Getting Pregnant
528
g ettin g pre g nant
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Getting Pregnant

gettingpregnant
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page i

Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page ii
This page intentionally left blank

gettingpregnant
A COMPASSIONATE RESOURCE TOOVERCOMING INFERTILITY
AND AVOIDING MISCARRIAGE
Second edition
PROF. ROBERT JANSEN MD, CREI
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page iii

First published by Allen & Unwin in 1997This edition first published by Allen & Unwin in 2003Copyright © Robert Jansen, 1997, 2003
All rights reserved. No part of this book may be reproduced ortransmitted in any form or by any means, electronic or mechanical,including photocopying, recording or by any information storageand retrieval system, without prior permission in writing from thepublisher.The Australian Copyright Act 1968 (the Act) allows amaximum of one chapter or 10 per cent of this book, whichever isthe greater, to be photocopied by any educational institution for itseducational purposes provided that the educational institution (orbody that administers it) has given a remuneration notice tocopyright Agency Limited (CAL) under the Act.
Allen & Unwin83 Alexander StreetCrows Nest NSW 2065AustraliaPhone: (61 2) 8425 0100Fax: (61 2) 9906 2218Email: [email protected]: www.allenandunwin.com
National Library of AustraliaCataloguing-in-Publication entry:
Jansen, Robert, 1946- .Getting pregnant : a compassionate resource to overcominginfertility and avoiding miscarriage.
2nd ed.Bibliography.Includes index.ISBN 1 74114 133 8.
1. Pregnancy. 2. Infertility. 3. Conception. I.Title.
616.692
Set in 11/14 pt Bembo by Midland Typesetters, Maryborough,VictoriaPrinted by McPherson’s Printing Group, Maryborough,Victoria
10 9 8 7 6 5 4 3 2 1
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page iv

ContentsPreface to second edition viiSection I: Nature What should be going right . . . how your body interacts
with nature 1
Chapter 1. Pregnancy and chance 3Chapter 2. Evolution and ‘infertility’ 10Chapter 3. Behind a successful conception 19Chapter 4. Establishing a successful pregnancy 39
Section II: Tests What tests to have done and when 57
Chapter 5. Making a diagnosis 59Chapter 6. When pregnancy’s not possible: Sterility 76Chapter 7. When pregnancy’s not probable: Subfertility 81Chapter 8. Tests for miscarriages 92
Section III: Special treatment Treatments matched to what’s wrong 115
Chapter 9. Preventing and treating miscarriage 117Chapter 10. A low sperm count 134Chapter 11. Not ovulating 152Chapter 12. Complications from FSH therapy 175Chapter 13. Blocked fallopian tubes and microsurgery 182Chapter 14. Ectopic pregnancy 197Chapter 15. Diagnosing endometriosis 208Chapter 16. Treating endometriosis 220Chapter 17. Fibroids and other problems in the uterus 228Chapter 18. Abnormalities present from birth 236
Section IV:Assisted conception Short-cuts to a baby 255
Chapter 19. Helping nature a bit 257Chapter 20. Helping nature a lot: Assisted conception 264Chapter 21. Storing embryos, sperm and eggs 297Chapter 22. Donation and surrogacy 305Chapter 23. ‘Designer babies’? Hardly . . . 321
Section V: Getting what you deserve Pregnant or not, what to expectfrom people around you 337
Chapter 24. Pregnancy 339Chapter 25. Relief from suffering 350
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page v

Chapter 26. Your doctor’s duties 356Chapter 27 Embryo research and society 375
Appendices The arithmetic of it all, and a bibliography 385
Appendix 1. The arithmetic of infertility 387Appendix 2. IVF results 393Appendix 3. More reading 400
Glossary 417
Index 503
VI � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page vi

Preface to second editionMuch has happened in the five years since the publication of the first edition of GettingPregnant, yet much has stayed the same.
Commanding the stage is the rise and rise of in vitro fertilization, or IVF as the canvasfor certainty when reproduction is in trouble. Pregnancy rates are twice what they were,and they continue to increase.The procedure of gamete transfer to the fallopian tubes, amainstay of assisted conception for subfertility in the mid-1990s, is now all but obsolete.
Improved diagnosis of early pregnancy, declining family size, and the heightened expec-tations of people in our community that events are or should be controllable, are allcontributing to greater and greater concern with fertility and normal pregnancy.Miscarriage,rather neglected in the closing stages of the last century, is gaining ground not just as anunhappy consequence in all too many cases of infertility but as a cause of reproductivedisappointment in its own right—one that needs better understanding and management.The last five years have seen steady progress in understanding the basis for the immuno-logical tolerance of the fetus by the pregnant woman. New insights into causes of recur-rent miscarriage are being published monthly.These advances have led to a substantialexpansion of my book’s account of early pregnancy and approaches to the genetics of recur-rent miscarriage.
Advancements in genetic diagnosis are bringing new clinical indications to IVF.Preimplantation genetic diagnosis (PGD) is still difficult, but in leading centers it is becomingroutine. As genetic testing in the community becomes more widely appreciated andrequested, following completion of the mapping and sequencing of the human genome,the field is extending to more widespread pre-pregnancy genetic diagnosis (P-PGD).
IVF with PGD, already a part of the management of miscarriages caused by balancedchromosomal translocations, but responsible for only a small minority of recurrent mis-carriages, will increasingly be used as new insights into genetic variants of immuno-protective molecules such as HLA-G promise embryo-biopsy management strategies tochoose embryos least likely to miscarry.
Meanwhile for society generally, a gradual move to more practical, evidence-based ethicsand evidence-based regulation has been welcome.The general and thorough revulsion feltby responsible biologists and reproductive physicians for the work of a small number of roguescientists who announced an intention to push the dangerous techniques of human cloninghas strengthened the community’s confidence that faith-based moral reasoning need not bethe only path to guide society forward in the complex fields of biotechnology.
Politicians who have taken the trouble to understand the biology of embryonic stemcells have delivered reasonably permissive legislation on embryo research in Britain andAustralia.No one doubts that the twenty-first century will be the century of human biolog-ical understanding.Yet other aspects of infertility medicine—and of course infertile people—have not changed so much.The anxieties and the stresses are no different, except that thepromise of cure for more and more makes the position of those who cannot be helped ifanything sadder and more frustrating.As a community we must come to better terms with
VII
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page vii

the declining fertility rates in Western societies resulting in part from postponement ofchildbearing to an age that, for some women, is too old for fertility to happen.The oopause,the irreversible cessation of fertility, is now more widely known to precede menopause byas much as a decade.At least it is getting better known that older eggs behave badly andthat IVF cannot overcome their bad behavior.
Paradoxically, the success of modern IVF is eclipsing our understanding of specific,cause-based infertility. It is harder to train young doctors and other health professionals inthe nuances of ovulation induction, fallopian tube microsurgery, adhesion prevention,endometriosis management, and uterine reconstruction these days—techniques that sawtheir widest usage in a pre-IVF age.
I have been most fortunate to have had a career in reproductive medicine and surgerythat has spanned this time. One function of this book is to preserve some of this under-standing in a generally accessible way.
I have enjoyed preparing the second edition of this book even more than I did the first.I hope it shows.
Thanks to the very many people who contacted me during the life of the first edition,with suggestions, questions and encouragement; to Annette Borlow and Alex Nahlous andthe first class editors and subeditors at Allen & Unwin, who are relentless in getting thebest out of a book and its author; to my friends and colleagues at Sydney IVF and at RoyalPrince Alfred Hospital in Sydney, who have made the experience of delivering goodmedicine and surgery in an ethical environment so fulfilling over the last 20 years; to Dianaand our children, for the stability that makes life at home a platform for intellectualendeavor; and to my late father, P.C. Jansen FRMS (1914–1971), who prepared me for a lifein medicine and biology in many ways, not least rebuilding for me the Reichert micro-scope his father had given him.
Robert JansenSydney
May 2003
VIII � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page viii

section I
nature
what should be going right . . . how your bodyinteracts with nature
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 1

Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 2
This page intentionally left blank

pregnancy and chance
At the best of timesit’s not 100 percent
There was an old woman,who lived in a shoe; she had so many children, she knew notwhat to do.
English nursery rhyme, from about the sixteenth century.
At the best of times, and perhaps at the worst, pregnancy is a matter of chance . . . ofluck, good or bad.
Normal fertility varies between couples, so the chance of getting pregnant whenyou have sex around the time you produce an egg can be high—or the chance can be low.If the chance of pregnancy is too low, we have the disability we call infertility.
This book’s about infertility. But, once upon a time, high fertility too was a curse.Thischapter considers:• High fertility;• Normal fertility;• Low fertility, or infertility; and• Psychological, or unexplained infertility.
HIGH FERTILITY, A DISABILITY?
After about the year 1500 in England among the emerging wealthier classes, a boombegan in the practice of wet-nursing. (Today we might call it surrogate breast-feeding.)For these women, recently mothers and concerned more with preserving their figuresthan with feeding their new infants, the social practice of wet-nursing put a stop to
3
1
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 3

thousands of years of what is nature’s best contraceptive: lactation, or the production ofmilk by the breasts.
Wet-nursing was at first confined to the aristocracy and the gentry, but by the early1700s many middle-class women were forgoing this natural brake on fertility, this naturalway of spacing the birth of children. Shortly after birth, mothers were sending their infantsoff to recently pregnant women in the countryside who’d lost their own infants in child-birth.This helped the city mothers conserve their busts. But it also meant they werepregnant again within a few months of delivering their babies.Well-to-do English womenof that time had anywhere from a dozen to 20 babies, and 30 babies was not rare.Childhood mortality was high and parents’ concern about it generally low, but with stillso many surviving offspring to be placed and educated, a family’s wealth could soon bediminished.
Making children a commodity is a reproach we hear today from some critics of modernreproductive technology. But if ever children were a commodity, it was in England andplaces like it several hundred years ago, when they came by the dozen and nurturing themwas contracted out commercially. High fertility, at this unique time in history, was a starkdisability. How envied were those who conceived only every five years! In modern soci-eties an unplanned five-year wait between children means four years of anguish.Today wewould call the couple’s state infertility.
Now that the misfortune of high fertility can be overcome easily by efficient contracep-tion, it’s less obvious that there’s a very wide range of fertility that nature regards as normal.
NORMAL FERTILITY
When it comes to fertility, how do we separate normal from abnormal? We’re used to seeingwhat’s normal spread across a wide range of possibilities. In nature there’s the large withthe small, the tall with the short, the high with the low.The normal and the abnormalblend, often with no clear separation between them.Attributes that have disadvantages inone context have advantages in others. In practice we loosely call something ‘abnormal’ ifour encounters with it are outside what we expect.
And what can a young couple embarking on a family expect? We need to get a bitcloser to just what the chance of getting pregnant is each month—or what the chanceof conceiving is in one menstrual or ovarian cycle.We can call this statistic monthly fertil-ity. Nature gives normal monthly fertility a wide range.A French demographer, HenriLeridon, has studied records from rural European societies from a hundred years ago,when there was little or no effective contraception (except for breast-feeding). He calcu-lated that the average normal chance of getting pregnant for a young couple living in theFrench countryside and embarking on a family was 20 percent per month.The normalrange of this statistic, he found, was from about 7 percent per month to about 45 percentper month (more on what we mean by ‘normal range’ later).Arithmetic can show thatthe expected time such normal couples take to achieve a pregnancy is then in the rangeof two to 18 months.
But how society has changed since the careful parish records of country England and
4 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 4

rural France were put together in the 1800s! We now see couples starting their families ata much older age—in their thirties instead of their twenties or teen years.We also have theeffects of the environment on fertility, particularly the social effects of sexually transmitteddisease and the effects of environmental pollutants, responsible it seems for a long-termtrend downwards in sperm counts (discussed in Chapter 10).
The result of these changes in society from a hundred years ago is that, with morecouples who are older, we should halve the average monthly expectation of fertility from20 percent to about 10 percent.This gives a normal range of monthly fertility in ourcommunity of about 1.5 percent to 25 percent.The expected time taken to achieve preg-nancy will then be in the range three months to four years.
Normal or abnormal?
Medicine,with its art and its science, exists to render the abnormal normal.This is why oursocieties train doctors (for more, see the box, Medicine’s perennial paradox).
But who’s to say where the distinction between normal and abnormal lies? If fertility islike height or weight—with no sharp distinction between normal and abnormal—and ifwe were to represent it on a graph, we’d be left with calling, say, the middle 90 percent ofthe population normal, and both the top 5 percent and the bottom 5 percent (with greatestand least fertility) abnormal. Right here and now we’re not bothered by the top 5 percentof the population (these couples today no longer have a problem). But the bottom 5 percentis surely an under-representation of the problem.There’s the perfectly understandable pressurefor everyone with below average fertility to be concerned and to seek help.
PREGNANCY AND CHANCE � 5
Medicine’s perennial paradox
The slighter the variation from normal, the more trouble medicine has in correct-ing an abnormality.
Returning a circumstance that’s a departure from normal back towards normal(which, after all, is why medicine exists) is most likely to be successful when thedeparture from normal is major.
Because any medical or surgical intervention risks introducing disturbancesattributable to the intervention, the less the departure from normal the less likelyit is that the intervention will improve the situation, and not make it worse.Thedifficulty is exaggerated when there’s more than one abnormality, and separate butsimultaneously effective maneuvers need to be devised.
Taking a mathematical approach to understanding infertility is essential to appre-ciate how malignantly a combination of separately mild disturbances thwarts gettingpregnant—and I do this in Appendix 1.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 5

The difficulties that this is capable of causing in the allocation of resources by societyare not hard to appreciate. It’s the arbitrariness and the capacity for exaggerating the medicalextent of childlessness that troubles administrators of health maintenance organizations(HMOs), politicians, the radical feminists of the 1990s, and others in our society who arecritics of modern reproductive medical practice.
Public funding for the overcoming of childlessness came under close scrutiny every-where at the close of the last century.The most this chapter can seek to contribute to thepublic debate is to make the facts regarding difficulties in getting pregnant more widelyavailable and accessible. Society must ultimately judge what forms of assistance for havingchildren it will pay for, or even condone.
Meanwhile most doctors tend sympathetically to define abnormal as something trouble-some enough to draw a patient into the chair with him or her in the office. For sure, somedoctors are also administrators and others are social scientists.They might even argue withtheir patients about what’s best for the community.But the doctor an infertile couple wantto see is a doctor who puts their interests first, or who at least tells them when there areconstraints that stop this being done.The infertility doctor and the patient become alliesin securing what’s wanted, which is usually a baby.This is the position I take in this book.
There’s more on what to expect of your doctor and how to get it in Chapter 26.
STERILITY, SUBFERTILITY AND UNEXPLAINED INFERTILITY
Most couples expect to get pregnant within about six months of trying. If it has taken ayear,most will have at least thought of seeing a doctor.The tests that are done on the doctor’srecommendation lead generally to one of three conclusions.
First, there could be a definite cause found for sterility, where no amount of time avail-able will enable pregnancy. (We’ll give excuses for using such a harsh word in Chapter 6.)Sterility can arise from a complete absence of sperm cells (spermatozoa) in the ejaculate. It canresult from a complete absence of ovulation (anovulation); in the worst case there may be noeggs left in the ovaries (premature ovarian failure). It can result from a complete obstruction tothe fallopian tubes,which prevents sperm from reaching an ovulated egg to fertilize it.Or theembryos that result from fertilization can repeatedly fail to develop—perhaps because theeggs are abnormal (the cause of sterility in the oopause, the time of normal sterility leadingup to the menopause) or, less commonly, because disease of the uterus ruins implantation.
Sterility is the subject of Chapter 6.Second, a cause may be found for subfertility—by which we mean fertility that’s low in
relation to what we expect, but is not zero.Examples include endometriosis; a low sperm count;irregular ovulation; a problem of anatomy or physiology that lowers the chance of sperm oregg arriving for fertilization at the right place at the right time, like an abnormal cervix oran immune reaction against sperm (sperm antibodies); or an abnormality in the uterus disturb-ing implantation.
Subfertility is the subject of Chapter 7.Third, tests may show nothing wrong whatsoever.Literally, the infertility is unexplained.
Unexplained infertility is dealt with here, and in Chapters 2 and 7.
6 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 6

The temptation with unexplained infertility is to try to discover new causes of infer-tility or, failing this, to think of the infertility as psychological. As it turns out, the onlymajor new cause of infertility that’s been discovered in the last 15 years is the harmful effectaging has on a woman’s eggs, a phenomenon we call the oopause.
To be sure, IVF technology has given us new insights into what can sometimes gowrong,but it is still uncommon to discover a definite and insurmountable barrier to gettingpregnant with IVF.To generalize, for women under 35 having IVF for unexplained infer-tility we often uncover a previously unsuspected sperm problem in their partner; for womenover 35 it more often turns out to be egg-related. I will return to the temptation to explainthe otherwise unexplainable as ‘psychological’ further on.Meanwhile, as researching doctorsand informed patients we are left with the conclusion that, biologically speaking, muchinfertility is not strictly abnormal.
We sometimes still hear calls for more research into the causes of infertility—into howwe can stop infertility from happening.The crunch is that the chief culprits for the infer-tility prevalent in today’s society are social ones.Although less often than before, we havesexually transmitted diseases as causes of sterility.We have the probable but unproven possi-bility of environmental toxins as potentially important contributors to relative subfertility.But numerically more important than these two environmental threats, at least in theWestern world, is the modern social custom of normal women postponing getting pregnantuntil they are older than their most fertile years.
PSYCHOLOGICAL INFERTILITY
When time goes by without a pregnancy, mental stress is not far behind.Can it be the other way around? What part do psychological factors play in causing
infertility or in causing infertility to persist? Does ‘having a good holiday’, such as cruisingin an ocean liner, really help? How valid are well-meant comments like,‘If you’d only stoptrying so hard you’d get pregnant’? Is it useful to hear that if you could only relax, if youcould only forget about infertility, everything would be all right? Should you avoid havingsex before ovulation ‘to save up the sperm’, but add to the stress?
Although there’s some evidence that stress can lower sperm counts and so contributeto male-related infertility, there is no evidence that stress in women causes infertility if themenstrual cycle is undisturbed and if having sex is not being overlooked. In fact the oppositemight be true.
One reason the mistaken notion that stress causes infertility is so widespread is thateveryone seems to have heard of couples who adopt a child and then promptly conceiveone of their own,despite years of infertility.We refer to such evidence as being ‘anecdotal’—relying on spectacular examples that blow you over instead of relying on boring, painstak-ing studies to work out what actually happens.
Remember Mark Twain, who said, ‘Get your facts first and then later, at your leisure,you can distort them as much as you please’? The facts are that there are only two goodpsychologically based reasons for a woman not getting pregnant: not ovulating properlyand not having sex.There have been no fewer than five careful studies on the real chance
PREGNANCY AND CHANCE � 7
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 7

of getting pregnant after adoption.These are studies that compare adopting couples withsimilar couples who have been trying for just as long but who are not adopting. In everyone of these five studies, it was obvious that couples who kept trying to get pregnant insteadof adopting had more chance of conceiving than those who adopted!
When you think about it the reasons are plain: once you adopt a baby the pressure tohave sex is off and you do it less often; you might even avoid it at midcycle on purpose.Acrying baby, your own or adopted, does disturb your sex life.
Psychological stress needs to be extreme if it’s to cause anovulation, that is, no ovula-tion, which is signaled by absent periods (amenorrhea). It’s most unusual for the ordinarystresses of modern life to be enough to stop ovulation completely, but stress around thetime of ovulation could make an ovulation less optimal than it might be (see the box,Stressedmonkeys). Certainly exercising too much or losing weight are important causes for ovula-tion to fail, and are discussed in Chapter 11. In fact, clinical psychologists have measuredstress among a sizeable group of women considering IVF for their infertility.Two years laterthe women with the most chance of having a baby were, on average, those who had shownthe highest stress levels in the earlier survey.
8 � GETTING PREGNANT
Stressed monkeys
Reid Norman works with rhesus monkeys at the Texas Tech University HealthSciences Center in Lubbock,Texas.
Monkeys are among our close relatives in the animal kingdom and in many waysresemble us in their reproductive physiology, including their 28-day menstrual cycle.Dr Norman has been investigating the effects of brief periods of mental stress onthe process of ovulation.
Norman and his colleagues have shown that six hours of physically constrain-ing female monkeys closely—the monkeys, for example, were strapped comfortablybut irritatingly to a chair—interferes with levels of luteinizing hormone (LH, whichcauses the mature ovarian follicle to ovulate—detailed in Chapter 3).The way thishappens seems to be a result of an increase in cortisol, the main hormone of theadrenal gland and commonly increased by physical or mental stress.
This inhibitory effect of cortisol on the monkeys’ LH was noticeable in the firsthalf of the menstrual cycle (the follicular phase) but not in the second half (the lutealphase). In extreme cases, suppressing LH by stress-induced increases in cortisol (orpossibly by other mental and neurological pathways in the brain that involve GnRH,the hormone directly responsible for production of LH) may stop ovulation alto-gether, disturbing the menstrual cycle rather obviously.
In less severe cases there may be enough LH to luteinize the mature follicle butnot enough to cause it to open and release the egg—resulting in what is known asthe luteinized unruptured follicle.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 8

We would not advise getting stressed for the sake of it: pregnancy can certainly happenif you’re not stressed but nevertheless committed to keep trying. So by all means avoid stressif you can (it’s what we all want to avoid), but if stress is part of your life don’t get extra-stressed worrying that stress is stopping you from conceiving. If you’re ovulating and you’rehaving sex, stress isn’t the cause of your infertility.
On the second psychologically related factor, you do need to have sex at more or lessthe right time.This is an area where many couples get into a vicious circle. Sex is post-poned in the hope of saving up for a heavy hit that’s meant to coincide with ovulation.Then the moment comes (or is thought to come) and stress or some other excuse gets inthe way.
Is having sex often ever bad for getting pregnant? No.No-one has ever shown that youcan have sex too often for fertility.What has been shown is that frequent ejaculation decreasesthe concentration of sperm in each ejaculate examined in a laboratory. But who cares?Research and common sense both point to the best place for sperm being not the labora-tory but the vagina—or,more exactly, the mucus of the cervix,where sperm are nourishedand stored over several days for steady release upwards towards the fallopian tube.The moresperm that get there, and the fresher they are, the better. If this is two or three times aday, then wow! And this will be true no matter what sperm count result you get from thelaboratory.
If, as a young couple, you’re living in a room at home with your parents or his—maybewith other children and with thin walls—having sex is going to be a stressful event, andalmost certainly is not going to be as frequent or successful as it would be otherwise. Ashort holiday—a weekend or a week away during ovulation—will tend to work wonders.A small amount of wine does no harm either. I go into what can help in more detail inChapter 19.
GOODBYE TO THE DO-GOODERS
To sum up, you can say goodbye to the do-gooders who tell you to relax and you’ll getpregnant.There’s just no evidence that for most people this is true.
Certainly it’s good for the chance of getting pregnant if you have sex more often, andno doubt it will help if it’s more fun, but you can forget the myth that there’s some myste-rious, psychological link between the stress of not getting pregnant and continuing not to.Thinking about infertility doesn’t stop you getting pregnant.
The fact is that what we today call unexplained infertility, as well as much ‘not-well-explained’ infertility, is a natural, normal phenomenon.We’ll look at why this distressingcondition has evolved to be so common in Chapter 2.
PREGNANCY AND CHANCE � 9
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 9

evolution and ‘infertility’
Why you are more normalthan you think
GETTING PREGNANT CAN BE TOO EASY
Iexplain here why nature often seeks to limit fertility—and why evolution has producedso much genetically determined infertility among humans. In doing so we willconsider:
• Reproductive strategies in nature;• Why nature puts a brake on fertility;• Why PCOS is good in a famine;• Why humans have high rates of miscarriage;• Why humans have low sperm counts;• Why humans get endometriosis; and• How unexplained infertility puts you at the top of the evolutionary tree.
FROM AMOEBAE TO HUMANITY
From single-celled animals such as the amoeba to complex multi-celled animals such asman, successfully reproducing organisms that are part of expanding populations gatherresources so that their progeny will outnumber their ancestors. In today’s society, humansneed to have an average of just over two children per couple to sustain the population.More than this will increase it.
But back in the fourteenth century, sustaining or growing the population meant havingsix or more children per couple.This was because of the high likelihood of death, not justof the children within families, but also of the adults before their dependent children were
10
2
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 10

grown up and able to have children of their own. (For a brief account of the transition, atleast how it was recorded in public by contemporary European artists, see the box, Thegrowing value of children in European history . . .)
For a species to succeed, it’s not enough just to give birth. For a human couple to bereproductively successful—for their reproductive strategy to triumph—they not only musthave children, they must also survive long enough to rear their offspring to an age at whichthe children become fertile adults. Children need to be nurtured to the point ofindependence, otherwise the reproductive effort is wasted.This principle lies behind thereproductive strategy of all large animals. (See the box, Of whales and women.)
EVOLUTION AND ‘INFERTILITY’ � 11
The growing value of children in European history . . .
Secular medieval paintings, when they are not depicting the Madonna and child,display the trials and tribulations of ordinary life. But children are rarely depicted.
Even the typical Madonna from the Middle Ages uncommonly pictures empathyfor the infant in her arms.
With the rise in wealth that accompanied the Renaissance, children began morecommonly to survive childhood, and came to be treasured as individuals from anearlier age, taught to be useful, and undoubtedly dressed up to be prized.
When you compare the medieval Madonna with a modern depiction of motherand child, today’s child is no commodity!
For more on the role of children in the family in the late Middle Ages, I recom-mend Barbara Tuchman’s book, The Calamitous 14th Century.
Of whales and women
Population scientists talk of two general strategies for achieving reproductive fitnessamong animals.
These two strategies are mutually exclusive.They mean that all-out reproduction(just having as many offspring as possible) is not always the best way for a populationto grow reliably and for a species to flourish in the long term.
r-selectionThe first reproductive strategy, r-selection, is contingent largely on the rate of repro-duction—how rapidly a species can produce offspring.
Key features are rapid sexual maturity, superabundant production of eggs by thefemale, low survival rates of offspring, and a short life for the parent. r-selection istypically favored by (or forced on by nature) smaller species, whose numbers wax
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 11

and wane dramatically with changes in the environment.When the environmentturns bad, numbers decline drastically.When it improves again, an explosive increasein numbers is needed for the species to exploit the opportunity quickly.Reproductive growth is highly leveraged . . . but adult life is brittle and short.Thinkof insects, butterflies and all sorts of other small animals.The mother might notsurvive more than a few hours after laying eggs. Relatively speaking, small mammalssuch as mice (and the mouse-like Australian native marsupial species Antechinus)show features of r-selection too, such as large litters, short times to maturity and ashort adult life, often with death after reproduction.The father might not survivemore than a few hours after copulation, all energy having been given to produc-ing sperm and competing with his rivals.
K-selectionThe second strategy, K-selection, shows sexual maturity gained slowly, limitedproduction of eggs, high survival rates of (usually single) offspring, and a longer lifefor the parent, generally with several episodes of gestation—and invariably with apremium placed on parental care of the young.This strategy witnesses competitionat the longer term capacity (K) of the environment.
It means that the offspring must reach first the size, then the sexual maturity, toreproduce, and thus for their parents’ genetic potential to be finessed.
In general, the larger the animal, the more it will rely on a K-selective strategyfor reproductive success: whales and elephants both have long gestation periods (15months for sperm whales, 22 months for elephants), long times from birth to adoles-cence and sexual maturity, and three- to five-year intervals between births, to protectthe parent and the existing offspring from the ravages frequent pregnancy otherwisewould have on the mother.
Our species, Homo sapiens, has become even more K-selected than the world’slargest mammals, despite our being physically much smaller.This is because the timethat our young need to grow to be independent has, for different purposes, becomethe same.
Our gestation periods are shorter, at nine months, so that our large-headed babiesdon’t get stuck during birth too often. So human infants are much more depend-ent at birth than whale calves or elephant calves are, with large brains anticipatingthe learning that will follow. Add to this the time it takes for the human brain tomature and be educated and we have in our species the longest times of childhooddependency and vulnerability seen on the planet.
Yet reproduction takes its toll on humans also.There is an ever-present risk ofdeath in childbirth, especially from bleeding, and in all but the most well-fed soci-eties aging occurs quickly during the child-bearing years.Correspondingly, in naturalcircumstances, graced by few trappings of civilization, the interval between humanbirths—the ‘birth interval’—is about the same as the three years or more foundamong whales and elephants.
12 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 12

In the course of our evolution towards bigger and better brains, the time from birth tomaturity has also increased considerably—spectacularly so for animals of our size.Theanatomy of the female pelvis eventually limited the size the fetus’s head could be at birthwithout getting stuck on the way out, so a lot of brain development had to occur after birth.This in turn meant that infants were born less and less mature, more and more vulnerableand reliant on their mothers, so a longer time came to be devoted to dependent infancy andchildhood.But childhood and adolescence also came to be extended with increasing ultimatebrain size and the time needed for the person to learn living skills.
In primitive human societies, menarche, the time of the first period (pronounced‘menarcky’), is at about 161/2 years. First pregnancy is not till about 18 years. (For more onthe consequences on the growing gap between menarche and the age of readiness to havechildren in modern societies, see the box, ’Twixt sex and reproduction.)
Pregnancies and bearing children wear a mother out. Having many children isextremely detrimental to a woman’s health, and also to her ability to raise the childrenshe’s got. Put simply, too much pregnancy can be bad for you and bad for the survival ofyour genes, especially if the environment is harsh and challenging, as it has probably beenfor most of human history and prehistory—indeed, as it has been right up to the mostmodern of times.
So, interestingly, we have a reproductive strategy in which delaying sexual maturityamong the offspring turns out to be an advantage for our species. (To understand howpopulation scientists distinguish r-selection and K-selection population strategies—and tounderstand where we as humans sit in the scheme of these things—see the box, Of whalesand women.)
During this time it’s important for the continuation of the species that childhood besecure: that parents in general, and mothers in particular, don’t wear themselves out bygetting pregnant too often.As a result, we have experienced much evolutionary pressurefor curbing fertility, for the birth of children to be spaced.
PUTTING A BRAKE ON FERTILITY
Spacing pregnancies in mammals—humans as well as the largest of them, whales andelephants—has come about in several ways.
One way is through ‘lactational amenorrhea’, the inhibition of ovulation, and for humans theinhibition of menstrual periods that’s caused by suckling the young at the breast.This is thechief natural contraceptive of the great apes and humans.To be an effective contraceptive,
A lengthening birth interval for our prehistorically evolving hominoid ances-tors depended on various natural ways—various biological devices—for spacingpregnancies.We need to understand the importance of long birth intervals and thenature of nature’s devices for achieving these long intervals if we’re to comprehendwhat today we call infertility.
EVOLUTION AND ‘INFERTILITY’ � 13
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 13

though, breast-feeding shouldn’t be diluted by other feeding.The hunter-gatherer !Kungnomads of the Kalahari Desert in southern Africa feed their babies several times an hour forthe first two or three years of life,and sleep with them at the breast; as a result, the average birthinterval among the !Kung is over four years, despite their natural, apparently high, fertility.There’s no way of knowing,though, for what time in human history and prehistory such inten-sive suckling has been usual.Modern but primitive societies such as the !Kung may have evolvedconsiderably from the early tribes we once had in common as ancestors.
Seasonal breeding among mammals is also associated with a lack of ovulation in theoff-season. It helps space pregnancies among the lesser apes, such as the lar gibbon ofthe Malayan rainforest. But among humans, other than the observation that we havehigher sperm concentrations in winter, seasonal changes in fertility are not conspicu-ous. (Probably men and women outside the tropics, through clothing, shelter, and some-times migration, have successfully adapted the environment to provide rough constancybetween the seasons.)
Environmental constraints on human fertility are seen, though, in the stop that occursto periods and to ovulation when a woman loses weight to below that at which, duringadolescence, menstruation began (explained further in Chapter 10).An intriguing excep-tion to this occurs with the polycystic ovary syndrome, in which fertility in the past mighthave been best during times of famine (see the box, PCOS: Fertility in famine).
But over the last several hundred thousand years, in environments less harsh than theKalahari Desert, suppressed ovulation from breast-feeding might not have been contraceptive
’Twixt sex and reproduction
Reproductive function in women is dependent on the production by the hypothal-amus of gonadotropin releasing hormone or GnRH (discussed in Chapter 3). GnRH isvery sensitive to body weight.The physiological result of this sensitivity is that theimprovement in human nutrition that’s taken place in many societies in the lasthundred years has produced an important lowering in the age at menarche from 15to 16 years in the mid-nineteenth century (and still today in primitive societies) to12 to 13 in today’s developed societies.
At the same time, the need for enculturation of our young is raising even furtherthe age at which emotional and educational maturity are reached.This counter-K-selective long-term trend in age at menarche has increased further the gap betweenthe ages of physical and mental maturity for adolescents—a gap that’s already hadclear and deep social consequences in the West.
Biology seems always to have been destined to play havoc with nineteenth-century morals and twentieth-century ideals. I explore the implications in an essaypublished in 1999 in the Medical Journal of Australia, called ‘Sex, reproduction andimpregnation: By 2099 we won’t confuse them’.
14 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 14

enough—as steadily evolving higher intelligence and increasing brain size and complexitydemanded co-evolution of longer and longer childhoods.
So what was it, then, that nature could turn to for evolving early humans to extendtheir birth interval and to increase the number of young raised safely to maturity? Howdid evolving humans, pressed to reproduce, unconsciously slow down their fertility toachieve an ultimately successful reproductive strategy?
Not by limiting sexuality—that is, not by getting rid of the pleasure of sex. DesmondMorris, among others, has argued convincingly in his book The Naked Ape that sexuality(probably a million or more years ago) had become—and remains today—the enjoyablecement needed for human relationships to be durable in the long term. Predictable sexualreward was presumably important to help make sure that females had the food supplied bytheir mates for themselves and for their dependent children.
Today, the lessons of medicine tell us that fertility in humans is not only rather low bythe standards of other primates, but that a number of conditions that diminish fertility havea genetic cause . . . an evolutionary cause.
PCOS: Fertility in famine
With the polycystic ovary syndrome (PCOS, discussed in Chapter 11) we have anotherexample of an at least partly inherited condition that diminishes fertility (by length-ening the menstrual cycle and reducing the frequency of ovulation), thus advantag-ing the evolution of reproductive success.
But Dr John Eden, a reproductive endocrinologist at the Royal Hospital forWomen in Sydney, believes that PCOS could have had more direct evolutionaryadvantages in some special circumstances.
In times of starvation, most women’s periods stop and they become infertile asthey lose weight.But would it be useful for some women to show the opposite? Saya famine went on for more than a generation—if all women stopped ovulating thepopulation would be wiped out!
You can imagine that at times of prolonged famine (and subnormal weight),some women—a minority, perhaps—would advantage the population by retain-ing their capacity to reproduce, even at the expense of decreased fertility in timesof plenty.
This is exactly what happens among women with PCOS, who may have irreg-ular periods (and ovulations) at normal body weight (and who stop ovulatingcompletely as they gain weight into the realm of obesity), but who will usuallyovulate well if their weight falls considerably below what we call normal.
This historical legacy could explain why perhaps as many as one in five ofall women have evidence of polycystic ovaries when the condition is looked forcarefully.
EVOLUTION AND ‘INFERTILITY’ � 15
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 15

SUBFERTILITY, A BENEFIT?
Any or all of the clinical conditions we can identify today with subfertility might have actedbeneficially to limit human fertility during our evolution, and thus to improve successivegenerations’ chance of reproductive success.
Any or all of these identifiable conditions we associate with clinical infertility might infact be inseparable from our species’ successful long-term reproductive strategy.
Many miscarriages
A high chance of miscarriage can serve a useful purpose in long-childhood species, accord-ing to Roger Short, a reproductive biologist at the University of Melbourne, and co-authorof Ever Since Adam and Eve. Short draws attention to the advantages brought by ‘a sprin-kling of genetically defective gametes [to produce] a measure of non-recurrent infertilitythrough early embryonic death’.Evidence of high rates of failure of early pregnancy amonghumans shows that no more than 25 percent to 50 percent of fertilizations will produce ahealthy pregnancy—a lower proportion than among the other primates.We see this inour IVF programs today: a majority of the embryos of normal women we test as part ourPGD/sex-selection/Down syndrome-prevention program at Sydney IVF have abnormalnumbers of chromosomes, or aneuploidy.Aneuploidy is usually of maternal origin and therisk of it increases with maternal age—or at least with a decline in the population of eggsremaining in the ovaries. It is by far the commonest genetic cause of human reproductivefailure.
There appear to have been similar evolutionary pressures among other species withlong childhoods because of the demands of huge adult size and hence a requirement formaternal longevity. According to Dr Short, whales too have high rates of embryonicdeath.
Low sperm counts
The inheritance of low sperm counts, or oligospermia (Chapter 10), has a similar effect todefective eggs in systematically diminishing fertility. Roger Short and others have shownthat variation in sperm counts and in the size of the testes in primates is determinedgenetically.
Before I had known about Roger Short’s work, I had an exciting encounter with theAmerican urologist Sherman Silber in an airport lounge in Singapore. I was explaining mytheories of evolutionary causes for the high prevalence of endometriosis in modern women(see the next section) when he drew my attention to the advantages that genetically deter-mined oligospermia may paradoxically have for men (at least men in monogamous rela-tionships).What we had in common—and, it turned out, in common with Dr Short—wasthat independently we had all reached the conclusion that by limiting fertility withoutlimiting sexuality, evolving humans (or more exactly groups of humans as societies) probablywere able to achieve greater ultimate reproductive fitness.
16 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 16

Endometriosis
Endometriosis (explained in detail in Chapter 15) is a condition in which tissue the sameas the lining membrane of the uterus, the endometrium, develops in locations outsidethe uterus, changing the environment for the woman’s pelvic organs and producingsubfertility.
Endometriosis becomes more common with age during the reproductive years, as themodern woman, generally neither pregnant nor breast-feeding (unlike her ancient prede-cessors), experiences an unprecedented number of ovulatory menstrual cycles—each oneincreasing the chance of new lining developing in the wrong place.
Endometriosis is rarely severe enough to be an undoubted cause of sterility, but severallines of evidence show that fertility is reduced even in mild endometriosis. Such informa-tion fits a theory that endometriosis reduces fertility in a manner that could be called ‘dose-dependent’—the more endometriosis, other things being equal, the greater the reductionin the chance each month of getting pregnant.
Endometriosis has been found in the other menstruating mammals, namely monkeysand apes, but only occasionally does it obviously disable them.Endometriosis could possiblyhave evolved independently in early humans,but more probably nature seized on this mostlyharmless consequence of menstruation in primates, opportunistically bestowing it with anadded responsibility.This would mean that endometriosis may date from at least 14 millionyears ago (which is when the Old World monkeys separated from the line destined tobecome humans).
Whether my exercise in theoretical anthropology is right or wrong, endometriosis isso common in women that, given its hereditary basis, it’s plausible that nature—at the cruelexpense of significant symptoms for many modern sufferers—kept it and developed it fora purpose.That purpose could have been to improve reproductive fitness through dimin-ishing fertility.
But, today . . .
Today there are three big problems in the way nature dumps you with the legacy of thisstrategy.
First, whereas a mild dose of an inherited infertility condition such as endometriosismight not be much more than a nuisance, remember that you get half your genetic inheri-tance from your mother and half from your father.While a single dose of endometriosis genesmight cause only minimal or mild endometriosis, every now and then, by chance, a womanwill get a double dose of the genes, producing crippling endometriosis and virtual sterility.
Second, again while a mild dose of endometriosis by itself, genetically determined andinherited, might not be much more than a nuisance, every now and then one of the othergenetically determined fertility restraints will be co-inherited (either by the woman herself,or by her partner).Thus oligospermia in the male and endometriosis in the female are acommon combination among infertile couples.Or you might see endometriosis and poly-cystic ovaries occurring in the one person.
EVOLUTION AND ‘INFERTILITY’ � 17
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 17

And that indeed is then a whole new ball game. It means that instead of, say, taking12 months to conceive rather than the more usual four months or so, it can take five orsix years. (If the arithmetic of this interests you, it’s in Appendix 1.)
And third, the physical or social environment can impact on what otherwise is a mildfertility restraint and again put you behind the eight ball. Examples include multiplying inthe effects of delayed child-bearing. By the thirties, not only is the endometriosis likely tohave developed somewhat further, but age-related effects on eggs are starting to show, andother age-dependent abnormalities such as fibroids are becoming more prevalent.
So there are three ways that a single ‘natural fertility restraint’, while of benefit to thespecies’ reproductive strategy on a population basis, can wreak havoc with individuals’ repro-ductive ambitions. If it were isolated and mild there would be no serious difficulty withconception, but the chance coming together of two factors, or the chance genetic exag-geration to a more severe form,or the impact of an added environmental factor, transformsthe desirable restraint it puts on fertility for the population into the unwelcome burden ofserious infertility for the individual.
YESTERDAY’S ADVANTAGE
You can conclude from this chapter that low human fertility is the result of a long andgenerally positive evolutionary sequence.What today we call unexplained infertility is by nomeans abnormal: it’s a highly evolved human condition.
But that’s not to say it ought not to be treated. Having to wait about five years to getpregnant is no longer considered the pinnacle of human reproductive achievement thatsociologically it once might have been. Just as we use contraception to minimize the socialdisadvantages of excessive fertility, so we’re justified in employing assisted conception tocope with insufficient fertility.
To appreciate the finer points of infertility and its effective treatment, Chapter 3 takesus into those normal workings of the body that lead to getting pregnant naturally.
18 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 18

behind a successful conception
How the ovaries, tubesand uterus work
While a girl may have her first menstrual period at 12 or 13, her ovaries have never-theless been functioning since before she was born.The eggs in each ovary weremade while she was a fetus, while she was still in her mother’s uterus, when her
mother was between about 14 and 20 weeks pregnant.The most eggs a woman will ever have, or have had—about seven million—is when
there’s still 20 weeks to go before birth. From this time on, there will be fewer and fewer,and none will be replaced. By the time of birth there are about two million eggs left in theovaries—a fraction of the original number.
Here we consider:• Eggs (ova and follicles) and what makes them grow and then ovulate during the ovarian
cycle;• Sperm and how they are produced;• The fallopian tube, the uterus and the cervix;• Conception, including fertilization and implantation; and• Establishment of pregnancy.
OVA AND FOLLICLES
As the eggs are made in the embryo (see the box, Laying down eggs for the future),they’re surrounded by a thin layer of cells to form a follicle.The follicle cells will support theegg they enclose for up to 50 years or more, providing it with nourishment, yet stoppingthe egg from maturing. Eggs that are left bereft of a follicle soon die and disappear.
19
3
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 19

When follicles grow inside the ovary, it’s because the follicle cells are multiplying,increasing in number from a handful to many thousands.
The great majority of follicles, however, never grow to maturity and ovulate; they startto develop,but then conditions for them to keep growing are not right; the egg they containloses its nourishment and dies; the follicle cells themselves die; and the tissue from the follicleis absorbed back into the ovary.We call this process atresia: the egg undergoes atresia andso does the follicle.
Atresia continues until all the follicles are gone.The younger a woman is, the more folli-cles at any one time are starting to develop, and hence the more follicles will be undergoingatresia.Atresia starts in the fetus, continues through childhood, adolescence and the reproduc-tive years, and finishes after the menopause,when finally there are no eggs left.Atresia marcheson at the same rate,heedless of pregnancy,heedless of using oral contraception (the birth controlpill), and heedless of conditions in which the periods stop (amenorrhea). Only during ovarianstimulation for assisted conception is it overcome . . . transiently and incompletely.
At the time of the first period, when reproduction first becomes possible, at least tech-nically, there are just 300 000 or so eggs left in the ovaries.
And so it continues. Every day, some resting, primordial follicles begin their growth withan increase in size of the egg (it ends up about 60 times bigger) and an increase in thenumber of follicle cells and in the size of the overall follicle. For those that escape earlyatresia, this long, slow growth, before they can be recruited into your menstrual cycle, beforethey can make estrogen and before they have a chance of being selected for ovulation, takeseight months.
20 � GETTING PREGNANT
Laying down eggs for the future
The process by which the eggs,or ova, are formed in the fetus is called oogenesis, and themultiplying forms of the eggs are the oogonia.The oogonia have all gone by birth.Fromthen on the eggs are in the form of primary oocytes,which cannot divide now except ina way called meiosis,by which the egg’s genetic complement (the chromosomes) is halved.
The equivalent of oogonia in males, the spermatogonia, persist in the testis through-out life, multiplying and replenishing themselves the way all other cells in the bodydo, by mitosis.
Why does nature insist that all the eggs are made before birth, whereas newsperm cells are usually made into old age? The reason must be important, because itseems to be true for much of the animal kingdom.Whether it be fish, frogs, reptiles,birds or mammals, the eggs are formed before the female of the species becomesfertile.
For some speculation on why eggs need to be laid down fast and then kept insuspended animation while waiting for their owner to grow up and reproduce, readthe Chapter 7 box, How eggs might get their ‘use-by’ date: Mishaps in the mitochondria.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 20

THE PITUITARY GLAND’S CONTROL OF THE OVARIES
The pituitary gland, lying under the brain behind the nose, produces two hormones thatthe ovary needs for ovulation: follicle stimulating hormone (FSH) and luteinizing hormone(LH), which in turn are controlled from higher up (see the box, Pituitary hormones dependon the brain).
The purpose of FSH, as the name indicates, is to keep follicles growing once they’vestarted.What makes a particular follicle start to grow after so many years of rest? This is stilla puzzle, but the number that will be getting going, say in one day or in one week or inone month (it’s a continuous affair), depends on how many follicles are still in the ovaries.
The purpose of LH (this hormone’s name can stay unexplained until later) is to pusha fully developed, large, preovulatory follicle into going further ahead and ovulating—whichwe’ll also get to further on.
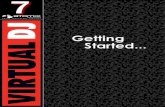
A resting follicle, or primordial follicle, is about one-eighth of a millimeter in diameter—only a little bigger than the egg it contains. It starts to grow, for a reason that’s still obscure,as the follicle cells begin to divide and increase in number (see Figure 3.1).As the folliclegrows, the follicle cells produce fluid, which forms an enlarging space, or antrum, amongthe cells, leaving the egg to one side attached to the wall of the follicle and still surroundedby a layer of follicle cells. (For a summary of what the follicles are called through thesestages see the box, Follicle talk.)
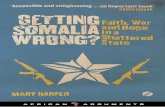
Figure 3.2 shows the changes in pituitary hormones and ovarian hormones during atypical ovarian cycle. Refer to it while we consider how a follicle does its amazing finalgrowth spurt and then ovulates.
An antral follicle that’s to have a chance of ovulating has to have been slowly growingfor about eight months and will be about 2 millimeters in diameter by the time the ovariancycle we’re about to focus on starts.Yet within two weeks at least one follicle will have adiameter 10 times greater—a thousand-fold increase in volume and a million-fold or moreincrease in cells.
BEHIND A SUCCESSFUL CONCEPTION � 21
Pituitary hormones depend on the brain
Production of FSH and LH by the pituitary gland demands stimulation from the partof the brain that lies immediately above it—the hypothalamus.The hypothalamus doesthis by means of gonadotropin releasing hormone (GnRH).
The hypothalamus secretes GnRH into special veins that go only to the pitu-itary gland.The pattern of this secretion is pulsatile, occurring as a spurt every 60 to90 minutes, continuing from the beginning of the cycle right through to the timeof ovulation.
Chapter 11 describes the pulsatile administration of GnRH intravenously toinduce ovulation in women in whom the hypothalamus isn’t working properly.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 21

As the woman’s period starts from the end of the previous cycle, there’s a small rise inFSH levels in the blood—enough to get this group,or cohort, of similar follicles being recruitedinto the cycle and growing further, instead of immediately undergoing atresia.The numberof follicles in the cohort (spread between the two ovaries) will depend inversely on thewoman’s age: at 20 years it could be about 50 or so; at 30 years, perhaps 20 to 30; at 40years, say five to ten; and at 45, maybe just one or two.This concept is important, becauseno amount of stimulating the ovaries can increase the number.The actual number at aparticular age will be different in different women, and to a small extent it may be differ-ent in a woman from one cycle to the next, especially when she gets older.
The follicle becomes visible on ultrasound scanning of the ovaries at about 3 milli-meters in size, a stage at which we refer to these follicles as ‘recruits’.As it grows, it secretesthe ovary’s important sex hormone, estrogen.The rise in estrogen in the blood is slow at first,but after the first week it goes up quickly. In response to this estrogen, the pituitary gland
22 � GETTING PREGNANT
Primordialfollicle
Primaryfollicle
(atresia)
Secondaryfollicle
Tertiaryfollicle
(atresia)
Graafianfollicle
(a) (b) (c) (d)
Figure 3.1 Stages of development of an ovarian follicle, showing the points at which atresia is likely:(a) a primordial follicle, with a thin layer of follicle cells, is the resting state for the egg overmany years; (b) a primary follicle, with still just one layer of follicle cells, is the first step todevelopment, but most follicles that start to develop quickly undergo atresia and are lostforever; (c) a secondary follicle has more than one layer of follicle cells, and most will go onto the next stage; (d) a tertiary follicle has formed an antrum, or space, filled with fluid (andhormones).At this stage the follicle is about one millimeter in diameter. Only follicles thatreach this point near the beginning of a new ovarian cycle have a chance to grow muchfurther.When they do grow, tissue around the follicles takes part in the function of thefollicle and is called the theca interna. If the woman is not on the birth control pill and is notpregnant or breast-feeding, ultimately one (or sometimes more) tertiary follicles will ovulateeach month after reaching the stage referred to as a preovulatory (or Graafian) follicle.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 22

cuts back its FSH production—and this soon sorts the sheep from the goats in the ovaries.One after the other, the follicles that by bad luck lag behind their fellows run out of
steam (or FSH) and undergo atresia. By the end of the first week, just one follicle is left—charged up with FSH and with its own capacity for making estrogen (and different in itscontent of hormones to other follicles: for more see the box, Hormones in follicles).
This dominant follicle, now about 8 to 10 millimeters in diameter, will keep growing,producing more and more estrogen,until it’s mature and approaching 2 centimeters in size.(Remember that the follicle, though it now has many thousands of follicle cells, consistslargely of fluid—it is, literally, a small cyst.)
The ovarian cycle
The first half of the ovary’s cycle, from menstruation to ovulation, is thus called the follic-ular phase. For the week before ovulation, the ovary (left or right) that contains the dominant
Follicle talk
We call the resting, unstimulated follicle the primordial follicle (see Figure 3.1).Theegg, or oocyte, it contains is small.
Primary follicles have just one layer of (multiplying) follicle cells.The egg it containshas already begun growing dramatically. Secondary follicles have more than one layerof follicular cells. It is a brief stage, usually, but in women with primary ovarian failuredue to the resistant ovary syndrome, this is where follicular development can get stuck.A tertiary follicle has formed a fluid-filled space, or antrum, among the follicle cells.An early tertiary follicle is about one millimeter across, and the egg is now about60 times the volume it was when its follicle was resting, containing very many moremitochondria in its cytoplasm. (‘Tertiary follicles’ and ‘antral follicles’ are the same thing.)
The term recruits usually means tertiary follicles a few millimeters across, largeenough to be recruited into an ovarian cycle, and just large enough to be discernibleon transvaginal ultrasound.This does not happen until about eight months have elapsedsince the primordial follicle began growing into a primary follicle.
A Graafian follicle is a larger tertiary follicle, a centimeter or more in diameter; it’snamed after Reijnier de Graaf (1641–1673), a Dutch microscopist and the first personto observe and to describe the ovarian follicle. In normal circumstances, each monthjust one Graafian follicle—the dominant follicle—will reach the stage of preovulatory follicle,about 2 centimeters in diameter, and capable of producing a mature secondary oocyte,itself capable of being fertilized after release from the follicle via ovulation or egg retrieval.
An atretic follicle is a degenerating primary or tertiary follicle (representing thetwo stages or decision points at which either continued growth of the follicle oratresia can happen).
BEHIND A SUCCESSFUL CONCEPTION � 23
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 23

follicle will become the sole producer of ovarian hormones for that cycle; the other ovarysleeps. But if, for one reason or another, a woman has only one ovary, then that ovary willnormally take over, providing a follicle for ovulation every month.
The length of the follicular phase is usually two weeks, but it varies. In young teenagers,when follicular development may not be sustained, one follicle can take another’s placewithout ovulation, giving cycles that can be long and unpredictable. Leading up to themenopause, there are few follicles left, and those that develop can have a head start fromhigher follicle stimulating hormone (FSH) levels. So the follicular phase can be short, some-times so short that ovulation takes place before the period is finished.
As the dominant follicle matures to become preovulatory, its follicular cells switch theirallegiance from FSH to LH.At the same time, the pituitary senses that the dominant follicle
24 � GETTING PREGNANT
7 14 21 2828-day menstrual cycle
(a)
28-day menstrual cycle(c)
28-day menstrual cycle(b)
28-day menstrual cycle(d)
7 14 21 28
7 14 21 28 7 14 21 28
FSH
LH
Estradiol
Progesterone
Figure 3.2 Hormone changes during a typical 28-day menstrual cycle in the pituitary hormones LHand FSH and in the ovarian hormones estradiol and progesterone.There is a small rise inFSH (a) at the end of the cycle, to push early tertiary follicles into growth.As the folliclesgrow, estradiol starts to rise (b), especially once the dominant follicle has been selected.The high level of estradiol at midcycle triggers a surge of LH (c), which causes the follicleto ovulate (release the egg) and to begin to secrete progesterone.When progesterone (andestradiol) fall (d) at the end of the cycle, menstruation starts in the uterus, FSH rises a littleagain, and a new cycle starts in the ovary.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 24

is ready to be ovulated by the high levels of estrogen now present in the blood (see Figure3.2).The pituitary then releases a surge of LH.This LH causes the follicular cells to start tosynthesize the ovary’s second main hormone, progesterone—the hormone that prepares thebody for pregnancy.Ovulation will take place 20 hours or so from the time LH levels peakin the blood, or about 36 hours after the LH surge starts.
For an account of the changes that occur to the chromosomes in the egg in the leadup to ovulation, see the box, Chromosomes in the egg.
Ovulation
During the hours leading up to ovulation, the follicular cells surrounding the egg secretemucus,which causes them to space themselves more widely, forming an expanding surround,or cumulus.Whereas the egg itself is too small to be seen by the naked eye, the structure thatthe follicle ovulates and presents to the fallopian tube is a millimeter or two in diameter—and it’s very sticky.The cumulus mass, as the egg plus its surround is called, adheres resolutelyto the opening of the tube when contact is made.We will move on to the tube shortly.
BEHIND A SUCCESSFUL CONCEPTION � 25
Hormones in follicles
As well as follicle cells (also called granulosa cells), the wall of the follicle is surroundedby a layer of special cells picked up as the follicle grows from the ovary’s substance,known as the theca interna. Its cells, the thecal cells, play an important part in the ovary’shormone manufacture.These cells, under the influence of a tiny amount of LH,make the male sex hormone androstenedione, which diffuses in among the folliclecells, where, under the stimulus of FSH, it’s converted to estradiol, the most potentand important of the estrogens.
Estradiol directly stimulates the follicle cells to divide and increase in number—andthe more follicle cells there are, the less the follicle needs to depend on FSH from theblood, and so the more likely it is to survive as falling FSH levels put the squeeze on.
Measuring the hormones in a follicle’s antrum can distinguish the three typesof follicle: a healthy, still-growing Graafian follicle will be rich in estradiol; an atreticfollicle will be dominated by androstenedione; and a preovulatory follicle will haveloads of progesterone as well as estradiol.
Tertiary follicles big enough to be recruited into ovarian cycles also produce aprotein hormone, inhibin B,which acts at the pituitary gland to decrease the produc-tion of FSH. At the end of a cycle, if there are fewer recruits available than anunknown critical number, inhibin B levels fall below a threshold, and serum FSHlevels at that time (during a period) will begin to rise earlier into the previous lutealphase, in turn bringing recruitment and follicular growth forward, and shorteningthe time between menstruation and ovulation—thus also shortening the ovariancycle as the woman gets older.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 25

As the follicle opens to release its fluid and its cumulus mass (which contains the egg),there is usually some bleeding from the ovary into the abdomen. (Rarely this is severe, causingan urgent clinical problem with pain and low blood pressure.) As the follicle caves in, thehigh levels of LH cause its follicular cells (or granulosa cells, as they tend to be called at aboutthis time), to get plumper as they get better at producing progesterone instead of estrogen.The follicle turns into a new structure, the corpus luteum. (This is how the LH that broughtit about gets its name, luteinizing hormone.) To move the progesterone out of the follicularcells and into the circulation, the collapsed follicle is invaded by blood capillaries.As thecorpus luteum matures into an efficient progesterone-producing structure it accumulatesfat, giving it a yellow color (hence the name corpus luteum,which is Latin for ‘yellow body’).
Progesterone is the ovarian hormone that dominates the second half of the ovariancycle, the luteal phase. Its levels in the blood (shown in Figure 3.2) reach a peak in the middleof the luteal phase, on about day 21. In the absence of a signal from an early pregnancy(through the pregnancy hormone human chorionic gonadotropin, or hCG), progesterone thenfalls, to reach again the low levels that characterize another follicular phase.
The length of the luteal phase is normally between 11 and 16 days. If pregnancy occursthen the life of the corpus luteum is extended for several weeks by being stimulated byhCG, until the placenta is producing enough progesterone to take over responsibility forsupporting the pregnancy.
For an account of how an early pregnancy is at risk from medical negligence duringthis time, see the box, Corpus luteum jeopardy—and a pregnancy or ovary in danger.
MEANWHILE, BACK IN THE MALE
The testes (singular: testis) in boys and men also begin to function during fetal life, whenthe male sex hormone testosterone is responsible for the normal development of the malesex glands and ducts shown in Figure 3.3. But mature sperm, like mature eggs, do not getmade and released until puberty (for more see the box, Nuts and bolts).
The spermatozoon is a long, slender cell,with chromosomes packed tightly into the sperm
26 � GETTING PREGNANT
Chromosomes in the egg
A few hours before ovulation, the primary oocyte completes the first division of meiosis,having first doubled its number of chromosomes the way a cell multiplying by mitosisdoes; the result is one secondary oocyte and one polar body—a tiny, discarded packetcontaining half the chromosomes.
The ovulated secondary oocyte remains suspended halfway through its secondmeiotic division until it’s fertilized,when it will release a second polar body to expelhalf of its chromosomes again, bringing it now from the diploid state with the fullcomplement of 46 chromosomes to the haploid state of 23 chromosomes, the samechromosome status as that of the sperm cell that fertilizes it.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 26

head, and equipped with a tail to propel it.The process by which the elongated spermato-zoa are formed from the round precursor cells, with their loosely packed chromosomes ina conventional, round nucleus, is called spermiogenesis.A tubule of the testis at any place alongits length or around its circumference will contain four generations of developing spermcells (pick any sector of the tubular clock stylized in Figure 3.4), and that sector will pushout a new batch of sperm every twelve days.
This means that it takes about 48 days for a sperm cell to form.The sperm will spendyet another 14 days or more in the male ducts (see Figure 3.3 and the box, Post-productionin the epididymis) to mature before ejaculation sends it and millions of its fellows on theirway. It’s important to know this, because if a man has a severe illness such as influenza asingle episode can disturb sperm production for more than two months.
At sexual intercourse, the sperm cells are ejaculated into the vagina,where the semen—the fluid holding the sperm and ejaculated by the man—comes into close contact with the
BEHIND A SUCCESSFUL CONCEPTION � 27
Bladder
Ampulla ofvas deferens
Seminalvesicle
Ejaculatoryduct
Prostategland
Rete testis
Epididymis
ScrotumTestis
Penis
Vas deferens
Urethra
Figure 3.3 Male sex organs. On each side in a man, the testis, rete testis, epididymis and vas deferenstransmit sperm cells (arrows) to the ampulla of the vas and the ejaculatory duct, locatedwithin the prostate gland, to await ejaculation.At ejaculation, secretions from the seminalvesicles and the prostate gland are added to the sperm cells to form the semen, whichspurts out through the urethra.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 27

mucus of the cervix. At ovulation the cervical mucus is receptive to the sperm: sperm cansurvive in it for several days or more, a steady stream being released upwards through theuterus and out along the fallopian tubes.
THE FALLOPIAN TUBE, UTERUS AND CERVIX
To understand what happens next, we turn now to the organs concerned: the fallopiantube, the uterus and the cervix.
The fallopian tube
The fallopian tubes connect the cavity of the abdomen (the peritoneal cavity, in which theovaries lie) with the cavity of the uterus (the uterine or endometrial cavity).The fallopian tubesin a woman thus link the woman’s insides directly with the world outside the body, by wayof a series of further hollow, tubular structures: the uterus, the cervix and the vagina. Byconducting eggs—or ova—from the ovary ultimately to the outside, the fallopian tube earnsits other name, the ‘oviduct’.
28 � GETTING PREGNANT
Corpus luteum jeopardy—and a pregnancy or ovary in danger
The corpus luteum is usually about 2 centimeters in diameter, like the follicle it springsfrom, but it can be a lot bigger if it gets cystic.A cystic corpus luteum usually func-tions normally—and grows still bigger if pregnancy happens. It can be painful for awhile, but otherwise a cystic corpus luteum has no medical importance . . . as longas it’s left alone.
Because the corpus luteum can have an astonishing range of appearances—itcan look for all the world like a particularly malignant tumor, both on ultrasoundand ‘in the flesh’ at operation!—insufficiently trained surgeons sometimes removethem (or, worse, they might remove the whole ovary).
The loss of a corpus luteum early in pregnancy deprives the uterus of progesterone,causing miscarriage. Likewise an operation involving the uterus, such as a laparoscopy, acurettage or a hysteroscopy, is liable to disrupt early pregnancy if scheduled after ovulation.
These elementary forms of negligence can be prevented by doctors always payingattention to the details and timing of a particular woman’s menstrual cycle in relationto her symptoms or procedures, if necessary verifying assumptions by performing atest for serum progesterone and, sometimes, a test for serum hCG.
Remember that for the first 10 days of conception the serum progesterone willbe raised while the pregnancy test is still negative. If you and your doctor want to besure you are not pregnant, the important test to do therefore is not a pregnancy testbut a serum progesterone—which needs then to be low (less than 2 nanograms permilliliter or less than 5 nanomoles per liter, where ‘nano’ means one billionth).
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 28

Each fallopian tube (illustrated in Figure 3.5) is about 10 to 12 centimeters long andconsists of an outer, wide, thin-walled part, the ampulla, close to the ovaries, leading to aninner, much narrower, more muscular part, the isthmus, close to the uterus.The isthmusconnects to the narrowest part of all, the interstitial segment, which passes for 1 to 2 centi-meters through the wall of the uterus to join the cavity of the uterus.
The fallopian tube is lined by two types of cells: secretory cells, which produce mucus,glucose and other substances important for nourishing the egg and embryo; and ciliated
BEHIND A SUCCESSFUL CONCEPTION � 29
Nuts and bolts
The testes develop in male fetuses a week or two after the ovaries develop in femalefetuses. Instead of follicles forming around oocytes, tubules form around the multi-plying male germ cells, the spermatogonia.
Unlike the ovaries’ oogonia, these spermatogonia keep reproducing themselvesfor life.They are nurtured in the tubules by supporting cells, the Sertoli cells.TheSertoli cells in fetal life produce anti-Müllerian hormone,which stops the male fetusfrom developing fallopian tubes, a uterus and a vagina.
Between the tubules are the ‘interstitial’ cells, the Leydig cells, which make testos-terone. In the fetus, enough of the mother’s hCG (which stimulates Leydig cells tomake testosterone in the same LH-like way it stimulates the mother’s corpus luteumto make progesterone) gets into the developing testes for lots of testosterone to beproduced. (It won’t be until puberty that the Leydig cells will become comparablyactive again.)
Fetal testosterone has important effects on the developing brain (boys’ brainsreally are different from this early time!), as well as on the internal sex glands andducts.
Externally, after conversion in the skin to dihydrotestosterone (DHT), fetal testos-terone causes what would otherwise be the labia (which in girls lie on each side ofthe opening to the vagina) first to fuse together into a scrotum and, second, to bringthe urethra out to the tip of the phallus.
At puberty, as testosterone increases, a proportion of the spermatogonia in thetubules of the testes begin entering meiosis as primary spermatocytes; the first meioticdivision then produces twice this number of secondary spermatocytes.The secondmeiotic division doubles the cells again, but now with just half the number of chro-mosomes in still round-shaped cells called spermatids.
Spermatids therefore contain the haploid number of chromosomes (23), andtypically eight spermatids will have come from one diploid (46-chromosome)spermatogonium, all lying as a cluster of still-connected round-shaped cells,enveloped by the arms of a Sertoli cell.With nurture and shaping from its Sertolicell, each spermatid will evolve from a round, tail-less cell to a missile-likespermatozoon.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 29

m3
m4
m5
m1
m2
XIV
XIIII
II
III
IV
V
VI
VII
VIII
IX
X
XI
XII
11
10
9
8
7
6
5
4
3
2
1
Sg(In)
Se
Sg(A)D
Sc2Sc (Z)
Sc(A)
A
RB
Sc (L)
Se
Se
Sc (R)
Sg(B)
Sg (In)
Sc (P)
30 � GETTING PREGNANT
Figure 3.4 Spermatogenic waves. Spermatogenesis is the process in mammals (in this case the rat) bywhich dividing spermatogonia in the tubules of the testis continuously produce spermcells.The process is set out here as a clock, with maturation through four layersproceeding clockwise for four revolutions. In reality, one cut across a tubule will usuallyall be at the same stage (one sector or slice of the clock), and what is shown here goingclockwise around the diagram would actually be occurring down the length of thetubule.The release of mature sperm in this way runs down the tubule, producing aspermatogenic wave—a perpetual moving harvest of mature sperm. Mature sperm leaveone spot in the tubule every 14 days (thus, in the diagram it takes 14 days to move aroundthe clock once), which means it takes 56 days for a newly formed spermatocyte to leavethe tissue as a spermatozoon. Source: B.Sc. (Med.) honours thesis.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 30

cells, which bear tiny hair-like structures, the cilia, beating in the direction of the uterusand carrying the still sticky cumulus mass down the ampulla soon after ovulation, towardsthe junction between the ampulla and the isthmus.
It’s at the fallopian tube’s ampullary–isthmic junction that fertilization takes place.The fertil-ized egg stays at the ampullary–isthmic junction for two to three days before the tubalisthmus loses its dense secretions, and the muscle in its wall relaxes, enabling the earlyembryo, now rid of its cumulus cells, to reach the uterus.The hormone that causes thesechanges in the tube is progesterone.
The uterus
The uterus consists of a body (the uterine fundus) and a neck (the cervix), which joins it tothe vagina. Its lining, the endometrium, grows to be one centimeter in thickness, as seen onan ultrasound scan.The wall of the uterus, the myometrium, is muscular and about twocentimeters thick. Outermost is a slippery layer similar to that which coats all the internalorgans, the uterine serosa. As Figure 3.5 shows, the endometrial, or uterine, cavity is anupside-down triangle in shape, with the tubes coming in on each side at the top; it’s alsoflat, with the front and the back surfaces touching, like a sandwich.
Post-production in the epididymis
From the hundreds of tubules in the testis, the sperm cells are pushed into severalvery fine ducts, the efferent ducts, lying in a connector called the rete testis, to enterthe epididymis.
The epididymis lies just next to the testis, in the scrotum, and is a single, long,coiled duct that would measure about 6 meters if laid out straight. It connects withthe vas deferens, a tube that takes the sperm up out of the scrotum (see Figure 3.3),and meets the male accessory glands, the seminal vesicles and the prostate gland, justbelow the bladder.
The sperm cells in the rete testis and the upper epididymis are as unpurposefulas newborn foals, staggering about in bewilderment, flicking their new-found tailsabout. Further down the epididymis they will mature, but they will also be coatedin special proteins that keep them subdued: there’s no point in wasting too muchenergy before the race starts.
As sperm come out of the epididymis and into the vas deferens (the long ductfrom the scrotum to the urethra), they will be mixed with the other components ofsemen (the fluid from the prostate and the seminal vesicles) and stored till ejaculation.
The sperm should have good motility for up to a week or two,but the epididymalproteins are there to stop them slipping into the energy-expensive hyperactivity thatthey will eventually need to force their way through the layers around an ovulated egg.
BEHIND A SUCCESSFUL CONCEPTION � 31
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 31

The endometrium grows under the influence of estrogen during the ovary’s follicularphase; in the uterus we therefore call this the proliferative phase and the uterus is lined thenby ‘proliferative endometrium’.
During the ovary’s luteal phase,progesterone causes the endometrium first to stop growingand then, instead, to make carbohydrate-rich secretions probably needed by an implantingembryo; in the uterus this is therefore called the secretory phase and the uterus is lined by‘secretory endometrium’.The day-to-day development of the endometrium is so precisethat you can set your calendar by it (see the box, The endometrial clock).
When estrogen levels, and especially progesterone levels, fall at the end of the ovariancycle (look at Figure 3.2 again), the endometrium breaks down and bleeds.This is themenstrual phase, during which, in the pituitary gland,FSH production rises to capture a newcohort of developing follicles, and, in the ovary, a new follicular phase starts.
32 � GETTING PREGNANT
Isthmus
Interstitialpart
Fundus ofuterus
Uterus
Cervix ofuterus
Vagina
Graafianfollicle
Fimbrial endAmpulla
Ovary
Figure 3.5 Internal female sex organs.The fallopian tubes connect the ovary on each side to theuterus (just one side is shown).The ovulating Graafian follicle releases the egg in itscumulus to the fimbrial end of the tube, from where it is carried quite quickly (half anhour) to the junction of the ampulla (which is wide) and the isthmus (which is narrow).Ferilization of the egg by sperm and cleavage of the pre-embryo occur at thisampullary–isthmic junction. Several days later, the developing pre-embryo is admitted tothe uterus, where it will implant, about a week after fertilization.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 32

The cervix
The cervix of the uterus does not show the same striking changes through the cycle thatthe endometrium does, but it does have important responses.
One of the jobs the cervix has is to keep sperm out if, higher up, there’s not going tobe an egg to be fertilized. In the follicular phase, under the effect of estrogen, the cervix opens,and the mucus becomes greater in amount, wateriness, stretchability (Spinnbarkheit), in itsferning (or forming a fern-like pattern when it’s dried on a microscope slide) and, mostimportantly, in its receptiveness to and penetrability by sperm. If estrogen levels fall—orwhen progesterone is produced to counteract the effect of estrogen—these changes are allquickly reversed and the mucus tightens up.Very soon into the luteal phase, therefore, themucus in the cervix once more keeps sperm out.
The endometrial clock
The sequence of changes in the endometrium, particularly in the secretory phase, isordered.
The first noticeable change, two days after ovulation (or day 16 of a typical28-day cycle), is for secretion to be visible in the endometrial gland cells under thenucleus (‘subnuclear vacuolation’); by day 18, secretion fills the cells and appearswithin the glands themselves; by day 21 there is a lot of watery-looking materialin the endometrial stroma between the glands; on day 24, the stromal cells getplumper, first around the spiral arteries of the endometrium, and then more gener-ally, to the virtual point of confluence—a state called the predecidual reaction in anon-pregnant cycle, which can go on to a fully developed decidual reaction if preg-nancy happens.
This sequence ticks like clockwork, to the point where a snapshot biopsy of theendometrium can tell a pathologist to within a day or two how long it has beensince ovulation occurred (or,more precisely, since exposure to progesterone began).If, at the end of a cycle, a well-developed predecidual reaction is seen on a biopsy,it can safely be inferred that the corpus luteum has produced enough progesterone,and produced it for long enough, for pregnancy to have been possible, at least so faras the endometrium is concerned.
But, also like a clock, the endometrium won’t tick backwards. If the endometriumis too developed for an embryo then bad luck—it won’t wait, the embryo can’t catchup, and the window of opportunity (the ‘implantation window’) will be closed.Thiscould be one reason why in vitro fertilization embryos sometimes have troubleimplanting, and I discuss this further in Chapter 20.On the other hand, if the embryois ahead of the endometrium, it can probably wait a little for the endometrium tocatch up.
BEHIND A SUCCESSFUL CONCEPTION � 33
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 33

34 � GETTING PREGNANT
Figure 3.6 Eggs and early embryos.
(a) Immature egg derived from an immature follicle, with the cumulus cells packed tightly aroundthe egg.
(b) Mature egg derived from a mature follicle, just before ovulation; the cumulus cells (the follicle cellsaround the egg) now have space between them, and the cumulus is said to be ‘expanded’.
(c) Fertilized egg, or zygote, at 20 hours; there are two pronuclei, one female and one male; the egg issurrounded by the zona pellucida.
(d) 2-cell embryo at 2 days; at this stage development of the embryo is still under the control of the egg’sgenome, as expressed before fertilization.
(e) 8-cell embryo at 3 days—the stage at which the new (embryonic) genome takes over control offurther development.
(f) Compacting morula at 4 days; individual cells (about 16) are no longer distinct as embryonic ‘tissue’ isforming.
(g) Early blastocyst at 5 days (about 64 cells); a cavity is forming, pushing the clump of cells of theemerging ‘inner cell mass’ to one side.
(h) Expanding blastocyst; later on day 5 (over 100 cells);most of the volume of the embryo is now fluid inthe blastocyst cavity; the compact inner cell mass (at 2 o’clock) will form the embryo (and eventuallythe fetus); the surrounding trophectoderm will form trophoblast (and eventually the placenta andmembranes); the zona pellucida is thinning as the embryo expands.
(i) Hatching blastocyst at 5 or 6 days (about 128 cells); the zona pellucida has opened (at 2 o’clock) andthe very fluid embryo, once free, can attach to the endometrium and implant [see Figure 4.2 for acontinuation].
Illustrations courtesy of Sydney IVF.
(a) (b) (c) (d) (e)
(f) (g) (h) (i)
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 34

CONCEPTION
Of the millions of sperm deposited in the vagina during sex, perhaps fewer than 200 reachthe fallopian tube.There might not be more than 10 sperm in the ampulla at the time theegg is fertilized.We suspect that the tube does a lot to move the egg and the few sperminto close contact for fertilization to become probable, but we don’t know how it does it.Fertilization needs to take place within about 10 hours of ovulation for the embryo later todevelop normally, so it’s best if the first sperm can get to the tube before the egg arrives.
Ejaculated sperm are motile (they swim), but they’re inhibited from displaying theirpeak performance by a surface layer of protein molecules (see the box,Post-production in theepididymis); if the proteins weren’t there, the sperm would run out of puff too fast.
The effect of taking off these brakes is to power up the sperm’s swimming speed andto give the cell membrane over the sperm head the stickiness the sperm needs to cling tothe egg’s outermost membrane—in all, a process called capacitation. Sperm that are beingstored in receptive mucus in the cervix are usually not yet in a capacitated state.Capacitationcan happen naturally, by having the sperm swim up through the uterus and out along thetube, or it can be made to happen in the laboratory, by spinning and washing the spermthrough a series of solutions (colloquially called sperm washing).
Fertilization
The ovulated egg has several layers that the capacitated sperm needs to power through;these are shown in Figure 3.6 and in Figure 3.7. First there is the jelly-like cumulus, whichthe sperm likes to get its tail into (the beating sperm tail gets a better grip in the cumulus,propelling it forwards more effectively). Second is a tough, glassy-looking membrane, thezona pellucida (Latin for ‘clear layer’), to which the sperm must successfully attach itself ifit’s to get through it.
What happens next is complicated but important.The sperm cell up to this point hasbeen wearing a crash-helmet, the acrosome. Imagine pushing your fist into a soft balloon:the fist is the sperm head’s nucleus (where its genetic material is packed densely into the23 chromosomes); the balloon is the acrosome.The outside of the sperm head, providedthe acrosome is intact (that is, the balloon hasn’t popped), is specifically sticky for the zonapellucida—the way Velcro is for its matching surface.The successful sperm binds tightly tothe zona (see Figure 3.7).This causes the acrosome to break open, releasing, instead of air(as a balloon would) a potent mixture of enzymes, which digest a path through the zona;these are helped by the capacitated sperm’s forcefully beating tail, itself with a good gripin what’s left of the cumulus.The process of the balloon bursting is called the acrosomereaction.
And so it is that the sperm, now bereft of its acrosome, finds itself next to the egg,within the perivitelline space; all it now needs to do is drift up to the vitellus—the egg itself.Covering the acrosome-reacted sperm head now is the inner layer of the acrosome,which,unlike the outer layers (now gone), is specifically sticky for the egg membrane. Contact ismade and the trap is sprung (see Figure 3.7 again).
BEHIND A SUCCESSFUL CONCEPTION � 35
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 35

Like nerve cells and muscle cells, the egg is electrically charged.The moment the spermfuses with it, an electrical signal causes several reactions inside the egg.Almost immediately(it takes about 15 seconds) the egg secretes what are called ‘cortical granules’,which containa mucus that fills the perivitelline space, smothering the egg membrane, and stopping anymore sperm that might be on their way in from attaching to the egg. (If another spermchances to reach the egg during this 15 seconds, more than one sperm will fertilize it andthe embryo will be ruined by having at least 23 too many chromosomes—a process calledpolyspermic fertilization, or simply ‘polyspermy’.)
At the same time, the egg finishes expelling its own extra chromosomes, reducing thenumber from 46 to 23, to match those of the sperm.
Third, the machinery of the egg starts preparing for it to become an embryo. In about24 hours it will divide into two cells, then four cells, and so on.
The sperm head, now inside the egg, falls apart, revealing all as the egg strips downto its chromosomes.This is no time for men to be bashful! At no other point are themale’s genes open to such scrutiny by his mate! Stripped bare, the egg fashions these malechromosomes to match its own: each set forms a watery blob within the substance of the
36 � GETTING PREGNANT
(a) (b) (c) (d) (e) (f)
Figure 3.7 Sperm attachment and fertilization of the egg: (a) the zona pellucida exhibits specialbinding sites complementary to those exhibited by the approaching capacitated spermcell; (b) binding between sperm cell and zona triggers the acrosome reaction in the sperm,(c) enzymes released from the acrosome digest a path through the zona; (d) the sperm cell,having penetrated the zona and entered the perivitelline space, has lost its plasmamembrane and outer acrosomal membrane and now displays new binding sitescomplementary to those on the membrane of the egg; (e) binding of the sperm to the eggis followed by release of material from the egg’s cortical granules into the perivitellinespace; this released material will coat the egg to prevent further sperm from binding;(f ) the sperm head, neck, and part of the tail enter the egg to fertilize it.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 36

egg (visible with the help of a microscope in Figure 3.6c)—the male and the femalepronuclei. This is the first definite sign of fertilization for the watching scientist, andis looked for in IVF laboratories between 16 and 20 hours after eggs are inseminatedin vitro.
The male and female pronuclei then join together so that the two sets of chromosomescan mingle and match, a process called syngamy.The chromosomes now number 46—thenormal complement again. If the sperm had an X-chromosome to pair with the egg’sX-chromosome the resultant chromosome count, or karyotype, will be 46,XX (female); ifthe sperm had a Y-chromosome the resultant karyotype will be 46,XY (male).
The fertilized egg then divides several times without increasing its overall size (seeFigure 3.6d and e), a process termed cleavage. Upon reaching about 16 cells, the cellsthemselves, till now just a loosely aggregated ball within the zona pellucida, for the firsttime begin to bind strongly together, in effect forming a tissue.We call this compaction.As a result, the embryo now has a homogeneous appearance, and is termed a morula(Figure 3.6f ).
The developing embryo enters the endometrial cavity three days after ovulation andfertilization. It is, or very soon will be, a blastocyst, a hollow ball of cells surrounding a cyst-like cavity, and soon to number a hundred or more cells (see Figure 3.6g and h).
The blastocyst’s cells have taken their first step towards differentiation, or specialization.A rim of outer cells is called the trophectoderm, and will give rise to the membranes andplacenta.The inner cells, which form a ball off to one side, called the inner cell mass, will,after implantation,give rise to the embryo proper,or fetus.These structures are more obviouswhen the blastocyst has expanded (Figure 3.6h).
Finally, the expanded blastocyst eases its way out of the now very thin and stretchedzona pellucida (we do call it ‘hatching’—see Figure 3.6i).The naked blastocyst is nowready to adhere to the surface of the endometrium.Already it is furiously signaling itspresence by producing many crucial substances, among which is that most ‘primitive’of the body’s proteins, human chorionic gonadotropin (hCG). hCG is the signal that tellsthe corpus luteum to keep producing progesterone and is, a little later, measurable in bloodor urine—the usual chemical basis for pregnancy tests.
Implantation
The blastocyst attaches to the endometrium on about day 21 of the menstrual cycle, orseven days after fertilization. It squeezes through the surface layer of the endometrium tolie within the endometrial stroma, the watery connecting substance between the endome-trial glands—which is what we mean by implantation. Nutrition comes from secretions ofthe endometrial glands.
The outer layer of the implanted blastocyst, the trophoblast, is soon in potential touchwith the mother’s blood, so oxygen diffuses through to the developing embryo. Sometimesas the blood first bathes the embryo (on about day 26 of the cycle), a small amount of bloodleaks out of the uterus into the vagina—this is implantation bleeding. If it occurs it’s nearlyalways much lighter than a menstrual period, so there should not be much confusion.
BEHIND A SUCCESSFUL CONCEPTION � 37
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 37

By day 28 a blood pregnancy test, set to measure serum hCG levels greater than 50 units,will be positive.
The stroma of the endometrium reacts to the presence of the pregnancy and to thecontinued production of progesterone from the corpus luteum in the ovary by forming athick, cell-filled layer, called the decidua (because like a deciduous tree’s leaves it will, eightor nine months later, be shed from the uterus at delivery along with the placenta as part ofthe afterbirth).The modified stromal cells, now called decidual cells, produce many impor-tant hormones, including relaxin,which helps stop the uterus from contracting prematurely,and prolactin,which in this location helps control the shifting of fluid into the gestational sac,the bag of fluid surrounding the embryo inside the pregnancy membranes.
The fetus, hopefully welcome, has thus positioned itself after a successful conceptionas snugly as any well-adapted parasite.But, like a more ordinary parasite, the fetus is biolog-ically a friendly foreigner to its host. Chapter 4 considers the details of how the motherand fetus adapt to each other to avoid miscarriage, and the tug-of-war that exists withinthe mother’s immune system.
38 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 38

establishing a successful pregnancy
How a pregnancy formsin the uterus
The chain of events we take for granted when a pregnancy is established is such a longone that I’m reminded of Tolstoy’s opening to his novel Anna Karenina, when he waswriting about what we take for granted in a successful marriage:
All happy families resemble one another, but each unhappy family is unhappy in its own way.
. . . which we might paraphrase as . . .
All successful pregnancies resemble one another, but each unsuccessful pregnancy is unsuccessful inits own particular way.
Just as many things need to go right, and to more or less keep going right, for a couple tostay in love and for their marriage to last, so it needs only one of the chain of many buildingsteps to go awry for a pregnancy to fail, and to miscarry.
How do we come to grips with this chain? In parallel with the biological account I willrun the metaphor of an international joint venture for a construction project.
AN OVERVIEW OF ‘PROJECT PREGNANCY’
For an insight into the key biological events that lead to successful pregnancy, let’s look atthe project as if it were a joint construction venture developing in a foreign country.Thereare benefits to the foreign, host country (playing the role of the mother), but there is alsosome cost Here are the key steps to the initiation of ‘Project Pregnancy’:
39
4
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 39

Step 1. The embryo forms, a deal is struck
Fertilization has occurred . . . by a genetically sound sperm, of an egg that is both geneti-cally normal and, in its cytoplasm, metabolically capable and resourceful.
We have the raw ingredients for the joint venture between Man Inc. and Woman Inc.Both have brought to the table a bundled set of instruction packs that will contribute to abalanced blueprint.The woman is supplying the resources to get started, the egg is packedwith nutrients, proteins, last-minute instructions to get through the first few days, as wellas an enormous supply of mitochondria to power things along, having pulled itself freefrom the energizing environment of the follicle and particularly the cumulus.
Step 2. Prior to implantation: the plan unfolds
Cleavage follows.The fertilized egg begins replicating, or dividing.By the third day the newgenome has become indispensable, and each of the eight cells is referring to it.By the fourthday, the 16 or so cells are cooperating to form the first tissue, as the morula undergoescompaction.Next the cells on the periphery differentiate slightly: these are the placental stemcells, or trophectoderm. By the fifth day, off to one side, on the inside of the blastocyst, isthe inner cell mass, destined to become the fetus and composed of embryonic stem cells, orES cells.We started with a single cell: we now have more than 100 cells.
The project is underway, controlled by a hopefully good partnership of smart maternaland paternal owners.Their wisdom and codified instructions comprise the DNA blueprintthat is being copied off, residing as a genome in each embryonic cell’s nucleus.Their jointcontributions to the developing idea are already being put to the test.
Step 3. Implantation: entry into foreign territory
The hatching blastocyst sheds its protective zona to expose itself to the intimacy of newsurroundings, sending signals to an endometrium made responsive by progesterone from thehost’s corpus luteum, and gaining entry (see Figure 4.1a).
The new project is hatched, admitted through the host country’s borders, and revealedto the host’s regulators.The regulators happen to be related to the maternal partner to theproject (a fact that might or might not prove helpful to the joint venture’s survival). Forthe duration of the project, the host will only support the project while there is an amplesupply of cash (progesterone) to keep everybody happy and cooperative.Where the prog-esterone comes from is a secondary consideration. It would have been supplied by the hostfor only another week without a great deal of cajoling from the pregnancy; even now thehost will provide it only for another few weeks, after which time it must all be generatedby the project itself.
The embryo’s surrounding trophectoderm starts budding off trophoblast,which extendsout into what should be a receptive endometrium, dissolving its carbohydrate, protein andnucleic acid-rich glands for nourishment, while the tissue between the glands, the endo-metrial stroma, is turned into decidua (see Figure 4.1b).
40 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 40

To pacify critical elements of the host’s blood coagulation system and the immunesystem, and to keep up the progesterone supply, the trophoblast is churning out humanchorionic gonadotropin (hCG) to push progesterone out of the gradually more reluctantcorpus luteum.To ensure that a bland, uniform, but persistent front is presented to thedecidua and its gathering white blood cells, the trophoblast that will surround the growinggestation consists only of a single, extraordinarily stretched, single cell, the syncytiotro-phoblast . . . crawling, growing . . . extending like an insatiable amoeba . . . fitting overthe whole pregnancy like a glove.
Outside this, individual cells of the extravillous trophoblast (the other executive arm ofthe underlying trophectoderm, now referred to as cytotrophoblast) venture deeply into thedecidua and beyond, preparing not just the neighbourhood for the pregnancy project butthe host’s immune system itself. For more on the remarkable properties of the trophoblast,see the box, The ‘ABCDEFG’ of tissue groups . . .
The host’s gathering militia comprises both a tolerant peace corps (resident, or uterine,NK cells to facilitate the project) and more aggressive itinerant peacekeepers (peripheral,or circulating, NK cells), as well as a few troopers (T cells), who are ready to call for rein-forcements and to start shooting if things go wrong or if there’s too much damage, eitherwithin the project or around it. As the infrastructure services begin developing, if theconstruction is too chaotic or if the policing immune system is provoked into a bad attitude,Project Pregnancy will be finished before it starts.
Communication helps the project take hold,but very many services need to be establishedsimultaneously and quickly for the sensitive, rapidly developing project to go ahead in thispotentially prickly environment.There’s more than just hCG and progesterone involved. Fordetails of the communication skills needed, see the box, . . . and shaking hands with HLA-G.
Meanwhile the roving members of the consular staff, the cells of the extravilloustrophoblast, are venturing deeply into host territory, concealing their foreignness whilepresenting a friendly face to the head honchos in the immune control centers, encourag-ing them to tolerate the project.
Step 4. Avoiding rejection
The surprise, you might think, is that in most cases the fetus is successful in keeping themother’s immune system so tolerant. Isn’t the fetus with its developing placenta a foreigner,getting half of its genes from a stranger (the father) or, in the case of gestational surrogacy, allof its genes from strangers? Why isn’t it rejected, like a poorly matched kidney or liver orheart transplant?
It seems the answer lies with the trophoblast on one side and, on the other, with theNK cells—white blood cells that in evolutionary time stretch back more than 500 millionyears, before the evolution of immune systems that have memory.This was a time whenthe planet’s oceans were inhabited only by invertebrates, animals accustomed to close prox-imity with each other, living communally as corals, sponges, molluscs and sea squirts. (Formore, see the box, Rejecting rejection: Pregnancy as a coral reef.)
ESTABLISHING A SUCCESSFUL PREGNANCY � 41
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 41

42 � GETTING PREGNANT
Figure 4.1 Implantation and the early establishment of pregnancy.
(a) The hatched blastocyst, free now of its zona pellucida, is trapped between the front and the back ofthe uterine lining, and implantation is under way, a week after ovulation and fertilization.
S the stroma of the endometrium is still loose and offers little resistance
ICM inner cell mass, composed of embryonic stem (ES) cells
CT cells of the trophectoderm (cytotrophoblast stem cells), which at the implantation sitemultiply into an amoeba-like tissue with many cell nuclei (shown) but no cell membranes,the syncytiotrophoblast, as well as releasing cells into the stroma as extravillous trophoblast(not shown)
SCT the syncytiotrophoblast pulls the embryo into the endometrium and, as it develops, willsurround the gestation, forming a layer that for the whole of the pregnancy will separatemother from fetus
Lac the first lacunar space is forming within the SCT: it is the forerunner of the intervillous space
(b) The embryo, growing fast and differentiating fast, has fully entered the lining of the uterus, and isnow enveloped by a shell of trophoblast (TB), at about the time the period will be missed; it is stilltoo small to be visible, but the trophoblast is releasing buckets of human chorionic gonadotropin, whichis the stuff that causes a positive pregnancy test. If the pregnancy fails now, this is all that it will havehad to show for it.
D the stroma has turned into decidua to react against the expanding gestation
ED the embryonic disk has formed three layers, the (upper) ectoderm, which will form skinstructures, and the (lower) endoderm, which will eventually line the digestive tract, and(through the process of gastrulation) the mesoderm, which forms the connective tissue,muscle, skeleton etc.
ICMCT
SCTLac
S
(a)
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 42

ESTABLISHING A SUCCESSFUL PREGNANCY � 43
AC the amniotic cavity, which starts small but eventually surrounds the fetus
CC the chorionic cavity forms the early gestational sac
YS the yolk sac is starting to form
EEM ‘extraembryonic mesoderm’ (mesoderm outside the embryo itself ) pushes into thetrophoblast to form chorionic villi (CV) while giving way to the rowing chorionic cavity(CC)
CV early chorionic villi, composed of EEM in the core and covered by cytotrophoblast andsyncytiotrophoblast (SCT)
Lac the lacunar spaces within the SCT begin to coalesce, a step closer to becoming theintervillous space; some have eaten into their blood vessels (BV) and endometrial glands(EG)
EVT extravillous trophoblast cells continue to cut loose from cytotrophoblast in direct contactwith decidua, to pass deep into the mother’s stroma, where they will later take command ofmaternal blood vessels (not shown); the EVT is engaging the mother’s immune system(NK)
EG some glands pour their nutritious contents into lacunar spaces (Lac) to reach the hungryembryo
MBV the maternal blood vessels will become plugged with EVT cells for the first 3 months ofpregnancy, after which they will flood the intervillous space
Redrawn from Hamilton, Boyd and Mosman’s Human Embryology.
EG EVT CT NK Lac D
TB
EG
UC
CC
AC
YS
ED
EEM
CV
SCT
CT
EVT
(b)
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 43

The ‘ABCDEFG’ of tissue groups . . .
We all know what blood groups are.They are the labels on red blood cells that dictatewhether a blood transfusion will be compatible or a disaster. Less well known aretissue groups.They are the labels attached to the other cells in the body that deter-mine whether an organ graft, like a kidney, a liver or a heart—or bone marrow—will ‘take’ or be rejected.
These tissue groups are called HLA molecules (HLA stands for human leukocyteantigen, an ‘antigen’ being any molecule that can elicit an immune, or antibodyresponse;‘leukocyte’ referring to white blood cells, which are much less compatiblebetween people than red blood cells can be; and ‘human’ . . . well, in other animalswe have to call it something else; thus the general name for this part of the genomein biology is the major histocompatibility complex, or MHC).
The MHC is dense with genes, and has a fascinating evolutionary history, havingbeen tightly retained through the evolution of the vertebrates. Its different genesform two main groups, the Class I genes (the first-discovered or ‘typical’ HLA-Aand HLA-B genes, and the ‘atypical’, still poorly understood, HLA-C, HLA-E,HLA-F and HLA-G genes), and the Class II genes (the HLA-D groups, compris-ing HLA-DR, HLA-DQ and HLA-DP), which are expressed only within theimmune system,but with a stronger policing role. Like all genes, they come in pairs,one from the mother and one from the father.
What’s their job description? For as long as animals have consisted of more thanone cell, there’s been a premium on recognizing, in the melee of the pond, whichcells are yours and which cells belong to someone else—a rival, or a threat.Any cellwith a different HLA ‘badge’ belongs to a rival club and should generally be elimi-nated if it gets too intimate. In complex organisms, NK cells, T cells and other whiteblood cells can do the job ruthlessly well.
But these policing cells also have to deal with invasions of tiny organisms, suchas viruses. For viruses to properly alert the immune system, for them to work asantigens, able to elicit a specific antibody response, they need to be presented to theimmune system in a special way.They need, in effect, to be suspended upon a back-ground that’s familiar to the police—and that background is the HLA moleculeitself. Unless the NK police recognize the HLA molecule as their own they do nottrust what they are seeing and will demolish the target grossly and non-specifically.The T cell police prefer to set the antigen up for a mug shot, parading it on an HLAbackground they are completely at home with, enabling it to be brought into veryclear focus, then retaining an image of the antigen in immunological memory for amore rapid response next time. And then they incarcerate and digest the antigenwithout too much of a fuss.
At least, that’s the theory. In practice, once a T cell is alerted it gets impatient. Notwanting to wait for the antigen to replicate faster than it can, the T cell swiftly recruits
44 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 44

any other T cell or NK cell in the vicinity (and a few other warrior white cells as well);justice is summary,and collateral damage is often considerable.But trouble is contained.
So far, so good; but it gets better.Because genes come in pairs, there can be different versions or polymorphisms of
the particular gene in a population, called alleles. (If you happen to get the same allelefrom your two parents you are homozygous for that gene; if the alleles are differentyou are heterozygous.) It so happens that different HLA alleles display a particularvirus or antigen in different ways. It depends on both the particular virus and theparticular allele, and the net effect determines how well the immune system willrespond. In other words, when a particular virus hits the village or valley you livein, you will be more or less likely to survive depending on which particular allelesyou happen to have.This means two things.
First, it pays to have two different alleles instead of an identical pair.There’s anobvious survival advantage for you as an individual to be heterozygous not homozy-gous, because your immune system can choose the better of two alleles instead ofthe better of one.
Second, the population you belong to—your village or your valley or yourtribe—will have a survival advantage if as wide a range of alleles as possible isrepresented among your group. So even if some individuals succumb to somenew scourge, others will survive to repopulate the village, the valley or the tribe.
The net result is that evolution has produced extraordinary diversity . . . andthere’s a huge range of possible HLA combinations.Theoretically there can be morethan 10 billion different combinations of the various HLA alleles—more than theworld’s population of humans! It’s no wonder it can be hard to secure a perfect, orsometimes even adequate, tissue match for a kidney transplant outside your ownfamily.And within your family, among your children, there will be as many as fourdifferent alleles to help at least some of them through the next dreadful epidemic,provided you have mated with someone not closely related to you (someone fromthe next valley or from a different tribe is ideal).
In fact, and as is well known, there are other advantages in outbreeding overinbreeding. Here’s how nature uses the HLA molecules to encourage it.
. . . the sweet smell of genetic diversity . . .
The HLA molecules, as well as providing the backdrop upon which antigens areheld conspicuous, also have a special affinity for all sorts of tiny volatile compoundsthat you can smell . . . that evaporate and tease the olfactory senses.These specialmolecules will be as personal as your HLA genes and as individual as your environ-ment.They can only be the same as someone else’s if you share HLA groups withthat person.And if you share HLA groups you will most likely share a heap of otherrecessive genes, and mating will mean inbreeding, and that will mean a much greaterrisk of inheriting two dud genes and developing a serious genetic disease.
ESTABLISHING A SUCCESSFUL PREGNANCY � 45
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 45

46 � GETTING PREGNANT
These HLA molecules can separate away from the cell surface to becomesoluble in the blood, able to be filtered out into the urine or through the sweatpores, and thus to enter the environment.The same process occurs in all verte-brates.The HLA molecules themselves are generally too big to be volatile andsmelly, but when a dog, say, marks its territory with a pee the soluble HLA mole-cules break down and release the volatile compounds the HLA molecule has snaredfrom the dog and its environment. Other dogs can tell the difference between theirown smell and another dog’s, and know to stay away (or sometimes to becomeespecially interested!).
In mice, these molecules—pheromones—are so powerfully linked to the repro-ductive system that when a pregnant female loses contact with her mate and consortswith a new male, the mismatch between his volatiles and those of her earlierboyfriend is enough to induce abortion of her embryos, so that she can go on tobear the new male’s young instead.
. . . and shaking hands with HLA-GNot surprisingly, prudent embryos keep their heads down, and display no HLA-A,HLA-B or HLA-D.The implanted gestation, gloved in HLA-free syncytiotro-phoblast, does the same, remaining stealthily invisible on the mother’s immune radarscreen.
The same applies to the cells of the extravillous trophoblast (see the main text) asthey venture deep into the mother’s decidua and body.What they do need to do (inorder to push the right buttons on potentially helpful maternal NK cells and Tcells) is to show HLA-E and HLA-G badges.Without some kind of HLA badgethey might be summarily expelled as total strangers.
And so, HLA-E and HLA-G have come to be two components of this amazingMHC gene group that are not polymorphic, but instead have been tightly conservedby evolution. Only a handful of different alleles are known.
What we know about them in pregnancy so far is that:• A small bit of HLA-G or HLA-C is needed for trophoblast to show its HLA-E
molecules—and that seems to be a good thing;• Although HLA-C comes in as many polymorphic forms as does HLA-A or
HLA-B, HLA-C does not upset the immune system in the same way: instead,it seems to be an advantage for the fetus to have different HLA-C alleles;
• Extravillous trophoblast cells, wearing their HLA-G on their sleeves, journeyinto the decidua and then far into the mother’s immune system; and
• Soluble forms of that same HLA-G from the fetus are increasingly concentratedin the mother’s circulation as pregnancy advances.
And how all this relates to miscarriage is one of the most exciting areas of researchin reproductive medicine today.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 46

If for any reason the development of the embryo falters, the trophoblast slows down,losing its capacity to sustain the rapid rise in hCG needed to maintain progesteroneproduction from the corpus luteum or, later, losing its own capacity to make progestrone.Bleeding will start and all the outside will know of the pregnancy will come from thetransient circulation of hCG . . . in other words, a transiently positive pregnancy test, abiochemical pregnancy, or what we call a subclinical miscarriage.
The trophoblast at first does not need much instruction for its own function and growth,out there on the periphery of the project. Its job description might be critical but it’s nottoo complicated. However, it does need plenty of support from the center.And it needs afriendly local militia.Without enough credibility at this early point, or with a too-pricklyconstabulary, the aggressive NK cells will take over from the facilitatory NK cells and willstick in the daggers, puncturing the trophoblast with molecules called perforins.The syncy-tiotrophoblast is only ever one big cell, stretched very thin, being fed by underlying cytotro-phoblastic stem cells. Prick it with perforins at this early stage and it will dissolve away,withnothing left as a legacy but some still-circulating, but dwindling, hCG, and a fast-fadingpregnancy test.
ESTABLISHING A SUCCESSFUL PREGNANCY � 47
Rejecting rejection: Pregnancy as a coral reef
Q. What does human pregnancy have in common with a coral reef?A. Living in intimate harmony with a foreign neighbor.
Cambridge immunologists Y.W. Loke and Ashley King have drawn an analogybetween invertebrate cooperation and the tolerance the mammalian mother showsto her immunologically different fetus. Remember that the make-up of fully half ofa fetus’s genes—and proteins—reflect those of its father, and will be largely foreignto the mother’s immune system. Loke and King, however, reject the metaphor thatcarrying a baby is like carrying a grafted kidney from a not-well-matched organdonor. Here’s why.
The vertebrate immune system has evolved over many millions of years. It consistsof three main components: (1) recognition that an organic substance is foreign, (2)reacting to the intrusion, and (3) remembering the challenge for a more efficientresponse next time (called immune memory).
Unlike their vertebrate descendants, invertebrates show just the first of the steps:they can recognize that a substance or organism is foreign (or ‘non-self ’), but willoften accommodate the guest or neighbor without hostility. Invertebrates do havewhite blood cells capable of dealing vigorously with an true intruder (they’re called‘natural killer’ or NK cells, and are part of what is called the innate immune system),but they also tend to injure themselves in the process, and so restrict this activity towhen it’s really necessary. So while their NK cells congregate at the front line, at theborder, ready to react, frequently the outcome is not warfare but rather the construc-tion of a wall, or fence, that leads to amicable co-existence.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 47

NK cells in the vertebrate world are different from more typical vertebrateimmune cells such as T cells, because NK cells develop no memory of past encoun-ters.The intruder is accommodated or rejected on present face value.The verte-brate lymphocyte system adapts as a result of such challenges; it demonstratesimmune memory in the form of specific antibodies. Previous intruders or antigensare remembered, so that a second exposure is dealt with even more quickly, specif-ically, violently, and generally more precisely (this is the basis for immunization).
Pregnancy, Loke and King suggest, has more in common with invertebratecooperation than with vertebrate adaptive immunity. Just as the myriad animalsbunched together on a coral reef shield themselves with limestone, so the motherand the fetus, to limit their contact, together build a barrier, the decidua (this isthe part of the mother that is literally deciduous and will be shed from the uteruswith the placenta at birth).
Nonetheless, the mother’s nutrient secretions and blood pass through this decidualbarrier, to bathe the chorionic villi in the intervillous space within the placenta. Soboth sides need to know what’s going on.Trophoblast cells behave inconspicuously,displaying non-challenging HLA-G rather than the provocative HLA-A, HLA-Band HLA-D (see the box, . . . and shaking hands with HLA-G).The language theycommunicate with, a robust ‘lingua franca’, is principally the language of the blood’scoagulation system (but that’s another story: see the box,Talking tough with thrombin).Maternal NK cells, which have no memory of past pregnancies, patrol this sensitiveborder region, appreciating the trophoblast’s HLA-G labels.
Nonetheless, adaptive immunity can’t be disinvented just because there’s a fetusin the uterus.The trophoblast sends emissaries, the extravillous trophoblast cells,whichmove into adjacent maternal tissues to re-mould them, even growing into the wallsof the arteries that supply the developing placenta, the so-called spiral arteries, tosoften them and ease down the force of flow into the placental vascular bed.TheT cells in the vicinity are from the peace corps; officially they are Type 2 helperT cells, or TH2 cells), and they either keep their distance or, when their buttons arepushed by HLA-G, tend to release friendly cytokines called interleukin 4 and inter-leukin 10 that keep the immune system reassured that all is basically well.
If for any reason this close relationship sours, the T cell peace corps is pulled outby the mother and replaced by T cells from the marines, the TH1 cells, which attackwith little further provocation.Employing the aggressive cytokines interferon-gammaand tumor necrosis factor, they have a licence to kill, both directly and by enlistingmacrophages.They also throw the blood clotting system out of balance, casing thenow unwelcome stranger in fibrin, the stuff of blood clots.The smoke arising fromthe battle contains many highly irritant chemicals.
Emerging from the molecular mayhem are special substances calledprostaglandins, which soften the cervix and stimulate the myometrium, the musclelayer of the uterus.The pregnancy is expelled—a miscarriage.
48 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 48

Step 5A. Placental construction: laying the project’s foundations
Around the growing embryo, spaces appear within the expanding syncytiotrophoblast calledlacunae, which, as the trophoblast continues eating into the endometrium, opens up theglands, nutritious secretions entering the spaces,which coalesce to shorten the path neededfor the nutrients to reach the embryo. Sometimes, a day or two before the missed periodthey eat into a blood vessel, manifesting to the outside world as implantation bleeding.
For the footings of the developing placenta between the lacunae, trunks of early chorionicvilli form.These villi grow like trees, the trunks growing thicker as they bud ever finerbranches into the coalescing lacunar spaces.At every stage, the lacunae (the developing inter-villous space) are lined by the omnipresent cell that is the syncytiotrophoblast. Down thetrack, about 12 weeks after the last menstrual period (LMP), these spaces will accept aregular flow of maternal blood. But for the first three months they are rather dry.
By the missed period, cytotrophoblast has replaced syncytiotrophoblast at the advanc-ing frontier, releasing extravillous trophoblast cells that travel in cognito, deep into thematernal decidua.
Having come to peaceful terms with the host officials, it’s hard now to see who iscontributing what to the scaffolding and support systems, so intermingled are the construc-tion molecules. But one thing is for sure: none of the extravillous cells belonging to theproject should wear military uniform.To display your unique tissue grouping molecules(such as HLA-A or HLA-B) is to attract instant reaction from the immune police.
So there is more to discretion than valor.Trophoblast and the mother’s blood and deciduaare from the start locked into a vigorous molecular negotiation to determine the spread anddetail of placental construction at the frontier.And the cut and thrust of the traveling extrav-illous trophoblast,as these fetal cells maneuver deep into the decidua,and as the gestation growsand grows, depends on maintaining an exquisite balance within the volatile milieu of themother’s blood coagulation system.Trophoblast even displays such potentially incendiary mole-cules as ‘tissue factor’,a molecule that is revealed in mature tissues only upon injury, so powerfulis it in activating the coagulation cascade of clotting factors.Bewilderingly, fibrin, the stuff thatbinds blood clots into a cohesive, adhesive plug, seems to be avoided during construction ofthe placenta,at least if everything is going according to plan.Yet defects in fibrinogen, from whichfibrin is derived, are capable of producing miscarriage, as are mutations that inactivate factorXIII, a molecule used to crosslink fibrin molecules: the placentas in affected women appearshonky and weak, defects that are overcome if activated factor XIII is administered to themother during placental formation. For more, see the box, Talking tough with thrombin.
Meanwhile the all-important exchange system of the developing placenta, the linkingspaces between the budding chorionic villi (the growing intervillous spaces), remainslined entirely by the living, breathing, growing syncytiotrophoblast, stretching over everylast branch.All the glucose, the oxygen, the nutrients the project needs pass through thesyncytiotrophoblast.And all the carbon dioxide and excrement the embryo or develop-ing fetus is ridding itself of pass through it in the opposite direction.
ESTABLISHING A SUCCESSFUL PREGNANCY � 49
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 49

Talking tough with thrombin
The centerpiece of the coagulation system is thrombin.Thrombin loves getting itsteeth into other proteins (it belongs to a family of enzymes called proteases). It’s theblood factor that converts the soluble, circulating protein fibrinogen into a networkof smaller fibrin molecules, which link to form the fabric of a blood clot.
Thrombin, the trigger for thrombosis, is itself derived from an inactive precur-sor, ‘prothrombin’, only when and where it’s needed, most commonly through abreech in integrity of the inside of blood vessels, exposing ‘tissue factor’.The systemof signals that pulls the trigger is potentially so powerful that just a milliliter of yourblood contains enough clotting potential, if unleashed, to coagulate all the blood inyour body within 15 seconds.
Mice that lack the enzyme to convert prothrombin into thrombin might bleedeasily, but they enjoy powerful protection against miscarriages of all sorts of causes.
On the basis that the devil otherwise makes work for idle hands, nature tiesthrombin up to pursue better ends, especially it seems at the trophoblastic frontier,according to a model published by Hartmut Weiler from the Medical College ofWisconsin and his colleagues in Nature Medicine.
We know that loose thrombin is gathered up by a molecule on the trophoblastsurface, thrombomodulin, and one in solution, antithrombin.
Thrombomodulin encourages thrombin to get its teeth out of fibrinogen andinto protein C, activating it to ‘activated protein C’ (APC), an important natural anti-coagulant that attacks clotting factor V (unless, that is, it’s the variant polymorphismknown as factor V Leiden, which resists APC and causes blood to like clotting morethan it should, a state called thrombophilia).
Antithrombin binds not just thrombin but also clotting factor Xa, again turningthrombin away from pro-coagulant temptations and giving it anticoagulant respon-sibilities instead.The drug heparin promotes this activity (for more on its role inpreventing miscarriage, see Chapter 9).
Thrombomodulin,APC and antithrombin are therefore important natural anti-coagulants responsible not just for keeping our blood flowing, but, when we werestarting off life as implanting embryos, stopping fibrin from getting between us andour mothers.
So, on the one hand,miscarriage is more likely if there is a deficiency of fibrino-gen or factor XIII. Somehow we do need to form fibrin somewhere in the placen-tal scaffold.
On the other, too much scaffold from thrombophilia and fibrin can separatemother and fetus and lead to miscarriage.Thrombophilia from any of (1) an increasedsusceptibility of prothrombin to form thrombin (the prothrombin G20210A poly-morphism), (2) resistance of factor V to APC, such as the factor V Leiden mutation,
50 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 50

Step 5B. Meanwhile embryonic development proceeds: Complicatedconstruction in the inner sanctum
Deep within the gestation, the purpose of the project,developing the fetus, should be progress-ing full steam.By the time of the missed period, an embryo that will be successful is formingits third definitive layer of tissue.What was the inner cell mass has become first a disk of twolayers, the ectoderm (or epiblast) on top, and the endoderm (or hypoblast) underneath (Figure4.1b).Then, in a move that creates a head-end and a tail-end to the embryo, an interveningtissue, the mesoderm, pushes between the two layers in a process called gastrulation.
Reading off the blueprint, the embryonic genome (copies of which are available inevery cell) already had 1600 separate genes functioning before the blastocyst had started toimplant. Since then new instructions have been requested almost by the hour, as the embryoprogresses through the remarkable changes that will give it functioning tissues and organsystems, as well as a human form.
Before long, as many as 30 000 instruction sets will be being followed.A majority ofthem comprise instructions for molecular signalling systems.
Above the embryonic disk the ectoderm is extending to form a bubble, a membranecalled the amnion, enclosing the at-first-tiny amniotic cavity.Below the disk, and more promi-nent, is the chorionic cavity, developing as mesoderm envelops the hollow insides of theblastocyst’s trophectoderm/cytotrophoblastic cavity with a new tissue called chorion.By a week after the missed period this growing cavity becomes the first visible sign of preg-nancy on transvaginal ultrasound: the gestational sac (see Figure 4.2a).
If all continues to go well, the yolk sac forms inside the chorionic cavity, connected tothe growing but still tiny embryo, and an early circulation system is developed, which willhelp carry nutrients from, and waste products to, the peripheral interface with the motherat the trophoblast surface.
Blood vessels will push into the trophoblastic columns as these columns bud intobranching trophoblastic villi (Figure 4.1b). Soon, the earliest blood cells are formed insidethem.Unlike later mature red blood cells, these primitive hemoglobin-containing red cellshave a nucleus.
The most prominent organ visible on transvaginal ultrasound after the yolk sac (seeFigure 4.3) will be the developing heart, beating at around 120 to 160 beats per minute,and visible by five and a half weeks from the LMP . . . if everything is going to plan.
and (3) a shortage of protein C all hobble thrombomodulin, allow thrombin tobehave badly, and make miscarriage more likely.
That most of us get through most of our adult lives without either bleeding todeath or suffering a major thrombosis seems remarkable, given the volatility of theblood coagulation system. Perhaps the fact that we proved ourselves in our first fewmonths of life after conception by constructing well-founded placentas sorted outthe women from the girls, the men from the boys, in terms of our ability to keep ourblood coagulation system in pretty good balance for so many years of our adult lives.
ESTABLISHING A SUCCESSFUL PREGNANCY � 51
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 51

With regard to the plan, consider the chromosomes as bound volumes of the blueprint.In the blueprint that every cell of the pregnancy is carrying, we need exactly two copiesof each instruction, or gene—one from each parent’s genome. If the instructions are iden-tical, then it’s an unambiguous,homozygous instruction; if not, it’s heterozygous, and the resultis less predictable (though usually the correct instruction wins out). If there’s only oneinstruction, it might not be heard. If there are three instructions, the action will be over-stated. But if both instructing genes for a particular step are faulty, and that step is a criticalpart of the plan that cannot be worked around, the project comes to a halt. Sometimes thishitch can affect genes on the host side . . . a failure of some maternal system within thedecidua that prevents the host uterus from ever accepting an ongoing pregnancy.
Step 6. A placental circulation
Meanwhile, at the periphery, the syncytiotrophoblast, the thin envelope of the placenta thateverywhere separates the mother from the gestation, is growing apace.By the time the babyis ready to be born, this single syncytiotrophoblast cell will have a surface area of 12 squaremeters. It grows because it is continuously fed by trophoblastic stem cells, the cytotrophoblast,fusing into it.About 15 percent of the bulk of the fusing cytotrophoblast is for growth, asthe placenta enlarges and extends and the villi keep branching.The other 85 percent is forturnover of the cell’s internal workings, its organelles. As bits of the syncytiotrophoblastwear out or get tired, they are pinched off and enter the mother’s circulation, reaching herlungs, where they stick and are broken down and absorbed. If this dynamic is disturbed,and the syncytiotrophoblast gets fatigued, miscarriage will not be far behind.
The syncytiotrophoblast has many functions. A crucial early one is to manufacturehCG in rapidly increasing amounts to push a more and more resistant corpus luteum intocontinuing the production of enough progesterone to reach the uterus. From six to eightweeks from the LMP, the syncytiotrophoblast takes over this responsibility. It feeds on choles-terol from the mother and turns it into progesterone, ensuring that there is plenty of itwhere it’s needed: at the interface with the host decidua.
Without continuous encouragement from fetal headquarters, represented both by thesupply of fusing cytotrophoblast cells and by various molecular messages from fetal tissues,the trophoblast loses its confidence in greasing the local immune system’s border officialswith progesterone, and diplomacy can fail.
The construction project,while it was still small,would just have dissolved away from hostil-ity expressed by the NK cells and T cells.But once it’s too big to be so ignominiously absorbed,an irritated host needs bigger guns as well as a way of physically pushing the project out.
Many,many developments (or developmental lack,or delay) can initiate the breakdownin communication that can sooner or later cause the host defense force to turn nasty.Whenit does become nasty it does so by turning on some bleeding and coagulation around theperimeter to seal the troublesome pregnancy off, followed by a call on the myometrium tocontract and to expel the doomed project.Only uncommonly does it send in much by theway of sacrificial T cell troops from the immune battalion.
For the pregnancy to be secure, the extravillous trophoblast, like the syncytiotrophoblast,
52 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 52

ESTABLISHING A SUCCESSFUL PREGNANCY � 53
Figure 4.2aThe first visible sign of pregnancy.A tiny gestational sac seen on ultrasound, 5 weeks fromthe LMP.
Figure 4.2b A ‘blighted ovum’ on ultrasound at 6 weeks from the LMP. The gestational sac has grown,but without an embryo or yolk sac, just a chorion. Note the easily visible decidua that hasformed around the gestational sac. Sooner or later, miscarriage is inevitable (see Figure 4.4c).Sonograms courtesy of Sydney Ultrasound for Women.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 53

54 � GETTING PREGNANT
(a) (b)
Figure 4.3 A twin pregnancy on ultrasound at 8 weeks and 4 days’ gestation, in which one fetus isdeveloping normally and one has died.
(c) (d)
(b) A close-up of the nonviable sac reveals a veryenlarged yolk sac, a classical sign that the fetuswill not survive. If this were a singletonpregnancy, miscarrriage would be inevitable.
(a) Both gestational sacs are visible.The uppersac was smaller in all the scans and the fetusvisible in this sac is not viable.The sac and itscontents will shrink and eventually disappear.
(d) The fetus, as well as having a heart beat on‘real-time’ ultrasound, is developing normally,with its head, body, upper and lower limbsalready visible.
(c) In contrast, the yolk sac of the healthy fetus isnow quite small.
Sonograms courtesy of Sydney Ultrasound for Women.Figure 4.4a–d is printed in color after Appendix 3.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 54

needs to achieve some key objectives.These covert operators, these ‘special forces’, are sentout into the decidua from those areas of trophoblast not in direct contact with the inter-villous space. Sometimes called ‘interstitial trophoblast’ or ‘intermediate trophoblast’, thesecells seek out the maternal host’s arteries that will be feeding the placenta.They enter themuscular walls of these arteries and subvert them, causing them to weaken and later todilate.They then enter the interior of the vessels, clogging them,before eventually forminga new lining that replaces the mother’s cells with the fetus’s cells.
All of this activity, remodelling the maternal host’s arterial supply to the placenta,meansthat just a trickle of maternal blood gets to the feto-maternal interface in the intervillousspace for the first three months of pregnancy. If everything is developing normally in a healthypregnancy,a transvaginal ultrasound will demonstrate an absence of flow through the placenta,if a Doppler study is done (see Figure 4.4a). (It’s the reason you can biopsy the placentaduring chorionic villus sampling, or CVS, without causing bleeding.)
On the other hand, a pregnancy that is not doing well will show maternal blood pulsinginto the intervillous space (Figure 4.4b).Miscarriage (Figures 4.4c and d) can follow withindays. If this conversion of the maternal arteries by the extravillous trophoblast is incom-plete but just enough to avert miscarriage, preeclampsia (pregnancy-associated high bloodpressure) is likely to occur later in the gestation.
Step 7. Serious growth and development
By the end of the first three months of pregnancy, construction of the supply systemis complete. The maternal arteries supplying the placenta have become large-volumecapacitance vessels, and it is time to open the faucets to the intervillous space, irrigating theplacental bed with maternal blood.
The embryo is now a fetus. It has a face, it has arms and legs, it has fingers and toes, it hasa brain and a spinal cord, it has testes or ovaries. Its critical organ systems are all close to beingfinalised, having formed in the lowest oxygen conditions imaginable—conditions that haveprotected the millions of copies of the project blueprint from replication errors,or mutations.
From now on, mistakes become a little less serious. Cells with errors can be replacedby cells that do not have those errors.
As blood circulates through the placental bed, the chorionic villi, still immature,gradually refine their architecture for greater efficiency, but it will the 23rd week beforefully mature ‘terminal’ villi form. It becomes more and more important that the ratherslowly flowing blood does not clot: to do so would cut off the oxygen supply and provefatal.To encourage the circulation, the tips of the villi produce a special anticoagulant,annexin V.
Delicate diplomacy continues regarding the mother’s white blood cells, but the groundrules of engagement are now well and truly established. Occasional roving white bloodcells from each side of the divide will travel deep into the others’ territory. Most will beleft behind long after the fetus and the host mother part company, to show up many yearslater as an occasional Y-chromosome-bearing cell line in the mother, or as an X-bearingcell line in a son (in an effect called microchimerism).
ESTABLISHING A SUCCESSFUL PREGNANCY � 55
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 55

What was once just a small blister, the amniotic cavity is now growing faster than the chori-onic cavity that surrounds it. Gradually the fluid between the chorionic membrane and theamniotic membrane (together ‘the membranes’) disappears, and the outside of the amnionfuses with the inside of the chorion.From 14 or 15 weeks from the LMP the fusion is completeand the fetus floats in its own amniotic cavity; amniocentesis becomes possible for sampling thefetus’s cells.The membranes fully occupy the uterus and seal the pregnancy off from the cervix.
Step 8. Surviving threats
Threats to Project Pregnancy remain. Even though the design features of the project andits host infrastructure are in place, the rapid growth taking place can strain the availableresources. If there is physical constraint, friction will occur at the boundary. If there is logis-tical constraint, problems with the supply line, the fetus’s growth will be restricted, especiallyin the closing stages of pregnancy. Sometimes the closing membranes trap organisms thatcan cause vaginosis inside the uterus, a subversion that at any time can trigger a late miscar-riage or premature labor. Occasionally a boundary gives way (see the discussion of cervicalincompetence in Chapter 8) and, to both sides’ dismay, the project falls apart physically.
Faulty aspects of the fetal blueprint can still be operative.An extra volume of instruc-tion set #21 (trisomy 21), for example (or of #13 or #18), may have permitted confidentbut abnormal development, escaping all internal checking procedures.The host mothercould demand a formal examination of the blueprint by karyotype, using a sample of chori-onic villi (CVS) or a specimen of fluid and cells from the amniotic cavity (amniocentesis).
The ever-present threat to the project from the host’s immune guard (its white bloodcells, or T cells) remains. Project Pregnancy must keep its own house in order or face theconsequences. Generally, however, the immune system is not out to cause trouble, but if itsniffs it will respond vigorously. If there is trouble—if, for example, the fetus is invaded byinfective organisms, or if shearing forces at the growth points provoke inflammation—themother will move quickly to safeguard her own future in a response that evolved millionsof years before there were doctors and nurses with antibiotics.The immune system is calledon and will go to work with a determination to protect the host. Collateral damage willbe severe and separation of the fetus from the mother is the usual result.
More often, by now, the host environment is tolerant and helpful, ensuring a steadilyincreasing stream of supplies as the fetus grows, providing a constraining but yielding neigh-borhood with room to grow without excessive friction or suffocation, and providingadequate waste removal, until the fetus is mature enough to separate from the host into anindependent life in a wider world.
Step 9. Birth
In the ideal pregnancy, the fetus signals to the host that he or she is ready to be born. Itdoes this by having its trophoblast convert fetal hormones to a special estrogen called estriol.The mother obliges by switching off her receptors to progesterone.This starts a cascade oflabour and birth, as she activates the powers to expel Project Pregnancy . . . powers that,until now, she has kept in reserve.
56 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 56

section II
tests
what tests to have done and when
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 57

Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 58
This page intentionally left blank

making a diagnosis
The first round of tests
There are just four things that stop a woman getting pregnant (see Table 5.1): no sperm;no eggs; a blockage stopping sperm getting to eggs; or a problem with implantationof the embryo in the uterus (usually through lack of oomph on the part of the embryo,
sometimes because something in the uterus is getting in the way).Here we look at the standard tests to distinguish these causes of infertility:
• Tests for sperm;• Tests for ovulation;• Tests for blockages; and• Tests for implantation.Except for the laparoscopy and hysteroscopy (which, being surgical operations, areoften postponed), these tests can be arranged by your family physician or generalpractitioner.
Chapter 6 will look at further testing and strategies if the preliminary tests appear toshow an abnormality capable of preventing pregnancy completely, called sterility.Chapter 7 willlook at further testing and strategies if the preliminary tests are normal or if they show anabnormality that might still allow pregnancy to take place, called subfertility.
SPERM COUNTS AND MUCUS TESTING
The two ways of looking at sperm are directly, under the microscope, which is called asemen analysis or a sperm count, or indirectly, by checking for the presence of sperm incervical mucus up to about 12 hours after having sex, a test called a postcoital test, or PCT.In practice, for reasons I’ll make clear, PCTs are not commonly done nowadays.
59
5
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 59

The semen analysis
A sperm count can be the simplest or the most difficult of tests, depending on how cooper-ative your partner is and, separately, how easy or hard it is for him to masturbate to providethe sample of semen needed. (See the box, Having a WHAT?)
The specimen also needs to be examined reasonably quickly—and generally duringthe ordinary working hours of the lab.He may need help from you, the woman, to overcomeany or all of these difficulties.
Laboratories will stress the need for the specimen to be complete—for none of theejaculate to be lost. A Sydney sperm expert, Dr John Tyler, has shown that an ejaculateobtained under stress might be very unrepresentative, mainly because its volume can below and sperm lying in the vas deferens might not be ejected into the semen effectively.Aspuriously low count can result, so a single low sperm count always warrants being doneagain, in better circumstances than before if these were strained.
Whether in a sterile container available from the laboratory or in a Silastic condom,the specimen should reach the lab within an hour or so. Keep it at ordinary room or bodytemperature to preserve the sperms’ movement, or motility. Sometimes it’s important forthe sperm to be fresher than this, especially if the sperm count is known to be low and thesample is to be used for special diagnostic or therapeutic maneuvers; in such a casethe semen is best collected at the IVF laboratory, which will have a special private areafor doing so.
A normal sperm count will have an overall volume of at least one milliliter; a spermdensity of more than 20 million sperm per milliliter; a motility of 50 percent or better (thepercentage of sperm cells present that are moving, preferably purposefully); and a propor-tion of abnormal forms (odd-shaped heads, deformities of the midpiece and abnormalitiesof the tail) at less than about 50 percent (or, using the World Health Organization’s so-called strict criteria for normal sperm appearance, of normal forms better than 14 percent).
60 � GETTING PREGNANT
Table 5.1 The four main reasons couples have trouble achieving a pregnancy, and thetests to have done
Sterility Subfertility Main tests
(no chance without help; details (reduced chance without help; details in Chapter 6) in Chapter 7)
no sperm (azoospermia) not enough sperm (oligospermia) • sperm count• postcoital test
no eggs (primary ovarian failure) eggs not ovulated normally or • serum progesteronefrequently (anovulation, or amenorrhea; • serum FSHoligomenorrhea)
complete blockage incomplete blockage (abnormal tubes; • chlamydial antibodiesabnormal cervix) • hysterosalpingogram
• laparoscopy
no implantation (oopause; reduced implantation (weak embryo; • transvaginal no uterus) abnormal uterus) ultrasound
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 60

But these are mostly arbitrary figures. Some couples have no trouble getting pregnantwith much lower sperm counts. Dr Sherman Silber, an American urologist and a worldleader in male infertility, has shown that almost no sperm count above a complete absenceof sperm is so bad that you can say that pregnancy is impossible.Ultimately it does just takeone sperm to make it.
MAKING A DIAGNOSIS � 61
Having a WHAT?
‘Yucky poo!’ is what I heard a grown man exclaim when one of my mentors in the1970s detailed the need for a sperm count by collecting a semen sample . . . bymasturbation into a clean, sterile,wide-open collecting jar. I thus had an insight intohow over-reaction to an adolescent indiscretion by a parental guardian had causeda scar.
Such social conditioning on the evils and perils of masturbation is fortunatelyrare nowadays, notwithstanding the sin of Onan and its broad interpretation in somereligions to mean that no semen should be released intentionally that does not entera vagina. (Disobedient Onan was struck dead by God in Genesis 38 for spilling hissemen onto the ground instead of into the wife of his brother, after he’d been toldby his father, Judah, to get her pregnant on his dead brother’s behalf.) The religioussystems that still insist on such biological and social folly are patriarchal to theextreme.
Still, not every male is experienced with masturbation. Producing a sample ofsemen on demand can be easier said than done, especially in a room that’s unfamil-iar, and especially if there’s not a total sense of privacy and security.
Most modern assisted conception (IVF) programs have well-designed, sound-proof facilities,where the wife or female partner can be present too (although moreoften she isn’t). Erotic literature helps some men, but not all.At Sydney IVF, to easethe tension,we also make whisky,wine and beer available—and we keep some Viagraclose by.
An acceptable alternative to masturbation is to collect semen during sex usinga special condom made of Silastic, which is an inert or chemically non-reactiveplastic. (Do not use an ordinary contraceptive condom: they’re usually made speciallyto be toxic to sperm cells.) Silastic condoms are thick and insensitive.One religiouslycorrect version has a tiny opening in the tip to avoid—just!—the contraceptive sinof Onan.
How long do you need to wait after a prior ejaculation to have a sperm countdone? Not long, but probably at least 24 hours. Don’t wait more than four or fivedays, though, unless you’re especially asked to. Sperm motility does not last foreverin the male reproductive organs. Sometimes a very short interval is unavoidable,particularly when there’s an unexpected shortfall in sperm cells at the time of an eggretrieval procedure for assisted conception.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 61

The postcoital test
We can get a better idea of how sperm are functioning in practice by looking at sperm inthe mucus of the cervix after sex.This is the postcoital test (PCT) or Sims-Huhner (or justHuhner) test.
Remember, though, that cervical mucus is only receptive to sperm during ovulation, sotiming the test correctly is critical.To do a PCT at any other time in the ovarian cycle ormenstrual cycle is meaningless, because it’s then normal for it to be negative (a negative testshows no sperm or no motile sperm; a positive test shows more than five normally motilesperm per microscopic field of examination). Indeed, it’s so important to time the testcorrectly that at Sydney IVF when we do this test we always measure serum estradiol, serumprogesterone and serum LH to confirm ovulation is occurring (often with prior ovarian moni-toring to anticipate the day of ovulation effectively).Referring back to Figure 3.2, at ovula-tion the estradiol should be high, luteinizing hormone (LH) should be high (the LH surgeshould be taking place), and progesterone should be low. If not, the test is being done tooearly or too late, or the ovulation isn’t strong enough for the PCT to be informative.
The cervix and its mucus should also look receptive: (1) the cervix should be open;(2) the volume of mucus should be good (every woman will be different for both theseparameters, but they will be consistent in one woman from ovulation to ovulation); (3) themucus should be clear,watery and stretchy (called its German name,Spinnbarkheit,meaning‘spinability’); and (4) the mucus should produce a complete ferning pattern when it’s allowedto dry on a microscope slide.A cervical score awards points from 0 to 3 for each of these fourparameters, the last two of which should be 3/3.
If the PCT is positive (motile sperm present in good numbers), then we can forget aboutthis aspect of getting pregnant. If the PCT is negative—and if it was done during a goodovulation—then interpretation gets complicated. Some infertile couples will go straight toassisted conception, either IVF or IUI (see Chapter 20) at this point: first, because of thepractical difficulty there can be in sorting out the cause; and second, because the treatmentfor whatever is found is often not successful.
In fact, many couples will quite correctly opt for IVF whether the PCT is positive ornegative.This is because, if the test is positive, we are no closer to explaining the infertility.IVF might be indicated for other obvious reasons at this stage, such as blocked fallopiantubes (see Chapter 6), or it might be used because we have unexplained infertility (seeChapter 7). I discuss the possible causes of a negative PCT carried out during a normalovulatory cycle on the day of ovulation in Chapter 7, but in practice, the complexities oftiming the PCT, the indirectness of the limited information it provides, and the probabil-ity of recourse to treatment such as IVF irrespective of its result, mean that many doctorsdispense with the PCT.
TESTS FOR OVULATION
Strictly, the only ways of being sure ovulation has taken place are by seeing the egg outsidethe ovary,or by inferring it got out of the preovulatory follicle because pregnancy has occurred.
62 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 62

Neither of these is usually very practical in investigating infertility. Generally we rely onindirect evidence of ovulation, detecting progesterone produced from the ovary after ovula-tion has taken place.
A single serum progesterone taken in the middle of the luteal phase can be all that’s neededto be practically sure that ovulation is taking place. (In a 28-day cycle, test on day 21; forcycles that are longer or shorter, assume a luteal phase length of 14 days with a varying follic-ular phase length, and therefore add to or subtract from day 21 the exact number of cycledays different from 28). At that time it should be more than 35 nanomoles per liter (ormore than 12 nanograms per milliliter, depending on which units are reported by the lab).
Preferably there should also be some sign that the length of the luteal phase is at least11 days, preferably about 14 days. Luteal phase length can be estimated by counting thedays between any clear indication of when ovulation occurs (such as experiencing ovulationpain, detecting an LH surge with a home-testing kit, or seeing a clear temperature dip on abasal body temperature chart, or BBT) and, to mark the end of the luteal phase, the onset offull menstrual bleeding (ignoring any premenstrual spotting). For more on the BBT see thebox, Hot for pregnancy, and for more on charting it, see the box, The BBT chart . . . obsolete?
Alternatively, the evaluation of the luteal phase can be done with more formal ovarianmonitoring, with hormone measurements and transvaginal ultrasounds leading up to ovula-tion and continuing in the luteal phase with, say, three evenly spaced measurements of serum
MAKING A DIAGNOSIS � 63
Hot for pregnancy
The rise in the basal body temperature, or BBT, with ovulation and for the duration ofpregnancy reflects the action progesterone has on the temperature-regulating centersin the hypothalamus in the brain.
Progesterone is an old molecule in nature, being found in fish, where it seemsto have no special purpose except as a jumping-off point for making other hormones.In mammals, however, nature employs progesterone to be the hormone that sustainspregnancy.
We may presume that the evolution of progesterone’s action on temperature wasnot just an accident—that, at least in our distant ancestors, it was an advantage forthe embryo, and then the fetus, to be in a somewhat warmer internal environmentthan was the case before ovulation.
Birds also have progesterone as an active hormone produced by the ovary,but birds function at a much higher body temperature than mammals do (about40 degrees Celsius, or 104 degrees Fahrenheit)—too high to be safe for aninternal embryo, but good if you’re sitting on your eggs in a nest.
Which is why chickens have to lay their fertilized eggs; which is why they haveto keep up their body heat;which is why they have to lay their fertilized eggs;whichis . . .
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 63

progesterone. Sometimes this will reveal that progesterone is being produced with a stronghint that the egg has not left the follicle. For more on what is called the luteinized unrup-tured follicle syndrome, or LUF, see the box, Fake ovulation.
Lastly, these estimates of progesterone are leading to more than just an answer to ques-tions concerning ovulation and length of the luteal phase.Progesterone, like other hormones,is what it does: its action on the endometrium must be adequate to support implantation andearly pregnancy.The adequacy of the luteal phase can therefore also be assessed by a premen-strual endometrial biopsy, which is discussed below under Tests for implantation.
TESTS FOR BLOCKAGES
The most common place where a blockage keeps egg and sperm apart is in the fallopiantube.There are two main ways the tubes can be checked for whether they’re open,or patent(called tests for tubal patency).The less intrusive method (though unquestionably still intrusive)is by a hysterosalpingogram or HSG, which involves a vaginal examination and injection ofradiographic fluid into the uterus and tubes to show them up on an x-ray (see Figures 5.1and 5.2).The more intrusive method is by laparoscopy, which is an operation requiring
64 � GETTING PREGNANT
The BBT chart . . . obsolete?
The place of the sometimes irksome basal body temperature chart in modern infertil-ity management is not as clear as it used to be.There are competing products on themarket to detect ovulation short of having blood tests done (Chapter 19 has thedetails). But there are clear cases when it’s useful—and it’s always cheap.
I advocate using the BBT when ovulation itself is in doubt or under investiga-tion and I am not using ovarian monitoring to follow the events of the ovarian cyclemore exactly.A series of charts over several months can indicate approximately whenin the cycle ovulation took place.This information can then be used in future tohelp time when to have sex.
Once the temperature is up, ovulation will be over and done with for that cycle.Where should the temperature be taken? Where in your body should you put
the thermometer? The temperature changes we’re looking for are subtle. And thetemperature as taken in the mouth bounces around a bit.You will get a clearer patternfrom measuring pelvic temperature, by placing the thermometer in the vagina.
But oral BBT charts can usually be revealing enough if taking the temperaturein the vagina is awkward, and if you’re not a mouth breather, and if you don’t havea glass of water before you take your temperature. (I know of no patients who preferto use the thermometer in their rectum, the way you take a baby’s temperature.)
Remember, too, that a thermometer for measuring the BBT, to be sensitiveenough, should not have the wider range that clinical thermometers designed todetect a fever have.You can buy a basal body thermometer at any chemist.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 64

general anesthesia. Laparoscopy, however, also enables endometriosis to be diagnosed, whichgives it a special advantage.
But because both tests are intrusive, you will be discussing with your doctor whetheryou do want to proceed with either or both at a relatively early stage of testing or whetheryou will wait to see what else does or doesn’t show up.
This could be a time for needing to be particularly candid with your doctor, as well ascalling for special diplomacy on his or her part, if you both want to be open about the reasonsfor doing tests (and so avoid professional paternalism, examined in Chapter 26).The majorcause of blocked fallopian tubes, at least if you have not had an operation on the pelvic organs,is prior salpingitis, nowadays typically from chlamydia, a sexually transmitted disease, or STD.
The good news—your doctor might or might not suggest it—is that you can stop shortof committing to an HSG or laparoscopy by having a blood test done for prior chlamydia,namely serum chlamydial antibodies.
Serum chlamydial antibodies
If these antibodies are not present—if it is a negative test—then there is virtually no chanceof having tubal obstruction, at least from chlamydia.This is where the test is very useful.Importantly, however, if chlamydial antibodies are present—if it is a positive test—it does notnecessarily mean that the tubes have been affected. Moreover, chlamydial antibodies can
MAKING A DIAGNOSIS � 65
Fake ovulation
It’s possible for a preovulatory follicle to form a corpus luteum and make progesteronewithout the egg escaping from it: this is the luteinized unruptured follicle, or LUF.
It’s detectable on careful ultrasound and hormone monitoring of ovulation. Insteadof the follicle collapsing or apparently disappearing on serial ultrasound examina-tions of the ovary, it keeps getting bigger as progesterone production gets underway.Typically, serum progesterone levels rise while the follicle on ultrasound grows to2.5 centimeters or more in diameter.
How often this happens normally is an open question.It’s more common in oligomenorrhea (described in Chapter 11), when it results
from diminished FSH drive of developing follicles during the follicular phase, andperhaps in endometriosis (described in Chapter 15) and during inadvertent use ofNSAIDs such as ibuprofen (Advil,Nurofen) and naproxen (Aleve,Naprosyn),whenit results from diminished effectiveness of the LH surge.
The progesterone produced in that cycle may be less than in an ovulatory cycle;the length of the luteal phase may be less than the normal 11 to 16 days; and there’sno egg released to enable conception to take place.
LUF forms part of the entity referred to as luteal phase insufficiency, or lutealphase defect.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 65

arise from non-chlamydial infections, or from chlamydial infections of a non-STD kind(including atypical pneumonia).
Depending on your past circumstances, a positive chlamydial antibody test might meanan earlier examination of the tubes.The choice of which test for tubal patency you shouldhave done is complicated and not all doctors have the same views.
Laparoscopy
Laparoscopy is an operation, usually carried out under full, or general, anesthesia, in whicha fiberoptic device (the laparoscope, about a centimeter in diameter) is passed into theabdomen through a small cut in the navel, or umbilicus. Before the laparoscope is passed(via a sharp trocar and a hollow cannula), carbon dioxide gas is instilled through a finercannula, to lift the abdominal wall from the intestines and give enough room in theabdomen to pass the larger instruments safely and to look about. One or, usually, twoother small incisions are made just above the pubic bone for other instruments to bepassed.
66 � GETTING PREGNANT
Figure 5.1 A normal hysterosalpingogram, or X-ray (roetgenogram), of the uterus and tubes.Appearing opaque (white) to X-rays are (a) the speculum in the vagina, (b) the cervix,(c) the triangular cavity of the uterus, (d) the narrow isthmus of the fallopian tube on eachside, (e) the wider ampulla of the fallopian tubes, and (f ) spill of the contrast dye out theend of the tube among the intestines.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 66

When investigating tubal patency (whether the tubes are open), some salt solution,perhaps with a dilute blue-colored dye, is instilled through the cervix into the cavity of theuterus. If everything is normal, the dye is then seen at laparoscopy to run from the uterusout through the ends of the fallopian tubes.
Laparoscopy takes about 20 minutes if it’s done just for diagnosis. Some conditions,such as endometriosis, may be able to be treated at once through the laparoscope; the oper-ation can then take longer, depending on the extent of the endometriosis.
Some surgeons have been using laparoscopy with a thin laparoscope under local anes-thesia (called minilaparoscopy), or even through the top of the vagina, behind the cervix.The view of the tubes can be excellent, especially if they have been suspended in warmsalt solution instead of carbon dioxide gas, but unfortunately it is not possible to deal effec-tively with endometriosis, or even to detect it reliably.
It’s usual to combine laparoscopy with hysteroscopy, which enables the uterotubal junc-tions to be inspected. A few years ago some colleagues and I became keen on passing aneven finer, flexible scope down the uterotubal junctions at hysteroscopy to inspect the insideof the tubes, a procedure called falloposcopy, but I rarely found it reliable enough to be useful.Alternatively, a better view can be obtained of the inside of the ampulla of the tube bypassing an intermediate-sized scope through the tube’s fimbrial end at the laparoscopy, aprocedure referred to as salpingoscopy, and well worthwhile in some circumstances.
MAKING A DIAGNOSIS � 67
Figure 5.2 An abnormal HSG.The left tube (on the right side of the X-ray) is blocked at the isthmus.The right tube shows a delicate filigree pattern in the isthmus called salpingitis isthmicanodosa (s.i.n.), which is a sign of long-standing inflammatory damage.The ampulla of theright tube is distended and without features, typical of a hydrosalpinx. Notice the unusualcup-shaped device used here to inject the contrast medium through the cervix.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 67

Like all surgery, laparoscopy carries hazards, such as bleeding, infection or damageto an internal organ.The risk of suffering these complications is low, usually less thanone in a thousand, but can be higher when there has been extensive previous surgery.You should schedule at least three days off work. Because some carbon dioxide can gettrapped under the diaphragm, and because nerves from the diaphragm mingle withnerves from the skin over the shoulders before they reach your brain, expect somediscomfort in the shoulders afterwards.You could have some bruising in the wall of theabdomen.
Hysterosalpingography
A hysterosalpingogram, or HSG, is (literally, if you understand Greek) an x-ray of the uterusand the fallopian tubes. Some gynecologists carry out HSGs themselves, but most areperformed by radiologists (specialist x-ray doctors).
Just about everyone who has had one says they hurt, but it’s rarely practical to offergeneral anesthesia—mainly because the best x-ray machines are not portable enough tomove into an operating room, where high standards of safety with anesthesia can beexpected.The pain,which has the characteristics of period pain, should not last longer thanthe time it takes for the x-rays to be done. It’s worth taking analgesics including whateverNSAIDs work for you and are readily available. I usually recommend two Naprogesic tablets(which combine naproxen and a small dose of dextropropoxyphene), about 30 minutesbefore the HSG is due to be done.
The HSG proceeds with a vaginal examination carried out with a speculum (as whenyou have a Pap smear of the cervix done).An instrument is fitted to the cervix by whichsome contrast medium (a liquid that to x-rays is dense, therefore visible) is slowly injectedinto the uterus and through the tubes.The test is judged normal if the medium passes outalong the tubes, demonstrating no obstruction or significant irregularities, then into theabdomen, where it disperses among the intestines (see Figure 5.1).
An HSG has three benefits laparoscopy does not have.First, it shows the lining of the tubes in a way that cannot be inferred by the tubes
simply being seen to be open at laparoscopy (see Figure 5.2, where the abnormal filigreepattern is important but would be missed at laparoscopy).
Second, when oil-soluble contrast medium is used—as Dr Alan DeCherney, at YaleUniversity in the 1980s, proved what gynecologists had long thought—some patientsgo on to conceive who would not have become pregnant otherwise. In other words,there’s something about the HSG medium that improves fertility for about four monthsafterward.
And third, there are circumstances in which, if you’re having a laparoscopy, you mightwant to have a more substantial procedure done on a form of blocked tube called a hydro-salpinx, but which should require specific informed consent.
For more on how even just a one-sided hydrosalpinx can cause sterility, see the box,Hydrosalpinx: Reintroducing a villain, in Chapter 20.A prior HSG allows this possibility tobe properly discussed beforehand.
68 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 68

If the HSG shows apparent obstruction of the narrow parts of the tubes, close to theuterus, some radiologists will pass a catheter into the uterotubal junction, or even downthe tube, to bring more pressure to bear in outlining the particular tube—a specializedmaneuver called a selective salpingogram.
Hysterosalpingograms have disadvantages too. If there is a hydrosalpinx, it’s possible forbacteria ordinarily resident in the vagina or cervix to be swept into the tube and, becausethere is no ready escape, the tube being a blind alley,multiply there to cause acute salpingitis,which if not promptly treated with antibiotics can turn into a pus-filled sac, or pyosalpinx,which can require surgery before it resolves.
The HSG is excellent for determining exactly where a tube is blocked, but if the tubesare open it’s not efficient at detecting adhesions on the outside of the tube (peritubaladhesions), which could be separating the tube from the ovary.
Lastly, the fat-soluble medium, if this is what is used to outline the tubes, can cause aninflammatory reaction in the abdomen in about 2 percent to 5 percent of people (this israrely harmful, but it can be).The radiologist must also be careful that the fat-solublemedium, during its instillation into the uterus, does not enter blood vessels, from wherethe oil might be transported to the lungs, causing breathlessness.A water-soluble mediumis used by many radiologists because of its lesser tendency to cause these reactions, butwater-based media do not cause the improvement in fertility that oily HSGs can some-times bring about.
In summary, hysterosalpingography and laparosocopy complement each other in eval-uation of tubal disease. Both investigations are useful in properly planning microsurgery torepair tubal blockages from salpingitis.
TESTS FOR IMPLANTATION
There are two requirements for successful implantation of an embryo in the uterus: a compe-tent blastocyst, and a receptive and nutrient endometrium.
Tests for the embryo
The importance of the embryo’s inherent metabolic strength is occasionally revealed by itsability to implant and grow as an ectopic pregnancy, in locations that are abnormal andinhospitable.We need to remember, though, that the ectopic embryo developing in thefallopian tube or even in the ovary or abdomen often has its growth stunted.The embryo,or later the fetus, forms abnormally. But this example from nature does demonstrate howan embryo that starts off vibrantly normal has much power to make its immediate envi-ronment provide what it needs.
We still have virtually no ways of investigating the health and vitality of embryos in vivo(that is, conceived and developing naturally in the body). And we still have only limitedways of testing embryos in vitro (that is, in the laboratory). For what we can do, see the box,Properly performing embryos.
MAKING A DIAGNOSIS � 69
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 69

70 � GETTING PREGNANT
Properly performing embryos
For an embryo at the stage of a blastocyst to be capable of becoming a healthy fetus,avoiding miscarriage, and resulting in a normal take-home baby, it has to be competentin three broad areas.
First, it needs to be chromosomally normal. In other words the embryo shouldhave a normal karyotype—with then an odds-on chance of being genetically normal.A conventional karyotype,however,which images the chromosomes directly, is diffi-cult to do on just one or two biopsied cells, so special DNA tests are being devisedto reveal the chromosome constitution indirectly.
The first of these has been a technique called fluorescent in situ hybridization (FISH).It is routine practice at Sydney IVF to look at chromosomes 13, 18, 21, X and Ywhen there is a special reason to do preimplantation genetic diagnosis (PGD, detailed inChapter 20 under heading,‘Embryo biopsy and preimplantation genetic diagnosis’).These are the five chromosomes that are capable of causing birth defects if presentin incorrect number (aneuploidy).A result is available on the day of embryo biopsy.
FISH does not ordinarily spot aneuploidies of the other chromosomes, whichwill result in miscarriage (or even a failure to develop at all beyond implanta-tion).
To look at all the chromosomes we use a more complex chromosome stainingtechnique called comparative genomic hybridization.Applied to embryos first by a groupof researchers at Melbourne IVF headed by Dr Leanda Wilton, CGH is now avail-able at Sydney IVF for PGD.
The difficulty with CGH is that it takes five or six days to obtain a resultfrom the tests—longer than we have available, unless the biopsied embryos arecryostored (frozen) for transfer to the uterus a month or so later (described inChapter 21).
With the help of a several million dollar industry grant, Sydney IVF is nowdeveloping multiplex gene amplification techniques to perform entire karyotypesas a DNA test—a technique comparable to CGH and involving rapid ascertain-ment of hundreds of gene sequences by reacting tiny samples with silicon-basedDNA arrays.
Second, the embryos need to be metabolically normal, or near-normal.Thismeans that they will be able to adapt well to culture conditions in vitro, producingall the myriad molecules they need to develop, and especially making a successfulshift, over the first few days following fertilization, from the genome of the preovula-tory egg, derived from the mother, to the combined genome of the new embryo,incorporating genes from the mother and father.
At Sydney IVF our research is examining which are the important early proteinsproduced by the new genome, and what metabolic conditions optimize this criticaltransition of the fertilized egg from one parent to two.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 70

Tests for the uterus
No single test tells us all we may need to know about the inside of the uterus, particularlyits lining, the endometrium. Having said that, though, the uterus is generally not as likelya place for there to be a problem in getting pregnant compared with other areas, such asthe fallopian tubes.Occasionally an unsuspected, retained intrauterine contraceptive device,or IUD, is discovered to have caused apparent infertility.
Abnormalities of the uterus that can cause infertility include uterine fibroids, adeno-myosis, intrauterine adhesions, and inflammation or infection of the endometrium (endometri-tis), endometrial polyps, and endometrial atrophy. For more on how these disturbances and othersprevent implantation, see the box, Thirsty for an embryo. The conditions themselves aredescribed in Chapter 17.
The uterus and endometrium can be studied in several ways.We shall start with theleast intrusive.
Transvaginal ultrasound scanning
Transvaginal ultrasound, using a high-frequency probe placed gently in the vagina, up againstthe cervix, gives very clear images of the uterus as well as of the ovaries.Ultrasounds of theuterus done abdominally, through a usually uncomfortably full bladder, do not generallyprovide the detail needed for accurate diagnosis in the uterus.Transvaginal ultrasound allowsthe thickness and appearance of the endometrium to be followed through the menstrualcycle. It thus enables polyps (which cause a thickened endometrium) and endometritis (which
Third, the mitochondria of the egg—the egg’s power supply—must be reasonablysound.At Sydney IVF we have developed a technique for sampling the fleshy partof the egg (the cytoplasm) without harming it.This enables us to analyze the mtDNA(mitochondria have their own, entirely maternally-derived, bit of DNA, importantfor metabolism), as well as analyzing the egg’s other gene expression patterns andparameters of metabolic health.
For more on mitochondria, see the Chapter 7 box, How eggs might get their ‘use-by’date: Mishaps in the mitochondria.
So there are many exciting areas to interest all of us, but we’re not ready yet toanalyze in vitro embryos routinely.
And when it comes to embryos that will not be in the lab, that remain in thebody, just about all we have available to guide us is an indirect measure of the metab-olism of the preovulatory follicle.Using transvaginal ultrasound with Doppler recordingsof blood flow, we can get an idea of the health, or otherwise, of the follicle’s rapidlydeveloping blood supply during the hours leading up to ovulation.This measure-ment has been linked with the subsequent embryo’s ability to turn carbohydratesinto energy.
MAKING A DIAGNOSIS � 71
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 71

72 � GETTING PREGNANT
Thirsty for an embryo
When we speak of the embryo in the ‘cavity’ of the uterus we might get a mislead-ing picture of an embryo rattling about in a cave, hoping to chance an encounterwith a wall it can attach to.
Instead, the space in the uterus, to steal an analogy conjured up by my colleagueDr Mark Bowman, is like the space in a bread sandwich.The front and the back arein contact.And whichever way you hold a sandwich with a small amount of jam inthe middle, the jam won’t fall out.
There are some disturbances possible, however.First, there should not be loose fluid in the space, washing the embryo about.
The endometrium, well into its secretory phase (the luteal phase, for the ovary), has beenunder the influence of progesterone for about a week at the stage that the embryo, nowa blastocyst, will be looking at implantation.
A responsive endometrium will be busy removing all residual fluid from theuterine cavity, sucking it almost dry, so that the front and back of the endometriumpress onto the blastocyst.
There is no routine test for this function, although researchers are looking withelectron microscopes at the endometrial cells ‘drinking’ the endometrial fluid by aprocess called pinocytosis—in which an endometrial cell takes small, membrane-bound gulps of fluid into its interior, while the top of the cell swells up, seen onelectron microscopy as a pinopode or ‘apical dome’, which also serves to extend thesurface of the endometrial cell into closer touch with the blastocyst.
To researchers, the appearance of pinopodes signifies a window of opportu-nity for implantation, sometimes called the implantation window, and supposedlythe only time the endometrium facilitates attachment and penetration by theblastocyst.
In any case, this process can be thwarted if there is a lump or tumor in the way,such as an endometrial polyp or a submucous fibroid. It can also be thwarted if theendometrium is not developing properly, either because of insufficient progesteroneor because of an inherent loss of progesterone responsiveness, as there is in endometri-tis, endometrial atrophy and intrauterine adhesions.
And it can be thwarted if too much fluid is coming down from a fallopian tubefor the endometrium to deal with, as there can be from a discharging hydrosalpinx(see the Chapter 20 box, Hydrosalpinx: Reintroducing a villain).
Second, the endometrial surface should not be too tough to resist the blastocystdissolving a small part of it in order to penetrate it.
Electron microscopy of the endometrium can also reveal what are called ‘tightjunctions’ between the surface cells of the endometrium, perhaps sometimes tootight to allow the blastocyst to squeeze past and to implant, particularly if for somereason it has not been shed properly by a recent completed menstruation.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 72

causes a thin endometrium) to be suspected, provided that the scan is timed for the mid-to-late proliferative phase, around day 7 of a 28-day menstrual cycle, when the normalendometrium is getting thicker but is still rather non-reflective to sound.
Ultrasound also reveals changes in the myometrium—the muscle of the wall of the uterus.Ultrasound is the best way of disclosing the position and size of uterine fibroids.Ultrasoundmight be the only way of suspecting adenomyosis (short of examining the whole uterus aftera hysterectomy).A retained IUD is clearly seen, even when it has lost its shadow or opaque-ness to x-rays.
Hysteroscopy
Hysteroscopy is a fiberoptic examination of the uterine cavity by an instrument that lookslike a short thin laparoscope—the hysteroscope. It complements the hysterosalpingogram inrevealing pathology that disturbs the shape of the endometrial cavity, especially intrauterineadhesions (scar tissue between the front and the back surface of the cavity), fibroids project-ing into the uterine cavity (submucous fibroids), and endometrial polyps.These can show up onHSG too, though hysteroscopy is still needed to locate the pathology accurately, and dealwith it.These conditions can thus often be treated during the diagnostic investigation, ifthe hysteroscopy is carried out under anesthesia (which it often is, together with alaparoscopy).
Hysteroscopy is also carried out without anesthesia as an office procedure, using a thinhysteroscope that doesn’t require the cervix to be dilated.
Curettage
Curettage or endometrial biopsy reveals the tissue structure of the endometrium. In the box,Estimating progesterone’s effectiveness, we consider this procedure in estimating normal ovula-tion, when the test is timed just before the date a period is expected.
The other side of the coin is that a total secretory phase picture of 14 or so days’exposure to progesterone says as much about the normal responsiveness of the endometriumas it does about the normal production of progesterone during the ovary’s luteal phase.This is a powerful way of ascertaining that the uterus can be expected to be normallyreceptive.
The main trap here, for you and your doctor, lies with mistaking any bleedingfrom the uterus as a full period, and expecting the lining of the uterus to have beenshed.This is not what happens, for instance, with anovulatory bleeding. For example,a normal, eventual ovulation on a background of previously untreated endometrialhyperplasia will rarely result in pregnancy.The likely reason is that, despite proges-terone exerting a normal-looking secretory effect, the background history of theendometrium is so chaotic that it remains resistant: it has to be got rid of for theuterus to move on.
MAKING A DIAGNOSIS � 73
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 73

As well, an endometrial biopsy or curettage can confirm or definitely exclude thepresence of endometritis; this is one reason why it’s usual, indeed almost invariable,for an endometrial biopsy to be done whenever there is the opportunity, such as atlaparoscopy.
It could also be an advantage, at some stage during the investigations, to have a full curet-tage done, to ensure that the lining of the uterus is fresh for subsequent cycles. For more,see the box, Curettage can be a good thing for infertility.
YOUR ROAD MAP FROM HERE
When you’ve had the tests described in this chapter, there’ll either be:• An abnormality found that means it’s impossible for you to get pregnant without help—
in which case study Chapter 6 and then go on to whichever chapter is relevant to yourdiagnosis and its treatment elsewhere in the book; or
• There’ll be a milder abnormality (or even no abnormality) found, which means you’retold that pregnancy can still happen; but because you know it’s already taken too long(and perhaps time is getting very short), you’d like to at least think about doing some-thing about it—in which case study Chapter 7 and then go on to the chapter on yourdiagnosis.
74 � GETTING PREGNANT
Curettage can be a good thing for infertility
When my colleagues and I were medical students, just about the only thing a familydoctor could (or did) do for infertility beyond a sperm count was a dilatation andcurettage (or D&C), in which the endometrium is scraped away and thereby forcedto grow again.
Because as students we couldn’t see the logic for it, and because family doctorsweren’t very adept at protecting their ideas against newly taught medical students,this (to us) rather drastic and senseless maneuver fell into disuse.
Now, however, we’re looking at it again.Curettage, timed at the onset of menstruation, ensures that for at least the partic-
ular cycle about to start there will be new endometrium developing.With a fullfollicular phase available for the endometrium to grow, giving it a full proliferativephase, endometrial freshness is assured.
And that is a good thing for implantation.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 74

MAKING A DIAGNOSIS � 75
Establishing progesterone’s effectiveness
A biopsy of the endometrium timed for the end of the menstrual cycle, just before aperiod starts (a premenstrual endometrial biopsy) can reveal how normally theendometrium has responded to progesterone.
If there is (1) obvious secretion in the endometrial glands (for nourishment ofthe implanting blastocyst), and (2) an extensive predecidual reaction between the glands,we can infer both that progesterone production from the ovary has been adequate,and that the endometrium has responded fully and appropriately.
This is true for whatever the serum progesterone levels might have been, and forwhatever concerns there might have been on the thickness, thinness or appearanceof the endometrium on transvaginal ultrasound scanning.
The biopsies are often done as office procedures in the USA.At Sydney IVF weperform endometrial biopsies under mild sedation and with local anesthesia aroundthe cervix, similar to what we do for an egg retrieval procedure. Either way, a thinendometrial biopsy curette is used that can be passed through an undilated cervix.
The chance of an early pregnancy being disturbed by taking the biopsy is small,but presumably it can happen; so if a biopsy is planned, either as an isolated test orin conjunction with a laparoscopy, pregnancy should be avoided during the monththe test is being done.
This test provides the ultimate standard for determining if there is a luteal phasedefect that affects the endometrium.
It also enables white blood cell populations to be looked at for cells that affectthe chance of the pregnancy ending in miscarriage.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 75

when pregnancy’s not possible:sterility
What to do when tests showno chance (without help)
Once the infertility tests described in Chapter 5 have been done, we know if thereare one or more obvious causes for not getting pregnant. Here we cover the situa-tions in which these tests show that pregnancy is impossible the way things stand
(see Table 6.1) . . . that there’s something wrong that no amount of time will overcome.In other words, the tests have shown one or more of:
• No sperm is being ejaculated;• No eggs are being ovulated;• The fallopian tubes are completely blocked, or they’ve been removed; or• The uterus is destroyed, missing or obstructed—from birth, from disease, or from a
hysterectomy.It means that something has to be done (and usually can be) or definitely there will be nobaby.
Sorry to possibly appear insensitive in using the word sterility.Though it sounds harsh,I have two excuses for employing it. First, words in medicine must be unambiguous (seethe box in the glossary under vocabulary), and the alternative term, complete infertility (whichI employed in the first edition of this book), is cumbersome and not widely used. Second,in lots of ways it’s better to have the tests show sterility than subfertility (which in the firstedition was relative infertility).
With sterility at least you have an unequivocal explanation, you gain in certainty, thereare definite treatments to consider, you can move forward.
76
6
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 76

NO SPERM
Very uncommonly, a sperm sample obtained under great stress for a sperm count can showa virtual exclusion of sperm; or, rarely, there just might have been a mix-up at the lab. Putsimply, a test result showing an absence of sperm, azoospermia, should mean examining asecond specimen, just to be sure.
Table 6.1 The four causes of sterility and what to find out next
Diagnosis Elaboration What next
no sperm azoospermia distinguish obstruction from poorproduction
no eggs anovulation distinguish primary ovarian failurefrom anovulation due to notenough FSH
no open fallopian tube what IVF was invented for distinguish obstructions close tothe uterus from those at theouter end
no uterus, or no cervix, amenorrhea despite ovulation if uterus present, how muchor no endometrium endometrial atrophy there is
Confirming azoospermia is an upsetting event that for weeks at least makes a man feelisolated, bereft and withdrawn, often with transient impotence and an understandable loss ofself-esteem. His partner can feel anger, guilt and a wish to make reparations, often switch-ing between these seemingly contradictory emotions, yet at times feeling them all at once.Sooner or later both will think of donor insemination and sperm banks (see Chapter 22),although modern technology—the hope that emerging microsurgical or IVF techniquesmight work—has made a decision to use donated semen even less straightforward than italready was on emotional grounds. In very many cases enough sperm cells can be obtainedfrom one or other testis for assisted conception to work, in the form of special variationsof in vitro fertilization (IVF) that involve surgical sperm cell recovery and ICSI—seeChapter 20 for the details.
The two of you could well still be able to have a baby that is entirely your own.Otherwise, the idea of using donated sperm will usually appeal sooner to the woman, butthis is rarely a straightforward decision for either partner.
An obstruction in supply or a manufacturing glitch?
The two reasons azoospermia comes about are: (1) a blockage on each side between the testisand the seminal vesicle, usually in the epididymis or the vas deferens; or (2) not producingenough mature sperm in the tubules of the two testes, known as ‘maturation arrest’.Theseconditions are talked about in detail in Chapter 10.A blockage can sometimes be overcomewith microsurgery, but if sperm are not being produced it’s rare for any treatment to work.So it’s important to make the distinction.
WHEN PREGNANCY’S NOT POSSIBLE: STERILITY � 77
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 77

The simplest way to find out if a blockage might be the cause for azoospermia is tomeasure FSH in the blood—by a serum FSH.
Nonobstructive azoospermia
If the serum FSH level is increased, there is irreversible damage to the tubules and,by impli-cation, no obstruction and no corrective treatment is available.
It might be possible, however, to recover enough reasonably mature cells from the testisdirectly to enable IVF and ICSI to be used to achieve pregnancy—a procedure called testicu-lar sperm extraction, or TESE. My colleague at Sydney IVF, Dr Jeffrey Persson, believes thefinding of useable sperm can be predicted if there is a positive test for serum inhibin B.Testsshould be done for genetic abnormalities that can be passed on to offspring conceived usingTESE and IVF.The details are in Chapter 10.
Obstructive azoospermia
If the serum FSH is normal, the cause could be an obstruction: a detailed review by a urol-ogist skilled in infertility microsurgery in men is called for, perhaps including a biopsy of thetestis to confirm that sperm production is normal. In this situation, pregnancy is certainlywithin reach using IVF and sperm obtained from the epididymis, with a procedure knownas epididymal sperm aspiration (ESA or MESA).The details are in Chapter 20. Depending onthe nature and extent of the obstruction,microsurgery might also be possible to permanentlyalleviate the obstruction.These details are in Chapter 10.
If the serum FSH is low, and especially if measurements of serum LH and serum testos-terone are also low, this might mean a loss of the pituitary gland’s drive to the testes; detailedreview by a specialist endocrinologist or andrologist is then warranted, because the situa-tion is potentially treatable with injections of gonadotropins.
IVF or donor insemination?
When IVF is used to overcome infertility from an absence of sperm it necessitates morephysical involvement for the woman than assisted insemination with donor sperm does. Onthe other hand, it will be the sperm of the man that the woman has chosen to marry orpartner that will get her pregnant, not that of a stranger.
Different couples will value the two sides to this equation differently. It’s usual for thecouple themselves to differ in their opinions.Time and a great deal of understanding mightbe needed to keep the relationship on an even keel. It helps most couples to be open buttactful about their thoughts. Skilled counselling (see Chapter 25) can help.
NO OVULATION
In contrast to an absence of sperm release, an absence of ovulation (called anovulation)is much less often due to a serious, untreatable abnormality. Chapter 5 explains how
78 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 78

anovulation is diagnosed.To distinguish the different conditions that can be responsible, wemeasure serum FSH, serum LH, serum prolactin and serum testosterone.
The common causes of anovulation fall into two important groups: those in which theserum FSH is elevated (primary ovarian failure), and those in which is low or normal (inwhich ovulation induction will be possible).
Primary ovarian failure
The serum FSH is increased because of a lack of follicles (which contain eggs) in the ovariesproducing estrogen and inhibin, inhibitory feedback by which normally keep FSH levels low.For the same reason, serum FSH levels increase dramatically after a woman goes throughher menopause.
The causes of primary ovarian failure are described in Chapter 11. Some have healthimplications beyond those caused by a lack of estrogen.The outlook for getting pregnantis not good. Pregnancy ordinarily requires egg donation, which means that a friend, relativeor other person agrees to undergo a cycle of IVF for this purpose, but meanwhile ovarianfailure is as disappointing and devastating a diagnosis as sperm failure.The issues associatedwith egg donation are discussed in Chapter 22.
Secondary anovulation
The causes of anovulation secondary to low or to too-constant levels of serum FSH are alsodescribed in detail in Chapter 10.The common ones are: (1) hypothalamic anovulation—a relativeor absolute lack of GnRH drive of the pituitary gland by the hypothalamus, with the result thatthe serum FSH and serum LH will be rather low; (2) hyperprolactinemia—an increase in theproduction of prolactin by the pituitary gland, so the serum prolactin will be high; and (3) thepolycystic ovary syndrome—an increase in ovarian production of testosterone increases the serumfree testosterone and free androgen index,with a fall in sex hormone binding globulin and a character-istic appearance of enlarged ovaries on transvaginal ultrasound scanning.There are rarer, moredangerous conditions that can mimic these dysfunctions; these are described in Chapter 11.In each of these conditions,ovulation can be induced.The details of ovulation induction regimensand how they are adapted to these different diagnoses are also in Chapter 11.
BLOCKED OR ABSENT TUBES
When blockages of the fallopian tubes are detected at laparoscopy or with a hysterosalpingogram(HSG), as described in Chapter 5,whichever of these two tests hasn’t been done yet shouldbe, to confirm and characterize the blockage.
Why does tubal blockage need confirmation? There is a small chance that apparentlyblocked tubes at HSG are the result of spasm—painful contractions of the uterus thatobstruct the tubes where they pass through the wall of the uterus: in this case a hysteroscopyand laparoscopy can clarify the situation.Alternatively, at laparoscopy,performed under generalanesthesia, there might have been technical difficulties injecting the salt solution or blue
WHEN PREGNANCY’S NOT POSSIBLE: STERILITY � 79
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 79

dye used for testing patency of the tubes through the cervix, thus not getting enoughpressure for it to pass down both tubes. Especially around the time of ovulation, plugs ofsecretion can block the narrow isthmus of the tubes and might not have been overcome byenough pressure.
A hysterosalpingogram, perhaps with a selective salpingogram, can clarify these equivocalsituations, and also determine how much open tube remains for possible microsurgery—andparticularly to see if a hydrosalpinx is going to complicate matters. For more on the perfid-ious effect of a hydrosalpinx, see the Chapter 20 box, Hydrosalpinx: Reintroducing a villain.
Unless the tubes have been removed or are totally destroyed, the choice will lie betweencorrective microsurgery (the operations are described in Chapter 13) and in vitro fertilization(the subject of Chapter 20). In practice, your decision will depend on the chance ofpregnancy with one or other approach, given the exact nature of the blockages and theavailable expertise; the relevant out-of-pocket costs after taking medical insurance plansinto account; and your personal view of minimally intrusive egg retrievals (but perhaps theneed for repeat treatments) versus major, if low-risk, abdominal surgery.
But, at the end of the day, the two approaches are not mutually exclusive.They can gotogether.
NO UTERUS, OR NO ENDOMETRIUM
Perhaps the starkest cause of sterility is the absence of a uterus.This can be the case frombirth, as in congenital absence of the uterus and vagina, described in Chapter 18. Morecommonly, in women of reproductive age, a hysterectomy has been carried out for a seriousunderlying condition, such as cancer. If the ovaries remain and are functioning (which isusually the case with congenital absence of the uterus, and often the case after hysterec-tomy) then stimulation of the ovaries and egg retrieval for in vitro fertilization should bepossible.
The embryos that result, however, will require gestational surrogacy—the help of asurrogate mother who receives the transferred embryos and bears the child for you.Thepractical and emotional issues involved with surrogacy are discussed in Chapter 22.
Surrogacy might also be necessary in cases of severe disease or other disturbance of theuterus, particularly if there has been extensive disruption or destruction of the endometrium.This is especially the case if there are intrauterine adhesions that have resisted correctionbecause of associated endometrial atrophy.These abnormalities and how to evaluate them arediscussed in Chapter 17.
While any of the conditions discussed in this chapter will mean that without treat-ment there’s sterility—unequivocal infertility that no amount of time will overcome—there are similar but less complete circumstances that leave you with a chance of gettingpregnant naturally.And because knowing what to do is then much less obvious, we devoteChapter 7 to this subject of subfertility.
80 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 80

when pregnancy’s not probable:subfertility
What to do when thetests show subfertility
Pregnancy could happen, but it isn’t.Your infertility tests (those described in Chapter 5)show that there are one or more abnormalities, which, though not totally definite,could explain why you’re not getting pregnant.You have what we call subfertility (see
Table 7.1); or perhaps the tests were all essentially normal—maybe completely normal—acondition called unexplained infertility.
Either way, you’re in a different, probably more frustrating situation than you are if thetests show a total barrier to pregnancy, or sterility (see Chapter 6).
Here we consider:• Evaluating causes of subfertility (oligospermia, ovulation disorders, partial obstructions,
endometriosis, cervical factors, sperm antibodies, uterine abnormalities, age effects);• How subfertility factors blow out the average time you’ll need to get pregnant;• Devising treatment strategies; and• Dealing with unexplained infertility.
CAUSES OF SUBFERTILITY
The basic infertility investigations described in Chapter 5 can show abnormalities that donot pose a total bar to getting pregnant. Some sperm are being produced; ovulation is happen-ing but could be defective; one fallopian tube is at least open and partially free; there’sendometriosis; the cervix is disturbed or there are sperm antibodies; the uterus is not too bad butnot normal; or you’re getting older.These are abnormalities that cause a delay in getting
81
7
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 81

pregnant, but which might still permit pregnancy if there’s enough time to keep givingpregnancy a chance.
But how do we know what that chance might be? And how can we improvethe odds?
Table 7.1 The main causes of subfertility
Culprit Elaboration Common reasons
sperm not enough sperm reach the tube • oligospermia
• sperm antibodies (male)
cervix sperm transport disrupted • cervicitis• previous cone biopsy• sperm antibodies (female)
eggs eggs not ovulated normally or frequently • oligomenorrhea• luteal phase defect• early ovarian failure
fallopian tubes sperm and eggs meet infrequently • peritubal adhesions• incomplete blockage
implantation weak embryos; or uterus not fully receptive • oopause *• endometritis• fibroids• endometrial polyps
mixed more than one of the above • includes endometriosi
unexplained apparently none of the above • natural genetic variation• effects of woman’s age *
* The metabolic weakness of eggs as women get older, while menstrual cycles are still regular, manifests asunexplained infertility until IVF is performed, after which it becomes apparent that embryos resultingfrom the eggs will not implant. Sooner or later this normal age-related development effectively becomessterility.
Oligospermia
Rather than being normal or revealing azoospermia, the sperm count can show oligospermia,a reduction in the number of sperm, usually associated with reduced sperm motility (thekicking motion the sperm are seen to have under the microscope) and with an increase inthe percentage of the sperm cells that have abnormal forms.
It’s not hard to understand how this decreases the chance of getting pregnant in anyparticular month.The lower the number of motile, normal-looking sperm in the ejaculate,the more hit-and-miss it is for one to get to the egg on time, and the lower the chance ofpregnancy happening quickly.
If you use marijuana or cocaine, don’t.They can interfere with sperm production.How to investigate and what to do about low sperm counts is discussed in Chapter 10.
82 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 82

Ovulation disorders
Infrequent or weak ovulation will often reveal itself as oligomenorrhea, or infrequent periods.The causes are the same as those for anovulation (the details are in Chapter 11).
But while the consequences are not as obvious as having no periods at all, there arestill hurdles to getting pregnant. First, less frequent ovulation means that fewer eggs arebeing released and therefore there are fewer opportunities to get pregnant over a periodof time. Second, in a long cycle, after a prolonged follicular phase, the development of theegg can be out of synch in relation to when ovulation happens, so while it may be releasedit might not be able to be fertilized or not be fertilized normally, making a miscarriage morelikely.Third, the preovulatory follicle can open but the egg not be released at all, insteadremaining within the follicle, within the corpus luteum, the luteinized unruptured follicle (formore, see the Chapter 5 box, Fake ovulation). And fourth, ovulation can be followed bytoo short a luteal phase to enable successful implantation of the embryo, even if the egg hasbeen fertilized normally (a luteal phase defect).
As with sperm counts, so-called recreational drugs, especially cocaine, can interfere witheffective ovulation.
The cervical factor
Sperm are intrepid, and if menstrual blood can get out through the cervix then sperm usuallyare able to get in. Nonetheless, it can’t help if the mucus in the cervix (cervical mucus) isinflamed due to infection (cervicitis) or if the cervix is scarred from previous surgery suchas a major cone biopsy. Modern methods of treating an abnormal Pap smear for cervicaldysplasia (also known as cervical intraepithelial neoplasia, or CIN) or for papilloma virusinfection—with cautery, cryotherapy (freezing) or laser—are unlikely to have a harmfuleffect on sperm getting through the cervix. By removing abnormal tissue in the canal ofthe cervix, these therapeutic maneuvers can sometimes improve sperm transit.
The effects of an abnormality of the cervix show up on a postcoital test (PCT) and inin vitro penetration tests that investigate sperm and mucus function in the laboratory.
What could be the causes of a negative PCT carried out during a normal ovarian cycleon the day of ovulation? First, the cervix can be resistant to estrogen as a result of earliersurgery, in which case the quantity of mucus can suffer. Second, the cervix can be infectedor inflamed, in which case the quality of the mucus sometimes (but by no means always)suffers. Cervicitis causes mucus to have a yellow color instead of being clear.
But there might be no apparent cause at all,with the mucus looking perfectly all right:in this case there could be poor sperm function or there could be antibodies to spermpresent (sperm antibodies), either in the mucus or in the semen. Before antibodies are lookedfor,or before significance is ascribed to detected antibodies, the mucus itself can be examinedmore systematically.
For resolving mucus versus sperm and timing issues, the classic in vitro penetration test isthe Kremer test, named after J. Kremer, Professor of Human Fertility at Utrecht andGroningen University Hospitals in the 1970s. It is a four-way test done between the
WHEN PREGNANCY’S NOT PROBABLE: SUBFERTILITY � 83
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 83

woman’s mucus,her partner’s fresh semen, a standard sample of normal mucus, and an appar-ently normal semen specimen.The possible outcomes and their interpretation are given inTable 7.2.
Table 7.2 Sperm–mucus interaction testing and its interpretation
Husband–wife Husband–donor Donor–wife Donor–donor
normal good good good good
sperm problem bad bad good good
mucus problem bad good bad good
sperm and mucus problem bad bad fair good
Penetration of sperm into the mucus is categorized as good, fair or bad. In practice, results are notalways clear cut.
In vitro penetration tests such as the Kremer test (like the postcoital test itself) are sodependent on normal prior estrogen exposure of the cervix that it’s best not to leave mattersto chance during a natural ovarian cycle.At Sydney IVF we give estrogen tablets from daytwo of the menstrual period (ethinylestradiol 75 micrograms per day works fine), both toproduce standard estrogen conditions for the mucus (obtained after about eight to ten days’exposure to the estrogens) and to stop natural ovulation—and the possibility of unwelcomeprogesterone that comes with it—from spoiling the test. If the mucus still isn’t good on thisdose of estrogen, we sometimes double it for another few days.
Not many cervical conditions are amenable to reliable correction, and the same is trueof most causes of the sperm malfunctions that might cause diagnostic confusion—and yetall these conditions are overcome with IVF. So the Kremer test, and indeed the postcoitaltest, are often dispensed with where recourse to IVF is readily available.
Sperm antibodies
Sperm antibodies occur when for some reason the man or the woman develops an immuneresponse against sperm cells.This potentially limits their movement and their ability to getto the egg.
Not all sperm antibodies are significant.The antibodies can be directed at any of threeparts of the sperm: the head, the middle or the tail (those directed at the tail are most likelyto stop movement, but most antibodies will slow sperm movement to some extent).Theantibodies can be agglutinating (and make sperm stick together in clumps), or immobiliz-ing (which are less common but are more deadly for sperm).The antibodies are looked forin both partners’ blood serum (serum sperm antibodies), in the semen (semen sperm antibodies)and in the mucus (cervical mucus sperm antibodies).
There’s generally no need to look for them if the PCT is normal.
84 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 84

Peritubal adhesions or one open tube
When there’s an adhesion, or scar tissue, around the fallopian tube separating the tube fromall of the surface of the ovary, or limiting the movement of the tube’s fimbrial end to touchthe ovary’s surface at ovulation, the chance of pregnancy is also reduced. By how muchdepends on the location and the extent of the adhesions.The worse the peritubal adhesionsare, the lower the chance of pregnancy happening quickly.
Because ovulation happens from just one ovary at a time, a woman who has had onetube removed or who has one tube blocked but the other open will on average take twiceas long to get pregnant. Ovulation is more likely than not to move alternately from oneovary to the other in successive months, especially in young women, but this is not a firmrule and sometimes it’s only the one ovary that ovulates consecutively for months on end—especially if part of the other ovary has been removed.
In younger women with otherwise normal fertility it might not matter at all havingtwo ovaries competing for the attention of one tube, but in older women (who have lesstime to spend), or if there are other reasons for not getting pregnant easily, doubling thetime needed to conceive can quickly matter a lot.
There’s detailed consideration of this problem in the Chapter 13 box, One ovary can beOK . . .
Disturbances of the uterus
Abnormalities of the uterus don’t often cause trouble actually getting pregnant—they’re morelikely to cause miscarriage once the pregnancy is underway (see Chapters 8 and 9).The moresevere forms of these abnormalities, though, will also delay or prevent conception.
The most common uterine cause of infertility is the presence of a fibroid or a polyp thatdistorts the cavity of the uterus (the endometrial cavity).The bigger the fibroid or polyp is,or the more of the cavity it occupies, the less will be the chance of successful implantationand pregnancy. Other causes of relative infertility in the uterus include inflammation(endometritis) and intrauterine adhesions (scar tissue affecting the uterine cavity).Their furtherevaluation and management are discussed in Chapter 17.
Endometriosis
This common condition seems to diminish fertility by limiting the life of sperm in thetube; causing defective ovulation; jeopardising egg pick-up from the ovary by the tube; andperhaps by compromising embryo implantation.The harm endometriosis does to fertilityseems to come from a chemical effect, a disturbance of the general internal environmentof the peritoneal cavity, so it’s unrelated to where the endometriosis is located among thepelvic organs. It’s only in the most severe cases that there is scarring that blocks the tubes—and then there can be sterility rather than subfertility.
In most cases it seems to be that the worse the endometriosis—particularly if it’s causingother symptoms—the longer it will take to get pregnant, but there are many exceptions,
WHEN PREGNANCY’S NOT PROBABLE: SUBFERTILITY � 85
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 85

and some women with apparently significant endometriosis get pregnant quickly, especiallyif the sperm count is excellent.
Endometriosis is discussed fully in Chapters 15 and 16.
Age
Whereas a measure of health in the uterus is essential for implantation and successful preg-nancy, so too is a genetically correct embryo with robust metabolism. In practice the embryofails much more often than the uterus does.
Age works in several ways. Creeping age can decrease the frequency with which acouple have sex. A man’s fertility decreases with age, as the sperm count usually decreases.Many of the causes of subfertility mentioned above become commoner as a woman getsolder. But even in the absence of these causes, what is increasingly clear is that it’s the ageof the woman that’s the critical factor in determining age-related fertility, subfertility and,sooner or later, sterility.
As a woman’s age advances beyond about 33, it becomes increasingly likely that heraging eggs will let the side down—at first just sporadically, but eventually so thoroughlythat sterility will occur, perhaps years before menopause (a phenomenon we call theoopause).
So, when a woman is up to about 10 years from the time when the menopause willhappen, she will be getting low on healthy eggs that are capable of producing a successfulpregnancy.Of course no-one can forecast when the menopause will take place for a partic-ular woman, and no-one can know when this rapid decrease in fertility will happen.Wedo know, though, that the average age at which Western women go through menopause is50 or 51, with a normal range from 40 years to 55 years.
This means that fertility falls fairly quickly at an average age of about 38 to 40, withthe range at which this fall in fertility can happen being from about 33 to 45.A late signthat this is taking place may be a shortening of the menstrual cycle (although this may notbe the only reason menstrual cycles can get shorter).
But a shortening menstrual cycle is more a test of the number of eggs still in the ovariesthan a test of their quality.The number of eggs can be tested indirectly by observing howmany tertiary follicles are visible in the ovaries on transvaginal ultrasound on about day 7 ofthe follicular phase, before the dominant follicle arises and puts paid to the others. Or it can betested less directly, by measuring serum FSH during a period,when low numbers of poten-tially responsive tertiary follicles cause a reflex high serum FSH result as the pituitary glandencounters resistance in the ovaries at the beginning of a new cycle, and tries to compen-sate by making more follicle stimulating hormone. Depending on chance events in theovaries (the number of responsive follicles at any particular time), serum FSH levels duringa period can vary from one cycle to the next.
At Sydney IVF we are attemping to estimate the stage of this age-related decline infemale fertility by looking at those quintessentially age-governed little structures inside cellsresponsible for providing a cell’s energy and potential for development, the mitochondria.For more, see the box, How eggs might get their ‘use-by’ date: Mishaps in the mitochondria.
86 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 86

WHEN PREGNANCY’S NOT PROBABLE: SUBFERTILITY � 87
How eggs might get their ‘use-by’ date: Mishaps in the mitochondria
Every cell in the body—including every egg cell and every sperm cell—needs asource of energy to power its functions.
The structures responsible for producing this energy are minute organelles insidethe cell called mitochondria.A mitochondrion looks, under the electron microscope,like a bacterium (and that’s what we think the mitochondrion evolved from,billionsof years ago). Every cell in the body contains hundreds of mitochondria, each busyburning up fat and sugar molecules with oxygen to release carbon dioxide as wellas usable energy (in the form of high-energy phosphate compounds called ATP,which are shifted around in the cell to where energy is needed for some criticalaction).
What makes these mitochondria fascinating is that each one has its own bit ofgenetic material—its own bit of DNA, just like each bacterium has its own DNA.This is the only place outside the cell’s nucleus (which is where the stick-likechromosomes are) that DNA is found.
Mitochondrial DNA (mtDNA) is different from nuclear, or chromosomal,DNAin a number of ways.
First, there are two of each particular stick-like chromosome, each with an incred-ibly long, double helix of DNA, which codes for different genes along the string.With two such chromosomes in each chromosome pair, there are two such strings,and so two copies of each gene, one maternal and one paternal.
But mtDNA is a circular molecule: the string becomes a ring.The genes are strungaround the string—all 13 of them, coding for proteins unique to mitochondria andtheir energy-generating apparatus. Moreover there are thousands of copies per cell.
Second, mutations (mistakes in the sequence contained in the DNA) are morefrequent. Repair of the genetic code does not take place, so that as cells get olderthey gradually accumulate more and more mitochondria that don’t work properly.Because of the large number of genes they compensate well for years, but eventu-ally there is a meltdown: age takes its toll.
Third, when you were conceived all of the mitochondria in your body camefrom the mitochondria in your mother’s egg—none came from the mitochondriain your father’s sperm cell that fertilized the egg. So mtDNA is a form of inheri-tance you get entirely from your mother.
So why do eggs all get produced before birth? (For details see Chapter 3.) Whydo new sperm cells keep forming, even into a man’s old age?
Consider that every time a cell divides the mitochondria will have divided moreoften—and every time a mitochondrion divides the several copies of mtDNA itcontains divide first.And each time DNA divides there’s an opportunity for a mistake,or mutation, in the genetic code to be propagated—which, in the long run, altersthe genome, a phenomenon we call genetic drift.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 87

HOW SUBFERTILITY FACTORS MULTIPLY
One of these subfertility factors on its own, if mild, won’t necessarily stop you havingchildren, even if it takes you longer than it otherwise would to get pregnant, as we beganto find out in Chapter 1.
But the effects are multiplied if there’s more than one abnormality.For example, if oligosper-mia decreases to one-fifth of normal the chance of getting pregnant in a particular month(monthly fertility rate), and endometriosis is also present,which by itself would also diminish themonthly chance to one-fifth of normal, then the overall decrease in the chance of pregnancyin one month equals one-fifth of one-fifth,or one-twenty-fifth of normal.Straight away there’slikely to be a real problem: there’s real infertility. (See the box, Mild problems go together . . .)
With more than two of these partial shortcomings—each, say, diminishing fertility toone-fifth per month, but all multiplying together—we can get to the situation where preg-nancy is no more likely than it is among couples using effective contraception! This effectis explained in Appendix 1 and summarized in the table there.
If egg cells kept dividing through life, then the older a woman became themore genetic drift there would be in the offspring—way beyond what nature isprepared to tolerate.That’s why nature puts all your eggs into long-term hiber-nation when you’re just a 20-week fetus. (This seems to be such an importantprinciple that it holds true for probably every vertebrate species of the animalkingdom: in all animals studied, all eggs are produced before the animal becomesfertile.)
Genetic integrity for sperm mitochondria? Forget it. Sperm mitochondria havea different, non-genetic job: providing the energy the sperm cell needs to swim tothe egg.
Capacitation of sperm (when they swim fastest to get through the egg’s cumulusand zona pellucida) probably represents firing sperm’s afterburners, deriving each lastounce of energy from the mitochondria before the successful sperm enters the egg,delivers its chromosomes, and tosses aside the depleted, exhausted, oxidized, maybeelectrocuted mitochondria that got it there.These defunct mitochondria wouldprobably be the last thing you’d choose to deliver pristine mtDNA.
But in none of the body’s tissues do mitochondria, and the integrity of theirDNA, last forever.
Aging of mitochondria in muscles, for example, accounts for the fact that noamount of training in middle age keeps your muscles as efficient as they were duringyour youth. Aging of mitochondria in heart muscle starts to happen later, duringyour forties.Aging of mitochondria in the cortex of the brain, on the other hand,doesn’t happen much until the seventies.
When does it happen in eggs? Several studies are starting to show that it occurs inthe thirties and forties—just the time that we know miscarriages get more commonand just the time that otherwise unexplainable infertility becomes prevalent.
88 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 88

But we should understand that in practice we have no sure way of knowing how mucha particular diagnosed mild abnormality or combination of mild abnormalities is actuallydiminishing the monthly chance of conceiving.
MANAGING SUBFERTILITY
The options for treating the subfertility that results comprise: (1) do nothing, just wait;(2) try to correct separately each problem that’s discovered; and (3) get around all theproblems at once with an appropriate form of assisted conception, such as IVF.
When is it best to do nothing? How do we judge what role a particular set of appar-ently mild or incomplete barriers to fertility is actually playing? How do we estimate theseverity of subfertility?
Mild problems go together . . .
Often a single mild subfertility factor will reach neither your awareness nor a doctor’s.This is because you are unlikely to have had tests done unless you’ve been trying ayear and one such factor is often not enough to stretch out the likely time you’llneed much past a year.
Pregnancy might take a few months longer; you may have worried for a while,but then it happens and all is well.The same thing happens a second time. By thenyou have your family and contraception instead of conception becomes thepriority.
No diagnosis will have been made. If there’s mild endometriosis, no-one will everknow. Likewise if, instead, there was mild oligospermia—or a mild or intermittentovulation disorder with some oligomenorrhea—or some mild peritubal adhesions froman earlier ovarian cystectomy. Et cetera.
But if two of these mild conditions had been present together it could well havebeen a different story.
The reason is, first, that people tend not to get tests for infertility done till they’vebeen trying a year or two. Second, it can take more than one mild subfertility factorto push the average time to conception past two years.
We consider the arithmetic in Appendix 1.Briefly, if a normal couple can achieve a conception in an average of three
months, then one mild subfertility factor will push the average to two years (so maybehalf or more go undiagnosed). But two factors acting moves the average time takento pregnancy to seven years—and few will escape detection.
For this reason, when we do tests for infertility, we more often see mild condi-tions in combination than we see them in isolation. Mild combinations occur moreoften in practice than in reality.
WHEN PREGNANCY’S NOT PROBABLE: SUBFERTILITY � 89
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 89

The worse the problem, the better the treatment
The more severe a subfertility factor is (and especially if it’s bad enough to cause sterility),the more likely it is that it will be the reason—and the only reason—why you’re not gettingpregnant.And, if it can be treated effectively, without the treatment itself introducing newsubfertility factors, it becomes highly likely that the treatment will lead to you gettingpregnant quickly.
Put simply, the worse the problem,provided it can be fixed, the better it can be to treatthe root cause, and the greater and more certain the improvement in your fertility thetreatment will bring.
For assessing mild subfertility factors, the duration of infertility is best
We saw earlier how several mild conditions can multiply to create a major problem. Buthow do we assess how such theory is translating into practice? What do we make of a situ-ation when there’s just one diagnosed cause of subfertility and it’s mild, or all the tests comeback normal (so-called unexplained infertility, see section below)?
The best guide when diagnosed subfertility factors are mild or trivial comes from thelength of time it has taken so far: the duration of infertility.You judge their effect by howlong it has taken to get pregnant so far (or how long it took to conceive a previous preg-nancy), and compare this with how long you have to conceive before you’re too old oryou think it’s taking unjustifiably long, called the time left for conception.The longer it’s takenso far, the less the chance per month of conceiving (the lower the monthly fertility rate, aneffect I explain in more detail in Appendix 1). So if it’s taken seven years (see the table inAppendix 1), then the monthly chance of getting pregnant if you continue to rely on luckcannot be more than 1 percent per month: anything higher than that is a statistical impos-sibility. Something has to change!
Remember, though, that pregnancy can happen any time by luck. Just because a coupleachieved pregnancy quickly the first time they tried—and only when the second preg-nancy took too long to happen were tests done that showed there were diagnosable problemspresent—doesn’t mean that those problems weren’t there all along. In such a situation thesubfertility factors are not necessarily new.
The second option—correcting each and every one of the separate, minor abnormal-ities found—can be a hard one.Why? It’s always the job of a doctor to try to return abnormalto normal.The art and science of medicine are most effective, though, when what we’retreating is a long way from what’s normal.For example, an operation for a ruptured appendixis life saving—it’s a highly efficacious thing to do. Bringing a blood sugar level back tonormal with insulin in someone in a diabetic coma is equally obviously effective. Butremoving the appendix in a patient with vague pain, or laboriously keeping a blood sugarlevel at 100 percent of normal instead of 110 percent of normal, is much less likely to makea big difference, especially if you remember that any form of medicine or surgery risksmaking the situation worse instead of better by introducing new, treatment-related abnor-malities to replace the abnormalities being treated.
90 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 90

In short, the more minor and the more numerous the abnormalities, the less likely itis that treating them will have a net beneficial effect.
These considerations make the third option, assisted conception, more attractive, espe-cially if you consider that endometriosis, say, usually has no harmful effect on gettingpregnant with IVF; that IVF readily compensates for moderate degrees of oligospermia oroligomenorrhea; that adhesions around the tube that don’t cause a hydrosalpinx are irrel-evant to the IVF process; and that the cervix becomes important to getting pregnant withIVF only if you can’t get an embryo transfer catheter through it.
Nonetheless, not everyone will decide at this point to pursue pregnancy.Whether youdo or not should be your choice—one you take with your partner, in full knowledge ofall the options and what these options involve.
Take your reading further with the specific chapters devoted to the diagnosis or diag-noses that have been made.
UNEXPLAINED INFERTILITY
It might by now becoming apparent that if the tests show little or no abnormality then it’sdoubtful that you will be very reassured.There are fewer options available than if a clearcause has emerged. It’s tempting to say it’s psychological or that medical science is stupidlymissing some exotic diagnosis that, if it were known, could be treated simply. Both theseconclusions are usually wrong, as I explain in Chapter 1. So don’t listen to people who tellyou it’s in your mind. It’s on your mind, for sure, but that’s not why you’re not gettingpregnant.
As far as exotic reasons for not getting pregnant are concerned—causes of infertilitythat are somehow out of reach—they do sometimes become apparent during IVF treat-ment, but I think they are rare. Chapter 2 makes it clear that it’s part of being human thatpregnancies should not happen too frequently. Unexplained infertility is a highly devel-oped evolutionary state, even if not desirable in modern society. Relatively untechnicalkinds of assisted conception such as GIFT work well; they would not work if there wassomething exotic stopping pregnancy. Our experience with IVF over the last 15 years hasshown us that, if anything, it’s usually a subtle difficulty with the sperm that stops womenunder about 38 years getting pregnant.
After 38 (though sometimes before) it’s more and more likely to be a subtle problemwith the eggs.This shows up during assisted conception cycles by there being fewer folli-cles and eggs than expected when the ovaries are stimulated.Exceptions to this rule, though,are common.
So where should you go from here? If no diagnosis has been made, take your explo-rations further with Chapters 19 and 20. If you do have a diagnosis, explore the specificchapters for your diagnosis or diagnoses first.
WHEN PREGNANCY’S NOT PROBABLE: SUBFERTILITY � 91
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 91

tests for miscarriages
There are many youcan have done
For most women most of the time, a miscarriage in isolation is sensibly regarded as justbad luck. Generally, a miscarriage is more likely to mean that the body’s reproductivesystem is working than that it is not—that next time, and without specific interven-
tion, a normal healthy pregnancy, and in due course a baby, will result.But a miscarriage that’s followed by a second one, and then perhaps a third—or a mis-
carriage that occurs after a long period of infertility—or a miscarriage in the middle threemonths of pregnancy—is another matter. Rather than being reassuring, such a miscarriageis a sign, perhaps a reminder, that all is not well and that tests should be done.
Here we consider:• The forms a miscarriage can take (what the symptoms and signs are);• How usual or common miscarriages are;• Recurrent miscarriages; and• Testing for the causes of miscarriage.
ARE YOU HAVING A MISCARRIAGE?
The first experience that a pregnancy is not doing as well as it should be doing usuallyconsists of some bleeding and then cramps. Eventually there can be an uncanny feeling ofwellness: the nausea of pregnancy disappears, the nipples lose their soreness. None of thesesymptoms is an invariable harbinger of doom. But they usually lead to tests—typically atransvaginal ultrasound, perhaps with a serum hCG (depending on the stage of the preg-nancy)—that will decide if all is well or not.
Miscarriages differ in the form they take, depending on how far the pregnancyhas developed.
92
8
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 92

Here we will look at:menstrual miscarriages,which occur with the period and without youknowing you have briefly been pregnant; subclinical miscarriages,which are like late and heavyperiods; clinical miscarriages,when you are likely to need a doctor;missed miscarriages (or missedabortion); and midtrimester, or late miscarriages, which are delivered with a mini-labor.
Menstrual miscarriages
A menstrual miscarriage is one that is so early that it does not delay the period.There areno symptoms of pregnancy. It’s not possible,without doing a blood pregnancy test late in theluteal phase, to distinguish a menstrual miscarriage from a normal period. (Remember thatthese symptoms—exaggerations of normal experiences—are also likely when a period islate and when the lining of the uterus—the endometrium—is thicker because of a prolongedfollicular phase and a late ovulation.) An ultrasound examination will not reveal a pregnancysac.
Some gynecologists call such a miscarriage a biochemical pregnancy, because the only hardevidence for pregnancy comes from a biochemical test (the pregnancy test, or level of serumhCG).
Subclinical miscarriages
A subclinical miscarriage is the miscarriage of an early pregnancy that delays the period aweek or two.As well as having a positive pregnancy test, a small gestational sac may developon transvaginal ultrasound (see Figure 4.2a); but when the miscarriage takes place it’s likea delayed period, though it can be heavier and longer than is normal for you.
No curettage of the cavity of the uterus is necessary. Not all gynecologists consider thisto be a separate category of miscarriage, so it too is sometimes called a biochemical preg-nancy, confirmable by pregnancy test or serum hCG.
Clinical miscarriages
The best-recognized sort of miscarriage can be called a clinical miscarriage, to set it apartfrom the other miscarriages we’ve talked about. In this case there’s a gestational sac presentif it’s looked for with a transvaginal ultrasound (see Figure 4.2b), and there can be symptomsof pregnancy.A fetal heart can develop and can be seen on ultrasound, but it might be latein appearing (more than six weeks after the last menstrual period—or, more accurately,longer than four weeks from conception) and, when the embryo doesn’t grow, the fetalheart slows and then it stops (Figure 4.3).
When miscarriage takes place, with bleeding and then pain, it’s common to have acurettage of the uterus to make sure the uterus has emptied and that bleeding or infectiondo not complicate matters. If a transvaginal ultrasound shows that miscarriage has beencomplete, curettage is not necessary.
Before the days of ultrasound, we used to distinguish a threatened miscarriage (bleeding,generally without pain, and a cervix that remained closed) from an inevitable miscarriage
TESTS FOR MISCARRIAGES � 93
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 93

(with painful contractions accompanying bleeding and with an opening cervix). Nowadaysa miscarriage will be regarded as inevitable if the gestational sac on ultrasound is smallerthan it should be and when the fetal heart is absent or is slow, at a time when it should bevisible and when it should be beating faster than about 120 beats per minute.
In cases of doubtful dates—and of course we usually give a much-wanted pregnancythe benefit of such doubt—a second ultrasound is carried out a week or two later: if thepregnancy has developed normally it’s likely to be normal; if growth has slowed furtherthen miscarriage will be inevitable.
The symptoms of miscarriage can sometimes be confused with the symptoms of anectopic pregnancy (discussed in Chapter 14).The ultrasound is useful in making this distinc-tion too.
Your doctor will be particularly interested in what parts of the pregnancy form beforemiscarriage takes place.The earlier the damage to the pregnancy the less developed theembryo or fetus will be, so that with many conceptuses (or ‘the product of the concep-tion’) there’s no embryo at all, just trophoblast (placenta) and chorion (membranes).
If embryonic structures are present, it’s the head-end of the embryo and the heart thatdevelop first; the tail can be very deficient (see Figure 4.4d).The further the pregnancy hasprogressed, the more complete the development will have been of the embryo or fetus. It’sunusual for a completely normally formed embryo to be lost in the first three months ofpregnancy. Just how complete the development of the pregnancy is at the time of miscar-riage can also be judged by having a pathologist examine the miscarriage tissue, either afterit’s been expelled from the uterus spontaneously (the natural process of miscarriage) or afterit has been proactively removed from the uterus by vacuum curettage.
The most useful test to do on miscarriage tissue (before it has been placed in a fixativesolution for the pathologist) is to send some trophoblast tissue for culture to permit a karyo-type,or analysis of the chromosomes.When a karyotype is done on incompletely formed miscar-riage tissue, in over 60 percent of cases the chromosome constitution will be abnormal.Viceversa, an abnormal chromosome constitution in the embryo means that, with a few excep-tions, the miscarriage will have been inevitable. If the chromosomal constitution is normal,on the other hand, there must have been another explanation for the miscarriage.Withrepeated miscarriages, therefore, or when a miscarriage looks inevitable after a period ofinfertility, a karyotype of the miscarriage tissue is an important test to determine the problem.I discuss this in more detail further on, under Chromosomal embryopathy.
A second useful test to do on the miscarriage tissue is a histopathology examination toexamine the site of implantation, looking for evidence of inflammation or thrombosis, andif possible judging the extent of spiral artery conversion by extravillous trophoblast (discussedin Chapter 4).
Missed miscarriage, or missed abortion
A pregnancy where there’s no embryo growing can persist into the second three months (thesecond, or middle, trimester) of pregnancy, especially if progesterone treatment has been usedto try to salvage the pregnancy but has succeeded only in delaying the natural process of
94 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 94

miscarriage, for example if there is a chromosome abnormality.A true missed abortion, as thispersistent state is known, is not a good thing to have happen,because the tissue of the miscar-riage hardens and can be difficult to curette from the cavity of the uterus, risking damage tothe endometrium in the form of intrauterine adhesions (discussed in Chapter 17).
Midtrimester miscarriages
Should a normally formed fetus miscarry, usually in the middle three months of pregnancy(the second,or mid, trimester), then the essential distinction for the cause of the miscarriageyou and your doctor will want to make is the one between cervical incompetence and prema-ture labor.The pattern of events is different—and the treatment of the two conditions isvery different—so careful recall of the order of events is important.
With cervical incompetence a normally formed fetus can be lost, after 14 weeks or moreof pregnancy, due to softening, shortening and then opening of the cervix. Such an ‘incom-petent’ cervix allows the membranes of the pregnancy to bulge through. Symptoms canbe minimal until it’s too late, consisting just of backache and an increase in wetness ordischarge from the vagina. In fact there might be no symptoms at all before the membranes(the waters) break, a rush of fluid is experienced, and the fetus is expelled into the vaginawith minimal bleeding and pain.The placenta will usually follow and bleeding is thencommon.
With premature or immature labor (if the fetus is still well short of viability), in the absenceof cervical incompetence the process is like labor—with the onset of painful, episodiccontractions of the uterus and bleeding before the waters break; the fetus and placenta arethen expelled.With such a pattern the common causes are an infection (sometimes, iron-ically, associated with the presence of a stitch in the cervix, or a cervical ligature, used to treatcervical incompetence); and abnormalities of the uterus (discussed in Chapter 18).
Sadly, it’s still not always possible to find a treatable cause even in repeated cases, andthen a variety of antibiotics, medications and hospitalization may be called for in trying tokeep the pregnancy in place until the newborn can be expected to be viable. I discuss thistreatment further in Chapter 9.
HOW USUAL ARE MISCARRIAGES?
Table 8.1 shows the average chance of a pregnancy ending in miscarriage according to theage of the woman. (The male partner’s age has very little, if any, effect.) There’s a steady risewith age from the early twenties (when it’s about 12 percent for clinically obvious miscar-riages), and a substantial increase in risk after the late thirties (when it’s about 20 percentto 25 percent for clinical miscarriages).After about the age of 42,more than half of all preg-nancies achieved will miscarry.
It used to be thought that it was the aging uterus that caused miscarriages to becomemore common in older women, but clinical studies with donated eggs and embryos fromyounger women to older women show that this is not the case.The aging process affects theeggs, leading to chromosomal or metabolic embryopathy,which I discuss further on (see also
TESTS FOR MISCARRIAGES � 95
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 95

the Chapter 7 box,How eggs might get their ‘use-by’ date:Mishaps in the mitochondria).As a result,many women in their forties, and some even in their fifties and sixties,have recently conceivedand successfully undergone pregnancy with eggs donated by much younger women.
RECURRENT MISCARRIAGE
Just as getting pregnant is a matter of chance, so is having a miscarriage. It’s uncommonfor every pregnancy to miscarry—although in some women it does seem to happenthis way.
Gynecology textbooks classically claim that repeated miscarriages should be investi-gated if a woman has had three or more of them in a row, a condition formerly called‘habitual abortion’ (nowadays,more gently, recurrent miscarriage).This is an old-fashionedperspective. It was 1982 before it was generally known that there’s an increased chance ofmiscarrying with just about every cause of subfertility (discussed in Chapter 7) and withmost treatments for infertility. If a miscarriage takes place with a background of infertility,it can help—in getting a total view of the reasons behind the disability—to investigate evenone miscarriage by sampling the miscarriage tissue and performing a karyotype. If the karyo-type is normal then the chances are that the miscarriage was caused by whatever is causingthe infertility.
Whether the karyotype of a miscarriage is normal or not,we can presently find a causefor about two-thirds of couples who have had three or more miscarriages; about half ofthese couples will have a successful pregnancy as a result of treatment.
There’s probably no medical condition that produces a longer list of tests than the inves-tigation of recurrent miscarriages calls for—although the good news is that most of themcan be done on the one sample of blood.Your doctor, however, might be selective, andexactly which tests are most likely to be helpful will depend on the circumstances. In thenext section I’ll approach the relevant tests according to a consideration of the possiblecauses of miscarriage. I should say straight away that these different categories are not wellknown outside Sydney IVF: your gynecologist might or might not consider or categorizethe causes of miscarriages this way.
96 � GETTING PREGNANT
Table 8.1 Effect of a woman’s age on the risk of her having a miscarriage
Age of woman Average chance of miscarrying
Younger than 20 years 12%
20 – 24 years 13%
25 – 29 years 14%
30 – 34 years 16%
35 – 39 years 19%
40 – 42 yeras 25%
43 years and older 50%
Source: Based predominantly on data from Dorothy Warburton and Clarke Fraser.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 96

But it’s a sensible approach, explaining miscarriages this way works, and it formsthe foundation of the comprehensive miscarriage management program developed atSydney IVF.
TESTING FOR THE CAUSES OF MISCARRIAGES
The key biological events that lead to successful pregnancy are fertilization (by a geneticallynormal sperm of an egg that is both genetically normal and, in its cytoplasm,metabolicallycapable), cleavage (as the egg becomes a ball of cells, now under the command of bothparents’ genes), implantation (by a hatched blastocyst into an adequately responsive endometrium),establishment of molecular dialogue between invading trophoblast and well-developed decidua(which includes critical elements of the blood coagulation system and the immune system—or immunological rejection occurs), and then what could be called the placental buildingindustry, the sound, earthquake-proof construction of chorionic villi to compose a matureplacenta and a reliable supply of placental perfusion (see Chapter 4 for an account of thesteps involved).
So the logistics are hugely important.But so too is the passenger, the developing embryo,which by the time it is a blastocyst is already making at least 1500 mostly indispensable mole-cules, with much more to come, involving switches on probably every chromosome.Thinkof chromosomes as racks of genes, so generally the bigger the chromosome the sooner itbecomes indispensable, requiring the right genes,without faults, and in the right dose (twocopies).
We’ll consider the causes of miscarriage in the following groups:• Chromosomal embryopathy, in which a genetic error at conception dooms the embryo;• Embryopathy before implantation, in which the gross genetic make-up of the embryo is
normal but there’s a harmful event that cripples the embryo before it has a chance toimplant properly (it can arise preconceptionally in the egg or sperm,or it can be a post-conceptional event affecting the cleaving embryo);
• Embryopathy after implantation, in which the embryo implants but fails to establish asubstantial placenta;
• Embryopathy after placentation, in which the placenta forms and there is some degree offetal development, but the pregnancy is then rejected; and
• Fetal loss,where a normal embryo or fetus is expelled from the uterus late in pregnancy
Chromosomal embryopathy
The condition described as chromosomal embryopathy produces miscarriages in which theembryo does not develop properly because of a gross genetic error present from conception.(The embryo is pathological, hence the term embryopathy; in these cases the karyotype ofthe pregnancy tissue is not normal—see Figure 8.1a.)
If the chromosomes are abnormally endowed at conception then often there’ll belittle or no chance of the pregnancy coming to term as a baby, especially if there are,
TESTS FOR MISCARRIAGES � 97
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 97

say, 69 chromosomes instead of the normal number of 46 chromosomes (triploidy—seeFigure 8.1b).
Likewise, if there is a chromosome missing there will sooner or later be a catastrophicshortage of genes, so that development will generally stop very early (resulting in a menstrualmiscarriage). Only a missing sex chromosome will permit, in some instances, development tothe point of birth and beyond (this karyotype 45,X results in Turner syndrome).
An extra chromosome is almost as harmful, with many trisomies causing menstrual orsubclinical miscarriages, but with trisomy 13, 18 or 21 (Down syndrome, see Plate 8.1c), aswell as trisomies of the sex chromosomes (for example, 47,XXX; 47,XYY; and 47,XXY,
98 � GETTING PREGNANT
Figure 8.1 Karyotypes. In a normal karyotype (a) there are 46 chromosomes; the presence of an X anda Y chromosome here indicates a male. In triploidy (b) there are three of every chromosomeand miscarriage is inevitable.With trisomy 21 (c) there are 47 chromosomes, with three ofchromosome 21 (arrow), indicative of Down syndrome; the presence of two X chromosomeshere indicates a female. If there is a balanced translocation (d) a part of a chromosome ismoved (here from the long arm of chromosome 11—arrow) to a different chromosome (hereon the short arm of chromosome 7—arrow); the fetus or person will be normal, but, at leasttheoretically, half of this woman’s eggs when fertilized will carry too much or too littlechromosomal material, resulting in implantation failure, miscarriage or a birth defect.(Karyotypes performed and photographed by Dr Cynthia Roberts, Sydney IVF.)
(a) (b)
(c) (d)
(enlarged)
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 98

or Klinefelter syndrome), sometimes not causing miscarriage, but instead developing to birthand resulting in a baby with a greater or lesser set of disabilities (generally soon fatal in thecase of trisomy 13 and trisomy 18).
Such aneuploidies can also arise after fertilization, during cleavage, producing a mixtureof normal and abnormal cells, a condition called mosaicism. Abnormalities that would belethal with all cells affected can be compatible with life if only a proportion of cells haveabnormal chromosomes.
Finally, a balanced translocation (see Figure 8.1d) is a well-recognized cause of recurrentmiscarriage.Here a part of a chromosome has moved to another site but is not yet missing,but when the chromosome pairs split up to form eggs or sperm these bits of chromosomecan either miss out or be present in the embryo’s cells to excess.
The more common abnormal karyotypes that cause miscarriages are listed in Table 8.2.Over 60 percent of such miscarriages have abnormal chromosomes.The table gives thebreakdown of these abnormalities. Because of the inevitability of miscarriage when thechromosome number is abnormal, knowing whether a pregnancy’s karyotype is or wasnormal or abnormal is fundamental to interpreting a miscarriage and estimating the like-lihood it will happen again.
How is a karyotype done? With difficulty and a lot of work (see the box, Karyotypingstep by step).We begin by getting some living tissue from the conception—in the form ofchorionic villi in early pregnancy, amniotic fluid cells later in pregnancy, or from either theplacenta or the fetus’s skin in the case of an immature delivery. In early miscarriages, trophoblasthas to be teased free from the mother’s decidua under a dissecting microscope, a difficultskill most pathology labs seem to have trouble with. (If decidual cells are inadvertently kary-otyped the not-useful result 46,XX is obtained, representing the karyotype of the motherinstead of the pregnancy.)
TESTS FOR MISCARRIAGES � 99
Table 8.2 Karotypes of miscarriages in the first three months of pregnancy
Abnormality Explanation Relative frequency
Aneuploidies
Monosomy One chromosome not enough 16%(particularly 45, X) i.e. 45 chromosomes
Trisomy One too many chromosomes 54%(especially trisomy 16) i.e. 47 chromosomes
Polyploidies
Triploidy 3 times the haploid number 20%i.e. 69 chromosomes
Tetraploidy 4 times the haploid number 6%i.e. 92 chromosomes
Unbalanced translocations
Unbalanced translocation Too much of part of a chromosome 4%
(at least)
Source: Adapted from figures published in 1975 by Boué and colleagues from France.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 99

This tissue then needs to be set up in tissue culture, so that the cells continue tomultiply in the laboratory. After this, the chromosomes are photographed through amicroscope while the cells are dividing. Even with the help of a computer, one highlytrained technician (a cytogeneticist) will be able to do no more than about 10 karyo-types per week.The karyotype is therefore a rather expensive test.
Unfortunately, though, by the time a miscarriage is expelled, the trophoblast tissuemight have degenerated too much for the cells to survive in tissue culture for karyotyp-ing. If finding a reason for a particular miscarriage is important enough, your doctormight recommend a curettage or a chorionic villus sampling (CVS) as soon as practicableafter a transvaginal ultrasound shows no surviving embryo.
100 � GETTING PREGNANT
Karyotyping step by step
In a culture, as in the body, cells divide by mitosis.Once the tissue culture for perform-ing the karyotype is underway,mitosis is stopped in its tracks by adding a drug calledcolchicine to part of the culture.This freezes mitosis at a stage of cell division calledmetaphase, when the chromosomes are separate and can be photographed.
Till the end of the last century they were then literally cut out from the photo-graph with scissors and pasted up in order.During the 1990s the cutting and pastingcame to be done on a computer screen, with each chromosome pair displayed insequence to check for completeness (see Figure 8.1).This is done for typically 20or so metaphases—an enormous amount of work, even for a computer.
Normal karyotypes are indicated this way: a normal female karyotype is 46,XX(to indicate 23 chromosome pairs, of which one pair comprises the sex chromo-somes and the other 22 pairs are autosomes, or non-sex chromosomes); a normalmale karyotype is 46,XY.
We have already encountered the term triploid, which means three times thehaploid number of chromosomes (see Chapter 3), and usually comes about if twosperm fertilize an egg.
The general term for the gain or loss of a single chromosome is aneuploidy.Themost common aneuploid chromosome complements are the trisomies, where thereis an extra chromosome because of incorrect movement of the chromosomes duringmeiosis into the egg or the sperm, for example, trisomy 21 (Down syndrome), in whichan extra chromosome 21 gets into egg or sperm and therefore into the embryo;and trisomies of the sex chromosomes (Klinefelter syndrome = 47,XXY; triple-Xsyndrome = 47,XXX; and extra-Y-chromosome syndrome = 47,XYY), in which theembryo is endowed with an extra sex chromosome.
The loss of one of a chromosome pair, a monosomy, is not compatible with evenearly embryo development—unless the chromosome lost is a sex chromosome, in acondition called Turner syndrome (45,X); even so a majority end as miscarriages,withonly a small proportion surviving as babies.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 100

Whether miscarriage tissue has been available for karyotyping or not, recurrentmiscarriages in the first trimester should mean the couple ought to have their karyotypechecked to exclude a balanced translocation (in which, as we saw above, a piece of one chro-mosome has been translocated to another position). Such a translocation does no harm tothe person concerned, because there’s no overall gain or loss of genetic material, but whenthe chromosome pairs split up and move into eggs or sperm (discussed in Chapter 3), there’llbe a shortage of genes for one egg or sperm, and an excess of genes for its sister egg orbrother sperm (shown in Figure 8.1d); other eggs and sperm can be normal (the ones thatreceive the normal member of the pair).
For more on balanced translocations of the chromosomes, see the box, Unbalancingtranslocations.
Other embryopathy arising before implantation
Injuries endowed prior to conception, or occurring between the time of conception andimplantation, that result in miscarriage are called preimplantational embryopathies.They canarise before conception in the egg or in the sperm, or after conception in the early embryo.
TESTS FOR MISCARRIAGES � 101
Unbalancing translocations
Balanced translocations (Figure 8.1d) should produce unbalanced, abnormal embryos25 percent of the time (because four different combinations are possible).
In practice the frequency is less than this.The reason must be either that thereis preferential selection of normal eggs or sperm cells somewhere along the line or,more likely (we believe), that syngamy fails more often than is usual and the embryo’sdevelopment is stopped before the pregnancy is revealed.
However,when there is a balanced reciprocal translocation (the ‘reciprocal’ refer-ring to the fact that two different chromosomes have swapped pieces), there is amuch, much greater chance of the fertilized egg having an abnormal amount ofchromosome material than 1 in 4, for two reasons.
First, there’s not just one chromosome that risks being unbalanced but two (witha third risk that both end up unbalanced).
Second, a translocated bit of chromosome can be so small that it doesn’t eversegregate properly, rattling about chaotically as chromosomes get distributed betweensperm cells in men and between egg cells in women, and ending up just aboutanywhere in the genome by random chance and disrupting the picture further.
The miscarriage rate with a balanced reciprocal translocation can therefore getrather close to 100 percent.
We have had many successful outcomes at Sydney IVF after using IVF withpreimplantation genetic diagnosis to work out which embryos are either normal orbalanced before we transfer them.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 101

Egg cytoplasm problems
The egg brings many resources to the post-conception partnership, particularly an endow-ment of proteins and protein-forming instructions (called messenger RNA) arising fromthe egg’s DNA, or genome, well before ovulation and packing the egg’s cytoplasm to thebrim. One reason eggs are so large compared with sperm is because they are packed withthese substances, which will be utilized by the daughter cells of the embryo for days orweeks into the pregnancy before, gradually, the embryo’s own genome, with the contri-bution derived from the sperm, takes over.More than anything else, the quality of the egg’scytoplasm will determine the early embryo’s metabolism.
Deficiencies of the egg cytoplasm can be inbuilt, with the egg faulty from the start, orthey can be acquired, with an inherently good egg not developing to its potential.
Although the details are not clear yet, defects of the egg cytoplasm might includeabnormalities of the mitochondria (see the Chapter 7 box, How eggs might get their ‘use-by’date: Mishaps in the mitochondria).The embryo’s mitochondria come entirely from themother and, indeed, the new embryo will not make any new mitochondria until twoweeks of development have occurred. So presumably an embryo that comes from an eggwith too few mitochondria will run out of them—and run out of energy—before it canimplant properly, becoming a blighted ovum (see Figures 4.2b, 4.4b and 4.4c).
Whether due to defective mitochondria or to some other deficiency within the cyto-plasm, sooner or later the effects of aging eggs will, for any woman continuing to put herreproductive ambitions to the test, result in blighted ovum-type miscarriages; as more timepasses there will be sterility.This sequence, this life-transition, we’ve labeled the oopause. It’sdescribed more completely in Chapter 7.
Unfortunately we do not have a reliable test yet for the quality of egg cytoplasm, so adiagnosis of oopause is a diagnosis we are left with when no other diagnostic leads lookplausible (what doctors call a ‘diagnosis of exclusion’).
At least as common, in programs of in vitro fertilization particularly, but also in manyovulation disorders accompanied by poor development of preovulatory follicles, is when theegg’s cytoplasm is spoiled because ovulation occurs without enough exposure to follicle stim-ulating hormone. Either the amount or the duration of FSH can be suboptimal.The resultwill be partial follicular atresia; it is usually possible to overcome this problem with adequateovulation induction. Some (probably most) of the miscarriages that we attribute to low levelsof serum progesterone in the luteal phase, so-called luteal phase defects, are actually due tospoiling of the follicle, and hence the egg, in the follicular phase.
Lastly, partial follicular atresia and poor eggs can result from certain genetic diseases thatit is important to uncover. Persisting with infertility or recurrent miscarriage treatment inthis situation can risk a serious handicap in male offspring called fragile-X syndrome.This isthe most common cause of serious mental deficiency in boys in the community.Womenwho are carriers of this sex-linked recessive condition can present with fewer and more poorlyresponding follicles during IVF treatments.
Tests for recurrent miscarriage where there is evidence of poor development of ovarianfollicles should include a transvaginal ultrasound on about day 7 of the follicular phase (to
102 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 102

look for development of follicles, see Chapter 7) and perhaps a PCR test for fragile-X DNAin the woman, in addition to the usual karyotype.
Sperm problems
As well as an abnormal karyotype (see earlier), the sperm can bring at least two furtherkinds of problem to the post-conception partnership, namely DNA breaks and adefective sperm centriole. For an explanation, see the box, Miscarriage tests men shouldhave . . .
TESTS FOR MISCARRIAGES � 103
Miscarriage tests men should have . . .
Your partner must not be left out of the evaluation. Sperm might be slippery littleswimmers but they shouldn’t escape responsibility for what needs to follow!
To begin with, he should have a blood test for a karyotype, to look for a balancedchromosomal translocation. But there are also more specialized tests that can be doneon the semen.
When sperm are formed (in the process called spermiogenesis, which transformsa round cell into one with the profile of a cruise missile; see Chapter 3), the DNAgets tightly packed, like a warhead.To do this, the chains of DNA in the chromo-somes need to form super coils, which involves breaking the chains and reformingthem.After the sperm fertilizes the egg this process has to be un-done (and resultsin the chromosomes forming the male pronucleus). Almost always, probably, someDNA breaks are left over that the egg has to repair as best it can.
If there’s too much DNA damage in the sperm head it swamps the egg’s abilityto repair it.As a result, the embryo won’t form properly. It doesn’t undergo cleavage,or it fails to undergo implantation, or it may go on to miscarry.
There is a test available at Sydney IVF to measure DNA breakage in sperm, thesperm chromatin structure assay, developed at the State University of South Dakota byDr Don Evenson. If the proportion of sperm cells in the sperm count showing DNAdamage is more than 15 percent, then subfertility or miscarriage is more likely. Morethan 30 percent of sperm cells damaged is likely to cause sterility or recurrent miscar-riage.This is a useful addition to just having a careful sperm count done (though thisis important also—with ‘strict criteria’ used for normality).
The second structural feature the fertilizing sperm endows to the embryo is thecentriole, a minute rod-shaped structure at the head-end of the sperm’s tail filament,or flagellum.After fertilization the centriole replicates, forming the two poles thatthe chromosomes are oriented towards in the cell divisions of mitosis. Faults in thecentriole mean faults in cell division, and faults in cell division mean faults in theembryo’s constitution.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 103

Embryo problems
It is nature’s way that injuries sustained by an embryo are usually ‘all or nothing’. Eitherthe injury will be mortal, ending in embryonic death or miscarriage, days or a week or twolater, or it will be shrugged off by the exuberance embryos show in growing.
Injuries suffered between the time of conception and implantation can include nutri-tional deficiencies and transport-timing problems within the fallopian tubes, as can happenwith disease of the fallopian tube and, to some extent, fertilization and development invitro (IVF). Recurrent miscarriage can occur with a one-sided hydrosalpinx (for more, seethe Chapter 20 box, Hydrosalpinx: Reintroducing a villain).
A noxious external event, such as a high fever or an alcoholic binge (it probablyneeds to be a real bender), might also injure an embryo sufficiently to cause a latermiscarriage.
Apart from tubal disease (see Chapters 5 and 13), these causes are generally one-off andno special tests are useful. Note, though, that if an episode such as a fever occurs, and if thepregnancy continues, the chance of a birth defect is just barely different from the gener-ally expected incidence of birth abnormalities.Most people, in other words,will not chooseto have an abortion just because they’ve experienced such an event.
No doubt many genetic conditions can also cause the embryo to fail at this point.Theembryo when it is ready to implant has already activated more than 1500 specific genes. Ifby chance both copies of one of these genes has an error, the deficiency could cause theembryo to fail and miscarriage to follow.This is even more so for the greater number ofspecific genes that are called to action after implantation.
Whether disorders of the centriole can cause miscarriage is not certain: mostdefects are probably so catastrophic that cleavage and implantation fail. Sperm affectedcan show increased breaks of the tail or abnormalities of the sperm midpiece oncareful semen analysis.
. . . and polymorphisms to watch out for
And finally,many causes of miscarriage are genetic, especially if both potential parentsare heterozygous for a genetic polymorphism that, in homozygous form, makes theembryo especially vulnerable.
Polymorphisms differ from ‘mutations’ by being much more common in the popu-lation, and by frequently showing some kind of advantage in certain circumstances(called heterozygous advantage), which promotes their inheritance.
Examples relevant to recurrent miscarriage may include HLA-G*01013 (whichdecreases the amount of soluble HLA-G soaking the mother’s immune system,possibly reducing tolerance) and the gene for folic acid metabolism, MTHFR, ab-normalities of which might affect the sperm count (in a way that can be overcomeby mega-supplements of 5 milligrams of folic acid a day).
104 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 104

Embryopathy after implantation
The possible reasons for an embryo or fetus to sustain injury after implantation are many.In general, we should also note, the later in fetal life such an injury occurs the more likelyit will be to reveal itself as an abnormality at birth rather than as a miscarriage.
We will look at this period in three stages.These categories are not fully separate, byany means, and causes applicable in one can also apply under the other headings.Nonetheless, to bring some order to the field we’ll consider the different causes just once,in the most typical stage at which they operate.
As the hatched blastocyst successfully attaches to the endometrium, it releases a gas, nitricoxide, that in the presence of progesterone signals the surface endometrium to dissolveunder it, and then it squeezes through, embedding into the endometrial stroma.
At least three things then need to be correct: the first is the decidual reaction, whichwe can test for, up to a point; the second two are much more difficult to explore, namelythe maternal genome (because we usually don’t know where to look or what to look for)and the fetal genome (which has the added difficulty of being physically inaccessible).
The maternal decidual reaction
Unless the lining of the uterus is hospitable to the penetrating blastocyst, the pregnancyhas no hope of becoming established properly.
One of the most important tests to do for investigating recurrent miscarriage, therefore,is to establish that there is a normal decidual reaction as seen on a premenstrual endometrial biopsy.We do the test in a month the woman is not trying for pregnancy (because we don’t wantinadvertently to disrupt an implantation, even if it would be a fluke to hit it). It’s carried outwith intravenous sedation and local anaesthetic, and takes just a few minutes in the day surgery.
This tells us:1. That progesterone production in the woman’s luteal phase has been adequate,2. That there is no disease of the endometrium such as endometritis that is limiting it or which
might indicate a infection that could cause miscarriage unless treated with antibiotics,3. That there is not an abnormal population of NK cells poised to mount an immune
reaction against the implanted embryo, and4. That the maternal genes for the decidual reaction are intact. (For the specialist, these
include genes for leukaemia inhibitory factor, or LIF, for interleukin 11, for prolactinand the prolactin receptor, for ‘tissue factor’, for various growth-promoting factors forblood vessels, and for structural cells called fibroblasts.)
But if the premenstrual biopsy is normal, we have little to go on in terms of checking formolecules that do their essential job later.
Maternal recessive genes
There are probably hundreds of maternal genes that are needed to work correctly beforethe woman’s side of the placenta develops properly. Before I categorize them, let’s brieflyconsider some facts about how you inherit most of them.
TESTS FOR MISCARRIAGES � 105
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 105

Production of correct proteins from the great majority of these genes is likely to dependon autosomal recessive inheritance.This means that you need just one normal allele of eachgene for it to function properly and code for a correct protein (which is just as well, becausethere are so many of them that the chances are we all carry a mutation in one or a few ofthem). For most people most of the time, therefore, a sprinkling of mutations among thesegenes is just part of being human.
Trouble, however, can come about in one of two ways.The first is if there is what couldbe called inbreeding, such as marrying your cousin.This makes it very much more likelythat a bad allele will team up with a bad allele. If this has been going on for centuries you’llbe safer, because harmful genes are likely to have been bred out over the generations. If it’sa recent thing in your family or town it dramatically increases the chance of homozygousinheritance of the faulty alleles and, because there’s no normal allele, the protein will beabnormal and genetic disease will follow.
The second way is more random,and there’s nothing you can do about it. Just by chance,even if you and your partner have quite different family and genetic backgrounds, youmight inherit a different bad allele from each parent but affecting the same gene.Geneticallyspeaking this is a heterozygous state, but for all intents and purposes the effect will be thatof homozygosity for a mutation.We call this compound heterozygosity. If the affected gene isneeded for a critical function in the uterus then recurrent miscarriage will be inevitable:every single pregnancy will be affected.
We think this could account for at least some situations of recurrent miscarriage whenthere are more than five more-or-less similarly timed recurrent miscarriages with no inter-vening normal pregnancy and the karyotypes for the parents are normal. Until we knowwhat the missing factor is and how we might replace it in the uterus, the pregnancies allfail and gestational surrogacy will be the only effective treatment (see Chapter 22 for theissues).Testing for these mutations is still very difficult, even though as a result of the HumanGenome Project we know what the correct DNA sequence should be for almost all ofthem.
Why is testing difficult? To begin with, there might be hundreds of proteins, any oneof which could be the culprit, so we really don’t know where to start looking. In manycases we hardly know yet what many of the proteins do.Moreover, even when we do thinkwe know which protein it is, and which gene to look at, most genes are huge, way too bigfor a non-research lab to sequence the DNA and to find the mistake, at least for a realisticamount of money (though such sequencing is fast becoming quicker and cheaper). Andlastly of course we can’t get to take samples where the implantation is going wrong beforeit’s all too late and the pregnancy has been lost.
Nonetheless we’re making progress.Among faulty proteins that can be corrected withadministered replacement proteins are rare errors in the blood coagulation proteins fibrino-gen and factor XIII (‘factor thirteen’), which are needed to provide the scaffolding for thenewly invading trophoblast and therefore for construction of the placenta.At Sydney IVF weare also interested in leukemia inhibitory factor (LIF), interleukin 10 (IL-10), regeneration andtolerance factor (RTF), vascular endothelial growth factor (VEGF), complement, and sticky adhesionmolecules called integrins (though the list is ever-changing).
106 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 106

Fetal genes
If the number of molecules that must work normally for the embryo, as a blastocyst, to hatch,attach and penetrate into the endometrium is large, then the number needed to build anormal maternal–fetal interface . . . the number needed to form the placenta . . . is evenbigger. Like the maternal molecules that need to be normal, many of these are also inher-ited with autosomal recessive inheritance. But unlike the maternal molecules, the fetus will getone from each parent, and even if each parent is a (heterozygous) carrier, the way the dicefall means that only one fetus in every four conceived will be homozygous recessive orcompound heterozygous.Only one in four fetuses will miscarry because of the recessive inher-itance of a bad protein.
So while this might explain quite a number of isolated miscarriages, it will not causelong strings of recurrent miscarriage.
More important, therefore,are the fetal genes that are not recessive—genes that are dominantor partially so,capable of causing at least some mischief when just one faulty allele is inherited—because then three out of four embryos a couple produces could have a tendency to miscarry.
Many of these alleles are rather common in the population, so common that they canscarcely be called abnormal.We refer to them as polymorphisms.
Examples include variations in the tissue-typing molecule HLA-G (see the Chapter 4box, . . . and shaking hands with HLA-G); a protein called TBP; the enzyme nitric oxidesynthetase, which produces nitric oxide, a messenger molecule; and a molecule that blocksthe action of immune cells, known as interleukin 1 receptor antagonist, as well as the genesthat cause the thrombophilias, discussed in the next section.To work out what the risk isthat the embryo or fetus inherits the polymorphism, in single or in double dosage, theprospective father should be tested as well as the prospective mother (see the box,Miscarriagetests men should have . . . and polymorphisms to watch out for).
When we learn more about these genes we will be able to help avoid miscarriages byusing IVF with preimplantation genetic diagnosis (a theme we will pick up in Chapter 9).
Embryopathy after placentation
The developing pregnancy needs the development of a quickly expanding blood supplythrough the wall of the uterus to the placenta.
As explained in Chapter 4,much needs to go right, in what’s sometimes a finely balancedstate.
We look here at tests probing the potential problems with anatomical constraints; thegeneral medical environment of the mother; the balance between immune tolerance andrejection; the blood clotting tendencies, or ‘thrombophilias’; and the association with foodintolerance, particularly celiac disease.
Anatomical constraints
The blood flow to the fetus can become insufficient in early pregnancy if implantation is:(1) on a uterine septum (a wall partly dividing the uterus in two—see Chapter 18); (2) over
TESTS FOR MISCARRIAGES � 107
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 107

a uterine fibroid (see Chapter 17); or (3) constrained by intrauterine adhesions or endometrialatrophy (Chapter 17).
These causes are best looked for with a hysterosalpingogram, a transvaginal ultrasoundof the uterus and/or a hysteroscopy (investigations described in Chapter 5).We will lookmore at anatomical (uterine) constraints later in pregnancy, below.
Medical constraints
An overactive thyroid gland (thyrotoxicosis) can cause miscarriages, perhaps because itincreases the rate of metabolism in the body generally and progesterone, needed for main-taining pregnancy, is got rid of too quickly.This is looked for with thyroid function tests,which comprise assays in blood of thyroxine and thyroid stimulating hormone (TSH). (Themiscarriage shown in Figure 4.4d resulted from an overactive thyroid gland: the embryo isalmost normal for its stage of development.)
Textbooks list diabetes as a cause of miscarriage, and women with recurrent miscarriageshave in the past undergone formal tests to exclude it.This is unnecessary. Diabetes causesmiscarriage only when it’s bad enough to need insulin for treatment and it’s under poorcontrol.The diagnosis, for these people,will have been made already. If in doubt, it’s simpleto test for sugar in the blood, with a plasma glucose level.
Any severe upset to the mother’s health or metabolism can affect the fetus. But theseupsets will generally be very obvious already. Failure of the kidneys, causing uremia, is oneexample, and is checked with a serum urea and creatinine.
One of the more subtle, though rare,metabolic causes of miscarriage is Wilson’s disease,in which there are high levels of copper in the serum (measured as serum copper), thoughusually in association with abnormal tests of liver function (and with a yellow ring visiblewithin the iris of the eye).
Immune tolerance or rejection, including the antiphospholipid syndrome
Remember that, from an immune perspective, the fetus is a foreigner (discussed in Chapter 4).The mother’s immune system usually learns to tolerate the fetus. If her immune system is tooreactive, the mother can reject the fetus—first by making antibodies and immune cells to it andthen through miscarriage.A lot is known about these events, though more is still to be learned.
We saw in Chapter 4 that the endometrium needs NK cells to recognize the implant-ing pregnancy—NK cells that are part of the ‘innate’ immune system.The NK cells normallyresident in the uterus are characterized as CD56-BRIGHT, in contrast with NK cells circu-lating in the blood (characterized as CD56-DIM, but also as being CD16-positive andCD57-positive).These circulating or ‘peripheral’ NK cells are more likely to turn on thefetus.They have been thought to circulate in higher numbers in women who later turnout to miscarry; they should not be present to any extent in the endometrium of normalwomen, but they are found there in some women who go on to miscarry.At Sydney IVFwe test for these CD57-positive cells, as well as for various T cells, in the blood and in thepremenstrual endometrial biopsy.
108 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 108

There is one blood-group antibody, or agglutinin, that causes recurrent miscarriages infamilies that have it—the rare anti-TjA antibody (also known as anti-PPIPk).Other agglu-tinins are looked for with a blood group and antibody screen.
Patients with the disorder known as systemic lupus erythematosus (SLE) form antibodiesagainst their own tissues.The antibody,or the group of antibodies,most likely to cause miscar-riages is known in several different guises as the lupus anticoagulant or lupus inhibitor (itslightly inhibits blood coagulation), and as antiphospholipid antibody or anticardiolipinantibody.The clinical syndrome that results is called the antiphospholipid syndrome and,typically but paradoxically,manifests with thrombosis.The tests we order to see if such anti-bodies can be implicated are the lupus anticoagulant and the serum anticardiolipin antibody; thesetests are important, because treatment is available with heparin and corticosteroid drugs.
Studies have suggested that antiphospholipid or anticardiolipin antibodies may (1) inearly pregnancy, decrease ‘conversion’ of maternal arteries to the placenta by extravilloustrophoblast cells (see earlier), and (2) in later pregnancy, inhibit the anticoagulant annexin V,which keeps blood flowing around the chorionic villi in the intervillous space of the placenta.This is a controversial area of miscarriage medicine, partly because there is still no standardway of measuring these antibodies.
Blood levels of antinuclear antibody (ANA) are often increased in women with recur-rent miscarriages and in patients with SLE, but unless there are other antibodies there invery high levels it will be unclear whether ANA is the cause or the result of the miscarriages,or whether the ANA is completely unrelated.
One of the most tantalizing hints about occasional primarily immunological causes forrecurrent miscarriages has come from the discovery that a proportion of women can betreated by being immunized to their partner’s (or to a stranger’s) white blood cells (thedetails are in Chapter 9).
The thrombophilias
Just as the normal immune system,particularly the ‘innate’ immune system, is poised betweentolerance and rejection, so also is the next cog in the rejection process, the blood coagula-tion system.
A number of polymorphisms cause the blood to clot more readily, a phenomenon calledthrombophilia.This can be an advantage if you’re having a baby in the bush, out in the wild,a long way from a blood transfusion service, but in the trigger-happy state of imminentmiscarriage it can be the final straw that puts a blood clot between the trophoblast and thedecidua (see the Chapter 4 box, Talking tough with thrombin).The clotting factor alleles thathave been thought to be behind an excessive tendency to miscarry, and for which DNAPCR tests are available, are factor V Leiden (the G1691A allele), prothrombin G20210A, andthe MTHFR C677T allele, if it is causing an increase in serum homocysteine.
Factor V Leiden is present in about 3 percent of Caucasians; it is almost never found inblack people and Asians. It is mainly implicated in late miscarriage and stillbirth,but a doubledose of the gene in the fetus (which can happen if both parents are carriers) might causecirculation failure in the placenta in earlier pregnancy.
TESTS FOR MISCARRIAGES � 109
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 109

MTHFR (which stands for methylene tetrahydrofolate reductase) is responsible forturning folic acid into metabolites that have several critical roles in the developing fetusand in the mother.The C677T allele is a very common variant, present in more than40 percent of Hispanics and Italians, about 35 percent of other Caucasians, and lessthan 10 percent of black people.
In the mother the C677T MTHFR allele predisposes the fetus to neural tube defects aswell as to miscarriage.This is the major reason why folic acid supplements are so importantfor pregnant women.If you have the allele, the dose of folic acid you should take is a minimumof 5 mg per day (which is 10 times the previously recommended dose for pregnant women).
The C677T allele in the father predisposes both to oligospermia (see the box,Miscarriagetests men should have . . . and Chapter 10) and to an increased risk of heart disease and stroke(which is why in surveys the gene becomes less common among men as they get older!).Men with the allele also benefit from high-dose supplements of folic acid.
Food intolerance and celiac disease
Another way the immune system can be tweaked to reject the fetus, it seems, is as collateraldamage when an immune reaction is induced by certain foods, particularly by a sensitiv-ity to gluten, as found in celiac disease. Difficulties getting pregnant or miscarrying repeat-edly can be the first symptoms of celiac disease, a disturbance of food absorption caused byan immune-based flattening of the surface folds within the intestine, and often occurringbefore symptoms of gastrointestinal disturbance.
The diagnosis can be screened for using blood tests (serum gliadin antibodies and serumtissue transglutaminase antibodies). If these are positive it is customary to confirm the presenceof celiac disease by performing a biopsy of the lining of the small intestine.
Fetal loss
In practice, a distinction between embryopathy arising after implantation and the loss of afully formed fetus is not always clear. But it helps to understand the things that can gowrong to an otherwise normally developing fetus and what tests can be done.
Cervical incompetence
The most common structural failure of the uterus in containing the pregnancy is a prema-turely opening (or dilating) cervix, called cervical incompetence. It requires careful and repeatedvaginal examinations during pregnancy to exclude it as an imminent cause of miscarriage.Sometimes a shortened, possibly incompetent cervix is seen on transvaginal ultrasound of apregnancy.
Treatment of an incompetent cervix involves placing a ligature or suture in the cervix(a cervical ligature, discussed further in Chapter 9), usually at about 12 weeks’ gestation sothat the suture won’t get in the way of an unrelated early miscarriage, for example from achromosomal cause.
110 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 110

If the incompetence is left untreated, miscarriages due to cervical incompetence tendto occur earlier and earlier (though never before about 14 weeks). Cervical incompetencemight be more common among infertility patients because the number of proceduresthey’ve had done through the cervix could have caused it to weaken. Most gynecologistswill be on the lookout for cervical incompetence in patients who have spent years tryingto get pregnant. Even if the chance (or risk) is low, the penalty for missing the diagnosiswhile it’s still treatable (the hazard) is severe.
Placing a suture or ligature in the cervix for an incompetent cervix is usually not adifficult operation, but if the earlier miscarriages were more of the immature labor varietythan true cervical incompetence, there’s a risk that the irritating presence of the suture inthe cervix, perhaps inevitably with some bacterial organisms,will make the situation worseinstead of better.This is why a rather definite diagnosis of cervical incompetence shouldbe made before a decision to place a suture is reached.At the end of the day it’s a matterof judgment and, in hindsight, it would be unfair to expect your obstetrician always to havebeen correct.
Uterine growth constraints
Abnormal constraint on the growing gestation can lead to miscarriage. Miscarriagescan thus result from abnormalities of the shape of the uterus, abnormalities that caneither result from disease of the uterus (see Chapter 17) or be present from birth (seeChapter 18).
Miscarriages due to a wall dividing the cavity of the uterus into two (a uterine septum)and miscarriages due to a fibroid, or benign tumor of the uterus, encroaching into the cavity(a submucous fibroid) typically happen in the first three months—usually after a fetal hearthas been detected—and are therefore of the postimplantational embryopathy kind.Miscarriages that are due to other birth abnormalities of the uterus, such as a bicornuateuterus or a unicornuate uterus (see Chapter 18), are typically of the premature labor and ‘fetalloss’ variety. Sometimes the run of miscarriages with these sorts of abnormal uterus getslater and later into the pregnancy each time, the uterus adapting more and more to accom-modate the pregnancy, and a viable pregnancy can eventually be expected without specialtreatment being necessary.These abnormalities are looked for before pregnancy with ahysterosalpingogram or by hysteroscopy.Treatment can be directed at the underlying abnor-mality (see Chapters 17 and 18) or at inhibiting contractions of the uterus that would expelthe fetus (see Chapter 9).
Constraint on the growing pregnancy can also come about if the gestation happens toimplant in the outer angle of the uterine cavity, close to where the fallopian tube enters it—this is called an angular pregnancy. If they do not miscarry early, angular pregnancies oftensettle into the cavity proper of the uterus as they grow and cause comparatively little furthertrouble (except perhaps for an increase in the likelihood of experiencing retention of theplacenta after the baby is born). I discuss the diagnosis of angular pregnancy in relation toectopic pregnancy in Chapter 14. Like an ectopic tubal interstitial pregnancy, an angularpregnancy can sometimes rupture the uterus, placing the mother in great danger.
TESTS FOR MISCARRIAGES � 111
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 111

Intrauterine infection
An infection of the fetus leading to miscarriage can happen in four ways: (1) the infectioncan have been there from the start, within the endometrial cavity, in the form of endometri-tis; (2) it can ascend through the cervix when the pregnancy is being established; (3) it canget to the fetus by way of the bloodstream, through the placenta; or (4) it can get there byway of a cervical ligature (posing a dilemma if the diagnosis of cervical incompetence isless than certain).
The most obviously infective or inflammatory cause of miscarriage is when pregnancyoccurs despite the use of an intrauterine contraceptive device, or IUD. Miscarriage is morecommon if the IUD is left in place than if it’s removed as soon as pregnancy is confirmedand before the IUD’s tail disappears into the uterus. If the IUD is left in place, not all preg-nancies miscarry (a majority won’t), but those that do can do so at any stage of gestation.
Endometritis of other infective cause before conception can cause miscarriages inthe same way, inflaming the fetal membranes and causing premature contractions of theuterus.
Once the pregnancy membranes have sealed off the uterine cavity from outside, earlyin the middle three months (or midtrimester), it’s much less common for infective organ-isms to gain entry.But organisms that got in earlier can gain hold, and the more they prolif-erate, and the more the immune system of the fetus matures, the more likely it is thatinflammation must sooner or later start, precipitating contractions and (very) prematuredelivery of the fetus.This is the mechanism behind the majority of ‘labor-like’miscarriages.The bacteria involved tend to be the same as those that are often found in the vaginabetween and during pregnancy, especially if they have been overwhelming the vagina’snormal acidity (called vaginosis).
If the membranes rupture prematurely, infection is sooner or later inevitable, followedby expulsion of the fetus.
The most prominent organisms that regularly reach a fetus by way of the blood-stream through the placenta include certain viruses (rubella—the German measles virus;the attenuated rubella virus used for immunization; cytomegalovirus; herpes zoster—the chickenpox virus; herpes simplex; and, although not considered to be a cause ofmiscarriages, HIV, which causes congenital AIDS). Certain bacteria (tuberculosis; syphilis;brucellosis) and certain parasites (malaria; toxoplasmosis) also cross the placenta to infectthe fetus.
Because blood-borne infections are typically followed by immunity, it’s rare for suchinfections to cause miscarriages repeatedly. Syphilis is an exception. Latent syphilis causesno symptoms but is nonetheless chronic and active, so a serological test for syphilis is a tradi-tional and still standard blood test done in pregnancy, and should especially be done forrecurrent miscarriages that take place in the second trimester. Some of these infections docause birth defects (rubella and syphilis being among the best known). If the infectionsare suspected clinically, prior exposure (and probable immunity) can be determined bymeasuring IgG antibodies in the blood, whereas a recent infection causes a distinguishabletransient rise of IgM antibodies.
112 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 112

How you should act on the information of a recent infection during early pregnancydepends on a number of things: the stage of the pregnancy; the likely involvement of thefetus; the circumstances of the conception; and the risk, not just of transmission ofthe organism to the fetus, but also of the likely severity of fetal damage.
We take the treatment of these conditions further in Chapter 9.
TESTS FOR MISCARRIAGES � 113
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 113

Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 114
This page intentionally left blank

section III
special treatment
treatments matched to what’s wrong
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 115

Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 116
This page intentionally left blank

preventing and treating miscarriage
It depends on the cause,and it’s getting better
Miscarriages are part of nature.But we want to keep them to a minimum. .Putting a stop to miscarriage is all the more imperative if the miscarriage is
taking place after a period of infertility or if it is one of a series (that is, thereis recurrent miscarriage).But let me say that in no area of reproductive medicine is there morecontroversy, over both the likelihood of miscarriages repeating themselves, and whattreatments are truly effective.A bit of good luck in pregnancy outcomes after several disap-pointments can make even charlatans look good.
Miscarriages can come about for genetic reasons, anatomical reasons, hormonal reasons,immune reasons, and from infections. Depending on the cause (and if you have two mis-carriages they might have different causes), interventions can be attempted:• Between pregnancies;• During conception (perhaps making use of IVF);• During implantation and early pregnancy;• During established pregnancy.
TREATMENT BETWEEN PREGNANCIES
In Chapter 8 I wrote that a miscarriage soon after a couple start putting their fertility tothe test is sensibly regarded as just bad luck: it’s reasonable to expect a normal next preg-nancy. A miscarriage after years of infertility, though, might not mean that cure is aroundthe corner.And when one miscarriage follows the other, and then there’s another, the searchfor treatment becomes urgent.
117
9
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 117

A possible cause for recurrent miscarriage (the causes are described in Chapter 8)will be found about half the time, although there’s usually some lingering doubt whetherthe apparent cause diagnosed will turn out to be the actual cause. Keep in mind too thatfew causes of miscarriage operate all the time; and that correcting a diagnosed causedoes not necessarily protect against a miscarriage from a different, incidental cause, suchas an isolated instance of chromosomal embryopathy or an unanticipated case of cervicalincompetence.
Here we examine: (1) antibiotic treatment of infections; (2) treatment of an abnormaluterus; (3) treatment for certain metabolic diseases; (4) immunotherapy; (5) other ‘empiri-cal’ treatment; and (6) supplementing your diet with folic acid before pregnancy.
Antibiotic treatment of infections
The infections most likely to cause miscarriages are those that start to fester in the spacebetween the decidua and the fetal membranes, having gained access to the endometrialcavity before pregnancy or during early pregnancy. Typically they begin to causemischief after about 15 weeks, when the membranes seal off the cervix, eventually result-ing in extreme prematurity (a ‘fetal loss’ kind of miscarriage, or premature labor; seeChapter 8).
The major kinds usually respond to a one-week course of metronidazole (Flagyl) anda tetracycline or erythromycin.
Bacterial vaginosis
A symptomatic vaginal discharge should be investigated and treated if you are trying toconceive.The commonest of these, monilia (or thrush), although irritating, with a some-times copious white, itchy discharge and inflamed vaginal mucosa, seems to be harmless;but it makes intercourse uncomfortable or painful, and can get worse in pregnancy. It is afungus which requires the use of a fungicidal vaginal pessary or cream (your partner shoulduse the cream too, especially under the foreskin).
More important in terms of pregnancy outcome are vaginitis caused by Trichomonas orthe bacterium Gardnerella vaginalis, both being common ‘overgrowths’ of organisms oftenpresent in the vagina overwhelming the physiological acid-producing species that keep thevaginal tissues healthy.They should respond to metronidazole (Flagyl) and to the antibioticclindamycin. Other organisms can also overgrow.
Non-symptomatic upper genital infections
Other bacteria are more silent, including the mycoplasmas Ureaplasma urealyticum andMycoplasma hominis. Sometimes they cause mild chronic endometritis, which might bedetected on premenstrual endometrial biopsy.They usually respond to the antibiotics tetracy-cline and erythromycin.
118 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 118

Surgical treatment of the uterus or fallopian tube
An anomaly or abnormality of the uterus, whether ‘congenital’ (present from birth,Chapter 18) or ‘acquired’ (that is, from a disease or injury, Chapter 17), can sometimes berepaired with a surgical operation.
A uterine septum can be treated by dividing the septum at hysteroscopy (see Chapter 18).A bicornuate uterus causes miscarriages less often; a corrective operation involves a laparotomy(opening of the abdomen) and plastic surgery to the uterus (metroplasty; see Chapter 18).
A submucous fibroid can often also be treated by resecting it at hysteroscopy, whereasmore extensive fibroids extending through the wall of the uterus need more extensivesurgery, involving laparotomy and excising of the fibroids (myomectomy; see Chapter 17).
Intrauterine adhesions can be difficult to treat, even with repeated hysteroscopies, but itis worth persisting until a good cavity of the uterus results (see Chapter 17).
A hydrosalpinx of one fallopian tube, an occasional and vexing cause of miscarriage, isreadily easily overcome by removing the tube (salpingectomy), repairing it with a salpingo-stomy (see Chapter 13), or placing a clip on the tubal isthmus (for more, see the Chapter20 box, Hydrosalpinx: Reintroducing a villain).
Metabolic diseases: Thyroid disease and celiac disease
There are several serious diseases in the mother in which miscarriage is more likely.Examplesinclude diabetes and chronic kidney disease. Generally the disease and its treatment willalready be a major part of the patient’s life.
Three exceptions—examples of a general illness that might first come to light throughcausing miscarriage—are an overactive thyroid gland,or thyrotoxicosis, sensitivity to dietarygluten, causing presymptomatic celiac disease, and a rare inherited disease of copper metab-olism affecting the liver,Wilson’s disease, which can manifest in women in their twentieswith miscarriages before signs of liver disease appear.
In these cases, if specific treatment can bring the disease under control before concep-tion occurs again, the outcome is generally more favorable. Respectively, such treatmentencompasses antithyroid drugs, a gluten-free diet, and a drug that binds spare copper andexcretes it.
Rarely, a dietary deficiency of selenium lies behind miscarriage; it responds to dietarysupplementation.
Immunotherapy: White blood cell inoculation
The analogy between a miscarriage and rejecting a transplanted organ is a strong one. Ifthe analogy is valid, then what they have in common is an overactive immune system.It becomes tempting, even apparently logical, to thwart the immune system somehow, inan attempt to re-set it to a more tolerant level.
One of the most tantalizing hints about possible immunological causes for recurrentmiscarriage has come from the discovery that a proportion of women seem to be successfully
PREVENTING AND TREATING MISCARRIAGE � 119
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 119

treated by being immunized to their partner’s (or to a stranger’s) white blood cells.A numberof studies, including one of our own in the early 1990s,have shown that the effect is strongerthan if the woman’s own white blood cells are used for the inoculation.The way it works isunknown (the NK cells that are presumably the target of the treatment are meant not to haveany immunological memory, so lingering benefits from treatment are hard to explain).Andfor all the controversy surrounding this immune treatment, there seems to be agreement thatit should not be used if anticardiolipin antibodies or the lupus inhibitor are present, as these canbe expected to be made worse. But even if these antibodies are not present the treatmentappears counterintuitive, because it seems designed to increase rather than decrease T cellimmune reactions to pregnancy (for an imaginative, if decade-old rationale, see the box, Alittle rejection).
120 � GETTING PREGNANT
A little rejection?
An ingenious theory was devised in the 1980s to account for the apparent benefitto the risk of miscarriage of immunization with white blood cells from the husband.Not all the facts fit, but for the moment at least let’s not have that stand in the wayof a good story.
It was proposed that if a man and a woman happen to share many of their HLAgroups (the tissue groups that decide the acceptance or rejection of donated kidneys,for example), the pregnant woman’s immune system will not recognize the fetus asbeing different early enough to mount what’s called immune tolerance to it. By thetime the minor immune differences are picked up, it’s too late, and the immuneresponse is one of rejection.
By sensitizing the mother to her partner’s tissue groups—through inoculationwith his white blood cells—her immune surveillance is sharpened, so the theorygoes, so that in a future pregnancy a response will take place more quickly, allowingtolerance to develop and enabling the fetus to survive without rejection.
Attractive though the story is, unfortunately no-one has ever been able to showthat the normal immune barriers of pregnancy breaking down is a common causefor miscarriage. If it happens, it does so without the overwhelming inflammationone sees, for example, in the rejection of a transplanted skin graft or kidney.
Dr Maria Teresa Illeni and her colleagues from Milan, Italy, published perhapsthe best-conducted study so far on immunotherapy for recurrent miscarriage.
Forty-four women with at least three straight miscarriages, all unexplained,entered the study and were either treated or not treated according to (figurativelyspeaking) the toss of a coin. Of the 22 women immunized, 16 became pregnant,and six of them (or 27 percent) miscarried. Of the 22 women who were notimmunized, 14 became pregnant (the difference between 16 and 14 is smalland almost certainly explainable by chance), among whom there were just twomiscarriages!
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 120

Having said that, the prevalent theory today on immune tolerance during pregnancydoes not invoke the ‘learned’ or ‘adaptive’ immune system represented by antibodies andimmunisation, but rather the ‘innate’ immune system of potentially friendly NK cells coop-erating with trophoblast cells, as I describe in the Chapter 4 box,Rejecting rejection:Pregnancyas a coral reef.
During 2001 the US Food and Drug Administration put a stop to white cell inocu-lation as a treatment for recurrent miscarriages in the United States, pending betterdocumentation of its effectiveness.
Other ‘empirical’ treatment
If no cause for miscarriage is found, or if miscarriages persist after a diagnosed ‘cause’ hasbeen treated, there’s much difference of opinion (or perhaps more frustrating,maybe muchlack of opinion) over what to do next.The range of possibilities—called empirical treatmentby some doctors—includes herbal remedies, acupuncture, hormone tablets or injections,and so-called ‘detoxification’ programs—removal of all contact from caffeine, alcohol, junkfood, nightclubs, and so on. Few of these corrections have been properly tested for effec-tiveness (and those that have been tested have generally been found to be wanting). For thebasis for why,historically, just about any treatment for recurrent miscarriage was more effec-tive than doing nothing, see the box, Malpas’s mistake.
I’m not out to persecute herbalists, naturopaths, acupuncturists and faith healers.Theyfill a need, especially when the attention they pay to you comes with compassion andpersonal understanding. Often they seem to have more time than busy family doctors orspecialists to look at the ‘whole you’. It’s just that they—like many gynecologists in thepast—have not put their remedies to the test of properly controlled research studies involv-ing control groups.
Supplements of folic acid
Why take folic acid before you get pregnant? Isn’t a balanced diet enough? In a word, no.And the usual recommended supplement might not be enough either.
First, we know that some cases of major abnormalities of the brain and spinal cord (thatis, anencephaly and spina bifida—the neural tube defects—which occur with an incidence
Based on these results, we can now safely say that treating recurrent miscarriagewith white blood cell inoculations no longer has a justifiable basis. (The US Foodand Drug Administration, or FDA, has reached the same conclusion.)
Incidentally, you might notice from Dr Illeni’s study that considering the wholegroup of 44 women with recurrent miscarriages, 30 became pregnant again, amongwhom just eight miscarried, and 22 were successful in having babies.
So don’t lose hope too quickly.
PREVENTING AND TREATING MISCARRIAGE � 121
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 121

122 � GETTING PREGNANT
Malpas’s mistake
In a proportion of cases,a series of miscarriages will simply be a confluence of bad luck.You can estimate that if a woman has a 10 percent chance of a miscarriage in
her first pregnancy, she’ll have a 10 percent chance of miscarrying a second preg-nancy, and a 1 percent (10 percent of 10 percent) chance of miscarrying the first twopregnancies.The chance of miscarrying the first three, just through bad luck,will be0.1 percent, or 1 in 1000 (rare, but it has to happen to someone).The same calcu-lations for a 40-year-old would give a chance of two miscarriages in a row as4 percent and three in a row of about 1 percent.
In real life the chance of a sequence of miscarriages taking place is higher, becausethere are real and persistent causes of miscarriage added to the chance of a miscar-riage caused simply by the way the odds fall.Truly empirical studies (studies based onobservation,on empirically derived facts) show that the risk after one or more miscar-riages can get high, but it’s rarely 100 percent.
With this as background, I can bring you to appreciate why there’s so muchquackery and witchcraft in the ‘treatment’ of recurrent miscarriage, even publishedin otherwise distinguished medical journals.There are two main reasons.
The first reason is the phenomenon that statisticians call ‘regression to themean’, meaning ‘a tendency for things to move towards the average as experienceaccumulates’.
If, for example, you take 100 couples who’ve had three successive miscarriages,do tests, find nothing especially wrong, then treat them with a special potion derivedfrom beetles’ wings, and then encourage them to conceive again, maybe half willmiscarry a fourth time, but the other half will have a baby.You could be tempted toattribute your success to the magic potion—and use statistics to prove that the miscar-riage rate that’s fallen from 100 percent (in the first three pregnancies) to 50 percent(in the fourth) is statistically significant. But all that’s really happened is that thecouples, who were selected because they had 100 percent miscarriages (ignoringthose who’d had fewer miscarriages and who broke the sequence through chancebefore reaching the number three), in their subsequent pregnancies behaved in theexpected, average way.
The second basis for error dates from 1938,when a statistician,P.Malpas,writingin the Journal of Obstetrics and Gynaecology of the British Empire, drew up a theoreticaltable of the likelihood of one miscarriage following the next, based on arguableassumptions of chance causes and 100 percent recurrent causes.An American, N.J.Eastman, revised the assumptions in 1956, but he reached similar conclusions.Theyended up with the following calculations for the risk of a fourth pregnancy miscar-rying, based respectively on their various assumptions and on an 18 percent first-pregnancy risk of miscarriage (from Malpas) and a 10 percent such risk (fromEastman):
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 122

Chance of next pregnancy according to according tomiscarrying . . . Malpas (1938) Eastman (1956)
after 1 previous miscarriage 22% 13%
after 2 previous miscarriages 38% 37%
after 3 previous miscarriages 73% 84%
For many years, study after study showed (jubilantly) that just about any kind oftreatment would reduce the risk of a further miscarriage quite markedly from thesegrim predictions.Among the more notorious of the drugs for which this claim wasmade was DES (diethylstilbestrol), later held responsible for frequent birth abnormal-ities of the vagina,cervix,uterus, and fallopian tubes in the babies who didn’t miscarry.
Eventually, in 1961,Dorothy Warburton and Clarke Fraser, then from the MontrealChildren’s Hospital,demolished the fallacy in Malpas’s and Eastman’s reasoning,namelythat there is (or was at that time) no evidence that there is an appreciable group ofwomen who throughout their lives have an indelible, 100 percent recurrent cause formiscarrying every pregnancy;rather, they correctly predicted that ‘the gestational processdepends on such a complex interaction between maternal and foetal factors, bothgenetic and environmental, that it must be susceptible to a very large number of agents’.
And the same statistical and Malpasian fallacies dog the reasoning of the naturopaths,herbalists and hypnotists (and so on) who claim to cure repeated miscarriage.
Dr Warburton in 1964, and again in 1979, studied miscarriage histories in womenwho’d had at least one baby. She showed, with her colleagues, that while the risk ofmiscarriage does rise appreciably after every further preceding miscarriage, the riskin fact is nowhere near as high as Malpas and Eastman had predicted in theory.
Still, through the bias she introduced by studying only fertile women (they allhad at least one baby),Warburton’s estimates might be low.The hardest studies to doare those which, instead of looking back at reproductive histories (retrospectivestudies), start by locating couples before they get pregnant and follow them up tosee what happens (prospective studies). Malcolm Macnaughton, from Aberdeen inScotland, was the first to do such a study.
Warburton’s and Macnaughton’s findings are set out below and serve as the bestguides we have to the true chance of miscarrying a further pregnancy after one ormore previous miscarriages. Note that these figures refer to clinical miscarriages, notsubclinical miscarriages or to so-called biochemical pregnancies (see Chapter 8 for moreon the distinction).
Chance of next pregnancy according to Warburton according tomiscarrying . . . (if you’ve previously had a baby) Macnaughton
(if no previous baby)
after 1 previous miscarriage 23% 20%
after 2 previous miscarriages 28% 44%
after 3 previous miscarriages 33% 58%
PREVENTING AND TREATING MISCARRIAGE � 123
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 123

of between one and five per thousand births) can come about because of a deficiency of folicacid in the diet, and can be protected against by taking folic acid at the time of conception.
Second, we know that women who’ve had a baby with such a neural defect are muchmore likely than other women to have had a miscarriage before. It’s therefore possible thatat least one kind of miscarriage actually represents an even grosser failure of developmentof the embryo than spina bifida or anencephaly, and could result from the same deficiency.
Thirdly, one group of women has an abnormal gene for an enzyme called methylte-trahydrofolate reductase, or MTHFR, which is needed to produce methylfolate, essentialfor amino acid metabolism. If you have the MTHFR C677T polymorphism, especially if youhave two copies (you are homozygous, not just heterozygous, for it, or have an increase inserum homocysteine), you may need 5 mg of folic acid a day or more to avoid an increasedrisk of pregnancy loss, neural tube defects and also thrombosis.This is 10 times the previ-ously recommended supplement.
Because deficiency of folic acid remains common in our society, and because taking folicacid supplements does no harm and is cheap, it’s reasonable to recommend 5 mg a day to allwomen attempting to get pregnant, including women who’ve had one or more miscarriages.
TREATMENT DURING CONCEPTION
Often the same reproductive disorder that causes infertility lies behind miscarriage whenconception does, by chance, happen. Medically, there’s no sharp distinction between notconceiving, and conceiving and miscarrying: managing the infertility properly can put anend to such miscarriages and lead to a healthy baby. In other circumstances there are specialopportunities for treating recurrent miscarriage with assisted conception maneuvers suchas IVF and even gestational surrogacy.
These figures provide guides for you, the reader, and for me, the explainer; buteven these data are not reliable enough for scientific studies of treatments.
What investigators should try to do is to divide couples randomly into twogroups, avoiding other variables like age and occupation that can cause bias, thentreat one group with the new potion or remedy and not treat the other group (thecontrol group).We can all then be convinced if there’s a difference in outcome betweenthe two groups.
Such controlled trials are difficult to mount and to pursue (and of course theymust have the approval of a human research ethics committee), but they have to be doneif we are to overcome quackery.They may seem unfair, in that half the couples don’tget the supposed benefit being tested, but in practice you would be surprised howoften the people in the control group end up doing better than people in the specif-ically treated group. Properly controlled trials have not shown, for example, thatinjections of human chorionic gonadotropin (hCG), still a part of some doctors’ prescrib-ing practice for prevention of recurrent miscarriage, are effective.
124 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 124

In this section we thus consider: (1) infertility and miscarriages (including ovulationinduction for defective ovulation, or luteal phase defects); (2) IVF with preimplantationgenetic diagnosis (for balanced chromosomal translocations and other reasons); and occa-sionally (3) IVF with egg donation or gestational surrogacy.
Infertility and miscarriages
The miscarriages common in infertility situations are usually early, including those dueto high concentrations of abnormal sperm (for treatment see Chapter 10), disorders ofovulation (see below), disease of the fallopian tubes (see Chapter 13) and, possibly,endometriosis (see Chapters 15 and 16).The best approach in these situations is to makean accurate diagnosis and then to carry out specific treatment, ensuring the best possiblestart to the pregnancy. Such treatment can include formal assisted conception with IVF(see Chapter 20).
Miscarriage is particularly common in women with defective ovulation, manifestingusually as oligomenorrhea and perhaps as a so-called luteal phase defect (in reality more of adeficiency of the follicular phase, as discussed further in Chapter 7).The ovulatory disordermost associated with miscarriage is undoubtedly the polycystic ovary syndrome, or PCOS. Itstreatment with metformin and clomiphene is discussed in Chapter 11. In more severe cases,when follicle stimulating hormone is needed, it is nowadays common to recommend IVF,bothto enable full maturation of the follicles without risking atresia and to avoid undue risk ofhigh multiple pregnancy (by limiting the numbers of embryos placed in the uterus).
IVF with preimplantation genetic diagnosis
Balanced chromosomal translocations
Nothing can be done to treat abnormalities of the chromosomes found by doing akaryotype on the prospective mother and father, of course. But if either partner carriesa balanced chromosomal translocation, there should, first, be a measure of reassurancethat not every pregnancy or embryo will have unbalanced chromosomes and bedoomed.
You need a lot of fortitude, though, to press on with successive pregnancies until, bychance,one is either genetically normal or has balanced chromosomes, and survives. (Indeed,the miscarriage rate can be much higher than the 50 percent rate you might at first expect—see the Chapter 8 box,Unbalancing translocations.) Should a pregnancy continue, the questioninevitably arises as to whether the chromosomes of the fetus should be looked at.The usualprocedures for this, chorionic villus sampling (CVS) and amniocentesis, themselves carry a smallrisk of causing miscarriage.
Today, in advanced IVF programs, many cases of balanced translocations are beingmanaged with preimplantation genetic diagnosis, or PGD. Embryos produced by IVF aresampled for one or more cells, which are then stained with specially selected FISH probes
PREVENTING AND TREATING MISCARRIAGE � 125
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 125

that can distinguish normal or balanced embryos on the one hand from unbalanced (hencedestined to miscarry) embryos on the other.The details are in Chapter 20.
Other miscarriage-based reasons for IVF and PGD
The most obvious reasons for invoking IVF in the treatment of recurrent miscarriage areto overcome an ovulation disorder requiring FSH therapy while avoiding multiple preg-nancy and to use PGD to safeguard against an unbalanced chromosomal translocation (aswe see above), but other reasons are also emerging.
First, no-one who is getting pregnant is safe from a miscarriage caused by a chromo-somal aneuploidy or polyploidy, events that, while sporadic, are numerically the major causeof miscarriage in younger and older women.The advent of molecular karyotyping (see theChapter 20 box, IVF-Plus™: Chromosome-checked embryos), in which all 24 chromosomesare counted, means that this major cause of miscarriage can be prevented from spoiling apregnancy for couples suffering from recurrent miscarriage generally, as well as improvingthe chance of a good outcome in couples intending to have special treatment to preventmiscarriage, such as heparin or corticosteroid therapy,which can have side-effects that haveto be weighed up against the likely benefit. IVF here increases the likelihood of the benefit.
Second, as we get to understand more about the genetic polymorphisms that affect thechance of pregnancy being successful, the more helpful it will be to select embryos thathappen to have polymorphisms most resistant to miscarriage (for more, see the Chapter 4box, The ‘ABCDEFG’ of tissue groups . . .’ )
The occasional need for egg donation or gestational surrogacy
Unfortunately, there may be a maternal genetic cause for the occasional long, unremittingsequence of miscarriages for which no chromosomal cause is obvious.There are severalpossibilities, affecting either the eggs or the uterus.
First, there could be an abnormality of the egg’s mitochondria (the little power-housesthat generate any cell’s energy), either through a mutation or set of mutations that occurredin the prospective mother’s cells when she was herself just an embryo—before her ovariesbecame populated by the eggs carrying the mutant mitochondrial DNA (mtDNA)—oraccumulating among the older eggs as the mother reached her late thirties and her forties(for more, see the Chapter 7 box, How eggs might get their ‘use-by’ date: Mishaps in the mito-chondria).This circumstance, if we could be sure of the diagnosis for a particular woman’smiscarriages, might lend itself to treatment with donated eggs (discussed in Chapter 22) orthe still experimental technique of cytoplasmic transfer, in which mitochondria are trans-fused from a normal egg to the older abnormal egg (discussed in Chapter 23).
Second, although we cannot yet usually prove it, there are surely instances of ‘doubledoses’ of rare mutations that affect some key molecule in the uterus needed for implantationto be successful. (Some,but not all,of these can be suspected by persistently inadequate deciduadespite more than adequate progesterone on premenstrual endometrial biopsy.) In such cases,at least until we know how we might replace a missing factor deep inside the uterus, the only
126 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 126

treatment might be to consider a relative or a good friend carrying the pregnancy and havingthe baby—gestational surrogacy.The same might apply in cases of persistently hostilematernal immune systems.
TREATMENT DURING IMPLANTATION AND EARLY PREGNANCY
There is probably no area of miscarriage management more controversial and unsettledthan that of attempting to alter the blood coagulation system or the immune system toprevent early (and even late) miscarriages.We look here at the pros and cons of low-doseaspirin, heparin (an anticoagulant), corticosteroid drugs such as prednisone, immunother-apy using gamma globulin infusions, and vaginally administered progesterone.We also lookat having a curette if miscarriage is inevitable.
Clearly a pregnancy that has an abnormal karyotype is beyond help, but in women whohave had many early miscarriages, repeated testing has generally revealed karyotypes thathave been monotonously normal.
It is still rare that specific treatment can be matched to a confident diagnosis.Whereone doctor or clinic might suggest one treatment for a particular set of test results, a seconddoctor or clinic will recommend another, and a third doctor might be adamant that noneof these measures will make any difference. But at a minimum, if we can relieve some ofyour stress and anxiety, this in itself can improve the balance of your immune system.
Historically, as mentioned before,much dodgy treatment has been invoked in the nameof treatment of early recurrent miscarriage. If you haven’t read the box Malpas’s mistake yet,now would be a good time.The studies on which the following treatments are consideredhave generally avoided his error.
Low-dose aspirin
For a drug that’s been in use for a hundred years, aspirin in ‘mini’ doses has been accumu-lating a heap of accolades: stroke and heart attack prevention, reduced risk of colon cancer,delaying the onset of Alzheimer’s dementia—the list goes on.And on top of that, it’s cheap,and you don’t need a doctor’s prescription. But does it work for miscarriage?
Although widely used for miscarriage prevention when anticardiolipin antibodies arepresent (and sometimes even to improve IVF results irrespective of antibodies), there is nogood evidence that aspirin is beneficial.
In an authoritative review of trials performed with an adequate control group,Dr MarianneEmpson, from the Clinical Immunology Service at Auckland Hospital,New Zealand,workedwith the international Cochrane database of clinical trials to make critical comparisons anddraw systematic conclusions.There were three well-carried-out trials involving aspirin (dose:50–80 mg per day), the larger two of which, from Helsinki, Finland, and Auckland, NewZealand, studied women who had had between three and eight miscarriages.Aspirin washelpful in none of the trials. It made no difference whether antiphospholipid antibodies suchas anticardiolipin antibodies were present or not. In fact, in both the larger studies there was aslight (but not statistically significant) increase in risk of another miscarriage if aspirin was used.
PREVENTING AND TREATING MISCARRIAGE � 127
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 127

I would speculate that aspirin could interfere with some molecular adhesion eventsimportant to early pregnancy. Otherwise the main risk with aspirin is gastric bleeding insensitive individuals.
Heparin
Heparin is a carbohydrate-rich anticoagulant that has almost as many uses as aspirin. It isgiven as injections under the skin.
In low dosage its molecules coat blood cells and blood vessels to make the blood more‘slippery’. In the usual therapeutic doses it interrupts blood coagulation, and so is the usual firstline of treatment to prevent thrombosis when there is a high risk of it. In fact, it makes senseto use it when the lupus anticoagulant is present (despite both the lupus inhibitor and heparinhaving ‘anticoagulant’ effects), as there is a significant risk of thrombosis in this condition.
Its credentials in miscarriage prevention are stronger than those of aspirin.But it requiresdaily or twice-daily injection and there is a risk of potentially serious side-effects, so itscredentials had better be good!
Regrettably, and probably spuriously, aspirin had already attracted considerable popu-larity as a gentle anticoagulant in its own right at the time the heparin trials were done.Typically, therefore, aspirin was used with heparin, which was then compared with aspirinalone.This was the case in each of the four studies in Dr Empson’s review.And in each ofthe four studies, heparin with aspirin was superior to aspirin alone, actually halving thenumber of miscarriages (a result that was highly statistically significant)—but unfortunatelywe cannot know how much better heparin, even in low dosage, might be than no therapy.
The side-effects of heparin, in addition to accidental or spontaneous bleeding, espe-cially at the injection sites, include a loss of some calcium from the bones during pregnancyand, rarely, a potentially serious depletion of blood platelets and kidney or liver failure.
When to use it? Certainly if the lupus anticoagulant is detected, and especially if therehas been thrombosis (together known as the antiphospholipid syndrome).The jury is stillundecided in cases where there is no history of thrombosis, and either there are low ordisputed levels of anticardiolipin antibody or one of the thrombophilias has been diagnosed.
Corticosteroid drugs
Cortisone-like drugs, including prednisone or prednisolone, are commonly used in medicineto suppress the immune system, so they jump to mind when immune rejection is blamedfor miscarriage.
In Chapter 4, I suggest that, in fact, the specific immune system rarely gets partic-ularly fussed by the so-called foreign graft a pregnancy represents, at least until a miscar-riage is well and truly underway.The component of the immune system most involvedin dealing with pregnancy is the innate immune system (the NK cells) and they areimportant in proactive ways—they should not be discouraged by immunosuppression.
The temptation to use prednisone is strongest when high levels of antibodies such as anti-cardiolipin and other antiphospholipid antibodies are present.But there is no evidence-based
128 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 128

support for any benefit. In the two properly conducted studies reviewed by Dr Empson, notonly did the prednisone not reduce the risk of miscarriage significantly, in each of them pred-nisone (regrettably used in conjunction with aspirin, again) increased the risk of prematurelabor from 12 percent to over 60 percent, and also increased the risks of high blood pressureand diabetes in late pregnancy.
Immune gamma globulin infusions
The last drug Dr Empson considered in her review was (and is) the most controversial:gamma globulin (read: ‘antibodies’) pooled from the blood of an enormous number ofdonors, but there were too few well-done studies for her to reach a firm conclusion.
How such immunotherapy might benefit pregnancy is conjectural.The therapeuticeffects reflect the functions of natural antibodies in healthy people,which probably includesstopping the immune T cells and the unfriendly NK cells from making as many hostilemolecules. But it is not known if the friendly NK cells might also be compromised.
Published results (mostly from enthusiasts) have at best been mixed.These infusions areextremely expensive. Blood products carry a small risk of hepatitis C and perhaps otherviral infections.
Vaginal progesterone
Progesterone is the hormone of pregnancy in all mammals.No pregnancy can survive withoutit, as I describe in Chapter 4. Moreover, in human pregnancy, it is made not in the ovariesbut right next to where it is doing its work: at the interface between fetal trophoblast andmaternal decidua.
As it turns out, progesterone has beneficial effects not just in keeping the uterus quiet;it also directly and potently suppresses the immune cells responsible for rejection (one ofthe aims of using corticosteroid drugs, just discussed), while at the same time promotingthe friendly NK cells, promoting the travelling extravillous trophoblast cells responsible forconversion of the maternal arteries feeding the placenta, and inhibiting the sequence ofinflammatory events that precede the muscle contractions in the uterus that push out thepregnancy. It’s indeed a good hormone to have plenty of.
Surprisingly, the most recent review of controlled trials involving progesterone treat-ment in early pregnancy in comparison with placebo treatment (to account for theundoubted benefit emotional support itself has in pregnancy outcome) was published wayback in 1989. Combining the figures from the only three well-done studies indicated apossible three-fold improvement in outcome after previous recurrent miscarriage.
On the other hand, studies on synthetic progestogens, usually taken as tablets by mouthfor other purposes, are less convincing—and some progestogens,particularly those that eithermimic or block the male hormone testosterone,have harmful effects on the developing fetus.
It is certainly high time for progesterone supplementation to be re-examined. Naturalprogesterone is available for use vaginally (needed to get high doses directly into the uterus)as pessaries or vaginal gel (for example, Crinone) and there is little downside to using it.
PREVENTING AND TREATING MISCARRIAGE � 129
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 129

Inevitable miscarriage: A curette, or let nature take its course?
Can we stop an early miscarriage once pregnancy is underway, or even once the first signsof miscarriage are present? The very great majority of early miscarriages are doomed fromconception or soon after. If a transvaginal ultrasound reveals a gestation with a slow orabsent fetal heart beat, and a reduced size compared with expected dates (illustrated inFigure 4.3), miscarriage is as inevitable as it would be if bleeding and an opening cervixwere present.
By the time a miscarriage threatens, especially in the first trimester, almost always thedie is well and truly cast and nothing—including hormone injections—will make a differ-ence to the outcome.The ‘ovum’ (for which, nowadays, read ‘embryo’) is ‘blighted’; typi-cally the trophoblast and gestational sac will develop but the embryo itself will not—there willbe no fetal heart beat, or it will be present only transiently.As we can read in Chapter 8,none of this tells us anything about the reason the pregnancy has gone awry, because manydifferent causes produce the all too common picture of such a blighted ovum. Once thesymptoms and signs of an inevitable miscarriage become apparent, it’s for the subsequentpregnancy that we can hope there will be a difference.
If getting pregnant has been difficult, however, or if this yet another miscarriage, thenbefore the miscarriage is over it will be important to obtain living placental tissue for akaryotype.The reason for getting a karyotype is to know if this miscarriage had to happen—that, whatever has come before, at least this miscarriage might have had a one-off cause.
Usually, getting a karyotype means having a curette before the miscarriage tissue isexpelled from the uterus naturally, because, by the time nature eventually pushes the preg-nancy out, the cells it contains that are still alive might be too few to enable a cell cultureto be set up to perform the karyotype. Having a curette is also useful for the pathologistto look for the implantation site among the curettings, to identify the activity of thetrophoblast within the decidua, and perhaps to characterize what kinds of white blood cells(NK cells,T cells, or inflammatory cells) have gathered around or within the pregnancytissues during the expulsion.
Having said this, there are many miscarriages where this information is not impor-tant. Whereas it was once considered necessary to have a curettage for a miscarriage(because of a risk otherwise of tissue being left behind or getting stuck, with suddenbleeding or a later infection), provided they are close to good medical care more womenare today choosing to let nature take its course.This enables you to come to terms withthe disappointment and grief more gradually, perhaps avoiding the heightened sense ofloss that may come from literally being pregnant one day and the next day, after a suddencurette, to seem to be left acutely with nothing. Discuss this option with your doctorbefore deciding.
TREATMENT DURING ESTABLISHED PREGNANCY
Envisage that the stage has been set, that your pregnancy appears completely normal on atransvaginal ultrasound scan carried out in the first three months.You have got through the
130 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 130

main danger time and while miscarriage is now uncommon there are several causes ofmiscarriage that can still bite.
The causes of miscarriage that operate during the middle three months (themidtrimester) include: (1) structural weakness of the cervix, or cervical incompetence; (2) irri-tability of the uterus (usually from a previously silent infection) precipitating premature labor;and (3) death of the fetus from a poor blood supply to the placenta, produced by increasedcoagulability of the mother’s blood and/or an inappropriate immune reaction in theplacenta.
Cervical weakness or incompetence
Very few symptoms herald the disaster of fetal loss from cervical incompetence. By thetime the woman notices a low ache in the back (common in pregnancy) and an increasein vaginal discharge (it can happen anyhow in pregnancy, but beware a sudden change),typically the membranes of the gestational sac are already bulging through a dilated cervix,and their rupture is not far off.As the waters break with a gush, the fetus almost falls out,with little in the way of contraction pains and little bleeding. Even if you can get to yourdoctor before the membranes break, and a valiant effort is made to tuck them backthrough the cervix before tying an urgently attempted cervical ligature, the membraneshave activated certain protein-destroying enzymes and are likely to give way within afew days.
Early diagnosis of cervical incompetence, in time to place a suture, depends on timelyexaminations of the cervix in women at risk of it (including previously infertile womenwho have had procedures done that could have weakened the cervix).More often the diag-nosis is made because previous pregnancies have been lost this way.
Treatment then consists of inserting a ligature or suture around the upper part ofthe cervix (the potential birth canal) at the end of the first three months of pregnancy,giving it support (a ‘stitch in time’).The operation is relatively simple, being performedthrough the vagina. The reason for this timing is two-fold: first, the gestational sacdoes not put pressure on the cervix until after 12 weeks of pregnancy; and, second,during the first three months many pregnancies miscarry for other reasons (especiallyan abnormal karyotype, see Chapter 8), and unless we wait for these to have happeneda suture placed too early in pregnancy might need urgently to be removed to avoida mess.
Occasionally the cervix has been so weakened that getting a ligature in place right up atthe top of what remains of it requires an abdominal operation. It is then typically inserted notduring pregnancy but before pregnancy takes place, taking into account the chance that itmight need to be removed in a hurry if an early miscarriage happens from another cause.
Uterine irritability and immature labor
Immature labor is like premature labor, but with a pre-viable fetus. (The absolute earliest afetus might survive early birth is now around 24 weeks,utilizing the most advanced neonatal
PREVENTING AND TREATING MISCARRIAGE � 131
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 131

intensive care facilities, but the mortality rate is significant and, in some ways worse, therisk of brain damage among survivors is high.)
The symptoms are those of a ‘mini-labor’.Painful uterine contractions occur,not neces-sarily very regularly,pushing the fetus against a slowly dilating cervix, generally with bleeding(because the placenta at these early stages very often still extends down into the region ofthe cervix).Unless this is the final pathway of a more fundamental cause for the midtrimestermiscarriage (see below), the fetus is usually normal at the start of the contractions, butsuccumbs during the labor, probably because the immature placenta is easily squashed ortorn loose.
For this reason there can be a real dilemma present if the fetus is between 23 and27 weeks and labor starts. Do you have a cesarean section to protect the fetus as muchas possible from trauma and a likely lack of oxygen during the labor, but hazard not justthe operation but also a brain-damaged infant after hugely expensive neonatal intensivecare? Or do you let nature take its course? This is a decision that you should make inclose consultation with the doctors available to you who will be looking after a surviv-ing baby.
Can the process be prevented or stopped? If ultrasound reveals the fetus to be normaland apparently healthy, sometimes the contractions of the uterus can be treated early enoughand vigorously enough to make a difference to the outcome.The drugs used include:(1) progesterone-like drugs such as 17-hydroxyprogesterone caproate, given as twice-weeklyinjections of Proluton Depot (Australia,UK) or Delalutin (USA); (2) prostaglandin-blockingdrugs such as the NSAIDs aspirin, mefanamic acid (Ponstan), indomethacin (Indocid), andchlorpromazine (Largactil); and (3) inhibitors of uterine muscle contractions such as salbu-tamol (USA: salbutarol;Ventolin). Many of these drugs have important side-effects for themother, the fetus, or both.
Even though an underlying infection is common, treatment with antibiotics at this latestage rarely helps, unfortunately.As described earlier, antibiotics for vaginosis, symptomaticor not, should be given before pregnancy or before the end of the first trimester.
Note also that the loss of a pregnancy this way can also be the first indication that thereis a congenital abnormality of the uterus present (see Chapter 8), such as a bicornuate uterus thatmight benefit from a corrective operation (see Chapter 18).
Fetal death in utero
In this group of situations a primarily normal fetus dies because the circulation in theplacenta fails.This can be because the mother’s blood coagulation system is too active (shemight suffer from an inherited thrombophilia) or because the immune system is too active(for example, she has the lupus anticoagulant or a significant antiphospholipid or anticar-diolipin antibody), which in turn activates the coagulation system.
In either case, the trouble is likely to have started when the placenta was beingformed, when incorrectly clotting blood plasma at the interface between implantingembryo and mother resulted in a faulty framework for the placenta to build on. In
132 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 132

technical terms, the extravillous trophoblast was deficient in converting the mother’sarteries to high volume, low resistance vessels, capable of delivering plenty of blood tothe intervillous space.
Preventative treatment, to have a chance of success, would have to be started early inpregnancy, while the placenta was still forming.
PREVENTING AND TREATING MISCARRIAGE � 133
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 133

a low sperm count
Treatment for men
Millions of sperm cells are ejaculated, yet just one’s needed to make it to the egg.That’s the way it needs to be, for a good chance of getting pregnant naturally. .
Here we look at the causes of:• No sperm at all, or azoospermia;• Reduced sperm, or oligospermia; and• Immunity to sperm, or sperm antibodies,and at treatment, particularly:• male-directed treatment, which is only occasionally fruitful; and• female-directed treatment, or assisted conception, particularly intrauterine insemination
(IUI) and sperm recovery procedures from men for in vitro fertilization using micro-epididymal sperm aspiration (MESA) and testicular sperm extraction (TESE).
The use of donated sperm for assisted insemination,or donor insemination (DI)—the ultimatefall-back for overcoming male infertility—is discussed in Chapter 22.
For a guide to a bunch of possibly new words, see the box, Sperm terms.
NO SPERM: AZOOSPERMIA
There are two main reasons and a minor one why sperm cells can be missing from the semen.The main reasons are either a failure of sperm production and release in the male sex
organs, the testes, or an obstruction in the male genital ducts that lead on each side fromthe testis to the penis, including the epididymis and the vas deferens.The least common reasonfor most of the sperm being missing is retrograde ejaculation.
The way to be sure of what’s happening is to measure a serum FSH,which if it’s increasedmeans for sure that sperm production is a problem (see the box, Follicle stimulating hormone,in men?), although normal levels do not rule out production problems.
134
10
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 134

A LOW SPERM COUNT � 135
Sperm terms
It’s useful to understand a few special terms properly.Semen refers to the milky fluid emitted at ejaculation, with male orgasm.The sperm cells account for only about 1 percent of the volume of the semen, so
there’s absolutely no way of knowing whether sperm are present in the semen unlessa microscope is used to examine the semen after a specimen is collected (essentiallya sperm count) or, if your partner is shy, your doctor examines your cervical mucus aftersexual intercourse (a postcoital test).
An inability to reach orgasm and thus to ejaculate is called impotence, and usuallymanifests in conjunction with an inability to obtain, or to sustain, erection of thepenis with sexual excitement.
In some diseases that affect nerves, including some cases of diabetes, ejaculationcan occur backwards, up into the urine lying in the bladder, instead of out the tipof the penis; this is called retrograde ejaculation.
Aspermia means that there’s no ejaculate with orgasm, usually indicatingmalfunction of the glands that provide the seminal fluid, the prostate and the seminalvesicles.
Spermatogenesis is the complete production line from dividing stem cells in thetubules of the testis (the spermatogonia), through the phases of meiosis, namely sper-matocytes and the spermatids, to mature, released sperm cells, or spermatozoa. Its durationis about two months.
Spermiogenesis is the last section of spermatogenesis, the remodelling process thatturns a round spermatid, already haploid, into an elongated swimming machine, thespermatozoon. It takes about two weeks.
When we perform a sperm count (the details are in Chapter 5), the result will beone of three:• It’s normal;• One or more parameters are below normal, loosely called oligospermia and
meaning not enough normal swimming sperm; or• No sperm are present at all—azoospermia.The technical term for having sperm with decreased average swimming ability, ormotility, is asthenozoospermia.
The technical term for having sperm with poor average appearance,or morphol-ogy, is teratozoospermia.
And if you have all three (decreased count, decreased motility and increasedabnormal forms) you therefore have . . . well, work it out for yourself. Because allthree often go together I lump them all into oligospermia.
An apparently normal sperm count does not always rule out a male contribu-tion to infertility.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 135

No sperm production
Sperm cells are nurtured to maturity in the tubules of the testis (the testicular tubules).These tubules are lined by Sertoli cells, which envelop the immature sperm cells, providingthem with the nutrition they need to develop.
Complete absence of sperm cells is surprisingly uncommon, but it does happen with,for example, errors of the chromosomes, such as with Klinefelter syndrome.The diagnosis of‘Sertoli-cell-only’ can be revealed by a biopsy of the testis (although there’s no need for this testif a karyotype shows the abnormality of Klinefelter,namely 47,XXY—an extra X-chromosome).
A more common difficulty in the tubules is when there are sperm cells present, buttheir numbers are reduced and most of those that are there don’t complete their develop-ment into mature sperm. About 1 million virtually mature sperm must be released fromthe tubules each day before sperm become detectable at all in the sperm count!
The serum FSH can be increased, although a late-stage arrest in the sperm’s development(maturation arrest) can show a normal serum FSH.A testicular biopsy is needed to define thediagnosis, but it might still miss some pockets of sperm production that could be enough toenable sperm cell recovery for assisted conception.Why some men have a maturation arrest hasbeen under active investigation for years.The causes in general seem to be the same as manyof those that result in less complete sperm-forming problems (see Oligospermia, further on).
If there’s a genetic cause for lowish sperm counts (see the box, Nature’s genes are callous,for why genetic causes of infertility evolve), then a random, unfortunate combination ofthe genes on a variety of chromosomes responsible for limiting sperm counts could produceazoospermia.These genetic causes are not yet able to be characterized, but because inher-itance is recessive they will rarely be passed on in severe degree.
A group of genetic causes on the Y-chromosome, however, can be detected withDNA tests, or PCR, and should be looked for. If assisted conception is successful theywill be passed on to every male offspring. For more, see the box, Microdeletions in theY-chromosome.
136 � GETTING PREGNANT
Follicle stimulating hormone, in men?
FSH is the hormone women make to stimulate follicles in the ovary (see Chapter 3for the details), from which it derives its name. FSH is just as important in men.
In women, the follicle cells nurture the developing egg. In men, it’s the Sertoli cellsthat nurture the sperm, and the same hormone, FSH, does the job.
Just as in women the serum FSH goes up when there are few or no eggs left inthe ovaries, so in men the serum FSH goes up when mature sperm are not beingproduced in the testis.
A high serum FSH in the absence of sperm in the ejaculate means that theproblem is substantial testicular damage and thus is not likely to be a blockage (or ifa blockage is present it’s not the only problem).
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 136

A shortage of follicle stimulating hormone, the testicles’ driving hormone in the pituitarygland (and a common cause of absent ovulation in women), is rare, though important todiagnose. It can be inherited or acquired. For more, see the box,FSH deficiency in men is rarebut important.
Maturation arrest and Sertoli-cell-only pathology can also be the result of radiationtreatment or drug treatment (chemotherapy) for cancer.Other environmental factors moreoften produce oligospermia and are discussed below.
Sperm obstruction
Obstructions lying between the testis and the urethra, which carries semen down thepenis at ejaculation, can be congenital (present before birth) or acquired later, mostcommonly through infection or surgery. Congenital forms of epididymal and vas deferens
A LOW SPERM COUNT � 137
Nature’s genes are callous
Why would nature allow inherited causes of oligospermia to gain ground whennature’s aim in evolution, on the face of it, ought to be to maximize reproductivepower?
I discuss this paradox in Chapter 2, where I show that there are advantages tothe species generally for reproduction to be limited.This limiting of fertility is moreimportant as couples get older,when they still enjoy,or perhaps require, sexual inter-course for their continued bonding, yet have children who need looking after.
While they depend on their mother, these children must not have her worn outthrough repeated bearing of more children, or have the bad luck to succumb froman obstetric accident during another childbirth; without a mother, there’s the riskthat none will survive to achieve sexual maturity and independence.
Remember that it’s not until your children grow up and themselves conceivethat you can truly say that you’ve successfully reproduced—that your genetic legacyhas been passed on.
So, nature will favor a sprinkling of genes that decrease fertility short of steril-ity, especially ones that operate as a couple gets a bit older.
And when by chance these same genes combine from two parents in a doubledose in an occasional hapless offspring—producing, say, severe oligospermia orazoospermia, unsympathetic nature regards it as a small price to pay.
Likewise, a couple can by chance be overdosed with infertility genes, for examplewhen a man with mild endometriosis is mating with a woman with mildendometriosis.
I deal further with the arithmetic in Appendix 1.Our purpose in reproductive medicine—as in medicine generally—is to soften
or reverse the personal effects of nature’s shortcomings and excesses.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 137

obstruction can arise genetically or through exposure to teratogens during fetaldevelopment.
Men with CBAVD (congenital bilateral absence of the vasa deferentia) can be carriers of oneor more genes for cystic fibrosis, a devastating disease of the lungs in children who inherit agene for it from both parents.They and their wives (female carriers are symptom free)should therefore be screened for the commonest and most serious alleles by DNA PCRtesting before a decision is made to have IVF.
Teratogenic causes of epididymal anomalies include exposure to environmental ormedically administered estrogens.The most notorious has been fetal exposure to diethyl-stilbestrol (DES), which was taken by many women in the 1950s and 1960s in an attemptto stop miscarriage, and which also caused reproductive anomalies in women.
Another situation known to have given rise to obstruction, from exposure duringinfancy, has an association with chronic bronchitis and sinusitis, and is known asYoung syndrome—probably a poisonous effect of the mercury formerly used in teeth-ing powders and, since mercury was removed from these products around 1960,getting rarer.
Absent or retrograde ejaculation
Absent ejaculation or backwards-directed, retrograde ejaculation can occur after spinal cordinjury (paraplegia) and after surgery to the bladder or prostate, as well as with diabetes.Thediagnosis is made by finding sperm in a sample of urine passed after orgasm in sexual inter-course or masturbation.
With absent ejaculation, sperm for use with assisted conception, including assistedinsemination, can be obtained by electroejaculation (whereby an electrical stimulus appliedunder anesthesia using a special probe is passed through the anus into the region of theprostate gland).
138 � GETTING PREGNANT
Microdeletions in the Y-chromosome
A number of the genes needed for sperm to form normally are located on theY-chromosome. If these genes are deleted in whole or part, they result in azoosper-mia (and so are referred to as DAZ genes, for ‘deleted in azoospermia’).
The Y-chromosome is susceptible to small deletions.These ‘microdeletions’ aretoo small to be seen on a karyotype: they require a DNA test such as a polymerase chainreaction, or PCR test, which (like a karyotype) is done on the man’s blood cells.
A microdeletion of the Y-chromosome is virtually certain to be passed on if thereare residual sperm cells in the testis suitable for TESE and ICSI—and means that amale offspring will have the same sterility.
Either this fact is accepted by the couple or preimplantation genetic diagnosis is usedto select for transfer only embryos that are 46,XX—in order to have a daughter.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 138

With retrograde ejaculation, sperm cells can be recovered from the urine, ‘washed’,concentrated, and then used for assisted insemination or for in vitro fertilization. If this is tobe done, the urine should first be de-acidified (rendered alkaline) in the body by taking atablespoon of baking soda dissolved in a small glass of water on three occasions over the24 hours before obtaining the specimen.
A LOW SPERM COUNT � 139
FSH deficiency in men is rare but important
In about one in 200 cases of male infertility, the testes are inactive because of a defi-ciency of FSH and LH from the pituitary gland (just as, much more frequently, thisdeficiency causes anovulation in women).
As well as inhibiting the maturing of sperm, such a deficiency causes the othermain tissue in the testes—the Leydig cells,which produce the male sex hormone testos-terone—to be inactive,which means the male sex characters are stopped from formingor from being maintained.
If the deficiency is present from birth or from childhood,puberty fails to happennormally.
If it’s acquired after puberty, there’ll be less of a need for shaving and, gradually,impotence or loss of sexual desire will follow.The abnormality is diagnosed by findinglow levels of serum FSH, serum LH and serum testosterone.
A deficiency of FSH and LH in men, as in women, may in turn be because ofa deficiency of the gonadotropin releasing hormone (GnRH), produced by the hypo-thalamus to drive the pituitary gland, as described in Chapter 3.
In some cases of FSH and LH deficiency present from birth there is a faultysense of smell (a physiological function also dependent on the hypothalamus)—an association known as Kallmann syndrome. Kallmann syndrome can occur ineither sex.
Deficiency of FSH can also be the result of disease of the pituitary gland itself,but this is even rarer.
A prolactin-producing tumor, also much less common in men than in women,generally produces profound impotence as the sperm count falls.The diagnosis is madeby finding a high serum prolactin, after which special tests for imaging the pituitarygland need to be carried out.
Although rare, these causes of azoospermia are important because they’re ableto be treated, using the same gonadotropin preparations that we use in women forovulation induction, namely human chorionic gonadotropin (hCG, such as Pregnyl andProfasi) and follicle stimulating hormone (such as Gonal F and Puregon).
Treatment is prolonged, though, and needs to be carried out over many monthsbefore adequate numbers of sperm are seen.
In between attempts at pregnancy, treatment with injections of testosterone isenough to support normal sexual function.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 139

REDUCED SPERM NUMBERS: OLIGOSPERMIA
A low sperm count is like greatness: some are born with it, others have it thrust upon them.
Inherited oligospermia
Many cases of low sperm counts are caused by inherited factors (a paradox discussed in thebox, Nature’s genes are callous).
In a study published in the British Medical Journal in 1994, Professor Richard Lilfordand colleagues showed that 17 of 148 men who attended either of two infertility clinics inLeeds had brothers who had also sought help for infertility, an incidence of over 11 percent;by contrast, of 169 men who were questioned while their wives were having babies or whowere requesting sterilization by vasectomy, none had a brother infertile from oligospermia.Careful analysis pointed to the likelihood that 60 percent of infertility in men was inher-ited by a recessive mode of inheritance (meaning that two abnormal genes are needed toinherit the oligospermia).The sorts of genes that could be involved are those that code forthe special structures in the sperm cells.About 1000 genes need to work well for sperma-tozoa to form in normal numbers.Although we don’t know much about these genes yet,we do know that the genes for decreased fertility in men are not the same as the genes fordecreased fertility in women.
Another prominent congenital cause of oligospermia is incomplete descent of the testis(or of both testes) into the scrotum.This condition is called cryptorchidism (from the Greekfor ‘hidden testicle’).The testis may lie anywhere from high in the abdomen, within thewall of the abdomen in the area of the groin, down to the soft tissues around the top ofthe scrotum.The higher the location, the higher the risk these testicles have of developingcancer. Diagnosis in early boyhood is important, because there’s evidence that the soonerthe situation is corrected by an operation (called an orchidopexy) the better for the laterproduction of sperm. Making a definite diagnosis in young boys can be difficult, however.(See the box, Hidden permanently, or just hiding?)
Environmentally caused oligospermia
If the genetics of oligospermia are still a little obscure, environmental causes of low spermcounts are even less understood.
Sperm experts don’t all agree that the average sperm count in men in Western societieshas fallen in the last generation or two, but the evidence that this has been happening isgetting stronger. In particular, there seems little doubt that the incidence of more seriousproblems with men’s testicles is increasing, such as a failure of one or both testes to descendinto the scrotum and, even more seriously, cancer of the testis,which can be associated withvery low sperm production.
What might the mechanisms be? An early favorite among clinicians has been theambient temperature the testes find themselves in. It’s well known that the normal temper-ature in the scrotum is several degrees lower than it is in the abdomen.The testes of many
140 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 140

mammals seem to need this lower temperature to work properly. I showed in 1967 (in myfirst published research) that an operation to pull rats’ testes back into the higher temper-ature of their abdomen with a suture caused the Sertoli cells to malfunction within24 hours, whereas the control group, whose testes were pulled up and then put back down,had undisturbed Sertoli cells.
So it’s wise to avoid hot baths and saunas if there’s any question about the sperm count.Hot showers are not a problem, as there’s enough evaporation over the scrotum whilestanding under the shower to keep the testes from heating up too much.Whether tightunderwear is a culprit remains to be proven.
One treatable cause of oligospermia is a varicocele—a varicose vein inside the scrotum,usually on the left side, which can allow blood at body temperature (too high), or bloodcontaining too much carbon dioxide or other substances, to spill backwards from theabdomen into the scrotum.Varicoceles can be felt in the upper part of the scrotum, typi-cally by noting more tissues between the fingers on the left side than can be felt on theright; the examining doctor might detect an impulse upon the man coughing, whichsends a spurt of blood backwards. The diagnosis of varicocele can be confirmed orexcluded by an ultrasound of the scrotum using Doppler studies to look at blood flowin the veins.
The treatment involves removing the abnormal vein or, better, tying it off higher upin the body, in the wall of the abdomen. (It means a day or two of discomfort, but it’s nomore than the discomfort a woman undergoes with a laparoscopy.)
The dilemma with treating varicoceles, however, is that not all detectable varicoceles areactually doing much harm—and treatment is not commonly followed by much improvement.
A LOW SPERM COUNT � 141
Hidden permanently, or just hiding?
Normal testes in young boys don’t spend all their time in the scrotum, so the diag-nosis of undescended testis or testes can be tricky.
The reason is that the tissues the testis hangs on include a muscle which cancontract, in a reflex reaction to anxiety or cold, to pull the testis up out of the scrotum.This is the so-called retractile testis, which needs no treatment and so needs to bedistinguished from a truly cryptorchid testis.
Experienced doctors sometimes advise the boy’s parents to gently feel for thetestes in the scrotum (with appropriate explanation to the boy!) while he’s relaxedin the bath; if they’re both in the scrotum at such a time, all’s well.
Likewise, if both testes have been noted to be present in the scrotum at birth,before the retractile reflex has developed, then all will be well too. Not all normaltestes are in the scrotum by birth, though, especially if birth has been premature.Careful examination over the few months after birth will usually confirm theirnormal arrival there.
Cryptorchidism is becoming more common, as is oligospermia generally.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 141

The sperm count is susceptible to environmental poisons, occupational toxins, and todrugs used for medical purposes. Chemotherapy drugs used for treating cancer can affectany tissue where cells are being made quickly, including the tubules of the testes; the detri-mental effects such cancer drugs have on the manufacture of sperm are often permanent.
Otherwise, little is known about which medical drugs are liable to depress spermproduction. Many of those used very commonly for high blood pressure and for pepticulcers can lower the sperm count, though not for everyone who takes them.
Sulfasalazine, used to treat colitis, is known to reduce the sperm count, sometimes toazoospermia. So do anabolic steroids, used for body-building. Never try to use androgensfor correcting oligospermia: administration of testosterone is so reliable at decreasing thesperm count that it is used in the male contraceptive (birth control) pill.
The substances polluting the environment are not well understood.Dioxin, an infamouscomponent of the defoliant known as Agent Orange, used for removing vegetation in theVietnam War,has been implicated in oligospermia, as it has in the causation of endometrio-sis (discussed in Chapter 15).
Industrial pollutants a man can be exposed to at work can be harmful; these includethe constituents of printing inks and adhesives, as well as paint pigments containing themetals lead, cadmium and mercury.The pesticides DDT, dibromochloropropane, chlorde-cone, and ethylenedibromide, among others, have also been blamed (see the box, Lessonsfrom wildlife . . .).
A group of researchers from Aarhus University in Denmark recently had the oppor-tunity to examine sperm counts from members of the Danish Organic Farmers Association.These farmers had significantly better sperm counts than comparable men who did not sofastidiously avoid potentially polluting chemicals.
Nicotine from smoking is probably the most avoidable of noxious environmentalsubstances. Harmful oxidation of sperm is typical in any situation where the sperm countis reduced environmentally and smoking can only make this worse. So-called recreationaldrugs are harmful too, including marijuana.
Alcohol in moderation probably does not affect the sperm count;wine,which containsmany natural anti-oxidants, could possibly turn out to be beneficial—in moderate amounts.
Infections of the male reproductive organs can be harmful, either by causing an obstruc-tion (discussed earlier) or by harming the sperm directly.A history of a discharge that stainsthe underclothes, of painful urination, or of unusual tenderness of the scrotal organs, are allreasons to have a specialist consultation with a urologist, with a view to treatment withantibiotics.
A particularly serious infection is one caused by the mumps virus, particularly if mumpsis contracted during adolescence and is associated with pain (hence inflammation) of thetestes. Permanent damage to the testis is likely, and azoospermia can result.Mumps in child-hood, well before the process of puberty starts, rarely affects the testis.
The testes can come to harm from injury to the scrotum.Torsion of the testis, or twistingon its blood supply, can cause substantial damage; although torsion is not very likely toaffect both testes, it happens more often than would be expected from pure chance. Painin the scrotum, spontaneously or after injury, is always a reason to seek medical help quickly.
142 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 142

A LOW SPERM COUNT � 143
Lessons from wildlife . . .
Human sperm counts seem to be more susceptible to harm than many animals’sperm counts.But studies on animals in the wild could be particularly useful in iden-tifying harmful pollutants in the environment.
Dr L.J. Guillette from the Department of Zoology at the University of Floridain Gainesville, in addressing the Fourteenth World Congress of Gynecology andObstetrics held in Montreal in 1994, argued convincingly that human agriculturaland industrial by-products and toxins are very widespread, even in environments wemight think are pristine. Measurable amounts of DDT, for example, are found evenin the polar regions.
Dangerous human-made contaminants share three special features, as well asbeing human in origin:• They evaporate easily;• They’re very poorly soluble in water, but soluble in fat; and• They’re not able to be metabolized or destroyed.They therefore disperse widely and get trapped in the fat stores of plants and animals,working their way thoroughly through the ecosystem.
Because of their persistence,organisms feeding on each other cause these substancesto accumulate and be magnified as they work up the food chain.Top-level predators,and this includes human consumers, can thus carry body burdens of contaminants atlevels a million or more times greater than the environmental background level.
The resulting reproductive disorders that have been found among wildlife, accord-ing to Dr Guillette, include reduced fertility, reduced ability to hatch (among birds),reduced viability of offspring,reduced hormone activity,and altered adult sexual behavior.
The detrimental effects of substances such as DDT, dioxin and polychlorinatedbiphenyls (PCBs) could arise because they and their metabolites act as estrogens andas anti-androgens.
. . . and from beef cattle
To add insult to this injury, synthetic estrogens active by mouth, such as diethyl-stilbestrol (DES), were for many years widely used to increase the weight of beef inthe livestock industry, before being banned in the 1980s.
Professor Niels Skakkebaek, of the University Department of Growth andReproduction in Copenhagen,has been a leader in drawing attention to what moreand more of us are convinced was a major decline through the second half of thetwentieth century in human sperm counts, alongside an increase in cryptorchidism,and an increase in cancer of the testis.
He, too, believes that estrogens and anti-androgens accumulating in the envi-ronment could be to blame.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 143

IMMUNE REACTIONS TO SPERM: ANTI-SPERM ANTIBODIES
The sperm-forming tubules in the testicles and the ducts that carry the sperm to the exteriorare physically isolated from the body’s immune system. Should the barrier between thebloodstream and the male’s reproductive tissues be breached, however, the immune systemis likely to form antibodies to the sperm cells.As we note in Chapter 7, sperm antibodies canbe formed to the head of the sperm, to its midpiece (its waist), or to its tail.
The antibodies can be ‘agglutinating’, causing the sperm to stick to each other and thusnot be able to swim properly, or they can be directly ‘immobilizing’, causing the sperm cellto die. More insidiously, they might just coat the sperm, producing no visible result, butblocking the sperm from attaching to the egg.
All these antibodies can be revealed by those sperm antibody tests that are carried outusing immunobeads.
The most common cause for sperm antibodies forming in men is the sterilizing oper-ation vasectomy.At the cut end of the vas deferens on the side of the testis (where, therefore,the sperm get obstructed), an irritation is set up, with inflammation and—inevitably—animmune reaction against the accumulating sperm, with production of sperm antibodies.Worse, at least for men who later want the sterilization to be reversed, the immune reactionpersists, permanently compromising sperm numbers and sperm motility, even when thevasectomy reversal procedure itself—the new plumbing—is a success. Sperm antibodies arealso likely to form when the epididymis or the vas deferens gets blocked from infection. Onthe other hand, they do not often form when these ducts have been blocked from birth.The reason for this discrepancy is not known.
Women too can develop sperm antibodies. Sperm are highly penetrative, routinelyreaching the peritoneal cavity after sexual intercourse. So the surprise is perhaps that anti-bodies do not form much more often than they do (see the box, Sperm in women, sperm inmen).A moderate level of sperm agglutinating antibodies is not uncommon in women aftermany years of infertility.
Curiously, sperm antibodies, if found in one partner, are more likely to be present alsoin the other partner. Even more curiously, sperm antibodies have also been discoveredamong women who have never had sex.The reason for the production of sperm anti-bodies in these situations is thought to be the coincidental resemblance some viruses orother infections have to the surface molecules on sperm cells—an immune phenomenonwe call cross-reactivity.
Because such an otherwise ordinary contagion is reasonably likely to affect cohabitingpartners, the common occurrence of antibodies that just happen to react also against spermis explained, and so too is the occasional development of sperm antibodies among virgins.
Why some men without blockages form sperm antibodies and why some women formserious levels of sperm antibodies that account for infertility is still obscure.Treatment isunsatisfactory short of assisted conception involving IVF and usually ICSI (see Chapter 20).
Immunosuppressive drugs, including the cortisol-like steroids cortisone, prednisone andprednisolone, are sometimes said to be effective, but when given in adequate amounts forlong enough there’s a small chance of a serious penalty: a crippling complication of the hip
144 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 144

joint, called aseptic necrosis of the femoral head (or noninfective tissue death of the top end ofthe thigh bone). Even a small risk of such a serious hazard keeps most doctors and mostpatients with sperm antibodies away from cortisone treatment for more than a short course,if not away from it completely.
TREATMENT OF MALE-FACTOR INFERTILITY
In reproductive medicine it’s not difficult to cause outrage among some more extremefeminists, such as a 1990s group who called themselves FINRRAGE (Feminist InternationalNetwork of Resistance to Reproductive and Genetic Engineering). Eating at their souls,it seems, was (maybe still is) the biological reality that it’s women who conceive childrenand in whom, through reproductive medicine, the proof of successful pregnancy needs to
A LOW SPERM COUNT � 145
Sperm in women, sperm in men
The body is no zoological fortress; if it were,we’d have no need for virologists, bacte-riologists and parasitologists.
Sperm in the body are intrepid—and rather long lasting.Sperm heads engulfed by macrophages (the body’s scavenging cells that ultimately
dispose of foreign material) last in recognizable form for a week or more. Inseminatedmice, for example, can reveal that genetic material from sperm cells ends up not justin the abdomen and the lymph glands, but eventually in far-off tissues such as theheart (though not, I should say, as identifiable sperm cells!).
Nature probably has a purpose in a woman getting to know her partner’s geneticmaterial first-hand before pregnancy. Studies show that there are fewer complica-tions in pregnancies that start after a suitable conditioning period of exposure tosperm.
Professor Ian Craft, an IVF doctor in London, found in the 1980s that a womanwho conceives by receiving donated embryos, and so has no prior exposure to therelevant male’s genetic material before she’s pregnant, runs a higher risk of experi-encing pregnancy-related high blood pressure than a woman who conceivesnaturally.
As well as sperm cells, semen contains white blood cells that can colonize therecipient,particularly if intercourse takes place in a way that causes abrasion or trauma.This is the way that the AIDS virus, HIV, is transmitted.
At vaginal sexual intercourse, male to female transmission of AIDS is twice aslikely to happen as female to male transmission.The risk could be higher with analintercourse and ejaculation.
So too,possibly,might be the risk of developing antibodies to sperm,when spermgain access to tissues in ways the reproductive system has not necessarily evolved tocope with.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 145

be achieved.Their gripe was the absence of available effective treatment for the greatmajority of men with low sperm counts, our efforts instead being directed at the woman,where with assisted conception we get by with smaller and smaller numbers of normal,even immature, sperm.
These methods of treatment, which involve fertilization of a woman’s egg or eggs invitro, have been a generally successful approach (and are discussed from a medical perspec-tive in Chapter 20 and from a more social perspective in Chapter 25).
Dr Renate Klein, from the Department of Women’s Studies at Deakin University,Victoria, maintains that too often the women in this situation are coerced into acceptingsuch intrusive treatments to gain ‘his’ child, instead of being given an even-handed choice.This choice includes the option of donor insemination, or assisted insemination using thesemen of a normal man who donates semen for the purpose (see Chapter 22).There is alsothe option of not having children at all.
How couples react to male infertility and how they then relate to each other is as variedas the couples who are affected by it. Discussion of this personal side is located elsewherein this book.My purpose here is to keep to the biological and medical facts as we presentlyunderstand them.
Male-directed treatment
The fact is that, with rare exceptions, the only effective options for treating men witholigospermia consist of surgical treatment of varicocele where appropriate, and some generalattention to not smoking and to avoiding more obvious workplace pollutants.
For most men with low sperm counts, orders of magnitude of improvement (10-fold,100-fold, 1000-fold) are needed to make a material difference to their partner’s conceivingeasily.This is a tall order for any treatment regimen when there is no hormonal deficiencyto be repaired. Only rarely is there a deficiency of FSH from disease of the pituitary glandor the hypothalamus that can be specifically overcome with gonadotropin therapy (see thebox, FSH deficiency in men is rare but important).
Drugs such as clomiphene (used to induce ovulation in women) have not been shown tobe effective in men, and they are expensive to use over any period of time.Treatment withmale hormones, androgens such as testosterone, should not be attempted.These hormones arecontraceptive in men; they will decrease the sperm count further.Anti-oxidant vitamins,such as vitamins A, C and E, might or might not be helpful, but most people are not shortof them or of other anti-oxidants found in the diet; the sperm count in any case is notlikely to be more than marginally improved.
Obstructive azoospermia is amenable to corrective surgery in men only when it’s the resultof a localized blockage of the epididymis or the vas deferens amenable to repair with micro-surgery. (Remember that a diagnosis of blockage is usually made by the doctor carefullyfeeling the structures in the scrotum. It’s confirmed by finding a normal serum FSH andperhaps by showing normal sperm-forming tubules in the testis on a testicular biopsy.Theducts are too fine to allow an x-ray to be done without risking a blockage resulting fromthe test itself.)
146 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 146

The surgery needed is highly specialized—don’t let just any urologist attempt it.He orshe must be particularly experienced in vasectomy reversal to even think of repairing obstruc-tions caused congenitally or through disease.
The success of such microsurgery depends on (1) the skill of the microsurgeon; (2) thelocation of the blockage (reversal of male sterilization by vasectomy—a vasovasostomy—isusually the most straightforward); and (3) the degree of problem caused by lingering spermantibodies.
Female-directed treatment, including assisted insemination
Beyond these forms of treatment, we have to move to the person in whom pregnancy isto happen and consider assisted conception.
In this chapter we’ll confine our attention to assisted insemination using the husband’ssemen (AIH) and, to prepare for the more substantial interventions that involve thewoman (and which are described in Chapter 20), we’ll consider the great progress that’sbeen made in recovering sperm cells for IVF from men with very few or no sperm inthe ejaculate.
AIH by intrauterine insemination (IUI) is the simplest and the oldest of the reproductivetechnologies.When impregnation through sexual intercourse fails to secure pregnancybecause of sexual impotence, very low semen volumes, retrograde ejaculation, severe hypospadias,or an abnormality in the woman in the region of the cervix,AIH using IUI can be carriedout with good effect.
Is there value in using AIH for couples whose infertility is mainly the result of oligosper-mia? Is it any better than similarly timed sexual intercourse (described in Chapter 19)?Many of us have long doubted that it is any better, especially with mere insemination ofthe ejaculate into the cervix.
Intrauterine insemination
If the sperm is prepared by washing it as if for use with IVF (by separating it from semen’sother components and resuspending the sperm in a special salt solution), then inseminatednot into the mucus of the cervix but up through the cervix, into the uterus itself—andthus called intrauterine insemination (IUI)—it might have some limited benefit.
In a study performed at the Free University Hospital in Amsterdam in the Netherlands,and published in 1990, Dr Antonio Martinez and colleagues randomly allocated womenwith either unexplained infertility or infertility associated only with oligospermia to oneof four treatments:1. Timed sexual intercourse;2. Timed IUI;3. Timed sexual intercourse after the woman had taken clomiphene (which induces ovula-
tion, perhaps of more than one follicle, but at the price of some negative effects onmucus in the cervix and on the lining of the uterus—see Chapter 11); and
4. Timed IUI after clomiphene.
A LOW SPERM COUNT � 147
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 147

148 � GETTING PREGNANT
From father to son
Can the genes for oligospermia or azoospermia be passed on? With modern assisted concep-tion technology, yes, in some instances at least. Just how this might happen depends onwhether the Y-chromosome is normal or abnormal,or where in the genome a respon-sible abnormal gene is located and whether it is dominant or recessive.
First, consider a whole additional sex chromosome, such as occurs in men with47,XXY, or Klinefelter syndrome. Although these men have azoospermia, there arereports that there can sometimes be small pockets of functioning tissue in the testi-cles from which sperm might be obtained using TESE. (Such men may have mosaicismof the chromosomes: two distinct cell lines, just one of which is 47,XXY.) Sperm inthis circumstance have an increased chance of carrying two sex chromosomes, result-ing in a fertilized egg, or zygote, perpetuating a sex chromosome trisomy, such as47,XXX or 47,XXY (depending on whether the sperm was 24,XX or 24,XY).
We thus screen men having TESE with a karyotype before proceeding. If anabnormal cell line is detected (typically, less than 100 percent of the man’s cells areabnormal, that is, there is mosaicism), it would be prudent, if TESE and ICSI stillgo ahead, for the sex chromosomes of a cell from the embryo(s) to be studied withFISH at preimplantation genetic diagnosis (PGD, see Chapter 20) or, if induced abortionis an acceptable option, for a karyotype to be done on the fetus during pregnancy(prenatal diagnosis), using either chorionic villus sampling (CVS) or amniocentesis toobtain fetal cells.
Second, there might be small deletions of genetic material from the Y-chromo-some that remove or disable one or more genes required for the manufacture ofsperm. In these cases, the microdeletions will inevitably be transmitted to all maleoffspring (see the box, Microdeletions in the Y-chromosome).
Third, many of the perhaps thousand or so genes required for normal spermproduction and normal structure and function of the tubules and epididymis arelocated among the non-sex chromosomes, the autosomes.Abnormal alleles can bedominant or recessive. Most autosomal gene mutations causing severe oligospermiaor azoospermia will be recessive, with a very small chance of the mother being acarrier for a similar abnormal gene.
Testing for the large number of possible genes is impossible for the time being,which means that this set of genetic conditions cannot reliably be distinguishedfrom environmental causes of testicular damage. In practice this does not matter.Environmental causes of infertility will naturally not be transmitted to theoffspring.And if it is genetic, then unless the parents are related it is unlikely thatthe child would be, like the father, homozygous or even compound heterozygous andhave two abnormal alleles of the same recessive gene (as this would require thetransmission of an abnormal allele of the very same gene from the mother—anunlikely coincidence).
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 148

According to this logic, a child conceived by ICSI ought to have almost as muchchance of being fertile and normal as anyone else.
We know enough to say that generally there is no substantial increase in abnor-malities among IVF and ICSI babies. But this is not to say that closer examination,as experience with such techniques increases,will not reveal differences, some subtle,some less so.
In the case of ICSI for severe oligospermia, at least, there does seem to be a signif-icant increase in the risk of a baby with an aneuploidy for an X- or a Y-chromo-some: karyotypes such as 45,X (Turner syndrome), 47,XXY (Klinefelter syndrome),47,XXX (triple-X syndrome) and 47,XYY (extra-Y-chromosome syndrome).The risk isperhaps one or two per 100 births,which is several times more than expected amongnatural conceptions.
It remains to be seen whether this represents an increased risk for the familiesinvolved (most of whom have naturally conceived pregnancies that are too fewand far between to be able to estimate the risk they would run with naturalconception).
Avoiding this risk, as discussed above, requires either PGD or prenatal diagno-sis. And for more on the risks of IVF and its laboratory add-on maneuvers, seeChapters 12 and 20.
Are there dangers for your children if the man has CBAVD?
Men born with blockages of the epididymis or an absent vas deferens (congenitalbilateral absence of the vas deferens, or CBAVD) might be carrying one or twopartially dominant genes for cystic fibrosis, a severe, usually fatal disease of the lungsin children who inherit a gene for it from each parent.
To be sure, if a male child inherits one abnormal cystic fibrosis gene he too mighthave CBAVD.But the even bigger worry is that the child might also inherit a secondabnormal allele from its mother, if she is a carrier (and about one in 25 mothers willbe carriers), catastrophically resulting in cystic fibrosis for the child.
CBAVD mandates a screening test for as many of the alleles as it is practica-ble to test of those known to cause cystic fibrosis, and particularly for delta F508.At Sydney IVF we can test for the commonest 30 or so of them, and plan toextend the testing to very many more with the introduction of DNA arraytechnology.
Both of you should be screened for the CF alleles, as a rare allele or set of allelesis more likely to be missed if testing is restricted to the male.
The presence of such alleles does not mean you can’t proceed with IVF withoutrisking a child with cystic fibrosis: screening of IVF embryos is possible using pre-implantation genetic diagnosis (PGD); or, anticipating induced abortion, prenataltesting can be performed during pregnancy.
A LOW SPERM COUNT � 149
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 149

The respective pregnancy rates were:1. None of 34 cycles (0.0 percent) of timed sex alone;2. Three of 32 cycles (9.4 percent) of IUI;3. One of 31 cycles (3.2 percent) of clomiphene + sex; and4. Five of 35 cycles (14.3 percent) of clomiphene + IUI.Dr Martinez concluded that there was significant value in intrauterine inseminationcompared with sexual intercourse, but not much, if any, additional benefit came from usingclomiphene, despite a significant increase in the number of eggs obtained. In none of thegroups was the pregnancy rate anywhere close to what can be achieved with IVF.
Intrauterine insemination plus superovulation
The benefit of ovulating multiple eggs (superovulation) in association with intrauterine insem-ination is demonstrated better by using follicle stimulating hormone instead of clomiphene.FSH avoids the negative effects clomiphene has on the uterus, and has become a popularform of assisting conception with IUI, whether there’s oligospermia or unexplained infer-tility. It also produces more ovulating eggs than clomiphene does.The arithmetic to justifyit is straightforward: if few sperm cells are reaching the fallopian tubes, the presence of twoeggs at the site of fertilization will double the chance of pregnancy; four eggs will just aboutquadruple it; and so on.
Californian studies in 1989 showed that AIH after treatment with FSH gave a preg-nancy rate of 7 percent per cycle, compared with 33 percent per cycle using gamete intra-fallopian transfer (GIFT), a more intrusive form of assisted insemination in which eggs areretrieved and placed along with the prepared sperm in a fallopian tube.
The Amsterdam doctors I referred to above achieved pregnancies with IUI only if morethan 2 million washed,normal,motile sperm were available for insemination into the uterus,and this is not achievable for many men with oligospermia.With GIFT, for instance, goodresults are possible with just 100 000 such sperm, and nowadays the results from IVF ingood laboratories are better than from GIFT.
I would conclude from this that the usefulness of AIH and IUI, with or without stim-ulation of the ovaries, is very limited for couples with significant oligospermia.
And a specific hazard remains whenever FSH is used without limiting the number ofeggs or embryos that can succeed, in that there is always some risk of higher-multiplepregnancy—triplets, quadruplets, quintuplets, and beyond—possibly then managed by fetalreduction, which has its own serious emotional dangers.
With any level of oligospermia, then, in vitro fertilization, if it can be afforded, is themedically preferable approach.
And with azoospermia, unless donor insemination is resorted to, in vitro fertilizationbecomes essential—if sperm can be recovered from your partner.
Sperm recovery operations in azoospermia
Overcoming the effects of extremely low and even zero sperm counts is the area wherehuge progress has been made with IVF. The breakthrough, which dates from the
150 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 150

mid-1990s, was the successful microscopic insertion of a single sperm directly into the eggto fertilize it—the procedure known as ICSI.
For non-obstructive azoospermia, and sometimes for severe oligospermia, the sperm arebeing obtained directly from the testis or from the ducts leading out of the testis, beforethey risk damage from oxidation and before they are exposed to sperm antibodies in theepididymis and the vas deferens.The operation is called testicular sperm extraction (TESE)and is carried out at Sydney IVF either with local or general anesthesia.
For obstructive azoospermia, sperm are obtained from the ducts on the testicular side ofthe obstruction, usually the epididymis, in an operation called epididymal sperm aspiration(ESA) or, if performed under magnification, microsurgical epididymal sperm aspiration(MESA). Both procedures are performed under either local or general anesthesia, depend-ing on the man’s preference.The recovered sperm can be used straight away for IVF orcryostored (frozen) for use later.
In other words, for the millions of ejaculated sperm nature needs in order to have oneegg fertilized, we’re able now to help to the extent that one egg and just one single recov-ered, normal sperm can mean an embryo more than half of the time.With several eggs andseveral sperm there are now almost always normal embryos to be transferred. But, as wesaw above on passing through our subject, there are genetic causes of both obstructive andnon-obstructive azoospermia and oligospermia. So see the box,From father to son, for a wordof caution, and a reminder that there are circumstances when genetic disease is likely to bepassed on to offspring.
Often there are genetic tests you can and should have done before you embark on yourhigh-tech pregnancy.
FINALLY . . .
Never say never. In medicine, as in life,we learn not to be too surprised by the unexpected.Provided there’s not a complete absence of sperm as the cause of sterility, pregnancy canand does sometimes happen. It really does ultimately take just one sperm to make it (and,despite the cynics, it’s usually not the milkman or the brush salesman). Experienced infer-tility doctors have seen pregnancies ensue with sperm counts of fewer than 1 million anddespite dismaying levels of sperm antibodies.
Whatever assistance and whatever intrusions you’re both enduring to get around theproblem of low sperm counts, try not to lose sight of this ever-present possibility.
A LOW SPERM COUNT � 151
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 151

not ovulating
Ovulation induction drugs
Menstruation, or bleeding from the lining of the uterus (the endometrium), is usuallybrought on by a fall in hormone support from the ovary.The timing of menstruationis determined by the cyclical activity or otherwise of the ovaries (the ovarian cycle).
If you’re not ovulating—a condition we call anovulation—or if your ovarian cycle isdisturbed, your menstrual cycle will also be disturbed or lost.
Here we will look at:• The symptoms of anovulation;• The readily treatable causes of anovulation and infertility—hypothalamic anovulation,
including weight loss, stress and too much exercise; raised prolactin levels (hyper-prolactinemia); the polycystic ovary syndrome; and their treatment (ovulation induction),with clomiphene and other drugs
• The untreatable cause, namely primary ovarian failure (premature menopause);• The dangerous causes: tumors of the pituitary gland,ovaries or adrenal glands; and finally,• The significance of anovulation following use of the birth control pill.
SYMPTOMS OF ANOVULATION
The most common menstrual sequel to anovulation is absent periods (amenorrhea), butsometimes there’s still enough estrogen being produced to cause irregular bleeding (anovu-latory periods, or anovulatory dysfunctional uterine bleeding).Anovulation is the main cause ofamenorrhea, but not the only one.Table 11.1 lists the main disturbances of the menstrualcycle, their association with ovulation or anovulation, and what can cause the disturbedmenstrual patterns.
You probably know what ovulatory periods are like: regular, often a bit painful withsome dysmenorrhea and even ovulation pain, and maybe with PMT and other cyclical features.
152
11
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 152

They are brought on by falling levels of progesterone and are much the same in durationfrom one period to the next.
But what are anovulatory periods like? Anovulatory menstrual periods, produced byfluctuating levels of estrogen alone, usually, but not always, occur irregularly.They are typi-cally painless (except if there are clots) and they vary a lot in length and amount from oneperiod to the next. PMT-like symptoms can occur.As a rule, anovulatory periods can causegreater loss of blood than ovulatory periods, so there can be a risk of anemia, even at ayoung age.
From a hormone perspective, there’s almost no difference between amenorrhea andanovulatory dysfunctional bleeding as manifestations of anovulation!
READILY TREATABLE CAUSES OF ANOVULATION
There are three common causes of amenorrhea due to anovulation that can be overcome bydrugs (or sometimes lifestyle changes):• Hypothalamic anovulation (exercise, stress, weight loss);• Hyperprolactinemia (raised levels of prolactin); and• Polycystic ovary syndrome or disease (which can also present with anovulatory dysfunctional
bleeding, see above).
NOT OVULATING � 153
Table 11.1 Patterns and causes of abnormal menstruation, including disturbances ofovulation
Technical name Meaning Reasons
amenorrhea absent periods (1) anovulation
(2) absent uterus (Ch. 18), obstructionin uterus or intrauterine adhesions(Ch. 17)
oligomenorrhea infrequent periods (1) infrequent ovulation
(2) anovulation, with varying estrogenlevels
irregular dysfunctional irregular heavy periods (1) anovulation, with varying estrogenuterine bleeding (DUB) levels
regular DUB regular, heavy periods (1) pathology of uterus (Ch. 17)
(2) bleeding tendency
hypomenorrhea regular, light periods (1) intrauterine adhesions (Ch. 17)
(2) oral contraceptive pill
(3) normal aging
intermenstrual bleeding or bleeding between or just before (1) pathology of the uterus (Ch. 17)
premenstrual spotting periods (2) pathology of the cervix
(3) endometriosis (Ch. 15)
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 153

The tests to distinguish them are described more fully in Chapter 5, and include serumFSH, serum LH, serum prolactin and serum testosterone, and either a serum free testosterone or thefree androgen index.
If there are infrequent periods, or oligomenorrhea, these tests are best done during thetime of the period. In any case, it’s best also to have a serum estradiol and serum proges-terone done, to know how active the ovaries were at the time the other hormones weretested.
The hormone changes of the ovarian cycle are described in detail in Chapter 3. Forhow these relate to menstrual disturbances, see the box, Hormones behind periods, or periodsbehind obstruction. Here we will look further into the biology of what’s gone wrong.
Hypothalamic anovulation
This condition is also known as ‘simple’hypothalamic amenorrhea and hypothalamic chronicanovulation (HCA).
Stress or losing weight (especially to a weight less than that at which, as a teenager, thefirst period, or menarche, took place), acting through the hypothalamus, reduce the brain’s
154 � GETTING PREGNANT
Hormones behind periods, or periods behind obstruction
Regular menstrual bleeding depends on a regular rise and fall in hormones from theovary, the details of which are in Chapter 3.
Briefly, this is achieved by development of follicles, which secrete the ovary’s firsthormone estrogen (specifically estradiol), followed by ovulation and production, by thecorpus luteum, of progesterone, the ovary’s second hormone.
Because it takes an average of about two weeks for a follicle to grow to the pointof ovulation (the follicular phase), and because the corpus luteum lasts about two weeks(the luteal phase), the ordinary ovarian cycle, and therefore the menstrual cycle, lasts aboutfour weeks (with a normal range that varies between 24 days and 35 days). Shorteror longer cycles are chiefly brought about by variation of the follicular phase.Theluteal phase is more constant.
The lining of the uterus, the endometrium, is built up by estrogen and is thentransformed to be receptive to pregnancy by progesterone.The follicular phase inthe ovary, during which only estrogen is released, is the proliferative phase in theendometrium (meaning that the endometrium proliferates, or grows, getting thickerand thicker).The luteal phase in the ovary, when progesterone is produced, is thesecretory phase in the endometrium, as further proliferation is inhibited and theendometrium transforms its energies from growth to differentiation, accumulatingsecretions to benefit an implanting embryo.
If there’s no ovulation—if there’s no progesterone or exposure to a progestogen—the endometrium can keep proliferating, getting thicker and thicker, and become
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 154

drive to the pituitary gland.This, in turn, reduces that gland’s drive of the ovaries, stoppingproper development of the follicles and causing ovulation to stop.The tests listed above willshow rather low levels of FSH, LH, prolactin, and testosterone.
For more on estimating what, for your height, a good weight would be for the ovariesto function, see the box, The body mass index, the stars and Monsieur Quetelet.The moreextreme weight loss of anorexia produces a doubly profound suppression of ovulation andperiods, and sooner or later there’s a combined effect of weight loss and psychologicalstress.
Substantial exercise, however, is capable of inhibiting ovulation whether weight lossoccurs or not. Dr P.T. Ellison, a Harvard (Massachusetts) anthropologist, has shown thathigh energy expenditure—the level of exercise associated with ballet dancing is a goodexample—is more likely to cause the periods to stop than weight loss alone.The same
‘hyperplastic’ (we call the condition endometrial hyperplasia). In the absence of ovula-tion (and in the absence of progesterone or a progestogen), the endometrium canbleed just from the loss of estrogen support.A swing up and down in estrogen canbe enough to cause serious bleeding when the endometrium is thick. Unlike anormal menstrual period at the end of exposure to progesterone (or progestogen),an anovulatory period does not cause the whole endometrium to be shed; often thebleeding occurs from patches of it; sooner or later it starts growing again and buildingup further.We call this anovulatory dysfunctional uterine bleeding.
There’s only a fine hormonal line between amenorrhea and anovulatory dysfunc-tional uterine bleeding: the hormonal disturbance underlying them can be virtuallythe same.
There will also be amenorrhea if there is no uterus (see Chapter 18), or if theendometrium in the uterus has been destroyed (endometrial atrophy) or replaced withintrauterine adhesions (see Chapter 17).
Cryptomenorrhea, or ‘hidden menstruation’, is apparent amenorrhea, resulting froman obstruction to menstruation such as an incompletely formed vagina or a trans-verse vaginal septum (see Chapter 18).Whereas amenorrhea itself is usually harmlessand painless, cryptomenorrhea is cyclically painful and can cause complications,including endometriosis, while it’s unrelieved.
Primary amenorrhea is when there have been no periods in a woman’s life.Themost common causes (beyond a simple delay from not having enough weight yetor exercising a lot) are primary ovarian failure (puberty fails as well) and congenital absenceof the uterus and vagina (breast and pubic hair development are normal; discussed inChapter 18).
Secondary amenorrhea is when the periods have stopped after having been present;its most common causes are hypothalamic anovulation, hyperprolactinemia, poly-cystic ovary syndrome and early menopause (all discussed in the main text), andintrauterine adhesions (discussed in Chapter 17).
NOT OVULATING � 155
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 155

happens with long-distance running, especially if it’s causing the sensation of ‘highs’.Thissensation is due to the production in the brain of endorphins, natural opium-like substancesthat confer a feeling of well-being.
Opium-derived drugs like heroin do the same thing more dangerously: amenorrhea ofthis kind is common among drug addicts.
By ‘simple’hypothalamic amenorrhea,we therefore mean that it’s not one of the remain-ing causes of amenorrhea, all of which show special characteristics in the blood tests otherthan just low levels of serum FSH. Here the underlying disturbances of physiology are notso simple and are elaborated in the box, GnRH has to be just right.
It’s also possible to be born with hypothalamic anovulation.This is one of the common-est causes of primary amenorrhea in which, at least until estrogen is administered, there is acomplete absence of sexual development—and, sometimes, a lack of any sense of smell!For the details, see the box, Kallmann syndrome and primary amenorrhea.
Hyperprolactinemia
Prolactin is a hormone produced by the pituitary gland, especially during and after pregnancy,when it prepares the breasts for lactation. Milk production then starts and is maintained
156 � GETTING PREGNANT
The body mass index, the stars and Monsieur Quetelet
There’s a normal range for the relationship between a person’s weight and height,calledthe body mass index (BMI),which gives a rough estimate of how much spare tissue thereis in the body,especially fat.The female body needs to have fat in reserve for pregnancyto be safe. Nature thus postpones menarche until this range is reached; and nature shutsoff the periods, and ovulation, if body fat falls below the range.The BMI—sometimescalled the Quetelet index—equals the weight (expressed in kilograms) divided by thesquare of the height (expressed in meters), and should be in the range 20 to 25.
A woman’s reproductive fortunes might or might not be determined by thepower of the constellations according to astrology.But why in the nineteenth centurya real star-gazer gave the matter of varying body fat his careful philosophical attentionis a puzzle. Lambert Adolphe Jacques Quetelet (1796–1874), a Brussels mathemati-cian and astronomer, possibly while he was thinking of Venus, made the rule that anadult’s body weight should be as many kilograms as that adult’s length in centime-tres exceeds 100.
Nowadays we overlook his arithmetic and instead confer his name on the BMI,which he did not invent. If the index is much under 20, ovulation suffers. Obesity,with a BMI greater than 25 or 30, can stop your periods too.
But unless there’s a tendency towards the polycystic ovary syndrome, for which it’sbetter to stay skinny (see the main text), a woman will probably be more fertile over-weight than underweight.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 156

once the high estrogen and progesterone levels of pregnancy disappear after delivery of thebaby and the placenta.
Unlike the other pituitary hormones, which are driven by ‘releasing factors’ from thehypothalamus such as GnRH, prolactin is controlled by an ‘inhibiting factor’, calleddopamine. Dopamine can be depressed by a range of conditions, although most dopamineshortages are idiopathic—meaning that no known cause can be invoked to explain them.The net effect of depressing dopamine is that production of prolactin from the pituitarygoes up.
Prolactin has a reflex action on the hypothalamus, decreasing its drive (via gonadotropin-releasing hormone) to the pituitary cells responsible for FSH and LH.Anovulation, and thenamenorrhea, follow.
The causes of hyperprolactinemia, which need to be looked for, include:• Drugs, among which are: (1) the major tranquilizers used for schizophrenia and other
causes of psychosis, such as chlorpromazine (Largactil); (2) some older antihyper-tensives (drugs used to lower blood pressure), including methyldopa (Aldomet);(3) antiemetics (drugs used to control nausea and vomiting) like metoclopramide(Maxalon); and (4) opium derivatives, such as heroin;
NOT OVULATING � 157
GnRH has to be just right
The common pathway through which the brain governs the way the pituitary glandcontrols the ovaries (and the testes in men) is by releasing, every 60 to 90 minutes, aburst or pulse of gonadotropin releasing hormone (GnRH, explained in Chapter 3).
In chronic hypothalamic anovulation, levels of GnRH are low, so the pituitary glanddoes not produce enough follicle stimulating hormone (FSH).This can come from changesin the balance between neurotransmitters (substances that mediate impulses acrossnerve junctions in the brain, particularly through the hypothalamus). Such imbalancesinclude insufficient levels of noradrenalin (norepinephrine), which is what mediatesamenorrhea associated with both weight loss and endorphin-releasing exercise (and thusalso lies behind the effects of opiates such as heroin in those addicted to it).
In anorexia nervosa there is both a shortage of noraderenalin and an excess in theneurotransmitter serotonin to shut off GnRH.
In hyperprolactinemic amenorrhea there is primarily a shortage in the neurotrans-mitter dopamine, a deficiency that permits increased production from the pituitarygland of prolactin, which in turn depresses GnRH.
On the other hand, either an excess of GnRH or an exaggeration of GnRHaction in the pituitary in the polycystic ovary syndrome causes the pituitary to produceluteinizing hormone (LH) at the expense of FSH, and again anovulation and amenor-rhea result.
In other words, if GnRH is insufficient or in excess, FSH suffers and ovulation(and the periods) stop.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 157

• The presence of tumors around or in the pituitary gland, which stop normal levels ofdopamine being produced or stop normally produced dopamine getting to all or partof the pituitary gland;
• Pregnancy and, later, normal lactation; reflexes from suckling travel from the nipple tothe hypothalamus, depressing dopamine; and
158 � GETTING PREGNANT
Kallmann syndrome and primary amenorrhea
Just about any cause of anovulation can come into effect before the periods are dueto begin, producing primary amenorrhea rather than secondary amenorrhea.
In some cases, the shortage of follicle stimulating hormone is so severe that theovaries, although loaded with primordial follicles, do not produce enough estrogenfor puberty to even start.Through the teenage years the affected girl gets taller, butno breast or pubic hair development takes place, and sooner or later tests will needto be done.
If the news is good, the serum FSH level will be low, and ovulation inductionwill be possible, one way or the other. If it is not, and the serum FSH is high, it meansprimary ovarian failure (see the main text) and then only egg donation can lead to preg-nancy.
There are a number of possible causes of hereditary deficiency of FSH (or ‘hypo-gonadotropic hypogonadism’),most of them passed on as recessive conditions,meaningthat both of the affected child’s parents,while themselves reproductively normal, arecarriers for the gene.
The least common causes are mutations of the gonadotropins FSH or LH.Morecommonly there is a mutation in the receptor for the hormone GnRH among thecells of the pituitary gland—or there is a congenital inability of cells in the hypothal-amus to produce GnRH effectively.When this is caused by a more general inheriteddeficiency in a part of the forebrain called the rhinencephalon, there is failure alsoof olfaction—an absence of a sense of smell—which is an otherwise curious asso-ciation first described in sexually immature adult men by F.J. Kallmann, in 1944.
Affected teenage girls are treated first with estrogens to enable the developmentof puberty.The birth control pill then works admirably well to keep the tissues andorgans in a healthy, sexually mature state. Menstrual periods will follow each pillcycle.
When ovulation induction is needed, clomiphene will not be effective, but pulsatileGnRH therapy works virtually 100 percent of the time. If facilities for GnRH therapyare not available, gonadotropin therapy can be used, but a full response requires at leasta small amount of LH (or hCG) to be present (see Chapter 3 to understand why).The older preparations of human menopausal gonadotropin (such as Humegon andPergonal) work better than the more modern pure FSH preparations such asMetrodin HP (Fertinex), Gonal-F and Puregon.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 158

• Chronic irritations or inflammations of the wall of the chest which may mimic thenervous reflexes otherwise produced by suckling.
The result of each of these conditions is not just the disappearance of the periods due tothe elevation of prolactin.Quite often the high levels of prolactin stimulate the productionof milk in the breasts, called galactorrhea—which is therefore an important symptom to tellthe doctor about if you’ve noticed it.
NOT OVULATING � 159
Big and bigger prolactin
Not all apparent hyperprolactinemia spells trouble with ovulation.We should appreciate that our measurements of hormones in the blood do
not necessarily measure what they’re actively capable of.We use immunity mole-cules called antibodies to detect hormones; they match the target hormone andbind them in a way that’s measurable. Now, the part of the hormone these anti-bodies react to is not necessarily the part of the hormone that binds to the receptorin the target tissue and which translates into hormone action. (There are assaysthat detect bioactivity—called bioassays or, in the laboratory, ‘receptor-basedassays’—but they are difficult and expensive, and are made use of only in medicalresearch.)
For most hormones most of the time, this difference between the part of thehormone that binds the measuring antibody and the part of the hormone that bindsthe hormone receptor doesn’t matter. But for prolactin it can matter dramatically, ifinnocently.
Some people make prolactin molecules that link together in pairs (dimers) orin fours (tetramers).These molecules, despite their bigger than normal size, functionperfectly normally. Only one part of the dimer (in the case of ‘big prolactin’) andonly one part of the tetramer (‘big, big prolactin’) binds to each receptor.Everythingfunctions as it should; there’s no abnormal milk production in the breasts (galactor-rhea) and there’s no problem with ovulation.The ovarian and menstrual cycles areregular.
All’s normal, that is, until someone measures prolactin with a conventionalantibody assay. Big prolactin will be measured as two prolactin molecules and big,big prolactin will be measured as four prolactin molecules—apparently revealinghyperprolactinemia of twice or four times the normal amount.
In principle, we could distinguish these states using chromatography, anexpensive and difficult test. In practice, we don’t bother. If ovulation is normalby other criteria (confirmed, say, by a normally elevated serum progesterone on day21 of the menstrual cycle) then an incidental finding of hyperprolactinemia canbe ignored.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 159

Curiously, it is possible to have—or to appear to have—hyperprolactinemia even thoughthere are regular, ovulatory menstrual cycles. In these cases the raised prolactin can beignored. For the explanation, see the box, Big and bigger prolactin.
Polycystic ovary syndrome
The polycystic ovary syndrome (PCOS, or polycystic ovary disease, PCOD) is a condition inwhich ovulation is rare and tiny cysts (actually 5 to 10 millimeter follicles) accumulate inthe ovaries.These follicles contain eggs, but instead of the follicles growing and going onto ovulate, they stall and secrete male hormones into the blood.The imbalance of pitui-tary hormones and male hormones in the blood perpetuate each other and the PCOSproblem.
Incidentally, it’s important not to think that this condition means ‘cysts’ in the conven-tional sense of biggish, abnormal structures that could require special treatment.The original,full name for PCOS was ‘micropolycystic ovary syndrome’ (a bit of a mouthful, so the‘micro’ has been lost).
If you have PCOS it will usually have been obvious for years, because of irregularperiods and, often, a tendency to acne and an increase in facial and body hair.Occasionally,PCOS first manifests during ovarian stimulation (either for ovulation induction, see furtheron, or as part of an IVF or GIFT cycle, see Chapter 20), when many more follicles thanusual start to grow.
The diagnosis of PCOS is made by finding a characteristic appearance of the ovaries ontransvaginal ultrasound.The ovaries are seen to be big and to have a peripheral ‘necklace’ ofrather uniformly sized, small follicles. On hormone testing, typically there is either or botha high ratio of serum LH to serum FSH and a high free androgen index or serum free testosterone.
The high levels of LH stimulate the cells around the follicles to produce too much inthe way of androgens (the male sex hormones, a little of which comes from all normalovaries).With PCOS the serum testosterone level therefore tends to be increased, or at leastbe towards the upper part of the normal range, whereas other causes of anovulation causeserum testosterone levels to be low.
Many people with PCOS have a tendency to diabetes, with resistance to the hormoneinsulin and raised sugar levels in the blood. Drugs that lower blood glucose, especiallymetformin, discussed below, have been shown to improve many features of PCOS.
A woman can have polycystic ovaries (PCO) while still ovulating normally and withoutshowing untoward symptoms (a normal condition discussed in Chapter 2 and in the box,Polycystic ovaries: Fertility in famine).We only call it PCOS—the PCO syndrome—if there’sa clinical disturbance such as irregular periods or abnormal hair growth,when some degreeof infertility is usual.
The disturbance to ovulation that PCO causes varies in degree.At one extreme there’samenorrhea or anovulatory bleeding (estrogen is abundant in PCOS).With mild cases, on theother hand, ovulation may be a bit less frequent than normal, or even completely normal,and provided that other aspects of reproductive functioning are good, fertility may be allright and the condition itself may go undiagnosed for a lifetime.
160 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 160

Indeed,PCO is so common that for an inherited condition (see the box,PCO is often gene-based) it’s hard to regard it as abnormal.
Why the birth control pill is good for PCOS if you don’t want to get pregnant yet
When you are not trying to get pregnant, the oral contraceptive (birth control) pill is goodtreatment for PCOS:• It stops the abnormal follicles causing male-hormone-producing tissue (thecal cells) from
accumulating in the ovaries, thus protecting future fertility;• It reduces complications such as abnormal hair growth (hirsutism);
NOT OVULATING � 161
PCO is often gene-based
At least some cases of PCO (some researchers think most cases) have an inheritedcause.
The condition is more common among women with a history of it in the family,and men in affected families have a tendency towards premature male-patternbaldness, with early receding of the hairline.
The abnormality is thought to be in a metabolic unit inside cells responsible forfine-tuning the production of the sex hormones, called cytochrome P450.
There is also a small proportion of women with PCOS (about one in 70) whohave a more clear-cut abnormality in the production of steroid hormones from theadrenal gland.As a result, the adrenals leak too much male sex hormone; the condi-tion is called attenuated or adult-onset congenital adrenal hyperplasia (CAH).
Adult-onset CAH is related to more severe forms of CAH that manifest at birthwith ambiguous genitals—intersex (discussed in Chapter 18)—due to excess malehormone exposure in the female fetus, and causing enlargement of the clitoris anda joining of the skin over the vagina.These abnormalities of the genitals don’t occurin adult-onset CAH. In CAH, as in other causes of PCOS, there’s an increase inserum testosterone and the free androgen index, as well as a diagnostic increase in a precur-sor substance, serum 17-hydroxyprogesterone.
In both the common (ovarian) variety and the adult-onset CAH (adrenal) varietyof PCOS, there is therefore a strong genetic component.
Why does nature allow such genes to evolve when they appear to be a disad-vantage for reproducing? Chapter 2 reveals the two reasons, but in summary thereare evolutionary advantages to reduced fertility generally, similar to the situation withendometriosis and oligospermia, either of which can have a hereditary basis; and secondly,women with PCO will ovulate best when they’re below otherwise ideal weight (abody mass index of less than 20), giving (at least in prehistoric times), the advantageof being able still to reproduce when they are short of food in times of famine, atime when most other women will be too thin to be fertile.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 161

• It provides you with regular periods, preventing overgrowth of the endometrium and therisk of endometrial hyperplasia; and
• It provides contraception (there’s always a risk, with so much LH about, that a folliclewill grow to the stage at which it might, unpredictably, ovulate).
If the pill is personally or culturally distasteful, however, the same ends can be achieved byseparately administering an estrogen and a progestogen (the male-hormone-blocking progesto-gen cyproterone acetate is especially useful).
TREATMENT BY INDUCING OVULATION
In conditions of amenorrhea or anovulation, there’s generally no point in undertaking ovula-tion induction unless there’s an immediate intention to conceive.This is for two reasons.
First, the complications of amenorrhea, such as low estrogen levels and osteoporosis,abnormal hair growth (hirsutism), anemia from anovulatory bleeding and endometrial hyper-plasia, are more cheaply and more directly dealt with by appropriate hormone treatment,especially the birth control (oral contraceptive) pill, as described in the last section.
Second, the drugs are expensive and the ovaries can become resistant to them.
Bromocriptine and cabergoline
One exception to this rule is the use of the drug bromocriptine (Parlodel) or its neweralternative, cabergoline (Dostinex), used to treat hyperprolactinemic amenorrhea.Thesedrugs are so specific for this condition—they precisely mimic the action of dopamine, thenatural inhibiting factor for prolactin in the pituitary—that they probably should be usedunless there’s a reason not to. By lowering prolactin at source, they not only prevent thecomplications of this form of amenorrhea due to low estrogen, they also preventthe prolactin-producing cells from growing into a tumor of such cells.
Bromocriptine (Parlodel), if given too suddenly, is likely to cause side-effects, includingdizziness (from low blood pressure), headaches and nausea. It should be started slowly,beginning with a low dosage. If side-effects still occur they can usually be avoided byadministering the tablets (not the capsules!) by placement in the vagina.Absorption fromthe vagina, across its moist, mucous surface, is excellent and, unlike the veins from thestomach and intestines, the veins from the vagina don’t go first to the liver (where mostside-effects originate).
Because ovulation nearly always returns quickly once treatment with bromocriptinehas begun, it’s often necessary to use contraception (the birth control pill is satisfactory).Otherwise the treatment can be safely continued for years. Bromocriptine should bestopped, though, when pregnancy is confirmed.
Whereas bromocriptine needs to be given once or twice a day, the newer,more potentdrug cabergoline (Dostinex) is more convenient, being administered just once or twice weekly.Cabergoline can be better tolerated, but it is also more expensive and there has been lessexperience with it. Ironically, because its effects could plausibly persist into pregnancy, themanufacturer still cautiously recommends that it be stopped a month before getting
162 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 162

pregnant! Nonetheless it has been used expressly for ovulation induction and there havenot been adverse effects.
Bromocriptine and cabergoline are very effective in infertility that is purely due to hyper-prolactinemic anovulation.Unless they have other reasons for infertility, up to 40 percent ofwomen taking it still don’t get a period—because they’re pregnant in the first month! Onlyintravenous GnRH treatment (see further on) approaches these drugs for effectiveness.
Metformin
Like bromocriptine and cabergoline for hyperprolactinemia, metformin can be used longterm to help overcome the basic hormone disturbance behind anovulation—in this casefor the raised androgens in the polycystic ovary syndrome.
Metformin is an ‘oral hypoglycemic agent’: it lowers blood sugar levels in mild andmoderate diabetes. By improving responsiveness to insulin, it also improves a number offeatures of PCOS, including lowering the serum LH and serum free testosterone.Women whoare overweight tend to lose more weight with a low calorie diet if metformin is added.Asa result of these actions, ovulation is improved naturally and, if ovulation induction is stillneeded, there is improvement also in the response of follicles to clomiphene or to FSH.Continuing metformin into the first three months of pregnancy, has been shown to reducethe chance of miscarriage. Moreover, metformin has long come off patent, so there aremany generic preparations available and it is reasonably priced.
Too good to be true? The downside is that you need to take several tablets at intervalsthrough the day: metformin does have side-effects and the dose that works is not far shortof where you get nausea and diarrhea.
Clomiphene
In hypothalamic anovulation and polycystic ovary syndrome, if you are attempting pregnancy thedrug clomiphene is the first choice for ovulation induction because of its inexpensivenessand the simplicity of using it. Clomiphene is marketed as Clomid by Merrill Dow and asSerophene by Serono.
Clomiphene acts by increasing the natural production of FSH, which is deficient inmost of the causes of anovulation we’re considering here. It does this because it’s an anti-estrogen, that is, it blocks the effect of estrogen on various tissues.This effectively tricks thepituitary gland into assuming that there’s not enough estrogen about, thereby pushing it intoincreasing its output of FSH. For clomiphene to work, the increase in FSH needs to beenough to get a group of follicles to grow, after which they reach maturity and ovulate inthe way described in Chapter 3, with a natural LH surge.
The dose of clomiphene you’ll need ranges from half a tablet (tablets are 50 mg) to fivetablets a day, always for five days, and generally starting on or between the second and thefifth day of a period.The dose depends on the severity of the anovulation (the degree ofsuppression of the hypothalamus) and on the woman’s body mass index.
Side-effects are common with the higher doses of clomiphene but not with the lower
NOT OVULATING � 163
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 163

ones. Metformin (see above) can decrease the dose of clomiphene needed in PCOS. Sucheffects include headache,depression,hot flushes or flashes (all symptoms of lack of estrogen),and temporary blurring of vision or an appearance of yellow coloration to things.Thesesymptoms pass after the five days of tablets finishes.
You need to be sure you’re not actually pregnant before you take clomiphene (see thebox, Beware clomiphene in pregnancy). Remember that because ovulation precedes a periodby two weeks, it’s possible for pregnancy to happen in a naturally resolving case of amen-orrhea without having an intervening period: you can go seamlessly from anovulatoryamenorrhea through a single ovulation to pregnancy, all without a period.
If you haven’t been ovulating, you need to have a proper period brought on by a courseof progestogen tablets, both to be sure no hidden ovulation leading to pregnancy has occurred,but also to shed the endometrium effectively before a new cycle starts. I use a progestogenknown to be innocuous in pregnancy for this purpose,medroxyprogesterone acetate (Provera),
164 � GETTING PREGNANT
Beware clomiphene in pregnancy
Clomiphene is probably not a safe drug in pregnancy, at least once the embryo’sgenital tract is developing, around eight to 10 weeks from the start of the concep-tion cycle (from the last menstrual period).
Although no birth defects have been reported with exposure of human fetusesto clomiphene, clomiphene as an estrogen-blocking drug happens to be very similarin structure to the estrogenic drug diethylstilbestrol (DES), which was widelyprescribed in the 1950s for miscarriages, and which is now notorious for havingcaused deformities of the upper vagina and uterus in female fetuses and of theepididymis and vas deferens in male fetuses.
Experiments show that clomiphene and DES do similar harm in pregnant mice.What they have in common, in disturbing these estrogen-sensitive events in theembryo, is prolonged attachment to the estrogen receptors, distorting the normalsequence of events in the development of the relevant organs and tissues.
I should stress—because it’s been seized on by some writers—that there’s nopractical possibility of enough clomiphene remaining in the body through the timeof ovulation and into pregnancy for there to be a risk of these harmful effects whenclomiphene is taken to induce ovulation. (And this is probably true even if a periodis misinterpreted and a course of clomiphene is mistakenly taken two weeks afterconception.)
Apart from being metabolized and excreted, clomiphene is so tightly attachedto existing receptors that even if some were to stick around this way there would benegligible amounts free to cross the placenta from the mother to her fetus weeksafter the last tablet was taken.
But this knowledge does serve to warn that it’s important not to use clomiphenein amenorrhea without first ruling out pregnancy.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 164

at a dose of, say, 5 milligrams per day for a full two weeks, which is the length of a normalluteal phase.
If there’s no bleeding within a few days of stopping the progestogen, we measure theserum estradiol as well as the serum progesterone and a pregnancy test.There could be a preg-nancy, but more often the hormone levels will be low and the explanation for the lack ofbleeding is that there was not enough endometrium present in the first place for it to beshed this way and thus for bleeding to occur.
If the serum progesterone is elevated, it’s possible to have a very early pregnancy evenif the pregnancy test is not positive yet.Whether pregnant or not, ovulation has occurred,so you should wait for a natural period before you start the clomiphene; you can then repeatthe serum progesterone and the pregnancy test if the period seems too light or too unusualto rule out pregnancy.
Once you’re ovulating regularly on a particular dose of clomiphene, you can repeat itfrom month to month without necessarily checking pregnancy tests each time, providedfirstly that the period that signals the repeat 5-day course is not unusual, and provided alsothat there is no pain in the region of the ovaries to indicate possible over-stimulation.
If you have PCOS and continue not to ovulate despite clomiphene, metformin can beadded (see earlier); if there is an elevation of an adrenal hormone called DHAS a night-time dose of a corticosteroid such as dexamethasone, 0.25 to 0.5 mg, can be given; or thedose of clomiphene can be increased.
Over the course of six months, pregnancy will happen in about half the women whorespond to clomiphene by ovulating. Of these pregnancies, about 20 percent end in mis-carriage, a particularly disappointing outcome.
The reason for the rather frequent lack of successful pregnancy despite apparently goodovulations is thought to be related to the estrogen-blocking effects of clomiphene.Especiallywith higher doses, such unwanted anti-estrogenic effects can spoil clomiphene’s beneficialeffects.These estrogen-blocking properties linger well past the useful rise in FSH thatclomiphene causes, interfering with the production of cervical mucus, and spoiling spermtransport, and also jeopardizing the normal growth of the endometrium, with the result thatthe periods become noticeably lighter and that, if it is checked, a luteal phase defect will beapparent on premenstrual endometrial biopsy.
If clomiphene doesn’t work, we have two more potent options for stimulating ovula-tion, both of them more complicated.We can provide gonadotropin releasing hormone(GnRH) by intravenous injections (it will not work in cases of PCOS). Or we can directlysubstitute for the absence of follicle stimulating hormone by giving daily injections of it.
Pulsatile GnRH
To use the FSH-regulating hormone GnRH clinically, we have to administer it in the wayit’s produced by the brain—that is, in spurts directly into the blood system.To do this, weload the GnRH into a portable, battery-operated, electronic syringe driver, preset to admin-ister an exact amount of the drug into a vein every 60 to 90 minutes, for about two weeks(the normal length of a follicular phase).
NOT OVULATING � 165
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 165

The GnRH stimulus to the pituitary gland to produce FSH needs to be in pulses, butit doesn’t have to be cyclical.The monthly pattern of the ovarian cycle (see Chapter 3 forthe details) is governed solely by the ovary. So the role of GnRH, though indispensable, isjust facilitatory, and simple to mimic.
It’s a wonderfully effective, if somewhat inconvenient, treatment, with no appreciablerisk of ovarian overstimulation (see Chapter 11) and no substantial risk of multiple preg-nancy.The rate of ovulation, with properly chosen cases of amenorrhea, is 100 percent(there’s not much in medicine you can say that about!) and the chance of pregnancy, if thereare no other reasons for infertility, is up to 40 percent per month.
(Note that the use of GnRH this way has nothing to do with the use of GnRH-agonistsin association with FSH injections for controlled superovulation in IVF programs.)
Special precautions need to be taken to change the intravenous site every four or fivedays, or at the first sight of inflammation of the vein.GnRH should not be used in patientswith heart murmurs because of the hazard of bacterial endocarditis, a condition in whichbacteria grow on the heart’s valves, damaging them catastrophically. Because of the smallrisk of infection, some doctors prefer to administer pulsatile GnRH under the skin (subcu-taneously), but it’s not so quickly absorbed there and treatment often fails. For the GnRHto work it needs a sharp upwards then downwards profile in the blood. If it’s administeredunder the skin, this profile is blunted.
Although pulsatile GnRH works extremely well in hypothalamic anovulation and alsoin hyperprolactinemia, it is not very effective in polycystic ovary syndrome.
Gonadotropin treatment
The other option, if clomiphene fails, is to stimulate the ovary directly with follicle stimu-lating hormone. Like GnRH,FSH also cannot be given by mouth, it has to be injected daily—generally intramuscularly into the arm or buttock for the old preparations of humanmenopausal gonadotropin (Humegon and Pergonal ), or subcutaneously with the new, pureFSH preparations—for about the two weeks it takes follicles to develop.
The newer FSH preparations are either highly purified from urine (Metrodin HP,whichis Fertinex in the USA, and Repromex) or synthetic, recombinant FSH (Gonal-F andPuregon), lacking the contaminating urine proteins that made the earlier preparationssuitable only for (rather uncomfortable) intramuscular injection and which caused occa-sional allergic reactions, but also lacking luteinizing hormone (LH).This lack of LH in modernpreparations of FSH matters only when natural LH is completely absent (as in cases ofcongenital FSH and LH deficiency: see the box, Kallmann syndrome and primary amenorrhea).
The same FSH preparations are used in IVF and GIFT to increase the proportion offollicles that grow and to become suitable for egg retrieval (see Chapter 20).
Using FSH to induce ovulation for getting pregnant naturally is tricky at the best oftimes (because of the risk of stimulating too many follicles and having a multiple preg-nancy), but the accumulation of very many little follicles that occurs in PCOS makes theuse of FSH even trickier for this condition: sometimes 20 or more follicles grow in eachovary! When bromocriptine, clomiphene or GnRH is used to induce ovulation, the
166 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 166

NOT OVULATING � 167
FSH and hCG administration, the day-by-day detail
To induce ovulation we typically start with 150 to 225 units of FSH each day, increas-ing the dose if necessary to get a rising level of serum estradiol, which we monitorfrequently, getting the result back a few hours after the blood test is taken. Once theserum estradiol gets to a concentration of about 1000 picomoles per liter, or about400 picograms per milliliter (a picogram is one-thousandth of a nanogram, whichis one-thousandth of a microgram, which is one-thousandth of a milligram, whichis one-thousandth of a gram!), we perform a transvaginal ultrasound scan to see howmany growing follicles we’ve produced that are contributing to the estrogen we’remeasuring.
The number of follicles that grow depends more on the number of respon-sive follicles that are present when FSH injections start than on how much FSHwe give—it’s largely a threshold effect on the follicles (below the FSH dosage-threshold the follicles compete and only one becomes a pre-ovulatory follicle;above the threshold they almost all do). If we’re inducing the development offollicles for superovulation (that is, for IVF, see Chapter 20) we will want a largenumber of follicles to get to be pre-ovulatory follicles (because we want a numberof eggs to work with), so we aim to keep the dose of FSH above the thresholddose.
But when we’re inducing ovulation in an anovulatory woman who is aimingto get pregnant by having sex, we need to aim for just one or two pre-ovulatoryfollicles, or there will be a risk of multiple pregnancy.
If the number of developing follicles is too high, we gradually reduce the dailyamount of FSH, mimicking the competition imposed on follicles that occurs innatural cycles as FSH levels fall during the follicular phase (see Chapter 3). If thenumber of follicles is way too high,we might have to stop altogether and, in consul-tation with the woman concerned, cancel the cycle.
Sometimes when we decrease the FSH dosage, all the follicles fall by the wayside(they become atretic), and the cycle is then also canceled.
Once the follicle or follicles have a mature size (about 2 centimeters diameter),we start the process of ovulation itself by administering hCG in a dose, depending onthe woman’s weight, of 3000 to 10 000 units.We know that ovulation will take placefrom follicles over about 1.5 centimeters in diameter about 38 hours after hCGadministration.
So, for conceiving naturally we usually give the hCG during the afternoon, inpreparation for intercourse the following evening. (See Chapter 19 for the OK ifyou want to have a glass of wine first.)
For IVF or IUI we fix the time at which we want to carry out the egg retrievalor the insemination (generally daytime), then count back 36 hours to set the timefor the hCG injection.This gives us an hour or two in reserve in case there are delays.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 167

normal feedback relationships between the follicles in the ovary and the FSH-produc-ing cells in the pituitary gland are more or less maintained.This means that there’s littleincreased risk of twins or of higher-number multiple pregnancies such as triplets orquadruplets. It also means that there’s little risk of serious enlargement of the ovaries,known as ovarian hyperstimulation syndrome (see Chapter 12).This, however, is not true oftreatment with FSH.
When FSH injections are used, the ovaries are stimulated directly.The only feedbackthat operates is what we get from the ovarian monitoring we do.We check on the appro-priateness of the doses by measuring the estrogens the follicles are producing (as serumestradiol) and by doing transvaginal ultrasounds to compare how many follicles are produc-ing the amount of estrogen we’re measuring.We therefore use these tests to limit theamount and duration of FSH, trying to get just one or two follicles to the point ofovulation.
Ovulation itself, including the final 38 hours or so of immediately pre-ovulatory changes
Supplementary doses of hCG (1000 units to 2000 units) are given four days andeight days after the initial ovulating dose to maintain drive to the corpus luteum, sothat it (or they, if there are more than one) will produce adequate progesterone forlong enough for pregnancy to become established—at which time hCG from thepregnancy itself will stimulate and ‘rescue’ the corpus luteum.Alternatively, proges-terone itself can be administered vaginally (this is more usual when there has beensuperovulation for IVF or IUI and there is a risk of ovarian hyperstimulation syndrome,discussed in Chapter 12).
Some nuances of treatment with FSH
In general, the dosages of FSH and hCG needed for ovulation induction, as withsuperovulation for IVF, depend on the body mass index.
In women over 100 kilograms (say 200 pounds), a daily dose of as much as600 units of FSH is typically needed, together with an hCG dose of 15 000 unitsto ovulate the follicles generated.
In the polycystic ovary syndrome, however, follicles are typically exquisitely sensi-tive to FSH, the dose of which might need to be much less than usual to avoid grossoverstimulation, despite a high BMI, whereas the hCG dose will be conventionalfor the woman’s particular weight.
In patients with absent pituitary production of LH (because of a deficiencyfrom birth, from disease of the pituitary gland, or because GnRH-agonists or antag-onists have dropped serum LH levels below 1.5 U/liter), a small amount of LHneeds to be added for pure FSH preparations to work properly. Recombinant LH isbeing marketed for this purpose: the recommended daily dose is 75 U.A consid-erably cheaper alternative is to use a similar low dose of hCG every day or everysecond day.
168 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 168

in the Graafian follicle, is triggered with an injection of human chorionic gonadotropin (hCG),acting like LH. hCG is marketed as Pregnyl (by Organon) and Profasi (by Serono). For thefull experience of treatment with gonadotropins, see the box, FSH and hCG administration,the day-by-day detail.
Even with the best of monitoring, though, more follicles can reach maturity than issafe to risk intercourse, and either the ovulation cycle that has been induced will need tobe canceled (it can seem to be a waste) or a last-minute suggestion might be made to carryout an assisted conception procedure such as IVF or GIFT instead (a compromise that’snot always ideal, because the decision is often made after the dose of FSH has been decreasedmore or less drastically, threatening the health of the extra eggs we like to have available inan IVF cycle).This is especially likely for ovulation induction for PCOS, in which responseto FSH is all too easily excessive.
UNTREATABLE ANOVULATION: PRIMARY OVARIAN FAILURE
Anovulation is generally one of the best-treated forms of infertility.There are exceptionsthough.When there are no responsive follicles in the ovaries, ovulation cannot be inducedwith the hormones or drugs described above. As discussed in Chapter 6, this happens inprimary ovarian failure (meaning that the ovarian failure is intrinsic and not secondary to aproblem mediated by the pituitary gland).
The diagnosis of primary ovarian failure is pointed to by serum FSH levels that arehigh, particularly if this has been the case on more than one occasion.Another name forit is premature menopause.The diagnosis will be the case in 5 percent to 10 percent ofpatients under the age of 40 investigated for absent periods and absent ovulation.Youmight have suspected it by the experience of menopause-like symptoms, such as hotflushes or flashes.
A biopsy of the ovary (a procedure carried out at the operation of laparoscopy) cansometimes be useful: it can reveal a complete absence of follicles (true premature menopause),the presence of many unstimulated follicles (called the resistant ovary syndrome) or, rarely,an inflammation of the follicles due to antibodies produced by the body against its owntissues (autoimmune oophoritis). For more, see the box, Special causes of primary ovarianfailure.
In cases of oligomenorrhea from impending primary ovarian failure, where serum FSHis already elevated, at least periodically, clomiphene or additional FSH will be of no use.Ovulation will happen intermittently when there is a sensitive follicle: no amount of FSHwill produce a follicle any faster.
Pregnancies can happen from these ovulations. Especially if the woman is still in hertwenties, the occasional follicle and its egg can be remarkably fertile. But are there dangersin pursuing pregnancy from these rare follicles and eggs? For a discussion, see the box,Special causes of primary ovarian failure (the section on X-chromosome anomalies). For adiscussion on the possible role of IVF, see the Chapter 20 box, IVF Lite™:More natural IVF.
Generally, though, we’re left with two therapeutic avenues, one discretionary and onemore or less compulsory.
NOT OVULATING � 169
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 169

170 � GETTING PREGNANT
Special causes of primary ovarian failure
Everyone’s ovaries will eventually fail.The younger a person is when depletion of eggs is complete, though, the more
likely it is that special tests can reveal a special reason for there being fewer sensitiveovarian follicles than expected.
We look here at three special causes of primary ovarian failure, in one of which,before depletion of eggs is complete,serious genetic disease can be passed on to offspring.
Special cause #1:The resistant ovary syndrome
Primordial follicles in the ovary (discussed in Chapter 3) start to grow for reasons thatseem to have nothing to do with FSH; it’s not until the secondary or tertiary folliclestage (eight months or so later) that follicles become sensitive to FSH.
This means that there’s an opportunity for things to go wrong that will frustrateFSH despite the presence of many small follicles.
In these situations a biopsy of an ovary (a procedure done at laparoscopy) can revealloads of primordial follicles instead of the expected picture with prematuremenopause,which is a virtual absence of such follicles.This is the appearance dubbed‘the resistant ovary syndrome’.
Behind the condition could be a shortage of any one of a number of unknowngrowth factor molecules.
Alternatively there could also be a mutation in the FSH receptors that folliclesneed to have to respond to FSH.
Or there could plausibly be a mutation in the FSH molecule itself that stops itbinding to FSH receptors while still permitting an assay for FSH to recognize theelevated level of serum FSH (serum ‘faulty FSH’) that would follow its lack of action.
In a condition called galactosemia, a number of things go wrong with folliclesand eggs from an early age, possibly affecting mitochondria as well as FSH receptors.In families with this disorder, sisters can have either the resistant ovary syndrome orpremature menopause on ovarian biopsy.
Treatment, for the moment, involves trying to sensitize the blocked follicles—using estrogen in an attempt to get them to grow to the point where they willrespond to FSH.This means we don’t give estrogen and progestogen together (thiswould be like being on the contraceptive pill). Instead, we give a small dose ofestrogen, say ethinyl estradiol (Estigyn, Progynon C) 10 to 20 µg per day, for four tosix weeks, interspersed with, say, medroxyprogesterone acetate (Provera) 5 mg per day,for two weeks.
This regimen can reasonably be used also in cases of apparently imminent ovarianfailure, when there is oligomenorrhea and intermittently elevated serum FSH levelsand, despite frequent symptoms of premature menopause, pregnancy is still beinghoped for.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 170

Special cause #2:Autoimmune oophoritis
There’s a class of diseases called autoimmune diseases in which the body’s immunesystem is driven to an attack, not on invading organisms, but on the body’s owntissues.Examples include attacks on the joints (rheumatoid arthritis), on the skin andthe muscles (dermatomyositis), on the arteries (polyarteritis nodosa), on the liver(autoimmune hepatitis), or on many tissues at once (in a disease called systemic lupuserythematosus).
The same can be true of the ovary in autoimmune oophoritis,which, in its earlystages, causes painful enlargement of the ovaries, visible on transvaginal ultrasound.Anovarian biopsy, taken at laparoscopy,will reveal inflammatory cells attacking the folli-cles, many of which can be cystic. Sometimes the only relief from the pain is toremove the ovaries at operation.
There’s a chance,still mainly theoretical, that early treatment with drugs that suppressthe immune system,such as cortisone and stronger drugs,might reverse the process;butthere’s been too little experience with them to know, as it’s a rare condition.
The end result is true premature menopause, with loss of all follicles.It’s usual to look for various tissue antibodies in all cases of primary ovarian
failure, because autoimmune oophoritis might not manifest until it has run its coursecompletely and all the follicles have been burned out by the immune process.
As well, autoimmune oophoritis tends to occur in association with some otherspecific autoimmune diseases of various glands.These other antibodies can be lookedfor in the blood to predict the later development of serious disease,which can there-fore be anticipated and treated before harm is done.
The other antibodies usually looked for include: thyroid antibodies (whichproduce an underactive thyroid, or hypothyroidism); adrenal antibodies (which causethe adrenal glands to fail, with weakness, low blood pressure and, often, increasedskin pigmentation); islet-cell antibodies (the islets of the pancreas produce insulin,so these antibodies anticipate diabetes); and gastric parietal cell antibodies (these cellsin the stomach produce ‘intrinsic factor’, which is needed for the lower intestine toabsorb vitamin B12—deficiency of B12 causes pernicious anemia and degenerativedisease of the spinal cord).
Although we tend to do these tests routinely, they are not often positive.
Special cause #3: X-chromosome anomalies
The younger a patient with primary ovarian failure, the more likely it is that there willbe an abnormality of the sex chromosomes to account for it detectable with a karyo-type, such as a partial Turner syndrome karyotype or triple-X karyotype.
Or the primary ovarian failure could be a manifestation of the woman being acarrier of an X-chromosome that is curiously fragile. If such an X-chromosome isinherited by a male child it causes a form of mental retardation known as fragile-Xsyndrome, which is the commonest cause of severe mental retardation in boys.
NOT OVULATING � 171
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 171

The medically important priority results from the inevitable shortage of estrogen produc-tion from the ovaries, which if not anticipated means that medical complications are likelyto happen eventually, comparable to those that follow the menopause (such as a lossof calcium from bones and an increased risk of heart disease), but at a younger age. It’simportant to prevent these complications by using estrogens, to which a progestogen tabletneeds to be added (for 11 days or more per month) to keep the endometrium from over-responding and overgrowing.
The discretionary avenue—the remaining hope for the young woman to have a baby—lies with egg donation, a subject covered in Chapter 22.
DANGEROUS CAUSES OF ANOVULATION
In every case of amenorrhea the careful physician will consider whether or not a potentiallydangerous tumor is lurking behind it.This is especially the case if there’s hyperprolactinemia(a substantial increase in serum prolactin, see below) or if there’s no obvious reason for theamenorrhea such as weight loss or PCOS.
Tumors affecting ovulation can grow in or above the pituitary gland (best revealed by aCAT scan or MRI scan of the pituitary gland and hypothalamus), or in the ovaries or adrenalglands (suspected on hormone testing and confirmed by imaging with a transvaginal ultra-sound, or a CAT scan or MRI scan of these organs).
Occasionally a hormonally active tumor in one or other ovary will be evident only bylocalizing the production of a high amount of a hormone such as estradiol, testosterone orandrostenedione to the affected ovary by selective catheterization, and sampling the ovarianand adrenal veins to assay these hormones.
Should a woman with primary ovarian failure have a karyotype and DNA studiesfor fragile-X done?
If there is no longer a hope of pregnancy, identifying a genetic abnormality couldhave little point, because reproduction is anyway prevented. It’s enough to cope withknowing that ovulation will never be possible without having to contend with thethought that one’s chromosomes are not normal.
On the other hand, if ovulation is still happening intermittently (a few folliclesstill remain) then active measures might still be pursued to make the most of ovula-tions still to come in the hope of achieving pregnancy.
Moreover, and especially if a second cause of subfertility or sterility has been diag-nosed, one possible therapeutic avenue to explore is IVF.
The best IVF technique to attempt is one in which the woman’s natural cycleis made use of, even though it is irregular. (For the details, see the Chapter 20 box,IVF Lite™: More natural IVF . . .).
In these situations further genetic testing for fragile-X (with DNA testing) andfor aneuploidy of the sex chromosomes (with a karyotype) becomes particularlyimportant.
172 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 172

If the serum prolactin is more than about twice normal, then it’s especially importantto look for a prolactin-secreting tumor in the pituitary gland. If the tumor is small, notdistorting the bone that contains the pituitary gland, it’s called a microadenoma; if biggerthan about 1 centimeter, it’s a macroadenoma. In either case, drug treatment withbromocriptine or cabergoline is the treatment of first choice, as it will shrink the tumor.Remember, though, that irrespective of the size of the tumor, bromocriptine or cabergo-line will cause ovulation and fertility to return very quickly.
Because prolactin-producing tumors are likely to grow during pregnancy, it’s not usuallywise to allow pregnancy before a macroadenoma has shrunk to the size of a micro-adenoma. Even then, complications from sudden growth or hemorrhage into the tumor(with compression of a surrounding structure such as the optic nerve) can occur duringpregnancy, needing urgent drug therapy or surgery (performed through the back of thenose) to take away the effects of the pressure.
‘POST-PILL’ AMENORRHEA
It’s commonly thought that the oral contraceptive, or birth control, pill can stop periodsfor months after its discontinuation. It’s now known that this is not true: the effect of thepill wears off in days.
The confusion began in the 1960s and 1970s, when not all the causes of amenorrheawere yet understood. In particular, the effects of weight loss on stopping periods was notappreciated until the late 1970s, after Dr Rose Frisch from the Harvard School of PublicHealth had drawn attention to it in a series of careful studies and publications.
We know now that virtually every instance of amenorrhea arising when the pill is stoppedcomes about because one of the conditions described above has developed coincidentally,buthas been masked because the pill will cause periods in anyone with a sensitive uterus andendometrium.The estrogen and progestogen the pill contains drive the uterus directly, irre-spective of what the pituitary gland and ovary might otherwise have been doing.
There is no relation, incidentally, between periods disappearing while on the pill andperiods not occurring after the pill’s stopped.‘Pill amenorrhea’, an absence of periods whileon the pill, is simply an exaggerated manifestation of what every pill user knows, namelythat periods are lighter while on the pill.This is because the progestogen in a pill cycle stopsthe endometrium from getting thicker much earlier than in the natural cycle; progesteronein the natural cycle does not take effect until after the first two weeks.
About 10 percent of women get extremely light periods (hypomenorrhea) or absentperiods (amenorrhea) while taking the pill.Apart from losing the reassurance that there’s nopregnancy, no harm comes from the periods being absent in this situation.
This is as good a place as any to dismiss the notion that the pill should be stopped forseveral months before attempting pregnancy ‘to get it out of the system’ (as if it were apoison).This advice is foolish.The pill, as demonstrated by the bleeding that follows itsbeing stopped, is out of the system within a few days.
At least one condition that can jeopardize the chance of getting pregnant—endometrio-sis—is usually suppressed on the pill, and stopping the pill for several months in favor of an
NOT OVULATING � 173
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 173

alternative contraceptive can be just long enough to allow endometriosis to get active againand spoil the chance of pregnancy.
In Chapter 12 we will focus on what can go wrong with ovulation induction before wemove on to the other specific causes of, and treatments for, infertility.
174 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 174

complications from FSH therapy
Especially OHSS
Dangers associated with inducing ovulation using gonadotropin treatment for ovulationinduction and,especially,multiple-ovulation induction (superovulation) for assisted conception(see Chapters 10 and 20), are dominated by the risk of over-enlargement of the ovaries.
The important condition that can result is the ovarian hyperstimulation syndrome (OHSS).Additional theoretical concerns with gonadotropin treatment—none of which has beenproven—include the possibilities of cancer, birth defects and infection.
OVARIAN HYPERSTIMULATION SYNDROME
It’s normal for the ovary to produce fluid in the abdomen (the peritoneal cavity) as a folliclegrows; it’s normal for the ovary to bleed at ovulation; and it’s normal for a corpus luteum toform in the ovary and to become cystic in the second half of the cycle, the luteal phase. Paincan accompany ovulation and the formation of a cystic corpus luteum. Premenstrual tensionat this time can cause bloating, irritability, depression and breast pain.When the ovaries arestimulated to increase the number of follicles, all these events and their symptoms can bemore than you would expect in a natural cycle.
There’s no sharp distinction between the expected and the unexpected when the ovariesare stimulated. It’s a matter of degree.The signs and symptoms usually get worse if there’ssuccessful conception, because the natural production of hCG will then be added to theinjected hCG that’s helped stimulate the ovaries up to that point.
In our experience of over 15 000 stimulations at Sydney IVF and at Royal Prince AlfredHospital, we would estimate that about one in 30 stimulations is accompanied by enoughpelvic pain in the luteal phase to cause a woman to want to rest in bed for a day or more(mild OHSS). In about one in 250 stimulations, rest in hospital results, mainly for obser-vation and to enable us to give adequate relief of discomfort or pain (moderate OHSS). In
175
12
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 175

about one in 1000 stimulations there’s enough fluid in either the abdomen or the chest tobe of serious medical concern: this is severe OHSS.
The main symptoms of dangerous degrees of hyperstimulation are difficulty in breath-ing, and vomiting or diarrhea. Breathing difficulties are caused by fluid accumulating inthe abdomen or in the chest and, if necessary, relief comes quickly (if temporarily) byaspirating the fluid. Removing fluid this way, or losing fluid through vomiting, can causedehydration, which, if it’s not recognized and not treated promptly, can lead to thickeningof the blood, slowing its flow, and hence to its clotting—a thrombosis.These are seriousconsequences. Strokes and even deaths have occurred in some centers. Further, the enlargedovaries can bleed, especially if they’re traumatized in any way.
Why do some women get severe OHSS while other women, with larger ovaries orhigher hormone levels, do not?
It’s clear that the fluid that accumulates is not coming directly from the ovaries; it’salso clear that it’s not a direct effect of high hormone levels on the tissues.After years ofspeculation, a study from Monash University in Melbourne pointed out the answer in themid-1990s. Dr Neil McClure and others reported in The Lancet that a protein is beingproduced in the ovary called vascular endothelial growth factor (VEGF), which increases thepermeability of capillaries to fluid as new capillary growth is stimulated.
VEGF is needed for new blood vessels to form in the pre-ovulatory follicle. If thequestion of why some women produce too much of this factor compared with others isstill obscure, at least we could have a more reliable way of predicting the development ofthis complication.
The ovaries will always recover completely from hyperstimulation, so long as they’renot operated upon and removed. Operation is rarely necessary for hyperstimulation, butone situation in which it is necessary is when the enlarged ovary rolls around and twistson its blood supply—a phenomenon known as torsion. Unless torsion is recognized andtreated quickly (see the box, Torsion of a rolling, twisting ovary), the ovary will not be able torecover and its eggs will be lost.
OVARIAN STIMULATION AND CANCER
There’s no direct evidence linking cancer to ovarian stimulation with gonadotropin (FSH)treatment, but in the 1990s there were suspicions of an association.There were three partic-ular areas of significant concern.
Breast cancer is the most common cancer of women during the reproductive years,especially if there’s a history of it in the family at a young age. It’s also more commonamong women who have not had children.There’s therefore a significant risk of breastcancer coinciding with infertility treatment, and the high levels of estrogen and proges-terone that go with stimulating the ovaries (and which also go with pregnancy) couldcause a cancer that’s already there to grow more quickly. For these two reasons, ovula-tion induction or assisted conception should not be undertaken, particularly by an olderwoman, if there’s an unresolved suspicion of breast cancer, such as a recently discoveredbreast lump.
176 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 176

Cancer of the cervix is another common malignancy in young women.Although it’s notcaused or aggravated by ovulation induction or by pregnancy, treatment of it during preg-nancy is difficult.Be careful to stay up to date with your cervical smears (Pap smears).Don’tassume because you’re having procedures done vaginally that check-ups of the cervix arebeing carried out: a cancer smear will not usually be taken during ovulation induction orassisted conception treatment unless you specially ask for it to be done.
Ovarian cancer is most often a tumor of older women, but by the mid-1990s about 10ovarian cancers in women who had been having ovulation induction had been reportedin the medical literature. In some of these women the cancer clearly preceded treatmentand was therefore a coincidence.The reported frequency has since been no higher thanmight be expected by chance, considering the huge numbers of treatments withgonadotropins that have been conducted around the world since the early 1960s.
An important on-going study of cancer incidence in women who had IVF in Victoriaduring the 1980s is being conducted by Dr Alison Venn of La Trobe University. She hasfound no increase.
Nonetheless, the association needs further research, not least because, like breastcancers that are already there before treatment, ovarian cancers can grow much morequickly during ovarian stimulation and during pregnancy. Individual women with infer-tility can be at particular risk of ovarian cancer, especially in later life.The reasons, andhow an ovarian cancer might be detected early, are described in the box, Infertility andovarian cancer.
COMPLICATIONS FROM FSH THERAPY � 177
Torsion of a rolling, twisting ovary
Torsion of an ovary occurs when an enlarged ovary, suspended on the comparativelyslender stalk of its blood vessels, rolls on itself to tightly twist this stalk, thus cuttingoff its own blood supply.
There is more or less sudden onset of severe continuous pain, usually accompa-nied, equally suddenly, by nausea and vomiting.
A useful study from Dr Gabriel Oelsner and others at the Chaim Sheba MedicalCenter in Israel has shown that most cases can be treated by simply untwisting theovary—even if the torsion is of more than a day’s duration, and even if the ovarylooks ugly from congested, old, unoxygenated blood.
Of 40 patients with ovarian torsion over a 10-year period, 14 were treated thisway at laparoscopy, saving not just the ovary and its eggs, but also the need for majorsurgery.
Torsion can sometimes happen without a prior major degree of hyperstimula-tion (it can occur without warning or antecedent interventions in girls passingthrough puberty, as a previously small ovary first enlarges with follicles).
With ovarian stimulation or superovulation it’s more common if pregnancy hashappened, as the enlarged ovary is lifted off its bed by the expanding uterus.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 177

OVARIAN STIMULATION AND BIRTH DEFECTS
The National Perinatal Statistics Unit, which for many years has collected data on birthdefects in the Australian population, cooperates with the Fertility Society of Australia topublish the birth outcomes of all pregnancies that happen as a result of IVF and GIFTprocedures.Although providing this information is voluntary for the 30 or so IVF programsin Australia, all centers or units take part.
In 1987 Dr Paul Lancaster, who then headed the NPSU, suspected that there could bea slight increase in birth defects after IVF. Given that miscarriages are more common in
178 � GETTING PREGNANT
Infertility and ovarian cancer
One reason to suspect that there could be a significant cause-and-effect relationshipbetween excessive ovulation and ovarian cancer is that it’s known that pregnancy orprolonged use of the oral contraceptive (birth control) pill—both of which inhibitovulation—protect for years afterwards against its later development.
In the case of the pill, using it for 10 years or more reduces the risk of ovariancancer after the menopause to about one-fifth of the incidence if the pill has neverbeen used. It’s therefore plausible that repeated multiple ovulations caused by repeatedcycles of FSH treatment will cause a similar increase in ovarian cancers.
This is not the same as saying that these hormones are carcinogens or that theyare the cause of the cancer (in, say, the way cigarette smoking is the cause of lungcancer).What’s likely is that the risk of cancer of the ovary depends in some way onthe total number of ovulations a woman has had. Ovulating 10 eggs at once wouldthen amount to 10 months’ worth of risk with single ovulations.
The big worry about ovarian cancer is the inaccessibility of the ovaries: a cancerin an ovary is usually rather extensive before symptoms alert you or your doctor tothe possibility.
Some women who, because of similar cancers in their family, are at particularlyhigh risk of ovarian cancer have therefore chosen after their menopause to have theirtwo ovaries removed surgically (the operation can usually be done at laparoscopy).
Short of such a radical step the best protection against ovarian cancer after themenopause is to have regular check-ups. Presently the best way of screening theovaries, before or after the menopause, is with transvaginal ultrasound and a specialblood test—a serum CA125 antigen level.
The ‘cost-effectiveness’ of screening the general population for ovarian cancerthis way has not been demonstrated to the satisfaction of our politicians,but for peoplewith special concerns it’s likely that such examinations will accompany Pap smearsand breast examinations after the menopause as routine screening maneuvers.
Meanwhile research is continuing on other blood tests that could indicate earlyovarian cancer.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 178

infertile women in general, but are particularly so in those conceiving with clomiphene(which was routinely used with FSH to stimulate the ovaries for IVF in the 1980s), DrLancaster’s proposal was, in a sense, not very surprising.
Of special concern was a possible several-fold increase in major deformities of thenervous system of the type called neural tube defects, which comprise anencephaly (anabsence of development of the brain, and not compatible with survival) and spina bifida (aserious defect of the spinal cord producing paralysis and a lack of bowel and bladder control).
Curiously, on the other hand, for a number of years no cases of cleft lip or palate (oneof the more common birth abnormalities) were encountered. If it is legitimate, just onthe basis of statistics, to suspect that IVF caused neural tube defects, it is equally justifiedto conclude that IVF protected embryos against cleft lip and palate.As you would expect,this is nonsense: I’m pointing it out to show the dangers of jumping to conclusions fromlimited data.
So many different birth defects are known that it was inevitable, just by chance, thatsome of them would be more common and some less common than expected. In bothcases, further experience has not supported the original conclusions. Cleft lip or palate hassince happened. It’s also been established that in fact there is no increased chance of neuraltube defects after ovulation induction or assisted conception.
The incidence of reportable birth defects has remained at about 2 percent of births,about the same as for the general population.What is more common (we discuss it in theChapter 10 box,From father to son) is an increase in some sex chromosome-based birth anom-alies when ICSI is used for extreme male-factor infertility.
INFECTION
Nowadays the follicle stimulating hormone (FSH) that is the essential ingredient of gonadotropintherapy for ovulation induction and stimulation protocols for IVF comes from two sources.
The first is from the urine of women who have been through the menopause and whoproduce large quantities of it.This is the source of human menopausal gonadotropin (hMG)preparations such as Humegon, Metrodin, Fertinex, Pergonal and Repromex.
Although some of these are now of merely historical importance, they remain morekeenly priced than their successors, the second group, the more or less synthetic recombi-nant follicle stimulating hormone (rFSH) preparations Follistim, Gonal-F and Puregon.Therecombinant FSH preparations are manufactured using gene technology methods, in whichthe DNA for making human-style FSH is inserted into the genome of hamster ovary cells,which are cultured in large vats and dedicated to churning out billions and billions of iden-tical FSH molecules (follitropin alpha or follitropin beta, depending on the manufacturer).
There are several reasons why the recombinant FSH preparations are favored over thepreparations extracted from human urine.
First, they are more reliable and consistent in potency.Second, the logistics of manufacture are much, much simpler and so they are cheaper
for the major drug companies to make (although this is not reflected in their price, whichis higher than for hMG preparations).
COMPLICATIONS FROM FSH THERAPY � 179
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 179

And third, although no infections have ever been reported from the human urine-derived hMG preparations, this remains a theoretical possibility. (For a cautionary tale ofthe potential seriousness of viral or prion transmission with human-derived FSH, see thebox, Creutzfeldt-Jakob disease and hPG.)
Meanwhile, the other gonadotropin needed for final maturation of the follicle and eggduring ovulation and stimulation for IVF, luteinizing hormone (or rather its usual substi-tute,human chorionic gonadotropin, hCG) was still, in 2002, available only from human urinarysources, in the form of Pregnyl and Profasi. It will not be long, however, before recombinanthuman chorionic gonadotropin and recombinant luteinizing hormone become available, as Ovidreland Luveris, respectively.
180 � GETTING PREGNANT
Creutzfeldt-Jakob disease and hPG
In the 1960s and 1970s, several countries established national programs in whichpituitary glands in their thousands were removed at all sorts of autopsies.The purposewas primarily to secure growth hormone for the treatment of growth-stuntedchildren who have growth hormone deficiency.
But secondarily there was an opportunity to save on the high cost of hMG byalso extracting the gonadotropins (as a mixture of FSH and LH), to yield a productcalled human pituitary gonadotropin (hPG), for ovulation induction.
All appeared to go well until the 1980s.Then several patients who had beentreated with growth hormone in different parts of the world (though not in Australia)developed a deadly brain disease, Creutzfeldt-Jakob disease (CJD), related to the‘mad-cow disease’ occurring in Britain from eating infected meat. hPG was imme-diately withdrawn from use, but it was too late.
CJD, once symptoms of dementia appear, is inexorably and rapidly fatal. In thelate 1980s in Australia (but, curiously, not in other countries), three women whoyears before had received hPG for amenorrhea related to FSH deficiency developedCJD and died.The contamination with the CJD prion probably occurred via thesmall amount of brain tissue that forms the neurohypophysis, the back part of the pitu-itary gland.
This tragic outcome to what were generally the best of intentions appears nowto have run its course, with no new cases turning up in the last 10 years.
It is important to note that CJD has not been reported to occur from the formsof gonadotropin used therapeutically today for ovulation induction and IVF. Noris there any reason to suppose that women who are being treated this way withhormones extracted from urine (the human menopausal gonadotropins) run such a risk.
For those connected with this awful turn of events—patients and doctors—theanguish has been considerable.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 180

Meanwhile also, doctors and infertile couples alike need to be aware of the uncertain-ties that are involved in some infertility treatments.These uncertainties need to be sharedbefore joint decisions are made on treatment.
We will take up the subject of communicating properly with your doctor later, inChapter 26.
COMPLICATIONS FROM FSH THERAPY � 181
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 181

blocked fallopian tubes andmicrosurgery
Microsurgical operationsand more
One or other fallopian tube is where sperm normally meets egg and where the embryobegins to form: the tubes are central to getting pregnant. For a summary of how thefallopian tubes perform their function, see the following box,Tubal function:Executive
summary (for more details see Chapter 3).Here we’ll examine the effects of the various causes of tubal blockages (for example,
previous operations, including intentional sterilization operations), but especially salpingi-tis, and how these lead to peritubal adhesions, or tissue growing around the tubes; hydro-salpinx, or obstruction of the outer,‘distal’ part of the tube, at the fimbrial end; and ‘proximal’tubal obstruction, or obstruction of the isthmus, close to the uterus.
We then look at preoperative evaluation and microsurgical treatment of these condi-tions, particularly salpingolysis and fimbriolysis, for treating peritubal adhesions; salpingostomy,for distal tubal obstruction; tubal resection and anastomosis, and tubal canalization, for proximaltubal obstruction; and finally, adhesion prevention, to stop adhesions from re-forming orfrom forming in the first place.
When both the tubes are blocked or missing, sperm can’t reach the ovulated egg, andsterility is inevitable. Pregnancy can’t happen without corrective surgery (the subject of thischapter) or IVF (see Chapter 20). However, a fallopian tube might be only partiallyblocked—or one tube can be blocked while the other tube is open. Pregnancy might bepossible but improbable.
Complicated combinations of one or two ovaries with tubes that cause subfertility are
182
13
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 182

common, and one of the circumstances in the box, One ovary can be OK . . . , might applyto you.
We’ll start by examining how tubal blockages come about.
CAUSES OF TUBAL BLOCKAGES
Tubes can be blocked from birth (as in congenital tubal obstruction), though this is rare.Tubescan also be blocked by intentionally cutting, tying or clipping them, for the purpose ofpreventing pregnancy (sterilization). Occasionally severe endometriosis can block a tube ortubes (discussed in Chapters 15 and 16.) More commonly, the tubes become damaged andobstructed because of a previous operation, such as an incautious operation on the intes-tines (a previous colectomy is notorious) or on an ovary (see the box, Expending the appendix)that leaves the tubes surrounded with adhesions.The majority, though,become blocked frominflammation, or salpingitis.
Salpingitis
Salpingitis means inflammation of the (trumpet-shaped) fallopian tube (the Greek for awar trumpet is ‘salpigx’). Inflammation can reach the tube from within, that is, from theuterus, as can occur with sexually transmitted diseases, including chlamydia and gonorrhea.
BLOCKED FALLOPIAN TUBES AND MICROSURGERY � 183
Tubal function: Executive summary
If you haven’t got time to revise Chapter 3, remember for now that each fallopiantube is about 10 to 12 centimeters long and consists of an outer, wide, thin-walledpart, the ampulla, and an inner, much narrower, more muscular part, the isthmus.
The isthmus connects to the narrowest part of all, the interstitial segment, whichpasses for 1 to 2 centimeters through the wall of the uterus to join the cavity of theuterus.
The tube is lined by two kinds of cells:‘secretory cells’, which produce mucus,glucose and other substances important for nourishing the egg and embryo; and‘ciliated cells’, which bear tiny hair-like structures, the cilia, beating in the directionof the uterus and carrying the still-sticky cumulus mass (the mucus-like blob insidewhich the egg is ovulated, or released, from the follicle) down the ampulla, towardsthe junction between the ampulla and the isthmus.
It’s at the fallopian tube’s ampullary–isthmic junction that fertilization takes place.The fertilized egg stays at the ampullary–isthmic junction for two to three days beforethe tubal isthmus loses its dense secretions, and the muscle in its wall relaxes, enablingthe early embryo, now rid of its cumulus cells, to reach the uterus.
The hormone that causes these changes in the tube is progesterone, production ofwhich by the ovary starts with ovulation.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 183

The acute salpingitis that follows can be without symptoms (clinically silent and unsuspected,as is often the case with chlamydia) or it can be accompanied by peritonitis (inflammationof the peritoneal cavity),with pain, tenderness, fever and a vaginal discharge (as is more usualwith gonorrhea).
If you are aware of these symptoms, even if they are mild, you should see a doctorurgently for antibiotics; if they are severe you could need hospital admission to receive
184 � GETTING PREGNANT
One ovary can be OK . . .
If you have just one ovary, it will normally take over completely from the one that’sbeen lost, ovulating every month instead of what on average would have been everysecond month before.
Generally you won’t run out of eggs and go through menopause any earlier: therate at which eggs are lost by atresia (see Chapter 3) is also halved. So your menstrualcycle generally stays the same.
. . . but two ovaries and one tube means subfertility . . .
However, if you have two ovaries, whether your tubes are normal or not, they willtend, from one cycle to the next, to take turns at ovulating. (Exceptions happen, andthe one ovary may dominate the other over shorter or longer periods of time, espe-cially if part of one ovary has been significantly reduced in size by previous surgery.)
If one tube becomes blocked, pregnancy will take, on average, twice as long tohappen.So,depending on the strength of your underlying fertility and on the amountof time you have left in which to get pregnant, having one blocked tube but twoovaries might critically reduce your chance of having a baby.
There’s also a risk of ectopic pregnancy in the blocked tube, because sperm can getout of the open tube, swim across to the other side, and fertilize an egg headed forthe blocked one, where the embryo then gets stuck.
In earlier days, before IVF made it wise to retain as much ovarian tissue as possiblefor egg retrievals (see Chapter 20), we sometimes intentionally removed an ovarynext to a hopelessly blocked tube if the other tube and ovary were normal—para-doxically but effectively doubling monthly fertility, the monthly chance of pregnancy.Such a ‘paradoxical ovariectomy’ can still occasionally be resorted to for improvingfertility in special circumstances.
. . . and one ovary and an opposite tube spells sterility
If you have one ovary (one having been removed for, say, a serious ovarian cyst), andthe only tube you have happens to be on the other side, conception is very unlikely(only a handful have been reported in the medical literature)—and a high propor-tion of the rare pregnancies that do occur turn out to be ectopic ones. IVF or GIFT(Chapter 20) is then a good option.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 184

antibiotics intravenously. If you have an IUD in place it usually should be removed whilethe infection is being treated (see the box, IUDs and salpingitis).
Inflammation can also reach the tube from its outside—by the spread, for example, ofinflammation from a neighboring organ such as the appendix (see the box, Expending theappendix).When this happens,most of the damage is on the outside,often sparing the delicatestructure of the inside of the tube.The tube and ovary can become separated by new tissue—referred to as peritubal adhesions if they surround the opening of the tube, and peri-ovarianadhesions if they enclose the ovary. (Usually both happens: tubo-ovarian adhesions.)
What is an adhesion? Think of an adhesion as a sheet of scar tissue. If you shaved offthe skin over the tips of your two index fingers, and held your fingers together long enough,an adhesion would grow between them to join them. So it is when the organs in theabdomen and pelvis lose their single-cell-thick lining and continue to lie close together—they become joined by an adhesion.The same can happen when scarring of the tube followssurgical operations in the pelvis for other conditions, resulting in ‘post-surgical’ adhesions.
Adhesions can also block the outer end of the tube as a result of endometriosis (seeChapter 15), especially when the neighboring ovary is affected. Rather less often, the tubecan be blocked by endometriosis of its wall, usually in the middle part of the tube, a locationfor a blockage different to that resulting from salpingitis. In other cases, the tube itself isspared from harm and the peritubal adhesion, by enveloping tubes and ovaries, prevents
Expending the appendix
Inflammation of the appendix (appendicitis) usually leaves the tubes and ovariesalone. But sometimes the inflammation is severe, an abscess forms in the pelvis, andone or both tubes and ovaries can get caught up in it.To stop this from happening,surgeons often err on the side of caution and remove a suspect appendix early.
If the appendicitis does involve the tube and ovary, it’s usually just the right tubethat gets involved in the inflammation and the adhesions that follow, but if a hydro-salpinx forms, even if only on one side, then sterility can result.
More general peritubal adhesions arising from neglected or advanced appendici-tis are rare in the USA, Australia and most other Western countries, where goodsurgeons and hospitals are easily and quickly available. It’s true that many appendixesare removed that turn out to be normal; but, for fertility, this is better than a generalpolicy of operating only when the diagnosis is certain.
What can be less fortunate, though, is mistaking a painful ovulation forappendicitis, operating, finding the appendix to be normal, then removing someincidental ‘cyst’ on the ovary (in reality almost always a normal corpus luteum), andcausing peritubal adhesions, not from the appendicitis or the appendicectomy butfrom the incautious surgical assault on an ovary, an ovary that almost always, in thesecircumstances, deserves to be left alone.
BLOCKED FALLOPIAN TUBES AND MICROSURGERY � 185
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 185

egg pick-up by the fimbrial end of the tube. In both these situations the damage is mainlyexternal and microsurgery (see below) can be particularly helpful.
Adhesions can be thick, fibrous and tough, or they can form thin, extensive sheets,and look like clear plastic wrap.The clingwrap-like adhesions look easy to treat, butunless very special precautions are taken (see below) they often re-form as tough, fibrousadhesions.
Chronic salpingitis (for chronic read ‘long-term’) can result either from repeated episodesof acute salpingitis or from the sort of infective organisms that elicit only a long-terminflammation. In many parts of the world, tuberculosis is the most common cause of chronicsalpingitis, and also one of the most common causes of sterility (see the box, Tuberculosis,in Chapter 17).
A tube acutely infected but treated promptly with antibiotics can recover completely,with no damage done. If the infection is repeated, or goes untreated, the inflammationbecomes chronic. All of the tube’s normal functions are disrupted by the scarring thatfollows: the hair-like cilia are lost; the muscle of the tube’s wall is disorganized; the secre-tions needed to nourish the embryo are spoiled; and the tube itself nearly always becomesblocked.
The blockage can be mostly at the outer, fimbrial end (resulting in a hydrosalpinx), ormostly at the inner end, close to the uterus, involving the isthmus and/or the interstitialsegment of the tube. A hydrosalpinx can form directly or it can follow a dramatic case ofacute salpingitis in which the tube has filled with pus. (For more, see the box, Salpinx,hydrosalpinx and pyosalpinx . . . ) A properly functioning tube is more likely to follow latermicrosurgery if the blockage has occurred in the isthmic or interstitial segment of the tube.(For more, see the section on salpingitis isthmica nodosa in the box, Salpinx, hydrosalpinxand pyosalpinx . . .)
186 � GETTING PREGNANT
IUDs and salpingitis
If the tubes become infected in the presence of an intrauterine contraceptive device,the IUD should be taken out while the salpingitis is treated.
IUDs can occasionally introduce an infection into the uterus at the time they’reinserted.This is most uncommon (it occurs in less than 2 percent of insertions).Moreoften, the presence of an IUD makes the uterus and tubes less resistant than theynormally are to STDs acquired at a later date.
Salpingitis in the presence of an IUD,as without it, can be acute or chronic.Whereassalpingitis usually affects both tubes more or less equally, salpingitis in the presenceof an IUD can be asymmetrical, affecting one side disproportionately.
Because of these considerations IUDs are best used for contraception inwomen who have had children, who are in stable, single-partner relationships,and who don’t want the intrusion or the permanence of a tubal ligation forsterilization.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 186

BLOCKED FALLOPIAN TUBES AND MICROSURGERY � 187
Salpinx, hydrosalpinx and pyosalpinx . . .
Like characters in Goscinny and Uderzo’s French comic-strip Asterix the Gaul, thesenames—or the prefixes—reflect their bearer’s treachery.
Salpinx is benevolent: it comes from the Greek for ‘war trumpet’, here thetrumpet-shaped fallopian tube.
Hydrosalpinx is a tube blocked from previous inflammation at the outer end andnow, months or years later, is filled with watery fluid.
But pyosalpinx, the worst villain, is an acutely inflamed, blocked tube filled withpus. It sometimes subsides with antibiotics, becoming a hydrosalpinx. Otherwise itcan rupture and form an abscess in the pelvis, much like a burst appendix, and thenit usually needs an operation to empty it (to drain it and the abscess).
A pyosalpinx can represent a tube infected for the first time, if the infection hasgone untreated, or it can represent a hydrosalpinx that has become reinfected.
A hydrosalpinx can have a particularly perverse and harmful effect on gettingpregnant—whether the opposite tube is normal and you’re trying naturally, orwhether you’re having IVF treatment.
How it does this has only been properly appreciated since 1994, when no fewerthan three articles were published showing that women having IVF had a muchlower chance of getting pregnant if their transvaginal ultrasounds (used for monitor-ing IVF treatment—see Chapter 20) disclosed one or two hydrosalpinges formingas the time for egg retrieval got closer.
What happens is that the high amount of estradiol coming from the ovary at thistime both stimulates production of more water in the tube and constricts the isthmusof the tube, trapping the fluid in the now swelling ampulla, which forms the hydro-salpinx.
Then, after ovulation and fertilization, while an embryo from either the good tubeon the other side or from the IVF embryo transfer is waiting in the uterus to implant(see Chapters 3 and 20 for the details), the rising amounts of progesterone comingfrom the ovary relax the isthmus, allowing the watery fluid to pass down throughthe uterus—often washing out the waiting embryo or embryos.The woman mayexperience fluid escaping through the vagina at this time.
This perfidious process accounts for not a few cases of persistent failure toconceive with IVF.The effect of the hydrosalpinx needs to be overcome.
Solutions include:• Removing the tube surgically (salpingectomy), at laparoscopy or laparotomy;• Opening the tube with microsurgery (salpingostomy); and• Placing an occlusive clip on the isthmus at laparoscopy,which won’t do anything
for the hydrosalpinx (except cause it to be swollen all the time), but effectivelyprevents the fluid entering the uterus, and so does the job.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 187

TUBAL MICROSURGERY
Depending on how much damage there is,and where in the tube or tubes the damage is located,the tube might be able to work again once the blockages are removed with microsurgery.
After the tubes have been evaluated, the operations available are salpingolysis and fimbri-olysis (removing peritubal adhesions from tubes that are intrinsically good); salpingostomy (anew opening in the outer end of a hydrosalpinx); tubal anastomosis (rejoining a tube aftercutting out a blocked part); and tubal canalization (pushing a wire through a blockage).
Although pregnancy rates of up to 70 percent can be expected from overcoming someinflammatory blockages, many tubes are so damaged that, even in the best microsurgeon’shands, the results are extremely poor (less than 10 percent pregnancy rates, a majority ofwhich are lost from miscarriage or tubal ectopic pregnancy). For this reason, since the 1970sIVF (see Chapter 20) has been developed as the only effective approach. Moreover, evenin the most straightforward cases the surgery can be spoiled by the subsequent formationof adhesions, despite making full use of the available techniques for preventing them formingor re-forming.
Preoperative evaluation of the tubes
Evaluating the tubes for microsurgery is a very specialized field.If the clinical history or infertility tests (see Chapter 4) suggest the possibility of tubal
damage, before I make a final decision on whether or not to recommend an operation,I will want to know what the tube looks like inside (first with a hysterosalpingogram), thenon the outside (with a laparoscopy) and maybe also on the inside again more directly (witha salpingoscopy or falloposcopy).These tests are described in Chapter 5.
The best situations for microsurgery are when the tube is only blocked close to the
. . . and salpingitis isthmica nodosa
A faithful companion and the least malicious character of the group,but an enigmaticone.
The three-part name means:• that it’s an inflammation of the tube (but there are none of the usual inflamma-
tory white blood cells visible to the pathologist);• that it affects the isthmus (nearly always on both sides); and• that it feels (and later looks) lumpy, or nodular.Salpingitis isthmica nodosa is best diagnosed with a hysterosalpingogram (see Chapter5),which reveals the basis for the lumpiness: tiny side channels off the isthmus’s mainchannel—which itself can still be open or, later in the pathological process, blocked.
The operation to correct it is a tubal anastomosis, after the abnormal part of theisthmus has been cut out.
188 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 188

uterus (and a resection of the blocked part and tubal anastomosis is possible) or when thereare thin,non-fibrous, sheet-like adhesions around the outside of an otherwise mainly normaltube: the operation for treating such peritubal adhesions is called a salpingolysis. If the adhe-sions include the fimbrial end, where treatment is more delicate, it is called fimbriolysis.
BLOCKED FALLOPIAN TUBES AND MICROSURGERY � 189
(a) (b)
Figure 13.1 Microsurgery of the fallopian tubes: reversal of sterilization by tubal anastomosis, at amagnification of 16 times.The two freshly cut ends of the tube have been joined bysix fine sutures.
(a) (b)
Figure 13.2 A hydrosalpinx (a), in which the tube is blocked at its outer end and, as a result, isdistended with fluid, and (b) the tube has been opened with a microsurgicalsalpingostomy.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 189

When the fimbrial end is completely scarred-over we have a hydrosalpinx.The micro-surgical operation to reverse this and re-open the end is a salpingostomy.When the tube isblocked at both ends, there’s usually disruption along its whole length and microsurgeryrarely leads to a successful pregnancy.
Salpingolysis and fimbriolysis
Salpingolysis is the microsurgical operation for releasing the tubes from adhesions by cuttingthe adhesions out, usually with a fine electrocautery needle. Electrocautery, or diathermy,uses a high-voltage electric current to evaporate tissue at the point of a fine surgical needle.Fimbriolysis is similar, but refers more precisely to removal of adhesions from the tube’sdelicate fimbrial end, near the ovary.
The surgery can, in principle, be done either at an open operation—a laparotomy—or at laparoscopy. Special skills are needed in either case.Laparotomy is a more major proce-dure in terms of recovery, but it’s more accurate and generally quicker. Laparoscopy has theadvantage of a short hospital stay, but the operation is technically much more difficult andusually takes longer; less drying-out of tissues occurs compared with laparotomy,but unex-pected difficulties with the operation are less readily dealt with (and in my experience manylaparoscopy surgeons underestimate the capacity of adhesions to form after extensive laparo-scopic surgical dissections).
Salpingolysis and fimbriolysis are helped by using the enlargement provided by thelaparoscope itself or, at laparotomy, by the operating microscope—with a magnification ofabout 6x.With either approach the surgeon should be able to see exactly where the adhe-sions are attached, and cut them free a millimeter or so from healthy tissue.
Salpingostomy
The operation in which a new opening is made in a tube completely blocked at its outer,fimbrial end is called a salpingostomy, or sometimes a ‘neosalpingostomy’. (If the tube is openbut the fimbriae are stuck together with fine adhesions, then the operation is a fimbriolysis,described above.) Carrying out a salpingostomy that gives the maximum chance of success,given the damage the tube has suffered, requires the surgeon to have had a great deal of expe-rience with tubal microsurgery.The most must be made of what fimbrial structures remain.
The ultimate result, however, is out of even the best surgeon’s hands.The scarring andthickening of the tube’s wall, the loss of the cilia (the fine hairs on the cells that propel theegg down the tube), the co-existence of other places of partial blockage along the tubefrom internal scarring—all will still be there after salpingitis has been cured and the mainblockage cleared.This damage continues to reduce the tube’s ability to transport eggs, spermand embryos even after a technically successful salpingostomy leaves the tube open andreasonably close to its ovary.
On average, only 5 percent to 10 percent of the women undergoing salpingostomieswill have a pregnancy that leads to a baby within a year of having the operation.The resultsare worse than this for women with badly damaged tubes and for women who’ve had a
190 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 190

previously unsuccessful attempt at the operation.The results are better if the lining of thetube has been well preserved, there is no internal scarring on salpingoscopy and falloposcopy,and the tube’s wall is not thickened. For more detail, see the box, Salpingostomy: Minutiae.
For most women, one cycle of IVF gives a better chance of pregnancy than a year ofwaiting and trying after salpingostomies. However, because an untreated hydrosalpinx canitself cause treatment with IVF to fail, it’s becoming more common again for such damagedtubes to be submitted to salpingostomy while still intending to have early treatment withIVF (see the box, Salpinx, hydrosalpinx and pyosalpinx . . .).
Tubal anastomosis
Removing a blocked part of the tube and rejoining the now freshly open ends is calledtubal anastomosis. It can be done for tubes blocked intentionally (for sterilization) oraccidentally (from salpingitis).
Previous sterilization
Blocking the fallopian tubes intentionally has become a popular form of permanent contra-ception. It’s not this book’s job to discuss the different ways this can be done, but it’s a fact
BLOCKED FALLOPIAN TUBES AND MICROSURGERY � 191
Salpingostomy: Minutiae
To open the hydrosalpinx, with the benefit of 6x magnification, the surgeon firstmakes a small opening at the point at which the fimbriae, or fingers, of the fimbrialend have come together. After this the operation involves dissecting between thefingers of the tube as seen from the inside.
In some cases the result is dramatic: the fimbriae themselves can be freed andthe tube soon looks almost normal. Perhaps one in three or one in two women willhave a baby.
In other cases there are adhesions between folds in the tubal lining, or the tube’swall is too thick, or there might be several complete blockages in the tube resultingin cystic spaces that can’t be made to communicate with each other—and which,therefore, need to be excised. In these cases the tube can usually be made to stayopen, but the opening that’s constructed is contrived, often limited in mobility, andlined by damaged tissue.
Once the tube is open, its damaged tissues do tend to recover, but the processtakes years rather than weeks or months, and in the meantime there’s more frustra-tion and disappointment.
Of the pregnancies that do occur when the tubes are so damaged, 25 percenttake place in the tube itself, as the fertilized egg gets stuck (an ectopic pregnancy,discussed in Chapter 14); and another 25 percent miscarry because of the poor nutri-
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 191

of life that at least two in 100 women will, for one good reason or another, change theirminds. Study after study has shown that, in practice, no amount of counseling at the timeof sterilization can predict this group: losing one or more of your children through accidentor disease is not something anyone expects; nor do many people, at the time the tubes aretied, expect to divorce and then remarry.
So it’s important that all sterilization operations are done in a way that’s at the sametime effective yet reversible with microsurgery.This means limiting the part of tube that’sremoved, tied or squashed to a centimeter or two, preferably in the region of the isthmus.
Fimbriectomy, which means removing the fimbrial end of each tube (and, incidentally,forming a hydrosalpinx), has the highest failure rate, is the most hopeless to reverse withmicrosurgery, stops IVF from working, and can be followed by complications after themenopause. So there are many good reasons why fimbriectomy should not be chosen as asterilization operation.
The word ‘anastomosis’, from the Greek ‘to make a mouth’, in surgical practice meansmaking two mouths and sewing them together,mouth-to-mouth.Tubal anastomosis is thus
192 � GETTING PREGNANT
Sterilization reversal: Minutiae
The most common and simple form of tubal anastomosis for sterilization reversal isfrom isthmus to isthmus on each side of the blockage (Figure 13.1).Typically five orsix sutures will be used in the muscle layer, with a separate closure of the overlyingserosal layer.The tube should almost always remain open and functional.
If the junction between isthmus and ampulla is missing after the sterilizationoperation, inevitably the join will be between two parts of the tube with differentdiameters, the narrow isthmus and the wider ampulla.The opening in the ampullais then made as small as practicable, and this form of join still works well, providedthat the sutures (typically from six to eight in the muscle layer) are accurately locatedaround corresponding parts of each freshened tube’s circumference.
The trickiest anastomoses are between ampulla and ampulla.Many sutures (often10 to 15) are needed. Because the wide ampulla has a very thin muscle wall it tendsto collapse in on itself.Too few stitches means narrowing at the site of the anasto-mosis and a risk of a later ectopic pregnancy.
Compared with anastomoses close to the uterus, the operated-on ampulla hasmore chance of sticking to the ovary, which lies alongside it, so we often carry outan early second-look laparoscopy to prevent adhesions after this kind of anastomo-sis, whereas it is not usually necessary after the others.
What kind of sterilization operation would the infertility microsurgeon choosefor the very best chance of later reversing it successfully?
My choice would be a single Filshie clip on each tube, placed about 2 or 3centimeters from the uterus,where the isthmus is getting a little bit wider, but beforeit becomes ampulla.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 192

the operation in which we cut out a blocked or diseased part of the fallopian tube and sewthe two healthy open ends on each side of the removed bit back together.The sutures weuse for tubal anastomosis are less than one-fifth of a millimeter in diameter, with a tinyneedle to match (see Figure 13.1a).The tube is brought back together with sutures in twolayers, the muscle layer just outside the tube’s inner lining, and the serosa, the outer liningof the tube.The details of the operation depend on just where and how much tube hasbeen lost. For these details, see the box, Sterilization reversal: Minutiae.
With accurate surgery, done at high magnification (typically 10x to 16x), the risk of alater pregnancy being an ectopic tubal one should be less than 2 percent and the risk ofmiscarriage no higher than for women of the same age with normal tubes.
The success rates for microsurgical sterilization reversal can be the highest of any formof infertility surgery. Pregnancy rates among the best surgeons are between 80 percent and90 percent within a year or two of the operation (though the majority occur within six to12 months). For women who are still under about 38, and who have fertile husbands, it’snowadays rare not to get pregnant. So IVF, in turn, is rarely needed.
The time between the sterilization operation and its reversal is not important, apartfrom the effects of increasing age. One patient I operated on had had her tubal ligation atthe time of her (second) cesarean section at the age of 19; she was 42 when the tubes wererejoined, and 43 when the baby was delivered.This differs from the situation of vasectomyreversals, in which there’s a strong negative correlation between the time elapsed and thechance of successfully fathering a pregnancy; the reason for the difference is men’s devel-opment of sperm antibodies after vasectomy.
Isthmic salpingitis
The same operation of tubal anastomosis can be used if the tube is blocked in the regionof the isthmus because of previous salpingitis. In some cases the condition that causes thiskind of blockage is the condition ‘salpingitis isthmica nodosa’ (see the box, Salpingitis,hydrosalpinx and pyosalpinx . . .). In this condition there is thickening of the wall of thetube due to tiny outgrowths from the inside of the tube; it feels lumpy when touchedwith the fingers at operation, as if it had little nodules in it.These nodules connect withthe tube itself and may cause a tubal ectopic pregnancy before the disease process completelyblocks the tube.
In other cases of salpingitis the tube is blocked at the isthmus or in its interstitial segment(where the tube passes through the wall of the uterus) simply by scar tissue. If the blockageis deep in the wall of the uterus it can be particularly tricky for surgeons not especiallyexperienced with this operation at this difficult site.
Overall, up to 70 percent of women with these forms of salpingitis-related tubalblockage can expect to conceive in the 12 months following tubal anastomosis if thereare no other infertility factors.This is not quite as good as the chance of pregnancyafter sterilization reversal (because the tube has been damaged more generally than itwould have been just from sterilization), but it is still good enough to be a good alter-native to IVF.
BLOCKED FALLOPIAN TUBES AND MICROSURGERY � 193
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 193

194 � GETTING PREGNANT
A critical balance: Healing or adhesions
When the coating of the abdominal cavity, the serosa, is injured—as it inevitably isat any pelvic operation—the blood on its surface soon clots.This superficial clotcauses nearby organs to stick together, at least temporarily.
Normally the clot dissolves in about six hours.The wandering cells of the abdom-inal cavity, the macrophages, form a protective coat over the raw and exposed tissues.Any blood clot that’s still left three days after the operation begins to form scar tissue.If there’s no blood clot left by this time, there’ll be no adhesions.
There’s still some doubt about where the new serosal cells of the peritoneumcome from, but it doesn’t much matter.The important point is that the new serosalining the peritoneum is fully formed by eight days after an operation—except inthose areas where a blood clot was left undissolved, and which, by eight days, arealready well on the way to forming scar tissue between organs such as the tube, theovary, the uterus, and the intestines.
This scar tissue is, then, the adhesion. Prevent the scar tissue forming and youprevent adhesions.The more often the scar tissue (the adhesions) has been operatedon, the more likely the adhesions are to regrow—and to be tough, thick ones ratherthan delicate, filmy ones.
Surgeons have long contrived to influence the outcome of peritoneal healingin favor of repair instead of scarring.
To be sure, if we were to use powerful drugs to completely stop blood fromclotting or scar tissue from forming we could stop adhesions, but for someonewho’s recovering from an operation such extreme drugs cause unacceptablecomplications.
We need something that either sticks around locally for the three days encour-aging the clot to dissolve, or that keeps all the surfaces apart for the eight days it takesall the serosa to reform.
For now, it’s just the second option we have the means for.The chief non-dissolv-able product available is Goretex (yes, the same stuff that ski clothing is made from,but spun a bit differently). Goretex has a long history of use in cardiac surgery, inwhich it is used to permanently replace the serosa around the heart where adhesionsare troublesome after inflammation or repeated operations.
Early laparoscopy
Eight to 10 days after the microsurgery,we can do a laparoscopy.This is after the serosahas healed.
At the laparoscopy we push apart all early points of adherence between the tubesand ovaries or other organs.This separates the very early scar tissue, on its way toforming an adhesion, and allows a few days for islands of new serosal cells to haveanother chance at linking up and completing the job of healing the peritoneum.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 194

TUBAL CANALIZATION
If the damage from salpingitis of the isthmus is limited, it might be possible to open theblockage permanently by pushing a catheter or wire through it.The procedure is donevaginally, through the cervix and the cavity of the uterus.The catheter or wire needs tobrought to the point at which the tube enters the cavity of the uterus.This can be doneeither by a gynecologist at hysteroscopy (so that the opening of the tube is actually seen whilethe catheter is passed into it) or by a radiologist at x-ray, while a hysterosalpingogram isattempted.The procedure is moderately painful, more so than with the usual hysterosalp-ingogram, though the pain should be brief.
Dr Amy Thurmond, a radiologist from Portland, Oregon, popularized the method.The good results she’s had with this technique have not always been reproduced in othercountries. I think this discrepancy means that different radiologists are being asked to see
Several different groups of infertility surgeons around the world, including somein Sweden, Holland and the USA, as well as me, have shown that carrying out suchan early (‘second-look’) laparoscopy is effective in diminishing eventual adhesionformation.
Enough ‘third looks’ have been done to know that adhesions are usually muchreduced by the maneuvers at the second look and often have been prevented alto-gether.
Surgical adhesion barriers
There are a number of products on the market that can be used at operation to forma barrier between organs. Some dissolve, and so can be left inside the body; othersdo not, so depending on where among the pelvic organs they are used they mightneed to be removed at the second-look laparoscopy.
The dissolvable adhesion barrier with which there has been the most experi-ence is Interceed (made by Johnson & Johnson).The material is woven from fibersof modified cellulose and, after being placed over damaged abdominal serosa, dissolvesin about eight days into simple sugar molecules (which are then absorbed by thebody and metabolized). During that time the cloth keeps the covered surfaces apartwhile the serosa reforms beneath it.
Clinical trials have shown Interceed to be effective in reducing or (sometimes)preventing adhesions, but an adhesion-free result is not guaranteed—and in my expe-rience a second-look laparoscopy is still advisable.
Its credentials in infertility surgery are not as good. If it’s used between the tubeand ovary (not clinically tested so far in published controlled trials), it obviouslyneeds to be removed after eight days, when the serosa has healed; removing it atlaparoscopy is possible. If it’s used on other surfaces, like the uterus or the side of thepelvic peritoneal cavity, it can in principle be left there, but studies on its usefulnessare still limited.
BLOCKED FALLOPIAN TUBES AND MICROSURGERY � 195
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 195

different types of conditions, and that not all the patients with tubes apparently blockedthis way are equally suitable for the procedure.
There seems little doubt that this approach works for cases of tubal spasm or for block-ages caused by plugs of secretion. But there’s doubt that these apparent blockages are, infact, real or permanent blockages. I’ve found the technique useful when a tubal anastomosishas for some reason become blocked. Being a new form of treatment, there’s still debateamong infertility specialists about the proper place of tubal canalization procedures.Undoubtedly part of the problem in evaluating it is that many of the cases treated this wayby some radiologists have not been properly investigated first.
I believe that true tubal blockages, especially if they extend over a centimeter or more,are best treated with a formal microsurgical tubal anastomosis.
PREVENTING ADHESIONS
From your reading up to this point you’ll know that adhesions are a menace to fertility.Theycan also cause pain from cramping of the intestines and from closely confining the processof ovulation.
The hunt for ways of stopping adhesions forming or re-forming after operations hasbeen accompanied by some research, a lot of speculation, and a bucketful of snake oil—magic remedies that are all promise and don’t deliver the goods.The way adhesions formis interesting (see the box, A critical balance: Healing or adhesions).The way to stop themgrowing back after they’re cut out is, first, to operate very carefully,with microsurgery; second,to carry out a laparoscopy eight to 10 days after the microsurgery, detaching adherencesbefore they become adhesions again; and third, to use one of the new adhesion barriersmade from woven, dissolvable material. For the science behind the second and third prin-ciples, read the box.
Not every infertility surgeon is convinced about the wisdom of the early ‘second-look’laparoscopy for stopping adhesions from growing back.There’s a lot of ‘out of sight, outof mind’ thinking about adhesions. On the negative side, it’s another operation, and it’s stillno total guarantee that adhesions won’t be back again.
A surgeon who tells you that you’ve got just six months to get pregnant after he or shehas ‘treated’ adhesions is misleading you badly. It’s an unfair and self-serving thing to say.Sure, if you do get pregnant quickly the surgeon probably did a good job and gets yourthanks; but if you’re not pregnant in that time the surgeon’s made it your fault! You had sixmonths and you didn’t try hard enough! But the fact is that if adhesions are going to growback they do so straight away—probably before you’ve even thought about having sex againafter your operation.
By not regularly doing early laparoscopies,most surgeons cannot know how often theiroperations fail to relieve adhesions or, indeed, how often they make your situation worse.
196 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 196

ectopic pregnancy
Pregnancy in the fallopiantube and other places
Apregnancy is ectopic (out of its usual place) when an embryo implants in a locationthat’s not the optimal place for it—that is, somewhere other than in the cavity of theuterus, well away from the fallopian tubes, and well away from the cervix.
Ectopic pregnancies can develop in the tubes, in the ovaries, in the cervix and even in theabdomen. Pregnancies in strange corners of the uterus can misbehave too, developing as aplacenta previa or as an angular pregnancy.
In this chapter we’ll look at treatment options for early ectopic pregnancies and late,or ruptured, ones.We will look at causes, including damaged tubes and hormone distur-bances. And we’ll consider what to do for fertility after you experience an ectopicpregnancy.
TUBAL PREGNANCIES
Most ectopic pregnancies are found in the fallopian tubes and are called ‘tubal pregnancies’.Most of these, in turn, are located in the outer part of the tube, the ampulla (see Chapter 3for a description of the parts of the tube).
Less often they occur in the narrow, inner part of the tube (the isthmus) or even in theinterstitial segment of the tube, which passes through the wall of the uterus (an interstitial or‘intramural’ pregnancy).
197
14
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 197

Symptoms
The classic tubal pregnancy first makes its presence felt by causing discomfort, then pain,low in the abdomen or pelvis, often (but not always) localized to one or other side.Therecan be symptoms of early pregnancy, such as nausea and tenderness of the nipples. Aperiod might or might not have been missed.There can be some irregular, dark bleeding.A period might simply seem to be lingering on.
If the ectopic pregnancy has been bleeding internally, there can be a general feeling offaintness, perhaps with spells of dizziness.There can also be a local feeling of discomfort inone or other shoulder. (The pain is felt in the shoulder because the internal bleeding irri-tates the under-surface of the diaphragm, nerves from which enter the spinal cord withthose that come from the shoulder, and the brain mixes up the messages it gets.)
Signs and tests
When the doctor carries out an examination, the abdomen low down can be sore to thetouch. Nearly always there’s tenderness on one side or the other on vaginal examination;pain on one side when the cervix is gently pushed each way is typical.
If the tubal pregnancy has burst through the tube’s wall and there’s bleeding, the pulsecan be either fast (from blood loss) or slow (a reflex from bleeding into the abdomen), butin either case there will be low blood pressure, or the result of ‘shock’).
198 � GETTING PREGNANT
Quantitative pregnancy testing
A blood pregnancy test gives a simple ‘yes’or ‘no’, an answer the lab can provide quickly.It does not measure the actual level of the pregnancy hormone, human chorionicgonadotropin (hCG), but signals whether it’s present in serum at a level greater or lessthan 50 units per liter (U/l). Although there’s a tiny amount of hCG present ineveryone’s blood (it’s such a basic hormone for human tissue to produce that our body’scells,many years after being derived from those present when we were early embryos,never completely forget how to make a bit of it—and they do, in a tiny amount), butthe concentration of hCG in non-pregnancy serum is much less than 5 U/l.
In the early stages of a pregnancy, before the missed period, hCG will bedetectable in blood at a concentration greater than 5 U/l, but perhaps not highenough to show up in a simple pregnancy test that’s set at 50.To detect the hCG, aquantitative serum hCG needs to be ordered from the pathologist.
Likewise, if serial measurements are to be done to track the levels, the same testshould be ordered twice, at least two or three days apart (during which,with a normalearly pregnancy, hCG should double). It’s best for serial measurements to be donein the same lab, for strict consistency of method.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 198

A blood pregnancy test will virtually always be positive.Characteristically,measuring serumhCG sequentially fails to show doubling of human chorionic gonadotropin levels every twoto three days—which is the way hCG goes up in a normal pregnancy (see the box,Quantitativepregnancy testing).The serum progesterone level will be lower than for a normal pregnancy.Theselast two tests, although they distinguish an abnormal pregnancy from a normal one, do notthemselves discriminate between an ectopic pregnancy and an imminent miscarriage.
The other test the doctor will arrange is a transvaginal ultrasound.This is sensitive enoughto show either what the ultrasonologists call ‘free fluid’ (in this case, blood) in the abdom-inal or pelvic cavity or, sometimes, among the echoes to one or other side of the uterus,to reveal the pregnancy itself (occasionally with a detectable fetal heart beat).
If left to nature, some tubal pregnancies will miscarry themselves out the end of thetube and everything settles down (a tubal abortion), in which case no further treatment isusually needed.And some ectopics soon stop growing and gradually fade away as the tissuedies and gets absorbed.Others, however, keep growing and, if not treated, rupture the tube,usually with considerable internal bleeding—a surgical emergency.
The most dangerous location to have an ectopic pregnancy is in that part of the tubethat passes through the wall of the uterus (an interstitial or intramural ectopic).Considerable
ECTOPIC PREGNANCY � 199
Particularly puzzling pregnancies
Diagnosing ectopic pregnancies can be tricky at the best of times: there are manycauses of pain and irregular bleeding, and an ectopic pregnancy can be missed if it’snot thought of in just about any such gynecological context.
But there are two special diagnostic conundrums.First, gynecologists have long observed that at operation for an ectopic preg-
nancy there can be a corpus luteum on the opposite side.This does not necessarilymean that the egg traveled across the pelvis to get into the tube. Rather, the signalsa tubal pregnancy sends about its presence (its production of hCG) can be marginal,perhaps not enough to stop menstruation and a further ovulation—in turn, perhapsmore often than not, from the opposite ovary.And this is one reason why a womanwho turns out to have an ectopic pregnancy may often believe she has not misseda period and so can’t be pregnant.
Second, there can be a pregnancy in the uterus and another in the tube or else-where: a condition called heterotopic pregnancy. In this case it’s possible that there wasa second ovulation perhaps a day or two after the main ovulation, with sperm stillaround to fertilize the egg but with a tube that’s lost its will to resist the intrepid, ifstraggling, embryo. In cases of tubes damaged by salpingitis, one embryo can make itsafely to the uterus while another gets caught somewhere in the tube.When thispicture is revealed on transvaginal ultrasound, early operation to remove the pregnancyin the tube can mean that the one in the uterus is saved.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 199

growth is supported by the surrounding tissue of the uterus until—ultimately and dramat-ically—rupture occurs, usually involving a main branch of the artery to the uterus.Fortunately, interstitial pregnancies are among the least common of ectopic pregnanciesand are plainly visible on transvaginal ultrasound.
Ectopic pregnancies in any location can be hard to diagnose, however, especially if theyco-exist with a normal pregnancy or there is a further ovulation despite their early presence(see the box, Particularly puzzling pregnancies).
Options for treating early ectopics: Laparoscopy and/or methotrexate
An ectopic pregnancy can’t be saved—it can’t be pulled out and placed in the uterus, unfor-tunately—but one can hope that the fallopian tube will be spared.
Nowadays, with early recourse to serial measurements of serum hCG and increasingaccuracy of transvaginal ultrasound in visualizing ectopic pregnancies early, two differentapproaches are making conservation of the tube more possible.
A laparoscopy in recent times has been the usual first line of treatment. If the tube hasnot ruptured it’s usually possible to remove the pregnancy sac from the tube without requir-ing laparotomy.The procedure in which the tube is slit open to reveal the pregnancy is calleda salpingotomy; the tube is then left open after the pregnancy has been pulled or washed out,to heal naturally. (Sometimes, at laparoscopy, the pregnancy will be seen to have endedalready, with a tubal abortion, discussed above.)
The second approach, using the drug methotrexate, is based on the fact that the cells ofthe trophoblast that surrounds the embryo grow quickly.This means that, like cancer cells,they can be rather selectively stopped in their tracks by drugs that focus on preventingfast-dividing cells from multiplying.These drugs are ‘cytotoxic’ drugs and are used forchemotherapy.
Methotrexate acts by blocking the availability of folic acid, a vitamin particularly impor-tant to developing trophoblast (see Chapter 7).The dose used to kill an ectopic pregnancyis much less than that used in treating cancer, so the typical side-effects suffered by peoplebeing treated by chemotherapy (nausea, vomiting, diarrhea, mouth ulcers, etc.) are lesscommon than they are in cancer patients.
The methotrexate can be used in different ways. Most commonly it is given alone at amoderate dosage (calculated at 50 milligrams per square meter of body surface area). It canalso be used in a high dose that is reversed some hours later with the administration offolinic acid, the active derivative of folic acid, which specifically antagonizes methotrex-ate’s lethal effect (it’s called ‘folinic acid rescue’).There are also satisfactory regimens usingrepeated low dosages.The best results occur in centers with significant experience and withwell-practiced protocols in place.
Some doctors have reported injecting methotrexate or other drugs directly into theectopic pregnancy by ultrasound-guided needle, but this seems to be less reliable.
Methotrexate is most effective when the ectopic pregnancy is small and not at the pointof rupturing (although some small ectopic pregnancies, particularly those with falling levelsof serum hCG,will resolve naturally).The aim with methotrexate is to leave the non-viable
200 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 200

embryo and trophoblast to be absorbed by the tube, a process that from my experience inobserving such tissue a year later by salpingoscopy tends to be incomplete.
Treating the ectopic by removing it from the tube at laparoscopy is quicker andsomewhat more certain, and so is preferable if the laparoscopy has already been decided onto confirm the diagnosis, but otherwise a surgical approach tends to be more expensive andcarries the usual hazards of general anesthesia and operations.
In either event you can generally leave hospital that evening or the next day, but it’sessential to be kept under observation with serial measurements of serum hCG levels,makingsure that they fall promptly and consistently. If hCG levels do not fall steadily over a weekor two the ectopic is persisting, in time to perhaps bleed again or even to rupture.Theconverse management can then be resorted to. Methotrexate can be administered if theprimary maneuver was laparoscopic removal; laparoscopy (though sometimes with sal-pingectomy) can be resorted to if the primary treatment was methotrexate.
If you have been taking folic acid for your pregnancy (see Chapter 7) you should stopit until your hCG levels have fallen to normal. Because folic acid is used to prevent certainbirth defects—preferably by commencing it several months before pregnancy is attempted—it would seem wise to wait this amount of time before re-embarking on pregnancy after acourse of methotrexate.
Surgical options for more advanced ectopics
If the clinical situation with a tubal pregnancy deteriorates, perhaps with collapse frominternal bleeding, an operation becomes urgent.Depending on the circumstances, a laparo-tomy is carried out as soon as possible. (If clinical conditions are less urgent, a laparoscopycan still be performed first, to confirm the diagnosis and perhaps to enable laparoscopictreatment.)
Whether at laparotomy or at laparoscopy, a decision will need to be made on whetherto remove just the gestational sac by way of a salpingotomy and conserving the tube; to removethe segment of the tube the pregnancy is implanted in (a partial salpingectomy), thusobstructing the tube but leaving it in a position for later repair with microsurgery; or toremove the whole tube (a salpingectomy).This last option is rarely an easy decision unlessthere’s too much bleeding for conserving the tube to be safe, or if you have had enoughectopic pregnancies to want no further risk of them—in which cases salpingectomy is thechoice.
Factors that bear on the decision of what to remove surgically include intentions regard-ing further attempts to get pregnant naturally: if a woman doesn’t really want more childrenthe tube is usually best removed.
But if further pregnancy is desired the factors that bear on the recommended surgeryinclude: the previous condition of the tube, especially whether it has contained an ectopicbefore; the practicality of later repairing the tube microsurgically (see Chapter 13); theapparent condition of the other tube; and the need to avoid leaving even a small hydro-salpinx (the presence of which can stop the other tube from working, as well as spoilingthe results of IVF; see Chapter 13).
ECTOPIC PREGNANCY � 201
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 201

It should rarely be necessary—and it’s certainly very undesirable—to remove the ovaryalong with the tube, even though it might be bleeding from a corpus luteum that’s beendisturbed.
ECTOPICS IN OTHER PLACES
There are locations for ectopic pregnancies within the body that cause them to behavedifferently from those in the fallopian tube. (For pregnancies that grow through the wallof the tube and develop in the abdomen, see the box, Abdominal pregnancy.)
Ovarian ectopic pregnancy
An ovulating egg can be fertilized while still in its follicle and then get stuck there. Such anovarian pregnancy accounts for about one in 200 ectopic pregnancies. It can be hard to distin-guish at laparoscopy from a bleeding corpus luteum—the structure that forms after a folliclehas ovulated.
The treatment has usually involved surgery to remove the ovary, but in early cases thatare not bleeding drug treatment with methotrexate is probably the best first choice.
Cervical ectopic pregnancy
Pregnancies that develop in the wall of the cervix, or cervical pregnancies, can also be a diag-nostic puzzle.The correct diagnosis might not be made until a biopsy is taken in theoperating room.
202 � GETTING PREGNANT
Abdominal pregnancy
In parts of the world where surgical treatment is not available, the clinical situationwhen a tube ruptures from an ectopic pregnancy often deteriorates to the point ofserious collapse and death. But sometimes it settles, and rarely the pregnancy cankeep growing—the trophoblast now extending out of the tube and across the surfaceof the peritoneal cavity. I managed such a case when I was training in Papua NewGuinea.
The woman believed she was normally pregnant, experiencing movements ofthe fetus as it grew; it was not until the fetus stopped kicking (and died) at 36 weeksthat she sought medical help.A laparotomy revealed the truth—after we suspectedit from where and how the baby was lying on x-ray—and I delivered a 2.8 kilogrambaby from the cavity of the abdomen, saw that I would experience a lot of diffi-culty removing the placenta from the loops of intestine it had attached to, anddecided to leave it there to absorb (which it did in due course and without furthercomplications).
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 202

Cervical pregnancies are rare and, to confuse matters, can look like a cancer of thecervix. If the correct diagnosis is not made by checking a pregnancy test then the surgeonand you can be in for trouble.The blood supply to such a pregnancy is greater than it iseven to a malignant tumor. Characteristically, bleeding begins during the surgical excisionprocess that is not easily brought under control.Tying off the major arteries to the uterus,or even a hysterectomy, can be necessary to stop the bleeding.
If bleeding does stop quickly after taking the biopsy the diagnosis might not be madeuntil the biopsy is examined by the pathologist: a further operation or drug treatment withmethotrexate should then be undertaken.
‘SLIGHTLY ECTOPIC’ PREGNANCIES
Within the cavity of the uterus itself there are locations for an embryo to implant that willcause it and its mother-to-be problems.These are not truly ectopic pregnancies becausethey are in the uterus—but because of their position complications are more likely.
Placenta previa
If the embryo attaches to the lining of the uterus, the endometrium, in the lower part of theuterus, the placenta will get into the way of the fetus during labor—a condition calledplacenta previa. Cesarean section can be needed for the baby to be delivered safely.
Angular pregnancy
The embryo can also implant just on the uterus’s side of where the tube joins the uterus—in a narrow, constricted region called the ‘angle’ of the uterus.A pregnancy here is calledan angular pregnancy. It is more likely to miscarry, as I explain in Chapter 8, often after thewoman has experienced cramping pain on the side where the pregnancy is located.
Occasionally the wall of the uterus is so stretched by the growing angular pregnancythat it ruptures, the way an interstitial pregnancy does. Early angular pregnancies and inter-stitial pregnancies can look the same on transvaginal ultrasound, lying in a space apparentlyseparate from the cavity of the uterus.They are therefore sometimes classified together (formore, see the box, Cornual pregnancy).
But usually an angular pregnancy behaves differently with further growth, settling intothe uterine cavity properly and progressing to term. (The placenta, imbedded in the angleof the contracted uterus that has just expelled a baby, can get stuck, or be ‘retained’, andmight need to be removed manually by the obstetrician.)
WHAT CAUSES ECTOPIC PREGNANCIES?
When it comes to explaining them, ectopic pregnancies are like miscarriages in the frus-tration they cause you and your doctor.We know what tends to cause them,but—with theexception of fallopian tubes that have obviously been damaged (see Chapter 13) and perhaps
ECTOPIC PREGNANCY � 203
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 203

those that occur while taking a progestogen-based contraceptive—we often can’t pin downthe cause in a particular instance.
To be sure, the relative incidence of ectopic pregnancies (compared with the number ofnormal pregnancies) has increased in many Western societies over the past 30 years or sofor two major reasons.
First is the wider occurrence of chronic salpingitis caused by chlamydia and gonorrheaacquired venereally, by sexual intercourse (see Chapter 13).
Second, those rare pregnancies that do occur despite normally effective contraception(intrauterine devices; and progestogen-based contraceptives, such as the minipill and implantsunder the skin such as Norplant) are more likely to be ectopic, because these contracep-tives are much less effective at preventing tubal pregnancies than they are at stoppingpregnancies in the uterus.
Damaged tubes
Chronic salpingitis or a previous surgical repair of the tube increases the risk of an ectopicpregnancy from less than 1 percent of pregnancies to 10 or 20 times that frequency.Aftertubal anastomosis (to reverse a sterilization procedure, see Chapter 13) the risk is about
204 � GETTING PREGNANT
Cornual pregnancy
Strictly speaking, a cornual pregnancy is one located in one horn of a bicornuate(‘two-horned’) uterus or in a unicornuate uterus (see Chapter 18). If the horn is ofgood size, a relatively normal pregnancy and delivery may follow, perhaps prema-turely, although it is more likely than on average to be a breech birth. If the horn issmall, and particularly if it does not communicate with the main part of the uterus,sooner or later it will rupture, like an interstitial pregnancy, and surgery is needed assoon as the condition is diagnosed.
The term cornual pregnancy is also loosely used to include angular pregnanciesand interstitial tubal pregnancies (see main text).An angular pregnancy may go to fullterm, whereas an interstitial pregnancy will rupture if not treated promptly.
The two conditions can be distinguished at laparoscopy by observing which sidea structure called the round ligament is pushed to. (The round ligament is well knownto all pelvic surgeons—it’s a cord of tissue that, in the embryo, runs from the devel-oping ovary down to the newly forming groin, pulling the ovary down into thepelvis as the embryo grows.) If the round ligament is pushed outwards it means thepregnancy is in the uterus; inwards means a pregnancy in the tube.
Both conditions might need surgery if the wall of the uterus looks set to tear,but an angular pregnancy—as is also true of some cornual pregnancies—can oftenthen be treated by vacuum curettage through the cervix rather than operating on itthrough a formal, open laparotomy.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 204

2 percent of pregnancies—rather low, because the health of the tube on each side of theplace at which it has been joined is usually normal.With operations for more serious disrup-tion of the tube, such as salpingolysis and, especially, salpingostomy, the risk is much higher,up to 25 percent or more of pregnancies.
Hormone disturbances
The human fallopian tube is very sensitive to hormones, as described in Chapter 3.Estrogen,produced by the maturing follicle, causes the tube to secrete mucus, which would normallybe protective against an implanting embryo.After ovulation, under the influence of proges-terone from the developing corpus luteum, this mucus quickly disappears.This is the probablereason why progestogen-based contraceptives, should a breakthrough conception occur, areassociated with an increased chance of ectopic pregnancy.
On the one hand,human embryos are especially invasive compared with those of otheranimals.On the other, the human tube has much less of this protective mucus than is foundin the tubes of other animals.
These two facts both contribute to the high frequency of ectopic pregnancies inhumans compared with other species. Rabbits and mice, with not-so-invasive embryosand with heaps of mucus on the surface of the tube’s cells throughout their ovariancycle, never have them, even when early embryos stripped of their zona pellucida (whichadds to the fertilized egg’s side of the lubrication needed for the embryo to slip downthe tube) are intentionally placed in the tube during experiments. Monkeys are in-between—they have a moderate amount of tubal mucus and occasionally get ectopicpregnancies.
If, while progesterone levels are going up after ovulation, the embryo’s transport downthe tube is interrupted, the tube will have lost much of its lubricating mucus and its resist-ance to implantation. This can be because of an adhesion in the tube from previoussalpingitis, as described already, but also because of a delay in the release of an egg fromthe ovary, or if an ovulated egg is missed by the tube on its own side and is, by chance,picked up later by the tube on the other side.
With the morning-after pill (postcoital contraception: for example, using two oral contra-ceptive pills in the morning and night after unanticipated sex), there’s a small increasedchance of ectopic pregnancy. Although this has been attributed to high estrogen levelskeeping the tube blocked with secretions, it seems to me at least equally plausible that alate ovulation has released the egg, which is then fertilized by remaining sperm. By thistime the tube’s well and truly under the influence of progesterone or progestogens (whichare present in the pill).
Similarly, the increased risk of tubal pregnancy with ovulation induction, particularly withfollicle stimulating hormone (see Chapter 11) and with IVF or GIFT (see further on),which also has been attributed to high levels of estrogen, can be explained by a later ovula-tion under progestogenized conditions. If there are lingering sperm about (which, giventhe usually excellent mucus in the cervix, there often are), an egg ovulated by a small follicleand fertilized a day or two late could be a perfect candidate for causing trouble.
ECTOPIC PREGNANCY � 205
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 205

Assisted conception
The risk of an ectopic pregnancy in the tube is higher after either GIFT or IVF, on top ofthe effects of the hormone disturbances we’ve just been talking about.With GIFT, whereeggs are placed in the fallopian tube to be fertilized, the risk is about 6 percent of preg-nancies.The reason is often unsuspected disease of the tube.
IVF too, even with transfer of fertilized eggs to the uterus rather than to the tube, canresult in an ectopic pregnancy, even if there’s only a stump of tube left after, say, salping-ectomy. If the tube itself is still present but is blocked only at its outer, fimbrial end (a hydro-salpinx) the risk is significant.
The reason for these ectopics could be that IVF embryos are always transferred with afew small bubbles of air (necessary to stop them drifting up or down the transfer catheterand getting lost).The embryos probably stick to these air bubbles, which in general can bea good thing as it keeps them up in the uterus rather than following the catheter back intothe mucus of the cervix (and into oblivion).But the same air bubbles can float up into what’sleft of one or other tube, carrying the hapless embryo with them.
If the tube is normal this might happen more often than we think, at least with day 2or day 3 embryos that aren’t really due to be in the uterus yet. It could even advantage theembryo, which then re-enters the uterus when it’s better prepared for it. But if the tube isnot normal, it will have little driving power to return an embryo to the uterus on schedule.What’s more, the embryo, snuggled into a niche of a damaged tube, is likely to escape thedischarge of fluid from a hydrosalpinx on the other side that can easily prevent normalimplantation in the uterus (for a discussion of this phenomenon, see the Chapter 20 box,Hydrosalpinx: Reintroducing a villain).
FERTILITY AFTER AN ECTOPIC PREGNANCY
How best to optimize fertility after an ectopic pregnancy is a difficult question.Too fewmodern clinical series have been published to go by, and the medical literature on the subjectsuffers from enthusiastic reports at the expense of more average results (see the box, Themisleading effects of selective publication).
Keeping options (and damaged tubes) open always runs the risk of a further ectopicpregnancy.Whether treated by methotrexate or salpingotomy, a tube that has carried anectopic pregnancy is never the same again: some internal scarring is inevitable, and can beseen via a salpingoscopy (Chapter 5).
Ironically, as ectopic pregnancies have come to be diagnosed earlier and as surgicalmethods have improved, so more women get pregnant again, but the proportion of thosepregnancies that once again are ectopic is also higher.The probable reason for this paradoxis that, in the past, results of surgery were mostly poor (no pregnancy) and only occasion-ally very good (normal pregnancy).
What tests should you have done after a tubal pregnancy? If you are planning to trygetting pregnant naturally again, a full investigation of both fallopian tubes is wise. Atminimum, I would suggest a hysterosalpingogram, and perhaps a laparoscopy and salpingoscopy.
206 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 206

ECTOPIC PREGNANCY � 207
The misleading effects of selective publication
When it comes to doctors or scientists reporting medical or scientific outcomes inthe journals that comprise the medical literature, it’s human nature to spend moreeffort reporting good results than bad ones.
True, a note of optimism lubricates the human spirit—both as patient and asphysician—and while that’s mostly a good thing, I can think of no clearer area thanectopic pregnancy where the tendency to report small series of good resultsand postpone reporting bad or even average results has so distorted the medicalliterature.
If there were some way of making sure that all results were reported—as is nowthe case, for example, with IVF outcomes in Australia and in the USA—this biaswould disappear.
But for now the bias persists and it’s only with time (and with particularly large,contradictory series described in the medical literature) that we’ll get the true picture:that successful pregnancy after one ectopic pregnancy is not rare; but that after twoectopics—whether in the same tube or in opposite ones—a normal pregnancy inthe uterus is decidedly uncommon, whatever method has been used for treatingthem.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 207

diagnosing endometriosis
What to look for
Endometriosis is the name given to tissue like the lining of the uterus (the endometrium)when it grows where it should not, in locations other than in the cavity of the uterusitself. It can affect the lining of the pelvis and abdomen (the peritoneal cavity), includ-
ing the surfaces of the pelvic and abdominal organs.This chapter considers:
• What endometriosis looks like;• How common endometriosis is;• The symptoms endometriosis causes;• What causes endometriosis;• How endometriosis develops; and• The ‘chicken and egg’ conundrum of how endometriosis relates to infertility.Chapter 16 will consider its treatment.
WHAT DOES IT LOOK LIKE?
To the gynecologist or surgeon looking inside your abdomen (at a laparotomy or a laparoscopycarried out for one reason or another), endometriosis typically has a dark brown appear-ance, in the form of spots or cysts.This color comes about because it bleeds each month atabout the same time that the lining of the uterus menstruates. Because the blood hasnowhere to go it gets stuck in the tissues, dries out and goes dark.
If the endometriosis has formed a cyst in an ovary (it happens to about one ineight women with endometriosis), the semi-fluid material in the cyst is rather like chocolatein its color and texture, which gives rise to its usual description as a ‘chocolate cyst’.
The tissues most affected by endometriosis are the serosa of the peritoneum, which
208
15
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 208

is the one-cell-thick, smooth membrane that lines all of the pelvic and abdominal cavityand its organs (see Chapter 13), and the soft supporting tissue just under the serosa.The peritoneum anywhere can be affected, even under the diaphragm, but in generalthe closer the peritoneum is to the ovaries the more likely it is to be affected by endo-metriosis. Behind the uterus, the surface of the bladder, and the ovaries themselves are allcommon locations.
In 1986 my friend and colleague Professor Peter Russell, a pathologist in Sydney,helped me to study a range of abnormal appearances in the peritoneal cavity to workout what they were.We took biopsies of more than 160 such lesions.The great majorityturned out to be endometriosis.We published our results in the American Journal ofObstetrics and Gynecology, and from this time on gynecologists have recognized whatwe called ‘nonpigmented endometriosis’—early endometriosis that has not developedyet to the point of bleeding and so does not have the usual brown color. Nonpigmentedendometriosis can have the appearance of thickened, white tissue; gland-like excrescencesthat look a bit like the endometrium itself; and red, flame-like lesions that are full ofblood vessels.
Researchers at the Gasthuisberg University Hospital in Leuven, Belgium, have sinceshown that these nonpigmented lesions can be just as chemically active as, or more activethan, more typical pigmented endometriosis, secreting substances capable of disturbingreproductive function.
HOW COMMON IS ENDOMETRIOSIS?
In the past about one in 100 women had very troubling symptoms of endometriosis, includ-ing severe pain and abnormal bleeding, symptoms bad enough to lead to an operation.Butendometriosis is a lot more common than this. Often it causes minimal or no symptoms.Many women have it without ever knowing about it. If it’s not causing symptoms there’sno need to worry about it (unless it’s discovered by accident, say, in someone very young,who might be likely to develop symptoms as she gets older).
Among women in their thirties whom I’ve operated on to rejoin tubes to reverse asterilization operation, about 20 percent have had some endometriosis, whether they havesymptoms or not. In women I investigate with a laparoscopy because they’re having troublegetting pregnant, the incidence is about 40 percent. This makes endometriosis verycommon—too common, strictly speaking, to justify calling it ‘abnormal’!
Nonetheless it’s a major cause of symptoms and suffering in women.
WHAT SYMPTOMS DOES IT CAUSE?
The symptoms that suggest endometriosis include pain, in the form of painful periods(dysmenorrhea) and painful sexual intercourse (dyspareunia), and abnormal bleeding,partic-ularly premenstrual spotting and, later, heavy periods (menorrhagia).
DIAGNOSING ENDOMETRIOSIS � 209
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 209

Pain
Dysmenorrhea should be suspected as being caused by endometriosis if it gets worse insteadof better as a woman grows out of her teens; if it starts to last longer than the first day ofmenstruation; or if it is increasingly felt in her back.
The pain of dysmenorrhea can be caused by the endometriosis bleeding as theendometrium does at menstruation, but with congestion and trapping of blood in theendometriosis tissue. More often, the same hormones—the endometrial prostaglandins—that cause normal, first-day menstrual cramps are released by the endometriosis at menstru-ation time, making the cramps coming from the uterus worse and more persistent thanthey would otherwise be.
Note, though, that menstrual cramps, especially in teenagers, can be severe withoutendometriosis being present; non-endometriosis dysmenorrhea, even though distressing,usually becomes less severe once a woman is in her late teens or early twenties, especiallyafter a pregnancy and childbirth.
A common site for endometriosis is on or below the ligaments that support the uterusfrom behind, at the level of the cervix, and which lie just below the ovaries. Theseuterosacral ligaments run from the sacrum (the lowest part of the backbone) to the uterus,and endometriosis affecting them is one reason why dysmenorrhea is often felt inthe back.
Because these ligaments are located behind and to the sides of the uppermost part ofthe vagina, pain with sex (dyspareunia) is another symptom of endometriosis; it’s character-istically felt deep inside the vagina, sometimes particularly after a period, when theendometriosis will have become congested.The dyspareunia might be felt from the timeof first intercourse or it can develop in sexually active women who previously had nosymptoms with sex.
If scarring occurs in the uterosacral ligaments from the repeated irritation and bleedingeach month, the uterus can be pulled backwards—producing a retroverted uterus—whichcan make dyspareunia worse.
Not all pain felt in the pelvis,whether or not it’s associated with your periods, is causedby endometriosis. (See the box, Is your pain really endometriosis?)
And many women with endometriosis will have no significant pain. Need they (oryou) worry? In general, no. Having endometriosis is not like, say, having a positive PAPsmear. Rarely does it lead to complications if it’s not causing pain.
Abnormal bleeding
Premenstrual spotting or premenstrual staining is the most characteristic symptom ofendometriosis. (I won’t abbreviate this to PMS,because it has nothing to do with the premen-strual tension syndrome; let’s call it PMSP instead.)
Periods start in a quite definite manner for most women. It’s usually abnormal to havespotting or staining—whether fresh or dark in character—that lasts more than about 12 to24 hours before menstruation begins properly. The association between PMSP and
210 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 210

endometriosis was discovered 25 years ago by Dr Anne Wentz and her colleagues inMemphis,Tennessee—but is still not well known among gynecologists.
We have since found that even a small amount of spotting or staining, sometimesseparated from the actual period by several days, correlates with the presence of endo-metriosis in more than 80 percent of patients—a surer correlation than for either dysmen-orrhea or dyspareunia, both of which can have other causes.This strong association wastrue both for infertile women and for women who had been referred for reversal of aprevious sterilization operation. PMSP is therefore an important clinical symptom; but
Is your pain really endometriosis?
Not all pelvic pain or back pain in women is due to endometriosis. Pain that’s feltat period time, or soon afterwards, is most typical of endometriosis pain.The paincan be spasmodic, but really only at period time. It can be accompanied by diarrheaand pain evacuating the bowel, but again really only around period time, exceptperhaps in particularly severe cases where endometriosis affects the tissue that liesbetween the vagina and the rectum (in which case it can be easily felt by the doctoron vaginal examination).More than a few hours of pain at ovulation can come fromendometriosis affecting the ovary.
Spasms of pain—rising, knife-like, to a crescendo, then sooner or laterabating—have to come from a muscular tissue that is contracting in an involun-tary way inside the abdomen.The organs that have such involuntary muscle tissueare the uterus, the fallopian tubes and the intestines. Spasms at times other thanaround period time and ovulation are almost always coming from the intestines,the bowel.
Because endometriosis is so common, very many women whose pain is reallyfrom abnormal contractions of the bowel and/or heightened sensations of pain fromthe bowel (together known generally as the irritable bowel syndrome), have the label‘endometriosis’ placed on their condition and go through an extraordinarily frus-trating time with their doctor trying to get relief from their symptoms throughtreatments that will work only for endometriosis.
Premenstrual tension (PMT) is another condition whose symptoms arecommonly confused with those of endometriosis. PMT symptoms usually precedethe period (though some women feel emotionally at their worst toward the endof menstruation).
Many women with endometriosis have both PMT and the symptoms ofendometriosis. Unless you and your doctor distinguish them carefully, treating onewithout the other will inevitably result in much dissatisfaction. (To be sure, this isone major reason hysterectomy has a bad name,because whatever hysterectomy doesfor symptoms of endometriosis, it does nothing for the monthly symptoms of PMT.)
DIAGNOSING ENDOMETRIOSIS � 211
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 211

PMSP is especially interesting scientifically because it may be a clue to explaining the fourthsymptom of endometriosis—infertility—which we’ll get to shortly.
In the absence of a desire for fertility, rarely is PMSP a troublesome enough symptomto need investigation and treatment. Bleeding between periods can, however, be substan-tial enough to be troublesome. It’s not always clear, though, whether such bleeding is dueto endometriosis or to a hormone imbalance associated with abnormal ovulation, partic-ularly in the case of teenagers and older women.
How do I know if I’ve got endometriosis?
There are three common ways endometriosis prompts you to see your doctor.Teenagers usually go, or get taken, because they have very painful periods, sometimes
with bleeding between them or with spotting before the periods. After visits to severaldoctors, each reluctant to take symptoms seriously, laparoscopy will eventually be decidedon, and the endometriosis revealed.
The most common way that endometriosis is discovered in women in their twentiesor thirties is during tests if they’re having trouble getting pregnant. Just how importantthe endometriosis actually is in causing the infertility varies a lot. In general, the moresubstantial the endometriosis, and the more associated symptoms there are such as increas-ing pain or premenstrual spotting, the more likely it is to be an important factor behindnot conceiving.
Older women—those in their later thirties or forties—are most likely to haveendometriosis discovered if they’re developing heavy and painful periods, troublesomeenough for them to see their doctor.Among the tests that will usually be done are a trans-vaginal ultrasound,which might show some other causes for the symptoms (such as fibroids,an endometrial polyp or, sometimes, adenomyosis; see Chapter 17), but which will notreveal endometriosis unless there’s a chocolate cyst visible in the ovary.
If you’re having an ultrasound done for these symptoms, make sure you have it duringor just after a period, so that the ultrasound appearance of a normal corpus luteum is notmistaken for an endometrioma (or vice versa). Just at the end of a period is the best timeto have this test.
So the diagnosis of endometriosis can sometimes be suspected if an abnormal cyst isseen on transvaginal ultrasound. But it can also be strongly suspected if a careful vaginalexamination reveals nodules, often tender, below or to the side of the cervix. (I should notethat detecting the signs of endometriosis in young girls is more difficult, because vaginalexamination, except gently, under anesthesia, is usually not an option.) Confirmation thencomes by looking for it and seeing it at laparoscopy.And that same laparoscopy can oftenbe used to treat it (see Chapter 16).
WHAT CAUSES ENDOMETRIOSIS?
Many diseases and disabilities are the result of hereditary and environmental causes actingtogether. Endometriosis is no exception.
212 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 212

Inheriting endometriosis
Professor Joe Leigh Simpson, now of the Baylor College of Medicine in Houston,Texas,but in 1980 at North Western University in Chicago, studied the families of 123 womenwith proven endometriosis. Nine of their 153 sisters (aged over 18) and 10 of their123 mothers had also had diagnoses of endometriosis made.This means that of the first-degree relations there was particularly substantial endometriosis in 19 of 276—a prevalenceof 17 percent. Furthermore, only one of 104 sisters of the patients’ husbands (their sisters-in-law) and only one of 107 husbands’mothers (their mothers-in-law)—non-genetic rela-tions used as a control group—had had endometriosis of similar severity.
So, if you have a positive history of endometriosis among your closest relations, you’reabout seven times more likely to have endometriosis.
This substantial increase in relative risk of endometriosis if you have a mother or sisterwith it is consistent with endometriosis being inherited by the interplay of several genes.
Environmental influences: Ovulations and menstruations
We know that different women are at different inherited risk of developing endometriosis.But there’s also a special risk factor for endometriosis apart from this hereditary tendency—and this is the number of ovulations and menstruations a woman has had.Two things happenin the ovarian or menstrual cycle that are crucial in the development of endometriosis.
First, the ovaries,with each ovulation, pour huge amounts of hormones, especially estro-gens, out of the follicle into the peritoneal cavity. If there’s tissue there that’s potentiallyeven a little bit sensitive to estrogens, it will respond and grow.With each ovulation thereis another chance of this.
Second, all women who menstruate and who have fallopian tubes that aren’t blockedwill bleed backwards during their menstrual period, out through the fallopian tubes andinto the abdomen. Menstrual blood, coming as it does from an endometrium that’s comeapart and is all set to regrow itself over the next few days, is presumably chock-full of growthfactors and other substances that the endometrium uses to rebuild itself. It could evencontain some viable endometrial gland cells.
So with each ovulation and each menstruation there’s another opportunity for abnormalgrowth. Modern women, who have many, many more ovarian and menstrual cycles thantheir predecessors through history and prehistory (see the box,Endometriosis and the modernwoman), are now sharing the effects in the form of endometriosis.
Thus we have two reasons so far as to why some women get endometriosis early, someget it late, and some never get it at all.We have the likelihood that women can have a varyinggenetic susceptibility to it.And we have this ‘environmental’ variable, the number of ovula-tory menstrual cycles a woman has had. It’s the accumulating effects of ovulatory menstrualcycles that’s the explanation for how the prevalence of endometriosis increases with ageand increases in women who delay having children.
It’s also clear from the genetic influences why some women develop endometriosis ata young age, whereas other women never develop it at all. It can cluster among close
DIAGNOSING ENDOMETRIOSIS � 213
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 213

relatives for genetic reasons, yet many affected people have no relatives affected by it (sistersor daughters are still more likely not to develop it than they are to develop it).
Once it’s present, continuing ovulation and/or menstruation usually makes it developfurther.
Environmental pollution too?
There are indications that endometriosis might be getting more and more common forreasons beyond the social circumstances that have increased the experience of ovulationand menstruation.Part of the increase, to be sure, is that many women are postponing havingchildren. Doubtless too, we’re more likely to diagnose it than we were in the past. Morelaparoscopies are now done for investigating the once more-tolerated symptoms of painand infertility.We’re also aware, now, of nonpigmented endometriosis, which a decade agowas often missed.
But still there’s the possibility that there might be other environmental factors that havechanged over the last generation or two, just as there seem to be more environmental contri-butions to oligospermia in men (discussed in Chapter 10).Recent discoveries in monkeys havepointed the finger at an industrial pollutant, the poison dioxin.While we all await more definiteinformation before we can be sure, the box, Dioxin gives the details of the studies so far.
HOW DOES ENDOMETRIOSIS DEVELOP? DOES IT SPREAD?
One theory on the way endometriosis gets going—the so-called implantation theory, firstdeveloped by Albany, New York, gynecologist John A. Sampson in the 1920s—has it thatlive cells from the endometrium in the uterus are shed into the menstrual flow.With passage
Endometriosis and the modern woman
From a functioning reproductive point of view, modern women are special not justbecause they tend to have children later than their predecessors; it’s also only in ratherrecent times in our history and prehistory that women have spent more than a fewmonths of their reproductive life ovulating and menstruating.
Over the last, say, 100 000 years, women have typically spent their reproductiveyears either pregnant or breast-feeding their infants.
The nine months of each pregnancy and the two or more years of (unsupple-mented) breast-feeding that followed each pregnancy stopped the ovaries fromovulating.
If each weaning was soon followed by another pregnancy, then the normal humanfemale condition biologically was—and arguably still is—to ovulate and to menstru-ate not more than 10 or 20 times in a lifetime.
There’s more on this in Chapter 2.
214 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 214

of menstrual flow back out through the tubes, surviving cells are said to attach themselvesto the serosa near the ends of the tubes to produce endometriosis. Further shedding fromthese ‘implants’ results in further implants, and so the endometriosis gets more extensive.Just how often this might happen is still debated.
The other main theory on how endometriosis gets started and develops is the meta-plasia theory, by which the body for some reason determines that there are patches ofsensitive tissue in the abdomen,or peritoneal cavity.These patches, it’s thought, then respondeither to the repeated huge amounts of estrogen with every ovulation or they respond torepeated exposure to menstrual blood with every menstruation and the growth factors itpresumably contains.
Metaplasia then involves the peritoneal tissues undergoing a metamorphosis from simpleserosa (with nondescript little blister-like blebs) to having the structure of endometrial-likeglands (clearly endometriosis), followed by dark pigmentation once bleeding has occurred.Any apparent spread of endometriosis, according to this theory, is just the slower develop-ment of some patches in comparison with others.
Traditionally, it’s been the implantation theory that’s captured the imagination, especiallyin North America—to the point that each ‘lesion’of endometriosis has rather presumptively
Dioxin
You may have read in Chapter 2 that endometriosis occurs in monkeys and apes,but it’s rarely severe. Researchers at the Harlow Primate Laboratory in Madison,Wisconsin, have been studying dioxin’s long-term effect on reproduction in femalerhesus monkeys.
In a systematic study that started 15 years ago, the Harlow researchers beganfeeding 16 monkeys small amounts of dioxin in their diet.This addition to their dietwas continued for four years.
Unexpectedly, six to 10 years afterward, three monkeys eventually died of debil-itation from endometriosis.
Tennessee gynecologist Dan Martin operated on the surviving monkeys and wasstaggered to find that there was severe endometriosis in most of those which hadbeen given the highest dose of dioxin (25 parts per trillion).A smaller proportion ofthe monkeys given 5 parts per trillion had moderate to severe disease.
None of the monkeys given no dioxin had moderate or severe endometrio-sis—they just had the mild or no endometriosis normally found in monkeysanywhere.
Several studies are now underway to correlate levels of dioxin and related chem-icals in women with the presence of endometriosis. If the association is confirmed,the search for other environmental toxins, and how they operate on an internal tissuethis way,will be on. Its importance for women of the future, as well as for our under-standing of endometriosis today and what causes it, is immense.
DIAGNOSING ENDOMETRIOSIS � 215
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 215

come to be called an ‘implant’. Since we’ve recognized the early, nonpigmented lesions ofendometriosis I mentioned at the beginning of the chapter, some gynecologists arebecoming convinced that endometriosis only very uncommonly seems to spread from onelocation to another, previously completely normal location.
Unlike cancer,which spreads and spreads,most cases of endometriosis, once the lesionshave matured, remain more or less restricted to the same locations throughout a woman’smenstrual years.This is not to say that cysts of endometriosis in the ovary don’t often growback after being removed, but if you’ve gone 20 years without having endometriosis cystsin the ovary, for example, it’s unlikely that they will suddenly start developing. (For more,see the box, Implantation or metaplasia?)
ENDOMETRIOSIS AND INFERTILITY: CHICKEN OR EGG?
How ironic! You’re more likely to have endometriosis if you delay having your first baby(because of all those ovulatory menstrual cycles over the years), yet once endometriosis isthere it contributes further to not getting pregnant.
216 � GETTING PREGNANT
Implantation or metaplasia?
In the developing female embryo,peritoneum close to the ovaries gives rise to special-ized hollow structures, the Müllerian ducts (discussed more in Chapter 18).
These hollow pipes grow to form the fallopian tubes, which will form a connec-tion from the peritoneal cavity to outside the body. Starting immediately next to theovaries, the Müllerian ducts meet in the middle to form the uterus and below it thecervix, and then connect with the lower vagina.
We know that, in adult life, tumors of the surface of the ovaries and of the peri-toneum close to the ovaries can mimic development of the lining tissues of theseMüllerian-derived organs. Often these cancers differentiate in the same way and atabout the same time in many locations in the pelvis.
Now, endometriosis has nothing at all to do with cancer, but perhaps the peri-toneum in some women retains the memory and the capacity to develop into theseMüllerian tissues?
The result would consist of a series of conditions—all of which, as it turns out,we do in fact find—ranging from ‘endosalpingiosis’ (growth of tissue like that of thefallopian tube, or salpinx) to ‘endocervicosis’ (growth of tissue like the lining of thecervix), as well as endometriosis (tissue like the endometrium), which is the mostcommon and most important of the three possibilities.
These observations thus underlie the metaplasia theory for endometriosis.The basis for the opposing implantation theory is given in the main text.Controversy between proponents of the implantation theory and the metapla-
sia theory continues.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 216

There are also special conundrums that need explaining. Every experienced gynecol-ogist knows of some paradoxes that just don’t seem to make easy sense. On the one hand,treating the mildest forms of endometriosis rarely seems to be followed quickly by preg-nancy. On the other, we’ve all seen examples of substantial endometriosis in whichpregnancy has happened without any apparent problem.
It’s like saying that curing a mild form of a disease is more difficult than curing a severecase! How do we explain these paradoxes?
The key to understanding endometriosis and infertility is to realize that it’s not likehaving blocked tubes, or not ovulating, or having no sperm.Unless the scarring that some-times goes with it obstructs the tubes (accounting for no more than 5 percent of womenwith endometriosis), there’s always a chance of getting pregnant: it’s a cause of subfertility,not sterility (discussed in Chapter 1). Instead, experience (and theory) is consistent withendometriosis gradually decreasing fertility as it becomes more extensive—or as it becomesmore active in whatever the ways are that it actually gets in the way of conception (see thebox, Mild or moderate endometriosis and infertility).
In practice, though, the chance of getting pregnant naturally, as with most of the reasonsfor decreased fertility, depends more on the length of time you’ve been trying, and on yourage, than it does on the ‘dose’ of the particular infertility factor that’s been discovered.
Endometriosis is sometimes found in women who were born without a uterusor vagina (a condition I discuss in Chapter 18), and who have thus never menstru-ated.This means that implantation of menstrual cells is not necessary in the causationof endometriosis.
As well, probably every woman with open fallopian tubes who menstruates willshed cells from the endometrium out through the tubes into the abdomen eachmonth. But not every woman gets endometriosis.This means that implantation ofendometrial cells is not sufficient to cause endometriosis.
In science, a theory that’s neither necessary nor sufficient is not usually a particularlystrong theory.
This was the belief of probably America’s greatest ever gynecological patholo-gist, Emil Novak. On his death in 1957, Novak took with him the conviction thatendometriosis was a metaplasia much more often than his contemporaries wereprepared to concede—despite attempts by two of Sampson’s implantation theorydisciples, Roger Scott and Richard TeLinde, to get him to change his mind.
Still, there are cases of endometriosis that are hard to explain by metaplasia ratherthan implantation.The most striking is the occurrence of endometriosis in scars inthe abdomen after operations done during pregnancy to open the uterus and removethe fetus (a mid-trimester abortion operation rarely done nowadays). For somepeculiar reason, such scar endometriosis complicates about one in 50 such opera-tions in the middle three months of pregnancy, but happens only rarely after cesareansection (C-section) in the last three months.
DIAGNOSING ENDOMETRIOSIS � 217
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 217

218 � GETTING PREGNANT
Mild or moderate endometriosis and infertility
Severe endometriosis can distort the tubes and ovaries so much that it’s not hard toimagine why fertility fails.With more moderate endometriosis, though, the tubesand ovaries are usually completely normal.What’s going wrong?
Recent speculations center on two things. First, there are wandering cells aboutthe body called macrophages, which surround and ingest all sorts of debris that oneway or another gets into the body.There are many macrophages in the peritonealcavity (probably because in women the peritoneal cavity, via the tubes, the uterusand the vagina, is open to the outside environment).Macrophages, for example, ulti-mately dispose of sperm cells that get into the body.
In endometriosis, these macrophages are known to be particularly aggressive—we call them activated macrophages.Activated macrophages may get into the fallop-ian tubes and dispose of sperm before they’ve had a chance of getting to the egg.This is one way endometriosis probably works in decreasing fertility—especiallyin a woman whose husband has a low sperm count or low sperm motility (seeChapter 10).
Activated macrophages also produce a variety of chemicals (called cytokines)that have been shown, at least in the laboratory, to interfere with sperm motility andalso with the survival of embryos.
Cytokines are also capable of causing normal tissues to bleed, perhaps explain-ing the premenstrual spotting that endometriosis so often causes.
Second—and this is still speculative—we know that the endometriosis that’sassociated with infertility is located very superficially in the peritoneal cavity, just onthe peritoneal surface, the serosa.According to Dr I.A. Brosens and his colleagues atthe Gasthuisberg University Hospital in Leuven, Belgium, this is different toendometriosis that’s causing pain,which is more likely to be several millimeters deep,growing into the underlying tissues.
We also know that superficial endometriosis has glands that secrete mucus, justlike the endometrium in the uterus secretes mucus in the second half of themenstrual cycle.This mucus, if it were to specially adhere to the fimbrial ends ofthe tubes (responsible for attracting the mucus-surrounded egg, which you mayremember is called the cumulus), could stop the egg from entering the tube, withthe egg more likely either to remain within the follicle or to float into oblivion inthe abdomen.
What’s the evidence that this might be taking place?Researchers have been working on endometriosis in hamsters. Hamsters are
rodents, like mice and rats. Rodents don’t develop endometriosis naturally but theycan be made to develop it by grafting endometrial tissue into their peritonealcavity.
The hamsters with endometriosis induced this way (but not normal hamsters)
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 218

Paradoxically, the more severe the endometriosis is, the more likely it is to be the chiefexplanation of a couple’s infertility and that successful treatment will be followed bypregnancy.The arithmetic of this paradox is explained in Appendix 1.
Briefly, because we don’t understand or can’t point the finger at all the reasons whynormal fertility varies between different couples, the more dramatic the cause for infertil-ity that’s found, the more likely it is that it will be the only cause, and that treating thatparticular recognized cause will lead to conception.
Treating endometriosis is the subject of Chapter 16.
Figure 15.1 is printed in color after Appendix 3.
have shown a mucous coating over the surface of the fimbrial ends of their fallop-ian tubes when looked at with great magnification using scanning electronmicroscopy.
This is just what one might expect if secretion of mucus from the endo-metriosis were to be getting in the way of ovulating eggs at the ends of thetubes.
We also know from extensive experience among women with endometriosisthat when we put lots of sperm directly into the tube (getting around a low spermcount), and we also put three or so eggs directly into the tube (getting around anypossible problem with egg pick-up by the tube’s fimbrial end), we have a very highchance of the woman getting pregnant. (This is the procedure of gamete intrafallop-ian transfer, or GIFT, discussed in Chapter 20.)
DIAGNOSING ENDOMETRIOSIS � 219
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 219

treating endometriosis
Hormones, operations, IVFand other symptomatic relief
Here I describe the various ways endometriosis can be treated—suppressing it, destroy-ing it, or ignoring it and just relieving symptoms.The symptoms of endometriosis andhow endometriosis comes about are discussed in Chapter 15.
TREATMENT—IF AND WHEN?
If endometriosis is not causing symptoms, especially if it’s not causing significant pain orinfertility, it might not need treatment at all. It will probably disappear after the menopause,when it stops being stimulated by ovulation or menstruation.
There are two main exceptions to this non-interventionist medical policy: when it’sdiscovered in a teenager and gentle suppression of the endometriosis is prudent to helpconserve fertility in the future; and when there’s a ‘chocolate’ cyst of the ovary (seeChapter 15), and suppression is important to stop the cyst getting bigger and perhapsbursting.
Remember that not everyone with endometriosis will have impaired fertility; untilfertility has been put to the test, no-one can know for sure if the endometriosis that’s beenseen will in fact result in infertility.
Table 16.1 summarizes the three main strategies for treating endometriosis that’s causing,or likely to cause, symptoms, namely:• Withdrawing the hormone support from the ovaries that endometriosis depends on;• Removing or destroying the abnormal endometriosis tissue; and• Alleviating the symptoms it’s causing while ignoring the endometriosis behind the
symptoms.
220
16
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 220

Table 16.1 Strategies for treating endometriosis
Take away the Destroy the target Just relieve the symptomshormone support endometriosis (the pain, the bleeding or
the infertility)
progestogens laparoscopy with non-steroidal anti-inflammatory drugsdiathermy or laser (NSAIDs) such as naproxen (for pain)
danazol birth control pill (for pain and bleeding)gestrinone assisted conception (for infertility)GnRH-agonists presacral neurectomy (for pain)
ovariectomy (remove the laparotomy and excision, hysterectomy (for pain and bleeding)ovaries) including ovarian
cystectomy
STRATEGY #1: STOPPING OVULATIONUsing drugs to suppress ovulation and cause endometriosis to regress, or shrink, has theadvantages of neither requiring anesthesia nor involving the hazards and discomfort of anoperation.The drugs are typically taken for a minimum of six months, during which timethere’s no possibility of pregnancy happening (because, intentionally, ovulation does nottake place). After the drugs are stopped it takes normal cycles about six weeks to comeback.With time, if pregnancy doesn’t happen, the endometriosis will become active again.
Drug treatment is best suited to younger women, women in their teens or twenties,for long-term control of endometriosis until fertility is to be put to the test.Once a womanhas known infertility, however, the time drug therapy takes is counterproductive and otherapproaches are better.
ProgestogensDrug treatment of endometriosis evolved from the observation that endometriosis oftenregresses in those women who get pregnant despite it—an effect attributed to the mainpregnancy hormone progesterone.There are several synthetic progesterone-like drugs (progesto-gens) available to mimic progesterone’s effect. Dr Robert Kistner, in Boston, began treatingendometriosis with medroxyprogesterone acetate (MPA, trade name Provera) in the late 1950s.Norethisterone (NET, trade name Primolut N; norethindrone in the USA) is also welltolerated and effective.MPA and NET are the hormone drugs I would choose for a womanif she has endometriosis diagnosed years before pregnancy’s wanted; the maintenance dosecan be very small, usually with no side-effects.
The hormone drugs we usually prescribe for shorter six-month courses of treatmentare, however, a little more powerful.They include the male hormone derivative danazol(Danocrine), gestrinone, and the class of substances called GnRH-agonists.
Danazol and gestrinoneDanazol works in several ways at once.First, it stops estrogen and progesterone being producedin the ovaries, decreasing the amounts of these hormones in the blood—and, especiallyimportant, in the fluid of the peritoneal cavity.
TREATING ENDOMETRIOSIS � 221
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 221

Second, it blocks the receptors to those hormones in responsive tissues.This means thatthe endometrium, as well as endometriosis tissue, cannot respond to whatever small amountof estrogen is still circulating. Menstruation stops and there is amenorrhea (absent periods)during treatment, although there can be breakthrough bleeding.
Third—and probably because of its resemblance to male sex hormones—danazol stopsthe pituitary gland from trying to compensate for the ovaries’ inactivity by increasing itsproduction of follicle stimulating hormone (FSH).
Because of its three-pronged action, danazol has been a little more effective at suppress-ing endometriosis than the progestogens, but its main advantage over the progestogens isthe comparative lack of breakthrough bleeding. I sometimes use a short course (two tothree months) of danazol to stop the periods effectively before switching to a progestogen.
Gestrinone, although technically not derived from male hormones, has male hormone-like side-effects similar to those of danazol, including acne and excessive facial hair.
The side-effects are generally slight, especially with short courses, but sometimes theycan be serious (see the box,Danazol mischief ).Unlike danazol, gestrinone needs to be takenjust two or three times a week.
Neither danazol nor gestrinone must ever be taken in pregnancy, because they cause
222 � GETTING PREGNANT
Danazol mischief
Thin women generally tolerate danazol better than fatter women do,because danazoloften stimulates the appetite. Danazol can also increase weight through retention offluid. Danazol is an anabolic steroid and develops the muscles. Muscle cramps canoccur during the first few weeks of treatment.
About 5 percent of patients starting danazol quickly develop a rash, usually overthe face and upper body; although the rash resembles an allergic reaction, allergy isprobably not its cause, and it subsides with continued treatment. Because danazol isa (weak) male sex hormone, it’s common for women to experience an increase infacial hair during treatment.Acne can be troublesome too.Although these reactionssubside after treatment is finished, other rarer reactions may not.
Enlargement of the clitoris occurs in about 1 percent of women taking the drug;noticeable change should mean stopping the danazol, because an increase in size canbe permanent.
Don’t take danazol if you sing
Women who sing for their career or for their pleasure should never use danazol.Sensitive testing shows that most women who take danazol will have a slight but
measurable decrease in the tone of their voice.Most people won’t notice a semitoneloss in vocal range, but the loss may be critical for a singer, who needs not just herbest vocal range but also confidence in the power of her voice over that range.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 222

abnormalities of the genital organs in female fetuses (of a kind described as intersex inChapter 18).To guard against inadvertently taking these drugs in pregnancy, a course ofdanazol or gestrinone should start only at the time of a normal menstrual period, follow-ing a pregnancy test if there are doubtful circumstances.
If there is doubt about whether ovulation is being suppressed in a sexually activewoman—for example, with low doses of danazol—a barrier method of contraception oran IUD should be used.
Other ways of suppressing the pituitary and ovary, and thus suppressing endometrio-sis, involve the use of GnRH-agonists.
GnRH-agonists
The GnRH ‘analogs’ are drugs that are similar to the body’s natural gonadotropin-releasinghormone (GnRH, see Chapter 3),which the hypothalamus produces to stimulate the pituitarygland.They either mimic the action of GnRH (GnRH-agonists) or block its action (GnRH-antagonists). (For more on the antagonists, see the Chapter 20 box, The long, short and ultra-short of GnRH-agonists.) GnRH-agonists first stimulate the pituitary, then soon exhaust thepituitary of its follicle stimulating hormone and luteinizing hormone.This means that the ovariesare also stimulated briefly, but then as FSH and LH levels fall they shrink from lack ofsupport, and withering with them are the tissues that depend on the ovaries’ hormones,including those affected by endometriosis.
This class of drugs has found an important place in reversibly removing the influenceof the ovaries: as well as being useful for endometriosis, we use GnRH-agonists for fibroidsand adenomyosis (see Chapter 17), and for controlling the pituitary during ovarian stimula-tion with injected FSH for assisted conception (see Chapter 20).
GnRH-agonists can be administered in several very different ways, probably equallyeffectively:• By daily injection under the skin using a very fine needle, such as leuprorelin (Lucrin;
known as leuprolide, or Lupron, in the USA);• By the several-times-a-day inhalation of a nasal spray, such as nafarelin (Synarel) or
buserilin, the drug being absorbed by the nasal mucosa to reach the pituitary glandthrough vascular channels in the intervening brain tissue; or
• By monthly depot injection of, for example, goserelin (Zoladex) and depot forms ofleuprolide.GnRH-agonists are so effective that the main side-effects of treatment come from the
inevitable lack of estrogen (see the box, GnRH-agonist mischief ). Like danazol andgestrinone, GnRH-agonists should only be started when you can be sure there’s no preg-nancy present.
So far, the quietening-down of the ovaries strategy for endometriosis I’ve describedhas been what we call ‘medical’, meaning that it uses drugs; this is in contrast to ‘surgical’,which implies a surgical operation and which is clearly a more radical order ofmagnitude.
TREATING ENDOMETRIOSIS � 223
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 223

Surgical removal of the ovaries
Ovariectomy (surgical removal of the ovaries) has an important place in the overall scheme ofendometriosis treatment.And the reason is the same as for drug treatments—the endometrio-sis that’s left behind after the operation is deprived of its support. Both ovaries need to be
224 � GETTING PREGNANT
GnRH-agonist mischief
Removing estrogen, specifically estradiol, is our intention when we use GnRH-agonists—and estrogen lack is precisely the basis of GnRH agonists’ commonside-effects: the symptoms are those of the menopause.
In the short term, within a month or two of starting, hot flashes or flushes arecommon, and there may be night sweats; headaches and loss of libido are much morecommon with GnRH-agonists than with danazol.Weight gain and increased bodyhair are rare though.
Over a six-month course, the estrogen deprivation the GnRH-agonists producecauses calcium to be lost from the bones—also similar to the situation after themenopause.The bone loss is mostly temporary, recovering over the six to 12 monthsafter the treatment finishes.The loss of bone can be prevented by giving a small dose ofestrogen and progestogen at the same time—a maneuver called ‘add-back’. Becauseovulation and the levels of estradiol in the abdomen are still so dramatically lowered, thesmall amounts of estrogen given with add-back do not stimulate the endometriosis.
All the GnRH-agonists release a small amount of histamine as a side-effect.Thiscan cause an annoying rash, for which an antihistamine can be tried.
Over the longer term (the information comes mainly from men having yearsof treatment with GnRH-agonists for cancer of the prostate gland), more bizarreside-effects may come to light.The fact is that the natural hormone GnRH isfound not just in the hypothalamus, from which it drives the pituitary gland, butoccurs all over the brain and the spinal cord, in places where we have no ideawhat its role is—and where we have no idea what the effects of GnRH-agonistsmight be (except that they are not obvious so far). However, some men on verylong-term treatment have developed nervous system side-effects, includingdementia and paralysis; whether these developments are truly complications oftreatment or whether, in these generally old people, they are coincidence is notcertain, but when things go wrong and a patient is on a drug, the drug is alwaysthe first suspect.
No harmful effects have been obvious in several newborn babies delivered afterGnRH-agonists were inadvertently used during early pregnancy, but because theagonist might interfere with the functioning of normal GnRH in the developingbrain it is best for GnRH-agonists be avoided in pregnancy.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 224

removed to get the effect, and the operation is rare without an accompanying hysterectomy(see further on).
Removing both ovaries is important not just for treating left-behind endometriosis butalso for removing the source of symptoms of PMT, if PMT is part of the problem and ifsurgery is being undertaken for endometriosis.
STRATEGY #2: REMOVING ABNORMAL TISSUE
The best time to destroy small areas of endometriosis is when it’s diagnosed at laparoscopy.
Laparoscopy
Effectiveness of treatment at laparoscopy with vaporization using a laser or with electro-cautery (diathermy, see Figure 16.1) is restricted by the closeness of other organs and therisk of damage to them,particularly the ureters (which carry urine from the kidneys downto the bladder) and the intestines.
Special experience is needed in performing this procedure.At the least, the gynecolo-gist diagnosing endometriosis at laparoscopy usually needs to remove the fluid normallypresent in the peritoneal cavity to be able to see all the candidate tissues deep in the pelvis,and a second or third instrument may need to be inserted to lift loops of intestine awayfrom the affected peritoneum to allow safe destruction of endometriosis tissue. If theendometriosis is either widespread or deep, then laparoscopic treatment becomes a veryspecialized, time-consuming treatment, for which great experience is required.
Operations for endometriosis must enhance fertility if they are to serve their purpose.This seems an obvious statement, but remember (see Chapter 13) that adhesions are a consid-erable hazard after any operation among a woman’s pelvic organs.The last thing we wantis for adhesions to replace the endometriosis as the cause of not getting pregnant.
Laparotomy
Laparotomy for endometriosis—formal opening of the abdomen, usually with a horizontalincision just above the pubic bone—is followed by cutting out the endometriosis lesions,and then closing, with sutures, the resulting gap in the peritoneal serosa. Becauseendometriosis often affects the ovaries or the peritoneal tissues close to the ovaries, adher-ence of the ovaries to underlying, operated-on peritoneum is almost inevitable, after eventhe most careful operations to excise the lesions.
If adhesions can be avoided, especially by early postoperative laparoscopy to treat adher-ences as they form (see Chapter 13), pregnancy rates after surgery are generally better thanafter drug treatment. Furthermore there is, practically speaking, little delay before the effectsof treatment are experienced.
‘Conservative surgery’ (meaning not involving hysterectomy or ovariectomy), withexcision of endometriosis tissue either at laparotomy or, depending on the gynecologist’sexperience, at laparoscopy, is therefore the ultimate treatment option for women withsymptoms in whom drugs have not worked—and it’s often the main option for older women.A short, preliminary course of danazol or progestogen for two or three months before the
TREATING ENDOMETRIOSIS � 225
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 225

operation is regarded by many endometriosis surgeons to be useful for consolidatingendometriosis lesions and improving the chance of removing all the abnormal tissue successfully.
In general, the use of ovary-suppressing drugs is avoided just after the operation,becausethey will have a contraceptive effect just when everyone’s feeling most optimistic aboutachieving pregnancy. But if aggressive-looking endometriosis has not been completelyremoved, there may be no alternative to using danazol, a GnRH-agonist or a progestogenfor several months after the operation.The nature of each particular operation is as variedas the distribution of the endometriosis, and more than the usual amount of surgical andgynecological experience is needed to obtain good results consistently.
The more substantial the endometriosis is, the more successful an operation will be inimproving fertility, provided all the endometriosis can be excised, and provided an adhesion-free result is gained.The reason for this paradox is that the more endometriosis that’s removedthe bigger the difference the operation will have made (see Chapter 7 and Appendix 1).
The expectation of pregnancy after technically successful treatment varies according toage and according to the couple’s duration of prior infertility.As a rough approximation,about 40 percent to 60 percent of couples conceive within 18 months after operation andabout 30 percent to 50 percent do so within 18 months of finishing a course of danazol.
Gynecologists should be aware of the results of their own operations and not rely onthe published results of others in advising operation for treatment. Insist on finding out whatthese results are for your gynecologist before you choose operation over medical treatment.
STRATEGY #3: SUPPRESSING SYMPTOMS
Endometriosis is not ordinarily a dangerous condition in the sense that it might lead tocancer. It usually leaves its mark through one of several symptoms, such as pain, abnormalbleeding or infertility.
In young people it’s important to bring endometriosis under control to stop it causingmore symptoms later, but for older women, in whom the endometriosis has taken manyyears to develop, a treatment approach directed purely at the symptoms may be best. In thisregard, the oral contraceptive (birth control) pill is safe and diminishes both bleeding andperiod pain (dysmenorrhea); it may also control painful intercourse (dyspareunia). (Stoppingthe periods altogether with a low dose of progestogen, as described earlier, achieves the samecontrol of symptoms and is probably better than the pill in preserving potential fertility.)
NSAIDs (nonsteroidal anti-inflammatory drugs) may be all that’s needed to controldysmenorrhea. In severe, intractable, pelvic pain, some gynecologists favor the operation ofpresacral neurectomy—dissecting out and cutting the nerves coming from the pelvis wherethey join together, just in front of the sacrum.
IVF (see Chapter 20) works at least as well with endometriosis as it does for anyother cause of infertility, provided the endometriosis has not caused chocolate cysts ofthe ovaries. Going straight to this approach is becoming popular among women in theirthirties and forties. Remember, though, that the ovarian stimulation that’s usually partof assisted conception will stimulate the endometriosis more than natural ovulations do,even though a successful pregnancy would in turn suppress it.
226 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 226

Hysterectomy,without removal of the ovaries, is no more likely to diminish endometrio-sis itself than is tying off the fallopian tubes (which, as it turns out, is of no help at all). Buthysterectomy reliably stops abnormal bleeding and dysmenorrhea. If you are past wantingto have children and if you have endometriosis or premenstrual tension that’s driving you todistraction, hysterectomy and ovariectomies, followed by estrogen replacement therapy (ERT),might be a good strategy for you.
Special information and precautions are needed before choosing a hysterectomy forrelief of your symptoms (see the box, Hysterectomy: Between a rock and a hard place), but Ihope that, by now knowing the medical facts, you will understand the ambiguous experi-ences other women have had with hysterectomy—and, on a confident medical basis, makeyour decision with your doctor.
Figure 16.1a–b is printed in color after Appendix 3.
TREATING ENDOMETRIOSIS � 227
Hysterectomy: Between a rock and a hard place
Whole books for consumers have lately been written on hysterectomies—especiallyon how to avoid them.
Why do some women intensely regret having an operation that to other womenhas meant peace and relief from symptoms?
Obviously a hysterectomy is not an option for someone intent on retaining thepotential for having children. Equally obviously there’s no question about the placeof hysterectomy for serious disease of the uterus when there’s no alternative satis-factory treatment available.Where’s the balance?
There are two reasons why removing the uterus has a place in the treatment ofendometriosis: first, the uterus is the source of bleeding and period pain, bothof which are symptoms that inevitably respond to hysterectomy; and second, thepresence of the uterus complicates estrogen replacement therapy (ERT) after the ovarieshave been removed, because a progestogen then needs to be taken in addition to theestrogen to prevent endometrial hyperplasia. And progestogens, in turn, have uncom-fortable side-effects that can mimic the very symptoms that led to the hysterectomy.
So, when a radical operation is planned for either endometriosis or premenstrualtension (or for both), it’s the removal of the ovaries that’s actually therapeutic; theuterus is removed so that ERT can be used without needing progestogens.
Still, you might ask, won’t ERT cause the endometriosis to flare up, especiallyin the absence of progestogens?
The reason why 95 percent or more of the time it doesn’t cause a flare-up is thatendometriosis depends so much on especially high levels of estrogen that comedirectly from the ovary during ovulation.Take the ovaries out, and this can’t happen.The amount of estrogen that gets to any remaining endometriosis through the blood-stream during ERT is very, very small in comparison.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 227

fibroids and other problemsin the uterus
Not as common asyou might think
For all its central importance for pregnancy, the uterus, or womb, is the least likelyorgan in which to find a problem when there’s trouble getting pregnant.When thingsgo wrong in the uterus,however, they’re often serious for fertility.Moreover, IVF won’t
overcome them. So overcoming pathology here can be a special challenge.Abnormalitiesof the uterus that are present at birth are discussed in Chapter 18.
We look here at disruption of the endometrium (the mucosal lining of the uterus) andof the myometrium (the muscular wall of the uterus), namely:• Endometritis, or inflammation of the endometrium;• Intrauterine adhesions, or distortion of the endometrium by scar tissue;• Endometrial atrophy, when the endometrium resists developing properly;• Endometrial polyps;• Fibroids, which are benign tumors of the myometrium; and• Adenomyosis: disruptions in which the glands of the endometrium grow in among the
myometrial fibers.In the absence of these specific diseases, the uterus can be expected to age well and to keepresponding to estrogen and progesterone (the details are in Chapter 3) after the menopause, longafter these hormones have stopped coming from the ovaries.
Experience with the donation of embryos from younger to older women has shownthat the decline in fertility that takes place as a woman gets older owes much more to whathappens in the ovaries than to what happens in the uterus.
228
17
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 228

For the conditions that we describe, remember that acute means ‘short-term’ and chronicmeans ‘long-term’.
DISRUPTION OF THE ENDOMETRIUM
In terms of regenerative powers and acceptance of implanting embryos the endometriumis rather forgiving.
Nonetheless infertility can result if there’s a general disturbance that seriously inhibitsits response to normal circulating levels of estrogen and progesterone; if there’s a substan-tial constraint on an implanted embryo and its placenta from expanding its contact withthe mother’s bloodstream; or if there’s a space-occupying lump that stops the front and theback of the endometrium from effectively trapping the implanting embryo.
Endometritis
Not to be confused with endometriosis (to which Chapters 15 and 16 are committed),endometritis means inflammation of the endometrium, usually from an infection.
To a pathologist, acute endometritis means a rapidly developing,usually short-term inflam-mation, and generally part of an overwhelming infection caused by chlamydia, gonorrheaor a pus-forming organism such as Streptococcus; the fallopian tubes then commonly carrythe brunt of the sepsis, as acute salpingitis.There’s pain, fever and a purulent discharge throughthe cervix.The treatment of such an acute infection is usually given in hospital, with anti-biotics administered intravenously.
Chronic endometritis, on the other hand, is long term and more insidious.There are oftenno symptoms. So little is known about it, and about its persistence from one cycle to thenext, that medical opinion is not unanimous on when or how to treat it.
The diagnosis is usually an incidental one, made at hysteroscopy or on biopsy of theendometrium, such as at curettage. Some cases, at least, are due to Mycoplasma, an organism
FIBROIDS AND OTHER PROBLEMS IN THE UTERUS � 229
Tuberculosis
In parts of the world where advanced tuberculosis is still common, tuberculousendometritis, a form of chronic endometritis and endometrial atrophy, is one of the mostfrequent causes of absent periods, or amenorrhea.Western specialists, though, comeacross it rarely.
The infertility that advanced tuberculosis causes comes also from damage to,and blockages of, the fallopian tubes—tuberculous salpingitis, a form of chronic sal-pingitis.The diagnosis is best made by hysterosalpingogram, which typically showsmyriad tiny side-channels off the main passage of the tube, as well as perhaps reveal-ing irregular compartmentalization of the cavity of the uterus from scarring.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 229

common in the vagina,which has gained access to the uterus through the cervix; it’s sensi-tive to the antibiotics tetracyclin and erythromycin, both of which are used to treat it—with a course for your partner, too, to stop re-infection.
Unless it is the result of tuberculosis (see the box, Tuberculosis), chronic endometritisdoes not usually cause scarring.
Intrauterine adhesions and endometrial atrophy
Partial or complete obliteration of the cavity of the uterus with scar tissue is a serious conse-quence of carrying out a curettage in circumstances in which the endometrium cannotregrow. In most clinical conditions that require curettage (a ‘curette’), the endometrium isin no danger.The surface layers only are removed and normal endometrium grows backin one cycle. It might be beneficial for fertility.
The times when it’s dangerous to curette the uterus are also, unfortunately, the timeswhen there’s little other option—usually after a recent pregnancy.The two situations arewhen retained bits of placenta cause bleeding a few weeks after the birth of a baby (calleda ‘secondary postpartum hemorrhage’); and when a missed abortion occurs and an unex-pelled fetus and trophoblast lie fixed in the uterus, becoming more and more compact andharder and harder to budge. In these two circumstances there is both a shortage of estrogen(the ovaries’ production of it still being suppressed by the recent pregnancy) and a likeli-hood of infection by bacteria—conditions that jeopardize the endometrium’s ability toregrow after the curettage. In some instances, the raw and damaged endometrium thendoes what two opposite and damaged surfaces anywhere else in the body would do if incontact, growing into each other with scar tissue and adhesions.
If the periods do not return (amenorrhea) or become much lighter (hypomenorrhea) afterthe pregnancy tissue has been removed, yet the woman is ovulating, the condition is knownas Asherman’s syndrome. Asherman’s syndrome is caused by blockages in the cavity of theuterus by scar tissue and adhesions, leading to replacement of the endometrium.
The diagnosis is made (preferably before hysteroscopy) by a combination of (1) reveal-ing periodic elevations of serum progesterone despite amenorrhea; (2) a hysterosalpingogram,showing constriction and irregularity (or sometimes absence) of the endometrial cavity;and (3) a transvaginal ultrasound, showing a reduced area of endometrium.
Treatment consists of painstaking separation of the adhesions accompanied by estro-gens to encourage the endometrium to regrow.
For the treatment to work, the adhesions need to be separated, generally at hysteroscopy,while the endometrium (or what’s left of it) is under the influence of estrogen, to promote itsgrowth.An intrauterine contraceptive device or something similar, such as a small ballooncatheter, can be left in the uterus for a few days (in the case of a balloon) or longer (in thecase of an IUCD) to keep surfaces apart (and, probably, to re-separate new adhesions whenit’s pulled out).
To correctly time the treating of intrauterine adhesions I first make sure the personis in the early follicular phase of the ovarian cycle (using ovarian monitoring if necessary), sothat there is no progesterone about to stop estrogen from stimulating the endometrium
230 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 230

that’s left.Then I use an eight-week or so course of estrogen treatment in high dosage,during the first two weeks of which I perform the first hysteroscopy and lysis of the adhe-sions.At the end of the eight weeks I then attempt to bring on a period by administer-ing a progestogen for 10 to 14 days—and hope that enough endometrium has reformedfor menstruation to follow. Treatment often needs repeating several times, with re-evaluation using hysterosalpingograms and ultrasounds between treatments. It is notalways completely successful.
The eventual outcome from treating intrauterine adhesions depends on how badly theendometrium has been damaged and on how well it recovers. Endometrium that has beenparticularly badly diminished can be beyond recovery, resulting in permanent endometrialatrophy. If treatment is successful to the point of a return of menstruation (especially if youget periods as heavy as they were before), and if the tubes are open, another pregnancy isusually possible. Such a pregnancy, however, has a greater chance than usual of ending earlyas a miscarriage or premature labor. More seriously still, the placenta of the new pregnancy cangrow deeply into the wall of the uterus (called placenta accreta), and might not come looseafter the fetus or baby has been delivered.The result of this can be bleeding that is some-times unstoppable short of an urgent hysterectomy.
Endometrial polyps
Polyps, as the name suggests, are benign tongues of tissue that seem to grow in theendometrium (as they do in other parts of the body) for no good reason.Symptoms includeheavy periods and bleeding between periods (including premenstrual spotting), as well asinfertility.The infertility probably comes about because fluid in the endometrial cavity poolsaround it, or to one side of it, as the front and back surfaces of the endometrium presstogether (see the box in Chapter 5, Thirsty for an embryo).The still free-floating embryo,ready to implant, can become ‘lost’ in this pool of fluid with none of the intimate contactwith the endometrium that’s the first step in its implantation.
The diagnosis is suspected at transvaginal ultrasound (polyps cause irregular thickeningand heightened echoes in the endometrium) and is confirmed at hysteroscopy. Althoughcurettage has been used for treatment, the curette often skates over and around the polyp,thus missing it. Resecting it under direct vision at hysteroscopy is reliable.
After treatment, however, polyps quite often grow back within a year or so.
DISRUPTION OF THE MYOMETRIUM
The muscular wall of the uterus, or myometrium, plays its greatest role at the end of preg-nancy, when it’s time for its coordinated contractions to expel the baby.The myometriumis usually quiet when it’s under the influence of progesterone—which it should be from soonafter ovulation, during implantation and during pregnancy.The two main abnormal condi-tions we encounter in the myometrium, fibroids and adenomyosis, often have little or noeffect on fertility, but they can lead to disturbance of an embryo or fetus once pregnancyis underway.
FIBROIDS AND OTHER PROBLEMS IN THE UTERUS � 231
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 231

Fibroids
Fibroids,known technically as myomas, are benign lumps of muscle tissue growing in or fromthe myometrium.The closer they are to the endometrium the more likely they are to causesymptoms such as heavy bleeding,dysmenorrhea and infertility (see the box,Mapping myomas,and Figure 17.1). Fibroids are best diagnosed before operation with transvaginal ultrasound.
The surgical operation for a fibroid that leaves the surrounding uterus intact is calleda myomectomy. Myomectomy is designed to conserve fertility.
232 � GETTING PREGNANT
Mapping myomas
Fibroids on the outside of the uterus are called subserous fibroids.They can be on along pedicle (‘pedunculated’)—which occasionally can twist, causing pain and eventualdegeneration of the fibroid;or they can be broad-based,a situation that’s usually troublefree unless the fibroid grows to a large size,when it can cause symptoms from pressure.
Within the wall of the uterus, fibroids are called intramural fibroids.They need tobe bigger than a few centimeters or be multiple before they cause symptoms,whichas well as dysmenorrhea and heavy periods can come to include an increased chanceof a pregnancy miscarrying, and even the prevention of successful implantation ofthe embryo—infertility.
The fibroids most likely to cause symptoms are those that project from themyometrium into the endometrial cavity—when they’re called submucous fibroids.Even a small submucous fibroid can project into the endometrial cavity enough tostop the endometrial surfaces coming together over the implanting embryo (seeEndometrial polyps in the main text), causing infertility, as well as often resulting inpronounced bleeding and cramping pain.
Fibroids present in pregnancy can occasionally degenerate rather suddenly andpainfully.
The presence of fibroids and their location are best determined, before opera-tion, with transvaginal ultrasound.
Malignant myomas, or myosarcomas
Cancer is rare in a fibroid.Textbooks say that one in 200 removed fibroids are malig-nant but, with more and more fibroids now diagnosed by transvaginal ultrasound,it’s more likely to be about one in 200 women with fibroids who turn out to havea fibroid that’s malignant. However, I have not encountered a case in a professionallifetime of infertility surgery.
The main sign of malignancy before operation—although it’s not completely tobe counted on—is a fibroid’s particularly rapid growth.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 232

For submucous fibroids, protruding into or lying in the endometrial cavity, the operationcan often be done at hysteroscopy, using a special instrument that shaves the fibroid away,strip by strip; this operation is a day-stay hospital procedure; there are no stitches.
For intramural fibroids, lying within the wall of the uterus, an open operation, or laparo-tomy, is usually necessary: the uterus is incised; the fibroid or fibroids are shelled out (theyusually grow with a compressed capsule around them and come out like peas from a pod);and the uterus is repaired in layers. If a myomectomy has involved dissection of the wall ofthe uterus, perhaps weakening it,most obstetricians will recommend that a later pregnancybe delivered by cesarean section.
Subserous fibroids, lying outside the uterus, might need no treatment; small ones cansometimes be removed at laparoscopy; large ones require laparotomy.
FIBROIDS AND OTHER PROBLEMS IN THE UTERUS � 233
Intramuralfibroid
Subserousfibroid
Submucousfibroid
Pedunculatedsubserous fibroid
Figure 17.1 Fibroids in the uterus.A subserous fibroid can twist and cause pain if it is pedunculatedbut it does not interfere with fertility.An intramural fibroid can disturb the supply ofblood to a developing pregnancy and thus may cause miscarriage.A submucous fibroidaffects the lining of the uterus directly and can cause infertility.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 233

Sometimes a course of GnRH-agonists (described in Chapter 16) is used to shrinkfibroids, especially large submucous ones, so that they can be more easily treated surgically.Occasionally, instigating GnRH-agonist treatment actually precipitates severe uterinebleeding from the fibroid.There is no lasting beneficial effect from these drugs, and thefibroid, after stopping treatment, quickly grows back to its previous size. GnRH-agonistsare not suitable for long-term use, partly because of cost, but mostly because of side-effects.Although many of the side-effects are preventable by adding back some estrogen in replace-ment therapy, in the case of fibroids (and unlike when it’s used for endometriosis) such add-back stops the treatment from working.
Several centers have now reported a non-operative treatment for fibroids in which acatheter is placed in the artery or arteries supplying blood to the fibroid and small plasticballs are injected—a process called embolization.The released balls get stuck in the branchesof the artery, depriving the target tissue of oxygen, and causing it to scar and contract.Collateral damage is common. Some patients having embolization treatment of fibroidshave developed primary ovarian failure, with premature menopause, presumably becauseof interference with its blood supply. Short of this, adjacent normal myometrium is as likelyas the fibroid to be killed by the embolization process. I would not recommend emboliza-tion of fibroids if you are wanting to get pregnant, although the technique could be usedto control heavy periods after you have finished your family.
Adenomyosis
As translation from the Latin might suggest, adenomyosis is the growth of glands from theendometrium in among the muscle of the myometrium. It can be diffuse, causing a gener-alized increase in size of the uterus, or it can be focal and cause lumps—in the form of oneor more ‘adenomyomas’.On transvaginal ultrasound, adenomyosis is not always visible; it cancause a generally uneven ultrasound echo from the myometrium, and if it is visible discretelyit can be difficult sometimes to distinguish it from a fibroid. Support for a diagnosis ofadenomyosis can come from finding an elevation of serum CA125 antigen levels (althoughovarian endometriosis, not uncommonly found in association with adenomyosis, can alsocause this test to be abnormal).
The distinction between a myoma and an adenomyoma is important, because conser-vative surgery is much trickier for adenomyomas than it is for myomas (there’s no clearseparation between the area of muscle containing the endometrial glands—the adenomy-oma—and the surrounding normal muscle). Such surgery is usually unrewarding in all butthe most limited and focal adenomyomas. Adenomyosis usually causes pain with periods(dysmenorrhea) and heavy periods (ovulatory dysfunctional uterine bleeding), just as fibroidscan. Often the correct diagnosis is not made until recalcitrant symptoms lead to a hyster-ectomy and the uterus is examined by a pathologist.
Adenomyosis will shrink (and serum CA125 levels will fall) with treatment usingGnRH-agonists or GnRH-antagonists, but the effect is short lived.
In one patient of mine, a woman in her early forties who had the second largest uterusI have seen from adenomyosis, we secured a pregnancy using donated eggs, IVF and a
234 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 234

challengingly difficult placement of three embryos guided by real-time ultrasound, morethan 15 centimeters from the cervix (the usual distance into the uterus for placing anembryo is about 6 centimeters).Although I had prepared the uterus for several months withGnRH-agonist, followed by our usual sequential regimen of estrogen and progesterone(described in Chapter 21), I had thought that we would have been lucky for even one ofthe embryos to implant in such an apparently abnormal environment, let alone all three.But she gave birth to triplets.
FIBROIDS AND OTHER PROBLEMS IN THE UTERUS � 235
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 235

abnormalities present from birth
Anomalies of the uterus, intersexand androgen-insensitivity syndromes
As a woman, you can expect to have two ovaries, two fallopian tubes, one uterus (andtherefore one cervix), and one vagina.The reality, however, can be more complex.Herewe look at:
• How these structures form in the fetus;• Symmetrical obstructive anomalies (imperforate hymen, absent uterus and vagina, absent
cervix);• Symmetrical duplications (septate uterus, bicornuate uterus, double uterus or vagina);• Asymmetrical anomalies (unicornuate uterus, blocked vagina on one side); and• Intersex states (girl or boy?).To begin with, we will go through how these structures were formed when you were anembryo.
THE MÜLLERIAN INHERITANCE
At about eight weeks of pregnancy (eight weeks from the last menstrual period, or LMP) thekidneys begin to develop in the fetus. For females, the ovaries then take shape just belowthem. For males, the testes form there. Going back to that early time, the embryo’s headhas taken shape; the heart is prominently responsible for the growing circulation. But thetail-end of the embryo is still rudimentary and rather plastic—able to end up in all sorts ofdirections.
In females, an open duct—the Müllerian duct (pronounce it ‘mool-air-ian’)—beginsto form near each ovary.As the tail-end of the embryo takes more shape, it passes overtowards the middle (see Figure 18.1). Here it will meet its companion duct from the
236
18
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 236

ABNORMALITIES PRESENT FROM BIRTH � 237
Cloaca
Metanephros
Mesonephros andmesonephric duct
Hindgut
Bladder
Urogenitalsinus
Ovary
Hindgut
Metanephric duct
Mesonephric duct
Urogenital sinus
Bladder
Ureter
Fused Müllerian duct
Paramesonephric(Müllerian) duct
(a)(Side view)
(b)(Side view)
(c)(Side view)
Figure 18.1 Development of the Müllerian ducts.These ducts develop in the fetus during the ninthand tenth weeks of pregnancy and form the fallopian tubes, the uterus and the uppertwo-thirds or so of the vagina.When the tail end of the embryo first forms (side view a), a‘cloaca’ receives (as it does, for example, in an adult frog) the urinary ducts, the bowel (or‘hindgut’) and the earliest sex ducts.The ‘mesonephros’ is the embryo’s temporarykidney, and its mesonephric duct on each side normally persists only in male fetuses, toform the male sex ducts.The ‘metanephros’ is the permanent kidney.As the tail end ofthe fetus grows (side view b), the cloaca divides into the rectum in back and the‘urogenital sinus’ in front (1); the ‘metanephric duct’ becomes the ureter, connecting thekidney to the bladder (2); and a new duct grows alongside the mesonephric duct oneach side, the ‘paramesonephric’ or Müllerian duct (3).With further development (frontview c), the Müllerian ducts meet and join in the middle before growing down to meetthe urogenital sinus, which will soon separate into the urethra in front and the lower partof the vagina behind. In this way the Müllerian ducts form the fallopian tubes, the uterusand the upper part of the vagina.The vulva and lowermost part of the vagina come fromthe urogenital sinus.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 237

238 � GETTING PREGNANT
Behind your PAP smear
Where the upper and lower vagina join turns out to be an important transitionbetween mucosa and skin: by birth the junction has shifted onto the cervix,forming a transformation zone that, as an adult, is checked regularly with PAPsmears.
Here’s how the vagina meets the skin and why you need to have PAP smears tocheck for early cancer of the cervix.
The tissue lining any surface or duct comes in a sheet called ‘epithelium’. Insidethe body, epithelium is usually just one cell thick; on the outside,where there’s morewear and tear, epithelium is many cells thick and is ‘stratified’—the skin is a toughexample (see Figure 18.2).
The epithelium of the Müllerian ducts, according to this rule, is ‘simple’, or one-celled.The cells are vertical in orientation, like columns, and so the epithelium isreferred to also as being ‘columnar’.
The urogenital sinus, the pouch of skin between the emerging leg buds referredto in the main text (and in Figure 18.1), and into which pass the bladder, the vaginaand the intestine,has epithelium like that of skin elsewhere, that is, stratified squamousepithelium.
Somewhere there must be a meeting of the two, the ‘squamo-columnar junction’.To begin with, this is at the lower end of the vagina, near the vestibule of the vulva(Figure 18.3a).A woman born with a hymen that has no opening in it (an imper-forate hymen) will have columnar epithelium above and squamous epithelium belowthe hymen (as shown in Figures 18.2 and 18.3a).Normally the connection betweenvagina and vulva is complete.
Further growth of this region in the fetus proceeds in a curious way: there’sslippage of neighboring tissues.The result is that squamous epithelium, rathersimilar to (but more moist than) skin, slides up to line the whole of the vaginaand a variable part of the vaginal side of the cervix (Figure 18.3b); if it didn’t,sexual intercourse would abrade the vaginal epithelium every time, causingbleeding and damage.
Ideally the squamo-columnar junction comes to be situated precisely at theopening of the cervix,with the columnar (or glandular) epithelium above it respon-sible for secreting the mucus of the cervical canal (Figure 18.3b).
But this is rarely the case.Usually it stops short, somewhere between the marginof the cervix and the opening of the canal (Figure 18.3c).This friable rim of columnartissue is called, disrespectfully, an ‘erosion’; it can bleed after intercourse; and, as ateenager matures, mildly acid fluid in the vagina causes it slowly to transform intostratified squamous epithelium, like the rest of the vagina.
This zone is thus called the transformation zone, and the normal metamorpho-sis of its epithelium from glandular to skin-like is called metaplasia. It provides an
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 238

other side, join, and then grow further downwards, opening into a space formed as apocket from the skin between the embryo’s leg buds (the urogenital sinus); this will laterbe distinguishable, from front to back, as the urethra, vagina and anus.Where these twoMüllerian ducts join, they thicken considerably to form the uterus.The parts of theducts on each side of the join become the fallopian tubes. The joined part of theMüllerian duct forms, from top to bottom, the body of the uterus (the uterine fundus),the neck of the uterus (the cervix) and the upper two-thirds of the vagina (see Figure18.1c and Figure 3.4, in Chapter 3).The lowermost part of the vagina derives from adimple in the skin. (For more on how the upper and lower vagina join, see the box,Behind your PAP smear.)
Congenital means something you are born with. If something can go wrong in the waythe body is put together, sooner or later, for someone, it will, and a baby will be born withan anomaly, or a variation from what’s normal. In most cases there is no obvious reason forthe anomaly; rarely a teratogenic drug may have been consumed during pregnancy (see thebox, The DES anomalies).The kidney system is close enough to the developing genitalsystem that anomalies of the two systems often go together.
For the Müllerian ducts and the internal sex organs, things may go wrong sym-metrically, in which case the kidneys are usually normal; or things may be lopsided, orasymmetrical, in which case commonly there’ll be a malformation of the kidney systemon the abnormal side.The following accounts are not complete—there’s no end to thepossibilities and the variations—but I’ll describe the more common and important condi-tions a family physician or a specialist gynecologist is likely to come across.The correctdiagnosis usually comes from a combination of imaging studies (such as transvaginal ultra-sound, especially ‘3-D’ ultrasound, MRI and hysterosalpingography) and endoscopy(hysteroscopy and laparoscopy).
In considering the congenital anomalies, let’s start with the symmetrical ones that causeobstructions, where a small part or a large part of the Müllerian duct system fails to formand open fully.
opportunity for things to go wrong—referred to as dysplasia (or more modernly,‘cervical intraepithelial neoplasia’, or CIN). Dysplasia (or CIN) can lead to overtneoplasia, or cancer, of the cervix—which for this reason almost always arises on theouter surface of the cervix.
The good news is that the transformation zone is easily observed.Wiping thecells off it for examination under the microscope is what a Pap (Papanicolaou)smear is.A positive smear means the presence of dysplastic or early cancerous cells(CIN). Looking at the transformation zone with a microscope is calledcolposcopy; it is used to confirm abnormal Pap smears and to judge the effectsof treatment of CIN.
ABNORMALITIES PRESENT FROM BIRTH � 239
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 239

SYMMETRICAL OBSTRUCTIVE ANOMALIES
Imperforate hymen
A transverse barrier across the lowermost part of the vagina can come about as an abnor-mality at birth or, rarely, after an inflammation in early childhood, causing the bits of anormal hymen to get stuck together. Either way, no-one usually knows about the problemuntil the periods are due to start at puberty.As the uterus bleeds, blood accumulates abovethe blockage and the vagina distends (see Figure 18.4a), causing cyclical episodes of painthat typically get worse each month.
The diagnosis can be made clinically by seeing a distended, dark membrane where thevagina should be. Carefully feeling the abdomen may reveal a tender lump coming upbehind the pubic bone, representing the uterus pushed up by the blood-filled upper vagina.If an ultrasound examination or a pelvic CT scan or MRI scan has been done, it will revealthe distended vagina above the blockage, filled with blood, and pushing the uterus upwards.
Treatment is in hospital, under anesthesia.The offending tissue is cut and the thick,trapped, chocolate-like blood escapes.To stop the hymen blocking up again the surgeonmakes a cross-shaped incision, cutting off four triangles of tissue between the arms of thecross. Recovery is usually immediate, complete and uneventful.
Absent uterus and vagina
In this case, two ovaries are present and are normal.They start producing hormones and ovulat-ing eggs, and so puberty takes place apparently normally.But the Müllerian ducts have almostcompletely failed to form, have failed to join, and have failed to meet the lower vagina (seeFigure 18.4b).There’s no menstruation because there’s no uterus to bleed. (There can be otherreasons, however,why puberty can be interrupted with an absence of menstruation—primaryamenorrhea—despite apparently normal development of the breasts and pubic hair; these otherconditions are associated with failure to ovulate, and are described in Chapter 11.)
The DES anomalies
In the 1950s,many pregnant women were given a new synthetic estrogen in an effortto lessen the chance of miscarriage.
This estrogen, diethylstilbestrol, or DES (pronounced ‘dee-ee-ess’), has left a legacyof uterine and vaginal anomalies that a generation of women now in their forties hashad to cope with.These legacies include cancer of the cervix and, ironically,miscarriage.
Although most women with DES abnormalities are now passing the age of child-bearing, the story of DES is notorious and should not be forgotten by anyone whouses unproven drugs for unproven reasons.
240 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 240

The diagnosis of congenital absence of the uterus and vagina is made clinically byrevealing just a dimple, or just firm tissue, where the opening of the vagina should be.An ultrasound or a CT or MRI scan confirms that there’s no uterus present, but theovaries are usually visible, located at the brim, or bony margin, of the pelvis. If a laparoscopywere to be done (it’s not really necessary), the ovaries would be seen to be making folli-cles and ovulating normally, but next to them would be just the beginnings of the fallop-ian tubes—they peter out towards the middle and there’s no swelling where the uterusshould be.
A teenager diagnosed with congenital absence of the uterus and vagina will need alot of understanding and help.A new uterus she cannot, of course, receive, so having ababy is not going to be possible.To enable her to have sex, a vagina will need to be fash-ioned from the soft and accommodating tissue that’s there in its place. On the positiveside, she has normal ovaries and normal hormones; there is no reason she should notfeel every bit a healthy woman.The first priority is to enable sexual intercourse to takeplace.
There are three ways in which a vagina can be made.The simplest is usually thebest. It helps if there’s a dimple in the vulva already, but it’s not essential.A set of strong,glass dilators is used progressively to push and stretch the skin into the soft space betweenwhere the bladder is in front and where the rectum is behind. It’s perfectly safe: nodamage can be done, and no detailed knowledge of anatomy is needed.The dilators willfollow the path of least resistance, the right path. Over weeks to months, every time sheshowers, the young woman pushes the dilator upwards for a few minutes, graduallystretching the skin to form a vagina. Eventually the process will be completed by having
ABNORMALITIES PRESENT FROM BIRTH � 241
Columnar epithelium
Connective tissue
Stratified epithelium
Figure 18.2 Collision! The Müllerian ducts are lined by a single layer of surface cells (‘epithelium’),which are column-like or columnar in shape.The urogenital sinus, like the skin generally,is lined by epithelium that has many layers; it is ‘stratified’ and flat in shape (or‘squamous’). Between the two there is connective tissue, which gets thinner and thinnerbefore it disappears, opening the vagina to the outside.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 241

sex regularly. But, for her confidence, it’s best to start treatment well before sex isexpected.
The second method is a simple surgical operation called a Williams operation, after theBritish gynecologist Arthur Williams, who devised it. A short pouch of skin is createdsurgically in the vulva, pointing backwards and opening forwards.As soon as surgical healingoccurs, after about three or four weeks, sex can start.With repeated sexual intercourse the
242 � GETTING PREGNANT
Uterus
Vagina
Vulva
Columnarepithelium
Stratifiedsquamousepithelium
Cervix
(a) (b) (c)
Figure 18.3 How the Müllerian junction migrates. Before the membrane between the vagina and theoutside disappears (a), the upper part of the vagina, like the rest of the Müllerian ducts, islined by columnar epithelium (see also Figure 18.2).After the vagina has opened (b), thejunction between the stratified squamous epithelium of the skin and the columnarepithelium of the Müllerian ducts migrates up the vagina—ideally to the point ofopening of the cervix (the ‘external os’).When this happens, the cervix is completelysmooth to look at, with a small opening, or canal, leading up the uterus (inset). Moreoften than not, the migration is not complete, and the ‘squamo-columnar junction’ endsup on the cervix somewhere (c) leaving a rather fragile, red-colored area around thecanal (inset). Because, with time, the exposed columnar epithelium transforms tosquamous epithelium, this zone is called the ‘transformation zone’—the site of interestwhen a PAP smear is done.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 242

pouch gets steadily bigger; instead of pointing backwards it becomes directed upwards—the path of least resistance again—the skin stretching into the proper place for the newvagina.What was ordinary dry skin becomes moist and very like the normal lining of thevagina.
The third way of producing the vagina is purposefully to dissect the tissues where thevagina should be and creating one artificially, with a skin graft placed over a mould—aprocedure called the McIndoe operation.The effect is immediate, but of all the methodsthis is the most hazardous.The danger comes from scar tissue forming in what should remaina soft and compliant part of the body.There also is a way of performing this operation withlaparoscopy.
ABNORMALITIES PRESENT FROM BIRTH � 243
(a) (b)
Figure 18.4 Müllerian atresia: failure of the Müllerian ducts to form properly. Blockage of the lowerpart of the vagina occurs (a) when the membrane between the Müllerian duct and theoutside persists.At puberty, menstrual blood accumulates above the blockage,considerably distending the vagina. (The fallopian tubes and ovaries have not beendrawn, but they are normal.) In virtually total failure of Müllerian duct development (b),there is congential absence of the uterus and vagina. In this case, only the outermost partof the fallopian tubes has formed.Any degree of abnormality between these twoextremes is possible.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 243

Having a baby with an absent uterus (but using your own eggs) requires gestationalsurrogacy, discussed in Chapter 22.
Absent cervix
Much less common than absence of the uterus and vagina, this less severe disturbance canbe more frustrating. First, as with the other conditions in this section, there is a failure ofthe periods to occur (primary amenorrhea), but periodic pain starts at about the time youwould expect menstruation to begin at puberty. But because the vagina does not fill withblood (only the less distensible uterus does), there is not the obvious swelling you get withan imperforate hymen.
Second, the uterus itself might be small and,while able to bleed and cause pain, it mightnot be enough to permit a pregnancy to develop, even if one way or the other a pregnancycan be achieved.
Third, it is a case of ‘so near and yet so far’.The operation to fix it seems so easy—somesimple plumbing to connect the uterus with the vagina.Yet the cervix is a sophisticatedorgan. In practice it is hard to keep a new connection between the vagina and uterus open,let alone for it to transmit sperm properly. Surgery is not uncommonly followed by severeinfections.To attempt a repair it is essential for the surgeon to be particularly experiencedwith surgery for such anomalies.
In pursuing a baby, it might ultimately be safer to suppress bleeding (what would be aperiod if the cervix was open) with a progestogen such as Primolut N, for many years ifnecessary, until IVF can be used, aiming then to implant an embryo directly into a preparedendometrial cavity.
SYMMETRICAL DUPLICATIONS
Imperfect joining between the Müllerian ducts from the two sides can produce any degreeof doubling.The possibilities range from a short wall dividing the body of the uterus intoright and left, to complete duplication of the uterus, cervix and vagina all the way downto the vulva, which is always single (see Figure 18.5).
Septate uterus
A wall between the right and left sides of the cavity of the uterus is called a uterine septum,and such a uterus is a septate uterus (Figure 18.5a). If the septum does not go all the waydown to the cervix, it’s a subseptate uterus (Figure 18.5b). In either case, there may be nosymptoms at all, except for a strong tendency for pregnancies to miscarry, usually in thefirst three months (and discussed in Chapter 8).The most minimal anomaly, really a vari-ation of normal, consists of a slight downwards indentation from the top, or fundus, of theuterus, called an ‘arcuate’ uterus.
In each case, the outer surface of the uterus shows little sign of the doubling.The diagnosisis made on x-ray (a hysterosalpingogram) or on hysteroscopy (both described in Chapter 4),
244 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 244

ABNORMALITIES PRESENT FROM BIRTH � 245
(a) (b) (c)
(d) (e) (f)
Figure 18.5 Müllerian duplications.The Müllerian ducts in these cases have reached the outside, butthey have not joined properly (tubes and ovaries are normal and have not been drawn):(a) septate uterus; (b) subseptate uterus; (c) bicornuate uterus; (d) double uterus, singlevagina; (e) single uterus, double vagina, also called a ‘longitudinal’ vaginal septum;(f ) double uterus, double vagina. In a, b and c the cervix looks normal at vaginalexamination and is not shown. In d, e and f the cervix has the appearances shown; notethat the cervix is double when the uterus is double.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 245

but needs a laparoscopy to confirm that the outside of the uterus looks single, not double.A septum or subseptum is treated at hysteroscopy by cutting its muscle in the same
(flat) plane as the cavity of the uterus (Figure 18.6); the cut muscle fibers fall away, frontand back, and the septum is gone with no scar in the uterus and no deficit of muscletissue.
Bicornuate uterus
A bicornuate uterus has the same division of the uterine cavity into right and left, but theoutside of the uterus, the fundus itself, is divided into two (Figure 18.5c).Again there maybe no symptoms—until pregnancy. Even then, pregnancies can grow normally, but theabnormal shape inside the uterus means that a breech birth is more common. Pregnanciesare less likely to miscarry early than they are with a septate uterus, but miscarriages in thesecond three months can be common; typically, successive pregnancies reach a more andmore mature stage.
Because there’s no simple operation to correct a bicornuate uterus, one approach,depending on the circumstances, is therefore to anticipate an immature but viable preg-nancy with no special intervention.The definitive operation to correct the abnormality—a metroplasty—is an open operation done at laparotomy, after which it takes a few monthsfor the uterus to heal before pregnancy should be attempted again.
Double uterus, cervix and/or vagina
English gives way to Latin as the more profound duplications of the Müllerian system aredescribed in gynecological textbooks.
A double uterus and cervix, each served by its own normal fallopian tube and ovary, iscalled a uterus bicornis bicollis (Figure 18.5d). Many women with such a uterus—or withsuch two uteruses—go through life unaware of a problem.There’s a greater chance ofprematurity among pregnancies. Occasionally the non-pregnant uterus gets in the wayof the pregnant uterus during childbirth. Breech births are more common, again becausethe effective space available for the baby to move about in has an odd shape.The divisionof the two uteruses is too great for repair to be feasible; but anyway there’s usually noneed for repair.
A double vagina is not particularly rare (Figure 18.5e). Sometimes it goes with a doubleuterus and cervix (Figure 18.5f).The way it declares itself can be startling, though charac-teristic. Often this is during the teenage years, when a girl begins to use a tampon formenstruation. Instead of stopping the menstrual blood, the tampon lets it go straight past,down the other vagina.Two tampons fixes the problem,but not before some puzzling expe-riences. Commonly one vagina comes to be preferred over the other, especially with sex.Sex is then sometimes comfortable; sometimes inexplicably it isn’t.With knowledge, thissymptom is straightforward to overcome.
If there’s a single cervix and uterus, the septum dividing the vagina into two willstop short of the top of the vagina (Figure 18.5e) and sperm during intercourse will get
246 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 246

ABNORMALITIES PRESENT FROM BIRTH � 247
(a)
(b)
(c)
Figure 18.6 Treatment for a uterine septum: transvaginal metroplasty: (a) front and side views of auterus with a septum.The septum is wide-based in the front view, but thin in the sideview; (b) special scissors are passed through the canal of the cervix to cut the septum inthe plane shown.The same can be achieved with very small scissors at hysteroscopy;(c) the cut muscle fibers pull back into the body of the uterus and the septum disappears.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 247

to the cervix whatever side of the septum is used for sex. On the other hand, if thepreferred side doesn’t communicate with the only functioning cervix, there will beinfertility.
More complicated is the double vagina that accompanies a double cervix and doubleuterus (Figure 18.5f). Conception will then only be possible when ovulation takes placeon the same side that sex does; most women will not be aware that it will have taken themtwice as long as it otherwise might have to get pregnant.
If it’s troublesome, the wall between such right and left vaginas can be removed by astraightforward operation.
NON-SYMMETRICAL ANOMALIES
With this group of anomalies, the two Müllerian ducts not only don’t join properly, butone or other side fails to develop as well as the other. The lesser side might be small(‘hypoplastic’) or blocked (‘atresic’). Co-existing abnormalities of the kidney system arecommon, such as a congenital blockage from kidney to bladder, doubling of the urinecollecting system, or perhaps a single or a horseshoe-shaped kidney, located lower in theabdomen than usual, perhaps within the pelvis.
Unicornuate uterus
With a unicornuate uterus there is one uterus and cervix, and usually one vagina (all normal-looking so far!). But on investigation with a hysterosalpingogram or laparoscopy (usually donefor other reasons), only one fallopian tube is found to be open (see Figure 18.7a).Development of the fallopian tube on the other side can be variable; the outer, open partis usually there, lying next to the ovary, but towards the middle it either dwindles intonothing (Figure 18.7a) or it expands to a more or less distinct uterus, partly joined ontothe main uterus (Figure 18.7b).
Usually there are no symptoms, but if the rudimentary uterus (or ‘horn’) is unrudi-mentary enough to have a cavity, pain can be felt on that side during periods; sometimesthis is bad enough to warrant an operation to remove the small uterus (leaving the bigone). On average a woman will take twice as long as she otherwise would to get pregnant,because conception is very unlikely when ovulation takes place on the closed side.Premature births and breech births are more common, as they are with the bicornuateuterus discussed before.
Occasionally a pregnancy will start in the closed side.When this happens it will bebecause sperm have passed up the open uterus, out along its fallopian tube and across theabdomen to the opposite, ovulating ovary, fertilizing an egg just as it is being picked upby a tube that leads nowhere.The result is a pregnancy in the tube or in the rudimen-tary uterus—in effect an ectopic pregnancy (see Chapter 14), and sooner or later a surgicalemergency.
248 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 248
Double uterus and vagina, with one vagina blocked
I have seen four teenagers with this distressing abnormality (see Figure 18.7c).There aretwo tubes and ovaries (as is normally the case), and two uteruses and cervixes (as with adouble uterus and cervix).As well there are two vaginas; but not only don’t they join, oneor other vagina does not open to the vulva. In each case the diagnosis had been missedbefore the girl had already been operated on by an uncritical general surgeon, and beforeshe’d been referred to a gynecologist. But the clinical symptoms and signs were the samewith each of the girls and were unmistakable.
At puberty, both uteruses begin to menstruate.As with an imperforate hymen,discussedbefore,menstrual blood accumulates in the blocked but distensible vagina, causing increas-ing pain with each period. As the vagina fills and swells it pushes the uterus up into theabdomen, producing a bigger and bigger lump—which is eventually noticed clinically, onultrasound, or on a CT or MRI scan.While these features are the same as for an imperfo-rate hymen, the puzzle and source of confusion is that menstrual periods are taking place,apparently normally and on time.The girl and her parents regard it all as a case of bad periodpain,dysmenorrhea.The examining doctor suspects a tumor in the pelvis and, all too typically,
ABNORMALITIES PRESENT FROM BIRTH � 249
(a) (b) (c)
Figure 18.7 Asymmetrical Müllerian abnormalities.The Müllerian ducts have not joined properlyand, moreover, the duct on one side has not formed or properly opened to the outside.In a unicornuate uterus (a) the uterus is ‘one-horned’, the Müllerian duct on theopposite side has formed only the very first part of the fallopian tube; in a unicornuateuterus with a rudimentary horn on the opposite side (b), there may or may not bebleeding each month in the rudimentary uterus; in a double uterus and vagina, with onevagina not in communication with the outside (c), blood accumulates in the closedvagina, distending it greatly (unlike in the situation in Figure 18.4a, periods occur, so thediagnosis can be missed for some time).
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 249

the general surgeon called in has not seen it before, operates, spots a mess, and takes some-thing out that would have been best left alone.
The correct treatment, under anesthesia, is to make a large opening between the twovaginas for the accumulated blood to discharge through.Later,when the tissues have settleddown, the remaining bits of wall between the two vaginas can be removed as well.
GIRL OR BOY? THE INTERSEX STATES
There’s almost no end to what can go awry ’twixt chromosomes and puberty.This takes usinto the highly specialized field of intersex or, in the USA, pseudohermaphrodism.
An hermaphrodite, like Hermaphroditus after his fusion with the nymph Salmacis, hasattributes that are at once female and male.We speak of a true hermaphrodite as one with bothovary and testis—sometimes on opposite sides, sometimes included in the one gland. For thebody, the net effect lies between almost normal male development (perhaps an abnormal testisin a hernia) and almost normal female development (with testicular tissue seen in part of aremoved ovary after an otherwise uneventful social history of sex, marriage and children). Inbetween,almost anything is possible,usually showing up at birth with genitals that are a puzzle.
True hermaphrodism is rare, though. Much more common is pseudohermaphrodism—patients with either testes or ovaries, but still with ambiguity on looking at the genitals orwith other confusion somewhere between maleness and femaleness.These are the intersexstates,which commonly are discovered at birth; occasionally they show up at puberty,whenexpected maleness or femaleness goes awry.The box, Nature’s children, goes into the details.
250 � GETTING PREGNANT
Nature’s children
Be warned: there’s no more complicated area in reproductive medicine than sexualdifferentiation.This is a lengthy and complex box.
We will discuss:• Chromosomal intersex (too few or too many sex chromosomes);• Male intersex (when male development is interrupted in a chromosomal male);• Female intersex (when male development is superimposed by hormones on a
chromosomal female); and• Behavioral gender.
In understanding these conditions one biological principle is paramount. In theabsence of sex chromosomes,or in the absence of testes, the fetus develops as a female.Even without sex chromosomes or gonads, the Müllerian ducts form (see the maintext) and the external genitalia take the shape of a vagina and vulva.
So you can regard immature female development as the blank canvas upon whicheither maleness or fertile femaleness must be painted (with the varying degrees ofcompleteness representing the intersex states).
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 250

Fertile femaleness simply requires a correct dose of X-chromosomes (two) result-ing in the presence in the ovaries of a normal number of oocytes.
Maleness is superimposed on femaleness through the effect of the Y-chromo-some causing the development of testes, which in turn produce the male hormonetestosterone as well as a substance that stops the Müllerian ducts from forming.
Chromosomal intersex
The chromosome pattern, or karyotype, of females is 46,XX and that of males is46,XY—as explained in Chapter 3.An extra chromosome disturbs the relationship.Nonetheless the rule is that one or more Y-chromosomes determines maleness.Twonormal X-chromosomes (no more, no less) are needed for females to be fully fertile.
The karyotype 47,XYY (a gratuitous Y-chromosome) might do little or no harm,though the jury is still out. Some say there’s a higher chance of antisocial, criminalbehavior.The karyotype 47,XXY (a gratuitous X-chromosome in a male) results inan infertile male with Klinefelter syndrome; most are tall; no sperm cells are formed,so there’s infertility (although in a proportion of cases rare sperm cells can be recov-ered from the testis—enough for ICSI, as discussed in Chapter 10).
Karyotypes 47,XXX and 48,XXXX result in women who might be normal,but can have fewer oocytes and hence can undergo premature menopause.
The pattern 45,X (a missing sex chromosome) produces a female. She will beboth infertile—from a lack of oocytes and hence primary ovarian failure (see Chapter11)—and short, a combination referred to as Turner syndrome.
So far, perhaps, so simple. But it’s only a small bit of the Y-chromosome thatcauses the maleness. Suppose just a tiny bit of the Y-chromosome (the relevant bit iscalled SRY) gets mislaid? The possibility now is that, despite a 46,XY karyotype, wecan have a normal-looking girl (if SRY is missing) and, despite a 46,XX karyotype,we can have a normal-looking boy (if SRY has found its way in). In both these casesthe ovaries and testes—the gonads—don’t form properly and puberty fails; as adoles-cents and adults they will be infertile.
Male intersex
Suppose now that the testis in an embryo is correctly determined, as planned, by a46,XY chromosome count. For things to go right, the internal ducts must be sensi-tive to the male hormone testosterone; sometimes they aren’t, so they disappear.
Add to this the fact that the external genitalia—the scrotum and penis—must besensitive to testosterone’s metabolic derivative, dihydrotestosterone; if there’s completeinsensitivity to it, a vagina and vulva form instead,with testes left high in the abdomen.
Because the breasts are not sensitive to testosterone, they flourish on the smallishamount of estrogen the testes make. At birth the girl looks normal. At puberty thebreasts develop well. Pubic hair is sparse. Of course there’s no menstruation becausethere’s no uterus (the testes have inhibited the development of the Müllerian ducts
ABNORMALITIES PRESENT FROM BIRTH � 251
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 251

normally).The condition is called testicular feminization, the children are (and shouldbe) raised as girls, and—the condition being genetic—sisters can also be affected.
Incomplete degrees of tissue insensitivity to male hormones take all manner offorms.As well, there’s a group of conditions in which tissue sensitivity to hormones is normal but testosterone production is too low.
In either case the result can range from the presence of a rudimentary vaginathat also receives the bladder, to an absent or small penis (‘microphallus’), perhapswith the urethra not quite getting to the tip of the penis (hypospadias). Assigning‘boy’ or ‘girl’ at birth can come to depend on a judgment as to whether the phalluscan be made competent with high doses of hormone cream rubbed on during child-hood. Fertility fails in the more severe forms.
In each of these examples the karyotype is that of a normal male, that is, 46,XY,but with full development of maleness interrupted.
Female intersex
Almost the same range of appearances can result from problems in the other direc-tion—when the karyotype is that of a normal female, 46,XX, but a degree of maledevelopment is imposed for other reasons.
Such imposed maleness can arise through nature in congenital adrenal hyperplasia(CAH), through production of testosterone by a tumor in a pregnant woman,or inad-vertently through administration of male hormones in pregnancy (for example, takingdanazol in pregnancy).
In each of these cases there’s exposure of the developing fetus to male hormones.Instead of the internal male ducts being suppressed by a lack of male sex hormonesthey persist. Moreover, instead of an open vulva and vagina, the labia fuse in themiddle, attempting to produce a scrotum.We now have ambiguous genitals with a46,XX karyotype. Surgery can help restore female anatomy—and usually the resultis at least workable. Pregnancy is often possible, but (in the case of CAH) can needovulation induction (see Chapter 11). In the past the enlarged phallus present in thiscondition was often surgically removed, but because both male and female sexual-ity can depend on it such surgery should not be carried out until adulthood, whenit often turns out not to be a good idea.
Gender
Unlike maybe a generation ago, few parents today believe giving a boy dolls to playwith will turn him into a girl, or giving a girl trucks to play with will make her aboy. Most people now accept that such elements of gender-characteristic behaviorare as much ‘in your genes’ as in your cultural environment.Although this is not theplace to take the matter much further, there is also now good evidence that homo-sexuality and heterosexuality are basically genetically determined. I would not besurprised to learn that this is also true of transsexualism.
252 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 252

What to do
In days gone by, if there was substantial doubt about ascribing sex at birth, ‘girl’ was thesafer choice,whatever the chromosomes and whatever the internal glands and organs mightsuggest, because, when it came to having sex, an absent vagina could be overcome withsurgery (see absence of the uterus and vagina, above), whereas the absence of a function-ing penis could not usually be corrected. In some cases surgery was carried out duringchildhood that involved enlarging a vagina and removing an enlarged clitoris.
Today we recognize that it is normal for human sexuality to have a wide range of expres-sion.What a generation ago was thoughtfully regarded as proactive surgical help in prepar-ing intersex children for a dichotomous sexual future today is seen as unwarranted andunconsented-to intrusion into sexual developmental possibilities, any of which could turnout to be satisfying.Distilling what we have learned from the anguished experience intersexchildren and young adults have had, I would say that there are today at least three stronggeneral principles regarding the intersex states.• Gender is a complex state, not always a simple distinction between male and female;
this complexity, and the ambiguities that are part of our sexuality and our relationships,have a natural, biological basis—one that deserves our understanding and acceptance.
But still it is not that simple. In the intersex states the gender one feels is depend-ent not on the sex chromosomes but on the exposure of the developing brain, beforebirth, to the male hormone testosterone.
The clearest example of its importance is the condition of testicular feminization(see also the main text), an extreme example of male intersex when there is totalinsensitivity in the tissues (brain included) to the action of testosterone. Invariablythese 46,XY people not only look female, they act female, they feel female—theyare female for all intents and purposes, except that they have no uterus and insteadof ovaries they have internal, undescended testes; naturally they cannot bear children,but they typically have a normal female sex life.As a fetus there was no ‘imprinting’of the brain by testosterone.
In the less complete (and much rarer) intersex state known as 5-alpha reductasedeficiency, there is a deficiency of the enzyme that turns testosterone into its activemetabolite, dihydrotestosterone (DHT).The lack of DHT is enough to prevent theexternal genital organs becoming male, and it is usual for these children to be assigneda female gender at birth.But notwithstanding the dresses they are then compelled towear, the developing brain responded enough to testosterone to make these childrenbehave as boys.When puberty gets underway there is no hiding these children’s correctgender: they become teenage boys in every sense other than anatomy.
There are isolated villages in South America where the genes for 5-alpha reduc-tase deficiency are so common that gender reversal at puberty is no big deal—whereintersex is accepted as a part of life.
ABNORMALITIES PRESENT FROM BIRTH � 253
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 253

• If there is doubt regarding ‘girl’ or ‘boy’ at birth, it is better to delay making or accept-ing a designation until full investigations have been carried out, instead of risking apremature assignment that may prove very difficult to live with.
• ‘Corrective’ surgery, no matter how well intentioned, should be avoided until adult-hood.A phallus, whether as clitoris, penis or in-between, is an important sexual organand should be left unoperated on, at least until the intersex child has reached adult-hood and matured sexually.
254 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 254

section IV
assisted conception
short-cuts to a baby
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 255

Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 256
This page intentionally left blank

helping nature a bit
Timing intercourseand orgasm, and more
Sex is important for getting pregnant, so it helps to talk about it.Not everyone, includ-ing your partner, will want to talk about it to the same extent though, or will wantto talk about it in the same way. But what none of us can get away from is that at
some stage your doctor, perhaps nurses, and at times laboratory technicians,will be sharingyour knowledge of when and how often you have sex—sometimes even how you havesex.What has generally been a private matter between the two of you can seem to becomeexcruciatingly public.
In this chapter we’ll look at:• How to have sex;• How often to have sex;• When to have sex; and• If you should have assisted insemination (IUI) as well as having sex.
It would be good if we could say that the professional people you need to talk to abouthelp with getting pregnant would always be sensitive,would be neither prudish nor flippant,would respect your personal situation, and would show a capacity for empathy. But themedical care involved with treating infertility is no different to other areas of medicine inthat you will probably have a person or several people relating to you on a very personalmatter who will differ in how they go about living up to that responsibility. Some will begood at it. Some won’t.
Put simply, you’ll find some people more helpful than others. Some, you’ll discover, aretactless; and some will turn out to be crass, rude or in other ways not the person for you.Depending on your personality you’ll face these difficulties in one of several ways:with sad
257
19
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 257

acceptance; with detached understanding and humor; with non-acceptance and rudenessin return; with carefully constructed criticism; or with non-acceptance and a change ofdoctor or pathology laboratory or infertility program.You might even make a phone callto your lawyer; or send a note to someone writing a book on infertility horror stories.Perhaps you might keep open the option of any one of these responses at different timesand in different circumstances.
Let me dispel some myths.
HOW TO HAVE SEX
Who am I to tell you how to have sex? Essentially it really doesn’t matter how you do.Usewhatever position you both feel comfortable with. Germaine Greer has written that themost appealing position for many women is with the man on his back and the woman ontop—the opposite to what has been called the missionary position (the traditional prescrip-tion for getting pregnant).
Either of these, and other positions too, can be perfectly satisfactory from the point ofview of reproductive biology.The only requirement is that it’s comfortable and that theejaculate ends up in the vagina, next to the cervix.The ejaculate coagulates next to thecervical mucus quite quickly; even if some of the semen seems to leak out, be reassured thatthis is not necessarily abnormal.
A woman needn’t orgasm to conceive. Although it’s fair to say that nature inventedorgasm for a reason, its evolutionary purpose was probably to make sex attractive at timesother than ovulation, encouraging bonding between partners.
Pleasure with sex has been around at least as long as the monkeys and apes. (There’s anintelligent and entertaining book by Meredith Small on the subject; see Appendix 3.) Evenamong the apes there are extraordinary differences between, say, the bonobo chimpanzees(they delight in it as often and in as varied ways as are possible!) and gorillas, among whomit’s an uncommon event and takes all of eight seconds. Both species are fertile.
If there’s one hint I can give, it’s that you can best avoid your partner seeing it asa chore by concentrating on enjoying it yourself, then your partner’s pleasure will lookafter itself.
Recent research, however, shows that an orgasm that follows ejaculation decreases theescape, or flow-back, of semen out of the vagina after sex. So a rather late orgasm mightwell be a good thing for retaining semen and for getting pregnant—at least when you’rehaving sex around the time of ovulation (see the box, Orgasm and retaining sperm in thevagina).
Smoking
Whether or not you have a cigarette after sex is up to you, although right now is a goodtime to say that smoking does decrease fertility, especially in women. How often smokingis the only reason for infertility is not certain, but I do know a couple who conceived withintwo months of stopping smoking, after about 10 years of tests and unsuccessful attempts at
258 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 258

treatment.The harmful effect of cigarette smoking is ‘dose-related’—the more you smoke,the more it decreases fertility.
Stress
How important it is to be free of stress is a question I’m asked almost every day. Stress canbe enough to interfere with proper ovulation (I discuss the way this can happen in Chapter 1),but this can be tested for in the usual way (see Chapter 4). If these tests are normal thenthere’s no evidence that the constant worry about not getting pregnant itself interferes withgetting pregnant unless you stop having sex. (I elaborate on the reasons for saying this inChapter 1.)
Alcohol
Alcohol has no harmful effects on getting pregnant, at least up to sensible, moderate levels.It will do you and your partner no harm, for example, to have a glass of wine before sex(unless, I suppose, it’s in the morning of a working day). I know that I might be puttingmyself out on a limb with this statement, so I should clarify it.
The facts are: first, that although claims have been made to the contrary, the (in myopinion) better, and better-controlled, studies have not shown that small to moderate amountsof alcohol are harmful to fertility; in fact a helpful effect on fertility has been reported.This
HELPING NATURE A BIT � 259
Orgasm and retaining sperm in the vagina
Researchers Dr Robin Baker and Dr Mark Bellis of the Department of EnvironmentalBiology at the University of Manchester,England, are quite categorical about it: femaleorgasm before ejaculation decreases the retention of sperm,whereas orgasm after ejac-ulation can reduce flow-back and increase sperm retention.
Dr Baker and Dr Bellis arrived at this conclusion with the help of 35 very coop-erative couples—couples who timed and measured their flow-back in relation tothe woman’s orgasm and to the man’s ejaculation in 323 copulations. (They also gotsimilar information from 3679 women who responded to a nationwide survey.)
Specifically, they claim that:• It makes no difference whether the orgasm happens during intercourse itself or
is initiated (by either partner) after it;• Extra sperm will be retained if orgasm happens at any time up to the time flow-
back starts;• Orgasm more than a minute before ejaculation reduces sperm retention and
increases later flow-back; and• Up to a few days, the longer it has been since a previous orgasm the more semen
is retained (I presume this is because the orgasm might be better).
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 259

is a conclusion consistent with wider experience in medicine, where, for example, alcoholhas been shown to have an important protective effect against heart disease. Many peopletake vitamins A, C and E because they are anti-oxidants, while one of the richest dietarysources of anti-oxidants is red wine.
Remember that men on average metabolize alcohol more efficiently than women, socan generally tolerate somewhat more alcohol than women can.Nothing I say here shouldbe construed as a license to get thoroughly drunk. Remember that overtly intoxicatinglevels of alcohol, especially those that result in a hangover, are harmful to health—and topregnancy once you are pregnant.
Whether you drink alcohol or not you will not be protected completely from the riskof having a baby with a birth defect, because defects come about from many other causes.The important point is that a lot of quarreling between partners can be avoided—and somefun can return to sex—by not taking a too restrictive view of alcohol consumption inrelation to getting pregnant.Alcohol is not like cigarette smoking, where any exposure isharmful.The medical evidence is that moderate amounts of alcohol, such as a glass or twoof wine, have not been associated with any special hazards—if drinking it is followed bygoing to bed with your usual partner.
HOW OFTEN TO HAVE SEX
Another question I’m asked a lot is how frequent intercourse should be to optimize thechance of conceiving. In particular I’m asked if it’s possible for fertility to suffer from havingsex too often.To deal with the second question first, the answer is no. Although we canshow that the density of sperm in the ejaculate diminishes with frequent ejaculation,remember that the mucus of the cervix at the time of ovulation is receptive to sperm tothe point of it being the best place for sperm to be—better than in the male ducts awaitingejaculation.
This is not to say that you should have,or you need to have, sex every day or even twicea day when attempting pregnancy. Every second day during the middle of the cycle isordinarily enough.With care in timing it (see below), it’s possible to have sex less frequently,and probably have more pleasurable and satisfying sex.Timing sex becomes more importantif there’s a decrease in the sperm count.When you have sex outside the time of ovulation,of course, it’s nothing to do with getting pregnant and everything to do with keeping yourrelationship pleasant and mutually supportive.
SEX OR INSEMINATION?
In some circumstances sex consistently fails to deliver the goods. Impotence, anatomicalproblems such as hypospadias, and physiological malfunction such as retrograde ejaculation areexamples of problems with sexual intercourse that can be overcome with masturbation,semen preparation in the laboratory and then assisted insemination, usually with ‘washed’semen into the uterus (intrauterine insemination, or IUI; see Chapters 10 and 20).
But is it any use to carry out such assisted insemination for low sperm counts
260 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 260

(oligospermia) or, for example, for unexplained infertility? Apart from these three well-defineddisturbances, the usefulness of IUI compared with having sex to get pregnant is contro-versial—despite IUI having become a medical industry.With proper timing in regard toovulation,Dr Gordon Baker in Melbourne and Dr Michael Hull in Bristol, among others,have shown in careful and purposeful studies (involving control groups of couples who hadsex normally for comparison) that sex is better than insemination.The Amsterdam studydescribed in Chapter 10 showed that IUI can have the edge if there are more than 2 millionwashed sperm available for the insemination procedure. See Chapter 10, too, for an accountof the limited place there is for IUI in association with injections of follicle stimulating hormonefor multiple-ovulation induction (superovulation).
WHEN TO HAVE SEX
Humans are not unique in pursuing sex for its own sake—we share it as a pastime withmonkeys, chimps and dolphins. Evolution has made it particularly pleasurable—althoughregimenting it when trying against the odds to get pregnant does lessen its appeal! Inwomen, sex drive or sexual willingness is not a reliable indicator of fertility, unlike the casein most other of the earth’s species. Sex-for-fun, sex-for-bonding is an evolutionary advance.
The functional price we pay for sex for reasons other than getting pregnant is that thefemale mating instinct (‘estrus’, or ‘heat’, among animals) is no longer synchronous withovulation, or with the chance of pregnancy.Your own symptoms of ovulation—and fertil-ity—are more subtle, but you can often recognize them.
For fertility, it’s better for sperm to be in the fallopian tube before ovulation takes place.The normally ovulated egg is poised to be fertilized as soon as it gets there. Its fertile lifeis then no more than about 10 to 12 hours, perhaps less. On the other hand, sperm willtake just two or three hours to reach the tube and be capacitated (see Chapter 3), that is, ina condition able to fertilize the egg.
The symptoms that precede ovulation include an increase in secretions in the vagina,when some women will detect particularly stretchable cervical mucus.Once these symptomsdisappear, the mucus will have tightened up to keep further sperm out of the uterus. So-called ovulation pain, or Mittelschmerz, in fact precedes ovulation by up to 24 hours; it’stherefore a good indication of when to time intercourse (provided it’s not so bad that itcauses intercourse itself to be painful—a rather cruel situation when it occurs).
Ovarian monitoring
Not uncommonly either you or your doctor will want to know precisely how long it takesfrom the start of your period until you ovulate (this is the follicular phase) and then howlong it takes until your period starts again (this is the luteal phase).This might be to checkhow well you are ovulating and to rule out a luteal phase defect (or the luteinized unrupturedfollicle syndrome, or LUF), or to time a diagnostic test that has to be done, say, as you areovulating (such as a postcoital test) or just before an anticipated menstrual period actuallybegins (such as a premenstrual endometrial biopsy).The monitoring this requires includes both
HELPING NATURE A BIT � 261
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 261

frequent measurements of hormones (in particular serum estradiol, serum LH and serumprogesterone), together with follicle tracking using transvaginal ultrasound. Chapter 3 describesthe sequence of events.
Generally speaking, though, this is all much too intrusive and expensive to go throughevery month, just to time when to have sex.What follows is the stuff you can do yourselfat home to improve your timing.
Temperature charting
The basal body temperature chart (see Chapter 5) is not a very efficient way to predictovulation: its main benefit is looking back on ovulation after the event. Here’s how it cancontribute to your cause.
First, once the temperature goes up it’s too late to conceive—so it’s useful in puttingan end to an exhausting regimen of sex-to-get-pregnant. Second, a dip in temperature canoccur with ovulation, so if you are deft this might be used as a signal. But third, and mostuseful, over several months it will give you and your gynecologist an idea of the time inthe cycle during which ovulation can occur, providing a general guide to when having sexwill give the best chance.
A temperature chart is not a hormone assay, though, and even the clearest chart can be24 hours or more out in revealing the day of ovulation.To do better than this means steppingup the technology a notch.
LH testing
When a follicle in the ovary is ready, the pituitary gland’s signal to ovulate consists of a surgeof luteinizing hormone (LH, explained in Chapter 3). More often than not it starts duringsleep, at about three or four in the morning, and will result in ovulation 36 to 40 hourslater. LH enters the urine within a few hours of the start of the surge, where it can bemeasured using a variety of kits bought over the counter from pharmacists or off the shelfat supermarkets. (Hint: supermarkets are much cheaper.Ask where the pregnancy tests are—they’ll be close by.)
The measuring technique varies a little: the package insert will explain how to use theparticular kit. I find that the urine sample to test is not the first one when you wake up.The bladder-full that’s there when you arise has the night’s accumulated urine, so it can betoo dilute.The urine to test is later that morning or at lunchtime. If the test is equivocal,test again the same day.A positive result (after negative results the day before) means thatovulation will take place in the next day and a half. Sex that night, and/or the followingmorning, will be well timed. However, with this schedule for testing it’s best to test thenext day as well: if it’s still positive, try that evening too.
The kits for testing urinary LH are not all that cheap, especially if you have any irreg-ularity to your cycle.To keep the cost down, you might either:• Keep a basal body temperature chart (described above) as well, first to show when
testing should start (about day 11 for a 28-day cycle; earlier for shorter cycles), and
262 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 262

second to show when to stop testing, should the LH surge signal have been missed andthe temperature be up; or
• Look for evidence of rising levels of estrogen, which always precede the LH surge(Chapter 3 describes the events of your cycle in detail).
You can detect rising estrogen levels either by being aware of changes in cervical mucus(discussed above) or by investing in a store-bought testing kit for detecting changes in yoursaliva.
Saliva testing for estrogen
Unlike tests for the LH surge, which are use-once and so are relatively expensive, a hometesting unit for estrogen (a rise in which always precedes the LH surge) can be used repeat-edly.These devices are based on a poorly understood phenomenon called ferning—thecrystallization of mucus molecules in a branching pattern when mucus (including saliva, asit turns out) that has been exposed to high levels of estrogen is allowed to dry on a glassslide and examined under a microscope.
Ferning has long been known to characterize cervical mucus that shows the effect ofestrogen at ovulation (it is one of the phenomena used to give the cervix a score, the cervicalscore or Insler score).Without understanding how, estrogen circulating in the blood can alsoaffect saliva this way.
Maybe Baby (not the movie) is a lipstick-sized personal microscope that lets you lookat your saliva for ferning. Designed for contraception (‘don’t have sex if there’s ferning’)it’s also good for getting pregnant (‘have sex if there’s ferning’, or ‘if there’s ferning, starttesting for your LH surge’). Look for it at your pharmacist, drug store or supermarket.
DO WE HAVE TO?
Timing sex this way might not seem much fun, but it’s worth trying to accept the disci-pline, rising above it, and then accepting the challenge together with a sense of humor.Adefinite seductive dinner once a month, even if timed with a clinical test, can be enticing.See the box, Champagne and candles, in Chapter 25, for how an LH test can help you plotand scheme for your evening!
Should this straightforward approach to timing when to have sex not produce apregnancy (after, say, six months), further help with a more formal program of assistedconception becomes the next option—and is the subject of the next chapter.
HELPING NATURE A BIT � 263
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 263

helping nature a lot:assisted conception
In vitro fertilization
What is meant by assisted conception? .Assisted conception procedures involve directly manipulating sperm, eggs or
embryos (any of which thereby spend at least a short time outside the body beforebeing returned) with the aim of increasing the chance of pregnancy in the month or ‘treat-ment cycle’ in which the assisted conception procedure is being carried out.
The main assisted conception maneuvers comprise:• Assisted insemination (also called intrauterine insemination, IUI);• Gamete intrafallopian transfer (GIFT, which is almost obsolete); and• In vitro fertilization (IVF, with its variants).In each case, the main steps in a cycle of treatment can consist of:• Controlled ovarian stimulation (sometimes known as superovulation);• Egg retrieval;• Sperm retrieval (see also Chapter 10);• Lab procedures, including ICSI, assisted hatching, PGD;• Embryo or gamete placement, or transfer;• Endometrial (‘luteal’) support; and• Working out what can or did go wrong.The chance of pregnancy will depend significantly on:• The age of the woman;• The diagnosis (ovarian status including PCO, male factor, tubal status, endometriosis,
uterine factors);
264
20
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 264

HELPING NATURE A LOT: ASSISTED CONCEPTION � 265
• The quality of the clinic; and• How strong the embryo is.
Rationale
In general, assisted conception increases the chance of pregnancy because: first, we increasethe number of sperm that get to where the egg is; and/or second, we increase the numberof eggs available for fertilization.
Unlike other treatments for infertility that are one-off (like surgery for blocked fallop-ian tubes or prescribing a course of treatment with drugs), assisted conception proceduresare not intended (at least without further intervention) to be effective past the particularcycle or month in which they’re used.Assisted conception procedures can be an alterna-tive approach or an additional approach to the more traditional, one-off (and meant-to-belasting) approaches to treatment.The correct place of assisted conception and its usefulnesscompared with these conventional methods of treatment depends on the cause of the infer-tility and also on your own special circumstances.
An assisted conception procedure is sometimes the only way infertility can be overcome,for example, in cases of sterility. More frequently they are the most expeditious path, as incases of subfertility. Increasingly, they are used to avoid transmission of genetic disease, usingembryo biopsy for preimplantation genetic diagnosis (PGD), to reduce the risk of miscarriageand even to enable a couple to choose the sex of their next child.
Here, at the beginning of the chapter, is a good place to point out that not everyonewill want—or can afford—to go to these lengths to get pregnant.
ASSISTED (OR INTRAUTERINE) INSEMINATION
Assisted insemination (AI) is the procedure in which sperm are delivered into the cervicalmucus, through the cervix into the uterus (also called intrauterine insemination, or IUI), orrarely through the uterus and out into the fallopian tube by ultrasound-guided catheter.Assisted insemination using the husband or male sexual partner’s sperm (AIH) is particu-larly efficient in only a few circumstances—when there’s physical difficulty with ordinarysexual intercourse (maybe due to impotence, paraplegia or severe hypospadias) or when there’sa specific and localized problem in the cervix of the uterus that the sperm otherwise can’tget past very well, such as a cervix badly scarred from a cone biopsy.
Even with controlled ovarian stimulation (superovulation) to increase the number ofeggs, AIH with intrauterine insemination (IUI) is not as effective as IVF for oligosper-mia (decreased sperm counts), for endometriosis or for unexplained infertility. Despite theselimitations, however, IVF is so expensive in many countries that IUI is neverthelessresorted to.There is more on IUI in Chapter 10.
Donor insemination (DI—assisted insemination using donor sperm, previously calledAID) is technically the same, and is typically accompanied by ovarian monitoring (seeChapter 19), although usually not by controlled ovarian stimulation.The special social andethical aspects of DI are described in Chapter 22.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 265

GAMETE INTRAFALLOPIAN TRANSFER
GIFT goes a step beyond IUI and is much more effective.After controlled ovarian stimula-tion and egg retrieval (see below), the gametes (eggs and sperm) are transferred together intoone or other fallopian tube, usually at laparoscopy.As with IUI, the fallopian tubes must benormal and the sperm count needs to be reasonably good (between 100 000 and 200 000motile sperm need to be transferred with the eggs). GIFT can work despite endometriosis.
IVF is nowadays more effective than GIFT in most labs, even if only one or two embryosare transferred. Because three or four eggs need to be transferred for a comparable chanceof pregnancy with GIFT, there is the hazard of high-multiple pregnancy.The need forgeneral anesthesia and laparoscopy add considerably to its cost. So GIFT is today of mostlyhistorical interest, except for people who for religious or moral reasons will not accept IVFbut can accept egg retrieval procedures.
IN VITRO FERTILIZATION
In vitro fertilization (IVF) means fertilization of eggs in the laboratory—literally, ‘in glass’(although nowadays in plastic). IVF requires fewer sperm than do IUI (about 1 million) andGIFT (at least 100 000), ranging down to 10 or less, for successful intracytoplasmic sperminjection, or ICSI.The fertilized eggs can be transferred to the fallopian tubes on the first orsecond day after retrieval, when with normal fertilization the embryo would still be in thefallopian tube (see Chapter 3).But, as with GIFT, such procedures—known as ZIFT,PROSTand TEST—require laparoscopy and are now obsolete,except for rare cases where the cervixis so disordered or damaged that conventional embryo transfer to the uterus is impossible.
More typically, the embryo or embryos are transferred to the uterus on the third dayas a 4- to 8-cell-plus cleavage-stage embryo, occasionally on the fourth day as a compactingmorula, and increasingly frequently on the fifth day as a blastocyst.
CONTROLLED OVARIAN STIMULATION (SUPEROVULATION)
There are several important components to controlled ovarian stimulation, whereby morethan one egg can be retrieved:
• Stimulating the ovaries with injections of FSH;• Preventing the LH surge with either a GnRH-agonist or a GnRH-antagonist;• Replacing the LH surge at midcycle with a ‘trigger’ injection of hCG;• Supporting the receptive state of the endometrium in the luteal phase with hCG or pro-
gesterone; and• Ovarian monitoring, with blood tests and ultrasounds.
Stimulating the ovaries with FSH
Normally, depending on a woman’s age, anywhere from one to 30 or more follicles (eachfollicle containing one egg) start to develop in each ovarian cycle (corresponding to a menstrual
266 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 266

cycle), by being sensitive to follicle stimulating hormone.These follicles are already partly devel-oped—they are tertiary follicles which started their development from primordial follicles abouteight months earlier.The older a woman is, the fewer primordial follicles she has left in herovaries, and the fewer small tertiary follicles (‘recruits’) are ready at the start of each newcycle to be recruited, as serum FSH levels transiently rise to begin driving their furthergrowth. No matter how many recruits are present at the beginning of the cycle, usually allbut one is lost on the way.This winning follicle goes on to ovulate.The others undergo
HELPING NATURE A LOT: ASSISTED CONCEPTION � 267
The wide range of available FSH preparations
The variety of follicle stimulating hormone preparations available in different partsof the world can be bewildering.Generally, and historically, they fall into three cate-gories, depending on how they are prepared and how much luteinizing hormoneactivity they contain.
A small amount of LH is needed for follicle development and proper develop-ment of the egg, so it has to be added for patients who for one reason or anotherstop producing LH themselves. Examples include when GnRH-agonists are stopped(see Ultrashort protocol, described in a later box); with overdosage of GnRH-antago-nists; when there is complete failure of the hypothalamus to produce GnRH (in casesof primary amenorrhea); and, rarely, with disease or absence of the pituitary gland.Toomuch LH, however, especially in long-acting form as human chorionic gonadotropin,might be harmful in some patients who already have high LH activity, as occurs inthe polycystic ovary syndrome.
The three kinds of FSH comprise:• Human menopausal gonadotropins with a high content of LH, such as Humegon
and Pergonal.These preparations contain contaminating urinary proteins thatsome people develop allergies to; they need to be given by muscular injection;and they can contain variable amounts of hCG to make up the required amountof LH activity (probably causing significant variation from batch to batch overtime).
• Purified human menopausal gonadotropins with low LH content, such asMetrodin and Menopur.
• Highly purified human menopausal gonadotropins with absent LH activity, suchas Metrodin HP (Fertinex in the USA) and Menogon (Repromex in the USA).These are the first truly modern FSH preparartions, not so much because (likethe recombinant FSHs) they contain no LH activity, but because they are highlypure and devoid of contaminating urinary proteins, so are easily self-adminis-tered by subcutaneous injection (injection under the skin).
• Recombinant FSH with absent LH activity, that is, follitropin alpha (Gonal-F) andfollitropin beta (Puregon, or Follistim in the USA).
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 267

atresia, and are lost forever (as did the many times greater number of potential recruits thatbecame sensitive to FSH at the wrong stages of the cycle).The reason this competitionbetween follicles takes place is that, in the natural cycle, FSH levels soon start to fall.Thepoint of the stimulated cycle is to keep FSH levels up, removing competition between folli-cles, enabling many more of the recruits to grow to the point of ovulating and able toprovide eggs for assisting conception in that cycle.
Follicle stimulating hormone (FSH) has to be given by injection, because it’s a complexprotein hormone that would be digested as food if given by mouth.For the different prepa-rations available, and what the differences between them are, see the box, The wide range ofavailable FSH preparations.
Counter-intuitive conclusions
With this information on board we can draw some important conclusions, conclusions thatare not otherwise intuitive.
First, no amount of FSH will stimulate more follicles than there are available to berecruited.The dose needs to be enough to stop the usual competition taking place amongthem.But once we reach this threshold, there’s not a lot of control possible over the numberof follicles that will grow.
Second, using FSH injections does not use up follicles any faster than they’re alreadybeing used anyway.They began their development in the ovaries eight months earlier, asmentioned before, and those that don’t produce eggs undergo atresia and are lost forever.
The dose of FSH
So if it’s not the intended number of follicles, what does determine the dosage of FSHinjections to be given? (This is important, because FSH is expensive, and giving moreFSH will not increase the number of eggs beyond the number of available recruits.)
The dosage depends on a woman’s weight,varying from about 100 units a day for a womanof 50 kilograms (110 pounds) to about 450 units a day for women over 100 kilograms (220pounds).The two other modifying factors are young age and the presence of PCOS.
Underlying these two modifying factors is the hazard that the ovaries become seriouslyenlarged, to the point of risking the complications of the ovarian hyperstimulation syndrome(OHSS). OHSS and other complications of ovarian stimulation are explained in Chap-ter 12. OHSS is more common in younger women (who have more follicles ready torespond to FSH) and in women with the polycystic ovary syndrome (see Chapter 11), so wheneither of these conditions is present the dosage of FSH is decreased in the hope of avoidingit. But it is very easy to overdo the decrease, producing widespread (if not immediatelyobvious) follicular atresia.
For many women there is no perfect dose: there is both too much follicular responseand too little FSH support of individual follicles, and OHSS will occur despite widespreadatresia. (In this case it can be best to continue stimulating the follicles properly but freezingall the embryos; see Luteal phase support, later on in this chapter.)
268 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 268

If no response occurs in about four days, as revealed by serum estradiol levels (see Ovarianmonitoring, further on in this chapter), the dose can be increased. Once the serum estradiol isrising steadily the dose must not be increased further—doing so won’t improve the respond-ing follicles and will increase the risk of OHSS. If the response seems too brisk, the dose ofFSH can be reduced, but it is important not to decrease it too suddenly.The follicles dependon FSH being maintained and, if it is not, can be tipped into undergoing atresia, a process thatcan be so slight that it goes unrecognized, except that the eggs don’t produce pregnancies.
Lastly, the duration of FSH administration is important.The normal length of the follic-ular phase generally needs to be made available to the growing follicles, that is, 11 days ormore.The follicles need to be brought past a diameter of 18 millimeters to reliably producefertilizable eggs.
Side-effects from FSH
Side-effects of FSH—apart from discomfort from the injection and the sheer inconven-ience of having an injection every day—come from the higher estrogen levels that occurcompared with normal cycles. Some people feel worse; some people feel better; probablyall feel different.
The other downside of administered FSH is that the higher number of developing folli-cles, producing higher levels of serum estradiol, can cause a premature release of luteinizinghormone from the pituitary gland. In an assisted conception cycle, such a premature LH surgeis likely to spoil everything.The follicles are not ready; the doctors are not ready; the eggsare not ready—and even if eggs are obtained, few are properly mature. So we go to sub-stantial lengths to stop such an LH surge from occurring.The two reliable ways are withGnRH-agonists and GnRH-antagonists.
Before we describe the use of these, however, we should point out that a prematureLH surge is not inevitable. It happens only about 10 percent or 20 percent of the time, andsome women (for an unknown reason) are more susceptible than others. Sometimes it’sbetter to cope with it rather than prevent it (see the box, IVF Lite™: More natural IVF ).
Preventing the LH surge: GnRH-agonists and GnRH-antagonists
The GnRH ‘analogs’ are a group of drugs all closely related to the natural hormonegonadotropin releasing hormone (GnRH), a small amount of which is released every hour ortwo by the hypothalamus of the brain to keep the pituitary gland active.They include twosubclasses of drug, the GnRH-agonists (which accentuate the duration of action of GnRH,‘down-regulating’ the response to it) and the newer GnRH-antagonists (which,more simply,block the effect of GnRH). Both have the purpose of preventing an unwanted LH surge.
GnRH-agonists
Exposure of the pituitary gland to a GnRH-agonist first stimulates it and then, paradoxi-cally but usefully, it inhibits it (called down-regulation).We can make use of both these
HELPING NATURE A LOT: ASSISTED CONCEPTION � 269
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 269

270 � GETTING PREGNANT
IVF Lite™: More natural IVF . . .
At Sydney IVF we’ve found that some women who for some reason repeatedly failto conceive with IVF using FSH/GnRH-agonist (or antagonist) combinations getpregnant quickly in a ‘more natural’ cycle.
In a young woman this can mean a totally natural (no added hormones) cycle;in an older woman, a cycle augmented with injections of FSH, but unaccompaniedby GnRH-agonists or GnRH-antagonists to suppress the LH surge.
Not all women receiving FSH alone have premature LH surges, so not all womenneed GnRH-agonists or antagonists during ovarian stimulation.The problem is, wecan’t predict the 20 percent or so who do, and there’s a lot invested in a treatmentcycle that’s at stake.That’s why using an agonist or antagonist is routine in IVF (andoverall their advent has made a huge difference to success rates).
Dr Cees Jansen (no relation, but we get on well!) is a gynecologist in Amsterdamwho specializes in using FSH alone—which means learning to deal with the prob-ability of an LH surge occurring. Indeed, this is what we all did before the late 1980s,before the GnRH-agonists were widely available.The same principles apply,whetherFSH is used to augment the number of developing follicles or this part of the ovariancycle is left entirely to itself.
Careful follicle tracking is needed, starting at the latest several days before the antic-ipated day of ovulation (anticipated on the basis of previous menstrual cycle length orexperience with detecting ovulation).
The aim is not to wait for the LH surge,but rather to get in first, once the leadingfollicle is 18 millimeters in diameter or bigger, with an ovulation-triggering dose ofhCG (Pregnyl or Profasi). If blood drawn at the time of the injection confirms thatserum estradiol has not yet fallen, that the serum LH has not started to rise significantly,and that the serum progesterone has not started to rise, then it’s reasonable to expectthat ovulation will not happen until at least 36 hours after the trigger. In practicethere is always some doubt, because the serum LH ordinarily fluctuates, even fromminute to minute.
So in a natural IVF or IVF Lite cycle at Sydney IVF, to be on the safe side wetime the egg retrieval for 34 hours after the trigger instead of the 36–37 hours custom-ary with regular IVF stimulations.
. . . especially when FSH is high
Natural cycle IVF can also be used for women in their twenties and thirties whoare close to premature menopause, with irregular ovulation (see Chapter 11) andelevated levels of serum FSH.
The reason for using IVF instead of timed intercourse might be the presence ofa factor adding to the infertility or to avoid leaving its timing to chance.
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 270

actions for ovarian stimulation, but the important one is the second: agonists effectively andreliably suppress the LH surge that can (prematurely) start the ovulation process in the stim-ulated ovaries.
The various GnRH-agonists may be administered differently but all work the sameway. Those that are available in Australia, Europe and the USA include:• Leuprorelin (Lucrin, and known as leuprolide under the tradename Lupron in the USA),
given by daily injection using a fine needle just under the skin;• Nafarelin (Synarel), given by nasal spray twice a day;• Buserilin (Suprefact), given by nasal spray four times a day; and• Goserelin (Zoladex) and triptorelin (Decapeptyl), both given as a monthly depot injec-
tion (and possibly less satisfactory for assisted conception).So, the GnRH-agonist first stimulates the pituitary gland to produce FSH and LH, therebystimulating the ovaries as well, then after a few days inhibits the pituitary and these twohormones fall to low (though still detectable) levels.This is what is so beneficial, partlybecause it stops the pituitary from competing with the FSH injections when these arestarted, but more importantly because it effectively prevents the LH surge,while still releas-ing enough LH to maintain hormone synthesis within the follicles.The upshot is that wecan continue the stimulation,without the risk of premature or unexpected ovulation, untilthe follicles are fully developed.
The main side-effect of the GnRH-agonists occurs as they start, an initial increase inFSH and LH referred to as a ‘flare’. For its importance, and for how it is managed, see thebox,The long, short and ultrashort of GnRH-agonists.Occasionally they cause a release of hista-mine in the body, causing an irritating skin rash in susceptible women soon after injection.
It’s probably important that GnRH-agonists are not taken during pregnancy. (Althoughwomen who’ve been kept on them for the first few weeks of pregnancy have not had babieswith obvious abnormalities, GnRH is normally present all over the baby’s developingnervous system, so it is safest to assume that exposing the fetus to high levels of GnRH-agonist could still turn out to be harmful in some subtle way.)
We stop the GnRH-agonist when ovulation of the stimulated follicles is triggered withhCG. Stopping the GnRH-agonist, again paradoxically, causes a further fall in LH (andprobably FSH) levels to extremely low, unrecordable levels, for about 10 to 14 days.
GnRH-antagonists
Several companies have now released an alternative to the GnRH-agonists, the GnRH-antagonists known as cetrorelix (Cetrotide) and ganirelix (Orgalutran).The antagonists havethe advantage that they drop levels of FSH and LH without first causing a flare (see above),
It is important in such cases,however, to first be sure that the woman has a normalkaryotype and is not a carrier for the heritable condition fragile-X syndrome, or seriousgenetic disease could be passed on to the next generation.
HELPING NATURE A LOT: ASSISTED CONCEPTION � 271
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 271

The long, short and ultrashort of GnRH-agonists
GnRH-agonists can be used in assisted conception programs in several different ways.
Short protocol
Starting the GnRH-agonist on day 1 or 2 of the menstrual period, with FSH injec-tions beginning within a day or two, is called the short protocol, and makes use of theflare of FSH activity that follows the first dose or two of GnRH-agonist to get thestimulation of the ovaries underway.The disadvantage of the short protocol is thatthe flare involves not just FSH (which normally flares at this time) but also LH.Andin some cycles, the corpus luteum from the previous cycle still has some life left in it,and responds to the LH flare with a surge of fresh progesterone production which canlast up to a week—and which could be harmful to the newly developing folliclesand their eggs, as well as to the endometrium.
Long protocol
The alternative is to start the GnRH-agonist many days, even weeks, before FSHinjections are started, allowing the pituitary to wind right down—and incidentallygiving great flexibility to timing the expected day of egg retrieval, which will beabout two weeks after the FSH injections are started.This is the long protocol. It canbe commenced at the start of menstruation (like the short protocol), in which caseserum estradiol and serum progesterone are monitored, and FSH is not begun untilthey are both suppressed. Or it can be started a week or so before the period is due,in the middle of the luteal phase.
Either way, the flare at the start of the long protocol is still capable of producingtransient ovarian cysts along with the developing follicles.These cysts are quite benign—they are either large old follicles without eggs (a ‘follicular cyst’producing estrogen,ora big atretic follicle, which produces no hormones) or a cystic and functionless corpusluteum.To say the least, though, they are a nuisance, confusing the picture whetherthey are producing hormones or not; in practice they often lead to cancellation of thecycle of treatment.Researchers in Bristol,England,have shown that such cysts can beprevented from forming by starting a week’s treatment with a progestogen a few daysbefore the GnRH-agonist is started, thus inhibiting the flare effect.
For long protocols at Sydney IVF we thus begin Provera 10 mg per day on aboutday 19 of the cycle before the one in which the ovaries will be stimulated.We thenstart the GnRH-agonist on day 23 (although it can be begun much later if desiredfor timing reasons).The Provera is stopped two days after the GnRH-agonist starts—usually after a week of administration, in which case the menstrual period should start at the expected time. The FSH injections can then start any time. Great
272 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 272

enabling them to be given for a much shorter time.They are typically started on aboutday 9 of the stimulated cycle and given for several days.
Flexible though the antagonists are in relation to timing, it seems they are less forgiv-ing in terms of dosage. Unlike the GnRH-agonists, which can be given in a wide range ofeffective dosages, underdosage and overdosage levels with GnRH-antagonists lie closetogether.Too little GnRH-antagonist and the LH surge will not be prevented.Too muchand the LH levels fall to unrecordable levels, perhaps jeopardizing the health of the folli-cles and the eggs they contain (comparable to the effects of the ultrashort protocol, discussedin the box,The long, short and ultrashort of GnRH-agonists). Such follicular atresia, even if slight,could be why direct comparisons between agonists and antagonists (studies involving closelycomparable control groups) have consistently shown slightly higher pregnancy rates amongthe agonists.
The other price to be paid for the apparent convenience of the GnRH-antagonists isthat they are more expensive to use, even though very many fewer doses are needed. At
flexibility can be achieved without sacrificing any benefit—either by extending thetime the Provera is given alone (the same effect can be achieved with birth control pillsor any other progestogen) or by extending the time the GnRH-agonist is given alone(this is more expensive).Remember, though,that in these extended regimens the periodmight or might not be delayed: it’s not important, but most people devote attention totheir period starting. If it’s substantially delayed, think of having a pregnancy test done.
Note that the Provera must be stopped before injections of FSH start. If theProvera is inadvertently continued there will be two problems: first, the follicles willnot respond properly to the FSH; and second, the endometrium won’t respondproperly to estradiol.
Ultrashort protocol
It’s also possible, in a variation of the short protocol, to stop the GnRH-agonist afterjust four or five days—the ultrashort protocol—without losing control over the pitu-itary gland.The LH surge will be prevented for at least a week after the GnRH-agonist is stopped. In fact, the pituitary during this time will be even furthersuppressed than it would have been had the GnRH-agonist been continued up tothe time ovulation is induced.
There are two problems with the ultrashort protocol. First, unless the folliclesare already well underway by the time the GnRH-agonist is stopped, it can be neces-sary to add LH (or low dose hCG, 50–100U per day) at a time when this is rarelynecessary with other protocols (because the woman’s small amount of residual LHproduction falls to nothing). Second, should a further dose of GnRH-agonist begiven after two days or more without it, a second flare of pituitary activity can beinduced, perhaps including the very LH surge we’re trying to stop.
HELPING NATURE A LOT: ASSISTED CONCEPTION � 273
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 273

Sydney IVF the antagonists are finding their place as emergency drugs in cycles where wehave used no agonists (see the box, IVF Lite™: More natural IVF . . . ).
hCG: The ‘trigger’
Human chorionic gonadotropin (hCG) is the hormone of pregnancy. In early pregnancyhCG acts like luteinizing hormone (LH) in stimulating the corpus luteum to makeprogesterone.
We can give an injection of hCG to replace the natural LH surge, and to set into motioneverything that will make ovulation happen, causing the egg in the mature follicle to be fertil-izable, and loosening it from the wall of the follicle so that it comes out with the aspiratedfollicular fluid at egg retrieval.
Why do we use hCG to mimic the LH surge? Why not use LH instead?Although synthetic, or recombinant LH (lutropin) is now available in some countries
(called Luveris by Serono), LH has a very short duration of action (measured in minutes),so to mimic the LH surge, which lasts more than 24 hours, more than one dose may haveto be administered.
hCG,on the other hand, lasts for days and a single injection can do the job.Presently hCGis still obtained by purifying it from the urine of pregnant women.Preparations of hCG includePregnyl (made by Organon in ampules of 500,1500 and 5000 units),Profasi (made by Seronoin ampules of 2000 and 5000 units) and Choragon (made by Ferring).They are ‘highly purified’and appear suitable to be self-injected under the skin, although product information stillsuggests deep injection into the buttocks.Recombinant hCG (Ovidrel by Serono) is availablein some countries.
The dose and timing of hCG
At Sydney IVF the usual dose of hCG to trigger ovulation is 5000 units. In women over80 kilograms (175 pounds), 10 000 units are given, and over 100 kilograms (220 pounds)we use 15 000 units. For women under 60 kilograms (130 pounds), 3000 units is usuallyenough.
In the USA the usual dose is 10 000 units.The reasons this higher dose is common arehistorical and relate to support for the corpus luteum during the luteal phase in ovulationinduction programs (see Chapter 11).
We know from experience that it takes just over 38 hours for ovulation to occur afteran injection of hCG. Eggs are mature and can float free in the follicle from about 34 hoursafter hCG, giving a four-hour ‘window’. Egg retrieval is typically scheduled 36 hours afterhCG (in practice, we schedule the retrieval and the hCG is self-administered 36 hoursbeforehand).
If a GnRH-agonist or GnRH-antagonist has not been used (see the box, IVF Lite™:Morenatural IVF . . . ), there’s a chance that the natural LH surge will have started before thehCG has been given—spoiling the cycle if it hasn’t been recognized or if a mistake is madein timing the egg retrieval.
274 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 274

Side-effects of hCG
The important and potentially dangerous side-effect of hCG is the ovarian hyperstimulationsyndrome (OHSS),which can begin to develop a week or so after the hCG trigger if a largedose has been used or if further doses have been given.
OHSS is discussed in detail in Chapter 12.
Luteal phase support
In the absence of LH, the corpora lutea that form in the ovary from the trigger dose of hCGwill have only a limited life.Once the hCG disappears from the circulation, typically withina week if the trigger dose has been kept low, the ovaries will stop producing progesterone,which is required to render the lining of the uterus, or endometrium, receptive to pregnancy.
In other words, there will be a luteal phase defect (a deficiency of the endometrium’ssecretory phase) unless:• A massive dose of hCG has been given for the trigger, enough to persist for two weeks
(or at least till implantation is secure);• Further doses of hCG are given, preferably with continued ovarian monitoring (see
below); or• Progesterone (or maybe a progestogen such as medroxyprogesterone acetate, though its use
is rare) is administered to replace the corpus luteum’s production of it.Of these options, the first two support the endometrium indirectly by stimulating the ovariesto make enough progesterone, and for long enough, to maintain the luteal phase untilimplantation occurs and the pregnancy itself makes enough hCG to take over. Both carrythe hazard of OHSS.
The third option is less likely to cause OHSS, but because the usual way of adminis-tering progesterone is by an oily intramuscular injection (for example, Proluton, typically50 mg daily or more) or as a vaginally admininistered cream or pessaries (for example,Crinone,200 mg daily or more), this option is more expensive, as well as either more painfulor more messy. OHSS can still occur when pregnancy happens and hCG from the preg-nancy restimulates the ovaries.
The only reliable way of preventing OHSS in situations where the risk is considered tobe high (such as with polycystic ovaries or in very young women) is to use a lowish trigger doseof hCG and then to cryostore all suitable embryos. In other words, to withdraw any chanceof pregnancy for that cycle of treatment and to withdraw all support for the corpora luteathat goes beyond a week from the retrieval. (Embryo cryostorage is discussed in Chapter 21.)
Minimizing the chance of OHSS during assisted conception treatment cycles involv-ing superovulation means monitoring ovarian response closely.
Ovarian monitoring
There’s normally an interactive, or feedback, relationship between the pituitary gland andthe ovaries.The pituitary’s production of FSH is controlled by the ovary’s response.
HELPING NATURE A LOT: ASSISTED CONCEPTION � 275
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 275

When FSH is administered this physiological control is abolished: we have to substi-tute our own feedback by recording the ovary’s response to the injections and, if necessary,varying how, or if, we give further injections of FSH in the follicular phase (called follicletracking) and injections of hCG in the luteal phase.
Follicle tracking
We learn how the ovary is responding to the injections by measuring and remeasuring theamount of estrogen in the blood (with serum estradiol levels) and by visualizing the numberand size of the ovarian follicles (with transvaginal ultrasounds).
There are two reasons why such ovarian monitoring is necessary during ovarian stimu-lation: first, to try to avoid dangerous degrees of stimulation that could lead to OHSS;second, so that hCG can be administered at the best time—with mature follicles—so that weget healthy eggs.
Monitoring usually starts on the first day of the menstrual period, when we measurethe levels of serum estradiol, serum progesterone and serum LH—to be sure that it’s truly amenstrual period that the bleeding represents, that it’s the start of a new cycle (and not,say, an ectopic pregnancy, a miscarriage or implantation bleeding). All three hormones shouldbe low.
(During treatment cycles involving a GnRH-agonist used according to the long protocol—see the box, The long, short and ultrashort of GnRH-agonists—your doctor may monitor theproper down-regulation of the pituitary gland with such tests over the course of a weekor more.)
At Sydney IVF we typically repeat the serum estradiol after several days’ stimulation withFSH injections to make sure that the dose of FSH, first, is enough to have achieved aresponse and, second, is not causing a grossly excessive response.
On the seventh or eighth day of FSH injections,we measure estradiol again, and performan ultrasound to see how many follicles are developing;on day 8, therefore,we know whethera certain level of estrogen is coming from a number of follicles still with further growthneeded before maturity, or whether that amount of estrogen is coming from just one ortwo follicles that are already mature.
From then until the follicles are close to 20 millimeters in diameter,we adopt a flexibleapproach in relation to the dosage of FSH, the duration of further stimulation, and thetiming of more estradiol measurements and ultrasounds.
If the LH surge has not been suppressed with a GnRH-agonist or GnRH-antagonist, weneed also to look for signs of the natural LH surge.This means more frequent blood tests,sometimes more than once per day, with measurements of serum progesterone and serum LHas well as estradiol.The last blood test is then taken at the time that hCG is given (for details,see the box, IVF Lite™: More natural IVF).
If these measurements are high, then an educated guess needs to be made as to whenthe LH surge probably began. In practice it can often be assumed to have started in theearly hours of the morning (see Chapter 19), which means timing the retrieval for aroundmidday—but there are exceptions.
276 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 276

Luteal phase monitoring
Sometimes dispensed with, especially if progesterone is being administered (see above), theessence of ovarian monitoring after ovulation is to ensure the adequacy of the ovaries’production of progesterone, so as to avoid a luteal phase defect.Thus frequent measurementsare made of serum progesterone.
Once levels of progesterone begin to fall, typically about five to eight days after thetrigger dose of hCG (see above), they fall very, very quickly.A further small dose of hCGshould then be administered (typically 1000 to 2000 units) in anticipation, or substitutiontherapy with progesterone should be commenced.
EGG RETRIEVAL
The culmination of ovarian stimulation and monitoring for IVF or GIFT is theegg pick-up (retrieval) procedure—the aspiration of the fluid from immediately preovu-latory follicles in which the eggs have detached themselves from the wall of the follicle,are surrounded by a mature cumulus (see Plate 2A), and are at the secondary oocyte stage,able to be fertilized.
The egg retrieval is carried out through the top of the vagina, to either side of the cervix,guided by transvaginal ultrasound (see Figure 20.1). It is also possible to aspirate the folliclesand retrieve the eggs at laparoscopy (this is how it was always done prior to the mid-1980s:see the box, Steptoe and Edwards).
Mild sedation administered intravenously, and local anesthesia, are generally all thatis necessary. General anesthesia can be avoided (although in cases where infertility iscomplicated by bad pelvic pain it is preferable). In this way Sydney IVF developedAustralia’s first ambulatory care IVF program in 1985, at Royal Prince Alfred Hospital.Follicle aspiration for IVF is thus carried out at a vaginal examination, usually whileyou are awake.The sedation is administered to take some of the anxiety out of theprocedure.
The ovaries will be scanned (you will have experienced this form of ultrasound duringthe monitoring of your ovarian stimulation program); local anesthetic will be infiltratedthrough the wall of the vagina around the ovaries; and the follicle or follicles will then beaspirated using a needle passed through the wall of the vagina beside the cervix, into theovary.
All that you will generally be aware of during the procedure is some pressure onthe ovary, followed by an ache that subsides.About one in 20 women experience consid-erable pain, however, so it’s best to have the option of general anesthesia available.There’s often a small amount of bleeding from the wall of the vagina. Other compli-cations, such as more major bleeding, damage to an internal organ or infection, arequite rare.
After the procedure you’ll spend a short time resting. Although you won’t generallyhave been anesthetized, the use of sedation means you should arrange for someone to takeyou home.
HELPING NATURE A LOT: ASSISTED CONCEPTION � 277
Getting Pregnant - prel, ch1-23 1/7/03 1:48 PM Page 277

SPERM COLLECTION
Usually your partner will collect a fresh sperm sample at the clinic (some of the nuancesof which are discussed in Chapter 10). Sometimes sperm will have been previously collected,prepared for freezing and stored.
Occasionally your partner will have required a surgical operation on the scrotum toobtain sperm from an obstructed epididymis (MESA) or, in cases of non-obstructive azoosper-mia, directly from a testicle (TESE).
278 � GETTING PREGNANT
Fallopian tubeUterus
To suctionpump
Vagina
Ultrasoundtransducer
Follicular fluidcollected
Ovarianfollicle
Figure 20.1 Ultrasound-guided follicle aspiration through the vagina for egg retrieval.The insertshows multiple follicular development after ovarian stimulation with FSH seen ontransvaginal ultrasound (the image has been inverted to correspond with thediagram).
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 278

IVF LAB PROCEDURES
We discuss:• Regular IVF and normal in vitro embryo development;• Sperm microinjection (ICSI);• Blastocyst culture;
Steptoe and Edwards
The inventors of human IVF were two Englishmen, Robert Edwards, a scientist atthe Physiological Laboratory at the University of Cambridge, and Patrick Steptoe,a gynecologist at Oldham and District General Hospital, 200 miles to the north.
It was Dr Steptoe’s special expertise with laparoscopy in the late 1960s, promis-ing practical access to ovaries and eggs, that led Dr Edwards to suggest to him theidea of collaborating to develop IVF into a clinical procedure for human infertility.
Their first scientific article was published (with tissue culture medium expert,Barry Bavister) in the prestigious journal Nature in 1969—as Professor Edwards waslater to put it, to ‘a world unaccustomed to the idea of human fertilization in vitro’.By 1971 human blastocysts had been developed in culture—still uncommon in clinicalIVF labs 30 years later!
Clinical work followed, but year after year of no success followed.There wasthen no way of knowing what was going wrong.And it could have been just aboutanything, ranging from the use of inappropriate progestogens such as norethisteronein attempts to prevent luteal phase defects to confining clinical embryo transfers towomen with hopelessly damaged fallopian tubes, no doubt including large hydro-salpinges now known to be especially inimical to embryo implantation (see the box,Hydrosalpinx: Reintroducing a villain).
Although the critics were calling the embryos duds, this turned out not to bethe case. Steptoe and Edwards were transferring single blastocysts that we now knowdo very, very well.Then, shortly after dispensing with the norethisterone, the firstpregnancy occurred. But elation turned to misery: it was a tubal ectopic pregnancy,reported in The Lancet in 1977.
Then, in 1978, came the birth of Louise Brown. Lesley Brown’s fallopian tubeshad been removed, so there was no hydrosalpinx and no chance of an ectopic.Another birth followed.The third and fourth births occurred at the Royal Women’sHospital in Melbourne,Australia in 1980.
It was to be 1984 before laparoscopy gave way to transvaginal egg retrieval guidedby ultrasound.The nefarious effect of a hydrosalpinx remained unsuspected until themid-1990s. It was to be the 2000s before single blastocyst transfers would againbecome routine.
HELPING NATURE A LOT: ASSISTED CONCEPTION � 279
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 279

• Assisted hatching; and• Embryo microbiopsy, for PGD.
Regular IVF
In conventional IVF, about 50 000 to 100 000 moving (motile) sperm are left in a smallplastic dish with the eggs.
The eggs, like all animal cells, are surrounded by their cell membrane, which enclosesthe egg cell cytoplasm, and also by a glassy membrane called the zona pellucida (describedin Chapter 3). Outside this there is a mucus-like layer that consists of cells derived fromthe follicle; this sticky layer is the cumulus, and its overall dimensions give the retrievedcumulus mass a diameter about 10 times that of the egg.The eggs are easily seen underthe microscope as the embryologist sifts through the aspirated fluid from the follicles (seeFigure 3.6b).
It’s these layers that sperm need to get through to reach the egg with ordinary IVF.It’s overcoming these layers that sperm microinjection—manipulating the sperm at amicroscopic level, or ‘micromanipulation’—seeks to do, described below under ICSI:Intracytoplasmic sperm insertion (see Figure 20.2d).
Contact with sperm soon disperses the cumulus. By the next day, some 15 hours afterintroducing the sperm to the eggs, the eggs are checked to see if they have fertilized byexamining them for the presence of pronuclei (see Figure 3.6c).
On the second day, the leading embryos will have divided twice, now containing fourcells. By the third day, there will be eight cells (see Figure 3.6e)—the stage at which oneor two of the cells may be removed for genetic diagnosis (discussed later in the chapter).
By the fourth day, the embryo consists of 16 cells or more. No longer individuallydistinct, they are fusing together to form a tissue.We call this process compaction and thesolid ball of cells forming the embryo at this stage is called a morula (see Figure 3.6f ).
On the fifth day an ultimately dramatic change takes place: the previously solid ball ofcells now has a hollow center, full of fluid.The process is called blastulation and the embryonow is a blastocyst (Figure 3.6g). Consisting maybe of 64 cells or more, the overall spheri-cal size of the early blastocyst is still no larger than the egg.
The blastocyst’s cells—called blastomeres—are not only getting smaller and smaller, theyare becoming specialized, differentiating into two main regions of the blastocyst.The blas-tocyst now begins to swell, stretching the zona pellucida to become thinner and thinner.
Figure 3.6h shows such an expanded blastocyst, differentiated into an inner cell mass (aball of cells destined to become the embryo proper—the fetus) and the outer trophectoderm(destined to become first the trophoblast, after implantation, and then the placenta and theplacental membranes, or ‘afterbirth’).
To culture embryos through to such expanded blastocysts requires special culture mediumand is discussed further below, under Blastocyst culture.
Even before embryo transfer, some blastocysts will start to escape from their zona pellu-cida.These are ‘hatching blastocysts’ (see Figure 3.6i).
280 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 280

The implantation rate after transferring expanded or hatching blastocysts at leadingIVF programs is 50 percent or more for women under 36 (see Appendix 2).At Sydney IVFthese embryos are doing so well that we prefer to transfer just one at a time.The risk ofmultiple pregnancy is otherwise too great.
ICSI: Intracytoplasmic sperm insertion
Sperm microinjection (ICSI) is a method of in vitro fertilization that puts only minimaldemands on the number of sperm available and their motility. ICSI is useful when there isthought to be a decreased chance of fertilization occurring with conventional IVF, eitherbecause of problems with low sperm numbers or low sperm motility (oligospermia orazoospermia), or because of other barriers to the fertilization process such as sperm anti-bodies.These conditions are discussed in Chapter 9.
Where to insert the sperm?
Before 1992, the sperm cell membrane was thought to have to merge with the egg cellmembrane for fertilization, whether naturally or with microinjection.The sperm cellswere injected through the zona pellucida, into the space immediately around the egg, theperivitelline space (Figure 20.2c)—a sperm microinjection technique called subzonal inser-tion, or SUZI. Fertilization then took place normally—sometimes (see the box, If youknew SUZI . . .).
At Sydney IVF in 1991 we had seven pregnancies from 59 cycles of SUZI(12 percent).At the time these results were unprecedented.The only alternative for preg-nancy among these couples had been donor insemination. Now the situation has changedgreatly for the better, with the advent in Belgium in 1992 of the sperm microinjectiontechnique ICSI, in which the sperm is inserted not into the space around the egg butright into the middle—into the cytoplasm—of the egg itself (see Figure 20.2d). UsingICSI, pregnancy rates for male infertility soon tripled at Sydney IVF and elsewhere whencompared with SUZI.
Typically, now, more than half the eggs retrieved will, with ICSI, be fertilizedsuccessfully, even with desperately low sperm counts.A revolution in overcoming male-related infertility has occurred.At Sydney IVF it no longer makes any difference howhigh or how low the sperm count is for an infertile couple: if we have as many indi-vidual sperm cells as we have mature eggs (even if we have fewer!), the chance of ababy is the same.
How to select the sperm?
Experience has shown that the genetic make-up of sperm cells—their ability ultimatelyto lead to a normal baby—is not related to motility.The presence of normal genes in thesperm cell seems to be more closely related to sperm shape than to sperm motility(although even with abnormal-looking sperm it seems the chromosomes are often still
HELPING NATURE A LOT: ASSISTED CONCEPTION � 281
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 281

282 � GETTING PREGNANT
Figure 20.2 Micromanipulation of eggs and embryos.
(a) The zona pellucida around an unfertilized secondary oocyte has been opened with a microlaser(at 2 o’clock), close to the polar body . . .
(b) . . . which is removed (inside the pipette, out of focus) for genetic diagnosis of a maternallyinherited condition.
(c) Subzonal insertion (of sperm) into the perivitelline space, inside the zona pellucida but outsidethe egg itself—the obsolete technique called SUZI.
(d) ICSI, or intracytoplasmic insertion of sperm (the sperm, circled, is still inside the pipette); afterinjection, the cytoplasm of the egg can be sampled for metabolic diagnosis, gene expressionstudies, or mitochondrial DNA analysis.
(e) Opening of the zona pellucida around an 8-cell (3 day) embryo for ‘assisted hatching’ (probablyineffective and not often performed) or, more frequently, for . . .
( f ) . . . embryo biopsy for preimplantation genetic diagnosis (PGD); generally just one cell isbiopsied (partially inside the pipette), representing 12.5% of the embryo’s tissue.
(g) Embryo biopsy at the (5-day) stage of a hatching blastocyst: several trophectoderm cells areavailable for PGD (just seen entering pipette), and the inner cell mass, or embryo, is leftuntouched; note that this blastocyst has already partially ‘hatched’ out of its zona pellucida (theonly cells that will be removed are already within the pipette).
Illustrations courtesy of Sydney IVF
Figure 20.3a–f is printed in color after Appendix 3.
(a) (b) (c) (d)
(e) (f ) (g)
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 282

normal), yet it’s sperm motility that’s most important in the race for the sperm to get tothe egg to fertilize it.
The sperm cell for microinjection is therefore selected mainly on the basis of its normalshape and size. Some motility is needed too (it shows that the particular sperm isn’t dead).
After insertion of the sperm into the egg with ICSI, as with SUZI, the biochemicalprocess by which the egg cell takes the sperm head apart and reassembles its chromosomes
HELPING NATURE A LOT: ASSISTED CONCEPTION � 283
If you knew SUZI …
Pregnancies from sperm microinjection around the world until 1993 were relativelyfew.The first baby born was in Singapore in 1988. In 1990, there were two babiesborn in England and two babies born from our program at Sydney IVF.
Only about 25 percent of the eggs we used to obtain at Sydney IVF would fertil-ize with the original sperm microinjection procedure known as subzonal insertion(SUZI). Not uncommonly, all eggs would fail to fertilize. For a practical chance ofsuccess we needed to get more than 10 eggs at the time of egg retrieval, and this meantthat the woman needed to be relatively young.
The barrier to fertilization rates with SUZI was the need for sperm placed inthe perivitelline space to bind to the egg cell membrane, something which requiredthe sperm head to get rid of its crash-helmet-like acrosome.The unpredictability ofthis meant putting 10 or more sperm in the space—and this in turn meant that alltoo often more than one sperm would fertilize the egg, ruining it.Too often it seemedthat it was all or nothing—polyspermy or fertilization failure.
The need for such an acrosome reaction (the process by which the sperm shedsits acrosome) became unnecessary when the sperm was injected into the egg itself.The first time this was done it was an accident: the embryologist slipped! To his (orwas it her?) amazement the egg not only survived the intrusion, it fertilized anddeveloped normally.The rest is history: ICSI has rendered SUZI obsolete.
The egg’s powerful disassembly machinery doesn’t seem to be put off by acro-somes.There is no question that ICSI has been the most amazing advance since theadvent of transvaginal egg retrieval.
The final chapter on ICSI, however, is still to be written. In Chapter 10 weconsider in detail the genetic conditions in men that might be passed on.There isevidence that, unlike regular IVF, a slightly higher proportion of babies conceivedwith ICSI have an aneuploidy of the sex chromosomes, congenital abnormalities ofthe male genitalia, and hereditary oligospermia.
Time and further experience should tell whether the more serious of theseabnormalities, uncommon but not rare, are due to the ICSI technique itself occa-sionally disrupting the internal architecture of the egg that holds its chromosomes orwhether it reflects the effect of a possible higher frequency of dodgy sperm in thesemen or testes of the men.
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 283

(and hence its genes) happens in the normal way. A risk that this might sometimes occurincorrectly with ICSI is discussed in the box, If you knew SUZI . . .
Blastocyst culture
After about three days of development in vitro, the embryo will fail to progress furtherif it is not receiving instructions from its new genome. Up to this point the egg’s geneshave been enough to carry its development, but from about the stage of four to eightcells the sperm’s genes, in combination with the genes the egg has been left with, musttake over.
At about this time there is also a change in the nutritional requirements of the embryo,which again shows a preference for glucose.The use of special, sequential culture solutionsfacilitates this metabolic appetite change.
If all these factors are favorable, the embryo goes on to compact and form a morula(Figure 3.6f ) and then a blastocyst (Figures 3.6g-i).
If this further development occurs on schedule, the embryo has a better chance ofimplanting and producing a pregnancy than an embryo transferred at any earlier stage,whenit has not had to pass this test.
Pregnancy rates for blastocyst transfers at Sydney IVF are given in Appendix 2.
Assisted hatching
After expansion (Figure 3.6g), the blastocyst must ‘hatch’ through its shell-like zona beforeit can attach to the lining of the uterus.This process is often seen to start in the lab duringblastocyst culture.
Some IVF scientists believe that the zona of eggs from older women is harder thannormal and may resist the hatching of the embryo.Attempts may be made to open the zonaand thus to assist hatching.This can be done with a microlaser such as is used for embryobiopsy (see below, and see Figure 20.2e).
Assisted hatching does not seem to be of any help in the eggs of younger women, andits place in women over 40 remains controversial.There is some evidence, however, thatassisted hatching could increase the chance of identical, or monozygotic twinning.
Embryo biopsy and preimplantation genetic diagnosis
There are three stages of egg and embryo development at which it is feasible to make agenetic diagnosis:• Before fertilization, the egg’s polar body, which is of no ongoing benefit to the egg or
embryo, can be removed and analysed (although only of course for maternally inher-ited chromosomes and genes) (Figure 20.2a, b);
• At the 8-cell cleavage stage, when removal of one cell will deplete the embryo of one-eighth (12.5 percent) of its cell mass, but permit analysis of the combined maternal andpaternal genome inherited by the particular embryo (Figures 20.2e, f ); and
284 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 284

• At the blastocyst stage, when several cells of the trophectoderm can be removed to enablegenetic testing that leaves the important inner cell mass undisturbed (Figure 20.2g)—akind of ‘mini’ chorionic villus sample.
Each of these techniques of embryo biopsy has its advantages and disadvantages for makingparticular genetic diagnoses. For more on the rapidly growing role for PGD in routine IVF,see the later heading,‘The special IVF needs of women over 35’ and the box, IVF Plus™:Chromosome-checked embryos.
EMBRYO TRANSFER, GAMETE TRANSFER
With successful fertilization, the resulting embryos can, in principle, be transferred the nextday, when they are at the stage of a zygote, or later, while they are in stages of cleavage orblastulation (see above and, to learn of the normal movement of the early embryo throughthe fallopian tube and into the uterus, see Chapter 3).
GIFT, ZIFT and TEST
Historically, before new culture media and improved in vitro methods greatly improved theresults from IVF, we gained benefit from transferring unfertilized eggs (with sperm) to thefallopian tubes (the procedure called GIFT), generally at laparoscopy.
When fertilization was in doubt, say with a low sperm count, and required the assuranceof IVF, benefit could also be had by transferring day 1 zygotes, or day 2 cleaving embryos toone or other fallopian tube (called ZIFT and TEST, respectively), also generally at laparoscopy.
GIFT and ZIFT continue to hold special appeal to those people who, for religious orother personal reasons, do not agree with fertilization or syngamy taking place outside thebody.TEST via laparoscopy remains an option for the occasional woman with a badlyscarred cervix that cannot be penetrated by an embryo transfer catheter.
Uterine embryo transfer
By the fourth day after fertilization, the developing early embryo expects to have reached theuterus. Just as improvements in embryo culture have led to longer times for keeping embryosunder laboratory conditions, materially improving the ability to chose between them andthus improving pregnancy rates, so also the need or the opportunity for transfer of embryosto a position other than in the uterus has all but disappeared (see above).
An embryo transfer to the uterus is mostly straightforward and painless, no more (orless) uncomfortable than having a Pap smear done. At a vaginal examination with aspeculum, a fine plastic catheter that has been loaded with the embryos is passed throughthe cervix into the uterus.
At Sydney IVF, we use a two-part catheter system consisting of a wider, outer cannulawith a bulbous tip to transit the cervix, and a narrower, very soft, inner catheter, whichcontains the embryo or embryos near its end, to pass down the cannula and beyond it, fora centimeter or two, into the cavity of the uterus.
HELPING NATURE A LOT: ASSISTED CONCEPTION � 285
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 285

We use ultrasound to make sure that the embryo transfer catheter is or has been posi-tioned correctly: the tiny amount of air on each side of the droplet of culture mediumcontaining the embryo or embryos is brightly visible in the endometrial cavity.
Should I lie around afterwards?
Many drawings of the uterus make it look as though it has a cave-like interior, in whichtransferred embryos might almost rattle about—float about, at least—before they might ormight not attach and implant! Intuitively this image makes you think it would be good tohang by your feet from the ceiling for an hour or so, to make sure the transferred embryosdon’t fall out.
The reality, luckily for the design of embryo transfer rooms, is otherwise. If you imagethe uterus side-on, you can see that the front and the back are close together.My colleague,Mark Bowman, likens it to a jam sandwich (a triangular one with just a tiny bit of jam inthe middle): no matter what way you hold it, the jam won’t fall out!
At Sydney IVF we have you get up pretty well immediately. Others have said that youcould probably go jump on a trampoline if you wanted to. (This might not be good foryour enlarged ovaries, though, so don’t do it!)
After the embryo transfer
Care of the ovaries and the developing secretory phase in the lining of the uterus (theendometrium), before and after the embryo transfer, is described above. The time afterthe embryo transfer is nerve-racking.You’re likely to feel at once elated (there’s a newchance of pregnancy) and deflated (you have lots less to do compared with before the eggretrieval—and, unless something is going wrong, you have much less contact with thepeople at the clinic).
And, looming, is the time at which a period might without warning start, or the bitter-sweet dawning of the day of the pregnancy test. Not since the day your high school resultscame out may you have had a day like it. Not everyone gets to this stage.
WHAT CAN UNEXPECTEDLY GO WRONG WITH IVF?
We look here at the unexpected:• No eggs;• No sperm; and• No fertilization, no cleavage or no implantation.
No eggs
An apparently unaccountable absence of eggs in the fluid from properly aspirated follicleshas been called the empty follicle syndrome (but I don’t think there is a mysterious ‘syndrome’).The cause is either follicular atresia or not enough hCG used to trigger final maturity of the
286 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 286

follicles (perhaps incorrectly prescribed; maybe incorrectly drawn up into the syringe; orpossibly, through a misunderstanding given, say, 12 hours instead of 36 hours before thescheduled egg retrieval).
Generally the embryologist will also remark that there is an absence of cumulus cells inthe fluid. If there are cumulus cells but no egg then the egg has simply been missed: goingback into the follicle once some bleeding has re-filled it a bit can produce the missing egg.
At Sydney IVF when there’s no egg and no cumulus from a series of follicles, theoperator stops aspirating them, leaving the remaining ones untouched until it’s establishedwhether or not the hCG trigger has been absorbed.This can be done within minutes, bytesting a specimen of urine with a sensitive pregnancy testing kit (which gives a positivereaction with detectable hCG).
If the urine test is negative, the remainder of the retrieval procedure is postponed whilea confirmatory blood test is done for serum hCG and for serum progesterone (the latter willhave failed to rise if hCG has not acted properly on the follicles). Instead of abandoningsuch a cycle, a further, higher dose of hCG can be given 36 hours before a rescheduled eggretrieval.This can lead to eggs being recovered even from the previously aspirated follicles.
If some mature eggs have been retrieved, but fewer than expected or hoped for, follicularatresia is likely.This might or might not relate to irregularities in the stimulation.Unfortunatelyit can be inherent in the follicles, although this is not a conclusion to jump to too readily.
No sperm
Your partner develops stage-fright and can’t collect a semen sample! Can you believe it!Whatever you do, don’t get mad . . .
Couples differ, obviously, but think twice before getting too intimately involved, as itwere.Especially if you’ve already had your egg retrieval you’re not going to be very convinc-ingly sexy. Generally he will need some space, geographically and time-wise.
At Sydney IVF we keep a stock of Viagra; this, and reassurance that there’s really nogreat hurry, can help heaps.The eggs will be fine for hours.
If the worst comes to the worst, and Viagra is not enough, sperm can be removed fromthe testis directly, using TESE. Desperate, perhaps, but better than a totally wasted cycle oftreatment. (Although we have had no direct experience with it, electroejaculation underanesthesia, a technique involving a probe in the rectum used to obtain semen in men withparaplegia, is another possibility.)
Prevention is better than cure, and most couples who have previous experience withdifficulty securing a sperm sample by masturbation take the precaution of obtaining a samplein less stressful circumstances, and placing prepared sperm in cryostorage.
No fertilization; no cleavage; no implantation
Second, fertilization can fail or fertilized eggs can fail to undergo cleavage properly.The reasoncan lie with the sperm (usually fertilization failure rather than cleavage failure) or with theegg (either or both), and of course it can lie with the lab.
HELPING NATURE A LOT: ASSISTED CONCEPTION � 287
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 287

Fertilization can fail when not enough sperm attach to the egg’s surrounding coat, thezona pellucida.This can happen because the number of healthy sperm available is too lowor because there are sperm antibodies present that block sperm from attaching. Either way,sperm not attaching to the zona means that future cycles should involve ICSI.
Fertilization and/or cleavage might fail if a substantial degree of atresia has occurredamong the follicles they were retrieved from.This can be an inherent shortcoming of awoman’s follicles or it can result from shortcomings in the FSH provided to stimulatefollicular development (see above); either way, it can be further aggravated by shortcom-ings in the lab’s culture systems (see the box, Embryo failure from follicular atresia: Nurture ornature?).
288 � GETTING PREGNANT
Embryo failure from follicular atresia: Nurture or nature?
For a tertiary follicle to develop normally, growing steadily from the 2 or 3 millimetersize it is at the start of the follicular phase to the 2 centimeter or so diameter it willbe when it is ready to release a mature secondary oocyte at ovulation or egg retrieval, itmust successfully fight off a strong propensity to fail—to fall into atresia.
In the natural ovarian cycle, follicular atresia is inevitable for all but the dominantfollicle.The point of ovarian stimulation with FSH is to fight the forces of atresia andthus to develop multiple dominant follicles. Success or failure depends on two factors:getting the FSH administration right; and having follicles capable of responding. Inother words, it depends not only on the nurture of the follicles but also on theirnature.
The nurture of follicles is more likely to be problematical in so-called high respon-ders. Paradoxically, the number of growing follicles is so great (say 20 or more)—andthe rise of serum estradiol levels becomes so alarming—that a high risk of OHSS isperceived,many days short of anticipated follicle maturity.Understandably, the physi-cian is tempted then to considerably reduce the dose of FSH. If the dose is reducedtoo drastically (though what reduction is acceptable has not been worked out) there’sthe risk that, critically deprived of support, all the follicles will tip into atresia, resultingat egg retrieval in oocytes that are no longer optimal or no longer even retrievable(the so-called empty follicle syndrome).
Alternatively, the recovered eggs, especially in a so-called low responder with fewfollicles, but also in some older women with still numerous follicles,might inherentlyfail to metabolize energy efficiently enough to carry them through fertilization,cleavage, implantation and formation of a healthy fetus (after what is known at SydneyIVF as the oopause).This is a manifestation of the effect of age in the woman and isthought possibly to be the result of increasingly faulty mitochondria in either the eggsor the granulosa cells (see the Chapter 7 box, How eggs might get their ‘use-by’ date:Mishaps in the mitochondria). Probably all women will have at least some follicles that,by nature, cannot avoid atresia.
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 288

In less severe instances, imperfect lab systems compound more naturally marginal situ-ations, insidiously resulting in pregnancy rates lower than they could be. For example,whereas a culture system involving levels of oxygen found in room air (about 20 percent,much higher than the 5 percent maximum found in the fallopian tubes) might work finefor the eggs of a 30-year-old, eggs from a 40-year-old might consistently fail to developadequately until the culture conditions are altered to avoid the toxic effects that 20 percentoxygen levels can engender.
To summarize, most embryos that fail to implant and/or fail to result in a baby, eventhough they might look normal in the lab, fail through combinations of intrinsic andextrinsic shortcomings, through the combination of nature and nurture. Inherent short-comings might be metabolically or genetically based. Extrinsic shortcomings might ariseduring stimulated follicular development (and thus be intrinsic by the time of eggretrieval) or subsequently, during laboratory handling.We believe that eggs from youngerwomen might recover from these shortcomings more readily than the eggs from olderwomen do.
The hot areas in IVF today comprise the development of ever more sophisticated culturemedia and embryo incubators, described in the section to follow, making sure the embryostransferred have the normal number of chromosomes by performing embryo biopsy and molec-ular karyotyping (see below), and the possibility of repairing metabolically defective eggsthrough still poorly understood maneuvers such as cytoplasmic transfer (see Chapter 23).
THE CHANCE OF IVF PREGNANCY
The chance of getting pregnant from a cycle of IVF treatment depends on:
• The age of the woman, particularly the age and number of her eggs;• The diagnosis (the reason for the infertility);
Furthermore, among egg-related factors, ovulation itself may have been triggered(by injection of hCG) too soon (or too late) in the follicular phase for the particularfollicle(s) concerned, resulting respectively in eggs that were substantially immature(and sometimes over-mature). It can be difficult to differentiate these states from theappearance of the recovered eggs in the laboratory, or to distinguish them from theeggs from early follicular atresia or from the oopausal eggs of older women describedabove.
Inevitably, a proportion of recovered eggs—usually from smaller aspirated folli-cles—will be immature at retrieval, will not reach the stage of secondary oocytes,and will fail to fertilize. If they do mature in the lab and fertilize, they might still failto undergo normal cleavage.This is part and parcel of every IVF treatment attempt.The proportion of embryos that make it to blastocysts in culture is usually well shortof the total.
HELPING NATURE A LOT: ASSISTED CONCEPTION � 289
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 289

• The quality of the program or clinic, especially the IVF lab,which becomes critical forolder women;
• The genetic normality of the embryo.
The age of the woman and her eggs
Age determines both the quantity and the quality of tertiary follicles available to be recruitedduring the beginning of any particular ovarian cycle.With age, the number steadily declines,as does the average quality. Quality will still vary between particular follicles in the groupof recruits available at the beginning of each cycle, so a larger group makes it more likelythat, by chance, one or more follicles and their eggs will be good enough to secure a preg-nancy resulting in a birth.
So age deals a double whammy:decreasing egg strength generally, and producing fewereggs at any one time to be lucky from.
Data from 1998 at Sydney IVF in which we looked at the overall chance of a babyfrom a single round of ovarian stimulation (see Figure A2.1), including babies from embryosnot immediately transferred but cryostored and transferred later, showed that age begandecreasing the pregnancy rate after the age of 34.Before 35, the chance of a baby,with twoday 3 embryos transferred, was almost constant among couples having a first or secondtreatment, irrespective of the woman’s age, at 60 percent per stimulation cycle.
After 35 the baby rate fell in a straight line: at 40 it was 25 percent; at 42 it was10 percent; by 45 it was zero. Clearly, special efforts are needed to give the older womanany real chance of success.
The impact of the cause of infertility
Our 1998 data was revealing of the impact of some diagnoses on a baseline of 60 percentchance of a baby in a first or second treatment under the age of 35. In summary, certaindiagnoses had no effect at all; others did.
Male-factor infertility
Low sperm counts could be completely compensated for with IVF, using ICSI when-ever necessary for oligospermia and with MESA, TESE or (rarely) DI with ICSI used forazoospermia.
Irrespective of the decrease in the sperm count the take-home baby rate was the same:60 percent per stimulation cycle.There’s more on male-factor infertility in Chapter 10.
Ovulation disorders
Couples with a mild degree of ovulation disorder, such as mild polycystic ovaries or oligomen-orrhea from weight loss, showed a slightly higher chance of having a baby than the average,about 65 percent per egg retrieval.
290 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 290

HELPING NATURE A LOT: ASSISTED CONCEPTION � 291
Hydrosalpinx: Reintroducing a villain
We met the hydrosalpinx in the box,Salpinx,hydrosalpinx and pyosalpinx, in Chapter 13.Whether present on one side or both sides, a hydrosalpinx spells trouble for gettingpregnant, either naturally or with IVF.The reason is complicated but important.
A hydrosalpinx forms when a fallopian tube, damaged from salpingitis, becomesblocked at the outer, fimbrial end, close to the ovary. Most hydrosalpinges, however,are not blocked at the inner, uterine end, remaining in direct communication withthe cavity of the uterus, the endometrial cavity.The isthmus of the hydrosalpinx isstill open, as is the isthmus of a normal tube.
So what? Well, the problem starts when a dominant follicle in either ovary startsproducing estradiol—either naturally or with superovulation. Estradiol causes theisthmus of the fallopian tube to become (temporarily) occluded, at the same timealso stimulating the hydrosalpinx to fill up with even more watery fluid.Ovulation—or follicle aspiration for egg retrieval—then takes place and the empty follicle beginsto produce progesterone.
As we see in Chapter 3, progesterone prepares the uterus for pregnancy, and doesso in many ways.One of these ways, in normal circumstances, is to cause the isthmusof the tubes to relax, admitting to the uterus an embryo previously held up at theampullary–isthmic junction, about three days after ovulation and fertilization (and thesame time that’s chosen in IVF programs to deliver IVF embryos to the uterusthrough the cervix).
The treachery occurs because it’s at this precise time, when the embryo orembryos should be gently held between the front and the back surface of theendometrium, that fluid from the hydrosalpinx trickles or gushes down through theendometrial cavity, inevitably posing a major threat to successful implantation.Pregnancy is lucky not to fail completely.Miscarriage is common among the implan-tations that survive the gush.
Remember, a hydrosalpinx affecting just one tube will cause this nasty trap tobe set, even if the other tube is completely normal and open.
What to do about it? At the least, the appearance of a previously unknownhydrosalpinx during follicle tracking with commitment to IVF should mean emptyingthe hydrosalpinx at the same time (and in the same way) that the fluid is collectedfrom the follicles to retrieve the eggs, and maybe repeating this at the embryo transfer.This might not be enough, however. Moreover, aspiration at embryo transfer couldcause some bleeding into the tube that might add to the embryo’s woes.
In the longer term, and preferably before IVF treatment starts, better optionsinclude removing the offending tube or tubes (salpingectomy), opening the tube witha microsurgical salpingostomy, or placing a clip on the tubal isthmus, as described inChapter 13.
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 291

More severe degrees of ovulation disorder, however, decreased the chance to about40 percent, reflecting the difficulty in dealing with the excessive reponse seen in moresevere cases of PCOS, and with dealing with some poorly understood ovulation disorderswith substantial disturbances of follicular development and proneness to follicular atresia.
There’s more on ovulation disorders in Chapter 11.
Fallopian tube disorders
When we consider that IVF was invented to overcome the effects of untreatably blockedfallopian tubes (see Chapter 13), it was a surprise to us that the more damaged the tubes werethe lower the chance of pregnancy with IVF.One possible reason is that we might not haverecognized all the circumstances in which a remnant of one or other fallopian tube includedsome of the tubal ampulla, leading to the presence of a hydrosalpinx. For the perfidious wayin which a hydrosalpinx stops fertility, either naturally or with IVF, see the box,Hydrosalpinx:Reintroducing a villain.
In my opinion it is essential to diagnose and treat a hydrosalpinx, even a small one,before commencing IVF.
Disorders of the uterus
Disorders that affect the endometrium (the lining of the uterus), such as submucous fibroids, anendometrial polyp, intrauterine adhesions, and endometritis or endometrial atrophy caused by tissuedisease, which cause trouble getting pregnant naturally, will be equally effective at prevent-ing pregnancy with IVF.These disorders need to be considered and be effectively treatedbefore starting any kind of assisted conception.There’s more about them in Chapter 17.Severe cases may be an indication for gestational surrogacy, discussed in Chapter 22.
The presence of endometrial overdevelopment, particularly the presence of any degreeof endometrial hyperplasia, is harmful to implantation, and can complicate some ovulation disor-ders, especially PCOS, in which estrogen is over-produced.The endometrium must be fullygot rid of before starting an assisted conception cycle, either with a full two-week course ofa progestogen to bring on proper menstruation or with a curettage.A curettage is generally helpfulprior to IVF. The best time for it (should the condition of the endometrium be in any doubt)is at the start of the FSH treatment discussed above.The endometrium will have plenty oftime to re-grow during the 10 or more days the ovarian stimulation will go on for.
Likewise, endometrial atrophy caused by a lack of estrogen, such as occurs in Turnersyndrome (but not endometrial atrophy caused by tissue destruction), is readily and quicklyovercome in the two weeks it takes to administer a course of estrogen in preparation foregg donation (discussed in Chapter 22).
Finally,what is the significance of having a ‘thin’ endometrium? We’ve had many normalpregnancies at Sydney IVF among women who never develop an endometrium thickerthan 4 or 5 millimeters on ultrasound, either with their own eggs or, in some cases, witheggs from younger donors. Likewise, it does not matter whether or not the endometriumadopts any particular ultrasound appearance. In any event, in neither case can much be done
292 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 292

about it. Bigger doses of estrogen make no difference. For some other ideas, see the box,Thin endometrium: Viagra or bust?
The quality of the clinic and lab
Attention to detail is everything, from a careful diagnostic work-up that excludes thoseconditions that prevent both natural conception and IVF-assisted conception, such as ahydrosalpinx or lesion of the endometrium (see below), through to careful regulation ofthe time and constancy of FSH dosages.
Assuming that the eggs that have been retrieved have been optimally nurtured through
HELPING NATURE A LOT: ASSISTED CONCEPTION � 293
Thin endometrium:Viagra or bust?
Much has been fretted about and written about a ‘thin’ endometrium visible ontransvaginal ultrasound during assisted conception cycles.
Occasionally due to endometritis or endometrial atrophy (discussed above), thesecauses can be confirmed or excluded by performing a premenstrual endometrial biopsy.Otherwise there is no good evidence that the endometrium needs to be any partic-ular thickness for implantation to occur. (Remember that ectopic pregnancies canimplant and develop quite readily in a diseased fallopian tube, which has noendometrium at all.)
If a premenstrual endometrial biopsy shows that the sequential action of estrogenand progesterone has produced a normal predecidual reaction in the endometrial stroma,the endometrium is responding properly for IVF to work, whatever its thickness.
If it does not respond fully, but reflects a luteal phase defect, then the problem mightor might not lie with the endometrium; it could just be poor hormone levels, aswith a disorder of ovulation (and readily overcome during ovarian stimulation forIVF; see main text).The test should be repeated with a full course of administeredestrogen and progesterone, the way these are used to prepare the endometrium forthe transfer of stored or donated embryos (Chapter 23). If the luteal phase defectpersists, the endometrial atrophy present can probably not be treated.
Dr Geoffrey Sher, an IVF doctor in San Francisco, several years ago published areport in which a thin endometrium in three of four patients seemed to improvewith adminsitration of a vaginal preparation of sildenifil (Viagra). In the patients wehave tried this technique on at Sydney IVF, it made no difference; and one of thempromptly conceived without Viagra when embryos from donated eggs were used.
In other words, it’s very tempting to attribute not getting pregnant despite thetransfer of normal-looking embryos to some shortcoming in your uterus.Your intu-itive feeling is that super-glue is the answer. But these shortcomings are rare. Much,much more often the fault lies with shortcomings in the embryos,which we discussin the box, Embryo failure from follicular atresia: Nurture or nature?
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 293

294 � GETTING PREGNANT
IVF-Plus™: Chromosome-checked embryos
Your embryo could be the best-looking blastocyst in the IVF lab, but it won’t keepgrowing normally unless it has the right genes in the correct balance. Basically thismeans it should have 46 chromosomes, in 22 pairs of non-sex chromosomes and a pairof sex chromosomes.Typically, half or more of all embryos are abnormal—they havetoo many or too few of one or more chromosomes (states known as aneuploidy andpolyploidy).
Unfortunately the classic display of the chromosomes we use for testing cells thathave been dividing and multiplying in culture—a standard karyotype (see Figure 8.1)—is not feasible on just one or a few cells taken fresh from an embryo. A differentapproach is needed, a recently developed technique known as molecular karyotyping.
The first way a chromosome was looked for was with gene-specific amplicationof DNA using the polymerase chain reaction (Figure 20.3a).The chromosome lookedfor was the Y-chromosome, which was of limited usefulness, but this is still more orless the way we still do preimplantation diagnosis, or PGD, for families with gene-specific genetic disease.
It’s been possible for several years to check a limited number of chromosomesusing fluorescent probes that attach to, typically, five target chromosomes, known as5-color FISH (Figure 20.3b), before selecting an embryo for transfer. But this leavesmost of the chromosomes unchecked, and capable of mischief.
Progress was made in 2000 by Dr Leanda Wilton at Melbourne IVF using atechnique called comparative genomic hybridization (CGH).What is it? Let’s look at itlaterally.
Imagine taking two supposedly identical pages from two telephone books, thensuppose that there’s one single letter or number that’s different, somewhere on thepage. How do you locate the error without going crazy?
Here’s a suggestion.Take a photocopy of each page on a transparent overhead,one in red ink and one in green ink.Carefully align the two sheets and project them.Almost every character will appear yellow-brown, except where they don’t exactlymatch. Standing out like a little beacon will be a small bit of unmatched red and/ora small bit of unmatched green.
That’s basically how CGH works.The sample DNA, or genome, is comparedwith a standard genome, one is dyed red, one is dyed green, and the two are fusedtogether, or hybridized.
Any significant amount of DNA (such as a piece of a chromosome) that’s missingin the sample will give a red signal; any significant amount of excess chromosomewill appear green. Figure 20.3c shows the result. It’s a great idea, but the trouble is,it takes one technician several days to get a result (Dr Wilton had to freeze theembryos after taking a cell for testing, transferring the normal embryo or embryosa month later, when the result for each embryo was eventually known).
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 294

follicular development, as stressed above,much will be determined by lab conditions as theembryos develop through to blastocysts.
An exceptionally stable culture environment should be provided for the egg and embryo,preferably by individualized incubators not subject to environmental swings of tempera-ture and gas as other people’s embryos are taken in and out.
The incubators should operate at 6 percent carbon dioxide and no more than 5 percentoxygen to minimize oxidizing conditions and to help the mitochondria. Embryos shouldbe at constant 37 degree Celsius temperature (about 98.6 degrees Fahrenheit) during allmanipulations outside the incubator, and finally a secure embryo transfer should be effectedusing a two-part catheter system and, if necessary, ultrasound control of embryo placement.
The culture conditions become especially important for older women and for womenwho are having their embryos tested using preimplantation genetic diagnosis (PGD).For more,see Figure 20.3 and the box, IVF-Plus™: Chromosome-checked embryos.
The special IVF needs of women over 35
The chance of pregnancy, both in natural circumstances and with assisted conception tech-niques, starts to fall from the age of about 35 (see Appendix 2).The chance of miscarriage
At Sydney IVF we have developed chromosome paints specific for every indi-vidual chromosome (Figure 20.3d) as well as adapting over 4000 specially mappedareas of chromosomes (Figure 20.3e). In each case we have created arrays (‘DNAchips’) that permit us to carry out two types of CGH reaction within a few hourson biopsied embryo cells (Figure 20.3f).
This is IVF-Plus . . . IVF in which each embryo is checked using molecularkayotyping for all its chromosomes before transfer.
But a note of caution: the proportion of human embryos that are shown to havean abnormal number of chromosomes is high … perhaps depressingly high. It canbe a shock when IVF-Plus reveals all the embryos to be abnormal, even though theyhave been growing well in the lab.
However, it is also possible to study the polar bodies of the eggs as they are collectedfrom the ovaries of older women (Figures 20.2a and b).The advantage of this is thatwhat’s in the polar bodies is the complement of what’s in the egg itself.And in most casesof aneuploid embryos it’s the egg that was the problem.For instance an egg with an extrachromosome 21 (which will cause trisomy 21 upon fertilization by a normal sperm) willhave one or other polar body lacking the displaced chromosome. So, by studying thepolar bodies with molecular kayotyping and finding that a chromosome 21 is missing,we can infer that the egg is abnormal. Of course polar body analysis will not discovertrisomy 21 embryos caused by a sperm cell with two copies of chromosome 21, butthese are a small minority.Most age-related trisomies take origin in the egg.
The end result in terms of a normal pregnancy and healthy birth might not bedifferent, but perhaps the emotional let-down, being earlier, will be a little less.
HELPING NATURE A LOT: ASSISTED CONCEPTION � 295
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 295

also rises among conceptions that do occur, and from the age of 42 more pregnanciesmiscarry than go to term, both with natural conception and with assisted conception.
The barrier to successful assisted conception is the nature of the woman’s eggs. InChapter 3, I describe how the eggs in the ovaries are all formed before birth: after 35 yearsor more, many of the eggs will have abnormalities of the chromosomes or the mitochondria,as well as other, yet-to-be-characterized metabolic shortcomings.The most rigorous, stable-environment and low-oxygen culture conditions are essential.
The association between a pregnant woman’s age and the risk of a fetal abnormality ofthe chromosomes, such as Down syndrome (trisomy 21), is well known.Although there aretests available to diagnose Down syndrome in early pregnancy (chorionic villus sampling,CVS,at about nine weeks, or amniocentesis at about 15 weeks), remember that it’s usual to transferthree eggs or embryos, so there’s a risk that a pregnancy may be multiple,with one or morenormal fetuses co-existing with an abnormal one.
There’s no satisfactory solution to this dilemma (one option, selective feticide, is discussedbriefly in the Glossary).
Not surprisingly, blastocyst culture and PGD (see earlier) is increasingly resorted to, tomake a diagnosis of trisomy 21 and other chromosomal abnormalities among embryoswhile still in the laboratory.
Sydney IVF, like many clinics, has no arbitrary policies that include or exclude any agegroup from assisted conception technology, but we try hard to dissuade women over theage of 42 or 43 from IVF. It’s ultimately the woman’s decision, taking into account themedical advice she gets from her doctor.Although there may be peace of mind to be hadfrom having tried IVF, there are reasons to be circumspect about embarking on assistedconception if you are a woman in your forties.
One novel way around the difficulties of older eggs—though easier said than done—is to use eggs donated by a younger woman. Egg donation, as well as embryo donation,sperm donation and surrogacy, is described in Chapter 22.
296 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 296

storing embryos, sperm and eggs
When your hopes arein the freezer
In the early 1980s, Professor Alan Trounson, working at the Centre for Early Humandevelopment at Monash University in Melbourne, began storing animal embryos fertil-ized in vitro at extremely low temperatures (cryostorage). In 1983 he reported the first
human pregnancy from a cooled-then-stored-then-warmed embryo.We know now that the risk of miscarriage, stillbirth and birth defects is no higher
with pregnancies established from transfer of frozen–thawed embryos than is the case withtransfer of fresh embryos. It could possibly even be lower.‘Embryo banking’ is today indis-pensable in making reproductive technology as effective as possible for infertile coupleshaving IVF.
This chapter considers:• Why embryo cryostorage is important;• What the dangers might be;• How long embryos can be stored for;• How a transfer is timed;• Storing sperm; and• Why storing eggs is so difficult.
FREEZING EMBRYOS
Ordinarily, lowering the temperature of tissues much below zero degrees Celsius causesfreezing. Ice crystals then form, crushing structures within the cells.The damage is irrepara-ble.When thawed, the cells do not survive.
297
21
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 297

Successful cryostorage of embryos has made use of ‘cryoprotectants’—substances that inhigh concentration cause solutions to become viscous and, at low temperatures, to solidifyin such a way that ice formation is minimal or absent (see the box, Nature’s antifreeze).
Why consider cryostorage?
Usually an IVF cycle will result in a number of apparently healthy early embryos additionalto the embryo or embryos that will be transferred ‘fresh’—that is, a few days after the eggretrieval.These extra embryos are then cryostored,usually still at the 2- to 4-cell stage, some-times at the pronuclear stage, but more and more often at the blastocyst stage.The storedembryos can be transferred at a later date, after thawing, producing a further chance ofpregnancy at a very much lower cost than the egg retrieval cycle.
298 � GETTING PREGNANT
Nature’s antifreeze
Many species of invertebrates—and, among the vertebrates, several species of frogsand at least one reptile—use dissolved chemicals of small molecular size such asglycerol and glucose to survive repeated freezing and thawing of their natural,Arctichabitats.
We use similar substances in the laboratory to enable embryos to be cooled toextremely low temperatures and ‘cryostored’.The antifreeze chemicals are calledcryoprotectants.The trick is to get them to replace the water that’s in the cells, other-wise when the water freezes it forms expanding ice crystals that crush the delicatecellular machinery.
There are two main ways the cryoprotectants work.With conventional cryo-storage of human embryos, we use a mixture of propanediol and sucrose. Thepropanediol penetrates the cells, pushing water out, while the sucrose stays outsidein high concentration, pulling water out.The embryo in its containing ‘straw’ isslowly cooled in the mixture, using a computer to gradually super-cool it to–7 degrees Celsius.Then, like throwing a stone into a calm, sub-zero lake, to instantlyfreeze it over the embryo is ‘seeded’ (by grasping it with even colder forceps), theremaining water forms microcrystals too small to cause trouble, and the embryo isplunged into liquid nitrogen.
A newer, more experimental technique goes further. Called vitrification, thepenetrant is dispensed with, sucrose being the sole chemical remaining outsidethe cell, but in even higher concentration than the sucrose used for conventionalcryostorage. Still as much an art as a science, vitrification may work better forunfertilized eggs and blastocysts.
Either way, the embryos’ environment is at the low temperature of liquidnitrogen, –192 degrees Celsius, which is two-thirds of the way down to the virtu-ally absolute zero of the furthest reaches of outer space.
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 298

The main reason for cryostoring embryos is thus to reduce the need to stimulate theovaries repeatedly, especially in young patients who produce large numbers of follicles andeggs in a conventional cycle of IVF.The temptation to transfer more than one or twoembryos, which carries with it the risk of twins or higher-multiple pregnancies, is thusconsiderably lessened. If pregnancy occurs in the egg retrieval cycle the spare embryos canbe kept several years (or longer), for a further attempt at pregnancy later on.
If we predict a substantial risk of ovarian hyperstimulation syndrome (OHSS), then allembryos produced from the retrieval can be cryostored,with no further injections of hCG,and with no chance of more hCG from the pregnancy itself continuing to stimulate theovaries, possibly dangerously.With such a ‘freeze all’ cycle, OHSS becomes rare.
Lastly, embryos are often stored after egg donation, enabling tests to be done to makesure the egg donor is not harboring a transmissible virus, before a final decision is made toproceed with the donation.
What are the dangers with cryostorage?
Not all embryos, or not all of an embryo’s cells, may survive cooling and warming.We cansee with the microscope how many of an embryo’s cells have survived. Prior to the stageof transfer to the uterus, the early embryo’s cells are ‘totipotent’ (in other words, each indi-vidual cell of the fertilized egg retains the same ability to develop into a complete embryo—a fetus, with all its supporting membranes).Theoretically, therefore, if say a 4-cell embryois cooled and thawed, only one cell needs to survive for a normal embryo still to result. Inpractice we would like to see at least three of the four cells make it, if it was a 4-cell embryothat was frozen.At Sydney IVF we would typically allow such a thawed embryo to demon-strate that it can begin dividing again before transferring it, ideally reaching the stage of blas-tocyst first.
Information accumulated by the National Perinatal Statistics Unit in Australia is showingno harmful difference in the outcomes of IVF pregnancies after cryostorage of embryos,and this appears to be true even when some cells survive and others don’t. Indeed, thereseems even to be a small trend to a better outcome compared with fresh embryos, maybeeven with a slightly lower risk of miscarriage and of birth defects.
How long can embryos be safely stored?
The temperature the embryos are stored at is that of liquid nitrogen, 192 degrees Celsiusbelow freezing.At such a low temperature,metabolism halts.The embryos are in suspendedanimation.They can remain in this state for hundreds of years. In practice, the time limitsto storage are not biological ones, they’re social (see the box, Embryo banks).
Transferring thawed embryos
Thawed embryos can be transferred to the uterus either in a natural cycle (in which themidcycle LH surge is looked for and the embryos transferred back three to six days
STORING EMBRYOS, SPERM AND EGGS � 299
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 299

afterwards) or in a cycle in which we take control over the endometrium by sequentiallyadministering estrogen then progesterone. For an example of how such a transfer cycle can becontrived, see the box, Priming the uterus for embryo transfer.
Our experience at Sydney IVF with treatment cycles where all the embryos have beencryostored has shown that the chance of frozen–thawed embryos implanting successfully
300 � GETTING PREGNANT
Embryo banks
How long might we store embryos? Biologically, certainly for hundreds of years.Butsocially?
In 1983,the year Professor Trounson achieved the world’s first human frozen embryopregnancy, we on the Australian Government’s Medical Research Ethics Committeesummed up the ethical position in the quotation below.Today I believe the questionsof inheritance are soluble, and I would be more relaxed about the 10-year limit (whichseems inappropriate for a 25-year-old confronted with sterilizing cancer treatment),butthe principles, I think, remain a sound anticipation of community concern.
Having accepted embryo freezing and thawing in principle, there is no timebeyond which the maintenance of the embryo in the cryostored state becomeslogically and unequivocally unethical.Yet,with time, the consequences are likelyto become increasingly distasteful to the community.There will also be legalproblems such as questions of property, inheritance, and control over the use ofand liability for loss of the embryos—any of which may increase with time.Arguments in favour of an agreed limitation thus become very strong. It wouldbe undesirable for embryos to be stored beyond the time of reproductive needor competence of the female donor; embryos that have not been implantedshould ordinarily be destroyed and discarded 10 years after freezing, or earliershould the donor(s) wish it or circumstances compel it.
National Health and Medical Research Council,Australia, 1983
The press and the politicians regularly re-open debate on the accumulating numberof embryos in storage, most of which will probably never been transferred. It is alegitimate community concern.
How much of an issue it is for the individuals whose embryos they are willdepend on their beliefs concerning the moral status of embryos (discussed in Chapter27). Should they be made available to other infertile couples? I discuss the consid-erable pitfalls with embryo adoption in Chapter 22.Couples who have embryos thatare to be discarded once their own reproductive needs are fulfilled could help othersindirectly by allowing them to be used for ethically approved embryo or stem cellresearch.
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 300

and leading to a baby is at least as good as it would have been had they been transferred asfresh, unfrozen embryos.
FREEZING SPERM
Compared with freezing embryos, freezing sperm is easy.Sperm are so small and robust that nospecial computer-driven equipment is needed, just the cryoprotectant and the liquid nitrogen.
The first sperm banks date from the 1960s, and were mostly used to store the sperm
STORING EMBRYOS, SPERM AND EGGS � 301
Priming the uterus for embryo transfer
Even women with regular menstrual cycles have a very narrow ‘window of opportu-nity’ during which thawed embryos can be transferred with a relatively high chanceof implantion. Getting the timing right depends on tracking the ovarian cycle. Butthat’s not all that has to be right: it has to be a ‘good’ ovulation, with a normal lutealphase, or the period could come early, carrying away an embryo that is otherwiseimplanting satisfactorily.
At Sydney IVF all this is generally too uncertain to be tolerable. Instead werecreate the ovary’s sequential production of estradiol and progesterone, which leavesmuch less to chance.
The estrogen we use is the closest orally active version of estradiol available,ethinylestra-diol (Estigyn or Progynon C), which is the same estrogen employed in the billions ofbirth control pills that women have taken since the 1950s.Because ethinylestradiol,evenalone, is contraceptive (but only by stopping ovulation),your ovaries will not be compet-ing with us for control of the lining of your uterus, or endometrium.We confirm thatthis is the case on the tenth day of treatment, with a measurement of estradiol (whichshould be low) and an ultrasound (which should show an absence of large follicles).
On the fourteenth day we decrease the estrogen and begin adding progesterone(generally as vaginally absorbed pessaries, but sometimes with the oral progestogenmedroxyprogesterone acetate, or Provera), thus mimicking the effects of ovulation onthe endometrium.
The cryostored embryos can then be transferred on precisely the right day fortheir particular stage of development.We can also know weeks in advance on whatday the embryo transfer will be.
And, in cases of egg donation when embryos have not been frozen but are beingtransferred fresh, we can use the same regimen to synchronize the recipient’s uterusto the donor’s stimulation treatment.We start the recipient’s estradiol with the donor’sFSH; the recipient’s progesterone we start 12 hours or so after the donor has her hCG.
If pregnancy happens, the estrogen and the progesterone are continued until weare sure they are being made by the placenta, when the hormone support can besafely withdrawn.
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 301

of sperm donors (I discuss donor insemination in Chapter 22).The sperm is prepared withthe antifreeze (in the early days the yolk from ordinary farm eggs was often used as well!),placed in small plastic straws that are frozen in the liquid nitrogen vapor and then plungedinto the –192 degree Celsius holding tank.When it is time for insemination, the straw istaken out of the liquid nitrogen and allowed to come to room temperature before thecontents are injected into the cervical mucus (‘intracervical’ insemination) or into the cavityof the uterus itself (intrauterine insemination, or IUI).
Increasingly in the 1970s and 1980s, men who were faced with sterilizing chemother-apy and radiotherapy for testicular cancer began storing some specimens in the hope thattheir sperm would later be enough to be used to impregnate a partner.Often, however, thesperm count was low and pregnancy did not happen. It was not until the 1990s, with theadvent of more widely available IVF programs, and particularly with the development ofICSI, that such stored semen became reliable as a form of reproductive insurance.Today,arguably, it would be medically negligent not to offer sperm cryostorage to a young manabout to undergo cancer treatment.
It is not so easy, however, for boys not accustomed to ejaculating on purpose or whoare still to reach adolescence, and who are faced with potentially sterilizing cancer treat-ment.The technical and social challenges are described in the box, Storing spermatogonia.
And if men faced with testis-threatening treatment can straightforwardly store theirsperm cells for later use, what about women and their eggs?
FREEZING EGGS
The best-proven option for women is to have their eggs fertilized and stored as embryos.For a woman who is about to receive chemotherapy or radiation treatment, however,she must first receive two weeks’ stimulation of the ovaries to bring follicles to the pointat which mature eggs can be obtained for their fertilization in vitro. Even if the woman
302 � GETTING PREGNANT
Storing spermatogonia
Unlike girls and women, whose ovaries contain eggs that have stopped replicatingand are all well into meiosis, the sperm cells in boys do not begin to replicate signif-icantly until the onset of puberty.
If a boy develops a childhood cancer that requires chemotherapy (leukemia, forexample), he cannot easily store sperm cells.Theoretically he could undergo treat-ment with FSH for six months or more to induce sperm formation, but the timeneeded would be entirely impractical and the precocious puberty it would invokewould be unacceptable.
Instead, research is progressing on the storage of spermatogonia from the tubulesof the testis that later can be thawed and reintroduced into the tubules to repopu-late the testes.
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 302

has a partner willing to provide the sperm to fertilize her eggs, this wait before eggs canbe obtained is often too long for her or for her physician to postpone the start of thetreatment.
The same applies if there is no partner for fertilizing the eggs—and the situation isfurther complicated by the fact that eggs about to ovulate do not freeze very reliably (seethe box, Poised to spring).
Immature egg freezing
If freezing unfertilized mature eggs does not work very well, resting eggs, in resting primor-dial follicles, unfortunately have so far done little better.At Sydney IVF and at many otherIVF programs, tiny ‘slices’ of ovarian surface—obtained by biopsy at laparoscopy (and usuallypacked with primordial follicles, at least in young women)—are frozen. Unfortunately thepieces must be very small for the cryoprotectant to diffuse into the tissue successfully.
STORING EMBRYOS, SPERM AND EGGS � 303
Poised to spring
At the time of ovulation, the unfertilized egg is a tensioned spring waiting to besprung.
Unlike sperm cells (and unlike fertilized eggs), recently ovulated eggs—and eggsobtained from follicles just before ovulation in the ordinary course of IVF—are tensewith electrical actions waiting to happen.When penetrated by a sperm, there’s anelectrical signal that spreads quickly through the egg to do several things:• Packets of mucus are released by the egg,producing a mucus coat that stops more
sperm getting too close;• The second division of meiosis is completed and the second polar body expelled;
and• The egg begins taking apart the sperm head to change it into the male pronu-
cleus, ready to merge with the female pronucleus (the process that ends insyngamy—see Chapter 3—by which 46 chromosomes are formed by the 23 fromthe sperm cell and the 23 from the egg cell).This vulnerable electric state of the egg—and the structures called spindles that
hold the egg’s chromosomes in the right place for completing meiosis and for fertil-ization—are vulnerable to a fall in temperature. For example, 10 minutes for an eggat ordinary lab temperature (say, 21°C or 70°F) instead of body temperature (37ºCor 98.6ºF) is enough to produce irrecoverable damage.
A Melbourne embryologist, Dr Deborah Gook, has had success with quicklyfreezing and thawing eggs to preserve these spindles (see ‘vitrification’ in the box,Nature’s antifreeze), but many scientists believe the spindles are too delicate—and theconsequences of disrupting them and producing chromosomal aneuploidy tooserious—for this procedure to be relied on and to become widely used.
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 303

This constraint severely limits the amount of tissue that can be stored, and it affects thenext step, because it’s one matter to freeze the tissues, store them and thaw them.What wecan do with the thawed tissue is quite another matter. How do we bring the thawed, still-immature eggs to the point at which they can be fertilized?
There are two possible ways we might try growing these tiny primordial follicles withtheir tiny eggs (resting eggs have only 1 to 2 percent of the volume of mature, ovulatingeggs, or secondary oocytes, so they have a long, long way to go). One is to try to developthe follicle and its egg in the laboratory, called in vitro maturation; the other is to trans-plant the stored ovarian tissue with its primordial follicles intact back into the ovary itself(see the Chapter 23 box, Trying to save your ovary for later).
The principle such egg storage depends on is the confidence that one or other of thesemethods for achieving maturation will, sooner or later, be perfected.As of now, unfortu-nately they have not.
Meanwhile, whether the two of you have stored sperm, eggs or embryos (see the box,‘By my testicles, I …’ )—remember to describe your preferred intention for their fate in yourwill.
304 � GETTING PREGNANT
‘By my testicles, I …’
‘Cross my heart’ we say in today’s polite times when we really want what we say tobe accepted by others as the truth.
In medieval times, though, the heart was not seen as housing the soul, rather itlay in the testicles (these were masculine times).To ‘testify’ meant taking the testi-cles in one hand and, under the pain of what can be imagined, the truth was sure tofollow.
So, if you have reproductive tissues stored, then in your last will and testament(yes,‘testament’ is also derived from testis) remember the testicles—and describe whatyou will and will not permit with your reproductive tissues after you have left thislife.
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 304

donation and surrogacy
Look for the trapsand pitfalls
Our society loves children.We place a high premium on being a parent. But society isstill ambivalent about creating families in ways that aren’t traditional. In Chapter 27,I question just how ‘traditional’ today’s so-called nuclear family really is.History shows
it only takes a generation or two of a certain kind of family structure prevailing in thecommunity for people to see it not just as normal, but possibly best.
People can understand and accept more easily what they have experienced and arefamiliar with.And because most people have not had to face the crisis of infertility, andso have little appreciation of the infertile couple’s plight, they won’t easily appreciate thatchildren can, in fact, be brought up stable and healthy in a very wide variety of familystructures.
Here we look at the vanguard in exploring the help—literally, the ‘surrogacy’—otherscan provide through:• Donating sperm;• Donating eggs;• Donating embryos;• Carrying a pregnancy and having a baby for you; and• When to tell your child his or her origins.To guide my way in this difficult moral and ethical field, I’ve found it most useful to considerhow each and every person involved can suffer (and then how to make sure they’reprotected) rather than to try and work it out from fundamentals, from theoretical, imper-sonal notions of people’s rights and obligations.
305
22
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 305

SPERM DONATION
When a man’s fertility fails because of a low sperm count, the personal consequences arecomplicated and sad. Impotence (usually temporary), loss of self-esteem and social withdrawalare common among husbands; anger, guilt and a wish to make amends are common amongwives. More and more, the couple will turn to doctors who can use reproductive technologysuch as IVF with intracytoplasmic sperm insertion (ICSI, discussed in Chapter 20) before theyaccept donor insemination (DI). Unfortunately, for many couples around the world, this tech-nology is often at or past the limit of what’s medically practicable and financially affordable.
What are the emotional issues?
Secrecy
Of the several people involved in any case of DI, it’s the infertile husband, more often thannot, for whom maintaining secrecy is most important. But this is more so in some culturesthan in others. For example, enlisting the help of a brother as sperm donor is an optiongenerally rejected in favor of maintaining secrecy in the USA,where modern family struc-tures are nuclear and insular. Among Indian Hindus, however, where more open andextended family networks persist, a brother’s fraternal semen donation can be an optionfavored on genetic and cultural grounds.
In Western societies in the 1970s, anonymous donor sperm banks replaced acceptanceof infertility, adoption, prudent adultery and divorce as the ways in which a woman mightadjust to her partner’s sterility.The ostensible reason for sperm donors to be anonymous isthe need to protect the social father, the recipient woman and the child from the embar-rassment of acknowledging—and somehow having to include—the child’s genetic fatherin their world.
In the 1990s increasing access to sperm banks came to be granted to women who didnot have husbands or male partners, in some cases because they were single, in some casesbecause they were in a lesbian partnership. Many Western countries had by then enactedlaws whereby the social father, after a birth resulting from DI, is recorded as the legal andonly father on the birth certificate.Whether he is known to the DI child or not, he cannotbe sued for maintenance. But in the 1990s also, we as DI professionals discovered moreabout two previously poorly considered aspects of DI practice.
First, it became increasingly obvious that children born of DI almost always found outsooner or later that they had a sperm donor as father, and that the older they were themore seriously they were hurt by the discovery. For more, see the box, Hazards and riskswith donor secrecy. And second, it became increasingly plain that we also have a duty tosperm donors, many of whom in surveys have said they’re willing to be approached bytheir DI offspring, even though their recruitment as donors had taken place with theexpectation and promise of being anonymous. For an elaboration on what drives men todonate sperm, see the box, What sperm donors think … But the first social experiment inremoving secrecy from sperm donation was not encouraging, as we see in the box, … andstopping sperm secrecy in Sweden.
306 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 306

Of course if sperm donation is resulting in children for women who have no malepartner, there will be no question that the child will sooner or later come to realize he orshe has a sperm donor for a biological father. As anti-discrimination laws are brought tobear on sperm bank practices, this is arising increasingly commonly.The issues are discussedin the box, Virgin births and lesbian motherhood.
The DI family
For the recipient couple, DI is a considerable challenge to the nature of their relationshipand marriage.The infertile woman generally accepts the idea of DI faster than her husbanddoes, although in my medical practice I sometimes hear descriptions of disquiet from apatient about the thought of a stranger’s sperm coursing through her body.The normal,social matter of choosing a genetic mate is effectively annulled; instead, with anonymoussperm banks, the reproductive choice passes to someone else.There’s more on the commer-cial side in the box, Mail order sperm.
Hazards and risks with donor secrecy
Having kept it a secret, even if you think the chance, or risk, of inadvertently disclos-ing a DI child’s true genetic paternity is small, the penalty, or hazard, when it allcomes out is great.
Remember that DI children in the twenty-first century will be adults at a timewhen genetic testing for heritable vulnerability to disease will be common.Comparedeven with today, the risk of accidental discovery can only increase.
In the 1980s and 1990s, social workers and counsellors working in the field ofadoption came to recognize the importance of genetic influences on childhoodpersonality and development.This typically followed separate meetings they hadwith the genetic parents and their adopted-out offspring, noting how alike motherand daughter so often were despite never having met.
Combined with the rising understanding of DNA in society generally, prevailingopinion has moved away from the notion that behavior and personality are mainly deter-mined culturally.More and more,we recognize the importance of genetic influences.
This is a change from the emphasis placed on ‘nurture’ over ‘nature’ in mostuniversity courses in the social sciences up to the 1990s.
This movement towards greater appreciation of the genetic determinants ofbehavior is increasing DI recipients’ desire to know more of sperm donors and isincreasing the wish of donor offspring to meet their genetic parents down the track.
As Western countries have moved increasingly towards recognizing the rights ofadopted children to discover their genetic parents, it is inconceivable that such rightswill forever be denied the children of sperm, egg or embryo donation.
DONATION AND SURROGACY � 307
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 307

308 � GETTING PREGNANT
What sperm donors think …
The motives behind a sperm donor’s decision to donate appear to vary accordingto the methods used within a community to recruit donors.
If donors are paid well (the USA is the one country where sperm donation isovertly commercial), most donors will at least seem to have donated for the money.
Outside the USA, sperm donation has mainly been an altruistic activity, with‘cost reimbursement’ common,but rarely to the extent that it is lucrative enough tobe a primary motivator. (Nevertheless, in the heyday of semen donation, the 1970sand 1980s, a small financial reimbursement seemed to have a facilitatory effect—perhaps justifying or ‘neutralizing’ an act that might otherwise have seemed a bit tooself-consciously altruistic.)
The nonfinancial motives recorded among sperm donors include:• Personal knowledge of and sympathy for infertile couples;• Especially among unmarried donors, a general desire to father a child or to pass
on genes;• Sometimes a simple curiosity about their own fertility; and• Occasionally, revenge!Unless they are specifically screened out, sperm donors as a group have alwaysincluded homosexual men.
In France, where DI is coordinated nationally through the Federation Françaisedes Centres d’Etudes et de Conservation du Sperme Humain (CECOS), only menwho are fathers are eligible to be sperm donors, a restriction that excludes well-motivated single men who want to be donors because they have no other hope ofsecuring genetic descendants.
Associate Professor Robyn Rowland of Deakin University’s Department ofWomen’s Studies, at an early stage of her career, found that the majority of donorswho already had children were separated from their wives at the time they becamesperm donors. From other sources we know that most marital separations in Australiaare initiated by the wife, who more often than not receives custody of the children.It seemed that in some way the men felt they were getting even.
The French experience with married donors also mentions semen donation as‘balm for a wounded ego’, confirming an element of compensation, spite or revengefor some sperm donors. In Professor Rowland’s study, a third of donors still livingwith a female partner had not told her and did not intend doing so.
Otherwise, however, secrecy may not be much of an issue. Dr Ken Daniels, aprofessor in social work at the University of Canterbury in Christchurch, revieweddonors on six New Zealand DI programs in the 1980s and found that 89 percentof donors had told other people of their involvement in sperm donation.
Irrespective of a donor’s main motive, studies in all countries where spermdonation is accepted show that donors show great interest in providing useful
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 308

information on their personal and professional characteristics—information beyondthe physical features that form the usual basis for matching donor with intendedsocial father.
There’s a complementary interest among sperm recipients, of course, to knowmore than just the medical and physical features of the donor. By the 1980s in ourown DI program at Royal Prince Alfred Hospital in Sydney,we were inviting donorsto write a paragraph or two to their anonymous offspring—a device that becamepopular among donors and recipients alike. But the high level of curiosity donorshave long shown in the outcome of their donations is still not often rewarded bymuch information about what’s happened.
In 1975, just a generation ago, Dr R. Schoysman, of the Brugmann UniversityHospital in Brussels, argued that ‘there is no reason whatsoever that he [the donor]should know the result’—and that donors whose own children had tragically diedwould be ‘troubled by the fact that somewhere there is another child alive’.This viewtoday seems antediluvian: surely most men would receive comfort or gratificationfrom such knowledge.
Times have changed since 1975, but donors are still mostly told nothing, unless acongenital abnormality or an inherited disease appears among the offspring, informa-tion about which can be medically important to the donor.Yet all the signs point tothe likelihood that today’s donors will sooner or later be approached by their offspring.
Curiously, in discussions of donors meeting ‘their child’,most people express theoffspring in the singular—in parallel, presumably,with the experience of an adoptedindividual seeking out his or her parents.But five or six such children is not unusualfor a sperm donor, in addition to his own natural ones. Sometimes it has measuredin the hundreds.
Whether or not all those offspring would want to make contact with theirgenetic father is beside the point: just knowing that there are so many children aboutcan itself be worrying.The student who goes through school selling his sperm repeat-edly may come to regret it.
So we badly need to develop more respect for non-commercially motivated spermdonors. Such new respect should have the immediate consequence of limiting thenumber of pregnancies attributable to each donor—or at least we should be askingdonors how many anonymous offspring they would be happy with.This principle isnot new,but the reason for the limit has generally been to reduce the chance of inad-vertent inbreeding (consanguinity) should any of the donor’s children happen to marry.
. . . and stopping sperm secrecy in Sweden
In 1985, new legislation in Sweden required openness concerning the identity ofsperm donors to recipients.A sharp decline in the use of DI followed immediately.The decline did not, however, come about because sperm donors were frightenedoff.While the legislation was no doubt the reason behind some individual spermdonors desisting, other men with different motives began volunteering.
DONATION AND SURROGACY � 309
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 309

For the infertile husband, the start of DI for his wife means an acknowledgment ofloss—a genetic dead end.The lasting importance of such a biological loss will depend onhis ideas of social and genetic fatherhood; it will depend on the supportive (or otherwise)attitude of his wife and friends; and,probably least but nonetheless important, it will dependon the compassionate approaches taken by the couple’s health professionals—the nurses,counselors and doctors.
Studies on the outcome for children born of DI show that they develop physically andmentally as well as or better than their naturally conceived peers.They’re usually healthy,wanted and loved.Their parents, in spite of their emotional strain and their psychologicaldramas, are less likely than average to separate and to divorce.
The anonymous side of DI has been made possible and prevalent by the physical simplic-ity of getting semen from men.
Programs of anonymous egg donation have, in contrast, been slow to develop,relying as they mostly have on spare eggs from women undergoing egg collection forIVF or on motivating amounts of commercial payment. But the rapidly developingexperience with egg donation from known donors has taught us a lot about donationin general.
EGG DONATION
For women who have no eggs of their own, receiving donated eggs that have been fertil-ized in vitro is the only way they’ll get pregnant. (The causes of such primary ovarian failureare discussed in Chapter 11.)
Egg donation, like sperm donation, can be motivated by sympathy for infertile women—whether they are known to the donors or not—and/or by commercial payments.Obtainingeggs for donation, unlike sperm donation, is necessarily an intrusive operation. In the past,before establishment of embryo freezing programs,many IVF programs encouraged womenaleady undergoing IVF to donate one or more eggs to other couples. Nowadays we
Rather, the wish for secrecy among couples using DI led them to seek treat-ment in neighbouring countries—abetted by traditionally minded doctors who werenot prepared to broker donations from donors who would be made known to thecouples. Dr Mats Ahlgren, a colleague of mine from Stockholm, Sweden, told mein the 1990s that couples were advised by their doctors to travel to Denmark orNorway for the sake of donors remaining anonymous.
Dr Ken Daniels of the University of Canterbury, New Zealand, who hasresearched sperm donation in Sweden, confirms that there is no shortage of donorshappy to be identified.
From my experience with sperm donation over the last 25 years, I believe thatit is usually the husbands who feel most comforted by never knowing the identityof the donor. Generally this represents a failure to come to grips with the issues.And, later on, this is likely to mean trouble for someone.
310 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 310

DONATION AND SURROGACY � 311
Virgin births and lesbian motherhood
Like celibate priests, devoted homosexual couples and committed virgins have beenpushed to the side in transmission of the human gene pool.
Now,with assisted insemination and with someone else’s help in providing sperm,the latter two of these three groups can bear genetic fruit without either pur-posefully transgressing their commitment or being blessed with divine intervention(occasionally known as ‘type 1 DI’).
Childlessness for an active heterosexual couple of reproductive age is a disabil-ity that calls for professional medical help.A normal expectation is being thwartedand a medical disability results. Such infertility is what our book is about.
In his or her professional medical practice, a doctor can and should be able torestrict professional obligations to treating medical infertility without venturinginto areas of considerable social controversy or moral uneasiness, and not be forcedto carry out procedures that are against his or her conscience.
But it is not only heterosexual couples who suffer when they are childless.Andassisted insemination itself needs no medical help:masturbation and injection of semeninto the vagina allows conception to take place with neither intercourse nor aninvoice for professional medical fees. Homosexuals, virgins and others can conceivein this way and have children without sex and without doctors.
Homosexuals face resistance in the community if they want to become parents.We often see that some male homosexuals wish to be sperm donors—and willbecome so unless prevented by legislation or regulation (in New South Wales, menwho try to be sperm donors to a medically administered sperm bank must by lawdisclose any history of male-to-male sexual activity, as well as other behavior consid-ered ‘at risk’ of contracting HIV).
Still, the technical simplicity of self-insemination means that women who seekpregnancy and children without ordinary sex can turn to homosexual men assources of semen. As a biosocial phenomenon, it’s inevitable.The compassionatedoctor concerned about the risk of infection with donations of fresh semenmight—if the law allows it—offer sperm-banking to quarantine any such dedi-cated semen while the donor is tested serially for the AIDS virus with serum HIVantibodies.
Do medical professionals—or does society—have other duties to a virgin’s or lesbianwoman’s desire to reproduce? We often hear the stable mother–father model advancedas essential for the psychological nurture of children: we hear the refrain ‘the child’sinterests must come first’ (as if we can really anticipate how the child will grow up).
This model is held as the disqualifying condition for virgins and lesbians. Butnowadays it’s a fractured model.
Whether it’s the resilience of children or the resourcefulness of single parents,today there are so many successful departures from the two-parent ideal that the
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 311

recognize more widely that this is rarely in the woman’s own interests, and generally, also,it was in reality too much a ‘spur of the moment’ decision to be comfortable.There was,moreover, the risk that the recipient might conceive while the principal patient did not.
In Assam in India, where the cost of IVF in relation to income is exceptionally highfor most women, several women commonly share the cost of one of them undergoing eggretrieval, and the eggs are then shared. Some programs in the developed world have givenwomen financial discounts if they will part with a proportion of their eggs.
In the USA and some other Western countries, payment of varying degrees is usual, typi-cally US$2500 to $5000,but sometimes much higher (see the box,Commerce in eggs . . .). A newindustry has been spawned,with brokers taking commissions for matching the wants of buyersand sellers, and women who have passed their natural menopause developing expectations thatmotherhood can again be theirs (see the box, … and pregnancy after the menopause).
In Australia,where commerce in human tissue is against Commonwealth law, the greatmajority of egg donations are by friends and sisters of women with primary ovarian failure.No payments are involved and it is everyone’s intention that the child or children will betold at a young age (see further on for a discussion of the principles). Secondarily, this meansthat the age of the donor is seldom a generational gap away from that of the recipient.Rarely do we see egg donation to women well past the normal age of pregnancy expec-tation.Occasionally Australian IVF programs receive requests from healthy, normal womenwho are prepared to undergo an IVF cycle purely so they can donate eggs to an unknownrecipient couple.The declining popularity of secrecy (see the box, Hazards and risks withdonor secrecy) is making such offers increasingly rare.
argument that nothing be done to facilitate breaks from this standard is unrealisticand unsympathetic. Just what the difference might be with or without an adult maleabout the household—and whether it makes a difference if the child without a malerole model in the family is a boy or a girl—needs more research.
Elsewhere I’ve written supportively about the biology of gay parenthood as away of increasing the realization of human potential (see ‘Bioethics of the sperma-tozoon’,Appendix 3), but I suspect that there’s still much to be learned in this areaof sociology.
Ultimately, however, it will be a matter for society to decide whether to applypublic resources to overcoming social childlessness; and it will be for individual doctorsto accommodate or reject such childlessness as part of their medical responsibilitytowards their patients or clients.
The question remains open whether the aloneness of a child brought up by apartnerless virgin—with, in some cases, firm ideas of the repulsiveness of sex—canbe overcome by the child’s peers and by education. Such fears might or might notturn out to be well founded.
Before pushing public policy one way or the other it will be important to havemore evidence on outcomes (see Bioethics of the spermatozoon,Appendix 3).
312 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 312

Legally, donating eggs is different from, and simpler than, donating sperm.Whereas newlaws have generally been needed to make sure that the social father with DI is also the legalfather, the connection between giving birth and being the legal mother does not ordinar-ily need special legislation.
In summary, egg donation in many ways is less complicated ethically than spermdonation.At least part of the reason is that secrecy tends to be much less of an issue, andthe donor is, or is readily regarded as, the child’s aunt or godmother, with a valid and easilyexplained interest in the child’s wellbeing.
Embryo donation is a different story.
EMBRYO DONATION
Embryos can be donated after eggs have been fertilized in vitro: the couple who donatespare embryos after their own procreative needs have been met can be portrayed as helpingothers with no physical risk to themselves. Or commercial clinics or brokers can beapproached who sell or broker sperm and eggs separately, enabling the incautious, with
DONATION AND SURROGACY � 313
Mail order sperm
There are commercial sperm banks in several countries, but only in the USA, withits strong national philosophy of pragmatism and commerce, is the sale of sperm forreproductive ends an industry.
Doctors can order semen through the mail for their infertile or childless clients,matched to order by physical and other attributes. Prepared semen costs aboutUS$150 to US$250 per 0.5 ml. In the USA, the presumption remains strong thatbuying sperm from a donor also buys off further duties towards the donor.Anonymityseems sacrosanct, and the price tends to be inversely proportional to popularity.
Already by 1980 a commercial sperm bank had been established where NobelPrize winners could bequeath their talents widely, if they wished, through selling theirsemen.At least two sperm banks in California in the 1990s were specializing in thesale of sperm from gifted men.At the Repository for Germinal Choice, described atthe time as a project of the Foundation for the Advancement of Man,‘approved’ appli-cants were (and maybe still are) given thorough descriptions of each available donor,from which they could make their selection.Writing in the Boston Globe on its firstand most famous donor, co-inventor of the transistor William Shockley, columnistEllen Goodman hoped that egotism was not transmitted along the DNA.
The Repository was not so fussy about the targets, however.Their first baby,conceived with the sperm of an IQ 200-plus mathematician, was born to 39-year-old Joyce Kowalski, who reportedly had done time in prison for fraud and whosetwo previous children had been removed from custody because of child abuse.
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 313

314 � GETTING PREGNANT
Commerce in eggs …
Because the procedure for obtaining eggs for donation is difficult physically, involv-ing superovulation, egg retrieval and IVF, you would expect the financial compensa-tion for egg donation to be greater than for sperm donation—and so it generally is.
A survey of 51 egg-donation programs by Dr Mark Sauer and Dr RichardPaulson in the US in the mid-1990s showed that 30 of them, or about 60 percent,used only donors designated and introduced by the recipient couples themselves,implying that there was a personally identified sympathy for the infertility of a closerelation on the part of the donors.The donors were usually sisters.
By 2000, however, most egg donations in the USA were commercial arrange-ments in which the donors were paid from US$2500 to US$5000 or more.
. . . and pregnancy after the menopause
Considerable controversy has arisen from the use of eggs from young women toenable pregnancy in women whose own eggs have long been gone.
A commercial clinic in Rome, Italy, has been behind women in their fifties andsixties getting pregnant and becoming mothers. Governments elsewhere have beenalarmed enough by this practice to legislate against it—generally using unfortunatelysimplistic, even arbitrary, logic.
Intuitively,most of us will be uncomfortable with the notion that women—partic-ularly just rich women—can buy the opportunity to get pregnant at any stage of theirlives.We can approach (and the popular press has approached) this issue from a numberof angles, including the welfare of the intended child, social equity and so on.
But the perspective that to me is the most clarifying has received scant atten-tion, perhaps because it’s at once more complicated and less emotional. For me thekey to the acceptability or otherwise of young eggs producing pregnancies for olderwomen lies in seeing the event from the perspective of the person who is going toprovide the eggs—the egg donor. Many of us are happy, in good circumstances, fora well-informed sister or friend of a woman with early menopause to go throughan IVF cycle, including stimulation and follicle aspiration for egg retrieval, out ofaffection and concern for the unfortunate woman in question.This can be an accept-able personal freedom to grant the donor, provided we can be sure that no undueor inappropriate coercion has occurred, and that she and the people important toher are properly informed and counseled, so that they won’t end up suffering regretabout their decision.
But can the same ever be true for a woman who is past her own normalmenopause asking this of a young stranger?
More often than not, such a woman’s own friends or sisters will themselves be ator beyond the menopause too, so for this purpose they won’t be useful to her.Her rela-tions, if they’re to be young enough to be helpful this way, will most likely be in some
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 314

the help of an IVF clinic, truly to design their own babies—or at least to pick certainattributes of both of their child’s gene-set donors.With rare exceptions, both practices aredangerous.
Altruistic donation is not likely to remain anonymous for long. Explanations aresooner or later required, not just to the children from the adopted embryos but also tothe extant children. News that you have full genetic siblings to be discovered living in astrange family might be almost as disrupting as news that you are yourself adopted. Suchembryo donation seems to have happened around the world quite often, using (withpermission, although there have been alleged exceptions) embryos placed in cryostorageafter IVF that have become surplus to the couple’s own reproductive needs. Experiencewith this practice in Australia does not encourage its continued practice. In a study ofembryo donations at Royal North Shore Hospital in Sydney, reported in 1999, inter-viewed women regretted their action, sometimes coming to tears in the presence of theinterviewing counselors.
In the case of embryos produced intentionally from unrelated and unknown spermdonor and egg donor, there is surely a heightened risk that the child will be alienated,should the social parents separate, should dissimilarity to the parents by chance be marked,or worse, should dissimilarity be the design.Acute observers have drawn analogies to thehatching of a cuckoo in the nest.
SURROGACY
For a woman to get pregnant and then to give her baby to an infertile couple can be thepinnacle of reproductive generosity—or, in some cases to date, reproductive folly. Broadly,the motivation can be altruistic (generally on the part of a sibling or close friend) or it canbe commercial (generally with no prior acquaintance).And the egg can be the surrogate’sor, through in vitro fertilization, that of the infertile woman.
Traditional surrogacy
It’s no new thing for a woman to conceive and to give birth to a baby she then gives away.Some Australian Aboriginal communities practice the custom as a treatment solution for
kind of dependent relationship to her, and ought to be disqualified on these grounds.(For sure,I would not be a party to a mother asking for egg donation from her daughter.)
Thus the only motive that remains viable for a ‘young stranger’ is commercial:the payment of money to the donor by the recipient, directly or indirectly, with thedoctor as the commissioning broker.
And this too is awkward.The average age of egg donors in some US egg donorprograms is just 21.This means that fully half the donors are still teenagers.
DONATION AND SURROGACY � 315
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 315

infertility to this day. If contact with the child is to be lost, however, no doubt the givingis not and never was easy.The custom by which an infertile wife could ‘give’ her maid toher husband for sexual intercourse and claim the subsequent child as her own is reportedin the biblical book of Genesis (16: 1–6).Nowadays, however, the surrogate is likely to havebeen inseminated medically.
The other modern difference is that most societies have legally codified marriage andthe legitimacy of children.This legal framework has developed to the point where thereare now formidable legal obstacles to recognizing as mother a woman other than the womanwho gives birth.
Although altruistic surrogacy isn’t novel—and it needs no special reproductive tech-nology—the surrogate runs the biological hazards of impregnation and pregnancy, and theemotional hazards of giving up both the product of her pregnancy and her genes—that is,both her genetic and gestational motherhood.Through history, the compensation for thesurrogate has come from her sense of generosity, added to by a continuing association withthe child, even if at some distance. But in forecasting the outcome it’s worth recalling thatHagar, the surrogate in Genesis 16, looked with contempt on her infertile mistress. Sarai,the previously barren mistress, in turn dealt so harshly with Hagar that Hagar had to flee.
Commercial surrogacy
In commercial surrogacy, an infertile couple commission a woman to have a baby for them,usually (in the USA) through the agency of a surrogacy brokerage, which typically retainsabout half of the fee paid.A legal and hopefully enforceable contract is signed, which to agreat extent limits the right of the surrogate to make decisions for herself concerningmedical and social matters while pregnant (such as smoking); and of course the contractwill endeavor to compel her to give up the baby at delivery.The USA is presently the onecountry in which the practice of commercial surrogacy is accepted.
At first the commonest form involved the woman’s own eggs,with assisted inseminationused for the surrogate to get pregnant.The egg, in other words, is the surrogate’s own.Atthe risk of unfairly diminishing her generosity, she is, in effect, selling her egg first, leasingher body for the pregnancy second, and, third, giving up a baby who differs from one moreconventionally ‘her own’ only by her not having chosen the mate to have sex with.Genetically and biologically the baby is the surrogate’s before and after she sells it.The firstsuch surrogate to try to have her contract overturned in the US courts and keep the babywas Mary Beth Whitehead. She was unsuccessful, but was granted visitation rights. In asimilar case in Australia, an appeal court has granted custody to the surrogate.
In the second form that surrogacy can take, the paid surrogate receives an embryo fertil-ized in vitro using the egg and sperm from the infertile couple.This is gestational surro-gacy, now the commonest form.Who the ‘biological’ mother is remains undefined, butunarguably the baby is genetically that of the commissioning parents and the surrogatemother is the gestational mother. Again perhaps unfairly diminishing her generosity, thesurrogate trades her body’s gestational function,much in the way that wet-nurses in the pastsold their ability to lactate.
316 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 316

Because there’s little recent example in society for not regarding as the natural motherthe woman who gives birth to the baby, the law in most countries would leave the surro-gate as the legal mother too, at least until the process of adoption transfers guardianship.Nevertheless, in the first case in the USA in which the gestational mother attempted tohave her contract overturned in the courts, brought by Anna Johnson, she was unsuccess-ful.At the time of this judgment,which was later upheld on appeal, newspapers, if they canbe accepted as a pointer to community attitudes, generally appeared content in theircommentaries to regard the genetic parents as the biological parents.
Medically justifiable surrogacy
In the 1970s and early 1980s in the USA,before IVF became effective and available, surro-gacy of the genetic plus gestational kind was extensively developed commercially as thetreatment for any difficult case of infertility. In this respect it resembled the ill-fated commer-cialization of uterine flushing in the USA to obtain embryos for sale (see the box, Wombflushing).The practice does not persist to any extent.
It’s when the commissioning infertile woman has no uterus (see Chapters 17 and 18),or when for some reason pregnancy would be exceptionally dangerous for her, or whenthere are genetic reasons in the uterus causing recurrent miscarriage (see Chapter 9), thatsurrogacy remains medically necessary for an infertile couple to secure genetic offspring.Several legislatures outside the USA have now started to respond to public opinion, whichhas consistently favored allowing altruistic surrogacy for valid medical reasons.
This move recognizes that when a relative or close friend is agreeable to bearing anIVF baby for a woman without a uterus of her own, she’s being given the opportunity tobe exceptionally generous. In carefully considered circumstances, there’s the prospect ofbenefit for everyone involved (except for paternalistic politicians who find the wholebusiness too distasteful or too morally hot to handle).The legislation that’s envisaged (butnot yet in Australia outside the ACT) will make easier what’s known as ‘parental orders’,in which a court can order, upon everyone’s agreement, that a child’s birth certificate recordthe commissioning mother instead of the birth mother.The need for lengthy adoptionprocedures to complete the surrogacy arrangement can in this way be overcome.
Just how morally hazardous the practice of commercial surrogacy is, I expect, willcontinue to be revealed.There will be the occasional sad eventuality of a baby born withan undiagnosed abnormality, wanted by no-one. More often, the hazards and the sufferingwill, in commercial terms, be revealed by the high price that successful parents will needto pay to keep their privacy from the relinquishing surrogate (for more, see the box,A poundof flesh: Exploitation and autonomy).Commercial surrogacy will always be limited by the veryreal suffering the surrogate bears after her separation from the child. Altruistic surrogacybetween the right people can get around this hazard.
What are the factors to consider in choosing a surrogate? The principles are much thesame as choosing a known egg donor or even semen donor; personal and personality factorsbeing favorable, the single most important factor—one the Sydney IVF Ethics Committeevalues particularly highly—is the length of time you have known and liked the person concerned.
DONATION AND SURROGACY � 317
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 317

WHAT TO TELL THE CHILD, AND WHEN?
One of the lessons we’ve learned from the practice of adoption is that accidental dis-covery by an adolescent of his or her true genetic origins is too serious a hazard to alloweven a small chance of it happening inadvertently. Such a discovery means that the quali-ties most expected by a child of its parents,openness and truthfulness,will have been assumedmistakenly—a dreadful revelation, whatever the child’s age.The same should be true ofchildren from donated sperm, eggs or embryos.
As a general principle, the longer you take to tell, the harder it is, both for you and forthe child.The alternative of not telling will sooner or later bear an awful harvest.
Make it a rule to pick up on it as early as the first opportunity arises—when the childdiscusses someone else’s parents (or lack of them), asks about where babies come from,picksup a related idea from The Simpsons or something else on television,or learns what an orphanis from a bedtime story. If that moment’s not right, it will be some time that evening, whenit’s quiet and restful and the day’s conversation can be revisited. It’s easier if they already knowas, say, an aunt or an uncle the person who helped mummy or daddy, but it’s not essential.
The younger your child is when this happens, the more likely she or he is to respondwith, ‘But you’re my real mummy and daddy, aren’t you?’ and the more easily you willanswer,‘Yes, of course, darling, you bet!’, and the quicker the conversation will turn to milkand cookies, or getting on with the bedtime story, leaving the gentle seeds sown to be devel-oped a little further next time.
Womb flushing
A novel way of donating an embryo while avoiding the full expense of an IVF proce-dure is for a woman to be inseminated with the semen of an infertile woman’shusband, to conceive, and then for the embryo to be washed out of the uterus andrecovered, just before implantation.
Around 1980 the technique was pushed in the USA by a venture capital fundedfirm, Fertility & Genetics Research Inc. of Chicago.
Womb flushing and embryo recovery, culture and transfer is a tricky and uncer-tain procedure. It carries medical as well as ethical hazards, including the possibilityof pushing the embryo out into the tubes, resulting in an ectopic pregnancy.
Ethics committees outside the USA have therefore generally not condoned thetechnique for embryo donation.
As IVF programs became prevalent in America during the 1980s, fewer and fewerclinical circumstances required womb flushing for treatment, so the method neverbecame popular. Fertility & Genetics Research Inc. went broke.
There are now no circumstances obvious where egg donation with IVF is nota better alternative for the prospective donor, ethically and medically.
318 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 318

DONATION AND SURROGACY � 319
A pound of flesh: Exploitation and autonomy
The criticism that commercial surrogacy promotes the exploitation of women andinfertile couples confuses the messenger (the surrogacy broker) with the message(the need of the infertile couples and the readiness of third parties to fill the need).Moreover, the fear that commercial surrogacy leads to the ‘commodification’ or‘dehumanization’ of babies is at odds with history.
The interpretation we might give on a couple’s commissioning a child from asurrogate when all else has failed is perfectly consistent with the historical trendtowards ascribing more and more individual value to children. It’s not the child butthe autonomous surrogate who risks the experience of being ‘dehumanized’—ultimately by a paid means to a lonely end. How can we estimate this haplessdehumanization—this possible resentment and suffering by the surrogate?
One measure of exploitation in the selling of body parts—whether it be blood,gametes (sperm or eggs), embryos, babies or body organs—is the relative size of thebroker’s commission in relation to his or her efforts, and, reciprocally, how much ofthe payment reaches the donor. In each case the people who commission the serviceare likely to be relatively wealthy, the person commissioned relatively poor.
It’s not clear in any of these cases, however, that what an outsider might callexploitation is particularly important to the people who opt to be commissionedthis way. In general it can be difficult to devise ways of dealing with the problem ofexploitation without seeming to wish to lock people into poverty. It could be arguedthat society has an obligation to better the economic position of the potentiallyexploited to the point where they would not be tempted by the money or be coercedor forced through their personal situation to accept the role—but society has thisobligation anyway; and besides, such betterment might simply bring a higher pricefor the donation.
Nonetheless, the rising price of wet-nursing led in part to its decline in popu-larity in England 300 years ago.
Society naturally aims to reduce the unfortunate circumstances in which peoplehave little alternative but to sell a part of themselves. In the meantime, making thepractice of surrogacy illegal is unlikely to work any better than its illegal status worksto suppress prostitution.Likewise, it may make it more difficult to police those whoseduty it should be to provide fair compensation.
Doing it voluntarily is an essential key to ethical donations of tissue and organs,whether the recipient is personally known to the donor or not, and whether or notthe donor is paid. But it’s clear from the distress of Mary Beth Whitehead and AnnaJohnson that bearing a child and giving it up—assuming there was and is no inten-tion to deceive from the beginning—can be very hard.An agreement to do so is notlike other commercial contracts, any more than was, say, Shylock’s demand inThe Merchant of Venice for the repayment of a debt with (should nothing more
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 319

negotiable be forthcoming) a pound of the hapless debtor’s flesh.The general unease that something so natural has become so unnatural—the
clue to the dehumanizing side of surrogacy—lies not with reproductive technologybut with the giving away of the child. It’s this loss that’s the source of the suffering,and it’s the surrogate’s suffering that is, or should be, a prime concern.
The fact remains that forewarning, payment and notions of autonomy are poorcompensation for loneliness and the loss of a baby.This sense of loss will happenoften with the rigidity of predominantly commercial surrogacy, in which I predictthat an ever-escalating price will need to be paid for privacy (to buy off the gesta-tional mother), in comparison with the usually more flexible circumstances of asurrogacy agreement that from the beginning is more obviously altruistic and whichretains personal contact between parents, surrogate and child, in an extended family.
For this is a circumstance which, when carefully planned, has the capacity toachieve lasting personal benefit for everyone concerned.
320 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 320

‘designer babies’? hardly …
The near future:A slope that’snot as slippery as it seems
Progress in medicine is driven by imagination, research, innovation and courage. Inthe last 20 years, reproductive medicine has depended on scientists, doctors and nursesdemonstrating these qualities—an interdependency that continues.
This chapter looks at the developments in reproductive medicine being activelyresearched today and examines what the technological keys might be to creating, ampli-fying, preserving or restoring a woman’s control over her reproduction when there’sinfertility or miscarriage, and when, for more personal, family-orientated reasons, tech-nological help in having a child is asked for.
I discuss:• Repairing older eggs: the oopause and cytoplasmic transfer;• Storing unfertilized eggs to postpone fertility: the promises and pitfalls;• Choosing your next baby’s sex;• Choosing which embryo to transfer: preimplantation genetic diagnosis, or PGD;• Why cloning won’t help infertile couples; and• Stem cell research.
OOCYTE COMPETENCE AND CYTOPLASMIC REPAIR
There are still many reasons embryos don’t do as well as we would like in the IVF laband, after embryo transfer, in a woman’s body. In many cases there can be an inherentembryopathy present, acquired from the sperm or, more often, from the egg before fertiliz-ation. In some cases this embryopathy will be chromosomal. In many cases we suspect
321
23
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 321

that it might be wear and tear of the egg’s, and hence the embryo’s, mitochondria.In vitro culture conditions can make a critical difference for these embryos (discussed
in Chapter 20), but the shortcomings of such eggs are still poorly understood.
The oopause
Human females, whose ovaries at birth contain all the eggs they will ever develop, usuallylose the ability to get pregnant in their late thirties or early forties, about a decade beforethe menopause, when the eggs are more or less finally depleted.This normal, physiologicalsterility is now unequivocally linked to a decline in the capacity of eggs from older womento develop, after fertilization, into viable embryos, and almost certainly this is in turn dueto a defect in the oocyte cytoplasm of the remaining eggs. At Sydney IVF we call thisphenomenon the oopause.
In modern society the reality of the oopause sits increasingly awkwardly with the long-standing, steady development of a rising age at first childbirth, which is leaving womenwho wish first to pursue a career with an ever shorter time in which to have children, anopportunity many inadvertently and lamentably miss.
Cytoplasmic transfer
A team of researchers in New Jersey led by Dr Jacques Cohen has demonstrated that thereis a small group of older women (late thirties, early forties) who still have apparently adequatenumbers of eggs, but who have consistently poor embryos.Dr Cohen showed that if a rela-tively small amount of cytoplasm is taken from apparently healthy donated eggs, and injectedinto the older eggs at the time of fertilization by ICSI, these people’s embryos look and domuch better.The chance of pregnancy increases significantly.
Dr Cohen’s team has also demonstrated, in some of the children of these women, thatmitochondrial DNA from the donor forms part of the inherited complement of mtDNA inthe cells of the offspring. Critics have called this ‘germ line gene therapy’, but I disagree(see the box, Possible hazards with cytoplasmic transfer).
It is not known whether the ooplasmic defect in the eggs of older women lies in aquantitative or qualitative deficiency in oocyte mitochondria or whether older eggs aremissing a critical factor in the cytoplasm, such as an enzyme or an RNA molecule.Thereare typically 400 000 or more mitochondria in a human egg at fertilization. Our work atSydney IVF reveals a range of mtDNA copy number between 100 000 and 5 million.Thesmall amount of cytoplasm shown to be beneficial, just 5 percent to 15 percent of the egg’svolume, points to a benefit more likely to be based on the addition of a missing catalystrather than adding to a lacking volume of material such as functioning mitochondria (akin,say, to replacing blood by transfusion in a person with anemia).
Where does the future of cytoplasmic transfer lie? The technique is promising. If onlywe knew how it worked, we might know what side-effects to look for.The children bornappear to have been clinically normal; the oldest (in 2003) is four. For now, however, cyto-plasmic transfer has been stopped in the USA by the Food and Drug Administration pending
322 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 322

‘DESIGNER BABIES’? HARDLY . . . � 323
Possible hazards with cytoplasmic transfer
The biological danger in germ-line gene therapy lies in the randomness of availablemeans of gene insertion, with its capacity to disrupt other genes and its capacity tooverdose the embryo.
To be sure, there are critics of reproductive technology who attach moral impor-tance to germ-line DNA generally and whose objections would persist no matterhow safe oocyte repair might be demonstrated to be.Ooplasmic transfer from healthydonated eggs does not involve altering genes.
But it does mean transferring some 13 genes that are contained within the small‘self-charging batteries’ we call mitochondria, and of which there are about a millionor so in an ovulated egg.Whether intentionally (for serious mitochondrial disease)or unintentionally (when for some reason an egg otherwise won’t start to developproperly), cytoplasmic transfer means transferring mitochondria—and that meanstransferring mitochondrial DNA.
For context,we should begin with the possible harms associated with the muchmore commonly practiced alternative to egg cytoplasm donation, the donation of awhole egg (see the Chapter 22 box, Commerce in eggs … and pregnancy after themenopause).
The mitochondrial DNA transferred—the mitochondrial genome—is unlikethe nuclear genome in several ways.To begin with, just 13 proteins are coded for,all concerned with a fundamental metabolic process called ‘oxidative phosphoryla-tion’within the mitochondrion,with little or no genetic difference from one healthyperson to the next.
Second, instead of the two alleles of each nuclear-encoded gene per cell, mito-chondrial alleles in a cell number in the hundreds or the thousands (hundreds ofthousands in the case of eggs), so any advertent or inadvertent ‘altering’ of the germ-line is at most a dilution effect, not a replacement.
Third, the mtDNA from the donor detectable in some of the offspring aftercytoplasmic transfer has little or nothing to do with mitochondrial genes. It’s in asmall area of the mtDNA molecule called the D-loop that does not code foranything (it was once called ‘junk DNA’; it is variable from family to family, evenmore so from racial group to racial group, etc; because you inherit mitochondriaand mtDNA only from your mother, anthropologists use it to trace matrilinealdescent).
There are, therefore, no novel or altered genes introduced by egg cytoplasmictransfer. So it is not gene therapy.
Those of us who are students of mitochondrial genetics are still cautious,however.There is no experimental animal to serve as a model for sterility fromooplasmic failure, because physiological sterility from dodgy egg function years beforeyou run out of eggs is, as far as we know, a peculiarly human phenomenon.
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 323

proper clinical trials and establishment of efficacy and safety, and in Australia by poorlyreasoned legislation prohibiting the creation of embryos with ‘genetic material’ (includingmt DNA) from more than two people.
Knowing the difficulties you can expect as you get older, the thought will occur thatmaybe you can store some eggs when you are young to make use of after a later birthday.
Some people argue that the cytoplasmic transfer of defective mtDNA mightenable propagation, in the rest of the child’s tissues years later, of deleted or other-wise mutated mtDNA, to result in mitochondrial disorders of a kind knownclinically to be associated with progressive, untreatable and ultimately fatal meta-bolic diseases.
But to invoke problems of this kind you first have to suppose that the donatedegg cytoplasm has a higher mutant mtDNA load than the recipient egg, otherwisethe situation will only be helped.
Obviously egg cytoplasm donors should in future be screened for mito-chondrial disease and, ideally, for mtDNA genomic integrity. But meanwhile, atleast as judged by the donor’s previous reproductive performance, you would havemore confidence in the oocyte mitochondria of the donors than in that of therecipients.
For rare families with mitochondrial DNA mutations there’s no other hope
Important as it is to improve the reproductive window for women in modernWestern society, there is more to consider medically—those families that suffer frommitochondrial genetic diseases.
Unlike conventional genetic disease,where a quarter to a half of all embryos willbe genetically normal (depending on whether the condition is recessive or dominant),with mutations of mitochondrial DNA up to 100 percent of offspring are affected,and the inherited diseases that result are among the most miserable infantile diseasesimaginable.An example is Leigh disease,with progressive and hopeless deteriorationof muscle and cerebral function from soon after birth until death, months or yearsinto infancy or childhood.
‘Conventional treatment’ for affected families consists of egg donation—a newset of mtDNA, to be sure, but also a new 32 000-plus nuclear alleles that are notfaulty in the affected woman.
There is a compassionate case here for nuclear transfer from the affected egg to adonated egg, in effect deliberately replacing the mitochondrial genome we shouldall have in common,while preserving the nuclear inheritance that characterizes ourdifferences.
I argue that we should proceed cautiously with clinical trials of cytoplasmictransfer for age-related female sterility and of nuclear transfer for families with mito-chondrial disease.The research should take place in centers equipped for adequatemitochondrial analyses of donors and the follow-up of infants and children.
324 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 324

USEFULLY CONSERVING YOUNG EGGS
There are two steps, neither of which is close to being perfected yet.
Safely freezing unfertilized eggs
As it was in the first edition of this book, the holy grail in the field of preserving femalereproductive potential is to reliably preserve eggs, first, without having to stimulate folli-cles to the point of ovulation, and second, without having to fertilize the recovered eggswith sperm before storage.This remains a woman’s present only hope if she wishes to leavehaving children until a later stage of her career or personal development, a time when herbiological clock may have taken her past the oopause.
Women about to receive potentially sterilizing chemotherapy for cancer or for seriousimmune diseases have a similar, even more urgent imperative.
The present emphasis in research is on freezing eggs well before ovulation—well beforethey acquire the delicate structure and machinery that enable them to receive a sperm celland complete the process of fertilization (for an explanation of the technical difficulties,see the Chapter 21 box, Poised to spring).
Resting eggs, in resting primordial follicles, may be the most stable of all to freeze. ManyIVF programs are freezing ‘slices’ of ovaries—obtained by biopsy at laparoscopy (and usuallypacked with primordial follicles)—for just this reason. But it’s one matter to freeze thetissues, store them and thaw them.This we can do. But there has been little or no successso far in bringing the thawed, still-immature eggs to the point of full development at whichthey can be fertilized.
In principle there are two ways we might try it: developing the follicle and its egg inthe laboratory, which is called in vitro maturation; or simply transplanting the stored ovariantissue with its primordial follicles intact back into the body (which is how it was originallydone in sheep).
Developing eggs from immature tertiary follicles
Take any egg out of its ovarian environment, separate it from its follicle cells, and it willmature spontaneously. It will complete the first division of meiosis and, theoretically at least,be ready to be fertilized. Researchers at Monash IVF, in Melbourne, have secured suchfertilization using IVF techniques on eggs removed from antral follicles down to just a fewmillimeters in size.A number of women have conceived and had babies from eggs obtainedthis way. But unlike the same procedure in cows—in which veterinary surgeons get preg-nancy rates of over 60 percent using IVF with eggs from small tertiary follicles—the chanceof a woman getting pregnant this way is still less than 2 percent.The smaller the follicle,the less likely it is that the egg will mature normally—and the more we have to learn aboutwhat’s needed to get it to a normal, fertilizable stage.
Much more work needs to be done before human in vitro maturation from tertiaryfollicles becomes reliable, but the project is worthwhile not just for reproductive
‘DESIGNER BABIES’? HARDLY . . . � 325
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 325

insurance—it would also be good not to have to stimulate the ovaries for superovulationin assisted conception programs.
Even more work is needed before eggs from primordial follicles will be able to be usedreliably after in vitro maturation.Remember this is a process that nature takes eight monthsto achieve within the ovary (see Chapter 3).
326 � GETTING PREGNANT
Trying to save your ovary for later
In the 1990s, in experiments involving sheep and mice, Dr Roger Gosden, workingat the Department of Physiology and the Centre for Reproductive Biology inEdinburgh, and Dr Jill Shaw, of the Centre for Early Human Development inMelbourne, succeeded in removing pieces of ovary, cutting the tissue into slices2 millimeters thick, freezing the slices and then transplanting the tissues back to thesame animal some time after that animal—in the course of the experiment—hadhad all other ovarian tissue removed.
Ordinarily this should have been the end of ovarian function (and of coursefertility) for these animals. In the majority of the animals the stored tissue, transferredeither to under the capsule of the kidney (a very vascular spot) or back to the regionwhere the ovaries had been, was able to regrow and to function normally, includ-ing ovulation.Some of the animals in which the tissue was put back where the ovariesshould have been were fertile.
The development of ‘ovarian slice freezing’ in the late 1990s promised the preser-vation of ovarian follicle function for women faced with a disease or treatment thatthreatens the survival of their ovaries, such as radiation treatment or chemotherapyfor cancer or even endometriosis (if it is bad enough to threaten the ovaries).
It was also hoped that preserving ovarian follicles at a young age might becomean option for women prescient enough to foresee a long career standing in the wayof early pregnancy and family building.
Although the numbers of follicles that survive the storage process represent justa fraction of those removed, the experiments with sheep show that fertility can follow.
Unfortunately, to date, no functionally successful regrafting of ovarian slices hasbeen reported in humans. Several researchers have shown that the follicles can, if leftlong enough (up to eight months after the graft) produce estrogen and even, occa-sionally, a retrievable egg; but normal fertilization and embryo development has notyet followed, nor (in 2003) has a baby.
Maybe, for humans, the number of primordial follicles in such a tiny slice is just toosmall to allow the probably tiny fraction that have full developmental potential enoughchance of being included in the sample.In other words,perhaps all that has been achievedfor these women so far is to put them from a menopausal situation into a perimenopause,when egg numbers are low, fertility is almost non-existent, and cycles are erratic.
Dr Gosden is now experimenting with freezing whole ovaries.
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 326

So far a normal embryo,with a successful birth,has been achieved with eggs from primor-dial follicles in just one mouse.Dr John Eppig and Dr Marilyn O’Brien,who research mouseeggs at the Jackson Laboratory,Bar Harbor,Maine,obtained this one normal pregnancy (andanother which miscarried) after transferring 190 two-cell embryos to the fallopian tubes ofproperly prepared mice.This is so far a rather discouraging result, given that conditions inmice can be much better standardized than they can be for women in clinical practice.
A better option for primordial follicles after storage seems to be to transplant themstraight back into the tissue of the animal or person they came from, and to allow natureto develop the follicles, but so far that too has not been successful in humans (for more, seethe box, Trying to save your ovary for later).
SEX AND GENETIC TRAIT SELECTION
As The Economist, a London-based weekly newspaper, has said,‘People are generally free tochoose how to bring up their children. If they want to choose their child’s sex as well,whynot?’The same could be said about choosing whether or not to try and suppress a familialtrait considered harmful or distressing.And, in both cases, it is not as if people haven’t tried.
For centuries, women and their husbands have visited witch doctors, astrologers andcharlatans aiming to control that quintessential matter of chance: whether the next babywill be a boy or a girl.And they have gone to churches and other places of worship andprayed, hoping for a modicum of spiritual intervention.And for probably much longer—perhaps since the origins of animal life generally—females have chosen consciously orunconsciously to mate with, and be impregnated by, males they perceive would enhancethe fitness of their offspring.
What’s new is that we are, today, starting to use reproductive technologies that makethese choices substantially more effective. I talk here about the present state of the tech-nology that’s needed to control sex and to screen embryos for genetic traits. Let me say atthe outset that I do not agree that this means we are designing babies.
‘Designer babies’ is a cliché that invokes thoughts of a blank canvas—one we start pastinggenes on . . . any genes.‘We’ll take a pair of these rare genes for green eyes; let’s go heterozy-gous for freckles; the newly discovered allele for dimples would be a cute touch … !’This isa long, long way from reality.
Reality used to be that a couple had maybe 10 children, among whom there wouldbe a wide assortment of genes—but only, of course, their genes, a reassortment of genesthe couple already had between the two of them.That much is the same today. It’s notan open canvas.Today, however, not many couples are going to have 10 children.Theymight only want one.And irrespective of how many children they’ve had, what’s wrongwith choosing the next child’s sex? Or making sure that some physical characteristic thatSam has always detested about himself or herself does not also trouble one or other oftheir children? It might sound trivial to someone else, but if it’s not trivial to Sam andSam—and if they’re not asking someone else to pay for it—why can’t they have theirIVF embryos checked for it (assuming the gene can be identified) and then just transferan embryo or embryos without it?
‘DESIGNER BABIES’? HARDLY . . . � 327
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 327

There are two important points to remember about the biology here. First, no gene(unless both parents have it) is going to appear in more than, on average, half the embryos.And we’re at least a generation away from even thinking of trying to repair a gene.It will alwaysbe easier to test for it (and to not use an embryo with it) than it will ever be to alter it.
Second, how the different genes (all 32 000 or more of them) assort with each otheris totally out of our hands, even in an IVF lab. In a restricted number of embryos, as isalways the case after egg retrieval and IVF, probably much less than half will even benormal (in terms of having the normal number of chromosomes); of these, on average nomore than half will have one wanted gene, no more than a quarter will have two wantedones, an eighth will have three—and so on. If you get too picky, you quickly run out ofembryos.
And a third point—a social one.We saw in Chapter 22 the extent to which, especiallyin the USA,babies are being born using sperm and/or eggs from anonymous donors,wherefully half (sometimes all) the genes in a baby are from a total stranger! It’s not illegal yet.(Some countries are starting to legislate that children must be able to track down theirgenetic parent or parents, the way the law is increasingly recognizing the rights of adoptedchildren.)
What, in this big picture, is the big deal about selecting one or two genes from withinyour family for your child? If this is ‘playing god’, then what god has been playing is dice(maybe he or she is relaxing with some trivial decision-making).At the very least, if youare into metaphysical power, the heavenly drama of whether Ms Jones has a boy or a girlnext time, or deciding which of her 300 000 eggs will become little Johnnie or Jeanie, willperhaps have been delegated for decision-making to a lesser immortal.
From hocus-pocus to sperm-cell sorting
Since the discovery that the X-chromosome is bigger than the Y-chromosome, scientists andothers have tried to exploit the difference by aiming to separate the supposedly heavierX-bearing sperm (destined to form girls) from the supposedly lighter Y-bearing sperm(destined to form boys).
To begin with,Y-bearing sperm have long been thought to swim faster—and so to getto the egg sooner. Following this premise, if you then conduct a race—by abstaining fromsex until the egg has been ovulated (‘late sex’)—you should increase the chance of havinga boy.On the other hand, if you want a girl, this theory has it that you should have sex wellbefore ovulation, let the Y-bearing sports jobs run out of puff, and the chances are that theslow but steady X-bearing sperm will be fittest to fertilize the egg by the time it appearsin the fallopian tube (‘early sex’). Landrum Shettles, a gynecologist from Alabama, popu-larized this principle in the 1970s, adding to the recipe a mildly alkaline vaginal douche(made by dissolving 5 grams of baking soda in half a liter of water) before intercourse forboy-selection, or adding a mildly acidic douche (20 ml of white vinegar in half a liter ofwater) before intercourse for girl-selection.
Some fantastic results have been claimed for Shettles’ method. For example, Dr CedricVear, a family physician from rural New South Wales, reported in The Medical Journal of
328 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 328

Australia in 1977 a perfect outcome among 10 consecutive couples. For some reason hestressed the need to avoid frivolity, to, as he put it,‘[impress] on both parties that the proce-dure is a scientific exercise and not an emotional or erotic skirmish’! What a killjoy! Whatwould Vear have thought of trying for a boy by holding off having sex till there’s a fullmoon shining through the window then timing a climax to coincide with the crow of arooster watching from the end of the bed? To be sure, Shettles advised avoiding orgasm forconceiving a girl, but I can’t work out the logic for that advice.Using the Shettles methods,and publishing in the MJA in 1985,Dr Barbara Simcock refuted Vear (and Shettles).Among73 women the success rate for choosing daughters was 50 percent; for choosing boys, sheconcluded that ‘the use of [a] modified Shettles’ method appeared to decrease the deliveryof a male child’.
More recently, attention has been focused on trying to separate X-bearing sperm fromY-bearing sperm in the lab, prior to assisted insemination. Most popular of the procedureshas been passing the sperm cells through a column made up of the human protein albumin,which was first reported in the distinguished British journal Nature in 1973, by R.H.Ericsson and others. Dr Ericsson has since been associated with a number of clinics in theUSA,Asia and Britain, at which it’s claimed that if couples use their albumin-based spermcell separation techniques they will conceive a child of the desired sex with more than thenormal approximately 50 percent probability.
Ericsson’s method, as published in 1973, reportedly produced a concentration ofY-bearing sperm.A number of investigators have explored this claim by testing the spermobtained with a fluorescent dye that stains part of the Y-chromosome (using a reliable tech-nique called fluorescent in situ hybridization, or FISH). Using FISH, investigators in labora-tories from South Australia to Barcelona, Spain, have been unable to show significantenrichment for either Y-bearing or X-bearing sperm using albumin separation columns.
So the effectiveness of sex selection clinics based on Ericsson’s sperm selection methodhas to be questioned.What we have learned from them,however, is how many people are afterboys and how many are after girls. (See the box, Should feminists be worried by sex selection?)
MicroSort
In 1990, patents were granted to the US Government for the technique of sperm-cellsorting to concentrate X-bearing and Y-bearing sperm using a separation technique basedon these cells’ different DNA content, and using a technology called flow cytometric sorting.Cell sorters based on flow cytometry are in wide usage in medicine. Blood transfusionservices, for example, use them to separate the different cells in donated human blood forspecific transfusions of red cells (for anemia), white cells (for infections) or platelets (forbleeding).
Dr Larry Johnson, working at the US Department of Agriculture laboratories inBeltsville, Maryland, successfully adapted cell sorters to deal with the unusual flat shapecharacteristic of sperm cell heads. He stains the cells with a special, non-toxic dye called afluorochrome, which emits light when excited by ultraviolet light from a laser. A spermcell passing through the sorter is shot by the laser; if a detector at right angles confirms that
‘DESIGNER BABIES’? HARDLY . . . � 329
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 329

the sperm’s flat surface is actually facing the laser then a detector in line with the laser ‘reads’the intensity of light radiation emitted.The sorter can be set to look for the slightly smalleramount of light a Y-bearing sperm emits or the slightly greater amount of light an X-bearingsperm emits. Either way, each sperm cell passing the test is then pushed electronically intoa separate path that leaves the cell sorter, for collection and later use.
Dr Johnson has used the fluorochrome-based cell sorting method with sperm from anumber of species, including rabbits, cattle and pigs.As well as testing the resulting Y- orX-enriched sperm populations with FISH, the sex of offspring produced from inseminat-ing the animals with these ‘sperm fractions’ has been studied.Proportions of females rangedfrom 75 percent in pigs to 94 percent in rabbits when the cell sorter was set for enrichingX-bearing sperm.Proportions of males,when the cell sorter was set for enriching Y-bearingsperm, ranged from 70 percent in pigs to 86 percent in rabbits.
Dr Ed Fugger and Dr Joseph Schulman, working at the Genetics & IVF Institute inFairfax,Virginia, outside Washington, DC, have successfully applied Dr Johnson’s methodto human sperm.Writing in the journal Human Reproduction in 1993, Johnson, Fugger,Schulman and others reported an average of 82 percent X-bearing sperm and 75 percentY-bearing sperm, depending on which type of sperm the machine was set to sort for. DrSchulman then went on to report the achievement of a pregnancy of the desired femalesex for most couples who were trying for a girl for family reasons or to avoid the risk of agenetic disease such as hemophilia (the gene for which is a recessive one found on theX-chromosome, the second of which in girls will usually be normal and thus stop expression
330 � GETTING PREGNANT
Should feminists be concerned by sex selection?
The enduring value of Dr Shettles’s work on sex selection, demonstrated also bythose who published both confirmatory and contradictory studies after him, is that,at least in Western countries, consistently more people seeking sex-selection wantgirls than want boys.
In Dr Barbara Simcock’s 1985 study in Sydney (see main text), fully 52 of the73 couples wanted a girl, compared with just 21 who sought a boy.
The same evidence of a preference for seeking females has been reported morerecently from Ericsson-associated clinics.
No doubt this preference for girls over boys does not hold true in all parts ofthe world. In India and China, for example, there is ample evidence that sons arefavored over daughters to such an extreme degree that abortion of female fetusesand even female infanticide are practiced.
Not just feminists are appalled by such brutality.Effective sperm selection would at the very least be preferable to abortion and
infanticide—until the social changes come about that might, with time, put an endto what is plainly an extraordinary pressure in these countries to have sons insteadof daughters.
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 330

of the disease). Because of the rather slow nature of the cell-sorting process (each spermhas to be electronically tested, one at a time, and then shunted to one side or the other), Ibelieve this technology is better suited for IVF with ICSI than for IUI, although it willdepend on the relative costs of these procedures. No doubt further developments of thetechnique at the Genetics & IVF Institute will improve its efficiency.
By the mid-1990s therefore, for the first time we had a technology for changing thechance of a wanted girl from one in two to four in five, and for changing the chance of awanted boy from one in two to two in three or better—but at a formidable price in dollarsand with odds that still fall well short of certainty.
To get better odds than this we move to IVF with PGD.
PREIMPLANTATION GENETIC DIAGNOSIS
Before cell-sorting technology was available to improve the chance of achieving femaleembryos, several British families at high risk of having children with hemophilia used IVFand biopsy of resultant embryos to work out which were male and which were female.The rationale was (and is still) that genetic diseases inherited by sex-linked recessive inheri-tance will manifest in boys but not in girls.The reason is that, being recessive, the abnormalgene will not be expressed (and therefore will not cause the disease) if there’s a normalsecond gene (or allele) present among the chromosomes. For such genes on the X-chromo-some, one allele or gene is enough: the Y-chromosome is too small to carry a comple-mentary savior gene.As well as hemophilia, sex-linked genetic diseases include Duchennemuscular dystrophy (a progressive weakness of the muscles) and Tay-Sachs disease (a seriousbrain disorder).
By using the polymerase chain reaction (PCR) to amplify pieces of DNA known tobe unique to the Y-chromosome, researchers led by Dr Alan Handyside at London’sHammersmith Hospital were able by the early 1990s to distinguish male from femaleembryos, and to transfer just those that were female.The alternative for these families wouldhave been to wait until pregnancy was established and then use either high-resolution trans-vaginal ultrasound or conventional karyotyping of cells obtained by chorionic villus sampling(CVS) or amniocentesis to discover the sex of the fetus, aborting it if it were male.
A number of IVF centers now have the capability of performing preimplantation geneticdiagnosis (PGD). Figure 20.2 shows such micromanipulation underway at Sydney IVF. Forchromosomal diagnoses, such as determining sex or discovering trisomies, including Downsyndrome (or trisomy 21), and Klinefelter syndrome (which is 47,XXY) and monosomies suchas Turner syndrome (45,X), FISH, CGH or molecular karyotyping can be used. For moleculardiagnosis of specific abnormal genes, such as the gene for cystic fibrosis,PCR is the method.
An increasing proportion of IVF eggs or embryos are being subjected to biopsy forPGD to exclude aneuploidy (see the Chapter 20 box, IVF-Plus™: Chromosome-checked embryos).For families affected by serious genetic diseases who have other reasons for consideringIVF, the ability to make diagnoses before embryos are transferred is an increasingly impor-tant development.Whether less serious genetic impairments will lead to the use of suchextreme technological intervention only time will tell.Recently, families planning a further
‘DESIGNER BABIES’? HARDLY . . . � 331
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 331

child in circumstances where an earlier child is terribly sick with, typically, a blood diseasefor which a bone marrow transplant has been advised, have considered IVF with PGD toensure that the newborn baby’s cord blood (from which bone marrow stem cells can beisolated) will match that of the older sibling.
Critics describe these situations as slippery slopes into designer embryos.Well, if thereis a slope, I think it’s got hills as well as dales and is not especially slippery: as genetic knowl-edge and methods for diagnosis and possible treatment slowly accumulate, societies willhave more time to debate these issues than prophets of doom would have us believe.
Couples have always had children for mixed reasons, and the love they end up showingfor their children might or might not have been what was on their separate minds whenconception occurred.The important issues are not new for experienced medical profes-sionals.We are not obliged to assist when it is plain that a planned pregnancy is evidentlyand solely a means to someone else’s end. Most requests for our help, be it for preventionof transmission of genetic disease, to achieve a balance of genders in the family, or to raisea new child who at birth unwittingly saves the life of an older sibling, arouse nothing butcompassion.
For certain, though, as sperm-cell sorting, ICSI and PGD raise the value of individualembryos, not only will our expectations of (and our identification with) a single embryogrow,we will want to be more certain than we can yet be that an apparently normal embryothat’s transferred will in fact implant to form an embryo, a fetus and then a baby.
And this means two things. First, we need to be sure that all the chromosomes arenormal, utilizing PGD with molecular karyotyping. Second, once we’ve established thatthe egg’s chromosomes are normal we need to be able to test the cytoplasm of the egg tocheck its metabolic status, to make sure it has the power it needs to propel itself into anormal implantation and gestation.
If an otherwise normal egg’s cytoplasmic metabolism is not up to speed, Dr Cohen’swork with cytoplasmic transfer, described earlier in the chapter, suggests that it might bepossible to repair it.
HOPE, HYPE AND CLONING
Transplant surgeons and their support staff today have the technical ability to graft a donateduterus to a man.Why don’t they do it? The world’s first male pregnancy could follow! Notsexy enough? Or is it too obviously freaky to risk a good professional reputation on?Cloning is more mysterious. It seems more attractive.
I’ll be direct here.There’s probably no better medical reason for cloning a human indi-vidual than there is for a man to bear a baby. (And the reason, such as it is, is that ‘surelyeveryone should have the chance of having his or her own child’!) Not everything in medicinethat can be done, is done. In practice there has to be a good reason to go to the trouble andexpense, especially when a team of skilled people needs to be assembled for the task.
The trouble with cloning is, first, the hype that clings to it.The hype is now such that,like unthinking moths to a flame, the limelight of fame beckons a class of doctor and scientistwhose work might otherwise attract little attention or respect. (More understandable is the
332 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 332

desperation of infertile couples or childless people, who are now beside themselves withhope.) The second problem with cloning is that you need to understand a lot of biologyto appreciate why cloning is never the answer to infertility.
‘Cloning’ entered the language in 1903, since which time the Oxford English Dictionaryrefers to it as reproduction by ‘budding’, splitting off part of what we now know is adiploid, multi-celled organism to form another.The word was first used in botany, inrelation to plants—that is, replicating a plant by taking a cutting.The word diploid is partof the key: it means two of each chromosome in each cell’s nucleus. In other words, higherplants and animals carry, in every cell other than the sex cells (the gametes), one of eachof their two parents’ chromosomes. In contrast, a sperm cell or an egg cell has half thisnumber (they are haploid), so that with fertilization the diploid state is reached again andthe unique new organism as an embryo has the double DNA code it needs to developsecurely, generally masking the few genetic imperfections we all carry on one or otherchromosome.
This process is called sexual reproduction. Forget whether the organisms had sex or not.IVF to a biologist is unequivocally sexual reproduction—even without the sex. Cloning,which involves no sperm, and uses an egg to put a budding nucleus into it, equivalent totaking a cutting, is asexual reproduction, just as practised by amoebas, yeasts and hopeful horti-culturalists.
Writing in the influential US journal Science in June 2000, Canberra cell biologistRobert Blanden and a colleague, Edward Steele, stated: ‘It comes as no surprise to plantbiologists that attempts to clone mammals [let alone people] from single body cells areplagued by high frequencies of developmental abnormalities and lethality.’
In other words, it was for good reason that, a billion years ago, nature took the ex-pensive step of doubling up on the chromosomes, just so that they could swap bits ofthemselves around, randomly recombining, before competing as eggs (and less probably assperm) for the privilege of passing to the next generation.While the eggs await this chancefor life in the next generation, the female body protects them from too much metabolismand cell division.That’s why all the eggs are formed in the fetus and then remain resting inthe ovaries as primordial follicles (see Chapter 3).
Not so for the body’s other cells. Hell-for-leather they divide, their DNA mutates andwears out—and some cells mutate enough to become cancers.And these are the cells thecloning doctors are trying to propagate as new people.
If cloning is a bit of a circus trick—remembering, though, that most circus tricks goright more regularly than cloning yields a healthy-enough offspring—where does the hypefall short of the hopes of the infertile?
The bounds of what IVF can achieve for the infertile lie, first, with sperm. Here hugeinroads have been made with ICSI: if there are even a few living sperm extractable fromthe depths of a testicle, healthy children can follow, as we see in Chapters 10 and 20. It’saging eggs—eggs from older women—that spell the practical limit to IVF treatment today,as we discussed above.
Cloning does not avoid the need for eggs, so it’s no substitute for tired eggs. It’s no curefor the oopause.
‘DESIGNER BABIES’? HARDLY . . . � 333
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 333

Is cloning a substitute for a sperm? Theoretically. But it supposes the woman’s chro-mosomes (in the form of a pronucleus) will be pulled out of her eggs to make way for adouble male set.And all so he can have a baby? It’s hard to imagine many women fallingfor this ruse.
Is it a substitute for a partner? Is this the way for a single woman to have a baby—ababy just like her mum or mom? Well, maybe, but one way or the other a vial of donatedsperm is not hard to come by (Chapter 22), and it’s much safer and cheaper.
Is cloning ethical? If something is stupid enough, as cloning is, it hardly matters if it’sethical or unethical, but the ethical objections to reproductive cloning are comprehensive: onfundamental biological grounds it’s the one technique described in this book that thwartssexual reproduction, a pervasive, hard-won evolutionary development; on consequentialgrounds it’s predicted to cause horrendous birth defects; and on social grounds it’s almostuniversally condemned for its lack of obvious compassionate purpose and its potential forabuse at the hands of the state. (For a discussion of the ethical principles involved in thesesituations (deontological, teleological and utilitarian), see the Chapter 26 box, Ethics: Moralimperatives, outcomes and equity.)
Should doctors like Professors Antinori and Zavos (who achieved notoriety in thepress during 2001 with claims they were to start human cloning, if necessary on an islandin the Mediterranean Sea) carry enough try-hards with them to push their plan to fruitionthey had better have paid careful attention to the forms their patients will need to signto give informed consent. Even the mildest of the abnormalities that most cloned animalsare showing will make for horrific press stories. Meanwhile, whatever happened to thelast guy who said he was going to clone humans—back in the year 2000? Where isDr Richard Seed today? When Antinori and Zavos go to the same place, there will besome disappointed lawyers.
EMBRYONIC STEM CELL RESEARCH
Ironically, a component of the cloning technology that gave rise to Dolly the sheep, and ofwhich I am so critical, could be the basis for the treatment of some difficult childhood andadult diseases, including diabetes and cancer.
Stem cells are ‘primitive’ or undifferentiated cells present in almost every tissue of thebody, capable of (1) continuing to divide (by mitosis) without wearing out the ends of thecell’s chromosomes, and (2) differentiating as required into mature, more differentiated,functional cells, to replace cells lost from tissue by wear and tear.
The most undifferentiated stem cells are found in the embryo, in particular the inner cellmass of the blastocyst.Many scientists would love to research with these cells, but their avail-ability is very restricted—partly because lab conditions for embryo culture need to be excel-lent to obtain the blastocysts from embryos donated for the purpose, and partly because oflimits on permissible embryo research (see Chapter 27).The hope is that these embryonicstem cells will be reliably induced to form more purposeful, differentiated cells that can betransplanted into diseased tissues or organs to replace faulty ones, thus enabling defectivetissues to be repaired.
334 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 334

At Sydney IVF we are working on such stem cells with the Diabetes TransplantationUnit of the Prince of Wales Hospital, Sydney, to develop insulin-producing cells that couldbe used to make up for a lack of them in children and young adults sick from juvenilediabetes, thus avoiding the need for frequent blood sugar measurements and insulin injec-tions through the day and night. Similar strategies have been proposed to treat depletedbone marrow after chemotherapy for cancer, as well as possibly for adult degenerativediseases such as Parkinson’s disease.
Critics of embryo research claim that the same or similar outcomes might be derivedfrom adult stem cells, which can, with some difficulty, be isolated from some tissues, andwhich might be able to be induced to de-differentiate further, then re-educated to developinto newly differentiated cell lines suitable for therapy. However, pursuing one researchavenue in an area that is still so poorly understood without the simultaneous benefit of thecomplementary approach is like trying to walk or run on one leg.To invoke a differentmetaphor, if you are a map-maker surveying a landscape, think of the map you could makeif you climb just one hill to look around at the surrounding valleys and hillocks.Then thinkof how much better a map you can make if you can climb a second hill to examine thesame ground from a different perspective.
The cloning technology that might be invoked involves somatic cell nuclear transfer, orSCNT—the isolation of a partly mature cell from a differentiated tissue somewhere inthe soma, or body, such as a breast cell (in the case of Dolly the cloned sheep) or acumulus or granulosa cell (in the case of Cumulina, the first cloned mouse).The scenarioI can envisage down the track involves, say, an 18-year-old woman, suffering fromdiabetes that requires five injections a day (or possibly recovering from leukemia andrequiring a bone marrow transplant that can’t be found because of tissue incompatibilitiesand likely rejection).
When SCNT becomes reliable and we know how to differentiate her embryonic stemcells, for the treatment of diabetes she would be able to undergo:• A single egg retrieval procedure, perhaps in her natural ovarian cycle;• Recovery of not just an egg (a secondary oocyte) suitable in other circumstances for
fertilization but, at the same time, granulosa cells from the cumulus mass surrounding herrecovered egg (the same cells that in the mouse resulted in Cumulina);
• Somatic cell nuclear transfer, followed by cleavage and formation of a blastocyst without theegg having been fertilized by a sperm;
• Isolation of cells from the inner cell mass, treated to produce embryonic stem cells, andallowing to multiply to a larger number, some of which are stored for future use;
• Programming the ES cells to differentiate into pancreatic islet stem cells, still capableof undergoing cell division, but now just a step away from becoming mature insulin-secreting cells;
• Injecting or otherwise placing the pancreatic cells back into the body, possibly in thepancreas itself, but more likely into the liver or another suitable location more acces-sible than the pancreas;
Implications would include:• Rejection does not occur, because the cells are her own;
‘DESIGNER BABIES’? HARDLY . . . � 335
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 335

• It would be possible to monitor the successful production of insulin as the need forinjections diminishes and then stops;
• Her ES cells could be kept in cryostorage to produce further pancreatic cells for repeattreatments, should they prove to be necessary.
And where is the ethical problem with that?
336 � GETTING PREGNANT
Getting Pregnant - prel, ch1-23 1/7/03 1:49 PM Page 336

section V
getting what youdeserve
pregnant or not, what to expectfrom people around you
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 337

Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 338
This page intentionally left blank

pregnancy
What to do and what toexpect when you are
When that hoped-for moment happens—a pregnancy test is positive, about twoweeks after the assisted conception procedure—the first response is relief. It’s over!The time and effort and money have paid off! Infertility is a memory! But you
soon realize that it’s not all over.There are still uncertainties.Things can still go wrong.Even when things go right (and they do go right more often than not) there are newchallenges.
Here we discuss:• What can go still go wrong?• Who is my doctor now?• What do I discuss with my obstetrician?• Prenatal testing: non-invasive, CVS, amniocentesis;• What will it be like after the delivery?
WHAT CAN GO WRONG?
Bleeding after a confirmed pregnancy might mean a miscarriage or it might mean that anectopic pregnancy is present.But it can also mean nothing at all other than a slight bleed withina normally pregnant uterus as new blood vessels form to support the developing fetus (calledimplantation bleeding, discussed in Chapter 3). If there’s bleeding, contact your gynecologistor your IVF center (if you’ve had assisted conception). Keep away from vigorous activity.Don’t have sex until it settles down.An ultrasound will probably be carried out sooner ratherthan later.
339
24
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 339

Miscarriage
A pregnancy conceived, but lost, can cause more distress than a pregnancy forever unattained.The most common way for a pregnancy to be lost is through a miscarriage, whether obvious(‘clinical’) or not (‘subclinical’, though ‘pre-clinical’ might be a gentler word).A subclinicalmiscarriage is when the pregnancy test is positive but no gestational sac becomes visible on transvaginalultrasound.Bleeding takes place sooner or later and can be heavier than a normal period.You donot need a curette.On the other hand, a clinical miscarriage is said to happen after an ultrasoundscan shows a gestational sac, inside which an embryo may (for a while), or may not, develop. Inthis case a curettage could be needed to empty the uterus and to keep it in best condition foranother pregnancy to be attempted down the track (a curette will be advised if bleeding is heavyand continues, or if a scan shows products of conception persisting inside the uterus).
Sometimes it’s advisable to have a karyotype, or chromosome study, done on the mis-carriage tissue.This can shed light on why the miscarriage happened (the details are inChapter 8). If this is not a priority,many women will prefer a natural wait-and-see approachto the miscarriage rather than having it curetted out so quickly after diagnosis that there isno time to come to terms with the impending loss.
The risk of miscarriage is related both to the woman’s age (see Table 8.1) and to the abnormalreproductive circumstances of the conception (see the box, Miscarriages and infertility).
340� GETTING PREGNANT
Miscarriages and infertility
With engaging candour—and from an era (1952) that preceded the developmentof most effective methods for treating infertility—Mr S.Bender, a surgeon and gyne-cologist then at the University of Liverpool, showed for the first time that the riskof miscarriage among infertile women is high.
Of 313 first pregnancies among women with primary infertility (they had notbeen pregnant before), 19.3 percent miscarried.This compares with a miscarriagerisk of 12 percent to 15 percent among women with no infertility. Miscarriages arethus more common after infertility than they are among pregnancies in women whohave no trouble getting pregnant.
In an article I published in the American Journal of Obstetrics and Gynecology in 1982(see the bibliography in Appendix 3 for Chapters 8 and 9), I analyzed most ofpublished articles on infertility and its treatment to that time. It became clear to methat both the reproductive abnormality behind the infertility and the new variablesintroduced by treatment could be responsible for this increase.
Whereas the karyotype, or chromosome composition,of miscarriages that happenin the first three months (which is when most take place) is abnormal in 65 percentof cases or more (see Chapter 9 for the details), it’s more likely to be normal in thecircumstances of infertility and its treatment. In other words, there are reasons ontop of the usual chromosomal mistakes at conception that can mar the environmentfor early embryos whenever fertility itself is reduced.
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 340

Ectopic pregnancy
An ectopic pregnancy is when the pregnancy develops in the fallopian tube instead of theuterus (explained in Chapter 14).This can happen after GIFT or even after IVF (eventhough embryos are usually transferred to the uterus after IVF, they can migrate into thetube). An ectopic pregnancy cannot keep developing: sooner or later internal bleedingoccurs. Its treatment is either by injections of the cytotoxic drug methotrexate or by an oper-ation (a laparoscopy or a laparotomy), at which the tube will be opened for the pregnancy tobe removed or, if damage is more substantial, the tube itself is removed.
Hydatidiform mole
Rarest of all the pregnancies that go wrong—assisted conception or not—are hydatidiformmoles, abnormal from conception, usually without an embryo or fetus, and resembling abunch of grapes when eventually expelled.
The word ‘hydatid’ means a little sac or fluid-filled vesicle. A ‘mole’ in medicine canmean any blemish or faulty structure that’s distinct from the normal tissue or organsurrounding it.The details are in the box, Molar pregnancy.
In my survey of infertility treatments in 1982, just three seemed to bring the riskof miscarriage back to normal: ovulation induction with bromocriptine for amenorrheadue to raised prolactin levels (see Chapter 11); operation for endometriosis (see Chapter16); and donor insemination for extremely low or zero sperm counts (see Chapter 21).(In each of these conditions, should pregnancy have occurred naturally, the risk ofmiscarriage was considerably increased.)
Most forms of assisted conception produce a rise in the risk of miscarriage overthat expected in normal women.The risk of miscarriage after IVF (or GIFT) hasbeen considerably decreased by abandoning the use of clomiphene (which can havedisadvantageous effects on the endometrium and hence on implantation of the embryo;see Chapter 11) in the superovulation regimen for stimulating the ovaries.
As it turns out,measuring the frequency of miscarriages—estimating the miscar-riage rate—can be a much more sensitive way of gauging the correctness of a partic-ular infertility treatment than measuring the pregnancy rate, or even the take-home babyrate.The reason is that there are too many variables that affect pregnancy rates andoverall take-home baby rates which have nothing to do with the treatment itself—especially the duration of the infertility and the age of the woman.
Infertility clinics and assisted conception programs can present good figuresby selecting carefully the patients whose results they report, but they cannot easilydo the same when reporting miscarriages as a proportion of the pregnanciesachieved.
The usefulness of using a low miscarriage rate as a signpost for good medicalpractice is not as well appreciated as it should be.
PREGNANCY � 341
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 341

WHO’S MY DOCTOR?
Let’s assume your pregnancy avoids these last pitfalls. If you’ve been having assisted concep-tion,you will have become used to the rather intense medical attention of the stimulation andthe egg pick-up.There’s something of a letdown for the next two weeks while waiting for aperiod or a pregnancy test. If the pregnancy test is positive it’s still another two weeks beforethe transvaginal ultrasound can show if the pregnancy is in the right place (the uterus) and ishealthy (of normal size for dates and with a beating fetal heart). During this time you mightsense some loneliness: you’re not ready yet to see an obstetrician for your pregnancy care; yousense your infertility doctor has done his or her job. But be reassured that, in fact, IVF clinicsand infertility nurses love hearing from their pregnant people—and your infertility doctorcertainly will be available for advice and to manage things if they go wrong. (Naturally youwon’t be bothered by these considerations if your infertility doctor is also your obstetrician.)
But only time will tell if all is well: no-one can further influence events to any extent. Inthe great majority of cases the die has been cast at conception (there’s either a normal embryo
Molar pregnancy
Hydatidiform moles are benign tumors of the placenta (the afterbirth) that look likebunches of grapes.They can be partial or complete (and for more on their interest-ing genetic causes see hydatidiform mole in the Glossary).
The grape-like sacs represent swollen tongues of trophoblast, or placental tissue,which distend because there is no embryo or fetus present to put embryonic bloodvessels into the trophoblast and, incidentally, to carry away the fluid the trophoblastabsorbs, sponge-like, from the mother’s circulation.
Nowadays most hydatidiform moles are easily diagnosed early in pregnancy ontransvaginal ultrasound,which confers a prolific pattern of echoes from the multiplefluid-filled sacs that compose the mole.
Hydatidiform moles occur naturally in fewer than one in 1200 pregnanciesamong European races; they can be much more frequent among some Asian popu-lations (the frequency in rural Indonesia is said to be one in a hundred pregnancies).In the USA, the incidence among African Americans is about half that in EuropeanAmericans.
The risk increases with the age of the woman (especially after 40).There arereports of hydatidiform moles after infertility and its treatment, including assistedinsemination, but it seems doubtful that there is any special association with infer-tility or assisted conception that is independent of the woman’s age.
Indeed the risk after IVF seems to be extraordinarily low, with fewer than fivereported despite over 100 000 IVF births to date.
342� GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 342

or not) and only time will reveal which is which. Nothing will rescue it if it’s a ‘blightedovum’.Normal embryos are generally built to survive, but be sensible.Don’t run 10 miles orgo scuba diving. But don’t encase yourself in cotton wool either. Sex is fine unless there’svaginal bleeding or painful spasms from the uterus; in these cases there is a threatened mis-carriage and sex with penetration or with orgasm may disturb the pregnancy further.
When should you get into touch with an obstetrician?
The temptation can be to see one as soon as possible. By all means phone as soon as seemssensible for an appointment eight to 10 weeks from the date of the last period—manyobstetricians are hard to get an appointment with at short notice. But it’s often better notto transfer to the care of an obstetrician until the pregnancy has been confirmed as healthy.
Instead, stay under the care of the gynecologist who assisted with the conception forthe time being. He or she may not be doing anything special, but knows what’s happenedso far and, as I said before, will be available if things don’t go right.
WHAT DO I DISCUSS WITH MY OBSTETRICIAN
Your pregnancy, if you’ve had assisted conception, is not the same as everyone else’s. Don’tlet anyone tell you anything different. For a start, you will probably be more used to sharingpersonal matters with your partner than with friends and relations (see Chapter 25). Forboth of you, involving your friends, relations and workmates in the pregnancy’s progress willprobably be less natural than it is for couples who got pregnant the straightforward way.
Second, you are going to be more anxious about your pregnancy.You already knowhow unkind nature can be.This feeling will diminish with time, and may disappear, butusually not until the baby’s born.
Third, your pregnancy could be multiple, with extra risks of prematurity. After IVF,even for single fetuses, there’s an extra risk of premature labor, small-for-dates gestation and still-birth (see the box, Birth defects and childhood development).There’s a small but real risk ofcervical incompetence—a symptomless weakening of the cervix (see Chapter 9)—that allowsthe pregnancy membranes to bulge through and then to break, almost always resulting inthe loss of the pregnancy (this weakness could be related to the large number of gynecol-ogical procedures that have at various times been done for most people who’ve taken along time to get pregnant).
What special precautions should my obstetrician take?
At Sydney IVF we recommend that all women who are pregnant after assisted concep-tion—whether the pregnancy is single or multiple (see further on)—have vaginal exami-nations between the twelfth and twenty-eighth weeks of pregnancy to detect cervicalincompetence early, or straight away if back pain or vaginal discharge occurs. If cervical incom-petence is detected (see earlier) then a protective stitch placed in the cervix is essential treat-ment (see Chapter 9).
PREGNANCY � 343
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 343

344� GETTING PREGNANT
Birth defects and childhood development
Birth defects . . .
In the broad scheme of things, IVF is safe—or at least it is approximately as safe asnature is.And if there is a higher risk of pregnancy going wrong after infertility, it isuncommon that this would be high enough to lead many people not to try over-coming the odds.
Birth abnormalities overall are about as frequent as occurs naturally according tothe great majority of studies. But the natural risk varies in different circumstances.
If you look carefully enough—if you look at birth defect incidences in enoughdifferent kinds of pregnancy,or in mothers of different ages, or among multiple preg-nancies, or in people with infertility conceiving naturally—differences that arerelatively small in general terms can in fact be different enough to become apparenteventually.
It might take even longer for certain specific but rare abnormalities to manifesta high relative risk, attributable perhaps to a special infertility circumstance or treat-ment technique.
It would be surprising to most reproductive biologists if there were not a slightincrease in risk of pregnancy going wrong after such a medically intrusive concep-tion in such difficult natural circumstances. Indeed, in the 1980s,many were surprisedthat there was not a large increase in birth abnormalities.
These birth abnormalities:• Might have happened because of reasons related to the reason for the infertility;• Might have happened because the pregnancy was multiple;• Might have happened because of the IVF or ICSI or PGD; or• Might have happened anyway to anyone, for reasons not understood.In most cases we cannot pin it down.But we are starting to get an idea of the relativestrength of the different possible contributions.
In 1991 and 1992, before IVF became tremendously popular, studies on birthoutcomes in infertility, either untreated or treated by methods other than IVF,were reported from many countries, including the USA, Britain, Sweden andIndia.
Generally these studies showed that among non-multiple births there was adoubling in low birthweight babies, principally from prematurity but also fromintrauterine growth restriction. This was in babies born to infertile couples ascompared with births to mothers in control groups with comparable age and numberof previous births.There was also a much higher risk of intrauterine fetal death andstillbirth.
Not surprisingly there was a much higher rate of birth by cesarean section amongpregnant, previously infertile women.
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 344

Similar findings were published in 2001 for women with unexplained infertil-ity in a series from the University of Aberdeen, after taking into account age,numberof prior births and type of treatment.
Meanwhile it is well known that the risks of prematurity, intrauterine growthrestriction and stillbirth, as well as birth abnormalities, are greatly increased amongtwin and higher multiple births.
As you would expect, studies on birth outcomes after IVF have shown thatthe same is true of twin and multiple births occurring from assisted conception.Although most IVF-related twin births are from more than one embryo implant-ing (non-identical twinning), there is also an increased risk of identical twinning,when an embryo divides into two, a form of twinning at even greater risk ofcomplications.
Therefore any study that looks at birth outcomes with a view to ascribing badpregnancy outcomes or birth defects to the IVF process itself needs (1) to take accountof the bad outcomes due to multiple pregnancy (while this is a problem, it is a differ-ent issue here) and (2) to take account of the bad outcomes due to whatever hascaused the infertility (which will be there whatever way the pregnancy takes place).
In the Chapter 10 box, From father to son, I deal with some of the specific, male-related conditions as well as chromosome abnormalities that can be passed from aninfertile or sterile man to his male offspring through ICSI.These abnormalities caninclude Turner syndrome and Klinefelter syndrome.
In most cases these specific abnormalities after ICSI have a genetic explanation(and would presumably occur naturally if natural conception were possible), but itis plausible that Turner syndrome might result occasionally from the ICSI proce-dure itself (for more on this, see the Chapter 23 box, Possible hazards with cytoplas-mic transfer).
During 2001–2002, studies from Western Australia and Sweden, reported in theprestigious journals The New England Journal of Medicine and The Lancet, claimedsubstantial increases in birth defects and neurological complications, including cerebralpalsy, among IVF and especially ICSI children.
Tellingly, these studies did not have matched control groups. Instead, they usedstatistical techniques to correct for the higher average age and fewer previous childrenamong the IVF/ICSI births.They also could not distinguish the effects of the labprocedures from the lingering effects of infertility. Furthermore, they both foundthat there was little or no effect of IVF or ICSI apparent among multiple births—meaning that the harm done by a multiple pregnancy was probably overwhelming,whether conception was natural or with IVF, compared with the other effects beingresearched.
The consensus among pediatricians is that avoiding multiple births is the singlegreatest contribution that can be made to reducing bad birth outcomes followingIVF. For more on how this might be done, see the box, Easy does it! Elective singleembryo transfer, in Appendix 2.
PREGNANCY � 345
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 345

Even if there’s no increased risk of things going wrong, the pregnancy may be practi-cally irreplaceable, so the hazard of pregnancy loss is by its nature a greater one than forsomeone who has no trouble getting pregnant.An ‘at risk’ approach to managing the preg-nancy and the labor is appropriate for your obstetrician.
Finally, nature’s not perfect and nor is medical care.The most painstaking attentioncannot stop the unexpected from happening and no amount of watchfulness will mean aperfect outcome. But everyone should do their best, from the moment you first contact aninfertility specialist or IVF center to when your baby goes home with you. If you thinkthis isn’t happening, start asking questions.
If you had the option of equally easily getting pregnant naturally or with IVF,any increase, or any uncertainty, might well sway you against IVF. But if there is agood reason for IVF (maybe you just have not been able to conceive naturally, oryou want to have an IVF pregnancy to avoid a genetic condition for which other-wise you might have an abortion, or you believe strongly enough that your familyneeds a further child of a different sex) then you need to accept the uncertainty andpossible increased risk.
Put simply, you should only have IVF or ICSI or PGD if you have a good reasonfor it.
Birth defects do occur after IVF. In some cases this will be because you can’t getpregnant quickly enough (or at all) in any other acceptable way. In some cases, suchas when you have PGD, this will be because you are having these procedures toreduce the risk of a particular birth defect for which you happen to be at high risk.
. . . and childhood development
Although concerns have also been expressed about childhood development afterIVF and ICSI, the choice of control groups has also been to blame in at least onestudy published prominently.
This study, carried out in Sydney and also published in The Lancet, claimedlanguage-based delays in very young infants after ICSI.The patients having ICSIwere from a more culturally diverse group than the control mothers,whose familieshad the advantage of living in one of the wealthiest parts of Sydney. Larger studieshave contradicted these findings.
More typical is the finding of high average achievement, with some studiesreporting significantly increased psychomotor development and mental develop-ment scores—although this also can probably be ascribed to external factors, in theform of the exceptional motivation of their parents.
Again, the greatest harm in school performance will occur among very prema-ture children.And the best way of reducing the risk of such prematurity is to reducethe risk of twin pregnancy during your infertility treatment.
346 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 346

Should we have antenatal diagnostic tests done?
There’s no universally correct answer, because ‘non-invasive tests’ (those that carry no riskfor the fetus) generally are not perfectly reliable,whereas the invasive tests that confer morecertainty (at least for genetic diseases) inevitably carry a small risk to the fetus from thesampling procedure.Recent history has shown that very many women are prepared to takea small risk (it is generally less than 1 percent) to achieve a measure of certainty that theirbaby will be normal, and will prefer to have an abortion if the fetus is abnormal.
Whether or not abortion is a morally acceptable option for you, if there is to be a babyborn with an abnormality there can be advantages in preparing yourself, your friends andyour relatives in advance.
Meanwhile it is important to remember that no single test can look for every possiblething that might be wrong.
Non-invasive testing: Blood tests and ultrasounds
Screening tests to estimate the risk of Down syndrome can be done by triple test and anultrasound for nuchal translucency at about nine weeks from the start of the last period. Spinabifida, a serious congenital abnormality of the spinal cord, can be detected by blood testsfor alpha fetoprotein. Major malformations can be seen on ultrasound after about 12 weeks.A formal malformation scan can be done on request at 19 weeks (in time in Australia foran induced abortion still to be legal).
Non-invasive testing for Down syndrome and other potential birth defects caused byan abnormal number of chromosomes is a rapidly advancing field—attractive because anyrisk to the fetus being tested is removed, and discomfort to the mother is minimized. (Fordetails on how these tests are advancing, see the box, Non-invasive testing for birth defects.)Because there’s no risk to the fetus in performing these tests, there’s also no reason (otherthan cost) not to consider having them done.
But for certainty, it’s still necessary to directly obtain a sample from the fetus, the placentaor the amniotic fluid in the gestational sac.
Chorionic villus sampling and amniocentesis
CVS involves obtaining a small sample of placenta (or chorionic villi) at about nine weeks’pregnancy, using ultrasound for guidance.The sample is obtained by inserting a catheterthrough the cervix into the layer between the membranes and the lining of the uterus tothe region of the placenta, then sucking out a small piece of placental tissue, or it can bedone with a needle passed through the abdomen and through the wall of the uterus directlyinto the placenta.My (very experienced) ultrasonologist colleagues tell me that there is lessdisturbance of the gestational sac, and hence a lower risk of miscarriage, with the needle.
Amniocentesis is done a little later in pregnancy, generally at about 14 to 16 weeks, andinvolves passing the needle through the abdomen and through the wall of the uterus intothe fluid surrounding the baby, avoiding the placenta, and sampling the cells floating about
PREGNANCY � 347
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 347

348 � GETTING PREGNANT
Non-invasive testing for birth defects
Today . . .
Today, non-invasive testing has two components.The first is the triple test,a blood test that measures three substances (sometimes more,
sometimes less) that change during pregnancy according to how many days have passedsince conception,but which,when the fetus is abnormal, tend to adopt higher or lower-than-normal profiles (or trajectories). Because the change from one week to the nextmeans a great deal in terms of whether the levels are normal or abnormal,accurate datingof the pregnancy is essential and a computer is used to calculate the risk of a defect.
The second component of early pregnancy screening is an ultrasound, to bothconfirm the gestational age of the fetus (to interpret the components of the tripletest) and measure the thickness (nuchal translucency) of the skin lying over the lowerpart of the fetus’s neck, as it is thicker here in very many cases of fetal abnormality.
Even taken together, however, the accuracy of these tests is not more than about80 percent.False positive tests (incorrectly predicting an abnormality) and false negative tests(incorrectly interpreting a birth defect as normal) are possible, so these tests do not todayreplace CVS and amniocentesis, followed by specific genetic testing such as a karyotype.
. . . and tomorrow
Tomorrow promises more.It seems that all fetuses, normal and abnormal, leak some of their cells and their
molecules into their mother’s circulation through the placenta. Just how long thesecells or these molecules stay in the mother’s circulation varies a great deal, but it canbe long enough for them to be detected using very sensitive methods of measurement.
Although still in research stages, machines called flow cytometers can already sortthrough samples of the mother’s blood to detect and isolate a few red or white bloodcells that have come from the fetus.Unlike the mother’s red blood cells, red cells orig-inating in the fetus contain a nucleus, so they are potentially very distinctive and useful.
These red cells have been used to determine the baby’s blood group, importantin cases of fetal anemia due to incompatibility with the mother’s blood group.Theyare also able to be studied using DNA-testing techniques such as PCR,which enablesall sorts of genetic conditions to be detected without having to obtain a sampledirectly from the fetus, the placenta or the gestational sac.
This raises the problem, which remains to be solved, that some cells from aprevious pregnancy might still be able to be isolated from the maternal blood duringa later pregnancy, perhaps even years later.
Even more exciting,perhaps, is the isolation and identification of individual placen-tal cells from the cervix—a test that could be as simple as having a PAP smear done.
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 348

in the amniotic fluid, cells that come from the skin, the mouth and the digestive tract ofthe fetus.
CVS has about a 1 percent to 2 percent chance of causing a miscarriage; the risk witha carefully directed amniocentesis, which avoids the placenta, is less, but the pregnancy ismore advanced and therefore the emotional trauma of terminating it, if it’s abnormal,is greater.Whether you have a CVS or an amniocentesis, the procedure should be done bya doctor who has had a lot of experience in performing them.
Twins or triplets can often be tested separately, but deciding what to do should one benormal and the other abnormal is an unenviable dilemma:once they were either all abortedor all delivered.Today there is a procedure called selective reduction available, in which justthe abnormal fetus is killed, or terminated, and (if there are no complications) the preg-nancy continues. As with abortion generally, not all women will regard this as a morallyacceptable alternative, but experience has shown that many women do choose it.
AFTER THE DELIVERY
The baby is born alive and she or he is well. Is this when the fun starts? Maybe! Certainlylife’s not the same, especially with twins or triplets! Babies are demanding and the changesto your life are just beginning. Not everyone adjusts readily. If you and your husband areolder, it can be harder to accommodate the changes, especially after years of being togetherwithout children.Those who cope best are those who share their feelings and anxietieswith their partner, their health professionals and their friends. Many IVF mothers havelearned to organize their life to cope with repeated cycles of assisted conception; whilethey might be well prepared in lots of organized ways, they may be less so when it comesto dealing with the degree of disorganization that a baby inevitably produces.
One important thing is to keep in touch—with each other and with those who helpedyou—and be easy on the infertile couples you’ve got to know but who haven’t made it yet.
PREGNANCY � 349
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 349

relief from suffering
Getting good counseling
Infertility, its investigation and its treatment are a rough ride. .Optimism takes turns with despair.The treadmill is worse if assisted conception
programs have been started,with their expensive promises and irregular, sometimes spec-tacular (sometimes multiple) successes.
Nothing disappoints the way a period does.Here we will look at:
• Your family and friends;• The threat to personal power;• The different effects on women and men;• Saying good-bye to privacy;• How to live for the present; and• Champagne and candles.Suffering comes not just from your childlessness; it threatens from every corner of yourrelationships with family, friends and acquaintances. It can come from your treatment despiteour best intentions.
On the other hand, relief from your suffering can come from changes, from opportu-nities and from luck other than pregnancy.With advice and help your suffering can becontained and in time displaced by newer challenges and achievements.
FAMILY AND FRIENDS
Infertility, as it develops, is profoundly isolating. In the beginning, as you don’t get pregnantas quickly as you expect, you might decide not to tell anyone outside the relationship.Youand your partner might even not reach the same conclusion about fertility at the same time.
350
25
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 350

Then, as month follows month, and as ovulation and menstruation follow each otheremptily, you cling together in mutual helplessness, often without seeking the support ofthose you’d normally confide in on less private matters—your workmates, your friends andyour less immediate family.Yet it’s a time when most couples’ relationships strengthen anddeep mutual commitment and empathy grow. I’ve been impressed—considering the levelof stress involved—by how few infertile marriages come unstuck, though undoubtedlysome do.
You will have debated whom to tell. Sex generally—and not getting pregnant in partic-ular—is such a personal and private matter between the two of you that it might seem toopainful to tell others.As time goes by, your sisters and friends conceive,but it gets harder andharder to share their joy. As their babies are born you might avoid family get-togethersand weekend barbecues with your friends, then chide yourself for being so upset when,youtell yourself, you should be happy for them.The hardest times for you will probably be whenclose friends announce news of their pregnancy, then visiting the hospital after their baby’sbirth, attending the religious ceremonies, and so on; there are surely other examples you cantell me about . . .
Before awareness of your infertility reaches friends and relations, their remarks can behurtful.You might be accused of being selfish, of not sharing your lives with children; ofbeing self-indulgent and antisocial.You’re thought to be too busy having a more privatecultural and social time,building a big house, taking exotic cruises and vacations.You’d swapthem all.
LOSS OF PERSONAL POWER
It’s common to question your own feelings about your sexuality.You may feel that you’renot a whole woman.You may feel angry with your body,which doesn’t seem to do anythingright.You might imagine a mystical but piercing punishment for a past abortion or a pastchild given up for adoption,or punishment for having intentionally put off having childrento develop a career.This could be the time when you (or your partner) confess to a pastindiscretion (or two), adding a new twist to the suffering.Our minds can function in strangeways and sometimes a foreign, illogical thought about ourselves lodges there and refuses toleave, hurting us when we are at our most depressed and vulnerable.You might sometimesfeel you are going mad: but such feelings are normal and counseling can help. Once suchbogus imaginings are out in the open—in the safety of a counseling session with a trueprofessional—they have less power over you.
There’s often a feeling of lack of control.With efficient contraception nowadays, havingchildren, for so many people, seems such a careful and precise decision. So much care istaken with not getting pregnant that no-one anticipates not being able to get pregnant.When infertility dawns it’s a devastating shock.Anger that the ability to have children hasbeen taken away can be overwhelming, sometimes frightening.
It seems that everywhere you go you’re surrounded by pregnant women or newmothers. Feelings of anger and unfairness overwhelm you. Other parents seem so callous,unsuited to the role, undeserving.The way they carelessly punish their child.You would
RELIEF FROM SUFFERING � 351
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 351

never do it. If only someone would give you a baby.You may feel like taking one.Two weeks of every four is spent in suspenseful hope. Nature makes most people feel
awful just before and during a menstrual period—the same bloody period that’s remind-ing you that nothing’s solved. It’s a double whammy, a double kick in the teeth. Out comethe cigarettes maybe, the cigarettes you promise you’ll toss out the second there’s a preg-nancy.Or,more positively, you might say to yourself,‘I must stay on an even keel, so I won’tbe disappointed if I’m not pregnant . . . if I remain positive it WILL happen’.
WOMEN AND MEN
Women and men do generally differ in the way they respond to the strain of infertility.There’s nothing too remarkable about being an exception to these generalizations, and weshouldn’t make too much of generalizations, but, in general . . .
Women are more likely to want to talk openly about their feelings.And, for women,so much more self-image is bound into the traditional role of bearing and nurturingchildren.Women are more likely to cry.Men have more opportunities to let off steam phys-ically and mentally, by playing sport, by aggressive pursuit of business. More of their goalsseem achievable.Talking a lot about the feelings infertility brings seems a waste of time formen, because it doesn’t change the situation.
Dr Ellen Freeman and her colleagues from the University of Pennsylvania evaluated200 infertile couples.They reported that more than 50 percent of infertile women regardinfertility to be the most upsetting experience of their lives, causing them at least as muchsuffering as divorce or the death of a close friend or family member. In contrast, the stressof infertility, or the suffering it causes,was rated this highly by just 15 percent of men.Giventhat so many couples experience it, infertility—its threat to reproductive choice and repro-ductive future—is probably the major cause of ‘psychological morbidity’ (as the socialscientists would call it), or suffering (as we’ll call it), among women in our community, anda lesser but still important one among men.
A destructive pattern can develop. As the realization of infertility sets in, as a coupleyou talk openly and understand and accept each other’s feelings.But as time goes by, anger,depression and guilt tend to take over.You, as husband,might grow tired of trying to supportand console your wife; you might withdraw, feeling the situation is out of your control;there’s helplessness and frustration.You, as wife, might be bitter and resentful, especially ofyour husband’s apparent other interests and protection from suffering. Before the fightingstarts is an important time to seek help and fresh understanding through counseling.Do consider it. Don’t be alone unnecessarily.
If you broke your leg you’d use a plaster cast, wouldn’t you? If your mind or your rela-tionship is breaking apart, let professional counseling help you keep it together.
Women bear the brunt of tests and treatment, even when a low sperm count seems tobe the reason.The subject of donor insemination might enter the conversation (its implica-tions are discussed in Chapter 22). It might have been brought up before, only to bedismissed, but it resurfaces. It might have been resisted in favor of complex TESE and ICSIprocedures (discussed in Chapters 10 and 20). Still the subject comes up again: it’s at this
352 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 352

time that the male partner’s feelings of inadequacy may first be thoroughly brought home—often acutely. Up to this point, many men will have escaped the full impact of infertility’spower to blame—consciously or unconsciously deflecting it, partly to their partner, partlyby replacing it with other achievements.Not all marriages survive the realignment of powerthat can occur at this point.
GOOD-BYE PRIVACY
The medical world intrudes.We met this phenomenon—this series of phenomena—explic-itly in Chapter 19. Sex is no longer a private matter. Everyone seems to get involved in it.How frequently? How frequent is frequent? Just for the heck of it—fending off embarass-ment—you throw in a few extra intercourse ticks on the temperature chart.Your husband’saffected by it too.Even masturbation is no longer private (see the box,Not for sensitive souls:Pushed to masturbate). Friends and family believe they have a duty to make suggestions andgive advice. In Chapter 19 we dismissed the notion that you can have sex too often; wedismissed the notion that it matters a scrap how you have it; we dismissed the notion thatorgasm for women is essential for conceiving. But by now, more often than not, sex is ashared chore.
RELIEF FROM SUFFERING � 353
Not for sensitive souls: Pushed to masturbate
Dr Aline Zoldbrod painted a piquant scene when she spoke in Sydney in 1993 atthe 12th annual meeting of the Fertility Society of Australia on the subject ‘Men,Women and Infertility’.
The couple had reached the infertility clinic,where the woman was greeted witheffusive salutations: ‘How are you? How are you bearing up? The blood tests havecome through very well, and you’ll be pleased that the ultrasound’s showing awonderful number of follicles. Please sit down and make yourself comfortable, weknow you’re having such a difficult time.We won’t keep you a minute.’
To the husband: ‘Here’s your container for the sperm sample.The toilet’s overthere.’
Exaggerated maybe,but not too foreign! Ejaculation can be easier said than done.Some disheveled magazines are not always the answer, especially when a need
for a (groan) second sample—already-collected eggs patiently waiting in the IVFlaboratory—follows hard or not so hard on the heels of the first. (Viagra canhelp.)
At Sydney IVF, as well as (of course) pristine, discreet cultural material in theprivate sperm-collecting rooms, we provide beer, whisky and wine, so as at least totake away some of the angst, and to dissolve some of the awesome sense of duty!
(Some men stay quite a while.)
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 353

You might start avoiding sex because it’s a reminder of your suffering.What’s the point ofit if you can’t get pregnant? Men can resent having to perform on demand at the ‘right time ofthe month’,with a partner who’s past enjoying it and just wants it to be over.Why are you takingso long? It’s depressing,with seemingly no way out.But there are things you can do to help.
LIVING FOR THE PRESENT
Use time between IVF cycles to strengthen your relationship.Make the most of the resourcesyou have. It may be cold comfort, but you are in a better position to do things sponta-neously than couples bound down with kids are.You do have more money to spend thancouples with children have—or than you’ll have when you’ve got them. It is interesting tofollow the theatre, to see new movies, to discover inexpensive restaurants, to get to knowwines and art, to go away for weekends.
Plan your life. Decide ahead which months will be set aside for assisted conception orinfertility treatment, which months for pleasure.With a plan of action that stretches formonths ahead you’re less likely to feel the bumps, month by disappointing month. Keepup the planning ahead, so if it’s disturbed by a pregnancy—well, that’s life!
Meanwhile consider plotting together. Defeat the calendar if need be, and schemetogether to avoid particularly painful family reunions. Everyone’s different, but conjointscheming is a positive way you can bolster your relationship.At times it will have a touch ofspice,of naughtiness, even humor! (For one elaboration, see the box,Champagne and candles.)
Remember,you’re not alone.Ten percent to 15 percent of couples take longer to achievea pregnancy than they think it should take: your neighbor, your boss, your colleague.Sometimes when you share your diagnosis you find others in similar situations—their closetsopen; their children turn out to be adopted; their children turn out to have come from donorinsemination.There’ll be couples who’ve been trying longer than you have.There are supportgroups formed by infertile couples and they can be a godsend.They can help the lonelinessand strike a note of fun.They stop you protecting yourself against some realities that willotherwise foment and later catch up with you. Many of the larger ones, such as Access inAustralia, and Resolve in the USA,publish useful and entertaining newsletters—a minimumlevel of involvement that you can turn on and off just by picking up the newsletter to browse.
Choose your local ‘consumer group’ carefully, though. Some smaller ones will havemoved from the common experience of infertility to the common experience of children.It’s human nature to parade your baby when it’s taken so long. (The maternity gear peoplewear can get a bit outrageous.)
Allow time for nurturing yourselves—time that’s not work, time that’s not focused onfertility.Listen to a relaxation tape, go to aerobics or yoga, take a walk.When you’re depressedthese actions will seem a chore, but good comes from them, so be firm with yourself.Don’tvolunteer to take on additional commitments with work or family while you are havingIVF, or at least during the months you’ve got IVF scheduled.You need time to cope withit properly, even though modern IVF centers, for the most part,will fit in with your workingday better than you might think.
Lean on your counselor, your nurse, your doctor. Don’t ever be afraid of asking
354 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 354

questions. (There’s more about your doctor in Chapter 26.) When all seems overwhelm-ing, remember the most potent suffering comes when you’re thinking about a childlessfuture. If you’re not successfully living for the present make some future plans. Recall howyou got on top of it before, how you successfully fought off those feelings last time.
Allow your partner to grieve the infertility in his or her own way. Don’t expect thesame feelings you have.Do take advantage of quiet times to communicate—but not alwaysabout infertility.A walk around the neighborhood together can, at a moment’s notice, bebetter than stewing and getting testy at home, even if it’s raining.
When a quarrel’s substantial, abstinence will make the heart fonder.Nature’s libidinoushelp will sooner or later be on the way! Keep an important fact in focus: fertile marriagesfail more often than infertile ones. For most couples, the shared experience of infertilityhas the power to bring you closer together than having children does.
Many of the ideas for this chapter, and their expression, came from Kerrie McGowan, infertilitycounselor at Royal Prince Alfred Hospital and Sydney IVF during the 1990s.
Champagne and candles
Among the myths dispelled in Chapter 19 is the one that a small amount of alcoholmight be harmful to getting pregnant.
Wine contains many natural antioxidants. People take the antioxidant vitaminsA, C and E to try to improve fertility, especially sperm counts. All the medicalevidence is showing that a sensible amount of wine—which includes enough tomake you feel good—is conducive to good health.
Never drink so much that it leaves a hangover, but a glass or two of wine cando wonders at midcycle. If having sex ‘at the right time’ has become a strain—partof the suffering instead of part of the solution—consider some private schemingbased on knowing early in the day when there’s to be an ovulation (with the urinaryLH testing we talk about in Chapter 19).
For a start, LH testing can give you both the confidence to not have sex moreoften than you both feel like, before and after ovulation.
The only cooperation you need for this plan to work is that on just one nightin the month you’re both to agree that there’s no going out with the boys or thegirls, there are to be no work-related dinners you’re not both at, and no-one’s tobring work home … and that it may be at rather short notice.
Then, whether it’s to be champagne, candles and your favorite food at home, oran intimate restaurant that’s on your short-list and where you’ve had no problemgetting a last-moment booking at mid-week, you can both do much to revitalizenumbed sexual appetites!
You’ve taken control.You’re having fun.Neither of you can do more than you’redoing.And neither of you need do more.
RELIEF FROM SUFFERING � 355
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 355

your doctor’s duties
What your doctor shouldbe doing to help you
Adoctor has a duty to do his or her best for patients—for an infertile couple—who askfor help.The General Medical Council in Britain, for instance, insists that a patienthas to be able to expect this of a doctor who’s consulted for any medical reason. In
responding to this obligation, doctors are accountable to their patients, to their peers andto the general community.
In this chapter we cover:• Moral dilemmas and ethical conflicts;• Moral imperatives, outcomes and equity (a framework for ethics);• Informed consent;• Responsibility in infertility research;• Ethical principles in practice (compassion, duties and rights, etc.);• Autonomy, professionalism, paternalism;• Ethics and ethics committees;• The Helsinki Declaration on the rights of patients;• From mercy to empathy;• Threatened values; and• Moral plurality versus Brave New Canada.
MORAL DILEMMAS AND ETHICAL CONFLICTS
In acknowledging a duty of care, a doctor is obliged to put the patient’s or the couple’sinterests ahead of other priorities, such as administration, profit or research.Where thismight not always be completely practicable, the doctor should tell the patient or couple
356
26
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 356

about the particular conflict of interest—and the couple should have the opportunity ofconsulting another doctor. For example, doctors who have administrative roles in publichospitals, if they also see patients professionally, have a special duty to make sure that theirpatients are aware of constraints on resources affecting what treatment they can offer, thatthey are accountable to managers as well as to their patients.
To some extent these conflicts affect the way every doctor practices. But how, in thecase of our example in a subsidized public hospital, should a doctor do his or her best forone patient who asks for more and more expensive assisted conception treatment, knowingthat to accede to such requests will straight away disadvantage others? It’s not easy. Moregenerally, authorities such as governments and HMOs can help in these ethical areas bymaking it clear how far society will fund such treatments or investigations, and where theline is to be drawn socially or medically.The aggrieved patient or couple may blame ananonymous bureaucrat, but the integrity of the doctor–patient relationship is preserved bythe doctor disclosing the limitations to the patient (and maybe arranging a second opinionwith another doctor).
Similarly, commercial considerations could tempt a doctor to ‘overservice’ or to ‘under-service’ (jargon for doing too much or too little), depending on whether the doctor is paidfee-for-service (especially if the health-care or diagnostic facility is owned by that doctor)or works for an HMO or within a system of global payment for a diagnosis-related groupof medical services (which is the way some governments and organizations pay for, or limittheir payments for, society’s medical ills).Again the patient or couple should be given theopportunity of consulting someone else after the doctor makes the disclosure.
A third example of conflict of interest is when matters of conscience, especially thedoctor’s own moral beliefs, clash with the patient’s wishes.The doctor’s duty then is todisclose what’s on his or her conscience—and that such considerations are influencingthe advice being given. It’s not right, for example, for a doctor working in a Catholichospital to offer only GIFT and not IVF for a couple with infertility due to fallopiantube problems or a particularly low sperm count.When IVF (which is undoubtedlymedically better in these cases), is available somewhere else, your doctor should make itvery clear how he or she is constrained by personal or local institutional views ofmorality. For sure, in some cases, the patient or the couple may share the doctor’s specialview that to create embryos and then not to transfer all of them to the uterus is immoral.The point is that the discussion should be an open one, not one pushed paternalisticallyby the doctor.
I propose that when there are unresolved differences of ethical opinion, provided thelaw is not broken, the responsibility for making ethical and moral decisions should restwith the people who most need to live with the consequences of the decision.Unfortunately, not everyone agrees with this notion. Society still has many people whowant to influence or to make decisions for others. (Typically they then walk away toanother case—to find someone else’s decision to make—instead of staying to sort out thepersonal consequences.) We still see this on the private matter of abortion.We still see itin questions of embryo research (see Chapter 27). For more, see the box, Ethics: Moralimperatives, outcomes and equity.
YOUR DOCTOR’S DUTIES � 357
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 357

358 � GETTING PREGNANT
Ethics: Moral imperatives, outcomes and equity
There is no one system of ethics that’s universally accepted.But one way that thoughtscan be ordered—and debate on matters of ethics disciplined—is by categorizingethical considerations into three groups.These are:• fundamental beliefs involving duty,which are seen by adherents to be self-evident
and not needing more basic proof (sometimes called deontological ethics);• the belief that goodness or badness of consequences, whether actual, intended or
predicted (sometimes called teleological ethics), is the basis for moral imperative;and
• a belief in social utility, which extends the idea of the benefit of consequencesaway from the individual to the whole of society (sometimes called utilitarian ethics).
We’ll begin with this last idea.Utilitarian ethics has been around in philosophical circles since the time of Jeremy
Bentham (1748–1832), a British philosopher writing during the time of the IndustrialRevolution. In its more refined form, Bentham’s proposal was that ultimate good isthat which promises or brings the greatest pleasure or benefit to the greatest numberof people.
Utilitarianism has since been more conspicuous in some societies than in others.Marxism, and the notion that ‘the end justifies the means’, brought notoriety to theprinciple of utilitarianism.
In Western society, utilitarian ethical principles and debate are surfacing againin the form of allocating finite, public resources among plural interests—in otherwords, ensuring equity among the community, or administrative fairness and justice.Modern examples of mainly utilitarian debate include political ones on society’sfunding for IVF.The ethical debate in Australia that preceded public payment forIVF, like the debate that preceded payment for induced abortions and for publicsponsoring of family planning associations, also drew on the other two categoriesof ethics.
But it can be useful to make cost-benefit analyses in the utilitarian area inde-pendently, before confusing the cost-benefit issue with moral prejudice (that is,withdeontological ethics) and with personal benefit or detriment (teleological ethics),and then having to reconcile the three—which is like mixing apples with pears andwith oranges.
Teleological ethical beliefs, or consideration of consequences, I regard here asrelating not to society as a whole but to individuals, which in practice means thewoman and her husband or reproductive partner. Such consequential considerationsare (or should be) objective—able to be identified, tested (if necessary experimen-tally) and then accepted or rejected.They should, at least potentially, be matters offact, and be verifiable or refutable through observation and experiment.
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 358

Take, for example, the proposition,‘Sperm microinjection is unethical as a tech-nique for IVF because there is or might be a high risk of producing babies withmajor deformities’.This becomes unacceptable as a teleological ethical argument ifexperience shows that the proposition is not true.
This is not to say that consequential arguments can only rest on facts and noton fears.Rather, consequential considerations need continually to take into accountnew empirical information as it becomes available. Because the data teleologicalconsiderations are based on can change with time, it’s legitimate (indeed it’s compul-sory) for ethical conclusions based on consequences to be ever open to rethinkingand to change.We might usefully call it evidence-based ethics.
Deontological ethical beliefs are by their nature the least flexible and the leastsubject to experiment. Either they’re innate or they’re instilled in people as childrenthrough teaching and observation.
The strength of a person’s convictions or character implies that his or herdeontological beliefs show substantial resistance to corruption by argument andobservation. (I sometimes think the most characteristic property of a deontolog-ically held belief is its perverse strengthening the better the evidence mountedagainst it.)
Incidentally, the similarity that the term ‘deontological’might have linguisticallyto ‘God-given’ is a coincidence, although religious beliefs are encompassed by theterm.The word’s origin is Greek, meaning ‘that which is binding, a duty’. So deon-tology is the philosophy of duty or moral obligation.
Although deontological principles include ethical positions that appear to beGod-given or derived from scriptures, they equally include a doctor’s fundamentalcompassion for, and belief that there is a fundamental duty to help, a couple madedistraught by their infertility.
Ethical debate soon spills over between these three categories. But the longer itis before this mixing starts, generally the more sensible the particular debate will be.
Consider, for example, the moral position that ‘life is sacrosanct from the momentof conception and that IVF, because it creates surplus embryos that will be deniedthe chance to survive, therefore ought not to be pursued’. (This is the standardposition of many fundamentalist Christians.)
Given that there are valid reasons for doubting the absolute truth of this positionin principle, what is the best approach to contradicting this deontological positionin practice?
Is it the argument that the number of children that result from IVF outweighsthe number of lost IVF embryos (a utilitarian argument)?
Is it the argument that nature wastes embryos in natural circumstances too sothe lost embryos are of no consequence (a teleological argument)?
Or is it the argument that infertility causes so much and such intense humansuffering that one has a compelling duty to invoke the only treatment that works(a deontological argument)?
YOUR DOCTOR’S DUTIES � 359
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 359

INFORMED CONSENT
In circumstances that are nearly always uncertain, the doctor and the couple need to workclosely to establish the ethical premises and the trust that’s needed to make good medicaldecisions.
Patients generally don’t like to risk losing the goodwill of their doctor.This is a pointthat should work to the advantage of the infertile couple and the doctor alike.The doctorought to be in a position to share uncertainty regarding the outcome of treatment withthe couple—they should form what the American physician Thomas Gutheil and others,writing in the New England Journal of Medicine in 1984, called the therapeutic alliance. It’s notso much the notion of a patient’s so-called autonomy (see the box, Autonomy and respect forpersons) but respect for each person that should lead the doctor to ensure that the couplebe presented with the advantages and disadvantages of alternative plans for treatment. Inmaking decisions that will affect them, the couple are invited to take as much responsibil-ity as suits their circumstances as they see them.This is where the purpose and value lie inobtaining informed consent for medical treatment.
In a case before the High Court in Australia in the 1990s, a young woman had lost thesight of her single good eye after an essentially elective operation on the diseased other one(Whittacker v.Rogers).The risk of such a complication occurring was extremely remote, butthe penalty she (and her doctor) paid was disastrous; she had not been told of this knownhazard even though, the court agreed, she had asked the doctor the right question.Thecourt affirmed the view that the information given in the process of consenting to medicaltreatment, at least in Australia, had to be be tailored to the patient’s enquiries in a givenmedical circumstance, and must not just be a reiteration of a list of probable or possiblecomplications.
Different countries might interpret the legal requirements of informed consent differ-ently, but the judgment in this Australian case illustrates an important obligation: whenoffering treatment for infertility the doctor is obliged to inform the couple of the
Individuals intuitively consider all three aspects in reaching a conclusion foraction or for a decision. It’s not uncommon, for example, for a couple who havemoral difficulties with embryos in vitro or in cryostorage to recruit financialconstraints and health fears from ovarian stimulation to help them rationalize thatenough is enough.But I think the most compelling argument is the one that matchesdeontology against deontology.
If the ethical question is serious enough in the community, a more formalaccommodation will ultimately need to be sought that crosses the three sets ofethical categories. In its rawest form, such an accommodation in a plural societymay consist of a vote on the matter, as occurred in Britain in 1990, when bothhouses of parliament voted with two-thirds majorities to approve IVF and embryoresearch.
360 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 360

consequences in as much detail as the couple want to hear. Printed information can help,to be sure, but the doctor must first anticipate a need for the most relevant informationand, should curiosity be slight, deliver it regardless (there’s basic information everyone must
YOUR DOCTOR’S DUTIES � 361
Autonomy and respect for persons
As a philosophical concept, a person’s autonomy derives from the system of ethicsdeveloped by the German philosopher Immanuel Kant (1724–1804). For Kant,morality was an ‘autonomous’ matter—the self-determination of the will. In thehistorical Age of Enlightenment, autonomy came to mean personal freedom. Now,since the late twentieth century, there’s a call for every decision that affects a personto be made by that person. (If more than one person is affected by that decision thenideally they take part jointly in making the decision.)
On the face of it, autonomy is a good thing, provided at least that one person’sautonomy does not infringe upon another’s. In clinical medicine, patient autonomybecomes identifiable—and problematic—when ethical justification for decisions onmedical care is based merely on the patient’s informed consent.
In the extreme case, the patient decides and the doctor complies.The risk is thatthe nature of the patient’s reasons for a certain decision become immaterial: thedecision is the patient’s to make and then the outcome of her or his decision becomeslegally irrelevant. In such an extreme situation, informed consent is a blanket thathides much uncertainty, responsibility for which is transferred from the doctor tothe patient.This transfer is ultimately unfair if insisted on by the doctor and unwiseif insisted on by the patient, because the doctor has been trained to have the knowl-edge sought by the patient or the couple.
So, autonomy is a goal rarely completely reached in medicine.And sometimesit’s completely lacking.There’s an inherent imbalance of power in all encountersbetween professional and lay people, between doctors and their patients (or in theextreme autonomy model,‘clients’).This after all is why the client seeks the adviceof a professional.
In other areas of medicine, a sick or incompetent patient has lost autonomy andwishes the professional to do his or her best on their behalf.This can be the situa-tion with infertility treatment too, but it shouldn’t be assumed by the doctor.
Professionalism can be described as the responsible practice of professional power;it implies involving the patient in making decisions where a choice exists and inexplaining the situation if there seems to be little choice.
Paternalism, on the other hand, can be defined as the irresponsible practice ofprofessional power, where the patient is kept in the dark or is pushed into accept-ing the treatment proposed.
Professionalism,by shunning paternalism, advances respect for persons and leadsto a sensible and balanced sharing of uncertainty.
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 361

have); and second, continue responding to it for as long as curiosity persists. If time constrainsthis at one professional consultation then another opportunity needs to be made.
So it’s you—the patient—who should decide how far discussion should go beforereaching a decision on medical treatment.A doctor should resist relying on only a signedconsent form ‘for protection’. All-encompassing forms for consenting to medical proce-dures seek to place too much weight on the patient. Such a form—and such a polarizedprofessional relationship—is good for neither the doctor nor the patient (who’s meant inthis way to be dumped with responsibility for whatever eventually happens).
Taking responsibility is a two-way thing.You need to take responsibility for whathappens too. Don’t expect your doctor to second-guess you: if you want to know morebefore starting an IVF treatment cycle, for example, after reading the information brochuresand signing the consent forms the IVF center provides, it’s your responsibility to postponestarting if you don’t feel ready.You have a right to know the chance of success, an estimatebased on various assumptions and generalizations. But when you do start, it’s your respon-sibility to share with your doctor the inevitable uncertainty concerning the outcome that’sa part of any medical treatment. (There’s more on this difficult concept of autonomy andgiving consent in the box, Autonomy and respect for persons.)
RESPONSIBILITY IN INFERTILITY RESEARCH
There’s probably no area in medicine where research and clinical practice are less distinctthan in reproductive medicine and the use of reproductive technology.This state of affairshas meant babies for infertile couples who otherwise would have outgrown their oppor-tunities. For them the rapidity of research becoming practice has been a blessing.For others,less successful, there is often a sense of bewilderment and resentment, when expensive,uncomfortable or even possibly dangerous maneuvers have failed to secure successful preg-nancy, especially when there has been a lingering atmosphere of experiment.This sectiondelves into the doctor’s duties and obligations to patients in an environment of research.
The widely accepted current minimum code of conduct for ethical clinical researchand human experimentation is the Helsinki Declaration of 1964 (in turn derived from theNuremberg Code of 1947, and amended in 1975 and in 1983), which established that, tobe ethical, medical research must be meaningful, scientifically based, medically supervised,consented to only after evaluation of risks, confidential, and truthfully reported. See thebox, The Helsinki Declaration, 1975.
Institutional review boards
Committees that review research protocols within institutions before they’re put into effecthave been established in most Western countries. Outside the USA they are called institu-tional ethics committees (or IECs); in the USA, institutional review boards (or IRBs). (Suchcommittees differ from those referred to in the USA as ethics committees: see the box,Ethics and ethics committees.) IECs or IRBs should be set up by all institutions that carry outa significant amount of research.They need to include lay men and women as members,
362 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 362

and often there are members with legal and ethical (sometimes theological) experience.Their membership might include specialist doctors and scientists, who are meant to rule aresearch protocol unethical if it’s not scientifically sound. (In some institutions the moraland scientific roles in judging a research proposal to be ethical are devolved to two commit-tees, which then liaise.)
IECs/IRBs are bound by the Helsinki Declaration.They cannot override laws andgovernment regulations, but they can impose narrower constraints—which they often do,depending on the nature of the institution (for example, hospitals run by religious orderscommonly limit the reproductive research they allow). Consciously or not, IECs/IRBsdraw on moral, consequential, and equity or resource-allocation considerations before theyapprove, improve or reject a research proposal. Members use their own ethical values asthey seek to put themselves in the place of the research subjects, so as to protect themwithout unduly standing in the way of medical progress.
YOUR DOCTOR’S DUTIES � 363
The Helsinki Declaration, 1975
The Helsinki Declaration on the rights of humans in the field of medical experi-mentation states that:• A fundamental distinction needs to be made between medical research in which the aim
is essentially diagnostic or therapeutic for a patient, and medical research in which theessential object is purely scientific.
• The responsibility for the human subject needs to rest with the medically qualified personinvolved and that [sic] it should never rest on the subject of the research, even though thesubject has given his or her consent.
• Every biomedical research project involving human subjects should be preceded by carefulassessment of predictable risks in comparison with foreseeable benefits to the subject or toothers; and that concern for the interests of the subject must always prevail over the inter-ests of science and society.
• The design and performance of each experimental procedure should be clearly formulatedin an experimental protocol, which should be transmitted to a specially appointed inde-pendent committee for consideration, comment and guidance.The Declaration goes on to say that, in principle, medical research can be
combined with professional medical practice:• The doctor can combine medical research with professional care, the objective being the
acquisition of new medical knowledge, only to the extent that medical research is justifiedby its potential diagnostic or therapeutic value for the patient.
• In any medical study, every patient—including those of a control group, if any—shouldbe assured of the best proven diagnostic and therapeutic method.
• The refusal of the patient to participate in a study must never interfere with thedoctor–patient relationship.
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 363

364 � GETTING PREGNANT
Ethics and ethics committees
More and more, ethical aspects of medical practice, as distinct from ethical aspectsof research protocols, are presented to institutional ethics committees for opinion.
In the USA, many institutions have set up rapid-response ethics committees,distinct from their institutional review boards, to which controversial medical deci-sions can be referred—sometimes by staff who have detected undue paternalism inclinical decisions made by colleagues.The danger is that ethical responsibility for thedecision, through such referral, becomes remote and diffuse, with diminished ratherthan improved accountability for the outcomes that result.
Nonetheless, ethics committees of both kinds can usefully help an individualresearcher or practitioner share a moral burden by providing a forum for formalethical consideration when that researcher or practitioner has doubts.
Institutional ethics committees haven’t evolved fully yet. Some shortcomings arequirky, others are pervasive.To start with, no committee will be better than themembers who compose it, and the committee will depend particularly on the expe-rience, intelligence and compassion of the person in the chair and the example heor she sets to the committee’s other members.
A more structural shortcoming of ethics committees finds its root in the follow-ing Helsinki principle:
In the treatment of the sick person, the doctor must be free to use a new diagnostic andtherapeutic measure, if in his or her judgment it offers hope of saving life, re-establishinghealth or alleviating suffering.
In other words, and in certain circumstances, a doctor should not necessarily beconstrained from introducing new treatments outside formal clinical trials, and a verylarge number of surgical and medical innovations involving operations and the useof therapeutic devices (indeed,most therapeutic medicine outside drug trials, includ-ing surgical operations on the fetus) have been introduced this way.By no means haveall IVF centers involved their ethics committees when introducing new (for them)treatment modalities that might or might not have worked well in other programs.
The irony for the doctor is that in many countries (but notably not in Australia),if he or she wishes to try a new treatment or operation, there’s presently no need torefer the matter to an ethics committee unless the practitioner wants to evaluate thenew treatment or operation in a controlled or randomized study of its efficacy.Thisinconsistency imposes a major practical disadvantage to constructing proper evalu-ations of new treatments by individual practitioners and within institutions.
The point,in practice,is so finely drawn that a decision made by an IVF center’s labo-ratory to use one embryo culture medium instead of another,on a trial and error basis, islikely to escape the attention of the IEC,whereas a better-designed,simultaneous,randomlyallocated comparison of culture media comes under full and critical external scrutiny.
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 364

Increasingly, IECs/IRBs are being brought together in different countries within aframework of national ethical policy, sometimes by a government-appointed ‘super ethicscommittee’, to which global or community-wide matters of ethical policy can be referred.In Australia, for example, a protocol was submitted to an IEC in the 1980s that involvedflushing pre-implantational embryos from the uterus of embryo donors impregnated byassisted insemination (see the Chapter 22 box, Womb flushing).
The then novel ethical hazards caused the IEC to refer womb flushing to the MedicalResearch Ethics Committee of Australia’s National Health and Medical Research Council,which published a paper discussing the ethical difficulties and recommended that studiesof this sort not proceed.The same national ethics committee was responsible for formu-lating general guidelines for the ethical conduct of research involving in vitro fertilizationand research involving the human fetus.The equivalent committee in Australia today is theAustralian Health Ethics Committee.
National ethics committees thus ordinarily build from a starting point enunciated inthe Helsinki Declaration to produce more country-specific sets of values, over which IECscan add their own institution-specific values.Thus there is a ‘ratchet function’ throughwhich, from Helsinki to the institution, ethical considerations can be tightened but notloosened.
ETHICAL PRINCIPLES IN PRACTICE
Whether infertility treatment is accepted medical practice or whether it is medical researchcan therefore be a vexed question. It’s often not possible to make the distinction.
What is there to guide the doctor and the patient?
Compassion
Treatment, whether established or relatively pioneering, should always be delivered withcompassion, whatever the level of autonomy or privacy the patient or couple choose at thatstage of their relationship with their doctor.The prudent doctor (or nurse or psychologistor social worker) will detect ‘the level of willingness to share feelings and emotions thecouple have’ and will respond to it. And complete doctors will make their capacity fordeeper feelings such as empathy known. (See the box, From mercy to empathy, for how thishuman hard-wired quality might have evolved.)
But these deeper shared feelings are delivered by the doctor to the patient at the patient’soption—only if the patient wants to share them.They are not necessarily appropriate toevery professional situation. In this way a patient’s privacy can be protected without standingin the way of good medicine.
As new options for treating infertility become available, there are other principles andvalues that are important for patients, doctors and other health professionals, researchers,ethics committees and governments to consider.This is especially so when the duties, obli-gations and rights of different people come into conflict.
YOUR DOCTOR’S DUTIES � 365
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 365

Duties, obligations and rights
The rights of the child should be paramountThis statement is presently popular in our society among social moralists when they considersuch complex situations as surrogacy (see also Chapter 22). It stems from Article 3 of theUnited Nations Convention on the Rights of Children. Unlike Article 3, however, therefrain is often used to refer to children who haven’t been born yet—or even to childrennot yet conceived, as if there were already a particular child to consider. Such a statementpromises a short-cut to ethical wisdom, a quick way out of the many moral entanglementsthat affect the family and the infertile couple in society.
But there are limits to its context and its power to illuminate moral and ethical values.Duties and rights are different perspectives of the same relationship. In a sense they workfrom opposite directions. One person’s right is meaningless without someone else’s duty orobligation. For example, the argument in a democracy that everyone has a right to vote reallymeans that governments are obliged to provide accessible polling stations and to countvotes honestly and accurately; if you choose to stay at home on election day, no-one has aduty to bring you the ballot papers, so your right to vote has lost its meaning. If a moralduty is perceived widely enough it gets to be seen as a right by the recipient—a right thatcould then spread to others in similar positions, producing a need to redefine others’ dutiesor obligations in an attempt to make everything seem fair and equitable.
From mercy to empathy
The words ‘sympathy’,‘compassion’ and ‘empathy’ have replaced the biblical expres-sions ‘mercy’ and ‘pity’ for giving meaning to important social feelings people showtheir fellows (falling deliberately short of the more psychologically invasive, some-times sexually invasive, emotion of love).
Empathy, despite its Greek appearance, is not an ancient word. It was coined in1912 to translate the German psychiatric term Einfühlung, or ‘feeling as one with’,which is a rather hazardous degree of psychotherapeutic identification a doctor,specifically a psychiatrist, can try to achieve with his or her patient.
The way we use empathy today probably more often represents the GermanMitgefühl, ‘feeling with’ someone, overlapping the word ‘compassion’, which datesfrom 1625 in English usage; but in either event we mean something deeper than‘sympathy’, the German for which is Sympathie.
Empathy does not need to characterize a health professional’s relationship withevery patient or client. It is neither practicable nor would it always be welcome.
Rather, the potential or capacity to show empathy is signaled in one way oranother and it is a reserve to draw on when the occasion calls for it.
Compassion, though, should be as obvious and as constant as bedrock.
366 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 366

Incompatibilities or conflicts can arise between, for example, a doctor’s duty to the wifeand to the husband (though it’s uncommon in practice).Perhaps more often, there’s conflictbetween the doctor’s sense of his or her own duty and the rights the couple have to securethe best medical advice and personal respect they consider should be on offer. If you as apatient think that your rights are at variance with a physician’s perceptions of his or herduties or obligations, then justice (see further on) is best brought about by openness: youshould be given the opportunity of seeking a second opinion and if conflicting expecta-tions persist you should take it.
There are instances where society, in seeking to accommodate rights, relies not just ondoctors’ self-motivated duties but adds to these duties by imposing obligations. In mostcountries, compulsory notification to public health authorities of certain infectious diseasessuch as hepatitis C and HIV are examples of such an extrinsic obligation. Reporting ofbirth defects is another.
Ethical duties can conflict in many ways in medicine—particularly in reproductivemedicine, because more than one client (or patient or autonomous person) is so commonlyinvolved.
Consider, for example, a sperm donor’s desire for news of his progeny versus the DIparents’ desire for privacy. In this example, different societies have (by regulation or by law)imposed different obligations: in Sweden the donor shares in the knowledge of the outcome;in the USA the donor signs away all such rights.
If society does not make obligations plain by regulation or law, a lot of thoughtfulnessand compassion is needed to reach an equitable solution. Ethical ‘through-ways’ or ‘short-cuts’ that insist on wisdom through one-eyed focusing on moral duties or obligations—such as obligations to children not yet conceived overriding the wishes of the prospectiveparents seeking reproductive help—can be a bullying form of paternalism, given that suchregulation of ordinary reproduction would not be acceptable.
Telling the truth, doing good and achieving justice
The bioethical principles that stand behind the notions of rights and duties between doctor andpatient or an infertile couple have much value and appeal.Telling the truth, doing goodand achieving justice would be almost universally supported but nevertheless they are princi-ples that can conflict.So a balance,which may sometimes be controversial,needs to be struck.
A place to start might be to look at these principles operating within each set of theethical systems (see the box, Ethics: Moral imperatives, outcomes and equity).We can thencompare strengths and weaknesses across the systems for society to come up with a compro-mise in public or professional policy.
In a pluralist society, ethical tensions will generally be least if these values are based onconsequences rather than on shared moral perceptions of duty, except when such moralpositions are virtually universal. (I explore this further in my paper,‘Evidence-based ethicsand the regulation of reproduction’.)
There is a widely recognized moral compulsion to tell the truth. Most agree that, asan ethical principle, truth should not be dispensed with simply for the sake of expediency,
YOUR DOCTOR’S DUTIES � 367
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 367

although occasionally for an individual the consequence or end (comfort) may justify unusualmeans (that is, withholding the truth). Integrity demands that truth not be dismissed forshort-term gains alone.
If, for a special reason, the truth is not told, the prudent doctor will share the real truth,and the responsibility for the untruth, with others, such as the patient’s husband or wife. Ishould add quickly that while this question might arise in dealing with terminal illnesses,the dilemma is not common among infertile couples: the trust they have in each other (seeChapter 25) should not be split.
Nonetheless it could be appropriate and kind, for example, to spare a 15-year-old fromknowledge of all the consequences of congenital absence of the uterus (Chapter 18) or prema-ture ovarian failure (Chapter 11) at first, while being more frank with her parents.
Integrity as a value means more than always telling the literal truth and keepingpromises. It calls for a consistency of approach that encourages faith in a doctor’s, a nurse’s,a psychologist’s, a social worker’s judgment.
The principle of non-maleficence, or not doing harm, has been made popular in theHippocratic Oath as ‘first, do no harm’.As an ethical principle it often has a strong moral,sometimes religious, basis.‘Thou shalt not kill’ is an ancient expression of non-maleficence.(Members of the Jainist religion in India take it to an extreme by breathing through a hand-kerchief, to avoid the accidental killing of flying insects, and by stepping carefully, so notto tread on ants.)
But taken to override other ethical principles within the doctor–patient relationship,non-maleficence is a prescription for doing nothing. In modern, powerful medical practicethe risk of doing harm has to be accepted—and the same is often true in reproductivemedicine.
Beneficence is the principle of doing good.Because to do powerful good may risk doingharm (maleficence), the two principles often conflict. In medicine nowadays beneficenceis the more widely observed principle, because it’s recognized that greater ultimate harmcan come from avoiding the risk of immediate harm. Instead, benefits are maximized whileharms are minimized. Multiple-ovulation induction for assisted conception (see Chapter 21) is agood example.
As an ethical principle, beneficence is determined largely by evidence, by the study ofconsequences for other individuals.As the Oxford (UK) moral philosopher R.M.Hare haspointed out, no serious addressing of beneficence in the political process can avoid ques-tions of equity. And controversy arises quickly in the political sphere if it means that ourduties to some individuals (in other words, these individuals’ rights) are diminished for agreater good. Non-maleficence then may properly become the basic moral obligation toeveryone, irrespective of how lucky or unlucky their station in society is.
Justice, as a principle,means giving every person his or her due.Distributive justice is thedistributing among members of our society those benefits (rights) and burdens (obligations)due to them.The basis of distributive justice is the notion of fairness, the criteria for whichinvolve equity and need, and debate over which is the very substance of our political process.
However unfairly treated they may feel personally, it’s a fact that, in comparison withinfertile couples in other countries,Australian infertile couples have done well in terms of
368 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 368

justice in society. Public subsidy for infertility operations and assisted conception proce-dures is better in Australia than it is in New Zealand,Asia, Britain, most European coun-tries and North America.
THREATENED VALUES
Nowadays there is a considerable call in Western countries for ‘evidence-based medicine’(as if it were something new).The modern concept of evidence-based medicine is essen-tially an attempt to ration medical treatments—or at least to ration publicly funded medicaltreatments—to those who have unequivocally been shown to benefit from the conditionbeing treated.
The ethical practice of medicine has always demanded that the doctor place highly theethical values of integrity, responsibility and accountability in his or her individual relationshipwith patients and with the community; and this has naturally meant employing treatmentsfor disease or suffering for which there is good evidence of efficacy. But in keeping withthe philosophy expressed in the Helsinki Declaration on innovative therapies, such medicalpractice has often paid scant regard to the financial cost of innovative treatment (at leastwhen the cost has been born by third parties).
An increasing focus on outcomes in medical practice generally—and in reproductivemedicine particularly—will be seen in the next few years, as those who ‘pay the pipers’increasingly ‘call the tune’—as HMOs and governments that fund health care define whattreatments they’re prepared to support.
Assisted reproductive technology has provided the excuse for rapid erosion of infertilitydoctors’ and patients’ rights by governments in many countries—at a rate much faster thanis taking place in other medical specialties, but specialties nonetheless susceptible to costrestraint through evidence-based financial pressures. It’s not hard to see why.
First, there’s very little limit to the number of people who are candidates for assistedconception in some form or other. Its public funding can obviously come under greatdemand without some form of rationing.
Second, there is the technology itself and its arousal of distrust. Distrust of science isnot far from the surface in today’s societies, no matter how much we seem to take scienceand technology for granted. (Many doctors inadvertently abet reproductive medicine’ssusceptibility to this degradation by themselves referring to the service they deliver as repro-ductive ‘technology’—implying that the technology is an end in itself rather than, as inother fields of medicine, just an aid to practicing exact medicine.)
And third, we are concerned here with an area of moral plurality of opinion—Whatare embryos? When do they have autonomy? When does life begin?—which has beenhijacked by moral conservatives and religious fundamentalists with agendas that tangle upIVF with the abortion debate. (For more on the polarisation of moral opinion, see the box,Moral plurality—and Brave New Canada.)
The consequence is that society’s trust in doctors—and often patients’ trust in theirdoctors—is, I think, under a threat greater than is seen in other areas of medicine. In the1990s several governments imposed or tried to impose on their infertile citizens the
YOUR DOCTOR’S DUTIES � 369
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 369

370 � GETTING PREGNANT
Moral plurality—and Brave New Canada
Moral plurality . . .
Equity has not been well served at the moral or social frontiers of reproductive medicine.Many governments,with scant regard for the opinions of their infertile patients,
have banned embryo research (discussed further in Chapter 27) on the basis of moralassumptions, and have banned gestational surrogacy (discussed in Chapter 22) on thebasis of what’s meant to be best for the family, but in each case patronizing theircitizens for doubtful cause.
A fetus is utterly dependent on its mother.An embryo in vitro is utterly depend-ent on the act of transfer into fallopian tube or uterus.Clearly neither the pre-viablefetus nor the embryo has autonomy.Yet it’s popular to extend the notion of autonomyto it, in the form of its potential for autonomy in the future.
A newborn child is dependent on its mother too, but respect for its potentialautonomy is so widespread that society confers on it some of the rights of an adult.This is achieved in practice by promoting the duties of some and enforcing theobligations of others towards ensuring its well-being.
Producing embryos for IVF or for research, then destroying those that aren’ttransferred, is equated with homicide by people who believe that human life startsat conception. For these people, producing embryos that will not or might not betransferred to a woman’s receptive reproductive organs is therefore morally unac-ceptable.This is what, for example, Cardinal Basil Hume, the (Roman Catholic)Archbishop of Westminster, said at the height of the IVF controversy in the 1980s—and it’s what many other ordinarily moral people still believe.
On the other hand there is the belief that humanness develops not instantly butin a sequence, a quick sequence,of fertilization, syngamy, cleavage, blastulation and implan-tation, followed seamlessly by embryonic development, neural responsiveness,movement and development of the senses.The moral position that obliges increas-ing protection of these stages accommodates IVF; it allows research on humanembryos in special circumstances; it allows contraception that operates after fertil-ization; and it allows abortion in other special circumstances without calling ithomicide or infanticide.This is what Dr John Habgood, the (Anglican) Archbishopof York, said during the height of the IVF controversy—and it’s what many otherordinarily moral people believe today.
Reconciling the two positions in the 1980s and 1990s, and in the twenty-firstcentury to date, has proved to be impossible.
A spiritual observer on another planet might scratch his or her head and marvel atthe energy that keeps such a trivial difference alive (trivial, at least, in comparison withthe brutality,homicide and genocide that’s still common over some parts of the globe).But the moral gulf persists. Reconciliation is a fantasy.Arguments are won, drawn orlost by passion, noise, numbers and—generally to no-one’s advantage—by legislation.
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 370

In the 1990s Britain led the world in embryo research—in purposefully studyingembryos in culture to determine their metabolism and their nutritional needs.Thiswas partly the result of legislation enacted in 1990—the first time plural differenceson the status of the embryo have been reconciled by a parliament or congress to theapparent advantage of the infertile.At that time, first the House of Lords and thenthe House of Commons voted (with two-thirds majorities) to approve, in principle,embryo research for the advancement of knowledge.
The price Britain’s infertile couples have had to pay, however, is substantial: theHuman Fertilisation and Embryo Authority, set up by the same Act of Parliamentthat approved embryo research, levies an additional £40 or more on the cost of everyIVF treatment cycle conducted in Britain.The government of Victoria has introduceda similar tax.
. . . and Brave New Canada
A squat grey building of only 34 stories.Over the main entrance the words,CENTRAL
LONDON HATCHERY AND CONDITIONING CENTRE, and, in a shield, the World State’smotto, Community, Identity, Stability.
The people who govern the Brave New World … are not madmen, and theiraim is not anarchy but social stability.
Aldous Huxley, Brave New World, 1932 (from which came the term ‘test-tube baby’)
Only a large scale movement toward decentralization and self-help can arrest thepresent tendency toward statism. Unless we choose to decentralize and to useapplied science … the social chaos resulting from rapid technological progressunder the need for efficiency and stability [will develop] into the welfare-tyrannyof Utopia.
Aldous Huxley, in a new foreword to Brave New World, 1946
There was old sex in the room.We still had our bodies.That was our fantasy.In the days of anarchy it was freedom to. Now you are being given freedomfrom.
Margaret Atwood,The Handmaid’s Tale, 1986(on the Republic of Gilead, in the near future)
The Supreme Court has decided that the peace, order, and good governmentpower can be invoked in support of federal legislative action.We are firmly ofthe belief that new reproductive technologies, as defined in our mandate, meetthe criteria established by the Supreme Court, so that federal intervention … isconstitutionally justified.
YOUR DOCTOR’S DUTIES � 371
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 371

More than any other aspect of health-related technology or service, theresearch and application of new reproductive technologies have significancebeyond the individuals directly involved.
Given rapidly expanding knowledge and rapid dissemination of technologies,immediate intervention and concerted leadership are required at the nationallevel … citizens in provinces with insufficient regulation may suffer harm.
The Royal Comission on New Reproductive Technologies recommends thatthe federal government establish an independent National ReproductiveTechnologies Commission charged with the primary responsibility of ensuringthat new reproductive technologies are developed and applied in the nationalpublic interest.
Royal Commission on New Reproductive Technologies,Ottawa, November 1993
In 1993, Canada’s Royal Commission on New Reproductive Technologiespublished a report that inadvertently—but chillingly—recalled Aldous Huxley’sBrave New World.
The Canadian commissioners’ words to justify central government control ofreproduction, of maintaining ‘the peace, order and good government power’, turnedout to have effectively paraphrased Huxley’s ‘Community, Identity, Stability’.
Interestingly, Canadian Margaret Atwood’s 1986 novel, The Handmaid’s Tale,concerned curtailment of random reproduction by a Christian fundamentalistgovernment bent on efficiently repopulating a genetically devastated Republic ofGilead, inhabitants of which were largely sterile after a nuclear war.There was nohigh technology involved, just pervasive central government with a desire to controlsex and getting pregnant. In other words, much the same theme as the RoyalCommission was pushing.
The Royal Commission—all six members of which were women—decidedwith ironic paternalism that they knew best what was in the ‘true interests’ ofCanadian women undergoing infertility treatment. In a closely argued (but in myopinion falsely premised) document, access to reproductive medical services—‘repro-ductive technology’, in the words of the Commissioners—would at once be restrictedyet universally available.
Upon establishment of an ‘independent’ (read ‘exclusive of doctors trained inreproductive medicine’) National Reproductive Technologies Commission, allCanadians with a defined need would have access to reproductive technology, suchas IVF (including anonymously donated sperm, eggs and embryos), whatever theirpartner status.
Private clinics were to be banned. At provincial clinics, treatment was to beallowed only for medical conditions where evidence-based certainty of efficacy hadbeen deemed by commissioners to be satisfactory. So IVF and assisted conception
372 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 372

guardianship of national statutory bodies to regulate what can or can’t be done with theirreproductive intentions—what may and may not be done (under penalties such as fines andimprisonment of doctors)—and, of course, curbing what might innovatively be done.
Whether composed of men or women—or with scrupulous attention paid to genderneutrality and every apparent interest group known to politics—these statutory authori-ties too often impose their priorities paternalistically.And, to add injury to the insult, theyfund their existence through a levy on patients’ cycles of assisted conception treatment.Noevidence has ever been published that patients want this protection or that they benefitfrom it.
These authorities do not restrict themselves to ensuring high standards of medicalpractice—there are heaps of accrediting bodies that do this more cheaply than governmentauthorities can.They are there to limit what takes place in the name of public opinion(rarely actually sought—and,when known,usually ignored, as in the case of altruistic surro-gacy in Australia) and in the name of what’s presented as the community’s moral values (orwhat a noisy group of people think the values should be).
generally were to be available for disease of the fallopian tubes (the subject of ourChapter 13) but not for oligospermia (our Chapter 10) or for endometriosis (Chapter15), let alone for subfertility of mixed cause (Chapter 6) or unexplained infertility(Chapters 2 and 6)—irrespective of the duration of infertility (see Appendix 1 forits importance).
On the other hand—and, according to the commissioners, in her own true inter-ests—a woman would have been prohibited from:• Voluntarily donating her eggs or embryos to another woman she knew;• Voluntarily undergoing an egg retrieval procedure for her sister or best friend;
and• Making use of her remaining frozen embryos should her husband die before she
considered her family complete (but instead, provided she had blocked tubes,she could have qualified for new embryos produced from anonymously donatedsemen!).
These prohibitions—these ‘freedoms from’, as Margaret Atwood might put it—werefounded not on evidence-based trials of personal good or personal harm done (socialtrials which in principle are as do-able as medical trials) but on what the commis-sioners believed to be Canadian women’s interests (or if not in their own interestthen in ‘the national interest’).
The price of Canada’s Royal Commission and its two-volume report in 1993was in excess of Can$27 million—more than a dollar for every man, woman andchild living in Canada.
Luckily it left more than a few Canadians with little stomach for what a perma-nent National Reproductive Technologies Commission would cost Canada and itsinfertile people. It has not been established.
YOUR DOCTOR’S DUTIES � 373
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 373

Would that today’s insistence on evidence-based medicine be joined by evidence-basedethics and evidence-based social policies!
I conclude this chapter by quoting The Reverend Gordon Dunstan,Professor Emeritusof Moral and Social Theology at the University of London, and a writer within the theo-logical tradition of the Church of England:
People who, as patients, experience a sensitive appreciation of human worth and dignity in theirown relationships with their doctors will the more readily credit medical [people] with respect forhuman worth and dignity in the embryo, and trust them accordingly.
Embryo research in Australia, in the USA and, when Dr Dunstan was writing in 1986,in Britain, had become problematical in the late 1970s and early 1980s not just because ofthe rather global fashion of not trusting science or doctors. It came about because therapidity of developments—and some public carelessness and inarticulateness on the part ofthe doctors concerned—enabled certain moral fundamentalists to succeed in confusingmany people about whose humanness needed protecting in IVF laboratories.
The resulting difficulties in conducting embryo research—and in properly exploringthe social innovations that reproductive medicine can bring to our notion of the family—are the subject of Chapter 27.
374 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 374

embryo research and society
Infertility research needseveryone’s support
Fertilize an egg in vitro. Look at the embryo that develops over the next week.Thendon’t eventually transfer it back to a woman’s reproductive tract (the uterus or thefallopian tubes).
To some critics of reproductive technology this is embryo research.Whether deliber-ate or not, an embryo is being created (see the box,Revision: What is an embryo?), an embryothat will not end up back in a woman’s body.Why do nature and IVF labs create manymore embryos than will ever become people? Do IVF labs have to create them? If so, doesit make a difference what happens in the lab over the few days they spend there beforethey’re discarded?
Here we examine:• Why, as long as we have IVF, there will always be ‘spare’ embryos;• The moral controversies of research with embryos and the production of embryonic
stem cells (ES cells);• Why objections to embryo research are fading; and• Why ‘test-tube babies’ do not mean for society what Aldous Huxley, back in 1932, is
meant to have prophesized in Brave New World.
SPARE IVF EMBRYOS
Just as nature makes use of many embryos that will never produce a pregnancy (see Chap-ter 8), so the quest for normal embryos in the lab that can reliably lead to pregnancy meansthat many more eggs are fertilized than will ever become babies. In practice, so-called spareembryos are produced in the ordinary course of IVF for two reasons.
375
27
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 375

First, unless you have special moral objections, it’s usual to try to fertilize all the eggswe get at your egg retrieval.This lessens the chance of having no embryos to transfer ifsome fail and gives the opportunity to store embryos for transfer later without operatingto get another egg. In short, fertilizing all available eggs minimizes the need to stimulatethe ovaries repeatedly. For most people, it’s common sense.
The second reason spare embryos come about is that there is harm in transferring allembryos to the uterus or to the tubes if more than one, two or three are available to transfer.The higher-number multiple pregnancy that results if more than two or three embryosimplant and develop is likely to end in miscarriage before the fetuses are viable.This lossis in no-one’s interest—not yours; not your doctor’s; not the community’s (which in somecountries shares the expense); and not the fetuses’.Yet limiting the number of eggs to befertilized to the maximum that can be transferred—generally three (as is the law inGermany)—is to seriously handicap the logistics of IVF.
The spare embryos that result are therefore usually discarded or stored (see Chapter
376 � GETTING PREGNANT
Revision:What is an embryo?
Regrettably, a working knowledge of biology is limited among the community atlarge, and to some people embryo research means keeping little fetuses in the labo-ratory for experiments such as connecting them to machines using electrodes.Whatactually happens in nature during early embryonic development (and for the firstweek in the lab) is described fully in Chapter 3. But here’s a good place for asummary.
The fertilized egg or zygote remains as a single cell for almost 24 hours.Whilein the fallopian tube it then divides into two, four, eight cells and so on until, afterabout four days’ development, it becomes a ball of 16 or 32 cells (a morula).Then—if all goes to plan—it hollows out to form a blastocyst; it’s at this stage that it’s normallyin the uterus.
As the blastocyst expands before hatching from its surrounding zona pellucida(up to about a week after fertilization), the first few cells in the middle of the blas-tocyst—the inner cell mass—take on the earliest features of what will become, afterimplantation, the embryo proper and, later, the fetus.The other cells—in fact mostof the cells that make up the embryo (and called the trophectoderm)—develop intothe placenta and the membranes that surround the fetus in the uterus, comprisingthe afterbirth at delivery of the baby.
The blastocyst then progressively hatches through an opening in its surroundingzona pellucida, so that it can come into direct contact with the lining of the uterusto implant. It’s at the stage of expanded or hatching blastocyst that most embryosare transferred at Sydney IVF.
Several weeks later, long after its time in the IVF lab, the embryo first becomesvisually recognizable as a fetus.
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 376

21). Sometimes a couple might ask that they be donated to another infertile couple (anethically dangerous course, discussed in Chapter 22).
WHY DO WE NEED MORE EMBRYO RESEARCH?
In the early days of IVF, before 1978 when the first IVF baby was born, there was littlechance that the eggs fertilized in vitro would develop into babies. In this sense, the IVFpractices of the 1980s could not have been worked out without embryo research in the1970s.We believe that IVF techniques into our new century will only improve further ifwe can continue to learn more about the early events after fertilization,not just by growingin culture for several days those embryos that are additional to the ones transferred, but(when conditions allow it and when providers of eggs and sperm approve) by fertilizingeggs for the special purpose of scientific investigation.
Let’s be clear about it: this is deliberately creating embryos for research and experi-menting with embryos. But just how big a moral question is it? And for whom is it somorally difficult?
The challenge
In most IVF cycles there are embryos that will not be used: they’ll be discarded. Sometimeswe know if they’re abnormal through preimplantation genetic diagnosis (PGD); usually wedon’t.
Before discarding them, how morally awkward is it then (1) to look at them (observa-tional research), (2) to study the effects of different culture medium on their capacity to keepgrowing a few days (interventional research), and (3) to isolate cells from them to study howembryonic cells differentiate (destructive research)?
And how morally awkward is it:• To fertilize eggs in different circumstances so that we can work out how eggs need to
be matured in vitro to save stimulating the ovaries, or to make sure that a metabolicdiagnostic test doesn’t cause subtle damage to eggs as embryos before we try the methodout in clinical practice (creating embryos for research)?
• To produce an embryo without sperm—by placing the nucleus of an ovarian cell insidea young woman’s own egg—to produce the stem cells we need to save her life (thera-peutic cloning)?
Interestingly, few people who have suffered infertility have a moral problem with the issueof embryo research. Experience in the UK in the early 1990s showed that even politicianscould be brought to understand embryology enough to become confident that humanitywould not be threatened by embryo research. But in the community there is still a differ-ence of opinion concerning embryo creation for any purpose.While there’s no sign of aconsensus developing, at Sydney IVF we believe that it’s your moral belief that should prevailfor your eggs, your sperm and your embryos.The principle we follow when we get consentfor IVF treatment or for research on embryos is that it’s the moral perspective of you-who-provide-the-embryo that’s overridingly important.
EMBRYO RESEARCH AND SOCIETY � 377
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 377

In Australia, the National Health and Medical Research Council (NHMRC) has, inprinciple, approved of research studies on embryos up to the stage of implantation, up totwo weeks after fertilization.Appropriately, all special studies involving embryos also needto be approved by an institutional ethics committee (see Chapter 26).
In the Australian state of Victoria, where most of the early Australian innovations inIVF such as embryo freezing and sperm microinjection took place, permission has, since1984, also been needed from the Victorian government’s Infertility Treatment Authority, agovernment body that has never given permission for meaningful embryo research beyondthe stage of syngamy. (Syngamy, as a moral milestone, is a peculiarly Victorian invention: itdefines human life as starting with contact between the sperm’s and the egg’s chromosomes,about 22 hours after the sperm enters the egg.) Clinical IVF research in Victoria has beenbrought to an effective stop—by a particularly paternalistic attitude of government towardits citizens.
In Britain, on the other hand, several centers have permission from the HumanFertilisation and Embryo Authority to conduct embryo research by fertilizing human eggsin vitro (with the permission of the ‘parents’) and to study the metabolism of humanembryos in vitro—what nutrients they need,when, and how much.For more, see the box,And where, exactly, do we see the continuity of life?
WHOSE HUMANNESS IS IN JEOPARDY?
It was once a virtue not to make an issue of a matter without good cause.Today, it seemsissues are often kept alive for the sake of it.
Embryo research in the 1980s and 1990s became popularly contentious. It remains sofor a minority, increasingly identified with radical opposition to abortion, who maintainthat human life, with its need for protection, come what may, is there from the moment ofconception (or, with a twist, under the Victorian Act described above, from the momentof syngamy). For such people, embryo research is, understandably, like homicide.
The two main moral positions on the matter—that human life starts at conception witha duty or obligation to protect life from that moment; or that life develops in stages, witha graded duty or obligation that unfolds according to the circumstances—have proved, aswe examine in more detail in Chapter 26, to be fundamentally irreconcilable. But perhapsthe chance of birth after an embryo’s few days of development following fertilization inthe lab was kept low in the 1990s through the starving of research more because of confu-sion in the wider community over whose humanness needed protecting in the IVF labo-ratory, thus amplifying beyond the importance of their numbers the arguments offundamentalists of the ‘right-to-life’movement or those adhering strictly to papal doctrine.
In the final analysis, the potential an embryo has depends on so many as yet unknownvariables that while we might consider it to be in the lap of the gods, a more secularposition is that, here and now, a particular embryo’s potential lies chiefly in the imagi-nation of the beholder (for a parable, read the box, The moral position of the embryo, andtales of mice). Although these feelings can clarify in support of embryo research, eitherwhen more information is made available or when the dehumanizing experience of
378 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 378

EMBRYO RESEARCH AND SOCIETY � 379
And where, exactly, do we see the continuity of life?
In condemning IVF and embryo research, right-to-life groups make much of theconclusion that if you trace the path a fertilizing egg makes to becoming a baby youfind no abrupt change that sets one stage apart from the next. Ergo, life starts whenthe sperm nudges the egg, and a human life, with all its profound need for protec-tion, is present from this earliest stage. Embryocide becomes homicide.
Leaving aside for a moment the fact that, arguably, there are some rather promi-nent steps (I can think of attachment of the blastocyst to the endometrium; theflooding of nutrient into the trophoblastic spaces; gastrulation, or the origin of a thirdlayer of cells, which is when the next generation’s germ cells form, and after whichidentical twins will be conjoined twins instead of completely separate individuals;and so on)—leaving these steps aside, with a bit of knowledge of human reproduc-tive biology you have to admit that the continuity of human development is a retro-spective diagnosis.
In other words, if you take a newborn baby and trace its roots, you can see amore or less smooth line of development in its past. But why then stop at fertiliza-tion, or when the sperm and the egg touch? Surely such a path just as easily extendsfurther back, to the production of the egg and of the sperm that fertilized it, andmaybe even to the hopes, wishes and intentions of the parents?
But on the other hand, if you work prospectively, looking for continuity forwardsfor every embryo (let alone every egg or every sperm), there are hiccups and dead-ends all over the place.A majority of early embryos have no hope of becoming babies,they just don’t have the DNA to do it.The fertilized eggs fail to develop. Or theyfail to implant. Or they miscarry.
Moreover, they might never have had anything to do with a sperm at all (and Idon’t mean the technique of nuclear transfer).
Ovulating eggs have such a strong job description to form embryo-like struc-tures that they will do it if they are pricked properly with a pin! That’s in the lab.They do it in nature also. In fact the commonest tumor of the ovary, a teratoma ordermoid cyst, is a disordered collection of every mature tissue you can think of—skin,hair, teeth, internal tissues—because a tumorous egg cell has developed throughembryonic stages, either on its own account or possibly because it has been ‘fertil-ized’ by another next to it.
There’s even a rare (and very malignant) cancer called a polyembryoma, whichmicroscopically resembles masses of two- to three-week embryos.
To me the only continuity that makes sense is the one we are striving for: ababy—a baby that starts with the hopes and aspirations of the woman and man weare treating, their valuable (often hard-won) eggs and sperm cells, and the earlyembryos we produce.The value we place on them before and after fertilization is,and should be, immense.
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 379

infertility happens close to home, it should still be asked,‘Whose humanity is threatenedby embryo research?’
It needs to be better known that what happens to embryos in the laboratory does notdehumanize or brutalize those who carry out embryo research. Our experience withnewcomers to embryo laboratories is that the opposite happens: IVF itself, embryo research,and knowing the couples whose hopes are present in vitro, all increase one’s awe of andrespect for that which is human. IVF and embryo experimentation is a very human andcaring experience for those directly involved with it.This fact in due course will put anend to doubts about its public morality in a plural society, just as moralists eventually gaveup on the supposed immorality of treating diphtheria with immune horse serum a hundredyears ago and maintaining that it was against God’s will to restart failing hearts with pace-makers 50 years ago.
For embryos, I believe that change is in the wind.Already we have seen the Australianand British governments signal to the community that the promise of embryonic stem cellresearch (discussed in Chapter 23) is of such commercial importance to their respective coun-tries’ emerging biotechnology industries that superficial queasiness about embryo researchought not to continue to elicit knee-jerk conservative rejection!
I would personally prefer to argue on moral grounds rather than commercial ones—but whatever! I think that our society will progress to embracing deliberate, unabashed,responsible embryo and fetal research in vitro, not because of cogent logic on its ethics orbecause the Pope changes his mind,but because the importance of such research for advanc-ing human health will outlive those who believe they should, for one reason or another,continue to oppose it.
That said, it’s obvious that there will still be reasonable and open-minded people whofeel that their sense of humanity is threatened by large-scale production and culturing ofhuman embryos in biotech labs for purposes other than the reproductive benefit of thepersons from whom the sperm and egg derive: that the creation of embryos for trivialcommercial purposes would be fundamentally out of step with progress to a more caringworld.
And I dare say I find myself in sympathy with this view.
BEYOND EMBRYO RESEARCH: BRAVE NEW WORLD?
For those reading these chapters sequentially, the most awkward issues in treating infertil-ity—commerce in third-party reproduction (in Chapter 22) and embryo research (this chapter)—have both now been discussed. Let me sum up their context in our society.
But,when the family is complete, to endow every remaining stored egg becauseit has incorporated a sperm, with importance beyond that which its owners wish toendow on it, is in my opinion a mystical, faith-based view that not every moralperson needs to take or to agree with.
The continuity of life is retrospective.
380 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 380

EMBRYO RESEARCH AND SOCIETY � 381
The moral position of the embryo, and tales of mice
The moral position of the embryo . . .
How is it that autonomy and notions of rights can be conferred on an embryo whileit consists still of undifferentiated cells, logically weeks or months from any notionof independence?
Let’s leave aside inspirations such as the soul, and when it might enter a body,because we saw in Chapter 26 how futile and unhelpful such philosophical maneu-vering has been in illuminating the morality of embryo research. Instead, a fableabout two mice might help.
. . . and tales of mice
The first mouse in the fable was a field mouse, genetically an outbred mouse, a free-range mouse,but he and his extended family lived on a farm,where they inhabited andpopulated a wheat silo.By prospering, father (later,grandfather) mouse and the growingfamily could remain out of neither sight nor mind.The farmer who owned the wheatsilo reached the inevitable conclusion that the mouse clan were vermin mice.
The mice were then exterminated by the farmer in the ordinary course of farmbusiness.The farmer’s children were aware of it but, being brought up on a farm,thought nothing of it. If pests, whether bugs, insects or mammals, get in the way ofproducing food efficiently and hygienically then, without fuss, they’re got rid of.No-one’s humanity suffers or is called into question.
The second mouse was a genetically inbred white mouse, identical to hundredsof thousands of other mice—a battery mouse, we might call it, if it were lined upwith others to test the safety of batches of drugs or perfumes.
This particular mouse’s misfortune was that it became an ephemeral celebrity—briefly a work of living art—sacrificed in public by an avant garde artist who hadno luck in convincing anyone crucial to his immediate fate that he was other thanculpably inhumane, that essentially there was something wrong with his head. In anycase, an indignant, revulsed community and judiciary saw to it that he paid for themouse’s glazed eyes and cold, stiffening little corpse with, I believe, a dissuasive fineand a period of community service.
Just as we are when children torment an animal to death (fortunately now notas popular as it was once), inherently compassionate people intimately concernedwith such an experience are saddened, perhaps a little brutalized.
What do these stories have in common, and in what ways do they differ? Andhow do they help us come to grips with human embryo research? Both are storiesof intentional rodenticide. But are the ethics of rodenticide immutable? Or are themoral circumstances of these two stories different?
Surely they are different. However inconsistent it is for mice, and however wemight luxuriate philosophically in the wrongs of rodenticide as our memories of
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 381

Since the late nineteenth century, there have been several medical and social waves ofliberation for women.Early in the twentieth century Sigmund Freud discouraged the inhi-bition of sexuality in the rearing of children.Through the century the women’s liberationmovement, latterly known as feminism, intensified the pressure for change.The results haveincluded (1) female emancipation (the vote for women); (2) development of effective pregnancyprevention; (3) better hygiene and the conquest of infection with antibiotics, leading to safechildbirth; (4) privacy and a tendency for the law to intrude less into bedroom matters; and(5) the option of divorce for marriages that no longer work.
The 1960s and 1970s—the two decades that followed the invention of the oral contra-ceptive or birth control pill—saw a rise in sexual permissiveness that was at last unshack-led from a corresponding risk of unwanted pregnancy.Abortion received widespread legalsanction in the 1970s in most Western countries. Only in the 1980s did the specter ofuntreatable, lethal venereal diseases from viruses begin to slow down the growth in popu-larity of premarital and extramarital sex.
Moral standards have waxed and waned throughout history, but the developments ofthe twentieth century brought to practical fruition trends that had been taking place forlonger than the 100-year-or-so moral cycle.These trends have included improving tech-nology, improving health and longevity, more effective personal freedoms and—veryconspicuously—a steady increase in the individual value placed upon children.
The present fortunate position is that the survival of children can be taken for grantedfrom infancy to old age; that we have command of contraception; and that we are nowcommanding conception—all of which means, or soon will mean, that reproduction, forthe first time in human evolution, is truly a matter of choice. Children are now regarded,perhaps sometimes overly so, as society’s most important members, with the popular claimthat, in matters of reproduction, the well-being of the child is important above all else.TheEnglish historian J.L. Stone, however, has demonstrated that today’s family in Western
mouse-traps and rat-catchers fall further into sociological and town-planning history,morality for most of us—our response to the deaths of the mice—will equate withhow we perceive our humanity to have been affected by their tales.
Rodenticide, at first sight, might not have much to do with embryo research.But it gives an insight into the projection of humanity and into what is dehuman-izing.The rights of these two mice turn out to be different because of the differentimpacts, the different duties we have to the two mice, have on how we sense ourhumanity.
The same is true of embryos, of their effect on us, on our duties toward them.It’s hard to see them in any perspective that does not depend utterly on their poten-tial—what they might become if a lot of things happen and if a lot of genetic codesand environmental circumstances are right.
But it is potential, not reality, and today their potential lies in the mind, the imag-ination, the hopes and aspirations of the beholder.
It is that which is the essence of humanity, of humanness, and which we respect.
382 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 382

societies, as a result of the cultural evolution that has elevated the child to such a pinnacle,is self-centred, inwardly turned, emotionally bonded, sexually liberated perhaps to a fault—and, though child-oriented, too often temporary.
Modern families, especially it seems in the USA and Scandinavia, but also in Australiaand other Western countries, are more loosely structured and less emotionally and sexuallycohesive than has been the case for centuries, according to Stone. In Chapter 22 we consid-ered how infertility can prove to be a better cement for a marriage under strain than fertil-ity provides.To the Indian social anthropologist Professor Prakash Reddy, accustomed toclose relations within his own extended family at home, the modern, sequestered, smallEuropean family of the type he studied in the Danish village of Hvilsager for his doctoralthesis lacks spirituality, overly emphasizes individualism, and has children brought up inde-pendent, alone and lonely.
Parents’ different, separate ambitions detach them from the home and from their depend-ence on each other.The guilt they feel over depriving children of adequate family life iscountered by concentrating too much on their children’s (very often on their one child’s)personal achievements. Children, according to Reddy, are becoming isolated within thefamily. For their socialization they depend not on their family but on their peer groups.(These trends are set to accelerate in countries such as the USA,where many children nowbeing conceived will have no hope of ever knowing one or both of their genetic parents—discussed further in Chapter 22.) As a ‘type’, this family has an impermanence, a transience,that for Stone recalls the chaos of earlier centuries.
Moreover there’s little reason to suppose that today’s Western ‘nuclear’ family modelhas a special claim to be the best—or that today’s typical small Western family will be morelasting than its predecessors. It’s been called ‘ethnocentric’ (overly regarding our own ethnicculture to be best) to assume that this one form of the family is crucial to the survival of asociety.This is the context in which we should examine gamete donation or sale, embryodonation and surrogacy. Cultural evolution, like biological evolution, works best if society,like nature, is rich enough and confident enough to accommodate diversity. In this way,changing circumstances bring adaptation, or more precisely they bring triumph for whatin retrospect are ‘preadaptations’: the luxury of diversity produces good results down thetrack that are not foreseen at the time the diversity is allowed to flower.With the twenti-eth-century nuclear family now fragile, we need to widen our concept of the family, toextend the notion of parenthood, to broaden our social options, to give people room tomove in finding solutions to society’s stresses and strains and how to bring up well-balancedchildren.This surely will value inclusiveness.
Looking into a future with the technology for ‘test-tube babies’ has brought manywriters to remember Aldous Huxley’s 1930s book Brave New World. It has brought some ofthese writers to be afraid of sliding down a slippery slope into the mechanical, oppressiveworld Huxley predicted for the future. It is timely to look again at Huxley’s background(a family of famous biologists, descended from Thomas Huxley, a friend of Charles Darwin)and purpose (which was not to halt technological development).
‘Sanity is a rare phenomenon in public life’, Huxley wrote in a new preface to BraveNew World in 1946, just after World War II. Huxley believed that governments would auto-
EMBRYO RESEARCH AND SOCIETY � 383
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 383

matically favor stability in society over truly responding to popular will, and would bureau-cratize reproduction. He believed this would cause powerful governments to become toobossy, too intrusive and too totalitarian, and that this situation would come about in thename of achieving ‘order’. Reproductive technology—maturation of eggs in vitro, in vitrofertilization and in vitro gestation—was the device Huxley used in Brave New World to illus-trate how a government could oppress.The danger was not the technology but the purposeit was put to.The remedy—the prophylaxis—Huxley advised, should be to decentralizecontrol over its application.
The reluctance of Australian politicians to grapple sensibly with altruistic surrogacy isa good example of government preferring order to change. (On the other hand, theAustralian government has been forward-looking in its provision of public funding for IVFand support for embryonic stem cell research.Generalizations can be unwise.) For anothertest of how those who govern us favor order for its own sake over change, watch howgovernments over the next decade deal with the personal matter of sex selection and so-called designer babies (discussed in Chapter 23).
So the sinister feature of the future in Aldous Huxley’s predictions was not what waspossible with IVF and embryonic life in test tubes. Rather, it was the total control thecentralized Utopian government of Brave New World had over people’s lives. (To imaginethe horrors that central-government control can have over sex and reproduction withoutany resort to technology read—or watch the video of—Margaret Atwood’s book TheHandmaid’s Tale.) It is surely a modern government’s proper job to foster tolerance and pluralopinions in society. It is not its role, gratuitously and paternalistically, to take personal deci-sions for its citizens.
In a tolerant society, decisions on assisting conception, like decisions on contraceptionand abortion, should be private and well-informed ones, taken by the people affected,helped by their professional advisors in a community framework of educated understand-ing.
By dealing explicitly with ethics, morality and suffering, as by explaining the physi-ology and medicine of infertility, I hope this book helps you to understand what’s happening,to talk with your doctor, and to voice your cause, your case and your concerns.
384 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 384

appendices
the arithmetic of it all, and a bibliography
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 385

Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 386
This page intentionally left blank

appendix 1
The arithmetic of infertility
The last 20 years have seen the physician’s approach to infertility transform.The devel-opment of IVF has so improved our capacity to overcome this most distressing ofdisabilities that we’ve had to overhaul many of our working ideas on how infertility
can come about. Some new causes have been discovered, generally of genetic origins. Butmore, we’ve come to appreciate how apparently minor disturbances can combine to causea major disruption in reproduction even when tests show that there’s no complete orabsolute barrier to getting pregnant.
A consequence of this change of approach is the need to change our way of explain-ing what’s happening to you. No longer is it good enough to say, ‘The chance of gettingpregnant after this operation is 60 percent.’This begs questions such as:‘Yes, but how longwill I have to wait?’; ‘Is that 60 percent in six months, a year or five years?’; ‘What effectwill my long periods (or my husband’s sperm count, or my endometriosis, or my age) haveon this chance?’;‘How will one or more cycles of IVF affect my chances of ending up witha baby?’
The first purpose of this appendix is to set out the arithmetic behind the new approachto appreciating fertility and infertility—an approach I introduce in Chapter 1. Its secondis to judge the place of various options for treatment when a couple has decided the preg-nancy has taken too long and the time remaining is getting short.
Before going on, it might be useful to reread Chapter 1. As I say there, at best—andsometimes, no doubt, at worst—getting pregnant is a matter of chance.The overall chancewill depend first on what the chance is biologically meant to be when you have sex at theright time; second, it will depend on the number of months (or cycles of ovulation) youcan keep trying, before you get too old or too fed up.
The statistic that describes this monthly chance is the monthly probability of conception,
387
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 387

known among population scientists as fecundability (abbreviated f): it’s the probability (thechance) of achieving pregnancy in one ovulation cycle. (You can express fecundability asa percentage, say 20 percent, or a proportion, 0.2—they mean the same thing.You mightremember from Chapter 1 that 20 percent represents normal average fecundability for apopulation of couples in their twenties when they first start trying to achieve a pregnancy.)Fecundability is similar to a number of other terms that are used, including ‘monthly fecun-dity’ (strictly speaking, the monthly probability of a live birth resulting from one cycleexposed to the possibility of pregnancy) and,more simply,monthly fertility. Like every statis-tic in biology, monthly fertility has a wide range of values in the population (shown inFigure A1.1). Figure A1.1 also represents,with an ellipse at the left end of the graph (markedS), a group of couples with a monthly fertility chance of zero—meaning sterility, whichaffects maybe 2 percent or 3 percent of couples trying to get pregnant: couples who havea complete barrier to getting pregnant that will always need more than just time toovercome.
Sterility is abnormal—that’s a statement that’s beyond argument (and diagnosing it isthe subject of Chapter 6).
Subfertility is a different matter. Population scientists—impersonal species that theyare!—might define subfertility as what the bottom 5 percent of the population have got—
388 � GETTING PREGNANT
S
RIN
HF
0% 10% 20% 30% 40% 50% 60% 70% 80%
Chance of getting pregnant each month
Figure A1.1 Distribution of monthly fertility in the population.A graph showing the wide range ofmonthly fertility in a large group of young people.The average for the group is 20%.The ellipse at the left end of the graph (S) represents the 2 or 3% of couples who havezero chance of pregnancy—meaning complete infertility, or sterility.To define normalfertility (N), we can separate the lowest 5% and the highest 5%, leaving the middle 90%as ‘normal’ (these cutoff points are arbitrary, however, and do not depend on any naturaldistinction). Couples in the ‘lower tail’ of the distribution then have abnormally lowfertility, or relative infertility (RI). Couples in the ‘upper tail’ (equally abnormal, youcould argue) have high fertility (HF).
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 388

corresponding with the bottom 5 percent of the area under the graph (marked RI, forrelative infertility). Fixing its limits within the normal range of monthly fertility shown inFigure A1.1 is quite arbitrary, as I discuss under Normal fertility in Chapter 1.You and Iwould probably put the cut-off rather higher than 5 percent.We would, instead, call thesituation subfertility or relative infertility whenever you think trying for pregnancy hasgone on long enough and you go to see your gynecologist for tests and advice. (Somepeople might say anything below average is enough to warrant having something doneabout it; again, your perception of how long it’s taken and how long you’ve still got arewhat’s important—but you might now be able to imagine the difficulty that arbitrarilydefining infertility like this causes for some administrators, politicians, radical feminists andothers who have been critical of expensive reproductive technology.)
In statistics, incidentally, it’s not just the bottom, say, 5 percent that’s abnormal. Logically,the top 5 percent of a statistical distribution curve such as Figure A1.1 is just as abnormal.It would correspond with ‘abnormally high fertility’ (HF).This phenomenon (it’s muchless of a problem than it used to be before the days of effective contraception) I discuss inChapter 1 under High fertility, a disability?
Tests for infertility can—and often do—give us results that are not conclusive.Pregnancyseems possible, but it hasn’t happened yet. Sometimes the investigations are all normal—unexplained infertility.But in practice the distinction between infertility of known cause andunexplained infertility is much less important than it used to be.Although IVF was devel-oped so that we could get around damaged fallopian tubes that were beyond repair—andundoubtedly this has transformed the treatment of sterility and serious infertility from thiscause—it’s in the modification of IVF to deal with subfertility and unexplained infertilitythat the second, bigger transformation in treatment is taking place.
APPENDIX 1 � 389
0 3 6 9 12 15 18 21 24 27 30 33 36
Months
Acc
umul
atin
g pr
opor
tion
pre
gnan
t 1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0
ƒ1 = 20%
ƒ1 = 5%ƒ1 = 1%
ƒ37 = 4.6%
ƒ37 = 3%
ƒ37 = 0.7%
Figure A1.2 Accumulating chance of having gotten pregnant. Modeling the cumulative chance ofhaving gotten pregnant over three years from average first-month fertilities ( f1) of 20%,5% and 1%.The right-hand figures give the residual average monthly fertility of thosestill not pregnant after the three years, that is, for month number 37 ( f37).
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 389

To understand relative infertility, and to understand when to use assisted conceptionmaneuvers to try to overcome it, I’ll make use of this special statistic—monthly fertility—and show you how with time monthly fertility mounts up to what’s called the cumulativechance of pregnancy.Take a first look now at Figure A1.2 for an introduction to this concept.
The classical causes of subfertility are described in Chapter 7, but experience has shownthat discovering a cause—and assessing the severity of it—is less important in determiningmonthly fertility (and hence the eventual chance of getting pregnant naturally as the monthspass) than is the duration of infertility.The other variable in determining the chance of achiev-ing pregnancy naturally in circumstances of relative infertility is the time available for chanceto have its way: the time left for conception.There are some other points I need to cover beforeI place assisted conception into this context.
We can show in theory and in practice that the worse a diagnosed cause of infertility is,the better the chance of getting pregnant naturally will end up being after treatment—provided that the treatment corrects the problem properly and that the treatment does not,through side actions, interfere with any other aspects of reproductive functioning. Mildabnormalities discovered while investigating infertility, on the other hand, may turn out tobe decoys, and attempts to treat them, especially if they’re multiple, not only lure attentionaway from whatever the undiscovered ‘real’ cause might be but risk introducing new dis-turbances that then take the distracting place of the original suspected abnormality orabnormalities. (In medicine generally, physicians or surgeons are most likely to achievebeneficial outcomes when departures from normal are more than slight, as I mention inthe box, Medicine’s perennial paradox, in Chapter 1. Most of our treatments can have side-effects and these side-effects are more likely to tip the balance unfavorably when the condi-tion being treated is relatively trivial.This principle is particularly prominent in reproductivemedicine and surgery.)
Frustration for you and your doctor in diagnosis and treatment is especially likely whenseveral abnormalities, possibly all individually mild, occur together.To demonstrate just howpowerful such multiple problems can be in preventing pregnancy we need to understandthe arithmetic of getting pregnant a bit better.
The now-standard medical way of judging the outcome of infertility treatment is what’scalled a life curve. Figure A1.2 shows an example of a life curve: in this case it’s the cumu-lative theoretical chance of having become pregnant during three years of trying to, based onthe average monthly fertility values for the start of the three years that are given in theboxed labels for each graph. Because these values are averages, as we progress along theparticular life curve the average monthly fertility of the couples who haven’t gotten pregnantfalls with each passing month (since it’s more likely that those with above-average monthlyfertility will conceive first). In constructing these graphs I’ve assumed that all the knowncauses of sterility (complete infertility not resolvable by time alone) have been excludedby the usual tests—so that, at least theoretically, everyone has a chance of getting pregnantif time can just go on and on.The figures to the right of Figure A1.2 give the remainingaverage monthly fertility rate of those couples who are still not pregnant after the threeyears.Notice, incidentally, that in this way three years of no pregnancy diminishes expectedmonthly fertility from 20 percent per month to 4.6 percent per month—which is
390 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 390

comparable to a fall that would be caused by introducing, at time zero, a disarrangementof anatomy or physiology that causes a 75 percent fall in monthly fertility (that is, from20 percent to 5 percent). Such is the power of ‘self-selection’.
Let me put this plainly and boldly: the longer the duration of the infertility hasbeen, the lower the chance each month of getting pregnant will be—whateverthe tests show.You would think that this principle would now be so well known that,when infertility treatments are being compared in clinical studies, getting a control group whohave spent the same time trying to get pregnant would be a necessity. But it’s quite rare inthe medical literature on treating infertility. Instead, study after published study still tries tocompare one treatment with another, or with no treatment, among patients who have acertain ‘dose’ of some deemed cause—such as a certain amount of endometriosis, a certainreduction in sperm count, and so on.This is fine in dramatically thorough causes of infer-tility—particularly it works with causes of sterility—but it doesn’t work for mild causes.
It’s not hard to imagine disturbances that cause the monthly chance of getting pregnantto fall in this way—that is, to about a quarter of what it otherwise should be. Mildendometriosis,mild oligospermia,mild abnormalities of the cervix and mild peritubal adhe-sions are all good examples. In combination, however, these decreases have to be multipliedtogether (see Table A1.1). In other words, whereas just one such abnormality is scarcelylikely to come to the surface and result in infertility (pregnancy is delayed but it still happensinside an acceptable time), combinations can be disastrous, with monthly fertility chancesthat are more like those of intentional and effective contraception! (This is also the reasonwhy,when we investigate infertility,we see combinations of mild abnormalities rather moreoften than we should if we were sampling the whole population.As a result, oligospermiaand endometriosis, for example, occur together more often among infertile couples thanthey would in a random sample of couples generally.)
But the proper conclusion is not to forecast virtually untreatable infertility when wefind such mixtures of disturbances. In reproductive medicine, correlating what we see inour tests with what is the real degree of disturbance is often unreliable.We cannot usuallyestimate, from the apparent or observed departure from normal disclosed by our investi-gations, just what the expected monthly fertility will be when a couple’s fertility has neveractually been put to the test. I’ve seen many young women with endometriosis, for example,
APPENDIX 1 � 391
Table A1.1 Modeling the effect of multiple minor abnormalities on monthly fertilityand on the likely time needed to get pregnant
Average monthly % Pregnant in % Pregnant in Average time neededNumber of factors fertility (%) 2 years 3 years to get pregnant
0 20 93.6 96.7 3 months
1 5 63.6 75.5 2 years
2 1 20.7 28.9 7 years
3 0.2 4.7 6.9 40 years
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 391

who’ve come to see me because of pain, but who then get pregnant quite quickly whenthey try. Instead, I emphasize again the duration of infertility and the time left for conception asbeing the important guides for estimating the chance of a pregnancy happening—moreimportant than working out the real or imagined, but capable of being labeled, diagnosis.
The technological interventions for assisting conception (described in Chapters 20 and22) share a capacity for increasing considerably the chance of getting pregnant in the monthin which they’re carried out.They achieve this by making much more likely the success-ful encounter of egg with sperm, resulting in fertilization, combined with multiplying thenumber of eggs or embryos in the reproductive tract.Their directness of approach to theproblem means that, very often, a whole series of diagnosed abnormalities can be got aroundin one maneuver.The same is true when there is no diagnosed abnormality.Depending onthe circumstances, pregnancy rates of between 5 percent and 40 percent per cycle are achiev-able; for many instances of subfertility or unexplained infertility this probably represents upto a 30-fold increase in monthly fertility.This then is how assisted conception finds itsrightful place in subfertility and unexplained infertility.
With assisted conception, pregnancy is thus still not certain, but the improvement seenover natural circumstances is considerable; and diagnosed causes of infertility, particularlyif they appear to be mild, are less important than they used to be.
I look at the results of treating infertility with IVF in Appendix 2.
392 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 392

appendix 2
IVF results
Not all IVF results are the same, not between women, not across town, nor amongdifferent countries. An analysis of the outcomes from our clinic, Sydney IVF, andcomparisons with national and international figures give useful insights that can be
used in a wide context.In Australia the National Perinatal Statistics Unit collates pregnancy data from all
Australian and New Zealand IVF clinics. In 1998, for example, there were over 14 000 eggretrieval cycles (and a further 1500 or so retrievals for the now much less frequentlyperformed procedure of gamete intrafallopian transfer, or GIFT). In that year at Sydney IVF,the second year of what are now at least four consecutive years during which the clinic hashad the highest IVF take-home baby rates in Australia, women under 35 had a greater than50 percent chance of having a baby from one round of IVF treatment.
A WOMAN’S AGE
Figure A2.1 shows the age distribution of the women treated at Sydney IVF in 1998 (thebar chart) as well as the chance of having at least one baby from one egg retrieval treat-ment (the line chart), irrespective of whether the pregnancy was immediate, using freshembryos, or with embryos stored and used after an interval.The chance of a woman under35 having a baby from one egg retrieval was better than 1-in-2 (52.4 percent). In this youngage group the great majority of embryo transfers, whether during the retrieval cycle orsubsequently, consisted of two embryos replaced (average 1.90). For women in their veryearly twenties the baby rate is even higher.
From the age of 34, however, there is an unremitting, straight-line decline in fertilityto reach zero before the age of 45, an age that is five or six years short of the median age
393
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 393

at menopause in Australia. It has long been recognized that fertility fails well before themenopause.This decline in IVF live births is about two years in advance of a similar naturalfall, which means that IVF cannot be relied on to overcome female age-related subfertil-ity (we call it the oopause) except by using donated eggs.
This early fall in fertility, and the fact that it cannot be overcome by IVF using thewoman’s own eggs, is important for society to take note of. Society must be encouragedto change, so that women can have children before they turn 34 without suffering thepenalty of gross or permanent jeopardy to their professional training and their career. It’simportant also to point out that the peak age of utilizing IVF (39 years) is six years after theage at which this decline in fertility starts. Investigating and treating infertility should getunderway at a younger age than it presently does.
THE IVF LAB: MISCARRIAGE OR LIVE BIRTH?
The average age of women attending Sydney IVF is 36, two years older than the nationalaverage of 34.We know from Chapter 8 that the chance of losing the baby from a miscar-riage depends a great deal on a woman’s age.
394 � GETTING PREGNANT
Figure A2.1 A histogram (bar chart) of the age women have IVF treatment at Sydney IVF in 1998,compared with the chance that one IVF treatment results in a baby (line chart).After avery high pregnancy rate in the early twenties, a plateau of over 50 percent is reachedthat lasts to the early thirties. From 34 the pregnancy rate steadily declines, to reach zeroby the early forties, for many women up to a decade before menopause. Note that IVFpeaks in popularity at the age of 39, six years after the decline in fertility starts.Reproduced with permission from the Medical Journal of Australia.
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 394

APPENDIX 2 � 395
Figure A2.2 Graph showing the increase in pregnancy rate at Sydney IVF that occurred with theintroduction of new embryo culture techniques during 1996.These involved highlystable temperature conditions, a low oxygen and high carbon dioxide environment, andspecially designed embryo transfer catheters.The improvements occurred both withfresh embryo transfers (Graph A) and with frozen embryo transfers (Graph B). In 2000the live birth rate stabilized despite moving from the usual two-embryos transferred toan increasing number of elective single embryo transfers (see text), greatly reducing twinpregnancies.
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 395

But despite this tendency for miscarriages to be commoner in older women, thechance of miscarriage from IVF is less at Sydney IVF than it is for many other clinics.Table A2.1 shows that the risk of having your pregnancy miscarry after IVF in 1998 was10.5 percent under the age of 35, and 16.1 percent between 35 and 40. After the ageof 40 it was over 40 percent, but this figure will come down significantly as preimplan-tation genetic diagnosis is used increasingly to screen embryos before transfer, using molecularkaryotyping.
This comparatively low risk of miscarriage is important for anyone hoping to have ababy, of course, but it’s a particularly important one if IVF with PGD is being used toovercome recurrent miscarriages (see Chapter 9).
The decreasing risk of miscarriage over the last decade at Sydney IVF has paral-leled the increase in the take-home baby rate from both fresh and frozen embryo transfers(Figure A2.2).The laboratory improvements that made this increase possible consist of:• A proprietary suite of stage-dependent embryo culture media made under license by
Cook IVF (Brisbane, Queensland) and Cook Urological (Bloomington, Indiana) andapproved by the US Food and Drug Administration in 2000;
• Mini- or desktop incubators (MINCs) with highly stable environmental conditions,including low oxygen levels comparable to the situation found deep inside the body,but with high carbon dioxide levels to supply the embryo with extra carbon atoms thatbuild up cellular structures; and
• Special embryo transfer systems that incorporate an outer cannula with a ‘Jansen-Anderson bulb tip’ (for negotiating the mucus-filled cervix) and a very soft innercatheter, brought no closer than 1 to 2 centimeters from the top of the uterine cavity.
For Sydney IVF’s international consulting projects the miscarriage rate is such a sensitiveyet robust indicator of good clinical and laboratory practice between clinics that we relyon it more than on overall pregnancy rates in assessing our client programs’ needs. (It canbe calculated from published data such as that from the National Perinatal Statistics Unitby subtracting the ‘viable’ pregnancies per embryo transfer from the ‘clinical’ pregnanciesand then dividing by the clinical pregnancies. Either the actual numbers or the percentagerates can be used in this calculation.)
INTERNATIONAL COMPARISONS: REDUCING LOST BABIES FROM TWINS ANDHIGHER MULTIPLES
You would think that the more embryos that are transferred at a time with IVF the greaterthe chance is that you’ll get pregnant. But getting pregnant, of course, is only the first step:you need to deliver your baby before you’ve got what you started IVF for in your hands.The other major factor that determines the chance of leaving the obstetric hospital witha baby is avoiding a high-risk multiple pregnancy.Table A2.1 shows that at Sydney IVF in1998, five of the seven pregnancies lost after 20 weeks from prematurity or stillbirth weretwin pregnancies. So there is—or should be—a much greater emphasis on transferring justone embryo at a time (called eSET, or ‘elective single embryo transfer’).
396 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 396

Differences in the recommended number of embryos transferred at a time is maybethe most obvious area of contrast in IVF practice between countries. But digging deeperinto the data shows that there are lab or clinical quality issues involved in the differencesas well.
National IVF results are reported as pregnancies per egg retrieval or embryo transfer.This information is a bit different from the figures I mentioned above (because it does notadd frozen embryo transfers to fresh transfers for each retrieval), but the data are widelyavailable and the overall delivery rate after IVF can easily be compared between countries(or clinics) or over time (Figure A2.2). In this respect, and counting women of all ages, in1998 the viable birth rate for IVF per embryo transfer in Australia was 17.4 percent (or16.8 percent if we take out Sydney IVF, where it was 29.9 percent). In Western Europein 1998, rates ranged from 16 percent in Germany (where legislation limits the numbersof eggs a woman may have fertilized), through 22 percent in the UK, to over 27 percentin Norway and Sweden. In the USA in 1998 the national delivery rate was 31 percent,but at the cost of a high multiple pregnancy rate of 38 percent, including triplets andhigher order multiples, reflecting the high number of embryos typically transferred at oncein that country.
Excepting the USA, these take-home baby rates are inversely related to these countries’proportion of embryo transfers involving more than two embryos (Germany, 59 percent;UK, 44 percent;Australia, 25 percent; Sweden, 4 percent), and hence not surprisingly alsoinversely related to their national IVF triplet pregnancy rates (Germany, 3.7 percent; UK,2.0 percent;Australia, 1.1 percent;Norway and Sweden,0.2–0.5 percent).Note that Norwayand Sweden obtain the highest take-home baby rates per procedure even though theytransfer the smallest number of embryos at a time.These differences are not explained byany possible differences in the woman’s age: the average age of women having IVF proce-dures in 1998 was 33.5 in Germany, 33.8 in the UK, and 34.2 in Sweden and in Australia(at Sydney IVF, 35.8). In other words, the countries and clinics best at carrying out IVFtend to transfer fewer embryos at a time.
So to boost the take-home baby rate further, since 1998 at Sydney IVF we have movedrapidly towards transferring just one embryo at a time (‘eSET’)—almost always after fiveor six days of culture, at the stage of blastocyst. Blastocysts can have a significantly increasedchance of producing a baby (see Table A2.2); there still seems to be about a one-in-20 riskof monozygotic twins.
Our latest statistics (see the box, Easy does it! Elective single embryo transfer) revealthe logic of this strategy: there’s at least as much chance of having a baby to show foryour one IVF treatment cycle if one embryo is transferred instead of two.And you arelikely to have more embryos in storage for subsequent pregnancies, so if you wanta family of more than one child, you’re more likely to get the family you want fromone IVF treatment cycle if the embryos are transferred one at a time rather than twoat a time.
APPENDIX 2 � 397
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 397

398 � GETTING PREGNANT
Table A2.1 Pregnancy outcome according to maternal age at egg retrieval for 1998 atSydney IVF
Age group All Ectopic Clinical Immature Single Twinpregnancies pregnancies miscarriages deliveries live births live
and stillbirths births
under 35 156/252 3/156 16/153 5 102 30c/132n=252 (61.9%) (1.9%)a (10.5%)b (22.7%)d
35-39 94/251 1/94 15/93 2 61 15/76
n=251 (37.5%) (1.1%)a (16.1%)b (19.7%)d
40-44 28/131 0/28 12/28 0 15 1/16
n=131 (21.4%) (42.9%)b (6.3%)d
Alle 278/634 4/278 43/274 7f 178 46/224
n=634 (43.9%) (1.5%)a (15.8%)b (20.5%)d
NotesCombined data for fresh and frozen embryo transfers.The average number of embryos transferred was 1.9.Outcomes audited by Ernst and Young. Reproduced with permission from the Medical Journal of Australia.a. Ectopic pregnancy rate denominator is all the pregnancies.b. Miscarriage rate denominator is those pregnancies that were in the uterus.c. One twin pregnancy was reduced from triplets by a feticidal operation.d. Twin pregnancy rate denominator is live births.e. Excludes 14 women aged 45 to 48, none of whom conceived.f. Two singleton pregnancies (in women under 35) were lost at 22 weeks; remaining five were twin
pregnancies lost between 21 and 32 weeks.
Table A2.2 Chance of one embryo resulting in a baby, depending on the stage ofdevelopment of the embryo.Year 1998 and 2001 information fromSydney IVF
one day 3 embryo one day 5 embryo(~8-cell embryo) (blastocyst)
under 35 22% 42%
35–39 11% 24%
40 plus 4% 12%
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 398

APPENDIX 2 � 399
Easy does it! Elective single embryo transfer
From 2001, women under 38 who had more than one suitable day-5 IVF embryofor transfer at Sydney IVF were encouraged to have a single blastocyst transferred,not two.By the time our analysis of birth outcomes began in 2002, 111 women hadagreed to eSET and 283 had chosen to have two embryos transferred.Here I analysewhere they have ended up, baby-wise.
Among the 111 eSET women, 46 became clinically pregnant with their freshembryo and another 17 were pregnant after a single stored embryo was transferred,representing 63 pregnancies (a clinical pregnancy rate of 57 percent), four of whichmiscarried (a miscarriage rate of just 6.4 percent).As a group, at the stage of this firstanalysis, their ongoing pregnancy rate is 53 percent, and there are still an average of3.6 stored blastocysts per woman.
Among the 283 women having embryos transferred two at a time, 154 becameclinically pregnant with fresh embryos, of whom 73,or 47 percent, conceived twins;another 19 conceptions followed frozen embryo transfers, representing a total of173 pregnancies (a clinical pregnancy rate of 61 percent, slightly higher than the57 percent of the eSET women), but 19 of which miscarried (a miscarriage rate of11 percent, almost twice as high as the eSET women). As a group, their ongoingpregnancy rate is a shade over 54 percent, just a percentage point higher than theeSET women, and with an average of only 2.5 blastocysts stored per woman.
Our second analysis, due in late 2003, will enable us to factor in the events oflater pregnancy and the delivery. If, as we expect,more twin pregnancies than single-ton births are lost around the time of birth, we will, for the first time in the historyof IVF, have shown that you are now more likely to have a baby or babies if yourblastocyst embryos are transferred one at a time.This is good news for everyone,including our colleagues working in the neonatal nurseries.
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 399

appendix 3
More reading
Abook written to be read by lay people and college students can’t have its textburdened by meticulous academic reference to the scientific literature.Yet, for manyreaders and students there will be opinions and statements in various chapters that
invite questions or which could tempt you out of interest to dig deeper.Where I’ve referredexplicitly to the work of others, I provide the source here. And to explain the basis forsome of the other material in the text, I list here what I’ve written before on the subjectscovered in each chapter, not to confer importance on them as articles, but because access-ing these earlier publications, each of which itself is properly referenced, can provide thepath for the curious—and the indignant—to delve further into sources. PDF files of mostof my articles can be downloaded free from www.jansen.com.au/author.htm.
Preface
Jansen, P.C. (1936) Microfotografische techniek.Antwerp: de Sikkel.
Chapter 1
Recommended general reading
Leridon, H. (1977). Human Fertility:The Basic Components. Chicago: University of ChicagoPress.
Stone, L. (1977). The Family, Sex and Marriage in England 1500–1800. London:Weidenfeldand Nicolson.
400
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 400

Bibliography
Jansen, R.P.S. (1983). ‘Peritoneal and plasma estradiol and progesterone levels in mild andmoderate endometriosis:A search for luteinized unruptured follicles’.Fertility and Sterility39: 394.
—— (1993). ‘Relative infertility: Modelling clinical paradoxes’. Fertility and Sterility 59:1041–5.
—— (1995).‘Elusive fertility: Fecundability and assisted conception in perspective’.Fertilityand Sterility 64: 252–4.
Selected other sources
Leridon, H., and Spira, A. (1984). ‘Problems in measuring the effectiveness of infertilitytherapy’. Fertility and Sterility 41: 580–6.
Norman, R.L. (1994). ‘Corticotropin-releasing hormone effects on luteinizing hormoneand cortisol secretion in intact female rhesus macaques’. Biology of Reproduction 50:949–55.
Norman, R.L., McGlone, J., and Smith, C.J. (1994).‘Restraint inhibits LH secretion in thefollicular phase of the menstrual cycle in rhesus macaques’. Biology of Reproduction 50:16–26.
Chapter 2
Recommended general reading
Morris, D. (1986). The Illustrated Naked Ape. London: Jonathan Cape.Potts,M., and Short,R. (1999).Ever Since Adam and Eve.Cambridge:Cambridge University
Press.Short, R.V. (1984). ‘Species differences in reproductive mechanisms’. In C.R. Austin and
R.V. Short (eds), Reproduction in Mammals. Book 4: Reproductive Fitness. (pp. 24–61).Cambridge: Cambridge University Press.
Silber, S.J. (1990).‘Why are humans so infertile?’ In S.J. Silber, How to Get Pregnant with theNew Technology. New York:Warner Books.
Tuchman,B. (1986).The Distant Mirror.The Calamitous Fourteenth Century.New York:PenguinPutnam.
Bibliography
Jansen, R.P.S. (1994). ‘Ovulation and the polycystic ovary syndrome’. Australian and NewZealand Journal of Obstetrics and Gynaecology 34: 277–85.
—— (1999).‘Sex, reproduction and impregnation:by 2099 we won’t confuse them’.MedicalJournal of Australia, 171: 666–7.
APPENDIX 3 � 401
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 401

Selected other sources
Short, R.V. (1984). ‘Species differences in reproductive mechanisms’. In C.R. Austin andR.V. Short (eds), Reproduction in Mammals. Book 4: Reproductive Fitness. (pp. 24–61).Cambridge: Cambridge University Press.
Chapters 3 and 4
Bibliography
Jansen, R.P.S. (1967) Light and electron microscopic studies on the effects of subcutaneousinjection of cadmium chloride and experimental cryptorehidism on the testis and adeno-hypophysis of the adult rat. B.Sc. (Med.) Thesis.The University of Sydney.
—— (1978).‘Fallopian tube isthmic mucus and ovum transport’. Science 201: 349–51.—— (1980). ‘Cyclic changes in the human fallopian tube isthmus and their functional
importance’. American Journal of Obstetrics and Gynecology 136: 292–308.—— (1984).‘Endocrine response in the fallopian tube’. Endocrine Reviews 5: 525–51.—— (1985).‘Endocrine response in the female genital tract’. In R.P.Shearman (ed.),Clinical
Reproductive Endocrinology. (pp. 109–64). Edinburgh: Churchill Livingstone.—— (1994). Follicles in competition [scientific correspondence]. Nature 367: 10.—— (1998).‘Effects of estrogen and progesterone on myometrium, cervix, fallopian tube,
vagina and vulva’. In I.S. Fraser, R.P.S. Jansen, R. Lobo and M. Whitehead (eds),Estrogens and Progestogens in Clinical Practice. (pp. 173–186). Edinburgh: ChurchillLivingstone.
Jansen, R.P.S., and Bajpai,V.K. (1982).‘Oviductal acid mucus glycoproteins in the estrousrabbit: An ultrastructural and histochemical study’. Biology of Reproduction 26:155–68.
—— (1983).‘Periovulatory glycoprotein secretion in the macaque fallopian tube’.AmericanJournal of Obstetrics and Gynecology 147: 598–608.
Jansen,R.P.S.,Turner,M., Johannisson,E.,Landgren,B.-M., and Diczfalusy,E. (1985).‘Cyclicchanges in human endometrial surface glycoproteins: A quantitative histochemicalstudy’. Fertility and Sterility 44: 85–91.
Jansen, R.P.S., and Ramsay, P. (1998). ‘Imaging in gynecological infertility’. In Anderson,J.C. (ed.), Gynecological Imaging. (pp. 567–580). London: Churchill Livingstone.
Ramsay, P. and Jansen, R.P.S. (1998). ‘Ultrasonography of the normal female pelvis’. InJ.C.Anderson (ed.),Gynecological Imaging. (pp. 567–580).London:Churchill Livingstone.
Selected other sources
Isermann,B.,others, and Weiler,H. (2003) ‘The thrombomodulin–protein C system is essen-tial for the maintenance of pregnancy’. Nature Medicine 9: 331–7.
402 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 402

Chapters 5, 6 and 7
Bibliography
Bowman, M., and Jansen, R. (1995).‘Modern management of infertility’. Modern Medicineof Australia October: 130.
Jansen, R.P.S. (1980). ‘Abortion incidence following fallopian tube repair’. Obstetrics andGynecology 56: 499–502.
—— (1982). ‘Spontaneous abortion incidence in the treatment of infertility’. AmericanJournal of Obstetrics and Gynecology 143: 451–73.
—— (1990). ‘Infertility and abortion’. In H.J. Huisjes and T. Lind (eds), Early PregnancyFailure. (pp. 196–211). Edinburgh: Churchill Livingstone.
Jansen, R. (1999). ‘Transmission of the mitochondrial genome’. In R. Jansen andD. Mortimer (eds), Towards Reproductive Certainty: Fertility & Genetics Beyond 1999.(pp. 333–47). London: Parthenon.
Jansen, R.P.S., and de Boer, K.A. (1998). ‘The bottleneck: Mitochondrial imperatives inoogenesis and ovarian follicular fate’. Molecular and Cellular Endocrinology 145: 81-88.
Jansen, R.P.S., and Elliott, P.M. (1981). ‘Angular intrauterine pregnancy’. Obstetrics andGynecology 58: 167–75.
Jansen,R.P.S., and Ramsay,P. (1998).‘Imaging in gynecological infertility’. In J.C.Anderson(ed.), Gynecological Imaging. (pp. 61–80). London: Churchill Livingstone.
Ramsay,P., and Jansen,R.P.S. (1998).‘Ultrasonography of the normal female pelvis’. In J.C.Anderson (ed.), Gynecological Imaging. (pp. 567–580). London: Churchill Livingstone.
Selected other sources
DeCherney, A.H., Kort, H., Barney, J.B., and DeVore, G.R. (1980). ‘Increased pregnancyrate with oil-soluble hysterosalpingography dye’. Fertility and Sterility 33: 407–10.
Gleicher, N., Pratt, D., Parrilli, M., Karande,V., and Redding, L. (1992).‘Standardization ofhysterosalpingography and selective salpingography:A valuable adjunct to simple opaci-fication studies’. Fertility and Sterility 58: 1136–41.
Handyside, A. (1992). ‘Prospects for the clinical application of preimplantation diagnosis:The tortoise or the hare’. Human Reproduction 7: 1481–3.
Kerin, J.,Anderson, R., Daykhovsky, L., Stein,A., Segalowitz, J.,Wade, M., Surrey, E., andGrundfest,W. (1990). ‘Falloposcopy: A microendoscopic technique for visual explo-ration of the human fallopian tube from the uterotubal ostium to the fimbria using atransvaginal approach’. Fertility and Sterility 54: 390–400.
O’Neill, C., Ryan, J.P., Collier, M., Saunders, D.M., Ammit, A.J., and Pike, I.L. (1989).‘Supplementation of in-vitro fertilisation culture medium with platelet activating factor’.Lancet ii: 769–72.
APPENDIX 3 � 403
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 403

Chapters 8 and 9
Bibliography
Jansen, R.P.S. (1980). ‘Abortion incidence following fallopian tube repair’. Obstetrics andGynecology 56: 499–502.
—— (1982). ‘Spontaneous abortion incidence in the treatment of infertility’. AmericanJournal of Obstetrics and Gynecology 143: 451–73.
—— (1990). ‘Infertility and abortion’. In H.J. Huisjes and T. Lind (eds), Early PregnancyFailure. (pp. 196–211). Edinburgh: Churchill Livingstone.
—— (2001).‘Germline passage of mitochondria: Quantitative considerations and possibleembryological sequelae’. Human Reproduction 15 (Suppl. 2): 112–28.
Selected other sources
Boué, J.G., and Boué,A. (1973).‘Increased frequency of chromosomal anomalies in abor-tions after induced ovulation’. Lancet 1: 679–80.
Illeni, M.T., Marelli, G., Parazzini, F.,Acaia, B., Bocciolone, L., Bontempelli, M., Faden, D.,Fedele, L., Maffeis,A., and Radici, E. (1994).‘Immunotherapy and recurrent abortion:A randomized clinical trial’. Human Reproduction 9: 1247–9.
Macnaughton,M.C. (1964).‘The probability of recurrent abortion’. Journal of Obstetrics andGynaecology of the British Commonwealth 71: 784.
Naylor, A.F., and Warburton, D. (1979). ‘Sequential analysis of spontaneous abortion. II.Collaborative study data’. Fertility and Sterility 31: 282–6.
Warburton,D., and Fraser, F.C. (1964).‘Spontaneous abortion risks in man:Data from repro-ductive histories’. American Journal of Human Genetics 16: 1–25.
Chapter 10
Recommended general reading
Silber, S.J. (1990).‘Why are humans so infertile?’ In S.J. Silber, How to Get Pregnant with theNew Technology. New York:Warner Books.
—— (1995).‘What forms of male infertility are there left to cure?’Human Reproduction 10:503–4.
Bibliography
Jansen, R.P.S. (1970). ‘Electronmicroscopic observations on the Sertoli cell in the experi-mentally cryptorchid rat testis’. Journal of Anatomy 106: 192.
Jansen,R.P.S.,Anderson, J.C.,Radonic, I., Smit, J., and Sutherland,P.D. (1988).‘Pregnanciesafter ultrasound-guided fallopian insemination with cryostored donor semen’. Fertilityand Sterility 49: 920–2.
Lippi, J.,Mortimer,D., and Jansen,R.P.S. (1993).‘Sub-zonal insemination for extreme malefactor infertility’. Human Reproduction 8: 908–15.
404 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 404

Selected other sources
Brahams, D. (1992).‘Chlorambucil infertility and sperm banking’. Lancet 339: 420.Guillette, L.J. Jr. (1995). ‘Endocrine-disrupting environmental contaminants and reproduc-
tion: Lessons from the study of wildlife’. In D.R. Popkin and L.J. Peddle (eds), Women’sHealth Today: Perspectives on Current Research and Clinical Practice. (pp. 201–7). London:Parthenon.
Klein,R.D. (1989). Infertility:Women Speak Out about Their Experiences of Reproductive Medicine.London: Pandora Press.
Liebaers, I., Bonduelle, M.,Van Assche, E., Devroey, P., and Van Steirteghem,A. (1995).‘Sexchromosome abnormalities after intracytoplasmic sperm injection’. Lancet 346: 1095.
Lilford, R., Jones,A.M., Bishop, D.T.,Thornton, J., and Mueller, R. (1994). ‘Case-controlstudy of whether subfertility in men is familial’. British Medical Journal 309: 570–3.
Martinez,A.R.,Bernardus,R.E.,Voorhorst,F.J.,Vermeiden, J.P.W., and Schoemaker, J. (1991).‘Pregnancy rates after timed intercourse or intrauterine insemination after humanmenopausal gonadotropin stimulation of normal ovulatory cycles:A controlled study’.Fertility and Sterility 55: 258–65.
Serhal, P., and Craft, I.L. (1987). ‘Immune basis for pre-eclampsia: Evidence from oocyterecipients’. Lancet ii, 744.
Sharpe, R.M. (1995).‘Another DDT connection’. Nature 375: 538–9.Sharpe,R.M., and Skakkebaek,N.E. (1993).‘Are oestrogens involved in falling sperm counts
and disorders of the male reproductive tract?’. Lancet 341: 1392–5.Skakkebaek, N.E., Giwercman, A., and de Kretser, D. (1994). ‘Pathogenesis and manage-
ment of male infertility’. Lancet 343: 1473–9.
Chapter 11
Bibliography
Handelsman, D.J., Jansen, R.P.S., Boylan, L.M., Spaliviero, J.A., and Turtle, J.R. (1984).‘Pharmacokinetics of gonadotropin-releasing hormone: Comparison of subcutaneousand intravenous routes’. Journal of Clinical Endocrinology and Metabolism 59: 739–46.
Jansen, R.P.S. (1993). ‘Pulsatile intravenous gonadotrophin releasing hormone for ovula-tion induction: Determinants of follicular and luteal phase responses’. HumanReproduction 8 (Suppl. 2): 193–6.
Jansen, R.P.S., Handelsman, D.J., Boylan, L.M., Conway,A., Shearman, R.P.S., and Fraser,I.S. (1987).‘Pulsatile intravenous gonadotropin-releasing hormone for ovulation induc-tion in infertile women. I. Safety and effectiveness with outpatient therapy’.Fertility andSterility 48: 33–8.
Jansen, R.P.S., Handelsman, D.J., Boylan, L.M., Conway,A., Shearman, R.P.S., Fraser, I.S.,and Anderson, J.C. (1987). ‘Pulsatile intravenous gonadotropin-releasing hormone forovulation induction in infertile women. II. Analysis of follicular and luteal phaseresponses’. Fertility and Sterility 48: 39–44.
APPENDIX 3 � 405
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 405

Selected other sources
Ellison, P.T., Panter-Brick, C., Lipson, S.F., and O’Rourke, M.T.O. (1993).‘The ecologicalcontext of human ovarian function’. Human Reproduction 8: 2248–58.
Frisch,R.E. (1987).‘Body fat,menarche, fitness and fertility’.Human Reproduction 2:521–33.Kallmann, F.J., Schonfield,W.A., and Barrera, S.E. (1944): ‘The genetic aspects of primary
eunuchoidism’. Am. J. Ment. Defic. 48:203.
Chapter 12
Selected other sources
Venn,A.,Watson, L., Lumley, J., Giles, G., King, C., Healy, D. (1995). ‘Breast and Ovariancancer incidence after infertility and invitro fertilization’. Lancet 346: 995–1000.
Chapter 13
Bibliography
Jansen, R.P.S. (1981). ‘Fallopian tube secretions: Implications for tubal microsurgery’.Australian and New Zealand Journal of Obstetrics and Gynaecology 21: 140–2.
—— (1993). ‘Medicine and surgery inside the fallopian tube’. Medical Journal of Australia158: 799–800.
—— (1995). ‘Ultrastructure and histochemistry of estrogen-dependent acid mucusglycoproteins in the mammalian oviduct’. Microscopy Research and Technique 32:29–49.
—— (1998).‘Sex steroid production from ovarian tumors’. In I.S. Fraser, R.P.S. Jansen, R.Lobo and M.Whitehead (eds),Estrogens and Progestogens in Clinical Practice. (pp. 745–60).New York: Churchill Livingstone.
Chapter 14
Bibliography
Franklin, R.R., Diamond, M.P., Malinak, L.R., Larsson, B., Jansen, R.P.S., Ronsenberg, S.,and Webster, B.W. (1995). ‘Reduction of ovarian adhesions by the use of Interceed’.Obstetrics and Gynecology 86: 335–40.
Jansen, R.P.S. (1980).‘Surgery–pregnancy time intervals after salpingolysis, unilateral salp-ingostomy, and bilateral salpingostomy’. Fertility and Sterility 34: 222–5.
—— (1982).‘Pelvic surgery in young women’. Medical Journal of Australia i: 525–6.—— (1985a). ‘Failure of intraperitoneal adjuncts to improve the outcome of pelvic
operations in young women’. American Journal of Obstetrics and Gynecology 153:363–71.
—— (1985b). ‘Early laparoscopy after infertility surgery’ [abstract]. Fertility and Sterility44: 8s.
406 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 406

—— (1986a).‘Tubal resection and anastomosis. I. Sterilization-reversal’.Australian and NewZealand Journal of Obstetrics and Gynaecology 26: 294–9.
—— (1986b).‘Tubal resection and anastomosis. II. Isthmic salpingitis’. Australian and NewZealand Journal of Obstetrics and Gynaecology 26: 300–4.
—— (1988a). ‘Early laparoscopy after pelvic operations to prevent adhesions: Safety andefficacy’. Fertility and Sterility 49: 26–31.
—— (1988b). ‘Failure of peritoneal irrigation with heparin during pelvic operationsupon young women to reduce adhesions’. Surgery, Gynecology and Obstetrics 166:154–60.
—— (1990a).‘Prevention and treatment of postsurgical adhesions’.Medical Journal of Australia152: 305–6.
—— (1990b).‘Controlled clinical approaches to investigating the prevention of peritonealadhesions’. Progress in Clinical and Biological Research 358: 177–92.
—— (1991). ‘Prevention of pelvic peritoneal adhesions’. Current Opinion in Obstetrics andGynecology 3: 369–74.
Selected other sources
Thurmond,A.S.,Novy,M.,Uchida,B.T., and Rosch, J. (1987).‘Fallopian tube obstruction:Selective salpingography and recanalization’. Radiology 163: 511–14.
Chapter 14
Bibliography
Jansen, R.P.S., and Elliott, P.M. (1981). ‘Angular intrauterine pregnancy’. Obstetrics andGynecology 58: 167–75.
Chapter 15
Bibliography
Jansen, R.P.S. (1983). ‘Peritoneal and plasma estradiol and progesterone levels in mild andmoderate endometriosis:A search for luteinized unruptured follicles’ [abstract].Fertilityand Sterility 39: 394.
—— (1986).‘Minimal endometriosis and reduced fecundability:Prospective evidence froman A.I.D. program’. Fertility and Sterility 46: 141–3.
—— (1992). ‘Nonpigmented endometriosis’. In D.C. Martin D.C. (ed.), Atlas ofEndometriosis. (pp. 5.1–5.4). London: Gower Medical Publishing.
—— (1993a). ‘Pathology and pathogenesis of endometriosis’. In C. Sutton and M.P.Diamond (eds),Endoscopic Surgery for Gynaecologists. (pp. 192–9).London:W.B.SaundersCompany Ltd.
—— (1993b).‘Endometriosis symptoms and the limitations of pathology-based classifica-tion of severity’. International Journal of Obstetrics and Gynecology 40 (Suppl.).
APPENDIX 3 � 407
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 407

Jansen, R.P.S., and Russell, P. (1986).‘Nonpigmented endometriosis. Clinical, laparoscopicand pathologic definition’. American Journal of Obstetrics and Gynecology 155: 1154–9.
Selected other sources
Brosens, I.A. (1993). ‘Endometriosis—narrow but deep—important’. Fertility and Sterility60: 201–2.
Brosens, I., Donnez, J., and Benagiano, G. (1993). ‘Improving the classification ofendometriosis’. Human Reproduction 8: 1792–5.
Gibbons,A. (1993).‘Dioxin tied to endometriosis’. Science 262: 1373.Nisolle,M.,Casanas-Roux,F.,Anaf,V.,Mine,J.-M.,and Donnez,J. (1993).‘Morphometric study
of the stromal vascularization in peritoneal endometriosis’.Fertility and Sterility 59: 681–4.Simpson, J.L., Elias, S., Malinak, L.R., and Buttram,V.C.J. (1980). ‘Heritable aspects of
endometriosis. I.Genetic studies’.American Journal of Obstetrics and Gynecology 137:327–31.TeLinde,R.W. (1978).‘The background of studies on experimental endometriosis’.American
Journal of Obstetrics and Gynecology 130: 570–1.TeLinde, R.W., and Scott, R.B. (1950). ‘Experimental endometriosis’. American Journal of
Obstetrics and Gynecology 60: 1147–73.Wentz,A.C. (1980).‘Premenstrual spotting: Its association with endometriosis but not luteal
phase inadequacy’. Fertility and Sterility 33: 605–7.
Chapter 16
Bibliography
Jansen, R.P.S. (1988).‘Endometriosis’. Australian Prescriber 11: 2–5.—— (1992).‘Principles of medical therapy for endometriosis pain’. Journal of Obstetrics and
Gynaecology 12 (Suppl. 2): s33–s37.Jansen,R.P.S., and Keogh,E.J. (1991).‘GnRH analogues in reproductive medicine’. Medical
Journal of Australia 154: 571–2.
Chapter 17
Bibliography
Fraser, I.S., Song, J.-Y., Jansen,R.P.S.,Ramsay,P., and Boogert,T. (1995).‘Hysteroscopic lysisof intra-uterine adhesions under ultrasound guidance’.Gynaecological Endoscopy 4:35–40.
Chapter 18
Bibliography
Jansen, R.P.S. (1997). ‘Intersex’. In P. Russell and A. Farnsworth (eds), Surgical Pathology ofthe Ovary. 2nd edn (pp. 81–90). Edinburgh: Churchill Livingstone.
408 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 408

Chapter 19
Recommended general reading
Small, M. (1993). Female Choices: Sexual Behavior of Female Primates. Ithaca, NY: CornellUniversity Press.
Bibliography
Jansen, R. (1987).‘The clinical impact of in vitro fertilization. I. Results and limitations ofconventional reproductive medicine’. Medical Journal of Australia 146: 342–53.
—— (1987).‘Assisted conception’. Modern Medicine of Australia June, 36–43.—— (1990).‘Unfinished feticide’. Journal of Medical Ethics 16: 61–5.
Chapter 20
Recommended general reading
Fraser, L.R. (2002).‘ART: boone or bane?’ Nature Medicine, 8 (Suppl. 1): S10–S13.
Bibliography
Jansen,R.(1988).‘Anaesthesia and assisted conception’.In:D.R.Kerr (ed.),Australasian Anaesthesia.(pp. 10–13). Sydney: Faculty of Anaesthetists,Royal Australasian College of Surgeons.
—— (1989a). ‘In vitro fertilization:A history of quality assurance in Australia, 1980–89’.Australian Clinical Review 9: 27–32.
—— (1989b).‘Gamete intra-fallopian transfer’. In C.Wood and A.O.Trounson (eds),ClinicalIn Vitro Fertilization. (pp. 63–80). Berlin: Springer-Verlag.
Jansen, R.P.S., and Anderson, J.C. (1987). ‘Catheterisation of the fallopian tubes from thevagina’. Lancet ii: 309–10.
—— (1993). ‘Transvaginal versus laparoscopic GIFT: A case-controlled retrospectivecomparison’. Fertility and Sterility 59: 836–40.
Jansen,R.P.S.,Anderson, J.C.,Birrell,W.R.S., Lyneham,R.C., Sutherland,P.D.,Turner,M.,Flowers, D., and Ciancaglini, E. (1990).‘Outpatient gamete intrafallopian transfer: 710cases’. Medical Journal of Australia 153: 182–8.
Jansen, R.P.S.,Anderson, J.C., and Sutherland, P.D. (1988).‘Nonoperative embryo transferto the fallopian tube’. New England Journal of Medicine 319: 288–91.
Jansen, R.P.S., Golovsky, D., Lippi, J., and Mortimer, D. (1993). ‘Pregnancy from subzon-ally-microinjected epididymal spermatozoa’. Medical Journal of Australia 158: 646–7.
Lippi, J.,Mortimer,D., and Jansen,R.P.S. (1993).‘Sub-zonal insemination for extreme malefactor infertility’. Human Reproduction 8: 908–15.
Lippi, J.,Turner, M., and Jansen, R.P.S. (1990). ‘Pregnancies after in vitro fertilization bysperm microinjection into the perivitelline space’ [abstract].Fertility and Sterility 54: s29.
Mortimer,D.,Catt, J.W.,Henman,M.,Bowman,M.C., and Jansen,R.P.S. (1998).‘Reducedembryo fragmentation leads to higher implantation and pregnancy rates using improvedIVF culture systems’ [abstract]. Fertility and Sterility.
APPENDIX 3 � 409
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 409

Sungurtekin,U., and Jansen,R.P.S. (1995).‘Profound luteinizing hormone suppression afterstopping the gonadotropin-releasing hormone-agonist leuprolide acetate’. Fertility andSterility 63: 663–5.
Selected other sources
Catt, J.W., and Henman,M. (2001).‘Toxic effects of oxygen on early human development’.Human Reproduction 15 (Suppl. 2): 199–206.
Colpin,H., and Soenen,S. (2002).‘Parenting and psychosocial development of IVF children:A follow-up study’. Human Reproduction 17: 1116–23.
Devroey, P., Liu, J., Nagy, Z., Goossens,A.,Tournaye, H., Camus, M.,Van Steirteghem,A.,and Silber, S. (1995). ‘Pregnancies after testicular sperm extraction and intracytoplas-mic sperm injection in non-obstructive azoospermia’.Human Reproduction 10:1457–60.
Edwards, R.G., Bavister, B.D., and Steptoe, P.C. (1969).‘Early stages of fertilization in vitroof human oocytes matured in vitro’. Nature 221: 632–5.
Edwards, R.G., Steptoe, P.C., and Purdy, J.M. (1980). ‘Establishing full-term human preg-nancies using cleaving embryos grown in vitro’. British Journal of Obstetrics andGynaecology 87: 737–56.
Fishel, S.,Antinori, S., Jackson, P., Johnson, J., Lisi, F., Chiariello, F., and Versaci, C. (1990).‘Twin birth after subzonal insemination’. Lancet 335: 722–3.
Fluker, M.R., Zouves, C.G., and Bebbington, M.W. (1993). ‘A prospective randomizedcomparison of zygote intrafallopian transfer and in vitro fertilization-embryo transferfor nontubal factor infertility’. Fertility and Sterility 60: 515–19.
Hansen,M.,Kurinczuk, J.J.,Bower,C., and Webb, S. (2002).‘The risk of major birth defectsafter intracytoplasmic sperm injection and in vitro fertilization’.New England Journal ofMedicine 346: 725–30.
Lalic, I.,Catt, J.W.,Henman,M.J., and Muir, S. (2000).‘Does short duration of sperm–oocyteincubation increase viability of embryos in human in vitro fertilization?’ ReproductiveTechnology 10: 62–9.
Mickle, J., Milunsky,A.,Amos, J.A., and Oates, R.D. (1995).‘Congenital unilateral absenceof the vas deferens:A heterogeneous disorder with two distinct subpopulations basedupon aetiology and mutational status of the cystic fibrosis gene’. Human Reproduction10: 1728–35.
Mortimer, D. (1986). ‘Comparison of the fertilizing ability of human spermatozoa prein-cubated in calcium- and strontium-containing media’. Journal of Experimental Zoology237: 21–4.
Mortimer,D.,Catt, J.W.,Henman,M.,Bowman,M.C., and Jansen,R.P.S. (1998).‘Reducedembryo fragmentation leads to higher implantation and pregnancy rates using improvedIVF culture systems’ [abstract]. Fertility and Sterility 70 (Suppl.).
Silber, S.J., Nagy, Z., Liu, J.,Tournaye, H., Lissens,W., Ferec, C., Liebaers, I., Devroey, P., andVan Steirteghem, A.C. (1995). ‘The use of epididymal and testicular spermatozoa forintracytoplasmic sperm injection:The genetic implications for male infertility’.HumanReproduction 10: 2031–43.
410 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 410

Silber, S.J.,Van Steirteghem, A.C., Liu, J., Nagy, Z.,Tournaye, H., and Devroey, P. (1995).‘High fertilization and pregnancy rate after intracytoplasmic sperm injection withspermatozoa obtained from testicle biopsy’. Human Reproduction 10: 148–52.
Steptoe, P.C., and Edwards, R.G. (1976).‘Reimplantation of a human embryo with subse-quent tubal pregnancy’. Lancet i: 880–2.
Steptoe, P.C., Edwards, R.G., and Purdy, J.M. (1980). ‘Clinical aspects of pregnanciesestablished with cleaving embryos grown in vitro’. British Journal of Obstetrics andGynaecology 87: 757–68.
Strömberg, B., Dahlquist, G., Ericson, A., Finnström, O., Köster, M., and Stjernqvist, K.(2002). ‘Neurological sequelae in children born after in-vitro fertilisation: A popula-tion-based study’. Lancet 359: 461–5.
Sutcliffe, A.G.,Taylor, B.,Thornton, S., Grudzinskas, J.G., and Lieberman, B.A. (1999).‘Children born after intracytoplasmic sperm injection’.British Medical Journal 348:704–5.
Venn,A.,Hemminki,E.,Watson,L.,Bruinsma,F., and Healy,D. (2001).‘Mortality in a cohortof IVF patients’. Human Reproduction 16: 2691–6.
Chapter 21
Selected other sources
Trounson, A.O., and Mohr, L. (1983). ‘Human pregnancy following cryopreservation,thawing and transfer of an eight-cell embryo’. Nature 305: 707–9.
Chapter 22
Bibliography
Handelsman, D.J., Dunn, S.J., Conway, A.J., Boylan, L.M., and Jansen, R.P.S. (1984).‘Psychological and attitudinal profiles in donors for artificial insemination’.Fertility andSterility 43: 95–101.
Jansen, R.P.S. (1985).‘Sperm and ova as property’. Journal of Medical Ethics 11: 123–6.—— (1995a).‘Bioethics of the spermatozoon’. In J.G.Grudzinskas, J.L.Yovich, J.L. Simpson
and T. Chard (eds), Cambridge Reviews in Human Reproduction.Volume 3. Gametes—TheSpermatozoon. (pp. 282–306). Cambridge: Cambridge University Press.
—— (1995b). ‘Bioethics of the oocyte’. In J.G. Grudzinskas, J.L.Yovich, J.L. Simpson andT.Chard (eds),Cambridge Reviews in Human Reproduction.Volume 2.Gametes—The Oocyte.(pp. 396–427). Cambridge: Cambridge University Press.
—— (1997). ‘Reproductive medicine and the social state of childlessness’. Medical Journalof Australia 167: 321–4.
Selected other sources
Daniels, K.R. (1987).‘Semen donors in New Zealand:Their characteristics and attitudes’.Clinical Reproduction and Fertility 5: 177–90.
APPENDIX 3 � 411
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 411

Daniels, K., and Lalos, O. (1995). ‘The Swedish Insemination Act and the availability ofdonors’. Human Reproduction 10: 1871–4.
Dunstan,G.R. (1975).‘Ethical aspects of donor insemination’. Journal of Medical Ethics 1:42–4.Huerre, P. (1980). ‘Psychological aspects of semen donation’. In G. David and W.S. Price
(eds),Human Artificial Insemination and Semen Preservation. (pp. 461–5).New York:PlenumPress.
Rowland, R. (1983). ‘Attitudes and opinions of donors on an artificial insemination bydonor (AID) program’. Clinical Reproduction and Fertility 2: 249–59.
Sauer,M.V., and Paulson,R.J. (1990).‘Human oocyte and preembryo donation:An evolvingmethod for the treatment of infertility’. American Journal of Obstetrics and Gynecology163: 1421–4.
Schoysman, R. (1975). ‘Problems of selecting donors for artificial insemination’. Journal ofMedical Ethics 1: 34–5.
Templeton, A. (1991). ‘Gamete donation and anonymity’. British Journal of Obstetrics andGynaecology 98: 343–50.
Chapter 23
Bibliography
Jansen, R.P.S. (1984).‘Fertility in older women’. International Planned Parenthood FoundationMedical Bulletin 18(2): 4–6.
—— (1995).‘Older ovaries:Ageing and reproduction’.Medical Journal of Australia 162:623–4.—— (2000). ‘Germline passage of mitochondria: quantitative considerations and possible
embryological sequelae’. Human Reproduction 15 (Suppl. 2): 112–28.
Selected other sources
Barnes, F.L.,Crombie,A.,Gardner,D.K.,Kausche,A., Lacham-Kaplan,O., Suikkari,A.-M.,Tiglias, J.,Wood,C., and Trounson,A.O. (1995).‘Blastocyst development and birth afterin vitro maturation of human primary oocytes, intracytoplasmic sperm injection andassisted hatching’. Human Reproduction 10: 101–5.
Eppig, J.J., and O’Brien,M.J. (1996).‘Development in vitro of mouse oocytes from primor-dial follicles’. Biology of Reproduction 54: 197–207.
Eppig, J.J., Schroeder,A.C., and O’Brien, M.J. (1992). ‘Developmental capacity of mouseoocytes matured in vitro: Effects of gonadotrophic stimulation, follicular origin andoocyte size’. Journal of Reproduction and Fertility 95: 119–27.
Gook,D.A., Schiewe,M.C.,Osborn, S.M.,Asch,R.H., Jansen,R.P.S., and Johnston,W.I.H.(1995).‘Intracytoplasmic sperm injection and embryo development of human oocytescryopreserved using 1,2-propanediol’. Human Reproduction 10: 2637–41.
Handyside, A. (1992). ‘Prospects for the clinical application of preimplantation diagnosis:The tortoise or the hare’. Human Reproduction 7: 1481–3.
Trounson,A.,Wood, C., and Kausche,A. (1994). ‘In vitro maturation and the fertilization
412 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 412

and developmental competence of oocytes recovered from untreated polycystic ovarianpatients’. Fertility and Sterility 62: 353–62.
Chapter 25
Recommended general reading
Cassell, E.J. (1991). The Nature of Suffering and the Goals of Medicine. New York: OxfordUniversity Press.
Bibliography
Jansen, R.P.S. (1994).‘Self-regulation or legislation in assisted reproductive technology’. InD.R.Popkin and L.J. Peddle (eds),Women’s Health Today:Perspectives on Current Researchand Clinical Practice. (pp. 343–51). London: Parthenon.
—— (1997). ‘Liberty or control in reproductive medicine’. In E. Porcu and C. Flamigni(eds), Human Oocytes: from Physiology to IVF. Bologna: Monduzzi Editore.
—— (1999).‘IVF and reproductive genetics in 1999: Biology, business, society and ethics’.In R. Jansen and D. Mortimer (eds), Towards Reproductive Certainty: Fertility & GeneticsBeyond 1999. (pp. 5–7). London: Parthenon.
Selected other sources
Freeman, E.W., Boxer, A.S., Rickels, K., Tureck, R., and Mastroianni, L.J. (1985).‘Psychological evaluation and support in a program of in vitro fertilization and embryotransfer’. Fertility and Sterility 43: 48–53.
National Health and Medical Research Council (1985). Embryo Donation by Uterine Flushing:Interim Report on Ethical Considerations.Canberra:Australian Government Publishing Service.
Chapter 26
Recommended general reading
Gutheil,T.G., Bursztajn, H., and Brodsky, A. (1984). ‘Malpractice prevention through thesharing of uncertainty. Informed consent and the therapeutic alliance’. New EnglandJournal of Medicine 311: 49–51.
Bibliography
Jansen, R.P.S. (1986). ‘Conflicts of interest and the physician entrepreneur’ [letter]. NewEngland Journal of Medicine 314: 252.
—— (1987).‘Ethics in infertility treatment’. In R.Pepperell,C.Wood and B.Hudson (eds),The Infertile Couple. 2nd edn (pp. 346–87). Edinburgh: Churchill Livingstone.
—— (1988). ‘Advantages and disadvantages of subspecialization’. International Journal ofObstetrics and Gynecology 27: 293–6.
APPENDIX 3 � 413
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 413

—— (1994). ‘Self-regulation or legislation in assisted reproductive technology’. In D.R.Popkin and L.J. Peddle (eds), Women’s Health Today: Perspectives on Current Research andClinical Practice. (pp. 343–51). London: Parthenon.
—— (1995). ‘Ethical principles and values’. In R.J.A.Trent (ed.), Handbook of AntenatalDiagnosis. (pp. 58–79). Cambridge: Cambridge University Press.
—— (1997).‘Evidence-based ethics and the regulation of reproduction’.Human Reproduction12: 2068–75.
—— (1999).‘Sex, reproduction and impregnation:By 2099 we won’t confuse them’.MedicalJournal of Australia 171: 166–7.
Chapter 27
Recommended general reading
Atwood, M. (1986) The Handmaid’s Tale. London: Jonathan Cape.Dunstan,G.R. (1984).‘The moral status of the human embryo:A tradition recalled’. Journal
of Medical Ethics 10: 38–44.—— (1986).‘In-vitro fertilization:The ethics’. Human Reproduction 1: 41–4.Huxley,A. (1932) Brave New World.Any edition after 1946.Singer,P. (1983).The Expanding Circle:Ethics and Sociobiology.Oxford:Oxford University Press.Singer,P.,Kuhse,H.,Buckle,K.,Dawson,K., and Kasimba,P. (1990).Embryo Experimentation.
Cambridge: Cambridge University Press.
Bibliography
Jansen, R.P.S. (1985). ‘A practical ethical framework for in vitro fertilization and relatedreproductive interventions’. Annals of the New York Academy of Science 442: 595–600.
—— (1987). ‘The clinical impact of in vitro fertilization. II. Regulation, money andresearch’. Medical Journal of Australia 146: 362–6.
—— (1988).‘Reproductive technology:Where to now?’ Healthright 7(2): 9–15.—— (1991).‘Mouse tales and embryo research’. In Proceedings of the First Annual Conference
of the Australian Bioethics Association. Melbourne:Australian Bioethics Association.Kola, I., Lacham, O., Jansen, R.P.S.,Turner, M., and Trounson, A. (1990). ‘Chromosomal
analysis of human oocytes fertilized by microinjection of spermatozoa into the periv-itelline space’. Human Reproduction 5: 575–7.
Selected other sources
Reddy, P. (1992). Saadan er Danskerne (‘Danes are like that’).Aarhus: Grevas Forlag.Stone, L. (1977). The Family, Sex and Marriage in England 1500–1800. London:Weidenfeld
and Nicolson.
414 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 414

Appendix 1
Bibliography
Jansen,R.P.S. (1993).‘Relative infertility:Modelling clinical paradoxes’.Fertility and Sterility59: 1041–5.
—— (1995).‘Elusive fertility: Fecundability and assisted conception in perspective’.Fertilityand Sterility 64: 252–4.
Appendix 2
Bibliography
Jansen, R.P.S. (2003). ‘The effect of female age on the likelihood of a live birth from oneinvitro fertilization treatment’. Medical Journal of Australia 178: 258–61.
Selected other sources
Coetsier,T. and the ESHRE Campus Course Report (2001). ‘Prevention of twin preg-nancies after IVF/ICSI by single embryo transfer’. Human Reproduction 16: 790–800.
APPENDIX 3 � 415
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 415

Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 416
This page intentionally left blank

glossary
In the following definitions, references to other glossary entries are in italics;within the defi-nitions, modifications of the defined term or alternative terms are given in bold,as are other glossary entries that do not provide additional information in the partic-ular context.
abdominal pregnancy An ectopic pregnancy located in the peritoneal cavity, or abdomen,usually having undergone implantation in the fallopian tube as a tubal pregnancy, thencontinuing to grow after the tube eventually ruptures. Rare in countries with readyaccess to medical care, as considerable symptoms have to have been ignored (andsurvived) during the tubal rupture part of the process.The fetus can grow almost to fullterm, but delivery of a live baby (delivered by operation) has never been reported.Sometimes (fancifully) thought of as a way men might bear children!
abnormal forms An estimate of the percentage of spermatozoa that have an abnormalshape of the head, mid-piece or tail. Part of the routine sperm count.
abnormality A departure from what’s normal—in a more or less exact medical sense.Anabnormality can be quantitative (or measurable with a number), qualitative (not measur-able but still apparent or obvious) or a matter of timing (temporal). Statistically,we definean abnormality as signifying either a measurement or a yes-or-no quality that is outsidewhat, for example, 90 or 95 or 99 percent of the population exhibits (see also statisticalsignificance). It’s a word without added value,unlike defect, for example,which has a negativeconnotation. So if you want to avoid a gratuitous, negative effect it’s preferable, usingthis example, to say ‘birth abnormality’ instead of ‘birth defect’. See also anomaly.
abortion Strictly, synonymous with spontaneous abortion or miscarriage. Loosely, an inducedabortion for early termination of pregnancy.
417
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 417

absolute infertility Synonymous with sterility, or 100 percent infertility; also called completeinfertility. See also relative infertility.
absolute risk Your actual chance of having something or being affected by something (soit does not usually mean ‘absolutely’ in the sense of ‘one hundred percent’, as in absoluteinfertility).Usually given as a ratio, proportion or percentage: for example, the (absolute)risk of having at least some visible endometriosis for a woman in her forties is about 20in 100, or 20 percent; the chance or the risk of pregnancy each month for a normalyoung couple (normal fecundability) is also about 20 percent, usually expressed as 0.2(that is, as a proportion); the risk of a woman developing cancer of the ovaries by thetime she reaches her seventies, in North America, Europe or Australia, is about one in90 (or about 1.1 percent).
accountability The sequel to responsibility, in which responsibility for the making of adecision continues to rest with the decision-maker as the effects or consequences fromthe decision unfold.
acrosome Consider it to be the mature spermatozoon’s crash-helmet, present over thesperm head until the successful sperm binds to the coating of the egg known as thezona pellucida; imagine it to be like a balloon into which your fist is pushed (the fistbeing the sperm’s head)—bursting only when bound like Velcro to the zona (seeacrosome reaction).
acrosome reaction If the acrosome is a balloon-like crash-helmet for the mature sperma-tozoon, the acrosome reaction is the bursting of that balloon, releasing enzymes thatdigest a path for the highly motile sperm (after capacitation) to push through the zonapellucida into the perivitelline space, where it can directly fertilize the egg.
acute Medically, means sudden and quick. An acute inflammation is usually red, tenderand may form pus. Opposite to chronic.
adenohypophysis The glandular part of the pituitary gland, lying toward the front, so inmedical-speak called the anterior pituitary.Produces follicle stimulating hormone, luteiniz-ing hormone and prolactin. Other hormones include hormones that: (1) cause normalchildhood growth (growth hormone); (2) drive the thyroid gland (thyroid stimulatinghormone, or TSH); and (3) drive the adrenal gland (adrenocorticotropic hormone, orACTH). See also hypothalamus and neurohypophysis.
adenomyoma See adenomyosis.adenomyosis An abnormal condition of the uterus in which glands from the endometrium
grow into the muscle of the wall of the uterus (the myometrium), causing local or generalenlargement of the uterus, pain with periods, and perhaps heavier periods.A localizedarea of adenomyosis is called an adenomyoma and can be hard to distinguish from afibroid on transvaginal ultrasound, although an increase in the serum CA125 antigen levelcan point to the correct diagnosis. Unlike a fibroid it is not easily removed at surgery,because it’s not clearly separable from surrounding tissue.There’s no satisfactory long-term treatment for adenomyosis: hysterectomy may be chosen if symptoms are badenough. GnRH-agonists give just temporary relief.
adhesion Scar tissue, in particular between the serosa (surface lining) of abdominal or pelvicorgans in the peritoneal cavity, which can interfere with the access the fallopian tube has
418 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 418

to the ovary at ovulation.Adhesions can be thin and transparent (sometimes called filmyor Grade 1), a little like thin plastic wrap; thicker, and containing more scar tissue andblood vessels (Grade 2); or thick, dense and tough (Grade 3).Adhesions are caused byinfections, endometriosis or a previous operation. Not all adhesions are important: itdepends on where they are. See also intrauterine adhesions.The treatment of adhesionsrequires microsurgery, and there are special steps that have to be taken to stop themcoming back again.
adrenal glandA paired gland lying above each kidney, responsible for the essential hormonecortisol. Equally important with the ovaries in producing androgens in women. See alsoserum 17-hydroxyprogesterone.
AFP See alpha fetoprotein.AI See assisted insemination.AID Artificial insemination, donor (or assisted insemination, donor); see donor insemination.AIDS Acquired immune deficiency syndrome (see HIV).AIH See assisted insemination, husband.alleles Because genes come in pairs, one on each of the chromosomes that make up a chro-
mosome pair, the two genes of the pair are not always identical.The many differentforms that a particular gene can take (and still function, for better or for worse, as agene within that gene’s job description) are referred to as its alleles. If the alleles areidentical, you are homozygous for that gene; if they are not, you are heterozygous.Abnormalalleles cause genetic disease or disability: if one allele is enough to cause abnormalitythen the gene is dominant (inherited with dominant inheritance) and the abnormality ispresent in the heterozygous and the homozygous state; if two alleles are needed to causeabnormality, then the gene is recessive (inherited with recessive inheritance) and the abnor-mality is present in the homozygous state and in a state where the two alleles are differ-ent but both are harmful (called compound heterozygosity. In the case of alleles found onX-chromosomes (see sex chromosome) but not on Y-chromosomes,which are smaller, a reces-sive gene will be unopposed in males (and so will act as a dominant gene), whereasfemale carriers of the allele will be unaffected except in the extremely unlikely eventthat they inherit (or gain by mutation) a second abnormal allele; this mode of inheri-tance is called sex-linked recessive inheritance.
alpha fetoprotein A form of albumin (a protein in the blood) produced only by the fetus,but which crosses the placenta and so is detectable in the mother’s blood (measured witha serum alpha fetoprotein, as well as being usefully measured in amniotic fluid obtained byamniocentesis. Detectable in higher than usual concentration with certain open abnor-malities involving the fetus’s brain and spinal cord (anencephaly and spina bifida).Presentin lower than usual concentration when there is a trisomy in the fetus, such as Downsyndrome (or trisomy 21), trisomy 18 or possibly Klinefelter syndrome—screening for allof which can be done with a triple test.
amenorrhea Absent menstrual periods, either because of absent ovulation (anovulation) orbecause of absence of, destruction of, or obstruction to the menstrual flow from theuterus, such as with intrauterine adhesions (when it’s known as Asherman’s syndrome).
AMH See anti-Müllerian hormone.
GLOSSARY � 419
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 419

amniocentesis Sampling the fluid from the amniotic cavity after about 14 or 15 weeks ofpregnancy. Cells from the fetus can be set up in culture for a karyotype, or for specialdiagnoses can be examined more quickly by fluorescent in situ hybridization (FISH), compar-ative genomic hybridization (CGH) or by polymerase chain reaction (PCR).Other substancesin the amniotic fluid (such as alpha fetoprotein, or AFP) can be measured to indicatewhether the fetus is normal or not.
amnion The membrane and cavity that encloses the developing embryo and fetus in fluid(essential for all vertebrates that reproduce out of the sea), cushioning the embryo andfetus from the effects of pressure. Unlike the chorion, contains cells that originate fromthe fetus itself.
amniotic cavity Cavity enclosed by the amnion, which grows from the embryo withinthe gestational sac, gradually catching up with it in size by about 14 weeks, when theamnion and chorion fuse, and after which amniocentesis becomes practicable. See alsoamniotic fluid.
amniotic fluidThe fluid in the amniotic cavity, or gestational sac,which contains cells derivedfrom the fetus. Sampled with amniocentesis. See also amnion.
amniotic membrane See amnion.ampulla The wide outer part of the fallopian tube, lying between the fimbrial end and the
narrow isthmus.ampullary-isthmic junction The point at which the wide ampulla of the fallopian tube
meets the narrow isthmus.The place where fertilization of the egg by a sperm cellnormally takes place.
ANA See antinuclear antibody.Androcur See cyproterone acetate.androgen insensitivity syndrome Complete or partial resistance to the action of andro-
gens in the body’s tissues. Prevents or limits the development of male characteristics inthe developing fetus, resulting in intersex. See also testicular feminization.
androgens Male sex hormones, including testosterone (the main androgen circulating inthe blood in men and in women) and androstenedione (which is weaker). Produced inwomen more or less equally by the adrenal glands and the ovaries (in thecal cells and hiluscells). Produced in much greater quantity in men by the testes (testicles).
androstenedione A weak androgen, produced in women by thecal cells in the ovary and bythe adrenal glands.
aneuploid See aneuploidy.aneuploidy The gain or loss of one or more chromosomes at meiosis, including trisomy (47
chromosomes) and monosomy (45 chromosomes).Caused by chromosomal nondisjunction.ANF Antinuclear factor; see antinuclear antibody.angular pregnancy When implantation occurs in one or other outer angle of the trian-
gular cavity of the uterus (that is, out to one side, very close to where the fallopian tubesenter the endometrial cavity).A miscarriage is common. Rupture of the uterus has beenreported.
annexin VA protein molecule with anticoagulant properties bound to chorionic villi, respon-sible for assisting maternal blood to circulate in the placenta.
420 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 420

anomaly Distinguishable from an abnormality in that the outcome in the case of an anomalymight not lead to disease or disability.An anomalous kidney, for example, is in the wrongplace but does its job perfectly well.The distinction between an anomaly and an abnor-mality, however, is loose and is not strictly observed.
anorexia See its more traditional name anorexia nervosa, although not all cases nowadaysare regarded as primarily ‘nervous’ conditions.
anorexia nervosa ‘Anorexia’means a profound loss of appetite, followed by loss of weight;‘nervosa’ means that there is a nervous or mental basis for the state, in this case a beliefby the person affected, and contrary to the perception of others, that she (very rarelyhe) is overweight. She stops eating,may induce vomiting, and uses laxatives to keep theintestines empty and the stomach flat.The menstrual periods stop (there is amenorrheafor two reasons: the weight loss and the underlying mental disturbance, both of whichcause hypothalamic anovulation). Medical complications from induced vomiting andlaxative abuse can be serious, occasionally fatal.Treatment, which includes psycholog-ical and psychiatric counseling, is difficult and is not always completely accomplished.It’s a condition chiefly of adolescent girls; the younger the patient the better the chanceof cure. For fertility, ovulation induction is often required.
anovulation Absence of ovulation.anovulatory cycles Menstrual cycles caused by ovarian activity (or ovarian cycles) not
accompanied by ovulation.The serum progesterone stays low, whereas some developmentof tertiary follicles and production of estradiol takes place. See also anovulatory dysfunctionaluterine bleeding.
anovulatory dysfunctional uterine bleeding Irregular and generally heavy bleedingcaused by anovulatory cycles.
Antagon The GnRH-antagonist ganirelix made by Organon. Called Orgalutran outsidethe USA.
anteflexed A forward angle of the fundus of the uterus in relation to the direction of thecervix. Usually only occurs when the uterus is anteverted. Opposite to retroflexed.
anteverted Refers to the (normal) position of the uterus, meaning that it is tilted forwardin relation to the direction of the vagina. Opposite to retroverted. See also transvaginalultrasound.
antibody A protein of the immune system capable of binding to an antigen.The bindingis specific to the particular antigen and often neutralizes its effects. Antibodies, orimmunoglobulins, account for almost half of the proteins circulating in the blood (mostof the rest being albumin).
anticardiolipin antibody (ACA) An antibody that acts against components in the cellmembranes (membranes that hold a cell together as well as surrounding some internalcell structures). Looked for in the blood (we ask for a serum anticardiolipin as a possibleimmune cause of recurrent miscarriages). Intriguingly, the membrane that contains mostcardiolipin is the membrane surrounding the mitochondrion (malfunction of which isimplicated in causing miscarriage, although how (or if) the antibody might get to themitochondria is not known. See also lupus anticoagulant and antiphospholipid antibody.
antigenAnything that stimulates the production of a specific antibody by the immune system.
GLOSSARY � 421
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 421

anti-Müllerian hormone A hormone produced by the Sertoli cells of the testes in a maleembryo to suppress the development of the Müllerian ducts.
antinuclear antibody (ANA) Antibody made by the body’s immune system that acts againstcomponents in the nucleus of the body’s own cells (thus sometimes producing an‘autoimmune disease’).Looked for in the blood as a screening test for a possible immunecause of recurrent miscarriages (for which also see anticardiolipin antibody) as well as for thepotentially serious autoimmune disease systemic lupus erythematosus (SLE; see alsolupus anticoagulant). Synonym: antinuclear factor.
antiphospholipid antibody An antibody directed at phosphate-containing fatty compo-nents of cell membranes, such as cardiolipin (see anticardiolipin antibody). Low levels areprobably common and harmless; in higher levels they can cause disease, particularlyduring pregnancy, including thrombosis, and also miscarriage.
anti-sperm antibodies Means the same as sperm antibodies.antral follicle A tertiary follicle.antrum A fluid-filled space between the follicle cells, the development of which marks the
transformation of a tertiary follicle from a secondary follicle. Composes the bulk of themature preovulatory follicle (sometimes called the Graafian follicle) and very obvious ontransvaginal ultrasound scanning during monitoring of follicular development as dark,‘echolucent’ spaces within the ovary.
apoptosisThe word for what scientists call programmed cell death, or cellular suicide.Thisis a normal—rather altruistic!—thing for a cell to do, as it purposefully switches onsome special genes that then alter its metabolism to dismantle itself and die, for thegreater good of the tissue or organ that it’s a part of. Pathologists distinguish apoptosisfrom necrosis. Examples of apoptosis include follicular atresia.
ART See assisted reproductive technology.artificial insemination See assisted insemination.artificial insemination, husband See assisted insemination, husband.aseptic necrosis of the femoral head Literally, noninfective death of the bone tissue
of the top end of the thigh bone (where it forms the hip joint).A rare but serious com-plication from continued high dosages of cortisone-like drugs, including cortisone,prednisone and prednisolone, sometimes used for treating, for example, sperm antibodies.See also necrosis.
asexual reproduction The opposite to sexual reproduction. See cloning.Asherman syndromeThe combination of intrauterine adhesions and amenorrhea, although
see also hypomenorrhea.aspermiaAn absence of semen despite male orgasm; thus, different to azoospermia, an absence
of sperm.assisted conceptionA group of medical treatments ranging from assisted insemination (IUI)
to in vitro fertilization (IVF), including its technical variants (such as GIFT, ICSI andPGD), and with the following common characteristics: (1) they are aimed at increasingthe chance of pregnancy each month, thus overcoming the medical disability of infertil-ity; (2) there is little or no ‘spillover’ of therapeutic effect beyond the cycle or month inwhich treatment is invoked; and (3) there is some form of procedural intervention,with
422 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 422

sperm, eggs or embryos spending some time outside the body. It’s not necessary for thereto be stimulation of the ovaries (superovulation) for multiple development of follicles.
assisted hatching An in vitro fertilization manipulation in which a small opening is madein the zona pellucida of the early embryo to help the blastocyst emerge prior to implanta-tion. Formerly carried out by judicious use of an enzyme to dissolve the zona (but riskingdamage to the embryo), leading IVF programs now use a microlaser.
assisted insemination Insemination, or injection of semen or prepared spermatozoa, intothe vagina, cervix, uterus (intrauterine insemination) or fallopian tube, to treat infertility. Abasic form of assisted conception.The husband’s (or male partner’s) sperm (AIH) or donatedsperm (DI) can be used. See also intrauterine insemination.
assisted insemination, husband (AIH) Assisted insemination in which the semen from thehusband or male partner is used.
assisted reproductive technology (ART) The term is essentially synonymous with assistedconception, but tends to emphasize the technology instead of the medical help to whichthe technology is put.The effects of unduly separate consideration of the technologyis discussed in the box, Moral plurality and Brave New Canada? in Chapter 26.
asthenozoospermia See oligospermia.atresia Process by which a tissue stops growing, loses its function and degenerates.
Synonymous with atrophy. See also follicular atresia and apoptosis.atretic follicle A tertiary follicle that: (1) is no longer growing; (2) is no longer secreting
estradiol; and (3) no longer contains a healthy oocyte, or egg. See also follicular atresia andfollicular recruitment.
atrophy Literally, an absence of nutrition,but in particular the result of such lack in a tissue,which shrinks and loses its normal function. For examples, see endometrial atrophy andfollicular atresia. Sometimes the end result of necrosis.
autonomy An ethical principle in which value is given to maximizing an individual’scontribution to the making of decisions that affect them. Can be overdone by abro-gating professional responsibility through misuse of informed consent.
autosome A chromosome other than one of the sex chromosomes (which are X or Y).Numbered from 1 to 22, and displayed in a karyotype.
Aygestin US trade name for norethindrone, made by Wyeth. See also Primolut N.azoospermia A complete absence of sperm (spermatozoa) in the semen.Detectable only by
performing a sperm count, as semen looks the same whether it contains sperm or not.Due either to an obstruction (usually in the epididymis or vas deferens), and called obstruc-tive azoospermia, or to failure of sperm to form or to mature in the testis and calledmaturation arrest. See also spermatogenesis and testicular sperm extraction (TESE).
B cellsWhite blood cells or lymphocytes that are part of the immune system and concernedwith the production of antibodies. See also T cells and NK cells.
balanced chromosomal translocation Remember chromosomes occur in pairs in all cellsexcept sperm and eggs. If part of one chromosome is found connected to a completelydifferent chromosome it is ‘translocated’. For that person there is no net gain or loss ofgenetic material, so the translocation is ‘balanced’ and there is no problem. But whenthat person makes eggs or sperm, some of these will have too much or too little genetic
GLOSSARY � 423
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 423

material.The same will be true for any embryo that results.The chromosomal translo-cation will then be ‘unbalanced’ and the embryo will sooner or later usually result in amiscarriage. If the two particular chromosomes have swapped parts,we call it a balancedreciprocal translocation. See also chromosomal cross-over and chromosomal embryopathy.
basal body temperature chart An inexpensive way of detecting ovulation through theeffect progesterone has on the hypothalamus, increasing the body’s temperature a few tenthsof a degree. Best recorded using a BBT thermometer (with a smaller scale than ther-mometers used to record fevers or high temperatures) first thing in the morning beforerising, and preferably in the vagina for accuracy. Day 1 of the chart is the first morningwhen there is menstruation (a period).Commonly there’s a dip in the temperature justbefore the sustained rise that indicates that ovulation has occurred (a ‘biphasic chart’).The chart typically records the days you are menstruating,when you have sex and whenyou’re aware of mucus and ovulation pain. Best used to document: (1) the presence andlength of the luteal phase, especially if clomiphene is being used for ovulation induction; and(2) the timing of symptoms such as premenstrual spotting. Not as good for predictingovulation as LH testing in urine.
BBT See basal body temperature chart.beneficence The ethical value that comes from doing good. See also non-maleficence and
suffering.bicornuate uterus A uterine anomaly in which the Müllerian ducts, before birth, do not join
completely, with the consequence that there is a double uterus, in which each of thetwo sides is smaller than a normal uterus and receives just one fallopian tube. Diagnosedby hysterosalpingogram, by hysteroscopy and laparoscopy, or by transvaginal ultrasound (prefer-ably three-dimensional ultrasound).
biochemical pregnancy A somewhat insensitive term for when conception and implan-tation have occurred, producing a positive pregnancy test, but without sign of a gestationalsac appearing on transvaginal ultrasound; in other words, a subclinical miscarriage or a menstrualmiscarriage.
biopsyTaking a small sample of tissue for diagnosis under the microscope. Biopsies of theendometrium can be done without anesthetic, through the cervix (see premenstrual biopsy).Biopsies of the ovary or of the lining of the peritoneal cavity (Such as to detect subtleendometriosis) are done at laparoscopy.A testicular biopsy is done to determine why there’sazoospermia. Using microscopic techniques, even an early embryo can be biopsied (seeembryo biopsy and preimplantation diagnosis).
blastocyst Stage of development of the early embryo that has undergone blastulation, inwhich a fluid-filled cavity forms in the formerly solid ball of cells (the morula), aboutfive days after fertilization. For the first time, a distinction can be made between a sheetof cells to one side, which will form the embryo proper, termed the inner cell mass,and the remaining, peripheral cells that constitute the trophectoderm, which—after theblastocyst ‘hatches’ through the zona pellucida and undergoes implantation—will formthe trophoblast.
blighted ovum An old-fashioned term for an inevitable miscarriage, meaning that the ovum(in its classical sense for professional embryologists) has not developed normally after
424 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 424

fertilization, there being present just the supporting tissues and no embryo.The term isdescriptive; it has no diagnostic value as to the cause of the miscarriage.
blood group and antibody screen Most commonly done before an operation that couldcause significant loss of blood, especially if an ectopic pregnancy is suspected, because ablood transfusion might be needed.Also done for investigation of recurrent miscarriages,when the rare but important antibody anti-TjA needs to be excluded or detected.Rh-negative women with an Rh-positive partner who are treated for miscarriage or forectopic pregnancy often require an injection of Rhogam or anti-D gamma globulinto avoid being sensitized (developing antibodies to) possibly Rh-positive red blood cellsfrom the embryo or fetus.
BMI See body mass index.body mass index (BMI) An estimate of the amount of fat a person has, calculated by
dividing his or her weight (expressed in kilograms) by the square of the height (expressedin meters).Normally between about 20 and 25, although the upper limit is higher withage.A BMI below 20 generally causes oligomenorrhea, then amenorrhea, through anovu-lation. A BMI much over 25 indicates obesity. Sometimes called the Quetelet index,although Quetelet actually devised a different formula (for the interesting back-ground to which see the box, The body mass index, the stars and Monsieur Quetelet, inChapter 11).
bowel The intestines.The small intestine (or small bowel) runs from the stomach to thewider large intestine (or large bowel),which starts with the cecum, in the region of theappendix on the right side of the lower abdomen, ascends (ascending colon), turns left(transverse colon), turns downward (descending colon), becomes the sigmoid colon (asit sweeps from side to side a bit), then the rectum, before emerging at the anus.
breakthrough bleeding Bleeding (usually irregular and light, that is,‘spotting’) while onthe birth control (oral contraceptive) pill or while taking a progestogen.With regard tothe pill, it is common (and of no sinister importance) in the first few months of pilluse; but if it happens after many months’ satisfactory use of the pill then it can signal:(1) interference with the efficacy of the pill (that is, a risk of ovulation and pregnancy) byan illness with diarrhea, simultaneously taking antibiotics, or a drug interaction (takingadditional medications that speed up the pill’s metabolism; or (2) co-existing pathol-ogy of the cervix or the uterus. Unexplained or persistent breakthrough bleeding meansyou should see your physician.
bromocriptine A drug that mimics dopamine, which is produced by the hypothalamus tonormally inhibit production of prolactin by the pituitary gland. Specific treatment forhyperprolactinemia: the tablets are given by mouth unless they cause side-effects, in whichcase the same tablets (but not the capsules) can be used vaginally! Made by Sandoz asParlodel.The use of bromocriptine for ovulation induction is discussed in Chapter 11.
buserilin A GnRH-agonist, made by Hoechst as Suprefact.Administered as a nasal spray.CA125 antigen A mucus-like protein produced in some circumstances by surface cells of
tissues derived from the Müllerian ducts. Its function is obscure but measurement as serumCA125 antigen can be useful in diagnosing adenomyosis, endometriosis and some cancersof the ovary.
GLOSSARY � 425
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 425

cabergoline Similar to bromocriptine, but more potent and with fewer side-effects; usedonce or twice weekly to lower production of prolactin in hyperprolactinemia. Not yetapproved for infertility treatment, but no adverse fetal effects have been reported whenused for ovulation induction.
caecum English spelling for cecum (see bowel).CAH See congenital adrenal hyperplasia.canalization See tubal canalization.capacitation An invisible change mature sperm (spermatozoa) undergo to acquire accel-
erated movement and the ability to undergo the acrosome reaction. Brought about natu-rally when sperm swim up through the uterus and fallopian tubes, or brought about inthe laboratory by spinning and washing the sperm through a series of solutions (inpreparation for assisted conception).
carrier Of a gene; see alleles.CAT scan A special form of x-ray taken with the person enveloped in the x-ray appara-
tus, which builds up a particularly good image of any cross-section or series of cross-sections through the body, by a process of computed tomography. Particularly usefulfor investigation of the anatomy of the pituitary gland and hypothalamus when a tumoris suspected or needs to be excluded. More widely available than an MRI scan, whichcan give even clearer results.
cautery Short for electrocautery, or diathermy.CAVD See congenital absence of the vasa deferentia.CBAVD Congenital bilateral absence of the vas deferens: see congenital absence of the vasa
deferentia.cecum See bowel.celiac disease A defect of intestinal absorption caused by abnormal sensitivity to gluten
in the diet that can first manifest with recurrent miscarriage or unexplained infertility, despitean absence of diarrhea or other disturbances of bowel function. Diagnosis is suggestedby serum antigliadin antibodies and serum tissue transglutaminase (or endomysial) antibodies,but requires biopsy of the lining of the small intestine via gastroscopy for confirma-tion. Responds to a gluten-free diet.
cervical incompetence Weakness of the cervix of the uterus revealed during pregnancy,usually because of previous operations on it, but sometimes without prior injury, leadingto miscarriage, typically in the second three months of the pregnancy. Diagnosed byexamining the cervix during the pregnancy, repeatedly if necessary. Often causes nosymptoms until the waters break (the pregnancy membranes from the gestational sacbulge through the opening cervix), when it’s usually too late to treat.Treated beforerupture of the membranes with a cervical ligature.
cervical ligatureA stitch or suture placed circumferentially around the cervix to strengthenand support it for the treatment of cervical incompetence.
cervical mucus Sticky secretion from the canal of the cervix, the job description of whichis to keep sperm (spermatozoa) out unless ovulation is about to take place,when it becomesvoluminous, watery, stretchable (Spinnbarkheit) and forms a crystalline ferning patternwhen allowed to dry on a glass slide. Natural family planning clinics can teach you to
426 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 426

look for it in the vagina—useful for getting pregnant as well as for avoiding it. See alsocervicitis, Kremer test, Insler score and postcoital test.
cervical mucus sperm antibodies Estimation of sperm antibodies in the cervical mucus.The presence of these antibodies can cause negative tests of cervical mucus–sperm inter-action, including a negative postcoital test.
cervical polyp A polyp of the canal of the cervix.A cause of bleeding after sex (postcoitalbleeding). Sometimes accompanied by an endometrial polyp, which can cause infertility,and which should thus be looked for with a transvaginal ultrasound.
cervical pregnancy An ectopic pregnancy located in the wall of the cervix. A particularlydangerous condition because of the risk of uncontrollable bleeding.
cervical score A score (out of 12) for the quality of cervical mucus, gauged by scoring eachof the following from 0 to 3: the cervix should be open and the volume of mucusshould be good (although every woman will be different for both these parameters,they will be consistent in one woman from ovulation to ovulation); the mucus shouldbe clear,watery and stretchy (Spinnbarkheit); and the mucus should produce a complete‘ferning’ pattern when it’s allowed to dry on a microscope slide.The first two criteriavary at ovulation in different women (so anything above a score of 9 or 10 can benormal), but the same woman should achieve the same Insler score from one ovula-tion to the next.Also called the Insler score.
cervical suture See cervical ligature.cervicitis Inflammation of the cervix, usually because of infection. Sperm might or might
not have trouble getting through the cervical mucus: this can be tested with a postcoitaltest. Occasionally cervicitis can mean that there is endometritis and salpingitis, in whichcase there will usually be pus present in the cervix.A cause of intermenstrual bleeding andpostcoital bleeding.Clinically there might be ‘contact bleeding’when taking a Pap smear.
cervix The ‘neck’ of the uterus, lying between the body of the uterus (its fundus) and thevagina. See also cervical mucus, cervical polyp, cervical pregnancy and cervicitis.The embry-ological development of the cervix and congenital abnormalities.
cetrorelix A GnRH-antagonist made by Serono.Approved for women undergoing in vitrofertilization, with good results when started on day 7 of the cycle, after five or six days’Gonal-F in suppressing the LH surge; the dosage,however, appears to be critical, to avoidover-suppressing natural luteinizing hormone. Marketed as Cetrotide.
CGH See comparative genomic hybridization.chiasmata See chromosomal cross-over.chimerism The condition when an individual shows two or more genetically different
cell lines that are derived from different zygotes, because of intermingling (see micro-chimerism). Chimerism on a micro scale is more common than generally appreciated,in the sense that most mothers who have had a child will, on careful investigation, beshown to have some white blood cells derived from their fetus or fetuses. See alsomosaicism and mixoploidy, although most cases of chimerism do not cause an abnor-mality of the karyotype.
chlamydiaA germ,or infective agent, responsible for infection of, and damage to, the fallop-ian tubes. In men particularly, chlamydial infection can cause nonspecific urethritis,
GLOSSARY � 427
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 427

with a feeling of burning during the passing of urine or with a yellow-colored dischargefrom the penis. In women, there can be a vaginal discharge or there can be mild ormoderate abdominal pain from acute salpingitis; it should be suspected whenever thereis yellow-colored mucus in the cervix during the taking of a PAP smear (that is, whenthere is cervicitis).There might be no symptoms in either sex.The diagnosis of a current,untreated infection is made by testing cell scrapings from the canal of the cervix or fromthe urethra.As a germ, Chlamydia is like a virus in some ways (it can grow only insidecells) and like a bacterium in others (it responds to some antibiotics—especially tetra-cyclines and erythromycin).When it’s diagnosed, both partners should be treated.Apast infection can be revealed by measuring serum chlamydial antibodies, although falsepositive tests can occur.
chocolate cyst A cyst of the ovary caused by endometriosis.The name comes from the old,dehydrated and thickened blood that it contains. Often causes an increase in serumCA125 antigen and can usually be seen on transvaginal ultrasound.
Choragon hCG made by Ferring.choriogonadotropin Generic name for recombinant human chorionic gonadotropin. See
Ovidrel.chorionThe outermost of the two membranes surrounding the gestational sac that encloses
the developing embryo. Separate from the amnion until about 14 weeks of pregnancy,after which the two membranes stick together without intervening fluid. Like theplacenta, with which at the margins it is joined seamlessly, derived from trophectoderm.See also amnion and chorionic villus.
chorionic gonadotropin A gonadotropin produced by the trophoblast of the placenta thatacts like luteinizing hormone. See human chorionic gonadotropin (hCG).
chorionic membrane See chorion.chorionic villus A tongue of tissue within the placenta composed of chorion and contain-
ing capillaries connected to the blood circulation in the fetus that laps the mother’sblood in the uterus, exchanging oxygen, nutrients and waste products between thefetus’s blood vessels (in the villi) and the mother’s blood.This tissue is sampled for genetictesting with a CVS (or chorionic villus sampling). See also intervillous space. Plural: chori-onic villi.
chorionic villus sampling (CVS) A test done at about nine weeks’ pregnancy at which,under the guidance of transvaginal ultrasound, a catheter is passed through the cervix ofthe pregnant uterus to obtain a small sample of tissue from the placenta (the afterbirth)for genetic testing, such as a karyotype.
chromatidThe name given to the products of a chromosome that has divided during meiosisor mitosis, before separating off as separate daughter chromosomes. See also chromoso-mal cross-over.
chromosomal cross-over Remember that the ordinary cells of the body have 46 chro-mosomes in 23 pairs.The members of each of the pair don’t contain the same genes (thisis why you can carry a gene for recessive inheritance without being sick, but if you haveboth genes there’s trouble). During the cell divisions that produce the germ cells (theprocess of meiosis), the 46 chromosomes first double to 92 before they end up with the
428 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 428

23 present in an egg or a sperm.Two of the four sibling chromosomes (we call themchromatids) then randomly exchange bits of themselves: there’s a ‘cross-over’.The pointsof junction where this happens are called chiasmata.Nature is jumbling up where thegenes will end up so that in the long run you don’t always have to inherit two partic-ular genes together just because they live next door to each other on a chromosome.Cross-over does not mean that genes can end up in any chromosome they like: unless‘translocated’, they will remain in pairs (of alleles) within a particular pair of chromo-somes. See also chromosomal nondisjunction, balanced chromosomal translocation and linkageanalysis. Chromosomal cross-over is the origin of what geneticists call hybrid vigor.
chromosomal embryopathyWhen the embryo or fetus is abnormal because of a mistakein its number of chromosomes (see aneuploid and polyploid), with too much or too littlegenetic material. Usually causes miscarriage. Revealed by performing a karyotype on theproducts of conception.
chromosomal nondisjunction Failure of chromatids to separate after chromosomal cross-over during meiosis.The origin of aneuploidy. More common in eggs, or oocytes, thansperm, and increases with age in women.
chromosomeThe mixture of a single (but double-stranded) long string of genetic material(DNA) wound around supporting proteins.There are 46 chromosomes (23 pairs) inevery normal human cell (other than the germ cells). Each cell therefore contains all thegenetic information needed to make a human being. But it’s only in the first few daysof the embryo that all of a cell’s DNA is accessible: once cells differentiate to have specialpurposes only the DNA they need remains unmasked. Chromosomes are located inthe cell’s nucleus and come in pairs, so that each cell has two alleles of each gene. See alsochromosomal cross-over.
chronic Medically,means slow to develop, and lingering or long-lasting.A chronic inflam-mation typically consists of fibrous (scar-like) tissue. Opposite to acute.
ciliumTiny hair-like projections on the surface of some cells,which are thus called ‘ciliated’.Coordinated beating of the cilia moves mucus and mucus-like substances (such as thecumulus mass) on the surface of ciliated cells in the direction of the cilial beat.An indi-vidual cilium has the same basic sub-microscopic structure as the tail (the flagellum) ofa sperm cell (a spermatozoon). See also immotile cilia syndrome. Plural: cilia.
cleavage Process by which a fertilized egg divides repeatedly over several days, forming(for a time) smaller and smaller cells; the process begins at the stage of the zygote andends with a morula.
Clomid Brand of clomiphene made by Marion Merrell.clomiphene A drug that blocks the action of estrogens and so tricks the pituitary gland into
thinking the ovary’s follicles are not producing enough estradiol, so that natural FSHproduction is temporarily increased, the ovaries thereby are stimulated, and folliclesgrow.The LH surge and ovulation usually follow naturally, but human chorionic gonadotropincan be given if monitoring is used to make sure the follicle is properly mature. Brandnames: Clomid (Marion Merrell) and Serophene (Serono).
cloning Originally a botanical term meaning asexual reproduction, or reproduction by‘budding’ rather than by genetic recombination involving an egg and a sperm.Animals
GLOSSARY � 429
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 429

can be cloned either by splitting an embryo during cleavage (nature does this in produc-ing monozygotic twinning) or by inserting an adult cell nucleus into a suitably primedsecondary oocyte, a process called somatic cell nuclear transfer (and generally still very inef-ficient, resulting in a new developing embryo in at most a few percent of attempts).See also therapeutic cloning and reproductive cloning.
coagulation system A complex set of blood and tissue components capable of a cascadeof events causing blood to clot.The central event is the conversion of soluble fibrino-gen to insoluble, polymerized fibrin through the action of thrombin. In a more moderateway, the coagulation system (and these molecules) lay down the scaffolding for normaldevelopment of the placenta, so that abnormalities of blood coagulation may contributeto recurrent miscarriages. See also thrombophilia.
coeliac disease See celiac disease.cohort See follicular recruitment.coitus Latin for having sex.colectomy An operation to remove the colon, performed in children for Hirschsprung’s
disease and in young women chiefly for ulcerative colitis and Crohn’s disease, and noto-rious for leaving the fallopian tubes caught up in ‘repaired’ serosa of the pelvic peritonealcavity, producing a hydrosalpinx on the left side, with resultant sterility, even though thetube on the right side might be normal.
collaborative reproductionAchieving pregnancy with the help of a third party to provideany of: the spermatozoa (see donor insemination); the oocytes (egg donation); or the uterus(surrogacy: see gestational surrogacy and traditional surrogacy). Current issues surround thequestion of whether or not to inform the child of his or her origins,whether the donoror surrogate should be anonymous or take some part in the child’s upbringing, exploita-tion and autonomy, and (in the case of sperm donation) access to sperm banks bywomen not in a heterosexual relationship with a sterile man.
colon See bowel.compaction Process by which the separate cells of the early embryo fuse together to form,
for the first time, a tissue.Typically occurs at the stage called the morula.With compaction,it becomes difficult to detach a cell for preimplantation genetic diagnosis.
comparative genomic hybridization (CGH) A molecular DNA diagnostic techniquewhereby a set of chromosomes (a genome) is compared with a standard set using differ-ent colored dyes (typically red and green), so that any areas that do not exactly matchwill appear green or red instead of brown; a sensitive technique that can be appliedto preimplantation genetic diagnosis as well as to chorionic villous sampling, or CVS, and toamniocentesis for prenatal diagnosis, yielding results much faster than is possible with aformal karyotype and more comprehensively than is possible with fluorescent in situhybridization.
compassion See empathy for a discussion of its place in the range of feelings one personcan have for another.
complement system A rapidly self-amplifying system of molecules in the body capable,when triggered by the immune system, of killing faulty or foreign cells or bacteria bypuncturing their membranes and dissolving their contents.
430 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 430

complete infertility See sterility.complete miscarriageTraditionally, any miscarriage revealed to be complete upon careful
inspection of the expelled pregnancy tissue (the ‘products of conception’, meaning that auterine curettage was not necessary to avoid the risk of retained tissue causing morebleeding or infection.Nowadays we can distinguish a complete from an incomplete miscar-riage (and whether or not a curettage should be done) with a transvaginal ultrasound,which can reveal significant retained tissue.
compound heterozygosityA heterozygous state in which the inherited alleles of the partic-ular gene are different and both harmful, with clinical effects similar to a homozygousstate.
conception The act of becoming pregnant.Traditionally, the fertilization of the egg (theoocyte) by a sperm (the spermatozoon) and the beginning of the growth of the embryo[Butterworths Medical Dictionary]. Since the advent of in vitro fertilization, conception issaid to have occurred only if the conceptus has undergone successful implantation, asevidenced by a positive pregnancy test. See also conception rate and pregnancy.
conception rate The percentage of months or treatment cycles that result in conception,including biochemical pregnancies, ectopic pregnancies, miscarriages and all potentially viablepregnancies (twins are not counted twice); less important for most purposes than theimplantation rate, pregnancy rate, viable pregnancy rate and the take-home baby rate.
conceptus The product of conception from fertilization.congenital An adjective meaning that something, especially an abnormality or anomaly, is
present from birth.The cause for such a condition can be hereditary (genetic) or it canbe an environmental factor operating before birth. See also congenital abnormality.
congenital abnormality Abnormal development of a body part during the life of theembryo or fetus, usually but not always apparent at or soon after birth. It can be geneti-cally inherited or be acquired by exposure to a physical or chemical insult, such as theaction of a teratogen (a drug or other substance in the environment), during develop-ment in the mother’s uterus. Few congenital abnormalities can be associated with aspecific cause, and an apparent cause might not be the true one.
congenital absence of the vasa deferentia (CBA) Congenital (present from birth)absence of the two vasa deferentia, which conduct sperm from the testes to the ejaculate;hence a cause of obstructive azoospermia. Because the vas deferens is usually affected onboth sides, the word ‘bilateral’ is often inserted, as CBAVD. Infertility is inevitable, butcan be overcome using in vitro fertilization with testicular sperm extraction (but see thecautionary box, From father to son, in Chapter 10).The cause, however, is usually thepresence among the man’s genes of one of the serious alleles for the genetic disease cysticfibrosis (which,having recessive inheritance, results when there are two such alleles present);it can also come about when there are one or two of the less serious abnormal allelesfor this condition.The more common of the abnormal alleles should therefore bescreened for (using a specially set up polymerase chain reaction on white blood cells):should an abnormal allele be present (delta F508 is the most common seriously abnormalone), the woman should be screened too, to predict the chance of cystic fibrosis occur-ring in the offspring.
GLOSSARY � 431
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 431

congenital adrenal hyperplasia (CAH) Enlargement and abnormal function of theadrenal glands, usually from before birth, owing to a genetically determined, partialblock in the production of cortisol, the adrenal glands’main hormone, resulting in over-production of subsidiary hormones, including androgens, tending to virilize the femalefetus, which can present at birth with intersex. In mild forms does not manifest untilpuberty, when the symptoms of oligomenorrhea and hirsutism mimic those of polycysticovary syndrome. See also serum 17-hydroxyprogesterone.
congenital anomaly See congenital abnormality.congenital bilateral absence of the vasa deferentia (CBAVD) See congenital absence of
the vasa deferentia.control group When a research study is done (an ‘experiment’, maybe), the procedure,
drug or process being tested or examined on the treatment group needs to be comparedwith a similar group that doesn’t receive the treatment; we call this group the controlgroup.The groups can consist of people, embryos or research animals, for example.
cornual pregnancy A commonly used term for an interstitial pregnancy, but can also referto an angular pregnancy, a pregnancy in a unicornuate uterus or a pregnancy in one side ofa bicornuate uterus.
corpus luteum Latin for ‘yellow body’, the description being that of the solid or cysticstructure in the ovary after ovulation. Derived from the ovulating Graafian follicle.At firstred and friable as arteries and veins invade the collapsed follicle, it soon matures into agland that is very efficient at producing progesterone, a hormone that’s soluble in the fatand which therefore gives the corpus luteum its yellow color. Provides its name to thesecond,or luteal phase of the ovarian cycle, as well as to luteinizing hormone,which causesthe corpus luteum to be formed and sustains it until, in the event of pregnancy, it issupported instead by human chorionic gonadotropin.The appearance of the corpus luteumon transvaginal ultrasound is so variable (and so able to be confused with a serious abnor-mality of the ovary) that for accurate diagnosis of such pathology it is best to scan inthe follicular phase or while taking a progestogen to prevent formation of this structure.Plural: corpora lutea.
corpus luteum defect See luteal phase defect.Crinone A vaginal gel that contains 8 percent progesterone.Well absorbed and with a potent
local effect on the endometrium.Used to mimic (or supplement) the ovarian luteal phase.A weaker (4 percent) formulation is available for long-term use in patients with poly-cystic ovary syndrome or after the menopause to prevent endometrial hyperplasia.
crossover See chromosomal cross-over.cryostorage Storage (at the very low temperature of liquid nitrogen) of sperm, embryos or
(very recently, but still controversially) unfertilized eggs, after special preparation of thesecells during cooling to replace much of the water they contain with a cryoprotectivesubstance such as dimethylsulfoxide, propanediol or glycerol. Storage is biologically safefor a decade or more, but the existence of banks (especially of embryos) has been aconcern of some in society.
cryptomenorrhea Literally, ‘hidden menstruation’. Apparent amenorrhea caused by anobstruction to the outflow of periodic bleeding from the uterus. Causes include an
432 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 432

obstruction in the vagina.Typically there is periodic pain coinciding with the timingof the hidden menstrual flow.The causes of cryptomenorrhea include an imperforatehymen.
cryptorchidism Literally (from the Greek),‘hidden testicle’.A condition in which thereis incomplete descent of the testis or testes from the abdomen into the scrotum.Synonymous with undescended testis. See also orchidopexy.
CT scan See CAT scan.culture mediumThe fluid in which cells or tissues, including eggs, sperm and embryos,
are grown. It consists of water, salts and nutrients.Different media have turned out bestfor different purposes. In the early days of in vitro fertilization, several different mediaseemed to produce equal results: examples included Ham’s F10 and Whittingham’s T6.Quinn’s medium (said to be based on human tubal fluid, though in reality different tothe fluid in the fallopian tube) produced better results than the first generation media.Today’s third generation media, or stage specific media, give superior results and are usedincreasingly. Plural: culture media.
cumulative chance of pregnancy The accumulating chance, month after month, ofsuccessfully having become pregnant.With a monthly fertility (a monthly chance of preg-nancy, or fecundability) of, say, 20 percent, there’s a 20 percent chance of pregnancy bythe end of the first month, a 20 percent of 80 percent (= 16 percent) chance of preg-nancy in the second month, and so a cumulative 36 percent (20 percent + 16 percent)chance by the end of the second month.Further accumulation lies behind the construc-tion of a life-table, as developed in Appendix 1.
cumulus mass A collection of specialized granulosa cells, surrounding the ovulating egg (orsecondary oocyte) in a sticky, mucus-like matrix. Sticks to the fallopian tube’s fimbrial endafter ovulation by a specific interaction with the tube’s cilia.
curettageThe operation of scraping out the contents of a hollow cavity (such as the endome-trial cavity of the uterus) with a curette, for making a diagnosis or for therapeuticallyremoving abnormal tissue. (D&C is abbreviated jargon for dilatation of the cervix andcurettage of the uterus.) When a curettage is done to empty the uterus of normal orabnormal pregnancy tissue, a special suction apparatus is used and we refer to the oper-ation as a vacuum curettage.
curette Spoon-shaped instrument for carrying out curettage.CVS See chorionic villus sampling.cyproterone acetate A progestogen that is particularly effective at blocking the effect of
male sex hormones (androgens) on the skin, and therefore reducing abnormal hair growth(hirsutism) and acne. Found singly in Androcur and in combination with an estrogen inDiane-35, a formulation used for oral contraception. Dangerous if taken in pregnancy,because it stops male fetuses from developing normal genital organs. Not available inthe USA.
cystic fibrosis A serious genetic disease (with a recessive inheritance pattern) characterizedby a major disturbance of the body’s mucus secretions, and thus a cause of incapacitat-ing disease of the lungs. Important in our context because the heterozygous (or carrier)state in men can manifest with azoospermia due to congenital absence of the vasa
GLOSSARY � 433
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 433

deferentia—the infertility of which is nowadays able to be overcome with testicular spermextraction and ICSI, thus risking inadvertent transmission. See also delta F508, and thebox, From father to son, in Chapter 10.
cytokines Soluble signaling molecules produced by cells to activate the immune system.cytoplasmThe part of a cell that is not the nucleus (the nucleus contains the chromosomes).
The cytoplasm is contained by the cell’s plasma membrane and contains all the othercellular structures, including the mitochondria. Genetic inheritance is mostly by way ofthe nucleus (with a contribution from mother and father); a small part is by way of thecytoplasm (with a contribution only from the mother). It is the cytoplasm of the egg(as a secondary oocyte) into which a sperm cell (spermatozoon) is injected in the processof intracytoplasmic sperm insertion. See also mtDNA.
cytotrophoblast Cells in the developing placenta that are derived from the early embryo’souter layer (the trophectoderm of the blastocyst) and then persist through pregnancy,producing either syncytiotrophoblast or extravillous trophoblast.
D&C See curettage.danazol A hormonal drug used for treating endometriosis. Related to male sex hormones
(it’s a weak androgen), it has occasional androgenic side-effects, including weight gainand increased muscle bulk (it’s also an anabolic steroid), and increased facial hair(hirsutism); less commonly there can be deepening of the voice or enlargement ofthe clitoris. For the details of its correct and incorrect use, see Chapter 16, especiallythe box, Danazol mischief. Made by Sanofi Winthrop as Danocrine.
Danocrine See danazol.Day-3 FSH See depletion of eggs and serum FSH.decapeptyl A GnRH-agonist, made by Ipsen Biotech as Triptorelin. Administered by a
monthly injection.decidua Differentiated endometrium of pregnancy which is shed (like a deciduous tree sheds
its leaves) at childbirth or miscarriage, as part of the afterbirth. During pregnancy it hasimportant hormonal functions (see decidual cells).
decidual cells Plump endometrial stromal cells, lying between the glands of the endometrium,formed under the prolonged influence of progesterone, especially with establishment ofpregnancy.Constitute the decidual reaction to form the decidua of pregnancy, and produceprolactin (important for regulating water entering the gestational sac) and relaxin, whichkeeps the myometrium quiet.
decidual reaction A transformation of the lining of the uterus (the endometrium) in preg-nancy. Complete confluence of endometrial stromal cells (lying between the endometrialglands) occurs, caused by prolonged (14 days or more) exposure to progesterone or aprogestogen; normally happens only with pregnancy.See also decidua and predecidual reaction.
delta F508 The commonest of the alleles to result in cystic fibrosis (when two delta F508alleles are present) or can occur when one F508 allele is present in a man.A womanheterozygous for this gene (with one F508 allele) will be a carrier for cystic fibrosis (andfor CBAVD) but will herself be otherwise normal.There are, however, many otherfaulty alleles that can also contribute to these clinical conditions.The most commonalleles can be looked for at preimplantation genetic diagnosis (PGD).
434 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 434

deontological ethics A set of ethical beliefs, in which principles and values are seen byadherents to be self-evident and not in need of more basic proof.The ethical princi-ples are duty-binding, innately known and by nature resistant to change. For practicalapplication, and a contrast to teleological ethics and utilitarian ethics, read the box, Ethics:Moral imperatives, outcomes and equity, in Chapter 26.
deoxyribonucleic acid See DNA.depletion of eggsThe natural process in which the older the female fetus, girl or woman
gets the fewer are the eggs (as primordial follicles) left in the ovaries; the huge majority ofeggs are lost because of atresia, only a tiny fraction by ovulation. Before the eggs aredepleted there is a mild or moderate elevation in serum FSH when measured duringthe menstrual phase (often called a day-3 FSH.When the eggs are more or less depletedthere will be primary ovarian failure and, in women who have had periods, the menopausewill take place, perhaps prematurely (premature menopause). Infertility, however, usuallyprecedes total egg depletion by up to 10 years. See also mitochondrion and oopause.
DHT See dihydrotestosterone.DI See donor insemination.Diane-35 A formulation of the oral contraceptive pill that contains, as well as an estrogen,
the progestogen known as cyproterone acetate, which is particularly effective at blockingthe effects of male hormones on the skin. Made by Schering.
diathermy Use of a high-voltage, high-frequency electric current to coagulate or evapo-rate tissue during surgery.Useful in reproductive medicine because it can be used duringlaparoscopy, particularly for stopping bleeding (by coagulation) and for treating endometrio-sis (by evaporation).
dihydrotestosterone (DHT) The most active male sex hormone or androgen; formed intarget tissues from testosterone (which is the main form of androgen circulating in theblood).Testosterone must be converted to DHT before it can do its job (the enzymefor which is 5-alpha reductase, and a deficiency of which is a cause of intersex).
dilatation and curettage Before curettage (of the uterus), the cervix is dilated to admit thecurette. Sometimes abbreviated as D&C.
Dimetriose See gestrinone.diploidThe full, normal complement of chromosomes, numbering 46 (as 23 pairs). See also
haploid.The noun form of this adjective is diploidy (the state of being diploid).distributive justice Justice dispensed in the community to confer maximum value to those
in need through the notions of fairness and consistency.dizygotic twins Twins formed from two fertilized eggs, or zygotes; non-identical twins.DNA The stuff of which genes are made. DNA is an abbreviation of deoxyribonucleic
acid, a molecule made of a variable sequence of units, the nature and order of whichforms the genetic code. DNA is located chiefly in the chromosomes, which form a cell’snucleus.A small amount of DNA (coding for about 13 genes) is found in the mitochon-dria (for which see also mtDNA).
DNA microarray Just as inkjet printers have revolutionized desktop publishing, so thesame technology has revolutionized genetic diagnosis, by miniaturizing hybridization,or fusion, between microspots of DNA printed onto a glass surface and a test sample
GLOSSARY � 435
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 435

of target DNA that binds when there is a perfect match.The resulting ‘DNA chips’can be ‘read’ to look for variations of DNA sequence (mutation screening), for meas-uring the degree of different gene activity in a cell (gene expression screening) or forestimating relative amounts of known DNA compared with the DNA standard genome(comparative genomic hybridization, or molecular karyotyping).
DNA testingTesting for the presence or absence of a particular sequence of DNA using molec-ular methods such as the polymerase chain reaction or, increasingly,with DNA microarrays.
dominant follicle The preovulatory follicle, or Graafian follicle, that has won the responsi-bility for producing estradiol for the rest of that particular ovarian cycle. Chosen by theend of the first week of the follicular phase. Its destruction (whether accidental or inten-tional) means that a new follicular phase must start, with ovulation two weeks later,whereas destruction of one of the tertiary follicles before one has become dominantcauses no interference with the timing of ovulation for that cycle.
dominant inheritance A pattern of inheritance of a characteristic (such as brown eyecolor) or abnormality in which just one gene or allele is needed to confer the character-istic or abnormality, in contrast to recessive inheritance,which requires two genes. See alsoheterozygous.
donor insemination (DI) Assisted insemination in which semen from a sperm donor (whois not the husband) is used.
Dostinex See cabergoline.Down syndrome Due to trisomy 21. Chromosome 21 is the smallest of the ‘autosomes’
(the non-sex chromosomes); trisomies of the other autosomes tend to be lethal at an earlierstage of embryonic or fetal development, and so are seen much more rarely. Diagnosisof Down syndrome requires a karyotype, obtainable from pregnancy tissue by chorionicvillus sampling (CVS) or amniocentesis. Screening for increased risk in pregnancy can beperformed by triple screen or by looking for nuchal translucency at transvaginal ultrasound.
DUB see dysfunctional uterine bleeding.duration of infertility One of the two most important variables (the other is time left for
conception) that determines the chance of still getting pregnant naturally in subfertility,including unexplained infertility.The longer the duration of infertility, the smaller thechance each month as time goes on. See also fecundability and time to pregnancy.
duty A moral compulsion for ethical action that is innate.The basis for deontological ethics.See also suffering. Generally synonymous with obligation. In Chapter 26, a duty isconsidered innate or intrinsic (it originates inside you),whereas an obligation is imposedextrinsically, by the enforcement of others’ rights (it originates outside you).
dysfunctional uterine bleeding (DUB) Heavy bleeding from the uterus. See anovulatorydysfunctional bleeding (often painless and irregular) and ovulatory dysfunctional bleeding(usually regular and can be associated with dysmenorrhea).
dysmenorrhea Painful menstruation. Can be primary, present in teenagers, generally inspasms around the start of the period; or it can be secondary, developing as a womangets older, and then typically lasting more than a day or so into the period, withprolonged aching as well as spasms. Primary dysmenorrhea might have no medicalimportance beyond the suffering the pain causes, and typically gets better as a woman
436 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 436

reaches her twenties; severe or persistent cases, however,warrant investigation.Secondarydysmenorrhea can signify, for example, endometriosis, fibroids, adenomyosis or peritubaladhesions.
dyspareunia Painful sexual intercourse that persists after the first few occasions or whichdevelops after months or years of painless sex.
eclampsia See preeclampsia.ectoderm The ‘upper’ layer of the embryo as the inner cell mass forms a circular disk two
cells thick, giving rise with further embryonic development to the skin, brain and spinalcord. Synonym: epiblast. See also endoderm and mesoderm.
ectopic pregnancy A pregnancy implanted in an abnormal location, such as the fallopiantube (see tubal pregnancy), the cervix (see cervical pregnancy), the ovary (see ovarian pregnancy)or the peritoneal cavity (see abdominal pregnancy). See also heterotopic pregnancy and cornualpregnancy.
ectopic pregnancy rate The percentage of ectopic pregnancies among total clinical preg-nancies (excluding ‘biochemical pregnancy’). Until a generation ago, the rate was about0.3 percent, which can be regarded as the incidence in normal women.The rate isincreased with abnormalities of the fallopian tubes, assisted conception and other cir-cumstances, so that nowadays ectopic pregnancies account for about 2 percent ofpregnancies in Western societies.
efferent ducts Fine passages in the rete testis conducting sperm cells (spermatozoa) from thetubules of the testis to the epididymis.
egg General term for oocyte.egg depletion See depletion of eggs.egg donation A form of collaborative reproduction comparable in some ways to sperm
donation (see donor insemination), but different in that eggs for donation are much harderto obtain physically than are ejaculated sperm; generally the egg donor undergoes allthe steps needed for in vitro fertilization up to the stage of egg retrieval.
egg pick-up See egg retrieval.egg retrieval Procedure for obtaining eggs (oocytes), involving the passing of a needle into
a mature (or preovulatory) follicle, either directly at laparoscopy or (more usually) via thevagina guided by transvaginal ultrasound.
electrocautery See diathermy.embryo The word is used loosely to describe everything from a fertilized egg (or zygote)
to a fetus, including the embryo.What nowadays we call the embryo has for long beencalled the ovum by professional embryologists!
embryo biopsy A biopsy, or removal of one or two cells, from an early IVF embryo forpreimplantation genetic diagnosis after in vitro fertilization.
embryo transfer (ET) Procedure by which the embryo is placed in the uterus or into thefallopian tube after in vitro fertilization.
embryonic stem cells See inner cell mass and stem cell.embryopathy Literally, pathology of the embryo (or fetus). Can underlie a miscarriage or, if
it reflects more or less permanent state, can cause unexplained infertility.empathy More than feeling compassion or sympathy ‘for’ another person, empathy puts you
GLOSSARY � 437
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 437

in their shoes to feel ‘with’ them or ‘as one’with them.First used in English in the earlytwentieth century to translate the German psychoanalytic term Einfühlung, meaning‘to feel as one with’, though in practice more closely translating the German Mitgefühl,‘to feel with’ someone.
empirical An awkward adjective that can have contrary meanings in medicine.Theword comes from the Greek for experience. On the one hand, empirical medicalpractice is that which is based only on observation and experiment (praiseworthy);on the other, it can refer to medical practice that’s based on very personal experi-ence without taking scientific principles into account (not praiseworthy); at worstit refers to treatment that’s chosen on no other basis than:‘Let’s see if it might work’.In this book I use it in its first sense unless I draw attention to a contrary use of itby others.
endocrine disrupter A natural or pollutant substance in the environment possibly capableof acting—alone or in combination with other substances—as an estrogen or as a blockerof androgens during development of the fetus. Suspected of causing endometriosis andoligospermia in later life.
endocrinology The study of hormones, including their production, their action and theirexcretion.
endoderm The ‘lower’ layer of the embryo, as the inner cell mass forms a circular disk twocells thick; with further embryonic development it gives rise to the digestive tract andits glands. Synonym: hypoblast. See also ectoderm and mesoderm.
endometrial atrophy Diminishment of the endometrium through lack of support by, espe-cially, the hormone estrogen or by the loss, through chronic endometritis and/or injury atcurettage under abnormally low estrogen conditions, of subsequent receptiveness toestrogen. Can cause light periods (hypomenorrhea) or absent periods (amenorrhea). Seealso Asherman syndrome and intrauterine adhesions.
endometrial biopsy See premenstrual endometrial biopsy.endometrial cavity The space inside the uterus lined by the endometrium.endometrial hyperplasia Overgrowth of the endometrium, caused usually by prolonged
action of estrogen unopposed by progesterone (that is, prolonged anovulation), as is the casein, particularly, the polycystic ovary syndrome. Potentially dangerous, because it can turnto cancer of the endometrium. Can be suspected by an echogenic appearance of theendometrium on transvaginal ultrasound and is confirmed by pathological examinationof tissue obtained at curettage.
endometrial polyp A polyp of the endometrium (lining of the uterus), sometimes withoutsymptoms, sometimes with abnormal bleeding such as intermenstrual bleeding, premen-strual spotting or heavy periods.A cause of infertility (and of failure of assisted conceptionto result in pregnancy). Diagnosable with transvaginal ultrasound.
endometrial resection An operation performed at hysteroscopy to treat menorrhagia byintentionally producing endometrial atrophy and intrauterine adhesions.
endometrial stroma Loose connecting-type (‘connective’) tissue that lies between glandsof the endometrium. Contains stromal cells that eventually respond to progesterone bybecoming plump to form a more or less continuous sheet towards the end of the
438 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 438

menstrual cycle (the predecidual reaction) or,more completely with successful implantationand pregnancy (the decidual reaction). See also decidua.
endometriosis A common condition in which tissue like the lining of the uterus (theendometrium), grows somewhere else, sometimes causing dysmenorrhea, premenstrual spotting,infertility, dyspareunia and ovulatory dysfunctional uterine bleeding. See also unexplained infertility.
endometritis Inflammation of the endometrium (the lining of the uterus). Can be acute orchronic. Not related to endometriosis.
endometrium The lining of the uterus, which contains the endometrial glands and theendometrial stroma. Distinct from the myometrium.
endorphins Opium-like substances produced naturally in the brain, which give a feelingof well-being. Production of endorphins is stimulated by many natural circumstances,and also by profound exercise (to which people can become ‘addicted’!). Depressed inpremenstrual tension.
environment The physical, chemical, biological and social milieu in which we live.Thisenvironment is sometimes called the external environment, in contrast to an internalenvironment that might describe the physical and chemical milieu inside the body,around a particular organ, tissue, cell or intracellular organelle. See also congenital andendocrine disrupter.
enzyme A protein found in cells and secretions that acts as a catalyst, greatly promoting achemical transformation for a special purpose. Enzymes are important in every aspectof biology, including the production (and destruction) of hormones.
epididymal sperm aspiration See microscopic epididymal sperm aspiration (MESA).epididymis A finely coiled tubular structure, lying next to each testis in the scrotum, which
connects the testis to the vas deferens, and through which sperm cells (or spermatozoa)pass and gain in maturity.
ERT See estrogen replacement therapy.ES cells Embryonic stem cells.eSET Elective single embryo transfer Choosing to have just one embryo transferred
after in vitro fertilization even though there is more than one embryo that is suitable; theother suitable embryos are frozen and stored.A strategy to increase the chance of takinghome a baby by minimizing the risk of multiple pregnancy,which carries a higher riskof miscarriage and stillbirth.
estradiol The most powerful natural estrogen. Produced by the ovarian follicle and corpusluteum in women, and (to a small extent) by the Sertoli cells in men.Also produced byfat cells (through conversion of testosterone) in older women, especially after themenopause. See also serum estradiol.
estriol A weak estrogen. Increased in pregnancy, especially late pregnancy. See also triple test.estrogenThe general name for one of the two principal female sex hormones (the other
is progesterone), responsible for stimulating growth of the female reproductive system(the vagina, the cervix, the uterus and the fallopian tubes) and growth of the breasts.Themain estrogen is estradiol, produced by the developing follicle (and to a lesser extent bythe corpus luteum) in the ovary; by the trophoblast of the placenta; and by the body’s fattissues (through conversion from male sex hormones, or androgens, in the blood).After
GLOSSARY � 439
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 439

the menopause the main estrogen is the weaker one, estrone, largely derived from conver-sion by the body’s fat of the weak androgen androstenedione.
estrogen replacement therapy (ERT) The therapeutic use of estrogen to stop theeffects of menopause after the ovaries have been removed or have stopped function-ing. If the uterus is still present the hormone regimen must include at least 11 days’progestogen usage each month, or there will be a risk of endometrial hyperplasia andhence endometrial cancer.
estrone A weak estrogen, which needs to be converted (in target tissues such as theendometrium) to the strong estrogen estradiol before, as a hormone, it causes an estrogeneffect.The main estrogen in blood after the menopause. Formed from estradiol when thathormone in tablet (or oral) forms is absorbed across the intestines.Abbreviated as E1.
ethical practice committeeA socially derived,multidisciplinary committee of a hospital.It meets irregularly, often at short notice, to help in the making of ethically difficultclinical decisions aimed at ascertaining and preserving the patient’s best interest. In theUSA generally called an ethics committee.
ethics A set of principles and values that govern behavior to accord with a notion ofmorality. See especially deontological ethics, teleological ethics and utilitarian ethics, and alsosee autonomy, beneficence, non-maleficence, justice and suffering.The ethics of assisted repro-ductive technology, collaborative reproduction, the doctor–patient relationship, informed consentand human embryo research are much debated.
ethics committeeA mandated committee of an institution (hence institutional ethics commit-tee, or IEC,or human research ethics committee, or HREC) that conducts medical research.It meets regularly and is composed of specialist and lay individuals who consider theethical implementation of protocols for research, according to the requirements of the1975 Declaration of Helsinki (on clinical research and human experimentation) and anyother official determinations relevant to the particular environment of the researchers.Its purpose is to gauge and to minimize risks run by the subjects of research. Its deci-sions are usually binding on researchers. In the USA this committee is called an institu-tional review board,or IRB. In the USA the term ethics committee denotes a committeedistinct from an IRB that considers clinical ethical matters (see ethical practice committee.
ethinylestradiol Orally effective form of estradiol that resists being converted to estroneafter ingestion. Generic (‘no frills’) name for Estigyn and Progynon C.
expanded blastocystThe last stage of development of the blastocyst before it hatches outof the zona pellucida prior to implantation.
extravillous trophoblast The outermost layer of trophoblast, produced by cytotrophoblastwhere there is direct contact with maternal decidua rather than blood.The EVT cellstravel into the decidua, reacting with NK cells and invading maternal blood vesselsfeeding the placenta, softening the walls and replacing the lining with fetal tissue, a processcalled ‘conversion’.Also known as interstitial or intermediate trophoblast.
extra-Y-chromosome syndrome A trisomy with a karyotype of 47,XYY—a male withan extra Y-chromosome.Affected men tend to be tall. Surveys of penal institutions haveindicated a higher than expected frequency, implying that affected men are at increasedrisk of being criminals.This assertion is controversial.
440 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 440

factor V Leiden A polymorphism for blood clotting factor ‘five’ that makes coagulationoccur more readily, therefore causing thrombophilia. Pronounced ‘Layden’.
factor XIII ‘Factor 13’.A component of the coagulation system. See fibrinogen.fallopian tube The hollow organ, about 10 to 12 centimeters long, that effectively joins
the ovary to the uterus on each side. Composed of the fimbrial end, the ampulla, theisthmus and the interstitial segment.
falloposcopy Looking inside the fallopian tube with a tiny (0.5 millimeter diameter), flexible,fiberoptic instrument, from the direction of the uterus. See also salpingoscopy.
fecundability Technical-speak for the monthly chance of pregnancy, or monthly fertilityrate,either for an individual (measured over time) or for a population (the number of concep-tions occurring in one month).For any individual with unexplained infertility, and in mildercases of subfertility, chiefly determined by the duration of infertility (or, in cases of secondaryinfertility, in which past fecundability is being estimated, determined by time to pregnancy).Once calculated this way (explained in Appendix 1),an estimate of the chance of still gettingpregnant naturally (as opposed to undergoing assisted conception) will chiefly be determinedby the time left for conception.See also normal monthly fertility and cumulative chance of pregnancy.
fertilization Entry of a sperm cell into an egg: their ‘marriage’.The egg is activated bythis event, so that: (1) ‘cortical granules’ are expelled that stop further sperm binding tothe egg; (2) the second division of meiosis is completed, with expulsion of the secondpolar body; and (3) the machinery of the egg is started, which will form pronuclei of themale and female chromosomes prior to syngamy.
Fertinex Highly purified Metrodin, with no residual luteinizing hormone, thus equivalent inactivity to recombinant FSH. Called Metrodin HP outside the USA. Made by Serono.
fetal reduction A controversial and emotionally hazardous way of dealing with a higher-order multiple pregnancy (such as quadruplets, quintuplets or higher) in which all theembryos or fetuses are at risk of being lost before viability.The technique involves carryingout transvaginal ultrasound and injecting a lethal substance (such as air or a solution ofpotassium) into the visibly beating heart of one or more of the embryos, so reducingthe number of surviving embryos to three, two or one. Generally regarded as a morestressful procedure than even an induced abortion, both for the person undergoing theoperation and for the ultrasound doctor asked to do it. Few people regard the avail-ability of fetal reduction to mean that the greatest care does not need to be taken toavoid higher-order multiple pregnancies in assisted conception programs.There’s a hazard:loss of the remaining fetuses from miscarriage; but the risk of this, with an experiencedultrasound doctor or fetal medicine specialist, is low.
fetus An unborn baby.The product of conception from the time the embryo is fully formed(from head to limbs—about eight weeks from the last menstrual period) until delivery.
fibrin A polymer that is formed from the circulating protein fibrinogen when blood clots(see coagulation system).Also important in the formation of the placenta, so abnormali-ties of fibrinogen can cause recurrent miscarriage.
fibrinogen A very soluble protein found in the blood that forms the progressively lesssoluble protein fibrin when blood clots, through the action first of thrombin and then offactor XIII. See also coagulation system.
GLOSSARY � 441
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 441

fibroidA benign ‘tumor’of the muscular wall of the uterus (the myometrium).More commonwith increasing age,but can occur in women in their twenties.Can be single or multiple,and can be located on the outside of the uterus (a subserous fibroid),within the wall of theuterus (an intramural fibroid), or protruding into the cavity of the uterus (a submucousfibroid.The closer it is (or they are) to the endometrial cavity, the more likely it is that afibroid will disturb reproduction (either as miscarriages or sometimes as infertility) and disturbmenstrual bleeding. Surgery for removal of a fibroid, or myoma, is called a myomectomy.
fimbria Latin for a fringe, particularly the fringed, open end of the fallopian tube referredto as the fimbrial end. Plural: fimbriae.
fimbrial end Also ‘fimbriated end’: the open, outside end of the fallopian tube in contactwith the surface of the ovary, from which it ‘picks up’ the ovulated egg from the rupturedfollicle. It’s composed of delicate fimbriae—finger-like projections of the tube lined bycells with tiny hairs (cilia),which beat towards the inside of the tube, carrying the stickycumulus mass containing the egg into the ampulla before fertilization. Easily damaged byinfection (salpingitis) or careless surgery, after which it may be blocked, resulting in ahydrosalpinx, or have its correct movement inhibited by adhesions.
fimbriectomy An operation for sterilization or ‘tubal ligation’ in which the fimbrial end ofeach fallopian tube is removed. It has a higher failure rate than most other sterilizationoperations on the tubes and also is more difficult to reverse if the woman intends toregain fertility. It can result in a hydrosalpinx, which can jeopardize success with in vitrofertilization (see the box, Hydrosalpinx: Reintroducing a villain, in Chapter 20), and themicrosurgery operation to reverse it, salpingostomy, is much less often followed by preg-nancy than tubal anastomosis operations are.
fimbriolysis Microsurgery of the fallopian tube’s fimbrial end, involving careful dissection offimbriae that have become stuck together from adhesions.Generally gives a better outcomethan salpingostomy (which must be resorted to if the fimbriae are too damaged to dissect).
FISH See fluorescent in situ hybridization.fluorescent in situ hybridization Known as ‘FISH’.A form of DNA testing for genetic
diagnosis in which a special region of a chromosome is stained with a dye that emitscolored light when exposed to ultraviolet light. For example, a marker for chromo-some 21 will normally show two spots of light, whereas three spots of light wouldindicate trisomy 21 (Down syndrome).Useful because the technique is accurate with just
442 � GETTING PREGNANT
Fetus or foetus?
Which spelling is correct? In the mistaken belief that the word fetus was derivedfrom the Latin foveo (to cherish), rather than feo (to beget), Isodurus (AD 560–636),Archbishop of Seville, started spelling it ‘foetus’. So, whether you are British orAmerican or Australian,‘fetus’ is etymologically better. (I’m indebted to Dr ThomasFirth Baskett, from 1988 to 1990 editor of the Journal of the Society of Obstetriciansand Gynaecologists of Canada, for this authoritative en passant.)
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 442

one cell, making diagnosis possible in an IVF embryo before transfer (see preimplanta-tion genetic diagnosis), and speeding up prenatal diagnosis while awaiting a full karyotype.Being replaced in some labs by comparative genomic hybridization.
foetus See fetus. For a discussion on the spelling, see the box, Fetus or foetus?folic acid Synonym: folate. A vitamin of the B group required for the synthesis of DNA.
Dietary deficiency is common, and leads, in pregnancy, to birth defects such as spinabifida, and ultimately to increased levels of serum homocysteine, especially in people withMTHFR C677T.
follicle Normal structure in the ovary that contains the egg, or oocyte. All are formed asprimordial follicles before birth and remain microscopic in size until growth starts (follicu-logenesis), a month or two before the cycle in which the particular follicle will be acandidate to ovulate.About 3 millimeters in diameter at the start of a cycle, and about2 centimeters in diameter when ready to ovulate.The follicle makes more and moreestrogen (particularly estradiol) as it grows. In ovarian monitoring for assisted conception, thenumber growing and their rate of growth are monitored by transvaginal ultrasound. Seealso primary follicle, secondary follicle, tertiary follicle, preovulatory follicle or Graafian follicle,atretic follicle and ovulation.
follicle aspiration Egg retrieval procedure for obtaining eggs (oocytes), involving the passingof a needle into a mature (or preovulatory) follicle, either directly at laparoscopy or (moreusually) via the vagina guided by transvaginal ultrasound.
follicle cells Cells of the follicle that surround the egg (the oocyte).An increase in numberis what causes the follicle to grow. In tertiary follicles they are responsible for convertingandrogens (from surrounding ovarian thecal cells) into estrogens, particularly estradiol. Atertiary follicle’s cells are also called granulosa cells.
follicle stimulating hormone (FSH) The hormone, or gonadotropin, produced by the pitu-itary gland that in women stimulates the tertiary follicle to grow; in men it stimulates sper-matogenesis. Obtained from human sources in a mixture with luteinizing hormone (LH)as: (1) human menopausal gonadotropin (hMG), extracted from the urine of women whohave been through the menopause (Humegon, Metrodin and Pergonal); and (2) humanpituitary gonadotropin (hPG), from human pituitary glands removed at autopsies (nowobsolete).Today, pure FSH is made synthetically with gene technology (recombinantFSH), such as Gonal-F and Puregon. See also serum FSH.
follicle tracking Serial transvaginal ultrasounds of the ovary during the follicular phase totrack the growth of one or more tertiary follicles, accompanied usually by serial esti-mations of serum estradiol, serum LH and serum progesterone, for the two-fold purposeof estimating follicular maturity (to time intercourse, a midcycle-dependent inves-tigation such as a postcoital test, or an egg retrieval) and identifying the onset of theLH surge, which can affect the timing of the intervention. Sometimes accompaniedby injection of human chorionic gonadotropin to trigger ovulation at a precisely antici-pated time.
follicular atresiaThe process by which a primary follicle or a tertiary follicle stops growing,leading to disappearance (apoptosis) of its follicle cells and the oocyte, or egg, each contains.Such a follicle is called an atretic follicle. See also follicular recruitment.
GLOSSARY � 443
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 443

follicular phaseThe part of the ovary’s monthly cycle before ovulation, dominated by thepresence of firstly, a cohort of growing tertiary follicles, then the dominant follicle, then theestradiol these follicles produce. Normally around 14 days in length, but quite variable,often being much longer for the first few menstrual cycles after the first period (menarche),and typically getting shorter in the months or years leading up to egg depletion andmenopause. Corresponds with the proliferative phase of the endometrial, or menstrualcycle.
follicular recruitment A follicle is ‘recruited’ at two distinct stages of development. Earlyor continuous recruitment refers to the ongoing, continuous recruitment of primordialfollicles to start their growth and become antral follicles, a process that is independent ofmajor hormones, starts before birth and ends when there are no follicles left, this takingplace around the time of menopause.Cyclical recruitment refers to the much later recruit-ment of medium-sized tertiary follicles into the ovarian cycle due to a temporary eleva-tion of follicle stimulating hormone, which occurs at the end of each luteal phase, thusinitiating a new follicular phase; the group of ‘recruits’ susceptible to this late recruitmentis called a cohort.Time-wise for a particular follicle, the two episodes of recruitmentoccur eight months apart: in other words, it takes eight months for a follicle to growfrom its resting state before it can have a chance of making estrogen and then undergo-ing ovulation. Not all early-recruited follicles undergo later cyclical recruitment: someare lost through early atresia, many others reach the stage at which they could be cycli-cally recruited at a stage when FSH is low (most stages of the ovarian cycle) and undergoatresia then.Readers will appreciate that ovulation induction, including intentional super-ovulation, can have no effect on the rate at which follicles are used up in ovaries or onthe age at which menopause will occur (the different recruitment points involved areeight months apart, with the early recruitment point governing the rate eggs are usedup and the late recruitment point deciding how many follicles can respond to provideuseable eggs).
folliculogenesis Strictly, the process by which follicles are first formed in the ovaries beforebirth; in the woman, it means the growth of a primordial follicle into an early tertiaryfollicle—a transition that confers receptiveness of the follicle to follicle stimulating hormone(FSH).The stimulus for initiation of follicular development and its timing for individ-ual follicles remain a mystery.
Follistim Recombinant follicle stimulating hormone made by Organon. Called Puregon inEurope,Australia and Asia. On an equivalent dose basis, produces serum FSH levels thatare somewhat slower to rise than with the use of hMG preparations, but which are ulti-mately higher: in other words, follicles and serum estradiol levels take a little longer torespond than they do to Humegon, but the number of mature, preovulatory follicles avail-able for egg retrieval is the same or more. I find that 200 U (units) of Puregon per dayproduces a similar result to 225 U of Humegon or Metrodin. Generically known asfollitropin beta.
follitropin Generic name for recombinant FSH, as found in Gonal-F (or follitropin alpha)and Puregon (Follistim), or follitropin beta.Although there are slight differences in thetwo preparations, their clinical action is equivalent.
444 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 444

fragile-X syndromeThe commonest cause of severe mental retardation in males, causedby a long ‘triple repeat sequence’ in a part of a gene for intelligence located on anX-chromosome, rendering this sex chromosome susceptible to breakage, which can berevealed either in a karyotype performed under special laboratory conditions or using aspecial PCR DNA test; females have two X-chromosomes and so may be carriers forthis devastating condition,which will affect one in two of their male children; the carrierstate in females can have clinical effects, namely a susceptibility to reduced numbers ofovarian follicles and hence primary ovarian failure and premature menopause, so should belooked for before assisted conception attempts are made in these clinical circumstances.
free androgen index Not often carried out at no cost—‘free’ here means the androgen(testosterone) in blood that is not bound to carrier proteins such as sex hormone bindingglobulin, and thus is immediately available for action in the tissues.A more sensitive testthan serum testosterone and likely to be increased in the polycystic ovary syndrome. Anindirect measure of serum free testosterone, which can be performed instead.
free testosterone index See free androgen index and serum free testosterone.FSH See follicle stimulating hormone.fundus The body, or the main part, of the uterus (that is, the part of the uterus that is not
cervix). Sometimes refers to the dome-shaped topmost part of the uterus.galactorrhea Demonstrable milk production from the breasts other than while purpose-
fully breast-feeding; caused by hyperprolactinemia or, sometimes, by disease in the breastor wall of the chest.
gamete A general term for a germ cell (that is, an egg or a sperm) that has been released orseparated from its gonad. See also haploid.
gamete intrafallopian transfer (GIFT) An assisted conception procedure in which unfer-tilized eggs plus sperm (that is, gametes) are transferred to the fallopian tube, so thatfertilization occurs in the normal place. Because in vitro fertilization is avoided, for somepeople GIFT is more morally acceptable than is IVF. The disadvantages are thatlaparoscopy is required and that for the pregnancy rate to be comparable to IVF toomany eggs need to be transferred, risking high-multiple pregnancy. See also zygoteintrafallopian transfer (ZIFT).
ganirelix A GnRH-antagonist made by Organon.The first to be FDA-approved for womenundergoing in vitro fertilization, with good results when started on day 7 of the cycle,after five or six days FSH in suppressing the LH surge; the dosage, however, appears tobe critical, to avoid over-suppressing natural luteinizing hormone.Marketed as Antagonin the USA and as Orgalutran elsewhere.
Gärtner’s duct See mesonephric duct.gastrulation A step of major reorganization of the developing embryo, coinciding time-
wise with the missing of the menstrual period in the early pregnant woman, in whichthe third, or ‘middle’ layer (the mesoderm) forms. Occurs after blastulation (the transfor-mation giving rise to the blastocyst) and before neurulation (the transformation formingthe brain and spinal cord).
gender Often a genteel term for distinguishing the male from the female sex.More precisely,the cultural attributes that attach to biological sex. In principle may be masculine
GLOSSARY � 445
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 445

(when more often than not it attaches to the male sex), feminine (more often thannot with the female sex) or neuter (the ‘gender’ non-sexual or inanimate objects have).Gender identity is not to be confused with heterosexual (opposite sex) or homosex-ual (same sex) preference. See also intersex and transsexualism.
geneThe smallest unit of inheritance coded by DNA. Generally, a single gene codes for asingle protein. Genes come in pairs of alleles (one inherited from each parent) in alltissues except the haploid cells, particularly the spermatozoon.
genes See gene.genetic-plus-gestational surrogacy See traditional surrogacy.genome A full set of DNA code (a full set of genes) for a whole animal or organism, or for
a defined component of an organism, such as a mitochondrion.germ cell Distinct from the somatic cells that compose most of the body’s tissues and organs,
germ cells form the eggs and sperm that will form the next generation. Early germ cellsare diploid and replicate by mitosis, but during their development they enter meiosis (foreggs this occurs before birth, for sperm it occurs after puberty), so that at the timeof fertilization the contributing sperm and egg are haploid. So also yolk sac, oogonium,spermatogonium, primary oocyte, secondary oocyte and spermatid.
gestation See pregnancy.gestational sac A fluid-filled bag of membranes in which the embryo forms during preg-
nancy.Visible on transvaginal ultrasound from about five weeks from the last menstrualperiod.Technically, the amniotic cavity (from which later in pregnancy the fluid is able tobe sampled with amniocentesis).
gestational surrogacy A form of collaborative reproduction in which the woman who is thesurrogate for the intended pregnancy receives embryos from the commissioning infertilecouple, who have undergone in vitro fertilization, then, by becoming pregnant, carries(or ‘gestates’) the pregnancy, gives birth and gives up the baby to the baby’s geneticparents. In principle the practice can be done for altruistic or commercial reasons. Itspitfalls and perils are described in Chapter 23.
gestrinone Generic name for Dimetriose, a drug used in the treatment of endometriosisthat inhibits ovulation and blocks the action of both estrogen and progesterone; risks andside-effects are similar to danazol; it is usually taken just twice weekly, by mouth.
GIFT See gamete intrafallopian transfer.glucose tolerance test See plasma glucose.GnRH See gonadotropin releasing hormone.GnRH-agonistA GnRH-analog that briefly stimulates the pituitary gland to release follicle stim-
ulating hormone (FSH) and luteinizing hormone (LH), then within a few days reduces thesehormones to low levels (you could say that the pituitary has had a clamp put on it), stoppingthem from competing with administered hormones—and,particularly in women,suppress-ing the LH surge that otherwise can spoil the timing of egg retrieval in an assisted conceptionprogram such as IVF or GIFT. Examples include: leuprorelin (Lucrin, made by Abbott,used in Australia and Europe) or leuprolide (Lupron,made by Abbott in the USA);nafare-lin (Synarel, by Syntex); goserelin (Zoladex, by ICI); triptorelin (Decapeptyl, by IpsenBiotech and used in Europe) and buserelin (Suprefact, by Hoechst, used in Europe).
446 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 446

GnRH-analog Synthetic hormones related to the natural hormone GnRH,or gonadotropinreleasing hormone. See GnRH-agonist and GnRH-antagonist.
GnRH-antagonist A GnRH-analog that (unlike GnRH-agonists) immediately stops thepituitary gland from releasing the gonadotropins follicle stimulating hormone (FSH) andluteinizing hormone (LH). Can substitute for GnRH-agonists for many gynecologicalpurposes (particularly to suppress the LH surge in assisted conception), although its usewith pure FSH preparations (such as Fertinex, Gonal-F, Metrodin HP or Puregon) canlead to poor egg quality unless the dosage is carefully controlled or some luteinizinghormone is added to the stimulation regimen. See cetrorelix and ganirelix.
gonad A gender-neutral word for an organ that contains germ cells and produces gametes,that is, the ovary and the testis.
gonadotrophin English spelling for gonadotropin.The etymological derivation of thespellings is different, though.A trophic effect of a hormone implies a nourishing action,whereas a tropic effect of a hormone implies a switching action; arguably it’s the latter(American) usage that is now known to be the more physiologically correct.
gonadotropin releasing hormone (GnRH) A hormone produced by the hypothalamusof the brain to regulate production and release of the gonadotropins follicle stimulatinghormone and luteinizing hormone.Can be administered to induce ovulation when it is defi-cient (particularly in amenorrhea due to weight loss or excessive exercise), but it has tobe given in small amounts directly into a vein every 60 to 90 minutes for the two weeksof a normal follicular phase (with an electronic syringe-driver), mimicking its naturalpattern of secretion (see Chapter 11 for details). See also GnRH-analog.
gonadotropinAny hormone that switches on the function of the gonads.There are two mainfamilies of gonadotropins: (a) the gonadotropin that stimulates the growth of the follicle,or follicle stimulating hormone (FSH); and (b) those that cause ovulation from the maturefollicle and stimulate the corpus luteum to develop and to produce progesterone, namelyluteinizing hormone (LH) and human chorionic gonadotropin (hCG).FSH will cause growingfollicles to produce the estrogen estradiol, provided that a small amount of LH (or hCG)is present.FSH and LH are produced in the pituitary gland,whereas hCG comes from theplacenta in pregnancy. In men, FSH stimulates the Sertoli cells of the testicular tubules, andhence drives spermatogenesis;LH and hCG stimulate the Leydig cells to produce testosterone.
Gonal-F Recombinant follicle stimulating hormone made by Serono. Generically known asfollitropin alpha.
good responder High responder; discussed under low responder.Goretex Not just the stuff of ski clothing:used in a special surgical specification as a barrier
to the formation of peritoneal adhesions.goserelin A GnRH-agonist, made by ICI as Zoladex.Administered by monthly injection.Graafian follicle Synonym for preovulatory follicle.A large, mature tertiary follicle that
will respond to an adequate LH surge or injection of human chorionic gonadotropin (hCG)by undergoing ovulation, releasing its egg. Produces estradiol and, with exposure to LHor hCG, progesterone. Named after Reijnier de Graaf (1641–1673), the first person tosee and to appreciate the importance of the ovarian follicle.
granulosa cells Ovarian follicle cells from a tertiary follicle.
GLOSSARY � 447
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 447

growth hormone One of the six main hormones that come from the front, glandularpart of the pituitary gland, the adenohypophysis.A small amount is needed in adults forthe follicle stimulating hormone to work properly.This led some doctors to add it to injec-tions of FSH in poor responders, but subsequent research has shown that increasing theamount of FSH does the same thing (and FSH is cheaper to buy than growth hormone).
habitual abortion A rather insensitive way of referring to recurrent miscarriage.haploidThe state of a cell with 23 chromosomes (half the normal diploid chromosome state),
found normally only in the spermatozoon and the egg (as the secondary oocyte). See alsomeiosis and gene.The noun form of this adjective is haploidy (the state of being haploid).
hatching blastocyst See blastocyst.hazard An event, usually unwanted, sometimes in the sense of a penalty.Unlike risk,which
has a number attached to it (it’s quantitative), a hazard is ‘yes’ or ‘no’: it’s either realized(experienced) or it’s not; although one hazard can be worse to experience than another,you can’t put a figure on it (it’s said to be qualitative). For more on the difference, readthe box, Risks and hazards.
hCG See human chorionic gonadotropin.heparin A naturally occurring anticoagulant, or substance that stops blood from clotting.
Used in medicine generally to prevent or to treat thrombosis, and sometimes in
448 � GETTING PREGNANT
Risks and hazards
For an intelligent assessment of the risks and benefits of multiple-ovulation induc-tion—as is the case so often with evaluating choices in treating infertility—we needto distinguish risk from hazard.
Strictly speaking, the risk of a high-multiple pregnancy with intrauterine insemi-nation (IUI) and superovulation (multiple-ovulation induction) is low—there’s a lowchance of it happening. But if it does happen the penalty is considerable—it’s aserious hazard.The hazard is such that one should accept it only if it has a very, verylow chance of eventuating.The difference between a risk and a hazard is that risk isa probability you can put a number on,whereas a hazard is an all-or-nothing event—it happens or it doesn’t.
For example,whether you sail a 4 meter boat across the Tasman Sea from Australiato New Zealand or whether you sail a 40 meter one, the ultimate hazard is the same(namely, drowning) but, other things being equal, the chance, or risk, of drowning ismuch less with the bigger boat. For another example of the distinction, the risk ofgetting caught shoplifting might be small, but the hazard, the penalty if you are caught,is prohibitive.
In practice it’s often not easy to balance the risk of not getting pregnant withthe hazards introduced by modern infertility treatment, such as high-multiple preg-nancy. Read more about the compromises in Chapter 20.
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 448

pregnancy to reduce the risk of miscarriage in someone who has had recurrentmiscarriages by improving blood flow in the placenta.Administered by injection underthe skin.
hermaphrodism See intersex.heterotopic pregnancyThe coexistence of a pregnancy in the uterus with an ectopic pregnancy.heterozygous An adjective to describe the genetic state when the pair of genes under
consideration consists of two alleles that are different. Disease or disability can follow ifone of the alleles is at once seriously abnormal and dominant (see dominant inheritance)over the other allele, or if the alleles are different but both are deleterious (a state calledcompound heterozygosity). See also homozygous.
high-multiple pregnancy An order of multiple pregnancy higher than twins.high responder See the description for low responder.hirsute See hirsutism.hirsutism Hair (particularly, terminal hair—hair that is thick and pigmented) on the face,
chest (between the breasts or around the nipples), abdomen or thighs that is gettingworse, or is worse than other family members, or is worse than usual for one’s race.More likely to be important medically if the periods are disturbed (if there is oligomen-orrhea or amenorrhea). See also polycystic ovary syndrome.
HIV Human immune deficiency virus, the virus that causes acquired immune deficiencysyndrome, or AIDS.Type 1 and type 2 viruses are recognized, and both are usuallytested for in serum HIV antibodies.
HLA molecules Also known as tissue typing molecules, human leukocyte antigens,responsible for acceptance or rejection of tissue grafts, and implicated in the survivalor rejection of the fetus in pregnancy.
hMG See human menopausal gonadotropin.homocysteine A metabolic substance important for the vitamin folic acid. Levels in the
blood (see serum homocysteine) are increased when there is not enough folic acid inthe tissues.
homozygous An adjective to describe the genetic state when the pair of genes underconsideration consists of two alleles that are the same. Disease or disability can followif both alleles are seriously abnormal—a condition known as recessive inheritance (and agood example of which is cystic fibrosis). See also heterozygous.
hormone replacement therapy (HRT) Literally the replacement of any naturally defi-cient hormone, but in practice it means estrogen replacement therapy.
hormone A chemical substance, natural or not, which acts as a signal from one part of thebody to another, via the bloodstream.The study of hormones is the science of endocrinol-ogy, and the hormone systems of the body are collectively known as the endocrine system.
hPG See human pituitary gonadotropin.hrFSH Human recombinant follicle stimulating hormone.HRT Hormone replacement therapy; see estrogen replacement therapy.HSG See hysterosalpingogram.HTF See Human Tubal Fluid.Huhner’s test See postcoital test.
GLOSSARY � 449
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 449

human chorionic gonadotropin (hCG) A gonadotropin produced by the placenta in preg-nancy (specifically it’s produced by the trophoblast of the chorionic villi); the hormonemeasured in performing a pregnancy test.The generic (‘no frills’) name for Pregnyl andProfasi, which are preparations of hCG obtained by extracting it from the urine ofpregnant women, and Ovidrel, which is made by recombinant gene technology. Mimics theaction of luteinizing hormone (LH),but has a very much longer duration of action—whichgives hCG considerable advantages over LH in clinical use.Given as an injection to leadto ovulation from a mature follicle 38 hours after the injection; or to stimulate ongoingfunction of the corpus luteum, particularly its production of progesterone. So it is typicallygiven after a course of follicle stimulating hormone (FSH) in assisted conception (IVF or GIFT)programs and ovulation induction programs 36 hours before the expected time of eggretrieval (or before having sex or IUI), and then sometimes in further, smaller doses tosupport the luteal phase that follows. Sometimes used with clomiphene. Ovarian monitor-ing is needed for its correct use with FSH or with clomiphene. hCG treatment canprecipitate the ovarian hyperstimulation syndrome (OHSS).The proper clinical use of hCGis described in Chapter 11.
human menopausal gonadotropin (hMG) A mixture of follicle stimulating hormone (FSH)and luteinizing hormone (LH) extracted for therapeutic use from the urine of menopausalwomen (women after the menopause normally produce these hormones in high concen-tration). Marketed as Humegon (Organon) and Pergonal (Serono). Metrodin (Serono) ishMG from which LH has been removed, and Metrodin HP (Serono) is Metrodin fromwhich other urinary proteins have been removed too, resulting in very pure FSH.Ferring market a highly purified hMG containing both FSH and LH, but not inAustralia (see Menogon or Repronex). No cases of transmitted (infectious) disease havebeen recorded after the use of hMG preparations, unlike human pituitary gonadotropin.See also recombinant FSH and recombinant LH.
human pituitary gonadotropin (hPG) A mixture of follicle stimulating hormone (FSH)and luteinizing hormone (LH) extracted directly from pituitary glands obtained at autop-sies; not used in Australia or elsewhere since 1986, when it was shown that Creutzfeldt-Jakob disease (CJD), a deadly form of dementia, had been transmitted from its use,presumably due to contaminating and infected brain tissue. Before 1986 it had beenused mostly for ovulation induction in women with amenorrhea (absent periods) for whichother hormones or drugs had not been effective, although sporadic instances of its usefor in vitro fertilization are known in Australia.No new cases of CJD have been reportedamong former users of hPG since the early 1990s.
human research ethics committee See institutional ethics committee and institutional reviewboard.
Human Tubal Fluid (HTF) Embryo culture medium formulated to resemble theconstituents found within the fallopian tube by Dr Patrick Quinn, an Australian scien-tist living in California, but differing in a number of respects.
Humegon Mixture of human menopausal gonadotropins containing follicle stimulating hormonemade by Organon; virtually equivalent to Pergonal.
hybrid vigor See chromosomal cross-over.
450 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 450

hydatidiform moleAn abnormal conceptus in which the chorionic villi of the placenta havebecome cystic and swollen, typically because the chorion has not developed in connec-tion with a fetus that has a properly functioning circulation.The placenta looks like abunch of grapes. See also hydatidiform mole, complete and hydatidiform mole, partial.
hydatidiform mole, complete A hydatidiform mole in which there is no embryo or fetus.The size of the uterus is often larger than expected from the date of the last menstrualperiod, often with a high level of serum hCG; there may be bleeding; and there is aclassic abnormal appearance on transvaginal ultrasound. Caused by pregnancy followingabnormal fertilization in which the oocyte is ‘empty’, that is, it loses its pronucleus, andeither (1) the male pronucleus from a single fertilizing sperm doubles (the karyotype ofthe mole is then always 46,XX, because 46,YY is immediately lethal) or (2) there aretwo male pronuclei from two fertilizing sperm (in which case the karyotype is either46,XX or 46,XY).Treatment is by vacuum curettage, but there is a persisting danger ofcancer (choriocarcinoma) and specialist medical follow-up is essential.
hydatidiform mole, partial Abnormal conceptus in which there is co-existence of a hyda-tidiform mole with a fetus; caused by triploidy. Not as dangerous as a molar pregnancywithout a fetus (see hydatidiform mole, complete), but medical follow-up is still necessary.
hydrosalpinx Blockage of the outer, or fimbrial end of the fallopian tube, usually as a resultof chronic salpingitis (but also sometimes from peritubal adhesions, from a salpingotomy orpartial salpingectomy for a tubal pregnancy, or from fimbriectomy), resulting in its distensionby watery contents.An untreated hydrosalpinx (even if only one tube is affected andthe other tube is normal) can cause infertility and failure to conceive even with in vitrofertilization (explained in the box, Hydrosalpinx: Reintroducing a villain, in Chapter 20).
hyperplasia Pathologists use this word to mean an abnormal increase in the number ofcells seen in a sample of tissue. See also endometrial hyperplasia.
hyperprolactinemiaAn increase in serum prolactin; can be accompanied by galactorrhea andamenorrhea; causes are described in Chapter 11.
hypomenorrhea Light periods, particularly in a woman who has previously had muchheavier periods.Occurs normally on the oral contraceptive (birth control) pill.Occursabnormally with intrauterine adhesions or endometrial atrophy; see also Asherman’s syndrome.
hypospadias A congenital abnormality in males in which the urethra does not reach the tipof the penis, but opens near its base.The penis is usually short and curved, which canmake sex difficult and can contribute to infertility.
hypothalamic anovulation Absence of ovulation caused by insufficient GnRH drive fromthe hypothalamus, so that the pituitary gland doesn’t produce enough follicle stimulatinghormone. Usually accompanied by absent periods (amenorrhea). Causes are described inChapter 11.
hypothalamic chronic anovulation See hypothalamic anovulation.hypothalamus Part of the brain lying immediately above (and connected to) the pituitary
gland; responsible for producing gonadotropin releasing hormone and dopamine, among otherhormones and substances (including the endorphins, serotonin, etc.). In women (whenconditioned to cyclical function by a lack of exposure to male sex hormones beforebirth) it resonates with the ovarian cycle and cooperates with the pituitary gland to cause
GLOSSARY � 451
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 451

corresponding cyclical production of follicle stimulating hormone and,particularly, a timelyLH surge. Responds to progesterone by raising the body’s temperature (see basal bodytemperature chart).
hysterectomyA surgical operation at which the uterus is removed,usually including the cervix(hence a ‘total hysterectomy’), but not necessarily including the fallopian tubes and ovaries.
hysterosalpingogram (HSG) An x-ray of the endometrial cavity and the inside (the lumen)of the fallopian tubes, thus outlining them. Performed by injecting a fluid medium thatblocks x-rays through the cervix, so that it first fills the endometrial cavity and thenflows out along the tubes, finally casting shadows between the loops of intestine if thetubes are open (illustrated in Chapter 5).The test is uncomfortable or painful to havedone, because of contractions of the uterus,which can be partially overcome by takingone of the same drugs that are used to overcome dysmenorrhea, the nonsteroidal anti-inflammatory drugs, or NSAIDs (I suggest taking two tablets or capsules 30 minutesbefore the test). See also selective salpingogram.
hysteroscopy An examination of the endometrial cavity of the uterus by a thin fiberopticinstrument, similar to the instrument used for laparoscopy.Hysteroscopy can be done inthe office, with or without sedation, to make a diagnosis, or in the operating roomunder general anesthesia, often in association with laparoscopy or to carry out a hystero-scopic operation, such as removal of an endometrial polyp, submucous fibroid or uterineseptum; see also endometrial resection.
ICSI See intracytoplasmic sperm insertion.IEC Institutional ethics committee (see ethics committee).IL-10 See interleukin 10.IMB See intermenstrual bleeding.IMC Abbreviation for inevitable miscarriage, or for an imminent or incomplete miscarriage.imminent miscarriage An alternative term for inevitable miscarriage.immotile cilia syndromeA disease syndrome caused by abnormal sub-microscopic struc-
ture of cilia, which therefore do not function properly during embryonic life, child-hood and adulthood.The consequences are situs inversus, in which the developinginternal organs in the embryo rotate randomly (so that 50 percent of affected peoplehave their heart on the right side of the chest and their liver on the left side of theabdomen), abnormal sinuses, a bad form of chronic bronchitis called bronchiectasis, causedby mucus not being cleared from the lungs properly, and male infertility, because thesperm tail (the flagellum) has the same sub-microscopic structure as the cilia and cannotpropel the spermatozoon. Curiously, female fertility is often normal or adequate: it seemsthe cilia of the fallopian tube’s fimbrial end still make useful contact with the cumulus massat ovulation, stopping the egg from getting lost and giving the muscular contractions ofthe tube the chance to carry the egg down to the ampullary–isthmic junction.Also calledKartagener syndrome, after the Swiss physician Manes Kartagener,who first describeda triad of situs inversus, abnormal sinuses and bronchiectasis.
immune system The body system devoted to resisting parasitic organisms (includingviruses, bacteria, fungi and parasitic animals) and to identifying altered body cells (suchas cancer) and destroying them. Includes nonspecific mechanisms (‘innate immunity’)
452 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 452

as well as, particularly, the lymphoid system vertebrates have evolved to recognize antigensand in response to produce specific, neutralizing antibodies. Excessive activity can leadto the immune system turning on normal tissues, or autoimmunity.
immunobead tests Tests that look for human antibodies attached to cells, especially (inour context) antibodies attached to sperm cells (see sperm antibodies).The test involvestiny plastic beads coated with antibodies to human antibodies: if they are seen to attachto sperm cells then the presence of antisperm antibodies on the sperm cells is inferred.
imperforate hymen See cryptomenorrhea.implantation The process by which the embryo’s trophoblast attaches to the mother’s
endometrium and penetrates it, establishing contact between the trophoblast’s develop-ing chorionic villi and the maternal blood. See also blastocyst. Signifies the commence-ment of gestation or pregnancy.
implantation bleeding A small to moderate amount of vaginal bleeding at the time thatimplantation becomes established.The physiology behind it is described in Chapter 3.Implantation bleeding can be confused with a menstrual period (particularly the lastmenstrual period) to give a false impression that pregnancy has not happened or, later, afalse estimate of the duration of the pregnancy.
implantation rate The proportion of transferred embryos in an in vitro fertilization proce-dure that produce a gestational sac visible on transvaginal ultrasound.Unlike for the concep-tion rate and the pregnancy rate, twins (with separate sacs) are counted separately. Animportant index of a clinic’s success rate with IVF because it reflects embryo qualityindependently of the number of embryos transferred.
impotence Inability to sustain an erection of the penis and hence to ejaculate.Occasionalimpotence is of no special psychological or medical importance. Although persistentimpotence is most often due to psychological causes, medical tests are important.
in vitro Latin for ‘in glass’,meaning ‘in the laboratory’. (In actual fact, these days, it’s usually‘in plastic’!) See also in vitro fertilization.
in vitro fertilization IVF,or fertilization of the egg (the secondary oocyte) by a sperm (a sper-matozoon) in vitro, that is, in the laboratory. Necessary if the fallopian tubes are diseasedor missing; useful if sperm fertilizing capacity is doubtful, because evidence of fertil-ization can be seen before the egg is transferred as an embryo.
in vitro maturation Maturation in the laboratory of the egg (as a primary oocyte) obtainedfrom an immature tertiary follicle until it becomes a secondary oocyte competent to befertilized by sperm using in vitro fertilization.The smaller the follicle, the lower the propor-tion of eggs that mature successfully. ICSI can be used to increase the proportion ofeggs that will fertilize, but the embryos on average do no better, and so no advantageis conferred by ICSI in this situation.
in vitro penetration test One of several tests of the ability of sperm to penetrate cervicalmucus at the time of ovulation or under the influence of estrogen. See Kremer test, post-coital test.
incomplete miscarriage (IMC) Any miscarriage before all miscarriage tissue has beenexpelled.Traditionally a uterine curettage was done after a miscarriage, in the belief (oftenaccurate) that there would still be some immature pregnancy tissue left in the uterus
GLOSSARY � 453
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 453

that could cause more bleeding and get infected. Nowadays we can distinguish anincomplete from a complete miscarriage (and whether or not a curettage should be done)with a transvaginal ultrasound, which is able to reveal significant retained tissue.Management is similar to the management of an inevitable miscarriage (and both areabbreviated IMC).
induced abortion See abortion.inevitable miscarriage (IMC) Traditionally any bleeding from the vagina during early
pregnancy with, on vaginal examination, opening of the cervix.Today, the diagnosis canbe made much sooner (and distinguished from a threatened miscarriage) by not detect-ing a normal embryo in a gestational sac on transvaginal ultrasound. Management is similarto the management of an incomplete miscarriage, often requiring curettage (and both areabbreviated IMC).
infertility Not getting pregnant as quickly as expected. See also sterility, subfertility or relativeinfertility, and suffering.
informed consentAn administrative and legal device by which approval to proceed basedon known or predicted consequences is obtained and recorded from a patient or froma volunteer for medical research, thus avoiding an accusation for what otherwise mightbe an assault. Just what ‘informed’ means can be the subject of much legal and ethicalwrangling. One modern interpretation is that it means as much as the person givingthe consent demonstrates that he or she wants to know (although most physicians, ethicscommittees, institutional review boards and courts underpin this with a minimum everyoneshould be told about the procedure being consented to). Discussed in Chapter 26 (seethe box, Autonomy and respect for persons).
inhibin A protein hormone produced in women by developing follicles as well as by thecorpus luteum, and in men by the testis in the presence of spermatogenesis, and acting onthe pituitary gland to inhibit the production of follicle stimulating hormone. In women,falling levels occur as the number of developing follicles reduces to low numbers leadingup to menopause, thus causing the elevation of serum FSH and shortening of the follicu-lar phase that characterizes the premenopause. In men, appreciable levels of serum inhibinB, a subclass of the inhibin family, predicts the presence of at least a small amount ofsperm production.
inner cell mass Group of cells that differentiates within (but to one side of) the devel-oping embryo when it is a blastocyst and which will, if all goes well after implantation,form the embryo proper, or fetus.Cells from the inner cell mass can be used to produceembryonic stem cells. See also trophectoderm.
Insler score See cervical score and monitoring.institutional ethics committee (IEC) See ethics committee.institutional review board (IRB) The US equivalent of an institutional ethics committee,
set up to govern the ethical conduct of medical research.integrins Proteins present on the surface of cells that are needed for cells to stick to each
other with the help of adhesion molecules. Important in implantation and in the properconstruction of the placenta; abnormalities or mutations can result in infertility or recur-rent miscarriage.
454 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 454

integrity A systematic ethical goal that preserves the values of truth, accountability, equityand consistency.
Interceed Used for minimizing adhesions in the peritoneal cavity after a surgical operationinvolving the fallopian tubes or ovaries.The material is woven from fibers of modifiedcellulose and, after being placed over abdominal surfaces the serosa of which are likelyto have been damaged, dissolves in about a week or two into simple sugar molecules(which are then absorbed by the body and metabolized); in the meantime, the clothkeeps the covered surfaces apart while the serosa reforms.Controlled trials have shownInterceed to be effective in preventing or reducing adhesions, but an adhesion-freeresult is not guaranteed. In my experience Interceed is exceptionally useful when denseadhesions resulting from previous operations are being treated. Made by Johnson &Johnson.The principles and practice of prevention of pelvic adhesions are described inthe box, Adhesions or healing, in Chapter 13.
interleukin 10 A signalling molecule that inhibits the immune system, so preventing rejec-tion of the fetus during pregnancy. It is thought that insufficient interleukin 10 is a causeof miscarriage.
intermediate trophoblast See extravillous trophoblast.intermenstrual bleeding (IMB) Bleeding between periods that are otherwise regular. If
it happens while on the oral contraceptive pill it’s called breakthrough bleeding; if it happensover a few days before a period starts properly it’s premenstrual spotting; if it happens aftersex it’s postcoital bleeding.These forms of IMB have different, usually important, causes.The formal term for it is metrorrhagia.
intersex A state of ambiguity regarding the assigning of sex or gender, usually because ofambiguity of the genital organs at birth.There is male intersex if the karyotype is46,XY, female intersex if it’s 46,XX. For a plain-speaking but carefully detailedaccount of this difficult area, read the box, Girl or boy?, in Chapter 18. Incorporateshermaphrodism and pseudohermaphrodism, terms that are not much used outside the USA.
interstitial cells See Leydig cells.interstitial pregnancy An ectopic pregnancy located in the interstitial segment of the fallopian
tube.An especially dangerous form of tubal pregnancy,because the surrounding myometriumof the uterus supports the pregnancy’s growth for weeks without causing symptoms;whenrupture eventually occurs it can be catastrophic,because a main branch of the main arteryto the uterus is torn, with sudden (sometimes fatal) bleeding into the peritoneal cavity.
interstitial segmentThe innermost part of the fallopian tube, passing through the wall ofthe uterus (the myometrium) to join the isthmus to the endometrial cavity.
interstitial trophoblast See extravillous trophoblast.intervillous space The space in the placenta in which the maternal blood flows.Washes
around the chorionic villi, which contain blood capillaries from the fetus, so that oxygenand nutrition pass to the fetus, while carbon dioxide and waste pass to the mother.Formed from lacunae and lined by the syncytiotrophoblast.
intracytoplasmic sperm insertion (ICSI) An in vitro fertilization technique for over-coming infertility due to oligospermia or azoospermia involving sperm microinjection (SMI),in which one or more sperm are injected through the zona pellucida, across the perivitelline
GLOSSARY � 455
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 455

space, through the vitelline membrane (the egg cell’s membrane), and into the substance(or cytoplasm) of the egg itself.Has completely replaced subzonal sperm insertion (SUZI).
intramural segment See interstitial segment.intrauterine adhesions Adhesions inside the endometrial cavity caused by prior infection
(endometritis), especially if there has been a curettage during the period of infection, orif curettage is performed in conditions of low estrogen.The circumstances in which thiscombination is most common are treatment for a missed abortion and treatment of apostpartum hemorrhage (bleeding a few weeks after the birth of a baby). See alsoAsherman syndrome and endometrial atrophy.A cause of absent periods amenorrhea, lightperiods (hypomenorrhea) or recurrent miscarriage.
intrauterine insemination (IUI) A form of assisted conception involving assisted inseminationinto the uterus,either for donor insemination (DI) or with husband’s or a male partner’s semen(AIH). IUI can be carried out with a woman’s natural cycles or with ovarian stimulation(superovulation) using clomiphene or follicle stimulating hormone, with ovarian monitoring.
IRB See institutional review board.irritable bowel syndrome A distressing dysfunction of the intestines, in which there’s
both overactivity of the involuntary contractions of the intestines’ muscular wall andincreased pain signals coming from those contractions.Treatment is based on decreas-ing the contractions (with a diet high in fiber, sometimes with antispasmodic drugs)and attempting to reduce the action of the pain-carrying nerves, both by sedating them(this means general sedation too, so it’s often not very acceptable) and by re-educatingthem to be less sensitive.Treatment is time consuming and, ultimately, not always satis-factory.The symptoms of the irritable bowel syndrome are often confused with thoseof endometriosis (to make the distinction read the box, Is the pain really endometriosis?, inChapter 15); they are sometimes made worse with, and at the time of, premenstrualtension, or, in my experience of patients with it, by performance of a laparoscopy.Typically(but not always), there is an alternating tendency towards diarrhea or constipation;sometimes there is nausea with the spasms.Also called spastic colon.
isthmus The narrow, inner part of the fallopian tube, about 3 to 4 centimeters long; liesbetween the ampulla and the interstitial segment.
IUD Abbreviation either for intrauterine death (death of a fetus, prefacing a stillbirth) orfor intrauterine (contraceptive) device, which, to resolve this ambiguity, is some-times (though not in this book) abbreviated as IUCD.
IUI See intrauterine insemination.IVF See in vitro fertilization.IVM See in vitro maturation.justice In this book, the ethical value to be had in a community from conferring rights and
obligations in a way that’s fair and accords to other ethical values (for example,non-malef-icence, beneficence). See also distributive justice.
Kallmann syndrome Congenital absence of gonadotropin releasing hormone in the hypothal-amus (causing, in women, primary amenorrhea and anovulation and in men, failure ofpuberty) in combination with a congenitally absent sense of smell.
Kartagener syndrome See immotile cilia syndrome.
456 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 456

karyotypeA test that displays the chromosome after relevant cells are grown in tissue culture.A normal female karyotype is designated 46,XX and a normal male karyotype 46,XY.Examples of karyotypes are illustrated in Chapter 8. See also molecular karyotyping.
Klinefelter syndrome A trisomy with a karyotype of 47,XXY, that is, a male with an extraX-chromosome.A cause of azoospermia.
Kremer testAn in vitro (laboratory) test of the interaction between sperm and cervical mucus,in which the mucus to be tested is drawn into two fine glass tubes (another two tubesare filled with mucus that is known to be good) to give a four-way test between:husband’s(or male partner’s) sperm and wife’s (or female partner’s) mucus; husband’s sperm andknown good mucus; known good sperm with wife’s mucus; known good sperm withknown good mucus. Because of the laboriousness of the test it’s usual to administerestrogen for at least a week in the follicular phase to ensure that the mucus is optimal.
K-selection A reproductive strategy where survival of a species is optimized by placing apremium on individual survival despite fluctuations of the environment. Favors largeanimals (and large animals favor this strategy)—animals that get pregnant more thanonce and the offspring of which require postnatal care before sexual maturity is reached.Spacing of pregnancy is important for survival of mother and offspring, and thus favorsthe evolution of a genetic basis for subfertility—an intriguing notion that’s the themeof Chapter 2.The opposite reproductive strategy to r-selection.The word comes fromthe environment’s Karrying capacity.
lacunae Latin for ‘lakes’: one lacuna, two lacunae. Refers particularly to spaces that formwithin the syncytiotrophoblast (which therefore continues to line the spaces), separatingthe SCT into strips of land and little peninsulas that will develop into chorionic villi, asthe lakes coalesce into one large intervillous space, into which maternal arteries will open,delivering blood to the placenta as it is being formed.
laparoscopy A ‘minimally invasive’ surgical operation at which instruments are passedthrough the wall of the abdomen: (1) for the diagnosis of abnormalities of the abdom-inal or pelvic organs (such as the fallopian tubes, ovaries and uterus) and to diagnoseendometriosis; or (2) therapeutically, to reach the fallopian tubes for certain assisted concep-tion procedures (see gamete intrafallopian transfer and zygote intrafallopian transfer). Carriesthe risks of surgery (damage to internal organs, hemorrhage, infection) and the risks ofgeneral anesthesia.
laparotomyA surgical operation in which the abdomen is opened.Needed for microsurgeryoperations on the fallopian tubes (although some operations formerly done only at laparo-tomy are now possible at laparoscopy). For infertility surgery, the scar from a laparotomyis usually a low, horizontal one, just above the pubic bone. Several days in hospital areneeded; most people are off work about three weeks; and some numbness or sensitiv-ity below the scar can be expected for several months, as nerves to the skin regrow.
large bowel The colon; see bowel.last menstrual period (LMP) The normal period immediately preceding conception. For
convenience, obstetricians calculate the duration of a pregnancy as starting with thisdate, even though of course it does not truly begin until fertilization (or, some wouldsay, implantation). See also implantation bleeding.
GLOSSARY � 457
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 457

leukemia inhibitory factor (LIF) A signalling molecule originally discovered in associ-ation with leukemia, but now known to have many functions, including the supportof pregnancy by the endometrium as it forms decidua.
leuprolide See leuprorelin.leuprorelin A GnRH-agonist made by Abbott and sold as Lupron in the USA. Called
leuprorelin in Australia and Europe, and sold there as Lucrin.Administered by dailyinjection under the skin or as a depot preparation once per month.
Leydig cells Cells of the testis lying between the testicular tubules in which sperm are formed(hence their other name, interstitial cells), and responsible for the production of themale sex hormone testosterone under the influence of luteinizing hormone.
LH surge A sudden and huge increase in production of luteinizing hormone by the pituitarygland in response to sustained and substantial levels of estradiol in the blood in women,midway through the ovarian cycle. Causes ovulation about 36 hours after it starts (about20 hours after its peak). If not suppressed during assisted conception (see GnRH-agonistsand GnRH-antagonists) it can start before human chorionic gonadotropin has been given,so spoiling the timing of egg retrieval.Timely production of the LH surge in adult womendepends on female conditioning of the hypothalamus and/or the pituitary gland beforebirth. Detectable by testing the urine with a special kit, described in Chapter 19. Seealso follicle tracking.
LH See luteinizing hormone.LIF See leukemia inhibitory factor.linkage analysis Read chromosomal cross-over first, then come back.Because it can take lots
of cross-overs (that is, lots of generations) to send two genes that live as neighbours ona chromosome into different directions (that is, they end up in different people), wecan do family studies to work out how closely people are related by seeing how longthe runs are of identical genes.
LMP See last menstrual period.long protocol A treatment protocol for using GnRH-agonists that involves their use for
more than a week before injections of follicle stimulating hormone (FSH) start for induc-tion of superovulation in assisted conception programs.The advantage is that any tempo-rary rise in luteinizing hormone levels and progesterone levels has dissipated before thedevelopment is under way of those ovarian follicles from which eggs will be obtainedat egg retrieval.The disadvantage, compared with the short protocol, is that higher (hencemore expensive) doses of GnRH-agonist and FSH are needed.The GnRH can bestarted with menstruation or during the luteal phase of the previous cycle. See also ultra-short protocol.The details are in the box, The long, short and ultrashort of GnRH-agonists,in Chapter 20.
low responder Early experience with superovulation for in vitro fertilization, particularly atthe original US program in Norfolk,Virginia, saw women patients classified into threeclasses of responders, depending on how many eggs were obtained at egg retrieval. Poorerthan usual outcomes could occur with either a low response or a high response (thehigh responders generally have polycystic ovaries, with a risk of ovarian hyperstimulationsyndrome, or OHSS). Many maneuvers have been used to try to retrieve more eggs
458 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 458

among low responders, such as starting high dose FSH on day 1, the adding of growthhormone, the avoidance of GnRH-agonists, etc., all generally without improving theresults. Day 3 serum FSH levels can be high in low responders, indicating a depletion ofeggs in the ovaries.
LPD See luteal phase defect.Lucrin See leuprorelin.LUF See luteinized unruptured follicle.lumenThe hollow center of a cylindrical organ or tissue, such as that of a fallopian tube or
a blood vessel.Adjective: luminal.Lupron See leuprorelin.lupus See systemic lupus erythematosus.lupus anticoagulant An antibody first noted in the disease systemic lupus erythematosus, or
‘lupus’, that has the ability to stop blood clotting.A cause of recurrent miscarriage.Closelyrelated to a family of anti-phospholipid antibodies, especially anticardiolipin antibody.Also called the lupus inhibitor.
luteal phaseThe part of the ovarian cycle between ovulation and the start of a new follicularphase, so dominated by the presence of the corpus luteum and the progesterone it produces.Normally between 11 and 16 days in length. Extended by the action on the corpusluteum of human chorionic gonadotropin (hCG) if implantation of the embryo is success-ful. Shorter cycles can interfere with implantation (a luteal phase defect). Correspondswith the secretory phase of the menstrual cycle.
luteal phase defect (LPD) A luteal phase that is shorter than optimal for a fertilized eggto undergo implantation.Very likely if the luteal phase is shorter than normal (11 to 16days), but not all luteal phases within this range are adequate. Often caused by a priordefect of the follicular phase or of the development of the ovulating tertiary follicle (thepreovulatory follicle) and hence there can be a defect of the egg itself (if ovulation hasactually occurred) or there can be a luteinized unruptured follicle—any of which willeither increase the risk of miscarriage or prevent pregnancy altogether for that cycle.Synonymous with luteal phase insufficiency.
luteinized unruptured follicle (LUF) Occurs when a reasonably mature tertiary follicle(or preovulatory follicle) receives an LH surge that’s enough to make it start producingprogesterone, but is not enough to cause it to release its egg through ovulation.The resultis that the egg is trapped in the follicle, which to a greater or lesser extent then func-tions like a corpus luteum, though this stage of the follicle’s life is often shorter, givingrise to a luteal phase defect (LPD). For more (and for the conditions in which it iscommon), see the box, Fake ovulation, in Chapter 7.
luteinizing hormone (LH) The hormone, or gonadotropin, produced by the pituitary glandto cause, in women, ovulation of a mature follicle in the ovary, resulting in formation ofthe corpus luteum; in men, stimulates the production of testosterone by the Leydig cells ofthe testis. Suppressed by GnRH-agonists and GnRH-antagonists, so that (for ovulationinduction) an injection of human chorionic gonadotropin (hCG), which acts the same way,has a predictable time course of action.A small amount of LH is essential for normalfunction of the tertiary follicle and the corpus luteum. See also LH surge and serum LH.
GLOSSARY � 459
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 459

Recombinant LH is under development by Serono as Luveris, but its clinical role inplace of hCG is not yet established.
lutropin Generic name for recombinant luteinizing hormone. See Luveris.Luveris Recombinant luteinizing hormone (rLH) made by Serono.macroadenoma See pituitary tumor.macrophage A cell in the body (a bit like the one-celled animal called an amoeba) that’s
able to: (1) wander about; (2) engulf and digest a huge range of foreign material andjunk that gets into the body’s tissues (including sperm cells). Macrophages are presentin almost every tissue in the body, especially if there is inflammation.We see them asscavenging cells—the cells that do the ultimate tidying up inside the body—but theycan be programmed to swallow very specific targets, sometimes committing suicide forthe greater good! There are normally lots of macrophages in the peritoneal cavity.
magnetic resonance imaging See MRI scan.major histocompatibility complex (MHC) An area of the genome where genes are found
that determine your ‘tissue type’, important in determining whether, for example,you canaccept or will reject an organ transplant from someone else.The genes in this area aretightly packed, show extreme polymorphism,and tend to be inherited together as a group.
maturation arrest See azoospermia and spermatogenesis.media Plural of medium. See culture medium.medical vocabulary See vocabulary.medium See culture medium.medroxyprogesterone acetate (MPA) A progestogen of a type related to progesterone itself.
Marketed as Provera (tablets) and Depo-Provera (injections) by Upjohn.meiosis A process similar to mitosis in which two successive divisions of a diploid cell’s
nucleus result in four ‘daughter’ cells, each with a haploid number of chromosomes. Unlikemitosis, each chromosome therefore duplicates just once (before the beginning ofmeiosis). Meiosis in humans (and other higher animals) takes place only among thegerm cells (oogonia and spermatogonia), which will have been multiplying by mitosis. Bydifferentiating into, respectively, primary oocytes or primary spermatocytes, each with 92chromatids, meiosis commences.With completion of the first meiotic division theproducts (including secondary oocytes and spermatocytes) each contain 46 chromosomes.With completion of the second meiotic division the haploid number (23) of chro-mosomes, suitable for fertilization, is reached. In the testis, meiosis and the productionof new sperm cells (spermatozoa) can continue throughout life, but in the ovary all eggcells that survive commence meiosis about 20 weeks before birth, spending the remain-ing time (up to 50 years or more) locked up in primordial follicles as primary oocytes.Whereas a primary spermatocyte gives rise to four haploid sperm cells, a primaryoocyte produces just one secondary oocyte (the spare 46 chromosomes are dumpedinto the first polar body just before ovulation), and then one egg cell (the spare 23chromosomes are dumped into the second polar body after fertilization). See also chro-mosomal cross-over.
membranes The amniotic membrane and the chorionic membrane attached to the placenta.menarche The first natural menstrual period (pronounced ‘menarcky’).
460 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 460

Menogon Highly purified human menopausal gonadotropin made by Ferring, and compara-ble to Metrodin HP. Called Repronex in the USA. Not available in Australia.
menopause The last natural menstrual period (so often a retrospective diagnosis); hencethe adjective menopausal, the natural state a woman is in after the ovaries have stoppedovulating because of depletion of eggs.The normal age of menopause is between 40 and55 years, with an average in Western societies of 50–51 years. See also perimenopause,premature menopause, oopause and estrone.
menorrhagiaTraditional medical term for dysfunctional uterine bleeding or, simply,heavy periods.menstrual abortion See menstrual miscarriage.menstrual cycleThe ovarian cycle as it’s expressed by the endometrium of the uterus. It consists
of the menstrual phase, the proliferative phase and the secretory phase. Like the ovarian cycleitself, it’s normally 24 to 35 days in length—typically 28 days, but there are lots of normalexceptions.
menstrual miscarriage For our purpose in the book, the loss of an early embryo at orbefore the expected time of a period.Not noticeable without specially measuring levelsof serum human chorionic gonadotropin One form of so-called biochemical pregnancy.
menstrual phase The phase of the menstrual cycle in the endometrium during which thereis menstruation, caused by withdrawal of progesterone at the end of the ovarian lutealphase as a new ovarian follicular phase starts; in anovulatory cycles or during treatment withestrogens, menstrual bleeding can occur from withdrawal, insufficiency or downwardfluctuations of estrogen alone.
MESA See microepididymal sperm aspiration.mesodermThe third, or ‘middle’ layer of the developing tissues of the early embryo, forming
between the ectoderm and the endoderm during the transformation of the embryo known asgastrulation;mesoderm gives rise to the body’s muscles,bones and various connecting tissues.
mesonephric duct cyst See mesonephric duct.mesonephric duct A duct on each side of the developing embryo or fetus that leads from
the embryo’s mesonephros, or temporary kidney. In male fetuses the duct persists as theWolffian duct to form the rete testis, the epididymis, the vas deferens and the seminalvesicle. In female fetuses it usually disappears completely (in favor of the paramesonephricduct, better known as the Müllerian duct), though portions of mesonephric duct canremain as harmless cysts, called Gärtner’s duct cysts.
mesonephric remnant See mesonephric duct.metaphaseThe third stage (of four stages) of mitosis (or meiosis), at which the chromosomes,
attached in a plate-like formation to a structure in the cell called a spindle, are easilydistinguished with a microscope, and can be photographed to construct a karyotype.
metaplasiaThe metamorphosis of a tissue to take on a different form,perhaps more char-acteristic of a tissue some distance away.One of the theories of the cause of endometrio-sis is based on metaplasia. The controversy is discussed in the box, Implantation ormetaplasia?, in Chapter 15.
metformin Oral anti-diabetic drug that improves many aspects of the polycystic ovarysyndrome, including lowering of androgens, serum LH, insulin levels and weight, in combi-nation with a low calorie diet; improves development of ovarian follicles and ovulation,
GLOSSARY � 461
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 461

as well as responsiveness to clomiphene or gonadotropins if ovulation induction or in vitrofertilization is necessary.
methotrexateA cytotoxic drug,originally developed for chemotherapy for certain cancers,used in the treatment of ectopic pregnancy, especially in the USA; side-effects can includebone marrow depression, gastrointestinal upset and mouth ulcers, among others.
Metrodin Human menopausal gonadotropin (hMG) from which luteinizing hormone (LH) haslargely been removed, leaving follicle stimulating hormone (FSH) as the active substance.Metrodin HP (Fertinex in the USA) is more purified, other urinary proteins having beenextracted too, and (unlike Metrodin) has no LH activity at all. Made by Serono.
Metrodin HP Called Fertinex in the USA. Metrodin that has been highly purified byremoving all contaminating urinary proteins and all luteinizing hormone, and is thussimilar in action to recombinant follicle stimulating hormone. See also serum estradiol andultrashort protocol.
metroplasty A plastic operation on the uterus to change the shape of its cavity, usually fora uterine septum or for a bicornuate uterus, if there have been a number of miscarriages.Illustrated and described in Chapter 18.
metrorrhagia Traditional medical term for intermenstrual bleeding.MHC See major histocompatibility complex.microadenoma See pituitary tumor.microarray See DNA microarray.microchimerism A state in an embryo, fetus, animal or person in which a small number
of cells that have a different genome occur.Arises naturally because cells (rarely, stem cells)can cross between a mother and her fetus, or experimentally by introducing foreignstem cells into an embryo, usually at the stage of blastocyst, when the introduced cellsbecome part of the inner cell mass.
microepididymal sperm aspiration (MESA) Using microsurgery to dissect the epididymisor rete testis (or sometimes the tubules of the testis itself—see also testicular sperm extrac-tion) to find motile sperm cells suitable to be aspirated, isolated and prepared for an invitro fertilization procedure, usually involving sperm microinjection, especially intracytoplas-mic sperm insertion.
microsurgery Literally, operating on small organs and tissues under the magnificationprovided by an operating microscope; the magnification is typically in the range of6x to 16x for infertility surgery.The term also implies keeping the tissues wet withphysiological salt solution during the operation, using fine, non-reactive stitches orsutures, being meticulous about stopping bleeding from small blood vessels andavoiding trauma to the serosa. See also fimbriolysis, microepididymal sperm aspiration, salp-ingolysis, salpingostomy and sterilization reversal (which includes tubal anastomosis andvasovasostomy).
minilaparoscope An instrument for carrying out laparoscopy that is just a few millimetersin diameter, making it possible to perform such operations in an ambulatory setting,without general anesthesia.The reliability of diagnoses made this way will need carefulevaluation, especially if done to exclude endometriosis, which can be difficult to findeven with conventional laparoscopy.
462 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 462

miscarriageThe delivery of (or the process of delivering) a conceptus before there is a viablefetus. See also threatened miscarriage, inevitable miscarriage, incomplete miscarriage, complete miscar-riage, menstrual miscarriage, subclinical miscarriage, missed abortion and recurrent miscarriages.
miscarriage rate The percentage chance that a pregnancy will end as a miscarriage.Thenormal rate of clinically apparent miscarriage for young women is about 12 percent.The rate rises independently with age, the number of previous pregnancies, and espe-cially the number of previous miscarriages experienced.The rate is also higher withmany causes of infertility when conception occurs with or without treatment.Thechance of having a second miscarriage after the first is described in the lengthy butimportant box, Malpas’s mistake, in Chapter 9.
missed abortion A miscarriage that should have happened but hasn’t.As a result, the preg-nancy tissue in the uterus gets tougher and more difficult to get out with a uterine curet-tage—which is the only treatment for it, but risks producing intrauterine adhesions.Thepregnancy test can stay positive for many weeks or even months.
missed miscarriage See missed abortion (in this context one still occasionally hears theword ‘miscarriage’).
mitochondrion A tiny structure inside the cell resembling a bacterium and responsiblefor burning food molecules with oxygen to produce carbon dioxide, and thus provid-ing energy for the cell’s use. Each cell has hundreds or thousands of mitochondria. Ifthere’s a single aspect of a cell that reveals the process of aging, it’s the mitochondria,which get less efficient as a person (and specifically a tissue) gets older. Mitochondrialaging in egg cells could be the reason why eggs in women over the age of 40 so oftenseem unable to produce healthy embryos—an intriguing area of current research (seemtDNA and read the Chapter 7 box, How eggs might get their ‘use-by’ date: Mishaps in themitochondria). Plural: mitochondria.
mitosis Usual process by which a cell (more strictly the nucleus of a cell) divides into two.Each chromosome duplicates before the beginning of mitosis, and mitosis involves sepa-ration of the resulting duplicates so that one goes into each ‘daughter’ nucleus [adaptedfrom The Penguin Dictionary of Biology, 6th edition, Penguin Books Australia Ltd,Ringwood,Victoria, 1973].At the third stage (of four stages) of mitosis, called metaphase,the chromosomes are easily distinguished with a microscope, and can be photographedto construct a karyotype. See also meiosis.
Mittelschmerz German for ovulation pain.mixed reproductive loss Repeated loss of pregnancies at different stages of development of
the embryo or fetus, that is, at different stages of pregnancy. Related to recurrent miscarriages.mixoploidy An abnormal state of the chromosomes seen on a karyotype in which cells from
an individual display two or more genetically different chromosome patterns. Can bethe result of mosaicism or chimerism.
molecular karyotyping A karyotype, or chromosome display,performed indirectly,by probinga tiny amount of DNA that has been extracted from a single cell or a tissue and ampli-fied using the polymerase chain reaction, tested in a very large number of locations incomparison with standard, normal DNA, to determine if any of the loci are increasedor decreased in number.The result is typically known within hours or at most a day
GLOSSARY � 463
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 463

of testing, unlike a conventional karyotype, which requires cells to be grown in tissueculture for a week or so before they are examined. Used with embryo biopsy for preim-plantation diagnosis (PGD) and also directly from tissue obtained at chorion villus sampling(CVS) and amniocentesis to provide a much quicker result. See also DNA microarray.
monitoring In our context, the frequent estimation of serum estradiol (or perhaps estimat-ing the cervical score) and performance of transvaginal ultrasound to estimate how close awoman is to ovulation. Monitoring is described in detail in Chapter 20. See also serumLH and serum progesterone.
monoamniotic twins Identical or monozygotic twins in which the split has occurred afterformation of the blastocyst, so that the twins share the same gestational sac (or amnioticcavity).There is a much higher risk of complications than in the more usual situationwhere twins do not share the same sac, because the fetuses or the umbilical cords canget tangled up.
monosomy An abnormality of the chromosome number due to a loss of one chromosomefrom a diploid set, resulting in 45 chromosomes instead of 46.The only mosomy compat-ible with fetal development and continued survival is that of Turner syndrome, the kary-otype of which is 45,X (that is, a monosomy of the sex chromosomes).
monozygotic twinsTwins formed from the splitting of a single fertilized egg, or zygote;identical twins; see also monoamniotic twins. IVF embryos have an increased chance offorming monozygotic twins.
monthly fecundity American for the monthly chance of conception, or monthly fertility rate.See also fecundability.
monthly fertility See monthly fertility rate.monthly fertility rateThe monthly chance of conception, the technical term for which
is fecundability. See also normal monthly fertility.morula A stage of the embryo that consists of a ball of cells, still enclosed by the zona pellu-
cida, preceding the stage of blastocyst. Formed from the fertilized egg, or zygote, by theprocesses of cleavage and compaction.
mosaicism The condition in which an individual shows two or more genetically differ-ent cell lines (generally with different karyotypes) that are derived from one zygote. Seealso chimerism and mixoploidy.
motility The quality of movement, especially forward propulsion, shown by sperm cells(spermatozoa) and caused by effective beating of their tail, or flagellum.Analyzed as partof the routine sperm count.
MRI scan Magnetic resonance imaging is a special form of imaging the body’s internal struc-tures, taken with the person enveloped in a huge and powerful magnet; a picture is builtup of any cross-section, or series of cross-sections, through the body, using a techniquethat detects and pictures structures by their different content of atoms with certain reso-nances to induced magnetic fields. Particularly useful for investigation of the anatomy ofthe pituitary gland and hypothalamus when a tumor is suspected. More expensive and lesswidely available than a CT scan, which gives adequate results in most cases.
mtDNA Mitochondrial DNA.The small amount of DNA found in the mitochondria.mtDNA is the genetic code for 13 proteins involved in metabolism. Because mtDNA
464 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 464

is much less stable than the DNA in the chromosomes (where the huge bulk of geneticcode is stored), mutations accumulate with time at a greater rate than that for chro-mosomal DNA—and eventually limit how well a particular cell or tissue can functionwith increasing age. Because all of the mtDNA you have you inherited from yourmother (you derive your mitochondria from the egg you came from), we could havean explanation of: (1) why all eggs are formed before birth (so the mitochondria don’thave to keep on dividing too often and risking genetic errors); and (2) why miscarriagesand infertility get commoner with age (as the egg’s several thousand mitochondriabegin to succumb to genetic errors).
MTHFR C677T A polymorphism affecting the metabolism of folic acid with a numberof possible consequences avoidable by increasing dietary supplements to mega-doses(5 mg to 10 mg per day), including: promotion of blood coagulation, or thrombophilia;abnormalities of the fetus (birth defects, especially neural tube defects such as spinabifida and anencephaly); recurrent miscarriage; an increased chance of heart disease andcoronary thrombosis; and in men, possibly contributes to oligospermia and infertility. Seealso serum homocysteine.
mucus Jelly-like secretion that is at once both sticky and slippery. See cervical mucus andcumulus mass.
Müllerian duct (pronounced ‘mool-air-ian’) Synonym for paramesonephric duct.The internalfemale sex duct, which forms on each side of a female embryo to connect the peritonealcavity with the outside of the embryo, starting at a point close to the ovary and formingfirst a fallopian tube then meeting its fellow from the other side to form the uterus, andthen extending downwards to form the upper part of the vagina before finally connect-ing with a little dimple between the urethra (in front) and the anus (behind) to reachthe exterior at the vulva. Passage of eggs from the ovaries (which ovulate into the peri-toneal cavity of all vertebrate species) to the outside world through this duct is howanimals, including humans, reproduce. Oddities in the development of the ducts causecongenital anomalies of any or all of these organs and are described in Chapter 18. Inmales the ducts do not develop because the Sertoli cells of the testes produce anti-Müllerianhormone. See also mesonephric duct.
Müllerian inhibiting factor See Müllerian duct.myoma See fibroid.myomectomy An operation to remove a myoma, or fibroid.A myomectomy for a submu-
cous fibroid is often possible at hysteroscopy; a myomectomy for an intramural fibroid (locatedwithin the wall of the uterus) usually requires an open operation, or laparotomy; amyomectomy for a subserous fibroid can be possible at laparoscopy.
myometriumThe muscular wall of the uterus, surrounding the endometrium.The myometriumcontracts (1) during menstruation, perhaps causing dysmenorrhea, and (2) during miscarriageor labor to deliver the conceptus. See also myoma (or fibroid) and adenomyosis.
nafarelin A GnRH-agonist, made by Syntex as Synarel and used as a nasal spray.natural killer cells See NK cells.naturalistic fallacyThe philosophical term coined by G.E. Moore early in the twentieth
century to devalue drawing ethical conclusions from empirical observation—that is, by
GLOSSARY � 465
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 465

moving from what is (facts that are observed) to what ought (morality). Moore felt thatethics should be intuitive, not inferred—therefore he presumably favored deontologicalethics over teleological ethics. Practical ethicists find this constraint unnaturally cripplingas it prevents them making a value judgment.
necrosis The word pathologists use when there is death of part or all of a tissue or organdue to an outside factor, such as cutting off the blood supply. If apoptosis is regarded ascellular suicide, then necrosis could be called cellular murder. Important examplesinclude aseptic necrosis of the femoral head and the loss of an ovary from untreated torsion,which is described in the box,Twisted ovaries, in Chapter 12 as a complication of ovarianhyperstimulation syndrome (OHSS).
negative history If you have a negative history for a disease or symptom it means thatyou do not have or have not had that disease or symptom.Compare with positive history.
negative test In medicine generally it may be best for tests to be negative (like tests forbrain tumors or tests for sexually transmitted diseases such as HIV—as for ‘histories’;compare negative history), but this is not always so in infertility. Infertility tests are gener-ally better if they’re positive, like the postcoital test, tests for ovulation, tests for tubal patencyand (not least) a pregnancy test (see also positive test).
NET See norethisterone.neurohypophysis The neural (nerve-containing tissue) part of the pituitary gland, lying
towards the back—and so, in medical-speak, called the posterior pituitary. Produces thehormones oxytocin (which acts on myometrium to cause contraction of the uterus) andvasopressin (which helps maintain blood pressure and conserves the body’s water in thekidneys).
NK cells White blood cells or lymphocytes that form part of the ‘innate’ immune systemcapable of recognizing foreign cells and dissolving them (hence their name: naturalkiller cells). Found normally, however, in the endometrium of the late secretory phase andin the decidua of pregnancy, where they have more friendly purposes in forming theboundary between mother and fetus. Unlike T cells and B cells, most NK cells do nothave ‘immunological memory’,whereby previous contact with a particular antigen causesa faster, more deadly immune response second time round.
non-maleficence The ethical principle that comes from not doing harm. See also bene-ficence and suffering.
non-obstructive azoospermia Azoospermia caused by low sperm production rates in thetestis, including maturation arrest. Can often be overcome with testicular sperm extraction(TESE) followed by in vitro fertilization utilizing intracytoplasmic sperm insertion (ICSI).
Norethindrone See norethisterone.norethisterone (NET) A progestogen of a type weakly related to the male hormone testos-
terone. Progestogens of this class are commonly found in the oral contraceptive pill.Norethisterone acetate is marketed as Primolut N and is made by Schering. Callednorethindrone in the USA and marketed as Aygestin by Wyeth.
normal monthly fertility Nature gives fertility a wide range, normally from about7 percent to 45 percent per month for women in their early twenties, to about 3 percentto 25 percent per month for women in their early thirties; for women in their early
466 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 466

forties it ranges from less than 1 percent to about 5 percent per month. See also monthlyfertility and fecundability.
Novarel Preparation of hCG made by Ferring. Similar to Pregnyl and Profasi.NSAIDs Nonsteroidal anti-inflammatory drugs, such as aspirin, ibuprofen (Advil,
Nurofen, etc.), mefanamic acid (Ponstan), naproxen sodium (Aleve, Naprosyn, orin Naprogesic in combination with dextropropoxyphene), which stop the produc-tion of prostaglandins; useful for dysmenorrhea and prior to a hysterosalpingogram.Excessive use at the time of ovulation might predispose to a luteinized unrupturedfollicle, so NSAIDs should not be used for ovulation pain if you are trying to getpregnant.
nuchal lucency See nuchal translucency.nuchal thickness See nuchal translucency.nuchal translucency A measurement done at transvaginal ultrasound of the thickness of the
tissue in the neck of the fetus; if excessive, it implies a substantially increased risk thatthe fetus is affected by Down syndrome and Turner syndrome.
nucleus Central structure within a cell that contains the chromosomes.The non-nuclear partof the cell is called the cytoplasm—which thus contains other cellular structures, includ-ing the mitochondria.Genetic inheritance is mostly by way of the nucleus (with a contri-bution from mother and father); a small part is by way of the cytoplasm (with acontribution only from the mother). See also mtDNA and mitosis. Plural: nuclei.
obligation A moral compulsion for ethical action, sometimes usefully distinguished from aduty by its derivation from example or external enforcement.According to this distinc-tion, obligations are derived chiefly from the considerations of teleological ethics and utili-tarian ethics,with duties derived from considerations of deontological ethics.See also rights.
obstructive azoospermia See azoospermia.oestrogen See estrogen.oestrone See estrone.office biopsy See premenstrual endometrial biopsy.OHSS See ovarian hyperstimulation syndrome.oligomenorrhea Infrequent menstrual periods. By convention, a menstrual cycle that is
consistently longer than 35 days. Oligomenorrhea always reflects irregularity ofhormonal events coming from the ovaries. See also anovulation and amenorrhea.
oligospermia Strictly, oligozoospermia, meaning a reduced number of sperm cells(spermatozoa) in the ejaculate (compared with azoospermia, which means no sperm inthe ejaculate). More generally, a decrease in normal, motile sperm, and more or lessencompassing laborious terms such as ‘asthenozoospermia’ (weak motility) and‘teratozoospermia’ (abnormal sperm), and even more laborious ones such as ‘oligo-asthenoteratozoospermia’, which do not reward the effort of concocting them.
oocyte The form of the ovum, or egg, which is undergoing a halving of the number ofchromosomes through the process of meiosis; see also primary oocyte and secondary oocyte.
oogenesisThe multiplication (by the process of mitosis) of ova, or eggs, in the ovaries of thefetus.
oogonium The earliest recognizable form of the ovum, or egg; present only in the ovaries
GLOSSARY � 467
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 467

of fetuses.Multiplies by the process of mitosis before developing into oocytes by the processof meiosis.The male equivalent (the spermatogonium) normally persists in the testicles tillold age. Plural: oogonia.
oopause A new term for the normal cessation of female fertility up to 10 years before themenopause, being apparent in some women after the age of 33 and in most women by45. Different from the perimenopause, which occurs as egg numbers fall far enough tocause shortening of the menstrual cycle, particularly the follicular phase, and accompaniedby elevation of serum FSH when measured during menstruation. If pregnancies areattempted through the oopausal transition, a woman who has had no prior reproduc-tive disturbance will typically experience recurrent miscarriages before developing other-wise unexplained infertility, manifesting in the IVF lab sequentially with unexplainedimplantation failure of apparently satisfactory embryos, then, in turn, a decreased rate offorming blastocysts, defective cleavage and then failure of fertilization.There is no knownmethod of overcoming its effects short of egg donation, except for some hope that theprocedure of cytoplasmic transfer might be helpful.
oophorectomy See ovariectomy.OPU Ovum pick-up; see follicle aspiration and egg retrieval.orchidopexy An operation to move an undescended testis into the scrotum, so that it has
more chance of developing normally and producing sperm cells (spermatozoa. See alsocryptorchidism.
OrgalutranThe GnRH-antagonist ganirelix made by Organon.Called Antagon in the USA.orgasm I don’t need to tell you what this is, you can find out for yourself! What you might
like to read about, though, is how having one, or not having one, or having one earlyor late, affects getting pregnant.Read the box,Orgasm and retaining sperm in the vagina, inChapter 19.
osteoporosis An abnormal condition of the bones, which are weakened by a loss ofcalcium.Deficient estrogen, such as after the menopause or after primary ovarian failure(premature menopause), eventually causes osteoporosis, with a tendency to bone frac-tures, especially of the wrist, the thigh and the backbone.
ovarian cycle The equivalent of the menstrual cycle in the ovary, comprising the follicularphase and the luteal phase.Thus the ordered sequence of timely development of tertiaryfollicles to a (usually) single dominant follicle or Graafian follicle, characterized by increas-ing production of the estrogen estradiol), through ovulation, when estradiol falls and prog-esterone starts to rise, followed by the development and then decline of the corpus luteum,with the further production of progesterone.Because estradiol and progesterone controlthe growth and development of the endometrium in the uterus, the ovarian cycle deter-mines the menstrual cycle (normally from 24 to 35 days in length, with a typical durationof about 28 days) and also the cycle of the normal female hypothalamus and pituitary gland.
ovarian hyperstimulation syndrome (OHSS) A complication of ovulation induction with,usually, follicle stimulating hormone, especially in cycles of superovulation for assisted concep-tion, when it is intended to retrieve more than one egg.The ovaries become large, theycan be painful, and there is excessive fluid released into the abdomen (the peritonealcavity). Either removing this fluid or the occurrence of vomiting can cause dehydra-
468 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 468

tion, thickening of the blood and, occasionally, a serious thrombosis, such as a stroke.Death has been reported.Moderate to severe OHSS is treated in hospital,with admin-istration of fluid intravenously, sometimes including albumin. See also vascular endothelialgrowth factor.
ovarian monitoringThe frequent estimation of serum estradiol (or perhaps estimating thecervical score) and performance of transvaginal ultrasound to estimate how close a womanis to ovulation. Monitoring is described in detail in Chapter 20. See also serum LH andserum progesterone.
ovarian pregnancy An ectopic pregnancy located in the substance of the ovary, presum-ably because an egg (an oocyte) has been fertilized while still in a follicle.
ovariectomy Surgical removal of the ovary. If the other ovary remains, the ovarian cycle,ovulation and the menstrual cycle usually continue as before.The place of ovariectomy inthe management of endometriosis and incapacitating premenstrual tension is discussed inChapter 16. Synonym: oophorectomy.
ovaries See ovary.ovary The female organ that produces eggs, or oocytes. Located on each side of the uterus,
to which the ovaries are functionally connected by way of the fallopian tubes (or oviducts).Ovidrel Recombinant human chorionic gonadotropin made by Serono. Called Ovitrelle in
Europe.oviduct Another name for fallopian tube (derived from its function of conducting, or trans-
porting, the ovum).ovulation Natural process by which a mature follicle in the ovary opens to release the second-
ary oocyte, or egg, enclosed in a sticky blob of mucus-like material, the cumulus mass. Seealso luteinizing hormone, LH surge, ovulation pain and human chorionic gonadotropin.Understanding the normal processes of reproductive physiology forms the basis forChapter 3.
ovulation inductionThe use of drugs to stimulate the development of follicles in the ovariesto undergo ovulation, such as clomiphene, various preparations containing follicle stimu-lating hormone (FSH), and human chorionic gonadotropin (hCG).The two main situationsfor it are: in the treatment of infertility due to anovulation (typically when there is oligo-menorrhea or amenorrhea (described in Chapter 11); and for superovulation in assistedconception (for example, in vitro fertilization and gamete intrafallopian transfer (described inChapter 20). See also ovarian hyperstimulation syndrome and ovarian monitoring.
ovulation pain A mild pain that precedes ovulation by about 12 hours, felt in the left orright side, but not by everyone nor in every ovarian cycle.A good indication of ovula-tion if it is felt.Can be exaggerated in endometriosis and in so-called ‘pelvic congestion’.The time from ovulation pain until the onset of menstruation (ignoring for this purposeany premenstrual spotting) is a good measure of the length of the luteal phase. Should notbe treated with NSAIDs such as Advil or Nurofen if you are trying to get pregnant,because these analgesics have been linked to the so-called luteinized unruptured folliclesyndrome, or LUF.
ovulatory dysfunctional uterine bleeding Heavy but generally regular bleeding causedeither by pathology in the uterus, such as fibroids, or by a generalized bleeding disorder,
GLOSSARY � 469
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 469

such as thrombocytopenia (a low platelet count), von Willebrand’s disease (can run infamilies) or treatment with anticoagulant drugs.The formal term for it is menorrhagia.
ovumThe female germ cell, or egg, from the earliest stage (the oogonium in the fetus), throughits release from the follicle (ovulation), and (to professional embryologists) through fertil-ization up to and sometimes beyond the stage of implantation. See also blighted ovum.Plural: ova.
ovum pick-up (OPU) See follicle aspiration and egg retrieval.PAPP-A ‘Pregnancy-associated plasma protein A’: a protein made by the syncytiotrophoblast
of the placenta to increase its sensitivity to growth signals. Found in increasing levels inthe pregnant woman’s serum as pregnancy develops. Decreased if the pregnancy isaffected by Down syndrome, therefore measured in the triple test used for fetal trisomy 21screening.
Parlodel See bromocriptine. Made by Sandoz.parthenogenesis Can occur when an egg (as a secondary oocyte) undergoes activation (by
itself, with some non-specific stimulus, or through fertilization by a sperm) and startsto divide (it undergoes cleavage), but the male chromosomes are not incorporated and theegg remains haploid; its further development will soon stop, probably well before implan-tation. Can be the cause of apparent (but false) late fertilization in the IVF lab.
partial mole See hydatidiform mole, partial and triploidy.paternalism A method of medical or administrative practice in which the values of the
practitioner or administrator are imposed upon the person most affected by the deci-sions to be made, without adequately heeding that person’s own values or power tomake decisions that directly affect them. For a discussion of paternalism in thedoctor–patient relationship, read the box, Autonomy and respect for persons, in Chap-ter 26. See also autonomy and professionalism.
PCB See postcoital bleeding.PCO See polycystic ovaries.PCOD Polycystic ovary disease. See polycystic ovary syndrome.PCOS See polycystic ovary syndrome.PCR See polymerase chain reaction and DNA testing.PCT See postcoital test.Percol A laboratory medium used for separating sperm. Not approved for human thera-
peutic use. See PureSperm.Pergonal Mixture of human menopausal gonadotropins containing follicle stimulating hormone
made by Serono; virtually equivalent to Humegon.perimenopause A time of intermittent symptoms of the menopause that first becomes
apparent as egg numbers in the ovaries fall far enough to cause shortening of themenstrual cycle, particularly the follicular phase, and accompanied by elevation of serumFSH when measured during menstruation.As it progresses,menstrual cycles can shortenconsiderably,while becoming interspersed unpredictably by unusually long cycles, some-times producing cystic follicles and even anovulatory dysfunctional bleeding, as well asepisodes of hot flashes (or flushes). Different from the oopause.
peritoneal adhesions See adhesions.
470 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 470

peritoneal cavityThe general abdominal cavity in which lie the stomach, the intestines,and the uterus, ovaries and fallopian tubes, each covered by a thin, moist, slippery surfacelayer, the peritoneal serosa (or peritoneum). An examination of the peritoneal cavity iscalled a laparoscopy. See also adhesions.
peritoneal serosaThe serosa of the peritoneal cavity.peritoneum The smooth, moist lining of the peritoneal cavity that forms the serosa of the
organs this cavity contains. For purists, such serosa is visceral peritoneum and the part ofthe peritoneum covering the wall of the abdominal cavity away from organs is calledthe parietal peritoneum.
peritubal adhesions Adhesions around the fallopian tube.perivitelline spaceThe space between the egg (the vitellus—the oocyte itself) and the zona
pellucida; sperm are injected into this space with subzonal insertion, or SUZI.PGD See preimplantation genetic diagnosis.phallus Generic term for the clitoris or penis; refers also to the early forms of these organs
in the embryo.pheromone A substance excreted by an organism that causes another member of the
particular species to behave or develop differently.Examples include substances excretedin the urine or sweat that affect mating behavior when detected through the sense ofsmell.
pituitary fossa See pituitary tumor.pituitary gland Gland located at the base of the brain and responsible (among other jobs)
for driving the ovaries in women and the testes in men by way of the pituitary hormonesfollicle stimulating hormone (FSH) and luteinizing hormone (LH),which are under the influ-ence of gonadotropin releasing hormone (GnRH) from the hypothalamus.Composed of twoparts, the adenohypophysis, or truly glandular part, in front, and the neurohypophysis,whichis a down-growth of the brain, behind.
pituitary tumor A tumor, usually benign, of the pituitary gland, usually resulting in amen-orrhea and anovulation.Often there is an increase (sometimes substantial) in serum prolactin.If the tumor is itself secreting prolactin it is called a prolactinoma. But other tumors canoccur, some of which secrete other pituitary hormones. The tumor grows inside aconfined space with walls of bone called the pituitary fossa: if it is still small and confinedto the fossa we call the tumor a microadenoma; if it enlarges the fossa or pushes out ofit, it is a macroadenoma, and is both more dangerous and capable of producing visualsymptoms and headaches. Diagnosed on a CAT scan or a MRI scan. Prolactin-secretingmicroadenomas can usually be treated just with drugs (see hyperprolactinemia).
placentaThat part of the ‘products of conception’ apart from the fetus where blood fromthe fetus and from the mother come into intimate contact to exchange nutrients andwaste. Composed of trophoblast.Together with the membranes (of the gestational sac) andthe umbilical cord composes the ‘afterbirth’. See also decidua.
plasma glucose A measurement of sugar (glucose) in the blood plasma to detect diabetes,an occasional cause of recurrent miscarriages. Usually checked a few hours after a mealor, more formally, with a glucose tolerance test that involves a standard drink of glucose(after prior fasting) followed by serial measurements of plasma glucose over three hours.
GLOSSARY � 471
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 471

PMS Either premenstrual spotting or premenstrual syndrome (see premenstrual tension, PMT).PMSP See premenstrual spotting.PMT See premenstrual tension.polar body A tiny, compact packet of excess chromosomes discarded first by the primary
oocyte as it becomes a secondary oocyte just before ovulation—the first polar body, with 46chromosomes; and second by the secondary oocyte immediately after fertilization (orafter activation by other means)—the second polar body,with 23 chromosomes.The polarbodies lie in the perivitelline space.The chromosome content of each polar body can betested as part of a preimplantation diagnosis maneuver to infer whether the correspon-ding oocyte has an aneuploidy: an extra chromosome in the polar body means a chro-mosome not enough in the oocyte, and vice versa; this is called polar body analysis.See also meiosis.
polycystic ovaries (PCO) The full name (almost never used) is micro-polycystic ovaries; it’sa diagnosis best made on transvaginal ultrasound,with lots of medium-sized follicles visiblearound the rim of the ovaries; can be part of the polycystic ovary syndrome. (The ‘cysts’ arenot real cysts.Think of them as stalled follicles.They don’t need to be treated.) A verycommon condition: about 20 percent of women have it, though only a few have thefull syndrome.
polycystic ovary syndrome (PCOS) A syndrome that consists of polycystic ovaries asso-ciated with any clinical symptom or sign of too much male hormone effect, such asacne, excess body hair (hirsutism), or long or absent cycles (oligomenorrhea or amenorrhea).Often called polycystic ovarian disease (PCOD) in the USA.
polymerase chain reaction (PCR) A method of amplifying (increasing in number) a singlepiece of DNA (the stuff of genes) to get enough of it to analyze physically or chemicallyfor DNA testing.A machine is used that uses alternate cycles of high temperature (toseparate DNA’s two strands) and medium temperatures (to combine each of the two singlestrands with free nucleic acids to make new complementary strands),doubling the amountof DNA in the machine’s ‘soup’ each cycle.A few hours in the machine automaticallycreates millions of identical DNA molecules from just one specimen. Needless to say, it’sextremely important that you start with the right bit of DNA, so you’re not inadvertentlyamplifying a bit of contamination! In the film Jurassic Park, PCR was used to amplify bitsof dinosaur DNA recovered from the bellies of contemporary insects, which had beentrapped and preserved for millions of years inside pieces of amber.A biopsy of a single cellfrom an embryo after IVF can, with PCR, produce enough DNA to test it for certaingenes that cause serious genetic disease. See also preimplantation genetic diagnosis.
polymorphisms Forms of a gene (that is, alleles) that are too prevalent in the populationto be called mutations or even, sometimes, to be regarded as abnormal. Often theyconfer an advantage in some special circumstance.
polyp A benign growth of tissue, usually of the lining of a hollow organ such as the intes-tine or the uterus. See cervical polyp and endometrial polyp.
polyploid A multiple of the haploid number of chromosomes in a cell other than the normaldiploid state. Includes triploid (three times the haploid number, or 69 chromosomes) andtetraploid (four times the haploid number, or 92 chromosomes).The noun form of this
472 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 472

adjective is polyploidy (the state of being polyploid).polyspermic fertilization See polyspermy.polyspermy Fertilization of an egg (a secondary oocyte) by more than one sperm (spermato-
zoon). In in vitro fertilization,more common if eggs are recovered that are either immatureor overly mature. Evident later, with the appearance of more than two pronuclei. Innatural conditions, a cause of a polyploid state in the embryo. See also triploid.Anothername for it is polyspermic fertilization.
poor responder See low responder.positive history If you have a positive history for a disease or symptom it means that you
have or have had that disease or symptom. Contrast with negative history.positive test In medicine, generally it might be best for tests to be negative (like tests for
brain tumors or tests for sexually transmitted diseases, such as HIV—as for medicalhistories, compare positive history), but this is not so in infertility. Infertility tests, such asthe postcoital test, tests for ovulation, tests for tubal patency, and (not least) a pregnancy test,are generally better if they’re positive.
postcoital bleeding (PCB) Bleeding after sex.Typically the result of abrasion of the cervix(which may be abnormal and you should have an examination and a PAP smear) or oftrauma to the vagina. Sometimes due to a cervical polyp.
postcoital contraception Using a contraceptive after sex instead of before it, to interruptimplantation of an embryo (if there is one).Taking two birth control (oral contraceptive)pills the morning and the night after the unanticipated opportunity for pregnancy isreasonably effective, but see your physician for details to carry this out safely and effec-tively.This maneuver might not protect against an ectopic pregnancy.
postcoital test (PCT) A test of: (1) receptiveness of the cervical mucus to sperm; and (2)sperm motility—both of which are needed for the test to be a positive test. It’s essentialthat the test be done to coincide with ovulation, tested with a urinary LH kit or meas-urements of serum estradiol (high), serum LH (preferably high) and serum progesterone (stilllow), because the job description of the cervical mucus at other times is to be impen-etrable to sperm (that is, the PCT will be negative for normal reasons).
postimplantational embryopathy An abnormality of the embryo (or fetus) that arisesafter implantation of the embryo in the endometrium (the lining of the uterus). Might,sooner or later, cause a miscarriage or birth abnormality. Discussed in Chapter 8.
Predalon Alternative name for Pregnyl used in Germany.predecidual reactionA partial confluence of stromal cells of the endometrium (lying between
the endometrial glands), caused by prolonged exposure (10 days or more) to proges-terone or a progestogen. See also decidual reaction.
preeclampsia A syndrome occurring in late pregnancy marked by an increase in bloodpressure, swelling of the ankles by fluid and the appearance of albumin in the urine,associated with reduced blood flow to the placenta, therefore putting the fetus at risk ofdeath, or stillbirth, and putting the mother at risk of complications from high bloodpressure, convulsions (eclampsia), kidney failure, liver failure and death.Treated withdrugs to lower the blood pressure and to prevent convulsions, while expediting thedelivery of the baby.
GLOSSARY � 473
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 473

pre-embryo A term sometimes used for the embryo or ovum from the stage of fertilizedegg (or zygote) up to the stage of the morula. During this time any of the cells of thefertilized ovum can develop into a whole new embryo—they are totipotent.As it becomesa blastocyst a proportion of the cells (the inner cell mass) commit to producing the embryoproper, while the remaining majority are destined to form trophoblast. Distinguishingpre-embryo from loose use of the term embryo has some value when debating themorality of embryo research, but it is not universal practice.
pre-embryo biopsy See embryo biopsy and preimplantation genetic diagnosis.pregnancyThe state of being with child [British Medical Dictionary]; specifically, the condi-
tion from implantation of the conceptus until its delivery.pregnancy rateThe percentage of months or treatment cycles that result in clinical preg-
nancy, excluding biochemical pregnancy, but including ectopic pregnancy, miscarriage and allpotentially viable pregnancies (twins are not counted twice; stillbirths and all live birthsare included). Less important for most patients’ purposes than the take-home baby rate.Less useful for embryologists intent on quality control in the laboratory than the implan-tation rate.
pregnancy test Nowadays a measurement of human chorionic gonadotropin in serum or urine,usually as a simple ‘yes’ or ‘no’ test. In principle a single test cannot distinguish a normalpregnancy from an ectopic pregnancy or one destined to miscarry (a miscarriage). See alsoserum hCG.
Pregnyl Human chorionic gonadotropin (hCG) made by Organon.preimplantation genetic diagnosis (PGD) Genetic diagnosis of an IVF embryo before
embryo transfer.Made possible by removing one or two cells of the embryo (embryo micro-biopsy).Typically performed on day 3 of embryo development in vitro, at the 8-cellstage, prior to compaction, or on day 5, as an expanding blastocyst. See also fluorescent insitu hybridization (FISH), comparative genomic hybridization (CGH) and polymerase chainreaction (PCR).
preimplantational embryopathyAn abnormality of the embryo (or fetus) that arises beforethe embryo undergoes implantation in the endometrium (the lining of the uterus).Usuallycauses miscarriage. Discussed in Chapter 8.
Premarin A mixture of estrogens in tablet form (from Ayerst Laboratories) with the repu-tation of being ‘natural’, though in reality extracted from the serum of pregnant mares(horses); the main human estrogen it contains is estrone.
premature labor The onset of labor, leading to delivery, before at least 37 weeks haveelapsed since the last menstrual period.The more prematurely babies are born, the greaterthe difficulty they have surviving, even with expert care; birth at 25–26 weeks is themost dangerous in terms of survival with serious disability.
premature menopauseWhen menopause occurs before the age of 40.See primary ovarian failure.premenstrual biopsy (PMB) See premenstrual endometrial biopsy.premenstrual endometrial biopsy A small sample (or biopsy) is taken of the lining of
the uterus (the endometrium) just before a period is expected, aiming to show advancedstages of progesterone’s effect on it, in the form of an adequate predecidual reaction.This avery sensitive test of the adequacy of the luteal phase—see the box,The endometrial clock,
474 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 474

in Chapter 3.The biopsy can be combined with a laparoscopy or carried out in isola-tion as an office procedure. It’s best to be sure that there is no possibility of pregnancyduring the cycle the test is conducted, as occasionally the biopsy jeopardizes an earlypregnancy (namely an early implantation, before the pregnancy test or serum hCG hasbecome positive). See also luteal phase defect.
premenstrual spotting A form of light intermenstrual bleeding consistently timed over afew days to a week before the period starts properly, although it might not happenevery month. About 80 percent of the time it signals the presence of endometriosis,making it the most predictive symptom for this condition; about 10 percent of the timeit means an abnormality of the uterus such as fibroids, an endometrial polyp or endometri-tis; the remaining 10 percent of the time there is no explanation found. It has nothingto do with premenstrual tension, which if present is a coincidence. For more on its asso-ciation with endometriosis, see Chapter 15.
premenstrual syndrome See premenstrual tension.premenstrual tension (PMT) A distressing group of symptoms usually timed for the lead-
up to a period, then relieved as menstruation takes place, although many women experi-ence different timing; includes downheartedness or depression (certainly an absence ofwell-being), aggression, fluid retention and weight gain, painful breasts (‘mastalgia’),headaches and pain in the pelvis; caused by a periodic fall in the brain’s endorphins, in turnusually precipitated by falling levels of progesterone in the second half of the luteal phase,although similar symptoms often accompany the use of progestogens, especially in olderwomen;may be better during superovulation cycles because of generally higher hormonelevels,but this is not always the case and PMT at the end of an unsuccessful cycle of assistedconception is particularly hard to put up with. Usually treated (up to a point) sympto-matically, with perhaps fluid tablets (diuretics) and analgesics, although it’s claimed thatthe drug Prozac has a specifically beneficial effect on mood,and encouragement of endor-phin release with exercise can also be useful. Because progesterone and progestogens arethe culprits, an operation to remove the ovaries (plus hysterectomy to simplify estrogen replace-ment therapy without needing progestogens) is usually curative, but drastic.
prenatal testing See chorionic villus sampling, amniocentesis and triple test.preovulatory Immediately prior to ovulation.preovulatory follicle A large, mature tertiary follicle that will respond to an adequate LH
surge or injection of human chorionic gonadotropin (hCG) by undergoing ovulation, releas-ing its egg. Produces estradiol and, with exposure to LH or hCG, progesterone. See alsoGraafian follicle.
primary In medicine the word ‘primary’ can denote primacy in one of three ways: (1)event-wise (for example, primary amenorrhea is when there has been no precedent—noprior period—whereas secondary amenorrhea follows prior periods, and likewise thedistinction between primary infertility and secondary infertility, a distinction based on priorsuccessful pregnancy); (2) developmentally or time-wise (for example, a primary folliclegives rise to a secondary follicle, then to a tertiary follicle); or (3) causally (for example,primaryovarian failure is based within the ovary itself,whereas secondary ovarian failure is second-ary to failure of gonadotropins). Getting to understand these sorts of distinctions is one
GLOSSARY � 475
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 475

reason why medical school takes a long time.primary amenorrhea Amenorrhea when a woman has never had a spontaneous menstrual
period, that is, a period not brought on by hormone treatment. See also primary.primary follicleThe first stage of growth or further development of the follicle, in which
the egg is enclosed by a single layer of round-shaped follicle cells, which are multi-plying. The majority of primary follicles undergo atresia; a minority develop intosecondary follicles.
primary infertilityTrouble getting pregnant (infertility) in someone who has never had asuccessful pregnancy (see primary).Although the exact definition can vary among gyne-cologists, in this book the differentiation between primary infertility and secondaryinfertility is most useful if a prior ectopic pregnancy or a prior miscarriage is consistent withthe state of primary infertility, whereas a prior induced abortion (which, the odds are,would otherwise have developed normally) means the state is secondary infertility.
primary oocyteThe form of the ovum, or egg, produced in the ovaries of fetuses by oogoniathat have begun the first part of the cell division known as meiosis (by which the chro-mosomes will eventually halve in number). Persists into childhood and adult life bycontainment in follicles.Gives rise to a secondary oocyte and the first polar body just beforeovulation. See also in vitro maturation.
primary ovarian failure Failure of the ovaries to produce enough follicles because of aproblem in the ovary itself, and resulting in depletion of eggs before the age of 40 years(known as premature menopause, a cause of secondary amenorrhea), or maybe even beforethe age puberty is expected (causing failure of puberty to happen, including primaryamenorrhea). Sometimes occurs in spite of good numbers of primordial follicles that (inex-plicably, so far) won’t develop (see the box, The resistant ovary syndrome, in Chapter 11).The younger the woman, the more likely that an aneuploidy will be found if a karyotypeis done on blood or on a biopsy of the ovary. Estrogen replacement therapy is important toprevent general jeopardy to health, including prevention of osteoporosis. See also Turnersyndrome, triple-X syndrome, fragile-X syndrome and primary.
primary spermatocyte The form of the sperm cell (or male gamete) at the first stage ofspermatogenesis, by which spermatogonia enter meiosis to start to reduce the number ofchromosomes for the more mature sperm cells (the spermatozoa) that will eventuate.
Primolut N The progestogen norethisterone acetate (UK, Australia) or norethindrone acetate(USA), made by Schering.
primordial follicle The resting, unstimulated stage of the follicle, in which the egg (as aprimary oocyte) is enclosed by just a few thinly stretched follicle cells. Primordial folliclespersist in the ovary from fetal life to the time of menopause, declining in number everyday during this time as some start to develop into primary follicles, most of which thenare lost through the process of follicular atresia.What the stimulus or signal is for a partic-ular primordial follicle to start growing remains completely unknown (it is independ-ent of FSH).
PRL See prolactin.Profasi Human chorionic gonadotropin (hCG) made by Serono. Nowadays highly purified
and should be suitable for subcutaneous injection.
476 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 476

professionalism As used in this book, the practice of maximizing the involvement of aclient or patient seeking the service of a professional in making decisions that willdirectly affect them.
progesteroneThe ovary’s second main hormone, produced only after ovulation and duringpregnancy (first by the corpus luteum, then by the placenta). Sometimes administered byinjection or by insertion into the vagina in the form of a pessary to supplement naturalproduction. See also estrogen, progestogen and serum progesterone.
progestin See progestogen. Strictly, the term progestin also encompasses progesterone (that is,‘progestins’ = ‘progesterone’ + ‘progestogens’).
progestogen A progesterone-like substance, usually more active when given by mouth thanis natural progesterone. Used with an estrogen in the birth control (oral contraceptive)pill. Commonly used examples have a structure like progesterone itself (for example,medroxyprogesterone acetate, or Provera; cyproterone acetate, or Androcur) or a structuredistantly related to the male hormone testosterone (for example,norethisterone, or PrimolutN; norgestrel).
Progynon C Schering’s preparation of ethinyl estradiol.prolactin (PRL) The hormone produced by the pituitary gland to stimulate the production
of milk in the breasts. Produced in increasing amount during pregnancy, although milksecretion is postponed until levels of estrogen and progesterone fall after the baby is born.For more on prolactin in the animal kingdom, and its importance in being producedby decidual cells in pregnancy, read the box, The fishy side of prolactin. See also bromocrip-tine, dopamine, hyperprolactinemia and serum prolactin.
proliferative phaseThe phase of development of the endometrium during which, after themenstrual phase, the endometrium grows to regain thickness under the influence of estra-diol (therefore it corresponds in time with the follicular phase in the ovarian cycle).
pronuclear stage transfer (PROST) A form of assisted conception in which in vitro fertil-ization (IVF) is used to produce fertilization of one or more recovered eggs (oocytes).Useful if the potential fertilizing ability of sperm (spermatozoa) is in doubt.Transfer ismade on the day after egg retrieval and IVF, before the fertilized egg divides (it’s at the
GLOSSARY � 477
The fishy side of prolactin
Prolactin is an old hormone in the animal kingdom. It has had many and varied roles.In fish it’s important in regulating water entering and leaving the tissues. In mammals,including humans, prolactin is well known for stimulating milk production, butprolactin produced by decidual cells in the endometrium during pregnancy seemsto be important in regulating the passage of water into the gestational sac—a functionthat seems to have been inherited down the millions of years since our ancestorswere fish.
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 477

pronuclear stage); the transfer is made to the fallopian tube to obtain advantages similar togamete intrafallopian transfer (GIFT) and is made possible by laparoscopy (with anesthesia)or, less successfully, by transvaginal ultrasound (without anesthesia). Synonymous withzygote intrafallopian transfer (ZIFT). See also pronucleus.
pronucleus A visible ‘blob’ (or vacuole)—there are usually two of them—inside an egg thathas undergone fertilization or activation by other means, and enclosing the chromosomesfrom the oocyte (the female pronucleus) and from the sperm (the male pronucleus). Plural:pronuclei. If three pronuclei are observed, the chances are that two sperm have enteredthe egg (polyspermy).
PROST See pronuclear stage transfer.prostaglandins Substances, first isolated from the prostate gland’s contribution to semen,
now known to be universally present throughout the body, being especially producedduring inflammation (when they cause pain). Drugs that stop prostaglandins beingproduced are used as analgesics (so called nonsteroidal anti-inflammatory drugs, orNSAIDs) and are also useful in minimizing contractions of the uterus in dysmenorrheaand premature labor.
prostate glandThe male sex gland located just below the bladder, in front of the rectum,through which the urethra runs; it contributes secretions to the semen.
prothrombin G20210A A polymorphism for the blood clotting factor prothrombin thatmakes coagulation occur more readily, therefore causing thrombophilia.
Provera The progestogen medroxyprogesterone acetate, made by Upjohn.pseudohermaphrodism Synonymous with intersex, except that intersex also includes true
hermaphrodism.Puregon Recombinant follicle stimulating hormone made by Organon.Called Follistim in the
USA. Generically known as follitropin beta.PureSperm A laboratory medium approved for separating human sperm, made by
Nidacom.pyosalpinx A fallopian tube obstructed at its outer, fimbrial end and containing pus as a result
of acute salpingitis. If the infection does not settle promptly with antibiotics, and becomesan abscess, surgical drainage can be needed (performed at transvaginal ultrasound in theoperating room or at laparoscopy, perhaps with a salpingectomy).
qualitative Something you can’t put a number on to give it its meaning or value, such assuffering. See also hazard. Opposite to quantitative.
quantitative Something you can give meaning or value to by giving it a number, such aspregnancy rate. See also risk. Opposite to qualitative.
Quetelet index See body mass index.Recagon Alternative name for Puregon used in India.receptor Consider a hormone to be a key; a receptor is then the lock. One is useless
without the other.A hormone cannot act on a cell (or a tissue) unless the cell displaysa receptor, which is linked to the internal machinery of the cell.
recessive inheritance A pattern of inheritance of a characteristic (such as blue eye color)or abnormality (such as congenital absence of the vas deferens) in which two genes oralleles are needed to confer the characteristic or abnormality, in contrast to dominant
478 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 478

inheritance,which requires just one gene. See also homozygous. In the case of alleles foundon X-chromosomes but not on the smaller Y-chromosomes, a recessive gene will beunopposed (and so will act as a dominant gene) in males, whereas female carriers ofthe allele will be unaffected except in the extremely unlikely event that they inherit(or gain by mutation) a second abnormal allele; this mode of inheritance is called sex-linked recessive inheritance.
recombinant follicle stimulating hormone (rFSH) Follicle stimulating hormone derivedfrom genetic engineering instead of being extracted from the urine of postmenopausalwomen (human menopausal gonadotropin, or hMG) or from the pituitary glands of cadavers(human pituitary gonadotropin, or hPG). Produced and marketed by the two pharma-ceutical companies,Organon (as Puregon, or Fertinex in the USA) and Serono (as Gonal-F), to replace their hMG preparations. Has the advantage over hMG (and its purifiedderivatives) of being standard in biological structure and activity, and of not being of ahuman source (hPG, but not hMG, having been implicated in transmission ofCreutzfeldt-Jakob disease).
recombinant FSH See recombinant follicle stimulating hormone.recombinant LH See recombinant luteinizing hormone.recombinant luteinizing hormone (rLH) Luteinizing hormone derived from genetic
engineering technology instead of being extracted from the urine.Marketed by Seronoas Luveris.
recruit See follicular recruitment.rectum Connects the large bowel (the colon) to the anus; lies behind the vagina in women.recurrent miscarriages A series of three or more consecutive miscarriages.regeneration and tolerance factor (RTF) A protein produced by the trophoblast that
reduces the tendency of the mother’s immune system to reject the pregnancy, apparentlyby increasing levels of interleukin 10, and thus reducing the tendency for miscarriage.
relative infertility Synonymous with subfertility.relative risk The chance of having something or being affected by something compared
with people in a comparable situation.Usually given as a ratio, a proportion or a percent-age, as in the chance of having endometriosis; if your sister has it, you have a relative riskof 7:1 (or seven times the risk) compared with the general population of women ofthe same age; your relative risk of developing cancer of the ovaries if you’ve accumu-lated 10 years on the oral contraceptive pill is 1:5, 0.2 or 20.
relaxin An insulin-like protein with quite different functions.As the name suggests, tissuessoften, relax or give way upon exposure to it. Produced, for example, in the wall of thepreovulatory follicle before ovulation,by the decidua to calm the myometrium of the pregnantuterus, and by the corpus luteum and the placenta to soften the ligaments of the pelvis inpreparation for labor and childbirth.
reproductive cloningThe use of somatic cell nuclear transfer (SCNT) or embryo splitting (seecloning) to secure pregnancy and a new individual intended to be virtually geneticallyidentical to the person who donated the cell nucleus used,or genetically identical siblingsresulting from embryo splitting (which in effect is the intentional creation of identicaltwins,or triplets, etc.).Practiced in animals, especially farm animals.Considered ethically
GLOSSARY � 479
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 479

abhorrent because of strong ethical arguments within the fields of deontologicalethics (including a duty not to intentionally violate the biological principle of sexualreproduction involving genetic reassortment and individual difference), teleological ethics(including the very high risk of severe birth defects with SCNT) and utilitarian ethics(where arguments are based on considerations by and for society generally).
Repronex Highly purified human menopausal gonadotropin made by Ferring. CalledMenogon or Menopur outside the USA.
resistant ovary syndrome See primary ovarian failure.responsibility See accountability.rete testisTiny ducts (about 20 in number) connecting the testicular tubules with the epididymis.retroflexed A backward angle of the fundus of the uterus in relation to the direction of the
cervix. Usually only occurs when the uterus is retroverted. Opposite to anteflexed.retroflexion See retroflexed.retrograde ejaculation Ejaculation in which semen, instead of spurting out from the penis
during male orgasm, spills upwards into the bladder. Usually has a medically importantcause, which requires investigation.Treatment can be successful by isolating spermato-zoa from the urine and carrying out some form of assisted conception, such as assistedinsemination or in vitro fertilization.
retroversion See retroverted uterus.retroverted Refers to the position of the uterus when it is tilted backward in relation to
the direction of the vagina. A retroverted uterus is not always abnormal. Sometimes,however, a uterus can be pulled into a retroverted position by endometriosis affecting theuterosacral ligaments. A sharply retroverted uterus can cause pain during and after sex(dyspareunia). Opposite to anteverted. See also transvaginal ultrasound.
retroverted uterus A uterus that lies more towards the back than the front. Retroversionof the uterus may be normal and, of itself, this is not a cause of infertility; rarely it canrepeatedly get in the way during sex and cause pain, in which case there are operationsavailable to bring it forward,out of the way.Retroversion can also develop from scarringcaused by endometriosis, in which case there can be pain with sex (dyspareunia) and infer-tility (caused by the endometriosis).
rFSH See recombinant follicle stimulating hormone.rightThe reciprocal, or other side, of a duty or obligation, often conferred by society on the
basis of equity or consistency, and matched either by intuitive duties or by conferredobligations.
risk Chance—expressed as a ratio, proportion or percentage. If the word is unqualified, itusually means absolute risk (the actual risk in a group of the population), in contrast torelative risk (which measures one person’s risk compared with another person’s). Seealso hazard.
ROSI See round spermatid injection.ROSNI See round spermatid nuclear injection.round spermatid injection (ROSI) Experimental form of testicular sperm extraction (TESE)
followed by intracytoplasmic sperm insertion (ICSI) in which a round (very immature) sper-matid is isolated for injection into the egg (or oocyte). Seems to be less successful than a
480 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 480

similar procedure in which the nucleus is isolated from the spermatid and used instead(see round spermatid nuclear injection). Not recommended clinically.
round spermatid nuclear injection (ROSNI) Experimental form of testicular spermextraction (TESE) followed by intracytoplasmic sperm insertion (ICSI) in which thenucleus of a round (very immature) spermatid is isolated for injection into the egg(or secondary oocyte). Intended to be used in treating non-obstructive azoospermia withsevere maturation arrest, when more spermatozoa are not obtainable. Animal studiesshow higher pregnancy rates than with round spermatid injection (ROSI), but limitedstudies in humans still indicate very high rates of embryopathy. Not recommendedclinically.
r-selection A reproductive strategy where survival of a species is optimized by explosiveincreases in numbers of animals whenever environmental circumstances are favorable;typically seen with small animals that reach sexual maturity quickly, which reproducejust once but with many progeny, and which do not need to tend to their progeny forvery long (if at all) after birth. In extreme cases (seen in many lower animals such asinsects), death of the father follows impregnation and death of the mother follows partu-rition (or giving birth).The opposite reproductive strategy to K-selection.
RTF See regeneration and tolerance factor.Rubin’s test See tests for tubal patency.rudimentary horn The small part of a bicornuate uterus in which one side is very small;
with regard to the side that is bigger (see unicornuate uterus), it can be called communi-cating or non-communicating depending on whether it has a cavity that joins with themain endometrial cavity. See also cornual pregnancy.
salpingectomy Surgical removal of the fallopian tube.salpingitis Inflammation of the fallopian tubes, usually due to infection. Can be acute (as in
gonorrhea, chlamydia and other infections) or chronic (as in persisting chlamydia, tuber-culosis, various fungus infections). Leads to blockage of the tubes and peritubal adhesionsif not treated promptly and effectively with antibiotics. See also pyosalpinx, hydrosalpinxand salpingitis isthmica nodosa.
salpingitis isthmica nodosaA nodular (‘nodosa’) thickening of the fallopian tube’s isthmus(‘isthmica’), probably due to previous salpingitis. Can cause localized obstruction of thetube and, if the obstruction is partial, an ectopic pregnancy can be caused.May be overcomewith microsurgery (see tubal anastomosis) or tubal canalization.
salpingogram An x-ray of the fallopian tubes. See hysterosalpingogram and selective salpin-gogram.
salpingolysis Microsurgery to remove peritubal adhesions or perifimbrial adhesions. See alsofimbriolysis, with which the term ‘salpingolysis’ overlaps. Sometimes carried out atlaparoscopy.A full description can be found in Chapter 13.
salpingoscopy Looking inside the fallopian tube with a fiberoptic instrument throughits relatively wide outer fimbrial end. Carried out at laparoscopy or laparotomy. See alsofalloposcopy.
salpingostomy Microsurgery to make a permanent, new opening at the outer fimbrial endof the fallopian tube after it has become blocked (see hydrosalpinx) from salpingitis or,
GLOSSARY � 481
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 481

uncommonly nowadays, from fimbriectomy. Sometimes attempted at laparoscopy, thoughmostly with a reduced chance of success. See also fimbriolysis.A description of the oper-ation is given in Chapter 13.
salpingotomy An operation involving a temporary opening length-wise along (usually)the ampulla of the fallopian tube, usually for the treatment of a (tubal) ectopic pregnancy.Occasionally performed for a pyosalpinx. Can be carried out efficiently at laparoscopy.
SCNT See somatic cell nuclear transfer.SCSA See sperm chromatin structure assay.secondary The word is used medically in one of three ways: (1) part of a sequence, as in
primary follicle, secondary follicle, tertiary follicle; (2) when a person has a precedent for acontrary state (for example, secondary amenorrhea, when a woman has had at least onespontaneous menstrual period,but then menstruation stops; secondary dysmenorrhea meansperiods that are painful after having been not so—or not so much; secondary infertilitymeans having trouble getting pregnant despite having become pregnant successfully inthe past); or (3) when the source of dysfunction lies elsewhere (for example, secondaryovarian failure means ovaries that do not function because, in this example, the pituitarygland on which the ovaries depend is not functioning). See also primary.
secondary amenorrhea Absent periods (amenorrhea) when a woman has had at leastone previous spontaneous menstrual period, but then menstruation stops. See alsosecondary.
secondary follicleThe second stage of growth of the follicle, in which the egg (as a primaryoocyte) is enclosed by a layer that’s more than one cell thick of round-shaped, multi-plying follicle cells.Virtually all secondary follicles will go on to become tertiary follicles.
secondary infertilityTrouble getting pregnant (infertility) in someone who has previouslyhad a successful or potentially successful pregnancy. Although the exact definition ofsecondary infertility can vary among gynecologists, for me the distinction betweensecondary infertility and primary infertility is most useful if the term secondary infertil-ity is restricted to when there has been a prior induced abortion (which, the odds are,would otherwise have developed normally) or a successful pregnancy; a prior ectopicpregnancy or a prior miscarriage is, in my view, still the state of primary infertility.
secondary oocyte The form of the oocyte, or egg, produced from the primary oocyte latein the life of the maturing follicle, just before ovulation.The egg stays at this stage untilfertilization by a sperm cell (spermatozoon). See also meiosis.
secondary ovarian failure Failure of ovulation along with low estrogen production fromthe ovaries because of insufficient signaling from the pituitary gland by its hormones, thegonadotropins.
secondary spermatocyte The form of the sperm cell in the second stage of spermato-genesis (through which the sperm cells are formed in the testes), produced from primaryspermatocytes in the first cell division of meiosis, and giving rise to spermatids, whichhave just half the normal cell’s complement of chromosomes, through the seconddivision of meiosis; enveloped by Sertoli cells in the testicular tubules.
secretory phase The phase of development of the endometrium during which, after theproliferative phase, the endometrium stops growing but starts producing secretions (which
482 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 482

nourish an implanting embryo) under the influence of progesterone, so it corresponds withthe luteal phase in the ovarian cycle.
selective catheterization An x-ray-directed technique for placing fine catheters in veinsof the body to sample the local production of hormones from a particular gland.
selective feticide See fetal reduction.selective salpingogram An x-ray like a hysterosalpingogram in which a catheter is passed
through the cervix and uterus, and then wedged into the fallopian tube to fill it with fluidvisible on x-ray. High pressure can be applied, so some tubes that seem blocked onhysterosalpingogram (or on passing dye at laparoscopy) can be shown in fact to be open.
semen Fluid produced by the male genital tract at ejaculation. Contains spermatozoa, as wellas many other substances, including those that make the ejaculate coagulate (and thencalled a coagulum, which is given time to liquefy before a semen analysis is done on it).Sperm cells account for only about 1 percent of the volume of the ejaculate, so it’s notpossible to be confident about a man’s sperm count just on the basis of the volume ofthe semen ejaculated.
semen analysis Formal name for a sperm count.semen sperm antibodies A test for detecting sperm antibodies in semen.seminal fluid See semen.seminal vesicles Male sex organs that are joined to the vas deferens on each side as they
enter the prostate gland to join the urethra; once thought to act as receptacles for storingsperm, they are now known to be more important for contributing constituents ofsemen.
septate uterus See uterine septum.septum Latin for ‘wall’. For an example, see uterine septum.serological test for syphilis One of a number of tests to detect previous or untreated
syphilis, an important (though nowadays rare) cause of birth defects and recurrent miscar-riages.The chance of detecting unsuspected syphilis might be very low, but the penaltyfor missing it is very high, so it’s still a routine test in early pregnancy.Tests are done onserum and include the Venereal Disease Research Laboratory (VDRL) test and theWasserman reaction (WR) test. Often tested as part of a screen for infectious diseasebefore assisted conception, although there is no evidence that syphilis is transmitted througheggs or sperm (it is caught from contact between the lining of the vagina and the surfaceof the penis).
Serophene Clomiphene made by Serono.serosaThe delicate, one-cell-thick outside lining of an organ in the body, particularly (for
our purposes in this book) the organs of the peritoneal cavity.Unlike other body surfacessuch as the skin and the lining of the stomach or intestines, an ulcer (or missing patch)of the peritoneal serosa always heals in eight days, however big the ulcer, or defect, is.See also peritoneal adhesions and peritoneum.
Sertoli cells Cells in the testis lining the testicular tubules that nurture the developing spermcells; responsible in fetal life for the production of anti-Müllerian hormone, which stopsthe male fetus from developing fallopian tubes, a uterus and a vagina.A source of estra-diol in men.
GLOSSARY � 483
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 483

serum That part of blood that’s left after it clots. Distinct from plasma, which is that partof unclotted blood that remains on top when blood is spun down in a centrifuge (whichwill still clot and leave serum unless an anticoagulant is added).Various serum tests (testsdone on serum, also called blood tests), are described in this glossary.
serum 17-hydroxyprogesterone 17-hydroxyprogesterone is formed from progesterone inthe adrenal glands (mostly as an intermediary substance on the way to making theadrenal’s main hormone, cortisol) and in the ovaries (on the way to making androgensand estrogens).A congenital lack of one or other of the enzymes needed to make cortisolin the adrenal causes androgens to be made instead, in turn causing hirsutism and oligomen-orrhea in women, maybe with the polycystic ovary syndrome (in mild cases) or (in severecases) causing intersex at birth.The adrenal glands enlarge in an attempt to maintainproduction of cortisol (hence congenital adrenal hyperplasia or CAH).An inappropriatelyhigh level of 17-hydroxyprogesterone in serum is diagnostic of CAH.
serum AFP See serum alpha fetoprotein.serum alpha fetoprotein Measurement of alpha fetoprotein in blood serum. High levels
can indicate a birth defect involving the brain or spinal cord, such as anencephaly orspina bifida (confirmed if amniocentesis shows high AFP levels in the amniotic fluid). Lowlevels can indicate an increased risk of Down syndrome (or trisomy 21), trisomy 18 and,occasionally, Klinefelter syndrome, signaling the need for a karyotype of the fetus’s tissuesby chorionic villus sampling (CVS) or amniocentesis.The formation of AFP in the earlyembryo is described in Chapter 4. See also triple test.
serum anticardiolipin antibody A test done to investigate recurrent miscarriages. See anti-cardiolipin antibody and lupus anticoagulant.
serum antigliadin antibodies Antibodies to gliadin, a component of dietary gluten, andpresent in wheat, barley, rice and oats, found in celiac disease, a defect of intestinal absorp-tion caused by abnormal sensitivity to gluten.
serum CA125 antigen Measurement of CA125 antigen in serum.A test done to investi-gate, particularly, adenomyosis and cancer of the ovary. Levels can also be increased withendometriosis (especially when there is a ‘chocolate cyst’ present), during normal menstru-ation and during normal early pregnancy.
serum chlamydial antibodiesA blood test to detect prior exposure to chlamydia.The anti-bodies commonly examined are not completely specific for the particular chlamydiaorganism that causes salpingitis and which is transmitted sexually: other chlamydia-likeinfections of the lungs and other regions of the body, and even some completely unre-lated infections with non-chlamydial organisms can produce false positive tests; a negativetest, that is an absence of detectable chlamydial antibodies, is however reassuring.
serum copper Done to screen for Wilson’s disease, in which there is abnormal retentionof copper in the body—a rare cause of recurrent miscarriages.
serum creatinine See serum urea and creatinine.serum estradiol Measurement of estradiol in blood serum. Used especially for monitor-
ing the development of ovarian follicles in assisted conception, usually together withtransvaginal ultrasound.The cycle might be a natural one or, more usually, one withovulation induction or superovulation.The result should be available within four hours
484 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 484

of the test for this purpose. For a diagram showing how serum estradiol levels changeduring the ovarian cycle, see Chapter 3.Abbreviated as serum E2.
serum free testosteroneThe direct measurement of the small proportion of testosterone thatis not bound in the blood to carrier proteins such as sex hormone binding globulin, and sois available directly to the tissues.A more sensitive and specific test than serum testosterone.
serum FSH Measurement of follicle stimulating hormone in serum. Useful at the time ofmenstruation for indicating a significantly decreased number of eggs in the ovaries inthe few years leading up to menopause (that is, indicative of depletion of eggs or primaryovarian failure); see also low responders. Continuously high in women after menopause,and then excreted in high amounts in the urine (from which, in turn human menopausalgonadotropin is derived). For a diagram of how serum FSH levels change during theovarian cycle, see Chapter 3.
serum hCG Measurement of human chorionic gonadotropin in serum: essentially a pregnancytest, but carried out more precisely (quantitatively) than is the case with a yes or no test(which is qualitative). Often carried out serially, to determine if a pregnancy is thriving(hCG levels double every two or three days in normal early pregnancy; languishing(levels rise more slowly, seen with an ectopic pregnancy and with an inevitable miscarriage);or resolving naturally (levels that are falling).Very high levels are seen with hydatidiformmole. Part of the triple screen used to screen for Down syndrome in early pregnancy.
serum HIV antibodiesA test for HIV, the virus that causes AIDS, and which comes in twostrains, type 1 and type 2.They need separate tests, but mostly both are done as a routine.The test looks for the development of an immune reaction against the virus, it does notlook for the virus itself, so it’s possible, for a few weeks, to have been infected (and to beinfective to others) with the test itself still a negative test, that is, apparently (but falsely) clear.
serum homocysteine Measurement of homocysteine in serum, used to detect majordeficiency of the vitamin folic acid. High levels make thrombosis more likely (see alsothrombophilia) and contribute also to recurrent miscarriage.
serum inhibin B In women, when measured during menstruation, inversely related tothe serum FSH (and probably provides no more information than the day 3 FSH levelin predicting depletion of eggs); in men with azoospermia, levels predict the likelihood ofbeing able to obtain sperm for ICSI at testicular sperm extraction. See also inhibin.
serum LH Measurement of luteinizing hormone in blood serum.Used in monitoring to judgethe occurrence of the LH surge, if GnRH-analogs have not been employed.The resultshould be available within four hours of the test for this purpose.For a diagram showinghow serum LH levels change during the ovarian cycle, see Chapter 3.
serum progesterone Measurement of progesterone in serum.The rise and fall of serumprogesterone in the ovarian cycle is shown in a diagram in Chapter 3: it is low in thefollicular phase, rises with ovulation, and is elevated through the luteal phase, falling priorto menstruation. Often measured to check the occurrence of prior ovulation (see alsopremenstrual endometrial biopsy). Used to infer the onset of ovulation in ovulation induc-tion or assisted conception programs, and attaches extra significance to an apparently raisedserum LH in judging the onset of the LH surge during monitoring.The result should beavailable within four hours for these purposes.Abbreviated as serum P4.
GLOSSARY � 485
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 485

serum prolactin Measurement of prolactin in serum.An increase is called hyperprolactinemia.serum sperm antibodies Estimation of sperm antibodies circulating in the blood.Generally
not as useful as estimating semen sperm antibodies (for men) or cervical mucus sperm anti-bodies (for women), as these fluids have more immediate contact with sperm cells.
serum testosterone Measurement of testosterone, the chief male sex hormone (androgen)circulating in the blood serum. If increased in women with oligomenorrhea or amenor-rhea, indicative of the polycystic ovary syndrome.The free androgen index and free testos-terone are more sensitive tests.
serum tissue transglutaminase antibodies See celiac disease.serum TSH Measurement of thyroid stimulating hormone in serum. See thyroid function tests.serum urea and creatinineA test of kidney function. Sometimes measured when screen-
ing for a kidney (renal) cause of recurrent miscarriages.
sex Sexual intercourse (coitus or having sex) or, gender or relating to it (as in sex chromosome).For more on what positions affect getting pregnant (most don’t!), see orgasm and thebox, Positioning missionaries for sex.
sex chromosome A chromosome that’s either the X-chromosome (a pair confers female-ness in a normal diploid complement of chromosomes) or the Y-chromosome (justone confers maleness in a normal diploid complement of chromosomes); distinct fromthe non-sex chromosomes, or autosomes (which are numbered from 1 to 22); aneuploi-dies give rise to Turner syndrome, Klinefelter syndrome, triple-X syndrome, extra-Y-chromo-some syndrome, etc.); examined in a karyotype.
sex hormone binding globulinThe main carrier protein in the blood for the hormonetestosterone;measured in conjunction with the serum testosterone to derive the free androgenindex.
sex-linked recessive inheritance See recessive inheritance.sexual reproduction Replication of a diploid organism after combination of haploid male
and female gametes, each of which has been produced through the process of meiosis,thus assuring a reassortment of the alleles present among the two parents, in the form
486 � GETTING PREGNANT
Positioning missionaries for sex
There’s much talk about the correct position to adopt for sex when you’re trying toget pregnant.You can forget most of it.The so-called missionary position works, there’sno doubt; but there’s no evidence that many other positions are not just as effective.With equally good credentials is the particularly comfortable one of the woman ontop and able to measure her own response. For each of you to lie on your side withintercourse from the rear can also be very satisfying for your husband,especially whenyou may be too tired to try for full orgasm yourself.All allow deep penetration atejaculation.There are others too. Getting pregnant doesn’t have to be tedious.
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 486

of a new,unique, individual genome. Preserved with in vitro fertilization despite the absenceof sexual intercourse.The opposite to cloning.
short protocolA treatment protocol for controlled stimulation of the ovaries using GnRH-agonists with injections of follicle stimulating hormone (FSH) for induction of superovulationin assisted conception programs that involves starting the GnRH-agonist a day ortwo before the injections of FSH start.The advantage is one of cost: less FSH (andless GnRH-agonist) are used compared with the long protocol.The disadvantage isthat luteinizing hormone levels and progesterone levels can rise, possibly (in some cycles oftreatment) spoiling optimal development of ovarian follicles.The GnRH-agonist iscontinued (in contrast to the ultrashort protocol) until follicles are mature and humanchorionic gonadotropin is given to start the process of ovulation.The details are in the box,The long, short and ultrashort of GnRH-agonists, in Chapter 20.
Simms-Huhner test See postcoital test.small bowelThe small intestine, leading out of the stomach; narrower but longer than the
large intestine (or colon), to which it connects. See also bowel.small-for-dates A general term used by obstetricians or pediatricians to refer to a fetus or
newborn baby that seems smaller than it should be for the assumed duration of thepregnancy so far.The three main causes are a genetic abnormality of the fetus; insuffi-cient nutrition for an otherwise normal fetus; and an incorrect calculation of the dates,maybe because ovulation and conception took place later than the usual two weeks afterthe last menstrual period. Recent research shows that women with infertility might be athigher risk of small-for-dates babies when they do get pregnant.
SMI See sperm microinjection.somatic cell Any cell that forms the tissues and organs of the body that is not a germ cell.
Derived from soma, the Greek for ‘body’.somatic cell nuclear transfer (SCNT) Transfer of the nucleus of a somatic cell into a second-
ary oocyte or zygote from which the chromosomes have been removed, in such a way thatcleavage still occurs, in effect causing the cell’s nucleus to ‘bud’, or reproduce withoutgenetic recombination, and hence a form of asexual reproduction or cloning; nowcommonly used for reproductive cloning in animals and, it is hoped, for therapeutic cloningto create embryonic stem cells for treatment of serious degenerative disease and cancers.
spastic colon syndrome See irritable bowel syndrome.sperm Common abbreviation for spermatozoon (or for the plural form spermatozoa).
Also used in the form sperm cell. For more on immature sperm cells, start with sper-matid. See also sperm count. Plural: sperm or spermatozoa.
sperm antibodiesThe result of a reaction of the immune system against sperm cells (sper-matozoa) and, by limiting the ability of sperm to show motility, a contributory (or occa-sionally the only) cause of infertility.Can be present in serum (see serum sperm antibodies),in cervical mucus or in semen. Can be agglutinating (which make sperm stick in clumps),immobilizing (which cripple sperm particularly effectively and kill them) or coating,which interfere with sperm attachment to the zona pellucida of the egg (the secondaryoocyte), preventing fertilization. The screening test for sperm antibodies involvesimmunobeads.To learn how virgins can develop antibodies to sperm, see Chapter 10.
GLOSSARY � 487
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 487

sperm chromatin structure assay (SCSA) A measurement of the proportion of spermcells that have damaged DNA. Fewer than 15 percent is consistent with normal fertil-ity; 15–30 percent can result in subfertility; and more than 30 percent may cause steril-ity or recurrent miscarriage.
sperm count A semen analysis, measuring the volume of the ejaculate, the density ofspermatozoa (‘sperm cells’, or just ‘sperm’) in it (expressed as so many million spermper milliliter), the proportion of sperm swimming normally (the motility), and the pro-portion with a normal shape.A normal sperm count consists of a volume of morethan 1 ml; a density of more than 20 million per ml; a motility of more than 50 percent;and normal forms of more than 50 percent (casual examination) or more than14 percent (critical examination by the strict criteria recently advocated by theWorld Health Organization). For the effects of frequent sex on sperm counts (aswell as other aspects of collecting semen for the test), see Chapter 5. For more onthe question of a possible worldwide decline in sperm counts over the last genera-tion, see Chapter 10.
sperm microinjection Either intracytoplasmic sperm insertion (ICSI) or subzonal insertion(SUZI,now obsolete). (Abbreviated SMI, although this is no longer in common usage.)
sperm wash See capacitation.spermatid The product of the spermatocyte in the testis when it has completed meiosis (by
which the number of chromosomes is halved, so it’s in the haploid state), and alsoenclosed in the testicular tubules by the Sertoli cells. Early spermatids are round-shaped,whereas late spermatids closely resemble mature spermatozoa. See also spermiogenesis.
spermatocyte The sperm cell equivalent to the oocyte stage of the egg. See also primaryspermatocyte, secondary spermatocyte and spermatogenesis. Further development in the testic-ular tubules results in a spermatid.
spermatogenesis Development of a sperm cell in the tubules of the testes (the testiculartubules), from spermatogonium and spermatocyte to spermatozoon (the last part of this process,from spermatid to spermatozoon, is called spermiogenesis).The process of spermatogen-esis takes 56 days.At any one location in a tubule there are cells at four different stagesof maturity (see Chapter 3), so mature sperm are released from a particular locationinto the lumen of the testicular tubules every 14 days.A systematic interruption of sper-matogenesis results in azoospermia and is called maturation arrest.
spermatogonium The replicating phase of the sperm cell in the testis, equivalent to theoogonium in the ovaries, but, unlike the oogonia, spermatogonia normally persist untilold age. Located among the supporting cells (Sertoli cells) in the testicular tubules.Dividesby the process of mitosis until it begins to undergo meiosis by changing into the primaryspermatocyte, the first step in the process of sperm cell formation, or spermatogenesis.Plural: spermatogonia.
spermatozoonThe final stage of development of the maturing sperm cell, as it leaves thetubules of the testis (the testicular tubules), to mature in the epididymis. Composed of ahead (including the acrosome), a midpiece loaded with mitochondria to provide energy, anda tail, or flagellum (see also cilium), for propulsion. Packed into the head of the sperma-tozoon is a haploid number of chromosomes (there are normally 23, including either an
488 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 488

X-chromosome or a Y-chromosome). See also sperm count and fertilization. Plural:spermatozoa.
spermiogenesisThe final part of the formation of a mature sperm cell, in which the round,early spermatid (already with a haploid number of chromosomes) loses its round shapeto acquire the features of the mature, elongated spermatozoon. Contrast with spermato-genesis, which encompasses spermiogenesis as it’s completed.
Spinnbarkheit One of the measurable qualities of cervical mucus that indicates receptive-ness to sperm. German for ‘ability to be spun’, meaning stretchability.
spontaneous abortion See miscarriage.statistical significance A point at which statistics indicate that a set of measurements or
observations does not just actually differ from normal (that is, it’s abnormal) or from acontrol group, but that the observed difference is unlikely (typically less than a one in 20risk) to have come about just by the effects of chance. (We then say that there is aP-value—for Probability—of less than 0.05,which is what one in 20 is when expressedas a proportion.) Note: One logical follow-on from this is that if you study 20 differentvariables for such statistical significance the odds are that one will have a P-value less than0.05, just by the expectations of chance! In practice,when multiple observations like thisare being made, statisticians will put a tougher criterion on what is ‘statistically signifi-cant’, such as P less than 0.02 or 0.01. For academic legitimacy, P-values should be setbefore looking at the data,not afterward.For more, see the box, ‘Significant’ or ‘important’?.
statistics (As in ‘lies’, ‘damned lies’ and ‘statistics’.) The science—and art—of using arith-metic and probability theory to work out how likely it is that an association betweensets of measurements or between sets of observations has happened by chance alone.See also statistical significance.
STDs Sexually transmitted diseases, such as gonorrhea, chlamydia and HIV.stem cell A relatively undifferentiated cell in any tissue responsible for replenishing cells
lost from that tissue through normal wear and tear, in the case of adult stem cells, orresponsible for virtually all of a fetus’s cells, in the case of embryonic stem cells; char-acterized by being able to replicate (through mitosis) seemingly for ever, either in thebody or in tissue culture, without wearing out the ends of the chromosomes. Embryonicstem cells are controversial because they are derived from human embryos, sometimesby the process of somatic cell nuclear transfer,which involves creating embryos or embryo-like forms of a kind that could be used for reproductive cloning.The word stem comes fromanalogy with the stem of a plant giving rise to branches and further branches, repre-senting the ever-increasing number of different paths a stem cell can differentiate into.
sterility The state of absolute infertility or complete infertility, with no chance of gettingpregnant without special help.Causes include azoospermia, anovulation (especially primaryovarian failure) and blocked fallopian tubes. (Although words like sterility and sterile soundinsensitive, especially for a book like ours, it’s important in medicine to avoid ambigu-ity; see the box, Medical vocabulary—sensitive, precise and correct?, for a discussion of themedical author’s dilemma.)
sterilization An operation designed to induce sterility. In men, usually carried out byremoving small segments of each vas deferens (vasectomy); in women, usually carried out
GLOSSARY � 489
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 489

490 � GETTING PREGNANT
‘Significant’ or ‘important’?
In considering statistical significance, we conventionally regard a one in 20 chance ofan association as being safe enough not to be just a coincidence.This represents aP-value, or probability estimate, of 0.05 or less, which is represented as P < 0.05.More conservative cut-offs (e.g. P < 0.02, or 1 in 50; or P < 0.01, or 1 in 100) needto be used: (1) if the data accumulating as a research study continues are examinedmore than once, rather than just at the end of the study; and (2) if more than oneassociation is being looked for at the same time.
For example, among the babies born from IVF in its earlier days, the frequencyof birth defects of the neural tube type (such as spina bifida) appeared to be increased(and cleft lip or palate appeared to be significantly decreased), but it was only becausemore than 100 individual birth defects were looked at, several of which you mightthen expect to have a one in 100 chance of being too high or too low; with morebabies born, the numbers slipped into statistical insignificance.
Showing that there is a statistically significant ‘association’ between one obser-vation and another does not of itself imply ‘cause’ and ‘effect’.The two observationsmay both be effects, with a yet-to-be-looked-for shared cause.
For a further example, there’s a statistical association between smoking and sal-pingitis (inflammation of the fallopian tubes), but no-one believes that one is thecause of the other.
In another example, we know that IVF is statistically associated with pre-termbirth (even when the effects of multiple births are excluded—see Chapter 20), butwe do not know that IVF causes premature birth: there can be a common reason forthe prematurity and for the need to employ IVF (various hypotheses, including pelvicadhesions or poor sperm, are under investigation).
The size of the statistical significance is quite different from the size of thedemonstrated difference (a large sample size can make even the most trivial differ-ence statistically significant at P < 0.01), although generally it’s easier to show signif-icance for a smallish sample if the difference itself is sizeable! Conversely, failing toshow a statistically significant difference is not the same as saying that there is nodifference: the size of the sample may just have been too small to draw a safe conclu-sion either way.
For other reasons too,‘statistical significance’ is not the same as ‘medical impor-tance’.Tall people might bump their heads significantly more often than short people,but that does not necessarily mean that tall people should wear crash helmets—letalone that wearing crash helmets should for this reason become a matter of publicpolicy (which we might distinguish as ‘administrative importance’).
In setting our clinical policies at Sydney IVF, we take more account of medicalimportance than statistical significance of certain outcomes, so that satisfying aprobability level of one in five (P < 0.2) is often enough for us to change our clinical
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 490

by removing, clipping or otherwise destroying a small segment of each fallopian tube,preferably close to the uterus (often called tubal ligation). See also fimbriectomy.
sterilization reversal An operation involving microsurgery to rejoin the healthy ends ofthe fallopian tubes or vasa deferentia to reverse the effects of a previous sterilization oper-ation. See also tubal anastomosis and vasovasostomy.
strict criteria See sperm count.subclinical miscarriage An early miscarriage, usually within a week or two of the period
that had been expected.Traditionally, one in which no curettage was needed; these daysa subclinical miscarriage is one that has not resulted in a gestational sac visible on trans-vaginal ultrasound.
subfertility Infertility that is not ‘absolute’ or ‘complete’ infertility (that is, there is a chanceof pregnancy; nor is it sterility; these last three terms are synonyms), but the chanceof getting pregnant each month (fecundability or monthly fertility) is reduced. Moreor less definite causes can include oligospermia, polycystic ovary syndrome and othercauses of oligomenorrhea, endometriosis, peritubal adhesions, fibroids (especially submucousfibroids) and increased age, especially of the woman. Subfertility is the subject ofChapter 7. See also cumulative chance of pregnancy and K-selection. Synonymous withrelative infertility.
submucous fibroid A fibroid (or myoma) that grows from the wall of the uterus inwardsto distort the endometrial cavity. Can be a cause of menorrhagia (heavy periods), inter-menstrual bleeding, premenstrual spotting, infertility and miscarriage. See also myomectomy.
submucous myoma See submucous fibroid.subseptate uterus See uterine septum.subserous fibroid A fibroid (or myoma) that grows from the outside surface of the uterus
into the cavity of the abdomen,or peritoneal cavity.The least likely of any sort of fibroidto affect reproduction, but can cause symptoms of pressure or pain should it twist ordegenerate suddenly. See also myomectomy.
subserous myoma See subserous fibroid.subzonal insertion (SUZI) An obsolete IVF technique involving sperm microinjection,
in which one or more sperm are injected through the zona pellucida into the periv-itelline space of the egg (the secondary oocyte). Not very effective, because its efficiencyis limited by sperm having to have undergone the acrosome reaction. Nowadayscompletely replaced by intracytoplasmic sperm insertion (ICSI), where the acrosomereaction is not a requirement.
suffering The prevention and alleviation of personal suffering by a patient is the physi-
laboratory practices (the different outcome thus becomes administratively impor-tant) if intuitively the change makes sense or if other effects from making the changeare likely to be trivial.
For these reasons, as medical writers who are proud of precision, we avoid theuse of the word ‘significant’ outside a statistical sense,when the word ‘important’willserve our purpose better.
GLOSSARY � 491
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 491

cian’s ultimate duty and the principal purpose of the professional practice of medicine.The suffering can be physical or mental.The ethical values of beneficence,non-maleficence,justice and equity, for many thoughtful physicians, become subordinate to the duty ofmaking the patient better. For the infertile couple, prevention or relief of suffering mostobviously means the physician helping them to have a baby; this is not always possible,however, in which case other medical and personal strategies need to be explored ifthe suffering is to be lessened.These themes are developed in Chapters 25 and 26.
superovulation Intentional induction of multiple ovulations at once, using injections offollicle stimulating hormone and human chorionic gonadotropin, for assisted conception. Inevitablythere is a risk of multiple pregnancy unless egg retrieval is performed. See also ovulationinduction, ovarian hyperstimulation syndrome (OHSS) and follicular recruitment (specifically,late or cyclical follicular recruitment).
Suprefact See buserilin.surrogate ‘A person who acts for or takes the place of another’ [Oxford English Dictionary].
In reproductive medicine, a woman who has a baby on another woman’s behalf. Seealso gestational surrogacy, traditional surrogacy and collaborative reproduction.
SUZI See subzonal insertion.sympathy See empathy for a discussion of its place in the range of feelings one person can
have for another.Synarel A GnRH-agonist, made by Syntex.Administered as a nasal spray.syncytiotrophoblast The component of the trophoblast bathed by maternal blood in the
placenta (and thus covering the chorionic villi). Derived by differentiation and fusion ofcytotrophoblast cells, so the syncytiotrophoblast only ever comprises just one cell (albeitwith very many cell nuclei), through which almost everything reaching or leaving theembryo or fetus must pass. By the end of normal pregnancy, its area is about 12 squaremeters, or over 100 square feet.Most hormones and proteins produced by the placenta,such as progesterone, hCG and PAPP-A, come from it. See also lacunae.
syngamy If fertilization is the ‘marriage’ between egg and sperm then syngamy is its‘consummation’, as the male and female pronuclei come together for the respectivehaploid sets of chromosomes to combine into a diploid set.An event of legislative impor-tance in the conservative Australian state of Victoria, after which permission for embryoresearch becomes much harder to obtain, whatever the views of the couple concernedor an ethics committee might be.
syphilis See serological test for syphilis.T cells White blood cells or lymphocytes that are part of the immune system concerned
with recognizing and dealing with foreign or abnormal cells discovered in the body’stissues. See also NK cells.
take-home baby rateThe percentage of treatment months (or treatment cycles in assistedconception) that result in the woman taking home one or more babies (twins are notcounted separately, though!); the statistic of most interest to patients and, in an age ofskepticism in the community, the most politically correct statistic for reproductivemedicine clinics to quote, but it’s less useful for clinics’ quality control purposes thanthe conception rate, the implantation rate, and the viable pregnancy rate, because: (1) it
492 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 492

excludes obstetric misadventures often beyond the control of the infertility clinic; and(2) there is a long lag before it can be calculated, making results at best about ninemonths old.
teleological ethics A set of ethical beliefs based on the goodness or badness of conse-quences, whether actual, intended or predicted. For purposes here, restricted to conse-quences to individuals, in contrast to utilitarian ethics. Open to change according toempirical observation of outcomes (hence ‘evidence based ethics’). For practical applica-tion, and a contrast to deontological ethics and utilitarian ethics, read the box, Ethics: Moralimperatives, outcomes and equity, in Chapter 26.
teratozoospermia See oligospermia.tertiary follicle The third stage of growth of the follicle, in which the egg is enclosed by
a thick layer of round-shaped follicle cells among which an antrum, or fluid-filled space,has formed; this antrum will come to dominate the size of the follicle.The first stageof the follicle visible with transvaginal ultrasound (when it reaches about 4 mm indiameter). Further growth of the early tertiary follicle is determined by follicle stimulat-ing hormone. Synonym: antral follicle.
TESE See testicular sperm extraction.TEST See tubal embryo-stage transfer.testicle Diminutive of testis: the terms are interchangeable.testicular biopsy A biopsy of the testis to work out the reason behind an absence of sperm
cells (azoospermia).Also used for testicular sperm extraction (TESE).testicular feminization A state of intersex in which the karyotype is male (46,XY), the
gonads are testes (hence also male), but the body is completely unresponsive to testos-terone and to its metabolite dihydrotestosterone, so it develops in the female way, with anormal vulva and vagina apparent at birth, and with normal development of the breastsat puberty. Because the testes still secrete anti-Müllerian hormone, there’s no uterus.Invariably these children are raised as girls, normal except for their primary amenorrheaand their infertility. Specialist medical supervision is needed,because there is an increasedrisk of cancer in the abnormal gonads. Synonymous with androgen insensitivitysyndrome (complete form).
testicular sperm extraction Dissection into the testis itself, in men with azoospermia dueto maturation arrest, to recover (by ‘teasing out’) immature sperm cells from the (often small)fraction of testicular tubules there which still contain such cells.The sperm cells are usedfor in vitro fertilization using intracytoplasmic sperm insertion (ICSI).Abbreviated as TESE.
testicular tubules The main constituent of the testis, lined by Sertoli cells and containingthe developing sperm cells. Lying between the tubules are the interstitial or Leydig cells.See also spermatogenesis.
testis The male gonad, located normally in the scrotum. Produces the hormone testosteroneas well as the male germ cells, or spermatozoa. Interchangeable with testicle. Plural: testes.
testosterone The main male sex hormone, or androgen, in the blood (where it is measuredas serum testosterone). Secreted in large amounts by the testis in a man. Before it acts onthe tissues it must be converted to dihydrotestosterone. Present also in women, beingconverted from the weaker androgen androstenedione.
GLOSSARY � 493
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 493

tests for tubal patency Tests that check whether the fallopian tubes are open, usually bypassing fluid through the cervix to fill the endometrial cavity and then demonstrate itcoming out the ends of the tubes.The two common tests are to pass a blue dye atlaparoscopy or a solution opaque to x-rays, namely a hysterosalpingogram. Once upon atime, carbon dioxide gas was used and listened for with a stethoscope (Rubin’s test); ahigh-tech version of Rubin’s test uses transvaginal ultrasound to show the gas. See alsofalloposcopy.The treatment of tubes shown to be obstructed on patency testing withmicrosurgery is detailed in Chapter 13.
494 � GETTING PREGNANT
Medical vocabulary—sensitive, precise and correct?
Innocent messengers can be shot for the message they deliver! Experienced and wisemessengers learn to give their message with discretion. Doctors, like other profes-sionals, sometimes have to deliver bad news.The judgment a doctor uses in his orher choice of vocabulary will affect how the information that’s there to be conveyedis received.This is part of the art of medicine: the adept doctor draws on a substan-tial vocabulary to match the message to the needs and receptiveness of the patientat the moment of the consultation, taking continuing account of how it’s beingunderstood.This flexibility is not as open to the author,who anticipates a wider andmore remote audience—a readership with a wide range of interests, experience,education and emotional states.
To soften an unwelcome message the language is sometimes softened.This canhappen systematically (being deaf becomes being ‘hearing impaired’), but in time,as the new vocabulary takes over, the realities of the message re-surface and there’sthe same temptation to come up with another substitute. Because this process canbe at a different stage for different people in different places and at different times,the vocabulary of a book can never be right for (or be to the taste of) every reader.So, however careful I am with vocabulary, I know I will never please everybody.
My priority is to be unambiguous. I take Mark Twain’s advice to find the factsfirst and then, at leisure, to rationalize them later. So I’m concerned in a book likethis to deliver a precise message first, and second to try to anticipate your responseto it. Having said this, many doctors will use vocabulary among themselves thatthey would not (or ought not) use with patients: habitual abortion is seen morecommonly in the medical literature than its kinder and no less precise synonym,recurrent miscarriages. Many stark descriptions come to us from a previous era—atime of less communication between doctors and patients than we expect today.But as medical language comes to be shared more with lay readers, doctors have tomodify their discussions.We do not want to exclude everyone without a medicaleducation, yet above all we should aim to remain exact.On the one hand this meansavoiding medical jargon; on the other hand it means avoiding oversensitivity if itjeopardizes clarity.
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 494

theca interna A layer of cells in the ovary lying immediately around the follicle; under theinfluence of luteinizing hormone it’s responsible for producing the weak male sex hormoneandrostenedione, which is then (1) converted by the follicle cells (the granulosa cells) intoestrogen, principally estradiol, or (2) converted by other tissues outside the ovary to testos-terone.
thecal cells Cells that make up, or come from, the theca interna.therapeutic cloningThe use of somatic cell nuclear transfer to produce embryonic stem cells
suitable for differentiation into tissues that are a perfect match to treat disease in theperson who provided the cell nucleus used. Ethically controversial.
threatened miscarriage (TMC) Traditionally, any bleeding from the uterus during preg-nancy while the cervix is (still) closed.Today, as well, there would need to be a normalembryo and, a little later, normal fetal heart movement pattern on transvaginal ultrasoundto separate it from an inevitable miscarriage.
three-dimensional ultrasound A computer-enhanced transvaginal ultrasound or a multi-probe abdominal ultrasound that produces a composite, constructed three-dimensionalimage of the uterus, which can then be viewed from any perspective. Excellent fordisplaying the form of the uterus in the investigation of uterine anomalies and recurrentmiscarriages.
thrombin An enzyme present in the blood that, when activated by tissue injury, causesblood to clot. See also coagulation system and fibrinogen.
thrombophilia An increase in the tendency of the blood to clot, as in ‘thrombosis’. Inprimitive, evolutionary times, a survival advantage for women giving birth, when lossof blood would on average be less, but exacting a price in terms of increased risk ofstroke or venous thrombosis.The thrombophilias are implicated in disturbances of preg-nancy, including recurrent miscarriage and stillbirth.
thyroid function tests (TFTs) Usually two tests: a serum thyroxine (low for underactiv-ity, high for overactivity) and a serum thyroid stimulating hormone (TSH,high for under-activity based primarily in the thyroid gland, low for overactivity based primarily inthe thyroid gland and low for underactivity based in the pituitary gland).As a screeningtest for malfunction of the thyroid gland a serum TSH will generally be enough.
thyroid stimulating hormone (TSH) A hormone produced by the adenohypophysis (thefront, glandular part of the pituitary gland) that switches on the thyroid gland, causingit to make and release thyroxine. See also thyroid function tests.
thyroxineThe main hormone of the thyroid gland, responsible for controlling the rate ofmetabolism in the body; activity of the thyroid gland is measured with thyroid functiontests.
time left for conception One of the two most important variables that determine thechance of still getting pregnant naturally in subfertility and unexplained infertility (theother is duration of infertility).The longer the time still available the better the chancethat, sooner or later, pregnancy will happen. Broadly limited by the female partner’sage, but personal circumstances and ambitions within the biologically available time-frame might shorten it, leading to a decision to seek treatment with assisted conception.Explained in Appendix 1. See also fecundability.
GLOSSARY � 495
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 495

time to pregnancy An estimate of likely fertility in secondary infertility, where the time ittook to get pregnant the first time is used as a very approximate guide to what mightbe expected next time round. Of limited usefulness, but if it took a long time to getpregnant the first time it will typically take at least as long the next time.Achieving apregnancy does not usually itself permanently cure subfertility.
TMC Abbreviation for threatened miscarriage.torsionTwisting of an organ on its vascular pedicle, risking necrosis.Can happen to the testis
in boys, especially after an injury to the scrotum,or to the ovary and fallopian tube, eitherspontaneously during adolescence or when enlargement from superovulation hasproduced ovarian hyperstimulation syndrome (OHSS), as described in the box, Twistedovaries, in Chapter 12.An operation to untwist it can save the affected organ, if carriedout quickly enough.
totipotent See pre-embryo.traditional surrogacy Surrogacy in which the woman who is the surrogate for the intended
pregnancy provides the eggs (through her own ovulation); is impregnated by assisted insemi-nation; carries (or ‘gestates’) the pregnancy; gives birth; and then gives up the baby tothe person who commissioned the surrogacy arrangement.Also known as genetic-plus-gestational surrogacy.The surrogate is as much the biological mother of the childas if she had conceived in natural circumstances, except that the male by whom she hasbeen impregnated has no prior social relationship with her. No countries other than theUSA,where commercial surrogacy can be legal,have encouraged the practice,whether foraltruistic or commercial reasons. For tribal society and biblical precedents, see Chapter 23.
transsexual An individual with a gender identity opposite to that conventionally associatedwith his or her biological sex.Not to be confused with intersex or with sexual preference.
transsexualism See transsexual.transvaginal ultrasound Ultrasound imaging of the pelvic organs for diagnosing abnor-
malities of (particularly) the uterus and the ovaries; for monitoring the development ofovarian follicles with ovulation induction and assisted conception programs; and for follow-ing the course of early pregnancy.Among the pioneers were Dr Karl Popp, who useda mechanical sector scanner vaginally in Hamburg in 1984, and Dr John Anderson,who used the first vaginal linear array scanner at Sydney IVF in 1985, leading to itswidespread use subsequently in Australia and the USA.
trial wash See sperm wash.Tridomose See gestrinone.trimester Literally, a three-month period of time; so the nine months of pregnancy are
divided into the first, second and third trimesters. Most miscarriages take place inthe first trimester (up to 12 or 13 weeks). Pregnancies that reach the third trimester(beyond 27 weeks) have an increasingly good chance of being viable (though nowadays,with intensive care, survival has occurred from about 24 weeks).
triple screen See triple test.triple testA screen for congenital abnormalities of the fetus done on the mother’s blood serum
during pregnancy to look for fetal trisomy, including Down syndrome.The original testcomprised measurements of: (1) serum alpha fetoprotein (decreased in the trisomies); (2)
496 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 496

serum hCG (increased in trisomy 21, decreased in trisomy 18); and (3) serum estriol(decreased in trisomy 21, increased in trisomy 18). Note that only 60 percent of preg-nancies with Down syndrome will be revealed by a triple test.Refinements have takenplace, with ‘free beta’ (part of the hCG molecule) replacing hCG itself, and with theaddition of PAPP-A replacing estriol, increasing the sensitivity and specificity of thetest. Further gains in sensitivity and specificity comes from adding an ultrasound testfor nuchal translucency. Even so, false positive tests are possible,which will be resolved onlyby performing CVS or amniocentesis, and so also are false negative tests,which means thatCVS and amniocentesis should still be considered in otherwise high-risk situations.
triple-X syndrome A trisomy with a karyotype of 47,XXX—a female with an extraX-chromosome.The old description of ‘super female’ is misleading, because fertility, ifaffected, is most likely reduced; primary ovarian failure is more common than with anormal chromosome complement and premature menopause then follows.
triploid A state of 69 chromosomes, or three times the haploid number, most commonlycaused by fertilization of the egg with two sperm; the embryo that results can develop asfar as a fetus, but is doomed to miscarry.The trophoblast of the placenta often undergoesthe partial changes of a hydatidiform mole.The noun form for this adjective is triploidy(the state of being triploid).
triptorelin A GnRH-agonist marketed by Ipsen Biotech as Decapeptyl.trisomy An abnormality of the chromosome complement in which there is an extra chro-
mosome seen on the karyotype.The extra chromosome can be an autosome, such as inDown syndrome (trisomy 21), or a sex chromosome, such as triple-X syndrome (47,XXX),Klinefelter syndrome (47,XXY) and extra-Y-chromosome syndrome (47,XYY).
trisomy 21 A trisomy for chromosome number 21, or an extra chromosome-21.This is themost common of the trisomies and gives rise to Down syndrome. Research has shownthat the commonest source of the extra chromosome is a mistake in the first divisionof meiosis in the egg cell (during the many years it rests as a primary oocyte).
trophectoderm Group of cells that differentiates around the periphery of the developingembryo when it is a blastocyst and which will, if all goes well after implantation, form theplacenta and membranes. See also inner cell mass and trophoblast.
trophoblast As the cells of the early embryo specialize, they soon differentiate into: (1)central ones that will form the embryo or fetus itself; and (2) peripheral ones (thetrophoblast) that will be responsible for invading the mother’s tissues (see implantation)and will form the placenta and the membranes. See also cytotrophoblast, syncytiotrophoblastand extravillous trophoblast.
true hermaphrodism Intersex when tissue typical of an ovary and a testis is found in theone person.The genital organs can appear to be normal female, normal male, or some-where in between. Intersex states where there are either normal ovaries or normal testes(but not both) are sometimes called pseudohermaphrodism.
truthA self-evident ethical principle,which has value provided no substantial harm is done;not to be dispensed with for expediency alone.
tubal abortion A tubal ectopic pregnancy that is in the process of being expelled out thefimbrial end of the fallopian tube.
GLOSSARY � 497
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 497

tubal anastomosis Microsurgery of the fallopian tubes in which an area of blockage is cutout and the healthy bits of tube on each side of the blockage are sewn back together.Can be done for localised salpingitis, including salpingitis isthmica nodosa, and for sterili-zation reversal.The operation is described in Chapter 13.
tubal canalization Overcoming a localized obstruction of the isthmus or the interstitialsegment of the fallopian tube by pushing a wire or a catheter through it, enabling (in somecases) the tube to be ‘re-canalized’ and so to remain open after being blocked before;it’s an attractive alternative to tubal anastomosis and can be performed either during theinvestigation of tubal infertility with hysteroscopy, laparoscopy and falloposcopy or at the timeof carrying out a hysterosalpingogram (see selective salpingography. Because not all tubesthat seem to be blocked are in fact blocked (sometimes a normal tube will not allowfluid to pass through it for hormonal reasons or because of a spasm), care needs to betaken to investigate the tube properly before canalization is undertaken.
tubal embryo-stage transfer (TEST) A variation of zygote intrafallopian transfer (ZIFT)in which, usually a day after when ZIFT (or PROST) would be carried out, cleavingembryos (at a two-cell to four-cell stage) are transferred to the fallopian tube as part of anin vitro fertilization program.
tubal ligationA sterilization operation in a woman involving interruption of the fallopian tubes.tubal patency See tests for tubal patency.tubal pregnancyAn ectopic pregnancy located in the fallopian tube;most occur in the ampulla,
but others can be located in the narrower isthmus or in the interstitial segment (see inter-stitial pregnancy).
tubule For those of the testis, see testicular tubules.Turner syndrome The combination of primary ovarian failure with constitutional (that is,
genetically determined) shortness; often with other clinical abnormalities, including‘webbing’of the neck; an increased ‘carrying angle’ at the elbow; short fourth metatarsal(foot) and metacarpal (hand) bones (the bone within the hand that leads to the ringfinger), and sometimes abnormalities of the heart and the thyroid gland.Associated witha karyotype that is 45,X (a monosomy, with one sex chromosome missing) or with partialloss (‘deletion’) of one of a pair of X-chromosomes.The single X-chromosome presentcan come from the mother or the father—and, interestingly, it behaves differently: if itcomes from the mother the girl is likely to be rather socially disruptive (the way littleboys often are), whereas if the X-chromosome comes from the father her behaviortends to be closer to that of most other girls!
ultrashort protocol A variation of the short protocol for using GnRH-agonists with injec-tions of follicle stimulating hormone (FSH) for controlled induction of superovulation inassisted conception programs.The GnRH-agonist is started with menstruation, a day ortwo before the injections of FSH start, and is discontinued after about five days fromstarting it (that is, often a week or more before ovulation).There are no special advan-tages, whereas there’s a potential disadvantage: a much more thorough suppression ofthe woman’s own luteinizing hormone (and maybe FSH) than if the GnRH-agonist iscontinued, potentially causing stimulated follicles to ‘run out of puff ’ before they arefully mature.The details are in the box, The long, short and ultrashort of GnRH-agonists,
498 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 498

in Chapter 20.The ultrashort protocol should not be used with pure forms of FSH,such as Fertinex,Gonal-F,Metrodin HP or Puregon, or poor egg quality will result if someluteinizing hormone is not administered.
ultrasound An imaging procedure like radar, but using high frequency sound waves; usedfor diagnosis (and, by physical therapists, in a different energy band, for treatment). Seealso transvaginal ultrasound.
unexplained infertility Infertility for which no obvious cause has been found after the follow-ing tests have been done with normal results: a sperm count or postcoital test; a test of ovula-tion, such as a serum progesterone that is satisfactorily high;and a laparoscopy (used to show thatthe tubes are open and that there is no endometriosis or other obvious abnormality).Althougha hysterosalpingogram (HSG) can substitute for laparoscopy in excluding blockage of thefallopian tubes,an HSG can miss peritubal adhesions and will miss endometriosis.Infertility shouldnot be considered unexplained unless a thorough, careful laparoscopy has been done.
unicornuate uterusA uterine anomaly that comes about when the uterus forms (in the embryo)from just one Müllerian duct; the uterus will be a little smaller than normal (making amiscarriage or premature labor more likely), and will be connected by a fallopian tube to justone ovary, contributing slightly to infertility (since,on average,only half of ovulations havea chance of resulting in pregnancy—see the box, One ovary can be okay … , in Chapter13). Reproduction, however, can be normal, and a woman might go through life with aunicornuate uterus and not know it.Diagnosed by hysteroscopy and laparoscopy,by hysteros-alpingogram or, particularly effectively, by three-dimensional ultrasound.There is more abutthis anomaly, including a diagram, in Chapter 18. Often there is a simultaneous abnor-mality of the kidneys, such as one kidney instead of two,diagnosable by abdominal ultra-sound or, more specifically, by a special kidney x-ray study called an intravenous pyelogram.
urinary LH-kitA home test for ovulation in which the urine is tested for luteinizing hormone.If the urine shows a positive test, ovulation will usually take place within 24 to 36 hours.Electronic devices that perform the same function are available (and are increasinglypopular in the UK). For more on making the most of your natural chances of gettingpregnant, read Chapter 19.
urofollitropin Generic name for FSH derived from the urine of menopausal womensources. See urinary menopausal gonadotropin, Fertinex, Humegon, Menogon and Metrodin.FSH of recombinant (synthetic) origin is called follitropin.
uterine anomalyAbnormality of the shape of the uterus a woman is born with (it is congen-ital); some uterine anomalies tend to cause recurrent miscarriages, premature labor or breechbirths; discussed in Chapter 18.
uterine curettage See curettage and vacuum curettage.uterine septumA septum or wall separating the cavity of the uterus into two halves; a cause
of recurrent miscarriages.uterusThe womb, in which pregnancy is gestated from the time of implantation of the embryo
until delivery or miscarriage; formed from the joining of the two Müllerian ducts (in theabsence of anti-Müllerian hormone); composed of the main,upper part (the uterine fundus)and a lower neck, or cervix, which connects it to the upper part of the vagina; most ofits wall is made of muscle tissue (the myometrium), but with an inner lining of glands
GLOSSARY � 499
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 499

(the endometrium) and, on the outer surface, a thin covering of uterine serosa. Best seenon transvaginal ultrasound, especially a three-dimensional ultrasound; its cavity is best displayedwith a hysterosalpingogram (or, strictly, a hysterogram).
utilitarian ethicsA set of ethical beliefs based on maximizing good for the greatest numberof people.For modern purposes, similar to teleological ethics (that is, consequential consid-erations) but with a community-wide reference instead of a context of individualpriority.Nowadays concerned with the equitable and consistent distribution of restrictedpublic resources. Open to change according to the systematic assessment of outcomes(and hence ‘evidence based’). For practical application, and a contrast to deontologicalethics and teleological ethics, read the box, Ethics: Moral imperatives, outcomes and equity, inChapter 26. Refer also to evidence based ethics.
vacuum curettage Curettage in which the contents of the early pregnant uterus are suckedout using a soft plastic catheter. Used in the treatment of miscarriage, in the treatmentof hydatidiform mole and to induce abortion.
vaginosis Colonization of the vagina with organisms that reduce the normally presentbacterium Lactobacillus, responsible for the vagina’s healthy acidity; there might be nosymptoms or there can be a vaginal discharge; the commonest offender is the bacteriumGardnerella vaginalis (also called Hemophilus vaginalis), which responds to the anti-biotics metronidazole (Flagyl) and clindamycin; if untreated by the end of the firsttrimester of pregnancy there is an increased risk of late miscarriage or premature labor.
value judgment A philosophical device for moving from what is to what ought. It bridgeswhat philosophers call the naturalistic fallacy—but not with the approval of some careerphilosophers.
values See ethics.varicocele A varicose vein in the scrotum, which in some cases can increase the temper-
ature of the testis, causing oligospermia; more common on the left side than on the right(because the left testicular vein is longer and more likely to have incompetent valves).One of the few treatable causes of male infertility (the treatment is to tie off the vein),although not all sperm counts improve.There’s more on varicocele, underwear designand avoiding saunas in Chapter 10.
vas deferensThe long duct that transports sperm cells (spermatozoa) from the epididymis to theseminal vesicles.Can be missing from birth (congenital absence of the vasa deferentia) or blockedas a result of infection or intentional interruption (vasectomy). Plural: vasa deferentia.
vascular endothelial growth factor (VEGF) A growth factor (or local hormone) neededfor new blood vessels to form in, for example, the corpus luteum, as it turns into an effi-cient hormone-producing gland making and releasing progesterone about a week afterovulation. Because such new blood vessels are rather leaky, excess VEGF from multiplecorpora lutea during ovulation induction or superovulation using gonadotropins can beassociated with new blood vessels trying to form in the general peritoneal cavity, leakageof fluid from which causes fluid to build up in the abdomen—a potentially dangerouscondition known as the ovarian hyperstimulation syndrome.VEGF is also important in theformation of the placenta, so mutations of VEGF or its target proteins can cause recurrentmiscarriage.
500 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 500

vasectomy Sterilization operation in a man involving surgical interruption of each vasdeferens in the upper part of the scrotum. See also vasovasostomy (for vasectomy reversal).
Vasectomy reversal See vasovasostomy.vasovasostomyVasectomy reversal, the operation for reversing a sterilization operation (a
vasectomy) in a man involving removal of the blocked part of each vas deferens, in theupper part of the scrotum, and joining by microsurgery one cut end of the vas to the othercut end. Generally not as successful at returning fertility as the equivalent operation inwomen (tubal anastomosis) because the development of sperm antibodies increases withthe length of time since sterilization and limits the effective sperm count after the reversal.Many clinics now carry out cryostorage of some sperm obtained at vasectomy reversalso that if pregnancy does not happen, or azoospermia persists, in vitro fertilization (IVF)can be carried out with ICSI without requiring a later operation (for MESA) on theman. MESA with ICSI and IVF can be used as an alternative to vasovasostomy.
VDRL See serological test for syphilis.VEGF See vascular endothelial growth factor.villus Plural: villi. See chorionic villus.vocabulary See the box, Medical vocabulary—sensitive, precise, and correct?Wasserman reaction (WR) See serological test for syphilis.Wilson’s disease See serum copper.Wolffian ductThe mesonephric duct.WR See serological test for syphilis.yolk sac A sac-like structure attached to the under-surface of the developing embryo.The
first part of the embryo to become visible on transvaginal ultrasound after the gestationalsac, but not by itself as reassuring as seeing a beating fetal heart that the pregnancy willmost likely avoid miscarriage. Not as important for a human embryo’s nutrition as it isfor a fertilized egg incubated by a hen, and in mammals contains no yolk, but the yolksac’s lumen is continuous with the lumen of the embryo’s developing gut, or intestine,and shares an absorptive function. Cells from the yolk sac become incorporated intothe fetus in many ways, including forming the primitive germ cells.
ZIFT See zygote intrafallopian transfer.Zoladex See goserelin.zona pellucida The tough but glassy-looking membrane that starts to surround the egg
(the primary oocyte) while it’s still in the follicle, protects it against sperm which have notundergone the acrosome reaction at its surface, and keeps the cells of the early embryotogether until the embryo, as a blastocyst, hatches through it in preparation for implan-tation.
zygote Fertilized egg or ovum up to the first cleavage division; this stage of development ofthe embryo takes about 22 hours, and for the last few of these hours it’s at the pronuclearstage. See also pronucleus.
zygote intrafallopian transfer (ZIFT) A form of assisted conception in which in vitro fertil-ization (IVF) is used to produce fertilization; transfer is made on the day after egg retrievaland IVF, before the fertilized egg divides (it’s at the zygote, or pronuclear stage). Useful ifthe potential fertilizing ability of sperm is in doubt.The transfer is made to the fallopian
GLOSSARY � 501
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 501

tube to obtain advantages similar to gamete intrafallopian transfer (GIFT) and is madepossible by laparoscopy (with anesthesia) or by transvaginal ultrasound (without anes-thesia). Synonymous with pronuclear-stage transfer (PROST).
502 � GETTING PREGNANT
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 502

5-alpha reductasedeficiency, and intersex253
abnormality 5, 416gcongenital 430gin fertility 388, 390
abortion 347, 382defined 416ghabitual 447gmissed 94–5, 230, 462gsee also miscarriage
absolute risk 417gAccess,Australia (support
group) 354accountability 364, 369
defined 417gacrosome 35, 283
defined 417gacrosome reaction 35, 283
defined 417gadenohypophysis 417gadenomyosis 71, 73, 228,
231, 234
503
defined 417gtreatment 234–5
adhesions 185–6, 194–5,230defined 417gpreventing 196surgical barriers 195
adolescence, length 13adoption 7, 8, 307adrenal gland 418gafterbirth 280agglutinins 109aging
effect on eggs 7, 18,102, 290, 296
and miscarriage 96, 102,398
and subfertility 86–8,393–6
see also oopauseAhlgren, Dr Mats 310AI see assisted inseminationalcohol 142, 355
and fertility 259–60
alleles 45, 418gsee also genes
alpha fetoprotein 418gamenorrhea 8, 153, 155–6
defined 418ghyperprolactinemic
155–60lactational 13–14post-pill 173–4primary 155, 156, 240,
475gsecondary 155, 481g
amniocentesis 56, 125,347, 349defined 419g
amnion 419gamniotic cavity 43, 51,
56, 419gamniotic fluid 419gampulla 29, 32, 419gampullary-isthmic junction
31, 419gANA see antinuclear
antibody (ANA)
index
Page numbers in italics indicate illustrations.
Page numbers followed by the letter g indicate glossary definitions.
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 503

anal intercourse 145androgens 419gandrostenedione 25anemia 162anencephaly 179aneuploidy 16, 70, 100,
126defined 419g
angular pregnancy 111,203, 419g
annexin V 55, 109, 419ganomaly 420ganorexia nervosa 155,
157, 420ganovulation 6, 8, 78–9,
152causes
dangerous 172–3readily treatable153–62
hypothalamic 79, 154–6secondary 79untreatable 169–72
anovulatory dysfunctionaluterine bleeding 73,152, 153, 155defined 420g
anti-Müllerian hormone29, 421g
antibodies 420ganticardiolipin antibody
420ganticoagulants 50, 55antigens 420gantinuclear antibody
(ANA) 109, 421gantiphospholipid syndrome
109, 421gantrum 21, 22, 23, 421gapes 14, 16, 17apoptosis 421gappendicitis 185artificial insemination see
504 � GETTING PREGNANT
assisted insemination (AI)asexual reproduction see
cloningAsherman’s syndrome
230, 421gaspermia 135, 421gaspirin, low-dose 127–8assisted conception 18,
20, 91, 264–5defined 264, 421gtubal pregnancy risk 206
assisted hatching 284assisted insemination (AI)
147, 150, 260, 265, 311defined 422gusing husband’s semen
(AIH) 147, 422gasthenozoospermia 135atresia 20, 23, 422g
partial follicular 102atrophy 422gAtwood, Margaret 371,
372, 384Australian Health Ethics
Committee 365autoimmune oophoritis
171autonomy 361, 365, 370,
381defined 422g
autosomal recessiveinheritance 106, 107
autosomes 97–100, 422gazoospermia 77–8, 134–9
defined 422ggenetic 148–9obstructive 146
B cell lymphocytes 422gbacterial vaginosis see
vaginosisBaker, Dr Gordon 261Baker, Dr Robin 259
balanced chromosomaltranslocation 99, 101,103, 125–6defined 422g
basal body temperature(BBT) chart 63–4, 262,423g
Bavister, Barry 279Bellis, Dr Mark 259Bender, S 340beneficence 368, 423Bentham, Jeremy 358biopsy 423g
embryo 282, 284–5,436g
ovaries 169, 170premenstrual
endometrial 64, 75testicular 136, 492g
birds, body temperature 63birth 56
multiple 150, 281, 296,345
birth defects 344–6non-invasive testing
347–9birth interval 12–13Blanden, Robert 333blastocyst 34, 37, 107,
280, 376culture 284, 397–8defined 423ghatching 34, 37, 40, 42,
280–1, 376assisted 284, 422g
inner cell mass 40, 453gblastulation 280bleeding
abnormal 210–12after pregnancy
confirmed 339anovulatory 73breakthrough 424g
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 504

chocolate cyst 208, 212,220defined 427g
chorion 43, 56, 427gchorionic villi 43, 49, 55,
427gchorionic villus sampling
(CVS) 55, 125, 347, 349defined 427g
Christian beliefs 359, 370chromosomal cross-over
427gchromosomal embryopathy
97–101, 428gchromosomes 20
balanced translocation99, 101, 103
defined 428gin embryos 70in oocyte 26, 97see also autosome; sex
chromosome;karyotyping
cilia 31, 428gCIN see cervical
intraepithelial neoplasia(CIN)
CJD see Creutzdeldt-Jakobdisease
cleavage 37, 40, 428gclomiphene 146, 147,
150, 163–5, 341defined 428gin pregnancy 164
cloning 332–4, 428greproductive 478gtherapeutic 494g
coagulation system 41, 49defined 429gthrombin 50–1
cocaine 82, 83Cohen, Dr Jacques 322,
332
INDEX � 505
intermenstrual 454gsee also amenorrhea;
cryptomenorrhea;dysmenorrhea;hypomenorrhea;oligomenorrhea
blighted ovum 53, 102,130, 423–4g
body mass index (BMI)156, 168, 424g
bonobo chimps 258bowel 424gBowman, Dr Mark 72brain, male 29Brave New World 371, 372,
375, 383–4breakthrough bleeding
424gbreast cancer 176breast-feeding 13–14breech birth 246bromocriptine 162, 173,
424Brosens, Dr IA 218buserilin 424g
cabergoline 162–3, 173,425g
CAH see congenitaladrenal hyperplasia(CAH)
cancer 216, 334breast 176cervix 177and ovarian stimulation
176–8ovary see ovarian cancerprostate 224testes 140, 143
capacitation 35, 88, 425gCAT scan 425CBAVD see congenital
bilateral absence of vasa
deferentia (CBAVD)celiac disease 110, 119,
425gcervical cancer 177cervical incompetence
95, 110–11, 131defined 425g
cervical intraepithelialneoplasia (CIN) 239
cervical ligature 95, 110,111, 112, 131defined 425g
cervical mucus 28, 62, 83defined 425g
cervical polyp 426gcervical score 263, 426gcervicitis 83, 426gcervix 28, 31, 32, 33, 242
abnormality 83absent 244defined 426gdouble 245, 246
CGH see comparativegenomic hybridization(CGH)
chemotherapy 137, 142drugs 200
childhood, length 13childhood development,
after IVF 346children
as commodity 4, 11historical mortality 10,
382isolation in modern
families 383rights 366
chimerism 426chlamydia 65, 183–4, 204
defined 426gtesting, for previous
infection see serumchlamydial antibodies
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 505

collaborative reproduction305-17, 429g
colposcopy 239compaction 37, 40, 280,
429gcomparative genomic
hybridization (CGH)70, 294–5, 429g
compassion 365–6, 429gcompound heterozygosity
106, 107, 430gconception 35, 430gconception rate 430gconceptus 94, 430gcongenital adrenal
hyperplasia (CAH) 252,431g
congenital anomalies ofuterus 239–250non-symmetrical 248–50symmetrical duplications
244–8symmetrical obstructive
240–4congenital bilateral absence
of vasa deferentia(CBAVD) 138, 149defined 430g
consent, informed 68,360–2, 453g
contraception 4, 18controlled ovarian
stimulation 150, 264,265, 266–9
corpus luteum 26, 28, 40,41cystic 28defined 431g
corticosteroid drugs128–9, 144–5
Craft, Professor Ian 145Creutzfeldt-Jakob disease,
and hPG 180
506 � GETTING PREGNANT
cross-reactivity 144cryoprotectants 298cryostorage 297
defined 431geggs 302–4
immature 303–4unfertilized 325
embryos 297–301ovaries 326slices of ovary 326sperm 301–2
cryptomenorrhea 155,431g
cryptorchidism 140, 141,143, 432g
cumulus cells 25, 34, 35,218
cumulus mass 25, 26, 31,34, 280defined 432g
curettage 28, 73–4, 130,340before IVF 292defined 432gand scar tissue 230–1
CVS see chorionic villussampling (CVS)
cystic fibrosis 138, 149,432g
cytokines 218, 433gcytoplasm 280, 433gcytoplasmic transfer 126,
322–4cytotrophoblast 41, 42,
43, 52defined 433g
D&C see curettagedanazol 221–3, 226, 433gDaniels, Dr Ken 308, 310DeCherney, Dr Alan 68decidua 38, 40, 43, 53,
433g
decidual cells 433gdecidual reaction 105, 433gdeontological ethics 359,
434gdesigner babies 327, 332,
384DHT see
dihydrotestosterone(DHT)
DI see donor insemination(DI)
diabetes 108, 119, 135and stem cells 334, 335
diagnostic tests, antenatal347
diathermy 434gfor cutting adhesions 190for endometriosis 221,
225 see also Figure16.1, printed in colorafter Appendix 3
diethylstilbestrol (DES)138, 143, 164anomalies 240
dihydrotestosterone (DHT)29
dioxin 142, 143, 214effect on monkeys’
reproduction 215diploidy 434gDNA 434g
amplifying, seepolymerase chainreaction
detecting in single cells,see fluorescent in situhybridisation
sequencing 106, 435gsee also preimplantation
genetic diagnosisdoctor-patient relationship
6, 360–2communication 493
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 506

development 37, 51,236, 376
early 34, 42, 43failed 86injuries to 104spare, after IVF 375–7tests for competence of
69–71thawed, transferring
299–301embryo banking 297, 300embryo donation 313–15embryo research 370,
371, 375, 377–80spare embryos 375–7
embryo transfer 285–6,299–301defined 436gpriming the uterus 301
embryonic stem cells (EScells) 40research 334–6, 380,
384see also stem cells
embryonic disk 42–3, 51embryopathy
after implantation 97,105–7, 472
after placentation 97,107–10
before implantation97–104, 473
chromosomal 97–101,428g
defined 436gempathy 366, 436gEmpson, Dr Marianne
127, 128, 129empty follicle syndrome
288endometrial atrophy 71,
72, 155, 228, 231, 292defined 437g
INDEX � 507
doctors 356duty of care 356–7ethical conflicts 356–60ethics in practice 365–9informed consent 360–2new treatments 364threatened values 369,
373–4dominant inheritance 435gdonor insemination (DI)
77, 78, 265, 306–10,352–3defined 435g
dopamine 157Down syndrome 98, 100,
295, 296, 347defined 435g
Duchenne musculardystrophy 331
Dunstan, ReverendGordon 374
duty 366–7, 435gdysfunctional uterine
bleeding (DUB) 153,155, 435g
dysmenorrhea 210, 226defined 435g
dyspareunia 210, 226defined 436g
dysplasia see cervicalintraepithelial neoplasia(CIN)
Eastman, NJ 122–3ectopic pregnancy 69, 94,
197, 203, 248, 341abdominal 202causes 203–6cervical 202–3defined 436gdiagnosis 199optimising fertility
afterwards 206
ovarian 202rate 436gtreatment 200–2
Eden, Dr John 15Edwards, Robert 279egg donation 79, 126,
296, 310, 312–13defined 436g
egg retrieval 23, 277, 278defined 436g
eggs 19–20, 34at ovulation 35, 261cytoplasm defects
102–3depletion of 434gdeveloping from
immature tertiaryfollicles 325–7
freezing 325–6mitochondria
abnormality 126number of 86use-by date 86–8see also blighted ovum;
oocytesejaculation 27, 353
absent 138frequent 9retrograde 134, 135,
138, 139, 260, 479gelectrocautery see
diathermyelectroejaculation 138,
287Ellison, Dr PT 155embolization, of fibroids
234embryo 205, 376, 381
biopsy 282, 284–5,436g
chromosome-checked294–5
defined 436g
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 507

endometrial biopsy seepremenstrual endometrialbiopsy
endometrial cavity 31, 32,437g
endometrial hyperplasia73, 155, 162, 292defined 437g
endometrial polyps 71,72, 73, 85, 228, 231, 292defined 437g
endometrial stroma 40,437gsee also decidua
endometriosis 17, 65, 67,85–6abnormal tissue removal
225–6appearance 208–9causes 212–14defined 438gdiagnosis 212effect on, of
contraceptive pill173–4
and infertility 216–19nonpigmented 209,
214, 216symptoms 209–12
suppression of 226–7theories about 214–17treatment 220–1
endometritis 71, 72, 74,85, 229–30, 292acute 229chronic 229, 230defined 438gand miscarriage 112
endometrium 17, 31, 32,40, 69defined 438gdisorders of 229–31,
292–3
508 � GETTING PREGNANT
secretory phase 32, 33,72
thin 292–3endorphins 156, 438gepididymal sperm
aspiration (ESA) 78, 151epididymis 27, 31, 438gepithelium 238, 241Eppig, Dr John 327equity 368, 370Ericsson, Dr RH 329, 330ERT see estrogen
replacement therapy(ERT)
ES cells see embryonicstem cells (ES cells)
estradiol 25, 224, 438gestriol 56, 438gestrogen 22, 32
defined 438gsaliva testing for 263
estrogen replacementtherapy (ERT) 439gafter hysterectomy 227in premature ovarian
failure 172ethics 358, 361
defined 439gdeontological 358evidence-based 359in practice 365–9teleological 358utilitarian 358
ethics committees 362,364, 439
evidence-based medicine369
extravillous trophoblastderivation from
cytotrophoblast 43,display of HLA-G 46occlusion of mother’s
arteries 52–56
factor V Leiden 50, 109,440
factor XIII 106, 440gfairness 368–9fallopian tubes 28–9, 31,66
blockages see tubalblockages
damaged 204–5defined 440gdisease 104formation 239function 183hormone disturbances
205patency tests 64–6peritubal adhesions 85,
182, 185falloposcopy 67, 440gfamilies 383fecundability 440g
see also monthly fertilityfemaleness, fertile 250–1feminism 382ferning 263fertility
after ectopic pregnancy206
environmentalconstraints 14
high 3–4normal/abnormal 4–6seasonal 14
Fertility Society ofAustralia 178
fertilization 31, 35–7, 40,36, 63defined 440gpolyspermic 36, 472gsee also in vitro
fertilizationfetal loss 97, 110–12fetal reduction 150, 296,
349, 440g
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 508

Fraser, Clarke 123Freeman, Dr Ellen 352freezing see cryostorageFreud, Sigmund 382Frisch, Dr Rose 173FSH see follicle stimulating
hormone (FSH)Fugger, Dr Ed 330fundus 444g
galactorrhea 159, 444ggalactosemia 170gamete 444ggamete intrafallopian
transfer (GIFT) 91,150, 206, 219, 264, 266,285defined 444g
gamma globulin infusions129
gastrulation 42, 51, 379,444g
gay parenthood 311–12gender 250, 252–3, 444ggenes 52, 97
defined 445gfetal 107recessive, maternal
105–6see also alleles; DNA;
mutations;polymorphisms
genetic diversity 45–6genetic drift 87–8genetic trait selection
327–31genome 445ggerm cells 445ggestation see pregnancygestational sac 38, 51, 53,
445ggestational surrogacy 41,
80, 127, 370
INDEX � 509
fetus 37, 38, 55, 280, 376avoiding rejection of
41, 47–8death in utero 132–3defined 440ggenes 107heartbeat 51infection of 112spelling of 441
fibrin 49, 50, 440gfibrinogen 49, 50, 106,
440gfibroids 18, 71, 73, 85, 228,
232–4, 233defined 441gintramural 232, 233, 233submucous 232, 233,
233, 292subserous 232, 233, 233treatment
embolization 234GnRH-agonists 234see also myomectomy
fimbriectomy 192, 441gfimbriolysis 188, 190,
441gFISH see fluorescent in situ
hybridization (FISH)flow cytometer 348fluorescent in situ
hybridization (FISH)70, 441g
foetus see fetusfolic acid
defined 442gsupplements in
pregnancy 104, 110,121, 124
follicle aspiration 442gsee also egg retrieval
follicle cells 24–25, 442gsee also granulosa cells;
cumulus
follicle stimulatinghormone (FSH) 21defined 442gdose 168, 268–9in men 136–7, 139range of preparations
267side effects 269to induce ovulation
166–9follicle tracking 276, 442g
see also ovarianmonitoring
follicles 19–20, 21–2atretic 23, 422defined 442gdevelopment 22dominant 23, 435gGraafian 22, 23, 25,
446ghormones 25preovulatory 21, 22,
23, 24, 71, 474gprimary 22, 23, 475gprimordial 20, 21, 22,
23, 170, 475gsecondary 22, 23, 170,
481gtertiary 22, 23, 25, 170,
288, 492gfollicular atresia 273, 287
defined 442gin IVF 288–9partial 102
follicular phase 32, 33, 261defined 443g
follicular recruitment443g
food intolerance 110,119
fragile-X syndrome 102,171–2, 271defined 444g
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 509

for recurrent miscarriage106, 126
defined 445ggestrinone 221, 222,
445gGIFT see gamete
intrafallopian transfer(GIFT)
GnRH see gonadotropinreleasing hormone(GnRH)
GnRH-agonists 221, 223,226complications 224defined 445geffect on endometriosis
223–6effect on fibroids 234preventing LH surge
269, 271treatment protocols
272–3, 276, 457g, 486g,497g
GnRH-antagonistsdefined 446gpreventing LH surge
269, 271, 273–4gonadotropin 446ggonadotropin releasing
hormone (GnRH) 8,14, 21, 157defined 446guse in ovulation
induction 165–6gonads 251, 446g
see also ovary; testisgonorrhea 183–4, 204Gook, Dr Deborah 303Goretex 194, 446ggorillas 258Gosden, Dr Roger 326Graafian follicles 22, 23,
25, 32, 446g
510 � GETTING PREGNANT
granulosa cells 25, 26,446g
Greer, Germaine 258growth hormone 447gGuillette, Dr LJ 143Gutheil,Thomas 360
Habgood, Dr John 370Handyside, Dr Alan 331haploidy 447gHare, RM 368hatching see under blastocysthazard, distinction from
risk 447hCG see human chorionic
gonadotropin (hCG)Helsinki Declaration 362,
363, 364, 365, 369hemophilia 331heparin 50, 109, 128,
447–8hermaphrodism
pseudo 250true 496gsee also intersex states
Hermaphroditus andSalmacis 250
heroin 156heterosexuality 252heterozygosity 45, 52,
448gcompound 106, 107,
430gHippocratic Oath 368hirsutism 162, 448ghistamine 224HIV/AIDS 145, 448gHLA molecules 44–6,
448ghMG see human meno-
pausal gonadotropinHomo sapiens 12homosexuality 252
homozygosity 45, 52,106, 448g
hormone replacementtherapy (HRT)see estrogen replacement
therapyhormones 448ghPG see human pituitary
gonadotropin (hPG)Hull, Dr Michael 261human chorionic
gonadotropin (hCG)26, 37, 41, 42defined 449gfor luteal phase support
275side effects 275to trigger ovulation
274–5Human Fertilisation and
Embryo Authority (UK)371, 378
Human Genome Project106
human leucocyte antigen(HLA) 44
human life 370, 378,379–80
human menopausalgonadotropin (hMG)179, 180defined 449g
human pituitarygonadotropin (hPG) 180defined 449g
Hume, Cardinal Basil370
Huxley,Aldous 371, 375,383–4
hydatidiform moles341–2complete 450gpartial 450g
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 510

infectionsantibiotic treatment
118blood-borne 112
infertility 3, 232absolute see sterilitydefined 453gduration of 90, 390,
435gliving for the present
354–5loss of personal power
351–2loss of privacy 353–4male-factor 281, 290
treatment 145–7and miscarriages 125,
340–1primary 475gpsychological 7–9relative see subfertilityresponse to strain
352–3secondary 481gstatistics 387–92strengthening
relationship 354–5suffering caused 350,
352, 490gtelling family/friends
350–1unexplained 6–7, 18,
81, 91, 261, 498ginfertility reseach
institutional reviewboards 362–3, 365
responsibility 362Infertility Treatment
Authority (Victoria)378
informed consent 68,360–2, 453g
inheritance
INDEX � 511
hydrosalpinx 182, 186,189, 190, 191defined 187, 450gone-sided 104, 119, 291surgery 68, 69, 80threatens implantation
72, 291, 292hymen, imperforate 238,
240see also cryptomenorrhea
hyperplasia 450ghyperprolactinemia 79,
156–60, 450ghypomenorrhea 153, 173,
450ghypospadias 252, 260,
450ghypothalamic anovulation
79, 450ghypothalamus 14, 21, 224
defined 450ghysterectomy 80, 211,
227, 451ghysterosalpingogram
(HSG) 64, 66, 68–9, 80abnormal 67defined 451gsee also selective
salpingogramhysteroscopy 28, 59, 67,
73defined 451g
ICSI see intracytoplasmicsperm insertion (ICSI)
Illeni, Dr Maria Teresa120–1
immotile cilia syndrome451g
immune systemdefined 451gmaternal 108, 119,
128
immunotherapy, forrecurrent miscarriage119–21, 129
implantation 6, 37–8,40–1, 42defined 452gtests for 69–74
implantation bleeding 37,49, 339, 452g
implantation rate 452gimplantation window 33,
72impotence 135, 139, 260,
452gin vitro fertilization (IVF)
78, 80, 206, 264chance of success
289–96, 393–9defined 266, 452gand endometriosis 226failure of fertilization
287–9lab conditions 293, 295lack of eggs 286–7lack of sperm 287and miscarriage 124–7,
394–6natural cycle IVF
270–1over 35, special needs
295–6problems 286–9regular procedure
280–1results 393–9spare embryos 375–7see also preimplantation
genetic diagnosisin vitro maturation 304,
325, 452gin vitro penetration tests
83–4, 452ginbreeding 45, 106, 309
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 511

autosomal recessive106, 107, 477g
sex-linked recessive477g
dominant 435ginhibin B 25, 453ginner cell mass 34, 40, 42,
51, 453ginsemination 260–1Insler score see cervical
scoreinstitutional ethics
committees seeinstitutional reviewboards
institutional review boards362–3, 365, 453g
integrity 368, 369, 454gInterceed 195, 454gintermenstrual bleeding
153, 454gintersex states 250–254
behavioural gender250, 252–3
chromosomal 250,251
defined 454gfemale 250, 252male 250, 251–2phallus, importance of
conserving 254intervillous space 454gintracytoplasmic sperm
insertion (ICSI) 151,280, 281–4, 282defined 454gsubzonal insertion
(SUZI) 281, 283,490g
intrauterine adhesions 71,72, 73, 80, 85, 95, 228,292and curettage 230–1
512 � GETTING PREGNANT
defined 455gtreatment 119
intrauterine contraceptivedevice (IUD) 112retained 71, 73and salpingitis 186
intrauterine infection 112intrauterine insemination
(IUI) see assistedinsemination
irritable bowel syndrome211, 455g
isthmic salpingitis 193isthmus 29, 32, 455IVF see in vitro fertilization
(IVF)IVF Lite 270–1IVF Plus 294–5
Jansen, Dr Cees 270Johnson, Dr Larry
329–30justice 367–9, 455g
distributive 368, 434g
K-selection reproductivestrategy 12–13, 456g
Kallmann syndrome 139defined 455gand primary amenorrhea
158Kant, Immanuel 361karyotype 37, 56, 70, 98,
340defined 456g
karyotypingafter miscarriage 94,
98–100, 130, 340molecular 294–5, 332
kidney failure 108, 119kidney system 239, 248King,Ashley 47–8Kistner, Dr Robert 221
Klinefelter syndrome 99,136, 148, 345, 456g
Kremer test 83–4, 456g
laborimmature 95, 131–2premature 56, 95,
473glactation 4lactational amenorrhea
13–14lacunae 42, 43, 49, 456gLancaster, Dr Paul 178–9laparoscopy 28, 59, 64–5,
66–8, 190appearance of
endometriosis see alsoFigure 15.1, printed incolor after Appendix 3
defined 456gfor ectopic pregnancy
200, 201to treat endometriosis
225laparotomy 190
defined 456gto treat endometriosis
225–6Leridon, Henri 4lesbian motherhood
311–12Leydig cells 29, 139, 457gLH see luteinizing
hormone (LH)LH surge 25, 262–3
defined 457ghome testing for 262–3preventing 269–275
life, human 370, 378,379–80continuity of 379–80
Lilford, Professor Richard140
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 512

microepididymal spermaspiration (MESA) 151,461g
microsurgery 461gfor tubal blockages
188–90, 189miscarriage 28, 52, 55,
92–3clinical 93–4, 340complete 430gand curette 130defined 462gand fibrinogen 49, 50and HLA molecules
44–6, 48incomplete 452ginevitable 93–4, 453gand infertility 340–1karyotyping 94,
98–100menstrual 93, 98midtrimester 95missed 94–5prevention/treatment
117–33recurrent see recurrent
miscarriagerejection of fetus 41,
47–8subclinical 47, 93, 340,
490gtesting for causes
97–113threatened 93, 494guseful purpose 16without intervention
130miscarriage rate 341, 462g
effects of age 95–6after IVF 394–6after previous
miscarriage 123miscarriage treatment
INDEX � 513
Loke,YW 47–8low birth weight 343,
344low responder 457–8g
IVF Lite, use of 270LPD see luteal phase defect
(LPD)lupus anticoagulant 109luteal phase 26, 32, 33, 261
defined 458gmonitoring 277support for 275
luteal phase defect (LPD)75, 83, 102defined 458g
luteinized unrupturedfollicle (LUF) 8, 64, 65,83defined 458g
luteinizing hormone (LH)8, 21, 26, 180, 267defined 458gLH surge 25, 262–3
defined 457ghome testing for262–3
preventing 269–275lymphocytes see B cells;
NK cells;T cells
McClure, Dr Neil 176McGowan, Kerrie 355McIndoe operation 243Macnaughton, Malcolm
123macrophages 218, 459gmagnetic resonance
imaging (MRI) 463gmajor histocompatibility
complex (MHC) 44,459see also HLA molecules
maleness 250–1
Malpas, P 122–3mammals 63, 129marijuana 82, 142Martin, Dan 215Martinez, Dr Antonio
147, 150Marxism 358masturbation 61, 353maturation arrest, in sperm
136, 137medical negligence 28medical practice
evidence-based 369threatened values 369,
373–4meiosis 20, 459gmenarche 13, 14, 459gmenopause 224, 460
premature see primaryovarian failure
menorrhagia 460gmenstrual cycle 24, 460g
shortening of 86menstruation 32, 152–3,
210–11backwards bleeding
213role of hormones
154–5MESA see microepididymal
sperm aspiration (MESA)metaplasia theory, for
endometriosis 215,216–17
metformin 163, 164, 165,460g
methotrexate 200–1, 461gmetroplasty 246, 461gMHC see major
histocompatibilitycomplex (MHC)
microchimerism 55,461g
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 513

between pregnancies117–24
during conception124–7
during establishedpregnancy 130–3
duringimplantation/earlypregnancy 127–30
empirical 121for men 134–51
missionary position 258,485g
mitochondriaaging of 88defined 462gof egg 71, 86–8, 126
mitochondrial DNA(mtDNA) 87
mitochondrial geneticdisease 324
mitosis 100, 462gMittelschmerz see
ovulation painmolecular karyotyping
126, 294–5, 332defined 462g
monilia (thrush) 118monkeys 205, 261
dioxin studies 214, 215effects of stress 8endometriosis 17
monosomy 463gmonosomy X see Turner
syndromemonthly fertility 4,
387–92moral plurality 370–1morning-after pill see
postcoital contraceptionMorris, Desmond 15morula 34, 37, 40, 280,
376
514 � GETTING PREGNANT
defined 463gmosaicism 99, 148, 463gmotility 35, 60, 82
decreased 135defined 463gand IVF 281, 283
MTHFR 104, 110, 124,464g
Müllerian ducts 216,236–7, 237, 238, 239,240, 248atresia 243, 243defined 464gduplications 245
mumps 142mutations 104, 106, 126,
148Mycoplasma 229–30myomas see fibroids
malignant seemyosarcomas
myomectomy 232, 464gmyometrium 31, 48, 73
defined 464gdisruption of 231–5
myosarcomas 232
National Health andMedical ResearchCouncil (NHMRC)378
National Perinatal StatisticsUnit 178, 299
natural killer cells see NKcells
necrosis 465gneural tube defects 121,
124, 179neurohypophysis 465gnicotine 142NK cells 41, 44, 47–8,
108, 120, 128, 129defined 465g
non-maleficence 368,465g
Norman, Reid 8Novak, Emile 217NSAIDs 226, 466gnuchal translucency 347,
348, 466g
obligations 366–7, 466gO’Brien, Dr Marilyn
327obstetricians 343, 346Oelsner, Dr Gabriel 177OHSS see ovarian
hyperstimulationsyndrome (OHSS)
oligomenorrhea 83, 125,466g
oligospermia 16, 17, 82,110, 150defined 135, 466genvironmental causes
140–3inherited 140, 148–9
oocytes 23, 251chromosomes 26competence 321–2defined 466gprimary 20see also eggs
oogenesis 20, 466googonia 20, 466goopause 6, 7, 86, 102,
288, 322defined 467g
oophoritis, autoimmune171
oral contraceptiveeffect on endometriosis
173–4effects of ceasing 173protection against
ovarian cancer 178
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 514

pheromones 46, 470gpinocytosis 72pinopodes 72pituitary gland 21, 470gplacenta 280, 470g
circulation 52, 55construction 49, 132–3
placenta accreta 231placenta previa 203PMT see premenstrual
tension (PMT)polar body 26, 471g
biopsy of 282, 284polycystic ovary syndrome
(PCOS) 125, 156,160–2and anovulation 79,
157defined 471gfertility in famine 14,
15gene-based 161
polyembryoma 379polymerase chain reaction
(PCR) 138, 471gpolymorphisms 104, 107,
471gpolyploidy 126, 471gpolyps 231, 471g
cervical 426gsee also endometrial
polypspolyspermy 36, 472gpopulation strategies
11–13postcoital bleeding 472g
see also intermenstrualbleeding
postcoital contraception205, 472g
postcoital test (PCT) 59,62, 135, 472g
preeclampsia 55, 472g
INDEX � 515
and sexualpermissiveness 382
orgasm 258, 467gafter ejaculation 258,
259ovarian cancer 177, 379
and infertility 178ovarian cycle 21, 23–5,
288defined 467gfollicular phase 32, 33,
261defined 443g
luteal phase 26, 32, 33,261defined 458gmonitoring 277support for 275
ovarian hyperstimulationsyndrome (OHSS) 168,175–6, 275, 299defined 467g
ovarian monitoring 168,261–2, 275–7, 468g
ovarian slice freezing326
ovarian stimulation 20,226–7and birth defects 178–9and cancer 176–8with FSH 266–9multiple follicles 278
ovariectomy 224–5, 468govaries 19, 184
biopsy 169, 170defined 468gremoval 224–5role of pituitary gland
21–6torsion 176, 177
oviduct see fallopian tubesovulation 23, 25–6, 85,
213
defined 468gdisorders 83, 290, 291effect of exercise 155–6lactational inhibition
13–14suppressing with drugs
221–5tests for 62–4
ovulation induction162–9complications of FSH
therapy 175defined 468ggonadotropin treatment
166tubal pregnancy risk
205–6ovulation pain 261, 468govum, blighted 53, 102,
130, 423–4g
PAP smear 238–9parthenogenesis 469gpartial follicular atresia
102paternalism 361, 364, 367,
372, 378defined 469g
Paulson, Dr Richard 314PCT see postcoital test
(PCT)perimenopause 469g
see also low responder;oopause
peritoneal cavity 470gperitubal adhesions 85,
182, 185perivitelline space 35,
470gPersson, Dr Jeffrey 78PGD see preimplantation
genetic diagnosis (PGD)phallus 252, 254, 470g
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 515

pregnancyabdominal 202, 416gafter menopause
314–15angular 111, 203, 419gbiochemical 47, 93,
423gcervical 202–3, 426gcornual 204, 431gcumulative chance of
389–92, 432gectopic see ectopic
pregnancyeffect on health 13heterotopic 199, 448ginterstitial 199–200,
454gmolar see hydatidiform
molemultiple 150, 281, 296,
345, 349see also twins
ovarian 202, 468gspacing 13–14time to 495gtubal 197–202, 497g
pregnancy, hazards 339birth defects 344–6bleeding 339cervical incompetence
343hydatidiform mole
341–2miscarriage 340prematurity 343
pregnancy rate 473gpregnancy test 28, 37, 38,
42defined 473gquantitative 198–9
preimplantation geneticdiagnosis (PGD) 70,284–5, 331–2
516 � GETTING PREGNANT
and balancedtranslocation 101,125–6
defined 473gDNA testing see also
Figure 20.3, printed incolor after Appendix 3
and embryo biopsy282, 284–5
polar body biopsy 282,284
see also IVF Plus; sexselection
premature labor 56, 95,473g
premature ovarian failure6
premenstrual endometrialbiopsy 64, 75, 473–4
premenstrual spotting153, 210–12, 218, 474g
premenstrual tension(PMT) 175, 211, 227defined 474g
presacral neurectomy226
primary ovarian failure23, 79, 158, 169–72defined 475ginforming child 368special causes 170–2
professionalism 361,476g
progesterone 25, 26, 31,40, 41, 52, 64action on temperature
63defined 476gvaginal 129
progestogens 129, 221,476g
prolactin 38, 156big prolactin 159
defined 476gpronuclear stage transfer
(PROST) 266, 476gpronuclei 34, 37, 280
defined 477gprothrombin
polymorphism 50, 477gPROST see pronuclear
stage transfer (PROST)prostaglandins 48, 477gprostate cancer 224prostate gland 27, 31,
477gpseudohermaphrodism see
intersex statespulsatile GnRH 165–6pyosalpinx 187, 477g
Quetelet index 156
r-selection reproductivestrategy 11–12, 480g
recombinant folliclestimulating hormone(rFSH) 179, 478g
recurrent miscarriage96–7, 478gchances of 122–3diagnosis 118fetal genes 107immunological causes
41, 47–8, 108–9, 110,119–20
karyotyping 96, 101Reddy, Professor Prakash
383relationship strengthening
354–5relative infertility see
subfertilityrelaxin 38, 478Repository for Germinal
Choice 313
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 516

Sertoli cells 29, 136, 141defined 482g
serum, defined 483gserum AFP 483gserum chlamydial
antibodies 65–6, 483gserum estradiol 24, 483gserum FSH 24, 25, 78,
134, 484gserum hCG 28, 484gserum inhibin B 484gserum LH 24, 484gserum progesterone 24,
28, 484gserum testosterone 485gsex chromosomes
abnormal number 100,251
defined 485gsize difference and
sperm selection 328sex see sexual intercoursesex organs, female, internal
32sex organs, male 26–8, 27
development 29infections of 142, 144
sex selection 327–31,384
sexual intercourse 9,27–8, 35, 145, 238,257–60bleeding after see
postcoital bleedingpreventing pregnancy
after see postcoitalcontraception
frequency for fertility260
painful see dyspareuniaposition 258, 485gorgasm 258, 467gtiming 261–6
INDEX � 517
reproductive cloning332–334, 478g
reproductive strategy11–13, 137
reproductive technology,and erosion of rights 369
resistant ovary syndrome170
Resolve, US (supportgroup) 354
responsibility 369and accountability 417gdefined 479gin research 362–5taking, patient and
doctor 362retrograde ejaculation
134, 135, 138, 139defined 479g
rFSH see recombinantfollicle stimulatinghormone (rFSH)
rights 366–7, 369, 381,479gpatients’ 367of the child 366versus duties or
obligations 366, 479risk 479g
absolute 417grelative 478gversus hazard 447
rodenticide 381–2rodents, endometriosis
studies 218–19Rowland, Professor Robyn
308Royal Commission on
New ReproductiveTechnologies (Canada)371–3
rubella (German measles)112
Russell, Professor Peter209
saliva testing, for estrogen263
salpingectomy 201, 480gsalpingitis 65, 69, 183–8,
199, 204acute 229defined 480gisthmic 193
salpingitis isthmica nodosa67, 188, 193defined 480g
salpingolysis 188, 190,480g
salpingoscopy 67, 480gsalpingostomy 188, 189,
190–1defined 480g
salpingotomy 200, 481gsalpinx 187Sampson, John A 214Sauer, Dr Mark 314scar tissue see adhesionsSchoysman, Dr R 309Schulman, Dr Joseph 330SCNT see somatic cell
nuclear transfer (SCNT)Scott, Roger 217secondary postpartum
hemorrhage 230selective feticide see fetal
reductionselective reduction see fetal
reductionselective salpingogram 69,
80, 482gsemen 27, 31, 135, 145
defined 482gsemen analysis see sperm
countseminal vesicles 31, 482g
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 517

testing for sperm aftersee postcoital test
sexual reproduction 333,485g
Shaw, Dr Jill 326Sher, Dr Geoffrey 293Shettles, Dr Landrum
328, 330Short, Roger 16Silastic condom 61Silber, Dr Sherman 16, 61sildenifil (Viagra) 293, 353Simcock, Dr Barbara 329,
330Simpson, Professor JL 213Sims-Huhner test see
postcoital test (PCT)singing, harmful effects of
danazol and gestrinone222
Skakkebaek, ProfessorNiels 143
small-for-dates 486gsmell, sense of 139, 156smoking, and sex 258–9somatic cell nuclear
transfer (SCNT) 335,486g
sperm 31, 83, 134–145capacitation 35, 88,
425gcentriole defects 103–4defined 486gDNA breaks 103fertilization by 35–6maturation arrest 136,
137production 27, 30
lack of 136see also spermatozoonterminology 135
sperm antibodies 83, 84,144–5
518 � GETTING PREGNANT
defined 486gsperm banks, commercial
313sperm chromatin structure
assay (SCSA) 103, 487gsperm collection 278sperm count 59, 60–1, 86,
103, 135abnormal forms 416defined 487glow see oligospermia
sperm donation 306donors
desire for information367
motives 308–9secrecy 306–7
ended in Sweden309–10
telling the child 318sperm microinjection see
intracytoplasmic sperminsertion (ICSI)
sperm obstruction 137–8sperm production 27, 30
lack of 136sperm recovery 150–1sperm washing 35, 139sperm-cell sorting
328–31spermatids 29, 487gspermatogenesis 30, 135,
487gspermatogenic waves 30spermatogonia 20, 29
defined 487gstorage 302
spermatozoon 26–7, 29,135defined 487g
spermiogenesis 27, 103,135, 488g
spina bifida 179, 347
Spinnbarkheit 33, 488gstatistical significance
488g, 489–90statistics 488gSteele, Edward 333stem cells 334, 488gSteptoe, Patrick 279sterility 6, 7, 17, 76, 80
causes 60, 77, 184defined 488gtests for 60see also infertility;
subfertilitysterilization 183, 488g
reversal 191–3, 490gStone, JL 382–3stress, and fertility 7–9,
259subfertility 6, 7, 16–18, 81
causes 60, 81–2, 184combined factors 88–9defined 490geffect of age on 86–8management 89–91tests for 60see also infertility; sterility
submucous fibroids 72,73, 111, 119defined 490g
subserous fibroids 232,490g
suffering 350, 352, 490gsulfasalazine 142superovulation 491g
see also controlledovarian stimulation
surrogacy 315altruistic 315, 316, 384commercial 316–17,
319exploitation 319–20gestational see gestational
surrogacy
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 518

truth 367–9, 496gtubal abortion 199, 200,
496gsee also tubal pregnancy
tubal anastomosis 188,189, 191–5, 204–5defined 497gsterilization reversal
191–3tubal blockages 79–80,
182–3, 292causes 183–8microsurgery 188–90,
189tubal canalization 188,
195–6, 497gtubal disease 104tubal embryo-stage transfer
(TEST) 266, 285, 497gtubal ligation 497g
see also sterilizationtubal patency 67
tests for 64–6, 493gtubal pregnancy 197–202,
497gtuberculosis 229Tuchman, Barbara 11tumors
affecting ovulation172–3, 379
pituitary 172, 470gTurner syndrome 98, 100,
251, 292, 345defined 497g
Twain, Mark 7, 493twin pregnancy 54twins
dizygotic (non-identical)434g
IVF-related 345, 396–9monoamniotic 463gmonozygotic (identical)
284, 397, 463g
INDEX � 519
medically justified 317traditional 315–16, 495g
SUZI see underintracytoplasmic sperminsertion (ICSI)
syncytiotrophoblast 41,42, 49, 52
syngamy 37, 378, 491gsyphilis 112systemic lupus
erythematosus (SLE)109
T cell lymphocytes 44–6,491g
take-home baby rate394–399, 491g
Tay-Sachs disease 331teleological ethics 358–9,
492gTeLinde, Richard 217teratozoospermia 135TESE see testicular sperm
extraction (TESE)TEST see tubal embryo-
stage transfer (TEST)testicular biopsy 136,
492gtesticular feminization
252, 253, 492gtesticular sperm extraction
(TESE) 78, 151, 492gtestis 26, 27, 29, 31
ambient temperature140–1
cancer of 140, 143defined 492gmaturation arrest 77retractile 141torsion 142
testosterone 26, 29, 142,146defined 492g
The Handmaid’s Tale 371,372, 384
theca interna 22, 25, 494gthecal cells 25therapeutic alliance 360thrombin 50–1, 494gthrombophilia, and
miscarriage 50–1, 107,109–10defined 494g
thrombosis 109, 176Thurmond, Dr Amy 195thyroid function tests
494gthyrotoxicosis 108, 119time left for conception
90, 390–2, 494gtime to pregnacy 390–2,
495gtissue factor 49tissue groups 44–5torsion 495
of ovary 176, 177of testis 142
transformation zone238–9, 242
transsexual 495gtransvaginal ultrasound
71, 73, 495gtriple test 347, 348, 495gtriple-X syndrome 496gtriploidy 496gtrisomy 98–9, 100, 496gtrisomy 21
defined 496gsee also Down syndrome
trophectoderm 34, 37, 40,496g
trophoblast 37, 40–1, 47,496g
Trounson, Professor Alan297, 300
trust 369
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 519

Tyler, Dr John 60
ultrasound 347, 348defined 498gthree-dimensional 494gtransvaginal 71, 73,
495guncertainty, sharing in
professional relationships361
uremia 108uterine anomaly 498guterine cavity see
endometrial cavityuterine embryo transfer see
embryo transferuterine fibroids see fibroidsuterine irritability 131–2uterine septum 111, 119,
244, 245defined 498gtreatment 246, 247
uterus 31–3, 32, 239,242absent 80, 240–4anatomical constraints
107–8, 111bicornuate 111, 132,
245, 246, 423congenital absence
240–4, 368congenital anomalies
239–250 defined 498gdisorders of 292–3double 246–8, 249–50,
249flushing of, for embryo
retrieval 317, 318, 365infection in 112
see also endometritis
520 � GETTING PREGNANT
menstrual phase 32problems 228retroverted 210, 479secretory phase 32,
286, 481–2septate 244–6, 245, 247subseptate 245, 246testing for abnormalities
71unicornuate 111, 248,
249, 498guterus bicornis bicollis
245, 246utilitarianism 358, 359,
499g
vagina 238, 239, 242abnormalities 245absent 240–4, 253creating 241–3double 246–8, 247,
249–50, 249vaginitis 118vaginosis 56, 112, 132
bacterial 118defined 499g
varicocele 141, 499gvas deferens 27, 31, 499gvascular endothelial growth
factor (VEGF) 176,499g
vasectomy 144, 500greversal 144, 147, 193,
500gVear, Dr Cedric 328–9VEGF see vascular
endothelial growth factor(VEGF)
Venn, Dr Alison 177Viagra see sildenifil (Viagra)virgin births 311–12
vocabulary, medical 493voice, harmful effects of
danazol and gestrinone222
Warburton, Dorothy 123weight loss 154–5, 173Weiler, Hartmut 50Wentz, Dr Anne 211wet-nursing 3–4, 319whales, and embryonic
deaths 16Whittacker v. Rogers 360Williams operation 242–3Wilson’s disease 108, 119,
483gWilton, Dr Leanda 70,
294womb see uteruswomb flushing 317, 318,
365
X-chromosome anomalies,causing ovarian failure171–2
Y-chromosome,microdeletions 138, 148
yolk sac 51, 54, 500gYoung syndrome 138
ZIFT see zygoteintrafallopian transfer(ZIFT)
zona pellucida 34, 35, 36,37, 280
zygote 34, 376, 500gzygote intrafallopian
transfer (ZIFT) 266,285, 500g
Getting Pregnant - Ch24 -end 1/7/03 1:46 PM Page 520