Utility of lung ultrasound scanning in neonatology
7
909 Woods PL. Arch Dis Child 2019;104:909–915. doi:10.1136/archdischild-2017-314538 Review Utility of lung ultrasound scanning in neonatology Patricia Lee Woods 1,2 To cite: Woods PL. Arch Dis Child 2019;104:909–915. ► Additional material is published online only. To view please visit the journal online (http://dx.doi.org/10.1136/ archdischild-2017-314538). 1 Neonatal Directorate, King Edward Memorial Hospital for Women Perth, Perth, Western Australia, Australia 2 Centre for Neonatal Research & Education, School of Paediatrics and Child Health, University of Western Australia, Perth, Western Australia, Australia Correspondence to Dr Patricia Lee Woods, Neonatal Directorate, King Edward Memorial Hospital, Perth, Western Australia 6008, Australia; [email protected]. gov.au Received 22 August 2018 Revised 14 October 2018 Accepted 18 October 2018 Published Online First 9 November 2018 © Author(s) (or their employer(s)) 2019. No commercial re-use. See rights and permissions. Published by BMJ. What is already known? ► Clinician-performed point-of-care ultrasound is widely used in neonatology for cardiac, cranial and abdominal assessments, but lung assessment is yet to become routine care. ► Principles of physics and artefact generation conform to that in adult and paediatric patients; however, interpretation within neonatal clinical context differs. What this study adds? ► Comprehensive evaluation of research and illustrated value of many current clinical applications used in tertiary neonatal intensive care. ► Consideration of the utility of point-of-care lung ultrasound as first-line investigation using appropriately focused clinical questions. ABSTRACT The utility of point-of-care lung ultrasound in neonatology is rapidly expanding. This review summarises current evidence of a diagnostic, procedural and observational tool valuable in the management of newborns requiring intensive care. Approaching a patient, probe in-hand with focused clinical question is essential, and barriers to implication together with important research questions are explored. INTRODUCTION Point-of-care lung ultrasound (LUS) has a widely established role in adult and paediatric critical care, emergency and prehospital medicine for the eval- uation of patients with respiratory and cardiovas- cular compromise. 1 2 Its use within neonatology is not new, 3–5 yet despite international consensus evidence-based recommendations, 6 why is it yet to be widely adopted? Why it is an attractive diagnostic tool almost goes without saying: rapid, simple to perform, non-inva- sive, radiation free and providing dynamic, real-time information without a radiological time lag using ultrasound equipment already in situ in neonatal intensive care unit (NICU) for clinician-performed cardiac, cranial and abdominal assessments. Equal if not superior validity to conventional radiology has been reported in most clinical settings in neonatal patients. 4 6–8 Consistent validation has been reported of a mean time of <5 min to perform and high reliability in interobserver agreement across the range of experienced to novice. 8–10 So, why sceptical? One could argue a lack of international conformity in scanning techniques, variation in ultrasound equipment and settings (there is no one agreed neonatal lung preset) and confusion in nomenclature have made things chal- lenging. Research declaring rapid summation of artefact interpretation into specific diagnostic state- ments and simplistic algorithms or lacking essential methodology warrant interpretation with caution. Even the term ‘Lung Ultrasound’ is not exactly correct; we are rarely ever observing actual lung parenchyma, just the interpretation based purely on artefact generation. 1 THE PHYSICS Multiple resources eloquently translate the prin- ciples of physics and artefact generation that we observe in LUS scanning 1–3 (online supplemen- tary video S1a–f) Artefacts are generated from the behaviour of ultrasound beams as they encounter variation in acoustic impedance between air/fluid/ tissue interfaces and represented by a combination of processes including shadowing, reverberation, mirroring, comet tail and ring down artefacts. There is literally an LUS alphabet of prescribed nomen- clature 1 starting with A lines (horizontal reverber- ation artefacts of the pleural tissue/air interface), B lines (discrete laser-like vertical reverberations originating from the pleural line moving synchro- nously with sliding) and C lines (fractal comet- tails radiating from an irregular air/tissue interface of consolidated lung), and although a few letters are missing, it does go up to and include Z lines. However, it is the interpretation of artefact genera- tion at the pleural surface that we strictly correlate with clinical, radiological and biological data. THE VERY FIRST BREATH To fully conceptualise the value of informa- tion gained from performing LUS, it is helpful to start from the moment of birth with initiation of breathing, clearance of lung fluid and transition to extrauterine life. Blank et al 11 characterised such ultrasound appearances in 63 healthy term and late preterm infants assigning a simple yet eloquent grading system type 0–3 (figure 1). Establishment of the pleural line was demonstrated within the first few breaths (median 4 breaths 3–6 ) consistent with aeration of distal lung units and substantial liquid clearance within 10–20 min in all infants. 11 DOES LABOUR MATTER? Studies comparing rate of fluid clearance in infants born via vaginal delivery, caesarean section (after labour) and elective caesarean section (without labour) have reported faster clearance within the Protected by copyright. on August 25, 2019 at King Saud University (KSU). http://adc.bmj.com/ Arch Dis Child: first published as 10.1136/archdischild-2017-314538 on 9 November 2018. Downloaded from
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Utility of lung ultrasound scanning in neonatology

909Woods PL. Arch Dis Child 2019;104:909–915. doi:10.1136/archdischild-2017-314538
Review
Utility of lung ultrasound scanning in neonatologyPatricia Lee Woods 1,2
To cite: Woods PL. Arch Dis Child 2019;104:909–915.
► Additional material is published online only. To view please visit the journal online (http:// dx. doi. org/ 10. 1136/ archdischild- 2017- 314538).1Neonatal Directorate, King Edward Memorial Hospital for Women Perth, Perth, Western Australia, Australia2Centre for Neonatal Research & Education, School of Paediatrics and Child Health, University of Western Australia, Perth, Western Australia, Australia
Correspondence toDr Patricia Lee Woods, Neonatal Directorate, King Edward Memorial Hospital, Perth, Western Australia 6008, Australia; Patricia. Woods@ health. wa. gov. au
Received 22 August 2018Revised 14 October 2018Accepted 18 October 2018Published Online First 9 November 2018
© Author(s) (or their employer(s)) 2019. No commercial re-use. See rights and permissions. Published by BMJ.
What is already known?
► Clinician-performed point-of-care ultrasound is widely used in neonatology for cardiac, cranial and abdominal assessments, but lung assessment is yet to become routine care.
► Principles of physics and artefact generation conform to that in adult and paediatric patients; however, interpretation within neonatal clinical context differs.
What this study adds?
► Comprehensive evaluation of research and illustrated value of many current clinical applications used in tertiary neonatal intensive care.
► Consideration of the utility of point-of-care lung ultrasound as first-line investigation using appropriately focused clinical questions.
AbsTRACTThe utility of point-of-care lung ultrasound in neonatology is rapidly expanding. This review summarises current evidence of a diagnostic, procedural and observational tool valuable in the management of newborns requiring intensive care. Approaching a patient, probe in-hand with focused clinical question is essential, and barriers to implication together with important research questions are explored.
InTRoduCTIonPoint-of-care lung ultrasound (LUS) has a widely established role in adult and paediatric critical care, emergency and prehospital medicine for the eval-uation of patients with respiratory and cardiovas-cular compromise.1 2 Its use within neonatology is not new,3–5 yet despite international consensus evidence-based recommendations,6 why is it yet to be widely adopted?
Why it is an attractive diagnostic tool almost goes without saying: rapid, simple to perform, non-inva-sive, radiation free and providing dynamic, real-time information without a radiological time lag using ultrasound equipment already in situ in neonatal intensive care unit (NICU) for clinician-performed cardiac, cranial and abdominal assessments. Equal if not superior validity to conventional radiology has been reported in most clinical settings in neonatal patients.4 6–8 Consistent validation has been reported of a mean time of <5 min to perform and high reliability in interobserver agreement across the range of experienced to novice.8–10
So, why sceptical? One could argue a lack of international conformity in scanning techniques, variation in ultrasound equipment and settings (there is no one agreed neonatal lung preset) and confusion in nomenclature have made things chal-lenging. Research declaring rapid summation of artefact interpretation into specific diagnostic state-ments and simplistic algorithms or lacking essential methodology warrant interpretation with caution. Even the term ‘Lung Ultrasound’ is not exactly correct; we are rarely ever observing actual lung parenchyma, just the interpretation based purely on artefact generation.1
The physICsMultiple resources eloquently translate the prin-ciples of physics and artefact generation that we observe in LUS scanning1–3 (online supplemen-tary video S1a–f) Artefacts are generated from the behaviour of ultrasound beams as they encounter variation in acoustic impedance between air/fluid/tissue interfaces and represented by a combination of processes including shadowing, reverberation,
mirroring, comet tail and ring down artefacts. There is literally an LUS alphabet of prescribed nomen-clature1 starting with A lines (horizontal reverber-ation artefacts of the pleural tissue/air interface), B lines (discrete laser-like vertical reverberations originating from the pleural line moving synchro-nously with sliding) and C lines (fractal comet-tails radiating from an irregular air/tissue interface of consolidated lung), and although a few letters are missing, it does go up to and include Z lines. However, it is the interpretation of artefact genera-tion at the pleural surface that we strictly correlate with clinical, radiological and biological data.
The veRy fIRsT bReAThTo fully conceptualise the value of informa-tion gained from performing LUS, it is helpful to start from the moment of birth with initiation of breathing, clearance of lung fluid and transition to extrauterine life. Blank et al11 characterised such ultrasound appearances in 63 healthy term and late preterm infants assigning a simple yet eloquent grading system type 0–3 (figure 1). Establishment of the pleural line was demonstrated within the first few breaths (median 4 breaths3–6) consistent with aeration of distal lung units and substantial liquid clearance within 10–20 min in all infants.11
does lAbouR mATTeR?Studies comparing rate of fluid clearance in infants born via vaginal delivery, caesarean section (after labour) and elective caesarean section (without labour) have reported faster clearance within the
Protected by copyright.
on August 25, 2019 at K
ing Saud U
niversity (KS
U).
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/archdischild-2017-314538 on 9 Novem
ber 2018. Dow
nloaded from

910 Woods PL. Arch Dis Child 2019;104:909–915. doi:10.1136/archdischild-2017-314538
Review
figure 1 Lung ultrasound grading during initiation of breathing at birth from Blank et al11 (reproduced with kind permission).
first 20 min in those born in presence of labour, irrespective of mode of delivery, but near complete clearance typically achieved within the first 4 hours in all healthy infants.11 12 One study of smaller sample size reported early differences observed in the rate of B line clearance between infants born via vaginal versus caesarean section resolved by 24 hours.13
WhAT hAppens When IT goes WRong?What are the sonographic observations when an infant fails to transition with delayed fluid clearance from alveoli and intersti-tium or born preterm with respiratory distress syndrome (RDS) secondary to surfactant deficiency and atelectasis? Copetti and Cattarossi14 described their observation of ‘Double Lung Point’ (DLP) in 32/60 infants within the first hour of birth demon-strating sharp transition of near normal in appearance (thin regular pleural line, A Line profile and few intermittent B lines) in superior regions versus a bright, coarse, irregular pleural line with densely compact B lines in inferior/lateral lung fields. Authors acknowledged an ambitious sensitivity and specificity of 100% of DLP for the diagnosis of transient tachypnoea of the newborn (TTN), not observed in healthy newborns or those with other respiratory pathology (including RDS). Early research drew scepticism regarding lack of clarity of case definitions, confounded by an absence of a validated clinical correlate14–16 and the need for further prospective and truly masked studies, which continue to date.
Blinded external evaluation of LUS performed within an hour of birth confirmed an extremely high diagnostic accuracy (~95% sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV)) for TTN and RDS in neonates with early respiratory distress.17 Their sonographic definition of TTN was a little broader with DLP not always observed (20/28 infants) but demonstration of a normal pleural line and numerous diffuse B lines seen in the remaining eight infants. A global observation of a thickened irregular pleural line, B line coalescence with absence of spared areas was documented in all infants with RDS.17 Precisely why DLP may be observed in some infants with TTN and not in others remains under scrutiny.18 The sonographic evolution of DLP is clinically consistent with recovery and gradual dissipation of B lines within 72–96 hours.17 However, a DLP appearance may be observed in preterm infants receiving respiratory support longer after recovery from RDS (figure 2A–C and online supplementary video S2a–c). From
our experience, this observation makes sense. RDS is a ‘global’ process of suboptimal aeration of the distal lung units across the lung fields where one would expect to observe pleural abnor-malities throughout, without regions of sparing. Interestingly, the sonographic appearance of RDS does not change immedi-ately after surfactant administration.15 17 19 While widespread, TTN does not impact all lung regions equally. With the process of fluid clearance and recovery, impact of gravity on extravas-cular/interstitial fluid and patient positioning (prone or supine) prior to scanning influences the pattern of aeration observed as in figure 2A–C, almost akin to a sponge semisaturated with water.
International evidence-based recommendations clearly state that LUS is a clinically useful diagnostic tool in neonates with suspected respiratory distress (strong level B), with a compar-ative accuracy to chest radiography, with most likely observa-tions of pleural line abnormalities, bilateral confluent B lines and absence of spared areas.6 Despite this statement, there is a lack of consensus between investigators presenting alternative sonographic criteria differentiating infants with TTN from RDS, making interpretation tricky. Liu et al16 categorised infants with TTN exhibiting an abnormal pleural line with a coalescent B line profile and absence of sparing (and associated pleural effusion in 20%) and characterised RDS features of an abnormal pleural line, generalised consolidation with air bronchograms, bilateral B line coalescence and presence of lung pulse, in preterm infants ranging 27–36 weeks’ gestation, including 40 controls (15 preterm 28–36 weeks gestation), without reported lung disease. Authors presented the sonographic finding of lung pulse specif-ically to a single pathological diagnosis of RDS (80% sensitive, 100% specific), which is disputed, together with the association of pleural line anomalies in infants with TTN.2 6
pRedICTIng pATIenT TRAjeCToRIes: hoW useful Is eARly lus In RegARds To dIAgnosTIC ACCuRACy And pRedICTIon of nICu AdmIssIon, RespIRAToRy suppoRT And RequIRemenT foR suRfACTAnT?The functional application and predictive value of point-of-care LUS in neonatology is where it gets exciting. LUS scoring systems have been validated worldwide with minor modifi-cations according to clinical context to evaluate these ques-tions.8 10 11 20 21
Protected by copyright.
on August 25, 2019 at K
ing Saud U
niversity (KS
U).
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/archdischild-2017-314538 on 9 Novem
ber 2018. Dow
nloaded from
911Woods PL. Arch Dis Child 2019;104:909–915. doi:10.1136/archdischild-2017-314538
Review
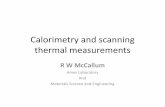
figure 2 LUS appearance of a 23-week gestation infant now corrected gestation of 34 weeks supported on continuous positive airway pressure (CPAP) 9 cm H2O fractional inspired oxygen .40. The infant was nursed in a prone position, and posterior, lateral and anterior chest regions were examined. (A) Posterior longitudinal view ‘Double Lung Point’ (DLP) appearance demonstrating a sharp transition of near normal aeration (thin regular pleural line, A Line profile and few intermittent B lines) in the superior/least dependent region versus a brighter, coarse, irregular pleural line with more compact B lines in the inferior/more dependent region. (B) Lateral longitudinal view in contrast shows a coarse pleural line with increasing B line coalescence (no DLP transition). (C) Anterior longitudinal view shows a bright, coarse, irregular pleural line with dense B coalescence (no DLP transition) and features consistent with reduced aeration and ‘Lung Pulse’ effect of adjacent cardiac motion. The sonographic representation of DLP is not truly specific to a diagnosis of TTN, as observed in this case in an extremely preterm infant at a postnatal age of 11 weeks. LUS, lung ultrasound.
Raimondi et al22 gave valuable insight into the extremely high predictive value of LUS in 60 late preterm and term infants at 60–120 min after birth, using a simple three-point classification score in predicting NICU admission and respiratory support (sensitivity: 77%, specificity: 100%, PPV: 100% and NPV:
97%). Both were required in all 14 babies with type 1 (‘white lung’) LUS appearance (4 ventilation and surfactant; 10 CPAP and oxygen). While 4/46 (8%) exhibiting type 2 (moderate B profile) required CPAP/oxygen, in contrast to none exhibiting a type 3 (A line profile). One caveat was lack of discrimina-tory power between milder and more severe conditions of RDS requiring mechanical ventilation. Signs of pulmonary adaptation were reported with serial ultrasounds demonstrating observation of an A line profile in 98% of infants at 36 hours, correlating with clinical improvement.22
Blinded analysis of LUS has been shown to reliably predict and outperform conventional radiographs for the failure of non-invasive ventilation after a 2-hour period of stabilisation and the need for intubation and surfactant administration within 24 hours.8 One acknowledged limitation was non-escalation of CPAP beyond 5 cm H2O prior to intubation, differing from most adopted clinical practice.
A strong correlation between bedside LUS reaeration scores and peep-induced lung recruitment (measured via pressure volume curves) in adult patients with ARDS is promising.23 However, authors report inability to accurately assess lung hyperinflation, which differs from our personal observations of a near perfect A line profile with reduced amplitude of pleural sliding, considered ‘too good’ in the context of respiratory distress in infants on positive pressure support (online supple-mentary video S3a,b).
Martelius et al24 reported no significant correlation between changes in static lung compliance (a measure of lung elasticity in mL/KPa/kg correlating with epithelial sodium transport and lung fluid resorption shown to increase significantly during postnatal adaptation25) and abundance of B lines on LUS during transi-tioning in healthy term infants. Observations in 130 term and preterm NICU infants with respiratory distress in the first hours of age demonstrated good correlation with oxygenation status irrespective of respiratory condition and good reliability to predict surfactant need in those <34 gestation receiving CPAP up to 6 cm H2O (AUC 0.93; 95% CI 0.86 to 0.99).10 Recent research has further demonstrated the value of LUS score to predict the need for a first surfactant dose (area under curve (AUC) 0.94; 95% CI 0.90 to 0.98; p<0.0001) in extremely preterm neonates with RDS, independent of gestational age.26 Major strengths of these studies include a comprehensive examination taking <5 min, standardised criteria for surfactant administration (Euro-pean consensus 201327) and application of a modified scoring system22 inclusive of consolidation.
RApId deTeCTIon of AIR leAkAnimal studies demonstrate precision in determining pneumo-thorax in the preterm lamb model using postmortem exam-ination as the gold standard.28 A very clear diagnostic pathway is illustrated in the 2012 international consensus recommen-dations6 and well accepted as a reliable and accurate tool in comparison to conventional radiography in adult critical care.1 2
In its simplest form, an indication of air leak comes from the observation of ‘standstill’ and lack of artefact generation from visceral pleural contact and movement on parietal. If you can observe horizontal pleural sliding, your question stops there; even the presence of one B line or transmission of lung pulse is enough to confirm direct pleural apposition at that point. Lung point is pathognomonic representing the limit of pleural separa-tion6 (figure 3 and online supplementary video S3c).
Differentiating true absence of observed pleural sliding from appearance of a vertical bounce and other ‘parasitic’ artefacts
Protected by copyright.
on August 25, 2019 at K
ing Saud U
niversity (KS
U).
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/archdischild-2017-314538 on 9 Novem
ber 2018. Dow
nloaded from

912 Woods PL. Arch Dis Child 2019;104:909–915. doi:10.1136/archdischild-2017-314538
Review
figure 3 Lung point illustrating sharp transition of a thin, regular pleural line with lack of sliding, absence of B lines or lung pulse in the superior lung field where pleura are separated by air leak, adjacent to region showing a bright, coarse, irregular pleural line with sliding, multiple B line artefacts, indicative of visceral and parietal pleural apposition.
figure 4 (A) Right anterior longitudinal view of pneumothorax in the inferior region in a 27-week gestation preterm infant supported on high-frequency jet oscillation showing a thin regular pleural line and mirror image artefact but lacking of horizontal sliding, B lines or lung pulse. Lung point identified in adjacent superior region with pleural apposition and associated artefacts generated (horizontal sliding of a coarse pleural line with synchronous movement of B lines). (B) Superior region using M-mode demonstrating a seashore sign (confirming pleural apposition and movement). (C) Inferior region using M-mode demonstrating the vastly different appearance of a stratosphere sign in presence of air leak. (D) anterior-posterior (AP) chest x-ray confirming persistent air leak in the right anterior lung regions despite an intercostal catheter in situ.
generated from chest wall excursion with marked recession or inadvertent movement of the probe can be challenging in neonates (online supplementary video S4a,b). Lichtenstein1 provides expert guidance on scrutinising artefact generation that is unchanged as it transcends the pleural line in M-mode in the presence of air leak generating an uninterrupted pattern from tissue recession that continues below the pleural line with abol-ished lung sliding (Avicenne sign, chapter 14, page 93–94 figure 14.3).
Cattarossi et al7 compared the performance of conventional chest radiographs, transillumination and LUS for the diagnosis of pneumothorax in 49 babies with respiratory distress. LUS outperformed both modalities, consistently diagnosing pneumo-thorax in all 23 babies with a sensitivity and specificity of 1, compared with 0.96 and 1 for chest x-ray and 0.87 and 0.96 for transillumination.7 Raimondi et al29 demonstrated high diag-nostic accuracy in detection of pneumothorax in the critically ill neonate outperforming clinical evaluation and reducing time to imaging diagnosis and drainage (mean time 5.3±5.6 min vs 19±11.7 min). Point-of-care ultrasound is thus extremely valu-able in clinical environments with foreseeable delay in obtaining and interpreting radiology. Successful ultrasound-guided emer-gency needle thoracocentesis of extremely preterm infants on respiratory support has been reported30 enables accurate delin-eation of the limit of pleural separation, without blind aspiration at a prescribed conventional landmark.
Surveillance of pleural recontact postprocedure necessitating further intervention or later facilitating timing of catheter removal is consistent with our experience in pneumothoraces in extremely preterm babies receiving high-frequency jet ventila-tion (figure 4A–D and online supplementary video S4c).
Pitfalls encountered with the detection of air leak are subtle transition in appearance to lung point in infants with hyperinfla-tion A line profile and reduced amplitude of sliding, in compar-ison with stark contrast with adjacent coalescent B line profile. Search for lung point may be unrewarding in an infant with massive tension pneumothorax separating visceral from parietal pleural as far as one can apply the probe. Differentiating small pneumothoraces in perihilar regions from pneumomediastinum may also be challenging but largely facilitated by lack of visual-isation of expected anatomical structures at that position, for example, thymus and cardiac vessels.2
Protected by copyright.
on August 25, 2019 at K
ing Saud U
niversity (KS
U).
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/archdischild-2017-314538 on 9 Novem
ber 2018. Dow
nloaded from
913Woods PL. Arch Dis Child 2019;104:909–915. doi:10.1136/archdischild-2017-314538
Review
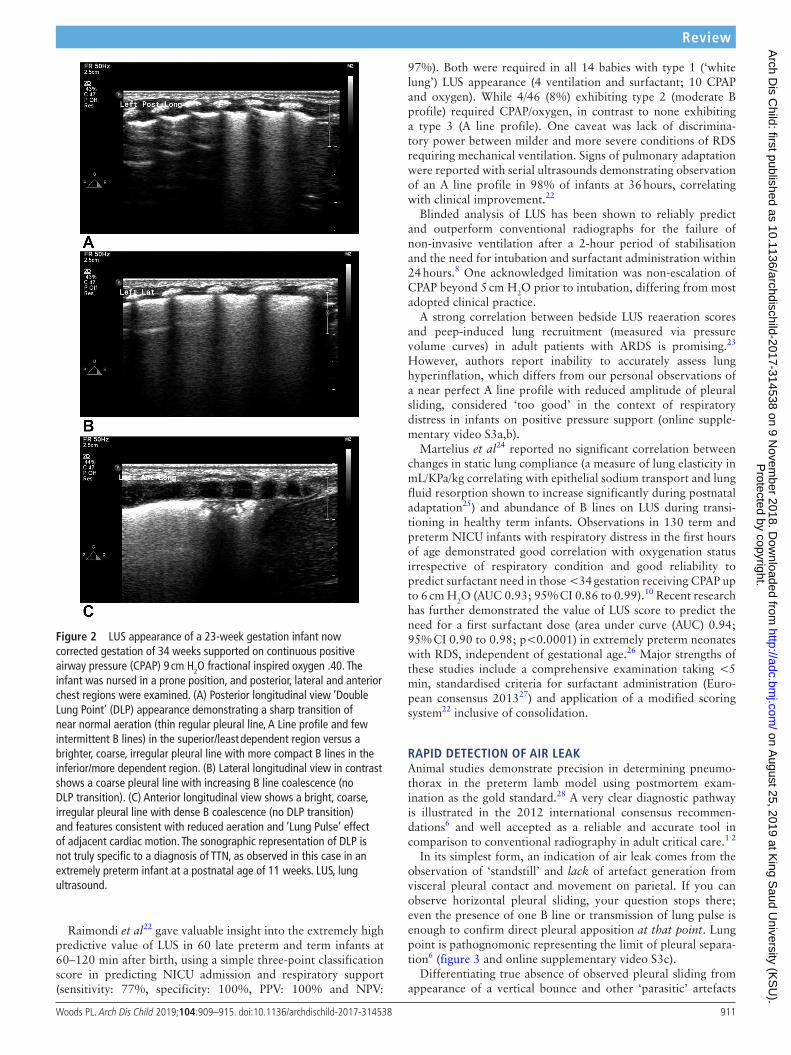
figure 6 Right posterior/lateral transverse view illustrating a fibrinous pleural effusion with extensive lung consolidation and evidence of poor aeration, with dynamic air bronchograms (hyperechoic, linear elements representing air in the bronchioles) within a vast hypoechoic region with irregular margins.
figure 7 Right posterior transverse view illustrating the sonographic appearance of non-translobar lung consolidation with transmission of ultrasound through the superficial lung interstitium and non-aerated air spaces at the pleural surface and disruption of the normal air/tissue/fluid interface that would generate a pleural line. Reduced sliding, with hypoechoic regions exhibiting a tissue-like appearance (‘Hepatization’) with a deep irregular boundary with adjacent aerated lung units, generates the ‘Shred Sign’ or fractal line.
figure 5 Left lateral longitudinal view of the costophrenic angle with a pleural effusion visualised as an anechoic space between the parietal pleura and the now non-apposed visceral pleural (lung line).
pleuRAl effusIonsPoint-of-care ultrasound literally outshines conventional radio-graphs when it comes to the diagnosis, assessment, procedural guidance and serial observation of pleural effusions.3 4 6 31 Pleural effusions are largely visualised as an anechoic space between the parietal pleura and the now non-apposed visceral pleural (lung line).1 Fluid collection is beautifully depicted in contrast to adjacent structures with dynamic visualisation of diaphragmatic activity and artefacts representing the lung line beneath during respiration. (figure 5 and online supplementary video S5) The clinical application of LUS has enormous potential from delivery room management of fetal hydrops enabling safe anatomical demarcation of diaphragm movement, guiding positioning and depth of percentesis. Serial three-dimensional (3D) assessment of the function of in situ intercostal catheters (complications of blockage or displacement) or guidance on timing of removal with clinical resolution that would otherwise mandate (yet another) static, two-dimensional CXR and unwelcome patient handling.
Can ultrasound reliably distinguish between transudate, exudate and haemorrhage? Probably not, but neither can a chest radiograph. Internal echo signals and fibrin deposition may be
observed more frequently in exudative effusions,6 (figure 6 and online supplementary video S6), but diagnostic analysis of fluid would provide such answers.
ConsolIdATIon And ATeleCTAsIsThe sonographic appearance of lung is well described with loss of acoustic reverberations of aerated lung and hence disrup-tion of the pleural line, hypoechoic areas exhibiting a tissue-like appearance (‘Hepatization’), often with irregular margins or wedge-shaped boarders.2 3 6 (figure 7 and online supple-mentary video S7). This appearance may represent a range of pathology including infectious exudate, meconium aspiration, pulmonary haemorrhage to name but a few. Contention arises where authors attribute a specific pathology to a sonographic appearance observed that may lack specificity in diagnosis, for example, a diagnostic flow diagram32 illustrating consolidation with dynamic air/fluid bronchograms equals pneumonia.
In adult and paediatric critical care, the presence of dynamic or static air bronchograms and regularity of the margin of hypoechogenicity have been useful in differentiating consolida-tion from atelectasis.1 33 Dynamic air bronchograms are hyper-echoic, linear elements representing air in the bronchioles that appear within an hypoechoic region (with irregular margins) observed mostly in the context of consolidated lung33 (figure 6 and online supplementary video S6). Dynamic describes a centrifugal movement in relation to respiration, while in static bronchograms, this is not observed and boarders are more regu-larly defined, suggestive of atelectasis.1
However, in the neonate, small hepatised regions moving in and out of ultrasound plane in the context of rapid tachy-pnoea can make accurate differentiation challenging. In a recent paper reporting 100% sensitivity and specificity of large regions of consolidation with irregular margins for the diagnosis of neonatal pneumonia, dynamic air bronchograms were only observed in 52% of confirmed cases.34
Lung pulse is the transmission of cardiac activity on adja-cent lung parenchyma and visceral pleura, replacing horizontal pleural sliding with a more vertical ‘bounce-like’ motion, which may be readily observed in both consolidated and atelectatic
Protected by copyright.
on August 25, 2019 at K
ing Saud U
niversity (KS
U).
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/archdischild-2017-314538 on 9 Novem
ber 2018. Dow
nloaded from

914 Woods PL. Arch Dis Child 2019;104:909–915. doi:10.1136/archdischild-2017-314538
Review
lung.1 2 In neonatal patients, it is not uncommon to observe a wide impact of cardiac pulsation over a large surface of the lungs given the relative size and relations of the organs within the small chest. A limitation of LUS is inability to identify deep regions of consolidation that do not reach the pleural surface.6
LUS has been valuable in the serial imaging and assessment of newborns with severe meconium aspiration, observing dynamic and heterogeneous patterns of B line coalescence, subpleural consolidations, atelectasis and bronchograms.5 35 In paediatric patients, it has an establishing role in the diagnosis and manage-ment of bronchiolitis and community-acquired pneumonia.36 37
A holistic approach is to perform LUS with a focused clin-ical question. In the case of an extremely preterm ventilated baby with raised inflammatory markers, increasing oxygen requirements and worsening ventilation, there would be value in performing a systematic and comprehensive ultrasound assessment, to provide dynamic, real-time information to assist 3D visualisation of the global status of lung aeration, presence of consolidations, effusions, air leak or potential iatrogenic pathology (eg, from endotracheal tube migration into the right main bronchus causing atelectasis of the right upper lobe). Only with appropriate correlation with clinical, biological and radio-graphical information is one in a position to narrow differen-tial diagnoses of reabsorptive atelectasis, infection, aspiration, pulmonary haemorrhage, air leak syndromes to optimise patient and respiratory management.
pRedICTIng developmenT of bRonChopulmonARy dysplAsIA (bpd) Three studies have specifically investigated the predictive value of LUS in the evolution of BPD in preterm babies with RDS.38–40 Each focused on the appearance of the lung bases using transabdominal windows, reporting either the earliest day at which persistence of retrodiaphragmatic hyperechogenicity (that otherwise resolved in unaffected infants) or transition to a non-homogenous BPD pattern of variable hyperechogenicity, with contiguous regions of sparing and pleural line anomalies (thickening, irregularity and subpleural consolidations) lent the greatest predictive value for development of BPD. Results vary between day 939 and day 1838 for persistence of retrodiaphrag-matic hyperechogenicity and given the majority of patients within each study did not develop BPD, authors highlight the NPV of this finding close to 95%. Ahuja et al40 reported presence of an abnormal pattern on day 14 had the greatest predictive value (94% accuracy) for development of clinical BPD (defined as oxygen dependency at 28 days) in infants <32 weeks’ gestation. Although impressive, conclusions are drawn from 6/33 babies demonstrating conversion from an hyaline membrane disease (HMD) to a persistent BPD pattern and clinical diagnoses of BPD. Of interest, three babies also demonstrating a conversion pattern between days 4 and 7 resolved to a normal pattern 3 days later and did not develop BPD. Specificity of persistent lung base hyperechogenicity for a diagnosis of BPD is questioned, exhibited in infants without supplemental oxygen requirements at 36 weeks postmenstrual age (PMA).15
Techniques in performing ultrasound now include more systematic interrogation of anterior/lateral lung regions in longitudinal and transverse planes.4 5 The definition of BPD is also evolving from a dichotomous outcome related to oxygen or respiratory support dependency at a precise chronological or PMA to a more meaningful physiological measurement of BPD as a continuous outcome (SHIFT), derived from single paired saturation of peripheral oxygen (SpO2)/partial pressure of
inspired oxygen (PiO2) measurement between 35 weeks and 36 weeks+6 days PMA.41 A prospective study is underway exam-ining the predictive value of early LUS for respiratory outcomes and the evolution of physiological BPD in 100 preterm infants with RDS <28 weeks’ gestation.[ANZCTR 1261 7000208303]
The concept of spared areas is contentious; BPD is described as a non-homogenous disease of the lung periphery, but are we really observing ‘normal’ patches? It is feasible that arte-facts generated are heavily dependent on on the relative angle of insonation to the pleural surface, when at precisely 90° at a given moment may act as a reflector, generating an A line profile, usually observed within a single intercostal space and inter-preted as ‘sparing’. Practically, scanning the preterm infant with an uneven chest curvature, marked recession, tachypnoea and comparatively large size ratio of linear probe can make image acquisition entirely free of parasitic movement challenging.
WIdeR ApplICATIonsThe potential utility of LUS in neonatology is exciting and evolving rapidly. A high diagnostic accuracy in assessing pulmo-nary overflow via abundance of B lines during the first days of life of infants with congenital heart disease has been reported, correlating well with echocardiography.42 Bedside imaging opportunities exist for infants with congenital malformations (congenital cystic adenomatoid malformation (CCAM), pulmo-nary sequestration and diaphragmatic hernia) and correlation with CT/MRI findings. Is LUS going to change our approach from counting anterior ribs on a static chest radiograph to a dynamic assessment of optimal targeted volume or mean airway pressure? Can we correlate LUS appearance with early successful extubation in the extreme preterm? Can we reliably inform bed and nursing resource planning in NICU in regards to predicted patient trajectories? Or avoid mother–infant separation in long-distance retrieval to tertiary NICU from remote clinical environments in cases predicted to require minimal respiratory support?
I doubt very much our radiographer colleagues are at immi-nent risk of redundancy, but there is opportunity in using LUS as a value-adding tool and reduce X-ray exposure with the appro-priately focused clinical question.43
WheRe nexT?Technological advances in image acquisition and quantitative texture analysis may dominate our future directions.44 The need for appropriately powered, prospective multicentred studies with sound correlation with clinical data has been recognised,45 together with standardisation and validation of point-of-care LUS techniques, evidence-based training programmes and accreditation standards. These may only be achieved with inter-national collaboration, robust discussion and consensus.46 The NeoLUS47 international expert group inaugural congress in Lung Ultrasound in Neonates and Children scheduled in Paris, 2019 (https://www. mcascientificevents. eu/ firstlaunch) and The Australasian Society of Ultrasound Medicine certification in clini-cian-performed ultrasound Certificate in Clinician Performed Ultrasound (CCPU) in neonatal lung are exciting developments as part of this journey ahead.
Contributors PLW is the sole author of this article and responsible for performing all original ultrasound studies presented herein. The author wishes to acknowledge Associate Professor Andrew Gill for his peer support and contribution to the implementation and teaching point-of-care neonatal lung ultrasound in neonatology at King Edward Memorial Hospital in Perth and as faculty of the Australasian Society
Protected by copyright.
on August 25, 2019 at K
ing Saud U
niversity (KS
U).
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/archdischild-2017-314538 on 9 Novem
ber 2018. Dow
nloaded from

915Woods PL. Arch Dis Child 2019;104:909–915. doi:10.1136/archdischild-2017-314538
Review
of Ultrasound Medicine. Mr Malcolm Bruce is also acknowledged for his assistance with medical illustrations.
funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests PLW is a co-author of the online learning package hosted by ASUM ’Lung Ultrasound In Neonatology’ with reference to illustrations provided in online supplementary video files S1a–f.
patient consent Not required.
provenance and peer review Commissioned; externally peer reviewed.
RefeRences 1 Lichtenstein DA. Lung Ultrasound in the Critically Ill: The BLUE Protocol: Springer
International Publishing, 2015. 2 RN Laursen CB, Volpicell G. Thoracic Ultrasound, 2018. 3 Lichtenstein DA, Mauriat P. LuNg ultrasound in the critically ill neonate. Curr Pediatr
Rev 2012;8:217–23. 4 Raimondi F, Cattarossi L, Copetti R, et al. International perspectives: Point-of-
care chest ultrasound in the neonatal intensive care unit: An italian perspective. Neoreviews 2014;15:e2–e6.
5 Cattarossi L. Lung ultrasound: its role in neonatology and pediatrics. Early Hum Dev 2013;89 Suppl 1(Suppl 1):S17–S19.
6 Volpicelli G, Elbarbary M, Blaivas M, et al. International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med 2012;38:577–91.
7 Cattarossi L, Copetti R, Brusa G, et al. Lung ultrasound diagnostic accuracy in neonatal pneumothorax. Can Respir J 2016;2016:1–5.
8 Raimondi F, Migliaro F, Sodano A, et al. Use of neonatal chest ultrasound to predict noninvasive ventilation failure. Pediatrics 2014;134:e1089–e1094.
9 Brusa G, Savoia M, Vergine M, et al. Neonatal Lung Sonography: Interobserver Agreement Between Physician Interpreters With Varying Levels of Experience. J Ultrasound Med 2015;34:1549–54.
10 Brat R, Yousef N, Klifa R, et al. Lung Ultrasonography Score to Evaluate Oxygenation and Surfactant Need in Neonates Treated With Continuous Positive Airway Pressure. JAMA Pediatr 2015;169:e151797.
11 Blank DA, Rogerson SR, Kamlin COF, et al. Lung ultrasound during the initiation of breathing in healthy term and late preterm infants immediately after birth, a prospective, observational study. Resuscitation 2017;114:59–65.
12 Blank DA, Kamlin COF, Rogerson SR, et al. Lung ultrasound immediately after birth to describe normal neonatal transition: an observational study. Arch Dis Child Fetal Neonatal Ed 2018;103:F157–F162.
13 Martelius L, Janér C, Süvari L, et al. Delayed lung liquid absorption after cesarean section at term. Neonatology 2013;104:133–6.
14 Copetti R, Cattarossi L. The ’double lung point’: an ultrasound sign diagnostic of transient tachypnea of the newborn. Neonatology 2007;91:203–9.
15 Copetti R, Cattarossi L, Macagno F, et al. Lung ultrasound in respiratory distress syndrome: a useful tool for early diagnosis. Neonatology 2008;94:52–9.
16 Liu J, Cao HY, Wang HW, et al. The role of lung ultrasound in diagnosis of respiratory distress syndrome in newborn infants. Iran J Pediatr 2015;25:e323.
17 Vergine M, Copetti R, Brusa G, et al. Lung ultrasound accuracy in respiratory distress syndrome and transient tachypnea of the newborn. Neonatology 2014;106:87–93.
18 Raimondi F, Yousef N, Rodriguez Fanjul J, et al. A multicenter lung ultrasound study on Transient Tachypnea of the Neonate. Neonatology 2018. accepted for publication Sep 2018.
19 Cattarossi L, Copetti R, Poskurica B, et al. Surfactant administration for neonatal respiratory distress does not improve lung interstitial fluid clearance: echographic and experimental evidence. J Perinat Med 2010;38:557–63.
20 Rodríguez-Fanjul J, Balcells C, Aldecoa-Bilbao V, et al. Lung Ultrasound as a Predictor of Mechanical Ventilation in Neonates Older than 32 Weeks. Neonatology 2016;110:198–203.
21 Rodríguez-Fanjul J, Balcells Esponera C, Moreno Hernando J, et al. Lung ultrasound as a tool to guide the administration of surfactant in premature neonates. Anales de Pediatría 2016;84:249–53.
22 Raimondi F, Migliaro F, Sodano A, et al. Can neonatal lung ultrasound monitor fluid clearance and predict the need of respiratory support? Crit Care 2012;16:R220.
23 Bouhemad B, Brisson H, Le-Guen M, et al. Bedside ultrasound assessment of positive end-expiratory pressure-induced lung recruitment. Am J Respir Crit Care Med 2011;183:341–7.
24 Martelius L, Süvari L, Janér C, et al. Lung ultrasound and static lung compliance during postnatal adaptation in healthy term infants. Neonatology 2015;108:287–92.
25 Helve O, Pitkänen O, Kirjavainen T, et al. Sodium transport in airway epithelium correlates with lung compliance in healthy newborn infants. J Pediatr 2005;146:273–6.
26 De Martino L, Yousef N, Ben-Ammar R, et al. Lung Ultrasound Score Predicts Surfactant Need in Extremely Preterm Neonates. Pediatrics 2018;142:e20180463.
27 Sweet DG, Carnielli V, Greisen G, et al. European consensus guidelines on the management of neonatal respiratory distress syndrome in preterm infants-2013 update. Neonatology 2013;103:353–68.
28 Blank DA, Hooper SB, Binder-Heschl C, et al. Lung ultrasound accurately detects pneumothorax in a preterm newborn lamb model. J Paediatr Child Health 2016;52:643–8.
29 Raimondi F, Rodriguez Fanjul J, Aversa S, et al. Lung ultrasound for diagnosing pneumothorax in the critically ill neonate. J Pediatr 2016;175:74–8.
30 Migliaro F, Sodano A, Capasso L, et al. Lung ultrasound-guided emergency pneumothorax needle aspiration in a very preterm infant. BMJ Case Rep 2014;2014:bcr2014206803.
31 Liu J, Ren XL, Li JJ. POC-LUS guiding pleural puncture drainage to treat neonatal pulmonary atelectasis caused by congenital massive effusion. J Matern Fetal Neonatal Med 2018;81:1–81.
32 Kurepa D, Zaghloul N, Watkins L, et al. Neonatal lung ultrasound exam guidelines. J Perinatol 2018;38:11–22.
33 Lichtenstein D, Mezière G, Seitz J. The dynamic air bronchogram. A lung ultrasound sign of alveolar consolidation ruling out atelectasis. Chest 2009;135:1421–5.
34 Liu J, Liu F, Liu Y, et al. Lung ultrasonography for the diagnosis of severe neonatal pneumonia. Chest 2014;146:383–8.
35 Piastra M, Yousef N, Brat R, et al. Lung ultrasound findings in meconium aspiration syndrome. Early Hum Dev 2014;90 Suppl 2(Suppl 2):S41–S43.
36 Basile V, Di Mauro A, Scalini E, et al. Lung ultrasound: a useful tool in diagnosis and management of bronchiolitis. BMC Pediatr 2015;15:63.
37 Shah VP, Tunik MG, Tsung JW. Prospective evaluation of point-of-care ultrasonography for the diagnosis of pneumonia in children and young adults. JAMA Pediatr 2013;167:119–25.
38 Avni EF, Cassart M, de Maertelaer V, et al. Sonographic prediction of chronic lung disease in the premature undergoing mechanical ventilation. Pediatr Radiol 1996;26:463–9.
39 Pieper CH, Smith J, Brand EJ. The value of ultrasound examination of the lungs in predicting bronchopulmonary dysplasia. Pediatr Radiol 2004;34:227–31.
40 Ahuja CK, Saxena AK, Sodhi KS, et al. Role of transabdominal ultrasound of lung bases and follow-up in premature neonates with respiratory distress soon after birth. Indian J Radiol Imaging 2012;22:279–83.
41 Quine D, Wong CM, Boyle EM, et al. Non-invasive measurement of reduced ventilation:perfusion ratio and shunt in infants with bronchopulmonary dysplasia: a physiological definition of the disease. Arch Dis Child Fetal Neonatal Ed 2006;91:F409–F414.
42 Rodríguez-Fanjul J, Llop AS, Balaguer M, et al. Usefulness of lung ultrasound in neonatal congenital heart disease (lusnehdi): Lung ultrasound to assess pulmonary overflow in neonatal congenital heart disease. Pediatr Cardiol 2016;37:1482–7.
43 Federici M, Federici PV, Feleppa F, et al. Pulmonary ultrasonography in the follow-up of respiratory distress syndrome on preterm newborns. Reduction of X-ray exposure. J Ultrasound 2011;14:78–83.
44 Palacio M, Bonet-Carne E, Cobo T, et al. Prediction of neonatal respiratory morbidity by quantitative ultrasound lung texture analysis: a multicenter study. Am J Obstet Gynecol 2017;217:196.e1–196.e14.
45 Raimondi F, Migliaro F, De Luca D, et al. Clinical data are essential to validate lung ultrasound. Chest 2016;149:1575.
46 Fraga MV, Stoller JZ, Lorch SA. Novel technologies for neonatal care: The case of point-of-care lung ultrasonography. Pediatrics 2018;142:e2018162:e20181621.
47 NeoLUS. Bedside lung ultrasound for the neonate and the small infant. https://wwwfacebookcom/groups/1493243264284547.
Protected by copyright.
on August 25, 2019 at K
ing Saud U
niversity (KS
U).
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/archdischild-2017-314538 on 9 Novem
ber 2018. Dow
nloaded from