Timothy M. Pawlik, Richard D. Schulick and ... - CiteSeerX
16
Timothy M. Pawlik, Richard D. Schulick and Michael A. Choti Expanding Criteria for Resectability of Colorectal Liver Metastases doi: 10.1634/theoncologist.2007-0142 2008, 13:51-64. The Oncologist http://theoncologist.alphamedpress.org/content/13/1/51 located on the World Wide Web at: The online version of this article, along with updated information and services, is by guest on March 1, 2014 http://theoncologist.alphamedpress.org/ Downloaded from by guest on March 1, 2014 http://theoncologist.alphamedpress.org/ Downloaded from
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Timothy M. Pawlik, Richard D. Schulick and ... - CiteSeerX

Timothy M. Pawlik, Richard D. Schulick and Michael A. ChotiExpanding Criteria for Resectability of Colorectal Liver Metastases
doi: 10.1634/theoncologist.2007-01422008, 13:51-64.The Oncologist
http://theoncologist.alphamedpress.org/content/13/1/51located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by guest on March 1, 2014
http://theoncologist.alphamedpress.org/
Dow
nloaded from
by guest on March 1, 2014
http://theoncologist.alphamedpress.org/
Dow
nloaded from

Expanding Criteria for Resectability of Colorectal Liver Metastases
TIMOTHY M. PAWLIK, RICHARD D. SCHULICK, MICHAEL A. CHOTI
Department of Surgery, Johns Hopkins University School of Medicine, Baltimore, Maryland, USA
Key Words. Colorectal cancer • Liver • Metastases • Resection • PrognosisDisclosure: No potential conflicts of interest were reported by the authors, planners, reviewers, or staff managers of this article.
LEARNING OBJECTIVES
After completing this course, the reader will be able to:
1. Identify the criteria for hepatic resection of colorectal metastases.
2. Describe strategies for expanding the number of patients who may potentially benefit from hepatic resection.
3. List the factors associated with poor prognosis following hepatic resection.
Access and take the CME test online and receive 1 AMA PRA Category 1 Credit™ at CME.TheOncologist.comCMECME
ABSTRACT
Surgical resection is the treatment of choice in patientswith colorectal liver metastases, with 5-year survivalrates reported in the range of 40%–58%. Over the past10 years, there has been an impetus to expand the crite-ria for defining resectability for patients with colorectalmetastases. In the past, such features as the number ofmetastases (three to four), the size of the tumor lesion,and a mandatory 1-cm margin of resection dictated whowas “resectable.” More recently, the criteria for resect-ability have been expanded to include any patient inwhom all disease can be removed with a negative mar-gin and who has adequate hepatic volume/reserve. Spe-cifically, instead of resectability being defined by what isremoved, decisions concerning resectability now centeraround what will remain after resection. Under this newparadigm, the number of patients with resectable dis-
ease can be expanded by increasing/preserving hepaticreserve (e.g., portal vein embolization, two-stage hepa-tectomy), combining resection with ablation, and de-creasing tumor size (preoperative chemotherapy). Thecriteria for resectability have also expanded to includepatients with extrahepatic disease. Rather than being anabsolute contraindication to surgery, patients with bothintra- and extrahepatic disease should potentially beconsidered for resection based on strict selection crite-ria. The expansion of criteria for resectability of colo-rectal liver metastases requires a much more nuancedand sophisticated approach to the patient with ad-vanced disease. A therapeutic approach that includes allaspects of multidisciplinary and multimodality care isrequired to select and treat this complex group ofpatients. The Oncologist 2008;13:51–64
INTRODUCTION
The incidence of colorectal cancer is approximately150,000 new cases per year in the U.S. [1]. Approximately
one half of these patients either present with hepatic metas-tases or develop them during the course of their disease [2].These hepatic metastases are discovered synchronously in
Correspondence: Timothy M. Pawlik, M.D., M.P.H., Department of Surgery, Johns Hopkins, 600 North Wolfe Street, Halsted 614, Bal-timore, Maryland 22187-6681, USA. Telephone: 410-502-2387; Fax: 410-502-2388; e-mail: [email protected] Received August 10,2007; accepted for publication November 30, 2007. ©AlphaMed Press 1083-7159/2008/$30.00/0 doi: 10.1634/theoncologist.2007-0142
TheOncologist®
Hepatobiliary
The Oncologist 2008;13:51–64 www.TheOncologist.com
by guest on March 1, 2014
http://theoncologist.alphamedpress.org/
Dow
nloaded from

15%–25% of patients [3–5], while 20%–25% of patientsmetachronously develop hepatic tumors [6 – 8]. In 30%–50% of patients with either synchronous or metachronousliver metastases, the liver is the only site of metastaticdisease [9]. Thus, 10,000–15,000 patients per year are can-didates for local therapy for colorectal metastases [8].
Although ablative therapies are frequently used, resec-tion of liver metastases, when possible, remains the pre-ferred therapy for potential cure [10]. The overall 5-yearsurvival rates are in the range of 35%–58% in the major se-ries reporting on the results of hepatectomy with curativeintent [10–19]. Patients with untreated metastatic colorec-tal cancer have a short median survival time of approxi-mately 12 months [20 –24]. Although the progress ofdeveloping effective agents has accelerated, the mediansurvival time of unresected patients is still in the range of16–24 months, and survival beyond 5 years is uncommon[25–36]. Given that surgical resection remains the bestchance for cure, there has been considerable interest in ex-panding the criteria for resectability of patients with colo-rectal metastasis using other adjunctive and adjuvantapproaches.
OLD PARADIGM: TRADITIONAL FACTORS
ASSOCIATED WITH RESECTABILITY
Previously, clinicopathologic factors were used to definethe appropriateness of attempting hepatectomy for colorec-tal metastases. These factors concentrated on the lesions tobe removed and patient factors rather than the liver thatwould remain. In a 1986 publication by Ekberg et al. [37],the authors proposed several general contraindications tohepatectomy for metastatic colorectal cancer. These criteriaincluded: four or more metastases within the liver, addi-tional extrahepatic metastatic disease, large size of hepaticmetastases, and the inability to achieve a resection marginof at least 1 cm. Multiple subsequent studies from othergroups then corroborated some or all of these findings.With time, these clinicopathologic factors were used to de-termine which patients with colorectal liver metastases had“resectable” disease.
Subsequently, these studies were criticized both on clin-ical and methodological grounds. One major problem isthat only a small number of patients who actually met all the“unresectable” criteria were included in the analyses. Ad-ditionally, most of these studies used only univariate (log-rank) analyses, which do not adjust for competing riskfactors that may have affected survival. Systemic chemo-therapy and the availability of adjunctive techniques suchas radiofrequency ablation (RFA) and portal vein emboli-zation (PVE) have greatly changed our management of pa-tients. These new techniques make the application of these
older data to current paradigms of treatment problematic.Community physicians, oncologists, and even some sur-geons still use these factors to determine resectability of pa-tients with colorectal metastases and fail to refer potentiallyresectable patients.
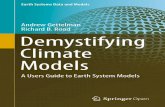
Tumor NumberPrevious studies have placed an inordinate emphasis on theassociation between the number of hepatic metastases andsurvival. For example, both Cady et al. [3] and Ekberg et al.[37] reported no disease-free survivors at 48 months, andHughes et al. [38] reported a 5-year survival rate of only18% for patients with four or more metastases. Many sur-geons interpreted these data to indicate four or more lesionsas a relative contraindication to hepatic resection, eventhough this survival rate exceeds what is reported followingpancreaticoduodenectomy for pancreatic cancer or transhi-atal esophagectomy for esophageal cancer. More recently,in an era of better adjuvant therapy and imaging modalities,Altendorf-Hofmann and Scheele [8] reported the lack of asurvival difference between patients who had one to threemetastases and patients who had four or more metastases aslong as they underwent an R0 (i.e., microscopically nega-tive) resection (Fig. 1). In another series of 159 patientswith four or more metastases who had a median of five he-patic metastases resected, Pawlik et al. [39] reported 5-yeardisease-free and overall survival rates of 22% and 51%, re-spectively. That study demonstrated that response to preop-erative chemotherapy was a much more robust factor inpredicting long-term survival than the number of hepaticmetastases. Specifically, analysis revealed that patientswho failed to have a measurable reduction in tumor size fol-lowing neoadjuvant chemotherapy had over a 2.5 timeshigher risk for cancer-related death following surgical treat-ment. These data suggest that higher tumor numbers shouldnot be used to deny patients a potentially curative resection.
Tumor SizeTumor size has been studied as a prognostic factor and re-sults have been mixed. Some studies [10, 14, 40] have re-ported tumor size to be important in regard to prognosis,whereas numerous other studies [9, 13, 41, 42] have failedto demonstrate this association. Given theses conflicting re-sults, the size of hepatic metastases cannot be accepted as acriterion for determining which patients should be taken tothe operating room. Size may negatively impact the sur-geon’s ability to gain negative margins or to leave an ade-quate remnant, but if a patient is potentially resectable theyshould not be denied the opportunity to have their diseasecompletely resected. Additionally, tumor size may be afunction of when the tumor is found during the disease
52 Colorectal Liver Metastases
by guest on March 1, 2014
http://theoncologist.alphamedpress.org/
Dow
nloaded from

course, rather than a true predictor of biological aggressive-ness.
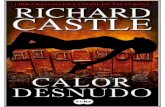
Surgical Margin <1 cmSurgical margin status has long been held as an importantcriterion for resectability and continues to be so. Cady et al.[43] reported that a surgical margin �1 cm was associatedwith a significantly shorter disease-free survival duration.Many centers adopted the “1 cm rule” as a minimal marginto obtain at the time of hepatic resection. They have sug-gested that an anticipated surgical margin �1 cm is an ab-solute or relative contraindication to surgery. The status ofthe surgical margin has been shown to be important in long-term outcomes following resection of colorectal liver me-tastases. Multiple studies [8, 13, 44, 45] have shown that anegative resection margin decreases local recurrence ratesand improves survival. Complete removal of all macro-scopic disease with negative microscopic resection marginsis a very strong determinant of long-term outcome in allstudies. In a study by Altendorf-Hofmann and Scheele [8],the median survival time of patients who underwent an R1or R2 resection was only 14 months, compared with 44months for those patients who underwent an R0 resection(Fig. 2a) [8].
In a more recent study by Choti et al. [13], patients whohad a positive microscopic resection margin had a mediansurvival time of only 24 months, compared with 46 monthsfor patients with a negative surgical margin. In that study, apositive surgical margin was associated with a 3.5 timeshigher relative risk for disease-specific death. Given theoverwhelming significance of a clear margin, then what isan acceptable negative microscopic margin? Early studies
[43, 46] suggested that patients with a margin �10 mm hadbetter outcomes than those with microscopically clear butcloser margins. On multivariate regression analysis withadjustment for other confounding risk factors, these find-ings have not been corroborated. Rather, more recent stud-ies [8, 44] have shown that survival was not associated withthe width of the negative surgical margin as long as theywere completely microscopically negative.
Pawlik et al. [44] reported on 557 patients in whom theinfluence of surgical margin status on survival and site of
Figure 1. Whereas in the past a tumor number greater thanfour was considered a relative contraindication to hepatic re-section, more recent data reveal no survival difference betweenpatients who had one to three metastases and those who hadfour or more metastases, all of whom had undergone an R0(i.e., microscopically negative) resection. From Altendorf-Hofmann A, Scheele J. A critical review of the major indica-tors of prognosis after resection of hepatic metastases fromcolorectal carcinoma. Surg Oncol Clin N Am 2003;12:165–192, xi, with permission.
Figure 2. Survival following hepatic resection of colorectalmetastases is not associated with the width of the negative sur-gical margin as long as the margin is completely microscopi-cally negative. (A): Complete removal of all macroscopicdisease and negative microscopic resection margins are verystrong determinants of long-term outcome. The median sur-vival time of patients who underwent an R1 or R2 resectionwas only 14 months, compared with 44 months for those pa-tients who underwent an R0 resection. From Altendorf-Hof-mann A, Scheele J. A critical review of the major indicators ofprognosis after resection of hepatic metastases from colorectalcarcinoma. Surg Oncol Clin N Am 2003;12:165–192, xi, withpermission. (B): However, the width of the surgical margindoes not appear to significantly affect survival in patients withnegative margins. That is, no significant difference in survivalwas seen in patients with a negative surgical margin, regardlessof the width of the margin. From Pawlik TM, Scoggins CR,Zorzi D et al. Effect of surgical margin status on survival andsite of recurrence after hepatic resection for colorectal metas-tases. Ann Surg 2005;241:715–722; discussion 722–724, withpermission.
53Pawlik, Schulick, Choti
www.TheOncologist.com
by guest on March 1, 2014
http://theoncologist.alphamedpress.org/
Dow
nloaded from

recurrence following curative hepatic resection was specif-ically evaluated. In that study, patients were classified ac-cording to the width of the resection margin, defined as theshortest distance from the edge of the tumor to the line oftransection. A positive margin was defined as the presenceof exposed tumor along the line of transection detected byhistologic examination, and margin recurrence was definedas evidence of new tumor involving the parenchymal tran-section line. On final pathologic analysis, margin status waspositive in 45 patients and negative by 1–4 mm in 129, 5–9mm in 85, and at least 1.0 cm in 298. Among the 45 patientswith a positive margin, the diagnosis of positive margin wasmade postoperatively in 34 patients and intraoperatively in11 patients. Of the patients who recurred, only 21 patients,or 4%, developed a recurrence at the site of the surgicalmargin. Among these 21 patients, only four had the surgicalmargin as the sole site of recurrence. With regard to factorspredictive of pattern of recurrence, patients with a positivesurgical margin had a higher overall recurrence rate, 51%,compared with about 40% for patients with a negative sur-gical margin. However, patients with a negative margin, re-gardless of the margin width, had similar overall recurrencerates. Only a positive surgical margin was associated withsurgical margin recurrence. The 5-year survival rate was17% for patients with a positive margin, compared with64% for patients with a negative surgical margin. The widthof the surgical margin did not significantly affect survival inpatients with negative margins. That is, no significant dif-ference in survival was seen in patients with a negative sur-gical margin, regardless of the width of the margin (Fig.2B). Furthermore, on multivariate analysis, margin statuswas not a significant predictor of survival.
It is clear that patients should be evaluated for resectionbased on the ability to resect all metastases with negativehistologic margins (along with preservation of adequate he-patic function). Patients should not be denied a potentiallycurative resection based on the prediction that a 1-cm mar-gin will not be obtainable.
Extrahepatic DiseaseThe presence of extrahepatic disease (exclusive of the pri-mary lesion and associated locoregional nodes) is acceptedto portend a worse prognosis following liver resection ofcolorectal metastases. Patients with extrahepatic diseasehave a significantly shorter overall survival time than pa-tients with liver-only disease (Fig. 3). The presence ofextrahepatic disease has become a well-accepted contrain-dication to liver resection for metastatic colorectal cancerbased on these patients having a worse prognosis. Initial re-ports by Adson et al. [15] and Hughes et al. [38] stated thatno patient with extrahepatic disease survived beyond 5
years. More recently, in the late 1980s and 1990s, othergroups [10, 14, 40] reported 5-year survival rates of 10%–20%. Interpretation of these studies should be done cau-tiously for multiple reasons. In many of these studies, directinvasion of adjacent structures was considered extrahepaticdisease. Although technically this may be true, direct inva-sion of a hepatic metastasis into an adjacent resectablestructure does not connote the same risk as a separate site ofextrahepatic metastasis. Many of these studies included toofew patients with extrahepatic disease to allow appropriatestatistical analysis. Lastly, all of these studies were carriedout before the current era of more active chemotherapyagents and more robust adjunctive techniques.
NEW PARADIGM: SHIFTING FOCUS ON HOW
RESECTABILITY IS DEFINED
Based on the currently available data, the prognostic impor-tance of clinicopathologic factors in deciding who is“resectable” is at best inconsistent and conflicting. Conven-tional clinicopathologic factors, although perhaps generallyinstructive with regard to prognosis, should not be used todefine resectability criteria in patients with colorectal livermetastases. Rather, current data have precipitated a shift inthe definition of resectability from criteria based on thecharacteristics of the metastatic disease (e.g., number, size,etc.) to new criteria based on whether a macroscopic andmicroscopic complete or R0 resection of the liver lesion, aswell as any extrahepatic disease, can be performed. In ad-dition, decisions on resectability are contingent on whetheran adequate liver remnant will be left following surgery.This notion of resectability represents a paradigm shift. In-stead of resectability being defined by what is removed, de-cisions concerning resectability now center around what
Figure 3. Patients with extrahepatic disease have a signifi-cantly shorter overall survival time than patients with liver-only disease. As such, the presence of extrahepatic disease hastraditionally almost universally been accepted as a contraindi-cation to hepatic resection of colorectal metastases. From Al-tendorf-Hofmann A, Scheele J. A critical review of the majorindicators of prognosis after resection of hepatic metastasesfrom colorectal carcinoma. Surg Oncol Clin N Am 2003;12:165–192, xi, with permission.
54 Colorectal Liver Metastases
by guest on March 1, 2014
http://theoncologist.alphamedpress.org/
Dow
nloaded from

will remain after resection, with a particular focus on thelack of residual disease as well as the volume and functionof the residual liver (Fig. 4). In this new paradigm, resect-ability is defined by four main criteria:
1. The disease needs to be completely resected. An R0 re-section of both the intra- and extrahepatic disease sitesmust be feasible.
2. At least two adjacent liver segments need to be spared.3. Vascular inflow and outflow, as well as biliary drainage
to the remaining segments, must be preserved.4. The volume of the liver remaining after resection (i.e.,
the future liver remnant) must be adequate (which usu-ally means at least 20% of the total estimated liver vol-ume for normal parenchyma, 30%–60% if the liver isinjured by chemotherapy, steatosis, or hepatitis [47], or40%–70% in the presence of cirrhosis, depending on thedegree of underlying hepatic dysfunction).
These new criteria of resectability depend less on dog-matic parameters such as tumor number, size, or locationand more on clinical judgment. As such, in difficult or bor-derline cases, resectability should be assessed by an expe-rienced hepatobiliary surgeon.
Armed with this new definition of resectability, we arefaced with the challenge of answering the question: howcan we increase the number of patients with resectable dis-ease? In general, there are three broad strategies: (a) in-crease/preserve hepatic reserve, (b) combined modalitylocal therapy, and (c) decrease tumor size.
INCREASING THE NUMBER OF PATIENTS WHO
HAVE RESECTABLE DISEASE
Increase/Preserve Hepatic Reserve
PVEIn general, 20% of the total liver volume appears to be theminimum safe volume that can be left following extendedresection in patients with a normal underlying liver. How-ever, the cutoff threshold for the future liver remnant (FLR)may need to be greater in those patients with underlying
liver injury secondary to steatosis or steatohepatitis (30%FLR) or cirrhosis (40% FLR). Computed tomography (CT)or magnetic resonance imaging can now provide an accu-rate, reproducible method for preoperatively measuringFLR volume [48]. The right liver (right lobe) accounts forabout two thirds of the total liver volume, and the left liver(left lobe) accounts for about one third. Often, patients withmultiple hepatic colorectal metastases are treated with re-section of the right hemiliver plus segment IV (termed ex-tended right hepatectomy or right trisectionectomy). Onaverage, this procedure removes 84% of the total liver vol-ume in the absence of compensatory hypertrophy resultingfrom tumor growth [49]. There is, however, considerablevariability in the lobar and segmental intrahepatic volumet-ric distribution. To avoid operating on patients with a low-volume FLR, any patient who fails to show compensatoryhypertrophy as a result of tumor growth and who has anFLR �20% (or 30% in patients with a very fatty liver)should be considered for PVE to induce hypertrophy of thecontralateral liver lobe [50].
PVE involves cannulating the left or right portal veinunder fluoroscopic guidance and embolizing the appropri-ate vessel(s) using embolic material (e.g., coils, thrombin,polyvinyl alcohol, cyanoacrylate, or tris-acryl gelatin mi-crospheres). The concept emerged from the recognition thattumor invasion of the portal vein causes contralateral lobarhypertrophy and ipsilateral atrophy. PVE is safe, with acomplication rate in the range of 5%–8%. PVE has beenshown to increase the size of the FLR from 8% to 16%, de-pending on the extent of the underlying liver disease (Fig.5) [51–53]. PVE has been shown to increase both the size of
Figure 4. Over the last decade, the criteria for resectability ofcolorectal liver metastases have been expanded and have un-dergone a paradigm shift. Instead of resectability being definedby what is removed, decisions concerning resectability nowcenter around what will remain after resection, with a particu-lar focus on the volume and function of the residual liver.
Figure 5. Portal vein embolization (PVE) can be used to ex-pand the number of potentially resectable patients who other-wise would have a marginal liver volume following hepaticresection. PVE has been shown to increase the size of the fu-ture liver remnant (FLR) from 8% to 16%, depending on theextent of underlying liver disease. From Vauthey JN, ChaouiA, Do KA et al. Standardized measurement of the future liverremnant prior to extended liver resection: Methodology andclinical associations. Surgery 2000;127:512–519, with per-mission.
55Pawlik, Schulick, Choti
www.TheOncologist.com
by guest on March 1, 2014
http://theoncologist.alphamedpress.org/
Dow
nloaded from

the FLR as well as the percentage of indocyanine green ex-cretion and bile volume flow in the remnant liver [54]. In2003, Farges et al. [53] published the results of a prospec-tive study of PVE performed in patients undergoing righthepatectomy for either primary liver cancer or metastaticliver disease. They demonstrated significantly fewer post-operative complications when PVE was used to increase theFLR volume in patients with chronic liver disease whoseanticipated FLR was �40%. In contrast, patients with nor-mal liver function who underwent a right hepatectomy didnot benefit from PVE. In general, PVE needs to be per-formed only in patients who have normal liver function whoare being considered for an extended right hepatic resec-tion; PVE is rarely necessary prior to extended left hepatec-tomy because the right posterior sector typically constitutesabout 30% of the total liver volume [49, 55]. The selectiveuse of PVE may enable safe and potentially curative hepaticresection in a subset of patients with advanced colorectalmetastases who would otherwise have been marginal can-didates for resection because of an inadequate FLR or sig-nificant underlying liver disease.
PVE is most useful as part of a multimodality approachthat includes preoperative chemotherapy and surgery. Che-motherapy in conjunction with PVE does not appear to bedetrimental to liver hypertrophy. Preoperative chemother-apy studies by both Elias and colleagues [56] and Bismuthand colleagues [57] included patients who underwent pre-operative PVE to increase the size of the FLR.
Two-Stage HepatectomyIn patients with multiple colorectal liver metastases in bothsides of the liver, a two-stage hepatectomy may be the besttherapeutic approach [58, 59]. Specifically, a two-stagehepatectomy approach may be the only potentially curativetherapeutic approach in those patients with extensive bilat-eral colorectal liver metastases that cannot be resected withor without ablation in a single procedure while sparing anadequate FLR. Initial experience with the two-stage hepa-tectomy procedure without PVE was associated with a rel-atively high incidence of liver failure resulting frominsufficient functional volume of the FLR and high mortal-ity (9%–15%) [59, 61]. More recently, two-stage hepatec-tomy combined with PVE was reported with no operativemortality and acceptable morbidity [59]. Because of con-cern that nodules in the FLR after PVE may progress morerapidly than those in the nontumoral remnant hepatic paren-chyma [61], metastases in the FLR (usually the left bilateralsectors) are usually resected in the first stage. PVE is thenperformed, if indicated, and the liver is allowed to hyper-trophy for 3–4 weeks. Another advantage of performing alimited resection in the first stage is the preservation of a
maximal amount of liver parenchyma that will hypertrophyafter PVE to become the FLR. The components of the twostages should, however, be individualized, depending onthe distribution of the tumor, liver volume, and otherneeded procedures. Similarly, as an alternative to PVE, por-tal vein ligation can sometimes be performed during thefirst-stage resection [62]. In the absence of any significanttumor progression, an extended hepatectomy (usually in-volving the right hemiliver) is performed as the secondstage.
Adam et al. [58] have reported a 3-year survival rate of35% in 13 patients undergoing two-stage hepatectomy.More recently, Jaeck et al. [59] reported 1- and 3-year sur-vival rates of 70.0% and 54.4%, respectively, in 25 patientsin whom a two-stage hepatic resection could be performed.The corresponding 1- and 3-year disease-free survival rateswere 35.2% and 14.1%, respectively. In that study, the au-thors reported no operative mortality and postoperativemorbidity rates of 15.1% and 56.0% after the first- and sec-ond-stage hepatectomies, respectively. A two-stage hepa-tectomy approach should be considered in patients withotherwise unresectable multiple bilateral hepatic metasta-ses. A two-stage hepatectomy should only be performed,however, with curative intent, and the application of thisstrategy must be carefully considered to avoid posthepa-tectomy liver failure.
Combined Local Therapy: Resection Plus RFAMethods for local ablation have been developed in recentyears with the goal of increasing the number of patients el-igible for liver-directed therapy. Combining hepatic resec-tion with ablation can expand the number of patients whomay be candidates for liver-directed surgical therapy, par-ticularly as larger lesions that are less effectively treatedwith ablation can be resected and small lesions can be ab-lated [63]. Although tumor ablation should not be viewed asa replacement to resection, it does have applicability in pa-tients who do not meet the criteria for resectability but arecandidates for liver-directed therapy based upon the pres-ence of liver-only disease.
Early experiences with ablation of metastases involvedhepatic cryosurgery, which relied on the destruction of a de-fined area within the liver by at least two cycles of freezing/thawing using probes cooled by liquid nitrogen or argon gasto subzero temperatures. Ice crystals form within the treatedcells leading to their destruction. Probably because of thesmaller size of the equipment, speed of use, lower cost, andfewer hepatic parenchymal complications (e.g., liver frac-turing, etc.), RFA was more recently adopted as the mostcommonly applied ablation method. Other interstitial localablative approaches have also been applied to liver metas-
56 Colorectal Liver Metastases
by guest on March 1, 2014
http://theoncologist.alphamedpress.org/
Dow
nloaded from

tases, including therapeutic high-intensity ultrasound abla-tion [64, 65], laser thermotherapy [66, 67], and yttrium-90seed implants [68], but these have not gained widespreadacceptance. More recently, thermal ablation using micro-wave emitting devices has been gaining in popularity[69, 70].
RFA involves the localized application of conductivethermal energy to destroy tumor cells. Specifically, alter-nating electric current in the range of radiofrequency waves(460 kHz) is applied from a generator through a needle elec-trode placed directly into the tumor [71]. As the tempera-ture within the tissue becomes elevated beyond 50–60°C,proteins are denatured, cells are destroyed, and a zone ofnecrosis surrounding the electrode develops [72]. A varietyof probe designs are available, including multielectrode de-ployable devices, cooled parallel probes, and saline infu-sion probes. These designs allow the capability ofincreasing the speed and size of the zones of ablation. Tu-mors �4 cm in greatest diameter can typically be ablatedwith a single placement of a multielectrode array, creating aspherical burn of up to 5–6 cm in diameter [73]. Larger tu-mors require multiple deployments of the needle electrode.Treatment should be planned such that the zones of coagu-lative necrosis overlap to ensure complete destruction of thetumor [73]. Ideally, a thermal zone of ablation measuring 1cm wide around the tumor should be created to ensure de-struction of the tumor as well as a rim of nonmalignant tis-sue. Tumors abutting major vascular structures can besafely ablated because the blood within these vessels acts asa heat sink to protect the vascular endothelium from thermalinjury while allowing complete coagulative necrosis of thetissue surrounding the vessel wall [73, 74]. However, thepresence of heat sinks from large vessels may result in in-complete ablation and higher local recurrence. RFA shouldnot, however, be applied to lesions near the hilum; althoughthe blood vessels can tolerate the heat generated from RFA,the large bile ducts in this area can be damaged, resulting inbiliary strictures [73].
Tumor ablation should not be viewed as a replacementfor resection, but more as a supplement or extension of lo-calized therapy in unresectable patients [11, 73, 75]. In gen-eral, patients with resectable colorectal liver metastasisshould undergo resection, not ablation. The main indicationfor ablation is in patients who do not meet the criteria forresectability, but are candidates for liver-directed therapybased upon the presence of liver-only disease. As with thecriteria for resectability, only those patients in whom com-plete margin-negative ablation can be achieved should beconsidered for this therapy. As with resection, incompleteor cytoreductive therapy should not be advocated outside aclinical trial.
Combining hepatic resection with ablation expands thenumber of patients who may be candidates for liver-di-rected surgical therapy, particularly as larger lesions thatare less effectively treated with ablation can be resected andsmall lesions can be ablated. Adding RFA to hepatic resec-tion has been reported to be well tolerated, with a perioper-ative morbidity and mortality comparable to those seenfollowing resection alone [75]. Procedure-related compli-cations were infrequent, with a complication rate �10%[75, 76]. Complications from RFA included bleeding, fe-ver, pain, biliary fistulae, and hepatic abscess [73, 75, 76].
Local recurrence following RFA is highly dependent ontumor size as well as location within the liver. While somestudies [11, 76–79] have reported recurrence or persistenceof metastatic disease at the site of the RFA to be �10%,other studies have reported local recurrence rates as high as47% [80, 81]. Survival following ablation is also difficult tointerpret, because many patients who undergo this therapyare characterized by a number of poor prognostic factors(e.g., “unresectable” disease, multiple tumors, bilobar loca-tion, etc.), thereby making comparisons with patients whohave undergone complete surgical resection difficult. Ingeneral, studies with isolated RFA show a median survivalduration of about 30–35 months and a 3-year survival rateof 20%–36% [75, 82–84]. In a recent study comparing re-currence and outcome following hepatic resection, RFA,and combined resection and RFA for colorectal liver me-tastases, Abdalla et al. [11] reported a significantly worsedisease-free and overall survival rate for patients treatedwith RFA. Some investigators, however, have questionedwhether patient selection for RFA may lead to biased ana-lytical comparisons. While prospective data are still neededto assess the comparability of RFA versus resection, RFAshould continue to be used in combination with resection asa means to achieve complete extirpation/destruction of alltumor-bearing liver in otherwise unresectable patients.
Reduce Tumor SizeWhereas in the past, bolus 5-fluorouracil and leucovorinhad reported response rates of only about 20%, over the pastdecade, additional chemotherapeutic and biologic agentshave been found that have significantly greater activityagainst colorectal cancer. These newer agents have led notonly to higher response rates, but also to a notable longersurvival time for patients with traditionally nonresectabledisease (Table 1). With combination therapies that includeoxaliplatin and irinotecan, response rates �50% can beachieved. This superior efficacy of chemotherapy agentshas led clinicians to treat a subset of previously unresect-able patients and “convert” them so that they can undergoliver surgery following tumor downsizing. Specifically,
57Pawlik, Schulick, Choti
www.TheOncologist.com
by guest on March 1, 2014
http://theoncologist.alphamedpress.org/
Dow
nloaded from

about 15%–20% of patients with initially unresectable dis-ease (defined as either the inability to resect all tumor whileleaving 20% of the total liver volume or by the concomitantpresence of extrahepatic metastases) have significant tumordownsizing to the point that the metastatic disease can ulti-mately be considered resectable. As such, patients with ex-tensive disease who respond to chemotherapy should bereassessed by a hepatic surgeon. By reconsidering the ini-tial unresectability of patients, hepatic resection, and long-term survival, may be achieved in a subgroup of patientswho otherwise would have a poor outcome [57, 85, 86].Adam et al. [85] reported that rescue surgery for unresect-able colorectal liver metastases downsized by chemother-apy resulted in a 5-year survival rate of 33%. Otherinvestigators [87– 89] have substantiated these findings,and resection of initially nonresectable liver metastases fol-lowing systemic chemotherapy has become increasinglymore common.
When treating patients with initially unresectable dis-ease with preoperative chemotherapy, the question oftenarises as to whether one should treat to “maximal effect” ordiscontinue chemotherapy once the disease within the liverhas been cytoreduced to the point where resection is feasi-ble. In the setting of unresectable disease, the goal of pre-operative chemotherapy is to convert the extent ofintrahepatic disease from unresectable to resectable basedon the criteria outlined above. As such, in general, preoper-ative chemotherapy should be stopped once the intrahepaticdisease has been downsized to the point where hepatic re-section is feasible. Not only does treating to maximal effectprior to surgery provide no measurable oncologic benefit,but prolonged courses of preoperative chemotherapy mayalso have a detrimental effect on the hepatic parenchyma.Some studies have associated the use of oxaliplatin with ahigher incidence of hepatic sinusoidal obstruction [90],while others have suggested that irinotecan may be associ-ated with steatosis [91, 92]. Fernandez et al. [91] reportedthat preoperative administration of oxaliplatin or irinotecanwas associated with a higher risk for steatohepatitis, espe-cially in the obese. Similarly, Vauthey et al. [93] reportedthat steatohepatitis was more common following preopera-tive treatment with irinotecan and was associated with ahigher 90-day mortality rate following hepatic surgery. Inaggregate, these data suggest that preoperative chemother-apy can potentially be a powerful tool to convert otherwiseunresectable patients, but its use should be individualized tothe specific circumstance. Chemotherapy that has effec-tively downsized previously unresectable lesions shouldnot be continued indefinitely. Rather, the patient should beseen by the hepatic surgeon or surgical oncologist on a reg-ular interval basis during chemotherapy. In this manner, the
surgeon can help continually assess disease response/pro-gression and reconsider resection if appropriate.
An important question arises when considering a patientfor surgery following response to preoperative chemother-apy: do all the original sites of disease need to be resected orablated in order to derive a survival benefit from local ther-apy? In general, the answer is yes. Benoist et al. [94] exam-ined metastatic sites in which complete radiologic responsewas achieved. Of the 66 lesions evaluated, the authors re-ported persistent tumor on pathology in 83% of cases.Based on these data, resection should be performed on alloriginal sites of disease. Local therapy of only residual sitesfollowing complete radiologic response of untreated sitesshould be considered cytoreductive therapy and avoided.These data serve to emphasize the importance of the sur-geon reviewing all cross-sectional imaging prior to plannedhepatic resection. In particular, it is critical to compare pre-therapy imaging including both the CT and positron emis-sion tomography (PET) scan with images obtainedfollowing chemotherapy. As noted, in general, all the orig-inal sites of disease that were noted on the initial pretherapyscans need to be resected or ablated, not just the residualdisease seen on post-therapy imaging.
EXTRAHEPATIC DISEASE
The role of hepatic resection in the setting of extrahepaticdisease was recently re-examined. Extrahepatic disease hastraditionally been considered a contraindication to resec-tion of hepatic colorectal cancer metastasis [9, 14, 15, 45].However, improvements in morbidity and mortality ratesfollowing hepatectomy, as well as the advent of more effec-tive systemic chemotherapy agents, have prompted severalinvestigators [95–98] to attempt surgery for some of thesepatients. Local extension to adjacent structures, intralumi-nal biliary tumor thrombus, and locoregional recurrenceshould not be considered true extrahepatic disease, andnone of these should be considered a contraindication tosurgery when an R0 resection is feasible. In contrast, therehas been significantly more controversy regarding hepaticresection for colorectal metastases in the presence of pul-monary metastases, hilar lymph node metastases, carcino-matosis, and metastasis of other extra-abdominal sites.
The lungs are the second most frequent site of metastaticdisease, accounting for roughly 20%–25% of the metasta-ses in patients who have undergone curative resection oftheir colorectal primary. Approximately 5%–10% of pa-tients who present with metastatic disease have a combina-tion of liver and lung metastases, and therefore there hasbeen interest in how this subset of patients should betreated. In the past, multiple studies [99–101] have reportedfavorable long-term survival rates after resection of local-
58 Colorectal Liver Metastases
by guest on March 1, 2014
http://theoncologist.alphamedpress.org/
Dow
nloaded from

ized lung-only disease. More recently, however, severalcenters have reported their results for patients undergoingcombined lung and liver resection [102–105]. These studieshave reported 5-year survival rates �30%. In fact, Shah etal. [105] reported a 5-year survival rate that exceeded 74%.In that study, although the median disease-free survival du-ration after initial metastasectomy was only 20 months, themedian overall survival time was 87 months. Roughly halfof the patients underwent repeat resections for recurrence,with the mean number of metastasectomies being 2.6 perpatient. There were no perioperative deaths. The authorsdemonstrated that an aggressive surgical approach, evenwith serial metastasectomies, can lead to significant long-term survival in a highly select group of patients—perhapsthose patients with a good response to chemotherapy andlonger disease-free intervals.
Prognosis following resection of pulmonary and livermetastases does not appear to be affected by synchronousversus metachronous presentation. Several studies have re-ported no significant difference in survival between pa-tients who present with simultaneous disease and those whopresent with synchronous disease [105, 106]. Thus, patientsshould not be denied a chance at curative hepatectomy sim-ply because of a history of pulmonary metastases, assumingall sites can be resected. There are, however, a number offactors that do appear to be associated with a particularlypoor prognosis. Patients with bilateral disease or whohave more than six pulmonary metastases were 50%–70% more at risk for disease-specific death than other pa-tients. Thus, particular attention must be paid whenconsidering these high-risk patients for combined liverand lung resection.
Unlike pericolic nodal disease, hilar lymph nodes arefelt to be “metastases from metastases” and are associatedwith a poor outcome. Because of this, some investigatorshave traditionally considered hilar nodal metastasis as acontraindication to hepatic resection of colorectal liver dis-ease. Although early studies [37, 107] reported few, if any,long-term survivors with hilar lymph node metastases,more recent studies [98, 108, 109] have reported long-termsurvival in some patients with hilar nodal metastases andhave concluded that this patient population may still benefitfrom hepatic resection.
When considering patients with hilar lymph node in-volvement, the location of the nodal metastases may be im-portant. Jaeck [109] distinguished two areas of hilar lymphnode involvement: the hepatoduodenal-retropancreaticarea and common hepatic artery/celiac-axis region.Whereas patients with positive hilar lymph nodes in the re-gion of the hepatic artery/celiac axis had a very poor prog-nosis, some patients with hilar lymph node metastases
involving the hepatoduodenal or retropancreatic areaachieved long-term survival. Specifically, the 3-year sur-vival rate following hepatectomy in patients with involve-ment of the hepatic pedicle lymph nodes limited to thehepatoduodenal-retropancreatic area was 38%, comparedwith 0% for patients with involvement of the common he-patic artery/celiac axis area [110]. Another critical factormay relate to whether the hilar lymph nodes are macroscop-ically positive. Although patients with microscopic in-volvement may derive a benefit from hepatic resection,gross involvement of the hilar nodes should be considered arelative contraindication to resection.
Peritoneal carcinomatosis is a common type of extrahe-patic disease in patients with colorectal liver metastasis,representing about one third of the cases of extrahepatic dis-ease. Although usually a particularly grave indicator ofpoor prognosis, some centers have reported success withdebulking and intraperitoneal chemotherapy [111, 112].However, such therapy is not the standard of care and, ingeneral, liver resection is not indicated in the presence ofdiffuse carcinomatosis. Specifically, patients who arefound to have unsuspected extrahepatic disease at the timeof laparotomy have a poor long-term prognosis [98]. Thus,in most cases, incidental peritoneal disease found at lapa-rotomy would contraindicate hepatic resection.
Elias et al. [98] reported that the 5-year survival rate fol-lowing hepatectomy for colorectal liver metastasis and si-multaneous resection of extrahepatic disease with curativeintent was 29%. The distribution of extrahepatic diseaseincluded hilar lymph nodes, peritoneal carcinomatosis,retroperitoneal nodes, and lung metastasis. No statisti-cally significant difference in outcome was found relat-ing to the site of extrahepatic disease; however, the studywas small and lacked statistical power. Patients withperitoneal carcinomatosis or extrahepatic disease at mul-tiple sites did tend to have a worse survival than patientswith single-site extrahepatic disease [98]. In contrast, pa-tients with only pulmonary metastasis as the type of ex-trahepatic disease had a particularly good outcomefollowing complete metastasectomy of both liver andlung disease [99, 101, 113, 114].
Not only is the site of the extrahepatic disease importantwith regard to prognosis, but perhaps more important is theadequacy of the resection. As with liver resection itself, theability to achieve a complete macro- and microscopic re-section of all known disease is critical to long-term out-come. In a study by Elias et al. [98], of those patients whounderwent resection of both intra- and extrahepatic metas-tases, the 5-year survival rate was 28% in those patientswho had an R0 resection, but was only 7% in those patientswho had an R1 or R2 resection. These data serve to empha-
59Pawlik, Schulick, Choti
www.TheOncologist.com
by guest on March 1, 2014
http://theoncologist.alphamedpress.org/
Dow
nloaded from

size that hepatic resection in the setting of extrahepatic dis-ease is warranted only when an R0 resection is feasible.Patients with disease not amenable to a complete resectionshould not be offered combined metastasectomies of intra-and extrahepatic disease. For those patients who can have acomplete microscopic resection, there are data to suggestthat long-term survival may be similar in patients with iso-lated liver metastases and in those with liver metastaseswith extrahepatic disease, when the extent of disease wassimilar. In the multivariate analysis from Elias et al. [98],the site of the metastatic disease had less prognostic impor-tance than the overall number of resected lesions, regard-less of site. Not surprisingly, patients with more overallmetastases have a worse survival than patients with fewerlesions—reflecting the worse overall tumor biology foundin those patients with multiple lesions. However, in thestudy by Elias et al. [98], when the number of lesions wascontrolled for, patients with and without extrahepatic dis-ease had similar overall survival times.
In addition to the extent of resection and the number ofmetastatic lesions, perhaps the most critical factor in help-ing to determine a patient’s eligibility for hepatic resectionin the presence of extrahepatic disease is the response topreoperative chemotherapy. Adam et al. [85] reported thatthe prognosis following hepatic resection is dependent onthe response to preoperative chemotherapy. Specifically,long-term survival is rare in patients who have disease pro-gression while on chemotherapy. While patients whoprogress on chemotherapy have only an 8% reported 5-yearsurvival rate following hepatic resection, those patientswho respond to chemotherapy have reported 5-year sur-vival rates of 37% [85]. Thus, the use of preoperative ther-apy may help to define those patients who will benefit froman aggressive surgical approach and those who may not (in-cluding those patients with extrahepatic disease). Whereasliver resection in patients with progressive disease on che-motherapy may not be warranted, an aggressive surgicalapproach may be appropriate in patients who have stabili-zation or responsive disease.
Therefore, based on the available data, a general treat-ment algorithm can be proposed. Patients with intra- andextrahepatic disease should initially be treated with sys-temic chemotherapy. Patients with progressive disease arenot candidates for surgery and should receive additionalchemotherapy and palliative support. Patients with stable orresponsive disease should be evaluated for surgery. Thosein whom an R0 resection is not possible are also not candi-dates for surgery and should go on to receive more chemo-therapy. However, patients in whom an R0 resection ispossible should be offered surgical resection followed byadjuvant chemotherapy. Patients with simultaneous hepatic
and extrahepatic colorectal metastases do, however, need tobe well selected for surgery. PET/CT can often be useful inevaluating the full extent of metastatic disease [115].
CONCLUSION
In summary, the criteria for resectability of colorectal livermetastases have been significantly revised and expandedover the course of the last decade. Clinicopathologic factorssuch as the tumor number, tumor size, presence of extrahe-patic disease, or width of the resection margin should nolonger be used to categorically exclude patients from con-sideration for surgical resection. Rather, assessment of re-sectability should take into account the ability to obtain anR0 resection of all known disease—whether it be intra- orextrahepatic. The feasibility of hepatic resection should bedetermined chiefly using three criteria: (a) the ability to pre-serve two contiguous hepatic segments, (b) the preservationof vascular inflow and outflow as well as biliary drainage,and (c) the ability to preserve an adequate FLR. In those pa-tients with extensive disease and limited hepatic reserve,PVE or a two-stage hepatectomy approach can sometimespermit surgical resection. Similarly, the use of preoperativechemotherapy can be associated with conversion of somepatients from unresectable to resectable. Preoperative che-motherapy may also be useful in the treatment of patientswith intra- and extrahepatic disease. In this setting, preop-erative chemotherapy can reduce disease volume so that anR0 resection is more feasible, but perhaps more impor-tantly, preoperative chemotherapy can help assess the un-derlying biology of the patient’s disease. Although thecriteria for resectability of colorectal liver metastases havebeen expanded to include patients with both intra- and ex-trahepatic disease, these patients must be very well se-lected. Patients with extensive extrahepatic disease, orthose who progress on systemic chemotherapy, shouldprobably not be considered for hepatic resection. The ex-pansion of criteria for resectability of colorectal liver me-tastases requires a much more sophisticated approach to thepatient with advanced disease. Patients require ongoing re-peat evaluations by a surgeon with expertise in hepatic re-section. Ultimately, a therapeutic approach that includes allaspects of multidisciplinary and multimodality care is re-quired to select and treat this complex group of patients.
AUTHOR CONTRIBUTIONSConception/design: Timothy M. Pawlik, Richard D. Schulick, Michael A.
ChotiCollection/assembly of data: Timothy M. Pawlik, Richard D. Schulick, Mi-
chael A. ChotiData analysis and interpretation: Timothy M. Pawlik, Richard D. Schulick,
Michael A. ChotiManuscript writing: Timothy M. Pawlik, Richard D. Schulick, Michael A.
ChotiFinal approval of manuscript: Timothy M. Pawlik, Richard D. Schulick, Mi-
chael A. Choti
60 Colorectal Liver Metastases
by guest on March 1, 2014
http://theoncologist.alphamedpress.org/
Dow
nloaded from

REFERENCES
1 Jemal A, Murray T, Ward E et al. Cancer statistics, 2005. CA Cancer
J Clin 2005;55:10–30.
2 Steele G Jr, Ravikumar TS. Resection of hepatic metastases from colorec-
tal cancer. Biologic perspective. Ann Surg 1989;210:127–138.
3 Cady B, Monson DO, Swinton NW. Survival of patients after colonic re-
section for carcinoma with simultaneous liver metastases. Surg Gynecol
Obstet 1970;131:697–700.
4 Blumgart LH, Allison DJ. Resection and embolization in the management
of secondary hepatic tumors. World J Surg 1982;6:32–45.
5 Jatzko G, Wette V, Muller M et al. Simultaneous resection of colorectal
carcinoma and synchronous liver metastases in a district hospital. Int J
Colorectal Dis 1991;6:111–114.
6 Finlay IG, McArdle CS. Occult hepatic metastases in colorectal carci-
noma. Br J Surg 1986;73:732–735.
7 Scheele J, Stang R, Altendorf-Hofmann A et al. Resection of colorectal
liver metastases. World J Surg 1995;19:59–71.
8 Altendorf-Hofmann A, Scheele J. A critical review of the major indicators
of prognosis after resection of hepatic metastases from colorectal carci-
noma. Surg Oncol Clin N Am 2003;12:165–192, xi.
9 Scheele J, Stangl R, Altendorf-Hofmann A et al. Indicators of prognosis after
hepatic resection for colorectal secondaries. Surgery 1991;110:13–29.
10 Fong Y, Fortner J, Sun RL et al. Clinical score for predicting recurrence
after hepatic resection for metastatic colorectal cancer: Analysis of 1001
consecutive cases. Ann Surg 1999;230:309–318; discussion 318–321.
11 Abdalla EK, Vauthey JN, Ellis LM et al. Recurrence and outcomes fol-
lowing hepatic resection, radiofrequency ablation, and combined re-
section/ablation for colorectal liver metastases. Ann Surg 2004;239:
818 – 825; discussion 825– 827.
12 Scheele J, Stangl R, Altendorf-Hofmann A. Hepatic metastases from colo-
rectal carcinoma: Impact of surgical resection on the natural history. Br J
Surg 1990;77:1241–1246.
13 Choti MA, Sitzmann JV, Tiburi MF et al. Trends in long-term survival
following liver resection for hepatic colorectal metastases. Ann Surg
2002;235:759–766.
14 Hughes KS, Rosenstein RB, Songhorabodi S et al. Resection of the liver
for colorectal carcinoma metastases. A multi-institutional study of long-
term survivors. Dis Colon Rectum 1988;31:1–4.
15 Adson MA, van Heerden JA, Adson MH et al. Resection of hepatic
metastases from colorectal cancer. Arch Surg 1984;119:647–651.
16 Schlag P, Hohenberger P, Herfarth C. Resection of liver metastases in colo-
rectal cancer—competitive analysis of treatment results in synchronous
versus metachronous metastases. Eur J Surg Oncol 1990;16:360–365.
17 Gayowski TJ, Iwatsuki S, Madariaga JR et al. Experience in hepatic re-
section for metastatic colorectal cancer: Analysis of clinical and patho-
logic risk factors. Surgery 1994;116:703–710; discussion 710–711.
18 Jenkins LT, Millikan KW, Bines SD et al. Hepatic resection for metastatic
colorectal cancer. Am Surg 1997;63:605–610.
19 Jamison RL, Donohue JH, Nagorney DM et al. Hepatic resection for met-
astatic colorectal cancer results in cure for some patients. Arch Surg 1997;
132:505–510; discussion 511.
20 Jaffe BM, Donegan WL, Watson F et al. Factors influencing survival in
patients with untreated hepatic metastases. Surg Gynecol Obstet 1968;
127:1–11.
21 Bengmark S, Hafstrom L. The natural history of primary and secondary
malignant tumors of the liver. I. The prognosis for patients with hepatic
metastases from colonic and rectal carcinoma by laparotomy. Cancer
1969;23:198–202.
22 de Brauw LM, van de Velde CJ, Bouwhuis-Hoogerwerf ML et al. Diag-
nostic evaluation and survival analysis of colorectal cancer patients with
liver metastases. J Surg Oncol 1987;34:81–86.
23 Bengtsson G, Carlsson G, Hafstrom L et al. Natural history of patients
with untreated liver metastases from colorectal cancer. Am J Surg 1981;
141:586–589.
24 Goslin R, Steele G Jr, Zamcheck N et al. Factors influencing survival in
patients with hepatic metastases from adenocarcinoma of the colon or rec-
tum. Dis Colon Rectum 1982;25:749–754.
25 Modulation of fluorouracil by leucovorin in patients with advanced colo-
rectal cancer: Evidence in terms of response rate. Advanced Colorectal
Cancer Meta-Analysis Project. J Clin Oncol 1992;10:896–903.
26 Saltz LB, Cox JV, Blanke C et al. Irinotecan plus fluorouracil and leuco-
vorin for metastatic colorectal cancer. Irinotecan Study Group. N Engl
J Med 2000;343:905–914.
27 de Gramont A, Bosset JF, Milan C et al. Randomized trial comparing
monthly low-dose leucovorin and fluorouracil bolus with bimonthly high-
dose leucovorin and fluorouracil bolus plus continuous infusion for ad-
vanced colorectal cancer: A French intergroup study. J Clin Oncol 1997;
15:808–815.
28 Douillard JY, Cunningham D, Roth AD et al. Irinotecan combined with
fluorouracil compared with fluorouracil alone as first-line treatment for
metastatic colorectal cancer: A multicentre randomised trial. Lancet 2000;
355:1041–1047.
29 Goldberg RM, Sargent DJ, Morton RF et al. A randomized controlled trial
of fluorouracil plus leucovorin, irinotecan, and oxaliplatin combinations
in patients with previously untreated metastatic colorectal cancer. J Clin
Oncol 2004;22:23–30.
30 de Gramont A, Figer A, Seymour M et al. Leucovorin and fluorouracil
with or without oxaliplatin as first-line treatment in advanced colorectal
cancer. J Clin Oncol 2000;18:2938–2947.
31 Cunningham D, Pyrhonen S, James RD et al. Randomised trial of irinote-
can plus supportive care versus supportive care alone after fluorouracil
failure for patients with metastatic colorectal cancer. Lancet 1998;352:
1413–1418.
32 Rougier P, Van Cutsem E, Bajetta E et al. Randomised trial of irinotecan
versus fluorouracil by continuous infusion after fluorouracil failure in pa-
tients with metastatic colorectal cancer. Lancet 1998;352:1407–1412.
33 Rothenberg ML, Oza AM, Bigelow RH et al. Superiority of oxaliplatin
and fluorouracil-leucovorin compared with either therapy alone in pa-
tients with progressive colorectal cancer after irinotecan and fluorou-
racil-leucovorin: Interim results of a phase III trial. J Clin Oncol 2003;
21:2059 –2069.
34 Hurwitz H, Fehrenbacher L, Novotny W et al. Bevacizumab plus irinote-
can, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl
J Med 2004;350:2335–2342.
35 Saltz LB, Meropol NJ, Loehrer PJ Sr et al. Phase II trial of cetuximab in
patients with refractory colorectal cancer that expresses the epidermal
growth factor receptor. J Clin Oncol 2004;22:1201–1208.
36 Moertel CG, Gunderson LL, Mailliard JA et al. Early evaluation of com-
bined fluorouracil and leucovorin as a radiation enhancer for locally un-
resectable, residual, or recurrent gastrointestinal carcinoma. The North
Central Cancer Treatment Group. J Clin Oncol 1994;12:21–27.
37 Ekberg H, Tranberg KG, Andersson R et al. Determinants of survival in
liver resection for colorectal secondaries. Br J Surg 1986;73:727–731.
38 Hughes KS, Simon R, Songhorabodi S et al. Resection of the liver for
61Pawlik, Schulick, Choti
www.TheOncologist.com
by guest on March 1, 2014
http://theoncologist.alphamedpress.org/
Dow
nloaded from

colorectal carcinoma metastases: A multi-institutional study of patterns of
recurrence. Surgery 1986;100:278–284.
39 Pawlik TM, Abdalla EK, Ellis LM et al. Debunking dogma: Surgery for
four or more colorectal liver metastases is justified. J Gastrointest Surg
2006;10:240–248.
40 Nordlinger B, Guiguet M, Vaillant JC et al. Surgical resection of colorec-
tal carcinoma metastases to the liver. A prognostic scoring system to im-
prove case selection, based on 1568 patients. Association Francaise de
Chirurgie. Cancer 1996;77:1254–1262.
41 Fortner JG, Silva JS, Golbey RB et al. Multivariate analysis of a personal
series of 247 consecutive patients with liver metastases from colorectal
cancer. I. Treatment by hepatic resection. Ann Surg 1984;199:306–316.
42 Doci R, Gennari L, Bignami P et al. One hundred patients with hepatic
metastases from colorectal cancer treated by resection: Analysis of prog-
nostic determinants. Br J Surg 1991;78:797–801.
43 Cady B, Jenkins RL, Steele GD Jr et al. Surgical margin in hepatic resec-
tion for colorectal metastasis: A critical and improvable determinant of
outcome. Ann Surg 1998;227:566–571.
44 Pawlik TM, Scoggins CR, Zorzi D et al. Effect of surgical margin status on
survival and site of recurrence after hepatic resection for colorectal me-
tastases. Ann Surg 2005;241:715–722; discussion 722–724.
45 Fong Y, Cohen AM, Fortner JG et al. Liver resection for colorectal me-
tastases. J Clin Oncol 1997;15:938–946.
46 Cady B, Stone MD, McDermott WV Jr et al. Technical and biological fac-
tors in disease-free survival after hepatic resection for colorectal cancer
metastases. Arch Surg 1992;127:561–568; discussion 568–569.
47 Ferrero A, Vigano L, Polastri R et al. Postoperative liver dysfunction and
future remnant liver: Where is the limit? Results of a prospective study.
World J Surg 2007;31:1643–1651.
48 Abdalla EK, Barnett CC, Doherty D et al. Extended hepatectomy in pa-
tients with hepatobiliary malignancies with and without preoperative por-
tal vein embolization. Arch Surg 2002;137:675– 680; discussion 680 –
681.
49 Abdalla EK, Denys A, Chevalier P et al. Total and segmental liver volume
variations: Implications for liver surgery. Surgery 2004;135:404–410.
50 Abdalla EK, Hicks ME, Vauthey JN. Portal vein embolization: Rationale,
technique and future prospects. Br J Surg 2001;88:165–175.
51 Madoff DC, Hicks ME, Abdalla EK et al. Portal vein embolization with
polyvinyl alcohol particles and coils in preparation for major liver resec-
tion for hepatobiliary malignancy: Safety and effectiveness—study in 26
patients. Radiology 2003;227:251–260.
52 Vauthey JN, Chaoui A, Do KA et al. Standardized measurement of the
future liver remnant prior to extended liver resection: Methodology and
clinical associations. Surgery 2000;127:512–519.
53 Farges O, Belghiti J, Kianmanesh R et al. Portal vein embolization before
right hepatectomy: Prospective clinical trial. Ann Surg 2003;237:208–
217.
54 Uesaka K, Nimura Y, Nagino M. Changes in hepatic lobar function after
right portal vein embolization. An appraisal by biliary indocyanine green
excretion. Ann Surg 1996;223:77–83.
55 Nagino M, Nimura Y, Kamiya J et al. Right or left trisegment portal vein
embolization before hepatic trisegmentectomy for hilar bile duct carci-
noma. Surgery 1995;117:677–681.
56 Elias D, Lasser P, Rougier P et al. Frequency, technical aspects, results,
and indications of major hepatectomy after prolonged intra-arterial he-
patic chemotherapy for initially unresectable hepatic tumors. J Am Coll
Surg 1995;180:213–219.
57 Bismuth H, Adam R, Levi F et al. Resection of nonresectable liver metas-
tases from colorectal cancer after neoadjuvant chemotherapy. Ann Surg
1996;224:509–520; discussion 520–522.
58 Adam R, Laurent A, Azoulay D et al. Two-stage hepatectomy: A planned
strategy to treat irresectable liver tumors. Ann Surg 2000;232:777–785.
59 Jaeck D, Oussoultzoglou E, Rosso E et al. A two-stage hepatectomy pro-
cedure combined with portal vein embolization to achieve curative resec-
tion for initially unresectable multiple and bilobar colorectal liver
metastases. Ann Surg 2004;240:1037–1049; discussion 1049–1051.
60 Bolton JS, Fuhrman GM. Survival after resection of multiple bilobar he-
patic metastases from colorectal carcinoma. Ann Surg 2000;231:743–
751.
61 Elias D, De Baere T, Roche A et al. During liver regeneration following
right portal embolization the growth rate of liver metastases is more rapid
than that of the liver parenchyma. Br J Surg 1999;86:784–788.
62 Kianmanesh R, Farges O, Abdalla EK et al. Right portal vein ligation: A
new planned two-step all-surgical approach for complete resection of pri-
mary gastrointestinal tumors with multiple bilateral liver metastases. J Am
Coll Surg 2003;197:164–170.
63 Elias D, Goharin A, El Otmany A et al. Usefulness of intraoperative
radiofrequency thermoablation of liver tumours associated or not with
hepatectomy. Eur J Surg Oncol 2000;26:763–769.
64 Yang R, Kopecky KK, Rescorla FJ et al. Sonographic and computed to-
mography characteristics of liver ablation lesions induced by high-inten-
sity focussed ultrasound. Invest Radiol 1993;28:796–801.
65 Sibille A, Prat F, Chapelon JY et al. Extracorporeal ablation of liver tissue
by high-intensity focused ultrasound. Oncology 1993;50:375–379.
66 Vogl TJ, Mack MG, Balzer JO et al. Liver metastases: Neoadjuvant down-
sizing with transarterial chemoembolization before laser-induced thermo-
therapy. Radiology 2003;229:457–464.
67 Christophi C, Nikfarjam M, Malcontenti-Wilson C et al. Long-term sur-
vival of patients with unresectable colorectal liver metastases treated by
percutaneous interstitial laser thermotherapy. World J Surg 2004;28:987–
994.
68 Buscombe JR. Interventional nuclear medicine in hepatocellular carci-
noma and other tumours. Nucl Med Commun 2002;23:837–841.
69 Simon CJ, Dupuy DE, Iannitti DA et al. Intraoperative triple antenna he-
patic microwave ablation. AJR Am J Roentgenol 2006;187:W333–W340.
70 Dong B, Liang P, Yu X et al. Percutaneous sonographically guided mi-
crowave coagulation therapy for hepatocellular carcinoma: Results in 234
patients. AJR Am J Roentgenol 2003;180:1547–1555.
71 Rhim H, Dodd GD 3rd. Radiofrequency thermal ablation of liver tumors.
J Clin Ultrasound 1999;27:221–229.
72 McGahan JP, Brock JM, Tesluk H et al. Hepatic ablation with use of radio-
frequency electrocautery in the animal model. J Vasc Interv Radiol 1992;
3:291–297.
73 Curley SA, Izzo F, Abdalla E et al. Surgical treatment of colorectal cancer
metastasis. Cancer Metastasis Rev 2004;23:165–182.
74 Curley SA, Davidson BS, Fleming RY et al. Laparoscopically guided bi-
polar radiofrequency ablation of areas of porcine liver. Surg Endosc 1997;
11:729–733.
75 Pawlik TM, Izzo F, Cohen DS et al. Combined resection and radiofre-
quency ablation for advanced hepatic malignancies: Results in 172 pa-
tients. Ann Surg Oncol 2003;10:1059–1069.
76 Curley SA, Izzo F, Delrio P et al. Radiofrequency ablation of unresectable
primary and metastatic hepatic malignancies: Results in 123 patients. Ann
Surg 1999;230:1–8.
62 Colorectal Liver Metastases
by guest on March 1, 2014
http://theoncologist.alphamedpress.org/
Dow
nloaded from

77 Wood TF, Rose DM, Chung M et al. Radiofrequency ablation of 231 un-
resectable hepatic tumors: Indications, limitations, and complications.
Ann Surg Oncol 2000;7:593–600.
78 Bilchik AJ, Wood TF, Allegra DP. Radiofrequency ablation of unresectable
hepatic malignancies: Lessons learned. The Oncologist 2001;6:24–33.
79 Machi J, Uchida S, Sumida K et al. Ultrasound-guided radiofrequency
thermal ablation of liver tumors: Percutaneous, laparoscopic, and open
surgical approaches. J Gastrointest Surg 2001;5:477–489.
80 Aloia TA, Vauthey JN, Loyer EM et al. Solitary colorectal liver metasta-
sis: Resection determines outcome. Arch Surg 2006;141:460–466; dis-
cussion 466–467.
81 van Duijnhoven FH, Jansen MC, Junggeburt JM et al. Factors influencing
the local failure rate of radiofrequency ablation of colorectal liver metas-
tases. Ann Surg Oncol 2006;13:651–658.
82 de Baere T, Elias D, Dromain C et al. Radiofrequency ablation of 100 he-
patic metastases with a mean follow-up of more than 1 year. AJR Am J
Roentgenol 2000;175:1619–1625.
83 Solbiati L, Ierace T, Tonolini M et al. Radiofrequency thermal ablation of
hepatic metastases. Eur J Ultrasound 2001;13:149–158.
84 Gillams AR. Thermal ablation of liver metastases. Abdom Imaging 2001;
26:361–368.
85 Adam R, Delvart V, Pascal G et al. Rescue surgery for unresectable colo-
rectal liver metastases downstaged by chemotherapy: A model to predict
long-term survival. Ann Surg 2004;240:644–657; discussion 657–658.
86 Adam R, Avisar E, Ariche A et al. Five-year survival following hepatic
resection after neoadjuvant therapy for nonresectable colorectal. Ann
Surg Oncol 2001;8:347–353.
87 Rivoire M, De Cian F, Meeus P et al. Combination of neoadjuvant che-
motherapy with cryotherapy and surgical resection for the treatment of un-
resectable liver metastases from colorectal carcinoma. Cancer 2002;95:
2283–2292.
88 Fowler WC, Eisenberg BL, Hoffman JP. Hepatic resection following sys-
temic chemotherapy for metastatic colorectal carcinoma. J Surg Oncol
1992;51:122–125.
89 Wein A, Riedel C, Kockerling F et al. Impact of surgery on survival in
palliative patients with metastatic colorectal cancer after first line treat-
ment with weekly 24-hour infusion of high-dose 5-fluorouracil and folinic
acid. Ann Oncol 2001;12:1721–1727.
90 Rubbia-Brandt L, Audard V, Sartoretti P et al. Severe hepatic sinusoidal
obstruction associated with oxaliplatin-based chemotherapy in patients
with metastatic colorectal cancer. Ann Oncol 2004;15:460–466.
91 Fernandez FG, Ritter J, Goodwin JW et al. Effect of steatohepatitis asso-
ciated with irinotecan or oxaliplatin pretreatment on resectability of he-
patic colorectal metastases. J Am Coll Surg 2005;200:845–853.
92 Pawlik TM, Olino K, Gleisner AL et al. Preoperative chemotherapy for
colorectal liver metastases: Impact on hepatic histology and postoperative
outcome. J Gastrointest Surg 2007;11:860–868.
93 Vauthey JN, Pawlik TM, Ribero D et al. Chemotherapy regimen predicts
steatohepatitis and an increase in 90-day mortality after surgery for he-
patic colorectal metastases. J Clin Oncol 2006;24:2065–2072.
94 Benoist S, Brouquet A, Penna C et al. Complete response of colorectal
liver metastases after chemotherapy: Does it mean cure? J Clin Oncol
2006;24:3939–3945.
95 Nagakura S, Shirai Y, Yamato Y et al. Simultaneous detection of colorec-
tal carcinoma liver and lung metastases does not warrant resection. J Am
Coll Surg 2001;193:153–160.
96 Elias D, Sideris L, Pocard M et al. Results of R0 resection for colorectal
liver metastases associated with extrahepatic disease. Ann Surg Oncol
2004;11:274–280.
97 Ferrero A, Polastri R, Muratore A et al. Extensive resections for colorectal
liver metastases. J Hepatobiliary Pancreat Surg 2004;11:92–96.
98 Elias D, Ouellet JF, Bellon N et al. Extrahepatic disease does not contra-
indicate hepatectomy for colorectal liver metastases. Br J Surg 2003;90:
567–574.
99 Inoue M, Kotake Y, Nakagawa K et al. Surgery for pulmonary metastases
from colorectal carcinoma. Ann Thorac Surg 2000;70:380–383.
100 Inoue M, Ohta M, Iuchi K et al. Benefits of surgery for patients with pul-
monary metastases from colorectal carcinoma. Ann Thorac Surg 2004;78:
238–244.
101 Sakamoto T, Tsubota N, Iwanaga K et al. Pulmonary resection for metas-
tases from colorectal cancer. Chest 2001;119:1069–1072.
102 Murata S, Moriya Y, Akasu T et al. Resection of both hepatic and pulmo-
nary metastases in patients with colorectal carcinoma. Cancer 1998;83:
1086–1093.
103 Kobayashi K, Kawamura M, Ishihara T. Surgical treatment for both pul-
monary and hepatic metastases from colorectal cancer. J Thorac Cardio-
vasc Surg 1999;118:1090–1096.
104 Headrick JR, Miller DL, Nagorney DM et al. Surgical treatment of hepatic
and pulmonary metastases from colon cancer. Ann Thorac Surg 2001;71:
975–979; discussion 979–980.
105 Shah SA, Haddad R, Al-Sukhni W et al. Surgical resection of hepatic and
pulmonary metastases from colorectal carcinoma. J Am Coll Surg 2006;
202:468–475.
106 Mineo TC, Ambrogi V, Tonini G et al. Longterm results after resection
of simultaneous and sequential lung and liver metastases from colorectal
carcinoma. J Am Coll Surg 2003;197:386–391.
107 Iwatsuki S, Dvorchik I, Madariaga JR et al. Hepatic resection for meta-
static colorectal adenocarcinoma: A proposal of a prognostic scoring sys-
tem. J Am Coll Surg 1999;189:291–299.
108 Nakamura S, Suzuki S, Konno H. Resection of hepatic metastases of colo-
rectal carcinoma: 20 years’ experience. J Hepatobiliary Pancreat Surg
1999;6:16–22.
109 Jaeck D. The significance of hepatic pedicle lymph nodes metastases in
surgical management of colorectal liver metastases and of other liver ma-
lignancies. Ann Surg Oncol 2003;10:1007–1011.
110 Jaeck D, Nakano H, Bachellier P et al. Significance of hepatic pedicle
lymph node involvement in patients with colorectal liver metastases: A
prospective study. Ann Surg Oncol 2002;9:430–438.
111 da Silva RG, Sugarbaker PH. Analysis of prognostic factors in seventy
patients having a complete cytoreduction plus perioperative intraperito-
neal chemotherapy for carcinomatosis from colorectal cancer. J Am Coll
Surg 2006;203:878–886.
112 Glehen O, Kwiatkowski F, Sugarbaker PH et al. Cytoreductive surgery
combined with perioperative intraperitoneal chemotherapy for the man-
agement of peritoneal carcinomatosis from colorectal cancer: A multi-
institutional study. J Clin Oncol 2004;22:3284–3292.
113 McAfee MK, Allen MS, Trastek VF et al. Colorectal lung metastases: Re-
sults of surgical excision. Ann Thorac Surg 1992;53:780–785; discussion
785–786.
114 Mansel JK, Zinsmeister AR, Pairolero PC et al. Pulmonary resection of
metastatic colorectal adenocarcinoma. A ten year experience. Chest 1986;
89:109–112.
115 Joyce DL, Wahl RL, Patel PV, Schulick RD, Gearhart SL, Choti MA. Pre-
operative positron emission tomography to evaluate potentially resectable
63Pawlik, Schulick, Choti
www.TheOncologist.com
by guest on March 1, 2014
http://theoncologist.alphamedpress.org/
Dow
nloaded from

hepatic colorectal metastases. Arch Surg 2006;141:1220–1226; discus-
sion 1227.
116 Giacchetti S, Perpoint B, Zidani R et al. Phase III multicenter randomized
trial of oxaliplatin added to chronomodulated fluorouracil-leucovorin as
first-line treatment of metastatic colorectal cancer. J Clin Oncol 2000;18:
136–147.
117 Kohne CH, van Cutsem E, Wils J et al. Phase III study of weekly high-
dose infusional fluorouracil plus folinic acid with or without irinotecan in
patients with metastatic colorectal cancer: European Organisation for Re-
search and Treatment of Cancer Gastrointestinal Group Study 40986.
J Clin Oncol 2005;23:4856–4865.
118 Tournigand C, Andre T, Achille E et al. FOLFIRI followed by FOLFOX6
or the reverse sequence in advanced colorectal cancer: A randomized
GERCOR study. J Clin Oncol 2004;22:229–237.
64 Colorectal Liver Metastases
by guest on March 1, 2014
http://theoncologist.alphamedpress.org/
Dow
nloaded from

Citations http://theoncologist.alphamedpress.org/content/13/1/51#otherarticles
This article has been cited by 9 HighWire-hosted articles: by guest on M
arch 1, 2014http://theoncologist.alpham
edpress.org/D
ownloaded from