Urinary concentrations of phthalates and phenols in a population of Spanish pregnant women and...
9
Urinary concentrations of phthalates and phenols in a population of Spanish pregnant women and children Lidia Casas a,b,c, ⁎, Mariana F. Fernández c,d , Sabrina Llop c,e,f , Mònica Guxens a,b,c , Ferran Ballester c,e,g , Nicolás Olea c,d , Mikel Basterrechea Irurzun c,h,i , Loreto Santa Marina Rodríguez c,h,i , Isolina Riaño j , Adonina Tardón c,k , Martine Vrijheid a,b,c , Antonia M. Calafat l , Jordi Sunyer a,b,c,m and On behalf of the INMA Project a Centre for Research in Environmental Epidemiology, Dr Aiguader 88, 08003 Barcelona, Catalonia, Spain b Hospital del Mar Research Institute (IMIM), Dr Aiguader 88, 08003 Barcelona, Catalonia, Spain c CIBER Epidemiología y Salud Pública (CIBERESP), Spain d Laboratory of Medical Investigations, San Cecilio University Hospital, University of Granada, Granada, Spain e Instituto de Salud Carlos III, Madrid, Spain f Center for Public Health Research (CSISP), Valencia, Spain g University of Valencia, Valencia, Spain h Subdirección de Salud Pública de Gipuzkoa. Departamento de Sanidad. Gobierno Vasco. San Sebastián, Spain i Instituto de Investigación Sanitaria BIODONOSTIA, San Sebastián, Spain j Hospital San Agustín, Avilés, Spain k University of Oviedo, Oviedo, Spain l National Center for Environmental Health, Centers for Disease Control and Prevention, Atlanta GA 30341, USA m Pompeu Fabra University, Barcelona, Catalonia, Spain abstract article info Article history: Received 1 September 2010 Accepted 18 February 2011 Available online 25 March 2011 Keywords: Phthalate Phenol Pregnancy Children Social class Exposure Background: Phthalate and phenol exposure is prevalent among the general population and of potential concern for pregnant women and children because of their suspected susceptibility to endocrine effects. Objectives: To evaluate the extent of exposure to several phthalates and phenols in a sample of Spanish pregnant women – according to their individual characteristics (age, social class, education, and body mass index) – and children who participated in the INMA — Infancia y Medio Ambiente (Environment and Childhood) project. Methods: One spot urine sample was taken during the third trimester of pregnancy from 120 pregnant women and from 30 4-year old children belonging to 5 Spanish birth cohorts, and analyzed for 11 phthalate metabolites and 9 phenols. Results: Three metabolites of di(2-ethylhexyl) phthalate, mono-2-ethyl-5-carboxypentyl phthalate, mono-2- ethyl-5-hydroxyhexyl phthalate, and mono-2-ethyl-5-oxohexyl phthalate; two metabolites of dibutyl phthalates, mono-isobutyl phthalate and mono-n-butyl phthalate; monoethyl phthalate (MEP), the main metabolite of diethyl phthalate; and two phenols, methyl paraben (M-PB) and 2,5-dichlorophenol were detected in the urine samples of all women. The highest urinary concentrations were for MEP and M-PB. Urinary concentrations of all phthalate metabolites and of 2,4-dichlorophenol, 2,5-dichlorophenol, and bisphenol A were lower in the pregnant women than in the children. Among women, a positive relationship with social class and education was shown for most of the phthalate metabolites and phenols. Almost all phthalate metabolites varied by region even after adjusting for social class and education. Conclusions: Phthalate and phenol exposures are prevalent in a group of pregnant women and young children, two susceptible populations, and these exposures might be positively related to social class. © 2011 Elsevier Ltd. All rights reserved. Environment International 37 (2011) 858–866 Abbreviations: MECPP, mono-2-ethyl-5-carboxypentyl phthalate; MEHHP, mono-2-ethyl-5-hydroxyhexyl phthalate; MEOHP, mono-2-ethyl-5-oxohexyl phthalate; MEHP, mono-2-ethylhexyl phthalate; MCPP, mono-3-carboxypropyl phthalate; MiBP, mono-isobutyl phthalate; MBP, mono-n-butyl phthalate; MBzP, monobenzyl phthalate; MEP, monoethyl phthalate; MCOP, mono(carboxy-isooctyl) phthalates; MCNP, mono(carboxy-isononyl) phthalates; BPA, bisphenol A; TCS, triclosan; M-PB, methyl paraben; P-PB, propyl paraben; B-PB, butyl paraben; E-PB, ethyl paraben; BP-3, benzophenone-3; 2.4-DCP, 2,4-dichlorophenol; 2.5-DCP, 2,5-dichlorophenol; LOD, limit of detection; BMI, body mass index. ⁎ Corresponding author at: Centre for Research in Environmental Epidemiology, Dr Aiguader 88, 08003 Barcelona, Catalonia, Spain. Tel.: + 34 932147314; fax: + 34 932147301. E-mail address: [email protected] (L. Casas). 0160-4120/$ – see front matter © 2011 Elsevier Ltd. All rights reserved. doi:10.1016/j.envint.2011.02.012 Contents lists available at ScienceDirect Environment International journal homepage: www.elsevier.com/locate/envint
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Urinary concentrations of phthalates and phenols in a population of Spanish pregnant women and...

Environment International 37 (2011) 858–866
Contents lists available at ScienceDirect
Environment International
j ourna l homepage: www.e lsev ie r.com/ locate /env int
Urinary concentrations of phthalates and phenols in a population of Spanishpregnant women and children
Lidia Casas a,b,c,⁎, Mariana F. Fernández c,d, Sabrina Llop c,e,f, Mònica Guxens a,b,c, Ferran Ballester c,e,g,Nicolás Olea c,d, Mikel Basterrechea Irurzun c,h,i, Loreto Santa Marina Rodríguez c,h,i, Isolina Riaño j,Adonina Tardón c,k, Martine Vrijheid a,b,c, Antonia M. Calafat l, Jordi Sunyer a,b,c,m
and On behalf of the INMA Projecta Centre for Research in Environmental Epidemiology, Dr Aiguader 88, 08003 Barcelona, Catalonia, Spainb Hospital del Mar Research Institute (IMIM), Dr Aiguader 88, 08003 Barcelona, Catalonia, Spainc CIBER Epidemiología y Salud Pública (CIBERESP), Spaind Laboratory of Medical Investigations, San Cecilio University Hospital, University of Granada, Granada, Spaine Instituto de Salud Carlos III, Madrid, Spainf Center for Public Health Research (CSISP), Valencia, Spaing University of Valencia, Valencia, Spainh Subdirección de Salud Pública de Gipuzkoa. Departamento de Sanidad. Gobierno Vasco. San Sebastián, Spaini Instituto de Investigación Sanitaria BIODONOSTIA, San Sebastián, Spainj Hospital San Agustín, Avilés, Spaink University of Oviedo, Oviedo, Spainl National Center for Environmental Health, Centers for Disease Control and Prevention, Atlanta GA 30341, USAm Pompeu Fabra University, Barcelona, Catalonia, Spain
Abbreviations: MECPP, mono-2-ethyl-5-carboxypenmono-2-ethylhexyl phthalate; MCPP, mono-3-carboxymonoethyl phthalate; MCOP, mono(carboxy-isooctyl) phparaben; B-PB, butyl paraben; E-PB, ethyl paraben; BP-3,⁎ Corresponding author at: Centre for Research in Env
E-mail address: [email protected] (L. Casas).
0160-4120/$ – see front matter © 2011 Elsevier Ltd. Aldoi:10.1016/j.envint.2011.02.012
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 1 September 2010Accepted 18 February 2011Available online 25 March 2011Keywords:PhthalatePhenolPregnancyChildrenSocial classExposure
Background: Phthalate and phenol exposure is prevalent among the general population and of potentialconcern for pregnant women and children because of their suspected susceptibility to endocrine effects.Objectives: To evaluate the extent of exposure to several phthalates and phenols in a sample of Spanishpregnant women – according to their individual characteristics (age, social class, education, and body massindex) – and children who participated in the INMA — Infancia y Medio Ambiente (Environment andChildhood) project.Methods:One spot urine sample was taken during the third trimester of pregnancy from 120 pregnant womenand from 30 4-year old children belonging to 5 Spanish birth cohorts, and analyzed for 11 phthalatemetabolites and 9 phenols.Results: Three metabolites of di(2-ethylhexyl) phthalate, mono-2-ethyl-5-carboxypentyl phthalate, mono-2-ethyl-5-hydroxyhexyl phthalate, and mono-2-ethyl-5-oxohexyl phthalate; two metabolites of dibutyl
phthalates, mono-isobutyl phthalate and mono-n-butyl phthalate; monoethyl phthalate (MEP), the mainmetabolite of diethyl phthalate; and two phenols, methyl paraben (M-PB) and 2,5-dichlorophenol weredetected in the urine samples of all women. The highest urinary concentrations were for MEP and M-PB.Urinary concentrations of all phthalate metabolites and of 2,4-dichlorophenol, 2,5-dichlorophenol, andbisphenol A were lower in the pregnant women than in the children. Among women, a positive relationshipwith social class and education was shown for most of the phthalate metabolites and phenols. Almost allphthalate metabolites varied by region even after adjusting for social class and education.Conclusions: Phthalate and phenol exposures are prevalent in a group of pregnant women and young children,two susceptible populations, and these exposures might be positively related to social class.© 2011 Elsevier Ltd. All rights reserved.
tyl phthalate; MEHHP, mono-2-ethyl-5-hydroxyhexyl phthalate; MEOHP, mono-2-ethyl-5-oxohexyl phthalate; MEHP,propyl phthalate; MiBP, mono-isobutyl phthalate; MBP, mono-n-butyl phthalate; MBzP, monobenzyl phthalate; MEP,thalates; MCNP, mono(carboxy-isononyl) phthalates; BPA, bisphenol A; TCS, triclosan; M-PB, methyl paraben; P-PB, propylbenzophenone-3; 2.4-DCP, 2,4-dichlorophenol; 2.5-DCP, 2,5-dichlorophenol; LOD, limit of detection; BMI, bodymass index.ironmental Epidemiology, Dr Aiguader 88, 08003 Barcelona, Catalonia, Spain. Tel.: +34 932147314; fax: +34 932147301.
l rights reserved.

859L. Casas et al. / Environment International 37 (2011) 858–866
1. Background
Some phthalates and phenols are used in the manufacture of poly-meric materials. High-molecular weight phthalates like di(2-ethylhexyl)phthalate (DEHP) act as plasticizers in the manufacture of flexible vinylplastic used in flooring, wall coverings, food contact applications andmedical devices. Low-molecular weight phthalates such as diethylphthalate (DEP) and dibutyl phthalate (DBP) can be used in personalcare products, lacquers, varnishes and coatings, including timedrelease polymeric coatings in some pharmaceuticals. Regarding phenols,bisphenol A (BPA) is one of themost largely studied compounds, and it isused in the manufacture of epoxy resins and polycarbonate plasticswhich, in turn, havemany commercial applications, including coatings offood cans as plastic baby bottles. Ingestion, inhalation and dermal contactare considered important routes of exposure for both phthalates andphenols in the general population. These contaminants are rapidlymetabolized, have short half-lives and are quickly excreted from the body(Meeker et al., 2009a; Talsness et al., 2009).
Experimental studies in rodents show that in utero exposure tohigh doses of some phthalates may result in adverse reproductiveeffects in adult males (Akingbemi et al., 2004; Dostal et al., 1988; Grayand Gangolli, 1986; Lin et al., 2008) as well as in fetuses and pups(Gray et al., 2000;Mylchreest et al., 1999). Non-human primates seemto be less sensitive to the exposure, and environmental exposures inhumans are generally several times lower than those experienced inlaboratory animals. Nonetheless, several studies in humans havereported significant associations between exposure to some phtha-lates and adverse reproductive health effects (Adibi et al., 2010; Dutyet al., 2003a,b, 2005; Hauser et al., 2006, 2007; Jonsson et al., 2005;Lomenick et al., 2010; Pan et al., 2006; Weuve et al., 2010; Wolff et al.,2010). For example, gestational exposure to some phthalates has beenassociated with reproductive effects in newborn boys such asdecreased anogenital distance (Swan et al., 2005), with inconsistentresults on gestational age (Adibi et al., 2009; Latini et al., 2003;Meeker et al., 2009b; Whyatt et al., 2009), and with a potential effecton neurodevelopment (Engel et al., 2009).
The associations between human exposures to phenols on humanreproductive health are largely unknown and the literature is mostlylimited to evaluations of BPA. A potential association between theexposure to BPA and serum androgen concentrations in women hasbeen described and this could affect the fetus following pregnancyexposures (Meeker et al., 2010, Mendiola et al., 2010; Mok-Lin et al.,2010; Takeuchi et al., 2004; Wolff et al., 2010).
Population levels of phthalates and phenols have been reported forseveral areas of USA and north of Europe, (Adibi et al., 2003, 2008;Becker et al., 2004, 2009; Berman et al., 2009; Calafat et al., 2008;Castorina et al., 2010; CDC, 2010; Koch et al., 2005, 2007; Peck et al.,2010; Wittassek et al. 2007; Wolff et al., 2008; Ye et al., 2008, 2009)but never in the south of Europe. In the present study, we aim todetermine the exposure status of phthalates and phenols amongpregnant women and children in Spain participating in the SpanishINMA — Infancia y Medio Ambiente (Environment and Childhood)project. A secondary objective is to evaluate whether maternal age,social class, education, and body mass index (BMI) predict urineconcentrations of these chemicals in these pregnant women.
2. Methods
2.1. Study population
One hundred and twenty pregnant women were selected atrandom from four birth cohorts (Asturias, Gipuzkoa, Sabadell andValencia) and 30 four-year old children (boys) from one birth cohort(Granada). These five birth cohorts belong to the INMA Project, apopulation-based birth cohort study conducted in Spain that has beendescribed in detail previously (Ribas-Fitó et al., 2006). Its main goal is
to investigate the role during pregnancy and early childhood ofenvironmental pollutants present in air, water, and diet in regard tochild growth and development. Based on knowledge from threeSpanish cohorts: Ribera d'Ebre and Menorca starting on year 1997,and Granada, starting on year 2000, a common protocol wasdeveloped by setting up 4 new birth cohort locations (Valencia,Sabadell, Asturias, and Gipuzkoa) unifying all 7 cohorts, whichrecruited mother–child pairs between 2004 and 2008. The researchprotocol was approved by the Ethics and Research Committees of allparticipating institutions. The involvement of the Centers for DiseaseControl and Prevention (CDC) laboratory was limited and determinednot to constitute engagement in human subjects' research.
2.2. Phthalates and phenols
Concentrations of phthalates and phenols were measured in spoturine samples collected from the women during the third trimester ofpregnancy (2004–2008), and from the children at the age of 4 years(2005–2006). Urine was collected in 100 mL non-vinyl and non-polycarbonate containers and stored at −20 °C. One aliquot of eachselected individual was shipped to the CDC Environmental HealthLaboratories, and aliquots were stored at or below −20 °C. All urinesamples were stored for a minimum of one year and a maximum of5 years before analysis. The samples were analyzed at the CDC for 11phthalate metabolites and 9 phenols: mono-2-ethyl-5-carboxypentylphthalate (MECPP),mono-2-ethyl-5-hydroxyhexyl phthalate (MEHHP),mono-2-ethyl-5-oxohexyl phthalate (MEOHP), mono-2-ethylhexylphthalate (MEHP), mono-3-carboxypropyl phthalate (MCPP), mono-isobutyl phthalate (MiBP), mono-n-butyl phthalate (MBP), monobenzylphthalate (MBzP),monoethyl phthalate (MEP),mono(carboxy-isooctyl)phthalates (MCOP), and mono(carboxy-isononyl) phthalates (MCNP),bisphenol A (BPA), triclosan (TCS),methyl paraben (M-PB), propyl para-ben (P-PB), butyl paraben (B-PB), ethyl paraben (E-PB), benzophenone-3 (BP-3), 2,4-dichlorophenol (2.4-DCP), and 2,5-dichlorophenol (2.5-DCP).
The concentrations of total (free plus conjugated) species ofurinary phenols and phthalate metabolites were quantified usingmodified high-performance liquid chromatography-isotope dilutiontandem mass spectrometry (HPLC-MS/MS) analytical methods de-scribed before (Silva et al., 2007; Ye et al., 2005). A subset of sampleswas also analyzed for free concentrations. The limits of detection(LOD) for each target compound are shown in Table 1.
2.3. Samples with potentially compromised integrity
All the urine samples were deep-frozen immediately aftercollection. They were stored in polypropylene tubes in a coolingchamber under conditions (−20 °C), which virtually exclude anychange in composition or chemical properties over a period of severalyears. Because the urine collection materials and storage containershad not been pre-screened for the presence of the target analytes andmost of the urine samples had been stored for up to 5 years before theanalyses for phenols and phthalate metabolites, we analyzed a subsetof 70 samples for both free and total concentrations of the compoundsof interest. The percentage of free species of several phthalatemetabolites (e.g., MBP and MEHP) in 13 of these samples was above90%. These findings are consistent with potential degradation of theurinary conjugates to free species (Samandar et al., 2009). Regardingthe phenol conjugated species, we did not observe unusual ratios inthe proportion of free and total concentrations for these chemicals(data not shown) probably due to the relatively higher stability ofphenolic conjugated species (Ye et al., 2007).
Therefore, the phthalate metabolite concentrations reported fromthe laboratory analyses for these 13 samples may not represent theactual concentrations at the time the samples were collected. Most ofthese samples (n=11) where from the Granada cohort, one was from

Table 1Limits of detection (LOD) for phthalate metabolites and phenols in urine (ng/mL).
Metabolite LOD
PhthalateDi(2-ethylhexyl) phthalate DEHP Mono-2-ethyl-5-carboxypentyl phthalate MECPP 0.6
Mono-2-ethyl-5-hydroxyhexyl phthalate MEHHP 0.7Mono-2-ethyl-5-oxohexyl phthalate MEOHP 0.7Mono-2-ethylhexyl phthalate MEHP 1.2
Di-n-octyl phthalate Mono-3-carboxypropyl phthalate MCPP 0.2Di-iso-butyl phthalate DiBP Mono-isobutyl phthalate MiBP 0.3Di-n-butyl phthtalate DBP Mono-n-butyl phthalate MBP 0.6Butylbenzyl phthalate BBzP Monobenzyl phthalate MBzP 0.3Diethyl phthalate DEP Monoethyl phthalate MEP 0.8Di-iso-nonyl pthalates DiNP Mono(carboxy-isooctyl) phthalates MCOP 0.7Di-iso-decyl phthalates DiDP Mono(carboxy-isononyl) phthalates MCNP 0.6
PhenolBisphenol A BPA 0.4Triclosan TCS 2.3Methyl paraben M-PB 1.0Propyl paraben P-PB 0.2Butyl paraben B-PB 0.2Ethyl paraben E-PB 1.0Benzophenone-3 BP-3 0.42,4-dichlorophenol 2,4-DCP 0.22,5-dichlorophenol 2,5-DCP 0.2
860 L. Casas et al. / Environment International 37 (2011) 858–866
Sabadell and another one from Gipuzkoa. Because we foundstatistically significant differences in the phthalate metabolite con-centrations between the samples with potentially compromisedintegrity and the other samples, but we did not observe theseconcentration differences for the phenols, we excluded these 13samples only for the phthalate statistical analyses.
2.4. Urinary creatinine and specific gravity
Creatinine was determined at the Normative Public Health Labora-tory of Bilbao, Basque Country by Jaffé method (kinetic with targetmeasurement, compensated method) with Roche reactives in a Hitachi911 auto-analyzer. Specific gravity was measured at CDC at roomtemperature using a handheld refractometer (The Science Company,Denver, CO, USA), which was calibrated with deionized water beforeeach measurement. Because results after adjustment for creatinine andfor specific gravity were identical, only adjustment for creatinine isshown.
2.5. Questionnaires
Variables assessed in this study as potential determinants forphthalate and phenol exposures were maternal age, maternal BMI,maternal education, and maternal social class. Face-to-face interviewquestionnaires were administered to themothers in the first and thirdtrimesters of pregnancy by trained interviewers, and these includedquestions on socio-demographic and health topics. Data on determi-nants of exposure described in the present study were collected in thefirst trimester questionnaire. Age at the time of the last menstrualperiod was recorded in years. BMI was obtained from self-reportedheight (in meters) and pre-pregnancy weight (in kilograms).Maternal social class was coded from the longest held job duringpregnancy; if the woman did not work during pregnancy, the lastjob before pregnancy was used. Occupations were coded using the 4-digit Spanish Codigo Nacional de Ocupaciones (CNO94), which isclosely related to the international ISCO88 coding system. Five socialclass categories were then created following the methodologyproposed by the Spanish Epidemiological Society (Domingo-Salvanyet al., 2000): SCI (managers of companies with≥10 employees, seniortechnical staff, higher independent professionals); SCII (managers of
companies with b10 employees, intermediate occupations); SCIII(administrative and financial management supporting personnel,other self-employed professionals, supervisors of manual workers,other skilled non-manual workers); SCIV (skilled and partly skilledmanual workers); and SCV (unskilled manual workers). Maternaleducation was classified in 3 categories: primary school or below,secondary school and university education or more.
2.6. Statistical analyses
Urinary concentrations of phthalate metabolites and phenols belowthe LODwere assigned a value equal to half of the LOD for the statisticalanalysis. Because the urinary concentrations of creatinine and the targetcompounds did not show a normal distribution, base 10 logarithmictransformation of the variables was computed. Bivariate and multivar-iate analyses were performed for the pregnant women subpopulation.ANOVA test was used to obtain urinary creatinine adjusted p-values forthe differences in the logarithmic transformation of contaminantconcentrations in urine between regions, and between categories ofmaternal socio-demographic characteristics andBMI. Twomultivariablelinear regression models were performed for each logarithmicallytransformed metabolite concentration, the first model included socialclass, age, BMI, region and logarithm of urinary creatinine, and thesecond one included the same variables except for social class that wasreplaced bymaternal education. Variables included in the models wereselected a-priori and not based on any threshold. Coefficients wereexponentially transformed to relative increases. We performed statis-tical analyses using STATA version 10.1 (Stata corporation, Collegestation, Texas).
3. Results
MECPP, MEHHP,MEOHPMiBP,MBP,MEP, 2,5-DCP, andM-BPweredetected in the urine samples of all women, TCS was only detected in59.5% samples (Table 2). The urinary concentrations of all phthalatemetabolites examined, and of 2,4-DCP, 2,5-DCP, M-PB and P-PB wereabove the LOD in the 4 year old children; TCS was only detected in36.7% of the children's samples. The highest median concentrations inboth pregnant women and children were observed for MEP andMECPP among the phthalate metabolites, and for M-PB, P-PB and 2,5-

Table 2Urinary concentrations of phthalate and phenol metabolites (ng/mL) during pregnancyand childhood.
Pregnant women Children
3rd trimester 4 years old
n %bLOD Median IQR n %bLOD Median IQR
PhthalatesMCNP 118 3.4 2.8 2.2 19 0.0 4.0 4.1MCOP 118 2.5 4.0 3.5 19 0.0 7.5 6.4MECPP 118 0.0 32.2 40.7 19 0.0 115.0 94.0MEHHP 118 0.0 17.3 21.6 19 0.0 57.4 56.6MEOHP 118 0.0 15.7 19.3 19 0.0 44.6 46.7MEHP 118 15.1 4.4 6.8 19 0.0 6.2 6.7MCPP 118 2.5 1.5 2.0 19 0.0 6.1 4.4MiBP 118 0.0 29.9 34.6 19 0.0 41.9 67.3MBP 118 0.0 27.5 39.0 19 0.0 30.2 35.7MBzP 118 0.8 10.5 12.7 19 0.0 33.0 32.6MEP 118 0.0 324 519.0 19 0.0 755.0 1282.0
Phenols2,4-DCP 120 9.1 1.1 1.8 30 0.0 3.1 5.52,5-DCP 120 0.0 16.5 29.5 30 0.0 55.6 167.1B-PB 120 9.9 2.4 10.3 30 16.7 1.2 3.7E-PB 120 12.4 8.8 25.7 30 20.0 8.1 26.2M-PB 120 0.0 191.0 415.5 30 0.0 150.0 427.8P-PB 120 1.7 29.8 61.3 30 0.0 21.5 56.4BP-3 120 9.9 3.4 15.5 30 3.3 1.9 3.2BPA 120 9.0 2.2 2.8 30 3.3 4.2 5.5TCS 120 40.5 6.1 84.7 30 63.3 1.2 3.9
861L. Casas et al. / Environment International 37 (2011) 858–866
DCP among the phenols. Median concentrations of all phthalatemetabolites examined and of 2,4-DCP, 2,5-DCP, and BPAwere lower inthe pregnant women than in the children (p-valuesb0.05); we didnot find statistically significant differences between the urinaryconcentrations of the remaining phenols.
Strong and statistically significant (p-valuesb0.05) correlationswere found between the creatinine-adjusted concentrations of thefour DEHP metabolites evaluated: MEOHP, MECPP, MEHHP, andMEHP (coefficient, r≥0.7), and between four of the phenols: 2.5-DCPand 2.4-DCP (r=0.9), and P-PB and M-PB (r=0.8) (Table 3). We didnot observe any statistically significant correlation between theconcentrations of phthalate metabolites and phenols.
Tables 4 and 5 show the phthalate metabolite and phenol urinaryconcentrations observed in the present study compared to thosereported before for women and children in other countries.
The age of pregnant women participating in the present studyranged from 17 to 43 years (43% were younger than 30), the youngestwomen were from Sabadell and Valencia (60% and 53% of womenyounger than 30, respectively). Regarding social class and education,half of the population was of low social class (VI and V) and 37% hadhigh education (university or more), a higher percentage of low social
Table 3Correlations of phthalate and phenol metabolites urinary concentrations, adjusted for logar
Phenols (n=150)
TCS BPA BP-3
Phthalates(n=137)
MCNP 1.0 1.0 −0.2 0.0MCOP 0.5 1.0 1.0 0.1MECPP 0.5 0.6 1.0 1.0MEHHP 0.5 0.6 0.9 1.0MEOHP 0.5 0.6 1.0 1.0 1.0MEHP 0.4 0.4 0.7 0.8 0.8MCPP 0.5 0.5 0.5 0.5 0.5MiBP 0.3 0.4 0.4 0.5 0.5MBP 0.4 0.4 0.5 0.4 0.4MBzP 0.5 0.6 0.3 0.5 0.6MEP 0.3 0.4 0.6 0.4 0.3
MCNP MCOP MECPP MEHHP MEOHP
class pregnant women was found in Valencia (60%), and a lowerpercentage of high education in Sabadell (27%). A quarter of thewomen was classified as overweight or obese (≥25 kg/m2) and thispercentage was higher in Asturias (40%).
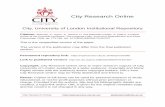
Phthalate metabolite and phenol urinary concentrations inpregnant women showed significant differences by region (Figs. 1and 2), social class, education, age, and BMI. Median concentrationsfor most phthalate metabolites were lower in Gipuzkoa than in otherregions. Women from Gipuzkoa also had the lowest concentrations ofsome phenols (2,4 DCP, 2,5 DCP, BP-3, BPA, and TCS). Women fromhigher social classes and higher achieved educational level had higherurinary concentrations of some phthalate metabolites (MCNP andMCOP) and parabens (B-PB, E-PB, and M-PB). After adjustment foreducation, age and BMI, higher social classes (I and II) remainedpositively associated with MCNP, E-PB and M-PB urinary concentra-tions (relative increases: 1.8, 2.5, and 2.3 referred to the lower socialclass, respectively) and positive associations were found additionallyfor MBP and TCS (relative increases: 1.7 and 3.0 referred to the lowersocial class, respectively) (Figs. 3 and 4). Multivariable modelsincluding education instead of social class showed increased con-centrations of MiBP and M-PB among university educated women(relative increases: 1.4 and 2.7 referred to primary education,respectively; p-valuesb0.05) and higher concentrations of MiBP,E-PB, and M-PB among women with secondary education (relativeincreases: 1.5, 2.4 and 2.3 referred to primary education, respectively;p-valuesb0.05).
4. Discussion
We found detectable concentrations of phthalate metabolites inmore than 84% of urine samples of pregnantwomen and in all samplesfrom children in a Spanish population. Phenols, excluding TCS, weredetected in urines of 68% of women and 73% of children. Concentra-tions of TCSwere detected in 59% and 37% of the pregnantwomen andchildren samples. MEP and M-PB were the compounds with thehighest concentrations in both pregnant women and children.Children presented higher median urinary concentrations thanpregnant women for all phthalate metabolites examined and forthree of the phenols (2,4-DCP, 2,5-DCP and BPA). Region of residencewas a determinant of concentrations of most phthalate metabolitesand three phenols (2,4-DCP, 2,5-DCP and BPA), and social class andeducation were positively related to concentrations of some of thephthalate metabolites and phenols.
There are many different known sources and routes of exposure tophenols and phthalates. Hence, determining the extent of exposure indifferent regions in Spain with different geography, climatology, andeven population lifestyle habits, as well as having different social classand education groups, can help in understanding exposure patterns.Moreover, exposure to phthalates and phenols is of potential concern
ithm of creatinine.
P-PB M-PB E-PB B-PB 2,5-DCP 2,4-DCP
0.1 0.1 0.2 0.1 −0.1 0.0 TCS−0.1 −0.1 0.1 0.0 0.3 0.3 BPA0.2 0.2 0.1 0.1 0.2 0.2 BP-31.0 0.8 0.6 0.3 0.1 0.0 P-PB
1.0 0.5 0.3 0.1 0.0 M-PB1.0 1.0 0.6 0.1 0.1 E-PB0.3 1.0 1.0 0.0 0.0 B-PB0.3 0.4 1.0 1.0 0.9 2,5-DCP0.3 0.7 0.4 1.0 1.0 2,4-DCP0.4 0.4 0.4 0.5 1.00.3 0.4 0.2 0.4 0.4 1.0MEHP MCPP MiBP MBP MBzP MEP

Table 4Comparison of the median and interquartile range (IQR) urinary concentrations of phthalate metabolites in women and children studies (ng/mL).
Phthalates
Study/region/year of sampling Population MECPP MEHHP MEOHP MEHP MCPP MiBP MBP MBzP MEP
WomenESBHum (Wittassek et al., 2007) 24.0 6.6 15.6 18.4 – 33.7 117.0 7.2 –
Germany 1988–2003 n=308 (–) (–) (–) (–) (–) (–) (–) (–) (–)NHANES (CDC forth National Report on Human Exposureto Environmental Chemicals)
31.3 19.4 13.7 1.8 3.0 4.1 24.4 13.3 182.0
USA 2003–2004 n=1355 (–) (–) (–) (–) (–) (–) (–) (–) (–)FRIENDS (Peck et al., 2010) 36.0 21.4 13.5 4.5 2.2 8.9 26.1 30.1 63.0USA 1999–2005 n=45 (65.6) (40.3) (27.9) (5.1) (2.7) (8.0) (41.0) (36.1) (84.0)
Pregnant womenINMA study 32.2 17.3 15.7 4.4 1.5 29.9 27.5 10.5 324.0Spain 2004–2008 n=120 (40.7) (21.6) (19.3) (6.8) (2.0) (34.6) (39.0) (12.7) (519.0)Generation R study (Ye et al., 2008) 18.4 14.0 14.5 6.9 1.0 42.1 42.7 7.5 117.0The Netherlands 2002–2006 n=100 (21.9) (23.1) (23.1) (14.0) (1.1) (51.1) (65.4) (13.2) (387.1)Children and Environmental Health Study (Wolff et al., 2008) 35.0 20.0 17.0 6.0 3.2 6.2 36.0 22.0 380.0USA 1998–2002 n=382 (54.0) (29.5) (27.7) (11.1) (4.2) (9.3) (59.0) (41.2) (873.0)CCCEH cohort (Adibi et al., 2008) 37.1 19.9 17.5 4.8 2.0 10.2 35.5 17.2 202.0USA n=246 (60.7) (33.0) (24.2) (11.4) (2.7) (11.7) (47.1) (35.6) (378.0)SFF (Adibi et al., 2009) – 11.2 9.9 3.5 – – – – –
USA 1998–2002 n=298 (–) (19.9) (19.5) (7.1) (–) (–) (–) (–) (–)
ChildrenINMA study 4 year old 115.0 57.4 44.6 6.2 6.1 41.9 30.2 33.0 755.0Spain 2004–2006 n=19 (94.0) (56.6) (46.7) (6.7) (4.4) (67.3) (35.7) (32.6) (1282.0)NHANES (CDC forth National Report on Human Exposureto Environmental Chemicals)
6–11 year old 51.6 36.5 25.8 2.7 7.1 7.0 36.7 35.0 81.7
USA 2003–2004 n=342 (–) (–) (–) (–) (–) (–) (–) (–) (–)GerES IV (Becker et al., 2009) 3–5 year old 68.2 51.7 37.9 4.6 – 97.8 100.0 19.7 –
Germany 2001–2002 n=137 (–) (–) (–) (–) (–) (–) (–) (–) (–)GerES IV (Becker et al., 2004; Koch et al., 2007) 2−4 year old – 54.3 44.4 6.8 – – 170.0 22.3 –
Germany 2001–2002 n=55 (–) (–) (–) (–) (–) (–) (–) (–) (–)
862 L. Casas et al. / Environment International 37 (2011) 858–866
for pregnant women and children because the developing fetus andyoung children are more susceptible to endocrine modulation effectsthan adults. This is, to our knowledge, the first study conducted inSpain to assess the exposure and the geographical and socio-demographical determinants to 11 different phthalate metabolitesand 9 phenols among pregnant women and children.
When interpreting these results, it is important to consider that thephthalates and phenols examined are rapidly metabolized, have short
Table 5Comparison of the median and interquartile range (IQR) urinary concentrations of phenols
Study/region/year of sampling
WomenNHANES (Calafat et al. 2008)USA 2003–2004 n=
Pregnant womenINMA studySpain 2004–2008 n=CHAMACOS (Castorina et al., 2010)USA 1999–2000 n=Health outcomes and measures of the environment study (Braun et al., 2009)USA 2003Generation R study (Ye et al., 2008)The Netherlands 2002–2006 n=Children and environmental health study (Wolff et al., 2008)USA 1998–2002 n=
ChildrenINMA study 4 ySpain 2004–2006 n=NHANES (Calafat et al. 2008) 6–1USA 2003–2004 n=
half-lives (i.e., few hours) and are quickly excreted from the body.Hence, any acute overexposurewithin a fewdays previous to sampling(e.g., medical intervention), could have increased abnormally theurinary concentration of some of the phthalate metabolites andphenols examined. Unfortunately we did not have any information onthe specific activities performed by the women and children duringthe days previous to the urine sample collection. Thus, we assumedthere was not any overexposure on the days previous to sampling.
in women and children studies (ng/mL).
Phenols
2,4-DCP 2,5-DCP BP-3 BPA TCS
– – – 2.4 –
1288 (–) (–) (–) (3.8) (–)
1.1 16.5 3.4 2.2 6.1120 (1.8) (29.5) (15.5) (2.8) (84.7)
1.1 18.5 – – –
478 (–) (–) (–) (–) (–)– – – 1.2 –
(–) (–) (–) (1.7) (–)– – – 2.2 –
100 (–) (–) (–) (2.0) (–)2.1 53.0 7.5 1.3 11.0
367 (4.0) (112.0) (28.4) (1.6) (39.1)
ear old 3.1 55.6 1.9 4.2 1.230 (5.5) (167.1) (3.2) (5.5) (3.9)1 year old – – – 3.7 –
328 (–) (–) (–) (5.0) (–)

MCNP MCOP MECP MEHHP MEOHP MEHP MCPP MiBP MBP MBzP MEP
PHTHALATES
0.0
0.2
0.4
0.6
0.8
1.0
3.6 ( 6.8 )
5.2 ( 6.8 ) 36.9
( 74.8 )19.1
( 52.7 )18.6 ( 41 )
4.6 ( 9.7 )
1.8 ( 2.3 )
47.1 ( 50.3 ) 34.1
( 42.3 )
14.5 ( 18.8 )
291.5 ( 329 )
2.3 ( 1.6 ) 2.2
( 2.7 ) 20.4 ( 28.3 ) 10.3
( 14.2 )10.5
( 10.5 ) 2.6 ( 4.1 )
0.6 ( 0.9 )
25.8 ( 23.2 )
10.4 ( 13.2 )
5.3 ( 10.5 )
94.5 ( 254.1 )
2.8 ( 1.5 )
3.6 ( 2.7 ) 31.5
( 31.6 )17.9
( 14.1 )
17.7 ( 21.6 ) 5
( 9.4 )1.9
( 2.8 )
31.5 ( 45.2 )
31.7 ( 49.7 )
14.6 ( 33.7 )
542 ( 834 )
2.5 ( 2.4 ) 4.3
( 3.7 )36.2
( 48.2 )19.5 ( 22 )
17.6 ( 21.1 )
5.2 ( 4.4 )
1.8 ( 1.9 )
24.8 ( 23.1 )
33.4 ( 47.3 )
8 ( 8 )
377.5 ( 511 )
* * * * * * * * *
* p<0.05Asturias Gipuzkoa Sabadell Valencia
Fig. 1. Description of third trimester of pregnancy phthalate metabolite urinary concentrations in each region (medians and interquartile ranges in ng/mL) and p values adjusted forlogarithm of creatinine.
863L. Casas et al. / Environment International 37 (2011) 858–866
Caution needs to be exercised when making comparisons acrossstudies that employ different study designs or target differentpopulations and different regions. Nonetheless, the present study
2,4-DCP 2,5-DCP B-PB E-PB M
PHEN
0.0
0.2
0.4
0.6
0.8
1.0
1 ( 1.5 )
15.2 ( 17.5 )
0.9 ( 2.9 )
7.6 ( 16.7 )
0.4 ( 0.6 ) 3.2
( 4.5 )
5 ( 15.8 )
13.9 ( 30.2 )
1.4 ( 1.8 )
21.6 ( 55.1 )
4.8 ( 10.2 )
16.2 ( 24.6 )
1.6 ( 2.2 ) 28.7
( 47.1 )
1.5 ( 7.5 )
6.3 ( 38.2 )
* *
Asturias Gipuzkoa S
Fig. 2. Description of third trimester of pregnancy phenol urinary concentrations in each regcreatinine.
confirms earlier reports in their observation that urinary phthalatemetabolites and phenols are commonly detected in the generalpopulation. Chemicals detected at the highest concentrations in our
-PB P-PB BP-3 BPA TCS
OLS
114.4 ( 269.5 ) 9.9
( 39.9 )
4.6 ( 18.7 )
3.3 ( 3.8 )
1.8 ( 23.6 )
219 ( 730 ) 36.8
( 56.4 )
1.4 ( 2.7 )
1.3 ( 3.1 )
1.1 ( 87.8 )
188 ( 229.2 )
36.2 ( 51.7 )
3.7 ( 9.4 )
1.5 ( 2.2 )
23.2 ( 106 )
222 ( 765.6 )
18 ( 115.4 )
4.8 ( 23.6 )
2.8 ( 3.6 )
5.2 ( 27.2 )
*
* p<0.05abadell Valencia
ion (medians and interquartile ranges in ng/mL) and p values adjusted for logarithm of

1
10
MEPMBPMiBPMCPPMEOHPMECPMCNP
Age (> 30 years old) High social class (I and II)Mid social class (III)
2
6
0.8
0.6
4
PHTHALATES
0.4
0.2
8
Fig. 3. Adjusted relative increases and 95% confidence interval of determinants of phthalate metabolite urinary concentrations in pregnant women. There is one model for each logtransformedmetabolite including all the determinants shown plus creatinine and region. Onlymodels with at least one coefficient p value below 0.25 in the determinants are shown.
864 L. Casas et al. / Environment International 37 (2011) 858–866
study populations were MEP and M-PB. MEP, a metabolite of diethylphthalate, and a compound used commonly in fragrances and otherpersonal care products, had also been detected at the highest medianconcentrations in previous studies performed in the USA and thenorth of Europe among the general population, (Calafat et al., 2008;CDC, 2010; Peck et al., 2010; Wittassek et al., 2007) pregnant women(Adibi et al., 2003, 2008; Castorina et al., 2010;Wolff et al., 2008; Ye etal., 2008, 2009), and children. (Becker et al., 2004, 2009; Koch et al.,
1
10 PHEN
0.4
0.6
0.8
2
4
6
0.2 EB-PB 2.5-DCP 2.4-DCP
8
Age (> 30 years old)
Fig. 4. Adjusted relative increases and 95% confidence interval of determinants of phenol urmetabolite including all the determinants shown plus creatinine and region. Only models w
2005, 2007; Wolff et al., 2010). Even so, MEP concentrations in ourstudy are significantly higher than those shown in other studies,except for one, the Children and Environmental Health Study in theUSA (Wolff et al., 2008) that reported higher urinary concentrations ofMEP in an ethnically diverse group of 404 pregnant women in NewYork City, NY. The urinary concentrations of all other phthalatemetabolites evaluated in our study were similar to the levels detectedin other studies. Regarding phenols, BPA urinary concentrations in our
OLS
TCSP-PB M-PB-PB
High social class (I and II) Mid social class (III)
inary concentrations in pregnant women. There is one model for each log transformedith at least one coefficient p value below 0.25 in the determinants are shown.

865L. Casas et al. / Environment International 37 (2011) 858–866
studywere similar to those reported for the USA general population in2003–4 (Calafat et al., 2008) but higher than in other USA studiesinvolving pregnant women (Castorina et al., 2010; Wolff et al., 2008;Ye et al., 2008). By contrast, 2,5-DCP, 2,4-DCP, TCS and BP-3 urinaryconcentrations in our study were lower than those reported before inother populations. These results suggest that some regional variabilityin the extent to phthalates and phenols exposure may exist. Thereported differences may be related to differences in the methodsused for analysis, to differences in study designs (e.g., timing ofsampling), to actual exposure differences across different geograph-ical regions, or to a combination of all of the above factors.
Several authors have discussed the inherent intra- and inter-variability of urinary phthalate and phenol concentrations mainly dueto the time of sample collection and measurement based on singlespot samples. For these reasons, Braun et al. (2011) propose usingseveral approaches to reduce or adjust for this variability: a) byadjusting for the time of urine collection, b) by collecting repeatedsamples to minimize biases (especially in pregnant women ideally itwould recommend using repeated measures taken over the pregnan-cy), and c) by correcting urine dilution using both specific gravity andcreatinine concentrations.
Furthermore, we found statistically significant differences for mostof the biomarkers examined between the four regions assessed in thecurrent study for pregnantwomen. Because these four cohorts followedthe same protocol, we assume this is not due to methodologicaldifferences but to actual geographical differences on exposure. Theseregional variations could be due to the observed differences in socialclass, education, and body mass index across regions, as well as todifferences in potential sources of exposure, such as packaged foodconsumption or body care products, that could not be assessed in thepresent study. The differences on individual characteristics togetherwith the regional climate differences (Atlantic in Asturias andGipuzkoa,and Mediterranean in Sabadell and Valencia) could lead to differentlifestyles across regions, and this could partly explain the regionalvariations in exposure we found. However, because of the relativelysmall number of samples per region evaluated (n=30), these resultsmust be interpreted with caution and cannot be generalized to thelarger population of pregnant women in Spain or even within the fourregions studied.
Previous studies have shown that urinary concentrations of certainphthalate metabolites in children may be two to four times higherthan in adults (Becker et al., 2009; Koch et al., 2005). The fact that inour study the children were not from the same region as the pregnantwomen, and that we observed significant differences in the women'surinary concentrations according to region, makes it difficult todetermine whether the differences we observed between children'sand pregnant women's urinary concentrations of some phthalatemetabolites and phenols are related to age or region. Because the timeperiod of children sample collection was included in the time periodof pregnant women sample collection (between years 2004 and2008), we can exclude this fact as a cause of the concentrationdifferences described between both population groups.
Regarding exposure determinants, several studies have suggestedassociations between exposure to phthalates and phenols and somesocio-demographical population characteristics (e.g., education andhousehold income), but results among studies are inconsistent. Forexample, some researchers have shown an inverse correlationbetween maternal education and phenol and phthalate metaboliteurinary concentrations (Adibi et al., 2009; Wolff et al., 2008), whileothers reported a positive correlation between the exposure to thesechemicals and household income (Ye et al., 2008). Further, a recentstudy conducted among Hmong women of reproductive age living inthe USA did not show any clear pattern between exposure tophthalates and education; women in the middle income categoryhad higher urinary concentrations of select phthalatemetabolites thanwomen in the high income category (Peck et al., 2010). In our study,
we observed a positive association between education and social class(based on occupation) and the concentrations of some phthalatemetabolites. However, given the small sample size these results mustbe interpreted cautiously. Thus, the small sample size might explainthe lack of associations between the biomarker levels and age or BMI.
The present study supports the evidence that environmentalphthalate and phenol exposures are prevalent in pregnant womenand children, two especially susceptible groups to the health effects ofthese contaminants; and this shows that this exposure might bepositively related to social class.
Disclaimer
The findings and conclusions in this report are those of the authorsand do not necessarily represent the views of the CDC. The authorsdeclare no competing financial interests.
Funding
This studywas fundedbygrants from InstitutodeSaludCarlos III (RedINMA G03/176 CB06/02/0041, FIS-FEDER 03/1615, 04/1509, 04/1112,04/1931, 05/1079, 05/1052, 06/1213, 07/0314 and 09/02647), SpanishMinistry ofHealth (FIS-PI041436, FIS-PI081151, FIS-PI06/0867, FIS-PS09/00090 FISS-PI042018, FISS-PI09/02311), Generalitat de Catalunya-CIRIT 1999SGR 00241, Obra Social Cajastur, Universidad de Oviedo,Department of Health of the Basque Government (2005111093 and2009111069), the Provincial Government of Gipuzkoa (DFG06/004and DFG08/001), Conselleria de Sanitat Generalitat Valenciana, andFundación Roger Torné.
Acknowledgments
We acknowledge Xiaoyun Ye, Amber Bishop, Xiaoliu Zhou, Tao Jia,Manori Silva, Ella Samandar, and Jim Preau (CDC, Atlanta, GA) formeasuring the urinary concentrations of phenols and phthalatemetabolites.
We would also like to thank all the participants in the INMAproject for their generous collaboration. A full roster of the INMAProject Investigators can be found at http://www.proyectoinma.org/presentacion-inma/listado-investigadores/en_listado-investigadores.html.
References
Adibi JJ, Hauser R,Williams PL,Whyatt RM, Calafat AM, Nelson H, et al. Maternal urinarymetabolites of di-(2-ethylhexyl) phthalate in relation to the timing of labor in a USmulticenter pregnancy cohort study. Am J Epidemiol 2009;169:1015–24.
Adibi JJ, Perera FP, Fedrychowski W, Camann DE, Barr D, Jackek R, et al. Prenatalexposures to phthalates among women in New York City and Krakow, Poland.Environ Health Perspect 2003;111:1719–22.
Adibi JJ, Whyatt RM, Hauser R, Bhat HK, Davis BJ. Transcriptional biomarkers ofsteroidogenesis and trophoblast differentiation in the placenta in relation toprenatal phthalate exposure. Environ Health Perspect 2010;118:291–6.
Adibi JJ, Whyatt RM, Williams PL, Calafat AM, Camann D, Herrick R, et al.Characterization of phthalate exposure among pregnant women assessed byrepeat air and urine samples. Environ Health Perspect 2008;116:467–73.
Akingbemi BT, Ge R, Klinefelter GR, Zirkin BR, Hardy MP. Phthalate-induced Leydig cellhyperplasia is associated with multiple endocrine disturbances. Proc Natl Acad SciUSA 2004;101:775–80.
Becker K, Göen T, Seiwert M, Conrad A, Pick-Fuss H, Müller J, et al. GerES IV: phthalatemetabolites and bisphenol A in urine of German children. Int J Hyg Environ Health2009;212:685–92.
Becker K, Seiwert M, Angerer J, Heger W, Koch HM, Nagorka R, et al. DEHP metabolitesin urine of children and DEHP in house dust. Int J Hyg Environ Health 2004;207:409–17.
Berman T, Hochner-Celnikier D, Calafat AM, Needham LL, Amitai Y, Wormser U, et al.Phthalate exposure among pregnant women in Jerusalem. Israel: results of a pilotstudy. Environ Int 2009;35:353–7.
Braun JM, Yolton K, Dietrich KN, Hornung R, Ye X, Calafat AM, et al. Prenatal Bisphenol AExposure and Early Childhood Behavior. Environ Health Perspect 2009;117:1945–52.

866 L. Casas et al. / Environment International 37 (2011) 858–866
Braun JM, Kalkbrenner AE, Calafat AM, Bernert JT, Ye X, Silva MJ, et al. Variability andpredictors of urinary bisphenol A concentrations during pregnancy. Environ HealthPerspect 2011;119:131–7.
Calafat AM, Ye X, Wong LY, Reidy JA, Needham LL. Exposure of the U.S population tobisphenol A and 4-tertiary-octylphenol: 2003–2004. Environ Health Perspect2008;116:39–44.
Castorina R, Bradman A, Fenster L, Barr DB, Bravo R, Vedar MG, et al. Comparison ofcurrent-use pesticide and other toxicant urinary metabolite levels among pregnantwomen in the CHAMACOS cohort and NHANES. Environ Health Perspect 2010;118:856–63.
CDC (Centers for Disease Control and Prevention). National report on human exposureto environmental chemicals. Available http://www.cdc.gov/exposurereport/. 2010[accessed 30 July 2010].
Domingo-Salvany A, Regidor E, Alonso J, Alvarez-Dardet C. Proposal for a social classmeasure. Working group of the Spanish Society of Epidemiology and the SpanishSociety of Family and Community Medicine. Aten Primaria 2000;25:350–63.
Dostal LA, Chapin RE, Stefanski SA, Harris MW, Schwetz BA. Testicular toxicity andreduced Sertoli cell numbers in neonatal rats by di(2-ethylhexyl)phthalate and therecovery of fertility as adults. Toxicol Appl Pharmacol 1988;95:104–21.
Duty SM, Silva MJ, Barr DB, Brock JW, Ryan L, Chen Z, et al. Phthalate exposure andhuman semen parameters. Epidemiology 2003a;14:269–77.
Duty SM, Singh NP, Silva MJ, Barr DB, Brock JW, Ryan L, et al. The relationship betweenenvironmental exposures to phthalates and DNA damage in human sperm usingthe neutral comet assay. Environ Health Perspect 2003b;111:1164–9.
Duty SM, Calafat AM, Silva MJ, Ryan L, Hauser R. Phthalate exposure and reproductivehormones in adult men. Hum Reprod 2005;20:604–10.
Engel SM, Zhu C, Berkowitz GS, Calafat AM, Silva MJ, Miodovnik A, et al. Prenatalphthalate exposure and performance on the neonatal behavioural assessment scalein multiethnic birth cohort. Neurotoxicology 2009;30:522–8.
Gray LE, Ostby J, Furr J, Price M, Veeramachanemi DN, Parks L. Perinatal exposure to thephthalates DEHP, BBP, and DINP, but not DEP, DMP, or DOTP, alters sexualdifferentiation of the male rat. Toxicol Sci 2000;58:350–65.
Gray TJ, Gangolli SD. Aspects of the testicular toxicity of phthalate esters. EnvironHealth Perspect 1986;65:229–35.
Hauser R, Meeker JD, Duty S, Silva MJ, Calafat AM. Altered semen quality in relation tourinary concentrations of phthalate monoester and oxidative metabolites.Epidemiology 2006;17:682–91.
Hauser R, Meeker JD, Singh NP, Silva MJ, Ryan L, Duty S, et al. DNA damage in humansperm is related to urinary levels of phthalate monoester and oxidativemetabolites. Hum Reprod 2007;22:688–95.
Jonsson BA, Richthoff J, Rylander L, Giwercman A, Hagmar L. Urinary phthalatemetabolites and biomarkers of reproductive function in young men. Epidemiology2005;16:487–93.
Koch HM, Becker K, Wittassek M, Seiwert M, Angerer J, Kolossa-Gehring M. D-n-butylbenzylphthalate— urinarymetabolite levels and estimated daily intakes: pilotstudy for the German environmental survey on children. J Expo Sci EnvironEpidemiol 2007;17:378–87.
Koch HM, Preuss R, Drexler H, Angerer J. Exposure of nursery school children and theirparents and teachers to di-n-butylphthalate and butylbenzylphthalate. Int ArchOccup Environ Health 2005;78:223–9.
Latini G, De Felice I, Presta G, Del Vecchio A, Paris I, Ruggieri F, et al. In utero exposure todi-(2-ethylhexyl)phthalate and duration of human pregnancy. Environ HealthPerspect 2003;111:1783–5.
Lin H, Ge RS, Chen GR, Hu GX, Dong L, Lian QQ, et al. Involvement of testicular growthfactors in fetal Leydig cell aggregation after exposure to phthalate in utero. ProcNatl Acad Sci USA 2008;105:7218–22.
Lomenick JP, Calafat AM,Melguizo CastroMS, Mier R, Stenger P. Phthalate exposure andprecocious puberty in females. J Pediatr 2010;156:221–5.
Meeker JD, Calafat AM, Hauser R. Urinary bisphenol A concentrations in relation toserum thyroid and reproductive hormone levels in men from an infertility clinic.Environ Sci Technol 2010;44:1458–63.
Meeker JD, Sthyanarayana S, Swan SH. Phthalates and other additives in plastics:human exposure and associated health outcomes. Philos Trans R Soc London B2009a;364:2097–113.
Meeker JD, Hu H, Cantonwine DE, Lamadrid-Figueroa H, Calafat AM, Ettinger AS, et al.Urinary phthalate metabolites in relation to preterm birth in Mexico City. HealthPerspect 2009b;117:1587–92.
Mendiola J, Jørgensen N, Andersson AM, Calafat AM, Ye X, Redmon JB, et al. Areenvironmental levels of bisphenol A associated with reproductive function in fertilemen. Environ Health Perspect 2010 [Epub ahead of print].
Mok-Lin E, Ehrlich S, Williams PL, Petrozza J, Wright DL, Calafat AM, et al. Urinarybisphenol A concentrations and ovarian response among women undergoing IVF.Int J Androl 2010;33:385–93.
Mylchreest E, Sar M, Cattley RC, Foster PM. Disruption of androgen-regulated malereproductive development by di(n-butyl) phthalate during late gestation in rats isdifferent from flutamide. Toxicol Appl Pharmacol 1999;156:81–95.
Pan G, Hanaoka T, Yoshimura M, Zhang S, Wang P, Tsukino H, et al. Decreased serumfree testosterone in workers exposed to high levels of di-n-butyl phthalate (DBP)and di-2-ethylhexyl phthalate (DEHP): a crosssectional study in China. EnvironHealth Perspect 2006;114:1643–8.
Peck JD, Sweeney AM, Symanski E, Gardiner J, Silva MJ, Calafat AM, et al. Intra- andinter-individual variability of urinary phthalate metabolite concentrations inHmong women of reproductive age. J Expo Sci Environ Epidemiol 2010;20:90-100.
Ribas-Fitó N, Ramón R, Ballester F, Grimalt J, Marco A, Olea N, et al. Child health and theenvironment: the INMA Spanish study. Paediatr Perinat Epidemiol 2006;20:403–10.
Samandar E, Silva MJ, Reidy JA, Needham LL, Calafat AM. Temporal stability of eightphthalate metabolites and their glucuronide conjugates in human urine. EnvironRes 2009;109:641–6.
Silva MJ, Samandar E, Preau JL, Reidy JA, Needham LL, Calafat AM. Quantification of 22phthalate metabolites in human urine. J Chromatogr B 2007;860:106–12.
Swan SH, Main KM, Liu F, Stewart SL, Kruse RL, Calafat AM, et al. Decrease in anogenitaldistance among male infants with prenatal phthalate exposure. Environ HealthPerspect 2005;113:1056–61.
Takeuchi T, Tsutsumi O, Ikezuki Y, Takai Y, Taketani Y. Positive relationship betweenandrogen and the endocrine disruptor, bisphenol A, in normal women and womenwith ovarian dysfunction. Endocr J 2004;51:165–9.
Talsness CE, Andrade AJM, Kuriyama SN, Taylor JA, vom Saal FS. Components of plastic:experimental studies and relevance for human health. Phil Trans R Soc London B2009;364:2079–96.
Weuve J, Hauser R, Calafat AM, Missmer SA, Wise LA. Association of exposure tophthalates with endometriosis and uterine leiomyomata: findings from NHANES,1999–2004. Environ Health Perspect 2010;118:825–32.
Whyatt RM, Adibi JJ, Calafat AM, Camann DE, Rauh V, Baht HK, et al. Prenatal di(2-ethylhexyl)phthalate exposure and length of gestation among an inner-citycohort. Pediatrics 2009;124:1213–20.
Wittassek M, Wiesmüller GA, Koch HM, Eckard R, Dobler L, Müller J, et al. Internalphthalate exposure over the last two decades — a retrospective humanbiomonitoring study. Int J Hyg Environ Health 2007;210:319–33.
Wolff MS, Engel SM, Berkowithz G, Ye X, Silva MJ, Zhu C, et al. Prenatal phenol andphthalate exposures and birth outcomes. Environ Health Perspect 2008;116:1092–7.
Wolff MS, Teitelbaum SL, Pinney SM, Windham G, Liao L, Biro F, et al. Investigation ofrelationships between urinary biomarkers of phytostrogens, phthalates, andphenols and puberal stages in girls. Environ Health Perspect 2010;118:1039–46.
Ye X, Bishop AM, Reidy JA, Needham LL, Calafat AM. Temporal stability of theconjugated species of bisphenol A, parabens, and other environmental phenols inhuman urine. J Expo Sci Environ Epidemiol 2007;17:567–72.
Ye X, Kuklenyik Z, Needham LL, Calafat AM. Automated on-line column-switchingHPLC-MS/MS method with peak focusing for the determination of nine environ-mental phenols in urine. Anal Chem 2005;77:5407–13.
Ye X, Pierik FH, Angerer J, Meltzer HM, Jaddoe VWV, Tiemeier H, et al. Levels ofmetabolites of organophosphate pesticides, phthalates, and bisphenol A in pooledurine specimens from pregnant women participating in the Norwegian Mother andChild Cohort Study (MoBa). Int J Hyg Environ Health 2009;212:481–91.
Ye X, Pierik FH, Hauser R, Duty S, Angerer J, Park MM, et al. Urinary metaboliteconcentrations of organophosphorous pesticides, bisphenol A, and phthalatesamong pregnant women in Rotterdam, the Netherlands: the generation R study.Environ Res 2008;108:260–7.