
Progression of Computational Thinking Skills Demonstrated ...
Upload
independentCategory
view
0download
0
Use of structural imaging to study theprogression of Alzheimer's disease
A David Smith and Kim A JobstOxford Project to Investigate Memory and Ageing (OPTIMA), University Departments ofPharmacology and Radiology, University of Oxford and Radcliffe Infirmary Trust, Oxford, UK
Computed tomographic scans in the temporal lobe orientation are a valuable wayof studying the medial temporal lobe. In patients with histopathologically-confirmed Alzheimer's disease the size of the medial temporal lobe is almost halfthat in age-matched controls and the rate of atrophy shown by yearly scans (15%per year) is 10-fold greater. Such a rapid rate of atrophy probably follows acatastrophic event in the brain indicating that Alzheimer's disease is distinct fromaccelerated normal ageing.The degree of medial temporal lobe atrophy is relatedto the density of neurofibrillary tangles in the hippocampus; it is a useful guide todiagnosis and has potential as a screening tool in populations. It is proposed thatmeasurement of the rate of atrophy in asymptomatic individuals may be a predictorof Alzheimer's disease and could be used to monitor the effectiveness of therapiesdesigned to retard the rate of neurodegeneration.
Postal address:Prof AD Smith,
University Departmentof Pharmacology,
Mansfield Road, OxfordOKI 3QT, UK
The diagnosis and assessment of dementia is still largely based uponclinical and neuropsychological criteria and Alzheimer's disease (AD), inparticular, is usually diagnosed by exclusion of other known causes ofdementia. The accuracy of clinical diagnostic procedures when assessedby subsequent histopathology is poor, since they either provide a highdiagnostic sensitivity but low specificity, or a high specificity but lowsensitivity1. The need for a biological marker is obvious: firstly, as a guideto diagnosis in life and, secondly, for monitoring the progression of thedisease and the effectiveness of any therapy. The discovery of mutationsin genes on chromosomes 1, 14 and 21 in the rare familial early-onsetforms of AD has identified 'trait' markers that will be of value incounselling (see chapter by Craddock & Owen). However, the search fora biological marker for the common non-familial (sporadic) form of ADis strewn with false trails and with misleading claims. A recent example isthe discovery that the epsilon 4 allele for apolipoprotein E is morecommon in subjects with sporadic AD than in the population as a whole.A dose-dependent effect of this allele upon the age of onset of AD hasbeen shown and it is clearly established as a powerful risk factor for AD(see chapter by Craddock &c Owen). However, it is not a biologicalmarker for the disease since about a quarter of those with pathologically-
Rritith M<H£COI Bulletin 1996;52 (No. 3):575-58<S ©Th« British Council 1996
by guest on July 13, 2011bm
b.oxfordjournals.orgD
ownloaded from

Biological psychiatry
confirmed AD do not have the epsilon 4 allele and not everyone whocarries this allele develops AD2. While the discovery of geneticallydetermined risk factors is very important for our understanding of ADand for the development of new therapies, such 'trait' markers are of novalue in the study of the progression of the disease and its response totreatment. Is it possible to identify a 'state' marker that is related to thedisease process itself? If so, how early can this marker be detected andhow is it related to the progression of the disease? In this chapter, weshow that neuroimaging methods can provide such markers and that, inparticular, a simple application of X-ray computed tomography (CT) hasclinical value in the assessment of dementia.
Early neuroimaging studies in Alzheimer's disease
Soon after their introduction to medicine, both functional and structuralimaging methods were applied to the study of patients with dementia.Differences were reported between subjects with dementia of Alzheimer'stype (DAT) and age-matched controls, but the field has not been withoutcontroversy. One of the main problems is that almost all studies haveused clinical criteria rather than histopathological criteria for diagnosisand, furthermore, the majority have been cross-sectional in nature. Weshall briefly summarise the salient features of early studies. Throughoutwe shall use DAT as an abbreviation for clinically diagnosed dementia ofAlzheimer's type and AD for histopathologically confirmed Alzheimer'sdisease.
Functional imaging (see chapter by Goodwin)
Early studies in Lund, followed by more recent tomographic studies,showed that patients with DAT had focal reductions in blood flow,glucose metabolism and oxygen uptake notably in the lateral temporaland inferior parietal lobes of the neocortex3-4. However, few functionalimaging studies have been longitudinal and fewer still have followed thesubjects to necropsy for definitive histopathological diagnoses. Accord-ingly, the precise diagnostic value of functional imaging remains to beestablished. OPTIMA'S ongoing studies5"7 show that single-photon-emission computed tomography (SPECT) evidence of hypoperfusion inthe parietotemporal region occurred in 87% of 54 cases with confirmedAD, that it was less common in other dementias and very rare inconfirmed controls. Thus, functional imaging has considerable potentialas a biological marker for AD.
5 7 6 BriHth Mmdical Bulletin 1996;52 (No. 3)
by guest on July 13, 2011bm
b.oxfordjournals.orgD
ownloaded from

Structural imaging in Alzheimer's disease
Structural imaging
Are the functional deficits in the parietotemporal cortex in AD simply theconsequence of focal atrophy of this region due to local pathology? Sincethe 1970s, there have been many CT studies that have searched forevidence of focal atrophy in the brains of subjects with DAT8'9. Thesearch was complicated by the overlap between changes common to ADand normal ageing and because cases were only diagnosed clinically. Theoverall conclusion from cross-sectional studies on standard axial CTscans is that focal atrophy is not consistently found, although subjectswith DAT may show a greater degree of generalised atrophy revealed bysulcul enlargement and ventricular dilatation, leading DeCarli et a/.8 toconclude in 1990: 'unfortunately, at present there is little definiteevidence for clear anatomic brain changes that accurately predict thecognitive dysfunction within a group of patients suffering with DAT...'.In studies where functional and structural imaging have been done in thesame subjects there is agreement that parietotemporal atrophy does notfully explain the selective functional deficit in this region4. The functionaldeficit is mainly due to a local reduction in metabolism in intact tissue4.We have suggested that the reduced metabolism in the parietotemporalregion might arise as a consequence of decreased synaptic activityfollowing the loss of afferent nerve fibres originating from projectionneurons in the medial temporal lobe that are known to degenerate inAD5.
The inability of standard axial CT scans reliably to differentiatesubjects with AD from elderly controls has had two consequences, onepractical and one conceptual. The practical consequence is thatphysicians and radiologists do not use CT scans to look specifically forAD but only to exclude other causes of dementia, such as cerebralinfarcts. The conceptual consequence has been a strengthening of theview that AD and ageing are part of a continuum and that AD is merelythe result of an acceleration of normal ageing processes. It is our beliefthat these views are no longer valid. We shall argue that structuralimaging of the medial temporal lobe shows, firstly, that AD can often bedetected by a simple CT scan and, secondly, that AD is distinct fromaccelerated ageing.
Importance of studying the medial temporal lobe
Neuropathological studies have consistently shown that the highestdensity of neurofibrillary tangles in patients with AD occurs in thehippocampus, subiculum, parahippocampal gyrus and amygdala, struc-
Brrtiih Medico/ Bulletin 199632 (No. 3) 577
by guest on July 13, 2011bm
b.oxfordjournals.orgD
ownloaded from

Biological psychiatry
Fig. 1 Lateraltopogram showing the
standard axial CTangleused internationally
{straight arrow: slices 10-26) and the angle used to
provide the temporallobe orientad view
(curved arrow: slices 2 -9). Note that the temporal
lobe oriented protocolprovides a series of 2 mm
thick contiguous slicesthat reveal the entire
medial temporal lobe inderail, (see Fig. 2).
tures that comprise the medial temporal lobe10. Furthermore, the loss ofneurons from the hippocampal formation is very pronounced11-12, whichleads to a reduction of up to 60% in the volume of this part of the medialtemporal lobe assessed in fixed brain sections13. These pathologicalfindings led Ball et al.XA to suggest that AD is a 'hippocampal dementia'.Why had such striking changes not been reported in the early CT studieson patients with DAT? The answer is that the standard axial CT usedinternationally does not show the medial temporal lobe at all well, mainlybecause of the scan angle used. Changes in the medial temporal lobe itselfhave to be inferred from dilatation of the temporal horns of the lateralventricles and enlargement of the suprasellar cisterns; such changes haveindeed been observed in DAT15-16. By 1988, an alternative camera anglewas in use for evaluating the hippocampus in patients with temporal lobeepilepsy and this angle was applied by de Leon et al.17 to study patientswith DAT. The angle is parallel to the long axis of the temporal lobe andscanning is carried out from below upwards until the inferior margin ofthe orbit is reached; in this way a complete series of images through thetemporal lobe is obtained without exposing the eyes (Fig. 1). Using this'temporal-lobe-oriented' CT procedure, de Leon and his colleagues17
Britith Medical Bulletin 199632 (No. 3)
by guest on July 13, 2011bm
b.oxfordjournals.orgD
ownloaded from

Structural imaging in Alzheimer's disease
~^> found that 8 7 % of patients with moderate to severe DAT showeddilatation of the hippocampal fissure, compared with 2 2 % of age-matched controls. Hippocampal atrophy was also more common in agroup that did not reach the clinical research criteria for DAT but whichshowed minimal memory impairments, leading these authors to suggestthat hippocampal atrophy might be a 'marker' for DAT which has beenshoum both to occur early in the course of the illness and to predictdeterioration in early cases before the diagnosis is established17.
This important preliminary report raised two key questions: first, ishippocampal atrophy as detected by neuroimaging in DAT a validmarker for histopathologically-confirmed AD; second, if so, how early inthe course of the disease can the atrophy be detected? We are well on theway to answering the first question, but to answer the second requireslongitudinal studies lasting many years; such studies are underway inNew York and Oxford.
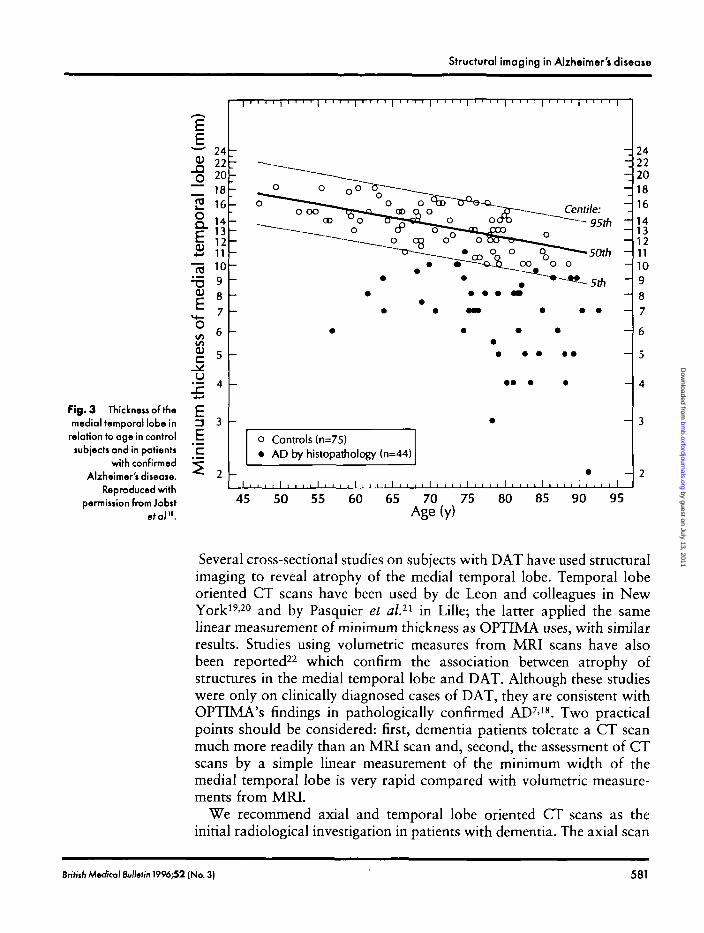
In 1988, the Oxford Project to Investigate Memory and Ageing(OPTIMA) began a longitudinal study in which patients with memoryproblems and age-matched controls, with no evidence of cognitive deficit,are studied by temporal-lobe-oriented CT scans at yearly intervals untildeath, when a definitive histopathological diagnosis is obtained.Assessment of the CT scans is done in as simple a way as possible inorder to obtain a linear measurement that could be applied in a busyradiological department18 . The measurement chosen was the minimumthickness (as judged by eye, but measured with callipers) of the medialtemporal lobe at the level of the brain stem (Fig. 2). A cross-sectionalanalysis in control subjects revealed a logarithmic age-related decline inthis thickness, indicating that the medial temporal lobe normally losesabout 1% of its thickness each year18. However, in 44 cases withpathologically confirmed AD the median thickness was 56% of that inage-matched controls (Fig. 3). The data for the two populations fittedGaussian distributions, which allowed us to predict the sensitivity andspecificity for the detection of AD in life using this measurement alone.The criterion used was a value below the 5th centile for controls of thesame age. Our most recent results, based upon 54 pathologically-confirmed AD cases, 20 cases of other dementias and 108 controls (100living, 8 dead) gave a sensitivity of 9 3 % and specificity of 8 1 % for AD7 .Thus, this very simple radiological procedure can be used as an aid in thediagnosis of AD. When the result from this structural imaging procedureis combined with the functional imaging criterion of a perfusion deficit inthe parietotemporal cortex on SPECT, the accuracy is even greater, witha sensitivity of 8 3 % and a specificity of 9 1 % in the same cohort7 . Inpractice, of course, the results of these radiological investigations and anyother changes revealed by the scans would be combined with detailedclinical findings before arriving at a final diagnosis.
British M«*co( Bulletin 1996^2 {No. 3) 579
by guest on July 13, 2011bm
b.oxfordjournals.orgD
ownloaded from

Biological psychiatry
Fig. 2 Temporal-lobe-oriented CTscans offemale patient with
histopatfiologicalh/-confirmed Alzheimer's
disease. (Note that left ofbrain is on the right.) Top:aged 62 with CAMCOG
score of 66.The minimumthickness of the medial
temporal lobe at the levelof the brain stem was
measured at trie pointsmarked by arrows: left 7.5
mm; right 14 mm. Bottom:same patient 3 years
later, with a CAMCOGscore of 29.
Measurements were left 2mm; right 3.5 mm.
(OPTIMA, unpublished).
580 Bn'h'th Mtdkal Bulletin 1996;52 (No. 3)
by guest on July 13, 2011bm
b.oxfordjournals.orgD
ownloaded from
Structural imaging in Alzheimer's disease
Fig. 3 Thickneu of themedial temporal lobe in
relation to age in controlsubjects and in patients
with confirmedAlzheimer's disease.
Reproduced withpermission from Jobst
efa l" .
<D_Q
0)
(U
E
inCDC
242220
18
16
1413121110
9
8
7
6
5
4
2
l • • ' ' i • ' ' ' l ' ' ' ' l ' '
—
t" ^ •—-•—r - 2 ° ° °̂ =- ° •
o oo or"**-— 0D O
h " °-—-
•-
•
—
—
o Controls (n=75)
• AD by histopathology
_I ' ' ' ' I ' ' ' ' I ' ' ' ' I ' '
OCD
o <
•
•
(n=44)
, I . ,
i I i i i
— - * - — . _
o 4B1 Oi o
°"""o'^ °
i | i . i i
oc- TI r"
oSo"- m °o
#•
, 1 , , ,
•
• • •mm
•••
•
, 1 , , , ,
l i • i . | . i
£——•—fb ^ ^
o
° %OO O
•
•
• a
• •
X J • • • I • •
i i l i i i i I
_
—
-
—
Centile: ~-~~—95th "
—50th -
o —
—
• • —
e • —
• —
• _
. i 1 i i i i 1
2422201816
14131211
10
9
8
7
- 6
- 5
- 4
- 3
- 2
45 50 55 60 65 70 75Age (y)
80 85 90 95
Several cross-sectional studies on subjects with DAT have used structuralimaging to reveal atrophy of the medial temporal lobe. Temporal lobeoriented CT scans have been used by de Leon and colleagues in NewYork19-20 and by Pasquier et al.n in Lille; the latter applied the samelinear measurement of minimum thickness as OPTIMA uses, with similarresults. Studies using volumetric measures from MRI scans have alsobeen reported22 which confirm the association between atrophy ofstructures in the medial temporal lobe and DAT. Although these studieswere only on clinically diagnosed cases of DAT, they are consistent withOPTIMA'S findings in pathologically confirmed AD7'18. Two practicalpoints should be considered: first, dementia patients tolerate a CT scanmuch more readily than an MRI scan and, second, the assessment of CTscans by a simple linear measurement of the minimum width of themedial temporal lobe is very rapid compared with volumetric measure-ments from MRI.
We recommend axial and temporal lobe oriented CT scans as theinitial radiological investigation in patients with dementia. The axial scan
British Medico/ Bulletin 1996;52 (No. 3) 581
by guest on July 13, 2011bm
b.oxfordjournals.orgD
ownloaded from

Biological psychiatry
can be used to look for other possible causes of dementia, such asmultiple infarcts, tumours and hydrocephalus, and the temporal lobe-oriented scan (in 1.5-2 mm slices) to reveal atrophy of the medialtemporal lobe. MRI volumetric acquisitions are useful in subjects whocan tolerate the procedure and these can be reconstructed in 1-2 mmslices along the long axis of the temporal lobe to give the best view of themedial temporal lobe, which can then be measured in exactly the sameway as from a temporal-lobe-oriented CT.
Longitudinal structural imaging
A question of considerable clinical importance is: how early in the courseof AD can structural imaging reveal a difference between age-relatedtissue loss and atrophy caused by the disease? If the atrophic process canbe detected early enough, before the symptoms are serious, a therapyaimed at arresting the neurodegeneration could then be applied.Longitudinal studies are needed to answer this question, with serialscans on subjects who should ideally be followed to necropsy.
The first detailed longitudinal studies were of the size of the lateralventricles. These showed a much greater rate of dilatation of theventricles in subjects with DAT than in age-matched controls23"26. Indeed,it was suggested that the rate of dilatation was a better discriminator ofDAT than the absolute size of the ventricle26. Clearly, once hydro-cephalus is excluded, the dilatation of the ventricles must be due to a lossof brain tissue. Indeed, comparison of longitudinal measurements of thethickness of the medial temporal lobe in controls and in subjects found tohave AD reveal a dramatic 10-fold greater rate of atrophy of the medialtemporal lobe in AD cases (Fig. 4). The average rate of atrophy in 47controls was 1.5% per year, while in 20 subjects with AD it was 15.1%per year27. An example of the change occurring over 3 years in a patientwith AD is shown in Figure 2. Such findings led us to suggest that AD-related atrophy follows a 'catastrophic event' in the brain and that it isdistinct from an acceleration of normal age-related atrophy27. Thisdistinction between AD and normal ageing was also made by West etal.n as a result of their finding that the CA1 pyramidal cell group in thehippocampus shows a marked loss of neurons in AD but not in normalageing. It is noteworthy that the neurofibrillary tangle density in thepyramidal cell layer of the hippocampus correlates both with the extentof atrophy assessed by CT scans in life and with the degree of memoryimpairment28. Thus, there is a direct correlation between a measurementmade by imaging in life and one of the principle histopathologicalmarkers for AD.
582 British Medical BulUtin 1996;52 (No. 3)
by guest on July 13, 2011bm
b.oxfordjournals.orgD
ownloaded from

Structural imaging in Alzheimer's disease
Fig. 4 Thickness of themedial temporal lobe inrelation to age at yearly
intervals in individualsubjects. Dotted lines
show 5% and 95%prediction limits Forage-
related atrophy from apopulation of 75 controls
(see Fig. 3). DAT: dementiaof Alzheimer's type,
clinical diagnosis; AD:histopathologicalhy-
confirmed Alzheimer'sdisease.Controls shown
are those who have diedand have no evident brainpathology. Modified from
Jobstef aF.
EE,0) 24
-D 22_2 20
1816
15
14fc 13
Si 12
_ 11.23 10"° 9E 8
^ 70)C 5
L 95f/i centile for controls
5th centile" 'for controls
D Control: no pathologyO Patient: not DAT• DAT* AD by histopathology
2422201816
1413121110987
45 50 55 60 65 70 75 80 85 90 95
Age (y)
Furthermore, the rapid atrophy of the medial temporal lobe in AD isassociated with a rapid rate of cognitive decline27, raising the questionwhether early detection of atrophy could be used to predict cognitivedecline in an individual subject. Cross-sectional studies show a greaterdegree of hippocampal atrophy in subjects with mild memoryimpairments than in age-matched normal controls29"31. A follow upof 32 such memory-impaired subjects showed that 23 (72%) reachedthe criteria for probable DAT after 4 years20. These findings areconsistent with the hypothesis that focal hippocampal atrophy insubjects with mild cognitive impairment is a predictor of DAT32, butthey do not tell us whether a rapid rate of atrophy in asymptomaticindividuals would be a predictor of DAT. Systematic longitudinalimaging studies in normal subjects over many years are needed toanswer this question.
Sn'hsh Medical Bulletin 1996^2 (No. 3) 583
by guest on July 13, 2011bm
b.oxfordjournals.orgD
ownloaded from

Biological psychiatry
Clinical value of the assessment of medial temporallobe atrophy
We believe that atrophy of the medial temporal lobe revealed bystructural imaging is a 'state' marker for AD and that its quantitativeassessment has several potential applications. Such measurements shouldalways be related to values for age-matched controls to avoid theconfounding effect of age-related tissue loss18'33 and should only be usedclinically in the context of the full clinical and radiological picture34.
Screening for AD in populations
Although AD is not the only cause of atrophy of the medial temporallobe18, it is likely to be by far the commonest cause in the elderly. Thus,screening for such atrophy could be used to estimate the prevalence ofAD in different populations. Such screening should use a cut-off valuethat gives a very low false-positive rate: e.g. for the linear measure ofmedial temporal lobe thickness from CT, a cut-off value yielding a 1 %false-positive rate will still detect 79% of cases of AD18. If the prevalenceof AD in one population is 5% and in another it is 10%, then it would besufficient to scan approximately 1000 subjects in each population todetect this difference at p<0.05 with a power of 0.85.
Diagnosis of AD
As described above, temporal lobe-oriented CT scans are a valuable aidto diagnosis and in our experience such scans are particularly useful insubjects with early symptoms and in those in whom it is difficult clinicallyto distinguish DAT from dementia associated with depression or otherpsychiatric or organic conditions.
Progression of Alzheimer's disease
The rapid rate of atrophy of the medial temporal lobe that ischaracteristic of AD may be a marker for the progression of the diseaseand so its measurement by CT or MRI would be a valuable way ofmonitoring the effectiveness of therapies designed to slow or arrest theneurodegenerative process.
5 8 4 Brihsh Mtdkal BulUtin 1996^2 (No. 3}
by guest on July 13, 2011bm
b.oxfordjournals.orgD
ownloaded from

Structural imaging in Alzheimer's disease
Prediction of AD
References
We suggest that a rapid rate of atrophy of structures in the medialtemporal lobe in asymptomatic individuals might be a marker for thesubsequent development of AD. Our suggestion is consistent withOPTIMA'S preliminary findings on asymptomatic subjects (̂ -B-27. andunpublished) and those of Fox et al.35 on two subjects with familial DAT.Further work is required to test this hypothesis.
1 Kukull WA, Larson EB, Reifler BV et al. The validity of 3 clinical diagnostic criteria forAlzheimer's disease. Neurology 1990; 40: 1364-9
2 Roses AD, Strittmatter WJ, Pericak-Vance MA et al. Clinical application of apolipoprotein Egenotyping to Alzheimer's disease. Lancet 1994; 343: 1564-5
3 Frackowiak S. Measurement and imaging of cerebral function in ageing and dementia. ProgBrain Res 1986; 70: 69-85
4 Waldemar G. Functional brain imaging with SPECT in normal aging and dementia:methodological, pathophysiological, and diagnostic aspects. Cerebrovasc Brain Metab Rev1995; 7: 89-130
5 Jobst KA, Smith AD, Barker CS et al. Association of atrophy of the medial temporal lobe withreduced blood flow in the posterior parietotemporal cortex in patients with a clinical andpathological diagnosis of Alzheimer's disease. / Neur.ol Neurosurg Psychiatry 1992; 55: 190—4
6 Jobst KA, Hindley NJ, King E., Smith AD. The diagnosis of Alzheimer's disease: a question ofimage?/ Clin Psychiatry 1994; 55 (suppl.): 22-31
7 Jobst KA, Smith AD, Shepstone BJ, Hindley NJ. The diagnosis of Alzheimer's disease: a matterof image? Alzheimer's Res 1995; 1 (suppl. 1): 8
8 DeCarli C, Kaye JA, Horwitz B et al. Critical analysis of the use of computer-assisted transverseaxial tomography to study human brain in aging and dementia of the Alzheimer type.Neurology 1990; 40: 872-83
9 Burns A, Pearlson G. Computed tomography. In: Burns A, Levy R (eds) Dementia. London:Chapman & Hall Medical, 1994; 407-26
10 Arnold SE, Hyman BT, Flory J et al. The topographical and neuroanatomical distribution ofneurofibrillary tangles and neuritic plaques in the cerebral cortex of patients with Alzheimer'sdisease. Cerebral Cortex 1991; 1: 103-16
11 Ball MJ. Neuronal loss, neurofibrillary tangles and granulovacuolar degeneration in thehippocampus with ageing and dementia. A quantitative study. Ada Neuropathol (Berl) 1977;37: 111-8
12 West MJ, Coleman PD, Flood DG et al. Differences in the pattern of hippocampal neuronal lossin normal ageing and Alzheimer's disease. Lancet 1994; 344: 769-72
13 Bobinski M, Wegiel J, Wisniewski HM et al. Atrophy of hippocampal formation subdivisionscorrelates with stage and duration of Alzheimer disease. Dementia 1995; 6: 205-10
14 Ball MJ, Hachinski V, Fox A et al. A new definition of Alzheimer's disease: a hippocampaldementia. Lancet 1985; i: 14-6
15 LeMay M, Stafford JL, Sandor T et al. Statistical assessment of perceptual CT scan ratings inpatients with Alzheimer's type dementia. / Comput Assist Tomomgr 1986; 10: 802-9
16 Kido DK, Caine ED, LeMay M et al. Temporal lobe atrophy in patients with Alzheimer disease:a CT study. Am J Neuroradiol 1989; 10: 551-5
17 de Leon MJ, George AE, Stylopoulos LA et al. Early marker for Alzheimer's disease: theatrophic hippocampus. Lancet 1989; ii: 672-3
Brihih Mtdical Suffah'n 1996;32 (No. 3) 585
by guest on July 13, 2011bm
b.oxfordjournals.orgD
ownloaded from

Biological psychiatry
18 Jobst KA, Smith AD, Szatmari M et al. Detecrion in life of confirmed Alzheimer's disease using asimple measurement of medial temporal lobe atrophy by computed tomography. Lancet 1992;340: 1179-83
19 George AE, de Leon MJ, Stylopoulos LA et al. CT diagnostic features of Alzheimer disease:importance of the choroidal/hippocampal fissure complex. Am J Neuroradiol 1990; 11: 101-7
20 De Leon MJ, Golomb J, George AE et al. The radiologic prediction of Alzheimer disease-theatrophic hippocampal formation. Am J Neuroradtol 1993; 14: 897-906
21 Pasquier F, Bail L, Lebert F et al. Determination of medial temporal lobe atrophy in earlyAlzheimer's disease with computed tomography. Lancet 1994; 343: 861—2
22 O'Brien JT. Is hippocampal atrophy on magnetic resonance imaging a marker for Alzheimer'sdisease? Int ] Geriatr Psychiatry 1995; 10: 431-5
23 Luxenberg JS, Haxby JV, Creasey H et al. Rate of ventricular enlargement in dementia of theAlzheimer type correlates with rate of neuropsychological deterioration. Neurology 1987; 37:1135^0
24 De Leon MJ, George AE, Reisberg B et al. Alzheimer's disease: longitudinal CT studies ofventricular change. Am J Neuroradiol 1989; 10: 371-6
25 Burns A, Jacoby R, Levy R. Computed tomography in Alzheimer's disease-a longitudinalstudy. Biol Psychiatry 1991; 29: 383-90
26 DeCarli C, Haxby JV, Gillette JA et al. Longitudinal changes in lateral ventricular volume inpatients with dementia of the Alzheimer type. Neurology 1992; 42: 2029-36
27 Jobst KA, Smith AD, Szatmari M et al. Rapidly progressing atrophy of medial temporal lobe inAlzheimer's disease. Lancet 1994; 343: 829-30
28 Nagy Z, Jobst KA, Esiri MM et al. Flippocampal pathology reflects memory deficit and brainimaging measurements in Alzheimer's disease: clinicopathological correlations using three sets ofpathologic diagnostic criteria. Dementia 1996; 7: 76-81
29 Convit A, de Leon MJ, Golomb J et al. Hippocampal atrophy in early Alzheimer's disease:anatomic specificity and validation. Psychiatry Q 1993; 64: 371-87
30 Convit A, Deleon MJ, Tarshish C et al. Hippocampal volume losses in minimally impairedelderly. Lancet 1995; 345: 266
31 Launer LJ, Scheltens P, Lindeboom J et al. Medial temporal lobe atrophy in an open populationof very old persons: cognitive, brain atrophy, and sociomedical correlates. Neurology 1995; 45:747-52
32 Convit A, de Leon M, Tarshish C et al. Hippocampal atrophy and cognitive impairment. Lancet1995; 345: 992
33 Smith AD. Hippocampal atrophy and cognitive impairment. Lancet 1995; 345: 99234 Philpot M, Bums A. Jobst et al. Detection in life of confirmed Alzheimer's disease using a simple
measurement of medial temporal lobe atrophy by computed tomography'. Br ] Psychiatry 1993163: 809-12
35 Fox NC, Warrington EK, Stevens JM, Rossor MN. Atrophy of the hippocampal formation inearly familial Alzheimer's disease: a longitudinal MRI study of at risk members of a family withan amyloid precursor protein 717va[_giy mutation. In: Growdon JH, Nitsch RM, Corkin S,Wurtman RJ (eds) The Neurobiology of Alzheimer's Disease. Proc 8th meeting Int Study Groupon Pharmacology of Memory Disorders. Zurich, Switzerland: 1995; 269-74
586 Bntiih Mtdical BuH.hn 1996^2 (No. 3)
by guest on July 13, 2011bm
b.oxfordjournals.orgD
ownloaded from
Copyright © 2022 FDOKUMEN




















