Thesis grand
78
INTRODUCTION “I firmly believe that if the whole materia medica could be sunk to the bottom of the sea, it would be all the better for mankind and all the worse for the fishes” . It is a broad term, includes all kinds of noxious effects- trivial, serious or even fatal. For the purposes of detecting and quantifying only those adverse effects of a drug which are of some important and occur in ordinary therapeutic setting, the term adverse drug reaction (ADR) has been defined as any ‘any noxious change which is suspected to be due to a drug, occurs at doses normally used in man, requires treatment or decrease in dose or indicates caution in the future use of the same drug’. This definition excludes trivial or expected side effects and poisonings or overdose. “Pharmacovigilance”, As per World Health Organization(WHO), “Pharmacoivigilance is the science and activities relating to the detection, assessment, understanding and prevention of adverse effects or any other drug related problems”. There is still a lack of understanding on this topic like how it functions, what are the benefits of sharing ADR knowledge and its purpose and importance. 2
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Thesis grand

INTRODUCTION
“I firmly believe that if the whole materia medica could be
sunk to the bottom of the sea, it would be all the better for
mankind and all the worse for the fishes”. It is a broad term,
includes all kinds of noxious effects- trivial, serious or
even fatal. For the purposes of detecting and quantifying only
those adverse effects of a drug which are of some important
and occur in ordinary therapeutic setting, the term adverse
drug reaction (ADR) has been defined as any ‘any noxious
change which is suspected to be due to a drug, occurs at doses
normally used in man, requires treatment or decrease in dose
or indicates caution in the future use of the same drug’. This
definition excludes trivial or expected side effects and
poisonings or overdose.
“Pharmacovigilance”, As per World Health
Organization(WHO), “Pharmacoivigilance is the science and activities relating
to the detection, assessment, understanding and prevention of adverse effects or
any other drug related problems”. There is still a lack of
understanding on this topic like how it functions, what are
the benefits of sharing ADR knowledge and its purpose and
importance.2

The pharmacovigilance concept rests on three pillars:
i) Collecting new information from reliable
scientific resources such as marketing
authorization holders, healthcare
professionals, consumers, international/public
bodies, journals, published and updated
literature etc.
ii) Classifying and analyzing the above
information.
iii) Calculating its contents as well as any action
taken on specific drug to all health sectors.
United Kingdom
The yellow card scheme for reporting suspected adverse
drug reactions (ADRs) was
introduced in 1964 and over 400,000 reports have now been
received by the
Committee on Safety of Medicines (CSM) / Medicines and
Healthcare products
Regulatory Agency (MHRA).3
Japan

From the perspective of identifying concerns for future
pharmacovigilance in Japan, safety measures for recent Adverse
Drug Reactions (ADRs) are compared between Japan and the
United States of America (U.S.A.) and are classified into the
following three main categories: category one for cases in
which ADR problems have not become apparent due to “drug lag”
in Japan, category two for cases in which Japanese
idiosyncrasies have become apparent, and category three for
adverse events for which assessment of the causal relationship
is difficult..4
The Central Drugs Standard Control Organisation (CDSCO), New
Delhi, under the aegis of Ministry of Health & Family Welfare,
Government of India has initiated a nation-wide
pharmacovigilance programme in July, 2010, with the All India
Institute of Medical Sciences (AIIMS), New Delhi as the
National Coordinating Centre (NCC) for monitoring Adverse Drug
Reactions (ADR) in the country to safe-guard Public Health. In
year 2010, 22 ADR monitoring centres (AMCs) including AIIMS,
New Delhi had been set up under this Programme. To ensure
implementation of this programme in a more effective way, the
National Coordinating Centre was then shifted from the All
India Institute of Medical Sciences (AIIMS), New Delhi to the
Indian Pharmacopoeia Commission (IPC), Ghaziabad, (U.P.) in
April, 2011.4
Realising the importance of the task, Medical Council OfIndia
(MCI) has made it mandatory for all medical colleges to have
an adverse drug reaction training, monitoring and reporting
program. There is still a lack of understanding on this topic
like how it functions, what are the benefits of sharing
Adverse Drug Reaction knowledge and its purpose and
importance.5To fulfil the above aim it is important to find out
the perception of doctors about ADR reporting and identify
steps which will improve adverse drug reaction reporting and
fulfil the goal of MCI.
There have been a study conducted in South India on knowledge,
attitude and Practices of physicians regarding ADR monitoring
which showed the poor knowledge of health care professionals
towards ADR monitoring and positive effect on spontaneous
reporting after educational interventions.6
Keeping these facts in mind, this study will be conducted to
assess awareness of pharmacovigilance among the healthcare

professionals and to evaluate the impact of an educational
intervention for improving awareness of pharmacovigilance
among physician and nurses in an Indian peripheral care
teaching hospital.
Review Of Literature
Adverse drug reaction (ADR) has been defined as ‘any noxious
change which is suspected to be due to a drug, occurs at doses
normally used in man, requires treatment or decrease in dose or
indicates caution in the future use of the same drug. 6
Pharmacovigilance has been defined by the WHO as the ‘science
and activities relating to the detection, assessment,

understanding and prevention of adverse effects or any other
drug related problems. 7
The risk of ADRs is necessarily an inherent risk of all
drug therapy and is modulated by several factors, including
dose and frequency of administration, genotype, and
pharmacokinetic characteristics of special populations, such
as pediatric and geriatric patients and those with hepatic or
renal impairment. Due to the high frequency and potentially
serious consequences, ADRs may have a dramatic impact in
clinical practice both from a clinical and economic
perspective. 8
Clinical trials often lack important information about rare
but serious adverse drug reactions, chronic toxicity, use in
special groups (such as children, women, elderly or pregnant)
or interactions with other drugs. 9 Therefore, post-marketing
surveillance activities are important to allow the early
detection of unexpected and/or serious adverse reactions. 10The
use of drugs in randomized controlled trials (RCTs) is
according to strict protocols, often in patients who are not
frail and in a very controlled environment , which is very

unlike the use of drugs observed in the more dynamic clinical
settings where the mode and consequences of drug use can be
more complex.11 RCTs also cannot detect ADRs due to
inappropriate drug use. ADRs arising from inappropriate drug
use can be due to inappropriate drug dosage, or duration of
treatment, drug interactions, off-label use or use in
contraindicated circumstances11, 12 all of which can occur in the
general population or in a hospital setting. This risk of
inappropriate drug use is compounded by patients self
medicating with over the counter medications. Therefore, the
role of pharmacovigilance in detecting and quantifying ADRs
due to inappropriate medication use in a clinical setting is
particularly important because such ADRs are potentially
preventable.13
Patrick K.J Crowley and co-workers discovered that drugs may
interact directly with excipients or with residues or
impurities therein. Such interactions may be modest, slow and
take time to be detected in conventional stability studies.
This can complicate and even delay project progression. When
designing dosage forms therefore it is important to be aware of
the potential for excipients to adversely affect quality.14

Peter Mansell et. al opined that pharmacovigilance had tended
to be a backroom function in the pharmaceutical industry, and a
largely reactive one too. Patient safety and public health
should sit at the heart of corporate social responsibility.15
Economic burden due to adverse drug reactions
The impact and the management of ADRs is complex and in the
USA may cost up to 30.1 billion dollars annually. ADRs may
increase costs due to increased hospitalization, prolongation
of hospital stay and additional clinical investigations in
more
serious cases.16 In addition ADRs may trigger prescription
cascades when new medications are prescribed for conditions
that are a consequence of another medication, which is often
an
unrecognized ADR. Examples include the use of antipsychotics
in Parkinson’s disease patients treated with dopaminergic
drugs or the use of anticholinergic drugs for urinary
retention
in Alzheimer’s disease patients treated with cholinesterase
inhibitors.17 This increases the costs of pharmacotherapy as
well as compounding the risk of further ADRs.
Epidemiology of adverse drug reactions in clinical practice
Several epidemiological studies have been conducted that give
an indication of the frequency of ADRs and the related health
care costs in clinical practice.16 Such consequences include
drug-related hospital admission, prolongation of hospital
stay, and emergency department visits. Estimates from France
suggest that upto 123,000 patients a year present to their
general practitioner with an ADR.18
ADRs account for 4.2-30% of hospital admissions in the
USA and Canada, 5.7-18.8% of admissions in Australia, and 2.5-
10.6% of admissions in Europe.19
Some studies focused on more vulnerable population such as
the pediatric and geriatric patients. Between 2.1% and 5.2% of
ADRs in children lead to hospitalization, and up to 39% of
ADRs in pediatric patients can be life threatening or fatal.20
A national study from the USA estimated that 11.4-35.5% of
emergency department visits in older adults are due to drug
related causes.21Studies from Europe similarly found out that
up to 20% of ambulatory patients experience ADRs and
approximately 10-20% of geriatric hospital drug admissions are
due to drug related causes.22. 23 Another consequence of ADRs is

the prolongation of hospital stay.24 A prospective study showed
that ADRs increased the mean hospital stay from a mean of 8
days in patients without ADRs to 20 days in patients with
ADRs.25 Davies et al also found an increased risk of mortality
in patients who experienced an ADR compared with those who did
not.
A high frequency of ADRs is also seen in nursing homes, with
32-65% of ADRs occurring in these populations.25
In general the role of drug surveillance measures is
highlighted considering that between 32% and 69% of drug
related admissions were reported as definitely or possibly
preventable.26 Through these pharmacovigilance and active drug
monitoring studies, potential general a priori predictors of drug
related adverse reactions such as female sex, increasing age
and polytherapy have been identified. In addition, the type of
drugs most likely to result in ADRs and the most common type
of ADRs observed have also been characterized facilitating
their recognition and prevention.27,28,29
RISE OF PHARMACOVIGILANCE

Until the thalidomide tragedy in 1961, when the devastating
adverse effects of the drug came to light, the systematic
collection and analysis of adverse drug events had not
received much attention, although there are several examples
of systematic attention to the (negative) effects of drugs
that go further back.31 In his article on 150 years of
pharmacovigilance Philip Routledge refers to a committee that was
set up by The Lancet to collect reports on mortalities
resulting from anaesthesia in Britain and its colonies, the
results of which were published.32,33 The formation of the
committee was a reaction to the death of a 15 year old girl in
1848 who had undergone chloroform anaesthesia for surgery of
an ingrown toenail.31
In 1950, reports of incidences of aplastic anaemia associated
with the use of chloramphenicol were received in the US.34 This
led the Council on Drugs of the American Medical Association
to set up a Blood Dyscrasia Registry.35
DRUG SAFETY SINCE 1960
In 1961, the Australian physician McBride published a letter
in which he suggested a connection between congenital
malformations in newly born infants and the hypnotic

thalidomide, which was marketed under various names in many
countries.36 Earlier on 19 November 1961, at a conference on
pediatrics, the German physician Dr Lenz from Hamburg argued
that there was a correlation between the many births of
children with congenital deformities and the use of
thalidomide.31 On 25 November 1961, the manufacturer Chemie
Grunenthal withdrew thalidomide from the market.31 The number
of children born with serious congenital malformations as a
result of maternal use of thalidomide is estimated between
6,000 and 12,000, the majority of whom were born in
Germany.37,38
It is noteworthy in this context that today toxicology and the
surveillance of congenital abnormalities frequently fall
outside the scope of the national pharmacovigilance centres,
and have become the designated field of separate specialized
organizations.31
In 1961, the US FDA started with the systematic collection
of reports on all types of adverse drug reactions, chiefly
through the Hospital Reporting Program.31 In various countries
the thalidomide tragedy prompted the immediate formulation of

criteria that new drugs needed to meet to receive marketing
authorization, and which standards, apart from quality, also
emphasized the safety and efficacy of new drugs.31 In addition
the governmental marketing authorization organizations were
commissioned to establish a post marketing surveillance system
to facilitate the early detection of adverse reactions in
order to prevent a similar tragedy from occurring in the
future.31 In 1968, ten countries that supported a spontaneous
reporting system for adverse drug reactions took the decision
to collaborate and join the WHO Pilot Research Project for
International Drug Monitoring.39 In 1971, a resolution of the
Twentieth World Health Assembly laid the foundations for the
WHO International Drug Monitoring Programme.40 In 1972, a
report was published that formed the basis of the current
international system of national centres collaborating in the
WHO Programme. 41,42
The WHO International Drug Monitoring Programme is supported
and coordinated by the WHO Collaborating Center for
International Drug Monitoring (the UPPSALA Monitoring Centre),
which maintains and implements the international database of
adverse drug events. Its activities are of major importance

and include providing active support to the pharmacovigilance
centres in low income countries, and the evaluation and
augmentation of pharmacovigilance in general. In 2000, the
Guidelines for Setting Up and Running a Pharmacovigilance Centre
appeared and in 2002 the importance of Pharmacovigilance was
published under the auspices of the WHO, which lays the
foundation for the further theoretical and practical
implementation of pharmacovigilance on an international
scale .43,44
The Uppsala Monitoring Centre (UMC), located in Uppsala,
Sweden is the field name for the WHO Collaborating Centre for
International Drug Monitoring. The UMC works by collecting,
assessing and communicating information from member countries'
National Pharmacovigilance Programs in regards to the
benefits, harm, effectiveness and risks of drugs.45
The functions of UMC are as follows:
1. To co-ordinate the WHO Programme for International Drug
Monitoring and its more than 100 member countries
2. To collect, assess and communicate information from
member countries about the benefits, harms and risks of

drugs and other substances used in medicine to improve
patient therapy and public health worldwide
3. To collaborate with member countries in the development
and practice of the science of pharmacovigilance.
4. The main focus and source of data
in pharmacovigilance are reports of ICSRs (individual
case safety reports) from healthcare providers and
patients in member countries of the WHO Programme. A WHO
global individual case safety report database (Vigibase)
is maintained and developed on behalf of the WHO by the
UMC.46 The UMC develops and provides several tools and
classifications for use by organisations involved in drug
safety, including the WHO Drug Dictionary, WHO
ART (adverse reaction terminology) – with a bridge to
the MedDRA terminology, tools for searching in the
database, and a program for case report management,
VigiFlow.47
MedDRA or Medical Dictionary for Regulatory Activities is
a clinically validated international medical
terminologydictionary (and thesaurus) used by regulatory
authorities in the pharmaceutical industry during the
regulatory process, from pre-marketing to post-marketing
activities, and for data entry, retrieval, evaluation,
and presentation. In addition, it is the adverse
event classification dictionary endorsed by
the International Conference on Harmonisation of
Technical Requirements for Registration of
Pharmaceuticals for Human Use (ICH).48
5. The Uppsala centre has also published books in the field
of drugs safety including a regular newsletter.49
6. Training Programs for ADR monitoring and reporting.
Pharmacovigilance in world
There are differences between countries ( and also between
regions within countries ( and also between regions within
countries) in the occurrence of ADRs and other drug related
problems. This may be due to many factors such as :50
1. Diseases and prescribing practices
2. Genetics, Diet and traditions of the communities
3. Processes of drugs’ production influencing the quality of
the pharmaceutical composition;

4. Drugs, distribution and use including indications , doses
and availability.51
5. The use of traditional medicines and supplements (for
example, herbal remedies), which may constitute specific
toxicological problems. 52,53
The data resulting from the whole country or single region
may have greater relevance and educational value and may
affect the national regulations.51
According to the circumstances, the information obtained
in a country (for example, the country of origin of the drug )
may not be relevant in other ones.52
ADR Monitoring and Pharmacovigilance in Selected
Countries
Australia
In Australia, healthcare professionals, pharmaceutical
companies and consumers can report suspected adverse drug
reactions to the Adverse Drug Reactions Advisory
Committee
(ADRAC). Healthcare professionals usually submit reports
on
the 'blue card' which accompanies the Australian Adverse
Drug
Reactions Bulletin and the Schedule of Pharmaceutical
Benefits.
Reports can also be made by letter, fax or electronically
to
http://www.tga.gov.au/problem/index.htm#medicines . 54
USA
The FDA(Food and Drug Administration) Adverse Event
Reporting System (FAERS) is a database that contains
information on adverse event and medication error reports
submitted to FDA. The database is designed to support the
FDA's post-marketing safety surveillance program for drug
and therapeutic biologic products. The informatic
structure of the FAERS database adheres to the
international safety reporting guidance issued by the
International Conference on Harmonisation (ICH E2B).
Adverse events and medication errors are coded to terms
in the Medical Dictionary for Regulatory Activities
(MedDRA) terminology.55
Europe
The European Medicines Agency is responsible for the
development, maintenance and coordination of EudraVigilance, a
system designed for the reporting of suspected side effects.
Reports submitted to EudraVigilance include suspected side
effects of medicines reported during both the pre- and post-
authorisation phases. The system allows the detection of
signals of suspected side effects that were previously
unknown, and of new information on known side effects.
EudraVigilance data for centrally authorised medicines
are analysed on a regular basis, with a two-week or four-week
frequency.
The European Medicines Agency's Committee for Medicinal
Products for Human Use (CHMP) and Pharmacovigilance Working
Party (PRAC) evaluate signals from EudraVigilance and may
recommend regulatory action as a result. EudraVigilance is
used by national medicines regulatory authorities, the Agency
and pharmaceutical companies.56
United Kingdom
The yellow card scheme for reporting suspected adverse
drug reactions (ADRs) was
introduced in 1964 and over 400,000 reports have now been
received by the
Committee on Safety of Medicines (CSM) / Medicines and
Healthcare products
Regulatory Agency (MHRA). 57
Brazil
The National System Of Pharmacovigilance, managed
by the Pharmacovigilance Unit(PVU), is a part of the Health
Products Post-Marketting Surveillance Department (HPPMSD).58
Jordan
The Jordanian Pharmacovigilance Center (JPC) was
established in January 2001 in cooperation with Sweden
International Development Agency (SIDA) and Higher Council for
Science and Technology.59
Pharmacovigilance in India

India is a vast country with pharmaceutical industry
valued at $18 billion and growing at the rate of 12-14%
per annum and exporting nearly 40% of generic medicines
worldwide. India is also emerging rapidly as a hub for
global clinical research and a destination for drug
discovery and development with several outsourced
projects in pharmacovigilance. In addition, new chemical
entities (NCEs) are being introduced into the country ,
which is reflected by the increased total number of
applications received and processed that doubled, from
10,000 in 2005, to 22,806 in 2009 at Central Drugs
Standard Control Organization (CDSCO), headquarters at
New Delhi.60
History of Pharmacovigilance in India
In India, consideration of the surveillance of ADRs
developed relatively late, as traditionally there was no
concept of surveillance of medicines in the country. Even
though, pharmacovigilance is still in its infancy, it is
not new to India. It was not until 1986 when a few
physicians, mainly from academic institutions, called

for greater attention to be devoted to the potential
adverse effects of prescription medicines and rational
prescribing of medicines.60 This led to formation of first
ADR monitoring program consisting of 12 regional centers,
each covering a population of 50 million, but was
unsuccessful. 61
Nothing much happened until a decade later when in 1997,
India formally joined the WHO ADR monitoring Program
based in UPPSALA, Sweden. Three centers for ADR
monitoring were identified, mainly based on the teaching
hospitals: A National Pharmacovigilance Center located in
the Department of Pharmacology, All India Institute of
Medical Sciences (AIIMS), New Delhi and two WHO special
centers in Mumbai (KEM Hospital) and Aligarh (JLN
Hospital, Aligarh Muslim University). These centers were
to report ADRs to the drug regulatory authority of India.
The major role of these centers was to monitor ADRs of
medicines marketed in India. However, this attempt was
also unsuccessful as information about the need to report
ADRs and about the functions of these monitoring centers

never reached the prescribers and there was lacking of
funding from the government.
From 1 January 2005, the WHO sponsored and World
Bank funded National Pharmacovigilance Program (NPVP) for
India was made operational,62 its work being overseen by the
National Pharmacovigilance Advisory Committee based at CDSCO.
Two zonal centers-the South West Zonal center (located in the
Department Of Clinical Pharmacology, Seth G S Medical College,
KEM Hospital, Mumbai) and the North east Zonal center (located
in the Department of Pharmacology, AIIMS, New Delhi)- were to
collate information from all over the country and send it to
the committee as well to the UPPSALA Monitoring Centre in
Sweden. Three regional centers would report to the Mumbai
center and two to the New Delhi one.
The five regional centers were located at Kolkata (IPGMR-
SSKM hospitals), Mumbai (T N Medical College& BYL Nair
Charitable Hospital), Nagpur (Indira Gandhi Medical
College), New Delhi (Lady Hardings Medical College) and
Pondicherry (JIPMER). Each regional center, in turn,
would have several peripheral centers (24 in total)
reporting to it.

The program had three broad objectives:- The short term
objective was to foster a reporting culture, the
intermediate objective was to involve large number of
healthcare professionals (HCPs) in the system in
information dissemination, and the long term objective
was for the program to be a benchmark for global drug
monitoring. However, this program also failed.63
Recently, Medical Council of India has also made it
mandatory for
all medical colleges to have an adverse drug reaction
training,
monitoring and reporting program. There is still a lack
of
understanding on this topic, what are the
benefits of sharing Adverse Drug Reaction knowledge ,its
purpose and importance and how Pvg centre functions. To
fulfill the above aim it is
important to find out the perception of doctors about
adverse
drug reaction reporting and identify steps which will
improve
adverse drug reaction reporting and fulfill the goals of
Medical Council Of India
The Current PV Program in India
Recognizing the need to restart the NPVP, in a brainstorming
workshop jointly organized by the Department of Pharmacology,
AIIMS and CDSCO in late 2009, the framework of the new and
current program was formulated. The program, now rechristened
as the PharmacovigilanceProgramme for India (PvPI), was made
operational from mid July 2010.64 Initially Department of
Pharmacology at AIIMS was nominated as the National
Coordinating Centre (NCC), which was later on changed to the
Indian Pharmacopoeia Commission (IPC), Ghaziabad (U.P.). The
main aim of the NCC is to generate an independent data on the
safety of medicines, which will be at par with global drug
safety monitoring standards.
ADR Monitoring Centres (AMCs) under PvPI play a vital role of
collection and follow-up of ADR reports from the patients. They
are set up across India to collect the adverse event
information from patients. These AMCs are the Medical Council
of India (MCI) approved medical colleges & hospitals,
medical/central/autonomous institutes, public health programmes
and corporate hospitals. They are responsible for collecting
the adverse event information from the patients, performing
follow up with them to check the completeness of the ADR
reports as per Standard Operating Procedures (SOPs), entering
information in the prescribed software (Vigiflow) and sending
them to NCC via the same software. Some AMCs are also
responsible for providing training and technical support at
regional level.
The PvPI started with the enrolment of 22 ADR monitoring
centres across the country in the year 2010, which has
increased to 90 by the end of 2012, 60 of which are phase I
(FY2010-FY2011) AMCs and 30 are phase II (FY2012-FY2013) AMCs.
All the 90 AMCs are categorised into four zones i.e. North,
South, East and West as per zonal offices of CDSCO in India and
are functioning under NCC.
There are more than 2000 pharmacy colleges 90 Institute of
Pharm.D, more than 200 dental institutes, 360 MCI approved

medical colleges, and more than 320 nursing institutes all over
India. These institutes are associated with patients care by
providing safe and effective medication. For robust
pharmacovigilance, all of these colleges will be included as
ADR Monitoring Centres under this programme in the years to
come. 65
ROLE OF TRAINING IN ADR REPORTING
Several studies world wide have helped in justifying the need
for continuous training for spontaneous adverse drug reaction
reporting. Spontaneous ADRs reporting represents a precious
resource for control and information about the drug’s safety,
since it allows the detection of potential warning signals
related to the use of all drugs available in a country.66,67
In order to inculcate the culture of spontaneous adverse
drug reaction reporting amongst the physicians there is a
necessity to first test the Knowledge, Attitude and Practices
(KAP)of physicians regarding adverse drug reaction monitoring
and then to train the physicians accordingly. A number of
studies have been carried out to test KAP of health

professionals regarding ADR monitoring and subsequently impart
training sessions for the same.
A study conducted in Portugal included in its training
program a workshop intervention with sessions giving a brief
introduction about the problem of ADR and its impact on
public health, followed by an approach of spontaneous
reporting of ADR. It also conducted telephonic interviews.
Educational interventions conducted in workshops or
telephone interviews significantly increased the number and
relevance of spontaneous ADR reports by the pharmacists of
Northern Portugal.68
A study was conducted in Manipal, India which included an
educational intervention, both theoretical and practical, to
improve ADR reporting. The theoretical part consisted of a
presentation on how to report a suspected adverse drug
reaction followed by economic and epidemiological importance
of reporting the ADRs and its effect on patient safety, as
well as the definition of pharmacovigilance, classification of
ADRs (i.e. in terms of causality assessment, seriousness and
severity, ADR reporting cards from various countries, ADR

alert cards, WHO online database for reporting adverse drug
reactions).
The practical part involved the health care professionals in
filling up the ADR forms. This study also utilized KAP
questionnaire to assess the knowledge of health care
professionals regarding ADR reporting and Pvg. The result of
this study showed increased awareness of pharmacovigilance
among health care professionals.5
Mala Kharkhar , Suresh Bowalekar conducted a study in Mumbai
on knowledge, attitude and perception of doctors on ADR
monitoring by designing a questionnaire.The study revealed
that practitioners were aware of ADR reporting; their
perception toward ADR reporting was right but it did not
reflected when it came to the act of reporting of ADRs..69
MrinMoyChakrabarty,VijayThawani in their study showed ensuring
proper education and frequent updating of health care
professionals by training them in data collection, filtration,
mining, verification, interpretation and coding of ADRs,
medicines coding, causality assessment, signal detection, risk
management, and action in case of serious/fatal adverse drug
events (ADE).70

P.Ravishankar, P.Subish, P.Mishra, A.K. Dubey in their study
showed that the theoretical information of pharmacovigilance
programme was to be covered (preferably small group briefings)
of 1 hr duration each. The first two activities (designing a
reporting form, and carrying out a severity and causality
assessment of a given ADR report.was done in a problem based
learning session of 2 ½ hr duration. The visit to the
pharmacovigilance centre and the presentation and discussion
of findings can be done in the second session.71
In a study conducted by Antonio Vallano and co-workers,
the pharmacovigilance sessions were held during scheduled
staff sessions and lasted about 45 to 60 minutes to ensure
that the greatest number of physicians could be present. The
presentations were given by clinical pharmacologists and
divided into three parts. The first part included a review of
all identified and reported ADRs throughout the hospital
(number of cases, type and severity of ADR, type of drug)
between 1 January 2003 and 31 December 2005.

The second part included a review of identified and reported
ADRs in each specific medical department where the sessions
were held.The main features of the cases and their
contribution to the overall results of the Pharmacovigilance
programme (PhVP) were openly discussed.
The third part provided general information on
pharmacovigilance issues such as signals generated by the the
PhVP, news about ADR warnings released by regulatory agencies
(Spanish Agency of Medicinal and Health Care Products, the
European Medicines Agency, the U.S.Food and Drug
Administration, and others), or drug toxicity problems
identified by published studies in medical journals, and all
the topics were discussed openly.
The study concluded that additional studies on the
development and effectiveness of educational activities in
pharmacovigilance are necessary. 72
ChetnaK.Desai and co-workers in their study used a pretested
KAP questionnaire comprising of 15 questions. The study showed
that physicians were aware of the ADRs and the importance of

their reporting. However, under reporting and lack of
knowledge about the reporting system were clearly evident.73
Roald Gerritsen and co workers compared the lecture-
based pharmacovigilance training methods with the practice
based method by analysing the number and quality of reports
sent in by graduate GPs who had been offered one of both
approaches during their vocational training. The practice
based methods resulted in significantly more and better
documented reports and more often concerned unlabelled events
than the lecture-based method.74
Mariam Molokhia and co workers collected data sources from
Medline, Embase, Cochrane Library and National Library for
health searches on ADR reporting (January 1997 to August 2007)
including cross-referenced articles and showed that
educational interventions combined with reminders and/or
prescription card reports can improve hospital-based ADR
reporting.75\\
Subharti Medical College & Hospital is a five hundred bedded,
multispecialty teaching cum tertiary hospital of western U.P,
India. Department of Pharmacology of the institute was one of
the 24 peripheral Pharmacovigilance center under NPVP

established in 2005 and is also one of the Pvg centre under
current Pvg programme of India (PvPI). The department is
actively involved in ADR reporting and pharmacovigilance but
still ADR reporting by physicians and surgeons is dismal and
disappointing. Disheartened by the low rate of spontaneous ADR
reporting in our institute, the present study was planned to
re-establish the culture of ADR reporting and to test current
KAP of physicians, surgeons, residents, interns and nursing
staff about ADR reporting and Pharmacovigilance.
AIMS & OBJECTIVES
1. To study knowledge, attitude and practice (KAP) of
doctors and health professionals about adverse drug
reaction monitoring.
2. To identify measures that will help in better adverse
drug reaction reporting.
3. To impart training of adverse drug reaction monitoring.
4. To study impact of training on adverse drug reaction
reporting in CSSH of Subharti Medical College.
Material and Methods
Design
A cross sectional survey to evaluate KAP among doctors,
dentists and nurses followed by intervention in the form of
training and observe impact of training and recording of
adverse effects in patients attending outpatient department
and admitted in the CSSH of Subharti Medical college.
Setting & Population:
The survey was conducted in a CSSH attached with Subharti
Medical College (b) Subharti Dental College (c) private
practitioners working in Meerut d) Fortis Hospital
Training of adverse drug monitoring
Training in the form of lectures and practical use of tools
for adverse drug reactions was given to Doctors, Dentists
and Nurses working in Subharti Medical College
Tools
Questionnaire to elicit KAP
CDSCO form for reporting adverse effects
Tool for Causality of ADR
Tool for Preventability of ADR
Tool for Severity of ADR
ICD Classification for adverse drug reactions (Y 40-59
& T36-50)
Procedure
1 .A survey was conducted on doctors, nurses, dentists of
Subharti Medical College. The Knowledge Attitude and
Practices (KAP) questionnaires was distributed and filled
by them.
The private practitioners in and around Meerut were given
KAP forms to fill in periodic professional meetings and also
by post and electronic forms.
The forms to physicians and pharmacologists from other
medical colleges were given in conferences, professional
meetings and by electronic means.
Total sample size of survey would be 500 health care
professionals. The survey was done by getting the forms
filled physically and via electronic mode through internet.
2. Training program was conducted for health care
professionals. It included lectures to sensitize them about
need of adverse drug reaction reporting (ADR reporting) as
per MCI guidelines, its impact on economy. The participants
were explained about their obligations and responsibilities
towards ADR reporting when prescribing new drugs.
They were trained on use of CDSCO form, Subharti Medical
College outpatient (OPD) forms for ADR, Subharti Medical
College indoor IPD forms of ADR and categories of ADR
according to international classification of diseases (ICD).

Training was given about the use of World Health
organisation forms on causality, severity and
preventability. Training on causality, severity and
preventability assessment was given with the help of lecture
and practical exercise. Regular training program were
conducted at periodic intervals.
3. ADR forms were distributed in all OPD’s as well as in
wards. The filled forms were collected.The adverse drug
reactions were scrutinised and adverse effect of new drugs
as well as serious adverse effects were reported by filling
of adverse drug reaction form of CDSCO. The adverse drug
reaction during the study period of 1 ½ yrs were.
4. The adverse drug reaction form for admitted patients
were attached with the patients treatment file. It was
initiated by staff nurse on duty, verified by resident and
then confirmed by crosschecking. All patients file was
cleared after scrutinising for filling of the forms for
admitted patients.
Statistical Analysis

All data was tabulated as Mean ± standard error. Nominal
data was analysed by using chi square test, ordinal data was
analysed by using appropriate non parametric tests and
interval data was analysed by parametric test. Comparison
between different groups was done by unpaired t-test and for
paired observation paired t-test was applied. Analysis of
variance was done where number of observations or groups is
more than 2.
Ethical justification
MCI has made it mandatory for all medical colleges to
have adverse drug reaction training, monitoring and
reporting program. This project will help in fulfilling
MCI regulations
No drug, surgery or procedure is being performed.
Only a survey was done followed by training and
reporting of ADRs.
The privacy of the participating doctors was maintained
throughout the work.
RESULTS

1
Fortis(n=105)
Subharti(n=210)
LLRM(n=123)
PP(n=62)
0
100
200
105209
120 621
Type of ADR reporting form used by the physicians?
NonePreventabilitySeriousnessSeverityCausality
Institution Group
No. Of Responses
Fig:1

Consultants(n=152) JRs(n=304) Interns(n=44)0
50
100
150
200
250
300
350
1 11
150
303
431
NonePreventabilitySeriousnessSeverityCausality
Fig:2
As seen in the fig:1 only 1 out of 210 (0.6%) doctors ofSubharti institute was aware about the causality assessmentform of ADR reporting while 2 out of 123(1.6%) doctors of LLRMwere about of severity form of ADR reporting, 1 (.8%)doctor ofLLRM was aware about seriousness form of ADR and none of thedoctors in Fortis and private practitioners were about any ofthe ADR reporting forms.
Fig:2 shows that (0.6%) 1 out of 152 consultants were awareabout the severity tool of assessment ADR form, 0.6% ofconsultants were aware of seriousness tool of adr assessment.1 out of 304 (0.32%) JRs were aware about causality assessment

form and 1 (2.27%) out of 44 interns were aware about thecausality assessment ADR form.
Q.2
Fortis(n
=105)
Subharti
(n=210) LLRM
(n=123) PP(n
=62)
0
100
200
105209
91 62
1
32
Are the physicians aware about the ADR form of CDSCO?
YesNo
Institution Group
No. Of Responses
Figure:3

Consultants(n=152) JRs(n=304) Interns(n=44)0
50100150200250300350
146278
43
6
26
1
Are you aware about the ADR reporting form of CDSCO?
YesNo
Participant Group
No of Responses
Figure:4
As see in Fig: amongst all the institutions, it was seen that32(26%) doctors of government institution LLRM were aware about the national CDSCO form of ADR reporting while only one(0.47%) of 210 doctors was aware about the CDSCO form. 100%doctors in Fortis and 100% private practitioners were aware about the CDSCO form.
Fig 4/ highlights the fact that 6 out of 152 (3.9%)consultantswere aware about the CDSCO form,26 out of 304 JRs(8.55%) were known to CDSCO form while only 1 out of 44(2.27%) intern was aware about the CDSCO form.

Fortis
(n=105
)
Subhar
ti(n=2
10)
LLRM(n
=123)
PP(n=6
2)0
100
200
105201
88 62
9
35
Q3) Have the ADR reporting forms made available to you?
YesNo
Institution Group
No. of Responses
Fig:5
Consultants(n=152) JRs(n=304) Interns(n=44)0
50100150200250300350
148273
44
4
31
Have the ADR reporting forms made available to you?
YesNo
Participant Group
Respondents
Fig:6
In Fig:5, it is seen that ADR reporting forms were available to 9 out of 210 (4.28%)doctors of Subharti, while 35 out of 123 (28.4%) doctors of LLRM were made available the ADR forms.100% of the doctors of Fortis and 100% private practitioners were not been given any ADR forms.
In Fig:6 4 out of 152(2.63%) consultants were been given the ADR forms, 31 out of 304(10.19%) JRs were made available with the ADR forms, while 100% of the interns got the ADR form.

Fortis(n
=105)
Subharti
(n=210)
LLRM(n=1
23) PP(n=62)
050
100150200250
105202
63 622
58
Q4) If Yes, which one?
NSNAWHOLocal/CDSCO
Institution Group
No. of Responses
Fig:7
Consultants JRs Interns0
50
100150
200250300350
1 1
143
253
44
8
40
If Yes, which one?
NSNAWHOLocal/CDSCO
Participant Group
Fig:8
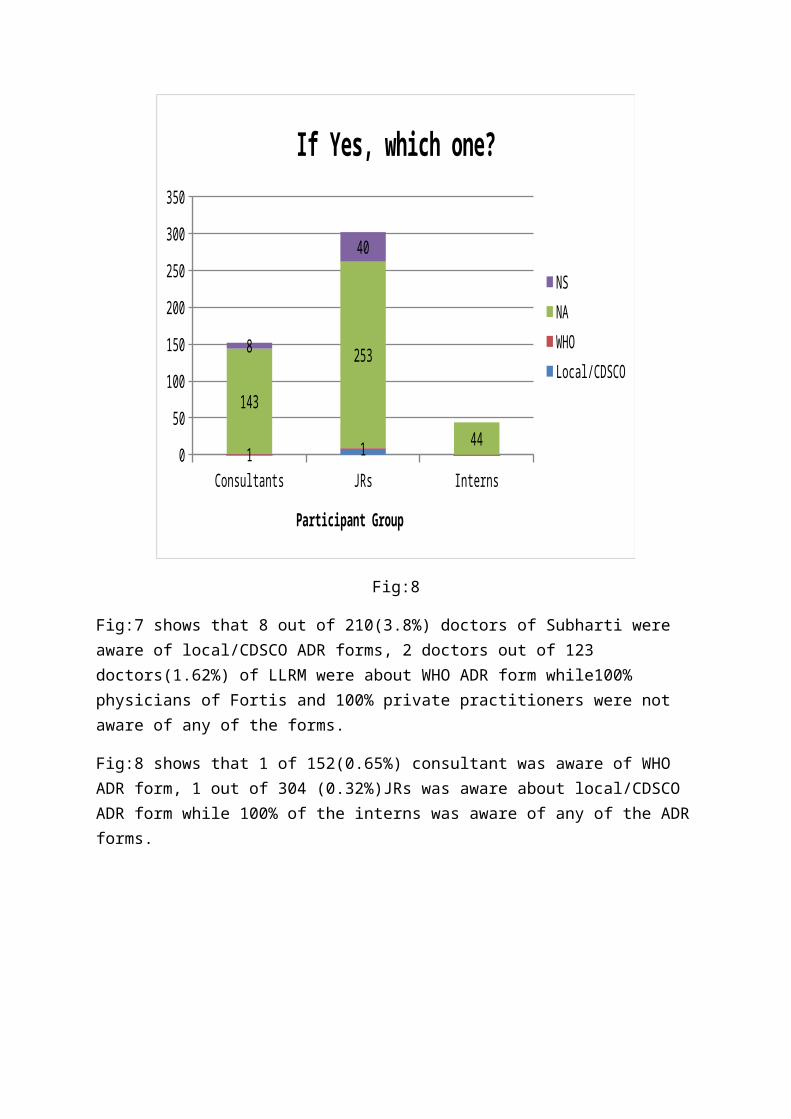
Fig:7 shows that 8 out of 210(3.8%) doctors of Subharti were aware of local/CDSCO ADR forms, 2 doctors out of 123 doctors(1.62%) of LLRM were about WHO ADR form while100% physicians of Fortis and 100% private practitioners were not aware of any of the forms.
Fig:8 shows that 1 of 152(0.65%) consultant was aware of WHO ADR form, 1 out of 304 (0.32%)JRs was aware about local/CDSCO ADR form while 100% of the interns was aware of any of the ADRforms.
Fortis
(n=105
)
Subhar
ti(n=2
10)
LLRM(n
=123)
PP(n=6
2)0
100
200
105210 60
621944
Q5) Was the ADR reporting form too complex to fill?
NANoYes
Institution Group
No.of Responses
Fig:9
Consultants(n=152) JRs(n=304) Interns(n=44)0
50100150200250300350
4 156 38142
251
44
Was the ADR reporting form too complex to fill?
NANoYes
Participant Group
No.of Responses
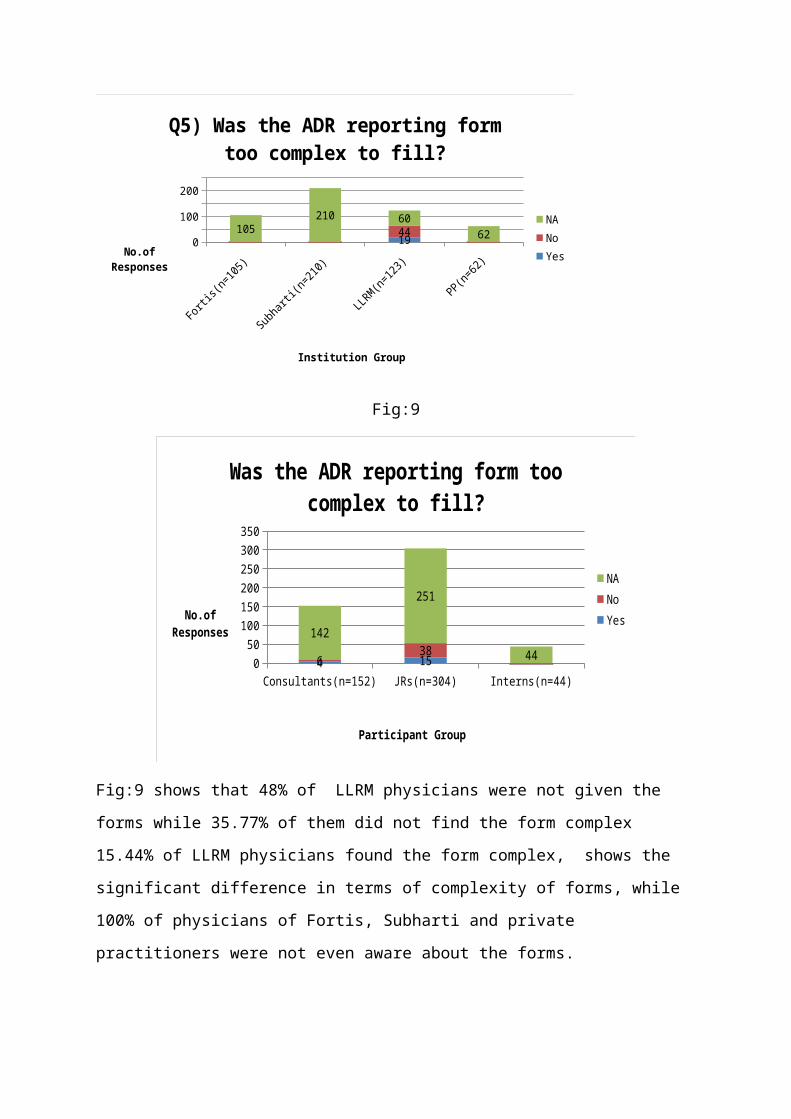
Fig:9 shows that 48% of LLRM physicians were not given the
forms while 35.77% of them did not find the form complex
15.44% of LLRM physicians found the form complex, shows the
significant difference in terms of complexity of forms, while
100% of physicians of Fortis, Subharti and private
practitioners were not even aware about the forms.
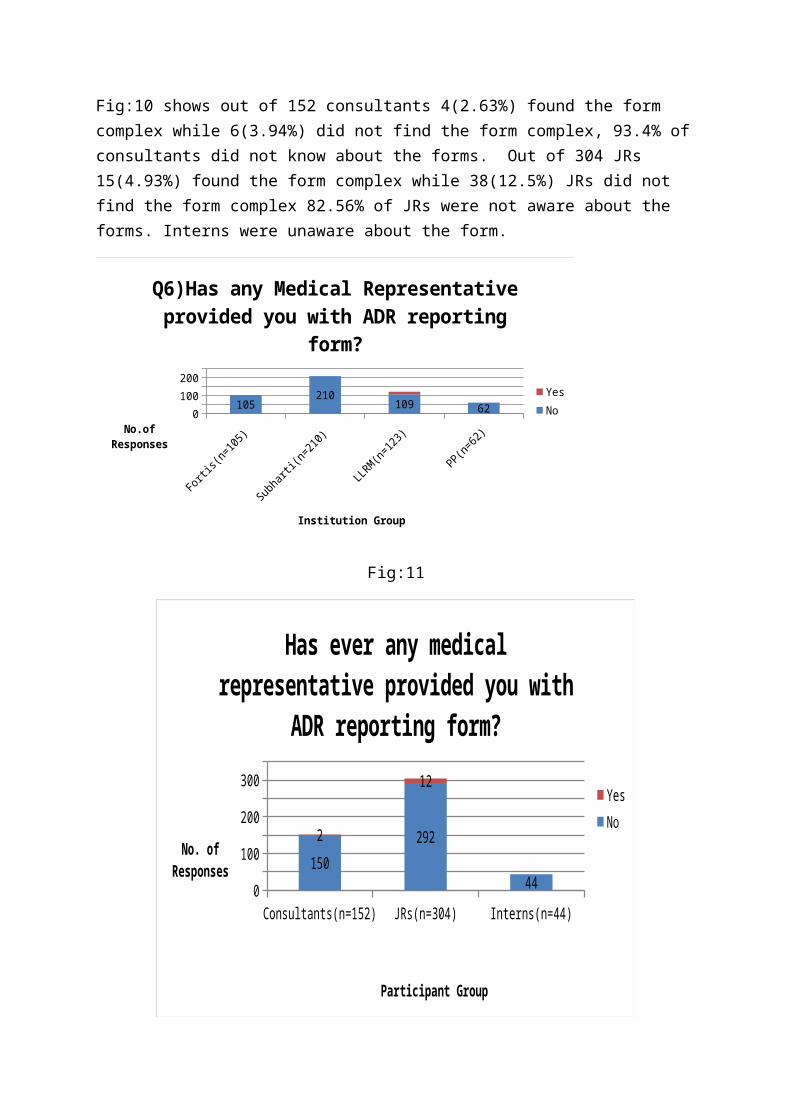
Fig:10 shows out of 152 consultants 4(2.63%) found the form complex while 6(3.94%) did not find the form complex, 93.4% ofconsultants did not know about the forms. Out of 304 JRs 15(4.93%) found the form complex while 38(12.5%) JRs did not find the form complex 82.56% of JRs were not aware about the forms. Interns were unaware about the form.
Fortis
(n=105
)
Subhar
ti(n=2
10)
LLRM(n
=123)
PP(n=6
2)0
100200
105210 109 62
Q6)Has any Medical Representative provided you with ADR reporting
form?
YesNo
Institution Group
No.of Responses
Fig:11
Consultants(n=152) JRs(n=304) Interns(n=44)0
100
200
300
150292
44
2
12
Has ever any medical representative provided you with
ADR reporting form?
YesNo
Participant Group
No. of Responses
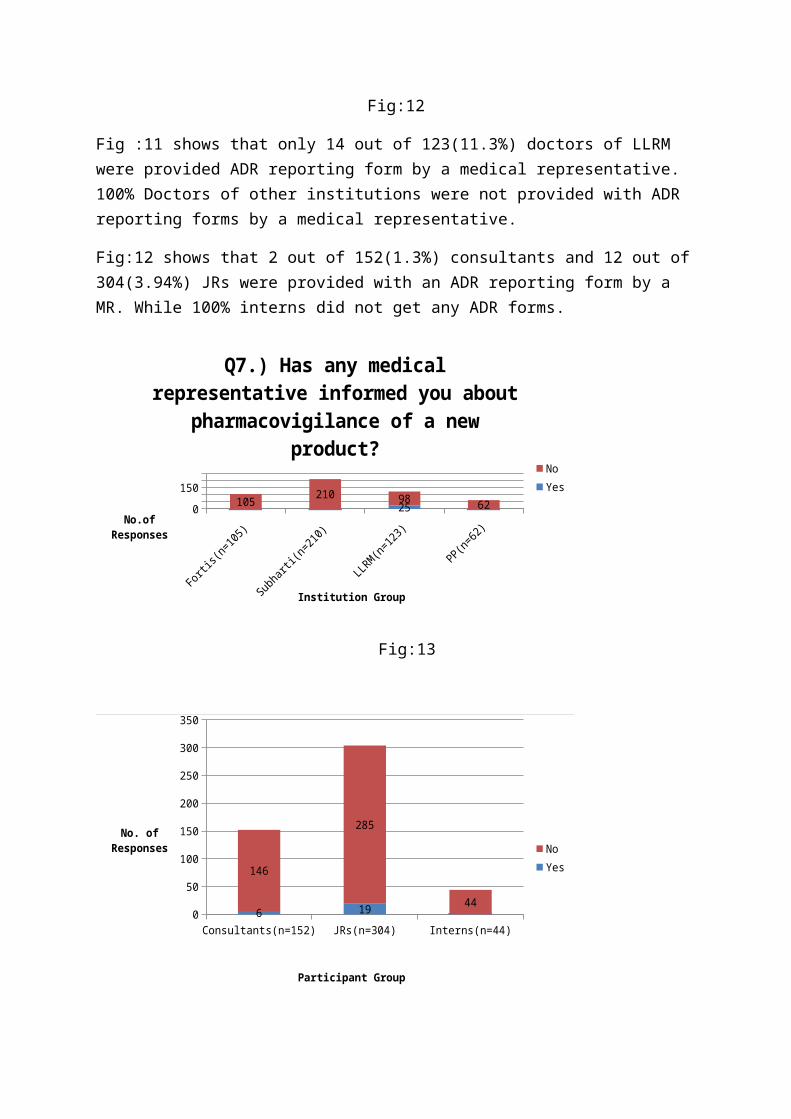
Fig:12
Fig :11 shows that only 14 out of 123(11.3%) doctors of LLRM were provided ADR reporting form by a medical representative. 100% Doctors of other institutions were not provided with ADR reporting forms by a medical representative.
Fig:12 shows that 2 out of 152(1.3%) consultants and 12 out of304(3.94%) JRs were provided with an ADR reporting form by a MR. While 100% interns did not get any ADR forms.
Fortis
(n=105
)
Subhar
ti(n=2
10)
LLRM(n
=123)
PP(n=6
2)0
150105 210 98 6225
Q7.) Has any medical representative informed you about
pharmacovigilance of a new product?
NoYes
Institution Group
No.of Responses
Fig:13
Consultants(n=152) JRs(n=304) Interns(n=44)0
50
100
150
200
250
300
350
6 19
146
285
44
NoYes
Participant Group
No. of Responses
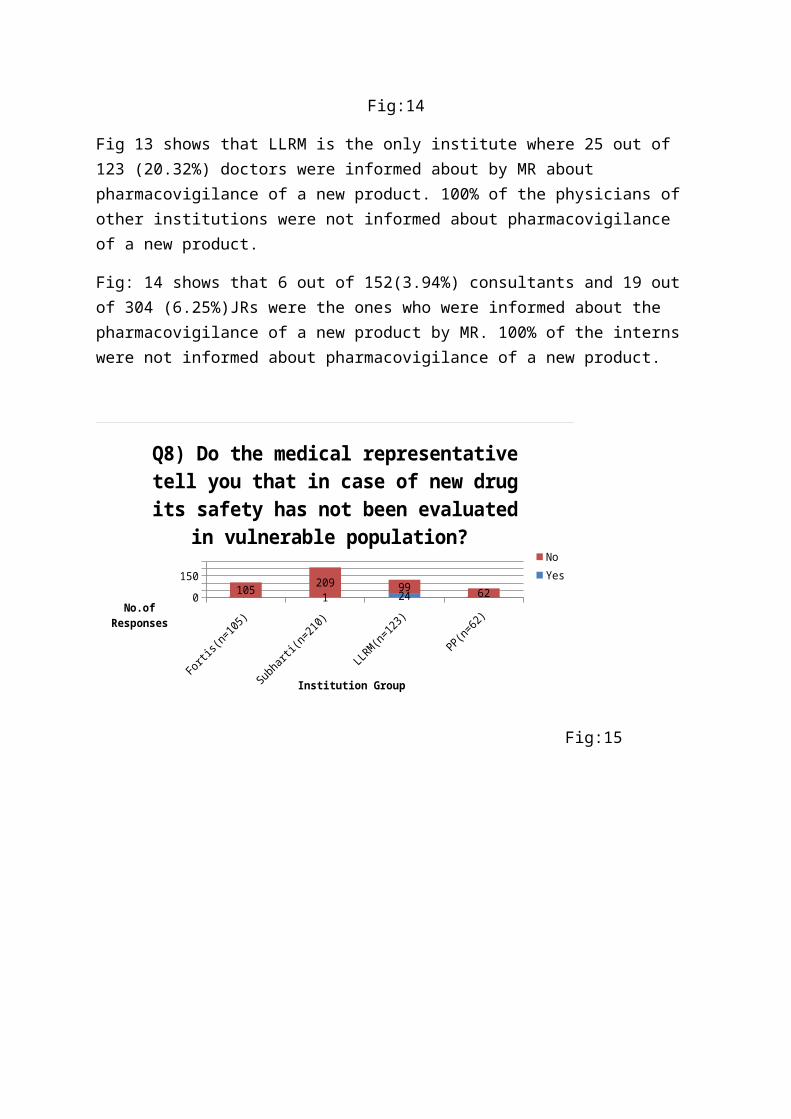
Fig:14
Fig 13 shows that LLRM is the only institute where 25 out of 123 (20.32%) doctors were informed about by MR about pharmacovigilance of a new product. 100% of the physicians of other institutions were not informed about pharmacovigilance of a new product.
Fig: 14 shows that 6 out of 152(3.94%) consultants and 19 out of 304 (6.25%)JRs were the ones who were informed about the pharmacovigilance of a new product by MR. 100% of the interns were not informed about pharmacovigilance of a new product.
Fortis
(n=105
)
Subhar
ti(n=2
10)
LLRM(n
=123)
PP(n=6
2)0
150105 209 99 621 24
Q8) Do the medical representative tell you that in case of new drug its safety has not been evaluated
in vulnerable population? NoYes
Institution Group
No.of Responses
Fig:15

Consultants(n=105) JRs(n=304) Interns(n=44)0
200400
5 19 1147 28543
Do the medical representative tell you in case of new drug the
safety issues in pregnancy, lacttion, children, old age and concurrent renal/hepatic disease? No
Yes
Participant Group
Respondents
Fig:16
Fig: 15 highlights the fact that 1 out of 210(0.47%) doctors of Subharti and 25 out of 123(20.3%) doctors of LLRM were toldabout effects of new drug on vulnerable population, while 100%doctors of Fortis and 100% private practitioners were not informed about effects of new drug on vulnerable population.
Fig:16 shows that 5 out of 152(3.28%) consultants, 19 out of 304 (6.25%) JRs were informed. 2.27% of the interns were informed.

Fortis
(n=105
)
Subhar
ti(n=2
10)
LLRM(n
=123)
PP(n=6
2)0
100200
105209 82
621 41
Q(9)Do you think a new drug would be safe from ADRs as it has been
thoroughly evaluated?
YesNo
Institution Group
No. of Responses
Fig:17
Consultants(n=152) JRs(n=304) Interns(n=44)0
100
200
300
19 22 1133
282
43
Do you think a new drug would be safe from ADRs as it has been
thorghly evaluated?
YesNo
Participant Group
Responses
Fig:18
Fig:17 shows that 41(33.3%) of doctors of LLRM and 0.47% of Subharti denies that new drug would be safe from ADRs. 100% ofthe doctors in Fortis, and 100% of the private practitioners believe that new drug would be safe from ADRs.
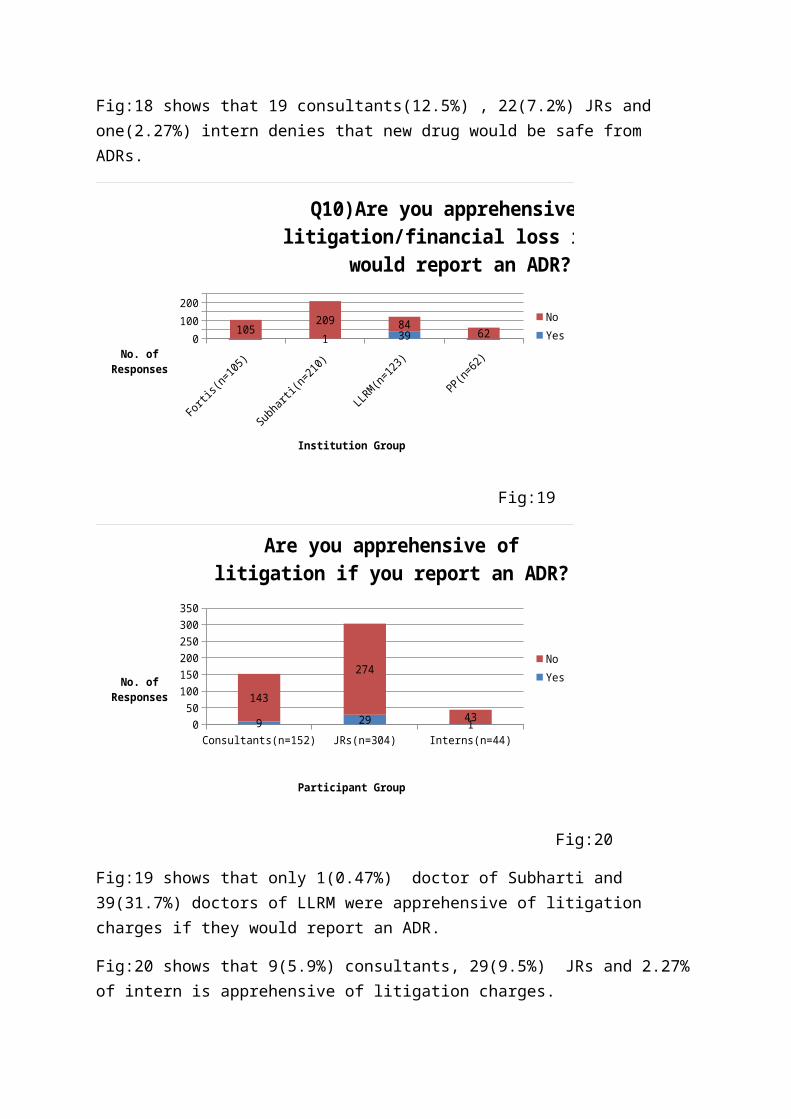
Fig:18 shows that 19 consultants(12.5%) , 22(7.2%) JRs and one(2.27%) intern denies that new drug would be safe from ADRs.
Fortis
(n=105
)
Subhar
ti(n=2
10)
LLRM(n
=123)
PP(n=6
2)0
100200
105209 84 621 39
Q10)Are you apprehensive of litigation/financial loss if you
would report an ADR?
NoYes
Institution Group
No. of Responses
Fig:19
Consultants(n=152) JRs(n=304) Interns(n=44)0
50100150200250300350
9 29 1
143
274
43
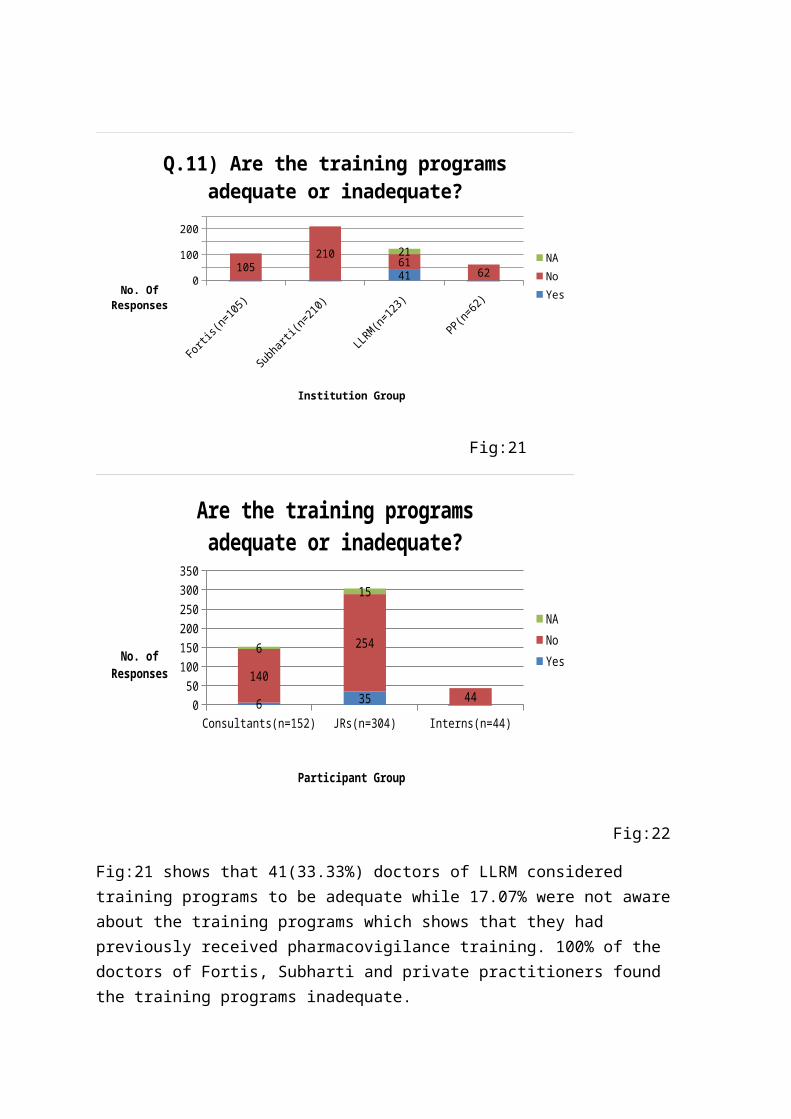
Are you apprehensive of litigation if you report an ADR?
NoYes
Participant Group
No. of Responses
Fig:20
Fig:19 shows that only 1(0.47%) doctor of Subharti and 39(31.7%) doctors of LLRM were apprehensive of litigation charges if they would report an ADR.
Fig:20 shows that 9(5.9%) consultants, 29(9.5%) JRs and 2.27%of intern is apprehensive of litigation charges.
Fortis
(n=105
)
Subhar
ti(n=2
10)
LLRM(n
=123)
PP(n=6
2)0
100
200
105210 61
6241
21
Q.11) Are the training programs adequate or inadequate?
NANoYes
Institution Group
No. Of Responses
Fig:21
Consultants(n=152) JRs(n=304) Interns(n=44)0
50100150200250300350
6 35140
254
44
6
15
Are the training programs adequate or inadequate?
NANoYes
Participant Group
No. of Responses
Fig:22
Fig:21 shows that 41(33.33%) doctors of LLRM considered training programs to be adequate while 17.07% were not aware about the training programs which shows that they had previously received pharmacovigilance training. 100% of the doctors of Fortis, Subharti and private practitioners found the training programs inadequate.

Fig:22 shows that 6(3.94%) consultants while 35(11.5%) JRs considered the training programs adequate. 100% of the internsfound the training programs inadequate.
Fortis
(n=105
)
Subhar
ti(n=2
10)
LLRM(n
=123)
PP(n=6
2)0
100200
105210 52
62566
Q12) Were You given repetitive training sessions on ADR
reporting?NANoYes
Institution Group
No. of Responses
Fig:23

Consultants JRs Interns0
50100150200250300350
1 413 53138
247
44
Were you given repetitive training sessions on ADR?
NANoYes
Participant Group
No. of Responses
Fig:24
Fig:23 shows 5 (4.06%) doctors of LLRM were given repetitive training sessions, 53.65% were not given repetitive training sessions in LLRM while 42.27% of the doctors in LLRM were not aware about the training sessions. 100% of the doctors in Subharti, Fortis and private practitioners did not know about the training sessions.
Fig:24 shows that 1(0.8%) consultant and 4 (1.31%)JRs were given repetitive training sessions. 100% of the interns were not given repetitive training sessions.

Fortis
(n=105
)
Subhar
ti(n=2
10)
LLRM(n
=123)
PP(n=6
2)
0100200
105210 96 62216
Q13) Is under reporting due to:a) lack of training, b) lack of time
c) BothBothLack of timeLack of regular training
Institution Group
No.of Responses
Fig:25

Consultant
s(n=152) JRs(n
=304)
Interns(n=
44)
050
100150200250300350
3 180 6149
280
44 BothLack of timeLack of regular training
Participant Group
No. ofResponses
Fig:26
Fig:25 highlights that 17.07% of doctors of LLRM consider lackof training to be the reason for under reporting, 4.87% doctors in LLRM consider lack of time to be the reason and 78.04% consider both lack of training and time to be the reasons for under reporting. !00% of the doctors in Fortis, Subharti and Private practitioners consider both the reasons for under reporting.
Fig 26 highlights the fact that 1.97% of the consultants consider lack of regular training training to be the reason for under reporting,98.02% of consultants take into account
both the factors for under reporting while 5.9% of JRs consider lack of regular training to be the reason for under reporting and 1.97% of the JRs consider lack of time to be thereason for under reporting, 92.1% of the JRs consider both thefactors reason for under reporting. 100% of the interns consider both the factors for under reporting.
Fortis
(n=105
)
Subhar
ti(n=2
10)
LLRM(n
=123)
PP(n=6
2)0
100200
105210
97 6226
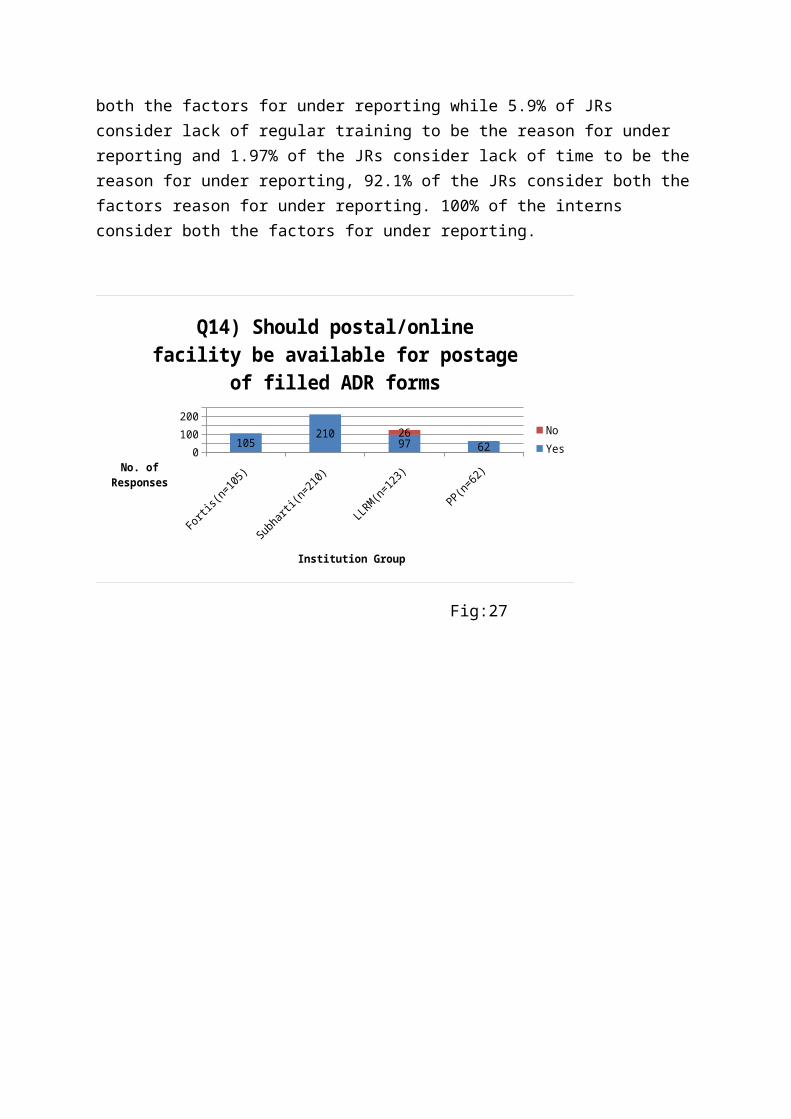
Q14) Should postal/online facility be available for postage
of filled ADR forms
NoYes
Institution Group
No. of Responses
Fig:27
Consultants(n=152) JRs(n=304) Interns(n=44)0
100
200
300
150280
44
2
24
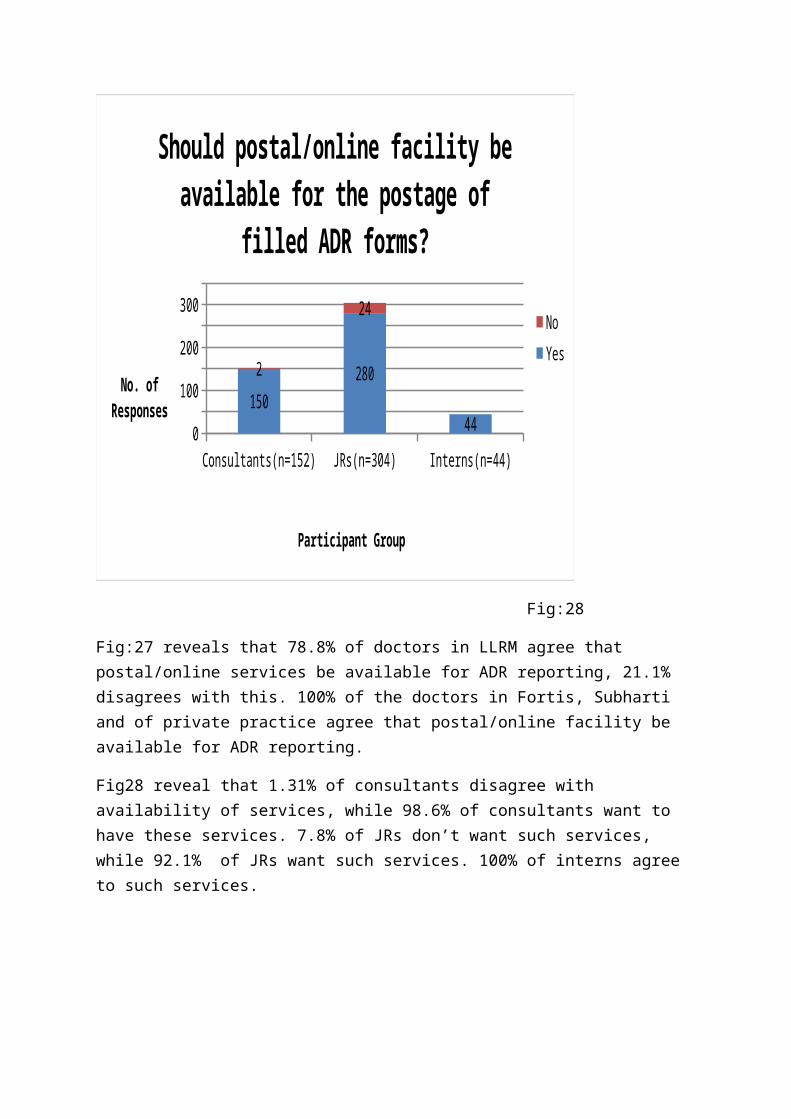
Should postal/online facility be available for the postage of
filled ADR forms?
NoYes
Participant Group
No. of Responses
Fig:28
Fig:27 reveals that 78.8% of doctors in LLRM agree that postal/online services be available for ADR reporting, 21.1% disagrees with this. 100% of the doctors in Fortis, Subharti and of private practice agree that postal/online facility be available for ADR reporting.
Fig28 reveal that 1.31% of consultants disagree with availability of services, while 98.6% of consultants want to have these services. 7.8% of JRs don’t want such services, while 92.1% of JRs want such services. 100% of interns agree to such services.

Fortis
(n=105
)
Subhar
ti(n=2
10)
LLRM(n
=123)
PP(n=6
2)0
100
200
105210
112 6211
15) Is there a lack of law to implement it?
NoYes
Institution Group
Respondents
Fig:29
Consultants(n=152) JRs(n=304) Interns(n=44)0
50100150200250300350
152
293
4411
Is there a lack of law to implement it?
NoYes
Participant Group
Respondents
Fig:30
Fig:29 highlights that 8.9% of doctors agree that there is a lack of law to implement ADR reporting while 91% disagree. 100% of the doctors in Fortis, Subharti and private practitioners disagree that there is a lack of law to implement ADR.
Fig 30 reveal that 3.6% of JRS agree that there is a lack of law to implement ADR reporting while 100% of consultants, 100%interns and 96.3% of JRs disagree that there is a lack of law to implement ADR reporting.
Fortis
(n=105
)
Subhar
ti(n=2
10)
LLRM(n
=12)
PP(n=6
2)
0
100
200
105210
85 6211
216
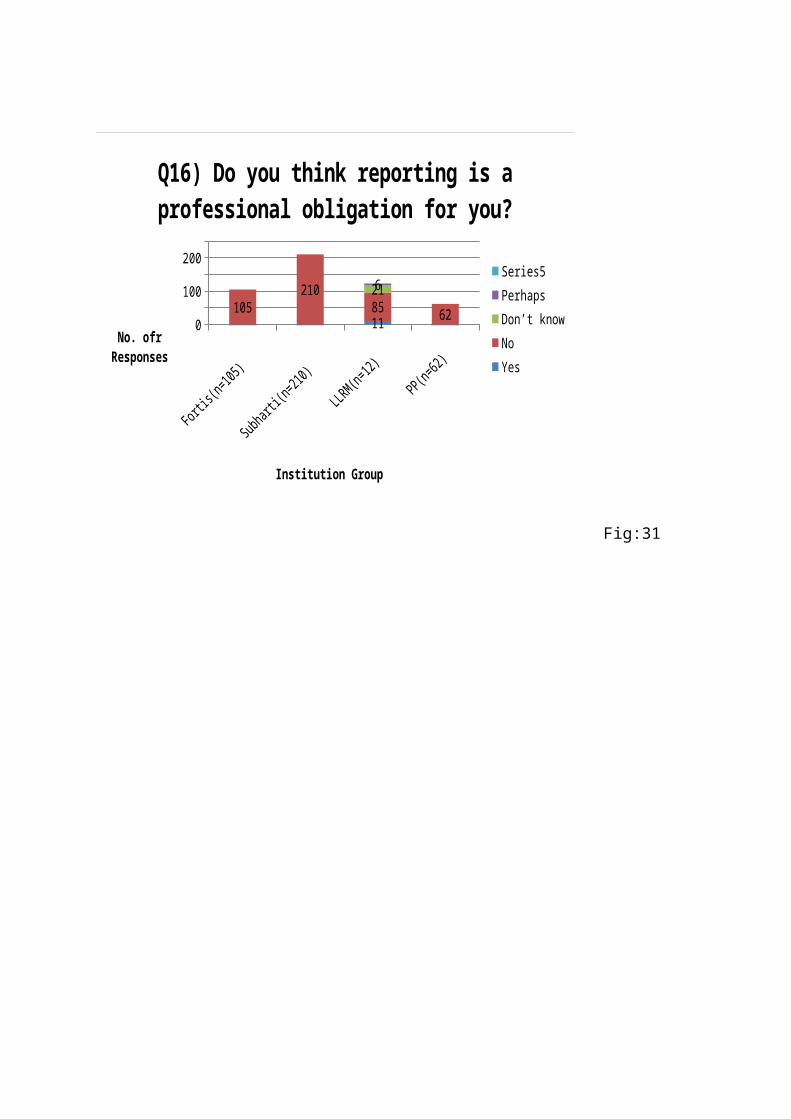
Q16) Do you think reporting is a professional obligation for you?
Series5PerhapsDon’t knowNoYes
Institution Group
No. ofr Responses
Fig:31
Consultants(n=152) JRs(n=304) Interns(n=44)0
50
100
150
200
250
300
350
144
274
44
3
18
3
3
2
9
PerhapsDon’t knowNoYes
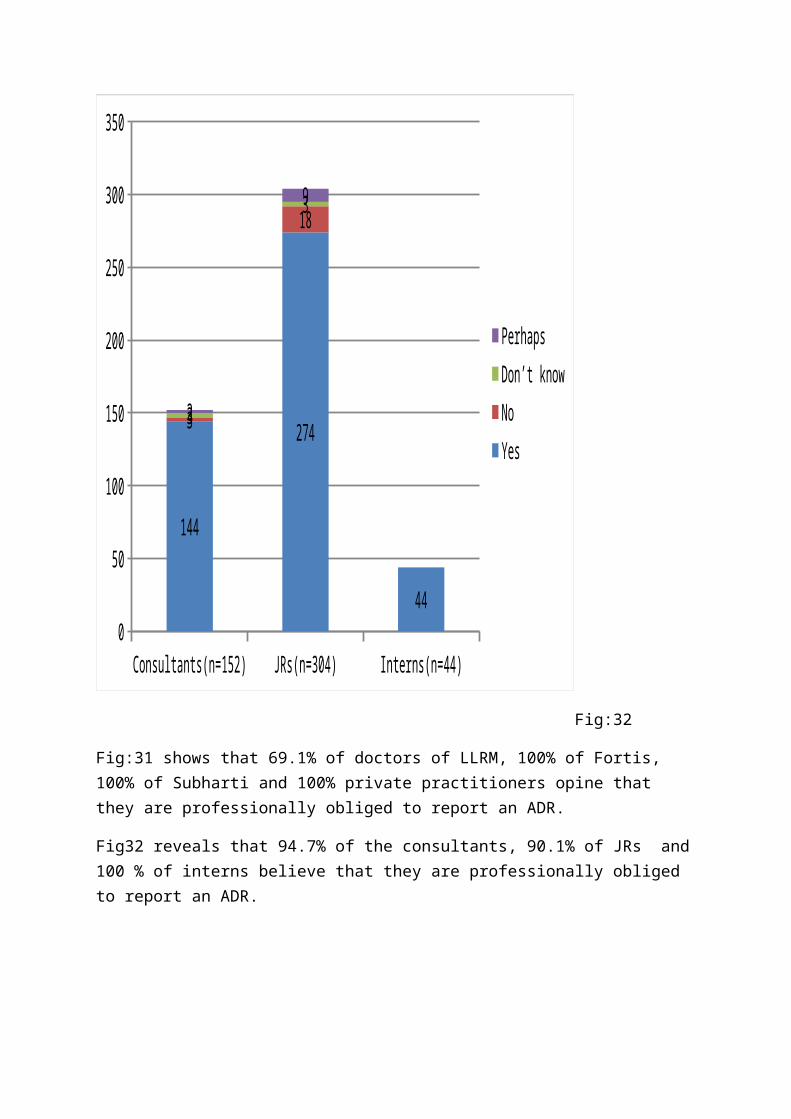
Fig:32
Fig:31 shows that 69.1% of doctors of LLRM, 100% of Fortis, 100% of Subharti and 100% private practitioners opine that they are professionally obliged to report an ADR.
Fig32 reveals that 94.7% of the consultants, 90.1% of JRs and100 % of interns believe that they are professionally obliged to report an ADR.
Fortis
(n=105
)
Subhar
ti(n=2
10)
LLRM(n
=123)
PP(n=6
2)0
100
200
105210
112 6211
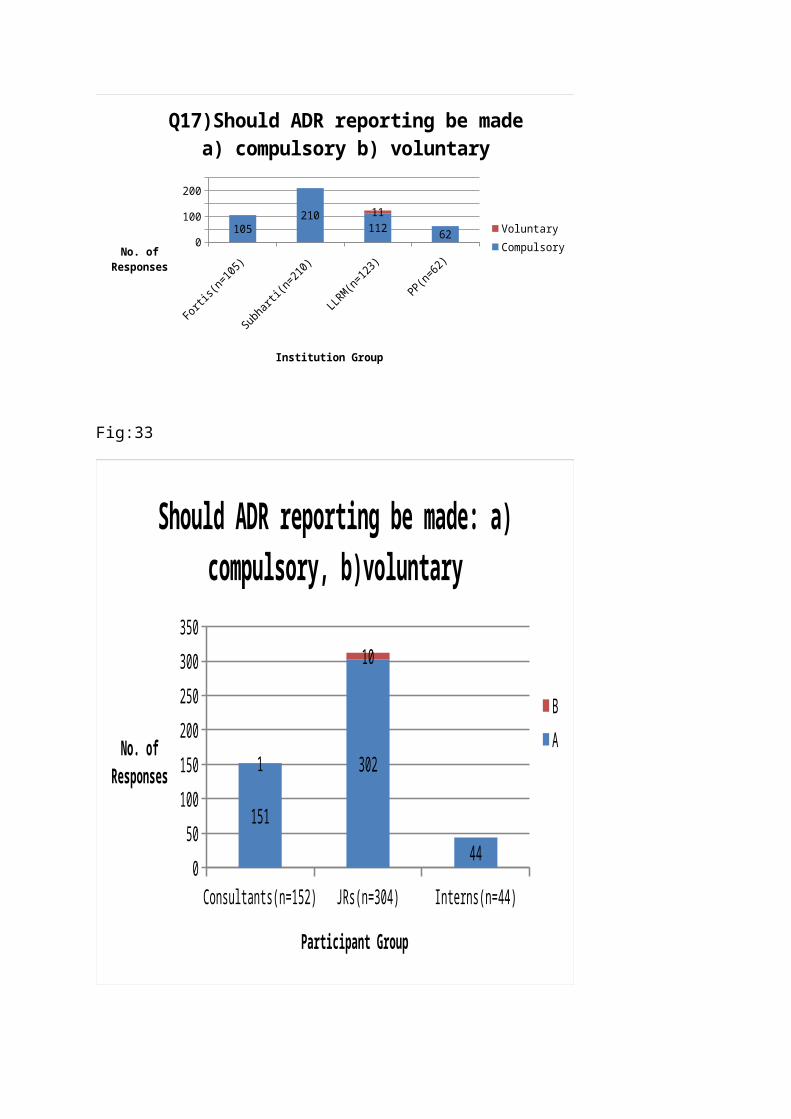
Q17)Should ADR reporting be made a) compulsory b) voluntary
VoluntaryCompulsory
Institution Group
No. of Responses
Fig:33
Consultants(n=152) JRs(n=304) Interns(n=44)0
50100150200250300350
151
302
44
1
10
Should ADR reporting be made: a) compulsory, b)voluntary
B A
Participant Group
No. of Responses

Fig:35
Fig34 shows that 91.0% of doctors in LLRM, 100% in Fortis, 100% in Subharti, and 100% private practitioners opine that ADR reporting should be made compulsory.
Fig35 reveals that 99.3% of the consultants, 96.7% of the JRs and 100% of interns agree that ADR reporting should be made compulsory.
Fortis
(n=105
)
Subhar
ti(n=2
10)
LLRM(n
=123)
PP(n=6
2)0
100
200
105210 99
6224
Q18)Do you get an ADR reporting bulletin/update?
NoYes
Institution Group
No. of Responses
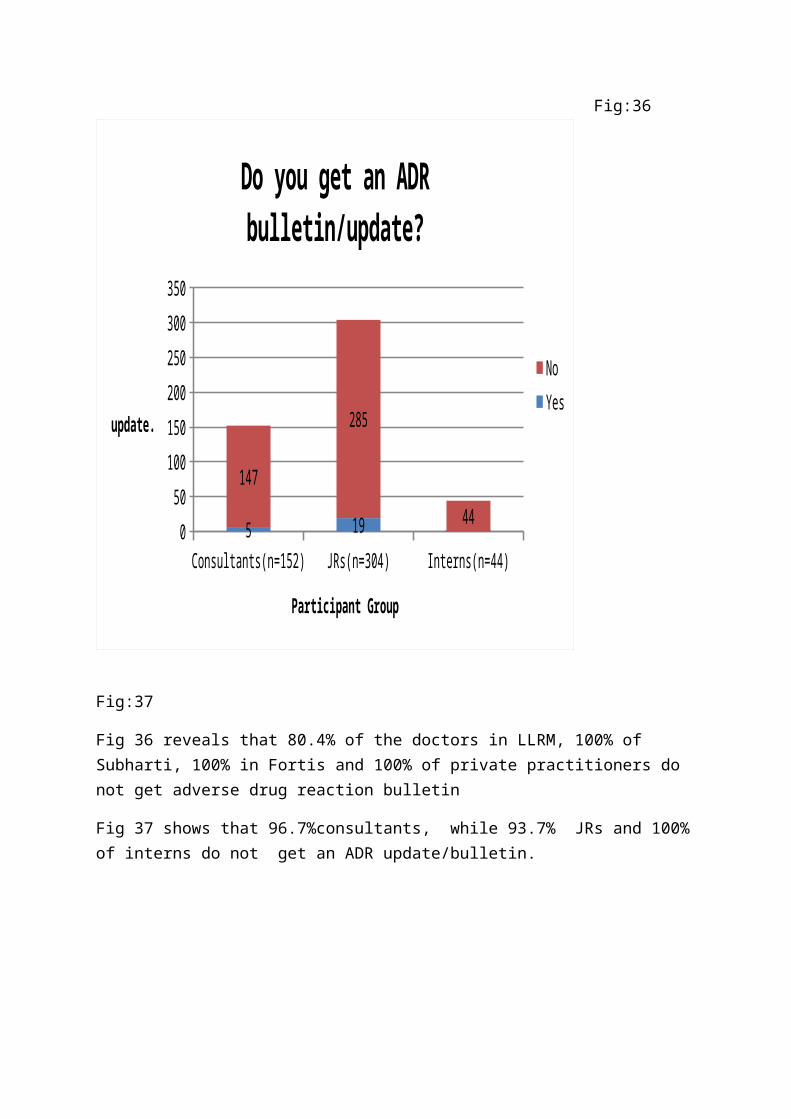
Fig:36
Consultants(n=152) JRs(n=304) Interns(n=44)050
100150200250300350
5 19
147
285
44
Do you get an ADR bulletin/update?
NoYes
Participant Group
update.
Fig:37
Fig 36 reveals that 80.4% of the doctors in LLRM, 100% of Subharti, 100% in Fortis and 100% of private practitioners do not get adverse drug reaction bulletin
Fig 37 shows that 96.7%consultants, while 93.7% JRs and 100%of interns do not get an ADR update/bulletin.

Fortis
(n=105
)
Subhar
ti(n=2
10)
LLRM(n
=123)
PP(n=6
2)0
100
200
105210
119 624
Q20) Is there a need for continuous medical education?
YesNo
Institution Group
No. of Responses
Fig:38
Consultants(n=152) JRs(n=304) Interns(n=44)050
100150200250300350
150
302
44
2
2
Is there a need of continuous medical education?
NoYes
Participant Group
No. of Responses
Fig:39
Fig:38 96.7% doctors of LLRM, 100% of Fortis, 100% of Subhartiand 100% of private practitioners opine that there is need forcontinuous medical education.

Fig:39 highlights the fact that 98.6%, 99.3% JRs and 100% interns agree that continuous medical education is needed.
Fortis(n
=105)
Subharti
(n=123)
LLRM(n=1
23)PP(n
=62)
0
100
200
83 132 65 6222
7838911
Q21)Have you ever come across an ADR?
Not surePerhapsNoYes
Institution Group
Respondents
Fig:4079,62.8, 52.8, 100
Consultants(n=152)
JRs(n=304) Interns(n=44)0
50
100
150
200
250
300
350
135200
7
12
89
37
2
7
0
3
8
Not surePerhapsNoYes
Participant Group
No. of Responses
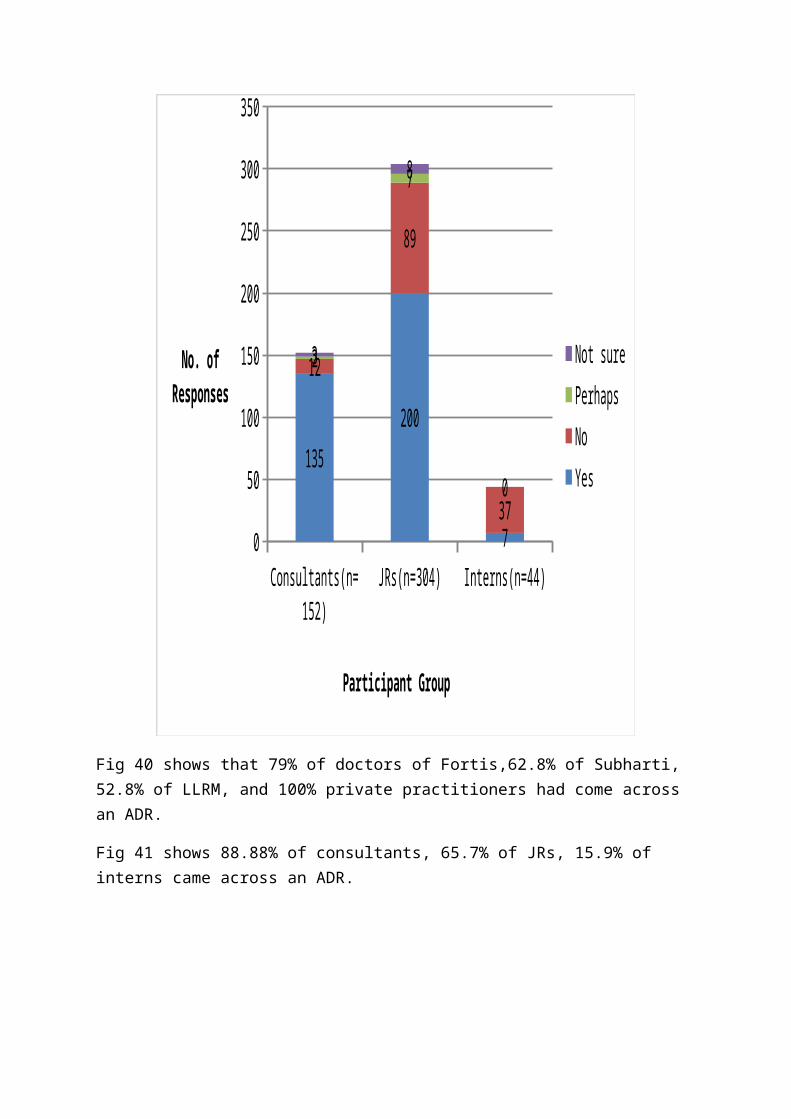
Fig 40 shows that 79% of doctors of Fortis,62.8% of Subharti, 52.8% of LLRM, and 100% private practitioners had come across an ADR.
Fig 41 shows 88.88% of consultants, 65.7% of JRs, 15.9% of interns came across an ADR.
Fortis
(n=105
)
subhar
ti(n=2
10)
LLRM(n
=123)
PP(n=6
2)0
100200
105210 91 6232
Is sufficient awareness created by print/electronic media for ADR
reporting?
NoYes
Institution Group
No.of Responses
Consultants(n=152) JRs(n=304) Interns(n=44)0
100
200
300
5 27147
277
44
Is sufficient awareness created by print/electronic media for ADR
reporting?
NoYes
Participant Group
No. of Responses
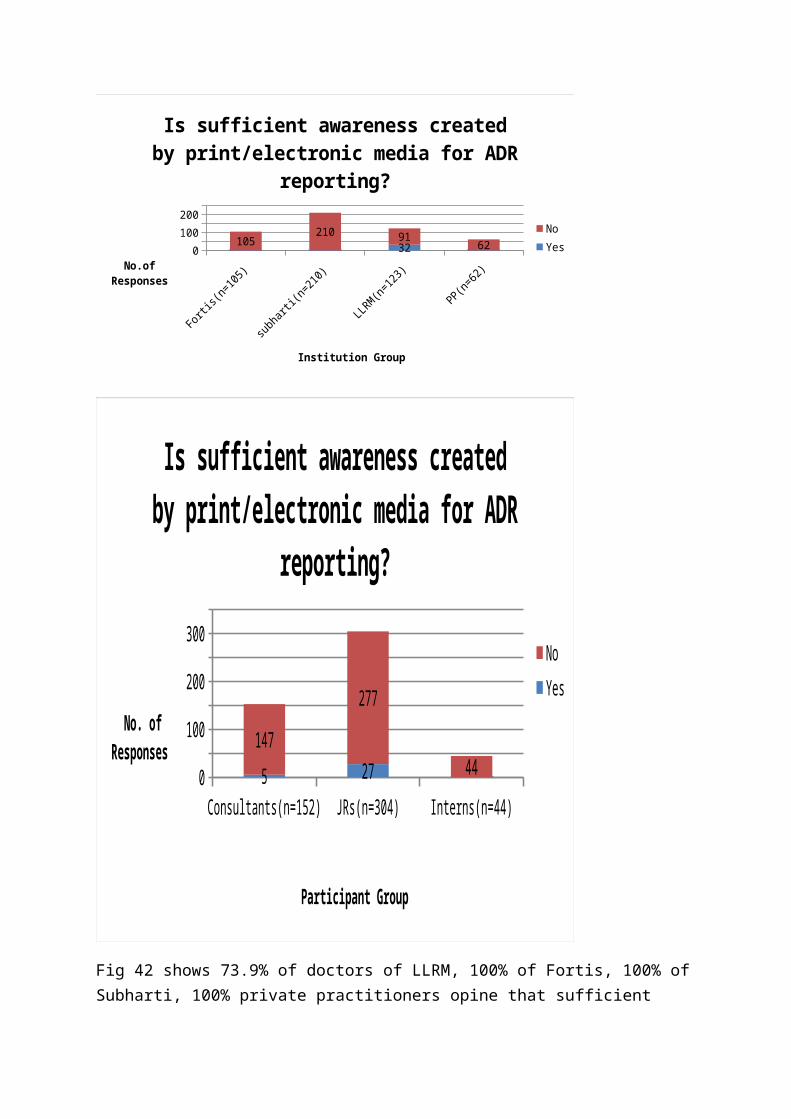
Fig 42 shows 73.9% of doctors of LLRM, 100% of Fortis, 100% ofSubharti, 100% private practitioners opine that sufficient

awareness in not available byn print/electronic media about ADR reporting.
Fig 43 shows that 96.7% of Consultants, 91.1% of JRs and 100% interns opine that sufficient awareness is not created by print/electronic media.
Fortis
(n=105
)
Subhar
ti(n=2
10)
LLRM(n
=123)
PP(n=6
2)0
100
200
105210
123 62
Should consumers be informed about ADR of drugs?
NoYes
Institution Group
No.of Responses
Consultants(n=152) JRs(n=304) Interns(n=44)0
50
100
150
200
250
300
350
152
304
44
NoYes
Participant Group
No.of Responses
Fig:44 shows that 100% of the doctors in LLRM, fortis, Subharti and private practitioners opine that consumers must be informed about ADR of drugs.
Fig 45 shows that 100% of Consultants, JRs and interns opine that consumers must be informed about ADR of drugs.

EFFECT OF TRAINING ON ADR REPORTING
During the course of 1 year of training sessions held in our institution positive outcomes were seen in the department of Psychiatry and Skin. From the Psychiatry dept 50 ADR reports were collected and from skin Department 60b ADR reports were collected.
DISCUSSION
Pharmacovigilance is still in its infancy in India. This has
led to lack of spontaneous adverse drug reaction reporting.
Lack of knowledge and education regarding importance of ADR
reporting play major roles in under reporting of ADRs. India
contributes only 2% overall ADRs to WHO in the world which is
a minute volume of the bulk. In the U.K., the number of ADR
reports has remained stable at 20,000 for the past 20 years.76
In Malaysia the number of reports has averaged at less than
2000 for the past 10 years.77 World wide, 95% of serious ADRs
do not get reported to health authorities78.
Majority of the physicians are not aware about the tools of
ADR assessment. Our study finds out that health care
professionals are unaware about the knowledge of
pharmacovigilance. This is supported by the study conducted in

Manipal where lack of knowledge of causality assessment tool
exists among the health care professionals.76
Almost all the physicians were unaware about the national
CDSCO form of India. We observed that doctors were less aware
of adverse drug reaction reporting systems. This is supported
by a study conducted by Madhan Ramesh et al.77 which stated
that doctors were less aware of the national and international
pharmacovigilance programs. Henceforth, the physicians did not
know whether the pattern of ADR reporting forms was complex or
easy.
The medical representatives did not provide adequate
information on pharmacovigilance of new product and its safety
concerns in vulnerable population. In a study by PipashaBiswas
et al,78 states that Pharmaceutical companies will need to show
both regulators and consumers that they are doing everything
possible to assure drug safety, while finding more effective,
while finding more effective approaches to manage drug safety
data. The companies need to be reassured that by reporting
adverse events and continuously monitoring for signals and
developing risk management plans for products. That is why
most of the physicians find a new drug to be safe from and

free from adverse drug reactions as they are not adequately
informed about the product.
From our study we found out that majority of doctors are not
apprehensive of litigation or financial loss if they would
report ADRs. This has proved to be a ray of hope towards
spontaneous adverse drug reaction reporting. If adequate
education is given to doctors then they would not be reluctant
to report ADRs. In a study conducted in Mumbai79, it states
that ignorance about the reporting is a major reason for under
reporting as compared to financial and legal aspects.
With regard to training of ADR reporting most of the doctors
have not attended any training sessions on pharmacovigilance
which highlights one of the causes for under reporting.
Studies80-82has shown that enhancing knowledge, attitude and
practice of improving awareness can increase the number of ADR
reports. Also a study conducted in Manipal76 reveals that
training and educational interventions markedly improved the
knowledge of pharmacovigilance among health care
professionals. Many studies have evaluated the effectiveness
of educational interventions aimed at increasing reporting
among physicians.83-87
Most of the doctors feel that there should be an online
facility for postage of filled ADR forms. This would make the
ADR reporting comparatively less tedious. In India an online
portal called “Vigiflow” is present through which all the AMCs
can report ADRs online. This is supported by some studies88-90
which state that in an era of established data and information
overload, medication administration and drug utilization are
significant factors in cost escalation, adverse outcomes, and
reduced quality in health care delivery. The availability and
use of large computerized clinical databases linked to
electronic medical records(EMR) now provide facilities for the
detection of adverse drug events and also the decision support
tools for clinicians to react appropriately to their
detection.
Majority of the doctors opine that there is no law which
compels the doctors for spontaneous ADR reporting. In a news
by CMAJ92 states that mandatory physician reporting of adverse
drug reactions could strengthen post market surveillance of
pharmaceuticals in Canada and provide an over haul of the
country’s “haphazard” drug safety database.A study by Kiran LJ
et al also found out thatcompulsory ADR reporting is important

in improving ADR reporting.93However, almost all the doctors
feel that they are professionally obliged to report ADRs.
Therefore if adequate training and sensitization of
pharmacovigilance is present implementation of law would not
be necessary. But the healthcare professionals do feel that
they should be compelled to fill ADR forms. Also, lack of time
and continuous medical education has led to under reporting
among the doctors. This was supported by the study conducted
by Chatterjee et.al92 which stated that a main reason for under
reporting of ADRs was the clinical negligibility of the
adverse reaction due to lack of time and little knowledge
about the types of reactions to be preferentially reported. In
the literature, a lack of time and knowledge about ADRs is
often considered to be a cause of under reporting.93-95Almost
all the doctors have encountered ADRs in their practice but
none of them have reported ADRs.The reasons for under
reporting of ADRs have been summarized by Inman96 as the “seven
deadly sins” . This includes financial incentives(rewards for
reporting), legal aspects(fear of litigation), complacency
(belief that the serious ADRs are already documented when a
drug is introduced in the market), diffidence(belief that
reporting should be done when there is certainty that the
reaction is caused by the use of a particular drug),
indifference (belief that a single report would make no
difference, ignorance (that only serious ADRs are to be
reported), lethargy (excuses about lack of time or
disinterestedness.
Majority of the doctors want consumers to be aware about the
adverse drug reactions of drugs. The IPC has a toll free
number for consumers in case patient suspects an adverse drug
reaction after consumption of a particular drug. In a study by
P. Ravishankar et al98 the health care professionals should
communicate the potential harm of drug-use to patients as a
matter of high priority. This would definitely contribute
towards effective ADR reporting in our country.
Despite the fact, that majority of the physicians lacked all
aspects (Knowledge, Attitude and Practices) of ADR monitoring
we found significant differences between the government
institution (LLRM) and private institutions(Subharti, Fortis
and private practitioners).Some of the doctors of LLRM were
known to the format of ADR reporting forms. Also significant
number of doctors of LLRM were informed about adverse drug
reactions by the medical representatives making it evident
that they are more interactive with medical representatives.
Our study showed that some of the doctors of LLRM have
undergone training for pharmacovigilance which we attribute to
the fact that when we contacted them retrospectively we found
out that they were given knowledge on pharmacovigilance in
their previous institutions
`