Time to first take-back operation predicts successful primary fascial closure in patients undergoing...
8
Time to first take-back operation predicts successful primary fascial closure in patients undergoing damage control laparotomy Matthew J. Pommerening, MD, a,b Joseph J. DuBose, MD, a Martin D. Zielinski, MD, d Herb A. Phelan, MD, e Thomas M. Scalea, MD, c Kenji Inaba, MD, f George C. Velmahos, MD, h James F. Whelan, MD, g Charles E. Wade, PhD, a,b John B. Holcomb, MD, a,b and Bryan A. Cotton, MD, MPH, a,b for the AAST Open Abdomen Study Group, Houston and Dallas, TX, Baltimore, MD, Rochester, MN, Los Angeles, CA, Richmond, VA, and Boston, MA Background. Failure to achieve primary fascial closure (PFC) after damage control laparotomy is costly and carries great morbidity. We hypothesized that time from the initial laparotomy to the first take-back operation would be predictive of successful PFC. Methods. Trauma patients managed with open abdominal techniques after damage control laparotomy were prospectively followed at 14 Level 1 trauma centers during a 2-year period. Time to the first take- back was evaluated as a predictor of PFC using hierarchical multivariate logistic regression analysis. Results. A total of 499 patients underwent damage control laparotomy and were included in this analysis. PFC was achieved in 327 (65.5%) patients. Median time to the first take-back operation was 36 hours (interquartile range 24–48). After we adjusted for patient demographics, resuscitation volumes, and operative characteristics, increasing time to the first take-back was associated with a decreased likelihood of PFC. Specifically, each hour delay in return to the operating room (24 hours after initial laparotomy) was associated with a 1.1% decrease in the odds of PFC (odds ratio 0.989; 95% confidence interval 0.978–0.999; P = .045). In addition, there was a trend towards increased intra- abdominal complications in patients returning after 48 hours (odds ratio 1.80; 95% confidence in- terval 1.00–3.25; P = .05). Conclusion. Data from this prospective, multicenter study demonstrate that delays in returning to the operating room after damage control laparotomy are associated with reductions in PFC. These findings suggest that emphasis should be placed on returning to the operating room within 24 hours after the initial laparotomy if possible (and no later than 48 hours). (Surgery 2014;156:431-8.) From the Department of Surgery a and the Center for Translational Injury Research, b The University of Texas Health Science Center, Houston, TX; The R Adams Cowley Shock Trauma Center, c University of Maryland Medical Center, Baltimore, MD; Department of Surgery, d Mayo Clinic, Rochester, MN; Department of Sur- gery, e University Of Texas Southwestern Medical Center, Dallas, TX; Department of Surgery, f Los Angeles County + University of Southern California Hospital, Los Angeles, CA; Division of Trauma, Critical Care, and Emergency Surgery, g Virginia Commonwealth University, Richmond, VA; and Division of Trauma, Emergency Surgery, and Critical Care, h Massachusetts General Hospital, Boston, MA DAMAGE-CONTROL LAPAROTOMY AND OPEN ABDOMINAL (OA) techniques offer a survival benefit in trauma patients; however, they are associated with a great deal of morbidity. 1-4 One of the primary end points of dam- age control, after the reversal of shock and comple- tion of necessary repairs, is to restore the integrity of the abdominal wall with primary fascial closure of the abdomen. Failure to achieve primary closure is a dreaded complication of OA management, after which secondary closure often is obtained with more complicated techniques, such as skin grafting or closure with mesh. Failed primary fascial closure is associated with longer hospital stays, increased complications, poor cosmesis, decreased functional quality of life, and, frequently, large ventral hernias requiring future operative reconstruction. 5,6 Presented at the 9th Annual Academic Surgical Congress in San Diego, CA, February 4–6, 2014. Accepted for publication April 14, 2014. Reprint requests: Bryan A. Cotton, MD, MPH, Center for Trans- lational Injury Research, 6410 Fannin St, UPB Suite 1100.20, Houston, TX 77030. E-mail: [email protected]. 0039-6060/$ - see front matter Ó 2014 Mosby, Inc. All rights reserved. http://dx.doi.org/10.1016/j.surg.2014.04.019 SURGERY 431
Transcript of Time to first take-back operation predicts successful primary fascial closure in patients undergoing...

PresenteDiego, C
Accepte
ReprintlationalHouston
0039-60
� 2014
http://d
Time to first take-back operationpredicts successful primary fascialclosure in patients undergoingdamage control laparotomyMatthew J. Pommerening, MD,a,b Joseph J. DuBose, MD,a Martin D. Zielinski, MD,d
Herb A. Phelan, MD,e Thomas M. Scalea, MD,c Kenji Inaba, MD,f George C. Velmahos, MD,h
James F. Whelan, MD,g Charles E. Wade, PhD,a,b John B. Holcomb, MD,a,b andBryan A. Cotton, MD, MPH,a,b for the AAST Open Abdomen Study Group, Houston and Dallas, TX,Baltimore, MD, Rochester, MN, Los Angeles, CA, Richmond, VA, and Boston, MA
Background. Failure to achieve primary fascial closure (PFC) after damage control laparotomy is costlyand carries great morbidity. We hypothesized that time from the initial laparotomy to the first take-backoperation would be predictive of successful PFC.Methods. Trauma patients managed with open abdominal techniques after damage control laparotomywere prospectively followed at 14 Level 1 trauma centers during a 2-year period. Time to the first take-back was evaluated as a predictor of PFC using hierarchical multivariate logistic regression analysis.Results. A total of 499 patients underwent damage control laparotomy and were included in thisanalysis. PFC was achieved in 327 (65.5%) patients. Median time to the first take-back operation was36 hours (interquartile range 24–48). After we adjusted for patient demographics, resuscitationvolumes, and operative characteristics, increasing time to the first take-back was associated with adecreased likelihood of PFC. Specifically, each hour delay in return to the operating room (24 hours afterinitial laparotomy) was associated with a 1.1% decrease in the odds of PFC (odds ratio 0.989; 95%confidence interval 0.978–0.999; P = .045). In addition, there was a trend towards increased intra-abdominal complications in patients returning after 48 hours (odds ratio 1.80; 95% confidence in-terval 1.00–3.25; P = .05).Conclusion. Data from this prospective, multicenter study demonstrate that delays in returning to theoperating room after damage control laparotomy are associated with reductions in PFC. These findingssuggest that emphasis should be placed on returning to the operating room within 24 hours after theinitial laparotomy if possible (and no later than 48 hours). (Surgery 2014;156:431-8.)
From the Department of Surgerya and the Center for Translational Injury Research,b The University of TexasHealth Science Center, Houston, TX; The R Adams Cowley Shock Trauma Center,c University of MarylandMedical Center, Baltimore, MD; Department of Surgery,d Mayo Clinic, Rochester, MN; Department of Sur-gery,e University Of Texas Southwestern Medical Center, Dallas, TX; Department of Surgery,f Los AngelesCounty + University of Southern California Hospital, Los Angeles, CA; Division of Trauma, Critical Care,and Emergency Surgery,g Virginia Commonwealth University, Richmond, VA; and Division of Trauma,Emergency Surgery, and Critical Care,h Massachusetts General Hospital, Boston, MA
DAMAGE-CONTROL LAPAROTOMYANDOPEN ABDOMINAL (OA)techniques offer a survival benefit in trauma patients;however, they are associated with a great deal of
d at the 9th Annual Academic Surgical Congress in SanA, February 4–6, 2014.
d for publication April 14, 2014.
requests: Bryan A. Cotton, MD, MPH, Center for Trans-Injury Research, 6410 Fannin St, UPB Suite 1100.20,, TX 77030. E-mail: [email protected].
60/$ - see front matter
Mosby, Inc. All rights reserved.
x.doi.org/10.1016/j.surg.2014.04.019
morbidity.1-4 One of the primary end points of dam-age control, after the reversal of shock and comple-tion of necessary repairs, is to restore the integrityof the abdominal wall with primary fascial closure ofthe abdomen. Failure to achieve primary closure isa dreaded complication of OA management, afterwhich secondary closure often is obtained withmore complicated techniques, such as skin graftingor closure with mesh. Failed primary fascial closureis associated with longer hospital stays, increasedcomplications, poor cosmesis, decreased functionalquality of life, and, frequently, large ventral herniasrequiring future operative reconstruction.5,6
SURGERY 431

SurgeryAugust 2014
432 Pommerening et al
As experience with OA has increased duringthe last several years, a clear association has beendemonstrated between the number of re-explorations and successful primary fascialclosure.7-11 That is, the longer the abdomen remainsopen, the less likely the patient will be primarilyclosed. Reasons for this might include that resuscita-tion of an open abdomen allows for increased third-spacing andbowel edema, retractionof fascial edges,and ultimately a loss of domain, resulting in failedfascial closure. As well, failure to close early maylead to increased complications (eg fistulae, anasto-motic failure), thereby preventing subsequentclosure. If either is true, a quick return to the oper-ating room after restoration of normal physiologymay reduce this phenomenon and improve overallprimary fascial closure rates.
The primary aim of this study was to evaluatewhether the time interval from initial laparotomyto the first re-exploration, or take-back (TB)operation, is predictive of primary fascial closureand whether there exists an optimal time to returnto the operating room to attempt definitiveclosure. We hypothesized that among adult traumapatients undergoing damage control laparotomy,increasing time to initial TB is negatively associ-ated with primary fascial closure.
METHODS
This study was conducted using data from theAmerican Association for the Surgery of Trauma(AAST) Open Abdomen registry, which was aprospective observational multi-institutional studythat enrolled patients during a 2-year period at 14trauma centers. The current study’s protocol wasapproved by the AAST Multi-Institution TrialsCommittee, and each participating center ob-tained approval from its own institutional reviewboard. Patients with an open abdomen after dam-age control laparotomy were enrolled prospec-tively from 2010 through 2011.
The inclusion criterion was nonclosure ofabdominal fascia after the initial trauma laparot-omy. Patients younger than 18 years of age andpregnant patients were excluded from the presentstudy. Participating centers on the AAST multi-center study portal securely uploaded data whichsubsequently were then collected at the end of thestudy period and analyzed by the principal in-vestigators. All patients included in the presentstudy had basic demographic data, admissionlaboratory values, intraoperative details, injurypatterns, fluid use (both intraoperatively and post-operatively for the first 48 hours), ventilatorsettings, and OA management variables
documented. All variables were defined using adata dictionary specifically designed for the studyto promote uniformity of data collection. Theseincluded the definition of intraoperative acidosisas any pH measurement of less than 7.35 intra-operatively and the definition of intraoperativehypothermia as a recorded temperature less than358C at any point during the initial operation. Pri-mary fascial closure was defined as simple, unassistedprimary reapproximation of the native abdominalfascia. Assisted primary closure techniques viaretention sutures or a Whitman patch were consid-ered secondary closures in this analysis.
Patients who died within 48 hours of admission orbefore the first TB were not included in the presentanalysis. Among those surviving to 48 hours whounderwent at least one repeat exploration, multivar-iate logistic regressionwas used to assess the relation-ship between time to initial TB and primary fascialclosure. Predicted probabilities of primary fascialclosure were then graphed over time to TB. Theinflection point with the greatest likelihood ofprimary fascial closure was then used to estimate anapproximate cutoff after which time to TB wasevaluated as a binary variable, early versus late TB.Patients who underwent early TB were thencompared with patients who underwent late TB. Allregressionwas performedusingmultivariable 2-levelhierarchical regression models to adjust for clus-tering of outcomes within hospitals. This approachallowed us to control formeasured and unmeasuredconfounding between hospitals and ensured thatpatients undergoing early TB were only comparedwith patients undergoing late TB from the samehospital.12-14 In cases in which likelihood ratiotesting indicated poor fit with hierarchical random-effects modeling, fixed-effects models were used.
All regression models included clinically impor-tant variables chosen a priori, and those associatedwith time to TB and primary fascial closure (P < .2)were included in the final model. The Wilcoxonrank sum test was used to compare continuous var-iables, and Pearson’s v2 or Fisher’s exact test wasused to compare proportions. Continuous vari-ables that were nonlinear with the primary and sec-ondary outcomes were log transformed prior tobeing used in the regression models. Two-tailedcomparisons were used for all analyses. Data man-agement and statistical analysis was performedusing STATA Statistical software (version 13.1; Col-lege Station, TX).
RESULTS
A total of 572 trauma patients from 14 level Itrauma centers underwent damage control

Table I. Basic demographics, injury severity and initial laboratory
Early TB # 48 hours (n = 412) Late TB > 48 hours (n = 87) P value
Age 37 (24–51) 33 (23–51) .696Age $55 y 81/412 (19.7) 16/87 (18.4) .786Male sex 324/412 (78.6) 71/87 (81.6) .536Blunt mechanism of injury 247/412 (60.0) 57/87 (65.5) .334Head AIS $3 81/341 (23.8) 19/72 (26.4) .635Chest AIS $3 219/372 (58.9) 48/80 (60.0) .852Abdominal AIS $3 342/397 (86.1) 60/85 (70.6) <.001Median ISS 27 (18–36) 25 (17–36) .397ISS $15 347/403 (86.1) 71/87 (81.6) .283Hemoglobin, g/dL 11.9 (9.8–13.3) 12 (10.1–13.6) .341
<7.0 19/410 (4.6) 2/87 (2.3) .5257.0–7.9 19/410 (4.6) 6/87 (6.9)8.0–9.9 70/410 (17.1) 12/87 (13.8)$10.0 302/410 (73.7) 67/87 (77.0)
pH 7.25 (7.16–7.33) 7.24 (7.16–7.31) .290<7.00 23/402 (5.7) 5/85 (5.9) .5077.00–7.19 114/402 (28.4) 30/85 (35.3)7.20–7.39 233/402 (58.0) 46/85 (54.1)$7.40 32/402 (8.0) 4/85 (4.7)
INR 1.2 (1.1–1.4) 1.2 (1.1–1.4) .083<1.20 180/405 (44.4) 42/83 (50.6) .5451.20–1.59 161/405 (39.8) 32/83 (38.6)1.60–1.99 42/405 (10.4) 7/83 (8.4)$2.00 22/405 (5.4) 2/83 (2.4)
Lactate, mg/dL 3.9 (2.6–6.3) 4.2 (3.1–6.1) .358<2.5 83/369 (22.5) 9/67 (13.4) .2352.5–4.9 153/369 (41.5) 33/67 (49.3)5.0–7.4 64/369 (17.3) 15/67 (22.4)$7.5 69/369 (18.7) 10/67 (14.9)
Median values represented with interquartile range (in parentheses) shown as 25th and 75th percentiles.AIS, Abbreviated Injury Score; INR, International Normalized Ratio; ISS, Injury Severity Score; TB, take-back.
SurgeryVolume 156, Number 2
Pommerening et al 433
operations and use of OA during the study period.Of those, 55 patients died within 48 hours ofinjury, and 12 patients died after 48 hours butbefore the initial TB and were excluded. Anothersix patients were excluded because the time to theinitial TB was not recorded. Therefore, a total of499 patients were included in the final analysis, ofwhich the majority was young to middle-agedmales and predominantly victims of blunt trauma.The median Injury Severity Score (ISS) was 26,indicating that the global injury burden in thiscohort was severe, and more than 83% of patientssustained severe abdominal injuries (AbbreviatedInjury Score $3) (Table I).
Univariate analysis. Patients were grouped ac-cording to whether they underwent early(#48 hours) or late (>48 hours) initial TB. Bothgroups were similar with respect to demographics,injury severity, and arrival laboratory values, with theexception that more patients in the early TB grouphad abdominal Abbreviated Injury Scores $3.Patients receiving early TB also more frequently
had evidence of clinical coagulopathy and hypo-thermia during the initial laparotomy (Table II), butboth groups received similar intraoperative and 24-hour resuscitation volumes. In addition, there wereno differences in types of abdominal injuries or re-pairs between the two groups. With respect to com-plications, there were no differences between thetwo groups (Table III). There was a trend, however,towards greater relaparotomy rates after primaryfascial closure among those with late first TB and,not surprisingly, longer ventilator days.
Damage control was the most common indica-tor for nonclosure (69%), followed by facilitationof early re-exploration (26%). The overwhelmingmajority of patients in the cohort (95%) had anegative pressure device used for temporaryabdominal closure, and this was similar in bothearly and late TB groups (95% vs 93%; P = .44). Awound-control device manufactured by K.C.I.Company (ABThera or Wound V.A.C.; KCI Inter-national, San Antonio, TX) was used in 303(61%) patients, whereas 170 (34%) patients

Table II. Intraoperative damage control indicators, operative interventions, and resuscitation propertiesand volumes
Early TB # 48 hours (n = 412) Late TB > 48 hours (n = 87) P value
Damage control indicatorsAcidosis 288/412 (69.9) 61/87 (70.1) .969Hypothermia (<358C) 134/412 (32.5) 20/87 (23.0) .080Clinical coagulopathy 187/412 (45.4) 26/87 (29.9) .008
Operative interventionGastric injury repair 54/412 (13.1) 8/87 (9.2) .315Hepatic injury repair 165/412 (40.0) 26/87 (29.9) .076Bowel resection 167/412 (40.5) 27/87 (31.0) .099Bowel left in discontinuity 107/412 (26.0) 13/87 (14.9) .090
Postoperative antibiotics 227/412 (55.1) 57/87 (65.5) .075Intraoperative crystalloids, L 3,000 (2,000–5,000) 3,219 (2,000–5,000) .619
<5 304/407 (74.7) 64/86 (74.4) .4195–10 87/407 (21.4) 16/86 (18.6)>10 16/407 (3.9) 6/86 (7.0)
Intraoperative blood products, L 2,458 (1,050–5,378) 2,090 (600–4,100) .141<5 297/412 (72.1) 67/86 (77.9) .5085–10 72/412 (17.5) 11/86 (12.8)>10 43/412 (10.4) 8/86 (9.3)
OR fluid balance, L 4,688 (2,975–7,848) 4,331 (2,580–7,855) .730<5 211/404 (52.2) 46/85 (54.1) .2015–10 137/404 (33.9) 22/85 (25.9)>10 56/404 (13.9) 17/85 (20.0)
24-hour crystalloids, L 4,573 (2,469–8,000) 5,583 (3,193–8,700) .110<5 218/408 (53.4) 40/87 (46.0) .4505–10 117/408 (28.7) 29/87 (33.3)>10 73/408 (17.9) 18/87 (20.7)
24-hour colloids, L 0 (0–2,053) 0 (0–570) .021<5 372/408 (91.2) 84/87 (96.55) .1305–10 17/408 (4.2) 0/87 (0)>10 19/408 (4.7) 3/87 (3.45)
24-hour fluid intake, L 6,025 (2,966–10,006) 5,893 (3,470–10,054) .714<5 168/408 (41.2) 36/87 (41.4) .9965–10 138/408 (33.8) 29/87 (33.3)>10 102/408 (25.0) 22/87 (25.3)
Median values represented with interquartile range (in parentheses) shown as 25th and 75th percentiles.TB, Take-back.
SurgeryAugust 2014
434 Pommerening et al
received a noncommercial apparatus, and all butone patient received continuous as opposed tointermittent negative pressure. Primary fascialclosure was achieved in 327 (65.5%) patients andvaried substantially among the 14 centers partici-pating in the study (range 25.5–85.2%), likelyowing to variations in patient demographics, sam-ple size, and clinical practice.
The median time to first TB was 36 (interquar-tile range 24–48) hours. One hundred seventy-eight (36%) patients returned to the OR for initialTB within the first 24 hours, 234 (47%) returnedbetween 24 and 48 hours, and 87 (17%) patientsreturned after 48 hours. Nearly 60% of patientswere admitted during the evening or early morn-ing hours (7 PM–7 AM). Median time to initial TB
was similar for both day and night admissions(33 hours versus 36 hours; P = .13), but patientsadmitted during the day were more likely to returnto the OR within 24 hours compared with night-time admissions (45% vs 29%; P < .001). This asso-ciation was only true, however, for the earliest ofTBs (<24 hours) because the proportion of initialTBs by 48 hours was similar in both day and nightadmissions (84% vs 81%; P = .327).
Multivariate analysis. Using hierarchical multi-variate logistic regression to adjust for potentialconfounders and variation by center, we foundtime to initial TB to be independently associatedwith primary fascial closure (Table IV). The proba-bility of primary fascial closure appeared to begreatest for TBs occurring 24–48 hours from initial

Table III. Outcomes, complications, and sequelae of open abdomens between groups
Early TB # 48 hours (n = 412) Late TB > 48 hours (n = 87) P value
Time to TB, h 30 (20–40) 59 (54–72) <.001Number of TBs 1 (1–3) 1 (1–3) .176Intra-abdominal complications 89/412 (21.6) 22/87 (25.3) .453
Intra-abdominal abscess/sepsis 81/412 (19.7) 21/87 (24.1) .347Enteric fistula 22/412 (5.3) 5/87 (5.7) .879
Extra-abdominal complications 229/412 (55.6) 49/87 (56.3) .900Acute renal failure 70/412 (17.0) 19/87 (21.8) .283Ventilator-associated pneumonia 64/412 (15.5) 18/87 (20.7) .283Sepsis 62/412 (15.0) 16/87 (18.4) .435ALI/ARDS 56/412 (13.6) 14/87 (16.1) .542DVT/PE 51/412 (12.4) 10/87 (11.5) .819Bloodstream Infection 45/412 (10.9) 9/87 (10.3) .875Catheter-associated UTI 46/412 (11.2) 9/87 (10.3) .824Hospital-acquired pneumonia 28/412 (6.8) 4/87 (4.6) .447
Any complication 254/412 (61.7) 56/87 (64.4) .635Primary fascial closure 276/412 (67.0) 51/87 (58.6) .136Early fascial closure (first TB) 179/411 (43.6) 38/87 (43.7) .983Relaparotomy after fascial closure 29/412 (7.0) 11/87 (12.6) .080ICU days 12 (6–21) 15 (6–30) .054Ventilator days 8 (4–16) 11 (4–19) .088Hospital days 21 (13–36) 24 (13–38) .381In-hospital mortality 50/412 (12.1) 14/87 (16.1) .316
Median values represented with interquartile range (in parentheses) shown as 25th and 75th percentiles.ALI, Acute lung injury; ARDS, acute respiratory distress syndrome; DVT, deep-vein thrombosis; PE, pulmonary embolism; TB, take-back; ICU, intensive careunit; UTI, urinary tract infection.
Table IV. Multivariate model predicting primaryfascial closure
VariableAdjusted OR(95% CI)
Pvalue
Time to TB, h 0.989 (0.978–0.999) .045*Abdomen AIS $ 3 0.700 (0.336–1.458) .340Bowel resection 0.614 (0.369–1.019) .059Postoperative antibiotics 1.533 (0.924–2.544) .098Intraoperative blood
products, mL0.814 (0.637–1.041) .101
24-hourcrystalloids > 10 L
0.509 (0.275–0.942) .032
Number of TBs 0.178 (0.108–0.293) <.001
*Statistically significant.AIS, Abbreviated injury score; CI, confidence interval; OR, odds ratio;TB, take-back.
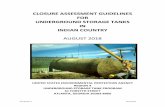
Fig. The predicted probability of primary fascial closurewith respect to time, in hours, from initial laparotomy tothe first TB after trauma. Successful primary fascialclosure was greatest in patients returning to the oper-ating room early. After approximately 24 hours, eachhour delay in first TB is associated with a 1.1% reductionin primary fascial closure.
SurgeryVolume 156, Number 2
Pommerening et al 435
laparotomy (Fig), after which each hour delay in re-turn to the operating room was associated with a1.1% reduction in primary fascial closure (odds ra-tio [OR] 0.989; 95% confidence interval [95% CI]0.978–0.999; P = .045).
When we controlled for confounders, late TBwas associated with a 47% decreased odds ofprimary fascial closure (OR 0.53; 95% CI 0.29–0.98; P = .04). This association was even more pro-nounced among severely injured patients with ISS
>15 (OR 0.38; 95% CI 0.20–0.74; P = .004). In bothmodels, increasing number of TBs and crystalloidinfusion > 10 L in the first 24 hours were alsoindependent predictors of primary fascial closure.Among patients with ISS > 15, bowel resection was

SurgeryAugust 2014
436 Pommerening et al
also negatively predictive of primary fascial closure(OR 0.59; 95% CI 0.35–0.98; P = .04).With respectto complications, early TB was not associatedwith fewer extra-abdominal complications; howev-er, there was a trend toward increased intra-abdominal complications in patients undergoinglate TB (OR 1.80; 95%CI 1.00–3.25; P = .05).
DISCUSSION
Until recently, much of the literature describingoutcomes after damage control was limited tosingle-center, retrospective reviews subject to sig-nificant potential for bias and confounding effects.The multicenter AAST Open Abdomen database isthe largest prospective, observational study oftrauma patients undergoing damage control lapa-rotomy and allowed us the opportunity to analyzeimportant components of OA management acrossa variety of populations and demographics. Wefound that increasing time to initial TB afterdamage control laparotomy is negatively associatedwith achieving primary fascial closure and, inparticular, that patients should return to theoperating room no later than 48 hours from theinitial laparotomy.
Several studies have identified the association offailed primary closure with increasing duration ofOA time.7-11,15-17 Our findings suggest that theimportant effects of this temporal relationshipoccur during the initial resuscitation period. Pa-tients may be particularly susceptible to fluid shiftsshortly after admission, and presumably it is dur-ing this time that patients are most likely to receivehigh volume and/or rapid infusion of resuscita-tion fluids. In the setting of inflammatory media-tors combined with endothelial injury andcapillary leak, fluid shifts and third-spacing resultin increased visceral edema.15,18 Given that fluidsfollow the path of least resistance, an open abdom-inal cavity may, in fact, facilitate increased boweledema and distention of abdominal contents,which might otherwise not occur in a closedabdominal cavity.19
In the initial publication from the AAST OpenAbdomen database, Dubose et al7 noted that thenumber of re-explorations was highly correlatedwith failure to achieve primary fascial closure,and this was seconded by Bradley et al20 in their ex-amination of the risk factors for development ofenterocutaneous fistulae.21 In the nontrauma pop-ulation, Zielinski’s group noted increased primaryfascial closure with fewer days of OA managementas well as fewer reexplorations.18 To our knowl-edge, this study is the first to identify the time in-terval from initial operation to initial TB as a
predictor of fascial closure. Not only is early TBpredictive of successful primary fascial closure,but this effect is independent of several importantconfounders, including the total number of re-explorations and the volume of resuscitation fluidinfused.
Many other risk factors for failure to achieveprimary fascial closure have been identified as well,particularly infectious complications.17,22 Themost commonly described complication associatedwith failed primary fascial closure is developmentof intra-abdominal abscess. Hatch et al9 evaluatedthe impact of closure at the first TB and notedthat early fascial closure was associated with adecrease in both infectious and noninfectiouscomplications. Although we did not find that earlyTBs necessarily achieved early fascial closure, wedid identify a trend towards reduced intra-abdominal complications for patients receivingearly TB.
High-volume resuscitation, particularly with lowblood ratios, has also been suggested to play a rolein increasing intra-abdominal pressure, secondaryabdominal compartment syndrome, and failure toprimarily close the abdomen. An increased orpositive fluid balance has been associated withthird space fluid accumulation and organ dysfunc-tion in animal models.18,23 Similarly, Ghneimet al24 demonstrated a reduction in OA days in pa-tients treated with goal-directed fluid resuscitation.In their updated clinical practice guidelines, the,the World Society of the Abdominal CompartmentSyndrome recommends the use of a protocol to tryto avoid a positive cumulative fluid balance in thecritically ill or injured and also suggests using anenhanced ratio of plasma/packed red blood cellsfor resuscitation of massive hemorrhage.11
Although this was not the primary outcome ofour study, in several of our multivariate analyses,high volumes of both crystalloids and blood prod-ucts were strongly associated with failed primaryfascial closure. Even after we controlled for thisassociation, time to TB remained independentlypredictive of primary fascial closure.
There are several limitations that are importantto consider in the interpretation of our results.Even though time to TB was prespecified andcollected prospectively, specific reasoning for whypatients returned for re-exploration at the timesthey did was not collected and may have beeninfluenced by other important unmeasured fac-tors, such as delays caused by increased intracra-nial pressures or refractory hypoxia. Similarly, theuse of diuretics, neuromuscular blockers, andother adjunctive therapies to assist abdominal

SurgeryVolume 156, Number 2
Pommerening et al 437
closure were not recorded and may have alsoinfluenced outcomes. In addition, previous studieshave reported higher primary closure rates thanwhat was observed in this study. Cothren et al25
were able to achieve 100% primary closure usinga modified vacuum-assisted closure technique. Ina prospective study by Miller et al,26 a primaryfascial closure rate of 88% was observed after im-plementation of a robust protocol using their pre-viously described vacuum-assisted fascial closuretechnique. Absence of standardized closure tech-niques and protocols among participating centersmay have contributed to the wide range of primaryclosure rates in this study.
Finally, a lack of uniformly agreed-on indica-tions for damage control and use of OA prior tothe study limits comparison in this cohort.Acidosis, hypothermia, and coagulopathy are oftencited as indications for damage control yet 15% ofthe patients in this cohort did not have any ofthese features, highlighting the possibility that OAmay have been overused in some patients. Not allof these patients achieved primary closure, howev-er, and nearly half went back for a second TB,indicating OA management may have been appro-priate and that there may be other importantindicators for the use of this technique. The lackof agreement on indications for OA is not limitedto this study and our results are, perhaps, morereflective of current practice than necessarily bestpractice. In addition, the prospective, multicenternature of this database and hierarchical statisticalmodeling to account for variations by centerstrengthen our results and improve the generaliz-ability of this study to a broad population oftrauma patients.
As our experience with OA management con-tinues to evolve, increased efforts must be under-taken to optimize primary fascial closure of theabdomen and avoid modifiable risk factors forfailed primary closure. Although conscious effortsshould be made to achieve early closure of theabdomen and minimize the number of TBs,emphasis should also be placed on returning tothe operating room as early as possible. Given ourfindings, this would mean returning to the oper-ating room within 24 hours after the initiallaparotomy if possible (and no later than48 hours). Each hour delay in first TB carrieswith it a real and increased risk of failure toachieve primary fascial closure (1.1% per hour).
The AAST Open Abdomen Study Group members arethe following: Binod Shrestha, MD, and John Holcomb,
MD, from the University of Texas Houston MedicalCenter; Kenji Inaba, MD, Obi Okoye, MD, and Agatho-klis Konstantinidis, MD, from the Los Angeles County +University of Southern California Hospital; Tom Scalea,MD, Jay Menaker, MD, and Joe DuBose, MD, from the RAdams Cowley Shock Trauma Center, University ofMaryland Medical Center; James F. Whelan, MD, RaoIvatury, MD, and Stephanie R. Goldberg, MD, from theVirginia Commonwealth University; Martin D. Zielinski,MD, and Donald Jenkins, MD, from the Mayo ClinicTrauma Centers; Stephen Rowe, MD, Darrell Alley, MD,John Berne, MD, and LaDonna Allen, RN, from the EastTexas Medical Center; Paola G. Pieri, MD, and StarreHaney, RN, MS, from the Maricopa Integrated HealthSystem; Jeffrey A. Claridge, MD, and Katherine Kelly,MD, from the MetroHealth Medical Center; Tiffany Bee,MD, and Timothy Fabian, MD, from the University ofTennessee Health Science Center; Raul Coimbra, MD,PhD, and Jay Doucet, MD, from the University ofCalifornia San Diego School of Medicine; Ben Coop-wood, MD, David Keith, MD, and Carlos Brown, MD,from the University of Texas Southwestern - Austin,University Medical Center Brackenridge; James M.Haan, MD, and Jeanette Ward, BA, from the Via ChristiHospital, St. Francis Campus; Stuart M. Leon, MD, EvertEriksson, MD, and Debbie Couillard, RN, BSN, fromThe Medical University of Southern Carolina; and MarcA. de Moya, MD, and Gwendolyn M. van der Wilden,MSc, from the Massachusetts General Hospital.
REFERENCES
1. Asensio JA, McDuffie L, Petrone P, Roldan G, Forno W,Gambaro E, et al. Reliable variables in the exsanguinatedpatient which indicate damage control and predictoutcome. Am J Surg 2001;182:743-51.
2. Burch JM, Ortiz VB, Richardson RJ, Martin RR, Mattox KL,Jordan GL Jr. Abbreviated laparotomy and planned reoper-ation for critically injured patients. Ann Surg 1992;215:476-83; discussion 483-4.
3. Germanos S, Gourgiotis S, Villias C, Bertucci M, Dimopou-los N, Salemis N. Damage control surgery in the abdomen:an approach for the management of severe injuredpatients. Int J Surg 2008;6:246-52.
4. Rotondo MF, Schwab CW, McGonigal MD, Phillips GR 3rd,Fruchterman TM, Kauder DR, et al. ’Damage control’: anapproach for improved survival in exsanguinatingpenetratingabdominal injury. J Trauma 1993;35:375-82; discussion 382-3.
5. de Vries Reilingh TS, van Goor H, Rosman C, BemelmansMH, de Jong D, van Nieuwenhoven EJ, et al. ‘‘Componentsseparation technique’’ for the repair of large abdominalwall hernias. J Am Coll Surg 2003;196:32-7.
6. Cheatham ML, Safcsak K, Llerena LE, Morrow CE Jr, BlockEF. Long-term physical, mental, and functional conse-quences of abdominal decompression. J Trauma 2004;56:237-41; discussion 241-2.
7. Dubose JJ, ScaleaTM,HolcombJB,ShresthaB,OkoyeO, InabaK, et al. Open abdominal management after damage-controllaparotomy for trauma: a prospective observational AmericanAssociation for the Surgery of Trauma multicenter study.J Trauma Acute Care Surg 2013;74:113-20; discussion 1120-2.

SurgeryAugust 2014
438 Pommerening et al
8. Hatch QM, Osterhout LM, Ashraf A, Podbielski J, Kozar RA,Wade CE, et al. Current use of damage-control laparotomy,closure rates, and predictors of early fascial closure at thefirst take-back. J Trauma 2011;70:1429-36.
9. Hatch QM, Osterhout LM, Podbielski J, Kozar RA, WadeCE, Holcomb JB, et al. Impact of closure at the first takeback: complication burden and potential overutilizationof damage control laparotomy. J Trauma 2011;71:1503-11.
10. Duchesne JC, McSwain NE Jr, Cotton BA, Hunt JP, Della-volpe J, Lafaro K, et al. Damage control resuscitation: thenew face of damage control. J Trauma 2010;69:976-90.
11. Kirkpatrick AW, Roberts DJ, De Waele J, Jaeschke R, Mal-brain ML, De Keulenaer B, et al. Intra-abdominal hyperten-sion and the abdominal compartment syndrome: updatedconsensus definitions and clinical practice guidelinesfrom the World Society of the Abdominal CompartmentSyndrome. Intensive Care Med 2013;39:1190-206.
12. Bingenheimer JB, Raudenbush SW. Statistical and substan-tive inferences in public health: issues in the applicationof multilevel models. Annu Rev Public Health 2004;25:53-77.
13. Behm JE, Edmonds DA, Harmon JP, Ives AR. Multilevel sta-tistical models and the analysis of experimental data. Ecol-ogy 2013;94:1479-86.
14. Lake ET. Multilevel models in health outcomes research.Part II: statistical and analytic issues. Appl Nurs Res 2006;19:113-5.
15. Shapiro MB, Jenkins DH, Schwab CW, Rotondo MF. Dam-age control: collective review. J Trauma 2000;49:969-78.
16. Shinall MC Jr, Mukherjee K, Lovvorn HN 3rd. Early fascialclosure of the damage control abdomen in children. AmSurg 2010;76:497-501.
17. Vogel TR, Diaz JJ, Miller RS, May AK, Guillamondegui OD,Guy JS, et al. The open abdomen in trauma: do infectiouscomplications affect primary abdominal closure? SurgInfect 2006;7:433-41.
18. Shah SK, Jimenez F, Walker PA, Xue H, Uray KS, Aroom KR,et al. A novel physiologic model for the study of abdominalcompartment syndrome (ACS). J Trauma 2010;68:682-9.
19. Hadeed JG, Staman GW, Sariol HS, Kumar S, Ross SE.Delayed primary closure in damage control laparotomy:the value of the Wittmann patch. Am Surg 2007;73:10-2.
20. Bradley MJ, Dubose JJ, Scalea TM, Holcomb JB, Shrestha B,Okoye O, et al. Independent predictors of enteric fistulaand abdominal sepsis after damage control laparotomy: re-sults from the prospective AAST Open Abdomen registry.JAMA Surg 2013;148:947-54.
21. Goussous N, Kim BD, Jenkins DH, Zielinski MD. Factorsaffecting primary fascial closure of the open abdomen in thenontraumapatient. Surgery2012;152:777-83; discussion783-4.
22. Holodinsky JK, Roberts DJ, Ball CG, Reintam Blaser A, Star-kopf J, Zygun DA, et al. Risk factors for intra-abdominalhypertension and abdominal compartment syndromeamong adult intensive care unit patients: a systematic reviewand meta-analysis. Crit Care 2013;17:R249.
23. Cordemans C, De Laet I, Van Regenmortel N, SchoonheydtK, Dits H, Huber W, et al. Fluid management in critically illpatients: the role of extravascular lung water, abdominalhypertension, capillary leak, and fluid balance. Ann Inten-sive Care 2012;2(Suppl 1):S1.
24. Ghneim MH, Regner JL, Jupiter DC, Kang F, Bonner GL,Bready MS, et al. Goal directed fluid resuscitation decreasestime for lactate clearance and facilitates early fascial closurein damage control surgery. Am J Surg 2013;206:995-1000.
25. Cothren CC, Moore EE, Johnson JL, Moore JB, Burch JM.One hundred percent fascial approximation with sequen-tial abdominal closure of the open abdomen. Am J Surg2006;192:238-42.
26. Miller PR, Meredith JW, Johnson JC, Chang MC. Prospec-tive evaluation of vacuum-assisted fascial closure afteropen abdomen: planned ventral hernia rate is substantiallyreduced. Ann Surg 2004;239:608-14; discussion 614-6.