
Use of Procalcitonin-Guided Decision-Making to Shorten Antibiotic Therapy in Suspected Neonatal...
10
Fax +41 61 306 12 34 E-Mail [email protected] www.karger.com Original Paper Neonatology 2010;97:165–174 DOI: 10.1159/000241296 Use of Procalcitonin-Guided Decision-Making to Shorten Antibiotic Therapy in Suspected Neonatal Early-Onset Sepsis: Prospective Randomized Intervention Trial Martin Stocker a Matteo Fontana a Salhab el Helou a Karl Wegscheider b Thomas M. Berger a a Neonatal and Pediatric Intensive Care Unit, Children’s Hospital of Lucerne, Switzerland, and b Department of Medical Biometry and Epidemiology, University Medical Center Hamburg-Eppendorf, Germany tors for early-onset sepsis, likelihood of infection as assessed by the attending physician and early conventional labora- tory findings. There was a significant difference in the pro- portion of newborns treated with antibiotics 672 h between the standard group (82%) and the PCT group (55%) (absolute risk reduction 27%; odds ratio 0.27 (95% CI 0.12–0.62), p = 0.002). On average, PCT-guided decision-making resulted in a shortening of 22.4 h of antibiotic therapy. Clinical outcome was similar and favorable in both groups but sample size was insufficient to exclude rare adverse events. Conclusion: Se- rial PCT determinations allow to shorten the duration of an- tibiotic therapy in term and near-term infants with suspect- ed early-onset sepsis. Before this PCT-guided strategy can be recommended, its safety has to be confirmed in a larger cohort of neonates. Copyright © 2009 S. Karger AG, Basel Introduction In neonates, clinical signs and symptoms associated with early-onset sepsis are non-specific and currently available laboratory tests have poor positive and negative predictive values. Delay in antibiotic treatment of infect- ed neonates carries a substantial risk, both in terms of mortality and morbidity. Therefore, newborns with sus- pected sepsis (based on clinical signs and/or perinatal/ Key Words Antibiotic therapy Early-onset sepsis Intervention study Procalcitonin Term and near-term neonates Abstract Background: Diagnosis of neonatal early-onset sepsis is dif- ficult because clinical signs and laboratory tests are non- specific. Early antibiotic therapy is crucial for treatment suc- cess. Objective: To evaluate the effect of procalcitonin (PCT)-guided decision-making on duration of antibiotic therapy in suspected neonatal early-onset sepsis. Methods: This single-center, prospective, randomized intervention study was conducted in a tertiary neonatal and pediatric in- tensive care unit in the Children’s Hospital of Lucerne, Swit- zerland, between June 1, 2005 and December 31, 2006. All term and near-term infants (gestational age 634 weeks) with suspected early-onset sepsis were randomly assigned either to standard treatment based on conventional labora- tory parameters (standard group) or to PCT-guided treat- ment (PCT group). Minimum duration of antibiotic therapy was 48–72 h in the standard group, whereas in the PCT group antibiotic therapy was discontinued when two consecutive PCT values were below predefined age-adjusted cut-off val- ues. Results: 121 newborns were randomly assigned either to the standard group (n = 61) or the PCT group (n = 60). The two groups were similar for baseline demographics, risk fac- Received: July 24, 2008 Accepted after revision: February 9, 2009 Published online: September 24, 2009 formerly Biology of the Neonate Martin Stocker, MD Pediatric Intensive Care Unit Royal Brompton Hospital, Sydney Street London SW3 6NP (UK) Tel. +41 79 373 67 19, E-Mail [email protected] © 2009 S. Karger AG, Basel 1661–7800/10/0972–0165$26.00/0 Accessible online at: www.karger.com/neo
Transcript of Use of Procalcitonin-Guided Decision-Making to Shorten Antibiotic Therapy in Suspected Neonatal...

Fax +41 61 306 12 34E-Mail [email protected]
Original Paper
Neonatology 2010;97:165–174 DOI: 10.1159/000241296
Use of Procalcitonin-Guided Decision-Making to Shorten Antibiotic Therapy in Suspected Neonatal Early-Onset Sepsis: Prospective Randomized Intervention Trial
Martin Stocker a Matteo Fontana a Salhab el Helou a Karl Wegscheider b
Thomas M. Berger a
a Neonatal and Pediatric Intensive Care Unit, Children’s Hospital of Lucerne , Switzerland, and b Department of Medical Biometry and Epidemiology, University Medical Center Hamburg-Eppendorf , Germany
tors for early-onset sepsis, likelihood of infection as assessed by the attending physician and early conventional labora-tory findings. There was a significant difference in the pro-portion of newborns treated with antibiotics 6 72 h between the standard group (82%) and the PCT group (55%) (absolute risk reduction 27%; odds ratio 0.27 (95% CI 0.12–0.62), p = 0.002). On average, PCT-guided decision-making resulted in a shortening of 22.4 h of antibiotic therapy. Clinical outcome was similar and favorable in both groups but sample size was insufficient to exclude rare adverse events. Conclusion: Se-rial PCT determinations allow to shorten the duration of an-tibiotic therapy in term and near-term infants with suspect-ed early-onset sepsis. Before this PCT-guided strategy can be recommended, its safety has to be confirmed in a larger cohort of neonates. Copyright © 2009 S. Karger AG, Basel
Introduction
In neonates, clinical signs and symptoms associated with early-onset sepsis are non-specific and currently available laboratory tests have poor positive and negative predictive values. Delay in antibiotic treatment of infect-ed neonates carries a substantial risk, both in terms of mortality and morbidity. Therefore, newborns with sus-pected sepsis (based on clinical signs and/or perinatal/
Key Words
Antibiotic therapy � Early-onset sepsis � Intervention study � Procalcitonin � Term and near-term neonates
Abstract
Background: Diagnosis of neonatal early-onset sepsis is dif-ficult because clinical signs and laboratory tests are non-specific. Early antibiotic therapy is crucial for treatment suc-cess. Objective: To evaluate the effect of procalcitonin (PCT)-guided decision-making on duration of antibiotic therapy in suspected neonatal early-onset sepsis. Methods: This single-center, prospective, randomized intervention study was conducted in a tertiary neonatal and pediatric in-tensive care unit in the Children’s Hospital of Lucerne, Swit-zerland, between June 1, 2005 and December 31, 2006. All term and near-term infants (gestational age 6 34 weeks) with suspected early-onset sepsis were randomly assigned either to standard treatment based on conventional labora-tory parameters (standard group) or to PCT-guided treat-ment (PCT group). Minimum duration of antibiotic therapy was 48–72 h in the standard group, whereas in the PCT group antibiotic therapy was discontinued when two consecutive PCT values were below predefined age-adjusted cut-off val-ues. Results: 121 newborns were randomly assigned either to the standard group (n = 61) or the PCT group (n = 60). The two groups were similar for baseline demographics, risk fac-
Received: July 24, 2008 Accepted after revision: February 9, 2009 Published online: September 24, 2009
formerly Biology of the Neonate
Martin Stocker, MD Pediatric Intensive Care Unit Royal Brompton Hospital, Sydney Street London SW3 6NP (UK) Tel. +41 79 373 67 19, E-Mail [email protected]
© 2009 S. Karger AG, Basel1661–7800/10/0972–0165$26.00/0
Accessible online at:www.karger.com/neo
Jana
Copyright hoch

Stocker /Fontana /el Helou /Wegscheider /Berger
Neonatology 2010;97:165–174166
neonatal risk factors) are commonly treated with broad-spectrum antibiotics (usually ampicillin and an amino-glycoside) until infection can be safely excluded [1] . ‘Rule out sepsis’ is one of the most common discharge diagno-ses in near-term and term infants admitted to the neona-tal intensive care unit [2] . Unnecessary long-term use of broad-spectrum antibiotics is a serious concern because it can promote the development of resistant bacteria, pro-long hospitalization and increase costs.
Procalcitonin (PCT) is a precursor peptide of the hor-mone calcitonin. The physiological function of PCT is unknown. In bacterial infections, plasma PCT concen-trations increase from 0.001–0.01 ng/ml (baseline range) to values ranging from 1 to 1,000 ng/ml. After injection of endotoxins, PCT concentrations rise within 6–8 h and reach a plateau after approximately 12 h. This is a faster response than that seen in C-reactive protein (CRP) which reaches maximal values after approximately 48 h [3] . Because of its kinetics, we hypothesize that PCT could be a better parameter than CRP to guide duration of an-tibiotic therapy.
In healthy adults, plasma PCT concentrations are very low, mostly ! 0.01 ng/ml. Normal birth and extrauterine adaptation stimulate an acute phase reaction in the new-born infant with release of PCT and other acute phase proteins [4] . In healthy neonates, plasma PCT concentra-tions increase gradually after birth, reach peak values at about 24 h of age (mean 1.5–2.5 ng/ml, range 0.1–20 ng/ml) and then decrease to normal values below 0.5 ng/ml by 48–72 h of age [4–6] . In newborns admitted to the neo-natal intensive care unit with clinical signs of respiratory distress without infection, peak plasma PCT concentra-tions at 48 h of age have been reported to be higher (mean 3–4 ng/ml) with large interindividual variations (range 0.2–20 ng/ml) [5, 7–10] .
Previous studies on the use of PCT as a marker of neo-natal sepsis suggested that PCT could be useful. However, the results of several observational studies are contradic-tory [5, 7, 8, 11–19] . With our prospective intervention study, we wanted to test the efficacy of PCT-guided deci-sion-making on the duration of antibiotic therapy and outcome in neonatal early-onset sepsis.
Methods
Study Design and Setting This study was designed as a single-center, prospective, ran-
domized intervention study. The study was approved by the local ethics committee for human studies. Parental informed consent was obtained for all study neonates. BRAHMS Diagnostica (Ber-
lin, Germany) provided the testing kits for PCT determinations but was not involved in any other aspects of the study and manu-script preparation. The study has been registered at ClinicalTrial.gov.
We hypothesized that PCT-guided decision-making allows to shorten the duration of empiric antibiotic therapy in suspected neonatal early-onset sepsis with unchanged outcome. The pri-mary endpoint was the proportion of infants treated with antibi-otics for 6 72 h (efficacy of study intervention). The co-primary endpoint was the absolute reduction of the duration of antibiotic therapy (quantitative version of the primary endpoint for estima-tion of effect size). Safety endpoints were survival and recurrence of infection requiring additional courses of antibiotic therapy in the first month of life. For comparison of recurrence of infection, the proportion of infants treated with antibiotics 6 120 h was cal-culated (non-inferiority test of the PCT group). Regardless of treatment duration, observation periods were the same in both groups with a minimum of 3 days of hospitalization and a follow-up interview after 1 month (telephone interview about intercur-rent illness, physician visits, medications and hospitalizations).
Patients Between June 1, 2005 and December 31, 2006, term and near-
term infants with a gestational age 6 34 weeks admitted to the Children’s Hospital of Lucerne (tertiary center adjacent to a ma-ternity hospital) with suspected early-onset sepsis in the first 3 days of life requiring empiric antibiotic therapy (ampicillin and gentamicin) were eligible for the study and randomly assigned either to standard care (standard group) or PCT-guided decision-making (PCT group). Randomization was accomplished by draw-ing group assignment cards in opaque-sealed envelopes. Exclu-sion criteria were severe congenital malformations, chromosom-al abnormalities and surgery in the first 3 days of life.
Laboratory Examinations The laboratory examinations were performed according to the
schedule shown in figure 1 . White blood count (WBC) with im-mature to total neutrophil ratio (I:T ratio) and CRP concentra-tions were obtained in all patients. Serial PCT measurements were only performed in patients assigned to the PCT group. Plasma PCT concentrations were measured using a time-resolved ampli-fied cryptate emission (TRACE) technology assay (Kryptor � PCT, BRAHMS, Henningsdorf, Germany). Assay time is 19 min, and in the clinical setting, results can be obtained within 1 h with 20–50 � l of plasma or serum [20] .
We defined age-adjusted PCT cut-off values according to the results of previous studies ( fig. 2 a) [5, 7–10] . To provide a margin of safety, the normal upper value of PCT at 18–36 h of age was defined as 10 ng/ml which is about 50% of the highest PCT con-centrations measured in neonates with respiratory distress not related to infection (approx. 20 ng/ml) [5] .
Probability of Infection and Duration of Antibiotic Therapy The probability of infection was assessed by the attending
physician during the hospitalization. Assessments according to predefined guidelines were not the results of a single evaluation but based on maternal risk factors (group B Streptococcus (GBS) positivity, prolonged rupture of membranes (PROM) 1 18 h, cho-rioamnionitis), the evolution of the patient’s clinical symptoms (6 predefined groups of clinical symptoms: (1) respiratory distress/
PCT and Antibiotic Therapy in Neonates Neonatology 2010;97:165–174 167
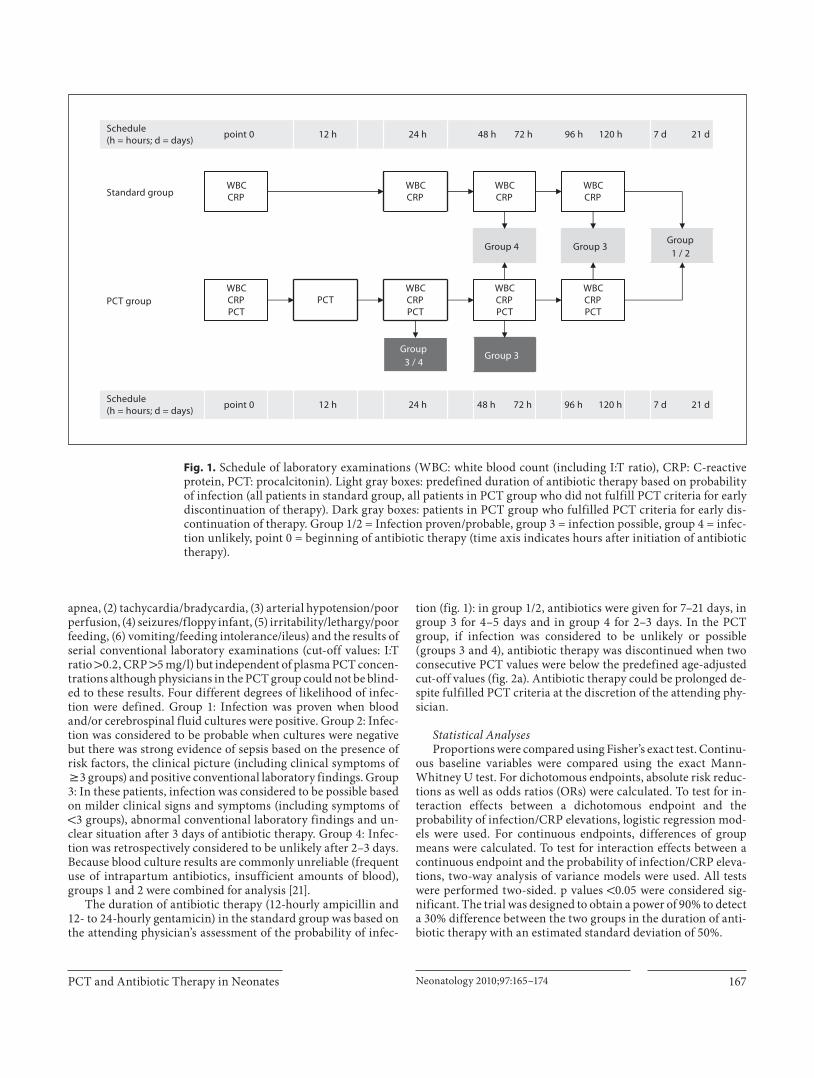
apnea, (2) tachycardia/bradycardia, (3) arterial hypotension/poor perfusion, (4) seizures/floppy infant, (5) irritability/lethargy/poor feeding, (6) vomiting/feeding intolerance/ileus) and the results of serial conventional laboratory examinations (cut-off values: I:T ratio 1 0.2, CRP 1 5 mg/l) but independent of plasma PCT concen-trations although physicians in the PCT group could not be blind-ed to these results. Four different degrees of likelihood of infec-tion were defined. Group 1: Infection was proven when blood and/or cerebrospinal fluid cultures were positive. Group 2: Infec-tion was considered to be probable when cultures were negative but there was strong evidence of sepsis based on the presence of risk factors, the clinical picture (including clinical symptoms of 6 3 groups) and positive conventional laboratory findings. Group 3: In these patients, infection was considered to be possible based on milder clinical signs and symptoms (including symptoms of ! 3 groups), abnormal conventional laboratory findings and un-clear situation after 3 days of antibiotic therapy. Group 4: Infec-tion was retrospectively considered to be unlikely after 2–3 days. Because blood culture results are commonly unreliable (frequent use of intrapartum antibiotics, insufficient amounts of blood), groups 1 and 2 were combined for analysis [21] .
The duration of antibiotic therapy (12-hourly ampicillin and 12- to 24-hourly gentamicin) in the standard group was based on the attending physician’s assessment of the probability of infec-
tion ( fig. 1 ): in group 1/2, antibiotics were given for 7–21 days, in group 3 for 4–5 days and in group 4 for 2–3 days. In the PCT group, if infection was considered to be unlikely or possible (groups 3 and 4), antibiotic therapy was discontinued when two consecutive PCT values were below the predefined age-adjusted cut-off values ( fig. 2 a). Antibiotic therapy could be prolonged de-spite fulfilled PCT criteria at the discretion of the attending phy-sician.
Statistical Analyses Proportions were compared using Fisher’s exact test. Continu-
ous baseline variables were compared using the exact Mann-Whitney U test. For dichotomous endpoints, absolute risk reduc-tions as well as odds ratios (ORs) were calculated. To test for in-teraction effects between a dichotomous endpoint and the probability of infection/CRP elevations, logistic regression mod-els were used. For continuous endpoints, differences of group means were calculated. To test for interaction effects between a continuous endpoint and the probability of infection/CRP eleva-tions, two-way analysis of variance models were used. All tests were performed two-sided. p values ! 0.05 were considered sig-nificant. The trial was designed to obtain a power of 90% to detect a 30% difference between the two groups in the duration of anti-biotic therapy with an estimated standard deviation of 50%.
12 h
PCT
24 h
Group 3 / 4
WBCCRPPCT
12 h 24 h
7 d 21 d
Group 1 / 2
7 d 21 d
96 h 120 h48 h 72 hpoint 0Schedule(h = hours; d = days)
Group 3
Group 3Group 4
WBCCRP
WBC CRP PCT
WBC CRP
96 h 120 h
WBC CRP PCT
WBC CRP
48 h 72 h
WBCCRPPCT
WBCCRP
point 0
Standard group
PCT group
Schedule (h = hours; d = days)
Fig. 1. Schedule of laboratory examinations (WBC: white blood count (including I:T ratio), CRP: C-reactive protein, PCT: procalcitonin). Light gray boxes: predefined duration of antibiotic therapy based on probability of infection (all patients in standard group, all patients in PCT group who did not fulfill PCT criteria for early discontinuation of therapy). Dark gray boxes: patients in PCT group who fulfilled PCT criteria for early dis-continuation of therapy. Group 1/2 = Infection proven/probable, group 3 = infection possible, group 4 = infec-tion unlikely, point 0 = beginning of antibiotic therapy (time axis indicates hours after initiation of antibiotic therapy).

Stocker /Fontana /el Helou /Wegscheider /Berger
Neonatology 2010;97:165–174168
Results
Between June 1, 2005 and December 31, 2006, a total of 126 term and near-term infants were admitted to the Neonatal and Pediatric Intensive Care Unit of the Chil-dren’s Hospital of Lucerne because of suspected early-on-set sepsis in the first 3 days of life and treated with em-piric antibiotic therapy. Of these, 5 were excluded because of missing parental consent (n = 2), protocol errors (n = 2) and surgery during the first 3 days (n = 1). Therefore,
121 patients were randomly assigned either to the stan-dard group (n = 61) or the PCT group (n = 60). The two groups were similar for baseline demographics and risk factors for early-onset sepsis without statistically signifi-cant differences ( table 1 ). Similarly, results of convention-al laboratory examinations and the proportions of in-fants belonging to groups 1–4 were comparable in the standard and the PCT group ( table 2 ).
6 12 18 24 30 36 42 48 54 60 66 72 96 120Hours of age
0.5
0.2
1.0
2.0
5.0
10.0
PCT
(ng
/ml)
sem
ilog
gra
ph 20.0
50.0
100.0Age-adjusted PCT cutoff values
a
6 12 18 24 30 36 42 48 54 60 66 72 96 120
Hours of age
0.5
0.2
1.0
2.0
5.0
10.0
PCT
(ng
/ml)
sem
ilog
gra
ph 20.0
50.0
100.0Infection proven/probable (n = 9)
b
Fig. 2. a Age-adjusted PCT cut-off values (gray boxes = predefined safety range; semilog graph). b PCT values of group 1/2 patients.

PCT and Antibiotic Therapy in Neonates Neonatology 2010;97:165–174 169
Primary Endpoint There was a significant difference in the proportion of
newborns treated with antibiotics 6 72 h between the standard group (82%) and the PCT group (55%) (absolute risk reduction 27%; OR 0.27, 95% CI 0.12/0.62, Fisher’s exact test (two-tailed) p = 0.002). The effect of PCT-guid-ed decision-making was dependent on the probability of infection (interaction p = 0.022) with the most pro-nounced effect in group 3 patients ( table 3 ).
Co-Primary Endpoint Overall, PCT-guided decision-making resulted in a
shortening of antibiotic therapy by an average of 22.4 h (exact Mann-Whitney U test p = 0.004; t test p = 0.012). This effect was also dependent on the probability of in-fection (interaction p = 0.024) ( table 4 ). For validation of these results, we also evaluated the doses of 12-hourly amoxicillin. The results were similar and showed an overall reduction of 1.8 doses of 12-hourly amoxicillin (exact Mann-Whitney U test p = 0.004; t test p = 0.013).
6 12 18 24 30 36 42 48 54 60 66 72 96 120Hours of age
0.5
0.2
1.0
2.0
5.0
10.0
PCT
(ng/
ml)
sem
ilog
grap
h 20.0
50.0
100.0Infection possible (n = 21)
c
6 12 18 24 30 36 42 48 54 60 66 72 96 120Hours of age
0.5
0.2
1.0
2.0
5.0
10.0
PCT
(ng
/ml)
sem
ilog
gra
ph 20.0
50.0
100.0Infection unlikely (n = 30)
d
Fig. 2. c PCT values of group 3 patients. d PCT values of group 4 patients (box-whisker plot: median, box marked by the first and third quartile, whiskers extended to the range, time axis indicates postnatal age in hours).

Stocker /Fontana /el Helou /Wegscheider /Berger
Neonatology 2010;97:165–174170
Table 1. Baseline demographics and risk factors for early-onset sepsis
Standard group(n = 61)
PCT group(n = 60)
p value
Gestational age, weeks, median (range)Birth weight, g, median (range)Female infantsSpontaneous vaginal deliveryVacuum/forceps deliveryPrimary C-sectionSecondary C-sectionArterial cord pH, median (range)Apgar scores, median
1 min5 min
10 minGBS positivePROM >18 hChorioamnionitsNo risk factorsIntrapartum antibioticsAge at initiation of antibiotic therapy, h
median (range)
39.7 (34.0–41.7)3,330 (1,800–4,900)
21 (35)31 (51)
4 (7)10 (16)16 (26)
7.25 (6.95–7.37)
899
19 (31)6 (10)2 (3)
36 (59)22 (36)
7 (2–68)
39.4 (34.4–42.0)3,200 (2,000–4,640)
25 (42)36 (60)
7 (12)6 (10)
11 (18)7.22 (6.97–7.37)
89
1017 (28)12 (20)
3 (5)31 (52)24 (40)
10 (1–60)
0.810.890.340.360.360.420.380.22
ns
0.840.130.680.470.81
0.23
Values are numbers with percentages in parentheses unless otherwise indicated.GBS = Group B Streptococcus; PROM = prolonged rupture of membranes.p values of two-sided Mann-Whitney U test (p < 0.05 = significant, ns = not significant).
Table 2. Assessment of probability of infection* and early conventional laboratory findings
Standard group(n = 61)
PCT group(n = 60)
p value
WBC in G/l at time point 0, mean [range]WBC in G/l at time point 24 h, mean [range]I:T ratio 1 0.2 at time point 0, n (%)I:T ratio 1 0.2 at time point 24 h, n (%)Platelets in G/l at time point 0, mean [range]Platelets in G/l at time point 24 h, mean [range]CRP 1 5 mg/l at time point 0, n (%) [range]CRP 1 5 mg/l at time point 24 h, n (%) [range]Infection probable/proven, n (%)Infection possible, n (%)Infection unlikely, n (%)
17.6 [4.9–41.0]17.4 [6.1–35.0]
43 (70)21 (34)
235 [89–473]247 [94–487]
20 (33) [6–45]37 (61) [6–116]
11/1* (20)19/1 (31)30/1 (49)
16.9 [3.1–35.0]15.9 [3.2–41.7]
40 (67)20 (33)
243 [102–385]262 [103–384]
21 (35) [6–180]42 (70) [6–159]
9/0 (15)21/ (35)30/ (50)
0.900.130.240.270.230.160.850.340.630.701.0
WBC = White blood cell count; CRP = C-reactive protein; I:T ratio = immature to total neutrophil ratio.* Infection proven with Staphylococcus hominis in blood culture. p values of two-sided Mann-Whitney U test (p < 0.05 = significant).

PCT and Antibiotic Therapy in Neonates Neonatology 2010;97:165–174 171
Because gentamicin dosing is gestational age specific, it was not possible to calculate reductions in gentamicin dosing.
Relation of PCT and CRP In an additional analysis, the clinical judgment of the
likelihood of infection was replaced by the observer-in-dependent 24-hour CRP level. In patients with a CRP concentration ̂ 5 mg/l, the proportion of newborns treated for 6 72 h was 63% in the standard group com-pared with 50% in the PCT group (absolute risk reduction 13%; OR 0.60, 95% CI 0.17/2.07; Fisher’s exact test (two-tailed) p = 0.533). In patients with a CRP concentration 1 5 mg/l, significantly more infants were treated with an-tibiotics 6 72 h in the standard group (95%) than in the PCT group (57%) (absolute risk reduction 38%; OR 0.076, 95% CI 0.016/0.359; Fisher’s exact test (two-tailed) p ! 0.001). However, neither the interaction test of CRP con-centrations and the primary endpoint within a logistic regression model nor the corresponding interaction test of CRP concentrations and the co-primary endpoint in a two-way analysis of variance model were significant (p = 0.098 and p = 0.150).
Possible Misclassifications Based on PCT In the PCT group, 1 near-term infant with a gestation-
al age of 35 6/7 weeks and a birth weight 2,520 g was treated with a second course of antibiotics. This infant required mechanical ventilation on the first day of life. The probability of infection was considered to be unlike-ly and antibiotic therapy was stopped after 24 h when two consecutive PCT values had been below the age-adjusted cut-off values. At 72 h of age, empiric antibiotic therapy was restarted because of clinical signs of infection and the detection of Escherichia coli in tracheal aspirates (blood cultures remained negative). Subsequently, the in-fant recovered rapidly following 7 days of antibiotic ther-apy and the clinical outcome was favorable. In 2 cases, antibiotic therapy was continued beyond 24 h despite ful-filled PCT criteria based on the attending physician’s de-cision. In 1 case, antibiotic therapy was stopped 24 h later, in the other 48 h later. In both cases, infection was ulti-mately considered to be unlikely (group 4).
Safety Endpoints Clinical outcome was similar and favorable in both
groups, with all patients surviving and recovering com-
Table 3. Primary endpoint: proportion of infants treated with antibiotics for ≥72 h (efficacy of study interven-tion)
Standardgroup
PCTgroup
Absoluterisk reduction
p value
All newbornsInfection probable/proven (group 1/2)Infection possible (group 3)Infection unlikely (group 4)
50/61 (82%)12/12 (100%)19/19 (100%)19/30 (63.3%)
33/60 (55%)9/9 (100%)
13/21 (61.9%)11/30 (36.7%)
27%0%
38.1%26.6%
0.002
<0.0010.038
The effect of PCT-guided decision-making is dependent on the probability of infection.
Table 4. Co-primary endpoint: absolute reduction of the duration of antibiotic therapy (quantitative version of the primary endpoint for estimation of effect size)
Standardgroup
PCTgroup
Absolutereduction
p value
All newborns, hInfection probable/proven (group 1/2), hInfection possible (group 3), hInfection unlikely (group 4), h
101.5170.8111.5
67.4
79.1177.8
83.446.5
22.47
28.120.9
0.0120.504
<0.0010.001
The effect is dependent on the probability of infection.

Stocker /Fontana /el Helou /Wegscheider /Berger
Neonatology 2010;97:165–174172
pletely. There was no significant difference in the propor-tion of newborns treated with antibiotics 6 120 h (group 1/2, patients with recurrence of infection) between the standard group (39%) and the PCT group (32%) (absolute risk difference 7%; OR 0.71, 95% CI 0.34/1.51, Fisher’s ex-act test (two-tailed) p = 0.45: non-inferiority test for the PCT group).
Plausibility of the Constructed Age-Adjusted PCT Cut-Off Values To evaluate the plausibility of the constructed age-ad-
justed PCT cut-off values, PCT values of group 1/2, 3 and 4 patients were superimposed on the nomogram ( fig. 2 b–d). Median PCT values in group 3 (possible infection: fig. 2 c) and group 4 (unlikely infection: fig. 2 d) patients were similar and close to the predefined threshold values. In contrast, median PCT concentrations of group 1/2 (probable or proven infection: fig. 2 b) patients were sig-nificantly higher. To evaluate the margin of safety, maxi-mal cut-off values were extended to 20 ng/ml. This would have led to an additional reduction of antibiotic therapy in 7 of 60 infants, but in 2 of these 7 patients infection was felt to be probable (group 1/2).
Discussion
In this prospective intervention study, we were able to show that PCT-guided decision-making significantly re-duces the duration of empiric antibiotic therapy in sus-pected early-onset sepsis of term and near-term infants. There was a significant difference in the proportion of newborns treated with antibiotics 6 72 h between the standard group (82%) and the PCT group (55%). On aver-age, PCT-guided decision-making resulted in a shorten-ing of 22.4 h of antibiotic therapy.
Results of previous studies on the use of PCT as an early marker of neonatal sepsis were contradictory, how-ever most studies were observational studies [5, 7, 8, 11–19] . It is essential for observational studies to compare the new marker with the gold standard. The gold standard for the diagnosis of neonatal early-onset sepsis, i.e. a positive blood culture, is often unreliable because of the frequent use of intrapartum antibiotics or insufficient amounts of blood available for culture [21] . Therefore, the problem of all observational studies of neonatal early-onset sepsis is the definition of sepsis. An intervention study offers a valuable alternative because the calculation of the main results is independent of the definition of sepsis. Recently, in an intervention study using serial PCT measurements,
Nobre et al. [22] showed a reduction of the duration of an-tibiotic therapy and intensive care unit stay in adult pa-tients with severe sepsis and septic shock. To the best of our knowledge, our study is the first PCT-guided inter-vention study in neonatal early-onset sepsis.
In the additional, CRP-stratified analysis, PCT-guid-ed reduction of the duration of antibiotic therapy was only statistically significant in the group with CRP values of 1 5 mg/l 24 h after initiation of antibiotic therapy. In these patients, PCT-guided decision-making appears most helpful. In contrast, no differences were found for patients with CRP concentrations ̂ 5 mg/l 24 h after an-tibiotics were started. However, these results have to be interpreted with caution since the differences between groups just missed statistical significance. Additional calculations of the impact of CRP are not possible be-cause of the study design and the fact that CRP was used in the assessment of probability of infection (CRP cut-off value 1 5 mg/l). The results of previously published stud-ies on the use of CRP as marker of neonatal sepsis are contradictory. Philip and Mills [23] were able to mini-mize antibiotic therapy using a clinical pathway for neo-natal sepsis. Decisions to start or discontinue of antibiot-ics were predominantly based on CRP determinations with a cut-off value of 10 mg/l. 216 out of 425 infants were treated because of risk factors without clinical findings and the mean duration of antibiotic therapy was 3.1 days. Ehl et al. [24] published an intervention study using CRP to guide duration of antibiotic therapy in suspected neo-natal bacterial infection. Lack of a randomized control group and false-negative CRP results (CRP ! 10 mg/l in the first 24–48 h after initiation of antibiotic therapy) in 2 out of 15 infants with positive blood cultures were the main limitations of this study. Finally, Benitz et al. [25] calculated and analyzed receiver-operator curves for CRP levels in proven neonatal sepsis and showed poor sensitivity of CRP measurements 24 h after initiation of antibiotic therapy. Elevated CRP levels were not observed in 18 out of 73 episodes in which blood cultures yielded pathogenic organisms.
In our study, 3 patients were possibly misclassified based on PCT determinations. In 1 patient, antibiotics were restarted when cultures of tracheal aspirates of the still intubated infant were positive for E. coli 48 h after early discontinuation of empiric antibiotic therapy. It is impossible to determine whether this was a primary in-fection (pneumonia) with false-negative PCT values or a secondary ventilator-associated nosocomial infection/colonization. The predictive value of PCT for local infec-tions is not conclusive. In a recently published study of

PCT and Antibiotic Therapy in Neonates Neonatology 2010;97:165–174 173
newborns with suspected pneumonia, Engle et al. [26] detected no additional predictive value of PCT compared to CRP. In 2 other patients, the attending physician con-tinued antibiotic therapy despite two consecutive normal PCT values based on his clinical assessment. Retrospec-tively, it seems unlikely that the PCT measurements were truly false-negative since antibiotics were stopped only 24 and 48 h later, respectively.
Clinical outcome (survival, recurrence of infection) was similar (no significant difference in the proportion of infants treated with antibiotics 6 120 h: non-inferior-ity test of the PCT group) and favorable in both groups with no deaths. Power calculation, however, was based on an expected reduction of the duration of antibiotic ther-apy and does not allow to exclude rare adverse events. This would require testing in a much larger patient popu-lation. Therefore, the safety of our PCT-guided strategy remains to be proven.
Several previous studies have described age-depen-dent normal values of PCT in the first 72 h of life [5, 7–10] . Based on these results, we constructed an age-adjusted PCT nomogram for the first 3 days of life and included an arbitrary margin of safety ( fig. 2 a) [5, 9] . This nomo-gram seems to be reasonable because median PCT values for patients with possible and unlikely infection (groups 3 and 4) were similar and close to the predefined thresh-old values and PCT concentrations for patients with probable or proven infection (group 1/2) were signifi-cantly higher. Since an extension of the safety cut-off lev-el to 20 ng/ml would have led to additional misclassifica-tions, a maximum PCT threshold concentration of 10 ng/ml seems to be rational.
There are several limitations to our study. First and most importantly, the small sample size does not allow to
prove the safety of our PCT-guided strategy. Second, be-cause of the single-center setting, our results cannot eas-ily be extrapolated to centers with different thresholds for initiation and discontinuation of empiric antibiotic ther-apy in newborns with non-specific signs and symptoms compatible with early-onset sepsis. Third, infection was proven in only 1 infant (positive blood culture), however, this is not uncommon in neonatal sepsis evaluations be-cause of the frequent use of intrapartum antibiotics or insufficient amounts of blood available for culture. Fi-nally, because of the study design, we were not able to calculate the effect for some interesting outcome vari-ables (length of hospitalization, costs, bacterial selec-tion).
Conclusions
PCT analysis is feasible in newborn infants. In our set-ting, serial PCT measurements allowed to significantly shorten the duration of empiric antibiotic therapy in term and near-term infants with suspected early-onset sepsis. The age-adjusted PCT nomogram with a safety cut-off value of 10 ng/ml seems to be reasonable. A multicenter study will be required to test the reliability and safety of a PCT-based strategy in a larger cohort of neonates.
Acknowledgement
BRAHMS Diagnostica (Berlin, Germany) provided the test-ing kits for PCT determinations but was not involved in any oth-er aspects of the study or manuscript preparation.
References
1 Polin RA: The ‘ins and outs’ of neonatal sep-sis. J Pediatr 2003; 143: 3–4.
2 Escobar GJ: The neonatal ‘sepsis work-up’: personal reflections on the development of an evidence-based approach toward new-born infections in a managed care organiza-tion. Pediatrics 1999; 103:e360–e373.
3 Gendrel D, Bohuon C: Procalcitonin as a marker of bacterial infection. Pediatr Infect Dis J 2000; 19: 679–688.
4 Marchini G, Berggren V, Djilali-Merzoug R, Hansson LO: The birth process initiates an acute phase reaction in the fetus-newborn infant. Acta Pediatr 2000; 89: 1082–1086.
5 Chiesa C, Panero A, Rossi N, Stegagno M, DeGiusti M, Osborn JF, Pacifico L: Reliabil-ity of procalcitonin concentrations for the diagnosis of sepsis in critically ill neonates. Clin Infect Dis 1998; 26: 664–672.
6 Assuma M, Signore F, Pacifico L, Rossi N, Osbron JF, Chiesa C: Serum procalcitonin concentrations in term delivering mothers and their healthy offsprings: A longitudinal study. Clin Chem 2000; 46: 1583–1587.
7 Guibourdenche J, Bedu A, Petzold L, March-and M, Mariani-Kurdjian P, Hurtaud-Roux M, Aujard Y, Porquet D: Biochemical mark-ers of neonatal sepsis: value of procalcitonin in the emergency setting. Ann Clin Biochem 2002; 39: 130–135.
8 Monneret G, Labaune JM, Isaac C, Beinvenu F, Puter G, Bienvenu J: Procalcitonin and C-reactive protein levels in neonatal infections. Acta Pediatr 1997; 86: 209–212.
9 Sachse C, Dressler F, Henkel E: Increased se-rum procalcitonin in newborn infants with-out infection. Clin Chem 1998; 44: 1343–1344.
10 Turner D, Hammerman C, Rudensky B, Schlesinger Y, Goia C, Schimmel MS: Pro-calcitonin in preterm infants during the first few days of life: introducing an age-related nomogram. Arch Dis Child Fetal Neonatal Ed 2006; 91:F283–F286.

Stocker /Fontana /el Helou /Wegscheider /Berger
Neonatology 2010;97:165–174174
11 Ballot DE, Perovic O, Galpin J, Cooper PA: Serum procalcitonin as an early marker of neonatal sepsis. S Afr Med J 2004; 94: 851–854.
12 Blommendahl J, Janas M, Laine S, Miettinen A, Ashorn P: Comparison of procalcitonin with CRP and differential white blood cell count for diagnosis of culture-proven neona-tal sepsis. Scand J Infect Dis 2002; 34: 620–622.
13 Distefano G, Curreri R, Betta P, Romeo MG, Amato M: Procalcitonin serum levels in perinatal bacterial and fungal infection of preterm infants. Acta Paediatr 2004; 93: 216–219.
14 Enguix A, Rey C, Concha A, Medina A, Coto D, Dieguez MA: Comparison of procalcito-nin with C-reactive protein and serum amy-loid for the early diagnosis of bacterial sepsis in critically ill neonates and children. Int Care Med 2001; 27: 211–215.
15 Franz AR, Kron M, Pohlandt F, Steinbach G: Comparison of procalcitonin with interleu-kin 8, C-reactive protein and differential white blood cell count for the early diagnosis of bacterial infections in newborn infants. Pediatr Infect Dis J 1999; 18: 666–671.
16 Gendrel D, Assicot M, Raymond J, Moulin F, Francouai C, Badoual J, Bohuon C: Procalci-tonin as a marker for the early diagnosis of neonatal infection. J Pediatr 1996; 128: 570–573.
17 Joram N, Boscher C, Denizot S, Loubersac V, Winer N, Roze JC, Gras-Le Guen C: Umbili-cal cord blood procalcitonin and C-reactive protein concentrations as markers for early diagnosis of very early onset neonatal infec-tion. Arch Dis Child Fetal Neonatal Ed 2006; 91:F65–F66.
18 Kordek A, Giedrys-Kalemba S, Pawlus B, Po-draza W, Czajka R: Umbilical cord blood se-rum procalcitonin concentration in the di-agnosis of early neonatal infection. J Perinatol 2003; 23: 148–153.
19 Resch B, Gusenleitner W, Müller WD: Pro-calcitonin and interleukin-6 in the diagnosis of early-onset sepsis of the neonate. Acta Paediatr 2003; 92: 243–245.
20 Meisner M: Pathobiochemistry and clinical use of procalcitonin. Clin Chim Acta 2002; 323: 17–29.
21 Connell TG, Rele M, Cowley D, Buttery JP, Curtis N: How reliable is a negative blood culture result? Volume of blood submitted for culture in routine practice in a children’s hospital. Pediatrics 2007; 119: 891–896.
22 Nobre V, Harbarth S, Graf JD, Rohner P, Pu-gin J: Use of procalcitonin to shorten antibi-otic treatment duration in septic patients. Am J Respir Crit Care Med 2008; 177: 498–505.
23 Philip AG, Mills PC: Use of C-reactive pro-tein in minimizing antibiotic exposure: ex-perience with infants initially admitted to a well-baby nursery. Pediatrics 2000; 106:e4.
24 Ehl S, Gering B, Bartmann P, Högel J, Poh-landt F: C-reactive protein is a useful marker for guiding duration of antibiotic therapy in suspected neonatal bacterial infection. Pedi-atrics 1997; 99: 216–221.
25 Benitz WE, Han MY, Madan A, Ramachan-dra P: Serial serum C-reactive protein levels in the diagnosis of neonatal infection. Pedi-atrics 1998; 102:e41.
26 Engle WD, Jackson GL, Sendelbach DM, Ste-hel EK, Ford DM, McHugh KM, Norris MR, Vedro DA, Velaphi S, Michelow IC, Olsen KD: Pneumonia in term neonates: laborato-ry studies and duration of antibiotic therapy. J Perinatol 2003; 23: 372–377.
Jana
Copyright hoch




















