Consumers' preference and perception of smoke-dried white ...
Upload
independentCategory
view
0download
0
doi: 10.1111/j.1529-8817.2005.00205.x
The Significant Increase in Cardiovascular Disease Riskin APOE ε4 Carriers is Evident Only in Men Who Smoke:Potential Relationship Between Reduced AntioxidantStatus and ApoE4
P. J. Talmud1,∗, J. W. Stephens1, E. Hawe1, S. Demissie2, L. A. Cupples2 , S. J. Hurel3,S. E. Humphries1 and J. M. Ordovas4
1Centre for Cardiovascular Genetics, British Heart Foundation Laboratories, Department of Medicine, Rayne Building, UniversityCollege London, 5 University St, London WC1E 6JF, United Kingdom2Boston University School of Public Health and School of Medicine, Boston, Mass 02111, USA3Department of Diabetes & Endocrinology, UCL Hospitals, London W1T 3AA, UK4Jean Mayer-U.S. Department of Agriculture Human Nutrition Research Centre on Ageing at Tufts University, Boston, Massachusetts02111, USA
Summary
Data from 1668 men (316 cardiovascular disease events) from the Framingham Offspring Study was reanalysed,specifically examining APOE:smoking interactions. Overall hazard ratio (HR) for smoking was 1.95 (1.52, 2.50)compared to non-smokers. Using ε3/3 as a referent group, in non-smokers HRs for ε2 carriers (ε2+; 1.04 (0.61,1.76) and ε4 carriers (ε4+; 1.04 (0.70, 1.54) showed no major risk increase. In smokers, HRs were 1.96 (1.26, 2.78)in ε3ε3 men, 3.46 (2.14, 5.60; p = 0.09 for interaction) in ε2+ and 3.81 (2.49, 5.84; p = 0.01 for interaction), witha significant interaction between daily cigarette consumption and APOE genotype on risk (p = 0.03). The potentialmechanism for this APOE ε4:smoking interaction was examined in a second study of 728 Caucasian patients withdiabetes, where markers of reactive oxygen species were available. APOE genotype was not associated with plasmaOX-LDL or total antioxidant status (TAOS) in non-smokers. However, in smokers ε4+ had 26.7% higher plasmaOX-LDL than other genotypes (APOE:smoking interaction p = 0.04), while ε2+ had 28.4% higher plasma TAOSthan ε3ε3 and ε4+ combined (APOE:smoking interaction p = 0.026). Although direct extrapolation needs to beconsidered with caution, these results identify that the cardiovascular disease risk-raising effect of ε4+ is confined tosmokers, and a feasible mechanism is presented by the reduced antioxidant capacity/increased OX-LDL of apoE4.
Keywords: TAOS, apolipoprotein E, cardiovascular diseases, diabetes mellitus, gene: environment interaction,smoking
Introduction
Almost all chronic disease results from gene: environ-ment interactions, and acknowledging and understand-ing this is the challenge that faces health scientists, andcardiovascular disease (CVD) is no exception (Sing et al.2003). It is one of the accepted tenets of cardiovascular
∗Corresponding author: Dr Philippa J Talmud, Fax: +44 207679 6212. E-mail: [email protected]
genetics that common variants of the apolipoprotein Egene (APOE), the ε2, ε3 and ε4 alleles, are associatedwith differences in coronary heart disease (CHD) andCVD risk. The 1996 meta-analysis estimated a sum-mary unadjusted odds ratio (OR) for ε4, compared toε3 homozygotes, as 1.38 (1.22, 1.57) in men and 1.82(1.30,2.54) in women, whereas the ε2 allele was not sig-nificantly associated with CHD risk in men, OR 0.94(0.79, 1.11), or in women, 1.07 (0.66, 1.76) (Wilsonet al. 1996). Thus while the ε4 allele was risk-enhancing
C© University College London 2005 Annals of Human Genetics (2005) 69,613–622 613

P. J. Talmud et al.
in both men and women, the effect of the ε2 allele wasnot (Wilson et al. 1996; Ioannidis et al. 2001). A recentmeta-analysis of studies published since 1996 concurredthat in men and women ε4 carriers (ε4+) had 42%higher CHD risk than ε3/3 individuals, while the risk-association for ε2 carriers was not consistent, but overallshowed risk effects that were no different from ε3 ho-mozygotes (Song et al. 2004).
Lahoz et al. (2001) examined the association of APOEgenotype and CVD risk in 3413 men and women partic-ipating in the Framingham Offspring Study (FOS). Afteradjustment for non-lipid risk factors including smoking,in the men alone both the ε2 [OR 1.79 (1.15, 2.77)],and ε4 [(OR 1.63 (1.13, 2.34)] alleles, were associatedwith an increased risk of CVD compared to ε3 homozy-gotes (Lahoz et al. 2001). In FOS, this atypical effect ofthe ε2 allele on risk was suggested to be due to the in-creased postprandial lipemia associated with the ε2 alleleand elevated fasting insulin levels in ε2 carriers (Lahozet al. 2001).
The modification of the CHD risk-associated effectsof smoking, by APOE genotype, was examined in theNorthwick Park Heart Study II (NPHSII), a prospectivestudy of CHD in over 3000 middle-aged UK men. Innever-smokers the CHD risk was similar in all APOEgenotypes. Compared to this reference group, ε3/3 cur-rent smokers had a hazard ratio (HR) of 1.68 (95%CI1.01, 2.83), which is within the range of the well-established doubling of risk linking cigarette smokingand CHD (Doll et al. 1994; Kannel et al. 2003). Carriersof the ε4 allele, however, showed significant interactionof genotype and smoking on risk (p < 0.007), with anHR of 3.17 (95%CI 1.82, 5.50). Thus the associationof the ε4 allele with CHD risk was confined to currentsmokers alone, and was independent of other classicalCHD risk factors, including plasma lipids (Humphrieset al. 2001).
We have reanalysed the FOS APOE data (Lahozet al. 2001), examining the potential interaction be-tween APOE and smoking on CVD risk. The studydid not have the power to examine the APOE: smokinginteraction in women, where CVD incidence was low;therefore the men alone were considered in this analysis.To explore the possible mechanisms for the interactionof smoking with APOE, and since smoking is a gen-erator of reactive oxygen species (ROS) (Churg, 2003),
we examined the relationship between APOE geno-type and markers of oxidative stress, namely oxidisedLDL (OX-LDL) and total antioxidant status (TAOS).Oxidative stress results from the excess of ROS over-whelming any endogenous antioxidant protection, andis well-documented in CVD (Harrison et al. 2003).ROS production promotes the formation of foam cellsdue to scavenger receptor-mediated uptake of OX-LDLby macrophages (Azumi et al. 2002). Since neither OX-LDL nor TAOS measures were available in FOS, we ex-amined their relationship with APOE in patients withdiabetes (University College London Diabetes and Car-diovascular Disease Study (Dhamrait et al. 2004)) whotypically display increased oxidative stress (Brownlee,2001), to determine whether there was a relationshipbetween these markers of ROS and APOE genotype,which would reflect the differing antioxidant capacityof the apoE isoforms.
Methods
Study Subjects
The details of the Framingham Offspring Study (FOS)and recruitment have been published previously (Kannelet al. 1979). Complete data was available on 1697 men.Between 1971–1994, there were 316 recorded CVDevents in these men during this 23 year follow-up. (Onehundred and twenty-two women had had an event, butbecause of the lack of power only the men were consid-ered for further analysis). CVD included CHD (MI,angina pectoris, coronary insufficiency and coronarydeath), stoke, peripheral vascular disease and congestiveheart failure, based on clinical information from physi-cian records and hospitalisation. The study had ethicalapproval from institutional review committees and thesubjects gave full informed consent.
Details of the University College Diabetes and Car-diovascular Study (UDACS) have been described else-where (Stephens et al. 2004). Briefly, this comprises1011 consecutive men and women (of whom 439 menand 284 women were Caucasian), recruited from thediabetes clinic at University College London Hospi-tals NHS Trust (UCLH) between the years 2001-2.All patients had diabetes according to WHO criteria(Alberti et al. 1998). Subjects were categorised by the
614 Annals of Human Genetics (2005) 69,613–622 C© University College London 2005

Relationship Between APOE ε4, Smoking and TAOS on CVD Risk
presence/absence of clinically manifest CVD. Ethicalapproval was obtained from the UCL/UCLH ethicscommittee.
APOE Genotyping
In the FOS, APOE genotyping was carried out byPCR and HhaI digestion (Lahoz et al. 2001; Hixsonet al. 1990). In the UDACS APOE genotyping wasperformed using a heteroduplex generator (Bolla et al.1999).
Measurement Of Plasma TAOS and OX-LDL
These measurements were performed on citrated plasmacollected at the time of recruitment. All samples wereimmediately placed on ice and underwent centrifugewithin one hour of collection. All samples were storedat −80◦C in aliquots and only defrosted for these mea-surements, and were analysed within 12 months of col-lection. OX-LDL was measure by ELISA (MercodiaAB, Uppsala Sweden). Plasma TAOS was measuredby a photometric microassay previously described bySampson et al. (2002) and is inversely related to oxida-tive stress (the higher the oxidative stress, the lower theTAOS). The inter-assay coefficient of variation (CV)was 14.1%, and the intra assay CV was 4.3%. CombinedAPOE genotype and OX-LDL, and APOE genotypeand TAOS levels were available for 282 males and 178 fe-males (63.6%) and 424 men and 277 women (96.9%), re-spectively. There was no difference in the APOE geno-type distribution or the baseline characteristics of thesetwo groups, despite the difference in participant num-ber, and thus does not represent selection bias (Supple-mentary Table 1).
Statistical Analysis
In the FOS skewed variables were log transformed tonormalise their distribution before analysis, while geo-metric means and approximate SD are presented. Dif-ferences in the baseline characteristics between thosemen who had a CVD event and those who were event-free were tested using the t-test for continuous variablesand χ 2 for categorical variables. Deviation from HardyWeinberg equilibrium using the χ 2 was assessed on the
Table 1 Baseline characteristic at exam 1 by CVD event statusat exam 6 in the Framingham Offspring Study (men)
No CVD CVDevent (1352) event (316) p-value
Age (years) 34.9 (10.1) 43.3 (8.8) 0.0032Smokers (number (%)) 528 (39.1%) 175 (55.4%) 0.0001BMI (kg/m2) 26.2 (3.5) 27.5 (3.9) 0.03Systolic BP (mm Hg) 124 (13) 132 (16) 0.0001Cholesterol (mg/dl) 196 (37) 218 (42) 0.005HDL (mg/dl) 44.9 (11.3) 41.7 (11.8) 0.31LDL (mg/dl) 130 (33) 147 (38) 0.004Triglyceride (mg/dl) 4.43 (0.657) 4.75 (0.679) 0.46
APOE genotype:∗ (number) (number )ε3ε3 915 182ε4+ 269 86ε2+ 168 48
∗29 ε2/4 not included
whole sample and included the ε2ε4 individuals. Base-line characteristics and exam 6 CVD prevalence data arepresented for descriptive purposes only. We used Cox’sregression models with time-dependent covariates, withsurvival time over the 23 year period (time to CVDor censoring) as a dependent variable; APOE geno-types and smoking as primary independent variables;and age, alcohol consumption, diabetes, hypertension,BMI, total cholesterol, HDL-C, and cholesterol treat-ment as covariates. Interactions between genotype andsmoking were considered using a likelihood ratio testto compare models with and without the interactionterm. Data on smoking and covariates were measuredat exams 1 through to 6 and value change over time.The models were specified such that the hazard at agiven exam depended on the values of smoking and co-variates prior to that exam. We used lagged covariatesto allow the proper time sequence of risk factors (ex-posure) and outcome. These analyses were performedusing the PHREG procedure in SAS.
In the UDACS, ANOVA was used to assess the asso-ciation between genotype and plasma TAOS/OX-LDL.The distribution of OX-LDL was normalised for analy-sis by using a square root transformation. The relation-ships between baseline parameters and plasma OX-LDLand TAOS were tested by Pearson’s correlation coeffi-cients. ANCOVA was performed to test the associationbetween genotype and plasma OX-LDL and TAOS, af-ter adjustment for potential confounders using multiple
C© University College London 2005 Annals of Human Genetics (2005) 69,613–622 615

P. J. Talmud et al.
regression analysis to obtain a residual. The interactionbetween genotype and smoking status in determiningplasma TAOS or OX-LDL (and adjusted measures) wasperformed using linear regression modelling, includingan interaction term for genotype and smoking status.For these analyses, since there was no heterogeneity ofeffect, to test the interaction between APOE genotypeand smoking on OX-LDL, ε3/3 and ε2+ were pooledand contrasted with ε4+, while to test the interaction ofgenotype and smoking on TAOS, ε3/3 and ε4+ geno-types were pooled and contrasted with ε2+. In all casesa p-value of less than 0.05 was considered statisticallysignificant.
Results
Framingham Offspring Study
Lipid profile, DNA and APOE genotypes were availableon 1668 men after exclusion of 29 ε2ε4 men. Geno-type distribution was in Hardy-Weinberg equilibriumand the allele frequencies were 0.80 for ε3, 0.12 forε4 and 0.079 for ε2. The baseline characteristics of thecohort are shown in Table 1. Compared to men freeof CVD, those men who had CVD were significantlyolder (p = 0.0032), more likely to be a current smoker(p = 0.0001), had a greater BMI (p = 0.03), and highersystolic BP (p = 0.0001), cholesterol (p = 0.005) andLDL (p = 0.004).
The Effects of Smoking on CHD RiskAccording to APOE Genotype
Forty-two percent of men smoked, and overall the ef-fect of smoking was to increase CVD risk almost twofold [crude HR 1.93 (1.50, 2.49)]. The smoking preva-lence according to APOE genotype is presented inTable 2. In a covariate-adjusted Cox’s regression model,smoking was associated with an increase in CVD risk inε3 homozygotes, HR1.96 (1.34, 2.77); in ε2+ smok-ers compared to ε2+ non-smokers the HR was 3.45(1.73, 6.45) and in ε4+ smokers compared to ε4+ non-smokers HR was 3.68 (2.22, 6.11). Thus in ε4+ andε2+, smoking was having an effect of a similar mag-nitude on CVD risk, which was about 70–80% higher
Table 2 Prevalence of smoking according to APOE genotype inthe FOS men
ε3/3 ε2/2+2/3 ε3/4+4/4(n)(n) (n) (n)
% prevalence 43% 40% 39%in whole group∗ 476/1097 87/216 140/355
% prevalence 42% 35% 33%in CVD-∗ 380/915 59/168 89/269
% prevalence 53% 58% 59%in CVD+∗ 96/182 28/48 51/86
∗Smokers/total
than in ε3/3 men who smoked, suggesting a potentialgene: environment/CVD risk interaction.
Combined Effects of Smoking and APOEGenotype on CHD Risk
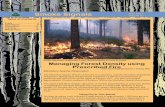
Compared to ε3/3 non-smokers, risk in ε2+ and ε4+non-smokers was not statistically different, HRs 1.04(0.61, 1.76) and 1.04 (0.70, 1.54), respectively. Forthe ε2+ men who smoked the HR was 3.46 (2.14,5.60; p = 0.09 for interaction), and for ε4+ HR 3.81(2.49, 5.84; p = 0.01 for interaction) compared to ε3/3non-smokers (Figure 1).
To assess the quantitative effect of smoking on thegenotypic effect on CVD risk, the interaction betweensmoking and APOE genotypes was evaluated usingsmoking as a continuous measure (number of cigarettessmoked per day). These results indicate a clear gradientof effect of smoking and genotype on risk (Figure 2),with an overall significant APOE: smoking interaction(p = 0.03).
University College Diabetes andCardiovascular Study (UDACS)
The baseline characteristics of the UDACS Caucasianmen and women by CVD status are presented inTable 3. In total 723 (100%) Caucasian men and womenwere successfully genotyped for the APOE genotype.Genotype distribution was in Hardy-Weinberg equilib-rium and the allele frequencies were 0.81 for ε3, 0.12for ε4 and 0.07 for ε2. Mean age was significantly higherfor those with CVD compared to those free of CVD.Total cholesterol and LDL cholesterol were significantlylower in those with CVD and this could be explained
616 Annals of Human Genetics (2005) 69,613–622 C© University College London 2005

Relationship Between APOE ε4, Smoking and TAOS on CVD Risk
Figure 1 Age adjusted CVD hazard ratios by APOE genotype in men stratified on the basis ofsmoking in the Framingham Offspring Study.ε2/4 men (n = 29) were excluded from the analysis.
by the significantly higher proportion of patients withCVD taking lipid lowering medications; ACE inhibitors(ACEI), aspirin, insulin and statins. HDL was lower andTGs higher in those with CVD compared to the CVDfree individuals.
Association of APOE Genotype and Smokingon TAOS and OX-LDL in UDACS
To test whether the genotype: smoking interactioncould be explained by measures of oxidative stress,which were not available in FOS, the association be-tween APOE and plasma OX-LDL and TAOS was ex-amined in UDACS. Only Caucasian men and womenwere considered, and since there was no significant ev-idence for heterogeneity of effect between men andwomen for these parameters (not shown) the analysiswas carried out in the group as a whole. Plasma TAOSwas correlated with glucose, triglycerides and HDL(r = −0.13 −0.14, 0.11, respectively; all p < 0.05) andOX-LDL with age, LDL and HDL (r = 0.31, −0.13,respectively; all p < 0.05) and these variables were ad-justed for in the analysis. No difference was observed inplasma TAOS and OX-LDL by pharmacological treat-ments with ACE inhibitors, statins, aspirin or insulin.Overall there was no significant association of genotypewith either plasma TAOS or OX-LDL and similarly,after stratification by smoking status, in non-smokers
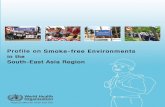
there was no association of genotype with either ad-justed TAOS or OX-LDL (Figure 3a, b). However, incurrent smokers ε2+ had 28.4% higher plasma TAOSthan ε3/3 and ε4+ combined (p = 0.026, Figure 3a),with a significant APOE: smoking interaction on plasmaTAOS (p = 0.026). Considering OX-LDL in smokers,ε4+ had 26.7% higher OX-LDL than ε3/3 and ε2+combined (p = 0.04, Figure 3b), displaying a significantAPOE: smoking interaction on OX-LDL (p = 0.04).
Discussion
Many studies, when analysing genotypic effects on CVDrisk, correct for all CVD risk factors, including smok-ing, to take into account any confounding chance dif-ferences in their prevalence by genotype. In doing so thepossibility of analysing for potential gene: environmentinteractions are removed. The studies included in the1996 meta-analysis (Wilson et al. 1996) corrected forconfounders, including smoking, and thus gave validityto the concept that APOE ε4 carriers were at increasedrisk of CHD compared to ε3/3 individuals, while ε2carriers were protected from risk. This concept of ε4-related risk became an accepted tenet of the field. Thedata from this present study are compelling, since theyhighlight two essential points. Firstly, reanalysis of theeffect of APOE genotype on CVD risk in the Fram-ingham Offspring Study, specifically testing for gene:
C© University College London 2005 Annals of Human Genetics (2005) 69,613–622 617

P. J. Talmud et al.
Figure 2 Age adjusted CVD hazard ratios by APOE genotype in men stratified on the basis of thenumber of cigarettes smoked per day in the Framingham Offspring Study compared to non-smoking ε3homozygotes:<1 cig = less than 1 cigarette per day; 10 cigs = 10 or less cigarettes per day; 20 cigs = 20 or lesscigarettes per day; 40 cigs = 40 or less cigarettes per daycompared to non-smoking ε3 homozygotesHR for ε3/3 smokers<1 cig HR 1.02 (1.01, 1.03 p = 0.0004),10 cigs HR 1.16 (1.08, 1.3, p < 0.0004)20 cigs HR 1.41 (1.17, 1.70, p < 0.0004)40 cigs HR 1.98 (1.36, 2.88 p < 0.0004)HR for ε2+ smokers<1 cig HR 1.15 (0.73, 1.80 p = 0.55)10 cigs HR 1.61 (1.09, 2.36, p < 0.02)20 cigs HR 2.34 (1.59, 3.44, p < 0.0001)40 cigs HR 4.97 (2.75, 8.90 p < 0.0001)HR for ε4+ smokers<1 cig HR 1.17 (0.83, 1.60 p = 0.69)10 cigs HR 1.60 (1.17, 2.20, p < 0.0003)20 cigs HR 2.27 (1.62, 3.17, p < 0.0001)40 cigs HR 4.53 (2.72, 7.55 p < 0.0001)Note: Hazard ratios (HRs) in the graph were not estimated from a categorical smoking variable. Theywere calculated from a model that was fitted assuming a log-linear relationship between smoking (numberof cigarettes smoked) and the underlying hazard function. Therefore it is inappropriate to report thenumber of individuals in each category.
smoking interactions, clearly demonstrates that whenstratified on the basis of smoking, the APOE ε4 and ε2carriers who do not smoke were at no greater CVD riskthan ε3/3 non-smokers. This is particularly powerfulsince a direct comparison can be made with the sameFOS data when smoking status was not considered, andwhere both ε4 and ε2 carriers showed increased CHDrisk (Lahoz et al. 2001). Secondly, compared to ε3/3men, ε4 men who smoked showed a significant inter-action of ε4 and smoking on risk (p = 0.01). Both ε4+
and ε2+ showed a clear cigarette/dose response, whichhas not been previously reported.
Significant effects of APOE genotype on risk re-mained even after adjustment for lipid variables in thepresent study (in smokers) and in several other stud-ies (Lahoz et al. 2001; Stengard et al. 1999; Humphrieset al. 2001). Taken together with the fact that the ε4non-smokers show no increased CVD risk, despite theirhigher lipid levels, this suggests that the APOE risk-associations are independent of lipids.
618 Annals of Human Genetics (2005) 69,613–622 C© University College London 2005

Relationship Between APOE ε4, Smoking and TAOS on CVD Risk
Table 3 Baseline characteristics of 723Caucasian subjects by CVD status in theUDACS
No CVD CVDTrait (n = 523) (n = 200) P Value
Age (years) 59.9 (14.0) 68.9 (10.1) <0.001Sex (F/M) 222/301 (42.4%/57.6%) 62/138 (31.0%/69.0%) 0.001Smokers (number %) 91 (17.2%) 30 (14.9%) 0.5Duration (years)+ 11 (5–11) 11 (6–18) 0.81Systolic BP (mmHg) 139.4 (19.75) 141 (21.8) 0.66Body mass index (kg/m2) 28.9 (6.1) 29.4 (5.9) 0.32Glucose (mmol/l) 10.1 (5.37) 9.6 (4.96) 0.39Cholesterol (mmol/1) 5.22 (1.0) 4.85 (1.1) <0.001LDL-C (mmol/1) 2.92 (0.9) 2.57 (0.9) <0.001HDL (mmol/1) 1.47 (0.5) 1.30 (0.4) <0.001Triglycerides (mmol/1) 1.95 (1.44) 2.25 (1.65) 0.02OX-LDL (u/l) 48.92 (17.6) 48.51(19.5) 0.82TAOS % 44.8 (12.8) 44.2 (13.10) 0.51ACEI (No/Yes) 314/215 (59.4%/40.6%) 87/115 (43.1%/56.9%) <0.001Aspirin (No/Yes) 348/181 (65.7%/34.3%) 53/149 (26.0%/74.0%) <0.001Insulin (No/Yes) 278/251 (52.7%/47.3%) 127/75 (62.9%/37.1%) 0.013Statin (No/Yes) 440/89 (83.1%/16.9%) 91/111 (45.2%/54.8%) <0.001APOE genotype:∗ (number) (number )ε3ε3 347 136ε4+ 111 39ε2+ 69 26
∗ε2/4 excluded from the start
APOE Genotype and Smoking Interactionon CVD Risk
In the FOS men, smoking per se was associated with a95% increase in risk. Compared to ε3/3 non-smokers,the effect of smoking was to increase risk by 96% inε3/3men, 246% in ε2+ and 281% in ε4+, with evi-dence of a significant interaction of ε4+ and smokingon risk. These results support the previous study, whichsuggested that the accepted observation of the universalrisk-association of ε4 needed re-assessment (Humphrieset al. 2001).
Two studies assessing the APOE: smoking interac-tion reported failure to confirm these findings. TheInternational Studies of Infarct Survival (ISIS), a largecase control study, demonstrated an incremental ORincrease of 1.17 for ε2ε3 to ε3ε3 to ε3ε4 subjects,but no ε4:smoking interaction was detected (Keavneyet al. 2003). ISIS used ε3ε2 subjects as the referencegroup, rather than ε3ε3, and excluded ε2ε2 (n = 78)and high-risk ε4ε4 individuals (n = 160). In re-analysis(Humphries et al. 2003) a significantly greater than ad-ditive effect of genotype and smoking on risk was seen,with a relative excess of risk interaction (RERI of 1.62
(0.4, 2.97), thus confirming APOE:smoking interac-tion on CHD risk in the ISIS. In the Physicians HealthStudy, a nested case: control cohort matched for smok-ing, neither an APOE genotype effect on risk nor anε4:smoking interaction were identified (Liu et al. 2003).As an indicator that this was a low-risk cohort, the ex-pected association of APOE genotype with plasma lipidlevels was not seen. Several studies using carotid arteryatherosclerosis (CAA) as an endpoint have identified anε4:smoking interaction (Djousse et al. 2002; Karvonenet al. 2002; Pezzini et al. 2004). Overall, these data sup-port an ε4: smoking interaction on risk, with the excep-tion of those studies where there is insufficient power,low smoking prevalence, or inappropriate analysis.
APOE ε2 Genotype and Smoking Interactionon CVD Risk
Lahoz et al. in reporting their initial findings of the asso-ciation of ε2 and ε4 alleles with increased risk in FOS,acknowledged that the ε2 findings were unusual andcontrary to the results from the meta-analysis (Lahozet al. 2001). Thus the FOS is atypical since ε2 carriers
C© University College London 2005 Annals of Human Genetics (2005) 69,613–622 619

P. J. Talmud et al.
Figure 3 Association of APOE genotype in non-smokers and smokers with (a) mean (± SE)adjusted percentage total antioxidant status (TAOS) and (b) mean (± SE) adjusted oxidised LDL inUDACS.TAOS was adjusted for TG, HDL and glucose. OX-LDL was adjusted for age, LDL and HDL.Numbers in the bars represent the number of individuals in each group.
usually show CVD risk protection compared to ε3/3men. In the present analysis, both ε2+ and ε4+ non-smokers showed hazard ratios which were not signifi-cantly different from ε3/3 non-smokers. However, inthe smokers both ε2 and ε4 carriers showed increasedrisk. While the interaction with smoking was signifi-
cant for ε4+ carriers it was not for ε2 carriers. In theFOS it is possible that this lack of interaction between ε2and smoking on risk merely reflects the smaller numberof ε2 carriers.
Two possible mechanisms for the increased risk-association of the ε2 allele, in the FOS men but not the
620 Annals of Human Genetics (2005) 69,613–622 C© University College London 2005

Relationship Between APOE ε4, Smoking and TAOS on CVD Risk
women were suggested by Lahoz et al. (2001); increasedpostprandial lipemia associated with the ε2 allele, and el-evated fasting insulin levels compared to ε3/3 and ε3/4men (Orchard et al. 1994).
Biological Basis for APOE:Smoking Interactions
In order to consolidate the statistically-establishedε4:smoking interaction with a biological mechanism,we examined two measures of oxidant stress in a sec-ond study (UDACS), taking APOE genotype and smok-ing into account in a study of patients with diabetes, agroup where increased ROS is typical. In the UDACS,ε4+ smokers had significant higher levels of OX-LDL(26.7%, p = 0.04) than the other genotypes combined,with significant APOE: smoking interaction on OX-LDL (p = 0.04). One mechanism causing this could bethe higher levels of ROS in ε4+ subjects, since apoE4 isacting as a poorer antioxidant. This is supported by thefact that recombinant apoE protection against oxidationin vitro is greater in ε2 > ε3> ε4 (Smith et al. 1998;Jolivalt et al. 2000), and could be explained by the factthat ε2 has two free SH-groups, ε3 has one and ε4none. Alternatively, subjects with the ε4 allele who haveamongst the lowest plasma levels of apoE (Davignonet al. 1988) have been reported to have a preponderanceof small dense LDL (Haffner et al. 1996). Since smalldense LDL is more susceptible to oxidation (Chait et al.1993; Sevanian et al. 1996), this would result in higherOX-LDL in ε4 carriers, particularly in those exposedto oxidative stress, namely smokers.
In the smokers, but not the non-smokers, carriers ofthe ε2 allele had 28% higher TAOS levels compared toboth ε3/3 and ε4+ subjects (p = 0.026), with a sig-nificant genotype: smoking interaction on TAOS. Highplasma TAOS implies reduced ROS and less oxidativestress, and goes some way to explain the protective na-ture of the ε2 allele in smokers, as seen in the NPHSII.In the FOS, although the ε2+ men had higher CVDrisk this showed no interaction with smoking, and thissupports the idea that increased risk in ε2+ in FOS is in-dependent of the higher antioxidant status of apoE2. Eventhough plasma TAOS is not a highly specific measureof plasma oxidative stress, for a large number of samplessuch as in the UDACS it is a practical and inexpensive as-
say. By comparison, assays of other plasma markers (e.g.plasma F2-isoprostanes) are time consuming and expen-sive. To test whether TAOS was an adequate measureof oxidative stress, we previously observed a significantcorrelation (r = −0.65; p = 0.003) between plasmaTAOS and esterified F2-isoprostane, supporting the useof plasma TAOS as an appropriate marker of reactiveoxygen species (Dhamrait et al. 2004; Stephens et al.2004).
Although direct extrapolation from one study to an-other needs to be considered with caution, these dataprovide a plausible explanation for the ε4:smoking in-teraction seen in the FOS and the lack of ε2:smokinginteraction reported elsewhere (Humphries et al. 2001).These data provide no additional insight into the ε2 ef-fect reported in the FOS (Lahoz et al. 2001).
These results provide strong confirmation that inmen, the ε4 association with CVD risk is essentiallyconfined to smokers. Since ε4 non-smokers show nomajor CVD risk, i.e. when the environmental insult isnot present, this has important public health implica-tions. No studies to date have examined this ε4: smok-ing effect in women, so it is not clear whether theseeffects are gender specific. The multifactorial nature ofCHD/CVD implies not only independent effects ofgenes and environmental factors but also their interac-tion on risk. Thus our study of ε4: smoking interactionand association with measures of ROS confirms andextends our understanding of the multifactorial basis ofCHD/CVD risk.
Acknowledgements
PJT, EH, and SEH are supported by the British Heart Foun-dation (RG2000/015). JWS is supported by Diabetes UK(BDA: RD01/0001357). This work was supported by grantsHL 54779 and HL35243 and NIH/NILBI contract NO1-38038 and contract 53-K06-5-10 from the US Departmentof Agriculture Research Services.
References
Alberti, K. G. & Zimmet, P. Z. (1998) New diagnostic criteriaand classification of diabetes–again? Diabet Med 15, 535–536.
Azumi, H. et al. (2002) Superoxide generation in directionalcoronary atherectomy specimens of patients with angina
C© University College London 2005 Annals of Human Genetics (2005) 69,613–622 621

P. J. Talmud et al.
pectoris: important role of NAD(P)H oxidase. Arteriosclero-sis, Thrombosis, and Vascular Biology 22, 1838–1844.
Bolla, M. K. et al. (1999) Rapid determination of apolipopro-tein E genotype using a heteroduplex generator. J Lipid Res40, 2340–2345.
Brownlee, M. (2001) Biochemistry and molecular cell biologyof diabetic complications. Nature 414, 813–820.
Chait, A. et al. (1993) Susceptibility of small, dense, low-density lipoproteins to oxidative modification in subjectswith the atherogenic lipoprotein phenotype, pattern B. AmJ Med 94, 350–356.
Churg, A. (2003) Interactions of exogenous or evoked agentsand particles: the role of reactive oxygen species. Free RadicBiol Med 34, 1230–1235.
Davignon, J. et al. (1988) Apolipoprotein E polymorphismand atherosclerosis. Arteriosclerosis 8, 1–21.
Dhamrait, S. S. et al. (2004) Cardiovascular risk in healthy menand markers of oxidative stress in diabetic men are associatedwith common variation in the gene for uncoupling protein2. European Heart Journal 25, 468–475.
Djousse, L. et al. (2002) Influence of apolipoprotein E, smok-ing, and alcohol intake on carotid atherosclerosis: NationalHeart, Lung, and Blood Institute Family Heart Study. Stroke1357–1361.
Doll, R. et al. (1994) Mortality in relation to smoking: 40years’ observations on male British doctors. British MedicalJournal 309, 901–911.
Haffner, S. M. et al. (1996) Apolipoprotein E polymor-phism and LDL size in a biethnic population Multilo-cus genetic determinants of LDL particle size in coronaryartery disease families. Arterioscler Thromb Vasc Biol 58, 585–594.
Harrison, D. et al. (2003) Role of oxidative stress in atheroscle-rosis. American Journal of Cardiology 91, 7A–11A.
Hixson, J. E. & Vernier, D. T. (1990) Restriction isotyping ofhuman apolipoprotein E by gene amplification and cleavagewith HhaI. Journal of Lipid Research 31, 545–548.
Humphries, S. E. et al. (2003) In search of genetic precision.Lancet 361, 1908–1909.
Humphries, S. E. et al. (2001) Apolipoprotein E4 and coro-nary heart disease in middle-aged men who smoke: aprospective study. Lancet 358, 115–119.
Ioannidis, J. P. et al. (2001) Replication validity of geneticassociation studies. Nat Genet 29, 306–309.
Jolivalt, C. et al. (2000) Differential oxidation of apolipopro-tein E isoforms and interaction with phospholipids. FreeRadic Biol Med 28, 129–140.
Kannel, W. B. et al. (1979) An investigation of coronary heartdisease in families. The Framingham offspring study. Am JEpidemiol 110, 281–290.
Kannel, W. B. et al. (2003) Latest perspective on cigarettesmoking and cardiovascular disease: the Framingham HeartStudy. J Cardiac Rehab 4, 267–277.
Karvonen, J. et al. (2002) Apolipoprotein E polymorphismaffects carotid artery atherosclerosis in smoking hypertensivemen. J Hypertens 20, 2371–2378.
Keavney, B. et al. (2003) Large-scale evidence that the car-diotoxicity of smoking is not significantly modified by theapolipoprotein E varepsilon 2/ varepsilon 3/ varepsilon 4genotype. Lancet 361, 396–398.
Lahoz, C. et al. (2001) Apolipoprotein E genotype andcardiovascular disease in the Framingham Heart Study.Atheroslcerosis 154, 529–537.
Liu, S. et al. (2003) A prospective study of the associationbetween APOE genotype and the risk of myocardial in-farction among apparently healthy men. Atherosclerosis 166,323–329.
Orchard, T. J. et al. (1994) Insulin as a predictor of coronaryheart disease: interaction with apolipoprotein E phenotype.A report from the Multiple Risk Factor Intervention TrialAnn Epidemiol 4, 40–45.
Pezzini, A. et al. (2004) Synergistic effect of apolipoprotein Epolymorphisms and cigarette smoking on risk of ischemicstroke in young adults. Stroke 35, 438–442.
Sampson, M. J. et al. (2002) Plasma F2 isoprostanes: directevidence of increased free radical damage during acute hy-perglycemia in type 2 diabetes. Diabetes Care 25, 537–541.
Sevanian, A. et al. (1996) Contribution of an in vivo oxidizedLDL to LDL oxidation and its association with dense LDLsubpopulations. Arterioscler Thromb Vasc Biol 16, 784–793.
Sing, C. F. et al. (2003) Genes, environment, and cardiovas-cular disease. Arteriosclerosis, Thrombosis, and Vascular Biology23, 1190–1196.
Smith, J. D. et al. (1998) The relationship between apolipopro-tein E and serum oxidation-related variables is apolipopro-tein E phenotype dependent. Int J Clin Lab Res 28, 116–121.
Song, Y. et al. (2004) Meta-analysis: apolipoprotein E geno-types and risk for coronary heart disease. Annals of InternalMedicine 141, 137–147.
Stengard, J. H. et al. (1999) Utility of the predictors of coro-nary heart disease mortality in a longitudinal study of elderlyFinnish men aged 65-84 years is dependent on context de-fined by Apo E genotype and area of residence. Clin Genet56, 367–377.
Stephens, J. W. et al. (2004) An interaction between theinterleukin-6 −174G>C gene variant and urinary proteinexcretion influences plasma oxidative stress in subjects withtype 2 diabetes. Cardiovasc Diabetol 3, 2-
Wilson, P. W. et al. (1996) Apolipoprotein E alleles and risk ofcoronary disease. A meta- analysis. Arterioscler Thromb VascBiol 16, 1250–1255.
Received: 11 March 2005Accepted: 24 May 2005
622 Annals of Human Genetics (2005) 69,613–622 C© University College London 2005
Copyright © 2022 FDOKUMEN