
The use of hydrophilic polymers as artificial vitreous
34
Pergamon Prog. Polym. Sci., Vol. 23,475-508 , 1998 Copyright 0 1998 Elsevier Science Ltd Printed in Great Britain. All rights reserved. 0079-6700/98 $19.00 SOO79-6700(97)00045-2 THE USE OF HYDROPHILIC POLYMERS AS ARTIFICIAL VITREOUS TRAIAN V. CHIRILA’,*, YE HONGB’b, PAUL D. DALTON’, IAN J. CONSTABLEa.b, MIGUEL F. REFOJO’ “Department of Biomaterials and Polymer Research, Lions Eye Institute, Perth, Western Australia, Australia bCentre for Ophthalmology and Visual Science, The University of Western Australia, Perth, Western Australia, Australia ‘The Schepens Eye Research Institute, Harvard Medical School, Boston, MA, USA CONTENTS 1. Introduction 1.1. The vitreous body of the eye 1.2. Need for vitreous substitution 1.3. Properties of an ideal substitute 2. Historical overview of non-polymeric and natural vitreous substitutes 3. Polymeric vitreous substitutes 3.1. Sernisynthetic polymers 3.1. I. Polysaccharides 3.12. Gelatin 3.2. Synthetic polymers 3.2.1. Poly( 1-vinyl-2-pyrrolidinone) 3.2.:2. Polyacrylamide 3.2..3. Poly(glycery1 methacrylate) 3.2.4. Poly(viny1 alcohol) 3.25. Poly(2-hydroxyethyl acrylate) 3.2.16. Poly(methy1 acrylamidoglycolate methyl ether) 4. Rheological studies on vitreous body and artificial substitutes 4.1. Rheology of the vitreous body 4.2. Oscillatory shear experiments as criteria for potential vitreous substitutes 5. Conclusions Acknowledgements References 475 475 477 481 482 486 487 487 491 491 491 493 494 495 496 496 497 497 499 501 502 502 1. INTRODUCTION 1.1. The vitreous body of the eye The vitreous body of the vertebrate eye should be regarded as a rather fascinating result of natural evolution. It consists almost exclusively of water, therefore appears like a very simple 475
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of The use of hydrophilic polymers as artificial vitreous
Pergamon Prog. Polym. Sci., Vol. 23,475-508 , 1998
Copyright 0 1998 Elsevier Science Ltd Printed in Great Britain. All rights reserved.
0079-6700/98 $19.00
SOO79-6700(97)00045-2
THE USE OF HYDROPHILIC POLYMERS AS ARTIFICIAL VITREOUS
TRAIAN V. CHIRILA’,*, YE HONGB’b, PAUL D. DALTON’, IAN J. CONSTABLEa.b, MIGUEL F. REFOJO’
“Department of Biomaterials and Polymer Research, Lions Eye Institute, Perth, Western Australia, Australia
bCentre for Ophthalmology and Visual Science, The University of Western Australia, Perth, Western Australia, Australia
‘The Schepens Eye Research Institute, Harvard Medical School, Boston, MA, USA
CONTENTS
1. Introduction 1.1. The vitreous body of the eye 1.2. Need for vitreous substitution 1.3. Properties of an ideal substitute
2. Historical overview of non-polymeric and natural vitreous substitutes 3. Polymeric vitreous substitutes
3.1. Sernisynthetic polymers 3.1. I. Polysaccharides 3.12. Gelatin
3.2. Synthetic polymers 3.2.1. Poly( 1-vinyl-2-pyrrolidinone) 3.2.:2. Polyacrylamide 3.2..3. Poly(glycery1 methacrylate) 3.2.4. Poly(viny1 alcohol) 3.25. Poly(2-hydroxyethyl acrylate) 3.2.16. Poly(methy1 acrylamidoglycolate methyl ether)
4. Rheological studies on vitreous body and artificial substitutes 4.1. Rheology of the vitreous body 4.2. Oscillatory shear experiments as criteria for potential vitreous substitutes
5. Conclusions Acknowledgements References
475 475
477 481
482 486 487 487 491 491 491
493 494 495 496 496 497 497 499 501 502 502
1. INTRODUCTION
1.1. The vitreous body of the eye
The vitreous body of the vertebrate eye should be regarded as a rather fascinating result of natural evolution. It consists almost exclusively of water, therefore appears like a very simple
475

476 T. V. CHIRILA et al.
element of the eye. Still, this highly hydrated material is structured in such a way that it behaves like a gel which, if dissected from the surrounding tissues, does not collapse under its own weight. This gel behaves as a solid and yet retains most of the properties of the fluid component (water) which are insignificantly altered. In fact, the very large amount of water is merely filling the interstitial spaces within a complicated scaffold made up of a protein
(collagen), a polysaccharide (hyaluronan), and proteoglycans. Although these biopolymers represent quantitatively a very minor fraction of the vitreous mass, their interpenetration results in a material with sufficient mechanical strength and elasticity to fulfil all functional
demands, and with remarkable optical clarity. The vitreous body (corpus vitreus), also termed vitreous humor, vitreus, or simply,
vitreous, is a clear and transparent jellylike mass filling the posterior cavity of the eye and occupying more than two-thirds of the ocular volume. The vitreous provides an adequate support for the retina, protects the surrounding ocular tissues from adverse circumstances, allows light to reach the sensory elements at the back of the eye, and allows the diffusion of metabolic solutes. According to Balazs, ’ the human vitreous consists of approximately 80% gel fraction and 20% liquid fraction, the latter increasing with age. Most other mammals have little or no liquid fraction.
The anatomy of the vitreous has been investigated for almost three centuries2’3 and led to many theories being advanced to explain its macroscopic structure, all widely divergent.
Closer to our time, Worst435 developed the concept of “cisternal system” which to date is probably the most appropriate anatomical description of the vitreous body.
The microscopic morphology of the vitreous and the relationship to its biological perfor- mance are not fully elucidated. There are currently two differing concepts on the nature of vitreous body. Some evidence supports the view that the vitreous is basically an extracellular matrix.6 Another model regards the vitreous as a specialized, albeit simple, connective
tissue. 7,8 Since the two theories are not yet reconciled, the structure and role of the vitreous are usually regarded from both points of view. 9 It is now accepted that the vitreous body is the result of a unique macromolecular organization, a double-network system consisting of a scaffold of randomly spaced rod-like collagen fibers, filled and entangled with a network of very large, coiled-up macromolecules of hyaluronan. The latter is present as its sodium salt (sodium hyaluronidate). The two biopolymers interact in such a manner that the resulting
body is a stable hydrogel in its normal state. In pathological conditions this hydrogel can undergo syneresis or mechanical collapse. The “mechanochemical model” proposed by Balazs’ is based on the double-network concept and explains satisfactorily the relation between some properties of the vitreous body and the physicochemical principles governing
its stability. Subsequent studies6 suggested that the Balazs model overestimated the impor- tance of hyaluronan, which should be rather regarded as a matrix-filler substance.
From the polymer scientist’s point of view, it is difficult to include correctly the natural vitreous within one of the known classes of multicomponent polymer materials such as blends, grafts, blocks, or interpenetrating polymer networks (IPNs). This is due to the uncertainty surrounding the presence of crosslinks, physical or covalent, either within any of the two components or between them. Based on rheological studies, Tokita ef al. lo con- cluded that the vitreous characteristics must be the result of a slight crosslinking between collagen and hyaluronan. The existence of interconnecting filaments between collagen fibrils and hyaluronan coils was demonstrated by transmission electron microscopy, l1 and digestion experiments using hyaluronidase indicated that these filaments are chemically different from

HYDROPHILIC POLYMERS AS ARTIFWIAL VITREOUS 477
hyaluronan. They may be “link” structures of a glycoprotein or proteoglycan nature.3*12*13
When a collagen fibril is common to two different bundles which are close to each other, as
surmised by Sebag and Balazs,14 it can conceivably act as a crosslink. However, Balazs recently concluded’ that the collagen network in the vitreous is not crosslinked, and that
the interaction between collagen and hyaluronan is based on very weak forces, likely mole- cular entanglements. The fact &at more than 90% of the hyaluronan in the vitreous gel can be separated frlom the collagen fibrils by using mechanical separation methods was regarded as a proof for the latter statement. It can be similarly argued that the remaining 10% of the hyaluronan could not be separated because it was retained by the collagen network through interactions stronger than entanglements.
1.2. Need for vitreous substitution
The vitreous body is an important intraocular element not only because of its optical and mechanical performances, but also due to its significant role in the pathogenesis and treat- ment of conditions affecting adjacent tissues or eventually the whole eye. There are two
situations in which the availability of an artificial vitreous, to be used as a supplement or as a total replacement, would significantly reduce the occurrence of blindness. In discussing this topic a specific terminology was unavoidable, and the majority of terms are explained in Table 1, in their approximate order of apparition.
First, the vitreous body can itself become dysfunctional either due to opacification or by its physical collapse and liquefaction. Pathological causes for dysfunctional vitreous include: i5-” developmental abnormalities, inflammatory processes (from infection, injury or retinal disease), hemorrhage, systemic diseases (e.g. tumors, diabetes mellitus), and degenerative processes (e.g. aging changes, myopia, hereditary hyaloideoretinopathies). The traumatic destruction of the vitreous body can be caused by mechanical, chemical and thermal trauma, or by the presence of intraocular foreign bodies. A collapsed or liquefied
vitreous has a great tendency to detach from the retina, and this change predisposes to damage of the retinal surface, vitreous bleeding or to retinal detachment, due to traction developing at any point of strong vitreoretinal adhesion.
All these conditions may result in extremely poor vision or even blindness. In principle, a total replacement of the afflicted vitreous with a biocompatible, transparent material would be desirable in such cases. However, the treatment of a dysfunctional vitreous is not the most important reason for which the vitreous substitutes are needed. In fact, the incidence of blindness in the world population due to an opaque vitreous is much lower than that due to cataract, cornea1 dysfunctionality, or retinal diseases. It is the surgical treatment of various complicated retinal detachments that mostly requires the availability of a vitreous substitute, either temporary or permanent, ideally to be injectable into the vitreous cavity at the time of surgery.
The retina is the eye’s sensory receptor for light. It is one of the three layers (Fig. 1) together constituting the wall which surrounds the vitreous cavity. This essential ocular element can be afflicted by many pathological conditions, as exemplified in Fig. 2, and most of them 1ea.d to blindness if not treated or if the treatment is not successful. Many of these afflictions are causally related to the detachment of the retina. A retinal detachment is the separation d the neural retina from the underlying pigment epithelium. The detachment of the vitreous (Fig. 3) may lead to tearing of the retina and the resulting holes, breaks or tears in

478 T. V. CHIRILA et al.
Table 1. Glossary
Term Explanation
Vitreous detachment
Vitreous traction
Cataract
Collapse of the vitreous body and its separation from the retinal surface. The pull of the retina by the vitreousIt can produce breaks or tears in the retinal tissue. Opacity of the crystalline lens.It prevents clear images forming on the retina and requires the surgical removal of the lens.
Macula
Diabetic retinopathy
A specialized small central area of the retina, devoid of blood vessels, which is responsible for acute central vision. An array of changes and disorders which develop in the retina of diabetic persons3 advances progressively to proliferative vitreoretinopathy, which consists of growth of new blood vessels and fibrous tissue.
Epiretinal membrane
Preretinal
Subretinal fluid
Choroidal detachment Vitrectomy
Transcleral vitrectomy
Scleral buckling
Pathologic formation of fibrocellular membranes causing the wrinkling of the retina. Pertaining to processes occurring immediately in front of the retina and behind the posterior vitreous face. Fluid that accumulates under the detached retinaIt can be drained by a hole made through the sclera and choroid. Separation of the choroid from the sclera. Removal of a portion of the vitreous, or of vitreous debris (blood, membranes), by surgical excision and/or suction. Vitrectomy performed by entering the vitreous cavity through the sclera. Surgical procedure for treating retinal detachment, designed to push the sclera and choroid against the retina.The sclera is indented or “buckled” inward by implanting a device made of an elastic material.
Uvea, uveitis Uvea is the generic term for the middle pigmented layer of the eye (iris, ciliary body, choroid), containing most of the blood vessel supplylnflammation of any of these elements is termed uveitis.
Rhegmatogenous retinal detachment
Glaucoma
Retinal detachment associated with, and usually caused by, a retinal break or tear. Group of diseases characterized by an increased intraocular pressure.Results in damage to the optic nerve and retinal nerve fibers.
Macrophages
Phagocytes
Cornea1 edema Vitritis
Ophthalmoscopy
Tonometry Chorioretinal
Large, mononuclear, highly active cells occurring in connective tissues.They become mobile when stimulated by inflammation. Also, they contribute to antibody production. Cells that ingest other cells or foreign bodies through a process called phagocytosis. Pathologic condition resulting in a hazy and swollen cornea. Inflammatory reaction in the vitreous accompanied by opacification and cellular invasion. Examination of the interior of the eye, especially the fundus (retina), using specific magnifying instruments called ophthalmoscopes. Measurement of intraocular pressure. Pertaining to pathological conditions afflicting the choroid and retina together.
Glial cells Cells of the supporting structure of any nervous tissue. Cytostatic agent An agent that suppresses the growth and proliferation of cells. Cytocidal agent An agent that kills cells.

HYDROPHILIC POLYMERS AS ARTIFICIAL VITREOUS 479
Fig. 1. Posterior ocular elements: 1 --sclera; 2-choroid; 3-retina; 3a-retinal pigment epithelium; 4-vitreous; S-blood vessels.
Fig. 2. A section through the posterior segment of the eye with a conceptual representation of pathological conditions affecting the retina: 1 -vitreous traction band; 2-fibrovascu- lar membrane; 3-macular edema; 4-submacular choroidal neovascularization; 5-dia- betic lretinopathy and vein branch occlusion; 6-epiretinal membrane; 7-retinal tear;
8-retinal detachment.
480 T. V. CHIRILA et al.
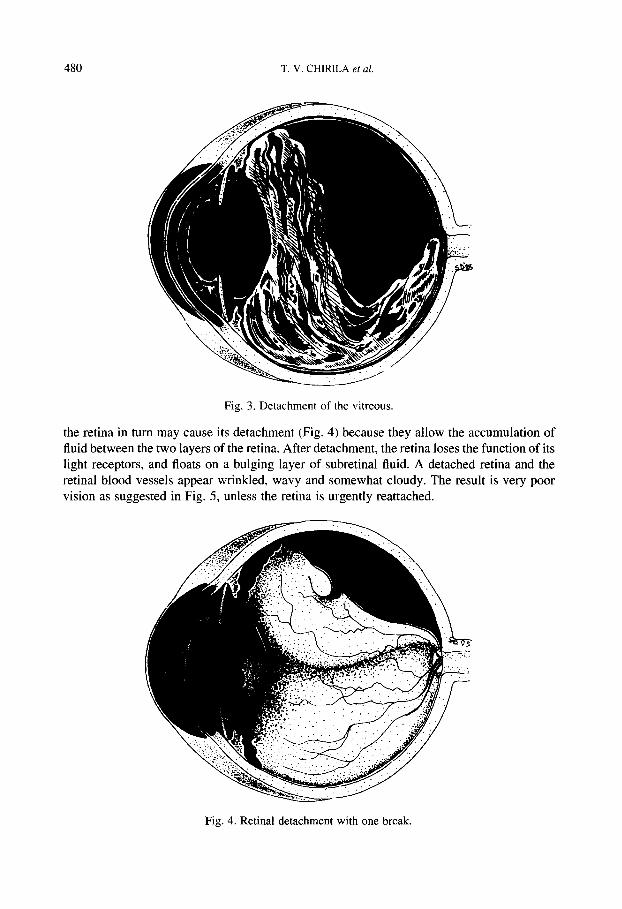
Fig. 3. Detachment of the vitreous.
the retina in turn may cause its detachment (Fig. 4) because they allow the accumulation of fluid between the two layers of the retina. After detachment, the retina loses the function of its light receptors, and floats on a bulging layer of subretinal fluid. A detached retina and the retinal blood vessels appear wrinkled, wavy and somewhat cloudy. The result is very poor vision as suggested in Fig. 5, unless the retina is urgently reattached.
Fig. 4. Retinal detachment with one break.

HYDROPHILIC POLYMERS AS ARTIFICIAL VITREOUS
@
a Fig. 5. Appearance of the same object to a person with normal vision (a) and to a person
with a detached retina (b).
Vitreous substitution is indicated in several vitreoretinal surgical procedures. The purpose of injecting a fluid substance into the vitreous cavity is the restoration of the volume and pressure of the eye globe, either as an adjunct to surgery or in order to replace or supplement a collapsed vi.treous body. The injected substitute should be able to exert a hydraulic pressure so as to provide tamponade to the retina against the choroid, and should alter the character- istics of the vitreous in order to relax the preretinal traction and to prevent the formation of new vitreoretinal traction which can occur due to cellular invasion laying down new scar tissue. Situations in which the vitreous substitution or supplementation are beneficial include: 18~*5’ after the drainage of the subretinal fluid during retinal detachment surgery; after
the fluid drainage in large choroidal detachments; for the maintenance of normal volume and pressure during transcleral vitrectomy; in cases of shallow, total retinal detachment where the small volume of subretinal fluid does not permit or justify extensive scleral surgery; during vitreoretinall surgery in presence of vitreous traction bands; in scleral buckling surgery with a collapsed vitreous; in surgery for the repair of penetrating injuries of the posterior segment; when the globe is still soft after repair of the eye wall.
1.3. Properties of an ideal substitute
To find a proper replacement for the natural vitreous is not an easy task. This has been proved by the numerous attempts made during this century in the hope that a truly functional substitute will eventually materialize. The situation was appropriately described by Sebag: 3 “History has witnessed the injection of nearly every imaginable substance into the vitreous.”
482 T.V.CHIRILA et al.
Both the characteristics displayed by the natural vitreous per se, as well as the experience so far with various materials suggest that an ideal substitute should fulfil the following
criteria:
1. it should be clear, transparent and colorless, and its density and refractive index should not be greatly different from those of the natural vitreous;
2. it should be storable and sterilizable, chemically and biologically inert, and non-toxic, hence would not trigger any undesirable biological responses (e.g. inflammation, cellular
invasion, scarring, neocollagen formation); 3. it should be biocompatible with the vitreous humor itself and with the adjacent tissues, and
should not affect their physiologic functions; 4. it should not be absorbable or biodegradable, in order to be maintained in the vitreous
cavity for a period as long as possible; 5. it should have lasting viscoelastic properties to avoid its own drainage through retinal
breaks, to push back the retina to proper position until secure adhesion is achieved, and to
prevent retinal redetachment; 6. it should have sufficient rigidity in order to assure proper tamponade of the retina against
the choroid and to counteract traction by vitreoretinal adhesions; 7. it must allow the transfer of necessary metabolites and proteins inside the vitreous, and to
or from the neighboring tissues, without disturbing the metabolic processes; 8. it should not lose transparency when procedures for closure of retinal breaks involving
high or low temperatures and light or laser beams are used; 9. preferably, it should be injectable through a small-gauge needle and all above properties
should be retained after injection; alternatively, it should be implantable through a small incision;
10. preferably, it should be a hydrophilic material with a high equilibrium water content, but must not be soluble in water.
The current unavailability of a material to replace successfully the vitreous body gives an indication of the difficulty in fulfilling this set of requisites.
2. HISTORICAL OVERVIEW OF NON-POLYMERIC AND NATURAL VITREOUS SUBSTITUTES
In 1890, Ford2’ treated the opaque vitreous in a human patient by partly removing it, but he did not replace the removed material. Deutschmann21g22 used healthy animal vitreous to treat retinal detachment in human patients, and he obtained improvement in 43% of cases. This
choice appeared reasonable since the vitreous is the normal inhabitant of the vitreous cavity. Gradenigo23 was the first to inject water into the vitreous, and others followed his example using physiological saline solutions. 24-26 Rosengren27-30 is credited with the first true scien- tific approach to the use of air tamponade in a large series of retinal detachments. Tables 2-7 summarize in a chronological order the various non-polymeric and natural agents used during this century as materials for vitreous substitution or supplementation. There is large variability in the reported performance of most of these agents. In many cases, certain materials were used with significant success in the treatment of retinal detachment. However, most of the agents failed in the long term due to their short-lived residence in the vitreous cavity and/or to postoperative complications such as inflammation, damage to lens and
HYDROPHILIC POLYMERS AS ARTIFICIAL VITREOUS 483
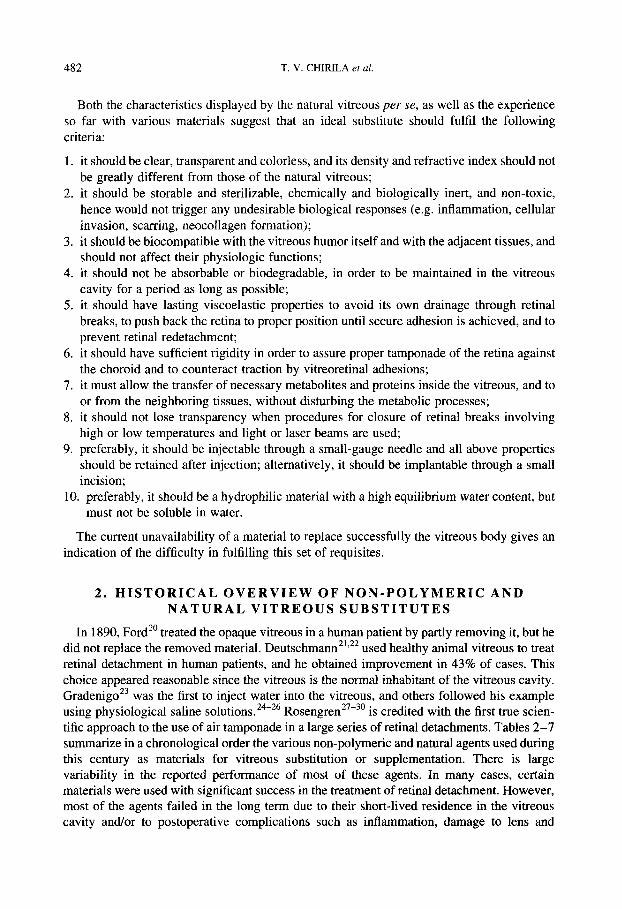
Table 2. Vitreous substitution with gases
Gas Recipient Pathological Clinical Remarks References (No. of cases) conditions follow-up
(months)
Air Air
Air Air
Air
Air/SF6 C~FIZ
Cat Human (2)
Human (300) Human (3)
Human (5)
Rabbit (24) Rabbit (14)
SF6 Monkey
Air, Air/SF6 Monkey (70%), Air/ C4F8 (70%) SF6 Human (69)
Xenon Human (4)
C3F8 Rabbit (8)
CzF6, C3F8 Human (56)
CZF6y C3Fs Human (87)
- n.a. Retinal detachment 0.5
Retinal detachment 12-96 Glaucoma, Injury 2-4
Retinal detachment 4
- na. - 6
- n.a.
- n.a.
Retinal detachment 6
Retinal detachment 6- 12
- 4
Retinal detachment 6
Retinal detachment 6-106
Short retention. 31 Reattachment 31
(1 case). 78% reattachment 27-29
Beneficial as a 32
surgical aid. Vision improved. 33 40% reattachment. No toxic effect. 34 No adverse reaction. 35 Some complications (cataract, glaucoma). No toxic effect. 36 Cataract.Transient rise in intraocular pressure. Mild irritation. 37
Vision improved. 38 65% reattachment. Mild cataract. Transient rise in intraocular pressure. Vision improved. 39 100% reattachment. Short retention. No toxic effect. 4o Transient cataract. 55% reattachment. 4’ Transient rise in intraocular pressure. Vision improved. 42
78% reattachment.
cornea, glaucoma, and various retinopathies. Most also lacked the viscoelastic properties of
the normal vitreous body. A special mention is due to the use of silicone oils as tamponade materials in vitreoretinal
surgery. Although they are formally synthetic polymers, the silicone oils will not be reviewed here, as the topic was treated in detail by Giordano and Refojo in this issue. so The silicone oils possess some important characteristics which singled them out as promising candidates for vitreous substitution: permanent retention in the vitreous cavity, remarkable optical clarity and chemic,al inertness. Since it was found that these materials were tolerated in the eye,91-93 their use in vitreoretinal surgery has been alternately advocated and castigated, and this controversy still lingers on. There is convincing evidence94-98 that the silicone oils in the

484 T. V. CHIRILA et al.
Table 3. Vitreous substitution with physiological saline solutions
Recipient (Number of cases)
Pathological conditions Remarks References
Rabbit (12)
Human (16)
Human (15)
Human (4)
Hemorrhagic vitreous Opaque vitreous Purulent infiltration Opaque and hemorrhagic vitreous Retinal detachment
Human (75) Retinal detachment
Well tolerated by tissues. 24 Transparency maintained. 25 100% vision recovered in cases of hemorrhage. 33% vitreous clarified. 27% vitreous clarified. 26
Well tolerated by tissues. 50% reattachment. Well tolerated by tissues. 4 1% reattachment.
eye can induce severe complications such as cataract, glaucoma, comeal damage, and “silicone retinopathy”. The post-surgical removal of a silicone oil is usually very difficult, and any remaining amount is retained indefinitely. In spite of this background, there has been a renewed interest in the use of silicone oil tamponade over the last decade,99-‘06 probably
stimulated by some doubts cast on the earlier reports on silicone-induced complications, by advances in surgical techniques and in the technology of oils purification, and by the view that most of the complications can be successfully treated. Recently, the Food and Drug Administration in the U.S.A. approved the use of a silicone oil with a kinematic viscosity of 50 St, manufactured by Adatomed, Germany, for certain complicated types of retinal detach- ment (Ophthalmology Times, August 7, 1995, pp. 10-l 1). However, silicone oils should be used mainly for desperate cases, and preferably as temporary replacements.
As a possible result of the controversy surrounding the effects of the injection of silicone oils into the vitreous cavity, the use of the silicone rubbers was proposed as an alternative. lo7 Balloons made of O.l-mm-thick silicone rubber sheets, glued together with silicone
adhesives, and provided with a silicone-made filling tube, were implanted in the vitreous cavity of 14 owl monkeys and six rabbits. After filling the balloon with saline, the tube was closed, sutured to the sclera, and covered with conjunctival tissue. The balloon and its contents were still transparent after 6 months, but transient lens opacities and retinal hemorrhage were noticed. The device was intended as a temporary implant, but the traumatic surgery required by the implantation of the empty balloon into the vitreous cavity and the hardness of the filled balloon, that could result in retinal damage, stopped further develop- ment of this device.
Perhaps the most important lesson on the replacement of the natural vitreous has come from the idea of using a mixture of collagen and sodium hyaluronidate, the so-called “reconstituted vitreous”, which was obviously based on the fact that these biopolymers are the two major structural components of the natural vitreous body itself. In an earlier study, lo8 the mixture was injected at a temperature of 10°C in monkey eyes and it became gel at body temperature. Within one month, the collagen disappeared completely and the concentration of sodium hyaluronidate became lower than before surgery. Transient fibrinous precipitation also occurred. Further experiments in primates’Og confirmed a complete

HYDROPHILIC POLYMERS AS ARTIFICIAL VITREOUS 485
Table 4. Vitreous substitution with halogenated liquids
Agent Recipient Pathological Clinical Remarks References (No. of follow-up cases) (months)
Perhuorinated polyether (Fomblin@-H)
(nGF&N
Rabbit
(27)
Rabbit
(38)
W3d3N Human Pertluorodecalin (4)
(C IOF 1s) (n-C4F9)sN, ClaFls Human Perfluorooctane (23) (CsF,,)
As above Human
(14)
(n-C4F&N, C taFta Human (17)
Perfluorophenan- Rabbit Irene (C 14F24) (22)
GF18 Human
(10) C t4F24 (Vitreon”) Human
(15)
As above Human
(1) Perfluorooctyl Monkey bromide (CsFtrBr) (4)
CIOFK? Rabbit
(34) Vitreon@ Human
(19)
Rabbit
(22)
- 6
- 5
Retinal detachment 2
Retinal detachment 6
Retinal detachment 6
Retinal detachment 6 with giant tears
- 1
Retinal tears 6
Retinal detachment 6
Retinal detachment 7
- 1.5
- L
Retinal detachment 9 and other vitreoretinal diseases
0.5
Severe complications. 45 Not suitable as a vitreous substitute. Complications. 46
Not suitable in the long term. 100% reattachment. 47
65% reattachment. 48 Useful for severe proliferative vitreoretinopathy. 49 All retinae were flattened. 73% reattachment. 55% vision improved. All retinae were 50
flattened. Residual agent. No inflammation. Well tolerated by 5’ tissues. 90% reattachment. 52 80% vision improved. 53 74% reattachment. Vision improved. Some complications. 100% reattachment. 54 Vision improved. 55 Transient inflammation. Severe complications. 56
100% reattachment. 57 80% vision improved. No toxic effect. No toxic effect. 58
Minor complications.
absorption of the original components within 4-5 months. The “reconstituted vitreous” became hazy after its injection and so remained indefinitely. Opacification, inflammation and formation of intravitreal strands were also reported. ‘lo The failure of the “reconstituted
vitreous” as a substitute showed that it is virtually impossible to duplicate Nature and make up a “natural” vitreous. The only alternative is to produce materials duplicating the properties of the natural vitreous, rather than its composition or structure. Ultimately,

486 T. V. CHIRILA ef al.
Table 5. Vitreous substitution with donor vitreous (human to human)
No. of cases Pathological conditions Clinical follow-up [months]
Remarks References
3 Hemorrhagic vitreous 12
13
2
72 Retinal detachment 84 105 Retinal detachment 6 34 Retinal detachment n.a.
35
3
Hemorrhagic vitreous n.a. Retinal detachment Retinal detachment l-30
74 Retinal detachment 24
Hemorrhagic vitreous (5 2- 15 cases) Retinal detachment (8 cases) Hemorrhagic vitreous 7-11
Vision improved (one case). Mild adverse reaction. 25% reattachment. Vision improved in hemorrhagic cases.
Vision improved (one case). Some complications. 40% reattachment. 33% reattachment. 17% reattachment. Some complications. Vitreous clarified. 50% reattachment. Vision improved (one case). Retinal reattachment (one case). Severe complications (one case). 20% reattachment. Severe complications (1 I cases).
59
60
61
62
63
64
65
66
61
the chemical structure of a successful vitreous substitute is irrelevant as long as it does not elicit a toxic response and fulfils as many as possible of the requirements itemized in
Section 1.3.
3. POLYMERIC VITREOUS SUBSTITUTES
The use of synthetic polymers for the supplementation or replacement of the vitreous body began in the mid- 195Os, a few years after poly(methy1 methacrylate) started to be used in the manufacture of prostheses for the intraocular lens and cornea. The earlier tentative reviews on vitreous substitution79*94,” ‘,‘12 scarcely mentioned the polymeric substitutes, but later reviews 110*‘13~“4 emphasized the growing importance of polymers in the surgical manage- ment of vitreoretinal pathologies. Two reviews 1’5~“6 were recently dedicated entirely to the polymeric vitreous substitutes, however they are still incomplete.
Both semisynthetic (i.e. modified natural polymers) and fully synthetic polymers have been proposed or tested as vitreous substitutes. With the exception of silicones, already mentioned, all these polymers were hydrophilic. The history of their performance and the knowledge gained from this experience are now exhaustively reviewed.

HYDROPHILIC POLYMERS AS ARTIFICIAL VITREOUS 487
Table 6. Vitreous substitution with treated collagen
Collagen treatment Recipient (No. of cases)
Clinical Remarks References follow-up (months)
Proctase digestion UV-irradiation As above
Proctase digestion
Proctase digestion UV-irradiation As above
As above
Proctase digestion
Proctase digestion UV-irradiation As above
Rabbit (72) 6 Well tolerated by tissues. ” Monkey (27) Retention: 60 days. Rabbit (28) 6 Transient inflammation. 69
Monkey (17) Retention: 60 days. Rabbit (24) n.a. The implant became cloudy 69 Monkey (10) and aggregated. Rabbit (20) 6 Mild transient complications. ” Monkey (21) Human (9) n.a. 50% vitreous clarified. 70
No reattachment. Monkey (23) 24 Mild inflammation. 71
Vitreous opacities. Fragmentation of implant.
Monkey (5) 24 Significant vitreous 71
opacification. Inflammation.
Monkey (45) 5 Mild inflammation. 72
Human (16) <l 19% reattachment. 13% 73
(Retinal detachment) vision improved. Mild vitreous opacification. Inflammation. Fragmentation of implant.
3.1. Semisynthetic polymers
Some derivatives of natural polymers that are soluble in water can be injected as aqueous solutions which, depending on their viscosity, are relatively rapidly eliminated from the
vitreous cavity. Although they have not been found useful as long-term vitreous substitutes, some of these materials have been developed as temporary viscoelastic fluid aids for ocular surgery, in both anterior and posterior segments of the eye. At present, the market of visco- elastic solutions is flourishing thanks to the good performance of water-soluble materials such as hyaluronan products, chondroitin sulfate, collagen, cellulose derivatives and some synthetic polymers, and the term “viscosurgery” was coined to describe the use of these solutions during surgery. “‘J’* Our literature search indicated that most of water-soluble
natural polymers which were tested as vitreous substitutes, were subjected to various levels of processing, i.e. from elaborate purification procedures to chemical modification.
3.1.1. Polysaccharides
Table 7 summarizes the use and performance of sodium hyaluronidate as a vitreous sub- stitute. The suggestion to use it as a vitreous substitute75,‘08 was justified by the presence of this biopolymer as a component of the natural vitreous body. The biocompatibility of the commercial products was progressively improved, and the currently available sodium

Tab
le
7. V
itreo
us
subs
titut
ion
with
so
dium
hy
alur
onid
ate
Age
nt
Rec
ipie
nt
Path
olog
ical
C
linic
al
follo
w-u
p (N
o. o
f ca
ses)
co
nditi
ons
(mon
ths)
R
emar
ks
Ref
eren
ces
Solu
tions
R
abbi
t ( 1
8)
(2-1
2 m
g m
l-‘)
E
tam
ucin
e@
Hum
an
(31)
E
tam
ucin
e@
Hum
an
(11)
Solu
tion
(2 m
g m
l-‘)
H
uman
(9
7)
Solu
tion
(2 m
g m
l-‘)
H
uman
(4
8)
Eta
muc
ine@
H
uman
(1
1)
- <
I
Ret
inal
de
tach
men
t V
aria
ble
(up
to
11)
Hem
orrh
agic
vi
treo
us
n.a.
R
etin
al
deta
chm
ent
Ret
inal
de
tach
men
t n.
a.
Ret
inal
de
tach
men
t V
aria
ble
(up
to 2
yea
rs)
Ret
inal
de
tach
men
t 2
Eta
muc
inem
H
uman
(8
9)
Hea
lon@
H
uman
(1
1)
Hea
lon@
H
uman
(2
5)
Solu
tion
(10
mg
ml-
‘)
Hum
an
(21)
Ret
inal
de
tach
men
t V
aria
ble
(up
to 5
yea
rs)
Ret
inal
de
tach
men
t Sh
ort
Eta
muc
inew
H
uman
(5
3)
Seve
re
retin
al
6 de
tach
men
t H
emor
rhag
ic
vitr
eous
n.
a.
(2 c
ases
) R
etin
al
deta
chm
ent
(19
case
s)
Ret
inal
de
tach
men
t n.
a.
Hea
lon@
H
uman
(4
1)
Ret
inal
de
tach
men
t na
.
Com
plic
atio
ns
(ret
inal
de
tach
men
t, ca
tara
ct).
50
% r
eatta
chm
ent.
67%
vi
treo
us
clar
ifie
d.
63%
rea
ttach
men
t. T
rans
ient
vi
treo
us
opac
ities
. 44
%
reat
tach
men
t. T
rans
ient
pr
ecip
itatio
n.
46%
re
atta
chm
ent.
Wel
l to
lera
ted
by t
issu
es.
73%
rea
ttach
men
t. 55
%
visi
on
impr
oved
. T
rans
ient
vi
treo
us
opac
ities
. N
o in
flam
mat
ion.
45
%
reat
tach
men
t. N
o in
flam
mat
ion.
G
ood
mat
eria
l pr
oper
ties.
55
% r
eatta
chm
ent.
Wel
l to
lera
ted
by t
issu
es.
72%
rea
ttach
men
t. Sl
ight
vi
treo
us
opac
ific
atio
n.
No
vitr
eous
cl
arif
icat
ion.
50
% r
eatta
chm
ent.
32%
rea
ttach
men
t. R
edet
achm
ent
with
in
14 d
ays.
W
ell
tole
rate
d by
tis
sues
. V
itreo
us
opac
ific
atio
n.
44%
rea
ttach
men
t. R
edet
achm
ent
with
in
14 d
ays.
Si
gnif
ican
t tis
sue
reac
tion.
14
75
65
76
77
78
79
80
81
82
83
83

HYDROPHILIC POLYMERS AS ARTIFICIAL VITREOUS

490 T. V. CHIRILA et al.
hyaluronidate pharmaceutical grade solutions are extensively used as viscoelastic agents in a
large range of ocular and other surgical procedures. Owing to a short longevity in the vitreous cavity and a poor tamponade effect, these solutions are not so successful as vitreous substitutes. The covalent crosslinking of sodium hyaluronidate was envisaged in order to
decrease its solubility in water, therefore to enhance its retention in the vitreous cavity. Such a material, known as “hylan”, was developed by Balazs and Leshchiner”9-122 by crosslinking with formaldehyde or divinyl sulphone. Two different forms of hylan are currently investi-
gated: 89,123-125 homogeneous “solution” and gel “slurry”. In some trials,89 the gel showed
encouraging results and a longer residence, but still could migrate to the subretinal space through retinal holes because of its insufficient coherence. 124
Kishimoto et al. ‘11 reported a study on the use as vitreous substitutes of other polysacchar- ides, such as dextran, alginic acid, chondroitin sulfate, guar gum (probably), methylcellulose and carboxymethylcellulose, which were all commercially available at that time. Some of the
materials used by these authors are difficult to identify owing to obsolete commercial names, restricted to the Japanese market. Equal volumes (0.3 ml) of diluted aqueous solutions of six different products were injected in the vitreous of 47 adult albino rabbits. Although the initial
inflammatory reaction subsided within 2 weeks, the vitreous body became opaque in more than half of the operated eyes. The histological examination of the eyes enucleated after 1 month revealed only slight damage to the posterior ocular segment. The authors wisely concluded that the results were insufficient for a decision on the use of these materials in the human eye. A year later, Mori’26 reported the results of injecting 0.8-1.2 ml of chondroitin sulfate or sodium alginate respectively into the vitreous cavity of albino rabbits. Opacity of the vitreous was again seen in more than half of the cases, although it disappeared almost entirely within a month. The retinae were slightly affected, and the author suggested that
these materials may be suitable for human trials. Clinical investigations on the use of a solution of sodium alginate in the treatment of retinal detachment were reported by M~ri’*~ in 1967. The material was injected into the vitreous cavity of five human eyes. It did not cause any postoperative inflammation, but it failed to reattach the retina. Gombos et al. 12’ injected dextrans into the cat vitreous cavity, including dextran 500 (MW 500 kDa, concentrations 0.004% and 1.5%), dextran 2000 (MW 2000 kDa, concentrations 0.004% and 0.8%), dextran sulfate 500 and dextran sulfate 2000, both at two different concentrations (0.004% and 1.5%, respectively). All the experimental eyes showed no postoperative complications in spite of some chemical changes in the vitreous composition observed after administration of dextran 500 and dextran sulfate 500. However, both dextran 2000 and dextran sulfate 2000 at low concentration induced opacity of the vitreous and the opacification was more severe when higher concentrations were used.
An aqueous buffered solution of sodium carboxymethylcellulose was tested as a vitreous substitute in four albino rabbits. lz9 It appeared to be well tolerated, with only transient inflam- mation observed. No data were given on the retention of this agent in the vitreous cavity.
A cellulose derivative, hydroxypropyl methylcellulose (HPMC), which is currently com- mercialized as Occucoat@ (Storz, U.S.A.), Ocugel@ (Surgidev, U.S.A.), Hymecel@ (Dispersa, Switzerland), Adatocelm (Adatomed, Germany), and Visilon@ (Shah and Shah, India) was recently evaluated as a possible vitreous substitute.‘30 The 2.2% solution of HPMC (MW 86 kDa) in water was injected into the vitreous cavity of 16 rabbits, following perfluoro- propane gas compression. The animals were sacrificed at various intervals up to 10 weeks. Hydroxypropyl methylcellulose was completely eliminated from the vitreous cavity within

HYDROPHILIC POLYMERS AS ARTIFICIAL VITREOUS 491
10 weeks; however, 80% of initial concentration was still present after 4 weeks. Its elimina-
tion probably took place through the aqueous humor. In an eye with a large retinal detach- ment, only 5% of the initial HPMC was left after 6 weeks, which suggested that it could have been eliminated through the choroidal circulation. Hydroxypropyl methylcellulose was also assayed for cytotoxicity on cultured retinal pigment epithelial cells and the cells maintained normal morphology after 4 weeks of microscopic observation. The results of this study
indicate that HPMC solutions are not able to function as long-term vitreous substitutes or to seal retinal holes in rhegmatogenous retinal detachment. However, as a short-term sub- stitute, HPMC appears to be more effective than other previously reported materials. Its lack
of cytotoxicity is encouraging and this could be an advantage if the material were to inadvertently enter the subretinal space through a retinal hole. Femandez-Vigo et al. 13’
demonstrated that it may be possible to control the retention time of the HPMC in the vitreous cavity by choosing a suitable molecular weight of the material. A product with MW of 86 kDa had a half life of 10.4 days in the vitreous, while another with MW of 120 kDa had a half life of 38.4 days.
3.1.2. GeZ&n
A group at the University of Amsterdam tested a modified gelatin, known as ‘ ‘polygeline’ ’ or Haemaccel@ (Hoechst AG, Germany), as a possible vitreous substitute, both in animals 13’ and human patients. 133 The product (MW 35 kDa) resulted by the thermal degradation of gelatin, and1 it was used before as a plasma volume expander with no reported allergenic or antigenic effects. A solution of 3.5% polygeline in water was indefinitely stable at room
temperature and had a refractive index very close to that of natural vitreous. The attempts to increase the viscosity of the injected material by increasing the concentration of polygeline or by mixing it with gelatin, agar, methylcellulose or poly(ethylene glycol) led to inflammation
and vitreous opacity. The polygeline solution was injected into the vitreous cavity of 120 rabbits, either with or without partial removal of the original vitreous. 13’ While no significant adverse reactions were noticed by clinical observation, it was quantitatively estimated that 77.5% of polygeline disappeared through diffusion within 10 days, which obviously pre- cludes its we as permanent substitute. However, the polygeline 3.5%-solution was subse- quently employed in 13 cases of human retinal detachment. 133 The material was tolerated
without adverse reaction in all cases followed between 2 and 17 months. The reattachment of the retina was achieved in most of the patients, but subsequent surgical treatment was gen- erally required due to certain long-term complications. The conclusion of these experiments was that polygeline solution is not a suitable long-term vitreous substitute because of its short retention and a rapid decrease in its viscosity. Although these investigators suggested that it could be useful in the short term, there was no further work reported on the use of polygeline as a vitreous substitute.
3.2. Synthetic polymers
3.2.1. Poly(‘l-vinyl-2-pyrrolidinone)
This polymer, known also as poly[ 1-(2-0x0-1-pyrrolidinyl)ethylene] or more commonly as polyvinylpyrrolidone (PVP), is soluble in water, if not crosslinked. It has many industrial
492 T.V.CHIRILA etal.
applications in areas such as cosmetics, adhesives, pharmaceuticals, paper manufacture, food processing, textiles, and photography. Aqueous solutions of PVP were also used for decades as blood plasma expanders. Polyvinylpyrrolidone induces only minor storage-related func-
tional changes in organs and its cytotoxicity is extremely low. ‘34 PVP has to be accoladed as the first synthetic polymer ever to be proposed and tested as a
potential vitreous substitute. In 1954, Scuderi reported’35 the replacement of 0.4-0.8 ml of the rabbit vitreous with several materials, including PVP. A commercial PVP product, Sub- tosan@ (Farmitalia, Italy) which is a solution of 3.5% PVP in aqueous salts, as well as a
solution of 90% PVP in pure water were injected in the vitreous cavity. Although no adverse reaction was noticed and the histology was unremarkable, all the eyes containing PVP became opaque and the opacity persisted till the end of the follow-up period (40 days). The author suggested that PVP was not a suitable vitreous replacement.
Chronologically, PVP was also the subject of the second attempt to use synthetic polymers as vitreous replacements. Apparently unaware of Scuderi’s work, Hayano and Yoshino136 reported in 1959 the use of diluted solutions of PVP in human eyes with rhegmatogenous retinal detachment and opaque vitreous. Although nothing was mentioned about the
postoperative retention of PVP in the vitreous cavity, the results were considered satisfactory, mainly due to the fact that PVP induced less inflammatory reaction than air or saline.
On the background of these rather incomplete investigations, no further reports on the use of PVP as a vitreous substitute could be found in the literature. Obviously, a short residence time in the eye is expected from an aqueous solution of PVP which is therefore unlikely to perform much better than, for instance, saline solutions. It was suggested’15 that its retention in the vitreous humor could be enhanced by crosslinking, based on the proven hypothesis’37 that if an uncrosslinked polymer is soluble in a liquid penetrant, the crosslinked version of the same polymer will only be swollen by that liquid (in this case, water), resulting in an
insoluble gel. From hundreds of crosslinked polymers of 1-vinyl-2-pyrrolidinone (VP), a few were selected for clinical evaluation, following a selection process based on the optical properties and injectability through small-gauge needles. 138~139 A homopolymer of VP cross-
linked with 0.25% 1,5-hexadiene-3,4-diol and a copolymer of VP with 1% 2-hydroxyethyl methacrylate (HEMA), crosslinked with the same agent (l%), were each injected into the vitreous cavity of six rabbits. The hydrated polymers retained a large amount of water (98- 99%) and behaved like viscoelastic gels. Clinically, the operated eyes were quiet, with the exception of transient opacities in the vitreous and cornea. The eyes were enucleated after 4 weeks and subjected to histopathological analysis. The common feature found in all eyes was the invasion of inflammatory cells. Vacuoles containing granular material, assumed to be polymer, were seen in the intercellular space of the neural retina, in the retinal pigment epithelium cells, and in macrophages, indicating the phagocytosis of polymer. ‘39 The finding deserves some comments, as PVP has so far been investigated only as an aqueous solution administered intravenously in animals or human patients. 134 When the uncrosslinked PVP possessed a molecular weight lower than 70 kDa, it was passively excreted by kidneys, but the polymers with higher molecular weights were distributed throughout the body and even- tually stored in various organs.134 This is an indication that some products of PVP bio- degradation are fragmented polymers that cannot be eliminated through renal filtration because of their size. For instance, the continuous intravenous administration of a PVP solution induced a heavy infiltration with phagocytic cells and the formation of granulomas

HYDROPHILIC POLYMERS AS ARTIFICIAL VITREOUS 493
in the normal rat liver. i40 The phagocytic cells contained vacuoles with PVP which was
internalized and apparently not further digested. Prior to these studies, 138*139 there were no data available on the biostability of crosslinked
PVP. Crosslinked polymers have in principle an infinite molecular weight, and consequently should be insignificantly fragmented by biological activity. However, the fragmentation of crosslinked PVP was clearly suggested by recent experiments, 138,139 and two factors might have contributed to it. First, the literature141-147 indicates the presence of a large variety of enzymes in the vitreous. Being substrate-specific, the enzymes cannot directly degrade a synthetic polymer, however they can reduce the activation energy of some chemical reac- tions, usually induced by heat or irradiation, which can then degrade polymers. 148*149 Second,
the retinal pigment epithelium cells are among the most metabolically active cells in the organism, l:jO-152 and the cells specific to the vitreous body (hyalocytes) are also phagocytic. *
It appears, therefore, that the native vitreous might be a hostile environment for synthetic polymers, and that the vacuoles found in retinal pigment epithelium and macrophages represent phagocytized polymeric material.138*139 Although it was shown153 that when the polymer particles are too large they cannot be completely engulfed by macrophages and a fibrous encapsulation will consequently result, the lack of fibrous capsules in the examined eyes indicates that the size of polymer particles may be sufficiently low to allow phago- cytosis. This raises the question of what is responsible for such a fine fragmentation of the gels. The process of injection through small gauge needles subjects the gels to enormous
shear stress which usually causes massive fragmentation leading to very poor optical char- acteristics. If the injection would have produced particles as small as those revealed by microscopy, the optical properties of the gels would have been poor enough to preclude their use as vitreous substitutes. It remains that the fragmentation of polymers must be caused by the excessive phagocytic activity in the vitreous body, but investigations within a larger time frame and involving the insertion of non-fragmented pieces of polymer are necessary to establish th.e fate of crosslinked PVP in the vitreous humor.
3.2.2. Polyacrylamide
Some details have to be mentioned here in order to evaluate properly the literature existing so far on the use of polyacrylamide (PAAm) as a vitreous substitute. Acrylamide as such is a
toxic and carcinogenic compound. However, if its polymerization is complete, the resulting polymers are not toxic, and display biocompatibility in various biological environments. It should also be emphasized that the uncrosslinked PAAm is a water-soluble polymer.
Miller-Jensen et al. 154~155 introduced PAAm as a potential artificial vitreous. In the first
report, 154 acrylamide was polymerized inside the vitreous of the eyes of 10 rabbits, as a diluted (3%) solution in water, containing initiator (probably ammonium persulfate). No mention of any crosslinking agent was made, still the result of the polymerization was a swollen gel, and not a solution of polymer. Aware of the serious effects of the residual monomer, the authors estimated that less than 1% of the lethal concentration of acrylamide was left unreacted in the vitreous cavity, a harmless concentration in their opinion. Irritation was observed in the operated eyes, but it subsided within days. In three animals, administered with the maximum amount of monomer solution (3 ml, which appears to be larger than the volume of the rabbit vitreous cavity), the vitreous became opaque. In the other animals, the clarity was maintained and the histology did not reveal any degeneration within 3 months postoperatively.
494 T. V. CHIRILA et al.
How wrong these investigators were in estimating the toxicity of residual acrylamide monomer has been shown in their own next report155 in which “disquieting” late manifesta-
tions of toxicity were acknowledged as a consequence of performing polymerization within the vitreous cavity. They proposed the implantation of a polymer with a high water content and investigated the conditions of polymerization of acrylamide in order to obtain such a gel. Again, no mention of any crosslinking was made and their claim to obtain a hydrogel, rather
than a water-soluble polymer, is questionable. They recommended that the “gel” with 98% (at least) equilibrium water content could be used as a vitreous substitute, after being sub-
jected to extensive dialysis. Such “gels” were tested by subcutaneous implantation in ani- mals, and no adverse reactions were noticed. Miller-Jensen reported later’56 more trials with PAAm in rabbits. This time, the polymer was crosslinked. In spite of some confusion due to the author’s statement that in some experiments aqueous solutions of crosslinked poly- acrylamide were used (which is anyway more credible than the previous allegation that uncrosslinked PAAm is not soluble in water), this report is more comprehensive. Intravitreal polymerization was again performed in 10 animals which were followed for 8 weeks, and extensive toxic uveitis was seen in all eyes. A gel obtained by polymerization of acrylamide (2% in water), crosslinked with N, N’-methylene-bis-acrylamide (0.02% of monomer), was selected for the vitreous replacement. Experiments with tritium-labeled PAAm injected in 40 eyes showed a retention of 55% after 4 weeks. Polyacrylamide gel injected in 60 rabbit eyes was well tolerated and the eyes remained clear until the end of the follow-up period
(14 months). Despite these optimistic findings, there is no subsequent indication that this or other groups have ever used PAAm as a vitreous substitute.
Refojo and Zauberman 157 used PAAm gel as a model for the optical performance of vitreous substitutes. They synthesized crosslinked PAAm, which is swellable, but not soluble, in water. Only the optical characteristics of such gels were assessed in their report; however, the authors supplied some very valuable considerations, applicable to any synthetic gel intended as a replacement for the vitreous body. For instance, it was demonstrated that gels that fragment owing to the injection process can provide media with a very poor optical quality. A low transparency is caused by the scattering of light at every interface between a gel particle and the surrounding aqueous medium. The larger the number of interfaces, the higher the scatter of light. The authors also drew attention to the possible effects of the so-
called “nude in the shower” phenomenon, I58 whenever the clarity of synthetic gels is
assessed in the vitreous cavity. This phenomenon has troubled the ophthalmic clinicians for years. While the person who examines a patient can see details behind a cataractous lens, or an edematous cornea, or a fragmented gel which resides in the vitreous cavity, the patient cannot see distinctly the outside world. This is analogous with the situation of a body behind the diffusing screen of a shower box. The closer the body to the screen, the more details can be seen by an observer located outside the shower box. While the target (e.g. the back of the eye) for the examining clinician is within a few millimeters from his diffusing screen (e.g. a diseased lens or cornea, or a fragmented gel in the vitreous), the patient still cannot see the visual acuity test chart because this is 6 m (a common standard) from his diffusing screen.
3.2.3. Poly(glycery1 methacrylate)
Hydrophilic gels obtained by the bulk polymerization of glyceryl monomethacrylate, or 2,3_dihydroxypropyl metbacrylate, have been firstly described in 1965 by Refojo. 159S’60 The

HYDROPHILIC POLYMERS AS ARTIFICIAL VITREOUS 495
polymer (PGMA) swells in water to 75% equilibrium water content. When polymerization is
carried out in solutions of increasing water concentrations, hydrogels with increasing water
contents (up to 95%) could be produced. An increase of the crosslinking agent content induced lower water uptakes.
Shortly afterwards, Refojo’s group demonstrated the biocompatibility of PGMA hydrogels in the eye,161 materials. 163
and proposed their use as vitreous substitutes, 16* and as scleral buckling Subsequently, Refojo 164 measured the swelling of PGMA in various solutions
of mineral salts and urea, in bovine serum, and in explanted bovine vitreous. While the
expected salting-out effects (in the salt solutions), and the osmotical dehydration (in the serum) were both clearly manifested, no changes in the swelling characteristics of PGMA gel were noticed when mixed with the explanted vitreous.
PGMA was tested as a vitreous substitute in 15 rabbit eyes.i6* Pieces of dehydrated gel were inserted into vitreous humor through a small incision. The implants swelled in the
surrounding fluid inside the cavity, reaching volumes 32 times greater than those in the dry state. No inflammatory reactions or complications were observed after 7 months of
clinical observation. Despite initial optimism, Refojo later acknowledged 113~1 l4 that the pro- cedure of :implanting dry gels had two main drawbacks: first, the surgery involved is too traumatic; second, the swelling of the implant proceeds at a relatively slow rate to attain the maximum volume of the gel at the operating table. In order to solve this problem, Hogen- Esch et al. ‘65 developed an injectable PGMA by performing polymerization in a large excess of water (oz. 90%) and using very low amounts of crosslinking agent. Upon swelling, this gel absorbed aqueous saline up to 96% of its weight. It was injected, very likely as a fragmented gel, into the rabbit vitreous cavity, and the results were reported as satisfactory. However, no other reports on the further use of PGMA as a vitreous substitute are available.
3.2.4. Poly(viny1 alcohol)
Poly(viny1 alcohol), henceforth PVA, is currently produced mostly by the saponification of
poly(viny1 acetate) with alkaline methanol or ethanol. The final content of residual acetoxy groups determines the solubility of resulting PVA. By crosslinking, the aqueous solutions of PVA can be transformed into insoluble hydrogels.
For many years, Yamauchi’s group in Japan has investigated the use of the crosslinked PVA hydrogel as a vitreous substitute. 166-175 The hydrogel was produced by the y-irradiation of a solution of 7% PVA in water with a dose of 0.6 Mrad from a 6oCo source. 166 After
aqueous extraction and sterilization the hydrogel, containing more than 99% water, was evaluated in vivo by injection into rabbit eyes.166-168 No inflammatory reaction or other complications were observed, except for some changes in the electroretinograms of a few animals. ‘68 In a later report, 174 inflammation and vitreous opacity occurred more frequently in the eyes injected with PVA than in those with saline. The optical properties of PVA
hydrogels iappeared quite suitable: 167,169 in a short time the gels became indistinguishable from the h.ost vitreous, as demonstrated by monitoring the refractive index and infrared spectrometric absorption characteristics. The rates of penetration into the PVA gel of some natural vitreous components (albumin, y-globulins, hyaluronan) were also evaluated in vivo by using UV spectrometric techniques, “’ and a crucial role of the level of polymer cross- linking was revealed. Allergic ocular inflammation was experimentally induced in eyes with or without IPVA. “‘J’~ Although the eyes containing PVA became preferentially opacified, no

496 T. V. CHIRILA et al.
definite conclusions were obtained because of “individual specificity” and because many of the unoperated eyes also developed opacities. One of the most intriguing results of this work was the behavior of the mixture PVA/chondroitin sulfate.170,173 The mixture displayed a better transparency than PVA, it could not be separated into components even after extraction in boiling water, and absorbed more water than PVA alone, but it was less compatible with the natural vitreous.
Yamauchi later summarized his group’s findings’75 and concluded that their PVA hydrogel should be considered as a suitable material for vitreous substitution in spite of more clinical
complications than those caused by saline solutions. This is probably a fair conclusion, but the residence of PVA in the vitreous cavity was not properly investigated.
Recently, Chinese researchers reported further work on the use of PVA hydrogels as
vitreous substitutes. 176 The hydrogels were produced by the y-irradiation of PVA (MW 77-79 kDa) as aqueous solutions. The experimental rabbit eyes were enucleated 2 months after injection, and no severe complications were observed. The authors suggested that the PVA hydrogels may need modification in order to improve their stability during the storage.
Crosslinked PVA hydrogels remain valid contenders for vitreous substitution. However, the users should be fully aware of the technology used for the manufacture of PVA. It was
shown”’ that commercial PVA obtained by methanolysis caused severe toxic response in the vitreous body and retina of animal eyes, while the product obtained by ethanolysis was
virtually non-toxic.
3.2.5. Poly(2-hydroxyethyl acrylate)
The development of poly(2-hydroxyethyl acrylate), henceforth PHEA, as a hydrogel for vitreous substitution is an example of a complete research, carried out from the early stage of the monomer purification to the final stage of histopathologic examination of the enucleated eyes, with honest, though negative, conclusions. ’ l4 Polymerization of 2-hydroxyethyl acry-
late was carried out in a large excess of water in the presence of redox initiators and 1% ethylene diacrylate as a crosslinking agent. The gel was dialyzed for 1 month, then placed in a syringe, and sterilized in an autoclave. Poly(2-hydroxyethyl acrylate) hydrogel displayed remarkable physical characteristics including good transparency, high viscosity, non-absorb- ability, cohesiveness, facile injectability, and good compatibility with the natural animal vitreous. The gel was injected both into the anterior and posterior segments of 12 rabbit eyes, and followed clinically for 6 weeks. In the anterior chamber, PHEA promoted fibrin forma- tion, transient formation of membranes around the gel, transient cornea1 edema, glaucoma
(two cases), and lens opacification (one case). In the vitreous cavity, PHEA induced transient opacity, membrane formation, and chorioretinal atrophy. Histopathologic examination of the enucleated eyes provided additional proof that PHEA was not tolerated in the rabbit eye. In the posterior segment, the evidence of severe complications such as extensive retinal disorganization with glial cell proliferation, chorioretinal scarring, and non-granulomatous vitritis suggests that PHEA should not be used as a vitreous substitute, in spite of its physical suitability.
3.2.6. Poly(methy1 acrylamidoglycolate methyl ether)
Methyl 2-methoxy-2-( 1-oxopropenylamino)acetate, better known as methyl acrylamido- glycolate methyl ether (MAGME), is used in a variety of industrial applications such as

HYDROPHILIC POLYMERS AS ARTIFICIAL VITREOUS 497
coatings (enamels, waterborne coatings, automative refinish coats), polymer products (graft
copolymers, elastomers, functionalized polymers), and in the mineral ore extraction. Copolymers of MAGME were proposed as supports for the immobilization of therapeutic
agents. 178J79 Over recent years, a large series of polymers of MAGME were produced as
potential vitreous substitutes. 115~1’6~180~‘81 Eventually, a homopolymer (PMAGME) synthe- sized in 80% water was selected for in viva evaluation. ‘*’ This gel was transparent, injectable, autoclavable, cohesive, and contained more than 99% water when fully hydrated. It was
injected intravitreally into six rabbit eyes and followed clinically by ophthalmoscopy, tonometry and fundus photography. The gel was initially well tolerated, but after 6 months the ophthalimoscopic analysis revealed progressive pallor of the optic nerve head. The eyes were enucl.eated 12 months after injection of polymer. Histopathological examination by light microscopy of retinal and vitreal sections revealed significant retinal disorganization, degeneration of the optic nerve and retinal neural elements, retinal detachment, and inflam-
matory changes. Analysis of immunohistochemically labeled retinal sections revealed loss of ganglion aells and extensive pathological reaction of the Miiller cells and astrocytes. The cytotoxicity of the hydrogel was then assessed in vitro by monitoring the proliferation of cultured mouse (Balb/c-3T3) fibroblasts using an immunocytochemical system. This bio-
assay showed both cytostatic and cytocidal effects of the polymer. The results indicated that PMAGME hydrogels cannot be used as vitreous substitutes because of a severe delayed toxic reaction elicited in the posterior segment of the eye. The toxic effect can be caused by the polymer itself or by residual contaminants such as acrylamide. The latter is indeed a neuro- toxic ageni, and specific damage caused by acrylamide to the neural elements of the visual system were proven experimentally. 182-185 The study on PMAGME’*l revealed for the first time the importance of performing in vitro cytotoxicity assaying as an eliminatory criterion in the selection of polymers as potential vitreous substitutes.
4. IRHEOLOGICAL STUDIES ON VITREOUS BODY AND ARTIFICIAL SUBSTITUTES
4.1. Rheology of the vitreous body
The view accepted on the vitreous body among the biomedical scientists is that the collagen fibers provide a rigid scaffold while the macromolecules of hyaluronan impart shock-absorbing properties to the whole system. Such a system would then possess visco- elastic properties.
At a time when very little was known about the structure and composition of the vitreous, Duke-Elder 186 concluded that the vitreous was a highly hydrated gel “in an unstable state of dynamic equilibrium, the consistence of which can be readily destroyed by mechanical trauma”. Robertson and Duke-Elder 187 measured the mechanical properties of the feline and bovine vitreous using an electromagnetic device to shift nickel microspheres through the vitreouls and measuring their displacement, and concluded that the vitreous has “viscous- elastic properties’ ’ , therefore it should be “composed of a mesh-work of elastic fibrae suspended in a viscous liquid”. Remarkably for these scientists with no background in polymer physics, they performed a creep analysis 187~188 of the vitreous based on a previously published experimental methodology. 189

498 T. V. CHIRILA et al.
Oscillatory shear experiments and the resulting plots of real (G’, the storage modulus) and
imaginary (G”, the loss modulus) parts of the complex dynamic shear modulus versus the frequency of oscillatory stress, termed sometimes as “mechanical spectra”, are currently
used to demonstrate the gel character, and to discriminate between different classes of gels such as entanglement networks or covalently crosslinked gels. 190-‘92 This methodology, as well as other mechanical tests, were used over the last three decades to describe the behavior of collagen, hyaluronan and vitreous.
Collagen behaved like a free-flowing liquid when subjected to high-frequency stress, and this behavior was strongly influenced by its water content 193-195 and by the ionic strength of its solutions. 196 Some pioneering work197-199 on the rheology of hyaluronan suggested a viscoelastic behavior (“flow elasticity”) which was explained by a large size of the macro-
molecules, their very high hydration and the interaction between biopolymer particles. In subsequent studies200~201 hyaluronan solutions were found to behave like entanglement gels, the plots of G’ and G” displaying a typical cross-over in the region 15-20 Hz. Balazs
obtained202 contradictory values for G’ and G” at two different frequencies and concluded
that the “the highly elastic hyaluronic acid putty . . . is not a gel of entangled or permanently crosslinked molecular networks”.
There are relatively few studies on the rheology of the vitreous body as such, probably owing to its destruction by conventional measuring methods. In 1963, Pfeiffer showed203 that the vitreous of mice and rats, when abruptly broken, displayed a measurable response which was considered “flow elasticity”. The viscoelastic properties of the intact bovine vitreous were evaluated by the dynamic compression moduli (storage and loss) and the loss tangent,204 and the resulting dependence of the moduli on frequency and their magnitude indicated that the vitreous is similar to hyaluronan, while their dependence on temperature is similar to that
found in collagen. It was also noticed204 that the rheological properties vary within different
regions of the vitreous body. The vitreous body appeared as a self-contained viscoelastic entity with a behavior different from either that of hyaluronan or collagen, or from any
weighted sum of these components. Zimmermanzo5 used a psychophysical method to record the movement of the vitreous body in human volunteers, resulting from eye and head move- ments as a response to the scattering pattern produced by a point light source. A damped oscillation of the vitreous was observed, and a value of 0.05 Pa (at 1.1 Hz) was determined for the shear modulus. Weber et ~1.~~~~~~ studied the behavior of pig and human isolated vitreous when a small metallic sphere was exposed to an external oscillating electromagnetic field. They used the Voigt-Kelvin model to describe the motion of the microsphere in the vitreous, characterized by a spring constant and a damping constant. The microsphere was displaced by the magnetic force but it tended to move back to the initial position when the force pulse had
ceased. The authors concluded that the vitreous is rubber-elastic rather than viscoelastic. The spring and damping constants in human eyes were significantly larger than in pig eyes, which was explained by the much higher concentrations of collagen and hyaluronan in the human vitreous. The shear stress analysis of the bovine vitreous revealed lo a viscoelastic behavior at frequencies between 3 and 100 mHz. The mechanical spectra suggested that the vitreous should be considered as a slightly crosslinked gel rather than an entanglement gel or a solution. In a psychophysical method recording the time-dependent changes in the position- ing of a point in the vitreous in relation to the motion of the eye as a whole, the vitreous body was modeled as a homogenous viscoelastic sphere.*‘* A quantitative study of the regional variations in the properties of the human vitreous was carried out recently by Lee et al.209 in
HYDROPHILIC POLYMERS AS ARTIFICIAL VITREOUS 499
which the four-parameter Burgers model was used to describe the viscoelastic behavior of the vitreous. The creep compliance response was composed of a retarded elastic region and an unrecovera.ble viscous flow region. Significant differences were found in the measured rheo- logical parameters between the anterior, central and posterior regions of the vitreous. In a
more detailed study,*” Lee compared rheologically the human and animal (pig, bovine)
vitreous humors and found significant differences between them in all three regions. The creep behawior of all samples was well fitted with the Burgers viscoelastic model. This behavior suggested that the vitreous can be described either as a dilute uncrosslinked polymer
system or as a dilute polymer solution which displays viscoelasticity as a perturbation of the
Newtonian behavior of the solvent. The graphic dependence of the storage (J’) and loss (J”) compliances on frequency indicated that the vitreous can be included rheologically within the class of amorphous polymers of high molecular weight, as defined by Ferry. *” The features of J” plots suggested an entanglement network in which the entanglements suppress long- range configurational rearrangements and act almost as though they were crosslinks.21o
4.2. Oscillatory shear experiments as criteria for potential vitreous substitutes
Ideally, a vitreous substitute should have rheological properties similar to those of the
natural vitreous. In other words, the material should have an elastic response at almost all frequencies in order to support the retina after the natural vitreous has failed this task. The mechanical energy generated at high frequencies by external forces acting upon the vitreous body such (as rubbing or hitting, and by heart beats and eye movements needs to be stored first and then dissipated s10wly.~ It has been shown that covalently crosslinked gels exhibit a storage modulus (G’) greater than the loss modulus (G”) and that their values are relatively frequency insensitive. 190 Mechanically, this class of gels should be suitable for vitreous substitution.
The problem becomes more complex as the only practical delivery system for the vitreous substitute to the eye is by injection through a small-gauge needle. The applied shear causes a large deformation of the polymer, and the degree of deformation under constant stress is
related to the structure of the polymer chains. The process of reptation, i.e. the snake-like motion of the chain, as a mechanism for stress relaxation in polymers, has been well docu- mented.*‘*,*13 The macromolecular chains overlap extensively creating a tunnel for each chain wherein the movement is restricted. The chain cannot move freely, because it cannot pass through or across other chains as this process would break other chains. The chain may,
however, move along its own tunnel, changing its position and conformation in time. If the polymer chains were joined through crosslinks, the stress relaxation mechanisms would also be affected. A covalently crosslinked polymer has an infinite molecular weight so diffusion of the chains ,will be limited. For a crosslinked gel to be injected or be able to experience a large deformation, some of the covalent bonds must be broken to allow chain movement. The covalent bonds, unlike the physical bonds, are not expected to form again once they were broken, so that the physical properties of the injected gel may be different from those displayed before injection. This will also alter the reptation process, the stress relaxation and other mechanical properties of the gel. The influence of injection process was demon- strated upon natural vitreous: when the human vitreous was removed using a 30-gauge needle, it was less viscous and visibly more homogenous than when removed using a larger 16-gauge needle.*14

500 T. V. CHIRILA et al.
Although quite relevant to the end use of materials designed as vitreous substitutes, their viscoelastic behavior was not contemplated as a selection criterion until recently, when synthetic gels based on VP were evaluated by dynamic shear analysis.“’ Following the
synthesis of more than 100 polymers, a small number were selected on the basis of their high equilibrium water content (above 95%) and good optical clarity, and subjected to
rheological evaluation by oscillatory shear experiments in a controlled stress rheometer. Potential vitreous substitutes included: homopolymers of VP crosslinked with 1,5-hexa- diene-3,4-diol(O.25 1%); copolymers of VP with HEMA (l-3%) crosslinked with ethylene dimethacrylate (O.l-0.25%); copolymers of VP with HEMA (7-10%) crosslinked with diallyl ether (0.25-0.75%); copolymers of VP with HEMA (l-5%) crosslinked with 1,5- hexadiene-3,4-diol(O.25- 1%); and a copolymer of VP with 10% HEMA with no crosslinking agent added. Representative samples from each group were characterized by their mechanical spectra, recorded before and after injection through a 30-gauge needle. All gels displayed before injection spectra typical of covalently crosslinked gels, i.e. G’ > G” and slopes approaching zero. The gels crosslinked with ethylene dimethacrylate dramatically changed
their characteristics following the injection process, as the values of shear moduli dropped substantially and the gels behaved like free-flowing fluids at higher frequencies (G” > G’). It is unlikely that these gels would be able to assure a proper tamponade to a detached retina. - _.
2 a G’
1 a b
B 0.5 0 77 G"
“i b
I I
0.01 0.02 0.05 0.1 0.2 0.5 1 F=w=Y t’W
Fig. 6. Mechanical spectra of a fully hydrated polymer of VP, crosslinked with 1,5- hexadiene-3,4-diol (0.25%), before (a) and after (b) injection through a needle.

HYDROPHILIC POLYMERS AS ARTIFICIAL VITREOUS
b 5.
501
Fig. 7. Mechanical spectra of a fully hydrated uncrosslinked copolymer VP/HEMA (90/ 10). before (a) and after (b) injection through a needle.
Their elastic response after only one injection is insufficient at high frequencies. The gels crosslinked. with diallyl ether or 1,5-hexadiene-3,4-diol displayed only minor changes in their viscoelastic behavior (Fig. 6). However, their moduli were very low both before and after injection, which suggests that these gels may not be able to provide a satisfactory tamponade. The gels that were produced without crosslinking agents maintained their properties virtually unchanged after injection, with no changes in the magnitude of G’ and G” (Fig. 7). These gels, which may be very lightly chemically crosslinked, owing to the presence of divinyl con- taminants, or merely physically crosslinked, displayed the most suitable mechanical characteristics as vitreous substitutes.
This study2r5 clearly indicated that rheological analysis should play a crucial role in the
selection of synthetic gels as vitreous substitutes, at least for two reasons: (1) the gels should display viscoelastic properties similar to those of the undisturbed natural vitreous body, and (2) the shearing history of the gels, i.e. the injection through small-gauge needles, has a fateful effect on their mechanical properties.
5. CONCLUSIONS
The substitution of the vitreous body of the eye is a complex issue. Many substances have been proposed and tested as vitreous substitutes during this century, but the criteria for

502 T. V. CHIFULA et al.
selecting most of these materials were ambiguously defined. Generally, they were chosen because of good optical clarity and ease of injection, and no systematic exploration of their toxicity, retention in the vitreous humor and injection-induced changes in their rheological properties was done prior to in viva experiments. The advent of synthetic polymers as
candidates for vitreous substitution did not much change this methodology (at least until recently), and incomplete research and lack of details in most of reports preclude definitive conclusions on their future as vitreous substitutes. The existing literature indicates that any
polymer in the form of an aqueous solution can function at best as a short-term substitute due to a rapid dissipation into the surrounding ocular tissues. On the contrary, the insoluble polymeric gels may function as long-term vitreous substitutes provided that a set of rather
stringent requirements is fulfilled. So far, a hydrogel able to do this has not been found.
ACKNOWLEDGEMENTS
This work was supported in part by grants from National Health and Medical Research Council of Australia (#/940707), and the Arnold Yeldham and Mary Raine Medical Research Foundation, Western Australia. The support from the Australian Foundation for the Preven-
tion of Blindness (Western Australia), Inc. and the Lions Clubs International Foundation (Oak Brook, IL, U.S.A.) is also acknowledged. We thank Cyanamid Australia Pty Ltd and
BASF Australia Ltd for supporting our research with gifts of monomers. This review would have never been accomplished without the generous assistance of the staff in the Medical Library of the University of Western Australia, Perth; we are especially indebted to Anne Batt, Georgiana Ananda and Danuta Michalak who made tremendous efforts to procure for us original articles from old or obscure publications. We thank Dr Hilda Bodnaras for translating the German articles. Dr Aizo Yamauchi (Hoya Corporation, Saitamaken, Japan) kindly provided copies of his articles published in Japanese journals. We thank Ruth Gutteridge and Susan Darrington for editorial assistance.
1.
2. 3.
4. 5.
6. 7.
8.
9.
10. 11. 12. 13.
REFERENCES
Balazs, E. A., in Duane’s Foundations of Clinical Ophthalmology, Vol. 1, ed. W. Tasman and E. A. Jaeger. J. B. Lippincot, Philadelphia, 1994, Ch.17. Redslob, E., Le Corps Vitro’. Masson, Paris, 1932, p. 160. Sebag, J., The Vitreous. Structure, Function, and Pathobiology. Springer, New York, 1989, pp. 1, 22, 146. Worst, J. G. F., Trans. Ophthalmol. Sot. UK, 1977, 97,550. Worst, J. G. F. and Los, L. I., Cisternal Anatomy of the Vitreous. Kugler Publications, Amsterdam, 1995. Swann, D.A , Int. Rev. Exp. Pathol., 1980, 22, 1. Balazs, E. A., in New and Controversial Aspects of Retinal Detachment, ed. A. McPherson. Harper & Row, New York, 1968, p. 3. Balazs, E. A. and Denlinger, J. L., in The Eye, 3rd edn, Vol. la, ed. H. Davson. Academic Press, Orlando, FL, 1984, p. 533. Constable, I. J., in New and Controversial Aspects of Vitreoretinal Surgery, ed. A. McPherson. The C.V. Mosby Co., Saint Louis, 1977, p. 11. Tokita, M., Fujiya, Y. and Hikichi, K., Biorheology, 1984, 21,751. Asakura, A., Nippon Ganka Gakkai Zasshi, 198589, 179. Mathews, M. B., Biochem. J., 1965, 96, 710. Serafini-Fracassini, A.P., Wells, J. and Smith, J. W., in Chemistry and Molecular Biology of the Intercellular Matrix, Vol. 2, ed. E. A. Balazs. Academic Press, London, 1970, p. 1201.

HYDROPHILIC POLYMERS AS ARTIFICIAL VITREOUS 503
14. Sebag, J. and Balazs, E. A., Invest. Ophthalmol. Vis. Sci., 1989, 30, 1867. 15. Cibis, P. A., Vitreoretinal Pathology and Surgery in Retinal Detachment. The C. V. Mosby CO.,
Saint ILouis, 1965, p. 28. 16. Shields, J. A., in Current Concepts ofthe Vitreous, ed. K. A. Gitter. The C. V. Mosby Co., Saint
Louis, 1976, p. 14. 17. Fuller, D. G. and Hutton, W. L., Presurgical Evaluation of Eyes with Opaque Media. Grune &
Stratton, New York, 1982, p. 2. 18. Shafer, D. M., in Controversial Aspects of the Management of Retinal Detachment, ed. C. L.
Schepens and C. D. J. Regan. Little, Brown and Co., Boston, 1965, p. 186. 19. Constable, I. J., in New and Controversial Aspects of Vitreoretinal Surgery, ed. A. McPherson.
The C. V. Mosby Co., Saint Louis, 1977, p. 387. 20. Ford, V., Lancet, 1890, 1,462. 21. Deutschmann, R., Beitr. Augenheilk., 1895,20, 1. 22. Deutschmann, R., Klin. Monatsbl. Augenheilk., 1906, 44,364. 23. Gradenigo, P., Ann. Ottalmol. Clin. Ocul., 1902, 31, 650. 24. Lowenstein, A. and Samuels, B., Graefes Arch. Ophthalmol., 1911, 80,500. 25. Elschnig, A., Graefes Arch. Ophthalmol., 1911, 80, 514. 26. Elschnig, A., Ber. Deut. Ophthalmol. Ges., 1911, 37, 11. 27. Rosengren, B., Acta Ophthalmol., 1938, 16, 3. 28. Rosengren, B., Acta Ophthalmol., 1938, 16, 573. 29. Rosen.gren, B., Acta Ophthalmol., 1952,30, 117. 30. Rosen.gren, B., Acta Ophthalmol. Suppl., 1966, 84, 156. 31. Ohm, J., Graefes Arch. Ophthalmol., 1911,79,442. 32. Hughes, W. L. and Cole, J. G., Arch. Ophthalmol., 1946, 35,525. 33. Smith, R., Br. J. Ophthalmol., 1952, 36, 385. 34. Van Horn, D. L., Edelhauser, H. F., Aaberg, T. M. and Pederson, H. J., Invest. Ophthalmol., 1972,
11, 1028. 35. Constable, I. J., Invest. Ophthalmol., 1974, 13,627. 36. Fineblxg, E., Machemer, R., Sullivan, P., Norton, E. W. D., Hamasaki, D. and Anderson, D., Am.
.I. Ophthalmol., 1975, 79,67. 37. Constable, I. J. and Swarm, D. A., Arch. Ophthalmol., 1975, 93,416. 38. Sabates, W. I., Abrams, G. W., Swanson, D. E. and Norton, E. W. D., Ophthalmology, 1981,88,
447. 39. Lincoff, H. and Kreissig, I., Arch.Ophthalmol., 1982, 100, 1083. 40. Thresher, R. J., Ehrenberg, M. and Machemer, R., Graefes Arch. Clin. Exp. Ophthalmol., 1984,
221, 192. 41. Chang, S., Lincoff, H. A., Coleman, D. J., Fuchs, W. and Farber, M. E., Ophthalmology, 1985,92,
651. 42. Lopez, R. and Chang, S., Am. J. Ophthalmol., 1992, 113,424. 43. Wood, D. J., Br. J. Ophthalmol., 1920,4,413. 44. Grafton, E. G. and Guyton, J. S., Am. J. Ophthalmol., 1948, 31, 299. 45. Miyamoto, K., Refojo, M. F., Tolentino, F. I., Foumier, G. A. and Albert, D. M., Retina, 1984,4,
264. 46. Chang, S., Zimmerman, N. J., Iwamoto, T., Ortiz, R. and Faris, D., Am. J. Ophthalmol., 1987,
103, 29. 47. Chang, S., Am. J. Ophthalmol., 1987, 103, 38. 48. Chang, S., Ozmert, E. and Zimmerman, N. J., Am. J. Ophthalmol., 1988, 106, 668. 49. Chang, S., Reppucci, V., Zimmerman, N. J., Heinemann, M. H. and Coleman, D. J., Ophthalmol-
ogy, 1.989, 96, 785. 50. Chang, S., Lincoff, H., Zimmerman, N. J. and Fuchs, W., Arch. Ophthalmol., 1989, 107,
761. 51. Nabih, M., Peyman, G. A., Clark, L. C., Hoffman, R. E., Miceli, M., Abou-Steit, M., Tawakol, M.
and Liu, K. R., Ophthalmic Surg., 1989, 20,286. 52. Glaser, R. M., Carter, J. B., Kuppermann, B. D. and Michels, R. G., Ophthalmology, 1991, 98,
1613.

504 T. V. CHIRILA et al.
53. Blinder, K. J., Peyman, G. A., Paris, C. L., Dailey, J. P., Alturki, W., Liu, K. R., Gremillion, C. M. and Clark, L. C., Br. J. Ophthalmol., 1991, 75,240.
54. Lee, K. J., Peyman, G. A., Paris, C. L., Alturki, W. A. and Desai, U. R., Ophthalmic Surg., 1992, 23, 553.
55. Conway, M. D., Peyman, G. A., Karacorlu, M., Bhatt, N., Soike, K. F., Clark, L. C. and Hoff- mann, R. E., Int. Ophthalmol., 1993, 17, 259.
56. Velikay, M., Wedrich, A., Stolba, U., Datlinger, P., Li, Y. and Binder, S., Am. J. Ophthulmol., 1993, 116,565.
57. Tanji, T. M., Peyman, G. A., Mehta, N. J. and Millsap, C. M., Ophthalmic Surg., 1993, 24, 681.
58. Bryan, J. S., Friedman, S. M., Mames, R. N. and Margo, C. E., Arch. Ophthalmol., 1994, 112, 1098.
59. Cutler, N. L., Arch. Ophthalmol., 1946, 35,615. 60. Cutler, N. L., Trans. Am. Acad. Ophthalmol. Otolaryngol., 1947, 52, 253. 61. Landegger, G. P., Am. J. Ophthalmol., 1950, 33, 915. 62. Shafer, D. M., Trans. Am. Acad. Ophthalmol. Otolaryngol., 1957, 61, 194. 63. Shafer, D. N. and Bussey, J. L., Arch. Ophthalmol., 1958, 60, 255. 64. Shapland, C. D., Arch. Sot. Amer. Oftal. Optom., 1959, 2, 299. 65. Castren, J. A., Acta Ophthalmologica, 1964, 42,427. 66. Seedorff, H. H. and Edmund, J., Acta Ophthalmologica, 1967, 45, 749. 67. Hudson, J. R., in New and Controversial Aspects of Retinal Detachment, ed. A. McPherson.
Harper & Row, New York, 1968, p. 365. 68. Stenzel, K. H., Dunn, M. W., Rubin, A. L. and Miyata, T., Science, 1969, 164, 1282. 69. Dunn, M. W., Stenzel, K. H., Rubin, A. L. and Miyata, T., Arch. Ophthalmol., 1969, 82, 840. 70. Dunn, M. W., Shafer, D. , Stenzel, K. H., Rubin, A. L., Miyata, T., Hopkins, L. and Powers, M. J.,
Trans. Am. Sot. Art6 ht. Organs, 1971, 17,421. 71. Pruett, R.C., Calabria, G. A. and Schepens, C. L., Arch. Ophthalmol., 1972,88,540. 72. Constable, I. J. and Swann, D. A., Arch. Ophthalmol., 1972, 88, 544. 73. Pruett, R. C., Schepens, C. L. and Freeman, H. M., Arch. Ophthaimol., 1974, 91,29. 74. Widder, W., Graefes Arch. Ophthalmol., 1960, 162,416. 75. Hruby, K., Klin. Monatzbl. Augenheilk., 1961, 138,484. 76. Hruby, K., Mod. Probl. Ophthaimol., 1966, 4, 228. 77. Hruby, K., Wiener Klin. Wochenschr., 1967,79,480. 78. Friedrich, H., An. Inst. Barraquer, 1969, 9,251. 79. Hruby, K., Buch. Augenarztes, 1970, 53,42. 80. Algvere, P., Acta Ophthalmologica, 1970, 49, 975. 8 1. Regnault, F., Bull. Mem. Sot. Fr. Ophtalmol., 197 1, 84, 106. 82. Kloti, R., Ophthalmologica, 1972, 165, 351. 83. Edmund, J., Mod. Probl. Ophthalmol., 1974, 12, 370. 84. Regnault, F. and Bregeat, P., Mod. Probl. Ophthalmol., 1974, 12, 378. 85. Kanski, J. J., Br. J. Ophthalmol., 1975, 59, 255. 86. Pruett, R. C., Schepens, C. L. and Swann, D. A., Arch. Ophthalmol., 1979,97,2325. 87. Denlinger, J. N., El-Mofty, A. A. M. and Balazs, E.A., Enp. Eye Res., 1980,30, 101. 88. Stenkula, S., Ivert, L., Gislason, I., Tomquist, R. and Weijdegard, L., Ophthalmic Surg., 1981,12,
435. 89. Nussbaum, J. J. and Roarty, J.,in Proceedings of Schepens International Society: Recent
Advances in the Research and Management of Vitreoretinal Disorders. Madrid, Spain, 1991, p. 71.
90. Giordano, G. G. and Refojo, M. F., Prog. Polym. Sci., 1998, 23,509-532. 91. Stone, W., New Engl. J. Med., 1958, 258, 486. 92. Armaly, M. F., Arch. Ophthalmol., 1962, 68, 390. 93. Cibis, P. A., Becker, B., Okun, E. and Canaan, S., Arch. Ophthalmol., 1962, 68,590. 94. Peyman, G. A., Ericson, E. S. and May, D. R., Sure. Ophthalmol., 1972,17,41. 95. Schepens, C. L., Retinal Detachment and Allied Diseases, Vol. 2. W. B. Saunders Co.,
Philadelphia, 1983, p. 747.

HYDROPHILIC POLYMERS AS ARTIFICIAL VITREOUS 505
96. Leaver, P. K., in Basic and Advanced Vitreous Surgery, ed. G. W. Blankenship, M. Stirpe, M. Gonvers and S. Binder. Liviana Press, Padova, Italy, 1986, p. 387.
97. Fedennan, J. L. and Schubert, H. D., Ophthalmology, 1988,95,870. 98. Leaver, P. K., in Retina, Vol. 3, ed. S. J. Ryan. The C. V. Mosby Co., Saint Louis, 1989, p. 293. 99. Gonvers, M., Bull. Mem. Sot. Fr. Ophtalmol., 1983, 94,441.
100. Miyamoto, K., Refojo, M. F., Tolentino, F. I., Fournier, G. A. and Albert, D. M., Arch. Ophthal- mol., 1986, 104, 1053.
101. Scott, J. D., in Retina, Vol. 3, ed. S. J. Ryan. The C. V. Mosby Co., Saint Louis, 1989, p. 307. 102. Nakamura, K., Refojo, M. F., Crabtree, D. V., Pastor, J. and Leong, F. L., Invest. Ophthalmol. Vis.
Sci., 1991, 32, 3007. 103. The Silicone Study Group, Arch. Ophthalmol., 1992, 110, 770. 104. The Silicone Study Group, Arch. Ophthalmol., 1992, 110,780. 105. The Silicone Study Group, Retina, 1993, 13,279. 106. Refojo, M., in Proceedings of the 206th ACS National Meeting: Polymers for Ophthalmic
Applications Symposium. Chicago, 1993, p. 545. 107. Tolentino, F. I., Liu, H. S., Refojo, M. F. and Freeman, H. M., in The Associationfor Research in
Vision and Ophthalmology (ARVO) Meeting Abstracts. Sarasota, FL, 1973, p. 30. 108. Balazs, E.A. and Sweeney, D. B., Mod. Probl. Ophthalmol., 1966, 4, 230. 109. Balazs, E. A. and Sweeney, D. B., in New and Controversial Aspects of Retinal Detachment,
ed. A. McPherson. Harper & Row, New York, 1968, p. 371. 110. Balazs, E. A. and Hultsch, E., in Advances in Vitreous Surgery, ed. A. R. Irvine and C. O’Malley.
C. C. Thomas, Springfield, IL, 1976, p. 601. 111. Kishimoto, M., Yamanouchi, U., Mori, S. and Nakamori, F., Nippon Ganka Gakkai Zasshi, 1964,
68, 1145. 112. Hruby, K., Mod. Probl. Ophthalmol., 1969, 8, 128. 113. Refojo, M. F., Polym. Sci. Technol., 1975, 8, 3 13. 114. Chan, I. M., Tolentino, F. I., Refojo, M. F., Foumier, G. and Albert, D. M., Retina, 1984,4,51. 115. Chiriba, T. V., Tahija, S., Hong, Y., Vijayasekaran, S. and Constable, I. J., J. Biomater. Appl.,
1994,9, 121. 116. Chiril,s, T. V., Hong, Y. and Dalton, P. D., in The Polymeric Materials Encyclopedia: Synthesis,
Properties a&Applications, Vol. 11, ed. J. C. Salamone. CRC Press, Boca Raton, FL, 1996, p. 8619. 117. Liesegang, T. J., Surv. Ophthalmol., 1990, 34, 268. 118. Liesegang, T. J., Int. Ophthalmol. Clin., 1993, 33, 127. 119. Balazs, E. A, and Leshchiner, A., U.S. Pat. 4 500 676, 1985, assigned to Biomatrix, Inc. 120. Balazs, E. A. and Leshchiner, A., U.S. Pat. 4 582 865, 1986, assigned to Biomatrix, Inc. 121. Balazs, E. A. and Leshchiner, A., U.S. Pat. 4605 691, 1986, assigned to Biomatrix, Inc. 122. Balazs, E. A. and Leshchiner, A., U.S. Pat. 4 636 524, 1987, assigned to Biomatrix, Inc. 123. Balazs, E. A. and Denlinger, J. L., in The Biology of Hyaluronan, ed. D. Evered and J. Whelan.
Wiley-Interscience, Chichester, UK, 1989, p. 265. 124. Chakrabarti, B., in Proceedings of the 206th ACS National Meeting: Polymers for Ophthalmic
Applications Symposium. Chicago, 1993, p. 547. 125. Larsen, N. E., Polk&, C. T., Reiner, K., Leshchiner, E. and Balazs, E. A., J. Biomed. Mater. Res.,
1993,27, 1129. 126. Mori, S., Nippon Ganka Gakkai Zusshi, 1965,69, 1441. 127. Mori, S., Nippon Ganka Gakkai Zasshi, 1967, 71, 22. 128. Gombos, G. M. and Berman, E. R., Acta Ophthalmologica, 1967,45,794. 129. Wilhelmus, K. R. and Moura, R. A., Ann. Ophthalmol., 1984, 16,350. 130. Femandez-Vigo, J., Refojo, M. F. and Verstraeten, T., Retina, 1990, 10, 148. 13 1. Fernandez-Vigo, J., Sabugal, J. F., Diaz Rey, A., Concheiro, A. and Martinez, R., J. Ocular
Pharmacol., 1990, 6, 137. 132. Oosterhuis, J. A., Van Haeringen, N. J., Jeltes, I. G. and G&us, E., Arch. Ophthalmol., 1966,76,
258. 133. Oosterhuis, J. A., Arch. Ophthalmol., 1966, 76,374. 134. Robinson, B. V., Sullivan, F. M., Borzelleca, J. F. and Schwartz, S. L., PVP: A Critical Review of
the Kinetics and Toxicology of Polyvinylpyrrolidone (Povidone). Lewis, Chelsea, MI, 1990.
506 T. V. CHIRILA et al.
135. Scuderi, G., Ann. Ottalmol. Clin. Ocul., 1954,80,213. 136. Hayano, S. and Yoshino, T., Rinsho Ganka, 1959, 13,449. 137. Peppas, N. A. and Barr-Howell, B. D., in Hydrogels in Medicine and Pharmacy, Vol. I, ed. N. A.
Peppas. CRC Press, Boca Raton, FL, 1986, p. 27. 138. Hong, Y., Chirila, T. V., Vijayasekaran, S. , Dalton, P. D., Tahija, S. G., Cuypers, M. J. H. and
Constable, I. J., J. Biomed. Mater. Res., 1996, 30, 441. 139. Vijayasekaran, S., Chirila, T. V., Hong, Y., Tahija, S. G., Dalton, P. D., Constable, I. J. and
McAllister, I. L., J. Biomater. Sci. Polym. Edn., 1996, 7, 685. 140. Van Den Bogert, C., Blaauw, E. H., Dontje, B. H. J., Hulstaert, C. E., Hardonk, M. J. and Kroon,
A. M., Virchows Arch., 1986, B 51, 39. 141. De Roetth, A., Arch. Ophthalmol., 1950, 43, 1004. 142. Gloster, J., Br. J. Ophthalmol., 1956, 40,487. 143. Freeman, M. I., Jacobson, B., Toth, L. Z. and Balazs, E. A., Exp. Eye Rex, 1968, 7, 113. 144. &terlin, S. E. and Jacobson, B., Exp. Eye Rex, 1968, 7,497. 145. &terlin, S. E. and Jacobson, B., Exp. Eye Rex, 1968, 7, 511. 146. Berman, E. R. and Voaden, M., in Biochemistry ofthe Eye, ed. C. N. Graymore. Academic Press,
London, 1970, p. 380. 147. Appleyard, M. E., McDonald, B. and Benjamin, L., Br. J. Ophthalmol., 1991, 75,276. 148. Salthouse, T. N., J. Biomed. Mater. Res., 1976, 10, 197. 149. Williams, D. F., J. Bioeng., 1977, 1, 279. 150. Bok, D. and Young, R. W., in The Retinal Pigment Epithelium, ed. K. M. Zinn and M. F. Marmor.
Harvard University Press, Cambridge, MA, 1979, p. 148. 15 1. Feeney, L. and Mixon, R. N., Exp. Eye Res., 1976,22, 533. 152. Bosch, E., Horwitz, J. and Bok, D., J. Histochem. Cytochem., 1993, 41, 253. 153. Beahan, P. G., in Techniques ofBiocompatibility Testing, Vol. I, ed. D. F. Williams. CRC Press,
Boca Raton, FL, 1986, p. 149. 154. Miiller-Jensen, K. and KGhler, H., Ber. Deut. Ophthalmol. Ges., 1969, 68, 181. 155. Miiller-Jensen, K., Klein, J. and Bauer-St%b, G., Ber. Deut. Ophrhalmol. Ges., 1969,69, 530. 156. Miiller-Jensen, K., Graefes Arch. Klin. Exp. Ophthalmol., 1974, 189, 147. 157. Refojo, M. F. and Zauberman, H., Invest. Ophthalmol., 1973, 12,465. 158. Miller, D., Surv. Ophthalmol., 1972, 16, 332. 159. Refojo, M. F., J. Appl. Polym. Sci., 1965, 9, 3161. 160. Refojo, M. F., J. Appl. Polym. Sci., 1965, 9, 3417. 161. Dohlman, C. H., Refojo, M. F. and Rose, J., Arch. Ophthalmol., 1967, 77, 252. 162. Daniele, S., Refojo, M. F., Schepens, C. L. and Freeman, H. M., Arch. Ophthalmol., 1968, 80,
120. 163. Calabria, G. A., Pruett, R. C., Refojo, M. F. and Schepens, C. L., Arch. Ophthalmol., 1970,83,
613. 164. Refojo, M. F., J. Biomed. Mater. Res. Symp., 1971, 1, 179. 165. Hogen-Esch, T. E., Shah, K. R. and Fitzgerald, C. R., J. Biomed. Mater. Res., 1976, 10,
975. 166. Yamauchi, A., Matsuzawa, Y., Nishioka, K., Hara, Y. and Kamiya, S., Kobunshi Ronbunshu,
1977, 34,261. 167. Nishioka, K., Hara, Y., Kamiya, S., Ikuno, T., Yamauchi, A. and Matsuzawa, Y., Rinsho Ganka,
1977, 31,907. 168. Hara, Y., Nishioka, K., Kamiya, S., Yamauchi, A. and Matsuzawa, Y., Nippon Ganka Kiyo, 1977,
28, 576. 169. Hara, Y., Nishioka, K., Kamiya, S., Yamauchi, A. and Matsuzawa, Y., Nippon Ganka Kiyo, 1977,
28, 1522. 170. Yamauchi, A., Matsuzawa, Y., Hara, Y., Matsushima, S., Nishioka, K., Nakao, S. and Kamiya, S.,
Nippon Ganka Kiyo, 1978,29,1922. 171. Yamauchi, A., Matsuzawa, Y., Hara, Y., Kamiya, S., Nishioka, K., Saishin, M. and Nakao, S.,
Nippon Ganka Kiyo, 1979,30,385. 172. Hara, Y., Kamiya, S., Nishioka, K., Saishin, M., Nakao, S. and Yamauchi, A., Nippon Ganka
Gakkai Zusshi, 1979, 83, 1478.

HYDROPHILIC POLYMERS AS ARTIFICIAL VITREOUS 507
173. Yamauchi, A., Nara Igakku Zasshi, 1982, 33, 349. 174. Hara, Y., Hara, T., Hatanaka, O., Hirai, H., Ichiba, S., Kamiya, S., Nakao, S., Saishin, M., Hiasa,
Y. and Yamauchi, A., Nippon Ganka Kiyo, 1984,35, 1340. 175. Yamauchi, A., in Polymer Gels. Fundamentals and Biomedical Applications, ed. D. DeRossi,
K. Kajiwara, Y. Osada and A. Yamauchi. Plenum Press, New York, 1991, p. 127. 176. Wang, B., Zhang, J., Wang, H., Mu, G., Wang, L. and Xu, J., in Polymers and Biomaterials.
Proceedings of the Chinese Materials Research Society 1990 International Symposia, Vol. 3, ed. H. Feng, Y. Han and L. Huang. North-Holland, Amsterdam, 1991, p. 397.
177. Rozenberg, M. E.and Sorokin, A. Y., in Polyvinyl Alcohol: Developments, ed. C. A. Finch. Wiley, Chichester, UK, 1992, p. 689.
178. Jarrett, R. D. and McCain, G. H., U.S. Pat. 4 687 808,1987, assigned to BioSpecific Technologies, Inc.
179. McCain, G. H. and Jarrett, R. D., U.S. Pat. 4 737 544, 1988, assigned to BioSpecific Technologies, Inc.
180. Chirila, T. V., Hong, Y. and Constable, I. J., The 3rd Pa& Polymer Conference, Preprints. Gold Coast, Australia, 1993, p. 373.
181. Chirila, T. V., Constable, I. J., Hong, Y., Vijayasekaran, S., Humphrey, M. F., Dalton, P. D., Tahija, S. G., Maley, M. A. L., Cuypers, M. J. H., Sharp, C., Moore, S. R. and Davies, M. J., Cells Mater., 1995, 5, 83.
182. Souyri. F., Chretien, M. and Droz, B., Brain Res., 1981, 205, 1. 183. Chretien, M., Patey, G., Souyri, F. and Droz, B., Brain Res., 1981, 205, 15. 184. Vidyasagar, T. R., Brain Res., 1981,224,452. 185. Merigan, W. H., Barkdoll, E. and Maurissen, J. P. J., Toxicol. Appl. Pharmacol., 1982, 62,
342. 186. Duke-Elder, W. S., J. Physiol., 1929, 68, 155. 187. Robertson, E.B. and Duke-Elder, W. S., Proc. Roy. Sot. London, Ser.B, 1933,112,215. 188. Duke-Elder, W. S. and Robertson, E. B., Br. J. Ophthalmol., 1934, 18,433. 189. Poole, J. H., Trans. Faraday Sot., 1925/1926, 21, 114. 190. Ross-hdurphy, S. B., in Viscoelasticity of Biomaterials, ed. W. G. Glasser and H. Hatakeyama.
ACS Symp. Series 489. American Chemical Society, Washington, DC, 1992, p. 204. 191. Ross-hdurphy, S. B., Polym. Gels Netw., 1994, 2, 229. 192. Almdal, K., Dyre, J., Hvidt, S. and Kramer, O., Polym. Gels Netw., 1993, 1,5. 193. Fukada, E. and Date, M., Biorheology, 1963, 1, 101. 194. Taniok:a, A., Jojima, E., Miyasaka, K. and Ishikawa, K., J. Polym. Sci., Polym. Phys. Edn, 1973,
11, 14r39. 195. Nguen, A. L., Vu, B. T. and Wilkes, G. L., Biopolymers, 1974, 13, 1023. 196. Rosenblatt, J., Devereux, B. and Wallace, D. G., Biomaterials, 1992, 13, 878. 197. Ogston, A. G. and Stanier, J. E., Biochem. .I., 1951, 49,585. 198. Ogston, A. G. and Stanier, J. E., J. Physiol., 1953, 119, 244. 199. Jensen, C. E. and Koefoed, J., J. Colloid Sci., 1954, 9,460. 200. Gibbs, D. A., Merrill, E. W., Smith, K. A. and Balazs, E. A., Biopolymers, 1968, 6,777. 201. Balazs, E. A. and Gibbs, D. A., in Chemistry and Molecular Biology of the Intercellular Matrix,
Vol. 3, ed. E. A. Balazs. Academic Press, London, 1970, p. 1241. 202. Balazs, E. A., Fed. Proc., 1966, 25, 1817. 203. Pfeiffer, H.H., Biorheology, 1963, 1, 111. 204. Bettelheim, F. A. and Wang, T. J. Y., Exp. Eye Res., 1976, 23,435. 205. Zimmerman, R. L., Biophys. J., 1980,29,539. 206. Weber, H. and Landwehr, G., Ophthalmic Res., 1982, 14, 326. 207. Weber, H., Landwehr, G., Kilp, H. and Neubauer, H., Ophthalmic Res., 1982, 14, 335. 208. Buchsbaum, G., Sternklar, M., Litt, M., Grunwald, J. E. and Riva, C. E., Biorheology, 1984,21,
285. 209. Lee, B., Litt, M. and Buchsbaum, G., Biorheology, 1992,29,521. 210. Lee, B., Comparative rheological studies of the vitreous body of the eye. Ph.D. Thesis 1992, UMI
Dissertation Services/Bell and Howell Co., Ann Arbor, MI, 1994. 211. Ferry, J. D., Viscoelastic Properties of Polymers, 3rd edn. Wiley, New York, 1980, p. 34.

508 T. V. CHIRILA et al.
212. Sperling, L. H., Introduction to Physical Polymer Science, 2nd edn. Wiley, New York, 1992, p. 181.
213. Mark, J. E., Eisenberg, A., Graessley, W. W., Mandelkern, L., Samulski, E. T., Koenig, J. L. and Wignall, G. D., Physical Properties of Polymers, 2nd edn. American Chemical Society, Washington, DC, 1993, p. 130.
214. Richards, 0. W. and Hague, E. B., Am. J. Ophthalmol., 1963,55, 15 1. 215. Dalton, P. D., Chirila, T. V., Hong, Y. and Jefferson, A., Polym. Gels Netw., 1995, 3,429.




















