The relationship of preoperative distress to endocrine and subjective responses to surgery: Support...
15
Journal of Behavioral Medicine, Vol. 11, No. 6, 1988 The Relationship of Preoperative Distress to Endocrine and Subjective Responses to Surgery: Support for Janis' Theory P. Salmon, ~ S. Pearce, I C. C. T. Smith, 2 A. Heys, 3 A. Manyande, ~ N. Peters, 4 and J. Rashid 4 Accepted for publieation." November 21, 1988 To test Janis" theory that preoperative worry can improve postoperative recov- ery, endocrine and subjective responses were measured in 2 7patients under- going major abdominal surgery which entailed threat to their health or longevity. Questionnaires to assess emotional and somatic state were com- pleted preoperatively and for 7 days postoperatively. Plasma cortisol, noradrenaline, adrenaline, and glucose were measured pre-, per-, and postoperatively. Preoperatively, noradrenaline correlated positively with pain and distress, and adrenaline negatively. Postoperatively, endocrine levels and distress were not clearly related. Nevertheless, preoperative pain negatively correlated with postoperative adrenaline and cortisol levels. This, and the negative correlation between preoperative distress and postoperative pain are consistent with Janis" theory. In addition, we found that the longer patients waited on the day of surgery, the greater were the cortisol, noradrenaline, and glucose responses. KEY WORDS: surgery; worry; anxiety; cortisol; noradrenaline; adrenaline; glucose. ~Department of Psychology, University College London, Gower Street, London, WC1E6BT, U.K. 2Department of Medicine, Rayne Institute, University College London, London, U.K. 3Department of Chemical Pathology, University College Hospital, Gower Street, London, U.K. 4Department of Anaesthetics, St. Mark's Hospital, City Road, London, U.K. 599 0160-7715/88/1200-0599506.00/0 1988 PlenumPublishing Corporation
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of The relationship of preoperative distress to endocrine and subjective responses to surgery: Support...
Journal o f Behavioral Medicine, Vol. 11, No. 6, 1988
The Relationship of Preoperative Distress to Endocrine and Subjective Responses to Surgery: Support for Janis' Theory
P. Sa lmon , ~ S. Pearce, I C. C. T. Smith, 2 A . Heys , 3 A . Manyande , ~ N. Peters, 4 and J. Rashid 4
Accepted for publieation." November 21, 1988
To test Janis" theory that preoperative worry can improve postoperative recov- ery, endocrine and subjective responses were measured in 2 7patients under- going major abdominal surgery which entailed threat to their health or longevity. Questionnaires to assess emotional and somatic state were com- pleted preoperatively and for 7 days postoperatively. Plasma cortisol, noradrenaline, adrenaline, and glucose were measured pre-, per-, and postoperatively. Preoperatively, noradrenaline correlated positively with pain and distress, and adrenaline negatively. Postoperatively, endocrine levels and distress were not clearly related. Nevertheless, preoperative pain negatively correlated with postoperative adrenaline and cortisol levels. This, and the negative correlation between preoperative distress and postoperative pain are consistent with Janis" theory. In addition, we found that the longer patients waited on the day of surgery, the greater were the cortisol, noradrenaline, and glucose responses.
KEY WORDS: surgery; worry; anxiety; cortisol; noradrenaline; adrenaline; glucose.
~Department of Psychology, University College London, Gower Street, London, WC1E6BT, U.K.
2Department of Medicine, Rayne Institute, University College London, London, U.K. 3Department of Chemical Pathology, University College Hospital, Gower Street, London, U.K. 4Department of Anaesthetics, St. Mark's Hospital, City Road, London, U.K.
599
0160-7715/88/1200-0599506.00/0 �9 1988 Plenum Publishing Corporation
600 Salmon et aL
INTRODUCTION
Although much evidence supports the claim that surgical patients' emo- tional state can influence their recovery from surgery, serious doubt remains about both the nature and the extent of this influence.
First, it is unclear whether certain aspects of preoperative emotional distress or arousal can promote recovery, as Janis (1958) proposed, or whether the effects are always harmful, as most subsequent evidence seems to sug- gest. Janis had argued that recovery was facilitated by an activity which he termed the "work of worry." An important limitation of many subsequent studies is that preoperative measures of anxiety have been regarded as the most appropriate indices of the work of worry. Nevertheless, in one report in which patients' preoperative anxiety predicted increasing postoperative pain and distress, preoperative feelings of "arousal" [measured by the Stress- Arousal Checklist (Mackay et al., 1978)] predicted the opposite (Ray and Fitzgibbon, 1981). Therefore while standard indices of anxiety may not reflect "worry" adequately, other measures-such as arousal -may be better indi- cators. There is a further reason why Janis' (1958) proposal is not necessari- ly refuted by the subsequent negative results. His theory was based on a view of surgery asa major crisis for patients; such traumas needed to be "worked through" in advance so as to minimize their impact. It is known that coping strategies differ between patients facing threatening and those facing non- threatening surgery (Feifel et al., 1987). Nevertheless, psychological research on postoperative recovery has involved relatively minor surgery and, hence, has not generally investigated patients whose health or lives are seriously threa- tened. More convincing benefits of preoperative emotional distress or arousal might be seen in such patients.
Second, another major area of doubt concerns the importance of emo- tional influences on recovery. Research, from Janis' onward, has concen- trated on patients' emotional state after surgery. Unfortunately, when other indices are recorded they often bear little relationship with emotional state, either pre- or postoperatively (Wolfer and Davis, 1970; Johnston and Car- penter, 1980; Wallace, 1986). Of course, there are reports that patients who were least anxious preoperatively or who had received special psychological preparation subsequently requested the least analgesic medication or were discharged from hospital the soonest (e.g., Wells et al., 1986). But such ef- fects may not necessarily benefit the patient's recovery. Moreover, these in- dices are open to so many extraneous influences that they cannot be regarded as direct indicators of patients' state (Johnston, 1978). The solution which we pursue in the present study is to measure more fundamental variables which might influence physical recovery and which themselves might be in- fluenced by emotional state.

Preop Distress and Responses to Surgery 601
One possible set of intervening variables is the endocrine responses to surgery. It has been argued that certain of these may slow down recovery (Ellis and Humphrey, 1982; Kehlet, 1984; Hall, 1985). The cortisol and catecholamine responses are of particular interest in view of these hormones' sensitivity to psychological factors (see Cox and Cox, 1985; Frankenhaues- er, 1980). It has been suggested that elevated circulating cortisol levels might impair immune function after surgery (Walton, 1978; Hole, 1984). The catecholamines, adrenaline and noradrenaline, are catabolic, contributing to muscle breakdown (see Kaufman, 1981) and have been implicated in the syndrome of "postoperative fatigue" (Rose and King, 1978). There is already suggestive evidence that levels of these hormones after surgery can be in- fluenced by psychological aspects of patients' care. Thus, increased levels of adrenaline (Wilson, 1981) or cortisol (Salmon et al., 1986) have been described in patients who had received preoperative preparation designed to reduce distress. In an earlier study, cortisol levels immediately postopera- tively correlated with a preoperative measure of anxiety, but the increase in steroid levels during the first 45 min of surgery correlated negatively (although only at p < .1) with preoperative interviewer ratings of "discomfort- involvement" made by one of two raters (Bursten and Russ, 1965).
In the present study, therefore, we measured patients' subjective phys- ical state after major surgery for serious disorders, which entailed threat to their physical well-being or longevity. Cortisol and catecholamine responses were measured, and emotional state assessed pre- and postoperatively so that we could test whether aspects of preoperative state would be associated, postoperatively, with a better physical state and a reduced endocrine response. We also measured circulating glucose, which has sometimes been used as an index of the stress response to surgery (e.g., Child and Kaufman, 1985).
METHOD
Patients
The patients studied were aged 18-77 years (mean, 42 years), were sched- uled for major abdominal or abdominal-perineal surgery at a specialist hospi- tal, and had been free of steroidal medication for at least 6 months. Of 30 patients recruited, 3 withdrew after surgery, saying that the questionnaires were too onerous or that they felt too unwell. Data were therefore analyzed for 27 patients: 9 male and 18 female. The main types of surgery were colec- tomy, proctocolectomy, colostomy, and ileostomy. The main disorders were colitis and cancer of the rectum. Surgery began between 8:15 AM and 3:30 PM.
602 Salmon et al.
Patients were routinely given benzodiazepine sedation on the evening before surgery. Anesthesia then followed standard procedures. Premedica- tion was by papaveretum and hyoscine or by pethidine and atropine; three patients received further opiate (fentanyl) during surgery. Anaesthesia was induced by thiopentone and maintained by N202/O2; halothane or isoflu- rane was administered as necessary. Endotrachial intubation was facilitated by suxamethonium; atracurium or acuronium was infused during surgery according to monitoring of neuromuscular function by a nerve stimulator. All patients received broad-spectrum antibiotics (metronidazole or gentamy- cin). For 24-48 hr postoperatively, continuous intravenous analgesia was provided by papaveretum, and antiemetics (metochlopramide or prochlor- perazine) were given routinely. Subsequently paracetamol or distalgesic was administered as required.
Patients were approached on the afternoon of the day of admission, which was either 1 day before surgery (for operations on Tuesday) or 3 days before (for those on Monday). They signed consent to take part in an inves- tigation of "how quickly patients get over the effects of surgery and anaesthesia."
Measurements
At the first meeting with the investigator (on the afternoon of admis- sion), the patients completed the first of eight identical sets of questionnaires which measured aspects of emotional and physical state (see below). The re- maining sets were left with the patients for completion daily at 12 noon for the first 7 postoperative days.
Blood Samples. The first sample was drawn from a peripheral vein at the time of consent; subsequent samples, through a central venous line in- troduced after induction by either internal jugular or subclavian routes. The peroperative sample was taken 90 min after incision; the "recovery room" sample, immediately after the patient had been removed to the recovery room. Postoperative samples were drawn, as close as possible to 12:00 noon, on the first, second, and third postoperative days. In the first 12 patients, an additional sample was taken from peripheral veins on the seventh postoper- ative day. Within 20 min of being drawn into heparanized tubes, samples were centrifuged at <0~ and the plasma was stored at -70~ until assayed.
Assays. Cortisol concentrations were measured in duplicate by radi- oimmunoassay (Farmos Diagnostica). Glucose was measured by a glucose analyzer (Landon Scientific Ltd.) based on an oxidase enzyme hydrogen peroxide sensor. Catecholamines were determined by high-performance li- quid chromatography (HPLC) with electrochemical detection (Smith et al., 1985).
Preop Distress and Responses to Surgery 603
Questionnaires. These included the State version of the STAI (Spiel- berger et at., 1970), the Stress-Arousal Checklist (Mackay et al., 1978), and the Recovery Inventory (RI; Wolfer and Davis, 1970). Although the last of these is a broad index of subjective physical state, a number of more specific indicators were included. These were the Modified Somatic Perception Ques- tionnaire (MSPQ; Main, 1983) and two visual-analogue scales (10-era lines), anchored at "None at all" and "The most I can imagine," on which patients answered "How intense has your pain been overall?" (Pain-intensity) and "How much distress has the pain caused you?" (Pain-distress). A third ques- tion, "How well have you coped with the pain?" was answered inconsistent- ly and is ignored. Finally, the questions "How much time have you spent thinking about your health?" (Worry) and "How frightened have you been about your health?" (Fright) were answered on 5-point scales. Instructions for State-anxiety and the Stress-Arousal Checklist were to record feelings "at this moment." The remaining repeated questionnaires referred to "how you have felt since bedtime last night."
Surgery. Volumes of blood lost and fluids replaced and times of inci- sion and entering the recovery room were noted from the routine records.
Statistical Methods
The biochemical indices were subject to log transformation to normal- ize their distributions. Relationships between measures were assessed by product-moment correlations; coefficients reaching significance at p < .05 are cited. Where isolated data were missing, degrees of freedom were cor- respondingly reduced for significance tests. Changes over time were assessed by repeated-measures analysis of variance, followed by post hoc t tests.
RESULTS
Biochemical Measures
Day-to-Day Changes. Analyses of variance confirmed that each meas- ure responded significantly to surgery (max p value of F ratios < .001), but Fig. 1 shows that the responses differed. All rise from the preoperative base- line to 90 rain after incision (although the rise in adrenaline did not reach significance) and from these levels to those in the recovery room. Although glucose tended to continue rising until the following day, the remaining meas- ures had fallen significantly by this time. The further gradual decline in cor- tisol, noradrenaline, and glucose contrasted with a nonsignificant rise in adrenaline. These differing trends continued until postop day 7, although this cannot be confirmed statistically because of the reduced N on this day.

604 Salmon et al.
3" I ,"'~" ~ Z _C~176 (n mot/, ~
2. ,r
0"5.
C 0
r
r OJ w t - O
=-0"5- O 1 O -J 0"5]
0
' , , , I Noradrenatine (n moll1) J g \
r Adrenatine (n mo[/~)
~ 1 O . . " ~
0"5 Glucose (m rno[/t')
Pre-op. Op. Pos~-op. Fig. 1. Mean transformed concentrations preoperatively, in theatre, and in the recovery room (Op 1 and 2), and on postoperative days. A broken line indicates a change of time scale. The N on postop day 7 is reduced. Bars show SED.
Intercorrelations. Although cortisol and the catecholamines intercor- related in the recovery room (Table I), correlations at other times were few. The negative correlation between the two catecholamines preoperatively (Ta- ble I) reappeared on the third postoperative day (r = - .60). The only correla- tions of glucose were with noradrenaline preoperatively and cortisol in the recovery room (Table I).
No biochemical measure correlated with volume of blood lost or fluid replaced. In contrast, there were extensive correlations with how late in the

Preop Distress and Responses to Surgery
Table I. Intercorrelations (p < .05) Between Transformed Plasma Hormone Levels Preoperatively (Below Diagonal) and in the Recovery Room (Above Diagonal)
605
Cortisol Noradrenaline Adrenaline Glucose
Cortisol ~ .55 .48 .52 Noradrenaline .41 . Adrenaline Glucose .56
day surgery began. This predicted cortisol levels peroperatively (r = .39) and in recovery (r = .43), as well as on the first and third days postoperatively (r's = .40 and .61, respectively); noradrenaline levels on the first and second postoperative days (r's = .48 and .52, respectively); and glucose levels in the recovery room (r = .48).
Questionnaires
The Stress-Arousal Checklist yielded little of interest and has, there- fore, been ignored.
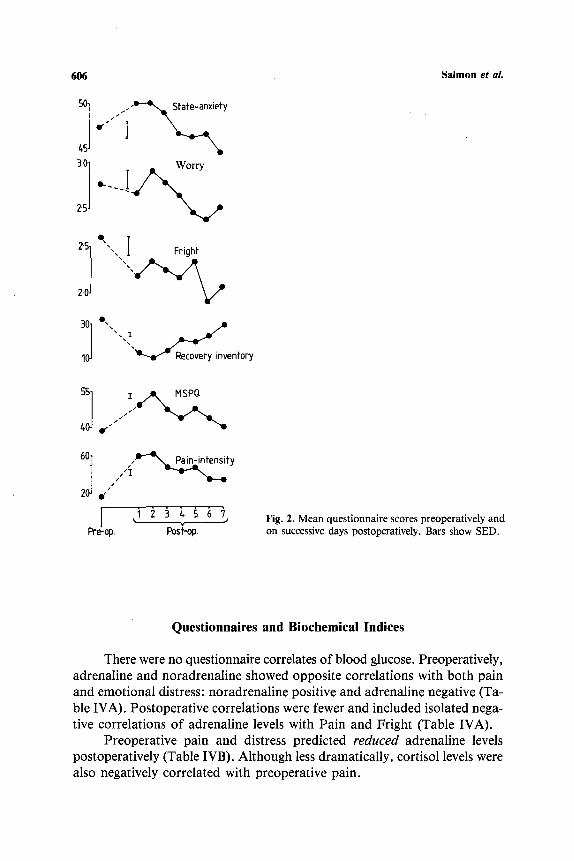
Day-to-Day Changes. Daily mean values are shown in Fig. 2. Pain- distress followed an identical time-course to Pain-intensity and is therefore not shown. All measures changed significantly (max p value of F ratios = .01). Those of distress were high preoperatively, declining to moderate lev- els over the postoperative week. The indicators of subjective physical state, in contrast, all deteriorated after surgery but fell within the week; Pain- intensity and Pain-distress at the end of the week remained significantly higher than preoperatively.
Interrelationships Between Questionnaires. These were calculated for the preoperative baseline and for selected postoperative days: 1, 3, and 7 (Table II). The indices of subjective physical state tended to intercorrelate throughout, as did Fright and Worry. Although subjective physical state was related to Fright and Worry preoperatively, they were subsequently uncor- related. State-anxiety was largely independent of all these measures.
Preoperative Predictors of Postoperative State. Postoperative State- anxiety, Recovery Inventory, and MSPQ showed few relationships with preoperative state apart from a tendency for the levels of each to correlate with its preoperative levels. Table IIIA shows significant negative correla- tions of preoperative State-Anxiety, Worry, and Fright with pain at the end of the postoperative week. This is despite Worry and Fright showing posi- tive correlations with pain preoperatively and on day 2 after surgery. In con- trast, patients who were most worried or frightened (Table IIIB) postoperatively had reported the poorest physical state and the most Worry and Fright preoperatively.
6O6
s . I I ir
3"01 _ Worry
25 ~
2s] "" ,,,,,,./~1 F,ight
20
60] ," ,~X.P_~i~iotensity~ -~'--"---, 20 e , /
Pre-op. Pos~-op.
Salmon et aL
Fig. 2. Mean questionnaire scores preoperatively and on successive days postoperatively. Bars show SED.
Questionnaires and Biochemical Indices
There were no questionnaire correlates of blood glucose. Preoperatively, adrenaline and noradrenaline showed opposite correlations with both pain and emotional distress: noradrenaline positive and adrenaline negative (Ta- ble IVA). Postoperative correlations were fewer and included isolated nega- tive correlations of adrenaline levels with Pain and Fright (Table IVA).
Preoperative pain and distress predicted reduced adrenaline levels postoperatively (Table IVB). Although less dramatically, cortisol levels were also negatively correlated with preoperative pain.

Tab
le
II.
Inte
rco
rrel
atio
ns
(p
< .0
5)
Bet
wee
n
Qu
esti
on
nai
re
Mea
sure
s P
reo
per
ativ
ely
an
d
on
P
ost
op
erat
ive
Day
s
RI
MS
PQ
P
ain
-in
ten
sity
P
ain
-dis
tres
s S
tate
-an
xie
ty
Tim
e-w
orr
yin
g
Pre
op
O
MS
PQ
Pai
n-i
nte
nsi
ty
- .7
4
.47
Pai
n-d
istr
ess
- .7
3
- .8
9
Sta
te-a
nx
iety
-
- -
Wo
rry
-
.48
-
.48
Fri
gh
t -
.34
.3
6
.56
Po
sto
p
day
1
MS
PQ
Pai
n-i
nte
nsi
ty
- .5
9
.76
Pai
n-d
istr
ess
- .5
7
.81
.8
7
Sta
te-a
nx
iety
-
- -
Wo
rry
-
- -
Fri
gh
t --
.4
7
-
Po
sto
p
day
3
MS
PQ
-
.53
Pai
n-i
nte
nsi
ty
- .4
8
.55
Pai
n-d
istr
ess
- .5
2
.63
.8
4
Sta
te-A
nx
iety
-
- -
Wo
rry
-
- -
Fri
gh
t -
- -
Po
sto
p
day
7
MS
PQ
-
.63
Pai
n-i
nte
nsi
ty
- .5
7
Pai
n-d
istr
ess
- .5
7
.86
Sta
te-a
nx
iety
-
- -
Wo
rry
-
- -
Fri
gh
t -
--
-
m m m
.39
.6
9
.53
.77
.69
= O

Tab
le I
II.
Cor
rela
tion
s (p
<
.05)
Bet
wee
n P
re-
and
Pos
tope
rati
ve S
tate
: C
orre
lati
ons
Am
ong
Pre
oper
ativ
e M
easu
res
Are
Rep
eate
d fr
om T
able
II
for
Com
pari
son
(m)
Pai
n-in
tens
ity
Pai
n-di
stre
ss
Pos
top
day
Pos
top
day
Pre
oper
ativ
e st
ate
Pre
op
1 2
3 4
5 6
7 P
reop
1
2 3
4 5
6 7
Rec
over
y in
vent
ory
.73
MS
PQ
.4
7 .5
2 P
ain-
inte
nsit
y .8
9 P
ain-
dist
ress
.8
9 .5
0 S
tate
-anx
iety
,4
9 -
.74
- .5
8 W
orry
.4
8 -
.58
- .6
8 .5
2 -
.62
Fri
ght
.56
- .5
1 .6
0 .5
5
B
Tim
e-w
orry
ing
Fri
ght
(B)
Pos
top
day
Pre
oper
ativ
e st
ate
Pre
op
1 2
3 4
5 6
7 P
reop
Pos
top
day
1 2
3 4
5 6
7
Rec
over
y In
vent
ory
-.4
8
-.5
3
-.4
6
-.4
6
-.4
8
.60
-.5
7
MSP
Q
Pai
n-in
tens
ity
.48
.50
.57
.49
.42
.64
Pai
n-di
stre
ss
.46
.60
.51
.54
.83
.68
Sta
te-a
nxie
ty
Wor
ry
.83
.62
.56
.55
.47
Fri
ght
.70
.57
.63
.59
,57
.45
- .3
5 .3
6 .5
6
.39
.70
-.42
-,
56
.41
.58
.57
,46
.53
.45
.67
.74
.59
.52
.49
.58
.54
,46
,54
Cg~
O
~t

Tab
le I
V.
Cor
rela
tion
s (p
<
.0
5) o
f T
ran
sfo
rmed
Pla
sma
Ho
rmo
ne
Lev
els
wit
h Q
uest
ionn
aire
Mea
sure
s M
ade
on t
he S
ame
Day
(C
oncu
rren
t) o
r P
reop
erat
ivel
y (P
redi
ctiv
e)
(A)
(B)
~d
gt.
Co
ncu
rren
t P
redi
ctiv
e
Po
sto
p d
ay
Rec
over
y P
ost
op
day
Pre
op
1
2 3
Pre
op
roo
m
1 2
3
0
Cor
tiso
l P
ain-
inte
nsit
y P
ain-
dist
ress
F
righ
t
Nor
adre
nali
ne
Pai
n-in
tens
ity
Pai
n-di
stre
ss
Sta
te-a
nxie
ty
Wor
ry
Fri
ght
Adr
enal
ine
Pai
n-in
tens
ity
Pai
n-di
stre
ss
Sta
te-a
nxie
ty
Wor
ry
Fri
ght
.44
.43
.55
.57
- .5
2
.89
- .4
8 --
.67
- .4
6
-.8
7
-.4
4
-.5
6
-.5
8
-,5
0
-.8
0
-.5
0
-.4
8
-.4
6
-,5
1
-.5
1
-.4
8
- .6
1

610 Salmon et ai.
DISCUSSION
Our results add to evidence that postoperative recovery cannot adequate- ly be described by a single index (Johnston, 1984). The two sets of measurements-questionnaires and biochemical-diverged substantially. Fur- thermore, the indices within each set did not cohere sufficently to suggest even a unitary endocrine or subjective response.
Only immediately postoperatively did the three endocrine measures closely correlate. They all peaked at this time, which has been reported be- fore (Nistrup Madsen et al., 1978; Child and Kaufman, 1985) and attributed to loss of the analgesic properties of the anaesthetic drugs (see Kaufman, 1981). The intercorrelation broke down by the first postoperative day; moreover, the preoperative levels showed no such interrelationship. Indeed, levels of adrenaline and noradrenaline were negatively associated preopera- tively and again by the third postoperative day. Divergence between these catecholamines is seen also in their relationships with the questionnaires (dis- cussed below). Glucose was a poor indicator of any of the hormones; preoper- ative levels were related to noradrenaline, and immediately postoperative levels to cortisol. It is likely that its levels are influenced by multiple endo- crine and other factors. This might also explain why, of all the biochemical measures, glucose levels alone showed no relationship with the questionnaires.
The questionnaires separated into three distinct sets: State-anxiety, those measuring subjective physical state, and the ratings of Worry and Fright. Although intercorrelating preoperatively, these dimensions were subsequently independent, which fits with previous reports that postoperative distress is unrelated to patients' physical state (Wolfer and Davis, 1970; Johnston and Carpenter, 1980). It is possible that the intercorrelation preoperatively, when physical trauma is relatively slight, arises because anxiety and worry worsen subjective physical state. Postoperatively, this effect would be overridden by the major physical trauma of surgery. (This would predict that, as physi- cal recovery proceeds beyond the period we investigated, the correlation should reappear.) Finally, the discordance between ratings of Worry and Fright, on the one hand, and State-anxiety, on the other, supports our sug- gestion that there may be different components to emotional state (cf. Bor- kovec et al., 1983).
There were marked differences between the hormones in the degree and nature of their relationship with subjective state. That cortisol levels on any day failed to correlate clearly with the questionnaires completed on that day is consistent with many previous studies which have found little or no corre- lation of cortisol with anxiety or other psychological states (Salmon et al., 1986; Brooks et al., 1986; Ho et al., 1988; cf. Bursten and Russ, 1965). The catecholamines were more sensitive to psychological state. Preoperatively
Preop Distress and Responses to Surgery 611
noradrenaline correlated with Pain, Fright, and Anxiety, and adrenaline with their absence. This pattern remained, although less consistent, postopera- tively. Notwithstanding the evidence that adrenaline and noradrenaline are associated with different emotional responses to stress (see Cox and Cox, 1985), the negative correlation of adrenaline with measures of distress is without precedent. It might, however, explain the apparent increase in adrena- line levels after the second postoperative day while Anxiety, Worry, and Fright, as well as the other biochemical indices, were declining.
In considering influences on recovery, the degree of independence be- tween the different sets of outcome indices requires us to examine each separately. From Janis' theory that preparatory worry can promote postoper- ative recovery, we predicted that preoperative distress or arousal would corre- late with postoperative somatic state, assessed subjectively in ratings of pain and symptoms or objectively in the endocrine responses. Our findings pro- vide some support for each prediction. Postoperative pain was least in pa- tients who had shown the most emotional distress preoperatively. Postoperative adrenaline and cortisol levels were highest in patients who had previously reported most pain and, in the case of adrenaline, emotional dis- tress. The involvement of preoperative pain is consistent with our sugges- tion above that it may be a reflection of patients' distress.
The effect on cortisol bears out an earlier finding (Bursten and Russ, 1965), but the reduction of postoperative adrenaline by preoperative discom- fort or distress has not previously been reported. Such an influence on adrena- line does, however, help to make sense of Wilson's (1981) report that preoperative relaxation training increased postoperative levels of adrenaline, and it is consistent with our own finding of negative correlations between adrenaline levels and emotional distress.
Our findings suggest one possible reason, in addition to our unusual choice of patients and measurements, why we have been able to identify benefits of preoperative distress and discomfort which have eluded many previous studies. We assessed our patients for longer postoperatively than has often been done. Effects became apparent only some days after surgery, when pain and emotional distress were already substantially reduced. It is possible that preoperative worry reduces the subjective stress of surgery, but only in the longer term. Indeed, this would be expected from the evidence that strategies involving denial of the stressor favor short-term coping, while those (such as worry) which entail acceptance promote long-term adapta- tion (Mullen and Suls, 1982).
Psychological processes seem unlikely, at first sight, to explain one fur- ther major influence on the endocrine responses. Cortisol, noradrenaline, and glucose responses were greater to operations which were performed later in the day. The effect on cortisol cannot be explained by diurnal variation
612 Salmon et al.
in its blood levels; the measurements on the day of surgery show the oppo- site trend to this (Weitzman et al . , 1971), and the samples on subsequent days were all drawn at noon, regardless of the time of surgery. Bursten and Russ (1965) reported a similar finding, that plasma cortisol levels after in- duction of anaesthesia (but before incision) were increased in patients whose operations began late in the day. They suggested a psychological explana- tion: that worry during this period of waiting increased the impact of sur- gery on cortisol levels. The implication is that this sort of worry is different in its effects from the state which t h e y - a n d w e - identified on preoperative days and which led to a r e d u c e d cortisol response.
Our results confirm the importance of discrete aspects of preoperative emotional state in predicting recovery. They also highlight the difficulty of identifying and describing those states within currently available theoretical frameworks. In particular, it is important to explore the different types of worry to which our results point: first, that measured preoperatively by the pain and other ratings, and that appeared to reduce stress responses; and second, the state of distress on the day of operation, which may be crucially different in its nature and biological effects.
ACKNOWLEDGMENTS
This work would not have been possible without the help of Dr. L. Kaufman and the active cooperation of the nursing staff at St. Mark's Hospi- tal. We are indebted to Mr. P. Hawley and Mr. J. Northover for allowing us to study their patients and to Professors Flynn and Prichard, who kindly provided facilities for the biochemical assays.
R E F E R E N C E S
Borkovec, T. D., Robinson, E., Pruzinsky, T., and DePree, J. A. (1983). Preliminary explora- tion of worry: Some characteristics and process. Behav. Res. Ther. 21: 9-16.
Brooks, J. E., Herbert, M., Walder, C. P., Selby, C., and Jeffcoate, W. J. (1986). Clin. En- docrinol. 24: 653-656.
Bursten, B., and Russ, J. J. (1965). Preoperative psychological state and corticosteroid levels of surgical patients. Psychosom. Med. 27: 309-316.
Child, C. S., and Kaufman, L. (1985). Effect of intrathecal diamorphine on the adrenocorti- cal, hyperglycaemic and cardiovascular responses to major colonic surgery. Br. J. Anaesth. 57: 389-393.
Cox, T., and Cox, S. (1985). The role of the adrenals in the psychophysiology of stress. In Karas, E. (ed.), Current Issues in Clinical Psychology, Plenum, New York, Vol. 2.
Ellis, F. R., and Humphrey, D. E. (1982). Endocrine and metabolic changes relating to anaesthesia and surgery. In Watkins, J., and Salo, M. (eds.), Trauma, Stress and Immunity, Buter- worth, London.
Preop Distress and Responses to Surgery 613
Feifel, H., Strack, S., and Nagy, V. T. (1987). Degree of life threat and differential use of cop- ing modes. J. Psychosom. Res. 31: 91-99.
Fell, D., Derbyshire, D. R., Maile, C. J. D., Larsson, I.-M., Ellis, R., Achola, K. J., and Smith, G. (1985). Measurement of plasma catecholamine concentrations. Br. J. Anaesth. 57:770- 774.
Frankenaueser, M. (1980). Psychobiological aspects of life stress. In Levine, S., and Ursin, H. (eds.), Nato Conference on Coping and Health, Academic Press, New York.
Hall, G. M. (1985). The anaesthetic modification of the endocrine and metabolic response to surgery. Ann. Roy. Coll. Surg. Eng. 67: 25-29.
Ho0 K. H., Hashish, I., Salmon, P., Freeman, R., Feinman, C., and Harvey, W. (1988). Reduction of post-operative swelling by a placebo effect. J. Psychosom. Med. 32: 197-205.
Hole, A. (1984). Per- and postoperative monocyte and lymphocyte functions: Effects of com- bined epidural and general anaesthesia. Acta Anaesthesiol. Scand. 28: 367-371.
Janis, I. L. (1958). Psychological Stress, Wiley, New York. Johnston, M. (1978). Assessing recovery from surgery. Paper presented at the Annual Confer-
ence of the British Psychological Society, York, U.K. Johnston, M. (1984). Dimensions of recovery from surgery. Int. Rev. Appl. Psychol. 33: 505-520. Johnston, M., and Carpenter, L. (1980). Relationship between pre-operative anxiety and post-
operative state. Psychol. Med. 10: 361-367. Kaufman, L. (1981). The endocrine response to surgery and anaesthesia. In Scurr, C. A., and
Feldman, S. (eds.), Scientific Foundations o f Anaesthesia, Heinneman, London. Kehlet, H. (1984). The stress response to anaesthesia and surgery: Release mechanisms and
modifying factors. Clin. Anaesthesiol. 2: 315-339. Mackay, C., Cox, T., Burrows, G., and Lazzerini, J. (1978). An inventory for the measure-
ment of self-reported stress and arousal. Br. J. Soc. Clin. Psychol. 17, 283-284. Main, C. (1983). The modified somatic perception questionnaire (MSPQ). J. Psychosom. Res.
27: 503-514. Mullen, B., and Suls, J. (1982). The effectiveness of attention and rejection as coping styles:
A meta-analysis of temporal differences. J. Psychosom. Res. 26: 43-49. Nistrup Madsen, S., Fog-Moiler, F., Christiansen, C., Vester-Andersen, T., and Engquist, A.
(1978). Cyclic AMP, adrenaline and noradrenaline in plasma during surgery. Br. J. Surg. 65: 191.
Ray, C., and Fitzgibbon, G. (1981). Stress arousal and coping with surgery. Psychol. Med. 11: 741-746.
Rose, E. A., and King, T. C. (1978). Understanding post-operative fatigue. Surg. Gynecol. Obstet. 147:97-101.
Salmon, P., Evans, R., and Humphrey, D. (1986). Anxiety and endocrine changes in surgical patients. Br. J. Clin. Psychol. 25: 135-141.
Smith, C. C. T., Curtis, L. D., Delamothe, A. P., Prichard, B. N. C., and Betteridge, D. J. (1985). The distribution of catecholamines between platelets and plasma in normal hu- man subjects. Clin. Sci. 69: 1-6.
Spielberger, C. D., Gorsuch, R. K. L., and Lushene, R. E. (1970). Manual for the State-Trait Anxiety Inventory, Consulting Psychologists' Press, Palo Alto, Calif.
Wallace, k. M. (1986). Pre-operative state anxiety as a mediator of psychological adjustment to and recovery from surgery. Br. J. Med. Psychol. 59: 253-261.
Wells, J. K., Howard, G. S., Nowlin, W. F. N., and Vargas, M. J. (1986). Presurgical anxiety and postsurgical pain and adjustment: Effects of a stress inoculation procedure. J. Consult. Clin. Psychol. 54: 831-835.
Weitzman, E. D., Fukushima, D. K., Nogeire, C., Roffwarg, H., Gallagher, T. F., and Hellman, L. (1971). Twenty-four hour pattern of the episodic secretion of cortisol in normal subjects. J. Clin. Endocrinol. Metab. 33: 14-22.
Wilson, H. F. (1981). Behavioral preparation for surgery: Benefit or harm? J. Behav. Med. 4: 79-102. Wolfer, J. A., and Davis, C. E. (1970). Assessment of surgical patients' pre-operative emotional
condition and postoperative recovery. Nursing Res. 19: 407-414.