Pharmacy Providers
41
April 2003 # 03-3 Kansas ansas ansas ansas Medical edical edical edical Assistance ssistance ssistance ssistance Programs rograms rograms rograms is the fiscal agent and administrator of the Kansas Medicaid Program for the Kansas Department of Social and Rehabilitation Services PREFERRED DRUG LIST – THIRD LISTING The third round of Preferred Drugs will become effective May 9, 2003. New prescriptions for non-preferred drugs will require prior authorization as of May 9, 2003. Dispense as written prescriptions, and existing refills on non-preferred drugs will override prior authorization requirements until date of service July 1, 2003. Physicians are encouraged not to use the dispense as written override unless there is a medical necessity for a non- preferred drug. If a non-preferred drug is prescribed without a DAW, written documentation will be required from the prescribing physician for consideration. The table(s) indicating preferred and non-preferred drugs within the therapeutic classes can be found in Appendix II of the Pharmacy Provider Manual. Prior authorization will be granted for one (1) year. Prior Authorization Request forms (which may be duplicated) have been updated since the initial mailing. Please use these new forms found in Appendix III of the Pharmacy Provider Manual or via the website listed below. Prior authorization forms may also be obtained by calling the Prior Authorization Unit at 1-800-285-4978. The non-preferred drug MUST be requested on the appropriate Prior Authorization Request form. Each form is specific for each group. Otherwise, these forms will be returned to the sender without initiation of the Prior Authorization process. Thank you for your cooperation and assistance. Request Forms Website: http://www.srskansas.org/hcp/medicalpolicy/pharmacy/ ___________________________________ PHARMACY PROVIDERS Policy and Procedure Update If you have any questions, please contact the Medical Assistance Customer Service Center at 1-800-933-6593 (in-state providers) or (785) 274-5990 between 7:30 a.m. - 5:30 p.m., Monday through Friday. Bulletins and manuals constitute proof of notification of program changes to Kansas Medical Assistance providers. Please read these publications carefully and keep them for future reference. BULLETIN
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Pharmacy Providers

April 2003 # 03-3
KKKKansas ansas ansas ansas MMMMedical edical edical edical AAAAssistance ssistance ssistance ssistance PPPProgramsrogramsrogramsrograms
P
The third round ofor non-preferredwritten� prescripauthorization reqnot to use the �dpreferred drug. Iwill be required preferred and nonof the Pharmacy P Prior authorizatio Prior Authorizatiinitial mailing. PManual or via thecalling the Prior A The non-preferrRequest form. Ereturned to the s Thank you for yo Request Forms W
BU
LL
ET
IN
If you have any 1-800-933-6593 Monday through Bulletins and mMedical Assistafor future refere
BU
LL
ET
IN
PHARMACY PROVIDERSPolicy and Procedure Update
is the fiscal agent and administrator of the Kansas Medicaid Program for the Kansas Department of Social and Rehabilitation Services
REFERRED DRUG LIST – THIRD LISTING
f Preferred Drugs will become effective May 9, 2003. New prescriptions drugs will require prior authorization as of May 9, 2003. �Dispense as tions, and existing refills on non-preferred drugs will override prior uirements until date of service July 1, 2003. Physicians are encouraged ispense as written� override unless there is a medical necessity for a non-
f a non-preferred drug is prescribed without a DAW, written documentation from the prescribing physician for consideration. The table(s) indicating -preferred drugs within the therapeutic classes can be found in Appendix II rovider Manual.
n will be granted for one (1) year.
on Request forms (which may be duplicated) have been updated since the lease use these new forms found in Appendix III of the Pharmacy Provider website listed below. Prior authorization forms may also be obtained by uthorization Unit at 1-800-285-4978.
ed drug MUST be requested on the appropriate Prior Authorization ach form is specific for each group. Otherwise, these forms will be ender without initiation of the Prior Authorization process.
ur cooperation and assistance.
ebsite: http://www.srskansas.org/hcp/medicalpolicy/pharmacy/
___________________________________
questions, please contact the Medical Assistance Customer Service Center at(in-state providers) or (785) 274-5990 between 7:30 a.m. - 5:30 p.m.,
Friday.
anuals constitute proof of notification of program changes to Kansasnce providers. Please read these publications carefully and keep themnce.

MARCH 2003 PAGE TWO
PROSPECTIVE DRUG UTILIZATION REVIEW (PRO-DUR) CHANGE Claims processed as of May 1, 2003, will begin auto-denying the Pro-DUR edit, Above Maximum Dose. The �Above Maximum Dose� edit occurs when the daily dose is greater than the recommended maximum dose for a beneficiary�s age. Providers may override the �Above Maximum Dose� edit if the patient meets the State-specified criteria by utilizing a combination of select NCPDP DUR Conflict, Intervention and Outcome Codes listed below: Criteria – Physician contacted and approved dose. DUR Conflict, Intervention and Outcome Codes – HD, M0 and 1G The provider must maintain documentation of override reason and codes. It is recommended this documentation is kept on the original prescription. For further details on auto-deny Pro-DUR edits, reference Section 8400 under �Prospective Drug Utilization Review� of the Pharmacy Provider Manual. ___________________________________ LIMIT OF 5 SINGLE-SOURCE PRESCRIPTION CLAIMS PER CALENDAR
MONTH
The limit of 5 single-source prescription claims per calendar month has been in effect as of April 1, 2003. Since then, many questions have been raised regarding this policy. Below are several clarifications for providers:
• Documentation of �Medical Necessity� is good for up to six (6) months. • The form in the March 2003 bulletin is an example and does NOT have to be used. Providers may
develop their own form, document the information on the back of the prescription or use any other means of documenting the �Medical Necessity� information.
• Providers may use one form documenting �Medical Necessity� for several of a beneficiary�s scheduled medications
• Every single-source prescription claim (except for the exclusions specifically outlined in the policy and in the March 2003 Bulletin) filled for a beneficiary within the same calendar month will count towards the limitation.
• Drug Utilization Review (DUR) edits take precedence over this edit. Therefore, if a beneficiary�s claim sets this edit and a DUR auto-deny edit, the provider must try and resolve the highest-ranking auto-deny DUR edit. If the patient does not meet the criteria to override the highest-ranking DUR edit, then the beneficiary may pay for the medication out-of-pocket.

MARCH 2003 PAGE THREE • The NCPDP Reject Code that appears when reaching this limit is �76� or �Plan Limitations
Exceeded�. • Even though the provider uses the NCPDP DUR Conflict Code of �AD� to override the 5 single-
source prescription claims per calendar month edit, KMAP does NOT send this Conflict Code value to providers in the NCPDP DUR Response area.
• Providers submitting claims on paper must document the �AD� override code in the �Remarks� section (field 16) on the paper claim form. The provider must link the line number to the code.
• Providers submitting via EMC may only resolve this edit issue via a paper claim form or POS. • There is NOT a list of NDCs considered single-source, multi-source or excluded. Providers may
contact the medical assistance number 1-800-933-6593 to inquire about an NDC. • NDCs may move back and forth between single-source, multi-source and excluded at any time.
PRIOR AUTHORIZATION OF COX II INHIBITORS
The Prior Authorization requirements for COX II Inhibitors are NOT related to the Preferred Drug List. All COX II Inhibitors for beneficiaries under the age of 65 require Prior Authorization. The COX II Inhibitors are not covered for Medikan beneficiaries.
FEDERAL UPPER LIMIT CHANGES
Effective with dates-of-service on and after May 11, 2003, the following products will have FUL changes from their current FUL pricing: Deletions: Desoximetasone 0.25%, Cream Diflunisal 500mg, Tabs Theophylline 100mg, Tabs, E.R. Theophylline 200mg, Tabs, E.R. Increases: Amiloride HCl; HCTZ 5mg/50mg, Tabs 0.06750 Amitriptyline HCl 150mg, Tabs 0.24300 Ampicillin/Ampicillin Trihydrate 250mg, Caps 0.17360 Ampicillin/Ampicillin Trihydrate 500mg, Caps 0.29910 Benzonatate 100mg, Caps 0.43870 Bumetanide 1mg, Tabs 0.28140 Bumetanide 2mg, Tabs 0.47080 Cholestyramine Light 4gm Resin, Packet 1.27670 Cholestyramine 4gm Resin, Packet 1.27670 Minocycline 50mg, Caps 0.90000 Minocycline 100mg, Caps 1.80000 Tolazamine 250mg, Tabs 0.40050 Verapamil 240mg, Tabs, E.R. 0.43500

MARCH 2003 PAGE FOUR Decreases: Amiodarone 200mg, Tabs 1.68750 Hydroxyzine Pam 50mg, Caps 0.10130 Methocarbamol 500mg, Tabs 0.19430
MAXIMUM ALLOWABLE COST (MAC) CHANGES The following MAC prices are effective for claims with dates-of-service on and after May 23, 2003. The prices may be a decrease (D), an increase (I) and/or new (N). Increases and/or decreases may be related to previous MAC or FUL prices. Refer to section 8400 of the Pharmacy Provider Manual under �Pharmacy Pricing� for additional reimbursement information. Amiodarone 200mg, Tabs 0.58000 D/N *
Amitriptyline 10mg, Tabs 0.04900 D/N Amitriptyline 25mg, Tabs 0.05300 D/N Amitriptyline 75mg, Tabs 0.11200 D/N Amphetamine Salt Mixture, 5mg, Tabs 1.12000 N Amphetamine Salt Mixture, 10mg, Tabs 1.12000 N Amphetamine Salt Mixture, 20mg, Tabs 1.12000 N Amphetamine Salt Mixture, 30mg, Tabs 1.12000 N Atenolol 25mg, Tabs 0.08200 D/N Benzonatate 100mg, Caps 0.28000 D/N * Cefadroxil 500mg, Caps 0.98000 D Clonidine 0.1mg, Tabs 0.07000 D/N Clonidine 0.2mg, Tabs 0.11200 D/N Clonidine 0.3mg, Tabs 0.14000 D/N Desoximetasone 0.25%, Cm, Gm 1.03000 N* Desoximetasone 0.25%, Oint, less than 60 Gms 1.20000 I Desoximetasone 0.25%, Oint, 60 Gms or greater 1.00000 I Furosemide 80mg, Tabs 0.09400 D/N Gemfibrozil 600mg, Tabs 0.30300 D/N Hydralazine 25mg, Tabs 0.05600 N Hydrocortisone 1%, Lotion 0.04000 D/N Hydroxyzine Pamoate 25mg, Caps 0.07000 D/N Hydroxyzine Pamoate 50mg, Caps 0.08400 D/N * Labetalol 100mg, Tabs 0.21000 D Labetalol 200mg, Tabs 0.33600 I Labetalol 300mg, Tabs 0.53200 I Lovastatin 10mg, Tabs 0.58000 D Lovastatin 20mg, Tabs 1.05000 D Lovastatin 40mg, Tabs 1.75000 D Methylprednisolone 4mg, Tabs 0.16800 D/N Methocarbamol 500mg, Tabs 0.15400 D/N * Methocarbamol 750mg, Tabs 0.28000 N Minocycline 100mg, Caps 1.40000 D/N *

MARCH 2003 PAGE FIVE
Naproxen 500mg, Tabs 0.12600 D/N Penicillin V Potassium 250mg/5ml, 200ml 0.02100 N Prednisone 5mg, Tabs 0.03400 N Prednisone 10mg, Tabs 0.04200 N Prednisone 20mg, Tabs 0.07000 N Propranolol 20mg, Tabs 0.06300 D/N
Propranolol/HCTZ 40/25mg, Tabs 0.08100 D/N Propranolol/HCTZ 80/25mg, Tabs 0.12100 D/N
Selenium Sulfide 2.5%, Lotion 0.03500 D/N Sulindac 200mg, Tabs 0.42000 D/N Tamoxifen 10mg, Tabs 0.54000 N Tamoxifen 20mg, Tabs 0.54000 N Theophylline 300mg, ER, Tabs 0.19600 N Thioradazine 10mg, Tabs 0.16800 I Thiothixene 1mg, Caps 0.11200 D/N Triamcinolone 0.1%, Paste 1.15000 N Valproic Acid 250mg, Caps 0.14000 D/N Verapamil 80mg, Tabs 0.07000 D/N * Price is affected by FUL change 5/11/2003, and will return to MAC pricing 5/23/2003. The most recent 2003 MAC and FUL price changes will be updated in Appendix I of the Pharmacy Provider Manual at a later date.
RETROACTIVE PRICE INCREASE - CYCLOBENZAPRINE 10MG TABS
On April 21, 2003, cyclobenzaprine 10mg was removed from FUL pricing of 0.08580 per tablet to a MAC price of 0.22000 per tablet EFFECTIVE FOR CLAIMS WITH DATES-OF-SERVICE ON AND AFTER APRIL 1, 2003. If you submitted claims for cyclobenzaprine 10mg tablets between April 1, 2003 and April 21, 2003, you may submit an adjustment for each claim.
PHARMACY PROVIDER MANUAL REVISIONS Remove: Replace With:
8-15 to 8-18 8-15 to 8-20 AI-1 to AI-26 AI-1 to AI-26 AII-1 AII-1


8400. Prospective Drug Utilization Review (PDUR) Kansas Medicaid is required through OBRA to perform PDUR. An incoming pharmacy claim goes through certain checks within the pharmacy system to determine if any potential problems exist by dispensing a medication. That information is then returned to the provider. The provider utilizes this information to determine the best course of therapy for the patient. In the past the PDUR edits only reported to the provider. As of October 2, 2000, Kansas Medicaid has PDUR edits that pay-but-report and auto-deny claims. For purposes of simplification, only the auto-deny DUR edits are discussed. A list of the pay-but-report edits can be obtained by contacting the Kansas Medicaid Provider Assistance Unit. Auto Deny DUR Edits: (These edits are in hierarchy order.)
PPI (Proton Pump Inhibitors) Acute Dosing Exceeds 60 Days: DUR auto-deny edit occurring when a patient�s Proton Pump Inhibitor (PPI) dosing is at or above acute dosing for greater than 60 days. Prior Authorization (PA) is required to continue at or above acute dosing. NOTE: If daily PPI dose is lowered to a maintenance dose, this edit will not post.
Exceeds 34 Days Supply: DUR edit that will auto-deny when the days supply on the current claim is greater than 34 days.
Refill Too Soon: DUR edit that will auto-deny when the same medication has been filled by the SAME provider and less than 80% of supply has been used.
Duplicate Therapy: DUR edit that will auto-deny when the same medication has been previously filled by ANOTHER provider and less than 80% of supply has been used.
Pregnancy Category X Drug With 650 (Pregnancy) Diagnosis: DUR edit that will auto-deny when claim for drug that is a category X is submitted for a female consumer who has a pregnancy diagnosis code in claims history within the past 280 days. Above Maximum Dose This DUR edit occurs when the daily dose is greater than the recommended maximum dose for the beneficiary's age.
Therapeutic Duplication: DUR edit that will auto-deny when a prescription is filled within 80% of the remaining supply of another prescription which is considered therapeutically equivalent by Kansas Medicaid. Including: (a) H2 Antagonists vs. PPIs (b) NSAIDS vs. Cox II Inhibitors
_________________________________
PHARMACY PROVIDER MANUAL 04/03 BENEFITS & LIMITATIONS
8-15

8400. Allowed Exceptions for Auto-Deny DUR Edits:
In order to override an auto-deny DUR edit, the provider must determine if the prescription meets the criteria in the following chart for the highest ranking edit listed in order under �Auto-Deny DUR Edits�. Patients that do not meet the criteria for the highest ranking auto-deny edit set may pay for the medication out-of-pocket. The provider must maintain documentation for the reason the denial was overridden and input the proper override values on the claim in the NCPDP DUR Conflict, Intervention, and Outcome fields.
NOTE: Overrides are not allowed for stolen or vacation medications.
DUR Edit Allowed Exceptions
Above Maximum Dose � Physician contacted and has approved dosage Duplicate Therapy * Therapy change, all consumers
* Lost/spilled medications, KBH ONLY
Exceeds 34 Day Supply * A single unit dispensed (such as Depo Provera® at 150 mg) exceeds 34 days.
* A child�s school requires a separate medication suppply * Primary insurance requires more than a 34 day supply to be
dispensed, AND the primary made a payment. (In this case if the other insurance makes a payment, then the system will automatically override this DUR edit.)
Pregnancy Category X * Patient is not pregnant
* Physician and patient are aware of the drug�s teratogenic effects and authorization to dispense has been given after the pharmacist consults with the physician.
Refill Too Soon * Therapy change, all consumers
* Lost/spilled medications, KBH ONLY
Therapeutic Duplication * Drug/dosage change verified by the physician Guidelines To Help Identify DUR Edits: Claims setting DUR edits can auto-deny and/or pay-but-report. Any set will return pertinent information to the provider, including the DUR Conflict Code, in the DUR Response Data fields. Providers can receive up to three edits in this area. The first edit returned to the provider in the DUR Response Data fields is considered the most significant. If more than three DUR edits set on a claim, the provider�s DUR Overflow indicator is populated. In this case the provider may contact the Provider Assistance Unit for further DUR information. Also, any auto-deny edit set will cause an NCPDP Reject Code to be returned to the provider. This reject code along with the DUR Response Data and Conflict Code helps a provider determine what edit set. ________________________________ PHARMACY PROVIDER MANUAL 04/03 BENEFITS & LIMITATIONS 8-16
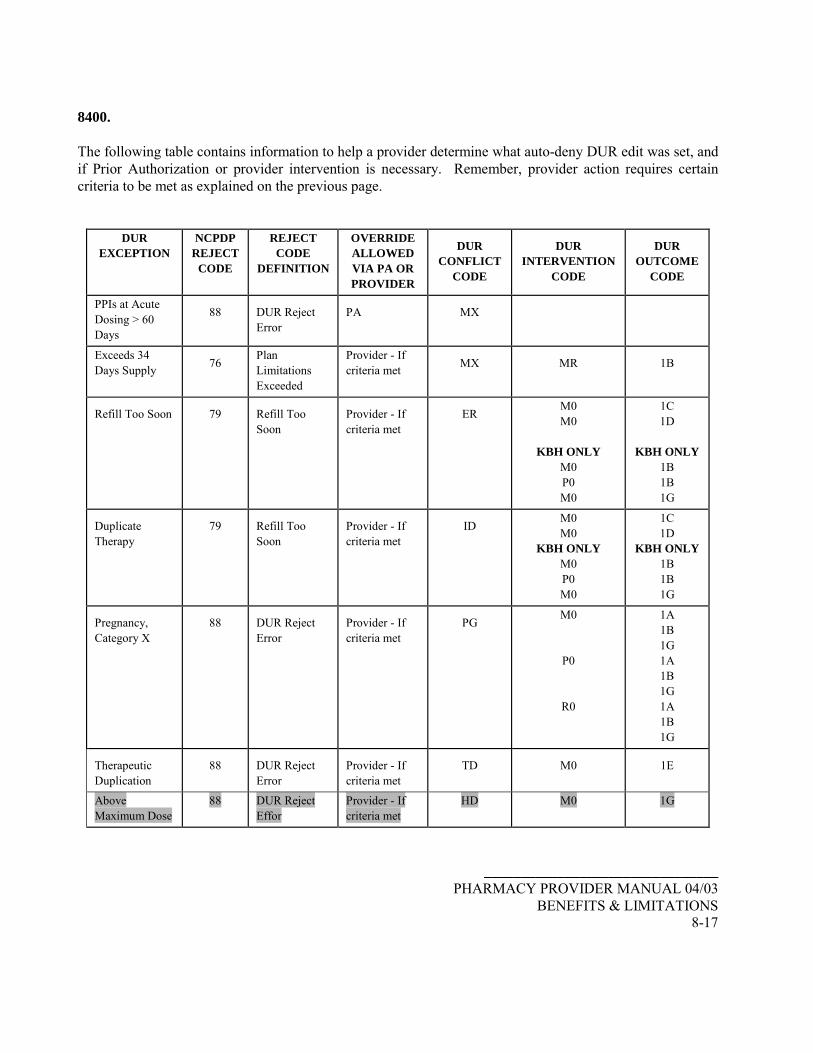
8400. The following table contains information to help a provider determine what auto-deny DUR edit was set, and if Prior Authorization or provider intervention is necessary. Remember, provider action requires certain criteria to be met as explained on the previous page.
DUR EXCEPTION
NCPDP REJECT
CODE
REJECT CODE
DEFINITION
OVERRIDE ALLOWED VIA PA OR PROVIDER
DUR
CONFLICT CODE
DUR
INTERVENTION CODE
DUR
OUTCOME CODE
PPIs at Acute Dosing > 60 Days
88
DUR Reject Error
PA
MX
Exceeds 34 Days Supply
76
Plan Limitations Exceeded
Provider - If criteria met
MX
MR
1B
Refill Too Soon
79
Refill Too Soon
Provider - If criteria met
ER
M0 M0
KBH ONLY
M0 P0 M0
1C 1D
KBH ONLY
1B 1B 1G
Duplicate Therapy
79
Refill Too Soon
Provider - If criteria met
ID
M0 M0
KBH ONLY M0 P0 M0
1C 1D
KBH ONLY 1B 1B 1G
Pregnancy, Category X
88
DUR Reject Error
Provider - If criteria met
PG
M0
P0
R0
1A 1B 1G 1A 1B 1G 1A 1B 1G
Therapeutic Duplication
88
DUR Reject Error
Provider - If criteria met
TD
M0
1E
Above Maximum Dose
88 DUR Reject Effor
Provider - If criteria met
HD M0 1G
________________________________ PHARMACY PROVIDER MANUAL 04/03
BENEFITS & LIMITATIONS 8-17

8400. Benefits Non-Covered:
The consumer is allotted money for miscellaneous expenditures within their monthly budget; consequently, some pharmacy items are not covered. The following represent examples of items that are not covered:
$ Medical supplies (as determined by FDA) $ Over-the-counter laxatives and stool softeners $ Over-the-counter nutritional supplements such as vitamins and minerals $ Routine feminine hygiene products $ Topical antiseptic and first aid preparations
Therapeutic categories generally not covered are drugs are:
DESI less-than-effective drugs and their Identical, Related, and Similar (IRS) drugs $ Benzodiazepines $ Cosmetic purposes $ Symptomatic relief of cough and colds $ Drugs designated by the Secretary of Health and Human Services $ Drugs with a manufacturer imposed restricted distribution system which requires the
additional purchase of associated tests or services from the manufacturer or its designee
$ Promotion of fertility $ Gender-specific medications if prescribed to the gender for which they are not FDA-
approved or medically necessary $ Hair growth $ Non legend (OTC) $ Weight reduction with exception of those requiring prior authorization $ Weight gain
_________________________________ PHARMACY PROVIDER MANUAL 04/03 BENEFITS & LIMITATIONS 8-18

8400
SINGLE-SOURCE PERSCRIPTION CLAIM LIMITATIONS Effective with DOS on or after April 1, 2003, there will be a limit of 5 single-source prescription drug claims allowed per beneficiary per calendar month. The following will be excluded from the limit edit: KBH beneficiaries Antiretroviral drugs State-specified anti-rejection drugs used for transplant patients State-specified anti-emetics State-specified chemotherapy drugs Interferons Immune Globulins Antihemophilic drugs Atypical antipsychotics All covered contraceptives All compound drug (until October 2003) Note: All prescriptions for insulin, Levothroid® , Synthroid® and Levoxyl® will price as single-source but be counted as multi-source for this policy (therefore, they are excluded from this edit). Note: PRESCRIPTION LIMIT OVERRIDE CODE AND CRITERIA Pharmacists should submit the prescription limit override code if:
1) Medical necessity from physician 2) The monthly prescription limit has been met
If a beneficiary meets the above criteria, the pharmacy provider should enter the “AD” DUR conflict code. No intervention and outcome codes are necessary. If a claim denies for DUR and this edit, the DUR takes precedence. In this case, the provider must see if the patient meets the criteria to override the highest-ranking DUR edit set on the claim. If so, the provider may override with the appropriate DUR override codes and document this intervention. If not, then the beneficiary may pay for the medication out-of-pocket. Pharmacists must not use the override code for a prescription until after the monthly prescription limit has been reached and medical necessity has been shown. Pharmacists will be audited for appropriate utilization of the prescription limit override code (“AD”).
_________________________________ PHARMACY PROVIDER MANUAL 04/03
BENEFITS & LIMITATIONS 8-19

8400 The limit of 5 single-source prescription claims per calendar month has been in effect as of April 1, 2003. Since then, many questions have been raised regarding this policy. Below are several clarifications for providers:
• Documentation of �Medical Necessity� is good for up to six (6) months. • The form in the March 2003 bulletin does NOT have to be used. This is an example providers may
use. Or, providers may develop their own form, document the information on the back of the prescription or use any other means of documenting the �Medical Necessity� information.
• Providers may use one form documenting �Medical Necessity� for several of a beneficiary�s scheduled medications. If a new single-source prescription claim is requested and denies for this edit, the provider must get �Medical Necessity� documentation. KEEP IN MIND the �blanket� form with �Medical Necessity� may be used ONLY for the patients regularly scheduled medications.
• Any time a single-source prescription claim is filled for a beneficiary within the same calendar month, regardless of if it is a refill or not, will count towards the limitation.
• The NCPDP Reject Code that appears when reaching this limit is �76� or �Plan Limitations Exceeded�.
• Drug Utilization Review (DUR) edits take precedence over this edit. Therefore, if a beneficiary�s claim sets this edit and a DUR auto-deny edit, the provider must try and resolve the highest-ranking auto-deny DUR edit. If the patient does not meet the criteria to override the highest-ranking DUR edit, then the beneficiary may pay for the medication out-of-pocket.
• Even though the provider uses the NCPDP DUR Conflict Code of �AD� to override the 5 single-source prescription claims per calendar month edit, KMAP does NOT send this Conflict Code value to providers in the NCPDP DUR Response area.
• Providers submitting claims on paper must document the �AD� override code in the �Remarks� section (field 16) on the paper claim form. The provider must link the line number to the code.
• Providers submitting via EMC may only resolve this edit issue via a paper claim form or POS. • There is NOT a list of NDCs considered single-source, multi-source or excluded. Providers may
contact the Medical Assistance Customer Service Center at 1-800-933-6593 (between 7:30 A.M & 5:30 P.M.) to inquire about an NDC.
• NDCs may move back and forth between single-source, multi-source and excluded at any time.
_________________________________ PHARMACY PROVIDER MANUAL 04/03 BENEFITS & LIMITATIONS 8-20
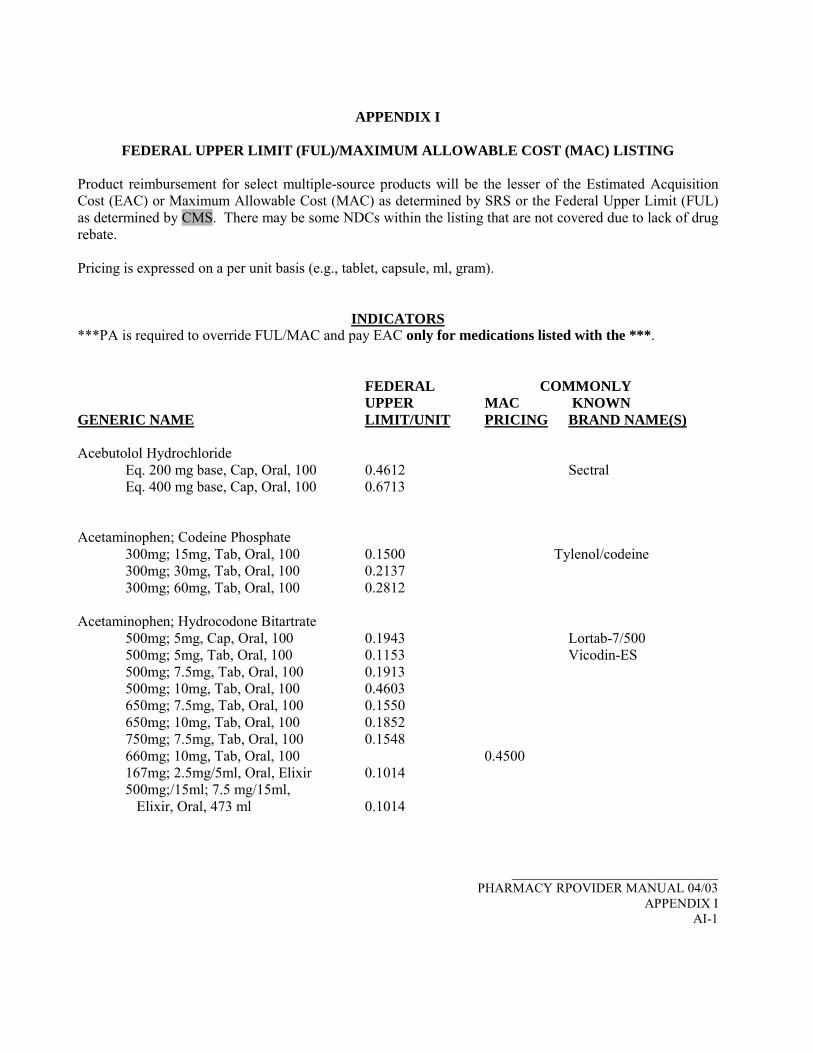
APPENDIX I
FEDERAL UPPER LIMIT (FUL)/MAXIMUM ALLOWABLE COST (MAC) LISTING Product reimbursement for select multiple-source products will be the lesser of the Estimated Acquisition Cost (EAC) or Maximum Allowable Cost (MAC) as determined by SRS or the Federal Upper Limit (FUL) as determined by CMS. There may be some NDCs within the listing that are not covered due to lack of drug rebate. Pricing is expressed on a per unit basis (e.g., tablet, capsule, ml, gram).
INDICATORS ***PA is required to override FUL/MAC and pay EAC only for medications listed with the ***.
FEDERAL COMMONLY UPPER MAC KNOWN
GENERIC NAME LIMIT/UNIT PRICING BRAND NAME(S) Acebutolol Hydrochloride
Eq. 200 mg base, Cap, Oral, 100 0.4612 Sectral Eq. 400 mg base, Cap, Oral, 100 0.6713
Acetaminophen; Codeine Phosphate
300mg; 15mg, Tab, Oral, 100 0.1500 Tylenol/codeine 300mg; 30mg, Tab, Oral, 100 0.2137 300mg; 60mg, Tab, Oral, 100 0.2812
Acetaminophen; Hydrocodone Bitartrate
500mg; 5mg, Cap, Oral, 100 0.1943 Lortab-7/500 500mg; 5mg, Tab, Oral, 100 0.1153 Vicodin-ES 500mg; 7.5mg, Tab, Oral, 100 0.1913 500mg; 10mg, Tab, Oral, 100 0.4603 650mg; 7.5mg, Tab, Oral, 100 0.1550 650mg; 10mg, Tab, Oral, 100 0.1852 750mg; 7.5mg, Tab, Oral, 100 0.1548 660mg; 10mg, Tab, Oral, 100 0.4500 167mg; 2.5mg/5ml, Oral, Elixir 0.1014 500mg;/15ml; 7.5 mg/15ml, Elixir, Oral, 473 ml 0.1014
_______________________________ PHARMACY RPOVIDER MANUAL 04/03
APPENDIX I AI-1
FEDERAL COMMONLY UPPER MAC KNOWN
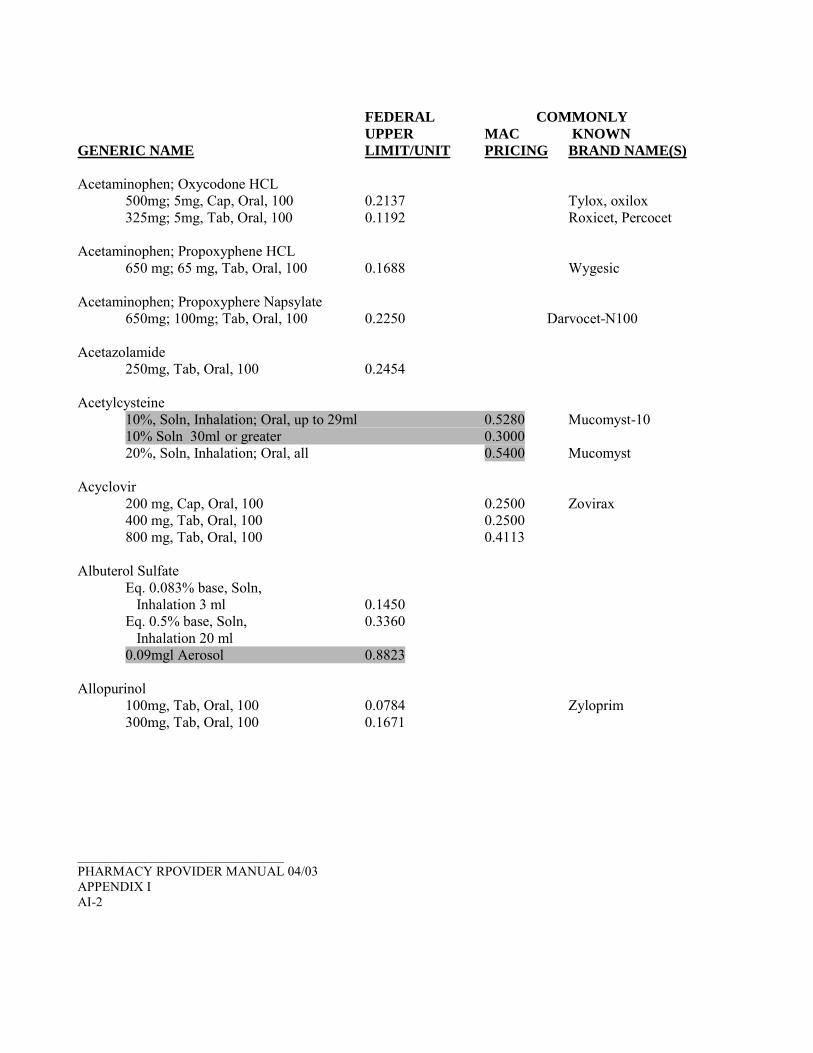
GENERIC NAME LIMIT/UNIT PRICING BRAND NAME(S) Acetaminophen; Oxycodone HCL
500mg; 5mg, Cap, Oral, 100 0.2137 Tylox, oxilox 325mg; 5mg, Tab, Oral, 100 0.1192 Roxicet, Percocet
Acetaminophen; Propoxyphene HCL
650 mg; 65 mg, Tab, Oral, 100 0.1688 Wygesic Acetaminophen; Propoxyphere Napsylate
650mg; 100mg; Tab, Oral, 100 0.2250 Darvocet-N100 Acetazolamide
250mg, Tab, Oral, 100 0.2454 Acetylcysteine
10%, Soln, Inhalation; Oral, up to 29ml 0.5280 Mucomyst-10 10% Soln 30ml or greater 0.3000 20%, Soln, Inhalation; Oral, all 0.5400 Mucomyst
Acyclovir
200 mg, Cap, Oral, 100 0.2500 Zovirax 400 mg, Tab, Oral, 100 0.2500 800 mg, Tab, Oral, 100 0.4113
Albuterol Sulfate
Eq. 0.083% base, Soln, Inhalation 3 ml 0.1450 Eq. 0.5% base, Soln, 0.3360 Inhalation 20 ml 0.09mgl Aerosol 0.8823
Allopurinol
100mg, Tab, Oral, 100 0.0784 Zyloprim 300mg, Tab, Oral, 100 0.1671
_______________________________ PHARMACY RPOVIDER MANUAL 04/03 APPENDIX I AI-2
FEDERAL COMMONLY UPPER MAC KNOWN
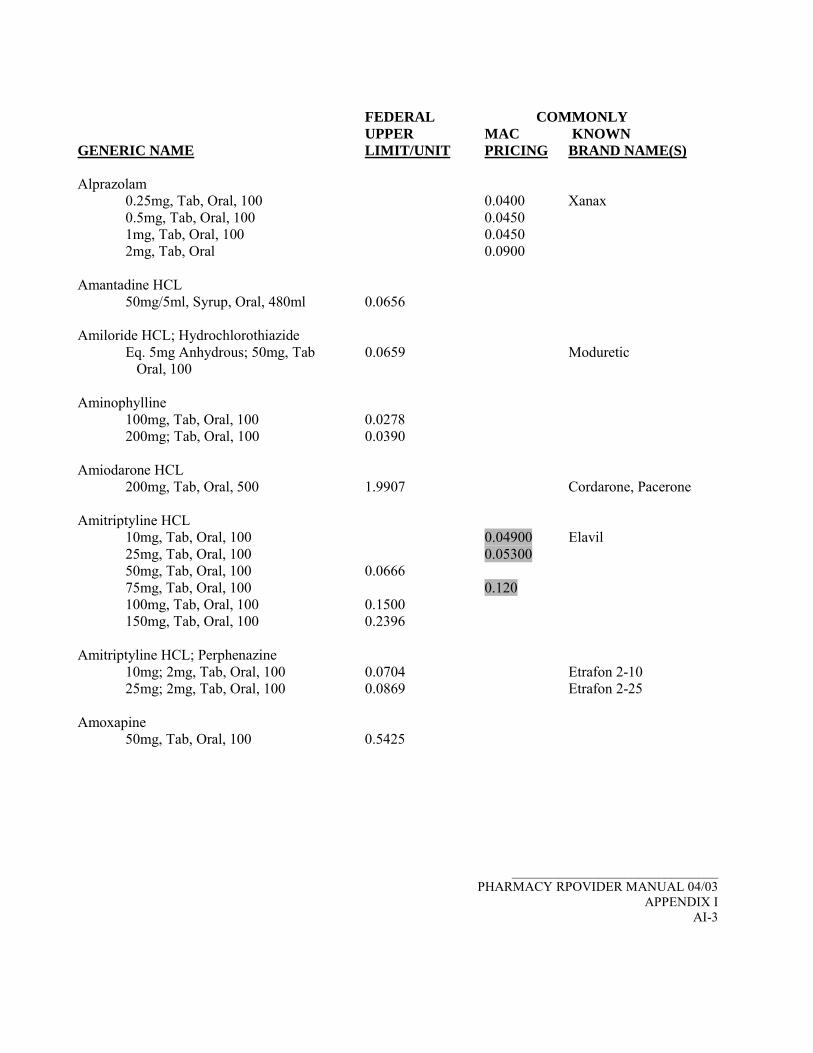
GENERIC NAME LIMIT/UNIT PRICING BRAND NAME(S) Alprazolam
0.25mg, Tab, Oral, 100 0.0400 Xanax 0.5mg, Tab, Oral, 100 0.0450 1mg, Tab, Oral, 100 0.0450 2mg, Tab, Oral 0.0900
Amantadine HCL
50mg/5ml, Syrup, Oral, 480ml 0.0656 Amiloride HCL; Hydrochlorothiazide
Eq. 5mg Anhydrous; 50mg, Tab 0.0659 Moduretic Oral, 100
Aminophylline
100mg, Tab, Oral, 100 0.0278 200mg; Tab, Oral, 100 0.0390
Amiodarone HCL
200mg, Tab, Oral, 500 1.9907 Cordarone, Pacerone Amitriptyline HCL
10mg, Tab, Oral, 100 0.04900 Elavil 25mg, Tab, Oral, 100 0.05300 50mg, Tab, Oral, 100 0.0666 75mg, Tab, Oral, 100 0.120 100mg, Tab, Oral, 100 0.1500 150mg, Tab, Oral, 100 0.2396
Amitriptyline HCL; Perphenazine
10mg; 2mg, Tab, Oral, 100 0.0704 Etrafon 2-10 25mg; 2mg, Tab, Oral, 100 0.0869 Etrafon 2-25
Amoxapine
50mg, Tab, Oral, 100 0.5425
_______________________________
PHARMACY RPOVIDER MANUAL 04/03 APPENDIX I
AI-3
FEDERAL COMMONLY UPPER MAC KNOWN
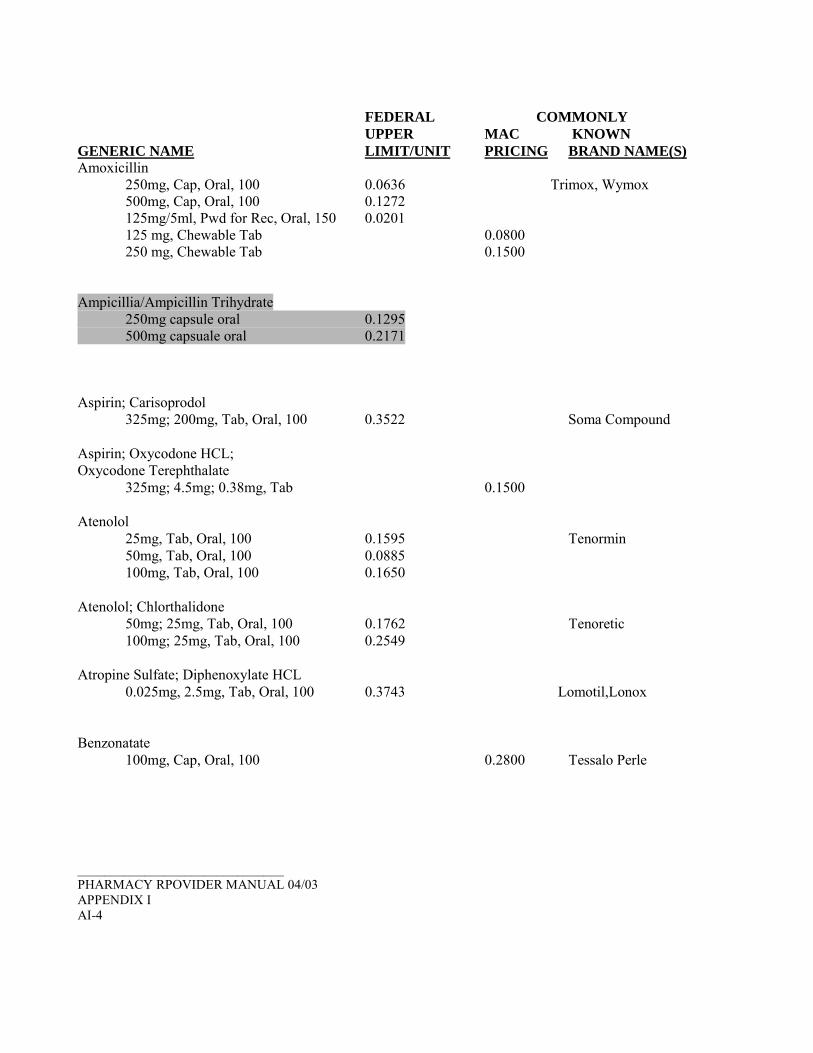
GENERIC NAME LIMIT/UNIT PRICING BRAND NAME(S) Amoxicillin
250mg, Cap, Oral, 100 0.0636 Trimox, Wymox 500mg, Cap, Oral, 100 0.1272 125mg/5ml, Pwd for Rec, Oral, 150 0.0201 125 mg, Chewable Tab 0.0800 250 mg, Chewable Tab 0.1500
Ampicillia/Ampicillin Trihydrate 250mg capsule oral 0.1295 500mg capsuale oral 0.2171
Aspirin; Carisoprodol
325mg; 200mg, Tab, Oral, 100 0.3522 Soma Compound Aspirin; Oxycodone HCL; Oxycodone Terephthalate
325mg; 4.5mg; 0.38mg, Tab 0.1500 Atenolol
25mg, Tab, Oral, 100 0.1595 Tenormin 50mg, Tab, Oral, 100 0.0885 100mg, Tab, Oral, 100 0.1650
Atenolol; Chlorthalidone
50mg; 25mg, Tab, Oral, 100 0.1762 Tenoretic 100mg; 25mg, Tab, Oral, 100 0.2549
Atropine Sulfate; Diphenoxylate HCL
0.025mg, 2.5mg, Tab, Oral, 100 0.3743 Lomotil,Lonox Benzonatate
100mg, Cap, Oral, 100 0.2800 Tessalo Perle _______________________________ PHARMACY RPOVIDER MANUAL 04/03 APPENDIX I AI-4
FEDERAL COMMONLY UPPER MAC KNOWN
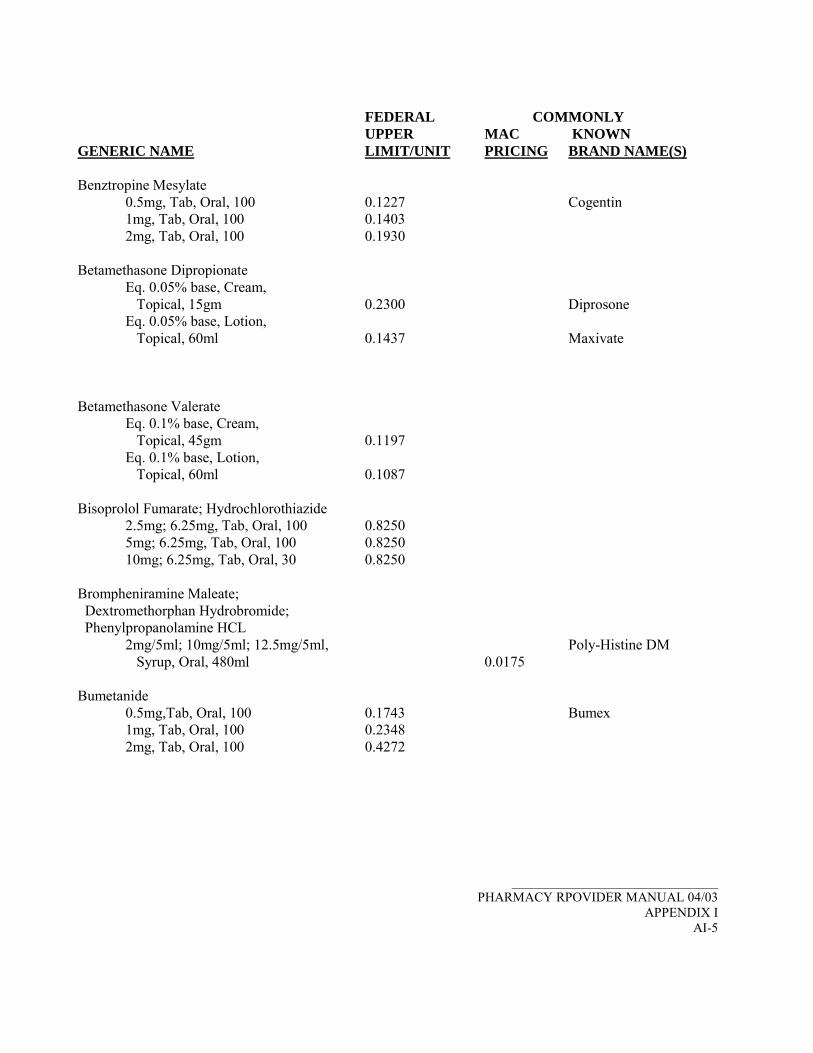
GENERIC NAME LIMIT/UNIT PRICING BRAND NAME(S) Benztropine Mesylate
0.5mg, Tab, Oral, 100 0.1227 Cogentin 1mg, Tab, Oral, 100 0.1403 2mg, Tab, Oral, 100 0.1930
Betamethasone Dipropionate
Eq. 0.05% base, Cream, Topical, 15gm 0.2300 Diprosone Eq. 0.05% base, Lotion, Topical, 60ml 0.1437 Maxivate
Betamethasone Valerate
Eq. 0.1% base, Cream, Topical, 45gm 0.1197 Eq. 0.1% base, Lotion, Topical, 60ml 0.1087
Bisoprolol Fumarate; Hydrochlorothiazide
2.5mg; 6.25mg, Tab, Oral, 100 0.8250 5mg; 6.25mg, Tab, Oral, 100 0.8250 10mg; 6.25mg, Tab, Oral, 30 0.8250
Brompheniramine Maleate; Dextromethorphan Hydrobromide; Phenylpropanolamine HCL
2mg/5ml; 10mg/5ml; 12.5mg/5ml, Poly-Histine DM Syrup, Oral, 480ml 0.0175
Bumetanide
0.5mg,Tab, Oral, 100 0.1743 Bumex 1mg, Tab, Oral, 100 0.2348 2mg, Tab, Oral, 100 0.4272
_______________________________ PHARMACY RPOVIDER MANUAL 04/03
APPENDIX I AI-5

FEDERAL COMMONLY UPPER MAC KNOWN
GENERIC NAME LIMIT/UNIT PRICING BRAND NAME(S) Buspirone
5mg, Tab 0.2200 10mg, Tab 0.2600 15mg, Tab 0.4000 30mg, Tab 0.9000
Captopril
12.5mg, Tab, Oral, 100 0.0398 Capoten 25mg, Tab, Oral, 100 0.0442 50mg, Tab, Oral, 100 0.0892 100 mg, Tab, Oral, 100 0.1867
Captopril; Hydrochlorothiazide
25mg; 15mg, Tab, Oral, 100 0.2359 Capozide 25mg: 25mg Tab Oral 0.2360 50mg; 25mg, Tab, Oral, 100 0.3702
Carbamazepine ***
200mg Tab, Oral, 100 0.1388 Tegretol Carbidopa; Levodopa
10mg; 100mg; Tab, Oral, 100 0.3644 Sinemet 25mg; 100mg; Tab, Oral, 100 0.3915 25mg; 250 mg, Tab, Oral, 100 0.4657
Carisoprodol
350mg, Tab, Oral, 100 0.3743 Soma Carteolol HCL
1% Soln Drops, Ophth, 10ml 3.6675 *** Requires PA to override FUL/MAC and pay at EAC _______________________________ PHARMACY RPOVIDER MANUAL 04/03 APPENDIX I AI-6

FEDERAL COMMONLY UPPER MAC KNOWN
GENERIC NAME LIMIT/UNIT PRICING BRAND NAME(S) Cefaclor
Eq. 250mg base, Cap, Oral, 100 0.3780 Ceclor Eq. 500mg base, Cap, Oral, 100 0.7490 Eq. 125mg base/5ml, Pwd for Rec, Oral 150 0.1107 Eq. 187mg base/5ml, Pwd for Rec, Oral 100 0.1661 Eq. 250mg base/5ml, Pwd for Rec, Oral 150 0.2995 Eq. 375mg base/5ml, Pwd for Rec, Oral 100 0.4492
Cefadroxil Hydrate
500mg, Cap, Oral 0.9800 Cephalexin
Eq. 250mg base, Cap 0.2513 Keflex Eq. 500mg base, Cap 0.4446
Chlorpheniramine Maleate
4mg, Tab, Oral, 100 0.0171 Chlor-Trimeton Chlorpropamide
100mg, Tab, Oral, 100 0.1837 Diabinese 250mg, Tab, Oral, 100 0.3885
Chlorthalidone
25mg, Tab, Oral, 100 0.0509 Hygroton 50mg, Tab, Oral, 100 0.0558
Chlorzoxazone
500mg, Tab, Oral, 100 0.1085
_______________________________ PHARMACY RPOVIDER MANUAL 04/03
APPENDIX I AI-7

FEDERAL COMMONLY UPPER MAC KNOWN
GENERIC NAME LIMIT/UNIT PRICING BRAND NAME(S) Cholestyramine (regular)
Eq. 4gm Resin/Packet, Pwd, Oral, 60pk 1.2212 Questran
Cholestyramine Aspartame (light)
Eq. 4gm Resin/Scoop, Prevalite Pwd, Oral 210gm or greater 0.15714 Locholest Light
Cimetidine
200mg, Tab, Oral, 100 0.1238 Tagamet 300mg, Tab, Oral, 100 0.1313 400mg, Tab, Oral, 100 0.1537 800mg, Tab, Oral, 100 0.2775
Cimetidine HCL
Eq. 300mg base/5ml Soln, Oral, 240ml 0.1139
Clindamycin HCL
Eq. 150mg base, Cap, Oral, 100 0.5000 Cleocin HCL Clindamycin Phosphate
Eq. 1% base, Soln, Topical 60ml 0.2060 Clobetasol Propionate
0.05%, Cream, Topical, 30gm 0.8315 Clomipramine HCL
25mg, Cap, Oral, 100 0.3322 Anafranil 50mg, Cap, Oral, 100 0.5138 75mg, Cap, Oral, 100 0.5772
Clonazepam***
0.5mg, Tab 0.2000 Klonopin 1mg, Tab 0.2100 2mg, Tab 0.3000
_______________________________ PHARMACY RPOVIDER MANUAL 04/03 APPENDIX I AI-8

FEDERAL COMMONLY UPPER MAC KNOWN
GENERIC NAME LIMIT/UNIT PRICING BRAND NAME(S) Clonidine HCL
0.1mg, Tab, Oral, 100 0.0700 Catapres 0.2mg, Tab, Oral, 100 0.1120 0.3mg, Tab, Oral, 100 0.1400
Clorazepate Dipotassium
3.75mg, Tab, Oral, 100 0.8350 Tranxene 7.5mg, Tab, Oral, 100 1.0388 15mg, Tab, Oral, 100 1.4094
Clozapine***
25mg 0.9000 Clozaril 100mg 1.9000
*** Requires PA to override FUL/MAC and pay at EAC Cromolyn Sodium
4% Soln/Drops, Ophth, 10ml 3.3750 Cyclobenzaprine HCL
10mg, Tab, Oral, 100 0.2200 Flexeril Cyclopentolate HCL
1%, per ml, up to 14ml 2.2700 Cyclogyl 1%, per ml, 15ml or greater 0.4500
Desmopressin spray, 0.1mg/ml 21.7500 DDAVP Desonide
0.05% Cream, per gram, up to 59 grams 0.4050 Tridesilon 0.05% Cream, per gram, 60 grams or greater 0.3000 0.05% Ointment, per gram, up to 59 grams 0.4050 Desowen 0.05% Ointment, per gram, 60 grams or greater 0.3000
Desoximetasone
0.25%, Cream, Topical 60gm 0.6180 Topicort 0.25% Oint, per gram, up to 59 grams 0.7500 0.25% Oint, per gram, 60 grams or greater 0.4500
_______________________________ PHARMACY RPOVIDER MANUAL 04/03
APPENDIX I AI-9

FEDERAL COMMONLY UPPER MAC KNOWN
GENERIC NAME LIMIT/UNIT PRICING BRAND NAME(S) Dexamethasone
0.5mg/5ml Elixir, Oral, 240ml 0.0625 Decadron Dexamethasone; Neomycin Sulfate; Polymyxin B Sulfate
0.1%; Eq. 3.5mg base/gm; 10,000u/gm, Oint, Ophth 3.5 gm 1.0713 Maxitrol
Diazepam
2mg, Tab, Oral, 100 0.0423 Valium 5mg, Tab, Oral, 100 0.0718 10mg, Tab, Oral, 100 0.1417
Diclofenac Potassium
50mg, Tab, Oral, 100 0.8625 Cataflam Diclofenac Sodium
50mg, Tab, Delayed Release, Oral, 100 0.4748 Voltaren 75mg, Tab, Delayed Release, Oral, 100 0.5850
Dicyclomine HCL
10mg, Cap, Oral, 100 0.1222 Bentyl 20mg, Tab, Oral, 100 0.1185
Diflunisal
500mg, Tab, Oral, 60 1.0000 Dolobid Diltiazem HCL
30mg, Tab, Oral, 100 0.1019 Cardizem 60mg, Tab, Oral, 100 0.1114 90mg, Tab, Oral, 100 0.2312 120mg, Tab, Oral, 100 0.2331
Diphenhydramine HCL
12.5mg/5ml, Elixir, Oral 120ml 0.0137
_______________________________ PHARMACY RPOVIDER MANUAL 04/03 APPENDIX I AI-10

FEDERAL COMMONLY UPPER MAC KNOWN
GENERIC NAME LIMIT/UNIT PRICING BRAND NAME(S) Dipivefrin HCL
0.1%, Soln/Drops, Ophth 5ml 0.8700 Propine Doxazosin Mesylate
1mg, Tab, Oral, 100 0.5918 2mg, Tab, Oral, 100 0.5918 4mg, Tab, Oral, 100 0.6210 8mg, Tab, Oral, 100 0.6518
Doxepin HCL
10mg, Cap 0.0600 Sinequan 25mg, Cap 0.0800 50mg, Cap 0.0900 75mg, Cap 0.2052 100mg, Cap 0.1500 150mg, Cap 0.3500 Eq. 10mg base/ml, Concentrate, Oral, 120ml 0.1145
Doxycycline Hyclate
Eq. 50mg base, Cap Oral, 50 0.0915 Eq. 100mg base, Cap, Oral, 50 0.1050 Vibramycin Eq. 100mg base, Tab, Oral, 50 0.1287
Enalapril
2.5mg, Tab 0.1100 Vasotec 5mg, Tab 0.1300 10mg, Tab 0.1400 20mg, Tab 0.1900
Erythromycin
250mg Cap, Delayed Release Pellets Oral, 100 0.1889 E-Mycin, Erygel, Ery C 2% Gel, Topical, per gram 0.5500 Up to 59 grams 2% Gel, Topical, per gram 0.6000 60 grams or greater 2% Soln, Topical 60ml 0.0687
Estradiol
0.5mg, Tab, Oral, 100 0.1791 1mg, Tab, Oral, 100 0.1932 2mg, Tab, Oral, 100 0.3060
_______________________________ PHARMACY RPOVIDER MANUAL 04/03
APPENDIX I AI-11
FEDERAL COMMONLY UPPER MAC KNOWN
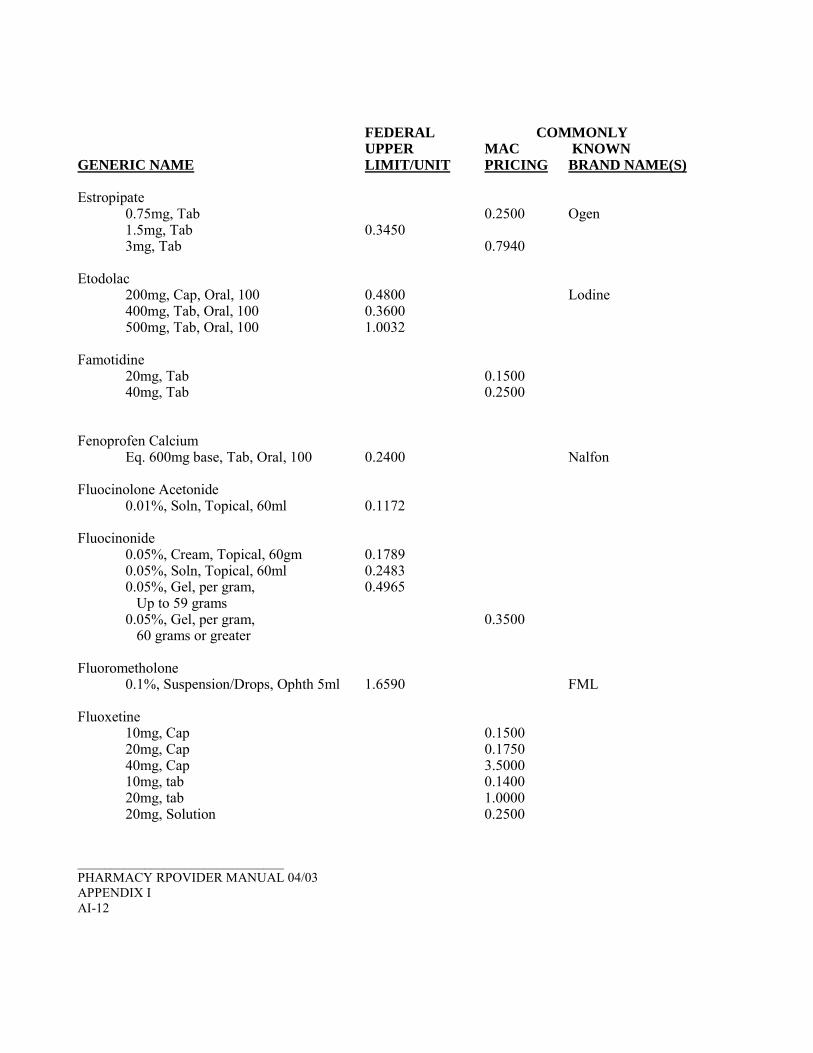
GENERIC NAME LIMIT/UNIT PRICING BRAND NAME(S) Estropipate
0.75mg, Tab 0.2500 Ogen 1.5mg, Tab 0.3450 3mg, Tab 0.7940
Etodolac
200mg, Cap, Oral, 100 0.4800 Lodine 400mg, Tab, Oral, 100 0.3600 500mg, Tab, Oral, 100 1.0032
Famotidine
20mg, Tab 0.1500 40mg, Tab 0.2500
Fenoprofen Calcium
Eq. 600mg base, Tab, Oral, 100 0.2400 Nalfon Fluocinolone Acetonide
0.01%, Soln, Topical, 60ml 0.1172 Fluocinonide
0.05%, Cream, Topical, 60gm 0.1789 0.05%, Soln, Topical, 60ml 0.2483 0.05%, Gel, per gram, 0.4965 Up to 59 grams 0.05%, Gel, per gram, 0.3500 60 grams or greater
Fluorometholone
0.1%, Suspension/Drops, Ophth 5ml 1.6590 FML Fluoxetine
10mg, Cap 0.1500 20mg, Cap 0.1750 40mg, Cap 3.5000 10mg, tab 0.1400 20mg, tab 1.0000 20mg, Solution 0.2500
_______________________________ PHARMACY RPOVIDER MANUAL 04/03 APPENDIX I AI-12

FEDERAL COMMONLY UPPER MAC KNOWN
GENERIC NAME LIMIT/UNIT PRICING BRAND NAME(S) Fluphenazine HCL
1mg, Tab, Oral, 100 0.2273 Prolixin 2.5mg, Tab, Oral, 100 0.2775 5mg, Tab, Oral, 100 0.3546 10mg, Tab, Oral, 100 0.5099
Flurbiprofen
100mg, Tab, Oral, 100 0.3600 Ansaid Flurbiprofen Sodium
0.03%, Soln/Drops, Ophth, 2ml 4.0679 Furosemide
10mg/ml, Solution, Oral 60ml 0.1300 Lasix 20mg, Tab, Oral, 100 0.0563 40mg, Tab, Oral, 100 0.0599 80mg, Tab, Oral, 100 0.09400
Gemfibrozil
600mg, Tab, Oral, 500 0.3030 Gentamicin Sulfate
Eq. 0.3% base, Soln/Drops, per ml 0.6000 Glipizide
5mg, Tab, Oral, 100 0.0699 Glucotrol 10mg, Tab, Oral, 100 0.0944
Glyburide
1.5mg, Tab, Oral, 100 0.2549 Glynase 3mg, Tab, Oral, 100 0.3202
Gramicidin; Neomycin Sulfate; Polymyxin B Sulfate
0.025mg/ml; Eq. 1.75mg base/ml 10,000 units/ml, Soln/Drops, Ophth 10ml 2.2185 Neoptic, Neosporin
_______________________________
PHARMACY RPOVIDER MANUAL 04/03 APPENDIX I
AI-13

FEDERAL COMMONLY UPPER MAC KNOWN
GENERIC NAME LIMIT/UNIT PRICING BRAND NAME(S) Guanfacine HCL
Eq. 1mg base, Tab, Oral, 100 0.5250 Tenex Eq. 2mg base, Tab, Oral, 100 0.7200
Haloperidol
2mg/ml, Conc., per ml, up to 119 ml 0.1500 2mg/ml, Conc., per ml, 120 ml or greater 0.0700
Homatropine Methylbromide; Hydrocodone Bitartrate
1.5mg/5ml, 5mg/5ml, Syrup, Oral 480ml 0.0280 Hycodan
Hydralazine HCL
10mg, Tab, Oral, 100 0.0354 Apresoline 25mg, Tab, Oral, 100 0.0560
Hydrochlorothiazide
25mg, Tab 0.1200 50mg, Tab 0.1200
Hydrochlorothiazide; Propranolol HCL
25mg; 40mg, Tab, Oral, 100 0.08100 Inderide 25mg; 80mg, Tab, Oral, 100 0.12100
Hydrochlorothiazide; Spironolactone
25mg; 25mg, Tab, Oral, 100 0.3463 Aldactazide Hydrochlorothiazide; Triamterene
25mg; 37.5mg, Cap, Oral, 100 0.3177 Dyazide 25mg; 37.5mg, Tab, Oral, 100 0.1932 Maxide 50mg; 75mg, Tab, Oral, 100 0.0488
Hydrocortisone
0.5%, Cream, Topical, 30gm 0.0375 Cortaid, Hytone 1%, Cream, Topical, 30gm 0.0585 2.5%, Cream, Topical, 30gm 0.1820 1% Lotion, Topical, 120ml 0.0400 2.5%, Lotion, Topical, 59ml 0.6814 1%, Oint, Topical, 30gm 0.0560 2.5% Oint, per gram, 0.1500 Up to 450 grams 2.5% Oint, per gram, 0.0881 451 grams or greater
_______________________________ PHARMACY RPOVIDER MANUAL 04/03 APPENDIX I AI-14

FEDERAL COMMONLY UPPER MAC KNOWN
GENERIC NAME LIMIT/UNIT PRICING BRAND NAME(S) Hydroxychloroquine Sulfate
200mg, Tab, Oral, 100 0.8535 Plaquenil Hydroxyzine Pamoate
Eq. 25mg HCL, Cap, Oral, 100 0.0700 Vistaril Eq. 50mg HCL, Cap, Oral, 100 0. 0.0840
Ibuprofen
400mg, Tab 0.0400 Motrin 600mg, Tab 0.0550 800mg, Tab 0.0800
Imipramine HCL
10mg, Tab, Oral, 100 0.2500 Tofranil 25mg, Tab, Oral, 100 0.3500 50mg, Tab, Oral, 100 0.4500
Indapamide
1.25mg, Tab, Oral, 100 0.1035 Lozol 2.5mg, Tab, Oral, 100 0.1125
Isoniazid
300mg, Tab, Oral, 100 0.0890 INH Isosorbide Dinitrate
5mg, Tab, Oral, 100 0.0242 Isordil 10mg, Tab, Oral, 100 0.0281 20mg, Tab, Oral, 100 0.0291 2.5mg, Tab, Sublingual, 100 0.0488
_______________________________ PHARMACY RPOVIDER MANUAL 04/03
APPENDIX I AI-15

FEDERAL COMMONLY UPPER MAC KNOWN
GENERIC NAME LIMIT/UNIT PRICING BRAND NAME(S) Isosorbide Mononitrate
10mg, Tab, Oral, 100 0.6110 ISMO 20mg, Tab, Oral, 100 0.4950 60mg, Tab, Extended Release Oral, 100 0.7492
Ketoconazole
200mg, Tab, Oral, 100 2.7750 Nizoral Ketoprofen
50mg, Cap, Oral, 100 0.4749 Orudis 75mg, Cap, Oral, 100 0.4058
Ketorolac Tromethamine
10mg, Tab, Oral, 100 0.6773 Toradol Labetalol HCL
100mg, Tab, Oral, 100 0.2813 Normodyne, Trandate 200mg, Tab, Oral, 100 0.2672 300mg, Tab, Oral, 100 0.4688
Lactulose
10gm/15ml, Soln, Oral 480ml 0.0219 Duphalac Levobunolol HCL
0.25% Ophth., ml 1.2600 Betagan 0.5%, Soln/Drops, Ophth 10ml 1.4925
Lidocaine HCL
2% Soln, Oral 100 ml 0.0278 Lisinopril 2.5mg, Tab 0.1000 5mg, Tab 0.1250 10mg, Tab 0.2000 20mg, Tab 0.2800 30mg, Tab 0.3000 40mg, Tab 0.4500 _______________________________ PHARMACY RPOVIDER MANUAL 04/03 APPENDIX I AI-16

FEDERAL COMMONLY UPPER MAC KNOWN
GENERIC NAME LIMIT/UNIT PRICING BRAND NAME(S) Lisinopril; HCTZ 10mg; 12.5mg Tab, Oral 0.645 20mg; 12.5mg, Tab, Oral 0.6983 20mg; 25mg, Tab, Oral 0.7065 Lovastatin
10mg, Tab 0.6500 20mg, Tab 1.1250 40mg, Tab 1.8750
Meclizine HCL
12.5mg, Tab, Oral, 100 0.0599 Antivert 25mg, Tab, Oral, 100 0.0717
Medroxyprogesterone Acetate
2.5mg, Tab, Oral, 100 0.2025 5mg, Tab, Oral, 100 0.3061 Provera, Cycrin 10mg, Tab, Oral, 100 0.2488
Megestrol Acetate
20mg, Tab, Oral, 100 0.3489 Megace 40mg, Tab, Oral, 100 0.6755
Meperidine HCL
50mg, Tab, Oral, 100 0.5370 100mg, Tab, Oral, 100 1.0347
Metformin
500mg, Tab 0.4000 850mg, Tab 0.4100 1000mg, Tab 0.4750
Methazolamide
25mg, Tab, Oral, 100 0.3150 Neptazane 50mg, Tab, Oral, 100 0.4650
Methenamine Mandelate
1gm, Tab, Oral, 100 0.2923 Methocarbamol
500mg, Tab, Oral, 100 0.1962 Robaxin _______________________________
PHARMACY RPOVIDER MANUAL 04/03 APPENDIX I
AI-17

FEDERAL COMMONLY UPPER MAC KNOWN
GENERIC NAME LIMIT/UNIT PRICING BRAND NAME(S) Methotrexate Sodium
Eq. 2.5mg base, Tab, Oral, 100 1.2637 Methylphenidate HCL
5mg, Tab, Oral, 100 0.3020 Ritalin 10mg, Tab, Oral, 100 0.3750 20mg, Tab, Oral, 100 0.6180
Methylprednisolone
4mg, Tab, Oral, 100 0.1680 Medrol Metoclopramide HCL
Eq. 5mg base/5ml, Soln, Oral, 480ml 0.0155 Eq. 5mg base, Tab, Oral, 100 0.1842 Reglan Eq. 10mg base, Tab, Oral, 100 0.1095
Metoprolol Tartrate
50mg, Tab, Oral, 100 0.0500 Lopressor 100mg, Tab, Oral, 100 0.0600
Metronidazole
250mg, Tab, Oral, 100 0.0849 Flagyl 500mg, Tab, Oral, 100 0.2184
Mexiletine HCL
200 mg, Cap, Oral, 100 0.9712 Minocycline HCL
Eq. 50mg base, Cap, Oral, 100 0.3936 Minocin Eq. 100mg base, Cap, Oral, 50 1.4000
Minoxidil
2.5mg, Tab, Oral, 100 0.3170 Loniten 10mg, Tab, Oral, 100 0.6000
Mirtazapine 15mg, Tab, Oral 2.000 30mg, Tab, Oral 2.100 _______________________________ PHARMACY RPOVIDER MANUAL 04/03 APPENDIX I AI-18

FEDERAL COMMONLY UPPER MAC KNOWN
GENERIC NAME LIMIT/UNIT PRICING BRAND NAME(S) Nadolol
20mg, Tab, Oral, 100 0.4650 Corgard 40mg, Tab, Oral, 100 0.4289 80mg, Tab, Oral, 100 0.8025 120mg, Tab, Oral, 100 0.5000 160mg, Tab, Oral, 100 0.6000
Naltrexone HCL
50mg, Tab, Oral, 100 4.0400 Naphazoline Hydrochloride Naphcon Forte
0.1%, Soln/Drops, Opcon Ophth 15ml 0.3140 Vasocon
Naproxen
250mg, Tab, Oral, 100 0.1044 Naprosyn 375mg, Tab, Oral, 100 0.1383 500mg, Tab, Oral, 100 0.1260 375mg, Tab, Delayed Release Oral, 100 0.6750
Naproxen Sodium
220mg, Tab (200mg base) 0.0800 Niacin
500mg, Tab, Oral, 100 0.0390 Nicolar Nicardipine HCL
20mg, Cap, Oral, 100 0.2000 Cardene 30mg, Cap, Oral, 100 0.3000
Nifedipine
10mg, Cap, Oral, 100 0.1237 Nitroglycerin
0.3mg SL, Tab 0.0700 0.4mg SL, Tab 0.0700
Nizatidine 150mg,Cap, Oral 1.8307 300mg, Cap, Oral 3.6615
_______________________________ PHARMACY RPOVIDER MANUAL 04/03
APPENDIX I AI-19

FEDERAL COMMONLY UPPER MAC KNOWN
GENERIC NAME LIMIT/UNIT PRICING BRAND NAME(S) Nortriptyline HCL
Eq. 10mg base, Cap, Oral, 100 0.1019 Pamelor Eq. 25mg base, Cap, Oral, 100 0.1406 Eq. 50mg base, Cap, Oral, 100 0.1722 Eq. 75mg base, Cap, Oral, 100 0.2203
Nystatin
100,000u/gm, Cream, Topical, 30gm 0.0755 Nilstat 100,000u/gm, Oint, Topical, 15gm 0.1019 100,000u/ml, Susp, Oral, 60ml 0.1757
Nystatin; Triamcinolone Acetonide
100,000u/gm 0.1% Cream, Topical, 30gm 0.0975 Mycotriacet II 100,000u/gm 0.1% Oint, Topical, 30gm 0.0975
Orphenadrine Citrate
100mg, Tab, Extended Release, Oral, 100 1.8225
Oxaprozine 600mg, Tab, Oral 100 0.6758 Oxybutynin Chloride
5mg, Tab, Oral, 100 0.1260 Ditropan 5mg/ml, Oral, Syrup 0.0500
Palivizumab
50mg, vial 573.5572 Synagis 100mg, vial 1050.000
Penicillin V Potassium
Eq. 250mg base/5ml, Pwd/Recon, Oral, 200 0.0210
Pentoxifylline
400mg, Tab, Ext. Release, Oral, 100 0.3000 Perphenazine
2mg, Tab, Oral, 100 0.2801 Trilafon 4mg, Tab, Oral, 100 0.3448 16mg, Tab, Oral, 100 0.6377
_______________________________ PHARMACY RPOVIDER MANUAL 04/03 APPENDIX I AI-20

FEDERAL COMMONLY UPPER MAC KNOWN
GENERIC NAME LIMIT/UNIT PRICING BRAND NAME(S) Pindolol
5mg, Tab, Oral, 100 0.1537 Visken 10mg, Tab, Oral, 100 0.1973
Piroxicam
10mg, Cap, Oral, 100 0.0788 Feldene 20mg, Cap, Oral, 100 0.0830
Polymyxin B Sulfate; Trimethoprim Sulfate
10,000u/ml, Eq. 1mg base/ml Soln/Drops, Ophth 10ml 1.2360
Potassium Chloride
8 Meq Tab, Ext. Release, Oral, 100 0.0772 Slow-K Prednisolone
15mg/5ml, Syrup, Oral, 480ml 0.2081 Prednisolone Acetate
1%, Suspension/Drops, Ophth 10ml 1.6950 Prednisone
5mg, Tab, Oral, 100 0.03400 Deltasone 10mg, Tab, Oral, 100 0.04200 Orasone 20mg, Tab, Oral, 100 0.0700
Primidone ***
250mg, Tab, Oral, 100 0.6405 Mysoline Probenecid
500mg, Tab, Oral, 100 0.7059 Prochlorperazine Maleate
Eq. 5mg base, Tab, Oral, 100 0.3986 Eq. 10mg base, Tab, Oral, 100 0.5766
Promethazine HCL
6.25mg/5ml, Syrup, Oral, 120ml 0.0264 Phenergan *** Requires PA to override FUL/MAC and pay at EAC
_______________________________ PHARMACY RPOVIDER MANUAL 04/03
APPENDIX I AI-21

FEDERAL COMMONLY UPPER MAC KNOWN
GENERIC NAME LIMIT/UNIT PRICING BRAND NAME(S) Propranolol HCL
10mg, Tab, Oral, 100 0.0585 20mg, Tab, Oral, 100 0.06300 40mg, Tab, Oral, 100 0.0848 80mg, Tab, Oral, 100 0.1140
Pseudoephedrine HCL; Triprolidine HCL
60mg; 2.5mg, Tab, Oral, 100 0.0336 Ranitidine HCL
150mg, Tab 0.1000 Zantac 300mg, Tab 0.2000 150mg, Cap 0.6500 300mg, Cap 1.2000
Selegiline HCL
5mg, Cap 1.7000 5mg, Tab 0.3500
Selenium Sulfide
2.5% Lotion/Shampoo, Topical 120ml 0.0350 Selsun
Silver Sulfadiazine
1%, Cream, 85gm 0.1100 Silvadene Spironolactone
25mg, Tab, Oral, 100 0.3000 Aldactone Sucralfate
1gm, Tab, Oral, 100 0.3690 Sulfacetamide Sodium
10%, Soln/Drops, Ophth 15ml 0.1530
_______________________________ PHARMACY RPOVIDER MANUAL 04/03 APPENDIX I AI-22

FEDERAL COMMONLY UPPER MAC KNOWN
GENERIC NAME LIMIT/UNIT PRICING BRAND NAME(S) Sulfamethoxazole; Trimethoprim
400mg; 80mg, Tab, Oral, 100 0.1325 Bactrim 800mg; 160mg, Tab, Oral, 100 0.1590 Septra
Sulfasalazine
500mg, Tab, Oral, 100 0.1757 Azulfidine Sulfinpyrazone
100mg, Tab, Oral 0.3000 Sulindac
150mg, Tab, Oral, 100 0.2625 Clinoril 200mg, Tab, Oral, 100 0.4200
Terazosin HCL
Eq. 1mg base, Cap, Oral, 100 1.5413 Eq. 2mg base, Cap, Oral, 100 1.5413 Eq. 5mg base, Cap, Oral, 100 1.5413 Eq. 10mg base, Cap, Oral, 100 1.5413
Tetracycline HCL
500mg, Cap, Oral, 100 0.0975 Sumycin Theophylline
100mg, Tab, Ext. Release, Oral, 100 0.1184 200mg, Tab, Ext. Release, Oral, 100 0.1607 300mg, Tab, Ext. Release, Oral, 100 0.1960
Thioridazine HCL
10mg, Tab 0.1680 15mg, Tab 0.1950 25mg, Tab 0.1090 50mg, Tab 0.3885 100mg, Tab 0.2250 150mg, Tab 0.9500 200mg, Tab 0.9000
Thiothixene
1mg, Cap, Oral, 100 0.1120 Navane 2mg, Cap, Oral, 100 0.1860 5mg, Cap, Oral, 100 0.2963 10mg, Cap, Oral, 100 0.4065
_____________________________ PHARMACY RPOVIDER MANUAL 04/03
APPENDIX I AI-23

FEDERAL COMMONLY UPPER MAC KNOWN
GENERIC NAME LIMIT/UNIT PRICING BRAND NAME(S) Ticlopidine HCL
250mg, Tab, Oral, 60 1.5119 Timolol Maleate Eq. 0.25% base, Soln/Drops 0.6975 Timoptic,Blocadren Eq. 0.5% base Soln/Drops 0.9000 Ophth 15ml Tizanidine HCL 2mg, Tab 0.8071 4mg, Tab 0.9520 Tobramycin
0.3%, Soln/Drops, Ophth 5 ml 1.1850 Tobrex
Tolazamide
250mg, Tab, Oral, 100 0.1864 Tolinase Tolmetin Sodium
Eq. 200mg, base, Tab, Oral 0.3000 Eq. 400mg base, Cap, Oral 0.6500
Tramadol HCL Ultram 50mg, Tab 0.2000 Trazodone HCL
50mg, Tab, Oral, 100 0.0684 Desyrel 100mg, Tab, Oral, 100 0.0952 150mg, Tab, Oral, 100 0.3113
Tretinoin 0.025% cream, Top 1.6000 Triamcinolone Acetonide
0.025%, Cream, Topical, 80gm 0.0364 Kenalog 0.1%, Cream, Topical, 80gm 0.0448 0.5%, Cream, Topical, 15gm 0.1889 0.1%, Oint, Topical, 80gm 0.0502 0.1%, Paste Dental 5gm 1.1500
Trifluoperazine HCL Eq. 1mg base, Tab, Oral, 100 0.2433 Stelazine Eq. 2mg base, Tab, Oral, 100 0.3552 Eq. 5mg base, Tab, Oral, 100 0.4271 Eq. 10mg base, Tab, Oral, 100 0.5403 ______________________________
PHARMACY RPOVIDER MANUAL 04/03 APPENDIX I AI-24

FEDERAL COMMONLY UPPER MAC KNOWN
GENERIC NAME LIMIT/UNIT PRICING BRAND NAME(S) Trihexyphenidyl HCL
2mg, Tab, Oral, 100 0.1275 5mg, Tab, Oral, 100 0.2580
0.7000
Tropicamide
0.5%, Soln/Drops, Ophth 15ml 0.6550 Mydriacyl 1%, Soln/Drops, Ophth 15ml Valproic Acid ***
250mg, Cap, Oral, 100 0.1400 Depakene 250mg/5ml Syrup, Oral, 480 ml 0.0594
Verapamil HCL
120mg, Cap, Ext. Release, Oral, 100 0.7500 Calan, Verelan, 180mg, Cap, Ext. Release, Oral, 100 0.8700 Isoptin SR 240mg, Cap, Ext. Release, Oral, 100 0.9900 40mg, Tab, Oral, 100 0.1963 80mg, Tab, Oral, 100 0.0700 120mg, Tab 0.1110 180mg, Tab, Ext. Release, Oral, 100 0.4350 240mg, Tab, Ext. Release, Oral, 100 0.3683
Vit. B-12-IF,C,Fe,FA, Cap 0.3500 Foltrin, Trinsicon Warfarin Sodium***
1mg Tab 0.3900 2mg, Tab 0.4500 2.5mg, Tab 0.4500 3mg, Tab 0.4500 4mg, Tab 0.4500 5mg, Tab 0.4500 6mg, Tab 0.5000 7.5mg, Tab 0.5000 10mg, Tab 0.5000
*** Requires PA to override FUL/MAC and pay at EAC
_______________________________ PHARMACY RPOVIDER MANUAL 04/03
APPENDIX I AI-25

ACE Inhibitors PRIOR AUTHORIZATION REQUEST FORM
Preferred Drug(s) that DO NOT require PA Non-Preferred Drug(s) that DO require PA Captopril(Capoten®), Enalapril(Vasotec®), Benazepril(Lotensin®), Fosinopril(Monopril®), Lisinopril(Zestril®& Prinivil®) Moexipril(Univasc®), Perindopril(Aceon®), Quinapril(Accupril®), Ramipril(Altace®), & Trandolapril(Mavik®)
** Indicates REQUIRED information
CONSUMER INFORMATION ** Name:__________________________________ **Medicaid Number: __________________
PHARMACY INFORMATION ** Name:__________________________________ **Phone Number: ____________________
Medicaid Number #:________________________ NDC:_____________________________
PRESCRIBING PHYSICIAN INFORMATION ** Name:__________________________________ **Medicaid Number: __________________
** Phone Number: __________________________
** Indicate: Non-Preferred Drug prescribed: ________________
Other:_____________________ ** Indicate: Preferred Drug tried: _________________________ Length of trial: _____________
** Check the appropriate box indicating medical necessity for the Non-Preferred Drug:
Medical intolerance to the Preferred Drug. Please specify:______________________________
_____________________________________________________________________________
Treatment failure to the Preferred Drug. Please specify:________________________________
_____________________________________________________________________________
** Prescribing Physician�s signature: _________________________________Date: ___________
FAX completed form to the Prior Authorization Unit @ 1-800-913-2229 (274-5956 Topeka). If the pharmacy provider has started a Prior Authorization request and this information is not received within 15 working days, the PA request will be denied for information not received.

ARB’s PRIOR AUTHORIZATION REQUEST FORM
Preferred Drug(s) that DO NOT require PA Non-Preferred Drug(s) that DO require PA Losartan(Cozaar®) & Telmisartan(Micardis®) Candesartan(Atacand®), Eprosartan(Teveten®), Irbesartan(Avapro®), Olmesartan(Benicar®), & Valsartan(Diovan®)
** Indicates REQUIRED information
CONSUMER INFORMATION ** Name:__________________________________ **Medicaid Number: __________________
PHARMACY INFORMATION ** Name:__________________________________ **Phone Number: ____________________
Medicaid Number #:________________________ NDC:_____________________________
PRESCRIBING PHYSICIAN INFORMATION ** Name:__________________________________ **Medicaid Number: __________________
** Phone Number: __________________________
** Indicate: Non-Preferred Drug prescribed: ________________
Other:_____________________ ** Indicate: Preferred Drug tried: _________________________ Length of trial: _____________
** Check the appropriate box indicating medical necessity for the Non-Preferred Drug:
Medical intolerance to the Preferred Drug. Please specify:______________________________
_____________________________________________________________________________
Treatment failure to the Preferred Drug. Please specify:________________________________
_____________________________________________________________________________
** Prescribing Physician�s signature: _________________________________Date: ___________
FAX completed form to the Prior Authorization Unit @ 1-800-913-2229 (274-5956 Topeka). If the pharmacy provider has started a Prior Authorization request and this information is not received within 15 working days, the PA request will be denied for information not received.

BETA-BLOCKERS PRIOR AUTHORIZATION REQUEST FORM
Preferred Drug(s) that DO NOT require PA Non-Preferred Drug(s) that DO require PA Atenolol(Tenormin®), Metoprolol(Lopressor®), Betaxolol(Kerlone®), Bisoprolol(Zebeta®), Propranolol(Inderal®), Sotalol(Betapace®), Carteolol(Cartrol®), Nadolol(Corgard®), Acebutolol(Sectral®), Metoprolol XL Penbutolol(Levatol®), Pindolol(Visken®), (Toprol XL®) Timolol(Blocadren®)
** Indicates REQUIRED information
CONSUMER INFORMATION ** Name:__________________________________ **Medicaid Number: __________________
PHARMACY INFORMATION ** Name:__________________________________ **Phone Number: ____________________
Medicaid Number #:________________________ NDC:_____________________________
PRESCRIBING PHYSICIAN INFORMATION ** Name:__________________________________ **Medicaid Number: __________________
** Phone Number: __________________________
** Indicate: Non-Preferred Drug prescribed: ________________
Other:_____________________ ** Indicate: Preferred Drug tried: _________________________ Length of trial: _____________
** Check the appropriate box indicating medical necessity for the Non-Preferred Drug:
Medical intolerance to the Preferred Drug. Please specify:______________________________
_____________________________________________________________________________
Treatment failure to the Preferred Drug. Please specify:________________________________
_____________________________________________________________________________
** Prescribing Physician�s signature: _________________________________Date: ___________
FAX completed form to the Prior Authorization Unit @ 1-800-913-2229 (274-5956 Topeka). If the pharmacy provider has started a Prior Authorization request and this information is not received within 15 working days, the PA request will be denied for information not received.
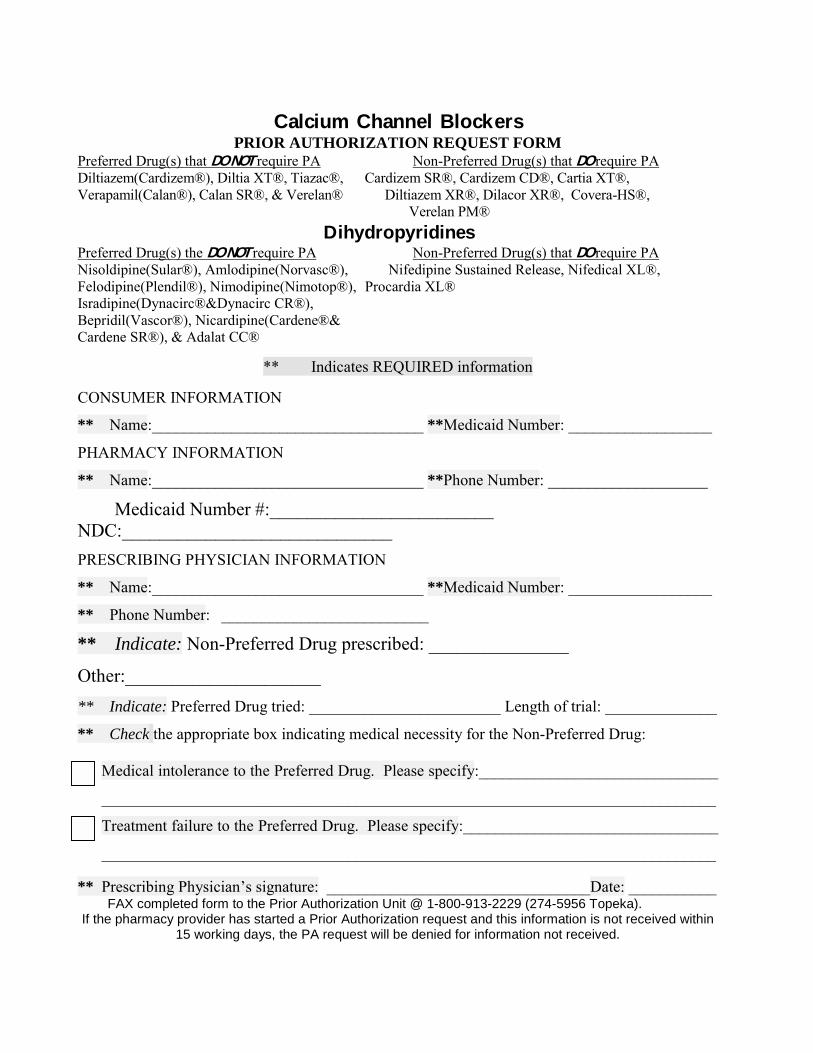
Calcium Channel Blockers PRIOR AUTHORIZATION REQUEST FORM
Preferred Drug(s) that DO NOT require PA Non-Preferred Drug(s) that DO require PA Diltiazem(Cardizem®), Diltia XT®, Tiazac®, Cardizem SR®, Cardizem CD®, Cartia XT®, Verapamil(Calan®), Calan SR®, & Verelan® Diltiazem XR®, Dilacor XR®, Covera-HS®, Verelan PM® Dihydropyridines Preferred Drug(s) the DO NOT require PA Non-Preferred Drug(s) that DO require PA Nisoldipine(Sular®), Amlodipine(Norvasc®), Nifedipine Sustained Release, Nifedical XL®, Felodipine(Plendil®), Nimodipine(Nimotop®), Procardia XL® Isradipine(Dynacirc®&Dynacirc CR®), Bepridil(Vascor®), Nicardipine(Cardene®& Cardene SR®), & Adalat CC®
** Indicates REQUIRED information CONSUMER INFORMATION
** Name:__________________________________ **Medicaid Number: __________________
PHARMACY INFORMATION
** Name:__________________________________ **Phone Number: ____________________
Medicaid Number #:________________________ NDC:_____________________________
PRESCRIBING PHYSICIAN INFORMATION
** Name:__________________________________ **Medicaid Number: __________________
** Phone Number: __________________________
** Indicate: Non-Preferred Drug prescribed: _______________
Other:_____________________ ** Indicate: Preferred Drug tried: ________________________ Length of trial: ______________
** Check the appropriate box indicating medical necessity for the Non-Preferred Drug:
Medical intolerance to the Preferred Drug. Please specify:______________________________
_____________________________________________________________________________
Treatment failure to the Preferred Drug. Please specify:________________________________
_____________________________________________________________________________
** Prescribing Physician�s signature: _________________________________Date: ___________ FAX completed form to the Prior Authorization Unit @ 1-800-913-2229 (274-5956 Topeka). If the pharmacy provider has started a Prior Authorization request and this information is not received within
15 working days, the PA request will be denied for information not received.