Typical and Atypical Perfusion Patterns in Periictal SPECT of Patients with Unilateral Temporal Lobe...
7
Clinical Research Typical and Atypical Perfusion Patterns in Periictal SPECT of Patients with Unilateral Temporal Lobe Epilepsy *Lauro Wichert-Ana, *Tonicarlo Rodrigues Velasco, *Vera Cristina Terra-Bustamante, *David Arau ´ jo Jr., *Veriano Alexandre Ju ´nior, ²Mery Kato, *Joa˜o Pereira Leite, ‡Joa ˜o Alberto Assirati, ‡He ´lio Rubens Machado, §Alexandre Cunha Bastos, and *Ame ´rico Ceiki Sakamoto *Department of Neurology–Center for Epilepsy Surgery (CIREP), ²Service of Nuclear Medicine, ‡Department of Surgery, and §Image Science and Medical Physics Center, Ribeira ˜o Preto Medical School, University of Sa ˜o Paulo, Ribeira ˜ o Preto, Brazil Summary: Purpose: To characterize perfusion patterns of periictal single-photon emission tomography (SPECT) in pa- tients with unilateral temporal lobe epilepsy (TLE) and to de- termine their relationship to the epileptogenic zone (EZ). Methods: We studied periictal SPECT scans of 53 patients after anterior mesial temporal lobectomy who had good seizure outcome after surgery. Ictal SPECT scans were performed dur- ing video-EEG monitoring. Typical SPECT patterns consisted of ipsilateral ictal hyperperfusion or ipsilateral postictal hy- poperfusion. Atypical ictal patterns included normal scans, bi- lateral temporal hyperperfusion, or contralateral patterns. These perfusion patterns were retrospectively analyzed searching for concordance rate with the EZ. Results: We obtained 51 ictal and two early postictal scans. In the typical group, 40 (75.4%) patients had ipsilateral ictal temporal lobe hyperperfusion, and one (1.9%) patient had ip- silateral postictal temporal lobe hypoperfusion. Twelve (22.7%) patients exhibited atypical perfusion patterns: seven (13.2%) patients had bitemporal ictal hyperperfusion (four cases showed asymmetric temporal lobe changes), four (7.6%) patients had contralateral hyperperfusion, and one (1.9%) pa- tient had a normal SPECT scan. All four patients with bitem- poral asymmetric hyperperfusions showed greater perfusion lateralized to the side of the EZ. Three of the four patients who had contralateral hyperperfusion also had a complex postictal- like pattern in the ipsilateral temporal lobe consisting of an- teromesial hyperperfusion with adjacent lateral hypoperfusion. Conclusions: This study analyzed typical and atypical per- fusion patterns in unilateral TLE, and suggested that not only typical, but also some atypical perfusion patterns may contrib- ute to the lateralization of EZ. Key Words: Epilepsy— Surgery—Temporal lobe epilepsy—SPECT—Perfusion pat- terns—rCBF. The multidisciplinary presurgical evaluation of pa- tients with medically intractable temporal lobe epilepsy (TLE) at many epilepsy surgery centers includes the ictal single-photon-emission computed tomography (SPECT) as an additional test that is considered a practical and highly sensitive method to localize the epileptogenic zone (EZ) (1–4). The initial studies of SPECT in epilepsy included only the interictal period, and the perfusion patterns then de- scribed in the TLE played only a modest role in the localization of the EZ (5–8). Later postictal SPECT had shown ipsilateral temporal lobe hypoperfusion or focal area of increased perfusion in the mesial and anterior parts of the ipsilateral temporal lobe, associated with decreased perfusion in the adjacent lateral temporal cor- tex. The adjacent hypoperfusion was considered to rep- resent the late evolution of the ictal state, called “post- ictal switch” (7), and this pattern has been considered a reliable diagnostic sign for the lateralization of the epi- leptogenic temporal lobe in postictal SPECT scans (5– 7,9,10). In the last two decades, several studies have confirmed the classic observation of ipsilateral ictal hyperperfusion as the hallmark SPECT finding for the lateralization of the epileptogenic temporal lobe (11–15). Some studies, however, have suggested that other complex ictal perfu- sion patterns, involving adjacent areas of the epilepto- Accepted February 14, 2001. Address correspondence and reprint requests to Dr. L. Wichert-Ana at Centro de Cirurgia de Epilepsia, CIREP–Hospital das Clı ´nicas da FMRP-USP, Av. Bandeirantes, 3900–CEP, 14.048-900 – Monte Alegre, Ribeira ˜o Preto, Sp, Brazil. E-mail: [email protected] Epilepsia, 42(5):660–666, 2001 Blackwell Science, Inc. © International League Against Epilepsy 660
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Typical and Atypical Perfusion Patterns in Periictal SPECT of Patients with Unilateral Temporal Lobe...

Clinical Research
Typical and Atypical Perfusion Patterns in Periictal SPECT ofPatients with Unilateral Temporal Lobe Epilepsy
*Lauro Wichert-Ana, *Tonicarlo Rodrigues Velasco, *Vera Cristina Terra-Bustamante,*David Araujo Jr., *Veriano Alexandre Ju´nior, †Mery Kato, *Joa˜o Pereira Leite,‡Joao Alberto Assirati, ‡He´lio Rubens Machado, §Alexandre Cunha Bastos, and
*Americo Ceiki Sakamoto
*Department of Neurology–Center for Epilepsy Surgery (CIREP), †Service of Nuclear Medicine, ‡Department of Surgery, and§Image Science and Medical Physics Center, Ribeira˜o Preto Medical School, University of Sa˜o Paulo, Ribeira˜o Preto, Brazil
Summary: Purpose: To characterize perfusion patterns ofperiictal single-photon emission tomography (SPECT) in pa-tients with unilateral temporal lobe epilepsy (TLE) and to de-termine their relationship to the epileptogenic zone (EZ).
Methods:We studied periictal SPECT scans of 53 patientsafter anterior mesial temporal lobectomy who had good seizureoutcome after surgery. Ictal SPECT scans were performed dur-ing video-EEG monitoring. Typical SPECT patterns consistedof ipsilateral ictal hyperperfusion or ipsilateral postictal hy-poperfusion. Atypical ictal patterns included normal scans, bi-lateral temporal hyperperfusion, or contralateral patterns. Theseperfusion patterns were retrospectively analyzed searching forconcordance rate with the EZ.
Results:We obtained 51 ictal and two early postictal scans.In the typical group, 40 (75.4%) patients had ipsilateral ictaltemporal lobe hyperperfusion, and one (1.9%) patient had ip-silateral postictal temporal lobe hypoperfusion. Twelve
(22.7%) patients exhibited atypical perfusion patterns: seven(13.2%) patients had bitemporal ictal hyperperfusion (fourcases showed asymmetric temporal lobe changes), four (7.6%)patients had contralateral hyperperfusion, and one (1.9%) pa-tient had a normal SPECT scan. All four patients with bitem-poral asymmetric hyperperfusions showed greater perfusionlateralized to the side of the EZ. Three of the four patients whohad contralateral hyperperfusion also had a complex postictal-like pattern in the ipsilateral temporal lobe consisting of an-teromesial hyperperfusion with adjacent lateral hypoperfusion.
Conclusions:This study analyzed typical and atypical per-fusion patterns in unilateral TLE, and suggested that not onlytypical, but also some atypical perfusion patterns may contrib-ute to the lateralization of EZ.Key Words: Epilepsy—Surgery—Temporal lobe epilepsy—SPECT—Perfusion pat-terns—rCBF.
The multidisciplinary presurgical evaluation of pa-tients with medically intractable temporal lobe epilepsy(TLE) at many epilepsy surgery centers includes the ictalsingle-photon-emission computed tomography (SPECT)as an additional test that is considered a practical andhighly sensitive method to localize the epileptogeniczone (EZ) (1–4).
The initial studies of SPECT in epilepsy included onlythe interictal period, and the perfusion patterns then de-scribed in the TLE played only a modest role in thelocalization of the EZ (5–8). Later postictal SPECT had
shown ipsilateral temporal lobe hypoperfusion or focalarea of increased perfusion in the mesial and anteriorparts of the ipsilateral temporal lobe, associated withdecreased perfusion in the adjacent lateral temporal cor-tex. The adjacent hypoperfusion was considered to rep-resent the late evolution of the ictal state, called “post-ictal switch” (7), and this pattern has been considered areliable diagnostic sign for the lateralization of the epi-leptogenic temporal lobe in postictal SPECT scans (5–7,9,10).
In the last two decades, several studies have confirmedthe classic observation of ipsilateral ictal hyperperfusionas the hallmark SPECT finding for the lateralization ofthe epileptogenic temporal lobe (11–15). Some studies,however, have suggested that other complex ictal perfu-sion patterns, involving adjacent areas of the epilepto-
Accepted February 14, 2001.Address correspondence and reprint requests to Dr. L. Wichert-Ana
at Centro de Cirurgia de Epilepsia, CIREP–Hospital das Clı´nicas daFMRP-USP, Av. Bandeirantes, 3900–CEP, 14.048-900 – MonteAlegre, Ribeira˜o Preto, Sp, Brazil. E-mail: [email protected]
Epilepsia,42(5):660–666, 2001Blackwell Science, Inc.© International League Against Epilepsy
660

genic temporal lobe or extending to another brain re-gion, may also contribute to the lateralization of the EZ(16–20).
In our surgical series of patients with TLE, we alsoobserved atypical perfusion patterns (APPs) that initiallydid not contribute to the lateralization of the EZ and evenrequired repetition of the SPECT scans. Careful analysisof these SPECT patterns may be of critical importance,especially in those cases with normal or mildly abnormalmagnetic resonance imaging (MRI) or nonlocalizing ic-tal electroencephalographic (EEG) changes.
In this study, we aimed to characterize the typical andatypical perfusion patterns of periictal SPECT scans in ahomogeneous group of patients with unilateral TLE, todetermine the relative frequency of these patterns, andfinally to analyze their relationship with the EZ.
PATIENTS AND METHODS
PatientsWe retrospectively analyzed 53 patients (23 male and
30 female patients) with medically intractable TLE,given video-EEG monitoring and periictal SPECT be-tween October 1996 and July 1998 in the Epilepsy Sur-gery Center (CIREP), at the Ribeira˜o Preto MedicalSchool, University of Sa˜o Paulo, Brazil. The presurgicallocalization of the EZ was based on the combined resultsof the multidisciplinary workup, which included long-term video-EEG monitoring, MRI and computed tomog-raphy (CT) scans, ictal and interictal SPECT, neuropsy-chologic evaluations, and the Wada test.
To characterize the perfusion patterns in TLE, we se-lected a homogeneous group of unilateral TLE patientsgiven anterior mesial temporal lobectomy. Only patientsin postsurgical seizure outcome Engel classes I and IIwere included (22). All subjects gave informed consentfor SPECT studies, and the presurgical protocol was pre-viously approved by the Ethics Committee of our insti-tution.
Presurgical workupPatients were given long-term video-EEG monitoring
through a digital video-EEG System (Vangard Systems,Cleveland Clinic Foundation, Cleveland, OH, U.S.A.).EEG records routinely included closed-spaced electrodesand bilaterally placed sphenoidal electrodes. Invasive re-cordings were performed whenever full convergence be-tween presurgical data was not achieved. A minimum ofthree seizures was required, and all EEG data wereevaluated by board-certified electroencephalographers.Imaging studies included CT and high-resolution MRIwith a 1.5-T Siemens Magneton Vision equipment.Neuropsychological testing was performed in all pa-tients, and the Wada test was applied whenever speechdominance and assessment of memory functions werenecessary.
SPECT methodsAll patients underwent periictal and interictal SPECT
scans. For the periictal SPECT, the tracer ethyl cystein-ate dimer (ECD) labeled with 3 GBq of99mtechnetium(99mTc) was injected immediately after the clinical orEEG seizure onset. The tracer was injected at a maximaldose of 1,295 MBq (35 mCi). The SPECT was consid-ered ictal whenever the injection of the tracer was com-pleted before clinical or EEG termination of the seizures.Postictal SPECT was considered whenever the injectionwas completed after the seizure termination, although itwas started during the ictal phase. In those cases of mul-tiple ictal SPECT, we considered for this analysis onlythe first ictal SPECT.
All interictal SPECT scans were performed using thesame tracer, when patients were free of seizures for$24h. The subjects were oriented to stay at rest, with theireyes open, in a quiet and dark room and required torefrain from talking and listening.
Ictal and interictal SPECT were carried out in a single-headed rotating gamma camera (Siemens Orbiter) usinga low-energy, high-resolution collimator (LEHR). It wasrecorded by 64 projections over 360° on a 64 × 64 ma-trix, acquisition time of 30 min, and 70,000 counts/frame. Projections were filtered with Butterworth filter4.25. Scans were reconstructed with a SOPHA NXTworkstation in transaxial slices parallel to a line drawnfrom the basis of the frontal lobe to the occipital lobe,and parallel to the long axis of the temporal lobe, fromwhich coronal sections were produced. Attenuation cor-rection was performed using first order Chang’s method(coefficient, 0.12/cm). The ictal perfusion patterns werevisually analyzed for the presence of hyper- or hypoper-fusion changes in the temporal lobes in comparison withthe interictal SPECT. Images were blindly and indepen-dently analyzed by two experienced specialists (L.W.A.,M.K.). Interobserver concordance was calculated forboth ictal and interictal scans (23).
Perfusion patterns definitionsTo determine the concordance rate of the perfusion
patterns, we mainly looked for hyperperfusions in theictal SPECT and hypoperfusions in the postictal SPECT.Typical perfusion patterns (TPPs) were defined as ipsi-lateral focal hyperperfusion in the ictal SPECT, and ip-silateral focal hypoperfusion in the postictal scan. Atypi-cal perfusion patterns (APPs) included all perfusion find-ings that did not exhibit the previously describedunilateral typical patterns.
RESULTS
Patient demographicsClinical and demographic data are shown in Table 1.
Fifty-three patients (mean age, 37 ± 9 years; age range,14–54 years) were included in this study. Mean age at
ICTAL SPECT PATTERNS IN TLE 661
Epilepsia, Vol. 42, No. 5, 2001

seizure onset was 6 years and 7 months (range, 1 monthto 32 years). Twenty-two patients had antecedent of fe-brile seizures. All patients had normal neurologic evalu-ation, except for one who had spastic paraparesis unre-
lated to the epilepsy. Video-EEG localized the EZ in allpatients, 26 patients on the right temporal lobe, and 27patients on the left. MRI imaging demonstrated hippo-campal atrophy in 51 (96%) of 53 patients and mesial
TABLE 1. Clinical characteristics and SPECT findings of the study patients
Pt/sex/age (yr)
Surgerysite MRI Outcome Pathology
Time of injection(s)a
Ictal/postictalSPECT findings
Perfusionpatterns
1/F/49 R T R HA I b HS 37.0 R T Hyper Ipsi2/F/21 R T R HA I b HS 28.0 R T Hyper Ipsi3/F/33 L T L HA I a HS 37.5 L T Hyper Ipsi4/F/48 L T L HA, L T Les I a HS 38.0 L T Hyper Ipsi5/M/14 R T R HA, R T Les I a HS, MD 31.0 R T Hyper Ipsi6/F/38 R T R HA I b HS, MD 50.0 Bi T Hyper & Hypo (R4 L) Bitemp7/M/41 R T R HA I a HS 44.0 Bi T Hyper (R4 L) Bitemp8/M/48 L T L HA, R T Les I a HS 48.0 L T Hyper Ipsi9/M/42 L T L HA I b HS 27.0 L T Hyper Ipsi10/F/36 R T R HA II b HS 34.5 Bi T Hyper (R > L) Bitemp11/M/47 L T L HA I b HS 21.5 L T Hyper Ipsi12/M/43 R T R HA, L F Ncc I a HS, MD 73.0 R T Hyper Ipsi13/M/27 L T L HA I b HS 68.0 L T Hypo Ipsi14/F/31 R T R HA I a HS 107.5 R T Hyper Ipsi15/F/16 L T Bilat HA, L < D II d HS, MD 44.0 L T Hyper Ipsi16/M/53 L T L HA, L T Les I a HS, MD 40.0 Normalb Normal17/M/41 R T R HA, Ncc I a HS, MD 46.0 R T Hyper Ipsi18/F/40 R T R HA I a HS 40.0 R T Hyper Ipsi19/F/35 L T L HA I a HS 38.0 L T Hyper Ipsi20/M/35 R T R HA I a HS 38.0 L T Hyper/R T Hypo Contra21/F/52 R T R HA I a HS 35.0 Bi T Hyper (R > L) Bitemp22/F/22 L T L HA I d HS 46.0 L T Hyper Ipsi23/M/28 R T R HA, R T Les I a HS 34.5 R T Hyper Ipsi24/M/30 R T R HA I d HS, MD 24.5 R T Hyper Ipsi25/M/54 L T L HA I a HS 41.5 L T Hyper Ipsi26/M/41 L T L HA I a HS, MD 57.0 L T Hyper Ipsi27/F/36 L T L HA I a HS, MD 15.0 L T Hyper Ipsi28/F/25 R T R T Les I b HS 25.5 R T Hyper Ipsi29/F/30 L T L HA I a HS 56.0 L T Hyper Ipsi30/F/39 R T R HA, R Ncc I a HS, Ncc, MD 71.0 Bi T Hyper (R > L) Bitemp31/F/33 L T L HA, Ncc I b HS, Ncc, MD 27.5 L T Hyper Ipsi32/M/30 L T L HA I b HS 65.0 L T Hyper Ipsi33/M/38 L T L HA II b HS 58.0 L T Hyper Ipsi34/F/32 R T R HA II b HS 34.0 R T Hyper Ipsi35/F/29 R T R HA I a HS 94.0 Bi T Hyper (R > L) Bitemp36/F/40 R T R HA I b HS, MD 33.0 R T Hyper Ipsi37/M/43 L T L HA I a HS 45.0 L T Hyper Ipsi38/M/38 R T R HA I a HS 26.0 R T Hyper Ipsi39/F/48 R T R HA I d HS, MD 58.0 R T Hyper Ipsi40/F/36 L T L HA I a HS 22.0 L T Hyper Ipsi41/F/34 L T L HA II b HS 25.0 L T Hyper Ipsi42/F/38 L T L HA I a HS 59.0 L T Hyper/R T Hypo Ipsi43/F/50 R T R HA I a HS, MD 59.0 R T Hyper Ipsi44/M/49 R T R mesial T Les I a ND 70.0 R T Hyper Ipsi45/M/34 L T L HA I d HS 51.0 Bi T Hyper (R4 L) Bitemp46/M/34 R T R HA, L FT Les I a HS 2.0 R T Hyper Ipsi47/M/30 R T R HA I a HS, Ncc, MD 34.0 L T Hyper/R T Hypo Contra48/F/49 L T L HA I a HS 40.0 R T Hyper/L T Hypo Contra49/M/28 L T L HA I a HS 29.5 L T Hyper Ipsi50/F/43 L T L HA, L O Ncc I b HS 72.5 R T Hyper/L T Hypob Contra51/F/32 R T R HA I a HS 43.5 R T Hyper Ipsi52/F/33 L T L HA I a MD 48.0 L T Hyper Ipsi53/F/40 L T L HA I b HS 77.5 L T Hyper IpsiMean 44.7SD 19.6
F, female; M, male; R, right; L, left; Bilat, bilateral; T, temporal; I and II, Engel classification; HA, hippocampal atrophy; HS, hippocampalsclerosis; MD, mycrodysgenesis; Les, lesions; Ncc, calcifications suggestive of neurocysticercosis; ND, mild findings suggesting but not defininghippocampal sclerosis; (s), seconds; Hyper, hyperperfusion; Hypo, hypoperfusion; Ipsi, ipsilateral to the epileptogenic temporal lobe; Bitemp,bilateraltemporal lobe hyperperfusion; Contra, contralateral temporal lobe hyperperfusion.
<, 4, and > means lower, equal, or higher volume or perfusion of one temporal lobe than the other.a Time of injection resulted from the mean between clinical and electroencephalographic delay for tracer injection.b Early postictal SPECT (patient 16 with 22 s and patient 50 with 12 s after seizure termination).
L. WICHERT-ANA ET AL.662
Epilepsia, Vol. 42, No. 5, 2001

temporal lesions suggestive of cortical dysplasia or low-grade tumor in two patients.
All patients underwent anterior mesial temporal lobec-tomy; three of them additionally had temporal lobe le-sionectomy (patients 16, 23, and 44). The follow-up pe-riod ranged from 10 to 32 months (mean, 18.6 ± 6.9months), and postoperative seizure outcome according toEngel’s classification is shown in Table 1. Pathology ofsurgical specimens demonstrated mesial temporal scle-rosis in all but two patients: one patient had microdys-genesis, and another one had mild and not defined patho-logic findings. Microdysgenesis was also the secondmost common pathologic finding associated with hippo-campal sclerosis.
SPECT and perfusion patternsFifty-one patients had ictal SPECT scans, and two
patients (13 and 50) had early postictal scans. Both TPPs
and APPs are described in Table 1 and exemplified inFig. 1. The difference between the means of time fortracer injection was not significant for TPPs (43.0 ± 19.7s) and ATT groups (50.3 ± 19.0 s; p4 0.26, independentsamplet test).
TPP was observed in 41 (77.3%) patients (see Table2), and comprised both ipsilateral ictal hyperperfusion(40 patients), and ipsilateral postictal hypoperfusion (onepatient). The ipsilateral hyperperfusion pattern achievedthe greatest concordance rate with the localization of theEZ (75.4%).
APP included several perfusion findings: (a) bitempo-ral symmetric hyperperfusion of the entire temporallobes (symmetric 1: two patients, 3.7%); (b) bitemporalsymmetric hyperperfusion restricted to the anteromesialand lateral regions, associated with bilateral hypoperfu-sion of the posterior temporal regions (symmetric two:one patient, 1.9%); (c) bitemporal asymmetric hyperper-
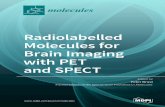
FIG. 1. Characterization of ictal SPECT perfu-sion patterns in unilateral temporal lobe epi-lepsy. ‘Typical ’ pattern with hyperperfusion onthe epileptogenic temporal lobe. ‘Atypical Bi-temporal Symmetric 1’ pattern with equal in-crease of perfusion on both whole temporallobes. ‘Atypical Bitemporal Symmetric 2 ’ patternsimilar to the type 1 except by additional andaccentuated hypoperfusion in posterior regionof both temporal lobes. ‘Atypical BitemporalAsymmetric’ pattern with bilateral hyperperfu-sion, but predominantly on the right epilepto-genic temporal lobe. ‘Atypical Contralateral’ pat-tern with contralateral hyperperfusion on theright temporal lobe, and ipsilateral complex per-fusion pattern comprising mild hyperperfusion inthe anteromesial temporal region with adjacentlateral hypoperfusion.
ICTAL SPECT PATTERNS IN TLE 663
Epilepsia, Vol. 42, No. 5, 2001

fusion, with greater perfusion ipsilateral to the EZ (asym-metric: four patients, 7.6%); (d) Contralateral hyperper-fusion associated either to ipsilateral hypoperfusion (onepatient, 1.9%) or ipsilateral hypoperfusion in the latero-posterior temporal region associated with a mild hyper-perfusion in the anteromesial temporal region (three pa-tients, 5.7%).
Interictal SPECT showed normal perfusion in 22(41.5%) patients, ipsilateral hypoperfusion in 20 (37.8%)patients, contralateral hypoperfusion in six (11.3%) pa-tients, bitemporal hypoperfusion in three (5.6%) patients,ipsilateral hyperperfusion in one (1.9%) patient, and con-tralateral hyperperfusion in one (1.9%) patient.
DISCUSSION
This study confirms the predominance of TPPs in theperiictal SPECT scans of unilateral TLE and their con-tribution to the localization of the EZ. However, our dataalso showed that APPs occur, and some of them mayplay a role in the lateralization/localization of the EZ.
TPPs were greatly represented by ipsilateral temporallobe hyperperfusion (40 of 41 patients), which showed aconcordance rate of 75.4% with the EZ. One patientshowed postictal ipsilateral hypoperfusion, similar toearlier-described localizing findings (5–7,9,10). TPPshave been previously described by several authors (12–15), and they mainly reflect the ictal increase in the re-gional cerebral blood flow (rCBF) in the epileptogenictemporal lobe. Other series further analyzed this typical
pattern by observing the relative distribution of the tracerin the different regions of the temporal lobe: mesial,lateral, and posterior regions (19). TPPs have been con-sidered a predictor of good surgical outcome (19), andthis fact has driven the efforts to optimize routines ofmonitoring and ictal tracer injections to improve the sen-sitivity of the ictal SPECT (24,25).
APPs were initially considered nonlateralizing find-ings for the purposes of selection of candidates for epi-lepsy surgery. However, retrospective review of two ofthese patterns demonstrated rCBF features that showed ahigh concordance rate with the EZ. First, thebitemporalasymmetricpattern was observed in seven patients, ofwhom four patients had bitemporal asymmetric hyper-perfusion, with the side of greater hyperperfusion alwaysconcordant with the localization of the EZ (100%). Thisfinding, as can be seen in Table 1 and Fig. 1, suggests apossible lateralizing role even in cases of bilateral ictalSPECT findings. Second, three of four patients withcon-tralateral hyperperfusionpattern (75%) showed addi-tional ipsilateral mild hyperperfusion in the mesial andanterior temporal regions, associated with a moderate tosevere hypoperfusion pattern in the adjacent areas. Thisipsilateral finding is similar to the previously describedpostictal pattern (5,10). A possible explanation for thisfinding may be that the tracer injection was relativelylate to record rCBF increase in the EZ, where a postictalpattern was then observed, and the contralateral hyper-perfusion may represent early seizure propagation to thecontralateral temporal lobe. In other words, this complexperfusion pattern suggests ipsilateral postictal and con-tralateral ictal perfusion states at the timing of the tracerinjection. One study (26) reported similar perfusion find-ings, but in a patient with bilateral independent temporallobe seizures, with the tracer injected in the interval be-tween two closely spaced seizures (one localized in theleft temporal lobe and the other in the right temporallobe). In this case, SPECT images showed hypoperfusionin the lateral, and hyperperfusion in the mesial region ofthe left temporal lobe (side of the first seizure), with apronounced hyperperfusion in the right anterior temporallobe (side of second seizure). In the fourth patient, whoalso had contralateral hyperperfusion but exclusively hy-poperfusion in the ipsilateral side, the same mechanismsprobably played a role, and one is tempted to assume thatthe tracer injection was even later during the course ofthat particular seizure, depicting a relative late postictalperfusion pattern in one temporal lobe (where the seizurestarted) and an ictal perfusion pattern in the other tem-poral lobe (where the seizure propagated to).
In TLE, several studies have already shown that per-fusion patterns and especially complex perfusion pat-terns may occur possibly because of the delay of tracerinjection (7,10,13), whereas others suggested that theymight reflect seizure propagation (18,19,30,31). Our
TABLE 2. Perfusion patterns in unilateral temporallobe epilepsy
Ictal/postictal SPECTNo. ofpatients
Concordancerate (%)
Typical 41 77.3Ipsilateral hyper 40 75.4Ipsilateral hypo (Postictal) 1 1.9
Atypical 12 22.7Bitemporal hyper 7 13.2
Symmetric 1 2 3.7Symmetric 2 1 1.9Asymmetric (Ipsilateral >
Contralateral) 4 7.6a
Contralateral hyper 4 7.6Contralateral 1: Contralateral
hyper with ipsilateral hypo 1 1.9Contralateral 2: Contralateral
hyper with ipsilateral temporalanteromesial hyper and adjacentposterolateral hypo 3 5.7b
Normal perfusion 1 1.9Total 53 100.0
Hyper, hyperperfusion; Hypo, hypoperfusion; <,4, and >, lesser,equal or greater perfusion.
a All patients with asymmetric bitemporal hyperperfusion hadgreater perfusion ipsilateral to the epileptogenic zone.
b Three of four patients that had contralateral hyperperfusion hadipsilateral complex perfusion pattern that suggested the lateralization ofepileptogenic zone.
L. WICHERT-ANA ET AL.664
Epilepsia, Vol. 42, No. 5, 2001

study, however, showed no significant difference in thedelay for tracer injection between the typical and atypicalgroups. Ho et al. (1996) (18) studied cerebral perfusionpatterns in four subgroups of patients with intractableTLE (with hippocampal sclerosis, with foreign-tissue le-sion in mesial temporal lobe, with foreign-tissue lesion inlateral temporal lobe, and with normal temporal lobetissue) and a good postsurgical outcome. They founddistinct patterns of cerebral perfusion in these subtypesof TLE. In groups 1 and 2, hyperperfusion was seen inthe ipsilateral mesial and lateral temporal regions. Ingroup 3, hyperperfusion was seen bilaterally in the tem-poral lobes, with predominant changes ipsilateral to thelesion, that can be explained by anatomic connectionsbetween the temporal lobes (32–34). They concludedthat the ictal perfusion patterns are helpful for subclas-sification of temporal lobe seizures and provide an in-sight into the preferential pathways of seizure propaga-tion in the subtypes of TLE. Markand et al. (1997) (3)performed ictal SPECT in 44 of 67 patients with medi-cally intractable TLE, and recorded in one patient an ictalhyperperfusion involving the contralateral temporal lobe,and in seven, a decreased rCBF in the epileptogenic fo-cus. They additionally described a patient with normalMRI and interictal and ictal EEG, suggesting seizureonset in the left temporal lobe, and ictal SPECT withrelative hyperperfusion in the right hemisphere. Positronemission tomography (PET) showed decreased meta-bolic activity in the left mesial temporal structures. In-terestingly, the reevaluation of the ictal SPECT studysuggested that there was a small area of hyperperfusionin the left mesial structures with an adjacent large area ofhypoperfusion, similar to our contralateral group.
Summarizing, our results suggest that one should notconsider the ictal contralateral hyperperfusion pattern asnoncontributory before attempting to carefully reevalu-ate the ipsilateral temporal perfusion pattern, looking es-pecially for restricted and discrete anteromesial hyper-perfusion and a lateral hypoperfusion pattern. Our studyin addition indicated that one should also carefully re-evaluate the bilateral hyperperfusion patterns looking forclear asymmetric findings, as they can still hold a later-alizing role.
We concluded that focal hyperperfusion ipsilateral tothe epileptogenic temporal lobe is the most common ictalperfusion pattern in unilateral TLE. However, ictal tracerinjections provide not only TPPs, but also APPs. Moreimportant, some types of APP may show conspicuousfindings that can additionally contribute to the lateraliza-tion of the epileptogenic zone in unilateral TLE. Furtherstudies focusing on ictal SPECT patterns in bilateral TLEor TLE with normal MRI are probably needed to evalu-ate the lateralizing role of those APPs, and more impor-tant, careful chronologic cross-analysis of ictal EEG andSPECT data may also ultimately be necessary to shed
light on the understanding of the dynamic electrophysi-ologic and rCBF phenomenology during the course ofepileptic seizures.
Acknowledgment: We thank Mr. Geraldo Ca´ssio dos Reisfor his statistics support and Dr. Roger Walz for his helpfulcomments. This study was supported by FAPESP, CAPES andFAEPA-HCFMRP/USP.
REFERENCES
1. Lee BI, Markand ON, Wellman HN, et al. HIPDM-SPECT inpatients with medically intractable complex partial seizures. Ictalstudy.Arch Neurol1988;45:397–402.
2. Shen W, Lee BI, Park HM, et al. HIPDM-SPECT brain imaging inthe presurgical evaluation of patients with intractable seizures.JNucl Med1990;31:1280–4.
3. Markand ON, Salanova V, Worth R, et al. Comparative study ofinterictal PET and ictal SPECT in complex partial seizures.ActaNeurol Scand1997;95:129–36.
4. Devous MD Sr, Thisted RA, Morgan GF, et al. SPECT brainimaging in epilepsy: a meta-analysis.J Nucl Med1998;39:285–93.
5. Rowe C, Berkovic S, Austin M, et al. Postictal SPECT in epilepsy.Lancet1989;1:389–90.
6. Rowe CC, Berkovic SF, Austin MC, et al. Visual and quantitativeanalysis of interictal SPECT with technetium-99m-HMPAO intemporal lobe epilepsy.J Nucl Med1991;32:1688–94.
7. Newton MR, Berkovic SF, Austin MC, et al. Postictal switch inblood flow distribution and temporal lobe seizures.J Neurol Neu-rosurg Psychiatry1992;55:891–4.
8. Duncan S, Gillen G, Adams FG, et al. Interictal HM-PAO SPECT:a routine investigation in patients with medically intractable com-plex partial seizures?Epilepsy Res1992;13:83–7.
9. Rowe CC, Berkovic SF, Sia ST, et al. Localization of epileptic fociwith postictal single photon emission computed tomography.AnnNeurol 1989;26:660–8.
10. Rowe CC, Berkovic SF, Austin MC, et al. Patterns of postictalcerebral blood flow in temporal lobe epilepsy: qualitative andquantitative analysis.Neurology1991;41:1096–103.
11. Lee BI, Markand ON, Wellman HN, et al. HIPDM single photonemission computed tomography brain imaging in partial onset sec-ondarily generalized tonic-clonic seizures.Epilepsia1987;28:305–11.
12. Berkovic S, Newton M, Chiron C, et al. Single photon emissiontomography. In: Engel JJ, ed.Surgical treatment of the epilepsies.New York: Raven Press, 1993:233–43.
13. Duncan R, Patterson J, Roberts R, et al. Ictal/postictal SPECT inthe pre-surgical localisation of complex partial seizures.J NeurolNeurosurg Psychiatry1993;56:141–8.
14. Spencer SS. The relative contributions of MRI, SPECT, and PETimaging in epilepsy.Epilepsia1994;35:S72–89.
15. Oliveira AJ, da Costa JC, Hilario LN, et al. Localization of theepileptogenic zone by ictal and interictal SPECT with 99mTc-ethylcysteinate dimer in patients with medically refractory epilepsy.Epilepsia1999;40:693–702.
16. Markand ON, Salanova V, Worth RM, et al. Ictal brain imaging inpresurgical evaluation of patients with medically intractable com-plex partial seizures.Acta Neurol Scand Suppl1994;152:137–44.
17. Ho SS, Berkovic SF, Berlangieri SU, et al. Comparison of ictalSPECT and interictal PET in the presurgical evaluation of temporallobe epilepsy.Ann Neurol1995;37:738–45.
18. Ho SS, Berkovic SF, McKay WJ, et al. Temporal lobe epilepsysubtypes: differential patterns of cerebral perfusion on ictalSPECT.Epilepsia1996;37:788–95.
19. Ho SS, Newton MR, McIntosh AM, et al. Perfusion patterns duringtemporal lobe seizures: relationship to surgical outcome.Brain1997;120:1921–8.
20. Spanaki MV, Zubal IG, MacMullan J, et al. Periictal SPECT lo-calization verified by simultaneous intracranial EEG.Epilepsia1999;40:267–74.
21. Avery RA, Spencer SS, Spanaki MV, et al. Effect of injection time
ICTAL SPECT PATTERNS IN TLE 665
Epilepsia, Vol. 42, No. 5, 2001

on postictal SPET perfusion changes in medically refractory epi-lepsy.Eur J Nucl Med1999;26:830–6.
22. Engel J Jr, Van Ness PC, Rasmussen TB, et al. Outcome withrespect to epileptic seizures. In: Engel J Jr, ed.Surgical treatmentof the epilepsies. New York: Raven Press, 1993:609–21.
23. Cohen J. A coefficient of agreement for nominal scales.EducPsychol Meas1960;20:37–46.
24. Newton MR, Austin MC, Chan JG, et al. Ictal SPECT usingtechnetium-99m-HMPAO: methods for rapid preparation and op-timal deployment of tracer during spontaneous seizures.J NuclMed 1993;34:666–70.
25. Smith BJ, Karvelis KC, Cronan S, et al. Developing an effectiveprogram to complete ictal SPECT in the epilepsy monitoring unit.Epilepsy Res1999;33:189–97.
26. Setoain FJ, Arroyo S, Lomena F, et al. Single photon emissioncomputed tomography (SPECT) in a patient with bilateral tempo-ral seizures: correlation between ictal EEG and postictal/ictalSPECT.Epilepsia1998;39:1001–5.
27. Runge U, Kirsch G, Petersen B, et al. Ictal and interictal ECD-SPECT for focus localization in epilepsy.Acta Neurol Scand1997;96:271–6.
28. Zubal IG, Spanaki MV, MacMullan J, et al. Influence oftechnetium-99m-hexamethylpropylene amine oxime injection timeon single-photon emission tomography perfusion changes in epi-lepsy.Eur J Nucl Med1999;26:12–7.
29. Avery RA, Zubal IG, Stokking R, et al. Decreased cerebral bloodflow during seizures with ictal SPECT injections.Epilepsy Res2000;40:53–61.
30. Lang W, Podreka I, Suess E, et al. Single photon emission com-puterized tomography during and between seizures.J Neurol1988;235:277–84.
31. Lee BI, Lee JD, Kim JY, et al. Single photon emission computedtomography-EEG relations in temporal lobe epilepsy [see com-ments].Neurology1997;49:981–91.
32. Amaral DG, Price JL. Amygdalo-cortical projections in the mon-key (Macaca fascicularis). J Comp Neurol1984;230:465–96.
33. McCulloch W, Garol H. Cortical origin and distribution of corpuscallosum and anterior commissure in the monkey (Macaca mu-latta). J Neurophysiol1941;5:555–63.
34. Turner BH, Mishkin M, Knapp ME. Distribution of the anteriorcommissure to the amygdaloid complex in the monkey.Brain Res1979;162:331–7.
L. WICHERT-ANA ET AL.666
Epilepsia, Vol. 42, No. 5, 2001