Fluorescence lifetime imaging by using time-gated data acquisition

Three-dimensionalElectrocardiographically GatedVariable Flip Angle FSE Imagingfor MR Angiography of theHands at 3.0 T: Initial Experience1
Ruth P. Lim, MBBS, M.Med, FRANZCRPippa Storey, PhDIliyana P. Atanasova, MSJian Xu, BSElizabeth M. Hecht, MDJames S. Babb, PhDDavid R. Stoffel, ARMRITHugo Chang, BSKellyanne McGorty, RTQun Chen, PhDHenry Rusinek, PhDH. Michael Belmont, MDVivian S. Lee, MD, PhD, MBA
After institutional review board approval and informedconsent were obtained for this HIPAA-compliant investiga-tion, a three-dimensional electrocardiographically gatedvariable flip angle (VFA) fast spin-echo magnetic reso-nance (MR) angiography technique was evaluated as anunenhanced method for imaging hand arteries in 13 sub-jects (including four patients) at 3.0 T; this included evalu-ation of vessel visualization with warming and cooling inseven subjects. Examinations were evaluated for imagequality and vessel conspicuity. Clear separation of arteriesfrom veins was achieved in all subjects, with excellentvessel conspicuity and depiction of stenoses. Warmingimproved vessel visualization in healthy volunteers. VFAMR angiography is a high-spatial-resolution technique thatenables the assessment of vascular reactivity in responseto temperature challenge.
� RSNA, 2009
1 From the Department of Radiology (MRI), New York Uni-versity Langone Medical Center, 530 First Ave, BasementSchwartz Bldg, New York, NY 10016 (R.P.L., P.S., I.P.A.,E.M.H., J.S.B., D.R.S., K.M., Q.C., H.R., V.S.L.); Depart-ment of Rheumatology, NYU Hospital for Joint Diseases,New York, NY (H.M.B.); and MR R&D Collaboration, NYUCenter for Biomedical Imaging, Siemens Medical Solu-tions, New York, NY (J.X., H.C.). Received February 15,2009; revision requested March 19; revision receivedMarch 27; accepted April 3; final version accepted April14. Address correspondence to R.P.L. (e-mail: [email protected] ).
� RSNA, 2009
ORIG
INAL
RESE
ARCH
�TE
CHNI
CAL
DEVE
LOPM
ENTS
874 radiology.rsnajnls.org ▪ Radiology: Volume 252: Number 3—September 2009
Note: This copy is for your personal, non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, use the Radiology Reprints form at the end of this article.

Imaging is vital in the work-up andmanagement of vascular hand abnor-malities, including thromboembolic
disease, vasculitides, trauma, and vascu-lar malformations. The standard of refer-ence for hand evaluation is digital sub-traction angiography (1). However,digital subtraction angiography has as-sociated risks of puncture site compli-cations, ionizing radiation, and iodinenephrotoxicity and can also be a pain-ful procedure for patients. In addition,vasodilators are frequently required foroptimal visualization of the small arteriesof the hand, which are highly reactive tonoxious stimuli (2). Contrast material–enhanced magnetic resonance (MR) an-giography has been advocated as a suit-able noninvasive alternative (3–5), butsmall vessel caliber, relatively slow arte-rial flow, and short arteriovenous transittimes can hamper arterial visualization(1,6). Attempts to shorten imaging timescan compromise spatial resolution or sig-nal-to-noise ratio.
An unenhanced technique is desir-able, particularly in patients with vasculit-ides or concurrent renovascular disease,in whom renal function may be compro-mised and nephrogenic systemic fibrosisbecomes a potential clinical concern (7).Time-of-flight and phase-contrast tech-niques have been reported (8) but arelimited by long imaging times and limitedcoverage (1).
An electrocardiographically gatedspin-echo–based MR angiographic tech-nique was initially described by Wedeenet al (9) and was later adapted into athree-dimensional (3D) single-shot fastspin-echo (FSE) technique by Miyazakiet al (10) on the basis of the principle thatblack blood images can be obtained infast-flowing blood with spin-echo se-quences.
Promising results have been obtainedwith this technique for the lower extrem-ities (11); however, vessel blur that is re-lated to echo train length and relative in-sensitivity to slow arterial flow could limitits use in the hand. Use of a variable flipangle (VFA) FSE-based MR angiographictechnique, sampling perfection with ap-plication of optimized contrasts using dif-ferent flip angle evolutions, or SPACE(12), has been described. The use of aVFA technique facilitates shorter inter-echo spacing and readout duration withsubsequently decreased vessel blurring;more accurate sampling of peak and slow-est flow in systole and diastole, respec-tively; and decreased radiofrequencydeposition compared with a constant flipangle single-shot FSE approach (13).
We hypothesize that VFA MR angiog-raphy will enable high-spatial-resolution,entirely noninvasive evaluation of the ar-teries of the hand. The primary purposeof this study was to develop and evaluatethe feasibility of the VFA MR angio-graphic technique for hand MR angiogra-phy at 3.0 T. A secondary aim was to usethe technique to evaluate the effects oftemperature challenge on visualization ofthe small vessels of the hand.
Materials and Methods
Two authors (J.X. and H.C.) are employ-ees of Siemens Medical Solutions, themanufacturer of the MR imaging systemused in this study. The other authors
(who are not Siemens employees) hadcontrol of the data and information thatmight present a conflict of interest for theemployee authors.
SubjectsThis prospective technical developmentstudy was approved by the institutional eth-ics committee of New York UniversityLangone Medical Center and was compli-ant with the Health Insurance Portabilityand Accountability Act. Informed consentwas obtained from all subjects. Unen-hanced hand MR angiographic examina-tions were performed in 13 subjects aged26–67 years (mean age, 47.3 years). Therewere six men with a mean age of 47.8 years(range, 26–62 years) and seven womenwith a mean age of 46.9 years (range,34–67 years). Nine of the subjects werehealthy volunteers (five men aged 26–62years [mean age, 46.8 years] and fourwomen aged 34–41 years [mean age, 37.5years]). Four of the subjects were patients(one man aged 53 years and three womenaged 45–67 years [mean age, 59.3 years]);all patients had a history of limited sclero-derma and secondary Raynaud disease. Atotal of 16 hands (nine right, seven left)were imaged; 10 hands were imaged with-out temperature challenge.
A subset of seven subjects (two men
Published online before print10.1148/radiol.2531090290
Radiology 2009; 252:874–881
Abbreviations:FSE � fast spin echoMIP � maximum intensity projection3D � three-dimensionalVFA � variable flip angle
Author contributions:Guarantor of integrity of entire study, R.P.L.; study con-cepts/study design or data acquisition or data analysis/interpretation, all authors; manuscript drafting or manu-script revision for important intellectual content, all au-thors; manuscript final version approval, all authors;literature research, R.P.L., I.P.A., V.S.L.; clinical studies,R.P.L., P.S., I.P.A., J.X., E.M.H., H.C., H.M.B.; statisticalanalysis, R.P.L., J.X., J.S.B.; and manuscript editing,R.P.L., P.S., E.M.H., J.S.B., H.C., Q.C., H.R., V.S.L.
Funding:This work supported by the National Institutes of Health(grant HL092439).
See Materials and Methods for pertinent disclosures.
Advances in Knowledge
� Three-dimensional electrocardio-graphically gated variable flip an-gle (VFA) fast spin-echo (FSE)MR angiography of the handsyields high-spatial-resolution im-ages with good arterial conspicu-ity, including visualization of thedigital arteries.
� Without the need for injectedcontrast material, this techniquecan be repeated and can consis-tently provide arterial phase im-ages without venous signal “con-tamination.”
� The noninvasive nature of thetechnique enables evaluation ofthe hand vasculature at baselineand after temperature challenge.
Implication for Patient Care
� Three-dimensional electrocardio-graphically gated VFA FSE MRangiography of the hands providesa noninvasive means of evaluatingarterial anatomy without the needfor injected contrast material.
TECHNICAL DEVELOPMENTS: MR Angiography of the Hands Lim et al
Radiology: Volume 252: Number 3—September 2009 ▪ radiology.rsnajnls.org 875
aged 39 and 53 years and five womenaged 34–66 years [mean age, 44.8years]) underwent imaging after temper-ature challenge. Of the subjects in thissubset, four were healthy volunteers andthree were patients. Two volunteers re-ported a history of digital color changewith exposure to cold, and two volunteershad no history of cold sensitivity. Sevenhands were imaged with temperaturechallenge. One volunteer’s hand was im-aged twice—once without temperaturechallenge and once with temperaturechallenge—resulting in a total of 16 handsimaged overall.
The average heart rate was 72.9beats per minute (range, 62–90 beats perminute), with irregular rhythm noted intwo patients (atrial fibrillation and fre-quent premature ventricular contractionsin one patient each).
MR Imaging ProtocolImaging was performed at 3.0 T (Trio;Siemens, Erlangen, Germany), with sub-jects imaged in the prone position witharms raised above the head in a “Super-man” posture (two volunteers) for simul-taneous bilateral hand imaging and in thelateral decubitus position for imaging ofthe contralateral hand (11 subjects).Foam wedges and a custom-designedhand holder were used to minimize sub-ject motion. Central electrocardiographicgating was used in all subjects. Examina-tions were tailored to hand size and to thesurface coil employed. For prone imag-ing, a six-element surface phased-arraycoil was used. For lateral decubitus imag-ing, a 12-channel head coil was used forlarger hands and an eight-channel kneecoil was used for smaller hands. VFA MRangiography is subtraction based, devel-oped from the 3D single-shot FSE MRangiographic technique, in which fast ar-terial flow (flow void) from systolic im-ages is subtracted from slow arterial flowthat appears bright on diastolic images(14). With cancellation of venous andbackground tissue, which are similar onboth systolic and diastolic images, abright-blood MR angiogram is obtained(Fig 1).
An oblique coronal acquisition cover-ing the entire hand in the plane of thepalm and fingers was performed with a
left-to-right phase-encoding direction. Im-aging parameters were as follows: repeti-tion time, two R-R intervals; effectiveecho time, 10 msec; variable flip angle;interecho spacing, 3.3 msec; voxel size,0.7 � 0.8 � 1–2 mm; bandwidth, 745Hz/voxel; 26–64 partitions (average,38.5 partitions); average acquisition time,2 minutes 52 seconds (1 minute 40 sec-onds to 4 minutes 30 seconds); and fieldof view, 240–280 � 156 � 252 mm. Tominimize readout duration, two echotrains per section were employed, for 43echoes per train with the use of parallelimaging (generalized autocalibrating par-tially parallel acquisitions, accelerationfactor 2–3) (15). Owing to the use of half-Fourier acquisition in the phase-encodingdirection, the echo train duration was 73msec. Centric encoding was employed.Although earlier studies using a single-shot FSE-based approach incorporatedadditional flow spoiling to achieve thenecessary degree of flow sensitivity forperipheral MR angiography (11,16), noadditional spoiling was required with ourtechnique because VFA MR angiographyis intrinsically more flow sensitive thansingle-shot FSE because of the lower flipangles of its refocusing pulses (17,18).
For systolic imaging, trigger delayswere based on a two-dimensional gradi-ent-echo phase-contrast scout sequencewith velocity encoding of 40 cm/sec, en-abling identification of the optimal triggertime, coinciding with peak systolic flowbased on a velocity-versus-time curve(Mean Curve, Leonardo; Siemens). A
0-msec trigger delay was used for dia-stolic imaging because it coincided withend diastole when velocity-versus-timecurves were reviewed for all subjects.Systolic and diastolic acquisitions wereacquired consecutively without pause.
For the subjects who underwent tem-perature challenge, images were acquiredafter cooling with hand immersion in coldwater (for 2 minutes at 10°C) for healthyvolunteers and after sitting in a tempera-ture-controlled room(13°C) for 20minutesfor patients. Healthy volunteers and pa-tients were then imaged a second time afterwarming for 10 minutes with saline bagsheated to 50°C.
Subjects were questioned (I.P.A.,D.R.S.) with regard to whether the imagingposition was comfortable or uncomfortableat the conclusion of imaging and wereasked to describe the nature of their dis-comfort if applicable. Imaging time for eachMR angiographic acquisition, average heartrate, and presence of arrhythmias were re-corded for each subject (R.P.L.).
Image AnalysisSubtracted 3D data sets were evaluatedby two radiologists (R.P.L. and E.M.H.,with 3 and 6 years of experience withvascular MR image interpretation, re-spectively) in consensus on a workstation(Leonardo, Siemens) and were reviewedby using multiplanar reconstruction andMIP. Overall image quality was assessedby using a four-point Likert scale, where ascore of 0 indicated nondiagnostic; ascore of 1, poor; a score of 2, satisfactory;
Figure 1
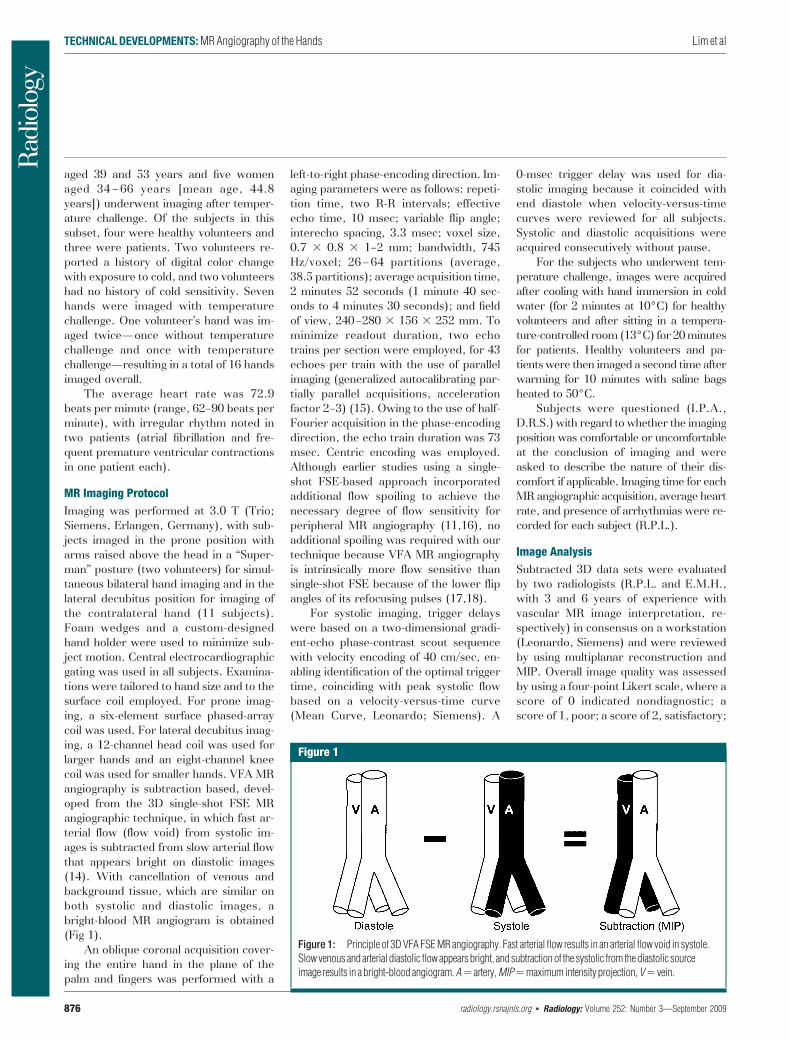
Figure 1: Principle of 3D VFA FSE MR angiography. Fast arterial flow results in an arterial flow void in systole.Slow venous and arterial diastolic flow appears bright, and subtraction of the systolic from the diastolic sourceimage results in a bright-blood angiogram. A� artery, MIP�maximum intensity projection, V� vein.
TECHNICAL DEVELOPMENTS: MR Angiography of the Hands Lim et al
876 radiology.rsnajnls.org ▪ Radiology: Volume 252: Number 3—September 2009

and a score of 3, excellent image quality.The number of vascular segments (pal-mar arches and metacarpal, common dig-ital, radialis indicis, princeps pollicis, andproper digital arteries) present and vesselsegment conspicuity (0 � nondiagnostic;1 � poor, impairing diagnosis; 2 � sub-optimal without diagnostic impairment;3 � good arterial signal intensity) wererecorded (19). For proper digital arter-ies, the number of digital arteries visibleto the terminal third was recorded. Visu-alization of terminal nutrient arteries wasalso recorded on a per-subject basis. Thepresence of venous signal (0 � absent;1 � present, not limiting interpretation;2 � present, affecting image interpreta-tion) was assessed. Motion artifact wasgraded separately for palmar (palmararches and metacarpal and common dig-ital arteries) and digital (radialis indicis,princeps pollicis, and proper digital arter-ies) segments as follows: a grade of 0indicated absent; a grade of 1, present,not affecting image interpretation; agrade of 2, present, affecting image inter-pretation; and a grade of 3, severe, ren-dering images nondiagnostic. Pathologicconditions and anatomic variants wererecorded qualitatively.
In subjects who underwent tempera-ture challenge, images were reviewed forimage quality, number of vessel seg-ments, and segment conspicuity for bothcool and warm image data sets. Anychange in the number of visualized seg-ments between cool and warm imagingwas recorded. The diameter of the super-ficial palmar arch was measured in sixsubjects who underwent provocative test-ing, and the diameter of the terminal ra-dial artery was measured in one subject inwhom the superficial palmar arch was notvisualized. Arterial caliber was measuredin millimeters at the same positions onmagnified coronal subtraction MIP im-ages, with cool and warm images viewedside-by-side for each subject.
Statistical AnalysisThe number of vessel segments visualized,systolic and diastolic acquisition times, andsegment conspicuity scores were summa-rized as means � standard deviations. Ananalysis of segmental conspicuity on the ba-sis of segment location, comparing palmar
vessels (palmar arches, metacarpal andcommon digital arteries) with digital vessels(radialis indicis, princeps pollicis, andproper digital arteries), was performed(J.S.B.). Generalized estimating equationsbased on a binary logistic regression modelwere used to compare palmar and digitalvessels and to derive confidence intervalsfor the percentage of vessels that could beexpected to show excellent conspicuity.The dependent variable was the binary in-dicator identifying vessels that received aconspicuity score of 3. The model includedhand (left vs right) and vessel position (pal-mar vs digital) as classification factors. Thecorrelation structure was modeled by as-suming that observations correlated onlywhen derived for the same patient, with thestrength of the correlation dependent onwhether vessels were from the samehand. Software (SAS, version 9.0;SAS Institute, Cary, NC) was used forstatistical computations. Results weredeclared significant when associatedwith a P value of less than .05.
Results
VFA MR angiography was well tolerated,with successful completion of the MR an-giographic examination in all cases. Imageacquisition in the lateral decubitus posi-tion was comfortable for all but one sub-ject, who reported pain in the dependentshoulder due to positional impingement.Both subjects who were imaged in theprone position reported bilateral armstiffness secondary to immobility and pro-longed bilateral arm extension, with par-esthesias also noted in one subject towardthe end of the examination. This position,however, enabled bilateral hand exami-nation in the same acquisition time.
Baseline Imaging without TemperatureChallengeImage quality was excellent for six sub-jects and was satisfactory for four, withno images considered poor quality ornondiagnostic. One hundred fifty-eightvascular segments were visualized in 10hands without temperature challenge: 19palmar arch, 30 common digital, 23 pal-mar metacarpal, 10 princeps pollicis, ninearteria radialis indicis, and 67 proper dig-ital artery segments. The mean number
of segments visualized per hand was15.8 � 2.3 (standard deviation). Fifty-seven (85%) of the 67 proper digital ar-teries were visualized to their terminalthird. High in-plane resolution enabled vi-sualization of terminal nutrient arteries inthree subjects (Fig 2).
There was high vessel segment con-spicuity, with scores as follows: palmararch, 2.9 � 0.5 (a score of 3 is consistentwith good arterial signal intensity); com-mon digital and metacarpal arteries,2.9 � 0.3; arteria radialis indicis and prin-ceps pollicis arteries, 2.5 � 0.6; andproper digital arteries, 2.7 � 0.6. Whensegments were stratified into palmar(proximal) and digital (distal) vessels, 66(92%) of the 72 palmar vessels receivedexcellent conspicuity scores (95% confi-dence interval: 72.5%, 97.9%). For digi-tal vessels, excellent conspicuity was re-corded in 59 (69%) of 86 segments (95%confidence interval: 48.0%, 83.8%). Thedifference between palmar and digitalvessel conspicuity was statistically signifi-cant (P � .01). The mean conspicuityscore was 2.9 � 0.34 for proximal vesselsand 2.6 � 0.60 for distal vessels.
There was no venous “contamina-tion” recorded for any subject (score of 0for all subjects). Mild motion artifact waspresent in the palmar segments of fivesubjects but did not affect image interpre-tation. For digital segments, motion arti-fact was noted in five subjects, limitingimage interpretation in two. One properdigital artery segment was partially ex-cluded from the imaging field of view.
Anatomic variations included a per-sistent median artery (Fig 3). The onepatient with scleroderma imaged at base-line had an abnormal image, with 12 ves-sel segments visualized overall—fewerthan for volunteers—and vessel tortuosityand irregularity were noted.
Temperature ChallengeProvocative testing of seven subjectsyielded differences in the number of visu-alized segments for volunteers versus pa-tients. For healthy volunteers, the transi-tion from cold to warm increased thenumber of visualized segments, whereasfor patients, minimal change was ob-served. With regard to vessel caliber, anincrease in caliber was noted in three vol-
TECHNICAL DEVELOPMENTS: MR Angiography of the Hands Lim et al
Radiology: Volume 252: Number 3—September 2009 ▪ radiology.rsnajnls.org 877

unteers and one patient, with no changefor the remaining subjects. These resultsare summarized graphically in Figure 4.
All images in healthy volunteers, con-sisting of cold and warm data sets foreach individual, were considered satisfac-tory (n � 5) to excellent (n � 3). Of thetwo volunteers who reported a history ofcold sensitivity, one had a history of fin-gertip cyanosis generalized to all digits oncold exposure. In this subject, four seg-ments were visualized when subjected tocold challenge; this increased to 14 seg-ments after warming. In the second sub-ject, who gave a history of left thumb coldsensitivity manifesting as blanching andnail bed cyanosis, 14 segments were visu-alized when cold, increasing to 17 withwarming. Beading of the princeps pollicisartery was also apparent in this subjectand persisted after warming (Fig 5).
In the patient group, image qualitywas considered satisfactory (with warm-ing) and excellent (with cooling) in onepatient and poor in the other two pa-tients. Fewer segments were visualizedoverall. The first patient, who had a his-tory of right index finger amputation forischemic gangrene and chronic right mid-dle fingertip ulceration, had nine arterialsegments visualized with cooling; eightsegments were visualized after warming(Fig 6). Of the patients with poor imagequality, the first was in atrial fibrillation atimaging; seven segments were visualized,increasing to eight segments with warm-ing. The superficial and deep palmararches and the princeps pollicis arterywere well seen, with poor conspicuity ofthe visualized common and proper digitalarteries. Motion artifact limited the inter-pretation of images of both palmar anddigital segments. The last patient had fre-quent ventricular ectopic beats, reporteddiscomfort with lateral decubitus posi-tioning, and had evidence of bulk motionon images. However, the deep arch andprinceps pollicis artery were visualized atboth cool and warm imaging, without al-teration in the number of visualized seg-ments or their caliber.
Discussion
Contrast-enhanced MR angiography ofthe hands is widely acknowledged as chal-
lenging owing to the competing demandsof high spatial resolution and short arte-riovenous transit time, which constrainsthe overall acquisition time (20). Venouscontamination in particular has beenproblematic, with use of centric reorder-ing timed to optimal arterial opacification(21), timed arterial compression (5), andsubsystolic cuff compression advocatedas means of minimizing venous overlay.Although not ideal, contrast-enhancedMR angiography has been preferred totraditional unenhanced techniques and tophase-contrast and time-of-flight MR an-giography, which suffer from long acqui-sition times for comparable spatial reso-
lution. Relatively slow flow and in-planesaturation offer challenges for time-of-flight imaging, and appropriate velocityencoding selection is a concern for phase-contrast MR angiography (1).
In our early experience, VFA MR an-giography offers the opportunity for un-enhanced pure arterial imaging. Becauseit is a subtraction technique, backgroundsignal is suppressed. It is relatively rapid,with submillimeter in-plane resolution im-aging achievable in approximately 3 min-utes. It is well tolerated, particularly whensubjects are imaged in the lateral decubi-tus position, and allows for repeated stud-ies if there is motion artifact or if temper-ature challenge is desirable. Decreasedradiofrequency deposition with the VFAapproach permits efficient imaging at 3.0T. The high signal-to-noise ratio availablewith 3.0-T imaging can be directly trans-lated into improved spatial resolution,
Figure 2
Figure 2: Coronal subtraction MIP VFA MRangiogram (repetition time, two R-R intervals;echo time, 10 msec; variable flip angle) of left handof 45-year-old man (healthy volunteer) clearlydepicts the hand arteries, including the terminalnutrient arteries. The inset is a magnified image ofthe distal left index finger and nutrient vessels.
Figure 3
Figure 3: Coronal subtraction MIP VFA MRangiogram (repetition time, two R-R intervals;echo time, 10 msec; variable flip angle) of left handof 38-year-old woman (healthy volunteer). Variantarterial anatomy, with a persistent median artery(arrow), is depicted.
TECHNICAL DEVELOPMENTS: MR Angiography of the Hands Lim et al
878 radiology.rsnajnls.org ▪ Radiology: Volume 252: Number 3—September 2009
with high conspicuity of the proper digitalarteries in our series and visualization ofthe terminal nutrient arteries in threesubjects.
Application of partial Fourier or par-allel imaging techniques in the phase-encoding direction enables shorter echotrain lengths and readout duration, mini-
mizing vessel blur and maintaining cleardemarcation between systolic and dia-stolic acquisitions. A segmented acquisi-tion was used to further minimize readout
Figure 4
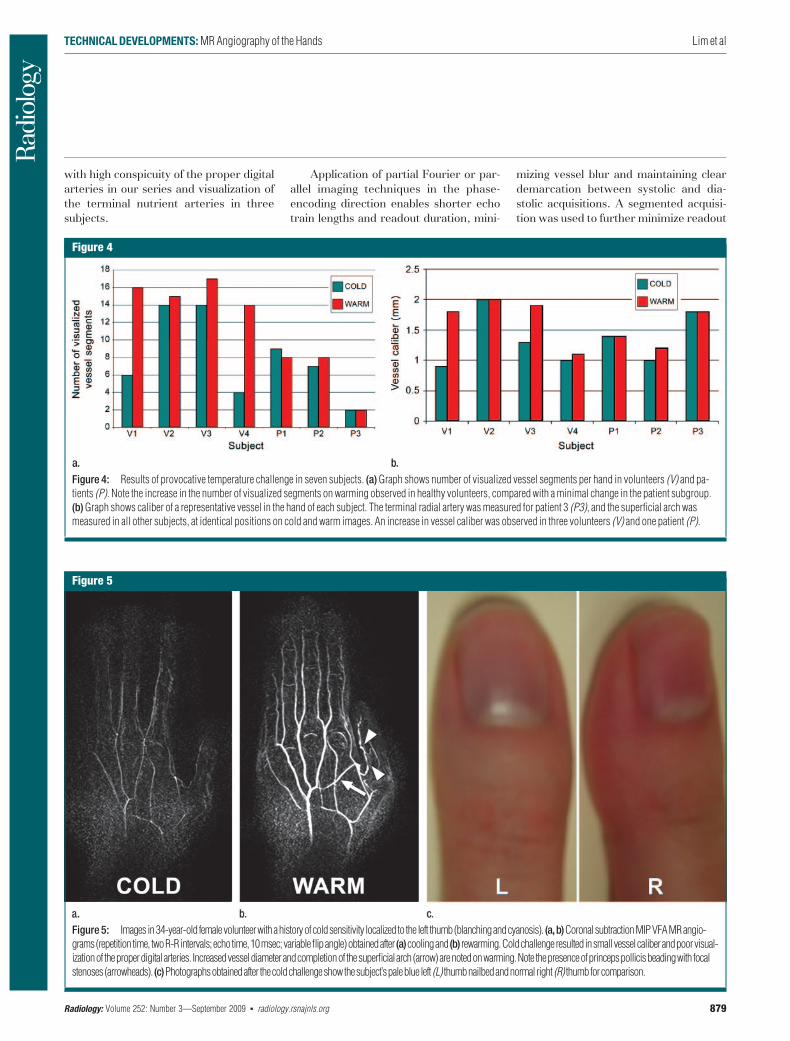
Figure 4: Results of provocative temperature challenge in seven subjects. (a) Graph shows number of visualized vessel segments per hand in volunteers (V) and pa-tients (P). Note the increase in the number of visualized segments on warming observed in healthy volunteers, compared with a minimal change in the patient subgroup.(b) Graph shows caliber of a representative vessel in the hand of each subject. The terminal radial artery was measured for patient 3 (P3), and the superficial arch wasmeasured in all other subjects, at identical positions on cold and warm images. An increase in vessel caliber was observed in three volunteers (V) and one patient (P).
Figure 5
Figure 5: Images in34-year-old femalevolunteerwithahistoryofcoldsensitivity localized to the left thumb(blanchingandcyanosis). (a,b)CoronalsubtractionMIPVFAMRangio-grams(repetitiontime, twoR-Rintervals;echotime,10msec;variableflipangle)obtainedafter (a)coolingand (b) rewarming.Coldchallengeresulted insmallvesselcaliberandpoorvisual-izationof theproperdigitalarteries. Increasedvesseldiameterandcompletionof thesuperficialarch(arrow)arenotedonwarming.Note thepresenceofprincepspollicisbeadingwith focalstenoses(arrowheads). (c)Photographsobtainedafter thecoldchallengeshowthesubject’spaleblue left (L) thumbnailbedandnormalright (R) thumbforcomparison.
TECHNICAL DEVELOPMENTS: MR Angiography of the Hands Lim et al
Radiology: Volume 252: Number 3—September 2009 ▪ radiology.rsnajnls.org 879
duration in our series because the differ-entiation of systolic and diastolic flow isparticularly important in the hand, wherepeak systolic velocities are as low as 23cm/sec � 12 for healthy subjects (22) andmay potentially be even lower when vas-culopathy is present.
We also noted marked changes invessel segment visualization and conspi-cuity after cold challenge and warming inhealthy subjects, including the two“healthy” volunteers with clinical symp-toms and examination findings of fingertipblanching and cyanosis at cold exposure.Conversely, little change in vessel visual-ization was observed in a small populationof patients with scleroderma. Cold stresstesting and rewarming have previouslybeen used to evaluate patients with pri-mary and secondary Raynaud phenome-non with a variety of techniques, includ-ing Doppler ultrasonography (US)(23,24), where decreases in digital andpalmar arch velocity, with increases inresistive and pulsatility indexes, weredemonstrated in patients with Raynaudphenomenon compared with healthy con-trol subjects. However, Doppler US is op-erator dependent and subject to acousticwindow limitations. Contrast-enhancedMR angiography can provide a high-spatial-resolution, reliable anatomic as-sessment, as has been shown withoutprovocative testing in scleroderma(25,26).
Unenhanced MR angiography offersthe added advantage of consistently purearterial phase imaging, allowing provoca-tive testing within a single visit. In sys-temic scleroderma, where secondaryRaynaud phenomenon is the presentingfeature in more than 90% of patients(27), endothelial dysfunction leads tostructural changes in the vessel wall thatare not seen in patients with primaryRaynaud phenomenon (27). Fixed versusreversible vascular abnormalities can bepotentially visualized, enabling simulta-neous anatomic and functional evalua-tion. Reliable evaluation of the presenceand degree of reversibility could provide abiomarker for differentiating primaryfrom secondary Raynaud phenomenon.With the development of medical thera-pies targeting the endothelium, includingendothelin receptor antagonists and �2c-
adrenoceptor antagonists (27,28), thereis exciting potential to evaluate the effi-cacy of therapeutic regimens in the pop-ulation of patients with scleroderma.
Our results are preliminary and illus-trate the promising nature of this unen-hanced MR angiography method for im-aging hand vessels. The main limitation ofour work was the lack of an imaging stan-dard for comparison. Because vasculopa-thy may decrease differences betweensystolic and diastolic velocities, this couldadversely affect vessel visualization with aflow-dependent technique such as ours,leading to disease overestimation—espe-cially in the patient group. In addition, astandardized cooling technique was notemployed, and this could partially ac-count for some of the observed differ-ences between volunteers and patientssubjected to temperature provocation.Further evaluation of the technique in alarger clinical population and with digital
subtraction angiography validation is re-quired.
Exploring the effect of cardiac ar-rhythmias on image quality is also war-ranted. Inaccurate triggering could causeinappropriate fast flow dephasing in somek-space partitions of the “diastolic” acqui-sition. Similarly, it could cause bright sig-nal from slow flow in some k-space parti-tions of the “systolic” acquisition. Suchinconsistencies in k-space will corrupt thereconstruction of the arteries on both im-age sets, causing signal loss and incoher-ent artifacts on the subtracted images.Inaccurate triggering could also causevariations in the degree of T1 relaxationbetween consecutive readout periods,which may contribute to incompletebackground suppression. Additional fu-ture work includes development of a cus-tom-designed hand coil by using elementsof appropriate size and with optimizedsensitivity profiles, engendering further
Figure 6
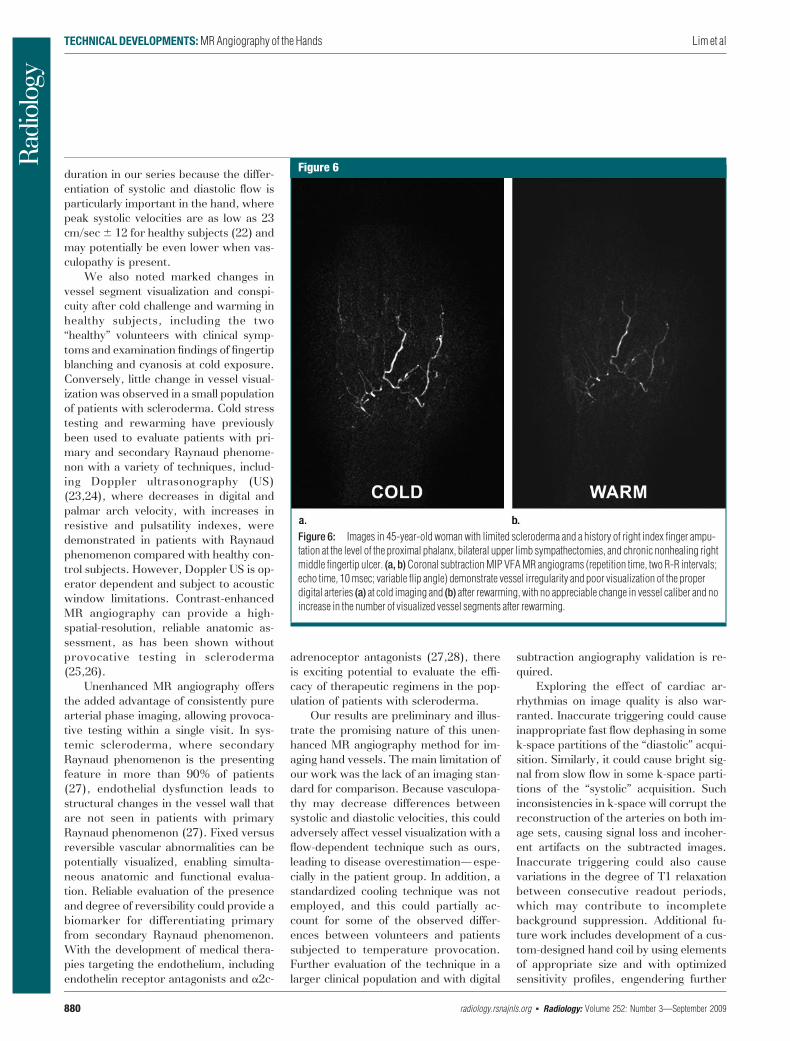
Figure 6: Images in 45-year-old woman with limited scleroderma and a history of right index finger ampu-tation at the level of the proximal phalanx, bilateral upper limb sympathectomies, and chronic nonhealing rightmiddle fingertip ulcer. (a, b) Coronal subtraction MIP VFA MR angiograms (repetition time, two R-R intervals;echo time, 10 msec; variable flip angle) demonstrate vessel irregularity and poor visualization of the properdigital arteries (a) at cold imaging and (b) after rewarming, with no appreciable change in vessel caliber and noincrease in the number of visualized vessel segments after rewarming.
TECHNICAL DEVELOPMENTS: MR Angiography of the Hands Lim et al
880 radiology.rsnajnls.org ▪ Radiology: Volume 252: Number 3—September 2009

gains in spatial resolution and imagingspeed. More aggressive k-space under-sampling techniques, particularly parallelimaging, could be explored, enabling asingle-shot acquisition with a minimizedacquisition window. This could poten-tially also increase the robustness of thesequence for arrhythmias.
Three-dimensional electrocardio-graphically gated unenhanced VFA MRangiography of the hands enables clearseparation of veins from arteries, withhigh in-plane resolution and excellentsmall vessel conspicuity. The techniquecan be repeated multiple times in a singlesession without the use of intravenouscontrast material, with potential clinicalapplication in the assessment of vascularreactivity with warming and cooling, suchas with the Raynaud phenomenon in apopulation of patients with connective tis-sue disease.
Acknowledgment: The authors thank MarthaHelmers, BS, for her expert assistance withpreparation of the figures.
References1. Rofsky NM. MR angiography of the hand and
wrist. Magn Reson Imaging Clin N Am 1995;3:345–359.
2. Loring LA, Hallisey MJ. Arteriography andinterventional therapy for diseases of thehand. RadioGraphics 1995;15:1299–1310.
3. Connell DA, Koulouris G, Thorn DA, PotterHG. Contrast-enhanced MR angiography ofthe hand. RadioGraphics 2002;22:583–599.
4. Lee VS, Lee HM, Rofsky NM. Magnetic res-onance angiography of the hand: a review.Invest Radiol 1998;33:687–698.
5. Wentz KU, Frohlich JM, von Weymarn C,Patak MA, Jenelten R, Zollikofer CL. High-resolution magnetic resonance angiographyof hands with timed arterial compression(tac-MRA). Lancet 2003;361:49–50.
6. Brauck K, Maderwald S, Vogt FM, Zenge M,Barkhausen J, Herborn CU. Time-resolvedcontrast-enhanced magnetic resonance an-giography of the hand with parallel imagingand view sharing: initial experience. Eur Ra-diol 2007;17:183–192.
7. Grobner T. Gadolinium: a specific trigger forthe development of nephrogenic fibrosingdermopathy and nephrogenic systemic fibro-
sis? Nephrol Dial Transplant 2006;21:1104–1108.
8. Krause U, Pabst T, Kenn W, Wittenberg G,Hahn D. MR angiography of the hand arter-ies. Angiology 2001;52:763–772.
9. Wedeen VJ, Meuli RA, Edelman RR, et al.Projective imaging of pulsatile flow with mag-netic resonance. Science 1985;230:946–948.
10. Miyazaki M, Sugiura S, Tateishi F, Wada H,Kassai Y, Abe H. Non-contrast-enhancedMR angiography using 3D ECG-synchro-nized half-Fourier fast spin echo. J MagnReson Imaging 2000;12:776–783.
11. Lim RP, Hecht EM, Xu J, et al. 3D nongado-linium-enhanced ECG-gated MRA of the dis-tal lower extremities: preliminary clinical ex-perience. J Magn Reson Imaging 2008;28:181–189.
12. Mugler JPI, Meyer H, Kiefer B. Practical im-plementation of optimized tissue-specificprescribed signal evolutions for improvedturbo-spin-echo imaging [abstr]. In: Pro-ceedings of the Eleventh Meeting of the In-ternational Society for Magnetic Resonancein Medicine. Berkeley, Calif: InternationalSociety for Magnetic Resonance in Medicine,2003; 203.
13. Xu J, Weale P, Laub G, et al. A novel non-contrast MR angiography technique usingtriggered non-selective refocused SPACE forimproved spatial resolution and speed [ab-str]. In: Proceedings of the Sixteenth Meet-ing of the International Society for MagneticResonance in Medicine. Berkeley, Calif: In-ternational Society for Magnetic Resonancein Medicine, 2008; 730.
14. Miyazaki M, Lee VS. Nonenhanced MR an-giography. Radiology 2008;248:20–43.
15. Griswold MA, Jakob PM, Heidemann RM,et al. Generalized autocalibrating partiallyparallel acquisitions (GRAPPA). Magn Re-son Med 2002;47:1202–1210.
16. Miyazaki M, Takai H, Sugiura S, Wada H,Kuwahara R, Urata J. Peripheral MRangiography: separation of arteries fromveins with flow-spoiled gradient pulses inelectrocardiography-triggered three-dimen-sional half-Fourier fast spin-echo imaging.Radiology 2003;227:890–896.
17. Atanasova IP, Storey P, Lim RP, et al. Effectof flip angle evolution on flow sensitivities inECG-gated fast spin echo MRA methods at3T [abstr]. In: Proceedings of the Seven-teenth Meeting of the International Societyfor Magnetic Resonance in Medicine. Berke-
ley, Calif: International Society for MagneticResonance in Medicine, 2009; 422.
18. Busse RF. Flow sensitivity of CPMG se-quences with variable flip refocusing and im-plications for CSF signal uniformity in 3D-FSE imaging [abstr]. In: Proceedings of theFourteenth Meeting of the International So-ciety for Magnetic Resonance in Medicine.Berkeley, Calif: International Society forMagnetic Resonance in Medicine, 2006;2430.
19. Gluecker TM, Bongartz G, Ledermann HP,Bilecen D. MR angiography of the hand withsubsystolic cuff-compression optimization ofinjection parameters. AJR Am J Roentgenol2006;187:905–910.
20. Goldfarb JW, Hochman MG, Kim DS,Edelman RR. Contrast-enhanced MR angiog-raphy and perfusion imaging of the hand.AJR Am J Roentgenol 2001;177:1177–1182.
21. Winterer JT, Scheffler K, Paul G, et al. Opti-mization of contrast-enhanced MR angiogra-phy of the hands with a timing bolus andelliptically reordered 3D pulse sequence.J Comput Assist Tomogr 2000;24:903–908.
22. Trager S, Pignataro M, Anderson J, KleinertJM. Color flow Doppler: imaging the upperextremity. J Hand Surg [Am] 1993;18:621–625.
23. Chikui T, Izumi M, Eguchi K, Kawabe Y,Nakamura T. Doppler spectral waveformanalysis of arteries of the hand in patientswith Raynaud’s phenomenon as comparedwith healthy subjects. AJR Am J Roentgenol1999;172:1605–1609.
24. Naidu S, Baskerville PA, Goss DE, RobertsVC. Raynaud’s phenomenon and cold stresstesting: a new approach. Eur J Vasc Surg1994;8:567–573.
25. Allanore Y, Seror R, Chevrot A, Kahan A,Drape JL. Hand vascular involvement as-sessed by magnetic resonance angiographyin systemic sclerosis. Arthritis Rheum 2007;56:2747–2754.
26. Wang J, Yarnykh VL, Molitor JA, et al. Mi-cro magnetic resonance angiography of thefinger in systemic sclerosis. Rheumatology(Oxford) 2008;47:1239–1243.
27. Sunderkotter C, Riemekasten G. Pathophysi-ology and clinical consequences of Raynaud’sphenomenon related to systemic sclerosis.Rheumatology (Oxford) 2006;45(suppl 3):iii33–iii35.
28. Henness S, Wigley FM. Current drug therapyfor scleroderma and secondary Raynaud’sphenomenon: evidence-based review. CurrOpin Rheumatol 2007;19:611–618.
TECHNICAL DEVELOPMENTS: MR Angiography of the Hands Lim et al
Radiology: Volume 252: Number 3—September 2009 ▪ radiology.rsnajnls.org 881
Radiology 2009This is your reprint order form or pro forma invoice
(Please keep a copy of this document for your records.)
Author Name _______________________________________________________________________________________________Title of Article _______________________________________________________________________________________________Issue of Journal_______________________________ Reprint # _____________ Publication Date ________________Number of Pages_______________________________ KB # _____________ Symbol RadiologyColor in Article? Yes / No (Please Circle)Please include the journal name and reprint number or manuscript number on your purchase order or other correspondence.
Order and Shipping Information
Reprint Costs (Please see page 2 of 2 for reprint costs/fees.)
________ Number of reprints ordered $_________
________ Number of color reprints ordered $_________
________ Number of covers ordered $_________
Subtotal $_________
Taxes $_________(Add appropriate sales tax for Virginia, Maryland, Pennsylvania, and the District of Columbia or Canadian GST to the reprints if your order is to be shipped to these locations.)
First address included, add $32 for each additional shipping address $_________
TOTAL $_________
Shipping Address (cannot ship to a P.O. Box) Please Print Clearly
Name ___________________________________________Institution _________________________________________Street ___________________________________________City ____________________ State _____ Zip ___________Country ___________________________________________Quantity___________________ Fax ___________________Phone: Day _________________ Evening _______________E-mail Address _____________________________________
Additional Shipping Address* (cannot ship to a P.O. Box)
Name ___________________________________________Institution _________________________________________Street ___________________________________________City ________________ State ______ Zip ___________Country _________________________________________Quantity __________________ Fax __________________Phone: Day ________________ Evening ______________E-mail Address ____________________________________* Add $32 for each additional shipping address
Payment and Credit Card DetailsEnclosed: Personal Check ___________
Credit Card Payment Details _________Checks must be paid in U.S. dollars and drawn on a U.S. Bank.Credit Card: __ VISA __ Am. Exp. __ MasterCardCard Number __________________________________Expiration Date_________________________________Signature: _____________________________________
Please send your order form and prepayment made payable to:
Cadmus ReprintsP.O. Box 751903Charlotte, NC 28275-1903
Note: Do not send express packages to this location, PO Box.FEIN #:541274108
Invoice or Credit Card InformationInvoice Address Please Print ClearlyPlease complete Invoice address as it appears on credit card statementName ____________________________________________Institution ________________________________________Department _______________________________________Street ____________________________________________City ________________________ State _____ Zip _______Country ___________________________________________Phone _____________________ Fax _________________E-mail Address _____________________________________
Cadmus will process credit cards and Cadmus Journal Services will appear on the credit card statement.
If you don’t mail your order form, you may fax it to 410-820-9765 with your credit card information.
Signature __________________________________________ Date _______________________________________Signature is required. By signing this form, the author agrees to accept the responsibility for the payment of reprints and/or all charges described in this document.
Reprint order forms and purchase orders or prepayments must be received 72 hours after receipt of form either by mail or by fax at 410-820-9765. It is the policy of Cadmus Reprints to issue one invoice per order.
Please print clearly.
Page 1 of 2RB-1/01/09
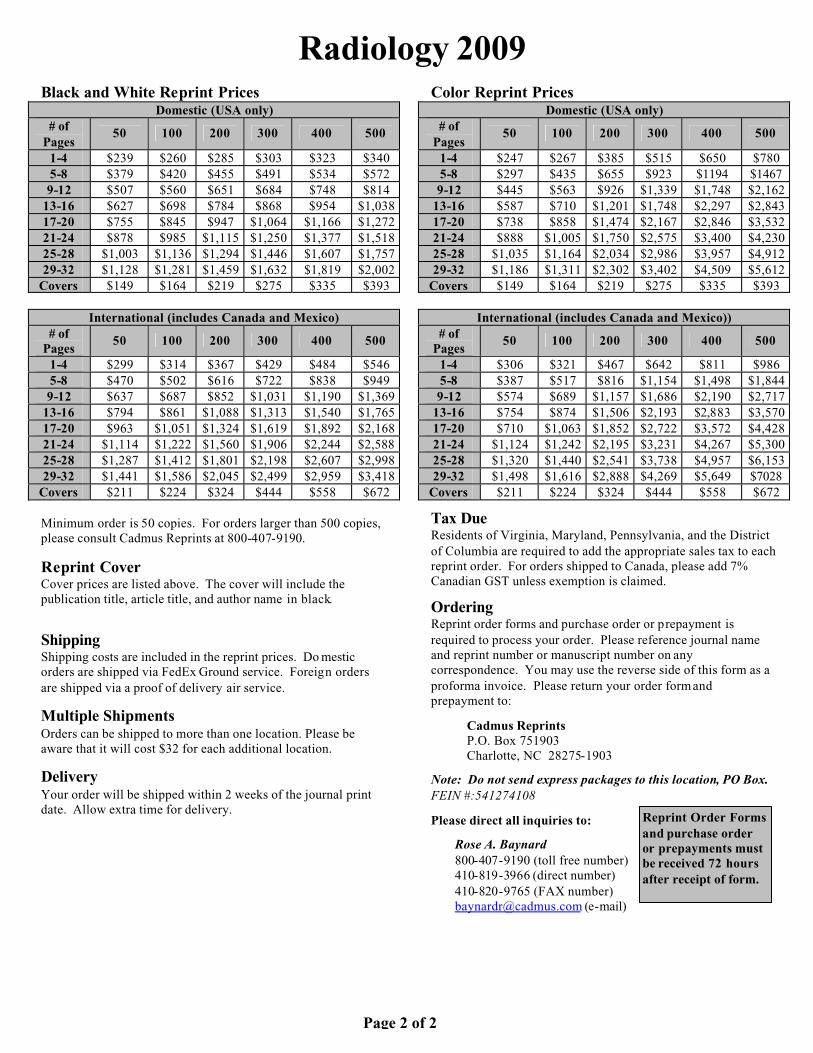
Radiology 2009Black and White Reprint Prices
Domestic (USA only)# of
Pages50 100 200 300 400 500
1-4 $239 $260 $285 $303 $323 $3405-8 $379 $420 $455 $491 $534 $5729-12 $507 $560 $651 $684 $748 $814
13-16 $627 $698 $784 $868 $954 $1,03817-20 $755 $845 $947 $1,064 $1,166 $1,27221-24 $878 $985 $1,115 $1,250 $1,377 $1,51825-28 $1,003 $1,136 $1,294 $1,446 $1,607 $1,75729-32 $1,128 $1,281 $1,459 $1,632 $1,819 $2,002
Covers $149 $164 $219 $275 $335 $393
International (includes Canada and Mexico)# of
Pages50 100 200 300 400 500
1-4 $299 $314 $367 $429 $484 $5465-8 $470 $502 $616 $722 $838 $9499-12 $637 $687 $852 $1,031 $1,190 $1,369
13-16 $794 $861 $1,088 $1,313 $1,540 $1,76517-20 $963 $1,051 $1,324 $1,619 $1,892 $2,16821-24 $1,114 $1,222 $1,560 $1,906 $2,244 $2,58825-28 $1,287 $1,412 $1,801 $2,198 $2,607 $2,99829-32 $1,441 $1,586 $2,045 $2,499 $2,959 $3,418
Covers $211 $224 $324 $444 $558 $672
Minimum order is 50 copies. For orders larger than 500 copies, please consult Cadmus Reprints at 800-407-9190.
Reprint CoverCover prices are listed above. The cover will include the publication title, article title, and author name in black.
ShippingShipping costs are included in the reprint prices. Do mesticorders are shipped via FedEx Ground service. Foreign orders are shipped via a proof of delivery air service.
Multiple ShipmentsOrders can be shipped to more than one location. Please be aware that it will cost $32 for each additional location.
DeliveryYour order will be shipped within 2 weeks of the journal print date. Allow extra time for delivery.
Color Reprint PricesDomestic (USA only)
# of Pages
50 100 200 300 400 500
1-4 $247 $267 $385 $515 $650 $7805-8 $297 $435 $655 $923 $1194 $14679-12 $445 $563 $926 $1,339 $1,748 $2,162
13-16 $587 $710 $1,201 $1,748 $2,297 $2,84317-20 $738 $858 $1,474 $2,167 $2,846 $3,53221-24 $888 $1,005 $1,750 $2,575 $3,400 $4,23025-28 $1,035 $1,164 $2,034 $2,986 $3,957 $4,91229-32 $1,186 $1,311 $2,302 $3,402 $4,509 $5,612
Covers $149 $164 $219 $275 $335 $393
International (includes Canada and Mexico))# of
Pages50 100 200 300 400 500
1-4 $306 $321 $467 $642 $811 $9865-8 $387 $517 $816 $1,154 $1,498 $1,8449-12 $574 $689 $1,157 $1,686 $2,190 $2,717
13-16 $754 $874 $1,506 $2,193 $2,883 $3,57017-20 $710 $1,063 $1,852 $2,722 $3,572 $4,42821-24 $1,124 $1,242 $2,195 $3,231 $4,267 $5,30025-28 $1,320 $1,440 $2,541 $3,738 $4,957 $6,15329-32 $1,498 $1,616 $2,888 $4,269 $5,649 $7028
Covers $211 $224 $324 $444 $558 $672
Tax DueResidents of Virginia, Maryland, Pennsylvania, and the District of Columbia are required to add the appropriate sales tax to each reprint order. For orders shipped to Canada, please add 7% Canadian GST unless exemption is claimed.
OrderingReprint order forms and purchase order or prepayment is required to process your order. Please reference journal name and reprint number or manuscript number on anycorrespondence. You may use the reverse side of this form as a proforma invoice. Please return your order form and prepayment to:
Cadmus ReprintsP.O. Box 751903Charlotte, NC 28275-1903
Note: Do not send express packages to this location, PO Box.FEIN #:541274108
Please direct all inquiries to:
Rose A. Baynard800-407-9190 (toll free number)410-819-3966 (direct number)410-820-9765 (FAX number)[email protected] (e-mail)
Reprint Order Forms and purchase order or prepayments must be received 72 hours after receipt of form.
Page 2 of 2
Copyright © 2022 FDOKUMEN