Twenty-year secular changes in sex specific lung cancer incidence rates in an urban Chinese...
7
Lung Cancer (2006) 51, 13—19 Twenty-year secular changes in sex specific lung cancer incidence rates in an urban Chinese population Kexin Chen a , Peizhong Peter Wang a,b,d,∗ , Baocun Sun a , Qiang Li a , Anthony Perruccio b , Denise Power b , Changli Wang a , Min He a , He M a , Yu Shibei c , Murray Krahn d , Angela Cheung d , Xishan Hao a a Tianjin Cancer Institute and Hospital, Tianjin Medical University, Tianjin, China b Division of Community Health, Faculty of Medicine, Memorial University of Newfoundland, Canada c Epidemiology Unit, Tianjin Centre for Disease Control, Tianjin, China d University Health Network, University of Toronto, Toronto, Canada Received 3 May 2005; received in revised form 18 August 2005; accepted 24 August 2005 KEYWORDS Lung cancer; Incidence; Chinese Summary The objective of this study was to describe trends in the incidence rates of primary lung cancer in a geographically defined Chinese population. Primary lung cancer cases (N = 40,022) diagnosed between 1981 and 2000 were identified by the Tianjin Cancer Registry. Age-specific and age-adjusted incidence rates to the world standard population were examined in both males and females. Age-period- cohort (APC) model and Poisson regression were used to assess the cohort effects and incidence trends. Crude and age-adjusted incidence rates in the study period were: 66.2/100,000 and 45.2/100,000 in males; and 47.7/100,000 and 28.2/100,000 in females, respectively. The major birth cohort effect can be described as for those born before 1940, in every age group lung cancer incidence rate increased as the birth years advanced. For those born after 1940, age specific incidence rates decreased as the birth years advanced. Results from the Poisson regression analyses suggested a statistically significant increasing trend of incidence rates of lung can- cer from 1981 to 1990 and changed little afterwards. Through first 10 years of the study period between 1981 and 2000, lung cancer incidence rates increased in both males and females. While the study results suggest that the age-adjusted incidence rates may have reached their peak and may even decline, as the Chinese population ages, and smoking prevalence remains high, the number of new lung cancer cases will continue to increase and overall burden of lung cancer will remain high. © 2005 Elsevier Ireland Ltd. All rights reserved. ∗ Corresponding author. Tel.: +1 709 777 8571 (Canada)/86 22 2334 0123x5226 (China); fax: +1 416 777 7382. E-mail address: [email protected] (P.P. Wang). 0169-5002/$ — see front matter © 2005 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.lungcan.2005.08.013
Transcript of Twenty-year secular changes in sex specific lung cancer incidence rates in an urban Chinese...

Lung Cancer (2006) 51, 13—19
Twenty-year secular changes in sex specificlung cancer incidence rates in anurban Chinese population
Kexin Chena, Peizhong Peter Wanga,b,d,∗, Baocun Suna, Qiang Lia,Anthony Perrucciob, Denise Powerb, Changli Wanga, Min Hea,He Ma, Yu Shibeic, Murray Krahnd, Angela Cheungd, Xishan Haoa
a Tianjin Cancer Institute and Hospital, Tianjin Medical University, Tianjin, China
b Division of Community Health, Faculty of Medicine, Memorial University of Newfoundland, Canadac Epidemiology Unit, Tianjin Centre for Disease Control, Tianjin, Chinad University Health Network, University of Toronto, Toronto, CanadaReceived 3 May 2005; received in revised form 18 August 2005; accepted 24 August 2005
KEYWORDSLung cancer;Incidence;Chinese
Summary The objective of this study was to describe trends in the incidencerates of primary lung cancer in a geographically defined Chinese population. Primarylung cancer cases (N = 40,022) diagnosed between 1981 and 2000 were identified bythe Tianjin Cancer Registry. Age-specific and age-adjusted incidence rates to theworld standard population were examined in both males and females. Age-period-cohort (APC) model and Poisson regression were used to assess the cohort effectsand incidence trends. Crude and age-adjusted incidence rates in the study periodwere: 66.2/100,000 and 45.2/100,000 in males; and 47.7/100,000 and 28.2/100,000in females, respectively. The major birth cohort effect can be described as forthose born before 1940, in every age group lung cancer incidence rate increasedas the birth years advanced. For those born after 1940, age specific incidence ratesdecreased as the birth years advanced. Results from the Poisson regression analysessuggested a statistically significant increasing trend of incidence rates of lung can-cer from 1981 to 1990 and changed little afterwards. Through first 10 years of thestudy period between 1981 and 2000, lung cancer incidence rates increased in bothmales and females. While the study results suggest that the age-adjusted incidencerates may have reached their peak and may even decline, as the Chinese populationages, and smoking prevalence remains high, the number of new lung cancer caseswill continue to increase and overall burden of lung cancer will remain high.© 2005 Elsevier Ireland Ltd. All rights reserved.
∗ Corresponding author. Tel.: +1 709 777 8571 (Canada)/86 22 2334 0123x5226 (China); fax: +1 416 777 7382.E-mail address: [email protected] (P.P. Wang).
0169-5002/$ — see front matter © 2005 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.lungcan.2005.08.013

14 K. Chen et al.
1. Introduction
Lung cancer is one of a few cancers with knowncauses; epidemiological data have consistentlyshown that exposure to tobacco smoke is the lead-ing cause of lung cancer [1—3]. Despite beinglargely preventable, lung cancer is one of the mostprevalent malignancy worldwide [4]. Where thegeographic and temporal patterns are correlatedwith tobacco consumption [5], there are notice-able variations in the attributable risk of tobaccofor lung cancer in different populations. For exam-ple, in most western countries it is believed thatabout 80% of lung cancers can be attributed totobacco products [6]. However, epidemiologicalstudies from some Asian countries suggest theattributable risk of tobacco for lung cancer is lower[7,8]; previous studies from China [7—9] suggestthat less than 50% of lung cancer cases can beexplained by tobacco consumption. These findingssuggest that non-tobacco risk factors may play dif-ferent roles in different parts of the world.
The incidence rate of lung cancer is higheramong males than in females. However, a largebody of research suggests that in most western
unit (DPHU) and the local police station. The DPHUroutinely reviews all death certificates and identi-fies deaths that are directly or indirectly caused bycancer. This study included all primary lung cancerpatients (ICD-9 codes 162). The Tianjin Cancer Reg-istry Centre is a member of the International Agencyfor Research on Cancer (IARC) of the World HealthOrganization and cancer incidence data have beenincluded in the IARC publication ‘‘Cancer Incidencein Five Continents’’ since 1981. A more detaileddescription of the registry can be found elsewhere[22,23]. The number of people in each age—sex spe-cific population for the six urban districts of Tianjinwas obtained from the Tianjin Police Head Office.This office enumerates the Tianjin urban populationbased on peoples’ unique resident cards, which aremandatory and cover all residents of Tianjin.
2.2. Descriptive analyses
Age—sex specific incidence rates were calculated.Age-adjusted incidence rates were calculated usingthe world standard population. Five-year age-gender specific incidence rates, beginning at 30years of age, were calculated per 5-year birthc
2
Tatsatg0wceaimafdlrf
3
Oli
countries the incidence is decreasing in men andincreasing in women [10—12]. Worldwide, thetotal consumption of tobacco is highest in China[13,14] and there have been several lung cancercase-control studies emerging from this country[7,8,15—18]. Despite this, few cancer registry-based epidemiological studies of incidence ratetrends have been undertaken in China. Such popu-lation based long-term studies would enable us toexamine the changing pattern of incidence ratesand aid us in predicting potential changing patternsin the future [19—21]. The objective of this studywas to describe the long-term incidence trends oflung cancer in an urban Chinese population usingdata from the Tianjin Cancer Registry.
2. Methods
2.1. Data
Since 1981, the Tianjin Cancer Registry has beencollecting data on all residents of Tianjin whodevelop cancer. The registry covers a populationof five million. Information collected on cancerreporting cards include name, sex, current age ordate of birth, address, reporting hospital or medicalinstitute, date (month and year) of diagnosis, fourdigit ICD-9 codes, and occupation. All death cer-tificates, the second source of cancer registration,are registered both at the district public health
ohort.
.3. Multivariate analyses
he observed number of lung cancer cases wasssumed to follow a Poisson distribution. Predic-ive variables included age, sex, year of diagno-is, and their interaction terms. Age was groupednd entered into models using dummy variables;he 40—49-year age-group was used as the referentroup given its greater stability as compared to the—19-year age-group. The coefficient for each termas the log-scaled relative risk. Age, period, andohort (APC) effects were fitted in log-linear mod-ls [24—29]. As the incidence rates of lung cancerre very low before 40 years of age, they were notncluded in the APC model. The maximum likelihoodethod was performed to estimate the parameters
ssociated with the APC model. The goodness-of-fitor the specified model was measured by devianceefined as twice the difference between the log-ikelihood of a perfectly fitting model and the cur-ent model. The SAS PROC GENMOD [30] was usedor model fitting.
. Results
ver the 20-year study period (1981—2000), 40,022ung cancer cases were identified; 58.5% occurredn males (Table 1). The mean age at diagnosis for the
Lung cancer incidence in China 15
Table 1 Characteristics of lung cancer cases diagnosed through 1981—2000; Tianjin, China
Variable Category Male Female Total
N Percent N Percent N Percent
Sex Male — — — — 23425 58.53Female — — — — 16597 41.47
Age (years) at diagnosis 0—19 7 0.03 6 0.01 13 0.0320—29 70 0.3 55 0.14 125 0.3130—39 375 1.6 223 0.56 598 1.4940—49 1438 6.14 820 2.05 2258 5.6450—59 4284 18.29 3067 7.66 7351 18.3760—69 9034 38.57 6686 16.71 15720 39.2870—79 6781 28.95 4682 11.70 11463 28.64>80 1436 6.13 1058 2.64 2494 6.23
Method of diagnosis Clinical only 2441 10.42 1744 10.51 4185 10.46Medical imaging 10635 45.40 8554 51.54 19189 47.95Histology at local site 10299 43.97 6244 37.62 16543 41.33Surgical examinationor autopsy
14 0.06 16 0.10 30 0.07
Death certificate only 2 0.01 2 0.01 4 0.01Unknown 34 0.15 37 0.22 71 0.18
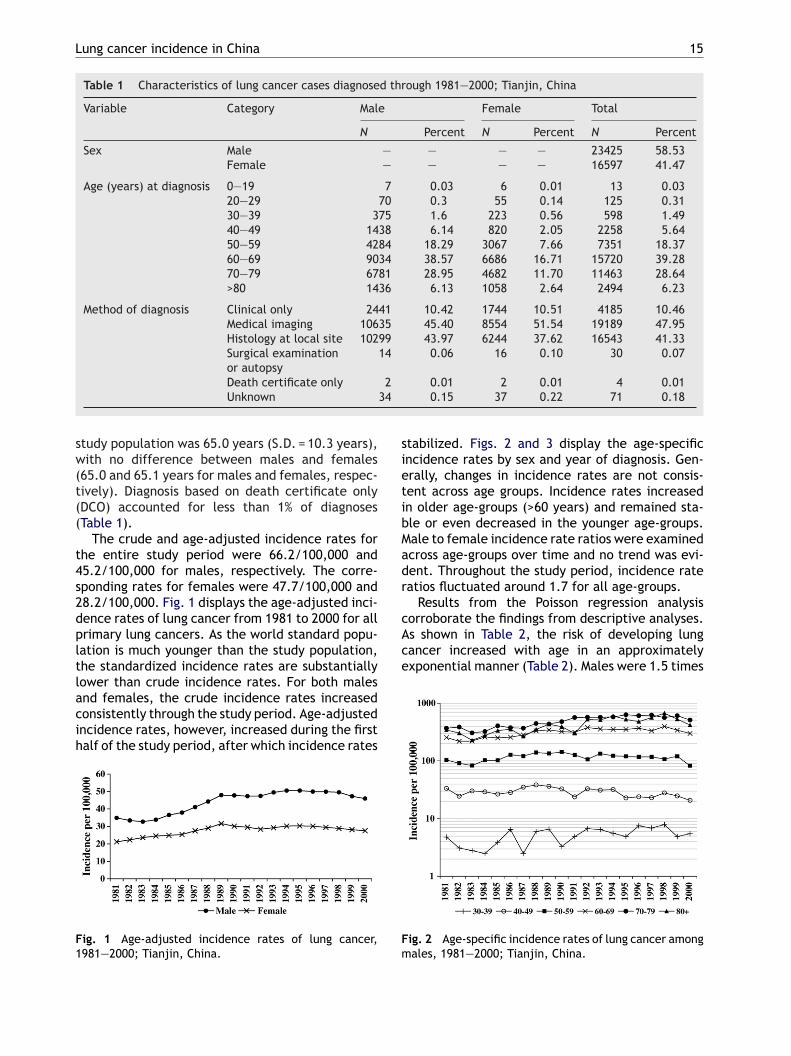
study population was 65.0 years (S.D. = 10.3 years),with no difference between males and females(65.0 and 65.1 years for males and females, respec-tively). Diagnosis based on death certificate only(DCO) accounted for less than 1% of diagnoses(Table 1).
The crude and age-adjusted incidence rates forthe entire study period were 66.2/100,000 and45.2/100,000 for males, respectively. The corre-sponding rates for females were 47.7/100,000 and28.2/100,000. Fig. 1 displays the age-adjusted inci-dence rates of lung cancer from 1981 to 2000 for allprimary lung cancers. As the world standard popu-lation is much younger than the study population,the standardized incidence rates are substantiallylower than crude incidence rates. For both malesand females, the crude incidence rates increasedconsistently through the study period. Age-adjustedincidence rates, however, increased during the firsthalf of the study period, after which incidence rates
F1
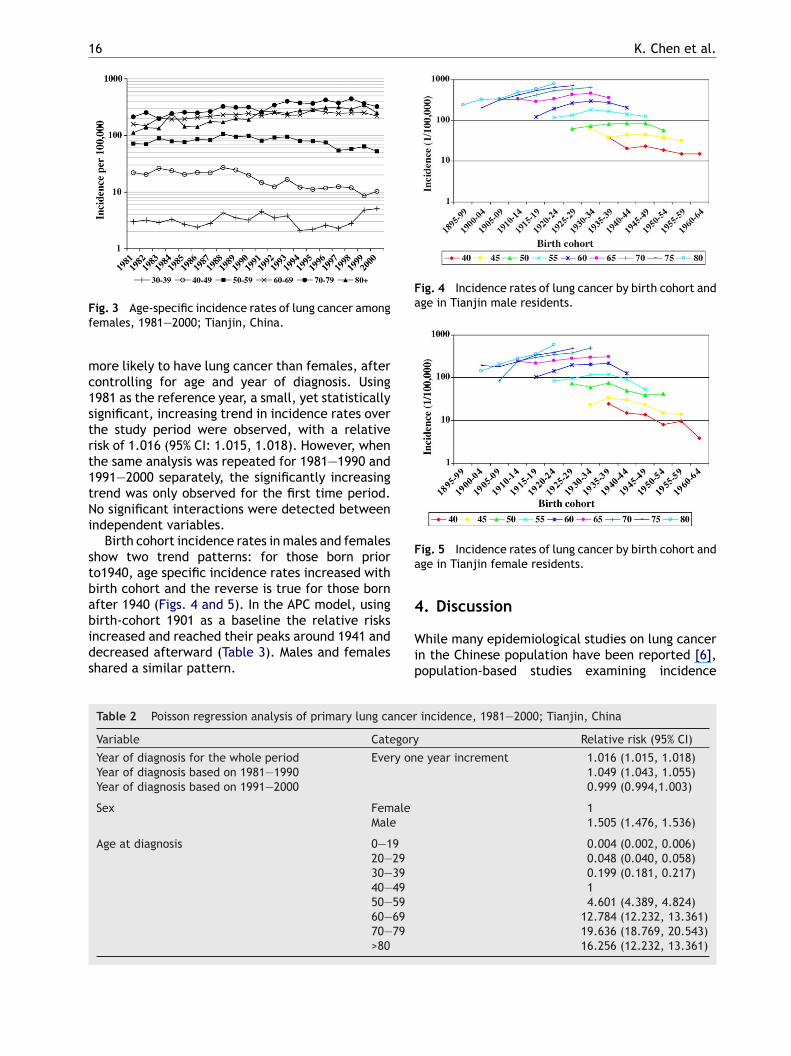
stabilized. Figs. 2 and 3 display the age-specificincidence rates by sex and year of diagnosis. Gen-erally, changes in incidence rates are not consis-tent across age groups. Incidence rates increasedin older age-groups (>60 years) and remained sta-ble or even decreased in the younger age-groups.Male to female incidence rate ratios were examinedacross age-groups over time and no trend was evi-dent. Throughout the study period, incidence rateratios fluctuated around 1.7 for all age-groups.
Results from the Poisson regression analysiscorroborate the findings from descriptive analyses.As shown in Table 2, the risk of developing lungcancer increased with age in an approximatelyexponential manner (Table 2). Males were 1.5 times
Fm
ig. 1 Age-adjusted incidence rates of lung cancer,981—2000; Tianjin, China.
ig. 2 Age-specific incidence rates of lung cancer amongales, 1981—2000; Tianjin, China.
16 K. Chen et al.
Fig. 3 Age-specific incidence rates of lung cancer amongfemales, 1981—2000; Tianjin, China.
more likely to have lung cancer than females, aftercontrolling for age and year of diagnosis. Using1981 as the reference year, a small, yet statisticallysignificant, increasing trend in incidence rates overthe study period were observed, with a relativerisk of 1.016 (95% CI: 1.015, 1.018). However, whenthe same analysis was repeated for 1981—1990 and1991—2000 separately, the significantly increasingtrend was only observed for the first time period.No significant interactions were detected betweenindependent variables.
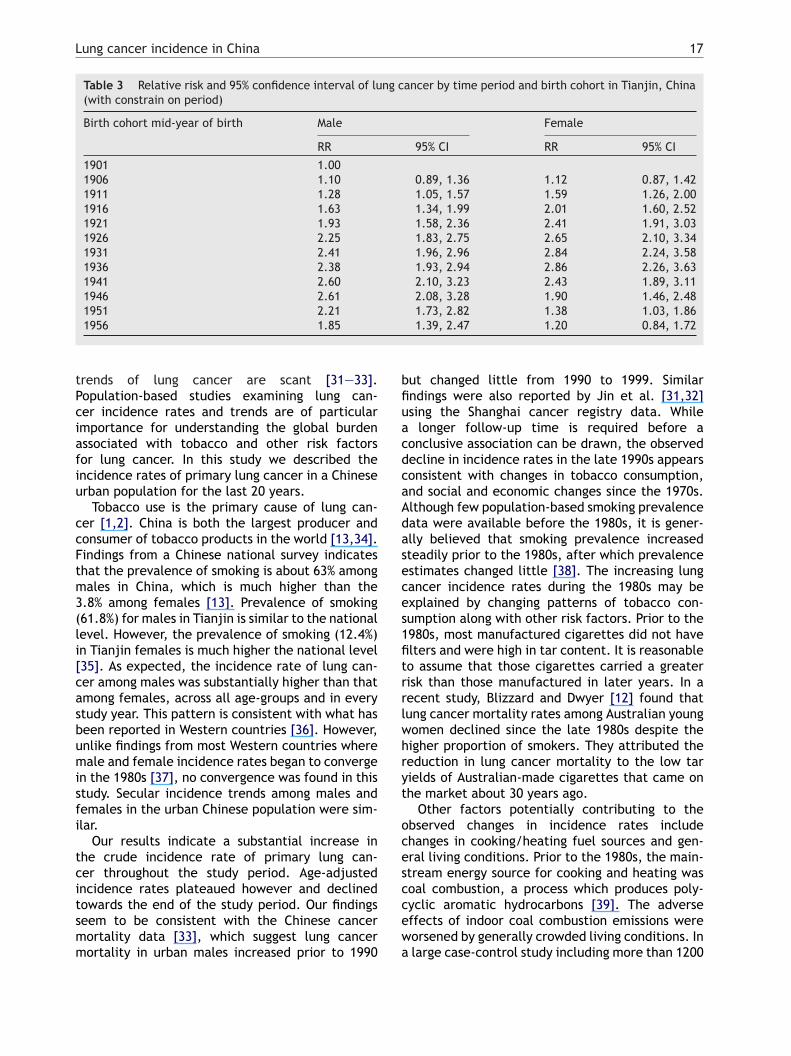
Birth cohort incidence rates in males and femalesshow two trend patterns: for those born priorto1940, age specific incidence rates increased withbirth cohort and the reverse is true for those bornafter 1940 (Figs. 4 and 5). In the APC model, usingbirth-cohort 1901 as a baseline the relative risksincreased and reached their peaks around 1941 anddecreased afterward (Table 3). Males and femalesshared a similar pattern.
Fig. 4 Incidence rates of lung cancer by birth cohort andage in Tianjin male residents.
Fig. 5 Incidence rates of lung cancer by birth cohort andage in Tianjin female residents.
4. Discussion
While many epidemiological studies on lung cancerin the Chinese population have been reported [6],population-based studies examining incidence
Table 2 Poisson regression analysis of primary lung cancer incidence, 1981—2000; Tianjin, China
Variable Category Relative risk (95% CI)
Year of diagnosis for the whole period Every one year increment 1.016 (1.015, 1.018)1.049 (1.043, 1.055)0.999 (0.994,1.003)
ale 11.505 (1.476, 1.536)
9 0.004 (0.002, 0.006)29 0.048 (0.040, 0.058)39 0.199 (0.181, 0.217)49 159 4.601 (4.389, 4.824)69 12.784 (12.232, 13.361)79 19.636 (18.769, 20.543)
16.256 (12.232, 13.361)
Year of diagnosis based on 1981—1990Year of diagnosis based on 1991—2000
Sex FemMale
Age at diagnosis 0—120—30—40—50—60—70—>80
Lung cancer incidence in China 17
Table 3 Relative risk and 95% confidence interval of lung cancer by time period and birth cohort in Tianjin, China(with constrain on period)
Birth cohort mid-year of birth Male Female
RR 95% CI RR 95% CI
1901 1.001906 1.10 0.89, 1.36 1.12 0.87, 1.421911 1.28 1.05, 1.57 1.59 1.26, 2.001916 1.63 1.34, 1.99 2.01 1.60, 2.521921 1.93 1.58, 2.36 2.41 1.91, 3.031926 2.25 1.83, 2.75 2.65 2.10, 3.341931 2.41 1.96, 2.96 2.84 2.24, 3.581936 2.38 1.93, 2.94 2.86 2.26, 3.631941 2.60 2.10, 3.23 2.43 1.89, 3.111946 2.61 2.08, 3.28 1.90 1.46, 2.481951 2.21 1.73, 2.82 1.38 1.03, 1.861956 1.85 1.39, 2.47 1.20 0.84, 1.72
trends of lung cancer are scant [31—33].Population-based studies examining lung can-cer incidence rates and trends are of particularimportance for understanding the global burdenassociated with tobacco and other risk factorsfor lung cancer. In this study we described theincidence rates of primary lung cancer in a Chineseurban population for the last 20 years.
Tobacco use is the primary cause of lung can-cer [1,2]. China is both the largest producer andconsumer of tobacco products in the world [13,34].Findings from a Chinese national survey indicatesthat the prevalence of smoking is about 63% amongmales in China, which is much higher than the3.8% among females [13]. Prevalence of smoking(61.8%) for males in Tianjin is similar to the nationallevel. However, the prevalence of smoking (12.4%)in Tianjin females is much higher the national level[35]. As expected, the incidence rate of lung can-cer among males was substantially higher than thatamong females, across all age-groups and in everystudy year. This pattern is consistent with what hasbeen reported in Western countries [36]. However,unlike findings from most Western countries wheremale and female incidence rates began to convergeisfi
tcitsmm
but changed little from 1990 to 1999. Similarfindings were also reported by Jin et al. [31,32]using the Shanghai cancer registry data. Whilea longer follow-up time is required before aconclusive association can be drawn, the observeddecline in incidence rates in the late 1990s appearsconsistent with changes in tobacco consumption,and social and economic changes since the 1970s.Although few population-based smoking prevalencedata were available before the 1980s, it is gener-ally believed that smoking prevalence increasedsteadily prior to the 1980s, after which prevalenceestimates changed little [38]. The increasing lungcancer incidence rates during the 1980s may beexplained by changing patterns of tobacco con-sumption along with other risk factors. Prior to the1980s, most manufactured cigarettes did not havefilters and were high in tar content. It is reasonableto assume that those cigarettes carried a greaterrisk than those manufactured in later years. In arecent study, Blizzard and Dwyer [12] found thatlung cancer mortality rates among Australian youngwomen declined since the late 1980s despite thehigher proportion of smokers. They attributed thereduction in lung cancer mortality to the low taryt
ocesccewa
n the 1980s [37], no convergence was found in thistudy. Secular incidence trends among males andemales in the urban Chinese population were sim-lar.
Our results indicate a substantial increase inhe crude incidence rate of primary lung can-er throughout the study period. Age-adjustedncidence rates plateaued however and declinedowards the end of the study period. Our findingseem to be consistent with the Chinese cancerortality data [33], which suggest lung cancerortality in urban males increased prior to 1990
ields of Australian-made cigarettes that came onhe market about 30 years ago.
Other factors potentially contributing to thebserved changes in incidence rates includehanges in cooking/heating fuel sources and gen-ral living conditions. Prior to the 1980s, the main-tream energy source for cooking and heating wasoal combustion, a process which produces poly-yclic aromatic hydrocarbons [39]. The adverseffects of indoor coal combustion emissions wereorsened by generally crowded living conditions. Inlarge case-control study including more than 1200
18 K. Chen et al.
lung cancer cases, Xu et al. [40] reported adjustedpopulation attributable risks associated with indoorair pollution of 13% among males and 17% amongfemales. Similar findings were also reported byother studies from China [41]. Since the early1980s, natural gas has gradually replaced coal asthe predominant fuel source for cooking and heat-ing.
Occupational exposures associated with lungcancer were substantive in China in the past[16,40]. However, their role appears to have dimin-ished, especially in urban cities like Tianjin. Manygovernment-owned chemical plants have closeddown and people are increasingly employed inthe hi-tech or service industries [22]. Additionally,plant workers tend to be better protected fromworkplace chemical exposures than they used tobe. These changes seem to be consistent with thefindings reported in this study.
Diet rich in vegetables and fruits has shown aprotective against lung cancer [42—47]. Over time,improvements in diet have been realized in China,as various fresh foods became more affordable andavailable to the general population. Living condi-tions also improved with the average per-person liv-
2 2
Chinese population ages, and smoking prevalenceremains high, the number of new lung cancer caseswill continue to increase and overall burden of lungcancer will remain high.
Acknowledgements
The Tianjin Cancer Registry is jointly funded bythe Tianjin Health Bureau and the Tianjin CancerInstitute. All computations were prepared at Tian-jin Cancer Institute and the responsibility for theuse and interpretation of these data is entirely thatof the authors. The authors thank the InternationalAgency for Research on Cancer (IARC) for their tech-nological support.
References
[1] Doll R, Peto R. The causes of cancer. Oxford, UK: CambridgeUniversity Press; 1981.
[2] Shopland DR, Eyre HJ, Pechacek TF. Smoking-attributablecancer mortality in 1991: is lung cancer now the leadingcause of death among smokers in the United States? J NatlCancer Inst 1991;83:1142—8.
[
[
[
[
[
ing space increasing from 6 m in the 1970s to 20 min 2000. Also, exposure to environmental tobaccosmoke (ETS) decreased with the increasing popu-larity of smoke-free environments. However, whilethe role of diet [40,43,48] and ETS [17,48] in lungcancer occurrence is uncertain, positive changes inthese factors should reduce lung cancer incidence.
There are a number of limitations that must beconsidered when interpreting the results of thisstudy. Histological classifications were not com-plete on some of the cancer registration cards.Thus, we were unable to examine the changesin lung cancer incidence rates by histologicaltypes. While in theory all cancer registration cardscould be cross-checked against hospital charts,such a procedure would require substantial inter-institutional coordination and financial resources.Future studies examining incidence trends by his-tological type may shed further insights. This studycovers a span of only 20 years and continued mon-itoring, over a longer period of time, is necessaryfor gaining a more comprehensive picture.
Despite being largely preventable, lung cancerremains a significant health threat to the Chinesepopulation. Based on 20 years of cancer registrationdata from a geographically defined area in China,the present results indicate a significant increas-ing trend of lung cancer incidence rates from 1981to 1990. While the study results suggest that theage-adjusted incidence rates may have reachedtheir peak and may even decline after 1990, as the
[3] Osann KE. Epidemiology of lung cancer. Curr Opin Pulm Med1998;4:198—204.
[4] Feraly J, Bray F, Pisani P, Parkin DM. GLOBOCAN 2000: Can-cer Incidence, Mortality and Prevalence Worldwide, Version1.0, IARC, Cancer Base No. 5. Lyon: IARC Press; 2001.
[5] Boffetta P, Trichopoulos D. Cancer of the lung, larynx, andpleura. In: Adami HO, Huter D, Trichopoulos D, editors. Thetextbook of cancer epidemiology. New York, NY: Oxford Uni-versity Press; 2002.
[6] Parkin DM, Pisani P, Lopez AD, Masuyer E. At least one inseven cases of cancer is caused by smoking Global estimatesfor. Int J Cancer 1994;59:494—504.
[7] Liu Z. Smoking and lung cancer in China: combinedanalysis of eight case-control studies. Int J Epidemiol1992;21:197—201.
[8] Yu SZ, Zhao N. Combined analysis of case-control stud-ies of smoking and lung cancer in China. Lung Cancer1996;14(Suppl. 1):S161—70.
[9] Zhao N. Meta-analysis of smoking and lung cancer in China:combined analysis of fifteen case-control studies. ZhonghuaLiu Xing Bing Xue Za Zhi 1993;14:350—4.
10] Jemal A, Travis WD, Tarone RE, Travis L, Devesa SS. Lungcancer rates convergence in young men and women in theUnited States: analysis by birth cohort and histologic type.Int J Cancer 2003;105:101—7.
11] Peto R, Darby S, Deo H, Silcocks P, Whitley E, Doll R. Smok-ing, smoking cessation, and lung cancer in the UK since1950: combination of national statistics with two case-control studies. BMJ 2000;321:323—9.
12] Blizzard L, Dwyer T. Declining lung cancer mortality ofyoung Australian women despite increased smoking islinked to reduced cigarette ‘tar’ yields. Br J Cancer2001;84:392—6.
13] Yang G, Fan L, Tan J, et al. Smoking in China: findings of the1996 National Prevalence Survey. JAMA 1999;282:1247—53.
14] Murray CJ, Lopez AD, Jamison DT. The global burdenof disease in 1990: summary results, sensitivity anal-
Lung cancer incidence in China 19
ysis and future directions. Bull World Health Organ1994;72:495—509.
[15] Liu ZY, He XZ, Chapman RS. Smoking and other risk fac-tors for lung cancer in Xuanwei, China. Int J Epidemiol1991;20:26—31.
[16] Xu ZY, Blot WJ, Xiao HP, et al. Smoking, air pollution, andthe high rates of lung cancer in Shenyang, China. J NatlCancer Inst 1989;81:1800—6.
[17] Zhang Y, Chen K, Zhang H. Meta-analysis of risk factors onlung cancer in non-smoking Chinese female. Zhonghua LiuXing Bing Xue Za Zhi 2001;22:119—21.
[18] Yuan JM, Ross RK, Wang XL, Gao YT, Henderson BE, Yu MC.Morbidity and mortality in relation to cigarette smokingin Shanghai China. A prospective male cohort study. JAMA1996;275:1646—50.
[19] Wang PP, Haines CS. Childhood and adolescent leukaemiain a North American population. Int J Epidemiol1995;24:1100—9.
[20] Wang PP, Cao Y. Incidence trends of female breast can-cer in Saskatchewan 1932—1990. Breast Cancer Res Treat1996;37:197—207.
[21] Haines CS, Tonita JM, Wang PP. Forty-two-year prostaticcancer incidence trends in a defined population of one mil-lion served by a reimbursement-linked cancer registry. JNatl Cancer Inst 1994;86:230—1.
[22] Hao XS, Wang PP, Chen KX, et al. Twenty-year trends ofprimary liver cancer incidence rates in an urban Chinesepopulation. Eur J Cancer Prev 2003;12:273—9.
[23] Hao XS, Chen KX, Wang PP, Rohan T. Changes in survivalpatterns in urban Chinese patients with liver cancer. World
[
[
[
[
[
[
[
[31] Jin F, Devesa SS, Zheng W, Blot WJ, Fraumeni Jr JF, Gao YT.Cancer incidence trends in urban Shanghai 1972—1989. IntJ Cancer 1993;53:764—70.
[32] Jin F, Devesa SS, Chow WH, et al. Cancer incidence trendsin urban shanghai 1972—1994: an update. Int J Cancer1999;83:435—40.
[33] Yang L, Parkin DM, Li L, Chen Y. Time trends in cancer mor-tality in China: 1987—1999. Int J Cancer 2003;106:771—83.
[34] Hu JF, Liu RZ, Zhang HL, et al. A survey of cigarette smok-ing among middle school students in 1988. Public Health1990;104:345—51.
[35] Song G, Li J, Zhang ZQ, Yu SB. Changes in smoking patternsin Tianjin between 1996 and 2000. Chi. J. Contro ChronNon-commun Dis 2002;10:126.
[36] Parkin DM. Trends in lung cancer incidence worldwide.Chest 1989;96:5S—8S.
[37] Sharp L, Brewster D. The epidemiology of lung cancer inScotland: a review of trends in incidence, survival and mor-tality and prospects for prevention. Health Bull (Edinb)1999;57:318—31.
[38] Weng XZ, Hong ZG, Chen DY. Smoking prevalence in Chineseaged 15 and above. Chin Med J (Engl) 1987;100:886—92.
[39] Lan Q, He X, Costa DJ, et al. Indoor coal combustion emis-sions, GSTM1 and GSTT1 genotypes, and lung cancer risk:a case-control study in Xuan Wei, China. Cancer EpidemiolBiomarkers Prev 2000;9:605—8.
[40] Xu ZY, Brown L, Pan GW, et al. Lifestyle, environmental pol-lution and lung cancer in cities of Liaoning in northeasternChina. Lung Cancer 1996;14(Suppl. 1):S149—60.
[41] Kleinerman RA, Wang Z, Wang L, et al. Lung cancer and
J Gastroenterol 2003;9:1212—5.24] Clegg LX, Feuer EJ, Midthune DN, Fay MP, Hankey BF. Impactof reporting delay and reporting error on cancer inci-dence rates and trends. J Natl Cancer Inst 2002;94:1537—45.
25] Clayton D, Schifflers E. Models for temporal variation in can-cer rates. I: Age-period and age-cohort models. Stat Med1987;6:449—67.
26] Clayton D, Schifflers E. Models for temporal variationin cancer rates. II: Age-period-cohort models. Stat Med1987;6:469—81.
27] Holford TR. Analysing the temporal effects of age,period and cohort. Stat Methods Med Res 1992;1:317—37.
28] Holford TR. Understanding the effects of age, period, andcohort on incidence and mortality rates. Annu Rev PublicHealth 1991;12:425—57.
29] Arbyn M, Van Oyen H, Sartor F, Tibaldi F, MolenberghsG. Description of the influence of age, period andcohort effects on cervical cancer mortality by loglinearPoisson models (Belgium 1955—94). Arch Public Health2002;60:70—100.
30] SAS Institute. SAS/STAT user’s guide, version 8. Cary, NC:SAS Institute; 1999.
indoor exposure to coal and biomass in rural China. J OccupEnviron Med 2002;44:338—44.
[42] World Cancer Research Fund. Food, nutrition and the pre-vention of cancer: a global perspective. Part II, Cancers,nutrition and food. Washington, DC: American Institute forCancer Research; 1997.
[43] Hu J, Johnson KC, Mao Y, et al. A case-control study ofdiet and lung cancer in northeast China. Int J Cancer1997;71:924—31.
[44] Zhou B, Wang T, Sun G, Guan P, Wu JM. A case-controlstudy of the relationship between dietary factors and riskof lung cancer in women of Shenyang, China. Oncol Rep1999;6:139—43.
[45] Swanson CA, Mao BL, Li JY, et al. Dietary determinants oflung-cancer risk: results from a case-control study in YunnanProvince, China. Int J Cancer 1992;50:876—80.
[46] Kumagai Y, Pi JB, Lee S, et al. Serum antioxidant vitaminsand risk of lung and stomach cancers in Shenyang, China.Cancer Lett 1998;129:145—9.
[47] Rylander R, Axelsson G, Andersson L, Liljequist T, BergmanB. Lung cancer, smoking and diet among Swedish men. LungCancer 1996;14(Suppl. 1):S75—83.
[48] Buiatti E, Geddes M, Arniani S. Epidemiology of lung cancer.Ann Ist Super Sanita 1996;32:133—44.