
Using ontologies for structuring organizational knowledge in Home Care assistance
18
international journal of medical informatics 79 ( 2 0 1 0 ) 370–387 journal homepage: www.intl.elsevierhealth.com/journals/ijmi Using ontologies for structuring organizational knowledge in Home Care assistance Aida Valls a,∗ , Karina Gibert b , David Sánchez a , Montserrat Batet a a Department of Computer Science and Mathematics, Universitat Rovira i Virgili, Av Països Catalans 26, 43007 Tarragona, Catalonia, Spain b Department of Statistics and Operational Research, Universitat Politècnica de Catalunya, C/ Jordi Girona 1-3, 08034 Barcelona, Catalonia, Spain article info Article history: Received 1 July 2009 Received in revised form 26 January 2010 Accepted 26 January 2010 Keywords: Medical informatics Telemedicine Organizational models Home Care services Knowledge representation Ontologies Distributed systems abstract Purpose: Information Technologies and Knowledge-based Systems can significantly improve the management of complex distributed health systems, where supporting multidisciplinar- ity is crucial and communication and synchronization between the different professionals and tasks becomes essential. This work proposes the use of the ontological paradigm to describe the organizational knowledge of such complex healthcare institutions as a basis to support their management. The ontology engineering process is detailed, as well as the way to maintain the ontology updated in front of changes. The paper also analyzes how such an ontology can be exploited in a real healthcare application and the role of the ontology in the customization of the system. The particular case of senior Home Care assistance is addressed, as this is a highly distributed field as well as a strategic goal in an ageing Europe. Materials and methods: The proposed ontology design is based on a Home Care medical model defined by an European consortium of Home Care professionals, framed in the scope of the K4Care European project (FP6). Due to the complexity of the model and the knowledge gap existing between the – textual – medical model and the strict formalization of an ontology, an ontology engineering methodology (On-To-Knowledge) has been followed. Results: After applying the On-To-Knowledge steps, the following results were obtained: the feasibility study concluded that the ontological paradigm and the expressiveness of mod- ern ontology languages were enough to describe the required medical knowledge; after the kick-off and refinement stages, a complete and non-ambiguous definition of the Home Care model, including its main components and interrelations, was obtained; the formalization stage expressed HC medical entities in the form of ontological classes, which are interrelated by means of hierarchies, properties and semantically rich class restrictions; the evaluation, carried out by exploiting the ontology into a knowledge-driven e-health application running on a real scenario, showed that the ontology design and its exploitation brought several ben- efits with regards to flexibility, adaptability and work efficiency from the end-user point of view; for the maintenance stage, two software tools are presented, aimed to address the incor- poration and modification of healthcare units and the personalization of ontological profiles. ∗ Corresponding author. Tel.: +34 977 55 96 88; fax: +34 977 55 97 10. E-mail address: [email protected] (A. Valls). 1386-5056/$ – see front matter © 2010 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.ijmedinf.2010.01.012
Transcript of Using ontologies for structuring organizational knowledge in Home Care assistance

i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f o r m a t i c s 7 9 ( 2 0 1 0 ) 370–387
journa l homepage: www. int l .e lsev ierhea l th .com/ journa ls / i jmi
Using ontologies for structuring organizational knowledgein Home Care assistance
Aida Vallsa,∗, Karina Gibertb, David Sáncheza, Montserrat Bateta
a Department of Computer Science and Mathematics, Universitat Rovira i Virgili, Av Països Catalans 26,43007 Tarragona, Catalonia, Spainb Department of Statistics and Operational Research, Universitat Politècnica de Catalunya,C/ Jordi Girona 1-3, 08034 Barcelona, Catalonia, Spain
a r t i c l e i n f o
Article history:
Received 1 July 2009
Received in revised form
26 January 2010
Accepted 26 January 2010
Keywords:
Medical informatics
Telemedicine
Organizational models
Home Care services
Knowledge representation
Ontologies
Distributed systems
a b s t r a c t
Purpose: Information Technologies and Knowledge-based Systems can significantly improve
the management of complex distributed health systems, where supporting multidisciplinar-
ity is crucial and communication and synchronization between the different professionals
and tasks becomes essential. This work proposes the use of the ontological paradigm to
describe the organizational knowledge of such complex healthcare institutions as a basis to
support their management. The ontology engineering process is detailed, as well as the way
to maintain the ontology updated in front of changes. The paper also analyzes how such
an ontology can be exploited in a real healthcare application and the role of the ontology
in the customization of the system. The particular case of senior Home Care assistance is
addressed, as this is a highly distributed field as well as a strategic goal in an ageing Europe.
Materials and methods: The proposed ontology design is based on a Home Care medical model
defined by an European consortium of Home Care professionals, framed in the scope of the
K4Care European project (FP6). Due to the complexity of the model and the knowledge gap
existing between the – textual – medical model and the strict formalization of an ontology,
an ontology engineering methodology (On-To-Knowledge) has been followed.
Results: After applying the On-To-Knowledge steps, the following results were obtained: the
feasibility study concluded that the ontological paradigm and the expressiveness of mod-
ern ontology languages were enough to describe the required medical knowledge; after the
kick-off and refinement stages, a complete and non-ambiguous definition of the Home Care
model, including its main components and interrelations, was obtained; the formalization
stage expressed HC medical entities in the form of ontological classes, which are interrelated
by means of hierarchies, properties and semantically rich class restrictions; the evaluation,
carried out by exploiting the ontology into a knowledge-driven e-health application running
on a real scenario, showed that the ontology design and its exploitation brought several ben-
efits with regards to flexibility, adaptability and work efficiency from the end-user point of
view; for the maintenance stage, two software tools are presented, aimed to address the incor-
poration and modification of healthcare units and the personalization of ontological profiles.
∗ Corresponding author. Tel.: +34 977 55 96 88; fax: +34 977 55 97 10.E-mail address: [email protected] (A. Valls).
1386-5056/$ – see front matter © 2010 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.ijmedinf.2010.01.012

i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f o r m a t i c s 7 9 ( 2 0 1 0 ) 370–387 371
Conclusions: The paper shows that the ontological paradigm and the expressiveness of
modern ontology languages can be exploited not only to represent terminology in a non-
ambiguous way, but also to formalize the interrelations and organizational structures
involved in a real and distributed healthcare environment. This kind of ontologies facilitates
the adaptation in front of changes in the healthcare organization or Care Units, supports
the creation of profile-based interaction models in a transparent and seamless way, and
increases the reusability and generality of the developed software components. As a con-
clusion of the exploitation of the developed ontology in a real medical scenario, we can say
that an ontology formalizing organizational interrelations is a key component for building
know
1
TliAanrbsci
iserofaip
wMpfrpiitahcaisg
aaftH
effective distributed
. Introduction
he care of senior patients suffering chronic diseases requiresife long treatments under continuous supervision, whichncreases the pressure on the public sector for long-term care.s a matter of fact, old people account for a high percent-ge of the hospitalizations in most European countries. It isow widely recognized that hospitalization is sometimes notelated to the patient’s acute medical condition, but for reha-ilitation needs or for social reasons, such as the lack of familyupport at home or difficult continuous access to specialistare facilities. In these cases, hospitalization is seen as bothnappropriate and costly [1].
Home Care (HC) is multidimensional and multidisciplinaryn its nature. It is conceived as the integration of medical,ocial and familiar resources addressed to the same goal:nabling the integral care of the patient in his own envi-onment [2]. HC is considered as a fundamental networkf long-term care facilities (e.g. rehabilitation units, nursingacilities and social services), capable of reducing institution-lization, expenses and risk of death. Home Care assistances a strategic goal in Europe because of the impact of seniorerson’s needs in public health systems [3].
Home Care assistance is especially effective for patientsho have complex medical, psychological and social needs.ultidisciplinar teams are more effective in assessing
atient’s needs and creating an effective care plan than pro-essionals working alone are. Those teams must communicateegularly in order to provide a comprehensive treatment of theatients, which usually have co-morbid diseases and require
ndividual intervention plans. In usual care settings (i.e. carenside hospitals and other institutions) team members workogether at the same site, so communication can be informalnd expeditious. This is not the case of providing the care atome, where the organization is distributed, team membersan belong to different institutions, depending on differentdministrations, they rarely meet each other and the flow ofnformation is neither constant nor complete. Thus, in the HCetting, the role of Information and Communication Technolo-ies becomes essential.
In European Countries, HC is structured in different waysccording to local rules, laws and funding. Thus, tradition-
lly the systems developed for HC are designed specificallyor each country, or even for a particular region or hospi-al [4,3], relying on local legacy systems such as Electronicealthcare records or Hospital Information Systems. Theseledge-driven e-health systems.© 2010 Elsevier Ireland Ltd. All rights reserved.
ad hoc systems have two main drawbacks: first, the lack ofgenerality and flexibility due to their dependency on non-standard healthcare models and already existing systems.This hampers their usefulness and limits their applicabilityand reusability to other medical contexts or to changes onthe healthcare workflows and regulations. Second, the needof developing new particular systems from scratch consumesenormous amounts of resources. The lack of a common HCmodel forces the implementation of many redundant mod-ules adapted to the concrete healthcare structure and requiresa financial effort that not all organizations are able to afford.
Even though the organizational model of Home Care maydiffer from one country to another, there are some basicaspects shared. Particularly, HC models are represented by thekind of services provided, human resources involved and theirorganization and dependences. The K4Care project (Knowledgebased Home Care eServices for an Ageing Europe) takes this intoconsideration. K4Care is a Specific Targeted Research of Inno-vation Project funded within the Sixth Framework Program ofthe European Commission that brings together 13 academicand medical institutions from 7 countries. The K4Care projectproposes a model which provides a HC paradigm easily adapt-able to any of the EU countries, including western and easternEuropean countries. It was designed to improve the capabil-ities of the new EU society to manage and respond to theneeds of the increasing number of senior population requir-ing personalized Home Care assistance. This has been doneby capturing and integrating the information, skills, expertiseand experiences of specialized centers and professionals of HCservices from several old and new EU countries. This medicalmodel is being supported by a web-based intelligent platformthat provides e-services to health professionals, patients andcitizens in general [5]. In fact, this system, denoted as K4CarePlatform, is a formalization in computational terms of the med-ical model proposed in the project.
The K4Care model proposes to distribute the HC ser-vices provision among local health units, which should beintegrated with the social services of municipalities and, even-tually, other organizations of care or social support. All theseorganizations must be coordinated in order to provide to thepatient the necessary sanitary and social support to be treatedat home. In these terms, the aim is to provide the so-called“unique access” for both social and sanitary services. The
common and basic Home Care structures shared by the mainsanitary systems in Europe have been identified in order topropose a model that may represent an incentive and enablesthe shift towards this European Home Care approach.
i c a l
372 i n t e r n a t i o n a l j o u r n a l o f m e dThis HC model is defined in a standard, modular andscalable manner, in order to improve the interoperability, flex-ibility and reusability against already existing systems. Thedefinition of such a model required a huge effort from themedical partners of the project. A panel of medical and socialexperts in the field of geriatrics and HC, from both old and newEuropean countries, was organized inside the K4Care projectto formalize the process of HC in a structured way, with thehelp of knowledge engineers.
As a result, the K4Care Home Care Model was proposed [5].It is mainly focused on the formalization of the HC organiza-tional structure of a medical institution and it is focused intwo basic entities: Actors and Services. On one hand, Actorsrefer to any person involved in HC (i.e. medical profession-als, continuous care providers, etc.). The model defines severalaspects of Actor’s interaction, duties and skills, in order toallow the detailed definition of medical roles. On the otherhand, care activities are organized into Services. Servicesmainly model the HC workflow to be followed during the exe-cution of HC, but also administrative processes. Services arecomposed by several Actions which should be performed byappropriate actors in a coordinated way. The results of theActions are typically stored in structured Documents, whichcompose the patient’s medical history and are the basis formedical professionals to decide upon the new services neededfor the patient. More details about the K4Care HC Model aregiven in Section 2.1.
Once the model was defined, it raised the question on howit should be formally represented in order to be exploited andadapted in a concrete e-health computer application. In orderto ensure the generality and flexibility of the approach, it wasdecided to separate the medical and organizational knowl-edge from the software components devoted to the executionof the system. This is a knowledge-driven approach, whichis more flexible and permits the update of the knowledge(and as a direct consequence, changes on the behaviour ofthe whole system) without requiring any change in the soft-ware tool. This is possible because the execution behaviouris decided at runtime upon the organizational knowledgestored in the system. In this manner, the system can be eas-ily adapted to changes in the corresponding organization,actor’s responsibilities and even the medical scope in which itis framed (e.g. geriatrics, oncology, rehabilitation, etc.), sim-ply by changing the knowledge information represented ina compliant way with respect to the structure of the HCmodel.
In order to fulfil those requirements, the HC organiza-tional model has been implemented as an ontology [6], aformalism widely used in Knowledge Engineering, AI andComputer Science, which provides a formal frame to representthe knowledge related with a complex domain in a computerreadable manner. As the K4Care HC model is centred on Actors,the developed ontology is called Actor Profile Ontology (APO).
It is worth to note that, in medicine, ontologies have beenusually employed as a mean to define a common termi-nology for a medical domain (as will be stated in Section
2.2). However, in our approach, the ontological paradigmand the possibilities of standard ontological languages areextensively exploited in order to define entities and complexinterrelationships among them, representing the structurei n f o r m a t i c s 7 9 ( 2 0 1 0 ) 370–387
and organization of the medical assistance. The proposedontology represents the general organizational model of HomeCare assistance with a role-based approach, which permitsthe use of this kind of ontology to design and develop user-oriented knowledge-based software systems. The modularapproach of the ontology facilitates the adaptation of the gen-eral model to each particular medical centre. Moreover, asdiscussed in Section 3.3, the Actor Profile Ontology can be tai-lored according to the user’s needs. This introduces flexibilityto the system to model the specific cases that appear in dailyassistance. All this features configure a novel approach whichbrings benefits from the knowledge exploitation point of view,as it will be described in a practical application.
So, in this paper, the design and engineering process fol-lowed to construct the Actor Profile Ontology is presented.Section 2 concerns materials and methods. First, the K4CareHC model is described (Section 2.1). Then, the ontologies arepresented as a formal framework to represent the organiza-tional knowledge of the K4Care HM model (Section 2.2). InSection 2.3, the On-To-Knowledge methodology is presentedas the formal knowledge engineering method used to prop-erly develop the Actor Profile Ontology from the K4Care HCmodel. Section 3 is divided in subsections according to the On-To-Knowledge steps. Each subsection provides results of thecorresponding step of the engineering method, giving the finalstructure of the Actor Profile Ontology and some details aboutthe design solutions proposed to face some of the intrinsicdifficulties raised when formalizing complex knowledge. Par-ticularly, Section 3.4 describes the exploitation of that kind ofontologies in a knowledge-driven multi-agent system for HCassistance as well as the results of the validation performedin the town of Pollenza (Italy) with real HC professionals andpatients. Section 3.3 is devoted to explain the maintenanceof the ontology. Finally, in Section 4 a discussion about theresults of the ontology development process are presented,with particular focus on explaining the advantages providedby the extensive use of ontologies in the particular context ofthe K4Care project.
2. Materials and methods
In this section, the Home Care model defined in the K4Careproject [7] is presented as the material used to develop theActor Profile Ontology. As it has been said in the introduc-tion, this model has been defined by integrating the knowledgeand experience of several Home Care centers and profession-als from different European countries. Thus, this medical HCmodel represents a shared view of how Home Care assistancecould be delivered in Europe, containing the knowledge aboutthe essence of the organizational structure of HC assistance.
Afterwards, the theoretical framework used to derive a for-mal ontology from the K4Care HC Model is introduced. First ofall, the ontological paradigm and its possibilities when formal-izing complex medical knowledge are discussed. Ontologicalfeatures of modern languages will be extensively exploited
in the design of the proposed ontology. Then, the On-To-Knowledge engineering method is presented as a suitableapproach to handle the required ontology construction pro-cess.
i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f o r m a t i c s 7 9 ( 2 0 1 0 ) 370–387 373
Table 1 – K4Care medical partners.
Partner Location
Centro Assistenza Domiciliare Azienda Sanitaria Locale (CAD) Rome, ItalyAmministrazione Comunale di Pollenza (COMPOL) Pollenza, ItalyUniversitá degli Studi di Perugia, Depart. of Geriatrics (UNIPG) Perugia, ItalyFundazione Santa Lucia (FSL) Rome, Italy
2
TpeniT
isia
scHssso
Hippt
as
•
General University Hospital in Prague (GUHP)“Ana Aslan” International Academy of Ageing (ANA)The Research Institute for the Care of Elderly (RICE)Szent Janos Hospital (SZH)
.1. The K4Care Home Care model
he K4Care HC Model was developed by the group of medicalartners of the K4Care project, with the help of knowledgengineers. The model integrates the best practices of old andew EU countries in a handbook of good medical assistance to
ll, disabled, chronic senior patients in a technological society.able 1 shows the medical partners of the K4Care project.
The generic structure of the model proposed in K4Care [5]ncorporates the common and basic Home Care structureshared by the main sanitary systems in Europe. In order to eas-ly implement its general design to a particular organization,modular structure is proposed.
As shown in Fig. 1, the K4Care HC Model is based on a nucleartructure (HCNS), which comprises the minimum number ofommon elements needed to provide a basic HC service. TheCNS can be extended with an optional number of accessory
ervices (HCAS) that can be modularly added to the nucleartructure. These services will respond to specialized cares,pecific needs, opportunities, means, etc. of either the usersr the health-care community where the model is applied.
The distinction between the HCNS and the complementaryCASs must be interpreted as a way of introducing flexibil-
ty and adaptability in the model and also as an attempt torovide practical suggestions for standards to be used whenrojecting and realizing new services in largely different con-exts.
Going into detail, each one of the HC care units (i.e. HCNSnd HCAS’s) consists of the same components: actors, actions,ervices, procedures and documents.
Actors are all the sort of human figures included in the struc-ture of HC.
Fig. 1 – The K4Care HC Model architecture.
Prague, Czech RepublicBucharest, RomaniaBath, United KingdomBudapest, Hungary
• Professional Actions and Liabilities are the actions that eachactor can perform to provide a service (or part of it) withinthe HC structure.
• Services are all the utilities provided by the HC structure forthe care of the HCP (Home Care patient).
• Procedures are the chain of events that leads actors in per-forming actions to provide services.
• Medical Information refers to the documents required and pro-duced by the actors to provide services in the HC structure.
As new HCAS’s are incorporated to the K4Care HC Model,new actors, actions, services, procedures and medical infor-mation enter to be part of the extended model. This way, theK4Care HC Model is compatible both with the current situationin the European countries, where the international, nationaland regional laws define different HC systems for differentcountries, and also with the forthcoming expected situationin which an European model for HC is desired.
2.2. Ontologies
In [6] an ontology is defined as “a formal, explicit specificationof a shared conceptualization”. Conceptualization refers to anabstract model of some phenomenon in the world by havingidentified its relevant concepts. Explicit means that the type ofconcepts identified, and the constraints of their use, are explic-itly defined. Formal refers to the fact that the ontology shouldbe machine-readable. Shared reflects the notion that ontologycaptures consensual knowledge, that is, not a personal viewof the target phenomenon of some particular individual, butone accepted by a group.
Ontologies are designed for being used in applications thatneed to process the content of information, as well as, to rea-son about it, instead of just presenting information to humans.They permit greater machine interpretability of content thanthat supported by XML, RDF and RDF Schema (RDF-S), by pro-viding additional vocabulary along with a formal semantics.
Because of the intrinsic complexity of the conceptsinvolved, the medical domain is one of the most activeones in defining and using ontologies [8]. They are mainlyemployed to define medical terminology with a clear andnon-confusing meaning, which facilitates the exchange ofinformation between different institutions, groups of profes-sionals, or systems. In complex domains, as the medical oneis, this is a crucial feature that permits to share a common
language and structured and well-defined concepts. Someexamples of widely used medical ontologies focused on struc-turing domain terminology are GALEN [9], MeSH (MedicalSubject Headings) [10], SNOMED (Systematized Nomenclature of
i c a l
374 i n t e r n a t i o n a l j o u r n a l o f m e dMedicine, Clinical Terms) [11], UMLS (Unified Medical Language Sys-tem) [12] and ON9 [13]. However, it is worth to note that mostof these domain ontologies focus only on the terminologicaland taxonomical aspects of the medical knowledge [14] (i.e.defining one or several concept hierarchies of diseases, syn-dromes, symptoms, treatments, etc.). However, this kind ofontologies does not exploit the whole potential of expressive-ness that modern ontological paradigms bring to knowledgeformalization.
From a structural point of view [15,16], an ontology is com-posed by disjoint sets of concepts, relations, attributes and datatypes. Concepts are sets of real world entities with commonfeatures. Relations are binary associations between concepts.There exist inter-concept relations which are common toany domain and domain-dependant associations. Attributesrepresent quantitative and qualitative features of particularconcepts, which take values in a given scale defined by thedata type.
Concepts are classes organized in one or several tax-onomies, linked by means of transitive is-a relationships.Multiple inheritance (i.e. the fact that a concept may haveseveral hierarchical ancestors or subsumers) is also supported.
Binary relations can be defined between concepts. In thosecases, the concept in the origin of the relation represents thedomain and those in the destination, the range. Those relation-ships may fulfil properties such as symmetry or transitivity.
By default, concepts may represent overlapping sets of realentities (i.e. an individual may be an instance of severalconcepts simultaneously). If necessary, ontology languagespermit to specify that two or more concepts are disjoint (i.e.individuals can only be instances of one of those concepts).
Some standard languages have been designed to codifyontologies. They are usually declarative languages based oneither first-order logic or on description logic. Some exam-ples are KIF, RDF (Resource Description Framework), KL-ONE,DAML + OIL and OWL (Web Ontology Language) [17]. The mostused are OWL [18] and RDF [19].
There are some differences between them according totheir supported degree of expressiveness. In particular, OWLis the most complete one, allowing the definition of logicalaxioms representing restrictions at a concept level (OWL-DLand OWL-Full). Axioms are expressed with a logical languageand contribute to define the meaning of the concepts, bymeans of specifying limitations on the concepts involved. Sev-eral restriction types can be defined:
• Cardinality: defines that a concept’s individual can be related(by means of a concrete relation type) to a minimum, maxi-mum or exact number of other concept’s instances.
• Universality: indicates that a concept has a local rangerestriction associated with (i.e. only a given set of conceptscan be the range of the relation).
• Existence: indicates that a least one concept must be therange of a relation.
All those restrictions can be defined as Necessary (i.e.an individual should fulfil the restriction in order to be aninstance of a particular class) or Necessary and Sufficient (i.e.in addition to the previous statement, an individual fulfilling
i n f o r m a t i c s 7 9 ( 2 0 1 0 ) 370–387
the restriction is, by definition, and instance of that class). Thisis very useful for implementing reasoning mechanisms whendealing with unknown individuals.
In addition, OWL also permits to represent more complexrestrictions by combining several axioms using standard log-ical operators (AND, OR, NOT, etc.).
Being the most expressive ontological language, OWL hasbeen selected to implement the Actor Profile Ontology. Con-cretely, OWL-DL form has been used, as it offers a highlevel of expressiveness (it supports all the ontological fea-tures described above) and it is based on Description Logics,permitting automatic reasoning to check and to detect incon-sistencies in the ontology. OWL-Full offers an increasedexpressiveness at the cost of the decidability and computa-tional completeness of the language (i.e. it is not possibleto perform automated reasoning). So, using OWL-DL, theAPO extensively exploits most of the possibilities offered bymodern ontological paradigms in order to design a highlyexpressive and realistic formal representation of the medicalHC model, and offers the possibility to perform automatedreasoning on the ontology. As it will be shown in Section 3.4,during the exploitation of the ontology in the developed HCsystem, ontological expressiveness contributes to improve thesystem’s flexibility and adaptability and permits to supportmany knowledge-driven medical tasks.
2.3. Ontology engineering
To build an ontology from a conceptual model of a real phe-nomenon as the one faced by the K4Care project is a complextask, as the completeness of the ontology should be ensuredeven when implicit knowledge makes difficult the formal-ization process. In this sense, Ontological Engineering providesmethodologies for building ontologies in a comprehensiveand structured way. In this field, there have been proposeddifferent methods for ontology construction [17], such asMethontology or On-To-Knowledge [20]. There are also semi-automatic techniques as TextToOnto [21] for ontology learningfrom text and tools to automatically learn domain ontologiesfrom the Web [22]. In addition, tools that permit the codifica-tion of ontologies are available, as Protégé [23].
In this research, the ontological engineering process forbuilding the APO has been performed under the On-To-Knowledge methodological approach. The design of thismethodology is focused on the creation of ontologies toimprove the knowledge management in large and distributedorganizations [20]. The On-To-Knowledge methodology isbased in five steps [20]:
1. Feasibility study: consists of carrying out a scoping andproblem analysis study to identify problem/opportunityareas and potential solutions, putting them into a widerorganizational perspective and deciding about economic,technical and project feasibility, in order to select the mostpromising focus area and target solution. Additionally, animpacts and improvements study for the selected solution
can be carried out.2. Kick-off: this step is devoted to establish the requirementsof the ontology specification. As a result, it is defined thedomain and the goal of the ontology, the design guidelines,

a l i n
3
4
5
vsnmb
3
Tliee
i n t e r n a t i o n a l j o u r n a l o f m e d i c
the available knowledge sources, the potential users andthe use cases. The outcome of this phase is a semi-formaldescription of the contents of the ontology, for example,using conceptual maps and descriptive text.
. Refinement: it is addressed to obtain a mature ontology intwo steps, taking as a basis the initial specification providedin the kick-off:• Knowledge elicitation with domain experts. This is a
very critical step, since lots of implicit knowledge isunconsciously used by experts in their daily reason-ing. This knowledge is crucial to obtain a correct modeland usually does not appear in the kick-off specifica-tion. This missing knowledge produces inconsistencies,redundancies or incompleteness that may cause wrongperformances of the Ontology. For knowledge elicitation,a top-down-approach is proposed in this particular case.One starts by modelling concepts and relationships on avery generic level. Subsequently these items are refined.This approach is typically done manually and leads to ahigh-quality engineered ontology.
• Formalization: Once a consistent, non-redundant and pre-sumably complete description of the domain is clear, theproper ontology elements to correctly formalize have tobe identified. The result of this stage is the ontology.The major decision that needs to be taken to completethis step is whether the ontology fulfils the requirementscaptured in the previous kick-off phase.
. Evaluation: a systematic evaluation of the ontologies mightlead to a consistent level of quality, which is very importantfor its acceptance in a real-world application. So, this stageis devoted to prove the correctness and usefulness of theontology by:• Checking the requirements and competency questions.• Testing the ontology in the target application environ-
ment.. Maintenance: On-To-Knowledge proposes to carry out ontol-
ogy maintenance as a part of the system softwareengineering process. Usually maintenance is devoted toclarify who is responsible for maintenance and how it isperformed and which time intervals are between two consec-utive maintenances. Moreover, there have to be strict rulesabout the update/insert/delete processes of the ontology.In this sense, enlargement and tailoring procedures can bedefined.
These five steps define a methodological approach that isery convenient for building high standard ontologies [20],uch as the one that was faced in the K4Care project. In theext section, the results of applying this methodology to for-alize the APO from the K4Care HC model are described step
y step.
. Results
he construction of the Actor Profile Ontology was done fol-
owing the steps of the ontological engineering methodologyntroduced in Section 2.3. During this process, knowledgengineers and medical experts worked together in order tonsure a complete transfer of the organizational medicalf o r m a t i c s 7 9 ( 2 0 1 0 ) 370–387 375
knowledge to the formal ontology, as well as the correctness ofthe representation of that information. In this section, thosestages are described, covering from the feasibility study andontological definition to its evaluation and maintenance.
3.1. Feasibility of using ontologies to represent HCorganizational knowledge
In the feasibility study, the main goals to be fulfilled by theActor Profile Ontology with regards to the Home Care modelformalization were identified:
1. To formalize the organizational knowledge in a languagethat can taxonomically represent the different elementsinvolved in the HC assistance and their organizationalinterrelations, as defined in the K4Care HC model.
2. To build a model centred in actor’s profiles to guaran-tee that the behaviour of the users involved in HC isconstrained according to their permissions, professionalliabilities, national and international legal rules and pri-vacy preserving.
3. The representation language for the knowledge structureshould be standard and recognizable by many different sys-tems in order to allow building interoperable informationsystems.
Ontologies are a formalism widely used in Knowledge Engi-neering, Artificial Intelligence and Computer Science, whichprovide a very suitable formal frame to represent the knowl-edge related to a complex domain, as a qualitative model [20].As introduced in Section 2.2, ontologies allow the definitionconcepts by means of classes, and those can be organized inone or several hierarchies and interrelated by means of labeledrelationships. Moreover, many different types of constraintscan be specified to give expressiveness to the modeled knowl-edge. Thus, it was concluded that ontologies were enough torepresent the HC organizational knowledge.
Regarding the second goal, a profile-based approach isappropriate to implement professional roles and user permis-sions in the system [24,25] and permits the implementation ofthe required authorization mechanisms as well as to adapt thesystem’s behaviour to the user’s profile. Profile-related struc-tures can be directly modeled by means of ontological conceptrestrictions defined at the Actor class level, indicating, for eachmedical role, their skills, allowed actions, permissions andaccess rights. Thus, ontologies also fulfill the second goal.
Finally, as stated in Section 2.2, the development ofstandard ontology languages and tools (such as editors orreasoners) facilitates the development and exploitation ofontologies in knowledge-based information systems.
3.2. Formalizing the K4Care HC model
The Kick-off stage of the ontology engineering process corre-sponds to the analysis of the K4Care HC model presented inSection 2.1, in order to identify the set of ontology require-
ments and an initial description of its content.The detailed description of this model is available as aproject deliverable in [7]. After analyzing it from the knowl-edge engineering point of view, it was concluded that the Actor

i c a l
376 i n t e r n a t i o n a l j o u r n a l o f m e dProfile Ontology structure should be able to identify and rep-resent:
• Which medical Services are provided by the system.• Which Actors participate in the provision of those Services.
An Actor will be associated with every sort of human figureincluded in the structure of the medical system.
• How Actors interact among them to provide those Services.Here Actions have to be defined, associated to every indi-vidual action that an actor can perform to contribute to theaccomplishment of a Service. Actions are combined into Pro-cedures to provide the desired Services. So one or severalProcedures will be linked to every Service.
• Which information is required and produced when per-forming the Service. It was decided that the basic unit ofinformation storage and exchange will be the Document,since it provides high flexibility.
• How the Actors interact with the stored information to pro-vide the Services. This means to define Actors access rightsto the Documents and the role of Documents in Procedures andActions.
• Which are the different Care Units (HCNS and HCAS) andwhich are their corresponding elements (services, actors,documents, etc.).
It was also decided not to store temporal constraints intoprocedure steps due to the limitations of OWL-DL when rep-resenting time-related restrictions [17]. This information (e.g.relative action orders, cycles of repetition, delays, etc.) is storedin specially designed structures represented using the SDA*language [26]. See [27] for details about how those structuresare created, managed and executed by the K4Care platform.
3.3. The Actor Profile Ontology construction
The next stage consisted in the refinement of the initial model.Two steps composed this phase:
• Elicitation: considering the basic specification obtained inthe previous stage, the knowledge entities required to for-malize de model were identified:o Actors implied in the model and their roles played inside
the system.o Services/procedures provided by the nuclear structure and
extensible via Care Units.o A general set of Actions and the list of Actions to be per-
formed during the execution of a Procedure.o The Actors implied in an Action. That is, who can per-
form each action. In a procedure, and action might beperformed by different actors.
o A general list of Documents and their associations to con-crete Actions. In K4Care, the result of an Action is storedin the form of one or several documents.
o The Actor’s permission to read/write the Documents. It isrequired to specify, for every actor, if he can create, modifyand consult a document.
The model specification proposed by medical partners wasthen analyzed by knowledge engineers to extract the requiredinformation to model the above entities. At this point, it was
i n f o r m a t i c s 7 9 ( 2 0 1 0 ) 370–387
detected some implicit and incomplete information due tothe semi-formal plain text definition of the model. Particu-larly, knowledge engineers found that many of Action-relatedknowledge (e.g. Actions composing a procedure, the docu-ments associated to an action) where missing in the originalmodel definition. To solve this lack of information doctorswere required to define structured tables indicating whichactors can start or perform each action and associating doc-uments with actions. Finally, they had to specify the actionsthat compose each procedure.
• Formalization: According to the specification provided bymedical experts, ontological entities were organized in sev-eral concept hierarchies (the top level elements of theseconcept hierarchies are shown in dark grey in Fig. 2),together with the relationships between them. A top-downdevelopment process was carried out in order to iterativelyrefine each general hierarchy identifying, for example, roletypes and concrete roles for the Actor hierarchy or group-ing Action according to their nature (e.g. back-office, nursing,patient-related, etc.). The ontology obtained after this processis coded in OWL-DL [18].
As a result of this engineering process, the main classes andinterrelations defined in the APO ontology were those shownin Fig. 2.
Formally, the ontology has six root classes (Action, Doc-ument, Entity, Procedure, Service and Care Unit), which aredefined as disjoint and specialized accordingly. In the follow-ing, their characteristics and interrelations defined by meansof OWL ontological restrictions are presented.
3.3.1. EntityIt refers to everyone which can perform an action. It is subdi-vided into two main classes:
(1) Group: representing teams with healthcare liabilities. Auniversal restriction is defined using the property hasMem-ber: Group → Actor (being Group the Domain and Actor theRange), which allows to indicate, at an instance level,which are the concrete members belonging to that group.A subtype of Group is also defined. Concretely, in the HCNSthere exist a group of actors called Evaluation Unit, whichis always composed by a Family Doctor, a Head Nurse,a Physician in Charge and a Social Worker, which are incharge of the care of a particular patient’s episode. In thiscase, an existential and an exact cardinality restrictions aredefined at a class level using the hasMember property, indi-cating that an Evaluation Unit is composed by the exactunion of those four actor types. The restriction is also asNecessary and Sufficient because any Group composed bythat set of actors must be an Evaluation Unit.
(2) Actor: representing individual participants (e.g. patient,nurse, physician in charge of the patient, head nurse andfamily doctor). On the other hand, Actors considered inthe HCNS are subdivided in the categories shown below:• Stable Members are professionals which usually are part
of the HC and they are directly employed by the health-care system. The stable members are: Physician inCharge, Head Nurse, Family Doctor, Nurse and SocialWorker.

i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f o r m a t i c s 7 9 ( 2 0 1 0 ) 370–387 377
logy
sH
weh
•
•
•
•
(scor
Fig. 2 – General structure of the Actor Profile Onto
• Additional Care Givers are professional and non-professional actors which usually are part of the HC,but they are not directly employed by the healthcaresystem. Additional care givers are Specialist Physicians,Social Operators, Informal Care Givers and ContinuousCare Providers.
• Patient is the object of the Home Care.
In addition to those basic actors, the K4Care HC model alsoupports the definition of new actors involved in the additionalCAS.
As a result of the functional analysis of the HC model,hich resulted in the set of knowledge requirements
nounced in Section 3.2, some properties between classesave been modelled:
doesAction: Entity → Action, indicates the Actions (joined byan OR operator) that an Entity can perform.initiatesService: Entity → Service, indicates the set of servicesan Entity can start.readDocument: Actor → Document, indicates read permissions(joining documents with an OR operator) to concrete actorroles.writeDocument: Actor → Document, express write permissions(joining documents also with an OR operator) to concreteactor roles.
Then, each concrete actor’s role defined in the ontologye.g. Head Nurse) exploits those properties by defining univer-
al class restrictions indicating the concrete Services that hean start, Actions that he can perform (e.g. Nurse doesActionnly (NursingActivity)) and the set of Document that he canead/write.. Inverse properties are not shown for simplicity.
3.3.2. ServiceFrom the K4Care HC Model analysis, Services have been spe-cialized in the following subclasses:
• Access Services consider the Actors as elements of the K4CareHC Model and address issues like patient’s admission or pro-fessional discharge.
• Patient Care Services consist of all the services needed for thepatient care, like for example consultation or prescriptionof pharmacological treatment.
• Information Services cover the needs of information that theactors require in the K4Care HC Model. Those services canaddress issues like guidelines consultation or overview ofwaiting lists.
The following properties are defined for the Service class:
• serviceIntiatedBy: Service → Entity, indicates the Entity that isable to activate the Service. This is the inverse to the initi-atesService property introduced above.
• hasProcedure: Service → Procedure, link Services to their cor-responding medical Procedures. A minimum cardinalityrestriction of 1 is defined for that property at a class level.This indicates that there may be at least one specific way –procedure – of performing a certain service.
Again, each concrete service of any of those three classes(e.g. HCPAdmission is a subclass of Access Service) uses those
properties to define universal restrictions indicating the set ofroles (union – OR – of Entities) that may start it (e.g. HCPAd-mission serviceInitiatedBy only (PhysicianInCharge OR HeadNurse))and the concrete Procedure used to execute that Service.
i c a l
tion behaviour and to properly manage actor’s competencies.Then, we comment the results obtained after its evaluation in
378 i n t e r n a t i o n a l j o u r n a l o f m e d
3.3.3. ProcedureA Procedure is related to a unique Service, but a Service mayhave several associated Procedures depending on external con-ditions, like the place where the care will be delivered. ForProcedures, the list of Actions or even additional Services whichshould be executed (i.e. nested Services are allowed) to accom-plish a Service should be specified.
The following properties are defined for the Procedure class:
• isProcedureOf: Procedure → Service, indicates to which Servicethe Procedure is linked. This property is the inverse ofhasProcedure and is defined with a restriction indicating exactcardinality of 1, because it can only correspond to one specificservice.
• hasStep: Procedure → Service U Action, indicates all the steps(Action or Service executions) required to complete a Pro-cedure, joining them with and AND operator. With thisproperty, for a concrete Procedure, the steps to be exe-cuted in order to fulfill the associated Service can bedefined by means of an existential restriction (i.e. contrar-ily to a universal restriction, in this case, all the steps aremandatory).
3.3.4. ActionDepending on the concrete Care Unit or medical organization,the ontology can include many subtypes of actions such associal actions, case management actions, back-office actions, nursingactions, etc.
The following properties are defined for the Action class:
• hasObject: Action → Patient, associates Actions to an objectthat receives it (a patient in medical systems). As the objectof a concrete action execution is unique, an exact cardinal-ity restriction is specified for that property (i.e. exactly oneobject should be defined for a concrete Action).
• hasSubject: Action → Entity, specifies the entity able to per-form that action. It is the inverse to the doesAction property.
• usesDocument: Action → Document, defines the result of anAction execution, with one or more Documents that shouldbe filled-out (joined with an AND operator).
Even though the object of a concrete Action is always aPatient, the specific set of Documents to be filled and the con-crete group of Entities who are able to execute the Actionmust be defined by means existential and universal restrictions,respectively.
3.3.5. DocumentDocuments have been specialized according the Service towhich they belong into Information, Access and Patient Care Doc-uments.
The following properties are defined for the Document class:
• isDocumentOf: Document → Service, relates each document tothe corresponding Service.
• isReadBy and isWrittenBy: Document → Actor, specifyread/write permissions for the different Actors. Theyare the inverse properties to readsDocument and writes-Document, respectively. Concrete documents may define
i n f o r m a t i c s 7 9 ( 2 0 1 0 ) 370–387
universal restrictions for the defined properties, indicatingspecific Services and Actor’s permissions.
3.3.6. Care unitAs introduced in Section 2.1, the K4Care HC Model distinguishesbetween Nuclear Services (which are common to any medicalcentre) and Additional Services (which are associated to a partic-ular Care Unit). In the latter case, a Care Unit may be modelledin the APO by specializing some of the basic classes and incor-porating appropriate class descriptions (as it will be discussedin Section 3.4).
In order to properly distinguish the Care Unit to whicheach ontological element belongs, a new class is introducedin the APO: Care Unit Element. For each Care Unit considered,a new subclass is added to that taxonomy (e.g. rehabilitation,oncology, etc.). So, every leaf of any of the Entity, Service andProcedure hierarchies also inherits from the appropriate sub-class of the Care Unit Element taxonomy, allowing an easy anddirect identification of the medical scope in which a particu-lar ontological element is framed. This is an example of howa multiple inheritance approach can help to model complexstructures of knowledge in a real domain.
The current APO structure incorporates the necessary enti-ties to deal with the basic services related to the Home Care ofelderly patients. Up to 49 HCNS Services have been defined,which are classified into Access Services (management ser-vices), Patient Care Services and Information Services. For everyservice, a decomposition in particular Actions is provided. Atotal of 118 individual Actions organized in several hierarchiesaccording to their scope (e.g. Back-office, Case Management,Evaluations, Nursing-care, etc.) were defined. For every action,the interaction between Actors is defined in the Procedures,as well as, which Documents are needed and the access per-missions of every actor to each kind of document. A totalof 119 organized according to the service in which they areframed. This gives an idea of the dimension of this ontol-ogy.
3.4. APO evaluation and exploitation in the K4Careplatform
Once a basic OWL ontology was built and checked via a rea-soner (FaCT++1), an evaluation process has been carried out.First, the logical consistency of the APO has been reviewed bya panel of experts. Then, the APO was introduced into a sys-tem prototype (the K4Care platform) aimed to prove that theproposed K4Care HC Model is able to provide real assistance inHC delivery. This software has been tested in Pollenza (Italy)involving real Home Care assistance organizations and a sam-ple of real elderly patients. In this section, we introduce the ICTplatform developed in the K4Care project and explain how theAPO can be exploited by a computer system to guide the execu-
a real setting.
1 http://owl.man.ac.uk/factplusplus/.

i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f o r m a t i c s 7 9 ( 2 0 1 0 ) 370–387 379
atfor
3WciatamsPtTtfkmzccsbdio
dt
raat
Fig. 3 – K4Care pl
.4.1. A brief outline of the K4Care platformhile the healthcare information system of a single medi-
al centre is usually rather centralized, medical assistancen Home Care naturally needs a distributed service-orientedrchitecture, as many kinds of actors from different institu-ions are involved. Thus, in the K4Care project a web-basedpplication has been designed in order to meet the require-ents of decentralization and remote access to distributed
ources by the involved actors. This system is called K4Carelatform and provides e-services for aiding the different insti-utions involved in the provision of Home Care assistance.his system implements the K4Care HC model according to
he design principles proposed in Section 2.1, especially theeature of decoupling the system’s implementation from thenowledge structures (ontologies) which represent the HCodel and its particular representation on a concrete organi-
ation. In this way, the medical and organizational knowledgean be modified by changing or extending the APO (e.g. HC pro-edures, actor’s responsibilities or even adding new care unitsuch as oncology). Those changes will immediately be adoptedy the actors of the system, as it is explained below. Thisesign of the K4Care Platform provides a high degree of flexibil-
ty, reusability and generality, which are fundamental aspectsf a system modelling complex and dynamic processes.
The architecture of K4Care Platform (shown in Fig. 3) isivided in three layers: the Knowledge Layer, the Data Abstrac-
ion Layer and the K4Care platform layer.The Knowledge Layer [28] includes all the knowledge sources
equired to specify the HC structure of a concrete organizationnd the data repositories to keep the medical data. It includesn electronic health record (EHR) which store patient data [29],he medical and organizational knowledge represented in the
m’s architecture.
Actor Profile Ontology (the APO presented in this paper), thedomain knowledge (terminology) stored in a domain ontologycalled Case Profile Ontology (CPO) [30] and a repository of care-flows and formal intervention plans represented in SDA* language[26].
As each knowledge base is expressed in a different format,the intermediate layer (Data Abstraction Layer [28]) objectiveis to decouple the generic execution of HC processes by theplatform from the way in which the data is stored in theKnowledge Layer, providing a transparent access to the data.
The upper layer of the K4Care Platform [27] is a web-basedapplication with a client side (a Web browser) and a serverside. The server is implemented using agent technology. Multi-agent systems [31] provide several advantages in comparisonto classical software paradigms when dealing with complexdistributed systems, such as modularity, flexibility and decen-tralization.
The agents of the multi-agent system of the K4Care Platformembed all the system logic by personifying the actors involvedin HC services. Agents act semi-autonomously, in the sensethat several actions, such as exchange of information, col-lection of heterogeneous data concerning a patient (results,current treatment, next recommended step, past history) orthe management of pending actions are performed by agentswithout the intervention of human users.
3.4.2. The APO as a source to implement agent’s codeEach real-world actor is represented in the system by a perma-
nent agent (generically represented as Actor Agents in Fig. 3).Those agents implement the functionalities of the corre-sponding user profile (e.g. a Head Nurse, a Patient, a FamilyDoctor, etc.). They have all the information related to the cur-
i c a l
380 i n t e r n a t i o n a l j o u r n a l o f m e drent activities of its particular user. For example, they knowwhich services are being executed and which are the pend-ing actions of the user. Moreover, the Actor Agent managesall queries and requests coming from the user or other ActorAgents.
The APO has an active role in making the implementationof the K4Care Platform as generic as possible and to ensurethat agent behaviour is coherent with the HC, because partof the agent code is automatically generated from the orga-nizational and user profile-related knowledge stored in theAPO. An especial module called code generator creates the basiccomponents needed to implement appropriate agent func-tionalities according to the knowledge stored in that ontology.Particularly, agent code for a certain user profile is createdtaking into account only the subset of actions that are associ-ated to that profile. So, each Actor Agent only incorporates thesource code associated to the skills and capabilities of its cor-responding user, avoiding that the system permits to the userto do any action which is out of his/her medical competencies.
With this approach, the APO is exploited as the basic sourceof information used to design and implement Actor Agents ina knowledge-driven fashion. In this way, if the organizationalknowledge may change (e.g. a particular profile should executean additional action), the implementation can be easily re-adapted in an automatic way. More details about automaticagent generation for the K4Care Platform are presented in [32].
3.4.3. The APO as a guide to agent’s executionIn addition to contribute to the static agent’s implementation,the APO is also used at execution time in order to dynami-cally guide the execution of HC processes and guide the user’sinteraction according to the K4Care HC Model.
Once the platform is physically deployed in a server, agentsare created and associated at execution time when the phys-ical user logs in. From that moment, the APO is consulted inorder to guide the system’s execution according to the pro-file of the corresponding actor role and the structure of themedical organization as defined in the ontology.
Particularly, the kind of information the agents may requestfrom the APO at execution time is:
• Which services a particular user may start (patient admis-sion or discharge, definition of formal intervention plans,follow-ups, nursing services, back-office activities, etc.).This is used to select only those aspects of the systemthe user can interact with. So, the user will have a partialand simplified view of the entire platform functionalitiesaccording to his/her profile.
• Which is the procedure (set of actions) needed to provide aparticular service (e.g. the execution of a medical treatment)and which types of actors must participate in the process.During the automatic management of the execution of ser-vices [27], the APO is consulted to delegate the actions (e.g.nursing activities) to available actors capable of performingthem. Then, a confirmation is requested both from the final
user and from the Head Nurse in order to delegate a par-ticular action. With this approach, services can be executeddistributedly, asynchronously and transparently among thesystem users.i n f o r m a t i c s 7 9 ( 2 0 1 0 ) 370–387
• In order to properly manage the EHR and maintain data pri-vacy, agents are also able to consult which are the read/writedocument permissions for each particular user and act inconsequence.
3.4.4. ValidationThe fireproof of both the HC model and its implementationvia the different components included in the K4Care Platformconsisted in an evaluation process carried out in a real insti-tution, involving HC medical staff which interacted with theplatform. The evaluation aimed to verify the adherence of thesystem to the needs and duties of Home Care, the possibil-ity of use it in daily activities, the capability of collecting andintegrating information from different sources and the pos-sibility of executing and personalizing healthcare proceduresand intervention plans [33].
The testing environment has been the community of thetown of Pollenza, a small town about 6000 inhabitants in cen-tral Italy, with about 22% of population older than 65 yearsand aging index of 156.7 in 2007. Due to the complexity of thesystem and the lack of IT skills of the evaluation staff, theplatform was presented as a final product in which evaluatorswere asked to rate the results and benefits observed from theirinteraction; however, they were not aware on the technolo-gies, components or design of the platform. It is importantto note that evaluators were regular healthcare members ofthe National Health Service and were not involved neither inthe K4Care research activities, the HC model design nor theplatform development.
The staff participating in the evaluation was composed byfour Geriatrician Physicians (GerP), one Physician in Charge(PC), four Nurses (N), being one the Head Nurse, one Geri-atrician and one Social Worker (SW). Patients used to testthe platform were selected from a group of volunteers. Eachof the four GerPs was asked to enrol al least five patientsrequiring Home Care services. As a result, 23 real patientswere chosen. All of them were Home Care patients defininga target population of mainly geriatric users, being the mostcommon diseases: Coronary Heart disease, Cerebrovasculardisease, Arthritis, Hip fracture, Diabetes and Hypertension.
Once the knowledge sources were set up for the testingenvironment, the platform was continuously applied in theusual care activity delivered by the involved staff during aweek. After that, all the participants provided a structuredevaluation of the system through validated questionnaires.Even though evaluators were not aware on the technical com-plexities and individual components of the platform and theevaluation was carried out from the final user point of view,one can extract conclusions regarding the adequacy of eachcomponent from the users’ ratings.
An initial stage involved several sessions and tutorials inwhich participant staff learned to use the platform with theassistance of IT experts and trained Geriatricians from theCAD and FSL medical research centres (see Table 1). After that,the platform interaction was completely transferred to thestaff who was asked to execute procedures of “usual care”
over the selected patients using, as much as possible, theK4Care platform to support their daily activities. Participantsremotely accessed the platform server via on-line connec-tion through laptops or desktops located at patient’s homes
a l i n
ofiwpoc4w
afpcow(aoaaasi
bwtfls5tioscP5r
fimtohvrvs
smtatp
uS
i n t e r n a t i o n a l j o u r n a l o f m e d i c
r professionals’ offices. As it is specified in the HC model andormally represented in the APO ontology, many of those activ-ties required the interaction of several groups of actors whichorked concurrently keeping track of each step of the carerocess. Quantitatively, the testing involved the introductionf 23 patients, the constitution of 10 Evaluation Units, the exe-ution of 184 Actions and the creation of 206 Documents of3 different types, values which usually represents months ofork.
After the testing, a structured evaluation was provided,sking the participants to fill in two questionnaires (adaptedrom the standard TAM questionnaire [34]). As, in some cases,rofessionals played several roles, nine questionnaires wereompleted: four from GerPs, one from a HN, two from Nurses,ne from a Geriatrician and one from a SW. Questionnairesere designed following the Technology Acceptance Model
TAM) which summarizes how users come to accept and usetechnology, focusing on the perceived usefulness and ease-f-use. It proposes a set of standardized items to be rated inscale from 1 to 7, from the perspective of the final user oftechnological product. Detailed results for each questions
nd questionnaire sheets are offered in [33]; in the rest of theection, we concentrate on the questions related to the APOnfluence in the system.
The first questionnaire evaluated the perceived ease of usey asking the user to rate if the operation with the platformas easy, if it was easy to make the system to perform what
he user wants to do, if the interaction was clear, if it wasexible enough and if it was easy to become skilful with theystem. The average score for this aspect of the system was.8 (SD 0.5). The APO, the knowledge-driven design and theailoring possibilities had a direct influence in the positive rat-ng of this aspect of the platform, incorporating a high degreef flexibility, adaptation and personalization possibilities andimplifying the interaction by presenting only options asso-iated to a professional profile. With respect to professionals,hysicians and the Head Nurse gave higher ratings (around.9) than other professionals (nurses and social workers whoated them around 5.6).
The perceived usefulness was evaluated by asking the pro-essionals to rate several items regarding the improvementn their job performance, the enabling to accomplish tasks
ore quickly, the potential increase of their productivity andhe enhancement of their effectiveness. The average scoref this aspect was 5.9 (SD 0.7). Again, professionals withigher responsibilities (Physicians and the Head Nurse) pro-ided higher ratings (6.1) than nurses (around 5.2), as they areesponsible of many daily management activities (such as ser-ice activation or actor assignments), which are assisted by theystem thanks to the APO.
The second questionnaire asked to evaluate the differentections of the K4Care platform from 1 to 7. The manage-ent of services (which takes advantage of the knowledge in
he APO) obtained the highest rate (5.7). Physicians rate thosespects much higher (5.9) than nurses (4.7) who may perceivehat the allowed actions were quite restricted due to their user
rofile.The final questions were about the general opinion of thesers: are K4Care tools needed in health care? (average 6.3,D 0.9); are you aware of similar tools? (1.9, SD 0.8); are you
f o r m a t i c s 7 9 ( 2 0 1 0 ) 370–387 381
aware of similar tools in use? (1.9, SD 0.8). Those results indi-cate that the healthcare professionals appreciate the noveltyof the knowledge-driven approach of the K4Care system andits necessity as a tool for assisting HC.
3.5. APO maintenance
The backbone of the Actor Profile Ontology represents theorganizational structure of the HCNS that is common to manyEuropean HC organizations. Additionally, some medical cen-tres have additional HCAS that respond to particular careactivities or needs of each organization. The modularity of theontology design facilitates the incorporation of new care units(e.g. oncology, rehabilitation, etc.) to the general model, havinga complete description of Home Care in Europe. Consideringthe importance of the ontology during the HC delivery, specialcare must be paid to its modification. As a result of the researchdevoted on ontology maintenance, three aspects have beenaddressed:
1. The enlargement of the APO with new care units that modelHCAS. It has been designed a tool for assisting the user inthe addition of new medical knowledge to the Actor ProfileOntology, called ISA (Intelligent Service Adder).
2. The structure of the APO also permits to automaticallyextract partial views of the model (called subAPOs) for eachcare unit, including only the part of the ontology that cor-responds to each particular centre. This provides a partialview of an HCAS and allows working in a modular way.
3. It is also possible to obtain role-centred sub-ontologies andto personalize them at a user level in order to customizethe system’s behaviour for final users. This is an impor-tant feature that has an impact on the acceptance of healthinformation systems [3,35]. The customization functional-ities are provided by a user-friendly tool called ATAPO.
3.5.1. Adding new care units to the APOIn order to make easier the ontology extension process, asoftware tool called Intelligent Service Adder (ISA) has beendesigned [36]. This tool exploits the well-defined and homo-geneous structure of the modelled knowledge to allow theincorporation of new care unit descriptions.
ISA is meant to be used by trained medical experts in astandalone way (i.e. the presence of a knowledge engineeris not required). In order to ensure the correctness of theincorporated knowledge with regards to the HC model, ISAguides the user along the definition of new elements. In thismanner, the user has to take the minimal possible decisionsconcerning the structure. ISA allows adding new care units ina semi-supervised fashion, and maintains the consistency ofthe resulting APO.
In order to define and to add new care units but avoidinginconsistencies, the system controls how the different ele-ments are introduced into the ontology. ISA starts from thedefinition of new Services by showing to the user all the dif-ferent Services types (e.g. Access Services) already defined into
the backbone APO. For every type, the system shows the exist-ing Services (e.g. HCP Admission) and it allows the user to linkthem with the new care unit or to create new ones if necessary(See Fig. 4).
382 i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f o r m a t i c s 7 9 ( 2 0 1 0 ) 370–387
mai
Fig. 4 – ISASecondly, the specification of Procedures for each new Ser-vice is requested. If none of the previously defined Procedurescan be reused, the user can create a new one using the toolsprovided by ISA. In this case, ISA is able to auto-complete thefollowing knowledge structures:
• The list of Actions and/or Services that compose the Procedure(hasSteps).
• The list of Documents to which an Action can interact to (uses-Document).
• The list of Actions that can be performed by an Actor (doe-sAction).
Optionally, after adding a Procedure, read/write permis-sions can be specified if new Actors and/or Documents arecreated.
As a result of this process, ISA outputs a new ontology withthe same core structure as the original APO but incorporat-ing the new Care Unit as new subclasses. As the consistencywith the original model is ensured, the K4Care Platform mayimmediately incorporate the new modelled knowledge with-out re-adapting and reprogramming its components (as it hasbeen explained in Section 3.4). ISA has been tested by addinga rehabilitation service to the K4Care nuclear structure [36].
3.5.2. APO tailoringThere are a number of aspects that could be tailored in theAPO, providing different degrees of flexibility and personaliza-tion to the system. In [37] those aspects have been discussed
together with the experts from a technical and functionalpoint of view. According to the requirements given by the med-ical experts, it was agreed to consider the following two typesof tailoring:n window.
1. Tailoring of Care Units: generates a subAPO with the infor-mation regarding a single care unit (e.g. subAPO of HCASoncology). This can be useful to automatically reduce theservices provided by the system in case of a Home Care cen-tre that only provides the basic HCNS but not the additionalHCAS or vice versa.
2. Tailoring of Entities: generates a subAPO with the informa-tion describing the role of a particular type of actor (e.g.subAPO of the Family Doctor, or subAPO of the EvaluationUnit). Once it is obtained, it can be modified by a particularuser to generate a personalized version. This type of ontol-ogy tailoring permits to adapt the behaviour of the systemto every particular user.
With respect to the first type of tailoring, the taxonomy ofCare Units is exploited in order to distinguish which elementsbelong to each particular care unit. So, the subAPO will onlycontain those concepts that inherit from the correspondingCare Unit. Additionally, is-a relations among those conceptsare kept in order to obtain a new ontology with the same tax-onomical relations of the original APO. Nevertheless, not allthe concepts are classified using the Care Unit taxonomy. Inthis case, in order to know whether they are related to a partic-ular care unit or not, non-taxonomic relations are taken intoaccount. If there exist some relation with a concept of the stud-ied Care Unit then, the concept is also stored into the subAPOof this Care Unit [37].
The second type of tailoring regards to the different Actorsor Groups in the HC model (Entities) and permits to customizethe K4Care Platform at a user level. In this case, the tailor-ing process creates particular views of the APO for each role
defined in the K4Care HC Model. Then, users have the pos-sibility to personalize their interaction with the HC systemin certain situations by building a personal and customizedsubAPO for a concrete role.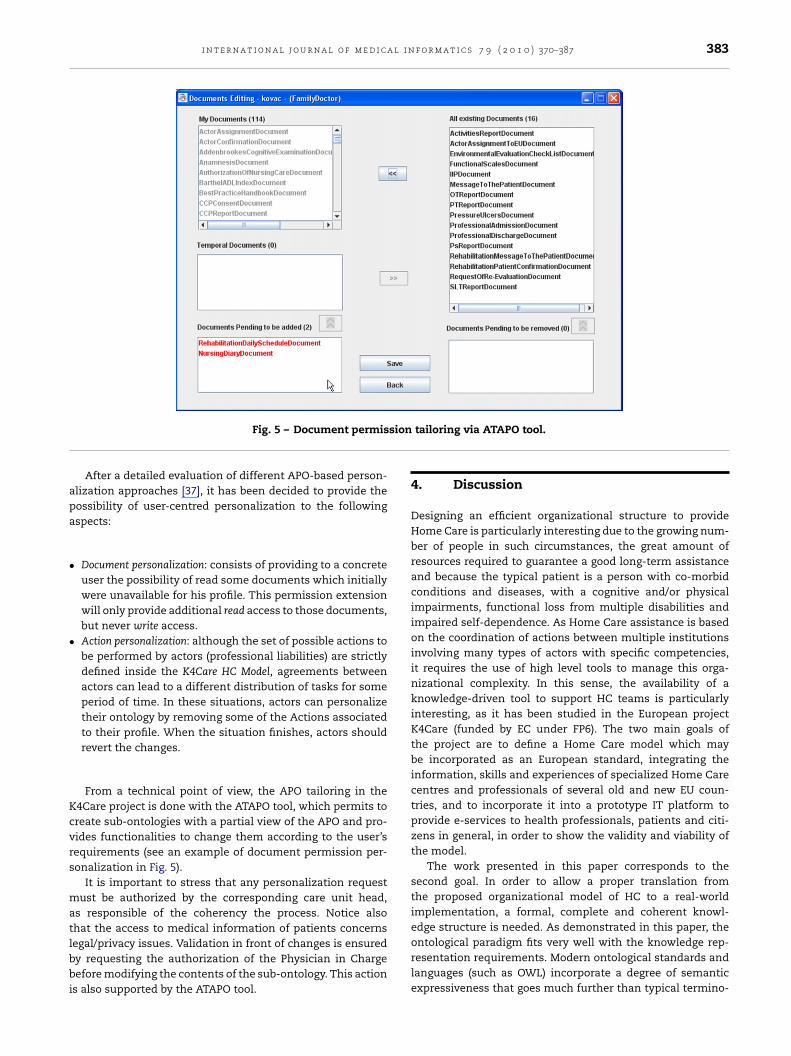
i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f o r m a t i c s 7 9 ( 2 0 1 0 ) 370–387 383
sion
apa
•
•
Kcvrs
matlbbi
Fig. 5 – Document permis
After a detailed evaluation of different APO-based person-lization approaches [37], it has been decided to provide theossibility of user-centred personalization to the followingspects:
Document personalization: consists of providing to a concreteuser the possibility of read some documents which initiallywere unavailable for his profile. This permission extensionwill only provide additional read access to those documents,but never write access.Action personalization: although the set of possible actions tobe performed by actors (professional liabilities) are strictlydefined inside the K4Care HC Model, agreements betweenactors can lead to a different distribution of tasks for someperiod of time. In these situations, actors can personalizetheir ontology by removing some of the Actions associatedto their profile. When the situation finishes, actors shouldrevert the changes.
From a technical point of view, the APO tailoring in the4Care project is done with the ATAPO tool, which permits toreate sub-ontologies with a partial view of the APO and pro-ides functionalities to change them according to the user’sequirements (see an example of document permission per-onalization in Fig. 5).
It is important to stress that any personalization requestust be authorized by the corresponding care unit head,
s responsible of the coherency the process. Notice alsohat the access to medical information of patients concerns
egal/privacy issues. Validation in front of changes is ensuredy requesting the authorization of the Physician in Chargeefore modifying the contents of the sub-ontology. This actions also supported by the ATAPO tool.
tailoring via ATAPO tool.
4. Discussion
Designing an efficient organizational structure to provideHome Care is particularly interesting due to the growing num-ber of people in such circumstances, the great amount ofresources required to guarantee a good long-term assistanceand because the typical patient is a person with co-morbidconditions and diseases, with a cognitive and/or physicalimpairments, functional loss from multiple disabilities andimpaired self-dependence. As Home Care assistance is basedon the coordination of actions between multiple institutionsinvolving many types of actors with specific competencies,it requires the use of high level tools to manage this orga-nizational complexity. In this sense, the availability of aknowledge-driven tool to support HC teams is particularlyinteresting, as it has been studied in the European projectK4Care (funded by EC under FP6). The two main goals ofthe project are to define a Home Care model which maybe incorporated as an European standard, integrating theinformation, skills and experiences of specialized Home Carecentres and professionals of several old and new EU coun-tries, and to incorporate it into a prototype IT platform toprovide e-services to health professionals, patients and citi-zens in general, in order to show the validity and viability ofthe model.
The work presented in this paper corresponds to thesecond goal. In order to allow a proper translation fromthe proposed organizational model of HC to a real-worldimplementation, a formal, complete and coherent knowl-edge structure is needed. As demonstrated in this paper, the
ontological paradigm fits very well with the knowledge rep-resentation requirements. Modern ontological standards andlanguages (such as OWL) incorporate a degree of semanticexpressiveness that goes much further than typical termino-
i c a l
384 i n t e r n a t i o n a l j o u r n a l o f m e dlogical and mainly hierarchical structures. As a result, an ActorProfile Ontology (APO) is proposed to represent the organiza-tional knowledge of HC assistance.
The paper addresses the issue of building such an ontologyusing a suitable knowledge engineering methodology. In par-ticular, the use of the On-To-Knowledge method is proposedand its application to the APO construction is detailed. In thissection, the results of the ontology engineering process arediscussed.
4.1. Ontologies as a paradigm to represent the HC in amedical organization
The study done in the feasibility stage analyzed if the ontolog-ical paradigm was appropriate to represent the organizationalmodel of Home Care assistance. Three main aspects werestudied, concluding that (1) the expressiveness of the ontologi-cal languages are enough to describe the entities and relationsof this model, (2) the actor’s liabilities and permissions canbe also represented using ontologies and (3) ontologies arespecially suitable to support distributed and interoperableinformation systems, modelling not only static knowledgebut also the interactions between actors. As a consequence,ontologies are an adequate approach to represent this kind ofknowledge.
In particular, it is worth to stress the fact that the ontologyproposed in this paper does not only define a common ter-minology (similarly to medical domain ontologies presentedin Section 2.2). In fact, the APO includes information aboutthe main entities involved in HC, but also represents com-plex interrelations and profile-related restrictions in order toformalize the organizational knowledge of a concrete medi-cal institution. This is particularly interesting for developingdistributed IT medical systems, as the one developed in theK4Care project, which must be easily adaptable to the dif-ferent legislations of each particular medical centre. In thismanner, the proposed ontology will become the key compo-nent to facilitate the integration and coordination of differentactors involved in HC in a concrete scenario (i.e. a particularcare unit of a concrete medical institution).
In order to have a formal representation of the organiza-tional model of HC assistance, in the so-called kick-off andelicitation stages (where a model of HC in EU countries wasdefined [5]), the proposal, manually elaborated by a panel ofexperts, was deeply analyzed. The definition of this model,which is proposed as a standard, required a huge effort fromthe medical partners of the project, identifying which arethe minimum elements needed to provide a basic HC ser-vice (HCNS). However, in Knowledge Engineering, it is wellknown that formalizing complex domains is a very difficulttask, mainly because of the existence of implicit knowledge,rarely expressed in a first expert’s specification. As usual, alsoin this particular research, the first specification provided bythe experts constituted a general view, which required deeperformalization at the engineering level, since some informationrelevant for designing the system was still missing.
In a knowledge-driven information system as the onedeveloped in the K4Care project, the correctness of the ontol-ogy is critical for two reasons: on one hand, the APO is used inthe implementation of the agent’s code; on the other hand, it
i n f o r m a t i c s 7 9 ( 2 0 1 0 ) 370–387
is a key element at runtime to ensure the provision of servicesaccording to the organizational rules represented in the ontol-ogy. In this sense, it was fundamental the use of KnowledgeEngineering techniques to refine and formally validate the ini-tial medical model in terms of correctness from a logical pointof view. A close interaction between experts and knowledgeengineers was required in this step. Non-trivial redundancies,inconsistencies and lacks of information were identified, as,for example, a clear specification of the documents involvedin each step of a medical procedure. This was a very valuableinformation that allowed to enhance the initial specificationof the organizational K4Care HC model, clearly identifying therelevant components and relations that must be representedin the Actor Profile Ontology.
4.2. Designing the Actor Profile Ontology
The ontology presented in this paper is particularly interestingbecause it incorporates most of the knowledge representa-tion possibilities offered by OWL, which gives an exampleof how those elements can be used in medical ontologies,but also in organizational ontologies for other domains. Onone hand, concepts are organized in several disjoint hierar-chies which constitute the core of the HCNS model. Each onecan be extensively refined by defining specializations and cre-ating subclasses according to the needs of a modelled CareUnit. Multiple-inheritance allows a properly classification ofeach component according to its nature (i.e. Document, Actor,Action, Procedure or Service) and, at the same time, accord-ing to the concrete Care Unit to which it belongs (e.g. Nuclear,Rehabilitation, Oncology, etc.). This allows managing the mod-elled knowledge from different points of view (i.e. from arole-centred view or from the Care Unit optics), as presentedduring the ontology maintenance and extension stages. Thisstructure is particularly interesting since it allows isolating thesub-ontology corresponding to a certain care unit obtaining,for example, the complete profile of the medical centre whererehabilitation services are offered.
On the other hand, in addition to class definition andstructuring, several properties have been introduced in orderto interrelate classes in a non-taxonomical way. Each addedproperty incorporates the semantics of the relation and allowsthe specification of concept restrictions at a class level. Usinglogic constraints and operators offered by OWL-DL, we wereable to define, for example, read/write access permissions inEHR documents for concrete user roles, the entities composingan Evaluation Unit, etc.
From the architectural point of view, the APO is internallyorganized to mimic the medical model of HC assistance pro-vided by the experts and to be flexible enough to support laterenlargements with new specialized services as oncology orrehabilitation (Care Units). The distinction between HCNS andHCAS permits to easily adapt the HC to the particular char-acteristics of different contexts (i.e. countries with differentorganizational structures or laws).
4.3. The ontology exploitation
Since the advantage of the ontological representation overother data representation structures is to be machine read-

a l i n
acKbpeitctatthcttwnCowo
cauAbCFtMEa
fictpgtaafripcsomw
cutwc
i n t e r n a t i o n a l j o u r n a l o f m e d i c
ble, the contents of the APO ontology, encoded in OWL,an be easily exploited in knowledge-based systems. In the4Care project, the APO is used to dynamically determine theehaviour of the K4Care platform according to a defined userrofile. So, when the user account is created, the code gen-rator creates a particular agent whose behaviour is definedn the APO according to a certain actor type. In other words,he knowledge stored in the APO is used to determine theapabilities and permitted actions of every agent created intohe system in such a way that the actions declared for thector type profile in the APO are the only ones allowed forhe corresponding user. With this approach, the APO makeshe system scalable and adaptable even to the evolutions ofealthcare management policies that the APO captures or mayapture in the future. The advantage of this approach is thathe APO represents all the structural knowledge of Home Care;his knowledge can be continuously updated and the systemill adapt in an automatic and seamless manner to new laws,orms, or ways of doing with a null reprogramming effort.onsidering that one of the main premises of K4Care is toffer a high degree of generality, flexibility and adaptabilityith respect to changes in HC, an ontology-based executionffered a very appropriate solution.
The K4Care platform has been presented to our health-are partners, which provided valuable feedback about thedherence of the implemented services to their daily HC, thesability of the interface and the functionality of the system.s a result, several revisions were made. The system has alsoeen presented in several events such as the 18th Europeanonference on Artificial Intelligence (ECAI 2008 [38]) and theifth Workshop on Agents Applied in Health Care, held withinhe 7th International Conference on Autonomous Agents andultiagent Systems (AAMAS 2008 [27]). Reviewers from the
uropean Commission also evaluated and approved the modelnd its ontology-based implementation.
The final version of the system which implements all theeedback and requests from the medical and technical staffnvolved in the evaluation was deployed and validated in theommunity of Pollenza (Italy). The K4Care Platform was appliedo the usual care activity of a heterogeneous set of healthcarerofessionals and real patients. The examiners provided a veryood overall score of 5.8/7, judging the platform as easy andhe usefulness as high. Detailed results show that Physiciansnd Head Nurses gave higher ratings than other profession-ls (i.e. nurses, social workers). This may be motivated by theact that physicians required a higher degree of flexibility andole adaptation due to their more variable duties and admin-strative responsibilities than nurses, who typically executehysical actions. From the answers, it is also possible to con-lude that the APO, which enables an efficient profile-basedystem interaction and assists in some tasks (i.e. managementf services and action delegation), had a crucial influence ininimizing the amount of time the user spends interactingith the system.
Users also perceived that there is a high need of health-are of tools like K4Care, even admitting their reluctance in
sing such IT tools. They also appreciated the possibilitieshat an ontology-based knowledge-driven approach providedith regards to improving the management support in such aomplex and distributed environment.
f o r m a t i c s 7 9 ( 2 0 1 0 ) 370–387 385
Maintenance is the last step of the engineering process,a stage which, in many cases, does not deserve the requiredattention. The availability of a well-defined and validatedontology is a good deal but, if it cannot be easily maintainedand updated, it gets impractical when the context changes.In this sense, our proposal addresses two issues: the immedi-ate and direct incorporation of new knowledge to the ontologyin order to support additional care units and the tailoring ofknowledge to particular situations.
Enlarging from scratch the basic APO with new specializedstructures in order to adapt it to other medical contexts hasan important risk of introducing redundancies or, even worse,inconsistencies. Due to this reason, a specific tool, called ISA,was designed and implemented to assist in this task, enablingthe user to reuse those concepts already existing in the APO ina coherent way, as well as ensuring that all new concepts intro-duced are correctly linked. As a result, by means of ISA, thereliability of the resulting structure is ensured, while incon-sistencies, redundancies and time devoted to the definition ofnew care units are minimized.
Going even further, the APO has been exploited as the baseto customize the system’s behaviour to specific situations. Thegeneration of subAPOs for Care Units is useful for the peo-ple in charge of the corresponding Care Unit, in order to havea complete description of the unit in a structured way. Thisinformation can also aid for management purposes. For exam-ple, the subAPO can indicate which actions are consideredand which actors perform them for a concrete care unit, orwhich are the actors with read/write permissions over eachdocument generated in the care unit.
In addition, each concrete user may create a tailoredversion of the whole ontology which incorporates only theentities and relations related to his/her profile for which duties(action performance) and document-related permissions canbe modified. In this sense, personalization acts as a filterof how the K4Care HC Model is perceived by each user. Forinstance, the APO of a particular orthopaedist will stress somehealthcare features that other APO users will ignore. In thisway, the same K4Care HC Model will have different interpreta-tions depending on the actor.
After the authorization of the changes in the profile, whichensures that the modifications made by actors follows theHome Care organizational model, Personal Agents will use thisupdated ontology instead of the general one to act according tothe individually modelled user’s profile. This is a transparentprocess which can be executed at runtime and results in animmediate adaptation of the system’s behaviour. In fact, thesystem is able to immediately detect changes in the ontology,which makes it able to negotiate the assignment of actionsto actors (Actor Agents) involved in a healthcare procedureaccording to the personalized subAPO. Moreover, ontology tai-loring permits to offer a personalized view of the platformaccording to the user profile (e.g. requested read permissionsover documents). This user-centered approach is strategic inmedical information systems, in order to improve their accep-tance [3,35].
As a final issue, it is worth to note that even though beingframed in the project’s scope, the presented ontology designcan be easily adapted to other Health Care domains. It isexpected that this kind of knowledge-driven approaches to

386 i n t e r n a t i o n a l j o u r n a l o f m e d i c a l
Summary pointsWhat was already known on the topic?
• There is a need of exploiting Information Technologiesin order to improve Home Care assistance at a Euro-pean level, because it is a continuously growing areawith great social and economical impact.
• Ontologies have been already used in medicine,mainly focused on the specification of medicalterminology.
• Ontologies are particularly useful for the develop-ment of distributed and interoperable systems, whichare especially interesting in complex and distributeddomains, such as Home Care assistance.
What this study added to our knowledge?
• The expressiveness of modern ontological models andlanguages offer an appropriate paradigm to formalizeand represent complex organizational knowledge of aspecific domain.
• Highly expressive ontologies formalizing in a non-ambiguous manner user profiles and organiza-tional interrelations can be exploited to implementknowledge-driven systems supporting health care,especially when coordination in multidisciplinarteams is required to provide the medical services, suchas the case of Home Care. Due to their knowledge-based execution, this kind of systems offers severaladded values with respect to classical ad-hoc medicalapplications, such as adaptability, reusability, flexibil-ity or customization possibilities.
• A particular ontology for Home Care, called ActorProfile Ontology, has been built on the base of aproposed European-level Home Care model. As aproof-of-concept, it has been successfully applied overa knowledge-based platform, aimed to improve the
r
delivery of Home Care.
information systems will deserve more attention in the futureof medical systems.
Conflict of interest statement
The authors of this paper are solely responsible for itscontent. It does not represent the opinion of the Euro-pean Community and the Community is not responsible forany use that might be made of the information containedherein.
Acknowledgments
The work presented in this paper has been developed inthe funded European IST project K4Care: Knowledge BasedHome Care eServices for an Ageing Europe (IST-2004-026968).The authors would like to acknowledge the work of the
i n f o r m a t i c s 7 9 ( 2 0 1 0 ) 370–387
other members of the K4Care consortium, especially Dr.David Riano (project co-ordinator) and the medical partners,led by Dr. Fabio Campana, who participated in the K4CareHC model definition and in the ontology validation. TheK4Care consortium has given their consent for submitting thispaper.
Contributions. The work presented in this paper is the resultof the research performed in collaboration with several peo-ple involved in the K4Care European project. Despite being ateam-work, each of the authors has clearly focused on onespecific part of the ontology engineering process presentedin the paper: Dr. Karina Gibert in the Feasibility and Kick-offstages, Dr. Aida Valls in the Ontology Construction, Dr. DavidSánchez in the Evaluation and Exploitation stages and Mrs.Montserrat Batet in the Maintenance stage. According to thisdistribution of work, each author has been in charge of writinghis/her corresponding part both in the results and discussionsections. The introduction and methods sections have beenwritten with the collaboration of all the authors. Finally, eachof them has reviewed the complete paper and agreed on thefinal version.
e f e r e n c e s
[1] F. Landi, G. Onder, A. Russo, S. Tabaccanti, R. Rollo, S.Federici, E. Tua, M. Cesari, R. Bernabei, A new model ofintegrated home care for the elderly: impact on hospital use,Journal of Clinical Epidemiology 54 (9) (2001) 968–970.
[2] M.H. Beers, in: M.H. Beers (Ed.), Geriatric InterdisciplinaryTeams in The Merck Manual of Geriatrics, Merck & Co, 2005(Chapter 7).
[3] S. De Rouck, A. Jacobs, M. Leys, A methodology for shiftingthe focus of e-health support design onto user needs: a casein homecare field, International Journal of MedicalInformatics 77 (2008) 589–601.
[4] A. Moreno, A. Valls, D. Riano, PalliaSys: agent-basedproactive monitoring of palliative patients, in: Proceedingsof the 4th International Workshop on Practical Applicationsof Agents and Multi-Agent Systems, Leon, Spain, October,2005.
[5] F. Campana, A. Moreno, D. Riano, L. Varga, Agent Technologyand e-Health, chap. K4Care: Knowledge-Based Homecaree-Services for an Ageing Europe, Software AgentTechnologies and Autonomic Computing, Birkhäuser Basel,Basel, Switzerland, 2008, pp. 95–115.
[6] R. Studer, V.R. Benjamins, D. Fensel, Knowledge engineering:principles and methods, IEEE Transactions on Knowledgeand Data Engineering 25 (1–2) (1998) 161–197.
[7] F. Campana, R. Annicchiarico, D. Riano, et al.Knowledge-Based Home Care eServices for an AgeingEurope. K4Care Deliverable D01, 2007. http://www.k4care.net/fileadmin/k4care/public website/downloads/K4CModel D01.rar.
[8] D. Pisanelly, Ontologies in Medicine, IOS Press, 2004.[9] A. Rector, J. Rogers, Ontological and practical issues in using
a description logic to represent medical concept systems:experience from GALEN, in: Proceedings of the Reasoning
Web, 2006, pp. 197–231.[10] S.J. Nelson, D. Johnston, B.L. Humphreys, Relationships inMedical Subject Headings. Relationships in the Organizationof Knowledge, Kluwer Academic Publishers, New York, 2001,pp. 171–184.

a l i n
[38] D. Isern, Knowledge based Homecare eServices for an ageing
i n t e r n a t i o n a l j o u r n a l o f m e d i c
[11] K.A. Spackman, K.E. Campbell, R.A. Cote, R.T. Snomed, Areference terminology for healthcare, Journal of theAmerican Medical Informatics Association (1997) 640–644(Special issue).
[12] S.J. Nelson, T. Powell, B.L. Humphreys, The United MedicalLanguage System (UMLS) Project. Encyclopedia of Libraryand Information Science, Marcel Dekker, Inc., New York,2002, pp. 369–378.
[13] A. Gangemi, D.M. Pisanelli, G. Steve, Some requirements andexperiences in engineering terminonolical ontologies overWWW, in: Proceedings of the 11th International Workshopof Knowledge Acquisition, Modelling and Management,1998, pp. 1–21.
[14] J. Dujmovic, H. Bai, Evaluation and Comparison of SearchEngines Using the LSP Method, Computer Science andInformation Systems 3 (2) (2006) 711–722.
[15] G. Stumme, M. Ehrig, S. Handschuh, S. Hotho, A. Madche, B.Motik, D. Oberle, C. Schmitz, S. Staab, L. Stojanovic, N.Stojanovic, R. Studer, Y. Sure, R. Volz, V. Zacharia, TheKarlsruhe View on Ontologies. Technical Report, Universityof Karlsruhe, Institute AIFB, Germany, 2003.
[16] P. Cimiano, Ontology Learning and Population from Text,Springer-Verlag, 2006.
[17] A. Gómez-Pérez, M. Fernández-López, O. Corcho, OntologicalEngineering, 2nd printing, Springer, Verlag, 2004.
[18] S. Bechhofer, F. van Harmelen, J. Hendler, I. Horrocks, D.McGuinees, D. Patel-Schneider, L. Stein, OWL Web OntologyLanguage Reference [http://www.w3.org/TR/owl-re].(Accessed May 2009).
[19] D. Fensel, The Semantic Web and Its Languages, IEEEIntelligent Systems 15 (6) (2000), pp. 67–63.
[20] S. Staab, H.P. Schnurr, R. Studer, Y. Sure, Knowledgeprocesses and ontologies, IEEE Intelligent Systems 16 (1)(2001) 26–34.
[21] A. Maedche, S. Staab, Ontology learning for the semanticweb, IEEE Intelligent Systems 16 (2) (2001) 72–79 (SpecialIssue on Semantic Web).
[22] D. Sánchez, A. Moreno, Learning non-taxonomicrelationships from web documents for domain ontologyconstruction, Data Knowledge Engineering 63 (3) (2008)600–623.
[23] N.F. Noy, R.W. Fergerson, M.A. Musen, The knowledge modelof Protégé-2000: combining interoperability, in: Proceedingsof the 12th International Conference in KnowledgeEngineering and Knowledge Management, Germany, 2000,pp. 17–32.
[24] K. Gibert, A. Valls, L. Lhotska, P. Aubrecht, Privacy preservingand use of medical information in a multiagent system, in:
A. Solanas, A. Martínez-Ballesté (Eds.), Advances in ArtificialIntelligence for Privacy Protection and Security, Series onIntelligent Information Systems, World Scientific, 2009, p. 1.[25] L. Lhotská, P. Aubrecht, A. Valls, K. Gibert, Securityrecommendations for implementation in distributed
f o r m a t i c s 7 9 ( 2 0 1 0 ) 370–387 387
healthcare systems, in: Proceedings of the 42th IEEEInternational Carnahan Conference on Security Technology,Czech Republic, October, 2008, pp. 76–83.
[26] D. Riano, The SDA* Model: a set theory approach, in:Proceedings of the 20th IEEE International Symposium onComputer-Based Medical Systems, Maribor, Slovenia, 2007,pp. 563–568.
[27] D. Isern, M. Millan, A. Moreno, G. Pedone, L. Varga,Agent-based execution of individual intervention plans, in:Proceedings of the 5th Workshop of Agents Applied inHealthcare collocated with AAMAS08, Estoril, Portugal, July,2008.
[28] M. Batet, K. Gibert, A. Valls, The data abstraction layer asknowledge provider for a medical multi-agent system,Lecture Notes on Artificial Intelligence: K4Care 2007 4924(2008) 86–100.
[29] P. Aubrecht, K. Matousek, L. Lhotská, On designing an EHCRrepository, in: Proceedings of the First InternationalConference on Health Informatics, vol. 2, Funchal, Madeira,January, 2008, pp. 280–285.
[30] F. Real, F. Campana, S. Ercolani, R. Annicchiarico, Anontology for the care of the elder at home, in: Proceedings ofthe Workshop K4HelP ECAI08, Patras, Greece, July, 2008.
[31] M. Wooldridge, An Introduction to Multiagent Systems, 2ndedition, John Wiley and Sons, Ltd., West Sussex, England,2009.
[32] A. Hajnal, A. Moreno, G. Pedone, D. Riano, L. Varga, The roleof knowledge in designing an agent platform for home care,in: Proceedings of the 2nd International Conference onKnowledge Management in Organizations, University ofLecce, Italy, September 10–11, 2007, p. 16.
[33] P. Tomassini, F. Campana, Validation and Assessment ofPlatform – II, Deliverable D12.2, 2009.
[34] Y. Malhotra, D.F. Galletta, Extending the technologyacceptance model to account for social influence: theoreticalbases and empirical validation, in: Proceedings of the 32ndHawaii International Conference on System Sciences, 1999.
[35] P. Yu, L. Haocheng, M.P. Gagnon, Health IT acceptancefactors in long-term care facilities: a cross-sectional survey,International Journal of Medical Informatics 78 (2009)219–229.
[36] J. Casals, K. Gibert, A. Valls, Enlarging a medical actor profileontology with new care units, Lecture Notes on ArtificialIntelligence: K4Care 2007 4924 (2008) 101–116.
[37] M. Batet, A. Valls, K. Gibert, S. Martínez, E. Morales,Automatic tailoring of an actor profile ontology, LectureNotes in Artificial Intelligence 5626 (2009) 104–122.
Europe: the K4Care platform, in: Proceedings of the 18thEuropean Conference on Artificial Intelligence, SystemDemonstrations, ECCAI, Patras, Greece, 2008,pp. 11–12.




















