
Synergistic Effects of Amiodarone and Fluconazole on Candida albicans
Upload
independentCategory
view
1download
0
The Use of the New Oral Antifungal Agents,Itraconazole, Terbinafine, and Fluconazole, to Treat
Onychomycosis and Other Dermatomycoses
Aditya K. Gupta, MD, FRCP(C)
Division of DermatologyDepartment of Medicine
Sunnybrook and Womens’ Health Sciences Center andthe University of Toronto Medical School
Toronto, Ontario, Canada
Douglas Albreski, DPM
Department of DermatologyUniversity of Connecticut Health Center
Podiatry SectionVA CT HSC Newington Campus
Newington, Connecticut
James Q. Del Rosso, DO, FAOCD
Department of DermatologyUniversity of Nevada School of Medicine
Las Vegas, Nevada
Nellie Konnikov, MD
Department of DermatologyNew England Medical Center
Boston, Massachusetts
Current Problems in
Dermatology®
Volume 13 Number 4 July/August 2001
Current Problems in
Dermatology®
INFORMATION FOR READERS
Current Problems in Dermatology (ISSN 1040-0486) ispublished bimonthly by Mosby. Corporate and editorialoffices: 11830 Westline Industrial Drive, St. Louis, MO63146-3318. Accounting and circulation offices: Mosby,6277 Sea Harbor Drive, Orlando, FL 32887-4800. Publishedin January, March, May, July, September, and November.Periodicals postage paid at Orlando, FL 32862, and at addi-tional mailing offices. POSTMASTER: Send addresschanges to Current Problems in Dermatology, Mosby,Periodicals Department, 6277 Sea Harbor Dr, Orlando, FL32887-4800.
Visit our Web site at www.mosby.com/cpderm.
Subscription Orders/Inquiries and Back Issues
Subscriptions may begin at any time. To enter a subscrip-tion to Current Problems in Dermatology, call 800-654-2452or 407-345-4000; fax 407-363-9661; or e-mail [email protected]. Remittances made by check, draft, post office,or express money order should be in US funds, drawn througha US bank, made payable to this Journal, and sent to Mosby,Subscription Customer Service, 6277 Sea Harbor Dr, Orlando,FL 32887, USA.
2001 US subscription rates: individual, $96.00; institution,$155.00; student and resident, $51.00; single issue, $28.00.Outside of the US and possessions: individual, $105.00; insti-tution, $164.00; student and resident, $60.00; surface deliv-ery, no additional charge. Airmail delivery to Canada andMexico, add $6.00; for all other international, add $12.00.Canadian customers, please add 7% GST to internationalprices. Prices subject to change without notice. Subscriptionrates include supplements. To receive student/resident rate,orders must be accompanied by name of affiliated institution,date of term, and the signature of program/residency coordi-nator on institution letterhead. Orders will be billed at indi-vidual rate until proof of status is received.
Single-copy prices will be charged on missing issues olderthan 3 months (6 months international) from mail date. Backissues generally are available for the previous 5 years.
Copyright
Copyright © 2001 by Mosby, Inc. All rights reserved. Nopart of this publication may be reproduced, stored in a re-trieval system, or transmitted in any form or by any means—electronic, mechanical, photocopying, recording, or other-wise—without prior written permission from the publisher,except in cases described below.
This journal has been registered with the CopyrightClearance Center, Inc., 222 Rosewood Drive, Danvers, MA01923. Consent is given for the copying of articles for per-sonal or internal use of specific clients. This consent is givenon the condition that the copier pay directly to the CCC thebase fee of $35.00 per article for copying beyond that per-mitted by U.S. Copyright Law: 1040-0486/2001 $35.00 + 0.This consent does not extend to other kinds of copying, suchas for general distribution, resale, advertising, and promo-tional purposes or for creating new collective works. Allinquiries regarding copyrighted material from this publica-tion other than those that can be handled through the CCCshould be directed, in writing, to Journals PermissionDepartment, Mosby, 6277 Sea Harbor Dr, Orlando, FL32887; fax 407-345-4058.
Additional Services
Reprints of single articles available online may be ob-tained by purchasing Pay-Per-View access for $25 per arti-cle on the journal Web site, www.mosby.com/cpderm.
Disclaimer
Statements and opinions expressed herein are those ofthe author(s) and not necessarily those of the editor(s) orpublisher. The editor(s) and publisher disclaim any respon-sibility or liability for such material and do not guarantee,warrant, or endorse any product or service advertised in thispublication, nor do they guarantee any claim made by themanufacturer of such product or service.
Abstract 220
Introduction 221
Onychomycosis 221Modified Classification of Toenail Onychomycosis 221
Distal and Lateral Subungual Onychomycosis 221Proximal Subungual Onychomycosis 221White Superficial Onychomycosis 222Candida Onychomycosis 222Endonyx Onychomycosis 222Total Nail Dystrophy 222
Differential Diagnosis of Onychomycosis 222Diagnosis of Onychomycosis 224
Distal and Lateral Subungual Onychomycosis 224Superficial Onychomycosis 224Proximal Subungual Onychomycosis 224Endonyx and Total Dystrophic Onychomycosis 224Microscopic Examination 224Culture 224Histopathologic Examination 225Immunohistochemistry 225Flow Cytometry 225
Use of the Newer Oral Antifungal Agents to Treat Onychomycosis 225and the Other Dermatomycoses
Pharmacokinetics of Itraconazole 225Pharmacokinetics of Fluconazole 225Pharmacokinetics of Terbinafine 226The Treatment of Onychomycosis and Other Dermatomycoses by Use of Itraconazole, 226
Terbinafine, and FluconazoleItraconazole 226
Tinea Corporis/Cruris/Pedis/Manus 226Tinea Versicolor 226Majocchi’s Granuloma 226Onychomycosis (Dermatophytes) 226
Curr Probl Dermatol, July/August 2001 215
Current Problems in
Dermatology®
served. Noed in a re-y means—
or other-publisher,
Copyrightnvers, MAes for per-nt is givene CCC thed that per-
$35.00 + 0.pying, suchnd promo-works. Allis publica-h the CCCPermissionlando, FL
may be ob-25 per arti-rm.
e those ofditor(s) orny respon-guarantee,sed in this
ade by the
The Use of the New Oral Antifungal Agents,Itraconazole, Terbinafine, and Fluconazole, to Treat
Onychomycosis and Other Dermatomycoses
216 Curr Probl Dermatol, July/August 2001
Onychomycosis (Nondermatophytes) 226Tinea Capitis 227
Fluconazole 227Tinea Corporis/Cruris/Pedis/Manus 227Cutaneous Candidiasis 227Tinea Versicolor 227Onychomycosis (Dermatophytes) 227Tinea Capitis 227
Terbinafine 227Tinea Corporis/Cruris/Pedis/Manus 227Onychomycosis (Dermatophytes) 227Onychomycosis (Nondermatophytes) 228Majocchi’s Granuloma 228Tinea Capitis 228Other Dermatophytosis 228
Factors Affecting the Response of Onychomycosis of the Toenails to 228Oral Antifungal Therapy
Genetic Predisposition 228Age and Sex 228Presence of Concomitant Tinea Pedis 228Environmental Factors 228Immunosuppression 228Immunodeficiency 228Diabetes Mellitus 229Psoriasis 229Local Factors 229
Safety Issues with the New Oral Antifungal Agents 229(Itraconazole, Terbinafine, and Fluconazole)
Gastrointestinal and Nervous System 230Hepatic Reactions 230Cutaneous Reactions 230
Laboratory Monitoring 230
Drug Interactions 230
Approach to Treating Fungal Infections of the Lower Extremity in Patients 230with Diabetes MellitusIntroduction 230Impact of Diabetes 231The Diabetic Foot 231Tinea Pedis 232
Interdigital Tinea Pedis 232Moccasin Tinea Pedis 233Vesicular or Acute Tinea Pedis 233
Treatment of Toenail Onychomycosis in Diabetic Patients 233Conclusions Regarding the Treatment of Superficial Fungal Infections in Diabetic Individuals 234
Strategies to Improve Cure Rates in the Treatment of Onychomycosis 234Choice of Oral Antifungal Agent 234
Measures Aimed at Optimizing Bioavailability of Drug 234
August 2001 Curr Probl Dermatol, July/August 2001 217
Compliance with Regimen 234Potential for Drug Interactions to Reduce Bioavailability 234A Poor Mycologic and Clinical Response May Be Associated with 235
Suboptimal Concentrations of Antifungal Agent in the Nail PlatePhysical Characteristics of the Nail Unit 235
Strategies to Reduce the Rate of Reinfection/Relapse 235
What Is the Yardstick of Successful Therapy for Onychomycosis of the Toenails: 237Clinical Versus Mycologic Cure
The Use of Oral Antifungal Therapy in Children 237
References 238
226227227227227227227227227227227228228228228
228
228228228228228228229229229
229
230230230
230
230
230
230231231232232233233233234
234234234
Access to Current Problems in Dermatology Online is now reserved for print subscribers!
Full-text access to Current Problems in Dermatology Online is now available for all print subscribers.To activate your individual online subscription, please visit Current Problems in Dermatology Online,point your browser to http://www.mosby.com/cpderm, follow the prompts to activate your onlineaccess, and follow the instructions. To activate your account, you will need your subscriber accountnumber, which you can find on your mailing label (note: the number of digits in your subscriberaccount number varies from 6 to 10). See the example below in which the subscriber account numberhas been circled:
Sample mailing label
This is your subscription account number
Personal subscriptions to Current Problems in Dermatology Online are for individual use only andmay not be transferred. Use of Current Problems in Dermatology Online is subject to agreement to theterms and conditions as indicated online.
****************************3-DIGIT 001SJ P1
FEB00 J054 C: 1 1234567-89 U 05/00 Q: 1J. H. DOE, MD531 MAIN STCENTER CITY, NY 10001-001

218 Curr Probl Dermatol, July/August 2001
Editorial
ONYCHOMYCOSIS represents a common and indolent superficial fungalinfection. Unlike superficial mycosis affecting the skin, onychomycosis, exceptin rare instances, requires oral therapy. Newer formulations with triazoles in lac-quer may prove to be useful in the topical treatment of onychomycosis. Beforethe advent of the new triazoles, or allylamines, dermatologists relied on therapywith griseofulvin or oral ketoconazole. Not only were these previous agents notterribly effective, but they were also fraught with significant side effects. Thenewer agents have significantly greater efficacy and require much shorter treat-ment periods. Itraconazole, fluconazole, and terbinafine are all well toleratedwith few major side effects. Dosage regimens for the 3 agents vary. Itraconazoleis used in pulse therapy 1 week per month for several cycles, depending on theindication. Terbinafine is used as continuous therapy, and fluconazole is used asweekly therapy. Whereas they were initially used in adults, there is now evidenceto suggest that these agents can be used in children in tinea capitis and othersuperficial infections.
Dr Gupta and colleagues have provided an in-depth review of this area that canserve as a reference source for these diseases.
Daniel N. Sauder, MD

Curr Probl Dermatol, July/August 2001 219August 2001
Aditya K. Gupta, MD, FRCP(C), went to medical school in the United Kingdom after receiving a master’s degree in engineering fromKing’s College, University of Cambridge, United Kingdom. He then obtained training in internal medicine at the University of Toronto,Canada. Subsequently, he completed a dermatology residency at the University of Michigan, Ann Arbor, followed by a fellowship inclinical pharmacology at the same program. He then went on to receive training at the National Institutes of Health, Bethesda, Md.Dr Gupta is currently an associate professor in the Division of Dermatology, Department of Medicine, Sunnybrook and Women’sCollege Health Sciences Centre (Sunnybrook site) and the University of Toronto. His main interest is clinical pharmacology and runsan active clinical trials unit. He is involved in clinical and basic research in this field. He is the director of a basic research labora-tory that has a special interest in mycology. He has written more than 250 articles in peer-review journals and 25 book chapters.He lectures extensively in Canada, the United States, and internationally. He is on the editorial/advisory boards of 16 journals includ-ing the International Journal of Dermatology, the Journal of the European Academy of Dermatology and Venereology, the Journal ofCutaneous Medicine and Surgery, Skin and Aging, Skin Therapy Letter, Dermatology, Pediatric Dermatology, Cutis, Medical Mycology,Mycoses, Mikologia Lekarska, Revista Iberamericana de Micologia, Clinics in Dermatology, and Podiatry Today. Dr Gupta has actedas consultant, received honoraria/study grants, and is on the speaker’s bureau for Janssen, Novartis, Pfizer, Medicis, and Dermik.
Douglas Albreski, DPM, is associate chief, podiatry section, and director of the Primary Podiatric Medical Residency Program at VAConnecticut Healthcare System, Newington. He is also an assistant professor in the Department of Dermatology at the University ofConnecticut School of Medicine in Farmington. He is a member of the American Podiatric Medical Association, the American PublicHealth Association, the Association of Military Surgeons in the United States, and the Council of Teaching Hospitals. In 1998 hebecame research committee chair for the Podiatry Division of the Federal VA Health Care System. He has been a principal investi-gator for several research grants and is currently involved in the development and design of a podiatric quality-of-life index. Dr Albreskiis a frequent lecturer and has published a number of scientific articles and abstracts. He received his DPM degree from the Collegeof Podiatric Medicine in Cleveland. He then completed a podiatric residency at Newington VA Medical Center in Newington, Conn.
James Q. Del Rosso, DO, FAOCD, is clinical assistant professor of dermatology at the University of Nevada School of Medicine andhas a private practice in dermatology in Las Vegas, Nev. Before that appointment, he practiced dermatology and was the director ofthe Dermatology Laboratory at the West Florida Medical Center in Pensacola. He also served as assistant professor of dermatologyand head of the Section of Dermatology at the Ohio University in Athens. A past president of the American Osteopathic College ofDermatology, Dr Del Rosso has lectured extensively on an international level on many issues related to antifungal therapy and iswell published. He was appointed a member of the West Florida Medical Center Clinic Honor Society. Other awards include theOutstanding Teacher Award of the Ohio State University College of Osteopathic Medicine and the Outstanding Volunteer ClinicalFaculty Teaching Award of the Ohio State University, Department of Dermatology. He received his DO degree from the Ohio UniversityCollege of Osteopathic Medicine. He completed a rotating internship at Doctors Hospital in Columbus, a residency in dermatologyat Atlantic Skin Disease and Skin Surgery Associates in Fort Lauderdale, Fla, and a fellowship in Mohs micrographic surgery andcutaneous oncology at the Ohio State University. He also received a pharmacy degree from St John’s University in Jamaica, NY, andcompleted a hospital pharmacy residency at Temple University Hospital in Philadelphia, Pa. Most recently, he was appointed to theBoard of Directors of the Council for Nail Disorders and the American Mohs Surgery, and to the American Osteopathic Board ofDermatology. He is board certified in both dermatology and Mohs micrographic surgery. Dr Del Rosso has served as a consultant oron the speaker’s bureau for Janssen Pharmaceutica, Bristol-Myers Squibb, Dermik, Ortho-Dermatology, and Medicis.
Nellie Konnikov, MD, received her MD degree from Moscow Medical School, Russia, and her postdoctoral training in internal medi-cine at Brigham and Women’s Hospital in Boston. She was a resident and chief resident in dermatology in the BU/Tufts combinedresidency training program. She was a recipient of the Dermatology Foundation fellowship award in cutaneous immunology and iscurrently a senior dermatologist and director of the dermatology residency training program at New England Medical Center in Boston.She is a clinical professor of dermatology at Tufts University School of Medicine. She is an active clinical investigator in the labora-tory and in the clinical setting. Her major research interests are cutaneous oncology, photoaging, cutaneous mycology, and ony-chomycosis. She has an extensive bibliography and actively participates as an invited faculty member and guest lecturer at numer-ous medical symposiums throughout New England and the United States. Dr Konnikov is a member of the Massachusetts MedicalSociety, the American Academy of Dermatology, the International Society of Dermatology, the New England Dermatological Society,the American Society for Dermatologic Surgery, and the Massachusetts Academy of Dermatology. She is a consultant for Janssen,Novartis, and Pfizer, has received honorariums and study grants from Block, Janssen, Novartis, and Pfizer, and is on the speaker’sbureau for Block, Janssen, and Novartis.
220 Curr Probl Dermatol, July/August 2001
The Use of the New Oral Antifungal Agents, Itraconazole,Terbinafine, and Fluconazole to Treat Onychomycosis
and Other Dermatomycoses
Onychomycosis refers to a fungal infection of the nail bed and secon-darily the nail plate. This could be caused by dermatophytes, Candidaspecies, and nondermatophyte molds. Tinea unguium is infection of thenail bed/plate by dermatophytes. The modified classification of ony-chomycosis is distal and lateral subungual onychomycosis, proximalsubungual onychomycosis, superficial onychomycosis, endonyx ony-chomycosis, and total dystrophic onychomycosis. In general, onlyabout 50% of all abnormal-appearing toenails can be attributed tomycologically proven onychomycosis. The other causes for abnormally-appearing nails include psoriasis, trauma, and lichen planus. Thenewer oral antifungal agents itraconazole, terbinafine, and fluconazolehave become primary treatments of onychomycosis and other superfi-cial fungal infections; however, griseofulvin, is widely used to treattinea capitis and ketoconazole, is preferred by some for the treatmentof tinea versicolor. Each of the new oral agents has been shown to beeffective and safe in dermatomycoses. Diabetic patients are more proneto development of onychomycosis compared with normal individuals.Because of the potential for morbidity, the feet in diabetic patients needto be examined carefully, with appropriate treatment of any fungal orbacterial infection. The management strategies with onychomycosisinclude no therapy, use of effective topical therapies if available,mechanical or chemical debridement, or oral antifungal therapy. Insome instances the most appropriate approach is a combination of twoof the above-mentioned therapy modes, for example, oral therapy andmechanical debridement. The preferred dosage regimens are itracona-zole (pulse), terbinafine (continuous), and fluconazole (once-weekly).Once a cure has been achieved, management includes education andcounseling of the patient to reduce the chances of recurrence of disease.There is a growing body of experience in which the new oral antifun-gal agents have been used to treat tinea capitis and other superficialinfections in children. The data suggest that itraconazole, terbinafine,and fluconazole are effective and safe in children. (Curr ProblDermatol 2001;13:213-48)
time. As the nail plate becomes progressively affected,it may become thicker and more crumbly. Microbio-logic flora such as Pseudomonas aeruginosa and Proteusvulgaris may be secondary invaders and can cause achange in the color of the nail plate.9 In North Americanepidemiologic studies, the causative agents of distal andlateral subungual onychomycosis (DLSO) includeTrichophyton rubrum, T mentagrophytes, T krajdenii,Epidermophyton floccosum, Candida species (C albi-cans, other Candida species), and nondermatophytemolds (eg, Scopulariopsis brevicaulis, Aspergillus sp,Acremonium sp, Scytalidium hyalinum, S dimidiatum).
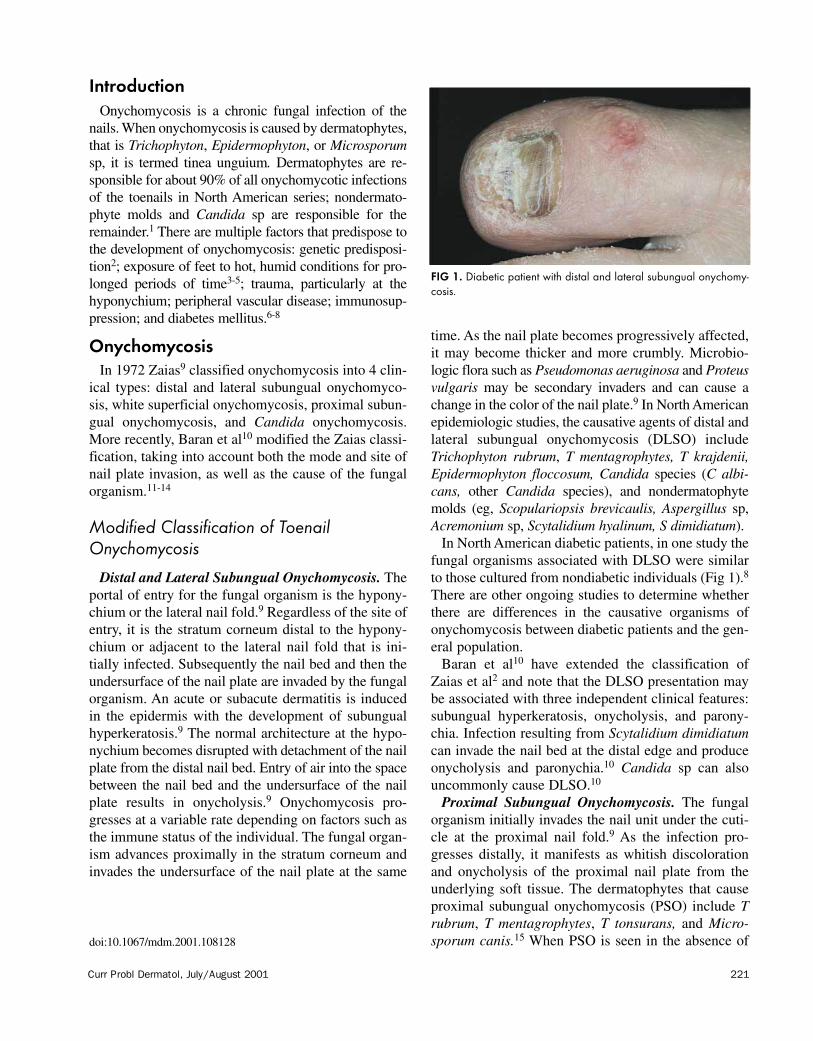
In North American diabetic patients, in one study thefungal organisms associated with DLSO were similarto those cultured from nondiabetic individuals (Fig 1).8
There are other ongoing studies to determine whetherthere are differences in the causative organisms ofonychomycosis between diabetic patients and the gen-eral population.
Baran et al10 have extended the classification ofZaias et al2 and note that the DLSO presentation maybe associated with three independent clinical features:subungual hyperkeratosis, onycholysis, and parony-chia. Infection resulting from Scytalidium dimidiatumcan invade the nail bed at the distal edge and produceonycholysis and paronychia.10 Candida sp can alsouncommonly cause DLSO.10
Proximal Subungual Onychomycosis. The fungalorganism initially invades the nail unit under the cuti-cle at the proximal nail fold.9 As the infection pro-gresses distally, it manifests as whitish discolorationand onycholysis of the proximal nail plate from theunderlying soft tissue. The dermatophytes that causeproximal subungual onychomycosis (PSO) include Trubrum, T mentagrophytes, T tonsurans, and Micro-sporum canis.15 When PSO is seen in the absence of
Curr Probl Dermatol, July/August 2001 221August 2001
IntroductionOnychomycosis is a chronic fungal infection of the
nails. When onychomycosis is caused by dermatophytes,that is Trichophyton, Epidermophyton, or Microsporumsp, it is termed tinea unguium. Dermatophytes are re-sponsible for about 90% of all onychomycotic infectionsof the toenails in North American series; nondermato-phyte molds and Candida sp are responsible for theremainder.1 There are multiple factors that predispose tothe development of onychomycosis: genetic predisposi-tion2; exposure of feet to hot, humid conditions for pro-longed periods of time3-5; trauma, particularly at thehyponychium; peripheral vascular disease; immunosup-pression; and diabetes mellitus.6-8
OnychomycosisIn 1972 Zaias9 classified onychomycosis into 4 clin-
ical types: distal and lateral subungual onychomyco-sis, white superficial onychomycosis, proximal subun-gual onychomycosis, and Candida onychomycosis.More recently, Baran et al10 modified the Zaias classi-fication, taking into account both the mode and site ofnail plate invasion, as well as the cause of the fungalorganism.11-14
Modified Classification of ToenailOnychomycosis
Distal and Lateral Subungual Onychomycosis. Theportal of entry for the fungal organism is the hypony-chium or the lateral nail fold.9 Regardless of the site ofentry, it is the stratum corneum distal to the hypony-chium or adjacent to the lateral nail fold that is ini-tially infected. Subsequently the nail bed and then theundersurface of the nail plate are invaded by the fungalorganism. An acute or subacute dermatitis is inducedin the epidermis with the development of subungualhyperkeratosis.9 The normal architecture at the hypo-nychium becomes disrupted with detachment of the nailplate from the distal nail bed. Entry of air into the spacebetween the nail bed and the undersurface of the nailplate results in onycholysis.9 Onychomycosis pro-gresses at a variable rate depending on factors such asthe immune status of the individual. The fungal organ-ism advances proximally in the stratum corneum andinvades the undersurface of the nail plate at the same
azole,sis
FIG 1. Diabetic patient with distal and lateral subungual onychomy-cosis.
doi:10.1067/mdm.2001.108128

222 Curr Probl Dermatol, July/August 2001
paronychia, the causative organism may be a dermato-phyte or even Candida sp.16
A distinct subtype is proximal white subungual ony-chomycosis (PWSO). This is often, but not invariably,seen in patients infected with the acquired immunode-ficiency syndrome (AIDS) virus.17-22 It may also be ob-served in other forms of immunosuppression, for example,lupus erythematosus and kidney transplant recipi-ents.23,24 Occasionally it has been seen in otherwiseimmunocompetent individuals.23 In patients with AIDSa combination of PSO and WSO has been reported.10
Proximal subungual onychomycosis may also developas a result of paronychia caused by C albicans.10 Inthis presentation onycholysis can be observed alongthe lateral edges of the nail plate. Nondermatophytemolds may also cause PSO, producing discoloration,(eg, Fusarium and Scopulariopsis sp [white or buffdiscoloration of the nail plate] and Aspergillus sp[green discoloration]).13,14,25,26
White Superficial Onychomycosis. WSO generallyappears as opaque white or yellow-colored superficialislands on the surface of the nail plate (Fig 2).9 In thistype of onychomycosis the fungal organism invadesthe nail plate directly; in contrast, in DLSO the nailbed is infected initially, followed by involvement of thenail plate. Superficial onychomycosis may not alwaysbe visible on cursory examination of the foot; some-times the islands are small and can be easily missed,and in other cases the onychomycosis is present on thesurface of a nail overlapped by another toe. The mostfrequent pathogen in this type of onychomycosis is Tmentagrophytes, which may be able to invade thesuperficial nail plate through enzymatic digestion.9
Nondermatophytes such as Aspergillus sp, Acremoniumsp, and Fusarium oxysporum can also produce thisclinical picture. Superficial onychomycosis can alsobe black in color (superficial black onychomycosis). T
rubrum may produce white or black superficial ony-chomycosis.27,28
Candida Onychomycosis. This form of onychomy-cosis was described by Zaias,9 with the clinical diseasebeing seen only in children and adults with “chroniccutaneous candidiasis syndrome.” The presentation wasalso termed “candidal granuloma.” The distal end ofthe digit may appear bulbous or “pseudoclubbed” withthickening of the nail bed.9 Pseudohyphae of C albi-cans would be expected to be present throughout theentire nail plate. In the revised classification proposedby Baran et al,10 there is no separate category for Can-dida onychomycosis because this organism may beassociated with different types of onychomycosis.
Endonyx Onychomycosis. This type of onychomy-cosis29 is not present in the Zaias classification but isan addition to the Baran et al10 revision. In this form ofonychomycosis, there is invasion of both the superfi-cial and deeper layers of the nail plate. Lamellar split-ting of the nail plate is observed. The causative organ-isms are those that produce endothrix scalp infection,for example, T soudanense and T violaceum. Invasionby T soudanense may reflect the high affinity of thisorganism to hard keratins.
Total Nail Dystrophy. Complete nail plate dystrophymay be classified into primary and secondary sub-types.10 The secondary type is the end point of any ofthe above forms of onychomycosis. The primary typeis seen in patients with chronic mucocutaneous can-didiasis where the entire nail unit may be simultane-ously infected, including the nail folds.10
Differential Diagnosis of OnychomycosisOnychomycotic nails may present with subungual
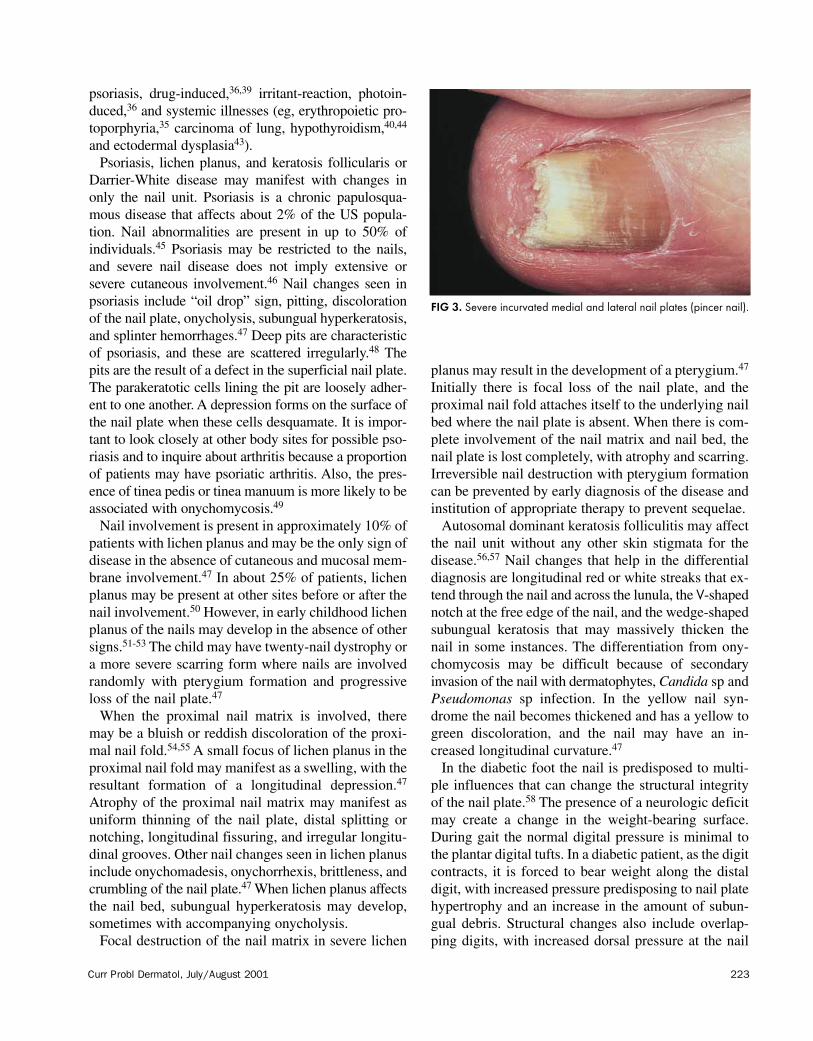
hyperkeratosis, onycholysis, nail plate discoloration, andloss of consistency of the nail plate. Not all abnormal-appearing nails are due to onychomycosis; in fact, onlyone half of all such nails may have mycologic evidenceof disease.1 The differential diagnosis includes anatomicabnormalities of nail, for example, pincer nail (Fig 3),psoriasis, trauma, lichen planus, Darrier-White disease(keratosis follicularis), and eczema. Paronychia may bedue to Candida sp or bacterial infection with the proxi-mal nail fold being infected initially in most instances.Application of cosmetics to nails can result in a varietyof changes, including onycholysis, paronychia, and aller-gic contact dermatitis.30-32 When only onycholysis ispresent, other nail dystrophies that produce this clinicalpicture should be considered,33-44 such as primary ony-cholysis,34 or secondary causes, such as cosmetics,38
FIG 2. White superficial onychomycosis.
Curr Probl Dermatol, July/August 2001 223
psoriasis, drug-induced,36,39 irritant-reaction, photoin-duced,36 and systemic illnesses (eg, erythropoietic pro-toporphyria,35 carcinoma of lung, hypothyroidism,40,44
and ectodermal dysplasia43).Psoriasis, lichen planus, and keratosis follicularis or
Darrier-White disease may manifest with changes inonly the nail unit. Psoriasis is a chronic papulosqua-mous disease that affects about 2% of the US popula-tion. Nail abnormalities are present in up to 50% ofindividuals.45 Psoriasis may be restricted to the nails,and severe nail disease does not imply extensive orsevere cutaneous involvement.46 Nail changes seen inpsoriasis include “oil drop” sign, pitting, discolorationof the nail plate, onycholysis, subungual hyperkeratosis,and splinter hemorrhages.47 Deep pits are characteristicof psoriasis, and these are scattered irregularly.48 Thepits are the result of a defect in the superficial nail plate.The parakeratotic cells lining the pit are loosely adher-ent to one another. A depression forms on the surface ofthe nail plate when these cells desquamate. It is impor-tant to look closely at other body sites for possible pso-riasis and to inquire about arthritis because a proportionof patients may have psoriatic arthritis. Also, the pres-ence of tinea pedis or tinea manuum is more likely to beassociated with onychomycosis.49
Nail involvement is present in approximately 10% ofpatients with lichen planus and may be the only sign ofdisease in the absence of cutaneous and mucosal mem-brane involvement.47 In about 25% of patients, lichenplanus may be present at other sites before or after thenail involvement.50 However, in early childhood lichenplanus of the nails may develop in the absence of othersigns.51-53 The child may have twenty-nail dystrophy ora more severe scarring form where nails are involvedrandomly with pterygium formation and progressiveloss of the nail plate.47
When the proximal nail matrix is involved, theremay be a bluish or reddish discoloration of the proxi-mal nail fold.54,55 A small focus of lichen planus in theproximal nail fold may manifest as a swelling, with theresultant formation of a longitudinal depression.47
Atrophy of the proximal nail matrix may manifest asuniform thinning of the nail plate, distal splitting ornotching, longitudinal fissuring, and irregular longitu-dinal grooves. Other nail changes seen in lichen planusinclude onychomadesis, onychorrhexis, brittleness, andcrumbling of the nail plate.47 When lichen planus affectsthe nail bed, subungual hyperkeratosis may develop,sometimes with accompanying onycholysis.
Focal destruction of the nail matrix in severe lichen
August 2001
planus may result in the development of a pterygium.47
Initially there is focal loss of the nail plate, and theproximal nail fold attaches itself to the underlying nailbed where the nail plate is absent. When there is com-plete involvement of the nail matrix and nail bed, thenail plate is lost completely, with atrophy and scarring.Irreversible nail destruction with pterygium formationcan be prevented by early diagnosis of the disease andinstitution of appropriate therapy to prevent sequelae.
Autosomal dominant keratosis folliculitis may affectthe nail unit without any other skin stigmata for thedisease.56,57 Nail changes that help in the differentialdiagnosis are longitudinal red or white streaks that ex-tend through the nail and across the lunula, the V-shapednotch at the free edge of the nail, and the wedge-shapedsubungual keratosis that may massively thicken thenail in some instances. The differentiation from ony-chomycosis may be difficult because of secondaryinvasion of the nail with dermatophytes, Candida sp andPseudomonas sp infection. In the yellow nail syn-drome the nail becomes thickened and has a yellow togreen discoloration, and the nail may have an in-creased longitudinal curvature.47
In the diabetic foot the nail is predisposed to multi-ple influences that can change the structural integrityof the nail plate.58 The presence of a neurologic deficitmay create a change in the weight-bearing surface.During gait the normal digital pressure is minimal tothe plantar digital tufts. In a diabetic patient, as the digitcontracts, it is forced to bear weight along the distaldigit, with increased pressure predisposing to nail platehypertrophy and an increase in the amount of subun-gual debris. Structural changes also include overlap-ping digits, with increased dorsal pressure at the nail
icial ony-
nychomy-al disease“chronic
tation wasal end ofbed” withof C albi-ghout theproposed
y for Can-m may becosis.nychomy-ion but isis form ofe superfi-ellar split-ve organ-infection, Invasionty of this
dystrophydary sub-of any of
mary typeeous can-imultane-
osissubungualation, andabnormal-fact, only evidenceanatomic
il (Fig 3),te diseaseia may bethe proxi-instances.
n a varietyand aller-holysis isis clinical
mary ony-smetics,38
FIG 3. Severe incurvated medial and lateral nail plates (pincer nail).

224 Curr Probl Dermatol, July/August 2001
plate that can cause hypertrophy and discoloration.Loss of protective sensation predisposes the nail plateto increased pressure and trauma from improper fittingshoes or compression of the nail unit.59
In a diabetic patient, because of the possibility ofperipheral neuropathy, it may not always be possibleto obtain an accurate history of trauma to the nail unit.Splinter hemorrhages can be associated with repetitivemicrotrauma. It is important to examine for digitalthrombi that have an increased incidence in elderly anddiabetic patients. Preliminary studies have demonstrat-ed slower growth of the nail plate in diabetic patientswith impaired lower extremity peripheral circulation.Also peripheral vascular disease can have an influenceon nail plate structure, including the thickness andopaqueness of the nail plate.60
An individual may receive a variety of medications,some of which may be associated with nail changes.Medications such as antibiotics and chemotherapeuticagents may be associated with nail changes.61,62
Diagnosis of OnychomycosisDistal and Lateral Subungual Onychomycosis. The
nail plate and the surrounding nail unit should be wipedclean with an alcohol swab. The distal-most portion ofthe nail plate should be discarded, thereby reducing thepossibility of contaminant inoculum. The diseased nailbed and the undersurface of the nail plate may be sam-pled with a variety of instruments, including a dual nailnipper, a 2-mm curette, or a number 15 scalpel blade.63-
66 Viable inoculum is most likely to be encounteredproximally near the junction between diseased andnormal-appearing nail. Whole nail clippings are notideal for light microscopic examination or culture andshould be reduced to a smaller size. Diabetic patientsmay have peripheral neuropathy, and therefore thesample should be obtained cautiously to ensure that thepatient does not incur trauma to the nail unit.67
Superficial Onychomycosis. The surface of the nailshould be disinfected with an alcohol swab. The ony-chomycosis affects the superficial surface, which maybe scraped off by use of a number 15 blade or curette.
Proximal Subungual Onychomycosis. After the sur-face of the nail is disinfected, the healthy uninvolvednail can be scraped off with a number 15 blade orcurette until the diseased proximal nail bed is reached.At this point the diseased nail plate and bed can besampled.
Endonyx and Total Dystrophic Onychomycosis. Theprocedure followed is similar to that for distal and lat-
eral onychomycosis. However, in endonyx onchomy-cosis no subungual debris would be expected.
Microscopic Examination. Direct microscopic ex-amination is an effective way to screen for the pres-ence of fungal organisms. False-negative results mayoccur in 5% to 15% of instances.66 The nail specimenmay be mounted in 20% to 30% potassium hydroxide(KOH) mixed with 5% glycerol and heated to emulsifylipids. Alternatively, a mixture of 20% KOH and 36%dimethyl sulfoxide can be used. A positive result ondirect microscopy signifies the presence of onychomy-cosis but does not reveal the identity of the organismor give an idea about its viability.
A KOH specimen is easier to interpret if a counter-stain such as chlorazol black E or Parker’s blue-blackink (1 part KOH/1 part ink) is used.68 Visualization isenhanced because chlorazol black E, which is chitin-specific, stains hyphae blue-black in color. Two tech-niques that may be used if a fluorescent microscope isavailable include the calcofluor white technique andthe Congo red technique. For a classification of struc-tures visualized under direct light microscopic exami-nation, the reader is referred to specialized texts.69-73
Culture. The identity of fungal nail pathogens canbe obtained by inoculating the sample onto a suitableculture medium and incubating the sample at 25°C to28°C. One medium that may be used is Sabouraudpeptone-glucose agar with cycloheximide and chlor-amphenicol. This may be available commercially asMycobiotic (Difco Laboratories, Detroit, Mich) andMycosel (BBL, Becton-Dickinson, Cockeysville, Md).66
Antibacterial agents such as chloramphenicol, chlorte-tracycline, and gentamicin inhibit bacterial overgrowth;cycloheximide inhibits molds. A cycloheximide-freemedium, such as Sabouraud glucose agar, Litmannoxgall medium, or inhibitory mold agar, should beused in addition to a cycloheximide-containing medi-um, especially because nondermatophyte molds oryeasts other than C albicans may be etiologic agents.66
The Dermatophyte Test Medium contains cyclohex-imide and chloramphenicol and is used by some physi-cians to screen for the presence of dermatophytes.74
When there is growth of a dermatophyte, alkalinity isgenerated that induces the phenol red indicator to turna red color. However, false-positive results can occurwhen some nonpathogenic fungi such as T terrestreinduce a similar color change. A false-negative reactionmay occur with some Microsporum sp and isolatescontaminated by bacteria. Another disadvantage of thedermatophyte test medium is that conidium develop-

Curr Probl Dermatol, July/August 2001 225
ment is not optimal, and visualization of colony reversepigmentation is difficult, thereby preventing identifica-tion of the causative fungal organism.75-77
Histopathologic Examination. Histologic techniquescan help demonstrate the presence of fungal organismsin the nail plate and subungual debris.78-80 The distrib-ution and density of the fungi, but not their identity,can be evaluated. Histologic specimens stained withperiodic acid-Schiff provide evidence of the invasive-ness of the fungal organisms. It may be possible toobtain an idea of the nature of the organism; for exam-ple, dermatophytes have regular, straight, septate hyphae;yeasts may appear as groups of cells or pseudohyphaepresent in an irregular distribution; and nondermato-phyte molds can have irregularly shaped hyphae.Bacteria can also be identified through periodic acid-Schiff staining methods.
Immunohistochemistry. Immunohistochemistry en-tails use of appropriate antibodies to the different fungalorganisms, thus enabling the hyphae to be labeled.81,82
In this manner the organism’s identity, location, anddensity could be confirmed. This technique could beused to demonstrate the presence of two or more inva-sive fungal organisms. Also, it would be possible todistinguish between an organism present on the nailsurface as a contaminant and one causing invasive dis-ease. Immunohistochemistry is currently a researchtechnique that is not widely available.
Flow Cytometry. With the use of flow cytometry,distinct “fingerprints” are produced for each fungalorganism.81,82 This technique provides informationabout the family to which the organism belongs andthe amount of fungal pathogen that is present. This isalso a research technique that is not widely available.
Use of the Newer Oral AntifungalAgents to Treat Onychomycosis and theOther Dermatomycoses
The new oral antifungal agents, itraconazole, terbi-nafine, and fluconazole, have provided significant
August 2001
advances in the treatment of superficial mycoticinfections.83-95 For many infections, a novel treatmentregimen relates to (1) an optimal pharmacokineticprofile (Table 1), (2) a shorter course of therapy, (3) highefficacy, and (4) a favorable safety profile. The efficacyof intermittent therapy regimens have been substantiat-ed, especially with the triazole agents. Continuous ther-apy is the preferred mode with terbinafine.
Pharmacokinetics of Itraconazole. The serum con-centration of itraconazole is influenced by severalparameters, including food and gastric acidity. Theamount of drug absorbed is markedly increased whenthe drug is administered postprandially.96,97 The ab-sorption and bioavailability of itraconazole depend onsaturation of the first-pass metabolism process thattakes place in the liver.98,99 In the plasma almost all(99.8%) of the itraconazole is bound to plasma pro-teins, mostly albumin. Itraconazole binds extensivelyto tissues, with some having concentrations 2 to 20times higher than the simultaneous concentration inthe plasma.99 The pharmacokinetic variables of itra-conazole are not affected in patients with renal insuffi-ciency and those undergoing hemodialysis.99 Absorp-tion is decreased in patients with neutropenia and inpatients with AIDS as a result of gastric hypochlorhy-dria.100
Pharmacokinetics of Fluconazole. The pharmaco-kinetic parameters of fluconazole are comparable aftereither intravenous or oral administration.101 There isextensive absorption (>90%) of drug that is similar inboth the postprandial and fasting states and is not de-pendent on stomach acidity.96,102 Fluconazole is onlyweakly bound to plasma proteins, with about 90% ofthe drug circulating free in the plasma. The drug appearsto be resistant to hepatic metabolism; approximately80% of fluconazole is excreted unchanged in urine, with2% in feces and about 11% as metabolites in urine.103
The levels of fluconazole in cerebrospinal fluid, saliva,vaginal tissue, sputum, skin, and blister fluid are com-parable with or exceed the simultaneous plasma con-centration.104 Decreased plasma clearance of the drug
onchomy-d.copic ex-the pres-
sults mayspecimen
hydroxide emulsifyand 36%result on
nychomy-organism
a counter-lue-blacklization isis chitin-
Two tech-roscope isnique andn of struc-ic exami-exts.69-73
ogens cana suitable
at 25°C toabouraudnd chlor-rcially as
Mich) andle, Md).66
l, chlorte-ergrowth;mide-freeLitmann
hould beng medi-molds oragents.66
cyclohex-me physi-ophytes.74
kalinity isor to turncan occur
T terrestree reactiond isolatesage of the
develop-
TABLE 1. Pharmacokinetic comparison of the new oral antifungal agents, itraconazole, terbinafine, and fluconazole
Itraconazole Terbinafine Fluconazole
Skin penetration Rapid (hours) Rapid (hours) Rapid (hours)Nail penetration 7-14 days 7-14 days <7 daysPost-therapy reservoir (epidermis) 2-4 weeks 2-4 weeks 16 daysPost-therapy reservoir (nail plate) 9 months 9 months 6 monthsHalf-life (serum) 64 ± 32 hours Distribution half-life 1.5 hours; elimination 30 hours
half-life 22 hours and 90 hours

226 Curr Probl Dermatol, July/August 2001
is seen in patients with liver cirrhosis and renal impair-ment, leading to delayed elimination.105
Pharmacokinetics of Terbinafine. Terbinafine iswell absorbed from the gut and extensively bound toplasma proteins. More than 99% of the drug is boundto albumin and lipoprotein fractions, including low-density lipoprotein, very low–density lipoprotein, andhigh-density lipoprotein.106,107 Terbinafine is highlylipophilic and keratinophilic and is therefore widelydistributed throughout skin and adipose tissue via der-mal-epidermal passive diffusion and sebum transport.The concentration of terbinafine is highest in sebumand hair samples compared with the simultaneous con-centration in plasma.108
Terbinafine is extensively biotransformed by the liver,mostly through oxidation into 15 metabolites. Morethan 80% of this drug is excreted in urine; the rest iseliminated with feces.106,107 In patients with renalinsufficiency, the absorption and distribution of terbina-fine are not affected, whereas elimination tends to beslower than in healthy individuals.106,108
The Treatment of Onychomycosis and OtherDermatomycoses by Use of Itraconazole, Terbinafine,and Fluconazole. The following summarizes suggest-ed treatment regimens with the three newer agents onthe basis of clinical studies and disease safety issuesrelated to adverse reactions and potentially significantdrug interactions.106-128
ItraconazoleItraconazole is effective in the treatment of dermato-
phyte infections of the skin, hair, and nails, Candida spinfections of skin and nails, tinea versicolor, and pity-rosporum folliculitis.127-132 In studies treating cuta-neous dermatoses, cure rates with itraconazole haveusually been determined 2 to 4 weeks after therapy. Finalcure rates in onychomycosis trials have usually beendetermined at 6 months after therapy for fingernailsand 9 months after therapy for toenails.
Tinea Corporis/Cruris/Pedis/Manus. In earlierstudies where itraconazole was used to treat cutaneousdermatophyte infections, lower daily doses and longerdurations of therapy were administered.133-135 Inter-mittent (pulse) regimens with higher daily doses usedfor shorter durations of therapy were subsequently shownto provide comparable or superior efficacy.136-141 Mostcutaneous infections respond to a 7-day course of ther-apy (single pulse); the daily dose varies with the siteand type of infection.86
A clinical response of approximately 90% and a
mycologic cure rate of 77% have been reported inassociation with the use of itraconazole 200 mg dailyfor 7 days for tinea corporis and cruris (n = 354).86
Comparable efficacy with 100 mg daily may require a15-day course of therapy.
Treatment of tinea pedis/manus with itraconazole200 mg administered twice daily for 7 days hasdemonstrated a clinical response of 90% and a myco-logic cure rate of 76% (n = 220).88 Other regimensused before the 1-week schedule were 100 mg dailyfor 30 days or 200 mg daily for 15 days.
Tinea Versicolor. Itraconazole 200 mg administereddaily for 7 days is effective for tinea versicol-or129,130,142-144; a clinical response of 94% and myco-logic cure rate of 89% have been reported.129 Highercure rates are achieved with a total dosage of at least1000 mg compared with a cumulative amount that isless than 1000 mg.130
Majocchi’s Granuloma. Itraconazole 200 mg ad-ministered twice daily for 7 days effectively cleared 7patients with Majocchi’s granuloma.120 In some cases,a second pulse of therapy may be needed 2 to 3 weeksafter completion of the first pulse.
Onychomycosis (Dermatophytes). Earlier trials wereat lower doses (50 to 100 mg) administered daily untilcure of fingernail and toenail disease. Subsequent stud-ies evaluated continuous and intermittent (pulse) dos-ing regimens for shorter durations of therapy.145 Theseregimens proved to be associated with higher curerates for both fingernail and toenail onychomycosis.
Short-course continuous therapy uses itraconazole200 mg administered daily for 12 weeks for toenailsand 6 weeks for fingernails.146 Intermittent (pulse)itraconazole uses repetitions of 200 mg twice daily for1 week of each month; consecutive pulses are separat-ed by a rest period of 3 weeks off the drug. Two puls-es are generally recommended for fingernail ony-chomycosis and three pulses for toenail disease. Fortoenails with dermatophyte onychomycosis, the myco-logic cure rate at follow-up 12 weeks from the start oftreatment with 3 to 4 pulses ranges from 38.3% to100%.147-160
Onychomycosis (Nondermatophytes). Itraconazolemay be effective for the treatment of onychomycosiscaused by some nondermatophyte molds, includingAspergillus sp, Scopulariopsis brevicaulis, Fusariumsp, and Alternaria sp.161 Continuous therapy withitraconazole 200 mg administered daily for 6 weeks iseffective for Candida sp fingernail onychomycosis.162
The pulse regimen may be effective for fingernail and

Curr Probl Dermatol, July/August 2001 227
toenail onychomycosis associated with Candidasp.163
Tinea Capitis. Itraconazole has been found to beeffective and safe when used to treat tinea capitis.
FluconazoleFluconazole has been reported to be effective for the
treatment of dermatophyte infections of the skin, hairand nails, cutaneous candidiasis, and tinea versicol-or.164-182 Many studies have evaluated once-weeklyintermittent therapy that was continued until clearanceof infection or for a maximum duration of up to 12months for toenail onychomycosis or 4 to 6 weeks forskin infection.
Tinea Corporis/Cruris/Pedis/Manus. Intermittentfluconazole 150 mg administered once weekly and re-peated for 2 to 4 weeks has been shown to produce amycologic cure rate of 78% to 93% for tinea cor-poris/cruris.166-172 A comparative study of 150 mg ad-ministered once weekly for up to 4 weeks and 50mg/daily for 4 weeks produced similar clinical andmycologic results.172 The intermittent regimen pro-duced a clinical response rate and mycologic cure rateof 91% for tinea corporis (n = 23) and a clinical re-sponse rate and mycologic cure rate of 100% for tineacruris (n = 14) at follow-up 1 month after therapy.172
In tinea pedis fluconazole 150 mg administered onceweekly for up to 6 weeks provided a mycologic curerate of 67% to 92%.169,171-173
Cutaneous Candidiasis. The data with intermittentfluconazole for cutaneous candidiasis are more limit-ed.171,172
Tinea Versicolor. A single dose of fluconazole 400mg produced clinical cure in 74% of patients exam-ined up to 6 weeks after therapy (n = 23).165 Anotherstudy evaluated fluconazole 600 mg administered dailyfor 15 days (n = 27).174 A clinical cure rate of 80% andmycologic cure rate of 88%, with a recurrence rate of14% were noted at 3 months after therapy.174
Onychomycosis (Dermatophytes). The dosage gen-erally used to treat onychomycosis is 150 mg adminis-tered once weekly until the abnormal-appearing nailhas grown out. This may take 4 to 9 months for fingernails and 9 to 12 months for toenails. Studies havebeen performed examining the efficacy of fluconazolefor treating toenail onychomycosis, with a range ofmycologic cure rates from 51% to 87%.176-181 In somepatients, adjunctive topical or surgical therapy wasused.176 A dosage finding study evaluated 150 mg (n =79), 300 mg (n = 75), and 450 mg (n = 80) of flucona-
August 2001
zole administered once weekly for a duration of therapyup to 12 months.179 Clinical success at 6 months aftertherapy in the 150-mg, 300-mg, and 450-mg groupswas reported as 77%, 79%, and 86%, respectively. Atthe end of treatment, the mycologic cure rate was re-corded as 47%, 59%, and 62%, respectively.179 Thetime to mycologic cure was 10.1 months in the 150-mg group, 8.8 months in the 300-mg group, and 9.6months in the 450-mg group.
Evaluation of nail plate concentrations of flucona-zole during and after once-weekly intermittent therapywith 150 mg, 300 mg, or 450 mg indicated persistenceof drug for 6 months after therapy.110 Nail plate levelsdeclined by half within 2.5 months, 2.4 months, and3.7 months, respectively.
Tinea Capitis. Fluconazole has been found to beeffective and safe when used to treat tinea capitis.
TerbinafineTerbinafine is effective in the treatment of dermato-
phyte infection of the skin, hair, and nails.182 Whengiven orally terbinafine is not effective against tineaversicolor; however, the topical and solution formula-tions are effective against this infection caused byMalassezia sp. In studies treating cutaneous derma-toses, cure rates with terbinafine have generally beendetermined 2 to 4 weeks after therapy. Final cure ratesin onychomycosis trials have usually been determinedat 6 months after therapy for fingernails and 9 monthsafter therapy for toenails.
Tinea Corporis/Cruris/Pedis/Manus. When used totreat tinea pedis, the regimen is 250 mg/d administeredfor 2 to 6 weeks, with mycologic cure rates at follow-up ranging from 71% to 100% (n = 90).183-190 Thedosage regimen for the treatment of tinea corporis is250 mg/d given for 2 to 4 weeks, with mycologic curerates at follow-up ranging from 68% to 100% (n =390).191-195
Onychomycosis (Dermatophytes). Terbinafine iseffective in the treatment of dermatophyte onychomy-cosis. The dosage regimen for fingernails and toenailsis 250 mg/d given for 6 and 12 weeks, respectively.When used for treating toenails, the mycologic curerate 12 months from the start of treatment varies from39.6% to 100%.* In comparative trials of dermatophytetoenail onychomycosis the mycologic cure rates are asfollows: itraconazole (pulse) vs terbinafine, 38.3% vs
ported inmg daily= 354).86
require a
aconazoledays has
d a myco-regimensmg daily
ministeredversicol-
nd myco-29 Higherof at leastunt that is
0 mg ad-cleared 7me cases,o 3 weeks
rials weredaily untiluent stud-ulse) dos-145 These
gher curemycosis.aconazoler toenails
nt (pulse)e daily fore separat-Two puls-nail ony-ease. For
the myco-he start of38.3% to
aconazoleomycosisincludingFusariumapy with
6 weeks isycosis.162
ernail and *References 117, 147-149, 153, 180, and 196-207.

228 Curr Probl Dermatol, July/August 2001
75.0%,153 itraconazole (pulse) vs terbinafine, 75.0 vs94.1%,158 itraconazole (pulse) vs terbinafine, 75.0%vs 76.%,147 and fluconazole vs terbinafine, 51.3% vs81.9%.180
Onychomycosis (Nondermatophytes). Terbinafinemay be effective in the treatment of some nonderma-tophyte mold onychomycosis.211,212 When usedagainst Candida sp, terbinafine may be more effectiveagainst C parapsilosis compared with C albicansinfections.208,209 In general, when terbinafine is usedagainst Candida sp, the dosage required may be high-er or the duration longer compared with its efficacyagainst dermatophytes.
Majocchi’s Granuloma. Terbinafine 250 mg/d givenfor 2 to 4 weeks has been reported to be effective in 2patients.213
Tinea Capitis. Terbinafine has been found to beeffective and safe when used to treat tinea capitis.
Other Dermatophytosis. Terbinafine has also beenshown to be effective against tinea imbricata,214 cuta-neous sporotrichosis,215 and black piedra.216
Factors Affecting the Response ofOnychomycosis of the Toenails to OralAntifungal Therapy
A body of evidence has accumulated that allows usto try and identify the factors associated with a subop-timal response to therapy with the new oral antifungalagents for onychomycosis of the toenails. The multiplefactors can be divided into genetic, environmental,systemic disease, and intrinsic nail characteristics.217
An understanding of the factors that may lead to sub-optimal response and decrease the rate of relapse ofonychomycosis might help improve the cost-effective-ness of new treatments for this chronic infection.
Genetic Predisposition. There may be a genetic pre-disposition to the development of tinea pedis and ony-chomycosis. An autosomal dominant trait of transmis-sion has been proposed for families predisposed to Trubrum infection.2 The practical implication of thiswould be early recognition and treatment of tinea pedisinfection before onychomycosis develops.
Age and Sex. In the general population the preva-lence of onychomycosis depends on the age and sex ofthe individual and has been reported to be 2% to8.4%.1,218-220 Onychomycosis is more frequent in indi-viduals older than 40 years.1 Men may be more likelyto have onychomycosis, possibly because of hormonaldifferences between the sexes.221 Children are less likely
to have onychomycosis compared with adults.222,223
The prevalence of the disease in children 18 years oryounger is between 0.16% and 0.3%.222-225
Presence of Concomitant Tinea Pedis. The inci-dence of onychomycosis correlates with the prevalenceof tinea pedis in some studies226-228 and has been re-ported to be significantly higher in individuals who livein a community setting or use communal washing facil-ities or swimming baths. Walking bare foot or sharingshoes that have high density of spores may predisposea healthy foot to fungal inoculum from skin scales andfragments shed by infected individuals.229 The lengthof the incubation period between inoculation, coloniza-tion, and invasion of fungal organisms leading to clini-cally evident onychomycosis is not known.
Environmental Factors. A number of environmentalfactors may play an important role in facilitating tineainfection and onychomycosis. A hot and humid micro-environment created by wearing shoes for prolongedperiods of time, tight shoes predisposing to pressure,and microtrauma to the feet have been shown to pre-dispose to the infection.226 It is not easy, however, toestablish tinea infection in subjects with completelynormal feet.230 In one study, the conditions for infec-tion were a heavy inoculum and a persistently wet en-vironment. The positive infectivity rate was at bestabout 50%, and infections tended to be transient andself-limiting.230
Immunosuppression. Certain patients with dermato-phyte infections may have a failed therapy, exhibit achronic course of the disease, or experience relaps-es.231,232 Although the exact relationship between theunderlying disease and dermatophyte infection is notclear, chronic infection with T rubrum may be associ-ated with atopy,233 diabetes mellitus,234 Cushing’s syn-drome,235 and lymphoma.236
It has been shown that 47% of patients chronicallyinfected with T rubrum had immediate hypersensitivi-ty responses to the intradermal Trichophyton test, 5%of patients had delayed type responses, and 11% of allpatients demonstrated both types of immune re-sponse.237
Besides T rubrum, the second most common causa-tive agent of onychomycosis in North America is Tmentagrophytes. Usually T mentagrophytes causes WSObut may also be associated with other types of ony-chomycosis, the vesicular type of tinea pedis, andinvolve the interdigital spaces or the arch of the foot.
Immunodeficiency. Patients with severe secondaryimmunodeficiency caused by human immunodeficiency

Curr Probl Dermatol, July/August 2001 229
virus (HIV) are more predisposed to superficial fungalinfection and onychomycosis compared with the gen-eral population. In individuals with a helper T-lym-phocyte count (CD4) of less than 400/mm3 (normalrange 1200 to 1400), the prevalence of onychomycosisis higher than the general age- and sex-matched popu-lation. PSO is considered to be suggestive of HIV dis-ease,17-21 although it has also been observed in otherimmunocompromised patients such as transplant re-cipients.24 In immunocompetent individuals, WSO isgenerally due to T mentagrophytes; in HIV-seroposi-tive patients the causative organism for WSO is morelikely to be T rubrum.238 Also, “one hand two feet”tinea infection, which is relatively uncommon in thegeneral population, is more likely to be present inpatients with HIV infection.238
Diabetes Mellitus. Patients with diabetes mellitus aremore likely to have development of onychomycosiscompared with the general population.8 In one study,onychomycosis was present in 26.2% of diabeticpatients (n = 550).8 After controlling for age and sex, therisk odds ratio for patients with diabetes to have ony-chomycosis of the toes was 2.77 times compared withnormal age- and sex-matched nondiabetic patients.8 Astepwise logistic regression demonstrated that signifi-cant predictors for onychomycosis included a family his-tory of onychomycosis, concurrent intake of immuno-suppressive therapy, and peripheral vascular disease.8
Psoriasis. The most prevalent papulosquamous dis-ease in the United States is psoriasis, affecting 2% ofthe US population. In patients with psoriasis, the pres-ence of an abnormal nail does not necessarily mean thatpsoriasis of the nail plate is causing the nail abnormal-ity; the possibility of onychomycosis coexisting withpsoriasis should be considered.239 In some instances,the nail abnormality may be due to onychomycosisalone. The odds of patients with psoriasis having ony-chomycosis was 56% greater than patiens without pso-riasis of the same age and sex (P = .02) in the sampleof 561 patients with psoriasis.239
Local Factors. Local factors play a role in modu-lating the response to the oral antifungal agentadministered for the treatment of toenail onychomy-cosis.217,240-244 To achieve the minimum inhibitory con-centration in the keratin of the affected nail plate, theantifungal agent has to be delivered by the circulationto the matrix site, the growth zone of the nail, or viadiffusion at the nail bed site. Poor penetration of theoral antifungal agent to the lateral nail plate from theunderlying nail bed may be present because of reduced
August 2001
adhesion between the lateral nail bed and the overly-ing nail plate.240
Patients appear to respond better to oral antifungaldrugs when there is minimal onycholysis. Possibly,there is reduced delivery of the drug from the nail bedto the ventral surface of the nail plate when extensiveonycholysis is present.242
Another presentation that may be a predictor of pooroutcome is the presence of a dermatophytoma, that is,a longitudinal yellow or whitish streak or spike alongthe nail plate or an oval-shaped mass in the middle ofthe nail.217,244 Usually, when this streak or mass is re-moved, it reveals a thick hyperkeratotic mass consis-tent of a dense collection of dermatophyte hyphae.244
A possible explanation of lower cure rates in suchpatients is that inadequate drug levels are reachedwithin the fungal mass. A logical therapeutic option isto surgically remove such a lesion.
When there is a total onychodystrophy involving thenail matrix, then optimal treatment may require a longercourse of continuous therapy or more pulses of inter-mittent treatment, compared with what would be suffi-cient to cure onychomycosis involving less than 75%of the nail plate and associated nail bed.154 A similarrecommendation may be true for onychodystrophicnails thicker than 2 mm compared with nails of normalthickness.242,243
Preexisting trauma to the nail unit leading to the per-manent dystrophy of the nail plate might be the reasonwhy the nail does not appear clinically normal evenafter a recommended course of oral antifungal therapyand in spite of negative mycologic study results (lightmicroscopy and culture).242,243 The patient has to becounseled about realistic expectations after oral anti-fungal therapy for pedal onychomycosis so that thereis an understanding that mycologic cure may notalways equate with clinical cure.217
Correct clinical diagnosis and mycologic confirma-tion of onychomycosis are essential to select theappropriate antifungal agent.217 There should be anappreciation of the factors that may predispose to ansuboptimal response to therapy so that extra antifungaltherapy can be administered, if clinically appropriate.
Safety Issues with the New OralAntifungal Agents (Itraconazole,Terbinafine, and Fluconazole)
Overall, the three newer oral antifungal agents areassociated with excellent safety profiles, especially
ults.222,223
8 years or
The inci-revalence been re-
s who livehing facil-or sharingredispose
scales andhe lengthcoloniza-g to clini-
ronmentalting tinea
mid micro-prolongedpressure,
wn to pre-wever, to
ompletelyfor infec-y wet en-
as at bestnsient and
dermato-exhibit a
ce relaps-tween theon is not
be associ-ing’s syn-
hronicallyrsensitivi-n test, 5%1% of all
mune re-
on causa-erica is Tuses WSOs of ony-edis, andthe foot.
secondarydeficiency

230 Curr Probl Dermatol, July/August 2001
with regimens used to treat superficial mycotic infec-tions.148,149,245-252 With each of the three oral antifun-gal agents, the attributable risk of adverse events isapproximately 5% to 10%.116,117,148,149,179 The risk ofdiscontinuation of therapy because of adverse reac-tions is low with itraconazole, terbinafine, and flu-conazole.245-248
Gastrointestinal and Nervous System. Most reac-tions are minor side effects such as gastrointestinalupset and headache, reported to occur with these agentsat rates only slightly higher than with placebo. Re-versal generally occurs on discontinuation of therapy.Taste change and taste loss have been reported in asso-ciation with terbinafine use in up to 2.7% of patientscompared with 0.8% in placebo.117 Changes in tastetend to develop early within the first few weeks oftherapy, whereas taste loss more often occurs after 1 to2 months of use.247,248 Women are affected more com-monly than men.249 Taste disturbance usually reverseswithin 2 to 10 weeks of stopping terbinafine.
Hepatic Reactions. The incidence of asymptomatichepatic enzyme elevations associated with the neweragents by use of regimens to treat superficial fungalinfections are generally less than 4%.88,117,179 Sporadicreports of reversible symptomatic hepatitis have beenreported in association with therapy with itraconazole,fluconazole, and terbinafine.148,149
Cutaneous Reactions. Transient skin eruptionsoccur in 2% to 4% of patients treated with itracona-zole, fluconazole, and terbinafine.148,149 The reactionsare generally reversible on discontinuing the oral anti-fungal agent.250 Serious cutaneous reactions have beenvery rarely reported with the new oral antifungal agents,itraconazole, terbinafine, and fluconazole.
Laboratory MonitoringSuggested laboratory monitoring guidelines for mon-
itoring of potential hepatic or hematologic reactions aregiven in the product monographs.116,117 The monitoringof the oral antifungal agents during therapy varies quitewidely among physicians.253 Patients should be coun-seled about what to look for that may indicate theonset of hepatic or hematopoietic dysfunction.
Drug InteractionsThe subject of drug interactions related to oral anti-
fungal agents has been extensively reviewed else-where.254,255 There are contraindicated drugs with itra-conazole and fluconazole but none with terbinafine.Examples of potentially important interactions are list-ed in Table 2. It is important to obtain a complete drughistory because this may affect the choice of antifun-gal agent.
Approach to Treating Fungal Infectionsof the Lower Extremity in Patients withDiabetes Mellitus.
Introduction
The prevalence of diabetes mellitus is increasing inthe United States and the remainder of the world, withdevastating consequences to the lower extremity insome instances. Presently there is an estimated popu-lation of 16 million people with diabetes in the UnitedStates, and it is projected that there will be 300 mil-lion people with diabetes worldwide by the year2025.256 In the diabetic patient, complications includeneuropathy, nephropathy, and ophthalmic disease. Acomplication of diabetes is lower extremity amputa-tion.257 Dermatologic complications of the lowerextremities in diabetic patients include fungal infec-tions and hypohydrosis, and these are risk factors forincreased morbidity, including superficial ulceration.Proper management of diabetic dermatologic infec-tions can help reduce the potential for serious compli-cations.256-262
TABLE 2. Some potentially significant drug interactions with itra-conazole, fluconazole, and terbinafine*
Contraindicateddrugs in the
United States Cautions
Itraconazole Astemizole FelodipineCisapride NifedipineLovastatin CyclosporineOral midazolam DigoxinSimvastatin WarfarinTriazolamTerfenadinePimozideQuinidineDofetilide
Fluconazole Cisapride Astemizole†
Terfenadine CyclosporinePhenytoinOral sulfonylurea hypoglycemic
agentsWarfarin
Terbinafine NortriptylineWarfarin
*Partial list. Refer to product monographs and reference texts for more com-plete list.†No longer available in the Unites States and many other countries.
Curr Probl Dermatol, July/August 2001 231
Impact of Diabetes
In people with juvenile-onset diabetes, the dermato-logic manifestations vary. In the study by Yosipovitchet al,262 the average age of diabetic patients was 23.5years, with the average duration of insulin-dependentdiabetes mellitus being 13 years.262 The prevalencerate of cutaneous disorders in this population includedichthyosis (48%), tinea pedis (32%), and onychomy-cosis (6%).262 In a study performed in patients withnon-insulin-dependent diabetes, Litzelman et al258
reported an incidence of the following: onychomyco-sis (67%), tinea pedis (12.3%) interdigital infection(18.8%), ulceration (10.5%), and amputation (2.9%).A comparison of the studies by Litzelman et al258 andYosipovitch et al262 demonstrates a higher prevalencerate of onychomycosis in the patients with non-insulin-dependent diabetes.
In the study by Evans et al,263 comparing nondiabeticwith diabetic patients with podiatric disorders, no sig-nificant differences were observed between these pop-ulations. The diabetic patients had an average age of76 years with a mean disease duration of 14.5 years.The prevalence of tinea pedis was 9% in the nondia-betic group and 7% in the diabetic group. No differ-ence was demonstrated in the prevalence of onycho-mycosis between the nondiabetic and diabetic groupswith prevalence rates of 43% and 45%, respectively.263
The Dermatophyte Test Medium was used to confirmthe diagnosis of onychomycosis, and this may accountfor lower rates in this study.
The Diabetic FootIn the diabetic foot the classic triad of neurologic,
vascular, and immune system deficit are observed.Neurologic complications are the most common; for
August 2001
example, peripheral neuropathy may result in the lossof sharp-dull sensation and two-point discrimination.As a result, the diabetic patient loses the protectivethreshold that enables reaction to plantar stimuli andabnormal forces. Without this protective sensation,traumatic injury through repetitive or direct trauma maycause laceration or abrasions to the epidermis. Otherneurologic changes include motor function deficit inthe intrinsic muscles of the foot, which results in mus-cular imbalance between the long flexor and extensormuscles of the foot and leg. These imbalances maycause contraction of the toes, leading to hammer toesand increased plantar pressure under the ball of thefoot. The structural changes along with loss of sensa-tion result in undue pressure to the skin, leading tohyperkeratosis and epidermal breakdown. The auto-nomic nervous system is also affected, predisposing tohypohydrosis and fissuring in the diabetic foot. Theepidermal breakdown in diabetic patients can facilitatethe development of increased bacterial infections andcellulitis. In addition, autonomic deficit may causearteriovenous shunting as blood is diverted from theskin, with resultant decrease in wound healing. Neuro-logic abnormalities can be more serious than initiallyanticipated for the diabetic patient, because they maypredispose to cutaneous breakdown (Fig 4).
Vascular insufficiency is a major cause of diabetic
eruptionsitracona-reactionsoral anti-
have beengal agents,
for mon-ctions are
monitoringaries quite
be coun-dicate then.
oral anti-wed else-with itra-rbinafine.
ns are list-plete drugf antifun-
ectionss with
reasing inorld, withremity inted popu-he United300 mil-the year
ns includeisease. A
y amputa-he lowergal infec-actors forlceration.gic infec-s compli-
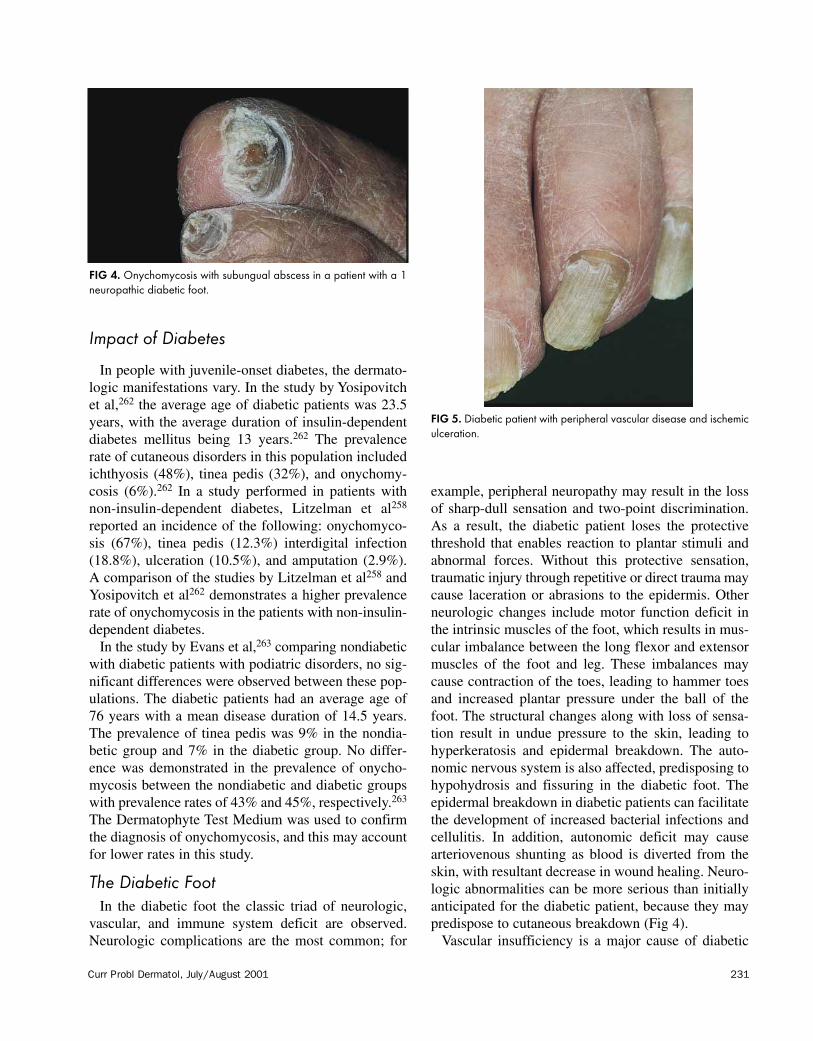
FIG 4. Onychomycosis with subungual abscess in a patient with a 1neuropathic diabetic foot.
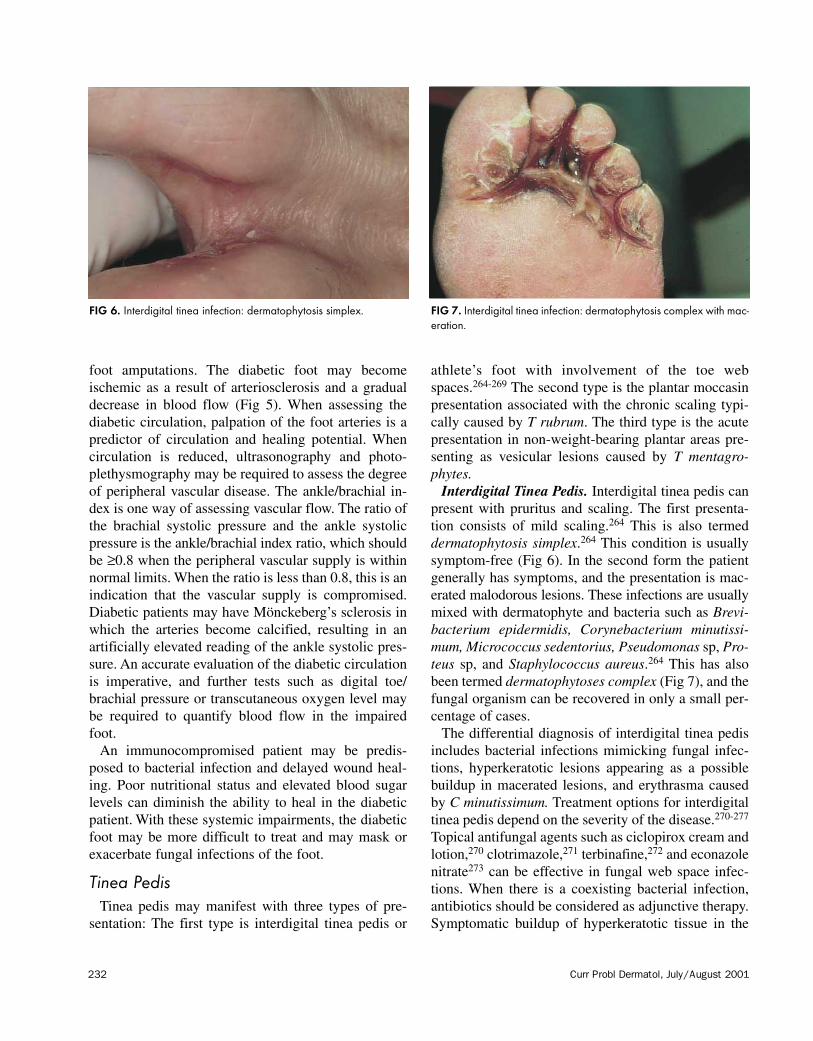
FIG 5. Diabetic patient with peripheral vascular disease and ischemiculceration.
232 Curr Probl Dermatol, July/August 2001
foot amputations. The diabetic foot may becomeischemic as a result of arteriosclerosis and a gradualdecrease in blood flow (Fig 5). When assessing thediabetic circulation, palpation of the foot arteries is apredictor of circulation and healing potential. Whencirculation is reduced, ultrasonography and photo-plethysmography may be required to assess the degreeof peripheral vascular disease. The ankle/brachial in-dex is one way of assessing vascular flow. The ratio ofthe brachial systolic pressure and the ankle systolicpressure is the ankle/brachial index ratio, which shouldbe ≥0.8 when the peripheral vascular supply is withinnormal limits. When the ratio is less than 0.8, this is anindication that the vascular supply is compromised.Diabetic patients may have Mönckeberg’s sclerosis inwhich the arteries become calcified, resulting in anartificially elevated reading of the ankle systolic pres-sure. An accurate evaluation of the diabetic circulationis imperative, and further tests such as digital toe/brachial pressure or transcutaneous oxygen level maybe required to quantify blood flow in the impairedfoot.
An immunocompromised patient may be predis-posed to bacterial infection and delayed wound heal-ing. Poor nutritional status and elevated blood sugarlevels can diminish the ability to heal in the diabeticpatient. With these systemic impairments, the diabeticfoot may be more difficult to treat and may mask orexacerbate fungal infections of the foot.
Tinea PedisTinea pedis may manifest with three types of pre-
sentation: The first type is interdigital tinea pedis or
athlete’s foot with involvement of the toe webspaces.264-269 The second type is the plantar moccasinpresentation associated with the chronic scaling typi-cally caused by T rubrum. The third type is the acutepresentation in non-weight-bearing plantar areas pre-senting as vesicular lesions caused by T mentagro-phytes.
Interdigital Tinea Pedis. Interdigital tinea pedis canpresent with pruritus and scaling. The first presenta-tion consists of mild scaling.264 This is also termeddermatophytosis simplex.264 This condition is usuallysymptom-free (Fig 6). In the second form the patientgenerally has symptoms, and the presentation is mac-erated malodorous lesions. These infections are usuallymixed with dermatophyte and bacteria such as Brevi-bacterium epidermidis, Corynebacterium minutissi-mum, Micrococcus sedentorius, Pseudomonas sp, Pro-teus sp, and Staphylococcus aureus.264 This has alsobeen termed dermatophytoses complex (Fig 7), and thefungal organism can be recovered in only a small per-centage of cases.
The differential diagnosis of interdigital tinea pedisincludes bacterial infections mimicking fungal infec-tions, hyperkeratotic lesions appearing as a possiblebuildup in macerated lesions, and erythrasma causedby C minutissimum. Treatment options for interdigitaltinea pedis depend on the severity of the disease.270-277
Topical antifungal agents such as ciclopirox cream andlotion,270 clotrimazole,271 terbinafine,272 and econazolenitrate273 can be effective in fungal web space infec-tions. When there is a coexisting bacterial infection,antibiotics should be considered as adjunctive therapy.Symptomatic buildup of hyperkeratotic tissue in the
FIG 6. Interdigital tinea infection: dermatophytosis simplex. FIG 7. Interdigital tinea infection: dermatophytosis complex with mac-eration.

Curr Probl Dermatol, July/August 2001 233
interdigital space may require debridement to reducepain and discomfort.
Moccasin Tinea Pedis. Moccasin tinea pedis causedby T rubrum may affect patients with long-term expo-sure to inoculum.274 The site of infection involves theplantar aspect extending to the dorsal-plantar junction.Other organisms that can cause moccasin tinea pedisinclude T mentagrophytes and Epidermophyton floc-cosum.
The differential of plantar tinea pedis includes chronicstasis dermatitis of the lower extremity caused byvenous insufficiency that extends beyond the plantarfoot and may present with fissures and ulceration.Psoriasis can manifest as patchy hyperkeratosis withscaling. A review of the past and family history may beof benefit. Hypohydrosis may present with similarfindings. The autonomic system in diabetic patients canbe denervated, resulting in decreased sweat production,which predisposes to dry skin. This condition is com-mon and needs to be differentiated from tinea pedis.
Treatments of tinea pedis include a variety of topicaland oral antifungal medications. Terbinafine 250 mg/dfor 1 to 2 weeks and itraconazole 400 mg/d for 1 weekin the pulse dosing protocol may be of benefit. Be-cause of the high recurrence rate of tinea pedis the useof powders and sprays can be helpful.139,276
Vesicular or Acute Tinea Pedis. The vesicular typegenerally involves a non-weight-bearing plantar aspectof the foot, commonly the medial arch. The skin spec-imen for KOH and culture examination should be per-formed from the roof of the vesicle; T mentagrophytesis the prominent organism cultured. A biopsy speci-men of the lesion may be required to confirm the diag-nosis. Contact dermatitis from allergens or irritantssuch as poison ivy or shoe material usually affects thedorsal aspect of the feet and is bilateral in presentation.Application of emollients may result in sensitization toperfumes, vitamin E, or other common additives.Pruritus and burning symptoms of contact dermatitismay be poorly recognized by the diabetic patient be-cause of neuropathy. Pustular psoriasis may presentwith diffuse redness, scaling, and lesions on the plan-tar aspect of the foot and palms; arthritis may be asso-ciated with the psoriasis.
Treatment modalities include topical and oral anti-fungal agents. Preventive care and education mustaccompany the treatment of tinea pedis infections; theuse of foot powders can reduce the risk for redevelop-ing infection.
August 2001
Treatment of Toenail Onychomycosis inDiabetic Patients
Onychomycosis has sometimes been referred to as acosmetic disorder, although mycotic infections of thenails can cause morbidity and reduce the quality of lifeand overall well being, especially in the diabetic patient.There are, to our knowledge, no published studies ex-amining the efficacy of the new oral antifungal agentsin treating toenail onychomycosis in diabetic patients.In the absence of such data, we suggest the followingapproach. Once the standard regimen for treating toe-nail onychomycosis has been completed, the patientshould return 6 to 9 months after the start of therapy.At that point, if clinically indicated, an extra pulse ofitraconazole or an additional month of terbinafinecould be administered.243
The adverse events in patients with diabetes melli-tus treated with terbinafine have been reported byPollak and Billstein.278 Of 77 patients with diabetesmellitus, 47 (61.0%) experienced one or more adverseevents. Those of definite or uncertain relationship toterbinafine were primarily of a gastrointestinal nature.Seven (9.1%) of the 77 patients had a serious adverseevent, but the investigators did not record a causalrelationship between the adverse event andterbinafine. Terbinafine is not known to have an inter-action with either insulin or the oral hypoglycemicdrugs.
The safety of itraconazole therapy for onychomyco-sis in diabetic patients has been reported by Albreskiand Gross.279 Fifty-two patients with onychomycosiswere randomly assigned to receive either itraconazoleor palliative therapy consisting of toenail trimming,cleaning, and soaking. Adverse events were reportedin 4 of 27 subjects treated with itraconazole (14.8%).One subject receiving itraconazole was withdrawnfrom the study because of elevated liver function testresults. In the other 3 patients the adverse events (rash,diarrhea, and pedal edema) were considered to be self-limiting and did not interfere with completion of thestudy. Separate analyses of prestudy and poststudyhemoglobin A1c and liver function levels in both thepalliative care and itraconazole treatment groups werecomparable, with no statistically significant differ-ences noted within the groups (P > .05). Data analysisperformed on the itraconazole group comparing pre-study and poststudy hemoglobin A1c levels, which re-flected the diabetic control, demonstrated a slightlyincreased trend in hemoglobin A1c levels in the oral
toe webmoccasinling typi-the acute
areas pre-mentagro-
pedis canpresenta-o termedis usuallyhe patientn is mac-re usuallyas Brevi-
minutissi-s sp, Pro- has also), and the
small per-
nea pedisgal infec-a possiblema causednterdigitalase.270-277
cream andeconazoleace infec-infection,e therapy.ue in the
ex with mac-

234 Curr Probl Dermatol, July/August 2001
hypoglycemic agent–controlled patients; this was notstatistically significant (P > .05).
The itraconazole package insert116 indicates thatsevere hypoglycemia has been reported in patientsconcomitantly receiving azole antifungal agents andoral hypoglycemics. However, the data from postmar-keting surveillance data over a period of 10 years280
suggest that there may be a lack of interaction betweenitraconazole and oral hypoglycemic agents that are notmetabolized through the CYP 3A4 system. In patientsreceiving itraconazole concomitantly with insulin oran oral antidiabetic agent, there were 14 reports sug-gestive of hyperglycemia and 9 reports of hypogly-cemia; most patients experienced no change in antidi-abetic effect.
Fluconazole is metabolized through the CYP 2C9pathway and to a lesser extent the 3A4 pathway.255
Severe hypoglycemia may be precipitated by the useof fluconazole with the oral hypoglycemic agents (eg,tolbutamide, glibenclamide, and glipizide) because theoral antifungal agent reduces the metabolism of theantidiabetic drugs.118 When fluconazole is used con-comitantly with these or other sulfonyl urea oral hypo-glycemic agents, blood glucose concentrations shouldbe carefully monitored, and the dose of the sulfonylurea should be readjusted as necessary.118
Conclusions Regarding the Treatment ofSuperficial Fungal Infections in DiabeticIndividuals
The diabetic patient undergoing treatment for ony-chomycosis may benefit from a team approach involv-ing an endocrinologist, podiatrist, and dermatologist.Once the fungal infection of the toenails has beencured, patient education is important to prevent rein-fection. Incorporating a preventive program of properdiabetic self-foot examination is extremely importantso early symptoms and signs of tinea pedis and ony-chomycosis can be identified by the patient and caregivers and treated appropriately at an early stage,thereby reducing the probability of secondary compli-cations from occurring.
Strategies to Improve Cure Rates in theTreatment of Onychomycosis
There should be mycologic confirmation of the clin-ical diagnosis of onychomycosis because a nonmy-cotic nail that has an abnormal appearance would not
be expected to improve after oral antifungal medica-tion.
Choice of Oral Antifungal AgentIn part this depends on the causative organism. Some
species of nondermatophyte molds, such as Scytalid-ium dimidiatum281 and possibly Onychocola canaden-sis,282 are resistant to the 3 newer oral antifungalagents, itraconazole, terbinafine, and fluconazole. Atthe moment there is only a limited role of standardizedantifungal susceptibility testing in evaluating the sen-sitivity of a causative dermatophyte to the differentantifungal agents. The assay approved by the subcom-mittee for antifungal susceptibility testing in 1997 isapplicable only for Candida sp infections.283 Work isin progress by a National Committee for ClinicalLaboratory Standards to develop susceptibility testingmethods for antifungal agents in dermatophytic infec-tions.
Measures Aimed at Optimizing Bioavailability ofDrug. For some oral antifungal agents it is recom-mended that the drug should be taken in a fed ratherthan a fasting state. Itraconazole capsules are absorbedbest when taken with a full meal. There is no such rec-ommendation for terbinafine or fluconazole.
Compliance with Regimen. Patients should be coun-seled about taking the correct amount of drug at theappropriate time points. It should be kept in mind thatthe preferred regimens for the 3 agents are itracona-zole (pulse therapy), terbinafine (continuous), and flu-conazole (once-weekly).
Potential for Drug Interactions to Reduce Bio-availability. The importance of obtaining a completedrug history from the patient and recognizing thatdrug interactions have the potential for decreasing orincreasing the plasma concentration of the antifungalagent cannot be underestimated. The amount of anti-fungal agent may be reduced at the site of the nailplate for reasons including the following: incom-plete absorption from the gastrointestinal tract (seeabove); distribution of drug to the anatomic site ofinterest (in this case the nail plate) is reduced, forexample, peripheral vascular disease may play a con-tributing role; induction of hepatic enzymes, forexample, with concomitant intake of a drug such asrifampin will reduce the plasma levels of the newantifungal agents. On the other hand an inhibitor ofthe cytochrome P450 3A4 enzyme system such asgrapefruit juice may increase the concentration ofitraconazole in the plasma.284 Drug interactions are

Curr Probl Dermatol, July/August 2001 235
generally predictable and therefore manageable inmany cases. Some drugs may be metabolized throughmore than one CYP 450 system, for example, war-farin has two enantiomers, with R-warfarin beingmetabolized by CYP 3A4 and CYP 1A2 and S-war-farin by CYP 3A4 and CYP 2C9.285-287
A Poor Mycologic and Clinical Response May BeAssociated with Suboptimal Concentrations of Anti-fungal Agent in the Nail Plate. With itraconazole theresponse is dependent on whether the itraconazoleconcentration in the nail plate is less than 100 ng/g,100 to 400 ng/g, or greater than 400 ng/g (verbal com-munication, Piet De Doncker, March 1999). We arenot aware of similar breakpoints being published forterbinafine. With fluconazole, a significant correlationwas observed between affected toenail steady-statefluconazole concentration and the clinical response atthe end of therapy.110 A significant correlation wasalso found for the cross-tabulation of global clinicalresponse (on the basis of response of all infected toe-nails) and affected toenail steady-state fluconazoleconcentration. At >7.5 µg/g there was a greater likeli-hood of improved response; however, no such correla-tion was seen between mycologic outcome and steady-state fluconazole concentration in affected nails.110
The concentration of 7.5 µg/g corresponds best with adose of 300 mg once weekly rather than the lower doseof 150 mg once weekly.
Because it is not a practical option to measure con-centrations of drug in the nail plate, one possibility isfor patients receiving itraconazole or terbinafine toreturn for reevaluation 6 to 9 months after the start oftherapy.243 The pharmacokinetic data indicate thatboth itraconazole and terbinafine may be detectable inthe toenail plate up to 12 months from the start oftherapy.112,146 In patients with dermatophyte pedalonychomycosis treated with itraconazole or terbina-fine, in whom the mycologic study result is still posi-tive 9 months from the start of therapy, there may bean advantage in treating this subgroup with an extrapulse of itraconazole or an extra 4 weeks of ter-binafine (depending on the drug used as initial thera-py).243
Physical Characteristics of the Nail Unit. The ap-pearance of the nail unit provides guidance about theneed for supplemental oral therapy or adjunctive mea-sures such as mechanical debridement.217,240,244
Patients with the following nail characteristics mayrequire oral antifungal therapy: slow outgrowth of nailplate (normal outgrowth of toenail plate is 1 mm/
August 2001
mo).217 Concomitant mechanical measures such asdebridement or excision of the affected nail plate maybe beneficial when: the nail plate is thickened (>2mm),217 lateral portion of the nail plate is diseased,extensive onycholysis and dermatophytoma (centrallongitudinal streak or central onycholytic mass be-tween the nail plate and the underlying nail bed).244
Strategies to Reduce the Rate ofReinfection/Relapse 242,243
With the introduction of the newer oral antifungalagents, it is possible to cure a greater proportion ofpatients with onychomycosis of the toenails comparedwith the era when griseofulvin alone was available.However, once cure of the disease has been achieved,it is important and prudent for the patient to take mea-sures to ensure that onychomycosis does not manifestagain.
When onychomycosis becomes clinically or myco-logically evident in a toenail that was regarded asbeing clinically and mycologically cured, then there is“recurrence” of onychomycosis. In some instances this
l medica-
sm. SomeScytalid-canaden-
antifungalnazole. Atndardizedg the sen-
differente subcom-n 1997 is3 Work isr Clinicalty testing
ytic infec-
ability ofs recom-
fed ratherabsorbedsuch rec-
d be coun-rug at themind thatitracona-
), and flu-
uce Bio-completezing thateasing or
antifungalnt of anti-f the nail: incom-tract (seeic site ofuced, foray a con-mes, forg such as
the newhibitor of
m such asration of
ctions are
TABLE 3. Measures to help prevent recurrence of onychomycosis243
1. Keep feet clean, cool, and dry.2. Wear socks made of cotton, wool, or similar absorbent material.3. Apply antifungal foot powders to shoes daily (eg, Zeasorb AF).4. Wear shoes of correct size and fit, and reduce biomechanical
stresses and microtrauma/macrotrauma to toenails; limit theuse of narrow-toed shoes and high heels.
5. Discard or rest footwear that may have a high density of fungalspores: old worn shoes, those worn without socks, or someoneelse’s shoes.
6. Avoid walking barefoot over surfaces that may have a high den-sity of fungal spores: carpeting, bathroom floors, showers,gymnasiums, locker rooms, and swimming baths. Wear san-dals or appropriate footwear, particularly when walking in anarea that may have a high density of fungal spores.
7. Keep toenails short, cutting them straight across. Do not roundout the edges.
8. Examine for and treat tinea pedis and other superficial mycoticinfections elsewhere on the body. Do not use the same clip-pers to cut normal and abnormal nails.
9. Family members and close friends/contacts should be treatedfor tinea pedis and onychomycosis.
10. Keep a high index of suspicion for recurrence of tinea pedis oronychomycosis: pruritus, erythema, maceration, vesicles involv-ing sole/toe web, or abnormal appearance in previously nor-mal-appearing nails.
11. Broad-spectrum topical antifungal treatments should be applied tonails and feet at appropriate times, such as when tinea pedis ispresent and also on a prophylactic basis. Also, 2% ketoconazoleshampoo can be applied to the feet once or twice a week as a pro-phylaxis for tinea pedis.

return of disease has been termed “relapse.” When dis-ease returns in a diseased nail that was successfullytreated and cured, there may be 2 possible explana-tions. First, when the patient was judged to be clini-cally and mycologically cured after treatment, therewere microscopic pockets or areas of the fungal organ-ism that were still present. With time the fungal burdenincreased and manifested either as clinical disease oras positive mycologic study result when the nail wassampled. This has been termed “relapse,” “recurrence,”or “delayed failure.”243,288-290 Second, the cause of thefungal organism of the now diseased nail that had beencured previously could be “reinfection” with the sameor different fungal organism compared with the initialcausative organism of onychomycosis. In other words,(Relapse or recurrence) = (Recurrence or relapse ordelayed failure) + Reinfection.
The rate of reinfection may be reduced if the patientis counseled about the following measures (Table
236 Curr Probl Dermatol, July/August 2001
3):243 (1) awareness of the symptoms and signs ofonychomycosis and tinea pedis realizing that tineapedis may predispose to onychomycosis, (2) recog-nizing that onychomycosis is an infectious diseaseand that the contagion may be spread to family mem-bers and other individuals, (3) noting that there maybe a genetic predisposition to onychomycosis andsome other chronic fungal syndromes, (4) takingappropriate measures to reduce the density of fungalorganisms that the foot comes into contact with. Thismay involve discarding, resting or disinfecting oldshoes, and (5) undertaking lifestyle modifications,such as taking measures to prevent microtrauma ormacrotrauma to the nail plate, in particular thehyponychium.
It is important for the patient to recognize the symp-toms and signs that may suggest early involvementwith tinea pedis and onychomycosis. Onychomycosisof mild severity is more likely to result in cure com-
TABLE 4. Dosage regimens for the treatment of tinea capitis in children298
Duration
Griseofulvin (continuous therapy with tablet or oral suspension, 125 mg/5 mL) 6 to 8 weeksMicrosize: 15-30 mg/kg/dayUltramicrosize: 8-17 mg/kg/day
Itraconazole (continuous therapy with capsules) Dosage: 5 mg/kg/day 2 to 4 weeks<10 kg: 50 mg/day or 5 mg/kg body weight/day10 to 20 kg: 1 capsule on alternate days21 to 30 kg: 1 capsule/day31 to 40 kg: 1 capsule/day or 1 capsule/day alternating with 2 capsules/day40 to 49 kg: 1 capsule/day alternating with 2 capsules/day or 2 capsules/day>50 kg: 2 capsules/day
Itraconazole (pulse therapy with capsules) During pulse therapy:* 5 mg/kg/day for 1 week 1 to 3 pulses>10 kg: 50 mg/day or 5 mg/kg body weight/day10 to 20 kg: 1 capsule on alternate days21 to 30 kg: 1 capsule/day31 to 40 kg: 1 capsule/day or 1 capsule/day alternating with 2 capsules/day40 to 49 kg: 1 capsule/day alternating with 2 capsules/day or 2 capsules/day>50 kg: 2 capsules/day
Itraconazole (pulse therapy with oral solution) During pulse therapy:* 3 to 5 mg/kg/day for 1 week 1 to 3 pulsesItraconazole oral solution (100 mg/10 mL)
Terbinafine (continuous therapy with tablets) 2 to 4 weeks<20 kg: 62.5 mg/day20-40 kg: 125 mg/day>40 kg: 250 mg/day
Fluconazole (tablet or oral suspension) 6 mg/kg given continuously or 8 mg/kg once weekly6 mg/kg/day 20 days6 mg/kg/day 2 weeks with an extra 1 week of
therapy two weeks later if clinically indicated when patient is evaluated 4 weeks from the start of therapy
5 mg/kg/day 30 days8 mg/kg once weekly 4 to 8 weeks
In many countries one or more of the above-mentioned agents may not be indicated for tinea capitis in children. This is a guideline only. An up-to-date referencesource must be consulted because the currently recommended treatment regimen may change as new data from clinical trials become available. With infectionsresulting from Microsporum sp, a longer duration of therapy may be required.*Pulse therapy is 1 week on active treatment and 3 weeks off drug.
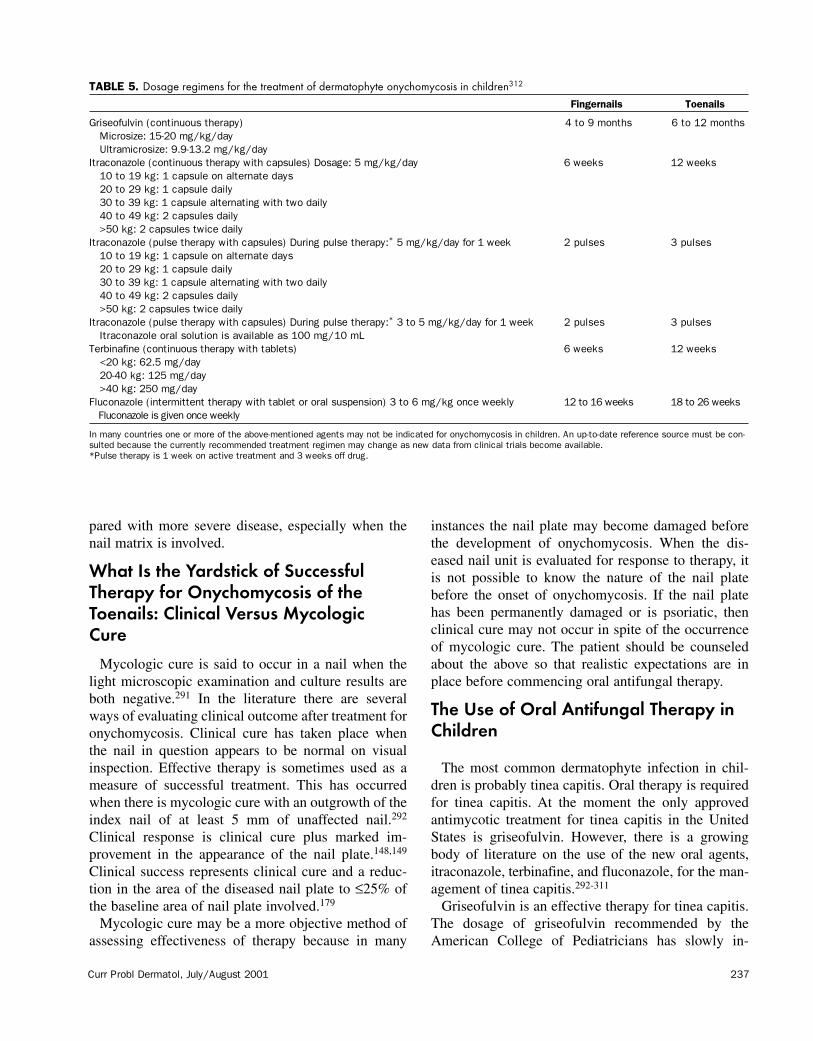
Curr Probl Dermatol, July/August 2001 237
pared with more severe disease, especially when thenail matrix is involved.
What Is the Yardstick of SuccessfulTherapy for Onychomycosis of theToenails: Clinical Versus MycologicCure
Mycologic cure is said to occur in a nail when thelight microscopic examination and culture results areboth negative.291 In the literature there are severalways of evaluating clinical outcome after treatment foronychomycosis. Clinical cure has taken place whenthe nail in question appears to be normal on visualinspection. Effective therapy is sometimes used as ameasure of successful treatment. This has occurredwhen there is mycologic cure with an outgrowth of theindex nail of at least 5 mm of unaffected nail.292
Clinical response is clinical cure plus marked im-provement in the appearance of the nail plate.148,149
Clinical success represents clinical cure and a reduc-tion in the area of the diseased nail plate to ≤25% ofthe baseline area of nail plate involved.179
Mycologic cure may be a more objective method ofassessing effectiveness of therapy because in many
August 2001
instances the nail plate may become damaged beforethe development of onychomycosis. When the dis-eased nail unit is evaluated for response to therapy, itis not possible to know the nature of the nail platebefore the onset of onychomycosis. If the nail platehas been permanently damaged or is psoriatic, thenclinical cure may not occur in spite of the occurrenceof mycologic cure. The patient should be counseledabout the above so that realistic expectations are inplace before commencing oral antifungal therapy.
The Use of Oral Antifungal Therapy inChildren
The most common dermatophyte infection in chil-dren is probably tinea capitis. Oral therapy is requiredfor tinea capitis. At the moment the only approvedantimycotic treatment for tinea capitis in the UnitedStates is griseofulvin. However, there is a growingbody of literature on the use of the new oral agents,itraconazole, terbinafine, and fluconazole, for the man-agement of tinea capitis.292-311
Griseofulvin is an effective therapy for tinea capitis.The dosage of griseofulvin recommended by theAmerican College of Pediatricians has slowly in-
signs ofthat tinea2) recog-s disease
mily mem-here maycosis and4) takingof fungal
with. Thiscting oldfications,rauma orcular the
the symp-volvementomycosis
cure com-
eek of if clinically s evaluated of therapy
ate referenceWith infections
TABLE 5. Dosage regimens for the treatment of dermatophyte onychomycosis in children312
Fingernails Toenails
Griseofulvin (continuous therapy) 4 to 9 months 6 to 12 monthsMicrosize: 15-20 mg/kg/dayUltramicrosize: 9.9-13.2 mg/kg/day
Itraconazole (continuous therapy with capsules) Dosage: 5 mg/kg/day 6 weeks 12 weeks10 to 19 kg: 1 capsule on alternate days20 to 29 kg: 1 capsule daily30 to 39 kg: 1 capsule alternating with two daily40 to 49 kg: 2 capsules daily>50 kg: 2 capsules twice daily
Itraconazole (pulse therapy with capsules) During pulse therapy:* 5 mg/kg/day for 1 week 2 pulses 3 pulses10 to 19 kg: 1 capsule on alternate days20 to 29 kg: 1 capsule daily30 to 39 kg: 1 capsule alternating with two daily40 to 49 kg: 2 capsules daily>50 kg: 2 capsules twice daily
Itraconazole (pulse therapy with capsules) During pulse therapy:* 3 to 5 mg/kg/day for 1 week 2 pulses 3 pulsesItraconazole oral solution is available as 100 mg/10 mL
Terbinafine (continuous therapy with tablets) 6 weeks 12 weeks<20 kg: 62.5 mg/day20-40 kg: 125 mg/day>40 kg: 250 mg/day
Fluconazole (intermittent therapy with tablet or oral suspension) 3 to 6 mg/kg once weekly 12 to 16 weeks 18 to 26 weeksFluconazole is given once weekly
In many countries one or more of the above-mentioned agents may not be indicated for onychomycosis in children. An up-to-date reference source must be con-sulted because the currently recommended treatment regimen may change as new data from clinical trials become available.*Pulse therapy is 1 week on active treatment and 3 weeks off drug.

238 Curr Probl Dermatol, July/August 2001
creased over the years, suggesting perhaps that theremay be increasing resistance of T tonsurans to griseo-fulvin.293,301 With T tonsurans tinea capitis, griseoful-vin has to be administered for 6 to 8 weeks. Themicrosize formulation in particular is absorbed bestwhen taken with a meal.
Itraconazole, terbinafine, and fluconazole are beingincreasingly considered to treat tinea capitis (Table 4).Studies with the newer agents suggest that with T ton-surans tinea capitis, a 2- to 4-week duration of activetherapy may be sufficient.302 The preferred mode oftherapy with the different agents is terbinafine (contin-uous), itraconazole (continuous or pulse), and flucona-zole (short-term continuous or once weekly). The effi-cacy rates of the newer antifungal agents appear to besimilar to those achieved with griseofulvin in spite ofthe shorter duration of therapy for T tonsurans tineacapitis. The data on the safety of the new antifungalagents in children indicate that itraconazole, terbina-fine, and fluconazole each have a favorable adverseeffects profile by use of the regimens outlined in Table5.223,298 Liquid formulations are available for griseo-fulvin (125 mg/5 mL), itraconazole (150 mg/10 mL),and fluconazole (40 mg/mL) in the United States, andthis may be of benefit in young children unable toswallow a capsule or tablet.
Onychomycosis is uncommon in children. In a NorthAmerican survey, the prevalence of onychomycosis inchildren ≤18 years old was 0.16% (95% confidenceinterval: 0% to 0.32%).223 If onychomycosis is sus-pected in a child, diligent search should be performedfor concomitant tinea pedis because in a large propor-tion of individuals, tinea pedis is believed to precedeonychomycosis. Also, in some patients the onychomy-cosis may exhibit an inherited pattern of autosomaldominance. If possible, other siblings and the parentsshould be examined for onychomycosis and tinea pedis.None of the newer antifungal agents (itraconazole,terbinafine, or fluconazole) are approved for the treat-ment of onychomycosis in children in the UnitedStates. Guidelines regarding the dosage regimens thatmay be used to treat onychomycosis in children aregiven in Table 6.223,312
When other superficial fungal infections, such astinea corporis/tinea cruris, tinea pedis/tinea manus,and tinea versicolor, are present in children, a topicalantifungal agent may be sufficient. An oral antifungalagent may need to be considered if the mycotic infec-tion is present over a large body surface area, topicaltherapy is unsuccessful, compliance is poor, or the
child is immunocompromised and the superficial fun-gal infection continues to recur.
Added at galley proof stage: Recently there havebeen labeling changes for itraconazole and terbinafine.Itraconazole should not be administered for the treat-ment of onychomycosis in patients with evidence ofventricular dysfunction such as congestive heart fail-ure (CHF) or a history of CHF. Pretreatment serumtransaminase tests are advised for all patients beforetaking terbinafine. For complete details of labelingchanges for both products, readers should review thelatest version of the relevant package inserts.
REFERENCES1. Gupta AK, Jain HC, Lynde CW, Watteel GN, Summerbell
RC. Prevalence and epidemiology of unsuspected onycho-mycosis in patients visiting dermatologists’ offices in Ontario,Canada—a multicenter survey of 2001 patients. Int JDermatol 1997;36:783-7.
2. Zaias N, Tosti A, Rebell G, Morelli R, Bardazzi F, Bieley H,et al. Autosomal dominant pattern of distal subungual ony-chomycosis caused by Trichophyton rubrum. J Am AcadDermatol 1996;34(Pt 1):302-4.
3. English MP, Gibson MD. Studies in the epidemiology oftinea pedis II: dermatophytes on the floors of swimming-baths. Br Med J 1959;1:1446-8.
4. English MP. Studies in the epidemiology of tinea pedis VII:the circulation of infection. Br Med J 1961;1:1086-9.
5. Gentles JC, Holmes JG. Foot ringworm in coal-miners. BrMed J 1957;14:22.
6. Aly R, Berger T. Common superficial fungal infections inpatients with AIDS. Clin Infect Dis 1996;22(Suppl 2):S128-32.
7. Matis WL, Triana A, Shapiro R, Eldred L, Polk BF, HoodAF. Dermatologic findings associated with human immuno-deficiency virus infection. J Am Acad Dermatol 1987;17:746-51.
8. Gupta AK, Konnikov N, MacDonald P, Rich P, Rodger NW,Edmonds MW, et al. Prevalence and epidemiology of toenailonychomycosis in diabetic subjects: a multicentre survey. BrJ Dermatol 1998;139:665-71.
9. Zaias N. Onychomycosis. Arch Dermatol 1972;105:263-74.10. Baran R, Hay RJ, Tosti A, Haneke E. A new classification of
onychomycosis. Br J Dermatol 1998;139:567-71.11. Baran R, Dawber RPR, Tosti A, Haneke E. Onychomycosis
and its treatment. In: Baran R, Dawber RPR, Tosti A,Haneke E. A text atlas of nail disorders: diagnosis and treat-ment. London: Martin Dunitz; 1996. p. 155-68.
12. Hay RJ, Baran R, Moore MK, Wilkinson JD. Candida ony-chomycosis—an evaluation of the role of Candida species innail disease. Br J Dermatol 1988;118:47-58.
13. Baran R, Tosti A, Piraccini BM. Uncommon clinical patternsof Fusarium nail infection: report of three cases. Br J Derma-tol 1997;136:424-7.
14. Tosti A, Piraccini BM, Stinchi C, Lorenzi S. Onychomycosisdue to Scopulariopsis brevicaulis: clinical features and re-
Curr Probl Dermatol, July/August 2001 239
sponse to systemic antifungals. Br J Dermatol 1996;135:799-802.
15. Piraccini BM, Morelli R, Stinchi C, Tosti A. Proximal sub-ungual onychomycosis due to Microsporum canis. Br J Der-matol 1996;134:175-7.
16. Baran R. Proximal subungual Candida onychomycosis: anunusual manifestation of chronic mucocutaneous candidosis.Br J Dermatol 1997;137:286-8.
17. Silva-Lizama E, Logemann H. Proximal white subungualonychomycosis in AIDS. Int J Dermatol 1996;35:290-1.
18. Noppakun N, Head ES. Proximal white subungual ony-chomycosis in a patient with acquired immune deficiencysyndrome. Int J Dermatol 1986;25:586-7.
19. Elewski BE. Clinical pearl: proximal white subungual ony-chomycosis in AIDS. J Am Acad Dermatol 1993;29:631-2.
20. Rongioletti F, Persi A, Tripodi S, Rebora A. Proximal whitesubungual onychomycosis: a sign of immunodeficiency. JAm Acad Dermatol 1994;30:129-30.
21. Dompmartin D, Dompmartin A, Deluol AM, Grosshans E,Coulaud JP. Onychomycosis and AIDS. Clinical and labora-tory findings in 62 patients. Int J Dermatol 1990;29:337-9.
22. Weismann K, Knudsen EA, Pedersen C. White nails inAIDS/ARC due to Trichophyton rubrum infection. Clin ExpDermatol 1988;13:24-5.
23. Weinberg JM, Koestenblatt EK, Don PC, White SM, SteinMN, Bamji M. Proximal white subungual onychomycosis inthe immunocompetent patient: report of two cases and re-view of the literature. Acta Dermatol Venereol 1999;9:81-2.
24. Chang P, Arenas R. Proximal white subungual onychomy-cosis in a kidney transplant patient. Int J Dermatol 1995;34:591.
25. Tosti A, Piraccini BM. Proximal subungual onychomycosisdue to Aspergillus niger: report of two cases. Br J Dermatol1998;139:156-7.
26. Contet-Audonneau N, Salvini O, Basile AM, et al. Ony-chomycosis provoked by moulds. Nouv Dermatol 1995;14:330-40.
27. Badillet G. Melanonychies superficielles. Bull Soc Fr MycolMed 1988;17:335-40.
28. Meisel CW, Quadripur. Onychomycosis due to Henderson-ula toruloidea. Hautnah 1992;6:232-4.
29. Tosti A, Baran R, Piraccini BM, Fanti PA. “Endonyx” ony-chomycosis: a new modality of nail invasion by dermato-phytes. Acta Derm Venereol 1999;79:52-3.
30. Woolf A, Shaw J. Childhood injuries from artificial nailprimer cosmetic products. Arch Pediatr Adolesc Med 1998;152:41-6.
31. Freeman S, Lee MS, Gudmundsen K. Adverse contact reac-tions to sculptured acrylic nails: 4 case reports and a litera-ture review. Contact Dermatitis 1995;33:381-5.
32. Barnett JM, Scher RK, Taylor SC. Nail cosmetics. DermatolClin 1991;9:9-17.
33. Daniel CR. Onycholysis: an overview. Semin Dermatol 1991;10:34-40.
34. Baran R, Badillet G. Primary onycholysis of the big toenails:a review of 113 cases. Br J Dermatol 1982;106:529-34.
35. Marsden RA, Dawber RPR Erythropoietic protoporphyriawith onycholysis. Proc R Soc Med 1977;70:572-4.
August 2001
36. Bethell HJ. Photo-onycholysis caused by demethylchlorte-tracycline. Br Med J 1977;2:96.
37. Voigt K, Holzegal K. [Permanent nail changes followinggold therapy]. Hautarzt 1977;28:421-3.
38. Goodwin P. Onycholysis due to acrylic nail applications.Clin Exp Dermatol 1976;1:191-4.
39. Baker H. Photo-onycholysis caused by tetracyclines. Br MedJ 1977;2:519-20.
40. Singchoovong L, Tandhanand S, Vannasaeng S, InturprapaM. Onycholysis in hyperthyroidism and hypothyroidism. JMed Assoc Thai 1976;59:143-5.
41. Manalo FB, Marks A, Davis HL Jr. Doxorubicin toxicity:onycholysis, plantar callus formation and epidermolysis.JAMA 1975;233:56-7.
42. Merrill RH. Fungal vs drug-induced onycholysis. South MedJ 1974;67:677-8.
43. Witkop CJ Jr, Brearley LJ, Gentry WC Jr. Hypoplasticenamel, onycholysis and hypohidrosis inherited as an auto-somal dominant trait: a review of ectodermal dysplasia syn-dromes. Oral Surg Oral Med Oral Pathol 1975;39:71-86.
44. Hamburger JI. Onycholysis in thyroid disease. JAMA 1970;213:1195.
45. Zaias N. Psoriasis of the nail: a clinical-pathologic study.Arch Dermatol 1969;99:567-79.
46. Calvert HT, Smith MA, Wells RS. Psoriasis and the nails. BrJ Dermatol 1963;75:415.
47. Baran R, Dawber RPR. The nail in dermatological disease.In: Baran R, Dawber RPR, editors. Diseases of the nail andtheir management. 2nd ed. Oxford: Blackwell ScientificPublications; 1994. p. 135-262.
48. Zaias N, Norton LA. In: Demis DJ, Dobson RL, McGuire J,editors. Clinical dermatology. 1980:3-4.
49. Scher RK, Ackerman AB. Subtle clues to diagnosis frombiopsies of nails: histologic differential diagnosis of onycho-mycosis and psoriasis of the nail unit from cornified cells ofthe nail bed alone. Am J Dermatopathol 1980;2:255-6.
50. Tosti A, Peluso AM, Fanti PA, Piraccini BN. Nail lichenplanus: clinical and pathological study of twenty-four patients.J Am Acad Dermatol 1993;28:724-30.
51. Burgoon CF Jr, Kostrzewa RM. Lichen planus limited to thenails. Arch Dermatol 1969;100:371.
52. Kanwar AJ, Govil DC, Singh OP. Lichen planus limited tothe nails. Cutis 1983;32:163-4,168.
53. Peluzo AM, Tosti A, Piraccini BM, Cameli N. Lichen planuslimited to the nails in childhood: case report and literaturereview. Pediatr Dermatol 1993;10:36-9.
54. Samman PD. The nails in lichen planus. Br J Dermatol 1961;73:288-92.
55. Ronchese F. Nail in lichen planus. Arch Dermatol 1965;91:347-50.
56. Ronchese F. The nail in Darier’s disease. Arch Dermatol1965;91:617-8.
57. Bingham EA, Burrow D. Darier’s disease. Br J Dermatol1984;111:88-9.
58. Caputo GM, Joshi N, Weitekamp MR. Foot infections inpatients with diabetes. Am Fam Phys 1997;56:195-202.
59. Bild DE, Selby JV, Sinnock P, Browner WS, Braveman P,
ficial fun-
here haverbinafine.the treat-idence ofheart fail-ent serumnts beforef labelingeview the
Summerbelled onycho-s in Ontario,ents. Int J
F, Bieley H,ungual ony-J Am Acad
miology ofswimming-
a pedis VII:86-9.-miners. Br
nfections inpl 2):S128-
k BF, Hoodan immuno-ol 1987;17:
Rodger NW,gy of toenaile survey. Br
05:263-74.sification of.chomycosis
R, Tosti A,s and treat-
andida ony-a species in
cal patternsBr J Derma-
chomycosisures and re-

240 Curr Probl Dermatol, July/August 2001
Showstack JA. Lower-extremity amputation in people withdiabetes. Diabetes Care 1989;12:24-31.
60. Lithner F. Purpura, pigmentation and yellow nails of thelower extremities in diabetics. Acta Med Scand 1976;199:203-8.
61. Daniel CR, Scher RK. Nail changes secondary to systemicdrugs and ingestants. In: Scher RK, Daniel CR, editors. Nails:therapy, diagnosis and surgery. 2nd ed. Philadelphia: WBSaunders; 1997. p. 251-61.
62. Tosti A, Baran R, Dawber RPR. The nail in systemic dis-eases and drug-induced changes. Baran R, Dawber RPR, edi-tors. Diseases of the nails and their management. 2nd ed.London: Blackwell Scientific Publications; 1994. p. 175-262.
63. Gupta AK, Sauder DN, Shear NH. Antifungal agents: anoverview. Part I. J Am Acad Dermatol 1994;30:677-98.
64. Hull PR, Gupta AK, Summerbell RC: Onychomycosis: anevaluation of three sampling methods. J Am Acad Dermatol1998;39:1015-7.
65. Daniel CR. The diagnosis of nail fungal infection. ArchDermatol 1991;127:1566-7.
66. Weitzman I, Summerbell RC. The dermatophytes. ClinMicrobiol Rev 1995;8:240-59.
67. Gupta AK, Scher RK. Management of onychomycosis: aNorth American perspective. In: Dermatology therapy.Elewski BE, editor. Copenhagen, Denmark: MunksgaardPress; 1997. p. 58-65.
68. Elewski BE. Diagnostic techniques for confirming ony-chomycosis. J Am Acad Dermatol 1996:S6-9.
69. Kane J, Summerbell RC, Sigler L, Krajden S, Land GA.Laboratory handbook of dermatophytes. Belmont, Calif: StarPublishing; 1997.
70. Kwon-Chung KJ, Bennett JE. Medical mycology. Philadel-phia: Lea and Febiger; 1992.
71. Rippon JW. The pathogenic fungi and the pathogenic actino-mycetes. 3rd ed. Philadelphia: WB Saunders; 1988.
72. Weitzman I, Kane J. Dermatophytes and agents of superfi-cial mycoses. In: Balows A, Hauseler WJ Jr, Herrmann KL,Isenberg HD, Shadomy HS, editors. Manual of clinicalmicrobiology. 5th ed. Washington, DC: American Societyfor Microbiology; 1991. p. 601-16.
73. Weitzman I, Rosenthal SA, Silva-Hutner M. Superficial andcutaneous infections caused by molds: dermatophytoses. In:Wentworth BB, editor. Diagnostic procedures for mycoticand parasitic infections. Washington, DC: American PublicHealth Association; 1988. p. 33-97.
74. Taplin D, Zaias N, Rebell G, Blank H. Isolation and recog-nition of dermatophytes on a new medium (DTM). ArchDermatol 1969;99:203-9.
75. St Germain G, Summerbell R. Identifying filamentous fungi:a clinical laboratory handbook. Belmont, Calif: StarPublishing Company; 1996. p. 1-314.
76. Crissey JT, Lang H, Parish LC. Manual of medical mycolo-gy. Cambridge, Mass: Blackwell Science; 1995. p. 1-263.
77. Kern ME. Medical mycology. Philadelphia Pa: FA DavisCompany; 1991. p. 1-239.
78. Suarez SM, Silvers DN, Scher RK, Pearlstein HH, AuerbachR. Histologic evaluation of nail clippings for diagnosingonychomycosis. Arch Dermatol 1991;127:1517-9.
79. Machler BC, Kirsner RS, Elgart GW. Routine histologicexamination for the diagnosis of onychomycosis: an evalua-tion of sensitivity and specificity. Cutis 1998;61:217-9.
80. Lee S, Bang D. Hyphae on the ventral nail plate as a clue toonychomycosis. Am J Dermato Pathol 1987;9:445-6.
81. Piérard GE, Arrese JE, De Doncker P, Piérard-FranchimontC. Present and potential diagnostic techniques in onychomy-cosis. J Am Acad Dermatol 1996;34:273-7.
82. Arrese JE, Piérard-Franchimont C, Greimers R, Piérard GE.Fungi in onychomycosis: a study by immunohistochemistryand dual flow cytometry. J Eur Acad Dermatol Venereol1995;4:123-30.
83. Gupta AK, Sauder DN, Shear NH. Antifungal agents: anoverview: part II. J Am Acad Dermatol 1994;30:911-33.
84. Shear NH, Gupta AK. Terbinafine for the treatment of pedalonychomycosis: a foot closer to the promised land of curednails? Arch Dermatol 1995;131:937-42.
85. Gupta AK, Scher RK, De Doncker P. Current managementof onychomycosis: an overview. Dermatol Clin 1997;15:121-35.
86. De Doncker P, Gupta AK, Marynissen G, Stoffels P,Heremans A. Itraconazole pulse therapy for onychomycosisand dermatomycoses: an overview. J Am Acad Dermatol1997;37:969-74.
87. Gupta AK, Shear NH. Terbinafine: an update. J Am AcadDermatol 1997;37:979-88.
88. Gupta AK, De Doncker P, Scher RK, et al. Itraconazole for thetreatment of onychomycosis. Int J Dermatol 1998;37:303-8.
89. Elewski BE. Onychomycosis: pathogenesis, diagnosis andmanagement. Clin Microbiol Rev 1998;11:415-29.
90. Hay RJ. Onychomycosis: agents of choice. Dermatol Clin1993;1:161-9.
91. Roseeuw D, De Doncker P. New approaches to the treatmentof onychomycosis. J Am Acad Dermatol 1993;29:S45-50.
92. Hay RJ. Risk/benefit ratio of modern antifungal therapy:focus on hepatic reactions. J Am Acad Dermatol 1993;29:S50-54.
93. Piérard GE, Arrese-Estrada J, Piérard-Francimont C.Treatment of onychomycosis: traditional approaches. J AmAcad Dermatol 1993;29:S41-45.
94. Meinhof W. Kinetics and spectrum of activity of oral anti-fungals: the therapeutic implications. J Am Acad Dermatol1993;29:S37-41.
95. Pollak R, Billstein SA. Safety of oral terbinafine for toenailonychomycosis. J Am Pod Med Assoc 1997;87:565-70.
96. Zimmermann T, Yeates RA, Laufen H, Pfaff G, Wilfeuer A.Influence of concomitant food intake on the oral absorptionof two triazole antifungal agents, itraconazole and flucona-zole. Eur J Clin Pharmacol 1994;46:147-150.
97. Barone JA, Koh JG, Bierman RH, et al. Food interactionsand steady-state pharmacokinetics of itraconazole capsulesin healthy male volunteers. Antimicrob Agents Chemother1993;37:778-84.
98. Hardin TC, Graybill JR, Fetchick R, Woestenborghs R,Rinaldi MG, Kuhn JG. Pharmacokinetics of itraconazole fol-lowing oral administration to normal volunteers. AntimicrobAgents Chemother 1988;32:1310-3.
99. Negroni R. Arechavala AI. Itraconazole: pharmacokineticsand indications. Arch Med Res 1993;24:387-93.
Curr Probl Dermatol, July/August 2001 241
100. Smith D, Vande Velde V, Woestenborghs R, Gazzard BG.The pharmacokinetics of oral itraconazole in AIDS patients.J Pharm Pharmacol 1992;44:618-9.
101. Montero-Gei F. Fluconazole: pharmacokinetics and indica-tions. Arch Med Res 1993;4:377-85.
102. Thorpe JE. Baker N, Bromet-Petit M. Effect of oral antacidadministration on the pharmacokinetics of oral fluconazole.Antimicrob Agents Chemother 1990;34:2032-3.
103. Dudley MN. Clinical pharmacology of fluconazole. Pharma-cotherapy 1990;10:1415-55.
104. Brammer KW, Farrow PR, Faulkner JK. Pharmacokineticsand tissue penetration of fluconazole in humans. Rev InfectDis 1990;12(Supp 3):S318-26.
105. Toon S, Ross CE, Gokal R, Rowland M. An assessment ofthe effects of impaired renal function and haemodialysis onthe pharmacokinetics of fluconazole. Br J Clin Pharmacol1990;29:221-6.
106. Jensen C. Clinical pharmacokinetics of terbinafine (Lamisil).Clin Exp Dermatol 1989;14:110-3.
107. Bulghur JA, Faulds D. Terbinafine. A review of its pharma-codynamic and pharmacokinetic properties, and therapeuticpotential in superficial mycoses. Drugs 1992;43:259-84.
108. Kovarik JM, Mueller EA, Zehender H, Denouel J, CaplainNH, Millerioux L. Multiple-dose pharmacokinetics and dis-tribution in tissue of terbinafine and metabolites. AntimicrobAgents Chemother 1995;39:2738-41.
109. De Doncker P. Pharmacokinetics of oral antifungal agents.Dermatologic Therapy 1997;3:46-57.
110. Rich P, Scher RK, Breneman D, et al. Pharmacokinetics ofthree doses of once-weekly fluconazole (150, 300 and 450mg) in the management of distal subungual onychomycosisof the toenail. J Am Acad Dermatol 1998;38:S103-109.
111. Jung EG, Haas PJ, Brautigam M, Weidinger G. Systemictreatment of skin candidosis: a randomized comparison ofterbinafine and ketoconazole. Mycoses 1994;37:361-5.
112. Schatz F, Bräutigam M, Dobrowolski E, et al. Nail incorpo-ration kinetics of terbinafine in onychomycosis patients. ClinExp Dermatol 1995;20:377-83.
113. Hay RJ. Pharmacokinetic evaluation of fluconazole in skinand nails. Int J Dermatol 1992;1:6-7.
114. Haneke E. Pharmacokinetic evaluation of fluconazole in plas-ma, epidermis and blister fluid. Int J Dermatol 1992;31:3-5.
115. Faergemann J, Laufen H. Levels of fluconazole in serum,stratum corneum, epidermis-dermis (without stratum corneum)and eccrine sweat. Clin Exp Dermatol 1993;18:102-6.
116. Itraconazole. In Physicians’ Desk Reference. 53rd ed. Mont-vale, NJ: Medical Economics Company Inc; 1999. p. 1436-9.
117. Terbinafine. In Physicians’ Desk Reference, 53rd ed. Mont-vale, NJ: Medical Economics Company In; 1999. p. 2038-9.
118. Fluconazole. In Physicians’ Desk Reference, 53rd ed. Mont-vale, NJ: Medical Economics Company Inc; 1999. p. 2379-83.
119. Cauwenbergh G, Degreef H, Heykants J, Woestenborghs R,Van Rooy P, Haeverans K. Pharmacokinetic profile of orallyadministered itraconazole in human skin. J Am Acad Derma-tol 1988;18:263-8.
120. Gupta AK, Groen K, Woestenborghs R, De Doncker P.Itraconazole pulse therapy is effective in the treatment of
August 2001
Majocchi’s granuloma: a clinical and pharmacokinetic eval-uation and implications for possible effectiveness in tineacapitis. Clin Exp Dermatol 1998;23:103-8.
121. Lever LR, Dykes PJ, Thomas R, et al. How orally adminis-tered terbinafine reaches the stratum corneum. J DermatolTreat 1990;1:23-5.
122. Faergemann J, Zehender H, Jones T, Maibach I. Terbinafinelevels in serum, stratum corneum, dermis-epidermis (withoutstratum corneum), hair, sebum and eccrine sweat. Acta DermVenereol 1991;71:322-6.
123. Faergemann J, Zehender H, Denouël J, Millerioux L. Levelsof terbinafine in plasma, stratum corneum, dermis-epidermis(without stratum corneum), sebum, hair and nails during andafter 250 mg terbinafine orally once per day for four weeks.Acta Derm Venereol 1993;73:305-9.
124. Faergemann J, Zehender H, Millerioux L. Levels of terbina-fine in plasma, stratum corneum, dermis-epidermis (withoutstratum corneum), sebum, hair and nails during and after 250mg terbinafine orally once daily for 7 and 14 days. Clin ExpDermatol 1994;19:121-6.
125. Wildfeuer A, Faergemann J, Laufen H, et al. Bioavailabilityof fluconazole in the skin after oral medication. Mycoses1994;37:127-30.
126. Yeates R, Laufen H, Zimmermann T, Scharpf F. Accumu-lation of fluconazole in scalp hair. J Clin Pharmacol 1998;38:138-43.
127. Del Rosso JQ, Gupta AK. The spectrum of utility of oralantifungal agents: from the Petri dish to the patient. Today’sTherapeutic Trends 1997;15:179-89.
128. Del Rosso JQ, Zellis S, Gupta AK. Itraconazole in the treat-ment of superficial cutaneous and mucosal Candida infec-tions. J Am Osteopath Assoc 1998;98:497-502.
129. Hickman JG. A double-blind, randomized, placebo-controlledevaluation of short-term treatment with oral itraconazole inpatients with tinea versicolor. J Am Acad Dermatol 1996;34:785-7.
130. Delescluse J. Itraconazole in tinea versicolor: a review. J AmAcad Dermatol 1990;23:551-4.
131. Del Rosso JQ, Gupta AK. The use of intermittent itracona-zole therapy for superficial mycotic infections: a review andupdate on the “one week” approach. Int J Dermatol 1999;38(Suppl 2):28-39.
132. Cauwenbergh G, De Doncker P. The clinical use of itra-conazole in superficial and deep mycoses. In: Fromtling RA,editor. Recent trends in the discovery, development andevaluation of antifungal agents. Barcelona: JR Prous SciencePublishers; 1987. p. 273-84.
133. Del Rosso JQ. Advances in the treatment of superficial fun-gal infections: focus on onychomycosis and dry tinea pedis.J Am Osteopath Assoc 1997;97:339-46.
134. Svejgaard EL. Recalcitrant dermatophyte infection. Derma-tol Therapy 1997;3:75-8.
135. Katsambas A, Antoniou CH, Frangouli E, Rigopoulos D,Vlachou M, Michailidis D, Stratigos J. Itraconazole in thetreatment of tinea corporis and tinea cruris. Clin Exp Derma-tol 1993;18:322-5.
136. Chow KW, Ting HC, Yap PY, Yee KC. Short treatmentschedules of itraconazole in dermatophytosis. Int J Dermatol1998;37:446-8.
e histologic: an evalua-217-9.as a clue to
45-6.ranchimontonychomy-
Piérard GE.tochemistryol Venereol
agents: an911-33.ent of pedalnd of cured
managementn 1997;15:
Stoffels P,chomycosisd Dermatol
J Am Acad
azole for the37:303-8.agnosis and9.rmatol Clin
he treatment9:S45-50.
gal therapy:ol 1993;29:
cimont C.ches. J Am
of oral anti-d Dermatol
e for toenail565-70.Wilfeuer A.l absorptionnd flucona-
interactionsole capsules
Chemother
nborghs R,onazole fol-Antimicrob
macokinetics
242 Curr Probl Dermatol, July/August 2001
137. Decroix J, Fritsch P, Picoto A, et al. Short term itraconazoleversus terbinafine in the treatment of superficial dermatomy-cosis of the glabrous skin (tinea corporis or cruris). Eur JDermatol 1997;7:353-7.
138. De Doncker P, Cauwenbergh G. Management of fungal skininfections with 15 days itraconazole treatment: a worldwidereview. Br J Clin Pract Suppl.1990;71:118-22.
139. Gupta AK, De Doncker P, Heremans A, et al. Itraconazole forthe treatment of tinea pedis: a dosage of 400 mg/day given for1 week is similar in efficacy to 100 or 200 mg/day given for 2to 4 weeks. J Am Acad Dermatol 1997;36:789-92.
140. Tausch I, Decroix J, Gwiezdzinski Z, et al. Short-term itra-conazole versus terbinafine in the treatment of tinea pedis ormanus. Int J Dermatol 1998;37:140-2.
141. Saul A, Bonifaz A. Itraconazole in common dermatophyteinfections of the skin: fixed treatment schedules. J Am AcadDermatol 1990;23:554-8.
142. Delescluse J, Cauwenbergh G, De Greef H. Itraconazole, anew orally active antifungal in the treatment of pityriasisversicolor. Br J Dermatol 1986;114:701-3.
143. Cauwenbergh G, De Doncker P, Stoops K, De Dier AM,Goyvaerts H, Schuermans V. Itraconazole in the treatment ofhuman mycoses: review of three years of clinical experience.Rev Infect Dis 1987;9:S146-52.
144. Del Palacio-Hernanz A, Delgado Vincente S, MenedezRamos F, Rodriguez-Noriega Belaustegui A. Randomized,comparative clinical trial of itraconazole and selenium sul-fide shampoo for the treatment of pityriasis versicolor. RevInfect Dis 1987;9:S121-7.
145. Willemsen M, De Doncker P, Willems J, et al. Post treat-ment itraconazole levels in the nail. J Am Acad Dermatol1992;26:731-5.
146. De Doncker P, Decroix J, Piérard GE, et al. Antifungal pulsetherapy for onychomycosis: a pharmacokinetic and pharma-codynamic investigation of monthly cycles of 1-week pulsetherapy with itraconazole. Arch Dermatol 1996;132:34-41.
147. Kejda J. Itraconazole pulse therapy vs terbinafine continuousdosing for toenail onychomycosis. Postgrad Med 1999;Specno:12-5.
148. Gupta AK, Shear NH. The new oral antifungal agents foronychomycosis of the toenails: a review. J Eur Acad Der-matol Venereol 1999;13:1-13.
149. Gupta AK, Shear NH. A risk-benefit assessment of thenewer oral antifungal agents used to treat onychomycosis.Drug Safety 2000;22:33-52.
150. Bonifaz A, Carrasco-Gerard E, Saúl A. Itraconazole in ony-chomycosis: intermittent dose schedule. Int J Dermatol1997;36:70-2.
151. Itraconazole package insert (Canada). Janssen Canada.August 1997.
152. De Doncker P, Van Lint J, Dockx P, Roseeuw D. Pulse ther-apy with one-week itraconazole monthly for three or fourmonths in the treatment of onychomycosis. Cutis 1995;56:180-3.
153. Evans EGV, Sigurgeirsson B, Billstein S. and the LIONstudy group. Double blind randomized study of continuousterbinafine compared with intermittent itraconazole in treat-ment of toenail onychomycosis. Br Med J 1999;318:1031-5.
154. Ginter G, De Doncker P. An intermittent itraconazole 1-
week dosing regimen for the treatment of toenail onychomy-cosis in dermatological practice. Mycoses 1998;41:235-8.
155. Haneke E, Abeck D, Ring J. The safety and efficacy ofintermittent therapy with itraconazole for finger- and toenailonychomycosis: a multicenter trial. Zeitschriftfuer Haut-krankheiten 1997;10:737-40.
156. Havu V, Brandt H, Heikkilä H, et al. A double-blind, ran-domized study comparing itraconazole pulse therapy withcontinuous dosing for the treatment of toe-nail onychomyco-sis. Br J Dermatol 1997;136:230-4.
157. Svejgaard E, et al. In De Doncker P, Van Custem J, PierardG, et al. Itraconazole compared to terbinafine in superficialfungal infections: From petri dish to patient! Poster P 206.Presented at The Fifty-sixth Annual American Academy ofDermatology Meeting, Orlando, Florida, USA, February 27-March 4, 1998.
158. Tosti A, Piraccini BM, Stinchi C, Venturo N, Bardazzi F,Colombo MD. Treatment of dermatophyte nail infections: anopen randomized study comparing intermittent terbinafinetherapy with continuous terbinafine treatment and intermit-tent itraconazole therapy. J Am Acad Dermatol 1996;34:595-600.
159. Wang DL, Wang AP, Li RY, Wang R. Therapeutic efficacyand safety of 1-week intermittent therapy with itraconazolefor onychomycosis in a Chinese patient population. Derma-tology 1999;199:47-9.
160. Wu J, Wen H, Liao W. Small-dose itraconazole pulse therapyin the treatment of onychomycosis. Mycoses 1997;40:397-400.
161. De Doncker P, Scher RK, Baran RL, et al. Itraconazole ther-apy is effective for pedal onychomycosis caused by somenondermatophyte molds and with mixed infection with der-matophytes and molds: a multicenter study in 36 patients. JAm Acad Dermatol 1997;36:173-7.
162. Kim JA, Ahn KJ, Kim JM. Efficacy and tolerability of itra-conazole in patients with fingernail onychomycosis: a 6-week pilot study. Curr Ther Res 1995;56:1066-75.
163. Rashid A, De Doncker P. Itraconazole one week pulse ther-apy in the management of Candida paronychia. PosterPresentation, 19th World Congress of Dermatology, SydneyAustralia, June 15-20, 1997.
164. Gupta AK, Scher RK, Rich P. Fluconazole for the treatmentof onychomycosis: an update. Int J Dermatol 1998;37:815-20.
165. Faergemann J. Treatment of pityriasis versicolor with a sin-gle dose of fluconazole. Acta Derm Venereol 1992;72:74-5.
166. Suchil P, Gei FM, Robles M, Perera-Ramierz A, Welsh O,Male O. Once weekly oral doses of fluconazole 150 mg inthe treatment of tinea corporis/cruris and cutaneous candidi-asis. Clin Exp Dermatol 1992;17:397-401.
167. Faergemann J, Mork NJ, Highland A, Odegard T. A multi-centre (double-blind) comparative study to assess the safetyand efficacy of fluconazole and griseofulvin in the treatmentof tinea corporis and tinea cruris. Br J Dermatol 1997;136:575-7.
168. Stary A, Sarnow E. Fluconazole in the treatment of tinea cor-poris and tinea cruris. Dermatology 1998;196:237-41.
169. Harmon TS, Asghar HA, Aman S, Jahangir M. Specialist1997;13:417-23.
Curr Probl Dermatol, July/August 2001 243
170. Papini M, Difonzo EM, Cilli P, et al. Itraconazole versus flu-conazole a double-blind comparison in tinea corporis. JMycologie Medicale 1997;7:77-80.
171. Kotogyan A, Harmanyeri Y, Tahsin Gunes A, et al. Efficacyand safety of oral fluconazole in the treatment of patientswith tinea corporis, cruris or pedis or cutaneous candidiasis:a multicentre, open, non-comparative study. Clin Drug In-vest 1996;12:59-66.
172. Nozickova M, Koudelkova V, Kulikova Z, Malina L,Urbanowski S, Silny W. A comparison of the efficacy of oralfluconazole, 150 mg/week versus 50 mg/day, in the treat-ment of tinea corporis, tinea cruris, tinea pedis, and cuta-neous candidosis. Int J Dermatol 1998;37:703-5.
173. Del Aguila R, Gei FM, Robles M, Perera-Ramirez A, MaleO. Once-weekly oral doses of fluconazole 150 mg in thetreatment of tinea pedis. Clin Exp Dermatol 1992;17:402-6.
174. Kose O. Fluconazole versus itraconazole in the treatment oftinea versicolor. Int J Dermatol 1995;34:498-9.
175. Amer MA and the Egyptian Fluconazole Study Group.Fluconazole in the treatment of tinea versicolor. Int JDermatol 1997;36:938-46.
176. Fräki J, Heikkila H, Kero M, et al. An open-label, non-com-parative, multicenter evaluation of fluconazole with or with-out urea nail pedicure for treatment of onychomycosis. CurrTher Res 1997;58:481-91.
177. Kuokkanen K, Alava S. Fluconazole in the treatment of ony-chomycosis caused by dermatophytes. J Dermatol Treat1992;3:115-7.
178. Montero-Gei F, Robles-Soto ME, Schlager H. Fluconazolein the treatment of severe onychomycosis. Int J Dermatol1996;35:587-8.
179. Scher RK, Brenneman D, Rich P, et al. Once-weekly flu-conazole (150 mg, 300 mg, or 450 mg) in the treatment ofdistal subungual onychomycosis of the toenail. J Am AcadDermatol 1998;38-77-86.
180. Havu V, Heikkila H, Kuokkenen K, et al. The study to com-pare the efficacy of Lamisil (terbinafine) and Diflucan (flu-conazole) in patients with onychomycosis. Poster 132. J EurAcad Dermatol Venereol 1996;7:154.
181. Sadeque Z, Rahmatullah H, Latif Khan A. A comparison ofthe efficacy of oral griseofulvin, fluconazole and terbinafinein the treatment of onychomycosis. Bangladesh J Dermatol1996;13:29-32.
182. Gupta AK. New strategies in the management of onychomy-cosis. West J Med 1996;164:521-2.
183. Savin RC. Oral terbinafine versus griseofulvin in the treat-ment of moccasin-type tinea pedis. J Am Acad Dermatol1990;23:807-9.
184. Hay RJ, Logan RA, Moore MK, Midgely G, Clayton YM. Acomparative study of terbinafine versus griseofulvin in “drytype” dermatophyte infections. J Am Acad Dermatol 1991;24:243-6.
185. Savin RC. Successful treatment of chronic tinea pedis (moc-casin-type) with terbinafine (Lamisil). Clin Exp Dermatol1989;14:116-9.
186. Savin RC. Terbinafine (Lamisil) versus griseofulvin in moc-casin type tinea pedis. J Dermatol Treat 1990;1:43-6.
187. White JE, Perkins PJ, Evans EGV. Successful 2-week treat-
August 2001
ment with terbinafine (Lamisil) for moccasin tinea pedis andtinea manuum. Br J Dermatol 1991;125:260-2.
188. De Keyser P, De Backer M, Massart DL, Westelinck KJ.Two-week oral treatment of tinea pedis, comparing terbina-fine (250 mg/day) with itraconazole (100 mg/day): a double-blind, multicentre study. Br J Dermatol 1994;130:22-5.
189. Hay RJ, McGregor JM, Wuite J, Ryatt KS, Ziegler C,Clayton YM. A comparison of 2 weeks of terbinafine 250mg/day with 4 weeks of itraconazole 100 mg/day in plantar-type tinea pedis. Br J Dermatol 1995;132:604-8.
190. Tausch I, Decroix J, Gwiezdzinski Z, et al. Short-term itra-conazole versus terbinafine in the treatment of tinea pedis ormanus. Int J Dermato 1998;37:128-44.
191. Cole GW, Stricklin G. A comparison of a new oral antifun-gal, terbinafine, with griseofulvin as therapy for tinea cor-poris. Arch Dermatol 1989;125:1537-9.
192. del Palacio Hernandez A, Lopez Gomez S, Gonzalez Lastra F,Moreno Palancar P, Iglesias Diez L. A comparative double-blind study of terbinafine (Lamisil) and griseofulvin in tineacorporis and tinea cruris. Clin Exp Dermatol 1990;15:210-6.
193. Farag A, Taha M, Halim S. One-week therapy with oralterbinafine in cases of tinea cruris/corporis. Br J Dermatol1994;131:648-86.
194. Decroix J, Fritsch P, Picoto A, Thurlimann W, Degreef H.Short-term itraconazole versus terbinafine in the treatment ofsuperficial dermatomycosis of the glabrous skin (tinea cor-poris or cruris). Eur J Dermatol 1997;7:353-7.
195. De Wit RFE. A randomized double-blind multicentre com-parative study of Lamisil (terbinafine) versus ketoconazolein tinea corporis. J Dermatol Treat 1990;1:41-2.
196. Alpsoy E, Yilmaz E, Basaran E. Intermittent therapy withterbinafine for dermatophyte toe-onychomycosis: a newapproach. J Dermatol 1996;23:259-62.
197. Arenas R, Dominguez-Cherit J, Fernández LM. Open ran-domized comparison of itraconazole versus terbinafine inonychomycosis. Int J Dermatol 1995;34:138-43.
198. Bräutigam M, Nolting S, Schopf RE, Weidinger G. Ran-domised double blind comparison of terbinafine and itra-conazole for treatment of toenail tinea infection—SeventhLamisil German Onychomycosis Study Group. BMJ 1995;311:919-22.
199. De Backer M, De Keyser P, De Vroey C, Lesaffre E. A 12-week treatment for dermatophyte toe onychomycosis: terbina-fine 250mg/day vs. itraconazole 200mg/day—a double-blindcomparative trial. Br J Dermatol 1996;134(Suppl 46):16-7.
200. Galimberti R, Kowalczuk A, Flores V, Squiquero L. Ony-chomycosis treated with a short course of oral terbinafine.Int J Dermatol 1996;35:374-5.
201. Goodfield MJD, Andrew L, Evans EGV. Short term treat-ment of dermatophyte onychomycosis with terbinafine. BMJ1992;304:1151-4.
202. Honeyman JF, Talarico FS, Arruda LHF, et al. Itraconazoleversus terbinafine (Lamisil): which is better for the treatmentof onychomycosis? J Eur Acad Dermatol 1997;9:215-21.
203. Svejgaard EL, Brandrup F, Kragballe K, et al. Oral ter-binafine in toenail dermatophytosis. Acta Derm Venereol1997;77:66-9.
204. Taush I, Bräutigam M, Weidinger G, Jones TC. Evaluationof 6 weeks treatment of terbinafine in tinea unguium in a
onychomy-41:235-8.efficacy ofand toenail
tfuer Haut-
-blind, ran-herapy withnychomyco-
m J, Pierardn superficialoster P 206.Academy ofebruary 27-
Bardazzi F,fections: anterbinafine
nd intermit-ol 1996;34:
utic efficacytraconazoleon. Derma-
ulse therapy997;40:397-
nazole ther-ed by someon with der-6 patients. J
ility of itra-ycosis: a 6-5.pulse ther-
hia. Posterogy, Sydney
he treatment998;37:815-
with a sin-92;72:74-5.
A, Welsh O,150 mg in
ous candidi-
T. A multi-s the safety
he treatmentl 1997;136:
of tinea cor-7-41.. Specialist
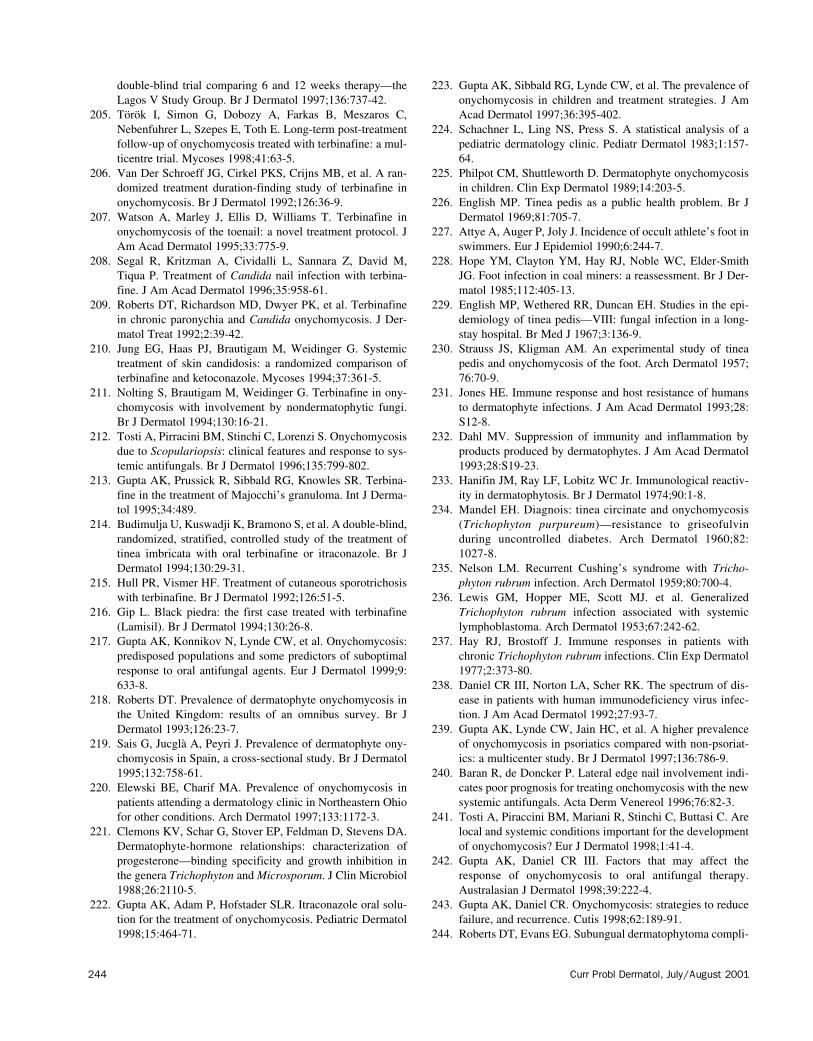
244 Curr Probl Dermatol, July/August 2001
double-blind trial comparing 6 and 12 weeks therapy—theLagos V Study Group. Br J Dermatol 1997;136:737-42.
205. Török I, Simon G, Dobozy A, Farkas B, Meszaros C,Nebenfuhrer L, Szepes E, Toth E. Long-term post-treatmentfollow-up of onychomycosis treated with terbinafine: a mul-ticentre trial. Mycoses 1998;41:63-5.
206. Van Der Schroeff JG, Cirkel PKS, Crijns MB, et al. A ran-domized treatment duration-finding study of terbinafine inonychomycosis. Br J Dermatol 1992;126:36-9.
207. Watson A, Marley J, Ellis D, Williams T. Terbinafine inonychomycosis of the toenail: a novel treatment protocol. JAm Acad Dermatol 1995;33:775-9.
208. Segal R, Kritzman A, Cividalli L, Sannara Z, David M,Tiqua P. Treatment of Candida nail infection with terbina-fine. J Am Acad Dermatol 1996;35:958-61.
209. Roberts DT, Richardson MD, Dwyer PK, et al. Terbinafinein chronic paronychia and Candida onychomycosis. J Der-matol Treat 1992;2:39-42.
210. Jung EG, Haas PJ, Brautigam M, Weidinger G. Systemictreatment of skin candidosis: a randomized comparison ofterbinafine and ketoconazole. Mycoses 1994;37:361-5.
211. Nolting S, Brautigam M, Weidinger G. Terbinafine in ony-chomycosis with involvement by nondermatophytic fungi.Br J Dermatol 1994;130:16-21.
212. Tosti A, Pirracini BM, Stinchi C, Lorenzi S. Onychomycosisdue to Scopulariopsis: clinical features and response to sys-temic antifungals. Br J Dermatol 1996;135:799-802.
213. Gupta AK, Prussick R, Sibbald RG, Knowles SR. Terbina-fine in the treatment of Majocchi’s granuloma. Int J Derma-tol 1995;34:489.
214. Budimulja U, Kuswadji K, Bramono S, et al. A double-blind,randomized, stratified, controlled study of the treatment oftinea imbricata with oral terbinafine or itraconazole. Br JDermatol 1994;130:29-31.
215. Hull PR, Vismer HF. Treatment of cutaneous sporotrichosiswith terbinafine. Br J Dermatol 1992;126:51-5.
216. Gip L. Black piedra: the first case treated with terbinafine(Lamisil). Br J Dermatol 1994;130:26-8.
217. Gupta AK, Konnikov N, Lynde CW, et al. Onychomycosis:predisposed populations and some predictors of suboptimalresponse to oral antifungal agents. Eur J Dermatol 1999;9:633-8.
218. Roberts DT. Prevalence of dermatophyte onychomycosis inthe United Kingdom: results of an omnibus survey. Br JDermatol 1993;126:23-7.
219. Sais G, Jucglà A, Peyri J. Prevalence of dermatophyte ony-chomycosis in Spain, a cross-sectional study. Br J Dermatol1995;132:758-61.
220. Elewski BE, Charif MA. Prevalence of onychomycosis inpatients attending a dermatology clinic in Northeastern Ohiofor other conditions. Arch Dermatol 1997;133:1172-3.
221. Clemons KV, Schar G, Stover EP, Feldman D, Stevens DA.Dermatophyte-hormone relationships: characterization ofprogesterone—binding specificity and growth inhibition inthe genera Trichophyton and Microsporum. J Clin Microbiol1988;26:2110-5.
222. Gupta AK, Adam P, Hofstader SLR. Itraconazole oral solu-tion for the treatment of onychomycosis. Pediatric Dermatol1998;15:464-71.
223. Gupta AK, Sibbald RG, Lynde CW, et al. The prevalence ofonychomycosis in children and treatment strategies. J AmAcad Dermatol 1997;36:395-402.
224. Schachner L, Ling NS, Press S. A statistical analysis of apediatric dermatology clinic. Pediatr Dermatol 1983;1:157-64.
225. Philpot CM, Shuttleworth D. Dermatophyte onychomycosisin children. Clin Exp Dermatol 1989;14:203-5.
226. English MP. Tinea pedis as a public health problem. Br JDermatol 1969;81:705-7.
227. Attye A, Auger P, Joly J. Incidence of occult athlete’s foot inswimmers. Eur J Epidemiol 1990;6:244-7.
228. Hope YM, Clayton YM, Hay RJ, Noble WC, Elder-SmithJG. Foot infection in coal miners: a reassessment. Br J Der-matol 1985;112:405-13.
229. English MP, Wethered RR, Duncan EH. Studies in the epi-demiology of tinea pedis—VIII: fungal infection in a long-stay hospital. Br Med J 1967;3:136-9.
230. Strauss JS, Kligman AM. An experimental study of tineapedis and onychomycosis of the foot. Arch Dermatol 1957;76:70-9.
231. Jones HE. Immune response and host resistance of humansto dermatophyte infections. J Am Acad Dermatol 1993;28:S12-8.
232. Dahl MV. Suppression of immunity and inflammation byproducts produced by dermatophytes. J Am Acad Dermatol1993;28:S19-23.
233. Hanifin JM, Ray LF, Lobitz WC Jr. Immunological reactiv-ity in dermatophytosis. Br J Dermatol 1974;90:1-8.
234. Mandel EH. Diagnois: tinea circinate and onychomycosis(Trichophyton purpureum)—resistance to griseofulvinduring uncontrolled diabetes. Arch Dermatol 1960;82:1027-8.
235. Nelson LM. Recurrent Cushing’s syndrome with Tricho-phyton rubrum infection. Arch Dermatol 1959;80:700-4.
236. Lewis GM, Hopper ME, Scott MJ. et al. GeneralizedTrichophyton rubrum infection associated with systemiclymphoblastoma. Arch Dermatol 1953;67:242-62.
237. Hay RJ, Brostoff J. Immune responses in patients withchronic Trichophyton rubrum infections. Clin Exp Dermatol1977;2:373-80.
238. Daniel CR III, Norton LA, Scher RK. The spectrum of dis-ease in patients with human immunodeficiency virus infec-tion. J Am Acad Dermatol 1992;27:93-7.
239. Gupta AK, Lynde CW, Jain HC, et al. A higher prevalenceof onychomycosis in psoriatics compared with non-psoriat-ics: a multicenter study. Br J Dermatol 1997;136:786-9.
240. Baran R, de Doncker P. Lateral edge nail involvement indi-cates poor prognosis for treating onchomycosis with the newsystemic antifungals. Acta Derm Venereol 1996;76:82-3.
241. Tosti A, Piraccini BM, Mariani R, Stinchi C, Buttasi C. Arelocal and systemic conditions important for the developmentof onychomycosis? Eur J Dermatol 1998;1:41-4.
242. Gupta AK, Daniel CR III. Factors that may affect theresponse of onychomycosis to oral antifungal therapy.Australasian J Dermatol 1998;39:222-4.
243. Gupta AK, Daniel CR. Onychomycosis: strategies to reducefailure, and recurrence. Cutis 1998;62:189-91.
244. Roberts DT, Evans EG. Subungual dermatophytoma compli-

Curr Probl Dermatol, July/August 2001 245
cating dermatophyte onychomycosis. Br J Dermatol 1998;138:189-90.
245. Pollak RA, Billstein SA. Safety of oral terbinafine for toenailonychomycosis. J Am Podiatr Med Assoc 1997;87:565-70.
246. Del Rosso JQ, Gupta AK, Conte ET. How to recognize andmanage adverse reactions to oral antifungals. Skin and Aging1999;May:48-56.
247. Hall M, Monka C, Krupp R, O’Sullivan D. Safety of oralterbinafine: results of a postmarketing surveillance study in25, 884 patients. Arch Dermatol 1997;133:1213-9.
248. O’Sullivan DP, Needham CA, Bangs A, Atkin K, KendallFD. Postmarketing surveillance of oral terbinafine in theUK: report of a large cohort study. Br J Clin Pharmacol1996;42:559-65.
249. Stricker BHC, Van Riemsdijk MM, Stunkenboom MCJM, etal. Taste loss to terbinafine: a case-control study of potentialrisk factors [abstract]. Pharmacoepidemiol Drug Safety1995;4:522.
250. Amichai B, Grunwald MH. Adverse drug reactions of thenew oral antifungal agents—terbinafine, fluconazole anditraconazole. Int J Dermatol 1998;37:410-5.
251. Gupta AK, De Doncker P, Heenen M. An overview and anassessment of the use of the antifungal agents itraconazole,terbinafine and fluconazole in dermatology. In: Korting HC,Schäfer-Korting M, editors. The benefit/risk ratio: a hand-book for the rational use of potentially hazardous drugs.Boca Raton: CRC Press; 1999. p. 263-85.
252. Gupta AK, Shear NH. Safety review of the new oral anti-fungal agents to treat superficial mycoses. Int J Dermatol1999;38(Suppl 2):40-52.
253. Gupta AK, Shear NH. A questionnaire study on the manage-ment of onychomycosis: Canadian perspective. Int J Derma-tol 1998;37:457-60.
254. Katz HI, Gupta AK. Oral antifungal drug interactions.Dermatol Clin 1997;15:535-44.
255. Gupta AK, Katz HI, Shear NH. Drug interactions with itra-conazole, fluconazole and terbinafine, and their manage-ment. J Am Acad Dermatol 1999;41:237-49.
256. Department of Health and Human Services, Centers forDisease Control and Prevention. National diabetes fact sheet:national estimates and general information on diabetes in theUnited States. Atlanta, GA: US Department of Health andHuman Services, Centers for Disease Control and Preven-tion; 1997.
257. Bild DE, Selby JV, Sinnock P, Browner WS, Braveman P,Showstack JA. Lower-extremity amputation in people withdiabetes. Epidemiology and prevention. Diabetes Care 1989;12:24-31.
258. Litzleman DK, Slemenda CW, Langefeld CD, et al.Reduction of lower extremity clinical abnormalities in patientswith non-insulin dependent diabetes mellitus. Ann InternMed 1993;119:36-41.
259. LeFrock JL, Joseph WS. Bone and soft-tissue infections ofthe lower extremity in diabetics. Clin Podiatr Med Surg1995;12:87-103.
260. Huse DM, Oster G, Killen AR, Lacey MJ, Colditz GA. Theeconomic costs of non-insulin-dependent diabetes mellitus.JAMA 1989;262:2708-13.
261. Trautner C, Haastert B, Giani G, Berger M. Incidence of
August 2001
lower limb amputations and diabetes. Diabetes Care 1996;19:1006-9.
262. Yopsipovitch G, Hodak E, Vardi P, Shraga I, Karp M,Sprecher E, David M. The prevalence of cutaneous manifes-tations in IDDM patients and their association with diabetesrisk factors and microvascular complications. Diabetes Care1998;21:506-9.
263. Evans SL, Nixon BP, Lee I, Yee D, Mooradian AD. Theprevalence and nature of podiatric problems in elderly dia-betic patients. J Am Geriatr Soc 1991;39:241-5.
264. Leyden JJ, Aly R. Tinea pedis. Semin Dermatol 1993;12:280-4.
265. Leyden JJ, Kligman AM. Interdigital athlete’s foot: newconcepts in pathogenesis. Postgrad Med 1977;61:113-6.
266. Leyden JJ, Klingman AM. Interdigital athlete’s foot. Theinteraction of dermatophyte and resident bacteria. Arch Der-matol 1978;114:1466-72.
267. Kates SG, Nordstrom KM, McGinley KJ, Leyden JJ.Microbial ecology of interdigital infections of the toe webspaces. J Am Acad Dermatol 1990;22:578-82.
268. Bolanos B. Dermatophyte feet infection among students en-rolled in swimming courses at a university pool. Bol AssocMed P R 1991;83:181-4.
269. Semel JD, Goldin H. Association of athlete’s foot with cel-lulitus of the lower extremities: diagnostic value of bacterialcultures of ipsilateral interdigital space samples. Clin InfectDis 1996;23:1162-4.
270. Aly R, Maibach HI, Bagatell FK, et al. Ciclopiroxolaminelotion 1%: bioequivalence to ciclopiroxolamine cream 1%and clinical efficacy in tinea pedis. Clin Ther 1989;11:290-303.
271. Smith EB, Graham JL, Ulrich JA. Topical clotrimazole intinea pedis. South Med J 1977;70:47-8.
272. Bergstresser PR, Elewski B, Hanifin J, et al. Topical terbina-fine and clotrimazole in interdigital tinea pedis: a multicen-ter comparison of cure and relapse rates with 1- and 4- weektreatment regimens. J Am Acad Dermatol 1993;28:648-51.
273. Kates SG, Myung KB, McGinley KJ, Leyden JJ. Theantibacterial efficacy of econazole nitrate in interdigital toeweb infections. J Am Acad Dermatol 1990;22:583-6.
274. Gupta AK, Einarson TR, Summerbell RC, Shear NH. Anoverview of topical antifungal therapy in dermatomycoses.Drugs 1998;55:645-74.
275. Leyden JJ, Kligman AM. Aluminum chloride in the treat-ment of symptomatic athlete’s foot. Arch Dermatol 1975;11:1004-10.
276. De Keyser P, DeBacker M, Massart DL, Westclinck KJ.Two-week oral treatment of tinea pedis comparingterbinafine (250 mg/day) with itraconazole (100 mg/day): adouble-blind, multicentre study. Br J Dermatol 1994;130:22-5.
277. Piérard GE, Wallace R, DeDoncker P. Biometrologicalassessment of the preventive effect of a miconazole spraypowder on athelete’s foot. Clin Exp Dermatol 1996;21:344-6.
278. Pollak R, Billstein SA. Safety of oral terbinafine for toenailonychomycosis. J Am Podiatr Med Assoc 1997;87:565-70.
279. Albreski DA, Gross EG. The safety experience of itracona-zole in the diabetic population: randomized, open-label
evalence ofgies. J Am
nalysis of a1983;1:157-
chomycosis
oblem. Br J
ete’s foot in
Elder-Smitht. Br J Der-
s in the epi-n in a long-
dy of tineamatol 1957;
of humansol 1993;28:
mmation byd Dermatol
cal reactiv--8.chomycosisriseofulvinl 1960;82:
ith Tricho-0:700-4.Generalizedh systemic2.atients withxp Dermatol
rum of dis-virus infec-
prevalencenon-psoriat-:786-9.ement indi-
with the new76:82-3.ttasi C. Areevelopment
affect theal therapy.
es to reduce
ma compli-
246 Curr Probl Dermatol, July/August 2001
study of itraconazole capsules versus palliative care for ony-chomycosis of the toenail in diabetic patients. J Am PodiatrMed Assoc 1999;89:339-45.
280. Verspeelt J, Marynissen G, Gupta AK, De Doncker P. Safetyof itraconazole in diabetic patients. Dermatology 1999;198:382-4.
281. Elewski BE, Greer DL. Hendersonula toruloidea andScytalidium hyalinum: Review and update. Arch Dermatol1991;127:1041-4.
282. Gupta AK, Horgan-Bell CB, Summerbell RC. Onychomyco-sis associated with Onychocola canadensis: 10 case reportsand a review of the literature. J Am Acad Dermatol 1998;39:410-7.
283. NCCLS. Reference method for broth dilution antifungal test-ing of yeasts; approved standard. NCCLS document M27-A.Wayne, PA: NCCLS; 1997 June.
284. Kawakami M, Suzuki K, Ishizuka T, Hidaka T, Matsuki Y,Nakamura H. Effect of grapefruit juice on pharmacokineticsof itraconazole in healthy subjects. Int J Clin Pharmacol Ther1998;36:306-8.
285. Kunze KL, Wienkers LC, Thummel KE, Trager WF.Warfarin-fluconazole—I: inhibition of the human cyto-chrome p450-dependent metablism of warfarin by flucona-zole: in vitro studies. Drug Metab Dispos 1996;26:414-21.
286. Black DJ, Kunze KL, Wienkers LC, et al. Warfarin-flucona-zole. II. A metabolically based drug interaction: in vivo stud-ies. Drug Metab Dispos 1996;24:422-8.
287. Kunze KL, Trager WF. Warfarin-fluconazole—III: a ratio-nal approach to management of a metabolically based druginteraction. Drug Metab Dispos 1996;24:429-35.
288. Hull PR. Onychomycosis—treatment, relapse and re-infec-tion. Dermatology 1997;194:7-9.
289. Tosti A, Piraccini BM, Stinchi C, Colombo MD. Relapses ofonychomycosis after successful treatment with systemicantifungals: a three-year follow-up. Dermatology 1998;197:162-6.
290. Gupta AK, Scher RK. Oral antifungal agents for onychomy-cosis. Lancet 1998;351:541-2.
291. Epstein E. How often does oral treatment of toenail ony-chomycosis produce a disease-free nail? an analysis of pub-lished data. Arch Dermatol 1998;134:1551-4.
292. Drake L, Shear NH, Arlette JP, et al. Oral terbinafine in thetreatment of toenails onychomycosis: North American mul-ticenter trial. J Am Acad Dermatol 1997;37:740-5.
293. Friedlander SF. The evolving role of itraconazole, flucona-zole and terbinafine in the treatment of tinea capitis. PediatrInfect Dis J 1999;18:205-10.
294. Friedlander SF, Suarez S. Pediatric antifungal therapy.Dermatol Clin 1998;16:527-37.
295. Blumer JL. Pharmacologic basis for the treatment of tineacapitis. Pediatr Infect Dis J 1999;18:191-9.
296. Tack DA, Fleischer A Jr, McMichael A, Feldman S. The epi-demic of tinea capitis disproportionately affects school-agedAfrican Americans. Pediatr Dermatol 1999;16:75.
297. Elewski BE. Treatment of tinea capitis with itraconazole. IntJ Dermatol 1997;36:539-41.
298. Gupta AK, Hofstader SL, Adam P, Summerbell RC. Tineacapitis: an overview with emphasis on management. PediatrDermatol 1999;16:171-89.
299. Frieden IJ, Howard R. Tinea capitis: epidemiology, diagno-sis, treatment and control. J Am Acad Dermatol 1994;31:542-6.
300. Aly R. Ecology, epidemiology and diagnosis of tinea capitis.Pediatr Infect Dis J 1999;18:180-5.
301. Committee on Infectious Diseases. Tinea capitis. In: Peter G,editor. 1997 Red Book: report of the Committee on Infec-tious Diseases. 24th ed. Chicago: American Academy ofPediatrics; 1997. p. 523-5.
302. Jahangir M, Hussain I, Hassan M, Haroon TS. A double-blind, randomized, comparative trial of itraconazole versusterbinafine for 2 weeks in tinea capitis. Br J Dermatol1998;139:672-4.
303. Elewski BE. Treatment of tinea capitis: beyond griseofulvin.J Am Acad Dermatol 1999;40:527-30.
304. Abdel-Rahman SM, Nahata MC. Treatment of tinea capitis.Ann Pharmacother 1997;31:338-48.
305. Jones, TC. Overview of the use of terbinafine (Lamisil) inchildren. Br J Dermatol 1995;132:683-9.
306. Sperling LC, Mezebish DS. Hair diseases. Med Clin NorthAm 1998;82:1155-69.
307. Noble SL, Forbes RC, Stamm PL. Diagnosis and manage-ment of common tinea infections. Am Fam Physician 1998;58:163-74.
308. O’Dell ML. Skin and wound infections: an overview. AmFam Physician 1998;57:2424-32.
309. Stein DH. Superficial fungal infections. Pediatric Clin NorthAm 1983;30:545-61.
310. Caputo RV. Fungal infections in children. Derm Clin 1986;4:137-49.
311. Gupta AK, Nolting S, deProst Y, et al. Itraconazole for thetreatment of dermatomycoses in children. 1999;199:248-52.
312. Gupta AK, Chang P, Del Rosso JQ, Adam P, Hofstader SLR.Onychomycosis in children: prevalence and management.Pediatr Dermatol 1998;15:464-71.
Copyright © 2022 FDOKUMEN




















