Prospects for ecological intensification of Australian agriculture
Upload
uni-duesseldorfCategory
view
4download
0
Annals of Oncology 19: 861–870, 2008
doi:10.1093/annonc/mdm551
Published online 3 January 2008original article
Triple-negative high-risk breast cancer derivesparticular benefit from dose intensification ofadjuvant chemotherapy: results of WSG AM-01 trial
O. Gluz1*, U. A. Nitz1, N. Harbeck3, E. Ting2, R. Kates3, A. Herr4, W. Lindemann5, C. Jackisch6,W. E. Berdel7, H. Kirchner8, B. Metzner9, F. Werner1, G. Schutt1, M. Frick1, C. Poremba2,R. Diallo-Danebrock2 & S. Mohrmann1
On behalf of the West German Study Group1West German Study Group, Breast Centre, Department of Gynecology and Obstetrics; 2Department of Pathology, University Hospital, Duesseldorf;3Department of Obstetrics and Gynecology, Technical University of Munich, Munich; 4Department of Clinical Genetics, University Hospital, Technical University,
Dresden; 5Department of Hematology/Oncology, Catholic Hospital, Hagen; 6Department of Gynecology and Obstetrics, City Hospital, Offenbach;7Department of Hematology/Oncology, University Hospital, Muenster; 8Department of Hematology/Oncology, Siloah Clinic, Hannover; 9Department of
Hematology/Oncology, City Hospital, Oldenburg, Germany
Received 28 July 2007; accepted 2 November 2007
Background: This paper evaluates the prognostic and predictive impact of protein expression of various molecular
markers in high-risk breast cancer (HRBC) patients with >9 involved lymph nodes, who received different
chemotherapy dose-intensification strategies within a prospective randomized WSG AM-01 trial.
Materials and methods: Paraffin-embedded tumors from 236 patients, who were randomly assigned to dose-
dense conventional chemotherapy with four cycles of E90C600 followed by three cycles of C600M40F600 every 2 weeks
(DD) or a rapidly cycled tandem high-dose regimen with two cycles of E90C600 every 2 weeks followed by two cycles of
E90C3000Thiotepa400 every 3 weeks (HD), were available for retrospective central pathological review (116 HD/120 DD).
Expression of estrogen receptor (ER), progesterone receptor (PR), MIB-1, epidermal growth factor receptor, and Her-
2/neu was evaluated immunohistochemically using tissue microarrays. Results were correlated with follow-up data
and treatment effects by proportional hazard Cox regression models (including interaction analysis).
Results: After a median follow-up of 61.7 months, 5-year event-free survival (EFS) as well as overall survival (OS) rates
for the 236 patients were significantly better in the HD arm: EFS: 62% versus 41% [hazard ratio (HR) = 0.60, 95% CI
0.43–0.85, P = 0.004]; OS: 76% versus 61% (HR = 0.58, 95% CI 0.39–0.87, P = 0.007). In multivariate analysis, HD,
tumor size <3 cm, positive PR, negative MIB-1 staining, and grade 1/2 were associated with favorable outcome.
Interaction analysis showed that regarding predictive effects, triple negative (ER/PR/Her-2/neu) and G3 tumors derived
most benefit from HD.
Conclusion: Tandem HD improves both EFS and OS in HRBC. This therapy effect may be partly attributable to
superior efficacy in the subgroup of triple-negative tumors and/or G3 with their poor prognostic marker profile.
Key words: basal-like, breast cancer, high dose chemotherapy, triple negative, breast cancer
introduction
Breast cancer patients with multiple positive lymph nodes(LNs) have a poor prognosis. The average annual lethalityrates in patients with ‡10 involved LNs are five times higherthan for N0 patients [1]. The 5-year event-free survival (EFS)without application of adjuvant therapy for this subgroup is<30% [2]. Anthracycline-containing adjuvant chemotherapyimproves outcome [3], but subgroup analysis shows that inthis high-risk subgroup few standard regimens have achieved
a 5-year EFS exceeding 40%–52% [4–6]. The benefit fromtaxanes in this subgroup remains unclear on the basis ofpublished retrospective, unplanned subgroup analyses fromtrials evaluating third-generation taxane combinations. Up tonow, findings from trials investigating the effects ofE90C3000Thiotepa400 every 3 weeks high dose chemotherapy(HD) in this high-risk group remain controversial. Somestudies have shown a significant superiority of HD in terms ofdisease-free survival, particularly in breast cancer patients with‡10 positive LN [7–9]. Other studies showed a trend to betterefficacy of HD but did not reach the level of significance [10,11], while other results did not reveal any advantage for HD [6,12, 13]. Up to now, our previously reported WSG AM-01 study
ori
gin
al
art
icle
*Correspondence to: Dr O. Gluz, West German Study Group, Breast Centre, University
Hospital of Duesseldorf, Moorenstrasse 5, 40225 Duesseldorf, Germany.
Tel: +49-2161-5662311; Fax: +49-2161-5662319; E-mail: [email protected]
ª The Author 2008. Published by Oxford University Press on behalf of the European Society for Medical Oncology.
All rights reserved. For permissions, please email: [email protected]
by guest on Decem
ber 18, 2015http://annonc.oxfordjournals.org/
Dow
nloaded from

is the only study demonstrating that the tandem HD armcompared with dose-dense Epirubicine and cyclophosphamide/cyclophosphamide, methotrexat and 5-fluoruracil therapy wassignificantly associated with reduced risk of both relapse anddeath [9]. Published trial designs are very heterogeneous interms of regimens, HD strategy, control arms, and patientselection criteria. Considering the heterogeneity of thepublished data, the aim should now be to identify promisingHD strategies and biological tumor subtypes derivingmaximum benefit from HD. To date, the predictive value ofestablished prognostic factors such as grade, estrogen receptor(ER), tumor size, Her-2/neu, or age is still under debate in theHD setting [14–16].Gene expression studies on the basis of DNA microarray
analysis have enabled molecular subtyping of breast tumorswith distinct patterns of proliferation, apoptosis, and DNArepair as well as with distinct prognostic implications [17].Luminal, hormone receptor expressing tumors have betterprognosis than Her-2/neu and triple-negative [ER-/progesterone receptor (PR)-/Her-2/neu]/basal-like subtypes.The management of triple-negative tumors poses a clinicalchallenge due to the limited therapeutic options in this subtype.The clinical relevance of the triple-negative subgroup wasreemphasized in the recent 2007 St Gallen conference (oralcommunication).Currently, there is only limited experience with regard to
the response of molecular subtypes to different cytotoxictherapies [18], but ER and growth factor such as Her-2/neu andepidermal growth factor receptor (EGFR) play a key role inboth molecular classification of breast cancer [17] and inprediction of chemotherapy effects [3, 19, 20].The aim of our study was to evaluate the benefits from HD
in clinically relevant subgroups, particularly triple-negativepatients, utilizing tumor samples from a retrospective, centralpathological blinded review with updated follow-up of therandomized prospective WSG AM-01 trial in high-risk breastcancer (HRBC).
materials and methods
patientsPatients included in our analysis took part at the randomized multicenter
WSG AM-01 trial, which compared tandem HD versus C600M40F600 every 2
weeks (DD) conventional chemotherapy. Eligible patients were 18–60 years
old, had histologically proven breast cancer, and ‡9 positive axillary LN.
Absence of distant metastases was verified by normal findings in chest
X-ray, liver ultrasonography, and bone scan.
The detailed protocol has been described elsewhere [9]. HD patients
received an induction regimen with two courses of E90C600 every 2 weeks
with granulocyte colony-stimulating factor (G-CSF) support from day 5 to
day 12. Patients received HD on day 25 to day 23. Peripheral blood
stem cells were given on day 0. DD consisted of four courses of E90C600
followed by three courses of DD with G-CSF support from day 5 to day 12.
Four weeks after completion of chemotherapy, all patients underwent
radiotherapy of the chest wall/breast and the infra- and supraclavicular
fossae at conventional doses and fractions. Tamoxifen 20 mg daily for 5
years was started in all patients with hazard ratio (HR)-positive disease
after the completion of chemotherapy.
The WSG AM-01 study was approved by the ethics committees of all
73 participating institutions. All patients provided written informed
consent. The trial was conducted according to the Helsinki Declaration
of 1975 as revised in 1983.
prognostic factors and histopathological analysisAt time of diagnosis, the following baseline characteristics were determined:
age, histopathology, tumor size, grade, number of examined and
positive LNs, and ER/PR status.
tumor samplesParaffin-embedded tumor blocks were requested from all 403 patients
participating in the trial. Representative sections from 252 of these
(63%) were received. Sufficient primary tumor tissue was available in
236 (59%) tumor samples; these sections were reviewed and analyzed at
our central laboratory by two experienced breast pathologists (RD-D and
CP) for specific morphologic features, including grade (based on the
criteria of Elston and Ellis) and vascular invasion.
tissue microarrays and antibodies forimmunohistochemistryExpression of ER, PR, Her-2/neu, MIB-1, and EGFR was analyzed
immunohistochemically using tissue microarrays, constructed from core
specimens (internal diameter 2 mm) of representative tumor areas.
Immunohistochemical staining was carried out on 3 lm paraffin
sections. Pretreatment for antigen retrievalwasmainly carried out by pressure
cooker except for EGFR, where pronase was used. After blockage of biotin
and peroxidase, immunohistochemical staining was carried out on an
automated immunostainer (Biogenex, i6000, San Ramon, CA) using the
standard labeled streptavidin–biotin method (UltraTek Reagent Detection
Kit, Scy Tek, Logan, UT) followed by 3,3-V-diaminobenzidine enzymic
development. Sectionswere counterstained bluewith hematoxylin.Omission
of the primary antibody served as negative control.
Consecutive sections were stained with antibodies against Her-2/neu
(polyclonal rabbit antibody c-erbB-2, dilution 1 : 500, DAKO, Glostrup,
Denmark), ER (rabbit monoclonal antibody, clone SP1, 1 : 800, DCS,
Hamburg, Germany), PR (rabbit monoclonal antibody, clone SP2, 1 : 800,
DCS), MIB-1/Ki-67 (mouse monoclonal antibody, MIB-1, 1 : 1000,
DAKO), and EGFR (mouse monoclonal antibody, clone E 30, 1 : 100,
Merck, Darmstadt, Germany).
immunohistochemical analysisExpression of Her-2/neu oncoprotein was categorized in three groups
according to the HercepTest score—score 0: no staining at all or membrane
staining in <10% of the tumor cells; score 1+: faint, incomplete
membranous staining; 2+: moderate, complete membranous staining; 3+:strong membranous staining, observed in >10% of the tumor cells,
respectively. A score of 3+ was designated as positive. Cases with 2+ scores
were further evaluated by FISH to evaluate Her-2/neu gene amplification.
Ki-67/MIB-1 expression was defined as a strong nuclear staining in at
least 10% of the tumor cells. ER and PR were scored by an intensity and
proportion score (1–3 negative and >4 positive).
statistical analysisBivariate correlations of individual markers were measured by Pearson’s
correlation. Association of markers with triple negativity was assessed
by Fisher’s exact test. Survival analysis was carried out using the
Kaplan–Meier method including the log-rank test group comparisons.
Uni- and multivariate analyses of EFS and overall survival (OS) used
proportional hazard Cox regression models. Multivariate analyses
(including treatment interaction analyses) were carried out by
backward elimination using the Wald test; HRs for borderline significant
factors and interactions are included; 95% confidence intervals are
original article Annals of Oncology
862 | Gluz et al. Volume 19 |No. 5 |May 2008
by guest on Decem
ber 18, 2015http://annonc.oxfordjournals.org/
Dow
nloaded from
reported. All data were analyzed using SPSS for Windows (SPSS,
Chicago, IL).
results
patient collective
From May 1995 to June 2002, 403 patients were randomlyassigned to receive to tandem HD (201 patients) or DDconventional chemotherapy (202 patients). From 236 patients(59%), paraffin-embedded tumor blocks with primary tumortissue were retrieved for central pathological review and furtherimmunohistochemical investigations (116 from HD and 120fromDD). Patient and tumor characteristics are detailed in Table1. The collective data available for the immunhistochemistryanalyses reported here were representative of the original study
population. There were no significant differences in thedistributions of clinicopathological factors.With regard to clinically interesting subgroups, 66 patients
had tumors that were triple negative, i.e. that stained negativefor ER, PR, and HER2. Triple-negative tumors weresignificantly associated with younger age (median: 45.2 years 69.0 versus 51.2 6 8.1; P < 0.001, Fisher’s exact test), G3(57% versus 31%; P = 0.001), and EGFR overexpression (34%versus 7%; P < 0.001). Moreover, HR-negative tumors asa whole were significantly associated with G3 (60% versus 23.2,P = 0.001), as well as overexpression of MIB-1 (67% versus52%, P = 0.028), Her-2/neu (31% versus 9.6, P < 0.001),and EGFR (28% versus 4%, P < 0.001).
patient outcome according to study arm
In all, 236 patients (116 HD and 120 DD) were followed upuntil November 2005, leading to a median follow-up time of61.7 months in patients still alive at time of analysis witha range of 4.2–121.9 months (HD: 67.9 months, DD: 56.3months). In all, 56 relapses were reported in the HD and 76in the DD group. Estimated 5-year EFS rates were 62% forHD group and 41% for DD (HR = 0.60, 95% CI 0.43–0.85,P = 0.004). A total of 99 deaths were reported (39 in HD; 60in DD); 5-year OS was 76% in HD arm and 61% in DD arm(HR = 0.58, 95% CI 0.39–0.87, P = 0.007) (Figure 1).
patient outcome according to prognostic factors
Tumors from 211 patients with available staining results forall protein markers were included in univariate andmultivariate analyses.In univariate analysis, the following factors were significantly
associated with better EFS: HD, positive PR status, tumorsize <3 cm, G1/2, and negative status of Her-2/neu and ofMIB-1. The same factors as well as positive ER status andnegative EGFR were significantly associated with longer OS.Multivariate analysis was carried out including the factors
therapy, tumor size, ER, PR, grade, HER-2/neu, MIB-1, andEGFR. HD therapy (HR = 0.48, P = 0.001) was significantlyassociated with reduced relapse risk. There was a similar butnonsignificant trend in positive PR status (HR = 0.65, P = 0.03).Positive MIB-1 status (HR = 1.90, P = 0.003) and largertumor size ‡3 cm (HR = 1.66, P = 0.008) were significantfactors for poor EFS.For OS, again HD therapy (HR = 0.43, P < 0.001) and
positive PR status (HR = 0.43, P = 0.001) were favorable,whereas in addition to positive MIB-1 status (HR = 1.73, P =0.03), G3 (HR = 1.64, P = 0.05) and larger tumor size ‡3 cm(HR = 1.76, P = 0.01) were associated with increased risk ofdeath. Detailed results for univariate and multivariateanalysis are shown in Table 2.
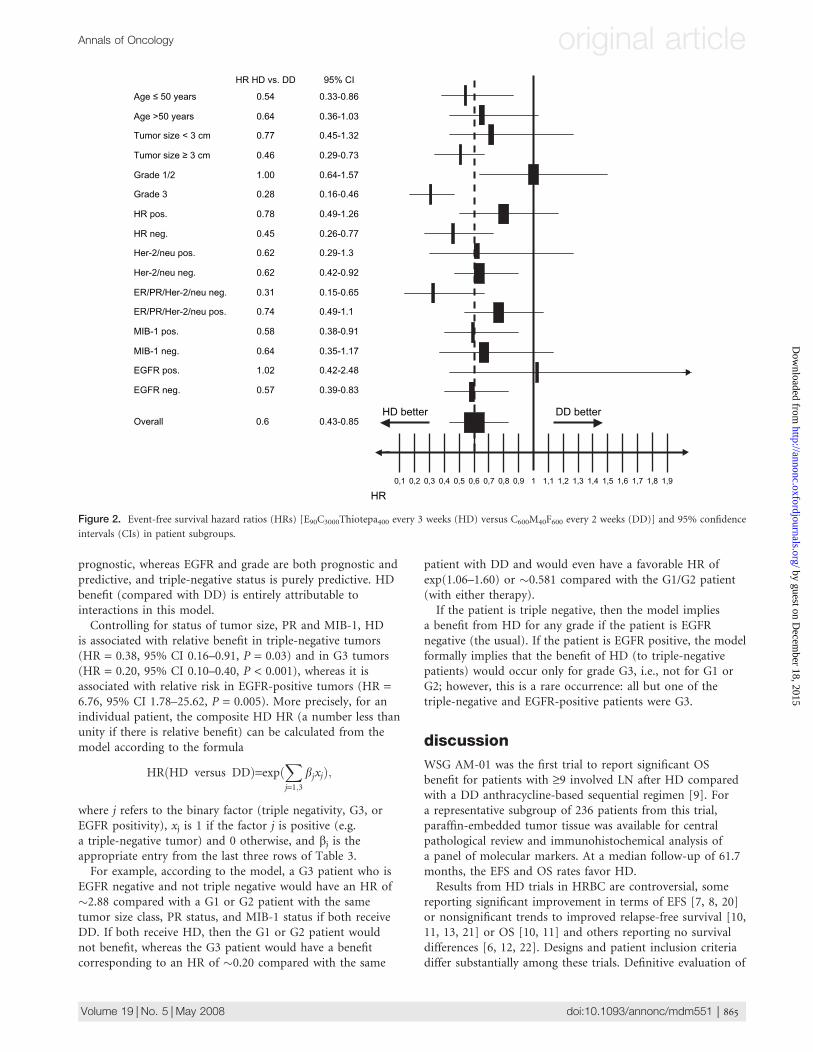
therapy effect in subgroups
Therapy efficacy was evaluated in clinically relevant subgroupsdefined according to clinicopathological criteria as well asprotein markers. HRs for EFS between the two treatmentgroups are displayed in Figure 2. The following parameterswere significantly associated with better outcome after HDversus DD: age £50 years; tumor size ‡3 cm; G3; negative
Table 1. Patient’s and tumor characteristics
Tandem HDC DD conventional
Characteristics n = 116 % n = 120 %
Age (years)
Median 6 SD 50.1 6 9.0 48.8 6 8.5
Menopausal status
Pre 63 54 59 49
Post 48 41 58 48
Unknown 5 5 3 3
Surgery
Breast-conserving therapy 39 34 47 39
Tumor size (cm)
Mean 6 SD 3.5 6 2.1 3.4 6 2.1
Median 2.8 3.0
Positive nodes
Mean 6 SD 17.3 6 7.5 16.9 6 6.9
Median 15.0 15.0
Receptor status
ER+ 51 44 49 41
PR+ 40 35 46 38
ER+ and/or PR+ 63 54 62 52
Unknown 2 2 4 3
Grading
G1 4 3 11 9
G2 61 53 66 55
G3 51 44 43 36
Her-2/neu staining
Positive 24 21 19 16
Negative 88 76 96 80
Unknown 3 2 5 4
Triple negative 30 26 36 30
EGFR staining
Positive 12 10 19 16
Negative 103 89 96 80
Unknown 1 1 5 4
MIB-1 staining
Positive 69 60 62 52
Negative 42 36 53 44
Unknown 5 4 5 4
HD, high-dose chemotherapy; DD, C600M40F600 every 2 weeks; SD,
standard deviation; ER, estrogen receptor; PR, progesterone receptor;
EGFR, epidermal growth factor receptor.
Annals of Oncology original article
Volume 19 |No. 5 |May 2008 doi:10.1093/annonc/mdm551 | 863
by guest on Decem
ber 18, 2015http://annonc.oxfordjournals.org/
Dow
nloaded from

HR, Her-2/neu, and EGFR status; and triple-negative tumors(ER/PR/Her-2/neu) as well as positive MIB-1 staining.As noted regarding Figure 2, significant benefits from HD
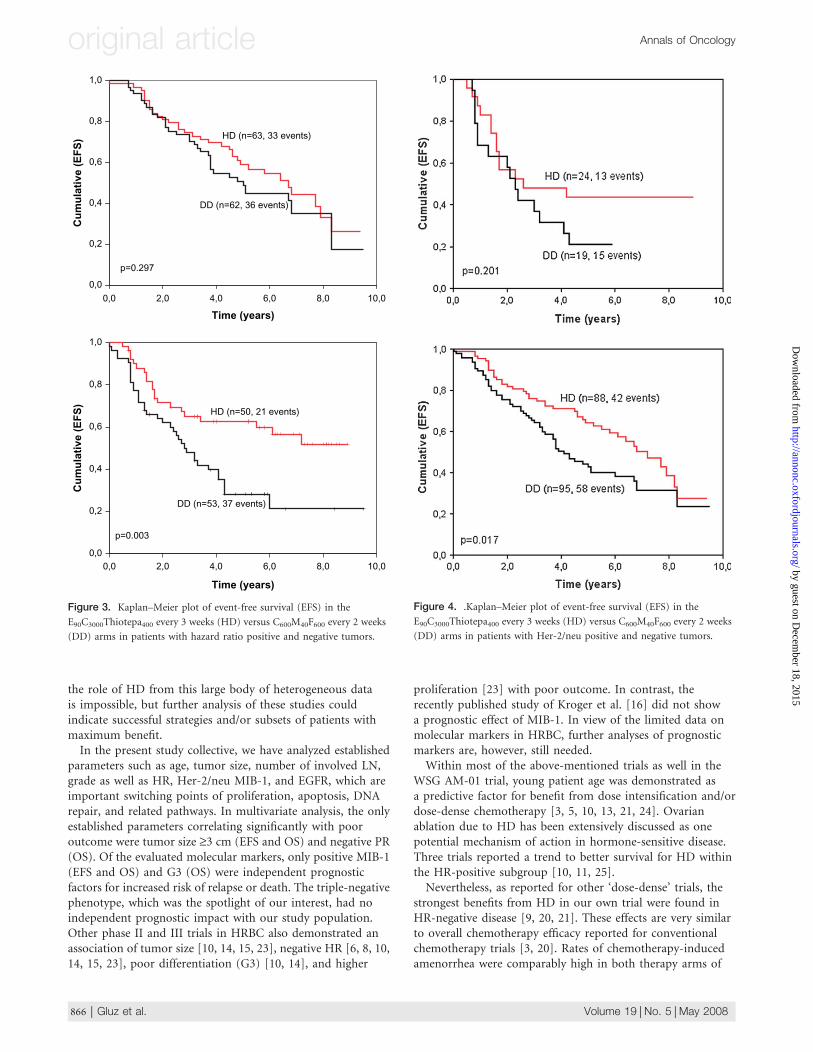
versus DD was seen in the HR negative but not in the HR-positive subgroup (see Figure 3). Within the HD arm, HRstatus did not have a significant impact on EFS (P = 0.592),whereas within the DD arm, HR-positive tumors hadsignificantly better EFS (P = 0.017). Her/2-neu-negativetumors were significantly associated with better EFS in boththerapy subgroups (Figure 4).In triple-negative tumors, the most pronounced effect of
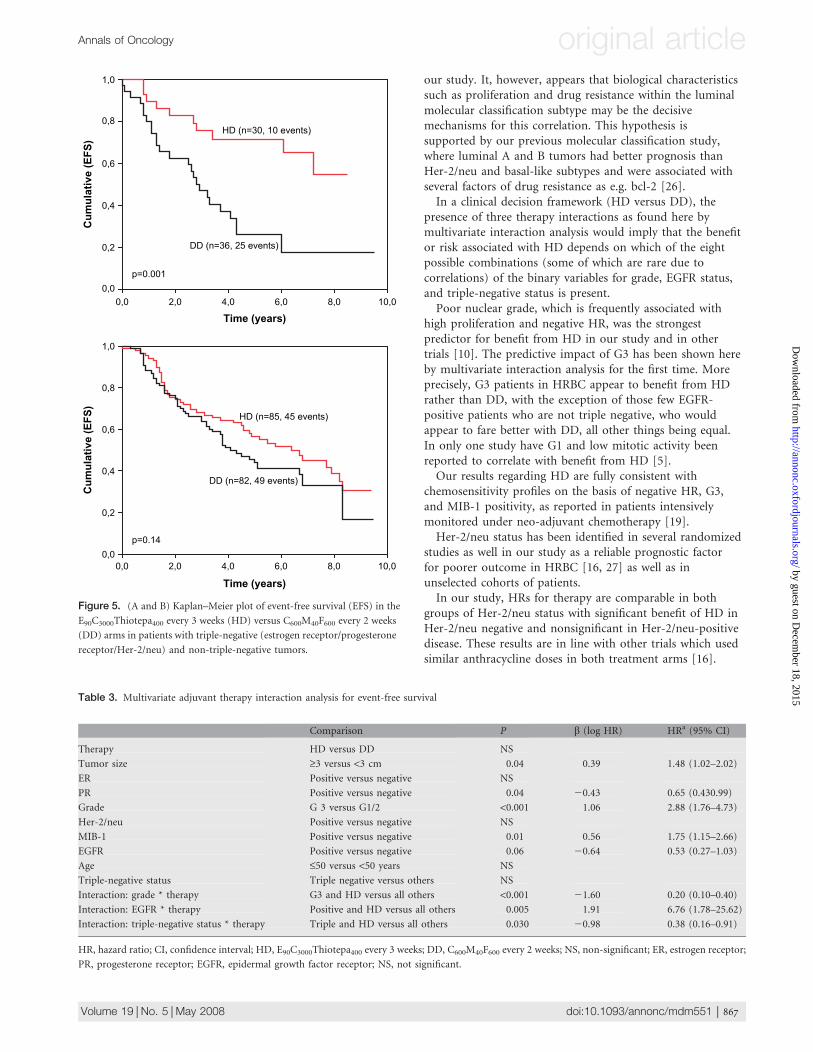
HD was observed. In this subgroup, median EFS was notreached in the HD arm, whereas it was only 32.3 months in theDD arm. This translates into an estimated 5-year EFS of 71% inthe triple-negative cohort treated by HD compared with only26% in the DD arm. There was no significant outcomedifference by therapy arm associated with the remainingtumors (see Figure 5).
adjuvant therapy interactions in multivariateanalysis
An additional perspective on predictive significance offactors for optimal individualized adjuvant therapy isprovided by multivariate interaction analysis: Each markerthat was significant in univariate Cox analysis wasconsidered both as a potential ‘main effect’ and asa potential interaction with adjuvant therapy (i.e. HDversus DD) in a proportional hazards model for EFS, theprimary end point of this randomized prospective trial.(Interaction analysis for EFS provides predictiveinformation about adjuvant therapy efficacy that is notconfounded by possibly differing palliative therapystrategies after relapse.)The resulting model is given in Table 3, which includes the
b coefficients of the underlying Cox model to aid in theinterpretation. We first note that according to the firstprognostic model, tumor size, PR, and MIB-1 are purely
Table 2. Multivariate analysis for event-free and overall survivals
Comparison Event-free survival Overall survival
Univariate Multivariate Univariate Multivariate
Pa P Hazard ratiob
(95% CI)
Pa P Hazard ratiob
(95% CI)
Therapy HD versus DD 0.004 0.001 0.48 (0.33–0.70) 0.008 <0.001 0.43 (0.28–0.74)
Tumor size ‡3 versus <3 cm 0.01 0.008 1.66 (1.14–2.22) 0.02 0.011 1.76 (1.14–2.72)
ER Positive versus negative 0.14 0.004
PR Positive versus negative 0.05 0.03 0.65 (0.44–0.96) <0.001 0.001 0.43 (0.26–0.70)
Grade G 3 versus G1/2 0.07 0.003 0.05 1.64 (1.01–2.57)
Her-2/neu Positive versus negative 0.048 0.005
MIB-1 Positive versus negative 0.01 0.003 1.90 (1.27–2.83) 0.005 0.032 1.73 (1.05–2.85)
EGFR Positive versus negative 0.12 0.005
Age £50 versus <50 years 0.45 0.69
aLog-rank testbCox proportional hazards model adjusted for age.
CI, confidence inetrval; HD, E90C3000Thiotepa400 every 3 weeks; DD, C600M40F600 every 2 weeks; ER, estrogen receptor; PR, progesterone receptor; EGFR,
epidermal growth factor receptor.
Figure 1. (A) Event-free survival (EFS) and (B) overall survival (OS).
original article Annals of Oncology
864 | Gluz et al. Volume 19 |No. 5 |May 2008
by guest on Decem
ber 18, 2015http://annonc.oxfordjournals.org/
Dow
nloaded from
prognostic, whereas EGFR and grade are both prognostic andpredictive, and triple-negative status is purely predictive. HDbenefit (compared with DD) is entirely attributable tointeractions in this model.Controlling for status of tumor size, PR and MIB-1, HD
is associated with relative benefit in triple-negative tumors(HR = 0.38, 95% CI 0.16–0.91, P = 0.03) and in G3 tumors(HR = 0.20, 95% CI 0.10–0.40, P < 0.001), whereas it isassociated with relative risk in EGFR-positive tumors (HR =6.76, 95% CI 1.78–25.62, P = 0.005). More precisely, for anindividual patient, the composite HD HR (a number less thanunity if there is relative benefit) can be calculated from themodel according to the formula
HRðHD versus DDÞ=expðX
j=1;3bjxjÞ;
where j refers to the binary factor (triple negativity, G3, orEGFR positivity), xj is 1 if the factor j is positive (e.g.a triple-negative tumor) and 0 otherwise, and bj is theappropriate entry from the last three rows of Table 3.For example, according to the model, a G3 patient who is
EGFR negative and not triple negative would have an HR of�2.88 compared with a G1 or G2 patient with the sametumor size class, PR status, and MIB-1 status if both receiveDD. If both receive HD, then the G1 or G2 patient wouldnot benefit, whereas the G3 patient would have a benefitcorresponding to an HR of �0.20 compared with the same
patient with DD and would even have a favorable HR ofexp(1.06–1.60) or �0.581 compared with the G1/G2 patient(with either therapy).If the patient is triple negative, then the model implies
a benefit from HD for any grade if the patient is EGFRnegative (the usual). If the patient is EGFR positive, the modelformally implies that the benefit of HD (to triple-negativepatients) would occur only for grade G3, i.e., not for G1 orG2; however, this is a rare occurrence: all but one of thetriple-negative and EGFR-positive patients were G3.
discussion
WSG AM-01 was the first trial to report significant OSbenefit for patients with ‡9 involved LN after HD comparedwith a DD anthracycline-based sequential regimen [9]. Fora representative subgroup of 236 patients from this trial,paraffin-embedded tumor tissue was available for centralpathological review and immunohistochemical analysis ofa panel of molecular markers. At a median follow-up of 61.7months, the EFS and OS rates favor HD.Results from HD trials in HRBC are controversial, some
reporting significant improvement in terms of EFS [7, 8, 20]or nonsignificant trends to improved relapse-free survival [10,11, 13, 21] or OS [10, 11] and others reporting no survivaldifferences [6, 12, 22]. Designs and patient inclusion criteriadiffer substantially among these trials. Definitive evaluation of
0,1 0,2 0,3 0,4 0,5 0,6 0,7 0,8 0,9 1 1,1 1,2 1,3 1,4 1,5 1,6 1,7 1,8 1,9
DD better
HR
HD better
Age ≤ 50 years
Age >50 years 0.64 0.36-1.03
Tumor size < 3 cm 0.77 0.45-1.32
Tumor size ≥ 3 cm 0.46 0.29-0.73
Grade 1/2
Grade 3
HR pos.
HR neg. 0.45 0.26-0.77
Her-2/neu pos. 0.62 0.29-1.3
Her-2/neu neg. 0.62 0.42-0.92
ER/PR/Her-2/neu neg. 0.31 0.15-0.65
ER/PR/Her-2/neu pos.
0.54
1.00
0.28
0.78
0.74
0.33-0.86
0.64-1.57
0.16-0.46
0.49-1.26
0.49-1.1
MIB-1 pos. 0.58 0.38-0.91
MIB-1 neg. 0.64 0.35-1.17
EGFR pos. 1.02 0.42-2.48
EGFR neg. 0.57 0.39-0.83
Overall 0.6 0.43-0.85
HR HD vs. DD 95% CI
Figure 2. Event-free survival hazard ratios (HRs) [E90C3000Thiotepa400 every 3 weeks (HD) versus C600M40F600 every 2 weeks (DD)] and 95% confidence
intervals (CIs) in patient subgroups.
Annals of Oncology original article
Volume 19 |No. 5 |May 2008 doi:10.1093/annonc/mdm551 | 865
by guest on Decem
ber 18, 2015http://annonc.oxfordjournals.org/
Dow
nloaded from
the role of HD from this large body of heterogeneous datais impossible, but further analysis of these studies couldindicate successful strategies and/or subsets of patients withmaximum benefit.In the present study collective, we have analyzed established
parameters such as age, tumor size, number of involved LN,grade as well as HR, Her-2/neu MIB-1, and EGFR, which areimportant switching points of proliferation, apoptosis, DNArepair, and related pathways. In multivariate analysis, the onlyestablished parameters correlating significantly with pooroutcome were tumor size ‡3 cm (EFS and OS) and negative PR(OS). Of the evaluated molecular markers, only positive MIB-1(EFS and OS) and G3 (OS) were independent prognosticfactors for increased risk of relapse or death. The triple-negativephenotype, which was the spotlight of our interest, had noindependent prognostic impact with our study population.Other phase II and III trials in HRBC also demonstrated anassociation of tumor size [10, 14, 15, 23], negative HR [6, 8, 10,14, 15, 23], poor differentiation (G3) [10, 14], and higher
proliferation [23] with poor outcome. In contrast, therecently published study of Kroger et al. [16] did not showa prognostic effect of MIB-1. In view of the limited data onmolecular markers in HRBC, further analyses of prognosticmarkers are, however, still needed.Within most of the above-mentioned trials as well in the
WSG AM-01 trial, young patient age was demonstrated asa predictive factor for benefit from dose intensification and/ordose-dense chemotherapy [3, 5, 10, 13, 21, 24]. Ovarianablation due to HD has been extensively discussed as onepotential mechanism of action in hormone-sensitive disease.Three trials reported a trend to better survival for HD withinthe HR-positive subgroup [10, 11, 25].Nevertheless, as reported for other ‘dose-dense’ trials, the
strongest benefits from HD in our own trial were found inHR-negative disease [9, 20, 21]. These effects are very similarto overall chemotherapy efficacy reported for conventionalchemotherapy trials [3, 20]. Rates of chemotherapy-inducedamenorrhea were comparably high in both therapy arms of
10,08,06,04,02,00,0
Time (years)
1,0
0,8
0,6
0,4
0,2
0,0
Cu
mu
lati
ve (
EF
S)
DD (n=62, 36 events)
HD (n=63, 33 events)
p=0.297
10,08,06,04,02,00,0
Time (years)
1,0
0,8
0,6
0,4
0,2
0,0
Cu
mu
lati
ve (
EF
S)
HD (n=50, 21 events)
DD (n=53, 37 events)
p=0.003
Figure 3. Kaplan–Meier plot of event-free survival (EFS) in the
E90C3000Thiotepa400 every 3 weeks (HD) versus C600M40F600 every 2 weeks
(DD) arms in patients with hazard ratio positive and negative tumors.
Figure 4. .Kaplan–Meier plot of event-free survival (EFS) in the
E90C3000Thiotepa400 every 3 weeks (HD) versus C600M40F600 every 2 weeks
(DD) arms in patients with Her-2/neu positive and negative tumors.
original article Annals of Oncology
866 | Gluz et al. Volume 19 |No. 5 |May 2008
by guest on Decem
ber 18, 2015http://annonc.oxfordjournals.org/
Dow
nloaded from
our study. It, however, appears that biological characteristicssuch as proliferation and drug resistance within the luminalmolecular classification subtype may be the decisivemechanisms for this correlation. This hypothesis issupported by our previous molecular classification study,where luminal A and B tumors had better prognosis thanHer-2/neu and basal-like subtypes and were associated withseveral factors of drug resistance as e.g. bcl-2 [26].In a clinical decision framework (HD versus DD), the
presence of three therapy interactions as found here bymultivariate interaction analysis would imply that the benefitor risk associated with HD depends on which of the eightpossible combinations (some of which are rare due tocorrelations) of the binary variables for grade, EGFR status,and triple-negative status is present.Poor nuclear grade, which is frequently associated with
high proliferation and negative HR, was the strongestpredictor for benefit from HD in our study and in othertrials [10]. The predictive impact of G3 has been shown hereby multivariate interaction analysis for the first time. Moreprecisely, G3 patients in HRBC appear to benefit from HDrather than DD, with the exception of those few EGFR-positive patients who are not triple negative, who wouldappear to fare better with DD, all other things being equal.In only one study have G1 and low mitotic activity beenreported to correlate with benefit from HD [5].Our results regarding HD are fully consistent with
chemosensitivity profiles on the basis of negative HR, G3,and MIB-1 positivity, as reported in patients intensivelymonitored under neo-adjuvant chemotherapy [19].Her-2/neu status has been identified in several randomized
studies as well in our study as a reliable prognostic factorfor poorer outcome in HRBC [16, 27] as well as inunselected cohorts of patients.In our study, HRs for therapy are comparable in both
groups of Her-2/neu status with significant benefit of HD inHer-2/neu negative and nonsignificant in Her-2/neu-positivedisease. These results are in line with other trials which usedsimilar anthracycline doses in both treatment arms [16].
10,08,06,04,02,00,0
Time (years)
1,0
0,8
0,6
0,4
0,2
0,0
Cu
mu
lati
ve (
EF
S)
HD (n=30, 10 events)
DD (n=36, 25 events)
p=0.001
10,08,06,04,02,00,0
Time (years)
1,0
0,8
0,6
0,4
0,2
0,0
Cu
mu
lati
ve (
EF
S)
HD (n=85, 45 events)
DD (n=82, 49 events)
p=0.14
Figure 5. (A and B) Kaplan–Meier plot of event-free survival (EFS) in the
E90C3000Thiotepa400 every 3 weeks (HD) versus C600M40F600 every 2 weeks
(DD) arms in patients with triple-negative (estrogen receptor/progesterone
receptor/Her-2/neu) and non-triple-negative tumors.
Table 3. Multivariate adjuvant therapy interaction analysis for event-free survival
Comparison P b (log HR) HRa (95% CI)
Therapy HD versus DD NS
Tumor size ‡3 versus <3 cm 0.04 0.39 1.48 (1.02–2.02)
ER Positive versus negative NS
PR Positive versus negative 0.04 20.43 0.65 (0.430.99)
Grade G 3 versus G1/2 <0.001 1.06 2.88 (1.76–4.73)
Her-2/neu Positive versus negative NS
MIB-1 Positive versus negative 0.01 0.56 1.75 (1.15–2.66)
EGFR Positive versus negative 0.06 20.64 0.53 (0.27–1.03)
Age £50 versus <50 years NS
Triple-negative status Triple negative versus others NS
Interaction: grade * therapy G3 and HD versus all others <0.001 21.60 0.20 (0.10–0.40)
Interaction: EGFR * therapy Positive and HD versus all others 0.005 1.91 6.76 (1.78–25.62)
Interaction: triple-negative status * therapy Triple and HD versus all others 0.030 20.98 0.38 (0.16–0.91)
HR, hazard ratio; CI, confidence interval; HD, E90C3000Thiotepa400 every 3 weeks; DD, C600M40F600 every 2 weeks; NS, non-significant; ER, estrogen receptor;
PR, progesterone receptor; EGFR, epidermal growth factor receptor; NS, not significant.
Annals of Oncology original article
Volume 19 |No. 5 |May 2008 doi:10.1093/annonc/mdm551 | 867
by guest on Decem
ber 18, 2015http://annonc.oxfordjournals.org/
Dow
nloaded from

Negative Her-2/neu status, however, correlates significantlywith benefit from HD, as reported by Rodenhuis et al. [7],who used a 25% lower cumulative anthracycline dose in the HDarm compared with the standard arm. The proposed explanationof this observation (as being due to associated Topo IIaamplification in Her-2/neu-positive disease as a target foranthracycline efficacy) was not confirmed in the recentlypublished study of Hannemann et al. [25]. Only 22% of thetumors in the Dutch study had coamplification of Topo IIaand Her-2/neu, and there were no survival differences betweenboth therapy groups in relation to Topo IIa status [25].In contrast to these results, patients with positive Her-2/neu
status and associated Topo IIa amplification (37%) had themost prolonged benefit from tailored dose-escalated 5-fluoruracil, epirubicine and cyclophosphamide compared withHD (cyclophosphamide, thiotepa and carboplatin) in thesubstudy of Tanner et al. [27] in 396 tumors (75%) from theScandinavian high-dose trial, where in the control arm themedian total anthracycline dose was 4.3 times higher than inthe HD arm. Several studies have identified positive Her-2/neustatus as a global marker, particularly for dose/schedule–response anthracycline sensitivity [21, 28] and for resistance toalkylating compounds [29], particularly in HD regimens inphase II trials [23, 30, 31]. A recently presented meta-analysis of5099 patients supports the conclusion of significant benefit ofanthracycline-based versus non-anthracycline-basedchemotherapy only in Her-2/neu-positive BC [32].Beyond trastuzumab, optimal chemotherapy regimens in
Her-2/neu-positive breast cancer and its combination withHD in HRBC [33] remain to be defined. In particular, furtherinvestigations of the impact of several cytotoxic agents andtheir interaction with Topo IIa are needed in Her-2/neu-positive HRBC, and this issue should preferentially beaddressed by randomized trials.In our study, young triple-negative (defined as ER, PR,
and Her-2/neu negative) patients benefited most from rapidlycycled tandem HD. This observation was confirmed atborderline significance by other research groups [25].Microarray and immunhistochemical studies as well ourrecent results of k-cluster analysis of protein profiling haveidentified triple-negative tumors as a biologically distinctbreast cancer entity, often associated with basal-like subtype[17, 26]. This subtype correlates with G3, p53 mutations,and poor prognosis [17, 26, 34], as well as with highersensitivity to neo-adjuvant chemotherapy [18, 35]. HDprovided an independent relative benefit in the triple-negativephenotype (as long as EGFR is negative) not attributable tothe association of grade with triple negativity. The finding ofa predictive impact of triple negativity is also remarkableconsidering the absence of a prognostic impact. Severalstudies have also identified it as a typical phenotype of BRCA1-associated tumors [36], especially in younger patients or inpatients with familiar history of breast cancer [37], whichare frequently associated with p53 mutations. Loss orinactivation of BRCA1 function is thought to be associatedwith sensitivity to DNA-damaging (e.g. alkylating)chemotherapy, which was used for dose intensification withinour study [38]. This association could be one hypotheticalexplanation for our results.
In our previous study, molecular classification has beenidentified as a very strong prognostic parameter, particularly inconventionally treated HRBC. Basal-like and Her-2/neusubtypes determined by k-clustering were strong predictorsfor poorer outcome [26], in line with other studies in HRBC[25]. HD efficacy was also more pronounced in thesesubtypes. No significant interaction between molecularsubtypes and dose intensification in HRBC has yet beenreported, possibly due to small subgroups. In contrast, bothtriple negativity and G3 status as assessed by standardclinical methodology were highly predictive for HD efficacyin HRBC, as shown in our study by interaction analysis. Thiseffect exceeds the predictive value of molecular subtypes forselection of patients for whom dose intensification could bewarranted. One possible explanation could be theheterogeneous biology within triple-negative breast cancer;these include a subset of nonbasal-like tumors, which arealso associated with proliferative patterns [39], but are negativefor basal markers (cytokeratin 5/6, vimentin, c-kit). Beforerobust and standardized subtyping using gene arrays isavailable, the immunhistochemical determination of triplenegativity in addition to routine tumor grade seems to befeasible for patient selection for dose-intense/dense regimensin clinical routine.In view of the clinical therapeutic challenges in management
of tumors with a triple-negative phenotype up to now, thefinding of a predictive impact of triple negativity bymultivariate interaction analysis with adjuvant HD versusDD therapy could have very important clinical consequences.The HD approach is intended to overcome somechemoresistance mechanisms and to target rapidly proliferatingtumor cells within a distinct molecular chemosensitivesubgroup and would provide further information fordefining of optimal chemotherapy regimen within triple-negative tumors.In EGFR-negative patients, either G3 or triple negativity
implies a benefit from HD. In EGFR-positive patients, who hadpoor outcome by multivariate analysis, a benefit from HD isapparent only for tumors (the large majority) that are bothtriple negative and G3. In view of the small numbers in thissubgroup and the methodological difficulties regarding EGFRtesting (e.g. determination activated/total expression) [40],our results, however, need to be substantiated before definiteconclusions are possible. Yet, our preliminary resultsindicate the need for additional targeted therapies, e.g. theuse of EGFR or multi-tyrosine kinase inhibitors in thissubgroup [41] particularly in combination with adequatechemotherapeutical options.In conclusion, tumor size, PR, and MIB-1 were identified as
independent prognostic factors in multivariate analysis withinour HRBC population for both EFS and OS. Age, tumor size,grade, HR, Her-2/neu, and EGFR status were predictive foreffects of HD with stem-cell support. All of the observed benefitfrom HD can be attributed to patients with triple-negativeand/or G3 tumors, as demonstrated by interaction analysis.Our results support design of randomized trials withina defined biological chemosensitive subtype, such as triple-negative breast cancer, and prospective implementation ofmolecular biological markers for HRBC.
original article Annals of Oncology
868 | Gluz et al. Volume 19 |No. 5 |May 2008
by guest on Decem
ber 18, 2015http://annonc.oxfordjournals.org/
Dow
nloaded from

authors contributions
Conception and design: OG, UAN, NH, SM, RD-D, RK, andCP. Financial support: UAN and NH. Administrative support:UAN, NH, and FW. Provision of study material or patients/collection of data: UAN, SM, GS, OG, RD-D, CJ, MF, WEB,BM, WL, and HK. Data analysis and interpretation: RK, OG,UAN, NH, AH, RD-D, CP, ET, SM, and MF. Manuscriptwriting: OG, UAN, NH, and RK. Final approval of manuscript:all authors.
acknowledgements
We thank all patients who participated in the trial andconsented to give their data. We thank all investigators fortreating the patients and reporting their data and allpathologists provided tumor material of study patients to thecentral tumor bank.Furthermore, we thank H. G. Bender for his support within
the Department of Gynaecology and Obstetrics and H. E.Gabbert for his support within the Department of Pathologyof the University of Duesseldorf.
references
1. Fisher B, Bauer M, Wickerham DL et al. Relation of number of positive axillary
nodes to the prognosis of patients with primary breast cancer. An NSABP
update. Cancer 1983; 52 (9): 1551–1557.
2. Montero AJ, Rouzier R, Lluch A et al. The natural history of breast carcinoma in
patients with > or = 10 metastatic axillary lymph nodes before and after the
advent of adjuvant therapy: a multiinstitutional retrospective study. Cancer 2005;
104 (2): 229–235.
3. Early Breast Cancer Trialists’ Collaborative Group and EBCTCG. Effects of
chemotherapy and hormonal therapy for early breast cancer on recurrence and
15-year survival: an overview of the randomised trials. Lancet 2005; 365 (9472):
1687–1717.
4. Buzdar AU, Kau SW, Hortobagyi GN et al. Clinical course of patients with breast
cancer with ten or more positive nodes who were treated with doxorubicin-
containing adjuvant therapy. Cancer 1992; 69 (2): 448–452.
5. Rodenhuis S, Bontenbal M, Beex LV et al. High-dose chemotherapy with
hematopoetic stem-cell rescue for high risk breast cancer. N Engl J Med 2003;
349 (1): 7–16.
6. Tallman MS, Gray R, Robert NJ et al. Conventional adjuvant chemotherapy with
or without high-dose chemotherapy and autologous stem-cell transplantation in
high-risk breast cancer. N Engl J Med 2003; 349 (1): 17–26.
7. Rodenhuis S, Bontenbal M, van Hoesel QG et al. Efficacy of high-dose alkylating
chemotherapy in HER2/neu-negative breast cancer. Ann Oncol 2006; 17 (4):
588–596.
8. Roche H, Viens P, Biron P et al. High-dose chemotherapy for breast cancer: the
French PEGASE experience. Cancer Control 2003; 10 (1): 42–47.
9. Nitz U, Mohrmann S, Fischer J et al. Comparison of rapidly cycled tandem high-
dose chemotherapy plus peripheral-blood stem-cell support versus dose-dense
conventional chemotherapy for adjuvant treatment of high-risk breast cancer:
results of a multicentre phase III trial. Lancet 2005; 366 (9501): 1935–1944.
10. Zander AR, Kroeger N, Schmoor C et al. High-dose chemotherapy with
autologous hematopoietic stem-cell support compared with standard-dose
chemotherapy in breast cancer patients with 10 or more positive lymph nodes:
first results of a randomized trial. J Clin Oncol 2004; 22 (12): 2273–2283.
11. Basser RL, O’Neill A, Martinelli G et al. Multicycle dose-intensive chemotherapy
for women with high-risk primary breast cancer: results of International Breast
Cancer Study Group Trial 15-95. J Clin Oncol 2006; 24 (3): 370–378.
12. Leonard R, Lind M, Twelves C et al. Conventional adjuvant chemotherapy versus
single-cycle, autograft-supported, high-dose, late-intensification chemotherapy
in high-risk breast cancer patients: a randomized trial. J Natl Cancer Inst 2004;
96 (14): 1076–1083.
13. Peters W, Rosner GL, Vredenburgh JJ et al. Prospective, randomized comparison
of high-dose chemotherapy with stem-cell support versus intermediate-dose
chemotherapy after surgery and adjuvant chemotherapy in women with high-
risk primary breast cancer: a report of CALGB 9082, SWOG 9114, and NCIC
MA-13. J Clin Oncol 2005; 23 (10): 2191–2200.
14. Faneyte IF, Peterse JL, Van Tinteren H et al. Predicting early failure after adjuvant
chemotherapy in high-risk breast cancer patients with extensive lymph node
involvement. Clin Cancer Res 2004; 10 (13): 4457–4463.
15. Nieto Y, Nawaz S, Shpall EJ et al. Long-term analysis and prospective validation
of a prognostic model for patients with high-risk primary breast cancer receiving
high-dose chemotherapy. Clin Cancer Res 2004; 10 (8): 2609–2617.
16. Kroger N, Milde-Langosch K, Riethdorf S et al. Prognostic and predictive
effects of immunohistochemical factors in high-risk primary breast cancer
patients. Clin Cancer Res 2006; 12 (1): 159–168.
17. Perou CM, Sorlie T, Eisen MB et al. Molecular portraits of human breast tumours.
Nature 2000; 406 (6797): 747–752.
18. Rouzier R, Perou CM, Symmans WF et al. Breast cancer molecular subtypes
respond differently to preoperative chemotherapy. Clin Cancer Res 2005; 11
(16): 5678–5685.
19. Colleoni M, Viale G, Zahrieh D et al. Chemotherapy is more effective in patients
with breast cancer not expressing steroid hormone receptors: a study of
preoperative treatment. Clin Cancer Res 2004; 10 (19): 6622–6628.
20. Berry DA, Cirrincione C, Henderson IC et al. Estrogen-receptor status and
outcomes of modern chemotherapy for patients with node-positive breast
cancer. JAMA 2006; 295 (14): 1658–1667.
21. Venturini M, Del Mastro L, Aitini E et al. Dose-dense adjuvant chemotherapy
in early breast cancer patients: results from a randomized trial. J Natl Cancer Inst
2005; 97 (23): 1724–1733.
22. Bergh J, Wiklund T, Erikstein B et al. Tailored fluorouracil, epirubicin and
cyclophosphamide compared with marrow-supported high-dose chemotherapy
as adjuvant treatment for high-risk breast cancer: a randomised trial. Lancet
2000; 356 (9239): 1384–1391.
23. Somlo G, Simpson JF, Frankel P et al. Predictors of long-term outcome following
high-dose chemotherapy in high-risk primary breast cancer. Br J Cancer 2002;
87 (3): 281–288.
24. Gianni AM, Bonadonna G. Updated 12-year results of the randomized clinical
trial comparing standard versus high-dose myeloablative chemotherapy in the
adjuvant treatment of breast cancer with >3 positive nodes (LN+). Cooperative
Group 2007 ASCO Annual Meeting Proceedings (Post-Meeting Edition) 2007; 25
(18 Suppl): (Abstr 549).
25. Hannemann J, Hannemann J, Kristel P et al. Molecular subtypes of breast cancer
and amplification of topoisomerase II alpha: predictive role in dose intensive
adjuvant chemotherapy. Br J Cancer 2006; 95 (10): 1334–1341.
26. Diallo-Danebrock R, Ting E, Gluz O et al. Protein expression profiling in high-risk
breast cancer patients treated with high-dose or conventional dose-dense
chemotherapy. Clin Cancer Res 2007; 13 (2): 488–497.
27. Tanner M, Isola J, Wiklund T et al. Topoisomerase IIalpha gene amplification
predicts favorable treatment response to tailored and dose-escalated anthracycline-
based adjuvant chemotherapy in HER-2/neu-amplified breast cancer:
Scandinavian Breast Group Trial 9401. J Clin Oncol 2006; 24 (16): 2428–2436.
28. Thor AD, Berry DA, Budman DR et al. erbB-2, p53, and efficacy of adjuvant
therapy in lymph node-positive breast cancer. J Natl Cancer Inst 1998; 90 (18):
1346–1360.
29. Paik S, Bryant J, Tan-Chiu E et al. HER2 and choice of adjuvant
chemotherapy for invasive breast cancer: National Surgical Adjuvant Breast and
Bowel Project Protocol B-15. J Natl Cancer Inst 2000; 92 (24): 1991–1998.
30. Nieto Y, Cagnoni PJ, Nawaz S et al. Evaluation of the predictive value of Her-2/
neu overexpression and p53 mutations in high-risk primary breast cancer
patients treated with high-dose chemotherapy and autologous stem-cell
transplantation. J Clin Oncol 2000; 18 (10): 2070–2080.
31. Hensel M, Schneeweiss A, Sinn HP et al. P53 is the strongest predictor of
survival in high-risk primary breast cancer patients undergoing high-dose
Annals of Oncology original article
Volume 19 |No. 5 |May 2008 doi:10.1093/annonc/mdm551 | 869
by guest on Decem
ber 18, 2015http://annonc.oxfordjournals.org/
Dow
nloaded from

chemotherapy with autologous blood stem cell support. Int J Cancer 2002; 100
(3): 290–296.
32. Gennari A, Sormani M, Puntoni M et al. A pooled analysis on the interaction
between HER-2 expression and responsiveness of breast cancer to
adjuvant chemotherapy. Breast Cancer Res Treat 2006; 100 (Suppl 1):
(Abstr 41).
33. Nieto Y, Vredenburgh JJ, Shpall EJ et al. Phase II feasibility and pharmacokinetic
study of concurrent administration of trastuzumab and high-dose
chemotherapy in advanced HER2+ breast cancer. Clin Cancer Res 2004;
10 (21): 7136–7143.
34. Sorlie T, Tibshirani R, Parker J et al. Repeated observation of breast tumor
subtypes in independent gene expression data sets. Proc Natl Acad Sci U S A
2003; 100 (14): 8418–8423.
35. Carey LA, Dees EC, Sawyer L et al. The triple negative paradox: primary tumor
chemosensitivity of breast cancer subtypes. Clin Cancer Res 2007; 13 (8):
2329–2334.
36. Lakhani SR, Van De Vijver MJ, Jacquemier J et al. The pathology of familial
breast cancer: predictive value of immunohistochemical markers estrogen
receptor, progesterone receptor, HER-2, and p53 in patients with mutations in
BRCA1 and BRCA2. J Clin Oncol 2002; 20 (9): 2310–2318.
37. Kandel MJ, Stadler Z, Masciari S et al. Prevalence of BRCA1 mutations in triple
negative breast cancer (BC). In Proceedings of the Annual Meeting of American
Society of Clinical Oncology, 2006; 24 (18 Suppl): (Abstr 508).
38. Kennedy RD, Quinn JE, Mullan PB et al. The role of BRCA1 in the cellular
response to chemotherapy. J Natl Cancer Inst 2004; 96 (22): 1659–1668.
39. Rakha E, El-Sayed M, Green A et al. Prognostic markers in triple-negative breast
cancer. Cancer 2007; 109 (1): 25–32.
40. Nicholson RI, Gee JM, Harper ME. EGFR and cancer prognosis. Eur J Cancer
2001; 37 (Suppl 4): S9–S15.
41. Huang F, Reeves K, Han X et al. Identification of candidate molecular markers
predicting sensitivity in solid tumors to dasatinib: rationale for patient selection.
Cancer Res 2007; 67 (5): 2226–2238.
original article Annals of Oncology
870 | Gluz et al. Volume 19 |No. 5 |May 2008
by guest on Decem
ber 18, 2015http://annonc.oxfordjournals.org/
Dow
nloaded from
Copyright © 2022 FDOKUMEN