CPD: Alopecia - Carrigtwohill Pharmacy
76
IRELAND’S OFFICIAL PHARMACY PUBLICATION MARCH 2019 CPD : Alopecia Economic backdrop for pharmacy sector IPU CONFERENCE – EARLY BIRD DEADLINE | EPILEPSY IRELAND Inhaler Technique Asthma Society and IPU launch awareness campaign
-
Upload
khangminh22 -
Category
Documents
-
view
8 -
download
0
Transcript of CPD: Alopecia - Carrigtwohill Pharmacy

IRELAND’S OFFICIAL PHARMACY PUBLICATION
MARCH 2019
CPD: AlopeciaEconomic backdrop for pharmacy sector
IPU CONFERENCE – EARLY BIRD DEADLINE | EPILEPSY IRELAND
Inhaler TechniqueAsthma Society and IPU launch awareness campaign

Our One-Day Review will include:■ Expert advice on your retail o� ering■ A complete review of the front-of-pharmacy including
category management and promotion planning■ Providing training in sales techniques■ Re-merchandising displays (interior and window) to
enhance the retail experience in your pharmacy■ Helping you and your sales team develop new sales ideas■ Using key performance indicators to help you
increase front-of-pharmacy business■ Motivating your sales team to be innovative,
sales focused and up-to-speed on product knowledge
A bespoke retail review of your front-of-pharmacy will give your pharmacy a facelift to boost your sales without overstretching your budget.
Darren Kelly, IPU Business Development Manager, has over 20 years of retail experience. If you would like further information on this service or would like to book a Retail Review, please contact Darren on (01) 493 6401 / 086 028 9825 / email: [email protected]
How we have helped ...
Perhaps the most e� ective part of the process was the
explanation given to the teams in store, the ownership they took of the ideas discussion and the speed of implementation of the change, which thankfully produced the
expected results.Tom Murray,
Murray’s Pharmacy, Co. Donegal
TAILOR-MADE JUST FOR YOUR PHARMACY
Retail Review A4 2017 ART.indd 1 02/05/2017 16:50

07 A Note from the Editor
MARCH 2019
The IPU Review is published monthly and circulated to Irish pharmacists. The views expressed by contributors are not those of the IPU nor is responsibility accepted for claims in articles or advertisements.
Subscription:€100 (Ireland North & South) and €150 (including postage overseas).
Publisher: Irish Pharmacy Union (IPU Services Ltd), Butterfield House, Butterfield Avenue, Rathfarnham, Dublin 14, D14 E126Tel: (01) 493 6401 Fax: (01) 493 6626 Email: [email protected]: www.ipu.ie
Editor: Jack Shanahan MPSI Editorial Associates: Sinéad Fennell, Ciara Browne and Jim Curran
Advertising: Sinéad Fennell Email: [email protected] Tel: (01) 493 6401 ©2019 Copyright: All Rights Reserved, Irish Pharmacy Union. Printed by Ryson Colour Printers Ltd.IPU Review is a Registered Trademark of the Irish Pharmacy Union.
08 Dates for your Diary
08 Pharmacy in the media
10 IPU Conference – Early Bird Deadline
10 Operation Transformation – Thank you
12 Urgent progress needed on resourcing healthcare in the community
14 Member Briefings – March 2019
14 Congratulations
IPU News The latest news and events from Butterfield House
16
Features16 Economic backdrop for pharmacy sector22 A community pharmacy-based
pilot project for BowelScreen25 IPU Conference30 Asthma Society
of Ireland34 An Analysis of
the Pharmacist Workforce Capacity in Ireland
34
30IPUREVIEW MARCH 2019 3

THE IPU CONTRACT UNIT IS HERE TO HELP YOUCONTACT DEREK OR AOIFE � For advice on any part of the pharmacy contract;� For advice on all aspects of processing claims;� For assistance in responding to direct correspondence from the HSE PCRS;� If you are called to a meeting with the HSE PCRS;� If your pharmacy is inspected by the HSE PCRS;� If you are subject to a claims investigation; and� If you are being investigated under the pharmacy contract.
Telephone: 01 406 1557 / 01 493 6401Derek Reilly, Contract Manager, [email protected] Garrigan, Contract Administrator, [email protected]
NEED HELP WITH THE HSE?
PCRS Claims 2019 ART.indd 1 24/01/2019 16:57

News66 PSI Strategy 2018 – 2020
67 IMVO – EU Falsified Medicines Directive (FMD)
68 HIQA announces public consultation on C-reactive protein point-of-care testing
69 National Cancer Strategy 2017 – 2026 Implementation Report 2018
70 Irish Skin Foundation Dermatology Study Day 2019 – 6 April 2019
70 Cystic Fibrosis Ireland to host national conference
70 9th All Ireland Pharmacy Conference – Call for Abstracts
71 Accord Healthcare launches High Tech Hub Demo Video with PharmaBuddy
71 Daffodil Day more important than ever
72 Ministers for Health and Agriculture publish report on antimicrobial use and resistance
72 Over 600 life-saving defibrillators across four manufacturers require urgent updates
73 Minister for Health appoints HSE Board
73 FSAI publishes updated guidelines
74 Irish Chemists’ Golfing Society News
74 Classifieds
39 Behaviour & Attitudes: Reframing Community Pharmacy
43 Epilepsy Ireland – Purple Day 26 March
45 CPD: Alopecia48 Assisted Decision-Making
(Capacity) Act 201551 Report of PSI Council Meeting
of 14 February 201953 Politics57 Obituary: Pádraig Ó Mathúna58 Studies60 High Tech Medicines Update:
Symkevi® Film-coated Tablets61 Clinical Tips: Restrictions
on the use of Quinolone and Fluoroquinolone Antibiotics
62 International Pharmacy News64 Product Information
THE IPU CONTRACT UNIT IS HERE TO HELP YOUCONTACT DEREK OR AOIFE � For advice on any part of the pharmacy contract;� For advice on all aspects of processing claims;� For assistance in responding to direct correspondence from the HSE PCRS;� If you are called to a meeting with the HSE PCRS;� If your pharmacy is inspected by the HSE PCRS;� If you are subject to a claims investigation; and� If you are being investigated under the pharmacy contract.
Telephone: 01 406 1557 / 01 493 6401Derek Reilly, Contract Manager, [email protected] Garrigan, Contract Administrator, [email protected]
NEED HELP WITH THE HSE?
PCRS Claims 2019 ART.indd 1 24/01/2019 16:57
45
48
39IPUREVIEW MARCH 2019 5

IPU PRODUCT FILE
ISO 9001Registered
QualityManagement
ISO 27001Registered
Information SecurityManagement
What is in the File?The File contains information on over 63,000 products, including:
Licensed medicinal products
Unlicensed medicinal products
Medical devices and sundries (bandages, dressings, ostomy equipment etc.)
Nutritional products, including foods for special diets
Veterinary products
Photographic products
Cosmetic products
Front of Shop products (shampoos, toothpastes, vitamins etc.)
In addition to pricing information, barcodes etc., the IPU Product File provides valuable professional information on health products. The professional information provided includes the Medicinal Product Name, PA/EU number, Generic Name, Pharmaceutical Form, Strength and Legal Status.
ISO CertifiedIn 2016, the IPU Product File achieved ISO Certification for 9001 (Quality) and 27001 (Information Security). The audit and certification process for ISO Certification emphasises the robustness of the IPU Product File and underpins its position as the definitive medicinal product catalogue in Ireland.
Easy to UseThe IPU Product File is an open system, so no matter what vendor you choose, the file can be adapted for your needs. The IPU Product File is available by electronic download, where you can log-in and download your monthly update.
Contact UsThe IPU Product File team are available to answer your queries, whether it’s on sourcing a product, pricing queries etc., the team will be able to assist you.
For any queries relating to the IPU Product File, please contact a staff member on 01 406 1550 or [email protected]
The IPU Product File has been in existence for more than 30 years and is an indispensable resource for community pharmacists. It was designed for pharmacists by pharmacists and is also used by doctors and hospital personnel. It is a vital support tool for prescribing, dispensing, claiming with PCRS, stock ordering, stock taking, price checking and product sourcing.

If you have any comments, queries or issues to raise, send your “Letters to the Editor” by email to [email protected].
No computer can take the place of a professional taking a compassionate and professional decision to avoid or minimise harm
On the face of it, pharmacists should not be sleeping too well at night. And this
would be true if you took a very functional look at some of our labours. It is evident that some of our processes can be automated. It would be fair to say that our Achilles Heel is the perception that our work is simply seen as a supply function. Yet, on any given day, while safe medicine supply is important, we are not automatons. We are professionals, exercising our judgement about where the patient benefits and risks lie. Even in the idyllic pastures and gently rolling verdant hills of the Kingdom, the winds of primary care change are blowing steadily.
Part of this is the gradual erosion and fragmentation of the traditional GP-patient relationship. As we move to large primary care centres, anonymity starts to follow. But this is only a minor part of the challenge. Above all else is the sheer volume of work faced by most GP practices. Most patients, and pharmacists, can attest to the sheer difficulty in getting a GP practice to even answer the phone. Most routine GP prescriptions are on a conveyor belt system. This has meant an increasing dependence on processes, many of which, with the best will in the world, don’t
always deliver optimal care. In addition, we now have the growth of remote prescription writing services, where the person signing the prescription will never examine, not to mind meet the patient under their care. And to cap it all, we have the arrival of ‘drop in’ clinics, large and small, where you will see an Irish registered doctor, but with few of the benefits of an overview of your clinical history. All reasons why you need a professional pharmacist acting in the best interest of the patient.
This is exactly what our code of conduct demands of us. The revised version, while varying in emphasis, still has this overarching concept at its core. For instance, the old chestnut, are pharmacists allowed to break the law? More specifically, are there times when, in a professional capacity, we are expected to supply controlled drugs outside legislative parameters? As we all should know, the legislation is very clear. There are no circumstances where you can supply a CD2/3/4.1 drug, with the honourable exception of phenobarbitone/phenobarbital in epilepsy, without a valid prescription. So, there it is. Black and white. Can’t be done. This is, of course, the answer that any computer can give. Technology is the master of the binary question, with everything coded in noughts and ones,
yes and no. This begs the question that arose earlier. If a pharmacist is simply an effector of a set of rules, then why not replace them with a machine? The technology is there. Dispensing robots are in many towns in Ireland. As electronic prescriptions become the norm, then there is an obvious progression. The reality is that there are times when it is necessary for pharmacists to break the law, purely in the patient’s best interest. These are exceptional circumstances. But they exist. And no computer can take the place of a professional taking a compassionate and professional decision to avoid or minimise harm.
FMD day passed with a splutter and a phut: nobody died and some actually had a working system in place by 9 February. As anticipated, plain sailing was not the order of the day. On a very positive note, the powers that be decided on a soft rollout. This meant that all medicines, in the initial period, are supposed to scan green. This does not mean that they all have a pass, in that if you adjudge a medicine to be suspicious, you should act. This is, of course, what would have happened previously. As I had done beta testing with one specific supplier, I decided to throw my lot in with them for going live. It would be fair to say that I wasn’t particularly enamoured with the live
offering. One of the major annoyances that I endured in the trial was the niggle of having to log-in every three hours. It says something about the quality of the product that this was my biggest issue. So, what did they do? They made everybody log-in every hour with the release version. Genius. It was no great consolation as I compared my setup with others. Of those that had a working system, it was clear, with two notable exceptions, that consultation with end-user needs was minimal. In many cases, you actually have to scan twice. Life is too short for these poorly designed and rushed FMD packages. Demand more.
A NOTE FROM THE EDITOR Jack Shanahan MPSI
One of the major societal issues facing us is the twin prongs of workplace and work evolution. While nobody has a crystal ball, the growth of artificial intelligence and self-styled expert systems are making many categories of workers nervous.
IPU PRODUCT FILE
ISO 9001Registered
QualityManagement
ISO 27001Registered
Information SecurityManagement
What is in the File?The File contains information on over 63,000 products, including:
Licensed medicinal products
Unlicensed medicinal products
Medical devices and sundries (bandages, dressings, ostomy equipment etc.)
Nutritional products, including foods for special diets
Veterinary products
Photographic products
Cosmetic products
Front of Shop products (shampoos, toothpastes, vitamins etc.)
In addition to pricing information, barcodes etc., the IPU Product File provides valuable professional information on health products. The professional information provided includes the Medicinal Product Name, PA/EU number, Generic Name, Pharmaceutical Form, Strength and Legal Status.
ISO CertifiedIn 2016, the IPU Product File achieved ISO Certification for 9001 (Quality) and 27001 (Information Security). The audit and certification process for ISO Certification emphasises the robustness of the IPU Product File and underpins its position as the definitive medicinal product catalogue in Ireland.
Easy to UseThe IPU Product File is an open system, so no matter what vendor you choose, the file can be adapted for your needs. The IPU Product File is available by electronic download, where you can log-in and download your monthly update.
Contact UsThe IPU Product File team are available to answer your queries, whether it’s on sourcing a product, pricing queries etc., the team will be able to assist you.
For any queries relating to the IPU Product File, please contact a staff member on 01 406 1550 or [email protected]
The IPU Product File has been in existence for more than 30 years and is an indispensable resource for community pharmacists. It was designed for pharmacists by pharmacists and is also used by doctors and hospital personnel. It is a vital support tool for prescribing, dispensing, claiming with PCRS, stock ordering, stock taking, price checking and product sourcing.
IPUREVIEW MARCH 2019 7

Pharmacy in the MediaAt the end of January, pharmacy students rallied outside the Dáil in protest at unpaid work placements. We were there to show our support to the students; there was media coverage on RTÉ Radio 1 and Darragh O’Loughlin was quoted in The Irish Times.
We were mentioned in the Irish Daily Star regarding the DPS Scheme and on Fora.ie regarding the new FMD legislation.
We were mentioned in the Mail on Sunday ahead of the launch of Operation Transformation’s nationwide Weigh Your Age campaign and our involvement this year. The campaign was announced on the programme on RTÉ One on Wednesday 6 February. There was significant national media around the campaign including The Irish Times, Irish Independent, The Herald and on RTÉ.ie. IPU member Sarah Breslin was quoted for an article in the Lifestyle section of the Irish Independent and there was coverage in the Donegal Democrat. Ann Marie Horan was also on RTÉ One’s Claire Byrne Live to discuss the campaign. There was a segment on Operation Transformation on 13 February to show footage from some of the pharmacies.
There was also coverage on RTÉ.ie, in two articles in the Irish Examiner, and in the Irish Daily Mirror regarding the IPU’s objection to VAT on food supplements.
Dates for your DiaryMARCH 2019
10 – 16 March World Glaucoma
Week, www.world
glaucomaweek.org/t
11 – 17 March National Brain
Awareness Week,
www.nai.ie/go/brain_
awareness_week
19 – 28 March IPU Member Briefings
22 March Daffodil Day,
www.cancer.ie
24 March World TB Day,
www.stoptb.org
26 March Purple Day, Epilepsy
Ireland, www.epilepsy.ie
29 March Early Bird Deadline
for IPU conference,
www.pharmacy
conference.ie
APRIL 2019
Bowel Cancer Awareness Month
www.cancer.ie
6 April ISF Dermatology Study
Day, www.irishskin.ie
12 April 65 Roses Day
(Cystic Fibrosis),
www.bit.ly/65Roses2019The � rst dedicated and No. 1 supplier of
unlicensed or di� cult to get medicines in Ireland.
Medisource is Irish-owned and has a team of pharmacist-led experts to deal with your enquiries.
We’re making it even easierto � nd unlicensed medicines. They’re now just a click away.
shop.medisource.ie
www.medisource.ie | Call 1890 2866366 | Fax 01 2866288 | Email [email protected]
Medisource is delighted to introduce our new online ordering system for exempt medicinal products. Pharmacists can register for online access at shop.medisource.ie
■ Real-time stock information
■ Easy search � lter
■ Tracking of online order history
■ Fast re-order option
■ Relevant product details e.g. HSE code, Fridge item, Foreign pack
■ No fax requirement
Medisource A4 Flyer ART.indd 1 25/02/2015 11:27
IPUREVIEW MARCH 20198

The � rst dedicated and No. 1 supplier of unlicensed or di� cult to get medicines in Ireland.
Medisource is Irish-owned and has a team of pharmacist-led experts to deal with your enquiries.
We’re making it even easierto � nd unlicensed medicines. They’re now just a click away.
shop.medisource.ie
www.medisource.ie | Call 1890 2866366 | Fax 01 2866288 | Email [email protected]
Medisource is delighted to introduce our new online ordering system for exempt medicinal products. Pharmacists can register for online access at shop.medisource.ie
■ Real-time stock information
■ Easy search � lter
■ Tracking of online order history
■ Fast re-order option
■ Relevant product details e.g. HSE code, Fridge item, Foreign pack
■ No fax requirement
Medisource A4 Flyer ART.indd 1 25/02/2015 11:27

IPU Conference – Early Bird DeadlineThe IPU National Pharmacy Conference is the ‘go-to’ event for community pharmacists in Ireland. The 9th annual conference will take place on 10 – 12 May 2019 in the Galmont Hotel, Galway. IPU Members can avail of a special Early Bird Rate – book before 29 March to secure the discounted rate.
The range of events held over the weekend ensures that there is something for everyone at this year’s conference. The conference is open to all registered pharmacists, as well as pharmacy staff and owners who are members of the IPU, and Pharmacy Interns.
10 educational sessions will be held over the weekend, providing you with the opportunity to enhance your skills, differentiate yourself from your peers and help you to stay up-to-date with current issues. The clinical sessions will focus on supporting a range of patients, thus improving patient outcomes and bettering the health of the communities you serve. Turn to pages 25-29 for more information about our 10 CPD sessions, along with a booking form you can use to book your place.
Your conference ticket gets you unlimited access to all the sessions, as well as the Exhibition Hall, Panel Discussion and Plenary Session. You can find full details of the conference at www.pharmacyconference.ie.
The Early Bird rate, available to IPU Members, is only €100. Sign-up and save before 29 March.
Operation Transformation – Thank you to all involved We want to thank all of you who took part in last month’s Operation Transformation Weigh Your Age campaign. It was a huge success and participating pharmacies were very busy all day. From feedback we have received from members, there was a great turnout in pharmacies and members were very happy with how everything went.
S U P P O R T E D B Y
As part of Operation Transformation, have your
metabolic age, visceral fat, fat percentage and weight
checked FOR FREE in this Pharmacy on 7 February 2019
WEIGHYOUR AGE
IPU NEWS
IPUREVIEW MARCH 201910

S U P P O R T E D B Y
As part of Operation Transformation, have your
metabolic age, visceral fat, fat percentage and weight
checked FOR FREE in this Pharmacy on 7 February 2019
WEIGHYOUR AGE
Hi Tech Portfolio
Further information is available on request from Accord Healthcare Ireland Ltd, Euro House |
Euro Business Park | Little Island | Cork | T45 K857 | Ireland. Tel: 021-461 9040 or from the SmPC available on www.accord-healthcare.ie
Date of Preparation: September 2018 UK&IE/HiT/0002/10-17a
Products subject to prescription. Supply through pharmacies only. Marketing Authorisation Holder for Actavis products Actavis Group PTC ehf, Reykavikurvegi, 76-78, 220 Hafnarfjordur, Iceland and for Accord products Accord Healthcare Limited, Sage House, 319 Pinner Road, North Harrow, Middlesex HAI 4HF, United Kingdom.
ONCOLOGY AGENT
BicalutamideBicalutamide
50 mg x 28 Film Coated Tablets
Capecitabine AccordCapecitabine
150 mg x 60 Film Coated Tablets300 mg x 60 Film Coated Tablets500 mg x 120 Film Coated Tablets
Accofil ▼Filgrastim
30 MU/0.5 ml Solution for Injection / Infusion in Pre-Filled Syringe x 5
48 MU/0.5 ml Solution for Injection / Infusion in Pre-Filled Syringe x 5
NEUTROPENIA
Imatinib AccordImatinib
100 mg x 60 Film Coated Tablets400 mg x 30 Film Coated Tablets
Temozolomide AccordTemozolomide5 mg x 5 Hard Capsules20 mg x 5 Hard Capsules100 mg x 5 Hard Capsules140 mg x 5 Hard Capsules180 mg x 5 Hard Capsules250 mg x 5 Hard Capsules
LinezolidLinezolid
600 mg x 10 Film Coated Tablets
ANTI-BACTERIAL AGENT
ANTI-FUNGAL AGENT
Voriconazole AccordVoriconazole
50 mg x 28 Film Coated Tablets 200 mg x 28 Film Coated Tablets
ANTI-VIRAL AGENT
ValganciclovirValganciclovir
450 mg x 60 Film Coated Tablets
IMMUNOSUPPRESSANT
Mycophenolate Mofetil AccordMycophenolate Mofetil
250 mg x 100 Capsules500 mg x 50 Film Coated Tablets
PULMONARY ARTERIAL HYPERTENSION
GranpidamSildenafil
20 mg x 90 Film Coated Tablets
HIV-1 INFECTION AND HEPATITIS B INFECTION
Tenofovir disoproxil Tenofovir disoproxil
245 mg x 30 Film Coated Tablets
Entecavir (Actavis)Entecavir
0.5 mg x 30 Film Coated Tablets
HEPATITIS B INFECTION
Pelgraz ▼Pegfilgrastim
6 mg Solution for Injection in Pre-Filled Syringe x1

Urgent progress needed on resourcing healthcare in the communityThe Government faces increasing and often competing demands from across the healthcare industry. In the face of these pressures the IPU has urged the Government to remain focussed on their primary care objectives and to deliver new and efficient ways to treat patients in their communities.
There are over 1,800 community pharmacies nationwide and the range of services they provide could be significantly enhanced. However, according to the IPU, the Government has consistently failed to progress a series of common-sense proposals, creating missed opportunities for patients and the system as whole.
Darragh O’Loughlin, Secretary General of the IPU said, “Community pharmacy is the most accessible part of our healthcare system, with four out of five members of the public visiting a pharmacy at least once a month. It is clear that our patients want to avail of more services from the convenience of their local pharmacy, but a lack of action from Government is consistently preventing us from doing so. Crucially, there are many people currently being treated by GPs, who could be treated in pharmacies. GP practices are already under severe pressure, with many reportedly unable to take on new patients. With GPs overwhelmed, it makes absolute sense to expand the scope of services provided by community pharmacists, which will reduce the burden on this overstretched part of the healthcare system.”
Services which the IPU recommend rolling out to Irish pharmacies include:
n Minor Ailment Scheme This scheme would enable medical card patients receive treatment for common illnesses such as hay fever, migraine or skin conditions free of charge direct from their local pharmacy. Currently medical card patients are required to visit a GP and obtain a prescription for treatments ordinarily available over the counter. Implementing this scheme prevent the requirement for up to 950,000 GP consultations each year.
n New Medicine Service A structured pharmacy-led monitoring service for patients on newly prescribed medications for long-term illnesses including COPD and Type 2 Diabetes. A pilot in Ireland has already shown this improves ‘optimal adherence’ to medications and could bring savings to the health system.
n Chronic Disease Management Envisaged as a collaborative initiative between GPs, Pharmacists and other healthcare providers this scheme would see pharmacists would monitor important health indicators and refer any concerns to GPs. A pharmacy-based blood pressure management service could for example save the state €1.36bn over 30 years.
“Irish pharmacists are ready, willing and waiting to enhance the levels of care they provide,” said Darragh O’Loughlin. “Unfortunately, time and again, despite all the successful pilots and studies, community pharmacists’ positive intentions and desire to help patients is left to gather dust on a shelf.”
Darragh O’Loughlin concluded that, “The time is right to optimise our delivery of primary care by providing appropriate convenient, accessible and cost-effective healthcare through pharmacies in communities throughout the country. Patients cannot afford to wait.”
IPU NEWS
IPUREVIEW MARCH 201912

RELIFE.MY SKIN SAYS
HOW I FEEL
IR-R
EL-
01-
2019
FE
B 2
019
P. 296 C
Uti l izzati 2 Colori Pantone:
P. 424 C
P. 296 C
Colore:
Relife advert._final.indd 1 15/02/2019 14:11

IPU NEWS
Member Briefings – March 2019 The IPU will be holding a series of member briefings in the last two weeks of March (see details below) to update you on all relevant current issues and to hear your views. Issues to be discussed will include the following:
n Current position regarding FEMPI;
n Falsified Medicines Directive / medicines authentication;
n Brexit;
n PCRS issues;
n Political lobbying campaign; and
n Any other issues arising.
Region Venue Time Date
Cork The Oriel House HotelBallincollig, Co. Cork
8.00pm 19 March
Limerick The Strand HotelEnnis Road, Limerick City
8.00pm 20 March
Kilkenny Newpark HotelCastlecomer Road, Kilkenny
8.00pm 21 March
Sligo Clayton HotelClarion Road,Ballytivnan, Sligo
8.00pm 25 March
Athlone Hodson Bay HotelRoscommon Road, Athlone
8.00pm 26 March
Galway Maldron Hotel Sandy Road(Formerly the Pillo Hotel)Headford Road, Galway
8.00pm 27 March
Dublin Crowne Plaza HotelBlanchardstown, Dublin 15
8.00pm 28 March
Congratulations Congratulations to Alma Barr, Education Coordinator, IPU, who gave birth to a baby boy last month. We wish Alma and Jonathan all the best with their new arrival!
GET THE RETAIL FACTOR IN YOUR PHARMACY.For further information on the IPU Retail Review service, please contact Darren Kelly on (01) 493 6401 / 086 028 9825 or email: [email protected]
IPU Retail Banners 190X45 MAR16 ART.indd 4 25/03/2016 17:55
IPUREVIEW MARCH 201914

DON’T LET PAIN HOLD YOU BACK
ESSENTIALINFORMATION
Solpa-Extra 500mg/65mg Soluble Tablets contain paracetamol and caffeine. For the treatment of mild to moderate pain. Adults and children over 16 years: 1-2 tablets dissolved in water every 4-6 hours. Max 8 tablets a day. Children 12-15 years: 1 tablet disolved in water every 4-6 hours. Max 4 tablets a day. Not suitable for children under 12 years. Contraindications: Hypersensitivity to the ingredients. Precautions: Particular caution needed under certain circumstances, such as renal or hepatic impairment, chronic alcoholism and malnutrition or dehydration. Precautions needed in asthmatic patients sensitive to acetylsalicylic acid, patients on a controlled sodium diet and with rare hereditary problems of fructose intolerance. Patients should be advised not to take other paracetamol containing products concurrently. Pregnancy and lactation: Not recommended during pregnancy and breastfeeding. Side effects: Rare: allergies. Very rare: thrombocytopenia, anaphylaxis, bronchospasm, hepatic dysfunction, cutaneous hypersentitivity reactions. Unknown: nervousness, dizziness. Further information is available in the SmPC. PA 1186/017/001. P. MAH: Chefaro Ireland DAC, Treasury Building, Lower Grand Canal Street, Dublin 2, Ireland. Date of preparation: April 2017.
Solpa-Extra New KV A4 Trade Ad.indd 1 01/02/2019 18:14

BUSINESS Jim Power, Economist
Trading conditions for the pharmacy sector continued to gradually improve in 2018 in line with most other parts of the economy. Sales of Pharmaceutical, Medical and Cosmetic items increased by 1.5% in value terms in 2018 and by a much stronger 5.5% in volume terms.
The pharmacy sector in 2018Trading conditions for the pharmacy sector continued to gradually improve in 2018 in line with most other parts of the economy. Sales of Pharmaceutical, Medical and Cosmetic items increased by 1.5% in value terms in 2018 and by a much stronger 5.5% in volume terms. Between 2015 and 2018, the volume of
sales increased by 17.1%, but the value of sales increased by a more modest 6.6%. This suggests that the pharmacy sector is still dealing with a financially pressurised consumer sector, with the ability to convert volume growth into value growth still challenging.
Economic backdrop for pharmacy sector
IPUREVIEW MARCH 201916

On the price side, compression is still a feature of the market. In 2018, the average consumer price of pharmaceutical products was 3.4% lower than the previous year and 10.5% lower than 2008; the average price of prescribed drugs declined by 5.3% in 2018 and was 19.7% lower than 2008; and the average price of other medicines declined by 0.1% in 2018, but prices were 1.8% higher than 2008.
The economy in 2018The Irish economy performed strongly in 2018, with almost all indicators of economic activity continuing to suggest solid levels of economic momentum.
GDP growthQuarterly national accounts data are available for the first nine months of 2018 and show that in the first three quarters of the year, real gross domestic product (GDP) expanded by 7.4% and real gross national product (GNP) expanded by 7.5%. Personal consumption increased by 3.1% and exports of goods and services expanded by 9.2%. Modified domestic demand expanded by 4.5%. This is an indicator of domestic demand where globalisation effects, such as trade in intellectual property products and trade in aircraft by leasing companies, are excluded. This is a more accurate representation of what happened on the ground in the real economy in 2018 and it describes an economy that experienced steady rather than dramatic growth as the GDP and GNP growth rates might appear to suggest.
Consumer dynamicsIn 2018, the volume of retail sales expanded by 3.8% but the growth in value terms was lower at 2.7%. The persistent gap between volume and value growth reflects the fact that retailers are still dealing with a personal sector that is resistant to higher prices and is continuously in search of value for money. This cautious consumer behaviour is due to
Figure 1: Retail Sales of Pharmaceutical, Medical & Cosmetic Items
Source: CSO
Figure 2: Consumer Price of Pharmacy Products
Source: CSO
the fact that personal finances are still stretched due to low wage growth for the past decade; a high personal tax burden; uncertainty relating to the impact of Brexit; and rapidly escalating house prices and rents that are soaking up disposable income, leaving less money available for other discretionary spending. The retail market is challenging, with the growth in online purchasing also a significant business challenge.
Consumer confidence recovered strongly in the aftermath of the recession
in 2008 but it has plateaued over the past three years and is proving quite volatile from month to month. In October, confidence dipped to a 46-month low but it improved modestly in January.
Issues such as Brexit, rapidly escalating house prices and rents, higher fuel costs, the high personal tax burden, and subdued wage growth are combining to have a somewhat sobering influence on the personal sector. However, this is not indicative of an impending sharp correction in consumer
spending, but rather reflects the financial strains that continue to pressurise the personal sector.
Labour marketIn the year to September 2018, the number of people in employment increased by 66,700 or 3% to reach 2.273 million. This is the highest level of employment ever achieved in Ireland. The growth in employment is broadly based from a sectoral perspective, and unlike the years leading up to 2007, it is not being driven primarily by
IPUREVIEW MARCH 2019 17

Figure 3: Consumer Confidence
Source: ESRI/KBC Bank
the construction sector and related activities. This makes it look more sustainable.
In the year to January 2019, the number of people officially registered as unemployed declined by 13,400, to reach 127,300. The unemployment rate stood at 5.3% of the labour force in January, which is down from 16% at the beginning of 2012.
TourismThe tourism performance continues to be very strong. In 2017, 9.93 million overseas visitors came to Ireland, which is the highest level ever recorded. The strong tourism performance continued in 2018. 10.6 million overseas visitors came into the country, which is 6.9% ahead of 2017. Visitor numbers from Great Britain increased by 0.8% to reach 3.76 million, and accounted for 35.4% of total overseas visitor numbers. This is down from 40.9% in 2016. Sterling weakness and slower UK growth have impacted on this market segment. Visitor numbers from North America increased by 13.4% to reach 2.38 million; and visitor numbers from the rest of Europe, excluding Great Britain, increased by 9.5% to reach 3.81 million.
Table 1: Employment Growth by Sector Q3 2012 – Q3 2018
Sector Q3 2012 (000S)
Q3 2018 (000S)
Change
Agriculture 110.1 104.9 -5,200
Industry 232.8 284.6 +51,800
Construction 82.8 146.5 +63,700
Retail & Wholesale 276.6 301.0 +24,400
Transportation 83.4 101.2 +17,800
Accommodation & Food Services
127.4 181.2 +53,800
ICT 91.2 124.1 +32,900
Financial Services 103.6 101.3 -2,300
Professional & Scientific
106.5 135.4 +28,900
Admin & Support Services
79.7 105.4 +25,700
Public Admin & Defence
89.3 104.1 +14,800
Education 134.2 170.6 +36,400
Health 258.4 282.1 +23,700
TOTAL 1,887.0 2,273.2 +386,200
Source: CSO, Labour Force Survey, 20 November 2018
The public financesThe Government recorded an Exchequer surplus of €106 million in 2018. This is the first budget surplus since 2006. The improvement in the public finances is due to tax revenue buoyancy rather than any serious efforts to control public expenditure. For the year as a whole, the Exchequer collected €55.6 billion in taxation, which is the highest level of tax revenues ever collected.
Tax revenues continued to grow strongly in January and were 7% ahead of January 2018. An Exchequer surplus of €1.64 billion was recorded in January.
The outlook for 2019The outlook for the Irish economy in 2019 looks reasonably good but the risks and challenges are clear.
As 2018 progressed, the external environment did give cause for concern. Growth in the Euro Zone lost considerable momentum; a number of emerging economies, such as Brazil, Argentina, Venezuela and Turkey, experienced considerable economic and political difficulties; UK growth was undermined by Brexit-related uncertainty and China lost considerable momentum. The US was the most notable exception, as the tax package implemented a year ago gave a significant boost to economic activity.
As we look ahead to 2019, many of the signs are pointing towards a more challenging year for the global economy and global geopolitics. It is unlikely that global recession will be experienced, but global growth looks set to be somewhat slower than in 2018 and there are considerable risk factors that will need to be watched closely.
n US growth is likely to ease over the coming months, as the fiscal stimulus package introduced a year ago dissipates. To date, the
IPUREVIEW MARCH 201918

Uncontrolled blood sugar
can’t wait
INVOKANA® (canagliflozin) 100 mg & 300 mg film-coated tablets. PRESCRIBING INFORMATION. Republic of Ireland. Please refer to Summary of Product Characteristics (SmPC) before prescribing. INDICATIONS: The treatment of adults with insufficiently controlled type 2 diabetes mellitus as an adjunct to diet and exercise as monotherapy when metformin is considered inappropriate due to intolerance or contraindications, or in addition to other medicinal products for the treatment of diabetes. DOSAGE & ADMINISTRATION: Adults: recommended starting dose: 100 mg once daily. In patients tolerating this dose and with eGFR ≥ 60 mL/min/1.73 m2 needing tighter glycaemic control, dose can be increased to 300 mg once daily. Caution increasing dose in patients ≥ 75 years old, with known cardiovascular disease or for whom initial canagliflozin-induced diuresis is a risk. Correct volume depletion prior to initiation. When add-on, consider lower dose of insulin or insulin secretagogue to reduce risk of hypoglycaemia. For oral use, swallow whole. Children: no data available. Elderly: consider renal function and risk of volume depletion. Renal impairment: not to be initiated with eGFR < 60 mL/min/1.73 m2. If eGFR falls below this value during treatment, adjust or maintain dose at 100 mg once daily. Discontinue if eGFR persistently < 45 mL/min/1.73 m2. Not for use in end stage renal disease or patients on dialysis. Hepatic impairment: mild or moderate; no dose adjustment. Severe; not studied, not recommended. CONTRAINDICATIONS: Hypersensitivity to active substance or any excipient. SPECIAL WARNINGS & PRECAUTIONS: Not for use in type 1 diabetes. Renal impairment: eGFR < 60 mL/min/1.73 m2: higher incidence of adverse reactions associated with volume depletion particularly with 300 mg dose; more events of elevated potassium; greater increases in serum creatinine and blood urea nitrogen (BUN); limit dose to 100 mg once daily and discontinue when eGFR < 45 mL/min/1.73 m2. Not studied in severe renal impairment. Monitor renal function prior to initiation and at least annually. Volume depletion: caution in patients for whom a canagliflozin-induced drop in blood pressure is a risk (e.g. known cardiovascular disease, eGFR < 60 mL/min/1.73 m2, anti-hypertensive therapy with history of hypotension, on diuretics or elderly). Not recommended with loop diuretics or in volume depleted patients. Monitor volume status and serum electrolytes. Haematocrit: careful monitoring if already elevated. Genital mycotic infections: risk in male and female patients, particularly in those with a history of GMI. Lower limb amputation: Consider risk factors before initiating. Monitor patients with a higher risk of amputation events. Counsel on routine preventative foot care and adequate hydration. Consider discontinuing Invokana when events preceding amputation occur (e.g. lower-extremity skin ulcer, infection, osteomyelitis or gangrene). Urine laboratory assessment: glucose in urine due to mechanism of action. Lactose intolerance: do not use in patients with galactose intolerance, total lactase deficiency or glucose-galactose malabsorption. Diabetic ketoacidosis (DKA): rare DKA cases reported, including life-threatening and atypical presentation cases. Where DKA is suspected or diagnosed, discontinue Invokana treatment immediately. Interrupt treatment in patients who are undergoing major surgical procedures or have acute serious medical illnesses. Consider risk factors for development of DKA before initiating Invokana treatment. SIDE EFFECTS: Very common (≥1/10): hypoglycaemia in combination with insulin or sulphonylurea, vulvovaginal candidiasis. Common (≥1/100 to <1/10): constipation, thirst, nausea, polyuria or pollakiuria, urinary tract infection (including pyelonephritis and urosepsis), balanitis or balanoposthitis, dyslipidemia, haematocrit increased. Uncommon (<1/100) but potentially serious: anaphylactic reaction, diabetic ketoacidosis, syncope, hypotension, orthostatic hypotension, urticaria, angioedema, bone fracture, renal failure (mainly in the context of volume depletion), lower limb amputations (mainly of the toe and midfoot, incidence rate of 0.63 per 100 subject-years, vs 0.34 for placebo). Refer to SmPC for details and other side effects. PREGNANCY: No human data. Not recommended. LACTATION: Unknown if excreted in human milk. Should not be used during breast-feeding. INTERACTIONS: Diuretics: may increase risk of dehydration and hypotension. Insulin and insulin secretagogues: risk of hypoglycaemia; consider lower dose of insulin or insulin secretagogue. Effects of other medicines on Invokana: Enzyme inducers (e.g. St. John’s wort, rifampicin, barbiturates, phenytoin, carbamazepine, ritonavir, efavirenz) may decrease exposure of canagliflozin; monitor glycaemic control. Consider dose increase to 300 mg if administered with UGT enzyme inducer. Cholestyramine may reduce canagliflozin exposure; take canagliflozin at least 1 hour before or 4-6 hours after a bile acid sequestrant. Effects of Invokana on other medicines: Monitor patients on digoxin, other cardiac glycosides, dabigatran. Inhibition of Breast Cancer Resistance Protein cannot be excluded; possible increased exposure of drugs transported by BCRP (e.g. rosuvastatin and some anti-cancer agents). LEGAL CATEGORY: POM. PACK SIZES & MARKETING AUTHORISATION NUMBER(S): Invokana 100 mg film-coated tablets: 30 tablets; EU/1/13/884/002. Invokana 300 mg film-coated tablets: 30 tablets; EU/1/13/884/006. MARKETING AUTHORISATION HOLDER: Janssen-Cilag International NV, Turnhoutseweg 30, B-2340 Beerse, Belgium. ® INVOKANA is a registered trade mark of Janssen-Cilag International NV and is used under licence. © 2017 Napp Pharmaceuticals Limited. FURTHER INFORMATION IS AVAILABLE FROM: Mundipharma Pharmaceuticals Limited, Millbank House, Arkle Road, Sandyford, Dublin 18. For medical information enquiries, please contact [email protected]. UK/INV-18203. Date of Preparation September 2018.
Adverse events should be reported to: HPRA Pharmacovigilance, Earlsfort Terrace, IRL - Dublin 2; Tel: +353 1 6764971; Fax: +353 1 6762517. Website: www.hpra.ie; E-mail: [email protected] events should also be reported to Mundipharma Pharmaceuticals Limited on [email protected] or by phone on 01 2063800 (1800 991830 outside office hours)
INVOKANA® is a registered trade mark of Janssen-Cilag International N.V. and is used under licence. MUNDIPHARMA® and the ‘mundipharma’ logo are registered trade marks of Mundipharma AG. Date of Item: November 2018. IRE/INVK – 18273
Distributed in Ireland by: Mundipharma Pharmaceuticals Limited, Millbank House, Arkle Road, Sandyford, Dublin 18, Ireland. Phone +353-1-2063800 www.mundipharma.ie
References: 1. Invokana SmPC www.medicines.ie 2. Davies MJ et al, Diabetes Care. 2018 Oct: 10.2337/dci18-0033 (http://diabetologia-journal.org/wp-content/uploads/2018/10/Consensus-Report-ADA-EASD.pdf). 3. Wilding JP et al J Diabetes Complications 2015; 29;438-44. 4. Neal B. et al. N Engl J Med 2017; 377:644-657. 5. Perkovic V. et al Lancet Diabetes Endocrinol. 2018 Sep;6(9):691-704
Seize the moment to make years of
difference
INVOKANA is indicated for the treatment of adults with insufficiently controlled type 2 diabetes mellitus (T2DM) as an adjunct to diet and exercise.1
The recommended starting dose of INVOKANA is 100mg once-daily.
* an SGLT2i for treatment of T2DM patients with ASCVD, HF, CKD and for use in patients where there is a compelling need to minimise hypoglycemia and those with a compelling need to minimise weight gain or promote weight loss
† Compared to standard of care
Lower HbA1c levelsIn patients with HbA1c higher than 9%, INVOKANA reduces HbA1c by 1.57% and 1.80% with its 100mg and 300mg doses respectively.3
Long-term cardiovascular benefits†
14% reduction in the risk of cardiovascular death, nonfatal myocardial infarction and nonfatal stroke (3-point MACE) HR 0.86 (95% CI 0.75-0.97).4
33% reduction in risk of hospitalisation for heart failure HR 0.67 (95% CI 0.52 - 0.87).4
Improved renal outcomes†
47% relative risk reduction in time to first adjudicated nephropathy event (doubling of serum creatinine, need for renal replacement therapy, and renal death) HR 0.53 (95% CI 0.33 - 0.84).5
27% reduction in the progression of albuminuria in patients with normo- or micro-albuminuria HR 0.73 (95% CI 0.67-0.79).4

economic momentum in the economy has been generally solid but there are definite signs of easing. There are also justifiable concerns about President Trump and his trade agenda. The growth of protectionism would not be good for global growth, and Ireland would be particularly vulnerable given the importance of external trade to the economy.
n Growth in the Euro Zone, the UK and China is likely to soften further, and emerging market economies are likely to continue to struggle.
n Global geopolitics also look risky, with Russia, the rise of the right in Italy, Hungary, Poland and Austria, the riots in France, and the relationship between the US and China being key issues of concern.
n US interest rates were increased four times during 2018. The Federal Reserve believes that rates will need to be increased by 0.5% over the coming year but this may not be needed. Based on recent slower growth in the Euro Zone and the complete lack of inflation, ECB rates are likely to remain unchanged for the duration of 2019. The ECB is currently very
relaxed about interest rates and a bit concerned by the slowdown in growth, particularly in Germany. This bodes well for interest rates.
n The outcome for Brexit remains deeply uncertain and will continue to represent a source of risk for Europe in general, but for Ireland and the UK in particular. A ‘soft Brexit’ would see sterling strengthen and a significant rebound in the UK economy, which would be very good news for Ireland. However, Brexit remains a source of considerable uncertainty and defeat for common sense.
The key domestic challenges include:
n The imbalance between demand and supply in the housing market is putting considerable upward pressure on house prices and rents and is undermining national competitiveness. It appears likely that house price inflation will moderate in 2019 due to affordability issues rather than adequate supply, but rents look set to remain under considerable upward pressure. Housing supply needs to increase as a matter of priority.
” It is unlikely that global recession will be experienced, but global growth looks set to be somewhat slower than in 2018 and there are considerable risk factors that will need to be watched closely.”
n The pressure to increase expenditure on public services, particularly health, will remain strong and will pressurise the public finances. Public sector pay pressures will be a particular challenge. Ireland still has a dangerously high level of Government debt that needs to be brought under control.
n As the economy steadily moves towards full employment, wage pressures are likely to intensify and the recruitment and retention of workers will become a significant challenge for all employers.
n The personal sector will remain pressurised due to a combination
of the high personal tax burden; subdued wage growth for the past decade, although wages will rise more strongly in 2019; rising house prices and rents will continue to soak up household disposable income; and Brexit will remain a source of deep concern and uncertainty.
Real GDP growth is forecast to expand by around 5% in 2019. Consumer spending is projected to grow by 3.2%; the unemployment rate is expected to fall below 5% but should average around 5% for the full year; and employment is expected to grow by 1.5% to average 2.29 million. A solid year looks in prospect, not least due to the strong momentum carrying forward from last year, but the risks and challenges will need to be watched very closely.
IPUREVIEW MARCH 201920
Challenging Times Ahead?Let Accord take care of you
Further information is available on request from Accord Healthcare Ltd Euro House I Euro Business Park I Little Island I Cork I T45 K857 I Ireland 021-461 9040
Date of Preparation: Jan 2019 NA-371-01
Damien McCormack
John MacHale
Martina Sweeney
David Lane
Gregg Farrell
Padraic O’Brien
Richard Doherty

PROFESSIONAL Jennifer Flaherty, ITT, Dan Ahern, Community Pharmacist Farranfore, Sinéad Flaherty, ITT and Tom Farrelly, ITT.
A community pharmacy-based pilot project for BowelScreen in County KerryBowel cancer is the second most common form of cancer in men, and third in women, diagnosed in Ireland. The most recent figure reported that 2,775 people were diagnosed with bowel cancer in 2017 (National Cancer Registry, 2018).
Individuals feel that bowel cancer is not as widely discussed or advertised as breast screening
and therefore do not see the importance of taking part in screening especially when they feel fine and do not have any symptoms (Wackerbarth et al, 2005). There is also an element of social embarrassment around bowel cancer, leading to it not being as freely discussed as other forms of cancer (Jones et al, 2010). The evidence would show that there is a concern amongst participants around the acceptability
of the screening test. Some people often believe the test is more complicated than it is and/or that it is quite distasteful. In recent years, there has been a shift from dispensing medication towards patient care, placing pharmacists in a prime position for delivering health messages and incorporating cancer screening initiatives into their existing practice (Havlicek and Mansell, 2016). Pharmacists are well placed to have open discussions with the public, as many people buy over-the-counter medication for common bowel issues such as irritable bowel
syndrome, altered bowel habits and hemorrhoids.
Mindful of looking for different ways of trying to promote cancer screening, the National Screening Service’s Bowel Screen approached researchers in the Institute of Technology Tralee (ITT) to investigate innovative ways of attracting people to participate in bowel screening. This study sought to assess the effectiveness of a community pharmacy based opportunistic bowel screening intervention. This study was a joint project between the National Screening Service (Ms Lynn Swinburne) and the
ITT with the support of the Irish Pharmacy Union, and in particular, Ms Pamela Logan, Director of Pharmacy Services with the IPU. The study was commissioned and carried out between March and July 2018 across six community pharmacies in county Kerry. The sites represented a mix of rural, medium and large towns in the county. In order to ensure a high level of consistency, pharmacists from the selected sites were invited to a training workshop in the delivery of the BowelScreen message and to educate them about how the bowel screening service operates.
IPUREVIEW MARCH 201922

“I quit smoking for her”Fergus O’Shea
FOR 24 HOUR CONTROL
Help smokers quit with an unbeatable combination* from
Now PCRSREIMBURSEABLE
ON THE GO CRAVING RELIEF Mini
*Provides significant improvements in quit rates vs patch alone.NiQuitin Clear 14mg Patches. Indication: Stop Smoking aid, Contains nicotine, Requires willpower. Always read the leaflet. Legal classification: GSL. PA 1186/18/5. MAH: Chefaro Ireland DAC, Treasury Building, Lower Grand Canal Street, Dublin 2, Ireland. Information about the product including adverse reaction, precaution, contra-indication and method of use can be found at: http://www.medicines.ie/medicine/12137/SPC/NiQuitin+CLEAR+14+mg+24+hours+transdermal+patch/ (14 mg). NiQuitin Mini Mint 1.5 mg Lozenges. Stop Smoking aid, Contains nicotine, Requires willpower. Always read the leaflet. Legal classification: GSL PA 1186/18/11 (1.5mg) PL. MAH: Chefaro Ireland DAC, Treasury Building, Lower Grand Canal Street, Dublin 2, Ireland. Information about the product including adverse reaction, precaution, contra-indication and method of use can be found at: http://www.medicines.ie/medicine/14493/SPC/NiQuitin+Mini+1.5mg+mint+lozenges (1.5mg). Date of preparation: 12/09/2018.
+ Patch
NiQuitin A4 Trade Ad (New KV Dad-Child) IRE v6 IPN.indd 1 24/10/2018 15:10

Patients aged between 60 to 69 years, presenting for prescriptions or other pharmacy items, were targeted to receive an intervention delivered by the pharmacist recommending the BowelScreen home test. In total, 85 people signed up to take part in the home test and of that number, 69 were deemed to be eligible to take part. Out of the 69 participants, 51 people returned the test kit, giving an overall uptake rate of 73.9%. For the purpose of illustration, the national return rates for the same time
period in 2017 and 2018 were compared with the return rates in this initiative. Given the wide disparity in sample sizes, it is difficult to make a direct comparison and as such should be treated with caution. Nonetheless, the kit return rates were very encouraging by comparison and certainly would suggest that community pharmacies are very well placed to assist with such health promotion initiatives.
Most people feel that they can appropriately self-care for these conditions at home and would not go to see the
GP until they are very unwell. Through these interactions, the community pharmacist therefore has the opportunity to raise awareness for bowel screening (Connolly, 2007). Pharmacists are in a prime position to aid with health screening, as they are one of the most accessible healthcare professionals to members of the general public and are already actively involved with health promotion and prevention as illustrated by their participation in the influenza vaccination programme.
09/04 – 06/05 2018 2017 Pilot Project Rates
No. Invited 28,879 22,985 69
Kits Returned 11,023 8,871 51
% Return Rate 38% 38.5% 73.9%
References1. Connelly, D., 2007. Community
pharmacists can play a key role raising awareness of bowel cancer. Pharmaceutical Journal, 278(7452), pp.580-580.
2. Havlicek, AJ. & Mansell, H. 2016. The community pharmacist’s role in cancer screening and prevention. Canadian Pharmacy Journal, 149(5),pp. 274-282.
3. Jones, R.M., Devers, K.J., Kuzel, A.J. and Woolf, S.H., 2010. Patient-reported barriers to colorectal cancer screening: a mixed-methods analysis. American journal of preventive medicine, 38(5), pp.508-516.
4. National Cancer Registry, 2018. Cancer Factsheet Colorectal. [Online]. Available at: https://www.ncri.ie/sites/ncri/files/factsheets/Factsheet%20colorectal.pdf [Accessed 26th December 2018].
5. Wackerbarth, S.B., Peters, J.C. and Haist, S.A., 2005. “Do We Really Need All That Equipment?” Factors Influencing Colorectal Cancer Screening Decisions. Qualitative Health Research, 15(4), pp.539-554.
6. World Health Organisation, 1994. The Role of the Pharmacist in the Healthcare System. [Online] Available at: http://apps.who.int/medicinedocs/pdf/h2995e/h2995e.pdf [Accessed 26th December 2018].
7. Winawer, S., Faivre, J., Selby, J., Bertaro, L., Chen, T.H., Kroborg, O., Levin, B., Mandel, J., O’morain, C., Richards, M. and Rennert, G., 2005. Workgroup II: the screening process. UICC International Workshop on Facilitating Screening for Colorectal Cancer, Oslo, Norway (29 and 30 June 2002). Annals of oncology, 16(1), pp.31-33.
IPUREVIEW MARCH 201924

CONFERENCE
10 CPD SESSIONS
TO CHOOSE FROM AND
MUCH MORE
IPU NATIONAL PHARMACY CONFERENCE 10 – 12 May 2019, The Galmont Hotel, Galwaypharmacyconference.ieThe face of community pharmacy is ever-changing with new initiatives always in the pipeline. The IPU National Pharmacy Conference ensures that you remain up-to-date with these developments through 10 informative educational sessions.
IPUREVIEW MARCH 2019 25

We have taken on valuable feedback from IPU members and worked with our Conference Subcommittee, IPU Academy, financial advisers, industry representatives and other organisations to develop a comprehensive and educational programme to support you with your CPD. We will provide you with a CPD template for each session which is designed to support your engagement with the CPD system developed by the IIOP. A certificate of attendance for your sessions will be sent to you after the conference. The conference programme features
professional and business sessions, covering a wide range of topics. See below information on all our sessions or for a full description, please visit www.pharmacyconference.ie.
Clinical Sessions5 Ways to Increase Your Wellbeing at Work (No Matter How Busy You Are) 4.00pm, Friday 10 May
This session will be delivered by Séamus Ruane, Galway-based contractor pharmacist with over 20 years’ experience in community pharmacy. This workshop will give you actionable, evidence-based steps to help you improve your wellbeing at work. It provides a clear template to help you consistently feel good and function effectively at work. Learn how to build positive emotion, increase engagement, and find meaning at work, all in an easy-to-apply format designed to make your changes last. Discover evidence-based, busy-proof wellbeing approaches that enable you to confidently handle common work challenges.
The Pharmacist in an Atrial Fibrillation Clinic . . . A Model of Care Sponsored by Bristol Myers Squibb 5.30pm, Friday 10 May
During this informative session, delivered by Edwina Morrissey, Senior Clinical Pharmacist at Tallaght University Hospital, you will gain a better understanding of atrial fibrillation, its diagnosis, complications and treatment. After this session you will be able to review and counsel a patient on a direct oral anticoagulant and understand the pharmacist’s role in the atrial fibrillation multidisciplinary clinic.
The Role of the Community Pharmacy Team in Supporting Palliative Care at Home 8.30am, Saturday 11 May
This exciting session is in association with Galway Hospice and will demonstrate how community pharmacy can play a big part in supporting Palliative Care in the home. This session will be delivered by Karen McKee, Chief Pharmacist, Galway Hospice Foundation.
Eczema Diagnosis and Treatment: Tips and Tricks for the Community Pharmacist / Sponsored by A.Menarini 12.30pm, Saturday 11 May
During this session, delivered by Dr Paul Ryan, Pharmacist and GP, the most recent prescribing guidelines on eczema are put into practice for the community pharmacist. Key learning points from this talk include pathophysiology of eczema, different types of eczema seen in community pharmacy as well as the treatment of the common eczema types.
The Challenges Presented by Breast Cancer Survivors Taking Antihormone Medication 10.00am, Sunday 12 May
This will be delivered by Elizabeth Summersby, RANP Oncology, Our Lady of Lourdes Hospital. Breast Cancer affects 1 in 9 Irish women and there are currently 2,883 new cases diagnosed annually1. With early detection and an increasing number of effective therapies, more women than ever are surviving breast cancer. Therapies such as Tamoxifen and Aromatase Inhibitors reduce the risk of recurrence by up to 50%2. These treatments may be used for up to 10 years3 and may result in long term side-effects.
1. National Cancer Registry, 2016. 2. Cahir et al. 2015. 3. Goss, 2016.
Business SessionsMaximising the Return from your Dispensary Data – a hmR Presentation 4.00pm, Friday 10 May
Health Market Research, for several years now, has been transforming your raw data into meaningful information to give your business the edge it needs in an extremely competitive environment. Using the most advanced technological solutions, we are helping you, the pharmacist to ‘maximise the return from your dispensary data’. hmR’s Pharmacy Platform identifies opportunities within the data and helps pharmacists unlock hidden profit potential including generic opportunities. This session will be delivered by Alan McCormick, Senior Manager – Pharmacy Business Intelligence, hmR Ireland.
Transform your Business using People, Process and Technology 8.30am, Saturday 11 May
We are looking forward to welcoming Jay Patel, Pharmacist and Executive Director, Day Lewis Plc, to speak on this topic at the conference. Pharmacy must adapt to the changing demands of both patients and commissioners. What innovation means however, is often misunderstood. This session describes what innovation actually is and how business owners can innovate leveraging three core assets (People, Process and Technology).
Economic Trends in 2019 and How they May Affect the Pharmacy Sector In Association with Moore Wealth Management 12.30pm, Saturday 11 May
This session will be delivered by Economist Jim Power where we will consider the Irish economic environment in general, the behaviour of consumers, the public finances, Brexit, interest rates and how all of these issues impact on the pharmacy business.
Leading Through Adversity 4.15pm, Saturday 11 May
Jack Kavanagh, Pharmacist and Motivational Speaker, will deliver on leading through adversity, which will reveal fundamental truths we can all relate to about the ebbs and flows of life as Jack relays his personal story of adversity and his journey from surviving to thriving in life. He will impart his biggest learnings in his journey of personal leadership, resilience and growth through the adversities we all encounter in our lives. Jack is set to inspire us at what is set to be an invigorating conference.
Leading, Delegating, Communicating – How will you Manage? 10.00am, Sunday 12 May
As a community pharmacist, you won’t just be a health professional – you will also be both a manager and a leader of a team of people within a pharmacy. The role of a pharmacist is a position of responsibility and with it comes assumed obligation; obligation to be in control, to be in authority, to solve problems, as well as to temporarily manage resources, people, compliance, targets and, above all, a health brand. There are three specific skills needed to manage the potential challenges which you may experience while working as a first-year pharmacist. These are; Communication Skills, Delegation Skills and Performance Management Skills. Join us in this session, delivered by Susan Madden, Principal, South East College – Further Education & Training, to discover how effective communication can help to foster a good working relationship between you and your team, which can in turn improve morale and employee efficiency.
IPUREVIEW MARCH 201926

Conference Information and RegistrationThe conference is open to all pharmacists, non-pharmacist pharmacy owners who are IPU Members, Pharmacy Interns and all pharmacy staff who work for members of the IPU.
You can register online at www.pharmacyconference.ie or by completing the form overleaf and faxing or posting it back to the details on the form.
Your registration fee includes
n Admission to all sessions
n Entry to Exhibition Hall
n Friday night dinner, with pre-dinner drinks
n Daily refreshments and lunches (Saturday and Sunday)
n Conference bag
Cancellations and refundsCancellations made prior to 19 April will be refunded in total. Refunds will not be processed after this date. Accommodation cancellations are at the discretion of the Galmont Hotel, Galway.
Condition of entryIt is a condition of entry that you may be photographed at the event and that your image may be used on IPU and IPU National Pharmacy Conference material. The IPU reserves the right to refuse entry to anyone it sees fit.
AccommodationThe Galmont Hotel (formerly the Radisson) is located in Galway city, just a three-minute walk from the central Eyre Square and overlooking Galway Bay. It is also just a short walk from the main railway and bus stations. Use code IPU2019 when making your reservation for a special conference rate. The hotel can be booked by contacting them on 091 538 300.
Please complete the form on the reverse and return it to the IPU to book your place for the 2019 IPU National Pharmacy Conference. You can also visit www.pharmacyconference.ie/Registration to book a place. The Early Bird rate for IPU Members is available until 29 March 2019.
We hope to see you there!
The conference also offers invaluable networking opportunities and face-to-face contact with your colleagues. There are numerous networking opportunities throughout the weekend, from the tea/coffee breaks in the Exhibition Hall to the IPU President’s Dinner & Ball – a key social event in the pharmacy calendar. This year’s President’s Dinner & Ball takes place on Saturday 11 May as part of the conference weekend. You can book your dinner ticket on the booking form provided for just €35.
Pharmacy StaffPharmacy staff and technicians can attend the conference for the full weekend for just €60! This includes admission to all sessions and the Exhibition Hall, as well as Friday night dinner and daily refreshments and lunches (Saturday and Sunday).
Pharmacy staff are a key asset to your pharmacy business and the conference is the ideal place for them to attend educational courses. To support the continuing education of pharmacy technicians, we will also hold a CPD for Pharmacy Technicians session on the Sunday morning entitled Support and Care for Cancer Patients.
One in three people in Ireland are given a diagnosis of cancer. This is almost always a life-changing event which poses challenges for patients. Pharmacy staff can offer advice and support about medication and lifestyle measures to help improve patient outcomes. At the end of this course, pharmacy technicians will be able to discuss the appropriate use of anti-emetics and other ancillary treatments prescribed for patients receiving chemotherapy or radiotherapy; advise patients on how to maintain good general health and what to do if they feel unwell; and offer practical advice on skin care and general appearance to help patients to look good and feel better.
APPEL Preceptor Training Pharmacists who would like to act as a Preceptor to a 4th-year pharmacy student under the new MPharm programme can undertake the required Preceptor training at this year’s IPU conference. These pharmacists will then be positioned to oversee four-month APPEL placements for 4th-year students in 2019. At the conclusion of the session, participants will understand the new role of the Preceptor, how placements are structured and assessed, and the learning outcomes set for students. The session will identify strategies to successfully facilitate experiential learning placements through effective feedback, resolving conflict and calibrating expectations. This training session will be delivered by Dr Maria Donovan, Practice Educator, University College Cork (UCC), and Eimear Ni Sheachnasaigh, Practice Educator, University Of Dublin, Trinity College (TCD). For more information on this session, please contact the APPEL Team at [email protected].
NEWLY QUALIFIED
PHARMACISTS!
If you first registered with
the PSI after 1 September
2016, you can attend the
conference for just
€80.
IPUREVIEW MARCH 2019 27

For further information please contactLaura Payne Brand and Trade Marketing Manager United Drug Wholesale
Mobile: 087 383 2297
Email: [email protected]
SAVE THE DATE!
14th-15th April
United, we do better
Brought to you by
14th - 15th April, Aviva Stadium, Dublin
16029 UD Pharmacy Show 2019_210mmx297mm Date In Diary AD.indd 1 15/02/2019 14:10

REGISTRATION FORMPlease complete this form in BLOCK LETTERS. Please mark below which events you would like to
attend. Please ensure you only select one option where there are parallel sessions.
Please return all forms to: Irish Pharmacy Union, Butterfield House, Butterfield Avenue, Rathfarnham, Dublin 14, D14 E126. If paying by credit card, you can also fax the form back to 01 493 6626. You will receive an email to confirm your registration and sessions booked. Alternatively, you can register online at www.pharmacyconference.ie.
FRIDAY 10 MAY12.30pm – o APPEL Preceptor Training – Supporting 3.30pm 4th-year Student Pharmacists on their Journey to Practice 4.00pm – o Maximising the Return from your 5.00pm Dispensary Data – a hmR Presentation OR o 5 Ways to Increase Your Wellbeing at Work (No Matter How Busy You Are)5.30pm – o The Pharmacist in an Atrial Fibrillation 6.30pm Clinic . . . A Model of Care8.00pm o Dinner SATURDAY 11 MAY8.30am – o Transform your Business using People, 9.30am Process and Technology OR o The Role of the Community Pharmacy Team in Supporting Palliative Care at Home10.00am – o Plenary Session 12.00pm 12.30pm – o Economic Trends in 2019 and How they 1.30pm May Affect the Pharmacy Sector OR o Eczema Diagnosis and Treatment: Tips and Tricks for the Community Pharmacist1.30pm – o Lunch 2.15pm3.00pm – o Panel Discussion: Sláintecare – 4.15pm the Future Shape of Healthcare 4.15pm – o Leading Through Adversity 5.15pm SUNDAY 12 MAY10.00am – o Leading, Delegating, Communicating – 11.00am How will you Manage? OR o The Challenges Presented by Breast Cancer Survivors Taking Antihormone Medication11.15am – o IPU AGM – Reports & Motions 1.15pm OR11.15am – o Support and Care for Cancer Patients 12.45pm (CPD for Pharmacy Technicians)1.15pm o Lunch
NAME:
PHARMACY:
ADDRESS:
PHONE NUMBER:
EMAIL:
Payment can be made by cheque or by supplying your credit card details below. Please make cheques payable to Irish Pharmacy Union and return with this form.
PRESIDENT’S DINNER & BALL Dinner €35
Name of Dinner Guest:
Dinner Guest €35
Attendance Fee €130
Pharmacy Staff €60
Early Bird Fee* €100 Non-Members €185
Pharmacy Interns €40
Newly Qualified Pharmacists registered after September 2016 €80
*The Early Bird Rate is for members only and is valid if booked and paid for before 29 March 2019.
CONFERENCE FEE
CREDIT CARD DETAILS
Name of Cardholder:
Card Number:
CVV Number:
Expiry Date:
IPU NATIONAL PHARMACY CONFERENCE 10 – 12 May 2019, The Galmont Hotel, Galway

How pharmacists can help to encourage good asthma managementThe Irish Pharmacy Union and the Asthma Society of Ireland have teamed up to encourage more people to take control of their asthma and practice proper inhaler technique. Sarah O’Connor, CEO of the Asthma Society of Ireland, details how pharmacists can help to encourage good asthma management and also outlines how pharmacists can team up with the Society to improve their own asthma knowledge.
PROFESSIONAL Sarah O’Connor, CEO, Asthma Society of Ireland
Ireland has the fourth highest rate of asthma in the world – 470,000 people in Ireland have asthma – one in five
children and one in ten adults. This makes asthma the most common chronic condition in the country. A person visits A&E in Ireland because of asthma every 26 minutes and the condition is responsible for 5,000 hospital admissions every year. Sadly, more than one person a week dies as a result of their asthma. Shockingly, 90% of asthma deaths are preventable and asthma deaths are on the rise.
The Asthma Society is the national charity dedicated to empowering Ireland’s people with asthma to take control of their asthma by providing them and their families with information, education, services and support.
The Asthma Society has a wealth of resources that allow people with asthma to take control of their condition and live a healthier life. The Society also has a number of resources that will be of benefit to pharmacists, including our inhaler technique videos, our Asthma E-Learning Programme, our Asthma in the Pharmacy Day clinics and our joint Asthma and COPD Adviceline.
IPUREVIEW MARCH 201930

Inhaler TechniqueProper inhaler technique is vital for people with asthma to properly manage their condition. It is estimated that 60% of people with asthma in Ireland are not managing their asthma as they should, putting about 280,000 people in danger of having an asthma attack, which in some cases can be fatal.
Poor inhaler technique is a major problem in managing asthma because the patient does not receive an optimal dose of the prescribed drug, resulting in reduced response to treatment and poor asthma control. As every pharmacist knows, even if the best medication is prescribed, if it is not used correctly it will not have any therapeutic effect. This is why proper inhaler technique is extremely important.
Pharmacists are in an excellent position to identify patients whose asthma may not be well controlled, due to poor inhalation technique. A
recent focus group, conducted by the Asthma Society of Ireland, showed that pharmacists are considered to have the highest satisfaction ratings of any kind of healthcare professionals in terms of the asthma supports provided.
Pharmacists can and do act as key educators for improving inhaler use. Patients using inhalation therapies need careful instruction, including step-by-step demonstration and observation of their technique when dispensing the medication. Pharmacists are available, not just when patients obtain their first inhaler, but also when they obtain refill inhalers, giving pharmacists the ideal opportunity to assess and educate their patients on an ongoing basis.
Pharmacists should also be aware of the inhaler technique videos which are available on www.asthma.ie. These videos are suitable for both patients and healthcare professionals and were recently updated to
include the newest inhalers on the market. Pharmacists should recommend these videos to people with asthma when purchasing medication but can also use these videos to brush up on their own knowledge of inhaler technique.
Asthma E-Learning ProgrammeAnother resource the Asthma Society offers that is extremely beneficial to pharmacists is the Care of Adults and Children with Asthma E-Learning Education Programme, which has been developed with clinical expertise from the National Clinical Programme for Asthma, patient and service user expertise from the Asthma Society of Ireland, healthcare delivery expertise from frontline staff and input from other stakeholders including ANAIL, Irish Thoracic Society and RCPI. The e-learning programme addresses key
issues in asthma care and provides excellent training in up-to-date best practise asthma management.
Pharmacists who undertake the programme will be able to enhance their skills and gain a comprehensive understanding of international best practices of asthma care including diagnosis, assessment, treatment and monitoring of adults and children with asthma.
This updated resource covers all aspects of asthma care and is designed to provide the confidence and skills necessary to provide best-practice care for people with asthma. The five modules within the resource are:
n Diagnosis and Assessment of Asthma;
n Treatment of Paediatric Asthma;
n Guided Self-Management/Asthma Action Plans; and
n Treatment of Asthma Attack.
Figure 1: Inhaler Technique Figure 2: Asthma E-Learning Programme
IPUREVIEW MARCH 2019 31

The programme takes approximately three hours to complete. This resource is geared towards self-directed learning, allowing learners to go through the modules at their own convenience with structured training and review exercises to reinforce the learning. The Asthma Society is encouraging all pharmacists to utilise this free cutting-edge training.
Asthma in the Pharmacy Day clinicsThe Asthma Society runs a number of Asthma in the Pharmacy Day clinics throughout the country. The Asthma Society’s nurse specialists are available at these events to provide advice, support, information and patient education on asthma. The nurse will typically see up to 11 patients over a period of six hours, usually 10.00am – 4.00pm.
The nurse will complete an asthma control test to gain an understanding of the patient’s asthma symptom control and discuss potential ways of improving this score if necessary, advise patients on medication usage and answer any questions they may have.
Where patients are identified as having poor asthma control, they will be advised to attend the appropriate healthcare professional, and the nurse will guide the patients on a range of topics including asthma in children, allergies, asthma management, inhaler technique, peak flow monitoring and smoking cessation.
There is a nominal fee of €90 paid by the pharmacy. However, all other costs are covered including the asthma nurse specialist and the provision of a box of literature. The Asthma Society will advertise the event on www.asthma.ie
and all their relevant social media channels. If you would like to book an Asthma in the Pharmacy Day clinic for your pharmacy, please contact the Asthma Society and we will arrange a date that suits your pharmacy. The Asthma Society would like to thank GSK for their kind support of this programme.
The joint Asthma and COPD AdvicelineThe joint Asthma and COPD Adviceline is a free service which users can call on 1800 44 54 64. The service involves a call back from an asthma respiratory nurse, who will undertake multiple calls with a person with asthma/COPD or their carer, to ensure that they are better informed and able to manage their asthma/COPD.
The Asthma Society’s respiratory nurse specialists work through every aspect of life with callers who have
asthma and/or COPD. They can help with what to do in the event of an asthma/COPD attack and the signs and symptoms of asthma/COPD, answer questions after a GP or consultant appointment, deal with triggers that may cause a serious escalation and help to put an Asthma Action Plan/COPD Self Management Plan in place. After speaking to one of these nurses, the user will be fully equipped with the information and skills they need to improve their health and to stay as well as possible.
In 2018, the joint Asthma and COPD Adviceline service was commended for Patient Education Project of the Year in the Irish Healthcare Awards and the feedback from service users has been very positive.
For more information about any of the above, please email [email protected] or contact the office on 01 817 8886.
IPUREVIEW MARCH 201932

The complete range of pain relief
2018/ADV/PAR/131H
Paralief Range Pain Relief - Full prescribing information is available on request. For retail sale through pharmacies only.
THE STATED DOSE SHOULD NOT BE EXCEEDED. Please refer to the individual product Summary of Product Characteristics.
PA Holder: Clonmel Healthcare Ltd., Clonmel, County Tipperary:Paralief 500 mg Tablets - Contains paracetamol PA 126/20/1 (24 pack size)
Paralief Cold+Flu Hard Capsules - Contains paracetamol, phenylephrine HCl and caff eine PA 126/272/1Paralief Hot Lemon 600 mg Powder for Oral Solution in Sachet - Contains paracetamol PA 126/20/6
Paralief 500 mg Eff ervescent Tablets - Contains paracetamol PA 126/20/4
PA Holder: Chanelle Medical, Loughrea, County Galway: Paralief Night Film-coated Tablets - Contains paracetamol and diphenhydramine HCl PA 688/38/1
Paralief Extra Film-coated Tablets - Contains paracetamol and caff eine PA 688/50/1
For more information go to www.clonmel-health.ie. Date prepared: January 2019

An analysis of the pharmacist workforce capacity in IrelandThis study examines pharmacist and pharmacy numbers in Ireland over the last 15 years, in conjunction with economic and demographic data to allow improved understanding and trending of pharmacy workforce descriptors in Ireland. By examining the evolution of the workforce, conclusions can be drawn regarding factors that have impacted the supply of pharmacists and forecasts can be made regarding factors that may impact pharmacist numbers into the future.
PROFESSIONAL Tara McMahon, Margaret Bermingham and Brendan T. Griffin, School of Pharmacy, University College Cork
Key findings
n The number of pharmacists in Ireland has increased by 90% over the last 15 years.
n There has been a 47% increase in the number of pharmacies in Ireland during the same time.
n Despite the opening of RCSI and UCC Schools of Pharmacy in 2002 and 2003 respectively, 57% of new PSI registrants over the last 15 years qualified via the EU route, predominately from the UK.
n Ireland’s output of pharmacy graduates per population is 40% lower than the UK and the number of pharmacy graduates per school of pharmacy in the UK is over twice that of Ireland.
n Any risk to the free movement and mutual recognition of pharmacists between the UK and EU as a result of Brexit would lead to significant shortages of pharmacists in Ireland.
n Of 10 comparator EU countries, Ireland has the joint highest number of pharmacists and the second highest number of pharmacies per head of population.
n Pharmacy workforce estimates in Ireland are based on total registrants on PSI, which may overestimate capacity given that 21.5% of pharmacists do not state their area of practice.
IPUREVIEW MARCH 201934

3000
3500
4000
4500
5000
5500
6000
0
100
200
300
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
Cum
ulat
ive
no. o
f pha
rmac
ists
Ann
ual a
dditi
ons
to r
egis
ter
Year
National Route EU Route Total number of pharmacists (cumulative)
Figure 1: Graph showing total number of pharmacists added to the PSI register annually via national and EU routes and total number of pharmacists in Ireland (cumulative) between 2003 and 2017
Data taken from PSI Annual Reports 2004 – 2016 and PSI Statistics.
Pharmacy workforce over the past 15 yearsThe total number of pharmacists in Ireland increased from 3,208 in 2002, to 6,097 in 2017 – an increase of 90%. On an annual basis, the average number of new additions to the PSI register is 341, qualifying by either the national, EU or third country routes. The number of pharmacists added via the national route has increased from an average of 71 annually from 2003 – 2006, to an average of 153 from 2007 – 2017. This is primarily a reflection of the increase in pharmacy graduates nationally coming from RCSI and UCC Schools of Pharmacy.
Under Directive 2005/36/EC, there is mutual recognition of professional qualifications which enables the free movement of pharmacists between EU member states. The number of pharmacists that registered with the PSI via the EU/EEA route has seen substantial fluctuation in recent years. Numbers increased dramatically from 2004, peaking in 2007 (306 registrants), most likely coinciding with the high demand for pharmacists, driven in no small part by the Celtic Tiger economy of the time. The numbers of EU registrants sharply declined from 2007 – 2009 as Ireland was hit by recession, healthcare budget cuts and net-migration out of Ireland. The number of EU pharmacists registering with the PSI fell by 66% between 2007 and 2009. Registrant numbers via the EU route have recovered since 2009 and stabilised at between 43% to 58% each year since.
Registrations via the third country route are relatively few, with an average of only four pharmacists per year registering via this route since 2010. The third country route of registration, through which pharmacists outside the EU/EEA register with the PSI, commenced in 2010. Prior to 2006, reciprocal registration agreements operated on the basis that pharmacist qualifications were mutually
IPUREVIEW MARCH 2019 35

recognised between Ireland-New Zealand and Ireland-Australia. Between 2003 and 2006, an average of 49 pharmacists per year registered via this reciprocal registration approach. However, this route was terminated in June 2006.
The total number of pharmacies in Ireland has consistently increased over the last 15 years. In 2003, there were 1,317 pharmacies; by the end of 2017 this number increased to 1,932 – an increase of 46%. As a result of this, the number of pharmacies per 100,000 of population has increased from 33 to 40.2. This has resulted in increased patient access to pharmacists in a community setting, facilitating greater provision of primary healthcare services, and has also increased competition in the sector.
Brexit: A potential risk to the Irish pharmacy workforceDespite the increase in pharmacists qualifying nationally in recent years, it is clear that the pharmacist workforce in Ireland is heavily reliant on pharmacists that qualify outside of Ireland. Since 2003, 62% of new registrants to the PSI qualified outside of Ireland, with 57% registering via the EU route and 5% via the third country route. The vast majority of EU-qualified new registrants are trained in the UK/Northern Ireland (in 2017, 113 out of 170 EU-qualified registrants were trained in UK/Northern Ireland) and it would seem reasonable to assume the majority are Irish students who studied pharmacy at a UK university.
Leaving aside the socioeconomic debate surrounding the national policy on limiting pharmacy places in Irish universities to less than 50% of the current labour market needs, it is clear that pharmacy services remain highly reliant on Irish students training at schools of pharmacy in the UK. It is unclear, as of yet, the extent to which the free movement
Figure 2: Number of pharmacists and pharmacies per 100,000 of population (2015) in comparison countries. Patient facing pharmacists in Ireland (i.e. community and hospital-based) also shown
Source: Organisation for Economic Co-operation and Development (OECD) Health Expenditure, Financing, Healthcare resources reports and Eurostat Health Personnel Statistics Reports
and mutual recognition of pharmacy qualifications will be upheld/withdrawn when the UK leaves the EU. However, any restrictions to this free movement will have a substantial impact on the pharmacist workforce. For this reason, Brexit poses a significant risk to the future capacity of the pharmacist workforce in Ireland.
The uncertainty around Brexit is also likely to impact on the numbers of Irish students applying to study in the UK through UCAS. Since June 2016, the overall number of applicants has fallen by 28%. While this study did not examine precise figures on the number of Irish students registering at schools of pharmacy in the UK, it is reasonable to assume that there will be a significant reduction in the number of Irish students qualifying as pharmacists in the UK from 2020/21 onwards. While the implications of Brexit are as of yet uncertain, the risk of
Brexit to pharmacy capacity is real given how reliant the pharmacist workforce in Ireland is on UK-trained pharmacists.
Pharmacy capacity in Ireland compared to other EU countriesWith the aim of benchmarking the pharmacist workforce in Ireland to other countries, a number of comparison countries were chosen based on a range of demographic and economic descriptors (population, GDP/capita, % GDP and % Government spending spent on healthcare, HDI values). This ensured that the chosen countries broadly share common goals in terms of economic, environmental, social and healthcare standards, therefore justifying that comparisons between these countries are appropriate.
Ireland and Belgium have the joint highest number of pharmacists per 100,000
of population (121), while the Netherlands has the lowest (21). However, it should be noted that the data for Ireland represents all pharmacists licenced to practise – i.e. all pharmacists on the PSI register. As a result, pharmacists that are not practising in patient-facing roles, such as industry, academia, regulation etc., are included, which may overestimate pharmacy workforce capacity. As of 1 October 2018, 70.5% of registered pharmacists identified as working in patient-facing roles (i.e. community or hospital pharmacy), 5.5% identified as working in non patient-facing roles (i.e. academic, industry, regulatory) and 2.5% identified as non-practicing or ‘other’. However, 21.5% of pharmacists did not state their area of practice. This is a substantial proportion and leaves much room for error when estimating the total percentage of patient-
IPUREVIEW MARCH 201936

79th FIP World Congress of Pharmacy and Pharmaceutical SciencesAbu Dhabi, United Arab Emirates22-26 September 2019
As we develop new skills to manage new technologies such as
robotics and the digitalisation of health care, it is important that
we do not compromise quality and safety.
Come to the Abu Dhabi congress, which will help you develop
the knowledge and attitudes to adapt to emerging new roles
through networking with pharmacists and scientists from all
areas of practice and from all around the world.
New horizons: Navigating winds of changeNew technologies, new roles, new opportunities for pharmacy
Do you want to be inspired to take on new roles and be prepared for success in a worldof change? Wherever you practise, FIP can help you stay ahead of the game so that you can provide the best care for patients.
A > New trends in science, practice
and education
Focuses on new technologies,
digitalisation of health care,
robotics, individualisation of
therapy, the provision of edu-
cation via virtual classrooms,
integrating science and practice
in teaching, communication,
people-centred care, and ethical
challenges.
B > New roles, opportunities and
responsibilities
Examines pharmacists’ roles and
the roles of individuals, looks
at new services and the skills
required to advance them, and
highlights the importance of
education and of collaboration
not only with pharmacy collea-
gues but also with other health-
care professionals.
C > Health now! Responding to the
challenges of today
Recognises that challenges can be
faced by looking at new research,
ethical considerations, new values,
access to health, health systems,
sustainability, environmental
sustainability, non-communicable
diseases, empowerment of patients,
empowerment of women, quality
and assessment.
D > Targeting special interests
Looks at special interests in the
different fi elds of pharmacy and
pharmaceutical sciences.
WELCOME TO ABU DHABI
Abu Dhabi is a modern, cosmopolitan city with an ancient heritage
where respect for the past informs the present and shapes the
future. There are historic buildings, engaging tours and a packed
calendar of events covering the arts, culture, sports and trade.
Visitors will encounter a diverse emirate, with deserts, beaches,
oases and mountains, and there are ultra-modern malls and small
souk-like stores to cater for their every (tax-free) shopping need.
CONGRESS STREAMS:
Please fi nd more information:
abudhabi2019.congress.pharmacy
NoteSome congress sessions are accredited for continuing education. Check our website.

facing and non patient-facing pharmacists in Ireland and pharmacy capacity predictions.
Therefore, using the total number of pharmacists when comparing to other countries leads to a misleading assessment of the capacity of the patient-facing sectors
of pharmacy practice. Based on the total number of registrants on the PSI register, Ireland is significantly above the median in terms of the number of pharmacists per population. Using the adjusted figure of 70% reporting as patient-facing brings the overall figure in line with the
comparison countries. It was unclear if the figures given for the comparison countries reflect all pharmacists registered with the national professional body or registered to practise in patient-facing roles, and is therefore a limitation of the current study. While non patient-facing
Figure 4: Number of pharmacy graduates per 100,000 population and average number of graduates per school of pharmacy (2014) in comparison countries
Sources: Number of pharmacy graduates (2014) - OECD. Number of Schools of Pharmacy - PHARMINE 2011 Number of pharmacy graduates/100,000 population (2014) - Calculated. Avg. number of graduates/School of Pharmacy -Calculated
0
10
20
30
40
50
60
Austri
a
Belgium
Denm
ark
Finlan
d
Germ
any
Irelan
d
Nethe
rland
s
Norway
Sweden UK
Num
ber
of p
harm
acie
s/10
0,00
0
Pharmacies/100,000 (2007) Pharmacies/100,000 (2015)
Figure 3: Number of pharmacies per 100,000 of population in 2007 and 2015 in comparison countries
Source: Organisation for Economic Co-operation and Development (OECD) Health Expenditure, Financing, Healthcare resources reports and Eurostat Health Personnel Statistics Reports
pharmacists’ roles are varied and may contribute indirectly to improving accessibility to medicines, clearly segmentation of the data to allow comparisons of patient-facing pharmacist density between countries will allow more reliable benchmarking in the context of access of patients to pharmacy-related services.
Belgium has the highest number of pharmacies per 100,000 of population, followed by Ireland. However, it is important to note that pharmacy numbers have decreased in Belgium between 2007 and 2015, while numbers are continuing to increase in Ireland. This illustrates that even though Belgium has the highest number of pharmacies currently, if current trends continue, Ireland will overtake it. Even though other countries (Norway, Sweden, UK) have shown increases in pharmacy numbers in recent years, their numbers are still far below Ireland. The total number of pharmacies per 100,000 of population in Ireland is still twice that of the UK.
Ireland lies exactly on the median set by the comparison countries in terms of pharmacy graduates per population. However, the number of graduates per school of pharmacy in Ireland is below the median at an average of 50 graduates per school. In the UK, the average number of graduates per school of pharmacy annually is around 114 – more than double the Irish figure. These two indicators of pharmacy education in Ireland show that despite the addition of RCSI and UCC Schools of Pharmacy, Ireland’s output of national pharmacy graduates is still low relative to other comparison countries.
The full report, including methods, bibliography and additional data, is published on the UCC Open Research Repository which can be accessed via https://cora.ucc.ie/handle/10468/7424.
IPUREVIEW MARCH 201938

BUSINESS Larry Ryan, Director, Behaviour & Attitudes
Early in 2018, the Irish Pharmacy Union (IPU) commissioned a project to understand why an increasing number of pharmacy students are opting for careers outside of community pharmacy. Working with Behaviour & Attitudes (B&A), a number of separate committees inputted at the project briefing phase, leading to a multi-stage project with qualitative and quantitative elements, which took a 360 degree look at pharmacy in Ireland today.
An extensive series of focus groups with students and pharmacists
at all levels (from recent graduates, right through to owners) was supplemented with interviews among key opinion leaders and educators. Having completed the qualitative phase in the Spring of 2018, a quantitative phase was rolled-out through the summer. This interviewed both IPU members and indeed co-operated with other representative groups and interests, so that the net could be cast more broadly to integrate the views of some who have already turned away from the sector.
Reframing community pharmacy
IPUREVIEW MARCH 2019 39
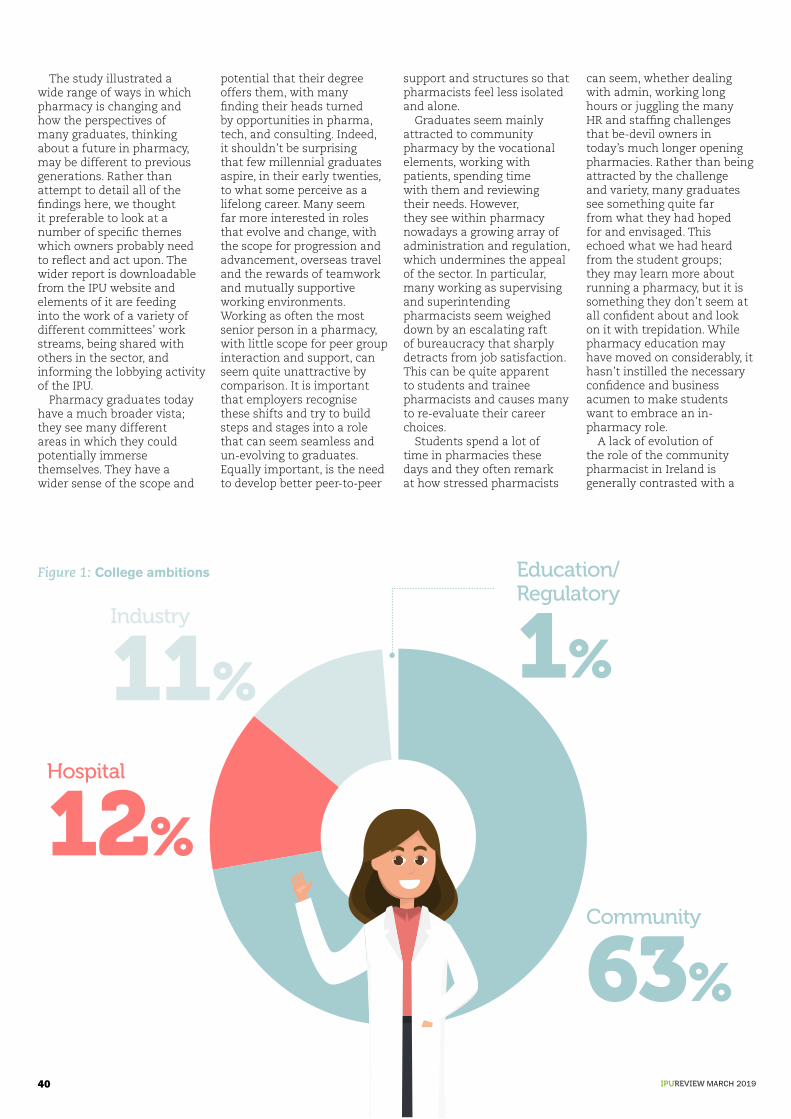
The study illustrated a wide range of ways in which pharmacy is changing and how the perspectives of many graduates, thinking about a future in pharmacy, may be different to previous generations. Rather than attempt to detail all of the findings here, we thought it preferable to look at a number of specific themes which owners probably need to reflect and act upon. The wider report is downloadable from the IPU website and elements of it are feeding into the work of a variety of different committees’ work streams, being shared with others in the sector, and informing the lobbying activity of the IPU.
Pharmacy graduates today have a much broader vista; they see many different areas in which they could potentially immerse themselves. They have a wider sense of the scope and
potential that their degree offers them, with many finding their heads turned by opportunities in pharma, tech, and consulting. Indeed, it shouldn’t be surprising that few millennial graduates aspire, in their early twenties, to what some perceive as a lifelong career. Many seem far more interested in roles that evolve and change, with the scope for progression and advancement, overseas travel and the rewards of teamwork and mutually supportive working environments. Working as often the most senior person in a pharmacy, with little scope for peer group interaction and support, can seem quite unattractive by comparison. It is important that employers recognise these shifts and try to build steps and stages into a role that can seem seamless and un-evolving to graduates. Equally important, is the need to develop better peer-to-peer
support and structures so that pharmacists feel less isolated and alone.
Graduates seem mainly attracted to community pharmacy by the vocational elements, working with patients, spending time with them and reviewing their needs. However, they see within pharmacy nowadays a growing array of administration and regulation, which undermines the appeal of the sector. In particular, many working as supervising and superintending pharmacists seem weighed down by an escalating raft of bureaucracy that sharply detracts from job satisfaction. This can be quite apparent to students and trainee pharmacists and causes many to re-evaluate their career choices.
Students spend a lot of time in pharmacies these days and they often remark at how stressed pharmacists
can seem, whether dealing with admin, working long hours or juggling the many HR and staffing challenges that be-devil owners in today’s much longer opening pharmacies. Rather than being attracted by the challenge and variety, many graduates see something quite far from what they had hoped for and envisaged. This echoed what we had heard from the student groups; they may learn more about running a pharmacy, but it is something they don’t seem at all confident about and look on it with trepidation. While pharmacy education may have moved on considerably, it hasn’t instilled the necessary confidence and business acumen to make students want to embrace an in-pharmacy role.
A lack of evolution of the role of the community pharmacist in Ireland is generally contrasted with a
Community
63%
Hospital
12%
Industry
11%
Education/ Regulatory
1%
Figure 1: College ambitions
IPUREVIEW MARCH 201940
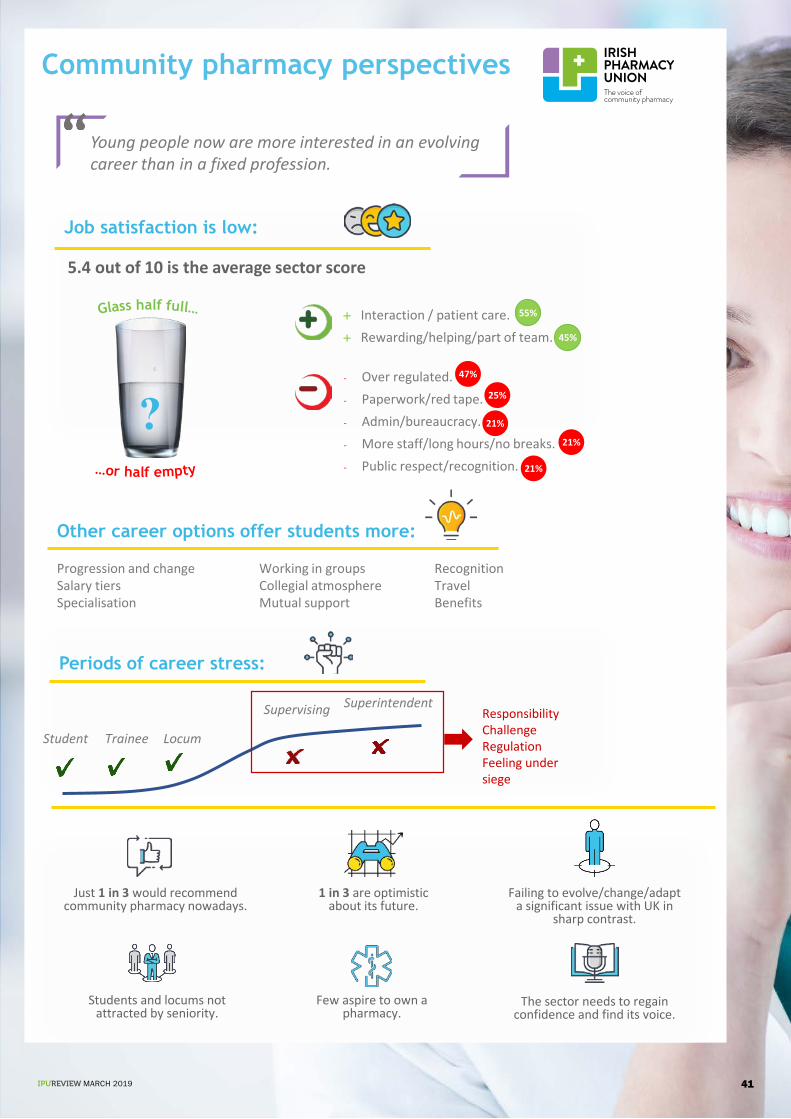
Community pharmacy perspectives
Young people now are more interested in an evolving career than in a fixed profession.
Other career options offer students more:
Progression and changeSalary tiersSpecialisation
Working in groupsCollegial atmosphereMutual support
RecognitionTravelBenefits
Job satisfaction is low:
Interaction / patient care. Rewarding/helping/part of team.
5.4 out of 10 is the average sector score
Periods of career stress:
Student Locum Trainee
Supervising SuperintendentResponsibilityChallengeRegulationFeeling under siege
Just 1 in 3 would recommend community pharmacy nowadays.
1 in 3 are optimistic about its future.
Failing to evolve/change/adapt a significant issue with UK in
sharp contrast.
Students and locums not attracted by seniority.
The sector needs to regain confidence and find its voice.
Few aspire to own a pharmacy.
- Over regulated.- Paperwork/red tape.- Admin/bureaucracy.- More staff/long hours/no breaks.- Public respect/recognition.
55%
45%
47%
25%
21%
21%
21%
?
IPUREVIEW MARCH 2019 41

much more developed role in Britain and elsewhere. Pharmacists in Britain are leading clinics, effectively prescribing and managing the care of patients, and equally are felt to have a much better and more consultative working relationship with GPs. This is sharply contrasted by a lack of change and development here and undoubtedly contributes to a sense among graduates that community pharmacy in Ireland may offer them less in the future. Unquestionably, those leading the sector need to agitate for change and evolution, not just to keep up with global shifts, but also to ensure that students perceive the role as more dynamic and capable of evolution.
The quantitative phase illustrated something that we had started to suspect during the initial groups and in-depth interview; that many pharmacists are bad at delegating and often don’t trust others to perform tasks that they can do themselves. For many, this leads them to micro-manage and become excessively embroiled in many administrative tasks that others could equally complete. Unquestionably, pharmacists need to learn how to delegate, but equally the sector needs to develop a cadre of workers who can complete the routine admin that relates to schemes, dealing with the PCRS and the other tasks that pharmacists need to shed to find the time to deal with patients.
The study highlighted some ancillary issues that gave cause for concern. In particular, morale and job satisfaction are poorer in the sector than they might be, with those in more senior and responsible roles seeming particularly bowed down.
The project has illustrated many issues which won’t come as a particular surprise to those working in the sector. What may be salutary, however, is the extent to which these may
be contributing to graduates deciding to look elsewhere.
Some key areas that need to be addressed include:
n Building more steps and stages into a pharmacy career, so that it loses a sense of seamlessness, of a lack of challenge, change and the potential for progression;
n Creating better peer-to-peer support networks so that young pharmacists don’t feel isolated;
n Working to reduce the amount of bureaucracy and admin and to shift the burden of what remains onto support staff;
n Developing more opportunities for patient interaction and ultimately convincing the authorities that pharmacists need to own more of this territory;
n Insinuating more business training into the pharmacy curriculum, so that young pharmacists are more enthusiastic about this important aspect; and
n Ensuring that placements in pharmacies are rewarding and stimulating and not leaving students with a fear of ancillary elements for which they feel unprepared.
The project was undertaken for the IPU by Behaviour & Attitudes with the generous help and participation of many across the sector. B&A and the IPU would like to pass on their thanks and to remind all that copies of the published research report are available to download from the website www.ipu.ie.
Larry Ryan is a Director of Behaviour & Attitudes and he takes charge of all studies undertaken for the IPU.
Likes about community pharmacy as a career (spontaneous)
%
Interaction with customers / community integration / community care
55
Helping people / rewarding / part of a dedicated team – making a difference
46
Health expertise / healthcare provision – providing good quality healthcare
10
Variety 9
Learning opportunities 6
Flexibility 6
Dislike profession / nothing appeals 6
Interesting 5
Self-employed / entrepreneurship / ability to run own business
5
Health / medicines / wellbeing of patient 5
Good money 4
“ Unquestionably, those leading the sector need to agitate for change and evolution, not just to keep up with global shifts, but also to ensure that students perceive the role as more dynamic and capable of evolution.”
IPUREVIEW MARCH 201942

Epilepsy is more common than you might think. Over 37,000 people in Ireland over the
age of five have epilepsy, making it one of the most common neurological conditions but, despite its prevalence, it remains a much misunderstood and often stigmatised hidden disability.
The word ‘epilepsy’ is used to describe a group of disorders, all of which are characterised by recurrent unprovoked seizures involving abnormal electrical activity in the brain. About one in every 20 people will have a seizure at some time during their lives.
For decades, the terms partial and generalised seizures were used to describe types of seizures. Partial seizures were those starting in one area or side of the brain, while generalised seizures were those occurring in both sides of the brain at the same time. In 2017, The International League Against Epilepsy revised its classification of seizures. The new classification is based on three key features: where seizures begin in the brain,
level of awareness during a seizure, and other features. This means that terms such as simple partial seizure and complex partial seizure are now replaced with Focal Aware and Focal seizure with impaired awareness respectively.
Epilepsy affects people of all ages, but is more prevalent in children, adolescents and those over 65 years. It is also more common in people with an intellectual disability. In about 60% of cases, no specific cause can be identified. In the remaining 40% of people, common causes include head injuries, strokes, brain infections, birth defects and genetic conditions.
With anti-epileptic drug (AED) treatment, up to 70% of people with epilepsy can achieve seizure control, while surgery or vagus nerve stimulation, as well as the ketogenic diet in children are also options that may be considered. Deep brain stimulation, cannabinoids and personalised therapy targeted to specific genetic mutations, are just three areas of current research that offer hope for the future.
PROFESSIONAL Peter Murphy, CEO, Epilepsy Ireland
26 March is Purple Day and Epilepsy Ireland CEO, Peter Murphy, discusses the condition and the work of the organisation across the country
Epilepsy Ireland: committed to meeting the needs of everyone with epilepsy
IPUREVIEW MARCH 2019 43

However, there are at least 10,000 people in Ireland living with uncontrolled seizures, and for this group in particular, the consequences of epilepsy can be long-lasting and significant. It can affect the person’s education, employment, psychological and social functioning, self-esteem and independent living. People with epilepsy must also cope with the physical impact of seizures, the side-effects of medications and for many, the social stigma and economic impact that can be associated with it. There is also an increased risk of mortality associated with epilepsy with an estimated 130 epilepsy-related deaths in Ireland each year.
Epilepsy Ireland‘s work Our support services, delivered through our offices in Dublin, Cork, Dundalk, Galway, Kerry, Kilkenny, Letterkenny, Limerick, Sligo and Tullamore are the core of our work and will be of interest to pharmacists across the country.
Our team of Community Resource Officers are key contacts for individuals or family members with epilepsy and depending on the need of the individual, can provide one-to-one support and advocacy, outreach services, educational programmes and self-management programmes. We also organise regular events and support groups in communities across the country.
STEPS is our six-session self-management programme for people with epilepsy. It supports people on a range of issues including seizure management, lifestyle issues, triggers and safety planning, managing moods and thoughts, communications and planning for the future. This course will help adults with epilepsy to meet others, manage their epilepsy and improve quality of life. We also offer a STEPS programme for parents as well as Innerwise, a follow-on programme designed to address stress management,
anxiety, wellness and personal confidence through meditation and personal development.
We also provide facilitated support sessions for those recently diagnosed with epilepsy, called the Living Well with Epilepsy Toolkit. The Toolkit is a comprehensive introduction to epilepsy management and includes handy resources such as a seizure diary, safety checklist and an epilepsy knowledge checklist. Demand for our services has grown by almost 40% over the past three years due to these new programmes and to strong links with clinical epilepsy services nationwide.
Another important service which continues to grow is our training programme in Epilepsy Awareness and the administration of Buccal Midazolam (BM) for healthcare professionals and those working in education or care settings. Over 2,000 people attended our training courses in 2018 and we also began providing BM demonstrations for parents and carers.
Epilepsy Ireland’s award-winning Training for Success course is currently recruiting for the upcoming one-year term starting in August 2019.
Based at the Institute of Technology Sligo, this one-year full time QQI Level 5 Access Programme has helped over 250 young people with epilepsy achieve life and career goals since its inception in 1998.
Our newly revamped website, www.epilepsy.ie, contains useful information for pharmacists and their patients alike, including a range of new epilepsy information booklets and our Epilepsy Management App for iPhone and Android, which can be downloaded from the site. The app helps record information about seizures (including video), identify potential triggers and seizure patterns, set important reminders, send emergency texts, organise medical appointments and measure missed medications.
In 2019, we hope to develop a new comprehensive guide
Purple Day 26 March Purple Day is an international grassroots effort dedicated to increasing awareness about epilepsy worldwide. Iconic buildings around Ireland will be lighting up purple to mark the occasion and we are inviting people to wear purple and host events in support of epilepsy awareness on this day.
To get a Purple Day wristband and for more information, visit www.epilepsy.ie or email [email protected].
to epilepsy for healthcare professionals, in association with our clinical care colleagues and we would welcome input from pharmacists who would like to contribute to the development of this important resource.
Likewise, if you are aware of a patient who would benefit from any of the supports outlined above, please do refer them to Epilepsy Ireland or contact us for more information.
Improving public understanding of epilepsy, supporting epilepsy research and advocating on behalf of people with the condition are also key objectives of our organisation. One of the most important issues in recent times relates to reducing the risks associated with in-utero exposure to sodium valproate. Children exposed to valproate in utero are at a high risk of serious developmental disorders (in up to 30 – 40% of cases) and congenital malformations (in approximately 10% of cases). While there is no official Irish data available, the FACS (Foetal Anti Convulsant Syndrome)
Forum estimates, based on international data, that at least 400 children in Ireland have been affected since the 1970s.
In February 2018, the European Medicines Agency put in place new risk minimisation measures which are being implemented in Ireland by the Health Products Regulatory Authority (HPRA). Epilepsy Ireland welcomes the strengthened warnings and educational resources which have been made available, which include patient and professional guides, alert cards, pharmacy posters and shelf barkers. These, and additional measures such as pregnancy prevention programmes, PL and SmPC updates, on-box and blister warnings, as well as reducing valproate pack sizes, will all combine to help to reduce the incidence of Foetal Valproate Syndrome in the years to come.
The role of pharmacists in educating and counselling patients will be a critical component in achieving this, building on the long-standing and vital role played by the profession in epilepsy care for generations in Ireland.
IPUREVIEW MARCH 201944

Types of AlopeciaAlopecia areata (AA) is a chronic inflammatory disease that affects the hair follicle and sometimes the nail. Alopecia areata usually presents as patches of hair loss on the scalp but any hair-bearing skin can be involved. The affected skin may be slightly reddened but otherwise appears normal. Short broken hairs (exclamation mark hairs) are frequently seen around the margins of expanding patches of alopecia areata. The nails are involved in about 10% of patients referred for specialist advice. In some people, larger areas are affected and occasionally it can involve the whole scalp (alopecia totalis) or even the entire body and scalp (alopecia universalis). Alopecia areata usually strikes before the age of 30. It can present at any age, and males and females are affected equally.
Androgenetic alopecia is a common form of hair loss in both men and women. In men, this condition is known as male pattern baldness. The prevalence and the severity of androgenetic alopecia is highest in white men, tends to occur less in black men, and later and more slowly in Asian men. By 30 years of age, it affects about a third of white men. This increases to around 80% in men older than 70 years of age. Men who present with thinning hair in their late teens or 20s are more likely to lose all their hair than those who have gradual thinning that is not obvious until their 30s or 40s. Hair is lost in a well-defined pattern beginning above both temples. Over time the hairline recedes to form a characteristic “M” shape. Hair also thins at the crown often progressing to partial or complete baldness.
In women, the hair becomes thinner all over the head and
the hairline does not recede, it rarely leads to complete baldness. The prevalence and severity of androgenetic alopecia in women increases greatly after menopause and affects about a third of white women aged 70 years and older.
Cicatricial alopecia is the loss of hair which is accompanied with scarring.
Traction alopecia is a gradual hair loss caused primarily by pulling force being applied to the hair.
Telogen effluvium is where physical, or emotional stress, may cause one half to three quarters of scalp hair to shed. Hair tends to come out in handfuls while you shampoo, comb or run your hands through your hair. Crash diets, especially those that do not contain enough protein, can be a contributory factor in this type of hair loss.
Risk FactorsRisk factors for hair loss include family history, nutrition and treatment of the hair. Family history of hair loss on either side of the family increases the risk of loss. It also affects the age at which hair loss begins and the extent of baldness. The risk of androgenetic alopecia is lower in men with a non-balding father and high in those with a balding father.
Diets low in iron and protein increase the risk of alopecia. The overuse of heat and products on the hair such as, straighteners and colouring agents, can all contribute to an increase in hair loss.
CausesCauses of alopecia include hormonal changes, medical conditions and some medications. Hormonal changes including factors
CPD Marie O’Brien MPSI
Document your learning Personal planEvaluate
Self-appraisal
Action
AlopeciaAlopecia is a condition resulting in hair loss from some, or all areas of the body. Approximately 2% of people are affected at some point in their lifetime. The onset may be at any age and there is no known race or sex predominance. Onset can be gradual or sudden and hair loss associated with alopecia can be temporary or permanent.
IPUREVIEW MARCH 2019 45

like pregnancy, childbirth or menopause in women can cause temporary hair loss. Medical conditions such as scalp infections, skin disorders, hair-pulling disorder (Trichotillomania) and thyroid problems can lead to alopecia. Finally, medications used for the treatment of cancer, arthritis, depression and high blood pressure (calcium channel blockers, beta blockers) can be linked with hair loss.
DiagnosisThe diagnosis of alopecia can be usually established based on clinical presentation. A complete blood count to include ferritin levels and thyroid function to determine any underlying issue is also helpful.
PrognosisPrognosis of alopecia areata is varied, in most cases which begin with a small number of patches of hair loss, hair grows back after a few months to a year, regardless of treatment. Some patients might experience only a single episode of hair loss during their lifetimes, while others experience multiple recurrences. Some patients have full hair regrowth, yet others remain the same or experience further hair loss. In general, hair regrowth is possible and known to be inversely correlated with the extent of hair loss, i.e. the greater the area of involvement (alopecia totalis or universalis), the less likely the chance of complete regrowth, and the more likely
alopecia areata will progress over time.
Other factors associated with poor prognosis include nail changes, early onset, family history and concomitant autoimmune diseases. In the absence of treatment, female pattern hair loss (FPHL) leads to progressive hair loss in affected areas, though not to complete baldness.
The progression of hair loss in androgenetic alopecia is unpredictable. In women, it rarely leads to complete baldness. In untreated men, hair loss progresses over time, with some going completely bald in as little as five years and others over 15 – 25 years. Often some hair is left at the base of the skull and areas above the ears.
TreatmentIf hair loss is caused by an infection or an underlying condition, then treatment of the infection or condition may help to prevent further hair loss. In the case of alopecia areata, if there are signs of regrowth then no treatment is necessary; however, if there is extensive involvement then specialist referral is required. There is no definitive cure and treatment is mainly focused on containing disease activity. Specialist treatments include corticosteroid injections, topical corticosteroids, immunotherapy, dithranol cream, UV light treatment (PUVA), oral ciclosporin, topical minodoxil, tattooing and wigs.
In the case of androgenetic alopecia, the treatments most commonly seen at pharmacy level are topical minodoxil and oral finasteride.
Minodoxil is available in 2% and 5% solutions (Regaine®) and is rubbed onto the scalp every day twice daily for male and female-pattern baldness. It can slow or stop hair loss, and may cause hair regrowth. The solution is a hair growth simulator and acts by activating potassium channels in follicular cells. Effects can take 12 to 16 weeks, and unfortunately, any new hair growth will fall out two months after treatment is stopped.
Most common side-effects include hypersensitivity reactions and headache. The patient should stop using Regaine® and see a doctor if hypotension is detected or if the patient is experiencing chest pain, rapid heartbeat, faintness or dizziness, sudden unexplained weight gain, swollen hands or feet, or persistent redness or irritation of the scalp or other unexpected new symptoms occur. Patients with known cardiovascular disease or cardiac arrhythmia should contact their GP before using Regaine®.
Finasteride is a 5-alpha-reductase-inhibitor prescribed at a 1mg dose (Propecia®). This is unlicensed in Ireland and is indicated for the treatment of men with male pattern hair loss (androgenetic alopecia) to increase hair growth and prevent further hair loss. Hair regrowth is not usually noticed for at least 4 – 6 months with finasteride. Usage is for men only and again once treatment is ceased, hair loss can reoccur. Breast tenderness and enlargement is an adverse effect of finasteride. Advise men taking finasteride to
promptly report to their GP of any changes in their breast tissue (such as lumps, pain, or nipple discharge). Depression, anxiety and suicidal thoughts with treatment have been observed. Men are advised to stop therapy if they develop depression and see their GP.
Unfortunately, such treatments can be disheartening for patients with slow results and the need to use medications long-term. In general, treatments are more effective the earlier they are started. Newer treatments include hair transplants, which have varying success and are an expensive solution. Hair transplantation is generally not an option for individuals with alopecia areata, as transplanted hairs are likely to be targeted by the immune system. Similarly, individuals with a remote history of alopecia areata who wish to undergo a hair transplantation for androgenic alopecia must be reminded that alopecia areata can occur again at any time in one’s life. If this happens, it could lead to loss of the transplanted hair.
Advicen An important function of
hair is to protect the scalp from sunlight. Patients should cover bald patches with a sun block or a hat to prevent sunburn and to reduce the chances of developing long-term sun damage;
n Some men and a few women with extensive alopecia find that shaving off the remainder of the hair provides a good solution;
“ In the case of alopecia areata, if there are signs of regrowth then no treatment is necessary; however, if there is extensive involvement then specialist referral is required.”
IPUREVIEW MARCH 201946

Self-appraisalWhat do I know about alopecia and the different types?
Am I aware of the long-term prognosis for an alopecia sufferer?
What treatments can I recommend in the pharmacy?
What support and advice can I offer patients?
Personal planIncluding a list of desired learning outcomes in a personal learning plan is a helpful self-analytical tool.
Create a list of desired learning outcomes.
How will I accomplish these learning outcomes?
Identify resources available to achieve learning objectives.
Develop a realistic timeframe for the plan.
ActionActivities chosen should be outcomes based to meet learning objectives.
Implement plan.
Read this article on alopecia.
CPD overviewEvaluate professional resource materials available in the pharmacy and source additional material if necessary.
Evaluate availability of patient support materials and source additional material if necessary.
EvaluateConsider outcomes of learning and impact of learning.
Have I met my desired learning outcomes?
Do I now feel confident to engage with prescribers on how to manage drug interactions affecting the drug excretion process?
Do I now feel confident to engage with and counsel patients about alopecia?
Provide example(s) of changes I have implemented in my pharmacy practice.
Have further learning needs been identified?
Document your learningCreate a record in my ePortfolio.
As part of this record, complete an evaluation, noting whether learning outcomes were achieved and identifying any future learning needs.
n Suggest joining a patient support group and meeting other people with alopecia areata. It will make it easier to adjust to the condition. Alopecia Ireland www.alopeciaireland.ie is an Irish patient support group;
n People with longer hair may find hair extensions help camouflage the problem. Some hairdressers become expert at this. It is important to avoid too much tension on any hair when this is done because this could cause hair loss;
n Artificial eyelashes, eyebrow pencils and eyebrow tattoos can help some people with problems in these areas; and
n Eat a well-balanced nutritional diet.
Pharmacist Supportn Hair loss can have profound
psychological effects on both patients and their families. It is important not to underestimate the patient’s distress and to provide reassurance;
n Recognise patterns of alopecia and recommend non-prescription treatment or refer where appropriate;
n Help identify the type of hair loss and assess if there could be an underlying treatable cause (e.g. diet); and
n Provide links to support groups available.
Further references available on request.
Your 5-minute assessment
Answer the following five questions true or false:
1. Almost 2% of people are affected by alopecia at some stage in their lifetime.
2. Alopecia always has a medical cause.
3. Alopecia can be cured with pharmacological intervention.
4. Propecia® (Finasteride) is for use by men only.
5. Alopecia areata affects men and women in equal numbers.
Answers:1. True. 2. False. 3. False. 4. True. 5. True.
IPUREVIEW MARCH 2019 47

HR Hazel Slevin, MPSI, Member of the IPU Employee Pharmacists’ Committee (EPC)
Assisted Decision-Making (Capacity) Act 2015
Historically there was a tendency for healthcare professionals to veer into
the territory of paternalistic healthcare, with the old adage “doctor knows best” underpinning many of the healthcare decisions and treatments which patients received. This protective attitude to patient wellbeing became increasingly at odds with the growing general recognition of a person’s right to autonomy, both in the context of healthcare decisions and the normal day-to-day interactions of individuals. A number of legal cases, both in Ireland and in other jurisdictions, highlighted the importance of patient consent to preserve and respect this right to
autonomy. These cases provided a cautionary warning to healthcare professionals that a procedure or treatment performed without consent could serve as a legal wrong against a patient and provide the basis of legal liability against the practitioner.
In response to this emerging patient-centric approach by the courts, many healthcare professions prioritised the development of communication skills and proactive dialogue with patients to obtain a gold standard of consent. Of course, this consent was dependent on the patient’s capacity to engage with the practitioner. Patients with questionable capacity continued to face the real risk that the old habits of paternalistic healthcare of
In this article Hazel Slevin examines the historical and legal context underpinning the recent Assisted Decision-Making (Capacity) Act 2015 enactment and consider its role in the future of pharmacy practice.
IPUREVIEW MARCH 201948

“minding” the patient would overcome their right to autonomy.
These cases of questioned capacity are not harking back to the dark ages. An example of paternalistic healthcare seeking to overbear a patient’s ability to self-determine is evident in the English case of Re C (Adult: refusal of treatment) [1994]. C was a patient who suffered from paranoid schizophrenia. During the course of his in-hospital treatment, he suffered an infection in his foot which resulted in the foot becoming gangrenous. The hospital doctors sought to amputate C’s foot, to which C vehemently objected. The case came before the courts and C was successful in his case. The court acknowledged, “[T]he presumption that C has the right to self-determination has not been displaced. Although his general capacity is impaired by schizophrenia, it has not been established that he does not sufficiently understand the nature, purpose and effects of the treatment he refuses.” This presumption of capacity is the bedrock of modern patient consent principles and was later accepted by the Irish courts and further enshrined in the 2015 Act.
While the general principle that a patient has a presumption of capacity is readily acceptable, there are of course cases in which patients’ capacity
to understand the “nature, purpose and effects of the treatment” may be questioned. These patients have what is described as “triggers”, which may require a healthcare professional to undertake an assessment of capacity. The method of assessment of capacity is another area in which the 2015 Act has provided clarity. In Medicine, Ethics and the Law (3rd edn, Bloomsbury 2016), one of Ireland’s leading medical law academics, Deirdre Madden, describes three methods of assessment which have generated much discussion; the status approach, the outcome approach and the functional approach.
The status approach allows the practitioner to assess the capacity of an individual based on their membership of a group. A common example used is people with dementia. Under the status approach, the presumption of capacity could be rebutted simply because an individual has a particular illness or medical condition. This, at face value, seems an over-generalised and simplistic tool given the myriad of individual patient factors which contribute to the prognosis and outcome of a condition. Two people with the same condition may have very different levels of capacity for a particular decision.
The outcome approach to capacity assessment considers the outcome achieved by the
decision made by the patient. The practitioner considers whether the decision made by the patient will achieve a good outcome. Again, this risked a foray by the practitioner into the murky waters of paternalistic healthcare. If the practitioner didn’t think it was a good outcome decision, a finding of impaired capacity could result.
The preferred method is the functional approach to the assessment of capacity. This is the method which has been embedded in the modern healthcare system by the 2015 Act. Madden describes the functional assessment, or decision-specific assessment, as “defining decision-making capacity in keeping with respect for the autonomy of the individual, so that the individual’s capacity is assessed in relation to a particular decision to be made, at the time it is to be made, rather than being a more general judgement about their cognitive ability”. From a very basic level, this assessment method balances the patient’s right to autonomy, with a recognition that the ability to self-determine is context and decision specific.
The functional approach to the assessment of capacity underpins much of the rationale for the 2015 Act. To put it simply, one size does not fit all. Each assessment is individual to the patient and cognisant of the patient’s capability at the time of the
decision to understand the relevant information, retain it for the period necessary to make the decision, weigh up the benefits and the consequences of that decision and communicate it effectively. Taking our earlier example of the patient with dementia, under the functional approach, the fact that a patient may not be able to retain the information long-term does not invalidate the decision, as long as the information is retained during the period of time in which the decision needs to be made.
A further motivator to the implementation of the new Act is that Ireland is a signatory to the UN Convention on the Rights of Persons with Disabilities. The 2015 Act was enacted to ensure compliance with the Convention and to give statutory effect to many of the decisions which the courts have reached regarding consent, capacity and the treatment of people with disabilities. While the 2015 Act has been signed into law, many of the sections have not yet been commenced. Nevertheless, it is worthwhile for pharmacists and other healthcare professionals to familiarise themselves with some of the sections which will guide their healthcare practice in the future.
As discussed, there is an underlying presumption that a patient has capacity unless the contrary is shown. In cases
” While the general principle that a patient has a presumption of capacity is readily acceptable, there are of course cases in which patients’ capacity to understand the “nature, purpose and effects of the treatment” may be questioned.”
IPUREVIEW MARCH 2019 49

of diminished capacity, the 2015 Act provides a range of supports that are in place to promote the autonomy and the dignity of the “relevant person”. The Act also addresses current lacunas in the law relating to Advanced Healthcare Directives and Power of Attorney decisions. For the purposes of this article, a focus will be placed on the support models which may be expected to be most commonly encountered in the pharmacy setting.
Part 3 of the 2015 Act provides for an assisted decision making whereby the appointer enters into an agreement with a Decision Making Assistant (DMA). This agreement is notified to the Director of the Decision Support Service. The DMA has a primary role to assist the appointer in obtaining information, assist in understanding the information, to ascertain the will of the appointer and aid in the clear communication of that decision. A key consideration of this role is that the DMA does not make the decision; it is the sole responsibility of the appointer. In the pharmacy setting, this may result in healthcare information being
communicated to the DMA at the request of the appointer.
Part 4 of the 2015 Act provides for a Co-Decision Maker (CDM). The CDM enters into an agreement with the appointer and, similarly to the DMA, facilitates in the obtaining and understanding of information. The appointment of a CDM must be registered. A key difference between the DMA and CDM is that the latter makes “a relevant decision jointly with the appointer”. In cases where the appointer and CDM differ in the decision outcome, the CDM must acquiesce to the appointer, unless there is a risk of serious harm to the appointer or another person. From a practice point of view, a co-decision maker will most likely be appointed by an individual who considers that their capacity is called into question or may soon be called into question.
The current ward of court system is also restructured under the 2015 Act. Part 5 allows the court to appoint a Decision Making Representative (DMR). The role of the DMR is identified as “a decision-making representative shall, insofar as this is possible, ascertain the will and preferences of the
relevant person on a matter the subject of, or to be the subject of, a relevant decision and assist the relevant person with communicating such will and preferences”. The representative has further authority “to make a relevant decision on behalf of the relevant person and shall act as the agent of the relevant person in relation to a relevant decision”. This is the highest level of support offered on foot of a court declaration that a person lacks capacity.
It is notable that the 2015 Act identifies a number of classes of individuals who are ineligible to act in these roles including, “the owner or registered provider of a designated centre or mental health facility in which the person who intends to appoint him or her as decision-making assistant resides”. This will prevent those operating or employed in nursing homes in which the appointer resides, from acting in these roles. This is a factor of consideration which may be particularly relevant in the community pharmacy setting.
While these support mechanisms have yet to be commenced, it is important that pharmacists are aware that the concept of patient-
centred care will be expanded through enhanced recognition and empowerment of autonomous decision-making. The person presenting at the counter may not be the person identified on the prescription. This is not an unusual concept in community pharmacy as it stands, yet there is understandable hesitancy and concern as to how much information can be disclosed or direction taken from this third party. The 2015 Act when fully commenced will help remove these grey areas of practice. The carefully designed support mechanisms will provide transparency for healthcare professionals as to who can obtain information on behalf of a patient, be counselled on behalf of a patient and, if capacity requires, engage in the decision-making process with that patient. This is a welcome development for all patients including those whose capacity may be called into question. It will also provide greater clarity to practitioners, at a time when there is increased scaremongering and uncertainty as to data protection and how it relates to third party representatives of patients.
What is in the File?The File contains information on over 63,000 products, including:
Licensed medicinal products Unlicensed medicinal products Medical devices and sundries (bandages, dressings,
ostomy equipment etc.) Nutritional products, including foods for special diets Veterinary products Photographic products Cosmetic products Front of Shop products (shampoos, vitamins etc.)
In addition to pricing information, barcodes etc., the IPU Product File provides valuable professional information on health products. The professional information provided includes the Medicinal Product Name, PA/EU number, Generic Name, Pharmaceutical Form, Strength and Legal Status.
ISO CertifiedIn 2016, the IPU Product File achieved ISO Certification for 9001 (Quality) and 27001 (Information Security). The audit and certification process for ISO Certification emphasises the robustness of the IPU Product File and underpins its position as the definitive medicinal product catalogue in Ireland.
Easy to UseThe IPU Product File is an open system, so no matter what vendor you choose, the file can be adapted for your needs. The IPU Product File is available by electronic download, where you can log-in and download your monthly update.
Contact UsThe IPU Product File team are available to answer your queries, whether it’s on sourcing a product, pricing queries etc., the team will be able to assist you. For any queries relating to the IPU Product File, please contact a staff member on 01 406 1550 or [email protected]
The IPU Product File has been in existence for more than 30 years and is an indispensable resource for community pharmacists. It was designed for pharmacists by pharmacists and is also used by doctors and hospital personnel. It is a vital support tool for prescribing, dispensing, claiming with PCRS, stock ordering, stock taking, price checking and product sourcing.
IPU PRODUCT FILE
ISO 9001Registered
QualityManagement
ISO 27001Registered
Information SecurityManagement
IPUREVIEW MARCH 201950

Report of PSI Public Council meeting of 14 February 2019
There was no gentle easing into the New Year for the PSI as its first Council Meeting of 2019 proved to be an eventful one. It was a full house in the Fenian Street HQ, with a full complement of Council members and standing room only in the public gallery, which was packed with pharmaceutical assistants who had come to learn their fate.
Registrar Niall Byrne began as usual with his comprehensive Registrar’s report. He updated members on the revised Code of Conduct, which the Competition and Consumer Protection Commission (CCPC) has concluded that implementing the draft Code does not result in competition “being prevented, restricted or distorted”. The PSI is now gearing up for the launch and roll-out of the new Code, pending its approval by the Minister for Health and the Oireachtas.
In addition, the Pharmacy Assessment System content has been updated in line with the review carried out in 2018, Mr Byrne outlined. Version 2 of the Pharmacy Assessment System will be sent to all pharmacies in the coming weeks.
The Registrar also outlined how the PSI had accepted a report and petition from the
Irish Pharmaceutical Students’ Association (IPSA), together with the Union of Students in Ireland (USI), in relation to the Masters in Pharmacy degree. A protest was recently held by these students, and the Council is currently considering the report and petition within its remit.
With the Brexit deadline looming, the PSI is being pro-active in terms of the potential consequences on pharmacy practice. The PSI now has a dedicated Brexit webpage on its site, and issues such as medicines supply and professional recognition are already being addressed. Damhnait Gaughan delivered an update on Brexit preparedness from the working group tasked with this, and explained that the PSI remains in close contact with their UK equivalent, the GPHC. The group is currently examining legislation in order to see how a “more streamlined” route for recognition of those holding third country qualifications could be introduced – the UK, of course, will become a third country following its exit on 29 March, deal or no deal.
Speaking of the EU, medicines authentication came into operation on 9 February; Mr Byrne explained to attendees that this had
been complex to implement, involving significant preparation, and should be considered to be in a “use and learn” phase for the initial period.
In relation to the forthcoming PSI Council elections, planning is now in progress for nominations and elections for pharmacist members to vacant Council seats in the coming months.
Pharmacist Sean Reilly saw fit to criticise the inspection activities of the Council, asking why these continued to be wholly unannounced, when Council had agreed to move towards a mixed of announced and unannounced inspections. Mr Byrne explained that while the PSI is working towards this, unannounced inspections remain a priority stating, “We are still finding unsatisfactory practices in retail pharmacies 11 years after the regulations were implemented.”
Also deemed unsatisfactory was the PSI’s failure to publish full documentation furnished to Council online; from now on, the various reports and presentations will be found online before the Council meeting.
In relation to the Business Transformation Programme, Fintan Foy presented the latest on the project, and the costings were discussed at
length. At €2.4 million over 10 years, Council members will be keeping a close watch on this, and indeed Mr Gorecki asked if there was a potential to “freeze the brief” if costs began to overrun.
The IIOP Strategic Review Working Group update was delivered by Mary Rose Burke, and led to dissent among members, who queried the value of establishing a separate pharmacy leadership organisation. Ms Burke argued that the PSI does have a legislative requirement to advise the Health Minister on the development of the profession. However, Vice President Nicola Cantwell voiced concerns regarding the funding of this.
Ms Burke summed it up by eloquently stating, “the interests of the profession are not always the interests of the regulator”. This could also be applied to the long-running saga regarding pharmaceutical assistants and changes to the draft rules on temporary absence. The findings of the recent public consultation were debated and discussed at length by Council members, with each member speaking at least once, if not twice, on the divisive issue. Graham Knowles stated that after a lengthy process, a decision is now required, but consensus
PROFESSIONAL Danielle Barron
IPUREVIEW MARCH 2019 51

was not forthcoming as a wide range of views were voiced by members. Marie Louisa Power described her dismay at the proposed rules, saying that as one of the new generation of young pharmacists, she believed it was a “retrograde step”, and asked if there was not another way to address this. Mr Gorecki admitted he had never seen such an overwhelmingly negative response from a public consultation and said it had given him “pause for thought”. In terms of patient safety, a
number of Council members queried the evidence base, asking where was the data on adverse events related to dispensing by pharmaceutical assistants.
The IPU submission to the public consultation was praised by many members who found it reasonable in its ask for a less restrictive process that would achieve the same result. Proposals for mandatory CPD for pharmaceutical assistants were dismissed, however, with Ms Gaughan explaining
this would require a change to primary legislation. Much discussion centred around what exactly the pharmaceutical assistants can dispense, and the rules surrounding repeat prescriptions and complex medicines such as those on the High Tech Medicines Scheme.
What most did agree on, however, is that the issue had been deferred by successive Councils and the can had been kicked as far down the road as it would go, as Hugo
Bonar put it. Following two adjournments, a vote took place on what exactly would be forwarded to Minister Harris. It was agreed that removal of Rule 8 (1) (a) (ii) (which excluded the dispensing of certain types of prescriptions) would satisfy the majority, and thus a revised set of rules was to be sent to the Minister for Health. It remains to be seen what will happen now.
” The PSI now has a dedicated Brexit webpage on its site, and issues such as medicines supply and professional recognition are already being addressed.”
Freephone: 1800 307777 Freefax: 1800 313395 Email: [email protected]
PROUDLY SUPPORTING MUNSTER RUGBY
PHX SPORTS STRAPPING TAPE A HEAVY DUTY, ULTRA-STRONG, TEARABLE TAPE, IDEAL
FOR COMPRESSION, SUPPORT & FIXATION USES
“ This tape is ideal for injuries both on and off the pitch”DAMIEN MORDAN Munster Rugby Head Physio
IPUREVIEW MARCH 201952

PROFESSIONAL
Concerns raised in Dáil over Falsified Medicines Directive
Sean Haughey TD (Dublin Bay North, Fianna Fáil) asked the Minister for Health, Simon Harris TD, “If his attention has been drawn to the concerns of dispensing pharmacists in relation to the Falsified Medicines Directive [and] if the concerns will be taken into account?” Similar questions were also put to the Minister from across the House, including from Tommy Broughan TD (Dublin Bay North, Independent); Tony McLoughlin TD (Sligo-Leitrim,
Fine Gael); Catherine Murphy TD (Kildare North, Social Democrats); Mattie McGrath TD (Tipperary, Independent); Louise O’Reilly TD (Dublin Fingal, Sinn Féin); and Róisín Shortall TD (Dublin North West, Social Democrats).
In responding to these questions Minister Harris explained, “The purpose of the Regulation is to benefit patient safety and maintain confidence in the safety of medicines supplied to them. He also committed to addressing
specific concerns saying, “I recognise concerns raised by stakeholders regarding the practical implementation of the Regulation. I also want to ensure that, above all, the normal supply of medicines to patients is maintained. I therefore intend to implement the system in a pragmatic manner and defer operating the offences provisions in the legislation for an initial period.”
On the same topic John Brassil TD (Kerry, Fianna Fáil) asked a series of detailed
POLITICS Brian Harrison
As the 9 February introduction of the new ‘Safety Features’ Delegated Regulations arising from the Falsified Medicines Directive approached, the concerns of pharmacists were raised by a number of Dáil members.
Sean Haughey Fianna Fáil
Tommy Broughan Independent
Tony McLoughlin Fine Gael
Catherine Murphy Social Democrats
Mattie McGrath Independent
Louise O’Reilly Sinn Féin
Róisín Shortall Social Democrats
John Brassil Fianna Fáil
Simon Harris Fine Gael
questions including, “the liability individual hospital pharmacists who are employees of the HSE and do not own the pharmacy in which they work?”
The subsequent guidance provided by the Minister included, “The liable parties and the corresponding offences for this Delegated Regulation are in line with existing legislative arrangements, governing the sale and supply of medicinal products to the public. There is nothing new in terms of the obligations under this legislation in terms of the focus of where the legal obligations lie. It is the responsibility of the body corporate to ensure that the infrastructure is in place and correctly functioning to facilitate the pharmacist decommissioning the medicinal product from the national repository prior to supplying to the patient. It is also the responsibility of the pharmacist that dispenses the medicinal product to comply with their requirements under this legislation.”
IPUREVIEW MARCH 2019 53

Gino Kenny People Before Profit Alliance
Richard Boyd Barrett People Before Profit Alliance
Victor Boyhan Independent
Michael D’Arcy Fine Gael
There has been widespread disquiet about the plans to standardise the rate of VAT on vitamins and food supplements at 23%. Gino Kenny TD (Dublin Mid-West, People Before Profit Alliance) described it as incongruous and likened it to a decision in 2014 to put VAT on herbal teas which he said, “the Minister at the time abandoned.”
Richard Boyd Barrett TD (Dún Laoghaire, People Before Profit Alliance) gave an example of a cancer patient called ‘Tony’ who “is paying €32.95 a month for a probiotic; €10 for thiamin; €10 for magnesium; and €20 for Vivioptal. Recommended by his doctor, he needs these products for his health and he is paying €70 a month for
them. He should not be paying that at all. If this VAT change goes ahead, he will be paying €86. He cannot afford that.”
Similar concerns were also raised in the Seanad, with Victor Boyhan (Independent) questioning whether a consultation process could be established to engage on this matter with stakeholders.
Speaking in the Dáil, Minister of State Michael D’Arcy TD (Wexford, Fine Gael) explained, “The standard rate of VAT applies to food supplements. However, there is a Revenue concession which allows a zero rate to be applied to certain types of food supplements such as vitamins, minerals and fish oils.
“Revenue published new guidance on 27 December
concerning the rate of VAT that applies to food supplements, announcing its intention to apply the 23% VAT rate to most food supplements with effect from 1 March 2019.
“It should be noted that human oral medicines, including certain folic acid and other vitamin and mineral products licensed by the Health Products Regulatory Association, will continue to apply at the zero rate of VAT. It is possible to retain these products at the zero rate because they qualify as oral medicines, which are charged to VAT at the zero rate in Ireland under an historical derogation to EU VAT law.”
Opposition protest VAT on vitamins and supplements
Ministers reassured about medical supply post-Brexit
Ensuring Ireland retains a continued supply of medicines following Brexit has been central to many discussions of Brexit planning. Tánaiste Simon Coveney TD (Cork South Central, Fine Gael) outlined the issue saying that, “between 70% and 80% of all medicines in Ireland will continue to come here from the UK or through the UK. After Britain leaves the EU, many of those products will need to have a different route into Irish pharmacies and Irish hospitals because they will no longer have the authorisation of the EU Medicines Agency in Britain.”
Minister Harris stated clearly that, “there is no need for hospitals, pharmacists or patients to order extra quantities of medicines, or for doctors to issue additional prescriptions. To do so could disrupt existing stock levels and hamper the supply of medicines for other patients.
“In 2018, the HPRA developed and launched a multi-stakeholder Medicine
Shortages Framework to anticipate and manage medicine shortages when they occur. This framework is used to manage and address an average of 45 shortage notifications a month. The health system is therefore well placed to anticipate and respond to any additional shortages, should they arise because of Brexit. As an additional safeguard, consideration is being given to those categories of medicines which are considered most essential to public health.”
The Secretary General for the Department of Health, Jim Breslin, also said, “There is no need for hospitals, pharmacists or patients to order extra quantities of medicines, or for doctors to issue additional prescriptions, as doing so could disrupt existing stock levels and hamper the supply of medicines to other patients.”
While the Taoiseach also outlined Ireland’s preparations stating, “A plan has been put in place and a
working group, comprising representatives from the Department of Health, the HSE, the Health Products Regulatory Authority and the Food Safety Authority, has met every week for nearly two years. It has advised against stockpiling because it believes stockpiling may cause a break in supply, although it is working closely with the pharmaceutical industry and the main wholesalers to ensure an adequate supply. It has identified a watch-list of approximately 24 medicines about which we are most concerned.”
Simon Coveney Fine Gael
IPUREVIEW MARCH 201954

Call for greater availability of smoking cessation aids under medical cardsLouise O’Reilly TD (Dublin Fingal, Sinn Féin) has questioned the Minister on the availability of smoking cessation aids and if it will be provided under the medical card.
Minister Harris responded that making nicotine replacement therapy (NRT) more widely available was a central recommendation of the policy document, Tobacco Free Ireland. He said that “NRT is available to medical card holders, on prescription, on the General Medical Services (GMS) Scheme. NRT products are also available as over the counter items, without the need for a prescription. In 2014, the Health Products Regulatory Authority announced that it had licensed some NRT items for sale in non-pharmacy outlets. In addition, two non-nicotine prescription medicines are authorised in Ireland to assist in smoking cessation, and these are available in the community drug schemes.”
However, he made no comment about whether NRT would be made available to medical card patients without the need for prescription.
TDs call for clarity on payments to pharmacy studentsA wide range of TDs have questioned the Ministers for Education and Health in relation to payments to pharmacy students. Michael Moynihan TD (Cork North West, Fianna Fáil) in one of many questions put to the Minister for Health asked the Minister if “he will ensure that pharmacy students will be in a position to be paid for their mandatory placement.” He similarly asked the Minister for Education, Joe McHugh TD, “if the issues faced by pharmacy students, who will now have enormous tuition fees for the fifth year of their course, will be addressed.”
Similar questions were also put to both Ministers by TDs including Margaret Murphy O’Mahony TD (Cork South West, Fianna Fáil); Brendan Griffin TD (Kerry, Fine Gael); Michael Healy-Rae TD (Kerry, Independent); Alan Kelly TD (Tipperary, Labour); Eugene Murphy TD (Roscommon-Galway, Fianna Fáil); Grace O’Sullivan TD (Green Party).
The response of both Ministers was that “Any students in third-level institutions experiencing exceptional financial need can apply for support under the Student Assistance Fund. This Fund assists students, in a sensitive and compassionate manner, who might otherwise be unable to continue their third level studies due to their financial circumstances. Details of this fund are available from the Access Office in the third level institution attended.”
Rural GP services debatedFianna Fáil deputy leader Dara Calleary TD (Mayo) has raised a topical issues debate in the Dáil in relation to GP services in rural areas. Deputy Calleary cited the areas of Kiltane and Bangor Erris where a current GP is moving positions leaving “members of the community concerned that they will be left without GP services.”
Deputy Calleary stated his view that the HSE should “step in and provide surgeries and facilities in the same way that IDA Ireland provides advance factories. The HSE should provide, through a public service obligation, a subsidy towards the employment and retention of staff.”
Responding to the concerns, Minister of State Finian McGrath TD (Dublin Bay North, Independent) assured the Dáil that “the Government is committed to enhancing primary care services, including general practice services. This is central to the Government objective of delivering a high-quality, integrated and cost-effective health service. Our goal is to ensure that patients throughout the country continue to have access to GP services, and that general practice is sustainable in all areas into the future.”
Minister McGrath also went on to outline how the number of GPs has increased in recent years stating, “The number of GPs on the Medical Council specialist register continues to increase. They have increased from 2,270 in 2010 to 3,723 as of 1 January 2019. The number of GPs holding General Medical Services (GMS) contracts has also risen from 2,098 in 2008 to almost 2,500 in 2019.”
Dara Calleary Fianna Fáil
Finian McGrath Independent
Michael Moynihan Fianna Fáil
Joe McHugh Fine Gael
Margaret Murphy O’Mahony Fianna Fáil
Brendan Griffin Fine Gael
Alan Kelly Labour
Eugene Murphy Fianna Fáil
Grace O’Sullivan Green Party
Louise O’Reilly Sinn Féin
IPUREVIEW MARCH 2019 55

Minister outlines response to Hydrocortisone shortageDeputies Charlie McConalogue TD (Donegal, Fianna Fáil) and Pearse Doherty TD (Donegal, Sinn Féin) questioned Minister Harris on the current shortage in Ireland of Hydrocortone. In response Minister Harris said, “The Department of Health is aware of a temporary shortage of Hydrocortone (hydrocortisone) 10mg tablets in Ireland. The marketing authorisation holder has notified the medicines regulator, the Health Products Regulatory Authority (HPRA), that the shortage of this medicine is due to manufacturing delays. In the interim, the Irish market is being supplied on a temporary basis with hydrocortisone 10mg tablets from other markets to meet the needs of Irish patients until supply of the Irish authorised medicine resumes.”
Calls for extension to Meningitis B vaccine programmeFollowing the concerns expressed by the HSE about the increase in Meningitis B cases, a number of politicians have called for an expansion to the existing vaccine programme.
Pearse Doherty TD (Donegal, Sinn Féin) expressed concern at the cost faced by families who have children born before 2016 who have “to pay for vaccination privately at a cost of between €300 and €450.” Fianna Fáil leader Micheál Martin TD (Cork South Central) said he was “perturbed” as to how the vaccine was being introduced citing the introduction of the Meningitis C vaccine which was provided to all children.
Responding to a similar question from Michael Healy-Rae TD (Kerry, Independent) Minister Harris said, “There are no plans to introduce a catch-up programme for the Meningitis B vaccine to older children. Those who have a medical card are eligible to have the vaccine administered by their GP free of charge. However, the purchase of the vaccine is not covered by the medical card scheme.”
Deputy Brassil queries HPRA fee increaseJohn Brassil TD (Kerry, Fianna Fáil) asked the Minister for Health a question about the planned 8% fee increase from the HPRA. The Minister stated that “the Authority’s last significant fee increase was in 2010. In 2011 and 2012, the HPRA reduced fees, and there were no fee increases between 2013 and 2017.”
In addition, he cited Brexit and the Falsified Medicines Directive as matters that will present significant challenges to both the pharmaceutical industry and the HPRA. The HPRA he said “plays a vital role in supporting this industry, and this fee increase is considered necessary in order to enable the Authority to continue to fulfil its public health remit.”
Methadone services outlined by Minister of State Catherine Byrne TDThe protocols for methadone strategy were explored in a Dáil discussion between John Curran TD (Dublin Mid West, Fianna Fáil) and Minister of State Catherine Byrne TD (Dublin South Central, Fine Gael). Curran asked the Minister “when the protocols on the methadone strategy were last reviewed and are they sufficient to ensure that those who want to progress from the methadone programme to become drug free can do so?”
Minister Byrne first of all outlined the uptake of methadone explaining that “Methadone prescribing for opioid dependence is a key element of the harm reduction approach to opioid use set out in the national drugs strategy. Methadone is one of the medications used in opioid substitution treatment, along with Suboxone. As of 30 November 2018, more than 10,000 people were in receipt of methadone maintenance treatment.”
She then outlined the protocols: “The guidelines are the first that specifically relate to opioid substitution treatment in HSE clinics and primary care settings. Opioid substitution treatment supports patients to recover from drug dependence. HSE addiction services work within the national drugs rehabilitation framework to support progression pathways. The framework ensures that individuals affected by drug misuse are offered a range of integrated options tailored to meet their needs and to create rehabilitation pathways.”
Treatment using Suboxone was also discussed, with the Minister stating, “Suboxone use has also been established as a treatment in Ireland. To facilitate the increase in the use of Suboxone, €750,000 was allocated in each of the years 2017 and 2018, giving us a sum of €1.5 million for the full year costs.”
While the Minister accepted Deputy Curran’s assertion that Ireland is “an outlier in comparison with most European countries that have 20% or 30% of those on opioid substitution treatment, OST, using Suboxone”, she did say that Ireland was “heading in the right direction.”
John Curran Fianna Fáil
Catherine Byrne Fine Gael
Michael Healy-Rae Independent
Micheál Martin Fianna Fáil
Charlie McConalogue Fianna Fáil
Pearse Doherty Sinn Féin
John Brassil Fianna Fáil
IPUREVIEW MARCH 201956

Pádraig Ó Mathúna was born in Cashel in October 1926. He received his early education at Cashel
C.B.S. and later at Rockwell College. After leaving school Pádraig embarked on a career in pharmacy. He studied at the School of Pharmacy, Mount Street, Dublin. He qualified as a pharmacist in 1955. He conducted his own pharmacy in Cashel from the early to the mid-1960’s. He subsequently managed a pharmacy in Kilfinane, Co Limerick for Dr Rosenstock. Later on he became the dispensary pharmacist in Carrick-on-Suir.
At this stage, Pádraig gravitated towards the artistic side of his being and became a full-time artist of exceptional talent and diversity. To say that he was multitalented would be a serious understatement. He became a silversmith and goldsmith of international repute. In his younger days he won the Oireachtas Gold Medal for the violin. He was also a noted philatelist, photographer, painter, historian and linguist.
The following excerpt of the eulogy delivered by his nephew, Cian O’Carroll, at his Requiem Mass illustrates the scope of Pádraig’s versatility.
“I doubt Pádraig Ó Mathúna passed an idle day in his life. His mind was constantly whirring, while juggling what seemed to be multiple strands of thought and argument and creativity. This was reflected in the sheer breadth of his accomplishments. It seemed that everything he turned his hands, or mind to, he excelled at and he was ready to turn those gifted hands to just about anything. From the violin and all forms of traditional music to photography, from stamp collecting, to archiving important aspects of our island’s struggle for real and meaningful independence and from genealogy, to pharmacy and on to his best known accomplishments, as an artist. He succeeded in his artistic expression across several media. From his goldsmith and silversmith creations, to his stunning enamelwork and, of course, his paintings,
Pádraig created an entire new yet distinctively modern and undeniably Celtic style in an authentic way. His metalwork is stunningly beautiful. He rejected the trend to adopt modern techniques and instead literally rediscovered the secrets of how ancient treasures of our culture were made. He then perfected those techniques and made extraordinary and beautiful objects with seemingly perfect proportions for both secular and sacred use – objects that surpass, not ape, the great treasures of the early Christian and Bronze ages. The whole nation and its visitors can enjoy the fine collection of some of his masterworks preserved for us all in the National Museum”.
About twenty years ago Pádraig moved to West Kerry, Dún Chaoin to be precise. Here he drew fresh inspiration from the natural beauty of his new surroundings, looking out as he was from his new abode, at the Blasket Islands. His home there was a veritable treasure chest of his varied art. He was happy to spend the last
chapter of his life in a totally Gaelic environment.
Pádraig was a close friend of mine for well-nigh three score years. Our common background in pharmacy, while it formed a certain bond between us, was overshadowed by our mutual love of our native language. In fact, we always conversed “as Gaeilge”.
Pádraig’s Requiem Mass in Cashel on 12 January last was attended by Uachtarán na hÉireann, Mícheál Dónal Ó hUigínn and was sung by Cór Chúil Aodha under the direction of Peadar Ó Riada. Some haunting airs were played by members of Cashel Comhaltas Ceoltóiri.
The chalice used in the mass was designed and made by Pádraig and presented to Cashel church in honour of his late wife, Siobhán.
Déanaim-se comhbhrón le iníonacha Phádraig – Siobhán agus Niamh agus lena gClann uiligh.
Ní imithe uainn, ach romhainn. I measc na nGael go rabh tú a chara.
OBITUARY Seán Ó Duibhir, MPSI
“A close friend for well-nigh three score years”: Pádraig Ó Mathúna –Obituary by Seán Ó Duibhir
IPUREVIEW MARCH 2019 57

CHMP recommends approval of Praluent® (alirocumab) to reduce cardiovascular risk in people with established atherosclerotic cardiovascular disease The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has adopted a positive opinion for Praluent® (alirocumab), recommending a new indication as an adjunct to correction of other risk factors. Praluent® should be used in addition to a maximally tolerated dose of statin or can be used alone in patients intolerant to or inappropriate for statin therapy.
The CHMP opinion is based on data from Odyssey Outcomes, a Phase 3 cardiovascular outcomes trial that assessed the effect of Praluent® in 18,924 patients who had an ACS between 1 – 12 months (median 2.6 months) before enrolling in the trial. Results from the Odyssey Outcomes trial were published in the New England Journal of Medicine in 2018.
The European Commission is expected to make a final decision in the coming months. Data from Odyssey Outcomes has also been submitted to the U.S. Food and Drug Administration (FDA), with a target action date of 28 April 2019.
For additional information about the company, please visit www.regeneron.com.
New Phase 3 data demonstrates superiority of TREMFYA®▼ (guselkumab) vs Cosentyx® (secukinumab) in delivering PASI 90 responses in the treatment of moderate to severe plaque psoriasis at week 48The Janssen Pharmaceutical Companies of Johnson & Johnson announced results from the ECLIPSE study demonstrating that TREMFYA® (guselkumab) was superior to Cosentyx® (secukinumab)* in treating adults with moderate to severe plaque psoriasis for the primary endpoint assessed at week 48. Data from the multicentre, randomised, double-blind head-to-head Phase 3 study demonstrated that 84.5% of patients treated with guselkumab achieved at least 90% improvement in their baseline Psoriasis Area Severity Index (PASI) score at week 48, compared with 70% of patients treated with secukinumab (p<0.001)1.
ECLIPSE incorporated six major secondary endpoints that used a fixed statistical sequence procedure to control for multiple comparisons and included both shorter and longer-term analyses. Guselkumab demonstrated non-inferiority to secukinumab in the first major secondary endpoint, with 84.6% of patients on guselkumab achieving a PASI 75 response at both weeks 12 and 48 versus 80.2% of those on secukinumab (p<0.001), however, it did not demonstrate superiority (p=0.062). Because superiority was not demonstrated for the first major secondary endpoint, p-values for all the subsequent major secondary endpoints were considered nominal1.
For more information, see www.janssen.com/ireland.
References1. Langley, RG et al. (2018) 3rd Inflammatory Skin Disease Summit 2018, 12–15 December;Vienna, Austria: LB4.
New England Journal of Medicine publishes positive results of the pivotal trial of Cablivi® (caplacizumab) for rare blood clotting disorderThe New England Journal of Medicine (NEJM) has published positive results of the Phase 3 trial of Cablivi® (caplacizumab) in adults with acquired thrombotic thrombocytopenic purpura (aTTP).
The current treatment for aTTP consists of daily plasma exchange, in which a patient’s blood plasma is removed and replaced with donor plasma, and immunosuppression. Even with currently available treatments, patients continue to be at risk of developing acute blood clotting conditions, such as stroke and heart attack, as well as recurrence of disease.
Cablivi demonstrated a safety profile consistent with what has been previously reported and in line with its mechanism of action; this included an increased risk of bleeding. The most frequently reported bleeding-related adverse events were epistaxis and gingival bleeding.
www.sanofi.us
STUDIES
IPUREVIEW MARCH 201958

FDA approves Cablivi® (caplacizumab-yhdp), the first Nanobody®-based medicine, for adults with acquired thrombotic thrombocytopenic purpura (aTTP)
The U.S. Food and Drug Administration (FDA) has approved Cablivi® (caplacizumab-yhdp) in combination with plasma exchange and immunosuppression for the treatment of acquired thrombotic thrombocytopenic purpura (aTTP) in adults. Cablivi is the first FDAapproved therapy specifically indicated for the treatment of aTTP.
Cablivi received FDA Fast Track designation and was evaluated under Priority Review, which is reserved for medicines that represent significant improvements in safety or efficacy in treating serious conditions.
The approval of Cablivi in the U.S. is based on the results of the pivotal multicentre, randomised, double-blind, placebo-controlled Phase 3 clinical study known as HERCULES. This trial evaluated the efficacy of Cablivi in combination with plasma exchange and immunosuppressive therapy (n=72) versus placebo, plasma exchange and immunosuppressive therapy (n=73) in 145 adults experiencing an episode of aTTP.
For full prescribing information, please visit www.cablivi.com
FDA advisory committee votes on Zynquista(TM) (sotagliflozin) as treatment for adults with type 1 diabetesThe Endocrinologic and Metabolic Drugs Advisory Committee of the U.S. Food and Drug Administration (FDA) voted eight to eight on the question of whether the overall benefits of Zynquista™ (sotagliflozin) outweighed the risks to support approval. Sotagliflozin is an investigational oral dual SGLT1 and SGLT2 inhibitor under regulatory review as an adjunct to insulin for the treatment of adults with type 1 diabetes (T1D). While the FDA is not required to follow the committee’s vote, the agency considers the committee’s recommendations when making its decision, which is anticipated by 22 March 2019.
Sotagliflozin, developed by Sanofi and Lexicon, has the potential to be the first oral antidiabetic drug approved in the United States together with insulin therapy to improve glycemic (blood sugar) control in adults with T1D.
The New Drug Application for sotagliflozin included data from the inTandem clinical trial programme, which included three Phase 3 clinical trials assessing the safety and efficacy of sotagliflozin in approximately 3,000 adults with inadequately controlled T1D. The safety and efficacy data has not yet been fully evaluated by any regulatory authority.
Sanofi also submitted a regulatory application to the European Medicines Agency (EMA) in 2018. An EMA approval decision is expected in the first half of 2019.
For more information, visit www.sanofi.us.
Bavarian Nordic Completes enrolment of first stage in Chordoma Phase 2 TrialBavarian Nordic A/S (OMX: BAVA, OTC: BVNRY) announced that the first stage of a Phase 2 study of its novel, targeted cancer immunotherapy candidate, BN-Brachyury in the treatment of advanced chordoma, has completed recruitment of the planned 10 patients ahead of schedule.
The multi-site trial, which holds the potential to serve as a registration trial, aims to determine if the combination of BN-Brachyury vaccine and the current standard of care, radiation therapy, results in a clinically meaningful objective response rate (ORR) within 12 months of radiation therapy, a timeframe during which historical controls show an ORR of less than 5% with radiation alone. Radiation has been shown to inflame the tumor, releasing cancer antigens. BN-Brachyury is designed to teach T cells to attack brachyury-expressing cells and kill the tumor cells.
For more information on the trial, please visit www.clinicaltrials.gov/ct2/show/NCT03595228.
STUDIES
IPUREVIEW MARCH 2019 59

HIGH TECH MEDICINES UPDATE Tara Kelly MPSI, Medicines Information Pharmacist, IPU
Symkevi® Film- coated Tablets
Symkevi 100mg/ 150mg film-coated tablets, indicated for the treatment of Cystic Fibrosis
(CF), have recently been added to the High Tech Medicines Scheme.
Symkevi tablets contain 100mg of Tezacaftor and 150mg of Ivacaftor and are indicated in combination with Ivacaftor 150mg tablets (Kalydeco) for the treatment of patients aged 12 years and older who are homozygous for the F508del mutation, or who are heterozygous for the F508del mutation with one of 14 other mutations in the cystic fibrosis transmembrane conductance regulator (CFTR) gene.
Symkevi should only be prescribed by physicians with experience in the treatment of CF, following confirmation of an indicated mutation using a genotyping assay.
Cystic Fibrosis Ireland welcomed this recent addition of Symkevi onto the High Tech Medicines Scheme, stating on their website, “This is the third in a series of groundbreaking and innovative drugs for CF in Ireland. These are precision CFTR drugs that treat the underlying cause of CF and are aimed at particular CF gene mutations – hence the need for more than one drug. The other two CFTR drugs that were previously approved by the Irish Government are Kalydeco (2013) and Orkambi (2017). The innovative deal struck in 2017 between Vertex and the HSE provided for both Orkambi, but also known drugs that were ‘in the pipeline’ (i.e. undergoing very positive clinical trials, such as Symkevi)”.
Mode of ActionThe CFTR protein is a chloride channel present at the surface of epithelial cells in multiple organs. The transport of
chloride ions helps control the movement of water in tissues, which is necessary for the production of thin, freely slowing mucus. Disease-causing mutations in the CFTR gene alter the production, structure, or stability of the chloride channel. All of these changes prevent the channel from functioning properly, which impairs the transport of chloride ions and the movement of water into and out of cells. Cells that line the passageways of the lungs, pancreas, and other organs produce mucus that is abnormally thick and sticky. The abnormal mucus obstructs the airways and glands, leading to the characteristic signs and symptoms of cystic fibrosis.
Tezacaftor is a selective CFTR corrector that binds to the first Membrane Spanning Domain (MSD-1) of CFTR. Tezacaftor facilitates the cellular processing and trafficking of normal or multiple mutant forms of CFTR to increase the amount of CFTR protein delivered to the cell surface, resulting in increased chloride transport in vitro.
Ivacaftor is a CRTR potentiator that facilitates increased chloride transport by potentiating the channel-open probability of the CFTR protein at the cell surface.
In most circumstances, Symkevi will be prescribed in combination with Kalydeco (Ivacaftor). The recommended dose is one Symkevi tablet taken in the morning and one Kalydeco 150mg tablet taken in the evening, approximately 12 hours apart.
The tablets should not be chewed, crushed, or broken before swallowing.
Both Symkevi and Kalydeco tablets should be taken with fat-containing food. Food or drink containing grapefruit or Seville oranges should be avoided during treatment, due to their inhibition of CYP enzymes.
Adverse Reactions and Drug InteractionsThe most common adverse reactions listed in the SmPC are headache and nasopharyngitis.
Liver function tests are recommended before initiating treatment every three months during the first year of treatment and annually thereafter.
The use of Symkevi is not recommended in patients with severe hepatic impairment unless the benefits are expected to outweigh the risks. Caution is recommended in patients with severe renal impairment or end-stage renal disease.
Exposure to Symkevi may be reduced by the concomitant use of CYP3A inducers. Therefore, co-administration with strong CYP3A inducers is not recommended, e.g. rifampicin, rifabutin, phenobarbital, carbamazepine, phenytoin, and St. John’s wort.
The dose of Symkevi should be adjusted when used with strong or moderate CYP3A inhibitors, e.g. ketoconazole, itraconazole, voriconazole, telithromycin, clarithromycin, fluconazole and erythromycin.
Ivacaftor may inhibit CYP2C9; therefore, INR monitoring is recommended during co-administration with warfarin. Glimepiride and glipizide should also be used with caution.
Tezacaftor metabolites have the potential to induce CYP1A2 and CYP2B6. Caution and appropriate monitoring should be used when Symkevi is administered with narrow therapeutic index substrates of CYP1A2 (such as theophylline) or CYP2B6 (such as bupropion).
Administration of Symkevi in combination with Ivacaftor may increase systemic exposure of medicinal products that are sensitive substrates of P-gp. Digoxin,
ciclosporin, everolimus, sirolimus and tacrolimus should be used with caution.
As a precautionary measure, it is preferable to avoid the use of Symkevi during pregnancy. A decision must be made whether to discontinue breast-feeding or to discontinue/abstain from therapy.
This product is under additional monitoring (black triangle). Patients and healthcare professionals are encouraged to report suspected side-effects seen with any medicine.
High Tech HubAs per HSE Circular 39/2018, hospitals have been requested to input prescriptions for Symkevi directly onto the High Tech Hub. If a patient presents with a High Tech prescription that is prefaced by ‘HTH’, the nominated pharmacy can access the prescription details and proceed to order. In the event that a patient presents with a handwritten High-Tech prescription, you may have to engage with the prescriber, or the High Tech Co-ordination Unit directly, as this patient may not meet the criteria for reimbursement.
As for Orkambi and Kalydeco, Symkevi can only be prescribed up to a maximum of three months, in line with the reimbursement protocol (see under the ‘Help’ Tab on the High Tech Hub).
The European Assessment Report and SmPC for Symkevi can be located on the EMA website (https://www.ema.europa.eu/en/medicines/human/EPAR/symkevi).
Symkevi tablets were granted a marketing authorisation valid throughout the EU in October 2018 and are listed on the IPU Product File since the January 2019 update (High Tech number: 88845).
IPUREVIEW MARCH 201960

CLINICAL TIPS Tara Kelly MPSI, Medicines Information Pharmacist, IPU
Restrictions on the use of Quinolone and Fluoroquinolone Antibiotics
The European Medicines Agency’s (EMA) safety committee reviewed some
serious, disabling and potentially permanent side-effects with quinolone and fluoroquinolone antibiotics given by mouth, injection or inhalation. (Ref: https://www.ema.europa.eu/en/medicines/human/referrals/quinolone-fluoroquinolone-containing-medicinal-products).
It was concluded that the licences for medicines containing cinoxcin, flumequine, nalidixic acid, and pipemidic acid should be suspended. There are no licensed products marketed in Ireland containing these particular agents.
However, use of the remaining fluoroquinolone antibiotics has been restricted.
The following fluoroquinolone antibiotics are licensed and marketed in Ireland at present:
n Ofloxacin: Tarivid;
n Ciprofloxacin: Ciproxin, Cifox, Truoxin, Cifloxager, Ciplox, Profloxin;
n Levofloxacin: Tavanic, Tavager; and
n Moxifloxacin: Avelox.
Additionally, norfloxacin and sitafloxacin are sometimes used as an Unlicensed/Exempt medicine in Ireland.
Adverse reactionsThe review found that these adverse reactions can involve several, sometimes multiple, systems, organ classes and senses. The serious side-effects include tendonitis, tendon rupture, arthralgia, pain in extremities, gait disturbance, neuropathies associated with paraesthesia, depression, fatigue, memory impairment, sleep disorders, and impaired hearing, vision, taste and smell. Tendon damage can occur within 48 hours of starting fluoroquinolone treatment but the damage may be delayed several months after stopping treatment. Patients who are older, have renal impairment or have solid organ transplantation, and those being treated with a corticosteroid are at higher risk of tendon damage.
Restrictions in useRestrictions on the use of fluoroquinolone antibiotics mean that they should not be used:
n To treat mild or self-limiting conditions, e.g. pharyngitis, acute bronchitis;
n To treat non-bacterial infections;
n To prevent traveller’s diarrhoea or to prevent recurring lower urinary tract infections; and
n To treat mild or moderate bacterial infections unless other antibiotics are contraindicated.
Fluoroquinolones should be avoided in patients who have previously had serious side-effects with a fluoroquinolone or quinolone antibiotic.
They should be used with caution in the elderly, patients with renal impairment and patients with solid organ transplants.
Concomitant use of corticosteroids should be avoided.
Advice for Patients
n Treatment should be discontinued and patient should be referred to the GP:
• At the first sign of tendon injury such as tendon pain or inflammation;
• If they experience pain, pins and needles, tingling, numbness, burning or weakness especially in the legs and arms; and
• If they feel depressed or have problems with memory, sleeping, or notice changes with
their vision, taste, smell or hearing.
n For patients with a serious infection that is susceptible to treatment with these antibiotics, fluoroquinolones remain an important treatment option.
n Patients should be informed of the risks associated with fluoroquinolones prior to initiating treatment and be advised to read the patient information leaflet.
All suspected adverse reactions associated with fluoroquinolones should be reported to the HPRA: http://www.hpra.ie/homepage/veterinary/safety-information/adverse-reaction-reporting
IPUREVIEW MARCH 2019 61

International Pharmacy NewsEU
PGEU publishes its vision for the pharmacy profession in a paper titled, Pharmacy 2030: A Vision for Community Pharmacy in EuropePGEU President Michał Byliniak stated, “This year, PGEU celebrates its 60th anniversary. It is time to acknowledge the pharmacy profession’s vital contribution to the health of people over the last decades and to look to the future to how the profession can further enhance this contribution and help to strengthen Europe’s health systems.
“In light of common challenges for European healthcare systems, such as financial sustainability, shortages of healthcare workers and the increasing burden of chronic diseases, we must recognise, support and develop the role of community pharmacists in providing highly accessible and quality patient care and prevention services.
“Community pharmacists want to use their position as highly skilled healthcare professionals, working at the heart of European communities, to further improve public health in a changing healthcare environment requiring more personalised, patient-centred and digital focus.”
Pharmacy 2030: A Vision for Community Pharmacy in Europe outlines 10 key recommendations:
1. Maximise the benefits of the community pharmacist’s intervention for patients and healthcare systems by promoting pharmaceutical services to improve treatment outcomes and adherence, and to minimise risks;
2. Involve community pharmacists in collaborative care models;
INTERNATIONAL NEWS Róisín Molloy, Membership & Secretary General’s Office Manager, IPU
3. Grant community pharmacists access to all relevant patients’ health information and the list of medications they are taking;
4. Consult pharmacists on the integration of new digital solutions in healthcare;
5. Allow pharmacists to help progress the digitalisation of healthcare as trusted sources for health information;
6. Support pharmacists in integrating pharmacogenomics, validated clinical rules and real-world data in their daily practice to improve patient safety;
7. Support community pharmacists in offering health screening, medicines management, health promotion and education to help reduce the overall burden of chronic diseases;
8. Establish regulatory frameworks to maximise the value of the highly-accessible community pharmacies network to the communities they serve;
9. Ensure that community pharmacists can provide patients with the full range of medicines and medical devices they need; and
10. Ensure that remuneration for community pharmacists properly reflects their contribution to improving pharmaceutical care, reducing the burden on other health services and supporting the sustainability of health systems.
Source: www.pgeu.eu/en/
Australia
Unmatched capacity and capability of community pharmacistsRecently released reports from the Productivity Commission and the Pharmacy Research Centre at the University of South Australia demonstrate that an increased commitment to medication management delivered through Australia’s 5,700 strong network of community pharmacies is required to reduce unnecessary hospital admissions and emergency department presentations.
The Productivity Commission found 2.9 million avoidable presentations at public hospital emergency departments in 2017 – 2018, while the Pharmacy Research Centre found 250,000 hospitalisations and 400,000 emergency department presentations annually due to medicine-related problems. These reports are the latest additions to the strong body of evidence about the need to invest in medication management delivered through Australia’s workforce of nearly 20,000 trusted medicines
PHARMACY 2030:
A Vision for Community
Pharmacy in Europe
IPUREVIEW MARCH 201962

experts who work as community pharmacists in suburbs and towns across Australia.
With some 450 million patient visits a year and dispensing over 300 million prescriptions to patients annually, Australia’s established community pharmacy network is the logical and practical means for delivering the medication management reviews, adherence support and expert medicines advice that will reduce unnecessary hospital admissions and take pressure off other already overstretched parts of the health system, such as general practice and aged care facilities.
With the large increase in the number of Australians living with chronic diseases and co-morbidities, patients’ medication-related needs have become more complex and require more intensive support. Investment in medication-related collaboration between GPs and community pharmacy needs to be enhanced and become more formalised, with funders recognising the significant net health and fiscal dividend from investing in medication management that is delivered through this established and reputable health infrastructure which underpins community-based healthcare.
This general practitioner community pharmacy based collaborative approach to medication management, developed through the Community Pharmacy in Health Care Homes trial, is also readily applicable to patients living in residential aged care facilities.
For these resident aged care patients, their local community pharmacy dispenses and undertakes, or arranges, the packing of the medicines which have been prescribed by their doctor. The community pharmacist takes responsibility for reconciling the patient’s medicines with their medication chart and liaises with the aged care facility, and the GP, if there are discrepancies, or the patient has urgent or emergency medicine needs.
However, this existing role can be significantly enhanced by investing in personalised medication management plans for residential aged care patients that include regular quality use of medicines support and medication management reviews which are undertaken by the patient’s community pharmacist working in collaboration with their GP. This approach will ensure continuity of care, timely interventions when problems arise, maintenance of the critical links with the patient’s prescribing doctor and dispensing pharmacist, and the ongoing provision of information to the patient’s healthcare team. This stands in stark contrast to the current medication management arrangements in aged care facilities which are ad hoc, often involve pharmacists with no links to the patient’s GP or community pharmacist, are not undertaken on a timely basis to prevent problems such as the overuse of anti-psychotics, and are largely divorced from the supply of medicines.
Source: www.guild.org.au
For further information on the IPU Retail Review service, please contact Darren Kelly on (01) 493 6401 / 086 028 9825 or email: [email protected]
THINKING OF A REFIT? HAVE THE RETAIL PLAN DONE FIRST.
Retail Review 190X135mm Ad ART *NEW*.indd 2 25/03/2016 16:37
IPUREVIEW MARCH 2019 63

PRODUCT INFORMATION
The Mundipharma network of independent associated companies has announced the launch of Pelmeg® (pegfilgrastim), a biosimilar of Neulasta® in Ireland following authorisation by the Health Products Regulatory Authority. The launch follows European Commission (EC) approval in November 2018.i Pelmeg is the fourth biosimilar medicine to be commercialised by Mundipharma (the third in Ireland), expanding its portfolio and commercial footprint across Europe. It was developed by Cinfa Biotech which was acquired by Mundipharma and announced in October 2018. Pelmeg® is indicated for the reduction of the duration of neutropenia and the incidence of febrile neutropenia in adult patients treated with cytotoxic chemotherapy for
malignancy (with the exception of chronic myeloid leukaemia and myelodysplastic syndromes).ii
Pelmeg® is a registered trademark of Cinfa Biotech, S.L. Herzuma®, Truxima® and Remsima® are all registered trademarks of Celltrion Inc. and are used under license.
For further information please contact, [email protected] or 01 206 3800.
i. European Medicines Agency. Pelmeg® (pegfilgrastim) European Public Assessment Report. Available at www.ema.europa.eu.
ii. European Medicines Agency. Pelmeg® (pegfilgrastim) Summary of Product Characteristics. Available at www.ema.europa.eu.
Mundipharma biosimilar Pelmeg® (pegfilgrastim) now available in Ireland
Accord Healthcare is delighted to announce the launch of Agomelatine Accord 25mg which is available in a pack size of 28 Film Coated Tablets.
This medicine is indicated for the treatment of major depressive episodes in adults.
Please refer to the Summary of Product Characteristics (SPC) available at www.hpra.ie or for Healthcare Professionals at www.accord-healthcare.ie for further information.
For further information please contact Accord in Cork on 021 461 9040 or visit www.accord-healthcare.ie.
Rowex Ltd. is pleased to announce the launch of Desogestrel Rowex 75 micrograms Film-coated tablets in a 28-pack size.
Desogestrel Rowex is indicated for contraception.For further information or to order contact our Rowex®
Telesales Team: Irene, Jeanne Marie or Rita on 1800 304 400.Product subject to medical prescription. Further information
and SPC are available from the Marketing Authorisation Holder: Rowex Ltd., Bantry, Co. Cork, P75 V009 Freephone: 1800 304 400 Fax: 027 50417 E-mail: [email protected].
Accord healthcare launch agomelatine 25mg
Rowex launch Desogestrel Rowex 75 micrograms Film-coated tablets
IPUREVIEW MARCH 201964

PHX sports strapping tapes are a heavy duty, ultra-strong, tearable tape, offering excellent performance for taping applications. Ideal for compression, support and fixation uses.The Physiologix range belongs to a stable of brands from Fleming Medical, which also includes Medicare, Irelands No. 1 pharmacy-only First Aid brand.
Munster Rugby uses Physiologix tapes and supports as their first choice for taping of players, both on and off the pitch. Each Physiologix product has been developed and designed to provide firm support that enables effective stabilisation and effective compression for the user.
Damien Mordan, head physio with Munster Rugby, believes that Physiologix PHX tapes are of the highest quality for the Munster squad. “The PHX Strapping tape range is ideal for compression and fixation injuries both on and off the pitch for our Munster squad.”
For further information, please contact Kieran Quinn, Fleming Medical 087 0624743 E-mail: [email protected].
Munster Rugby’s head physio recommends Physiologix PHX tapes for Munster Rugby players
PRODUCT INFORMATION
Pictured: Damien Mordan, Munster Rugby Head Physio and Jean Kleyn, Munster Rugby.
STOCKTAKING SERVICESPHARMACY SPECIALISTS | SAME DAY AUDITABLE REPORTS
LIVE STOCK INTEGRATION WITH:
44 Church Street, Tullamore, Co. Offaly Phone/Fax 057 93 20045Alan Daly – Director 087 2666431 Darren Donoghue – Manager 086 3809082
BCAC
M
Y
CM
MY
CY
CMY
K
ABC Advert JULY2014.pdf 1 28/07/2014 14:41
IPUREVIEW MARCH 2019 65

NEWS
The PSI has published its new Corporate Strategy 2018 – 2020 outlining a programme of activities intended to further develop the regulator’s important contribution to assuring trust in pharmacists, in pharmacy services and the achievement of better public health outcomes. Through its role in regulating 6,050 pharmacists and over 1,900 pharmacies, the PSI will work to improve public understanding of what good pharmacy practice looks like and to assure the high standards that can be expected by everyone availing of pharmacist-provided care. This is reflected in the proposal to publish more extensive information gathered in the course of its monitoring of pharmacy services through its inspection function.
This year also sees the review of the PSI’s professional Code of Conduct for pharmacists to ensure it continues to reflect the changing healthcare environment and the evolving role of pharmacists within the wider health service. As healthcare professionals, there is a need for each pharmacist to manage potential conflicts which may arise between business and organisational goals, and their own professional ethics. The Code sets out the ethical standards which govern the practice of pharmacy and which the public, patients and other healthcare professionals require and expect of pharmacists.
PSI President, Rory O’Donnell, spoke about the new Corporate Strategy starting at a crossroads to change. “In less than 10 years, we have seen significant achievements in establishing clear structures of regulation. We have moved towards a more risk-based approach to inspection, for example. The education and training of pharmacy students has been radically reformed along with the requirements for the continuous professional development of existing registrants. The PSI has also supported the expansion of vaccination services within pharmacies and we have undertaken a major programme of research and stakeholder engagement, through the Future of Pharmacy Practice Report, to assess how pharmacy can help meet the future needs of patients and members of the public. Now we are going to build on our work to date, ensuring a regulatory system that affirms the trust that the public places in it and is capable of meeting future patient and health service needs.”
While the implications of Brexit for the sector are still uncertain, the PSI acknowledges within the Strategy that it may be required to allocate additional resources, during the term of the plan, to manage the effects of the UK’s decision to leave the EU. The possible implications for the PSI include the movement of pharmacists between jurisdictions and the facilitation of cross-border healthcare. The PSI manages different routes of registration for pharmacists to practice in Ireland, with a large cohort coming each year from the UK, including returning Irish students. “As the impact of Brexit becomes clearer, we will work closely with the Department of Health, and other healthcare regulators in Ireland and across Europe, to minimise the negative impact on Ireland,” said Niall Byrne, PSI Registrar.
Find annual service plans, reports and strategy on the PSI website, www.psi.ie.
PSI Strategy 2018-2020: Assuring trust in pharmacy through effective regulation
IPUREVIEW MARCH 201966

NEWS
A new national and European system, giving patients further protection from the threat of counterfeit medicines came into effect on 9 February 2019. Throughout Europe, medicine packs will have enhanced tamper-proof measures and will now carry a barcode with a unique serial number so that each pack can be scanned in a pharmacy. It will be checked against a central database to ensure the product is legitimate before handover to a patient. Established and managed by the Irish Medicines Verification Organisation (IMVO), the new national system provides an additional layer of security to protect the supply of medicines at pharmacy and patient level. Ireland is now in compliance with the EU Falsified Medicines Directive (FMD), which provides more safeguards and security to ensure Irish patients will continue to have absolute confidence in the medicines they receive from their pharmacy.
According to Pat O’Mahony, Chair, IMVO, “Setting up this advanced and robust verification system is a significant undertaking as a result of over three years of collaboration by the key Irish stakeholders including pharmaceutical manufacturers, parallel distributors, wholesalers, as well as community and hospital pharmacists. Substantial work and investment has been required by everyone in the medicines supply chain to have the system up and running and in place as appropriate to the legislation coming into effect. Although there has been no risk or reported incidents at pharmacy level from counterfeit or falsified medicines in Ireland, other countries have had issues so this new system provides further security and protection for Irish patients now and into the future. Counterfeit medicines can pose serious risks to health, as there is no guarantee of their quality or safety.”
continued overleaf
New medicines security features further protect supply chain for medicines
Pictured above using the new system at Conefrey’s Care Plus Pharmacy, Pearse Street, Dublin 2, are: (main pic) Amy Brophy and her children Amelia and Tommy Andrews, Leonie Clarke, General Manager IMVO; (inset pic) Leonie Clarke and pharmacist Tomás Conefrey.
IPUREVIEW MARCH 2019 67

NEWS
continued from previous page
The initiative has involved the collaboration of over 2,000 pharmacies, hospitals and wholesalers in Ireland who distribute and dispense over 95 million prescription medicines every year, as well as the manufacturers who make the products. Each pharmacy now has a scanner to check each pack before it is dispensed to the patient. The scanner connects to a central database of prescription-only medicines manufactured, distributed and supplied for sale in Ireland.
Patients will see the new safety features appear on medicine packs as they come onto the market this year. Each pack will have a:
n Barcode (2D matrix barcode) containing data unique to that pack; and
n Anti-tamper device to provide assurances that the pack has not been interfered with, e.g. glued flap, sticky seal, plastic break-seal.
Minister for Health, Simon Harris TD, said, “The purpose of the regulation is to improve patient safety and maintain confidence in the safety of medicines supplied to patients. Nothing in the new regulations seeks to alter the existing legal and regulatory responsibilities of persons authorised to place medicinal products on the market or supply them to the public. It will apply to manufacturers, wholesalers, pharmacy owners and pharmacists equally. This new national system provides further security and protection for Irish and European patients now and into the future.”
The system is based on providing an alert if the barcode is not identified when scanned. A clear protocol then follows to investigate these alerts, involving the location where the pack was scanned, the manufacturer, the Health Products Regulatory Authority (HPRA), IMVO and its European counterpart, the European Medicines Verification Organisation (EMVO). For the next number of months, medicine packs with and without the individual serial number will be available at the same time as the existing stocks are gradually replaced by new packs with safety features. There is also a period of time allowed to bed in the new system across the country so alerts will be monitored and managed without any impact on medicine supply during this ‘use and learn’ phase.
IMVO advises that purchasing prescription-only medicines from the internet or other unauthorised sources is illegal and there is a high risk that these products are counterfeit, not safe for use, and do not contain the active ingredient required to make the medicine work. When you receive medicines from your pharmacist, always listen to their advice and follow the steps outlined in the package leaflet.
Counterfeit medicinal products are now officially known as ‘falsified medicinal products’ under EU medicines legislation. Falsified medicines may contain ingredients which are of poor quality or in the wrong dose.
HIQA announces public consultation on C-reactive protein point-of-care testing to guide antibiotic prescribing in primary careThe Health Information and Quality Authority (HIQA) has commenced a national public consultation on a Draft Health Technology Assessment of C-reactive protein point-of-care testing (CRP POCT) to guide antibiotic prescribing for acute respiratory tract infections in primary care settings.
The objective of CRP POCT is to assist the clinician in ruling out serious bacterial infection, thereby supporting a decision not to prescribe an antibiotic to those who are unlikely to benefit from treatment. HIQA’s health technology assessment reviews the clinical and cost-effectiveness of CRP POCT. The assessment will inform a decision as to whether CRP POCT should be used to support antibiotic prescribing in primary care for patients presenting with symptoms of acute respiratory tract infection. The assessment also considers the organisational implications associated with introducing CRP POCT in primary care.
HIQA’s Chief Scientist, Dr Conor Teljeur, said, “In European terms, Ireland has a moderate to high rate of antibiotic prescribing. A large proportion of those prescriptions are initiated in primary care for patients with acute respiratory infections. Most respiratory tract infections are self-limiting and caused by viruses. Antibiotics are only useful for patients with bacterial infections. It is not always clear if a patient presenting with a respiratory tract infection has a bacterial or viral infection. C-reactive protein point-of-care testing can support a GP in deciding not to prescribe an antibiotic. In clinical trials, C-reactive protein point-of-care testing in primary care has been shown to be effective in reducing antibiotic prescribing without affecting patient safety.”
The review concluded that the use of CRP POCT to inform antibiotic prescribing in primary care for acute respiratory tract infections leads to a significant reduction in antibiotic prescribing without compromising patient safety. While there is evidence that CRP POCT has a short-term effect on antibiotic prescribing, it is unclear whether that effect is sustained over the longer term. The draft findings of HIQA’s report have been published for public consultation.
HIQA invites members of the public to give feedback on the draft report until Friday 15 March 2019.
You can read the draft report and take part in the public consultation on www.hiqa.ie.
IPUREVIEW MARCH 201968

NEWS
The first implementation report on the National Cancer Strategy 2017 – 2026, launched by the Minister for Health, sets out the progress achieved on the implementation of the 52 recommendations of the Strategy and the degree to which the key performance indicators are being met.
Prevention and Early Diagnosis highlights include:
n Legislation on standardised retail packaging for tobacco;
n The passage of the Public Health Alcohol Act 2018;
n The integration of cancer prevention into the messaging under the Healthy Ireland Initiative;
n Progress towards a national skin cancer prevention plan; and
n The uptake rates for cancer screening.
Highlights in Treatment and Survivorship include:
n New posts in medical and surgical oncology;
n The commissioning of two new linear accelerators in St Luke’s Hospital;
n The progress of construction work on a new radiation oncology centre in Cork University Hospital towards completion in Q1 2019;
n Publication of a Model of Care for Oral Anti-Cancer Medications;
n The commencement of the roll-out of a National Cancer Information System;
n The progress being made by Working Groups on Survivorship and Psycho-Oncology;
n The appointment of a National Clinical Lead for psycho-oncology; and
n Establishment of a Cancer Patient Advisory Committee.
Minister Harris said, “The challenges facing us in cancer are significant. The recent annual report of the National Cancer Registry indicated that approximately 22,640 cases (excluding non-melanoma skin cancers and non-invasive cancers) are diagnosed each year. While projections indicate that the number of people with cancer will increase significantly with our increasing and our ageing population, we have a pathway laid out in the Strategy that will lead to many potential cancers being prevented, and to continuous improvements in the treatment and follow-up services available to patients with cancer. The past year also brought significant challenges with regards to cervical cancer. We will take a number of very important steps this year towards achieving our goal of effectively eradicating this cancer.”
The Implementation Report 2018 can be found at www.health.gov.ie.
National Cancer Strategy 2017 – 2026 Implementation Report 2018
NATIONAL CANCER
STRATEGY2017 - 2026
IPUREVIEW MARCH 2019 69

NEWS
Irish Skin Foundation Dermatology Study Day 2019 – 6 April 2019 The Irish Skin Foundation (ISF) has announced details of its 4th annual Dermatology Study Day which takes place on 6 April 2019 in the Ashling Hotel, Parkgate Street, Arran Quay, Dublin 8, from 9.00am – 3:55pm.
The 2019 programme is designed for hospital and community-based pharmacists, GPs, public health nurses and others involved in providing first-line management of skin conditions/diseases. The programme will cover first-line management of: Burns and Abrasions; Paediatric Skin Conditions; Rosacea; Alopecia; Hidradenitis Suppurativa (HS); and Skin Cancer Recognition.
The Dermatology Study Day will be chaired by Carmel Blake, Dermatology ANP at Tallaght University Hospital and ISF Helpline Clinical Manager.
Registration Fee: €75 including tea/coffee and lunch. For details on the full programme, please visit www.irishskin.ie.
9th All Ireland Pharmacy Conference – Call for Abstracts The All Ireland Pharmacy Conference now invites submission of abstracts for the 2019 conference.
The 9th All Ireland Pharmacy Conference will be held at Ballymascanlon House Hotel, Dundalk on 14 and 15 October 2019.
The conference is themed around the FIP Pharmaceutical Workforce Development Goals. Abstracts are invited that deal with a broad range of pharmacy practice, including (but not limited to) the following areas:
n Competency development (FIP Goal 5);
n Advanced practice and specialisation (FIP Goal 4);
n Workforce impact (FIP Goal 11); and
n Working with others (FIP Goal 8).
Abstracts can be submitted on the IIOP website, www.IIOP.ie/AIPC2019. The closing date for receipt of abstracts is Friday 10 May 2019 and authors will be notified regarding acceptance by Friday 21 June 2019.
The organising bodies will cover the conference costs for the main presenter of each oral presentation. For those presenting posters, the day delegate fee will be covered.
Registration is now open for Cystic Fibrosis Ireland’s (CFI) annual conference, which will take place in the Mount Wolseley Hotel, Carlow, on Saturday 30 March, entitled 2009 – 2019: A Decade of Progress, but many Challenges Ahead.
The conference takes place ahead of CFI’s annual fundraising flag day, 65 Roses Day, on Friday 12 April, when people are urged to buy a purple rose for €2 or donate online at www.65RosesDay.ie.
Among the speakers will be Prof. Barry Plant, Cork University Hospital, who will address new CF drug therapies in the pipeline, while Dr Michelle Murray, Mater Hospital, will update on transplants and organ donor consent developments.
For further information and to register, please visit www.cfireland.ie.
The conference will also be streamed online at www.cfireland.ie.
Cystic Fibrosis Ireland gets set to host national conference for CF Community – 12 April 2019
IPUREVIEW MARCH 201970

Daffodil Day more important than everDaffodil Day 2019 takes place on 22 March and members of the public are urged get involved by volunteering to help fundraise on www.cancer.ie and donating what they can on the day.
RTÉ Weather and National Lottery presenter Nuala Carey has appealed to the public to shower Daffodil Day with donations, in the wake of her father’s death from cancer in November. “Pancreatic cancer currently has the lowest survival rate for all major cancers, with just one in ten people alive five years after diagnosis. We can, and must, change this, but it will require much more investment in cancer research and services. That’s why I am appealing to everyone to get involved and help make Daffodil Day 2019 bigger than ever. Your donations will also fund vital supports for patients and their families, so no one has to go through cancer alone.”
Averil Power, Chief Executive of the Irish Cancer Society, said, “Last year, our nurses, staff and volunteers reached thousands of patients affected by cancer, but we didn’t reach everyone in need. We don’t just want to provide an excellent service to some cancer patients, we want to provide it to all cancer patients. As 98% of our funding comes from the public, we simply can’t do that without more donations.”
To view the Irish Cancer Society’s Research Plan 2019 or for further information on Daffodil Day, please see www.cancer.ie.
NEWS
The High Tech hub was introduced to all pharmacists by the HSE in March 2018 in an effort to streamline administration of the scheme for pharmacists and to provide enhanced visibility of stock management and spending on this scheme to the HSE. After speaking to customers, Accord Healthcare identified that many pharmacists have concerns with using the Hub. Accord therefore approached PharmaBuddy with the idea of creating a demonstration video and answering any queries pharmacists may have in relation to the High Tech Hub.
Marguerite Tierney, Accord’s PR & Marketing Manager, explains, “PharmaBuddy, the online resource for Irish pharmacists, conducted further research with their pharmacist members. They received a number of queries from pharmacists such as ‘how to tell if stock is dispatched’, ‘what happens if the Hub generates a warning’ or ‘can the user dispense a medicine from the Hub if the prescription was written inside the EU but out of the State’; from there, a short demonstration video which covers all the aforementioned issues and many more, was created.”
The video will sit on the PharmaBuddy website, accessible to all registered pharmacist members, and also on the High Tech page of the Accord Healthcare website www.accord-healthcare.ie.
Accord Healthcare launches High Tech Hub Demo Video with PharmaBuddy
Pictured at the launch of the Accord Healthcare High Tech Hub Demo video are Marguerite Tierney, Accord Healthcare and Dr Paul Ryan, Pharmacist, GP & founder of PharmaBuddy.
IPUREVIEW MARCH 2019 71

NEWS
The Department of Health and the Department of Agriculture, Food and the Marine have published the Ireland – One Health Report on Antimicrobial Use & Antimicrobial Resistance. This report provides, for the first time, a snapshot of the antimicrobial use (AMU) and antimicrobial resistance (AMR) in both humans and food-producing animals in Ireland.
The World Health Organisation defines antimicrobial resistance as the resistance of a micro-organism to an antimicrobial drug that was originally effective for treatment of infections caused by it.
This One Health report shows that data in Ireland on AMU for humans and food-producing animals is improving all the time. However, gaps remain in the information available, namely;
n Although data for approx. 90% of acute hospital and 95% of public prescription antimicrobial use is available, there is no data for available for private prescription antimicrobial use;
n Surveillance of human AMR reflects invasive infections only (Blood Stream Infections (BSIs) in acute settings) and not on other infections (Urinary Tract Infections (UTIs) and wound infections) outside of the acute setting;
n Currently, information from national surveillance of AMU does not include information on the appropriateness of the antimicrobials used in either sector;
n There is no specific surveillance for AMR in imported food products; and
n There is also no systematic surveillance for AMR in the environment.
Commenting on the publication of the report, Minister for Health Simon Harris TD said, “We know that the emergence of AMR worldwide is a real and growing public health crisis and we are likely approaching a tipping point if antibiotic resistance continues unchecked. There are some stark reminders of the consequences of AMR when we consider the outbreaks of Carbapenemase producing Enterobacteriaceae (CPE). In adopting the One Health approach, it is acknowledged that sectors on their cannot properly address this concern in isolation and a joint, co-ordinated approach is required.”
Further information is available at www. health.gov.ie.
Ministers for Health and Agriculture publish report on antimicrobial use and resistance
IrelandOne Health Report on Antimicrobial Use & Antimicrobial Resistance
16
Ireland’s first One Health Report on Antimicrobial Use and Antimicrobial Resistance 2016 January 2019
Over 600 life-saving defibrillators across four manufacturers require urgent updates The Health Products Regulatory Authority (HPRA) is urging owners of automated external defibrillators (AEDs) to check that the recommended safety and maintenance updates on their device have been undertaken. All individuals who are in possession of an AED are advised to urgently check if their device is one of the models below. If they have an affected AED, the HPRA urges the owners to contact the manufacturer or the HPRA to ensure their AED receives all necessary updates.
An estimated 614 AEDs by four different manufacturers require urgent updates in Ireland to ensure they will work correctly in an emergency situation. Without these updates, the AED may not work as intended. The devices may require a software upgrade – similar to upgrading software on your phone or computer – or the replacement of a component part within the AED.
Since the HPRA’s previous announcement in November 2017, 95 AEDs have had completed updates that were outstanding at that time and the HPRA is now calling on other owners to do the same. Commenting, Anne Tobin, Medical Devices Vigilance Manager of the HPRA, highlighted the positive progress made by owners who are proactively liaising with the manufacturers. “It is very encouraging to see that manufacturers are reviewing their devices, identifying shortcomings, and taking action. We are urging owners of AEDs to be vigilant and to check if they have one of the affected AEDs and, if they do, to liaise with manufacturers to ensure the devices are updated without delay. This year, 614 automated external defibrillators in Ireland required an urgent update, without which the devices may not perform in a life-threatening emergency’’.
Further information may be found on the HPRA’s website, www.hpra.ie.
IPUREVIEW MARCH 201972

NEWS
The Minister for Health, Simon Harris TD, announced eight new appointees to the Board of the HSE. The Board will be appointed on an administrative basis until the legislation has passed. These positions were advertised through the State Board process operated by the Public Appointments Service. They will join Ciarán Devane, announced as Chair of the HSE Board in September 2018.
The new appointees are:
n Fergus Finlay, former CEO of Barnardos;
n Tim Hynes, Group Chief Information Officer, AIB;
n Prof. Deirdre Madden, Professor of Law at UCC and Chair of the Commission on Patient Safety and Quality Assurance. Dr Madden will be appointed Deputy Chair of the HSE Board;
n Dr Sarah McLoughlin, Science and Communication Officer at Retina International and patient advocate;
n Mark Molloy, Quantity Surveyor, member of the Expert Group on Tort Reform and Management of Clinical Negligence Claims and patient advocate;
n Aogán Ó Fearghail, former GAA President;
n Fiona Ross, Chair of CIE and Mental Health Ireland; and
n Dr Yvonne Traynor, Vice President of Regulatory and Scientific Affairs with Kerry Group.
At the time of printing there remained one final position on the Board to be filled which will have particular relevance to the competency area of financial planning and management.
Minister for Health appoints HSE board members on administrative basis
FSAI publishes updated national healthy eating guidelines The Food Safety Authority of Ireland (FSAI) has published the updated Healthy Eating, Food Safety and Food Legislation – a Guide Supporting the Healthy Ireland Food Pyramid.
According to Dr Pamela Byrne, CEO, FSAI, “The guide is a combination of international best practice with up-to-date Irish research to ensure the advice meets the specific dietary needs of the Irish population. It provides food-based advice that protects people from five years of age onwards against diet-related ill health such as heart disease, cancer, obesity and diabetes, which are major causes of ill health in Ireland. It gives this advice across four age groups from five to 51+ years with distinct information for those leading active and non-active lifestyles.”
Developed in conjunction with the Department of Health and the Health Service Executive, the guide covers portion sizes and servings, tips for choosing the healthiest types of foods, as well as reducing risks during cooking. It also covers:
n Nutritional composition – how various foods best meet different people’s needs;
n Food safety – microbiology, harmful bacteria, viruses and how these can be minimised; and
n Food law – to ensure businesses are aware of legal requirements to provide consumers with accurate information on nutritional labelling and allergen declarations.
The Guide is available on the FSAI website, www.fsai.ie.
IPUREVIEW MARCH 2019 73

CLASSIFIEDS
FULL-TIME CHIEF 1 PHARMACIST REQUIRED – DUBLIN
St Patrick’s Mental Health Services requires a full-time Chief 1 Pharmacist
The successful applicant must: • Be a registered Pharmacist with the Pharmaceutical
Society of Ireland (PSI) or be entitled to be so registered • Have at least five years satisfactory post registration
hospital experience • Possess a high standard of administrative, managerial or business ability • Possess
the requisite knowledge and ability (including a high standard of suitability and management ability) for the
proper discharge of the duties of the office.
Contact Brian Davitt: [email protected] ph: 01 249 3639
FULL-TIME PHARMACIST REQUIRED – TIPPERARY
Costigan’s Pharmacy, Blind Street, Tipperary Town, requires a full-time Pharmacist.
Recently relocated pharmacy, with a busy dispensary and innovative design. Heavily
health-care focused. Two pharmacists on duty, as well as experienced technicians. 30 minutes
from Limerick, 60 minutes from Cork.No late nights. Working one Saturday in three.
Excellent package for the right candidate.
Email Siobhán: [email protected] or phone 086 880 4924
PROPERTY FOR SALE. TIPPERARY (Large town). Great potential as pharmacy / health centre. Near four nursing homes. Enquiries in confidence to PO Box 119
PHARMACY FOR SALE. CORK. Excellent business opportunity.Enquiries in confidence to PO Box 718
PHARMACIST SEEKS TO PURCHASE PHARMACY. CORK CITY OR COUNTY. All options considered. Reply in confidence to PO Box 818
ALL BOX NUMBER REPLIES SHOULD BE POSTED TO: Irish Pharmacy Union, Butterfield House, Butterfield Avenue, Rathfarnham, Dublin 14.
This independent service is free to IPU members. Entries will be deleted after three months.
Advertisements should be forwarded to Sinéad Fennell by email to [email protected].
Want to increase your Pharmacy’s margins?
Xsulent Consultancy specialise in the area of drug pricing and
purchasing, working with wholesalers and manufacturers to get the best deal for your pharmacy.
For professional advice and a free consultation, contact David Murnane on 0851157435 or [email protected]
Irish Chemists’ Golfing Society NewsThe new season of the ICGS Golf outings will get underway in March. Please find below the fixtures for 2019:
Tuesday 26 March The Island Golf Club
Monday 15 April Naas Golf Club
Sunday 19 May Tramore Golf Club
Monday 20 May Tramore
Tuesday 21 May Tramore (Captain’s Prize)
Sunday 16 June Druids Glen Hotel & Golf Club (ICGS VsUCGA)
Monday 17 June Druids Glen
Thursday 11 July Carlow Golf Club
Tuesday 13 August Portmarnock Golf Club
Sunday 8 September Killarney Golf & Fishing Club (President’s Prize)
Monday 9 September Killarney
Sunday 29 September Rosapenna Hotel & Golf Resort (GOY Finals)
Monday 30 September Rosapenna
Incoming Captain for the year is Mr Patrick Digan, and newly elected President is Mr Frank Reen. New members are always welcome, and all standards of golf are catered for.
IPUREVIEW MARCH 201974

CLASSIFIEDS
To advertise here, contact Sinéad at [email protected]
FULL-TIME DISPENSING TECHNICIAN REQUIRED
– DUBLINExperienced technician required for South Co. Dublin pharmacy (near Dun Laoghaire). Four days per week, with one Saturday in
four. Experience with OTC also helpful. Pharmacy open 9.00am – 7.00pm, Monday to Friday, and 9.00am – 6.00pm, Saturdays.
Email CV to May Gallagher [email protected]
FULL-TIME SUPERVISING PHARMACIST REQUIRED
– CORKHaven Pharmacy Burke’s, Macroom,
Co. Cork, requires a full-time Supervising Pharmacist.
Excellent conditions. No late nights or Sundays.
Contact Seamus on 087 698 1634 or email CV to [email protected]
SUPPORT PHARMACIST REQUIRED
PHARMACY PLUS BIRR9.30am – 6.00pm, Monday – Saturday.
No Sundays. No Bank Holidays. No Late Nights. Lunch Break Everyday.
Excellent Work Systems. Award Winning Team. Full-time available but Part-time will also be
considered.
Email: [email protected] David 087 232 2905
FULL-TIME PHARMACIST
REQUIRED – DUBLIN
Foxrock Pharmacy, Dublin, requires a full-time Pharmacist. Busy pharmacy
and very pleasant place to work.
Enquiries by email to [email protected]
IS THE JOB DONE?Achieving Tax-efficient financial security for Pharmacy Owners using Company Cash,
Property, Pensions and investments.Contact: Joanne Fenelon or Jim Doyle on 01 526 7770
Enquiries to: [email protected] Wealth Limited trading as Guardian Wealth, t/a ARF Ireland,is regulated by the Central Bank Of Ireland 40569. Guardian Wealth Limited is registered in
Ireland at 3 Upper George Street, Wexford. Company Registration Number 399683
Have You Consideredthe Value ofYour Pharmacy?JPA Brenson Lawlorcan independently value yourbusiness so that you canascertain how much it is worth.
Telephone Jason Bradshawor Padraic Ferguson on01-6689760
www.brensonlawlor.ie
Contact Us Today forA Free Consultation.
C
M
Y
CM
MY
CY
CMY
K
Brenson Lawlor Box Advert option 2.pdf 1 12/06/2017 08:28
Untitled-1 1 12/06/2017 12:05
IPUREVIEW MARCH 2019 75

2019
www.cosmeticassociation.ie
CHRISTMASCosmetic & Gift Trade Fair
The Main Hall, RDS,Ballsbridge, Dublin
Sunday 19th May10am - 6pm
Monday 20th May9am - 6pm
Tuesday 21st May9am - 6pm
The Main Hall, RDS,Ballsbridge, Dublin
Sunday 19th May10am - 6pm
Monday 20th May9am - 6pm
Tuesday 21st May9am - 6pm
CA Advert A4 2019.pdf 1 26/10/2018 10:45

![HKIFM CPD MVAC.ppt [\254\333\256e\274\322\246\241]](https://static.fdokumen.com/doc/165x107/63175591c72bc2f2dd056c30/hkifm-cpd-mvacppt-254333256e274322246241.jpg)