
The role of childhood sexual abuse sequelae in the sexual revictimization of women
35
The role of childhood sexual abuse sequelae in the sexual revictimization of women An empirical review and theoretical reformulation Terri L. Messman-Moore a, * , Patricia J. Long b a Department of Psychology, Benton Hall, Miami University, Oxford, OH 45056-1601, USA b Department of Psychology, Oklahoma State University, Stillwater, Oklahoma, USA Received 1 March 2002; received in revised form 21 June 2002; accepted 22 July 2002 Abstract There is now widespread empirical evidence that child sexual abuse (CSA) survivors are at greater risk for sexual revictimization in adulthood, but less is known of the mechanisms underlying this relationship. Despite the lack of a conceptual framework to guide research, there has been a recent influx of studies examining explanatory variables, with most focusing on the psychological sequelae of CSA: alcohol and drug use, sexual behavior, dissociation, posttraumatic symptomatology, poor risk recognition, and interpersonal difficulties. With the exception of sexual behavior, the studies reviewed here provide limited or mixed support for the role of intrapersonal factors in revictimization. Future research may benefit from a focus on the function of psychological distress that is expressed as psychological vulnerability, as opposed to individual forms of psychopathology or maladaptive behavior. An ecological framework may be useful as a guide to future investigations, as this model focuses on factors outside of the victim, including childhood factors such as family environment, contextual factors including the behavior of the perpetrator, and societal and cultural factors that impact revictimization. Future investigations should focus on the interaction between victim vulnerability and perpetrator behavior. Implications for prevention programming, clinical intervention, and future research are discussed. D 2002 Elsevier Science Ltd. All rights reserved. Keywords: Revictimization; Child sexual abuse; Rape; Review; PTSD; Alcohol abuse; Risk recognition; Interpersonal functioning 0272-7358/02/$ – see front matter D 2002 Elsevier Science Ltd. All rights reserved. doi:10.1016/S0272-7358(02)00203-9 * Corresponding author. Tel.: +1-513-529-2403; fax: +1-513-529-2420. E-mail address: [email protected] (T.L. Messman-Moore). Clinical Psychology Review 23 (2003) 537 – 571
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of The role of childhood sexual abuse sequelae in the sexual revictimization of women
The role of childhood sexual abuse sequelae in the sexual
revictimization of women
An empirical review and theoretical reformulation
Terri L. Messman-Moorea,*, Patricia J. Longb
aDepartment of Psychology, Benton Hall, Miami University, Oxford, OH 45056-1601, USAbDepartment of Psychology, Oklahoma State University, Stillwater, Oklahoma, USA
Received 1 March 2002; received in revised form 21 June 2002; accepted 22 July 2002
Abstract
There is now widespread empirical evidence that child sexual abuse (CSA) survivors are at greater
risk for sexual revictimization in adulthood, but less is known of the mechanisms underlying this
relationship. Despite the lack of a conceptual framework to guide research, there has been a recent
influx of studies examining explanatory variables, with most focusing on the psychological sequelae of
CSA: alcohol and drug use, sexual behavior, dissociation, posttraumatic symptomatology, poor risk
recognition, and interpersonal difficulties. With the exception of sexual behavior, the studies reviewed
here provide limited or mixed support for the role of intrapersonal factors in revictimization. Future
research may benefit from a focus on the function of psychological distress that is expressed as
psychological vulnerability, as opposed to individual forms of psychopathology or maladaptive
behavior. An ecological framework may be useful as a guide to future investigations, as this model
focuses on factors outside of the victim, including childhood factors such as family environment,
contextual factors including the behavior of the perpetrator, and societal and cultural factors that
impact revictimization. Future investigations should focus on the interaction between victim
vulnerability and perpetrator behavior. Implications for prevention programming, clinical intervention,
and future research are discussed.
D 2002 Elsevier Science Ltd. All rights reserved.
Keywords: Revictimization; Child sexual abuse; Rape; Review; PTSD; Alcohol abuse; Risk recognition;
Interpersonal functioning
0272-7358/02/$ – see front matter D 2002 Elsevier Science Ltd. All rights reserved.
doi:10.1016/S0272-7358(02)00203-9
* Corresponding author. Tel.: +1-513-529-2403; fax: +1-513-529-2420.
E-mail address: [email protected] (T.L. Messman-Moore).
Clinical Psychology Review 23 (2003) 537–571

1. Introduction
Sexual revictimization occurs when a survivor of sexual abuse or rape during childhood is
victimized again (i.e., revictimized) during adulthood (Messman & Long, 1996). Evidence of
the revictimization of child sexual abuse (CSA) survivors has been found among different
populations of women, including college samples (Gidycz, Coble, Latham, & Layman, 1993;
Gidycz, Hanson, & Layman, 1995; Mayall & Gold, 1995; Messman-Moore & Long, 2000;
Urquiza & Goodlin-Jones, 1994), clinical samples (Briere & Runtz, 1987; Bryer et al., 1987;
Shields & Hanneke, 1988), military samples (Merrill et al., 1999), and community samples
(Fergusson, Horwood, & Linskey, 1997; Messman-Moore & Long, 2002; Wyatt et al., 1992).
CSA survivors are between 2 and 11 times more likely to experience adult assault as compared
to nonvictims (Fergusson et al., 1997; Wyatt, Guthrie, & Notgrass, 1992). A recent meta-
analysis (Roodman & Clum, 2001) found that between 15% and 79% of women with histories
of CSAwere raped as adults and reported an overall moderate effect size for revictimization.
It is important to recognize and understand revictimization because sexual victimization
experiences often involve significant, negative psychological, and interpersonal distress that
is frequently long lasting. Traumatic sexual experiences, such as CSA and rape, are associated
with numerous acute and chronic psychological difficulties, including PTSD, depression,
suicidality and self-harm behaviors, anxiety, substance abuse, dissociation, interpersonal
difficulties, low self-esteem, and feelings of guilt and self-blame (for reviews, see Goodman,
Koss, & Russo, 1993; Polusny & Follette, 1995; Resick, 1993). Women with histories of
victimization are also likely to suffer from physical difficulties related to victimization such as
chronic pelvic pain (Goodman et al., 1993) and serious reproductive and sexual health
problems (Bohn & Holz, 1996). Further, repeated traumatic experiences, such as revictim-
ization, may be more likely than a single traumatic incident to involve such negative
psychological sequelae, as there is growing evidence that the psychological effects of
interpersonal violence are cumulative in nature (Follette, Polusny, Bechtle, & Naugle,
1996; Messman-Moore, Long, & Siegfried, 2000).
Now that the vast majority of recent empirical studies are in agreement concluding that
revictimization does occur, researchers are turning their attention toward attempts to explain
the CSA survivor’s increased vulnerability for future sexual assault. Answers to the question
‘‘Why?’’ are important because such information can be used to develop well-informed rape
prevention programming that effectively reduces rates of sexual assault for all women and for
CSA survivors in particular. Further, it is known that prevention and risk reduction programs,
although efficacious for women without histories of assault, are not always helpful for
revictimized women (Breitenbecher & Gidycz, 1998; Hanson & Gidycz, 1993; Marx,
Calhoun, Wilson, & Meyerson, 2001). Therefore, it is imperative that mechanisms leading
to revictimization be identified and understood, as such information will inform programming
tailored specifically to this population.
Several factors, mostly of an intrapersonal nature (e.g., alcohol problems, dissociation, and
sexual behavior) have been investigated as factors contributing to the CSA-revictimization
relationship. Other factors have been investigated as well, including characteristics and severity
of CSA (Wind & Silvern, 1992), negative or dysfunctional childhood family environment
T.L. Messman-Moore, P.J. Long / Clinical Psychology Review 23 (2003) 537–571538

(Fergusson et al., 1997; Koverola, Proulx, Battle, & Hanna, 1996), and other forms of
childhood abuse such as physical abuse or combined physical and sexual abuse (Cloitre,
Tardiff, Marzuk, Leon, & Portera, 1996; Schaaf & McCanne, 1998). Recently, two reviews on
this subject critiqued the empirical literature. Breitenbecher (2001) conducted a narrative
review of empirical investigations and briefly addressed numerous possible causes of
revictimization. Roodman and Clum’s (2001) quantitative review and meta-analysis discussed
methodological considerations relevant to this topic. However, neither review discussed at
length overarching theoretical models nor underlying causal mechanisms (as opposed to
numerous individual factors) that may address the possible interrelationship between causal
factors. Given the recent increase in research on this topic, and because of the important
preventive and clinical implications of identifying and understanding the underlying mecha-
nisms related to revictimization, another review of the recent literature appears necessary. In
contrast to these two recent reviews (see Breitenbecher, 2001; Roodman & Clum, 2001), this is
not an exhaustive review of all investigations that study revictimization; rather, there are two
areas of focus. First, the empirical literature focusing on the role of intrapersonal psychological
factors in sexual revictimization is presented. This focus on intrapersonal factors will allow for
greater detail and depth in the discussion of empirical studies. Theoretical explanations for
sexual revictimization are then examined and an overarching model is identified that would
encompass many of the causal factors discussed previously by Breitenbecher. This model could
serve as a conceptual framework to guide future investigations.
Despite a recent influx of empirical examinations focusing on sexual revictimization, there
continues to be a variety of definitions for this phenomenon (e.g., multiple incidents of abuse in
childhood, multiple incidents in adulthood, at least one incident of abuse in childhood and
adulthood). Discussion of how methodology influences the study of revictimization is beyond
the scope of this article and has been covered elsewhere (Roodman & Clum, 2001). However,
we must recognize that definitions of revictimization impact the investigation of what causes
revictimization. Although we acknowledge other definitions, for purposes of this review, revic-
timization is limited to the experience of sexual abuse in childhood (or adolescence) and sexual
assault or rape in adulthood, with the caveat that definitions of childhood and adulthood vary.
2. Review of the empirical literature
Despite absence of an overarching theoretical framework, research examining contrib-
uting or explanatory factors regarding the CSA survivor’s increased vulnerability has
moved forward. The majority of factors investigated thus far appear to be the psycho-
logical sequelae of the earlier sexual trauma,1 indicating that negative psychological effects
1 It is important to note that much of what is considered to be the negative sequelae of CSA is in fact a
‘‘correlate’’ of CSA (for discussion, see Polusny & Follette, 1995); due to the nature of this topic, the causal
effects of such factors can never be proven. However, it is widely accepted that the experience of childhood sexual
abuse plays an important role in the development of psychopathology and maladaptive behavior patterns. This is
assumed here as well.
T.L. Messman-Moore, P.J. Long / Clinical Psychology Review 23 (2003) 537–571 539

Table 1
Summary of studies examining the psychological sequelae of CSA as risk factors for sexual revictimization
Authors Population n Abuse definition Design Variables Findings
Retrospective
Arata (1999) College women with
histories of CSA
and revictimization;
mean age = 24; 71%
Caucasian 76% single
41 CSA: < 14 years
(Finkelhor, 1979).
Adult: � 14 years.
Unwanted contact (SES;
Koss & Oros, 1982)
Retrospective PTSD: Structured Clinical
Interview for DSM-III-R;
Posttraumatic Stress
Disorder (SCL-90-R;
Crime-Related PTSD Scale)
RV women more likely
than non-RV women to have
lifetime diagnosis of PTSD;
not more likely to have
current diagnosis
Classen, Field,
Koopman,
Nevill-Manning,
and Spiegel (2001)
Treatment-seeking CSA
survivors with PTSD;
mean age = 38; 66%
Caucasian, 54% married;
moderate to low SES
52 CSA: < 16 years, >5 years
age difference b/t
perpetrator and victim;
>2 events b/t ages 3 and
15, genital contact.
Adult: >18 years in past 6
months; coercion, attempted
rape or rape (SES;
Koss & Gidycz, 1985)
Retrospective Interpersonal problems:
Interpersonal problems
(Inventory of Interpersonal
Problems, IIP); PTSD
(Clinician Administered
PTSD Scale for DSM-IV)
RV greater interpersonal
diff. than non-RV;
RV greater difference
with assertive behavior,
overly nurturing behavior,
and social avoidance
Cloitre, Cohen,
and Scarvalone
(2002)
Treatment-seeking
rape survivors and
non-assaulted
community women;
70% Caucasian,
53% b/t ages 31 and 50;
50% low SES;
58% some college or
college graduate
69 CSA: < 18 years; contact
abuse by family or trusted
adult; coerced or forced or
� 5 years age difference b/t
victim and perpetrator (Child
Maltreatment Interview
Schedule; Briere, 1992).
Adult: � 18 years; forced
completed/attempted oral –
genital contact, intercourse, or
penetration (Sexual Assault
History Initial Interview
Schedule; Resick, 1987)
Retrospective Interpersonal Schemas:
Beck Depression
Inventory; Brief
Symptom Inventory;
Interpersonal Schema
Questionnaire (ISQ)
RV generalize from
childhood to adult schemas;
schemas generally negative,
portray parents as hostile
and controlling. RV showed
more limited range of
interpersonal expectations,
tended to expect others to
be hostile and dominant;
non-RV also generalize from
childhood to adult schemas;
schemas generally positive,
portray parents as warm
and noncontrolling;
Non-RV CSAS didn’t
generalize schemas
from childhood.
Cloitre, Scarvalone,
and Difede (1997)
Treatment-seeking
rape victims and
nonvictimized
control group;
mean age = 33.5;
76% Caucasian,
92% employed,
92% educated
56 CSA: < 18 years; contact by
family or trusted adult;
coerced or unwanted
experiences by perpetrator
5 years older than victim.
Adult: � 18 years; completed
or attempted intercourse,
oral – genital contact
Retrospective PTSD and dissociation:
Structured Clinical
Interview for DSM-II-R;
Dissociative Experiences
Scale (DES); Inventory for
Interpersonal Problems (IIP)
RV more likely to meet
criteria for a dissociative
disorder. RV reported more
difficulties interpersonal
functioning. No differences
between RV and single adult
assault for levels of PTSD
symptomatology.
T.L.Messm
an-M
oore,
P.J.
Long/Clin
icalPsych
ologyReview
23(2003)537–571
540
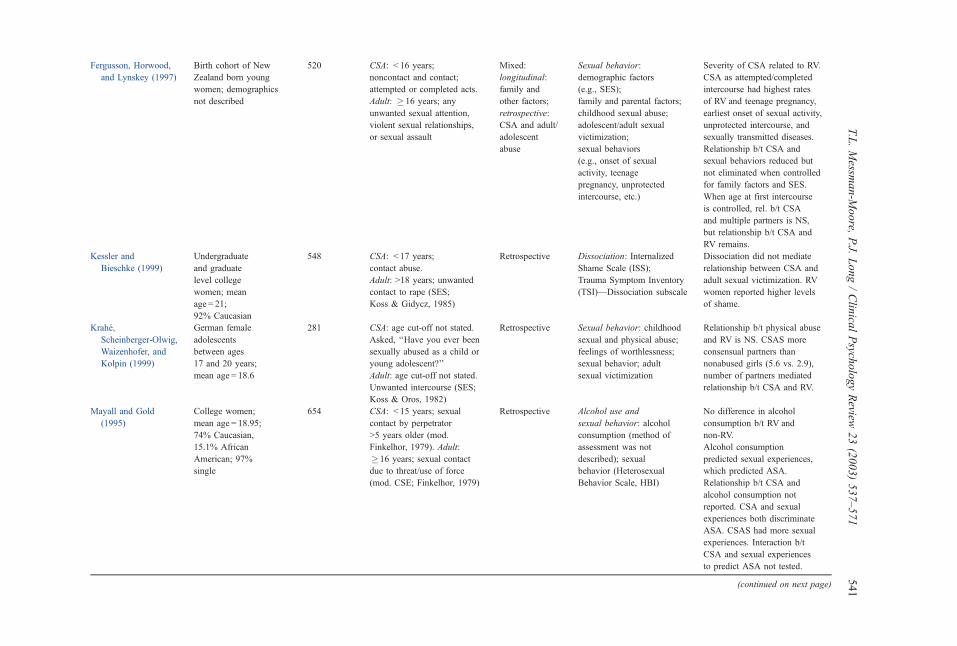
Fergusson, Horwood,
and Lynskey (1997)
Birth cohort of New
Zealand born young
women; demographics
not described
520 CSA: < 16 years;
noncontact and contact;
attempted or completed acts.
Adult: � 16 years; any
unwanted sexual attention,
violent sexual relationships,
or sexual assault
Mixed:
longitudinal:
family and
other factors;
retrospective:
CSA and adult/
adolescent
abuse
Sexual behavior:
demographic factors
(e.g., SES);
family and parental factors;
childhood sexual abuse;
adolescent/adult sexual
victimization;
sexual behaviors
(e.g., onset of sexual
activity, teenage
pregnancy, unprotected
intercourse, etc.)
Severity of CSA related to RV.
CSA as attempted/completed
intercourse had highest rates
of RV and teenage pregnancy,
earliest onset of sexual activity,
unprotected intercourse, and
sexually transmitted diseases.
Relationship b/t CSA and
sexual behaviors reduced but
not eliminated when controlled
for family factors and SES.
When age at first intercourse
is controlled, rel. b/t CSA
and multiple partners is NS,
but relationship b/t CSA and
RV remains.
Kessler and
Bieschke (1999)
Undergraduate
and graduate
level college
women; mean
age = 21;
92% Caucasian
548 CSA: < 17 years;
contact abuse.
Adult: >18 years; unwanted
contact to rape (SES;
Koss & Gidycz, 1985)
Retrospective Dissociation: Internalized
Shame Scale (ISS);
Trauma Symptom Inventory
(TSI)—Dissociation subscale
Dissociation did not mediate
relationship between CSA and
adult sexual victimization. RV
women reported higher levels
of shame.
Krahe,
Scheinberger-Olwig,
Waizenhofer, and
Kolpin (1999)
German female
adolescents
between ages
17 and 20 years;
mean age = 18.6
281 CSA: age cut-off not stated.
Asked, ‘‘Have you ever been
sexually abused as a child or
young adolescent?’’
Adult: age cut-off not stated.
Unwanted intercourse (SES;
Koss & Oros, 1982)
Retrospective Sexual behavior: childhood
sexual and physical abuse;
feelings of worthlessness;
sexual behavior; adult
sexual victimization
Relationship b/t physical abuse
and RV is NS. CSAS more
consensual partners than
nonabused girls (5.6 vs. 2.9),
number of partners mediated
relationship b/t CSA and RV.
Mayall and Gold
(1995)
College women;
mean age = 18.95;
74% Caucasian,
15.1% African
American; 97%
single
654 CSA: < 15 years; sexual
contact by perpetrator
>5 years older (mod.
Finkelhor, 1979). Adult:
� 16 years; sexual contact
due to threat/use of force
(mod. CSE; Finkelhor, 1979)
Retrospective Alcohol use and
sexual behavior: alcohol
consumption (method of
assessment was not
described); sexual
behavior (Heterosexual
Behavior Scale, HBI)
No difference in alcohol
consumption b/t RV and
non-RV.
Alcohol consumption
predicted sexual experiences,
which predicted ASA.
Relationship b/t CSA and
alcohol consumption not
reported. CSA and sexual
experiences both discriminate
ASA. CSAS had more sexual
experiences. Interaction b/t
CSA and sexual experiences
to predict ASA not tested.
(continued on next page)
T.L.Messm
an-M
oore,
P.J.
Long/Clin
icalPsych
ologyReview
23(2003)537–571
541

Table 1 (continued)
Authors Population n Abuse definition Design Variables Findings
Retrospective
Merrill et al. (1999) US Navy recruits;
mean age = 21;
63% Caucasian,
22% Black,
8% Hispanic,
84% single, 53% HS,
40% some college
1093 CSA: < 14 years;
contact with perpetrator
� 5 years older (mod.
Finkelhor, 1979).
Adult: � 14 years.
Rape—intercourse,
oral – genital contact
by force, threats,
or use of alcohol/drugs.
Attempted rape—
attempted unwanted
intercourse (SES;
Koss & Woodruff, 1991)
Retrospective Alcohol use and
sexual behavior:
Alcohol Abuse—
Michigan Alcoholism
Screening Test;
Childhood Physical
Abuse—Conflict;
Tactics Scale Parent –
Child Version; number
of sexual partners
CSA, alcohol problems,
and number of sexual
partners predicted adult
rape (controlling for
child physical abuse).
No significant interaction
between alcohol problems,
number of sexual partners,
or CSA in predicting
adult rape.
Messman-Moore
and Long (2002)
Community women;
mean age = 37;
92% Caucasian,
52% married
300 CSA: < 17 years;
contact by relative,
person � 5 years older,
or due to threat/
force (Finkelhor, 1979;
Wyatt, Lawrence,
Vodounon, & Mickey, 1992).
Adult: � 17 years.
Rape—intercourse by
force or use of alcohol/
drugs. Coerced
intercourse—unwanted
intercourse due to
verbal coercion, misuse
of authority (mod. SES;
Koss & Oros, 1982)
Retrospective Alcohol/drug use
diagnosis: Lifetime
Alcohol Abuse/
Dependence, Substance
Abuse/Dependence—
Structured Clinical
Interview for Diagnosis
(SCID-IV-NP)
CSA, alcohol-related
diagnoses and
substance-related
diagnoses each
predicted rape and
coerced intercourse.
No significant
interaction between
CSA and either
diagnostic status
in predicting rape or
coerced intercourse.
Wyatt, Notgrass,
and Gordon (1995)
African American
community sample;
46% age 18–26,
54% age 27–36,
42% never married,
34% HS educ.,
37% some college
126 CSA: < 18 years;
noncontact and contact,
unwanted or coercive
incidents (Wyatt, 1985).
Adult: >18 years;
noncontact, attempted
and completed rape
Retrospective Sexual behavior:
frequency of sexual
behavior; frequency
of unintended and
aborted pregnancies;
number of sex
partners and brief
relationships (WSHQ;
Wyatt et al., 1992)
RV and women victimized
during adulthood more
likely to report multiple
partners and brief
relationships compared to
CSA only or nonabused.
RV women more likely than
others to report unintended
pregnancies or abortions.
T.L.Messm
an-M
oore,
P.J.
Long/Clin
icalPsych
ologyReview
23(2003)537–571
542

Gidycz, Hanson,
and Layman
(1995)
College women;
mean age = 18–19;
92% Caucasian,
39% moderate
to high SES,
18% low to
moderate SES
N = 796,
T1 = 667
(85%)*,
T2 = 178
(75%),
T3 = 65
(85%);
* percent
return-rate
CSA: < 14 years
(Finkelhor, 1979);
noncontact, fondling,
rape, or attempted rape.
Adolescent: � 14 years
prior to participation;
unwanted fondling,
verbally coerced
intercourse, rape, or
attempted rape
(SES; Koss &
Oros, 1982). Both
CSA and adolescent
victimization ranked
according to severity,
moderate to severe
Prospective
9 months
Alcohol use, sexual
behavior, and
interpersonal
problems: previous
sexual victimization;
number of sexual
partners; alcohol use
(typical use);
psychological
adjustment (Beck
Depression Inventory,
Beck Anxiety
Inventory);
interpersonal
functioning (IIP)
CSA correlated
with adolescent
victimization,
adolescent victimization
correlated with RV
at 3, 6, and 9 months.
Alcohol use to
intoxication predicted
adolescent victimization
but not RV. CSA and
adolescent victimization
correlated with
interpersonal problems.
Interpersonal problems
did not predict RV.
Number of sex partners
at Time 1 predicted
RV at Time 3
(9 months). Number
of partners did not
mediate b/t CSA and
RV. CSA correlated
with number of partners
during adolescent
and at Time 1;
adolescent victimization
correlated with number
of sexual partners at
Times 1, 2, and 3.
Greene and
Navarro (1998)
College women;
95% Caucasian,
40% high SES,
31% moderate
SES, 69%
first-year students
T1 = 274,
T2 = 88,
T3 = 105
CSA: < 14 years
(Finkelhor, 1979).
Adolescent:
age 14 until
beginning of
study (SES;
Koss &
Gidycz, 1985).
Adult: (SES)
Prospective
9 months
Alcohol use and
sexual behavior:
alcohol consumption;
level of sexual
activity; psychological
adjustment (Beck
Depression Inventory
and Beck Anxiety
Inventory)
Prior victimization
most consistent
predictor of future
victimization; alcohol
use correlated
with victimization
at all intervals, but
did not predict RV.
(continued on next page)
T.L.Messm
an-M
oore,
P.J.
Long/Clin
icalPsych
ologyReview
23(2003)537–571
543

Table 1 (continued)
Authors Population n Abuse definition Design Variables Findings
Prospective
Himelein (1995) College women; mean
age: T1 = 18.4 years,
T2 = 21.0 years; 73%
Caucasian, 24%
Black, 4% other
minority
T1 = 330,
T2 = 100
CSA: < 16 years;
noncontact and
contact experiences
with anyone except
dating partner (mod.
Finkelhor, 1979).
Pre-college/adolescent
victimization: no age
stated; unwanted
contact with dating
partner regardless of
age (mod. SES; Koss &
Gidycz, 1985). Sexual
victimization: no age
stated; unwanted contact
since beginning
college (mod. SES)
Longitudinal
32 months
Alcohol use and
sexual behavior:
consensual sexual
experiences; alcohol
use in dating;
assertiveness; attitudes
towards rape
CSA correlated with
adolescent victimization;
adolescent victimization
correlated with adult
victimization, CSA not
correlated with adult
victimization; adolescent
victimization correlated
with consensual sexual
experiences, alcohol use in
dating, and sexual victimization
during college; adolescent
victimization strongest
predictor of college victimization.
Sandberg,
Matorin, and
Lynn (1999)
College women;
*mean age� 18.5;
* predominantly
Caucasian
*(demographic
information not collected)
T1 = 349,
T2 = 338
CSA: < 16 years;
contact only
(Finkelhor, 1979).
Adult: � 16 years;
unwanted contact
(SES; Koss & Oros, 1982)
Prospective
10 weeks
PTSD and dissociation:
Dissociative Experiences
Scale (DES); Impact
of Events
Scale—Revised (IES-R)
All variables were related.
Dissociation and PTSD did
not mediate RV. PTSD
moderated RV.
Siegel and
Williams
(2001)a
Community females;
93% African American;
low SES; age: T1 = 8.4
T1 = 206,
T2 = 411,
T3 = 249;
206 CSAS
and controls
CSA: < 18 years;
documented by
hospital records
or contact by force
or by perpetrator
� 5 years older.
Adult: not described
Longitudinal
20 years;
wave 1—
1973–1975,
wave 2—1990–
1991, wave 3—
1996–1997
Alcohol use and
sexual behavior:
Michigan Alcohol
Screening Test (MAST;
Selzer, 1971); sexual
behavior and beliefs
(Belief Inventory;
Jehu, 1988)
CSA did not predict RV,
but CSA prior to and after
age 13 did predict RV.
Multiple sexual partners
and alcohol abuse predicted
ASA, only alcohol abuse
predicted ASA when all factors
considered together.
West, Williams,
and Siegel
(2000)a
Black women with
documented histories
of CSA; mean
age = 25.2; 61%
never married,
50% HS educ., low SES
113 CSA: see Siegel
and Williams (2001)
above. Adult: >18 years;
any unwanted sexual
experience (Russell, 1984)
Prospective Sexual behavior:
age at first consensual
intercourse; number of
consensual partners;
prostitution
No difference b/t RV and non-RV
for age at first intercourse or
number of partners. RV more
likely than non-RV to report
engaging in prostitution.
Summary of abbreviations: CSA= child sexual abuse, CSAS=CSA survivors, b/t = between, rel = relationship, adol = adolescent, vic = victimization, NS = nonsignificant.a These studies utilized the same sample.
T.L.Messm
an-M
oore,
P.J.
Long/Clin
icalPsych
ologyReview
23(2003)537–571
544

of the earlier abusive experience may actually create or increase vulnerability for later
victimization.
Given this, the role of several psychological correlates of CSA, including posttraumatic
stress disorder (PTSD), dissociation, alcohol and drug use, sexual behavior, risk recognition
difficulties, and interpersonal difficulties, will be examined. Only studies designed specif-
ically to examine revictimization are included. To ease comparison of studies, specific
information as definitions of CSA, adolescent and adult sexual assault, and rape are included
if available. Although investigations of single variables will be insufficient to fully explain
the CSA survivor’s vulnerability, the majority of studies discussed examine only one or a few
variables. To date, no studies that examine large, complex models are available. A brief
summary of all the studies reviewed can be found in Table 1.
2.1. Posttraumatic symptomatology, dissociation, and revictimization
PTSD and dissociation may contribute to revictimization because these problems are not
uncommon chronic reactions for survivors of CSA (Polusny & Follette, 1995), and such
difficulties can interfere with information processing of relevant danger cues (Sandberg,
Matorin, & Lynn, 1999). Rates of PTSD among CSA survivors in clinical samples range from
33% to 86% (Polusny & Follette, 1995). In a community sample, Saunders et al. (1992) found
that between 8.8% and 17.9% of CSA survivors met criteria for PTSD. Further, likelihood of
developing PTSD appears related to severity of the childhood abuse, with higher rates among
those experiencing contact sexual abuse and childhood rape (Saunders et al., 1992).
Several aspects of PTSD may be important with regard to revictimization. Re-
experiencing symptoms, such as intrusive thoughts (and the emotional distress accom-
panying those symptoms), may interfere with the ability to perceive or act upon potential
risk or danger when a situation contains cues that remind the CSA survivor of prior
abuse. Chu (1992) has proposed that during the numbing phase of PTSD, an individual
may be more vulnerable due to decreased awareness of potential danger. Arousal
symptoms, such as sustained hypervigilance and exaggerated startle response, can
generalize from the CSA scenario to ‘‘safer’’ situations in the survivor’s everyday life
and create within the abuse survivor a constant state of ‘‘being on alert.’’ However, while
hyperarousal is sometimes positively correlated with threat perception (Wilson, Calhoun,
& Bernat, 1999), continual arousal symptoms may actually desensitize the survivor to real
threat and decrease the likelihood that she will respond to perceived danger. A survivor
who frequently feels afraid in situations that she labels ‘‘intellectually’’ as safe may learn
to cope with overwhelming affect by ignoring her emotional response if it involves fear.
This may result in increasing difficulty distinguishing between true alarms and learned
alarms (Barlow, 2002). The perpetrator, in turn, may recognize her inability to accurately
assess risk and act upon this vulnerability. Dissociation affects information processing in a
similar capacity. Dissociation may also increase risk for revictimization because sexual
predators may learn to recognize such confusion or distractibility as signs of a woman’s
vulnerability and be more likely to attack such women (Cloitre, Scarvalone, & Difede,
1997).
T.L. Messman-Moore, P.J. Long / Clinical Psychology Review 23 (2003) 537–571 545

2.1.1. Empirical studies
Despite the theoretical links between PTSD, dissociation, and revictimization, few studies
that examine these relationships are available. Four studies were located which were designed
specifically to examine the role of PTSD and/or dissociation in relation to sexual revictim-
ization. Arata (1999) proposed that PTSD would be a precursor to, and a possible risk factor
for, revictimization among college women. She found that although revictimized women
were significantly more likely to have a lifetime diagnosis of PTSD than women with a
history of CSA only, they were not significantly more likely to have a current diagnosis.
However, PTSD was generally identified as having begun following the CSA experience
(63% of revictimized women reported a childhood onset, while 38% reported an adult onset).
Although not statistically significant, differences between these two groups regarding onset of
PTSD approached statistical significance (P < .07), indicating that PTSD is a precursor and
possible risk factor for revictimization. Kessler and Bieschke (1999) examined dissociation
and revictimization in a large retrospective investigation of college women. While approx-
imately 70% of CSA survivors were revictimized, dissociation was not statistically related to
adult victimization, thus precluding any mediating effects. Sandberg et al. (1999) conducted
the most methodologically rigorous study to date, which examined the role of dissociation
and posttraumatic symptomatology in relation to sexual revictimization in a 10-week
prospective study of college women. While dissociation and PTSD were related to
victimization both in childhood and adulthood, neither dissociation nor PTSD symptoms
mediated the relationship between CSA and adult sexual assault. However, while dissociation
also failed to moderate this relationship, PTSD symptoms did have a significant moderating
effect. Previous sexual victimization was more strongly associated with subsequent sexual
victimization in the context of high levels of posttraumatic symptomatology.
Only one study is available that examines these issues with a clinical sample (Cloitre et al.,
1997). Rates of PTSD were high in the revictimized (75%) and adult sexual assault only
(70%) groups. However, a significantly larger number of revictimized women met criteria for
a dissociative disorder (46%) as compared to the women who reported adult assault only
(13%). The lack of differences between groups regarding PTSD symptomatology may be due
to ceiling effects and the high level of psychological distress exhibited by all of the
participants who were seeking treatment.
2.1.2. Summary
Conclusions drawn from such a small and diverse group of studies are tentative at best.
Although revictimization is associated with PTSD and related symptomatology, given that
most studies are retrospective, it is still unknown if PTSD operates as an underlying causal
mechanism rather than an outcome of revictimization. One prospective study (Sandberg et
al., 1999) did find that revictimization is more likely for CSA survivors who suffer from
PTSD and related symptoms, implying that PTSD may play a causal role. The role of
dissociation in relation to revictimization is unclear given that a clinical sample found
dissociation to be important, while college studies did not. This may due to an interaction
between the nature of the sample (e.g., college students) and level of psychological distress
(e.g., nonclinical levels). More information is needed to conclude that dissociation might
T.L. Messman-Moore, P.J. Long / Clinical Psychology Review 23 (2003) 537–571546

create risk for revictimization among women who experience clinically significant
psychological distress. Because these studies are comprised of predominantly Caucasian,
educated, young women from college samples, additional investigations are needed with
large diverse community samples focusing on PTSD and related symptomatology such as
dissociation and dissociative disorders with prospective, and ideally longitudinal designs.
Further, the discrepancy in findings between different types of samples may indicate that
studies of psychological distress would be most appropriate with community or clinical
samples, rather than college samples, given the level of functioning of women in these
groups.
2.2. Alcohol and substance abuse and revictimization
Alcohol abuse and substance abuse as factors in revictimization have also been studied. It
is known that women with a history of CSA are more likely to have problems with alcohol
and other substances as compared to women with no history of CSA (Briere & Runtz, 1987;
Mullen et al., 1996; Silverman, Reinherz, & Giaconia, 1996; Wilsnack et al., 1997). It has
been hypothesized that increased use of alcohol and other drugs by survivors may help
alleviate the distress associated with victimization experiences. Many researchers have
conceptualized substance abuse by survivors as a form of emotional or experiential avoidance
(e.g., Briere, 1992; Briere & Runtz, 1993; Follette, 1994; Polusny & Follette, 1995). Use of
alcohol or other substances may help CSAS to numb negative feelings associated with CSA,
to forget the abuse experience, and to avoid abuse-specific memories and affective responses
characteristic of PTSD (Briere & Runtz, 1993; Follette, 1994). Briere and Runtz (1987, p.
374) have suggested that alcohol and drug intoxication function as forms of ‘‘chemically
induced dissociation, invoked as a chronic coping response to aversive affects, memories, and
situations.’’
Not only are alcohol and drug use associated with CSA, but they have also been identified
as factors involved in adult sexual assault (for review, see Testa and Parks, 1996). Use of
alcohol by the rape victim as well as the perpetrator has been identified as a situational
variable that may increase the likelihood of rape and other forms of sexual assault (Marx, Van
Wie, & Gross, 1996), and some studies have found that more than half of female rape
survivors report using alcohol before their assault (Frinter & Rubinson, 1993; Harrington &
Leitenberg, 1994; Muehlenhard & Linton, 1987). Fewer studies are available examining the
use of substances (other than alcohol) and rape, although theoretically effects of substance use
and related problems would be similar to those of alcohol. Burnam et al. (1988) found that
sexually assaulted individuals were 1.8 times more likely to report a history of alcohol abuse
or dependence and 2.6 times more likely to report a history drug abuse or dependence prior to
the assault as compared to a control group. The risk for sexual assault likely increases for
intoxicated women because this condition impairs problem solving and escape behaviors.
Further, women who drink may be more likely to encounter potential perpetrators in the
setting in which alcohol is consumed (e.g., bars, fraternity parties, etc.) and may be at
increased risk for sexual victimization because of the way they are perceived by men (Testa &
Parks, 1996). Men perceive women who are drinking as more sexually responsive (George et
T.L. Messman-Moore, P.J. Long / Clinical Psychology Review 23 (2003) 537–571 547

al., 1995) and are less likely to view forced or coerced sex with an intoxicated woman as rape
(Norris & Cubbins, 1992).
2.2.1. Empirical studies
There are seven studies available which focus on the role of alcohol or substance use as
factors in revictimization. Three studies utilizing a retrospective design examine these issues.
Messman-Moore and Long (2002) examined the role of both alcohol and substance use
disorders in relation to revictimization of CSA survivors in a community sample. Both CSA
and diagnostic status (DSM-IV diagnoses of alcohol/substance abuse/dependence) predicted
rape and coerced intercourse, but there was no significant interaction between CSA and
diagnostic status. Merrill et al. (1999) investigated the relationship between childhood abuse
(physical and sexual) and sexual revictimization, as well as two mediating factors, number of
sexual partners, and alcohol problems, in a sample of US Navy recruits. CSA was a
significant predictor of adult rape (even when controlling for childhood physical abuse).
Alcohol problems and number of sexual partners also predicted adult rape even when
considered with the childhood abuse variables. Although CSA survivors had a higher
number of sexual partners, controlling for this factor did not eliminate the association
between CSA and adult rape, suggesting that the number of sexual partners does not mediate
revictimization. Further, there was no significant interaction between CSA and alcohol
problems in relation to adult rape (revictimization), indicating that CSA and alcohol
problems constitute two independent risk factors for adult rape (as in the Messman-Moore
and Long study). Mayall and Gold (1995) examined the relationship among adult sexual
assault, CSA, sexual activity, and alcohol use in a large college sample. There was a
significant relationship between contact CSA and adult sexual assault, but there was no
evidence for a direct relationship between alcohol consumption and adult sexual assault.
Sexual experience was the strongest predictor in the model that discriminated between
women who were and were not assaulted during adulthood. Further, sexual experience was
significantly but weakly correlated with CSA. Women with histories of CSA reported more
sexual experiences during adulthood than women without a history of CSA. The association
between alcohol consumption and adult sexual assault was mediated by amount of adult
sexual experience.
Four studies are available that use a longitudinal or prospective design to examine the role
of alcohol use in revictimization. Siegel and Williams (2001) examined drinking and sexual
behavior in relation to revictimization risk in a longitudinal study following girls with
documented CSA and a matched control group for approximately 20 years. They found that a
history of problem drinking significantly increased the odds of revictimization. When
considered together, presence of CSA and adolescent sexual abuse together (abuse both
before and after age 13) increased the likelihood of adult victimization by almost five times,
while alcohol problems increased risk 2.5 times. Although the number of sexual partners was
positively correlated with revictimization, such behavior did not increase risk of assault
substantially. In another longitudinal study, Himelein (1995) followed college women over a
period of 32 months and examined both alcohol use and sexual behavior as risk factors for
sexual victimization. She found evidence of revictimization from adolescence to adulthood
T.L. Messman-Moore, P.J. Long / Clinical Psychology Review 23 (2003) 537–571548

(but not from childhood to adulthood). Later victimization was positively correlated with
number of sexual partners, and women were more likely to be victimized in college dating
situations if they reported greater use of alcohol in dating situations. However, prior
victimization in dating was the strongest predictor of subsequent sexual victimization, and
alcohol use was no longer related to later victimization in a multivariate model. Greene and
Navarro (1998) investigated alcohol consumption and sexual behavior in relation to
revictimization in a prospective study of female college students. Results supported existence
of revictimization, but alcohol use did not mediate the effects of previous victimization.
Alcohol use was a significant predictor in the path analysis in relation to prior victimization
but not revictimization. However, the number of sexual partners was positively correlated
with adolescent and later victimization. Sexual behavior accounted for almost 13% of the
variance predicting later victimization, but did not consistently predict sexual revictimization.
Gidycz et al. (1995) examined alcohol use, sexual behavior, and interpersonal difficulties in
relation to revictimization among college women with a prospective design. Typical alcohol
use was related to adolescent victimization only, and was not a significant predictor of sexual
revictimization. Number of sexual partners at the initial assessment was related to CSA,
adolescent and later victimization at a 3-month follow-up period, but was not related to
victimization assessed at 6 and 9 months. Initial interpersonal functioning was correlated with
CSA and adolescent victimization, but was not correlated with subsequent victimization at 3,
6, and 9 months. Later interpersonal functioning was not correlated with subsequent
victimization either.
2.2.2. Summary
The role of alcohol-related problems in revictimization is still obscure despite seven
studies available examining these problems. What is clear is that alcohol related factors are
related to sexual victimization, regardless of how alcohol-related factors are assessed (i.e.,
measures of consumption vs. psychological diagnosis) and regardless of the population
surveyed (i.e., college vs. community samples). However, despite these findings, it does not
appear that alcohol-related factors consistently explain the relationship between prior and
subsequent victimization. The one study (Mayall & Gold, 1995) that tested for mediation did
not find that alcohol use mediated the relationship between CSA and revictimization. The
failure of some studies to find interactions between CSA and alcohol-related factors (Merrill
et al., 1999; Messman-Moore & Long, 2002) does not support the idea that alcohol moderates
the CSA-revictimization relationship. Results of all prospective studies indicate that prior
victimization is the strongest predictor of later victimization. Further, with the exception of
Siegel and Williams (2001), most prospective studies indicate that alcohol use is not a
significant predictor of later victimization when in a model containing multiple factors
(Gidycz et al., 1995; Greene & Navarro, 1998; Himelein, 1995). These inconsistencies across
studies may be due to an interaction between type of sample and severity of psychological
problems, which may impact nonsignificant findings. However, it may be that there are no
mediating effects for alcohol or drug-related problems, but because CSA survivors are more
likely than nonsurvivors to have such problems, they continue to be at increased risk for
revictimization.
T.L. Messman-Moore, P.J. Long / Clinical Psychology Review 23 (2003) 537–571 549

2.3. Risk recognition and revictimization
Some researchers have discussed the possibility that revictimization occurs because
revictimized women may have deficits in their abilities to perceive or act upon threat in
potentially dangerous situations (Chu, 1992; Kluft, 1990; Nurius & Norris, 1996). Failure
to engage in self-protective behavior may be related to several factors including low self-
esteem, assertiveness deficits, or lack of skill in avoiding or escaping risky situations.
Impediments to accurate risk recognition or responses should be considered within an
interpersonal and social context, however. Nurius (2000) emphasizes that risk perception
also includes the application of such knowledge to the self, which means that a woman
might identify a risky scenario but discount this information if she beliefs these risk
factors do not apply to her for one reason or another. A second important issue is that
with each appraisal a woman must consider both the possible positive and negative
consequences of a self-protective response. Risky scenarios are often the very same
situations in which women are pursuing the goals of entertainment, friendship, or
intimacy, which may take precedence over concerns for safety and self-protection
(Nurius, 2000). A woman may not engage in self-protective behavior if she has concerns
about how she might be viewed or perceived by her partner (as well as her peer group)
if she rejects the sexual advances. When compared to women without a history of sexual
abuse, CSA survivors might be more concerned about being rejected by a person they
care about, or conversely, from potential embarrassment that could occur in reaction to
public resistance, or be more likely to have a general fear of being stigmatized or judged
by others.
Research conducted thus far on risk recognition or perception has focused on repeated
adult sexual victimization, rather than child to adult sexual revictimization. Several studies
examined the relationship between adult sexual assault and identification of threat cues in a
dating situation using an analogue design. Neither retrospective designs (e.g., Cue, George, &
Norris, 1996) nor prospective designs (e.g., Breitenbecher, 1999) found a relationship
between threat perception and prior adult sexual victimization, while Breitenbecher (1999)
also found no relationship between threat perception and adult victimization during a 5-month
follow-up period.
Most studies, including those reviewed above, focus on recognition of risk and less on how
women respond to perceived risk. However, Meadows, Jaycox, Orsillo, and Foa (1997)
conducted a study of college students that differentiated between recognizing and acting on
potential risk. While no differences were found between previously victimized and non-
victimized women (physical or sexual assault at any age) for risk recognition, individuals
with histories of assault reported that they would leave a hypothetical scenario significantly
later than did individuals without a history of sexual assault, even when controlling for
severity of dissociation. Scenes with an acquaintance or someone known to the subject (rather
than a stranger) were ‘‘left’’ significantly later by subjects with a history of assault. Further,
subjects without a history of assault also endorsed leaving the scene prior to physical contact,
in contrast to previously abused subjects who usually did not endorse leaving until after
physical contact had been made.
T.L. Messman-Moore, P.J. Long / Clinical Psychology Review 23 (2003) 537–571550

2.3.1. Empirical studies
While the topic of risk recognition in relation to repeated victimization has received some
attention, there is relatively little known about risk recognition in relation to revictimization
that occurs for CSA survivors. Meadows, Jaycox, Stafford, Hembree, and Foa (1995)
examined the relationship between childhood abuse (either physical or sexual), risk
recognition, and adult revictimization (physical or sexual assault) with a sample of
treatment-seeking women diagnosed with PTSD and found that women who reported only
a single assault had significantly better risk recognition than revictimized women. However,
poor risk recognition was not associated with child sexual or physical abuse.
While not limiting revictimization to only CSA survivors, Wilson et al. (1999) did include
women with child to adult revictimization as well as women who reported repeated adult
sexual victimization. They investigated revictimization, PTSD, and perceptions of risk
among college women with an analogue study utilizing an audiotaped date rape vignette.
Participants were instructed to stop the audiotape ‘‘if and when they believed the man had
gone too far’’ (p. 707). Longer response latencies indicated poorer risk recognition. Overall,
revictimized women had longer response latencies than women who were victimized on a
single occasion. One interesting incidental finding concerns the role of symptomatology in
risk recognition. While overall levels of PTSD symptomatology did not mediate the
relationship between prior victimization and revictimization, symptomatic women, particu-
larly those with high levels of hyperarousal PTSD symptoms, detected risk earlier than
nonsymptomatic women.
2.3.2. Summary
Despite the assumption that risk perception is an important factor in sexual assault, there is
much less known about how this factor may impact child to adult sexual revictimization.
Future research must examine this question in relation to CSA, as only two studies included
CSA survivors (e.g., Meadows et al., 1995; Wilson et al., 1999). Unfortunately, neither of
these studies examined the specific role of childhood sexual abuse, although Meadows et al.
(1995) concluded that childhood abuse (both physical and sexual) did not have an important
role in risk recognition. Further, there are no studies available that examine the relationship
among CSA, risk recognition, behavioral responses, and revictimization. Findings from the
later Meadows et al. (1997) study indicate that behavioral responses, rather than risk
recognition per se, may be an important causal factor in revictimization, but this possibility
remains unexamined in the case of child to adult sexual revictimization. Additional study is
needed to determine if CSA survivors are at risk for revictimization not only because of deficits
in risk recognition, but also because of internal barriers to their escape from this situation.
2.4. Sexual behavior and revictimization
Another factor that may be important in explaining the problem of revictimization is the
sexual behavior pattern of survivors. The current literature suggests that CSA survivors display
different patterns of sexual behavior compared to women with no history of CSA. Sexual
behavior such as precocious and/or coercive sexual behavior (Bonner, Walker, & Berliner,
T.L. Messman-Moore, P.J. Long / Clinical Psychology Review 23 (2003) 537–571 551

1999), younger age at first intercourse (Fergusson, et al., 1997; Fiscella, Kitzman, Cole,
Sidora, & Olds, 1998; Stock, Bell, Boyer, & Connell, 1997), and greater number of sexual
partners (Fergusson et al., 1997; Fehrenbach & Long, 2001; Krahe, Scheinberger-Olwig,
Waizenhofer, & Kolpin, 1999) are more common among survivors. There is also some
evidence that women with a history of CSA have more permissive attitudes about participation
in sexual behavior (Miller et al., 1995), are both more accepting of the sexual behavior of
others and themselves (Fehrenbach & Long, 2001), have more negative attitudes towards
sexual behavior (Orr & Downs, 1985), have different reasons for engaging in sexual
intercourse (Fehrenbach & Long, 2001), and may be more likely to label themselves as
promiscuous as compared to peers with similar types and rates of sexual behavior (Fromuth,
1986). Sexual guilt, sexual anxiety, fear of intimacy, and low sexual self-esteem have also been
found among women with a history of CSA (Fehrenbach & Long, 2001; Fromuth, 1986).
Researchers have proposed that CSA survivors may engage in sexual behaviors as a way of
avoiding emotional distress (Briere, 1996). Engaging in sexual behaviors may help survivors
to avoid the negative feelings associated with CSA and to forget the abuse experience and
avoid abuse-specific memories, even temporarily. Increased sexual behavior evident among
CSA survivors may place them at greater risk for revictimization because they are exposed to a
greater number of sexual partners (some of whom may sexually assault them).
Also increasing the risk of revictimization may be the CSA survivor’s self-perception. As
noted previously, women with a history of CSA are more likely to have permissive attitudes
about participation in sexual behavior and are more likely to label themselves as promiscuous
as compared to peers with similar types and rates of sexual behavior. Such self-perceptions
may be apparent to potential perpetrators and may influence the decision to target these
women for sexual coercion. These self-perceptions may also make it more difficult for these
women to leave sexually abusive relationships after an assault has occurred (i.e., in the
context of a marriage or dating relationship). Women with a history of CSA may not perceive
better alternatives as they have come to expect violence in sexual relationships based on their
prior experiences.
Given that there are a number of reasons to believe that revictimization may be related to a
survivor’s sexual behavior, it is not surprising that the relationship between sexual behavior
and revictimization has been studied extensively. Overall, nine studies were found that focus
on some aspect of sexual behavior in relation to revictimization, including five retrospective
and four prospective studies.
2.4.1. Empirical studies
Krahe et al. (1999) examined the relationship between adult sexual victimization,
childhood sexual and physical abuse, and sexual behavior in a sample of German female
adolescents. Women with histories of CSA and those who were ‘‘not sure’’ whether they
experienced CSAwere more likely than nonabused to women to report unwanted intercourse.
The number of partners predicted sexual victimization; women who reported CSA had a
significantly higher number of sexual partners (5.6 vs. 2.9 reported by women without
histories of CSA), which was in turn related to higher rates of later victimization. There was
no relationship between age at first intercourse and sexual victimization. When CSA was
T.L. Messman-Moore, P.J. Long / Clinical Psychology Review 23 (2003) 537–571552

considered together with consensual sexual activity, the relationship between CSA and
revictimization was reduced, but not eliminated, indicating that the link the CSA and
subsequent victimization is not exclusively attributable to the mediating effect of sexual
activity.
Fergusson et al. (1997) investigated sexual behaviors in relation to revictimization among a
birth cohort of New Zealand born young women who were studied from birth to the age of 18
(although reports of CSA were retrospective). Those reporting CSA involving attempted or
completed intercourse had the earliest onset of sexual activity and the highest rates of sexual
revictimization after the age of 16. After adjustment for childhood and family factors, the
relationships between CSA and sexual outcomes tended to reduce. Further, it appears that the
direct impact of CSA on sexual risk taking behaviors is mediated by the impact of CSA on
age at first consensual intercourse. CSA is associated with an increased rate of early onset
consensual intercourse that acts to increase the individual’s risk of multiple sexual partners.
However, independent of age at first intercourse and family background, CSA increases
likelihood of sexual revictimization, particularly the risk of rape/attempted rape during late
adolescence.
Two studies are available that examine the role of sexual behavior in sexual revictimization
among more diverse samples including African American women. West, Williams, and Siegel
(2000) investigated the relationship between CSA, sexual behaviors, and sexual revictimiza-
tion among African American women with documented histories of CSA. They failed to find
any differences between revictimized and nonrevictimized CSA survivors for age at first
consensual sexual experience or for number of consensual partners. However, revictimized
survivors were more likely to report engaging in prostitution as compared to nonrevictimized
survivors. In another study focusing on African American women, Wyatt, Notgrass, and
Gordon (1995) found that women who were revictimized or women with only adult
victimization were more likely to have multiple sexual partners and brief sexual relationships
than women who experienced only CSA or who were not abused.
Three prospective studies and one longitudinal study were discussed previously in
regard to alcohol use (Gidycz et al., 1995; Greene & Navarro, 1998; Himelein, 1995;
Siegel & Williams, 2001). Overall, these studies found a relationship between sexual
behavior and later victimization. In prospective studies with college women that spanned
9–32 months, number of sexual partners consistently predicted later victimization (Gidycz
et al., 1995; Greene & Navarro, 1998; Himelein, 1995), although when assessed in shorter
intervals (3, 6, or 9 months), number of sexual partners did not always predict
revictimization (Gidycz et al., 1995; Greene & Navarro, 1998). Further, although number
of sexual partners was positively correlated with revictimization in a 20-year longitudinal
community study, such behavior did not increase risk of assault substantially (Siegel &
Williams, 2001).
2.4.2. Summary
Many studies are available that examine sexual behaviors in relation to the revictimization
of CSA survivors with different populations. Results of most studies presented here support
the idea that sexual behaviors are related to revictimization, but the role of each type of
T.L. Messman-Moore, P.J. Long / Clinical Psychology Review 23 (2003) 537–571 553

behavior in relation to revictimization is mixed. In some studies, CSA and adult sexual
victimization appear related to the number of consensual sexual partners, with victimized
women reporting more partners. Some report that the number of sexual partners mediates the
relationship between CSA and revictimization (e.g., Himelein, 1995; Krahe et al., 1999;
Wyatt et al., 1995). Others, however, indicate that additional variables such as age at first
intercourse, mediate the relationship between CSA and number of partners (Fergusson et al.,
1997). While it is logical that women who begin sexual activity at earlier ages will likely have
more sexual partners across their lifespan, it is unknown which of these factors (early
intercourse vs. number of partners) is the more important contributor to revictimization.
Further, several studies find either mixed or no support for the role of sexual behavior in
revictimization (Gidycz et al., 1995; Siegel & Williams, 2001). Nonetheless, overall these
findings suggest that sexual behavior is an important factor in the revictimization of CSA
survivors. Additional studies with more diverse samples are needed to examine multiple
aspects of sexual behavior, including self-perceptions and attitudes regarding sexuality.
2.5. Interpersonal difficulties and revictimization
Another aspect of the traumatic effects of CSA potentially related to revictimization is the
negative impact of CSA on interpersonal relationships. The experience of CSA may
interfere with the development of self-concept and sexual identity, and may distort basic
beliefs about trust, safety, and control in significant relationships (Cole & Putnam, 1992;
Trickett & Putnam, 1993; for review, see DiLillo, 2001). For instance, DiLillo and Long
(1999) found that CSA was associated with less satisfaction, trust, and poorer communica-
tion in couple relationships, and Hunter (1991) found that CSA survivors reported lower
relationship satisfaction with their partners and poorer sexual adjustment. In a clinical
sample, Jehu (1988) found that all of the CSA survivors surveyed reported problems in both
general social relationships and with partners, and half of survivors reported interpersonal
problems with other women. Harter, Alexander, and Neimeyer (1988) also found that CSA
was associated with poor social adjustment among college women. Browne and Finkelhor
(1986) describe the problematic interpersonal relations that can result from four different
traumagenic dynamics—traumatic sexualization, betrayal, stigmatization, and powerless-
ness. Messman and Long (1996) speculate that the traumagenic dynamic of betrayal could
impact judgment regarding the trustworthiness of others. Gelinas (1983) has observed that
survivors of CSA tend to place the needs of others before their own and have difficulty
saying ‘‘no’’ in intimate relationships, perhaps creating risk for revictimization. Further,
revictimization may occur through a variety of mechanisms that impact interpersonal
relatedness including a maladaptive learning history or beliefs regarding interpersonal
relationships that result from the CSA experience, gender role socialization and sex role
stereotypes, poor relationship choices, and learned helplessness (Messman & Long, 1996).
However, there are currently only a few studies available that examine whether certain types
of interpersonal difficulties are associated with revictimization (Classen, Field, Koopman,
Nevill-Manning, & Spiegel, 2001; Cloitre et al., 1997; Cloitre, Cohen, & Scarvalone, 2002;
Gidycz et al., 1995).
T.L. Messman-Moore, P.J. Long / Clinical Psychology Review 23 (2003) 537–571554

2.5.1. Empirical studies
In a prospective study discussed earlier, Gidycz et al. (1995) examined interpersonal
functioning as a potential mediator of revictimization. Initial interpersonal functioning was
correlated with CSA and adolescent victimization, but was not correlated with subsequent
victimization at 3, 6, and 9 months. Later interpersonal functioning was not correlated with
subsequent victimization either. However, in a retrospective study, Classen et al. (2001) found
that treatment-seeking women with histories of CSA and current PTSD and who had also
been sexually revictimized in the previous 6 months reported greater interpersonal problems
than those who were not sexually revictimized during that period. Revictimized women were
more likely to describe themselves as overly responsible and as having greater difficulty
being assertive in interpersonal relationships than those who were not revictimized.
Revictimized women also described themselves as being overly nurturing and socially
avoidant. In another retrospective study discussed earlier, Cloitre et al. (1997) investigated
interpersonal functioning in relation to revictimization among a clinical sample. The
interpersonal functioning of revictimized women differed significantly from women with
only adult assault. Overall, revictimized women exhibited and reported significantly greater
difficulties regarding self- and interpersonal dysfunction as compared to women with a
history of sexual assault only during adulthood. Cloitre et al. (2002) also examined the
interpersonal schemas of revictimized women. Revictimized women had the tendency to
generalize their predominant parental schemas to their current relationships, particularly the
schemas that their parents were hostile and controlling. Women with histories of CSA but
who were not revictimized tended to view their parents in a similar light, but did not
generalize from parental to current schemas. Finally, women who were never abused or
assaulted generalized warm and noncontrolling schemas of their parents to their current
schemas.
2.5.2. Summary
Researchers are only recently beginning to explore the impact of CSA on interpersonal
functioning in relation to revictimization. The studies discussed above provide a starting-
point for further investigations given the consistent finding of disturbed relatedness
among CSA survivors, particularly those who are revictimized. Revictimized women tend
to view themselves in a more negative light, seeing themselves as less assertive and more
likely to provide care for others rather than consider their own needs. Further, these
women also seem to generalize negative interpersonal schemas from childhood to
adulthood, expecting others to treat them in a hostile, controlling and domineering man-
ner, even if there is evidence to the contrary (Cloitre et al., 2002). However, despite
these observations, not all studies find interpersonal functioning related to revictimization
(Gidycz et al., 1995).
2.6. Summary of research on revictimization factors
All studies examined here focused on the psychological problems of CSA survivors as
factors in revictimization. From this review, we can draw several conclusions, but several
T.L. Messman-Moore, P.J. Long / Clinical Psychology Review 23 (2003) 537–571 555

limitations should be acknowledged. First, most studies examining these phenomena utilize
college samples that are predominantly Caucasian and middle- to upper-class (e.g., Gidycz
et al., 1995; Greene & Navarro, 1998; Himelein, 1995; Mayall & Gold, 1995). Evidence
of revictimization is stronger among samples that include older women (Roodman &
Clum, 2001), while studies reviewed here tended to include young samples. Because most
studies focus on middle- to upper-class, educated, young, Caucasian, college women,
findings from these studies might not apply to non-Caucasian women, or to women living
in crime-ridden inner cities or within substandard financial means. However, studies of
young, Caucasian, college students are still important because findings indicate that
revictimization does occur within all socioeconomic strata, and protective factors, such
as higher socioeconomic status and education, do not always protect women from
revictimization. Despite the emphasis on college populations, some studies including
noncollege samples were available. Unfortunately, they usually had a much smaller sample
size that might have impacted statistical findings (e.g., Classen et al., 2001; Cloitre et al.,
1997, 2002).
Second, lack of diversity with regard to psychological functioning also creates problems
when examining psychological distress as a factor in revictimization, as individuals from
college samples have on average significantly better psychological adjustment than
individuals from clinical and community samples. The severity of psychological distress
is important to consider because it may be that only clinically significant psychological
problems would be severe enough to interfere with functioning and affect vulnerability. An
overview of findings suggests that, for many studies discussed here, psychological
functioning is confounded with sample type (i.e., college), limiting conclusions regarding
psychological distress variables. For studies reviewed here, the relationship between
psychological problems and revictimization was stronger in clinical (e.g., Cloitre et al.,
1997) or community samples (e.g., Merrill et al., 1999; Siegel & Williams, 2001) rather
than college samples (e.g., Gidycz et al., 1995; Greene & Navarro, 1998; Sandberg et al.,
1999).
Third, and very importantly, the vast majority of research to date consists of retrospective
studies that are unable to determine causality, and findings from retrospective investigations
often differ from prospective or longitudinal studies. For example, two prospective studies
(Gidycz et al., 1995; Greene & Navarro, 1998) reported results from retrospective data that
identified a relationship between alcohol use and revictimization, however, results from
prospective data failed to support this factor as a consistent predictor of later sexual
victimization (i.e., revictimization). This is further complicated because most prospective
studies used college samples. Finally, although many studies discuss possible mediating roles
for these psychological factors, few studies actually tested for mediation. Despite these
problems however, there are several tentative conclusions.
Of all the types of psychological distress reviewed, only one factor, sexual behavior,
predicts revictimization on a fairly consistent basis. Most studies find a relationship between
revictimization and the level of sexual activity (number of partners), and this factor
sometimes mediates the relationship between CSA and revictimization. However, given that
the link between CSA and later victimization is never completely eliminated, sexual behavior
T.L. Messman-Moore, P.J. Long / Clinical Psychology Review 23 (2003) 537–571556

does not fully explain revictimization. These findings indicate that sexual behavior cannot by
itself explain the phenomenon of revictimization.
Evidence for the role of other psychological problems is often mixed, prohibiting strong
conclusions regarding any causal role in revictimization. Although PTSD symptomatology is
associated with revictimization among retrospective studies, its role as a causal mechanism is
still unclear. Arata (1999) found an apparent temporal relationship between CSA and PTSD,
implicating PTSD as possible causal factor, although the retrospective design precludes this
conclusion. However, results from one prospective study (Sandberg et al., 1999) suggest that
PTSD might better be conceptualized as playing a moderating, rather than mediating role.
Given these positive findings, PTSD should likely be examined further as a causal factor in
revictimization. An association between revictimization and dissociative phenomena is not
consistently found. Only retrospective studies using clinical samples (e.g., Cloitre et al.,
1997) find that dissociation and related problems are related to revictimization (as opposed to
college samples), and there have been no tests of mediating models or use of prospective
designs with clinical or community samples.
There is also mixed evidence that alcohol-related factors directly affect revictimization, as
some retrospective studies report independent effects for CSA and alcohol use (e.g., Merrill et
al., 1999; Messman-Moore & Long, 2002), and alcohol use often fails to consistently predict
revictimization in prospective studies (e.g., Gidycz et al., 1995; Himelein, 1995). The one study
examining the role of substance abuse (Messman-Moore & Long, 2002) found no evidence of
an interaction between such problems, and both factors were strong predictors when in the
model together, which suggests that mediation could not have held.More information is needed
to determine if alcohol-or substance-related factors explain the relationship between CSA and
revictimization, or if these factors contribute to revictimization independently.
Analogue studies examining risk recognition find that risk recognition is not consistently
associated with revictimization, but this concept may be important in conjunction with
information about escape behaviors and PTSD symptomatology (see Meadows et al., 1997;
Wilson et al., 1999). Interpersonal difficulties and beliefs about relationships do appear to be
consistently related to revictimization (Classen et al., 2001; Cloitre et al., 1997, 2002), but the
causal role of these factors has not yet been explored. The findings of one study examining
the response to risk recognition (Meadows et al., 1997) and studies focusing on interpersonal
difficulties (Classen et al., 2001; Gelinas, 1983) overlap, indicating that poor assertiveness
within relationships may serve as an internal barrier to acting upon risk. Examining the
intersection between these concepts may prove fruitful.
Although there may be some methodological explanations for inconsistencies among the
findings discussed above, wemust also acknowledge other reasons why intrapersonal problems
do not consistently explain revictimization. It could be that these variables are not critical to the
process of revictimization, but they are correlated with factors that are explanatory. For
instance, alcohol expectancies might be more important than alcohol use itself with regard to
revictimization (Nishith, Bazile, Clum, Messman-Moore, & Resick, 2001). It may be that only
women who abuse alcohol solely because they expect use to enhance sexuality, sociability, etc.,
are at increased risk for revictimization, because they are most likely to abuse alcohol in a
scenario that is risky for acquaintance rape (e.g., parties, fraternity houses, or bars). Other
T.L. Messman-Moore, P.J. Long / Clinical Psychology Review 23 (2003) 537–571 557

factors correlated with psychological distress, such as coping strategies or access to social
support, may also be important to explore. Previous studies have found that effective coping
strategies are an important factor in recovery from adult rape and incest, while disengagement
and avoidant methods of coping lead to increased psychological distress (Burt & Katz, 1987;
Drauker, 1989). One study examining revictimization and coping (Gibson & Leitenberg, 2001)
found that revictimized women usedmore disengagement methods to cope with an adult sexual
assault than women without a history of CSA. Reactions to disclosure of abuse and available
social support may also play an important role (Messman-Moore & Resick, 2002).
We must also recognize that it is very possible that the focus should not be on intrapersonal
psychological factors at all. However, to support this conclusion, we need additional research
based upon a guiding theoretical model that captures the complexity of this issue, including
not only victim characteristics, but also perpetrator behavior and societal and cultural factors
that operate to increase risk.
3. Theoretical explanations of revictimization
There is no empirically validated theoretical model of revictimization, although several have
been proposed (e.g., Gold, Sinclair &Balge, 1999; Grauerholz, 2000;Messman&Long, 1996).
Without a guiding theory, the same question continues to be asked: ‘‘Why are these women at
increased risk?’’ The search for an answer to this question has led most researchers to focus on
the victim, i.e., ‘‘Is there something about the CSA survivor as an individual that places her at
greater risk?’’ Some have asked, ‘‘Do these women choose sexually abusive partners as some
unconscious desire for a ‘mastery’ experience?’’ (Chewning-Korpach, 1993; Chu, 1992; van
der Kolk, 1989). It has been proposed that the psychodynamic concept of repetition compulsion
explains revictimization in that ‘‘many traumatized people expose themselves, seemingly
compulsively, to situations reminiscent of the original trauma’’ (van der Kolk, 1989, p. 389).We
argue that the phenomenon of repetition compulsion as an explanation of revictimization is
unsatisfactory because it is difficult to study empirically, and because the theory is often
misinterpreted to blame the victim.
In an effort to understand revictimization, most theories focus exclusively on the CSA
survivor or characteristics of her abuse. This is problematic, however, because previous
research has found that few, if any, victim characteristics besides previous victimization
predict rape (Koss & Dinero, 1989; Koss & Harvey, 1991). Focusing on the victim and her
behavior is also problematic because there is no consideration of the behavior and motivation
of the perpetrator. While there has been research on the characteristics of sexually aggressive
perpetrators (for review, see Berkowitz, 1992), we must also examine the role of perpetrators’
behaviors and motivations in models of revictimization. Theories of revictimization should
also consider the importance of societal and cultural factors including devaluation of women
and children, patriarchal systems, gender-related social roles, sexual scripts, and cultural
myths as factors potentially contributing to revictimization (Koss et al., 1994).
There is a need for an all encompassing, theoretical framework to guide empirical studies of
revictimization, its causes and effects. This theory should be complex and broad enough to
T.L. Messman-Moore, P.J. Long / Clinical Psychology Review 23 (2003) 537–571558

encompass intrapersonal, interpersonal, and societal issues, should organize the inchoate
literature and explain disparate empirical findings. While we encourage a focus on factors
outside the victim, we are not arguing that theories should not address the circumstances and
context of sexual victimization in relation to the victim.Wemust learn more about the factors or
mechanisms that contribute to the increased vulnerability of CSA survivors. However, instead
of focusing solely on the vulnerability of these women, theories should include the interaction
of two factors: (1) the vulnerability of CSA survivors and (2) the presence of an opportunistic
perpetrator. To date, most theories and empirical research focus on the first half of this formula
without acknowledging the importance of a second necessary factor, the perpetrator.
3.1. An ecological model
Given these criteria, an ecological model may be a good way to understand the relationship
between CSA and revictimization. Grauerholz (2000) discusses such a model, developing
ideas first presented by Bronfenbrenner (1977, 1979) and Heise (1998). This model proposes
that revictimization can be understood within a system of four levels, illustrated as four
concentric circles that consider four levels of factors: ontogenic development factors related
to the initial victimization experience (e.g., personal history of the victim, psychological
sequelae of CSA or early family environment), microsystem factors considering the context
of abuse (e.g., perception by the perpetrator that the victim is an easy target, victim’s
decreased ability to respond assertively and effectively to unwanted sexual advances),
exosystem factors such as lack of resources or alternatives (e.g., low socioeconomic status,
unsafe living conditions, etc.), and macrosystem factors such as cultural norms and
institutions (e.g., cultural tendency to blame victims).2
The ecological model provides an overarching, guiding theory, and is the most inclusive
and far-reaching available, allowing integration of research conducted from various theor-
etical perspectives. The majority of research on revictimization has focused on variables such
as characteristics of the initial CSA experience (e.g., physical force, penetration, relationship
to the perpetrator), other forms of childhood abuse (e.g., physical abuse), and the psycho-
logical sequelae of the childhood abuse (e.g., dissociation), factors which fall within the two
innermost circles of Grauerholz’s model: ontogenic development and microsystem. The
interpersonal, contextual, and cultural factors considered as the exosystem and macrosystem
in this model have not received as much attention. Focusing exclusively on intrapersonal or
2 Those familiar with the Bronfenbrenner model might note that Grauerholz’s definitions of ontogenic
development and microsystem are not consistent with the original ecological model. Grauerholz has grouped
together historical factors including the family environment during childhood as part of ontogenic development,
while Bronfenbrenner’s model would consider the family environment as part of the microsystem. Further,
Grauerholz considers the interaction between the perpetrator and the psychological problems of CSA survivors as
part of the microsystem, which is also not entirely consistent with the original ecological model. Despite these
differences, however, this model may still be a useful heuristic if adapted as a guiding framework because this
model considers the behavior of the perpetrator, the context in which victimization occurs, and the psychological
vulnerability of the CSA survivor.
T.L. Messman-Moore, P.J. Long / Clinical Psychology Review 23 (2003) 537–571 559

microsystem factors ignores important information such as perpetrators’ perceptions of
victims, or cultural forces that likely contribute to continued victimization of CSA survivors.
Research focusing on revictimization, and explanatory factors in particular, is clearly in
initial, early stages of development. Utilizing the ecological model as a theoretical or
conceptual framework would provide scholars with a sense of direction, as well as a
framework within which to interpret findings.
Although much research on revictimization focuses on the two innermost circles of the
Grauerholz (2000) model, ontogenic development and microsystem, we believe that the
empirical studies reviewed here would best fit within a single level, the microsystem, the
context in which revictimization occurs. To fully understand the phenomenon of revictimiza-
tion, we must move beyond a focus on the victim’s personal characteristics or history and
widen our perspective to the microsystem, the first level that examines the context of
victimization, including both the perpetrator and the victim. Further, it may be beneficial to
move away from conceptualizing psychological problems of the victim as intrapersonal, to
viewing these problems as interpersonal, when considered in conjunction with revictimiza-
tion. Revictimization is an interpersonal process. Indeed, despite the importance of PTSD,
dissociation, or alcohol abuse, such problems do nothing to increase risk for victimization
unless there is a perpetrator present who will ‘‘take advantage of’’ the victim’s vulnerability.
Further, contextual factors might be more amenable to change. Ontogenic factors, by
definition, occur earlier in the survivor’s life and often cannot be altered. However, we can
change the context in which revictimization is more likely by focusing on the interaction
between victim vulnerability and perpetrator behavior.
We also should consider the possibility that risk for revictimization might vary within
different levels of this model depending on the identity of the perpetrator. For instance, while
macrosystem factors such as patriarchal views would influence revictimization by all types of
perpetrators, exosystem factors such as poverty and unsafe neighborhoods might contribute
more significantly to revictimization by a stranger. Further, certain risk factors may be more
salient than others for revictimization perpetrated by different types of perpetrators (e.g.,
partners vs. acquaintances vs. strangers). Future research should also consider not only
victim-related factors, but perpetrator-related factors as well. The perpetrator can be examined
at each level of the ecological system as well as the victim.
3.2. Underlying causal mechanisms
Although intrapersonal factors such as sexual behavior and alcohol use appear important to
the process of revictimization, we still need a unifying framework to increase our under-
standing of how the interaction between victim characteristics and perpetrator behavior leads
to revictimization. The psychological sequelae of CSA discussed previously can be
conceptualized as two mechanisms within the microsystem that increase vulnerability of
CSA survivors for revictimization (see Fig. 1). These two mechanisms operate in different
ways to increase risk for revictimization, and may help explain why certain factors do not
consistently predict revictimization. The first mechanism operates to increase risk for
revictimization through increased contact with potential rapists. Here, the victim’s sexual
T.L. Messman-Moore, P.J. Long / Clinical Psychology Review 23 (2003) 537–571560

behavior (e.g., number of sexual partners) or problems such as alcohol or drug use increase
the likelihood of revictimization because these behaviors operate to increase contact with
potential perpetrators, or because these behaviors actually create a context where victimiza-
tion is more likely (e.g., in situations where alcohol is consumed by both the victim and
perpetrator). For instance, women who drink may be more likely to encounter potential
perpetrators in settings such as bars or fraternity parties where alcohol is likely to be
consumed (Testa & Parks, 1996). Promiscuous sexual behavior could increase revictimization
risk simply because women who have more sexual partners are more likely to encounter a
potential perpetrator. This mechanism would also explain why women who abuse alcohol or
substances, but whose use occurs only in their own home or in situations where potential
perpetrators are not present, would be at lower risk. For such women, problematic alcohol or
substance use would not increase risk for revictimization.
The second mechanism operates in a different manner to increase risk for revictimization
because it involves factors that increase the likelihood that the perpetrator will choose to act
aggressively. The second mechanism reflects the psychological and social vulnerability
within the victim that potential perpetrators are likely to identify and act upon. According to
this mechanism, women are at increased risk because psychological difficulties (e.g.,
dissociation, frequent intoxication, or risk recognition deficits) decrease awareness or the
ability to respond to dangerous situations, resulting in a vulnerable state to which a
perpetrator might respond with aggression. Risk increases because a potential perpetrator
would identify and act upon the woman’s vulnerability, not just because such problems
increase the likelihood of encountering a perpetrator.
Fig. 1. Microsystem mechanisms within an ecological framework of revictimization.
T.L. Messman-Moore, P.J. Long / Clinical Psychology Review 23 (2003) 537–571 561

Because psychological correlates of CSA (e.g., dissociation, PTSD, alcohol abuse, sexual
behavior, risk recognition, interpersonal difficulties) have mostly been examined in isolation,
one could infer that they are considered to be completely separate factors with different
underlying mechanisms, or assume that such factors operate in different ways to create risk
for revictimization. However, such factors probably do not operate independently. For
example, Epstein et al. (1998) found that PTSD mediated the relationship between childhood
rape and alcohol use. Therefore, examination of factors in combination appears to be
important. However, few studies that empirically examine more than a single variable are
available. We propose that these factors are related, not simply because of the high rates of
comorbidity among such problems, but because underlying mechanisms and processes may
operate in very similar ways to increase vulnerability and increase risk for revictimization
among CSA survivors.
For instance, alcohol abuse and dissociation, two distinct phenomena, do have functional
aspects that overlap (e.g., both intoxication and dissociation lead to decreased awareness of
surroundings and ability to respond to danger—both factors serving as vulnerabilities that
potential perpetrators may act upon). Briere and Runtz (1987) identified the functional
similarity between substance intoxication and dissociation when they concluded that alcohol
and drug intoxication function as forms of ‘‘chemically induced dissociation, invoked as a
chronic coping response to aversive affects, memories, and situations’’ (p. 374). Further,
although interpersonal difficulties do not operate in ways similar to PTSD and dissociation,
these sequelae can also serve to increase vulnerability to revictimization because of an
increased possibility that the CSA survivor will be manipulated within an interpersonal
context. In all cases, the psychological sequelae would operate to increase risk because a
perpetrator perceives the victim’s reduced awareness, her inability to respond assertively and
effectively, or both.
Similarly, alcohol use and certain patterns of sexual behaviors may share a common
underlying mechanism that leads to revictimization. Contact with a greater number of sexual
partners may place a woman in contact with more potential perpetrators. Consuming alcohol
and substances in social settings involving others may also serve to increase contact with
sexual perpetrators. Thus, while these two factors may not occur simultaneously within any
one woman, the presence of either factor may increase her risk for revictimization by
increased exposure to perpetrators.
Several different types of psychological difficulties can increase risk for revictimization
because perpetrators identify or recognize this psychological vulnerability and act upon it.
Different types of psychological difficulties can also increase risk for revictimization because
they increase contact with potential perpetrators. Focusing on the function or outcome of this
symptomatology (e.g., decreased awareness and ability to respond to danger leading to
vulnerability to a potential perpetrator or increased contact with potential perpetrators), rather
than the distinct symptomatology itself (i.e., dissociation vs. drug abuse vs. interpersonal
dysfunction vs. sexual behaviors) may help explain contradictory findings. Some women may
be more vulnerable because they abuse alcohol or drugs, and others may be more vulnerable
because of their tendency to dissociate, but neither alcohol abuse nor dissociation will fully
explain revictimization for all women. Further, increased numbers of sexual partners or
T.L. Messman-Moore, P.J. Long / Clinical Psychology Review 23 (2003) 537–571562

greater use of alcohol, often in social settings, may increase contact with perpetrators. Neither
one alone will explain this increased potential for victimization, and these factors must be
considered in the context of increased vulnerability as well.
The state of the current literature on this subject could be compared to the story of the blind
men and the elephant. As researchers, some of us are focusing on the trunk, some of us are
focusing on the tail, and others are focusing on the leg of the elephant, without realizing that
in actuality we are all studying different parts of the same beast. Rather than construing that
the entire elephant is a rope (as did the blind man examining the tail), the blind man must
communicate with his peers about their experiences. Here, rather than concluding, for
example, that alcohol abuse is the only important explanatory factor (or conversely, that it
is not important because it is not consistently related to revictimization), we must also
consider that sexual behavior, interpersonal problems, and each of the other correlates of CSA
are part of this problem. Alcohol abuse, dissociation, PTSD, risk recognition, and interper-
sonal problems may simply be different ways in which vulnerability is expressed, but are
actually different aspects of the same mechanism that increases risk for revictimization:
psychological vulnerability. Increased numbers of sexual partners and alcohol or substance
use in social settings may similarly be different aspects of the second mechanism: increased
risk through contact with perpetrators. These variables may not consistently predict
revictimization if they are examined separately or in isolation (i.e., alcohol abuse or PTSD,
alcohol use or sexual behavior patterns), rather than as the concept of psychological
vulnerability. Given this, we propose a shift from examining individual types of psycho-
logical distress to a focus on the function or outcome of such problems: increased contact with
potential perpetrators and psychological vulnerability acted upon by perpetrators. Such
mechanisms may be best examined as a composite of several other individual factors.
It is necessary to assess not only the individual contribution of each risk factor, but also
the importance of a composite variable that reflects the functional aspects of these factors
that increase risk and vulnerability. This composite variable may be comprised of an
accumulation of different types of risk (e.g., engaging in high risk sexual behavior and
abusing alcohol), or may be comprised of an severity index of problems, with more severe
problems creating risk regardless of the type of problem (e.g., engaging in high risk sexual
behavior is sufficient to increase risk by itself if such behavior reaches a certain threshold).
Assessing increased risk and psychological vulnerability is important because it is very
likely that this risk and vulnerability, rather than the psychological problems from which
these mechanisms are derived, are the essential factors with regard to increased likelihood of
revictimization.
While not an attempt to explain revictimization, one study (Koss & Dinero, 1989) utilized
this approach to examine risk for sexual victimization among college women. Risk was
operationalized according to three vulnerability-enhancing mechanisms: vulnerability-cre-
ating traumatic experiences (e.g., family violence, family instability, CSA), social–psycho-
logical vulnerability (e.g., sexual attitudes, rape myth acceptance), and situational
vulnerability (e.g., alcohol use, sexual activity). Although these three mechanisms failed to
predict victimization (only vulnerability-creating experiences such as CSA appeared import-
ant in this model), this may still be a valuable approach. These mechanisms may have been
T.L. Messman-Moore, P.J. Long / Clinical Psychology Review 23 (2003) 537–571 563

unable to predict victimization simply because the wrong risk factors were selected for
inclusion.
Future attempts to quantify psychological vulnerability as a composite variable may
benefit from an ‘‘in depth case study approach,’’ utilizing qualitative analysis to identify
salient risk factors. A qualitative examination could focus on the presence and intensity of
different factors, identify common patterns or combinations of factors, and consider the
context of victimization in relation to revictimization. Qualitative analyses can also examine
the relative importance or frequency of many ‘‘subclinical’’ problems as opposed to the
presence of a single ‘‘clinically significant’’ problem, as well as provide data for formulating
profiles of revictimized women, and future studies may determine whether certain patterns
emerge as more prevalent. Qualitative findings may ultimately impact which factors are the
focus of future investigations.
4. Conclusion
The negative long-term impact of childhood sexual abuse is irrefutable. Most mental
health professionals agree that such experiences are related to acute and chronic psycho-
logical (and physical) difficulties, and that such difficulties often continue into adulthood.
Those searching for an explanation of the CSA survivor’s increased vulnerability for later
victimization have sought answers in several realms, most recently focusing on the
psychological sequelae of CSA as a possible contributor to the increased vulnerability for
revictimization. However, although the focus of current empirical research intuitively ‘‘makes
sense,’’ the area continues to suffer from lack of a guiding theoretical model. What has
resulted is a disconnected literature. Although attention focused on this topic has grown
considerably in the past several years, little has been accomplished by way of identifying
overarching explanatory models.
We are beginning to discover important factors contributing to revictimization. The
research conducted so far has provided us with some limited information, but also with
clues for the direction of future research. The ecological framework provides an appropriate
setting for the study of revictimization, and future investigations should include a focus on the
microsystem level of this model, which emphasizes the interaction of attributes, behaviors,
and beliefs of the victim and the perpetrator. We must focus less on individual factors and
instead examine mechanisms that increase vulnerability and risk within the context of the
microsystem. In all studies of revictimization, we must recognize the importance of factors
besides the victim and her behavior. We hope that a general acceptance of an ecological
model will spur interest in factors outside the victim and her behavior, including the behavior
of the perpetrator and our society’s response to the sexual victimization of children and
women. However, we also must not shy away from the study of victims’ characteristics or
behaviors (which are targeted by perpetrators) for fear of blaming the victim. This, too, would
impede progress in the development of effective risk reduction programming and treatment
for survivors. Focusing on how abuse affects victims to make them more vulnerable does not
mean that we believe victims intentionally place themselves in dangerous situations.
T.L. Messman-Moore, P.J. Long / Clinical Psychology Review 23 (2003) 537–571564

Furthermore, while important, focusing on women’s behaviors and risk reduction program-
ming will only help some individual women some of the time (i.e., those who participated in
such programs, and then only under some sets of circumstances) to reduce their risk.
However, to truly reduce the incidence of sexual victimization for all women, global change
can only occur through prevention programming with men. Effective risk reduction
programming for women does not equal rape prevention.
Much of the current research seeking to explain revictimization focuses on the victim and
the psychological effects of CSA. The function of the psychological effects of CSA can be
described by two separate mechanisms at the microsystem level. The first mechanism—
exposure risk—includes factors that increase contact with potential perpetrators, such as
engaging in high-risk sexual behaviors, or using alcohol or other substances in situations
where perpetrators are likely to be present. The second mechanism increases vulnerability to
potential perpetrators because such factors increase the likelihood that a perpetrator will act
aggressively. PTSD, dissociation, alcohol use, risk recognition, or interpersonal difficulties
can all function to increase the likelihood that a perpetrator will view the victim as ‘‘an easy
target.’’ Although these two mechanisms are promising as potential explanations, we should
recognize that they are just two of many mechanisms underlying the process of revictimiza-
tion. Research on revictimization must also address the macrosystem and exosystem because
these systems encapsulate our society’s devalued view of women and children; such
devaluation may increase sexual aggression and the acceptability of violence towards women
and children. Research on macrosystem and exosystem factors might benefit from the
inclusion of theories such as routine activities theory (Finkelhor & Asdigian, 1996; Schwartz
& Pitts, 1995), and other ideas from disciplines such as victimology, sociology, and
criminology. For instance, according to routine activities theory, (Finkelhor & Asdigian,
1996) certain aspects of the victim, including victim vulnerability, increase risk because such
characteristics are ‘‘congruent’’ with the motives or needs of offenders. This idea seems
particularly relevant to the study of revictimization.
Conclusions of studies examining mediating and moderating factors in revictimization
are important to development of effective risk reduction programs. If future research
would utilize the ecological model to focus on the perpetrator as well as the victim,
information gleaned from such studies might contribute positively to the development of
effective prevention programs for men. Risk reduction programming may need to extend
programs designed for all women, to include components tailored to women with histories
of CSA. Programs for women with histories of victimization may benefit from focusing
on the victim’s personal attributes and skill deficits as well as focusing on reduction in the
psychological sequelae of CSA such as dissociative tendencies. Clinicians are in a unique
position to ameliorate the effects of, or even reduce the likelihood of, victimization. If
revictimization is related to vulnerability created by the psychological sequelae of previous
victimization experiences, mental health providers will be able to decrease risk for
revictimization if therapy successfully resolves such issues. Psychotherapy may decrease
vulnerability if the survivor’s psychological symptoms of PTSD or dissociation are
decreased or eliminated, if a survivor’s self-esteem improves, or if self-protective
behaviors are modeled and learned (for example, see Messman-Moore & Resick, 2002).
T.L. Messman-Moore, P.J. Long / Clinical Psychology Review 23 (2003) 537–571 565

Psychotherapy could also help survivors develop safer, more appropriate repertoires of
sexual behavior, to examine beliefs about interpersonal relationships, particularly intimate
relationships, and to examine the impact of interpersonal dynamics in relation to
revictimization.
Finally, scholars must recognize the impact of our work and accept responsibility for
where our questions, and the answers to those questions, lead us. Our theories of
revictimization will shape what we will find empirically. If we focus on the victim, we
will find within her and her behavior explanations for revictimization. However, we must
recognize the interpersonal context in which revictimization takes place, and choose to also
focus on the perpetrator and cultural factors within our society. The study of revictimiza-
tion should focus on the intersection between the victim and the perpetrator. We will never
fully understand revictimization while the microscope remains focused solely on the
victim.
Acknowledgements
This research was supported by a grant awarded to the first author from the College of
Arts and Sciences at Miami University. Earlier versions of this article were presented at the
7th International Family Violence Research Conference, July 2001, in Portsmouth, NH and
the 35th Annual Meeting of the Association for Advancement of Behavior Therapy,
November 2001, in Philadelphia, PA. The authors would like to thank Margaret
O’Dougherty Wright and Sarah Ullman for comments and suggestions on earlier versions
of this manuscript.
References
Arata, C. M. (1999). Sexual revictimization and PTSD: an exploratory study. Journal of Child Sexual Abuse, 8(1),
49–65.
Barlow, D. H. (2002). Anxiety and its disorders: the nature and treatment of anxiety and panic (2nd ed.). New
York: Guilford Press.
Berkowitz, A. (1992). College men as perpetrators of acquaintance rape and sexual assault: A review of recent
research. Journal of American College Health, 40(4), 175–181.
Bohn, D. K., & Holz, K. A. (1996). Sequelae of abuse: health effects of childhood sexual abuse, domestic
battering, and rape. Journal of Nurse–Midwifery, 41, 442–456.
Bonner, B., Walker, G., & Berliner, L. (1999). Children with sexual behavior problems: assessment and treatment.
Final Report, Grant No. 90-CA-1469.
Breitenbecher, K. H. (1999). The association between the perception of threat in a dating situation and sexual
victimization. Violence and Victims, 14 (2), 135–146.
Breitenbecher, K. H. (2001). Sexual revictimization among women: a review of the literature focusing on
empirical investigations. Aggression and Violent Behavior, 6 (4), 415–432.
Breitenbecher, K. H., & Gidycz, C. A. (1998). An empirical evaluation of a program designed to reduce the risk of
multiple sexual victimization. Journal of Interpersonal Violence, 13, 472–488.
Briere, J. (1992). Child abuse trauma: theory and treatment of the lasting effects. Newbury Park, CA: Sage.
T.L. Messman-Moore, P.J. Long / Clinical Psychology Review 23 (2003) 537–571566

Briere, J. (1996). Therapy for adults molested as children: beyond survival (2nd ed.). New York: Springer
Publishing.
Briere, J., & Runtz, M. A. (1987). Post sexual abuse trauma: data and implications for clinical practice. Journal of
Interpersonal Violence, 2, 367–379.
Briere, J., & Runtz, M. A. (1993). Childhood sexual abuse: long-term sequelae and implications for psychological
assessment. Journal of Interpersonal Violence, 8, 312–330.
Bronfenbrenner, U. (1977). Toward an experimental ecology of human development. American Psychologist, 32,
513–531.
Bronfenbrenner, U. (1979). The ecology of human development. Cambridge, MA: Harvard Univ. Press.
Browne, A., & Finkelhor, D. (1986). Impact of child sexual abuse: a review of the research. Psychological
Bulletin, 99, 66–77.
Bryer, J. B., Nelson, B. A., Miller, J. B., & Krol, P. A. (1987). Childhood sexual and physical abuse as factors in
adult psychiatric illness. American Journal of Psychiatry, 144, 1426–1430.
Burnam, M. A., Stein, J. A., Golding, J. M., Siegel, J. M., Sorenson, S. B., Forsythe, A. B., & Telles, C. A. (1988).
Sexual assault and mental disorders in a community population. Journal of Consulting and Clinical Psy-
chology, 56(6), 843–850.
Burt, M. R., & Katz, B. L. (1987). Dimensions of recovery from rape. Journal of Interpersonal Violence, 2,
57–81.
Chewning-Korpach, M. (1993). Sexual revictimization: a cautionary note. Eating Disorders, 1(3/4), 287–297.
Chu, J. A. (1992). The revictimization of adult women with histories of childhood abuse. Journal of Psycho-
therapy Practice and Research, 1, 259–269.
Classen, C., Field, N. P., Koopman, C., Nevill-Manning, K., & Spiegel, D. (2001). Interpersonal problems and
their relationship to sexual revictimization among women sexually abused in childhood. Journal of Inter-
personal Violence, 16 (6), 495–509.
Cloitre, M., Cohen, L. R., & Scarvalone, P. (2002). Understanding revictimization among childhood sexual abuse
survivors: An interpersonal schema approach. Journal of Cognitive Psychotherapy: An International Quar-
terly, 16 (1), 91–112.
Cloitre, M., Scarvalone, P., & Difede, J. (1997). Posttraumatic stress disorder, self- and interpersonal dysfunction
among sexually retraumatized women. Journal of Traumatic Stress, 10 (3), 437–452.
Cloitre, M., Tardiff, K., Marzuk, P. M., Leon, A. C., & Portera, L. (1996). Childhood abuse and subsequent sexual
assault among female inpatients. Journal of Traumatic Stress, 9 (3), 473–482.
Cole, P. M., & Putnam, F. W. (1992). Effect of incest on self and social functioning: a developmental psycho-
pathology perspective. Journal of Consulting and Clinical Psychology, 60 (2), 174–184.
Cue, K. L., George, W. H., & Norris, J. (1996). Women’s appraisals of sexual-assault risk in dating situations.
Psychology of Women Quarterly, 20 (4), 487–504.
DiLillo, D. (2001). Interpersonal functioning among women reporting a history of childhood sexual abuse:
empirical findings and methodological issues. Clinical Psychology Review, 21(4), 553–576.
DiLillo, D., & Long, P. J. (1999). Perceptions of couple functioning among female survivors of child sexual abuse.
Journal of Child Sexual Abuse, 7, 59–76.
Drauker, C. (1989). Cognitive adaptation of female incest survivors. Journal of Consulting and Clinical Psy-
chology, 57, 668–670.
Epstein, J. N., Saunders, B. E., Kilpatrick, D. G., & Resnick, H. S. (1998). PTSD as a mediator between childhood
rape and alcohol use in adult women. Child Abuse and Neglect, 22(3), 223–234.
Fehrenbach, T., & Long, P. J. (2001). Sexual functioning of college females following child sexual abuse. Manu-
script in preparation, Oklahoma State University.
Fergusson, D. M., Horwood, L. J., & Lynskey, M. T. (1997). Childhood sexual abuse, adolescent sexual behaviors
and sexual revictimization. Child Abuse and Neglect, 21(8), 789–802.
Finkelhor, D. (1979). Sexually victimized children. Jefferson, NC: McFarland & Company, Inc., Publishers.
Finkelhor, D., & Asdigian, N. L. (1996). Risk factors for youth victimization: beyond a lifestyles/routine activities
theory approach. Violence and Victims, 11(1), 3–19.
T.L. Messman-Moore, P.J. Long / Clinical Psychology Review 23 (2003) 537–571 567

Fiscella, K., Kitzman, H. J., Cole, R. E., Sidora, K. J., & Olds, D. (1998). Does child abuse predict adolescent
pregnancy? Pediatrics, 101(4), 620–664.
Follette, V. M. (1994). Acceptance and commitment in the treatment of incest survivors: a contextual approach. In
S. C. Hayes, N. S. Jacobson, V. M. Follette, & M. Dougher (Eds.), Acceptance and change: content and
context in psychotherapy (pp. 285–268). Reno, NV: Context Press.
Follette, V. M., Polusny, M. A., Bechtle, A. E., & Naugle, A. E. (1996). Cumulative trauma: the impact of child
sexual abuse, adult sexual assault, and spouse abuse. Journal of Traumatic Stress, 9, 25–35.
Frinter, M. P., & Rubinson, L. (1993). Acquaintance rape: the influence of alcohol, fraternity membership, and
sports team membership. Journal of Sex Education and Therapy, 19, 272–284.
Fromuth, M. E. (1986). The relationship of childhood sexual abuse with later psychological and sexual adjustment
in a sample of college women. Child Abuse and Neglect, 10, 5–15.
Gelinas, D. J. (1983). The persisting negative effects of incest. Psychiatry, 46, 312–332.
George, W. H., Cue, K. L., Lopez, P. A., Crowe, L. C., & Norris, J. (1995). Self-reported alcohol expectancies and
postdrinking sexual inferences about women. Journal of Applied Social Psychology, 25, 164–186.
Gibson, L. E., & Leitenberg, H. (2001). The impact of child sexual abuse and stigma on methods of coping with
sexual assault among undergraduate women. Child Abuse and Neglect, 25, 1343–1361.
Gidycz, C. A., Coble, C. N., Latham, L., & Layman, M. J. (1993). Sexual assault experience in adulthood and
prior victimization experiences: a prospective analysis. Psychology of Women Quarterly, 17, 151–168.
Gidycz, C. A., Hanson, K., & Layman, M. J. (1995). A prospective analysis of the relationships among sexual
assault experiences. Psychology of Women Quarterly, 19, 5–29.
Gold, S. R., Sinclair, B. B., & Balge, K. A. (1999). Risk of sexual revictimization: a theoretical model. Aggression
and Violent Behavior, 4 (4), 457–470.
Goodman, L. A., Koss, M.P, & Russo, N. F. (1993). Violence against women: physical and mental health effects.
Applied and Preventive Psychology, 2, 79–89.
Grauerholz, L. (2000). An ecological approach to understanding sexual revictimization: linking personal, inter-
personal, and sociocultural factors and processes. Child Maltreatment, 5 (1), 5–17.
Greene, D. M., & Navarro, R. L. (1998). Situation-specific assertiveness in the epidemiology of sexual victim-
ization among university women: a prospective path analysis. Psychology of Women Quarterly, 22, 589–604.
Hanson, K. R., & Gidycz, C. A. (1993). Evaluation of a sexual assault prevention program. Journal of Consulting
and Clinical Psychology, 6, 1046–1052.
Harrington, N. T., & Leitenberg, H. (1994). Relationship between alcohol consumption and victim behaviors
immediately preceding sexual aggression by an acquaintance. Violence and Victims, 9, 315–324.
Harter, S., Alexander, P. C., & Neimeyer, R. A. (1988). Long-term effects of incestuous child abuse in college
women: social adjustment, social cognition, and family characteristics. Journal of Consulting and Clinical
Psychology, 56, 5–8.
Heise, L. (1998). Violence against women: an integrated, ecological framework. Violence Against Women, 4,
262–290.
Himelein, M. J. (1995). Risk factors for sexual victimization in dating: a longitudinal study of college women.
Psychology of Women Quarterly, 19, 31–48.
Hunter, J. A. (1991). A comparison of the psychosocial maladjustment of adult males and females sexually abused
as children. Journal of Interpersonal Violence, 6, 205–217.
Jehu, D. (1988). Beyond sexual abuse: therapy with women who were childhood victims. New York: Wiley.
Kessler, B. L., & Bieschke, K. J. (1999). A retrospective analysis of shame, dissociation, and adult victimization in
survivors of childhood sexual abuse. Journal of Counseling Psychology, 46 (3), 335–341.
Kluft, R. P. (1990). Dissociation and subsequent vulnerability: a preliminary study. Dissociation, 3(3), 167–173.
Koss, M. P., & Dinero, T. E. (1989). Discriminant analysis of risk factors for sexual victimization among a
national sample of college women. Journal of Consulting and Clinical Psychology, 57 (2), 242–250.
Koss, M. P., & Gidycz, C. A. (1985). Sexual experiences survey: reliability and validity. Journal of Consulting
and Clinical Psychology, 53, 422–423.
Koss, M. P., Goodman, L. A., Browne, A., Fitzgerald, L. F., Ketia, G. P., & Russo, N. F. (1994). No safe haven:
T.L. Messman-Moore, P.J. Long / Clinical Psychology Review 23 (2003) 537–571568

male violence against women at home, at work, and in the community. Washington, DC: American Psycho-
logical Association.
Koss, M. P., & Harvey, M. R. (1991). The rape victim: clinical and community interventions (2nd ed.). Newbury
Park, CA: Sage Publications.
Koss, M. P., & Oros, C. J. (1982). Sexual experiences survey: a research instrument investigating sexual aggres-
sion and victimization. Journal of Consulting and Clinical Psychology, 50, 455–457.
Koss, M. P., & Woodruff, W. J. (1991). Emerging issues in women’s health. In J. J. Sweet, & R. H. Rozensky
(Eds.), Handbook of clinical psychology in medical settings (pp. 201–221). New York: Plenum Press.
Koverola, C., Proulx, J., Battle, P., & Hanna, C. (1996). Family functioning as predictors of distress in revicti-
mized sexual abuse survivors. Journal of Interpersonal Violence, 11, 263–280.
Krahe, B., Scheinberger-Olwig, R., Waizenhofer, E., & Kolpin, S. (1999). Childhood sexual abuse and revictim-
ization in adolescence. Child Abuse and Neglect, 23 (4), 383–394.
Marx, B. P., Calhoun, K. S., Wilson, A. E., & Meyerson, L. A. (2001). Sexual revictimization prevention: an
outcome evaluation. Journal of Consulting and Clinical Psychology, 69 (1), 25–32.
Marx, B. P., Van Wie, V., & Gross, A. M. (1996). Date rape risk factors: a review and methodological critique of
the literature. Aggression and Violent Behavior, 1, 27–45.
Mayall, A., & Gold, S. R. (1995). Definitional issues and mediating variables in the sexual revictimization of
women sexually abused as children. Journal of Interpersonal Violence, 10 (1), 26–42.
Meadows, E. A., Jaycox, L. H., Orsillo, S. M., & Foa, E. B. (1997, November). The impact of assault on risk
recognition in ambiguous situations. Presented at the 31st annual meeting of the Association for Advancement
of Behavior Therapy, Miami Beach, FL.
Meadows, E. A., Jaycox, L. H., Stafford, J., Hembree, E. A., & Foa, E. B. (1995, November). Recognition of risk
in revictimized women. Presented at the 29th annual meeting of the Association for Advancement of Behavior
Therapy, Washington, DC.
Merrill, L. L., Newell, C. E., Thomsen, C. J., Gold, S. R., Milner, J. S., Koss, M. P., & Rosswork, S. G. (1999).
Childhood abuse and sexual revictimization in a female Navy recruit sample. Journal of Traumatic Stress, 12
(2), 211–225.
Messman, T. L., & Long, P. J. (1996). Child sexual abuse and its relationship to revictimization in adult women: a
review. Clinical Psychology Review, 16 (5), 397–420.
Messman-Moore, T. L., & Long, P. J. (2000). Child sexual abuse and revictimization in the form of adult sexual
abuse, adult physical abuse, and adult psychological maltreatment. Journal of Interpersonal Violence, 15 (5),
489–502.
Messman-Moore, T. L., & Long, P. J. (2002). Alcohol and substance use disorders as predictors of child to adult
sexual revictimization in a sample of community women. Violence and Victims, 17 (3), 319–340.
Messman-Moore, T. L., Long, P. J., & Siegfried, N. J. (2000). The revictimization of child sexual abuse survivors:
an examination of the adjustment of college women with child sexual abuse, adult sexual assault, and adult
physical abuse. Child Maltreatment: Journal of the American Professional Society on the Abuse of Children, 5
(1), 18–27.
Messman-Moore, T. L., & Resick, P. A. (2002). Brief treatment of complicated PTSD and peritraumatic responses
in a client with repeated sexual victimization. Cognitive and Behavioral Practice, 9 (2), 89–99.
Miller, B. C., Monson, B. H., & Norton, M. C. (1995). The effects of forced sexual intercourse on white female
adolescents. Child Abuse and Neglect, 19 (10), 1289–1303.
Muehlenhard, C. L., & Linton, M. A. (1987). Date rape and sexual aggression in dating situations: incidence and
risk factors. Journal of Counseling Psychology, 34, 186–196.
Mullen, P. E., Martin, J. L., Anderson, J. C., Romans, S. E., & Herbison, G. P. (1996). The long-term impact of the
physical, emotional, and sexual abuse of children: a community study. Child Abuse and Neglect, 20, 7–21.
Nishith, P., Bazile, A., Clum, G. C., Messman-Moore, T., & Resick, P. A. (2001, November). Alcohol expectancies
in treatment-seeking female rape victims with a history of childhood sexual abuse. In T. Messman-Moore
(Chair), Risk for sexual revictimization: examination of cognitive and behavioral factors. Symposium conduc-
ted at the 35th annual meeting of the Association for the Advancement of Behavior Therapy, Philadelphia, PA.
T.L. Messman-Moore, P.J. Long / Clinical Psychology Review 23 (2003) 537–571 569

Norris, J., & Cubbins, L. A. (1992). Dating, drinking, and rape: effects of victim’s and assailant’s alcohol
consumption on judgments of their behavior and traits. Psychology of Women Quarterly, 16, 179–191.
Nurius, P. S. (2000). Risk perception for acquaintance sexual aggression: a social-cognitive perspective. Aggres-
sion and Violent Behavior, 5 (1), 63–78.
Nurius, P. S., & Norris, J. (1996). A cognitive ecological model of women’s response to male sexual coercion in
dating. Journal of Personality and Human Sexuality, 8 (1/2), 117–139.
Orr, D. P., & Downs, M. C. (1985). Self-concept of adolescent sexual abuse victims. Journal of Youth and
Adolescence, 14 (5), 401–410.
Polusny, M. A., & Follette, V. M. (1995). Long-term correlates of child sexual abuse: theory and review of the
empirical literature. Applied and Preventive Psychology, 4, 148–166.
Resick, P. A. (1987). Reactions of female and male victims of rape and robbery (Final Report, NIJ Grant No.
MH37296). Washington, DC: National Institute of Justice.
Resick, P. A. (1993). The psychological impact of rape. Journal of Interpersonal Violence, 8 (2), 223–255.
Roodman, A. A., & Clum, G. A. (2001). Revictimization rates and method variance: a meta-analysis. Clinical
Psychology Review, 21 (2), 183–204.
Russell, D. (1984). Sexual exploitation: rape, child sexual abuse, and sexual harassment. Beverly Hills, CA:
Sage.
Sandberg, D. A., Matorin, A. I., & Lynn, S. J. (1999). Dissociation, posttraumatic symptomatology, and sexual
revictimization: a prospective examination of mediator and moderator effects. Journal of Traumatic Stress,
12 (1), 127–138.
Saunders, B. E., Villeponteaux, L. A., Lipovsky, J. A., Kilpatrick, D. G., & Veronen, L. J. (1992). Child sexual
assault as a risk factor for mental health disorders among women: a community sample. Journal of Inter-
personal Violence, 7, 189–204.
Schaaf, K. K., & McCanne, T. R. (1998). Relationship of childhood sexual, physical, and combined sexual and
physical abuse to adult victimization and posttraumatic stress disorder. Child Abuse and Neglect, 22 (11),
1119–1133.
Schwartz, M. D., & Pitts, V. L. (1995). Exploring a feminist routine activities approach to explaining sexual
assault. Justice Quarterly, 12 (1), 9–31.
Selzer, M. L. (1971). The Michigan alcoholism screening test: the quest for a new diagnostic instrument.
American Journal of Psychiatry, 127, 1653–1658.
Shields, N. M., & Hanneke, C. R. (1988). Multiple sexual victimization: the case of incest and marital rape. In
G. T. Hotaling, D. Finkelhor, J. T. Kirkpatrick, & M. A. Straus (Eds.), Family abuse and its consequences:
new directions in research (pp. 255–269). Newbury Park, CA: Sage Publications.
Siegel, J. A., & Williams, L. M. (2001). Risk factors for sexual victimization of women: results from a prospective
study. Manuscript under review.
Silverman, A. B., Reinherz, H. Z., & Giaconia, R. M. (1996). The long-term sequelae of child and adolescent
abuse: a longitudinal study. Child Abuse and Neglect, 20, 709–723.
Stock, J. L., Bell, M. A., Boyer, D. K., & Connell, F. A. (1997). Adolescent pregnancy and sexual risk-taking
among sexually abused girls. Family Planning Perspectives, 29 (5), 200–203.
Testa, M., & Parks, K. A. (1996). The role of women’s alcohol consumption in sexual victimization. Aggression
and Violent Behavior, 1, 217–234.
Trickett, P. K., & Putnam, F. W. (1993). Impact of child sexual abuse on females: toward a developmental,
psychobiological integration. Psychological Science, 4, 81–87.
Urquiza, A. J., & Goodlin-Jones, B. L. (1994). Child sexual abuse and adult revictimization with women of color.
Violence and Victims, 9, 223–232.
van der Kolk, B. A. (1989). The compulsion to repeat the trauma: re-enactment, revictimization, and masochism.
Psychiatric Clinics of North America, 12, 389–411.
West, C. M., Williams, L. M., & Siegel, J. A. (2000). Adult sexual revictimization among black women sexually
abused in childhood: a prospective examination of serious consequences of abuse. Child Maltreatment, 5(1),
49–57.
T.L. Messman-Moore, P.J. Long / Clinical Psychology Review 23 (2003) 537–571570

Wilsnack, S. C., Vogeltanz, N. D., Klassen, A. D., & Harris, T. R. (1997). Childhood sexual abuse and women’s
substance abuse: national survey findings. Journal of Studies on Alcohol, 58, 264–271.
Wilson, A. E., Calhoun, K. S., & Bernat, J. A. (1999). Risk recognition and trauma-related symptoms among
sexually revictimized women. Journal of Consulting and Clinical Psychology, 67 (5), 705–710.
Wind, T. W., & Silvern, L. (1992). Type and extent of child abuse as predictors of adult functioning. Journal of
Family violence, 7 (4), 261–281.
Wyatt, G. E. (1985). The sexual abuse of Afro-American and White-American women in childhood. Child Abuse
& Neglect, 9 (4), 507–519.
Wyatt, G. E., Guthrie, D., & Notgrass, C. M. (1992). Differential effects of women’s child sexual abuse and
subsequent sexual revictimization. Journal of Consulting and Clinical Psychology, 60, 167–173.
Wyatt, G. E., Lawrence, J., Vodounon, A., & Mickey, M. R. (1992). The Wyatt Sex History Questionnaire: a
structured interview for female sexual history taking. Journal of Child Sexual Abuse, 1(4), 51–68.
Wyatt, G. E., Notgrass, C. M., & Gordon, G. (1995). The effects of African American women’s sexual revictim-
ization: strategies for prevention. In C. F. Swift (Ed.), Sexual assault and abuse: sociocultural context of
prevention (pp. 111–134). New York: Haworth Press.
T.L. Messman-Moore, P.J. Long / Clinical Psychology Review 23 (2003) 537–571 571




















