Total Page.cdr
40
Journal of Diabetic Association Medical College, Faridpur Vol. 3, No. 1, January 2019 Official Journal of Diabetic Association Medical College, Faridpur (An Institution of Faridpur Diabetic Association) Web Address: www.damcf.org; http://damcf.org/site/journal; E-mail: [email protected] ISSN No. 2663-8312 Contents Editorial: Childhood Obesity 9 Biswas B K Original Articles: Mothers Knowledge on EPI and Immunization Status of Their Under Five Children 11 Huda S M N, Asaduzzaman A K M, Latif A, Akhiruzzaman, Zaman F, Islam MA, Forhad C M R Q Ultrasonographic Evaluation in the Diagnosis of Acute Appendicitis with Histopathological Correlation 15 Saiham K S, Hossain R, Halder B A, Satter A, Yesmin L, Naz F M, Alam S, Ahmad M R, Hossin I A Study on Environmental Sanitation in Some Selected Villages of Bhanga, Faridpur 20 Rahman M T, Asaduzzaman A K M Operative outcomes of Laparoscopic Cholecystectomy 24 Rahman M M, Rahman M S, Chowdhury A A M A M, Rahman M M, Qaiyum M A, Ahmed S, Hasan T M Mammographic Evaluation of Breast Mass & Comparison with Histopathological Findings 28 Yesmin L, Hossain R, Saiham K S, Naz F M, Alam S, Ahmad M R, Hossain M I Review Article: Environmental Sanitation: The Public Health Challenge 33 Tarafdar M A, Rahman M T Case Report: Female Genital Tuberculosis 36 Ahmed S, Shaha D R, Begum P, Akter T, Akter H
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Total Page.cdr

Journal of Diabetic Association Medical College, Faridpur
Vol. 3, No. 1, January 2019
Official Journal ofDiabetic Association Medical College, Faridpur
(An Institution of Faridpur Diabetic Association)
Web Address: www.damcf.org; http://damcf.org/site/journal;E-mail: [email protected]
ISSN No. 2663-8312
Contents
Editorial:Childhood Obesity 9Biswas B K
Original Articles:Mothers Knowledge on EPI and Immunization Status of Their Under Five Children 11Huda S M N, Asaduzzaman A K M, Latif A, Akhiruzzaman, Zaman F, Islam MA, Forhad C M R Q
Ultrasonographic Evaluation in the Diagnosis of Acute Appendicitis with Histopathological Correlation 15Saiham K S, Hossain R, Halder B A, Satter A, Yesmin L, Naz F M, Alam S, Ahmad M R, Hossin I
A Study on Environmental Sanitation in Some Selected Villages of Bhanga, Faridpur 20Rahman M T, Asaduzzaman A K M
Operative outcomes of Laparoscopic Cholecystectomy 24Rahman M M, Rahman M S, Chowdhury A A M A M, Rahman M M, Qaiyum M A, Ahmed S, Hasan T M
Mammographic Evaluation of Breast Mass & Comparison with Histopathological Findings 28 Yesmin L, Hossain R, Saiham K S, Naz F M, Alam S, Ahmad M R, Hossain M I
Review Article:Environmental Sanitation: The Public Health Challenge 33Tarafdar M A, Rahman M T
Case Report:Female Genital Tuberculosis 36Ahmed S, Shaha D R, Begum P, Akter T, Akter H
Journal of Diabetic Association Medical College, Faridpur (JDAMC)Vol. 3, No. 1, January 2019
Advisory BoardChairman, Gorverning Body
Professor Dr. Dipti Pramanik
Professor Dr. Jamal Uddin Ahmed
Professor Dr. Md. Nasir Uddin
ChairpersonProfessor Dr. Md. Zohirul Islam Miah
Editor-in-ChiefProfessor Dr. Jitesh Chandra Saha
Executive EditorProfessor Dr. AKM Asaduzzaman
EditorsProfessor Dr. Md. Harunur Rashid
Professor Dr. Sk. Yunus Ali
Professor Dr. Nasiruddin Ahmad
Professor Dr. Md. Yusuf Ali
Assistant EditorsDr. Muhammad Nazrul Islam
Dr. Bijoy Kumar Shaha
Dr. Akhiruzzaman
MembersProfessor Dr. Shipra Sinha Roy
Professor Dr. Sudhendu Prakash Biswas
Professor Dr. Barun Kanti Biswas
Professor Dr. Md. Rafiqul Islam
Professor Dr. Khandaker Anowar Hossain
Dr. Md. Saiful Arifin
Dr. Md. Mesbah Uddin Khan
Dr. Mohammad Saiful Hoque
Dr. Dilip Kumar Das
Dr. Md. Fazlul Hoque
Dr. Khalifa Mahmud Walid
Dr. Muhammad Asaduzzaman Biswas
Dr. Hasnina Akter
TreasurerDr. Md. Isahaque Ali Khan
Editorial StaffAshikuzzaman Suzan
General InformationThe Journal of Diabetic Association Medical College, Faridpur (JDAMC) is the official journal of Diabetic Association Medical College, Faridpur. The journal is published twice in a year i.e. January and July. It accepts original articles, review articles, and case reports. Complimentary copies of the journal are sent to libraries of all medical and other relevant academic institutions in the country and selected institutions abroad.
Papers for publication should be sent to Editor-in-Chief, JDAMC, Diabetic Association Medical College, Faridpur, Bangladesh. Only Scientific papers written in English will be accepted. While every effort is always made by the editorial board to avoid inaccurate or misleading information appearing in JDAMC, information within the individual article are the responsibility of its author(s), JDAMC and its editorial board accept no liability whatsoever for the consequences of any such inaccurate and misleading information, opinion or statement.
Published by: Professor Dr. Jitesh Chandra Saha Editor-in-Chief, JDAMC
Designed by : Nizam KhanPrinted by : Radiant Printing & Packaging 27, Nilkhet Babupura, New Market Dhaka-1212. Phone: 01712571681
Address of correspondence: Editor-in-Chief, JDAMC 1st Floor, Room No-204, Diabetic Association Medical College, Faridpur. Jheeltuly, Faridpur-7800, Bangladesh. Cell: +8801711431902 Web Address: www.damcf.org; E-mail: [email protected]
Editorial Board
1
2

Congratulations All praises to the Almighty. It is a great pleasure that Diabetic Association Medical College, Faridpur is the first private medical college in the South part of Bangladesh, going to publish it’s 5th scientific journal. I solely praise our devoted researchers and doctors who contribute themselves to achieve this great task.
The aim of this journal is to enhance and upgrade the research work of our teachers in the field of medical science. It provides an integrative forum for medical researchers across the globe to exchange their knowledge and views. It also helps us to promote communication among fellow academicians and researchers worldwide. It provides an opportunity to academicians in exchanging their knowledge that is directly relevant to all domains of health sciences.
I would like to congratulate our journal committee and all concerned personnel for the publication of this first issue. I hope this journal will develop a new channel for authors for disseminating their research findings. Honorable medical researchers are invited to submit their research paper for the next issues.
Lastly, I express my heartfelt gratitude to all the researchers for their cordial Endeavour. I expect regular publication of the biannual issues of this journal would brighten the academic and research environment of this institution. I am very much hopeful for the better outcome of this journal.
Professor Dr. Jitesh Chandra Saha Editor-in-Chief, JDAMC
From the Desk of the Editor-in-Chief
3

4
General InformationAims & Scope:The Diabetic Association Medical College journal is a scientific journal dealing with clinical medicine, basic sciences, epidemiology, public health and various health care specialities. It is an official organ of Diabetic Association Medical College and going to be published bi-annually (January and July).
The journal publishes articles of authors from any part of the globe/country. It intends to publish the highest quality material on all aspects of medical science. It accepts original research articles, review articles, short communications, case reports and letters to editor. In addition, it provides readers with opinion regarding the articles published in the journal. Complimentary print copies of the journal are sent to libraries of all medical colleges and other relevant academic institutions in the country.
Instruction to authors:Manuscript written in English on bio-medical topics will be considered for publication provided these have not been published previously and are not under consideration for publication elsewhere.
Conditions for manuscript submission:l All manuscripts will be subjected to peer and editorial
review.
l Accepted manuscript will become the property of Diabetic association medical college journal.
l The author should obtain written permission from appropriate authority if the manuscript contains any table, data or illustration previously published in other journals. The letter of permission should be submitted with manuscript.
l If the photographs are identified, permission from the patient or parents/guardians should accompany the manuscript. Otherwise identity will be blackened out.
l The materials submitted for publication may be in the form of an original research, review article, special article, a case report, recent advances, new techniques, brooks review on clinical/medical education, adverse drug reaction or a letter to the editor.
l The authors should sign a covering letter mentioning that final manuscript has been seen and approved by all authors. Relevance and contributions of coauthors should be clearly mentioned by principal author. Irrelevant person or without any contribution should not be entitled as coauthors.
l All rights are reserved to the journal. No part may be reproduced or transmitted in any form or by any means without written permission form editors.
l We strongly encourage authors to pay careful attention to the instruction to the “Instruction for authors” which will be found in this section of each issue.
l The editorial board reserves the right to edit and if necessary, shorten any material accepted for publication. All manuscript will go through a peer-review process.
l Editors are not responsible for currier/postal failure.
Manuscript preparation:l It should be typed in English and on one side of A4
(290×210 cm) size white paper, using Times New Roman font size 12, with double space throughout. All pictures should be in 300 dpi.
l The widely accepted “Vancouver style” should be followed in reference section.
l There should be one original, two paper copies and one IBM Compatible electronic copy.
l There should be a margin of 2.5 cm at both top and bottom and 1.2 cm left and right.
l Pages should be numbered in English numerical at the upper right hand corner of each page.
l Each of the following section should be in separate page:
¡ Title page
¡ Abstract
¡ Text-Introduction, Materials & Methods, Result & Discussion
¡ References
¡ Tables and legends
¡ Acknowledgement
Title page: Title page should include the title of the paper, name of the authors, name of the department they worked, email address & phone number. Title should be concise, informative and self-explanatory (not exceed 100 characters). Title should provide a reasonable indications of the contents of the paper.
Abstract:It should be structured as introduction with objectives, materials and methods, result, discussion with conclusion including key words, number of figures, tables, references & correspondence (about 350 words maximum).
Text: The text should be presented in the form of-l Introduction: Provide background of the study. It
should be very specific & reasoning. It should include
Information for Authors
5
the purpose of the article. The rational for the study or observation should be summarized. Only strictly pertinent references should be cited. Data or conclusion from the work being reported should not be presented in the introduction.
l Materials and Methods: Provide technical information about the study. Study design & sampling method should be mentioned. Describe your section of subjects (patients or laboratory animals) clearly. Consent from respondents/patients should be taken in a form before interview/study. All drugs & chemicals used should be identified precisely, including generic name, dose and route of administration. For all quantitative measurements SI unit should be used.
l Results: This should be presented in logical sequence in the text, table and illustration, for statistical analysis standard procedure should be maintained.
l Discussion: Author's comment on the result supported with contemporary references including arguments and analysis of identical work done by other workers may be elaborately discussed. A summary is not required. Describe the implication of the findings for future research.
l Conclusion: Link the conclusion with the goals of the study but avoid unqualified statements and conclusion no t comple te ly suppor ted by your da ta . Recommendation when appropriate may be included.
l Tables: Number and titles of tables to be clearly written in Arabic numerical.
l Source: Source of illustrations & figures should be mentioned.
l Abbreviations and symbols: Use only standard abbreviations, avoid abbreviation in the title of the article.
Acknowledgement: 1. Contributions that need acknowledgement but do not
justify authorship, such as general support by a dept. or dept. chairman.
2. Acknowledgement of technical help.
3. Acknowledgement of financial & material support.
4. Author should obtain written permission for everyone acknowledged by name.
Reference: These should be given in the text using the Vancouver system. They should be numbered consecutively in the order in which they first appear in the text using superscript. If a reference is cited more than once the same number should be used each time. References cited only in tables and figures and not in the text should be numbered in sequence from the last number used in the text and in the order of mention of the individual tables and figures in the text. At the end of the paper, on a page (s) separate from the
text, references should be listed in numerical order. The journal adheres closely to the Vancouver style of references (See ht tp: / / www.nlm. nih.gov/bsd/uniform_ requirements. html, updated 2013).
Sample references are given below-
1. Standard Journal Article
List the first six authors followed by et al: Halpern SD, Ubel PA, Caplan AL. solid-organ
transplantation in HIV-infected patients. N Engl J Med. 2002 Jul 25;347(4):284-7
As an option, if a journal carries continuous pagination throughout a volume (as many medical journals do) the month and issue number may be omitted:
Halpern SD, UP PA, Caplan AL. Solid-organ transplantation in HIV-infected patients. N Engl J Med. 2002;347:284-7
More than six authors: Rose ME, Huerbin MB, Melick J, Marion DW, Palmer
AM, Schiding JK, et al. Regulation of interstitial excitatory amino acid concentrations after cortical contusion injury. Brain Res. 2002; 935(1-2):40-6
Optional addition of a database's unique identifier for the citation:
Helpern SD, Ubel PA, Caplan AL. Solid-organ transplantation in HIV-infected patients. N Engl Med. 2002 Jul 25;347(4):284-7. PubMed PMID:12140307
Organization as author: Diabetes Prevention Program Research Group.
Hypertension, insulin's and proinsulin In participants with impaired glucose tolerance Hypertension. 2002;40(5) :679-86
No author given: 21st century heart solution may have a sting in the tail
BMJ. 2002;325(7357):184
Volume with supplement: Geraud- G, Spierings EL, Keywood C. Tolerability
and safety of frovatriptan with short- and long-term use for treatment -of migraine and in comparison with sumatriptan. Headache. 2002,42 Suppl 2:S93-9.
Issue with supplement: Glauser TA. Integrating clinical trial data into clinical
practice. Neurology. 2002;58(12 Suppl 7):S6-12.
Article published electronically ahead of the print version:
Yu WM, Hawley TS, Hawley RG, Qu CK. Immortalization of yolk sac-derived precursor cells. Blood. 2002 Nov 15; 100(10):3828-31. Epub 2002 Jul 5.
2. Books and Other Monographs Personal authore(s): Murray PR, Rosenthal KS, Kobayashi GS, Pfaller
MA. Medical microbiology. 4th ed. St. Louis: Mosby, 2002.
6

3. Other Published Material Newspaper article: Tynan T. Medical improvements lower homicide rate: study sees drop in assault rate. The Washington Post.
2002 Aug 12; Sect. A: 2 (col.4). Dictionary and similar references:
Dorland's illustrated medical dictionary. 29th ed. Philadelphia: W.B. Saunders; 2000. Filamin; p. 675.
4. Unpublished Material In press or Forthcoming: Tian D, Araki H, Stahl E, Bergelson J, Kreitman M.
Signature-of balancing selection in Arabidopsis. Proc Natl Acad Sci U S A. Forthcoming 2002.
5. Journal Article on the Internet Abood S. Quality improvement initiative in nursing
homes: the ANA acts in an advisory role. Am J Nurs [Internet]. 2002 Jun [Cited 2002 Aug 12] 102(6): [about 1, p.]. Available from: http://www.annals.org/ cgi/reprint/145/1/62.pdf
IllustrationAll drawings should be made with black Indian ink on white paper. Photographs and photomicrographs should be supplied as glossy black and white prints unmoundted. All
photographs, graphs and diagrams should be referred to as figures numbered consecutively in the text in Arabic numerals-.
Drug namesGeneric name should generally be used. When proprietary brands are used in research, include the brand name in parentheses in the methods section.
PermissionMaterials taken from other source must be accompanied by a written statement from both author and publishers giving permission to the journal for reproduction Obtain permission in writing from at least one author of papers that is still in press, unpublished data and personal communications.
The editor of Journal of Diabetic Association Medical College reserves the customary right to style and if necessary shortens the material accepted for publication and to determine the priority and time of publication. Editor assumes that the manuscript submitted by the author is based on honest observations. It is not a task of the editor to investigate scientific fraud paper.
7

8

IntroductionPaediatricians have been facing a very common complaints: ‘‘Look doctor, my child is thin & has been becoming thinner day by day and not eating enough.” Although their kids achieved almost all the parameters of normal growth & development. Traditionally, a fat child is considered as an ‘‘attractive’’ child and is often referred to as an ‘‘healthy” child. However, the adverse effects and serious consequences of childhood obesity are now proven beyond doubt. At least 30% of obesity begins at childhood. Conversely 50 to 80% of obese children, become obese adults Many longitudinal studies have demonstrated 1.convincingly, the higher risks of child onset obesity In 2,3 .the Harvard study, morbidity from cardiovascular disease, diabetes, obesity related cancers and arthritis was 50 to 100% higher in obese individuals who were also obese as children and the cardiovascular mortality in such individuals was doubled 4.
Obesity has become a pandemic and it has been estimated that about 13% of the world's population (11% of men and 15% of women) are obese. The increased economic 5
development and nutrition transition has led to a dramatic increase in the prevalence of obesity in children, especially in developing countries. Over 340 million children and adolescents aged 5-19 years are reported to overweight and obese. The prevalence of overweight and obesity among 5-19 years has risen dramatically from just 4% in 1975 to just over 18% in 2016.The rise has occurred similarly both boys and girls 5.
According to the Centre for Disease Control and Prevention (CDC), overweight is defined as a body mass index (BMI)
th that or above 85 percentile and below 95 percentile for children and teens of the same age and sex. Obesity is
thdefined as a BMI at or above 95 percentile for children and teens for the same age and sex. Due to the increasing trend of higher BMIs in children around the world, it is not possible to have any ideal population on whom ideal weight/BMI charts can be constructed. Country specific growth charts have been designed to assess the development of children between 5 and 18 years of age 6.
Some documented risk drivers of childhood obesity related to food, eating behavior, intake, and feeding practices are as follows: shorter duration of breastfeeding or no breastfeeding; ready availability of calorie-dense food;
preference to and increased consumption of sweet and fatty/fried food snacks; skipping the breakfast; and the child food environment at home. (7,8,9,10). Food related risk drivers are also very closely related to social structures; urbanization (urban residence; rural-to-urban migration; and psychological stress in urban settings); increasing affluence; and child targeted market. For 7,11,12
children, prime movers in the domain of social structures are family related attributes. The correlates emerging through a study conducted in urban school children in central India are father and/or mother involved in service/business; and English medium schools (which again may be a proxy of higher economic strata. Risk 13
drivers associated with physical activity are motorized transport; increased mechanization of day-to-day activities; and child playing outdoor games for <30 min. 11,13
Decreased duration of sleep (<8.5h/day) and increased television viewing (>3h/day) have also been documented as significant risk drivers.14
Almost all households in Bangladesh are entertaining televisions; the facilities dramatically increased in last two decades. The children along with their parents/family members engaged in television viewing for a long period which creates a significant barrier for health promotion. Even when they are dealing with health-related issues, they frequently end up promoting a product goaded by some quasi-scientific misinformations. With their near universal reach and traction ,the market forces are exerting an overreaching influence to sustain this seemingly unidirectional mass movement toward their construct of ‘‘modernity’’.14
According to WHO, childhood obesity is one of the most stserious public health challenges of the 21 century.
Prevention of obesity in children is vital because the treatment is extremely difficult. The following strategies should be taken to address the complex problem-
l Balanced nutrition to pregnant mothers
l Encourage exclusive breastfeeding
l High importance on physical activity
l Making healthier choice available and banning un-healthy food in cafeteria,(sweetened beverages and energy-dense junk food)
l Screen-time (TV, Computer, Smartphones) to be restricted to maximum 2h/day
l Mandatory 60 min of physical activity daily supervised by parents
l Restriction on eating out at weekends and restricting availability of junk foods at home
Editorial
Childhood ObesityBiswas B K
9
Journal of Diabetic Association Medical College 2019;3(1)9-10
Correspondence to:
Prof. Barun Kanti BiswasDepartment of PaediatricsDiabetic Association Medical College, Faridpur, Bangladesh.E-mail: [email protected]
l Restriction on advertisement of commercial foods on television at prime time and during children's programs and ban on unfair nutrition claims for commercial products
15l Prohibition of promotional gifts with junk foods.
Effectively addressing the complex problem of childhood obesity calls for a sustained, muti-sectoral response involving the public, private, health professional and non-governmental sectors. The role primary and secondary prevention is the mainstay plan for controlling the epidemic. These strategies can be initiated at home and in preschool institutions, schools and after-school care services. However further research needs to be done to examine the most effective strategies of intervention,
15prevention and treatment of obesity in children.
The impact of overweight and obesity in children on lives and economies offers a serious signal and cautionary tale as these health problems rapidly expand into low-and-middle income countries like Bangladesh. So, we should start early actions to prevent obesity in our future generation.
References1. Styne DM. Childhood and Adolescent Obesity.
PCNA2001;48:823-847.
2. Guo SS,Huang C,Maynard, LM,Demerath E,Towne B,Chumlea WC,et al .Body mass index during childhood,adolescene and young adulthood in relation to adult overweight and adiposity.The Fels Longitudinal Study.Int J Obes Relat Metlab Disord 200;24:1628-1635.
3. Neita FJ,Szklo M,Comstock CW. Childhood weight and growth rate as predictors of adult mortality.Am J Epidemiol 1992;136:80-86.
4. Must A,PF Jacques.GE Dallal,CJ Bazema,WH Dietz.Long -term morbidity and mortality of overweight adoloscents.A follow-up of the Harvard Growth Study of 1992 to 1935.N Engl J Med 1992;327:1350-1355.
5. Available from:http://www.who.int/news-room/fact-sheets/detail/obesity –and-overweight[last accessed on 2018 Dec 23].
6. Khadilkar VV,Khadlikar AV.Revised Indian Academy of Pediatrics 2015 growth charts for height,weight and body mass index for 5-18 year-old Indian children.Indian J Endocr Metab 2015;19:470-6.
7. Ahmed QI,Ahmed CB,Ahmed SM.Childhood obesity.Indian J Endocrinol Metab2010;14:19-25
8. Kiranmala N,Das MK,Arora NK.Determinants of childhood obesity: Need for a transsectoral convergent approach.Indian J Pediatr 2013;80 Suppl 1:538-47.
9. Raj M,Kumar RK.Obesity in children & adolescents.[PUBMED] [FULL text]
10. Arora M,Nazar GP,Gupta VK,Perry CL,Reddy KS,Stigler MH. Association with breakfast intake with obesity,dietary and physical activity behavior among urban school-aged adolescents in Delhi,India :Resuts of a cross-sectional study.BMC Public Health 2012;12:881
11. Misra A,Khurana L.The metabolic syndromes in South Asian: Epidemiology,determinants,and prevention.Metab Syndr Relat Disord;7:497-514
12. Raychoudhuri M,Sanyal D. Childhood Obesity: Determinants,evauation and prevention. Indian J Endocrinol Metab 2012;16:192-4
13. Bharati DR,Deshmukh PR,Garg BS. Correlates of overweight & obesity among school going children of Wardha city,central India. Indian J Med Res 2008;127:539-43.
14. Chaturvedi S.Silent drivers of childhood obesity in India. Indian J Public Health 2019;63:91-3
15. Kar SS,Kar SS.Prevention of childhood obesity in India:Way forward .J Nat Sc Biol Med 2015;6:12-7
10
Childhood Obesity Biswas B K

Abstract The Expanded Programme on Immunization is a World Health Organization programme with the goal to make vaccines available to all children. The objective of this study is to find out "Mothers knowledge on immunization of children and immunization status of under five children in selected villages of Modhukhali". For this purpose a descriptive type of cross sectional study was conducted during the period of November 2017 to march 2018. During the survey data were collected from 370 conveniently selected mothers who had at least one child under 5 years. After taking verbal consent a face to face interview was conducted through a pretested questionnaire
The result showed that mean(±SD) age of mother was 26.71(±6.43) years. Most(46.49%) of the respondents have completed primary education and 5.67% have completed graduation. The study revealed that about 98.64% people have knowledge about immunization, 96.46% of people know when to start vaccination of their child, 85.31% population accomplished EPI schedule. About 99% people gave BCG vaccine, 95.40% people gave pentavalent vaccine, 91.62% people gave PCV vaccine and 94.87% people gave OPV vaccine to their child.
EPI services of the country have been improved by some years but yet there are some gaps in rural areas. The health education programme about EPI should be run in the rural areas in a proper organized way. There is also need for strong supervision & monitoring of EPI services throughout the country.
Key word: EPI, Vaccine, Knowledge on Immunization, Immunization status, Under 5 children.
IntroductionExpanded programme on immunization is one of the world health organization programmes which have a goal to make vaccines available to all the children throughout the world.
Globally, immunization currently averts an estimated 2 to 3 million deaths every year. In Bangladesh it has prevented an estimated 2 million deaths from 1987- 2000, and continues
1to prevent approximately 200,000 deaths each year . WHO introduced EPI (Expanded Programme on Immunization) in 1977 at Alma-Ata, the capital of Kazakhastan for the underdeveloped countries. Subsequently Bangladesh has launched EPI. In our country immunization coverage was 52% in 1991, 53% in 2000, 79% in 2010, 80% in 2011and 81% in 2013 which signifies our excellent success for
1prevention of communicable diseases in successive years . So, EPI in Bangladesh has been recognized for its sustained high coverage and great contribution to the reduction of childhood morbidity and mortality and it received two
1GAVI best performance award in 2009 and 2012.
A recent estimate suggest that immunization programmes annually prevent 3.2 million child deaths,and represent one of the most cost effective health intervention. Data indicate that more extensive delivary of EPI could further improve
2,3,4,5,6the survival and health status of children.
Bangladesh officially initiated EPI activities in 1979, but EPI efforts were seriously considered only after 1985 when the country made its commitment at the United Nations to reach universal child immunization by 1990.
The intensified immunization program was expanded in phases. In 1985 the first phase of EPI commenced in 8 thana; it expanded to 190 thana in 1988, and near universal access
7to immunization service was achieved by the end of 1989.
Timely vaccination, i.e., the receipt of all scheduled vaccinations in an age-appropriate fashion, is critical for the prevention of deadly diseases in infants and achievement of the UN Millennium Development Goal to reduce infant
Original Article
Mothers Knowledge on EPI and Immunization Status of Their Under Five Children
1 2 3 4 5 6 7Huda S M N , Asaduzzaman A K M , Latif A , Akhiruzzaman , Zaman F , Islam M A , Forhad C M R Q
1. Dr. S.M. Nazmul Huda, Lecturer, Department of Community Medicine, Diabetic Association Medical College, Faridpur.
2. Professor Dr. AKM Asaduzzaman, Professor, Department of Community Medicine, Diabetic Association Medical College, Faridpur.
3. Dr. Md. Abdul Latif, Consultant Radiology and Imaging Department, General Hospital, Madaripur.
4. Dr. Akhiruzzaman, Assistant Professor, Department of Community Medicine, Diabetic Association Medical College, Faridpur.
5. Dr. Fouzia Zaman, Lecturer, Department of Community Medicine, Diabetic Association Medical College, Faridpur.
6. Dr. Mohammad Alimul Islam, Assistant Registrar, Medicine, Faridpur Medical College Hospital.
7. Dr. C.M. Reza Qureshi Forhad, Professor (CC), Department of Biochemistry, US Bangla Medical College, Dhaka.
Correspondence to:Dr. S.M. Nazmul Huda; MBBSLecturer, Department of Community MedicineDiabetic Association Medical College, Faridpur.Email: [email protected]
11
Journal of Diabetic Association Medical College 2019;3(1)11-14
Mothers Knowledge on EPI and Immunization Status of Their Under Five Children Huda S M N
mortality. Infants, especially in rural or underprivileged settings often receive delayed vaccinations leaving them susceptible to vaccine-preventable illnesses early in the
8first year of life.
More research can help to find out the laps and gaps of immunization coverage in rural area and helps to strength the programme throught the country.
Methodology:This cross sectional study was conducted in selected villages of modhukhali upazilla during the period of November 2017 to March 2018 to assess the Mothers Knowledge on Immunization of Children and Immunization Status of Their Under Five Children. During the survey data were collected from 370 conveniently selected mothers who had at least one child under 5 years. After taking verbal consent a face to face interview was conducted through a pretested questionnaire. At first the interview questionnaire were checked and rechecked to reduce the errors if any. Secondly necessary corrections were made. Thirdly the responses were coded adequately. Fourthly a master sheet was prepared based on variables used in the study. Finally necessary calculations were made from the master sheet and were presented data by tabulations and charts.
Result:The findings of the survey have been presented in the following section.
Table 1: Socio demographic status of the respondents (n=370)
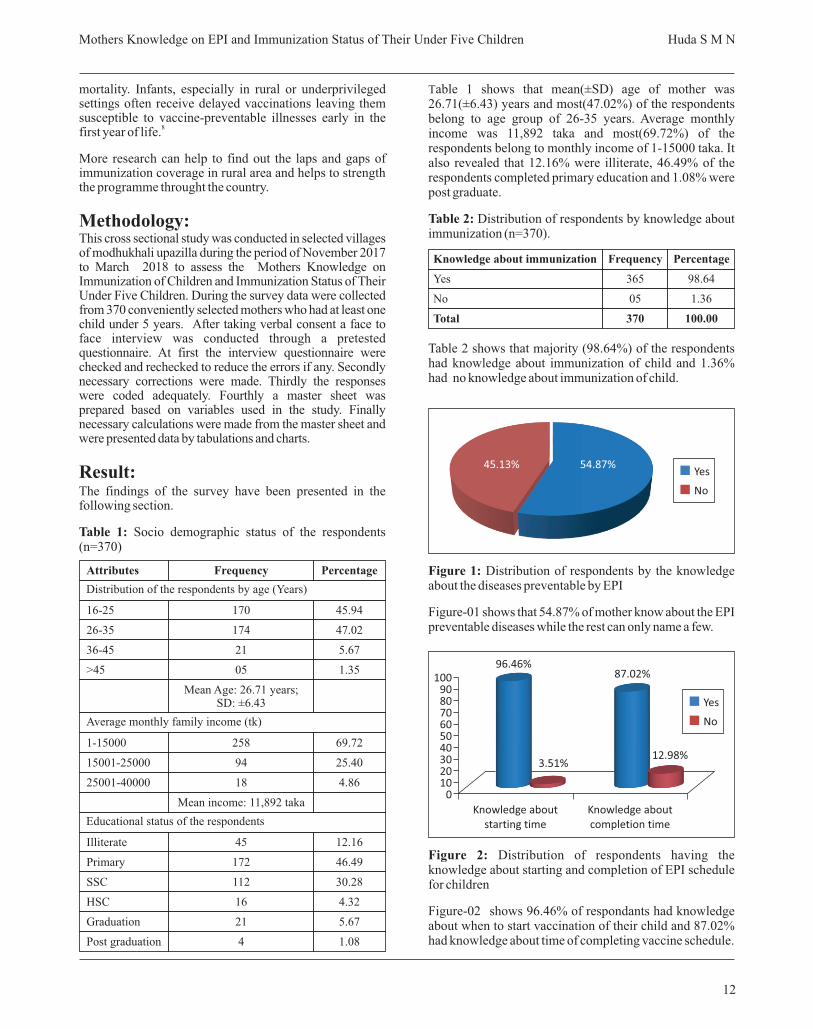
Table 1 shows that mean(±SD) age of mother was 26.71(±6.43) years and most(47.02%) of the respondents belong to age group of 26-35 years. Average monthly income was 11,892 taka and most(69.72%) of the respondents belong to monthly income of 1-15000 taka. It also revealed that 12.16% were illiterate, 46.49% of the respondents completed primary education and 1.08% were post graduate.
Table 2: Distribution of respondents by knowledge about immunization (n=370).
Table 2 shows that majority (98.64%) of the respondents had knowledge about immunization of child and 1.36% had no knowledge about immunization of child.
Figure 1: Distribution of respondents by the knowledge about the diseases preventable by EPI
Figure-01 shows that 54.87% of mother know about the EPI preventable diseases while the rest can only name a few.
Figure 2: Distribution of respondents having the knowledge about starting and completion of EPI schedule for children
Figure-02 shows 96.46% of respondants had knowledge about when to start vaccination of their child and 87.02% had knowledge about time of completing vaccine schedule.
12
Attributes
16-25
26-35
36-45
>45
1-15000
15001-25000
25001-40000
Illiterate
Primary
SSC
HSC
Graduation
Post graduation
Frequency
170
174
21
05
Mean Age: 26.71 years; SD: ±6.43
258
94
18
Mean income: 11,892 taka
45
172
112
16
21
4
Percentage
45.94
47.02
5.67
1.35
69.72
25.40
4.86
12.16
46.49
30.28
4.32
5.67
1.08
Distribution of the respondents by age (Years)
Average monthly family income (tk)
Educational status of the respondents
Knowledge about immunization
Yes
No
Total
Frequency
365
05
370
Percentage
98.64
1.36
100.00
Yes
No
45.13% 54.87%
100908070605040302010
0
3.51%12.98%
87.02%96.46%
Knowledge about starting time
Knowledge about completion time
Yes
No
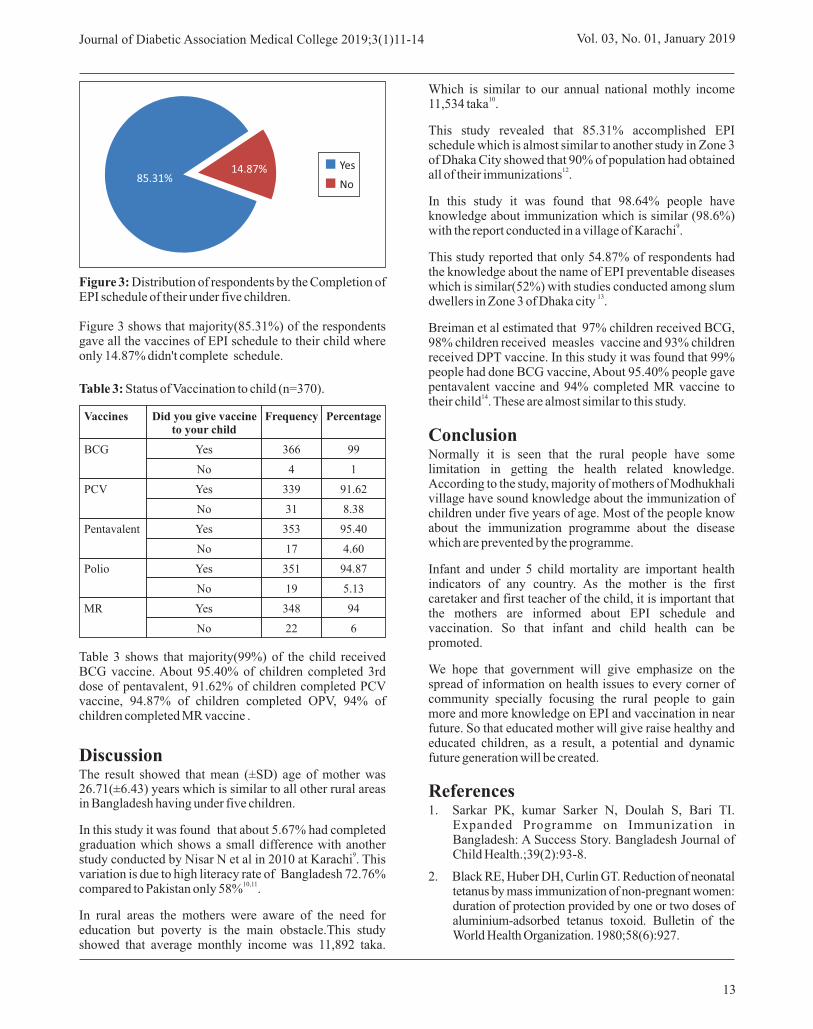
Figure 3: Distribution of respondents by the Completion of EPI schedule of their under five children.
Figure 3 shows that majority(85.31%) of the respondents gave all the vaccines of EPI schedule to their child where only 14.87% didn't complete schedule.
Table 3: Status of Vaccination to child (n=370).
Table 3 shows that majority(99%) of the child received BCG vaccine. About 95.40% of children completed 3rd dose of pentavalent, 91.62% of children completed PCV vaccine, 94.87% of children completed OPV, 94% of children completed MR vaccine .
DiscussionThe result showed that mean (±SD) age of mother was 26.71(±6.43) years which is similar to all other rural areas in Bangladesh having under five children.
In this study it was found that about 5.67% had completed graduation which shows a small difference with another
9study conducted by Nisar N et al in 2010 at Karachi . This variation is due to high literacy rate of Bangladesh 72.76%
10,11compared to Pakistan only 58% .
In rural areas the mothers were aware of the need for education but poverty is the main obstacle.This study showed that average monthly income was 11,892 taka.
Which is similar to our annual national mothly income 1011,534 taka .
This study revealed that 85.31% accomplished EPI schedule which is almost similar to another study in Zone 3 of Dhaka City showed that 90% of population had obtained
12all of their immunizations .
In this study it was found that 98.64% people have knowledge about immunization which is similar (98.6%)
9with the report conducted in a village of Karachi .
This study reported that only 54.87% of respondents had the knowledge about the name of EPI preventable diseases which is similar(52%) with studies conducted among slum
13dwellers in Zone 3 of Dhaka city .
Breiman et al estimated that 97% children received BCG, 98% children received measles vaccine and 93% children received DPT vaccine. In this study it was found that 99% people had done BCG vaccine, About 95.40% people gave pentavalent vaccine and 94% completed MR vaccine to
14their child . These are almost similar to this study.
ConclusionNormally it is seen that the rural people have some limitation in getting the health related knowledge. According to the study, majority of mothers of Modhukhali village have sound knowledge about the immunization of children under five years of age. Most of the people know about the immunization programme about the disease which are prevented by the programme.
Infant and under 5 child mortality are important health indicators of any country. As the mother is the first caretaker and first teacher of the child, it is important that the mothers are informed about EPI schedule and vaccination. So that infant and child health can be promoted.
We hope that government will give emphasize on the spread of information on health issues to every corner of community specially focusing the rural people to gain more and more knowledge on EPI and vaccination in near future. So that educated mother will give raise healthy and educated children, as a result, a potential and dynamic future generation will be created.
References1. Sarkar PK, kumar Sarker N, Doulah S, Bari TI.
Expanded Programme on Immunization in Bangladesh: A Success Story. Bangladesh Journal of Child Health.;39(2):93-8.
2. Black RE, Huber DH, Curlin GT. Reduction of neonatal tetanus by mass immunization of non-pregnant women: duration of protection provided by one or two doses of aluminium-adsorbed tetanus toxoid. Bulletin of the World Health Organization. 1980;58(6):927.
13
Journal of Diabetic Association Medical College 2019;3(1)11-14 Vol. 03, No. 01, January 2019
85.31%14.87% Yes
No
Vaccines
BCG
PCV
Pentavalent
Polio
MR
Did you give vaccine to your child
Yes
No
Yes
No
Yes
No
Yes
No
Yes
No
Frequency
366
4
339
31
353
17
351
19
348
22
Percentage
99
1
91.62
8.38
95.40
4.60
94.87
5.13
94
6

14
3. Koenig MA, Khan MA, Wojtyniak B, Clemens JD, Chakraborty J, Fauveau V, Phillips JF, Akbar J, Barua US. Impact of measles vaccination on childhood mortality in rural Bangladesh. Bulletin of the World Health organization. 1990;68(4):441.
4. Arya SC. Human immunization in developing countries: practical and theoretical problems and prospects. Vaccine. 1994 Jan 1;12(15):1423-35.
5. Pan American Health Organization. The Impact of the Expanded Program on Immunization and the Polio Eradication Initiative on Health Systems in the Americas. Final Report of the 'Taylor Commission' 1995. Vol. PAHO Document No. 1995-00003.
6. Ginneken JV, Bairagi R, Francisco AD, Sardar AM, Vaughan P. Health and demographic surveillance in Matlab: past, present and future. Dhaka: International Centre for Diarrhoeal Disease Research, Bangladesh 1998.
7. Talukdar LR, Basu RN, Shareef M, Khan MR. The near miracle: how immunization services are delivered. In: Huq M (ed), Near Miracle in Bangladesh. Dhaka: University Press Limited; 1991, 57-74
8. Vasudevan L, Labrique AB, Mehra S, Wu L, Levine O, Feikin D, Klemm R, Christian P, West Jr KP. Maternal determinants of timely vaccination coverage among infants in rural Bangladesh. Vaccine. 2014 Sep 22;32(42):5514-9.
9. Nisar N, Mirza M, Qadri MH. Knowledge, Attitude and Practices of mothers regarding immunization of one year old child at Mawatch Goth, Kemari Town, Karachi. Pak J Med Sci. 2010 Jan 1;26(1):183-6.
10. Department of Film and Production. Government of the Peoples Republic of Bangladesh 2017.
11. Pakistan Literacy Rate stands at 58pc, International The News, April 27,2017.
12. Perry H, Weierbach R, Hossain I, Islam RU. Childhood immunization coverage in zone 3 of Dhaka City: the challenge of reaching impoverished households in urban Bangladesh. Bulletin of the World Health Organization. 1998;76(6):565.
13. Quaiyum A, Tunon C, Hel Baqui A, Yum ZQ, Khatun J. Impact of national immunization days on polio-related knowledge and practice of urban women in Bangladesh. Health Policy and Planning. 1997 Jan 1;12 (4):363-71.
14. Breiman RF, Streatfield PK, Phelan M, Shifa N, Rashid M, Yunus M. Effect of infant immunisation on childhood mortality in rural Bangladesh: analysis of health and demographic surveillance data. The Lancet. 2004 Dec 18;364(9452):2204-11.
Mothers Knowledge on EPI and Immunization Status of Their Under Five Children Huda S M N

Abstract Ultrasonogram is a useful tool in providing valuable information for the diagnosis of of acute appendicitis. Ultrasound could increase the diagnostic accuracy in those patients presented with unclear symptoms and signs of acute appendicitis . The aim of this study is to evaluate the effectiveness of U/S in the diagnosis of acute appendicitis. This cross sectional study was carried out in the department of Radiology & Imaging, Sir Salimullah Medical College, Dhaka during the period of January'2016 to December'2016. It included 40 patients suspected to have acute appendicitis. Ultrasound (U/S) was done for all these patients. There were (18) males represent (45%) and (22) females represent (55%). These patients are grouped according to gender, age, signs & symptoms, the result of U/S examination and histopathological result. Ultrasound was positive in (33) patients (82.5 %) and negative in (07) patients (17.5%). Four patients out of (07) had true negative results while (03) patients were false negative. Ultrasound sensitivity was (91.4 %) in diagnosing acute appendicitis, specificity was (80%), accuracy rate was (92.5%), positive predictive value (96.7%) and negative predictive value (57.1%). As abdominal ultrasound showed high validity parameters for the diagnosis of acute appendicitis, the study concluded that ultrasonogram is a useful diagnostic modality in preoperative evaluation of acute appendicitis and can be used for planning of appropriate management.
Keyword: Ultrasonographic Evaluation, Acute Appendicitis, Histopathological Correlation.
IntroductionAcute appendicitis is still one of the most common surgical abdominal emergencies. In 70% of patients with acute appendicitis, the diagnosis is made clinically based on
classic sign and symptoms. In the remaining 30% of patients with uncertain clinical finding radiological imaging
1is needed to establish the diagnosis. In acute appendicitis, the preoperative diagnosis is wrong in 30% and despite the improvement in surgical techniques, the negative
2appendicectomy rate continues to be as high as 25%. Even despite the uncertainty of diagnosis, appendicitis demands prompt treatment in order not to be neglected and misdiagnosed leading to progression of the disease with associated morbidity and mortality that may include the risk of perforation which happens in approximately
3one third of the cases. The newer techniques of ultrasonography (US) and computed tomography (CT) have shown great promise in evaluation of patients with
4suspected acute appendicitis. The advantages of ultrasound examination to diagnose appendicitis is well known; the study is quick, widely available in most cases, non-invasive, repeatable and has been known to be accurate. High resolution ultrasound enables visualization of the inflamed appendix and can assess a variety of relevant disease. Bed-side ultrasound in evaluation of patients with suspected
5appendicitis is used nowadays as preliminary test. One expert team has identified three criteria for diagnosis of appendicitis by ultrasound examination which include; tender non compressible appendix, no peristalsis of the appendix and the overall diameter of the appendicular
6lumen is greater than 6mm. Demonstration of 7appendicolith alone does not suggest acute appendicitis.
Computed tomography (CT) had a good role in the diagnosis of acute appendicitis but ionizing radiation and the use of intravenous contrast made it a relatively invasive
8test. It is also not avaiable in all centres. It should be emphasized that USG does not replace clinical diagnosis, but is a useful adjunct in the diagnosis of acute appendicitis. Studies have demonstrated the potential to achieve higher diagnostic accuracy with imaging techniques than may be
9achieved with clinical acumen alone.
Original Article
Ultrasonographic Evaluation in the Diagnosis of Acute Appendicitis with Histopathological Correlation
1 2 3 4 5 6 7 8 9Saiham K S , Hossain R , Halder B A , Satter A , Yesmin L , Naz F M , Alam S , Ahmad M R , Hossin I
1. Dr. Kazi Shantono Saiham Consultant, Radiology and Imaging, Doctors Care General Hospital & Diagnostic Center, Brahmanbaria.
2. Md. Rued Hossain Associate Professor & Head of the department, Department of Radiology and Imaging, Sir Salimullah Medical College, Dhaka.
3. Dr. Bibekananda Halder Associate Professor, Department of Radiology and Imaging Sir Salimullah Medical College, Dhaka.
4. Dr. Asifa Satter Associate Professor, Department of Radiology and Imaging Sir Salimullah Medical College, Dhaka.
5. Dr. Lovely Yesmin Medical officer, NITOR, Dhaka
6. Dr. Fouzia Mujib Un Naz, Assistant Professor Department of Radiology & Imaging, Dhaka Dental College.
7. Dr. Md. Shafiul Alam Assistant Professor, Department of Dental Radiology & Imaging Dhaka Dental College.
8. Dr. Md. Rasel Ahmad Medical Educationist and Dental Surgeon, Consultant United Oro-Dental & Maxillofacial Surgery.
9. Dr .Md. Immam Hossin Lecturer, Department of Radiology & Imaging Dhaka Dental College
Correspondence to:Dr. Kazi Shantono SaihamConsultant, Radiology and Imaging, Doctors Care GeneralHospital & Diagnostic Center, Brahmanbaria.Email: [email protected]
15
Journal of Diabetic Association Medical College 2019;3(1)15-19
Ultrasonographic Evaluation in the Diagnosis of Acute Appendicitis with Histopathological Correlation
Saiham K S
Objectives of the study:This study was designed to a) evaluate the validity of ultrasonography (USG) in the diagnosis of acute appendicitis. Specific objectives were to b) diagnose clinically suspected acute appendicitis based on ultrasonographic findings, c) compare the ultrasonological diagnosis with that of histopathological diagnosis and to find out d) the sensitivity, specificity, positive predictive value, negative predictive value and accuracy of transabdominal ultrasuond in the diagnosis of acute appendicitis.
Materials and MethodsThis cross sectional study was conducted in department of Radiology & Imaging, Sir Salimullah Medical College, Dhaka in collaboration with the department of Pathology of the same institute from January 2016 to December 2016. Patients attended at the General Surgery department with clinically suspected acute appendicitis referred to the Department of Radiology and Imaging, Sir Salimullah Medical College, Dhaka was included in the study. A total of 40 patients were included in this study after taking written informed consent, who could fulfill the selection criteria as defined below.
Inclusion criteria: l Patients of both sexes and of all ages having clinical
suspicion of acute appendicitis referred for USG examination.
Exclusion criteria:l Patients unwilling to give consent.
l Patients who are unwilling or unfit for surgery.
l Non availability of biopsy report.
l Diagnosis of any disease other than acute appendicitis.
Transabdominal ultrasonography was performed by Logiq P5 GE healthcare ultrasound Machine.A linear array transducer ; 11L Linear Probe (5-13 MHz) and convex Probe 4C (1.4-5MHz) used in examination.Patients were followed up upto their final diagnosis by histopathology. Their ultrasonogram and histopathological diagnoses were compared to find out the the validity of USG in the diagnosis of acute appendicitis. Appropriate data were collected by using a preformed data sheet. All the relevant collected data were compiled on a master chart and statistical analyses were done by computer software SPSS-19.0. The results were presented as text, tables, figures, charts, diagrams and the validity test was done.
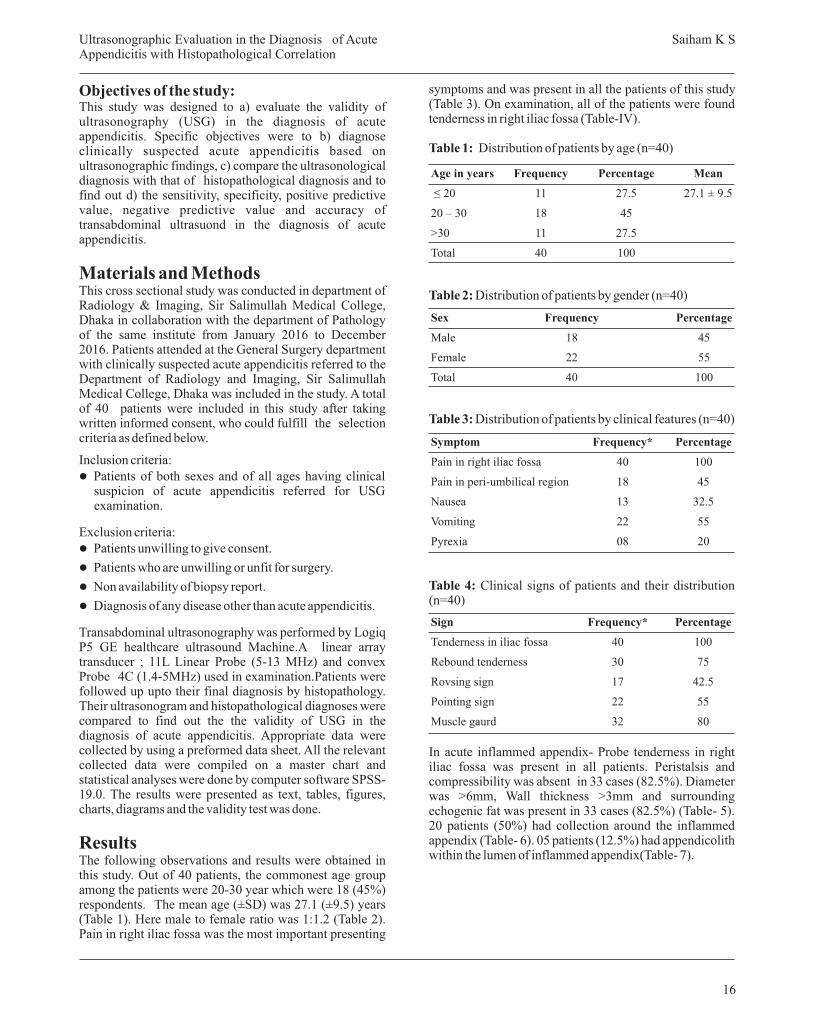
ResultsThe following observations and results were obtained in this study. Out of 40 patients, the commonest age group among the patients were 20-30 year which were 18 (45%) respondents. The mean age (±SD) was 27.1 (±9.5) years (Table 1). Here male to female ratio was 1:1.2 (Table 2). Pain in right iliac fossa was the most important presenting
symptoms and was present in all the patients of this study (Table 3). On examination, all of the patients were found tenderness in right iliac fossa (Table-IV).
Table 1: Distribution of patients by age (n=40)
Table 2: Distribution of patients by gender (n=40)
Table 3: Distribution of patients by clinical features (n=40)
Table 4: Clinical signs of patients and their distribution (n=40)
In acute inflammed appendix- Probe tenderness in right iliac fossa was present in all patients. Peristalsis and compressibility was absent in 33 cases (82.5%). Diameter was >6mm, Wall thickness >3mm and surrounding echogenic fat was present in 33 cases (82.5%) (Table- 5). 20 patients (50%) had collection around the inflammed appendix (Table- 6). 05 patients (12.5%) had appendicolith within the lumen of inflammed appendix(Table- 7).
16
Age in years
≤ 20
20 – 30
>30
Total
Frequency
11
18
11
40
Percentage
27.5
45
27.5
100
Mean
27.1 ± 9.5
Sex
Male
Female
Total
Frequency
18
22
40
Percentage
45
55
100
Symptom
Pain in right iliac fossa
Pain in peri-umbilical region
Nausea
Vomiting
Pyrexia
Frequency*
40
18
13
22
08
Percentage
100
45
32.5
55
20
Sign
Tenderness in iliac fossa
Rebound tenderness
Rovsing sign
Pointing sign
Muscle gaurd
Frequency*
40
30
17
22
32
Percentage
100
75
42.5
55
80
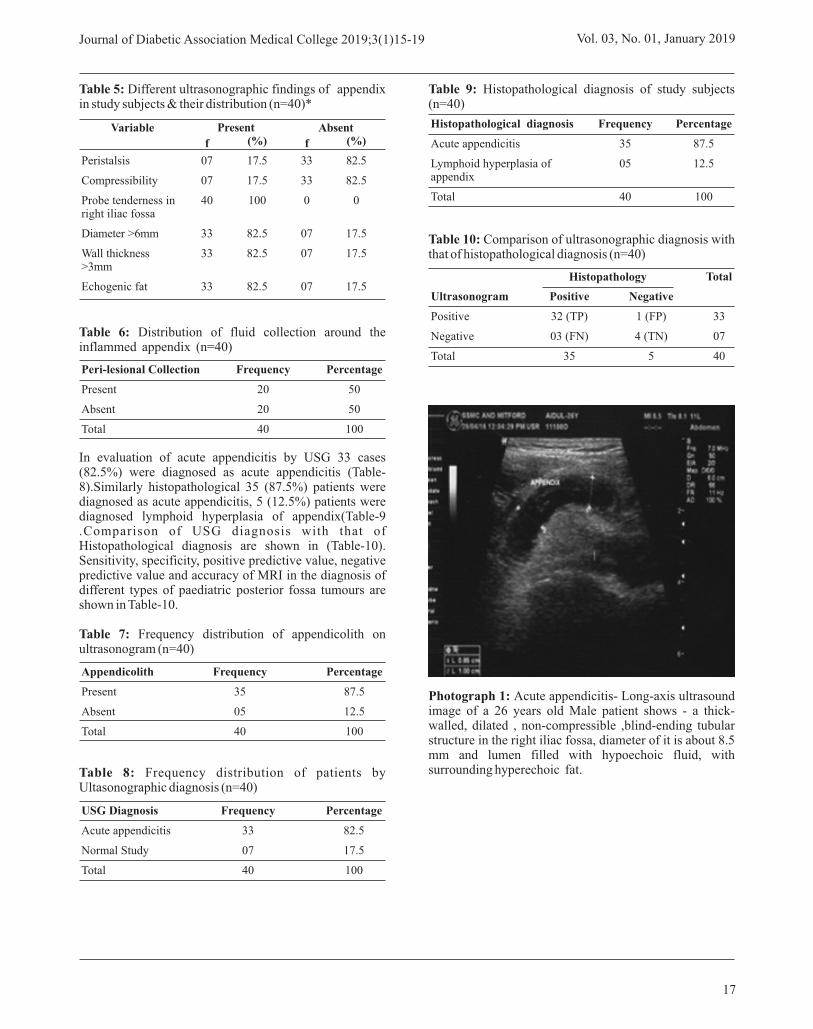
Table 5: Different ultrasonographic findings of appendix in study subjects & their distribution (n=40)*
Table 6: Distribution of fluid collection around the inflammed appendix (n=40)
In evaluation of acute appendicitis by USG 33 cases (82.5%) were diagnosed as acute appendicitis (Table-8).Similarly histopathological 35 (87.5%) patients were diagnosed as acute appendicitis, 5 (12.5%) patients were diagnosed lymphoid hyperplasia of appendix(Table-9 .Comparison of USG diagnosis with that of Histopathological diagnosis are shown in (Table-10). Sensitivity, specificity, positive predictive value, negative predictive value and accuracy of MRI in the diagnosis of different types of paediatric posterior fossa tumours are shown in Table-10.
Table 7: Frequency distribution of appendicolith on ultrasonogram (n=40)
Table 8: Frequency distribution of patients by Ultasonographic diagnosis (n=40)
Table 9: Histopathological diagnosis of study subjects (n=40)
Table 10: Comparison of ultrasonographic diagnosis with that of histopathological diagnosis (n=40)
Photograph 1: Acute appendicitis- Long-axis ultrasound image of a 26 years old Male patient shows - a thick-walled, dilated , non-compressible ,blind-ending tubular structure in the right iliac fossa, diameter of it is about 8.5 mm and lumen filled with hypoechoic fluid, with surrounding hyperechoic fat.
17
Journal of Diabetic Association Medical College 2019;3(1)15-19 Vol. 03, No. 01, January 2019
Ultrasonogram
Positive
Negative
Total
Positive
32 (TP)
03 (FN)
35
Negative
1 (FP)
4 (TN)
5
33
07
40
Histopathology Total
Histopathological diagnosis
Acute appendicitis
Lymphoid hyperplasia of appendix
Total
Frequency
35
05
40
Percentage
87.5
12.5
100
USG Diagnosis
Acute appendicitis
Normal Study
Total
Frequency
33
07
40
Percentage
82.5
17.5
100
Appendicolith
Present
Absent
Total
Frequency
35
05
40
Percentage
87.5
12.5
100
Peri-lesional Collection
Present
Absent
Total
Frequency
20
20
40
Percentage
50
50
100
Peristalsis
Compressibility
Probe tenderness in right iliac fossa
Diameter >6mm
Wall thickness >3mm
Echogenic fat
07
07
40
33
33
33
17.5
17.5
100
82.5
82.5
82.5
33
33
0
07
07
07
82.5
82.5
0
17.5
17.5
17.5
Present AbsentVariable
ff (%)(%)

18
Photograph 2: Long-axis & cross-sectional transabdominal ultrasound image of acute appendicitis of 44 yrs male shows- a thick-walled, dilated, non-compressible ,blind-ending tubular structure in the right iliac fossa, diameter of it is about 8.3 mm and lumen filled with hypoechoic fluid .
Photograph 3: Acute appendicitis in a 22 yrs old female- long axis & cross-sectional image of ultrasound shows a distended, fluid-filled appendix that measured 6.9 mm in diameter. Echogenic fecolith with posterior shadowing within a fluid-filled dilated appendix.
Photograph 4: Long-axis & cross-sectional transabdominal ultrasound image of acute appendicitis of 15 yrs old male shows- a thick-walled, dilated, non-compressible ,blind-ending tubular structure in the right iliac fossa, diameter of it is about 7.8 mm and lumen filled with hypoechoic fluid, with surrounding hyperechoic fat.
DiscussionIn this study it was observed that most common age group among the patients were 20-30 year which were 18 (45%) respondents. Mean ± SD of age of the patients was 27.1 ± 9.5 years. Adesunkanmi,1993 observed 90% of the cases
10had the commonest age group of 10-30 years.
The incidence of acute appendicitis is variable in both sexes. Male to female ratio in the present study was 1:1.2. A study was done by Barber et al., 1997 and according to his study male to female ratio was 2.2:1.2. It can be seen from the given statistics, that there are no set patterns for incidence of the disease in both sexes and it is highly
11variable.
Acute appendicitis has been found to presenting with typical symptoms. Pain was the most important presenting symptoms and was present in all the patients of this study. This similar observation might be explained by the study done by Sharma et al., 2007 who reported lower abdominal pain in all cases of appendicitis. In this study 13 (32.5) patients experienced nausea and 22(55.0%) had vomiting,
13once or twice usually in the early part of disease. Barber et al, 1997 observed that 51-69% of patients with appendicitis
11vomit.
Regarding the tenderness in acute appendicitis right iliac fossa tenderness was found in all the patients of this study. Incidence of tenderness in this study compares well with other studies where tenderness could be elicited in 96-100% patients with appendicitis (Adesunkanmi,1993;
10,11Barber et al.,1997). Muscle guarding was found in
Ultrasonographic Evaluation in the Diagnosis of Acute Appendicitis with Histopathological Correlation
Saiham K S

32(80.0%) of the patients which matched with other studies. A study by Adesunkanmi et al.,1993 observed
10muscle guarding was present in 81% cases. This present study showed that rebound tenderness in 30 (75.0%) cases, which shows similiarity with two different studies done by
10Adesunkanmi,1993.
Peristalsis and compressibility of appendix was absent in 33 (82.5%) cases of this study and Probe tenderness in right iliac fossa was present in all patients. In a study by Sharma et al., 2007 found graded tenderness 54.2% which
13is not similar with present study .In this study diameter of the lumen of appendix was >6mm,Wall thickness >3mm and echogenic fat was present in 82.5% 82.5% and 17.5% cases respectively. In a study by Helo et al., 2012 found diameter >6mm in 47% and Echogenic fat in 66% cases, which is not similar to my study findings. In this current study it was observed that 50% of the patients had collection around the inflammed appendix. Sharma et al., 2007 study findings regarding fluid collection didn't match
13with our study which was 19.4%.
Among 40 patients in this study, 05 patients (12.5%) had appendicolith seen within the lumen of appendix . On the other hand study done by Sharma et al., 2007 among 118
13patients, no patient was found with appendicolith.
This present study showed that ultrasound was able to find appendicitis in 33 (82.5%) patients while 7 (17.5%) were negative for appendicitis. The diagnosis of all the patients has been confirmed by histopathology to elucidate the disease. Histopathology was taken as the gold standard test for the comparison. USG diagnosis was weighted against the histopathological diagnosis of the disease. Total 35 (87.5%) cases were confirmed on histopathology while 5 (12.5%) were found negative. Out of 35 positive cases on histopathology, 32 were positive on ultrasound that reveals 91.4% sensitivity, which is comparable with the study by
12Qureshi et al., 2014 that shows sensitivity of 91.5%. This study findings was higher than some other study where
13sensitivity was 63.3% in the study of Sharma et al., 2007. Out of 5 negative cases on histopathology 4 were negative on ultrasound which shows specificity of 80.0 % which match with a study by Sharma et al., 2007 which shows specificity
1382.1%. Our findings was lower than the study observeb by 12Qureshi et al., 2014 that shows specificity 87.5%.
The sensitivity of ultrasound in the diagnosis of acute appendicitis in the present study was 91.4%, specificity 80%, positive predictive value 96.7%, negative predictive value 57.1% and accuracy 92.5%, which might be comparable with the study by Qureshi et al., 2014 which reported about the specificity 80%, positive predictive value 96.4%, negative predictive value 73.7% and
12accuracy 90.7%.
ConclusionAs abdominal ultrasound showed high validity parameters for the diagnosis of acute appendicitis, the study concluded
that ultrasonogram is a useful diagnostic modality in preoperative evaluation of acute appendicitis and can be used for planning of appropriate management.
References1. Orr RK, Porter D, Hartman D: ultrasonography to
evaluate adults for appendicitis: decision making based on meta-analysis and probabilistic reasoning. Academic Emerg Med 1995 Jul;2(7);644-50
2. Parulekar SG. Ultrasonographic finding in disease of the appendix. J ultrasound Med. 1993; 2: 59.
3. Flum DR, Koepsell T: The clinical and economic correlates of misdiagnosed appendicitis: Nationwide analysis. Arch Surg 2002,137:799-804
4. Adams DH, Fine C, Brooks DC. High-resolution real-time ultrasonography. A new tool in the diagnosis of acute appendicitis. Am J Surg 1988; 155:93-7
5. Pieper R, Kager L,. Acta Chir-Scand 1982, Fischer T, Filimonow S, Petersein J, Beyersdorff D, Muhler M, Hamm B. Ultraschall Med 2002
6. Jeffery RB JR, Laing FC, Townsend RR. Acute appendicitis. Sonographic criteria based on 250 cases. Radiology 1998;167: 357-359.
7. Lowe LH, Penney MW, Scheker LE, et al. Appendicolith revealed on CT in children with suspected appendicitis: how speci fi c is it in the diagnosis of appendicitis? AJR Am J Roentgenol 2000; 175:981-4
8. Rao PM, Rhea JT, Novelline RA, McCabe CJ, Lawrason JN, Berger DL. Helical CT technique for the diagnosis ofappendicitis prospective evaluation of a focused appendix CT examination. Radiology 1997; 202:139-144.
9. Malik K , Khan A, Waheed I. Evaluation of the Alvarado score in the diagnosis of acute appendicitis. J Coll Physicians Surg Pak 2000; 10: 392-4
10. Adesunkanmi, AR. Acute appendicitis: a prospective study of 54 cases. West Afr J Med, 1993; 12 (4),pp. 197-200.
11. Barber, MD., Mclaren, J., Rainey, JB. Recurrent appendicitis. Br J Surg. 1997; 84.pp. 110-112.
12. Qureshi, A., Sultan, N., Aziz, A., Sheikh, B. Sensitivity of Ultrasonography in the Diagnosis of acute appendicitis as compared to clinical, per operative and histopathologic findings. Pak J Surg. 2014; 30(3).pp.205-210.
13. Sharma, R., Kasliwal, DK., Sharma, RG. Evaluation of negative appendicectomy rate in cases of suspected acute appendicitis and to study the usefulness of ultrasonography in improving the diagnostic accuracy. Indian J. Surg. 2007; 69.pp.194-197.
19
Journal of Diabetic Association Medical College 2019;3(1)15-19 Vol. 03, No. 01, January 2019

Abstract This descriptive type of cross sectional study was conducted during the period of September 2017-February2018 to assess the status of environmental sanitation and the level of literacy and practices of hygiene of rural mothers in selected villages of Bhanga, Faridpur. Sample size was 190 and the respondents were rural mothers. Data were collected from 190 rural mothers through convenient sampling. After taking verbal consent, a face to face interview was conducted through a pre-tested semi-structural questionnaire. The study revealed that majority of the respondents (56.32%) was illiterate. The study showed that all most all (97.36%) respondents used tube well water for drinking purpose. The study also showed that majority (91.57%) had knowledge about safe water. It was also revealed from the study that majority of the respondents had the idea about water borne diseases caused by consumption of unsafe water. Majority 73.68% respondents lived in Kacha house and only 18.95% respondents had sanitary latrines. It is concluded from the study that there is inadequate knowledge about environmental sanitation particularly housing and disposal of human excreta and also the rate of illiteracy is significantly high amongst respondents.
Keyword: Environmental sanitation, rural mothers.
IntroductionThe world Health Organization defines environmental sanitation as "the control of all those factors in man's physical environment which exercise or may exercise a deleterious effect on his physical development, health and survival”. Of the three ecological factors (agent, host and environment) responsible for disease, the disease agent is usually identified with the help of the laboratory, the host is available for study but the environment from which the patient comes is largely unknown. Yet frequently, the key to the nature, occurrence, prevention and control of disease lies in the environment. Without this knowledge, this key may not be available to the physician who desires to cure disease, prevent or control it. The United Nations conference on the Human Environment, held in Stockholm in 1972 stressed the need to improve health by improving
1environmental sanitation .
Our Country is still lagging far behind many countries in the field of environmental sanitation. The basic problems of safe water supply end sanitary disposal of human excreta are yet to be solved. Much of the ill-health in the country is due to defective environment. Since more than 80 percent of the population live in rural areas the problem is one of
rural sanitation.
Studies in Matlob have shown that safe drinking water alone was not enough to control cholera and even water use
2for other domestic purpose was also important . Improvements in both water supply and sanitation are necessary if health in developing countries is to be
3improved .
Adverse environmental conditions affect health status of its inhabitants. In order to find out the status of environmental sanitation in rural areas the present study was under taken.
Methodology This cross sectional study was conducted at two purposively selected villages (namely RASIBPUR and SHARIFABAD) of GHARUA Union of BHANGA Upazila, Faridpur. Study period was from 10.09.2017 to 12.02.2018 to assess the status of environmental sanitation, level of literacy and practices of hygiene of rural mothers. All the 778 households of the two selected villages constituted the study population. During the survey, data were collected from the rural mothers of 190 households through convenient sampling after taking a verbal consent. So the total sample size was 190. Data were collected through a pretested questionnaire by face to face interview. At first the interview questionnaire were checked and rechecked to reduce the errors if any. Then necessary corrections were made. Thirdly the responses were coded properly. Finally a master sheet was prepared based on variables used in the study. Finally necessary calculations were made from the master sheet and data were presented by tables and charts.
Original Article
A Study on Environmental Sanitation in Some Selected Villages of Bhanga, Faridpur
1, 2Rahman M T Asaduzzaman A K M
1 Mohammad Tanvir Rahman, psc,Engrs Major,Utility Shifting Officer, Service Area-3 Padma Bridge Rail Link Project (PBRLP), Jajira, Shariatpur, Bangladesh.
2 Dr. AKM AsaduzzamanProfessor and Head, Department of Community Medicine Diabetic Association Medical College, Faridpur.
Correspondence to:Mohammad Tanvir Rahman, psc, EngrsMajor,Utility Shifting Officer, Service Area-3Padma Bridge Rail Link Project (PBRLP), Jajira, Shariatpur, Bangladesh. Email: [email protected]
20
Journal of Diabetic Association Medical College 2019;3(1)20-23
A Study on Environmental Sanitation in Some Selected Villages of Bhanga, Faridpur Rahman M T
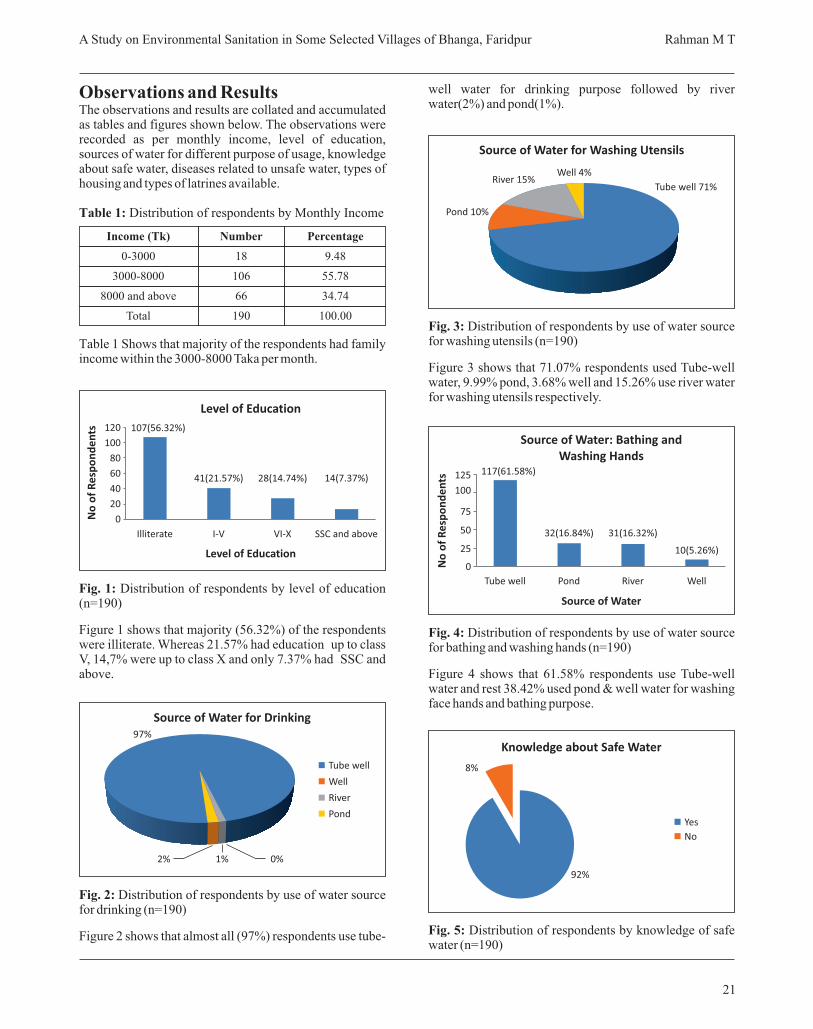
Observations and ResultsThe observations and results are collated and accumulated as tables and figures shown below. The observations were recorded as per monthly income, level of education, sources of water for different purpose of usage, knowledge about safe water, diseases related to unsafe water, types of housing and types of latrines available.
Table 1: Distribution of respondents by Monthly Income
Table 1 Shows that majority of the respondents had family income within the 3000-8000 Taka per month.
Fig. 1: Distribution of respondents by level of education (n=190)
Figure 1 shows that majority (56.32%) of the respondents were illiterate. Whereas 21.57% had education up to class V, 14,7% were up to class X and only 7.37% had SSC and above.
Fig. 2: Distribution of respondents by use of water source for drinking (n=190)
Figure 2 shows that almost all (97%) respondents use tube-
well water for drinking purpose followed by river water(2%) and pond(1%).
Fig. 3: Distribution of respondents by use of water source for washing utensils (n=190)
Figure 3 shows that 71.07% respondents used Tube-well water, 9.99% pond, 3.68% well and 15.26% use river water for washing utensils respectively.
Fig. 4: Distribution of respondents by use of water source for bathing and washing hands (n=190)
Figure 4 shows that 61.58% respondents use Tube-well water and rest 38.42% used pond & well water for washing face hands and bathing purpose.
Fig. 5: Distribution of respondents by knowledge of safe water (n=190)
21
Income (Tk)
0-3000
3000-8000
8000 and above
Total
Number
18
106
66
190
Percentage
9.48
55.78
34.74
100.00
Level of Education
Level of Education
No
of
Re
spo
nd
en
ts
Illiterate
120
100
80
60
40
20
0
I-V VI-X SSC and above
107(56.32%)
41(21.57%) 28(14.74%) 14(7.37%)
Source of Water for Drinking
2% 1%
97%
0%
Tube well
Well
River
Pond
Tube well 71%
Pond 10%
River 15%Well 4%
Source of Water for Washing Utensils
Source of Water: Bathing and Washing Hands
Source of Water
No
of
Re
spo
nd
en
ts 125
100
75
50
25
0
Tube well Pond River Well
117(61.58%)
32(16.84%) 31(16.32%)
10(5.26%)
8%
92%
Yes
No
Knowledge about Safe Water
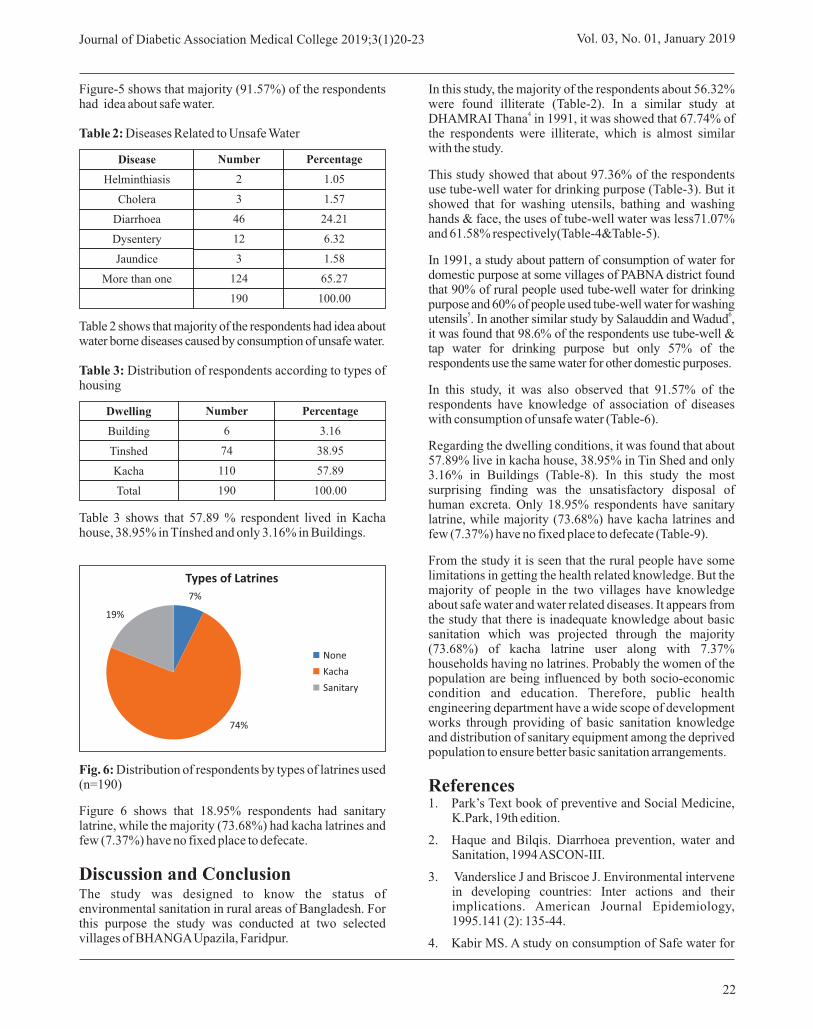
Figure-5 shows that majority (91.57%) of the respondents had idea about safe water.
Table 2: Diseases Related to Unsafe Water
Table 2 shows that majority of the respondents had idea about water borne diseases caused by consumption of unsafe water.
Table 3: Distribution of respondents according to types of housing
Table 3 shows that 57.89 % respondent lived in Kacha house, 38.95% in Tínshed and only 3.16% in Buildings.
Fig. 6: Distribution of respondents by types of latrines used (n=190)
Figure 6 shows that 18.95% respondents had sanitary latrine, while the majority (73.68%) had kacha latrines and few (7.37%) have no fixed place to defecate.
Discussion and ConclusionThe study was designed to know the status of environmental sanitation in rural areas of Bangladesh. For this purpose the study was conducted at two selected villages of BHANGA Upazila, Faridpur.
In this study, the majority of the respondents about 56.32% were found illiterate (Table-2). In a similar study at
4DHAMRAI Thana in 1991, it was showed that 67.74% of the respondents were illiterate, which is almost similar with the study.
This study showed that about 97.36% of the respondents use tube-well water for drinking purpose (Table-3). But it showed that for washing utensils, bathing and washing hands & face, the uses of tube-well water was less71.07% and 61.58% respectively(Table-4&Table-5).
In 1991, a study about pattern of consumption of water for domestic purpose at some villages of PABNA district found that 90% of rural people used tube-well water for drinking purpose and 60% of people used tube-well water for washing
5 6utensils . In another similar study by Salauddin and Wadud , it was found that 98.6% of the respondents use tube-well & tap water for drinking purpose but only 57% of the respondents use the same water for other domestic purposes.
In this study, it was also observed that 91.57% of the respondents have knowledge of association of diseases with consumption of unsafe water (Table-6).
Regarding the dwelling conditions, it was found that about 57.89% live in kacha house, 38.95% in Tin Shed and only 3.16% in Buildings (Table-8). In this study the most surprising finding was the unsatisfactory disposal of human excreta. Only 18.95% respondents have sanitary latrine, while majority (73.68%) have kacha latrines and few (7.37%) have no fixed place to defecate (Table-9).
From the study it is seen that the rural people have some limitations in getting the health related knowledge. But the majority of people in the two villages have knowledge about safe water and water related diseases. It appears from the study that there is inadequate knowledge about basic sanitation which was projected through the majority (73.68%) of kacha latrine user along with 7.37% households having no latrines. Probably the women of the population are being influenced by both socio-economic condition and education. Therefore, public health engineering department have a wide scope of development works through providing of basic sanitation knowledge and distribution of sanitary equipment among the deprived population to ensure better basic sanitation arrangements.
References1. Park’s Text book of preventive and Social Medicine,
K.Park, 19th edition.
2. Haque and Bilqis. Diarrhoea prevention, water and Sanitation, 1994 ASCON-III.
3. Vanderslice J and Briscoe J. Environmental intervene in developing countries: Inter actions and their implications. American Journal Epidemiology, 1995.141 (2): 135-44.
4. Kabir MS. A study on consumption of Safe water for
22
Journal of Diabetic Association Medical College 2019;3(1)20-23 Vol. 03, No. 01, January 2019
Disease
Helminthiasis
Cholera
Diarrhoea
Dysentery
Jaundice
More than one
Number
2
3
46
12
3
124
190
Percentage
1.05
1.57
24.21
6.32
1.58
65.27
100.00
Dwelling
Building
Tinshed
Kacha
Total
Number
6
74
110
190
Percentage
3.16
38.95
57.89
100.00
Types of Latrines
None
Kacha
Sanitary
74%
19%
7%

23
domestic purpose in a rural area of Bangladesh: 1990; Vol-III, ENHR,Dhaka.
5. Sutradhar and Ramapa da. A study on the pattern of consumption of water for domestic purpose in selected rural areas of Bangladesh; 1991: Vol-III, ENHR, Dhaka.
6. Salauddin and Wadud. Environmental sanitation in Semi-urban areas, JOPSOM, 1986; Vol-I, No-I: 25-28.
A Study on Environmental Sanitation in Some Selected Villages of Bhanga, Faridpur Rahman M T

Abstract Background: Laparoscopic cholecystectomy is the most commonly performed operation of the digestive tract. It is considered as the gold standard treatment for cholelithiasis.
Aim: To evaluate the outcome of it regarding length of hospital stay, complications, morbidity and mortality at a secondary hospital.
Materials and Methods: Data ware collected by retrospective record review method from 200 patients who underwent laparoscopic cholecystectomy. Patients' demographics, co-morbid diseases, previous abdominal surgery, conversion to open cholecystectomy, operative time, postoperative complications, and hospital stay were collected and analyzed.
Results: Out of 200 patients, 165 (82.5%) were females and 35 (17.5%) males. The mean age of the patients was 49.35±8.68 years. Mean operative time was 65.94±11.52 min. Five cases (2.5%) were converted to open surgery, one due to obscure anatomy (0.5%) 2 due to acute cholecystitis and oedematous gall bladder (1.0%) and one by bleeding (0.5%) one for bile duct injury. Two (1.0%) cases had biliary leakage. Mean hospital stay was 2.6±1.5 days. Sixteen (8.0%) developed wound infection. There was no case of port site hernia, bowel injury or spilled gallstones. There was no mortality recorded in this series.
Conclusions: Laparoscopic cholecystectomy is a safe and effective line for management of gallstone disease that can be performed with acceptable morbidity at a secondary hospital.
Keywards: Cholecystectomy, Laparoscopy, Cholelithiasis, Complications.
IntroductionLaparoscopic cholecystectomy (LC) represents a significant change in the management of gallbladder disease and it is the most commonly performed operation of the digestive tract. It is considered as the gold standard
1,2treatment for cholelithiasis. It replaced open cholecystectomy as the first choice of treatment for gallstones and inflammation of the gallbladder. It was made for the first time in 1987 by Muret. Despite many modified methods (natural orifice transluminal endoscopic surgery- NOTES, single-incision laparoscopic surgery), LC is still
4the gold standard for symptomatic gallstone disease. The risk of intraoperative injury during laparoscopic
3,4cholecystectomy is higher than in open cholecystectomy. It has been anticipated that this will diminish with
3increasing surgeon experience in the use of LC. In USA approximately one million patients are newly diagnosed annually with gall stone disease and approximately 600,000 operations are performed a year more than 75% of them by
5laparoscopy.
Laparoscopic cholecystectomy offers the patients the advantages of minimal invasive surgery. However with the widespread acceptance of LC the spectrum of complications in gallstone surgery has changed. The intraoperative complications of LC like bowel and vascular injury (trocar site), biliary leak and bile duct injuries decrease with the passage of time, because of increased experience of the surgeons, popularity of the
5procedure and introduction of new instruments. This study was the exploration of laparoscopic cholecystectomy with the aim to evaluate the complications of laparoscopic cholecystectomy in cholelithiasis, both in symptomatic and asymptomatic patients, including co-morbidity and conversion of laparoscopic to open cholecystectomy.
Original Article
Operative outcomes of Laparoscopic Cholecystectomy1 2 3 4 5 6 7Rahman M M , Rahman M S , Chowdhury A A M A M , Rahman M M , Qaiyum M A , Ahmed S ,Hasan T M
1. Dr. Md. Mazedur Rahman Associate Professor, Department of Surgery President Abdul Hamid Medical College, Kishoreganj.
2. Dr. Md. Siddiqur Rahman Associate Professor, Department of Urology, Women's Medical College, Sylhet.
3. Dr. A.A.M.A. Mumit Chowdhury Assistant Professor, Department of anesthesia President Abdul Hamid Medical College, Kishoreganj.
4. Dr. Md. Mushfiqur Rahman Associate Professor, Department of Surgery Prime Medical College, Rangpur.
5. Dr. Md. Abdul Qaiyum, Senior Consultant (Surgery), Shahid Shamsuddin Ahmed Hospital, Sylhet.
6. Dr. Shahana Ahmed Associate Professor, Department of Obstetrics and Gynaecology Diabetic Association Medical College, Faridpur
7. Dr. Md. Tarek Hasan Medical Officer, 250 Bedded Sadar Hospital, Patuakhali.
Correspondence to:Dr. Md. Mazedur RahmanAssociate professor, Department of SurgeryPresident Abdul Hamid Medical College, Kishoreganj. E-mail: [email protected]
24
Journal of Diabetic Association Medical College 2019;3(1)24-27
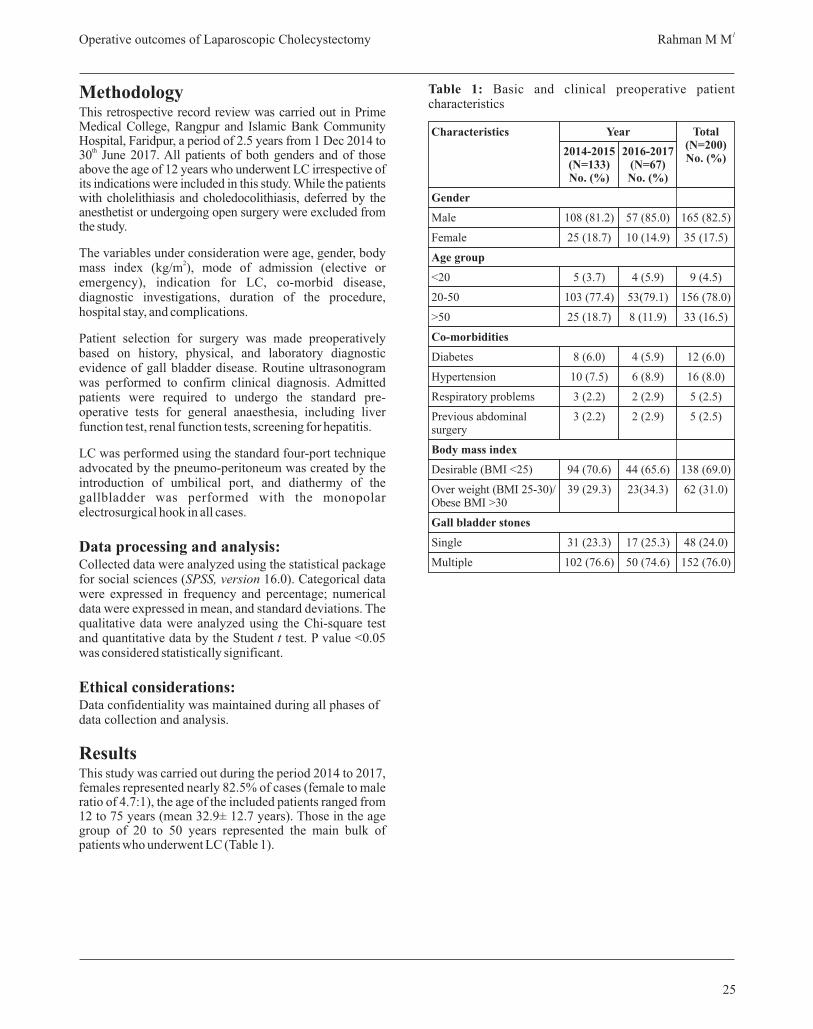
Operative outcomes of Laparoscopic Cholecystectomy1 Rahman M M
MethodologyThis retrospective record review was carried out in Prime Medical College, Rangpur and Islamic Bank Community Hospital, Faridpur, a period of 2.5 years from 1 Dec 2014 to
th30 June 2017. All patients of both genders and of those above the age of 12 years who underwent LC irrespective of its indications were included in this study. While the patients with cholelithiasis and choledocolithiasis, deferred by the anesthetist or undergoing open surgery were excluded from the study.
The variables under consideration were age, gender, body 2mass index (kg/m ), mode of admission (elective or
emergency), indication for LC, co-morbid disease, diagnostic investigations, duration of the procedure, hospital stay, and complications.
Patient selection for surgery was made preoperatively based on history, physical, and laboratory diagnostic evidence of gall bladder disease. Routine ultrasonogram was performed to confirm clinical diagnosis. Admitted patients were required to undergo the standard pre-operative tests for general anaesthesia, including liver function test, renal function tests, screening for hepatitis.
LC was performed using the standard four-port technique advocated by the pneumo-peritoneum was created by the introduction of umbilical port, and diathermy of the gallbladder was performed with the monopolar electrosurgical hook in all cases.
Data processing and analysis:Collected data were analyzed using the statistical package for social sciences (SPSS, version 16.0). Categorical data were expressed in frequency and percentage; numerical data were expressed in mean, and standard deviations. The qualitative data were analyzed using the Chi-square test and quantitative data by the Student t test. P value <0.05 was considered statistically significant.
Ethical considerations:Data confidentiality was maintained during all phases of data collection and analysis.
ResultsThis study was carried out during the period 2014 to 2017, females represented nearly 82.5% of cases (female to male ratio of 4.7:1), the age of the included patients ranged from 12 to 75 years (mean 32.9± 12.7 years). Those in the age group of 20 to 50 years represented the main bulk of patients who underwent LC (Table 1).
Table 1: Basic and clinical preoperative patient characteristics
25
Gender
Male
Female
Age group
<20
20-50
>50
Co-morbidities
Diabetes
Hypertension
Respiratory problems
Previous abdominal surgery
Body mass index
Desirable (BMI <25)
Over weight (BMI 25-30)/ Obese BMI >30
Gall bladder stones
Single
Multiple
2014-2015 (N=133) No. (%)
108 (81.2)
25 (18.7)
5 (3.7)
103 (77.4)
25 (18.7)
8 (6.0)
10 (7.5)
3 (2.2)
3 (2.2)
94 (70.6)
39 (29.3)
31 (23.3)
102 (76.6)
2016-2017 (N=67) No. (%)
57 (85.0)
10 (14.9)
4 (5.9)
53(79.1)
8 (11.9)
4 (5.9)
6 (8.9)
2 (2.9)
2 (2.9)
44 (65.6)
23(34.3)
17 (25.3)
50 (74.6)
165 (82.5)
35 (17.5)
9 (4.5)
156 (78.0)
33 (16.5)
12 (6.0)
16 (8.0)
5 (2.5)
5 (2.5)
138 (69.0)
62 (31.0)
48 (24.0)
152 (76.0)
Total (N=200) No. (%)
Characteristics Year
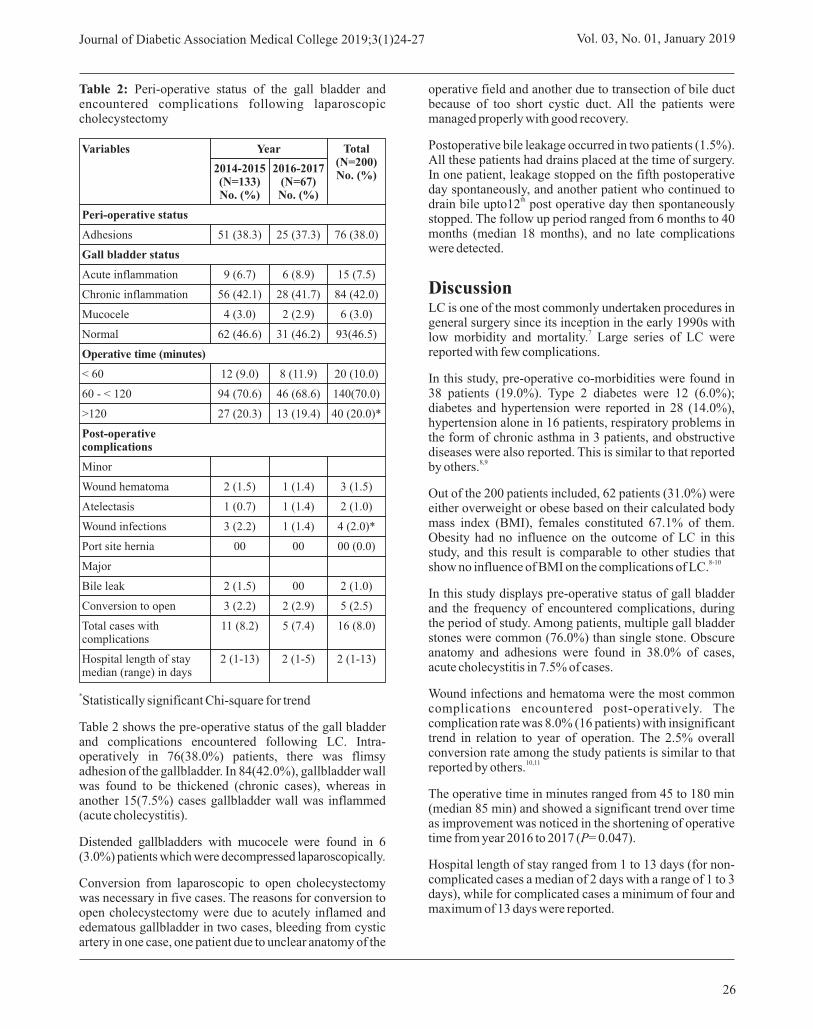
Table 2: Peri-operative status of the gall bladder and encountered complications following laparoscopic cholecystectomy
*Statistically significant Chi-square for trend
Table 2 shows the pre-operative status of the gall bladder and complications encountered following LC. Intra-operatively in 76(38.0%) patients, there was flimsy adhesion of the gallbladder. In 84(42.0%), gallbladder wall was found to be thickened (chronic cases), whereas in another 15(7.5%) cases gallbladder wall was inflammed (acute cholecystitis).
Distended gallbladders with mucocele were found in 6 (3.0%) patients which were decompressed laparoscopically.
Conversion from laparoscopic to open cholecystectomy was necessary in five cases. The reasons for conversion to open cholecystectomy were due to acutely inflamed and edematous gallbladder in two cases, bleeding from cystic artery in one case, one patient due to unclear anatomy of the
operative field and another due to transection of bile duct because of too short cystic duct. All the patients were managed properly with good recovery.
Postoperative bile leakage occurred in two patients (1.5%). All these patients had drains placed at the time of surgery. In one patient, leakage stopped on the fifth postoperative day spontaneously, and another patient who continued to
thdrain bile upto12 post operative day then spontaneously stopped. The follow up period ranged from 6 months to 40 months (median 18 months), and no late complications were detected.
DiscussionLC is one of the most commonly undertaken procedures in general surgery since its inception in the early 1990s with
7low morbidity and mortality. Large series of LC were reported with few complications.
In this study, pre-operative co-morbidities were found in 38 patients (19.0%). Type 2 diabetes were 12 (6.0%); diabetes and hypertension were reported in 28 (14.0%), hypertension alone in 16 patients, respiratory problems in the form of chronic asthma in 3 patients, and obstructive diseases were also reported. This is similar to that reported
8,9by others.
Out of the 200 patients included, 62 patients (31.0%) were either overweight or obese based on their calculated body mass index (BMI), females constituted 67.1% of them. Obesity had no influence on the outcome of LC in this study, and this result is comparable to other studies that
8-10show no influence of BMI on the complications of LC.
In this study displays pre-operative status of gall bladder and the frequency of encountered complications, during the period of study. Among patients, multiple gall bladder stones were common (76.0%) than single stone. Obscure anatomy and adhesions were found in 38.0% of cases, acute cholecystitis in 7.5% of cases.
Wound infections and hematoma were the most common complications encountered post-operatively. The complication rate was 8.0% (16 patients) with insignificant trend in relation to year of operation. The 2.5% overall conversion rate among the study patients is similar to that
10,11reported by others.
The operative time in minutes ranged from 45 to 180 min (median 85 min) and showed a significant trend over time as improvement was noticed in the shortening of operative time from year 2016 to 2017 (P= 0.047).
Hospital length of stay ranged from 1 to 13 days (for non-complicated cases a median of 2 days with a range of 1 to 3 days), while for complicated cases a minimum of four and maximum of 13 days were reported.
26
Journal of Diabetic Association Medical College 2019;3(1)24-27 Vol. 03, No. 01, January 2019
Peri-operative status
Adhesions
Gall bladder status
Acute inflammation
Chronic inflammation
Mucocele
Normal
Operative time (minutes)
< 60
60 - < 120
>120
Post-operative complications
Minor
Wound hematoma
Atelectasis
Wound infections
Port site hernia
Major
Bile leak
Conversion to open
Total cases with complications
Hospital length of stay median (range) in days
2014-2015 (N=133) No. (%)
51 (38.3)
9 (6.7)
56 (42.1)
4 (3.0)
62 (46.6)
12 (9.0)
94 (70.6)
27 (20.3)
2 (1.5)
1 (0.7)
3 (2.2)
00
2 (1.5)
3 (2.2)
11 (8.2)
2 (1-13)
2016-2017 (N=67) No. (%)
25 (37.3)
6 (8.9)
28 (41.7)
2 (2.9)
31 (46.2)
8 (11.9)
46 (68.6)
13 (19.4)
1 (1.4)
1 (1.4)
1 (1.4)
00
00
2 (2.9)
5 (7.4)
2 (1-5)
76 (38.0)
15 (7.5)
84 (42.0)
6 (3.0)
93(46.5)
20 (10.0)
140(70.0)
40 (20.0)*
3 (1.5)
2 (1.0)
4 (2.0)*
00 (0.0)
2 (1.0)
5 (2.5)
16 (8.0)
2 (1-13)
Total (N=200) No. (%)
Variables Year
27
ConclusionThe results of this study confirm that LC at a secondary level of care is a safe and effective intervention in selected patients with symptomatic gallstones. Most of the complications are due to lack of experience or knowledge of typical error. It has several advantages compared with open cholecystectomy; however, when there is a major complication a multidisciplinary approach should be performed at a tertiary hospital.
References1. Reynolds W. , J r The f i r s t l aparoscopic
cholecystectomy. JSLS. 2001;5:89-94.
2. Mouret P. Celioscopic surgery: Evolution or revolution? Chirurgie. 1990;116:829-32.
3. Livingston EH, Rege RV. A nationwide study of c o n v e r s i o n f r o m l a p a r o s c o p i c t o o p e n cholecystectomy. Am J Surg. 2004;188:205-11.
4. Simopoulos C, Botaitis S, Polychronidis A, Tripsiani G, Karayiannakis AJ. Risk factors for conversion of l a p a r o s c o p i c c h o l e c y s t e c t o m y t o o p e n cholecystectomy. Surg Endosc. 2005;19:905-9.
5. Russell EM, Bruce J, Krukowski ZH. Systematic review of the quality of surgical mortality monitoring. Br J Surg. 2003;90:527-32.
6. Martin RC 2nd, Brennan MF, Jaques DP. Quality of complication reporting in the surgical literature. Ann Surg. 2002;235:803-13.
7. Reddick EJ. Laparoscopic cholecystectomy in freestanding outpatient centers. J Laparoendosc Surg. 1992;2:65-7.
8. Osborne DA, Alexander G, Boe B, Zervos EE. Laparoscopic cholecystectomy: Past present, future. Surg Technol Int. 2006;15:81-5.
9. Al-Mulhim AA. Male gender is not a risk factor for the outcome of laparoscopic cholecystectomy: A single surgeon experience. Saudi J Gastroenterol. 2008;14:73-9.
10. Angrisani L, Lorenzo M, De Palma G, Sivero L, Catanzano C, Tesauro B, et al. Laparoscopic cholecystectomy in obese patients compared with nonobese patients. Surg Laparosc Endosc. 1995;5:197-201.
11. Bittner R. Laparoscopic surgery: 15 years after clinical introduction. World J Surg. 2006;30:1190-203.
12. Giger UF, Michel JM, Optiz I, Th Inderbitzin D, Kocher T, Krahenbühl L. Risk factors for perioperative complications in patients undergoing laparoscopic cholecystectomy: Analysis of 22,953 consecutive cases from the Swiss Association of Laparoscopic and Thoracoscopic Surgery.
Operative outcomes of Laparoscopic Cholecystectomy1 Rahman M M

Abstract
Objective: To evaluate the diagnostic performance of Mammography in the diagnosis of benign and malignant breast mass.
Method: This Cross-sectional type of study was carried out in the Radiology & Imaging department of Sir Salimullah Medical College and Mitford Hospital, Dhaka, during July 2013 to June 2015, to determine the value of mammography in evaluation of breast mass, and also to determine the sensitivity, specificity, accuracy, PPV and NPV of mammography in the diagnosis of benign and malignant breast mass in comparison to the histopathological findings. For this purpose clinically suspected as having breast mass, referred in the above mentioned hospitals and enrolled for surgical management were included in this study. Mammography were done in all these patients and they were followed up from the admission upto the post operative tissue diagnosis of breast mass in respective pathology departments for histopathological correlation
Results: Almost one third (31.6%) patients were age belonged to 46-50 years and the mean age was found 47.8±6.4 years. A total of 41 patients had mass only among them, 3 (7.3%) were malignant and 38 (92.7%) were benign patients. Six patients were mass with spiculation, among them all (100.0%) were malignant patients. Five patients were mass with macro calcification; among them all (100.0%) were benign patients. Two patients were mass with micro calcification, among them all (100.0%) were malignant patients. Three patients were mass with spiculation, micro calcification and enlarged axillary lymph node; among them all (100.0%) were malignant patients. Out of 57 patients, on histopathological diagnosis 29 (50.9%) were firbroadenoma, 6 (10.5%) were fibrocystic change, 4 (7.0%) were cyst, 4 (7.0%) were abscess and 1(1.8%) were galactocele. They were benign lesion of breast. Histopathological diagnosis of invasive ductal carcinoma, invasive lobular carcinoma and medullary carcinoma were 8 (14. %), 4 (7.00%) and 1 (1.8%) respectively. Mammography malignant was found 14 cases out of which 10 (76.9%) malignant and 4 (9.1%) benign evaluated by histopathology. Mammography benign was found 43 cases out of which 3 (23.1%) malignant and 40 (90.9%) benign evaluated by histopathology. The sensitivity was 76.9%, specificity 90.9%, accuracy 87.7%, positive predictive values 71.4% and negative predictive values 93.0% in mammography for identification of breast mass.
Conclusion: Mammography is a cost effective, available and less time consuming procedure to see location of lesion, density of the lesion, margin of the lesion, glandular pattern of the breast etc and thereby to help a surgeon for operative planning and thus decreasing patient's morbidity and mortality. Mammography is highly sensitive, specific, reliable and useful method in the differentiation of malignant and benign breast masses. It can be used to plan subsequent appropriate management in majority of cases. Further studies can be undertaken by including large number of patients.
IntroductionBreast cancer is one of the common diseases among the females in the world. Generally about 25% of woman's are affected by breast cancer, in that 20% leads to lethal cancers. It is one the leading cause of death due to cancer in women. Breast cancer can be reduced by: giving birth to child before 30, Breast-feeding, Limiting alcohol intake, maintaining a healthy weight, exercising regularly. Breast cancer that forms in tissues of breast, usually ducts (tubes that carry milk to nipple) and lobules (glands
1that make milk).
In Bangladesh remarkable increase of breast cancer has occurred in recent year. National Institute of cancer research from 1996 to
st2000 showed cervical cancer as ranked 1 and breast cancer ndranked 2 in females. The management of patients with carcinoma
Original Article
Mammographic Evaluation of Breast Mass & Comparison with Histopathological Findings
1 2 3 4 5 6 7Yesmin L , Hossain R , Saiham K S , Naz F M , Alam S , Ahmad M R , Hossain M I
1. Dr. Lovely Yesmin Medical officer, Department of Radiology & Imaging, National institute of Traumatology and Orthopedic Rehabilitation (NITOR) Dhaka.
2. Dr. Rued Hossain, Associate professor, Radiology & Imaging SSMC, Dhaka.
3. Dr. Kazi Shantono Saiham, Consultant, Doctors Care General Hospital & Diagnostic Center Brahmanbaria.
4. Dr. Fouzia Mujib Un Naz Assistant Professor Department of Radiology & Imaging Dhaka Dental College.
5. Dr. Md. Shafiul Alam Assistant Professor Department of Dental Radiology & Imaging Dhaka Dental College.
6. Dr.Md. Rasel Ahmad Medical Educationist and Dental Surgeon, Consultant United Oro-Dental & Maxillofacial Surgery.
7. Dr .Md. Immam Hossin Lecturer, Department of Radiology & Imaging Dhaka Dental College.
Correspondence to:Dr. Lovely YesminMedical officer, Department of Radiology & ImagingNational institute of Traumatology and Orthopedic Rehabilitation(NITOR) Dhaka. Email: [email protected]
28
Journal of Diabetic Association Medical College 2019;3(1)28-32

Mammographic Evaluation of Breast Mass & Comparison with Histopathological Findings Yesmin L
breast can be improved if a definitive diagnosis is obtained preoperatively by Radiological examination and/ or needle biopsy/cytology. Public awareness of the potential benefits of early detection of breast cancer has increased dramatically in recent years, and more women are now seeking the advice of a physician immediately after
2detecting a breast mass.
Among these the common causes of breast masses are 3fibroadenoma, fibrocystic disease and carcinoma. Breast
carcinoma is the most common cancer among women between 40 to 55 years of age. Common forms of breast cancer are medullary carcinoma, mucinous carcinoma, tubular carcinoma, inflammatory breast cancer, Paget's disease of the nipple, phylloides tumor, lipoma, galactocele
4etc.
Mammography has been the “gold standard” in breast cancer detection for >40 years. Limitations in its ability to detect both small and lobular breast cancers, poor resolution in dense breasts, and a lack of significant improvement in cancer detection, despite digital mammography and computer aided diagnosis, has inevitably lead to a search for other modalities to improve
5the detection of breast cancer.
Although it is seen as the best examination technique for the early detection of breast cancer reducing mortality rates by up to 25%, their interpretation requires skill and
6experience by a trained radiologist.
Women who present with breast symptoms or who have palpable findings on clinical examination are usually investigated with breast imaging, which generally consists of mammography or breast sonography or both. The choice of primary breast imaging in examining women with symptoms is partly based on age. However, despite the importance of age in clinical practice, little evidence exists as to the appropriate age (or age range) that delineates the choice of initial diagnostic breast imaging in symptomatic women. In the absence of evidence, experts suggest that women younger than 35 years be examined with sonography, and women 35 years and older be examined with mammography,
7as the primary breast imaging modality.
A comprehensive review of the literature found little evidence about the comparative age-specific accuracy of mammography and breast sonography in symptomatic
8women. That study found that sonography was more sensitive than mammography in women younger than 62 years, the so-called crossover age, and mammography was more sensitive than sonography in women older than 62 years. However, the study's authors acknowledged that the nonindependent interpretation of the two tests and the analysis used may have led to underestimation of the sensitivity of mammography, and that the crossover age
9may be as early as 48 years. For a valid comparison of the accuracy of two tests, the tests need to be interpreted independently (without knowledge of each other) in the
10same subjects.
Houssami et al. reported that the sensitivity of mammography increased substantially in women older than 50 years. Sonographic sensitivity of 81.7% was not significantly greater than mammographic sensitivity of 75.8%. However, in women 45 years old or younger, the sensitivity of sonography was 13.2% (95% confidence interval, 2.1-24.3%) greater than that of mammography.
11The specificity of both tests was approximately 88.0%.
MethodologyThis cross sectional study was carried out in the Radiology and imaging department of Sir Salimullah Medical College, Dhaka from July 2013 to June 2015 after approval of ethical committee. During the study period 57 patients from 35 to 60 years of age, referred for mammographic evaluation of breast mass, which were further evaluated with histopathological findings. Mammographic findings were evaluated by the researcher and a senior Radiologist. Patients who underwent operation, histopathological reports were collected. Out of 60 patients, two patients refused to undergo operation and one patient lost histopathology report. Finally mammographic findings of 57 patients were compared with histological findings.
Data were collected in a pre-tested questionnaire by taking history, examining the patients clinically, the finding and interpretation of the Mammography. Histopathological diagnoses were considered as gold standard of diagnostic criteria. The data were collected by the researcher herself. Statistical analyses were carried out by using the Statistical Package for Social Sciences version 20.0 for Windows (SPSS Inc., Chicago, Illinois, USA).
Procedure for mammography: The women was escorted to the changing room, where she was undressed from the waist up and change into the screening center gowns after taking proper history and clinical examination. She was asked to wipe off any deodorants, perfumes or powders that she had used that day, as these can mimic micro calcification on the film. The peak kv used for mammogram was low of kvp of around 24-30 kv and mAs varies depending on the breast tissue density. All mammogram were done using the film screen technique and consist of at least 2 views for each breast (CC & MLO). Supplemental views were obtained when considered necessary for adequate visualization. Markers were used to indicate the side and view demonstrated on that particular film. This was done for a reference point to understand the orientation of the breast, especially in the CC view. Compression paddle was handled carefully to reduce the discomfort level of the patient. After processing of film mammogram was viewed in optimum lighting condition. A powerful magnifying glass was used to get a better look at suspected pathology. Final interpretation of mammogram was taken with the help of radiologist of department of Radiology and Imaging (SSMCH). All patients were undergoing excision or biopsy of the mass lesion. Histopathological slides was prepared and
29
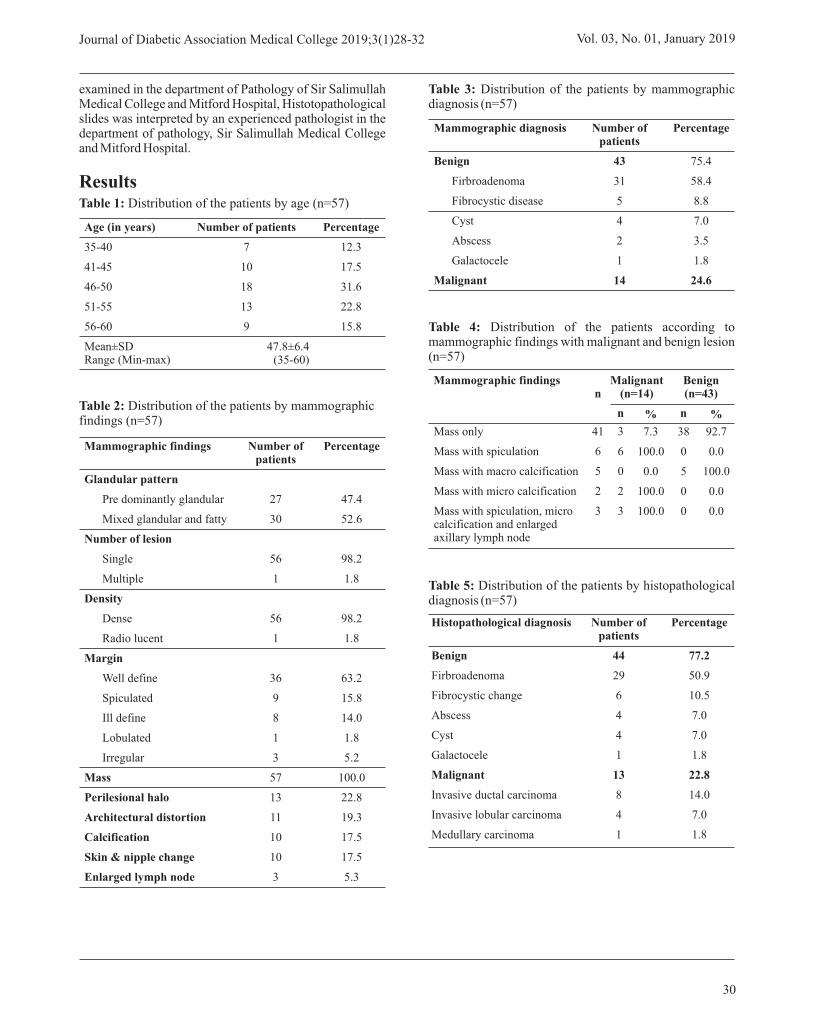
examined in the department of Pathology of Sir Salimullah Medical College and Mitford Hospital, Histotopathological slides was interpreted by an experienced pathologist in the department of pathology, Sir Salimullah Medical College and Mitford Hospital.
ResultsTable 1: Distribution of the patients by age (n=57)
Table 2: Distribution of the patients by mammographic findings (n=57)
Table 3: Distribution of the patients by mammographic diagnosis (n=57)
Table 4: Distribution of the patients according to mammographic findings with malignant and benign lesion (n=57)
Table 5: Distribution of the patients by histopathological diagnosis (n=57)
30
Age (in years)
35-40
41-45
46-50
51-55
56-60
Mean±SDRange (Min-max)
Number of patients
7
10
18
13
9
Percentage
12.3
17.5
31.6
22.8
15.8
47.8±6.4(35-60)
Mammographic findings
Glandular pattern
Pre dominantly glandular
Mixed glandular and fatty
Number of lesion
Single
Multiple
Density
Dense
Radio lucent
Margin
Well define
Spiculated
Ill define
Lobulated
Irregular
Mass
Perilesional halo
Architectural distortion
Calcification
Skin & nipple change
Enlarged lymph node
Number of patients
27
30
56
1
56
1
36
9
8
1
3
57
13
11
10
10
3
Percentage
47.4
52.6
98.2
1.8
98.2
1.8
63.2
15.8
14.0
1.8
5.2
100.0
22.8
19.3
17.5
17.5
5.3
Mammographic diagnosis
Benign
Firbroadenoma
Fibrocystic disease
Cyst
Abscess
Galactocele
Malignant
Number of patients
43
31
5
4
2
1
14
Percentage
75.4
58.4
8.8
7.0
3.5
1.8
24.6
Mass only
Mass with spiculation
Mass with macro calcification
Mass with micro calcification
Mass with spiculation, micro calcification and enlarged axillary lymph node
41
6
5
2
3
3
6
0
2
3
7.3
100.0
0.0
100.0
100.0
38
0
5
0
0
92.7
0.0
100.0
0.0
0.0
Malignant (n=14)n
Benign (n=43)
n % n %
Mammographic findings
Number of patients
44
29
6
4
4
1
13
8
4
1
Percentage
77.2
50.9
10.5
7.0
7.0
1.8
22.8
14.0
7.0
1.8
Histopathological diagnosis
Benign
Firbroadenoma
Fibrocystic change
Abscess
Cyst
Galactocele
Malignant
Invasive ductal carcinoma
Invasive lobular carcinoma
Medullary carcinoma
Journal of Diabetic Association Medical College 2019;3(1)28-32 Vol. 03, No. 01, January 2019

31
Table 6: Comparison between mammography with histopathology (n=57)
Table 7: Sensitivity, specificity, accuracy, positive and negative predictive values of the mammography evaluation for prediction of breast mass.
DiscussionThis cross-sectional type of study was carried out with an aim to determine the benign and malignant nature of breast mass by mammography and diagnosis of breast mass by histopathology and also to evaluate the diagnostic performance of mammography in the evaluation of benign and malignant breast mass in comparison to the histopathological findings. In this present study, a total of 57 patients were included, among which almost one third (31.6%) patients were age belonged to 46-50 years. The mean age was found 47.8±6.4 years with range from 35 to
11 1260 years. Houssami et al. and Nascimento et al. found that the mean age of subjects was 44.9±8.7 years varied from 27 to 55 years and 49±12 years varied from 37 to 61 years respectively, which are is consistent with the current
13study. Yunus et al. showed the mean age was 48 years varied from 30-80 years. The above findings are comparable with the current study Out of 57 patients, 43 (75.4%) were benign lesions and only 14 (24.6%) malignant lesions. Mammographic findings of 31 (54.4%) patients were firbroadenoma, 5 (8.8%) were fibrocystic disease, 4 (7.0%) were cyst, 2 (3.5%) were abscess, 1 (1.8%) were galactocele and 14 (24.6%) were malignant lesions. Firbroadenoma 12.7%, simple cyst 4.8%, Breast Abscess 1.2%. Galactocele 1.2%, Breast malignancies
14 12cases 18.1%. In another study Nascimento et al. found that 58.3% lesions were benign and 41.7% were malignant. In this present study it was observed that 41 patients had only mass among them, 3 (7.3%) were malignant and 38
(92.7%) were benign patients. Six patients were mass with spiculation, among them all (100.0%) were malignant patients. Five patients were mass with macro calcification, among them all (100.0%) were benign patients. Two patients were mass with micro calcification, among them all (100.0%) were malignant patients. Three patients were mass with spiculation, micro calcification and enlarged axillary lymph node, among them all (100.0%) were malignant patients.
In this current study it was observed that benign and malignant lesion were 44 (77.2%) and 13 (22.8%) respectively. Out of 57 patients, histopathological diagnosis of 29 (50.9%) were firbroadenoma, 6 (10.5%) were fibrocystic change, 4 (7.0%) were cyst, 4 (7.0%) were abscess and 1 (1.8%) were galactocele. All of them are benign lesion of breast. Histopathological diagnosis of invasive ductal carcinoma, invasive lobular carcinoma and medullary carcinoma were 8 (14.0%), 4 (7.0%) and 1
11 (1.8%) respectively. In Houssami et al. study reported that the histologic types of cancer in the 240 patients were invasive ductal 70.0%, ductal in situ 14.0%, invasive lobular 9.0%, tubular 4.0%, medullary 1.0%, and other types 1.2% and no histology 0.8%. Biopsies of 115 breast masses detected at mammography were performed by
12Nascimento et al. and found sixty-seven of these lesions (58.3%) were benign and 48 (41.7%) were malignant.
In this series out of all cases 14 were diagnosed as malignant breast mass by mammography, among them 10 (76.9%) were confirmed by histopathology. They were true positive. Four cases were diagnosed as having as malignant breast mass by mammography but not confirmed by histopathology. They were false positive. Out of 43 cases of benign breast mass which were confirmed by mammography, three (23.1%) were confirmed as malignant breast mass and 40 (90.9%) were benign breast mass by histopathological findings. They were false negative and
12true negative respectively. Nascimento et al. found 58.3% and 41.7% lesions were benign and malignant respectively.
In this current study evaluation of breast mass by mammography showed that the sensitivity was 76.9%, specificity 90.9%, accuracy 87.7%, positive predictive values 71.4% and negative predictive values 93.0%.
11Houssami et al. mentioned that mammographic sensitivity was 75.8%. Mammography is nearly 87%
15,16,17accurate in detecting cancer its specificity is 88% and its positive predictive value may be as high as 22% (Barlow et al. 2002). But the false negative findings in mammography in evaluation of palpable breast mass is
18high, estimated between 4.0% & 12.0% . Nascimento et 12al. mentioned in their study that the sensitivity was 68%,
specificity 76%, and accuracy 75%. NPV 76% and PPV was 51% observed by first observer. Another observed found sensitivity 87.0%, specificity 44.0%, accuracy 62.0%, NPV was 83% and PPV 53% observed by second observer. So, overall diagnostic accuracy correlates well with other studies.
Malignant
Benign
Total
10
3
13
76.9
23.1
4
10
14
9.1
90.9
Malignant (n=14)
Benign (n=43)
n % n %
Mammography
Histopathology
14
43
57
Total
Sensitivity
Specificity
Accuracy
Positive predictive value
Negative predictive value
76.9%
90.9%
87.7%
71.4%
93.0%
Mammography
Mammographic Evaluation of Breast Mass & Comparison with Histopathological Findings Yesmin L
ConclusionIt was found that mixed glandular and fatty, single lesion, dense, and well defined margin were commonly found in mammography. Firbroadenoma was more common in benign lesion. Firbroadenomas were more common among the benign lesions and invasive ductal carcinoma among the malignant lesions in Histopathological diagnosis. Mammography is cost effective, available and less time consuming procedure to see location density, margin of lesion, glandular pattern of the breast etc. and thereby helping surgeon for operative plan and decreases patient's morbidity and mortality. Therefore it can be concluded that mammography is highly sensitive, specific and useful method in the differentiation of malignant and benign breast masses. It can be used to plan the subsequent appropriate management in majority of cases. Further studies can be undertaken by including large number of patients.
References 1. Abinaya, S, Sivakumar, R, Karnan, M, Shankar, M,
Karthikeyan, M, ‘Detection of breast cancer in mammograms - a survey’, International Journal of Computer Application and Engineering Technology, 2014; vol. 3, no. 2, pp. 172-178.
2. WHO, ‘Cancer Registry Report: National Institute of Cancer Research and Hospital 2005-2007’, National Institute of Cancer Research and Hospital, 2009; pp. 1-21.
3. Cotran, RS, Kumar, V & Robbins, SL, ‘The breast’, In: thRobbin's Pathological Basis of Disease, 6 edition,
W.B Saunders company, Philadelphia; 1999; pp. 1093-1114.
4. Imaginis, ‘Advanced in mammography and other breast imaging methods’, 2006; Available from http://www.imaginis.com/mammography/advances-in-mammography-and-other-breast-imaging-methods-1
5. Malik, SS, Akhter, T & Malik, SA, ‘Mammographic- sonographic co-relation in the diagnosis of breast lump’, Biomedica. 2008; vol. 24, pp. 147-151.
6. Bovis, K and Singh, S, ‘Detection of Masses in Mammograms Using Texture Features’, Proceedings of the International Conference on Pattern Recognition (ICPR’00), IEEE, 2000; pp. 267-270.
7. Dixon, JM & Mansel, RE, ‘Symptoms, assessment, and guidelines for referral’, In: Dixon JM, ed. ABC of breast diseases, 2nd ed. London: BMJ, 2000; pp. 3-7.
8. Irwig, L & Macaskill, P, ‘Evidence relevant to guidelines for the investigation of breast symptoms’, Sydney, Australia: National Breast Cancer Centre, 1997; pp. 5-18.
9. Houssami, N, Ciatto, S, Irwig, L, Simpson, JM & Macaskill, P, ‘The comparative sensitivity of mammography and ultrasound in women with breast symptoms: an age-specific analysis’, Breast, 2002; vol. 11, pp. 125-130.
10. National Health and Medical Research Council, ‘How to review the evidence: systematic identification and review of the scientific literature’, Canberra, A.C.T, Australia: Commonwealth of Australia, 2000; pp. 62-63.
11. Houssami, N, Irwig, L, Simpson, JM, McKessar, M, Blome, S & Noakes, J, 'Sydney Breast Imaging Accuracy Study: Comparative Sensitivity and Specificity of Mammography and Sonography in Young Women with Symptoms', AJR, vol. 180, 2003; pp. 935-940.
12. Nascimento, JHR, Silva, VD & Maciel, AC, 'Accuracy of mammographic findings in breast cancer: correlation between BI-RADS classification and histological findings', Radiol Bras. vol. 43 no. 2, 2010; pp. 91-96.
13. Yunus, M, Ahmed, N, Masroor, I & Yaqoob, J, 'Mammographic Criteria for Determining the Diagnostic Value of Microcalcifications in the Detection of Early Breast Cancer', J Pak Med Assoc. vol. 54, no. 1, 2004; pp. 24-29.
14. Taori, K, Dhakate, S, Rathod, J, Hatgaonkar, A, Diswal, A & Wavare, P et al., 'Evaluation of Breast Masses Using Mammography and Sonography as First time Line Investigations', Open Journal of Medical Imaging, 2013; vol. 3, no. 1, pp. 40-49.
15. Osuch, JR, Reeves, MJ, Pathak, DR and Kinchelow, T, 'BREASTAID: Clinical Results from Early Development of a Clinical Decision Rule for Palpable Solid Breast Masses,' Annals of Surgery, 2003; vol. 238, no. 1, pp. 728-737.
16. Berg, WA, Campassi, CI and Ioffe, OB, 'Cystic Lesions of the Breast: Sonographic-Pathologic Correlation', Radiology, vol. 227, no. 1, 2003; pp. 183-191.
17. Kolb, TM, Lichy, J and Newhouse, JH, 'Comparison of the Performance of Screening Mammography, Physical Examination, and Breast US and Evaluation of Factors that Influence Them: An Analysis of 27,825 Patiluations,' Radiology, vol. 225, no. 1, 2002; pp. 165-175.
18. Dennis, MA, Parker, SH, Klaus, AJ, Stavros, AT, Kaske, TI and Clark, SB, 'Breast Biopsy Avoidance: The Value of Normal Mammograms and Normal Sonograms in the Setting of a Palpable Lump', Radiology, vol. 219, no. 1, 2001; pp. 186-191.
32
Journal of Diabetic Association Medical College 2019;3(1)28-32 Vol. 03, No. 01, January 2019

IntroductionThe term 'environment' is widely used and has a broad range of definitions, meanings and interpretations. What does the term 'environment' mean? In popular usage, for some people, the term 'environment' means, simply, 'nature': in other words, the natural landscape together with all of its non-human features, characteristics and processes. However, for other people, the term 'environment' includes human elements to some extent - the surroundings or conditions in which a person, animal, or plant lives or operates, the natural world, as a whole or in a particular geographical area, especially as affected by human activity.1
An ecosystem (also called as environment) is a natural unit consisting of all plants, animals and micro-organisms (biotic factors) in an area functioning together with all of the non-living physical (abiotic) factors of the environment. The natural environment encompasses all living and non-living things occurring naturally, meaning in this case not artificial. The term is most often applied to the Earth or some parts of Earth. This environment encompasses the interaction of all living species, climate, weather and natural resources that affect human survival
2and economic activity. Therefore, it is not particularly helpful to conceptualize the ‘environment’ without including in that conceptualization some notion of relationship. Individual, objects, elements and systems influence and are in turn influenced by their surroundings.
Indeed, the networks of relationships that exist between different entities may, in some cases, be extensive and highly complex. Thus the 'environment' may be regarded as a 'space' or a 'field' in which networks of relationships, interconnections and interactions between entities occur.3
Sanitation is the conditions relating to public health, especially the provision of clean drinking water and adequate sewage disposal and can be defined as the provision of facilities and services for the safe disposal of human urine and feces. As WHO declares “Sanitation refers to the provision of facilities and services for the safe management of human excreta from the toilet to
containment and storage and treatment onsite or conveyance, treatment and eventual safe end use or disposal. More broadly sanitation also included the safe management of solid waste and animal waste”. 4
"Environmental sanitation" means the art and science of applying sanitary, biological and physical science principles and knowledge to improve and control the environment and factors therein for the protection of the health and welfare of the public. This article highlights the burden of 5
environmental sanitation as well as implication of sanitation problems.
The burden of environmentThe issues of sanitation and hygiene are closely related to perceptions of pollution and dirt, as well as wholesomeness or cleanliness. Scientists refer sanitation (as well as food-hygiene rules) to a universal human activity of classification. This implies that there is no universal specification of dirt itself; rather, what are considered dirty are items out of place in that society's classification system or hierarchies. Hence, dirt is referred to as “disorder” and exists only “in the eye of the beholder”. Such values are of immense importance for how sanitation can be organized and upheld in a society.6
Globally, 946 million people still open defecate (9 out of 10 live in rural areas), 2.4 billion people lack access to basic sanitation (7 out of 10 in rural areas), 663 million lack access to basic water sources, and diarrhea is the second leading cause of death in children under five much of which is preventable by clean water and sanitation. 7,8
Though Bangladesh has for many years enjoyed almost universal access to drinking water, arsenic contamination of 22 percent of the country's tube wells lowered the service coverage to below 80 percent. Bangladesh has made significant progress in reducing open defecation, from 34 percent in 1990 to just one percent of the national population in 2015.However, the current rate of improved sanitation is 61 percent, growing at only 1.1 percent annually. Still, the quality of sanitation coverage is an emerging area of concern, with more than 40 percent of all latrines classified as “unimproved.” Drinking water access is widespread, but half of the drinking water consumed fails to meet water safety standards. In urban areas of Bangladesh, piped water supply reaches only about one-third of the population, and there is no systematic sewer disposal and treatment system. Only Dhaka, Bangladesh's capital city, has a sewer system, and it serves just 18 percent of the city.9
Bangladesh has made remarkable progress to in eliminating the practice of open defecation. But climbing the 'sanitation ladder' still represents a challenge. Access to sanitation remains moderate at 55.9 per cent. The knowledge of key
Review Article
Environmental Sanitation: The Public Health Challenge1 2Tarafdar M A , Rahman M T
1 Monowar Ahmad Tarafdar Professor, Department of Community Medicine Z H Sikder Women's Medical College, Dhaka.
2 Mohammad Tanvir Rahman, psc, Engrs Major,Utility Shifting Officer, Service Area-3 Padma Bridge Rail Link Project (PBRLP), Jajira, Shariatpur, Bangladesh.
Correspondence to:Monowar Ahmad TarafdarProfessor, Department of Community MedicineZ H Sikder Women's Medical College, Dhaka.Email: [email protected]
33
Journal of Diabetic Association Medical College 2019;3(1)33-35

Environmental Sanitation: The Public Health Challenge Tarafdar M A
hygiene messages is high in Bangladesh, but the practice of effective handwashing, the most effective hygiene behaviour, is very low. Conventional sewerage systems are absent in all urban areas except Dhaka. But even in the capital city, only 1 in 5 people are served by a sewer network. The safe disposal of faecal matter generated in rural and urban areas is recognised as a major challenge by the Bangladesh government. Only about two out of five households practice safe disposal of child faeces, despite implications that lead to illness and death of children. There are solid links among diarrhoeal diseases, stunting and sanitation. Unimproved sanitation can lead to faecally transmitted infections like diarrhoea, intestinal
10inflammation and worms.
To minimize environmental burden the country is having activities aimed at improving or maintaining the standard of basic environmental conditions affecting the well-being of people. These conditions include (1) clean and safe water supply, (2) clean and safe ambient air, (3) efficient and safe animal, human, and industrial waste disposal, (4) protection of food from biological and chemical contaminants, and (5)
11adequate housing in clean and safe surroundings.
Environmental sanitation was defined as “the control of all those factors in man's physical environment which exercise or may exercise a deleterious effect on his physical, mental or social well-being.” Methods for the safe and adequate disposal of excreta and sewage and clean and ample water
12supplies were among the priorities.
Improving health is one of the main goals of water and environmental sanitation interventions. Despite this, many aid and development workers working in the field of water and environmental sanitation have only a limited knowledge of the infections they try to prevent. Although the relevant information does exist, it is often scattered in specialized literature and rarely finds its way into the
13field. In recent years, there has been increasing pressure, particularly in the underdeveloped nations, for bettering
14the rural sanitary environment.
Implication of Sanitation problem'The sanitary revolution' of introducing piped water and waterborne sewerage to people's homes in 19th Century Europe was voted the most important medical milestone since 1840, beating even the discovery of antibiotics and
15the development of anesthesia.
In many developing nations dry onsite sanitation systems are the norm and hence there is no direct requirement for
16water (other than for personal and domestic hygiene).
Sustainability has become a central theme of environmental, human development and resource use studies. Although the idea of sustainability has many facets, the central idea is that we should use resources in ways that do not diminish them. An important question in environmental studies today is how continuous improvements can be made in human
welfare within the limits of the earth's natural resources. This is because the problem of environmental pollution has assumed a serious and gigantic proportion and this threatens
17the very existence of human society.
Poor sanitation resulting from the practice of widespread open defecation and indiscriminate dumping of refuse have negative health and social impacts on communities with negative health consequences. Sanitation service provision is known as a “Top-Down” approach at the central, regional, district and/or municipal levels to the neglect of community members who are beneficiaries of the project. This resulted in a poor maintenance of the services
18provided.
Sanitation can be said to be the state of cleanliness. It is a broad concept and connotes the process of keeping something clean. Sanitation is the arrangement for protecting the health, especially the removal of the human, industrial and domestic wastes. Sanitation is also a process embarked upon to keep the total of man's environment
19hazard free.
Slum dwellers are likely to be among the most deprived people in urban areas. Poor hygiene practices and inadequate sanitary conditions play major roles in the increased burden of communicable diseases within developing countries and continuous community hygiene education along with adequate access to water supply and
20sanitation improves hygiene behavior.
In areas where a large proportion of the population is not served with adequate water supply and sanitation, sewage flows directly into streams, rivers, lakes, and wetlands, affecting coastal and marine ecosystems, fouling the environment and exposing millions of children to disease. Particularly, in the context of urbanization, domestic wastewater, sewage, and solid waste improperly discharged presents a variety of concerns from providing breeding grounds for communicable disease vectors to contributing to air, water, and soil pollution. The results of poor waste management also contribute to a loss of valuable biodiversity. Improved sanitation reduces environmental burdens, increases sustainability of environmental resources and allows for a healthier, more
21secure future for the population.
Implementation of low-cost sanitation system with lower subsidies, greater household involvement, range of technology choices, options for sanitary complexes for women, rural drainage systems, IEC and awareness building, involvement of NGOs and local groups, availability of finance, human resource development, and emphasis on school sanitation are the important areas to be considered. Also, appropriate forms of private participation and public private partnerships, evolution of a sound sector policy in Indian context, and emphasis on sustainability with political commitment are prerequisites to bring the change.22
34
There are serious scientific grounds for concern, and a need for objective evidence. However there is often a perverse preference for alarm rather than reassurance. 'They are poisoning us' is a favorite refrain of the media, but only
23because people want to hear it.
A growth in population creates more work for the administration. To deal with the problems of population growth, various organizations need to work together; for example, water, sanitation and health service providers, and non-governmental organizations (NGOs). When growth is rapid, these organizations can be overwhelmed and so coordination can break down. This may mean that in some cases, efforts are duplicated, and sometimes there will be gaps in addressing some aspects of the programme. If public administration and regulation is already weak, the entire system can fail. In the absence of good regulation, standards of sanitation and waste provision can fall, increasing pressures in other areas such as health services.24
References1. Dictionary online. Available from: URL:
www.dictionary.com
2. Johnson, D. L.; Ambrose, S. H.; Bassett, T. J.; Bowen, �M. L.; Crummey, D. E.; Isaacson, J. S.; Johnson, D. N.; Lamb, P.; Saul, M.; Winter-Nelson, A. E. Meanings of Environmental Terms. Journal of Environmental Quality. 1997, 26 (3): 581–589.
3. What is 'the environment'. The Earth System and its �Components. Available from: https://www.soas.ac.uk/ cedep-demos/000_P500_ESM_K3736-Demo/unit1/ page_08.htm
4. WHO. Available from: URL: https://www.who.int/ �topics/sanitation/en/
5. Oregon Legal Glossary. Available from: URL:https:// �www.o regon laws .o rg /g lo s sa ry /de f in i t i on / environmental_sanitation
6. Jiménez A, Cortobius M and Kjellén M. Water, �sanitation and hygiene and indigenous peoples: a review of the literature, Water International, 2014, 39:3, 277-293.
7. WHO/UNICEF JMP. WHO/UNICEF Joint �Monitoring Program (JMP) for Water Supply and Sanitation. 2015
8. WHO. Safely managed drinking water- thematic �report on drinking water 2017. World Health Organization. Geneva, Switzerland.2017.
9. World Bank October 8, 2016. Bangladesh: Improving �Water Supply and Sanitation. Available From: URL: https://www.worldbank.org/en/results/2016/10/07/bangladesh-improving-water-supply-and-sanitation
10. UNICEF. Safer sanitation and hygiene: Quality, �equitable access and sustainability. https://www. unicef. org/bangladesh/en/better-access-safe-drinking- water/safer-sanitation-and-hygiene
11. Available from: URL: http://www.businessdictionary. �com/ definition/environmental-sanitation
12. WHO. https://www.who.int/water_sanitation_health/ �environmentalsanitation.pdf
13. Control ing and prevent ing disease. Erik �Rottier,Margaret Ince. Available from: URL: https://ec.europa.eu/echo/files/evaluation/watsan2005/annex_files/WEDC/diseases/cpd01.pdf
14. World Health Organization. Sanitation and Hygiene �policies. Available from: https://www.who.int/ water_ sanitation_health/hygiene/sanhygpromo3.pdf?ua=1
15. BMJ. Editorial . Brit ish Medical Journal. �2007;334:111. [PMC free article] [PubMed] [Google Scholar]
16. Peter A. Harvey. Environmental Sanitation Crisis: �More than just a health issue Environtal Health Insights. 2008; 2: 77–81. Available from: URL: ht tps: / /www.ncbi .nlm.nih.gov/pmc/art icles/ PMC3091339/
17. Sadiq Q. O., Ezeamaka C. K.*, Daful M. G., Anjide T. �W., Sani H. and Ogbole M. Environmental sanitation practices in Kuchigworo and Garamajiji along airport road, Abuja; Journal of Geography and Regional Planning December 2018; Vol. 11(11):172-182
18. Abalo E M, Agyemang S, Atio S, Ofosu-Bosompem D, �Peprah P and Ampomah-Sarpong R. Environmental sanitation unleashed: Effectiveness and challenges of the National Sanitation Day as a community sanitation participatory approach in Aboabo, Ghana; Cogent Environmental Science, 2017, 3:1, 1405888. Available from: URL: https://doi.org/10.1080/23311843. 2017.1405888
19. Smart N U. Environment, Sanitation, and Health. �Environmental Review Journal. 2000, 3: 206-214.
20. Farah S, Karim M, Akther N, Begum M, Begum N. �Knowledge and Practice of Personal Hygiene and Sanitation: A Study in Selected Slums of Dhaka City; Delta Med Col J. Jul 2015; 3(2): 68-73
21. Shaikh BT, Hatcher J. Health seeking behaviour and �health service utilization in Pakistan: Challenging the policy makers. J Public Health (Oxf) 2005;27:49-54.
22.� Kumar S G, Kar SS, Jain A. Health and environmental sanitation in India: Issues for prioritizing control strategies. Indian J Occup Environ Med [serial online] 2011 [cited 2020 Feb 18];15:93-6. Available from: http://www.ijoem.com/text.asp?2011/15/3/93/93196
23.� Rose G. Environmental health: problems and prospects Journal of the Royal College of Physicians of London January 1991, 25 (1): 48-52
24.� Introduction to Sanitation and Waste Management. Available from: URL: https://www.open.edu/ openlearncreate/mod/oucontent/view.php?id=80395&printable=1
35
Journal of Diabetic Association Medical College 2019;3(1)33-35 Vol. 03, No. 01, January 2019

Abstract The incidence of genital tuberculosis varies widely with the social status of the patient and her environment. The incidence is about 1% amongst gynaecological patients attending the outpatient department in the developing country. Genital TB may be asymptomatic and the majority of women are diagnosed during investigations of infertility. Genital system TB represents 15-20% of extrapulmonary TB and is usually asymptomatic affecting mainly young women in the reproductive age group. Here we presented a case of genital TB which was diagnosed during laparotomy. After confirmation of diagnosis by histopathology, the case was successfully managed by antitubercular therapy for 9 months.
Keywords: Genital tuberculosis.
IntroductionTuberculosis is a worldwide disease with greater prevalence where the population is concentrated in areas with poor sanitation and unfavorable social and economic condication. Genital TB is one form of extra pulmonary TB and is not uncommon.
The incidence is about 1% among gynaecological patients attending the outpatient department in the developing
1countries. The causative organism is M. tuberculosis human type.
Genital TB occurs mostly secondary to pulmonary tuberculosis. Commonly by the haematogenous route in a manner similar to spread to other extra pulmonary sites like urinary tract, bones and joints etc.
The fallopian tubes are affected in almost 100% of cases followed by the endometrium in 50%, ovaries in 20%, cervix in 5% and vulva and vagina1%.1
The initial sites of infection is in the submucosal layer of
the ampullary part of the tube. Direct inoculation of tubercle bacilli can also take place over vulva or vagina during sexual intercourse with a partner suffering from tuberculous lesion of genitalia.
The infection is restricted mostly (80%) to childbearing period (20-40 years). Genital tuberculosis occurs in 10-20% of patients who have pulmonary tuberculosis in adolescence . The symptoms of genital tuberculosis are 1
infertility, menstrual abnormality, amenorrhoea or oligomenorrhoea, chronic pelvic pain. Tubo-ovarian mass, vaginal discharge in the form of postcoitalbleeding or blood stained discharge and constitutional symptoms such as loss of weights, malaise, anorexia, pyrexia and anemia etc.
Case ReportLuchita, 16 years old unmarried young girl presented of outpatient department of Diabetic Association Medical College Hospital with the complaints of abdominal pain, generalized weakness, per vaginal whitish discharge. Her menstrual cycle was regular with average flow and duration. Her age of menarche was at 13 years of age. Her grandfather sufferings from TB 2 years back. On examination her weight was 47 kg, BP- 100/70 mmHg. On per abdominal examination there was a lump 8×10 cm in diameter. Occupying partly left iliac, left lumber, umbilical and hypogastrium region. Margin was irregular, smooth surface, firm in consistency and mobility was restricted. She was admitted for further evaluation with a plan of laparotomy. Her USG report revealed thick wall septated cyst with floating low level internal echoes (9.9cm×5.5cm; approx. vol. 132ml) is noted in pelvic region. Her CA-125 was 98.5 µ/ml. chest x-ray was normal. Other investigation shows no abnormality.
Her laparotomy was done. After opening of abdomen there was dense adhesion of left adnexa with surrounding structure with intestine and omentum.
Adhesiolysis was done as per as possible after taking biopsy and peritoneal toileting abdomen was closed in layers.
Case Report
Female Genital Tuberculosis1 2 4 4 5Ahmed S , Shaha D R , Begum P , Akter T , Akter H ,
1. Dr. Shahana Ahmed; FCPS (Obst And Gynae) Associate Professor, Department of Obstetrics and Gynaecology Diabetic Association Medical College, Faridpur.
2. Prof. Dr. Dipti Rani Shaha; FCPS (Obst and Gynae) Professor & Head, Department of Obstetrics and Gynaecology Diabetic Association Medical College, Faridpur.
3. Dr. Poly Begum; FCPS (Obst and Gynae) Associate Professor, Department of Obstetrics and Gynaecology Diabetic Association Medical College, Faridpur.
4. Dr. Tahmina Akter, MD (Paediatric Medicine) Associate Professor, Department of Paediatrics Diabetic Association Medical College, Faridpur.
5. Dr. Hasnina Akter, MPhil (Radiotherapy) Assistant Professor, Department of Oncology Diabetic Association Medical College Hospital, Faridpur.
Correspondence to:Dr. Shahana Ahmed, MBBS, FCPS (Obst & Gynae) Assistant Professor, Department of Obstetrics & GynecologyDiabetic Association Medical College, Faridpur. E-mail: [email protected]
36
Journal of Diabetic Association Medical College 2019;3(1)36-38

Female Genital Tuberculosis Ahmed S
Biopsy report showed tissue from ovarian cystic mass showing granulomatous inflammation, section from the piece of tissue reveal granulation tissue. The granulation tissue contains granulomas. The granuloma was composed of epitheloid cells containing Langhan’s type of giant cell.
The treatment consists of Isoniazide plus Rifampicin plus Ethambutol plus Pyrazinamide orally. In addition pyridoxin 300 mg a day was also administered to prevent neuropathy. Antitubercular therapy was continue for 9 months and hepatic and renal function tests and periodical eye fundus, visual acuity and visual fields examinations were normal during follow up.
Discussion Although genital TB can occur in any age group. The majority of patients are in the reproductive age group. 75% 2
of them being in the 20-45 years age . Postmenopausal 2
women accounts for 7-11% of cases of genital TB.
Genital TB may be asymptomatic and the majority of women are diagnosed during investigations of infertility. 3
Systemic constitutional symptoms of weight loss, feeling unwell and night sweats may be resemble classical acute pelvic inflammatory disease (PID). M. tuberculosis is the 4 causative organism in 90-95% of cases where as Mycobacterium bovis can also causes the disease.5
Infection of the female genital tract with TB is relatively rare entity. There are two main routes for the infection, the first is blood borne from a primary site such as the lungs, or kidneys. The other route is through sexual intercourse where the infection can manifest itself as local lesions. Infection of the vulva, vagina and cervix can be caused by direct inoculation in the lower female reproductive tract if the sexual partner has genital and/or urinary TB infection. In that respect genital TB can be considered a sexually transmitted disease.6
Endometrial TB and involvement of the fallopian tubes are obvious explanations in relation to infertility as these conditions can interfere with implantation and sperm/zygote transport. In a study concerning the effect of genital TB on fertility hysterosalpingogram (HSG) revealed tubal abnormalities in 17 (95.2%) out of 21 patients. The most common abnormality was a bilateral tubal blockage and deformity of the uterine cavity was found to be as 54.4% of cases. TB can also affect the ovaries and cervix and this 7
may have an impact on fertility as well. Another important manifestation of genital TB is menstrual irregularities. Irregularities may include oligomenorrhoea or amenorrhoea. An important pathological finding in women with genital TB in Asherman's syndrome that explains the menstrual irregularities and infertility as well. Intra and postoperative complications are increased after surgery in women with genital TB.8
General abdominal and pelvic examination findings are normal in majority of genital tuberculosis patients. A 9,10
pelvic mass may be identified and adnexal tenderness may be elicited.
Diagnosis is achieved most effectively through a combination of a high index of suspicion especially in areas of low prevalence through initial clinical assessment and the case of appropriate investigations. High risk factors include a history of previous pulmonary TB infection. Contact with a pulmonary TB sufferer, recent travel to or migration from high prevalence countries.11
Chest X-ray is aimed at demonstrating current or past TB lesions in the lungs, which are a common site for primary infection. However, most chest X-ray are normal.12
Whenever feasible, every effort should be made to send specimens and tissue for culture, In order to confirm diagnosis and establish drug sensitivities. Suspected tuberculous lesions in accessible sites such as the vagina, cervix and the vulva may be biopsied directly. Endometrial tissue may be obtained by aspiration biopsy or dilatation and curettage or directly at hysteroscopy. Endometrial biopsy is best performed in the premenstrual period. Menstrual fluid can be obtained from the vagina during the first menstruation for culture and microscopy.13
Histology demonstrates the typical caseous granulomatous lesion with giant epitheloid cells. Rapid nucleic acid amplification techniques such as polymerase chain reaction (PCR) allow direct identification of M. tuberculosis in clinical specimens. Such methods can detect fewer than ten organisms in clinical specimens compared with 10000 necessary for smear positivity. Although PCR is more sensitive (85-95%) than microscopy and bacteriological culture on pulmonary specimens. It does not distinguish live from killed bacilli.12,13
Abdominal and pelvic ultrasound, computed tomography (CT) and magnetic resonance imaging (MRI) are employed in circumstance where an abdominal or pelvic mass is present.14
ConclusionThe incidence of female genital TB is increasing. So gynaecologists will be increasingly faced with cases of TB and its consequences. Genital TB may be asymptomatic or may present with atypical symptoms or mimic other conditions. It is imperative to consider the possibility of TB in women in the reproductive age group, who present with the symptoms of infertility, chronic pelvic pain and menstrual dysfunction. Where other causes have been excluded. This is particularly important when these women full into the high risk category for TB infection.
Referencesth1. DC Dutt's Textbook of Gynecology, Hiralal konar, 7
Edition, Genital Tuberculosis, Page-113-115.
2. Has DW. Mycobacterial diseases. In: Mandell GL,
37

Bennet JE, Dolin R, editors. Principles of Practice of Infectious Diseases. Philadelphia, PA: Churchill Livingstone;2000.p. 2576-607.
3. Aka N,Vural TZE. Evaluation of patients with active pulmonary tuberculosis for genital involvement. J ObsetetGynaecol Res 1997;23:337-40.
4. Rajamaheswari N. Pelvic tuberculosis [www.Sunned. org/pelvictb.html].
5. Cow TWP, Lim KB,Valliparim S. The masquerades of female pelvic tuberculosis: case reports and review of literature on clinical presentation and diagnosis. J ObstetGynaecol Res 2002;28:203-10.
6. Chowdhury NN. Overview of tuberculosis of the female genital tract. J Indian Med Assoc 1996;94:345-6.
7. LambaH,Bryne M. GoldinR,Jenkins C Tuberculosis of the cervix: case presentation and a review of the literature. Sex transm Infect 2002;78:62-3.
8. Qureshi RN, Sanmad S, Hamd R, Lakha SF. Female genital tuberculosis revisited. J Pak Med Assoc 2001;51:16-18.
9. Gaur BM, Megashwari B, Lal N. Tuberculosis Endometritis: a clinic-pathological study of 1000 cases. Br JObsetetGynaecol 1983;90:84-6.
10. Samal S, Gupta U, Agarwal P. Menstrual disorders in genital tuberculosis. J Indian Med assoc 2000;98:126-7.
11. Muechler E, MinkowitzS.Postmenopausal endometrial tuberculosis. ObsetetGynaecol 1971;38:768-70.
12. Health protection agency. Preliminary Annual Report on Tuberculosis Reported in 2002 I England, Wales and Northern Ireland. London: HPA; 2004 [www.hpa.org.uk/infections].
13. Rose AMC, Sinka K, Watson JM, Mortimer JY, CarlettA.An estimate of the contribution of HIV infection to recent rise in tuberculosis in England and Wales. Thorax 2002;57:442-5.
14. Raut VS, Mahasvir AA, Sheth SS. The Montoux test in the diagnosis of genital tuberculosis in women. Int J GynaecolObstet 2001;72:165-9.
38
Vol. 03, No. 01, January 2019Journal of Diabetic Association Medical College 2019;3(1)36-38
Diabetic Association Medical College, Faridpur