The potential offered by real-time, high-sensitivity monitoring of ethane in breath and some pilot...
9
INSTITUTE OF PHYSICS PUBLISHING JOURNAL OF OPTICS A: PURE AND APPLIED OPTICS J. Opt. A: Pure Appl. Opt. 7 (2005) S376–S384 doi:10.1088/1464-4258/7/6/019 The potential offered by real-time, high-sensitivity monitoring of ethane in breath and some pilot studies using optical spectroscopy Kenneth D Skeldon 1,4 , Claire Patterson 1 , Cathy A Wyse 2 , Graham M Gibson 1 , Miles J Padgett 1 , Chris Longbottom 3 and Lesley C McMillan 3 1 Department of Physics and Astronomy, Kelvin Building, University of Glasgow, G12 8QQ, UK 2 Institute for Comparative Medicine, Garscube Campus, University of Glasgow, UK 3 Division of Community Health Sciences, University of Dundee, Dundee, UK E-mail: [email protected] Received 25 November 2004, accepted for publication 18 April 2005 Published 12 May 2005 Online at stacks.iop.org/JOptA/7/S376 Abstract Breath analysis applied to biomedical applications has gained much momentum is recent years due to the growing research demonstrating that breath gas can provide clinically useful data. Particularly exciting is the area of real-time breath analysis which, when coupled with appropriately chosen target species, can offer a novel method for non-invasive patient monitoring. Here we describe the role of ethane, a breath gas of universal appeal in assessing in vivo oxidative stress (cell damage). We first present a review of emerging applications where real-time ethane monitoring could yield original new results for healthcare. We then report on results from a portable ethane spectroscopy system (accuracy better then 100 parts per trillion (1 part in 10 10 ) over a 1 s time response) that we have developed to exploit some of these applications. By presenting some initial results from pilot studies in the life sciences, we comment on the requirements that the next stage of optical spectroscopy technology has to meet in order to benefit clinical end-users. Keywords: ethane, trace gas spectroscopy, lead salt laser, breath analysis, oxidative stress (Some figures in this article are in colour only in the electronic version) 1. Introduction It has long been recognized that the profile of volatile organic compounds (VOCs) in exhaled breath could be useful in the diagnosis and monitoring of disease [1]. The development of breath analysis has steadily progressed despite the complex and variable chemical composition of the breath and the technological challenges of measuring trace concentrations of many of the components [2]. 4 Author to whom any correspondence should be addressed. One approach to breath analysis, given this variability, has been to focus on hydrocarbons in the range C4– C20, looking for characteristic combinations of these VOCs that might uniquely indicate the presence of a range of diseases [3–6]. However, while results have been encouraging, unique fingerprint combinations remain elusive despite nearly 400 components being investigated and sophisticated computational methods being employed [7, 8]. This is possibly explained, in that a given sample of breath merely represents a ‘snapshot’ of the volatile products generated by on-going physiological processes, so the relative proportions 1464-4258/05/060376+09$30.00 © 2005 IOP Publishing Ltd Printed in the UK S376
Transcript of The potential offered by real-time, high-sensitivity monitoring of ethane in breath and some pilot...
INSTITUTE OF PHYSICS PUBLISHING JOURNAL OF OPTICS A: PURE AND APPLIED OPTICS
J. Opt. A: Pure Appl. Opt. 7 (2005) S376–S384 doi:10.1088/1464-4258/7/6/019
The potential offered by real-time,high-sensitivity monitoring of ethane inbreath and some pilot studies usingoptical spectroscopyKenneth D Skeldon1,4, Claire Patterson1, Cathy A Wyse2,Graham M Gibson1, Miles J Padgett1, Chris Longbottom3 andLesley C McMillan3
1 Department of Physics and Astronomy, Kelvin Building, University of Glasgow, G12 8QQ,UK2 Institute for Comparative Medicine, Garscube Campus, University of Glasgow, UK3 Division of Community Health Sciences, University of Dundee, Dundee, UK
E-mail: [email protected]
Received 25 November 2004, accepted for publication 18 April 2005Published 12 May 2005Online at stacks.iop.org/JOptA/7/S376
AbstractBreath analysis applied to biomedical applications has gained muchmomentum is recent years due to the growing research demonstrating thatbreath gas can provide clinically useful data. Particularly exciting is the areaof real-time breath analysis which, when coupled with appropriately chosentarget species, can offer a novel method for non-invasive patient monitoring.Here we describe the role of ethane, a breath gas of universal appeal inassessing in vivo oxidative stress (cell damage). We first present a review ofemerging applications where real-time ethane monitoring could yieldoriginal new results for healthcare. We then report on results from a portableethane spectroscopy system (accuracy better then 100 parts per trillion(1 part in 1010) over a 1 s time response) that we have developed to exploitsome of these applications. By presenting some initial results from pilotstudies in the life sciences, we comment on the requirements that the nextstage of optical spectroscopy technology has to meet in order to benefitclinical end-users.
Keywords: ethane, trace gas spectroscopy, lead salt laser, breath analysis,oxidative stress
(Some figures in this article are in colour only in the electronic version)
1. Introduction
It has long been recognized that the profile of volatile organiccompounds (VOCs) in exhaled breath could be useful in thediagnosis and monitoring of disease [1]. The development ofbreath analysis has steadily progressed despite the complexand variable chemical composition of the breath and thetechnological challenges of measuring trace concentrations ofmany of the components [2].
4 Author to whom any correspondence should be addressed.
One approach to breath analysis, given this variability,has been to focus on hydrocarbons in the range C4–C20, looking for characteristic combinations of these VOCsthat might uniquely indicate the presence of a range ofdiseases [3–6]. However, while results have been encouraging,unique fingerprint combinations remain elusive despitenearly 400 components being investigated and sophisticatedcomputational methods being employed [7, 8]. This ispossibly explained, in that a given sample of breath merelyrepresents a ‘snapshot’ of the volatile products generated byon-going physiological processes, so the relative proportions
1464-4258/05/060376+09$30.00 © 2005 IOP Publishing Ltd Printed in the UK S376

The potential offered by real-time, high-sensitivity monitoring of ethane in breath and some pilot studies using optical spectroscopy
of VOCs are dependent on the underlying kinetics. Forexample, the solubility of hydrocarbons in the blood increaseswith increasing chain length, and so there is a chain-length-dependent time delay between their generation in vivo andtheir exhalation in the breath.
An alternative approach has been to focus on singlecommon components in breath that have proven clinicalsignificance. In this paper we discuss the potential offeredby the monitoring of ethane gas in real time and the roleof optical spectroscopy in realizing this. Exhaled ethane(C2H6) is produced in vivo by the oxidation of cell membranelipids [9] as a consequence of free radical mediated attack [10].Antioxidant defences counter this free radical attack, resultingin a state of dynamic equilibrium in healthy individuals.Oxidative stress (OS) was defined in 1985 as ‘a disturbancein the pro-oxidant–antioxidant balance in favour of theformer’ [11]. Since disease is often accompanied by raisedlevels of OS, exhaled ethane is a potential biomarker of disease.Ethane has advantages over other volatile markers of oxidativestress in that it is highly volatile (boiling point = −88.6 ◦C), itis not metabolized significantly [12] and it is poorly soluble inboth oil and water. Therefore, when free radicals are releasedinto the tissue, the ethane generated is rapidly lost in exhaledbreath [13], making it a readily accessible and effective markerfor oxidative stress in real time.
However, the real-time measurement of ethane has onlybecome possible relatively recently. Optical spectroscopytechniques are likely to open up a new window on non-invasiveoxidative stress measurement for a whole range of clinical andlife science applications, although the technology must achieveambitious targets. First, it must be sensitive, since ethane istypically present in breath at part per billion (ppb) levels (1 partin 109). Second, the technology must be able to chart ethaneexpiration in real time in order to probe alveolar gradients.Third, and perhaps most importantly, any instrumentation mustbe portable in order that it can be conveniently used on-site.
The ethane spectroscopy system we describe below hasachieved many of these goals. Before we discuss the designand performance of the technology, we will summarize someof the medical motivation for the development of an oxidativestress monitor.
2. The importance of oxidative stress
Free radical induced oxidative stress has been recognizedas playing a role in the development of a wide range ofdiseases. These include respiratory diseases such as lungcancer [3, 4, 7, 8], cystic fibrosis [14], chronic obstructivepulmonary disease (COPD) [15–17], acute respiratory distresssyndrome (ARDS) [18], and asthma [15, 19]. Other conditionswhere an elevation in oxidative stress has been reportedinclude breast cancer [20], ulcerative colitis [21], inflammatorybowel disease and HIV infection [22] and pre-eclampsia inpregnancy [23, 24]. It has also been reported that severeoxidative stress in critical illness [25] can lead to organfailure [26].
Any condition where there has been ischaemia andreperfusion injury is associated with breakdown of cellularlipids and so will lead to a resulting increase in oxidativestress. This includes cardiopulmonary bypass [27–29],
haemodialysis [30–33], and organ transplantation [34].Recent publications discuss the role of oxidative stress inrenal [35–39], pancreatic [40], liver [41], lung [42] andheart [43] transplantation, and specifically, the use of exhaledbiomarkers has been discussed in relation to the heart, liver andlung. Oxidative stress has also been found to increase duringperiods of maximal exercise [44, 45].
Another known cause of elevated oxidative stress isexposure to ionizing radiation. Radiotherapy can be regardedas a cause of oxidative stress since ionizing radiation exerts itsbiological effects, at least in part, through physico-chemicalinteractions which cause the production of free radicals.Recent data from the Oncology Department of NinewellsHospital, using reflectance spectrophotometry, showed awidely varying range of values for radiation induced reddeningof the skin (erythema) [46, 47], and so any test that couldhelp optimize dosage could be clinically useful. This mayhelp the problem of dose threshold where too high a dosecan cause normal tissue damage but too low a dose candeny patients with more radioresistant tumours the chanceof efficient cure [48]. The techniques currently in use havebeen proved too cumbersome and/or unreliable for routineclinical use in assessing this balance [49] and could constitutean important application of an ethane test.
Having highlighted many of the possible applications fora convenient breath assessment of oxidative stress we shouldstress that a rigorous sampling protocol must be employedin order to minimize errors [2]. Breath gas levels areaffected by smoking habit, duration after eating and drinking,medication history and also issues regarding the effects ofthe ambient background. For example, proper assessment ofthe air being inhaled by subjects, whether it be the normalroom background or air from a hydrocarbon-free source, ismandatory. Consistent sample collection regarding tidal airversus alveolar breath must also be considered, involvingperhaps carbon dioxide expiration as a dynamic tag.
Above all, the ability to measure exhaled breath in realtime with an on-site analyser will always prove better thandiscrete methods involving sample collection devices. We willdescribe an ethane spectroscopy system based upon technologyfirst developed for use in the oil industry [50], and thathas now been developed into a dedicated healthcare sensorwith the potential to exploit some of the clinical applicationsdiscussed [51].
3. Ultra-sensitive wavelength modulationspectroscopy for ethane
Optical absorption spectroscopy systems for gas analysis havebrought about new opportunities in recent years, while theincreased sensitivity available with modulation techniquesoffers particular potential for trace species measurement [52].Although the high resolution optical techniques are necessarilymore specific to target species than mass spectrometry andits variants, they offer much faster evaluation of samples andthe advantage of real-time use. Although many techniquesare available for gas analysis, many of which rely on massspectrometry and variants thereof [53], we are aware of notechniques that can offer sub-ppb, real-time measurement ofethane, other than optical spectroscopy.
S377
K D Skeldon et al
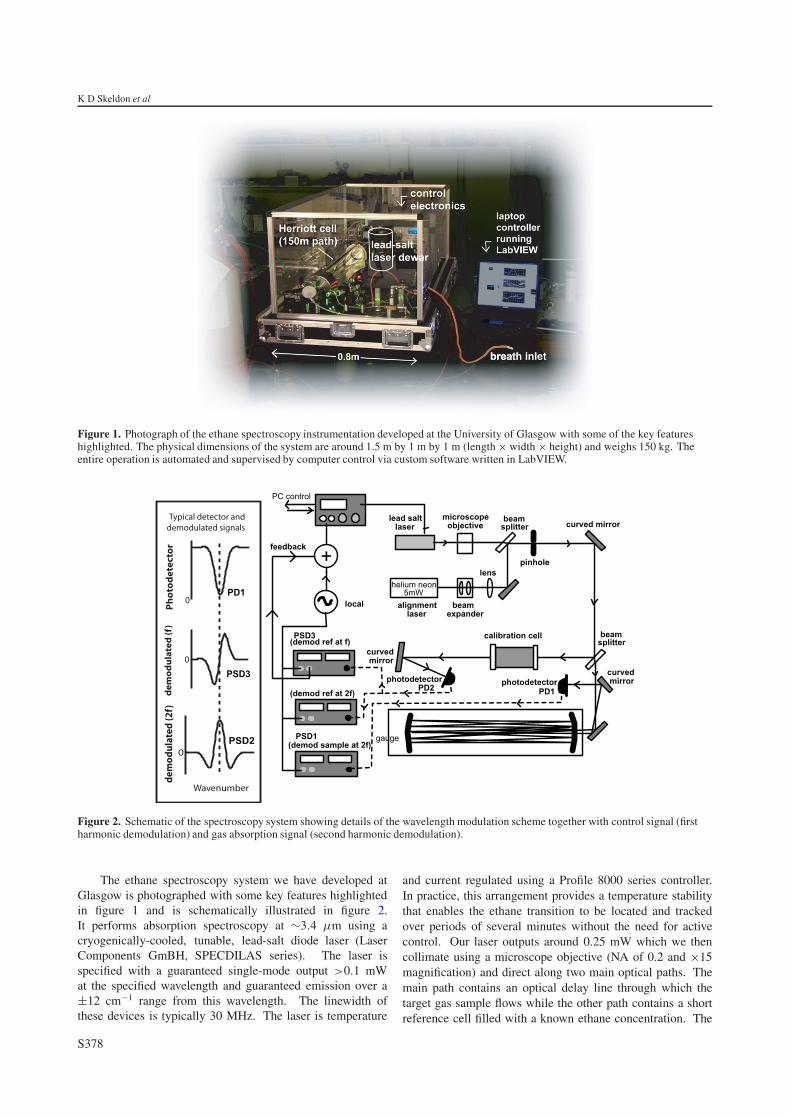
Figure 1. Photograph of the ethane spectroscopy instrumentation developed at the University of Glasgow with some of the key featureshighlighted. The physical dimensions of the system are around 1.5 m by 1 m by 1 m (length × width × height) and weighs 150 kg. Theentire operation is automated and supervised by computer control via custom software written in LabVIEW.
Figure 2. Schematic of the spectroscopy system showing details of the wavelength modulation scheme together with control signal (firstharmonic demodulation) and gas absorption signal (second harmonic demodulation).
The ethane spectroscopy system we have developed atGlasgow is photographed with some key features highlightedin figure 1 and is schematically illustrated in figure 2.It performs absorption spectroscopy at ∼3.4 µm using acryogenically-cooled, tunable, lead-salt diode laser (LaserComponents GmBH, SPECDILAS series). The laser isspecified with a guaranteed single-mode output >0.1 mWat the specified wavelength and guaranteed emission over a±12 cm−1 range from this wavelength. The linewidth ofthese devices is typically 30 MHz. The laser is temperature
and current regulated using a Profile 8000 series controller.In practice, this arrangement provides a temperature stabilitythat enables the ethane transition to be located and trackedover periods of several minutes without the need for activecontrol. Our laser outputs around 0.25 mW which we thencollimate using a microscope objective (NA of 0.2 and ×15magnification) and direct along two main optical paths. Themain path contains an optical delay line through which thetarget gas sample flows while the other path contains a shortreference cell filled with a known ethane concentration. The
S378
The potential offered by real-time, high-sensitivity monitoring of ethane in breath and some pilot studies using optical spectroscopy
higher response, lower integration time lower response, higher integration time
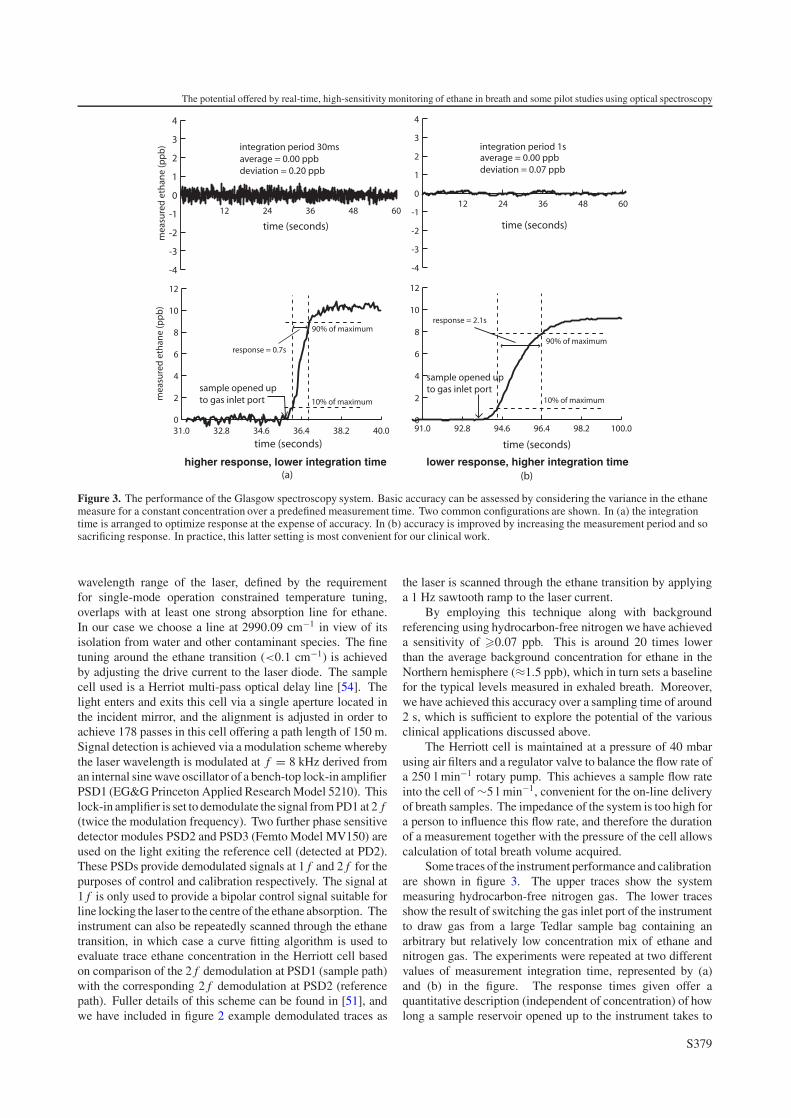
Figure 3. The performance of the Glasgow spectroscopy system. Basic accuracy can be assessed by considering the variance in the ethanemeasure for a constant concentration over a predefined measurement time. Two common configurations are shown. In (a) the integrationtime is arranged to optimize response at the expense of accuracy. In (b) accuracy is improved by increasing the measurement period and sosacrificing response. In practice, this latter setting is most convenient for our clinical work.
wavelength range of the laser, defined by the requirementfor single-mode operation constrained temperature tuning,overlaps with at least one strong absorption line for ethane.In our case we choose a line at 2990.09 cm−1 in view of itsisolation from water and other contaminant species. The finetuning around the ethane transition (<0.1 cm−1) is achievedby adjusting the drive current to the laser diode. The samplecell used is a Herriot multi-pass optical delay line [54]. Thelight enters and exits this cell via a single aperture located inthe incident mirror, and the alignment is adjusted in order toachieve 178 passes in this cell offering a path length of 150 m.Signal detection is achieved via a modulation scheme wherebythe laser wavelength is modulated at f = 8 kHz derived froman internal sine wave oscillator of a bench-top lock-in amplifierPSD1 (EG&G Princeton Applied Research Model 5210). Thislock-in amplifier is set to demodulate the signal from PD1 at 2 f(twice the modulation frequency). Two further phase sensitivedetector modules PSD2 and PSD3 (Femto Model MV150) areused on the light exiting the reference cell (detected at PD2).These PSDs provide demodulated signals at 1 f and 2 f for thepurposes of control and calibration respectively. The signal at1 f is only used to provide a bipolar control signal suitable forline locking the laser to the centre of the ethane absorption. Theinstrument can also be repeatedly scanned through the ethanetransition, in which case a curve fitting algorithm is used toevaluate trace ethane concentration in the Herriott cell basedon comparison of the 2 f demodulation at PSD1 (sample path)with the corresponding 2 f demodulation at PSD2 (referencepath). Fuller details of this scheme can be found in [51], andwe have included in figure 2 example demodulated traces as
the laser is scanned through the ethane transition by applyinga 1 Hz sawtooth ramp to the laser current.
By employing this technique along with backgroundreferencing using hydrocarbon-free nitrogen we have achieveda sensitivity of �0.07 ppb. This is around 20 times lowerthan the average background concentration for ethane in theNorthern hemisphere (≈1.5 ppb), which in turn sets a baselinefor the typical levels measured in exhaled breath. Moreover,we have achieved this accuracy over a sampling time of around2 s, which is sufficient to explore the potential of the variousclinical applications discussed above.
The Herriott cell is maintained at a pressure of 40 mbarusing air filters and a regulator valve to balance the flow rate ofa 250 l min−1 rotary pump. This achieves a sample flow rateinto the cell of ∼5 l min−1, convenient for the on-line deliveryof breath samples. The impedance of the system is too high fora person to influence this flow rate, and therefore the durationof a measurement together with the pressure of the cell allowscalculation of total breath volume acquired.
Some traces of the instrument performance and calibrationare shown in figure 3. The upper traces show the systemmeasuring hydrocarbon-free nitrogen gas. The lower tracesshow the result of switching the gas inlet port of the instrumentto draw gas from a large Tedlar sample bag containing anarbitrary but relatively low concentration mix of ethane andnitrogen gas. The experiments were repeated at two differentvalues of measurement integration time, represented by (a)and (b) in the figure. The response times given offer aquantitative description (independent of concentration) of howlong a sample reservoir opened up to the instrument takes to
S379
K D Skeldon et al
fill the sample cell. We define the T90 interval as the timetaken for the measured concentration to vary from 10% to90% of the final steady state value. The integration periodof 30 ms offers basic accuracy of 0.2 ppb and T90 time of0.7 s, and is a typical operating point for our clinical samplemeasurements. The basic accuracy is limited by technicalnoise sources (dynamic optical fringing and electronic noiseassociated with the PSDs). Estimates of the laser light levelsat the photodetectors suggest that we are around a factor offour from the fundamental sensitivity limit set by photon shotnoise.
It should be noted that contamination due to other speciesis not problematic in our technique, since the only othergas in close proximity to our chosen ethane transition ismethane, albeit separated by more than the typical width ofboth transitions. This can be used to our advantage as bothgases can be simultaneously measured over a ∼0.5 cm−1 range(and we routinely do this by applying a suitable ramp signalto the laser current controller). Indeed it is sometimes usefulto monitor methane in breath studies in order to screen forextremely high concentrations that might indicate the presenceof contaminants.
Several groups have reported ethane measurement in thepast, for example using photoacoustic technology [55, 56]or cavity decay-time techniques [57, 58]. However, sinceour technology was motivated by an industrial applicationrequiring field use in a hostile environment [59], it hasintrinsic technical attributes that make for a robust instrumentin the present application. For example, in contrast toresonant optical cavity based systems our technique is firstorder insensitive to mirror contamination. We routinelyuse it to directly analyse breath with no need for samplefiltering or pre-preparation and with no evident degradationin performance over months of operation. Furthermore,although others have reported sensitivities for ethane that areextremely low, the issue of measurement integration time mustbe considered. We believe our present configuration to offer thebest reported combination of high sensitivity and low responsetime while requiring no preprocessing of the breath sample. Ofcourse, there is a user-dictated trade-off between measurementintegration time and basic accuracy. The operating pointchosen is to some extent influenced by the particular clinicalapplication. As we indicated above, for many of the pilotexperiments described below, we have operated the instrumentat a setting corresponding to ∼0.2 ppb accuracy and ∼0.7 sresponse (T90) time.
The operation of our technology is turn-key, automatedby control software written in LabVIEW. This oversees allaspects of instrument operation, including laser management,cell pressure control, data acquisition and calibration issues.This combination of features lends itself to direct clinical use.Having said this, a key feature limiting convenient on-site use isinstrument bulk. We will comment later on some current workto miniaturize the technology and so begin to push forward theboundaries of the real-time clinical applications.
4. Pilot studies in monitoring and diagnosticapplications
We have conducted pilot studies in a range of clinical andlife-science fields. Here we present snapshots of the most
time (minutes)
reperfusion
reperfusion (~1hour)
anhepatic
pre-reperfusion
pre-hepatectomy
ethane (ppb)
0 15 30 45 60-15-30
A
B
0
10
20
30
40
50
60
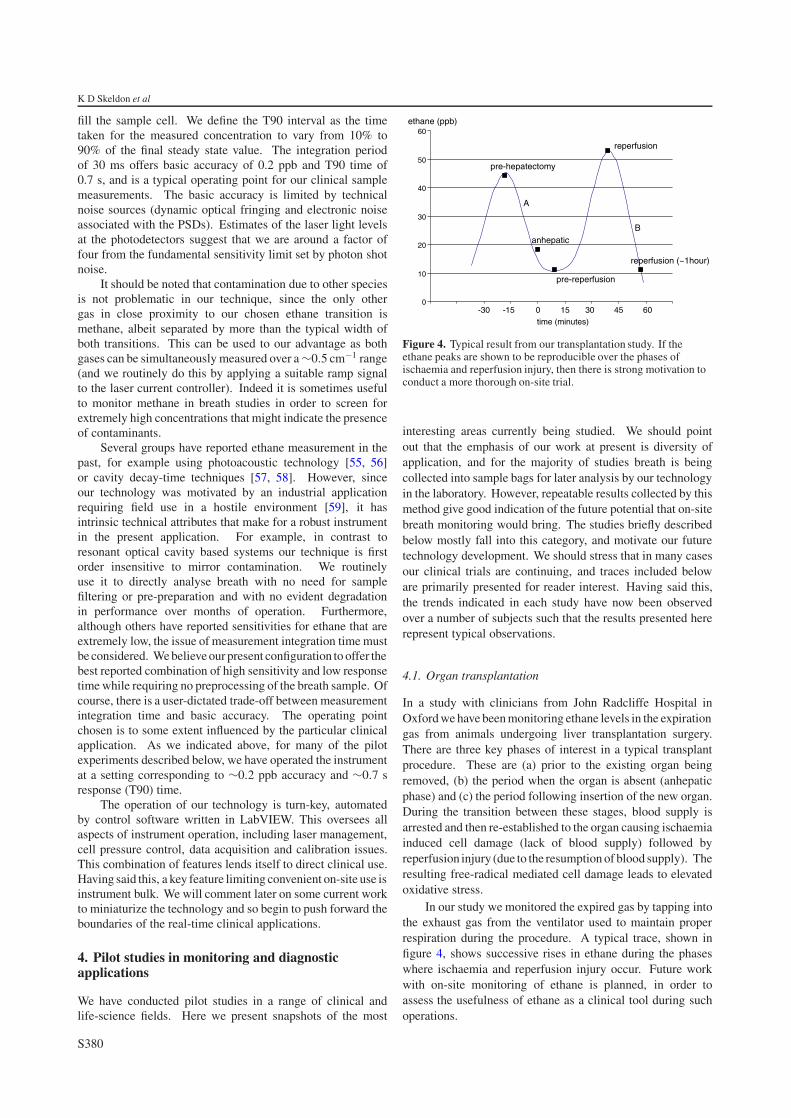
Figure 4. Typical result from our transplantation study. If theethane peaks are shown to be reproducible over the phases ofischaemia and reperfusion injury, then there is strong motivation toconduct a more thorough on-site trial.
interesting areas currently being studied. We should pointout that the emphasis of our work at present is diversity ofapplication, and for the majority of studies breath is beingcollected into sample bags for later analysis by our technologyin the laboratory. However, repeatable results collected by thismethod give good indication of the future potential that on-sitebreath monitoring would bring. The studies briefly describedbelow mostly fall into this category, and motivate our futuretechnology development. We should stress that in many casesour clinical trials are continuing, and traces included beloware primarily presented for reader interest. Having said this,the trends indicated in each study have now been observedover a number of subjects such that the results presented hererepresent typical observations.
4.1. Organ transplantation
In a study with clinicians from John Radcliffe Hospital inOxford we have been monitoring ethane levels in the expirationgas from animals undergoing liver transplantation surgery.There are three key phases of interest in a typical transplantprocedure. These are (a) prior to the existing organ beingremoved, (b) the period when the organ is absent (anhepaticphase) and (c) the period following insertion of the new organ.During the transition between these stages, blood supply isarrested and then re-established to the organ causing ischaemiainduced cell damage (lack of blood supply) followed byreperfusion injury (due to the resumption of blood supply). Theresulting free-radical mediated cell damage leads to elevatedoxidative stress.
In our study we monitored the expired gas by tapping intothe exhaust gas from the ventilator used to maintain properrespiration during the procedure. A typical trace, shown infigure 4, shows successive rises in ethane during the phaseswhere ischaemia and reperfusion injury occur. Future workwith on-site monitoring of ethane is planned, in order toassess the usefulness of ethane as a clinical tool during suchoperations.
S380
The potential offered by real-time, high-sensitivity monitoring of ethane in breath and some pilot studies using optical spectroscopy
Figure 5. Typical trace based on repeated delivery of samples frompatients undergoing radiation treatment. The trial is in its earlystages, but the ability to correlate ethane production with dose wouldbe significant. Note that the data line is smoothed, and the nature ofthe ethane variation between the concentrations collected can onlybe assessed with on-site monitoring. Error bars represent theinstrument accuracy over the measurement period taken to emptyeach sample bag. Patients tended to provide smaller post-treatmentsamples and hence the error values increase in this regime.
4.2. Radiation therapy
We have commenced a pilot trial involving twenty newlyreferred patients for radiation treatment at Ninewells Hospitalin Dundee. The aim is to investigate whether ethane in thebreath of the patients was elevated due to the oxidative stresscaused directly by the radiation dose. Sampling of the breathis done pre-treatment and immediately post-treatment by thedelivery of breath samples into collection bags (Tedlar, 5 l).Initial results, an example of which is shown in figure 5, showincreased ethane a few minutes following the radiation dose,but it is too early in the trial to draw firm conclusions on whethersuch elevations are correlated to the radiation dose. As thetrial progresses, factors such as individual patient sensitivityto radiation and the proportionality between observed ethaneand integral dose will be examined more fully.
If the ethane is shown to be reproducible given consistentpatient and dose parameters then on-site monitoring of breathcould provide a novel method of optimizing the radiotherapydoses for individual patients.
4.3. Exercise induced oxidative stress
In conjunction with sports science physiologists at theUniversity of Glasgow we have conducted pseudo-real-timemeasurements of exhaled ethane in human, equine and canineathletes. Breath samples were collected at 20 and 30 minprior to the commencement of exercise. Human subjects thenran on a treadmill at a pre-determined speed (which eliciteda stable heart-rate of 140–160 bpm and at which the subjectfelt comfortable) on the flat for two minutes, and followingthis, the gradient was increased stepwise every 2 min at a rateof 1◦ min−1. Once the subjects reached volitional exhaustionthe treadmill was returned to a walking pace on the flat for6 min. During both the incremental and recovery phases onthe treadmill expired gas was collected every 2 min for analysisof ethane content.
The canine athletes (racing greyhounds) were testedbefore and after a competitive race over a distance of 480 m
0
25
50
75
100
125
150
ethane (pmol/min/kg)
exercise recoverystage
pre-exercise (~12 minutes)
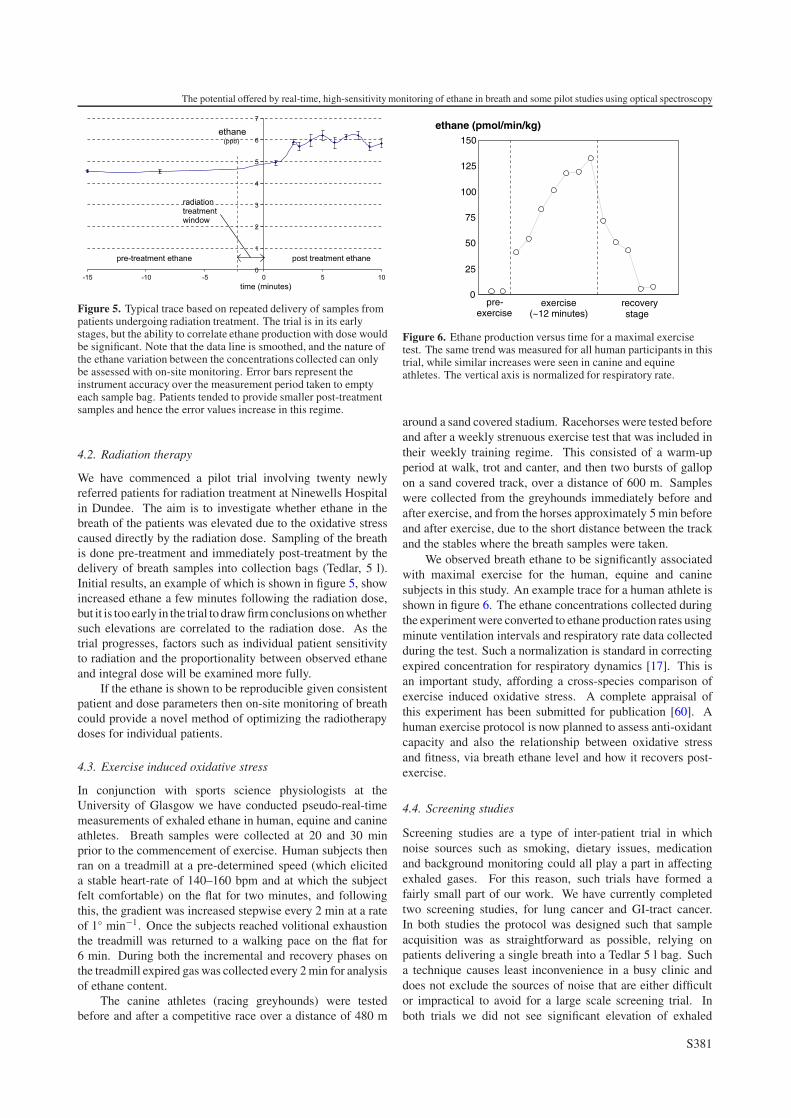
Figure 6. Ethane production versus time for a maximal exercisetest. The same trend was measured for all human participants in thistrial, while similar increases were seen in canine and equineathletes. The vertical axis is normalized for respiratory rate.
around a sand covered stadium. Racehorses were tested beforeand after a weekly strenuous exercise test that was included intheir weekly training regime. This consisted of a warm-upperiod at walk, trot and canter, and then two bursts of gallopon a sand covered track, over a distance of 600 m. Sampleswere collected from the greyhounds immediately before andafter exercise, and from the horses approximately 5 min beforeand after exercise, due to the short distance between the trackand the stables where the breath samples were taken.
We observed breath ethane to be significantly associatedwith maximal exercise for the human, equine and caninesubjects in this study. An example trace for a human athlete isshown in figure 6. The ethane concentrations collected duringthe experiment were converted to ethane production rates usingminute ventilation intervals and respiratory rate data collectedduring the test. Such a normalization is standard in correctingexpired concentration for respiratory dynamics [17]. This isan important study, affording a cross-species comparison ofexercise induced oxidative stress. A complete appraisal ofthis experiment has been submitted for publication [60]. Ahuman exercise protocol is now planned to assess anti-oxidantcapacity and also the relationship between oxidative stressand fitness, via breath ethane level and how it recovers post-exercise.
4.4. Screening studies
Screening studies are a type of inter-patient trial in whichnoise sources such as smoking, dietary issues, medicationand background monitoring could all play a part in affectingexhaled gases. For this reason, such trials have formed afairly small part of our work. We have currently completedtwo screening studies, for lung cancer and GI-tract cancer.In both studies the protocol was designed such that sampleacquisition was as straightforward as possible, relying onpatients delivering a single breath into a Tedlar 5 l bag. Sucha technique causes least inconvenience in a busy clinic anddoes not exclude the sources of noise that are either difficultor impractical to avoid for a large scale screening trial. Inboth trials we did not see significant elevation of exhaled
S381
K D Skeldon et al
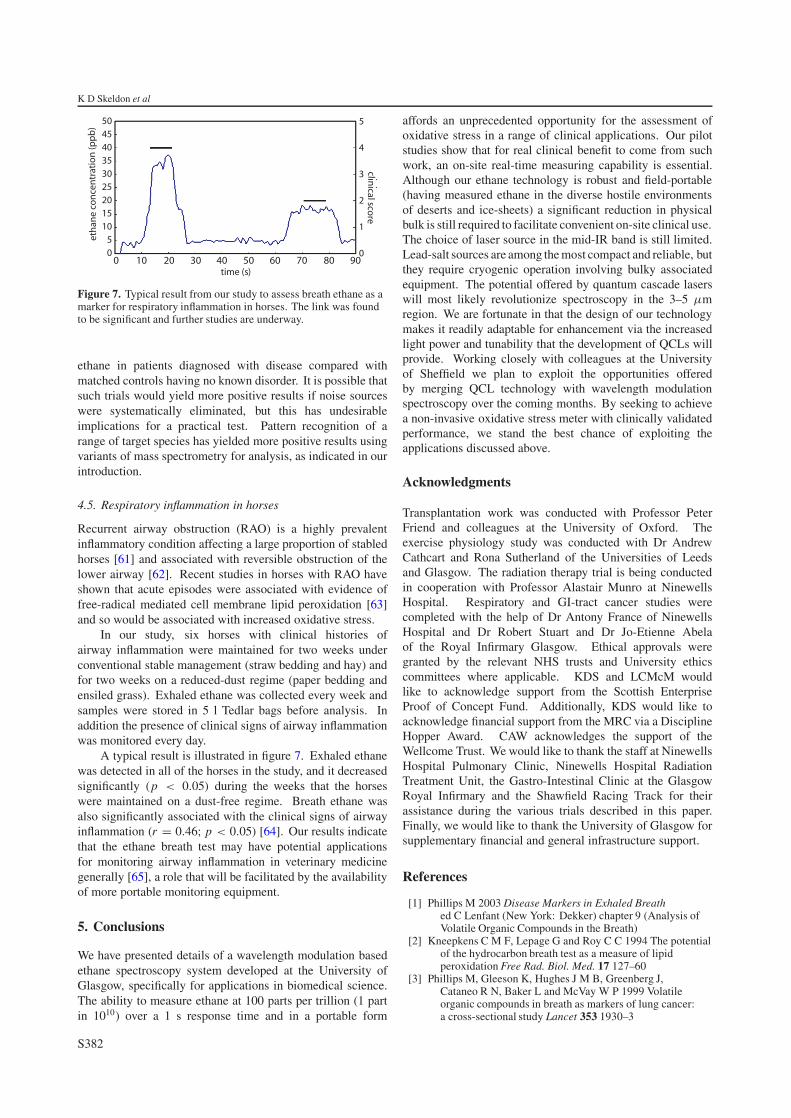
Figure 7. Typical result from our study to assess breath ethane as amarker for respiratory inflammation in horses. The link was foundto be significant and further studies are underway.
ethane in patients diagnosed with disease compared withmatched controls having no known disorder. It is possible thatsuch trials would yield more positive results if noise sourceswere systematically eliminated, but this has undesirableimplications for a practical test. Pattern recognition of arange of target species has yielded more positive results usingvariants of mass spectrometry for analysis, as indicated in ourintroduction.
4.5. Respiratory inflammation in horses
Recurrent airway obstruction (RAO) is a highly prevalentinflammatory condition affecting a large proportion of stabledhorses [61] and associated with reversible obstruction of thelower airway [62]. Recent studies in horses with RAO haveshown that acute episodes were associated with evidence offree-radical mediated cell membrane lipid peroxidation [63]and so would be associated with increased oxidative stress.
In our study, six horses with clinical histories ofairway inflammation were maintained for two weeks underconventional stable management (straw bedding and hay) andfor two weeks on a reduced-dust regime (paper bedding andensiled grass). Exhaled ethane was collected every week andsamples were stored in 5 l Tedlar bags before analysis. Inaddition the presence of clinical signs of airway inflammationwas monitored every day.
A typical result is illustrated in figure 7. Exhaled ethanewas detected in all of the horses in the study, and it decreasedsignificantly (p < 0.05) during the weeks that the horseswere maintained on a dust-free regime. Breath ethane wasalso significantly associated with the clinical signs of airwayinflammation (r = 0.46; p < 0.05) [64]. Our results indicatethat the ethane breath test may have potential applicationsfor monitoring airway inflammation in veterinary medicinegenerally [65], a role that will be facilitated by the availabilityof more portable monitoring equipment.
5. Conclusions
We have presented details of a wavelength modulation basedethane spectroscopy system developed at the University ofGlasgow, specifically for applications in biomedical science.The ability to measure ethane at 100 parts per trillion (1 partin 1010) over a 1 s response time and in a portable form
affords an unprecedented opportunity for the assessment ofoxidative stress in a range of clinical applications. Our pilotstudies show that for real clinical benefit to come from suchwork, an on-site real-time measuring capability is essential.Although our ethane technology is robust and field-portable(having measured ethane in the diverse hostile environmentsof deserts and ice-sheets) a significant reduction in physicalbulk is still required to facilitate convenient on-site clinical use.The choice of laser source in the mid-IR band is still limited.Lead-salt sources are among the most compact and reliable, butthey require cryogenic operation involving bulky associatedequipment. The potential offered by quantum cascade laserswill most likely revolutionize spectroscopy in the 3–5 µmregion. We are fortunate in that the design of our technologymakes it readily adaptable for enhancement via the increasedlight power and tunability that the development of QCLs willprovide. Working closely with colleagues at the Universityof Sheffield we plan to exploit the opportunities offeredby merging QCL technology with wavelength modulationspectroscopy over the coming months. By seeking to achievea non-invasive oxidative stress meter with clinically validatedperformance, we stand the best chance of exploiting theapplications discussed above.
Acknowledgments
Transplantation work was conducted with Professor PeterFriend and colleagues at the University of Oxford. Theexercise physiology study was conducted with Dr AndrewCathcart and Rona Sutherland of the Universities of Leedsand Glasgow. The radiation therapy trial is being conductedin cooperation with Professor Alastair Munro at NinewellsHospital. Respiratory and GI-tract cancer studies werecompleted with the help of Dr Antony France of NinewellsHospital and Dr Robert Stuart and Dr Jo-Etienne Abelaof the Royal Infirmary Glasgow. Ethical approvals weregranted by the relevant NHS trusts and University ethicscommittees where applicable. KDS and LCMcM wouldlike to acknowledge support from the Scottish EnterpriseProof of Concept Fund. Additionally, KDS would like toacknowledge financial support from the MRC via a DisciplineHopper Award. CAW acknowledges the support of theWellcome Trust. We would like to thank the staff at NinewellsHospital Pulmonary Clinic, Ninewells Hospital RadiationTreatment Unit, the Gastro-Intestinal Clinic at the GlasgowRoyal Infirmary and the Shawfield Racing Track for theirassistance during the various trials described in this paper.Finally, we would like to thank the University of Glasgow forsupplementary financial and general infrastructure support.
References
[1] Phillips M 2003 Disease Markers in Exhaled Breathed C Lenfant (New York: Dekker) chapter 9 (Analysis ofVolatile Organic Compounds in the Breath)
[2] Kneepkens C M F, Lepage G and Roy C C 1994 The potentialof the hydrocarbon breath test as a measure of lipidperoxidation Free Rad. Biol. Med. 17 127–60
[3] Phillips M, Gleeson K, Hughes J M B, Greenberg J,Cataneo R N, Baker L and McVay W P 1999 Volatileorganic compounds in breath as markers of lung cancer:a cross-sectional study Lancet 353 1930–3
S382
The potential offered by real-time, high-sensitivity monitoring of ethane in breath and some pilot studies using optical spectroscopy
[4] Phillips M, Cataneo R N, Cummin A R C, Gagliardi A J,Gleeson K, Greenberg J, Maxfield R A and Rom W N 2003Detection of lung cancer with volatile markers in the breathChest 123 2115–23
[5] Phillips M, Cataneo R N, Ditkoff B A, Fisher P, Greenberg J,Gunawardena R, Kwon C S, Rahbari-Oskoui F and Wong C2003 Volatile markers of breast cancer in the breath Breast J.9 184–91
[6] Phillips M, Cataneo R N, Greenberg J, Grodman R andSalazar M 2003 Breath markers of oxidative stress inpatients with unstable angina Heart Dis. 5 95–9
[7] Gordon S M, Szidon J P, Krotoszynski B K, Gibbons R D andO’Neill H J 1985 Volatile organic compounds in exhaled airfrom patients with lung cancer Clin. Chem. 31 1278–82
[8] O’Neill H J, Gordon S M, O’Neill M H, Gibbons R D andSzidon J P 1998 A computerized classification techniquefor screening for the presence of breath biomarkers in lungcancer Clin. Chem. 34 1613–8
[9] Riely C A, Cohen G and Lieberman M 1974 Ethane evolution:new index of lipid peroxidation Science 183 208–10
[10] Halliwell B and Gutteridge J M C 2001 Free Radical Biologyand Medicine 3rd edn (Oxford: Oxford Science) p 246
[11] Sies H (ed) 1985 Introductory remarks Oxidative Stress(London: Academic) pp 1–8
[12] Burk R, Ludden T and Lane J 1982 Pentane clearance frominspired air by the rat: dependence on the liverGastroenterology 84 138–42
[13] Brown R H and Risby T H 2003 Disease Markers in ExhaledBreath ed C Lenfant (New York: Dekker) chapter 13
[14] Brown R K and Kelly F J 1994 Role of free radicals in thepathogenesis of cystic fibrosis Thorax 49 738–42
[15] Rahman I, Morrison D, Donaldson K and MacNee W 1996Systemic oxidative stress in asthma, COPD and smokersAm. J. Respir. Crit. Care Med. 154 1055–60
[16] Repine J E, Bast A and Lankhorst I 1997 Oxidative stress inchronic obstructive pulmonary disease: oxidative stressstudy group Am. J. Respir. Crit. Care Med. 156 341–57
[17] Paredi P, Kharitonov S A, Leak D, Ward S, Cramer D andBarnes P J 2000 Exhaled ethane, a marker of lipidperoxidation, is elevated in chronic obstructive pulmonarydisease Am. J. Respir. Crit. Care Med. 162 369–73
[18] Gutteridge J M and Mitchell J 1999 Redox imbalance in thecritically ill J. Br. Med. Bull. 55 49–75
[19] Barnes P J 1990 Reactive oxygen species and airwayinflammation Free Radic. Biol. Med. 9 235–43
[20] Li D, Zhang W, Sahin A A and Hittelman W N 1999 DNAadducts in normal tissue adjacent to breast cancer: a reviewCancer Detect. Prev. 23 454–62
[21] Sedghi S, Keshavarzian A, Klamut M, Eiznhamer D andZarling E J 1994 Elevated breath ethane levels in activeulcerative colitis: Evidence for excessive lipid peroxidationAm. J. Gastroenterol. 89 2217–21
[22] Aghdassi E and Allard J P 2000 Breath alkanes as a marker ofoxidative stress in different clinical conditions Free Rad.Biol. Med. 28 880–6
[23] Hubel C A 1999 Oxidative stress in the pathogenesis ofpreeclampsia Proc. Soc. Exp. Biol. Med. 222 222–35
[24] Bilodeau J F and Hubel C A 2003 Current concepts in the useof antioxidants for the treatment of preeclampsia J. Obstet.Gynaecol. Can. 25 742–50
[25] Goodyear-Bruch C and Pierce J D 2002 Oxidative stress incritically ill patients Am. J. Crit. Care 11 543–51
[26] Lovat R and Preiser J C 2003 Antioxidant therapy in intensivecare Curr. Opin. Crit. Care 9 266–70
[27] Barsacchi R, Pelosi G, Maffei S, Baroni M, Salvatore L,Ursini F, Verunelli F and Biagini A 1992 Myocardialvitamin E is consumed during cardiopulmonary bypass:indirect evidence of free radical generation in humanischaemic heart Int. J. Cardiol. 37 339–43
[28] Angdin M, Settergren G, Starkopf J, Zilmer M, Zilmer K andVaage J 2003 Protective effect of antioxidants on
pulmonary endothelial function after cardiopulmonarybypass J. Cardiothorac. Vasc. Anesth. 17 314–20
[29] Andreoni K A, Kazui M, Cameron D E, Nyhan D, Sehnert S S,Rohde C A, Bulkley G B and Risby T H 1999 Ethane:a marker of lipid peroxidation during cardiopulmonarybypass in humans Free Radic. Biol. Med. 26 439–45
[30] Giardini O, Taccone-Gallucci M, Lubrano R,Ricciardi-Tenire G, Bandino D, Silvi I, Ruberto U andCasciani C U 1984 Evidence of red blood cell membranelipid peroxidation in haemodialysis patients Nephron 36235–7
[31] Dursun E, Ozben T, Suleymanlar G, Dursun B andYakupoglu G 2002 Effect of hemodialysis on the oxidativestress and antioxidants Clin. Chem. Lab. Med. 40 1009–13
[32] Capodicasa E, Trovarelli G, De Medio G E, Pelli M A,Lippi G, Verdura C and Timio M 1999 Volatile alkanes andincreased concentrations of isoprene in exhaled air duringhemodialysis Nephron 82 331–7
[33] Handelman G J et al 2003 Breath ethane in dialysis patientsand control subjects Free Radic. Biol. Med. 35 17–23
[34] Phillips M et al 2004 Heart allograft rejection: detection withbreath alkanes in low levels (the HARDBALL study)J. Heart Lung Transpl. 23 701–8
[35] Abdelfatah A, Ducloux D, Toubin G, Motte G, Alber D andChalopin J M 2002 Treatment of hyperhomocysteinemiawith folic acid reduces oxidative stress in renal transplantrecipients Transplantation 73 663–5
[36] Kosieradzki M, Kuczynska J, Piwowarska J,Wegrowicz-Rebandel I, Kwiatkowski A, Lisik W,Michalak G, Danielewicz R, Paczek L and Rowinski W A2003 Prognostic significance of free radicals: mediatedinjury occurring in the kidney donor Transplantation 751221–7
[37] De Vega L, Perez Fernandez R, Martin Mateo M C,Bustamante J, Bustamante A, Herrero A M and BustamanteMunguira E 2003 Study of the activity ofglutathione-peroxidase, glutathione-transferase andglutathione-reductase in renal transplants Transpl. Proc. 51346–50
[38] Przekwas M, Malgorzewicz S, Zdrojewski Z,Debska-Slizien A, Lysiak-Szydlowska W andRutkowski B 2003 Influence of predialysis oxidative stresson peroxidation processes after renal transplantationTranspl. Proc. 35 2170–3
[39] Campise M, Bamonti F, Novembrino C, Ippolito S,Tarantino A, Cornelli U, Lonati S, Cesana B M andPonticelli C 2003 Oxidative Stress in kidney transplantpatients Transplantation 76 1474–8
[40] Li X, Chen H and Epstein P N 2004 Metallothionein protectsislets from hypoxia and extends islet graft survival byscavenging most kinds of reactive oxygen species J. Biol.Chem. 279 765–71
[41] Risby T H et al 1994 Evidence for free radical-mediated lipidperoxidation at reperfusion of human orthotopic livertransplants Surgery 115 94–101
[42] Studer S M, Orens J B, Rosas I, Krishnan J A, Cope K A,Yang S, Conte J V, Becker P B and Risby T H 2001 Patternsand significance of exhaled-breath biomarkers in lungtransplant recipients with acute allograft rejection J. HeartLung Transpl. 20 1158–66
[43] Schimke I, Schikora M, Meyer R, Dubel H P, Modersohn D,Kleber F X and Baumann G 2000 Oxidative stress in thehuman heart is associated with changes in the antioxidantdefence as shown after heart transplantation Mol. Cell.Biochem. 204 89–96
[44] Ashton T, Rowlands C C, Jones E, Young I S, Jackson S K,Davies B and Peters J R 1998 Electron spin resonancespectroscopic detection of oxygen-centred radicals inhuman serum following exhaustive exercise Eur. J. Appl.Physiol. 77 489–502
[45] Leaf D A, Kleinman M T, Hamilton M and Barstow T J 1997The effect of exercise intensity on lipid peroxidation Med.Sci. Sports Exerc. 29 1036–9
S383
K D Skeldon et al
[46] Munro A 2004 personal communication, Radiation Oncology,Ninewells Hospital, Dundee
[47] Wells M, Macmillan M, Raab G, MacBride S, Bell N,MacKinnon K, MacDougall H, Samuel L and Munro A2004 Does aqueous or sucralfate cream affect the severity oferythematous radiation skin reactions?A randomised controlled trial Radiother. Oncol. 73 153–62
[48] Mackay R I and Hendry J H 1999 The modelled benefits ofindividualizing radiotherapy patients’ dose using cellularradiosensitivity assays with inherent variability Radiother.Oncol. 50 67–75
[49] West C M et al 1998 The intrinsic radiosensitivity of normaland tumour cells Int. J. Radiat. Biol. 73 409–13
[50] Gibson G, Monk S D and Padgett M 2002 A field-portable,laser-diode spectrometer for the ultra-sensitive detection ofhydrocarbon gases J. Mod. Opt. 49 769–76
[51] Skeldon K D, Gibson G M, Wyse C A, McMillan L C,Monk S D, Longbottom C L and Padgett M J 2004Development of high resolution real-time sub-ppb ethanespectroscopy and some pilot studies in life science Appl.Opt. at press
[52] Silver J A 1992 Frequency modulation detection for tracespecies detection: theory and comparison amongexperimental methods Appl. Opt. 31 707–17
[53] Cheng W-H and Lee W-J 1999 Technology development inbreath microanalysis for clinical diagnosis J. Lab. Clin.Med. 133 218–28
[54] Herriott D R, Kogelnik H and Kompfner R 1964 Off-axispaths in spherical mirror resonators Appl. Opt. 3 523–6
[55] Kuhnemann F, Schneider K, Hecker A, Martis A A E,Urban W, Schiller S and Mlynek J 1998 Photoacoustictrace-gas detection using a CW single-frequency parametricoscillator Appl. Phys. B 66 741–5
[56] van Herpen M M J W, Li S, Bisson S E and Harren F J M2002 Photoacoustic trace gas detection of ethane using acontinuously tunable continuous-wave optical parametricoscillator based on periodically poled lithium niobate Appl.Phys. Lett. 81 1157–9
[57] Dahnke H, Kleine D, Hering P and Murtz M 2001 Real-timemonitoring of ethane in human breath using mid-infraredcavity leak out spectroscopy Appl. Phys. B 72 971–5
[58] von Basum G, Halmer D, Hering P and Murtz M 2004 Partsper trillion sensitivity for ethane in air with an opticalparametric oscillator cavity leak-out spectrometer Opt. Lett.29 797–9
[59] Hirst B, Gibson G, Gillespie S, Archibald I, Podlaha O,Skeldon K, Courtial J, Monk S and Padgett M 2004 Oil andgas prospecting by ultra-sensitive optical gas detection withinverse gas dispersion modelling Geophys. Res. Lett. 31L12115
[60] Wyse C A, Cathcart A, Sutherland R, Ward S A, Padgett M J,McMillan L and Skeldon K D 2005 Effect of maximalexercise on exhaled ethane and carbon monoxide in human,equine and canine athletes Comp. Biochem. Physiol.at press
[61] Bracher V, von Fellenberg R, Winder C N, Gruenig G,Hermann M and Kraehenmann A 1991 An investigation ofthe incidence of chronic obstructive pulmonary disease(COPD) in random populations of Swiss horses EquineVeterinary J. 23 136–41
[62] Robinson N E 2001 International workshop on equine chronicairway disease Equine Vet. J. 33 5–19
[63] Kirschvink N, Art T, Smith N and Lekeux P 1999 Effect ofexercise and COPD crisis on isoprostane concentration inplasma and bronchoalveolar lavage fluid in horses EquineVet. J. 30 (Suppl.) 88–91
[64] Wyse C A et al 2004 The effect of environmental modificationon exhaled ethane, carbon monoxide and hydrogen peroxidein horses with respiratory inflammation Vet. Rec. at press
[65] Wyse C A, Skeldon K S, Gibson G, McMillan L C,Padgett M J, Preston T, Yam P S and Love S 2005 Potentialapplications of exhaled breath analysis in veterinarymedicine Breath Analysis for Medical Diagnosis andTherapeutic Monitoring (Proc. 1st Int. Conf. on BreathAnalysis) ed A Amann and D Smith (Singapore: WorldScientific)
S384