know about ASC benchmarking . . . . . . .29
AT A GLANCE . . . . . . . . . . .36
ASC section on page 29
When it comes to staffing, ORmanagers may feel they�rerunning faster to stay in the
same place.Managers say recruitment and reten-
tion are their greatest challenges. Effortsthey are making to prepare their ownOR staff may be a major reason vacancyrates and turnover rates have remainedfairly steady over the past 4 years.
Just over half of managers�51%�are faced with a nursing shortage intheir ORs. A little less than half�46%�have a shortage of anesthesia providers.
Managers cover for shortages primari-ly with overtime and extended hours forsurgery. A few have had to close ORs.
In all, 57% have vacancies for RNs,
and 48% have vacancies for surgicaltechnologists (STs), roughly the same aslast year.
The average vacancy rate for thosewith openings is 8.6%, on a par with the8.4% average for all RNs reported by theAmerican Hospital Association.
The findings are from OR Manager�s2004 Salary/Career Survey. Results onthe staffing portion of the survey arereported in this issue. This is the fourthyear staffing questions have been asked.The rest of the survey results will be inthe October issue.
The survey was mailed in May to1,229 OR Manager subscribers and had areturn rate of 34%. A separate survey
Vacancy, turnover rates stablein face of staffing challenges
The staff are volunteering for com-mittees, seeking out education,and stepping up to mentor new
staff. They willingly sign up to give in-services and join in performance im-provement committees. When they havetime, they ask if there are patient chartsthat need auditing.
What made the difference? Managersattribute the enthusiasm to their clinicalladders for RNs and surgical technolo-gists (STs).
�The staff tend to be much moreinvolved, volunteer more, and takeresponsibility for things,� says KarenDumond, RN, MSN, CNOR, nursingdirector of the Bramhall Campus OR atMaine Medical Center (MMC) in Port-land, Maine.
A community hospital system in cen-tral California also finds participation isup among RNs in its clinical ladder pro-gram.
�The staff will say, �Sure, I�ll float tothat unit. I can get clinical ladder pointsfor that,�� says Marilyn Harris, RN,MSN, CNOR, director of surgical ser-vices for Hanford Community MedicalCenter and Central Valley GeneralHospital in Hanford, Calif. �You hope italso is because they want to help theirfellow nurses, but it adds an extra incen-tive.�
Though the hospitals don�t have datalinking the ladders to improved recruit-ment and retention, both ORs are fullystaffed.
Clinical ladders ramp up staff’senthusiasm and participation
Continued on page 19
Salary/Career Survey
Continued on page 13
Recruitment & retention

2
Full Page Ad
2
Please see the ad for 3M HEALTHCAREin the OR Manager print version.

3September 2004
UpcomingSalary/Career Survey
Learn what your colleagues aremaking and what they see as theirbiggest rewards and challenges.
A leadership gapWhy recruiting perioperative direc-
tors is difficult and what�s needed tohelp.
OR Manager Vol 20, No 9
Editorial
September 2004 Vol 20, No 9OR Manager is a monthly publication forpersonnel in decision-making positions inthe operating room.
Elinor S. Schrader: PublisherPatricia Patterson: EditorJudith M. Mathias, RN, MA:
Clinical editorBillie Fernsebner, RN, MSN:
Consulting editorJanet K. Schultz, RN, MSN:
Consulting editorKathy Shaneberger, RN, MSN, CNOR:
Consulting editor
OR Manager (USPS 743-010), (ISSN8756-8047) is published monthly by ORManager, Inc, 1807 Second St, Suite 61,Santa Fe, NM 87505-3499. Periodicalspostage paid at Santa Fe, NM and addi-tional post offices. POSTMASTER: Sendaddress changes to OR Manager, PO Box5303, Santa Fe, NM 87502-5303.
OR Manager is indexed in the CumulativeIndex to Nursing and Allied HealthLiterature and MEDLINE/PubMed.
Copyright © 2004 OR Manager, Inc. All rightsreserved. No part of this publication may bereproduced without written permission.
Subscription rates: $86 per year. Super sub-scriptions (electronic) $129 per year.Canadian, $98. Foreign, $115. Single issues$10. Address subscription requests to POBox 5303, Santa Fe, NM 87502-5303. Tele:800/442-9918 or 505/982-0510. Web site:www.ormanager.com
Editorial Office: PO Box 5303, Santa Fe, NM87502-5303. Tel: 800/442-9918. Fax: 505/983-0790. E-mail: [email protected]
Advertising Manager: Anthony J. Jannetti,Inc, East Holly Ave/Box 56, Pitman, NJ08071. Telephone: 856/256-2300; Fax:856/589-7463. John R. Schmus, nationaladvertising manager. [email protected]
The monthly publication for OR decision makers
OR managers seem to be dealingwith a �new normal� in staffing.From the numbers, it looks like
staffing is holding on. The vacancy rate,turnover rate, and use of temporary staffhaven�t changed substantially for the past4 years, according to the staffing portionof the annual OR Manager Salary/CareerSurvey reported in this issue.
But the numbers tell only part of thestory. A lot is going on behind the scenes.
A few years ago, much of the newswas about bonuses. You still see head-lines about big sign-on bonuses, but inthe OR, it appears leaders have movedon to more creative strategies.
Indeed, if survey respondents weregoing to give themselves a �GoldenScalpel� award this year, many said itwould be for recruitment and retention.
One manager wrote that her organi-zation has developed an elective coursefor credit with the local university.Another, as a result of education provid-ed to inexperienced OR RNs over thepast 3 years, is using only 1 agencynurse�a big change from 5 years agowhen this facility was down 8 nursingpositions out of 20.
One manager said she would give theaward to her orientation team. �Theyworked very diligently to create a posi-tive, progressive orientation programthat keeps the orientees interested andhappy to be here,� she said.
Still another wrote, �There actually isa waiting list to work in our OR. Moraleis very high.� She credits a unit-basedcouncil and positive relations with physi-cians as some of the reasons.
A new level for laddersRead about other creative programs
in this issue. Two organizations have taken their
clinical ladder programs to a new level(p 1). Maine Medical Center has set up aladder for surgical technologists in addi-tion to RNs. Two community hospitals inrural California have a well-thought-outRN ladder with a user-friendly format.
The Mayo Clinic Hospital in Phoenixhas a new Perioperative EducationPipeline that not only provides educationto RNs who want to move into the ORbut also offers a career track to entry-level employees (p 21).
One of the nation�s fast-growing
cities, Phoenix is attracting a lot of newresidents, many of them retirees whobring along their needs for health care.Meanwhile, as in the rest of the country,the nursing population is movingtoward retirement.
But managers aren�t wringing theirhands.
�Our secret is to train, train, train. Onceyou get short staffed, you never recover,�says Rita Borden, RN, BSN, executivedirector of surgical services for the SunHealth system based in Sun City, Ariz, andthe 2003 OR Manager of the Year.
Sun Health facilities currently have 4surgical technologists (STs) and 3 RNs ina periop education program. Borden isparticularly proud of a program that pro-vides training for central service techs tobecome STs. Two OR employees, an STand a secretary, recently completed studyto become RNs.
Sun Health also pays for RN employ-ees to continue on to get their BSNs.
For many of you, there�s probablynothing new in these stories. You mayhave equally creative programs. It�s like-ly to be a theme for years to come.
It�s heartening to know that managersare building seawalls to help keep theworst of the tidal wave at bay. ❖
�Pat Patterson
Orientation without aneducator
In the staffing survey, 43% of commu-nity hospitals do not have an OR educa-tor, yet most are hiring nurses withoutOR experience.
How are you managing orientationwithout an educator? Share your experi-ence. E-mail [email protected] a possible interview.
“
“Our secret is
train, train,train.

4
Please see the ad for ADVANCED STERILIZATION PRODUCTSin the OR Manager print version.

The Joint Commission on Accredi-tation of Healthcare Organiza-tions announced its 2005 National
Patient Safety Goals July 20. For the first time, goals are specific to
the type of setting, such as hospitals, crit-ical access hospitals, ambulatory careorganizations, and office-based surgeryfacilities, among others. There continueto be 7 goals in all.
Two new goals have been added forhospitals:� Reconciling medications across the
continuum of care. This requires plan-ning a process in 2005 for full imple-mentation in 2006.
� Reducing the risk of patient harmfrom falls.Two of the 2004 goals are no longer
National Patient Safety Goals:
� Requirements for surgical site verifi-cation are now covered under theUniversal Protocol for preventingwrong surgery, which took effect July1. The protocol applies to hospitals aswell as ambulatory surgery andoffice-based surgery facilities.
� The goal on clinical alarms has been
dropped because of progress towardmeeting this goal. Three goals have been reworded or
expanded:� The goal on patient identifiers now
applies not only to giving medicationsand blood and taking blood samplesbut also to other specimens and anyother treatments or procedures.
� The goal on improving communica-tion has a new requirement for care-givers to measure, assess, and if need-ed, take action to improve timelinessof reporting of critical test results andvalues.
� The goal on medications has a newrequirement for organizations toreview a list of look-alike/sound-alike drugs annually and take actionto prevent errors for these drugs.The goals for critical access hospitals
are identical to those for hospitals.
Surgical fire goal forambulatory care
The goals for ambulatory care organi-zations, including ambulatory surgerycenters (ASCs), and office-based surgeryfacilities are the same as the hospitalgoals�with 2 important differences: � Reducing the risk of surgical fires is a
new goal for ASCs and office facilitiesbut not for hospitals.
� The goal on patient falls applies tohospitals but not to ASCs and offices.For 2005, ambulatory organizations
and office-based surgery facilities arerequired to educate their staff about fires.This includes �operating licensed inde-pendent practitioners� (like doctors) andanesthesia providers.
Why isn�t this a goal for hospitalsalso?
This year, the goals were specificallydeveloped and ranked for each type oforganization, explains Michael Kulc-zycki, MBA, executive director ofJCAHO�s Ambulatory Care Accredita-tion Program. For hospitals, the surgical-fire goal did not rank as high as othersthat were selected.
�This does not mean hospitals shouldignore the issue of preventing surgicalfires,� he said. �However, the JointCommission will not be surveying forthat in the hospital setting for 2005.�
There is no readily available data onhow many surgical fires occur in ASCs
JCAHO issues 2005 Patient Safety Goals
5OR Manager Vol 20, No 9September 2004
Continued on page 8
Amy Bethel, RN, MPA, CNAExecutive director, surgical servicesIowa Health, Des Moines
Mark E. Bruley, EITVice president of accident & forensic investigation, ECRIPlymouth Meeting, Pa
Judith Canfield, RNC, MNA, MBAAssociate administrator of surgical servicesUniversity of Washington MedicalCenter, Seattle
Christy Dempsey, RN, BSN, CNORVice presidentSt John�s Regional Health CenterSpringfield, Mo
Franklin Dexter, MD, PhDAssociate professorDepartment of AnesthesiaUniversity of Iowa, Iowa City
Mary Diamond, RN, MBA, CNORDirector of surgical servicesSharp Healthcare, San Diego
Marion L. Freehan, RN, MPA/HA,CNORNurse manager, main operatingrooms, Massachusetts GeneralHospital, Boston
William J. Mazzei, MDMedical director, perioperative services, University of California,San Diego
Mary M. Murphy, RN, BSN, CNORDirector, surgical servicesMunson Medical CenterTraverse City, Mich
Barbara Pankratz, RN, MSNDirector, surgical servicesUniversity of Wisconsin Hospital &Clinics, Madison
Robert V. Rege, MDProfessor and chairmanDepartment of surgeryUT Southwestern Medical CenterDallas
Marimargaret Reichert, RN, MAAdministrator, Surgical Care CenterSouthwest General Health CenterMiddleburg Heights, Ohio
Kathy E. Shaneberger, RN, MSN,CNORDirector, perioperative services and ortho/neuro service lineMercy General Health PartnersMuskegon, Mich
Allen WarrenBusiness manager, surgical servicesMission St Joseph�s HospitalAsheville, NC
Advisory Board
“
“Two new goals have
been added forhospitals.

6
Please see the ad for SURGICAL INFORMATION SYSTEMSin the OR Manager print version.
Visit us at Managing Today’s OR Suite Booth #313 in Chicago.

7OR Manager Vol 20, No 9September 2004
2005 National Patient Safety GoalsHospitals & Ambulatory
critical access care andhospitals office-based
surgicalfacilities
Goal: Improve the accuracy of patient identification. X X•Use at least 2 patient identifiers (neither to be the patient’s
physical location) whenever administering medications or blood products, taking blood samples and other specimens for clinical testing, or providing any other treatments or procedures.
•What’s new? Goal is expanded to include other specimens or other treatment or procedures.
Goal: Improve effectiveness of communication among X Xcaregivers.•For verbal or telephone orders or for telephonic reporting of critical
test results, verify the complete order or test result by having the person receiving the order or test result “read back” the complete order or test result.
•Standardize a list of abbreviations, acronyms, and symbols that are not to be used throughout the organization.
•Measure, assess, and if appropriate, take action to improve the timeliness of reporting, and timeliness of receipt by the responsible licensed caregiver, of critical test results and values.
•What’s new? First requirement has been reworded. Third requirement is new.
Goal: Improve safety of using medications. X X•Remove concentrated electrolytes (including, but not limited to,
potassium chloride, potassium phosphate, sodium chloride >0.9%) from patient care areas.
•Standardize and limit the number of drug concentrations available in the organization.
•Identify and, at a minimum, annually review a list of look-alike/sound-alike drugs used in the organization and take action to prevent errors involving the interchange of these drugs.
•What’s new? Requirement on look-alike/sound-alike drugs is new.
Goal: Improve safety of using infusion pumps. X X•Ensure free-flow protection on all general-use and PCA (patient-
controlled analgesia) intravenous infusion pumps used in the organization.
•This goal is unchanged.
Goal: Reduce the risk of health care-associated infections. X X•Comply with current U S Centers for Disease Control and Prevention
(CDC) hand hygiene guidelines.•Manage as sentinel events all identified cases of unanticipated death
or major permanent loss of function associated with health care-associated infections.
•This goal is unchanged.
(Continued on page 8)

and offices, noted Mark Bruley, vice pres-ident of accident and forensic investiga-tion for ECRI, an expert on surgical fires.ECRI is a nonprofit organization thatspecializes in health care technology.
ECRI estimates 50 to 100 surgical firesoccur each year in the U S, with 1 to 2patient deaths. �Most of the cases wehave investigated have involved ambula-tory surgery, regardless of the type offacility,� Bruley said.
Approximately 75% of surgical firesinvolve oxygen-enriched atmospheres,Bruley noted. Oxygen-enriched atmos-pheres are most common under the sur-gical drapes when an oxygen source isused on the face during monitored anes-thesia care (MAC). This is very commonin ambulatory surgery.
�The fact that the Joint Commissionhasn�t made this a National Patient SafetyGoal for hospitals doesn�t remove the bur-den to be proactive about preventingfires,� he said. �It�s a huge risk manage-ment issue regardless of whether it�s agoal targeted at your type of facility.�
Reconciling medicationsThe purpose of the new goal on rec-
onciling medications across the continu-um of care is to prevent medicationerrors that can occur if clinicians aren�taware of all of the medications patientsare taking, Kulczycki noted.
How will this goal apply to surgicalfacilities?
�The expectation is that the surgerycenter will get as accurate a list as possi-ble from patients both of their medica-tions and herbal products they may beusing,� Kulczycki said.
�If they discharge the patient to anyother provider setting, they need tomake sure they provide as complete a listas possible to the other setting.� Thatincludes postoperative pain medications.An example is a patient having orthope-dic surgery who is released to home care.
For 2005, surveyors will be lookingfor some evidence that organizations areplanning for this goal. Full implementa-tion is not required until 2006.
JCAHO has answers to frequentlyasked questions about the 2005 goals on itsweb site. Go to www.jcaho.org and lookunder the National Patient Safety Goals. ❖
The Joint Commission will present a ses-sion on the National Patient Safety Goals at
the Managing Today�s OR Suite conferenceOct 6 to 8 in Chicago. Mark Bruley of ECRIwill present a session, Surgical Fires:Awareness of a Continuing Risk. A confer-ence brochure is at www.ormanager.com
ECRI resourcesFree poster: Only You Can Prevent
Surgical Fires, plus other publications onfires are at www.ecri.org, ProfessionalInformation, Medical Device SafetyReports.
A clinician�s guide to surgical fires:How they occur, how to prevent them,how to put them out. Health Devices.2003; 32(1):5-24. Article rates 8 OR firesafety videos, finding 3 worth considera-tion. Contact ECRI at 610/825-6000 ext5888.
Joint Commissionresources
�Preventing surgical fires.� JointCommission Perspectives on Patient Safety.October 2003.
�Train staff to prevent surgical fires.�Joint Commission: The Source. April 2004.Both available from Joint CommissionResources at www.jcrinc.com
8 OR Manager Vol 20, No 9 September 2004
Continued from page 5
Goal: Accurately and completely reconcile medications X Xacross continuum of care.•During 2005, for full implementation by January 2006, develop
a process for obtaining and documenting a complete list of the patient’s current medications upon the patient’s entry to the organization and with the involvement of the patient. This process includes a comparison of the medications the organization provides to those on the list.
•A complete list of the patient’s medications is communicated to the next provider of service when it refers or transfers a patient to another setting, service, practitioner, or level of care within or outside the organization.
•What’s new? This is a new goal. During 2005, surveyors will look for evidence that planning is underway for implementation in 2006.
Goal: Reduce the risk of patient harm resulting from falls. X•Assess and periodically reassess each resident’s risk of falling,
including the potential risk associated with the resident’s medication regimen, and take action to address any identified risk.
•What’s new? This is a new goal for hospitals.
Goal: Reduce the risk of surgical fires. X•Educate staff, including operating licensed independent practitioners
and anesthesia providers on how to control heat sources and manage fuels and establish guidelines to minimize oxygen concentration under drapes.
•What’s new? This is a new goal for ambulatory care organizations and office-based surgical facilities.

9
Please see the ad for MEDLINE INDUSTRIES INC
in the OR Manager print version.

10
Please see the ad for INTEGRATED MEDICAL SYSTEMSin the OR Manager print version.

Career strategist Marilyn MoatsKennedy will lead an all-day pre-conference seminar on managing
today�s diverse generations at theManaging Today�s OR Suite conferenceOctober 6-8 in Chicago. OR Managerasked her how to keep Boomers, Busters,and Netsters working harmoniously.
What are the age-relatedissues in OR nursingtoday?
Kennedy: The shortfall of nursesafter the Baby Boomers retire. The aver-age OR nurse is 52; the average nurse is47. The five highest birthrate years were1946 through 1950. Hospitals are goingto have to keep this whole group intheir 50s and 60s happy because thereare no replacements. You can�t hirewhat wasn�t born. Nursing will nevermake up for the shortages, so you�vegot to keep the older ones working andkeep stirring the pot for the young oneswith incentives.
What incentives can youoffer different agegroups?
Kennedy: Younger people want timeoff. Older people want money. Rewardthem appropriately.
How do we recruitbodies that don’t exist?
Kennedy: Give up the assumptionthat there is only one time to get them.You need to hit them at different pointson the age spectrum. Start in juniorhigh, then high school, then at the endof college. These are choice points topresent your arguments.
Another great time is when womendivorce in their 60s. It�s the age with thehighest rate of divorce right nowbecause it�s when their husbands retire.These women may have said, �for bet-ter or worse� but not �for lunch.�
Describe the nurse of thefuture.
Kennedy: He�there will be a lot moremen�will be in his late 20s or early 30sand becomes a nurse as a second career.First, he has to get rid of his college debtwith a well-paying but less meaningfuljob. Then he will choose nursing becausepeople under 30 are obsessed with pur-pose and making a difference.
I’m in my late 50s andinterviewing for a newposition in a smaller
facility. The pay isn’t great soI’m asking for more benefits.Is that OK?
Kennedy: Sure, as long as youunderstand that you cannot work forless than you earned before withoutputting a serious dent in your career.Once you take a step back in pay fordoing the same job, they�re going tojump on you: �Here�s someone with adamaged ego; let�s give him or her lessmoney.� In your situation, I would askfor time off or a performance bonus.
I’m 62, and my boss is32. She has an MBA andruns our surgery center.
What’s the secret to workingwith Busters?
Kennedy: Respect your boss�s skillset even though it is different than yourown. Hers is much more technological.Also, don�t expect her to chit-chat.Work is not social for people in their30s; she�s moving an agenda. If it�s toouncomfortable, keep this in mind: She�llbe moving on shortly and you canprobably outlast her.
I have some staff in theirlate 20s. The older nursesresent them because
we’re short staffed, and theywon’t work more than 3 shiftsa week. How do I deal withthese conflicts?
Kennedy: You can�t. But you canshow that each group brings somethingspecial to a collaborative�but not nec-essarily cooperative�relationship.
Managing a cross-generational work-force is like conducting an orchestra.Each age group brings different skillsand attitudes. In the end, you get theintended result.
I manage several nursesin their 20s and mostly30s. When I tell them a
task needs to be done, theylook at me with a blank stare.Obviously, my priority isn’ttheir priority. How do Imanage this generation?
Kennedy: Do not hint or suggest.This age group is Teflon coated. You say,�Jane, do X.� They resent it when peopletry to manipulate them. To a Boomer youcould say, �This needs to be done,� andshe will get up and do it. ❖
�Leslie Flowers
The conference brochure is at www.ormanager.com. Or call 800/442-9918.
Marilyn Moats Kennedy is founder andmanaging partner of Career Strategies, amanagement consulting firm in Wilmette,Ill. She publishes Kennedy�s CareerStrategist, a newsletter on career planning,job hunting, and office politics. Her webaddress is www.moatskennedy.com
11OR Manager Vol 20, No 9September 2004
Building a cross-generational workforce
Marilyn Moats Kennedy
Q
Q
Q
Q
Q
Q
Q
Q
Medicare changespolicy on obesity
A new policy on obesity by the federalgovernment may pave the way for studiesto determine whether Medicare shouldpay for obesity treatments, ranging fromsurgery to diets to psychotherapy.
The policy, announced July 15 byHealth and Human Services SecretaryTommy G. Thompson, removes lan-guage in the Medicare coverage manualthat said obesity is not an illness.
The new policy is not expected tohave an immediate effect on Medicarecoverage. But as a first step, officialsplan to convene a Medicare coveragecommittee in the fall to evaluate the evi-dence on obesity surgery for reducingheart disease and other illnesses.
Information about the policy is atwww.hhs.gov/news ❖

12
Please see the ad for SKYTRON, INC.in the OR Manager print version.

was conducted for ambulatory surgerycenters.
Recruiting gets tougher each year.More than 80% of managers say recruit-ing perioperative RNs has become moredifficult in the past year�and 87% said itgot more difficult the year before.
OR managers accept the fact that hir-ing experienced perioperative nurses islargely a thing of the past. Over 80%often hire RNs without OR experience�double the percentage of 1991�and
expect to provide them with additionalpreparation for the OR.
OR vacancies, turnoverFor those with RN openings, overall,
the vacancy rate was highest in teachinghospitals (10.1%) and in the West (10.5%).
Vacancy rates are lower than in 2001and about the same as in 2003.
On average, RN positions were openfor 12.3 weeks and ST positions for 10.1weeks. There was little difference byregion. The time is not as long as in 2001,when the average was 16.5 weeks forRNs and 15.2 weeks for STs.
Vacancy rates for the OR are lowerthan the 14% for RNs in general reportedby JWT Specialized CommunicationsHealthcare Group, which consults onrecruitment and retention.
Temps and travelersReliance on contract workers has been
relatively steady over the past 4 years.This year, 23% report they routinely useagency staff and travelers to fill budgetedOR positions, similar to previous years.
When temps are used, they fill onaverage 7.8% of budgeted FTE positions.Of those who rely on temps, 77% usethem for less than 10% of their budgetedFTEs. Two facilities reported 50% ormore of their staff are travelers. Both arecommunity hospitals, one in the Westand one in the East.
Use of temporary staff is highest inthe West, where 36% use them routinely.In the South, only 14% regularly useagency staff or travelers.
Larger departments are more likely torely on temporary staff:
13OR Manager Vol 20, No 9September 2004
Salary/Career Survey
Continued on page 15
Open positions in ORs
Is recruiting experienced OR nurses difficult?Overall East Central South West
Very 40% 35% 41% 40% 42%
Somewhat 47% 56% 41% 50% 45%
Not at all 13% 9% 18% 9% 14%
Numbers may total more than 100% due to rounding.
Has recruiting becomemore difficult in thepast year?
Yes85%
No15%
Perioperative RNs
Surgical technologists
Continued from page 1
Hospital respondentsto survey
Region Distribution Response
East 204 (17%) 20%South 421 (34%) 27%Central 355 (29%) 36%West 249 (20%) 21%
Yes60%
No40%
OR staffing trends2004 2003 2002 2001
Average staff turnover rate
RNs 7.3% 6.8% 10.5% 13.0%
STs 7.1% 7.0% 8.4% 10.0%
% of FTE positions open
RNs 8.6% 5.4% 9.5% 9.4%
STs 6.4% 6.6% 9.3% 11.7%
Routinely use agency/travelers
23% 25% 27% 19%
Source: OR Manager, Inc.
No openings
RNs 43%
STs 52%

14 OR Manager Vol 20, No 9 September 2004
Salary/Career Survey
Average staff turnover rateType of facility Region
Overall Community Teaching
RNs 7.3% 7.2% 7.8%STs 7.1% 7.6% 5.4%
East Central South West
5.6% 7.7% 8.0% 7.5%7.3% 6.0% 8.3% 6.4%
Average number of open positions in ORsType of facility Region
Overall Community Teaching
RNs 1.8 1.4 2.8STs 1.1 0.9 1.7
East Central South West
1.4 1.2 1.8 2.81.0 0.9 1.2 1.4
What percentage of budgeted FTE positions are open?Type of facility Region
Overall Community Teaching
RNs 8.6% 7.8% 10.1%STs 6.4% 6.1% 6.4%
East Central South West
7.0% 8.2% 8.2% 10.5%4.6% 8.4% 5.1% 6.5%
Average number of weeks positions have been openType of facility Region
Overall Community Teaching
RNs 12.3 12.3 12.3STs 10.1 10.5 8.8
East Central South West
13.1 11.4 11.2 14.010.7 10.7 8.6 10.3
Do you routinely use agency/travelers to fill budgeted OR positions?Type of facility Region
Overall Community Teaching
23% 21% 26%
East Central South West
21% 22% 14% 36%
Note: Turnover was defined as the percentage of staff who have left and been replaced in the past year.
What percentage of FTEs are agency/travelers?Type of facility Region
Overall Community Teaching
7.8% 8.1% 7.7%
East Central South West
4.9% 6.1% 2.3% 13.0%
15OR Manager Vol 20, No 9September 2004
Salary/Career Survey
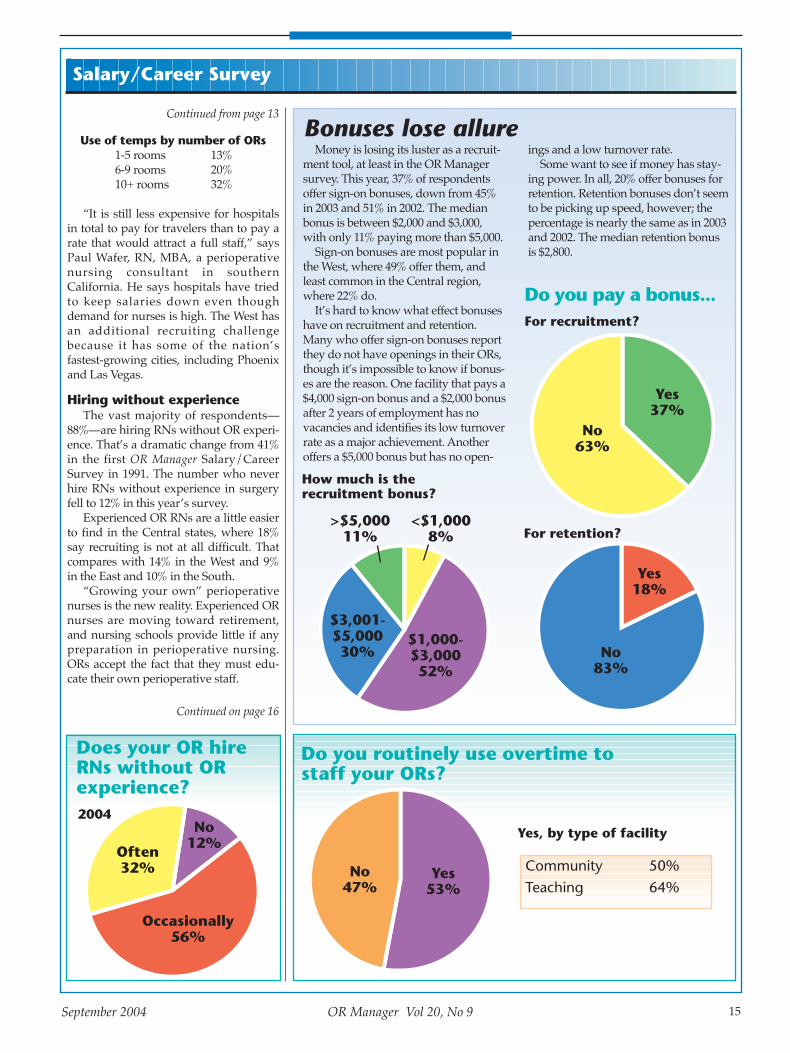
Use of temps by number of ORs1-5 rooms 13%6-9 rooms 20%10+ rooms 32%
�It is still less expensive for hospitalsin total to pay for travelers than to pay arate that would attract a full staff,� saysPaul Wafer, RN, MBA, a perioperativenursing consultant in southernCalifornia. He says hospitals have triedto keep salaries down even thoughdemand for nurses is high. The West hasan additional recruiting challengebecause it has some of the nation�sfastest-growing cities, including Phoenixand Las Vegas.
Hiring without experienceThe vast majority of respondents�
88%�are hiring RNs without OR experi-ence. That�s a dramatic change from 41%in the first OR Manager Salary/CareerSurvey in 1991. The number who neverhire RNs without experience in surgeryfell to 12% in this year�s survey.
Experienced OR RNs are a little easierto find in the Central states, where 18%say recruiting is not at all difficult. Thatcompares with 14% in the West and 9%in the East and 10% in the South.
�Growing your own� perioperativenurses is the new reality. Experienced ORnurses are moving toward retirement,and nursing schools provide little if anypreparation in perioperative nursing.ORs accept the fact that they must edu-cate their own perioperative staff.
Continued from page 13
Bonuses lose allureMoney is losing its luster as a recruit-
ment tool, at least in the OR Managersurvey. This year, 37% of respondentsoffer sign-on bonuses, down from 45%in 2003 and 51% in 2002. The medianbonus is between $2,000 and $3,000,with only 11% paying more than $5,000.
Sign-on bonuses are most popular inthe West, where 49% offer them, andleast common in the Central region,where 22% do.
It�s hard to know what effect bonuseshave on recruitment and retention.Many who offer sign-on bonuses reportthey do not have openings in their ORs,though it�s impossible to know if bonus-es are the reason. One facility that pays a$4,000 sign-on bonus and a $2,000 bonusafter 2 years of employment has novacancies and identifies its low turnoverrate as a major achievement. Anotheroffers a $5,000 bonus but has no open-
Do you pay a bonus...
Yes37%
No63%
For retention?
For recruitment?
Yes18%
No83%
$1,000-$3,00052%
$3,001-$5,00030%
<$1,0008%
>$5,00011%
Do you routinely use overtime to staff your ORs?
No47%
Yes53%
Does your OR hireRNs without ORexperience?
Often32%
No12%
Occasionally56%
2004Yes, by type of facility
Community 50%Teaching 64%
How much is the recruitment bonus?
ings and a low turnover rate.Some want to see if money has stay-
ing power. In all, 20% offer bonuses forretention. Retention bonuses don�t seemto be picking up speed, however; thepercentage is nearly the same as in 2003and 2002. The median retention bonusis $2,800.
Continued on page 16

16 OR Manager Vol 20, No 9 September 2004
Salary/Career Survey
What effect has the nursing and anesthesiashortage had on your OR?
Nurses AnesthesiaProviders
Do not have a shortage 49% 54%
Day of surgery cancellations NA 3%
One or more ORs closed for more than 1 week 6% 14%
Loss of surgical cases to other facilities 5% 7%
Longer patient waits for elective surgery 11% 17%
Extended hours for scheduled cases 33% 31%
Increased use of overtime to complete schedule 47% 31%
Increased use of agency/traveler nurses 16% NA
Extended hours for PACU 31% 24%
Patients discharged home or to surgical floor later in day 23% 17%
Enough educators in OR?Educators are taking on an increas-
ingly important role as ORs hire moreinexperienced staff and try to keepemployees up to speed with new tech-nology.
For the first time this year, the surveyasked how many educators ORs haveand whether they think their education-al resources are adequate.
The range in the number of educa-tors varies widely�36% have none,while 1 teaching hospital has 10. Mostwith no educator are community hospi-tals. In all, 42% of community hospitalshave no educator, but only 15% ofteaching hospitals have none.
For those with an educator, 73% had1 person in that role.
Managers are split on whether theyhave enough educational support.About half of community hospitals saytheir resources are adequate, comparedto two thirds of teaching hospitals.
Smaller departments especially feelstretched:
Are educational resourcesadequate?
1-5 ORs 6-9 ORs 10+ ORs43% 51% 66%
Do you consider youreducational resourcesadequate?
How many educators/staffdevelopment staff do youhave in the OR?
1-5 ORs 6-9 ORs 10+ ORs
0.5 0.8 1.5
Impact of shortagesThough about half of respondents say
they have a shortage of RNs or anesthesiaproviders, few have closed ORs for thatreason. Only 6% (24 facilities) closed ORsfor more than 1 week because they did nothave enough nurses, and 14% (56 facili-ties) closed ORs because of a lack of anes-thesia coverage. One facility reported clos-ing a room every Monday because of theanesthesia shortage. Another managerwrote the hospital does not have a short-age because of its high pay for nurse anes-thetists at $109 an hour.
The main ways of coping with theshortages are to have the staff worklonger hours and to add hours to the sur-gical schedule. The majority of respon-dents�53%�routinely use overtime tostaff their ORs.
ORs also are extending hours in thepostanesthesia care unit and dischargingpatients later. ❖
�Billie Fernsebner, RN, MSN, and Pat Patterson
Stayed the same
81%
Decreased7%
Increased13%
Yes54%
No46%
In the past 2 years, the number of educators has…
Continued from page 15

17OR Manager Vol 20, No 9September 2004
Salary/Career Survey
Fewer staffing challenges for ASCsAmbulatory surgery centers
(ASCs) are having an easiertime with recruitment and
retention than hospitals.A lower percentage of ASCs have
vacancies, and it takes them less time tofill a position. They rely less on over-time, perhaps because most ASCs per-form short cases during the day shiftonly.
The results are from staffing ques-tions in the OR Manager Salary/Careersurvey, which was sent in May to 583ASC managers with a return rate of23%.
Some highlights:� More than half of ASCs�58%�
report no RN openings, compared to43% of hospitals. And 75% have noopenings for surgical technologists(STs), whereas 52% of hospitals do.
� Twenty five percent still have noproblems recruiting experienced ORnurses, which is true for only 13% ofhospitals.
� About half (49%) do not hire RNswithout OR experience, while 12%of hospitals do not.Still some have done a lot of work to
prepare new recruits. One manager wasproud that her center has offered thePerioperative Nursing 101 course fromthe Association of periOperativeRegistered Nurses to 3 nurses.
�We provided preceptors within theASC. This took exceptional time andinvolvement of all senior staff,� saysthis manager of a 2-OR eye clinic.
The pick of nursesASC managers are less likely than
hospital managers to name recruitmentand retention as their greatest achieve-ments or challenges.
Attracting and keeping RNs is easierin a surgery center than a hospital ORfor a number of reasons, according toOR Manager interviews with ASC man-agers.
�The procedures are easier, therearen�t as many procedures to train on,you rarely have an emergency, thephysicians are in a better mood�andthe hours are awesome,� says MindyHoffman, RN, CNOR, manager of theSurgery Center for Sharp Chula Vista
Medical Center in San Diego.Effingham Ambulatory Surgery
Center in rural Effingham, Ill, has awaiting list of nurses who want to workthere. The center does not hire nurseswithout OR experience.
Though the local hospital gives largerraises and better benefits, nurses are will-ing to give up a little for a better qualityof work life, says the center�s administra-tor, Leanne Bales, RN, CNOR.
Though the median age of nurses inthe area is about 40 years, Bales saysshe also has her choice of 20-somethingnurses.
Though RNs may be attracted toASCs, the true test is retention, notesDiana Procuniar, RN, BA, CNOR, nurs-ing administrator at the Winter HavenAmbulatory Surgical Center in WinterHaven, Fla.
Not every nurse is a good fit,whether OR experienced or not. ASCsare fast paced with an increasing num-ber of technologically sophisticatedcases. At Winter Haven, all nurses mustbe ACLS and PALS certified and will-ing to cross train.
Strong orientation needed�No matter how much you explain
the intensity and the pace in the inter-view, they don�t have an appreciationfor it until they are in the middle of it,�Procuniar says.
To help nurses get a good start, shesays an ASC needs a strong orientation
What percentage ofbudgeted FTEpositions are open?RNs 7.1% (n=36)STs 10.5% (n=28)
Has recruiting becomemore difficult in thepast year?
No36%
Yes62%
No52%
Yes36%
Noanswer
12%
RNs
STs
Does your OR hireRNs without OR experience?
Often7%
No49%
Occasionally45%
Average weeks ASC positions havebeen open
RNs 7.0 (n=47)STs 7.6 (n=37)
Numbers do not equal 100% due torounding
Continued on page 18

18 OR Manager Vol 20, No 9 September 2004
Salary/Career Survey
Do you routinely use overtime tostaff your ASC ORs?
No65%
Yes35%
Does your ASC pay a bonus to recruitclinical staff?
No82%
Yes19%
Thank youOR Manager thanks its subscribers
who generously took time to com-plete this year’s survey.
We appreciate your part in gather-ing this information, which will beuseful to your colleagues around thecountry.
Average staffturnover rate
RNs 7.0% (n=124)STs 5.5% (n=101)
Do you offer ORtraining for nurses?
Yes, atthe ASC
65%
No27%
Yes,elsewhere
8%
Numbers do not equal 100% due torounding
Is recruitingexperienced ORnurses more difficult?
Very 26%Somewhat 49%Not at all 25%
Average number of open positions
RNs 0.6 (n=56)STs 0.3 (n=30)
No open positions
RNs 58% (n=77)STs 75% (n=89)
Open positions in ASC ORs
Salary/Career Survey director
Billie Fernsebner, RN, MSN, education director for OR Manager,Inc, has coordinated the OR ManagerSalary/Career Survey for the past 8years.
program tailored to each nurse�sstrengths as well as insecurities.
�Bonuses, hourly pay, and stafflunches�none of that really mattersunless your staff is happy,� she says.
In her experience, an OR backgroundis not as important to a nurse�s successin an ASC as enthusiasm, autonomy, astrong focus on customer service, and asense of humor.
Fewer candidatesIn Southeastern Michigan a nursing
shortage is affecting ASCs.�We are seeing fewer candidates
even for Monday-through-Friday posi-tions,� says Cheryl Dendy, RN, admin-istrative director for the AmbulatorySatellites at St John Hospital andMedical Center, St Clair Shores, Mich.
�There are fewer nurses available inour market, and the economy still hasnot been poor enough to lure a lot offolks out of the home.�
The situation is frustrating becauselocal nursing schools have a waiting listof people wanting to enroll. There arenot enough slots because of a facultyshortage.
St John�s ambulatory units stillrequire a minimum of 3 years of ORexperience.
�We have a high standard for main-taining our patient and surgeon satis-faction scores,� which are in the top 2%to 8% nationally, Dendy says. St Johnhas an extensive interview process thatincludes observation time in the center,which shrinks the pool further.
She is looking to retired nurses tocome in during crunches. Though somemay not be physically capable of han-dling the pace, they can run the surgicalboard and help with other projects.
Also difficult to find are experiencedpostanesthesia nurses.
�I rarely find one and have to do alot of training,� she says. This isdemanding in a multispecialty centerthat serves pediatric patients andrequires a high level of skill.
Though the center could lower itshiring requirements, �we feel we havetoo much at risk. All of us are willing todo what it takes to keep the center run-ning until we can best fill a vacancy,�she says. ❖
Continued from page 17

Something to reach forMMC, a teaching center with 21 ORs
on the main campus, a 5-OR surgery cen-ter, and a surgical volume of about18,000 cases a year, introduced its ST lad-der about 2 years ago, in addition to itsRN ladder. The staff is 50% RNs and 50%STs.
�We are equally in need of recruitmentand retention for techs as for RNs,� says
Dumond. �Wewanted to givethem somethingto reach for ifthey don�t wantto go back toschool.� All STsmust be certifiedwithin 3 monthsof employment.
The ST ladder has 3 rungs: � CST I: Entry level. Performs scrub
role on core cases for assigned ser-vices.
� CST II: Automatic advancementafter 2 years as a CST I with a 2%increase in pay. Performs core andspecialty procedures in assigned ser-vices.
� CST III: 5 years of experience plusapproval of application with a 4%increase in pay. CST IIIs are expectedto work at least 32 hours a week andfunction independently and profi-ciently in the scrub role in complexcases in their assigned area andmaintain competency in other spe-cialties. CST III candidates must doc-ument 20 hours of continuing educa-tion a year, including some classesoutside the hospital. �We also look for them to give in-ser-
vices themselves,� adds Dumond. �Weask them to teach the difficult learner,such as the person who is having a hardtime with orientation.� CST III applicantsalso must document participation in adepartment quality or improvementcommittee or community involvement,such as visiting schools to talk aboutcareers in the OR.
Submitting a portfolioThe clinical ladder pay increases are
in effect as long as STs stay at their level. �In their yearly evaluation, if at Level
III, they have to continue to meet the cri-
teria for a Level III, or they drop back alevel�you have to live up to that levelon a yearly basis,� Dumond notes.
To advance from CST II to CST III, STssubmit a portfolio, similar to what thenurses compile for their ladder. In theportfolio are letters of recommendation,proof of educational credits, a letter fromthe candidate addressing how he or shehas fulfilled the requirements, and aninterview with the review committee.
The review committee is made upentirely of STs. Dumond has beenimpressed with their leadership andimpartiality. �They make decisions aboutpeople they work with every day, andthey really do hold people to the line,�she says.
It took some time for the committee tolearn to make decisions based on thedocumentation presented to them, suchas peer reviews and recommendationsfrom managers, rather than adding theirown impressions about applicants ortheir performance.
In organizing the committee,Dumond asked for volunteers. It waskey that the STs who volunteered hadthe respect of the staff and could drivethe process.
A role for lead techsLead techs are an additional advance-
ment opportunity for STs but are not partof the ladder. Lead techs assist with tech-nical management of a cluster and earn2% more than a CST III.
�Lead techs are viewed as leaders,even by the nurses. They are a greatresource and are willing to share theirinformation,� Dumond says.
Among their functions are to knowthe competencies of other STs in theircluster and give assignment advice toRN leaders, give input on STs� perfor-mance evaluations, order instrumentsand equipment, send equipment out for
repair, communicate with surgeonsabout instrument and supply needs, andhelp to arrange in-services. In the cardiacservice in particular, the lead tech �hasprovided a huge role in keeping the teamtogether,� Dumond says.
Tips for successShe finds the clinical ladder process
has elevated the STs� involvement andinitiative.
�They have been more willing toaddress issues with each other ratherthan going to management. They arelooking for ways to improve the system,and they are more interested in takingadvantage of educational opportunities.�
Dumond�s tips for being successfulwith ST ladders:� Be clear if seniority is not a qualifica-
tion for advancement. �Even thoughwe were clear, we had excellent techsapply because they had 20 years ormore of experience but didn�t neces-sarily meet all of the criteria,� shenotes.
� If applicants are turned down, beclear about how soon the person canreapply and exactly which criteriamust be addressed.�We learned we needed to be really
clear about the expectations, how theycould succeed, and when they couldreapply,� she says.
Fine tuning an RN ladderHanford and Central Valley have
worked to refine their nursing clinicalladder for 4 or 5 years. The system, with2 small hospitals and an ambulatorysurgery center, is in a rural communitysouth of Fresno.
Simple at first, the ladder has�evolved into something that is a lotmore meaningful,� says Harris. One ofthe changes was to award bonuses forladder advances instead of increases inhourly pay. That avoids the problem ofhaving to take back pay if a nursedecides to drop back a level.
The ladder, with 4 steps for RNs and 3steps for LVNs, is based on a point sys-tem that is clearly spelled out in a packetnurses receive. The packet has ladderpolicies and procedures as well as work-sheets for recording achievements ineach category of the ladder�s profession-al development process:
19OR Manager Vol 20, No 9September 2004
Recruitment & retention
Continued on page 20
Continued from page 1
“
“Nurses often go above andbeyond the
requirements.

� development of self
� development of others
� commitment to patient care needs
� improvement of patient care
� improvement of unit or organization
� advancement of nursing/perfor-mance improvement.�The ones who are the most success-
ful fill out the worksheets as they com-plete the activities. We thought it wasimportant to make it user friendlybecause nurses are so busy,� Harris says.
New employees can apply for the lad-der immediately if they work at least 40hours per pay period and have at least 2years� experience as a nurse. Experiencednurses are hired as an RN II, while newgraduates are hired as an RN I.
Nurses can apply for advancement bythe first of every quarter, submitting 12months of documentation. Applicationsare reviewed by the system�s clinical lad-der committee, chaired by Harris.
Nurses often go above and beyondthe requirements. An RN IV requires 150points, but some applicants have 180points.
The bonus for advancing is $1,000 perstep. Thus, a nurse who moves from
Level II to III receives $1,000. A nurse canearn an additional $1,000 for moving onto Level IV in the same year. Levels mustbe renewed each year, and nurses receivebonuses for renewing. For example, anRN IV who wants to stay at that levelmust accumulate enough points torenew at Level IV for the next year. If sherenews both Level III and IV, she receivesa $2,000 bonus. But if the nurse decidesto renew only at Level III, she receives a$1,000 bonus. The amount of the bonus istied to the hospital�s financial status.
�We have found that a lot of nursesare doing the work already. All they aredoing is documenting it and presentingit to the ladder committee,� Harris says.�It�s a nice way for them to capture itand showcase it.
�It�s so heartwarming to see thedevelopment,� she adds. �We have nurs-es signing up to give in-services forCEUs. They also are doing the staffschedule. If they have time, they ask meif there are charts that need auditing.�They are taking the initiative to �closethe loop� on performance improvementactivities.
Fully staffed ORsMMC and Hanford/Central Valley
have no vacancies in the ORs. �We are fully staffed, and we have
been for about 3 years�we have not hada traveler in 3 years,� says Dumond. Ithelps that Portland has an ST education-al program, and the hospital has aninternship program for OR RNs. TheOR�s turnover rate is about 3%, and thewhole hospital�s turnover rate is underthe national average.
MMC�s administration strongly sup-ports clinical ladders and other educa-tion efforts. Says Dumond, �Education isa priority here. It�s not easy to get peoplefree, but we will struggle for education.�
Hanford/Central Valley also have noOR vacancies and have not used a travel-er since 1994.
�We have been blessed. Our folks aretenured, and we have hired new grads,who have worked out beautifully,�Harris says. As a rural community,Hanford tends to have a staff that staysin the area. And with 3 facilities, she hasthe flexibility to move staff around if nec-essary to cover peak times. ❖
20 OR Manager Vol 20, No 9 September 2004
Recruitment & retention
Continued from page 19
Clinical ladder criteria for MaineMedical Center and Hanford/CentralValley are in the OR Manager Toolbox atwww.ormanager.com
Most hospitals to get full update, CMS says
Urban hospitals will see a 5.7%average increase in inpatientpayments for fiscal 2005, and
rural hospitals will receive a 6.2% aver-age increase, in a final rule the Centersfor Medicare and Medicaid Services(CMS) issued Aug 3.
For the first time in 2005, Medicarewill link payments to participation inquality measurement.
Hospitals that report quality data toCMS will receive a full inflation update,while those that do not will receive 0.4percentage points less than the fullupdate.
CMS said the �overwhelming major-ity� of hospitals will be eligible for thefull update but did not have a numberas of Aug 6. Congress passed a law lastyear requiring hospitals to report on 10quality measures or receive a lowerpayment update.
In May, 70% of hospitals had signed
up to report data, and 40% had submit-ted data on at least one measure.
CMS also pledged to be more openin its decisions on paying for new med-ical technology, with more opportuni-ties for public input.
Changes in technologypayments
Among changes for 2005 are add-onpayments for 2 technologies:� an implantable neurostimulator for
deep-brain stimulation for patientswith essential tremor and Parkin-son�s disease
� A device that provides cardiac re-synchronization therapy with defib-rillation.Add-on payments will continue for
bone morphogenic protein (BMP). In addition, heart-assist devices,
including left-ventricular assist devices(LVADs), will be assigned to the DRG
for heart transplants, which will pro-vide higher payment. LVADs originallywere approved as a �bridge� therapy totransplant but are now approved as a�destination� therapy for patientsrequiring permanent mechanical car-diac support.
Also, a spinal fusion procedure requir-ing only a single incision is beingremoved from the DRG for spinal fusionsrequiring 2 incisions, resulting in a higherpayment for the latter procedures.
The final rule also addresses theimpact of changes in geographic classi-fication of hospitals, with phase-ins forhospitals that would see a decrease intheir wage index.
There also are provisions to aid criti-cal access hospitals that serve Medicarepatients in rural areas. ❖
Information on the rule is at www.cms.gov

21OR Manager Vol 20, No 9September 2004
Perioperative Education Pipeline gives Mayo staff a career path
Perioperative managers have beenreaching out to other nursing unitsto recruit RNs for the OR.
One hospital is reaching even furtherinto its ranks.
As part of the Perioperative Educa-tion Pipeline at the Mayo Clinic Hospitalin Scottsdale, Ariz, a person with a highschool education or GED who hires on inan entry-level position can follow a 9-year program to become a periopera-tive RN with a BSN. With 2 more yearsof education, the person can become acertified registered nurse anesthetist(CRNA) or a perfusionist.
The pipeline is a career pathway thatsupports the education of employeesfrom the entry level on up.
�We are a high acuity, tertiary care facili-ty, and we need to have folks in thepipeline,� says Karen Biel, RN, BSN, direc-tor of perioperative services. The 200-bedhospital has 15 ORs in the main hospitaland 4 ORs in an ambulatory surgery center.
The pipeline is one way of meetingthe Phoenix area�s fast-growing need forhealth care. This year, 750 hospital bedsare opening. Mayo�s beds are full, and itis adding new ORs. At this point, theORs are fully staffed.
�This concept evolved because wewant to give opportunities to peoplewithin our institution who want to fur-ther their education,� says CarolynLeslie, RN, MS, CPAN, CNOR, one of theOR�s 2 perioperative education coordina-tors with Brad Haase, RN, MS, CNOR.For Mayo, a teaching institution, educa-tion is a primary mission and value.
Mayo provides tuition reimburse-ment for all employees from the day theyare hired and arranges their schedules sothey can take classes.
Entering the pipelineA person can enter the pipeline at any
point. An entry-level person accepted intothe program begins taking communitycollege courses in subjects such as medicalterminology and basic life support.
From there, the person can move onto become a central service (CS) techni-cian, taking more courses at the commu-nity college and gaining clinical experi-ence at the hospital. A CS position pro-vides a basic knowledge of surgical
instrumentation, tray assembly, and ster-ilization practices.
With additional education, a CS techcan progress to become a surgical tech-nologist (ST). Mayo partners with 2 STeducational programs.
�They go to school for the didacticportion and come here for their clinicalexperience,� notes Haase.
An ST can continue on to pursue aBSN and become an RN.
Currently, several people have com-pleted the CS track, and several othersare in the ST program. Some STs havegone on to become RNs, and a PACUnurse is enrolled in a CRNA program.
Courses for nursesFor nurses who want to come to work
in the OR, the hospital has offered a peri-operative nursing course annually forthe past 5 years. The course is based onPerioperative Nursing 101 from theAssociation of periOperative RegisteredNurses (AORN). The 12-week coursetypically has 3 to 5 students. Instructionis provided by the educators, with teamleaders and guest lecturers providingsome of the content.
Most of the staff serve as preceptors.They are required to take a 6-hour pre-ceptor training program, which is a mod-ule in the AORN course.
�That�s critical for the success of theprogram,� Haase notes.
The staff really enjoy precepting, headds. �They will ask, �When are wegoing to get our next students?��
OR orientation is conducted in phas-es. The basic orientation is 90 days for allnew RN employees, including thosewith experience. After that, they areexpected to take call in their specialty.Nurses orient to a primary specialty ini-tially because Mayo�s ORs are organizedby specialty.
A nurse who orients to orthopedics,for example, might work solely in thatspecialty for the first year because theservice takes its own call. For generalsurgery, initial orientation might take 2weeks to 2 months, depending on thenurse�s experience. After that, nursesrotate to other specialties they mightencounter on call, such as gynecology,urology, and neurosurgery. ❖
Recruitment & retention Share yoursuccesses at2005 meetings
Share your successes with your col-leagues at the conferences of ORManager, Inc. Send proposals of
about 500 words describing the sessionyou wish to present. Sessions areapproximately 1 1/2 hours long.
Managing Today’s OR Suite Oct 19 to 21, 2005, San Diego
Managing Today�s OR Suite focuseson practical topics related to manage-ment of surgical services, such asachieving greater efficiency, manage-ment of information, leading and devel-oping staff, and keeping costs undercontrol.
The keynote address and generalsessions feature nationally knownspeakers who have important messagesfor surgical services directors. If youwish to suggest a general session speak-er, please obtain as much informationabout the person as you can, such as thespeaker�s title, organization, address,and phone number.
OR Business ManagementConferenceMay 2 to 4, 2005, Tampa, Fla
The OR Business Management Con-ference emphasizes financial manage-ment, materials management, OR tech-nology/equipment management, andOR design and construction.
The deadline for proposals and sug-gestions for both conferences is Nov 1.
Fax or e-mail proposals to BillieFernsebner, RN, MSN, education direc-tor, OR Manager, Inc, at 303/442-5960or [email protected]. If youhave questions, please call 303/442-1661. ❖
Have an idea?Do you have a topic you’d liketo see covered in OR Manager?Have you completed a projectyou think would be of help to
others? We’d be glad to consider your suggestions.
Please e-mail Editor PatPatterson at

One staff nurse has frequent coldsand calls in sick. She complainsabout her patients and the
administration, feels overwhelmed byher duties, and overeats when she feelsstressed.
Another staff nurse bounces intowork. She is enthusiastic, supportive toher peers, serves on hospital committees,and is a loving caregiver. Other thanvacations, she�s missed work in the pastyear only when her child was ill and fora funeral. She works out at a gym at least3 times a week.
What�s the difference between thesetwo nurses?
�Hardiness. Just like hardy plants aremore likely to survive in tough environ-ments, so will hardy nurses, � says LeslieFurlow, RN, PhD, of AchieveMentors, Inc,and HardinessMentors, LLC, Tolar, Tex.
Hardiness in health careThe concept of hardiness in health
care workers emerged in the mid-1980safter a landmark study at Illinois BellTelephone (IBT) during the breakup ofthe telephone giants.
Salvatore R. Maddi, PhD, and histeam of researchers at the University ofChicago studied 400 IBT employees over12 years. In the most stressful years ofthe divestiture, during layoffs and reor-ganizations, they found almost two-thirds of the participants showed signifi-cant wellness breakdowns, includingheart attacks, cancer, suicide, depression,anxiety, or divorce. But the remainingone-third maintained their health andperformance and actually thrived.
�These hardy individuals had the atti-tude of �When the going gets rough, getmore involved,�� says Maddi. �Theyeither rose within IBT, left and startedtheir own businesses, or rose up theranks of a competitor.�
Since then, more than 600 studiesrelated to hardiness have been conduct-ed around the world, and Maddi�s trade-marked hardiness survey has been trans-lated into 15 languages, he says. Maddiis the founder and director of TheHardiness Institute, Inc, Newport Beach,Calif.
�Hardiness is a combination of atti-tudes and skills that help you be resilientand turn stressful situations from poten-
tial disasters into growth opportunities,�Maddi says.
In nursing, studies over the last 2decades have demonstrated that high-hardy nurses are more resistant to stress,strain, and burnout.
Sharon Judkins, RN, PhD, director ofnursing administration at the Universityof Texas and Furlow�s research partner,showed in her study that for nurse man-agers, high hardiness is linked to lowerlevels of stress and higher problem-solv-ing skills.
�Hardiness has emerged as a bufferstrategy not only to diminish the nega-tive effects of stress, but also to helpdevelop coping skills that will benefitboth individuals and organizations,�says Furlow.
3 C’s of HardinessAccording to Maddi�s original
research and later work by nurseresearchers, hardy nurses share these 3personality attributes:
CommitmentHardy nurses are deeply involved in
life�s activities and have a knack of find-ing something interesting or importantabout whatever it is they are doing, sayJudkins and Furlow. They do not give upeasily under pressure and possess astrong sense of purpose and direction.They stay useful and don�t pull back intoisolation and alienation.
ControlHardy nurses believe they have great
control over their lives and act to createbetter life situations. Consequently, theysee workplace stressors as nonthreaten-ing, natural, and meaningful, noteauthors Fox, Fox, and Wells. Nurse man-
agers who are high-hardy often createfun, positive work environments. Theydon�t waste time on feelings of power-lessness or passivity. They keep trying tohave an influence on their environment.
�Staff is empowered to make a differ-ence because the manager believes boththe manager and staff do make a differ-ence,� says Judkins.
ChallengeHardy nurses see change, pressures,
and disruptions, however painful, asopportunities for learning and growth.They tend to see the opportunity andexcitement in change, while low-hardynurses feel threatened and frequentlyrespond with negativity, criticism, andeven sabotage.
�If you�re hardy, you�re someone whodeals with issues,� Furlow says. �And ifyou want to succeed in nursing, youneed to be able to deal with conflict andchallenge because change is the onlyconstant in health care.�
Hardiness can be learnedHardiness can be learned, says
Furlow, who provides hardiness trainingover a period of 18 months.
�Research has shown that hardinesstraining that takes place in a few days isnot retained,� she says.
HardinessMentors first provides a 3-day intensive for groups of no more than10 people. They come back weekly for 6weeks, then return at 3, 6, 12, and 18months for 2- to 3-hour sessions.Participants are assessed on a hardinessscale at the beginning and end of eachsession.
The training builds skills in commu-nication, conflict management, problemsolving, anger management, and stressmanagement, Furlow says.
Participants usually are nursing direc-tors or middle-level managers��thelevel that was devastated by reengineer-ing in the �90s and is lacking in manager-ial skills,� she says.
Maddi�s group, The HardinessInstitute, also provides training anddeveloped the original HardiSurveyassessment, which is available throughThe Hardiness Institute�s website (www.hardinessinstitute.com).
22 OR Manager Vol 20, No 9 September 2004
“Hardy nurses” less likely to burn out
Recruitment & retention
“
“Hardiness helps you be moreresilient.

Hardiness retains nurses The best way to teach hardiness is
through emulation, says Furlow.�Hardy managers transfer these skillsto their staff.�
Results from hardiness training for 12nurse managers who cover 20 depart-ments at Osteopathic Medical Center inFort Worth, Tex, showed that 6 monthsafter the initial training by Hardi-nessMentors, nursing staff turnover wasreduced 63%. Moreover, this was at atime the hospital was for sale.
�The data reinforce our belief that ifwe made nurse managers more hardy,their staff would not turn over as quicklybecause managers would be able to dealwith issues and emulate hardy behav-
ior,� Furlow says.As organizations strive to become
hardy, they attract and retain a higherproportion of hardy individuals,reports Maddi.
A 1987 study by Rich and Rich foundthat some of the least hardy nurses arethe youngest. They have higher burnoutrates because they lack experience inhandling stress, and the job may notmeet their initial expectations.
A hardiness scale can help determinea nurse�s hardiness level and need fortraining. Less hardy nurses can then bedeveloped and/or assigned to less stress-ful environments.
Furlow does not advise administeringthe hardiness assessment during the
interview process for new employeesunless it is used with every applicantbecause there could be equal opportuni-ty issues.
Furlow concludes that fostering a cul-ture of hardiness is the greatest deterrentto the negative effects of stress�staffburnout, poor work performance, acuteand chronic health problems and highturnover.
�Many organizations pay consultantsenormous fees to change the culture. Bydeveloping a high-hardy environment,administrators can reap the same bene-fits at a fraction of the cost.� ❖
�Leslie Flowers
Leslie Flowers is a freelance writer inIndianapolis, Ind.
Salvatore Maddi can be reached at TheHardiness Institute at 949/252-0580 [email protected].
Leslie Furlow can be reached at Har-dinessMentors at 877/331-4321 or [email protected]
ReferencesCollins M A. The relationship of work
stress, hardiness, and burnout amongfull-time hospital staff nurses. Journalof Nursing Staff Development. 1996;12(2):81-85.
Fox R T, Fox D H, Wells P J. Performanceof first-line management functions onproductivity of hospital unit person-nel. Journal of Nursing Administration.1999;29(9):12-18.
Judkins S, Furlow, L. Creating a hardywork environment: Can organizationalpolicies help? Texas Journal of RuralHealth. 2003; 21(4):11-17.
Judkins S K, Ingram M. Decreasing stressamong nurse managers: A long-termsolution. Journal of Continuing Educa-tion in Nursing. 2002:33(6):259-264.
Rich V I, Rich A R. Personality hardinessand burnout in female staff nurses.Image: Journal of Nursing Scholarship.1987;19(2):63-66.
Simoni P S, Paterson J J. Hardiness, cop-ing, and burnout in the nursing work-place. Journal of Professional Nursing.1997;13(3):178-185.
23OR Manager Vol 20, No 9September 2004
Recruitment & retention
Commitment� Encourage personal involvement
in daily organizational life.
� Mentor protégés by sharing per-sonal successes and failures.
� Establish interdepartmental men-tors by pairing new managers withseasoned managers in otherdepartments.
� Provide conflict management andassertiveness training to promotehealthy group interaction andcohesiveness.
� Role-play and offer scenarios todiscuss how staff as a group cancommit to solving problems andissues together.
Control� Provide an environment in which
nurses feel a sense of influenceover their practice.
� Create physician and nurse prac-tice committees to establish stan-dards of care collaboratively anddetermine how and when nursinginterventions will be taken.
� Develop policies to allow nurses topractice to the extent of their skillsand abilities.
� Provide open communicationchannels between administrationand staff for sharing informationand requesting input.
� Advocate manager participation inhospital budget preparation.
� Encourage and reward creativityamong staff to generate ideas andimplement new practices, such assolving scheduling issues.
� Discuss opportunities to increase asense of autonomy, such as sharedgovernance and self-scheduling.
� Discuss case studies to reinforceproblem-solving strategies ratherthan fire fighting.
� Create a fun work environment.
Challenge� Develop policies that promote par-
ticipation in change, such asencouraging and rewarding activeparticipation in committees andgroups.
� Promote change as constructive�an evolution rather than a negativeintrusion.
� Promote new learning experiencesamong staff.
� Engage staff in the change processand reward positive changes inbehavior and practices.
� Encourage and reward risk-takingrather than risk-avoiding behav-iors. Link risk-taking behaviorswith patient outcomes.
Source: Judkins & Ingram, 2002; Judkins& Furlow, 2003.
Strategies to encourage hardiness

OR managers are just starting totalk about a new technology�radiofrequency identification, or
RFID�that is expected to replace manytypes of bar codes in 5 years and makepatient identification and other functionsmore effective.
Two pilot studies are underway inORs to evaluate the use of radiofrequen-cy identification wristband technology inblood transfusions and surgical site veri-fication.
Georgetown University Hospital inWashington, D C, a 609-bed teachingcenter, began its 100-patient study in
March to com-pare bar-codetechnology withRFID to verifyt r a n s f u s i o n sfrom donor topatient, saysGerald Sandler,MD, director oft r a n s f u s i o n
medicine at Georgetown, who is con-ducting the study.
In the second study, surgical nurses at300-bed Valley Presbyterian Hospital inVan Nuys, Calif, will use readers to scanpatients with RFID wristbands beforesurgery to ensure the correct body part isoperated on, says Irwin Thall, managerfor RFID in health care with PrecisionDynamics Corp, a San Fernando, Calif-based wristband identification company.
Both studies are testing Precision�sRFID �Smart Band� wristbands.
�We are looking to prove severalthings,� Thall says. �We want to showthe clinical efficacy of RFID technologyand how it can make things in the ORwork more smoothly, with improvedrecord keeping and reduction of errors.�
Georgetown studyLike a growing number of hospitals,
Georgetown�s OR has been using barcodes to track blood transfusions.Hospital studies have shown bar codesreduce medication error rates by asmuch as 85%, according to the U S Foodand Drug Administration.
In Georgetown�s study, patients havebeen given wristbands embedded withboth bar codes and RFID chips. Dual-usescanners have been specially developed for
the study, Dr Sandlersays.
Before a bloodtransfusion, nursesscan the bar code onthe wristband to deter-mine the patient�sidentity. If the bar-codescanning fails, thenurse flips a switch onthe reader and collectsthe patient identifica-tion using RFID.
�My intent is to tryto find the optimal cir-cumstances when barcodes should be usedfor patient, lab, andspecimen identificationand the optimal condi-tions to use RFID,� saysDr Sandler.
The FDA will re-quire pharmaceutical companies to placebar codes on all hospital drugs by 2007.The agency says less than 1% of all UShospitals have bedside barcoding sys-tems. If all hospitals use the technology,the FDA estimates bar codes could pre-vent more than 25,000 medical errorseach year and save about $4.5 billionover the same time period.
In February, the FDA also backed useof RFID as an alternative to bar codesthroughout the medication distributionsystem and as a tool to help reduce drugcounterfeiting.
While bar codes can help reduceerrors, Dr Sandler says the accuracy ofreading bar-coded wristbands dependson the age of the patient and how longthe patient has been wearing them.
�Scanning a patient�s wristband isn�tas easy as scanning a flat Wheaties box ina grocery store,� he says. �We have identi-fied problems using bar codes. When weuse bar codes in the outpatient depart-ment, it is 100% successful. But if a patienthas been in the hospital 3 days, slept on(the wristband), and taken showers, it isnot as effective. There are nonread errors.This has led us to test RFID.�
Another purpose of the study is totest a dual-use�bar code and RFID�reader system. �Once the FDA requiresbar codes on medications, there is no rea-son to have another system for blood
bags. We want one platform that can beused for both blood and medications,�he says.RFID versus bar codes
Unlike bar codes, RFID�s signal cantransmit through human bodies, cloth-ing, and nonmetallic materials withoutthe reader having a direct line of sightwith the tag, Precision�s Thall says.
RFID also can have larger memorycapacities, wider reading ranges, andfaster processing than bar codes, he says.Combining a microchip and antenna,RFID provides wireless communicationfor accurate identification, tracking, andprocessing, he says.
Precision�s Smart Band�s RFID chipalso can contain patient information suchas name, blood type, allergies, and med-ications, Thall says.
Depending on signal strength, RFIDchips have 5 feet to 25 feet of read range.RFID wristbands cost about $1.10 to$1.25 each, he says.
At Georgetown, nurses use a scannerattached to a portable digital assistant(PDA) to read the wristband chip, whichdisplays the data on the screen andallows nurses to check the transfusionorder and the actual blood product to beadministered. �Sometime in the futurewe also may place an RFID reader along
24 OR Manager Vol 20, No 9 September 2004
Patient safety
“Smart” wristbands tested for patient ID
A nurse scans a patient�s RFID wristband. Courtesy PrecisionDynamics Corp.
Continued on page 26

25
Please see the ad for KARL STORZ ENDOSCOPY �AMERICA
in the OR Manager print version.

the door of a patient�s room,� Dr Sandlersays. �It can be programmed for the indi-vidual patient. When an incorrect bloodbag enters the room, an audible alertwould sound off. This system also can beused for medications.�
Valley Presbyterian studyThe pilot study at Valley Presbyterian
Hospital will evaluate use of the wrist-bands on patients in the outpatientsurgery department. If the study is suc-cessful, the hospital plans to expand useof RFID wristbands to inpatient surgery.
�With RFID, you can store informa-tion on the patient, the site of surgery,and treatment. You can�t do that with barcodes because you can�t store enoughinformation,� Thall says. �We believe
this will reduce the incidence of wrong-site surgeries.�
Once the pilot studies are completedlater this year, Precision wants to expandpilots to up to 50 hospital ORs and devel-op partnerships with medical devicemanufacturers.
Technology for tracking While RFID is seen as the next gener-
ation of bar codes, or at least more effec-tive in some health care situations, RFIDhas a limited range, which restricts it usein applications like patient tracking, saysJohn Pantano, vice president of sales andmarketing with Radianse, a Lawrence,Mass-based indoor positioning solutionscompany.
For tracking patients, staff, and equip-ment, a growing number of hospitalsand surgery centers use a combination ofradiofrequency (RF) and infrared (IR)technology, says Todd Brown, vice presi-dent of products with PeriOptimum, aPittsburgh-based OR software develop-ment company.
Providence St Vincent Medical Centerin Portland, Ore; Spectrum HealthEndoscopy Center, Grand Rapids, Mich,and Massachusetts General Hospital(MGH), Boston, are some organizationsthat use a combination RF/IR trackingsystem for patients and equipment.
MGH has been studying Radianse�sRF/IR badges for about 19 months tohelp them reengineer their perioperativeprocess, says Pantano. In MGH�s proto-type OR of the Future, the system is usedto measure patient flow time, wait time,resource utilization, and their variances.(See June OR Manager.)
The passive tags continuously trans-mit RF and IR waves to receivers con-nected to MGH�s local area network. Thesystem also tracks medical devices suchas external pacers, infusion pumps, andtelemetry transmitters.
The savings from RF/IR or RFIDtracking technology come not simplyfrom deploying the systems but fromusing the information to improve theentire OR process, says H. T. Snowday,vice president of product developmentwith Versus Technology, a Traverse City,Mich-based company that makes wire-less locating systems.
�ORs are experimenting with the ideathat they can use the tracking system tobe notified when a patient moves fromone area to the next,� Snowday says. Forexample, when a patient moves out ofthe preoperative area, the next staff per-son to see that patient would be notifiedthrough the computer system, he says.
�This automates the process andincreases throughput,� Snowday says.�In the future, when you integrate sched-uling with tracking, you can also use theinformation to change schedules on thefly. If a procedure is late, you can movearound ORs to make sure you don�t haveto cancel a surgery at the end of the day.�
Versus provides an RF/IR systemwith its Versus Information System (VIS),Snowday says.
When patients check in at the OR reg-istration center, they are given a VISbadge to wear so they can be trackedthrough the surgery process.
Next stepsOne of the challenges over the next 2
years is to integrate wireless trackingsystems�both RFID and RF/IR�withsurgical scheduling and billing systems,says Pantano.
�We will see more software applica-tions to help track patients in real time,maintain schedules, or help determine ifschedules are falling behind or if thereare problems or bottlenecks that can beadjusted,� he says.
Tracking systems also can be connectedwith billing systems to speed reimburse-ment. �You put a (RF/IR) tag on an infu-sion pump, and you can track how longthat pump is infusing a drug into apatient. Once the pump is removed, [thepatient is] no longer using the therapy, andyou can bill for that time,� Pantano says.
Versus also is evaluating use of RFIDchips on medications, injectables, andsmall equipment. ❖
�Jay Greene
Jay Greene is a freelance writer in StPaul, Minn.
26 OR Manager Vol 20, No 9 September 2004
Patient safety
What is RFID?Radiofrequency identification
(RFID) is an emerging technology thatuses small, dime-sized chips to track avariety of supplies, equipment,patients, and staff.
Wal-Mart became the first majorretailer to announce plans to requiresuppliers to put RFID tags on ship-ping crates and pallets by 2005.Gillette plans to purchase 500 millionRFID tags for its consumer products.The U S Department of Defenseannounced similar requirements forits suppliers.
When the RFID chips are placed onproducts, electronic readers send outsignals that activate the chip, whichresponds by transmitting identifyinginformation back to the reader. Themicrochips within the tags containmore than 10 times the information ofbar codes.
Unlike bar codes, RFID-taggeditems do not have to be individuallyscanned. The chips also can be readwithin containers and from a distancein a passive, non-line-of-sight manner.
�We expect to see active RFID tagsfor larger equipment and passive tagsfor smaller pieces like catheters andsutures,� says Erin Sparnon projectengineer with ECRI, PlymouthMeeting, Pa. Some companies also areinstalling RFID chips in medicalequipment like endoscopic instru-ments, she says.
Continued from page 24
“
“We’ll see more softwareto help track
patients.

ManagingToday’s OR Suite
SeventeenthAnnual
Chicago HyattRegencyOctober 6–8, 2004General session speakers� Carl Hammerschlag, MD, The Way it Was is Not
The Way it Is� Amanda Gore, Communicating Your Way to Success� Michael Roberto, Harvard Business School, Leader-
ship Lessons Learned from the Everest Disaster� Steve Lundin, PhD, Go Fish!� Mary Murphy, RN, 2002 OR Manager of the Year
You’ll have eight all-day seminars and more breakout sessions to choose from.
All-day seminars� Transformational Leadership � Six Sigma for Process Improvement� Building a Cross-Generational Work Force� Managing a Central Processing Department� Supply Chain Management
Breakouts� Implementing a Just Culture� Ambulatory Track: Holistic Patient-Centered Model,
Physician Credentialing� Fire Safety� Pain Management� Improving Patient Flow� Managing Intraoperative Medication� Service Recovery Programs� OR of the Future
And much, much more…Networking, receptions, exhibits, and other educational opportunities
The brochure for the conference is available atwww.ormanager.com or by calling 800/442-9918.

28 OR Manager Vol 20, No 9 September 2004
Half Page AdOLYM0904
4/c(New)
Hospitals invest to save nurses’ backs
Duke University Hospital in Durham,N C, spent $670,000 in the first phase of aprogram to install patient lifts and teachnursing staff to use them, reports the Aug8 News & Observer, a North Carolina news-paper. WakeMed, based in Raleigh, N C,has spent more than $650,000 on inflatablemats and lifts. A recent study found thatevery day the hospital has at least onepatient who weighs more than 350pounds. Rex Healthcare, also in Raleigh,has invested what it said was �significantmoney� on ergonomic devices.
They�re all part of an effort to improvecare for heavier patients and save wearand tear on the nursing staff.
Nurses have one of the highest occu-pational injury rates of any profession�12.5 per 100 workers, according to theBureau of Labor Statistics. The AmericanNurses Association estimates more thanone third of nurses suffer from back-relat-ed injuries and that 12% of nurses leavethe profession annually for that reason.
�www.newsobserver.com
A “mommy and daddy” trackto attract nurses
Though it will be no surprise to manymanagers, Vanderbilt Children�s Hospitalin Nashville, Tenn, is offering flexibleshifts as short as 4 hours. The family-friendly schedule is intended to lure par-ents of young children back into nursing,reports the Aug 9 Tennessean. Nurses canbe eligible for benefits at 30 hours a week.
Several other Nashville-area hospitalsoffer flexible scheduling. At CentennialMedical Center and Southern Hills, partof HCA Inc�s TriStar Health System, nurs-es who work 20 hours a week can qualifyfor health benefits. Job sharing is popularat Williamson Medical Center in Franklin,Tenn, with 2 nurses sharing one full-timeposition. Nurses there also qualify forbenefits by working 20 hours a week.
As in many areas, though more stu-dents want to enroll, nursing schools haveturned away applicants because they didnot have enough faculty or clinical train-ing programs.
�www.tennessean.com
Residency programs complyingwith work-hour limits
Physician training programs aredoing a pretty good job at staying with-in new resident work limits imposedlast year. In all, 95% of 2,000 programswere in compliance.
Many programs used schedulechanges, night float, and other modifica-tions to bring duty hours below the limits,the Accreditation Council for GraduateMedical Education reported Aug 4. Somereplaced residents� services with care bynurse practitioners, physician assistants,or hospitalists.
The council turned down a request toincrease surgical chief residents� limit to88 hours, citing a lack of data to show thelimit was having a negative effect.
The limits restrict residents to 80hours of work averaged over 4 weeks,and 10 hours of rest between dutyhours, among other rules. ❖
�www.acgme.org
Workplace

29OR Manager Vol 20, No 9September 2004
There are a number of reasons whyan ambulatory surgery center(ASC) might want to benchmark�
physician owners want to know if rev-enue is on target, you think you needmore staffing, or your accreditation sur-vey is coming up. You want to knowwhere you stand, and someone suggestssigning up for a benchmarking program.
Before jumping in, you need a goodunderstanding of what benchmarkingcan do and can�t do for your ASC. Youneed to know the benefits and limita-tions so you know you are being com-pared appropriately.
Independent ambulatory surgery cen-ters (ASCs) are small businesses thatneed a basis for comparison, and bench-marking is a good way to achieve that,says Susan Kizirian, RN, MBA, directorof the Southeastern Surgery Center inTallahassee, Fla.
Benchmarking can provide guide-posts for budgeting and forecasting.
For example, the Ambulatory SurgeryPerformance Survey by the MedicalGroup Management Association(MGMA), conducted in collaborationwith the American Association ofAmbulatory Surgery Centers (AAASC),has data on measures such as revenueper case and total operating cost percase.
The Federated Ambulatory SurgeryAssociation (FASA) provides bench-marking to its members on financial aswell as clinical indicators.
Learning from othersProbably the most important bene-
fit�and best reason to benchmark�is tolearn from others so you can improve.
�If you�re benchmarking just becauseof accreditation standards, you�re notgetting out of it all that you could. Thereason to benchmark is to find out who�sdoing things differently and getting bet-ter results,� comments Jennifer Green ofSurgical Outcomes Information Ex-change (SOIX), a not-for-profit organiza-tion that provides benchmarking forASCs.
Benchmarking can also help withinsurance contracting, particularly if
your ASC does especially well on mea-sures such as complication rates or effi-cient patient flow.
Another benefit is to build strongerworking relationships within the ASC.
�Like QI, benchmarking can be ateambuilding activity,� says NaomiKuznets, PhD, director of the Accredi-tation Association for AmbulatoryHealthcare�s Institute for QualityImprovement (AAAHC IQI), a nonprofitorganization that provides clinicalbenchmarking for ASC procedures.Comparing your center�s performancewith others injects a spirit of competitionthat motivates people to work together.
Benchmarking can also be a manag-er �s ally. Perhaps you have startedreporting to a new boss who is not fromthe ASC industry, and you need to pro-vide information on the median days inaccounts receivable and other businessmeasures. Or a new investor has signedon, and you want to educate that personabout ambulatory surgery.
There may be the need to counterwhat Kizirian calls �fish stories,� talesabout how much money someone hasmade investing in another ASC or howlow someone else�s supply costs are.Benchmarking can give you a factualbasis for responding to anecdotes.
Of course, benchmarking and qualityimprovement are also accreditationrequirements of AAAHC and the JointCommission on Accreditation of Health-care Organizations.
What to look for Independent ASCs have several
benchmarking programs to choose from(sidebar). Corporate-owned centers usu-ally participate in their company�s ownprogram. Some consultants and manage-ment companies also have their ownbenchmarks.
Criteria to consider in assessing abenchmarking program:
1. Will the program protect your facility’sconfidentiality?
What to know about ASC benchmarking
Continued on page 30
“
“The most important
benefit is to learnfrom others.
Gwendolyn Grothouse, RNAdministrative directorApple Hill Surgical CenterYork, Pa
Barbara Harmer, RN, BSN, MHASenior consultantHealthCare Consultants, IncCelebration, Fla
Jerry Henderson, RN, MBA, CNOR,CASCExecutive directorThe SurgiCenter of BaltimoreOwings Mills, Md
Diana Procuniar, RN, BA, CNORNursing administratorWinter Haven Ambulatory Surgical
CenterWinter Haven, Fla
Donna Gelardi-Slosburg, RN, BSN, CASCNational surgery specialistHealthSouthSt Petersburg, Fla
Rhonda Tubbe, RN, CASC, CNORAdministratorThe Surgery Center of NacogdochesNacogdoches, Tex
Ambulatory Surgery Advisory Board

A benchmarking organization shouldbe able to assure you that only aggregateresults will be reported, and individualparticipants� identities will be protected.
2. Are facilities participating similar toyours in size and patient population?
�There are organizations that willgive you broad-brush measures,� saysKuznets. But that may not provide anaccurate comparison. Comparing multi-specialty centers to single-specialty cen-ters, for example, may not be useful.
�If you are looking at turnover timefor knee arthroscopy in a multispecialtycenter, results will be different than in anorthopedic center,� she notes.
AAAHC is developing some nonclini-cal measures such as staffing costs. Theaim is to break these down by the type ofprocedure, specifically by CPT code.
�If you are looking at staffing costs,
you don�t want to compare cataract pro-cedures with knee arthroscopy orcolonoscopy,� she notes, because theseprocedures may be staffed differently.
The AAAHC IQI studies have focusedon the top 3 ASC procedures�cataractremoval, arthroscopy, and colonoscopy�because most facilities have enough dataon those to be able to participate in bench-marking. SOIX provides benchmarking in35 procedural categories and is launchingfacility-level benchmarking.
3. Does the program focus on topics thatare relevant to you?
Are you looking for clinical measures,financial measures, or both? Which pro-grams focus on topics that are in linewith your improvement objectives?Kizirian described how some centershave used information from the MGMAreport (sidebar).
4. Is the data relatively easy to obtain?
How much time will it take to collectinformation for benchmarking? Will youhave to go back to patient charts to col-lect data, or will the study be prospec-tive? Will you be able to obtain the finan-cial data from your accounting systemand standard reports?
The MGMA benchmarking question-naire requires financial data and otherstatistics on performance. Though theassociation believes the questionnaire isstraightforward, some ASCs say theyhave found it time-consuming to com-plete. In all, 120 facilities out of 1,138returned the questionnaire for the latestreport, for a return rate of 9.5%, whichMGMA is trying to improve. Kiziriannotes that MGMA has been working tosimplify the survey tool. She has givenpresentations at national meetings tocoach ASCs on how to organize theirinformation for the survey instrument.
5. Will the organization provide a samplereport you can look at?
Is the information reported in a waythat will be useful to you? Ask for a sam-ple report to see whether the informationwould assist your center in makingchanges.
6. Do the reports include informationabout best performers?
Learning from best performers abouthow they achieved their results is one ofthe chief benefits of benchmarking.AAAHC IQI includes information frombest performers in its reports. SOIX facili-tates networking among its members sothey can learn, for example, how a best-performing center achieved its outcomesfor pain management after arthroscopy.
Fear factorsManagers may feel their anxiety lev-
els rising when the subject of bench-marking is raised. What if the center�sperformance isn�t in line with others?Will they be held accountable?
Kuznets cautions against usingbenchmarking results for accountabilitybecause most studies aren�t large enoughto provide statistical power. Instead, thefocus should be on quality improvement.
Kizirian recommends that managers
30 OR Manager Vol 20, No 9 September 2004
AmbulatorySurgery Centers
Continued on page 32
How 3 ASCs used benchmarkingresults:Support for more nursingstaff
The nurse manager of an indepen-dent multispecialty ASC with 4 ORsperforming 6,000 cases a year was hav-ing difficulty staffing the ORs duringvacations and providing lunch relief.Turnover time was slowing on busydays. Surgeon satisfaction was drop-ping, and morale was sinking. YoungerGen X and Y employees wanted a morebalanced life, with more time off andless overtime.
Using data from a benchmarkingreport, she showed the center�s boardthat the center�s staffing was below themedian by 2.5 FTEs for the size andtype of facility. The board agreed toincrease staffing. How many staff for thebusiness office?
An ASC administrator hired a newbusiness manager from another settingwho wanted to hire more employeesfor the business office because that is
what she was used to. He showed herthe benchmarking report, whichshowed the center actually was staffedat the 75th percentile for centers of itssame surgical volume. The businessmanager agreed to make adjustments.Getting real on revenue
The administrator of a large multi-specialty ASC was being held to unre-alistic goals for gross revenue and netprofit by the center�s governing board.He was restricted in the new surgeonshe could recruit to bring in more rev-enue. The administrator showed theboard a benchmarking report showingthat the center�s gross revenue was atthe 75th percentile, net income was atthe 90th percentile, and operating costswere below the median. The boardaccepted the findings and reset thegoals to more realistic levels.
Source: Susan Kizirian, RN, MBA, inter-viewed on use of the Medical GroupManagement Association�s AmbulatorySurgery Center Performance Survey.
Benchmarking success stories
Continued from page 29

31
Please see the ad for ADVANCED STERILIZATION PRODUCTS
in the OR Manager print version.

32 OR Manager Vol 20, No 9 September 2004
prepare by understanding how thebenchmarking study is conducted andwhat the results mean. For example, sheis director of a urology center, and only 3urology centers participated in the cur-rent MGMA report.
�The data for the urology centers is soskewed that it is not useful for me,� shesays. If her center �s board membersasked about the data, she would explainthat not enough urology centers partici-pated for it to be meaningful.
�Eventually, more urology centerswill participate, and the data will bemore useful to me,� she says.
She does find the MGMA surveyhelpful for aggregate numbers, such asstaffing levels per OR or accounts receiv-able data per 1,000 cases.
A benchmarking conundrumA dilemma in benchmarking is bal-
ancing the need for detailed data withthe limited time and resources ASCshave for filling out questionnaires.
�Regardless of how you do it, perfor-mance measurement takes time,� saysGreen. �Some centers have made perfor-
mance measurement part of their day-to-day activities with regular feedback tothe staff� to see if the center�s perfor-mance stacks up with others�. For exam-ple, your revenues may be up and com-plication rates down. But you might findyour recovery time is longer than others�,and you may still find room for improve-ment.
Participating in benchmarking createsa conundrum, Kizirian notes: The moredetailed the data a report requires, themore useful a report can be. To achievethat level of detail, participants must bewilling to collect the information. But themore data they must look up, the lesslikely they are to want to participate�and the less valid the results.
One barrier is the variation in ASCs�accounting systems.
�The most common obstacle is thatpeople don�t collect their financial datain such a way that they can report it easi-ly on our survey,� Kizirian says.
She is helping to address this in pre-sentations at AAASC and MGMA meet-ings.
If your center plans to participate inbenchmarking, the best advice is to lookat the program in depth so you under-stand how you will be compared andhow you can be prepared to understandand explain the results.
It�s also helpful if you accept a QI phi-losophy, seeing benchmarking as onepiece in the continuing effort to improveyour center�s performance. ❖
AAAHC IQI has a new publication toguide ASCs in quality improvement andbenchmarking at the basic, intermediate, orexpert level. Quality Improvement andBenchmarking: A Workbook of Strategiesand Tools for Success can be ordered byphoning 847/853-6079 or visitingwww.aaahciqi.org. Price is $85.
AmbulatorySurgery Centers
The following programs providebenchmarking for ambulatory surgerycenters.
Accreditation Association forAmbulatory Health Care.Institute for QualityImprovement
Clinical benchmarking studies forsurgery centers include cataract extrac-tion and lens insertion, colonoscopy,knee arthroscopy, and liposuction.Studies are open to all ambulatory careorganizations, whether AAAHCaccredited or not.
847/853-6079. www.aaahciqi.org
Federated AmbulatorySurgery Association
The Outcome Monitoring Project is afree quarterly benchmarking study forFASA members. Studies includestaffing, financial, and procedural indi-cators as well as patient satisfaction.Breakdowns for multispecialty and sin-gle-specialty facilities.
703/836-8808. www.fasa.org
Medical Group ManagementAssociation
Ambulatory Surgery Center
Performance Survey: 2003 Report Based on2002 Data.
Survey conducted in collaborationwith the American Association ofAmbulatory Surgery Centers.Information on staffing, accountsreceivable, clinical facility, charges, rev-enue, and expenses. Participantsinclude MGMA and AAASC members.
877/275-6462. www.mgma.com
OR BenchmarksA service of OR Manager, Inc.
Surgical procedure studies look atdirect costs for supplies, anesthesia,and labor and procedure and turnovertimes. Also conducts surgeon satisfac-tion surveys.
800/442-9918. www.orbenchmarks.com
Surgical OutcomesInformation Exchange
Benchmarking studies for ASCs com-pare information on 10 quality indica-tors for 35 procedural categories.Indicators range from complicationrates to overall patient satisfaction.Membership includes networking withbest performers.
877/602-0156. www.soix.com
Continued from page 30
Benchmarking programs
“
“People have to be willing
to put the timeinto it.
Check our web site for the latest news, meetingannouncements, and other
practical help. www.ormanager.com

33
Please see the ad for SPECTRUM SURGICAL
in the OR Manager print version.

34 OR Manager Vol 20, No 9 September 2004
Quarter Page AdB&W
DANB0904(New)
Quarter Page AdB&W
TVL0104(Pickup)
Senate passes bill forvoluntary error reporting
The U S Senate on July 23 passedlegislation to set up a confidential vol-untary system for physicians and hos-pitals to report medical errors withoutfacing legal ramifications. Errors wouldbe reported to groups called PatientSafety Organizations, which wouldanalyze the information to offer feed-back on how to improve the health sys-tem. The U S House approved a similarmeasure in March. The two bills mustnow be reconciled. The legislation hasbipartisan support.
U S links immigrant patients’status to hospital aid
The federal government is offering$1 billion to hospitals that provideemergency care to undocumentedimmigrants. But to get the money, hos-pitals would have to ask patients abouttheir immigration status, �a prospectthat alarms hospitals and advocates for
immigrants,� The New York Times (Aug10) reports.
The largest allocations would go toCalifornia, Texas, Arizona, New York,Illinois, and Florida.
When Congress decided to providethe money last year, state officials andhospitals saw it as a breakthrough. Buthospital execs and immigrant rightsgroups say questioning patients abouttheir status would keep immigrantsfrom seeking care and might cost hospi-tals more than they gain.
�www.nytimes.com
Hospital outpatient paymentupdate proposed
Hospitals would get a 3.3% inflationupdate for outpatient services in fiscal2005 under a proposed rule issued Aug9 by the Center for Medicare andMedicaid Services (CMS).
The rule would reduce a patient�smaximum copayment to 45%, downfrom 50% this year. Medicare is gradu-
ally reducing coinsurance to 20% of thetotal payment.
For the first time, new Medicare ben-eficiaries would be entitled to a wel-come physical, a service approved byCongress last year. Medicare would paya physician fee plus $75 to hospitals forthe exam. Hospitals also would get apay boost for routine screening alreadycovered by Medicare. For example, flex-ible sigmoidoscopy payments wouldincrease by 7.42% and screeningcolonoscopies by 9.9%.
Under new technology, the rulewould continue to set rates for brachy-therapy on charges adjusted to cost andcreate new definitions for new codes forhigh-activity brachytherapy.
CMS would extend a program toprotect payments for small rural hospi-tals with fewer than 100 beds and forsole community hospitals in rural areas.
Comments will be accepted until Oct8 with a final rule expected by Nov 1.
�www.cms.hhs.gov
Health Policy & Politics

35
Please see the ad for LAWSON SOFTWARE
in the OR Manager print version.

36 OR Manager Vol 20, No 9 September 2004
P O Box 5303Santa Fe, NM 87502-5303
The monthly publication for OR decision makers
At a Glance
The monthly publication for OR decision makers
Periodicals
National consensus on antibioticprophylaxis for surgery
In general, the first dose of antibioticsshould begin 60 minutes before the sur-gical incision, and antibiotics should bediscontinued within 24 hours after thesurgery, according to a national work-group on antimicrobial prophylaxis toprevent surgical site infection. Their con-sensus statement has specific recommen-dations for gynecological and obstetricalsurgery, total hip and knee replacement,cardiothoracic and vascular surgery, andcolorectal surgery.
Endorsing the statement were theAmerican Academy of OrthopaedicSurgeons, the American College ofSurgeons, the American Society ofAnesthesiologists, the Association ofperiOperative Registered Nurses, andthe Association for Professionals inInfection Control and Epidemiology,among many others.
�Bratzler D W, Houck P M. ClinicalInfectious Diseases, June 15, 2004;38:1706-1715. Download for free at
http://www.journals.uchicago.edu/CID/journal/contents/v38n12.html
JCAHO needs more oversight,GAO says
The Joint Commission�s pre-2004 hos-pital accreditation process did not identi-fy most of the hospitals that state sur-veys found had deficiencies in Medicarerequirements, the General AccountingOffice (GAO), a government watchdog,reported July 20. The review conducted
from 2000 to 2002 identified 31% (157) ofhospitals with deficiencies. Of these,JCAHO did not identify 78% as havingdeficiencies.
The GAO recommends that Congressconsider giving the Centers for Medicareand Medicaid Services (CMS) the samekind of oversight over JCAHO�s hospitalaccreditation program that it has overother accreditation programs. GAO saidit did not evaluate the new processJCAHO implemented this year. JCAHOtook issue with GAO�s methodology. Abill has already been introduced inCongress. �www.gao.gov. Look under reports by date.
Massachusetts panel issuesadvice on obesity surgery
An expert panel formed by theMassachusetts Department of Healthissued recommendations for weight-losssurgery for the state�s hospitals Aug 4.The panel was formed after severalpatients died last year.
Among highlights:� Institutions performing weight-loss
surgery should perform more than100 cases a year and have high-vol-ume surgeons who perform 50 to100 cases a year.
� Surgeons seeking provisional privi-leges for open obesity surgeryshould be proctored for 10 cases by asurgeon with full privileges for openweight-loss surgery. For laparoscop-ic surgery, surgeons should be proc-tored for 25 cases by a fully privi-
leged surgeon in laparoscopicweight-loss surgery.
� Surgeons seeking full privileges forboth open and laparoscopic surgeryshould have their first 15 casesreviewed by a committee, whichshould include the chief of surgeryand an experienced weight-loss sur-geon.
� Nurses who care for patients withsevere obesity should complete acompetency-based orientation thatenables them to identify potentialcomplications and prevent adverseoutcomes. ❖
�The report is available atwww..mass.gov/dph
JCAHO alert on infant deathsand injury during delivery
Team training should be held in peri-natal areas to teach staff to work togethermore effectively, the Joint Commissionon Accreditation of Healthcare Organiza-tions recommends in a July 21 SentinelEvent Alert. Teams also should hold clin-ical drills for high-risk events such asshoulder dystocia, emergency c-section,maternal hemorrhage, and neonatalresuscitation, JCAHO advises. In 47cases of perinatal death or permanentdisability reported to JCAHO since 1996,72% identified communication as theroot cause, with 55% saying organiza-tional culture was a barrier to teamwork.
�www.jcaho.org. Look under SentinelEvent Alerts.