
The role of rehabilitation providers Part 2
24
1 Running head: PERCEPTIONS OF REHABILITATION PROVIDERS The Role of the Rehabilitation Provider in Occupational Rehabilitation: Providing for Whom? Part 2: Perceptions of Key Stakeholders Dianna T. Kenny The University of Sydney Australia In Australian Journal of Rehabilitation Counselling, 1998, 4 (2), 11-122 Key words: rehabilitation provider, occupational rehabilitation, injured worker, workers’ compensation Correspondence and reprints: Associate Professor Dianna Kenny PhD, School of Behavioural and Community Health Sciences, Faculty of Health Sciences, The University of Sydney, PO Box 170, Lidcombe, NSW, AUSTRALIA 2141 This research was funded by a grant from the WorkCover Authority of NSW, Australia (Grant No 30 303 010)
Transcript of The role of rehabilitation providers Part 2

1
Running head: PERCEPTIONS OF REHABILITATION PROVIDERS
The Role of the Rehabilitation Provider in Occupational Rehabilitation: Providing for
Whom? Part 2: Perceptions of Key Stakeholders
Dianna T. Kenny
The University of Sydney
Australia
In Australian Journal of Rehabilitation Counselling, 1998, 4 (2), 11-122
Key words: rehabilitation provider, occupational rehabilitation, injured worker, workers’
compensation
Correspondence and reprints: Associate Professor Dianna Kenny PhD, School of Behavioural
and Community Health Sciences, Faculty of Health Sciences, The University of Sydney, PO
Box 170, Lidcombe, NSW, AUSTRALIA 2141
This research was funded by a grant from the WorkCover Authority of NSW, Australia
(Grant No 30 303 010)

2
ABSTRACT
This paper is the second part of a two part series that examines the perceived roles and
effectiveness of rehabilitation providers. The first paper examined the perceptions of
rehabilitation providers regarding their roles in, and perceived barriers to, occupational
rehabilitation. In this paper, key stakeholders’ perceptions of the role of rehabilitation
providers in the management of workplace injury were assessed via interviews and surveys.
Forty-nine injured workers were interviewed and 407 returned a survey questionnaire. Two
surveys of employers were conducted: one in the Newcastle/Hunter region of NSW,
Australia, the other a state-wide survey (N=612) of a representative sample of employers in
NSW. In addition, nine treating doctors and 14 insurers were interviewed. Results indicate
two thirds of workers were satisfied with the service they had received from the rehabilitation
provider. The major concerns of injured workers were the rehabilitation providers’ lack of
knowledge of the demands of particular workplaces, the problems associated with particular
injuries and the pressure on rehabilitation providers from employers and insurers to return the
injured worker to work.. Sixty percent of employers reported that rehabilitation providers
were effective in restoring injured workers to work. Treating doctors were generally hostile
to
rehabilitation providers, claiming that they were unprofessional, inexpert and poorly trained.
Finally, insurers complained of stereotypical case management plans, role confusion, and
over-servicing.

3
An increasing number of injured workers are referred to rehabilitation providers to
assist them and their employers to achieve a safe, timely and durable return to work. In the
previous paper in this series, the perceptions of rehabilitation providers were canvassed via in
depth semi-structured interviews to elucidate the major barriers to occupational rehabilitation
and their possible solutions. Three major barriers to occupational rehabilitation that were
identified by rehabilitation providers. These were: (i) problems associated with defining their
core business and client group; (ii) misconceptions, lack of information and failure of
communication; and (iii) lack of co-operation and overt and covert obstruction to the
rehabilitation process by other key stakeholders. Each of these barriers were experienced
with each of the nominated stakeholder groups. Solutions offered included: i) forming a
trusting relationship with the injured worker; ii) enhancing employer knowledge of, and
commitment to rehabilitation; iii) enlisting the support of treating doctors as team players in
the injury management process; iv) early referral of the injured worker to rehabilitation; and
v) finding better ways to resolve disputes between insurers and injured workers.
In this paper, using both data (ie using a variety of data sources) and methodological
(using qualitative data, content analysis and statistical analyses of survey questionnaires)
triangulation (Patton, 1990), the perceptions of key stakeholders about the practices and
effectiveness of rehabilitation providers are reported. The aim of this study is to determine
the degree of concurrence between the self-perceptions of rehabilitation providers and the
perceptions of stakeholders who use their services. This process is a necessary precursor to
improving the management of occupational injury.
METHOD
Participants
The stakeholders who provided commentary on the practices of rehabilitation
4
providers included 456 injured workers, 49 of whom were interviewed and 407 of whom
responded to a survey; and two groups of employers (N=93 and N=614) who responded to
surveys. In addition, the views of nine general practitioners and 14 insurers who participated
in in-depth semi-structured interviews are also presented. The demographic characteristics of
the sample have been described in detail elsewhere (see Kenny, 1994; 1995a; 1996), but are
briefly summarised for each sub-sample in the subsequent sections.
Procedure and Instruments
Interviews
All interviews were conducted by the author and trained interviewers, and were
recorded and transcribed verbatim for coding (for details, see Kenny, 1995a). The semi-
structured interview protocols for each stakeholder can be found in Kenny (1995). Interviews
for injured workers were conducted in their homes, and interviews for the other stakeholders
were conducted at their workplaces. The interviews were between one and two hours long.
In the interview protocols of all stakeholders, two open-ended questions ie "What are
the major barriers to the return to work and occupational rehabilitation of injured workers?"
and "How might these barriers be overcome?" formed the basis of a coding scheme designed
to elucidate the roles that each stakeholder played as perceived by the other stakeholders.
Only stakeholder comments related to the role of rehabilitation providers are reported in this
paper.
The purpose of the interviews was to identify the major themes relating to the
perceived role and effectiveness of rehabilitation providers and to assess the commonality of
emergent themes across the stakeholder groups. In the following results section, issues were
identified as common themes if they were present in 50% or more of the interview responses
for each of the stakeholder groups. The surveys of injured workers and employers assessed
5
the degree to which the results of the interview studies were representative of injured workers
and employers who use rehabilitation services.
Injured worker questionnaire
Questions for the injured workers’ survey questionnaire were developed from
discussions with rehabilitation personnel from the WorkCover Authority of New South
Wales and from detailed analyses of in-depth semi-structured interviews of 49 injured
workers who had been purposefully sampled from the original sample of 3 041 workers (see
Kenny, 1995a for details of sampling). These interviews identified what workers perceived to
be the major barriers to occupational rehabilitation following a workplace injury or illness.
The questionnaire comprised 6 sections as follows: Demographic information, nature and
outcome of injury, job and workplace characteristics, the claim for workers compensation,
injury management and personnel involved, and an open-ended section inviting workers'
comments about what was most helpful and what was least helpful in assisting them to return
to work following their injuries. The survey was pilot tested on 30 injured workers who did
not form part of the study population, and modified according to feedback from this group
before distribution to the study sample.
Employer Questionnaires
Questions for the initial survey [Work and Rehabilitation Survey for Employers
(Kenny, 1996)] were developed from discussions with rehabilitation personnel from the
WorkCover Authority of New South Wales and from detailed analyses of in-depth semi-
structured interviews of the 23 employers of the 49 injured workers described above. These
in-depth interviews assessed employer knowledge about occupational rehabilitation,
workplace practices and perceived barriers to occupational rehabilitation following a
workplace injury or illness. The Work and Rehabilitation Survey consisted of 45 questions
6
distributed among seven sections as follows: industry demographics, injury characteristics,
occupational health and safety and rehabilitation policies, policies and practices regarding
suitable duties, workers' compensation, injury management and personnel involved, and an
open-ended section inviting employers' comments about what was most helpful and what was
least helpful in assisting their injured workers to return to work following their injuries.
Questions for the statewide survey were based on questions used in the Work and
Rehabilitation Survey for Employers (Kenny, 1996).
Treating doctor interview protocols
The interview protocol for general practitioners covered issues related to their
perceived roles and responsibilities in treating workers' compensation claimants, the
difficulties they encountered, their perceptions of other stakeholders, and of the workers'
compensation system and their views regarding the role of worker and workplace
characteristics in contributing to the outcome of the injury.
Insurer interview protocols
The interview protocol for insurers covered issues related to workers’ compensation
in general, their perceived role in the injury management process, communication with
stakeholders and the criteria they used to select rehabilitation providers and medical
practitioners to whom they referred injured workers.
RESULTS AND DISCUSSION
Stakeholders’ Perceptions of Rehabilitation Providers
Injured Workers (N=49 interviewed)
The 49 injured workers who were interviewed were selected using a stratified
purposeful sampling technique of an original population of 3,041 workers to adequately
represent sex, industry, injury type, amount of time lost (all exceeding one week), and
7
employer size. Back injuries (34%) sprains and strains (21%) and occupational overuse
(17%) accounted for 72% of all injuries. Twenty six (53%) of these workers had been
referred to a rehabilitation provider. Of these, 18 (69.2%) had a back injury, five had a sprain
or strain, and three had an overuse injury. Data presented in this section refer only to this sub-
group of 26 workers.
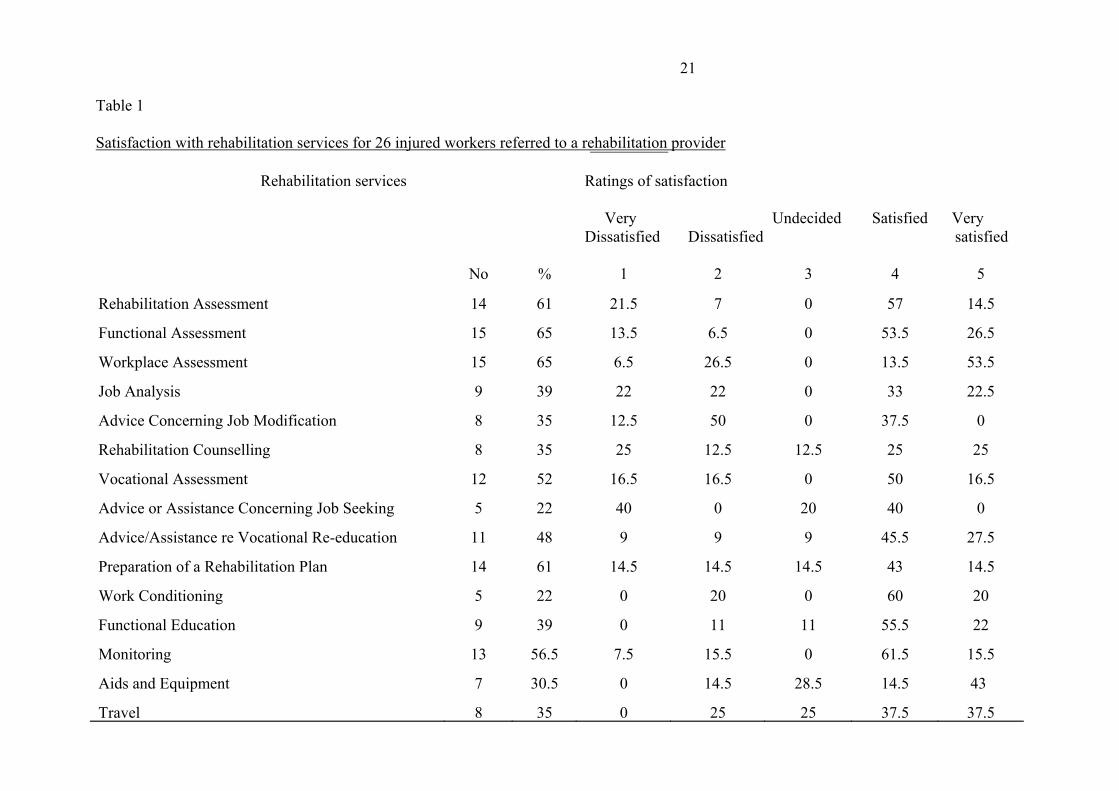
Rehabilitation providers offer a range of services to injured workers that are codified
by the WorkCover Authority. Table 1 sets out the type of service offered, the number and
percentage of workers who received each service and their satisfaction rating of the service
provided.
____________________________________________________
Insert Table 1 here
_____________________________________________________
The most frequently offered services to this group were rehabilitation assessments,
functional assessments, workplace assessments, and the preparation of rehabilitation plans.
Rehabilitation providers were perceived to perform some of their functions well and others
poorly. Satisfaction ratings for all services ranged from 80% very satisfied/satisfied for
functional assessments and work conditioning, to 37.5% - 40% very satisfied/satisfied for
advice concerning job modification, and advice or assistance concerning job seeking. The
numbers are small and should be interpreted cautiously, and used only as a basis for seeking
further feedback from users of these services. Below are examples of satisfied and
dissatisfied injured workers’ responses to the role of the rehabilitation provider in injury
management. Positive experiences with the rehabilitation provider were often juxtaposed
with negative experiences with other stakeholders, as exemplified in the scenarios below.
“The injury took place in a coal mine and their safety officer rang me once and asked
8
how I was going. He told me he wanted to see me some time and wanted me to make
suggestions on how the accident could have been avoided and any improvements
needed to make safer working conditions. I never heard from him again. I felt my
employer and insurance company knew everything that was going on and didn't want
to tell me much at all. I felt the injured worker was the forgotten person in all that was
going on. If I didn't see a rehabilitation provider, the situation would have been a
disaster and I would have lost my job.”
“I didn’t get any decent help from anyone until I saw the rehabilitation provider. I had
tried quite a few different jobs at work after my injury, but they all put too much
strain on my knee. So we (worker and rehabilitation provider) put our heads together
and discussed what I’d like to do. She said, ‘This is what you can do and this is what
you can’t do.’ So I decided to do a business operations course at Tech, and now I am
assistant manager of a tyre place. It could easily have been the scrap heap.”
“My rehabilitation provider was an occupational therapist. I was referred about a
month after my injury (ie herniated L4/L5 disc). She was able to give me a lot of
directions as to what I was supposed to do, not just to manage my injury, but to
manage the process as well. She talked to the physiotherapist and my employer and
helped out with the paperwork. She worked out a coherent treatment plan. That took
some of the pressure off me at a time when I wasn’t coping very well.”
Negative experiences with rehabilitation providers centred around their perceived
inexperience or lack of knowledge of the demands of particular workplaces, the problems
associated with particular injuries and the pressure on rehabilitation providers from the
9
employer and the insurer to return the worker to work as quickly as possible, the latter
problem clearly associated with the issue of core business and client identification
highlighted in the interviews.
“My employer was of little help to me. The rehabilitation co-ordinator had no time for
follow-up and was totally inefficient. As a result I have now exacerbated my back
injury. Also, this was due to an inexperienced rehabilitation provider who did not
realise the amount of heavy work involved in the area where I work. Good luck in
your survey. I hope some help can result. We need it.”
“The rehab provider was just a yes man. The insurer said, ‘Jump!’ and she said, ‘How
high?’ She pushed me from day one to go back to work. I was in too much pain, but
that didn’t get factored into the argument. She said that there was always something
that you could do, it didn’t matter how much pain you were in.”
“Some rehab providers have a ‘one size fits all’ policy. Our company used the same
rehab provider for all the workers on compo, and you could see that we were all
steered through the same process line, with no consideration for individual needs.”
Injured Worker Survey
Qualitative methods are ideal for identifying and specifying problems in the operation
of a system. Quantitative data are then required to assess the extent of the problems.
Accordingly, a survey based on interview and consultation data was designed and distributed
to 1,229 workers who could be located from the original population of 3,041 injured workers.
Of the 407 workers who responded to the survey questionnaire, 137 (33.7%) had been
referred to a rehabilitation provider. More than half (54%) of this group of referred workers
10
had suffered a back injury, of which 72% involved disc pathology. The majority (64.7%)
were male, from labouring, machine operating, or trade occupations (70%). Half of those
referred felt permanently unable to do some (34.3%) or all (16.1%) of their pre-injury duties.
At the time of completion of the questionnaire, 53.3% had returned to work full-time, and
10.2% had returned part-time.
Employers were the source of referral for 41.6% of injured workers, treating doctors
referred 23.4%, rehabilitation co-ordinators referred 17.5%; 8.8% were self-referrals, with
the remaining 8.8% referred from other sources, including the insurer. Forty-two percent
(41.9%) were referred within four weeks of their injury, 27.9% within 12 weeks, 11% within
26 weeks and the remainder (11.8%) were referred more than 26 weeks after they were
injured or could not remember when they were referred.
There was a statistically significant association between referral to a rehabilitation
provider and return to work outcome, with those referred much less likely to have returned to
work (χ2 =17.63, df=1, p=.0003). This finding reflects the referral bias to rehabilitation
providers, with more seriously or permanently injured workers being more likely to be
referred to rehabilitation providers than those who were temporarily unable to perform their
normal work duties (Kenny, 1995d). Poor outcome of rehabilitation may also be related to
the delay in referral noted above. Of workers referred to rehabilitation providers, more than
half were not referred within four weeks of injury, a time frame currently considered to be
best practice by WorkCover and insurers. There is ample evidence in the literature supporting
early intervention and early referral to rehabilitation (Ehrmann-Feldman, et al, 1996;
Gardner, 1991; Lechner, 1994; Lusted, 1993; Ryan et al, 1995).
The failure to provide information and the presence of misinformation were major
foci of the interviews with rehabilitation providers and were perceived by them to constitute
11
substantial barriers to the success of occupational rehabilitation. To assess the extent of the
perceived problem, injured workers were asked about their information source and
knowledge of the workers’ compensation system. At the time of their injury, only 13% of
workers believed that they knew everything that they needed to know about workers'
compensation; 53.3% said that they knew a little and 33.7% said that they knew nothing
about how the system worked. Twenty-five percent (24.8%) were informed about their rights
and procedures by their employers, 17.2% reported that they gained the necessary
information by their own efforts, 12% received information from their union representative or
workmates, 12.2% from friends or family members, and the remainder cited treating doctors
(8.8%), rehabilitation co-ordinators (5.7%), solicitors (5.7%), rehabilitation providers (2.7%)
and others (including the insurer, the WorkCover Authority of New South Wales,
pamphlets/brochures at work) (10.9%) as their major source of information. These figures
vindicate the perception of rehabilitation providers that dissemination of accurate information
is a problem that requires attention.
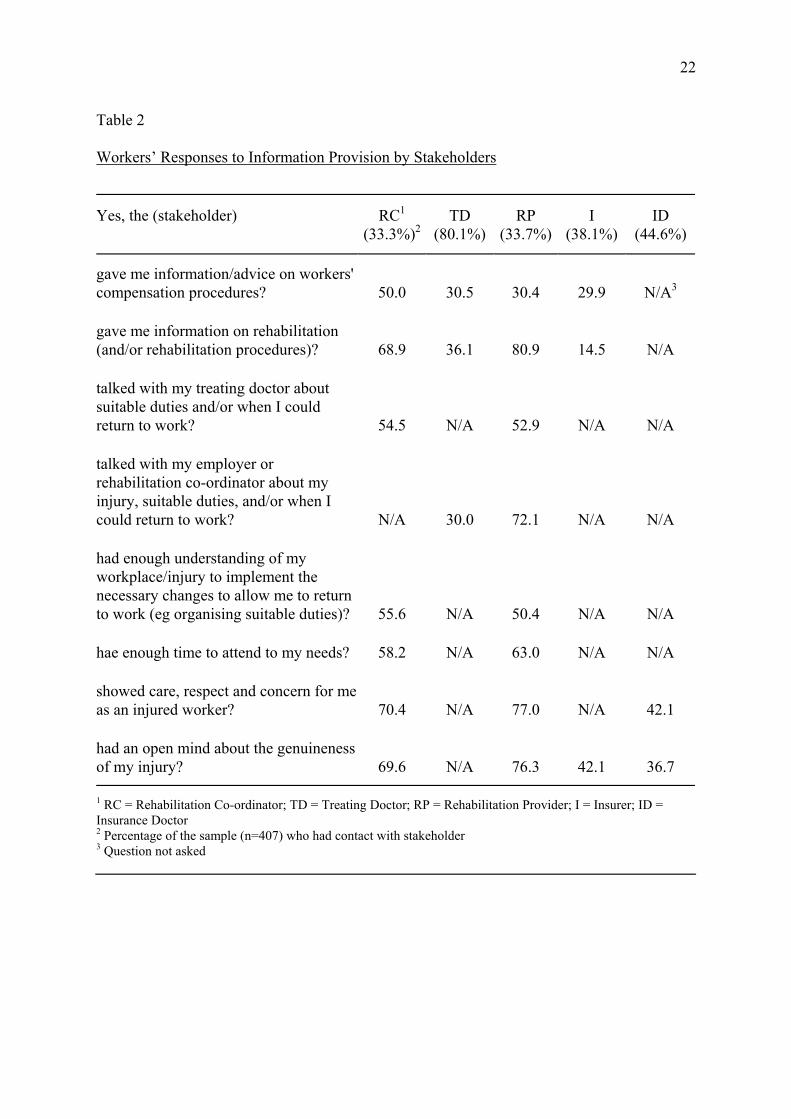
Injured workers were also asked about information provision from five key
stakeholders. Table 2 summarises the findings.
_________________________
Insert Table 2 here
_________________________
Rehabilitation providers were significantly more likely (p<.05) than treating doctors and
insurers to provide information on rehabilitation, and significantly less likely than
rehabilitation co-ordinators to provide advice on workers’ compensation procedures. They
were also perceived to have a more open mind on the genuineness of the injury than either
the insurer or the insurance doctor, although one quarter of those workers who saw a

12
rehabilitation provider also felt that the rehabilitation provider doubted the genuineness of
their injury. Only half of the workers interviewed thought that the rehabilitation provider had
sufficient understanding of their workplace and injury to advise on suitable duties. Between
25% - 50% of injured workers were dissatisfied with some component of their suitable
duties, including a lack of support from both the worker’s supervisor and co-workers.
To test the view of rehabilitation providers that doctors often sabotaged their attempts
to return injured workers to work, injured workers were asked about the advice given to them
by their treating doctors. Of the workers who continued to work while they were undergoing
occupational rehabilitation (n=70), 61.5% reported that their treating doctor had advised them
to discontinue work until they were completely fit. For the workers who were temporarily
unable to perform their normal work duties (n=235), 56.7% reported that their treating
doctors had advised them not to return to work until they were completely fit. There was a
trend that indicated that workers so advised by their treating doctors were less likely to return
to work than workers who were not given this advice (χ2 = 3.48, df=1, p=.06). These data
support the views of rehabilitation providers, who perceived that doctors often worked
against the principles and goals of occupational rehabilitation.
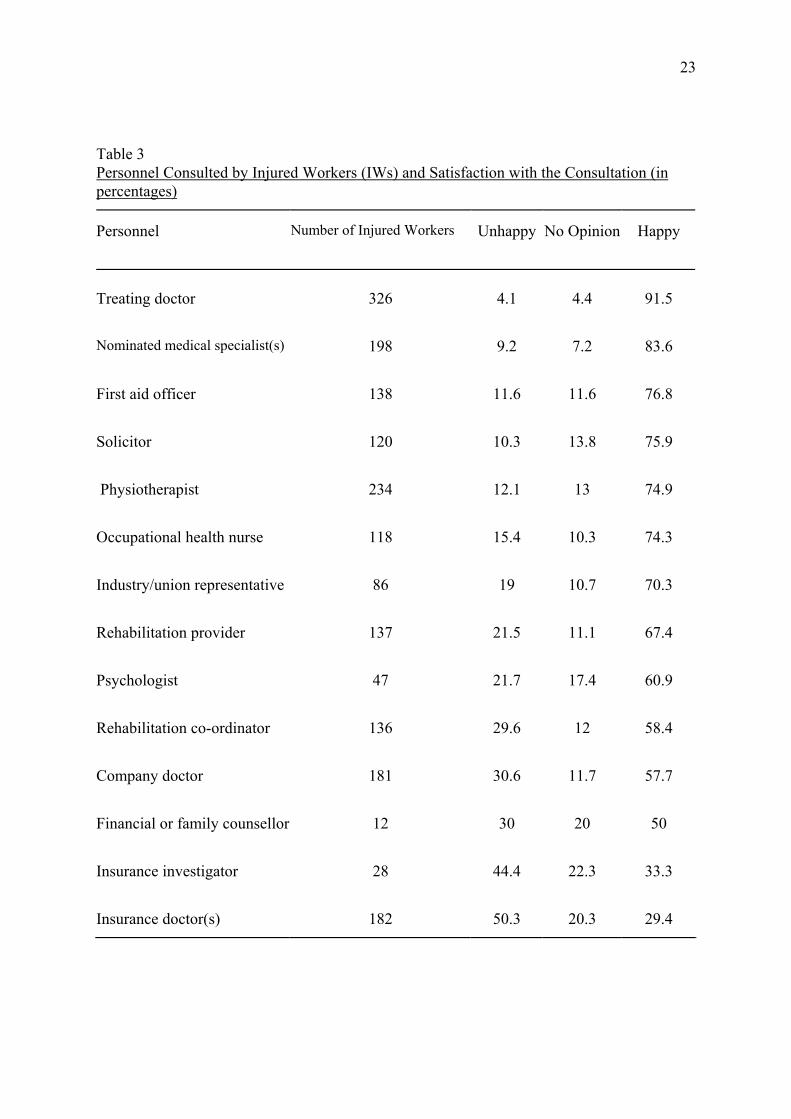
Injured workers may consult with many stakeholder groups in the post injury period.
Table 3 presents the range of personnel consulted by injured workers together with
satisfaction ratings with the service provided.
_____________________________
Insert Table 3 here
______________________________
The table indicates that 67.4% of injured workers who consulted a rehabilitation provider
were satisfied with their consultation. This compares poorly with satisfaction with the

13
treating doctor, with whom 91.5% of injured workers expressed satisfaction. It has been
argued that high satisfaction ratings for treating doctors are related to the collusion of the
treating doctor with the injured worker (Kenny, 1996). The data do not provide insight into
the basis on which satisfaction ratings were made. However, 81.1% injured workers who saw
a rehabilitation provider reported that the provider had consulted them about the development
of a return to work plan and 86% said that the provider followed through on the plan.
Although only 49.5% of workers expressed any confidence that the plan would be successful,
60.4% found that the provider had been helpful in either assisting them to return to work or to
retrain for another job (31% of referrals to rehabilitation providers retrained).
Employers: Newcastle/Hunter Survey (N=93)
Of the 93 employers who responded to the survey questionnaire, 58.6% reported that
rehabilitation providers were effective (48.3%) or very effective (10.3%) in assisting injured
workers return to work. Rehabilitation providers were ranked in a similar way with respect to
effectiveness to rehabilitation co-ordinators (60.7%) and the workplace rehabilitation
program (53.5%) in assisting injured workers return to work.
Employers: State Wide Survey (N=612)
The majority of respondents (71.3%) indicated that their organisations used the
services of an accredited rehabilitation provider. One-tailed tests indicated that there was a
consistent relationship between the size of the employer and the use of an accredited
provider. The proportions of organisations utilising a rehabilitation provider were as follows:
53.6% of organisations with 20 or fewer employees, 69.3% of those with 21-100 employees,
80.8% of those with 101-500 employees, and 95.4% of those with over 500 employees.
Pairwise comparisons of these data were all statistically significantly (Z > 1.65). Respondents
who reported that their organisations referred workers to an accredited rehabilitation provider
14
(n = 427) were asked to indicate their reasons for this practice. The most common reasons
were the “length of time off work” (73.1%) and the “severity of the injury” (72.1%). Table 4
presents the percentage frequencies of reasons for referring to an accredited rehabilitation
provider, in total and by the size of the organisation. One-tailed tests indicated that
organisations with more than 500 employees were more likely; (1) than organisations with 20
or fewer (Z > 1.68) or 101-500 (Z = 1.68) employees to report “when a person needs
retraining” as a reason; (2) than organisations with 20 or fewer (Z = 2.04) or 21-100 (Z =
1.79) employees to report “when the employee requests referral” as a reason; and, (3) than
organisations with 20 or fewer employees (Z = 1.68) to report “severity of injury” as a
reason. No other significant differences were identified.
____________________________________________________
Insert Table 4
_____________________________________________________
Treating doctors
Treating doctors were generally hostile to rehabilitation providers, claiming that they
were unprofessional, inexpert, and poorly trained. Accordingly, treating doctors perceived
part of their role with injured workers was to advise and guide them through the
compensation system, and to protect them from potentially unhelpful interventions from
rehabilitation providers. Below are some comments from treating doctors reflecting this
perception. “I have to guide workers through the whole confusing system because there are a
plethora of rehabilitation providers out there who are not supplying the goods.....” “There is
an enormous amount of money being wasted on rehabilitation providers. The main problem
is that they do not have a sufficient comprehension of the workplace.” This comment is
particularly intriguing as it is a criticism that most stakeholders have levelled at the treating

15
doctor (Kenny, 1996).
Insurers
Insurers identified a number of issues that concerned them about rehabilitation
provider practice. These included “stereotyped case management plans” (about which injured
workers also complained), a lack of mutual respect and co-operation between insurers and
providers, role confusion between rehabilitation co-ordinators and rehabilitation providers
that resulted in lack of ownership and/or responsibility for case management, unnecessary
prolongation of the history of the claim, and over-servicing.
CONCLUSIONS AND RECOMMENDATIONS
The triangulation of data sources in this study offers important insights into the roles
and functions of rehabilitation providers in injury management. The perceptions of the
different stakeholders converged on several issues related to the services of rehabilitation
providers. There was also mutuality in stakeholder accounts with the self-perceptions of
rehabilitation providers. These data provide a basis upon which the role of the rehabilitation
provider can be clarified, and service provision improved.
One of the key barriers identified by rehabilitation providers was the definition of
their core business and identification of their client group. The tension created by the
problem of serving multiple masters (ie insurer, employer, injured worker) simultaneously
was also felt by injured workers, some of whom perceived rehabilitation providers to be ‘yes
men’ to either or both the employer and the insurer. Insurers described role confusion
between providers and rehabilitation co-ordinators which resulted in the abrogation of the
role of case manager by both, leaving the injured worker stranded in the system without a
guide.
The second barrier identified by rehabilitation providers was the problem related to

16
transmission of information and misinformation. This barrier was borne out by the finding
that only 13% of injured workers reported that they had sufficient information to deal
effectively with their injury and workers’ compensation claim. Injured workers filled the
information gap by talking to union representatives, work colleagues, family and friends,
doctors and solicitors, among others. These sources are fertile ground for the distribution of
misinformation, particularly about their rights and entitlements, that may perpetuate the
belief in the “pot of gold” notion that mitigates against early return to work.
The third concern of rehabilitation providers, that there was a lack of co-operation and
overt and covert obstruction to the rehabilitation process by different stakeholders was
supported in this study. In the survey of injured workers, it was apparent that doctors were
advising workers to either discontinue working, or to not return to work until they were
“100% fit.” This advice is contrary to the model of active rehabilitation practised by
rehabilitation providers and was not only perceived, but demonstrated, to undermine their
efforts to achieve return to work for some workers.
Loss of respect for the services of rehabilitation providers ensued from the perception
of both injured workers (“one size fits all”) and insurers (“stereotyped case management
plans”) that rehabilitation plans were formulaic and did not address the needs of individual
workers. Doctors also questioned the technical competence of rehabilitation providers. Both
doctors and injured workers complained that rehabilitation providers did not have sufficient
knowledge of the workplace to prescribe appropriate suitable duties. The injured worker
survey confirmed that this was a pervasive concern. Fewer than 40% reported feeling
satisfied with the advice concerning job modification that was offered by rehabilitation
providers.
Rehabilitation providers stressed the importance of developing a trusting relationship

17
with the injured worker as a basis for a successful outcome. One third of workers expressed
satisfaction with their contact with their rehabilitation provider, and a quarter stated that the
rehabilitation provider doubted the genuineness of their injury. This is a poor foundation
upon which to build a trusting relationship.
The results of this study indicate that for this sample of injured workers, between a
quarter and a half experienced some difficulty with the process of occupational rehabilitation,
including dissatisfaction with the services provided by rehabilitation providers. However, for
the group who were happy with the service they received from rehabilitation providers, the
role of the provider was often pivotal in their return to work. We can learn from this group
how to improve the practice for all workers. In these cases, the rehabilitation provider
assumed an assertive case management role, negotiated with key stakeholders to achieve
consensus on goals, took a role in information dissemination, devised a plan in consultation
with the injured worker and the treating doctor, and followed through on its implementation.
These findings indicate the minimum requirements for effective rehabilitation
provider practice in the complex task of assisting injured workers to return to work in a safe
and timely manner. The current practice arrangements for rehabilitation providers are
problematic and need to be addressed at the pre-practice training, systemic and policy levels.
Clear guidelines for each stakeholder, and clear definition of roles and responsibilities must
also be formulated and/or negotiated on an individual basis to mitigate the competing forces
that appear to be operating within the current system, that serve to undermine the common
goals of occupational rehabilitation.
REFERENCES
Crisson, J. E., & Kneefe, F. J. (1988). The relationship of locus of control to pain
coping strategies and psychological distress in chronic pain patients. Pain, 35, 147-154.
18
Duncan, G. (1996). Is compensation bad for your back? The Australian Journal of
Rehabilitation Counselling, 2 (2). 128-139.
Ehrmann-Feldman, D., Rossignol, M., Abenhaim, L., and Gobeille, D. (1996).
Physician referral to physical therapy in a cohort of workers compensated for low back pain.
Physical Therapy, 76 (2), 150-56.
Edwards, J. R. (1988). The determinants and consequences of coping with stress. In
G. L. Cooper & R. Payne (Eds). Causes, coping and consequences of stress at work.
Chichester: Wiley.
Gardner, J. A. (1991). Early referral and other factors affecting vocational
rehabilitation outcome for the workers’ compensation client. Rehabilitation Counseling
Bulletin, 34 (3), 197-209.
Hart, P. M.., Wearing, A. J., & Headey, B. (1993). Assessing police work
experiences: Development of the Police Daily Hassles and Uplifts Scales. Journal of
Criminal Justice, 21, 553-572.
Kable, S., Kenny, D. T., Kroon, M., Quinn, S., & Edwards, S. (1997). Employer work
and rehabilitation survey 1997. Sydney, NSW: WorkCover Authority of New South Wales.
Kenny, D.T. (1994). Determinants of time lost from workplace injury: The impact of
the injury, the injured, the industry, the intervention and the insurer. International Journal of
Rehabilitation Research, 17 (4), 333-342.
Kenny, D.T. (1995a). Common themes, different perspectives: A systemic analysis of
employer-employee experiences of occupational rehabilitation. Rehabilitation Counseling
Bulletin, 39 (1), 54-77.
Kenny, D.T. (1995b). Failures in occupational rehabilitation: A case study analysis.
Australian Journal of Rehabilitation Counselling, 1 (1), 33-45.
19
Kenny, D.T. (1995c). Case management in occupational rehabilitation: Would the
real case manager please stand up? Australian Journal of Rehabilitation Counselling, 1 (2),
104-117.
Kenny, D. T. (1995d). Patterns of referral to accredited rehabilitation providers and
outcomes of service. Journal of Applied Rehabilitation Counselling,26 (4), 46-52.
Kenny, D. T. (1996). The roles, functions and effectiveness of treating doctors in the
management of occupational injury: Perceptions of key stakeholders. The Australian Journal
of Rehabilitation Counselling, 2 (2), 86-98.
Lechner, D. E. (1994). Work hardening and work conditioning interventions: Do they
affect disability? Physical Therapy, 74 (5), 471-93.
Lusted, M. (1993). Predicting return to work after rehabilitation for low back injury.
Australian Journal of Physiotherapy, 39 (3), 203-1.
Mehler, P. J., & Wodtke, K. H. (1990). A survey of unethical practices in
rehabilitation counseling using the randomized response method. Paper presented at the
Annual Convention of the American Psychological Association, Boston, MA.
Millon, T. (1990). Towards a new personology: An evolutionary model. New York:
Wiley.
Murphy, G. C., Young, A. E., & Vo, K. (1995). Using locus of control to predict the
return-to-work achievements of back-injured occupational rehabilitation clients. The
Australian Journal of Rehabilitation Counselling, 1 (2), 83-92.
Quebec Taskforce on Spinal Disorders (1987). Scientific approach to the assessment
and management of activity-related spinal disorders: A monograph for clinicians. Spine, 12
(Supplement).
Patton, M. Q. (1990). Qualitative evaluation and research methods. London: Sage.
20
Ryan, W. E., Krishna, M. K., and Swanson, C. E. (1995). A prospective study
evaluating early rehabilitation in preventing back pain chronicity in mine workers. Spine, 20
(4), 489-91.
Tarvydas, V. M., & Cottone, R. R. (1991). Ethical responses to legislative,
organizational, and economic dynamics: A four level model of ethical practice. Journal of
Applied Rehabilitation Counselling, 22 (4), 11-18.
Turk, D., & Rudy, T. (1991). Persistent pain and the injured worker: Integrating
biomedical, psychosocial and behavioural factors in assessment. Journal of Occupational
Rehabilitation, 1, 159-179.
WorkCover Authority of New South Wales (1994). Workers’ Compensation
Statistics. Sydney, NSW: Author.
21
Satisfaction with rehabilitation services for 26 injured workers referred to a rehabilitation provider
Rehabilitation services Ratings of satisfaction Very Undecided Satisfied Very Dissatisfied Dissatisfied satisfied
No
%
1
2
3
4
5
Rehabilitation Assessment
14
61
21.5
7
0
57
14.5
Functional Assessment
15
65
13.5
6.5
0
53.5
26.5
Workplace Assessment
15
65
6.5
26.5
0
13.5
53.5
Job Analysis
9
39
22
22
0
33
22.5
Advice Concerning Job Modification
8
35
12.5
50
0
37.5
0
Rehabilitation Counselling
8
35
25
12.5
12.5
25
25
Vocational Assessment
12
52
16.5
16.5
0
50
16.5
Advice or Assistance Concerning Job Seeking
5
22
40
0
20
40
0
Advice/Assistance re Vocational Re-education
11
48
9
9
9
45.5
27.5
Preparation of a Rehabilitation Plan
14
61
14.5
14.5
14.5
43
14.5
Work Conditioning
5
22
0
20
0
60
20
Functional Education
9
39
0
11
11
55.5
22
Monitoring
13
56.5
7.5
15.5
0
61.5
15.5
Aids and Equipment
7
30.5
0
14.5
28.5
14.5
43
Travel
8
35
0
25
25
37.5
37.5
Table 1
22
Table 2
Workers’ Responses to Information Provision by Stakeholders
Yes, the (stakeholder)
RC1
(33.3%)2
TD
(80.1%)
RP
(33.7%)
I
(38.1%)
ID
(44.6%) gave me information/advice on workers' compensation procedures?
50.0
30.5
30.4
29.9
N/A3
gave me information on rehabilitation (and/or rehabilitation procedures)?
68.9
36.1
80.9
14.5
N/A
talked with my treating doctor about suitable duties and/or when I could return to work?
54.5
N/A
52.9
N/A
N/A
talked with my employer or rehabilitation co-ordinator about my injury, suitable duties, and/or when I could return to work?
N/A
30.0
72.1
N/A
N/A
had enough understanding of my workplace/injury to implement the necessary changes to allow me to return to work (eg organising suitable duties)?
55.6
N/A
50.4
N/A
N/A
hae enough time to attend to my needs?
58.2
N/A
63.0
N/A
N/A
showed care, respect and concern for meas an injured worker?
70.4
N/A
77.0
N/A
42.1
had an open mind about the genuineness of my injury?
69.6
N/A
76.3
42.1
36.7
1 RC = Rehabilitation Co-ordinator; TD = Treating Doctor; RP = Rehabilitation Provider; I = Insurer; ID = Insurance Doctor 2 Percentage of the sample (n=407) who had contact with stakeholder 3 Question not asked
23
Table 3 Personnel Consulted by Injured Workers (IWs) and Satisfaction with the Consultation (in percentages) Personnel
Number of Injured Workers
Unhappy
No Opinion
Happy
Treating doctor
326
4.1
4.4
91.5
Nominated medical specialist(s)
198
9.2
7.2
83.6
First aid officer
138
11.6
11.6
76.8
Solicitor
120
10.3
13.8
75.9
Physiotherapist
234
12.1
13
74.9
Occupational health nurse
118
15.4
10.3
74.3
Industry/union representative
86
19
10.7
70.3
Rehabilitation provider
137
21.5
11.1
67.4
Psychologist
47
21.7
17.4
60.9
Rehabilitation co-ordinator
136
29.6
12
58.4
Company doctor
181
30.6
11.7
57.7
Financial or family counsellor
12
30
20
50
Insurance investigator
28
44.4
22.3
33.3
Insurance doctor(s)
182
50.3
20.3
29.4

24
Table 4
Employer Reasons for Referring Injured Workers to Rehabilitation Providers (N = 427)
Reason
Total(%)
referred
Size of employer
1-20
21-100
101-500
501+
Length of time off work
73.1
72.2
74.2
73.2
72.9 No suitable duties
37.0
42.3
33.3
33.1
42.1
When a person needs retraining
40.0
30.7
36.5
36.0
50.0
When an employee requests referral
35.6
21.2
29.0
33.1
47.9
Severity of injury
72.1
61.5
64.5
74.6
78.6
Other
26.9
19.2
28.0
28.2
27.9




















