Synthesis of Semliki Forest virus RNA requires continuous lipid synthesis

The Medicalization of Education: AHistoriographic Synthesis
Stephen Petrina
We believed we had overwhelming evidence that to know a child better is tolove it more.
G. Stanley Hall (1923)1
Sol Cohen was right and wrong. Education was medicalized but thisprocess occurred much earlier and not necessarily in the way he explainedit. Today, psychotherapeutic knowledge is nevertheless commonlyaccepted as central or natural to administrative offices and classrooms ofNorth American schools. But this medicalization of classroom policies,practices, and schools was not a progressive process of the medicalestablishment securing its hegemony over the jurisdiction of moderneducation. Rather, the medicalization of education was much lessdetermined and much more contingent than medicalization thesessuggest. Medical practices were constructed in schools through complexand subtle interrelationships among the likes of janitors, nurses,pediatricians, pathologists, pharmacists, psychologists, psychiatrists,social workers, and teachers during the late nineteenth and first threedecades of the twentieth century. These interrelationships were reinforcedby practices of eugenics, hygiene, and public health. In material forms,these interrelationships were manifested within architectural spaces,discourses, and practices in clinics, courts, hospitals, prisons, andschools. Education is just one of a variety of social practices thatembraced the power of psychotherapeutic values, and where a variety ofhealth interventions were administered and politicized. There arecountless redundancies across diverse social practices in the ‘‘psychiatricsociety,’’ ‘‘therapeutic state,’’ ‘‘medicalization of life,’’ or what Cohen calledthe ‘‘triumph of the therapeutic.’’2
History of Education Quarterly Vol. 46 No. 4 Winter 2006
Stephen Petrina is associate professor of curriculum studies at the University of BritishColumbia. He is at work on a book on the automation of education, 1924–1984.
1G. Stanley Hall, Life and Confessions of a Psychologist (New York: Appleton, 1923),392.
2Sol Cohen. ‘‘The Mental Hygiene Movement, The Development of Personalityand the School: The Medicalization of American Education.’’ History of EducationQuarterly, 23 (Summer 1983): 123–149; idem, ‘‘The Triumph of the Therapeutic:Essay Review.’’ History of Education Quarterly, 30 (1990): 371–79; Robert Castell,Francoise Castell and Ann Lovell, The Psychiatric Society trans. Arthur Goldhammer(New York: Columbia University Press, 1982); Ronald Leifer. ‘‘Introduction: TheMedical Model as the Ideology of the Therapeutic State.’’ The Journal of Mind and
Medicalization refers to a process whereby nonmedical problemsare defined and treated as medical problems. The medicalization thesisderives from the work of sociologists of the 1930s to 1950s, such asKingsley Davis, C. Wright Mills, and Talcott Parsons, who linked socialcontrol to an increasing dominance of medicine over individual andsocial problems. In the 1970s, sociologists referred to this increasingdominance as medicalization. Irving Zola, one of the first to use theterm, defined medicalization as a ‘‘process whereby more and more ofeveryday life has come under medical dominion, influence andsupervision.’’ When Ivan Illich published Medical Nemesis in 1975 andits expanded edition, Limits to Medicine in 1976, ‘‘the medicalization oflife’’ thesis emerged from academic to popular discourse. Critics reactedto this ‘‘medical imperialism’’ narrative, leaving medicalization theoriststo refine their conceptual work. This challenged historians, such asCohen, to specify the ways in which practices were medicalized. By theearly 1990s, sociologists such as Peter Conrad limited medicalization tothe process of ‘‘defining a problem in medical terms, using medicallanguage to describe a problem, adopting a medical framework tounderstand a problem, or using medical intervention to ‘treat’ it.’’ Theuniqueness of education as a psychotherapeutic practice demands morethan a footnote to Cohen’s medicalization thesis.3
For Cohen, the mental hygiene movement in the 1920s was a formof medicalizationFpsychiatrists and psychologists entered the schoolsand rendered student personality and behavioral disorders into medicalproblems.4 Although Cohen noted that this process began in the 1890s,
Behavior, 11 (Autumn 1990): 247–258; Andrew J. Polsky, The Rise of the Therapeutic State(Princeton, NJ: Princeton University Press, 1991); Philip Reiff, The Triumph of theTherapeutic (New York: Harper & Row, 1966); Christine Mary Shea, ‘‘The Ideology ofMental Health and the Emergence of the Therapeutic Liberal State.’’ PhD diss.,University of Illinois at Urbana-Champaign, 1980.
3Peter Conrad. ‘‘Medicalization and Social Control.’’ Annual Review of Sociology 18(April 1992): 209–232; Peter Conrad and Joseph Schneider. ‘‘Looking at Levels ofMedicalization.’’ Social Science and Medicine (January 1980): 75–79; Renee Fox. ‘‘TheMedicalization and Demedicalization of American Society.’’ Daedalus 106 (January 1977):9–22; Ivan Illich, Medical Nemesis (London: Calder & Boyars, 1975), 31; Ivan Illich, Limitsto Medicine (London: McClelland & Stewart, 1976); Irving K. Zola. ‘‘Medicine as anInstitution of Social Control.’’ Sociological Review 20 (October 1972), 487–504; P.M.Strong. ‘‘Sociological Imperialism and the Profession of Medicine: A CriticalExamination of the Thesis of Medical Imperialism.’’ Social Science and Medicine 13(February 1979): 199–215; Irving K. Zola, Socio-Medical Inquiries (Philadelphia: TempleUniversity Press, 1983), 295.
4On mental hygiene, see Cohen. ‘‘The Mental Hygiene Movement’’; Idem, ‘‘TheMental Hygiene Movement and the Development of Personality: Changing Conceptionsof the American College and University, 1920–1940.’’ History of Higher Education Annual 2(1982): 65–93; Idem, ‘‘the School and Personality Development: Intellectual History,’’ inHistorical Inquiry in Education ed. John H. Best (Washington, DC: American EducationalResearch Association, 1983), 109–137; Idem, ‘‘Every School a Clinic: A Historical
504 History of Education Quarterly

his cases deal with mental hygiene in the 1920s and the medicalization ofpersonality in schools and universities. This medicalization thesisremains productive and extremely relevant to understanding moderneducation and life in schools. Other historians support this link betweenmedicalization and psychiatry or mental hygiene as well. For example,French historical sociologist Robert Castell and his colleaguesconcluded that ‘‘not only was psychiatry involved in the general trendtoward the medicalization of childhood, it was the driving force in thewhole process.’’ Cohen, Castell, and others generally date the be-ginnings of the medicalization of education with the arrival of theneurologist Sigmund Freud to America in 1909, the founding of theNational Committee for Mental Hygiene that same year, and thefounding of the American Psychoanalytic Association in 1910. Histo-rians document the confluence of mental hygiene, psychoanalysis,and child guidance, which also had its psychiatric beginnings in 1909with the founding of William Healy’s Juvenile Psychopathic Institutein Chicago. By the 1920s, permutations of psychoanalysis, viamental hygiene and child guidance, were introduced into NorthAmerican schools to attend to both normal and abnormal studentproblems.5
I argue, however, that the medicalization of education occurred inmore complex and subtle ways than recognized by Cohen, Castell, andother historians following their leads. Whereas Theresa Richardson andChristine Shea documented the power of industrial philanthropists,such as the Rockefellers, to control social welfare through practices suchas mental hygiene, I argue that this power responded to a politics ofmedicine already embedded in the designs and policies of the schools.Contrary to theses that limit medicalization to mental hygiene or ableist‘‘special education,’’ I argue that the ‘‘common’’ classroom provides
Perspective on Modern Education,’’ in From the Campus: Perspectives on the School ReformMovement eds. Sol Cohen and Lewis C. Solmon (New York: Praeger, 1989), 18–33;Gerald N. Grob, Mental Illness and American Society, 1875–1940 (Princeton, NJ:Princeton University Press, 1983), 144–78; Fred Mathews, ‘‘In Defense of CommonSense: Mental Hygiene as Ideology in Twentieth-Century America,’’ Prospects 4 (Fall1979): 459–516; Theresa Richardson, The Century of the Child: The Mental HygieneMovement and Social Policy in the United States and Canada (Albany: State University of NewYork Press, 1989); Shea, ‘‘The Ideology of Mental Health.’’
5Of course, in the 1920s and 1930s, at $10.00 per hour, or an average of $3,000 to$6,000 for two years of treatment, psychoanalysis was quite limited as a therapeuticprocedure. As a result, permutations, rather than strict, technical forms of psychoanalysis,were popularized in sectors such as education. On this, see Stephen Petrina, ‘‘Luella Cole,Sidney Pressey and Educational Psychoanalysis, 1921–1931,’’ History of EducationQuarterly 44 (Fall 2004): 524–53. For fees and services, see Harold T. Hyman. ‘‘TheValue of Psychoanalysis as a Therapeutic Procedure.’’ Journal of the American MedicalAssociation 107 (August 1936): 326–29.
The Medicalization of Education 505
clues to a form of medicalization typically overlooked.6 Disabilityhistorians, such as Elizabeth and Philip Safford, documented theinterdependencies between medical intervention and the managementof training and custodial care institutions for the blind and deaf, andintellectually and physically disabled.7 Although the medicalization ofdisability and special education has its logical conclusion in eugenics andsocial Darwinism, the sciences of the well-born fail to inform thenormalizing and regulating practices of common, modern
6Gerald Coles, The Learning Mystique (New York: Ballantine, 1987); BarryFranklin, From ‘‘Backwardness’’ to ‘‘At-Risk’’ (New York: State University of New YorkPress, 1994); Peter Conrad, Identifying Hyperactive Children: The Medicalization of DeviantBehavior (London: Lexington, 1976); Jeroen Decker. ‘‘An Educational Regime: MedicalDoctors, Schoolmasters, Jurists and the Education of Retarded and Deprived Children inthe Netherlands around 1900.’’ History of Education 25 (July 1996): 255–268; Gerald M.Erchak, and Richard Rosenfeld, ‘‘Learning Disabilities, Dyslexia, and the Medicalizationof the Classroom,’’ in Images of Issues: Typifying Contemporary Social Problems ed. Joel Best(New York: Aldine De Gryter, 1989), 79–97; Steve Harlow. ‘‘The Medicalization of theClassroom: The Constriction of Difference in Our Schools.’’ Holistic Education Review 2(Summer 1989): 12–17; Bernard Harris, The Health of the School Child: A History of theSchool Medical Service in England and Wales (Philadelphia: Open University Press, 1995);John S. Hurt, Outside the Mainstream: A History of Special Education (London: B.T.Batsford, 1988); Marvin Lazerson, ‘‘The Origins of Special Education,’’ in SpecialEducation Policies: Their History, Implementation and Finance eds. Jay Chambers andWilliam T. Hartman (Philadelphia: Open University Press, 1983), 15–47; DavidParker, ‘‘‘A Convenient Dispensary’: Elementary Education and the Influence of theSchool Medical Service, 1907–39,’’ History of Education 27 (February 1998): 59–83;Maynard C. Reynolds. ‘‘An Historical Perspective: The Delivery of Special Education toMildly Disabled and At-Risk Students.’’ Remedial and Special Education 10 (November1989): 7–11; Scott Sigmond, Radical Analysis of Special Education: Focus on HistoricalDevelopment and Learning Disabilities (New York: Routledge, 1987); Gerald Thompson.‘‘A Fondness for Charts and Children: Scientific Progressivism in Vancouver Schools,1920–50.’’ Historical Studies in Education 12 (Spring/Fall, 2000): 111–128; MargaretWinzer, The History of Special Education: From Isolation to Integration (Washington, DC:Galludet University Press, 1994); David Wright and Anne Digby, eds., From Idiocy toMental Deficiency: Historical Perspectives on People With Learning Disabilities (New York:Routledge, 1996). On the sociology of medicalization, see Peter Conrad. ‘‘Medicalizationand Social Control.’’ Annual Review of Sociology 18 (Spring 1992): 209–232; Renee Fox.‘‘The Medicalization and Demedicalization of American Society.’’ Daedalus 106 (January1977): 9–22; Ivan Illich, Medical Nemesis (London: Calder & Boyars, 1975); Ivan Illich,Limits to Medicine (London: McClelland & Stewart, 1976).
7Elizabeth Bredberg, ‘‘Writing Disability History: Problems, Perspectives andSources,’’ Disability & Society 14 (June 1999): 189–201; James G. Carrier, ‘‘Sociology andSpecial Education: Differentiation and Allocation in Mass Education,’’ American Journalof Education 94 (May 1986): 281–312; Aude de Saint-Loup, ‘‘A History ofMisunderstandings: A History of the Deaf,’’ Diogenes 44 (Summer 1996): 1–25; PhilipL. Safford and Elizabeth Safford, A History of Childhood and Disability (New York: TeachersCollege Press, 1996); Geraldine T. Scholl, Ed., Foundations of Education for Blind andVisually Handicapped Children and Youth: Theory and Practice (New York: AmericanFoundation for the Blind, 1986); Rosemarie Garland Thomson, Extraordinary Bodies:Prefiguring Physical Disability in American Culture and Literature (New York: ColumbiaUniversity Press, 1997); Winzer, ibid; David Wright and Ann Digby, From Idiocy to MentalDeficiency: Historical Perspectives on People with Learning Disabilities (New York: Routledge,1996).
506 History of Education Quarterly
classrooms.8 Joanne Brown offered a history and theory of the rhetoricalpower behind medical language and stopped there, but we have to startwith medicine as an idiom in science and follow psychologists intoclinics and hospitals to attend to their training and socialization inmedical practice.9 Historians such as Margo Horn, Kathleen Jones, andAnthony Platt documented the gradual medicalization of childguidance, but I suggest that compulsory vaccination clinics anddispensaries were more obvious forms of medicalization and predatedchild guidance clinics of the 1910s by two decades.10 And wherehistorians documented the process of medicalizing education throughmedical inspections during the 1900s and 1910s, I argue that there arenumerous sites that supported a more subtle form of medicalization atthat time.11 Although historians place the origins of psychotropic drug
8Ian R. Dowbiggin, Keeping America Sane: Psychiatry and Eugenics in the United Statesand Canada, 1880–1940 (Ithaca: Cornell University Press, 1997); Paul Lombardo.‘‘Medicine, Eugenics and the Supreme Court: From Coercive Sterilization toReproductive Freedom.’’ Journal of Contemporary Health Law and Policy 13 (Fall 1996):1–25; Roy A. Lowe. ‘‘Eugenicists, Doctors and the Quest for National Efficiency: AnEducational Crusade, 1900–1939.’’ History of Education 8 (April 1979): 293–306; Philp R.Reilly, The Surgical Solution: A History of Involuntary Sterilization in the United States(Baltimore: Johns Hopkins University Press); Steven Selden, Inheriting Shame: Eugenicsand Race in America (New York: Teachers College Press, 1999).
9JoAnne Brown, The Definition of a Profession (Princeton, NJ: Princeton UniversityPress, 1992).
10Margo Horn, Before It’s Too Late: The Child Guidance Movement in the United States,1922–1945 (Philadelphia: Temple University Press, 1989); Kathleen W. Jones, Taming theTroublesome Child: American Families, Child Guidance, and the Limits of Psychiatric Authority(Cambridge: Harvard University Press, 1999; Anthony Platt, The Child Savers: TheInvention of Delinquency (Chicago: University of Chicago Press, 1969); TheresaRichardson, ‘‘Revisiting the Medicalization of Childhood and the Colonization ofChildren’s Policy by Psychologists and Psychiatrists, Review of Kathleen W. Jones’Taming the Troublesome Child’’ H-Net Reviews in the Humanities & Social Sciences (February2000): http://www.h-net.org; Steven Schlossman, Love and the American Delinquent: TheTheory and Practice of Progressive Juvenile Justice, 1825–1920 (Chicago: University ofChicago Press, 1977). See also Jane Addams, The Child, the Clinic and the Court (New York:New Republic, 1925); William Healy, The Individual Delinquent (Boston: Little, Brownand Company, 1922).
11N.D. Daglish. ‘‘Robert Morant’s Hidden Agenda?: The Origins of the MedicalTreatment of Schoolchildren.’’ History of Education 19 (February 1990): 139–148; JohnDuffy. ‘‘School Vaccination: The Precursor to School Medical Inspection.’’ Journal of theHistory of Medicine and the Allied Sciences 33 (July 1978): 344–355; Mona Gleason. ‘‘Race,Class and Health: School Medical Inspection and ‘‘Healthy Children’’ in BritishColumbia, 1890 to 1930.’’ Canadian Bulletin of Medical History 19 (January 2002): 95–112; David Kirk. ‘‘Foucault and the Limits of Corporeal Regulation: The Emergence,Consolidation and Decline of School Medical Inspection and Physical Training inAustralia, 1909–1930.’’ International Journal of the History of Sport 13 (August 1996): 114–131; David Kirk and Karen Twigg. ‘‘Regulating Australian Bodies: Eugenics,Anthropometrics and School Medical Inspection in Victoria, 1900–1940.’’ History ofEducation Review 23 (February 1994): 19–37; Patricia Potts. ‘‘Medicine, Morals, andMental Deficiency: The Contribution of Doctors to the Development of SpecialEducation in England.’’ Oxford Review of Education 9 (April 1983): 181–196; Stephen T.
The Medicalization of Education 507

control of hyperactive children in the 1930s, this blatant form ofmedicalization is located in the discovery of the nervous child in thelate 1800s and early 1900s and its treatment through dispensaries, patentmedicines, and vivisection techniques.12
In summary, the practices documented by historians are accuratebut, individually, inadequate to account for the medicalization ofeducation. To comprehend the scope of this process, one has tointegrate histories of deviant students (e.g., Conrad, Horn and Jones),hyperactive children (e.g., Conrad), medical inspections (e.g., Gleason),mental hygiene (e.g., Cohen and Richardson), disability (e.g., Safford &Safford, Saint-Loup), and special education (e.g., Erchak and Rosenfeld,Franklin, and Harlow). Even if one undertook this task, the full scope ofthe medicalization process would not be appreciated. In this article, Isynthesize this historiography by describing the medicalization ofeducation as a diversification of educational hygiene during the 1890sand early 1900s. Within eight unique sitesFintelligence tests, medicalinspections, physical education and instruction in hygiene, schoollunches, hygiene of instruction, school sanitation, clinical psychology,etiology of nervous children, and vivisectionFin the 1890s and early1900s developed a well-articulated modern, psychotherapeuticdiscourse and practice of schooling. These sites constituted, in 1915,what educator Louis Rapeer called ‘‘educational hygiene.’’ Hedivided this into intellectual disability training, medical supervisionor mental hygiene, school sanitation or school hygiene, physical dis-ability training, physical education, instruction in hygiene orphysical hygiene, and the hygiene of instruction or what I callneoscholastic hygiene. These sites suggest a thorough practice of medicalintervention and an aggressive subjugation of education to allopathicmedicine. Already by 1917, Life Magazine depicted the public school as aclinic, monitored by medical inspections, sanitized and charged with themandate of ‘‘medical moralization’’ (Figure 1). Medicine providedpowerful discourses, procedures, and strategies for educators andinterventionists in schools. Education came under the influence ofallopathic physicians in the 1890s and, increasingly through the early1910s, under the influence of psychiatrists, psychologists, andpsychiatric social workers. Schooling was reconstructed as medicinewas reoriented toward scientific laboratory and clinical practices or
Woolworth, ‘‘Conflict, Collaboration and Concession: A Study of the Rise and Fall ofMedical Authority in the Seattle Public Schools, 1892–1922.’’ PhD diss., University ofWashington, 2002.
12Peter Conrad. ‘‘The Discovery of Hyperkinesis: Notes on the Medicalization ofDeviant Behavior.’’ Social Problems 23 (October 1975): 12–21; Idem, Identifying.
508 History of Education Quarterly
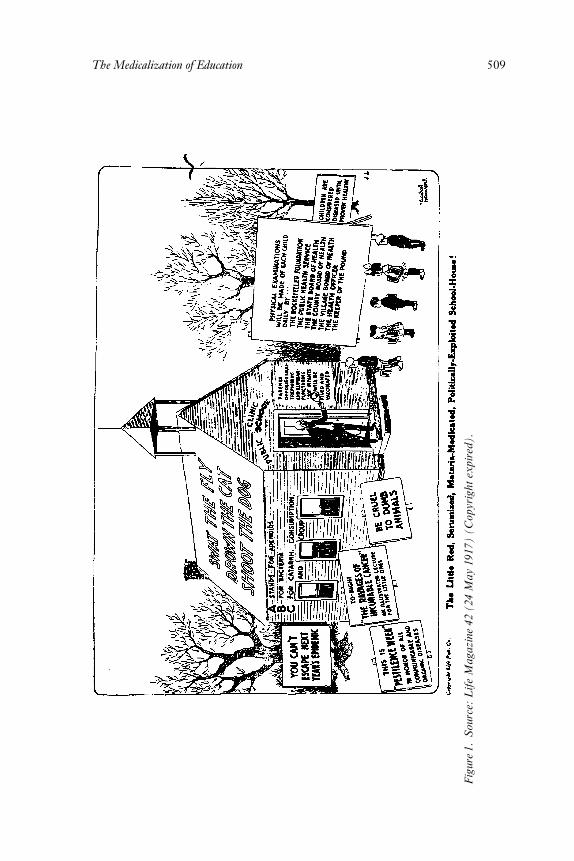
Figure1.Source:
LifeMagazine42(24May1917)(Copyrightexpired).
The Medicalization of Education 509

methods also common to changes in business, corrections, jurispru-dence, and health.13
In 1908, Clark University President G. Stanley Hall outlined theprogress through which scientific medicine and psychology came toregulate each day of development in childhood and adolescence.Speaking at a gathering to celebrate the centennial of the MedicalSchool at the University of Maryland, Hall noted a number of the highpoints in what he called ‘‘social therapeutics.’’ He acknowledged thedoctors’ unprecedented progress from the early days of child study in thelate 1880s to current psychotherapeutic practices in mental, physical,and school hygiene, and the hygiene of school subjects. ‘‘The doctor nowfollows the child into the school’’ he exclaimed, opening ‘‘a tiny healthbook’’ for each of the young scholars. In addition to laying down therules of life in each tiny health book, he continued, physicians adopted a‘‘pastoral function to youth’’ to keep them pure and liberate them from‘‘the quacks that play upon’’ adolescence and young adulthood. Thesefunctions marked a battle against the evils of ignorance and quackery,and something that knowledge in the name of liberty could cure. Hallpracticed psychology for thirty years and saw an inseparableinterrelation between the psychic and the somatic. The boundariesbetween medicine and psychology in his own life were blurred, as heserved as medical superintendent of the Bay View Hospital for theInsane while practicing the ‘‘new psychology’’ at Johns HopkinsUniversity in the 1880s. He held weekly clinics for his students in thehospital, providing training in both medical therapeutics and science. AtClark, he practiced and lectured at the Worcester State Hospital untilthe mid 1890s. With the authority of his MD granted at Johns Hopkins,Hall never reduced himself to a ‘‘mere psychologist’’ as his peer did adecade earlier while bowing in the presence of medical practitioners. ForHall, medicine and psychology were equally powerful in their guidanceover education. By the time he hosted Freud’s visit to the U.S. in 1909,the medicalization of education was extensive and diversified.14
13Louis Rapeer, Essentials of Educational Hygiene (New York: Scribners, 1915), 130–1. See also William Burnham, ‘‘Outlines of School Hygiene,’’ Pedagogical Seminary 2(February 1892): 9–71; Lester King, Transformations in American Medicine (Baltimore:Johns Hopkins University Press, 1991), 218–225; George Rosen, The Structure ofAmerican Medical Practice, 1875–1941 (Philadelphia: University of Pennsylvania Press,1983), 13–36; Paul Starr, The Social Transformation of American Medicine (New York: BasicBooks, 1982), 180–196.
14This integration of medicine and psychology partially underwrote the reasonwhy Hall went out of his way to host Freud during his first American visit in 1909. G.Stanley Hall. ‘‘The Medical Profession and Children.’’ Pedagogical Seminary 15 (February1908): 207–218, 209, 215; Boris Sidis. ‘‘The Nature and Principles of Psychology.’’American Journal of Insanity 56 (July 1899): 41–52, 41. On Hall and Medicine, see DorothyRoss, G. Stanley Hall: The Psychologist as Prophet (Chicago: University of Chicago Press,
510 History of Education Quarterly

Intelligence Tests and Medical Inspections
At the 225-year-old renowned Salpetriere Hospital in Paris during 1881,Jean Martin Charcot established an outpatient clinicFa consultationexterne or Policlinique. In his clinical practice in the hospital, the famousneuropathologist and chef de clinique Charcot attended to the ‘‘neurosesand psychoses’’ of women confined to the hospital. He demonstrateddaily in front of students and each Friday to the public within theteaching theater built in the early 1880s. The outpatient clinic, or whatwas called the Policlinique, extended Charcot’s reach into Paris and wasopened for therapeutically treating working-class men and women for avariety of mild mental disorders. Scientific laboratories, social services,and the teaching theater tied to the Policlinique formed a hugepsychotherapeutic complex. By the early 1890s, the Policlinique wasattracting 5,000 patients per year and was the main source of Charcot’sclinical practice until his death in 1893. In 1889, Pierre Janet, Charcot’sstudent and Parisian psychiatrist, was appointed head of the psychologieclinique, another arm of what came to be known as the notorious CliniqueCharcot.15 Another of Charcot’s students, Alfred Binet, left theSalpetriere in 1890 after studying for seven years, and similar to Janet,moved from neuropathological studies to a more psychotherapeuticapproach to treating individual mental ‘‘abnormalities.’’ In 1892, Binetaccepted a post as associate director of the Sorbonne Laboratorie dePsychologie Physiologique, but continued to spend a few days per week atthe Salpetriere clinic.
In the Sorbonne clinic, Binet and Victor Henri, a clinician andpsychopathologist, began a series of psychophysical examinations onyoung boys from the local schools, using a range of apparatus borrowedfrom the Salpetriere or contrived to detect differences in attention span,character, memory, judgment, and self-confidence. Binet’s and Henri’saccess to school children was carefully monitored, and headmastersrefused to allow examinations of young women, as they recollectedCharcot’s dramatic demonstrations at the Salpetriere. By 1895 and 1896,after examining about 400 boys, Binet and Henri outlined an entirediscourse on psychologie individuelleFan individual psychology where
1972), 393–97; William H. Burnham, Great Teachers and Mental Health: A Study of SevenEducational Hygienists (New York: Appleton, 1926), 189–247.
15Christopher Goetz, Michel Bonduelle and Toby Gelfand, Charcot: ConstructingNeurology (New York: Oxford University Press, 1995); Jan Goldstein, Console and Classify:The French Psychiatric Profession in the Nineteenth Century (Cambridge: CambridgeUniversity Press, 1987); Pierre Janet, ‘‘Pierre Janet,’’ in A History of Psychology inAutobiography ed. Carl Murchison (Worcester, MA: Clark University Press, 1930),123–133; Mark S. Micale. ‘‘The Salpetriere in the Age of Charcot.’’ Journal ofContemporary History 20 (October 1985): 703–731; Mark S. Micale. ‘‘Hysteria and itsHistoriography: The Future Perspective.’’ History of Psychiatry, (March 1990): 33–124.
The Medicalization of Education 511

the objective was comparisons of mentally ‘‘abnormal’’ with mentally‘‘normal’’ individuals. Four years later, Binet and Theodore Simon, amedical student and budding psychologist, refined psychologie individuellewith young boys confined to Perray-Vauclue, an institution for mentally‘‘abnormal’’ adolescents. They described their psychophysicalprocedures for ‘‘diagnostic du niveau intellectuel des abnormaux’’ in 1905as a way of detecting degrees of difference in abnormality and normalityfor eventual medical, pedagogical, or psychological treatment of indi-viduals. In 1908, Henry Goddard, director of the Vineland TrainingSchool for the Feeble-minded in the U.S, translated Binet and Simon’sapparatus and procedures to English, and proceeded to administer the‘‘intelligence examinations’’ to his young Training School charges andabout 2,000 children in local New Jersey schools in 1909 and 1910.16
Signifying an increasing confidence in allopathic methods andmarking the twenty-year anniversary of the Association of MedicalOfficers of American Institutions for Idiotic and Feeble-minded, theJournal of Psycho-Asthenics was established in 1896. ‘‘Psycho-Asthenics’’was coined at this time to refer to the etiology, diagnosis, and treatmentof ‘‘idiocy or feeble-mindedness’’ and epilepsy while the journalcommunicated the progress of institutional practice and the arts andsciences of medicalizing the abnormal or pathological mind. Trials todiagnose mental abnormalities with psychophysical performance testapparatus (i.e., reaction time) were conducted in France, Germany, andthe U.S. throughout the late 1800s, but physicians and psychiatrists hadmore routinely relied on medical inspections and observations toidentify mental abnormality in individuals.17
In Boston, fifty ‘‘medical visitors’’ were appointed in 1894 to visitthe city schools to examine ‘‘all children thought by their teachers to beailing.’’ Chairman of the Board of Health and physician Samuel H.Durgin assigned each medical visitor, or doctor, to an urban district.Acting on a recent epidemic of diphtheria, Durgin ordered each of hisphysicians to visit schools each morning to make routine inspections ofthe school children and enforce necessary sanitary precautions.
16Stella E. Sharp. ‘‘Individual Psychology: A Study in Psychological Method.’’American Journal of Psychology, (April 1899): 329–391; Theta H. Wolf, Alfred Binet(Chicago: University of Chicago Press, 1973), 143–89; Leila Zenderland, MeasuringMinds: Henry Herbert Goddard and the Origins of American Intelligence Testing (Cambridge:Cambridge University Press, 1998), 71–120. For historiography of intelligence testing,see Stephen Petrina. ‘‘Getting a Purchase on ‘The School of the Future’ and ItsConstituent Commodities: Histories and Historiographies of Technologies.’’ History ofEducation Quarterly 42 (Spring 2002): 75–111, on 86–91; idem, ‘‘‘The Never-To-Be-Forgotten Investigation’: Luella W. Cole, Sidney L. Pressey and Mental Surveying inIndiana, 1918–1921,’’ History of Psychology 4 (August 2001): 245–271.
17Editors, ‘‘Announcement,’’ Journal of Psycho-Asthenics 1 (September 1896): 34–35.
512 History of Education Quarterly

Authority over who to examine was renegotiated and as the superin-tendent of schools noted, ‘‘the doctors inspect not only the pupilsselected by the teachers, but also many others.’’ He also noted that theydid much ‘‘more than inspect’’ in that they treated, taught, andintroduced an allopathic point of view to health. Through establishing‘‘pleasant relations with the boys and girls,’’ they were able to implementhygienic and sanitary practices that provided continuity from visit tovisit. They also used their authority to send students home from schooland follow-up with visits to the children’s home. A large number of theinspectors were agents of the Board of Health and had ‘‘doubleauthority’’; hence, they could order the parent(s) to keep the childisolated in the home until recovery was approved. Approximately 5,000children were inspected over four months, uncovering fifty-eight casesof diphtheria and a number of other illnesses. Eventually, the physiciansaccepted as their charge the diagnosis of normality based on a physicalexaminationFthe ‘‘mental and the physical are mutually inter-dependent’’ commented one proponent in 1903. ‘‘The medicalinspector should always be psychologist as well as physician,’’ hecontinued, so ‘‘that he may assist the teacher in determining howmuch mental exertion should be required of each age or period ofdevelopment, that evil may not result from overexertion at criticalperiods. He should assist the teacher in classifying the pupils’’ andregulating body, mind, and soul. Chicago followed suit with inspectorsappointed in 1895, and in 1898 in a seven-month period, 115,000students were examined at a cost of $13,000, or about half of what it costNew York City for the same practice.18
Physical Education, Dietetics, and School Hygiene
About the time Durgin was appointing medical inspectors to the schoolsof Boston, a physician from the Boston General Hospital was declaring
18Edwin Seaver. ‘‘Medical Inspection in Public Schools: Discussion.’’ Journal ofProceedings and Addresses of the National Education Association 40 (July 1901): 238–39, 239;Homer W. Zirkle. ‘‘Discussion.’’ Journal of Proceedings and Addresses of the NationalEducation Association 42 (July 1903): 784–85, 784; Edwin P. Seaver. ‘‘The MedicalVisitors.’’ Superintendent’s Report, (1895): 76–79, Boston Archives and RecordsManagement Division; Stratton D. Brooks, ‘‘Report of the Director of SchoolHygiene,’’ Superintendent’s Report (1908): 102–48, Boston Archives and RecordsManagement Division; John Duffy. ‘‘The Early Days of the School HealthMovement.’’ Conspectus of History 1 (October 1981): 43–54; George Rosen, A History ofPublic Health, expanded edition (Baltimore: John Hopkins University Press, 1993), 340–41; Luther H. Gulick and Leonard Ayres, Medical Inspection of Schools (New York: RussellSage Foundation, 1908). See also John C. Burnham. ‘‘Medical Inspection of Prostitutes inAmerica in the Nineteenth Century.’’ Bulletin of the History of Medicine 45 (January 1971):203–211; Elizabeth Yew. ‘‘Medical Inspection of Immigrants at Ellis Island, 1891–1924.’’Bulletin of the New York Academy of Medicine 56 (June 1980): 488–503.
The Medicalization of Education 513

the benefits of a full regimen of exercise and physical education forstudents. Speaking in front of the Boston Society for MedicalImprovement, W.M. Conant outlined two inseparable goals forphysical education. Hygienically, regulated programs of fitness offeredprocedures whereby students corrected deformities of the body,prevented the onset of certain physical ailments, and maintained ahealthy physiology and moral outlook. Educationally, physicaleducation offered procedures for developing agility, discipline,endurance, expression, judgment, posture, strength, and powers ofself-control. Physically and morally fit young bodies were, accordingto Conant, prepared to carry the load of business, labor, marriage,professions, war, or other demanding callings. Conant summarized thedeclaration of the professionalization of physical education that NewYork physician Luther Halsey Gulick crafted in 1890. At the time,Gulick was founding president of the Playground Association ofAmerica, which stood for the lessons of self-governance nurtured byunstructured play. As director of the Young Men’s Christian AssociationGymnasium in Jackson, Michigan, Gulick was a devotee of ‘‘muscularChristianity,’’ where physical education was an instrument for morallessons that would dissipate evils rooted in criminal intentions.Convinced of links between physiology, emotional control, andmorality, he agitated for the widespread adoption of medicalinspections of all school children in the mid to late 1890s and for theNational Education Association’s institution of a Physical EducationDepartment in 1895.19 Fitness in young body, mind, and soul made for acapillary, responsive discipline and prompt obedience, which easedteachers’ ‘‘mass control of large bodies of children’’ in classrooms.20
19Laura Azzarito, Poetra Munro and Melinda Soloman. ‘‘Unsettling the Body: TheInstitutionalization of Physical Activity at the Turn of the 20th Century.’’ Quest 56(November 2004): 377–396; Dominick Cavallo, Muscles and Morals: OrganizedPlaygrounds and Urban Reform, 1880–1920 (Philadelphia: University of PennsylvaniaPress, 1981), 32–38; W.M. Conant, ‘‘The Educational Aspects of College Athletics,’’Boston Medical and Surgical Journal 18 (February 1894): 20; Luther H. Gulick. ‘‘PhysicalEducation: A New Profession.’’ Proceedings of the American Association for the Advancementof Physical Education 5 (July 1890): 59–66; Harvey Green, Fit For America: Health, Fitnessand Sport in American Society (New York: Pantheon, 1986), 181–215; James Hughes.‘‘Physical Training as a Factor in Character Building.’’ Journal of Proceedings and Addressesof the National Education Association 40 (July 1896): 911–18; Roberta Park. ‘‘Science,Service and the Professionalization of Physical Education, 1885–1905.’’ ResearchQuarterly in Exercise and Sport 57 (Spring 1987): 7–20; Roberta Park. ‘‘Physiologists,Physicians, and Physical Educators: Nineteenth Century Biology and Exercise,‘Hygienic and Educative’.’’ Journal of Sport History 14 (Spring 1987): 28–60; MarthaVerbrugge. ‘‘Recreating the Body: Women’s Physical Education and the Science of SexDifferences in America, 1900–1940.’’ Bulletin of the History of Medicine 71 (1997): 273–304.
20N.D. Kimberlin. ‘‘Physical Training in Public Schools.’’ Journal of Proceedings andAddresses of the National Education Association 39 (July 1895): 296–97, on 297.
514 History of Education Quarterly
Physical exercise supplemented instruction in hygiene, which wasmade part of the public school curriculum during the 1880s and 1890sprimarily due to agitation by the Women’s Christian Temperance Union(WCTU). By the early 1890s, nearly every state in the United Statespassed legislation requiring the instruction of hygiene in some shape orform. The WCTU endorsed physician Eli Brown’s Young TemperanceManual (1888) and other popular textbooks such as physician AlbertBlaisdell’s The Child’s Book of Health (1894), which offered students clearlessons on hygiene, nutrition, and the evils of alcohol, narcotics, andtobacco. The didactics of anatomy and physiology gave way to theformation of health habits. Hygiene and health primers, textbooks, andsimilar publications, including Bernarr Macfadden’s monthly periodicalPhysical Culture (ca., 1899), linked older discourses of moral temperancewith newer ideas about virility, care of the body and dietetics. Now, theabled body was instructed on avoiding the disabled body.21
In 1894, the New England Kitchen petitioned the Boston SchoolCommittee to provide lunches for students in the city’s nine highschools. As the first school lunch program, it became a model forother cities across the country. The New England Kitchen, underdirection of chemist-cum-domestic scientist Ellen Richards, openedits doors for patrons in 1890 to demonstrate modern notions of nutritionalong with the prophylactic and therapeutic value of food. There was aconnection, the Kitchen’s advocates argued, between diet, hygiene,mental performance, and moral temperance. ‘‘Good thinking, likegood rowing,’’ said Richards, ‘‘requires proper feeding.’’ The lunchprogram effectively linked scientific nutrition with medical dietetics,opening children’s mouths for medicine’s entry into the public schools.
21The Child Health Organization, formed in 1918, coined the phrase ‘‘healtheducation’’ in 1919 to distinguish new practices from the older instruction in hygiene.Charles Woodward and Pauline Williamson, The Laws of Health and How to Teach Them(New York: Charles E. Merril, 1925). On the history of health education, see HowardConrad. ‘‘Historical Steps in the Development of Health Education.’’ Mind and Body 42(May 1935): 81–82; Richard K. Means, A History of Health Education in the United States(Philadelphia: Lea & Febiger, 1962); Idem, Historical Perspectives on School Health (Auburn:Auburn University Press, 1975); John Taylor, ‘‘A History of the Formation,Development, and Growth of the Department of Health Education at SouthernIllinois University at Carbondale, 1921 to 1993.’’ PhD diss., Southern IllinoisUniversity at Carbondale, 1996. On the history of the body and physical culture, seeJeanette Rhedding-Jones. ‘‘History and Critical Theories: Discursive Play and BodyWork.’’ Pedagogy, Culture and Society 8 (2000): 249–261; William Joyce, ed. The IllustratedHistory of Physical Culture (London: Alan Radley, 2001); David Kirk, Schooling Bodies: SchoolPractice and Public Discourse, 1880–1950 (London: Leicester University Press, 1998); JohnMassey, American Adonis: Tony Sansone, the First Male Physique Icon (New York: Universe,2004); Roberta Park. ‘‘History of Research on Physical Activity and Health: SelectedTopics from 1867 to the 1950s.’’ Quest 47 (August 1995): 274–287; Idem, ‘‘A Decade of theBody: Researching and Writing About the History of Health, Fitness, Exercise and Sport,1983–1993.’’ Journal of Sport History 21 (Spring 1994): 59–82.
The Medicalization of Education 515

The Boston school lunch program was initiated in 1894 under protest ofthe school janitors, who were entrepreneurial in selling snacks (cocoa,crackers, milk) or home-baked goodies (cakes, cookies) to the students inbasement corners. Protecting their interests, the janitors complained tothe school committee and generated resistance outside the schools.Local push-cart owners felt their small businesses were threatened, anddime store merchants placed signs in windows stating: ‘‘Don’t LetAnyone Tell You What You Should Eat!’’ Parents inquired whethertheir children were guinea pigs for dietetic experiments. The BostonSchool Committee intervened, and proceeded to supervise the selling ofall food in schools. Persuaded by Richards’ notions that good behaviorand thought were linked to good food, the committee approved anddemanded that the city’s nine high schools be served. About 2,500students opted for lunches each day. For five cents, they received a lunchof bread with butter, crackers, and soup. Richards calculated the caloricvalue of the new lunches, and monitored the carbohydrate, fat, andprotein content of the food. She also tied the value of teaching propertable manners and the hygienic handling of food to the nutritional valueof the lunches. Within a few years, similar lunch programs were initiatedin New York and other large cities. The program in Boston continueduntil 1907, when it was turned over to the Women’s Educational andIndustrial Union. Local physicians approved, and as one specialist ofdietetics put it in 1893: Doctors will soon prescribe what foods studentsshould eat. ‘‘Physicians,’’ he said, ‘‘are to be the teachers and authoritieson foods.’’22
22Rima Apple, ‘‘Science Gendered: Nutrition in the United States, 1840–1940,’’ inThe Science and Culture of Nutrition eds. Harmke Kamminga and Andrew Cunningham(Atlanta, 1995), 129–154; L. Margaret Barnett, ‘‘Every Man His Own Physician: DieteticFads, 1890–1914,’’ in Science and Culture of Nutrition eds. Harmke Kamminga & AndrewCunningham (Atlanta: Roclopi, 1995), 155–178; Robert Clarke, Ellen Swallow: TheWoman who Founded Ecology (Chicago: Follett, 1973), 123–140; Ephraim Cutter. ‘‘Addresson DieteticsFMedical Food Ethics Now and to Come.’’ Journal of the American MedicalAssociation 20 (March 1893): 238–244, on 242; Caroline Hunt, The Daily Meals of SchoolChildren, U.S. Bureau of Education Bulletin No. 3 (Washington, DC: GovernmentPrinting Office, 1909); Caroline Hunt, The Life of Ellen H. Richards (Boston: Whitcomband Barrows, 1912), 215–229; Charles G. Kerley, ‘‘The Nutrition on School Children,’’Teachers College Record 6 (March 1905): 85–89; Harry Levenstein, Revolution at the Table:The Transformation of the American Diet (New York: Oxford University Press, 1988), 44–59; Horace Makechnie. ‘‘Problems in Feeding School Children.’’ Journal of the AmericanMedical Association 30 (January 1898): 56–57; A.E. Miller. ‘‘Hygienic Management ofChildren.’’ Journal of the American Medical Association 31 (December 1898): 1556–58;Mary H. Moran. ‘‘Boston High School Lunches.’’ Journal of Home Economics 2 (April1910): 181–84; Mary H. Moran and Julia Pulsifer, Boston’s Public School Lunches (Boston:Women’s Educational and Industrial Union, 1908); Nathan Oppenheim, The Care of theChild in Health (New York: Macmillan, 1900); Ellen H. Richards, ‘‘The Food of SchoolChildren and Young Students,’’ in Plain Words About Food: The Rumford Kitchen Leaflets ed.Ellen Richards (Boston: Home Science Publishing Company, 1893/1899), 89–103; Idem,
516 History of Education Quarterly

In the midwestern United States in 1896, the Indiana State Board ofHealth passed nine rules addressing a far-reaching hygiene of publicschool practice. Written under the insistence of John Hurty, thesecretary of the Board of Health in Indianapolis, the rules wereimmediately dubbed the ‘‘Magna Carta’’ of school hygiene in Indiana.Rule number one empowered school officials to refuse admittance ofchildren from households that were infected with contagious diseases orchildren suspected of infection until an examination was made by acertified physician and approved by a state Health Officer. Explicitlylinking morality, sanitation, and the science of germ theory, the nextseven rules spelled out in no uncertain terms the governance andmaintenance of classroom apparatus, furniture, and physical plants.School and township trustees and janitors were required to put physicalcomponents such as desks, floors, pencils, tablets, and water fountains in‘‘sanitary condition’’ before opening their schools. As his friend andbiographer put it, Hurty stood for better hygiene through ‘‘bettersanitation, better preparation of teachers, school health examinations,better textbooks and better everything.’’ ‘‘Better everything’’ meant thatarchitecture and interior effects were governed by codes of hygiene.School hygiene transformed the work of the educational architect andinterior designer and generously elevated the power and status of theschool janitor. As school hygiene leader Fletcher Dressler concluded,‘‘the janitor of the modern school building is, next to the principal,perhaps the most important officer in the school.’’ Now, the janitor sethousekeeping standards, safeguarded valuable property, exerted moralauthority over students, regulated the conditions for safety, andgoverned the entire health environment of the school and its premises.23
‘‘The Prophylactic and Therapeutic Value of Food,’’ in Plain Words About Food: TheRumford Kitchen Leaflets ed. Ellen H. Richards (Boston: Home Science PublishingCompany, 1893/1899), 104–114; Idem, ‘‘Public Kitchens in Relation to SchoolLunches and to Restaurants,’’ Plain Words About Food: The Rumford Kitchen Leaflets ed.Ellen H. Richards (Boston: Home Science Publishing Company, 1893/1899), 161–65;Idem, ‘‘Luncheons for School Children.’’ New England Kitchen Magazine 3 (May 1895):51–54.
23Thurman B. Rice, The Hoosier Health Officer: A Biography of John N. Hurty(Indianapolis: Indiana State Board of Health, 1946), 134–35; Gilbert B. Morrison,‘‘School Architecture and Hygiene,’’ in American Education ed. Nicholas Murray Butler(New York: L.B. Lyon Company, 1900), 430; Dressler quoted in John A. Garber, ‘‘TheSchool Janitor,’’ U.S. Bureau of Education Bulletin 24 (1922): 3; May Ayres, Jesse Williamsand Thomas Wood, Healthful Schools (New York: Houghton Mifflin, 1918); SeveranceBurrage and Henry T. Baily, School Sanitation and Decoration (New York: D.C. Heath,1899); W. Kilham, ‘‘The Hygienic Construction of Schoolhouses from an Architect’sStandpoint,’’ Fourth International Congress on School Hygiene Transactions, Vol. II (1914):35–38. On the history of school sanitation, see John Duffy, The Sanitarians: A History ofAmerican Public Health (Urbana: University of Illinois Press, 1990), 175–220; Idem,‘‘School Buildings and the Health of American School Children in the NineteenthCentury,’’ in Healing and History ed. Charles Rosenberg (New York: Dawson, 1979), 161–
The Medicalization of Education 517

Hygiene of Instruction, Clinical Psychology, and the Nervous Child
Elsewhere on the Atlantic coast and about the time doctors entered theBoston schools, a pediatrician from New York brought clinical scienceto bear on the whole of classroom practice. In the early 1890s, JosephMayer Rice made headlines in the popular and academic presses for hissurvey of elementary schools in thirty-seven city school districts on theeast coast and in the midwestern United States. Rice summarized thehealth of the schools in The Forum in 1892 and 1893: most of the classeshe observed, and generally the schools he surveyed, were sick; evils wereevident, and there was some tough scientific medicine to take. Whileaggressively criticized for locating the ‘‘roots of all educational evils’’ inan old regime of pedagogy and corrupt governance, his work came to berepresented as the first large-scale practice of the new social science ofschooling. Rice returned to some of these schools again in 1895 and1896 and examined nearly 100,000 students to attend to knowledge andpractice in arithmetic, English composition, penmanship, and spelling.More interested in conditions under which students learned than in howwell individuals added or spelled, he contrived his test apparatus toexamine the students’ ‘‘mental labor.’’ Rice argued that there werehygienic principles to the design of schoolrooms and texts, and to howand what should be taught, and at what age and speed it could be learned.For Rice, the new pedagogy was governed by knowledge of thesehygienic principles and a psychotherapeutic detection of errors inpractices like adding and spelling. Without this psychotherapeuticknowledge and the skills to diagnose errors, teachers were ‘‘fully asliable to prosecution for malpractice as the physician who has bungled insetting a bone.’’ He proposed a practice where teachers clinicallyexamined students to provide an idea of their attainment of schoolknowledge and forwarded standardized test results to centrallaboratories for analysis. Time and time again, Rice was recognizedfor exercising clinical science in his hygiene of instruction.24
178: Suellen Hoy, Chasing Dirt: The American Pursuit of Cleanliness (Oxford: OxfordUniversity Press, 1995), 87–149; Petrina, ‘‘Getting a Purchase’’; Nancy Tomes, Gospel ofGerms: Men, Women and American Life (Cambridge: Harvard University Press, 1998);Idem, ‘‘The Private Side of Public Health: Sanitary Science, Domestic Hygiene, andGerm Theory, 1870–1900,’’ Bulletin of the History of Medicine 64 (Winter 1990): 509–539.
24Rice’s work through the 1890s was published in two volumes. J.M. Rice, The PublicSchool System of the United States (New York: Century, 1893), 9; J.M. Rice, ScientificManagement in Education (New York: Hinds, Noble & Eldridge, 1914), 55, 27, 136. OnRice, see Lawrence Cremin, The Transformation of the School: Progressivism in AmericanEducation, 1876–1957 (New York: Knopf, 1961), 3–8; Murray Levine, ‘‘The AcademicAchievement Test: Its Historical Context and Social Functions,’’ American Psychologist 31(June 1976): 228–238. See also, Edward L. Thorndike. ‘‘Educational Diagnosis.’’ Science 37(January 1913): 133–142. On malpractice, see William F. Foster. ‘‘Educational Malpractice:Educate or Litigate.’’ Canadian Journal of Education 11 (March 1986): 122–29.
518 History of Education Quarterly
In Philadelphia, Lightner Witmer modeled educationaland psychological practices after institutions common to medicineFthe clinic and dispensary. If other practitioners, such as Rice, shiftedbut respected boundaries among education, medicine, and psycho-logy, Witmer removed any boundaries that impeded psycho-therapeutic practice in education. In what became a manifesto for‘‘clinical psychology,’’ Witmer made a pitch at the fourth annualmeeting of the American Psychological Association for pedagogicaland psychological practices that were clinical in outlook andscope. The following year, 1897, he opened a ‘‘psychological clinic’’at the University of Pennsylvania. Attending to ‘‘abnormal’’and ‘‘normal’’ children from the local Philadelphia publicschools, Haddonfield Training School, Miss Marvin’s HomeSchool, and the Pennsylvania Training School, he set out to treatwhatever ailed his young subjects. A ‘‘medical and psychologicalexamination’’ led to a ‘‘diagnosis of the child’s mental andphysical condition and the recommendation of appropriate medicaland pedagogical treatment.’’ Witmer often referred to his firstcase where an ailment of reading difficulty was treated with a pairof eyeglasses. He routinely prefaced this case by remarking that hiswork was for abnormal and normal children alike. The young boywas brought to his office by a local school teacher, as Witmer describedthe meeting: ‘‘She was imbued with the idea that a psychologistshould be able, through examination, to ascertain the causes of adeficiency in spelling and recommend the appropriate pedagogicaltreatment for its amelioration or cure.’’ And so it would be in clinicalpsychology. ‘‘As the physician examines his patient and proposestreatment with a definite purpose in view, namely the patient’s cure,’’he explained, ‘‘so the clinical psychologist examines a child with a singledefinite object in viewFthe next step in the child’s mental and physicaldevelopment.’’ Admitting that while ‘‘clinical psychology’’ and‘‘psychological clinic’’ were odd juxtapositions of concepts, they werenonetheless the best choices to indicate the ‘‘character of the method’’ heused. Clinic referred to medical, or hygienic and therapeutic, methodrather than medical space. Like Hall, Witmer trained a number ofstudents in psychotherapeutic practiceFhe called his ‘‘psychologicaltraining school’’ the ‘‘hospital school.’’ Indeed, the renownedpsychoclinicist J.E. Wallace Wallin asserted in 1920 that ‘‘schoolsmust be organized more or less on the plan of the modern hospital.That is, the pupils should first be carefully examined and diagnosedbefore any attempt is made to differentiate the instruction y in orderthat remediable defects may be discovered and corrected whenpossible.’’ As Maud Merrill noted upon writing a history of the clinic,‘‘the training program for ‘psychoclinicists’ was to fit them to become
The Medicalization of Education 519

examiners in psychological clinics which functioned as ‘educationaldispensaries.’’’25
In Boston, again during the mid-1890s, physician Philip Knappisolated 150 ‘‘nervous children’’ from the city schools to investigate theetiology of what appeared to be an increasing number of cases. Althoughhis colleague argued, ‘‘much of our school system seems almost expresslydesigned for the manufacture of nervous invalids,’’ Knapp found thatschoolwork accounted for only a small part of nervousness in children.‘‘If under any school regime only a part of the scholars break down,’’ hereasoned, ‘‘there must be some reason other than school work why theysuccumb while their comrades are unaffected.’’ If schoolwork ‘‘rarelyoccasions nervous disease,’’ Knapp concluded, then the etiology is morelikely pathological and attributed to functions of the central nervoussystem. Arriving at a similar conclusion on nervous or precociouschildren a few years earlier, another physician suggested the new termaprosexia to refer to ‘‘the inability to fix the attention on any more or lessabstract subject.’’ With ‘‘hyperactivity of function’’ now named andisolated as a pathological, neurophysiological symptom, physiciansfocused on cure and prevention. By the 1900s, physicians were moreconfident of the etiology of the nervous child than earlier physicians.Punton, for example, unequivocally declared, ‘‘precocity is a sure sign ofbiological inferiority.’’ ‘‘The belief that the child will outgrow itsnervousness and consequently there is no cause for alarm when a childsuffers from the various forms of nervous weakness y is not onlymisleading, but absolutely false, and contrary to all medical knowledgeand experience.’’ He continued: ‘‘the sooner this fact is well understoodby both parent and teacher, the better, for it may save many a boy or a girlfrom becoming a confirmed neuroasthenic, hysteric or epileptic.’’Nervous children were ‘‘more curable than any other time, but whenneglected,’’ developed ‘‘serious permanent disabilities.’’ Somephysicians recommended a ‘‘prescription for the mother,’’ such asCarter’s Little Nerve Pills, linking the pharmaceutical industry to the
25Lightner Witmer. ‘‘The Organization of Practical Work in Psychology.’’ ThePsychological Review 4 (January 1897): 116–17; Idem, ‘‘Clinical Psychology,’’ ThePsychological Clinic 1 (March 1907): 1–9, 4, 1, 8. For Witmer see Joseph French. ‘‘Onthe Conception, Birth, and Early Development of School Psychology.’’ AmericanPsychologist 39 (September 1984): 976–987; Paul McReynalds, Lightner Witmer: His Lifeand Times (Washington, DC: American Psychological Association, 1997); JohnO’Donnell. ‘‘The Clinical Psychology of Lightner Witmer.’’ Journal of the History of theBehavioral Sciences 15 (Winter 1979): 3–17; Barry Richards. ‘‘Lightner Witmer and theProject of Psychotechnology.’’ History of the Human Sciences 1 (Winter 1988): 201–219;J.E.Wallace Wallin. ‘‘Handicapped Children.’’ American Journal of School Hygiene 4(September 1920): 29–48, on 44; Maud Merrill. ‘‘Oscillation and Progress in ClinicalPsychology.’’ Journal of Consulting Psychology 15 (July 1951): 281–89, on 284.
520 History of Education Quarterly

public school system. Eventually, in the 1930s, drug trials with nervousschool children emerged as legitimate and socially acceptable.26
The vivisection of school children was sporadic throughout the1800s but became increasingly common in the twentieth century. By thelate nineteenth century, vivisection referred to any experimental,invasive manipulation of animal and human subjects. In Boston during1896, Arthur Wentworth performed lumbar punctures on thirtychildren under his care in the Children’s Hospital, primarily to testthe diagnostic value of withdrawing spinal fluid. Labeled humanvivisection, Wentworth’s work inspired similar experiments onchildren in orphanages and institutions for the ‘‘feebleminded’’ andwayward youth during the early 1900s.27 The first clinical drug trialswith children who demonstrated ‘‘educational disabilities’’ were direct-ed by Charles Bradley in the mid- to late 1930s. The thirty children(twenty-one boys, nine girls) used in the Benzedrine trials were confinedto the Emma Pendleton Bradley Home in Providence, Rhode Island. Ofthe 270 students cared for, the group chosen for the trials demonstrated arange of behavioral problems and nervous disorders. Bradley claimed‘‘striking changes’’ and ‘‘spectacular improvement in schoolperformance in half of the children,’’ and proceeded to sponsor andinspire similar studies through the 1950s. Ciba Pharmaceutical ProductsInc. patented methylphenidate hydrochloride in 1950, trialed andmarketed it as Ritalin in the mid-1950s, and in 1970 finally ran upagainst mass protest and accusations that students were ‘‘drugged intoconformity in the classroom.’’28
26Philip C. Knapp. ‘‘The Influence of Overwork in School in the Production ofNervous Diseases in Childhood.’’ Boston Medical and Surgical Journal 85 (July 1896): 37–39, on 37, 38; D. Guye. ‘‘On Aprosexia and Headache in School Children.’’ Practitioner 47(September 1891): 198–201, on 198; John Punton. ‘‘Nervous Disorders of Children:Their Relation to School Life and Work.’’ American Medicine 13 (February 1907): 79–86,on 84; William B. Pritchard. ‘‘The Hygiene and Management of Nervous Children.’’Archive of Pediatrics 27 (July 1910): 499–505, on 503. See also Archibald Church,‘‘Nervous Children.’’ Archives of Pediatrics 23 (September 1906): 678–681, 700–705;Editor, Precocious Children.’’ Archive of Pediatrics 14 (February 1897): 116–18.
27On the vivisection of children, see Diana Belais. ‘‘Vivisection Animal andHuman.’’ Cosmopolitan 49 (July 1910): 267–273; Susan Lederer. ‘‘Hideyo Noguchi’sLuetin Experiment and the Antivivisectionists.’’ Isis 76 (March 1985): 31–48; Idem,‘‘Orphans as Guinea Pigs: American Children and Medical Experimenters, 1890–1930,’’in In the Name of the Child: Health and Welfare, 1870–1940 ed. Roger Cooter (New York:Routledge: 1992), 96–123; Idem, Subjected to Science: Human Experimentation in AmericaBefore the Second World War (Baltimore: Johns Hopkins University Press, 1995), 40–46,79–85; Susan Lederer and Michael Grodin, ‘‘Historical Overview: PediatricExperimentation,’’ in Children as Research Subjects eds. Michael Grodin and Leonard H.Glantz (Oxford: Oxford University Press, 1994), 3–28; G.M. Searle, ‘‘Murder in theName of Science,’’ Catholic World 70 (July 1903): 493–504.
28Charles Bradley. ‘‘A Children’s Hospital for Neurologic and BehaviorDisorders.’’ Journal of the American Medical Association 107 (August 1936): 650–653;
The Medicalization of Education 521
Neoscholastic Hygiene
Beginning in the early 1890s, there was fierce resistance to the pro-cesses of medicalization, most aggressively demonstrated by anti-vaccinationists, antivivisectionists, alternative healers, and proponentsof ‘‘medical freedom.’’ Opposition groups and many of the lay publicbelieved that education was medicalized through the hegemony ofallopathic practices. As Woolworth documented, parents combinedwith Christian Scientists to contain allopathic practices in cities suchas Seattle during the early 1920s.29 The director of hygiene for Bostonschools reported in 1908 that he and his officers encountered‘‘opposition from teachers who feared that pedagogy was to bemedicalized, from parents who resented any usurpation of homeauthority, from physicians who feared their private practice might beinvaded, and from certain members of the public at large who sawdangers of paternalism in the movement.’’ Initial ‘‘fears,’’ he emphasized,paled in light of the inroads of medicine into schooling. By 1910, 337cities across the United States employed 1,194 doctors and 371 nurses toadminister medical practices. In 1912, seven states had compulsorymedical inspection laws like Massachusetts and another twelve states
Idem, . ‘‘The Behavior of Children Receiving Benzedrine.’’ American Journal of Psychiatry94 (November 1937): 577–585, on 578, 584; Idem, Charles Bradley and M. Bowen.‘‘Amphetamine (Benzedrine) Therapy of Children’s Behavior Disorders.’’ AmericanJournal of Orthopsychiatry 11 (January 1941): 92–103; Idem, ‘‘Benzedrine and Dexedrinein the Treatment of Children’s Behavior Disorders.’’ Pediatrics 5 (January 1950): 24–37;Lester Grinspoon and Susan B. Singer. ‘‘Amphetamines in the Treatment of HyperkineticChildren.’’ Harvard Education Review 43 (November 1973): 515–555; Mathew Molitchand John Sullivan. ‘‘The Effect of Benzedrine Sulfate on Children taking the NewStanford Achievement Test.’’ American Journal of Orthopsychiatry 7 (October 1937): 519–522; Max Hartmann and Leandro Panizzon, assignors to Ciba Pharmaceutical ProductsInc., ‘‘Pyridine and Piperdine Compounds and Process of Making Same,’’ U.S. Patent2,507,631 (May 1950): 1–3; ‘‘Ritalin (methylphenidate),’’ Physician’s Desk Reference, 11thed. (Oradell, NJ: Medical Economics, 1956), 441–42. On the history of Ritalin and thetreatment of Attention-Deficit Hyperactivity Disorder, see Conrad, ‘‘The Discovery ofHyperkinesis’’; Idem, Identifying Hyperactive Children: the Medicalization of DeviantBehavior (Toronto: D.C. Heath, 1976); Toby Miller and Marie C. Leger, ‘‘A VeryChildish Moral Panic: Ritalin,’’ Journal of Medical Humanities 24 (Summer 2003): 9–33.For Ritalin controversy, Harlan Vinnedge, ‘‘Drugs for Children: Politicians Who WouldPractice Medicine,’’ New Republic 164 (March 1971): 13–15.
29Woolworth, ‘‘Conflict,’’ 278–298; On antivivisection, see Lederer, ‘‘HideyoNoguchi.’’ For anti-vaccination, see Nadav Davidovich, ‘‘Homeopathy and Anti-Vaccinationism at the Turn of the Twentieth Century,’’ in The Politics of Healing ed.Robert D. Johnston (New York: Routledge, 2004), 11–28; Martin Kaufman. ‘‘TheAmerican Anti-Vaccinationists and Their Arguments.’’ Bulletin of the History of Medicine41 (September 1967): 463–478; Dorothy Porter and Roy Porter. ‘‘The Politics ofPrevention: Anti-Vaccinationism and Public Health in Nineteenth-Century England.’’Medical History 32 (July 1988): 231–252. On Medical Freedom and allopathic hegemony,see Stephen Petrina, Medicalizing Liberty in the Kingdom of Evils: Education, Medicine,Psychotherapeutics, Foucault (unpublished manuscript).
522 History of Education Quarterly
had somewhat more permissive laws. At the Fiftieth Annual NationalEducation Association (NEA) Meeting in Chicago in 1912, CharlesReed, a physician from Cincinnati, announced that despite two decadesof medical progress in the schools, opposition was collective andsystematic. The United States now had the ‘‘peculiar and questionabledistinction,’’ Reed announced, of a ‘‘nation-wide movement to defeat,not only the medical inspection of schools, but all other statutory effortsto prevent diseasey thru observance of hygienic law.’’ ‘‘These people intheir organized capacity,’’ he warned the NEA crowd, ‘‘having raised theshibboleth of ‘‘Medical Freedom,’’ are engaged in an active propagandato impose the tyranny of their selfish interests upon the people.’’ ‘‘Theyhave raised the cry that the meaning of all this health legislation is todeprive the individual his right to employ the physician of his choice, andon this falsehood, they have solicited and received contributions to theircorruption fund.’’ Reed spoke for the medical profession andrepresented the resistance to allopathic medicine as dangerously naiveand selfish. ‘‘It finally became evident,’’ explained Reed, that ‘‘the healthof the rising generation involves an intimate technical and professionalknowledge of anatomy, physiology, hygiene, the causes and preventionof disease, and the art to determine and define the physiologicallimitation of each individual pupil.’’30
By 1910, there were at least eight different sites and trajectoriesthrough which education was medicalized. The medicalization ofeducation was popularized through the training of new practitionersin these sites. G. Stanley Hall held weekly clinics for students at BayView Hospital for the Insane while at Johns Hopkins in Baltimore.Lightner Witmer’s efforts in training practitioners were tightly tied to
30Charles A. Reed. ‘‘The Medical Inspection of Children and Medical Freedom.’’Journal of Proceedings and Addresses of the National Education Association 50 (1912): 273–78;‘‘News and Comment: The School Hygiene Department of Boston, Mass.’’ PsychologicalClinic 2 (1908): 251–52, 251. On the progress of medicine in schools, see Julia GrahamLear. ‘‘School Based Services and Adolescent Health: Past, Present and Future.’’Adolescent Medicine 7 (June 1996): 163–180; Lawrence A. Averill. ‘‘The Present Statusof School Health Work in the 100 Largest Cities of the United States.’’ American Journalof School Hygiene 1 (February 1917): 30–38, 53–62; Idem, Educational Hygiene (BostonHoughton Mifflin, 1926); Josephine Baker, Child Hygiene (New York: Harper & Brothers,1925); Gulick and Ayers, Medical Inspection, 167–180; Ernest B. Hoag and Lewis M.Terman, Health Work in the Schools (Boston: Houghton Mifflin, 1914); Philip van Ingen,‘‘History of Child Welfare in the United States,’’ in A Half Century of Public Health ed.Mazyk P. Ravenel (New York: Public Health Association, 1921), 290–334; Rapeer,Essentials; Marie M. Ready, ‘‘Hygiene and Physical Education,’’ Biennial Survey ofEducation, 1928–1930, U.S. Office of Education Bulletin No. 20 (1931): 353–380; James F.Rogers, School Health Activities in 1930, U.S. Office of Education Pamphlet No. 21 (May1931); Idem, ‘‘Health Services in City Schools,’’ in Biennial Survey of Education in theUnited States, 1938–40 (Washington, DC: U.S. Government Printing Office, 1942), 1–50; Willard Small, Educational Hygiene, Bureau of Education Bulletin No. 33 (1923).
The Medicalization of Education 523

the medical department at the University of Pennsylvania. HenryGoddard, at the Vineland Training School in New Jersey, waspersistent in offering internships in psychotherapeutic training andcare for the disabled during the 1910s. Opportunities for interning andinvestigative work in hospitals were typical of changes occurring inscientific psychology in the U.S. during the 1900s and 1910s. Amongchanges that took place in medical training during the late 1880s andearly 1900s was the decrease in apprenticeships with generalpractitioners and an increase in clinic and hospital internships.Abraham Flexner’s report on medical education published in 1910helped increase the rate of this change. Flexner, a young physiciantrained at Johns Hopkins, argued that in clinics and hospitals, medicalstudents should be placed in positions of both observer and clinician.Clinics and hospitals provided settings for close personal contactsbetween interns and patients, and a setting for observing a range ofmedical practices. Appointments and internships in clinics and hospitalshelped psychologists repudiate philosophical psychology, orintrospectionism, and materialize scientific psychology. Thegeneration of psychologists that included Walter Dearborn andRobert Yerkes at Harvard and Arnold Gesell at Yale opened the doorsto medical institutions with their newfound interests in clinical andabnormal psychology. Yerkes spearheaded psychological internships forhis Harvard students in Boston’s hospitals and clinics. Luella Cole,Norman Fenton, Florence Goodenough, Sidney Pressey, Leta StetterHollingworth, and David Shakow were among those whose rite ofpassage into educational or school psychology was through hospitals inthe 1910s and early 1920s.31
Reflecting Flexner’s recommendations, there was a sharp increasein the number of ‘‘teaching hospitals’’ in the United States during the1910s. The Boston Psychopathic Hospital, for example, was a relatively
31For Cole and Pressey’s training, see Petrina, ‘‘Luella Cole, Sidney Pressey.’’ Onpsychological internships and training, see Loyal Crane. ‘‘A Plea for the Training ofPsychologists.’’ Journal of Abnormal Psychology 20 (July 1955): 228–233; SamuelFernberger. ‘‘The Training of Mental Hygienists.’’ Psychological Clinic 14 (October1930): 137–142; William Morrow. ‘‘The Development of Psychological InternshipTraining.’’ Journal of Consulting Psychology 10 (July 1946): 165–183; John O’Donnell,The Origins of Behaviorism: American Psychology, 1870–1920 (New York: New YorkUniversity Press, 1985), 195–97; David Shakow. ‘‘An Internship for Psychologists(with Special Reference to Hospitals).’’ Journal of Consulting Psychology 2 (April 1938):73–76; Lewis Terman. ‘‘Professional Training for Mental Hygiene.’’ Popular ScienceMonthly 80 (March 1912): 289–297; Robert I. Watson. ‘‘Training of ClinicalPsychologists.’’ American Journal of Orthopsychiatry 22 (Spring 1952): 140–152; RobertI. Watson. ‘‘A Brief History of Clinical Psychology.’’ Psychological Bulletin 50 (September1953): 321–346; Lightner Witmer. ‘‘The Hospital School.’’ Psychological Clinic 1 (July1907): 138–146; Idem, ‘‘Courses in Psychology at the Summer School of the University ofPennsylvania.’’ Psychological Clinic 4 (November 1911): 245–273.
524 History of Education Quarterly

small, four-story, brick building built to function as a research laboratoryand temporary care and outpatient facility. This ‘‘charitable’’ institutionopened its doors in June 1912 and was modeled after Kraepelin’s dem-onstration clinic in Munich and somewhat after the Clinique Charcot atthe Salpetriere in Paris. Arrangements with local universities, such as theBoston School of Social Work, Harvard, Smith College and Tufts, madethe Boston Psychopathic Hospital a convenient institution for studentsneeding short-term apprenticeships and residences. Cole and Pressey’straining at the Psychopathic Hospital in 1917 and 1918 preparedthese two educational psychologists to specialize in mental hygieneand the hygiene of instruction. They readily integrated the lab-oratory techniques of behaviorism with the clinical procedures ofpsychoanalysis.32 They popularized psychotherapeutic knowledgeand products in university courses and workshops for teachers.Like medical practitioners, they adopted dispositions towardtreatment and assumed the authority to manage and control in-dividual cases through the hygiene of instruction or ‘‘neoscholastichygiene.’’33
The hygiene of instruction reaffirmed the authority of disciplinarycontent (i.e., neoscholasticism) common to the school curriculum (i.e.,art, English, history, math, science, etc.) and its maintenance throughstandardized tests. Neoscholastic hygiene regulated how and what tothink about subjects such as art or science and was, in effect, a way ofregulating normality from early ages. Educational psychologists such asCole and Pressey recognized that the minutiae of everyday schoolinggoverned the students’ mental health as well as mobility. Theycalled their ‘‘diagnostic or teach-test procedure’’ ‘‘EducationalPsychoanalysis,’’ or ‘‘the problem of finding out why pupils make theerrors they do.’’ ‘‘What makes a child begin common nouns withcapitals? Why does a given pupil put commas where they are not
32Who is qualified to administer examinations, make diagnoses, and prescribetreatments? Of course, the relations between medicine and psychology were not withoutdisputes. See for example John C. Burnham. ‘‘Psychiatry, Psychology and the ProgressiveMovement.’’ American Quarterly 12 (October 1960): 457–465; Idem, ‘‘The StruggleBetween Physicians and Paramedical Personnel in American Psychiatry, 1917––41.’’Journal of the History of Medicine 29 (January 1974): 93–106; William J. Goode.‘‘Encroachment, Charlatanism, and the Emerging Profession: Psychology, Sociology,and Medicine.’’ American Sociological Review 25 (October 1960): 902–914; David Shakow.‘‘Psychology and Psychiatry: A Dialogue.’’ American Journal of Orthopsychiatry 19 (March1949): 191–210, 381–396; Robert I. Watson. ‘‘Historical Perspectives on the relationshipof Psychologists to Medical Research.’’ Neuropsychiatry 6 (January 1960): 51–59.
33Neoscholastic hygiene is a derivative of the hygiene of instruction and refers tothe use of clinical methods to reaffirm the authority of disciplinary content of schoolsubjects. Lawrence A. Averill, The Hygiene of Instruction (New York: Houghton Mifflin,1928); Harry N. Rivkin, Educating for Adjustment: The Classroom Applications of MentalHygiene (New York: D. Appleton-Century, 1936).
The Medicalization of Education 525
needed? How do children arrive at their queer conclusions in regard tocausal relationships in history?’’ The ‘‘hygiene of instruction’’ oreducational psychoanalysis meant that the facts and figures enteringyoung minds were controlled and monitored for potential adverseeffects. Art, science, and social studies books, for example, paidhomage to the past and patriotism. Regulations and publisheragreements basically ensured that only ‘‘healthy’’ content and imagesentered the minds of young scholars. Educational psychologists furtherrationalized the curriculum through clinical methods.34
For educators, the clinical method underwrote what psychologistGiles Ruch called the ‘‘complete act of instruction’’:
1 Initial presentation of materials to be mastered. This phaseconsists of setting problems to be solved, textbook readingsand discussion, teachers’ comments on persistent difficul-ties in learning, etc.
2 Drill to support the temporary mastery gained under thefirst phase of instruction. This may be drill proper or it maymean applications and reviews.
3 Diagnostic measurement at the period when phases one andtwo are thought to be complete.
4 Reteaching or remedial instruction upon any weakness re-vealed under the third phase.
5 Final measurement and evaluation of a more general andless detailed character than that of phase three. This con-stitutes the final survey of achievement and leads to a judg-ment as to whether the individual or class is ready toproceed to new work.
34On educational psychoanalysis, see Petrina, ‘‘Luella Cole, Sidney Pressey’’; LeoBrueckner. ‘‘Diagnostic Analysis of Classroom Procedures.’’ Elementary School Journal 27(January 1926): 25–40; Leo Brueckner and Ernest Melby, Diagnostic and Remedial Teaching(New York: Houghton Mifflin, 1931); Luella Cole, ‘‘The Use of QuantitativeMeasurement in Educational Diagnosis and in Evaluating Remedial Instruction,’’ inQuantitative Measurement in Instruction in Higher Education ed. Stuart Courtis (Chicago:University of Chicago Press, 1930), 164–177; Carter Good. ‘‘Research in SecondarySchool Methods.’’ Journal of Educational Research 22 (January 1930): 9–30; Arthur A.Metcalf. ‘‘Diagnostic Testing and Remedial Teaching.’’ School Executives Magazine 49(June 1930): 358–360; Marion Monroe. ‘‘Diagnostic and Remedial Procedures inReading.’’ Educational Record 19 (February 1938): 105–113; Emanuel Paulu, DiagnosticTesting and Remedial Teaching (New York, D.C. Heath and Company, 1924); BerthaRogers and Teresa Baker. ‘‘A Diagnostic and Remedial Activity in Supervision.’’ Journal ofEducational Research 5 (January 1922): 21–26; Eugene Smith. ‘‘The Use of Tests andMeasurements in the Three R’s: A Symposium.’’ Progressive Education 5 (March 1928):136–152; Thorndike, ‘‘Educational Diagnosis.’’ On textbook histories, see StephenPetrina. ‘‘Getting a Purchase on ‘The School of Tomorrow’ and Its ConstituentCommodities: Histories and Historiographies of Technologies.’’ History of EducationQuarterly 42 (April 2002): 75–111.
526 History of Education Quarterly

In 1939, Charlotte Easby Grave, Principal of the Woods Schools inRoslyn, Pennsylvania, summarized this progressive pedagogy: ‘‘thelearning pill was sugar coated, which made it a little easier to swallow,but it was still medicine. No longer did the teacher say, ‘Take thisbecause I told you so.’ She said, ‘You want to be well and strong, don’tyou?’Fthen take this medicine, it’s good for you.’’ The school hadbecome an educational dispensary or ‘‘therapeutic milieu’’ andinstruction was no exception. The clinical, ‘‘diagnostic-remedialapproach [to instruction],’’ one analyst concluded in 1969, ‘‘is themost frequently used in schools today.’’35
Although medical intervention was what, in 1913, a neurologistrecognized as a ‘‘veritable medicosociological problem,’’ up until the1930s the relation between medicine and sociology was limited toclinical sociology and psychiatric social work. In the 1930s,sociologists began to study systematically the ‘‘medico-authoritarianmantle’’ associated with clinical and associated allopathic, medicalpractices.36 These studies and others through the 1960s were theinspiration behind the medicalization thesis. In the late 1960s and1970s, sociologists of medicine and medicalization describedallopathic practices from a perspective of ‘‘mentalities.’’ To understandmedical practice in the schools, it is worth attending to sociological aswell as historical descriptions. Eliot Freidson observed, for example,that clinical practitioners share a common ethos or mindset conditionedthrough work with patients or students. He described the allopathicethos as a ‘‘clinical mentality,’’ characterized by commitments to actionas opposed to inaction, individualism, faith in procedure, perceptiontrained to illness as opposed to health, pragmatism and firsthandexperience, subjectivism in that the use of senses are important to
35On clinical methods, see Robert I. Watson, Readings in the Clinical Method inPsychology (New York: Harper & Brothers, 1949); Idem, The Clinical Method in Psychology(New York: Harper & Brothers, 1951). On the complete act of instruction, see Giles M.Ruch, The Objective or New-Type Examination (Chicago: University of Chicago Press,1929), 9; Charlotte E. Grave, ‘‘Twenty-Five Years of Progress at the Woods Schools,’’ inTwenty-Five Years of Progress in Education eds. (Langhorne, PA: Child Research Clinic ofthe Woods Schools, 1939), 12; Bruno Bettelheim and Emmy Sylvester. ‘‘A TherapeuticMilieu.’’ American Journal of Orthopsychiatry 18 (April 1948): 191–200; Thomas Oakland,‘‘Diagnostic Help 5b: Examiner Is In,’’ Psychology in the Schools 6 (1969): 359–367, on 360.
36Mary Sutton. ‘‘Medical Sociology in the Public Schools.’’ New York MedicalJournal 108 (December 1913): 1164–66, on 1164. On early medical sociology, seeKingsley Davis. ‘‘Mental Hygiene and the Class Structure.’’ Psychiatry 1 (January1938): 55–65, on 65; Harold D. Laswell, Psychopathology and Politics (New York: Viking,1930); C. Wright Mills. ‘‘The Professional Ideology of Social Pathologists.’’ AmericanJournal of Sociology 49 (1943): 165–180; Talcott Parsons. ‘‘Illness and the Role of thePhysician: A Sociological Perspective.’’ American Journal of Orthopsychiatry 21 (October1951): 452–460; Louis Wirth. ‘‘Clinical Sociology.’’ American Journal of Sociology 27(January 1931): 49–66.
The Medicalization of Education 527

practice, and an emphasis on indeterminacy or uncertainty. The termclinical literally refers to ‘‘bedside’’ or personal, practical psycho-therapeutic attention to patientsFmedical practice in the presence ofpatients, or practice at the ‘‘sick-bed.’’ Eventually, the connotationencompassed diagnosis and treatment with the patient present,whether bedridden or not. Freidson suggested: ‘‘Clearly, neithermedicine nor the physician may be characterized as passive y
medicine is committed to treating rather than merely defining andstudying y It has a mission of active intervention guided by what, inwhatever time and place it exists, it believes to be ill in the world.Furthermore, it is active in seeking out illnessyAnd insofar as illness isdefined as something badF[a weakness] to be eradicated or containedFmedicine plays the role of what Becker called the ‘moralentrepreneur.’’’37
If teachers share this moral entrepreneurialism and clinicalmentality with medical practitioners, then students identify withpatients. Talcott Parsons noted that the North American ‘‘pattern forillness is focused on the capacity for achievement for the individual.’’Therapeutic recovery for a patient is defined as a ‘‘job to be done incooperation with those who are technically qualified to help. The focusthen operates to polarize the components of the ‘problem’ in such a waythat the primary threat to [the patients’] achievement capacity which must beovercome is dependency.’’ These accounts are insightful but, for somehistorians and sociologists, fail to account adequately for science andtechnology. An ‘‘objective’’ bedside attention paid by medicalpractitioners to their patients, and a new precision in diagnosis andtreatment through laboratory medical science marked clinical practicesmore and more throughout the nineteenth century. According tohistorian John Harley Warner, new laboratory-based, clinicalknowledge was a product of ‘‘privileged epistemology.’’38
37Eliot Freidson, Profession of Medicine: A Study of the Sociology of Applied Knowledge(New York: Dodd, Mead and Company, 1971), 172, 252. See also, Andrew Abbott, TheSystem of Professions (Chicago: University of Chicago Press, 1988); Paul Atkinson, MedicalTalk and Medical Work: The Liturgy of the Clinic (London: Sage, 1995); Caroline Cox andAdrienne Mead, eds., A Sociology of Medical Practice (London: Collier-Macmillan, 1975);Amatai Etzioni, The Semi-Professions and Their Organization: Teachers, Nurses, SocialWorkers (New York: Free Press, 1969); Eliot Freidson, Doctoring Together: A Study ofProfessional Social Control (New York: Elsevier, 1975); Idem, Medical Work in America:Essays on Health Care (New Haven, CT: Yale University Press, 1989); Eliot Freidson andJudith Lorber, eds., Medical Men and Their Work (Chicago: Aldine, 1972); Robert K.Merton, Sociological Ambivalence and Other Essays (New York: Free Press, 1976).
38Talcott Parsons, ‘‘Definitions of Health and Illness in Light of American Valuesand Social Structure,’’ in Patients, Physicians and Illness ed. E. Gartly Jaco (London CollierMacmillan, 1973), 140–41; John H. Warner, ‘‘The Fall and Rise of Professional Mystery,’’in The Laboratory Revolution in Medicine eds. Andrew Cunningham and Perry Williams(Cambridge: Cambridge University Press), 141.
528 History of Education Quarterly
What emerged from clinical practice, says Michel Foucault, was‘‘medical perception.’’ For Foucault, the patient’s ‘‘bed’’ became ‘‘a fieldof scientific investigation and discourse.’’ ‘‘This new structure isindicatedFbut not of course exhaustedFby the minute but decisivechange, whereby the question: ‘What is the matter with you?’y wasreplaced by that other question: ‘Where does it hurt?’, in which werecognize the clinic and the principle of its entire discourse.’’ Clinicalpractice involves a mode of saying and seeingFa productive,pedagogical gaze. In education, a unique arrangement ofpsychotherapeutics was practiced at the ‘‘deskside.’’ Teaching was notso much a dialogue as a ‘‘deskside’’ practice. This clinical ‘‘deskside’’practice was, according to progressive practitioner Arthur Metcalf, thekeynote of progressive education: ‘‘find the weakness of the child andapply the teaching effort at the point of weakness.’’ At the ‘‘deskside,’’one metaphorically asks this child, ‘‘where is your weakness?’’ revealingas Foucault suggested, a modern discourse of clinical practice. The firsttask of this practice, said Foucault, ‘‘is therefore political: the struggleagainst disease’’ is a struggle ‘‘against bad government.’’ From medicinecame knowledge of illness, but also knowledge of ‘‘healthy man, that is, astudy of non-sick man and a definition of the model man’’ or student.39
Medicating Kids
I described eight, distinct practices through which schools weremedicalized during the last decade of the nineteenth century and thefirst three decades of the twentieth century. The medicalization ofeducation was summarized in expanding definitions of educationalhygiene, encompassing mental, neoscholastic, physical, and schoolhygiene by the mid-1910s. Mental hygiene, as noted by Cohen,attended to the maintenance of normality as well as the diagnosis andtreatment of abnormality and disability in personality and intelligence.The hygiene of instruction or neoscholastic hygiene expanded fromconcerns with fatigue induced from academic studies to the detection ofpathologies behind adding or spelling and the psychotherapeutics ofreaffirming the authority of school subjects. The medical practices ofphysical hygiene, such as medical inspections, physical education, andinstruction in hygiene, were primarily concerned with interrelationsamong ability and body, mind, and soul. Through the sanitation ofbuilding and fixture design and maintenance, schools were physically
39Michel Foucault, The Birth of the Clinic trans. A.M. Sheridan Smith (New York:Vintage, 1973/1994), xii, xv, xviii, 33–34; Metcalf, ‘‘Diagnostic Testing,’’ 360; Foucaultquoted in Colin Gordon, ed., Power/Knowledge (Brighton: Harvester, 1980), 166.
The Medicalization of Education 529

modeled on the clinic and hospital in the name of school hygiene. Thehygienic practices and texts of dietetics, health education, and physicalculture responded to new alignments among anatomy, anthropometry,chemistry, eugenics, medicine, physiology, and psychology.
I argued that in the aggregate, our histories of the medicalization ofeducation account somewhat for the diversification of educationalhygiene but individually are incomplete in that they fail to account forthe articulation of its practices.40 I offered a synthesis and demonstratedthat the medicalization of education was material inasmuch as it wasideological. By providing a detailed narrative of interdependenciesbetween allopathic medicine and education, I suggested that themedicalization of education was basically a historical accomplishmentestablished on contingencies. During the late 1800s, clinical, scientificmedicine provided a ‘‘privileged epistemology’’ for allopaths interestedin extending their authority into the full range of modern life. Besidestraditional systems of church-sponsored benevolence, newinterventionistsFdieticians, clinical nurses, physicians, psychiatrists,psychologists, psychiatric social workersFhelped popularize aseemingly secular system of expertise for treating everyday problems.Of course, philanthropy, policy, and the legal system shored up long-term allopathic intervention in the schools. Indeed, the modernclassroom was constructed through models of the clinic and dispensaryFinstitutions toward which educators and psychologists turned toenforce the rudiments of liberal, progressive practiceFeven asadministrators ran their offices and hallways on models of the efficientbusiness establishment.
Why does it matter whether we recognize how, when, and whyeducation was medicalized? If we fail to recognize that merit and theregulation of mobility only partially account for the persistence andpower of examination and remediation industries in North Americaneducation, we cannot understand the increasingly complex role thatmedicine plays in the lives of students.41 We will merely wonder at the
40On diversification of educational hygiene, see Kenneth E. Veselak. ‘‘HistoricalSteps in the Development of the Modern School Health Program.’’ Journal of SchoolHealth 29 (July 1959): 262–69.
41Signifying the marketability of psychotherapeutic knowledge for education, 650Sylvan Learning Centers are operating in Canada and the United States and competingwith the Educational Testing Service (ETS) to provide computerized testing andremedial services to place students on the road to good academic health. Companiessuch as Sylvan and the ETS’s Princeton Review are coordinating their services with publicschools to exploit the $2.5 billion test preparation market. Denise Hawkins. ‘‘Multiple-Choice Mushroom.’’ Black Issues in Higher Education 11 (February 1995): 8–10, 12;Marguerite Clark, George Madaus, Catherine Horn and Miguel Ramos. ‘‘TheMarketplace for Educational Testing.’’ Statements 2 (April 2001): 1–10; Walter M.Haney, George F. Madaus and Robert Lyons, The Fractured Marketplace for
530 History of Education Quarterly
fact that between 5 and 10 percent of North American school-agestudents are diagnosed with ADHD and about three million areprescribed Ritalin and generic derivatives of methylphenidate.Historians and educators ought to understand that a process ofmedicating kids for school is completely interdependent with acomplex of psychotherapeutic practices and historical contingencies.This historiographic synthesis should leave little doubt that this practicehas a deep and complex history that demands sustained attention. Largerhistorical and moral problems are how and why allopathic physicianswon school privileges and rights over a variety of alternativepractitioners contesting access to the body, minds, and souls ofstudents.42
Standardized Testing (Boston: Kluwer, 1993); Richard P. Phelps. ‘‘Estimating the Cost ofStandardized Student Testing in the United States.’’ Journal of Educational Finance 24(Winter 2000): 343–380; Peter Saks, Standardized Minds (Cambridge: Perseus, 1999),221–230.
42The U.S. Congress passed The Child Medication Safety Act of 2003 ‘‘to protectchildren and their parents from being coerced into administering a controlled substancein order to attend, and for other purposes.’’ On trends in methylphenidate uses, seeWilliam Cooper, Gerald Hickson, Catherine Fuchs, Patrick Arbogast and Wayne Ray.‘‘New Users of Antipsychotic Medications Among Children Enrolled in TennCare.’’Archives of Pediatrics & Adolescent Medicine 158 (August 2004): 753–59; Lawrence H.Diller, Running on Ritalin (New York: Bantam, 1998); Idem, ‘‘Lessons from Three YearOlds,’’ Developmental and Behavioral Pediatrics 23 (February 2002): S10–S12; SvetlanaKolchik, ‘‘Use of Ritalin to Control Kids’ Behavior,’’ Honolulu Advisor (13 November2002), http://the.honoluluadvertiser.com/article/2002/Nov/13/hf/hf01a.html; AntonMiller, Christopher Lalonde, Kimberlyn M. McGrail and Robert Armstrong.‘‘Prescription of Methylphenidate to Children and Youth, 1990–1996.’’ CanadianMedical Association Journal 165 (November 2001): 1489–494; Miller and Leger, ‘‘A VeryChildish Moral Panic’’; Linda M. Robison, David Sclar, Tracy L. Sclar and RichardGalin. ‘‘National Trends in the Prevalence of Attention-Deficit/Hyperactivity Disorderand the Prescribing of Methylphenidate Among School-Age Children: 1990–1995.’’Clinical Pediatrics 38 (April 1999): 209–217; Julie M. Zito, Daniel Safer, Susan dosReis,James Gardner, Myde Boles and Frances Lynch. ‘‘Trends in the Prescribing ofPsychotropic Medications to Preschoolers.’’ Journal of the American Medical Association283 (February 2000): 1025–030.
The Medicalization of Education 531
Copyright © 2022 FDOKUMEN