Twelve-month neurofunctional assessment and cognitive performance at 36 months of age in extremely...
10
DOI: 10.1542/peds.2006-3364 2007;120;1012 Pediatrics Fumagalli and Fabio Mosca Maria Lorella Giannì, Odoardo Picciolini, Chiara Vegni, Laura Gardon, Monica Months of Age in Extremely Low Birth Weight Infants Twelve-Month Neurofunctional Assessment and Cognitive Performance at 36 http://pediatrics.aappublications.org/content/120/5/1012.full.html located on the World Wide Web at: The online version of this article, along with updated information and services, is of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275. Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2007 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Point publication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly by guest on June 13, 2013 pediatrics.aappublications.org Downloaded from
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of Twelve-month neurofunctional assessment and cognitive performance at 36 months of age in extremely...
DOI: 10.1542/peds.2006-3364 2007;120;1012Pediatrics
Fumagalli and Fabio MoscaMaria Lorella Giannì, Odoardo Picciolini, Chiara Vegni, Laura Gardon, Monica
Months of Age in Extremely Low Birth Weight InfantsTwelve-Month Neurofunctional Assessment and Cognitive Performance at 36
http://pediatrics.aappublications.org/content/120/5/1012.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2007 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by guest on June 13, 2013pediatrics.aappublications.orgDownloaded from

ARTICLE
Twelve-Month Neurofunctional Assessment andCognitive Performance at 36 Months of Age inExtremely Low Birth Weight InfantsMaria Lorella Giannı, MD, Odoardo Picciolini, MD, Chiara Vegni, MD, Laura Gardon, PT, Monica Fumagalli, MD, Fabio Mosca, MD
Neonatal Intensive Care Unit, Institute of Pediatrics and Neonatology, Fondazione IRCCS “Ospedale Maggiore Policlinico, Mangiagalli e Regina Elena” University MedicalSchool, Milan, Italy
The authors have indicated they have no financial relationships relevant to this article to disclose.
ABSTRACT
OBJECTIVE. The objective of this study was to investigate whether an early neuro-functional assessment (at 12 months’ corrected age) is predictive of cognitiveoutcome at 36 months of age in extremely low birth weight infants.
METHODS.We conducted an observational longitudinal study. Neurodevelopmentaloutcome by means of a neurofunctional assessment was evaluated at 12 months’corrected age and 36 months’ chronological age in 141 extremely low birth weightchildren. Cognitive outcome was assessed with use of the Griffiths Mental Devel-opmental Scale.
RESULTS.A significant association was found between the 12-month neurofunctionalstatus and cognitive performance at 36 months. A higher general quotient on theGriffiths Mental Developmental Scale at 36 months was observed in infants whoexhibited normal (score: �1) neurodevelopment compared with children whoexhibited minor (score: 2) and major (score: �3) dysfunctions at the 12-monthneurofunctional evaluation (99 � 6.8 vs 85.3 � 16.3 vs 57.3 � 22.0). A score of�2 at the 12-month neurofunctional assessment, abnormal brain MRI results atterm, and chronic lung disease remained predictive of cognitive delay at 36months of age and also after adjustment for confounders.
CONCLUSIONS. The 12-month neurofunctional evaluation may be an additional usefulclinical tool in predicting later cognitive outcome in extremely low birth weightchildren.
www.pediatrics.org/cgi/doi/10.1542/peds.2006-3364
doi:10.1542/peds.2006-3364
KeyWordsneurofunctional assessment, cognitiveoutcome, extremely low birth weightinfants
AbbreviationsVLBW—very low birth weightELBW—extremely low birth weightSGA—small for gestational ageNEC—necrotizing enterocolitisROP—retinopathy of prematurityCLD—chronic lung diseaseHC—head circumferenceGQ—general quotient
Accepted for publication May 29, 2007
Address correspondence to Maria LorellaGiannı, MD, Neonatal Intensive Care Unit,Clinica Mangiagalli, IRCS, University MedicalSchool, Via Commenda 12, 20122 Milano, Italy.E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005;Online, 1098-4275). Copyright © 2007 by theAmerican Academy of Pediatrics
1012 GIANNI et al by guest on June 13, 2013pediatrics.aappublications.orgDownloaded from

SURVIVAL OF VERY low birth weight (VLBW; �1500 g)infants has recently improved as a result of advances
in perinatal care.1 Major disabilities occur in 15% to 20%of the VLBW population, with a higher prevalence ininfants with the youngest gestational age and the lowestbirth weight.2 A high rate of learning difficulties, behav-ioral problems, and lower IQ scores, compared with thepopulation mean, is reported in survivors without majordysfunctions, especially extremely low birth weight(ELBW; �1000 g) infants.3 Early detection of infants whoare at high risk for poor neurodevelopmental outcomeremains a challenge for clinicians to make referral for in-tervention and optimize potential outcome. Several au-thors4,5 have investigated the relationship between motorability, mainly investigated by a developmental assessmentof movement, and cognitive performance in ELBW, sug-gesting that early movement problems may be predictiveof later cognitive adverse outcome even in the absence ofdefined neurologic problems.
We previously reported that an early neurofunctionalevaluation in VLBW infants may be an additional usefultool in reassuring parents on the integrity of centralnervous system function.6 Few data are available in theliterature on any hypothetical relationship between cog-nitive outcome of ELBW infants and early neurofunc-tional assessment.7,8 The aim of this study was to exam-ine whether a neurofunctional evaluation at 12 monthsis predictive of cognitive outcome at 36 months of age inELBW infants.
METHODSAmong all consecutive newborn infants who were ad-mitted at the same Institution from 1996 to 2001, 159infants entered the study. Inclusion criterion was birth
weight �1000 g. Exclusion criteria were presence ofcongenital diseases and/or chromosomal abnormalitiesor infant death during postpartum hospital stay. Infantswere scheduled to be prospectively followed up to 36months of age. The Consolidated Standards of ReportingTrials (CONSORT) flowchart of the study is shown in Fig1. Written informed consent was obtained from thenewborns’ parents, and the departmental ethics commit-tee approved the study design.
Presence of gestational hypertension and/or pre-eclampsia, steroids received before delivery, and educa-tional level were investigated as maternal variables. Ges-tational hypertension and preeclampsia were defined,respectively, as de novo hypertension (systolic bloodpressure � 140 mm Hg or diastolic BP � 90 mm Hg)arising after midpregnancy and gestational hypertensionassociated with new-onset proteinuria (�300 mg/24hours). The educational level of mothers was evaluatedand categorized as low (�13 years) or high (�13 years).
Neonatal characteristics (gestational age, being appro-priate or small for gestational age [SGA], birth weight,length, and head circumference); need for mechanicalventilation; and the occurrence of sepsis, necrotizingenterocolitis (NEC; classified as stage 3 according to theclassification of Bell et al9), bronchopulmonary dyspla-sia, and retinopathy of prematurity (ROP) of stage 3 orhigher were recorded prospectively. Gestational age wasbased on the last menstrual period and first-trimesterultrasonogram. Infants with birth weights of �10th or�10th percentile for gestational age, according to theNorth-Italian growth charts, were classified as appropri-ate for gestational age or SGA, respectively.10 Sepsis wasdefined by the presence of a positive blood culture.Patients with NEC were pooled together with those who
FIGURE 1Consolidated Standards of Reporting Trials (CONSORT) flowchart.
PEDIATRICS Volume 120, Number 5, November 2007 1013 by guest on June 13, 2013pediatrics.aappublications.orgDownloaded from

had sepsis because of the strong association of NEC withinfection. Chronic lung disease (CLD) was defined byuse of supplemental oxygen at 36 weeks’ postconcep-tional age. Corrected age was calculated, up to 24months of life, from the chronologic age adjusting forgestational age. Brain MRI was performed at a mean of40 � 2 weeks’ postconceptional age in all newborns. Anabnormal MRI result was defined by the presence ofmajor brain lesions (eg, ventriculomegaly, cystic andnoncystic periventricular leukomalacia, focal parenchy-mal brain lesions).
Infants entered a follow-up program that consisted ofperiodic pediatric visits at 3, 6, 12, and 24 months’corrected age and 36 months’ chronological age and ofevaluation of neurodevelopmental outcome by means ofthe neurofunctional evaluation at 12 months’ correctedage and 36 months’ chronological age. Cognitive out-come was assessed with use of the Griffiths Mental De-velopmental Scale at 36 months’ chronological age.
Weight, length, and head circumference (HC) weremeasured using standardized procedures.11 Growth zscores were then calculated by EuroGrowth 2000 soft-ware (EuroGrowth Study Group, Vienna, Austria).Catch-up growth was defined by a growth z score ofmore than �2 SD.
The neurofunctional evaluation6 was based on thestudy of evoked and spontaneous motility, posturaladaptability, variability of motor patterns, and neuromo-tor and behavioral skills. A detailed description of theneurofunctional assessment is reported in the Appendix.Infants were categorized into 3 groups, according to theneurofunctional status, as normal (score: 0–1), exhibit-ing minor dysfunctions (score: 2), or exhibiting majordysfunctions (score: 3–4). The Griffiths Mental Develop-ment Scale12 and related subscales (locomotor, personalsocial, hearing and speech, hand and eye coordination,performance, and practical reasoning) were adminis-tered by the same expert trained examiner, who wasblind to the neurofunctional evaluation. A general quo-tient (GQ) was then calculated. The mean value of GQwas 100 with an SD of 12. A GQ of �70 was classified assevere developmental delay.
Statistical AnalysisDescriptive data are shown as means � SD or number ofobservations (percentage). Comparison among groupswas performed by the �2 test for discrete variables or byanalysis of variance for continuous variables. Signifi-cance of multiple comparisons was adjusted by the leastsignificant difference test correction. Differences withinpatients in repeated measurements of growth parame-ters were assessed by analysis of variance. Logistic re-gression analysis was used to identify determinants ofdevelopmental delay (GQ � 88) at 36 months of age.Maternal and neonatal characteristics that are known tobe associated with adverse cognitive outcome were en-
tered in the model. Factors examined included maternaleducation, prenatal steroids, maternal hypertension,multiple birth, gender, birth weight, gestational age, be-ing SGA, sepsis, ROP of stage 3 or higher, HC catch-upgrowth at 12 months, neurofunctional status at 12months’ corrected age, CLD, and cranial MRI status atterm.
All statistical analyses were conducted at the � � .05level and were 2-tailed. Statistical analysis was per-formed by using SPSS 12 (SPSS Inc, Chicago, IL).
RESULTSFollow-up data at 36 months’ chronological age wereavailable for 141 (70 girls; 71 boys) infants. One infantdied through the follow-up. No differences in the char-acteristics at birth and in the developmental measures,when last assessed, were observed between infants whowere lost at follow-up and those who were evaluated.The characteristics of the studied population at birth areshown in Table 1.
Maternal hypertension occurred in 35.1% and 39.4%of mothers with infants who exhibited a GQ of �88 and�88, respectively, at 36 months’ chronological age (P �.39). Antenatal steroids were administrated to 50% and59.5% of mothers with infants who exhibited a GQ of�88 and �88, respectively, at 36 months’ chronologicalage (P � .2). Maternal educational level was low in73.1% and 83.8% of mothers with infants who exhib-ited a GQ of �88 and �88, respectively, at 36 months’chronological age (P � .2). The characteristics of thestudied population according to cognitive outcome at 36months’ age are shown in Table 2.
Younger gestational age, being male, ROP of stage 3or higher, and CLD were associated with a GQ of �88 at36 months of age. A GQ of �70 was found in 14.2% (n� 20) of children. Abnormal MRI status was found in72.4% and in 27.6% of infants who exhibited a GQ of�88 and �88, respectively, at 36 months’ chronologicalage (P � .0001).
Mean (SD) weight, length, and HC z scores rangedthrough the first 36 months of life from �2.62 (1.7) at 3months to �1.77 (1.3) at 36 months (P � .0001), from�2.67 (1.5) to �1.01 (1.07; P � .0001), and from �1.57(1.38) to �1.57 (1.03; P � 0.9), respectively. At 36months, 38%, 17%, and 34% of infants had weight,
TABLE 1 Characteristics of the Studied Population at Birth
Infant Characteristics at Birth (N � 141) Value
Birth weight, mean (SD), g 839.5 (122.8)Birth length, mean (SD), cm 33.9 (2.4)Birth HC, mean (SD), cm 24.6 (1.6)Gestational age, mean (SD), wk 28 (1.9)Boys, n (%) 71 (50.4)SGA, n (%) 56 (39.7)Infants ventilated, n (%) 117 (83.0)Multiple birth, n (%) 39 (27.7)
1014 GIANNI et al by guest on June 13, 2013pediatrics.aappublications.orgDownloaded from

length, and HC z score less than �2 SD, respectively.Absence of HC catch-up growth at 36 months was asso-ciated with a GQ of �88 at 36 months (P � .05).
Neurofunctional Assessment at 12 Months’ Corrected Age andat 36 Months’ Chronological AgeAt 12 months’ corrected age, the neurofunctional scorewas �1 in 82 (58.2%) infants, 2 in 41 (29%), and �3 in18 (12,8%). The corresponding values at 36 months’chronological age were 67 (47.5%), 52 (36.9%), and 22(15.6%) infants. At the age of 36 months, the neuro-functional status improved, unchanged, or deterioratedin 7 (5%), 108 (76.6%), and 26 (18.4%) infants, respec-tively; 73% and 100% of infants with a score of �1 or�3, respectively, at 12 months’ corrected age had un-changed functional status at 36 months of age. Theclinical disabilities of infants who had a neurofunctionalscore of 2 at 36 months of age were learning disabilitiesand dyspraxia (23%), clumsiness (23%), behavioralproblems (30%), language impairment (10%), psy-chomotor retardation (12%), and hypoacusia (2%). Theclinical features of the infants who had a neurofunc-tional score of �3 at 36 months of age were cerebralpalsy (63%), mental retardation (22%), visual impair-ment (5%), deafness (5%), and autism spectrum (5%).
Neurofunctional Status at 12 Months’ Corrected Age andGriffiths Mental Development Scale at 36 Months’Chronological AgeA significant statistical association between the 12-month neurofunctional status and the GQ assessed at 36months (P � .0001) was found. On posthoc analysis, allcomparisons were significant.
Predicting GQ at 36 Months’ Chronological Age From the 12-Month Neurofunctional AssessmentA logistic regression analysis was performed to identifydeterminants of developmental delay at 36 months (Ta-ble 3). For statistical analysis, patients who had a score of�2 at the 12-month neurofunctional evaluation were
pooled. Abnormal cranial MRI results at term, CLD, anda score of �1 at the neurofunctional evaluation at 12months were found to be independently associated withcognitive delay at 36 months.
DISCUSSIONIn this study, the 12-month neurofunctional assessment,MRI status at term, and CLD remained predictive ofcognitive development at 36 months in ELBW infants,also after adjusting for confounders. In addition, wefound that children who were assessed as normal (score� 1) at the 12-month neurofunctional assessmentshowed significantly higher GQ at 36 months of agecompared with infants who exhibited dysfunctions(score � 2). This finding could be explained by the factthat the detection of dysfunctions at 12 months of agemay reflect the difficulty that the infant experiences inthe learning process and in the development of newtasks, as a result of impairment of the emerging func-tions at that age, evaluated by the neurofunctional ap-proach. As a consequence, the normal process of cogni-tion may be impaired.
Several authors have found an association betweenmotor function assessed at 12 months and cognitiveoutcome at school age. Burns et al4 reported that groupclassification of motor development at age 1 year, inves-tigated using the neurosensory motor developmentalassessment, is predictive of cognitive outcome in ELBWinfants at age 4 years. Jeyaseelan et al5 reported thatmotor difficulties, assessed by use of neurosensory motordevelopmental assessment, in ELBW infants at 2 yearsare strongly associated with later clinical measures ofattention. Roth et al13 and Stewart et al14 found a closerelationship between neuromotor impairment, investi-gated by standardized neurologic examination, and cog-nitive defects at age 4 years. The results of these studiesare consistent with Piaget’s theory15 and the mirror neu-ron system.16,17 According to Piaget, there is a strict in-terrelation between motor and cognitive development:action is considered the foundation of knowledge as it is,
TABLE 2 Characteristics of the Studied Population According to Cognitive Outcome at 36 Months of Age
Characteristic Cognitive Assessment at 36 mo
GQ � 88 (n � 37) GQ � 88 (n � 104) Pa
Birth weight, mean (SD), g 827.8 (143.0) 843.6 (115.0) NSBirth length, mean (SD), cm 33.6 (2.6) 34.1 (2.3) NSBirth HC, mean (SD), cm 24.1 (1.9) 24.7 (1.5) NSGestational age, mean (SD), wk 27.2 (1.8) 28.2 (1.9) �.05Males, n (%) 24.0 (64.9) 47 (45.2) �.05SGA, n (%) 10 (27.0) 46 (44.2) .05Multiple birth, n (%) 12 (32.4) 27 (26.0) NSSepsis, n (%) 8 (22.9) 30 (29.1) NSROP stage 3 or higher, n (%) 10 (27.8) 9 (8.7) �.05CLD, n (%) 25 (67.6) 17 (16.3) �.001
NS indicates not significant.a t or �2 test.
PEDIATRICS Volume 120, Number 5, November 2007 1015 by guest on June 13, 2013pediatrics.aappublications.orgDownloaded from

at first, physical and then it is transformed into mentalaction and representation. Also, the mirror neuron sys-tem, which activates when an individual performs anaction, as well as when he or she observes a similaraction done by another individual, seems to play animportant role in the social cognition process: it seemsnot only to provide an action recognition mechanismbut also to constitute a neural system for coding theintentions of others and allowing imitation learning.18 Inaddition, according to Hadders-Algra,19 both primary(the phase in which the variation in motor behavior isnot geared to external conditions) and secondary (thephase in which the motor performance can be adaptedto specific situations) variability and, consequently, themotor repertoire can be reduced in preterm infants as aresult of perinatal lesions or abnormal cerebral corticaldevelopment. Consistent with these findings, the asso-ciation of the 12-month neurofunctional evaluationwith cognitive performance at 36 months of age may beto some extent explained by the fact that a neurofunc-tional approach includes the evaluation of evoked andspontaneous motility, postural adaptability, and variabil-ity of motor patterns, according to the emerging func-tions of each age.6 The finding of lower GQ at 36 monthsin infants who exhibited minor dysfunctions at the 12-month neurofunctional assessment highlights the im-portance of additional implementation of individualizedcare plans both during hospital stay and in the postdis-charge period because a limited motor repertoire, evenin the absence of brain lesions, may result in deficit ofprocessing information and solving problems throughthe selection of the most appropriate strategies andadaptive solutions. In addition, promoting the infant’sneurobehavioral together with motor organization hasbeen reported to be associated with both medical and
developmental advantages20; therefore, detection of dys-functions at the 12-month neurofunctional evaluationmay represent an additional clinical tool in identifyinginfants who are at risk for poor later cognitive outcomeand could benefit from early intervention.
Although efforts have been made to eliminate theartificial division between the neurologic and the behav-ioral approach to the neurodevelopmental assessment ofpreterm infants, few studies have investigated the rela-tionship between the cognitive outcome of ELBW in-fants and the neurofunctional evaluation. Wallace et al8
reported that preterm neonates who had poor neurobe-havioral performance, assessed as visual-following andauditory-orienting, had significantly lower cognitive testscores at age 1 and 6 years. Costantinou et al7 found thatthe Neurobehavioral Assessment of the Preterm Infants,evaluated before hospital discharge, correlates with cog-nitive outcome at 30 months of age.
There is increasing evidence that cognitive domain inpreterm infants is one of the most common areas of poorfunctioning.21 The prevalence of severe developmentaldelay found in our study is 14.2%. Several multicentertrials2,22–25 reported different rates of developmental dis-abilities in very preterm infants, ranging from 15% to20% up to 35% to 40%. In a meta-analysis, Bhutta etal26 reported that mean cognitive scores of preterm in-fants at school age were 10.9 lower compared with thoseof control subjects, showing a linear correlation withbirth weight and gestational age. In this study, a youngergestational age, being male, absence of HC catch-upgrowth at 36 months, and severe ROP were associatedwith developmental delay at 36 months at univariateanalysis. No association with birth weight was found,probably because in our study, infants with birth weight�600 g were unrepresented. Being male, having poorpostnatal growth, especially of the head, and havingsevere ROP have been reported as risk factors for devel-opmental delay by other authors.2,27,28
In this study, at logistic regression analysis, also ab-normal MRI status at term and the presence of CLDremained predictive of cognitive outcome at 36 months.Abnormal MRI status at term has been reported as astrong predictor of adverse neurodevelopmental out-come by other authors,29 suggesting a role for MRI atterm in risk stratification for preterm infants. There isagreement on the unfavorable effect of CLD, even in theabsence of severe brain lesions, on cognitive outcome inchildren who are born very preterm, which seems topersist into school age.30
In our study, maternal education and being SGA werenot predictive of later cognitive outcome. The effect ofmaternal education on cognitive outcome in ELBW in-fants remains in question. Although several authorshave reported lack of maternal education as a risk factorfor poor cognitive development,2 others did not observeany effect.4,5 Current literature is inconclusive also about
TABLE 3 Variables AssociatedWith a GQ of <88 at 36 Months ofAge: Logistic Regression Analysis
Parameter Adjusted OR(95% CI)
Gestational age (�28 vs �28 wk) 1.70 (0.30–8.40)Birth weight (�800 vs �800 g) 2.70 (0.50–14.00)Gender (male vs female) 1.40 (0.40–5.40)Being SGA (yes vs no) 0.70 (0.10–4.70)Multiple birth (yes vs no) 0.90 (0.20–4.60)Sepsis (yes vs no) 0.50 (0.10–2.40)ROP stage 3 or higher (yes vs no) 0.60 (0.08–3.90)CLD (yes vs no) 8.80 (1.80–42.90)a
HC z score at 12 mo (absence vs presence of catch-upgrowth)
2.30 (0.60–9.70)
Neurofunctional status at 12 mo (normal vs impaired) 0.15 (0.03–0.70)a
MRI status at term (abnormal vs normal) 16.70 (3.30–84.30)b
Maternal hypertension (yes vs no) 0.80 (0.20–3.70)Prenatal steroids (yes vs no) 0.70 (0.20–2.90)Maternal education (low vs high) 1.60 (0.30–8.40)
OR indicates odds ratio; CI, confidence interval.a P � .05.b P � .005.
1016 GIANNI et al by guest on June 13, 2013pediatrics.aappublications.orgDownloaded from

the role of being SGA in determining neurodevelopmentoutcome. Some studies31 reported no effect of SGA statuson cognitive outcome, whereas others found a modestassociation between SGA and IQ.32
We did not find any association between sepsis anddevelopmental delay. This finding is in agreement withVohr et al,2 who did not identify sepsis as predictive ofcognitive impairment, whereas Stoll et al33 found a rateof cognitive developmental disability of 33% to 42% ininfants with infection versus 22% in infants withoutinfection.
A potential limitation of the findings of this study isthe loss to follow-up, which was �10%; however, be-cause the patients who were lost to follow-up had sim-ilar characteristics at birth and in the developmentalmeasures, when last assessed, to those reported, this lossis unlikely to bias substantially the associations reported.An additional limitation of this study was that, despite arelatively large sample size, the low rate of severe cog-nitive impairment precluded a separate analysis to iden-tify the variables that were predictive of a GQ of �70.
Because disability, defined as impairment of function,has been recognized to be multidimensional,34,35 thechoice of outcome classifications and assessments re-mains difficult. Additional investigations are warrantedto identify additional, simple methods of neurodevelop-mental assessment in clinical practice that may betterreflect the emerging concept of disability and focus theattention on the consequences of disease rather than ondisease itself. A functional approach to the neurodevel-opmental evaluation that actually investigates not onlyan infant’s motor but also neuromotor and behavioralskills may well relate to later outcomes and focus on theoutcome potential of the infant.
CONCLUSIONSAccording to our findings, the presence of a score of �2at the 12-month neurofunctional assessment representsan early clinical marker of adverse later cognitive out-come. This study suggests that an early neurofunctionalevaluation could be an additional useful tool in alertingclinicians to follow up neurodevelopment strictly to ini-tiate early intervention programs. Additional, largerstudies are desirable to clarify better the role of theneurofunctional assessment in the early identification ofchildren who are at risk for poor later cognitive perfor-mance.
REFERENCES1. Draper ES, Manktelow B, Field D, James D. Prediction of
survival for preterm births by weight and gestational age: ret-rospective population based study. BMJ. 1999;319:1093–1097
2. Vohr BR, Wright LL, Dusick AM, et al. Neurodevelopmentaland functional outcomes of extremely low birth weight infantsin the National Institute of Child Health and Human Develop-ment Neonatal Research Network, 1993–1994. Pediatrics. 2000;105:1216–1226
3. Taylor Hg, Klein N, Hack M. School-age consequences of birthweight less than 750 g: a review and an update. Dev Neuropsy-chol. 2000;17:289–321
4. Burns Y, O’Callaghan M, McDonnel B, Rogers Y. Movementand motor development in ELBW infants at 1 year is related tocognitive and motor abilities at 4 years. Early Hum Dev. 2004;80:19–29
5. Jeyaseelan D, O’Callaghan M, Neulinger K, Shum D, Burns Y.The association between early minor motor difficulties in ex-tremely low birth weight infants and school age attentionaldifficulties. Early Hum Dev. 2006;82:249–255
6. Picciolini O, Giannı ML, Vegni C, Fumagalli M, Mosca F. Use-fulness of an early neurofunctional assessment in predictingneurodevelopment outcome in very low birth weight infants.Arch Dis Child Fetal Neonatal Ed. 2006;91:F111–F117
7. Costantinou JC, Adamson-Macedo EN, Mirmiran M, AriagnoRL, Fleiser BE. Neurobehavioral assessment predicts differen-tial outcome between VLBW and ELBW preterm infants. JPerinatol. 2005;25:788–793
8. Wallace IF, Rose SA, McCarton CM, Kurtzberg D, Vaughan HG.Relations between infant neurobehavioral performance andcognitive outcome in very low birth weight preterm infants. JDev Behav Pediatr. 1995;16:309–317
9. Bell MJ, Temberg JL, Feigin RD, et al. Neonatal necrotizingenterocolitis: therapeutic decisions based on clinical staging.Ann Surg. 1978;187:1–7
10. Robertson C. Catch-up growth among very-low-birth-weightpreterm infants: a historical perspective. J Pediatr. 2003;143:145–146
11. Agostoni C, Grandi F, Scaglioni S, et al. Growth pattern ofbreastfed and nonbreastfed infants with atopic dermatitis inthe first year of life. Pediatrics. 2000;106(5). Available at: www.pediatrics.org/cgi/content/full/106/5/e73
12. Griffiths R. The Abilities of Young Children: A Comprehensive Sys-tem of Mental Measurement for the First 8 Years of Life—ChildDevelopment Research Centre London. London, England: Youngand Son; 1970
13. Roth SC, Baudin J, Pezzani-Goldsmith M, Townsend J, Reyn-olds EO, Stewart AL. Relation between neurodevelopmentalstatus of very preterm infants at one and eight years. Dev MedChild Neurol. 1994;36:1049–1062
14. Stewart AL, de Costello AM, Hamilton PA, et al. Relationshipbetween neurodevelopment status of very preterm infants atone and four years. Dev Med Child Neurol. 1989;31:756–765
15. Piaget J. The Origins of Intelligence in the Child. London, England:Penguin Educational; 1977
16. Iacoboni M, Dapretto M. The mirror neuron system and theconsequences of its dysfunctions. Nat Rev Neurosci. 2006;7:942–951
17. Rizzolatti G, Craighero L. The mirror neurons system. Annu RevNeurosci. 2004;27:169–192
18. Iacoboni M, Molnar-Szakacs I. Grasping the intentions of oth-ers with one’s owns mirror neuron system. PLOS Biol. 2005;3:529–535
19. Hadders-Algra M. Early brain damage and the development ofmotor behavior in children: clues for therapeutic intervention?Neural Plast. 2001;8:31–49
20. Als H, Lawhon G, Brown E, et al. Individualized behaviouraland environmental care for the very low birth weight preterminfant at high risk for bronchopulmonary dysplasia: neonatalintensive care unit and developmental outcome. Pediatrics.1986;78:1123–1132
21. Marlow N. Introduction: neurodevelopmental follow-up afterpreterm birth. Early Hum Dev. 2006;82:149–150
22. Finnstrom O, Otterblad O, Sedin G, et al. Neurosensory out-come and growth at three years in extremely low birth weight
PEDIATRICS Volume 120, Number 5, November 2007 1017 by guest on June 13, 2013pediatrics.aappublications.orgDownloaded from

infants: follow-up results from the Swedish national prospec-tive study. Acta Paediatr. 1998;87:1055–1060
23. Doyle LW; Victorian Infant Collaborative Study Group. Out-come at 5 years of age of children 23 to 27 weeks’ gestation:refining the prognosis. Pediatrics. 2001;108:134–141
24. Wood NS, Marlow N, Costeloe K, Gibson AT, Wilkinson AR.Neurologic and developmental disability after extreme pretermbirth. N Engl J Med. 2000;343:378–384
25. Schmidt B, Asztalos EV, Roberts RS, et al. Impact of broncho-pulmonary dysplasia, brain injury, and severe retinopathy onthe outcome of the extremely low birth weight infants at 18months: results from the trail of indomethacin prophylaxis inpreterms. JAMA. 2003;289:1124–1129
26. Bhutta AT, Cleves AM, Casey PH, Cradock MM, Anand KJ.Cognitive and behavioural outcomes of school-aged childrenwho were born preterm. JAMA. 2002;288:728–737
27. Msall ME, Phelps DL, DiGaudio KM, et al. Severity of neonatalretinopathy of prematurity is predictive of neurodevelopmen-tal functional outcome at age 5.5 years. Pediatrics. 2000;106:998–1005
28. Latal-Hajnal LH, von Siebenthal K, Kovari H, Bucher HU,Largo RH. Postnatal growth in VLBW infants: significant asso-ciation with neurodevelopmental outcome. J Pediatr. 2003;143:163–170
29. Woodward LJ, Anderson PJ, Austin NC, Howard K, Inder TE.Neonatal MRI to predict neurodevelopmental outcomes in pre-term infants. N Engl J Med. 2006;355:685–694
30. Bohm B, Katz-Salamon M. Cognitive development at 5.5 yearsof children with chronic lung disease of prematurity. Arch DisChild Fetal Neonatal Ed. 2003;88:F101–F105
31. Martyn CN, Gale CR, Sayer AA, Fall C. Growth in utero andcognitive function in adult life: follow up study of people bornbetween 1920 and 1943. BMJ. 1996;312:1393–1396
32. Hollo O, Rautava P, Korhonen T, Helenius H, Kero P, SillanpaaM. Academic achievement of small-for-gestational age chil-dren at age 10 years. Arch Pediatr Adolesc Med. 2002;156:179–187
33. Stoll BJ, Hansen NI, Adams-Chapman I, et al. Neurodevelop-mental and growth impairment among extremely low birthweight infants with neonatal infection. JAMA. 2004;292:2357–2365
34. Msall ME. Neurodevelopmental surveillance in the first 2 yearsafter extremely preterm birth: evidence, challenges, and guide-lines. Early Hum Dev. 2006;82:157–166
35. World Health Organization. International Classification of Func-tioning, Disability and Health. Geneva, Switzerland: WorldHealth Organization; 2001
1018 GIANNI et al by guest on June 13, 2013pediatrics.aappublications.orgDownloaded from
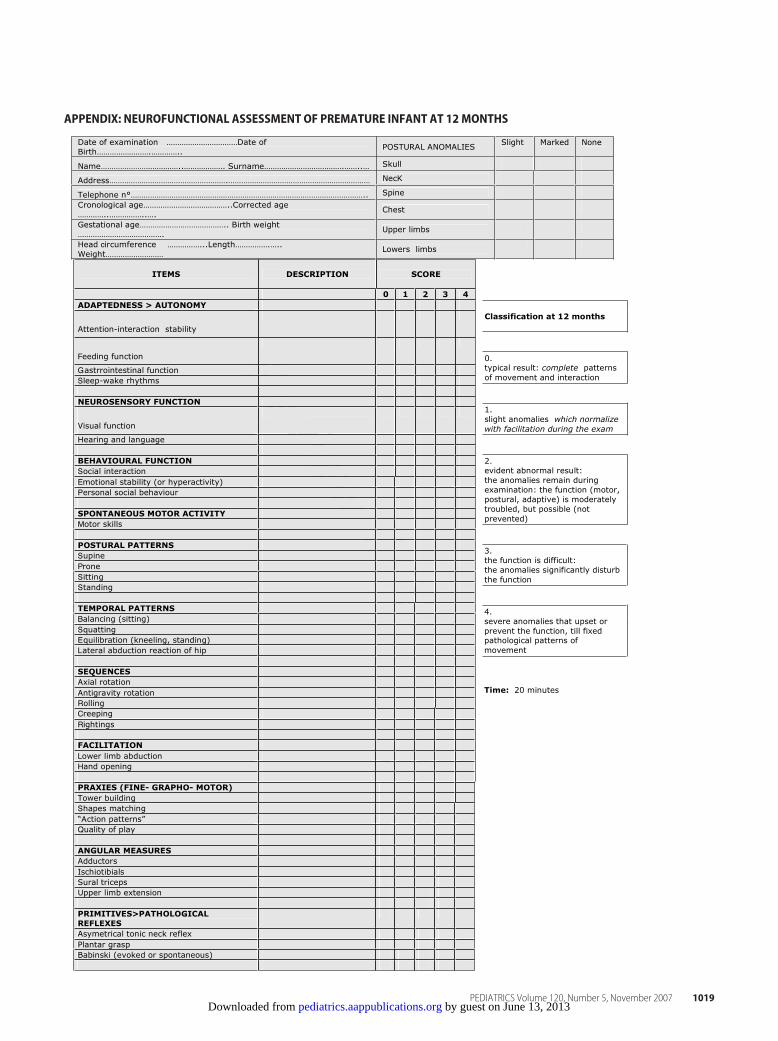
APPENDIX: NEUROFUNCTIONAL ASSESSMENT OF PREMATURE INFANT AT 12MONTHS
Review Copy
Classification at 12 months
0.typical result: complete patterns
of movement and interaction
1.
slight anomalies which normalize
with facilitation during the exam
2. evident abnormal result:
the anomalies remain during
examination: the function (motor,
postural, adaptive) is moderately
troubled, but possible (not
prevented)
3. the function is difficult:
the anomalies significantly disturb
the function
4.
severe anomalies that upset or
prevent the function, till fixed pathological patterns of
movement
Time: 20 minutes
Date of examination ……………………………Date of
Birth…………………….………….. POSTURAL ANOMALIES
Slight Marked None
Name………………………………..………………. Surname……………………………….……..… Skull
Address……………………………………………….………………………………………………………… NecK
Telephone n°……………………………………………………………………………………………….. Spine
Cronological age…………………………………..Corrected age
…………..……………..…. Chest
Gestational age………………………………….. Birth weight
…………………………………. Upper limbs
Head circumference ……………...Length…………….…..
Weight……………………… Lowers limbs
ITEMS DESCRIPTION SCORE
0 1 2 3 4
ADAPTEDNESS > AUTONOMY
Attention-interaction stability
Feeding function
Gastrrointestinal function
Sleep-wake rhythms
NEUROSENSORY FUNCTION
Visual function
Hearing and language
BEHAVIOURAL FUNCTION
Social interaction
Emotional stability (or hyperactivity)
Personal social behaviour
SPONTANEOUS MOTOR ACTIVITY
Motor skills
POSTURAL PATTERNS
Supine
Prone
Sitting
Standing
TEMPORAL PATTERNS
Balancing (sitting)
Squatting
Equilibration (kneeling, standing)
Lateral abduction reaction of hip
SEQUENCES
Axial rotation
Antigravity rotation
Rolling
Creeping
Rightings
FACILITATION
Lower limb abduction
Hand opening
PRAXIES (FINE- GRAPHO- MOTOR)
Tower building
Shapes matching
“Action patterns”
Quality of play
ANGULAR MEASURES
Adductors
Ischiotibials
Sural triceps
Upper limb extension
PRIMITIVES>PATHOLOGICAL
REFLEXES
Asymetrical tonic neck reflex
Plantar grasp
Babinski (evoked or spontaneous)
PEDIATRICS Volume 120, Number 5, November 2007 1019 by guest on June 13, 2013pediatrics.aappublications.orgDownloaded from

DOI: 10.1542/peds.2006-3364 2007;120;1012Pediatrics
Fumagalli and Fabio MoscaMaria Lorella Giannì, Odoardo Picciolini, Chiara Vegni, Laura Gardon, Monica
Months of Age in Extremely Low Birth Weight InfantsTwelve-Month Neurofunctional Assessment and Cognitive Performance at 36
ServicesUpdated Information &
tmlhttp://pediatrics.aappublications.org/content/120/5/1012.full.hincluding high resolution figures, can be found at:
References
tml#ref-list-1http://pediatrics.aappublications.org/content/120/5/1012.full.hat:This article cites 31 articles, 8 of which can be accessed free
Subspecialty Collections
_subhttp://pediatrics.aappublications.org/cgi/collection/neurologyNeurology
orn_infant_subhttp://pediatrics.aappublications.org/cgi/collection/fetus:newbFetus/Newborn Infant
velopment_milestones_subhttp://pediatrics.aappublications.org/cgi/collection/growth:deGrowth/Development Milestones
nt:behavioral_issues_subhttp://pediatrics.aappublications.org/cgi/collection/developmeDevelopment/Behavioral Issuesthe following collection(s):This article, along with others on similar topics, appears in
Permissions & Licensing
mlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhttables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2007 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by guest on June 13, 2013pediatrics.aappublications.orgDownloaded from