
Analysis of trends and prospects regarding stents for human ...
Upload
independentCategory
view
3download
0
European Heart Journal (2004) 25, 920–925
Clinical research
Treatment of in-stent restenosis using apaclitaxel-eluting stent: acute results andlong-term follow-up of a matched-pair comparisonwith intracoronary b-radiation therapy
http://eurheD
ownloaded from
Peter W. Radkea,*, Stefan Kobellaa, Axel Kaisera, Andreas Frankea,Daniela Schubertb, Eberhard Grubec, Peter Hanratha, Rainer Hoffmanna
a Medical Clinic I, RWTH University Hospital, Pauwelsstraße 30, 52057 Aachen, Germanyb Department of Radio-Oncology, University Hospital of Aachen, Aachen, Germanyc Heart Centre Siegburg, Siegburg, Germany
Received 30 October 2003; revised 5 February 2004; accepted 13 February 2004Available online 17 April 2004
See Page 898 for the editorial comment on this article�
by guest on June 2, 2013artj.oxfordjournals.org/
Aims Intracoronary radiation therapy (ICR) has significantly improved the long-termoutcome after treatment of diffuse in-stent restenosis (ISR). The efficacy of drugeluting stents in this setting remains less well defined. This matched-pair analysiscompared the procedural and long-term clinical and angiographic outcome aftertreatment of diffuse ISR using a paclitaxel-eluting stent (PES) with intracoronary b-radiation therapy.Methods and Results Twenty-two patients receiving 25 PES (ACHIEVETM, Cook, 3.1 lgpaclitaxel per square millimeter, non-polymer based coating) for ISR underwent 6-month angiographic and 12-month clinical follow-up. From a database including 141patients (174 lesions) undergoing intracoronary b-radiation for ISR, 25 lesions (25patients) were pair-matched with the former group for lesion length and vessel size.PES implantation and ICR were successfull in all patients with a significantly lowerpostprocedural in-stent diameter stenosis in the PES group (8± 12% vs. 18± 8%,p < 0:01). Angiographic binary in-lesion restenosis at 6 month was 20% (5/25 lesions)in the PES group and 16% (4/25) in the ICR group (p ¼ 1:0). PES implantation resultedin significantly higher in-stent MLD at FU (2.10± 0.71 vs. 1.75± 0.36, p ¼ 0:03) and ahigher in-stent net gain (PES: 1.19± 0.69, ICR: 0.84± 0.49, p ¼ 0:04). Two patientsin the PES group and 6 patients in the ICR group experienced a target lesion revas-cularisation at 12-month follow-up (p ¼ 0:25).Conclusion Implantation of a non-polymer based paclitaxel-elution stent and con-ventional ICR therapy for complex ISR lead to comparable acute and long-termclinical and angiographic follow-up results.
�c 2004 The European Society of Cardiology. Published by Elsevier Ltd. All rightsreserved.
KEYWORDSStent;
Restenosis;
Brachytherapy;
Drug-eluting stent;
Paclitaxel
* Corresponding author. Tel.: þ49-241-8089301; fax: þ49-241-8880209.
E-mail address: [email protected] (P.W. Radke).� doi:10.1016/j.ehj.2004.04.008.
0195-668X/$ - see front matter �c 2004 The European Society of Cardiology. Published by Elsevier Ltd. All rights reserved.doi:10.1016/j.ehj.2004.02.014
Treatment of in-stent restenosis using a paclitaxel-eluting stent 921
Introduction
The prevention and treatment of in-stent restenosis (ISR)remain among the most challenging problems in inter-ventional cardiology. The introduction of drug-elutingstents has significantly reduced the incidence of ISR ascompared to bare metal stents in de novo lesions.1;2
Regarding the treatment of ISR, intracoronary radiationtherapy (ICR) seems to be the only modality to effec-tively reduce the rate of recurrent restenosis.3 Radiationtherapy, however, has potential side effects and requiresa specific infrastructure.4;5 The efficacy of drug-elutingstents for the treatment of ISR lesions remains less wellestablished. This study compared the acute procedural,6-month angiographic, and 1-year clinical follow-upresults after treatment of diffuse ISR using paclitaxel-eluting stents (PES) with intracoronary b-radiation ther-apy in a matched-pair analysis.
by gueshttp://eurheartj.oxfordjournals.org/
Dow
nloaded from
Methods
Patients and procedures
Forty-seven symptomatic patients (60± 11 years, 79% male)presenting with 50 ISR lesions (>50% diameter stenosis) in nativecoronary arteries treated at the Aachen University Hospitalformed the study population.
Initially, 27 consecutive lesions in 24 patients were treatedwith a PES (AchieveTM, Cook, 3.1 lg paclitaxel per squaremillimeter, non-polymer-based coating). These patients wererecruited from the DELIVER II trial, a prospective, non-rando-mised, multicentre, consecutive enrolment study evaluatingnon-polymer PES in the treatment of patients with lesions athigh risk for revascularisation. The primary study endpoint wastarget-lesion revascularisation at 180 days. For the purpose ofthis comparative study, all patients underwent 6-month angio-graphic and 12-month clinical follow-up assessment. Inclusion
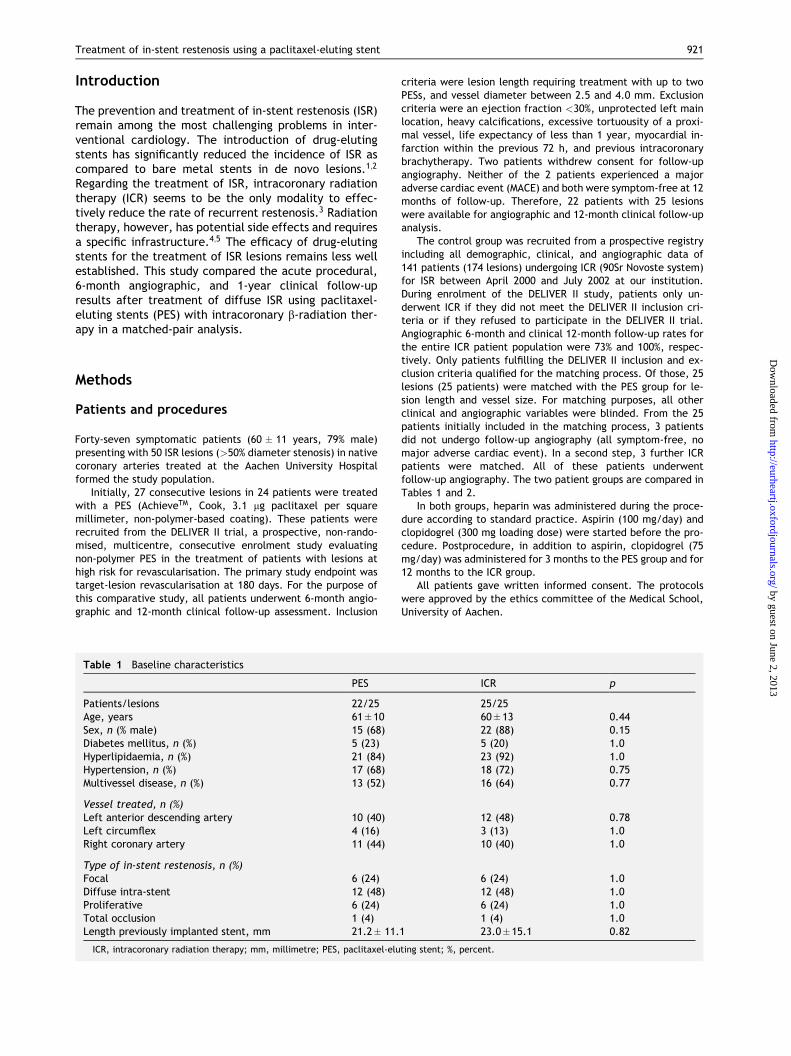
Table 1 Baseline characteristics
PES
Patients/lesions 22/25Age, years 61±10Sex, n (% male) 15 (68)Diabetes mellitus, n (%) 5 (23)Hyperlipidaemia, n (%) 21 (84)Hypertension, n (%) 17 (68)Multivessel disease, n (%) 13 (52)
Vessel treated, n (%)Left anterior descending artery 10 (40)Left circumflex 4 (16)Right coronary artery 11 (44)
Type of in-stent restenosis, n (%)Focal 6 (24)Diffuse intra-stent 12 (48)Proliferative 6 (24)Total occlusion 1 (4)Length previously implanted stent, mm 21.2± 11.
ICR, intracoronary radiation therapy; mm, millimetre; PES, paclitaxel-elu
criteria were lesion length requiring treatment with up to twoPESs, and vessel diameter between 2.5 and 4.0 mm. Exclusioncriteria were an ejection fraction <30%, unprotected left mainlocation, heavy calcifications, excessive tortuousity of a proxi-mal vessel, life expectancy of less than 1 year, myocardial in-farction within the previous 72 h, and previous intracoronarybrachytherapy. Two patients withdrew consent for follow-upangiography. Neither of the 2 patients experienced a majoradverse cardiac event (MACE) and both were symptom-free at 12months of follow-up. Therefore, 22 patients with 25 lesionswere available for angiographic and 12-month clinical follow-upanalysis.
The control group was recruited from a prospective registryincluding all demographic, clinical, and angiographic data of141 patients (174 lesions) undergoing ICR (90Sr Novoste system)for ISR between April 2000 and July 2002 at our institution.During enrolment of the DELIVER II study, patients only un-derwent ICR if they did not meet the DELIVER II inclusion cri-teria or if they refused to participate in the DELIVER II trial.Angiographic 6-month and clinical 12-month follow-up rates forthe entire ICR patient population were 73% and 100%, respec-tively. Only patients fulfilling the DELIVER II inclusion and ex-clusion criteria qualified for the matching process. Of those, 25lesions (25 patients) were matched with the PES group for le-sion length and vessel size. For matching purposes, all otherclinical and angiographic variables were blinded. From the 25patients initially included in the matching process, 3 patientsdid not undergo follow-up angiography (all symptom-free, nomajor adverse cardiac event). In a second step, 3 further ICRpatients were matched. All of these patients underwentfollow-up angiography. The two patient groups are compared inTables 1 and 2.
In both groups, heparin was administered during the proce-dure according to standard practice. Aspirin (100 mg/day) andclopidogrel (300 mg loading dose) were started before the pro-cedure. Postprocedure, in addition to aspirin, clopidogrel (75mg/day) was administered for 3 months to the PES group and for12 months to the ICR group.
All patients gave written informed consent. The protocolswere approved by the ethics committee of the Medical School,University of Aachen.
ICR p
25/2560±13 0.4422 (88) 0.155 (20) 1.023 (92) 1.018 (72) 0.7516 (64) 0.77
12 (48) 0.783 (13) 1.010 (40) 1.0
6 (24) 1.012 (48) 1.06 (24) 1.01 (4) 1.0
1 23.0±15.1 0.82
ting stent; %, percent.
t on June 2, 2013
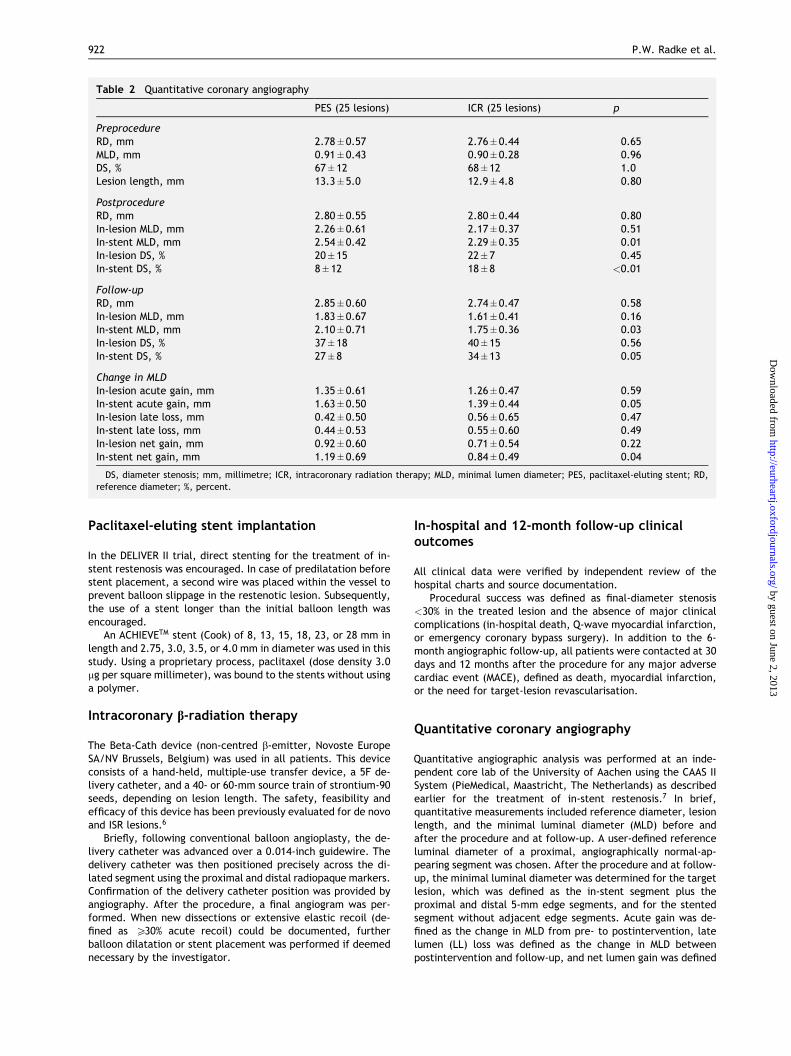
Table 2 Quantitative coronary angiography
PES (25 lesions) ICR (25 lesions) p
PreprocedureRD, mm 2.78±0.57 2.76±0.44 0.65MLD, mm 0.91±0.43 0.90±0.28 0.96DS, % 67±12 68±12 1.0Lesion length, mm 13.3±5.0 12.9±4.8 0.80
PostprocedureRD, mm 2.80±0.55 2.80±0.44 0.80In-lesion MLD, mm 2.26±0.61 2.17±0.37 0.51In-stent MLD, mm 2.54±0.42 2.29±0.35 0.01In-lesion DS, % 20±15 22±7 0.45In-stent DS, % 8±12 18±8 <0.01
Follow-upRD, mm 2.85±0.60 2.74±0.47 0.58In-lesion MLD, mm 1.83±0.67 1.61±0.41 0.16In-stent MLD, mm 2.10±0.71 1.75±0.36 0.03In-lesion DS, % 37±18 40±15 0.56In-stent DS, % 27±8 34±13 0.05
Change in MLDIn-lesion acute gain, mm 1.35±0.61 1.26±0.47 0.59In-stent acute gain, mm 1.63±0.50 1.39±0.44 0.05In-lesion late loss, mm 0.42±0.50 0.56±0.65 0.47In-stent late loss, mm 0.44±0.53 0.55±0.60 0.49In-lesion net gain, mm 0.92±0.60 0.71±0.54 0.22In-stent net gain, mm 1.19±0.69 0.84±0.49 0.04
DS, diameter stenosis; mm, millimetre; ICR, intracoronary radiation therapy; MLD, minimal lumen diameter; PES, paclitaxel-eluting stent; RD,reference diameter; %, percent.
922 P.W. Radke et al.
by guest on June 2, 2013http://eurheartj.oxfordjournals.org/
Dow
nloaded from
Paclitaxel-eluting stent implantation
In the DELIVER II trial, direct stenting for the treatment of in-stent restenosis was encouraged. In case of predilatation beforestent placement, a second wire was placed within the vessel toprevent balloon slippage in the restenotic lesion. Subsequently,the use of a stent longer than the initial balloon length wasencouraged.
An ACHIEVETM stent (Cook) of 8, 13, 15, 18, 23, or 28 mm inlength and 2.75, 3.0, 3.5, or 4.0 mm in diameter was used in thisstudy. Using a proprietary process, paclitaxel (dose density 3.0lg per square millimeter), was bound to the stents without usinga polymer.
Intracoronary b-radiation therapy
The Beta-Cath device (non-centred b-emitter, Novoste EuropeSA/NV Brussels, Belgium) was used in all patients. This deviceconsists of a hand-held, multiple-use transfer device, a 5F de-livery catheter, and a 40- or 60-mm source train of strontium-90seeds, depending on lesion length. The safety, feasibility andefficacy of this device has been previously evaluated for de novoand ISR lesions.6
Briefly, following conventional balloon angioplasty, the de-livery catheter was advanced over a 0.014-inch guidewire. Thedelivery catheter was then positioned precisely across the di-lated segment using the proximal and distal radiopaque markers.Confirmation of the delivery catheter position was provided byangiography. After the procedure, a final angiogram was per-formed. When new dissections or extensive elastic recoil (de-fined as P30% acute recoil) could be documented, furtherballoon dilatation or stent placement was performed if deemednecessary by the investigator.
In-hospital and 12-month follow-up clinicaloutcomes
All clinical data were verified by independent review of thehospital charts and source documentation.
Procedural success was defined as final-diameter stenosis<30% in the treated lesion and the absence of major clinicalcomplications (in-hospital death, Q-wave myocardial infarction,or emergency coronary bypass surgery). In addition to the 6-month angiographic follow-up, all patients were contacted at 30days and 12 months after the procedure for any major adversecardiac event (MACE), defined as death, myocardial infarction,or the need for target-lesion revascularisation.
Quantitative coronary angiography
Quantitative angiographic analysis was performed at an inde-pendent core lab of the University of Aachen using the CAAS IISystem (PieMedical, Maastricht, The Netherlands) as describedearlier for the treatment of in-stent restenosis.7 In brief,quantitative measurements included reference diameter, lesionlength, and the minimal luminal diameter (MLD) before andafter the procedure and at follow-up. A user-defined referenceluminal diameter of a proximal, angiographically normal-ap-pearing segment was chosen. After the procedure and at follow-up, the minimal luminal diameter was determined for the targetlesion, which was defined as the in-stent segment plus theproximal and distal 5-mm edge segments, and for the stentedsegment without adjacent edge segments. Acute gain was de-fined as the change in MLD from pre- to postintervention, latelumen (LL) loss was defined as the change in MLD betweenpostintervention and follow-up, and net lumen gain was defined

Treatment of in-stent restenosis using a paclitaxel-eluting stent 923
as the change in MLD from preintervention to follow-up. In-stentrestenosis was classified as previously described.8 Recurrentrestenosis was defined as diameter stenosis P50% within thetarget lesion at follow-up angiography.
Statistical analysis
Due to the exploratory nature of this study, no adjustments tothe significance level were made. Data were not normally dis-tributed, but departures from the normality assumption weremodest. All continuous data are presented as mean± SD for theconvenience of the reader. All tests were two-sided. Compari-sons between groups were performed with the paired Student ttest for continuous variables. Qualitative data are presented asfrequencies and quantitative data were compared using Fisher’sexact test. A p-value of <0.05 was considered statisticallysignificant.
by guest on June 2, 2013http://eurheartj.oxfordjournals.org/
Dow
nloaded from
Results
Patient characteristics
A comparison of the two patient populations is providedin Tables 1 and 2. Both groups were well balanced forlesion length and vessel size as a result of the matchingprocess. In addition, further preprocedural angiographicvariables, demographic data, type of ISR, and length ofthe primarily implanted stent were also comparable.Seventy-six percent lesions in either group were classi-fied as “diffuse.”
In the PES group, predilatation was performed in 20lesions and direct stenting in 5 lesions. Four lesions (16%)were each treated with 2 paclitaxel-eluting stents.
In the ICR group, the mean prescribed dose was21.1± 3.1 Gy at a distance of 2 mm from the radiationsource (range 16.0–25.3 Gy); the dwell time was 228±45 s. Atheroablative techniques and the cutting balloonwere not used. Three patients (12%) received an addi-tional bare-metal stent at the stent margins due todissection.
Clinical outcome
Clinical 30-day and 12-month follow-up data wereavailable for all patients. The procedural success was100% and there was no MACE at 30 days in both groups.No subacute stent thrombosis occurred in either group.During the 12-month follow-up, 2/22 (9%) patients in thePES group and 6/25 (24%) patients in the ICR group ex-perienced a MACE due to recurrent restenosis (all target-lesion revascularisations, p ¼ 0:25). One of the patientsundergoing ICR and receiving additional stents at themargins experienced a MACE due to recurrent restenosis(85% diameter stenosis at angiographic follow-up) andsubsequent target-lesion revascularisation. There wereno deaths and no myocardial infarctions.
Angiographic outcome
All 47 patients underwent 6-month follow-up angiogra-phy (100%, Table 2). Binary restenosis was documented
in 5/25 lesions (20%) treated with a PES and in 4/25 le-sions (16%) receiving ICR (p ¼ 1:0). Paclitaxel-elutingstent implantation lead to a higher postproceduralin-stent lumen diameter (2.54± 0.42 vs. 2.29± 0.35,p ¼ 0:01) and less in-stent diameter stenosis (8± 12 vs.18± 8, p < 0:01). With a comparable late lumen loss inboth treatment groups, this resulted in a significantlyhigher in-stent minimal lumen diameter (2.10± 0.71 vs.1.75± 0.36, p ¼ 0:03) and a higher net lumen gain(1.19± 0.69 vs. 0.84± 0.49, p ¼ 0:04) in the PES group.
Discussion
This study compared a non-polymer-based paclitaxel-eluting stent (PES) with intracoronary b-radiation for thetreatment of complex ISR.
Recent reports have suggested beneficial effects ofsirolimus9;10 and paclitaxel-eluting stents11 in the treat-ment of ISR. At present, however, only intracoronaryradiation therapy has been shown to effectively reducethe incidence of recurrent ISR.3;12 Intracoronary radia-tion therapy, however, requires a specific infrastructureand carries the risk of potentially fatal side effects (i.e.,late thrombosis5) Given the ease of use and availabilityof drug-eluting stents, they are likely to become thepredominant treatment for diffuse in-stent restenosis,even when angiographic and clinical results obtained arecomparable to ICR. Despite a lack of randomised trialsthus far, this matched-pair analysis provides furthersupport for the potential benefit of drug-eluting stents inthe treatment of ISR.
This study was neither randomised nor powered todetect clinical treatment differences. In the PES group,however, the MACE rate was very low (9%). It is inter-esting that the clinical event rate in the TAXUS III studyusing a polymer-bound, paclitaxel-eluting stent for thetreatment of diffuse in-stent restenosis was higher thanin this series (29%). Differences in study populations(i.e., 18% bypass interventions in the TAXUS III study) anda higher proportion of patient in TAXUS III receiving 2 ormore stents (46% vs. 16%) probably account for this.Notably, the size of the study population in both trialswas relatively small.
Clinical long-term follow-up in this study identifiedonly 2 PES patients who experienced a MACE (both tar-get-lesion revascularisation). Both patients showed an-giographic restenosis at 6 months of follow-up and eventsoccurred in the first 7 months after the index procedure(5 and 7 months, respectively). In the ICR group, how-ever, 4 patients with angiographic restenosis at 6 monthswere identified. Of those, 3 patients had to undergotarget-lesion revascularisation and 1 patient showed anon-significant 60% stenosis. In addition, 3 further pa-tients without angiographic restenosis at 6 months offollow-up required target-lesion revascularisation due todelayed restenosis in the first year after the index pro-cedure (10–12 months). Indeed, recent preclinical datasuggest that clonogenic inactivation is the mechanism bywhich radiation therapy significantly delays the recur-rence of ISR rather than completely preventing this

924 P.W. Radke et al.
by guest on June 2, 2013http://eurheartj.oxfordjournals.org/
Dow
nloaded from
process.13 These findings are further supported by clini-cal observations showing a late catch-up phenomenon inpatients undergoing ICR for ISR.14 Of note, this phe-nomenon has also been described in a paclitaxel-deri-vate-eluting polymer stent system (QuaDS),15 but wasnot observed in this study using a paclitaxel-eluting (non-polymer-based coating) stent. Clearly, this observationunderscores the complexity of drug-eluting stent sys-tems. Both the drug carrier systems (i.e., polymers) andthe antiproliferative substances used (i.e., paclitaxel,paclitaxel-derivatives, sirolimus) determine the thera-peutic potential of the stent system to reduce/suppressneointimal hyperplasia.
Regarding the clinical long-term outcome, PES im-plantation not only compares favourably to the matchedICR group (24% MACE), but also to (1) previously reporteddata from randomised trials using b- and c-radiation(15–28% MACE3;12) and to (2) stent-in-stent therapy usinguncoated stents (22–44% MACE16).
The angiographic analysis showed a significantly lowerpostprocedural in-stent diameter stenosis in the PESgroup compared to the ICR group (8± 12% vs. 18± 8%,p < 0:01). This observation deserves special attention asa recent meta- regression analysis has revealed thatpostprocedural diameter stenosis is the strongest pre-dictor of the frequency of MACE in patients undergoingtreatment for in-stent restenosis.16 This may not applyfor ICR as a recent report has suggested that the residualstenosis after angioplasty preceding ICR does not affectclinical outcome, at least until 6 months after theprocedure.17
In-lesion angiographic analyses did not show differ-ences between treatment groups. A significant edge-stenosis phenomenon, however, was not observed in thePES group. As a result of small patient numbers, theadvantageous procedural result for the PES group prob-ably did not translate into a superior long-term outcomein this study. Of note, previous studies have also shownbetter postprocedural lumen dimensions using the stent-in-stent technique as compared to balloon angioplastyalone.18
Lumen loss, as a surrogate for the amount of recurrentneointimal hyperplasia, was 0.44± 0.53 mm in the PESgroup and, thus, comparable to the ICR group(0.55± 0.60 mm). In addition, these data are also well inline with the findings of large ICR trials (i.e., 0.44± 0.69mm in the INHIBIT trial3) or recently published data usinga slow-release, polymer-bound, paclitaxel-coated stent(0.54± 0.51 mm11).
As the implantation of additional stents should beminimised when using ICR due to an increased rate ofadverse events,12;19 PES implantation for ISR seems toparticularly benefit from improved procedural results incombination with antiproliferative effects, leading to asignificantly higher in-stent net lumen gain in this study.
Finally, this study has intrinsic limitations. First, thestudy was not randomised, but both study groups wererecruited from prospective registries with prespecifiedendpoints. Furthermore, the group sizes are relativelysmall. The next level of evidence supporting the use ofdrug-eluting stents for the treatment of in-stent reste-
nosis, however, will likely be obtained by randomisedstudies rather than an increase in patient populations ofcase-control studies. Intravascular ultrasound was notroutinely performed during the procedures. Therefore,further information regarding the mechanism of acutelumen gain and recurrent restenosis in the PES group isnot available.
In summary, PES implantation combines advantageousprocedural results with a low late lumen loss. Eventhough total patient numbers treated with drug-elutingstents for diffuse ISR are small at the moment, thesefavourable mechanistic results clearly warrant reason-ably powered randomised trials with clinically relevantendpoints. If comparable results are confirmed, drug-eluting stents may become the preferred treatmentmodality for patients with diffuse in-stent restenosis.
Acknowledgements
The expert statistical assistance of Robert Kwiecien,PhD, Institute for Medical Statistics, University Hospitalof Aachen, is gratefully acknowledged.
References
1. Morice MC, Serruys PW, Sousa JE et al. A randomized comparison of asirolimus-eluting stent with a standard stent for coronary revascu-larization. N Engl J Med 2002;346:1773–80.
2. Park SJ, Shim WH, Ho DS et al. A paclitaxel-eluting stent for theprevention of coronary restenosis. N Engl J Med 2003;348:1537–45.
3. Waksman R, Rainzer AE, Yeung A et al. Use of localised intracoronaryb-radiation in treatment of in-stent restenosis: the INHIBIT rando-mised controlled trial. Lancet 2002;359:551–7.
4. Sabate M, Costa MA, Kozuma K et al. Geographic miss: a cause oftreatment failure in radio-oncology applied to intracoronary radia-tion therapy. Circulation 2000;101:2467–71.
5. Costa MA, Sabate M, van der Giessen WJ et al. Late coronaryocclusion after intracoronary brachytherapy. Circulation1999;100:789–92.
6. Latchem DR, Urban P, Goy JJ et al. Beta-radiation for coronary in-stent restenosis. Cathet Cardiovasc Intervent 2000;51:422–9.
7. Radke PW, Klues HG, Haager PK et al. Mechanisms of acute lumengain and recurrent restenosis after rotational atherectomy of diffusein-stent restenosis: a quantitative angiographic and intravascularultrasound study. J Am Coll Cardiol 1999;34:33–9.
8. Mehran R, Dangas G, Abizaid AS et al. Angiographic patterns of in-stent restenosis: classification and implications for long-term out-come. Circulation 1999;100:1872–8.
9. Degertekin M, Regar E, Tanabe K et al. Sirolimus-eluting stent fortreatment of complex in-stent restenosis. J Am Coll Cardiol2003;41:184–9.
10. Sousa JE, Costa MA, Abizaid A et al. Sirolimus-eluting stent for thetreatment of in-stent restenosis: a quantitative coronary angiographyand three-dimensional intravascular ultrasound study. Circulation2003;107:24–7.
11. Tanabe K, Serruys PW, Grube E et al. TAXUS III Trial. In-stentrestenosis treated with stent-based delivery of paclitaxel incorpo-rated in a slow-release polymer formulation. Circulation2003;107:559–64.
12. Leon MB, Teirstein PS, Moses JW et al. Localized intracoronarygamma-radiation therapy to inhibit the recurrence of restenosis afterstenting. N Engl J Med 2001;344:250–6.
13. Brenner DJ, Miller RC. Long-term efficacy of intracoronary irradiationin inhibiting in-stent restenosis. Circulation 2001;103:1330–2.
14. Regar E, Kozuma K, Sianos G et al. Routine intracoronary beta-irradiation. Acute and one year outcome in patients at high risk forrecurrence of stenosis. Eur Heart J 2002;23:1038–44.

Treatment of in-stent restenosis using a paclitaxel-eluting stent 925
15. Liistro F, Stankovic G, Di Mario C et al. First clinical experience with apaclitaxel derivate-eluting polymer stent system implantation for in-stent restenosis. Immediate and long-term clinical and angiographicoutcome. Circulation 2002;105:1883–6.
16. Radke PW, Kaiser A, Frost C et al. Outcome after treatment ofcoronary in-stent restenosis: results from a systematic review usingmeta-analysis techniques. Eur Heart J 2003;24:266–73.
17. Chenau E, Ajani AE, Leborgne L et al. Relation of residual stenosisafter angioplasty to long-term outcome of patients treated for in-
stent restenosis with intravascular radiation therapy. Am J Cardiol2002;89:1426–8.
18. Elezi S, Kastrati A, Hadamitzky M et al. Clinical and angiographicfollow-up after balloon angioplasty with provisional stenting forcoronary in-stent restenosis. Catheter Cardiovasc Interv 1999;48:151–6.
19. Cha DH, Malik IA, Cheneau E et al. Use of restenting should beminimized with intracoronary radiation therapy for in-stent resteno-sis. Catheter Cardiovasc Interv 2003;59:6–7.
by guest on June 2, 2013http://eurheartj.oxfordjournals.org/
Dow
nloaded from
Copyright © 2022 FDOKUMEN


















![[Characteristics of encrustation of ureteric stents in patients with urinary stones]](https://static.fdokumen.com/doc/165x107/633645e7cd4bf2402c0b6fc8/characteristics-of-encrustation-of-ureteric-stents-in-patients-with-urinary-stones.jpg)

