The relationship between chronic fatigue and somatization syndrome: A general population survey
10
The relationship between chronic fatigue and somatization syndrome: A general population survey Alexandra Martin a, 4 , Trudie Chalder b , Winfried Rief a , Elmar Braehler c a Section for Clinical Psychology and Psychotherapy, Philipps University, Marburg, Germany b Academic Department of Psychological Medicine, Weston Education Center, King’s College London, Strand, London, United Kingdom c Medical Faculty, University of Leipzig, Leipzig, Germany Received 26 June 2006; received in revised form 14 May 2007; accepted 15 May 2007 Abstract Objective: The objective of this study was to assess the prevalence of chronic fatigue (CF) and its association with somatization syndrome [Somatization Syndrome Index (SSI) 4/6: z4 somatoform symptoms in men, 6 in women] in the general population. Methods: A representative sample of the German population (N=2412) completed a fatigue questionnaire and a screening instrument for current somatoform symptoms (Screening for Somatoform Symptoms 7). Results: The prevalence rate of CF was 6.1% (n =147). Females were affected significantly more often as compared with males (7% vs. 5.1%). The mean number of somatoform symptoms was higher in CF cases than in control subjects without CF (11 vs. 2; Pb.001). Seventy-two percent of the subjects with CF fulfilled the SSI4/6 criterion for somatization syndrome. Quality of life (EUROHIS-QOL and 8-item Short-Form Health Survey) and well-being (5-item WHO Well-Being Index) were markedly decreased in CF and SSI4/6. The results of regression analyses suggest that fatigue and somatization severity had a similar impact on quality of life. Conclusions: The results suggest that CF is relevant in the general population. Its substantial overlap with somatization syndrome supports the hypothesis that the two syndromes are only partially different manifestations of the same under- lying processes. D 2007 Elsevier Inc. All rights reserved. Keywords: Chronic fatigue; Epidemiology; Prevalence; Somatoform disorder; Somatization syndrome Introduction Chronic fatigue (CF) is characterized by enduring fatigue, tiredness, lack of energy, and weakness resulting in severe impairment in daily functioning. Prevalence rates of CF suggest that the syndrome is important especially in clinical settings [1–3] but also in the general population [4–9]. Chronic fatigue is not a specific illness, but it is occurring with a wide range of somatic conditions or mental disorders. There is still no commonly accepted definition of CF; generally, an explicit assumption is not made about the existence or nonexistence of medical conditions that could explain the fatigue. Some recent evidence suggested that it was not possible to identify an organic condition to explain the fatigue in most subjects with CF [10]. In this study, we assumed that CF is a syndrome defined as a set of symptoms indicating the existence of a problem. Chronic fatigue syndrome (CFS) is defined as unexplained fatigue lasting for 6 or more months [refer to the U.S. Centers for Disease Control and Prevention (CDC) [11] for further criteria]. It has been suggested that the CDC’s definition of CFS is too restrictive and that some classification criteria seem to be arbitrary [12]. Some evidence suggest that fatiguing 0022-3999/07/$ – see front matter D 2007 Elsevier Inc. All rights reserved. doi:10.1016/j.jpsychores.2007.05.007 4 Corresponding author. Section for Clinical Psychology and Psycho- therapy, Philipps University, Gutenbergstr. 18, D-35032 Marburg, Ger- many. Tel.: +49 6421 282 3656; fax: +49 6421 2828904. E-mail addresses: [email protected] (A. Martin)8 [email protected] (T. Chalder)8 [email protected] (W. Rief)8 [email protected] (E. Braehler). Journal of Psychosomatic Research 63 (2007) 147 – 156
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of The relationship between chronic fatigue and somatization syndrome: A general population survey

Journal of Psychosomatic Res
The relationship between chronic fatigue and somatization syndrome:
A general population survey
Alexandra Martina,4, Trudie Chalderb, Winfried Rief a, Elmar Braehlerc
aSection for Clinical Psychology and Psychotherapy, Philipps University, Marburg, GermanybAcademic Department of Psychological Medicine, Weston Education Center, King’s College London, Strand, London, United Kingdom
cMedical Faculty, University of Leipzig, Leipzig, Germany
Received 26 June 2006; received in revised form 14 May 2007; accepted 15 May 2007
Abstract
Objective: The objective of this study was to assess the
prevalence of chronic fatigue (CF) and its association with
somatization syndrome [Somatization Syndrome Index (SSI) 4/6:
z4 somatoform symptoms in men, 6 in women] in the general
population. Methods: A representative sample of the German
population (N=2412) completed a fatigue questionnaire and a
screening instrument for current somatoform symptoms (Screening
for Somatoform Symptoms 7). Results: The prevalence rate of
CF was 6.1% (n=147). Females were affected significantly more
often as compared with males (7% vs. 5.1%). The mean number
of somatoform symptoms was higher in CF cases than in
control subjects without CF (11 vs. 2; Pb.001). Seventy-two
0022-3999/07/$ – see front matter D 2007 Elsevier Inc. All rights reserved.
doi:10.1016/j.jpsychores.2007.05.007
4 Corresponding author. Section for Clinical Psychology and Psycho-
therapy, Philipps University, Gutenbergstr. 18, D-35032 Marburg, Ger-
many. Tel.: +49 6421 282 3656; fax: +49 6421 2828904.
E-mail addresses: [email protected] (A. Martin)8
[email protected] (T. Chalder)8 [email protected] (W. Rief)8
[email protected] (E. Braehler).
percent of the subjects with CF fulfilled the SSI4/6 criterion
for somatization syndrome. Quality of life (EUROHIS-QOL and
8-item Short-Form Health Survey) and well-being (5-item
WHO Well-Being Index) were markedly decreased in CF and
SSI4/6. The results of regression analyses suggest that fatigue
and somatization severity had a similar impact on quality of
life. Conclusions: The results suggest that CF is relevant in the
general population. Its substantial overlap with somatization
syndrome supports the hypothesis that the two syndromes
are only partially different manifestations of the same under-
lying processes.
D 2007 Elsevier Inc. All rights reserved.
Keywords: Chronic fatigue; Epidemiology; Prevalence; Somatoform disorder; Somatization syndrome
Introduction
Chronic fatigue (CF) is characterized by enduring
fatigue, tiredness, lack of energy, and weakness resulting
in severe impairment in daily functioning. Prevalence
rates of CF suggest that the syndrome is important
especially in clinical settings [1–3] but also in the general
population [4–9].
Chronic fatigue is not a specific illness, but it is occurring
with a wide range of somatic conditions or mental disorders.
There is still no commonly accepted definition of CF;
generally, an explicit assumption is not made about the
existence or nonexistence of medical conditions that could
explain the fatigue. Some recent evidence suggested that it
was not possible to identify an organic condition to explain
the fatigue in most subjects with CF [10]. In this study, we
assumed that CF is a syndrome defined as a set of symptoms
indicating the existence of a problem. Chronic fatigue
syndrome (CFS) is defined as unexplained fatigue lasting
for 6 or more months [refer to the U.S. Centers for Disease
Control and Prevention (CDC) [11] for further criteria]. It
has been suggested that the CDC’s definition of CFS is
too restrictive and that some classification criteria seem to
be arbitrary [12]. Some evidence suggest that fatiguing
earch 63 (2007) 147–156

Table 1
Description of the study sample collectively and separately for CF cases and control subjects
Study sample
(N=2412, 100%)
CF cases
(n=147, 6.1%)
Control subjects
(n=2265, 93.9%) Statistics
Sex [n (%)]
Male 1147 (47.5) 58 (39.5) 1087 (48.0) v2(1)=4.04
Female 1267 (52.5) 89 (60.5) 1178 (52.0)
Age [years, mean (S.D.)] 47.9 (18.2) 57.9 (17.4) 47.3 (19.0) t(2410)=�7.0444d=0.58 (95% CI=0.4–0.75)
Age group [years, n (%)]
b35 638 (26.5) 19 (12.9) 619 (27.3) v2(2)=45.444
35–64 1230 (51) 63 (42.9) 1167 (51.5)
N64 544 (22.5) 65 (44.2) 479 (21.1)
Family status [n (%)]
Single 590 (24.5) 21 (14.3) 569 (25.1) v2(2)=20.0444
Married/Living together 1243 (51.5) 70 (47.6) 1173 (51.8)
Separated/Divorced/Widowed 579 (24) 56 (23.1) 523 (38.1)
Education [n (%)]
Secondary school,b10 years 1127 (46.7) 86 (58.5) 1041 (46) v2(3)=12.144
Intermediate school leaving
certificate, b12 years
874 (36.3) 47 (32) 827 (36.5)
High school or higher 350 (14.5) 14 (9.5) 336 (14.8)
Still in school 61 (2.5) 0 (0.0) 61 (2.7)
Family income per month
[Euro, n (%)]
b750 105 (4.6) 13 (9.0) 92 (4.3) v2(3)=15.744
750–1249 515 (22.3) 44 (30.3) 471 (21.8)
1250–1999 901 (39.1) 53 (36.6) 848 (39.3)
z2000 784 (34) 35 (24.1) 749 (34.7)
Somatization syndrome [n (%)]
Fulfilled/Yes 392 (16.3) 106 (72.1) 286 (12.6) v2(1)=358.4444
95% CI=14.8%–17.7%
Somatoform symptom count
(SOMS-7) 0–53 [mean (S.D.)]
2.6 (5.1) 10.6 (8.0) 2.1 (4.4) t(151.9)=12.8444
d=1.35 (95% CI=1.2–1.5)
SOM [mean (S.D.)] 0.21 (0.31) 0.69 (0.27) 0.18 (0.45) t(152.7)=13.6444
d=1.37 (95% CI=1.2–1.6)
4 CF cases vs. control subjects, Pb.05.
44 CF cases vs. control subjects, Pb.01.
444 CF cases vs. control subjects, Pb.001.
A. Martin et al. / Journal of Psychosomatic Research 63 (2007) 147–156148
illnesses can be at best viewed on a continuum with CF
at the one end and CFS at the more severe end of the
spectrum [13,14].
Aside from these, CFS as a discrete nosological entity
has been questioned [15,16]. A number of studies have
shown that CFS often co-occurs with other medically
unexplained bodily syndromes (e.g., fibromyalgia, irritable
bowel syndrome, and multiple chemical sensitivity) [17].
There is also a body of evidence showing the associations
among CF as well as CFS and somatization disorder (SD) as
well as subthreshold somatization syndromes [18,19].
Somatization disorder, according to the Diagnostic and
Statistical Manual of Mental Disorders, Fourth Edition and
the International Statistical Classification of Diseases, 10th
Revision (ICD-10), is not defined by a specific target
symptom but is characterized by a history of multiple
disabling somatic symptoms that cannot be fully explained
by any medical factor. Somatization disorder is rarely found
in the community, and the diagnostic criteria have also been
considered to be too restrictive. Escobar et al. [20]
suggested the concept of an abridged SD—the Somatization
Syndrome Index (SSI4/6)—and showed that this syndrome
was associated with similar risk factors, service use patterns,
and disabilities as found in the full SD. The condition is
characterized by four medically unexplained symptoms in
men and six in women without the SD’s restrictions about
symptom distribution across body sites and long timeline
criteria. In research, especially in epidemiological studies,
this somatization concept is widely accepted [21].
Wessely et al. [15] argued that in addition to a substantial
overlap between functional somatic syndromes and case
definitions, there are also similarities in patient character-
istics and treatment approaches. Because the similarities in
functional syndromes outweigh the differences, it has been
suggested that they are different manifestations of the same
biomedical and psychosocial processes [15,16].
Current knowledge about CF is mainly derived from
treated populations and may be biased (e.g., by the
differential help-seeking behavior linked with sex and
socioeconomic status) [22,23]. The co-occurrence rates of
various medically unexplained syndromes may also be an
overestimation, particularly if assessed in clinical settings

A. Martin et al. / Journal of Psychosomatic Research 63 (2007) 147–156 149
[24]. To date, it is unclear as to how CF and somatization
syndrome overlap and as to what extent the two syndromes
have a differential effect on quality of life.
We therefore assessed CF in a representative general
population sample. We decided to investigate CF as a
broader category (without evaluation of possible organic
factors that might explain the fatigue) to preclude the
possible impact of too many restrictions made by the criteria
(such as in CFS). The first aim of the study was to assess the
point prevalence of CF and its sociodemographic character-
istics in the German general population. The second aim
was to examine the overlap of CF and somatization
syndrome SSI4/6 with respect to symptomatology. Third,
we aimed to examine the associations between CF and
somatization syndrome with various indicators of quality of
life because the latter factor can be considered to be an
important indicator of functioning.
Methods
Design and subjects
A cross-sectional survey of a random general population
sample of Germany was conducted based on face-to-face
contacts using questionnaires and with the assistance of an
independent demography consulting company (USUMA,
Berlin, Germany). The random selection was based on
multistage sampling with three stages (according to the
typical random selection procedure in national surveys in
Germany). First, 258 sample point regions were randomly
drawn from the last political election register, covering rural
and urban areas from all regions in Germany. The second
stage was a random selection of households using the
random route procedure (based on a starting address). The
third stage was a random selection of household respondents
with the Kish selection grid. The inclusion criterion was
being aged 14 years or older. Data collection took place
between September and October 2004.
The initial sample consisted of 4156 subjects, of whom
62.3% participated (n=2591). Reasons for dropout included
the following: three unsuccessful attempts to contact the
household or selected household member (12.6%); the
household or selected household member disagreed to
participate (23.6); and the household member was on a
holiday break or absent as a result of an illness (1.4%).
Some of the information could not be used because of
incomplete data collection during the interview (n=39,
0.9%) or self-report when completing the Fatigue Ques-
tionnaire (FQ; n=140, 5.5%). The final sample consisted of
2412 subjects (52.5% were females). The patients’ ages
ranged from 14 to 99 years (mean=47.9, S.D.=18.2);
approximately 52% were married (or living together with
a partner), 51% had 10 or more years of education (e.g.,
high school or college degree), and 27% were living in
households earning less than 1250 Euro per month (see
Table 1 for study sample characteristics). The sample had
the typical characteristics of the German population in terms
of sex, age, and level of education (see the 2004 population
report of the Federal Statistical Office of Germany, http://
www.destatis.de/themen/e/thm_bevoelk.htm: 51.4% were
females, 22% were older than 64 years, and 48.8% had
secondary school as their highest level).
All participants were visited personally, were informed
about the study procedures, and signed an informed consent
form (in minors, informed consent was obtained from the
parents). They were instructed that several rating scales
would follow, without informing them about the special
focus on CF and somatoform symptoms. Thereafter,
subjects completed the following self-rating scales:
– a demographic information sheet;
– the FQ to identify CF cases and noncases [25];
– a screening questionnaire on somatoform symptoms
[Screening for Somatoform Symptoms 7 (SOMS-7)]
[26] to assess somatization syndrome SSI4/6; and
– some rating scales to assess different aspects of
quality of life and well-being: EUROHIS-QOL [27],
8-item Short-Form Health Survey (SF-8) [28], and
5-item WHO Well-Being Index (WHO-5) [29].
Assessment instruments and case identification
The German version of the FQ presented by Chalder et al.
[25] was used. The FQ is a self-report questionnaire
inquiring about the various physical and mental fatigue
symptoms specifically related to CF. The FQ has been tested
in large community samples [8,22]. The internal consistency
of the German FQ was high (Cronbach’s a=.93), and the
factor structure of the original version was replicated [30].
The FQ consists of 11 items rated as less than usual, no
more than usual, more than usual, or much more than
usual—offering the option of binary (0 0 1 1) or Likert
(0 1 2 3) scoring. In the present study, we used the binary
scoring for CF case identification (score range=0–11)
according to Chalder et al. [25]: A score of 4 or higher
represents severe fatigue, whereas that of 4 or higher for 6 or
more months indicates caseness for CF. The FQ total score
(FQ-T) is the sum of the Likert-scored items (range=0–33)
and indicates severity of the fatigue symptoms.
The state version of the SOMS-7 [26,31] was used to
identify the number and severity of current somatoform
symptoms. It lists 53 bodily symptoms, covering all
somatoform symptoms mentioned in the Diagnostic and
Statistical Manual of Mental Disorders, Fourth Edition and
ICD-10 SD as well as somatoform autonomic dysfunction.
Subjects were asked to indicate the symptoms that were
present during the past 7 days and for which physicians had
not been able to find a clear organic cause. The intensity of
symptoms was Likert scaled from 0 (not at all) to 4 (very
strongly). The scale has high internal consistency (a=.92)and is valid in discriminating SD, somatization syndrome
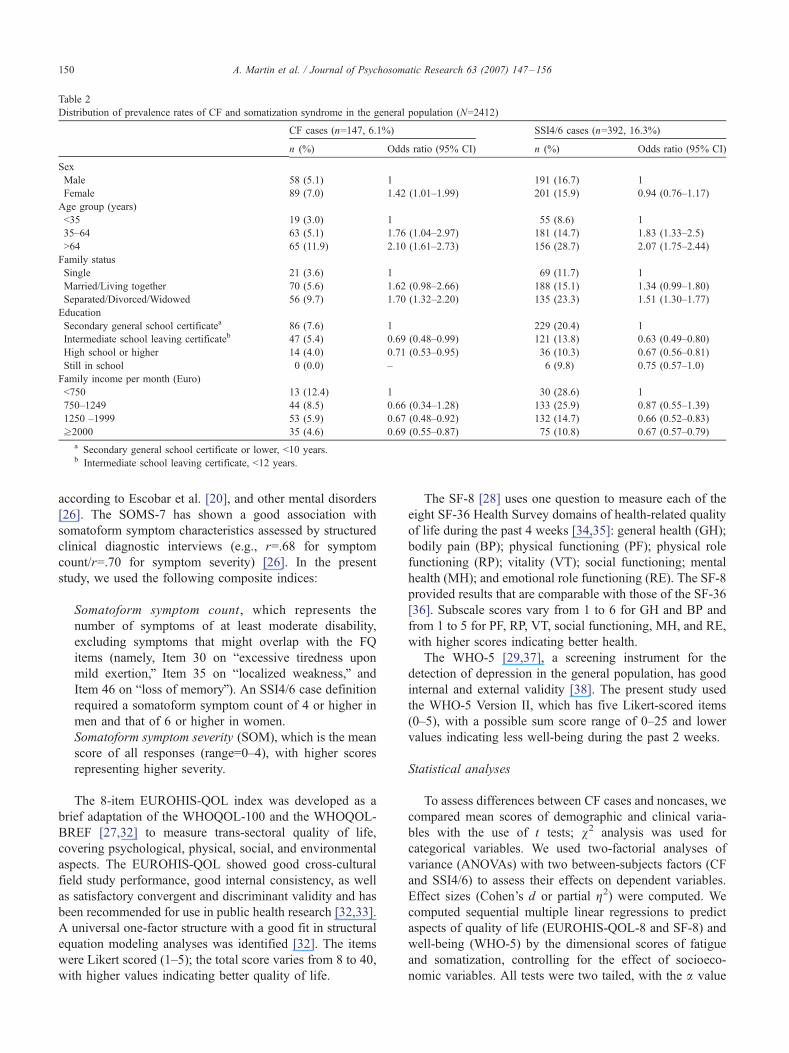
Table 2
Distribution of prevalence rates of CF and somatization syndrome in the general population (N=2412)
CF cases (n=147, 6.1%) SSI4/6 cases (n=392, 16.3%)
n (%) Odds ratio (95% CI) n (%) Odds ratio (95% CI)
Sex
Male 58 (5.1) 1 191 (16.7) 1
Female 89 (7.0) 1.42 (1.01–1.99) 201 (15.9) 0.94 (0.76–1.17)
Age group (years)
b35 19 (3.0) 1 55 (8.6) 1
35–64 63 (5.1) 1.76 (1.04–2.97) 181 (14.7) 1.83 (1.33–2.5)
N64 65 (11.9) 2.10 (1.61–2.73) 156 (28.7) 2.07 (1.75–2.44)
Family status
Single 21 (3.6) 1 69 (11.7) 1
Married/Living together 70 (5.6) 1.62 (0.98–2.66) 188 (15.1) 1.34 (0.99–1.80)
Separated/Divorced/Widowed 56 (9.7) 1.70 (1.32–2.20) 135 (23.3) 1.51 (1.30–1.77)
Education
Secondary general school certificatea 86 (7.6) 1 229 (20.4) 1
Intermediate school leaving certificateb 47 (5.4) 0.69 (0.48–0.99) 121 (13.8) 0.63 (0.49–0.80)
High school or higher 14 (4.0) 0.71 (0.53–0.95) 36 (10.3) 0.67 (0.56–0.81)
Still in school 0 (0.0) – 6 (9.8) 0.75 (0.57–1.0)
Family income per month (Euro)
b750 13 (12.4) 1 30 (28.6) 1
750–1249 44 (8.5) 0.66 (0.34–1.28) 133 (25.9) 0.87 (0.55–1.39)
1250 –1999 53 (5.9) 0.67 (0.48–0.92) 132 (14.7) 0.66 (0.52–0.83)
z2000 35 (4.6) 0.69 (0.55–0.87) 75 (10.8) 0.67 (0.57–0.79)
a Secondary general school certificate or lower, b10 years.b Intermediate school leaving certificate, b12 years.
A. Martin et al. / Journal of Psychosomatic Research 63 (2007) 147–156150
according to Escobar et al. [20], and other mental disorders
[26]. The SOMS-7 has shown a good association with
somatoform symptom characteristics assessed by structured
clinical diagnostic interviews (e.g., r=.68 for symptom
count/r=.70 for symptom severity) [26]. In the present
study, we used the following composite indices:
Somatoform symptom count, which represents the
number of symptoms of at least moderate disability,
excluding symptoms that might overlap with the FQ
items (namely, Item 30 on bexcessive tiredness upon
mild exertion,Q Item 35 on blocalized weakness,Q and
Item 46 on bloss of memoryQ). An SSI4/6 case definition
required a somatoform symptom count of 4 or higher in
men and that of 6 or higher in women.
Somatoform symptom severity (SOM), which is the mean
score of all responses (range=0–4), with higher scores
representing higher severity.
The 8-item EUROHIS-QOL index was developed as a
brief adaptation of the WHOQOL-100 and the WHOQOL-
BREF [27,32] to measure trans-sectoral quality of life,
covering psychological, physical, social, and environmental
aspects. The EUROHIS-QOL showed good cross-cultural
field study performance, good internal consistency, as well
as satisfactory convergent and discriminant validity and has
been recommended for use in public health research [32,33].
A universal one-factor structure with a good fit in structural
equation modeling analyses was identified [32]. The items
were Likert scored (1–5); the total score varies from 8 to 40,
with higher values indicating better quality of life.
The SF-8 [28] uses one question to measure each of the
eight SF-36 Health Survey domains of health-related quality
of life during the past 4 weeks [34,35]: general health (GH);
bodily pain (BP); physical functioning (PF); physical role
functioning (RP); vitality (VT); social functioning; mental
health (MH); and emotional role functioning (RE). The SF-8
provided results that are comparable with those of the SF-36
[36]. Subscale scores vary from 1 to 6 for GH and BP and
from 1 to 5 for PF, RP, VT, social functioning, MH, and RE,
with higher scores indicating better health.
The WHO-5 [29,37], a screening instrument for the
detection of depression in the general population, has good
internal and external validity [38]. The present study used
the WHO-5 Version II, which has five Likert-scored items
(0–5), with a possible sum score range of 0–25 and lower
values indicating less well-being during the past 2 weeks.
Statistical analyses
To assess differences between CF cases and noncases, we
compared mean scores of demographic and clinical varia-
bles with the use of t tests; v2 analysis was used for
categorical variables. We used two-factorial analyses of
variance (ANOVAs) with two between-subjects factors (CF
and SSI4/6) to assess their effects on dependent variables.
Effect sizes (Cohen’s d or partial g2) were computed. We
computed sequential multiple linear regressions to predict
aspects of quality of life (EUROHIS-QOL-8 and SF-8) and
well-being (WHO-5) by the dimensional scores of fatigue
and somatization, controlling for the effect of socioeco-
nomic variables. All tests were two tailed, with the a value

Fig. 1. Overlap of cases with CF and somatization syndrome.
A. Martin et al. / Journal of Psychosomatic Research 63 (2007) 147–156 151
set at .05. All analyses were conducted with the SPSS
Version 12.0 (Chicago, IL, USA) statistical package.
Results
Prevalence rates of CF in the general population
Severe fatigue (FQ symptom score of 4 or higher) was
reported by a total of 342 subjects [14.2%, 95% confidence
interval (CI)=12.8–15.6]. Of these, 193 subjects reported the
onset of their fatigue to be less than 6 months ago (shorter
fatigue at b3 months: n=146, 6%, 95% CI=5.1–7.0;
prolonged fatigue at 3–6 months: n=46, 1.9%, 95%
CI=1.4–2.6%). One hundred forty-seven subjects reported
that their fatigue lasted for at least 6 months and were
diagnosed as having CF. Thus, the prevalence rate of CF
Fig. 2. Pattern of somatoform symptoms in subjects with CF (n=147), subjects wi
(no CF, n=2265). The graph shows the symptoms that were reported by at least
cases was 6.1% (95% CI=5.1–7.1) in the German general
population (N=2412). Most CF cases reported that they
were tired at least half of the time (n=114/147, 80.3%).
Table 2 presents the point prevalence rates of CF for
socioeconomic subgroups and shows that females were
affected significantly more as compared with males (7% vs.
5.1%). The prevalence of CF increased with age: only 3% of
the subjects younger than 35 years reported CF, in contrast
to almost 12% of the population aged 65 years or older. The
prevalence rates differed with family status, with the highest
rates in the group of divorced or widowed subjects.
Prevalence rates were two times higher in the group with
a low family income than those in the groups with a
monthly income of at least 1250 Euro.
Socioeconomic characteristics of persons with CF as
compared with control subjects
Chronic fatigue cases were compared with the subjects
who did not meet the CF criteria [control group (CG)] on
socioeconomic and clinical characteristics (Table 1). The
two groups differed significantly with respect to all
variables. The CF group subjects were more likely to be
female as well as older and less likely to be single. The CF
group also had lower educational degrees and lower income
as compared with the CG.
Chronic fatigue and somatoform symptoms
The point prevalence rate of somatization syndrome SSI4/
6 was 16.3% in the general population sample (Table 1). The
distribution of somatization syndrome across the socio-
th somatization syndrome (SSI4/6, n=392), and control subjects without CF
30% of the subjects with CF.
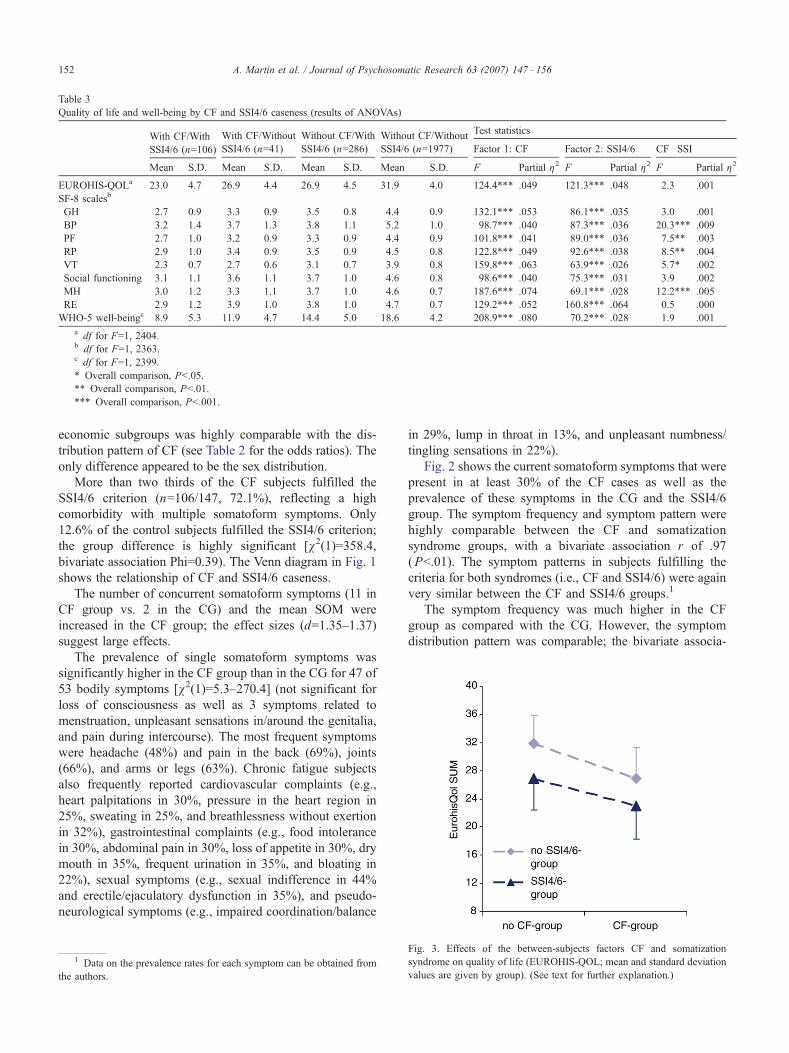
Table 3
Quality of life and well-being by CF and SSI4/6 caseness (results of ANOVAs)
With CF/With
SSI4/6 (n=106)
With CF/Without
SSI4/6 (n=41)
Without CF/With
SSI4/6 (n=286)
Without CF/Without
SSI4/6 (n=1977)
Test statistics
Factor 1: CF Factor 2: SSI4/6 CF�SSIMean S.D. Mean S.D. Mean S.D. Mean S.D. F Partial g2 F Partial g2 F Partial g2
EUROHIS-QOLa 23.0 4.7 26.9 4.4 26.9 4.5 31.9 4.0 124.4444 .049 121.3444 .048 2.3 .001
SF-8 scalesb
GH 2.7 0.9 3.3 0.9 3.5 0.8 4.4 0.9 132.1444 .053 86.1444 .035 3.0 .001
BP 3.2 1.4 3.7 1.3 3.8 1.1 5.2 1.0 98.7444 .040 87.3444 .036 20.3444 .009
PF 2.7 1.0 3.2 0.9 3.3 0.9 4.4 0.9 101.8444 .041 89.0444 .036 7.544 .003
RP 2.9 1.0 3.4 0.9 3.5 0.9 4.5 0.8 122.8444 .049 92.6444 .038 8.544 .004
VT 2.3 0.7 2.7 0.6 3.1 0.7 3.9 0.8 159.8444 .063 63.9444 .026 5.74 .002
Social functioning 3.1 1.1 3.6 1.1 3.7 1.0 4.6 0.8 98.6444 .040 75.3444 .031 3.9 .002
MH 3.0 1.2 3.3 1.1 3.7 1.0 4.6 0.7 187.6444 .074 69.1444 .028 12.2444 .005
RE 2.9 1.2 3.9 1.0 3.8 1.0 4.7 0.7 129.2444 .052 160.8444 .064 0.5 .000
WHO-5 well-beingc 8.9 5.3 11.9 4.7 14.4 5.0 18.6 4.2 208.9444 .080 70.2444 .028 1.9 .001
a df for F=1, 2404.b df for F=1, 2363.c df for F=1, 2399.
4 Overall comparison, Pb.05.
44 Overall comparison, Pb.01.
444 Overall comparison, Pb.001.
A. Martin et al. / Journal of Psychosomatic Research 63 (2007) 147–156152
economic subgroups was highly comparable with the dis-
tribution pattern of CF (see Table 2 for the odds ratios). The
only difference appeared to be the sex distribution.
More than two thirds of the CF subjects fulfilled the
SSI4/6 criterion (n=106/147, 72.1%), reflecting a high
comorbidity with multiple somatoform symptoms. Only
12.6% of the control subjects fulfilled the SSI4/6 criterion;
the group difference is highly significant [v2(1)=358.4,
bivariate association Phi=0.39). The Venn diagram in Fig. 1
shows the relationship of CF and SSI4/6 caseness.
The number of concurrent somatoform symptoms (11 in
CF group vs. 2 in the CG) and the mean SOM were
increased in the CF group; the effect sizes (d=1.35–1.37)
suggest large effects.
The prevalence of single somatoform symptoms was
significantly higher in the CF group than in the CG for 47 of
53 bodily symptoms [v2(1)=5.3–270.4] (not significant forloss of consciousness as well as 3 symptoms related to
menstruation, unpleasant sensations in/around the genitalia,
and pain during intercourse). The most frequent symptoms
were headache (48%) and pain in the back (69%), joints
(66%), and arms or legs (63%). Chronic fatigue subjects
also frequently reported cardiovascular complaints (e.g.,
heart palpitations in 30%, pressure in the heart region in
25%, sweating in 25%, and breathlessness without exertion
in 32%), gastrointestinal complaints (e.g., food intolerance
in 30%, abdominal pain in 30%, loss of appetite in 30%, dry
mouth in 35%, frequent urination in 35%, and bloating in
22%), sexual symptoms (e.g., sexual indifference in 44%
and erectile/ejaculatory dysfunction in 35%), and pseudo-
neurological symptoms (e.g., impaired coordination/balance
1 Data on the prevalence rates for each symptom can be obtained from
the authors.
in 29%, lump in throat in 13%, and unpleasant numbness/
tingling sensations in 22%).
Fig. 2 shows the current somatoform symptoms that were
present in at least 30% of the CF cases as well as the
prevalence of these symptoms in the CG and the SSI4/6
group. The symptom frequency and symptom pattern were
highly comparable between the CF and somatization
syndrome groups, with a bivariate association r of .97
(Pb.01). The symptom patterns in subjects fulfilling the
criteria for both syndromes (i.e., CF and SSI4/6) were again
very similar between the CF and SSI4/6 groups.1
The symptom frequency was much higher in the CF
group as compared with the CG. However, the symptom
distribution pattern was comparable; the bivariate associa-
Fig. 3. Effects of the between-subjects factors CF and somatization
syndrome on quality of life (EUROHIS-QOL; mean and standard deviation
values are given by group). (See text for further explanation.)

Table 4
Sequential multiple regression to predict quality of life (EUROHIS-QOL)
Model Predictor variable b (Model 4)a DR2b R2
1 Sex �.005 – –
Age �.021 – –
Family status �.05944 – –
Education .028 – –
Income .2014 – .1454
2 FQ-T �.2684 .1644 .3104
3 SOM �.3644 .0824 .3924
4 FQ-T�SOMS-7 .037 .001 .3934
2V SOM �.3644 .1954 .3414
3V FQ-T �.2684 .0514 .3924
Sample population=2301. For further explanation, see text.a Standardized b weights of the final regression model.b Incremental.
4 Pb.001
** Family status is significant at Pb.01.
2 Data not reported but can be requested from the authors.
A. Martin et al. / Journal of Psychosomatic Research 63 (2007) 147–156 153
tion r of the symptom patterns in the CF group and the CG
was .93 (Pb.01). Therefore, the patterns of bodily symp-
toms did not appear to be qualitatively different among the
CF group, SSI4/6 group, and CG and differed only in terms
of general symptom probability.
Quality of life and well-being
We analyzed the effects of CF and SSI4/6 caseness on
aspects of subjective quality of life and well-being
(ANOVAs with two between-subjects factors; see Table 3
for the mean scores by each factor value and test
statistics). The trans-sectoral quality of life (EUROHIS-
QOL) was markedly decreased in the CF and SSI4/6
groups and was the lowest for those subjects with CF and
SSI4/6. Mean scores did not differ between the CF-only
and SSI4/6-only conditions. The dotted lines in Fig. 3 are
almost parallel, illustrating that the two between-subjects
factors had an independent and additive effect on quality
of life, whereas the interaction of CF and SSI4/6 was
not significant.
A similar pattern of results was obtained for the SF-8
dimensions with the tool’s various aspects of health-related
quality of life. First, a multivariate ANOVA was computed
to control for inflation of Type I error. The main effects of
the two group factors were highly significant, suggesting the
health-related quality of life to be decreased in CF [�=0.89,F(8, 2356)=34.9, Pb.001] and SSI4/6 [�=0.92, F(8,
2356)=14.4, Pb.001]. There was an overall significant
CF�SSI4/6 caseness interaction for the SF-8 [�=0.98,F(8, 2356)=5.6, Pb.001]. Univariate ANOVAs showed that
the main effects for CF and SSI4/6 were significant across
all eight SF-8 dimensions; that is, health-related quality of
life was lower for those who fulfilled CF or SSI4/6 criteria,
very comparable in both conditions, and lowest in the case
of both syndromes. The interaction effects were significant
in five of the eight variables; however, the effect sizes were
very small for the interactions (partial g2=.000–.009).
The analysis of the WHO-5 scores also showed a
significant reduction of well-being in CF and somatization
syndrome. Again, the effects of CF and SSI4/6 were
additional, and the interaction of the two factors was
not significant.
The previous analyses compared the effects of CF and
somatization syndrome based on the case categories. We
conducted additional sequential multiple regressions using
the dimensional predictors FQ-T and SOM as well as
controlling for the impact of possibly influential socio-
demographic variables. Table 4 presents details of the
regression analysis predicting quality of life (EUROHIS-
QOL) as a criterion variable. Sociodemographic variables
were entered as the first predictors’ block, together explain-
ing 14.5% of the variance. The second block included the
FQ-T, resulting in 16.4% of incremental explained variance.
Somatoform symptom severity was entered as the third
block, adding 8.2% of the variance. The interaction of the
two latter variables was entered next, but this did not
contribute significantly to the total explained variance of
almost 40%. We then reanalyzed the multiple regression by
changing the order of the second and third blocks (i.e.,
entering SOM first and FQ-T only at the next block). Again,
both variables changed R2 significantly, but this time, with
the incremental R2 of SOM being .195 and the R2 of FQ-T
being .05 (Psb.001).
According to this procedure, multiple regression analyses
were also computed for the indicators of health-related
quality of life and well-being. Overall, the same pattern of
results was obtained.2 In summary, some of the sociodemo-
graphic variables, particularly family income and family
status, affected quality of life significantly. In addition,
fatigue severity and SOM significantly predicted quality of
life, namely in an additive way.
Discussion
Our study confirms high prevalence rates for CF and
somatization syndrome. Subjects were asked to report the
somatic symptoms for which physicians had not been able
to find a clear organic cause. The pattern of these self-
reported symptoms in CF cases was similar to the
distribution pattern in the general population, albeit symp-
tom prevalence rates were on a much higher level in CF.
Chronic fatigue and somatization syndrome were associated
with an almost comparable reduction in various aspects of
quality of life.
Prevalence of CF
The point prevalence of CF was high, with 6.1% of the
German population reporting significant fatigue lasting for

A. Martin et al. / Journal of Psychosomatic Research 63 (2007) 147–156154
at least 6 months. To compare the prevalence estimation
with figures of previous studies, one needs to keep in mind
that the prevalence of self-reported fatigue varies widely,
depending on how it is defined [5]. The point prevalence
rates in general population samples have been consistently
higher for CF, ranging from 4.3% to 18.3% [7–9,39],
than for CFS-like syndromes, ranging from 1.8% to 3.6%
[4–6,9], and lowest for CFS, ranging from 0.037% to 0.42%
[22,40,41]. Reported prevalence rates also depend on how
they were assessed. Studies based on questionnaire assess-
ments have yielded higher prevalence rates as compared
with studies based on interviews [9]. Two former studies
used the same instrument (i.e., the FQ) to investigate CF in
community populations. Both studies showed a higher
prevalence of CF in Norway (11.4%, sample age
range=19–80 years) [7] and the United Kingdom (18.3%,
sample age range=18–45 years) [8]. Because these studies
did not include adolescents, we reanalyzed our data for
subjects aged 18 years or older, resulting in a CF prevalence
rate of 6.3% (147/2330 subjects). Considering only subjects
aged between 19 and 80 years (as in Reference [7]), we
again obtained a point prevalence rate of 6.1% (138 CF
cases among 2251 subjects). A direct comparison of this
study with the results of the former studies is nonetheless
difficult because of differences in methodology (e.g., survey
methods and sample characteristics).
Sociodemographic characteristics
We found the highest CF prevalence rates among
females, persons of older age, those who are widowed or
divorced, and those with a lower family income. There is
almost consistent evidence that women are more often
affected by CF as compared with men, both in clinical and
population-based samples [4,5,7–9]. Some previous studies
found a similar age effect, with more severe fatigue in older
age groups [7], and very low prevalence rates in people
younger than 18 years [9]. Based on the present study, it
cannot be ruled out that the increasing probability of
reporting CF in older age groups might be related to other
diseases. However, it remains unclear whether higher
comorbidity of medical conditions and CF in the elderly
population is based on a causal relationship or just a
coincidence. Our results further suggest an inverse relation-
ship of CF with socioeconomic status. This is consistent
with previous findings of an association with lower income
[9] and higher CFS levels in people with lower levels of
education and occupational status [7,22]. All together, these
findings do not support the assumption that CF or CFS is a
syndrome of primarily middle-class patients.
Relationship of CF and somatization syndrome
The results show a substantial overlap of CF and
somatization syndrome; almost three quarters of CF cases
also met SSI4/6 criteria (72%). This cannot be explained by
similarities of the syndrome criteria because we defined
SSI4/6 based on somatoform symptoms only, which do not
include the FQ items that we used to define CF. The CF
group reported many additional somatoform symptoms of at
least moderate intensity, and the comparison with the CG
revealed large effect sizes. The distribution pattern of the
symptoms in CF resembled the pattern in the SSI4/6 group
(r=.97). The latter condition was defined by the number of
medically unexplained symptoms, not special target symp-
toms. Similarities were also evident for the distribution
pattern in control subjects without CF (r=.93). This
relationship indicated that the very frequent symptoms in
CF were also the symptoms with the highest frequencies in
the general population, although absolute base rates
differed. Overall, these results suggest that the somatic
symptom pattern in CF is not specific.
For at least 30% of the CF cases, 14 somatoform
symptoms were prevalent. Highest frequencies were
reported for back pain, pain in arms or legs, joint
pain, and headache; these pain complaints are also
among the CDC criteria for CFS. However, symptoms
related to sexual, cardiovascular, and gastrointestinal
functions were among the most frequently reported
symptoms in CF. Recent studies have found comparable
results in CFS, showing a greater prevalence of some
atypical symptoms as compared with some of the typical
CFS symptoms [9,42,43].
In addition, we compared the impact of CF and SSI4/6
on measures of quality of life. Both clinical syndromes
were associated with a reduction in cross-sectoral and
health-related quality of life, as well as lower reports of
well-being. The effect sizes regarding the two syndromes
were shown to be substantial, whereas the interaction of
the two syndromes added little or no variance. Thus,
the effect is mainly additive, showing that subjects with
CF and multiple somatoform symptoms reported the
poorest quality of life and well-being. The results of
regression analyses suggest that fatigue and somatization
severity had a similar impact on quality-of-life outcomes,
even when controlling for the impact of sociodemo-
graphic variables.
Our results confirm previous findings that highlight the
need to consider the number and severity of somatoform
symptoms in subjects presenting with CF. Katon and Russo
[44] showed that the extent of impairment in daily activities
and the tendency to amplify symptoms increased linearly
with the number of lifetime physical symptoms that a
patient with CF experienced.
Limitations
Our findings are limited by difficulties associated with
studying fatigue and somatoform complaints in a represen-
tative general population survey. Both clinical syndromes
assessed were based on self-reports. The design of the
survey precluded an independent medical assessment to rule

A. Martin et al. / Journal of Psychosomatic Research 63 (2007) 147–156 155
out organic causation. The study’s classification of soma-
tization syndrome was based on the subjects’ recall of the
somatic symptoms for which a physician was unable to
identify a clear organic causation. Ideally, a physical origin
of the symptoms by medical investigations would be ruled
out to classify them as somatoform symptoms, although the
interrater reliability of doctors’ ratings about the medical
causality of symptoms is low [45]. At least, the SOMS is a
questionnaire with well-established psychometric proper-
ties, and its indices were shown to be closely associated
with data of diagnostic interviews [26].
The definition of CF cases used in this study was not
identical to other definitions used in the literature and
was not limited to medically unexplained CF. It is not
possible to generalize the results obtained to the group of
CFS patients. However, we intended not to be too restrictive
in our case definition, and some evidence suggest that the
difference between CFS and CF is more quantitative than
qualitative [13,14].
The cross-sectional nature of the study limited our ability
to determine whether the sociodemographic factors (e.g.,
lower family income) were actual risk factors, correlates, or
a result of CF presence and severity. Overall, the response
rate (62.3%) was satisfactory and similar to other GH
surveys [46]. However, this still leaves 37.7% of people for
whom data can only be estimated.
Conclusions and practical implications
The results suggest that CF is a relevant syndrome in the
general population. Its substantial overlap with somatoform
syndrome supports the hypothesis that the two syndromes
are only partially different manifestations of the same
underlying processes. These processes could be cognitive–
perceptual, psychophysiological reactivity, and/or related to
illness behavior [47].
Previous results showed that specialists tend to focus on
symptoms according to their area of specialization and tend
to ignore symptoms of other body sites [48,49]. As a result,
coexisting conditions may be overlooked and patients may
try to get assistance from several specialty clinics, with a
potential cumulative effect on health care costs, resulting in
the risks of overinvestigation and iatrogenesis [50]. The
presence of fatigue and that of somatic symptoms not only
impair quality of life and functional abilities but also affect
treatment response (multiple symptom syndromes may be
more difficult to treat as compared with single symptom
conditions) [51]. It is important that clinicians of all
specialties inquire about additional medically unexplained
bodily symptoms beyond a patient’s initial presenting
complaint. Our data show that this is particularly important
if patients present with fatigue. Furthermore, clinicians need
to offer a comprehensive treatment approach with the aim of
providing general coping strategies, rather than offering
interventions focused on a specific symptom.
References
[1] Bates DW, Schmitt W, Buchwald D, Ware NC, Lee J, Thoyer E, et al.
Prevalence of fatigue and chronic fatigue syndrome in primary care
practice. Arch Intern Med 1993;153:2759–65.
[2] Kim CH, Shin HC, Won CW. Prevalence of chronic fatigue and
chronic fatigue syndrome in Korea: community-based primary care
study. J Korean Med Sci 2005;20:529–34.
[3] Kroenke K, Wood DR, Mangelsdorff AD, Meier NJ, Powell JB.
Chronic fatigue in primary care Prevalence, patient characteristics, and
outcome. JAMA 1988;260:929–34.
[4] Evengard B, Jacks A, Pedersen NL, Sullivan PF. The epidemiology of
chronic fatigue in the Swedish Twin Registry. Psychol Med 2005;35:
1317–26.
[5] Furberg H, Olarte M, Afari N, Goldberg J, Buchwald D, Sullivan PF.
The prevalence of self-reported chronic fatigue in a US twin registry.
J Psychosom Res 2005;59:283–90.
[6] Huibers MJ, Kant IJ, Swaen GM, Kasl SV, Med OE. Prevalence of
chronic fatigue syndrome-like caseness in the working population:
results from the Maastricht cohort study. J Occup Environ Med
2004;61:464–6.
[7] Loge JH, Ekeberg O, Kaasa S. Fatigue in the general Norwegian
population: normative data and associations. J Psychosom Res 1998;
45:53–65.
[8] Pawlikowska T, Chalder T, Hirsch SR, Wallace P, Wright DJM,
Wessely SC. A population based study of fatigue and psychological
distress. BMJ 1994;308:763–6.
[9] Steele L, Dobbins JG, Fukuda K, Reyes M, Randall B, Koppelman M,
et al. The epidemiology of chronic fatigue in San Francisco. Am J
Med 1998;105:83–90.
[10] Kelsall H, Sim M, McKenzie D, Forbes K, Leder D, et al. Medically
evaluated psychological and physical health of Australian Gulf War
veterans with chronic fatigue. J Psychosom Res 2006;60:575–84.
[11] Fukuda K, Straus SE, Hickie I, Sharpe MC, Dobbins JG, Komaroff A,
et al. The chronic fatigue syndrome: a comprehensive approach to its
definition and study. Ann Intern Med 1994;121:953–9.
[12] Sullivan PF, Pedersen NL, Jacks A, Evengard B. Chronic fatigue in a
population sample: definitions and heterogeneity. Psychol Med 2005;
35:1337–48.
[13] Darbishire L, Ridsdale L, Seed PT. Distinguishing patients with
chronic fatigue from those with chronic fatigue syndrome: a
diagnostic study in UK primary care. Br J Gen Pract 2003;53:441–5.
[14] Wessely S, Chalder T, Hirsch S, Wallace P, Wright D. Psychological
symptoms, somatic symptoms, and psychiatric disorder in chronic
fatigue and chronic fatigue syndrome: a prospective study in primary
care. Am J Psychiatry 1996;153:1050–9.
[15] Wessely S, Nimnuan C, Sharpe M. Functional somatic syndromes—
one or many? Lancet 1999;354:936–9.
[16] Wessely S, White PD. There is only one functional somatic syndrome.
Br J Psychiatry 2004;185:95–6.
[17] Aaron LA, Buchwald D. A review of the evidence for overlap among
unexplained clinical conditions. Ann Intern Med 2001;134:868–81.
[18] Afari N, Buchwald D. Chronic fatigue syndrome: a review. Am J
Psychiatry 2003;160:221–36.
[19] Johnson SK, DeLuca J, Natelson BH. Assessing somatization disorder
in the chronic fatigue syndrome. Psychosom Med 1996;58:50–7.
[20] Escobar JI, Rubio-M Stipec G, Canino M. Somatic Symptoms Index
(SSI): a new and abridged somatization construct—prevalence and
epidemiological correlates in two large community samples. J Nerv
Ment Dis 1989;177:140–6.
[21] Creed F, Barsky A. A systematic review of the epidemiology of
somatisation disorder and hypochondriasis. J Psychosom Res 2004;
56:391–408.
[22] Jason LA, Richman JA, Rademaker AW, Jordan KM, Plioplys AV,
Taylor RR, et al. A community-based study of chronic fatigue
syndrome. Arch Intern Med 1999;159:2129–37.
A. Martin et al. / Journal of Psychosomatic Research 63 (2007) 147–156156
[23] Wessely S, Chalder T, Hirsch S, Wallace P, Wright D. The prevalence
and morbidity of chronic fatigue syndrome: a prospective primary care
study. Am J Public Health 1997;87:1449–55.
[24] Jason LA, Taylor RR, Kennedy CL. Chronic fatigue syndrome,
fibromyalgia, and multiple chemical sensitivities in a community-
based sample of persons with chronic fatigue syndrome-like symp-
toms. Psychosom Med 2000;62:655–63.
[25] Chalder T, Berelowitz G, Pawlikowska T, Watts L, Wessely S, Wright
D, et al. The development of a fatigue scale. J Psychosom Res
1993;37:147–53.
[26] Rief W, Hiller W. A new approach to the assessment of the
treatment effects of somatoform disorders. Psychosomatics 2003;44:
492–8.
[27] Power M. Development of a common instrument for quality of life. In:
Nosikov A, Gudex CI, editors. EUROHIS: developing common
instruments for health surveys. Amsterdam7 IOS, 2003. pp. 145–63.
[28] Ware JE, Kosinski M, et al. How to score and interpret single-item
health status measures: a manual for users of the SF-8k Health
Survey. Lincoln, RI7 Quality Metric Incorporated, 2001.
[29] Bech P. Measuring the dimensions of psychological well-being by the
WHO-5. Qol Newsl 2004;32:15–6.
[30] Martin A, Rief W, Gaab J, Br7hler E. Messung chronischer
Erschfpfung—Teststatistische Prqfung und Normierung der deut-
schen Version der Chalder Fatigue Skala {The measurement of
chronic fatigue: psychometric properties and normative data of the
German version of the Chalder Fatigue Questionnaire} [submitted
for publication].
[31] Rief W, Hiller W, Heuser J. SOMS—Das Screening fqr Somatoforme
Stfrungen Manual zum Fragebogen [SOMS—The Screening for
Somatoform Symptoms]. Bern7 Huber-Verlag, 1997.
[32] Schmidt S, Muehlan H, Power M. The EUROHIS-QOL 8-item index:
psychometric results of a cross-cultural field study. Eur J Public
Health 2005 doi:10.1093/eurpub/cki155.
[33] Br7hler E, Mqhlan H, Albani C, Schmidt S, Teststatistische Prqfungund Normierung der deutschen Versionen des EUROHIS-QOL
Lebensqualit7ts-Index und des WHO-5 Wohlbefindens-Index. Diag-
nostica 2007;53:83–96.
[34] Ware JE, Sherbourne CD. The MOS 36-item Short-Form Health
Survey (SF-36) Conceptual framework and item selection. Med Care
1992;30:473–83.
[35] Bullinger M, Kirchberger I. Der SF-36 Fragebogen zum Gesund-
heitszustand-Handanweisung [SF-36 questionnaire concerning health
status]. Goettingen7 Hogrefe, 1998.
[36] Ellert U, Lampert T, Ravens-Sieberer U. Messung der gesundheitsbe-
zogenen Lebensqualit7t mit dem SF-8-Eine Normstichprobe fqrDeutschland [Measuring health-related quality of life with the
SF-8]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheits-
schutz 2005;48:1330–7.
[37] Bech P, Olsen RL, Kjoller M, Rasmussen NK. Measuring well-being
rather than the absence of distress symptoms: a comparison of the SF-
36 mental health subscale and the WHO-Five Well-Being Scale. Int J
Methods Psychiatr Res 2003;12:85–91.
[38] Bonsignore M, Barkow K, Jensen F, Heun R. Validity of the five-item
WHO Well-Being Index (WHO-5) in an elderly population. Eur Arch
Psychiatry Clin Neurosci 2001;251(Suppl 2):II27–II31.
[39] Skapinakis P, Lewis G, Meltzer H. Clarifying the relationship between
unexplained chronic fatigue and psychiatric morbidity: results from a
community survey in Great Britain. Int Rev Psychiatry 2003;15:57–64.
[40] Lloyd AR, Hickie I, Boughton CR, Spencer O, Wakefield D.
Prevalence of chronic fatigue syndrome in an Australian population.
Med J Aust 1990;153:522–8.
[41] Reyes M, Nisenbaum R, Hoaglin DC, Unger ER, Emmons C, Randall
B, et al. Prevalence and incidence of chronic fatigue syndrome in
Wichita, Kansas. Arch Intern Med 2003;163:1530–6.
[42] Nisenbaum R, Reyes M, Unger ER, Reeves WC. Factor analysis of
symptoms among subjects with unexplained chronic fatigue—what
can we learn about chronic fatigue syndrome? J Psychosom Res
2004;56:171–8.
[43] Wilson A, Hickie I, Hadzi-Pavlovic D, Wakefield D, Parker G, Straus
SE, et al. What is chronic fatigue syndrome? Heterogeneity within
an international multicentre study. Aust N Z J Psychiatry 2001;35:
520–7.
[44] Katon W, Russo J. Chronic fatigue syndrome criteria A critique of the
requirement for multiple physical complaints. Arch Intern Med
1992;152:1604–9.
[45] Fink P, Rosendal M, Olesen F. Classification of somatization and
functional somatic symptoms in primary care. Aust N Z J Psychiatry
2005;39:772–81.
[46] Jacobi F, Wittchen H, Holting C, Sommer S, Lieb R, Hffler M, et al.
Estimating the prevalence of mental and somatic disorders in the
community: aims and methods of the German National Health
Interview and Examination Survey. Int J Methods Psychiatr Res
2002;11:1–18.
[47] Kirmayer LJ, Looper KJ. Abnormal illness behaviour: physiological,
psychological and social dimensions of coping with distress. Curr
Opin Psychiatry 2006;19:54–60.
[48] Aaron LA, Burke MM, Buchwald D. Overlapping conditions among
patients with chronic fatigue syndrome, fibromyalgia, and tempor-
omandibular disorder. Arch Intern Med 2000;160:221–7.
[49] Nimnuan C, Hotopf M, Wessely S. Medically unexplained symptoms
An epidemiological study in seven specialities. J Psychosom Res
2001;51:361–7.
[50] Fink P. Surgery and medical treatment in persistent somatizing
patients. J Psychosom Res 1992;36:439–47.
[51] Looper KJ, Kirmayer LJ. Behavioral medicine approaches to somato-
form disorders. J Consult Clin Psychol 2002;70:810–27.