
Determinants of ageism against older adults: a systematic ...

This article appeared in a journal published by Elsevier. The attachedcopy is furnished to the author for internal non-commercial researchand education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling orlicensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of thearticle (e.g. in Word or Tex form) to their personal website orinstitutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies areencouraged to visit:
http://www.elsevier.com/copyright

Author's personal copy
The SeniorWISE Study: ImprovingEveryday Memory in Older Adults☆
Graham J. McDougall Jr, Heather Becker, Keenan Pituch,Taylor W. Acee, Phillip W. Vaughan, and Carol L. Delville
We testedwhether at-risk older adults receivingmemory training showed bet-termemoryself-efficacy,metamemory,memoryperformance,and function ininstrumental activities of daily living than participants receiving a health pro-motion training comparison condition. We followed participants for 26months. The sample was mostly female (79%) and Caucasian (71%), with17% Hispanics and 12% African Americans; average age was 75 years, andaverage education was 13 years. The memory training group made greatergains on global cognition and had fewer memory complaints, but both groupsgenerally maintained their performance on the other cognitive measures andinstrumental activities of daily living (IADLs) throughout the 24-month studyperiod.Black andHispanic participantsmadegreater gains thanWhites did onsome memory performance measures but not on memory self-efficacy. Theunexpected finding that minority eldersmade the largest gainsmerits furtherstudy.Thisstudycontributedtotheknowledgebaseofgeropsychiatricnursingby providing evidence for an effective psychosocial intervention that could bedelivered byadvancedpractice nurses.© 2010 Elsevier Inc. All rights reserved.
O LDER ADULTS ARE often aware, or aremade aware, of cognitive slips, euphemisti-
cally called senior moments (Carey, 2006). Suchmemory complaints have been identified as pre-dictors ofmild cognitive impairment (MCI), and theycan set off a diagnostic cascade, leading ultimately toa conversion to dementia for some individuals(Comijs, Deeg, Dik, Twisk, & Jonker, 2002; Pear-man & Storandt, 2004; Winblad et al., 2004; Zandi,2004; Zeintl, Kliegel, Rast, & Zimprich, 2006). Arecent U.S. study concluded that 22% of adults olderthan 71 years might have MCI (Plassman et al.,2008). Because the number of new cases ofAlzheimer's disease (AD) is expected to increasethreefold to 13.2 million by 2050, the developmentof preventive interventions is urgent (Hayslip,Maloy, & Kohl, 1995; Hebert, Scherr, Bienias,Bennett, & Evans, 2003; Morgan et al., 2007).
Individuals' subjective evaluations of theirmemories may be cause for concern, but numerousstudies suggest their perceptions may be modifiable
because memory complaints are often associatedwith anxiety and depression (Cockburn & Smith,1994; Dux et al., 2008; Fiocco, Wan, Weekes, Pim,& Lupien, 2006; McDougall, Strauss, Holston, &Martin, 1999). Adults at risk for impaired episodicmemory and executive function are often 65 yearsand older and have depressive symptoms (Butters etal., 2008; Carlson, Xue, Zhou, & Fried, 2009;Federal Interagency Forum on Aging Related
Available online at www.sciencedirect.com
☆Trial Registration ClinicalTrials.gov NCT00094731.
From the The University of Texas at Austin, School ofNursing, Austin, TX; The University of Texas at Austin,Department of Educational Psychology, Austin, TX; andTexas State University - San Marcos, Department ofCurriculum and Instruction, San Marcos, TX.
Corresponding Author: Graham J. McDougall Jr. TheUniversity of Texas at Austin, School of Nursing, 1700Red River, Austin, TX 78701.
E–mail address: [email protected]© 2010 Elsevier Inc. All rights reserved.0883-9417/1801-0005$34.00/0doi:10.1016/j.apnu.2009.11.001
Archives of Psychiatric Nursing, Vol. 24, No. 5 (October), 2010: pp 291–306 291
Author's personal copy
Statistics, 2008; Herrmann, Goodwin, & Ebmeler,2007. Additional risk factors include living aloneand multiple comorbidities, which may lead tosocial isolation (Finkel, Reynolds, McArdle, &Pedersen, 2007; Mendes de Leon, Gold, Glass,Kaplan, & George, 2001; Michael, Berkman,Colditz, Holmes, & Kawachi, 2002; Salthouse,2003; Wilson et al., 2002).
Memory performance varies as a function ofindividuals' self-efficacy beliefs (Artistico, Cervone,& Pezzuti, 2003; Bandura, 1989; Berry, 1989; Berry,West, & Dennehey, 1989; Jennings, & Darwin,2003; Lachman, Steinberg, & Trotter, 1987;McDougall, 2004). A recent study of older adultsfound consistent decline in memory self-efficacywith age (McDougall, 2009); chronological age inyears was significantly inversely related to memoryself-efficacy. Memory self-efficacy may mediatememory performance, and interventions designed toimprove self-efficacy may be as important asteaching compensatory mnemonic strategies (Berry& West, 1993; Lachman, Weaver, Bandura, Elliott,& Lewkowicz, 1992; Rebok & Balcerak, 1989;West, Bagwell, & Dark-Freudeman, 2008).
Although not uniformly accepted, mental stim-ulation, or “use it or lose it” emphasizes thatengagement in novelty and innovation may helpreverse decline in cognitive function and help anindividual maintain cognition (Light, 1991; Salt-house, 1991). This disuse hypothesis is driving theinterest in whether brain exercises can prevent ordelay what is considered “normal” decline inmemory (Boron, Willis, & Schaie, 2007; Salthouse,2006; Salthouse, Berish, & Miles, 2002; Vergheseet al., 2003). Interventions have included theplasticity-based adaptive cognitive training of theImprovement in Memory with Plasticity-basedAdaptive Cognitive Training study and computertraining (Slegers, van Boxtel, & Jolles, 2009; Smithet al., 2009). A recent meta-analytic review foundno evidence that cognitive intervention programsslow or delay the progression of AD (Papp, Walsh,& Snyder, 2009).
Nevertheless, psychosocial interventions devel-oped to prevent memory decline have also targetedfunctional ability, loneliness, isolation, physicalactivity, and the social and/or physical environment(Cattan, White, Bond, & Learmouth, 2005;McDougall, 2002; Oswald, Rupprecht, Gunzel-mann, & Tritt, 1996; Phelan, Williams, Penninx,LoGerfo, & Leveille, 2004). The Advanced Cog-
nitive Training for Independent and Vital Elderly(ACTIVE) trials (Ball et al., 2002; Jobe et al., 2001)found that participants in each intervention groupimproved their targeted cognitive abilities andmaintained these gains for 5 years (Willis et al.,2006). The ACTIVE trials, however, did notaddress the subjective aspects of memory self-efficacy and metamemory (Lachman, Andreoletti,& Pearman, 2006; Scogin, 1997; West et al., 2008).
The ability to perform independent living skillsis dependent on intact executive function (Dodge,Du, Saxton, & Ganguli, 2006; Johnson, Lui, &Yaffe, 2007). As age and memory loss increase,cognitively demanding instrumental activities suchas remembering to take medications, managingmoney, or using the telephone may becomedifficult to perform (Royall, Palmer, Chiodo, &Polk, 2005). The focus of this study was everydaymemory—the day-to-day operations of memory inreal-world ordinary situations (West & Sinnott,1991; West, Crook, & Barron, 1992). The goal wasto improve everyday memory and ultimatelyperformance of IADLs.
The Cognitive Behavioral Model of EverydayMemory (CBMEM) tested here was derived fromBandura's self-efficacy theory (Bandura & Locke,2003; Dellefield & McDougall, 1996; McDougallet al., 1999; McDougall, 1998; McDougall, 2009).We tested the hypothesis that older adults whoreceived the CBMEM-based memory trainingintervention would show significantly better mem-ory self-efficacy, memory strategies, and memoryperformance, and better function in IADLs thanparticipants in a health promotion training condi-tion at postclass (2 months after baseline) and overthe remaining three assessment points: postbooster(6 months), postclass follow-up (14 months), andend of study (26 months). This article reports thefindings from baseline to postclass and frombaseline to end of study.
METHODS
Settings and Sample
Independent adults were recruited from a metro-politan area in Central Texas via print and televisionmedia, as well as directly from city-run senioractivity centers, churches, health fairs, and festivals.The trainings were implemented at seven sites in thecommunity: four senior centers, a university-based
292 MCDOUGALL ET AL

Author's personal copy
wellness clinic, and two apartment complexes forlow-income older adults.
Eligibility criteria included age 65 years or more,ability to speak and understand English, no sensoryloss or cognitive impairment, and willingness toparticipate in the study for 24 months. Sensory losswas determined over the telephone or in person byself-report evaluation of hearing and vision. Visualand hearing acuity were further evaluated at the“in-person” eligibility screening by evaluatorobservation and by a self-report checklist devel-oped for the study.
Ability to communication in English wasassessed using a checklist designed for the studyand completed by a team member at the initialscreening. We asked seven questions to determineeligibility in this order: Are you able to hearconversations on the phone? Are you able tocomprehend English conversations? Are you ableto articulate enough to be understood? Are youable to participate in two-sided conversations?Can you decipher concrete and abstract conversa-tional content? Are you able to make anappointment for follow-up testing? Can you repeatback the appointment time and place? If anyquestion was answered incorrectly, the individualwas deemed ineligible.
The Mini-Mental State Examination (MMSE;Folstein, Folstein, & McHugh, 1975) was used toscreen for cognitive impairment and monitorcognitive decline throughout the study. Onlythose with scores 23 or higher were eligible toparticipate in the study. However, the eligibilityscore was reduced to 20 or higher at one seniorcenter to recruit Hispanics with low education. Fourfemales and one male were recruited using thisadjusted screening protocol. In addition, theControlled Oral Word Association Test from theMultilingual Aphasia Examination (Sumerall, Tim-mons, James, Ewing, & Oehlert, 1997) and TheTrail-Making Test were administered duringscreening (Reitan, 1958), and participants wererequired to pass Trails A and/or Trails B at or abovethe 10th percentile for their age group for inclusionin the study.
Those with AD or other dementia, Hodgkin'sdisease, neuroblastoma, or cancer of the liver,lung, or brain were excluded from the study.Medical eligibility was assessed verbally using afour-item health status checklist designed for theproject. Three hundred forty-six adults were
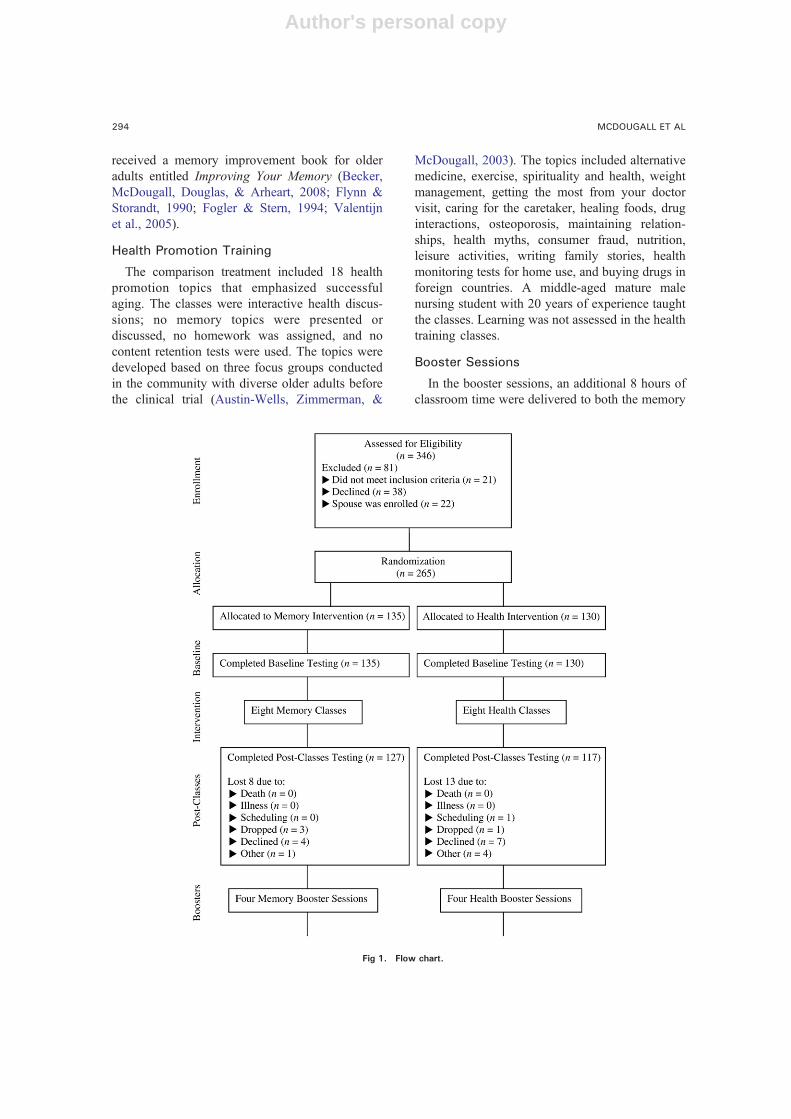
recruited, but 81 did not participate: 21 did notmeet inclusion criteria, 38 declined, and 22 werefemale spouses in a couple, who were excluded sothat adequate numbers of males would be repre-sented in the sample (Figure 1). The final sample(N = 265) was 72% non-Hispanic White, 17%Hispanic, and 11% African American. The averageage was 75 years. Most of the participants werefemale (77%). The university's institutional reviewboard approved the study.
Once participants were screened and consented,they were randomly assigned numeric codescorresponding to either the memory or healthpromotion training interventions. Randomizationwas separate for each of the sites. One hundredthirty-five individuals were assigned to memorytraining and 130 were assigned to health training.Eleven groups met at seven sites in the community.Both training groups participated in 12 sessions.
Memory Training
The CBMEM-based intervention consisted ofeight classes and four booster sessions (McDougall,1998, 1999, 2000, 2002). The memory training wasbased on the four components of self-efficacytheory: enactive mastery experience, vicariousexperience, verbal persuasion, and physiologicarousal. A female septuagenarian role model taughtthe memory training classes. In each memory class,the first 20 minutes were dedicated to guidedpractice of stress inoculation that included aprogressive muscle relaxation exercise with visual-ization. Next, homework from an earlier sessionwas discussed. Class topics included memory andhealth, memory functions and mechanisms, factorsaffecting memory for people of all ages, memorybeliefs and aging, and use of internal and externalmemory strategies (McDougall, 2009). During theeight-session classroom component of the memorytraining, 30 minutes of practice with memorystrategies were allocated during each class tostrengthen enactive mastery experience, the stron-gest component of self-efficacy. After each mem-ory training class, participants wrote down someaspect of their learning or an essential point fromthe class, such as a memory strategy. Eachparticipant was given a plus or minus (0, 1) forthe class session. Between the eight-sessionCBMEM, and the four booster sessions, a partic-ipant would have a possible score between 0 and12. On completion of the study, participants
293SENIORWISE STUDY
Author's personal copy
received a memory improvement book for olderadults entitled Improving Your Memory (Becker,McDougall, Douglas, & Arheart, 2008; Flynn &Storandt, 1990; Fogler & Stern, 1994; Valentijnet al., 2005).
Health Promotion Training
The comparison treatment included 18 healthpromotion topics that emphasized successfulaging. The classes were interactive health discus-sions; no memory topics were presented ordiscussed, no homework was assigned, and nocontent retention tests were used. The topics weredeveloped based on three focus groups conductedin the community with diverse older adults beforethe clinical trial (Austin-Wells, Zimmerman, &
McDougall, 2003). The topics included alternativemedicine, exercise, spirituality and health, weightmanagement, getting the most from your doctorvisit, caring for the caretaker, healing foods, druginteractions, osteoporosis, maintaining relation-ships, health myths, consumer fraud, nutrition,leisure activities, writing family stories, healthmonitoring tests for home use, and buying drugs inforeign countries. A middle-aged mature malenursing student with 20 years of experience taughtthe classes. Learning was not assessed in the healthtraining classes.
Booster Sessions
In the booster sessions, an additional 8 hours ofclassroom time were delivered to both the memory
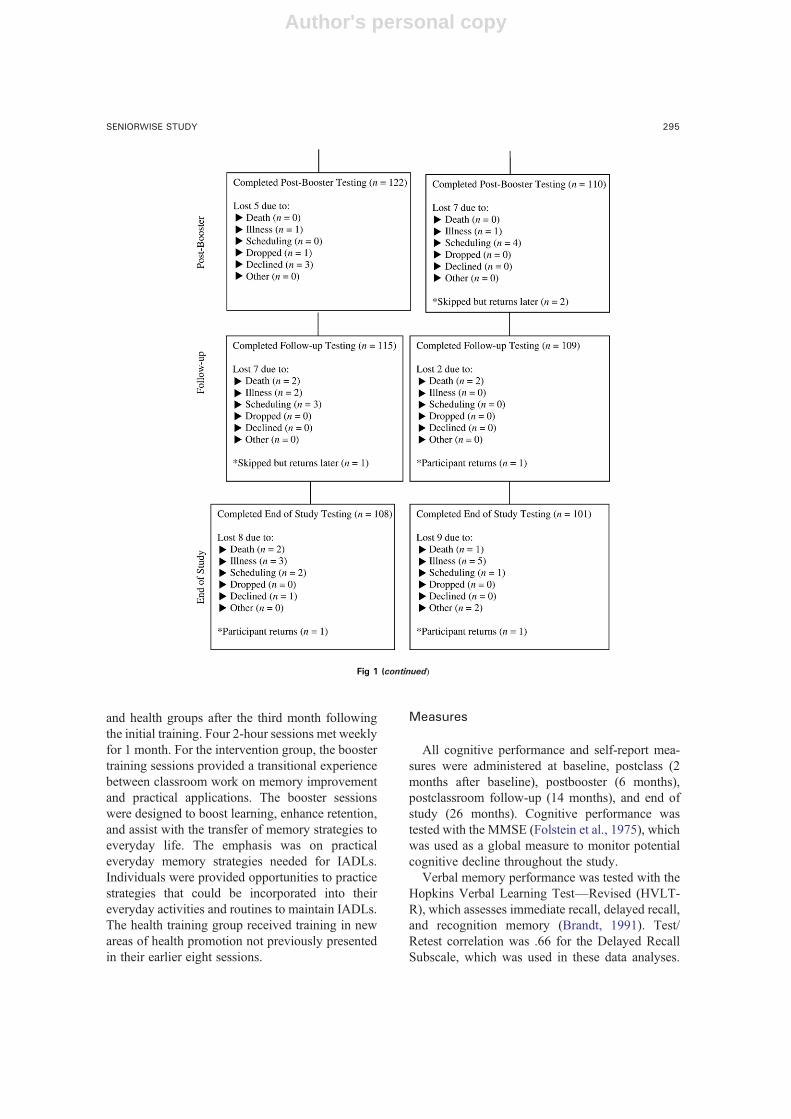
Fig 1. Flow chart.
294 MCDOUGALL ET AL
Author's personal copy
and health groups after the third month followingthe initial training. Four 2-hour sessions met weeklyfor 1 month. For the intervention group, the boostertraining sessions provided a transitional experiencebetween classroom work on memory improvementand practical applications. The booster sessionswere designed to boost learning, enhance retention,and assist with the transfer of memory strategies toeveryday life. The emphasis was on practicaleveryday memory strategies needed for IADLs.Individuals were provided opportunities to practicestrategies that could be incorporated into theireveryday activities and routines to maintain IADLs.The health training group received training in newareas of health promotion not previously presentedin their earlier eight sessions.
Measures
All cognitive performance and self-report mea-sures were administered at baseline, postclass (2months after baseline), postbooster (6 months),postclassroom follow-up (14 months), and end ofstudy (26 months). Cognitive performance wastested with the MMSE (Folstein et al., 1975), whichwas used as a global measure to monitor potentialcognitive decline throughout the study.
Verbal memory performance was tested with theHopkins Verbal Learning Test—Revised (HVLT-R), which assesses immediate recall, delayed recall,and recognition memory (Brandt, 1991). Test/Retest correlation was .66 for the Delayed RecallSubscale, which was used in these data analyses.
Fig 1 (continued)
295SENIORWISE STUDY

Author's personal copy
Visual memory performance was measured withthe Brief Visuospatial Memory Test–Revised(Brief Visuosp), which asks the individual toreproduce a series of geometric designs (Benedict,1997). Test/Retest correlation was .72.
The Rivermead Behavioural Memory Test(RBMT), which was used to test everyday memorybridges laboratory-based measures of memory andassessments obtained by self-report and observa-tion. The standardized profile score has a possiblerange from 0 to 24 and is sometimes interpreted withcutoff points for four groups of memory function:normal (22–24), poor (17–21), moderately im-paired (10–16), and severely impaired (0–9). Alphareliability was .73 (Cockburn & Smith, 1989;Wilson, Cockburn, Baddeley, & Hiorns, 1989).
The Direct Assessment of Functional Status(DAFS) was used to assess ability to functionwith IADLs. The DAFS measures performance intest time orientation, communication abilities,transportation, and financial, shopping, eating,and dressing/grooming skills (Loewenstein et al.,1989, 1992). The DAFS demonstrated high inter-rater and test–retest reliabilities for patients at amemory disorder clinic (English and Spanishspeaking) and normal controls. Alpha reliabilitywas .79.
Memory self-efficacy was measured by theMemory Self-Efficacy Questionnaire (MSEQ),which asks respondents to predict their perfor-mance level and estimate their strength andconfidence in performing 10 everyday tasks(Berry et al., 1989). The 35-item version of theMSEQ was used; alpha reliability was .95.
The Spielberger State-Trait Anxiety Inventory(STAI) was used to measure anxiety. The STAI wasdeveloped to differentiate the temporary conditionof “state anxiety” and the chronic condition of “traitanxiety” in adults (Spielberger, Gorsuch, & Lush-ene, 1970). Alpha reliabilities were .85 and .89.
The Centers for Epidemiologic Studies Scale(CES-D), which emphasizes somatic complaints(rated on a 4-point Likert scale), was used to evaluatedepressive symptoms (Radloff & Teri, 1986). Inolder adults, reliability coefficients were from .85 to.91. Alpha reliability in this study was .78.
The Metamemory in Adulthood (MIA) question-naire was used to measure aspects of memoryknowledge (Dixon, Hultsch, & Hertzog, 1988). TheMIA questionnaire consists of 108 statements inseven subscales, and responses are rated on a 5-
point Likert scale. Within the Strategy subscale (18items), we differentiated how often participantsused both internal memory strategies (elaboration,rehearsal, and so on) and external strategies (lists,notes, and so on) to enhance their everyday memoryfunction. Alpha reliabilities were .78 and .77,respectively. Memory complaints were measuredwith a revised MIA questionnaire based on aconceptual item analysis and a factor analysis of690 older adults. The revised MIA questionnairecomplaint subscale consists of 21 items andcaptures individuals' perceptions of their memoryabilities as generally stable or subject to long-termdecline. A higher average item score (N2.5)indicates greater stability and fewer complaintsabout failing memory (McDougall, Becker, &Arheart, 2006). Mean scores range from 0 to 5.Alpha reliability was .91.
Statistical Analysis
Hierarchical linear models (HLM) were used totest the efficacy of the intervention (Bryk &Raudenbush, 1992). Age, education, and racial/ethnic group were included as covariates. Numberof classes attended was also entered as a covariateto control for dosage effects. Two HLM analyseswere conducted for each outcome measure: one toevaluate treatment and covariate effects, includingeffects of ethnicity, from baseline to the end ofclasses and a similar analysis to evaluate effectsfrom baseline to end of study. The three-levelanalysis models included repeated measures atLevel 1. At Level 2, participants were modeledwithin sites. Because time was included as a Level 1explanatory variable and the treatment variable wasentered in the model at Level 2 for the gains (as wellas in the model for initial status), the model testedwhether the “treatment” or “control” group madegreater gains across time.
In the Level 3 model, between-site variableswere identified. Because of the limited number ofsites, we did not attempt to explain variation acrosssites but controlled for it in the analyses. Weexamined relative gains from beginning to end ofclasses and from beginning to end of the 26-monthstudy. Other analyses, including all five time pointsand allowing for a nonlinear trajectory, yieldedsimilar results. For each of the analyses in which thememory treatment effect was not statisticallysignificant, we performed an additional HLManalysis that did not include the treatment effect
296 MCDOUGALL ET AL

Author's personal copy
or covariates. The purpose was to examine thedirection and statistical significance of overallchange over time from baseline to end of classesor baseline to end of study when the memory groupdid not differ significantly from the health group.
RESULTS
Baseline Comparisons
The analytic sample consisted of 265 randomizedparticipants: 135 in the memory training and 130 inthe health promotion training (Figure 1, Table 1).Eight deaths occurred during the study unrelated tothe protocol. Ninety-five percent of participantscompleted the memory training; 87% completed thehealth promotion training (six or more of the eighttraining sessions). At the final testing, 108 and 101individuals were in the memory training and thehealth promotion groups, respectively. Eighty-fourpercent in the memory training and 78% in thehealth promotion completed three or more boostersessions. The memory and health groups did notdiffer significantly at baseline on either the outcomemeasures or demographics (t test). When gender,education, age, MMSE score, health status, andmemory versus health training group were entered
simultaneously into a logistic regression as pre-dictors of finishing the study, being female (P =.03) and reporting better perceived health (P = .04)were the only significant predictors. Cronbach'salphas ranged from .73 to .95. Means and standarddeviations for outcome measures are in Table 2.
The HLM results for measures of cognitiveabilities and instrumental functional abilities areshown in Table 3. At baseline, older, less-educated,Black, and Hispanic participants had significantlylower scores on visual memory. Less-educated,Black, and Hispanic participants also had lowerbaseline scores on verbal memory. At baseline,scores on the MMSE were positively associatedwith years of education and negatively associatedwith being Hispanic or Black.
Lower DAFS scores at baseline were related tobeing older, less educated, Hispanic, and Black.Although in preliminary univariate tests the mem-ory and health promotion groups did not differ atbaseline on outcome measures, the HLM resultssuggested that the memory group scored signifi-cantly higher at baseline on everyday memory thandid the health promotion group.
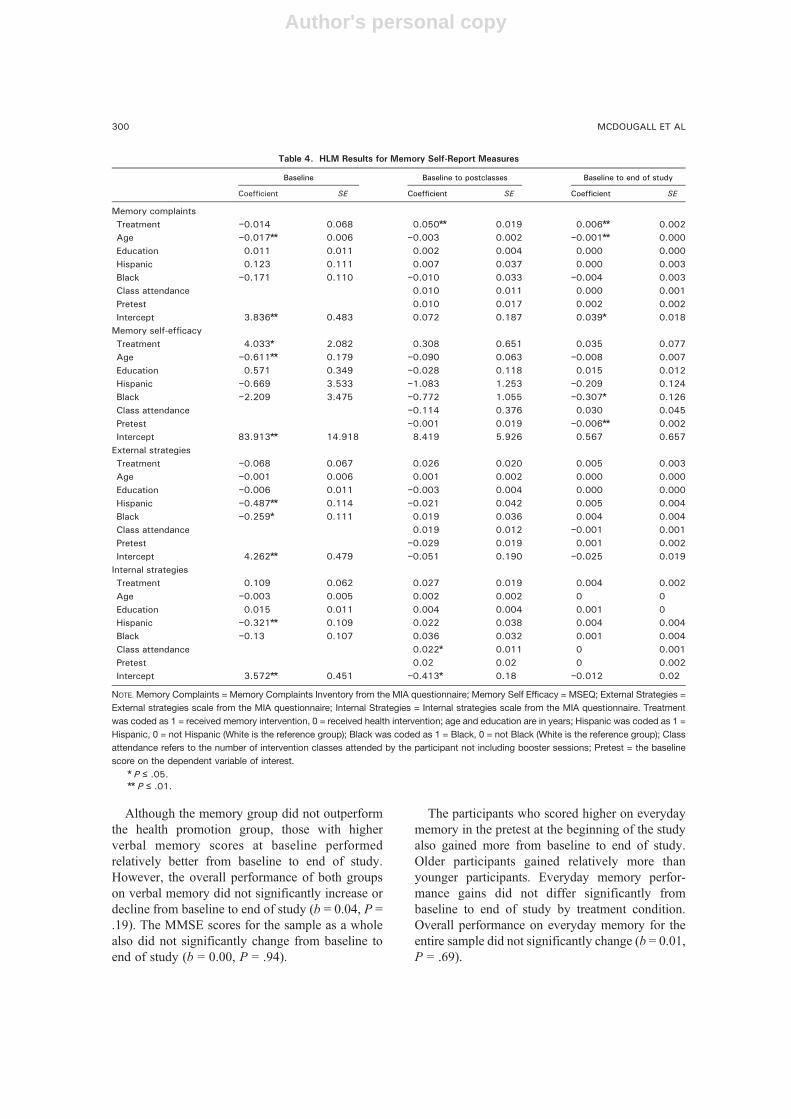
Younger participants reported fewer memorycomplaints at baseline than older participants
Table 1. Demographics and Screening Measures at Baseline
Variables Score range
Comparison group (n = 130) Intervention group (n = 135)
M ± SD or n (%) M ± SD or n (%)
Age 65–94 74.83 ± 6.22 74.69 ± 5.74Education 0–22 13.81 ± 3.71 13.39 ± 3.9No. of people in house 1–6 1.65 ± 1.42 1.53 ± .81Attention 0–324 45.53 ± 36.73 44.95 ± 34.16Cognitive flexibility 0–630 134.91 ± 98.62 125.3 ± 74.27Organizational strategy 0–79 40.58 ± 11.16 41.27 ± 11.46Depression 0–60 9.47 ± 6.87 9.13 ± 6.71State anxiety 20–80 29.32 ± 8.12 29.72 ± 8.18Trait anxiety 20–80 32.15 ± 8.55 31.90 ± 9.24GenderMale 30 (23.1) 30 (22.2)Female 100 (76.9) 105 (77.8)RaceWhite 93 (71.5) 96 (71.1)Black 15 (11.5) 15 (11.1)Hispanic 22 (16.9) 24 (17.8)Marital statusMarried 37 (28.5) 45 (33.8)Never married 3 (2.3) 5 (3.8)Divorced 26 (20) 25 (18.8)Widowed 64 (49.2) 58 (43.6)
NOTE. Attention = Trail-Making Test A; Cognitive Flexibility = Trail-Making Test B; Organizational Strategy = Controlled Oral Word Association
Test; Depression = CES-D; State and Trait Anxiety = STAI.
297SENIORWISE STUDY
Author's personal copy
(Table 4). In addition, younger participants ratedtheir memory self-efficacy higher than olderparticipants did. In addition, the memory traininggroup reported significantly higher memory self-efficacy at baseline than the health promotiongroup. Hispanics and Blacks reported using fewerexternal memory strategies than Whites did atbaseline. In addition, Hispanics used fewer internalstrategies than Whites did.
TRAINING EFFECTS FROM BASELINE TOPOSTCLASS: PERFORMANCE MEASURES
The memory and health promotion groups didnot differ significantly in gains on visual memoryfrom baseline to postclasses (Table 3). Performancefor the entire group also did not change signifi-cantly (b = −0.20, P =.50). The memory and healthgroups did differ significantly in gains frombaseline to postclasses on the DAFS performancemeasure, although both groups improved on the
DAFS (b = 0.23, P = .04). On verbal memory,overall performance did not significantly changefrom baseline to end of classes (b = 0.36, P = .10).However, the memory group showed greater gainsfrom baseline to postclasses on MMSE scores, ameasure of global cognition. On everyday memoryperformance, there were no significant gains for thememory group from baseline to end of classes (b =0.14, P = .07).
TRAINING EFFECTS FROM BASELINE TO ENDOF STUDY: PERFORMANCE MEASURES
Overall performance on visual memory did notsignificantly increase or decline for the sample as awhole (b = −0.08, P = .11). Hispanic and Blackparticipants gained more than Whites did, andindividuals with less education also gained rela-tively more.
Participants showed no significant changes inDAFS scores from baseline to end of study (b =
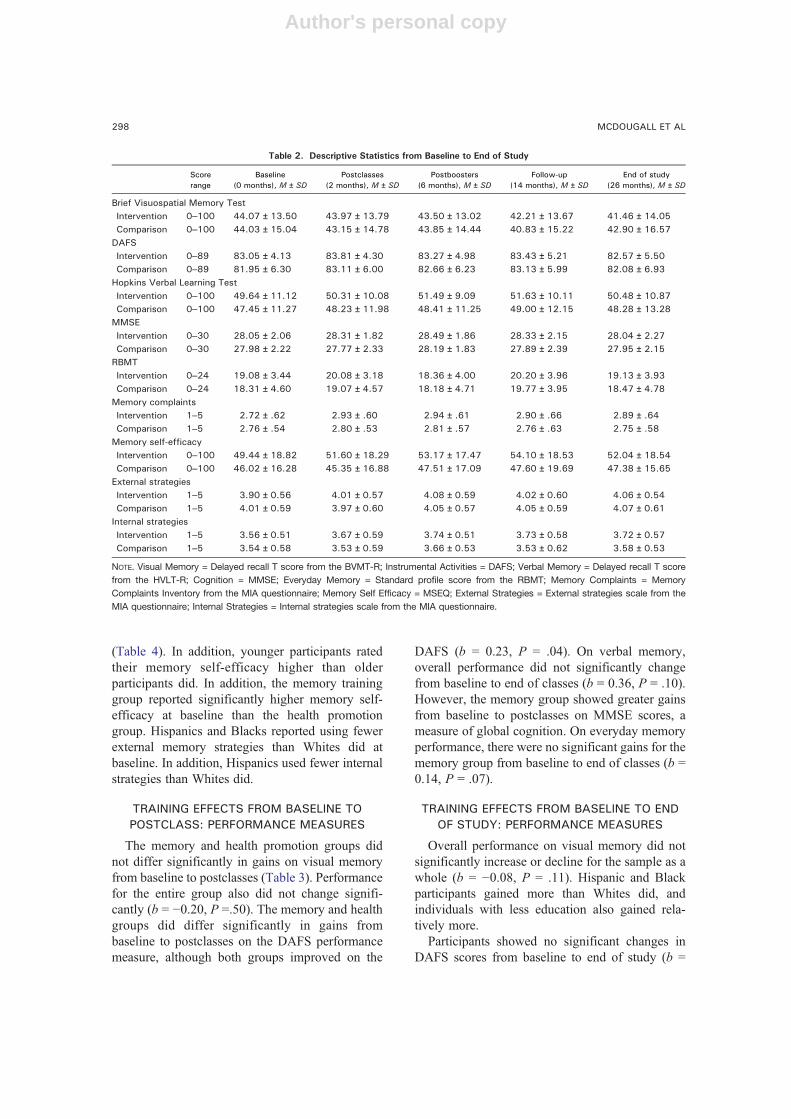
Table 2. Descriptive Statistics from Baseline to End of Study
Scorerange
Baseline(0 months), M ± SD
Postclasses(2 months), M ± SD
Postboosters(6 months), M ± SD
Follow-up(14 months), M ± SD
End of study(26 months), M ± SD
Brief Visuospatial Memory TestIntervention 0–100 44.07 ± 13.50 43.97 ± 13.79 43.50 ± 13.02 42.21 ± 13.67 41.46 ± 14.05Comparison 0–100 44.03 ± 15.04 43.15 ± 14.78 43.85 ± 14.44 40.83 ± 15.22 42.90 ± 16.57
DAFSIntervention 0–89 83.05 ± 4.13 83.81 ± 4.30 83.27 ± 4.98 83.43 ± 5.21 82.57 ± 5.50Comparison 0–89 81.95 ± 6.30 83.11 ± 6.00 82.66 ± 6.23 83.13 ± 5.99 82.08 ± 6.93
Hopkins Verbal Learning TestIntervention 0–100 49.64 ± 11.12 50.31 ± 10.08 51.49 ± 9.09 51.63 ± 10.11 50.48 ± 10.87Comparison 0–100 47.45 ± 11.27 48.23 ± 11.98 48.41 ± 11.25 49.00 ± 12.15 48.28 ± 13.28
MMSEIntervention 0–30 28.05 ± 2.06 28.31 ± 1.82 28.49 ± 1.86 28.33 ± 2.15 28.04 ± 2.27Comparison 0–30 27.98 ± 2.22 27.77 ± 2.33 28.19 ± 1.83 27.89 ± 2.39 27.95 ± 2.15
RBMTIntervention 0–24 19.08 ± 3.44 20.08 ± 3.18 18.36 ± 4.00 20.20 ± 3.96 19.13 ± 3.93Comparison 0–24 18.31 ± 4.60 19.07 ± 4.57 18.18 ± 4.71 19.77 ± 3.95 18.47 ± 4.78
Memory complaintsIntervention 1–5 2.72 ± .62 2.93 ± .60 2.94 ± .61 2.90 ± .66 2.89 ± .64Comparison 1–5 2.76 ± .54 2.80 ± .53 2.81 ± .57 2.76 ± .63 2.75 ± .58
Memory self-efficacyIntervention 0–100 49.44 ± 18.82 51.60 ± 18.29 53.17 ± 17.47 54.10 ± 18.53 52.04 ± 18.54Comparison 0–100 46.02 ± 16.28 45.35 ± 16.88 47.51 ± 17.09 47.60 ± 19.69 47.38 ± 15.65
External strategiesIntervention 1–5 3.90 ± 0.56 4.01 ± 0.57 4.08 ± 0.59 4.02 ± 0.60 4.06 ± 0.54Comparison 1–5 4.01 ± 0.59 3.97 ± 0.60 4.05 ± 0.57 4.05 ± 0.59 4.07 ± 0.61
Internal strategiesIntervention 1–5 3.56 ± 0.51 3.67 ± 0.59 3.74 ± 0.51 3.73 ± 0.58 3.72 ± 0.57Comparison 1–5 3.54 ± 0.58 3.53 ± 0.59 3.66 ± 0.53 3.53 ± 0.62 3.58 ± 0.53
NOTE. Visual Memory = Delayed recall T score from the BVMT-R; Instrumental Activities = DAFS; Verbal Memory = Delayed recall T score
from the HVLT-R; Cognition = MMSE; Everyday Memory = Standard profile score from the RBMT; Memory Complaints = Memory
Complaints Inventory from the MIA questionnaire; Memory Self Efficacy = MSEQ; External Strategies = External strategies scale from the
MIA questionnaire; Internal Strategies = Internal strategies scale from the MIA questionnaire.
298 MCDOUGALL ET AL

Author's personal copy
−0.01, P = .68). However, those with initiallyhigher DAFS scores and those who attended moreclasses gained more from baseline to end of study.
Those with fewer years of education gained moreon the DAFS from baseline to end of study, andBlacks gained more than Whites.
Table 3. HLM Results for Memory Performance Measures
Baseline Baseline to postclasses Baseline to end of study
Coefficient SE Coefficient SE Coefficient SE
BVMT-RTreatment 0.758 1.437 0.122 0.483 −0.062 0.080Age −0.495⁎⁎ 0.123 0.121⁎ 0.051 0.022⁎⁎ 0.007Education 0.811⁎⁎ 0.236 −0.071 0.093 −0.016 0.013Hispanic −8.901⁎⁎ 2.399 −0.612 1.002 0.336⁎ 0.132Black −12.818⁎⁎ 2.329 0.307 0.984 0.538⁎⁎ 0.134Class attendance 0.105 0.279 0.040 0.038Pretest 0.007 0.023 0.027⁎⁎ 0.003Intercept 71.030⁎⁎ 10.295 −9.294 4.744 −2.992⁎⁎ 0.672Direct Assessment Functional StatusTreatment 0.952 0.523 −0.028 0.149 −0.031 0.023Age −0.119⁎⁎ 0.045 −0.008 0.015 −0.002 0.002Education 0.490⁎⁎ 0.085 −0.020 0.029 −0.008⁎ 0.004Hispanic −3.305⁎⁎ 0.862 0.189 0.302 0.016 0.039Black −4.842⁎⁎ 0.844 0.072 0.275 0.104⁎⁎ 0.040Class attendance 0.105 0.087 0.026⁎ 0.013Pretest −0.001 0.020 0.011⁎⁎ 0.002Intercept 85.012⁎⁎ 3.741 0.375 2.161 −0.890⁎ 0.293HVLT-RTreatment 1.778 1.174 0.173 0.372 −0.008 0.051Age −0.081 0.101 −0.039 0.037 −0.006 0.004Education 0.594⁎⁎ 0.195 0.037 0.071 −0.006 0.008Hispanic −5.997⁎⁎ 2.013 −0.380 0.726 0.041 0.086Black −12.157⁎⁎ 1.967 0.156 0.700 0.168 0.090Class attendance 0.098 0.216 0.031 0.029Pretest – – −0.031 0.018 0.009⁎⁎ 0.002Intercept 47.193⁎⁎ 8.455 3.406 3.473 −0.062 0.439MMSETreatment 0.270 0.197 0.208⁎⁎ 0.079 −0.006 0.010Age −0.010 0.017 −0.014 0.008 −0.002 0.001Education 0.210⁎⁎ 0.034 −0.033⁎ 0.016 −0.005⁎ 0.002Hispanic −0.878⁎ 0.364 −0.327⁎ 0.161 0.003 0.017Black −2.095⁎⁎ 0.350 0.106 0.145 0.028 0.017Class attendance – – 0.010 0.044 0.001 0.005Pretest – – 0.004 0.022 0.009⁎⁎ 0.003Intercept 26.086⁎⁎ 1.440 1.257 0.934 −0.086 0.109RBMTTreatment 0.847⁎ 0.412 0.136 0.139 −0.011 0.018Age −0.154⁎⁎ 0.036 −0.012 0.015 0.000 0.002Education 0.224⁎⁎ 0.069 −0.017 0.026 −0.005 0.003Hispanic −2.713⁎⁎ 0.720 0.482 0.282 −0.003 0.032Black −3.578⁎⁎ 0.696 0.089 0.268 0.037 0.033Class attendance – – 0.121 0.081 −0.002 0.010Pretest – – −0.026 0.022 0.008⁎⁎ 0.002Intercept 27.517⁎⁎ 2.969 0.671 1.422 −0.076 0.163
NOTE. VisualMemory = Delayed recall T score from theBVMT-R; Instrumental Activities = DAFS; VerbalMemory =Delayed recall T score from the
HVLT-R; Cognition = MMSE; Everyday Memory = Standard profile score from the RBMT. Treatment was coded as 1 = received memory
intervention, 0 = received health intervention; age and education are in years; Hispanic was coded as 1 = Hispanic, 0 = not Hispanic (White is the
referencegroup); Blackwascoded as 1=Black, 0 = notBlack (White is the reference group); Class attendance refers to the number of intervention
classes attended by the participant not including booster sessions; Pretest = the baseline score on the dependent variable of interest.⁎ P ≤ .05.⁎⁎ P ≤ .01.
299SENIORWISE STUDY
Author's personal copy
Although the memory group did not outperformthe health promotion group, those with higherverbal memory scores at baseline performedrelatively better from baseline to end of study.However, the overall performance of both groupson verbal memory did not significantly increase ordecline from baseline to end of study (b = 0.04, P =.19). The MMSE scores for the sample as a wholealso did not significantly change from baseline toend of study (b = 0.00, P = .94).
The participants who scored higher on everydaymemory in the pretest at the beginning of the studyalso gained more from baseline to end of study.Older participants gained relatively more thanyounger participants. Everyday memory perfor-mance gains did not differ significantly frombaseline to end of study by treatment condition.Overall performance on everyday memory for theentire sample did not significantly change (b = 0.01,P = .69).
Table 4. HLM Results for Memory Self-Report Measures
Baseline Baseline to postclasses Baseline to end of study
Coefficient SE Coefficient SE Coefficient SE
Memory complaintsTreatment −0.014 0.068 0.050⁎⁎ 0.019 0.006⁎⁎ 0.002Age −0.017⁎⁎ 0.006 −0.003 0.002 −0.001⁎⁎ 0.000Education 0.011 0.011 0.002 0.004 0.000 0.000Hispanic 0.123 0.111 0.007 0.037 0.000 0.003Black −0.171 0.110 −0.010 0.033 −0.004 0.003Class attendance 0.010 0.011 0.000 0.001Pretest 0.010 0.017 0.002 0.002Intercept 3.836⁎⁎ 0.483 0.072 0.187 0.039⁎ 0.018
Memory self-efficacyTreatment 4.033⁎ 2.082 0.308 0.651 0.035 0.077Age −0.611⁎⁎ 0.179 −0.090 0.063 −0.008 0.007Education 0.571 0.349 −0.028 0.118 0.015 0.012Hispanic −0.669 3.533 −1.083 1.253 −0.209 0.124Black −2.209 3.475 −0.772 1.055 −0.307⁎ 0.126Class attendance −0.114 0.376 0.030 0.045Pretest −0.001 0.019 −0.006⁎⁎ 0.002Intercept 83.913⁎⁎ 14.918 8.419 5.926 0.567 0.657
External strategiesTreatment −0.068 0.067 0.026 0.020 0.005 0.003Age −0.001 0.006 0.001 0.002 0.000 0.000Education −0.006 0.011 −0.003 0.004 0.000 0.000Hispanic −0.487⁎⁎ 0.114 −0.021 0.042 0.005 0.004Black −0.259⁎ 0.111 0.019 0.036 0.004 0.004Class attendance 0.019 0.012 −0.001 0.001Pretest −0.029 0.019 0.001 0.002Intercept 4.262⁎⁎ 0.479 −0.051 0.190 −0.025 0.019
Internal strategiesTreatment 0.109 0.062 0.027 0.019 0.004 0.002Age −0.003 0.005 0.002 0.002 0 0Education 0.015 0.011 0.004 0.004 0.001 0Hispanic −0.321⁎⁎ 0.109 0.022 0.038 0.004 0.004Black −0.13 0.107 0.036 0.032 0.001 0.004Class attendance 0.022⁎ 0.011 0 0.001Pretest 0.02 0.02 0 0.002Intercept 3.572⁎⁎ 0.451 −0.413⁎ 0.18 −0.012 0.02
NOTE. Memory Complaints = Memory Complaints Inventory from the MIA questionnaire; Memory Self Efficacy = MSEQ; External Strategies =
External strategies scale from the MIA questionnaire; Internal Strategies = Internal strategies scale from the MIA questionnaire. Treatment
was coded as 1 = received memory intervention, 0 = received health intervention; age and education are in years; Hispanic was coded as 1 =
Hispanic, 0 = not Hispanic (White is the reference group); Black was coded as 1 = Black, 0 = not Black (White is the reference group); Class
attendance refers to the number of intervention classes attended by the participant not including booster sessions; Pretest = the baseline
score on the dependent variable of interest.⁎ P ≤ .05.⁎⁎ P ≤ .01.
300 MCDOUGALL ET AL

Author's personal copy
TRAINING EFFECTS FROM BASELINE TOPOSTTEST CLASSES: SELF-REPORT MEASURES
Table 4 presents the HLM results for the self-report measures of memory complaints, self-effica-cy, and strategies. Memory group participantsreported a greater reduction in memory complaintsfrom baseline to postclasses. Memory self-efficacygains, however, did not significantly differ bytraining group (b = 0.53, P = .17). For internalstrategies, scores for the sample did not significantlyincrease or decline (b = 0.01, P = .33). However,those who attended more classes reported greateruse of internal strategies over time. Similarly,overall scores for external strategies did not changesignificantly (b = 0.00, P = .79). On the psycholog-ical measures of anxiety (state/trait) and depression,controlling for education, there were no significanteffects of time, ethnic group, or intervention.
TRAINING EFFECTS FROM BASELINE TO END OFSTUDY: SELF-REPORT MEASURES
Memory training participants who were youngerreported a greater reduction in memory complaintsthan older participants. On the memory self-efficacy measure, Whites made relatively greatergains than Blacks did, but neither group changedsignificantly (b = 0.07, P = .33). Both groupsimproved their use of external and internal memorystrategies over time. Internal strategies increasedsignificantly (b = 0.004, P b .01), as did externalstrategies (b = 0.004, P = .03). The memory groupdid not make significantly greater gains than thehealth promotion group in strategy use.
DISCUSSION
This study had many strengths. First, the triethnicsample was recruited in the community, andvolunteer participants were highly motivated andmaintained their interest in the study, as evidencedby a 79% retention rate over the 26-month study.The ACTIVE trials reported 80% retention at 24-month follow-up (Ball et al., 2002). Further, derivedfrom Bandura's (1997) self-efficacy theory,CBMEM intervention provided a unique packageof cognitive skills development in exposure,repeated practice, relevant modeling from an olderadult facilitator, cognitive skills modeling, anddesensitization. Using booster sessions for habitu-ation of learning, our intentionwas the integration ofdidactic content with practical application. Finally,
the range of outcomes was comprehensive andadministered at each measurement occasion. Studylimitations included the lack of a no-treatmentcontrol group. Further, the generalizability of thefindings from the minority sample is not clear.
The participants in both the memory and healthpromotion groups improved their use of externaland internal memory strategies. This is a uniquefinding for an intervention that did not place anyemphasis on memory strategies in the healthtraining (Lachman et al., 1992; Lachman, Andreo-letti, & Pearman, 2006). However, both groupsreceived mental stimulation and social engagementin part that may explain the benefits to memory.Participants may have engaged in self-study toimprove memory strategies as a result of theirparticipation in the study. Health promotiontraining is not a normative intervention in people'sdaily lives. When this study was launched in 2001,evidence of the effectiveness of memory trainingwith older adults was known (Floyd & Scogin,1997; Verhaeghen, Marcoen, & Goossens, 1992),but the benefits of health promotion as mentalstimulation were less well known. Nevertheless, thehealth promotion group's maintenance of cognitivefunctioning is consistent with growing scientificevidence that health promotion interventions,including physical activity, may prevent decline(Abbott et al., 2004; Boron et al., 2007; Salthouse,2006; Salthouse et al., 2002; Verghese et al., 2003;Weuve et al., 2004).
In the analyses, race and ethnicity were covari-ates, which suggests that memory performance maychange differently over time based on demographiccharacteristics. Both Hispanics and Blacks tendedto make greater gains than Whites on visualmemory; Blacks also performed better over timeon instrumental functional abilities, although His-panics performed worse on the memory measure inthe short run. These results raise the question: Areminorities more likely to gain from health promo-tion or memory training interventions? Becausepretest scores were included in the model ascovariates, the differential changes over time forBlack and Hispanic participants as compared toWhites were not due to lower pretest scores.
The participants improved on the DAFS perfor-mance measure from baseline to end of classes, butthere was no significant change in scores at the endof the study. Transfer of learning or practice effectsmay have occurred as a result of taking the DAFS
301SENIORWISE STUDY
Author's personal copy
repeatedly. Although our participants were screenedout for dementia, we found that the DAFS (evenexcluding the eating and dressing/grooming skillssubscales) had a nonnormal distribution and aceiling effect despite the fact that two thirds ofthese same respondents scored in the poor orimpaired ranges of a test of everyday memoryperformance. This pattern of results suggested thatthe DAFS might not be sensitive to the early deficitsin functioning exhibited by older adults who areexperiencing poor memory performance but are stillliving independently in the community.
In addition, our study included four required 90-minute booster sessions at 3 months posttraining forall participants. These additional sessions may haveincreased learning and retention through practiceeffects with everyday activities. The four boostersessions for the health promotion group may haveincreased the mental stimulation for this group(Austin-Wells, McDougall, & Becker, 2006).
Less-educated, Black, and Hispanic participantshad lower scores than Whites on verbal memory atbaseline. In our HLM analyses, we examined theverbal memory delayed recall T-score as anoutcome at Times 2 and 5. Controlling for ethnicity,age, education, and verbal memory scores at Time1, there were no treatment effects. However, testingwith Hispanic elders was often done over manydays to accommodate their low literacy skills andlevel of frustration with the complex battery ofmeasures. Practice effects may have been greaterfor Blacks and Hispanics, or the interventions mayhave been more effective for minority participants(McDougall, Holston, & Wilke, 2001; McDougallet al., 2008). Because different patterns wereobserved for Blacks and Hispanics, future researchshould examine ethnic/racial groups separately andconsider the moderator effects of race and ethnicityon memory training.
Following the training, we observed an improve-ment in global cognition; however, there was nochange from baseline to end of study. The initialimprovement may reflect a practice effect inducedby repetition because the period between baselinetesting and postclass was approximately 8 weeks.The MMSE has a documented selective bias towardepisodic memory and visuospatial skills in normalelderly adults without dementia (Hill & Backman,1995). In addition, in a longitudinal analysis,Rabbitt, Diggle, Holland, and McInnes (2004)found that practice improvements were greatest
between the first and second experiences with acognitive task.
The memory group showed no greater gains ineveryday memory performance than the healthpromotion group. These findings contrast with theACTIVE trial findings, in which the participants ineach intervention group improved targeted cognitiveabilities by an amount approximately equal to thecognitive decline that would naturally occur in olderadults without dementia and maintained these gainsfor 5 years (Ball et al., 2002; Willis et al., 2006).
The participants in our study did not havedementia. However, 169 (64%) individuals hadmeasurable problems in one or more domains ofeveryday function, and 46 (17%) had problems thatwould be of serious enough concern for furtherneuropsychological referral and would potentiallymeet the criteria for MCI. The MCI prevalence ratein a nationally representative sample was 22%(Plassman et al., 2008). In recent studies, indivi-duals with MCI might have received differentialbenefits from cognitive training (Belleville, 2008;Unverzagt et al., 2007). The issue of memorycomplaints deserves further discussion becausethese subjective concerns are often predictive of afuture diagnosis of MCI (Pearman & Storandt,2004; Purser, Fillenbaum, & Wallace, 2006;Winblad et al., 2004; Zandi, 2004; Zeintl et al.,2006). We found a reduction in memory complaintsfor participants in the memory group. At 26months, they continued to report fewer complaints.
Whites made relatively greater gains than Blacksdid in memory self-efficacy. We expected memoryself-efficacy to improve based on evidence fromprevious studies with diverse older adults (Ditt-mann-Kohli et al., 1991; Lachman et al., 1992;McDougall, 1998; 1999; 2000; 2002; Rebok, &Balcerak, 1989; West et al., 2008). However, allprevious intervention studies used different mem-ory efficacy questionnaires. Difficulty in compre-hending the MSEQ was reflected in our findings.Future studies will require further adjustment of thismeasure, and possibly other measures, to accom-modate the literacy level of participants (Institute ofMedicine, 2004; Scott et al., 2002).
In a recent study, Algase, Souder, Roberts, &Beattie (2006) elevated the urgency to prepareadvanced practice geropsychiatric nurses to care forthe projected 15 million older adults by 2030 withmajor psychiatric illness. The CBMEM provides aframework for intervening with the everyday
302 MCDOUGALL ET AL

Author's personal copy
memory concerns of older adults striving forindependence. Nevertheless, the findings thatBlack and Hispanic elderly persons made greatergains than Whites on some memory performancemeasures merit further study.
ACKNOWLEDGMENT
Support for this research was provided by NIAGrant R01 AG 15384.
REFERENCES
Abbott, R. D., White, L. R., Ross, G. W., Masaki, K. H., Curb, J.D, & Petrovitch, H. (2004). Walking and dementia inphysically capable elderly men. Journal of the AmericanMedical Association, 292(12), 1447–1453.
Algase, D. L., Souder, E., Roberts, B., & Beattie, E. (2006).Enriching geropsychiatric nursing in advanced practicenursing programs. Journal of Professional Nursing, 22(2), 129–136.
Artistico, D., Cervone, D., & Pezzuti, L. (2003). Perceived self-efficacy and everyday problem solving among you andother adults. Psychology and Aging, 18, 68–79.
Austin-Wells, V., McDougall, G. J., & Becker, H. (2006).Recruiting and retaining an ethnically diverse sample ofolder adults in a longitudinal intervention study.Educational Gerontology, 32, 159–170.
Austin-Wells, V., Zimmerman, T., & McDougall, G. J. (2003).An optimal delivery format for lectures targeting matureadults. Educational Gerontology, 29(6), 493–501.
Ball, K., Berch, D. B., Helmers, K. F., Jobe, J. B., Leveck, M. D.,Marsiske, M., et al. (2002). Effects of cognitive traininginterventions with older adults: A randomized controlledtrial. Journal of the American Medical Association, 288(18), 2271–2278.
Bandura, A. (1989). Regulation of cognitive processes throughperceived self-efficacy. Developmental Psychology, 25(5), 729–735.
Bandura, A., & Locke, E. A. (2003). Negative self-efficacy andgoal effects revisited. Journal of Applied Psychology, 88(1), 87–99.
Becker, H., McDougall, G. J., Douglas, N., & Arheart, K. L.(2008). Comparison of the impact of an eight-session andfour-session memory intervention. Archives of Psychiat-ric Nursing, 22(2), 87–94.
Belleville, S. (2008). Cognitive training for persons with mildcognitive impairment. International Psychogeriatrics, 20(1), 57–66.
Benedict, R. H. B. (1997). Brief Visuospatial Memory Test—Revised: Professional manual. Odessa, FL: Psycholog-ical Assessment Resources, Inc.
Berry, J. M. (1989). Cognitive efficacy across the life span:Introduction to the special series. Developmental Psy-chology, 25, 683–686.
Berry, J. M., & West, R. L. (1993). Cognitive self-efficacy inrelation to personal mastery and goal setting across thelife span. International Journal of Behavioral Develop-ment, 16, 351–379.
Berry, J. M., West, R. L., & Dennehey, D. M. (1989). Reliabilityand validity of the memory self-efficacy questionnaire.Developmental Psychologist, 25, 701–713.
Boron, J. B., Willis, S. L., & Schaie, K. W. (2007). Cognitivetraining gain as a predictor of mental status. The Journalsof Gerontology Series B, Psychological Sciences andSocial Sciences, 62(1), P45–P52.
Brandt, J. (1991). The Hopkins Verbal Learning Test: Develop-ment of a new memory test with six equivalent forms.The Clinical Neuropsychologist, 5, 125–142.
Bryk, A. S., & Raudenbush, S. W. (1992). Hierarchical linearmodels. Newbury Park, CA: Sage Publications.
Butters, M. A., Young, J. B., Lopez, O., Aizenstein, H. J.,Mulsant, B. H., Reynolds III, C. F., et al. (2008).Pathways linking late-life depression to persistentcognitive impairment and dementia. Dialogues inClinical Neursoscience, 10(3), 345–357.
Carey, B. (2006). A ‘senior moment’ or a self-fulfillingprophecy? The New York Times, D6.
Carlson, M. C., Xue, Q. L., Zhou, J., & Fried, L. P. (2009).Executive decline and dysfunction precedes decline inmemory: The women's health and aging study. TheJournals of Gerontology Series A, Biological Sciencesand Medical Sciences, 64(1), 12–18.
Cattan, M., White, M., Bond, J., & Learmouth, A. (2005).Preventing social isolation and loneliness among olderpeople: A systematic review of health promotioninterventions. Ageing & Society, 25, 41–67.
Cockburn, J., & Smith, P. T. (1989). The Rivermead BehaviouralMemory Test. Supplement 3: Elderly people. Bury St.Edmonds, Suffolk: Thames Valley Test Company.
Cockburn, J., & Smith, P. T. (1994). Anxiety and errors ofprospective memory among elderly people. BritishJournal of Psychology, 85, 273–282.
Comijs, H. C., Deeg, D. J., Dik, M. G., Twisk, J. W., &Jonker, C. (2002). Memory complaints: The associ-ation with psycho-affective and health problems andthe role of personality characteristics. A 6-yearfollow-up study. Journal of Affective Disorders, 72,157–165.
Dellefield, K. S., & McDougall, G. J. (1996). Increasingmetamemory in older adults. Nursing Research, 45(5),284–290.
Dittmann-Kohli, F., Lachman, M. E., Kliegl, R., & Baltes, P.(1991). Effects of cognitive training and testing onintellectual efficacy beliefs in elderly adults. Journal ofGerontology, 46(4), 162–164.
Dixon, R. A., Hultsch, D. F., & Hertzog, C. (1988). TheMetamemory In Adulthood (MIA) questionnaire. Psy-chopharmacology Bulletin, 24, 671–688.
Dodge, H. H., Du, Y., Saxton, J. A., & Ganguli, M. (2006).Cognitive domains and trajectories of functional inde-pendence in nondemented elderly persons. The Journalsof Gerontology Series A, Biological Sciences andMedical Sciences, 61(12), 1330–1337.
Dux, M. C., Woodard, J. L., Calamari, J. E., Messina, M., Arora,S, Chik, H., et al. (2008). The moderating role of negativeaffect on objective verbal memory performance andsubjective memory complaints in healthy older adults.Journal of the International Neuropsychological Society,14(2), 327–336.
303SENIORWISE STUDY
Author's personal copy
Federal Interagency Forum on Aging Related Statistics (2008).Older Americans 2008: Key indicators of well being.Washington, DC: U.S. Government Printing Office.
Finkel, D., Reynolds, C. A., McArdle, J. J., & Pedersen, N. L.(2007). Cohort differences in trajectories of cognitiveaging. The Journals of Gerontology Series B, Psycho-logical Sciences and Social Sciences, 62(5), P286–P294.
Fiocco, A. J., Wan, N., Weekes, N., Pim, H., & Lupien, S. J.(2006). Diurnal cycle of salivary cortisol in older adultmen and women with subjective complaints of memorydeficits and/or depressive symptoms: Relation to cogni-tive functioning. Stress, 9(3), 143–152.
Floyd, M., & Scogin, F. (1997). Effects of memory training onthe subjective memory functioning and mental health ofolder adults: A meta-analysis. Psychology and Aging, 12(1), 150–161.
Flynn, T., & Storandt, M. (1990). Supplemental group discus-sions in memory training for older adults. Psychologyand Aging, 5(2), 178–181.
Fogler, J., & Stern, L. (1994). Improving your memory: How toremember what you are starting to forget. Baltimore:John Hopkins University Press.
Folstein, M. F., Folstein, S. E., & McHugh, P. R. (1975). ‘Mini-Mental State’: A practical method for grading thecognitive state of patients for the clinician. Journal ofPsychiatric Research, 12, 189–198.
Hayslip, B., Maloy, R. M., & Kohl, R. (1995). Long-termefficacy of fluid ability interventions with older adults.Journal of Gerontology: Psychological Sciences, 50B(3),P141–P149.
Hebert, L. E., Scherr, P. A., Bienias, J. L., Bennett, D. A., &Evans, D. A. (2003). Alzheimer disease in the U.S.population: Prevalence estimates using the 2000 census.Archives of Neurology, 60(8), 1119–1122.
Herrmann, L. L., Goodwin, G. M., & Ebmeler, K. P. (2007). Thecognitive neuropsychology of depression in the elderly.Psychological Medicine, 37(12), 1693–1702.
Hill, R. D., & Backman, L. (1995). The relationship between theMini-Mental State Examination and cognitive function-ing in normal elderly adults: A componential analysis.Age and Ageing, 24, 440–446.
Institute of Medicine, J (2004).Health literacy: A prescription toend confusion. Washington, DC: The National Acade-mies Press.
Jennings, J. M., & Darwin, A. L. (2003). Efficacy beliefs,everyday behavior, and memory performance amongolder elderly adults. Educational Gerontology, 29,71–91.
Jobe, J. B., Smith, D. M., Ball, K., Tennstedt, S. L., Marsiske,M, Willis, et al. (2001). ACTIVE: A cognitiveintervention trial to promote independence in olderadults. Controlled Clinical Trials, 22, 453–479.
Johnson, J. K., Lui, L. Y., & Yaffe, K. (2007). Executivefunction, more than global cognition, predicts functionaldecline and mortality in elderly women. Journals ofGerontology Series B, Biological Sciences and MedicalSciences, 62(10), M1134–M1141.
Lachman, M. E., Andreoletti, C., & Pearman, A. (2006).Memory control beliefs: How are they related to age,strategy use and memory improvement? Social Cogni-tion, 24(3), 359–385.
Lachman, M. E., Steinberg, E. S., & Trotter, S. D. (1987).Effects of control beliefs and attributions on memoryself-assessments and performance. Psychology andAging, 2(3), 266–271.
Lachman, M. E., Weaver, S. L., Bandura, M., Elliott, E., &Lewkowicz, C. J. (1992). Improving memory andcontrol beliefs through cognitive restructuring and self-generated strategies. Journal of Gerontology, 47(50),P293–P299.
Light, L. L. (1991). Memory and aging: Four hypotheses in searchof data. Annual Review of Psychology, 42, 333–376.
Loewenstein, D. A., Amigo, E., Duara, R., Guterman, A.,Hurwitz, D., Berkowitz, N., et al. (1989). A new scale forthe assessment of functional status in Alzheimer'sdisease and related disorders. Journal of Gerontology,44, P114–P121.
Loewenstein, D. A., Ardila, A., Rosselli, M., Hayden, S., Duara,R, Berkowitz, N., et al. (1992). A comparative analysis offunctional status among Spanish- and English-speakingpatients with dementia. Journal of Gerontology, 47,P389–P394.
McDougall, G. J. (1998). Increasing memory strategy use andself-efficacy in Hispanic elders. Clinical Gerontologist,19(2), 57–76.
McDougall, G. J. (1999). Cognitive interventions among olderadults. In J. J. Fitzpatrick (Ed.), Annual review of nursingresearch, 17th ed. New York: Springer.
McDougall, G. J. (2000). Memory improvement in assistedliving elders. Issues in Mental Health Nursing, 21(2),217–233.
McDougall, G. J. (2002). Memory improvement in octogenar-ians. Applied Nursing Research, 15(1), 2–10.
McDougall, G. J. (2004). Memory self-efficacy and memoryperformance among Black and White elders. NursingResearch, 53(5), 323–331.
McDougall, G. J. (2009). A framework for cognitive interven-tions targeting everyday memory performance andmemory self-efficacy. Family and Community Health,Supplement 1, 32(18), S15–S26.
McDougall, G. J., Becker, H., & Arheart, K. L. (2006). Olderadults in the SeniorWISE study at-risk for mild cognitiveimpairment. Archives of Psychiatric Nursing, 20(3),126–134.
McDougall, G. J., Becker, H., Pituch, K., Acee, T. W., Vaughan,P., & Delville, C. L. (2008, June). Emerging evidence formemory training with community-residing minorityolder adults. Research poster presented at the annualmeeting of Academy Health, Washington, DC.
McDougall, G. J., Holston, E. C., & Wilke, P. (2001). RecruitingAfrican-Americans into cognitive aging research. Eth-nicity & Disease, 11, 124–133.
McDougall, G. J., Strauss, M. E., Holston, E., & Martin, M.(1999, November). Memory self-efficacy and memoryanxiety as predictors of memory performance in at-riskelderly. S. Kwon (Chair), Memory and cognition:Theoretical and methodological approaches to self-ratings, control beliefs, and self-efficacy. Symposiumconducted at the annual meeting of the GerontologicalSociety of America, San Francisco, CA.
Mendes de Leon, C. F., Gold, D. T., Glass, T. A., Kaplan, L., &George, L. K. (2001). Disability as a function of social
304 MCDOUGALL ET AL
Author's personal copy
networks and support in elderly African Americans andWhites: The Duke EPESE 1986–1992. The Journals ofGerontology Series B, Psychological Sciences and SocialSciences, 56(3), S179–S190.
Michael, Y. L., Berkman, L. F., Colditz, G. A., Holmes, M. D.,& Kawachi, I. (2002). Social networks and health-relatedquality of life in breast cancer survivors: A prospectivestudy. Journal of Psychosomatic Research, 52(5),285–293.
Morgan, M. D., Mielke, M. M., O'Brien, R., Troncoso, J. C.,Zonderman, A. B., & Lyketsos, C. G. (2007). Rates ofdepression in individuals with pathologic but not clinicalAlzheimer disease are lower than those in individualswithout the disease: Findings from the BaltimoreLongitudinal Study on Aging (BLSA). AlzheimerDisease & Associated Disorders, 21(3), 199–204.
Oswald, W. D., Rupprecht, R., Gunzelmann, T., & Tritt, K.(1996). The SIMA-project: Effects of 1 year cognitiveand psychomotor training on cognitive abilities ofelderly. Behavioural Brain Research, 78, 67–72.
Papp, K. V., Walsh, S. J., & Snyder, P. J. (2009). Immediate anddelayed effects of cognitive interventions in healthyelderly: A review of current literature and futuredirections. Alzheimers and Dementia, 5(1), 50–60.
Pearman, A., & Storandt, M. (2004). Predictors of subjectivememory in older adults. Journals Gerontology BPsychological Sciences Social Sciences, 59(1),P4–P6.
Phelan, E. A., Williams, B., Penninx, B. W. J. H., LoGerfo, J. P.,& Leveille, S. G. (2004). Activities of daily livingfunction and disability in older adults in a randomizedtrial of the health enhancement program. The Journals ofGerontology Series A, Biological Sciences and MedicalSciences, 59(8), M838–M843.
Plassman, B. L., Langa, K. M., Fisher, G. G., Heeringa, S. G.,Weir, D. R., Ofstedal, M. B., et al. (2008). Prevalence ofcognitive impairment without dementia in the UnitedStates. Annals of Internal Medicine, 148(6), 427–434.
Purser, J. L., Fillenbaum, G. G., & Wallace, R. B. (2006).Memory complaint is not necessary for diagnosis of mildcognitive impairment and does not predict 10-yeartrajectories of functional disability, word recall, or shortportable mental status questionnaire limitations. Journalof the American Geriatrics Society, 54(2), 335–338.
Rabbitt, P., Diggle, P., Holland, F., & McInnes, L. (2004).Practice and drop-out effects during a 17-year longitu-dinal study of cognitive aging. Journal of Gerontology:Psychological Sciences, 59B, 84–97.
Radloff, L. S., & Teri, L. (1986). Use of the Center forEpidemiological Studies—Depression Scale with olderadults. Clinical Gerontologist, 5, 119–136.
Rebok, G. W., & Balcerak, L. J. (1989). Memory self-efficacyand performance differences in young and old adults: Theeffect of mnemonic training. Developmental Psychology,25(5), 714–721.
Reitan, R. M. (1958). Validity of the Trail Making Test as anindicator of organic brain damage. Perceptual and MotorSkills, 8, 271–276.
Royall, D. R., Palmer, R., Chiodo, L. K., & Polk, M. J. (2005).Declining executive control in normal aging predictschange in functional status: The Freedom House study.
Journal of the American Geriatrics Society, 52,346–352.
Salthouse, T. A. (1991). Theoretical perspectives on cognitiveaging. Hillsdale, NJ: Lawrence Erlbaum Associates.
Salthouse, T. A. (2003). Memory aging from 18 to 80. AlzheimerDisease Associated Disorders, 17(3), 162–167.
Salthouse, T. A. (2006). Mental exercise and mental aging:Evaluating the validity of the “use it or lose it”hypothesis. Perspectives on Psychological Science, 1(1), 68–87.
Salthouse, T. A., Berish, D. E., &Miles, J. D. (2002). The role ofcognitive stimulation on the relations between age andcognitive functioning. Psychology and Aging, 17(4),548–557.
Scogin, F. M. (1997). Effects of memory training on thesubjective memory functioning and mental health ofolder adults: A meta-analysis. Psychology and Aging, 12(1), 150–161.
Scott, T. L., Gazmararian, J. A., Williams, M. V., & Baker, D. W.(2002). Health literacy and preventive health care useamong Medicare enrollees in a managed care organiza-tion. Medical Care, 40(5), 395–404.
Slegers, K., van Boxtel, M., & Jolles, J. (2009). Effects ofcomputer training and internet usage on cognitiveabilities in older adults: A randomized controlled study.Aging Clinical and Expirmental Research, 21(1), 43–54.
Smith, G. E., Housen, P., Yaffe, K., Ruff, R., Kennison, R. F.,Mahncke, H. W., & Zelinski, E. M. (2009). A cognitivetraining program based on principles of brain plasticity:Results from the Improvement in Memory with Plastic-ity-based Adaptive Cognitive Training (IMPACT) study.Journal American Geriatrics Society, 57(4), 594–603.
Spielberger, C. D., Gorsuch, R. L., & Lushene, R. E. (1970).Manual for the State-Trait Anxiety Inventory (Self-Evaluation Questionnaire). Palo Alto, CA: ConsultingPsychologists Press.
Sumerall, S. W., Timmons, P. L., James, A. L., Ewing, M. J. M.,& Oehlert, M. E. (1997). Expanded norms for theControlled Oral Word Association Test. Journal ofClinical Psychology, 53, 517–521.
Unverzagt, F. W., Kasten, L., Johnson, K. E., Rebok, G. W.,Marsiske, M., Koepke, K. M., et al. (2007). Effect ofmemory impairment on training outcomes in ACTIVE.Journal of the International Neuropsychological Society,13, 953–960.
Valentijn, S. A., Van Hooren, S. A., Bosma, H., Touw, M. S.,Jolles, J., Van Boxtel, M. P., et al. (2005). The effect oftwo types of memory training on subjective and objectivememory performance in healthy individuals aged 55years and older: A randomized controlled trial. PatientEducation and Counseling, 57, 106–114.
Verghese, J., Lipton, R. B., Katz, M. J., Hall, C. B., Derby, C. A.,Kuslansky, G., et al. (2003). Leisure activities and therisk of dementia in the elderly. New England Journal ofMedicine, 348(25), 2508–2516.
Verhaeghen, P., Marcoen, A., & Goossens, L. (1992). Improvingmemory performance in the aged through mnemonictraining: A meta-analytic study. Psychology and Aging, 7(2), 242–251.
R. L. West & J. D. Sinnott (Eds.). (1991), Everyday memory andaging. New York: Springer-Verlag.
305SENIORWISE STUDY
Author's personal copy
West, R. L., Bagwell, D. K., & Dark-Freudeman, A. (2008).Self-efficacy and memory aging: The impact of amemory intervention based on self-efficacy. Neuropsy-chology Development and Cognition B Aging Neuropsy-chology and Cognition, 15(3), 302–329.
West, R. L., Crook, T. H., & Barron, K. L. (1992). Everydaymemory performance across the life span: Effects of ageand noncognitive individual differences. Psychology andAging, 7(1), 72–82.
Weuve, J., Kang, J. H., Manson, J. E., Breteler, M. M. B., Ware,J., & Grodstein, F. (2004). Physical activity, includingwalking, and cognitive function in older women. Journalof the American Medical Association, 292(12),1454–1461.
Willis, S. L., Tennstedt, S. L., Marsiske, M., Ball, K., Elias, J.,Koepke, K. M., et al. (2006). Long-term effects ofcognitive training on everyday functional outcomes inolder adults. Journal of the American Medical Associa-tion, 296(23), 2805–2814.
Wilson, B., Cockburn, J., Baddeley, A., & Hiorns, R. (1989). Thedevelopment and validation of a test battery for detecting
and monitoring everyday memory problems. Journal ofClinical andExperimentalNeuropsychology, 11, 855–870.
Wilson, R. S., Beckett, L. A., Barnes, L. L., Schneider, J. A.,Bach, J., Evans, D. A., et al. (2002). Individualdifferences in rates of change in cognitive abilities ofolder persons. Psychology and Aging, 17(2), 179–193.
Winblad, B., Palmer, K., Kivipelto, M., Jelic, V., Fratiglioni, L.,Wahlund, L. O., et al. (2004). Mild cognitive impairment—Beyond controversies, towards a consensus: Report ofthe International Working Group on Mild CognitiveImpairment. Journal of Internal Medicine, 256(3),240–246.
Zandi, T. (2004). Relationship between subjective memorycomplaints, objective memory performance, and depres-sion among older adults. American Journal of Alzhei-mer’s Disease and Related Disorders, 19(6), 353–360.
Zeintl, M., Kliegel, M., Rast, P., & Zimprich, D. (2006).Prospective memory complaints can be predicted byprospective memory performance in older adults.Dementia and Geriatric Cognitive Disorders, 22(3),209–215.
306 MCDOUGALL ET AL
Copyright © 2022 FDOKUMEN



















