University of Gondar Institutional Repository
59
I University of Gondar College of Medicine and Health Sciences School of Biomedical and Laboratory Sciences Department of Medical Microbiology Multi-drug resistant and Extended-spectrum β-lactamases producing bacterial uropathogens among pregnant women at the University of Gondar Teaching Hospital, Northwest Ethiopia. By: Sirak Biset (BSc) Advisors: Prof. Feleke Moges (PhD) and Setegn Eshetie (MSc) A thesis submitted to the Department of Medical Microbiology, College of Medicine and Health Sciences, University of Gondar for partial fulfillment of the requirements for the degree of Master of Sciences in Medical Microbiology. June, 2017 Gondar, Ethiopia
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of University of Gondar Institutional Repository
I
University of Gondar
College of Medicine and Health Sciences
School of Biomedical and Laboratory Sciences
Department of Medical Microbiology
Multi-drug resistant and Extended-spectrum β-lactamases producing bacterial
uropathogens among pregnant women at the University of Gondar Teaching Hospital,
Northwest Ethiopia.
By: Sirak Biset (BSc)
Advisors:
Prof. Feleke Moges (PhD) and
Setegn Eshetie (MSc)
A thesis submitted to the Department of Medical Microbiology, College of Medicine and
Health Sciences, University of Gondar for partial fulfillment of the requirements for the
degree of Master of Sciences in Medical Microbiology.
June, 2017
Gondar, Ethiopia

II
University of Gondar
College of Medicine and Health Sciences
School of Biomedical and Laboratory Sciences
Department of Medical Microbiology
CERTIFICATE
This is to certify that the thesis entitled “Multi-drug resistant and Extended-spectrum β-
lactamase producing bacterial uropathogens among pregnant women at the University
of Gondar Teaching Hospital, Northwest Ethiopia.” done by Sirak Biset for the Masters of
degree in Medical Microbiology was carried out under our supervision and the thesis has not
been previously submitted in part or full for any degree or diploma in this or any other
University.
Advisors Sign Date
1. Prof. Feleke Moges ___________ ___________
2. Mr. Setegn Eshetie ___________ ___________
June, 2017
Gondar, Ethiopia
I
ACKNOWLEDGMENT
Foremost, I would like to express my sincere gratitude to my advisors Prof. Feleke Moges and
Mr. Setegn Eshetie for the continuous support of my MSc study and research, for their
understanding, inspiration, and massive learning. Their guidance helped me in all the time of
research and writing of this thesis.
Besides my advisors, I would like to thank all the staff members and lab technicians of
Microbiology Department for their encouragement, and profitable remarks. I would like also
to thank all study participants for their leading contribution in this study. I thank my fellow
classmates for the inspiring discussions, for the sleepless nights we were working together in
the lab, and for all the fun we have had in the last two years. Last but not the least, I would like
to thank my family for supporting me spiritually throughout my life.
This project was supported by the mega project of the University of Gondar in Reference
number of VP/RCS/05/192/2015.

II
LIST OF TABLES
Table 1: Socio demographic characteristics of pregnant women attending ANC clinic at the
UoGTH, March to May, 2017. .................................................................................. 17
Table 2: Pregnancy and clinical related factors among pregnant women attending ANC clinic
at the UoGTH, March to May, 2017.......................................................................... 18
Table 3: The prevalence of MDR, ESBLs producing and MR (Methicillin resistant) bacteria
among uropathogens isolated from pregnant women attending ANC clinic at the
UoGTH, March to May, 2017. .................................................................................. 19
Table 4: Pregnancy and clinical related factors against significant bacteriuria and MDR
bacteria among pregnant women attending the ANC clinic at the UoGTH, March to
May, 2017. ................................................................................................................. 20
Table 5: Distribution of drug resistance pattern among uropathogens isolated from pregnant
women attending ANC clinic of the UoGTH, March to May, 2017 ......................... 21
Table 6: Distribution of multiple drug resistance among uropathogens isolated from pregnant
women attending ANC clinic at the UoGTH, March to May, 2017.......................... 22
Table 7: The distribution of antibiotic resistance among ESBLs producing and non ESBLs
producing gram negative bacteria isolated from pregnant women attending ANC at
the UoGTH, January to May, 2017. .......................................................................... 23
Table 8: Bi-variable and multi-variable analysis of factors associated with the presence of
MDR bacteria among pregnant women attending at the UoGTH, March to May, 2017.
................................................................................................................................... 24

III
TABLE OF CONTENTS
ACKNOWLEDGMENT ....................................................................................................................... I
LIST OF TABLES ................................................................................................................................ II
TABLE OF CONTENTS .................................................................................................................... III
LIST OF ABBRIVIATION .................................................................................................................. V
ABSTRACT .......................................................................................................................................... VI
1. INTRODUCTION ......................................................................................................................... 1
1.1 Background ........................................................................................................................... 1
1.2 Statement of the problem ..................................................................................................... 3
1.3 Literature review .................................................................................................................. 5
1.4 Significance of the study ....................................................................................................... 9
2. OBJECTIVES ............................................................................................................................. 10
2.1 General Objective ............................................................................................................... 10
2.2 Specific Objectives .............................................................................................................. 10
3. MATERIALS AND METHODS ............................................................................................... 11
3.1 Study Area ........................................................................................................................... 11
3.2 Study design and period ..................................................................................................... 11
3.3 Population ............................................................................................................................ 11
3.3.1 Source population ......................................................................................................... 11
3.3.2 Study population ........................................................................................................... 11
3.4 Inclusion and Exclusion criteria ........................................................................................ 11
3.4.1 Inclusion criteria ........................................................................................................... 11
3.4.2 Exclusion criteria .......................................................................................................... 11
3.5 Sample size and sampling procedures ............................................................................... 11
3.5.1 Sample size ................................................................................................................... 11
3.5.2 Sampling technique ....................................................................................................... 12
3.6 Study Variables ................................................................................................................... 12
3.6.1 Dependent variable ....................................................................................................... 12
3.6.2 Independent variables ................................................................................................... 12
3.6.3 Operational definitions .................................................................................................. 12
3.7 Data collection procedures ................................................................................................. 13
3.7.1 Socio-demographic and clinical data ............................................................................ 13
3.7.2 Sample collection .......................................................................................................... 13
3.7.3 Culture and identification techniques............................................................................ 13
3.7.4 Drug Susceptibility Testing (DST) ............................................................................... 14
IV
3.7.5 Extended Spectrum β-Lactamase Detection ................................................................. 14
3.7.6 Quality control .............................................................................................................. 15
3.8 Data processing and Analysis............................................................................................. 15
3.9 Ethical consideration .............................................................................................................. 16
4. RESULTS .................................................................................................................................... 17
5. DISCUSSION .............................................................................................................................. 25
6. LIMITATION OF THE STUDY ............................................................................................... 28
7. CONCLUSION ........................................................................................................................... 29
8. RECOMMENDATION .............................................................................................................. 30
9. REFERENCES ............................................................................................................................ 31
ANNEX ................................................................................................................................................ 37
Annex I: Study information sheet and consent form ................................................................... 37
Annex III: Questionnaire ............................................................................................................... 41
Annex IV: Procedures .................................................................................................................... 45

V
LIST OF ABBRIVIATION
ABR: Antibiotic Resistance
ANC Anti-natal care
ASB Asymptomatic Bacteriuria
ASP Antimicrobial Susceptibility Pattern
AST Antimicrobial Susceptibility Testing
ATCC American Type Culture Collection
CDC Communicable Diseases Control
CLSI Clinical and Laboratory Standards Institute
CoNS Coagulase Negative Staphylococcus
ESBLs Extended-Spectrum β-Lactamases
GNB Gram Negative Bacteria
HIV Human Immuno-deficiency Virus
MDR Multi-drug Resistant
MDROs Multi-drug Resistance Organisms
MHA Muller Hinton Agar
MRCoNS Methicillin resistant coagulase negative staphylococcus
MRSA Methicillin resistant staphylococcus aureus
SOPs Standard Operating Procedures
SPSS Statistical Package for Social Sciences
UPEC Uropathogenic Escherichia coli
UTIs Urinary Tract Infections
WHO World Health Organization

VI
ABSTRACT
Introduction: Urinary tract infections (UTIs) are the most common bacterial infections during
pregnancy. Above 80% of those infections are caused by enteric bacteria, which are known for years
by their drug resistant ability, especially those producing extended-spectrum β-lactamases (ESBLs).
Though the prevalence of multi-drug resistant (MDR) strains, including ESBLs are increasing in the
world, their prevalence is not well understood especially in low income countries including Ethiopia.
Objectives: To assess Multidrug resistance, ESBLs production, and associated risk factors for the
presence of MDR uropathogen among pregnant women attending the University of Gondar Teaching
Hospital (UoGTH), Gondar North-west Ethiopia.
Materials and Methods: A hospital based cross-sectional study was conducted among pregnant
women from March to May, 2017. A pre-tested and structured questionnaire was applied to collect
data on socio-demographic, pregnancy and clinical related factors. A total of 384 early morning mid-
stream urine sample was collected from study participants and the culture, gram staining, biochemical
and drug susceptibility testing were done following standard microbiological techniques. Most
importantly, ESBL production was screened using disk diffusion test and confirmed by a double disk
diffusion test. The data were entered and analyzed by using SPSS version 20 and a p-value of less than
0.05 was considered as statistically significant.
Result: The overall prevalence of UTI was 15.9% (95%CI = 12.8% -20.1%). E.coli (49.2%), CoNS
(27.9%), and S.aureus (18%) were the predominant uropathogens isolated from pregnant women. About
60.65% (95%CI = 45.3 – 72.1) of isolates were MDR. The prevalence of ESBLs production among
cases infected with Enterobacteriaceae was 18.2%. The drug resistance rate of gram negative isolates
was higher for ampicillin (90.9%), cephalothin (84.8%), and augmentin (57.6%). Gram positive isolates
were showed low susceptibility to penicillin (89.3%) and cotrimoxazole (75%). Nitrofurantoin showed
the highest activity (100%) against gram negative isolates. The susceptibility rate of gram positive
isolates was 100% for gentamicin and amikacin, and 98.36% for nitrofurantoin. Prior antibiotic therapy
(AOR = 5.46, 95%CI = 1.38 – 21.65) was associated with the presence of MDR bacteria.
Conclusion and recommendation: Since MDR prevalence was high among uropathogens, treatment
of UTI during pregnancy should be based on the antibacterial susceptibility testing result. The isolation
of highly drug resistant strains like ESBLs and MR staphylococcus spps in this study calls for the need
of antibiotic surveillance study in the study area. Nitrofurantoin and ciprofloxacin or norfloxacin
showed higher activity against uropathogens. Gentamicin and amikacin could also be used to treat gram
positive bacterial infections.
Key words: ESBL, uropathogens, pregnant women, UTI, MDR, Northwest Ethiopia

1
1. INTRODUCTION
1.1 Background
Urinary tract infection (UTI) is an infection involving structures (kidneys, ureters, bladder, or
urethra) that the urine passes through before being eliminated from the body (1). Urinary tract
infection can occur anywhere along the urinary tract, divided into upper tract infections
(pyelonephritis), and lower tract infections ( cystitis), which are commonly caused by bacteria
(2). Urinary tract can be infected in different ways such as due to haematogenous or lymphatic
spread of uncommon organisms like S.aureus, but the ascent of microorganisms from the
urethra is the common path way that leads to UTI (3).
Urinary tract infection is the most common public health problem worldwide, and females are
more likely to be infected due to their physiological conditions, proximity of the urethral
opening to the anus, the presence of vagina which can serve as a reservoir for bacterial
pathogens and the shorter length of the urethra (about 3 cm) (4, 5). Urinary tract infection be
presented with symptomatic and asymptomatic forms (6). Asymptomatic bacteriuria (ASB)
means an isolation of a specified quantitative count of bacteria in an appropriately collected
urine specimen obtained from a person without symptoms or signs referable to urinary
infection(7). Symptomatic UTI can be defined as a positive urine culture (significant
bacteriuria) with typical symptoms of a UTI like urinary frequency or urgency, dysuria,
suprapubic pain or fever (8). It is recommended to treat symptomatic UTI in all patients
according to local guidelines, but there is no need to treat ASB unless they are pregnant or
undergoing invasive urologic procedures (7, 8). Even if the prevalence of ASB is the same or
slightly higher in pregnancy (4-7%) than those without pregnancy, the risk of developing
pyelonephritis with bacteriuria during pregnancy is 25–30% (9), which has been linked to
maternal sepsis, respiratory distress, and an increase in the preterm birth rate (10).
Urinary tract infections during pregnancy can cause many complications both to mothers and
neonates. It is known that pre-term delivery, low birth weight, pre-eclampsia, intra uterine
growth retardation and cesarean delivery have been associated with maternal UTIs (11-13).
There is also a report about the effect of maternal UTIs on the increase incidence (by 5.9 fold)
of neonatal UTIs (14). In order to prevent these complications UTI during pregnancy has to be
treated (7, 8, 12-15). However, high prevalence of UTI during pregnancy in conjunction with
inappropriate and excessive antibacterial treatment are risk factors of increasing antibiotic
resistance (ABR) (16).

2
Antibiotic resistance is a growing problem across the world, and is the ability of a bacteria to
stop an antibiotics from working against it (17), or the ability of bacterial strains to survive
concentrations of antibiotics that kill sensitive cells of the same strain (18). Though,
antibacterial drugs have played a pivotal role in reducing the burden of infectious diseases,
indiscriminate use of drugs could leads for the rapid evolution of resistance strains due to a
lack of competition from susceptible ones (19). The development of ABR is a natural
evolutionary phenomenon, but it is largely accelerated by the selective pressure exerted by
widespread use of antibiotics as it has been extensively misused in both humans and food-
producing animals (20-22).
There are different mechanisms of ABR that the bacteria use to defend for its survival. One
mechanism is through the production of enzymes with the ability to hydrolyze antibiotics,
notably; beta lactam agents. These agents can stop bacterial cell wall synthesis (23), but there
are smart bacteria that have evolved enzymes like extended spectrum β-lactamases (ESBLs)
which can break down the amide bond of the antibiotic’s β-lactam ring and made them
ineffective (24). Extended-spectrum β-lactamases are capable of conferring bacterial resistance
to the penicillins, 1st, 2nd, and 3rd generation cephalosporins, and monobactams, but not the
cephamycins or carbapenems, and which are inhibited by β-lactamase inhibitors such as
clavulanic acid (25). These organisms also carry genes encoding resistance to other classes of
antibiotics, e.g. aminoglycosides, and quinolones. As a result, most of them are classified as
multi-drug resistance organisms (MDROs) (26). It has been also reported that these enzymes
and other ABR phenotypes can be transferred to drug susceptible strains (27). Multi-drug
resistant organisms such as ESBLs producing strains are associated with institutionalization,
previous use of any antibiotics, age, chronic underlying disease, urinary catheters, abdominal
surgery, ICU stay and gut colonization (28).
Because β-lactam antibiotics are well tolerated, efficacious, and currently most used classes of
antibacterial drugs in the infectious disease treatment (29), the emergence and rapid spread of
MDR mainly ESBL producing strains in different parts of the world is a night-mare, especially
for developing countries as they are usually relying on these drugs.

3
1.2 Statement of the problem
As it is stated above, UTIs represent the most common bacterial infections during pregnancy.
Pregnancy induces urinary retention due to the weight of the enlarging uterus, urinary stasis
due to progesterone-induced ureteral smooth muscle relaxation, increase in calyceal and
ureteral dilatation which is parallel to the incidence of pyelonephritis and the presence of
glycosuria and an increase in level of urinary amino acids. These changes, along with difficulty
with hygiene due to a distended pregnant belly could increases the frequency of UTIs (30).
Urinary tract infections during pregnancy are commonly caused by Gram-negative pathogens
with Enterobacteriaceae, in particular Escherichia coli (E.coli) accounting for about 90% of
these infections (31). Multi-drug resistant determinants like extended-spectrum β-lactamases
expressed in gram negative bacteria (GNB) influences the degree of resistance to antibiotics.
The family Enterobacteriaceae are typical ESBL producers with E.coli, K.pneumoniae and
K.oxytoca are common carriers of this enzyme. However, ESBL production has also been
observed in other Enterobacteriaceae (32). Since the family Enterobacteriaceae are the
commonly isolated strains from urine of pregnant women and are known for years due to their
ESBLs production characteristics, the consequence of UTIs can be greatly increased.
Urinary tract infections caused by MDR and ESBLs producing enterobacteriaceae are
associated with different problems during pregnancy, including the development of
pyelonephritis and cystitis in mother, pre-eclampsia, preterm delivery and having low birth
weight infant which makes the infant susceptible to infection (33, 34). Urinary tract infection
also found to be one of the main reasons causing cesarean deliveries with K.pneumoniae and
E.coli infections are the main causes, according to a study in Iran (35). Vertical transmission
of MDR bacteria or genes codes for drug resistance from mothers to their neonates also
documented. Extended spectrum β-lactamase producing organisms found to be vertically
transferred from mothers to neonates, early colonization of neonates with a significant number
of E.coli has been reported and drug resistance genes also found to be transferred from mothers
to both vaginal and cesarean delivered neonates (36). This types of scenario forces us to think
on how to prevent mother’s drug resistant genes before transferred to their neonates, and
screening mothers and treating them with appropriate medicine can give us a positive result.
The incidence of UTI among pregnant women has been reported in different parts of Ethiopia,
by 2010, it was 9.2% in Jimma (37), by 2011, 10.4% in Gondar (38) and 9.5% in Bahir Dar
(39), by 2012, 12% in Gondar (40) and 18.8% in Hawassa (41) and by 2015, it was 14% in
Dire Dawa . From these different findings, we can see that UTI is the common infection of

4
Ethiopian’s pregnant women with its incidence is slightly increased from year to year. In
Ethiopia, Enterobacteriaceae family especially E.coli and K.pneumoniae, which are common
ESBL producers, are also the leading causes of UTI among pregnant women (37-42).
It is reported that the rapid evolution of ESBL producing or other MDR bacteria is directly
associated with over use of antibiotics. Unless appropriate action taken, these bacteria may
soon out-numbered drug susceptible strains in the world. This situation will bring very serious
problem to the world, like a massive increase in morbidity and mortality due to ineffective
treatment and minimum availability in drugs and/or in resources. So it is important that each
health facility in once country has to know what is happening in their environment as it can
help the world to prevent new infections and control spread of present infections.
5
1.3 Literature review
I. Prevalence of MDR and ESBLs producing uropathogens
Bacteria move toward becoming MDR by means of accumulation of multiple genes as well as
increased expression of genes that code for multi-drug efflux pumps (43). The reported
prevalence of multi-rug resistant bacteria is vary with in different parts of the world. As a study
in Iran documented, the overall prevalence of MDR among UPEC isolates was 63% with 68%
and 61% among in-patients and out-patients, respectively (44).
Extended-spectrum β-lactamase production in bacteria especially Enterobacteriaceae family
has been reported in different parts of the world, and its occurrence is widely vary (45).
According to a study from Pakistan, the prevalence of MDR among uropathogens was
379/1000 (37.9%) and overall ESBL production was 58/100 (5.8%). The prevalence of ESBL
producing strains among MDR bacteria isolated from females was 32/172 (18.6%) (46).
In India, study on UTI of pregnant women showed that 87% of urine isolates were from
Enterobacteriaceae family, with 65.15% of them were ESBL producers. Proportion of ESBL
production in Klebsiella spp., E.coli, and Enterobacter spps. were 86.36% and 64.51%, and
30%, respectively. ESBL producing organisms had higher resistance to antibiotics than non-
producers (47). In another study on antibiotic susceptibility pattern (ASP) of ESBL
uropathogens from pregnant women, E.coli (44.4%), and K. pneumoniae (37.0%) were
common ESBL producing pathogens (48). Again a study on a wide range of urine sample from
pregnant women in India showed that 51.2% bacteriuria, of which 74.8% were from pregnant
women with asymptomatic bacteriuria. ESBL production has been observed in 47% and 36.9%
of E.coli and K.pneumonia isolates (49).
There is also a report in Nepal on prevalence of ESBL in pregnant women. In this study 91.33%
isolates were GNB, 72% of them were MDR, and E.coli (52%) and K.pneumoniae (17.3%)
were common isolates. The prevalence of ESBL production in GNB isolates were 7.3%.
Incidence of ESBL production were higher in K.pneumoniae (15.38%) than E.coli (7.69%)
(50).
According to the study from Bangladesh on prevalence of Extended Spectrum β-Lactamases
(ESBLs) producers among GNB in UTIs, the predominant urine isolates were E.coli,
K.pneumoniae and Enterococci spps, are accounts for 90.14% of all isolates. ESBL production
has been seen in 53.03% of isolates among all gram negative isolates from urinary tract

6
infections. Higher rate of ESBLs were seen in K.pneumoniae and E.coli isolates, which was
57.14% and 53.33%, respectively (51).
In Africa, Enterobacteriaceae family, especially E.coli and K.pneumoniae are the common
uropathogens, but proportion of ESBL producing Enterobacteriaceae isolated from UTI cases
is greatly vary with in countries; for example, one review documented the proportion as 4.3%-
20.2%, 1.5%-7.5% and 3.8% to 22.8% in countries with high, medium and low human
development index, respectively (52). Another review on proportion estimates of ESBL
producing Enterobacteriaceae in East Africa hospitals showed that the overall pooled
proportion of ESBL producing Enterobacteriaceae were 0.42 (42%), with 0.30 in Ethiopia,
0.42 in Kenya, 0.39 in Tanzania, and 0.62 in Uganda (53).
In a retrospective study from Central African Republic, the prevalence of ESBLs producing
strains was reported as 3.7%, 8.9%, and 19.3% in 2004, 2005, and 2006, respectively. It was
reported that these strains were common in patients under 15 years old (54). A study from
Madagascar highlights a significant prevalence of ESBL producer colonization among
pregnant women in the community with 18.5% prevalence of ESBL producing
Enterobacteriaceae (66.7% were E.coli and 16.67% were K.pneumoniae). This high rate of
maternal carriage of strains with a resistant ability to commonly used antibiotics may increase
the transmission of MDR stains to neonates (55).
In Nigeria, one study on ESBL producing uropathogens among asymptomatic pregnant women
found that E.coli (40%), K.pneumoniae (20%), and Enterobacter spp. (14%) were common
urine isolates. The prevalence of ESBL production were 20% among all isolates, with
Klebsiella spp. 9(56%), E.coli 6(38%), and Enterobacter cloacae 1(6%) (56). Almost similar
findings were reported in another study, 80 clinical isolates were isolated from 300 urine
samples of pregnant women, with Escherichia coli (42%), Klebsiella pneumoniae (21%),
Klebsiella oxytoca (12%), and Enterobacter spp. (12%) were common isolates. Among these
isolates 20% of them were ESBL producers, with 56% of Klebsiella spp.38% of E.coli, and
6% of E. cloacae were producers (57). Another study in the Nigerian University of Uyo
teaching hospital indicates that prevalence of E.coli and K.pneumoniae in urine of pregnant
women is 40% and 20% with 32% and 50% of each isolates were ESBL producer, respectively
(58).
A study from Tanzania on antimicrobial resistance among producers and non-producers of
ESBL in urinary isolates documented that 45.2% of the isolates were ESBL producers, with
39.1% and 51.1% of E.coli and K.pneumoniae isolates were producers of the enzyme (59).
7
In Ethiopia, there are a limited number of studies about ESBL producing organisms. A study
done from Jimma revealed that, all E.coli isolates were MDR. Among them, 36% were ESBL
producers. In another study, ESBL producing E.coli and K.pneumoniae were detected in
38.4% of all isolates, with 72.1% of ESBL producing pathogens were from female patients,
and 70.4% of K.pneumoniae isolates were ESBL producers (60, 61). A study conducted in
Bahirdar, reported that 57.6% and 9.4% prevalence of ESBLs producing Enterobacteriaceae
among clinical and drinking water samples, respectively (62).
II. Antibiotic resistance in uropathogens
The family Enterobacteriaceae are the most and frequently isolated bacteria from UTI which
is one of the most treated cases in the world. This scenario can tell us how much the
Enterobacteriaceae group are exposed to different antibiotics which actually help resistant
strains to greatly multiply. As a result economic cost, morbidity, and mortality become
prevalent. Other uropathogens mainly staphylococcus species are also known in the field of
multi drug resistance; for instance methicillin resistant staphylococcus spps.
A study from Pakistan on MDR E. coli and K. pneumoniae causing UTI in pregnant women
documented that these strains showed a high rate of resistance, which was >50%, to ampicillin,
nalidixic acid, cefotaxime, norfloxacin, ceftriaxone and ceftazidime. Resistance to ampicillin
was actually 100% in these isolates (63).
In Sri Lanka, ESBL producing E.coli and K.pneumoniae uropathogens were highly resistance
to commonly used oral antibiotics (ampicillin 100%, nalidixic acid 98%, norfloxacin 97% and
cotrimoxazole 79%). These stains also had resistance rates of 72%, 61% and 94% for
gentamicin, amoxicillin/clavulanate, and ciprofloxacin, respectively compared to isolates that
were negative for ESBL with resistance rates of 2%, 2%, and 8%, respectively. Nitrofurantoin
were effective treatment for infections (64).
A cross sectional study from Nigeria on ASP of uropathogens from pregnant women with UTI
found that isolated uropathogens showed a high rate of resistance to cotrimoxazole (99.6%),
amoxicillin (98.8%), cloxacillin (95.6%), tetracycline (84.1%), chloramphenicol (81.2%),
nalidixic acid (78.6%) nitrofurantoin (66.3%) and streptomycin (61.9%). They were sensitive
to levofloxacin, cefpodoxime, ofloxacin, ciprofloxacin and ceftriaxone (65). Another study
from Nigeria showed that E.coli isolates were less susceptible to ceftriaxone (15.8%),
cefuroxime (14%) and amoxicillin (2.3%), K.pneumoniae was completely resistant to
ampicillin (66). Again in another study, gram negative isolates from urogenital samples showed

8
a high degree of resistance to gentamicin (84%), streptomycin (91%), aztreonam (96%), and
erythromycin (98%). K.pneumoniae and E.coli were resistant to cefoxitin (67% and 58%) and
cefepime (67% and 61%) (67).
A reviewed article from Southern and Eastern Africa showed that a high resistance to
antibiotics especially by GNBs; for example, 84.5% to ampicillin, 68.5% to cotrimoxazole and
over 90% to trimethoprim /sulfamethoxazole from Tanzanian isolates with E.coli was the
commonest one. Higher resistance to antibiotics in Ethiopia have been documented with
multiple resistance rates to erythromycin (89.4%), amoxicillin (86.0%) and tetracycline
(72.6%) by Enterobacteriaceae isolates from different clinical samples (68).
A study from Gondar documented that uropathogens showed a high rate of resistance to
ampicillin (91.7%), amoxicillin (79.1%), tetracycline (52.3%) and cotrimoxazole (50%), but
sensitive to ceftriaxone (87.5%) amoxicillin/clavulanic acid (83.3%), ciprofloxacin (75%),
norfloxacilin (70.8%) and chloramphenicol (66.7%) (40).
III. Risk factors for the presence of MDR bacterial infection.
Risk factors for the occurrence of UTIs during pregnancy which might be caused by MDR
bacteria have been documented. A study in USA documented that usage of invasive devices,
antibiotic therapy and longer hospitalization were associated factors for the presence of MDR
E.coli isolates (69). The use of broad spectrum antibiotic therapy was reported as a risk factor
for the presence of MDR bacterial infection A study in Ethiopia also documented that previous
use of antibiotics, hospitalization, and history of catheterization were risk factors for the
presence of MDR bacterial infection (70)

9
1.4 Significance of the study
Since UTI is higher in pregnant women and most cases are related to bacteria, there is a chance
that complication may occur to mothers and neonates. Because Enterobacteriaceae are the
most common isolates in UTIs and are the leading candidate for production of ESBLs, there is
a reasonable chance of resistance to penicillin and other derivatives including cephalosporins
and monobactams (commonly used to treat UTIs).
In developing world especially in Africa, because of financial problems in conjunction with
negligence, many UTIs during pregnancy are diagnosed clinically and treated empirically.
Hence, lack of specific diagnostic tools like culture and sensitivity testing leads to blind
treatment, in turn it could promote the rapid spread of MDR strains including ESBLs producing
strains.
A WHO global report has revealed the overall epidemiology of ESBL producing bacteria have
not been well understood in resource limited countries like Ethiopia (20). Therefore, this study
is aimed at, to determine MDR and ESBL production in bacterial uropathogens isolated from
pregnant women; and to identify associated risk factors with MDR bacterial infection. As a
result, this study will help for clinicians in the drug prescription practice towards UTIs
treatment during pregnancy especially in the study area. Additionally, it may open the door for
other researchers interested in the same field.

10
2. OBJECTIVES
2.1 General Objective
To assess Multi-drug resistance, extended spectrum β-lactamase (ESBL) production and
associated risk factors with MDR uropathogens isolated from pregnant women at the UoG
Teaching Hospital, Gondar, Ethiopia.
2.2 Specific Objectives
To determine the prevalence of Multi-drug resistant bacterial isolates among culture
positive pregnant women.
To determine the prevalence of extended spectrum β-lactamase production among gram
negative uropathogens isolated from pregnant women
To identify factors associated with the presence of MDR bacterial infection among
pregnant women

11
3. MATERIALS AND METHODS
3.1 Study Area
The study was conducted at the University of Gondar teaching hospital, Gondar, Amhara,
Northwest Ethiopia. Gondar teaching hospital is found in Gondar town, with a distance of 747
km from Addis Ababa (capital city of the country) and 182 km far from Bahir Dar (capital city
of Amhara regional state). The hospital is one of the biggest tertiary level referral and teaching
hospital in Amhara region. An estimated of 5 million people from the surrounding zones and
nearby regions visit for different medical services.
3.2 Study design and period
A hospital based cross-sectional prospective study was conducted among pregnant women
from March to May, 2017
3.3 Population
3.3.1 Source population
The source population was all pregnant women seeking medical help at the UoGTH.
3.3.2 Study population
The study population was all pregnant women visiting the ANC unit of the UoGTH during the
study period.
3.4 Inclusion and Exclusion criteria
3.4.1 Inclusion criteria
All pregnant women who visited the ANC unit at the UoGTH and were eligible for this study.
3.4.2 Exclusion criteria
All pregnant women on antibiotic treatment for the last two weeks from data collection and
during data collection were excluded from the study as therapy may disrupt the number of
bacteria in the urine sample.
3.5 Sample size and sampling procedures
3.5.1 Sample size
The sample size was calculated based on single population proportion formula as shown below.
The value of p was taken as 50% (0.5) because as to the best of our knowledge, there was no
local data available on the prevalence of ESBL producing bacterial isolates among pregnant
women.

12
𝑛 =𝑍2𝑃(1 − 𝑃)
𝑑2=(1.96)2(0.5)(1 − 0.5)
(0.05)2= 384
Where n = sample size, Z = Z statistic for a level of confidence, P = expected prevalence or
proportion, and d = precision (d = 0.05), Z = Z statistic: Standard normal distribution value at
95% CI, which is 1.96.
3.5.2 Sampling technique
After obtaining the average number of pregnant women (900) visiting the antenatal clinic of
the UoG Teaching Hospital per month (registration book from the hospital), the number of
source subjects who were possibly visit the clinic within the study period were estimated
(2700). The sampling interval k = 7 were determined by dividing this estimated number by the
study sample size which is 384. The first unit (which was 4) were selected at random (using
lottery method) and other units were selected systematically by taking every 7th unit after the
4th unit.
3.6 Study Variables
3.6.1 Dependent variable
Presence of Extended spectrum beta lactamase producing bacterial infection
Presence of MDR bacterial infection among pregnant women
3.6.2 Independent variables
Socio demographic characteristics
Pregnancy related characteristics
Previous hospitalization,
Previous antibiotic usage
Presence of diabetes,
Presence of HIV
Past history of UTI.
3.6.3 Operational definitions
Previous hospitalization: defined as participants experienced hospitalization for a medical
condition in the last twelve months, and before the date of this study
Previous antibiotic usage: defined as participants using any antibiotics before two weeks from
the day on which they gave their urine sample for this study.
13
Previous history of urinary tract infection: defined as participants had confirmed urinary
tract infection in the last twelve months, and before the date of this study.
MDR: a bacterial isolate which is resistant to one or more antibiotics in three or more classes
of antimicrobials that the isolate is expected to be susceptible is said to be MDR bacteria.
ESBLs: are enzymes that can hydrolyze penicillins, 1st, 2nd, and 3rd generation cephalosporins,
and monobactams, but not the cephamycins or carbapenems, and which are inhibited by β-
lactamase inhibitors such as clavulanic acid.
3.7 Data collection procedures
3.7.1 Socio-demographic and clinical data
A structure and pre-tested questionnaire were used to collect data on socio demographic
characteristics (age, educational status, etc.), clinical characteristics (Previous hospitalization,
history of UTI, history of antibiotic use, etc.) and pregnant related issues (gestation period,
parity, etc.). Data were gathered from each study subjects, and carried out by trained data
collectors (midwives).
3.7.2 Sample collection
After giving professional instruction to pregnant women on how to collect clean-catch mid-
stream urine sample, about 20 ml of urine specimen were collected in a sterile screw-capped,
wide-mouthed container from each pregnant woman. After labelling the container with unique
sample number, date and time of collection, it was placed in to the refrigerator (4–6 °C) until
it was ready for processing, which were obviously done within 1-2 hours of collection (71).
3.7.3 Culture and identification techniques
Urine specimen was first inoculated on Cysteine Lactose Electrolyte Deficient (CLED) agar
using sterile loop measuring 0.01µl then later colonies from CLED agar were subjected to gram
staining procedure and then sub-cultured on MacConkey and Blood agar plates. The plates
were incubated in appropriate atmosphere at 37OC for 24-48 hrs overnight. The numbers of
culture grown bacteria were estimated by using a calibrated loop that can hold a specified
amount of bacterial suspension and by accepting that a single colony growth represents a single
organism. The result was reported as number of colony forming unit (CFU) per ml of urine. A
count of ≥ 105 CFU/ml of urine was considered as a true infection (significant bacteriuria).
Each significant bacteria was identified by colony characteristics on the respective media, gram
14
staining and the pattern of biochemical reactions (71). The API 20E also used to support the
bacterial identification process (bioMerieux, France).
3.7.4 Drug Susceptibility Testing (DST)
Antibiotic susceptibility testing and screening of potential ESBLs were carried out using disk
diffusion method. The bacterial suspension were made and incubated at 37°C for about 4 to 5
hours then its turbidity were adjusted to a 0.5 McFarland turbidity standard. The turbidity of
suspension was adjusted by adding sterile saline to the bacterial suspension if the suspension
is more turbid or incubate the suspension further if the turbidity is lower than the standard (71).
Muller Hinton Agar (MHA) was used for doing antimicrobial susceptibility test. Antimicrobial
disks used in this study include: ampicillin (10µg), cephalothin (30µg), nalidixic acid (30µg),
cefepime (30µg), augmentin (30µg), ceftazidime (30µg), cefotaxime (30µg), cefuroxime,
cefoxitin (30µg), cefixime, norfloxacin (10µg), ciprofloxacin (5µg), ceftriaxone (30µg),
nitrofurantoin (300µg), Trimethoprim-sulfamethoxazole (1.25/23.75µg), gentamicin (10µg),
amikacin (30µg), tetracycline (30µg), chloramphenicol (30µg), doxycycline (30µg). Plates
were inverted and incubated at 37 OC for 18 - 24 hrs. Growth inhibition was measured to the
nearest whole millimeter using a calliper. The zone diameter was interpreted according to the
Clinical and Laboratory Standards Institute (CLSI) guideline as susceptible (S), intermediate
(I), or resistant (R) (72).
3.7.5 Extended Spectrum β-Lactamase Detection
Extended spectrum β-lactamase production was detected using two steps; screening, and
confirmatory.
I. Screening procedure
All isolates showing reduced susceptibility to either of the 3rd generation cephalosporins
(Cefpodoxime zone: ≤17 mm; Ceftazidime zone: ≤22 mm; Cefotaxime zone: ≤27 mm;
Ceftriaxone zone: ≤25 mm) were selected after performing initial antibiotic susceptibility
testing on MHA using CLSI (2017) recommended Disk-Diffusion methods. Those isolates then
subjected to phenotypic confirmatory test to confirm the possible presence of ESBL enzyme
(73).
II. Confirmatory procedure
Double disk (Combination disk) diffusion test: This test was done using CLSI, 2017
recommendations as a reference (73). We used ceftazidime (30µg) and cefotaxime (30µg) disks
15
with and without clavulanate (10µg) in order to confirm whether the bacteria were ESBL
producers or not. After the bacterial suspension were adjusted in a way that it gives confluent
growth on MHA using 0.5 McFarland standard suspension as a reference, cefotaxime (30µg),
ceftazidime (30µg), ceftazidime-clavulanate (30/10µg) and cefotaxime-clavulanate (30/10µg)
disks were plated on MHA that was inoculated with a single bacterial suspension. After
overnight incubation for about 16-18 hours at 37oC, a ≥ 5mm increase in a zone diameter for
either cefotaxime or ceftazidime tested in combination with clavulanate Vs the zone diameter
of the agent (ceftazidime or cefotaxime) when tested alone was taken as positive for the
presence of ESBLs in bacterial isolates.
3.7.6 Quality control
Pre-tested and structured questionnaire was used to collect socio-demographic, pregnancy, and
clinical related factors. Standard Operating Procedures (SOPs) were strictly followed during
pre-analytical, analytical and post-analytical stages of sample collection and laboratory work.
The quality of each of the culture media were checked using reference strains (E.coli ATCC
25922, P.aeruginosa ATCC 27853 and S.aureus ATCC 25923) before starting to use them for
growing bacterial isolates from urine sample. The sterility of the prepared media were also first
checked by incubating 5% of the batch overnight at 37oC and confirm its sterility before using
the batch for our sample. For ESBL positive control, K.pneumoniae ATCC 700603 and ESBL
negative control, E.coli ATCC 25922 strains were used (73).
3.8 Data processing and Analysis
The data was entered in to Statistical Package for Social Sciences (SPSS) version 20 and was
double checked before analysis. Appropriate descriptive statistics for demographic and clinical
characteristics were calculated. Factors suspected to be a risk for the emergence of MDR
bacteria were analyzed by bivariate analysis and multivariate logistic regression analysis to
assess the association between dependent and independent variables. Variables with a p- value
of < 0.2 in the bi-variate analysis were included in the multivariate logistic regression analysis.
Odds ratio was calculated with a confidence interval of 95% and a p-value < 0.05 was
considered as statistically significant. Study findings were explained in words, tables and
graphs.

16
3.9 Ethical consideration
Prior to the commencement of the study, ethical clearance was obtained at the University of
Gondar, School of Biomedical and Laboratory Sciences ethical review committee and official
letter of co-operations was provided to UoGTH. Written and informed consent was obtained
from study participants after explaining the purpose and objective of the study. Any patient
who was not willing to participate in the study had the right to decline from the study and her
treatment procedure was never be affected by this decision. They were informed that all data
and sample obtained from them was kept confidential by using codes instead of any personal
identifiers and was meant only for the purpose of the study. The result from the study
participant was sent to their physicians for appropriate treatment.

17
4. RESULTS
Sociodemographic characteristics
A total of 384 pregnant women were participated in the present study. The minimum and the
maximum ages of the study subjects were 15 and 45 years with a mean age of 26.27 and a
standard deviation of 5.4. About 349 (90.9%) of the study subjects were Orthodox Christians,
305 (79.4%) were urban, and 365 (95%) were married. About 128 (33%) of the participants
were illiterate, 167 (43.5%) were house wife, and 110 (28.6 %) had monthly income ≤1000
birr (Table 1).
Table 1: Socio demographic characteristics of pregnant women attending ANC clinic at the
UoGTH, March to May, 2017.
Socio-demographic characteristics Frequency Percentage
Age (in years)
15 – 19 21 5.5
20 – 24 127 33.1
25 – 29 141 36.7
30 – 34 51 13.3
>34 44 11.5
Religion
Orthodox 349 90.9
Muslim 31 8.1
Protestant 2 0.5
Others 2 0.5
Residence
Urban 305 79.4
Rural 79 20.6
Marital status
Currently single 19 4.9
Currently married 365 95.1
Level of Education
Not read and write 128 33.3
Primary 71 18.5
Secondary 99 25.8
College/university 86 22.4
Occupation
House wife 167 43.5
Farmer 37 9.6
Merchant 46 12
Employed 96 25
Daily laborer 21 5.5
Others 17 4.4
Monthly Income (in birr)
≤1000 110 28.6
1000 – 1800 86 22.4
1801 – 2800 98 25.5
≥2801 90 23.4

18
Pregnancy and clinical related factors
Of the total participants, 190 (49.5%), and 119 (31%) were on their 3rd, and 2nd trimester,
respectively. Of the total study participants, 224 (58.3%) of the pregnant mother had more than
one pregnancy experience, 176 (45.8%) of the women were nulliparous (a women who had no
given birth before). Of the total study subjects, 26 (6.8%) had a history of prior hospitalization,
62 (16.1%) had history of previous UTI, and 88 (22.9%) had prior antibiotic therapy. The 3.4%
of pregnant women had HIV infection. Number of pregnant women with symptom of UTI were
122 (31.8%) (Table 2).
Table 2: Pregnancy and clinical related factors among pregnant women attending ANC clinic
at the UoGTH, March to May, 2017.
Pregnancy related characteristics Frequency Percentage
Gestation period
<3 months 55 14.3
3 – 6 months 119 31
>6 months 190 49.5
Don’t know 20 5.2
No of Pregnancy
Prim-gravida 160 41.7
Multi-gravida 224 58.3
No of times giving birth
Nulliparous 176 45.8
Primiparous 98 25.5
Multiparous 110 28.6
Previous Hospitalization
Yes 26 6.8
No 358 93.2
History of UTI
Yes 62 16.1
No 322 83.9
Antibiotic therapy
Yes 88 22.9
No 296 77.1
HIV
Yes 13 3.4
No 371 96.6
Participant status for UTI
Symptomatic 122 31.8
Asymptomatic 262 68.2

19
Prevalence
The overall prevalence of UTI among study participants was 61 (15.9% (95%CI = 12.8 - 20.1)).
Of all isolated uropathogens, E.coli (30 (49.2%)) was the most common cause of urinary tract
infection followed by CoNS (17 (27.9%)) and S.aureus (11 (18%)). The prevalence of MDR
among uropathogens was 37/61 (60.65% (95%CI = 45.3 – 72.1)). About 13 (76.47%) of the
CoNS and 17 (56.67%) of the E.coli isolates were MDR. The prevalence of ESBLs production
among gram negative bacteria isolated from pregnant women found to be 6/33 (18.2%). E.coli
and E.clocae were the two ESBL producing isolates. Methicillin resistant among gram positive
isolates were done and 4 (36.36%) of the S.aureus were MRSA and 8 (47.06%) of the CoNS
were MRCoNS (Table 3).
Table 3: The prevalence of MDR, ESBLs producing and MR (Methicillin resistant) bacteria
among uropathogens isolated from pregnant women attending ANC clinic at the UoGTH,
March to May, 2017.
Isolates
Number (%)
Frequency and percentage (prevalence)
MDR ESBL MR
E.coli 30 (49.2%) 17 (56.67%) 5 (16.67%) -
K.pneumoniae 2 (3.3%) 1 (50%) 0 -
E.clocae 1 (1.6%) 1 (100%) 1 (100%) -
S.aureus 11 (18%) 5 (45.45%) - 4 (36.36%)
CoNS 17 (27.9%) 13 (76.47%) - 8 (47.06%)
Total 61 (100%) 37/61 (60.65%) 6/33 (18.18%) 12/28 (42.85%)
Key; MDR: Multi-drug resistant, ESBL: Extended spectrum β-lactamase, MR: Methicillin resistant
The prevalence of urinary tract infection among symptomatic and asymptomatic pregnant
women was 38/122 (31.1%) and 23/262 (8.8%), respectively. The Fisher’s exact test showed
that history of hospitalization, previous history of UTI, and prior antibiotic therapy were
associated with the presence of UTI. Study subjects who had sign and symptom of UTI had
significantly higher UTI infection than those without sign and symptoms. The prevalence of
MDR bacteria was 25/38 (65.8%) among culture positive symptomatic pregnant women and
12/23 (52.2%) among culture positive asymptomatic subjects. The prevalence of MDR was
significantly higher (p < 0.05) among study participants who had a history of antibiotic therapy
than those who hadn’t. (Table 4).

20
Table 4: Pregnancy and clinical related factors against significant bacteriuria and MDR bacteria among pregnant women attending the ANC
clinic at the UoGTH, March to May, 2017.
Variables Significant bacteriuria MDR bacteria
Yes No Total p- value Yes No Total p- value
Gestation period
<3 months 6 (10.9%) 49 (89.1%) 55 0.219 3 (50%) 3 (50%) 6 0.808
3 – 6 months 24 (20.2%) 95 (79.8%) 119 15 (62.5%) 9 (37.5%) 24
>6 months 30 (15.8%) 160 (84.2%) 190 18 (60%) 12 (40%) 30
Don’t know 1 (5%) 19 (95%) 20 1 (100%) 0 1
No of Pregnancy
Prim-gravida 29 (18.1%) 131 (81.9%) 160 0.383 21 (72.4%) 8 (27.6%) 29 0.127
Multi-gravida 32 (14.3%) 192 (85.7%) 224 16 (50%) 16 (50%) 32
No of times giving birth
Nulliparous 31 (17.6%) 145 (82.4%) 176 0.501 21 (67.7%) 10 (32.3%) 31 0.492
Primiparous 12 (12.2%) 86 (87.8%) 98 6 (50%) 6 (50%) 12
Multiparous 18 (16.4%) 92 (83.6%) 110 10 (55.6%) 8 (44.4%) 18
Hospitalization
Yes 15 (57.7%) 11 (42.3%) 26 <0.001 10 (66.67%) 5 (33.3%) 15 0.807
No 46 (12.8%) 312 (87.2%) 358 27 (58.7%) 19 (41.3%) 46
History of UTI
Yes 27 (43.5%) 35 (56.5%) 62 <0.001 20 (74.07%) 7 (25.93%) 27 0.099
No 34 (10.6%) 288 (89.4%) 322 17 (50%) 17 (50%) 34
Antibiotic therapy
Yes 27 (30.7%) 61 (69.3%) 88 <0.001 22 (81.5%) 5 (18.5%) 27 0.007
No 34 (11.5%) 262 (88.5%) 296 15 (44.12%) 19 (55.88%) 34
HIV
Yes 4 (30.8%) 9 (69.2%) 13 0.135 3 (75%) 1 (25%) 4 1
No 57 (15.4%) 314 (84.6%) 371 34 (59.65%) 23 (40.35%) 57
Participant status for UTI
Symptomatic 38 (31.1%) 84 (68.9%) 122 <0.001 25 (65.8%) 13 (34.2%) 38 0.433
Asymptomatic 23 (8.8%) 239 (91.2%) 262 12 (52.2%) 11 (47.8%) 23
Key; MDR: Multi-drug resistant, UTI: Urinary tract infection, HIV: Human immuno-deficiency virus
Note: The percentage displayed under positive culture and MDR was calculated using the frequency of each classes of the variable group that
were enrolled in this study, and positive for culture as a denominator, respectively

21
Antimicrobial susceptibility pattern
Antibiotic susceptibility testing showed a high resistance rate of ampicillin 27 (90%), cephalothin 25
(83.33%), and augmentin 17 (56.7%) among E.coli isolates. None of the gram negative isolates were
resistant to nitrofurantoin. Resistance rate for ampicillin and cephalothin was 100 % among
K.pneumoniae isolates. There was only one uropathogen found to be resistant to nitrofurantoin which
was one of the CoNS. Among the gram positive isolates, 4 (36.4%) of the S.aureus and 8 (47%) of the
coagulase negative staphylococcus (CoNS) were resistant to cefoxitin. None of the gram positive isolates
were resistant to gentamicin and amikacin, but a high penicillin (90.9% and 88.2%) and cotrimoxazole
(63.63% and 82.35%), resistance rate among S.aureus and CoNS were observed, respectively (Table 5)
Table 5: Distribution of drug resistance pattern among uropathogens isolated from pregnant women
attending ANC clinic of the UoGTH, March to May, 2017
Antibiotics
tested
Isolated organisms
Total (61) E.coli
(n = 30)
K.pneumoniae
(n = 2)
E.clocae
(n = 1)
S.aureus
(n = 11)
CoNS
(n = 17)
AUG 17 (56.67%) 1 (50%) 1 19/33 (57.6%)
FEP 6 (20%) 0 1 7/33 (21.2%)
CFM 6 (20%) 0 1 7/33 (21.2%)
CRO 5 (16.67%) 0 1 6/33 (18.2%)
FOX 3 (10%) 0 1 4 (36.36%) 8 (47.05%) 18/61 (26.2%)
CXM 5 (16.67%) 0 1 6/33 (18.2%)
AMP 27 (90%) 2 (100%) 1 30/33 (90.9%)
NAL 5 (16.67%) 0 1 6/33 (18.2%)
CF 25 (83.33%) 2 (100%) 1 28/33 (84.8%)
CPD 5 (16.67%) 0 1 6/33 (18.2%)
CAZ 5 (16.67%) 0 1 6/33 (18.2%)
NOR 4 (13.33%) 0 0 1 (9.1%) 8 (47.05%) 13/61 (21.3%)
F 0 0 0 0 1 (5.9%) 1/61 (1.64%)
CIP 4 (13.33%) 0 0 1 (9.1%) 8 (47.05%) 13/61 (21.3%)
CTX 5 (16.67%) 0 1 6/33 (18.2%)
GEN 0 0 0/28 (0.0%)
PEN 10 (90.9%) 15 (88.2%) 25/28 (89.3%)
TE 2 (18.18%) 9 (52.9%) 11/28 (39.3%)
COT 7 (63.63%) 14 (82.35%) 21/28 (75%)
AMK 0 0 0/28 (0.0%)
DOX 2 (18.18%) 10 (58.82%) 12/28 (42.68%)
C 3 (27.27%) 9 (52.9%) 12/28 (42.68%)
ERY 2 (18.18%) 9 (52.9%) 11/28 (39.3%)
Key: “”: Not done, AUG: Amox-clavulanic acid, FEP: Cefepime, CFM: Cefixime, CRO: Ceftriaxone, FOX: Cefoxitin,
CXM: Cefuroxime, AMP: Ampicillin, NAL: Nalidixic acid, CF: Cephalothin, CPD: Cefpodoxime, CAZ: Ceftazidime, NOR:
Norfloxacin, F: Nitrofurantoin, CIP: Ciprofloxacin, CTX: Cefotaxime, PEN: Penicillin, TE: Tetracycline, COT:
Cotrimoxazole, AMK: Amikacin, DOX: Doxycycline, C, Chloramphenicol, and ERY: Erythromycin.

22
Only 2/61 (3.28%) of bacterial isolates were sensitive to all antibiotics used in this study. The 16 (26.23%)
of the isolates were resistant to three of the antibiotics tested. The 14 (22.95%) of the isolates were
resistant to two of the antibiotics tested. About 19 (31.15%) of the isolates were resistant to at least five
of the antibiotics tested (Table 6).
Table 6: Distribution of multiple drug resistance among uropathogens isolated from pregnant women
attending ANC clinic at the UoGTH, March to May, 2017.
Isolated organisms
Number of drugs affected by the isolate
Total R0 R1 R2 R3 R4 R5
E.coli (n = 30) 2 (6.67%) 1(3.33%) 8 (26.67%) 10 (33.33%) 2 (6.67%) 7 (23.33%) 30
K.pneumoniae (n = 2) 0 (0.0%) 0 (0.0%) 1 (50%) 1 (50%) 0 (0.0%) 0 (0.0%) 2
E.clocae (n = 1) 0 (0.0%) 0 (0.0%) 0 (0.0%) 0 (0.0%) 0 (0.0%) 1 (100%) 1
S.aureus (n = 11) 0 (0.0%) 3 (27.27%) 3 (27.27%) 2 (18.18%) 1 (9.09%) 2 (18.18%) 11
CoNS (n = 17) 0 (0.0%) 2 (11.76%) 2 (11.76%) 3 (17.65%) 1 (5.88%) 9 (52.94%) 17
Total (61) 2 (3.28%) 6 (9.84%) 14 (22.95%) 16 (26.23%) 4 (6.56%) 19 (31.15%) 61
Key: R0: Resistant to none (Sensitive to all), R1: Resistant to one, R2: Resistant to two, R3: Resistant to three, R4: Resistant
to four and R5: Resistant to five and more antibiotics tested.

23
ESBLs producing strains showed a 100% resistance rate to all of the 3rd generation cephalosporin and,
cefuroxime, and cefepime, and the difference was significant (p< 0.001) when compared to resistance
rates by non ESBLs producing bacterial isolates. Ampicillin and cephalothin were also ineffective against
all ESBLs and most non-ESBLs producing strains and the difference was not significant. Nitrofurantoin,
norfloxacin and ciprofloxacin were batter in clearing ESBLs producing uropathogens than other classes
of antibiotics used in this study. (Table 7)
Table 7: The distribution of antibiotic resistance among ESBLs producing and non ESBLs producing
gram negative bacteria isolated from pregnant women attending ANC at the UoGTH, January to May,
2017.
Antibiotics tested
ESBL
p-value No (27) Yes (6)
Cephalothin 22 (81.5%) 6 (100%) 0.556
Cefpodoxime 0 (0.0%) 6 (100%) < 0.001
Amox-clavulanic acid 15 (55.6%) 4 (66.7%) 0.618
Cefepime 1 (3.7%) 6 (100%) < 0.001
Cefixime 1 (3.7%) 6 (100%) < 0.001
Ceftriaxone 0 (0.0%) 6 (100%) < 0.001
Cefoxitin 1(3.7%) 3 (50%) 0.014
Cefuroxime 0 (0.0%) 6 (100%) < 0.001
Ampicillin 24 (88.9%) 6 (100%) 0.392
Nalidixic acid 2 (7.4%) 4 (66.7%) 0.005
Ceftazidime 0 (0.0%) 6 (100%) < 0.001
Norfloxacin 2 (7.4%) 2 (33.33%) 0.142
Nitrofurantoin 0 (0.0%) 0 (0.0%) -
Ciprofloxacin 2 (7.4%) 2 (33.33%) 0.142
Cefotaxime 0 (0.0%) 6 (100%) < 0.001
24
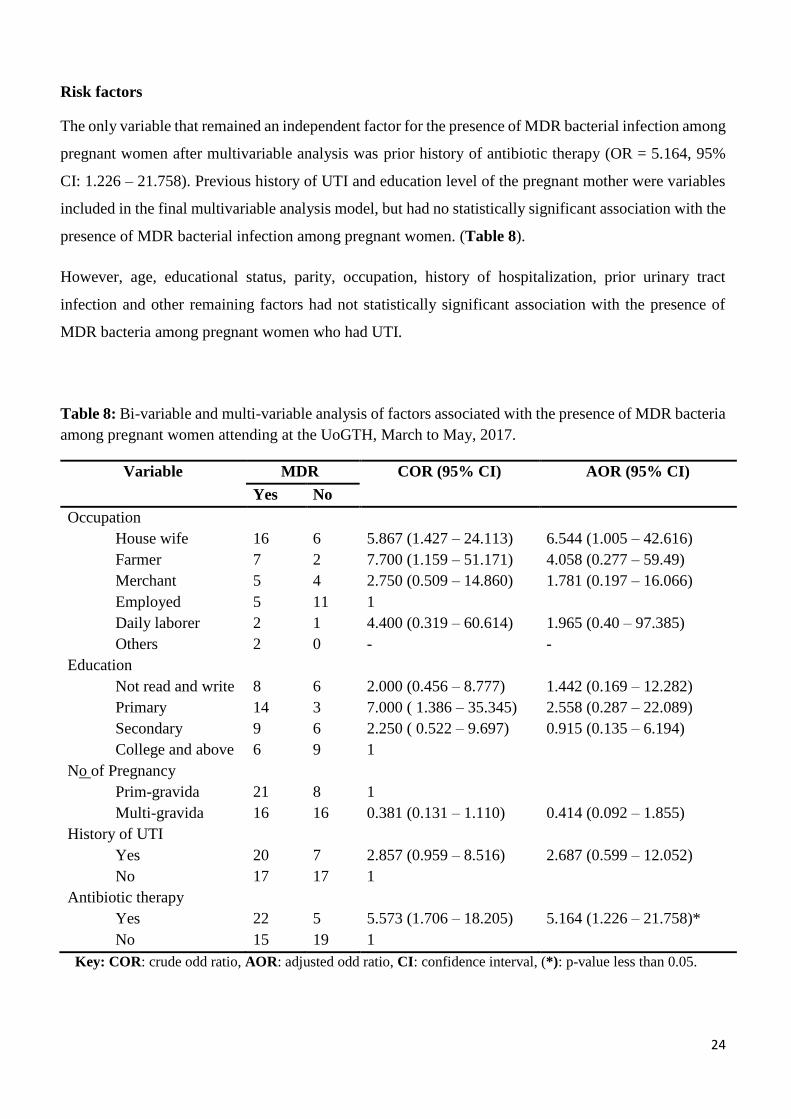
Risk factors
The only variable that remained an independent factor for the presence of MDR bacterial infection among
pregnant women after multivariable analysis was prior history of antibiotic therapy (OR = 5.164, 95%
CI: 1.226 – 21.758). Previous history of UTI and education level of the pregnant mother were variables
included in the final multivariable analysis model, but had no statistically significant association with the
presence of MDR bacterial infection among pregnant women. (Table 8).
However, age, educational status, parity, occupation, history of hospitalization, prior urinary tract
infection and other remaining factors had not statistically significant association with the presence of
MDR bacteria among pregnant women who had UTI.
Table 8: Bi-variable and multi-variable analysis of factors associated with the presence of MDR bacteria
among pregnant women attending at the UoGTH, March to May, 2017.
Variable MDR COR (95% CI) AOR (95% CI)
Yes No
Occupation
House wife 16 6 5.867 (1.427 – 24.113) 6.544 (1.005 – 42.616)
Farmer 7 2 7.700 (1.159 – 51.171) 4.058 (0.277 – 59.49)
Merchant 5 4 2.750 (0.509 – 14.860) 1.781 (0.197 – 16.066)
Employed 5 11 1
Daily laborer 2 1 4.400 (0.319 – 60.614) 1.965 (0.40 – 97.385)
Others 2 0 - -
Education
Not read and write 8 6 2.000 (0.456 – 8.777) 1.442 (0.169 – 12.282)
Primary 14 3 7.000 ( 1.386 – 35.345) 2.558 (0.287 – 22.089)
Secondary 9 6 2.250 ( 0.522 – 9.697) 0.915 (0.135 – 6.194)
College and above 6 9 1
No of Pregnancy
Prim-gravida 21 8 1
Multi-gravida 16 16 0.381 (0.131 – 1.110) 0.414 (0.092 – 1.855)
History of UTI
Yes 20 7 2.857 (0.959 – 8.516) 2.687 (0.599 – 12.052)
No 17 17 1
Antibiotic therapy
Yes 22 5 5.573 (1.706 – 18.205) 5.164 (1.226 – 21.758)*
No 15 19 1
Key: COR: crude odd ratio, AOR: adjusted odd ratio, CI: confidence interval, (*): p-value less than 0.05.

25
5. DISCUSSION
The high prevalence of UTI during pregnancy and fear of its complication on both mothers and their baby
(11, 35) encourages the irrational use of antibiotics (74) especially in the developing world where
empirical treatment is prevalent. This indiscriminate use of antibiotics could be responsible for the
emergence of drug resistance strains. Having the prevalence of drug resistant strains among pregnant
women at hand could help clinicians in improving the wise use of antibiotics during pregnancy and
preventing and controlling infections.
The reported prevalence of UTI (15.9%) in this study was in agreement with previous study in eastern
Ethiopia (42) which was 14%, in Tanzania by Masinde et al (75) which was 14.6%. But it was higher
than the studies conducted in Bahir Dar by Tazebew D et al (39) which were 9.5% and in Gondar by
Alemu et al (38) which were 10.4%. This difference might be due to the higher proportion of symptomatic
study participants in the present study.
In the present study, E.coli was the predominant isolate among uropathogens with a prevalence of 49.2%
followed by CoNS (27.9%), and S.aureus (18.03%). Previous reports from regions of Ethiopia have also
shown that E.coli was the commonly isolated uropathogen from pregnant women (38, 39, 42) where
E.coli, CoNS, and S.aureus as the three predominant bacterial isolates among pregnant women. The
result, however, was slightly different from the study from Hawassa (41) where CoNS were frequently
isolated than E.coli. This difference might be due to the difference in hygienic practices between study
participants and climate and temperature factors.
The prevalence of MDR among uropathogens in the present study was 60.65%. This is in line with the
study done in the same area back in 2002 with a reported prevalence of 68% (70), but another study done
in 2012 showed a higher prevalence of MDR bacteria (95%) (38). Lower MDR prevalence in this study
might be due to the difference in a MDR definition. In this study MDR was defined as any organism that
was resistant to at least 3 different antibiotics of different classes whereas the previous study in Gondar
used MDR as organisms resistant to two or more antibiotics. However, this figure was higher than the
study result from Pakistan where MDR prevalence was (37.9%) (46). This is significantly lower than a
finding reported in the present study. This discrepancy might be due to difference with study participants
where male patients other than females were included in the previous study.
Interestingly, the present study was also aimed to assess the presence of prevalence of ESBLs production
among enterobacteria. Hence, the prevalence of ESBLs was 18.2%. This was lower than results reported
in Ethiopia, which was ranged from 25% to 38.4% (61, 76, 77). Reasonably, difference in study setting,
sampling protocol and study population could have an impact on the isolation rate of ESBLs. The above

26
mentioned studies used clinical samples like surgical specimen, wound swabs and ear discharges which
are highly exposed to the outside condition within the hospital. Besides, in-patients were also part of the
study subjects in the previous studies, and it is known that hospitalized patients are at high risk of
acquiring drug resistant strains in the hospitals.
Likewise, the finding of this study was lower than the study done in India by Selvakumar et al. (78) that
the prevalence of ESBLs producing enterobacteria was 25.2%. On the other hand, it was higher than the
study done in Nepal by Thapa et al. that was 7.3% (50) and Pakistan by Iqbal et.al. that was 5.8% (46).
This difference of prevalence might be due to the great difference in number of bacterial isolates, and the
difference in geographical area.
At species level, this study has also revealed that the prevalence of ESBLs producing E.coli was 16.7%
and it is incompatible with a report by Olufunke et al. on prevalence of ESBLs producing UPEC among
symptomatic pregnant women in Nigeria (27). This might be due to the fact that our study includes those
women without symptom of UTI in addition to those having UTI symptoms. This result also lower than
previous study results in Ethiopia, for instance 36%, and 28.2% of ESBL producing E.coli was identified
in Jimma by 2012 and 2015, respectively.
In the present study about 90%, 84.8% and 57.6% of gram negative uropathogens were resistant to
ampicillin, cephalothin, and augmentin, respectively. Previous report from different part of Ethiopia also
showed high resistance rate to ampicillin and augmentin (37, 39). The possible explanation of ampicillin
and augmentin resistance might be due to its extensive use in the health facilities as this may boost the
selection of uropathogens harboring β-lactamase enzyme that can easily hydrolyze penicillins.
In this study, drugs like, nitrofurantoin, gentamicin, and amikacin were effective against uropathogens
followed by norfloxacin and ciprofloxacin. Thapa et.al (49) reported the same antibiotics as the effective
drugs to clear uropathogens. All ESBLs producing bacterial isolates in this study were completely
resistant to 9 out of 15 antibiotics tested especially to 3rd generation cephalosporins. This finding was in
line with previous studies done by Onwuezobe et.al. in Nigeria (54) and by Kumar Yadav et.al. in Nepal
(79). This higher antibiotic resistance rate among ESBLs producing isolates may be due to the fact that
the already in place plasmid could carrying genes other than those coding ESBLs which are responsible
for resistant to other classes of antibiotics like fluoroquinolones.
In the present study, nitrofurantoin was the only drug that clears all ESBLs producing strains. This result
was in line with the study done in Nepal by Thapa et.al. (49) and Sri Lanka by Dissanayake et al. (64)
where nitrofurantoin also showed minimum resistance among ESBLs producing strains. This similarity

27
in nitrofurantoin sensitivity rate between studies might be because of its narrow range of clinical
indications which results in less usage compared to other UTI drugs.
This study showed that prior antibiotic usage was an independent risk factor for the presence of MDR
bacteria among pregnant women. Previous study in Ethiopia also reported use of antibiotics as the same
risk factor for MDR bacteria (70). Other studies were also reported it as a risk factor for the presence
ESBLs producing strains which are usually MDR (80, 81). However, these studies also reported
hospitalization and catheterization as a risk factor for the presence of multidrug resistant bacteria. It is
known that antibiotics are used to clear infection causing pathogenic bacteria. However, the usage of
antibiotics also increases the prevalence of antibiotic resistance strains via selective pressure where
antibiotics kill susceptible bacteria and leave the resistant one to survive and multiply (82, 83)

28
6. LIMITATION OF THE STUDY
The study was done at the hospital setting so that the result may not be representative to other pregnant
women attending another health sectors in the same area. Associated factors for MDR bacterial infection
were not fully addressed because of the absence of participants with factors like catheterization, diabetes
mellitus and etc. The number of isolates were small, and this may affect the estimation of prevalence of
ESBL producing strains among pregnant women.
29
7. CONCLUSION
In conclusion, in the present study. Though the prevalence of ESBLs producing gram negative
uropathogens isolated from pregnant women was not as high compared to other studies in Ethiopia, high
rate of MDR infection was detected. High level of resistant to all of the 3rd generation cephalosporin and
other classes of antibacterials by ESBLs producing strains was observed. Antibiotics, like; nitrofurantoin,
ciprofloxacin and norfloxacin were effective against gram negative uropathogens including ESBL
producers. Gentamicin, amikacin and, nitrofurantoin were also effective against staphylococcus spps that
caused UTI. Antibiotic therapy was associated with the presence of Multi-drug resistant bacterial
infection among pregnant women.

30
8. RECOMMENDATION
Based on the result of the present study the following points can be recommended;
Since MDR prevalence was high among uropathogens isolated from pregnant women, treatment
of urinary tract infection during pregnancy should be based on the antibacterial susceptibility
testing result.
The isolation of highly drug resistant strains like ESBLs and Methicillin resistant staphylococcus
spps in this study calls for the need of antibiotic surveillance study in the study area. Moreover,
conducting molecular studies will help to characterize the various drug resistant strains.
Drugs like ampicillin, cephalothin, cotrimoxazole, penicillin, erythromycin, chloramphenicol,
and augmentin cannot be used as an empirical treatment, whereas nitrofurantoin and ciprofloxacin
or norfloxacin could be used as the treatment of UTI during pregnancy with a great care.
Gentamicin and amikacin could also be used to treat gram positive bacterial infections of the
urinary tract.
31
9. REFERENCES
1. Sheerin NS. Urinary tract infection. Medicine. 2011;39(7):384-9.
2. Talha H. Imam. Introduction to Urinary Tract Infections (UTIs) - Genitourinary Disorders -
Merck Manuals Professional Edition; 2016 [updated May 2016; cited 2016 November, 01].
Available from: http://www.merckmanuals.com/professional/genitourinary-disorders/urinary-
tract-infections-utis/introduction-to-urinary-tract-infections-utis.
3. Grabe M, Bartoletti R, Bjerklund-Johansen TE et al. Guidelines on Urological Infections.
European Association of Urology; 2015. p. 86.
4. Cynthia NC, Bruce DF, Harvey RA. Lippincott’s Illustrated Reviews: Microbiology Third ed.
Harvey RA, editor2013. 438 p.
5. McGuire L. A Seat on The Aisle, Please! The Essential Guide to Urinary Tract Problems in
Women. Mayo clinic proceedings. 2007;82(1):130.
6. McCormickT, Ashe RG, PM K. Urinary tract infection in pregnancy. The Obstetrician &
Gynaecologist. 2008;10:156-62.
7. Nicolle LE, Bradley S, Colgan R, Rice JC, Schaeffer A, Hooton TM. Infectious Diseases Society
of America guidelines for the diagnosis and treatment of asymptomatic bacteriuria in adults.
Clinical infectious diseases. 2005;40(5):643-54.
8. Andrea Green H, Mark E Rupp, Schooneveld TCV. Urinary Tract Infection and Asymptomatic
Bacteriuria Guidance. Omaha, Nebraska, USA: Nebraska Medical Center; 2014.
9. Nicolle LE. Asymptomatic bacteriuria: review and discussion of the IDSA guidelines.
International journal of antimicrobial agents. 2006;28 Suppl 1:S42-8.
10. Nadeau HC, Subramaniam A, Andrews WW, editors. Infection and preterm birth. Seminars in
Fetal and Neonatal Medicine; 2016: Elsevier.
11. Mazor-Dray E, Levy A, Schlaeffer F, Sheiner E. Maternal urinary tract infection: is it
independently associated with adverse pregnancy outcome? J Matern Fetal Neonatal Med.
2009;22(2):124-8.
12. Mittendorf R, Williams MA, Kass EH. Prevention of preterm delivery and low birth weight
associated with asymptomatic bacteriuria. Clinical infectious diseases. 1992;14(4):927-32.
13. Minassian C, Thomas SL, Williams DJ, Campbell O, Smeeth L. Acute maternal infection and risk
of pre-eclampsia: a population-based case-control study. PloS one. 2013;8(9):e73047.
14. Emamghorashi F, Mahmoodi N, Tagarod Z, Heydari ST. Maternal urinary tract infection as a risk
factor for neonatal urinary tract infection. Iranian journal of kidney diseases. 2012;6(3):178-80.
15. Mazor-Dray E, Levy A, Schlaeffer F, Sheiner E. Maternal urinary tract infection: is it
independently associated with adverse pregnancy outcome? The Journal of maternal-fetal &
neonatal medicine. 2009;22(2):124-8.
16. Axel S. Merseburger MAKa, Moul JW. Urology at a Glance: Springer; 2014.

32
17. WHO. Antimicrobial resistance U.S.A: WHO; 2016 [updated September 2016; cited 2016
11/3/2016]. Available from: http://www.who.int/mediacentre/factsheets/fs194/en/.
18. AAM. Antibiotic Resistance: An Ecological Perspective on an Old Problem. 1752 N Street, NW,
Washington, DC 20036: American Academy of Microbiology; 2009.
19. O'Neill J. Tackling Drug-resistance infections globally: Final Report and Recommondations.
London: Wellcome Trust & HM Government; 2016 May, 2016.
20. WHO. Antibiotic Resistance: Global Report on Surveillance. Geneva: World Health
Organization; 2014.
21. Stephan Harbarth, Hanan H. Balkhy, Herman Goossens, Vincent Jarlier, Jan Kluytmans,
Ramanan Laxminarayan, et al. Antimicrobial resistance: one world, one fight! Antimicrobial
Resistance and Infection Control. 2015;4(49):1-15.
22. CDC. Antibiotic resistance threats in the United States, 2013: Centres for Disease Control and
Prevention, US Department of Health and Human Services; 2013.
23. Rawat D, Nair D. Extended-spectrum β-lactamases in Gram Negative Bacteria. Journal of Global
Infectious Diseases. 2010;2(3):263-74.
24. Thenmozhi S, Moorthy K, Sureshkumar B, Suresh M. Antibiotic resistance mechanism of ESBL
producing Enterobacteriaceae in clinical field: A review. Int J Pure Appl Biosci. 2014;2(3):207-
26.
25. Paterson DL, Bonomo RA. Extended-spectrum beta-lactamases: a clinical update. Clinical
microbiology reviews. 2005;18(4):657-86.
26. S. Thenmozhi, K. Moorthy, B. T. Sureshkumar, Suresh M. Antibiotic Resistance Mechanism of
ESBL Producing Enterobacteriaceae in Clinical Field: A Review. International Journal of Pure
& Applied Bioscience. 2014;2(3):207-26.
27. Olufunke OA, Abiodun AO, Dunah FC. Extended Spectrum Beta-Lactamase-Producing
Uropathogenic Escherichia coli in Pregnant Women Diagnosed With Urinary Tract Infections in
South-Western Nigeria. Journal of Molecular Biology Research. 2014;4(1):34.
28. Sophia Fircanis M, Maria McKay R, MA, CIC. Recognition and Management of Extended
Spectrum Beta Lactamase Producing Organisms (ESBL). In: Ana Tuya Fulton M, editor.
Geriatrics for the Practicing Physician. Rhode Island: the warren alpert medical school of brown
university; 2010. p. 161-2.
29. Bush K, Bradford PA. β-Lactams and β-Lactamase Inhibitors: An Overview. Cold Spring Harbor
Perspectives in Medicine. 2016;6(8):a025247.
30. Johnson E. Urinary Tract Infections in Pregnancy: Practice Essentials, Pathophysiology, Etiology:
Emedicine.medscape.com; 2016 [updated July 24, 2016; cited 2016 November 01]. Available
from: http://emedicine.medscape.com/article/452604-overview#a4.
31. Gilstrap LC, 3rd, Ramin SM. Urinary tract infections during pregnancy. Obstetrics and
gynecology clinics of North America. 2001;28(3):581-91.

33
32. Fircanis S, McKay M. Recognition and management of extended spectrum beta lactamase
producing organisms (ESBL). Medicine and health, Rhode Island. 2010;93(5):161-2.
33. Denkel LA, Schwab F, Kola A, Leistner R, Garten L, von Weizsacker K, et al. The mother as
most important risk factor for colonization of very low birth weight (VLBW) infants with
extended-spectrum beta-lactamase-producing Enterobacteriaceae (ESBL-E). The Journal of
antimicrobial chemotherapy. 2014;69(8):2230-7.
34. Rettedal S, Lohr IH, Bernhoff E, Natas OB, Sundsfjord A, Oymar K. Extended-spectrum beta-
lactamase-producing Enterobacteriaceae among pregnant women in Norway: prevalence and
maternal-neonatal transmission. Journal of perinatology. 2015;35(11):907-12.
35. Amiri M, Lavasani Z, Norouzirad R, Najibpour R, Mohamadpour M, Nikpoor AR, et al.
Prevalence of Urinary Tract Infection Among Pregnant Women and its Complications in Their
Newborns During the Birth in the Hospitals of Dezful City, Iran, 2012 - 2013. Iranian Red
Crescent medical journal. 2015;17(8):e26946.
36. Seale J, Millar M. Perinatal vertical transmission of antibiotic‐resistant bacteria: a systematic
review and proposed research strategy. BJOG: An International Journal of Obstetrics &
Gynaecology. 2014;121(8):923-8.
37. Beyene G, Tsegaye W. Bacterial uropathogens in urinary tract infection and antibiotic
susceptibility pattern in jimma university specialized hospital, southwest ethiopia. Ethiopian
journal of health sciences. 2011;21(2):141-6.
38. Alemu A, Moges F, Shiferaw Y, Tafess K, Kassu A, Anagaw B, et al. Bacterial profile and drug
susceptibility pattern of urinary tract infection in pregnant women at University of Gondar
Teaching Hospital, Northwest Ethiopia. BMC Research Notes. 2012;5:197.
39. Demilie T, Beyene G, Melaku S, Tsegaye W. Urinary bacterial profile and antibiotic susceptibility
pattern among pregnant women in north west ethiopia. Ethiopian journal of health sciences.
2012;22(2):121-8.
40. Ferede G, Yismaw G, Wondimeneh Y, Sisay Z. The prevalence and antimicrobial susceptibility
pattern of bacterial uropathogens isolated from pregnant women. Eur J Exp Biol. 2012;2(5):1497-
502.
41. Tadesse E, Teshome M, Merid Y, Kibret B, Shimelis T. Asymptomatic urinary tract infection
among pregnant women attending the antenatal clinic of Hawassa Referral Hospital, Southern
Ethiopia. BMC Research Notes. 2014;7:155.
42. Derese B, Kedir H, Teklemariam Z, Weldegebreal F, Balakrishnan S. Bacterial profile of urinary
tract infection and antimicrobial susceptibility pattern among pregnant women attending at
Antenatal Clinic in Dil Chora Referral Hospital, Dire Dawa, Eastern Ethiopia. Therapeutics and
Clinical Risk Management. 2016;12:251-60.
43. Nikaido H. Multidrug Resistance in Bacteria. Annual review of biochemistry. 2009;78:119-46.
44. Dehbanipour R, Rastaghi S, Sedighi M, Maleki N, Faghri J. High prevalence of multidrug-
resistance uropathogenic Escherichia coli strains, Isfahan, Iran. Journal of natural science,
biology, and medicine. 2016;7(1):22-6.
34
45. Tham J. Extended-Spectrum Beta-Lactamase-Producing Enterobacteriaceae: Epidemiology, Risk
Factors, and Duration of Carriage. 1 ed. Lund: Faculty of medicine, Lund University; 2012. 85 p.
46. Iqbal R, Majid A, Alvi IA, Hayat A, Andaleeb F, Gul S, et al. Multiple drug resistance and ESBL
production in bacterial urine culture isolates. Am J BioSci. 2014;2(1):5-12.
47. Jain K, Rajput MS, Chavan N, Jain S, Tripathi S, Niyati P. ESBL-A Great Concern in Urinary
Tract Infections in Tertiary Care Hospital, Indore. International Journal of Health Sciences and
Research (IJHSR). 2015;5(8):217-23.
48. Krishnakumar S, Rajan RA, Babu MM, Bai VDM. Antimicrobial susceptibility pattern of
Extended Spectrum of Beta Lactamase (ESBL) producing uropathogens from pregnant women.
Indian Journal of Medicine and Healthcare. 2012;1(8):189-92.
49. Rizvi M, Khan F, Shukla I, Malik A, S. Rising prevalence of antimicrobial resistance in urinary
tract infections during pregnancy: Necessity for exploring newer treatment options. Journal of
Laboratory Physicians. 2011;3(2):98-103.
50. Thapa R, Lamichhane P, Banjara MR, Acharya GP. Prevalence of extended spectrum
betalactamse producing uropathogens in pregnant women. Asian Journal of Pharmaceutical and
Clinical Research. 2015;8(1):207-10.
51. Chowdhury AH, Husain MA, Akter N, Mazed MA, Ahmed S, Sultan T, et al. Prevalence of
Extended Spectrum b-Lactamases (ESBLs) Producers Among Gram-Negative Bacilli in Urinary
Tract Infections. Chattagram Maa-O-Shishu Hospital Medical College Journal. 2015;14(2):17-
20.
52. Tansarli GS, Poulikakos P, Kapaskelis A, Falagas ME. Proportion of extended-spectrum β-
lactamase (ESBL)-producing isolates among Enterobacteriaceae in Africa: evaluation of the
evidence—systematic review. The Journal of antimicrobial chemotherapy. 2014:dkt500.
53. Tolbert Sonda, Happiness Kumburu, Marco van Zwetselaar, Michael Alifrangis, Ole Lund,
Gibson Kibiki a, et al. Meta-analysis of proportion estimates of Extended-Spectrum-Beta-
Lactamase- producing Enterobacteriaceae in East Africa hospitals. Antimicrobial Resistance and
Infection Control. 2016;5(18):1-9.
54. Bercion R, Mossoro-Kpinde D, Manirakiza A, Le Faou A. Increasing prevalence of antimicrobial
resistance among Enterobacteriaceae uropathogens in Bangui, Central African Republic. The
Journal of Infection in Developing Countries. 2009;3(03):187-90.
55. Chereau F, Herindrainy P, Garin B, Huynh BT, Randrianirina F, Padget M, et al. Colonization of
extended-spectrum-beta-lactamase- and NDM-1-producing Enterobacteriaceae among pregnant
women in the community in a low-income country: a potential reservoir for transmission of
multiresistant Enterobacteriaceae to neonates. Antimicrobial agents and chemotherapy.
2015;59(6):3652-5.
56. Onwuezobe A, Orok F. Extended spectrum beta-lactamase producing Uropathogens in
Asymptomaticpregnant women attending antenatal care in an urban community secondary health
facility. African Journal of Clinical and Experimental Microbiology. 2015;16(2):49-53.
57. Onwuezobe IA, Orok FE. The Bacterial Isolates and Plasmid Profile of Extended Spectrum Beta-
Lactamases Producers Causing Urinary Tract Infection among Pregnant Women in Uyo, Nigeria.
Journal of Biosciences and Medicines. 2015;3(07):25.

35
58. Azekhueme I, Moses AE, Abbey SD. Extended Spectrum Beta-Lactamases in Clinical Isolates of
Escherichia coli and Klebsiella pneumoniae from University of Uyo Teaching Hospital, Uyo-
Nigeria. Journal of Advances in Medical and Pharmaceutical Sciences. 2015;2(3):117-235.
59. Moyo SJ, Aboud S, Kasubi M, Lyamuya EF, Maselle SY. Antimicrobial resistance among
producers and non-producers of extended spectrum beta-lactamases in urinary isolates at a tertiary
Hospital in Tanzania. BMC Research Notes. 2010;3:348.
60. Shewki Moga Siraj, Solomon Ali, Wondafrash B. Extended-spectrum β-lactamase production in
Klebsiella pneumoniae and Escherichia coli at Jimma University Specialized Hospital, South-
West, Ethiopia. Molecular Microbiology Research. 2015;5(1):1-9.
61. Yohannes Mulualem, Tesfaye kasa, Zeleke Mekonen, Suleman S. Occurrence of Extended
spectrum beta (β)-lactamases in multi-drug resistance Escherichia coli isolated from a clinical
setting in Jimma University Specialized Hospital, Jimma, southwest Ethiopia. East African
Journal of Public Health. 2012;9(2).
62. Abera B, Kibret M, Mulu W. Extended-Spectrum beta (β)-Lactamases and Antibiogram in
Enterobacteriaceae from Clinical and Drinking Water Sources from Bahir Dar City, Ethiopia.
PloS one. 2016;11(11):e0166519.
63. Qadeer N, Durrani MA, Iqbal SM. Multidrug Resistant Escherichia coli and Klebsiella
pneumoniae Causing Urinary tract Infection in Pregnant Women. Int j pathol. 2013;11(2):45-9.
64. DMBT Dissanayake, SSN Fernando, Chandrasiri N. The distribution and characteristics of
Extended-Spectrum β-Lactamase (ESBL) producing Escherichia coli and Klebsiella species
among urinaryisolates in a tertiary care hospital. Sri Lanka Journal of Infectious Diseases.
2012;2(2):30-6.
65. Onoh R, Umeora O, Egwuatu V, Ezeonu P, Onoh T. Antibiotic sensitivity pattern of uropathogens
from pregnant women with urinary tract infection in Abakaliki, Nigeria. Infection and Drug
Resistance. 2013;6:225-33.
66. Akobi O.A, Inyinbor H.E, Akobi E.C, Emumwen E.G, Ogedengbe S.O, Uzoigwe E.O Amlscn, et
al. Incidence of Urinary Tract Infection among Pregnant Women Attending Antenatal Clinic at
Federal Medical Centre, Bida, Niger-State, North Central Nigeria. American Journal of Infectious
Diseases and Microbiology. 2014;2(2):34-8.
67. Tijjani J, Arzai A, Sadiq N. Antimicrobial susceptibility pattern of extended spectrum
betalactamase producers in gram-negative urogenital isolates in Kano, Nigeria. Bayero Journal
of Pure and Applied Sciences. 2012;5(1):20-5.
68. Kimang'a AN. A Situational Analysis of Antimicrobial Drug Resistance in Africa: Are We Losing
the Battle? Ethiopian journal of health sciences. 2012;22(2):135-43.
69. Uzodi AS, Lohse CM, Banerjee R. Risk Factors For and Outcomes of Multidrug-Resistant
Escherichia coli Infections in Children. Infectious Diseases and Therapy. 2017;6(2):245-57.
70. Moges F, Mengistu G, Genetu A. Multiple drug resistance in urinary pathogens at Gondar College
of Medical Sciences Hospital, Ethiopia. East African medical journal. 2002;79(8):415-9.
71. Cheesbrough M. District Laboratory Practice in Tropical Countries -Part 2. Second ed. New York,
USA: Cambridge University Press; 2006. 442 p.

36
72. CLSI. Performance Standards for Antimicrobial Susceptibility Testing; Twenty-Fourth
Informational Supplement. CLSI document M100-S24. Wayne, PA: Clinical and Laboratory
Standards Institute; 2014.
73. CLSI. Performance Standards for Antimicrobial Susceptibility Testing. CLSI supplement M100.
Wayne, PA: Clinical and Laboratory Standards Institute; 2017.
74. Anick Berard, Fabiano Santos, Ema Ferreira, Perreault S. Urinary Tract Infections During
Pregnancy. In: Tenke DP, editor. Urinary Tract Infections: InTech; 2011. p. 360.
75. Masinde.A, Gumodoka.B, Kilonzo.A, Mshana.S.E. Prevalence of urinary tract infection among
pregnant women at Bugando Medical Centre, Mwanza, Tanzania. Tanzania Journal of Health
Research. 2009;11(3).
76. Siraj SM, Ali S, Wondafrash B. Extended-spectrum β-lactamase production in Klebsiella
pneumoniae and Escherichia coli at Jimma University Specialized Hospital, South-West,
Ethiopia. Molecular Microbiology Research. 2015;5.
77. Mulisa G, Selassie L, Jarso G, Shiferew T, Zewdu A, Abebe W, et al. Prevalence of Extended
Spectrum Beta-lactamase Producing Enterobacteriaceae: A Cross Sectional Study at Adama
Hospital, Adama, Ethiopia. J Emerg Infect Dis. 2016;1(1):2-6.
78. Selvakumar B, Jasmine R. Prevalence & Antibacterial resistance of ESBLs among Pregnant
Women with UTI. International Journal of Pharmaceutical Sciences and Research.
2011;2(11):2846.
79. Yadav KK, Adhikari N, Khadka R, Pant AD, Shah B. Multidrug resistant Enterobacteriaceae and
extended spectrum β-lactamase producing Escherichia coli: a cross-sectional study in National
Kidney Center, Nepal. Antimicrobial Resistance and Infection Control. 2015;4(1):42.
80. Colodner R, Rock W, Chazan B, Keller N, Guy N, Sakran W, et al. Risk factors for the
development of extended-spectrum beta-lactamase-producing bacteria in nonhospitalized
patients. European Journal of Clinical Microbiology & Infectious Diseases. 2004;23(3):163-7.
81. Lautenbach E, Patel JB, Bilker WB, Edelstein PH, Fishman NO. Extended-spectrum beta-
lactamase-producing Escherichia coli and Klebsiella pneumoniae: risk factors for infection and
impact of resistance on outcomes. Clinical Infectious Diseases : 2001;32(8):1162-71.
82. Read AF, Woods RJ. Antibiotic resistance management. Evolution, medicine, and public health.
2014;2014(1):147.
83. Wiesch PA, Kouyos R, Engelstadter J, Regoes RR, Bonhoeffer S. Population biological principles
of drug-resistance evolution in infectious diseases. The Lancet Infectious diseases.
2011;11(3):236-47.
37
ANNEX
Annex I: Study information sheet and consent form
Study Title: Multi-drug resistant and Extended-spectrum β-lactamase production in bacterial
uropathogens isolated from pregnant women attending university of Gondar teaching hospital,
northwest Ethiopia.
Name of the Sponsor: Amhara Regional Health Bureau and Mega project of University of Gondar.
Name of the Organization: School of Biomedical and Laboratory Sciences, College of Medicine and
Health Sciences, University of Gondar.
1. Purpose of the Research Project: The result of this study will help the In line with this the findings
will also provide baseline information for health sector administrators, concerned bodies and the patients
themselves in planning and managing of drug resistance that further reduce the morbidity and mortality
associated with the disease.
2. Procedure: In order to perform the indicated study at Gondar referral hospital you are invited to take
part in this project. If you are willing to participate, you need to understand the purpose of the study and
give your consent .The required clinical sample will be collected by laboratory professionals who are
currently working in the laboratory department of this hospital. Then, you will be requested to give your
consent to the sample collector. Socio-demographic, associated factors and clinical information will be
collected from the study participants using structured questionnaires via interview technique; since you
fulfil the criteria you are kindly requested to give the required sample and genuine answers to the
prepared questionnaire.
3. Risk associated with the study: You will not be at any physical or psychological risk and no damage
resulting from the research procedures.
4. Benefits of the study: Based on the diagnosis result you will be treated accordingly. Moreover, this
study will have a great value on preventive measures in hospitals and in the community. The results of
this study have importance to treat the patients
5. Compensation for participation: You will not receive any payment for your participation in this
research study.
6. Confidentiality of your information- All information gathered from the study participant will remain
confidential. Your participation in this study is strictly anonymous. Personal information will be treated
confidentially and under no circumstances will it be transmitted to any person or organization. The results

38
of this study will be evaluated and summarized, and a feedback of the results to the study participants
will be given by principal investigator.
7. Right to Refusal or Withdraw: Your participation in the study is absolutely voluntary; you have
full right to refuse from participating in this research. You can refuse to give sample and not to respond
any or all the questionnaires and this will not affect you on using any kind of services from the hospital.
8. Person to Contacts: This research project will be reviewed and approved by Ethical clearance
committee of School of Biomedical and laboratory Sciences, College of Medicine and Health Sciences,
University of Gondar. If you want to know more information, you can contact the following individuals
and you may ask at any time you want.
School of Biomedical and Laboratory Sciences, UoG P.Box-196, Gondar, Ethiopia
Mr. Sirak Biset, principal investigator, UoG Mobile: +251911754344/ e-mail: [email protected]
Prof. Feleke Moges, (advisor), UoG Mobile: +251918778160/ e-mail: [email protected]
Mr. Setegn Eshetie, (advisor), UoG Mobile: +251947050546/ e-mail: [email protected]
Participant consent form
Serial No-----------Name of health institution----------Card No--------- Date-----------
I the undersigned study participant have been well informed about the objective of the study entitled
“Multi-drug resistant and Extended-spectrum β-lactamase production in bacterial uropathogens
isolated from pregnant women attending university of Gondar hospital, Gondar, Northwest
Ethiopia.”January to May, 2017.
I am also told that all the information obtained at any course of the study is to be kept confidential.
Moreover, I have also been well informed of my right to keep hold of, decline to cooperate and drop out
of the study if I want and none of my actions will have any bearing at all on my overall health care and
hospital access.
I agreed voluntarily to provide the requested sample.
Name and signature of study participant _________________ Date______
Name and signature of investigator ________________ Date_________

39
የመረጃና የስምምነት ዉል ቅጽ (Amharic version)
የጥናቱ ርእስ - ሶስትና ከዚያ በላይ የሚሆኑ ፀረ- ባክቴሪያዎችን እንዲሁም ፔንሲሊን እና ሴፋሎስፖሪን በሚባሉት ፀረ-ባክቴሪያዎች
ዉሰጥ የሚመደቡትን ብዛት ያላቸዉ ፀረ-ባክቴሪያዎች መቋቋም የሚችሉ የባክቴሪያ ዝርያዎችን በጎንደር ሪፈራል ሆስፒታል ክትትል
በሚያደርጉ ነፍሰ-ጡር እናቶች ውስጥ መኖራቸውን በማረጋገጥ በምን ያህል መጠን እንዳሉ ፣ የትኛዉን መድሃኒት በምን ያህል መጠን
መቋቋም እንደቻሉ እና በእነርሱ ለመያዝ ምክንያት ሊሆኑ የሚችሉ ነገሮችን ለይቶ ማወቅ
የጥናቱ ደጋፊ :- የአማራ ብሔራዊ ክልላዊ መንግስት ጤና ቢሮ እና የጎንደር ዩኒቨርሲቲ ሜጋ ፕሮጀክት
የድርጅቱ ስም :-ጎንደር ዩኒቨርሲቲ ህክምናና ጤና ሳይንስ ኮሌጅ የላቦራቶሪ እና ባዮሜዲካል ትምህርት ቤት
የጥናቱ ዓላማ- የዚህ ጥናት አላማ በዋናነት ሶስትና ከዚያ በላይ የሚሆኑ ፀረ- ባክቴሪያዎችን እንዲሁም ፔንሲሊን እና ሴፋሎስፖሪን
በሚባሉት ፀረ-ባክቴሪያዎች ዉሰጥ የሚመደቡትን ብዛት ያላቸዉ ፀረ-ባክቴሪያዎች መቋቋም የሚችሉ የባክቴሪያ ዝርያዎችን በጎንደር
ሪፈራል ሆስፒታል ክትትል በሚያደርጉ ነፍሰ-ጡር እናቶች ውስጥ መኖራቸውን መለየትና በምን ያህል መጠን እንደሚገኙ ማሳወቅ
ነው፡፡ ከጥናቱ የሚገኘውን ውጤት ለጤና ተቋም አስተዳዳሪዎች ፣ ለሚመለከታቸው አካላት እና ለጥናቱ ተሳታፊዎች በማሳዎቅና በዚህ
ጀርም ምክንያት የሚመጣዉን ችግር ለመቆጣጠር እና ለመከላከል የሚያስችሉ መሠረታዊ መረጃዎችን በመጠቆም ችግሩ እንዲቀረፍ
ይረዳል፡፡
የአሰራር ሂደት- ይህን ጥናት በጎንደር ሪፈራል ሆስፒታል ለመስራት የጥናቱ ተሳታፊ እንዲሆኑ ተጋብዘዋል፡፡ ለመሳተፍ ፍቃደኛ ከሆኑ
የጥናቱን ዓላማ መረዳትና ፍቃደኝነትዎን መግለፅ ይጠበቃል፡፡ለዚህ ጥናት የሚያስፈልገው የሽንት ናሙና የሚሰበሰበው በጥናቱ ወቅት
በላቦራቶሪ ክፍል ዉስጥ የሚሰሩ የሆስፒታሉ ባለሙያዎች ይሆናሉ፡፡ እንዲሁም በተጨማሪ ሙሉ ማህበራዊ ነክ የሆኑ ጥያቄዎች እና በ
ጀርሙ ለመያዝ እነዲሁም እንዲፈጠር ለሚያደርጉ ሁኔታዎች ከእያንዳንዱ የጥናቱ ተሳታፊ በመጠይቁ መሰረት ይሰበሰባል፡፡ እርስዎም
መስፈርቱን እስካሟሉ ድረስ የሚያስፈልገዉን ናሙና ለመስጠት እንዲሁም ለተዘጋጀው ጥያቄ ትክክለኛ ምላሽ እንዲሰጡ በትህትና
ይጠየቃሉ፡፡
ከጥናቱ ጋር ተያይዞ የሚመጣ ጉዳት - በዚህ ጥናት ዝርዝር ኣሰራር ሂደት ውስጥ አካላዊ ወይም አዕምሮአዊ ጉዳት አይኖርም፡፡
ጥቅሞች - በምርመራ ውጤትዎ መሠረት ሕክምና ያገኛሉ በተጨማሪም ይህ ጥናት ያለዉን ችግር ለመቆጣጠርና በሚወለዱት ጨቅላ
ህፃናት፣ በሆሰፒታል እና በማህበረሰቡ ዘንድ የመከላከል ስራ እንዲሰራ ያደርጋል፡፡ በተጨማሪም ሆስፒታሉ ለቀጣይ ስራዎቹ አመች
መንገድን እንዲያዘጋጅ ያደርጋል፡፡
ለተሳትፎ የሚሰጥ ማካካሻ- ምንም አይነት የካሳ ክፍያ የለዉም
የጥናቱ መረጃ ሚስጥራዊነት ሁሉም ከተሳታፊዎች የሚሰበሰቡ መረጃዎች በሚስጢር የሚያዙ እና የሚጠበቁ ይሆናሉ፡፡ በማንኛውም
ምክንያት ተሳታፊዎች እነማን መሆናቸውን የሚያሳይ በመጠይቁ ይሁን በሌላ ነገር አይኖርም፡፡ የተሰበሰቡ መረጃዎች ለሶስተኛ ወገን
ተላልፎ አይሰጡም፡፡ በተጨማሪም ውጤቱ የሚለካዉም ሆነ ተሰብስቦ የሚያዘው በዋና ተመራማሪዉ ብቻ ነው፡፡
የመዉጣት (የማቋረጥ) መብት - በዚሀ ጥናት ላይ መሳተፍዎ በሙሉ ፍቃደኝነት ላይ የተመሰረተ ነው :: ጥናቱን የማቋረጥ ሙሉ መብት
አለዎት፡፡ ናሙናም ሆነ ለመጠይቁ መልስ ያለመስጠት ከሆስፒታሉ የሚያገኙትን ማነኛውንም አገልግሎት አይገድብም ፡፡
የሚያገኙዋቸው ሰዎች- ይህ ጥናት በጎንደር ዪኒቨርሲቲ የስነምግባር ምርምር ኮሚቴና ሕክምናና ጤና ሳይነንስ ኮሌጅ የላቦራቶሪ
ባዮሜዲካል ትምህርት ክፍል ተዕልኮ የፀደቀ ነዉ፡፡ ጥያቄ ካለዎት እነዲሁም ተጨማሪ መረጃ ከፈለጉ በማንኛዉም ጊዜ ከዚህ በታች
የተጠቀሰዉን አድራሻ መጠቀም ይችላሉ፡፡
ባዮሜዲካል እና ላቦራቶሪ ሳይንስ ፖ.ሳ.ቁ-196, ጎንደር, ኢትዮጵያ
አቶ ሲራክ ቢሰጥ: ዋና ተመራማሪ: ጎንደር ዩኒቨርሲቲ ስ.ቁ: +251911754344/ ኢ.ሜል፡ [email protected]
ፕ/ር ፈለቀ ሞገስ: አማካሪ፡ ጎንደር ዩኒቨርሲቲ ስ.ቁ: +251918778160/ ኢ.ሜል፡ [email protected]
አቶ ሰጠኝ እሸቴ- አማካሪ፡ ጎንደር ዩኒቨርሲቲ ስ.ቁ: +251947050546/ ኢ.ሜል፡ [email protected]

40
የተሳታፊዎች የስምምነት ማረጋገጫ
ተራ ቁጥር-----------የሚታከምበት ጤና ተቋም--------------የካርድ ቁጥር---------------ቀን-------
እኔ ከዚህ በታች ስሜ የተጠቀሰዉና የፈረምኩት የጥናቱ ተሳታፊ ሶስትና ከዚያ በላይ የሚሆኑ ፀረ- ባክቴሪያዎችን እንዲሁም ፔንሲሊን
እና ሴፋሎስፖሪን በሚባሉት ፀረ-ባክቴሪያዎች ዉሰጥ የሚመደቡትን ብዛት ያላቸዉ ፀረ-ባክቴሪያዎች መቋቋም የሚችሉ የባክቴሪያ
ዝርያዎችን በጎንደር ሪፈራል ሆስፒታል ክትትል በሚያደርጉ ነፍሰ-ጡር እናቶች ውስጥ መኖራቸውን በማረጋገጥ በምን ያህል መጠን
እንዳሉ ፣ የትኛዉን መድሃኒት በምን ያህል መጠን መቋቋም እንደቻሉ እና በእነርሱ ለመያዝ ምክንያት ሊሆኑ የሚችሉ ነገሮችን ለይቶ
ለማሳወቅ የሚደረገውን ጥናት አላማና ጥቅም በሚገባ ተረድቻለሁ፡፡ በጥናቱ ላይ መሳተፍም ሆነ አለመሳተፍ በራሴ ፍቃድ የሚወሰን
መሆኑንም ተገልጾልኛል፡፡ በተጨማሪም በጥናቱ ባልሳተፍም ሆነ አቋርጨ ብወጣ ከሆስፒታሉ በማገኘዉ የህክምና አገልግሎት ላይ
ምንም አይነት ችግር እንደማያደርስብኝ ተነግሮኛል፡፡
በመሆኑም ከእኔ የሽንት ናሙና እና ሌሎች መረጃዎችን መዉሰድ አስፈላጊ መሆኑን ስለተገነዘብኩኝ ለጥናቱ አስፈላጊ የሆንዉን ሁሉ
ለመስጠት ሙሉ ፈቃደኛ መሆኔን በፊርማዬ አረጋግጣለሁ፡፡
የተሳታፊ ስምና ፊርማ ________________ ቀን _____________________
የተመራማሪ ስምና ፊርማ ______________ ቀን _________________
41
Annex III: Questionnaire
I. English version
Study title: Multi-drug resistant and Extended-spectrum β-lactamase producing bacterial uropathogens
among pregnant women at University of Gondar Teaching Hospital, Northwest Ethiopia.
Questionnaire code no
100: Socio-demographic characteristics.
I would like to start by asking you some background questions before asking you questions on your health
related issues. This information is confidential and will only be used for research purposes.
S.no Question Answer code Remark
Q100 Age in years
Q101 Religion 1. Orthodox
2. Muslim
3. Protestant
4. Others specify ……………..
Q102 Residence 1. Urban
2. Rural
Q103 Marital status 1. Never married
2. Currently married
3. Separated/Divorced
4. Widowed
5. Others
Q104 Educational level 1. Not read and write
2. Read and write
3. Primary education
4. Secondary education
5. College/University
Q105 Monthly income 1. ≤1000
2. 1001-1800
3. 1801-2800
4. ≥2801
Q106 Occupation 1. Housewife
2. Farmer
3. Merchant
4. Gov’t/private employer
5. Daily laborer
6. Others specify…………………..

42
200. Pregnancy related information’s
S.no Question Answer code Remark
Q200 Gestation period 1. <3 months
2. 3-6 months
3. >6months
4. Don’t know
Q201 How many pregnancies do you
have including the present one
1. Primigravida
2. Multigravida
Q202 How many children do you have 1. Nulliparous
2. Primiparous
3. Multiparous
300. Risk factors for acquisition of ESBL producing uropathogens
S.no Questions Code Remark
Q300 History of previous hospitalization 0. No
1. Yes
Q301 Prior UTI infection for the last 12 months 0. No
1. Yes
Q302 Prior antibiotic therapy 0. No
1. Yes
Q303 Does the patient has diabetes mellitus
(look the patient history)
0. No
1. Yes
Q304 Does the patient has affected by HIV infection
(look the patient history)
0. No
1. Yes
Q305 Presence of sign and symptom of UTI 0. No
1. yes

43
II. የአማረኛ መጠይቅ
የጥናቱ ርዕስ፡- ሶስትና ከዚያ በላይ የሚሆኑ ፀረ- ባክቴሪያዎችን እንዲሁም ፔንሲሊን እና ሴፋሎስፖሪን በሚባሉት ፀረ-ባክቴሪያዎች
ዉሰጥ የሚመደቡትን ብዛት ያላቸዉ ፀረ-ባክቴሪያዎች መቋቋም የሚችሉ የባክቴሪያ ዝርያዎችን በጎንደር ሪፈራል ሆስፒታል ክትትል
በሚያደርጉ ነፍሰ-ጡር እናቶች ውስጥ መኖራቸውን መለየትና በምን ያህል መጠን እንደሚገኙ ማወቅ
የመጠይቁ መለያ ቁጥር
ክፍል 1. የማህበረሰብ ነክ ባህርያት ጥያቄዎች
ተ.ቁ ጥያቄ የመልስ መለያ ምርመራ
ጥ100 እድሜ
ጥ101 የሚከተሉት ሃይማኖት 1. ኦርቶዶክስ
2. እስልምና
3. ፕሮቴስታንት
4. ሌላ ይጠቀስ …………………
ጥ102 ነዋሪነት (መኖሪያ ቦታዎ) 1. ከተማ
2. ገጠር
ጥ103 የጋብቻ ሁኔታዎት 1. ያላገባች
2. ያገባች
3. የፈታች
4. ባሏ የሞተባት
ጥ104 የትምህርት ደረጃዎት 1. ማንበብና መፃፍ የማትችል
2. ማንበብና መፃፍ የምትችል
3. አንደኛ ደረጃን የተከታተለች
4. ሁለተኛ ደረጃን የተከታተለች
5. ኮሌጅ/ ዩኒቨርሲቲን የተከታተለች
ጥ105 የገቢዎት መጠን በወር 1. ≤1000
2. 1001-1800
3. 1801-2800
4. ≥2801
ጥ106 ስራዎት 1. የቤት እመቤት
2. ገበሬ
3. ነጋዴ
4. የመንግሰት/ የግል ድርጅት ተቀጣሪ
5. የቀን ሰራተኛ
6. ሌላ ካለ ይጠቀስ

44
ክፍል 2፡ ከእርግዝናዎ ጋር ተያያዥነት ያላችዉ ጥያቄዎች
ተ.ቁ ጥያቄ የመልስ መለያ ምርመራ
ጥ200 የስንት ወር ነፍሰ-ጡር ነዎት ሀ. ከ3 ወር በታች
ለ. 3-6 ወር
መ. ከ6 ወር በላይ
ሠ. አይታወቅም
ጥ201 ይህ ሰንተኛ እርግዝናዎ ነዉ ሀ. የመጀመሪያ
ለ. ሁለትና ከዚያ በላይ
ጥ202 አጠቃላይ ስንት እርስዎ የወለዷቸዉ
ልጆች አሉዎት
ሀ. የለኝም
ለ. አንድ
መ. ሁለትና ከዚያ በላይ
ክፍል 3. አሁን ደግሞ ፔንሲሊን እና ሴፋሎስፖሪን በሚባሉት ፀረ-ባክቴሪያዎች ዉሰጥ የሚመደቡትን ብዛት ያላቸዉ ፀረ-ባክቴሪያዎች
መቋቋም በሚችሉ የባክቴሪያ ዝርያዎች ለመያዝ አጋላጭ ሊሆኑ የሚችሉ ነገሮች እርስዎ ጋር ያላቸዉን ዝምድና ለማወቅ የሚከተሉትን
ጥያቄዎች አጠይቀወታልሁ
ተ.ቁ ጥያቄ የመልስ መለያ ምርመራ
ጥ300 በአለፉት 12 ወራት ዉስጥ ሆስፒታል ተኝተዉ ያዉቃሉ ሀ. አላዉቅም ለ. አዎ
ጥ301 በአለፉት 12 ወራት ዉስጥ የሽንት ቧንቧ ኢንፌክሽን
አጋጥሞወት ያዉቃል
ሀ. አያዉቅም ለ. አዎ
ጥ302 ከአሁን በፊት መድሃኒት (ፀረ-ባክቴሪያ) ወስደዉ ያዉቃሉ ሀ. አላዉቅም ለ. አዎ
ጥ303 ነፍሰ-ጡር እናቷ በስኳር በሽታ የተጠቁ ናቸዉን
(መረጃቸዉን አይተዉ ይሙሉ)
ሀ. የለም ለ. አዎ
ጥ304 ነፍሰ-ጡር እናቷ በ ኤች አይ ቪ የተጠቁ ናቸዉን
(መረጃቸዉን አይተዉ ይሙሉ)
ሀ. የለም ለ. አዎ
ጥ305 ነፍሰ-ጡር እናቷ የሽንት ቧንቧ ኢንፌክሽን በሽታ ምልክት
ይታይባቸዋልን
ሀ. የለም ለ. አዎ

45
Annex IV: Procedures
Clean-catch midstream urine collection.
This method helps protect the urine sample from germs that are normally found on the penis or vagina.
The pregnant women were told to follow the following procedures in order to collect urine sample.
1. Wash your hands first and then remove the lid of the container carefully and do not touch the
inside of the cup with your fingers.
2. Clean the area around your genitals.
3. Spread open the folds of skin around the vagina with one hand. Then use the other hand to clean
the area around the vagina and urethra thoroughly using sterilized swabs soaked with
appropriate disinfectant.
4. Wipe the area from front to back to avoid spreading bacteria from the anus to the urethra.
5. Start to urinate into the toilet or urinal. Participants should keep holding apart the
folds of skin around the vagina while they urinate.
6. After the urine has flowed for several seconds, place the collection cup into the stream. Collect
about 20 ml of this "midstream" urine without stopping the flow.
7. Do not touch the rim of the container to your genital area. And don't get toilet paper, pubic hair,
stool (faces), menstrual blood, or other foreign matter in the urine sample.
8. Finish urinating into the toilet or urinal.
9. Carefully replace the lid on the cup. Wash your hands. Return the cup to the lab.
Culture media preparation
1. Read the label on a bottle of dehydrated agar media. It specifies the amount of dehydrated powder
required to make 1 litter (1,000 ml) of medium. Calculate the amount needed for 1/2 litter and weigh
out this quantity.
2. Place 500 ml of distilled water in an Erlenmeyer flask. Add the weighed, dehydrated agar while
stirring with a glass rod to prevent lumping.
3. Set the flask on a tripod over an asbestos mat.
4. When the agar mixture is completely dissolved, remove the flask from the flame or hot plate, close it
with the cotton plug or cap, and it has to be sterilized in the autoclave.
5. When the flask of sterilized agar is returned to you, allow it to cool to about 50°C (the agar should be
warm and melted, but not too hot to handle in its flask). Remove the plug or cap with the little finger
of your right hand and continue to hold it until you are sure it won’t have to be returned to the flask.
46
Quickly pour the melted, sterile agar into a series of Petri dishes. The petri dish tops are lifted with
the left hand and the bottoms are filled to about one-third capacity with melted agar.
6. Replace each Petri dish top as the plate is poured. When the plates are cool (agar solidified), invert
them to prevent condensing moisture from accumulating on the agar surfaces.
7. Place inverted agar plates in the 35°C incubator. They should be incubated for at least 24 hours to
ensure they are sterile (free of contaminating bacteria) before you use.
Gram stain procedures
1. Prepare a thin smear of the culture and allow to air-dry
2. Fix the dried smear
3. Cover the fixed smear with crystal violet stain for 30–60 seconds.
4. Rapidly wash off the stain with clean water.
5. Tip off all the water, and cover the smear with Lugol’s iodine for 30–60 seconds.
6. Wash off the iodine with clean water.
7. Decolorize rapidly (few seconds) with acetone–alcohol. Wash immediately with clean water.
8. Cover the smear with neutral red stain for 2 minutes.
9. Wash off the stain with clean water.
10. Wipe the back of the slide clean, and place it in a draining rack for the smear to air-dry.
11. Examine the smear microscopically, first with the 40x objective to check the staining and to see
the distribution of material, and then with the oil immersion objective to report the bacteria and
cells
Results
Gram positive bacteria . . . . . . . . . . . . . Dark purple
Yeast cells . . . . . . . . . . . . . . . . . . . . . . . Dark purple
Gram negative bacteria. . . . . . . . . . Pale to dark red
Nuclei of pus cells . . . . . . . . . . . . . . . . . . . . . . . Red
Epithelial cells . . . . . . . . . . . . . . . . . . . . . . . . Pale red

47
Biochemical testing procedures
Identification of Gram negative bacteria: was based on their test result with a series of biochemical
tests.
Procedure
1. Prepare a suspension of the test organism with nutrient broth. 3-4 colony of test organism in 5 ml
nutrient broth.
2. A loop full of the bacterial suspension was inoculated in to indole, citrate agar, triple sugar iron agar,
lysine decarboxylase agar, mannitol, urea agar and motility medium.
3. Incubate at 35-37oc for 18-24 hours.
4. Look for color change (turbidity for motility) of the medium
5. Identify the test organism by considering the result of the six biochemical tests
For example,
An isolate was considered as E. coli when it was Indole positive, citrate negative, lysine positive, gas and
acid producer, ferments mannitol, urea negative and motile.
An isolate was be identified as K. pneumoniae when it was indole negative, citrate positive, ferments
mannitol, lysine positive, urea slow producing and non-motile.

48
API 20e test procedure:
This test was used to identify gram negative bacteria, especially for Enterobacteriaceae family.
Test procedure includes
A. Preparation of the strip
1. Prepare an incubation box (tray and lid) and distribute about 5 ml of distilled water or
demineralized water into the honeycombed wells of the tray to create a humid atmosphere.
2. Record the strain reference on the elongated flap of the tray.
3. Remove the strip from its packaging.
4. Place the strip in the incubation box
B. Preparation of the inoculum
1. Use any tube containing 5 ml of sterile saline or sterile distilled water, without additives.
2. Using a pipette, remove a single well isolated colony from an isolation plate. It is recommended
to use young cultures (18-24 hours old).
3. Carefully emulsify to achieve a homogeneous bacterial suspension.
4. This suspension must be used immediately after preparation.
C. Inoculation of the strip
1. Using the same pipette, fill both tube and cupule of the tests [CIT], [VP] and [GEL] with the
bacterial suspension.
2. Fill only the tube (and not the cupule) of the other tests. Create an aerobiosis in the tests ADH,
LDC, ODC, H2S and URE by overlaying with mineral oil.
3. Close the incubation box and Incubate at 36°C ± 2°C for 18-24 hours.
D. Reading the strip
1. After the incubation period, read the strip by referring to the Reading Table.
2. If 3 or more tests (GLU test + or –) are positive, record all the spontaneous reactions on the result
sheet and then reveal the tests which require the addition of reagents:
a. TDA Test: add 1 drop of TDA reagent. A reddish brown color indicates a positive
reaction to be recorded on the result sheet.
b. IND Test: add 1 drop of JAMES reagent. A pink color developed in the whole cupule
indicates a positive reaction to be recorded on the result sheet.

49
c. VP Test: add 1 drop each of VP 1 and VP 2 reagents. Wait at least 10 minutes. A pink
or red color indicates a positive reaction to be recorded on the result sheet. If a slightly
pink color appears after 10 minutes, the reaction should be considered negative.
3. If the number of positive tests (including the GLU test) before adding the reagents is less than 3.
a. Re-incubate the strip for a further 24 hours (± 2 hours) without adding any reagents.
b. Reveal the tests requiring the addition of reagents
E. Interpretation
Identification is obtained with the numerical profile.
1. Determination of the numerical profile: On the result sheet, the tests are separated into groups of
3 and a value 1, 2 or 4 is indicated for each. By adding together the values corresponding to
positive reactions within each group, a 7-digit profile number is obtained for the 20 tests of the
API 20 E strip. The oxidase reaction constitutes the 21st test and has a value of 4 if it is positive.
2. Identification: With the identification software: Enter the 7-digit numerical profile manually via
the keyboard.
Antimicrobial susceptibility testing
Procedure
1. Prepare a suspension of the test organism by emulsifying several colony of the organism in a sterile
saline until it matches with a turbidity of 0.5 McFarland standard
2. Take a sample from the suspension with a sterile swab (squeeze the swab against the side of the test
tube to remove the excess fluid).
3. Spread the inoculums evenly over the Muller-Hinton agar plate with the swab and wait for about 30
minutes
4. Using a sterile forceps or needle, place the antimicrobial disc on the inoculated plate
5. Incubate the plate aerobically at 35-37oC for 18-24 hours
6. Read the test and measure the radius of the inhibition zone.
7. Interpret the reaction of the test organism to each antibiotics used as sensitive, intermediate, or
resistance as per the standard
Sensitive – zone of radius is wider or equal to the control
Intermediate –zone of radius is more than three mm smaller than the control
Resistance – no zone of inhibition.

50
Annex IIb: Laboratory Data Collection Form: Patient ID.______________
Negative culture Positive culture
Put a sign here…. Isolated uropathogen/s MDR ESBL production
0. No
1. Yes
0. No
1. Yes
ESBL= Extended-Spectrum Beta Lactamase, MDR= Multi-drug Resistant
Antibiotic Susceptibility Pattern
Name of
Antibiotic
Sensitivity Results: Zone diameter breakpoints nearest to whole mm
Content S I R Zone diameter(mm) Final result (S or I or R)
S= susceptible, I= intermediate, R= resistant
Susceptible (S): implies that isolates are inhibited by the usually achievable concentrations of
antimicrobial agent when the dosage recommended to treat the site of infection is used.
Intermediate (I): implies that clinical efficacy in body sites where the drugs are physiologically
concentrated or when a higher than normal dosage of a drug can be used.
Resistant (R): implies that the isolates are not inhibited by the usually achievable concentrations of the
agent with normal dosage schedules (CLSI).
51
University of Gondar
College of Medicine and Health Sciences
School of Biomedical and Laboratory Sciences
Department of Medical Microbiology
DECLARATION
The research work in this thesis entitled “Multi-drug resistant and Extended-spectrum β-lactamase
producing bacterial uropathogens among pregnant women at the University of Gondar Teaching
Hospital, Northwest Ethiopia.” was carried out by me under the supervision of Prof. Feleke Moges and
Mr. Setegn Eshetie at the University of Gondar, College of Medicine and Health Sciences, School of
Biomedical and Laboratory Sciences, Department of Medical Microbiology, for the award of MSc
Degree in Medical Microbiology. I declare that this work is original and has not been submitted to any
other University or institution.
Name of student: Sirak Biset Tel: +251911598568 Email: [email protected]
Place: Gondar, 2017 Sign: Date: __________
Advisors Sign Date
1. _______________________
2. _______________________
Examiner Sign Date
1._____________________ _____________ _____________________