The prevalence of person-perceived participation restriction in community-dwelling older adults
9
The prevalence of person-perceived participation restriction in community-dwelling older adults Ross Wilkie, George Peat, Elaine Thomas & Peter Croft Primary Care Sciences Research Centre, Keele Universtity, Keele, Staffordshire, ST5 5BG, United Kingdom (E-mail: [email protected]) Accepted in revised form 4 May 2006 Abstract Objective: To estimate the prevalence, nature and distribution of person-perceived participation restriction, in community-dwelling older adults. Method: Population based cross-sectional postal survey of 11,055 adults aged 50 years and over in North Staffordshire, United Kingdom. Person-perceived participation restriction was measured using the Keele Assessment of Participation which covers 11 different aspects of life mapped to the World Health OrganizationÕs International Classification of Functioning. Four-week period prevalence was calculated for restriction in any, multiple and for each aspect separately. Prevalence estimates were calculated for the total sample, and for each age and gender stratum. Results: A total of 7,878 subjects responded (adjusted response – 71.3%). The 4-week period prevalence of any participation restriction was 51.8%; 3.3% had substantial restriction. Participation restriction increased with age (p<0.001) and, for moderate and substantial restriction, was more frequent in women. The prevalence of restricted participation in individual aspects of life ranged from 3.8% (work) to 25.9% (mobility outside the home). Conclusion: Some restriction of participation ‘as and when we want itÕ is common in the general population and increases with age, although severe restriction only affects a minority. The distribution of person-perceived participation restriction is similar to that of impairments and activity limitation in community-dwelling older adults. Key words: General population, Elderly, Participation restriction, Person-perceived, ICF Introduction As the proportion of older adults in the general population rises, ill-health and disability associ- ated with old age will increasingly influence the overall picture [1]. There are many different approaches to measuring disability, and the World Health Organization (WHO) has endorsed the International Classification of Functioning, Dis- ability and Health (ICF) with the aim of facili- tating a consistent approach [2]. This framework uses disability as an umbrella term for abnormal functioning at three separate levels; anatomical/ physiological level – impairment; individual level – activity limitation; societal level – participation restriction [2]. Of the three levels of disability proposed in the ICF, we know least about participation restriction. Participation restriction refers to the societal con- sequences of health conditions and is defined as ‘problems an individual may experience in involvement in life situationsÕ [2]. Participation restriction is hypothesised to result from the complex interaction between a health condition, the individual, and contextual factors such as the physical, social and cultural environment [2]. In attempting to measure it directly, we recognise that how people function in the context of their Quality of Life Research (2006) 15:1471–1479 Ó Springer 2006 DOI 10.1007/s11136-006-0017-9
Transcript of The prevalence of person-perceived participation restriction in community-dwelling older adults

The prevalence of person-perceived participation restriction
in community-dwelling older adults
Ross Wilkie, George Peat, Elaine Thomas & Peter CroftPrimary Care Sciences Research Centre, Keele Universtity, Keele, Staffordshire, ST5 5BG, United Kingdom(E-mail: [email protected])
Accepted in revised form 4 May 2006
Abstract
Objective: To estimate the prevalence, nature and distribution of person-perceived participation restriction,in community-dwelling older adults. Method: Population based cross-sectional postal survey of 11,055adults aged 50 years and over in North Staffordshire, United Kingdom. Person-perceived participationrestriction was measured using the Keele Assessment of Participation which covers 11 different aspects oflife mapped to the World Health Organization�s International Classification of Functioning. Four-weekperiod prevalence was calculated for restriction in any, multiple and for each aspect separately. Prevalenceestimates were calculated for the total sample, and for each age and gender stratum. Results: A total of7,878 subjects responded (adjusted response – 71.3%). The 4-week period prevalence of any participationrestriction was 51.8%; 3.3% had substantial restriction. Participation restriction increased with age(p<0.001) and, for moderate and substantial restriction, was more frequent in women. The prevalence ofrestricted participation in individual aspects of life ranged from 3.8% (work) to 25.9% (mobility outside thehome). Conclusion: Some restriction of participation ‘as and when we want it� is common in the generalpopulation and increases with age, although severe restriction only affects a minority. The distribution ofperson-perceived participation restriction is similar to that of impairments and activity limitation incommunity-dwelling older adults.
Key words: General population, Elderly, Participation restriction, Person-perceived, ICF
Introduction
As the proportion of older adults in the generalpopulation rises, ill-health and disability associ-ated with old age will increasingly influence theoverall picture [1]. There are many differentapproaches to measuring disability, and the WorldHealth Organization (WHO) has endorsed theInternational Classification of Functioning, Dis-ability and Health (ICF) with the aim of facili-tating a consistent approach [2]. This frameworkuses disability as an umbrella term for abnormalfunctioning at three separate levels; anatomical/physiological level – impairment; individual level –
activity limitation; societal level – participationrestriction [2].
Of the three levels of disability proposed in theICF, we know least about participation restriction.Participation restriction refers to the societal con-sequences of health conditions and is defined as‘problems an individual may experience ininvolvement in life situations� [2]. Participationrestriction is hypothesised to result from thecomplex interaction between a health condition,the individual, and contextual factors such as thephysical, social and cultural environment [2]. Inattempting to measure it directly, we recognisethat how people function in the context of their
Quality of Life Research (2006) 15:1471–1479 � Springer 2006DOI 10.1007/s11136-006-0017-9

lives (e.g., work and social activities) may be ofmore concern to them than actual impairments ordifficulties with individual tasks [3]. Participationrestriction is an appealing concept for thoseinterested in older populations and the impact ofchronic diseases because, even when health con-ditions and activity limitations are irreversible,there may still be the potential to maintain par-ticipation [4].
Population studies indicate that the prevalenceof many health conditions and impairments [5],and of activity limitation (measured by self-report[5–7] or by objective methods [8]) rises withincreasing age and is higher in women. Whetherthe same pattern exists for participation restrictionis less clear. Population studies of participationrestriction or handicap – the concept from whichparticipation restriction evolved – are not easy toidentify from the health literature. Certain aspectsof them have been measured in population studiesof disability [e.g., 9–12] but are seldom describedas handicap or participation restriction nor fullyevaluated within the ICF framework. An excep-tion is the Gospel Oaks project, where an attemptwas made to measure handicap in its entirety.Their results suggested that handicap did increasewith age, but was reported equally by men andwomen [13].
There are several reasons why the pattern ofparticipation restriction in the population may notsimply follow that of impairments and activitylimitation. Environmental factors may eitherfacilitate or obstruct participation in those with agiven health condition, impairment or degree ofdifficulty. When allowed to judge for themselveswhether they are restricted or not (as opposed tousing some external standard), individuals with thesame health condition, impairment or degree ofdifficulty in a certain task might arrive at differentinterpretations based on experience and expecta-tions. ‘Paradoxical� ratings of good quality of lifehave been found in people with more severe dis-ease and poorer objective function [14, 15] and asimilar phenomenon may exist for rating partici-pation restriction.
Factors both from the environment and behindthe subjective appraisal of participation may alter
over the course of middle and old age. As a simpleexample, the prevalence of lower limb osteoar-thritis increases with age [16], as does difficultywith walking [17]. However, a similar age-relatedincrease in the prevalence of feeling restricted ingetting around outside the home may be offset byenvironmental facilitators such as availability anduptake of public and private transport, or bychanges in how mobile individuals with osteoar-thritis expect to be as they get older.
We have estimated participation restriction in apopulation survey, choosing to measure it fromthe individual�s perspective by enquiring whetherthey take part ‘as much as they want� in a range oflife situations. We present here an estimate of theprevalence and nature of participation restrictionin a cross-sectional sample of older adults in thegeneral population, and its association with ageand gender in this sample.
Methods
Study design and participants
The North Staffordshire Osteoarthritis Project(NorStOP) is a population-based prospectivecohort study of community-dwelling adults aged50 years and over registered with three generalpractices (regardless of the extent or nature of anycontacts with the practice) in North Staffordshire.Ethical approval for the study was obtained fromthe North Staffordshire Local Research EthicsCommittee. Full details of the study protocol havepreviously been reported [18]. In March 2002,baseline self-complete questionnaires about healthwere mailed to all adults aged 50 years and overregistered with the three participating practices. Astandard mailing procedure was used, in which areminder postcard was sent to non-responders2 weeks after the initial mailing, and a repeatquestionnaire sent to remaining non-responders afurther 2 weeks after this. Ninety-eight percent ofthe general adult population in North Stafford-shire is Caucasian with levels of health deprivationand disability below the average for England andWales [19, 20].
1472

Data collection
The questionnaire collected information ondemographic, socioeconomic and general healthcharacteristics, including Short Form-12 instru-ment (SF-12) [21]. Participation restriction wasmeasured by the Keele Assessment of Participa-tion (KAP) [22]. This is a recently developed11-item self-complete instrument, designed tomeasure participation in a number of areas of lifefrom the perspective of the individual. It covers thefollowing aspects, mapped to domains and sub-domains of the World Health Organization�sInternational Classification of Functioning:mobility within the home, mobility outside thehome, self-care, looking after belongings, lookingafter the home, looking after dependants, inter-personal interaction, managing money, work,education, and social activities [22]. Items arephrased to capture performance (‘I have�), indi-vidual judgement and the nature and timeliness ofparticipation (‘as and when I have wanted�).Responses were on a five point ordinal scale(i.e., ‘All of the time� ‘Most of the time� ‘Some ofthe time� ‘A little of the time� ‘None of the time�).Filter questions are included in four items (lookingafter dependants, work, education and socialactivities) to allow responders to indicate if theseitems were relevant or not, since in pilot studiesthese were identified as not applying to everyone�slives. The reliability and validity of the KAP hasbeen established as adequate for providing esti-mates of person-perceived participation restrictionin population studies [22].
Statistical analysis
Participation restriction was defined by a responseof ‘some of the time� or less and calculated forresponders who had completed all KAP items. The4-week period prevalence of participation restric-tion was calculated overall and within age andgender specific strata for (i) any participationrestriction (participation restriction in at least oneaspect of life), (ii) minimal (1–3 restricted aspectsof life), moderate (4–6 aspects of life) and sub-stantial (7–11 aspects of life) amounts of partici-pation restriction and (iii) each of the 11 aspects oflife separately.
Differences between age groups in each of theabove prevalence estimates of participationrestriction were tested using a chi-square test (v2),and, if significant, followed by a chi-square test forlinear trend. Gender differences were examined bypercentage difference with 95% confidence inter-vals.
To estimate the effects of age on the gender-specific prevalence estimates of the amounts ofparticipation restriction, age-specific prevalencewas calculated separately for men and women foreach category of participation restriction. A crudesummary ratio of the observed prevalence in wo-men to men was also calculated and expressedrelative to a figure of 100 as representing no dif-ference between men and women. Indirect stan-dardisation was used to calculate an age-adjustedratio of female to male prevalence [23].
Results
A total of 11,055 questionnaires were mailed, and7,878 completed forms returned (adjustedresponse = 71.3%). Of the non-responders, 255people declined to take part, 109 did not completethe questionnaire due to ill health, and no contactwas received from 2,813 people. Responders weremore likely to be female than were non-respond-ers. Non-response was highest in the youngest(50–59 years) and oldest (80+ years) age groups.However, survey responders as a whole were verysimilar in general health, age, gender and maritalstatus to UK norms, suggesting that there was nosubstantial non-response bias [24, 25].
Fifty-six percent of responders were female [26].The overall mean (standard deviation) age was66.3 years (10.3 years). The mean age of femaleresponders was slightly higher (66.9 years) thanthat of male responders (65.5 years). Twenty-sixpercent of the sample were currently working,proportionately more males than females (differ-ence 9.1%; 95% CI: 7.1%, 11.1%). Males weremore likely to be in higher managerial/professionaloccupations and less likely to be in semi-routineoccupations, when compared with females. Themean SF-12 mental and physical health scoreswere 48.8 (SD: 11.2) and 40.7 (SD: 12.5), respec-tively, similar in men and women. Physical healthSF-12 scores fell (indicating poorer health) with
1473

increasing age for men and women (e.g., 44.7 forwomen aged 50–59 years, 31.6 for women aged80+ years). However, mental health scores didnot change with age in either gender.
Prevalence of any participation restriction
A total of 7,259 (92.1%) responders completed allKAP items. A total of 3,759 reported participationrestriction in one or more aspects of life (4-weekprevalence of any participation restriction =51.8%) (Table 1). This increased linearly with age(p<0.001) and was more common in women thanin men (% difference: 6.6% [95% CI: 4.2, 8.9]).
Prevalence of participation restriction in multipleaspects of life
A total of 2,697 (37.2%) indicated participationrestriction in one-to-three (minimal), 822 (11.3%)in four-to-six (moderate) and 240 (3.3%) in seven-to-eleven (substantial) (Table 1). For all threecategories, prevalence increased linearly with age(p<0.001) in both men and women. There was nodifference in the prevalence of minimal amounts ofrestriction between men and women (% difference:0.9% [95% CI: 1.4, 3.1]). However, moderate andsubstantial amounts of participation restriction
were significantly more common in women than inmen (% difference: 3.4 [95% CI: 1.9, 4.8] and 2.3[95% CI: 1.5, 3.1]).
These patterns were confirmed after indirectstandardisation for age, the ratios of female:maleprevalence of minimal, moderate and substantiallevels of participation restriction being 101, 129,205, respectively (Table 2). Gender differences in-creased with age.
Prevalence of participation restriction in each aspectof life
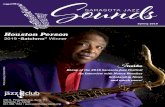
The most common participation restriction was inmobility outside the home (25.9%). The preva-lence estimates for the other aspects of life were:managing money (19.2%), interpersonal interac-tion (16.2%), looking after the home (15.8%),mobility within the home (14.1%), social activities(13.6%), looking after belongings (11.5%), self-care (10.6%), looking after dependants (5.4%),education (4.1%), and work (3.8%).
The prevalence of participation restriction in-creased with age in seven of the items, but in two(work and education) the prevalence was highestin the 50–59 age group and decreased at older ages(Figure 1). For social activities and looking afterdependants, there was no change with age.
Table 1. Four-week period prevalence of participation restriction; overall and stratified by age and gender
Categories of
amounts of
participation
restriction
All responders
(n = 7259)
Age group Gender
50–59 60–69 70–79 80+ v2 (trend)* p Female Male % difference
(95% CI)a
Any (‡1 aspect)
No. 3759 1051 1029 1057 548 265 <0.001 2218 1541
% 51.8 44.0 46.9 57.2 75.5 54.7 48.1 6.6 (4.2, 8.9)
Minimal (1–3 aspects)
No. 2697 788 779 743 387 59.6 <0.001 1523 1174
% 37.2 32.8 35.5 40.2 46.7 37.5 36.6 0.9 ()1.4, 3.1)
Moderate (4–6 aspects)
No. 822 195 193 245 189 121.0 <0.001 520 302
% 11.3 8.1 8.8 13.3 22.8 12.8 9.4 3.4 (1.9, 4.8)
Substantial (7–11 aspects)
No. 240 68 57 69 69 14.1 <0.001 175 65
% 3.3 3.3 2.6 3.7 3.7 4.3 2.0 2.3 (1.5, 3.1)
*v2 (trend) calculated with 1 degree of freedom.aCI, Confidence interval.
1474
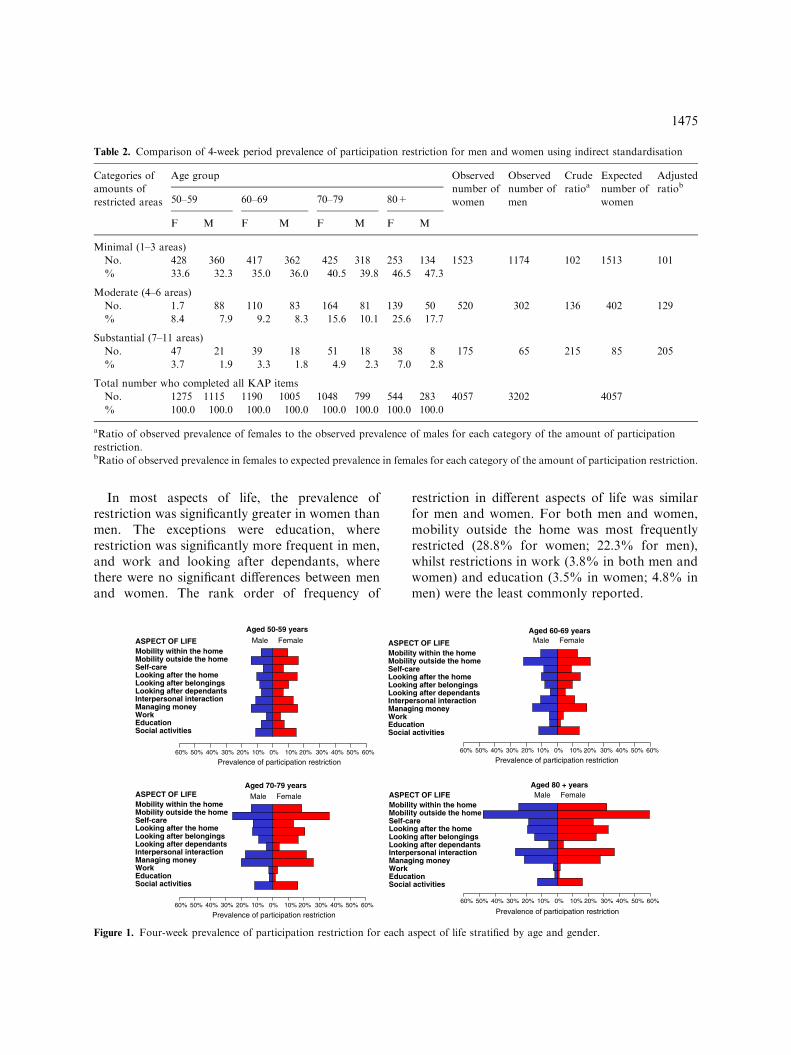
In most aspects of life, the prevalence ofrestriction was significantly greater in women thanmen. The exceptions were education, whererestriction was significantly more frequent in men,and work and looking after dependants, wherethere were no significant differences between menand women. The rank order of frequency of
restriction in different aspects of life was similarfor men and women. For both men and women,mobility outside the home was most frequentlyrestricted (28.8% for women; 22.3% for men),whilst restrictions in work (3.8% in both men andwomen) and education (3.5% in women; 4.8% inmen) were the least commonly reported.
0% 10% 20% 30% 40% 50% 60%10%20%30%40%50%60%
Prevalence of participation restriction Prevalence of participation restriction
Prevalence of participation restrictionPrevalence of participation restriction
Male Female Male Female
Male FemaleMale Female
Aged 70-79 years
0% 10% 20% 30% 40% 50% 60%10%20%30%40%50%60%
Aged 80 + years
0% 10% 20% 30% 40% 50% 60%10%20%30%40%50%60%
Aged 60-69 years
Mobility within the homeMobility outside the home
Managing money
Education
Interpersonal interaction
Work
Looking after dependants
Self-careLooking after the homeLooking after belongings
Social activities
0% 10% 20% 30% 40% 50% 60%10%20%30%40%50%60%
ASPECT OF LIFE
Mobility within the homeMobility outside the home
Managing money
Education
Interpersonal interaction
Work
Looking after dependants
Self-careLooking after the homeLooking after belongings
Social activities
ASPECT OF LIFE
Mobility within the homeMobility outside the home
Managing money
Education
Interpersonal interaction
Work
Looking after dependants
Self-careLooking after the homeLooking after belongings
Social activities
ASPECT OF LIFEMobility within the homeMobility outside the home
Managing money
Education
Interpersonal interaction
Work
Looking after dependants
Self-careLooking after the homeLooking after belongings
Social activities
ASPECT OF LIFE
Aged 50-59 years
Figure 1. Four-week prevalence of participation restriction for each aspect of life stratified by age and gender.
Table 2. Comparison of 4-week period prevalence of participation restriction for men and women using indirect standardisation
Categories of
amounts of
restricted areas
Age group Observed
number of
women
Observed
number of
men
Crude
ratioaExpected
number of
women
Adjusted
ratiob
50–59 60–69 70–79 80+
F M F M F M F M
Minimal (1–3 areas)
No. 428 360 417 362 425 318 253 134 1523 1174 102 1513 101
% 33.6 32.3 35.0 36.0 40.5 39.8 46.5 47.3
Moderate (4–6 areas)
No. 1.7 88 110 83 164 81 139 50 520 302 136 402 129
% 8.4 7.9 9.2 8.3 15.6 10.1 25.6 17.7
Substantial (7–11 areas)
No. 47 21 39 18 51 18 38 8 175 65 215 85 205
% 3.7 1.9 3.3 1.8 4.9 2.3 7.0 2.8
Total number who completed all KAP items
No. 1275 1115 1190 1005 1048 799 544 283 4057 3202 4057
% 100.0 100.0 100.0 100.0 100.0 100.0 100.0 100.0
aRatio of observed prevalence of females to the observed prevalence of males for each category of the amount of participation
restriction.bRatio of observed prevalence in females to expected prevalence in females for each category of the amount of participation restriction.
1475

Discussion
We have used a simple self-report instrument toestimate participation restriction in an older pop-ulation sample. We measured participationrestriction from the perspective of the individual asit potentially gives a more accurate account andgreater understanding of participation restrictionthan a societal perspective in which participation iscompared against a normative objective standard[27]. We have shown that it is common and ishigher in the oldest ages and in women. However,the extent to which different areas of life are af-fected varies greatly, with restriction in some areasrather low. Although some restriction is common,25% of those aged 80 years and over remain freeof participation restriction in most areas of theirlife.
Despite their conceptual contrasts, participationrestriction appears to have a similar prevalenceand distribution in the older population as thatreported for activity limitation and impairments[5–7]. Referring to the conceptual model of par-ticipation restriction, the age-related increase inchronic disease and activity limitation does notappear to be offset by environmental factors (e.g.,the provision of assistance or assistive-devices) andpersonal factors (e.g., expectations that function-ing should be difficult), sufficiently to maintainparticipation to the extent that older people wish;participation restriction also increases with age.However, participation restriction offers a per-spective different to measures of impairment andactivity limitation alone, and provides one way inwhich the impact of health conditions on thefunctioning of older adults in the contexts of theireveryday lives can be described.
Our study provides evidence that the oldest oldand women are more vulnerable with respect totheir participation in everyday life, and highlightsthe large number of older adults who may benefitfrom interventions designed to improve participa-tion. Mobility outside the home was the mostcommon area of participation restriction and,however measured, is clearly a major concern inthis age-group, warranting specific investigationsinto this form of disability [28, 29]. Work was theleast common area of participation restriction andthe decreasing prevalence with increasing age mayreflect the increasing proportion of older adults
who are retired and no longer consider engaging inemployment.
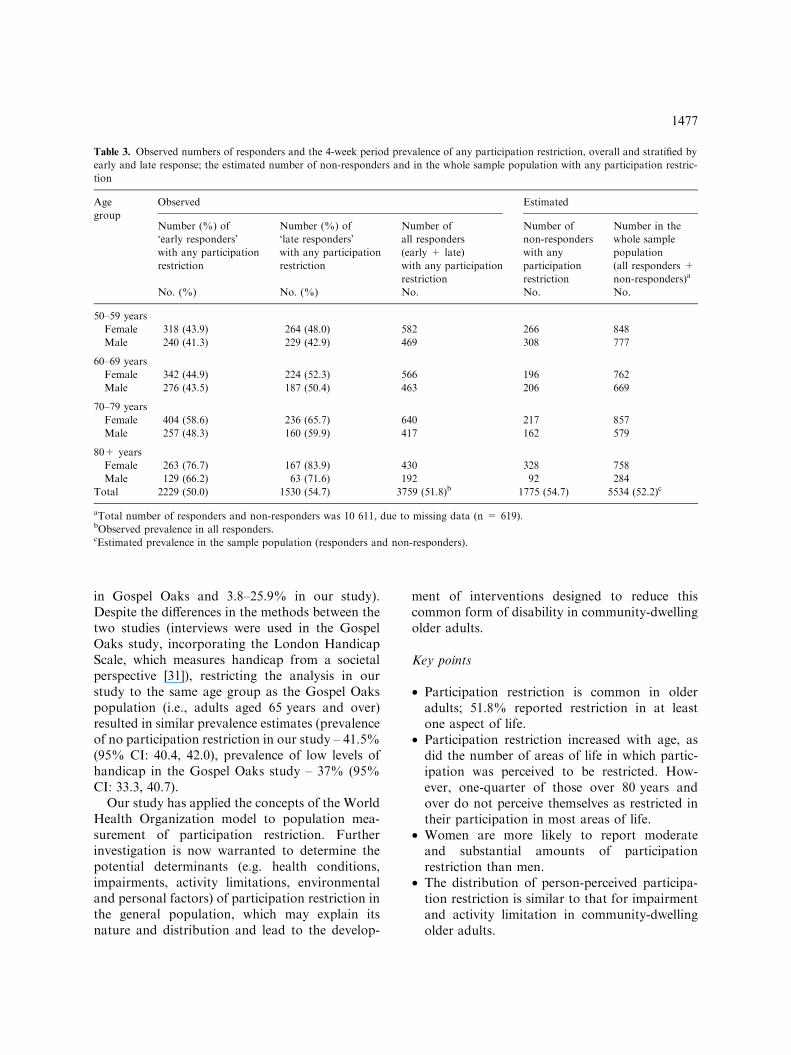
The general practices used in this study werelocated in urban areas and the number ofnon-white groups were small, limiting the gener-alizability of these estimates of participationrestriction. The postal method may have preventedcollection of information from those with cogni-tive or physical impairment, who may participateless than those able to complete questionnaires.We estimated the effects of non-response, byregarding ‘late� responders (those who respondedafter receiving a reminder postcard or question-naire) as a representative sample of non-respond-ers [30]. The prevalence of participation restrictionwas higher in the ‘late� responders than in ‘early�responders, suggesting that our reported preva-lence of any participation restriction was indeed anunderestimate (Table 3).
Missing data (619 (7.9%) of 7,878 participantsdid not complete all KAP items) may also have ledto an underestimate of prevalence, although theeffects of this are likely to be small. In comparisonto those included in the analysis, those who did notcomplete all KAP items were older (mean age(years): 70.2 cf 70.0), were more likely to be female(58.0% cf 55.9%) and had lower general health(mean SF-12 physical functioning score: 38.6 cf40.8; mean SF-12 mental functioning score: 46.3 cf48.9).
The prevalence in four areas (looking after de-pendants, work, education and social activities)may have been affected by the inclusion of ascreening question. Responders who indicated inthe screening question that they chose not toparticipate in these areas are classified as partici-pating. However, misclassification can occur, forexample, responders may choose not to work dueto a health condition or working conditions actingas a barrier, and are erroneously classified asparticipating in work ‘as and when they want.�Therefore, the screening questions may lead to anunderestimate of prevalence in these aspects of life.
The estimates of participation restriction werelower than those reported for handicap in theGospel Oaks project [13], overall (63% indicatedmore than low levels of handicap in the GospelOaks compared with 51.8% indicating some par-ticipation restriction in at least one aspect of life inour study) and for individual items (range: 38–75%
1476
in Gospel Oaks and 3.8–25.9% in our study).Despite the differences in the methods between thetwo studies (interviews were used in the GospelOaks study, incorporating the London HandicapScale, which measures handicap from a societalperspective [31]), restricting the analysis in ourstudy to the same age group as the Gospel Oakspopulation (i.e., adults aged 65 years and over)resulted in similar prevalence estimates (prevalenceof no participation restriction in our study – 41.5%(95% CI: 40.4, 42.0), prevalence of low levels ofhandicap in the Gospel Oaks study – 37% (95%CI: 33.3, 40.7).
Our study has applied the concepts of the WorldHealth Organization model to population mea-surement of participation restriction. Furtherinvestigation is now warranted to determine thepotential determinants (e.g. health conditions,impairments, activity limitations, environmentaland personal factors) of participation restriction inthe general population, which may explain itsnature and distribution and lead to the develop-
ment of interventions designed to reduce thiscommon form of disability in community-dwellingolder adults.
Key points
• Participation restriction is common in olderadults; 51.8% reported restriction in at leastone aspect of life.
• Participation restriction increased with age, asdid the number of areas of life in which partic-ipation was perceived to be restricted. How-ever, one-quarter of those over 80 years andover do not perceive themselves as restricted intheir participation in most areas of life.
• Women are more likely to report moderateand substantial amounts of participationrestriction than men.
• The distribution of person-perceived participa-tion restriction is similar to that for impairmentand activity limitation in community-dwellingolder adults.
Table 3. Observed numbers of responders and the 4-week period prevalence of any participation restriction, overall and stratified by
early and late response; the estimated number of non-responders and in the whole sample population with any participation restric-
tion
Age
group
Observed Estimated
Number (%) of
‘early responders�with any participation
restriction
Number (%) of
‘late responders�with any participation
restriction
Number of
all responders
(early + late)
with any participation
restriction
Number of
non-responders
with any
participation
restriction
Number in the
whole sample
population
(all responders +
non-responders)a
No. (%) No. (%) No. No. No.
50–59 years
Female 318 (43.9) 264 (48.0) 582 266 848
Male 240 (41.3) 229 (42.9) 469 308 777
60–69 years
Female 342 (44.9) 224 (52.3) 566 196 762
Male 276 (43.5) 187 (50.4) 463 206 669
70–79 years
Female 404 (58.6) 236 (65.7) 640 217 857
Male 257 (48.3) 160 (59.9) 417 162 579
80+ years
Female 263 (76.7) 167 (83.9) 430 328 758
Male 129 (66.2) 63 (71.6) 192 92 284
Total 2229 (50.0) 1530 (54.7) 3759 (51.8)b 1775 (54.7) 5534 (52.2)c
aTotal number of responders and non-responders was 10 611, due to missing data (n = 619).bObserved prevalence in all responders.cEstimated prevalence in the sample population (responders and non-responders).
1477

Acknowledgements
This study is supported financially by a Pro-gramme Grant awarded by the Medical ResearchCouncil, UK (Grant code: G9900220) and byfunding secured from the North StaffordshirePrimary Care R&D Consortium for NHS servicesupport costs. The authors would like to thankthe administrative and health informatics staff atKeele University�s Primary Care SciencesResearch Centre. We would also like to thankthe doctors, staff and patients of the participat-ing general practices and Professor Carol Jaggerfor her helpful comments on the drafting of thispaper.
References
1. Robine JM, Jagger C, Mathers CD, Crimmins EM,
Suzman RM, Peron Y. Introduction. In: Robine JM, Jagger
C, Mathers CD, Crimmins EM, Suzman RM (eds),
Determining Health Expectancies. Chichester: John Wiley
and sons, 2003.
2. World Health Organization. International Classification of
Functioning, Disability and Health. Geneva: World Health
Organization, 2001.
3. Harwood RH, Jitapunkul S, Dickinson E, Ebrahim S.
Measuring handicap: Motives, methods, and a model. Qual
Health Care 1994; 3: 53–57.
4. Harwood RH, Prince M, Mann A, Ebrahim S. Associa-
tions between diagnoses, impairments, disability and hand-
icap in a population of elderly people. Int J Epidemiol 1998;
27: 261–268.
5. Moore EG, Rosenberg MW, Fitzgibbon SH. Activity
limitation and chronic conditions in Canada�s elderly,
1986–2011. Disabil Rehabil 1999; 21: 196–210.
6. Martin J, Meltzer H, Elliot D. OPCS Surveys of Disability
in Great Britain: The Prevalence of Disability Among
Adults. London: OPCS, HMSO, 1987.
7. Beckett LA, Brock DB, Lemke JH, Mendes de Leon CF,
Guralnik JM, Fillenbaum GG, Branch LG, Wetle TT,
Evans DA. Analysis of change in self-reported physical
function among older persons in four population studies.
Am J Epidemiol 1996; 143: 766–778.
8. Ferrucci L, Penninx BW, Leveille SG, Corti MC, Pahor M,
Wallace R, Harris TB, Havlik RJ, Guralnik JM. Charac-
teristics of non-disabled older persons who perform poorly
in objective tests of lower extremity function. J Am Geriatr
Soc 2000; 48: 1102–1110.
9. Badley EM, Tennant A. Impact of disablement due to
rheumatic disorders in a British population: Estimates of
severity and prevalence from the Calderdale Rheumatic
Disablement Survey. Ann Rheum Dis 1993; 52: 6–13.
10. Bebbington AC, Darton RA. Healthy Life Expectancy in
England and Wales: Recent Evidence. London: PSSRU,
1996.
11. Cousins C, Jenkins J, Laux R. Disability data from the
Labour Force Survey: Comparing 1997–1998 with the past.
In: Office for National Statistics. Labour Market Trends
(June edition). HMSO: London, 1998.
12. Fried LP, Bandeen-Roche K, Kasper JD, Guralnik JM.
Association of comorbidity with disability in older women:
The Women�s Health and Aging Study. J Clin Epidemiol
1999; 52: 27–37.
13. Harwood RH, Prince MJ, Mann AH, Ebrahim S. The
prevalence of diagnoses, impairments, disabilities and
handicaps in a population of elderly people living in a
defined geographical area: The Gospel Oak project. Age
Ageing 1998; 2: 707–714.
14. Schwartz CE, Rapkin BD. Reconsidering the psychomet-
rics of quality of life assessment in light of response shift
and appraisal. Health Qual Life Outcomes 2004; 2: 14.
15. Carr AJ, Gibson B, Robinson PG. Measuring quality of
life: Is quality of life determined by expectations or
experience? Br Med J 2001; 322: 1240–1243.
16. Doherty M. Risk factors for progression of knee osteoar-
thritis. Lancet 2001; 358: 775–776.
17. Freedman VA, Martin LG. Understanding trends in
functional limitations among older Americans. Am J Public
Health 1998; 88: 1457–1462.
18. Thomas E, Wilkie R, Peat G, Hill S, Dziedzic KS, Croft
PR. The epidemiology and management of clinical osteo-
arthritis in the older population: Prospective 3-year study
of natural history and health care utilisation in the general
population. BMC Musculoskel Disorders 2004; 5(1): 2.
19. Trinder P. South Stoke Primary Care Trust. Demography
and Deprivation Profile. Directorate of Health Policy and
Public Health, North Staffordshire Health, 2002 http://
www.nsha.co.uk/home/library/hp/hp.
20. Trinder P. Newcastle-under-Lyme Primary Care Trust.
Demography and Deprivation Profile. Directorate of
Health Policy and Public Health, North Staffordshire
Health, 2002 http://www.nsha.co.uk/home/library/hp/hp.
21. Ware J Jr, Kosinski M, Keller SD. A 12-item short-form
health survey: Construction of scales and preliminary tests
of reliability and validity. Med Care 1996; 34: 220–233.
22. Wilkie R, Peat GM, Thomas E, Hooper H, Croft PR. The
Keele Assessment of Participation: A new instrument to
measure participation restriction in population studies.
Combined qualitative and quantitative examination of its
psychometric properties. Qual Life Res 2005; 14(8): 1889–
1899.
23. Bland M. An Introduction to Medical Statistics, 2nd ed.,
Oxford: Oxford Medical Publications, 1995.
24. Office for National Statistics. Health Quarterly 20. London:
Office for National Statistics, 2002.
25. Pettit T, Livingston G, Manela M, Kitchen G, Katona C,
Bowling A. Validation and normative data of health status
measures in older people: The Islington study. Int J Geriatr
Psychiatr 2001; 16: 1061–1070.
26. Thomas E, Peat G, Harris L, Wilkie R, Croft PR. The
prevalence of pain and pain interference in a general
1478

population of older adults: Cross-sectional findings from
the North Staffordshire Osteoarthritis Project (NorStOP).
Pain 2004; 110: 361–368.
27. Ueda S, Okawa Y. The subjective dimension of functioning
and disability: What is it and what is it for. Disabil Rehabil
2003; 25: 596–601.
28. Leveille SG, Penninx BW, Melzer D, Izmirlian G, Gurali-
nik JM. Sex differences in the prevalence of mobility
disability in old age: The dynamics of incidence, recovery,
and mortality. J Gerontol B Psychol Sci Soc Sci 2000; 55:
S41–50.
29. Odding E, Valkenburg HA, Stam HJ, Hofman A. Deter-
minants of locomotor disability in people aged 55 years and
over: The Rotterdam study. Eur J Epidemiol 2002; 17:
1033–1041.
30. Papageourgiou AC, Croft PR, Ferry S, Jayson MI, Silman
AJ. Estimating the prevalence of low back pain in the
general population. Evidence from the South Manchester
Back Pain Survey. Spine 1995; 20: 1889–1894.
31. Harwood RH, Rogers A, Dickinson E, Ebrahim S.
Measuring handicap: The London Handicap Scale, a new
outcome measure for chronic disease. Qual Health Care
1994b; 3: 11–16.
Address for correspondence: Primary Care Sciences Research
Centre, Keele Universtity, Keele, Staffordshire, ST5 5BG,
United Kingdom
Phone: +44-1782-593927; Fax: +44-1782-583911
(E-mail: [email protected])
1479