trainee handbook 2 - Alive & Thrive
186
Ha Noi, July 2011 TRAINEE HANDBOOK 2: Counseling on infant and young child feeding at a health facility
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of trainee handbook 2 - Alive & Thrive

Ha Noi, July 2011
TRAINEE HANDBOOK 2: Counseling on infant and young child feeding
at a health facility


ACKNOWLEDGEMENT
Alive & Thrive (A&T) acknowledges the special cooperation of the National Institute of Nutrition (NIN)in reviewing and giving helpful feedback on the three training manuals on Infant and Young Child
Feeding (IYCF) for health-facility and community-based health workers.
We would like to express our sincere gratitude to the following experts in Infant and Young Child
Nutrition (IYCN), training and behavior change communication (BCC), without whose support, the
development of these training manuals would not have been possible:
1. Dr. Pham Thi Thuy Hoa, Director of Food and Nutrition Training Center - NIN
2. MA. Huynh Nam Phuong, Specialist of Food and Nutrition Training Center - NIN
3. MA. Trinh Ngoc Quang, Head of Education and Training Department - Center for Health Education and Communication - Ministry of Health (MoH)
4. MA. Tran Thi Nhung - Center for Health Education and Communication - MoH
We would also like to express our appreciation to health workers and Viet Nam Women’s Union
members from fourteen provinces for participating in our training to become the provincial trainers for
A&T and for contributing useful comments that enabled the finalization of these manuals.
We extend our gratitude to A&T team members in Viet Nam who worked closely with the consultant
team to review and provide comments on these training manuals. The special support of the A&T
monitoring and evaluation team in developing the pre and post-tests and effectively evaluating the
trainings of trainers has been critical in finalization of these manuals.
We thank Maryanne Stone-Jimenez, Technical Consultant, for her comments on the technical content
and layout of the training manuals.
We would also like to thank the World Health Organization (WHO), the United Nations Children’s Fund
(UNICEF), the Pan American Health Organization (PAHO), and other organizations whose training
materials and references made our task of putting this manual together a great deal easier.
Finally, we would like to express our sincere gratitude to the Department of Maternal and Child Health,
MoH Viet Nam for their support and guidance in the development of these training manuals.
A&T is grateful for the financial support from the Bill & Melinda Gates Foundation.
Acknowledgement
Counseling on infant and young child feeding at health facility .i

INTRODUCTION
Addressing child nutrition, particularly stunting among children under two years old, is a high priority
for the Government of Viet Nam. In recent years, Viet Nam has made substantial efforts to reduce the
malnutrition rate among children under five years old - reducing this rate from 38.7% in 1999 to 31.9%
in 2009 (NIN). However, underweight and, in particular, stunting among children under two years old
remain high in Viet Nam in comparison to countries with the same economic status in the region. An
extremely low rate of exclusive breastfeeding (EBF) for the first six months, and poor complementary
feeding (CF) practices are the main reasons for this high stunting rate among children under two years
old in Viet Nam.
To support the government’s efforts to reduce the high malnutrition rate among children under five
years old, Save the Children (SC), through a partnership with the Academy for Educational Develop-
ment (AED), GMMB, the International Food Policy and Research Institute (IFPRI) and the University
of California Davis, is implementing the A&T project in Viet Nam over a period of five years (2009-2013). The project goal is to reduce malnutrition and death caused by sub-optimal IYCF practices by
improving the rate of EBF and CF practices for children aged 0 up to 24 months.
In order to achieve this, A&T will support health facilities in fifteen provinces to establish IYCF coun-
seling services in rural and urban areas using a social-franchise model. In addition, A&T will establish
IYCF support groups will be established in mountainous areas. to guide this work, A&T produced a
package of training manuals on IYCF and counseling skills for health-facility managers and staff and
community-based workers, including nutrition collaborators, village health workers, and Viet Nam
Women’s Union members. The participants who are trained using these manuals will be able to provide
IYCF counseling services in health facilities and in the community. The package includes a set of four
manuals and four trainee handbooks as follows:
Introduction
Counseling on infant and young child feeding at health facilityii.
MANUALNO.
TOPICTRAINERMANUALS
TRAINEEHANDBOOKS
1.Management and Operation of IYCF Franchise Model(Mat troi be tho) ü ü
2. Counseling on IYCF at Health Facility ü ü
3. BCC on IYCF at Community (Franchise Model) ü ü
4. BCC on IYCF in Remote Areas (IYCF Support Group Model) ü ü

* This fourth manual is designed for use only in project area where residents have difficulty accessing
health facility and where IYCF Support Groups are already established.
This book you are reading is Trainee Handbook Two, which will be used as a reference for health-
facility workers who have been trained to provide IYCF counseling services at the franchise “M t tr ibé th ”.
We would appreciate any comments and suggestion users have about this trainee handbook. Kindly
direct comments, suggestions, and questions to Mrs. Tran Thi Kiem - A&T Office - E4B Trung Tu
Diplomatic Compound, 6 Dang Van Ngu, Dong Da, Ha Noi or via email:
This handbook may be reproduced in part or full with prior permission from A&T.
Thank you.
Introduction
Counseling on infant and young child feeding at health facility .iii
ACRONYMS
A&T Alive and Thrive
AED Academy for Educational Development
AV Audio-visual
BCC Behavior Change Communication
BF Breastfeeding
BMI Body Mass Index
CBW(s) Community-based worker(s)
CF Complementary Feeding
CHC(s) Commune Health Center(s)
EBF Exclusive Breastfeeding
HIV/AIDS Human Immunodeficiency Virus/ Acquired Immune Deficiency Syndrome
IFPRI International Food Policy Research Institute
IYCF Infant and Young Child Feeding
M&E Monitoring and Evaluation
MoH Ministry of Health
NIN National Institute of Nutrition
NGO(s) Non-governmental organization(s)
PR Public Relations
SC Save the Children
SL Slide
UN United Nations
VWU Viet Nam Women’s Union
WHO World Health Organization
Acronyms
Counseling on infant and young child feeding at health facilityiv.
CONTENTS
ACKNOWLEDGEMENT...........................................................................................................i
INTRODUCTION .....................................................................................................................ii
ACRONYMS ...........................................................................................................................iv
IYCF INDICATORS ................................................................................................................vii
TRAINING SCHEDULE ........................................................................................................viii
Session 1: Introduction - Ice-breaker ............................................................................................1
Session 2: Objective - Training Schedule .....................................................................................2
Session 3: Introduction of IYCF ....................................................................................................3
Session 4: Current Situation of IYCF in Viet Nam.........................................................................7
Session 5: Introduction of A&T and the Social-Franchise Model on Infant and Young Child Nutrition Counseling ..............................................................................10
Session 6: IYCF Franchise Services: Opportunities of Individual and Group Contacts..............15
Session 7: Behavior Change Communication.............................................................................18
Session 8: Good Communication Skills ......................................................................................23
Part 1 – Listening, Learning, and Observing .............................................................23
Session 9: Good Communication Skills ......................................................................................26
Part 2 - Building Confidence and Giving Support. How to Use Counseling Cards....26
Session 10: Individual Counseling for Mothers and Caregivers..................................................28
Session 11: Group Counseling for Mothers on IYCF ..................................................................31
Session 12: Health and Nutrition Care for Pregnant Women and Lactating Mothers .................35
Session 13: The Significance of BF ............................................................................................39
Session 14: Nutrient Demands of Children under Six Months ....................................................46
Session 15: Breastmilk Production .............................................................................................50
Session 16: In-classroom Practice - Individual Counseling on BF..............................................55
Session 17: In-classroom Practice Group-Counseling on BF .....................................................58
Session 18: Positioning and Attachment.....................................................................................60
Session 19: Assessing a Breastfeed...........................................................................................66
Session 20: Expressing and Storing Breastmilk .........................................................................70
Session 21: Common BF difficulties............................................................................................75
Session 22: Field Practice...........................................................................................................84
Contents
Counseling on infant and young child feeding at health facility .v
Session 23: Importance of CF.....................................................................................................87
Session 24: CF - Quantity and Quality........................................................................................91
Session 25: Feeding Technique ................................................................................................103
Session 26: In-classroom Practice - Appropriate CF Promotion and Management ..................105
Session 27: Preparing a Hygiene Meal and Food Safety .........................................................108
Session 28: Feeding Ill (Sick) Children and Children With HIV-infected Mothers .....................113
Session 29: Assessing Nutrition Status ....................................................................................120
Session 30: Decree 21..............................................................................................................130
APPENDICES .....................................................................................................................143
Appendix 1: Roles of Community-Based Worker, Health-facility Worker and Health-Facility Managers ......................................................................................144
Appendix 2: Client Recording and Reporting Forms ................................................................147
FIGURES
Figure 1: Tools Diagram.............................................................................................................147
Figure 2: Form Y1 - List of Women 7-9 Months Pregnant and Mothers with Children under 2 Years ...............................................................................................149
Figure 3: Form YB – Monthly CBW report.................................................................................152
Figure 4: PYB – Summary CBW report .....................................................................................154
Figure 5: Franchise Management Book P1 - Form P1.1 - Franchise Staff’s Training follow-up (Franchise staff and counselor) ..................................................................156
Figure 6: Franchise Management Book P1 - Form P1.2 - Franchise’s BCC material Management Follow-up Card (Franchise manager) ..................................................157
Figure 7: Franchise Management Book P1 - Form P1.3 - Franchise Item Half Year count, Page 1 (Franchise manager) ..................................................................158
Figure 8: Franchise Management Book P1 - Form P1.3 - Franchise ItemHalf Year Count, Page 2 (Franchise manager) .................................................................159
Figure 9: Form P2 - Mother Card at the Franchise, Page 1 ......................................................161
Figure 10: Form P2 - Mother Card at the Franchise, Page 2 ....................................................162
Figure 11: Form P3 - Daily Service Records at the Franchise ..................................................165
Figure 12: Form P4 - Group Counseling and Baby Competition (Franchise manager) ............168
Figure 13: Form P5 - Client Referral Form................................................................................170
Figure 14: Form PB - Franchise Monthly Report (Franchise manager) ....................................172
Figure 15: Form M2 - Client Satisfaction Questionnaire ...........................................................174
Contents
Counseling on infant and young child feeding at health facilityvi.
IYCF indicators
Counseling on infant and young child feeding at health facility .vii
IYCF INDICATORS
Breastfeeding (BF) Indicators
1. Initiation of BF: The proportion of infants who are breasted within the first hour after delivery.
2. EBF under 6 months: The proportion of infants who are fed exclusively with breastmilk for the
first six months (180 days). That means an infant receives only breastmilk and no other liquids or
solids, not even water, with the exception of drops or syrups consisting of vitamins, minerals
supplements or medicine according to health-worker instructions.
3. Continued BF at 1 years: The proportion of children 12-15 months of age who are fed breastmilk.
4. Continued BF at 2 years: The proportion of children 20-23 months of age who are fed breastmilk.
CF Indicators
5. Introduction of complementary foods: The proportion of infants 6-8 months of age who receive
solid, semi-solid, or soft food.
6. Dietary diversity: The proportion of children 6-23 months of age who receive foods from four or
more food groups.
7. Consumption of iron-rich or iron-fortified foods: The proportion of children 6-23 months of age
who receive iron-rich food or iron-fortified food that is specially designed for infants and young
children, or that is fortified in the home.
Types of Malnutrition
8. Underweight: refers to humans who are considered to be under a healthy weight. The definition
is usually made with reference to the body mass index (BMI). (Weight-for-age Z score <-2).
9. Stunting: is a reduced growth rate in human development. It is a primary manifestation of malnu-
trition in early childhood, including malnutrition during fetal development brought on by the
malnourished mother. (Height-for-age Z score <-2).
10. Wasting: refers to the process by which a debilitating disease causes musclehttp: muscle and fat
tissue to "waste" away. Wasting is sometimes referred to as "acute malnutrition" because it is be-
lieved that episodes of wasting have a short duration, in contrast to stunting, which is regarded as
chronic malnutrition. (Weight-for-height Z score <-2).
11. Overweight: refers to the process when accumulated muscle and fat tissue causes the body
weight to be over the standard of the same age and gender. Overweight is identified when weight-
for-age Z score >2.

Training schedule
Counseling on infant and young child feeding at health facilityviii.
TIM
ED
AY
1D
AY
2 (
BF
)D
AY
3 (
BF
)D
AY
4 (
CF
)D
AY
5 (
CF
)
7:30
- 8:
00P
re-t
est
Revi
ew
Revi
ew
Revi
ew
Revi
ew
8:00
- 8:
30Se
ssio
n 1:
In
troduct
ion –
Ice
-bre
ake
r
Sess
ion
12:
Health
and n
utr
ition c
are
for
pre
gnant
wom
en &
lact
atin
g m
oth
ers
Sess
ion
18:
Posi
tionin
g &
attach
ment
Sess
ion
23:
Import
ance
of C
F
Sess
ion
29:
Ass
ess
ing n
utr
itional
statu
s
8:30
- 9:
00Se
ssio
n 2:
Obje
ctiv
e –
Tra
inin
g S
chedule
Sess
ion
13:
Sig
nifi
cance
of B
FE
arly
initi
atio
n a
nd E
BF
defin
ition
Com
posi
tion o
f bre
ast
milk
– c
olo
stru
m,
matu
re m
ilk
Sess
ion
19:
Ass
ess
ing a
bre
ast
feed
Sess
ion
24:
CF
– q
uantit
y and q
ualit
yQ
&A
:CF
9:00
- 9:
30Se
ssio
n 3:
Intr
oduct
ion o
f IY
CF
Win
dow
of
Opport
unity
Key
IYC
F p
ract
ices
9:30
- 10
:00
Sess
ion
4: IY
CF
in V
iet N
am
Sess
ion
20:E
xpre
ssin
g a
nd
st
oring b
reast
milk
10:0
0 - 1
0:30
TE
A B
RE
AK
10:3
0 - 1
1:00
Sess
ion
5:In
troduct
ion o
f A&
Tpro
ject
and the s
oci
al f
ranch
ise
model o
n IY
CF
counse
ling
Sess
ion
14:
Nutr
ition d
em
and o
f ch
ildre
n u
nder
six
month
sSe
ssio
n 21
: C
om
mon B
F D
iffic
ulti
es
Sess
ion
24:
CF
– q
uantit
y and q
ualit
y(c
ont.)
Post
-test
and
train
ing e
valu
atio
n
11:0
0 - 1
1:30
Sess
ion
6:IY
CF
fra
nch
ise s
erv
-ic
es.
Opport
uniti
es
for
indiv
idual &
gro
up c
onta
cts
Sess
ion
15:
Bre
ast
milk
pro
duct
ion
Sess
ion
25:
Feedin
g tech
niq
ue
LU
NC
H
13:3
0 - 1
4:00
Sess
ion
7:
BC
C S
tages
of C
hange
Sess
ion
16:
In c
lass
-room
pra
ctic
e : in
div
idual
counse
ling o
n B
F
Sess
ion
30: D
ecr
ee 2
1
Sess
ion
27:
Pre
paring a
hyg
ienic
meal
and food s
afe
ty
Sess
ion
28:
Feedin
g il
l (si
ck)
child
ren
and c
hild
ren h
avi
ng H
IV-in-
fect
ed m
oth
ers
Sess
ion
26:
In c
lass
-room
pra
ctic
e: A
p-
pro
priate
CF
Pro
motio
n &
Managem
ent
Intr
oduct
ion o
f re
cord
-in
g form
s and b
ooks
at fr
anch
ise
Pla
nnin
g for
the im
ple
-m
enta
tion o
f fr
anch
ise
model a
t lo
calit
y
14:0
0 - 1
4:30
Sess
ion
8:
Good c
om
munic
atio
n s
kills
14:3
0 - 1
5:00
Sess
ion
9:
Good C
om
unic
atio
n S
kills
(con
t.)Se
ssio
n 22
: Pra
ctic
e
15:0
0 - 1
5:30
Sess
ion
10:
Indiv
idual c
ounse
l-in
g for
moth
ers
& c
are
giv
ers
Sess
ion
17:
In c
lass
-room
pra
ctic
e: gro
up c
ounse
l-in
g o
n B
F
15:3
0 - 1
6:00
TE
A B
RE
AK
Pre
- and p
ost
-test
re
sults
Cert
ifica
tes
Clo
sing
16:0
0 - 1
7:00
Sess
ion
11: G
roup c
ounse
ling for
moth
ers
on IY
CF
Sess
ion
17: I
n c
lass
-room
pra
ctic
e :
gro
up c
ounse
ling o
n B
F (
cont.)
Revi
ew
of F
ield
Pra
ctic
eQ
&A
on B
F
Sess
ion
26:
In c
lass
-room
pra
ctic
e(c
ont.)
17:0
0 - 1
7:15
DA
ILY
EV
AL
UA
TIO
N
TR
AIN
ING
SC
HE
DU
LE
Session 1: Introduction – Ice-breaker
Counseling on infant and young child feeding at health facility .1
SESSION 1: INTRODUCTION – ICE-BREAKER
Objectives
1. Introduce participants.
2. Create a warm and friendly training atmosphere.
Session 2: Objective – Training Schedule
Counseling on infant and young child feeding at health facility2.
SESSION 2: OBJECTIVE – TRAINING SCHEDULE
Objectives
After completing this training, trainees will be able to:
1. State the concepts of social franchising and the A&T franchise model on IYCF counseling
services.
2. Understand key concepts of BCC.
3. Understand the key content of IYCF counseling at a health facility.
4. Develop skills to provide individual counseling for clients (mothers, fathers, and caregivers) on
IYCF.
5. Develop skills to provide group counseling on IYCF.
6. Develop plans to apply knowledge and skills to conduct IYCF franchise services at a health
facility.
Session 3: Introduction of IYCF
Counseling on infant and young child feeding at health facility .3
SESSION 3: INTRODUCTION OF IYCF
Objectives:
After completing this session, trainees will be able to:
1. Point out the importance of IYCF and the significance of the Window of Opportunity.
2. Provide current nutritional recommendations for children from 0-24 months of age.
Importance of IYCF
It is estimated that up to 150 million children under five years are malnourished worldwide (WHO 2004).Child malnutrition leads to the decreased mental and physical development capacity of children, the
national future generation, thus affecting the capacity to attain Millennium Development Goals 1, 4,
and 5 of reducing fatality and disease in children. Moreover, child malnutrition also affects the socio-
economic development of a country in the long run.
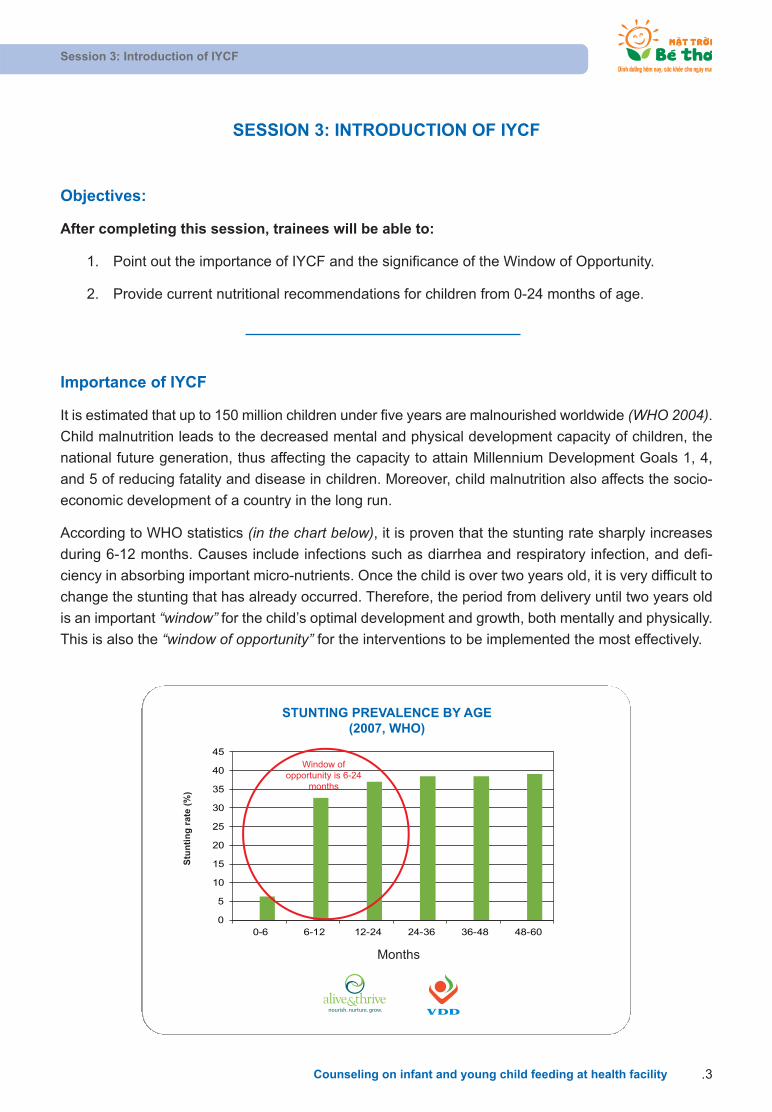
According to WHO statistics (in the chart below), it is proven that the stunting rate sharply increases
during 6-12 months. Causes include infections such as diarrhea and respiratory infection, and defi-
ciency in absorbing important micro-nutrients. Once the child is over two years old, it is very difficult to
change the stunting that has already occurred. Therefore, the period from delivery until two years old
is an important “window” for the child’s optimal development and growth, both mentally and physically.
This is also the “window of opportunity” for the interventions to be implemented the most effectively.
0
5
10
15
20
25
30
35
40
45
0-6 6-12 12-24 24-36 36-48 48-60
Window ofopportunity is 6-24
months
Months
Stu
nti
ng
rat
e (%
)
STUNTING PREVALENCE BY AGE(2007, WHO)
nourish. nurture. grow.

Session 3: Introduction of IYCF
Counseling on infant and young child feeding at health facility4.
Research shows that a child’s height at three years is highly related to his/her height as an adult – by
adding about 77 cm to a child’s height at age three you can predict their height as adults. Therefore
someone who is severely stunted as a child will be a short adult while someone who is well nourished
as a child will be a tall adult.
Hence, in order to ensure all children will become tall and healthy adults in the future, we need to focus
on improving IYCF practices to prevent stunting from a very early age. This intervention needs to be
implemented by appropriate activities at different ages: from the seventh month of pregnancy until the
child is 24 months old.
The “Window of Opportunity” and appropriate times for the most effective IYCF interventions
The “Window of Opportunity” period (from the time of delivery until 24 months) is an important period
to implement appropriate activities to prevent child malnutrition. However, for each of these times, there
are different messages on behavior change communication to suit the child’s needs at different ages.
Therefore, there are three windows of opportunity as follows:
Severe Moderate Mild Well-nourished
94.589.585.3
81.2
158.0162.5
167.3
170.9
Average growth from 3-18 years 77cm
Heightat 18 y
Heightat 3 y
STUNTED 3 YEAR OLD - STUNTED ADULT(GUATEMALA, INCAP ORIENTE STUDY)
nourish. nurture. grow.
Impact of the “Window of Opprtunity” to the child development

Session 3: Introduction of IYCF
Counseling on infant and young child feeding at health facility .5
Each “window” has specific intervention activities:
In pregnancy, a mother needs to be cared for and receive good nutrition. Especially in the
last trimester of pregnancy, a mother needs to be provided with knowledge on BF.
When the child is 0- 6 months, a mother needs support to ensure that the child is breastfed
immediately after birth, and exclusively for the first six months.
When the child is 6 -24 months, a mother needs to know how to give age-appropriate CF
and continue BF until the child is 24 months.
In conclusion, 0-24 months is the critical period during a child’s development. We call it the “Windowof Opportunity”, which is the ideal time to implement the most effective interventions.
Ideal practices on child feeding
Poor BF and CF practices are leading reasons for child malnutrition during the first two years of life.
Therefore, IYCF plays a critical role in improving a child’s health and survival. WHO and UNICEF
recommend that a child needs EBF for the first six months and adequate and appropriate CF along
with continued BF until the child is two years old or beyond (WHO/PAHO).
Preconception through
pregnancy
0-6 mo: Exclusive
Breastfeeding
6-24 mo: Complementary
feeding and continued BF
WINDOWS OF OPPORTUNITY
nourish. nurture. grow.

Session 3: Introduction of IYCF
Counseling on infant and young child feeding at health facility6.
Fifteen ideal IYCF practices include:
1. All infants are breastfed for the first time within the first hour after birth.
2. No infants are given prelacteals before BF.
3. All infants are fed colostrum.
4. All infants and young children are breastfed on demand, during the day and night.
5. All infants are exclusively breastfed for the first 6 months.
6. No children are weaned before 24 months of age.
7. Children are not fed with a bottle and pacifiers.
8. All infants are fed complementary food after the first six months (180 days).
9. All infants and young children are fed the recommended number of meals daily.
10. All infants and young children meet their recommended daily energy requirements.
11. All infants and young children are fed nutrient- and energy-dense food.
12. Children are given diverse food (with four food groups or more).
13. Children are given iron-rich food or an iron supplement daily.
14. All infants and young children are fed meat, fish, or poultry daily.
15. All the children are supported and motivated to eat to satiety during meal times.
WHO age calculation
Zero-month-old baby: children from the time of delivery until 29 days old.
One- month-old baby: children from 30 to 59 days old.
Five- month-old baby: children from five months to five months and 29 days old.
Children under six months: children under 180 days old.
Thus, EBF in the first six months means in the first 179 days.

Session 4: Current situation of IYCF in Viet Nam
Counseling on infant and young child feeding at health facility .7
SESSION 4: CURRENT SITUATION OF IYCF IN VIET NAM
Objectives:
After completing this session, trainees will be able to:
• Point out IYCF problems in Viet Nam in general and in provinces selected by A&T.
Current situation of IYCF in Viet Nam
Though Viet Nam has been recognized as a country that has experienced significant economic devel-
opment in the past years, child malnutrition still exists.
• More than 7 million children under 5 years old*.
• One in five children: underweight (18.9%)#.
• One in three children: stunted (31.9%)#.
Despite:
• Food security.
• 90% literacy*.
Source: * Health Statistics Yearbook (2009), # NIN Surveillance: 10 A&T provinces (2009)
Antenatal care and postnatal care (ANC & PNC)
• More than 90% of women receive ANC but no/little counseling on BF.
• 80-90% of women have a skilled attendant at birth but no/few have support at delivery for the
initiation of BF.
• No PNC visits except for complications.
BF
Ideal Practice 1: Initiate BF within an hour of birth
• Only 55% of children are breastfed within the first hour after birth.
• The rate is highest in mountain areas (70%), lowest in urban areas (30%).
• The rate is higher for community health centers (CHCs) (70%) compared to hospitals and private
clinics (40%).
Session 4: Current situation of IYCF in Viet Nam
Counseling on infant and young child feeding at health facility8.
Ideal Practice 2: No prelacteals
• Two out of three mothers (60%) give something beside breastmilk during first three days.
• One out of three mothers (30%) bring formula to the health facility for delivery (in Hanoi as manyas 87% mothers bring formula with them).
Ideal Practice 3: Give colostrum
• Almost one out of three mothers (27%) squeeze out some colostrum.
• In some provinces this rate is as high as 90%.
Ideal Practice 4: BF on demand, day and night
• 85% mothers breastfeed on demand.
Ideal Practice 5: EBF tills 6 months
• 10% EBF up to 6 months of age.
• Only of 50% of mothers and 30% of pregnant women know what EBF means.
• Most health workers know what EBF means but believe EBF is required for only four months.
Ideal Practice 6: BF up to 24 months of age
• 60 - 90% of mothers BF up to 12 months.
• On average most mothers stop BF at 15 -18 months.
Ideal Practice 7: No feeding with bottles and pacifiers
• 75% of children are not fed with bottles and pacifiers (0-24 months).
Barriers to BF
• Perception of insufficient milk quality and quantity.
• Separation of mother and child.
• Perception that water is needed to clean a baby’s mouth and quench thirst.
• Availability of formula milk.
• Maternity-leave policy.
• Lack of appropriate information and support.

Session 4: Current situation of IYCF in Viet Nam
Counseling on infant and young child feeding at health facility .9
CF indicators
Indicator
Ideal practice 8: Children aged 6-8 months given complementary food 90%
Ideal practice 9: Children given the recommended number of meals per day No data
Ideal practice 10: Children meet the recommended daily energy requirements Yes, if BF
Ideal practice 11: Children fed nutrient- and energy-dense food No data
Ideal practice 12: Children 6-23 months given diverse food 50%
Ideal practice 13: Children given iron-rich food 79%
Ideal practice 14: Children fed meat, fish, or poultry daily 3-4 times/week
Ideal practice 15: Children supported and motivated to eat Yes
CF
• Complementary food is given as early as 2-3 months (urban: 4-5 months).
• Consistency and quality of complementary food is an issue.
• Diets are highly iron-deficient.
Communication findings
• The rate of TV, radio, and mobile ownership is high, but very few called/used a hotline. In urban
areas, computer ownership is more than 60%, access to the Internet 26%. Less than 25% of moth-
ers read newspapers.
• Only 30% of mothers attended group sessions on nutrition counseling.
• 75% are willing to pay for effective nutrition counseling – on average 30,000- 50,000 VND.
Session 5: Introduction of A&T and the Social-Franchise Model on Infant and Young Child Nutrition Counseling
Counseling on infant and young child feeding at health facility10.
SESSION 5: INTRODUCTION OF A&T AND THE
SOCIAL - FRANCHISE MODEL ON INFANT AND
YOUNG CHILD NUTRITION COUNSELING
Objectives:
After completing this session, trainees will be able to:
1. Clarify the main content of the A&T project.
2. State the concept of the franchise model on IYCF.
A&T project
• Five-year initiative (2009-2013).
• Bangladesh, Ethiopia, and Viet Nam
• Improving BF and CF policies and practices at scale and preventing child deaths.
• Funded by the Bill & Melinda Gates Foundation.
International partners
• Academy for Educational Development – Lead, Communications, Private Sector.
• GMMB – Policy and PR.
• International Food Policy Research Institute – M&E, Operations Research.
• Save the Children – Community interventions.
• University of California, Davis – Small-grants program.
Vietnamese partners
• MoH– Department of Maternal and Child Health.
• NIN.
• Provincial Department of Health.
• Viet Nam Women’s Union.
• UN Agencies.
• NGOs – Marie Stopes International, Plan International, World Vision, etc.

Session 5: Introduction of A&T and the Social-Franchise Model on Infant and Young Child Nutrition Counseling
Counseling on infant and young child feeding at health facility .11
Program areas
• North: Hanoi, Hai Phong, Thai Nguyen, Thanh Hoa.
• Central: Danang, Quang Tri, Quang Ngai, Quang Nam, Quang Binh.
• South: Khanh Hoa (Nha Trang), Vinh Long, Tien Giang, Ca Mau, Dak Lak, Dak Nong.
Project objectives
1. Double EBF rates (0 - 6 months) by the end of the project.
2. Improve CF practices (6-24 months) in both quality and quantity by the end of the project.
3. Reduce the stunting rate for children under 2 years old by at least 2% per year.
Intervention strategies
• Improve the policy and regulatory environment to support IYCF interventions.
• Shape, create, and support demand for IYCF through the franchise model on IYCF.
• Increase supply and demand and encourage the use of fortified complementary food through co-
operation with the private sector.
Franchise model
Overview of franchising
“Franchising” is a business model that enables rapid and effective expansion of a product and/or service
of a specified standard by transferring daily management responsibility for other independent
enterprises.
In the commercial sector, franchising is used to expand a franchisor’s business with the aim of quickly
increasing profits. For society, social franchising is used to expand a “business” but for the purpose of
increasing the impact of a social initiative as opposed to generating revenues for the franchisors.
Benefits of social franchising
FRANCHISOR FRANCHISEE
• Rapid growth of service through a network offranchisees
• Increasing access to services for people
• Quality assurance
• Enhanced reputation with certificates of servicequality and brand name
• Supported in marketing services
• Supervised to support service quality
• Updated technical expertise
• Increased number of clients and revenue
Social welfare
• Public receives a high-quality service with appropriate price
• In the health sector, it is able to manage service quality and improve income for staff
• Health indicators are improved
Session 5: Introduction of A&T and the Social-Franchise Model on Infant and Young Child Nutrition Counseling
Counseling on infant and young child feeding at health facility12.
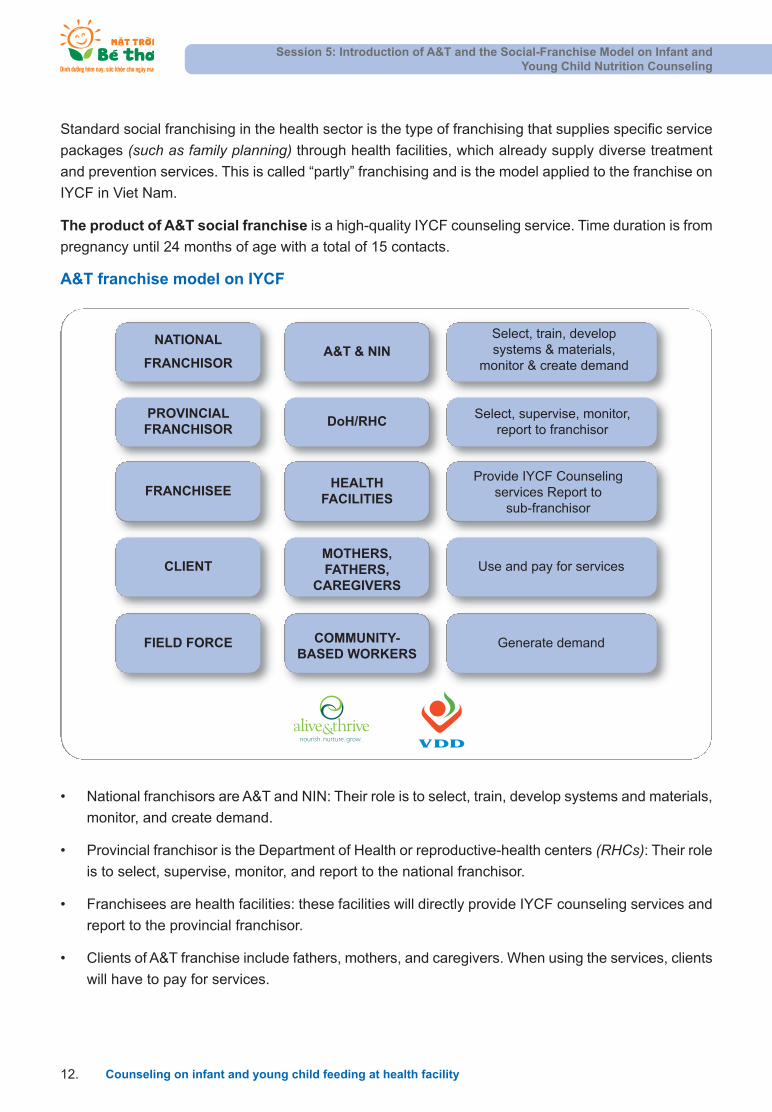
• National franchisors are A&T and NIN: Their role is to select, train, develop systems and materials,
monitor, and create demand.
• Provincial franchisor is the Department of Health or reproductive-health centers (RHCs): Their role
is to select, supervise, monitor, and report to the national franchisor.
• Franchisees are health facilities: these facilities will directly provide IYCF counseling services and
report to the provincial franchisor.
• Clients of A&T franchise include fathers, mothers, and caregivers. When using the services, clients
will have to pay for services.
Standard social franchising in the health sector is the type of franchising that supplies specific service
packages (such as family planning) through health facilities, which already supply diverse treatment
and prevention services. This is called “partly” franchising and is the model applied to the franchise on
IYCF in Viet Nam.
The product of A&T social franchise is a high-quality IYCF counseling service. Time duration is from
pregnancy until 24 months of age with a total of 15 contacts.
A&T franchise model on IYCF
NATIONAL
FRANCHISOR
PROVINCIALFRANCHISOR
FRANCHISEE
CLIENT
A&T & NIN
DoH/RHC
HEALTH FACILITIES
MOTHERS,FATHERS,
CAREGIVERS
Select, train, develop systems & materials,
monitor & create demand
Select, supervise, monitor, report to franchisor
Provide IYCF Counseling services Report to
sub-franchisor
Use and pay for services
FIELD FORCE COMMUNITY-BASED WORKERS
Generate demand
nourish. nurture. grow.

Session 5: Introduction of A&T and the Social-Franchise Model on Infant and Young Child Nutrition Counseling
Counseling on infant and young child feeding at health facility .13
• In the community, the CBWs include village health workers, nutrition collaborators, and members
of village WU : their role is to generate demand for services.
Components of a franchise
• High-quality standardized service.
• Fee for services.
• Franchise-branded commodities.
• Operator-owned outlets.
A&T franchise model
• Standardized service:
Good-quality IYCF counseling services.
9-15 contacts over 27 months (3rd trimester pregnancy –24 months).
• Fee for services:
To be established by provinces.
Dependent on level of facility.
• Brand:
Easily identifiable, gains equity over time.
Recognized.
• Ownership:
Public Health facilities (province, district, commune).
Private Health facilities.
Session 5: Introduction of A&T and the Social-Franchise Model on Infant and Young Child Nutrition Counseling
Counseling on infant and young child feeding at health facility14.
A&T brand
A&T FRANCHISE BRAND
nourish. nurture. grow.
• Professional
• Trustworthy
• High quality
• Functional
• Welcoming
• Child-friendly
The logo set is composed of three elements:
• The logo: The beaming sun both symbolizes a blooming sunflower as well as a smiling child in
good care. The sun represents vitality while the two leaves stand for nurturing hands. The overall
meaning is caring for a healthy, happy child and for the future generation.
• The clinic name: The clinic name “Mat troi be tho” is synonymous with the above meaning and
emphasizes “child” as the prime target of the clinic. The clinic name is short and easy to remember
and understand. It is highly indicative of the nature of the project as well as its target.
• The project slogan: “Nutrition today, health tomorrow” – The slogan emphasizes the importance
of appropriate nutrition for babies to create a foundation for their future development, and for the
future of Viet Nam.
Value of the brand name:
• Professional
• Trustworthy
• High-quality
• Functional
• Welcoming
• Child-friendly

Session 6: IYCF Franchise Services: Opportunities of Individual and Group Contacts
Counseling on infant and young child feeding at health facility .15
SESSION 6: IYCF FRANCHISE SERVICES: OPPORTUNITIES
OF INDIVIDUAL AND GROUP CONTACTS
Objectives:
After completing this session, trainees will be able to:
1. State IYCF Service Packages provided at a health facility
2. Point out proper timing to access mothers for IYCF counseling
The A&T Model is a social-franchise model and its product is “High-quality IYCF counseling services”.
Full IYCF service package
SERVICE METHOD TIME
1) Package 1 (G1): EBF promotion (as pregnancy)
1 group/class counseling 3rd trimester of pregnancy
2 individual counseling 3rd trimester of pregnancy
2) Package 2 (G2): EBF support (at delivery)
Individual support At delivery
3) Package 3 (G3): EBF management
2 (the first two) individualcounseling
1 week after birth
2 weeks after birth
2 Group/class counseling 1-6 months after birth
4) Package 4 (G4): CF education
1 individual counseling 4-6 months after birth
5) Package 5 (G5): CF management
Combination of individual- and group-coun-seling sessions, totaling 6 contacts
One between 6-8 months
One between 9-12 months
Four between 12-24 months

Session 6: IYCF Franchise Services: Opportunities of Individual and Group Contacts
Counseling on infant and young child feeding at health facility16.
Service packages depending on types of health facility:
In general, these components will be available at health facilities as follows:
TYPES OF HEALTH FACILITY FRANCHISE SERVICE PACKAGE
Commune Health Centers
EBF promotion
EBF support (for CHCs that do deliveries)
EBF management
CF education
CF management
Provincial Reproductive-Health-Care Centers
EBF promotion
EBF management
CF education
CF management
Hospital (where deliveries occur)EBF promotion
EBF support
Paediatric facilities
EBF management
CF education
CF management
Session 6: IYCF Franchise Services: Opportunities of Individual and Group Contacts
Counseling on infant and young child feeding at health facility .17
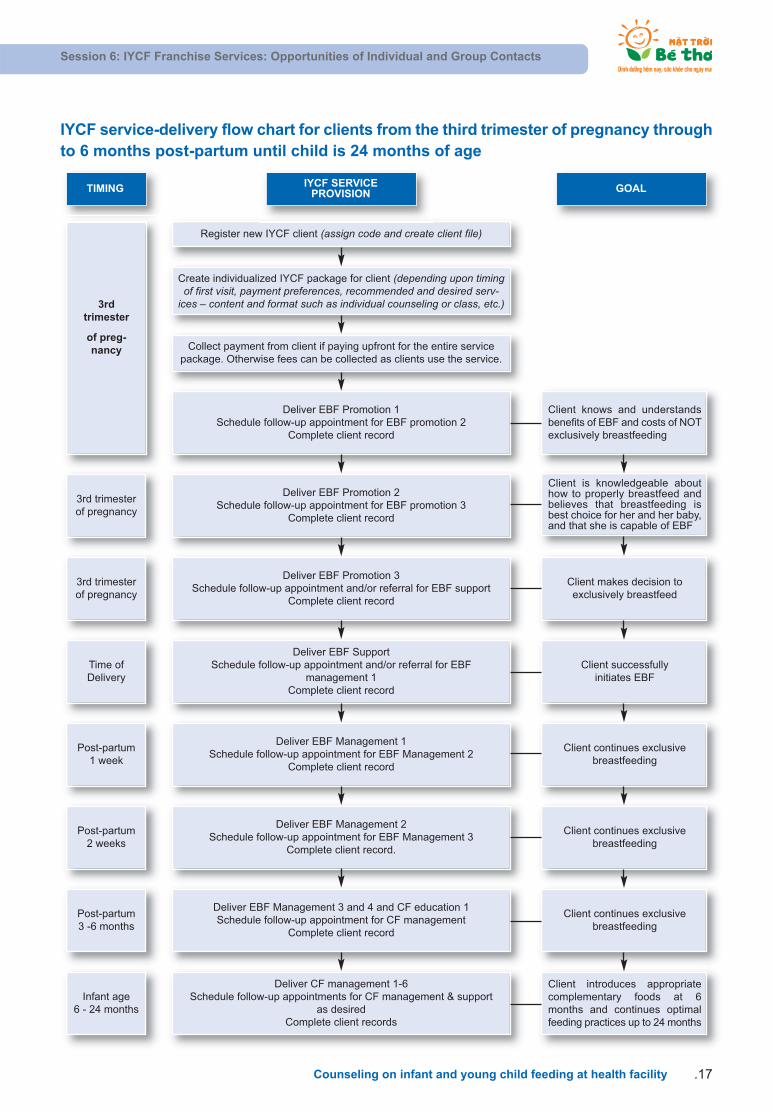
IYCF service-delivery flow chart for clients from the third trimester of pregnancy throughto 6 months post-partum until child is 24 months of age
Register new IYCF client (assign code and create client file)
Create individualized IYCF package for client (depending upon timingof first visit, payment preferences, recommended and desired serv-
ices – content and format such as individual counseling or class, etc.)
Collect payment from client if paying upfront for the entire servicepackage. Otherwise fees can be collected as clients use the service.
Deliver EBF Promotion 1 Schedule follow-up appointment for EBF promotion 2
Complete client record
Client knows and understandsbenefits of EBF and costs of NOTexclusively breastfeeding
Client is knowledgeable abouthow to properly breastfeed andbelieves that breastfeeding isbest choice for her and her baby,and that she is capable of EBF
Client makes decision to exclusively breastfeed
Client successfully initiates EBF
Client continues exclusivebreastfeeding
Client continues exclusivebreastfeeding
Client continues exclusivebreastfeeding
Client introduces appropriatecomplementary foods at 6months and continues optimalfeeding practices up to 24 months
Deliver EBF Promotion 2 Schedule follow-up appointment for EBF promotion 3
Complete client record
3rd trimesterof pregnancy
3rd trimesterof pregnancy
Time of Delivery
Post-partum1 week
Post-partum2 weeks
Post-partum3 -6 months
Infant age 6 - 24 months
Deliver EBF Promotion 3 Schedule follow-up appointment and/or referral for EBF support
Complete client record
Deliver EBF Support Schedule follow-up appointment and/or referral for EBF
management 1Complete client record
Deliver EBF Management 1 Schedule follow-up appointment for EBF Management 2
Complete client record
Deliver EBF Management 2 Schedule follow-up appointment for EBF Management 3
Complete client record.
Deliver EBF Management 3 and 4 and CF education 1 Schedule follow-up appointment for CF management
Complete client record
Deliver CF management 1-6Schedule follow-up appointments for CF management & support
as desiredComplete client records
3rdtrimester
of preg-nancy
TIMING IYCF SERVICE PROVISION GOAL

Session 7: Behavior Change Communication
Counseling on infant and young child feeding at health facility18.
• There is behavior that is good for health and there is behavior that is not good for health.
Examples of healthy behavior in IYCF:
• Useful healthy behavior
Eat and drink sufficiently when pregnant.
Consume iron tablets according to a health worker instruction.
Feed your baby colostrum.
Exclusively breastfeed for the first 6 months.
Appropriate CF.
Provide Vitamin A for babies.
Monitor the child’s weight.
Increase BF if the baby is ill.
Wash your hands with soap before feeding children.
Etc.
SESSION 7: BEHAVIOR CHANGE COMMUNICATION
Objectives:
After completing this session, trainees will be able to:
1. Identify basic concepts of behavior and BCC.
2. Explain the steps of behavior change.
3. Describe BCC interventions and strategies at different levels.
1. Definition of healthy behavior:
• Healthy behavior is a daily practice or action that is positive to health.
• Healthy behavior is affected by ecological, environmental, social, economic, cultural, and political
elements.
• Behavior consists of the following sections: knowledge, attitude, belief, and practice.
BEHAVIOR = KNOWLEDGE + ATTITUDE + BELIEF + PRACTICE

Session 7: Behavior Change Communication
Counseling on infant and young child feeding at health facility .19
• Harmful behaviors (risky behaviors)
Squeezing out colostrum.
Feeding children with liquorices right after birth.
Giving complementary food to children under 6 months of age.
Letting babies go on a diet when they get diarrhea.
• Behaviors that are not good but not harmful for child health:
Putting a silver ring on a child’s wrist.
2. What is BCC?
Behavior change communication is comprised of communication activities that are planned to create
sustainable behavior of individuals and the community based on the understanding of practices among
the community, sharing appropriate information to help an individual and the community develop new
skills or beliefs and encouraging them to overcome difficulties to practice and maintain new behavior.
BCC on IYCF aims to change/create new community norms on IYCF.
For example: BCC on IYCF will help pregnant women and mothers feeding children under 2 years
old practice and maintain behaviors such as: coming to a health facility to be counseled on IYCF,
practicing right IYCF behaviors (feeding children with colostrum, EBF for the first sixth months, appro-priate CF...)
The aim of any BCC activity is not just to improve knowledge but to ensure that the knowledge
becomes an action – i.e., behavior changes and is maintained. It is also important that most people in
the community (70-80%) start practicing the behavior so that it becomes a norm or standard
practice in the community. Only then can we consider behavior change communication successful.
3. Process of behavior change
Behaviors of person can be changed, sometimes quickly, sometimes slowly and due to many reasons.
The behavior of a person is complicated, so it’s very difficult to change it. However, to accept practicing
and maintaining a good behavior compared to a harmful behavior, a person needs to experience a
process of the five summarized steps:
Step 1: Pre-awareness
Step 2: Awareness
Step 3: Intention
Step 4: Trials - Assessment
Step 5: Maintenance / Relapse

Session 7: Behavior Change Communication
Counseling on infant and young child feeding at health facility20.
4. Stages of behavior change communication
BCC of IYCF includes four stages: the household stage, the community stage, the health-facility stage,
and the policy stage. For each stage, there is different access to IYCF behavior change communication
but the messages should be consistent at all levels.
• In the household: negotiate behavior change with individuals
Health workers, village heath staff, Viet Nam women’s union... (generally called communicators)will counsel, encourage, and convince mothers and family members to change inappropriate IYCF
behaviors and to practice appropriate ones.
STEPS OF BEHAVIOR-CHANGE PROCESS AND INTERVENTIONS BY
COMMUNITY-BASED WORKERS
3. Provide basic information
2. Explain/analyze the positive/negative effects of the behavior
1. Identify knowledge, belief and practice
9. Provide/support resources needed
8. Support to address barriers
7. Discuss implementation and analyze barriers /motivators
6. Encourage and motivate
5. Give examples of positive deviants
4. Provide knowledge and skills
Pre-awareness
Awareness
Intention
Trials - Assessment
Maintenance Relapse
11. Follow up, support, and encourage maintenance
10. Discuss experience and make a decision
Community-based workers’ interventions
Session 7: Behavior Change Communication
Counseling on infant and young child feeding at health facility .21
• In the community: changing community norms and problem solve
The communicators in the community can organize group sessions and clubs, combining with
community meetings to carry out group counseling on IYCF. In group-counseling sessions,
communicators will help local people recognize harmful behavior and customs, and then prioritize
issues to influence and gradually change old practices related to IYCF and accept and practice
new behaviors.
• In the health facility: training and building capacity for health workers
When health workers are trained and their capacity to train others on IYCF improved, they will start
group and individual counseling, open IYCF classes for mothers, and help and support mothers to
change IYCF behaviors. In cases that exceed the health facility’s capacity, health workers will refer
mothers and babies to appropriate health facilities to be given appropriate counseling and care.
Research has indicated that mothers usually believe, and want to receive information from, health
workers. Therefore, counseling and training activities for mothers at health facilities will urge them
to change behaviors.
• Policies: advocacy
Authorities receive information in many ways, such as through documents, newspapers, confer-
ences, meetings, or the mass media. If they accept IYCF information, leaders and policy makers
will issue policies creating a favorable environment or promoting practical actions to support and
to raise concerns about IYCF. For example, actions such as: regulations about maternity leave for
mothers to take care and breastfeed their children; arrangements for mothers to work near home;
putting malnutrition prevention into the socio-economic development targets of each locality;
strengthening economic development and hunger eradication; poverty reduction; and supporting
communication on IYCF in each community, etc.

Session 7: Behavior Change Communication
Counseling on infant and young child feeding at health facility22.
BCC INTERVENTIONS AT DIFFERENT LEVELS
Home
Community
Negotiate individualbehavior change
Change communitynorms & problem solve
Training &capacity building
AdvocacyPolicy
Healthcenter/PVO
nourish. nurture. grow.
The stages of BCC are shown by BCC Pyramid below:
Session 8: Good communication skills
Counseling on infant and young child feeding at health facility .23
SESSION 8: GOOD COMMUNICATION SKILLS
PART 1 – LISTENING, LEARNING, AND OBSERVING
Objectives:
After completing this session, trainees will be able to:
1. List basic skills in interpersonal communication on IYCF.
2. Practice the skills of listening and learning and observing.
1. Listening and learning skills
• Listen carefully to get information on mothers’ IYCF practices
Show appropriate gestures, eyes, smile, facial expression, and posture (sitting, standing,
moving…).
Remove barricades between communicators and mothers.
Maintain eye contact and use non-verbal communication effectively.
Sit in line with participants. Keep a proper distance between communicators and mothers.
Do not appear in a hurry.
Do not grumble, sigh, or yawn.
• Pay attention and encourage mothers to share their thoughts and feelings
Look at the participant, nod, smile, or use simple words such as “well”, “yeah”, “really”...
Do not argue or interrupt mothers if it is unnecessary.
Do not do personalize things as mothers are talking.
Minimize factors causing distraction (TV, phone, noise...).
• Ask questions on unclear points or repeat the key points that mothers have just discussed
using similar language but also to briefly check whether you understand mothers or not. If you mis-
understand them, you can correct them again. For example: you can repeat “Is that what youmean...”, “In other words,...”
• Use non-verbal communication effectively.
• Avoid judging words such as: not right, wrong, not good, bad... If you use these words when
discussing with mothers, you will make them feel that they have made mistakes or something is
wrong, and therefore they will be afraid to open up to you.
• Maintain eye-contact.
• Use a lot of open-ended questions.
Essentially, there are three types of questions:
• A closed-ended question:
A closed-ended question is the type of question that limits the answer content to one wordsuch as “yes” or “no”, “right” or “wrong”, “already” or “not yet”, etc...
For example: Question: “Did you go for a pregnancy test?”
The mother will answer: “Yes” or “No”.
The answer is short and provides little information, so you need to ask more questions. Limitthe use of closed-ended questions in the communicating process.
• An open-ended question:
An open-ended question is a type of question that requires mothers to think and to give an an-swer with more information.
An open-ended question usually starts with words such as: Why? When? How? What?Where?... You should use a lot of open-ended questions in the communicating process togather more information.
For example: What difficulties do you have when BF?
• An oriented question (leading question).
A leading question is a type of question where the communicator orients the trainees to givethe answer he wants. Avoid using this type of question in the communicating process.
For example: “You understand that breastmilk is very important to children, don’t you?”
How to ask questions:
• Ask one question at a time.
• Ask short and clear questions.
• Ask relevant questions.
• Use open-ended questions to help trainees talk about their emotional states, conditions, and
behaviors (to understand what they know, trust, and do).
• Avoid leading questions.
2. Observation skills
How to observe
• Observe all aspects carefully: facial expression, gestures, responses, behaviors, context, a baby’s
status, etc.
Session 8: Good communication skills
Counseling on infant and young child feeding at health facility24.

Session 8: Good communication skills
Counseling on infant and young child feeding at health facility .25
• Choose an appropriate position.
• Observation is carried out in a sensitive way, politely, continuously, and with a motivating and
encouraging attitude.
• Observe objectively, do not judge subjectively.
Don’ts during observation
• Observe with neglect, indifference, or lack of concentration.
• Scrutinize with unsympathetic and insensitive eyes.
• Use disrespectful and impolite non-verbal language.

Session 9: Good communication skills
Counseling on infant and young child feeding at health facility26.
SESSION 9: GOOD COMMUNICATION SKILLS
PART 2 - BUILDING CONFIDENCE AND GIVING SUPPORT.
HOW TO USE COUNSELING CARDS
Objectives:
After completing this session, trainees will be able to:
1. Describe the skills of providing information; building confidence and giving support.
2. Describe how to use counseling cards.
1. Providing information skills
• Provide specific and relevant information.
• Use simple words that are easy to understand.
• Speak clearly and concisely.
• Make one to two recommendations only – recommendations should be practical.
• Use counseling cards as a support.
• Demonstrate the skill/recommendation if required.
• Ask the mother to repeat/demonstrate recommendations to ensure she completely understands.
• Negotiate and ensure that the mother agrees to try out the recommendations.
• Arrange follow-ups if needed.
2. Skills for building confidence and providing support
• Accept what mothers think and feel, avoid being judgmental: Sometimes you can not be sat-
isfied with what mothers tell you but if you show your disagreement or do not want to listen, they
will feel hurt, sad, uncomfortable, unconfident, and not want to tell to you anything else. Do not
oppose and criticize, but accept what they tell you neutrally (neither agree nor oppose).
• Empathize with the mother and let her know how you feel.
• Identify and compliment good practices, praise the mothers: When people are praised about
what they did, they will be confident and encouraged to try other things. We learn how to identify
an issue and what mothers do wrong, then help them correct it. However, it is also necessary to
identify what mothers do well to compliment them.
Session 9: Good communication skills
Counseling on infant and young child feeding at health facility .27
• Provide practical help: Showing your support will help mothers feel confident in the things they
are doing and continue maintaining those good behaviors. Your support is shown through many
aspects such as: providing appropriate information and arranging follow-ups to practice new
behavior.
• Encourage mothers to ask questions and clarify any doubts.
• Use non-verbal communication effectively.
• Create a friendly and reliable atmosphere.
3. Use counselling cards
Purposes of using counseling cards in communication sessions on IYCF
• Counseling cards are tools that support interpersonal communication and counseling.
• Counseling cards consist of many pictures, therefore:
They are attractive and draw the mother’s attention.
They help mothers to easily remember for a long time, especially for mothers who have low
literacy.
They help mothers better understand what they were verbally instructed to do.
• It is necessary to know how to use counseling cards during behavior change communication on
IYCF to achieve a high level of efficiency.
How to use counseling cards
• Counseling cards are only used with individuals or small groups (6-10 persons).
• Health workers should select cards and review them in advance. In each session, communicators/
counselors should choose two to three cards only.
• When providing information, it is necessary to hold the cards so that the mothers can see them
clearly.
• Let mothers view the cards and share what they see in the cards.
• Discuss the content of the cards and ask mothers to relate them to their situation.
• Explain and provide additional information if required. Health workers may refer to information from
text pages.
• Summarize and come to an agreement on recommendations that the mothers should try.
• At the end of the session, place the cards back in order and check to be sure the set is complete.
Session 10: Individual counseling for mothers and caregivers
Counseling on infant and young child feeding at health facility28.
SESSION 10: INDIVIDUAL COUNSELING FOR MOTHERS
AND CAREGIVERS
Objectives:
After completing this session, trainees will be able to:
1. Explain how to apply communication skills to counseling.
2. Describe steps of individual counseling on IYCF.
How to give counseling to mothers and caregivers to help them change old practices, accept and maintain new behavior on IYCF and to help their children grow well? This is the question that is posedhere for health workers and communicators.
To help mothers change IYCF behaviors, health workers and communicators need to have good communication skills (listening and learning skills, observation skills, information-provision skills, andskills on building confidence and giving support) to apply in counseling steps.
Six steps of individual counseling
Step 1: Introduce – create a warm and friendly atmosphere
• Greet mother.
• Introduce yourself.
• Make eye contact.
• Smile.
• Show respect.
Step 2: Identify current problems/issues
• Listen.
• Be non-judgmental.
• Ask open-ended questions to learn about current situation/issue.
• Accept what a mother says.
Step 3: Analyze and assess
• Be non-judgmental.
• Identify the problem / issue.
• Respond to the mother’s questions.

Session 10: Individual counseling for mothers and caregivers
Counseling on infant and young child feeding at health facility .29
Step 4: Make practical recommendations
• Provide relevant information (use simple language).
• Build confidence.
• Make one to two practical recommendations.
• Be non-judgmental.
Step 5: Negotiate behavior – get commitment
• Discuss different solutions - small practical solutions.
• Let mothers choose the solution.
• Get commitment to try one to two recommendations.
• Use simple language and be non-judgmental.
Step 6: Summarize – closing
• Ask the mother to repeat the recommendation.
• Correct the recommendation if required.
• Arrange follow-ups with mothers.
• Praise and thank the mothers.
Notes: In order to help counselors at the franchise “M t tr i bé th ” comply with these six steps of
individual counseling and apply appropriate skills for each step, the following checklist will help:
• The counselor to self-check when providing the counseling services.
• The manager and supervisor to use when evaluating counseling skills of health
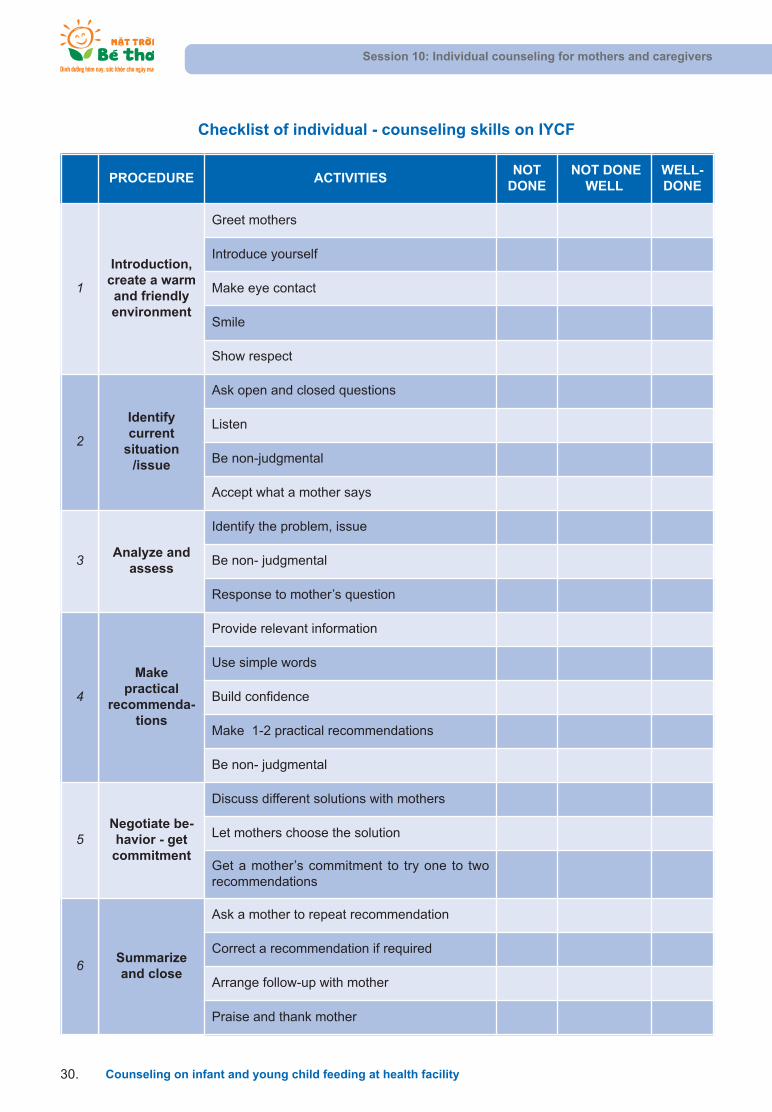
Checklist of individual - counseling skills on IYCF
Session 10: Individual counseling for mothers and caregivers
Counseling on infant and young child feeding at health facility30.
PROCEDURE ACTIVITIESNOT
DONENOT DONE
WELLWELL-DONE
1
Introduction,create a warmand friendly environment
Greet mothers
Introduce yourself
Make eye contact
Smile
Show respect
2
Identifycurrent
situation/issue
Ask open and closed questions
Listen
Be non-judgmental
Accept what a mother says
3 Analyze andassess
Identify the problem, issue
Be non- judgmental
Response to mother’s question
4
Makepractical
recommenda-tions
Provide relevant information
Use simple words
Build confidence
Make 1-2 practical recommendations
Be non- judgmental
5Negotiate be-havior - getcommitment
Discuss different solutions with mothers
Let mothers choose the solution
Get a mother’s commitment to try one to tworecommendations
6 Summarizeand close
Ask a mother to repeat recommendation
Correct a recommendation if required
Arrange follow-up with mother
Praise and thank mother
Session 11: Group counseling for mothers on IYCF
Counseling on infant and young child feeding at health facility .31
SESSION 11: GROUP COUNSELING FOR
MOTHERS ON IYCF
Objectives:
After completing this session, trainees will be able to:
1. Describe what preparation is needed for organizing a group-counseling session.
2. escribe steps for conducting a group-counseling session on IYCF.
Why group counseling is needed
• Access to a greater number of clients than that of individual counseling.
• Clients have an opportunity to learn from each other and support each other.
• Provide information and instruction on new behaviors and discuss how to solve problems
on IYCF.
• Identify client difficulties and encourage clients to come for individual counseling and
better care.
When to conduct a group-counseling session
• Communicator may organize a group-counseling session for pregnant women or mothers in the
village, usually once a month in the communes where the health facility has no “franchise modelon IYCF”.
• May integrate with community meetings, including women’s and village meetings etc.
• May integrate with club activities.
Prepare for a group-counseling session
• Review time that clients need to receive counseling on IYCF to identify the appropriate participants
for the counseling session
• Select topic of the counseling session, prepare appropriate information and counseling cards
• Identify appropriate time and location for counseling session (no more than 60 minutes from startto finish).
• Invite participants.
• The counselor should come early to check seats, drinks, etc.
Steps of conducting a counseling session for a group
Step 1: Introduction
• Greet mothers.
• Introduce yourself.
• Ask mothers to introduce themselves.
• Introduce the topic.
• Do a quick warm-up to create a friendly atmosphere and attract participation (sing songs, warm-up games, etc.).
Step 2: Identify attitudes, understanding, and practices of mothers on a counseling topic
• Use open-ended questions to find out what mothers know, believe, do, and are interested in.
• Listen carefully to what mothers share.
• Accept what mothers think and do.
• Identify and praise what mothers understand and do right.
Step 3: Analyze and assess
• Identify difficulties mothers are having in practicing the current topic.
Step 4: Provide information and negotiate change
• Provide information related to the counseling topic.
• Use relevant counseling cards to help mothers understand and remember information.
• Discuss solutions to overcome difficulties.
• Make practical recommendations on what mothers can do.
• Encourage and negotiate with mothers to select one to two actions to try.
• Come to an agreement on practicing new behavior and get commitment from mothers.
• Ask one to two mothers to repeat the recommendations.
• Correct the recommendations if required.
• Inform mothers that they can be counseled privately at CHCs.
Step 5: Summarize and closing
• Summarize main points of the counseling session
• Identify the need for individual home visits if required
• Agree on a plan of the next counseling session
• Thank mothers
The checklist of group counseling skills on IYCF is a tool that helps:
• The counselor to self-check whether s/he provided appropriate counseling services.
• The manager and supervisor to use when evaluating counseling skills of health staff.
Session 11: Group counseling for mothers on IYCF
Counseling on infant and young child feeding at health facility32.

Session 11: Group counseling for mothers on IYCF
Counseling on infant and young child feeding at health facility .33
Checklist of individual - counseling skills on IYCF
PROCESS ACTIVITYNOT YET
DONENOT DONE
WELLWELL-DONE
Step 1: Introduction
Greet mothers
Introduce yourself
Mothers introduce themselves
Introduce the topic
Warm-up to a create happy atmosphere involvingtrainee participation (singing, games…)
Step 2: Identify atti-
tudes, under-standing, andpractices ofmothers onthe counsel-
ing topic
Use open-ended questions to see what mothersknow, believe, do, and are interested in
Listen to mothers sharing
Accept what mothers think and do
Identify and praise what mothers understand anddo right
Step 3: Analyze and
assess
Identify the mothers’ difficulties in practicing thecurrent topic
Step 4: Provide infor-
mation andnegotiatechange
Give information that is relevant to the counselingtopic
Use the counseling card properly to help the mothers understand and remember information
Discuss solutions to overcome difficulties
Make practical suggestions on what mothers can do
Encourage and negotiate with each mother to select one to two actions to try
Come to an agreement on implementing new behavior
Inform mothers that they can be counseled privately at CHCs
Step 5: Summarize –get commit-
ment
Summarize main points of the counseling session
Agree on the plan for the next meeting
Arrange a follow-up about the mother practicingthe new behavior
Say “thank you” to the mothers.

Notes: Each franchise will be provided with BCC materials to support counseling sessions. Detailed
list of BCC materials provided is as follows:
Session 11: Group counseling for mothers on IYCF
Counseling on infant and young child feeding at health facility34.
JOB AIDS /COUNSELING MATERIAL
nourish. nurture. grow.
At village level:
• Invitation card
• Loudspeaker scripts
At franchise:
• Counseling cards
• Posters; Leaflet
• Mother-and-child booklet
• Franchise promotional items
• Educational CD/DVDs
In which:
• Invitation cards: are designed as leaflets and contain IYCF messages. The invitation cards are
managed by community-based workers (CBWs). As pregnant women and mothers who are eligible
for franchise services are identified, community-based workers are required to give them invitation
cards and motivate them to go to the franchise “M t tr i bé th ” to receive the services.
• Loudspeaker scripts: every 2-3 months, CBWs will be given a CD with messages to be played on
the village loudspeakers.
• Mother-and-child booklet: is designed as a health book and contains information on IYCF practices.
During the first visit to the “M t tr i bé th ” franchise, pregnant women/mothers will be registered
and given a mother-child book. CBWs must ensure that the pregnant women/mothers keep these
books safe and use them.
• Counseling cards: are a set of cards illustrating IYCF messages. Each franchise will get two to
three sets that can be used by health-facility workers for individual and group-counseling sessions.
• Posters, leaflets: during visits to the “M t tr i bé th ” franchise, pregnant women/mothers, fathers,
and caregivers will be given leaflets on a variety of topics. Once they return to the village, they
may consult CBWs on the content of these leaflets.

Session 12: Health and nutrition care for pregnant women and lactating mothers
Counseling on infant and young child feeding at health facility .35
SESSION 12: HEALTH AND NUTRITION CARE
FOR PREGNANT WOMEN AND LACTATING MOTHERS
Objectives:
After completing this session, trainees will be able to:
1. Present the importance of nutrition care for pregnant women and lactating mothers.
2. State the proper dietary requirements for mothers during pregnancy and lactation.
3. Point out necessary health care for women during pregnancy and lactation (breast care, immu-nization, supplementation of iron, hygiene, working and resting routines, mental support, etc.).
4. List out the types of food and appropriate dishes for pregnant women and lactating mothers at
their localities.
Importance of nutrition
• Meet demand for the body’s activities and the mother’s physiological changes such as metabolism
transformation, fat accumulation, weight gain, increased uterus volume, fetus growth, and milk pro-
duction later on.
• Inappropriate nutrition for pregnant women will affect infant’s development later on:
Undernutrition in the first period of pregnancy: newborn is not underweight but is at high riskof obesity and cardiovascular diseases later.
Undernutrition in the last period of pregnancy: newborn is at high risk of underweight and diabetes.
You need to understand the importance of nutrition for pregnant women to meet the demands of the
fetus’s development as well as mother’s nutrition needs during pregnancy and lactation.
Changes in mother’s body during pregnancy
• Body-weight changes (mother and fetus’s weight gain) during pregnancy:
AMOUNT OF WEIGHTGAIN
1ST TRIMESTER 2ND TRIMESTER 3RD TRIMESTER
Mother 1000 gram 4000 – 5000 gram 5000 – 6000 gram
Fetus 100 gram 1000 gram 2000 gram
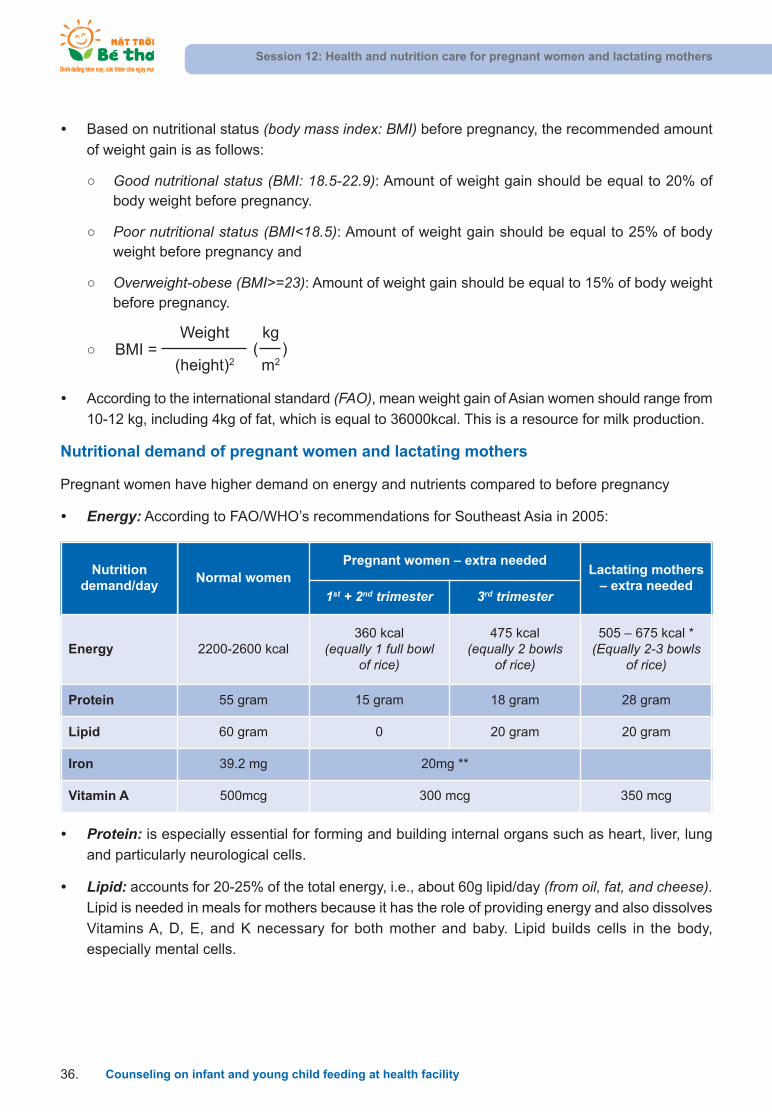
• Based on nutritional status (body mass index: BMI) before pregnancy, the recommended amount
of weight gain is as follows:
Good nutritional status (BMI: 18.5-22.9): Amount of weight gain should be equal to 20% ofbody weight before pregnancy.
Poor nutritional status (BMI<18.5): Amount of weight gain should be equal to 25% of bodyweight before pregnancy and
Overweight-obese (BMI>=23): Amount of weight gain should be equal to 15% of body weightbefore pregnancy.
• According to the international standard (FAO), mean weight gain of Asian women should range from
10-12 kg, including 4kg of fat, which is equal to 36000kcal. This is a resource for milk production.
Nutritional demand of pregnant women and lactating mothers
Pregnant women have higher demand on energy and nutrients compared to before pregnancy
• Energy: According to FAO/WHO’s recommendations for Southeast Asia in 2005:
Session 12: Health and nutrition care for pregnant women and lactating mothers
Counseling on infant and young child feeding at health facility36.
Weight
(height)2(
kg
m2)BMI =
• Protein: is especially essential for forming and building internal organs such as heart, liver, lung
and particularly neurological cells.
• Lipid: accounts for 20-25% of the total energy, i.e., about 60g lipid/day (from oil, fat, and cheese).Lipid is needed in meals for mothers because it has the role of providing energy and also dissolves
Vitamins A, D, E, and K necessary for both mother and baby. Lipid builds cells in the body,
especially mental cells.
Nutritiondemand/day
Normal womenPregnant women – extra needed
Lactating mothers– extra needed
1st + 2nd trimester 3rd trimester
Energy 2200-2600 kcal360 kcal
(equally 1 full bowl of rice)
475 kcal (equally 2 bowls
of rice)
505 – 675 kcal *(Equally 2-3 bowls
of rice)
Protein 55 gram 15 gram 18 gram 28 gram
Lipid 60 gram 0 20 gram 20 gram
Iron 39.2 mg 20mg **
Vitamin A 500mcg 300 mcg 350 mcg
Session 12: Health and nutrition care for pregnant women and lactating mothers
Counseling on infant and young child feeding at health facility .37
• Vitamins, minerals, and micro-nutrients:
Vitamins and minerals are necessary for the body’s normal metabolism and building internal organs.
In addition to its increasing eyesight and immune resistance, Vitamin A creates long bones forinfants, helping them to potentially reach optimal height.
Vitamin D supports absorption and metabolism of calcium, forming a child’s skeleton.
Vitamin C increases resistance to infection and supports iron absorption.
Acid folic helps produce blood and neurological tubes.
Other vitamins support the body’s ability to absorb nutrients and strengthen the body’s functions.
Iron helps to produce blood, and is available in solid blood, red-colored meat, soy beans, anddark-green leaves.
Calcium helps in forming the skeleton.
Zinc increases an infant’s height during pregnancy and an infant’s immune system.
Nutrients are available in food consumed daily. However, each type of food will contain more of some
nutrients than others. Therefore, food diversification is needed to receive sufficient nutrients.
Appropriate diet for mothers during the pregnancy period
A meal for a pregnant woman should provide sufficient nutrients by providing all four food groups; her
meal should contain more food than before pregnancy. In this way the mother receives:
• Sufficient energy by consuming rice, noodles, corn, sweet potato, cassava, and its processed
products.
• Protein: from animal-source food such as meat, fish, egg, and milk containing precious protein.
Also, she should eat more beans, peas, sesames, peanuts, and plant oils to provide more protein.
• Lipid: provided from oil, fat, peanuts, sesames, etc.
• Vitamins and minerals by eating green vegetables and fruit (popular vegetables available in VietNam such as spinach, “rau ngot”, “rau cai xoong”, “rau den”, etc. are rich in Vitamin C, carotene,B12, B2, iron, folic acid, etc.) Ripe fruit such as banana, papaya, orange, mango, etc. are also es-
sential for mothers. She should eat ripe fruit daily if possible.
Foods and drinks that should be limited
• Do not use stimulating beverages/food such as alcohol, coffee, cigarettes, and thick tea.
• Reduce condiments such as chili, pepper, and garlic.
• Reduce salty food, especially for edematous mothers, to diminish edema and avoid problems
at birth.
Other health care
• Antenatal care: every three months in three trimesters during pregnancy
Purposes:
1st trimester: identify pregnancy and receive counseling on nutrition, consume an iron tablet,and monitor weight.
2nd trimester: monitor the fetus’s development, receive a tetanus vaccine, monitor the amountof weight gain, and receive counseling on nutrition.
3rd trimester: monitor the fetus’ development, receive tetanus vaccine, monitor the amount ofweight gain, receive counseling on nutrition, and make prognosis of delivery.
• Consume an iron tablet to prevent iron-deficiency anemia as instructed by health staff.
• Breast care: Breast care, especially nipple sanitation, is very important to ensure that the lactiferous
duct is unblocked after delivery. Gently cleaning during bathing is recommended.
Advice to mothers during breast sanitation:
Do not continuously rub a dry milk drop, clean and gently get it out.
In case of flat or inverted nipples: stretching nipples is only allowed for full-term pregnancy(from 38 weeks of pregnancy) because early stretching leads to uterus contraction, affectingthe development of the fetus.
• Appropriate schedule of work and rest:
Do not work hard during pregnancy, to avoid miscarriage and premature delivery.
Do moderate exercises for smooth circulation, but do not participate in extreme sports or athletics.
Relaxation is necessary for mother and unborn baby; however only relaxing and not workingmakes a mother unhealthy and she will have difficulty delivering her baby. The last month isthe period of greatest weight gain, resulting in the mother having difficulty moving. Therefore,stopping work one month before delivery is helpful to both mother and baby
Mental factors are very important to the pregnant mother and fetus’s development. A happyfamily and a well-cared-for mother will help the fetus develop well, prepare for a smooth delivery, and enable sufficient milk production.
Session 12: Health and nutrition care for pregnant women and lactating mothers
Counseling on infant and young child feeding at health facility38.
Session 13: The significance of BF
Counseling on infant and young child feeding at health facility .39
SESSION 13: THE SIGNIFICANCE OF BF
Objectives:
After finishing this session, trainees will be able to:
1. State the concept and definition of EBF.
2. Point out the benefits of early and EBF.
3. State the components of breastmilk.
4. Describe major differences between breastmilk and other milk.
1. Definition of EBF:
EBF means giving a baby only breastmilk, and no other liquids or solids, not even water. Drops or
syrups consisting of vitamins, mineral supplements, or medicines are permitted.
2. Benefits of BF
Benefits of BF – for infants
• Provides a superior source of nutrients, meets all of the baby’s demands for the first 6 months.
• Promotes optimum growth and development.
• Stimulates optimum development of the brain.
• Protects against infections, especially diarrhea and respiratory infections.
• Easy to digest and effectively used.
• Provides adequate water for the baby in the first 6 months.
• Ensures nutrition, especially in emergencies (natural disaster, war, etc.).
• Clean, always ready, and of appropriate temperature.
Benefits of BF – for mothers
• Helps expel placenta and reduces the risk of bleeding.
• BF stimulates good uterus contraction.
• Early and frequent BF stimulates breastmilk production.
• Prevents engorgement (early and frequent BF).
• Provides good economic benefit (cost-effective).
FURTHER READING
Protecting a baby against infections
• Breastmilk contains white blood cells and a number of anti-infection factors, which help
to protect a baby against infections. Breastmilk helps the baby fight against infections
such as diarrhea, respiratory infection, otitis, meningitis, and urinary infections.
• This diagram shows that: when the mother develops an infection (1), white blood cells
• Promotes bonding and motherhood.
• Good for a mother’s health (decreases ovarian cancer, breast cancer, and cervical cancer).
• Improves nutrition metabolism for mothers.
• Delays a new pregnancy and menstruation.
Benefits of BF – for the family
• Reduces illness.
• Reduces health expenses.
• Prevents the mother from getting pregnant again soon after birth.
3. Disadvantages of artificial feeding
• For babies:
Interferes with bonding between mothers and babies.
More diarrhea and persistent diarrhea.
More frequent respiratory infections.
Malnutrition and Vitamin A deficiency.
More allergies and milk intolerance.
Increased risk of some chronic diseases.
Obesity.
Lower IQ.
• For mothers:
Mothers may become pregnant sooner.
Increased risk of anemia, ovarian cancer, and breast cancer for mothers.
Session 13: The significance of BF
Counseling on infant and young child feeding at health facility40.
4. Composition of breastmilk
Differences between colostrum and mature milk
• Colostrum is the special breastmilk that is available in the mother’s breast from the 14th to 16th
week of pregnancy and is produced in the first one to three days after delivery. Colostrum is thick
and yellowish or clear in color. It contains more protein than mature milk.
in her body become active and make antibodies against infections to protect her; (2)
some of these white blood cells go to her breasts and make antibodies; and (3) these
are secreted into breastmilk to protect her baby.
• Therefore a baby should not be separated from his mother when she has an infection
because her breastmilk also protects him against infection.
Psychological benefits of BF
• BF has important psychological benefits for both mothers and babies. Close contact im-
mediately after delivery helps the mother and baby to bond and helps the mother to feel
emotionally satisfied.
• The child who is breastfed tends to cry less and may be more emotionally secure. Some
studies suggest that BF may help a child develop intellectually. Low-birth-weight babies
fed breastmilk during the first weeks of life perform better on intelligence tests in later
childhood than children who are formula-fed.
Session 13: The significance of BF
Counseling on infant and young child feeding at health facility .41
COLOSTRUM
Property Importance
• Antibody-rich • Protects against allergies and infection
• Many white cells • Protects against infection
• Mild purgative effect• Clears meconium
• Helps to prevent jaundice
• Growth factors• Helps intestine to mature
• Prevents allergies and food intolerance
• Rich in Vitamin A • Reduces severity of infection
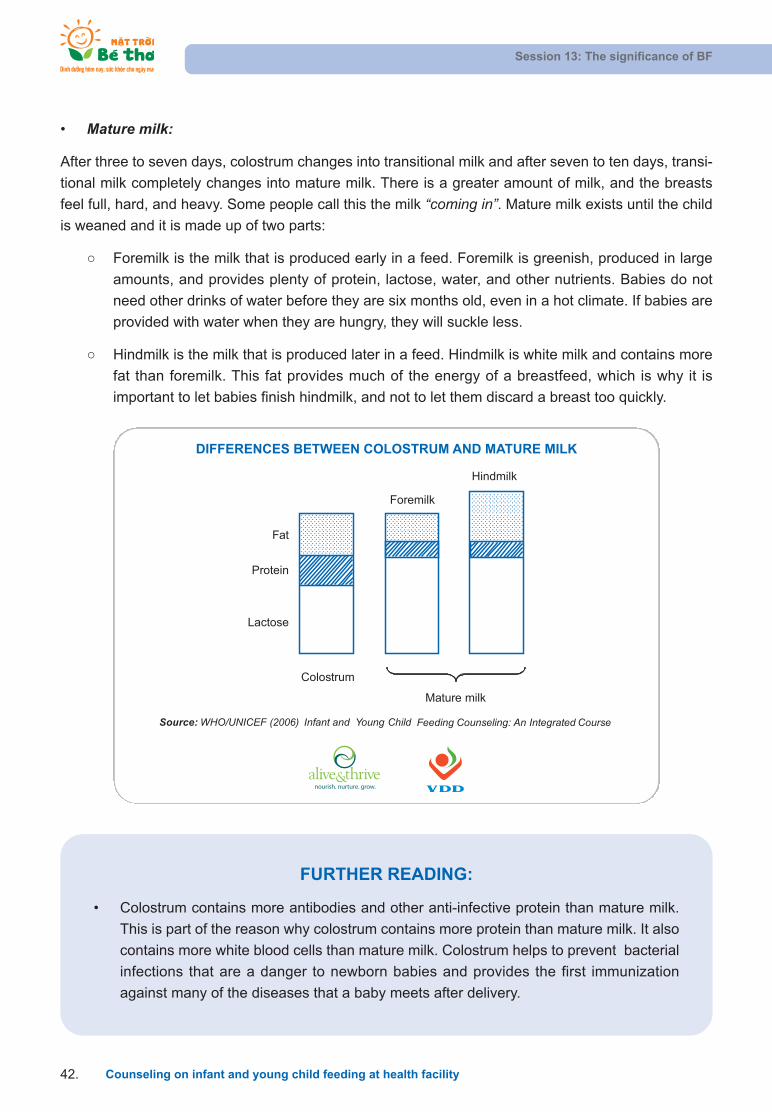
• Mature milk:
After three to seven days, colostrum changes into transitional milk and after seven to ten days, transi-
tional milk completely changes into mature milk. There is a greater amount of milk, and the breasts
feel full, hard, and heavy. Some people call this the milk “coming in”. Mature milk exists until the child
is weaned and it is made up of two parts:
Foremilk is the milk that is produced early in a feed. Foremilk is greenish, produced in large
amounts, and provides plenty of protein, lactose, water, and other nutrients. Babies do not
need other drinks of water before they are six months old, even in a hot climate. If babies are
provided with water when they are hungry, they will suckle less.
Hindmilk is the milk that is produced later in a feed. Hindmilk is white milk and contains more
fat than foremilk. This fat provides much of the energy of a breastfeed, which is why it is
important to let babies finish hindmilk, and not to let them discard a breast too quickly.
Session 13: The significance of BF
Counseling on infant and young child feeding at health facility42.
DIFFERENCES BETWEEN COLOSTRUM AND MATURE MILK
Source: WHO/UNICEF (2006) Infant and Young Child Feeding Counseling: An Integrated Course
Fat
Protein
Lactose
Foremilk
Hindmilk
Colostrum
Mature milk
nourish. nurture. grow.
FURTHER READING:
• Colostrum contains more antibodies and other anti-infective protein than mature milk.
This is part of the reason why colostrum contains more protein than mature milk. It also
contains more white blood cells than mature milk. Colostrum helps to prevent bacterial
infections that are a danger to newborn babies and provides the first immunization
against many of the diseases that a baby meets after delivery.
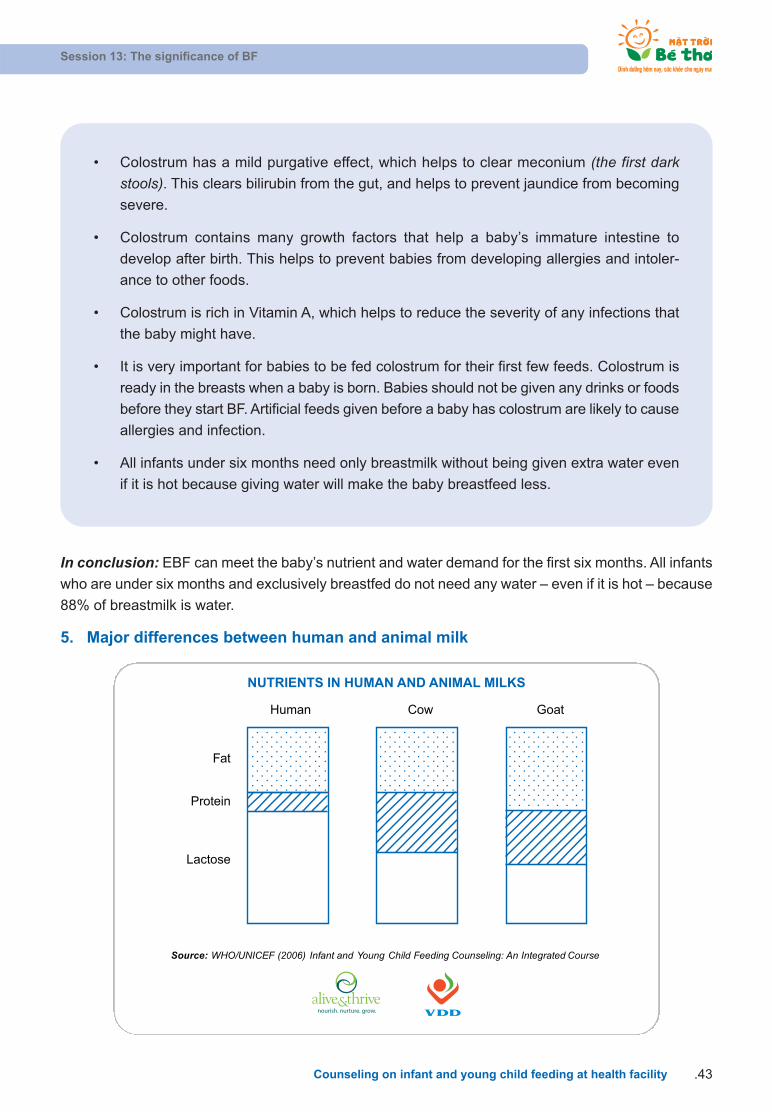
In conclusion: EBF can meet the baby’s nutrient and water demand for the first six months. All infants
who are under six months and exclusively breastfed do not need any water – even if it is hot – because
88% of breastmilk is water.
5. Major differences between human and animal milk
Session 13: The significance of BF
Counseling on infant and young child feeding at health facility .43
NUTRIENTS IN HUMAN AND ANIMAL MILKS
Source: WHO/UNICEF (2006) Infant and Young Child Feeding Counseling: An Integrated Course
Fat
Protein
Lactose
Human Cow Goat
nourish. nurture. grow.
• Colostrum has a mild purgative effect, which helps to clear meconium (the first darkstools). This clears bilirubin from the gut, and helps to prevent jaundice from becoming
severe.
• Colostrum contains many growth factors that help a baby’s immature intestine to
develop after birth. This helps to prevent babies from developing allergies and intoler-
ance to other foods.
• Colostrum is rich in Vitamin A, which helps to reduce the severity of any infections that
the baby might have.
• It is very important for babies to be fed colostrum for their first few feeds. Colostrum is
ready in the breasts when a baby is born. Babies should not be given any drinks or foods
before they start BF. Artificial feeds given before a baby has colostrum are likely to cause
allergies and infection.
• All infants under six months need only breastmilk without being given extra water even
if it is hot because giving water will make the baby breastfeed less.
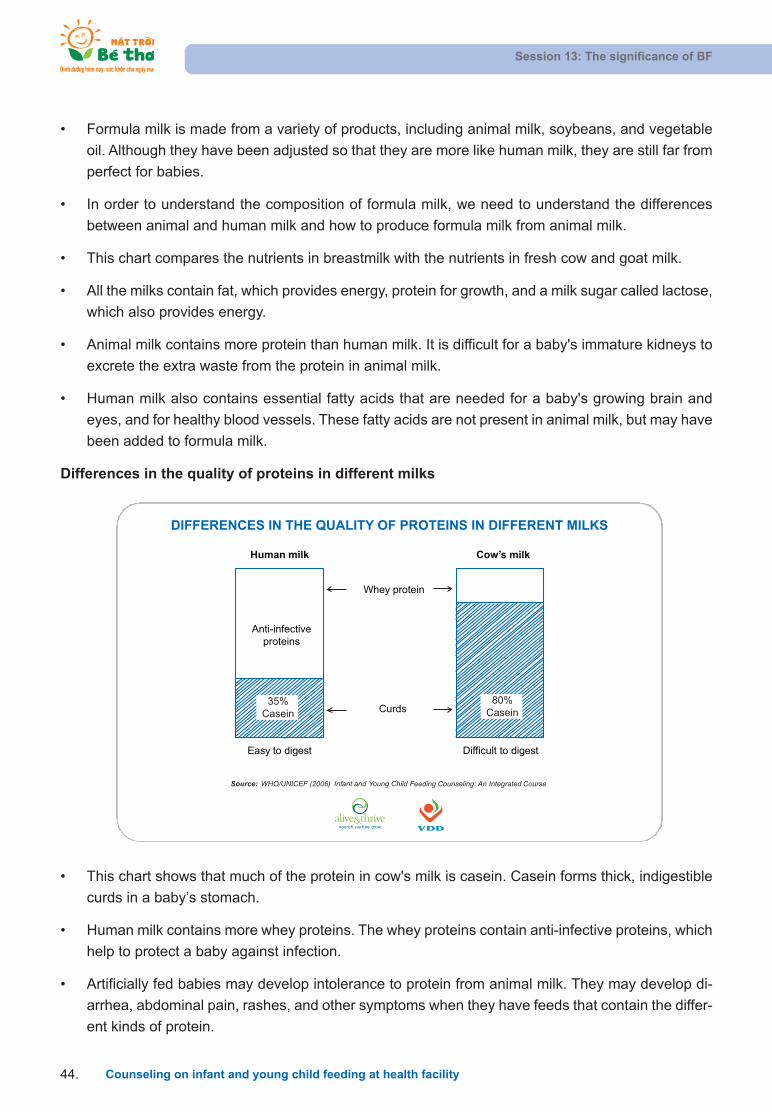
• This chart shows that much of the protein in cow's milk is casein. Casein forms thick, indigestible
curds in a baby’s stomach.
• Human milk contains more whey proteins. The whey proteins contain anti-infective proteins, which
help to protect a baby against infection.
• Artificially fed babies may develop intolerance to protein from animal milk. They may develop di-
arrhea, abdominal pain, rashes, and other symptoms when they have feeds that contain the differ-
ent kinds of protein.
• Formula milk is made from a variety of products, including animal milk, soybeans, and vegetable
oil. Although they have been adjusted so that they are more like human milk, they are still far from
perfect for babies.
• In order to understand the composition of formula milk, we need to understand the differences
between animal and human milk and how to produce formula milk from animal milk.
• This chart compares the nutrients in breastmilk with the nutrients in fresh cow and goat milk.
• All the milks contain fat, which provides energy, protein for growth, and a milk sugar called lactose,
which also provides energy.
• Animal milk contains more protein than human milk. It is difficult for a baby's immature kidneys to
excrete the extra waste from the protein in animal milk.
• Human milk also contains essential fatty acids that are needed for a baby's growing brain and
eyes, and for healthy blood vessels. These fatty acids are not present in animal milk, but may have
been added to formula milk.
Differences in the quality of proteins in different milks
Session 13: The significance of BF
Counseling on infant and young child feeding at health facility44.
DIFFERENCES IN THE QUALITY OF PROTEINS IN DIFFERENT MILKS
35%Casein
80%Casein
Cow’s milkHuman milk
Whey protein
Curds
Anti-infectiveproteins
Easy to digest Difficult to digest
Source: WHO/UNICEF (2006) Infant and Young Child Feeding Counseling: An Integrated Course
nourish. nurture. grow.
Session 13: The significance of BF
Counseling on infant and young child feeding at health facility .45
FURTHER READING: TEN STEPS FOR SUCCESSFUL BF
Every facility providing maternity services and care for newborn infants should:
1. Have a written BF policy that is routinely communicated to all health-care staff.
2. Train all health-care staff in skills necessary to implement this policy.
3. Inform all pregnant women about the benefits and management of BF.
4. Help mothers initiate BF within half an hour of birth.
5. Show mothers how to breastfeed and how to maintain lactation even if they are separated from
their infants.
6. Give newborn infants no food or drink other than breastmilk, unless medically indicated.
7. Practice rooming-in – allow mothers and infants to remain together 24 hours a day.
8. Encourage BF on demand.
9. Give no artificial teats or pacifiers (also called dummies or soothers) to BF infants.
10. Foster the establishment of BF support groups and refer mothers to them upon discharge from
the hospital or clinic.

SESSION 14: NUTRIENT DEMANDS OF CHILDREN
UNDER SIX MONTHS
Objective:
After this session, trainees will be able to:
1. Describe the size of a baby’s stomach.
2. Describe the nutrient demands of a BF baby.
3. State frequency and duration of BF.
1. Size of baby’s stomach
Parents often worry about whether their babies eat sufficiently or not. With bottle-fed babies, it is easy
to quantify compared to BF babies; the amount of breastmilk they eat is unknown. To know if babies
suckle sufficiently or not, we should study the size of baby’s stomach, especially in the first few weeks.
Day 1 and 2: the size of a small grape
Mothers still ask themselves why colostrum is too little. It is simple: a newly born baby’s stomach only
can store a liquid amount equivalent to a small grape. In addition, in the first two days, a baby’s stomach
is not able to stretch to store more than that. Mothers see that if babies are fed too much, they will
burp. Burping in children is due to many reasons, among which the small size of baby’s stomach is a
common one.
At this time, a baby’s stomach only can store about 5 to 7 ml. Therefore, a mother’s body only produces
the amount of colostrum that a baby’s stomach can store. The size of a baby’s stomach and the amount
of colostrum and suckling frequency (about 10 to 12 times per day) all combine to ensure that the baby
gets enough colostrum on day 1 and day 2.
Day 3: the size of a lemon
A baby’s stomach expands in the first three days until it reaches the size of a lemon (22 to 27 ml). Until
the third day, babies should be breastfed 8 to 12 times/day.
Breastfeeding a baby frequently is better than BF large amounts infrequently. This is because a baby’s
stomach cannot store much. In addition, a long breastfeed can cause nipple pain. Long BF periods
should only be applied later when baby’s stomach is big enough to store more milk.
Day 10: the size of a big egg
Until breastmilk is “coming in” around the tenth day of BF, a baby’s stomach can only store an amount
equivalent with 60 to 81 ml and equal in size to a big egg.
Session 14: Nutrient Demands of Children under Six Months
Counseling on infant and young child feeding at health facility46.
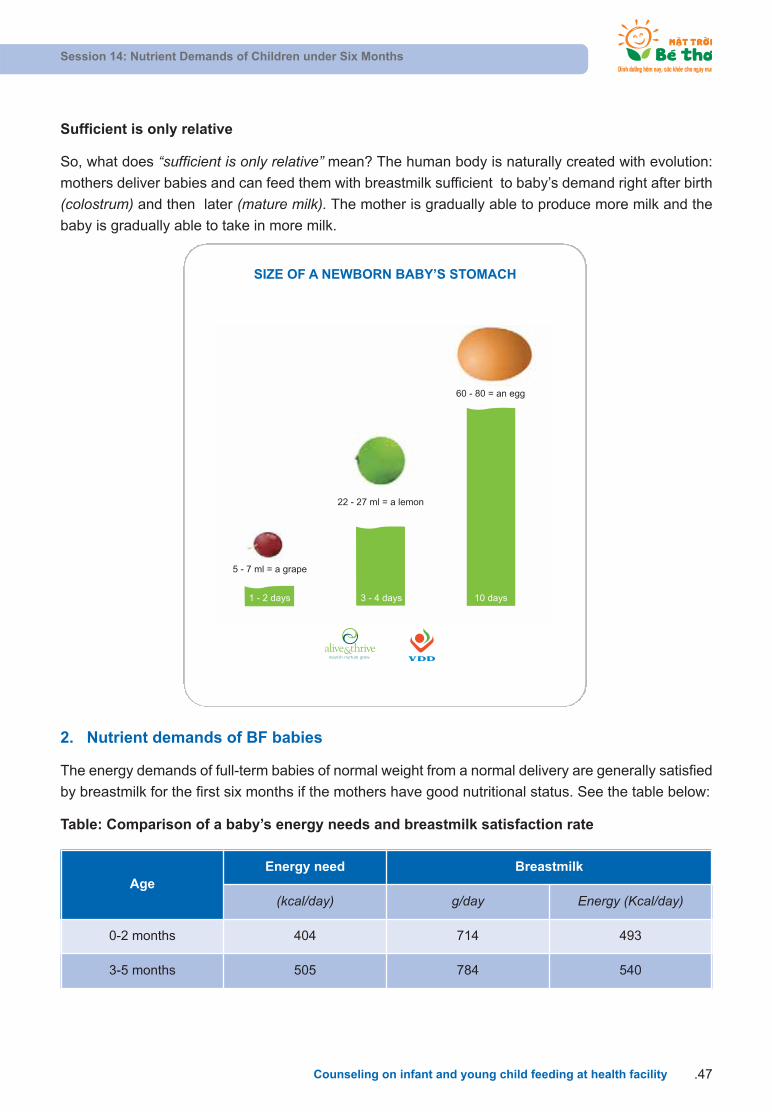
Sufficient is only relative
So, what does “sufficient is only relative” mean? The human body is naturally created with evolution:
mothers deliver babies and can feed them with breastmilk sufficient to baby’s demand right after birth
(colostrum) and then later (mature milk). The mother is gradually able to produce more milk and the
baby is gradually able to take in more milk.
Session 14: Nutrient Demands of Children under Six Months
Counseling on infant and young child feeding at health facility .47
SIZE OF A NEWBORN BABY’S STOMACH
5 - 7 ml = a grape
1 - 2 days 3 - 4 days 10 days
22 - 27 ml = a lemon
60 - 80 = an egg
nourish. nurture. grow.
2. Nutrient demands of BF babies
The energy demands of full-term babies of normal weight from a normal delivery are generally satisfied
by breastmilk for the first six months if the mothers have good nutritional status. See the table below:
Table: Comparison of a baby’s energy needs and breastmilk satisfaction rate
AgeEnergy need Breastmilk
(kcal/day) g/day Energy (Kcal/day)
0-2 months 404 714 493
3-5 months 505 784 540

• On this graph, each column represents the total amount of energy needed at that age. The taller
columns indicate that more energy is needed as the child becomes older, bigger, and more active.
The dark part shows how much of this energy is supplied by breastmilk.
• This graph shows that breastmilk supplies sufficient energy and nutrients for the baby for the first
six months. In this period, the child’s digestive system is not mature enough to manage formula
milk or complementary food. Breastmilk helps the child’s digestive system to mature.
• From the age of six months, breastmilk is no longer sufficient by itself. In addition to breastmilk, all
babies need complementary food from six months of age.
• However, breastmilk continues to be an important source of energy and high-quality nutrients be-
yond six months of age. From 6-12 months, breastmilk still continues to provide more than half of
the child’s energy needs. From 12 – 24 months, breastmilk continues to provide about one third of
the child’s energy needs. Breastmilk also helps to complete the child’s brain development and
provides antibodies. No food or formula can serve as a substitute. Hence, we must encourage and
support mothers to continue to breastfeed up to 24 months or beyond.
Milk production of mothers is adjusted appropriately according to a baby’s demand. This is clearly
shown in mothers who have twins or triplets and still practice EBF for the first six months or more.
When a baby’s demand increases, breastmilk production also increases within a few days, even in a
few hours. See the chart below to see more about a baby’s energy demands and the nutrient supply
from breastmilk.
Session 14: Nutrient Demands of Children under Six Months
Counseling on infant and young child feeding at health facility48.
00-2 m 3-5 m 6-8 m 9-11 m 12-23 m
200
400
600
800
1000 Energy Gap
Energy frombreast milk
Energ
y (k
cal/d
ay)
ENERGY REQUIRED BY AGE AND THEAMOUNT SUPPLIED FROM BREAST MILK
Age (months)
nourish. nurture. grow.
Source: WHO/UNICEF, IYCF Counseling: An Integrated Course (2006)

3. Frequency and duration of BF
• BF on demand:
Signs that a baby wants to suckle (turns over, opens its mouth and turns its head from oneside to another, moving its tongue in and out, sucking its fingers or fist).
Continue BF until the baby comes off the breast itself, at least 15-20 minutes each breast.
• Finish one breast before shifting to another.
• BF both day and night, that is, 8-12 times/24 hours.
• Frequent suckling maintains breastmilk production.
• A baby gets enough milk when s/he passes urine at least six times/day.
• BF up to 24 months or beyond.
Session 14: Nutrient Demands of Children under Six Months
Counseling on infant and young child feeding at health facility .49
FURTHER READING:
Practice frequent BF and BF on demand during the day and night
• Babies need to be breastfed on demand and frequently, both during the day and night.
The frequency of suckling is about 8-12 times within 24 hours. The gap between each
feed may be more or less two to three hours.
• A baby’s stomach is small and needs frequent feeds. Breastmilk amounts are totally ap-
propriate with that size, breastmilkis easy to digest.
• Babies should be fed before they cry. Crying is a sign of being hungry.
• Each feeding time should last until the baby wants to stop and come off the breast
him/herself. If the feeding duration lasts for more than half an hour or two successive
feeds are too close (the gap between each time is only 1-1.5 hours), it shows that babies
do not attach well to the breast and suckle ineffectively, so mothers should double check.
• Frequent BF maintains milk secretion, delays a new pregnancy, and provides
immune substances in each feed. Frequent BF also helps to prevent breast problems
like engorgement that make mothers feel uncomfortable and not want to continue
BF their baby.
• If babies urinate at least six times within 24 hours, it is a sign of sufficient BF (in the firsttwo days when babies drink colostrum, mothers may only need one to two nappies/day).If not, babies should be breastfed more or mothers need to check their BF technique
again.
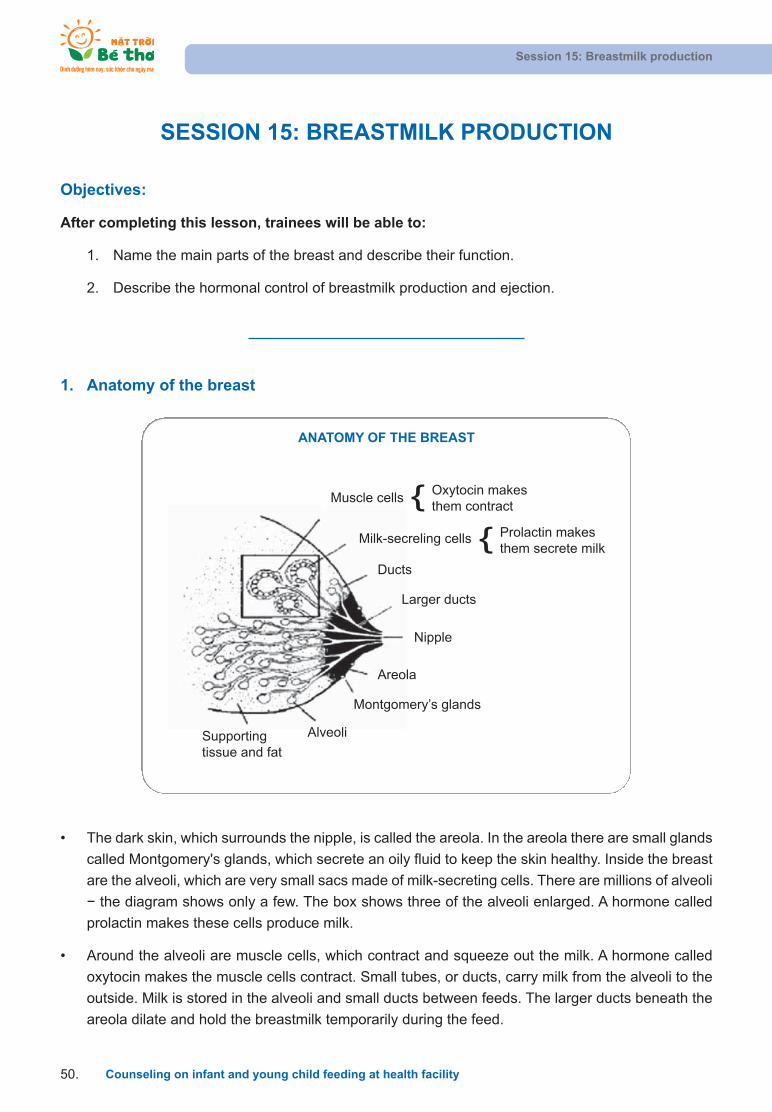
• The dark skin, which surrounds the nipple, is called the areola. In the areola there are small glands
called Montgomery's glands, which secrete an oily fluid to keep the skin healthy. Inside the breast
are the alveoli, which are very small sacs made of milk-secreting cells. There are millions of alveoli
the diagram shows only a few. The box shows three of the alveoli enlarged. A hormone called
prolactin makes these cells produce milk.
• Around the alveoli are muscle cells, which contract and squeeze out the milk. A hormone called
oxytocin makes the muscle cells contract. Small tubes, or ducts, carry milk from the alveoli to the
outside. Milk is stored in the alveoli and small ducts between feeds. The larger ducts beneath the
areola dilate and hold the breastmilk temporarily during the feed.
SESSION 15: BREASTMILK PRODUCTION
Objectives:
After completing this lesson, trainees will be able to:
1. Name the main parts of the breast and describe their function.
2. Describe the hormonal control of breastmilk production and ejection.
1. Anatomy of the breast
Session 15: Breastmilk production
Counseling on infant and young child feeding at health facility50.
Supportingtissue and fat
Alveoli
Montgomery’s glands
Areola
Nipple
Larger ducts
Ducts
Milk-secreling cells Prolactin makesthem secrete milk{
Muscle cellsOxytocin makesthem contract{
ANATOMY OF THE BREAST
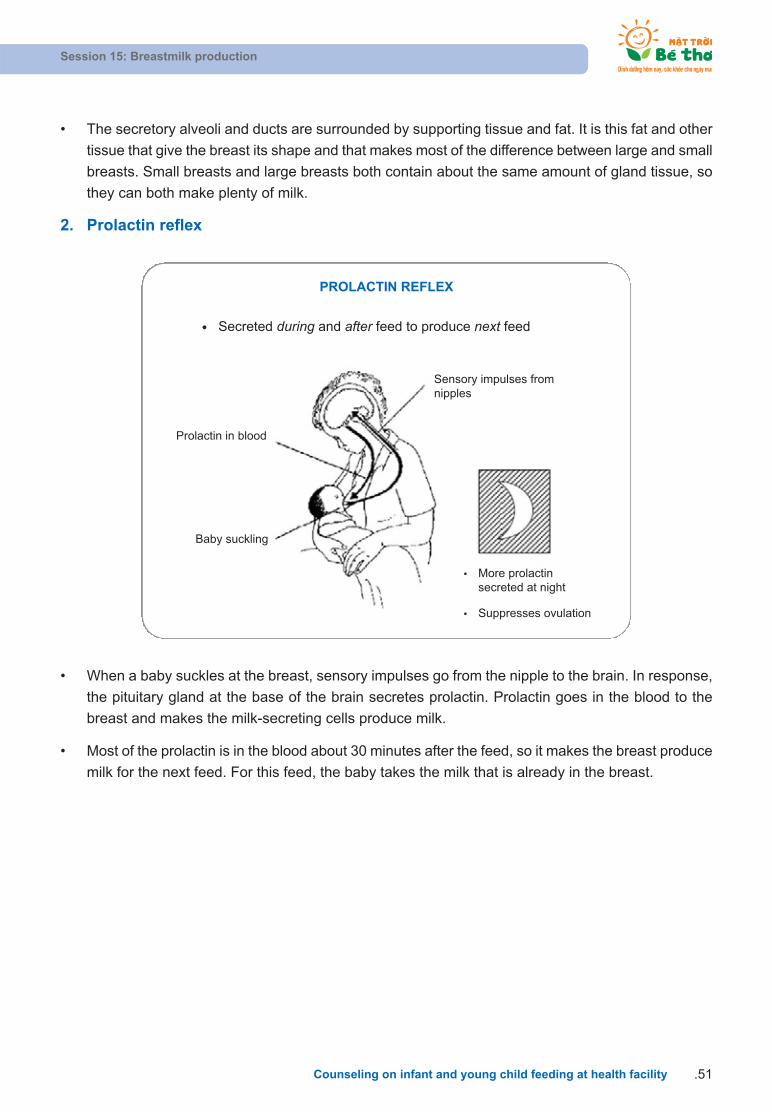
• The secretory alveoli and ducts are surrounded by supporting tissue and fat. It is this fat and other
tissue that give the breast its shape and that makes most of the difference between large and small
breasts. Small breasts and large breasts both contain about the same amount of gland tissue, so
they can both make plenty of milk.
2. Prolactin reflex
Session 15: Breastmilk production
Counseling on infant and young child feeding at health facility .51
Prolactin in blood
Baby suckling
Sensory impulses fromnipples
More prolactinsecreted at night
Suppresses ovulation
Secreted during and after feed to produce next feed
• When a baby suckles at the breast, sensory impulses go from the nipple to the brain. In response,
the pituitary gland at the base of the brain secretes prolactin. Prolactin goes in the blood to the
breast and makes the milk-secreting cells produce milk.
• Most of the prolactin is in the blood about 30 minutes after the feed, so it makes the breast produce
milk for the next feed. For this feed, the baby takes the milk that is already in the breast.
PROLACTIN REFLEX
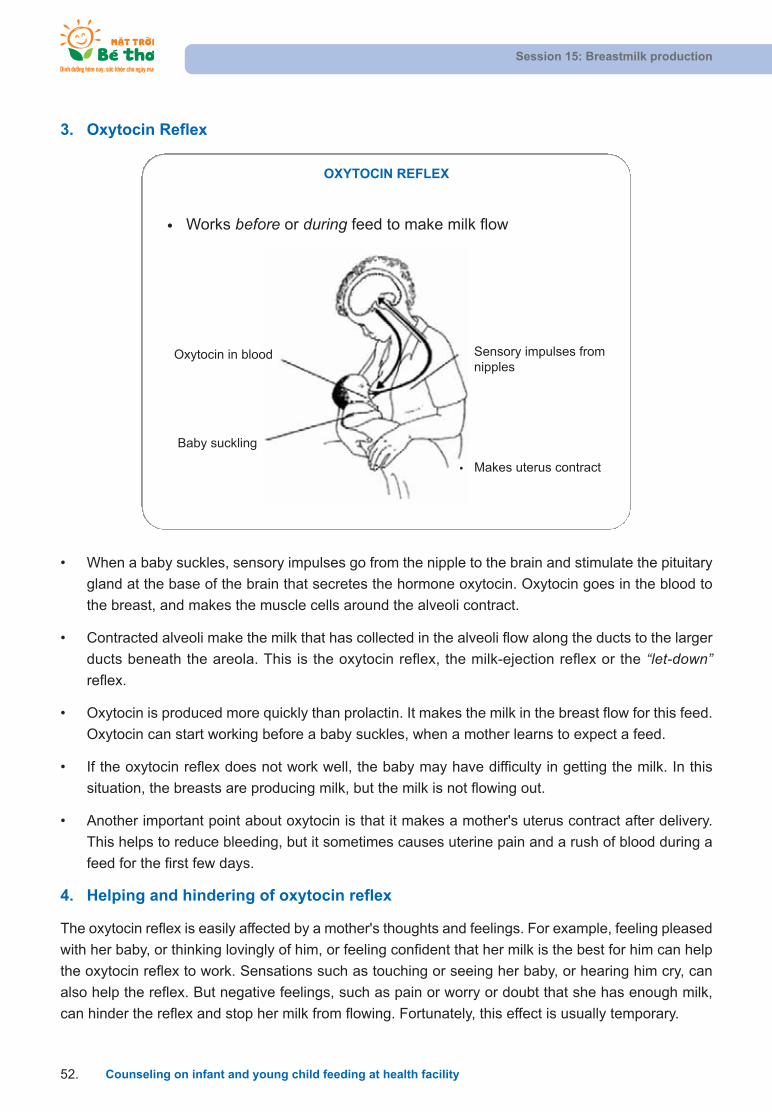
• When a baby suckles, sensory impulses go from the nipple to the brain and stimulate the pituitary
gland at the base of the brain that secretes the hormone oxytocin. Oxytocin goes in the blood to
the breast, and makes the muscle cells around the alveoli contract.
• Contracted alveoli make the milk that has collected in the alveoli flow along the ducts to the larger
ducts beneath the areola. This is the oxytocin reflex, the milk-ejection reflex or the “let-down” reflex.
• Oxytocin is produced more quickly than prolactin. It makes the milk in the breast flow for this feed.
Oxytocin can start working before a baby suckles, when a mother learns to expect a feed.
• If the oxytocin reflex does not work well, the baby may have difficulty in getting the milk. In this
situation, the breasts are producing milk, but the milk is not flowing out.
• Another important point about oxytocin is that it makes a mother's uterus contract after delivery.
This helps to reduce bleeding, but it sometimes causes uterine pain and a rush of blood during a
feed for the first few days.
4. Helping and hindering of oxytocin reflex
The oxytocin reflex is easily affected by a mother's thoughts and feelings. For example, feeling pleased
with her baby, or thinking lovingly of him, or feeling confident that her milk is the best for him can help
the oxytocin reflex to work. Sensations such as touching or seeing her baby, or hearing him cry, can
also help the reflex. But negative feelings, such as pain or worry or doubt that she has enough milk,
can hinder the reflex and stop her milk from flowing. Fortunately, this effect is usually temporary.
3. Oxytocin Reflex
Session 15: Breastmilk production
Counseling on infant and young child feeding at health facility52.
Oxytocin in blood
Baby suckling
Sensory impulses fromnipples
Works before or during feed to make milk flow
Makes uterus contract
OXYTOCIN REFLEX

Session 15: Breastmilk production
Counseling on infant and young child feeding at health facility .53
These help reflex These hinder reflex
Thinks lovingly of baby
Sounds of baby
Sight of baby
Touches baby
Confidence
Worry
Stress
Pain
Doubt
FURTHER READING: SIGNS AND SENSATIONS OF AN ACTIVE OXYTOCIN REFLEX
A mother may notice:
• A squeezing or tingling sensation in her breasts just before she feeds her baby or during a feed.
• Milk flowing from her breasts when she thinks of her baby or hears him crying.
• Milk dripping from her other breast when her baby is suckling.
• Milk flowing from her breasts in fine streams if her baby comes off the breast during a feed.
• Pain from uterine contractions, sometimes with a rush of blood, during feeds in the first week.
• Slow deep sucks and swallowing by the baby, which show that breastmilk is flowing well into his
mouth.
HELPING AND HINDERING OF OXYTOCIN REFLEX
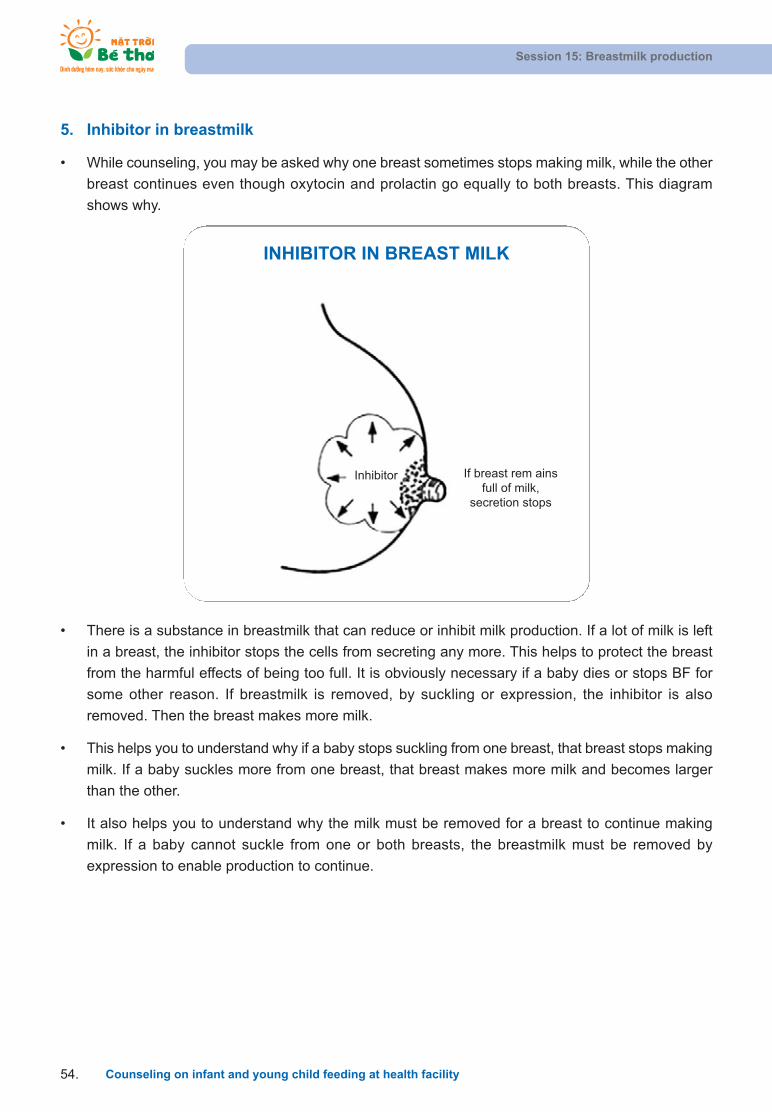
5. Inhibitor in breastmilk
• While counseling, you may be asked why one breast sometimes stops making milk, while the other
breast continues even though oxytocin and prolactin go equally to both breasts. This diagram
shows why.
Session 15: Breastmilk production
Counseling on infant and young child feeding at health facility54.
INHIBITOR IN BREAST MILK
If breast rem ainsfull of milk,
secretion stops
Inhibitor
• There is a substance in breastmilk that can reduce or inhibit milk production. If a lot of milk is left
in a breast, the inhibitor stops the cells from secreting any more. This helps to protect the breast
from the harmful effects of being too full. It is obviously necessary if a baby dies or stops BF for
some other reason. If breastmilk is removed, by suckling or expression, the inhibitor is also
removed. Then the breast makes more milk.
• This helps you to understand why if a baby stops suckling from one breast, that breast stops making
milk. If a baby suckles more from one breast, that breast makes more milk and becomes larger
than the other.
• It also helps you to understand why the milk must be removed for a breast to continue making
milk. If a baby cannot suckle from one or both breasts, the breastmilk must be removed by
expression to enable production to continue.
SESSION 16: IN-CLASSROOM PRACTICE - INDIVIDUAL
COUNSELING ON BF
Objectives:
After completing this session, trainees will be able to:
1. Practice individual BF-counseling skills.
2. Apply knowledge on BF into counseling practice for mothers.
• Read carefully “the case studies on BF individual counseling” below and determine:
Who are the clients? What are their problems?
Which behaviors need to be changed?
What are the difficulties when practicing new behaviors?
Which information is necessary during the counseling session?
Which counseling cards should be used?
• Use the checklist of individual counseling on IYCF as a self-observing and monitoring tool to see
if the counseling session provides enough information.
Session 16: In-classroom practice - Individual Counseling on BF
Counseling on infant and young child feeding at health facility .55
CASE STUDIES ON BF INDIVIDUAL COUNSELING
AT A HEALTH FACILITY
Case study 1: Ms. Phuong is in the seventh month of pregnancy. This is her first child. When
talking to her, you learn that her mother-in-law does not let her eat crabs, shellfish, and buf-
falo meat because she said that this food could make the baby get diarrhea easily. Please
counsel her mother-in-law.
Case study 2: You are in the ninth month of pregnancy, this is your first time. You intend to
breastfeed your baby but many people say that breastmilk often comes in late so you should
bring formula milk when coming to the hospital for delivery. You don’t want to feed your baby
formula milk but are afraid that he will be hungry when he is born.
You can start the conversation with: “I don’t know whether I should bring formula milk whencoming to hospital for delivery.”

Session 16: In-classroom practice - Individual Counseling on BF
Counseling on infant and young child feeding at health facility56.
Case study 3: Ms. Huong gave birth to her first baby two days ago and she does not know
how to breastfeed her baby properly. She hears that if she does not breastfeed properly, her
baby may not be able to suckle and will get hungry. Please counsel her on how to attach the
baby to her breast and how to breastfeed properly.
Case study 4: Ms. Nhung delivered a baby two months ago. You visit her house and see
her breastfeed her baby but there is still a tin of milk powder for babies and a feeding bottle,
teat, etc. Ms. Nhung says that she has a lot of breastmilk but she hears that feeding infants
with powdered milk will make them chubbier. Therefore, she is going to feed her baby with
powdered milk next week. Please counsel her.
Case study 5: Ms. Ngan is BF her baby who is three months old. She feels that she does
not have enough milk to breastfeed her baby exclusively. She would like to start giving her
child other food as she feels her child is hungry all the time. Please counsel her.
Case study 6: Ms. Chung is BF her baby who is four months old. However, she is going to
return to work in a few weeks. She wants to start giving her child half a bowl of bot (ricegruel) twice a day. Please counsel her.

Session 16: In-classroom practice - Individual Counseling on BF
Counseling on infant and young child feeding at health facility .57
SKILLS ACTIVITIESNOT
DONENOT DONE
WELLWELL-DONE
1
Introduction – a create warmand friendly environment
Greet mothers
Introduce yourself
Make eye contact
Smile
Show respect
2Identify
current prob-lems /issues
Listen
Be non-Judgmental
Ask open-ended questions
Accept what a mother says
3 Analyze/assess
Identify the problem, issue
Identify priority if there is more than one problems
Ask more open-ended questions to identify barriers
Respond to mother’s question
4Make practicalrecommenda-
tion
Provide relevant information
Build confidence
Make 1-2 practical recommendations
Use counseling cards/ materials
5Negotiate
behavior – getcommitment
Discuss different solutions with mothers
Let mothers decide the solution
Get mother’s commitment to try 1-2 recommendations
6 Summary -Closing
Ask mother to repeat recommendation
Correct recommendation as appropriate
Arrange follow-up with mothers
Praise and thank mothers
CHECKLIST OF INDIVIDUAL COUNSELING SKILLS ON IYCF

Session 17: In-classroom practice Group-counseling practice on BF
Counseling on infant and young child feeding at health facility58.
SESSION 17: IN-CLASSROOM PRACTICE
GROUP - COUNSELING PRACTICE ON BF
Objectives:
After completing this session, trainees will be able to:
1. Practice group-counseling skills on BF.
2. Apply knowledge on BF in counseling practice for mothers.
• Read carefully “the case studies for BF group counseling” below and determine:
Who are the clients? What are their problems?
Which behaviors need to be changed?
What are the difficulties when practicing new behaviors?
Which information is necessary during the counseling session?
Which counseling cards should be used?
Case studies for BF group counseling
Case study 1: In your village, local residents live far from the health station. They live hardlives. Mothers often work hard and do not receive nutrition care during the pregnancy andBF period. Organize a group discussion with pregnant women on nutrition care for pregnantwomen.
Case study 2: You have organized a group-counseling session for pregnant women. Youraim is to talk about the immediate initiation of BF. As you discuss this with the mothers, youlearn that in this community they believe that the first few drops of colostrum are not goodfor the baby. Please conduct the counseling session.
Case study 3: You have organized a group-counseling session on EBF for mothers of children aged 3-4 months. Some mothers say that they have to go to work and so they haveto give their children some other food besides breastmilk. Please conduct the counseling session.
Case study 4: It is the summer season and you receive feedback from the village healthworkers that many mothers are giving water to their children because they believe the chil-dren will get dehydrated. You organize a counseling session for mothers to talk about EBF.
• Use the checklist of group counseling on IYCF as a self-observing and monitoring tool to see if thecounseling session provides enough information

Session 17: In-classroom practice Group-counseling practice on BF
Counseling on infant and young child feeding at health facility .59
CHECKLIST OF GROUP COUNSELING ON IYCF
PROCESS ACTIVITYNOT YET
DONENOT WELL
DONEWELLDONE
Step 1: Introduction
Greet mothers
introduce yourself
Mothers introduce themselves
Introduce the topic
Warm-up to create happy atmosphere, involvingtrainee’s participation (singing, games…)
Step 2: Identify atti-
tudes, under-standing, andpractices ofmothers onthe counsel-
ing topic
Use open-ended questions to know what mothersknow, believe, do and are interested in
Listen to mothers’ sharing
Accept what mothers think and do
Identify and praise what mothers understand anddo right
Step 3: Analyze and
assess
Identify mothers’ difficulties in practicing the current topic
Step 4: Provide infor-
mation andnegotiatechange
Give information that is relevant to the counselingtopic
Use counseling cards properly to help mothers understand and remember information
Discuss solutions to overcome difficulties
Make practical suggestions on what mothers can do
Encourage and negotiate with each mother to select one to two actions to try
Come to an agreement on implementing new behavior
Inform mothers that they can be counseled privately at CHCs
Step 5: Summarize –get commit-
ment
Summarize main points of the counseling session
Agree on the plan for the next meeting.
Arrange follow-up on mothers’ practicing new behavior
Say “thank you” to mothers
Session 18: Positioning and attachment
Counseling on infant and young child feeding at health facility60.
SESSION 18: POSITIONING AND ATTACHMENT
Objectives:
After completing this lesson trainees will be able to
1. Explain the four key points of positioning.
2. Describe how a mother should support her breast for feeding.
3. Help a mother to position her baby at the breast.
4. Help the baby to attach to the breast.
5. Demonstrate the main positions – sitting, lying, underarm, and across.
Note:
• Always assess a mother BF before you help her. Take time to observe what she does so that you
can understand her situation clearly. Do not rush to make her do something different.
• Give a mother help only if she has difficulty. Some mothers and babies breastfeed satisfactorily in
positions that would be difficult for others. This is especially true with babies more than about two
months old. There is no point trying to change a baby’s position if he is getting breastmilk effectively,
and his mother is comfortable.
• Let the mother do as much as possible herself. Be careful not to ‘take over’ from her. Explain what
you want her to do. If possible, demonstrate on your own body to show her what you mean.
• Make sure that she understands what you do so that she can do it herself. Your aim is to help her
to position her own baby. It does not help if you can get a baby to suckle but his mother cannot do
it on her own.
Help a mother who is sitting to position her baby
• Greet the mother, introduce yourself, and ask for the mother and baby’s name. Ask how the mother
feels and one to two more open-ended questions on BF.
• Assess a breastfeed. Ask if you may see how baby breastfeeds and ask the mother to put him to
the breast in her usual way. (If the baby has just been breastfed many times, arrange a time tocome back.) Observe the breastfeed.
• If you identify that the mother needs help to improve the baby’s attachment at the breast, say some-
thing encouraging like: “He really wants your breastmilk, doesn’t he?”
• Then explain what to do to help and ask if the mother agrees or not. For example, say: “BF might
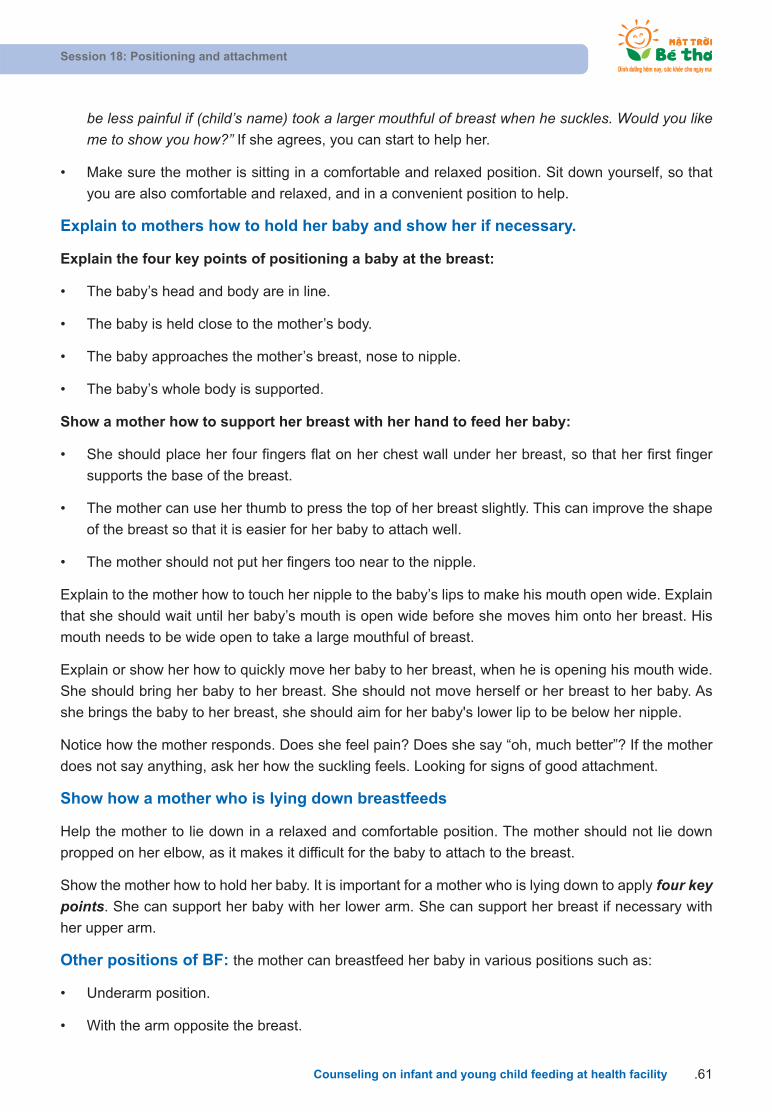
Session 18: Positioning and attachment
Counseling on infant and young child feeding at health facility .61
be less painful if (child’s name) took a larger mouthful of breast when he suckles. Would you likeme to show you how?” If she agrees, you can start to help her.
• Make sure the mother is sitting in a comfortable and relaxed position. Sit down yourself, so that
you are also comfortable and relaxed, and in a convenient position to help.
Explain to mothers how to hold her baby and show her if necessary.
Explain the four key points of positioning a baby at the breast:
• The baby’s head and body are in line.
• The baby is held close to the mother’s body.
• The baby approaches the mother’s breast, nose to nipple.
• The baby’s whole body is supported.
Show a mother how to support her breast with her hand to feed her baby:
• She should place her four fingers flat on her chest wall under her breast, so that her first finger
supports the base of the breast.
• The mother can use her thumb to press the top of her breast slightly. This can improve the shape
of the breast so that it is easier for her baby to attach well.
• The mother should not put her fingers too near to the nipple.
Explain to the mother how to touch her nipple to the baby’s lips to make his mouth open wide. Explain
that she should wait until her baby’s mouth is open wide before she moves him onto her breast. His
mouth needs to be wide open to take a large mouthful of breast.
Explain or show her how to quickly move her baby to her breast, when he is opening his mouth wide.
She should bring her baby to her breast. She should not move herself or her breast to her baby. As
she brings the baby to her breast, she should aim for her baby's lower lip to be below her nipple.
Notice how the mother responds. Does she feel pain? Does she say “oh, much better”? If the mother
does not say anything, ask her how the suckling feels. Looking for signs of good attachment.
Show how a mother who is lying down breastfeeds
Help the mother to lie down in a relaxed and comfortable position. The mother should not lie down
propped on her elbow, as it makes it difficult for the baby to attach to the breast.
Show the mother how to hold her baby. It is important for a mother who is lying down to apply four keypoints. She can support her baby with her lower arm. She can support her breast if necessary with
her upper arm.
Other positions of BF: the mother can breastfeed her baby in various positions such as:
• Underarm position.
• With the arm opposite the breast.
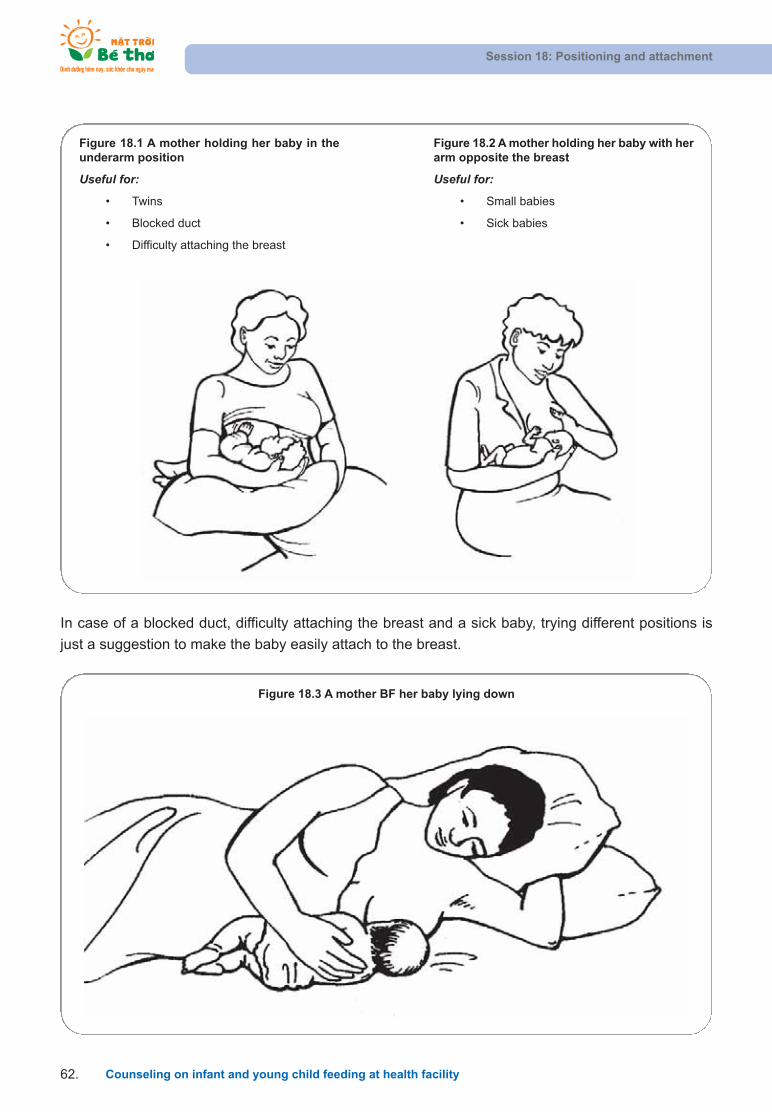
Figure 18.1 A mother holding her baby in theunderarm position
Useful for:
• Twins
• Blocked duct
• Difficulty attaching the breast
Figure 18.3 A mother BF her baby lying down
Figure 18.2 A mother holding her baby with herarm opposite the breast
Useful for:
• Small babies
• Sick babies
Session 18: Positioning and attachment
Counseling on infant and young child feeding at health facility62.
In case of a blocked duct, difficulty attaching the breast and a sick baby, trying different positions is
just a suggestion to make the baby easily attach to the breast.

HELPING A MOTHER TO POSITION HER BABY
• Greet the mother and ask how BF is going.
• Explain what might help, and ask if she would like you to show her.
• Make sure that she is comfortable and relaxed.
• Sit yourself down in a comfortable and convenient position.
• Explain how to hold the baby and show her if necessary.
The four key points are:
The baby’s head and body in line.
The baby is held close to the mother’s body.
The baby’s face approaches the breast, nose to nipple.
The baby’s head, shoulders, and bottom held.
Show her how to support her breast:
With her fingers against her chest wall below her breast.
With her first finger supporting the breast.
With her thumb above her breast.
Her fingers should not be too near to the nipple.
• Explain or show her how to help the baby to attach:
Touch her baby's lips with her nipple.
Wait until her baby's mouth is wide open.
Move her baby quickly onto her breast, aiming his lower lip below the nipple.
• Notice how she responds and ask her how she feels when her baby is suckling.
• Look for signs of good attachment. If the attachment is not good, try again.
Session 18: Positioning and attachment
Counseling on infant and young child feeding at health facility .63
Attachment
Look at pictures on attachment from the inside and outside and explain with picture one “correct attachment” and picture two “incorrect attachment”.
Good and poor attachment
What differences do you see?
Attachment (outside appearance)
What differences do you see?
1 2 1 2

Four signs of correct attachment
1. More of the areola is visible above the baby’s top lip than below the lower lip.
2. The baby’s mouth is wide open.
3. The baby’s lower lip is curled outwards.
4. The baby’s chin is touching or almost touching the breast.
Causes of poor attachment
1. Use of a feeding bottle – nipple confusion.
2. Inexperienced mother – first baby, bottle feeding.
3. Functional difficulty – small/weak babies, poorly protractile nipple/underlying tissues, engorged
breasts, BF delay.
4. Lack of skilled support –from the community, experienced women, birth attendants, etc.
Result of poor attachment
If a baby is poorly attached, and he ‘nipple sucks’, it is painful for his mother. Poor attachment is the
most important cause of sore nipples. As the baby sucks hard to try to get milk he pulls the nipple in
and out. This makes the nipple skin rub against his mouth. If a baby continues to suck this way, he can
damage the nipple skin and cause cracks (also known as fissures). As the baby does not drink breast-
milk effectively the breasts may become engorged. As s/he does not get enough breastmilk, s/he may
be unsatisfied and cry a lot. He may want to feed often or for a very long time at each feed. Eventually
if breastmilk is not removed, the breasts may make less milk. A baby may fail to gain weight and the
mother may feel she is failing at BF.
To prevent this from happening all mothers need help to position and attach their babies. Also babies
should not be given feeding bottles. If a baby feeds from a bottle before BF is established, he may
have difficulty suckling effectively.
Session 18: Positioning and attachment
Counseling on infant and young child feeding at health facility64.

Session 18: Positioning and attachment
Counseling on infant and young child feeding at health facility .65
How to attach a baby at the breast
Position baby’s nose level to the nipples. Use a
finger or nipple to lightly touch the baby’s lips
so that the baby opens his mouth.
Wait until the baby’s mouth is wide open, then
bring the nipple right onto his mouth.
Ensure that the baby takes a mouthful of breast,
nearly covering all of the areola.
When a baby is attached well• More areola is seen above baby’s upper
lip• Baby’s mouth is wide open • Lower lip is turned outwards• Baby’s chin is touching the mother’s
breast
When the baby is full, hold him tightly in your
arms.
When finished, BF will bring a satisfactory
feeling to both mother and baby.

Session 19: Assessing a Breastfeed
Counseling on infant and young child feeding at health facility66.
SESSION 19: ASSESSING A BREASTFEED
Objectives:
After completing this lesson, trainees will be able to:
1. Explain the content of and the use of the Breastfeed Observation Job Aid
2. Assess a breastfeed by observing a mother and baby.
3. Recognize signs of good and poor attachment and positioning.
Assessing a breastfeed helps you to decide if a mother needs help or not, and how to help her. Before
asking questions, you can learn a lot about how well or badly BF is going just by observing. There are
some signs you can observe when a baby is not BF. However, there are signs you can only observe
when a baby is BF.

Session 19: Assessing a Breastfeed
Counseling on infant and young child feeding at health facility .67
BREASTFEED OBSERVATION JOB AID
Mother's name ________________ Date ______________
Baby's name ___________________ Baby's age ________
Signs that breastfeeding is going well:
GENERAL
Mother:
¨ Healthy
¨ Relaxed and comfortable
¨ Signs of bonding between mother and baby
Signs of possible difficulty:
Mother:
¨ Ill or depressed
¨ Tense and uncomfortable
¨ No mother/baby contact
Baby:
¨ Healthy
¨ Calm and relaxed
¨ Reaches or moves for breast if hungry
Baby:
¨ Sleepy or ill
¨ Restless or crying
¨ Does not reach or root
BREASTS
¨ Healthy
¨ No pain or discomfort
¨ Breast well supported with fingers away from nipple
¨ Breasts look red, swollen, or sore
¨ Breast or nipple painful
¨ Breasts held with fingers on areola
BABY’S POSITION
¨ Baby’s head and body in line
¨ Baby held close to mother’s body
¨ Baby’s head and neck supported
¨ Baby approaches breast, nose to nipple
¨ Baby’s neck and head twisted to feed
¨ Baby not held close
¨ Baby not supported
¨ Baby approaches breast, lower lip/chin to nipple
BABY’S ATTACHMENT
¨ More areola seen above baby’s top lip
¨ Baby’s mouth open wide
¨ Lower lip turned outwards
¨ Baby’s chin touches breast
¨ More areola seen below bottom lip
¨ Baby’s mouth not open wide
¨ Lips pointing forward or turned in
¨ Baby’s chin not touching breast
SUCKLING
¨ Slow, deep sucks with pauses
¨ Cheeks round when suckling
¨ Baby releases breast when finished
¨ Mother notices signs of oxytocin reflex
¨ Rapid shallow sucks
¨ Cheeks pulled in when suckling
¨ Mother takes baby off the breast
¨ No signs of oxytocin reflex noticed
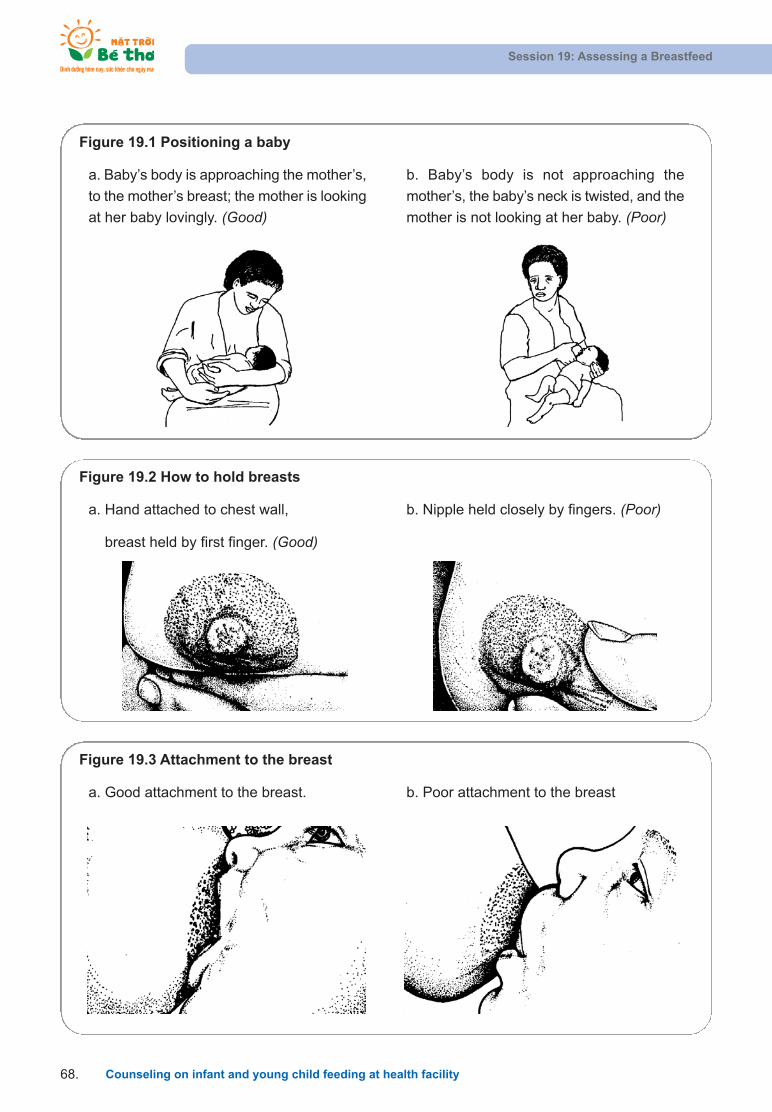
Session 19: Assessing a Breastfeed
Counseling on infant and young child feeding at health facility68.
Figure 19.1 Positioning a baby
a. Baby’s body is approaching the mother’s,
to the mother’s breast; the mother is looking
at her baby lovingly. (Good)
b. Baby’s body is not approaching the
mother’s, the baby’s neck is twisted, and the
mother is not looking at her baby. (Poor)
Figure 19.2 How to hold breasts
a. Hand attached to chest wall,
breast held by first finger. (Good)
b. Nipple held closely by fingers. (Poor)
Figure 19.3 Attachment to the breast
a. Good attachment to the breast. b. Poor attachment to the breast

Session 19: Assessing a Breastfeed
Counseling on infant and young child feeding at health facility .69
Exercise: Using the Breastfeed Observation Job Aid
In this exercise, you will practice identifying signs of good and poor attachment through some slides
showing a baby suckling. In some pictures, you will also see signs of correct and wrong positioning.
• If you see a sign on the slide, make a in the box next to the sign.
• If you do not see a sign, leave the box empty.
BREASTFEED OBSERVATION JOB AID
Mother's name ________________ Date ______________
Baby's name ___________________ Baby's age ________
Signs that breastfeeding is going well:GENERALMother:
¨ Healthy
¨ Relaxed and comfortable
¨ Signs of bonding between mother and baby
Signs of possible difficulty:
Mother:¨ Ill or depressed
¨ Tense and uncomfortable
¨ No mother/baby contact
Baby:¨ Healthy
¨ Calm and relaxed
¨ Reaches or moves for breast if hungry
Baby:¨ Sleepy or ill
¨ Restless or crying
¨ Does not reach or root
BREASTS¨ Healthy
¨ No pain or discomfort
¨ Breast well supported with fingers away from nipple
¨ Breasts look red, swollen, or sore
¨ Breast or nipple painful
¨ Breasts held with fingers on areola
BABY’S POSITION¨ Baby’s head and body in line
¨ Baby held close to mother’s body
¨ Baby’s head and neck supported
¨ Baby approaches breast, nose to nipple
¨ Baby’s neck and head twisted to feed
¨ Baby not held close
¨ Baby not supported
¨ Baby approaches breast, lower lip/chin to nipple
BABY’S ATTACHMENT¨ More areola seen above baby’s top lip
¨ Baby’s mouth open wide
¨ Lower lip turned outwards
¨ Baby’s chin touches breast
¨ More areola seen below bottom lip
¨ Baby’s mouth not open wide
¨ Lips pointing forward or turned in
¨ Baby’s chin not touching breast
SUCKLING¨ Slow, deep sucks with pauses
¨ Cheeks round when suckling
¨ Baby releases breast when finished
¨ Mother notices signs of oxytocin reflex
¨ Rapid shallow sucks
¨ Cheeks pulled in when suckling
¨ Mother takes baby off the breast
¨ No signs of oxytocin reflex noticed

Session 20: Expressing and storing breastmilk
Counseling on infant and young child feeding at health facility70.
SESSION 20: EXPRESSING AND STORING BREASTMILK
Objectives:
After completing this lesson, trainees will be able to:
1. List the situations when expressing breastmilk is needed.
2. Explain and practice ways to stimulate the oxytocin reflex.
3. Explain to a mother the steps of expressing breastmilk by hand.
4. Introduce some other tools for expressing milk.
5. Explain how to store breastmilk.
Introduction
• There are many situations in which expressing breastmilk is necessary and important to enable a
mother to initiate or to continue BF.
Expressing milk is needed to:
Leave breastmilk for a baby when the mother goes out or goes to work.
Feed a low-birth-weight baby who cannot breastfeed.
Feed a sick baby, who cannot suckle enough.
Keep up the supply of breastmilk when a mother or baby is ill.
Prevent leaking when a mother is away from her baby.
Help a baby to attach to a full breast.
Help with breast-health conditions, e.g., engorgement.
Facilitate the transition to another method of feeding or to heat-treat breastmilk.
• All mothers should learn how to express their milk, so that they know what to do if the need arises.
All maternal-health workers should be able to teach mothers how to express their milk.
• Many mothers are able to express plenty of breastmilk using their own techniques. If a mother's
technique works for her, let her continue. But if a mother is having difficulty expressing milk, teach
her a more effective technique.

Session 20: Expressing and storing breastmilk
Counseling on infant and young child feeding at health facility .71
Stimulate the oxytocin reflex
The oxytocin reflex may work well if a mother expresses breastmilk as it does when a baby suckles. A
mother needs to know how to facilitate her oxytocin reflex, or she may find it difficult to express
her milk.
HOW TO STIMULATE THE OXYTOCIN REFLEX
1. Help the mother psychologically:
• Build her confidence.
• Try to reduce any sources of pain or anxiety.
• Help her to have good thoughts and feelings about the baby.
2. Help the mother practically. Help or advise her to:
• Sit quietly and privately or with a supportive friend.
• Some mothers can express easily in a group of other mothers who are also expressing for their babies.
• Hold her baby with skin-to-skin contact if possible:
She can hold her baby on her lap while she expresses. If this is not possible, she can look at the babyor a photograph of her baby.
• Warm her breasts
She can apply a warm compress, or warm water, or have a warm shower.
• Stimulate her nipples
She can gently pull or roll her nipples with her fingers.
• Massage or stroke her breasts lightly
Some women find that it helps if they stroke the breast gently with their finger tips or with a comb.
Some women find that it helps to gently roll their closed fist over the breast towards the nipple.
• Ask a helper to rub her back.
Figure 20.1 A helper rubbing a mother's back to stimulate the oxytocin reflex
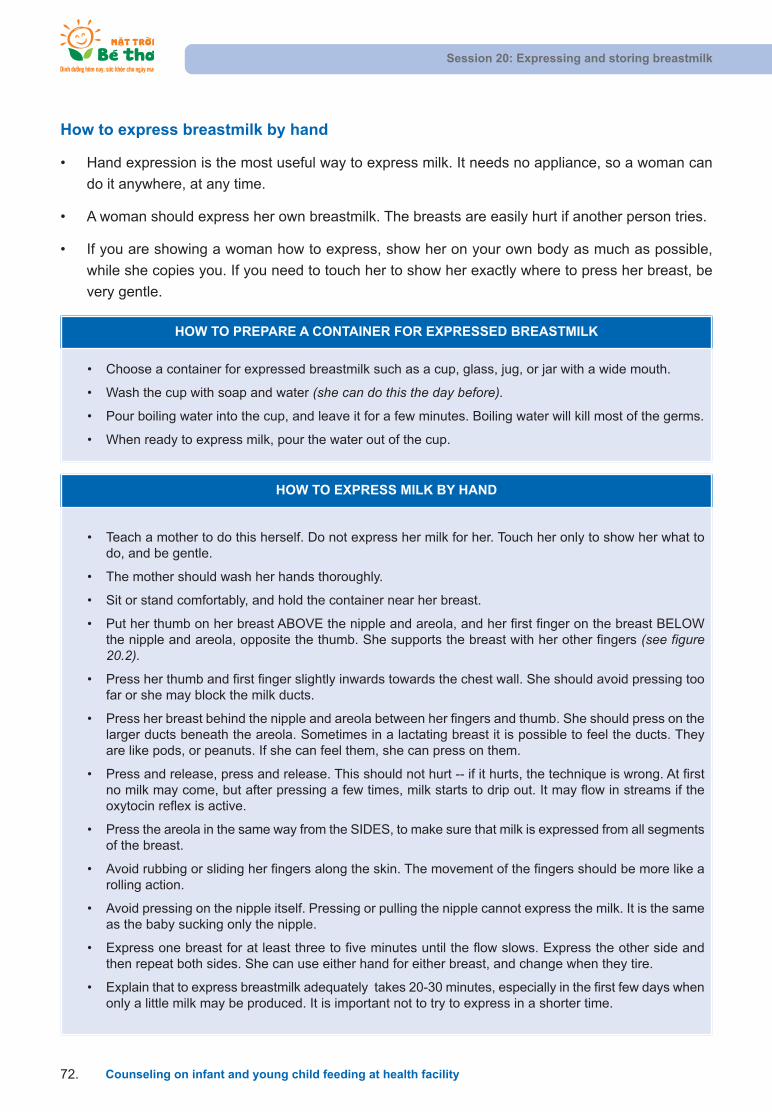
How to express breastmilk by hand
• Hand expression is the most useful way to express milk. It needs no appliance, so a woman can
do it anywhere, at any time.
• A woman should express her own breastmilk. The breasts are easily hurt if another person tries.
• If you are showing a woman how to express, show her on your own body as much as possible,
while she copies you. If you need to touch her to show her exactly where to press her breast, be
very gentle.
Session 20: Expressing and storing breastmilk
Counseling on infant and young child feeding at health facility72.
HOW TO PREPARE A CONTAINER FOR EXPRESSED BREASTMILK
• Choose a container for expressed breastmilk such as a cup, glass, jug, or jar with a wide mouth.
• Wash the cup with soap and water (she can do this the day before).
• Pour boiling water into the cup, and leave it for a few minutes. Boiling water will kill most of the germs.
• When ready to express milk, pour the water out of the cup.
HOW TO EXPRESS MILK BY HAND
• Teach a mother to do this herself. Do not express her milk for her. Touch her only to show her what todo, and be gentle.
• The mother should wash her hands thoroughly.
• Sit or stand comfortably, and hold the container near her breast.
• Put her thumb on her breast ABOVE the nipple and areola, and her first finger on the breast BELOWthe nipple and areola, opposite the thumb. She supports the breast with her other fingers (see figure20.2).
• Press her thumb and first finger slightly inwards towards the chest wall. She should avoid pressing toofar or she may block the milk ducts.
• Press her breast behind the nipple and areola between her fingers and thumb. She should press on thelarger ducts beneath the areola. Sometimes in a lactating breast it is possible to feel the ducts. Theyare like pods, or peanuts. If she can feel them, she can press on them.
• Press and release, press and release. This should not hurt -- if it hurts, the technique is wrong. At firstno milk may come, but after pressing a few times, milk starts to drip out. It may flow in streams if theoxytocin reflex is active.
• Press the areola in the same way from the SIDES, to make sure that milk is expressed from all segmentsof the breast.
• Avoid rubbing or sliding her fingers along the skin. The movement of the fingers should be more like arolling action.
• Avoid pressing on the nipple itself. Pressing or pulling the nipple cannot express the milk. It is the sameas the baby sucking only the nipple.
• Express one breast for at least three to five minutes until the flow slows. Express the other side andthen repeat both sides. She can use either hand for either breast, and change when they tire.
• Explain that to express breastmilk adequately takes 20-30 minutes, especially in the first few days whenonly a little milk may be produced. It is important not to try to express in a shorter time.

Session 20: Expressing and storing breastmilk
Counseling on infant and young child feeding at health facility .73
How often should a mother express her breastmilk?
It depends on the reason for expressing the milk, but usually as often as the baby would breastfeed.
To establish lactation, to feed a low-birth-weight (LBW) or a sick newborn she should start to
express milk on the first day, as soon as possible after delivery. She may only express a few drops of
colostrum at first, but it helps breastmilk production to begin, in the same way that a baby suckling
soon after delivery helps breastmilk production to begin.
She should express as much as she can as often as her baby would breastfeed. This should be at
least every three hours, including during the night. If she expresses only a few times, or if there are
long intervals between expressions, she may not be able to produce enough milk.
To keep up her milk supply to feed a sick baby: she should express at least every three hours.
To build up her milk supply, if it seems to be decreasing after a few weeks: express very often for
a few days (every two hours or even every hour), and at least every three hours during the night.
To leave milk for a baby while she is out at work: express as much as possible before she goes to
work, to leave for her baby. It is also very important to express while at work to help keep up her
supply.
Figure 20.2 How to express breastmilk
a. Place a finger and thumb each side of the areola and press inwards towards the chest wall.
b. Press behind the nipple and areola between your finger and thumb.
c. Press from the sides to empty all segments.
a b
c
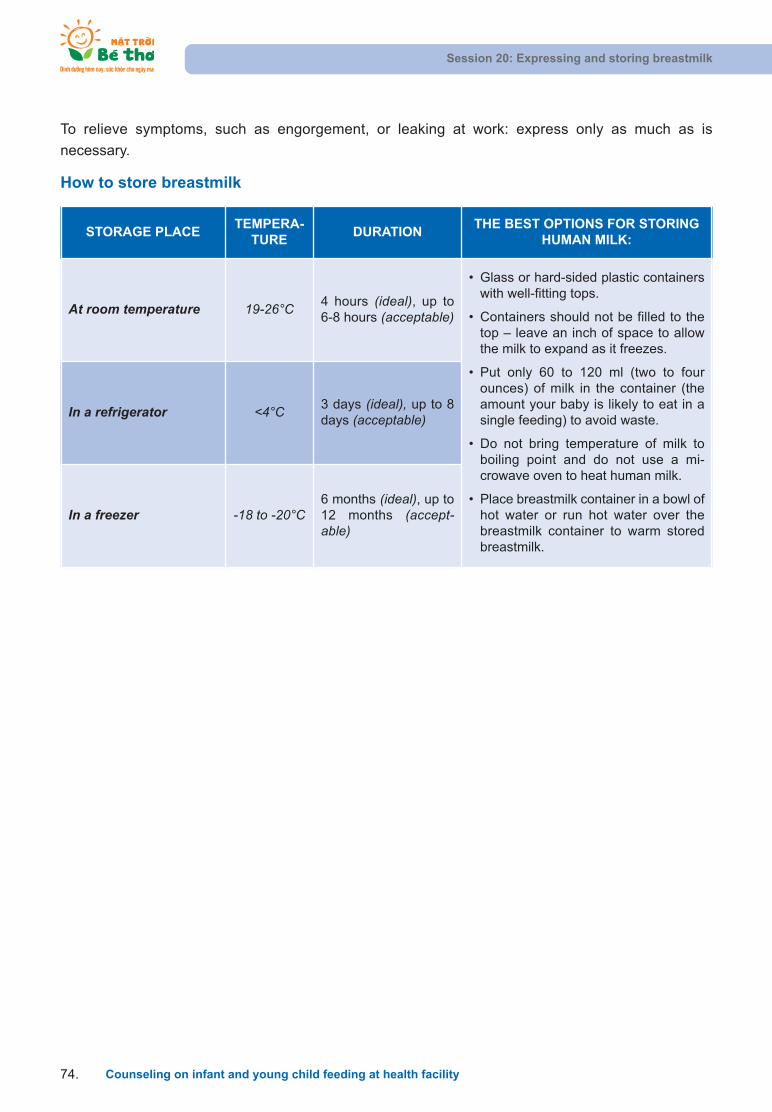
To relieve symptoms, such as engorgement, or leaking at work: express only as much as is
necessary.
How to store breastmilk
Session 20: Expressing and storing breastmilk
Counseling on infant and young child feeding at health facility74.
STORAGE PLACE TEMPERA-
TUREDURATION
THE BEST OPTIONS FOR STORINGHUMAN MILK:
At room temperature 19-26°C 4 hours (ideal), up to 6-8 hours (acceptable)
• Glass or hard-sided plastic containerswith well-fitting tops.
• Containers should not be filled to thetop – leave an inch of space to allowthe milk to expand as it freezes.
• Put only 60 to 120 ml (two to fourounces) of milk in the container (theamount your baby is likely to eat in asingle feeding) to avoid waste.
• Do not bring temperature of milk toboiling point and do not use a mi-crowave oven to heat human milk.
• Place breastmilk container in a bowl ofhot water or run hot water over thebreastmilk container to warm storedbreastmilk.
In a refrigerator <4°C 3 days (ideal), up to 8days (acceptable)
In a freezer -18 to -20°C6 months (ideal), up to12 months (accept-able)
Session 21: Common BF difficulties
Counseling on infant and young child feeding at health facility .75
SESSION 21: COMMON BF DIFFICULTIES
Objectives:
After completing this lesson, trainees will be able to:
1. Identify symptoms and causes of common BF difficulties and know how to support mothers in treatment and prevention.
Introduction:
• In previous sessions we have discussed ways to help mothers with BF.
• When helping mothers with difficulties you will need to use all the skills you have learned so far.Counselors and community health workers have important roles to support mothers through thesedifficulties, as mothers may not visit a health facility to seek help.
• The most commonly encountered BF difficulties include:
Insufficient milk.
Flat and inverted nipple.
Cracked nipple.
Engorgement.
Mastitis.
Crying baby – breast refusal.
Difficulty one: At a mother’s side
1. Not enough milk
SIGNS WHAT TO DO PREVENTION
Reliable signs
• Poor weight gain: less than500 grams per month
• Small amount of concen-trated urine: less than 6times per day
Possible signs
• Baby not satisfied afterbreastfeeds and cries often
• Very frequent breastfeeds
For mothers who really do not have enough milk
• Use your counseling skills to compile a goodfeeding history.
• Observe and assess a breastfeed to check po-sitioning and attachment
• Listen to the mother and family to identify if thereis any psychological problem or wrong belief.
• Solutions that you suggest to the mother mustdepend upon the cause of the insufficient milk.
• If possible, visit the mother and baby daily untilthe baby is gaining weight
• Disseminate andeducate motherson BF from preg-nancy.
• Skin-to-skin con-tact with motherto start BF withinan hour after birth
• Support motherwith correct posi-tioning right fromthe first breast-

2. Breast conditions
Session 21: Common BF difficulties
Counseling on infant and young child feeding at health facility76.
SIGNS WHAT TO DO PREVENTION
• Baby refuses to breastfeedor has very long breastfeeds
• Baby has hard, dry, or greenstools
• No milk comes out when themother expresses
• Breasts did not enlarge dur-ing pregnancy
• Milk did not ‘come in’ afterdelivery
For mothers who perceive that their babies donot get enough milk but in fact, they do getenough.
• Signs of the child: no signs detected as identifiedin the left column. The child gains weight well,passes urine regularly, and does not cry often.
• Identify the reasons why the mother doubts herability to produce enough milk.
• Based on what is being identified, provide appro-priate solutions and support.
• Arrange follow-ups with mothers as soon as pos-sible and provide more support to prevent moth-ers from giving complementary foods.
feed.
• Breastfeed exclu-sively on demandduring the dayand night.
• Encourage agood diet for themother from preg-nancy and duringthe BF period.
PROBLEMS - SIGNS WHAT TO DO PREVENTION
Flat and inverted nipple • Build confidence for the mother by explainingthat a baby suckles from the breast – not fromthe nipple; that the mother should breastfeedmore because, when the baby breastfeeds, hewill stretch her nipple out.
• Encourage the mother to position the baby atthe breast early after delivery, and urge her tobe patient before the milk comes in and herbreasts are full.
• Show the mother how to make the nipple stretchout by herself before a feed; this will help a babyto attach better.
• Show the mother how to shape the breast bysupporting her breast from underneath with herfingers, and press the top of the breast gentlywith her thumb; this will help the areola and nipple to stretch out so that the baby can attachbetter.
• If the breasts are full of milk: express breastmilkand feed it to the baby with a cup. Continue tobreastfeed the baby until the breasts are released (the baby attaches better and nipplecondition is improved).
• In complicated cases, use the syringe method(cut through the barrel of the syringe at the nozzle end, place the plunger in the cut end, restthe uncut end on top of the nipple and pull theplunger to protract your nipple).
Before delivery:
• If inverted nipple is iden-tified early during preg-nancy, instruct mothershow to stretch the nippleor wear nipple shells.
• Most nipples improvearound the time of deliv-ery without any treat-ment.
• Help a mother to initiateBF early after delivery.

Session 21: Common BF difficulties
Counseling on infant and young child feeding at health facility .77
PROBLEMS - SIGNS WHAT TO DO PREVENTION
Sore or cracked nipple
• Cracks across top of nipple or around base
• Occasional bleeding• May become infected
• Do not stop BF.• Improve attachment. Begin to breastfeed on the
side that hurts less.• Vary BF positions.• Let the baby come and attach to the breast by
him/herself.• Apply drops of breastmilk to nipples and allow
them to air dry.• Do not use soap or cream on nipples.• Do not wait until the breast is full to breastfeed.• Continue to breastfeed the baby and do not use
bottles.
• Good attachment. • Do not use feeding
bottles (suckling from abottle is easier than suck-ling from a mother’sbreasts so the baby mayrefuse the breast).
• Do not let the breasts gettoo full.
• Do not use soap orcreams on nipples.
Engorgement – blocked duct
Symptoms:• Swelling
• Warmth
• Slight redness
• Pain
• Skin shiny and tight andnipple flattened
• Usually begins on the 3rd-4th day after birth
• Apply cold compresses to breasts to reduceswelling.
• Breastfeed more frequently and offer bothbreasts.
• Improve attachment.• Gentle stroking of breasts helps to stimulate milk
flow (in the community, mothers often use acomb and gently comb the breast towards thenipple).
• Press around the areola to reduce edema andto help baby to attach.
• Express milk to relieve pressure until baby cansuckle.
• Help the baby to attachwell in the first breast-feed.
• Put the baby skin-to-skinwith the mother and startBF within an hour of birth.
• Breastfeed frequently ondemand/cue both dayand night: 10 -12 timesper 24 hours.
• Express unused breast-milk after each breast-feed.
Plugged Ducts and Mastitis
Symptoms of Mastitis• Hard lump, severe pain,
redness in one area,swelling, and no fever.
Symptoms of pluggedducts• Hard swelling. • Severe pain. • Redness in one area.• Generally not feeling well. • Fever.
• Continue BF (if breastmilk is not near the ab-scess let the baby feed more frequently and asoften as s/he will).
• Apply a warm compress (if mastitis is not de-tected).
• Hold the baby in different positions, so that thebaby’s tongue/chin is close to the site of theplugged duct/mastitis (the reddish area). Thetongue/chin will massage the breast and releasethe milk from that part of the breast.
• Ensure good attachment.• Apply gentle pressure to the breast with the
palm of your hand, rolling fingers towards nipple.Then express milk or let the baby feed every twoto three hours day and night.
• Rest (mother).• Drink more liquids (mother).• If there is no improvement in 24 hours, refer the
mother to a health facility.
• Ensure good attachment.• Breastfeed on demand/
cue, and let infants finish/come off the breastby him/herself.
• Avoid tight clothing. • Get support from the fam-
ily to perform non-infant-care chores so that themother has more timewith her baby – ensurethat the baby is breastfedon demand.
• Avoid holding the breastwith a scissors hold be-cause this will preventmilk flow.
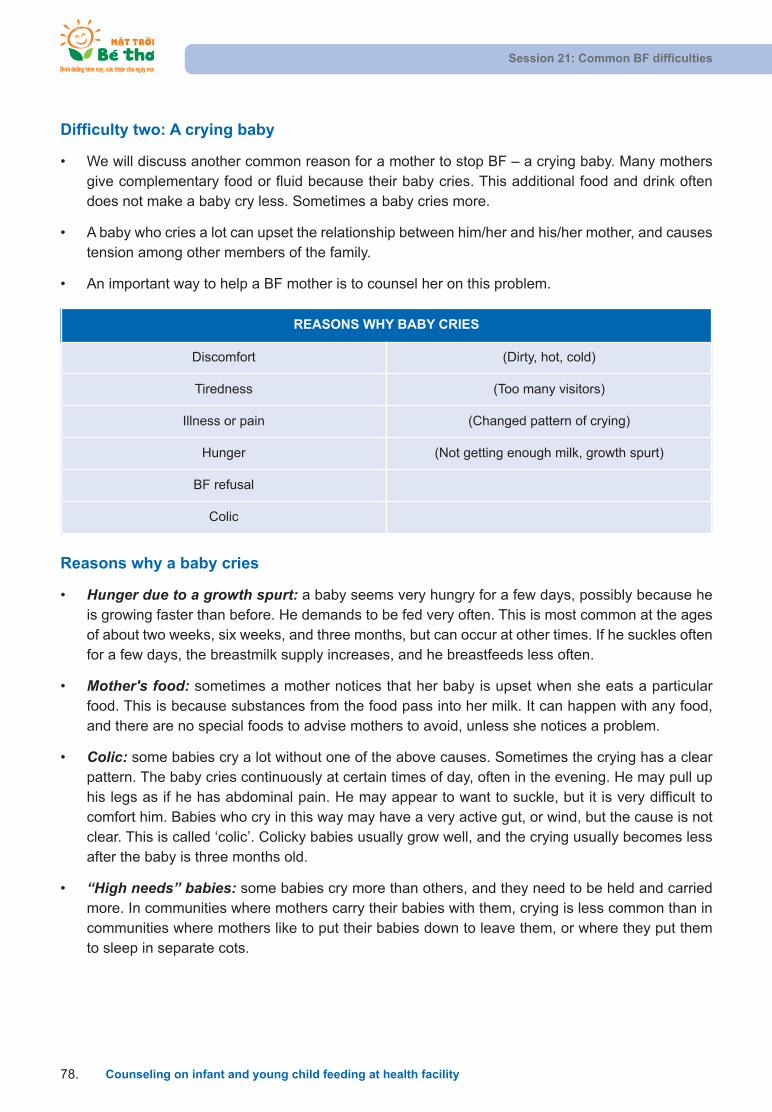
Difficulty two: A crying baby
• We will discuss another common reason for a mother to stop BF – a crying baby. Many mothersgive complementary food or fluid because their baby cries. This additional food and drink oftendoes not make a baby cry less. Sometimes a baby cries more.
• A baby who cries a lot can upset the relationship between him/her and his/her mother, and causestension among other members of the family.
• An important way to help a BF mother is to counsel her on this problem.
Session 21: Common BF difficulties
Counseling on infant and young child feeding at health facility78.
REASONS WHY BABY CRIES
Discomfort (Dirty, hot, cold)
Tiredness (Too many visitors)
Illness or pain (Changed pattern of crying)
Hunger (Not getting enough milk, growth spurt)
BF refusal
Colic
Reasons why a baby cries
• Hunger due to a growth spurt: a baby seems very hungry for a few days, possibly because heis growing faster than before. He demands to be fed very often. This is most common at the agesof about two weeks, six weeks, and three months, but can occur at other times. If he suckles oftenfor a few days, the breastmilk supply increases, and he breastfeeds less often.
• Mother's food: sometimes a mother notices that her baby is upset when she eats a particularfood. This is because substances from the food pass into her milk. It can happen with any food,and there are no special foods to advise mothers to avoid, unless she notices a problem.
• Colic: some babies cry a lot without one of the above causes. Sometimes the crying has a clearpattern. The baby cries continuously at certain times of day, often in the evening. He may pull uphis legs as if he has abdominal pain. He may appear to want to suckle, but it is very difficult tocomfort him. Babies who cry in this way may have a very active gut, or wind, but the cause is notclear. This is called ‘colic’. Colicky babies usually grow well, and the crying usually becomes lessafter the baby is three months old.
• “High needs” babies: some babies cry more than others, and they need to be held and carriedmore. In communities where mothers carry their babies with them, crying is less common than incommunities where mothers like to put their babies down to leave them, or where they put themto sleep in separate cots.
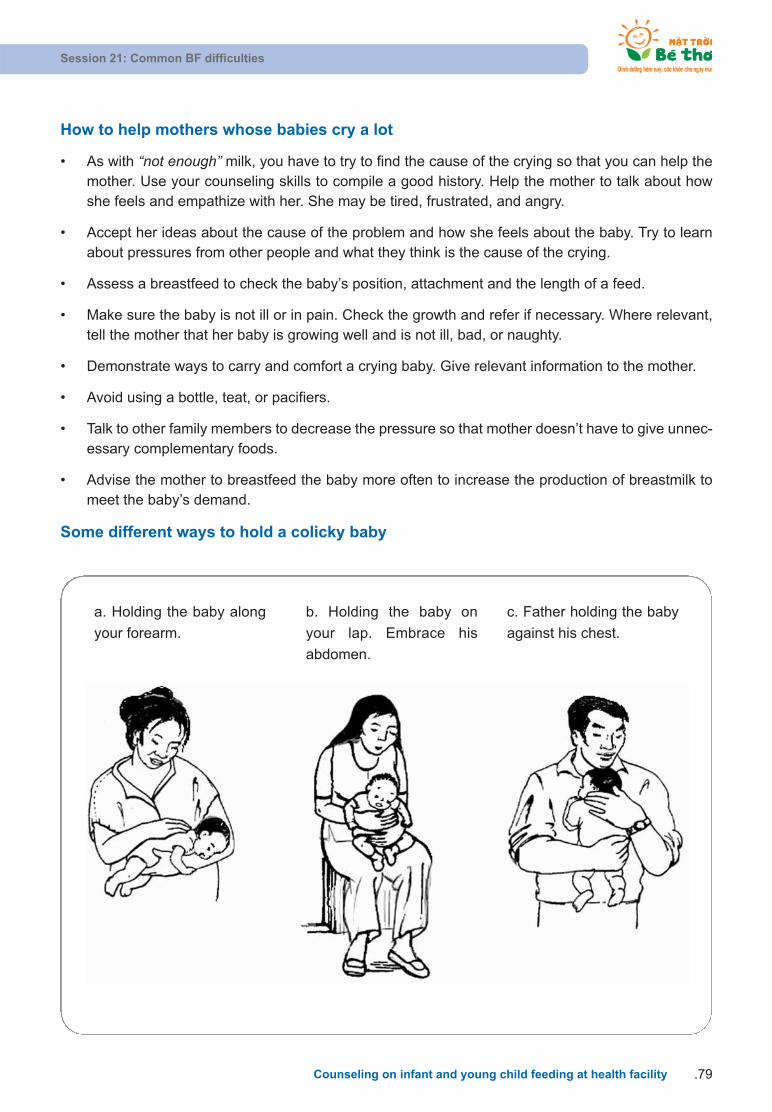
Session 21: Common BF difficulties
Counseling on infant and young child feeding at health facility .79
a. Holding the baby along
your forearm.
b. Holding the baby on
your lap. Embrace his
abdomen.
c. Father holding the baby
against his chest.
How to help mothers whose babies cry a lot
• As with “not enough” milk, you have to try to find the cause of the crying so that you can help themother. Use your counseling skills to compile a good history. Help the mother to talk about howshe feels and empathize with her. She may be tired, frustrated, and angry.
• Accept her ideas about the cause of the problem and how she feels about the baby. Try to learnabout pressures from other people and what they think is the cause of the crying.
• Assess a breastfeed to check the baby’s position, attachment and the length of a feed.
• Make sure the baby is not ill or in pain. Check the growth and refer if necessary. Where relevant,tell the mother that her baby is growing well and is not ill, bad, or naughty.
• Demonstrate ways to carry and comfort a crying baby. Give relevant information to the mother.
• Avoid using a bottle, teat, or pacifiers.
• Talk to other family members to decrease the pressure so that mother doesn’t have to give unnec-essary complementary foods.
• Advise the mother to breastfeed the baby more often to increase the production of breastmilk tomeet the baby’s demand.
Some different ways to hold a colicky baby
Session 21: Common BF difficulties
Counseling on infant and young child feeding at health facility80.
FURTHER READING:
Breast refusal
• In some communities breast refusal is a common reason for stopping BF. However, it need notlead to the complete cessation of BF, and can often be overcome. Refusal can cause great distress to the baby's mother. She may feel she has failed at BF.
• There are different kinds of refusals as follows:
Sometimes a baby attaches to the breast, but then does not suckle, or suckles very weakly.
Sometimes a baby cries and fights at the breast, when his mother tries to breastfeed him.
Sometimes a baby suckles for a minute and then comes off the breast crying. He may dothis several times during a single feed.
Sometimes a baby takes one breast, but refuses the other.
• You need to know why a baby is refusing to breastfeed, before you can help the mother andbaby to enjoy BF again.
• Reasons why babies refuse to breastfeed:
The baby is ill, sedated, or in pain.
Difficulty with BF technique.
Changes which upset the baby.
Apparent, not real, refusal.
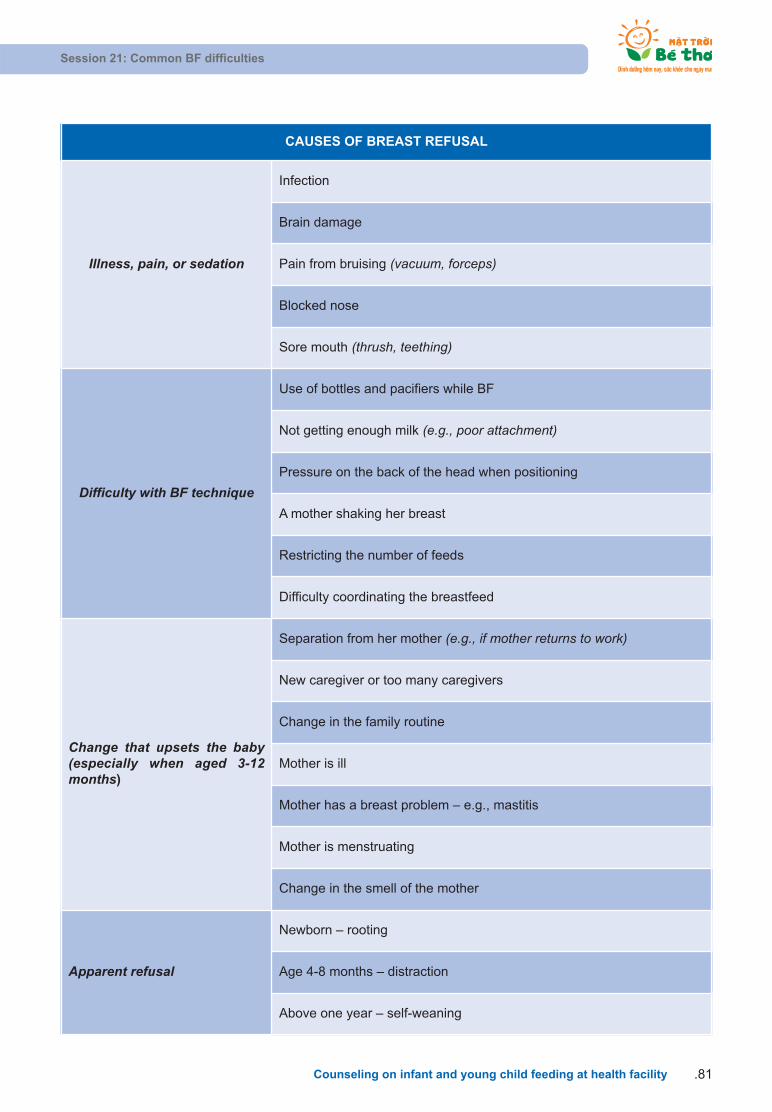
Session 21: Common BF difficulties
Counseling on infant and young child feeding at health facility .81
CAUSES OF BREAST REFUSAL
Illness, pain, or sedation
Infection
Brain damage
Pain from bruising (vacuum, forceps)
Blocked nose
Sore mouth (thrush, teething)
Difficulty with BF technique
Use of bottles and pacifiers while BF
Not getting enough milk (e.g., poor attachment)
Pressure on the back of the head when positioning
A mother shaking her breast
Restricting the number of feeds
Difficulty coordinating the breastfeed
Change that upsets the baby(especially when aged 3-12months)
Separation from her mother (e.g., if mother returns to work)
New caregiver or too many caregivers
Change in the family routine
Mother is ill
Mother has a breast problem – e.g., mastitis
Mother is menstruating
Change in the smell of the mother
Apparent refusal
Newborn – rooting
Age 4-8 months – distraction
Above one year – self-weaning
How to help mothers whose babies refuse the breast
Session 21: Common BF difficulties
Counseling on infant and young child feeding at health facility82.
HELPING A MOTHER AND BABY TO BREASTFEED AGAIN
Help the mother to do these things:
• Keep her baby close – no other caregivers: Give plenty of skin-to-skin contact at all times, not just at feeding times.
Sleep with her baby.
Ask other people to help with housework.
• Offer her breast whenever her baby is willing to suckle:When her baby is sleepy, or after a cup-feed.
When she has time.
• Help her baby to take the breast using the following ways:Express breastmilk into his mouth.
Position him so that he can attach easily to the breast – try different positions.
• Feed her baby by cup:Give her own expressed breastmilk if possible. If necessary, give artificial feeds.
Avoid using bottles, teats, or pacifiers.
Other situations that can affect BF
1. The mother is sick:
• When a mother has a headache, pain in her back, a flu, diarrhea, or other common diseases(malaria, anemia, cholera, etc.), she SHOULD CONTINUE BF.
• The mother should relax and drink more water to help her body recover.
• If there is no improvement, she should go for a health check and tell the health staff that she is BF.
2. Light-weight baby:
• The mother needs to help her baby attach well to the breast and hold her baby.
• How to breastfeed: breastfeed long and slowly, keep the baby near the breast.
• In the first few weeks, the baby may not be able to suckle directly from mother’s breast so themother is encouraged to express breastmilk and feed her baby by cup and spoon
• If the baby sleeps too much, pick him up gently in order to wake him up for BF.
• Crying is the last sign of hunger. Early signs of hunger include the combination of the followingthings: alertness and restless, mouth open and head moving, tongue turning outwards and inwards,sucking his/her fingers. If there is only one of these signals, it is not certain that the baby is hungry.
3. The mother has malnutrition:
• She should eat more to get better (the mother eats to breastfeed her baby).
Session 21: Common BF difficulties
Counseling on infant and young child feeding at health facility .83
• She needs vitamin A within six weeks after delivery and micronutrient supplements daily if available.
• The mother secretes more breastmilk if she breastfeeds her baby frequently.
4. Twins:
• The mother can exclusively breastfeed both babies if they are frequently breastfed and well attached to the breast.
• The more the baby suckles, the more breastmilk is secreted.
• Twins need early BF after delivery, if the babies are unable to latch on immediately, help the motherto express her breastmilk and feed them by a cup. Try to stimulate breastmilk production early tomake sure the breasts can secrete enough milk for both babies.
5. The mother becomes pregnant again:
• In most countries, when a mother gets pregnant again, she often stops BF her baby. She usuallythinks that BF during the pregnancy period can affect one of the two babies. Sometimes, a mother’snipple is sensitive when she is pregnant. However, BF both babies is completely safe and has noharm to them and the mother has enough breastmilk for both of them.
• If the baby is under one year old, continued BF is good for him/her in order to maintain good health,growth, and development.
• The mother is encouraged to eat more meals per day to have good health, support BF and nurturethe fetus.
6. The mother is stressed
• The quality of breastmilk is not affected and milk secretion is not reduced if the mother is stressed.However, breastmilk can temporarily come in infrequently.
• If she continues BF, milk flow will recover.
• Often keep the mother and baby together if the mother agrees
• Comfort and encourage the mother, enable her to talk, and provide spiritual and practical support.
• She should rest and breastfeed her baby.
• She should drink warm water to relax and support breastmilk secretion.
7. Mother is away from the baby
• When the mother is not at home, she should express and store breastmilk to feed her baby at timeof a normal breastfeed.
• Instruct the caregiver to feed the baby with safely expressed breastmilk
• The mother should sleep with her baby in order to frequently BF at night when she is at home
• If the mother can take her baby to her work place, continue BF frequently.
Session 22: Field practice
Counseling on infant and young child feeding at health facility84.
SESSION 22: FIELD PRACTICE
Objectives:
After completing this session, trainees will be able to:
1. Use appropriate listening and learning skills when counseling mothers on IYCF.
2. Assess a breastfeed with a Breastfeed Observation Job Aid.
3. Illustrate how to help a mother with good positioning and attachment.
The following notes summarize the instructions for your tasks in a field practice that the trainer will tell
you about. Try to spend some time reading these notes to remind youself of what you have to do during
the practice. In the field practice, you will work in a small group and take turns talking to mothers while
the others observe.
Trainees should bring:
• Four Breastfeed Observation Job Aids.
• Four counseling-skills checklists.
• Pencils, notebooks.
• No books.
If you are the one who talks to the mother:
• Introduce yourself and ask for the mother’s permission to talk to her. Introduce your group and
explain to the mother that you are interested in child feeding. Find a chair to sit down. You can sit
on mother’s bed if needed and if allowed.
• If the baby is suckling, ask the mother to continue BF. If not, ask the mother to breastfeed as usual
whenever the baby wants to suckle. Ask for the mother’s permission so that the whole group can
observe a breastfeed.
• Before or after a breastfeed, you should ask the mother several open-ended questions to start
such as: how the mother feels, how the baby is, how a breastfeed works. Encourage the mother
to talk about herself and her baby. Praise two things that the mother and baby do right. Provide
two necessary bits of information relevant to her situation. Practice counseling skills as much as
possible.
• Helping the mother to position her baby and to overcome difficulties is an important part of field
practice. Usually, the baby feels sleepy. In case that a baby is sleeping, you can say that “I knowthat your baby is sleepy but can we talk about how to hold a baby until he wakes up?” Then show

Session 22: Field practice
Counseling on infant and young child feeding at health facility .85
Summary
Remember all skills learned so that you can help mothers in different situations: listening and learning,
building confidence and giving support, assessing a breastfeed, helping a mother with positioning and
attachment, and taking details of feeding history.
In many cases, there is no treatment. Therefore, it is important that you give appropriate suggestions
and information to help mothers.
the mother four key points of positioning. By doing so, the baby may wake up and want to suckle
when his nose touches the mother’s breast.
If you are an observer:
• Stand and keep quiet. Try to be as quiet as possible. Give no comments and do not talk.
• Generally observe the mother and baby. Pay attention to: is the mother happy? Does she have
formula milk or is she bottle-feeding? Generally observe the conversation between the mother and
the trainee. Pay attention to: who talks the most? Is the mother comfortable and interested?
• Specifically observe the counseling skills of the trainee who is practicing, including non-verbal com-
munication. Mark with a ( ) in the checklist of counseling skills if any skill is in use in order to help
the discussion. Notice if the trainee makes any mistakes – for example, using judging words or
asking a lot of closed-ended questions that the mother can only answer with “yes” or “no”.
• Keep quiet while observing the mother and baby during a breastfeed. When observing, make
notes in the Breastfeed Observation Job Aid. Write the mother and baby’s names, mark a ( ) beside
each sign that you see and note down the duration of the breastfeed.
• Thank the mother after the conversation and say something to praise and support her.
MISTAKES TO AVOID
Do not tell her that you are paying attention to her BF
The mother’s behavior may change and she may feel uncomfortable if she feeds her baby formula milk.You should say that you are interested in “child feeding” or “child- feeding techniques”.
Be careful not to turn forms into barriers
While talking to the mother, do not note down anything. Trainees should use forms to remind themselvesof what to do and to record later what they want to remember. Trainees who are observing are allowed tonote things down.

CHECKLIST OF INDIVIDUAL-COUNSELING SKILLS ON IYCF
Session 22: Field practice
Counseling on infant and young child feeding at health facility86.
SKILLS ACTIVITIESNOT
DONENOT DONE
WELLWELL-DONE
1
Introduction–
a createwarm andfriendly
environment
Greet mothers
Introduce yourself
Make eye contact
Smile
Show respect
2Identify
current prob-lems /issues
Listen
Be non-Judgmental
Ask open-ended questions
Accept what a mother says
3 Analyze/assess
Identify the problem, issue
Identify priority if there is more than one problems
Ask more open-ended questions to identify barriers
Respond to mother’s question
4
Makepractical
recommen-dation
Provide relevant information
Build confidence
Make 1-2 practical recommendations
Use counseling cards/ materials
5
Negotiatebehavior –
get commit-ment
Discuss different solutions with mothers
Let mothers decide the solution
Get mother’s commitment to try 1-2 recommen-dations
6 Summary -Closing
Ask mother to repeat recommendation
Correct recommendation as appropriate
Arrange follow-up with mothers
Praise and thank mothers
SESSION 23. IMPORTANCE OF CF
Objectives:
After completing this lesson, trainees will be able to:
1. Explain the importance of continued breastfeeding.
2. Define complementary feeding (CF).
3. Explain why there is an optimal age for children to start CF.
Definition of CF
• CF means giving other soft, semi-solid, or solid foods in addition to breastmilk.
• These foods are called complementary foods.
Note: Powdered milk (formula) and other fruit juice are not considered to be complementary foods.
• These additional foods and liquids are called complementary foods, because they are complemen-
tary to breastmilk and do not totally replace breastmilk. Complementary foods must be nutritious
and in adequate supply so the child can continue to grow.
• During the CF period, the young child gradually becomes accustomed to eating family foods. Feed-
ing includes more than just the foods provided for the child. How the child is fed can be as important
as what the child is fed.
The optimal age to start CF
• Our body uses food for energy to keep it alive, to grow, to fight infection, to move around, and to
be active. Food is like the wood for the fire – if we do not have enough good wood, the fire does
not provide good heat or energy. In the same way, if young children do not have enough good
food, they will not have the energy to grow and to be active.
• The following chart demonstrates the daily energy demands of a child by age.
Session 23. Importance of CF
Counseling on infant and young child feeding at health facility .87
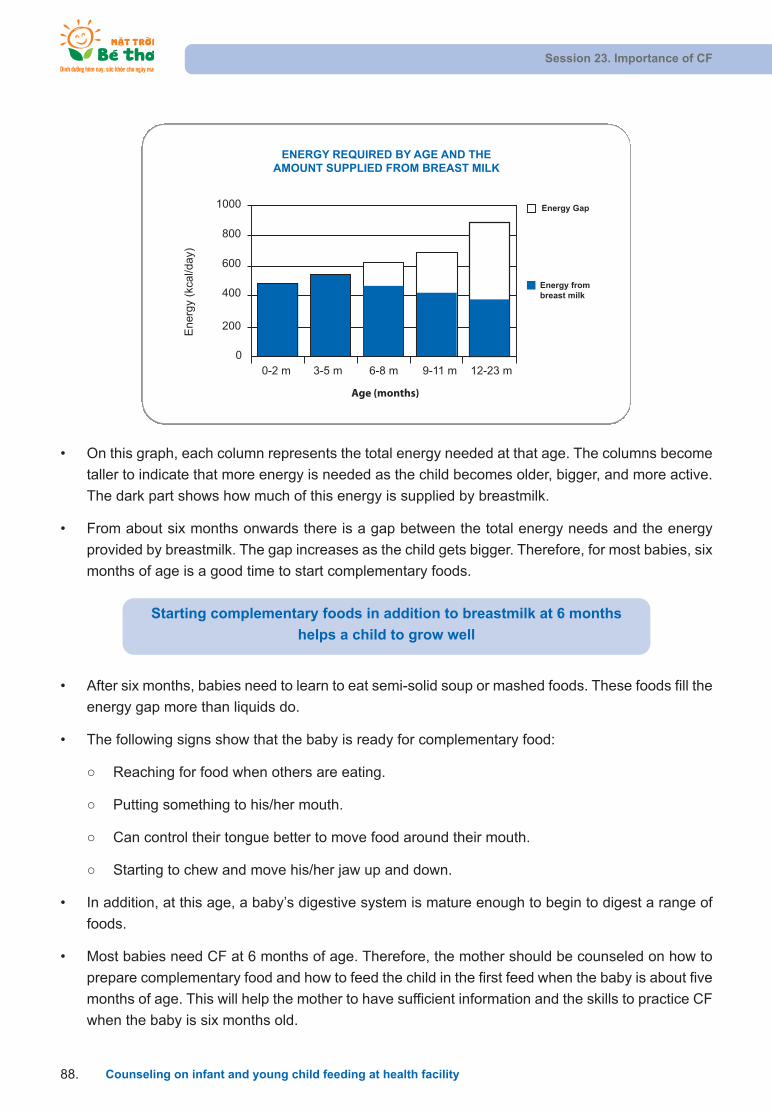
• After six months, babies need to learn to eat semi-solid soup or mashed foods. These foods fill the
energy gap more than liquids do.
• The following signs show that the baby is ready for complementary food:
Reaching for food when others are eating.
Putting something to his/her mouth.
Can control their tongue better to move food around their mouth.
Starting to chew and move his/her jaw up and down.
• In addition, at this age, a baby’s digestive system is mature enough to begin to digest a range of
foods.
• Most babies need CF at 6 months of age. Therefore, the mother should be counseled on how to
prepare complementary food and how to feed the child in the first feed when the baby is about five
months of age. This will help the mother to have sufficient information and the skills to practice CF
when the baby is six months old.
• On this graph, each column represents the total energy needed at that age. The columns become
taller to indicate that more energy is needed as the child becomes older, bigger, and more active.
The dark part shows how much of this energy is supplied by breastmilk.
• From about six months onwards there is a gap between the total energy needs and the energy
provided by breastmilk. The gap increases as the child gets bigger. Therefore, for most babies, six
months of age is a good time to start complementary foods.
Session 23. Importance of CF
Counseling on infant and young child feeding at health facility88.
00-2 m 3-5 m 6-8 m 9-11 m 12-23 m
200
400
600
800
1000 Energy Gap
Energy frombreast milk
Energ
y (k
cal/d
ay)
ENERGY REQUIRED BY AGE AND THEAMOUNT SUPPLIED FROM BREAST MILK
Age (months)
Starting complementary foods in addition to breastmilk at 6 months
helps a child to grow well
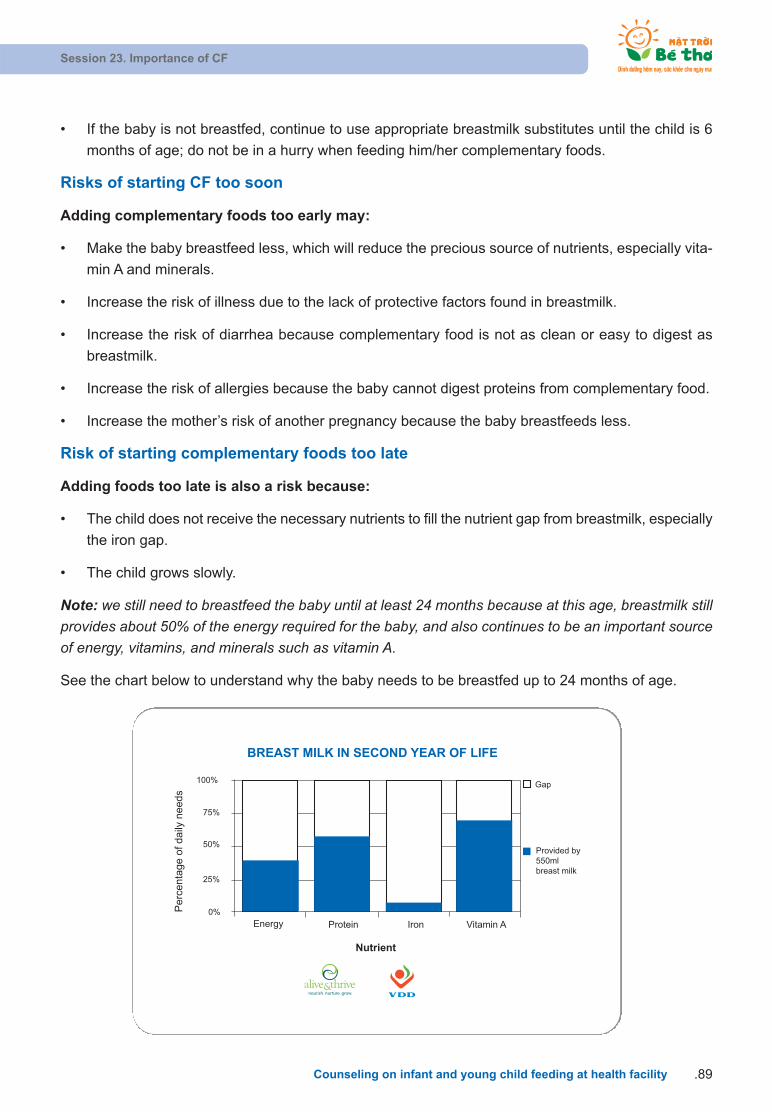
• If the baby is not breastfed, continue to use appropriate breastmilk substitutes until the child is 6
months of age; do not be in a hurry when feeding him/her complementary foods.
Risks of starting CF too soon
Adding complementary foods too early may:
• Make the baby breastfeed less, which will reduce the precious source of nutrients, especially vita-
min A and minerals.
• Increase the risk of illness due to the lack of protective factors found in breastmilk.
• Increase the risk of diarrhea because complementary food is not as clean or easy to digest as
breastmilk.
• Increase the risk of allergies because the baby cannot digest proteins from complementary food.
• Increase the mother’s risk of another pregnancy because the baby breastfeeds less.
Risk of starting complementary foods too late
Adding foods too late is also a risk because:
• The child does not receive the necessary nutrients to fill the nutrient gap from breastmilk, especially
the iron gap.
• The child grows slowly.
Note: we still need to breastfeed the baby until at least 24 months because at this age, breastmilk stillprovides about 50% of the energy required for the baby, and also continues to be an important sourceof energy, vitamins, and minerals such as vitamin A.
See the chart below to understand why the baby needs to be breastfed up to 24 months of age.
Session 23. Importance of CF
Counseling on infant and young child feeding at health facility .89
Gap
Provided by550mlbreast milk
0%
25%
50%
75%
100%
Pe
rce
nta
ge
of
da
ily n
ee
ds
Energy Protein Iron Vitamin A
Nutrient
BREAST MILK IN SECOND YEAR OF LIFE
nourish. nurture. grow.

Continued BF
• Babies should be exclusively breastfed for the first 6 months.
• From 6-12 months, BF continues to provide half or more of the child’s nutritional needs, and from
12-24 months, at least one-third of their nutritional needs. In addition, breastmilk continues to
provide protection for the child against many illnesses and provides more than 50% of the total
amount of vitamin A that a child needs each day.
Session 23. Importance of CF
Counseling on infant and young child feeding at health facility90.
BF for two years or longer helps a child to develop and to grow
strong and healthy
Summarize the lesson
• A baby’s nutritional status affects his/her health. A baby’s health condition includes not only devel-
opment and growth but also the baby’s ability to fight against diseases and recover after illness.
• In order to ensure that a baby is always healthy and grows well, the mother needs to ensure:
All infants are breastfed for the first six months.
All infants and young children are given complementary food at six months.
All young children continue to be breastfed up to 24 months.

SESSION 24: CF - QUANTITY AND QUALITY
Objectives:
After completing this lesson, trainees will be able to:
1. Present the quantity of complementary foods, including frequency and amount.
2. Explain reasons for using foods of a thick consistency.
3. Describe ways to enrich foods.
4. Explain the importance of using a variety of foods, including iron- and vitamin A- rich foods.
1. Principles of CF
• Start giving complementary food at an appropriate age (start at 6 months – 180 days), not too early
or too late. Continue BF as much as possible.
• Start with liquid food and move to solid food, from a little to bigger amounts, and help the baby get
acquainted with new food (not providing diluted food for more than two weeks).
• Number of meals should increase according to the child’s age. Ensure that the food suits the baby’s
appetite.
• Make the food tender for easy eating and swallowing.
• Prepare mixed food rich in nutrients using locally available food. Add different food to the baby’s
semi-solid soup and porridge to make the food colorful, delicious, attractive, and sufficient in
nutrients. For example, add egg yolk for a yellow color, add vegetables for a green color, add meat,shrimp, or crab for a brown color. You should not give the baby the same food more than once ina day.
• Thicken the complementary food. Add oils, fat, sesame, or peanut in the complementary foods to
provide more energy, helping the baby to grow fast or add micronutrient powder.
• The cooking tools must be clean and hands must be washed before preparing meals and feeding
the child.
• Give the child more complementary food during and after the child’s illness and give the child more
liquid food/drink especially after a bout of diarrhea or a high temperature.
• You should not give MSG to a child; MSG is not nutritious.
• Do not give the child confectionery sugars or soft drinks before meals because the sweetness will
increase blood sugar, inhibiting the extracting enzyme so that child lose his/her appetite and skips
the meal or takes less food.
Session 24: CF - Quantity and Quality
Counseling on infant and young child feeding at health facility .91
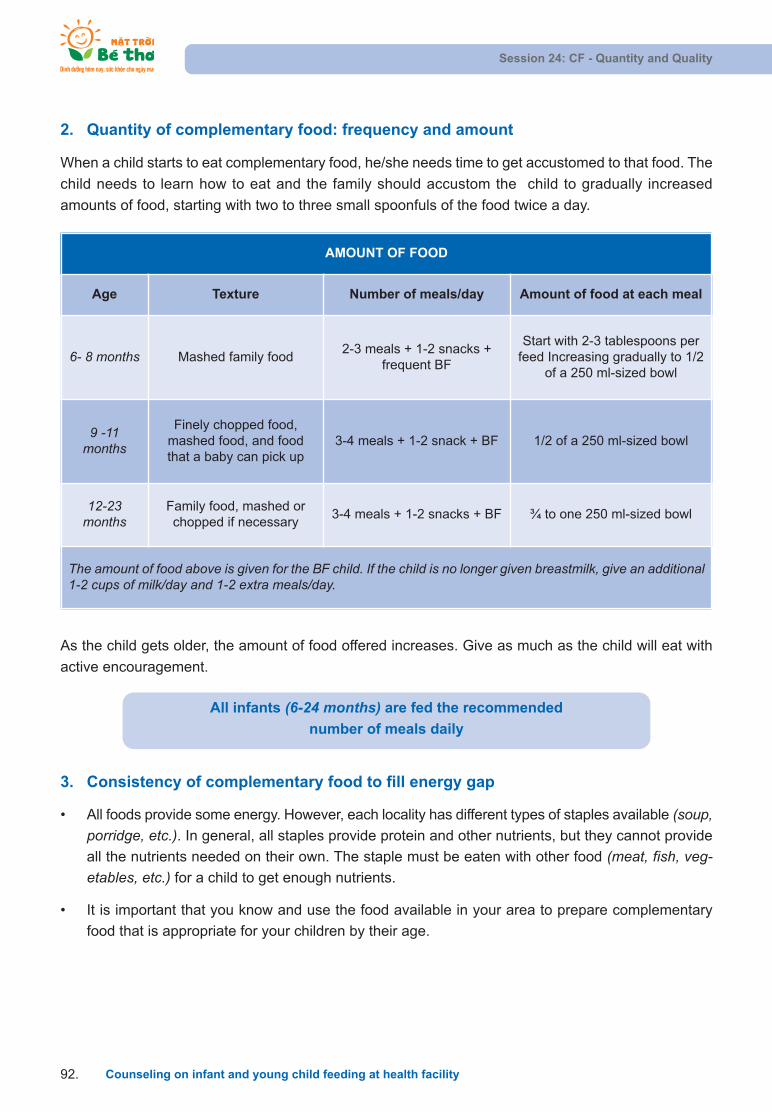
3. Consistency of complementary food to fill energy gap
• All foods provide some energy. However, each locality has different types of staples available (soup,porridge, etc.). In general, all staples provide protein and other nutrients, but they cannot provide
all the nutrients needed on their own. The staple must be eaten with other food (meat, fish, veg-etables, etc.) for a child to get enough nutrients.
• It is important that you know and use the food available in your area to prepare complementary
food that is appropriate for your children by their age.
As the child gets older, the amount of food offered increases. Give as much as the child will eat with
active encouragement.
2. Quantity of complementary food: frequency and amount
When a child starts to eat complementary food, he/she needs time to get accustomed to that food. The
child needs to learn how to eat and the family should accustom the child to gradually increased
amounts of food, starting with two to three small spoonfuls of the food twice a day.
Session 24: CF - Quantity and Quality
Counseling on infant and young child feeding at health facility92.
AMOUNT OF FOOD
Age Texture Number of meals/day Amount of food at each meal
6- 8 months Mashed family food 2-3 meals + 1-2 snacks +
frequent BF
Start with 2-3 tablespoons perfeed Increasing gradually to 1/2
of a 250 ml-sized bowl
9 -11months
Finely chopped food,mashed food, and foodthat a baby can pick up
3-4 meals + 1-2 snack + BF 1/2 of a 250 ml-sized bowl
12-23months
Family food, mashed orchopped if necessary
3-4 meals + 1-2 snacks + BF ¾ to one 250 ml-sized bowl
The amount of food above is given for the BF child. If the child is no longer given breastmilk, give an additional1-2 cups of milk/day and 1-2 extra meals/day.
All infants (6-24 months) are fed the recommended
number of meals daily
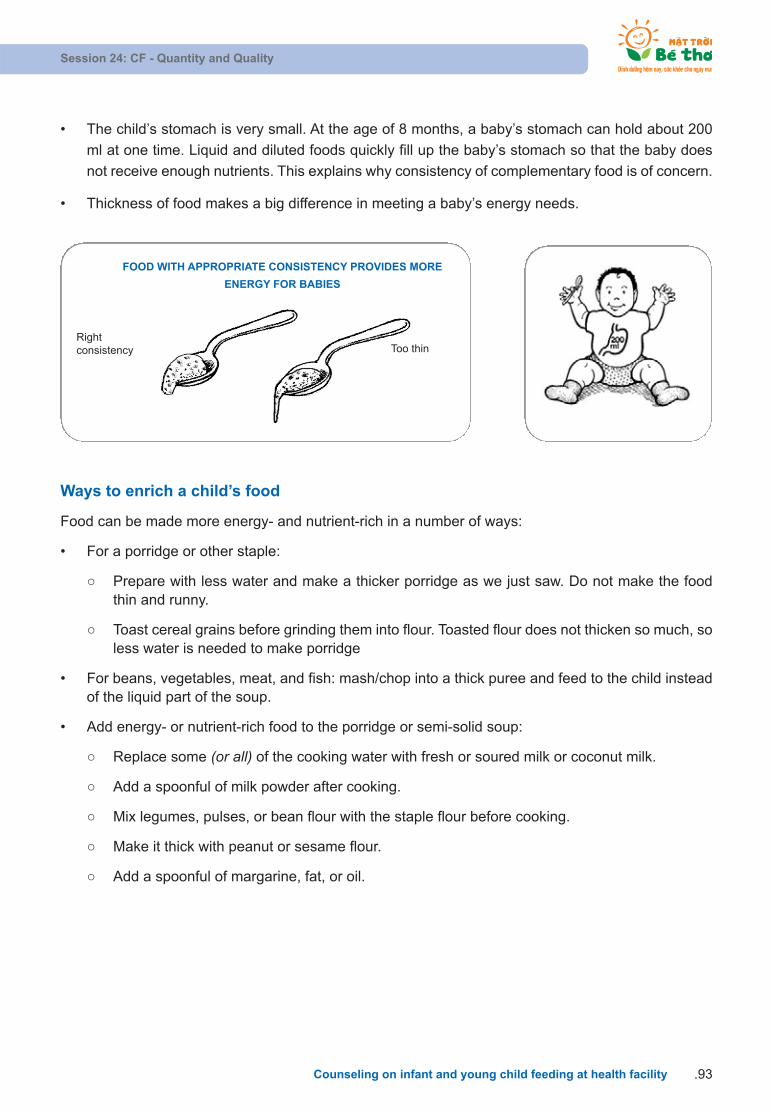
• The child’s stomach is very small. At the age of 8 months, a baby’s stomach can hold about 200
ml at one time. Liquid and diluted foods quickly fill up the baby’s stomach so that the baby does
not receive enough nutrients. This explains why consistency of complementary food is of concern.
• Thickness of food makes a big difference in meeting a baby’s energy needs.
Session 24: CF - Quantity and Quality
Counseling on infant and young child feeding at health facility .93
FOOD WITH APPROPRIATE CONSISTENCY PROVIDES MORE
ENERGY FOR BABIES
Rightconsistency Too thin
Ways to enrich a child’s food
Food can be made more energy- and nutrient-rich in a number of ways:
• For a porridge or other staple:
Prepare with less water and make a thicker porridge as we just saw. Do not make the foodthin and runny.
Toast cereal grains before grinding them into flour. Toasted flour does not thicken so much, soless water is needed to make porridge
• For beans, vegetables, meat, and fish: mash/chop into a thick puree and feed to the child insteadof the liquid part of the soup.
• Add energy- or nutrient-rich food to the porridge or semi-solid soup:
Replace some (or all) of the cooking water with fresh or soured milk or coconut milk.
Add a spoonful of milk powder after cooking.
Mix legumes, pulses, or bean flour with the staple flour before cooking.
Make it thick with peanut or sesame flour.
Add a spoonful of margarine, fat, or oil.

FURTHER READING:
Fats and oils
• Oils and fats are concentrated sources of energy. A little oil or fat, such as one-half
teaspoon, added to the child’s bowl of food, gives extra energy in a small volume. The
addition of fatty/oily foods also makes thicker porridge or other staples softer and
easier to eat.
• Fats and oils can also be used for frying foods, or spreading on foods such as bread.
The fat or oil should be fresh because fats and oils can go bad when stored.
• If a large amount of oil is added, the child may become full before he has eaten all of
the food. This means the child may get the energy from the oil but less of the other
nutrients because the child eats less food overall.
• If a child is growing well, extra oil is usually not needed. A child who eats too much oil
or fried foods can become overweight.
• Sugar and honey are also energy-rich and can be added to foods in small quantities
to increase the energy concentration. However, these foods do not contain any other
nutrients.
• Caregivers need to watch that sugary foods do not replace other foods in the diet. For
example, sweets, sweet biscuits, and sugary drinks should never be used instead of
a meal for a young child.
• Essential fatty acids are needed for a child’s growing brain and eyes, and for healthy
blood vessels. These essential fatty acids are present in breastmilk.
• For children over six months old, who are not breastfed, good sources of essential
fatty acids are fish, seeds, and vegetable oil. Animal-source foods also provide
essential fatty acids.
Fermented or germinated flour
• Fermented porridge can be made in two ways – the grain can be mixed with water
and set to ferment overnight or longer before cooking, or the grain and water are
cooked into porridge and then fermented. Sometimes some of a previous batch of the
fermented porridge is added to speed up the process of fermentation. Porridge made
from germinated grain can also be fermented.
• The advantages of using fermented porridge are:
Session 24: CF - Quantity and Quality
Counseling on infant and young child feeding at health facility94.
It is less thick than plain porridge so more grain/flour can be used with the same
amount of water. This means each cupful of porridge contains more energy and
nutrients than plain (unfermented) porridge.
Children may prefer the taste of “sour” porridge and therefore eat more.
The absorption of iron and some other minerals is better from fermented porridge.
It is more difficult for harmful bacteria to grow in fermented porridge, so it can be
kept for a day or two.
• Grain is also fermented to make alcohol. However, the short fermentation period talked
about here to make fermented porridge will not make alcohol or make the child drunk!
Germinated or sprouted flour
• Cereal or legume seeds are soaked in water and then left to sprout. The grains are
then dried (sometimes toasted) and ground into flour. A family can do this at home but
it is more common to buy flour already germinated.
• Mixed flours that include germinated flour in addition to the main flour may be available
in the store.
• If families in your area use germinated flour, the following ways can make a thicker
and more nutritious semi-solid soup:
Use this germinated flour to make semi-solid soup. This type of flour does not
thicken much during cooking so less water can be used.
Add a pinch of the germinated flour to cooked thick semi-solid soup that has
cooled a little bit. Semi-solid soup should be boiled again for a few minutes after
adding the germinated flour. This addition will make the semi-solid soup softer and
easier for the child to eat.
• Germinated flour also helps more iron absorption.
Session 24: CF - Quantity and Quality
Counseling on infant and young child feeding at health facility .95
4. Components of complementary food
To ensure that all children receive diverse foods, each complementary feed should include the following
food groups:
• Basic food: include food that provides the main calories in the diet. In our country, rice, corn, and
sweet potato are often made into paste for the child to eat.
• Food rich in protein:
Animal-source food: rich in nutrients, including eggs, milk, meat, shrimp, crab, eel, pupa, and
organs such as liver. Pork, beef, chicken, not necessarily lean meat, can be given to a baby
but it is better to give children both lean and fat meat.
Food from plants: including all kinds of pulses such as black beans, green beans, soy beans,
etc., of which soy beans are the richest in protein and lipid. When these foods are mixed with
cereals, they become as nutrient-rich as animal-source foods – but are cheaper.
• Food rich in energy: including oil, butter, fat, sugar, etc. Oil and fat provides energy for the child’s
meal. They also make food softer and easy to swallow. In addition to animal fat, a child should be
given more peanut oil, sesame oil, soya oil, and so on. Oil contains more unsaturated fatty acids
than fat does so it is easily absorbed. Feeding a child with fat and oil helps him easily absorb vita-
mins saturated in oil such as vitamin A, E, D, K, etc.
• Food rich in vitamins, minerals, and fiber: Green vegetables and ripe fruit have a significantly
abundant supply of vitamins and minerals. This is a very good source of food for children. Dark-
green leaves such as “rau ngot”, “rau muong”, “rau den”, “mong toi”, “rau cai”, etc. are all rich in
vitamin C and micronutrients like beta-caroten (pre-vitamin A) and iron, preventing a baby from
having dry eyes and anemia. Ripe fruit (papaya, mango, banana, orange, mandarine, sapodilla...)is rich in micro-nutrients, which are not lost because no cooking is needed.
Food selection and substitution
For areas with disadvantaged economic conditions such as remote and mountainous areas, compo-
nents of complementary food for babies can be replaced as follows:
• Rice replaced by corn or sweet potato.
• In protein-rich foods: meat and eggs replaced by shrimps, crabs, fish, and cow milk replaced with
soya milk.
• Animal-protein substitution: protein from meat, eggs, milk, shrimps, crabs, or fish can replaced by
protein from plants: soy-beans, green beans, black beans, sesame, or peanuts.
• Oil replaced by fat.
5. Importance of using diverse foods
• Most adults and older children eat a mixture or a variety of foods at mealtimes. In the same way,
it is important for young children to eat a mix of good complementary foods.
• To give more energy to children, snacks can be given to them in addition to meals. Good snacks
– such as yoghurt and other milk products, bread or biscuits spread with butter, margarine, nut
paste or honey, fruit, bean cakes and cooked potatoes, etc. –provide both energy and nutrients.
Note: snacks should not be confused with junk food such as sweets, fried potatoes, or other products.
Session 24: CF - Quantity and Quality
Counseling on infant and young child feeding at health facility96.
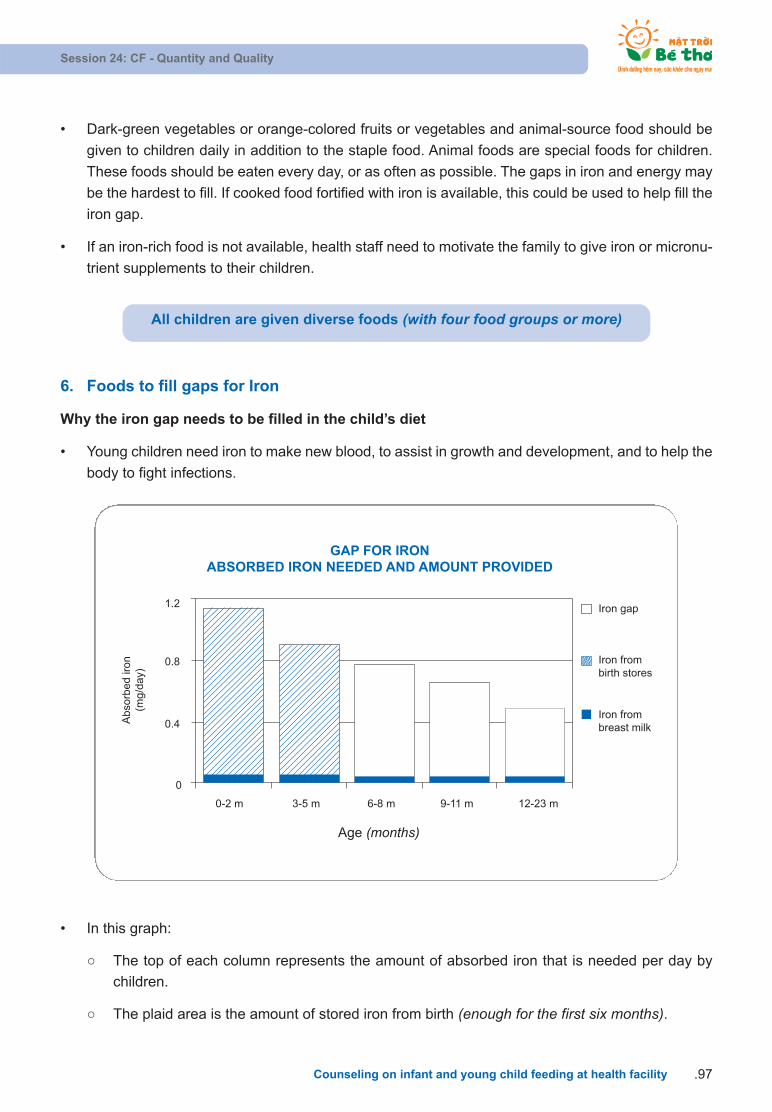
• Dark-green vegetables or orange-colored fruits or vegetables and animal-source food should be
given to children daily in addition to the staple food. Animal foods are special foods for children.
These foods should be eaten every day, or as often as possible. The gaps in iron and energy may
be the hardest to fill. If cooked food fortified with iron is available, this could be used to help fill the
iron gap.
• If an iron-rich food is not available, health staff need to motivate the family to give iron or micronu-
trient supplements to their children.
Session 24: CF - Quantity and Quality
Counseling on infant and young child feeding at health facility .97
All children are given diverse foods (with four food groups or more)
6. Foods to fill gaps for Iron
Why the iron gap needs to be filled in the child’s diet
• Young children need iron to make new blood, to assist in growth and development, and to help the
body to fight infections.
Abso
rbed ir
on
(mg/d
ay)
0
0-2 m 3-5 m 6-8 m 9-11 m 12-23 m
0.4
0.8
1.2
Age (months)
Iron gap
Iron frombirth stores
Iron frombreast milk
GAP FOR IRONABSORBED IRON NEEDED AND AMOUNT PROVIDED
• In this graph:
The top of each column represents the amount of absorbed iron that is needed per day by
children.
The plaid area is the amount of stored iron from birth (enough for the first six months).
FURTHER READING:
Iron absorption: The amount of iron that a child absorbs from food depends on:
• The amount of iron in the food.
• The type of iron (iron from meat and fish is better absorbed than iron from plants).
• The types of other food present in the same meal (some increase iron absorption andothers reduce absorption).
• Whether the child has anemia (more iron is absorbed if anemic).
Eating these foods at the same meal increases the amount of iron absorbed from eggsand plant foods such as cereals, pulses, seeds, and vegetables:
• Food rich in vitamin C such as tomato, broccoli, guava, mango, pineapple, papaya,orange, lemon, and other citrus fruit.
• Small amounts of the flesh or organs/offal of animals, birds, fish, and other sea foods.
Iron absorption is decreased by:
• Drinking tea and coffee.
• Eating food high in fiber.
The black area along the bottom of the columns shows the iron provided by breastmilk (thebaby must be breastfed).
The white area illustrates the iron gap that needs to be filled with complementary food.
• A full-term baby is born with good stores of iron to cover his needs for the first 6 months.
• The young child grows faster in the first year than in the second year. This is why the need for iron
is higher when the child is younger.
• The iron store is gradually used up over the first 6 months. So after that time we see a gap between
the child’s needs and the iron they receive from breastmilk.
• Zinc is another nutrient that helps children to grow and stay healthy. It is usually found in the same
foods as iron, so we assume that if they are eating food rich in iron they are also receiving zinc.
Health workers’ aims are:
• To identify locally available food that is rich in iron.
• To instruct families to use these iron-rich foods to complement the food for their young children.
Iron absorption
Pulses and dark-green leaves are sources of iron. However, it is not enough that a food has iron in it.
The iron must also be in a form that the child can absorb and use.
Session 24: CF - Quantity and Quality
Counseling on infant and young child feeding at health facility98.
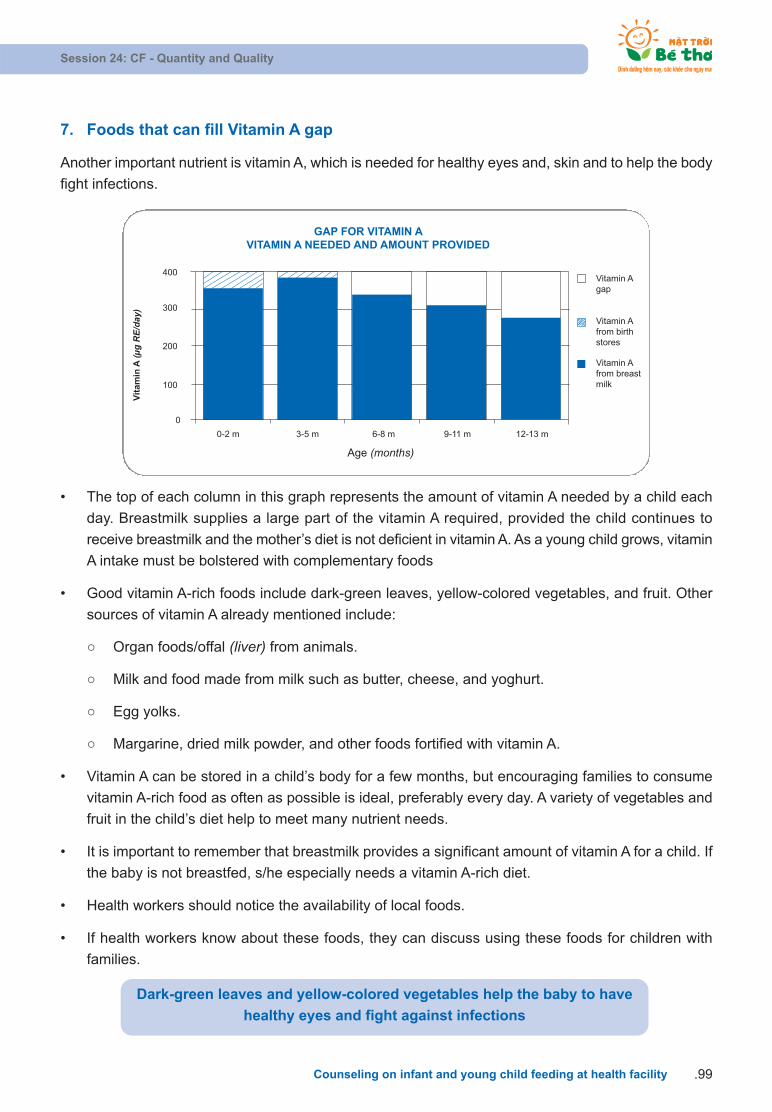
Session 24: CF - Quantity and Quality
Counseling on infant and young child feeding at health facility .99
7. Foods that can fill Vitamin A gap
Another important nutrient is vitamin A, which is needed for healthy eyes and, skin and to help the body
fight infections.
Vit
amin
A (
g R
E/da
y)
0
0-2 m 3-5 m 6-8 m 9-11 m 12-13 m
100
200
300
400
Age (months)
Vitamin Agap
Vitamin Afrom birthstores
Vitamin Afrom breastmilk
GAP FOR VITAMIN AVITAMIN A NEEDED AND AMOUNT PROVIDED
• The top of each column in this graph represents the amount of vitamin A needed by a child each
day. Breastmilk supplies a large part of the vitamin A required, provided the child continues to
receive breastmilk and the mother’s diet is not deficient in vitamin A. As a young child grows, vitamin
A intake must be bolstered with complementary foods
• Good vitamin A-rich foods include dark-green leaves, yellow-colored vegetables, and fruit. Other
sources of vitamin A already mentioned include:
Organ foods/offal (liver) from animals.
Milk and food made from milk such as butter, cheese, and yoghurt.
Egg yolks.
Margarine, dried milk powder, and other foods fortified with vitamin A.
• Vitamin A can be stored in a child’s body for a few months, but encouraging families to consume
vitamin A-rich food as often as possible is ideal, preferably every day. A variety of vegetables and
fruit in the child’s diet help to meet many nutrient needs.
• It is important to remember that breastmilk provides a significant amount of vitamin A for a child. If
the baby is not breastfed, s/he especially needs a vitamin A-rich diet.
• Health workers should notice the availability of local foods.
• If health workers know about these foods, they can discuss using these foods for children with
families.
Dark-green leaves and yellow-colored vegetables help the baby to have
healthy eyes and fight against infections

FURTHER READING:
The importance of animal-source foods
• Foods from animals, meat, and organs such as liver, heart, and blood, as well as milk,yoghurt, cheese, and eggs are rich sources of many nutrients.
• The meat and organs of animals, birds, and fish (including shell fish and tinned fish),as well as blood-source foods, are rich in iron and zinc. Liver is not only a good sourceof iron but also of vitamin A.
• Animal-source foods should be eaten daily or as often as possible. This is especiallyimportant for the non-breastfed child.
• Foods from animals such as milk and eggs are good for children because they arehigh in protein and other nutrients. However, milk and milk products, such as cheeseand yoghurt, are not good sources of iron.
• Milk fat contains vitamin A. Therefore, foods made from whole milk are good sourcesof vitamin A.
• Foods made from milk (whole milk, skim milk, or powdered milk) and any food containing bones, such as pounded dried fish, are good sources of calcium to helpbones grow strong.
• Egg yolk is another source of nutrients and rich in vitamin A.
• Only animal-source foods can provide enough iron needs for children. Foods suchas flour, pasta, and instant cereals are also a good iron source for children. Some children may need supplements if they do not eat enough food containing iron, or ifthey have particularly high iron needs.
• Ideal practice: All infants and young children are fed meat, fish, or poultry daily. Allchildren are given iron-rich food and iron supplements daily.
The importance of legumes
Legumes or pulses such as beans, peas, and lentils, as well as nuts and seeds, are goodsources of protein. Legumes are a source of iron as well. Beans, peas, lentils, nuts, orseeds are all good for children.
Some ways these foods could be prepared that would be easier for the child to eat and digest are:
• Soak beans before cooking and throw away the water.
Session 24: CF - Quantity and Quality
Counseling on infant and young child feeding at health facility100.
• Remove skins by soaking raw seeds and then rub the skins off before cooking them.
• Boil beans, then sieve to remove coarse skin.
• Toast or roast nuts and seeds and then pound them into a paste.
• Add beans/lentils to soups or stews.
• Mash cooked beans.
Eating a variety of foods in the same meal can improve the way the body uses the nutrients. For example, combining a cereal with a pulse (e.g., rice and beans), or addinga milk product to a cereal or grain (maize meal with milk).
Foods fortified with micro-nutrients
In some countries, there are fortified complementary foods available cheaply – e.g., flouror a cereal product with added iron and zinc for children. These products are convenientto use and provide nutrients that families may be interested in.
Note: when discussing fortified complementary foods with caregivers, there are somepoints to consider:
• What are the main ingredients?
• Is the product fortified with micronutrients such as iron, vitamin A, or other vitamins?
• Does the product contain ingredients such as sugar and/or oil to add energy?
• What is the cost compared to similar home-produced foods?
• Does the label or other marketing imply that the product should be used for childrenof a specific age or how to use it? Does it have an expiry date?
• Do not use products that have written on them “a breast-milk substitute” or “for childrenunder six months only”.
Session 24: CF - Quantity and Quality
Counseling on infant and young child feeding at health facility .101
8. Fluid needs of the young child
• A baby who is exclusively breastfeeding receives all the liquid he/she needs. However, he/she
needs extra water when given complementary food. Likewise, a baby who is under six months of
age and only receiving replacement milk does not need extra water.
• Offer a drink when the child seems thirsty. Extra fluid is needed if the child has a fever or diarrhea.
Session 24: CF - Quantity and Quality
Counseling on infant and young child feeding at health facility102.
FLUID NEEDS OF THE YOUNG CHILD
• Water is good for thirst. A variety of pure fruit juices can also be used.
Note: Too much fruit juice may cause diarrhea and may reduce the child’s appetite.
• Drinks that contain a lot of sugar may actually make the child thirstier as his body has to
deal with the extra sugar. Fizzy drinks (sodas) are not suitable for young children.
• Sometimes a child is thirsty during a meal. A small drink will quench the thirst and they
may then eat more.
• Remember that children who are not receiving breastmilk need special attention and
special recommendations. A non-breastfed child aged 6-24 months of age needs
Approximately two to three cups of water per day (1 cup = 250ml) in a moderate
climate.
Four to six cups of water per day in a hot climate.
This water can be incorporated into porridge or stews, but clean water should also be
offered to the child several times a day to ensure that the infant’s thirst is satisfied.

SESSION 25: FEEDING TECHNIQUE
Objectives:
After completing this lesson trainees will be able to:
1. Describe feeding patterns and influences on children’s feeding activity
2. Explain to family members how to encourage the children to eat
• A child needs to be fed, to be taken care of, and to have good health in order to grow and develop
well. Even when food is limited, good care can help make the best use of these limited resources.
• Good care here refers to the behavior and practice of caregivers and family members who provide
food, health care, stimulation, and emotional support necessary for the child’s growth and
development.
• An important time to use good care practices is at meal times – when helping young children
to eat.
• A child needs to learn how to eat, to try new foods (not breastmilk), to chew, to move food around
the mouth, and to swallow food. A child needs to learn how to get food effectively into his/her mouth,
how to use a spoon, how to drink, and to hold a spoon and a cup.
• Therefore, it is very important to show how a mother can encourage her child and to feed him. This
can help families to enjoy a happy atmosphere at mealtimes.
• Feeding needs to occur in response to the child’s cues or signals using encouragement and praise.
Session 25: Feeding technique
Counseling on infant and young child feeding at health facility .103
RESPONSIVE FEEDING TECHNIQUES
• Respond positively to the child with smiles, eye-to-eye contact, and encouraging words.
• Feed the child slowly and patiently with love.
• Try to feed a variety of food to encourage eating.
• Cease temporarily when the child stops eating, and then continue later on
• Give the child finger food that the child can feed him/herself.
• Minimize distractions in the meal.
• Stay with the child through the meal and be attentive.
Talk to the child with eye-to-eye contact during feeding
Mealtime is when children learn to eat and they will eat more if a happy and comfortable atmosphere
is created. Feed the child when he is alert and happy. If the child is sleepy, upset, or over-hungry, he
may not eat well. Regular mealtimes and the focus on eating may also help a child learn to eat.
Session 25: Feeding technique
Counseling on infant and young child feeding at health facility104.
All infants and young children (6-24 months) are supported and
motivated to eat to satiety during meal times

SESSION 26: IN-CLASSROOM PRACTICE APPROPRIATE
CF PROMOTION AND MANAGEMENT
Objectives:
After completing this session, trainees will be able to:
1. Apply counseling skills to the promotion and management of appropriate CF.
1. Instructions for food demonstration
The trainer needs to prepare:
• Essential cooking utensils: Gas cooker, three pots, bowls, chopsticks, plates, spoons (5 ml), knife,
cutting board, clean towel, fresh water, etc.
• Food: adequate to prepare three different types of CF (first processed, cleaned)
• Cooking process
• Age-appropriate CF recipes
• Get food and utensils ready
Food demonstration:
• The trainer practices first: prepare CF for seven-month-old children and explain to mothers what
s/he is doing:
How to measure water, “bot” exactly?
What is the right order of food?
Add rice flour (Starch) + meat/shrimp/fish (Protein) + water and stir until they are well-cooked,
then add vegetables, fish sauce and oil at last.
Ensure hygiene and food safety while preparing food and store dry food (“bot”) after use
• Ensure hygiene and food safety while preparing complementary food (four “clean”)
• Demonstrate and give further explanation:
A seven month-old child needs how many calories? How much food does he need? Etc.
Energy demand by age?
How to check the consistency of food?
Session 26: In-classroom practice Appropriate CF Promotion and Management
Counseling on infant and young child feeding at health facility .105
How to reduce the consistency of “bot”/”chao”?
How to increase the density of food?
What to note while preparing food for sick children?
• When the food is ready: ask the mothers to taste and give comments
• Ask if the mothers have any questions
2. Apply the skills that you have learned to counsel mothers in the following case studies
• Greet the “caregiver” and introduce yourself. Ask his/her name and use his/her name during the
conversation.
• Ask one or two open-ended questions to start the conversation and identify why he/she needs
counseling.
• Use the skills that you have learned to encourage the “caregiver” to talk to you.
Case studies on CF:
Your baby is 6 months of age and grows well. This is your second baby. You come to the health facility
to enquire about how to feed your baby.
Some of your friends advise you to bottle feed because you can put the watery food into a bottle and
your baby can eat him/herself.
You are not sure whether this is good or bad.
You can start the conversation with:
“I wonder if I could give my baby thin semi-solid soup by bottle so that he can eat on his own?”
Case study two:
You come to the health facility because you think your baby grows slowly and often gets sick. Your
baby is 8 months of age. This is your first baby.
You are confused from the different information you have heard. You do not know what to follow. You
do some things that you think are correct and some things that your husband and mother-in-law advise
you to.
You do not give your baby meat and mashed vegetables but only use the water after you boil these
foods because you think it is too early to give him these foods.
You can start the conversation with:
“I do not give my baby mashed vegetables or meat – my mother-in-law said that they are not good foryoung children.”
Session 26: In-classroom practice Appropriate CF Promotion and Management
Counseling on infant and young child feeding at health facility106.

Case study three:
You come to the health facility for a regular weight check-up. Your baby is 18 months of age and grows
very slowly. You are very worried, anxious, and tired. This is your first child.
You feed your baby diverse foods (semi-solid soup, mashed fruit, vegetables, and beans) but he only
eats a bit and then cries and throws it away. You feed him daily and do not breastfeed him.
You can start the conversation with:
"Why my baby is not gaining weight?"
"I try to feed my baby but he refuses"
"Please tell me what I should do to make my baby eat".
Case study four:
Your baby is 7 months of age. This is your first child. Your friends advise you to come to a health facility
to receive counseling on CF. You are surprised because you think your baby is too young – less than
one year old – for complementary food.
Your baby is breastfed and growing well. You do not particularly care, but are curious and want to know.
You can start the conversation with:
“I haven’t thought of giving my baby complementary foods; he does not need that until he is one yearold. Is that right?”
Session 26: In-classroom practice Appropriate CF Promotion and Management
Counseling on infant and young child feeding at health facility .107
SESSION 27. PREPARING A HYGIENE MEAL AND FOOD SAFETY
Objectives:
After completing this lesson, trainees will be able to:
• Explain the ways to keep a child’s meal hygienic and safe.
Requirements for clean and safe feeds
A baby who is not breastfed is at increased risk of illness for two reasons:
Replacement feeds may be contaminated with organisms that can cause infection.
The baby lacks the protection provided by the breastmilk.
• After six months (180 days) of age all children require complementary food. Clean and safe prepa-ration and feeding of complementary food is essential to reducing the risk of infection and itscauses.
• The main points to remember for clean and safe preparation of food are:
Clean hands.
Clean utensils.
Clean food and water.
Safe storage
Clean hands
Session 27. Preparing a hygiene meal and food safety
Counseling on infant and young child feeding at health facility108.
CLEAN HANDS
Wash hands with soap andwater
• Before holding food andreguarly when preparing a meal
• After using the toilet, cleaning ababy’s bottom, or holding pets/animals
• Wash hands and the child’shands before feeding
nourish. nurture. grow.
• You must regularly wash your hands after using the toilet, after washing the baby, after disposing
of the baby’s stools and changing the nappies, and after preparing food because your hands may
be easily contaminated with organisms such as: raw meat, poultry. Also after touching animals,
before preparing or serving food and before eating and feeding the baby.
• It is important to wash your hands with soap, running water, or clean water, washing the palms,
the space between the fingers and nails, and the back of the hands. Let the hands dry naturally or
wipe the hands with a clean towel. Do not wipe your hands on the clothes you are wearing or a
towel you share with others.
Clean utensils
Session 27. Preparing a hygiene meal and food safety
Counseling on infant and young child feeding at health facility .109
CLEAN UTENSILS
• Keep knives, chopping boards,containers, and the kitchenclean
• Wash all the surface and uten-sils for cooking and food con-tainer before and after usingthem
• Use clean utensils and coveredcontainers for the baby
• Separate raw meat, poultry,and sea food from other food
• Use separate containers andchopping board for cooked foodand raw food
• Use covered containers tostore food
nourish. nurture. grow.
• You should keep clean all the utensils and the surfaces used for preparing food. If possible, use
a soft brush to reach all the corners. Use covered utensils to avoid insects and dust. Use a clean
spoon to feed the baby semi-solid soup and a clean cup to give the baby milk or fruit juice. The
caregiver needs to use another spoon when tasting the baby food.
• Bring the water to a rolling boil before using it. This will kill most harmful micro-organisms. A rolling
boil is when the surface of the water is moving vigorously for a second or two. The water can cool
down naturally in a clean covered container. The best kind of container has a narrow top, and a
tap through which the water comes out. This prevents people from dipping cups and hands into
the water, which can make it unsafe. If the water has been stored for more than 48 hours it is better
to use it for something else, for example, cooking or give it to older children to drink.
Safe storage
Safe water and food
Session 27. Preparing a hygiene meal and food safety
Counseling on infant and young child feeding at health facility110.
SAFE FOOD AND WATER
Water
• Use clean or filtered water
• Give the baby boiled water
Food
• Use fresh food
• Do not use expired/old food
• Wash and clean the raw foodbefore cooking
• Cook food well
• Eat immediately affter cooking
• Stored food needs to be re-heated
nourish. nurture. grow.
SAFE STORAGE
• Keep the food in a coveredcontainer
• Keep food in dry, clean places
• Preserve dry food carefully
• Use cooked food within onehour
nourish. nurture. grow.
FURTHER READING:
Cleaning a cup: A cup does not need to be boiled. To clean a cup, wash it and scrub it
with hot soapy water each time it is used. If possible, dip the cup into boiling water, or pour
boiling water over it just before use, but this is not essential. An open, smooth surfaced
cup is easiest to clean. Avoid tight spouts, lids, or rough surfaces where milk could stick
and allow bacteria to grow.
Five key points for safe food
Keep clean
• Wash your hands before handling food and often during food preparation.
• Wash your hands after going to the toilet, changing the baby, or coming in contact
with animals.
• Wash all surfaces and equipment used for food preparation or serving.
• Protect kitchen areas and food from insects, pests, and other animals.
Separate raw and cooked food
• Separate raw meat, poultry, and seafood from other food.
• Use separate equipment and utensils such as knives and cutting boards for han-
dling raw food.
• Store food in covered containers to avoid contact between raw and prepared food.
Cook thoroughly
• Cook food thoroughly, especially meat, poultry, eggs, and seafood.
• Bring food like soups and stews to a boil. For meat and poultry, make sure juices
are clear, not pink.
• Reheat cooked food thoroughly. Bring to a boil or heat until it is too hot to touch.
Stir while re-heating.
Keep food at safe temperatures
• Do not leave cooked food at room temperature for more than two hours.
• Do not store food too long, even in a refrigerator.
Session 27. Preparing a hygiene meal and food safety
Counseling on infant and young child feeding at health facility .111
• Do not thaw frozen food at room temperature; thaw in a refrigerator.
• Food for infants and young children should ideally be freshly prepared and not
stored at all after cooking.
Use safe water and raw materials
• Use safe water or treat it to make it safe.
• Choose fresh and wholesome foods.
• Use pasteurized milk.
• Wash fruit and vegetables in safe water, especially if eaten raw.
• Do not use food beyond its expiry date.
Session 27. Preparing a hygiene meal and food safety
Counseling on infant and young child feeding at health facility112.

SESSION 28: FEEDING ILL (SICK) CHILDREN AND
CHILDREN WITH HIV-INFECTED MOTHERS
Objectives:
After completing this lesson, trainees will be able to:
1. Explain the importance of feeding children during illness.
2. Present how to feed the child during illness and recovery and how to feed a child with an
HIV-infected mother.
3. State the danger signs in young children and how to handle them.
Introduction
• During infections, the child needs more energy and nutrients to fight the infection. If they do not
get extra food, their fat and muscle tissue is used as fuel. This is why they lose weight, look thin,
and stop growing.
• The goal in feeding a child during and after illness is to help him to return to the weight he had
before he was ill.
Session 28: Feeding ill (sick) children and children with HIV-infected mothers
Counseling on infant and young child feeding at health facility .113
Encourage children to drink and eat during illness and provide
extra food after illness to help them recover quickly
1. Feeding a child during illness
A child who is ill needs extra food. In this period, the child normally only wants breastmilk and no other
food. Although the child does not want to eat, you should not restrict his food.
FEEDING A SICK CHILD
For children < 6 months
• Continue to breastfeed.
• Breastfeed more frequently.
For children > 6 months
• Continue to breastfeed.
• Encourage the child to drink and eat – with lots of patience.
• Feed them small amounts frequently.
• Give food that the child likes.
• Give a variety of nutrient-rich food.
• The food should be tender and easily digestible.

2. Some guidance for feeding child having diarrhea and infection
When a child is sick, it is important to take care of and feed him/her properly - in addition to getting
medical treatment to help him/her recover quickly from illness. Common diseases among young chil-
dren are diarrhea and respiratory infection. In this section, we focus on introducing care and on feeding
a child who has diarrhea and a high fever. These are also common principles of feeding a child during
any illness.
Diet for a child who has diarrhea
• To treat diarrhea, the most important thing is to prevent dehydration; quickly handle dehydration if
it occurs and monitor the child’s diet.
• Prevent dehydration at home by giving the child more clean water than usual or an oral rehydration
salts (ORS) drink along with liquid made from food like porridge, salted porridge water, roasted
rice water, and rice water.
• In case of dehydration, take the child to health staff or health stations for treatment. The best way
to deal with dehydration is to give an ORS drink and liquid from cooking food.
• The common principle is to give the child more to drink than usual whenever he wants and to
continue providing the child with something to drink until he no longer has diarrhea. For children
under two years old, they cannot ask for water themselves so they express their thirst by stimulation
and looking uncomfortable. Therefore, you should bring water to him/her to see whether s/he is
thirsty and wants to drink or not. When s/he does not want more to drink, it means that s/he is
getting enough water to compensate lost liquid.
• How to give a child a drink: do not bottle-feed. Feed him/her by spoon every 1-2 minutes and use
a cup for older children. If the child vomits, stop giving him anything to drink for ten minutes, then
• During illness, a child has little appetite even though the family tries to encourage him to eat. The
child’s appetite usually increases after the illness so it is important to continue to pay extra attention
to feeding after the illness. This is a good time for families to give the child extra food so that lost
weight is quickly regained.
• Young children need extra food until they have regained all their lost weight and are growing at a
healthy rate.
Session 28: Feeding ill (sick) children and children with HIV-infected mothers
Counseling on infant and young child feeding at health facility114.
FEEDING DURING RECOVERY
• Give extra breastfeeds.
• Feed an extra meal.
• Give an extra amount.
• Use extra-rich food.
• Feed with extra patience and love.

continue, but more slowly, for example, a spoon every 2-3 minutes. The amount of water a child
needs after going to toilet is:
Children under 2 years old: 50-100 ml
Children from 2-10 years old: 100-200 ml
Children over 10 years old and adults: drink on demand
• Take the child to a health worker or health facility for treatment if there is sign of severe
dehydration.
Session 28: Feeding ill (sick) children and children with HIV-infected mothers
Counseling on infant and young child feeding at health facility .115
FURTHER READING:
Types of drinks used in diarrhea treatment:
a) ORS: is the best drink to treat dehydration
• How to prepare an ORS drink: wash your hands with soap and clean water before
preparing it.
• Pour the powder from the package into a clean jar or pot. Get a liter of clean water (or
suitable amount of water for each package used). Cooling boiled water is the best,
but if it is not available, use the cleanest water. Pour the water into the container and
stir carefully until the powder is completely dissolved. Cover the jar and give it to the
child within 24 hours. If all the ORS has not been used up within 24 hours, throw it
away and prepare a new batch.
b) How to prepare salted porridge: Cook a handful of rice with a pinch of salt and clean
water, and then filter it though a closely woven basket to get the water for the child to
gradually drink .
c) Water from rice roasted with salt and sugar: 50g rice (one handful) roasted until it
turns yellow and water. Cook them together, then filter the mixture though a closely
woven basket and add eight teaspoons of sugar, one teaspoon of salt, then boil it
again. When it is cool the child can drink it gradually.
d) Banana water or sapodilla water: grind or smash five bananas or sapodillas with one
liter of cooling boiled water and one teaspoon of salt, for the child to drink gradually.
e) Carrot soup with salt and sugar: 500g of carrot, one teaspoon of salt, eight spoon-
fuls of sugar. Rub well-cooked carrot in a closely woven basket or mash in a blender,
add salt and sugar, then boil it again.
Diet of a child with diarrhea:
• Feeding a child who has diarrhea is very important to prevent weight loss and possible
malnutrition.
• A child under 6 months old who is breastfed: continue BF with increased frequency of breastfeeds.
• A child over 6 months old: Foods that are recommended for a child who has diarrhea include: rice
(rice flour), potato, lean chicken, lean pork, soya milk, oil, carrot, sapodilla, and banana.
• In addition, feed the child more often, little by little, with other nutrient-rich foods such as meat,
egg, milk, fish, etc. and add oil or fat to enrich the energy of the food. The food should be tender,
well cooked, thinner than usual, and fed to the child right after cooking to ensure hygiene and
reduce risk of infection. If only processed food is available, re-cook it before feeding the baby. A
baby should be given ripe fruit or ripe fruit juice such as banana, orange, lemon, mango, papaya,
etc. to increase the amount of potassium. Avoid giving them soft drinks because they may lead to
more serious diarrhea.
Avoid using high-fiber or nutrient-poor food such as high-fiber vegetables, grain starch (corns,beans, etc.); they are difficult to digest.
Avoid using food containing too much sugar, which may cause more serious diarrhea.
The amount of food: encourage the child to eat as much as possible, six times a day or morefor younger children.
After the diarrhea is over, a child should be given one more meal per day for two weeks inorder to help him quickly recover and prevent malnutrition. A child with prolonged diarrheashould be given one more meal per day for at least one month.
When to take a child to health facility
After two to three days treated at home without improvement or if the following symptoms are noticed,
a child should be taken to health facility:
• Urinating many times with watery stools.
• Continuous and multiple vomiting.
• Increased signals of thirst.
• Fever.
• Eating and drinking less than usual.
• Blood in stools.
Prevention of diarrhea
• A child should be exclusively breastfed in the first six months and continued to be breastfed until
the child is two years old.
Session 28: Feeding ill (sick) children and children with HIV-infected mothers
Counseling on infant and young child feeding at health facility116.
• A child should be given complementary food from the seventh month. Porridge for the child should
be prepared with colorful food of all four food groups, especially oil. The food should be well cooked,
mashed, and served right after cooking.
• The food must be clean.
• Use a clean bowl, cup, and spoon to feed the child.
• Family members need to wash their hands after going to the toilet and before cooking and feeding
the child.
• Use a hygienic toilet. Let the child use a chamber pot and throw stools into the toilet.
• Give the child all scheduled vaccinations. Give the child the measles vaccination when he is nine
months old.
3. Diet for a child who has a high fever after developing infections
When children develop an infection, they often have a high fever, increased basic metabolism of ten
percent in accordance with one increased degree of fever. Therefore; demand for fluid, energy, protein,
vitamins, and minerals rise significantly. High fever often makes digestive enzymes become inhibited,
leading to the child losing appetite, which is why the child should be given food that is easy to digest.
Foods recommended for a child having high fever due to infection: ripe fruit, especially fruit rich
in vitamin C, such as orange, lemon, mandarin, grapefruit, etc. and food rich in protein, such as breast-
milk, cow milk, soya milk, egg, meat, and fish
Diet for a child who has a high fever due to infection
• A young child who is still breastfed: continue to breastfeed with increased frequency. If the child
cannot suckle, feed him expressed breastmilk with a spoon.
• An older child who is eating complementary food: give him tender, various, and easily digestible
food and divide this food into many small meals such as semi-solid soup and, porridge, thinner
soup cooked with meat, egg, fish, vegetable, and oil. Feed the child his favorite foods to encourage
him to eat more.
• Give the child more fruit, drinks, and fruit juices to compensate fluids lost due to fever and to provide
him with more vitamins.
• After the child recovers from illness, give him one extra meal per day and feed him food rich in nu-
trients to help him recover quickly .
4. For children of an HIV-infected mother
• Most mothers with HIV are appropriately counseled by specially trained health workers. Therefore,
franchise staff only need to note that mothers should not practice mixed feeding, that is, should
not give breastmilk and other food at the same time.
Session 28: Feeding ill (sick) children and children with HIV-infected mothers
Counseling on infant and young child feeding at health facility .117

Replacement feeding is the process of feeding a child who is not breastfed with a diet that provides
all the nutrients the child needs until the child is fully fed with family food.
The five requirements include:
1. Acceptable: the mother perceives no barrier to replacement feeding. Barriers may have cul-
tural or social reasons, or be due to fear of stigma or discrimination.
2. Feasible: the mother (or family) has adequate time, knowledge, skills, hours, and resources
to prepare the replacement food and feed the infant up to 12 times in 24 hours.
3. Affordable: the mother and family, with community or health-system support if necessary, can
pay for the cost of purchasing/producing, preparing, and using replacement food, including all
ingredients, fuel, clean water, soap, and equipment, without compromising the health and nu-
trition of the family.
4. Sustainable: availability of a continuous and uninterrupted supply and a dependable system
of distribution for all ingredients and products needed for safe replacement feeding, for as long
as the infants need, up to one year of age or longer.
5. Safe: replacement food is correctly and hygienically prepared, stored, and fed in nutritionally
adequate quantities with clean hands and using clean utensils, preferably by cup.
Session 28: Feeding ill (sick) children and children with HIV-infected mothers
Counseling on infant and young child feeding at health facility118.
Options for feeding 0-6 month old babies
Replacement feeding (milkpowder, home-modified ani-mal milk with a micronutrientsupplement) if 5 requirementsare met
5 requirements
- Acceptable
- Feasible
- Affordable
- Sustainable
- Safe
Early cessation as replacementfood meets 5 requirements
Exclusive breastfeeding

5. Danger signs in children
When a child is sick, the family should pay more attention to recognize danger signals. When a
caregiver sees the child having one of the following danger signs, it is necessary to bring him to the
health facility for treatment:
• A baby cannot breastfeed.
• A baby has diarrhea and is thirsty.
• A baby cannot drink or has difficulty drinking.
• A baby vomits a lot.
• A baby’s stool is mixed with blood.
• A baby has a fever (high temperature, higher than 380C).
• A baby has convulsions.
• A baby sleeps soundly and is hard to wake up.
• A baby has abnormal signs (fast breathing, difficultly breathing, sunken rib-cage).
• Hypothermia.
Session 28: Feeding ill (sick) children and children with HIV-infected mothers
Counseling on infant and young child feeding at health facility .119
SESSION 29: ASSESSING NUTRITION STATUS
Objectives:
After completing this lesson, trainees will be able to:
1. State the concept of nutrition status.
2. Categorize and assess nutrition status with anthropometrical methods.
3. Practice techniques of weighing with scales and height and arm- circumference measures.
4. Practice using a growth chart in counseling.
Definition:
Nutrition status is a set of functional, structural, and biochemical characteristics reflecting the satisfac-tion level of the body’s demands.
Nutrition status of individuals is the outcome of eating and using the body’s nutrients. Good nutrition
status reflects balance between food intake and health condition. When the body is in nutrient deficiency
or excess, it means the individual has health or nutrition problems.
Types of malnutrition
• Underweight: refers to humans who are considered to be under a healthy weight. The definition
is usually made with reference to the body mass index (BMI). (Weight-for-age Z score <-2).
• Stunting: is a reduced growth rate in human development. It is a primary manifestation of malnu-
trition in early childhood, including malnutrition during fetal development brought on by the
malnourished mother. (Height-for-age Z score <-2).
• Wasting: refers to the process by which a debilitating disease causes muscle and fat tissue to
"waste" away. Wasting is sometimes referred to as "acute malnutrition" because it is believed that
episodes of wasting have a short duration, in contrast to stunting, which is regarded as chronic
malnutrition. (Weight-for-height Z score <-2).
Some methods to assess nutrition status
Major methods used include:
1. Anthropometry, using scales and tape measures
2. Survey of diet or eating customs.
3. Clinical check-up, paying particular attention to implicit or explicit symptoms of nutrient
deficiency.
Session 29: Assessing nutrition status
Counseling on infant and young child feeding at health facility120.

4. Tests, especially biochemical tests (blood, urine tests, etc.).
5. Function tests to identify functional disorders caused by nutrient deficiency.
6. Survey of sickness and fatality to study relations between sickness and nutrition status.
7. Assessment of ecological factors related to nutrition status and health.
Nutrition anthropometric method
Nutrition anthropometry is a technique to measure body size and structure and to assess nutritional
status. Nutritional status results from both hereditary and environmental factors, in which nutritional
factors play a critical role.
Anthropometric sizes can be classified into the following groups:
a) Body mass, characterized by weight
b) Length sizes, specifically lying length and standing height
c) Body structure, energy and protein storage via surface soft tissues: skin and muscle beneath fat
Techniques to collect anthropometric measures
Following is the WHO standards (1883) that are currently applied:
Month calculation (for babies under 5 years old):
• 0 month: from the time of delivery till before first completed month day (from day 1 to day 29).
• 1 month: from the first completed month until the day before the second completed month (fromday 30-day 59).
• 12 months: from 12 completed months until 12 months and 29 days.
Year calculation:
• 0 years or under 1 year: from the time of delivery until the day before the completed year (1st year).
• 1 year: from the day of first completed year until the day before the second birthday (2nd year).
When we say children under 5 years old, we mean children from 1-60 months.
Session 29: Assessing nutrition status
Counseling on infant and young child feeding at health facility .121

Measuring technique
Note:
• When measuring height is impossible, measure him lying down and subtract 0.7 cm from the result.
• When a baby is 24 months old, s/he can both stand or lie down to be measured, but it should be
noted that if you measure the height, compare it to classification for height measuring and if you
measure his length, then compare it to classification for length measuring.
• When the child is 24 months old or over, measure height only.
Figure 29.2: Equipment and method for measuring the lying length of a child under 25 months old
Weighing technique
Figure 29.1: Weighing a baby
Session 29: Assessing nutrition status
Counseling on infant and young child feeding at health facility122.
MEASURING PERSON
Using right handto pull the footboardagainst thechild’s feet
Left hand tohold the child’sknees
SUPPORTERUsing two handsto hold thechild’s head
The child lies straight along the board
Movablefootboard
Reading results Movableheadboard
Foldingdirection

Figure 29.3: Measuring the standing height of a child from 25 months old or over.
Session 29: Assessing nutrition status
Counseling on infant and young child feeding at health facility .123
Measuring arm circumference: Poor development or muscular wasting is the main symptom of mal-
nutrition caused by protein and energy deficiency, especially in young children.
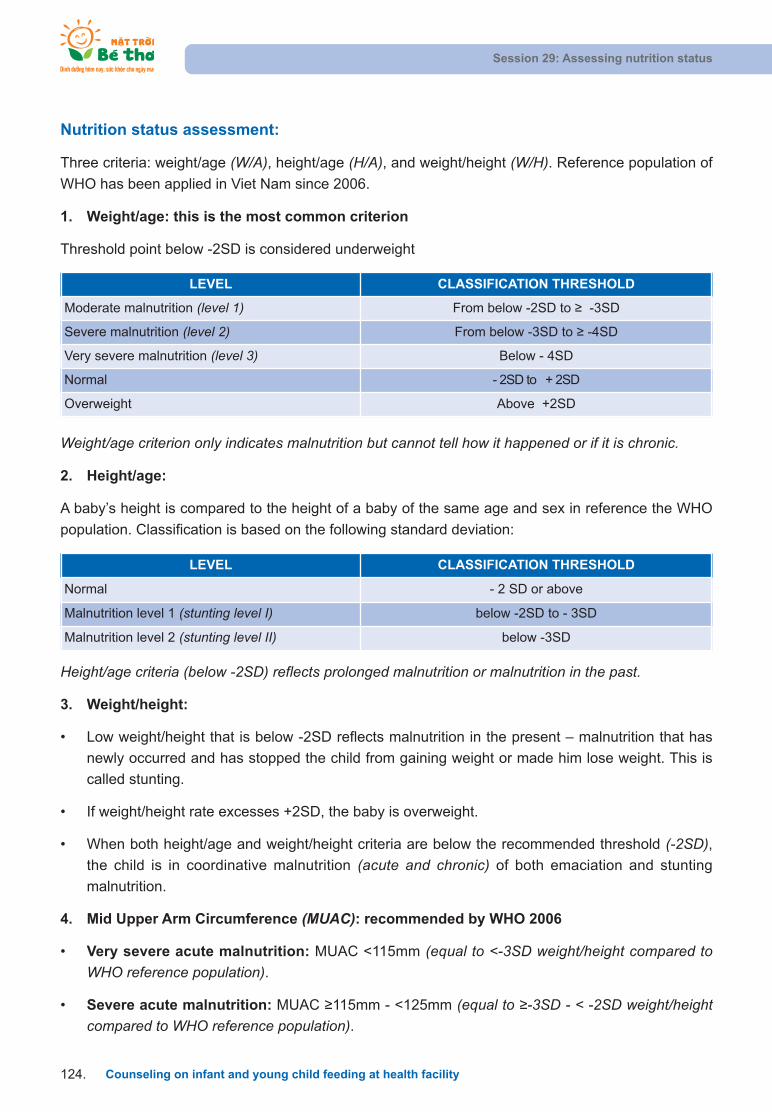
Height/age criteria (below -2SD) reflects prolonged malnutrition or malnutrition in the past.
3. Weight/height:
• Low weight/height that is below -2SD reflects malnutrition in the present – malnutrition that has
newly occurred and has stopped the child from gaining weight or made him lose weight. This is
called stunting.
• If weight/height rate excesses +2SD, the baby is overweight.
• When both height/age and weight/height criteria are below the recommended threshold (-2SD),the child is in coordinative malnutrition (acute and chronic) of both emaciation and stunting
malnutrition.
4. Mid Upper Arm Circumference (MUAC): recommended by WHO 2006
• Very severe acute malnutrition: MUAC <115mm (equal to <-3SD weight/height compared toWHO reference population).
• Severe acute malnutrition: MUAC 115mm - <125mm (equal to -3SD - < -2SD weight/heightcompared to WHO reference population).
Weight/age criterion only indicates malnutrition but cannot tell how it happened or if it is chronic.
2. Height/age:
A baby’s height is compared to the height of a baby of the same age and sex in reference the WHO
population. Classification is based on the following standard deviation:
Nutrition status assessment:
Three criteria: weight/age (W/A), height/age (H/A), and weight/height (W/H). Reference population of
WHO has been applied in Viet Nam since 2006.
1. Weight/age: this is the most common criterion
Threshold point below -2SD is considered underweight
Session 29: Assessing nutrition status
Counseling on infant and young child feeding at health facility124.
LEVEL CLASSIFICATION THRESHOLD
Moderate malnutrition (level 1) From below -2SD to -3SD
Severe malnutrition (level 2) From below -3SD to -4SD
Very severe malnutrition (level 3) Below - 4SD
Normal - 2SD to + 2SD
Overweight Above +2SD
LEVEL CLASSIFICATION THRESHOLD
Normal - 2 SD or above
Malnutrition level 1 (stunting level I) below -2SD to - 3SD
Malnutrition level 2 (stunting level II) below -3SD
Practice using a growth chart in counseling
• Divide the class into small groups of three to four members: one member plays the role of a
counselor, one plays the role of the mother/ caregiver, the others observe and comment.
• Each group is given a growth chart and draws one of those situations.
Session 29: Assessing nutrition status
Counseling on infant and young child feeding at health facility .125
Situation 1
Minh 3 months age, male
Birth weight: 3.4kg
1 month : 4.2 kg
2 months: 5 kg
3 months: 5.7 kg
Situation 2
Vân 6 months age, female
Birth weight: 3.1 kg
2 months: 4.5 kg
3 months: 4.7 kg
4 months: 4.7 kg
Situation 3
Nga 9 months age, female
Birth weight: 4 kg
6 months: 8 kg
7 months: 7.8 kg
9 months: 7.9 kg
Situation 4
Lan 13 months age, male
Birth weight: 3.5 kg
10 months: 9.3 kg
9 months: 9.6 kg
12 months: 10.1 kg
Situation 5
Hoa 15 months age, male
Birth weight: 2.5 kg
12 months: 12 kg
13 months: 12.5 kg
14 months: 13.5 kg
• Groups start the counseling role-play:
The person who plays the role of the mother: study the child’s weight gain to set up the situation(the diet, care, disease...).
The counselor completes the growth chart and uses it in counseling.
The observers use the Checklist of Counseling Skills to assess.
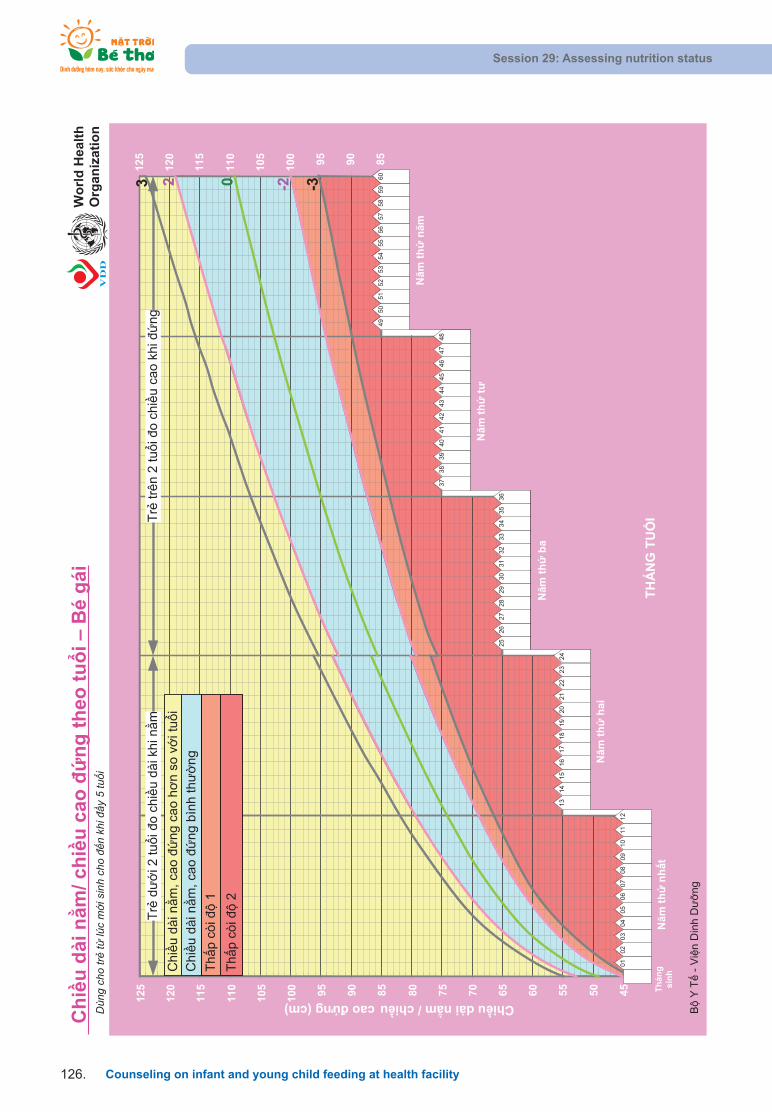
Session 29: Assessing nutrition status
Counseling on infant and young child feeding at health facility126.

Session 29: Assessing nutrition status
Counseling on infant and young child feeding at health facility .127

Session 29: Assessing nutrition status
Counseling on infant and young child feeding at health facility128.

Session 29: Assessing nutrition status
Counseling on infant and young child feeding at health facility .129

SESSION 30: DECREE 21
Objectives:
After completing this session, trainees will be able to:
1. Point out the importance of Decree 21.
2. State the main points stated in Decree 21 related to health facilities and health workers.
What is Decree 21/2006/ND-CP?
Decree 21/2006/ND-CP (“Decree 21”), issued in 2006, aims to promote optimal IYCF practices by
restricting methods and scopes in which breastmilk substitutes are marketed.
Decree 21 stipulated that information and communication related to infant feeding should clearly state
that breastmilk is an optimal choice compared to breastmilk substitutes. The Decree indicated how
nutrition products can be marketed, where they can be sold and roles of major related target groups,
including product producers and traders, health facilities, and medical workers.
Scope of the Decree includes
Milk and food for infants under 6 months old
Milk for infants from 6 to 24 months of age
Feeding bottles
Pacifiers
Why Decree 21 is so important?
One consequence of poor nutrition for infants that can be clearly seen in Viet Nam is a high stunting
rate. Thirty-three percent of children under five are stunted. Good nutrition for babies from birth until
24 months is critical for his/her physical development. Appropriately nutritious diets in this period will
improve the child’s growth and physical development, learning achievements, and even future
economic conditions. Vice versa, poor nutrition in the first months of life will slow down the child’s
physical development to a point where poor growth becomes irreversible.
Research conducted by A&T has shown that the majority of children in Viet Nam do not receive
sufficient nutrition. Although there are many factors that influence what and how infants and young
children are fed, prevalent incorrect information about BF and the rampant advertisement of breast-
milk-substitutes is regarded as having huge impact on the nutrition decision of many families and the
consequent poor nutritional status of so many children.
Session 30: Decree 21
Counseling on infant and young child feeding at health facility130.

Conforming to Decree 21 will contribute to the promotion of optimal IYCF practices in Viet Nam. This
will help reduce malnutrition and stunting, which then increases national labor productivity through
reducing the burden of diseases and contributing to the abundance and vigor of the labor force.
Management and Implementation responsibility
The MoH is in charge of managing and implementing Decree 21, simultaneously coordinating with the
Ministry of Trade, Ministry of Culture and Information, Committee for Population, Family and Children,
and related Ministries and Departments.
• The food administration is responsible for screening and licensing advertisements related to formula
milk and nutrition products for young children in the mass media before these advertisements are
printed or broadcast.
• The Maternal and Child Health Department coordinates all programs targeting mothers with young
children.
• The Department of Health Inspection supervises the implementation of the Decree. Health
Inspectors cooperate with other departments in MoH to supervise and monitor the implementation of
this Decree nation-wide annually. (At the provincial level, the Health department is in charge of this).
Penalties given to violating milk companies are subject to Decree 45. This Decree was issued in 2005,
a year before Decree 21 was issued. As a result, the violations listed in Decree 21 do not necessarily
correspond to the penalties listed in Decree 45.
The government is currently considering revisions to these decrees.
Decree 21 and role of health facilities, physicians and medical workers
Health facilities and medical workers are responsible for encouraging and promoting optimal IYCF, and
can do this by conforming strictly to Decree 21:
Each health facility should:
• Encourage BF.
• Organize educational materials on BF.
• Enable mothers to breastfeed their babies within the first hour after delivery.
Health facilities should not:
• Sell or allow the selling of milk for infants less than 12 months of age or food for infants less than
6 months of age, except for drugstores at hospitals.
• Allow manufacturers and traders of nutrition products for infants to display products, except for
drugstores at hospitals.
Session 30: Decree 21
Counseling on infant and young child feeding at health facility .131

Physicians and medical workers should:
• Encourage BF.
• Organize materials to promote BF.
• Instruct mothers and caregivers about correct usage of nutrition products for infants in those special
cases that require the use of these products.
Physicians and medical workers should not:
• Receive material benefits or products labeled with names or logos of milk products for infants less
than 12 months of age or food for infants less than 6 months of age.
• Help manufacturers and traders give sample products or presents related to nutrition products for
infants.
• Instruct or, counsel women in childbirth to use nutrition products for infants except in situations that
require the use of these products.
Information, education, and communication
Doctors and health workers at health facilities are the only channels to provide information and educa-
tional material on IYCF to pregnant women, mothers, and their families.
1. Information, education, and communication on the benefits of breastfeeding and on methods
of nurturing infants must be given priority in programs on information, education, and commu-
nication on the protection of mother and on child health, and on child-malnutrition prevention
and control.
2. Messages about the superiority of breastmilk must be clear and must point out the disadvan-
tages of not BF.
3. Information about BF and CF must be accurate and easy to understand.
Information, education, and communication documents on nurturing infants that have the following
content are prohibited:
1. Pictures or words to encourage bottle-feeding.
2. Discourage breastfeeding infants.
3. Comparisons of nutrition products for infants with breastmilk.
4. Names or logos of infant-nutrition products.
Decree 21 and the role of companies producing and distributing nutrition products forinfants:
Companies producing nutrition products for infants have an important role to play in ensuring the health
and development of young children. Establishments that produce or distribute nutrition products must
ensure that all products comply with relevant food safety, quality, and hygiene standards and that health
workers have information on how to properly use these products.
Session 30: Decree 21
Counseling on infant and young child feeding at health facility132.
In regard to food for infants under 6 months old or milks for infants under 12 months old, or-
ganizations that produce or sell nutrition products for infants MAY NOT:
1. Use forms of sale promotion.
2. Contact mothers, pregnant women, or family members working in health facilities to promote
products.
3. Provide health workers or health facilities with food products for infants under 6 months old or
milk products for infants under 12 months old.
4. Provide health workers or health facilities with any material benefits, nor can the company
provide groups with items featuring the name or logo of products.
5. Grant scholarships or funds for research, training, counseling services, or other uses to
promote products.
6. Display products in health facilities. (The one exception where this is allowed is in a hospitaldrugstore)
Advertising
1. Advertising milk or food products for infants under 6 months old is prohibited.
2. Advertising of milk for children aged 12-24 months is allowed, but the first part of the
advertisement must state that breastmilk is the best food for the health and growth of infants.
3. All advertisements must be reviewed and approved by the MoH.
4. No advertisements may promote the abandonment of BF, promote bottle feeding, or compare
milk products with breastmilk.
Labeling of nutritious products for infants
1. Labels cannot imply that the product is equal to or better than breastmilk.
2. Labels must include the text: “breastmilk is the best food for the health and growth of infants.Antibacterial elements, especially antibodies, available in breastmilk only, help prevent andcontrol diarrhea, respiratory infections, and several other infectious diseases for infants”.
3. Labels must include the text: “Use this product only under physicians’ instructions. Strictlyfollow preparation instructions. Feed children with clean cups and spoons”.
4. Instructions on how to prepare the food should be in Vietnamese, be easy to follow, and be
accompanied by simple tables.
5. The age of the child that the product is designed for must be clearly indicated.
6. Product labels may not feature pictures or drawings of infants under the age of 12 months,
bottles, or dummies.
Session 30: Decree 21
Counseling on infant and young child feeding at health facility .133
7. Laws on the labeling of products for domestic, imported, or exported goods must be adhered
to, and production and expiration dates must be included.
Labeling of Feeding Bottles and Dummies
1. Labels for bottles must include the text: “strictly following the instructions on hygiene and sterilization. The use of feeding-bottles may make children refuse breastfeeding, or cause diarrhea”.
2. Bottle labels must also include instructions on proper use and sterilization.
3. Packages or labels stuck on dummies must include the text: “using dummies will negativelyaffect BF”.
4. Labeling regulations for bottles and dummies also apply to products imported into Viet Nam.
Session 30: Decree 21
Counseling on infant and young child feeding at health facility134.

THE GOVERNMENTSOCIALIST REPUBLIC OF VIET NAM
Independence – Freedom – Happiness
No.: 21/2006/ND-CP
Hanoi, February 27th 2006
Decree on the trading in and use of nutritious products for infants
THE GOVERNMENT
Pursuant to the December 25, 2001 Law on Organization of the Government;
Pursuant to the June 15, 2004 Law on Child Protection, Care and Education;
Pursuant to the June 14, 2005 Commercial Law;
Pursuant to the November 16, 2001 Ordinance on Advertisement;
Pursuant to the December 24, 1999 Ordinance on Goods Quality;
Pursuant to the July 26, 2003 Ordinance on Food Hygiene and Safety;
At the proposal of the Minister of Health,
DECREE:
Chapter I
GENERAL PROVISIONS
Article 1.- Scope of regulation and subjects of application
1. This Decree provides for information, education and communication on, advertisement for, trading
in, and use of, nutritious products for infants, feeding bottles and dummies.
2. This Decree applies to Vietnamese and foreign organizations and individuals in Viet Nam.
Article 2.- Interpretation of terms
In this Decree, the terms below are construed as follows:
1. Nutritious products for infants include milk and food produced by industrial methods, which are up
to the set standards and suitable to the special physiological conditions and each period of growth
of infants, including:
a) Milk and food of animal or plant origin, for under-6 month infants;
b) Milk for infants aged between 6 months and 24 months.
Session 30: Decree 21
Counseling on infant and young child feeding at health facility .135

2. Supplementary food means food processed for additional use together with breastmilk, and milk
for infants aged between 6 months and 24 months.
3. Infants mean children who are from newborn to 24 months old.
4. Labels of nutritious products for infants means pictures, drawings or other illustrations; words,
prints or embossed images, affixed to or presented on packages of nutritious products for infants.
5. Giving of samples of nutritious products for infants means the free-of-charge supply of a small
quantity of nutritious products for infants.
6. Advertisement for nutritious products for infants means the introduction of nutritious products for
infants in any forms for profit-making purposes.
7. Medical examination and treatment establishments include general hospitals, obstetric or pediatric
hospitals, maternity homes; general clinics, obstetric or pediatric clinics; regional general clinics,
and commune, ward and township health stations.
8. Physicians and medical workers mean those who have medical professional qualifications, includ-
ing doctors, intermediate-level physicians, convalescence workers and midwives working at med-
ical examination and treatment establishments.
Chapter II
INFORMATION, EDUCATION, COMMUNICATION AND ADVERTISEMENT
Article 3.- Information, education and communication on the benefits of breastfeeding
1. Information, education and communication on the benefits of breastfeeding and on methods of
nurturing infants must be given priority in programs on information, education and communication
on the protection of mothers' and children's health, and on child malnutrition prevention and
control.
2. The MoH shall coordinate with the Ministry of Culture and Information, the Ministry of Trade, the
Ministry of Education and Training, the Committee for Population, Family and Children, the Central
Committee of the Viet Nam Fatherland Front, the Central Committee of the Viet Nam Women's
Union, the Central Committee of the Ho Chi Minh Communist Youth Union, the Central Committee
of the Viet Nam Peasants' Association, the Viet Nam Labor Confederation, and other agencies and
social organizations in communicating and educating about the superiority of breastmilk, the
importance of breastfeeding and the continuation of breastfeeding.
Article 4.- Information, education and communication documents on nurturing infants
1. Contents of information, education and communication documents on nurturing infants must be
clear, easy-to-read, easy-to-understand, objective and scientific.
2. Information, education and communication documents on nurturing infants must cover the following
contents:
Session 30: Decree 21
Counseling on infant and young child feeding at health facility136.
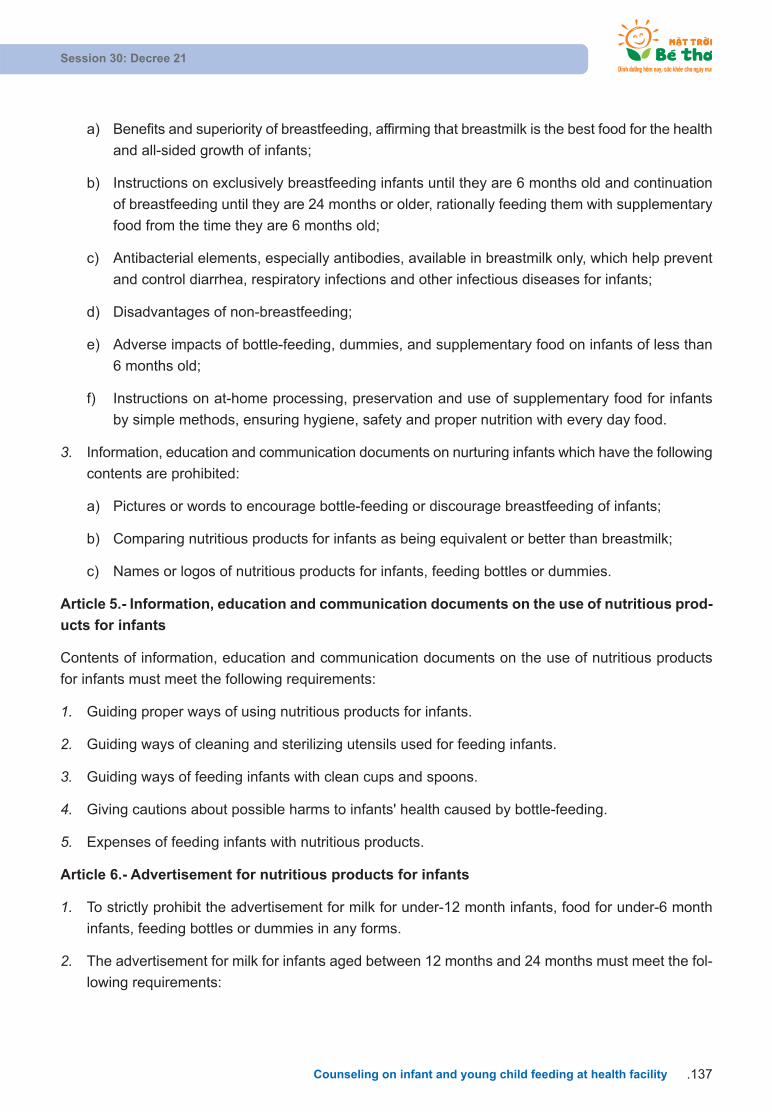
a) Benefits and superiority of breastfeeding, affirming that breastmilk is the best food for the health
and all-sided growth of infants;
b) Instructions on exclusively breastfeeding infants until they are 6 months old and continuation
of breastfeeding until they are 24 months or older, rationally feeding them with supplementary
food from the time they are 6 months old;
c) Antibacterial elements, especially antibodies, available in breastmilk only, which help prevent
and control diarrhea, respiratory infections and other infectious diseases for infants;
d) Disadvantages of non-breastfeeding;
e) Adverse impacts of bottle-feeding, dummies, and supplementary food on infants of less than
6 months old;
f) Instructions on at-home processing, preservation and use of supplementary food for infants
by simple methods, ensuring hygiene, safety and proper nutrition with every day food.
3. Information, education and communication documents on nurturing infants which have the following
contents are prohibited:
a) Pictures or words to encourage bottle-feeding or discourage breastfeeding of infants;
b) Comparing nutritious products for infants as being equivalent or better than breastmilk;
c) Names or logos of nutritious products for infants, feeding bottles or dummies.
Article 5.- Information, education and communication documents on the use of nutritious prod-
ucts for infants
Contents of information, education and communication documents on the use of nutritious products
for infants must meet the following requirements:
1. Guiding proper ways of using nutritious products for infants.
2. Guiding ways of cleaning and sterilizing utensils used for feeding infants.
3. Guiding ways of feeding infants with clean cups and spoons.
4. Giving cautions about possible harms to infants' health caused by bottle-feeding.
5. Expenses of feeding infants with nutritious products.
Article 6.- Advertisement for nutritious products for infants
1. To strictly prohibit the advertisement for milk for under-12 month infants, food for under-6 month
infants, feeding bottles or dummies in any forms.
2. The advertisement for milk for infants aged between 12 months and 24 months must meet the fol-
lowing requirements:
Session 30: Decree 21
Counseling on infant and young child feeding at health facility .137

a) The first part of the advertisement must have the content: "Breastmilk is the best food for thehealth and all-sided growth of infants";
b) Advertisement contents must comply with the provisions of Articles 4 and 5 of this Decree and
other provisions of law on advertisement.
3. Before putting advertisement for milk for infants aged between 12 months and 24 months, organ-
izations or individuals must send advertisement registration dossiers to the MoH according to the
provisions of law on advertisement.
Chapter III
TRADING IN NUTRITIOUS PRODUCTS FOR INFANTS
Article 7.- Publication of food quality, hygiene and safety standards
Nutritious products for infants, before being marketed, must have their quality, hygiene and safety stan-
dards published according to the provisions of law on goods quality and food hygiene and safety.
Article 8.- Regulations on labels of nutritious products for infants
1. Labels of nutritious products for infants must meet the following requirements:
a) There must be the words "CHU Y" (attention) (in upper case), followed by the words (in lowercase) with the following contents: "Breastmilk is the best food for the health and all-sided growthof infants. Antibacterial elements, especially antibodies, available in breastmilk only, help prevent and control diarrhea, respiratory infections and several other infectious diseases for infants." The height of letters must not be less than 2 mm;
b) There must be the words (in lower case): "Use this product only under physicians' instructions.Strictly follow preparation instructions. Feed children by clean cups and spoons." The height
of letters must not be less than 1.5 mm;
c) Infants' age groups suitable for use of the product must be clearly written;
d) Product labels must be printed with the number of the certificate of published food quality,
hygiene and safety standards.
2. Other contents of labels of nutritious products for infants shall comply with the provisions of law on
labeling of domestically circulated, imported or exported goods, and must meet the following
requirements:
a) Guiding proper ways of preparation, illustrated with simple and easy-to-understand tables in
Vietnamese;
b) Giving full and accurate introduction of origin, date of production, expiry date, ingredients, serial
number of the certificate of published food quality, hygiene and safety standards, and informa-
tion on nutritious value of the product;
Session 30: Decree 21
Counseling on infant and young child feeding at health facility138.
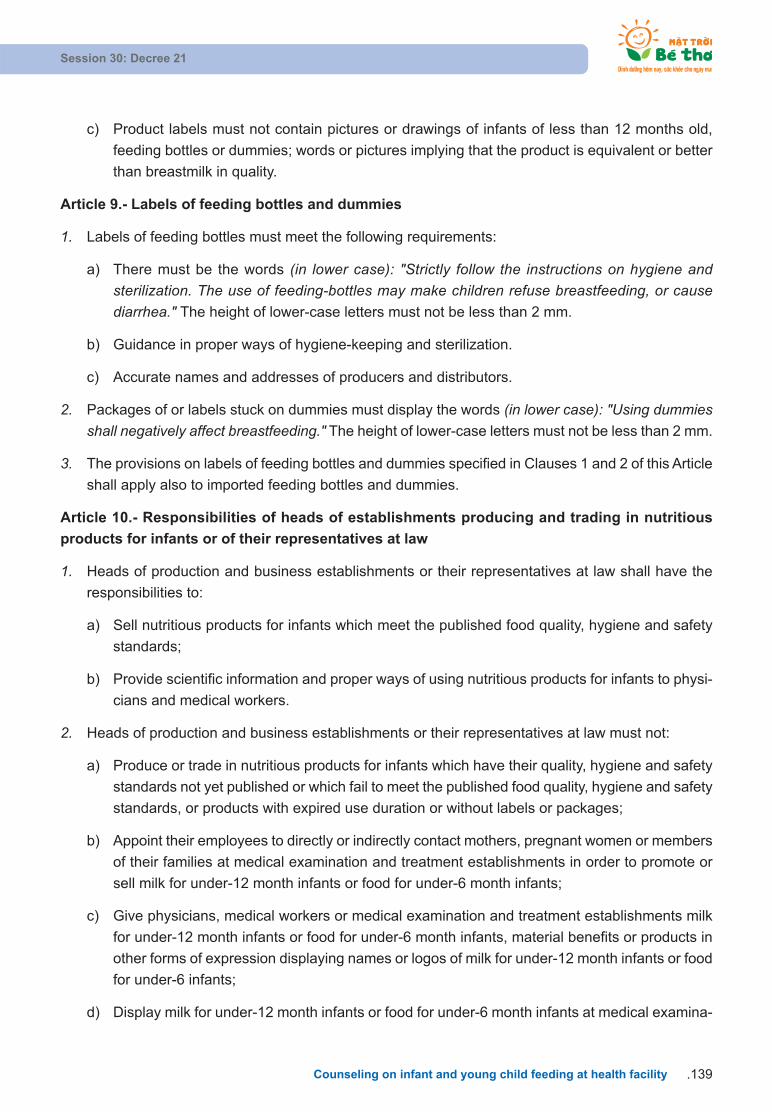
c) Product labels must not contain pictures or drawings of infants of less than 12 months old,
feeding bottles or dummies; words or pictures implying that the product is equivalent or better
than breastmilk in quality.
Article 9.- Labels of feeding bottles and dummies
1. Labels of feeding bottles must meet the following requirements:
a) There must be the words (in lower case): "Strictly follow the instructions on hygiene and sterilization. The use of feeding-bottles may make children refuse breastfeeding, or cause diarrhea." The height of lower-case letters must not be less than 2 mm.
b) Guidance in proper ways of hygiene-keeping and sterilization.
c) Accurate names and addresses of producers and distributors.
2. Packages of or labels stuck on dummies must display the words (in lower case): "Using dummiesshall negatively affect breastfeeding." The height of lower-case letters must not be less than 2 mm.
3. The provisions on labels of feeding bottles and dummies specified in Clauses 1 and 2 of this Article
shall apply also to imported feeding bottles and dummies.
Article 10.- Responsibilities of heads of establishments producing and trading in nutritious
products for infants or of their representatives at law
1. Heads of production and business establishments or their representatives at law shall have the
responsibilities to:
a) Sell nutritious products for infants which meet the published food quality, hygiene and safety
standards;
b) Provide scientific information and proper ways of using nutritious products for infants to physi-
cians and medical workers.
2. Heads of production and business establishments or their representatives at law must not:
a) Produce or trade in nutritious products for infants which have their quality, hygiene and safety
standards not yet published or which fail to meet the published food quality, hygiene and safety
standards, or products with expired use duration or without labels or packages;
b) Appoint their employees to directly or indirectly contact mothers, pregnant women or members
of their families at medical examination and treatment establishments in order to promote or
sell milk for under-12 month infants or food for under-6 month infants;
c) Give physicians, medical workers or medical examination and treatment establishments milk
for under-12 month infants or food for under-6 month infants, material benefits or products in
other forms of expression displaying names or logos of milk for under-12 month infants or food
for under-6 infants;
d) Display milk for under-12 month infants or food for under-6 month infants at medical examina-
Session 30: Decree 21
Counseling on infant and young child feeding at health facility .139

tion and treatment establishments, except hospital drugstores; or apply forms of sale promotion
to milk for under-12 month infants or food for under-6 month infants;
e) Grant scholarships, provide funds for scientific research, training courses, conferences, work-
shops, concerts, telephone counseling services or other forms in order to directly or indirectly
introduce products, aiming to promote the trading in or use of milk for under-12 month infants
or food for under-6 month infants.
Chapter IV
USE OF NUTRITIOUS PRODUCTS FOR INFANTS
Article 11.- Responsibilities of heads of medical examination and treatment establishments
1. Heads of medical examination and treatment establishments shall have the responsibilities to:
a) Organize communication on and encourage breastfeeding;
b) Create conditions for mothers to breastfeed their newborns within one hour after birth.
2. Heads of medical examination and treatment establishments must not:
a) Sell, or permit the sale of, milk for under-12 month infants or food for under-6 month infants at
medical examination and treatment establishments, except hospital drugstores;
b) Permit establishments producing or trading in nutritious products for infants to display, or post
up names of nutritious products for infants, feeding-bottles or dummies at medical examination
and treatment establishments, except hospital drugstores.
Article 12.- Responsibilities of physicians and medical workers in medical examination and
treatment establishments
1. Physicians and medical workers in examination and treatment establishments shall have the re-
sponsibilities to:
a) Organize communication on and encourage breastfeeding;
b) Provide guidance on proper ways of using nutritious products for infants for mothers or mem-
bers of their families in special cases where it is necessary to use such products.
2. Physicians and medical workers in examination and treatment establishments must not:
a) Receive directly or indirectly milk for under-12 month infants or food for under-6 month infants,
other material benefits or products in other forms of expression displaying names or logos of
milk for under-12 month infants, which are given by establishments producing or trading in nu-
tritious products for infants or their representatives;
b) Help production and business establishments give sample products or gifts related to nutritious
products for infants;
Session 30: Decree 21
Counseling on infant and young child feeding at health facility140.

c) Provide guidance or advice or make prescriptions for pregnant women to use nutritious prod-
ucts for infants in cases where it is unnecessary to use these products.
Chapter V
IMPLEMENTATION PROVISIONS
Article 13.- Management responsibilities
1. The MoH shall assume the prime responsibility for, and coordinate with the Ministry of Trade, the
Ministry of Culture and Information, the Committee for Population, Family and Children, and
concerned ministries and branches in, managing the use of nutritious products for infants; manage
quality, hygiene and safety of nutritious products for infants; inspect and examine the implementa-
tion of the provisions of law on trading in and use of nutritious products for infants.
2. The Ministry of Culture and Information shall assume the prime responsibility for, and coordinate
with the Ministry of Trade and the MoH in, managing communication on and advertisement for
nutritious products for infants according to their assigned competence.
Article 14.- Implementation effect
This Decree takes effect 15 days after its publication in "CONG BAO".
To annul the Government's Decree No. 74/2000/ND-CP of December 6, 2000, on the trading in and
use of breastmilk substitutes to protect and encourage breastfeeding.
Article 15.- Implementation responsibilities
1. The Minister of Health shall assume the prime responsibility for, and coordinate with the Minister
of Trade, the Minister of Culture and Information and the Minister-Director of the Committee for
Population, Family and Children in, guiding the implementation of this Decree.
2. Ministers, heads of ministerial-level agencies, heads of Government-attached agencies, and
presidents of provincial/municipal People's Committees shall have to implement this Decree.
ON BEHALF OF THE GOVERNMENT
PRIME MINISTER
PHAN VAN KHAI
Session 30: Decree 21
Counseling on infant and young child feeding at health facility .141

Counseling on infant and young child feeding at health facility .143
APPENDICES
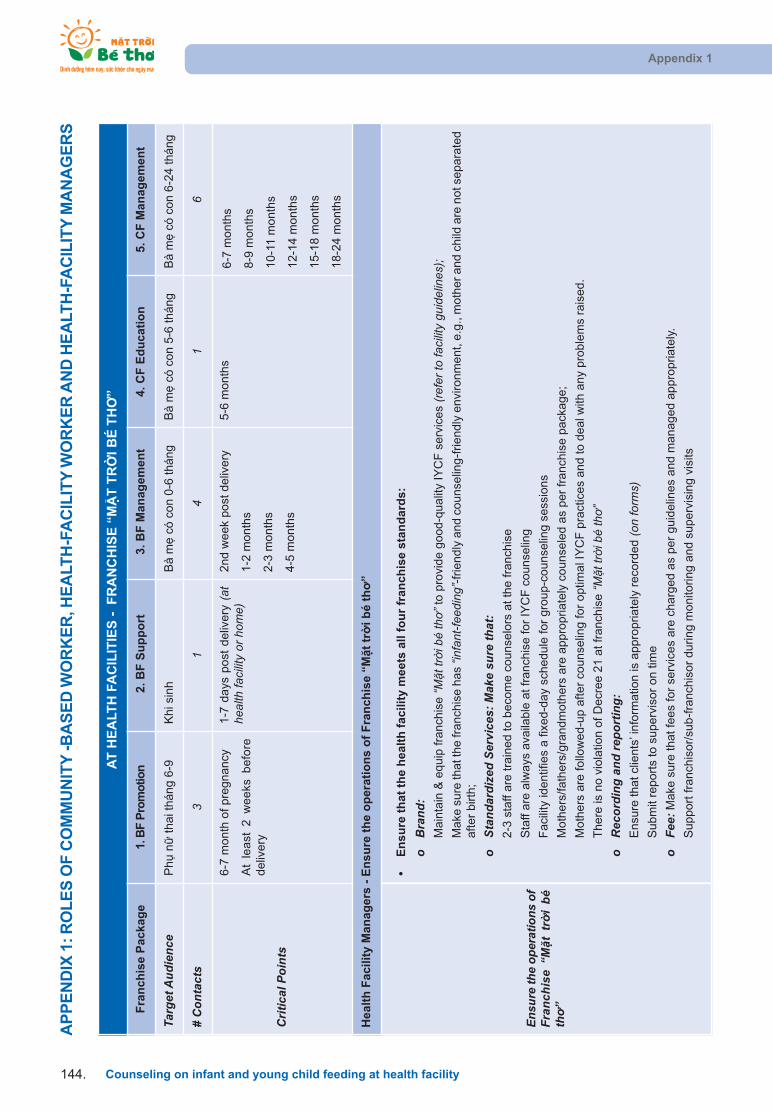
AP
PE
ND
IX 1
: RO
LE
S O
F C
OM
MU
NIT
Y -B
AS
ED
WO
RK
ER
, HE
ALT
H-F
AC
ILIT
Y W
OR
KE
R A
ND
HE
ALT
H-F
AC
ILIT
Y M
AN
AG
ER
SAppendix 1
Counseling on infant and young child feeding at health facility144.
AT
HE
ALT
H F
AC
ILIT
IES
- F
RA
NC
HIS
E “
MT
TR
I BÉ
TH
”
Fra
nch
ise
Pac
kag
e1.
BF
Pro
mot
ion
2. B
F S
up
po
rt3.
BF
Man
agem
ent
4. C
F E
du
cati
on
5. C
F M
anag
emen
t
Targ
et A
udie
nce
Ph
n thai t
háng 6
-9
Khi s
inh
Bà m
có c
on 0
-6 t
háng
Bà
m c
ó c
on
5-6
th
án
gB
à m
có
co
n 6
-24
th
án
g
# C
onta
cts
31
41
6
Crit
ical
Poi
nts
6-7
month
of pre
gna
ncy
At
lea
st 2
we
eks
be
fore
deliv
ery
1-7
da
ys p
ost
de
live
ry (
athe
alth
faci
lity
or h
ome)
2nd w
eek
post
deliv
ery
1-2
month
s
2-3
month
s
4-5
month
s
5-6
mo
nth
s6
-7 m
on
ths
8-9
mo
nth
s
10
-11
mo
nth
s
12
-14
mo
nth
s
15
-18
mo
nth
s
18
-24
mo
nth
s
Hea
lth
Fac
ility
Man
ager
s -
En
sure
th
e o
per
atio
ns
of
Fra
nch
ise
“Mt
tri b
é th
”
Ensu
re th
e op
erat
ions
of
Fran
chis
e “M
t tr
i bé
th”
•
En
sure
th
at t
he
hea
lth
fac
ility
mee
ts a
ll fo
ur
fran
chis
e st
and
ard
s:
oB
rand
: M
ain
tain
& e
quip
fra
nch
ise “M
t tr
i bé
th”t
o p
rovi
de g
ood-q
ualit
y IY
CF
serv
ice
s (re
fer t
o fa
cilit
y gu
idel
ines
);M
ake
sure
that t
he fr
anch
ise h
as
“infa
nt-fe
edin
g”-f
riendly
and c
ounse
ling-f
riend
ly e
nvi
ron
me
nt,
e.g
., m
oth
er
an
d c
hild
are
no
t se
pa
rate
dafter
birth
;
oSt
anda
rdiz
ed S
ervi
ces:
Mak
e su
re th
at:
2-3
sta
ff are
tra
ined t
o b
eco
me c
ounse
lors
at
the f
ranch
ise
Sta
ff are
alw
ays
ava
ilable
at
franch
ise f
or
IYC
F c
ounse
ling
Faci
lity
identif
ies
a f
ixed-d
ay
schedule
for
gro
up-c
ounse
ling s
ess
ions
Moth
ers
/fath
ers
/gra
ndm
oth
ers
are
appro
priate
ly c
ounse
led a
s per
franch
ise p
ack
ag
e;
Moth
ers
are
follo
wed-u
p a
fter
counse
ling f
or
optim
al I
YC
F p
ract
ices
and t
o d
ea
l with
an
y p
rob
lem
s ra
ise
d.
There
is n
o v
iola
tion o
f D
ecr
ee 2
1 a
t fr
anch
ise “M
t tr
i bé
th”
oR
ecor
ding
and
repo
rtin
g:
Ensu
re that cl
ients
’ info
rmatio
n is
appro
priate
ly r
eco
rded (o
n fo
rms)
Subm
it re
port
s to
superv
isor
on t
ime
oFe
e:M
ake
sure
that
fees
for
serv
ices
are
charg
ed a
s per
guid
elin
es
and m
ana
ge
d a
pp
rop
ria
tely
.
S
upport
fra
nch
isor/
sub-f
ranch
isor
during m
onito
ring a
nd s
uperv
isin
g v
isits

Appendix 1
Counseling on infant and young child feeding at health facility .145
Hea
lth
fac
ility
wo
rker
s -
Ind
ivid
ual
an
d g
rou
p c
ou
nse
ling
Org
aniz
e in
divi
dual
-and
grou
p-co
unse
ling
ses-
sion
s fo
r m
othe
rs/h
us-
band
s/gr
andm
othe
rsfr
om th
e th
ird tr
imes
ter
of
preg
nanc
y til
l th
ech
ild is
24
mon
ths
of g
e
•F
or
pre
gn
ant
wo
men
oId
entif
y pre
gn
ant
wom
en d
uring r
egula
r A
NC
check
ups
and g
ive in
vita
tion c
ard
s to
co
me
fo
r “M
t tr
i bé
th”s
erv
ice
s
oR
egis
ter
pre
gnant
wom
en a
s cl
ients
of
the “M
t tr
i bé
th”f
ranch
ise s
ince
the
3rd
trim
est
er
of
pre
gn
an
cy
oG
ive e
ach
pre
gnant
wom
an a
moth
er-
child
book
oC
ounse
l the m
oth
er
on th
e in
itiatio
n o
f BF
; motiv
ate
the m
oth
er
to b
ring h
er
husb
an
d/m
oth
er-
in-la
w to
the
“Mt t
ri b
é th
”fra
nch
ise
for
counse
ling
oF
ollo
w-u
p the
moth
er
via t
ele
phone t
o r
em
ind h
er
of
the n
ext
vis
it
•D
uri
ng
del
iver
y:
oE
nsu
re that th
e m
oth
er
initi
ate
s B
F w
ithin
one h
our
aft
er
birth
; ensu
re s
kin-t
o-s
kin
co
nta
ct
oP
ract
ice “r
oom
ing-
in”,
no s
epara
tion o
f m
oth
er
and b
aby
oE
nco
ura
ge a
nd s
upport
the m
oth
er
to b
reast
feed p
roperly
(pos
ition
ing
and
atta
chm
ent)
oE
nsu
re n
o w
ate
r, li
quid
s, o
r pre
lact
eals
to b
e g
iven t
o t
he c
hild
befo
re t
he f
irst
bre
ast
fee
d
oE
nsu
re n
o fo
rmula
to
be g
iven t
o t
he c
hild
befo
re t
he f
irst
bre
ast
feed o
r w
hile
mo
the
r is
at
he
alth
fa
cilit
y
•E
BF
:
oE
nsu
re that m
oth
ers
com
e t
o “M
t tr
i bé
th”f
ranch
ise f
or
EB
F c
ounse
ling b
y co
nta
ctin
g m
oth
ers
via
te
lep
ho
ne
;
osc
hedule
indiv
idual-co
unse
ling s
ess
ions
on E
BF
on d
em
and;
oO
rganiz
e fix
ed-d
ay
gro
up-c
ounse
ling s
ess
ions;
oLin
k w
ith c
om
munity
-base
d w
ork
ers
for
follo
w-u
ps
of
moth
ers
.
•C
F:
oC
onduct
Indiv
idual c
ounse
ling o
n C
F o
n d
em
and.
oE
nsu
re fix
ed-d
ay
CF
gro
up-c
ounse
ling s
ess
ions
and c
onduct
food d
em
onst
ratio
ns.
oF
ollo
w u
p w
ith m
oth
ers
thro
ugh c
om
munity
-base
d w
ork
ers
and v
ia t
ele
phone;
rem
ind
mo
the
rs o
f re
gu
lar
visi
ts.
•C
on
du
ct q
uar
terl
y h
ealt
hy-
bab
y co
mp
etit
ion
s at
hea
lth
fac
iliti
es
•P
rovi
de
smal
l gif
ts/p
rize
s fo
r m
oth
ers
wh
o e
xclu
sive
ly b
reas
tfee
d a
nd
fo
llow
CF
rec
om
men
dat
ion
s.
•E
nsu
re c
om
mu
nic
atio
n m
ater
ials
are
dis
pla
yed
an
d u
sed
, an
d t
hat
co
rrec
t IY
CF
scr
ipts
/tap
es a
re p
laye
d o
n v
illag
e lo
ud
spea
k-er
s.
•S
up
ervi
se c
om
mu
nit
y-b
ased
wo
rker
s, a
sk t
hem
to
pro
vid
e m
on
thly
up
dat
es, a
nd
co
nso
lidat
e th
ese
into
a r
epo
rt.
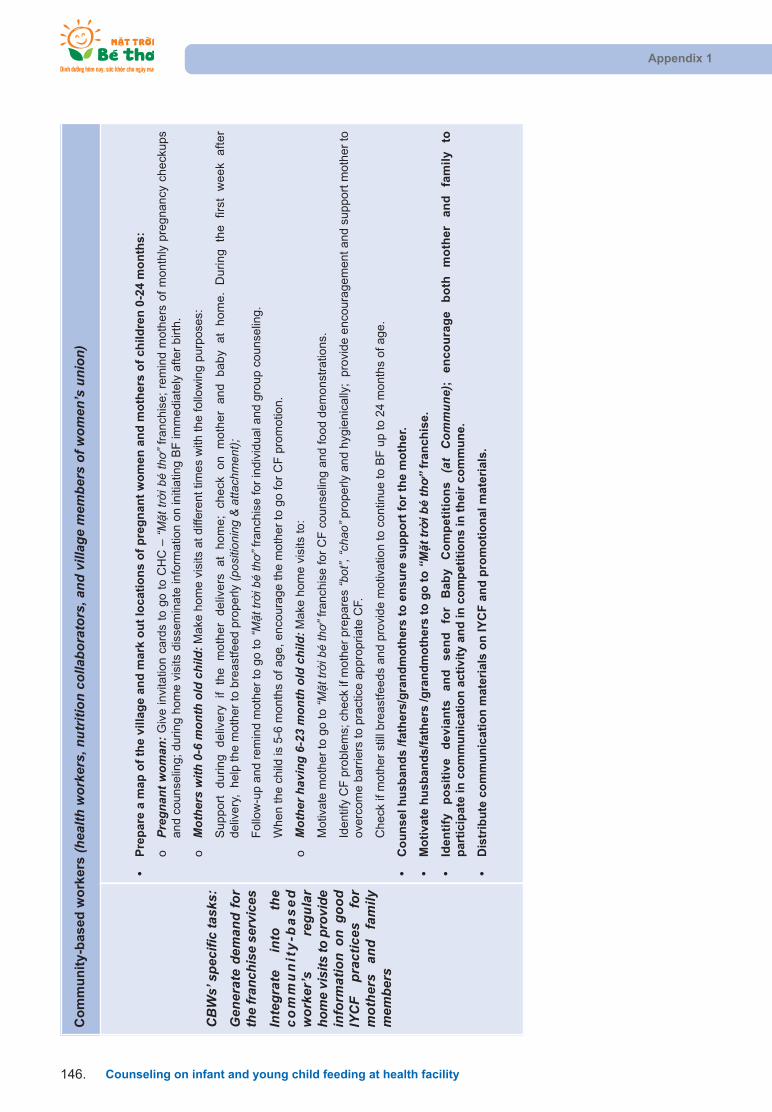
Appendix 1
Counseling on infant and young child feeding at health facility146.
Co
mm
un
ity-
bas
ed w
ork
ers
(hea
lth w
orke
rs, n
utrit
ion
colla
bora
tors
, and
vill
age
mem
bers
of w
omen
’s u
nion
)
CB
Ws’
spe
cific
task
s:
Gen
erat
e de
man
d fo
rth
e fr
anch
ise
serv
ices
Inte
grat
e in
to
the
com
mu
nit
y-b
ased
wor
ker’
s re
gula
rho
me
visi
ts to
pro
vide
info
rmat
ion
on g
ood
IYC
F pr
actic
es
for
mot
hers
an
d fa
mily
mem
bers
•P
rep
are
a m
ap o
f th
e vi
llag
e an
d m
ark
ou
t lo
cati
on
s o
f p
reg
nan
t w
om
en a
nd
mo
ther
s o
f ch
ildre
n 0
-24
mo
nth
s:
oPr
egna
nt w
oman
:Giv
e in
vita
tion c
ard
s to
go t
o C
HC
– “M
t tr
i bé
th”f
ran
chis
e;
rem
ind
mo
the
rs o
f m
on
thly
pre
gn
an
cy c
he
cku
ps
and c
ounse
ling;
during h
om
e v
isits
dis
sem
inate
info
rmatio
n o
n in
itiatin
g B
F im
me
dia
tely
aft
er
birth
.
oM
othe
rs w
ith 0
-6 m
onth
old
chi
ld:M
ake
hom
e v
isits
at
diff
ere
nt
times
with
th
e f
ollo
win
g p
urp
ose
s:
Su
pp
ort
d
uri
ng
d
eliv
ery
if
the
m
oth
er
de
live
rs
at
ho
me
; ch
eck
o
n
mo
the
r a
nd
b
ab
y a
t h
om
e.
Du
rin
g
the
fir
st
we
ek
aft
er
deliv
ery
, h
elp
the m
oth
er
to b
reast
feed p
roperly
(pos
ition
ing
& at
tach
men
t);
Follo
w-u
p a
nd r
em
ind m
oth
er
to g
o t
o “M
t tr
i bé
th”f
ranch
ise f
or
indiv
idual a
nd
gro
up
co
un
selin
g.
When the c
hild
is 5
-6 m
onth
s of
age,
enco
ura
ge t
he m
oth
er
to g
o f
or
CF
pro
mo
tion
.
oM
othe
r hav
ing
6-23
mon
th o
ld c
hild
: Make
hom
e v
isits
to:
Motiv
ate
moth
er
to g
o t
o “M
t tr
i bé
th”f
ranch
ise f
or
CF
counse
ling a
nd f
ood
de
mo
nst
ratio
ns.
Identif
y C
F p
roble
ms;
check
if m
oth
er
pre
pare
s “b
ot”,
“cha
o”pro
perly
and h
ygie
nic
ally
; p
rovi
de
en
cou
rag
em
en
t an
d s
up
po
rt m
oth
er
toove
rcom
e b
arr
iers
to p
ract
ice a
ppro
priate
CF.
Check
if m
oth
er
still
bre
ast
feeds
and p
rovi
de m
otiv
atio
n t
o c
ontin
ue t
o B
F u
p to
24
mo
nth
s o
f a
ge
.
•C
ou
nse
l hu
sban
ds
/fat
her
s/g
ran
dm
oth
ers
to e
nsu
re s
up
po
rt f
or
the
mo
ther
.
•M
oti
vate
hu
sban
ds/
fath
ers
/gra
nd
mo
ther
s to
go
to
“Mt t
ri b
é th
”fr
anch
ise.
•Id
enti
fy
po
siti
ve
dev
ian
ts
and
se
nd
fo
r B
aby
Co
mp
etit
ion
s (a
t C
omm
une)
; en
cou
rag
e b
oth
m
oth
er
and
fa
mil
y to
p
arti
cip
ate
in c
om
mu
nic
atio
n a
ctiv
ity
and
in c
om
pet
itio
ns
in t
hei
r co
mm
un
e.
•D
istr
ibu
te c
om
mu
nic
atio
n m
ater
ials
on
IYC
F a
nd
pro
mo
tio
nal
mat
eria
ls.
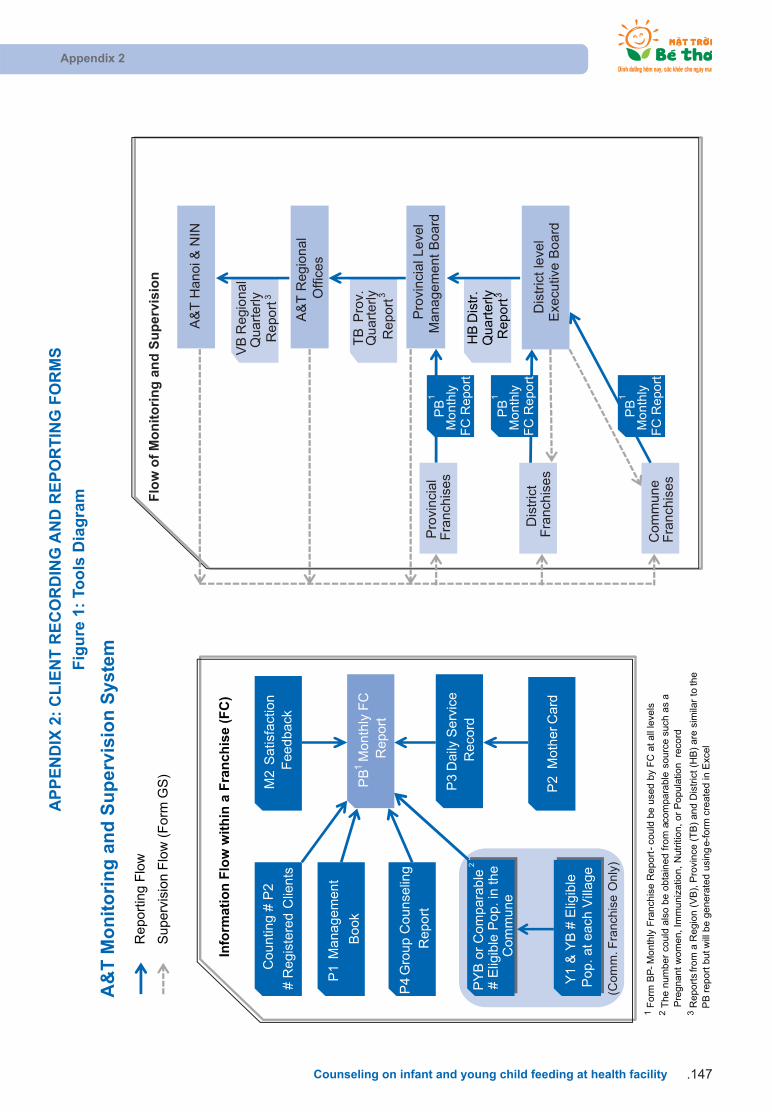
AP
PE
ND
IX 2
: C
LIE
NT
RE
CO
RD
ING
AN
D R
EP
OR
TIN
G F
OR
MS
Fig
ure
1:
Too
ls D
iag
ram
Appendix 2
Counseling on infant and young child feeding at health facility .147
(Com
m. F
ranc
hise
Onl
y)
P3
Daily
Serv
ice
Reco
rd
P2
Mo
the
r Ca
rd
P1
Ma
na
ge
me
nt
Bo
ok
PY
B o
r C
om
pa
rab
le2
# E
ligib
le P
op
. in
the
C
om
mu
ne
Co
un
ting
# P
2
# R
egis
tere
d C
lients
Y1 &
YB
# E
ligib
le
Po
p. a
t ea
ch V
illa
ge
PB
1M
on
thly
FC
R
ep
ort
Pro
vin
cial L
eve
lM
an
ag
em
en
t B
oa
rd
Dis
tric
t le
vel
Exe
cutiv
e B
oard
A&
T H
an
oi &
NIN
Com
mu
ne
Fra
nch
ises
Dis
tric
t F
ranch
ises
Pro
vin
cia
l F
ranch
ises
M2
Sa
tisfa
ctio
n
Feed
ba
ck
HB
Dis
tr.
Quart
erly
Rep
ort
3
TB
Pro
v.
Quart
erly
Repo
rt3
Info
rmat
ion
Flo
w w
ith
in a
Fra
nch
ise
(FC
)
Flo
w o
f M
on
ito
rin
g a
nd
Su
per
visi
on
1F
orm
BP
-M
ont
hly
Fra
nch
ise R
epo
rt -
coul
d b
e u
sed b
y F
C a
t all
leve
ls
2T
he n
um
ber
could
als
o b
e o
btain
ed f
rom
a co
mpara
ble
sourc
e s
uch
as
a
Pre
gnant
wo
men, I
mm
uniz
atio
n,
Nutr
itio
n,
or
Po
pula
tion
reco
rd3
Repo
rts
from
a R
egio
n (V
B),
Pro
vinc
e (
TB
) and D
istr
ict (H
B)
are
sim
ilar
to th
e
PB
repo
rt b
ut w
ill b
e g
enera
ted u
sing e
-fo
rm c
reate
d in
Exc
el
A&
T R
egio
nal
Offi
ces
VB
Reg
iona
lQ
uart
erly
Repo
rt3
P4
Gro
up
Co
un
selin
g
Re
po
rt
Re
por
ting
Flo
w
Superv
isio
n F
low
(F
orm
GS
)
PB
1
Mo
nth
ly
FC
Rep
ort
PB
1
Mo
nth
ly
FC
Rep
ort
PB
1
Mo
nth
ly
FC
Rep
ort
A&
T M
on
ito
rin
g a
nd
Su
per
visi
on
Sys
tem
Fig
ure
2:
Fo
rm Y
1 -
Lis
t o
f w
om
en 7
-9 m
on
ths
pre
gn
ant
and
mo
ther
s w
ith
ch
ildre
n u
nd
er 2
yea
rsFigure 2
Counseling on infant and young child feeding at health facility148.
Y1.
LIS
T O
F P
RE
GN
AN
T W
OM
EN
7 -
9 M
ON
TH
AN
D
MO
TH
ER
S W
ITH
CH
INL
DR
EN
UN
DE
R 2
YE
AR
S
CB
W n
am
e:........................................................................................................................
.................
Vill
age:........................................................................................................................
.........................
Com
mune:........................................................................................................................
...................
Dis
tric
t:........................................................................................................
...............
.........................
Pro
vince
:........................................................................................................................
.....................
nour
ish. n
urtu
re. g
row
.

Figure 2
Counseling on infant and young child feeding at health facility .149
Y1.
Lis
t o
f p
reg
nan
t w
om
en 7
-9 m
on
ths
and
mo
ther
s w
ith
ch
ildre
n u
nd
er 2
yea
rs
89
1011
121
23
45
67
89
1011
121
23
45
67
89
1011
12
(1)
(2)
(3)
(4)
(5)
(6)
(7)
(8)
No
Mo
ther
's n
ame
Mo
th
er's
age
Ch
ild d
ate
of
bir
th
1st
Invi
tati
on
ca
rd r
ecei
ved
d
ate
Writ
e do
wn
child
's a
ge b
y m
onth
. Use
this
form
to c
ompl
ete
YB fo
rm.
Yea
r 20
11Y
ear
2012
Yea
r 20
13

Figure 2
Counseling on infant and young child feeding at health facility150.
Name List of pregnant women 7-9 months and mothers with children under 2 years
Symbol Y1
Purpose
To keep track of mothers from the 7th month of pregnancy until the child is 24months
Provide information to the YB form
Level/Location Hamlets/villages
Implimentor Demand generators (CBW)
Data source List of pregnant women from CHCs or CBWs which they manage themselves
Time/frequency Update monthly or whenever a new mother/pregnant woman comes to the center
Management/ Archives Form Y1 is filled and kept by CBW.
Steps to fill out theform
Fill all information one the cover page: CBW name, village, commune, districtand province name
Collumn (2) The mother’s fullname. Can add the names of their husbands or par-ents in parenthese to distinguish. For example: Nguyen Thi Thanh (Hoa). Note:Write in order of the mother who has the oldest child to pregnant women
Collumn (3) Mother’s date of birth (if known)
Collumn (4) The child's date of birth:
• Write the expected date of birth for the pregnant women update it with actual
date of birth of the child upon delivered.
• In case of premature death or neonatal motality, write down the status at birth
and cross out the rest of the form.
Collumn (5) Date received the first invitation card: The date CBW gives the firstinvitation card to the mother and introduce the Franchise - MTBT.
Collumns (6,7,8): 1 column stands for 1 month: CBW write down the child's ageby month.
Note:
• If the child is more than 24 months old then cross out the rest of the calendar
• If the mother moves to another region or the child has died then note this and
cross out the rest of the calendar.
INSTRUCTION FOR Y1 FORM

Figure 2
Counseling on infant and young child feeding at health facility .151
Validation/ supervision,support
A) Supervisor (frequency)
1. Franchise management (quarterly)
2. Supervisors from upper level (randomly)
B) Testing method:
Number of mothers matchs the information in A3 and PEMC books
C) Checklist
1. Fill out name of CBW, village, general information
2. Write down the child's age by month
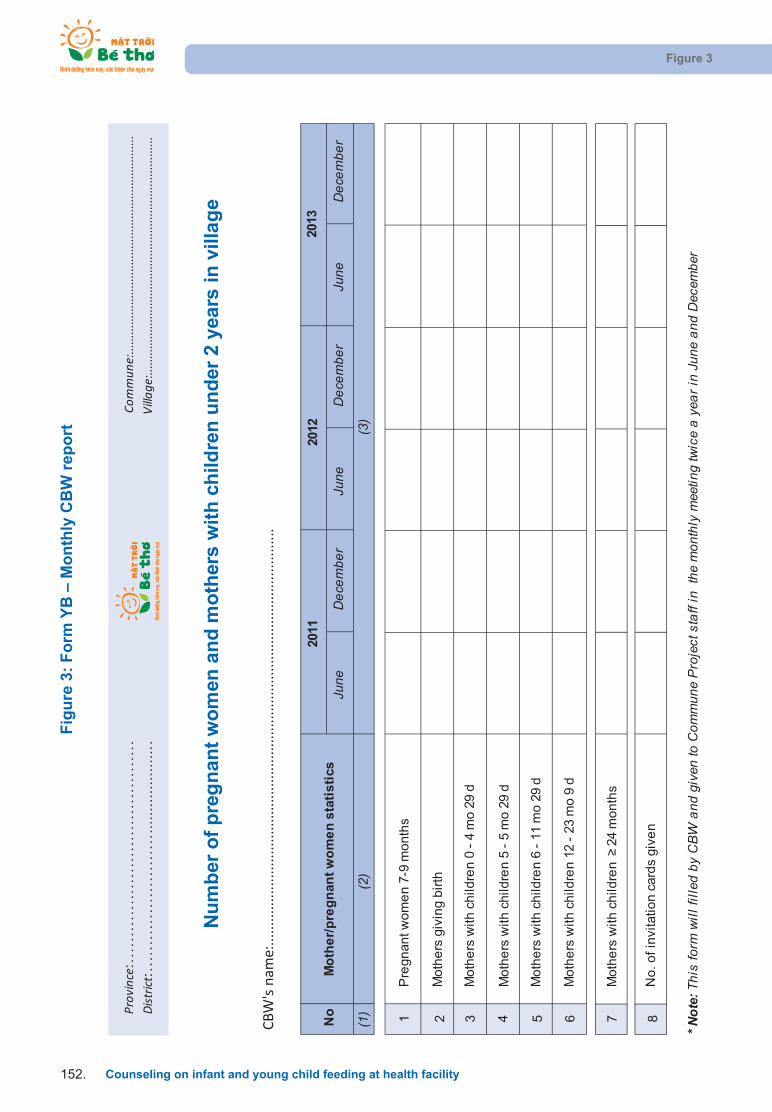
Fig
ure
3:
Fo
rm Y
B –
Mo
nth
ly C
BW
rep
ort
Figure 3
Counseling on infant and young child feeding at health facility152.
Commun
e:..................................................................
Villag
e:........................................................................
CBW
's n
ame:
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
...
Province
:...
....
....
....
....
....
....
....
....
....
...
District:
....
....
....
....
....
....
....
....
....
....
....
...
June
Dec
embe
rJu
neD
ecem
ber
June
Dec
embe
r
1P
regn
ant w
om
en
7-9
mo
nth
s
2M
oth
ers
giv
ing
bir
th
3M
oth
ers
with
ch
ildre
n 0
- 4
mo
29
d
4M
oth
ers
with
ch
ildre
n 5
- 5
mo
29
d
5M
oth
ers
with
ch
ildre
n 6
- 1
1 m
o 2
9 d
6M
oth
ers
with
ch
ildre
n 1
2 -
23 m
o 9
d
7M
oth
ers
with
ch
ildre
n
24
mo
nth
s
8N
o. o
f in
vita
tion
car
ds
give
n
* Not
e: T
his
form
will
fille
d by
CBW
and
giv
en to
Com
mun
e P
roje
ct s
taff
in t
he m
onth
ly m
eetin
g tw
ice
a ye
ar in
Jun
e an
d D
ecem
ber
Nu
mb
er o
f p
reg
nan
t w
om
en a
nd
mo
ther
s w
ith
ch
ildre
n u
nd
er 2
yea
rs in
vill
age
No
Mo
the
r/p
reg
nan
t w
om
en
sta
tist
ics
2011
(1)
(2)
(3)
2012
2013
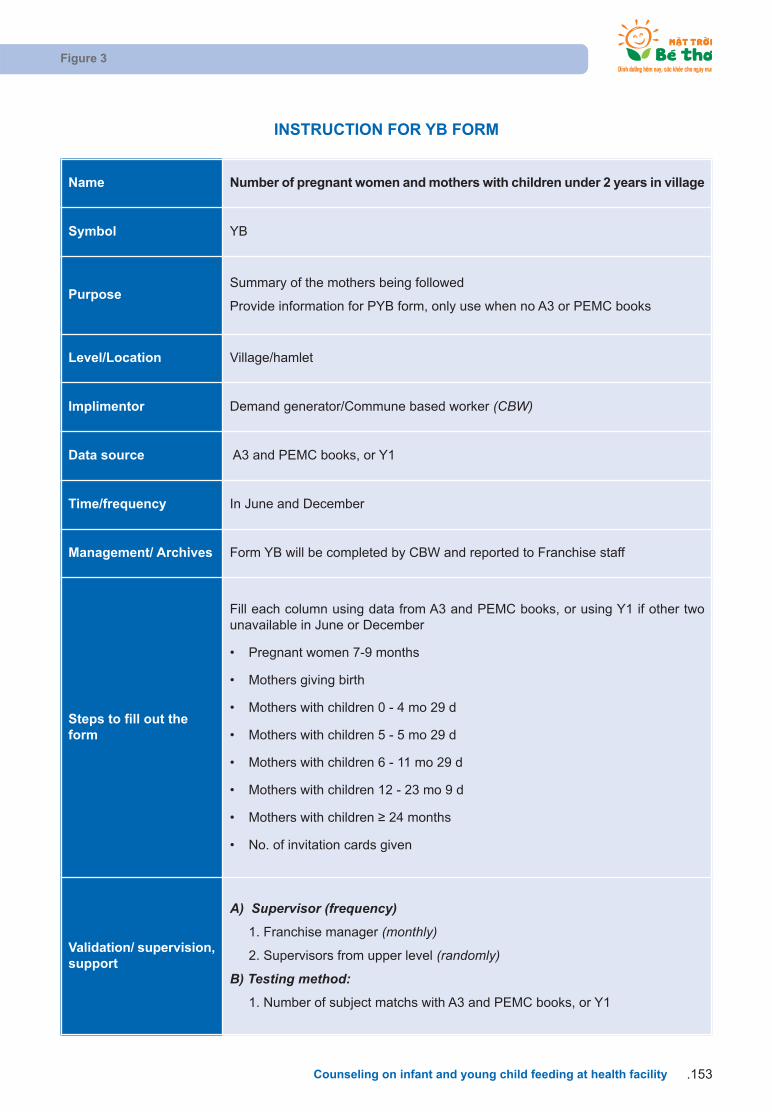
Figure 3
Counseling on infant and young child feeding at health facility .153
Name Number of pregnant women and mothers with children under 2 years in village
Symbol YB
PurposeSummary of the mothers being followed
Provide information for PYB form, only use when no A3 or PEMC books
Level/Location Village/hamlet
Implimentor Demand generator/Commune based worker (CBW)
Data source A3 and PEMC books, or Y1
Time/frequency In June and December
Management/ Archives Form YB will be completed by CBW and reported to Franchise staff
Steps to fill out theform
Fill each column using data from A3 and PEMC books, or using Y1 if other twounavailable in June or December
• Pregnant women 7-9 months
• Mothers giving birth
• Mothers with children 0 - 4 mo 29 d
• Mothers with children 5 - 5 mo 29 d
• Mothers with children 6 - 11 mo 29 d
• Mothers with children 12 - 23 mo 9 d
• Mothers with children 24 months
• No. of invitation cards given
Validation/ supervision,support
A) Supervisor (frequency)
1. Franchise manager (monthly)
2. Supervisors from upper level (randomly)
B) Testing method:
1. Number of subject matchs with A3 and PEMC books, or Y1
INSTRUCTION FOR YB FORM
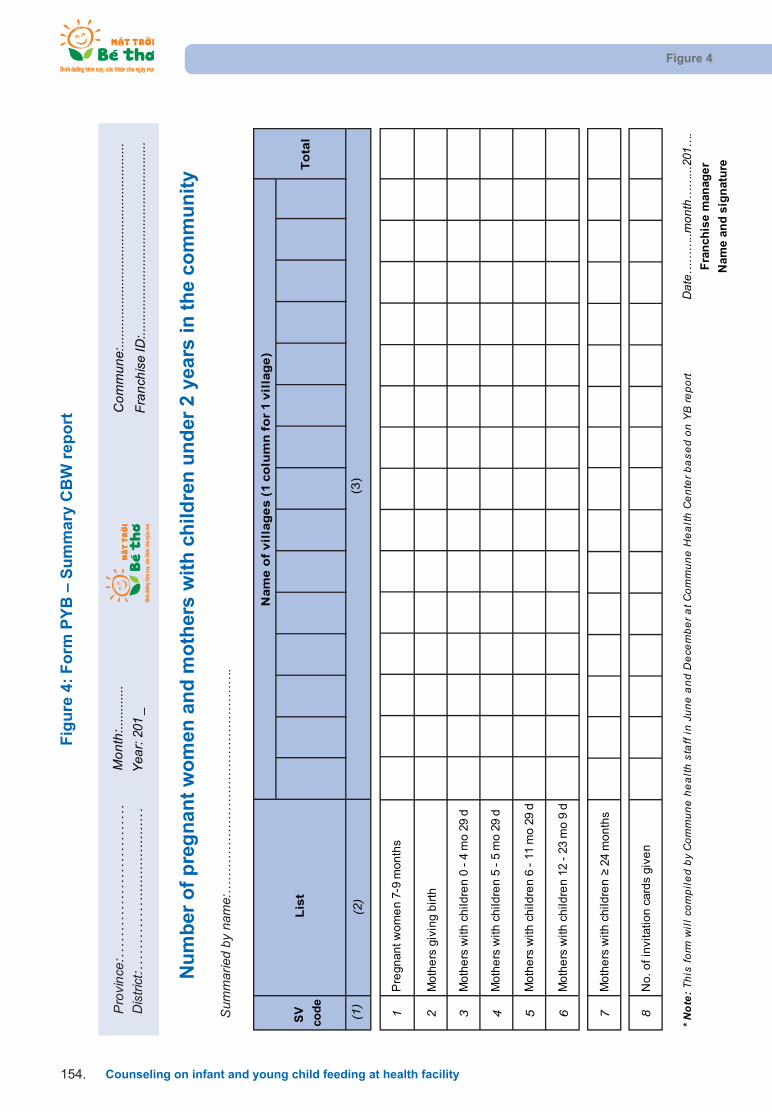
Fig
ure
4:
Fo
rm P
YB
– S
um
mar
y C
BW
rep
ort
Figure 4
Counseling on infant and young child feeding at health facility154.
Com
mun
e:...
......
......
......
......
......
......
......
......
.....
Pro
vinc
e:..
....
....
....
....
....
....
...
Dis
trict
:...
....
....
.....
......
......
.....
.
Nu
mb
er o
f p
reg
nan
t w
om
en a
nd
mo
ther
s w
ith
ch
ildre
n u
nd
er 2
yea
rs in
th
e co
mm
un
ity
Mon
th:..
......
....
Yea
r: 20
1 _
Fran
chis
e ID
:.....
......
......
......
......
......
......
......
......
Sum
mar
ied
by n
ame:
……
……
……
……
……
……
……
……
….
Pre
gnan
t wo
me
n 7
-9 m
on
ths
Mo
the
rs g
ivin
g b
irth
Mo
the
rs w
ith c
hild
ren
0 -
4 m
o 2
9 d
Mo
the
rs w
ith c
hild
ren
5 -
5 m
o 2
9 d
Mo
the
rs w
ith c
hild
ren
6 -
11
mo
29
d
Mo
the
rs w
ith c
hild
ren
12
- 23
mo
9 d
Mo
the
rs w
ith c
hild
ren
2
4 m
on
ths
No
. of
invi
tatio
n c
ard
s giv
en
* Not
e: T
his
form
will
com
pile
d by
Com
mun
e he
alth
sta
ff in
Jun
e an
d D
ecem
ber a
t Com
mun
e H
ealth
Cen
ter b
ased
on
YB
repo
rtD
ate…
……
..mon
th…
…...
201…
.F
ran
chis
e m
anag
er
Nam
e a
nd
sig
nat
ure
Nam
e o
f v
illa
ge
s (
1 c
olu
mn
fo
r 1 v
illa
ge
)
SV
cod
e
(1)
1 2 3 4 5 6 7 8
(2)
To
tal
(3)
Lis
t
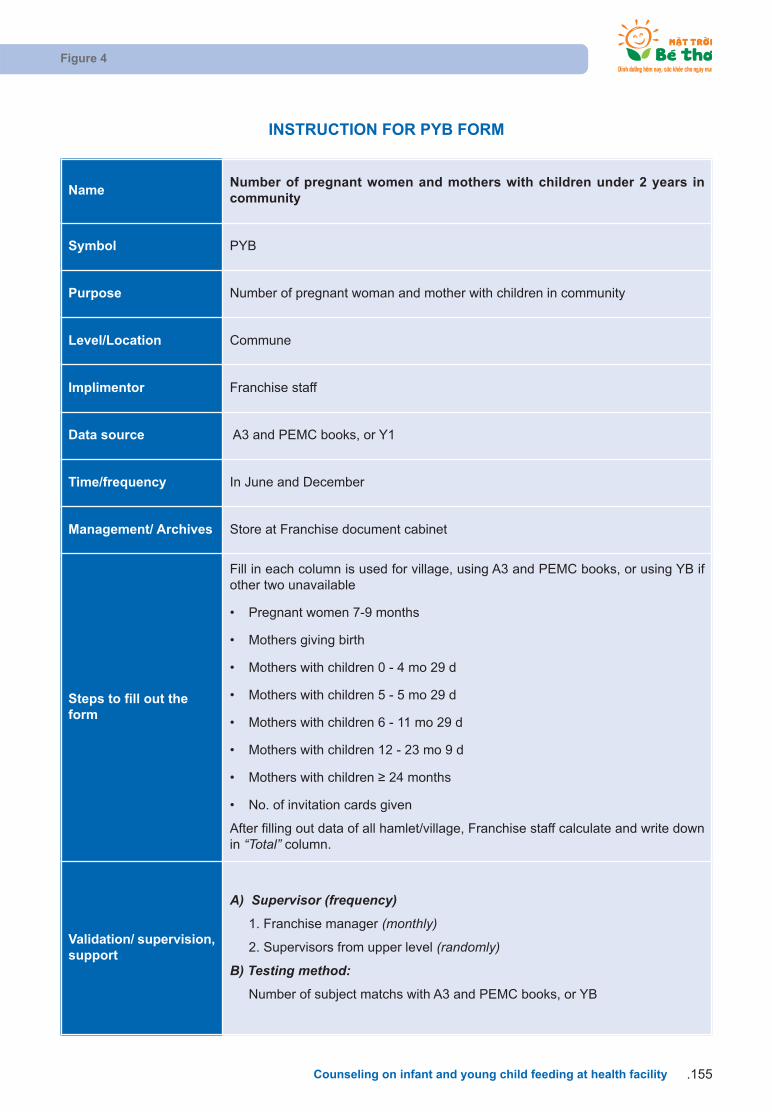
Figure 4
Counseling on infant and young child feeding at health facility .155
NameNumber of pregnant women and mothers with children under 2 years in community
Symbol PYB
Purpose Number of pregnant woman and mother with children in community
Level/Location Commune
Implimentor Franchise staff
Data source A3 and PEMC books, or Y1
Time/frequency In June and December
Management/ Archives Store at Franchise document cabinet
Steps to fill out theform
Fill in each column is used for village, using A3 and PEMC books, or using YB ifother two unavailable
• Pregnant women 7-9 months
• Mothers giving birth
• Mothers with children 0 - 4 mo 29 d
• Mothers with children 5 - 5 mo 29 d
• Mothers with children 6 - 11 mo 29 d
• Mothers with children 12 - 23 mo 9 d
• Mothers with children 24 months
• No. of invitation cards given
After filling out data of all hamlet/village, Franchise staff calculate and write downin “Total” column.
Validation/ supervision,support
A) Supervisor (frequency)
1. Franchise manager (monthly)
2. Supervisors from upper level (randomly)
B) Testing method:
Number of subject matchs with A3 and PEMC books, or YB
INSTRUCTION FOR PYB FORM

Fig
ure
5:
Fra
nch
ise
Man
agem
ent
Bo
ok
P1
- F
orm
P1.
1 –
Fra
nch
ise
staf
f’s
trai
nin
g f
ollo
w-u
p
(Fra
nchi
se s
taff
and
coun
selo
r)
Figure 5
Counseling on infant and young child feeding at health facility156.
NO
NA
ME
TIT
LE
TR
AIN
ED
OR
GA
NIZ
ER
NO
TT
RA
INE
DR
EM
AR
KD
ate
Topi
cVD
DA
&T
Oth
er
Prov
ince
:.....
......
......
......
......
......
..H
ealth
faci
lity:
......
......
......
......
...
Dis
trict
:.....
......
......
......
......
......
.....
Fran
chis
e’s
ID:..
......
......
......
.....
1. S
TAF
F T
RA
ININ
G F
OL
LO
W-U
P O
N IY
CF

Figure 5
Counseling on infant and young child feeding at health facility .157
Fig
ure
6:
Fra
nch
ise
Man
agem
ent
Bo
ok
P1
- F
orm
P1.
2 –
Fra
nch
ise’
s B
CC
mat
eria
l man
agem
ent
follo
w-u
p c
ard
(F
ranc
hise
man
ager
)
Prov
ince
:.....
......
......
......
......
......
..
Ye
ar: 2
01__
Hea
lth fa
cilit
y:...
......
......
......
......
Dis
trict
:.....
......
......
......
......
......
.....
Fran
chis
e’s
ID:..
......
......
......
.....
NO
DA
TE
RE
CE
IVE
DD
IST
RIB
UT
ED
BA
LA
NC
ES
IGN
RE
MA
RK
Qua
ntity
From
Qua
ntity
To
2. B
CC
AN
D O
TH
ER
PR
OM
OT
ION
AL
MA
TE
RIA
LS
Item
:....
......
......
......
......
......
......
......
......
......
......
......
......
.

Figure 7
Counseling on infant and young child feeding at health facility158.
Fig
ure
7:
Fra
nch
ise
Man
agem
ent
Bo
ok
P1
– F
orm
P1.
3 –
Fra
nch
ise
item
hal
f ye
ar c
ou
nt,
pag
e 1
(Fra
nchi
se m
anag
er)
ITE
MQ
UA
NT
ITY
RE
CE
IVE
D
JUN
E'S
CO
UN
TD
EC
EM
BE
R'S
CO
UN
T
Goo
dN
ot g
ood
Rem
ark
Goo
dN
ot g
ood
Rem
ark
BC
C m
ater
ials
Counse
ling C
ard
s
Post
er
1: N
urs
e m
ore
Post
er
2: N
o w
ate
r
Post
er
3: N
o form
ula
Loudsp
eake
r sc
ripts
Vid
eo c
lip 1
: N
urs
e m
ore
Vid
eo c
lip 2
: N
o w
ate
r
Vid
eo c
lip 3
: N
o form
ula
3D
Vid
eo: B
reast
-milk
and F
eedin
g
Fu
rnit
ure
Wooden C
hair
5
Pla
stic
Sto
ols
5
Table
1
Docu
ment ca
bin
et
1
Cooki
ng d
em
onst
ratio
n m
odule
1
TV
& D
VD
Shelf
1
Dis
pla
y sh
elf
1
IEC
mate
rials
hold
er
dis
pla
y unit
1
Ch
ildre
n P
lay
Are
a
Boxe
s2
Mats
12
Toy
set 1
1
Toy
set 2
1
3. F
RA
NC
HIS
E IT
EM
(USI
NG
TH
IS C
OPY
FO
R R
EPO
RT)
F
ran
chis
e co
de:
__
__ _
_ __
__
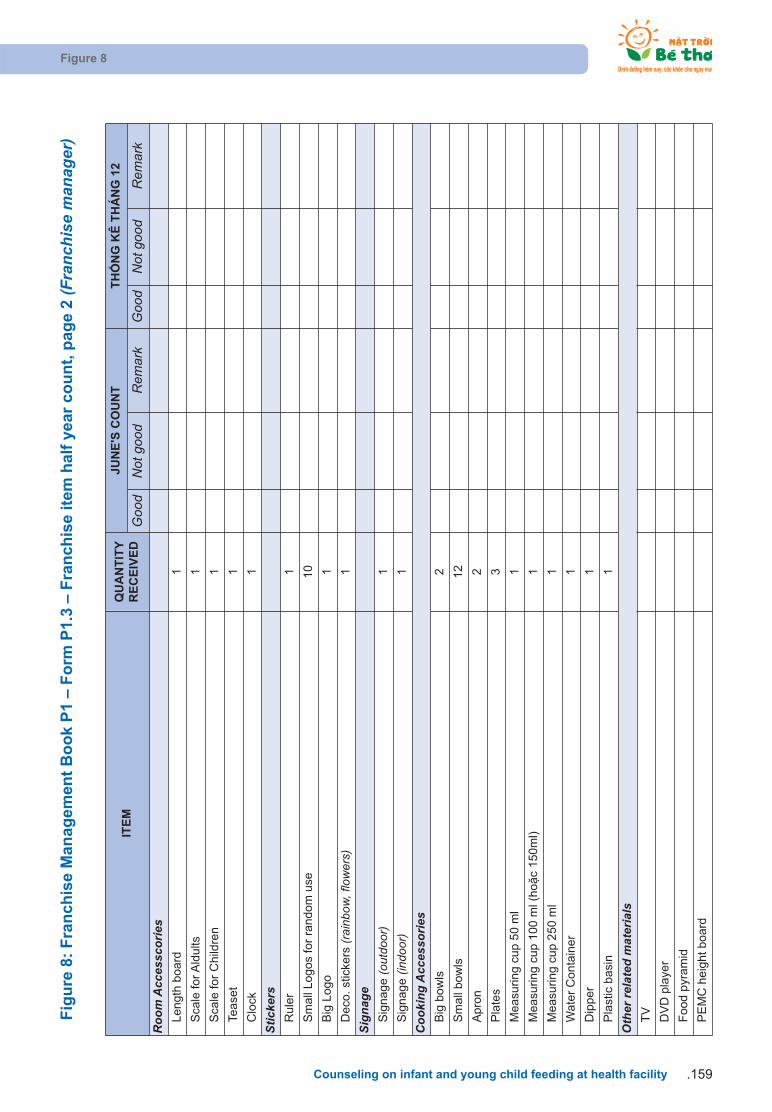
Figure 8
Counseling on infant and young child feeding at health facility .159
Fig
ure
8:
Fra
nch
ise
Man
agem
ent
Bo
ok
P1
– F
orm
P1.
3 –
Fra
nch
ise
item
hal
f ye
ar c
ou
nt,
pag
e 2
(Fra
nchi
se m
anag
er)
ITE
MQ
UA
NT
ITY
RE
CE
IVE
D
JUN
E'S
CO
UN
TT
HN
G K
Ê T
HÁ
NG
12
Goo
dN
ot g
ood
Rem
ark
Goo
dN
ot g
ood
Rem
ark
Roo
m A
cces
scor
ies
Length
board
1
Sca
le for A
ldults
1
Sca
le for
Child
ren
1
Tease
t1
Clo
ck1
Stic
kers
Rule
r1
Sm
all
Logos
for
random
use
10
Big
Logo
1
Deco
. st
icke
rs (r
ainb
ow, f
low
ers)
1
Sign
age
Sig
nage
(out
door
)1
Sig
nage
(indo
or)
1
Coo
king
Acc
esso
ries
Big
bow
ls2
Sm
all
bow
ls12
Apro
n2
Pla
tes
3
Measu
ring c
up 5
0 m
l1
Measu
ring c
up 1
00 m
l (ho
c 150m
l)1
Measu
ring c
up 2
50 m
l1
Wate
r C
onta
ine
r1
Dip
per
1
Pla
stic
basi
n1
Oth
er re
late
d m
ater
ials
TV
DV
D p
laye
r
Food p
yram
id
PE
MC
heig
ht board

Figure 8
Counseling on infant and young child feeding at health facility160.
INSTRUCTION FOR P1 BOOK
Name Management book
Symbol
YBP1.1 Franchise staff follow-up IYCF training
P1.2 BCC and promotional materials
P1.3 Franchise item half year count
Purpose
Franchise manager use this book when:• Reporting and planning
• Auditing of property periodically
Level/Location Franchises in provinces, districts and communes
Implimentor Franchise staff
Data source Counting
Time/frequency
• Staff training follow-up on IYCF: update when ever staff change (staff move to otherCHC, new staff…)
• BCC and other promotional material management follow-up card: update wheneversomething changes (receive, distribute or report)
• Franchise item half year count: twice a year (in June and December) - Copy this pageattach to Monthly report to management board
Management/ Archives Franchise manager stores P1 book in document cabinet/folder
Steps to fill out the form
P1.1 Staff training follow-up on IYCF• Name column: Staff’s fullname. Addition will be filled at the end of the list
• Title at Franchises and health facilities
• Training: Write training time & topic.
• Cross “X” in column “Not trained” if they have not been trained
• Organizer: Multiple choice. For example: A&T and NIN
P1.2 BCC and other promotional material management follow-up cards• Use one form P1.2. for each BCC material. for example: Invitation cards, mother & child
book, posters, leaflets...
• Each time a BCC material is received or distributed, Franchise staff fill out information in1 row
• When there is no more space, start a new form, staff write down “Stored” number in to“Store” in the first row of the new form.
P1.3 Franchise item half year count (Copy for report)• This is the franchise item list for each facility
• In June and December annually, Franchise staff check the facility item and write downnumber of each item into columns: "Good" - available for using "Not good" for broken ifmissing write into "Remark". And then Franchise manager sign and attach a copy withmonthly report to managerment board.
Validation/ supervision,support
A) Supervisor (frequency)1. Franchise manager (monthly, quaterly)2. Supervisors from the management board (monthly, quarterly)
B) Supervise method:1. Check is data is filled out on all forms
2. Randomly choose 1 BCC material: compare the stored number in form and realstored number.
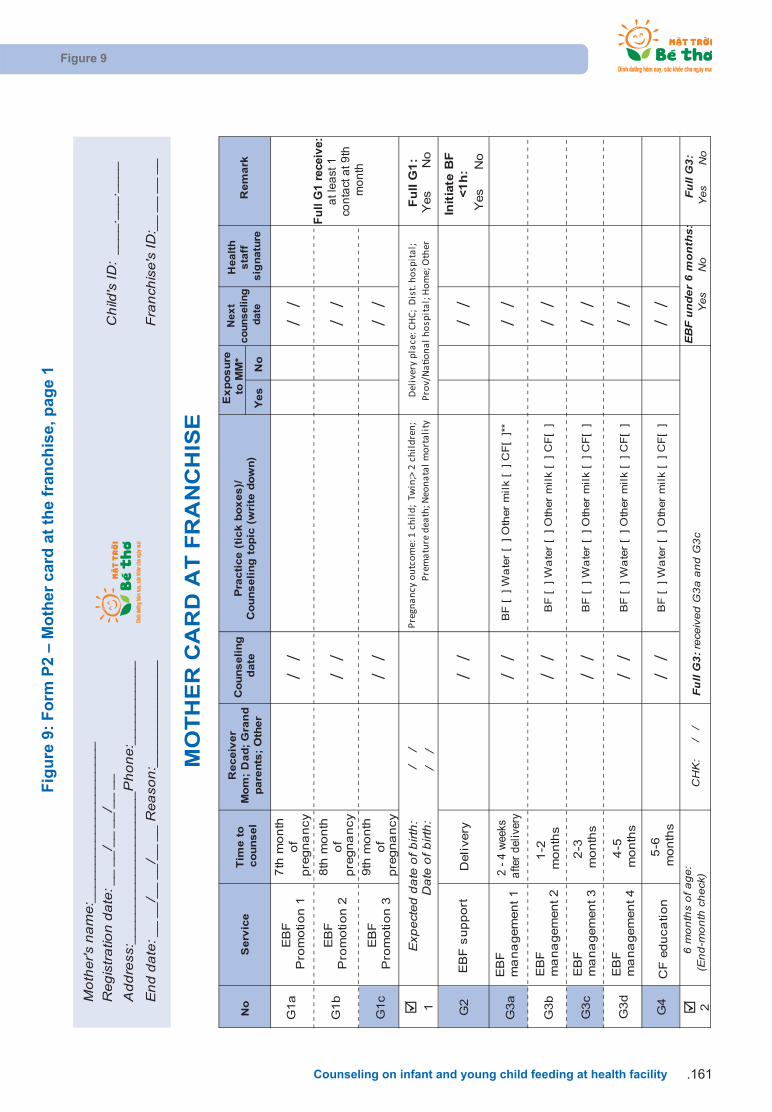
Figure 9
Counseling on infant and young child feeding at health facility .161
Fig
ure
9:
Fo
rm P
2 –
Mo
ther
car
d a
t th
e fr
anch
ise,
pag
e 1
G1
a
G1
b
G1
c
G2
G3
a
G3
b
G3
c
G3
d
G4
NoM
othe
r's n
ame:
____
____
____
____
____
_
Add
ress
:___
____
____
____
____
_Pho
ne:_
____
____
__C
hild
's ID
: __
__._
__._
___
Reg
istra
tion
date
: __
__/_
_ __
/__
__
End
dat
e: _
_ __
/__
__/_
_ __
Rea
son:
____
____
____
__F
ranc
hise
's ID
:__
__ _
_ __
Yes
No
EB
F
Pro
mo
tio
n 1
EB
F
Pro
mo
tio
n 2
EB
F
Pro
mo
tio
n 3
7th
mo
nth
o
f p
regn
an
cy
8th
mo
nth
o
f p
regn
an
cy
9th
mo
nth
o
f p
regn
an
cy
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
1 2
Preg
nanc
y ou
tcom
e: 1
chi
ld;
Twin
;> 2
chi
ldre
n;
Prem
atur
e de
ath;
Neo
nata
l mor
tali
tyF
ull G
1:
Yes
N
o
EB
F s
up
po
rtD
eli
very
Init
iate
BF
<1
h:
Yes
No
EB
F
ma
na
gem
en
t 1
2 -
4 w
eeks
a
fter
deli
very
BF
[
] W
ate
r [
] O
ther
mil
k [
]
CF
[ ]
**
EB
F
ma
na
gem
en
t 2
1-2
m
on
ths
BF
[
] W
ate
r [
] O
ther
mil
k [
]
CF
[ ]
EB
F
ma
na
gem
en
t 3
2-3
m
on
ths
BF
[
] W
ate
r [
] O
ther
mil
k [
]
CF
[ ]
EB
F
ma
na
gem
en
t 4
4-5
m
on
ths
BF
[
] W
ate
r [
] O
ther
mil
k [
]
CF
[ ]
CF
ed
uca
tio
n5
-6
mo
nth
sB
F [
]
Wa
ter
[ ]
Oth
er
mil
k [
]
CF
[ ]
CH
K:
/
/Fu
ll G
3:
Yes
No
Fu
ll G
1 r
ecei
ve:
a
t lea
st 1
co
nta
ct a
t 9th
m
on
th
/
/
/
/
Exp
ecte
d da
te o
f birt
h:D
ate
of b
irth:
Del
iver
y pl
ace:
CH
C; D
ist.
hosp
ital
; Pr
ov/N
aon
al h
ospi
tal;
Hom
e; O
ther
6 m
onth
s of
age
:(E
nd-m
onth
che
ck)
Full
G3:
rece
ived
G3a
and
G3c
EB
F un
der
6 m
onth
s:
Yes
No
Serv
ice
Tim
e t
o
co
un
sel
Receiv
er
Mo
m;
Da
d;
Gra
nd
pa
ren
ts;
Oth
er
Co
un
seli
ng
d
ate
MO
TH
ER
CA
RD
AT
FR
AN
CH
ISE
Pra
cti
ce (
tick
bo
xes
)/C
ou
ns
eli
ng
to
pic
(w
rite
do
wn
)
Ex
po
su
re
to M
M*
Nex
t co
un
sel
ing
d
ate
Hea
lth
s
taff
s
ign
atu
reR
em
ark

Figure 10
Counseling on infant and young child feeding at health facility162.
Fig
ure
10:
Fo
rm P
2 –
Mo
ther
car
d a
t th
e fr
anch
ise,
pag
e 2
G5a
G5b
G5c
G5d
G5e
G5f
G5
a
G5
b
G5
c
G5
d
CF
ma
na
gem
en
t 1
CF
ma
na
gem
en
t 2
CF
ma
na
gem
en
t 3
CF
ma
na
gem
en
t 4
CF
ma
na
gem
en
t 5
CF
ma
na
gem
en
t 6
6-7
m
on
ths
BF
[
] I
nfa
nt fo
rmu
la [
]
CF
8-9
m
on
ths
BF
[
] C
F: Q
ua
nt (2
mea
ls,1
/2 b
ow
l) [
]
Va
riety
[
]
10
-11
m
on
ths
BF
[
] C
F: Q
ua
nt (2
mea
ls,1
/2 b
ow
l) [
]
Va
riety
[
]
12
-14
m
on
ths
BF
[
] C
F: Q
ua
nt (3
mea
ls,3
/4 b
ow
l)[
]V
ari
ety
[
]
15
-18
m
on
ths
BF
[ ]
CF
: Q
ua
nt (3
-4 m
ea
ls,3
/4 b
ow
l) [
]
Va
riety
[ ]
18
-24
m
on
ths
BF
[
] C
F: Q
ua
nt (
3-4
mea
ls,1
bo
wl)
[
]V
ari
ety
[
]
CH
K:
/ /
Fu
ll G
5:
Yes
N
o
___ _
__
Fu
ll 5
p
ackag
es:
Yes
N
o
Ab
bre
via
tio
ns:
BF
=B
rea
stf
eed
ing
CF
=C
om
ple
men
tary
feed
ing
CH
C=C
om
mu
ne h
ea
lth c
en
ter
Dis
t.=D
istr
ict; P
rov.=
Pro
vin
ce
EB
F=E
xcl
isiv
e b
rea
stf
eed
ing
G=C
on
su
ltin
g p
ack
ag
e
3
24 m
on
ths o
f a
ge:
(End
-mon
th c
heck
)F
ull G
5: re
ceiv
ed G
5a, G
5b, G
5c &
G5d
BF
un
til 2
4 m
on
ths
Yes
N
o
To
tal n
um
ber
of
sevic
es
pro
vid
ed
Ful
l 5 p
acka
ge if
mot
her g
ot fu
ll G
1, G
2, G
3, G
4 an
d G
5
*E
xp
osu
re to
mass m
ed
ia o
f th
e m
oth
er:
** T
ick b
ox [
]:
X -
yes, 0 -
no
In th
e la
st 30 d
ays, h
ave y
ou
exp
osu
red
to
IY
CF
info
r. f
rom
TV
, ra
dio
, lo
ud
sp
ea
ker,
new
sp
ap
ers
,
inte
rnet?
(N
ot in
clu
de f
om
ula
pro
mo
tion
)
No
Yes
No
Serv
ice
Tim
e t
o
co
un
sel
Receiv
er
Mo
m;
Da
d;
Gra
nd
pa
ren
ts;
Oth
er
Co
un
seli
ng
d
ate
Pra
cti
ce (
tick
bo
xes
)/C
ou
ns
eli
ng
to
pic
(w
rite
do
wn
)
Ex
po
su
re
to M
M*
Nex
t co
un
sel
ing
d
ate
Hea
lth
sta
ff
sig
na
ture
Rem
ark
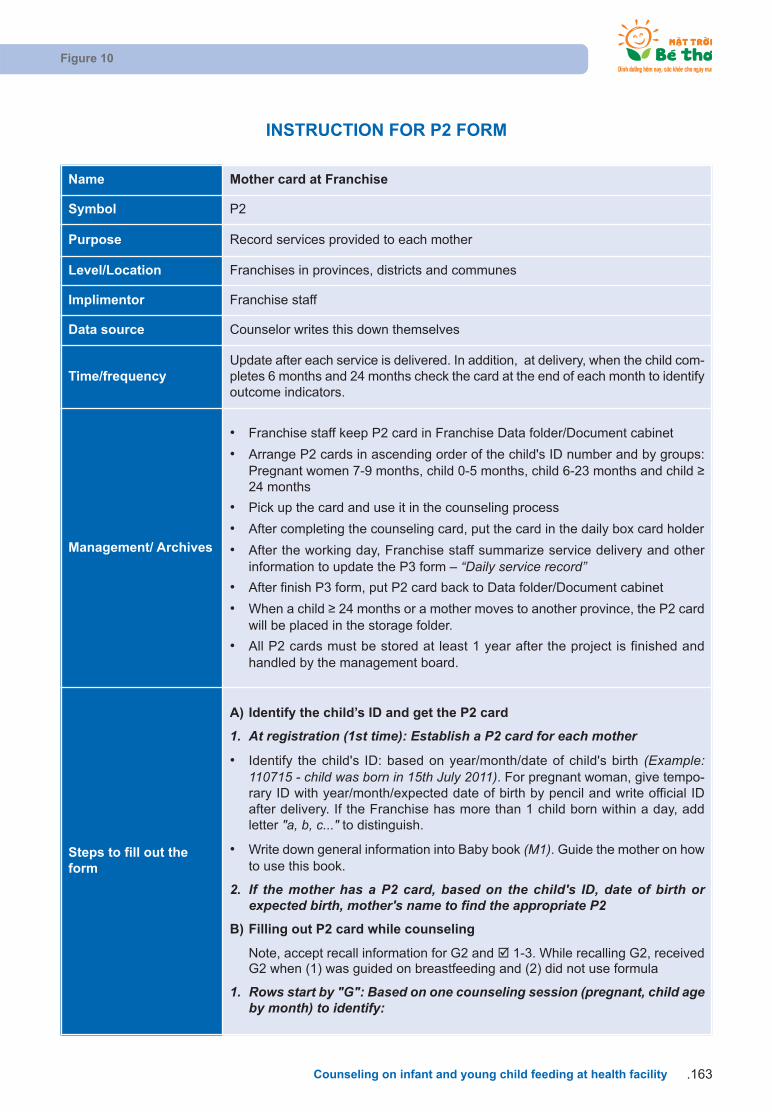
Figure 10
Counseling on infant and young child feeding at health facility .163
INSTRUCTION FOR P2 FORM
Name Mother card at Franchise
Symbol P2
Purpose Record services provided to each mother
Level/Location Franchises in provinces, districts and communes
Implimentor Franchise staff
Data source Counselor writes this down themselves
Time/frequencyUpdate after each service is delivered. In addition, at delivery, when the child com-pletes 6 months and 24 months check the card at the end of each month to identifyoutcome indicators.
Management/ Archives
• Franchise staff keep P2 card in Franchise Data folder/Document cabinet
• Arrange P2 cards in ascending order of the child's ID number and by groups:Pregnant women 7-9 months, child 0-5 months, child 6-23 months and child 24 months
• Pick up the card and use it in the counseling process
• After completing the counseling card, put the card in the daily box card holder
• After the working day, Franchise staff summarize service delivery and other information to update the P3 form – “Daily service record”
• After finish P3 form, put P2 card back to Data folder/Document cabinet
• When a child 24 months or a mother moves to another province, the P2 cardwill be placed in the storage folder.
• All P2 cards must be stored at least 1 year after the project is finished and handled by the management board.
Steps to fill out theform
A) Identify the child’s ID and get the P2 card
1. At registration (1st time): Establish a P2 card for each mother
• Identify the child's ID: based on year/month/date of child's birth (Example:110715 - child was born in 15th July 2011). For pregnant woman, give tempo-rary ID with year/month/expected date of birth by pencil and write official IDafter delivery. If the Franchise has more than 1 child born within a day, addletter "a, b, c..." to distinguish.
• Write down general information into Baby book (M1). Guide the mother on howto use this book.
2. If the mother has a P2 card, based on the child's ID, date of birth or expected birth, mother's name to find the appropriate P2
B) Filling out P2 card while counseling
Note, accept recall information for G2 and þ 1-3. While recalling G2, receivedG2 when (1) was guided on breastfeeding and (2) did not use formula
1. Rows start by "G": Based on one counseling session (pregnant, child ageby month) to identify:

Figure 10
Counseling on infant and young child feeding at health facility164.
Steps to fill out theform
1.1. Counseling receiver: write down all receivers by group: mother, father,grandsparents or other.
1.2. Counseling date: Date of counseling
1.3. Practice (tick boxes)/Counseling topic (write down): the day before counseling
• Tick practice boxes [ ] (X for yes and 0 for no)• Example: in G3c row: Child receiving breast milk, water and formula and not
yet receiving complementary foods, please fill in: BF [X] Water [X] Formula milk[X] CF[0]
• Write down counseling topic, note for follow-up
1.4. Mass media exposure: Ask mother about mass media exposure on infant andyoung child feeding in last 30 days if yes cross X into Yes column, if not, crossX into No column.
1.5. Next counseling date: write the next counseling date.
1.6. Health staff signature: counselor signs
1.7. Remark: Counselor writes down other criteria information
2. Rows start at tick box þ:þ 1. End of pregnancy:
Ask and write tentative birth date
When mother delivered, circle appropriate words in Pregnant outcome and
Delivery place
þ 2. Child is 6 month of age:
Exclusive breastfeeding in the first 6 months: Based on actual practice in rows G3a-d: Circle Yes if all are only BF and no water, no infant formula and no CF otherwise circle No
Call to get this information if the mother doesn't come in for counseling
Full G3: received G3a and G3c
þ 3. Child is 24 month of age:
Continue BF at 24 months: At the last contact G5f, child is still BF
Call to get this information if the mother doesn't come in for counseling
Full G5: received G5a, G5b, G5c & G5d
Count and write down total number of services provided
Full received: the mother receive G1, G2, G3, G4 and G5 when child is 24 months of age
Write the end date and reason. Common reasons for the completion of follow up are: 24 months, out migration, and death
Validation/ supervision,support
A) Supervisor (frequency)1. Franchise manager (weekly, monthly)2. Supervisor from a district or province (monthly, quarterly)
B) Supervise method:1. Supervisor get 3 P2 forms randomly, check general information and
counseling information
2. Compare P2 form and service row of P3
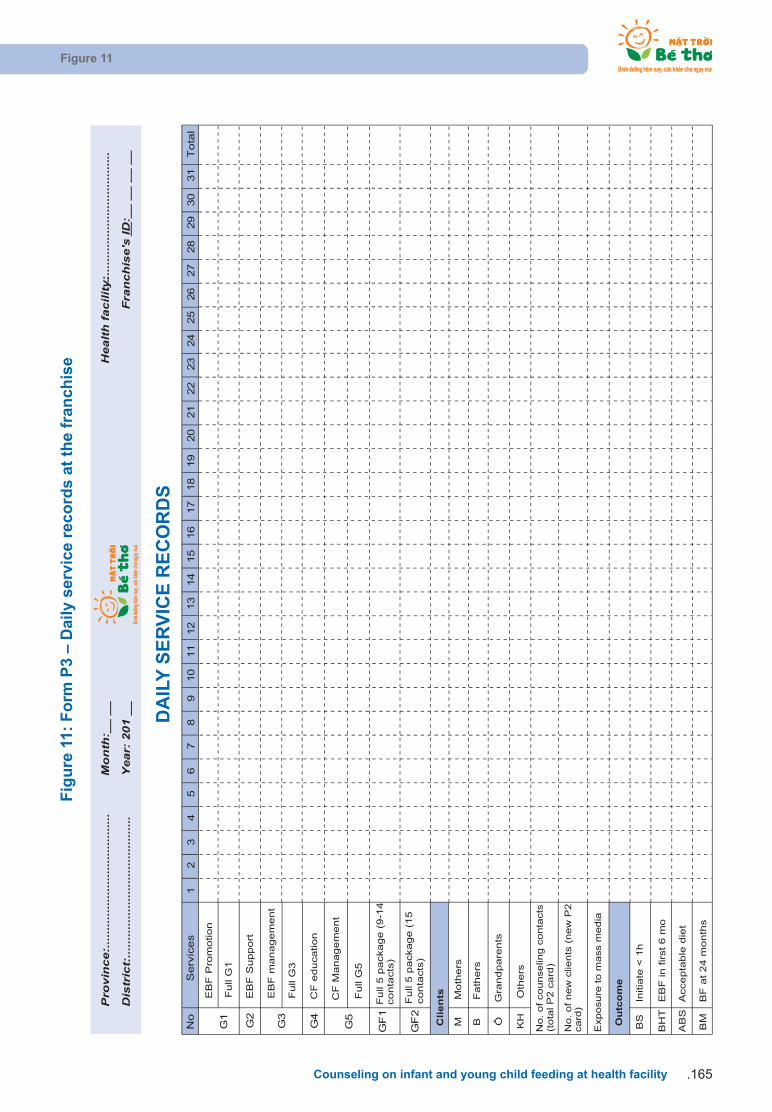
Figure 11
Counseling on infant and young child feeding at health facility .165
Fig
ure
11:
Fo
rm P
3 –
Dai
ly s
ervi
ce r
eco
rds
at t
he
fran
chis
e
No
12
34
56
78
910
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
Tota
l
G1
G3
G2
G4
G5
GF
1
GF
2
Pro
vin
ce:.
......
......
......
......
......
......
.M
on
th:_
_ __
H
ealt
h f
acili
ty:
......
......
......
......
......
......
...
Dis
tric
t:...
......
......
......
......
......
......
.Y
ear:
201
__
Fra
nch
ise'
s ID
: __
__
__ _
_ __
Se
rvic
es
EB
F P
rom
otio
n
Full
G1
EB
F S
up
po
rt
EB
F m
an
agem
en
t
Full
G3
CF
ed
uca
tio
n
CF
Man
agem
en
t
Full
G5
Fu
ll 5
pa
cka
ge
(9
-14
co
nta
cts
)
Fu
ll 5
pa
cka
ge
(1
5
co
nta
cts
)
MM
oth
ers
BF
ath
ers
ÔG
ran
dp
are
nts
KH
Oth
ers
BS
Initia
te <
1h
BH
TE
BF
in f
irst
6 m
o
AB
SA
cce
pta
ble
die
t
BM
BF
at
24
mo
nth
s
No.
of
new
clie
nts
(new
P2
ca
rd)
O
utc
om
e
DA
ILY
SE
RV
ICE
RE
CO
RD
S
Clien
ts
No
. o
f co
un
se
ling
co
nta
cts
(t
ota
l P
2 c
ard
)
Exp
osu
re t
o m
ass m
ed
ia
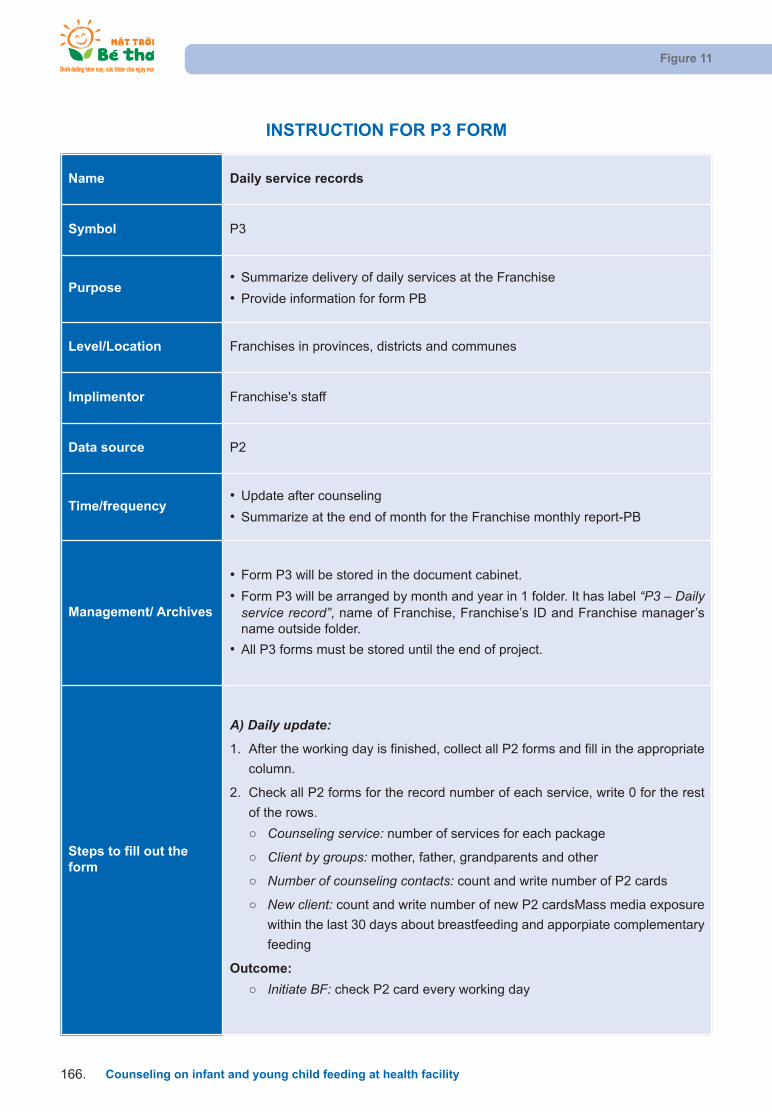
Figure 11
Counseling on infant and young child feeding at health facility166.
INSTRUCTION FOR P3 FORM
Name Daily service records
Symbol P3
Purpose• Summarize delivery of daily services at the Franchise
• Provide information for form PB
Level/Location Franchises in provinces, districts and communes
Implimentor Franchise's staff
Data source P2
Time/frequency• Update after counseling
• Summarize at the end of month for the Franchise monthly report-PB
Management/ Archives
• Form P3 will be stored in the document cabinet.
• Form P3 will be arranged by month and year in 1 folder. It has label “P3 – Dailyservice record”, name of Franchise, Franchise’s ID and Franchise manager’sname outside folder.
• All P3 forms must be stored until the end of project.
Steps to fill out theform
A) Daily update:
1. After the working day is finished, collect all P2 forms and fill in the appropriate
column.
2. Check all P2 forms for the record number of each service, write 0 for the rest
of the rows.
Counseling service: number of services for each package
Client by groups: mother, father, grandparents and other
Number of counseling contacts: count and write number of P2 cards
New client: count and write number of new P2 cardsMass media exposure
within the last 30 days about breastfeeding and apporpiate complementary
feeding
Outcome:
Initiate BF: check P2 card every working day

Figure 11
Counseling on infant and young child feeding at health facility .167
Steps to fill out theform
EBF in first 6 months: Count P2 card record "Yes" in þ 2. Accept calling for information
Continue BF at 24 months: Count P2 card record "Yes" in þ 3. Accept callingfor information if the mother doesn't come
Acceptable diet: Count P2 card is acceptable (meal frequency, size and variety) the day before counseling
B) Summary at the end of monthSummarize by rows in the table to complete Franchise Monthly report -PB.
Validation/ supervision,support
A) Supervisor (frequency)
1. Franchise manager (weekly, monthly)
2. Supervisor from a district or province (monthly, quarterly)
B) Supervise method:
Check rows and columns summary with Franchise Monthly report -PB.
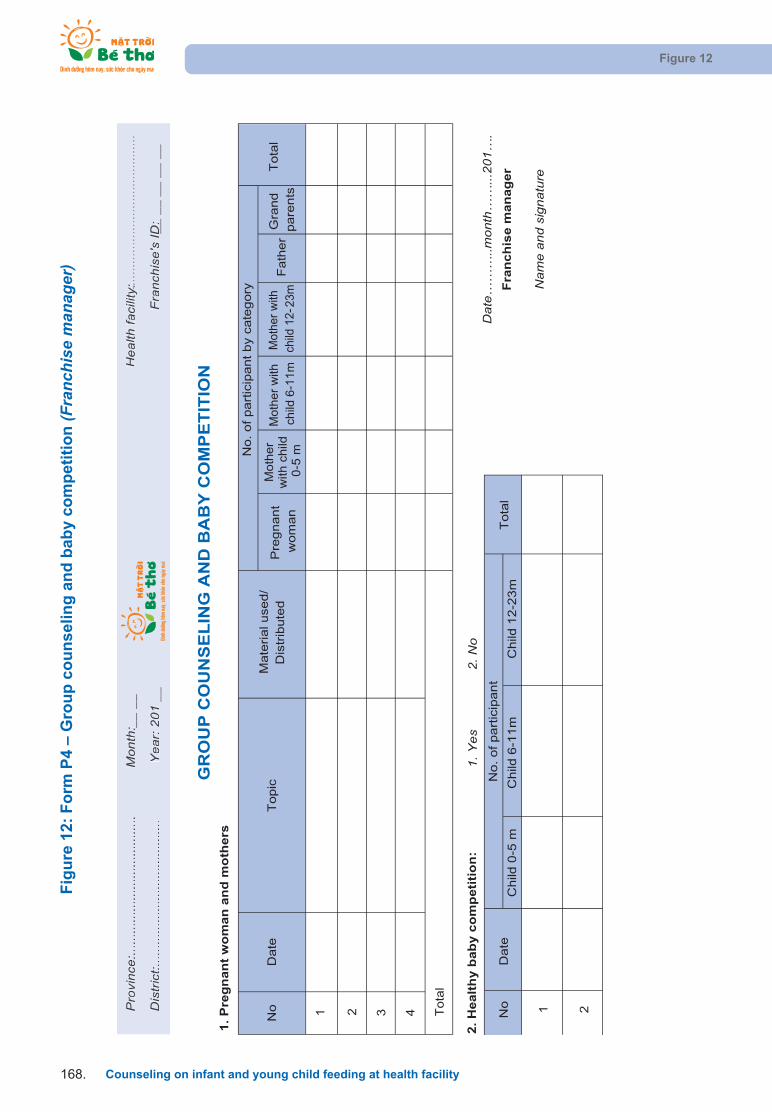
Figure 12
Counseling on infant and young child feeding at health facility168.
Fig
ure
12:
Fo
rm P
4 –
Gro
up
co
un
selin
g a
nd
bab
y co
mp
etit
ion
(Fra
nchi
se m
anag
er)
Pro
vinc
e:...
......
......
......
......
......
.....
Mon
th:_
_ __
H
ealth
faci
lity:
......
......
......
......
......
......
......
Dis
tric
t:....
......
......
......
......
......
......
Yea
r: 2
01 _
_F
ranc
hise
's ID
: __ _
_ __
__
__
1.
Pre
gn
an
t w
om
an
an
d m
oth
ers
Pre
gnant
wom
an
Moth
er
with
child
0
-5 m
Moth
er
with
ch
ild 6
-11
m
Mot
her
with
ch
ild 1
2-23
mF
ath
er
Gra
nd
pare
nts
2.
Healt
hy b
ab
y c
om
peti
tio
n:
1. Y
es
2. N
o
Child
0-5
mC
hild
6-1
1m
Child
12
-23
m
Dat
e……
…..m
onth
……
...20
1….
Fra
nc
his
e m
an
ag
er
Nam
e an
d si
gnat
ure
GR
OU
P C
OU
NS
EL
ING
AN
D B
AB
Y C
OM
PE
TIT
ION
Date
No.
of part
icip
ant
Topic
Date
Mate
rial used/
Dis
trib
ute
dN
o
No.
of part
icip
ant by c
ate
gory
Tota
l
Tota
l
Prorr
vivvniice
:.....
......
......
......
......
......
...M
onthtt
:___
___H
ealthtt
faffci
liiilltyt
:yyy:yyy.::....
......
......
......
......
......
......
Disii
trttirrc
t:....
......
......
......
......
......
......
Ye
YYar
:rr20
1___
Fr
FFarrnc
hisiie'
s'ID
:______
______
___
1 2No
1 2 3 4 To
tal
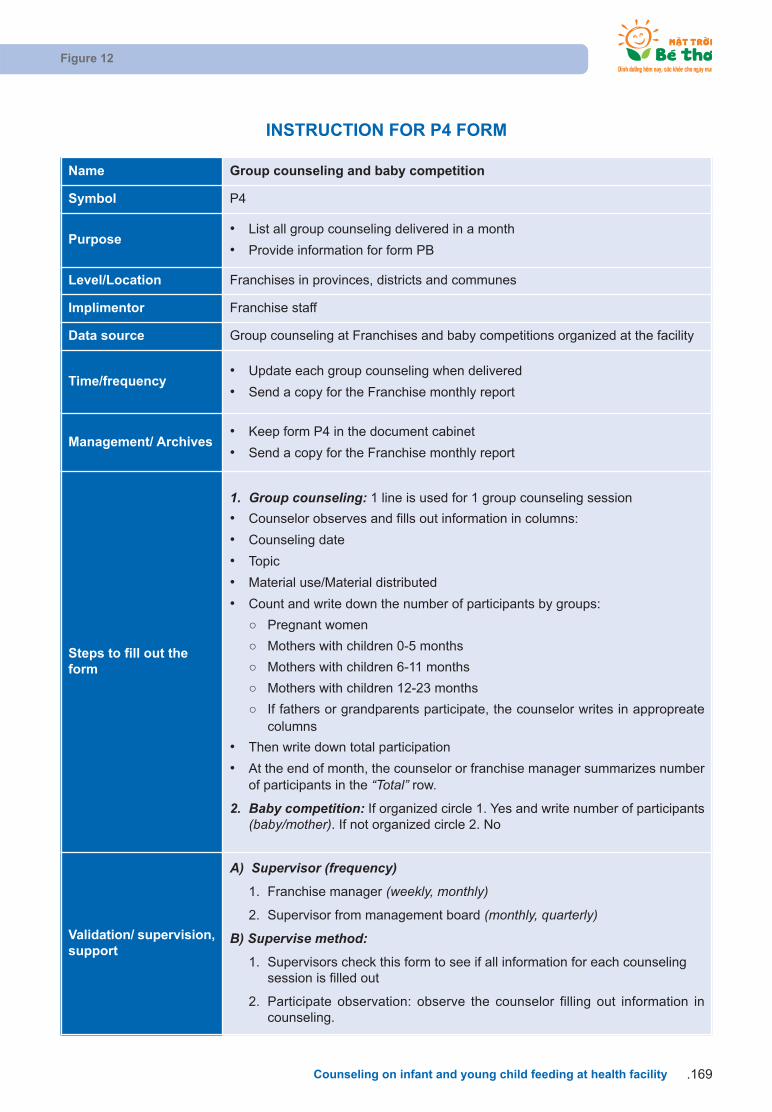
Figure 12
Counseling on infant and young child feeding at health facility .169
INSTRUCTION FOR P4 FORM
Name Group counseling and baby competition
Symbol P4
Purpose• List all group counseling delivered in a month
• Provide information for form PB
Level/Location Franchises in provinces, districts and communes
Implimentor Franchise staff
Data source Group counseling at Franchises and baby competitions organized at the facility
Time/frequency• Update each group counseling when delivered
• Send a copy for the Franchise monthly report
Management/ Archives• Keep form P4 in the document cabinet
• Send a copy for the Franchise monthly report
Steps to fill out theform
1. Group counseling: 1 line is used for 1 group counseling session
• Counselor observes and fills out information in columns:
• Counseling date
• Topic
• Material use/Material distributed
• Count and write down the number of participants by groups:
Pregnant women
Mothers with children 0-5 months
Mothers with children 6-11 months
Mothers with children 12-23 months
If fathers or grandparents participate, the counselor writes in appropreate columns
• Then write down total participation
• At the end of month, the counselor or franchise manager summarizes numberof participants in the “Total” row.
2. Baby competition: If organized circle 1. Yes and write number of participants(baby/mother). If not organized circle 2. No
Validation/ supervision,support
A) Supervisor (frequency)
1. Franchise manager (weekly, monthly)
2. Supervisor from management board (monthly, quarterly)
B) Supervise method:
1. Supervisors check this form to see if all information for each counseling session is filled out
2. Participate observation: observe the counselor filling out information in counseling.

Figure 13: Form P5 – Client Referral Form
Figure 13
Counseling on infant and young child feeding at health facility170.
Mother's name:....................................... Child's ID: ___.___.___
Address:..................................................
Child's name:.......................................... Franchise's ID:__ __ __
Child's (tentative) birthday: ....../....../......
1. Name of facility making the referral: _______________________________________
2.
3.
Referal date: __ __/__ __/_________
Services received at this facility: (Circle, multiple response)
3.1. EBF promotion 3.3. EBF management
3.2. EBF support (at delivery) 3.4. CF education
3.5. CF management
4. Facility referred to: _____________________________________________________
5. Service(s) for which client is being refered: (Circle, multiple response)
5.1. EBF promotion 5.3. EBF management
5.2. EBF support (at delivery) 5.4. CF education
5.5. CF management
6. Reason for referal: (Eg: No delivery facility at health centre, high risk case, illness, etc…)
……………………………………………………………………………………………………
……………………………………………………………………………………………………
7. Outcome of referance : ……………………………………………………………………..
8. Other comments: …………………………………………………………………………….
_____, date___ month ___ year 201__ _____, date___ month ___ year 201__
Referry facility Referry facility
Franchise staff
Name and signature
Franchise staff
Name and signature
CLIENT REFERAL FORM

Figure 13
Counseling on infant and young child feeding at health facility .171
INSTRUCTION FOR P5 FORM
Name Client referral form
Symbol P5
Purpose To refer client to other Franchise to receive counseling service
Level/Location Franchises at province, district and commune
Implimentor Franchise staff
Data source Counselors write it themselves base on information in P2 card
Time/frequency Refer a mother to another Franchise each form is used for 1 client
Management/ Archives• Give this form for client bring to other Franchise
• Record into P2 card
Steps to fill out theform
• Complete general information: Mother’s name address child’s name and birth-day (if delivered) child’s ID and Franchise ID
• Name of facility, referral date
• Counselor circles the number of service(s) that mothers received at this Fran-chise and service(s) that mothers need to receive at the new Franchise
• Give this form to mother and she will send to new Franchise
Validation/ supervision,support
A) Supervisor (frequency)
1. Franchise manager (monthly, quarterly)
2. Supervisor from district or province (monthly, quarterly)
B) Supervise method:
1. Supervisors check this form for filling out all information on P5 and P2 forms
2. Participate observation: observe counselor filling out information in counseling.
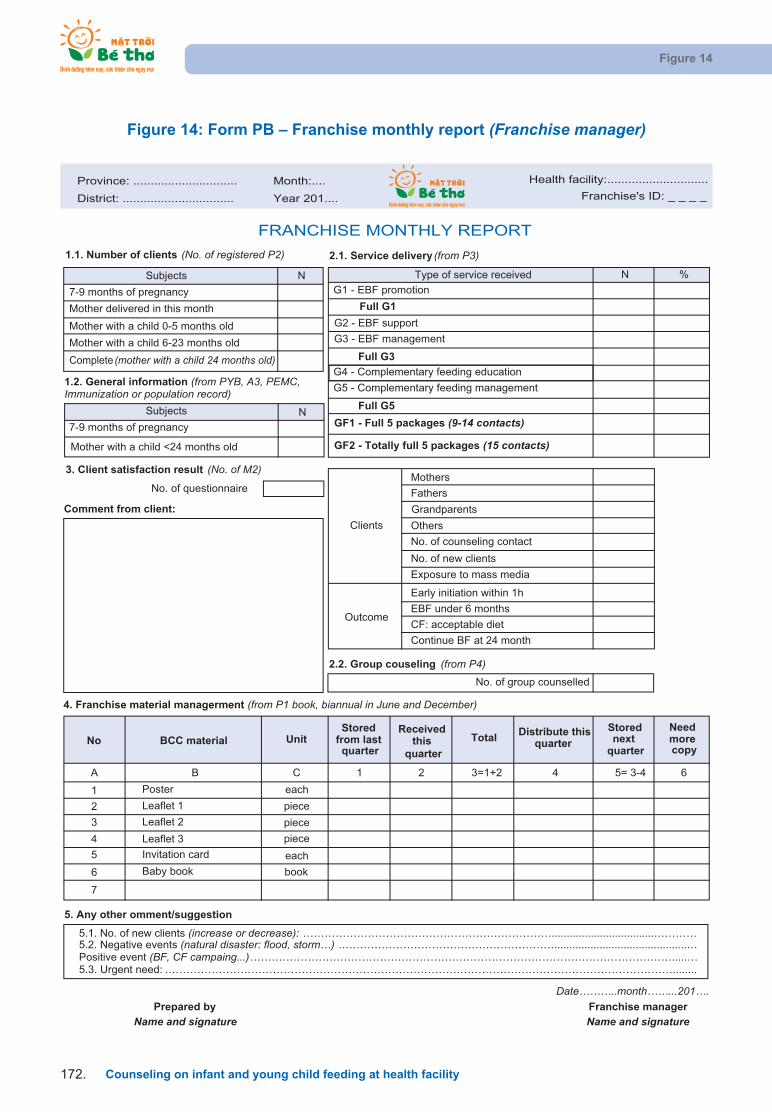
Figure 14: Form PB – Franchise monthly report (Franchise manager)
Figure 14
Counseling on infant and young child feeding at health facility172.
Province: .............................. Month:.... Health facility: .............................
District: ................................ Year 201.... Franchise's ID: _ _ _ _
2.1. Service delivery (from P3)
N
N
N %
7-9 months of pregnancy
7-9 months of pregnancy
Mother with a child 6-23 months old
Clients
Mothers
Fathers
Others
Mother with a child <24 months old
No. of counseling contact
No. of new clients
3. Client satisfaction result (No. of M2)
Exposure to mass media
No. of questionnaire
Outcome
Early initiation within 1h
Comment from client:
EBF under 6 months
CF: acceptable diet
Continue BF at 24 month
2.2. Group couseling (from P4)
4. Franchise material managerment (from P1 book, biannual in June and December)
No BCC materialStored
from last quarter
Receivedthis
quarter
Total Distribute this quarter
Stored next
quarter
Need morecopy
A B 1 2 3=1+2 4 5= 3-4 6
1 Poster
2 Leaflet 1
3 Leaflet 2
4 Leaflet 3
5 Invitation card
6 Baby book
7
5. Any other omment/suggestion
5.1. No. of new clients (increase or decrease): ……………………………………………………………..................................…………5.2. Negative events (natural disaster: flood, storm…) ……………………………………………………............................................…Positive event (BF, CF campaing...)……………………………………………………………………………………………………….....…5.3. Urgent need: ……………………………………………………………………………………………………………………………........
Date………..month……...201….Prepared by
Name and signatureFranchise managerName and signature
book
C
each
piece
piece
piece
each
Unit
No. of group counselled
1.2. General information (from PYB, A3, PEMC, Immunization or population record) G5 - Complementary feeding management
Complete (mother with a child 24 months old)
Full G5
GF1 - Full 5 packages (9-14 contacts)
GF2 - Totally full 5 packages (15 contacts)
G4 - Complementary feeding education
Mother with a child 0-5 months oldG3 - EBF management
G2 - EBF support
Full G3
FRANCHISE MONTHLY REPORT
Subjects
Subjects
Type of service received
G1 - EBF promotion
Mother delivered in this month Full G1
1.1. Number of clients (No. of registered P2)
Grandparents

Figure 14
Counseling on infant and young child feeding at health facility .173
INSTRUCTION FOR PB FORM
Name Franchise monthly report
Symbol PB
PurposeSummary Franchise activities of the report month Include PYB and P1.3 with thereports for June and December
Level/Location Franchises in provinces, districts and communes
Implimentor Franchise staff
Data sourceForms: P1, P3, P4, M2, PYBAlternative to form PYB, franchises at the commune level can use available infor-mation from the pregnancy book (A3) and PEMC for report to complete form PYB
Time/frequency On the 5th of every month
Management/ Archives
Save 1 copy at the FranchiseFranchise at commune and district levels send the report to the District manage-ment board, Franchise at province level send the report to the Province manage-ment board.
Steps to fill out theform
1.1. Number of clients (count number of P2 card are follow-up at Franchise) bygroups.
1.2. General information: from "Total" column in PYB form, which might gather fromthe Pregnant book (A3) for PEMC report. Photocopy and include PYB form.
2.1. Service delivery (from P3 form): Get data from "Total" column of P3 form tofill this session % = Service delivery / Client are followed
2.2. No. of group counseling sessions: from P4 form3. Client satisfaction results: write no of forms M2 received4. Franchise material managerment based on P1.2 report in June and Decem-
ber Copy P1.3 form and attach to this report5. Any other comments/suggestions:
• No. of new clients (increase or decrease)• Negative events (natural disaster: flood, storm…)• Positive events (BF, CF campaing...)• Urgent need
Validation/ supervision,support
A) Supervisor (frequency)
1. Supervisor from management board (quarterly)
B) Supervise method:
1. Compare report with P3 card and management book.
Denominator Numerator
- Pregnant women 7th-9th months pregnant G1
- Delivery Full G1 or G2
- Mother with a child 0-5 months G3, full G3 or G4
- Mother with a child 6-23 months G5
- Complete (Mother with a child 24 months old) Full G5, GF1, and GF2

Figure 15: Form M2 – Client satisfaction questionnaire
Figure 15
Counseling on infant and young child feeding at health facility174.
Province: .............................. Health facility: ..........................................District: ................................Year: 201__ Franchise's ID: __ __ __ __ __
Date of Service ___/ ____/______
Service Received ……………………………………………………………………………
1. How did you hear about the IYCF franchise? (Multiple response)Circle
a. Health staff d. Leaflet, TV chanelsb. Community based workers e. Franchise sign at gatec. Other mother/s f. Others (specify)..............................................
2. How many minutes did you wait for counseling? Note your waiting time (in minutes)
...........................................................................................................................................................................
3. Do you feel that the counselor
a. Was friendly to you?
b. Gave enough information for you to make a decision about infant feeding: 1. YES 2. NO
c. Listened to you:
d. Responded to your concerns or problems:
e. Was supportive with no judgment:
4. Overall, how would you rate the quality of IYCF services at this facility?
Circle one: 1. POOR 2. FAIR 3. GOOD 4. EXCELLENT
Comments:…………………………………………………………..……………………………………………………………………
…………………………………………………………..……………………………………………………………………
5. Your comments and suggestions to improve the quality of the IYCF services at this facility
…………………………………………………………..……………………………………………………………………
…………………………………………………………..……………………………………………………………………
6. Will you recommend the IYCF service at this facility to a friend or family member?
Circle one: 1. YES 2. NO
If NO, please explain:…………………………………………………………..……………………………………………………………………
…………………………………………………………..……………………………………………………………………
THANK YOU VERY MUCH!
CLIENT SATISFACTION QUESTIONNAIRE
Yourhelp in completingthis questionnaireis valuablefor us to provideour clientswith the bestquality of care.Please leave the completed questionnaire in the designated box. Your responses are confidential. Thank you!
1. YES 2. NO
1. YES 2. NO
1. YES 2. NO
1. YES 2. NO

TRAINEE HANDBOOK TWO
Counseling on Infant and Young Child Feeding
at Health Facility
Ha Noi, July 2011
Alive & Thrive Vietnam203 - 204, E4BTrung Tu Diplomatic CompoundNo 6 Dang Van Ngu, Ha Noi
Tel: +84-4-3573 9066Fax: +84-4-3573 9063www.aliveandthrive.org