The Maternal Lifestyle Study: Drug Use by Meconium Toxicology and Maternal Self-Report
11
DOI: 10.1542/peds.107.2.309 2001;107;309 Pediatrics Marilyn A. Huestis, Loretta P. Finnegan and Penelope L. Maza Verter, Charles R. Bauer, Seetha Shankaran, Henrietta S. Bada, H. Chip Walls, Barry M. Lester, Mahmoud ElSohly, Linda L. Wright, Vincent L. Smeriglio, Joel Self-Report The Maternal Lifestyle Study: Drug Use by Meconium Toxicology and Maternal http://pediatrics.aappublications.org/content/107/2/309.full.html located on the World Wide Web at: The online version of this article, along with updated information and services, is of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275. Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2001 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Point publication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly at Indonesia:AAP Sponsored on May 31, 2013 pediatrics.aappublications.org Downloaded from
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of The Maternal Lifestyle Study: Drug Use by Meconium Toxicology and Maternal Self-Report
DOI: 10.1542/peds.107.2.309 2001;107;309Pediatrics
Marilyn A. Huestis, Loretta P. Finnegan and Penelope L. MazaVerter, Charles R. Bauer, Seetha Shankaran, Henrietta S. Bada, H. Chip Walls,
Barry M. Lester, Mahmoud ElSohly, Linda L. Wright, Vincent L. Smeriglio, JoelSelf-Report
The Maternal Lifestyle Study: Drug Use by Meconium Toxicology and Maternal
http://pediatrics.aappublications.org/content/107/2/309.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2001 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Indonesia:AAP Sponsored on May 31, 2013pediatrics.aappublications.orgDownloaded from

The Maternal Lifestyle Study: Drug Use by Meconium Toxicology andMaternal Self-Report
Barry M. Lester, PhD*; Mahmoud ElSohly‡; Linda L. Wright, MD§; Vincent L. Smeriglio, PhDi;Joel Verter, PhD¶; Charles R. Bauer, MD#; Seetha Shankaran, MD**; Henrietta S. Bada, MD‡‡;
H. Chip Walls, BA§§; Marilyn A. Huestis, PhDii; Loretta P. Finnegan, MD¶¶; andPenelope L. Maza, PhD##
ABSTRACT. Objective. The objective of this studywas to describe drug use by pregnant women participat-ing in the 4-site Maternal Lifestyle Study of in uterococaine and/or opiate exposure.
Methods. Meconium specimens of 8527 newbornswere analyzed by immunoassay with GC/MS confirma-tion for metabolites of cocaine, opiates, cannabinoids,amphetamines, and phencyclidine. Maternal self-reportof drug use was determined by hospital interview.
Results. The prevalence of cocaine/opiate exposure inthe 4 sites was 10.7% with the majority (9.5%) exposed tococaine based on the combination of meconium analysisand maternal self-report. However, exposure status var-ied by site and was higher in low birth weight infants(18.6% for very low birth weight and 21.1% for low birthweight). Gas chromatography/mass spectrometry (GC/MS) confirmation of presumptive positive cocainescreens was 75.5%. In the cocaine/opiate-exposed group,38% were cases in which the mother denied use but themeconium was positive. There was 66% agreement be-tween positive meconium results and positive maternalreport. Only 2% of mothers reported that they used onlycocaine during pregnancy and mothers were 49 timesmore likely to use another drug if they used cocaine.
Conclusion. Accurate identification of prenatal drugexposure is improved with GC/MS confirmation andwhen the meconium assay is coupled with a maternalhospital interview. However, the use of GC/MS mayhave different implications for research than for publicpolicy. We caution against the use of quantitative analy-sis of drugs in meconium to estimate the degree of expo-sure. Our study also highlights the polydrug nature ofwhat used to be thought of as a cocaine problem.Pediatrics 2001;107:309–317; cocaine, opiates, polydruguse, pregnancy substance abuse, meconium, self-report,
multisite, gas chromatography/mass spectrometry, lowbirth weight, prenatal drug exposure.
ABBREVIATIONS. LBW, low birth weight; NICHD, NationalInstitute of Child Health and Human Development; VLBW,very low birth weight; NBW, normal birth weight; EMIT,enzyme-multiplied immunoassay technique; THC, cannabinoids;PCP, phencyclidine; GC/MS, gas chromatography/mass spec-trometry; BE, benzoylecgonine; CE, cocaethylene; HBE, m-hydroxy-benzoylecgonine; 6MAM, 6-monoacetylmorphine; HYM, hydro-morphone; HYC, hydrocodone; QNS, quantity not sufficient; OR,odds ratio; CI, confidence interval.
The accurate identification of prenatal cocaineexposure is critical for 2 reasons: 1) to fullyunderstand the nature and magnitude of the
problem, and 2) to determine appropriate medicaland psychosocial intervention. Methods used toidentify prenatal cocaine exposure vary and includeinterview, self-administered questionnaire, intakehistory, urine testing of mother and infant, and test-ing of infant hair and meconium, resulting in widelydisparate estimates of rates of cocaine use by preg-nant women. Maternal self-report of drug use isproblematic because of the fear of the consequencesof admitting to the use of an illegal substance, andthe inaccuracy of recall, especially when details suchas when, how often, and how much are asked. Un-derreporting of drug use by pregnant women hasbeen documented in several studies.1–3 In a sampleof over 3000, in which 43% were positive for illegalsubstances, Ostrea et al1 found that only 11% of themothers admitted to illicit drug use. Frank et al3found that self-report misclassified 24% of cocaineusers identified by urine toxicology.
Biomarkers of in utero cocaine exposure in theneonate include measurement of the drug in blood,urine, hair, and meconium and, recently, in gastricaspirate and amniotic fluid.13 Urine has been themost widely used specimen; however, Ostrea et al4,5
reported meconium to be more suitable than urinefor detecting fetal exposure to cocaine. Urine detec-tion underestimates exposure because cocaine me-tabolites are measurable in urine for no more than 96to 120 hours after the last cocaine use in contrast tomeconium, which can detect cocaine use throughoutthe second half of pregnancy. In addition, the con-centration of drugs may be higher in meconium thanin urine.5 A number of studies suggest that meco-
From *Brown Medical School, Women and Infants’ Hospital and BradleyHospital, Providence, Rhode Island; ‡ElSohly Laboratories, Inc, Oxford,Mississippi; §National Institute of Child Health and Human Development,Bethesda, Maryland; iNational Institute on Drug Abuse, Bethesda, Mary-land; ¶George Washington University, Biostatistics Center, Rockville,Maryland; #University of Miami School of Medicine, Miami, Florida;**Wayne State University School of Medicine, Detroit, Michigan; ‡‡Univer-sity of Tennessee Memphis, College of Medicine, Memphis, Tennessee;§§Forensic Toxicology Laboratory, University of Miami, Miami, Florida;iiNational Institute on Drug Abuse, Baltimore, Maryland; ¶¶Center forSubstance Abuse Treatment, Rockville, Maryland; and ##Administration onChildren, Youth and Families, Washington, DC.Received for publication Dec 10, 1999; accepted Jun 1, 2000.Reprint requests to (B.M.L.) Infant Development Center, Women and In-fants’ Hospital, 101 Dudley St, Providence, RI 02905-2499. E-mail:[email protected] (ISSN 0031 4005). Copyright © 2001 by the American Acad-emy of Pediatrics.
PEDIATRICS Vol. 107 No. 2 February 2001 309 at Indonesia:AAP Sponsored on May 31, 2013pediatrics.aappublications.orgDownloaded from

nium is the most useful specimen for the detection ofprenatal cocaine exposure.1,6,7–11 Lewis et al12 foundthat meconium detected 2.7 times more instances ofcocaine use than urine. However, these studies havebeen criticized by Casanova et al13 who argue thatthe methods used for the meconium measurementdiffered in analytic sensitivity and specificity fromthe urine screening methods, precluding a directcomparison of the performance of urine versusmeconium as matrices for the detection of cocaine. Inaddition to the choice of specimen, the detection ofcocaine exposure is influenced by the choice of initialscreening test and confirmation procedure. In severalstudies, urine toxicology was used to corroborateself-report.14–16 The importance of using both self-report and a biomarker was illustrated by Frank etal.3 Although self-report misclassified 24% of cocaineusers identified by urine toxicology, 51% of thosewho admitted use were negative for cocaine in theurine.
Estimates of cocaine exposure also vary dependingon the population studied. The 1988 National Mater-nal and Infant Health Survey,17 a mail survey, re-ported cocaine use during pregnancy by .4% ofwomen. The more recent National Pregnancy andHealth Survey18 based on questionnaire responsesestimated cocaine use by pregnant women at 1.1%.However, the National Pregnancy and Health Sur-vey also included urine test results from a subsampleand found significant underreporting of cocaine use.Higher prevalence rates of cocaine use during preg-nancy were reported in 2 high-risk population hos-pital surveys. In a 36-hospital review of dischargerecords, 10% to 17% of the women used cocaineduring pregnancy.19 The US Government Account-ing Office20 reviewed medical records in 10 hospitalsand reported prenatal cocaine exposure rangingfrom .3% to 11.6%. Prevalence rates of cocaine useduring pregnancy in 5 state studies21–25 ranged from.8%22 to 2.6%.23 Studies conducted at the local levelreveal a broader range: .4% in 26 hospitals in 1county in California,26 3.4% in 1 county in Florida,27
and 18.4% to 31% in single hospitals.1,28 Other factorsthat may account for the variability in estimates ofcocaine use by pregnant women are whether thesample is from a clinic,27 inner-city,3 or private hos-pital,23 or whether samples were highly selected toinclude women in drug treatment,29 or whether onlywomen enrolled in prenatal care3 were included.
We report the results of drug use by pregnantwomen from a study conducted in 4 sites that variedin racial and ethnic characteristics, social class, geo-graphic region, and that included public and privatehospitals. We used self-report and a meconium assaywith confirmation to determine exposure status tococaine and opiates, and we included the use of otherlicit and illicit drugs. We also studied low birthweight (LBW) infants and report our results by birthweight and by study site. Our intent is not to provideprevalence estimates for public health or public pol-icy purposes but to provide a description of prenataldrug exposure in the sites and to discuss some of theissues in the detection of prenatal cocaine exposure.
METHODSThe Maternal Lifestyle Study is a prospective multisite longi-
tudinal study on the association of drug use during pregnancywith acute neonatal events and long-term neurodevelopmentalchild outcome conducted under the auspices of the National In-stitute of Child Health and Human Development (NICHD) Neo-natal Research Network. The NICHD developed a fiscal and sci-entific collaboration with the National Institute on Drug Abuse,the Administration on Children, Youth, and Families, and theCenter for Substance Abuse Treatment to design and fund thestudy. Four clinical centers were selected: Brown University, theUniversity of Miami, the University of Tennessee at Memphis, andWayne State University. George Washington University served asthe Biostatistical Coordinating Center. The study was approved bythe institutional review board at each center and recruitmentoccurred between May 1993 and May 1995. In addition, a NationalInstitute on Drug Abuse Certificate of Confidentiality was ob-tained by each center that ensured confidentiality of informationregarding the participant’s drug use. The certificate supersededthe mandatory reporting of illegal substance use that was in effectin the Florida and Rhode Island centers. The certificate was ex-plained to the mother during the recruitment and informed con-sent procedure including the fact that the certificate did not ex-clude reporting of evidence of child abuse or neglect. Testing ofthe infant’s meconium for drugs was included as part of theinformed consent.
Mothers were recruited shortly after delivery and recruitmentstrategies varied among the 4 centers to maximize enrollment. Therecruitment strategy was designed to identify and recruit allwomen delivering very low birth weight (VLBW) infants of 501 to1500 g. For mothers delivering LBW (1501–2500 g) and normalbirth weight (NBW; .2500 g) infants, recruitment varied by cen-ter. Maternal exclusion criteria included age ,18 years, identifiedpsychosis, history of institutionalization for retardation or emo-tional problems, or language barriers that prevented her fromunderstanding the study. Infant exclusion criteria included out-born birth, multiple gestation, birth weight ,501 g, gestational age.42 weeks based on obstetrical estimate, or if in the judgment ofthe attending physician, the infant was unlikely to survive.
After informed consent, a maternal interview was conducted inhospital to determine past and current drug use and sociodemo-graphic information. The interview was structured, based on awritten script, and conducted by social workers or nurses whowere trained and certified to administer the interview. The inter-view was conducted in privacy after the mother had delivered andwas comfortable. A physical examination of the infant was con-ducted and the infant’s meconium was collected and refrigerated.Specimens were collected from more than 1 diaper and pooled ifthe quantity of meconium was small, as often occurred in thepreterm infants. Before discharge, maternal and infant charts wereabstracted to collect selected medical data. Meconium sampleswere processed, refrigerated, batched, and express shipped to acentral laboratory (ElSohly Laboratories, Oxford, MS), where theywere frozen at 220°C for analysis of metabolites of illicit drugs.The assay consisted of an initial enzyme-multiplied immunoassaytechnique (EMIT) screen for cocaine, opiates, cannabinoids (THC),amphetamines, and phencyclidine (PCP) with cutoff concentra-tions of 20 ng/g for THC and PCP, and 200 ng/g for the cocaine,opiate, and amphetamine metabolites. Presumptive positivescreens were confirmed with gas chromatography/mass spec-trometry (GC/MS) with cutoffs at the limit of detection of theassays. These were 50 ng/g for the cocaine, opiate, and amphet-amine metabolites, 5 ng/g for THC-COOH, and 3 ng/g for PCP.Details of the assay method are reported by ElSohly et al.30 Thecocaine metabolites included in the GC/MS confirmation werecocaine, benzoylecgonine (BE), cocaethylene (CE), and m-hy-droxybenzoylecgonine (HBE). HBE was added midway throughthe screening phase. The opiate metabolites included morphine,codeine, 6-monoacetylmorphine (6MAM), hydromorphone(HYM), and hydrocodone (HYC). THC, amphetamine, and meth-amphetamine and PCP were also confirmed by GC/MS, althoughamphetamines and PCP analysis were discontinued because oflow prevalence.
A mother–infant dyad was defined as exposed if either themother admitted using cocaine or opiates during the pregnancyhospital interview or if the infant’s meconium was positive for oneof the indicated metabolites of cocaine or opiates in the EMIT
310 MATERNAL LIFESTYLE STUDY OF DRUG USE BY MECONIUM AND MATERNAL SELF-REPORT at Indonesia:AAP Sponsored on May 31, 2013pediatrics.aappublications.orgDownloaded from

screen and by GC/MS confirmation. A dyad was categorized asnonexposed if the mother denied using both cocaine and opiatesduring the pregnancy on the hospital interview and the infant’sEMIT meconium screen was negative for both cocaine and opiates.Maternal use of alcohol, marijuana, and nicotine during the preg-nancy were treated as background variables in both the exposedand unexposed groups.
RESULTSDuring the 2-year recruitment period, 19 079
mothers were screened in the 4 centers. Of these,16 988 met the eligibility criteria, and 11 811 (70%)consented to participate in the study. The 5177 eligi-ble mothers who were not included are those whorefused consent, those not available, and those withlanguage barriers. Meconium was collected and cen-trally assayed on 8805 of the infants. Of the 8805meconium samples collected 277 (3.1%) had quantitynot sufficient (QNS) to perform the EMIT screen.QNS varied for the 3 birth weight groups from 7.1%for the VLBW group to 2.7% for the NBW group.Birth weight was missing for 1 infant, resulting in afinal sample of 8527 specimens on which all analysesare reported. The demographic characteristics of the8527 mothers in the final sample and the 3284 moth-ers who had consented but meconium was not col-lected or QNS are shown in Table 1. The demo-graphic characteristics were similar between these 2groups, suggesting that the sample in which themeconium was collected was representative of thesample of mothers who consented to participate inthe study.
Screening ResultsThe results of the EMIT meconium screen by clin-
ical center and birth weight group are summarizedin Table 2. The overall percentage of presumptivepositive cocaine screens by EMIT was 9.5%. How-ever, this varied considerably between centers andbirth weight groups. For VLBW infants, the EMITscreen was positive for cocaine in 18.2% of infants atWayne State, but only 4.8% at Miami. A similarvariation was seen for each of the 2 other birthweight groups: 26.6% to 12.0% in the LBW group and10.0% to 4.3% for the NBW group.
Although the prevalence of opiate use was less(2.3%), we still observed center variation (7.2% atBrown to 1.6% at Tennessee for LBW infants). Theresults for the cannabinoid screen also showed bothcenter (Wayne State was the highest and Miami wasthe lowest) and birth weight variation (VLBW infantsshowed the lowest positive rate except at Brown).The overall EMIT estimated prevalence of THC usewas 7.2%; however, only 36.5% of these were con-firmed positive by GC/MS. This low confirmationrate resulted in too small a sample for proper eval-uation and the THC screen was dropped midwaythrough the recruitment period. The EMIT-estimatedprevalence of amphetamine was .8% and no positivescreens were confirmed. Three percent of the meco-nium specimens screened positive for PCP but only4% of these were confirmed by GC/MS.
GC/MS ResultsThe meconium samples for 809 infants screened
positive for cocaine use. Of these, 22 (2.8%) wereQNS for GC/MS confirmation. The data in Table 3summarize the results of the GC/MS testing on theremaining 787 samples. Of these, 556 (70.6%) werepositive for at least 1 of the 3 metabolites: BE, co-caine, and CE. In addition, after ;50% of the screenshad been completed we added a fourth metabolite(HBE) to the confirmation process. For the 382 in-fants where confirmation was possible for all 4 me-tabolites, 287 (75.1%) were confirmed for BE, cocaine,or CE. An additional 38 (10%) were confirmed onlyfor HBE. Thus, in the subset in which all 4 metabo-lites were assessed, 325 of 382 or 85.1% were con-firmed by GC/MS.
As in the screening results, we report both a centerand birth weight variation in the type(s) of metabo-lites that were confirmed. For all birth weightgroups, BE and later, HBE was more likely to be theconfirming metabolite. CE was least likely (,10%) tobe identified in all birth weight groups. In each of thebirth weight groups, the use of BE alone would haveidentified 86.5% (VLBW), 98.7% (LBW), and 98.6%
TABLE 1. Demographic Characteristics (%) of Mothers in Each Site Who Consented
Wayne State Tennessee Miami Brown
In Final Sample
Yes No Yes No Yes No Yes No
GA ,32 wk 9 13 11 8 6 10 3 10Education ,12 y 38 41 34 33 44 47 18 20Insurance
Medicaid 86 91 88 88 62 63 25 28Private/HMO 11 8 7 7 3 3 70 67Self-pay 1 1 5 5 35 34 5 5
Married 17 17 24 24 37 37 67 64Maternal age 18–25 y 57 57 63 63 45 44 32 35Race
Black 83 84 81 85 30 33 9 10White 14 14 18 14 5 6 77 75Hispanic 3 2 1 1 65 61 14 16
TotalIn final sample: 8527Not in final sample: 3283
ARTICLES 311 at Indonesia:AAP Sponsored on May 31, 2013pediatrics.aappublications.orgDownloaded from

(NBW) of all samples confirmed positive for cocaineexposure.
Of the 200 positive screens for opiates, 18 (9.0%)were QNS for GC/MS confirmation. Overall, 70% ofthe 182 presumptive positive samples were con-firmed positive by GC/MS. Morphine accounted for46% to 62% of the birth weight-specific confirma-tions, while codeine was confirmed in 43% to 47% ofthe cases. The 6MAM, HYM, and HYC metaboliteswere identified in only 5 of the cases (2.7%). Thenumbers of cases at the specific sites and birthweight groups were too small to draw inferencesabout variability in drug exposure.
The variation in cocaine exposure by birth weightbased on the meconium results is shown in Table 4.Dividing the infants into 500-g birth weight groupsshows that the rate of cocaine exposure increasesthrough 2500 g both for the positive screens and forthose with positive GC/MS confirmation.
Maternal ReportTable 5 summarizes the results of the in-hospital
maternal interview reported use of cocaine and/oropiates during the pregnancy. Of the 8805 mothersfor whom there was an infant’s meconium available,619 (7.3%) reported using cocaine and 100 (1.2%)
TABLE 2. Number and Percent Positive Meconium Drug Screen (EMIT) for Metabolites of Cocaine, Opiates, and THC by Center andBirth Weight Group (n 5 8527)
Center Birth Weight Cocaine Opiates THC
No. (%)
Wayne State University 501–1500 g 32 (18.2) 7 (4.0) 10 (5.7)1501–2500 g 151 (26.6) 30 (5.3) 82 (14.5).2500 g 162 (10.0) 55 (3.4) 182 (11.2)Total 345 (14.6) 92 (3.9) 274 (11.6)
University of Tennessee 501–1500 g 24 (15.3) 3 (1.9) 10 (6.4)1501–2500 g 81 (18.2) 7 (1.6) 45 (10.1).2500 g 94 (8.5) 17 (1.5) 96 (8.6)Total 199 (11.7) 27 (1.6) 151 (8.8)
University of Miami 501–1500 g 4 (4.8) 2 (2.4) 2 (2.4)1501–2500 g 33 (13.0) 5 (2.0) 9 (3.6).2500 g 102 (6.0) 21 (1.2) 68 (4.0)Total 139 (6.8) 28 (1.3) 79 (3.9)
Brown University 501–1500 g 7 (10.4) 3 (4.5) 6 (9.0)1501–2500 g 30 (12.0) 18 (7.2) 24 (9.6).2500 g 89 (4.3) 32 (1.5) 82 (3.9)Total 126 (5.3) 53 (2.2) 112 (4.6)
Total 501–1500 g 67 (13.9) 15 (3.1) 28 (5.8)1501–2500 g 295 (19.5) 60 (4.0) 160 (10.6).2500 g 447 (6.9) 125 (1.9) 428 (6.6)Total 809 (9.5) 200 (2.3) 616 (7.2)
TABLE 3. Number and Percent Positive GC/MS Confirmation of EMIT–Positive Meconium Samples by Center and Birth WeightGroup
Cocaine OpiatesCenter Birth
WeightBE* Cocaine* CETH* HBE† BE/
Cocaine/CETH*
Morphine Codeine 6MAM HYM HYC AnyOpiate
No. (%)
Wayne State 501–1500 g 13 (43.3) 7 (23.3) 1 (3.3) 6 (60.0) 14 (46.7) 4 (80.0) 1 (20.0) 0 0 0 4 (80.0)University 1501–2500 g 114 (76.5) 76 (51.0) 22 (14.8) 55 (77.5) 114 (76.5) 19 (65.5) 13 (44.8) 0 0 0 21 (72.4)
.2500 g 135 (83.9) 91 (56.5) 16 (9.9) 63 (87.5) 136 (84.5) 37 (69.8) 29 (54.7) 1 (1.9) 1 (1.9) 0 47 (88.7)Total 262 (77.1) 174 (51.2) 39 (11.4) 124 (81.0) 264 (79.0) 60 (69.0) 43 (49.4) 1 (1.1) 1 (1.1) 0 72 (82.8)
University ofTennessee
501–1500 g 14 (58.3) 11 (45.8) 1 (4.2) 6 (54.5) 14 (58.3) 1 (33.3) 1 (33.3) 0 0 1 (33.3) 3 (100.0)1501–2500 g 69 (87.3) 53 (67.1) 7 (8.9) 40 (87.0) 72 (91.1) 4 (80.0) 2 (40.0) 0 0 0 4 (80.0).2500 g 72 (77.4) 55 (59.1) 15 (16.1) 43 (76.8) 73 (78.5) 8 (47.1) 10 (58.8) 0 1 (5.9) 0 12 (70.6)Total 155 (79.1) 119 (60.7) 23 (11.7) 89 (78.8) 159 (81.1) 13 (52.0) 13 (52.0) 0 1 (4.0) 1 (4.0) 19 (76.0)
University ofMiami
501–1500 g 2 (50.0) 1 (25.0) 0 2 (50.0) 3 (75.0) 0 2 (100.0) 0 0 0 2 (100.0)1501–2500 g 20 (62.5) 8 (25.0) 0 13 (76.5) 20 (62.5) 0 0 0 0 0 0.2500 g 51 (51.0) 38 (38.0) 9 (9.0) 30 (50.0) 52 (52.0) 2 (11.1) 2 (11.1) 0 0 0 3 (16.7)Total 73 (53.7) 47 (34.6) 9 (6.6) 45 (55.6) 75 (55.1) 2 (8.0) 4 (16.0) 0 0 0 5 (20.0)
BrownUniversity
501–1500 g 3 (42.9) 4 (57.1) 7 (100.0) 1 (16.7) 6 (85.7) 1 (33.3) 2 (66.7) 0 0 0 3 (100.0)1501–2500 g 21 (75.0) 7 (25.0) 28 (93.3) 16 (84.2) 21 (75.0) 10 (66.7) 8 (53.3) 0 0 0 10 (66.7).2500 g 30 (37.5) 19 (23.8) 80 (89.9) 14 (70.0) 31 (38.8) 15 (53.6) 13 (46.4) 0 1 (3.6) 0 18 (64.3)Total 54 (47.0) 30 (26.1) 115 (91.3) 31 (68.9) 58 (50.4) 26 (56.5) 23 (50.0) 0 1 (2.2) 0 31 (67.4)
Total 501–1500 g 32 (49.2) 23 (35.4) 2 (3.1) 15 (48.4) 37 (56.9) 6 (46.2) 6 (46.2) 0 0 1 (7.1) 12 (92.3)1501–2500 g 224 (77.8) 144 (50.0) 29 (10.1) 124 (81.0) 227 (78.8) 33 (62.3) 23 (43.4) 0 0 0 35 (66.0).2500 g 288 (66.4) 203 (46.8) 40 (9.2) 150 (75.8) 292 (67.3) 62 (53.4) 54 (46.6) 1 (.9) 3 (2.6) 0 80 (69.0)Total 544 (69.1) 370 (47.0) 71 (9.0) 289 (75.7) 556 (70.6) 101 (55.5) 83 (45.6) 1 (.6) 3 (1.7) 1 (.5) 127 (69.8)
* Total n 5 787.† Total n 5 382.
312 MATERNAL LIFESTYLE STUDY OF DRUG USE BY MECONIUM AND MATERNAL SELF-REPORT at Indonesia:AAP Sponsored on May 31, 2013pediatrics.aappublications.orgDownloaded from
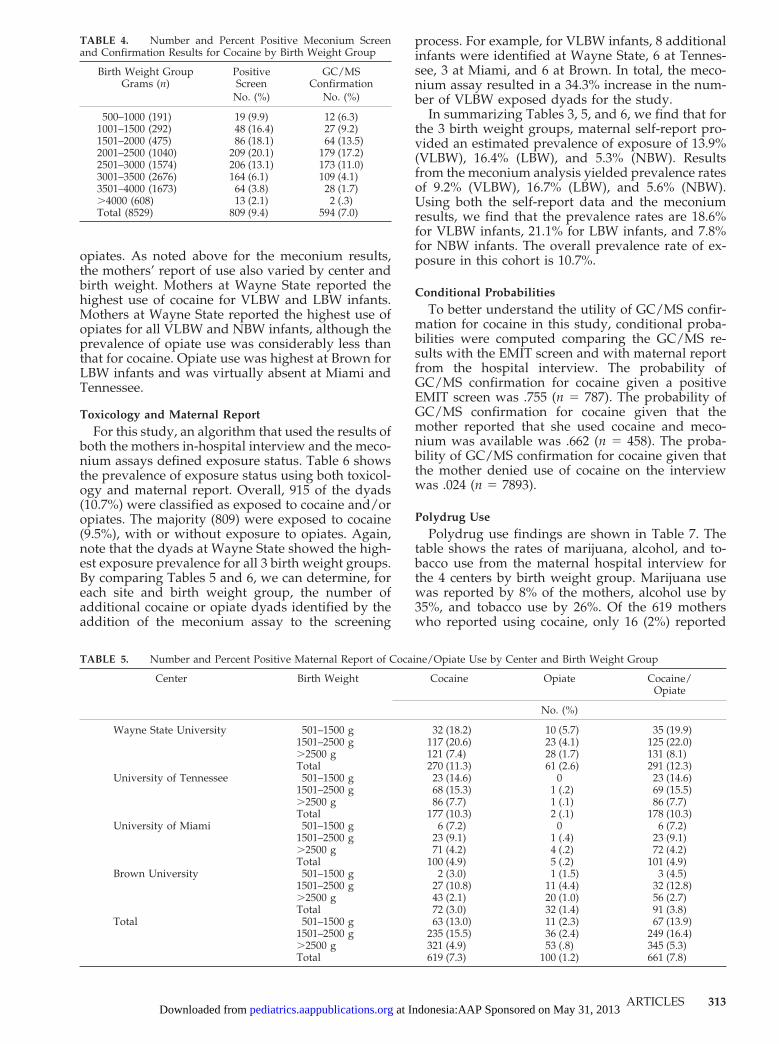
opiates. As noted above for the meconium results,the mothers’ report of use also varied by center andbirth weight. Mothers at Wayne State reported thehighest use of cocaine for VLBW and LBW infants.Mothers at Wayne State reported the highest use ofopiates for all VLBW and NBW infants, although theprevalence of opiate use was considerably less thanthat for cocaine. Opiate use was highest at Brown forLBW infants and was virtually absent at Miami andTennessee.
Toxicology and Maternal ReportFor this study, an algorithm that used the results of
both the mothers in-hospital interview and the meco-nium assays defined exposure status. Table 6 showsthe prevalence of exposure status using both toxicol-ogy and maternal report. Overall, 915 of the dyads(10.7%) were classified as exposed to cocaine and/oropiates. The majority (809) were exposed to cocaine(9.5%), with or without exposure to opiates. Again,note that the dyads at Wayne State showed the high-est exposure prevalence for all 3 birth weight groups.By comparing Tables 5 and 6, we can determine, foreach site and birth weight group, the number ofadditional cocaine or opiate dyads identified by theaddition of the meconium assay to the screening
process. For example, for VLBW infants, 8 additionalinfants were identified at Wayne State, 6 at Tennes-see, 3 at Miami, and 6 at Brown. In total, the meco-nium assay resulted in a 34.3% increase in the num-ber of VLBW exposed dyads for the study.
In summarizing Tables 3, 5, and 6, we find that forthe 3 birth weight groups, maternal self-report pro-vided an estimated prevalence of exposure of 13.9%(VLBW), 16.4% (LBW), and 5.3% (NBW). Resultsfrom the meconium analysis yielded prevalence ratesof 9.2% (VLBW), 16.7% (LBW), and 5.6% (NBW).Using both the self-report data and the meconiumresults, we find that the prevalence rates are 18.6%for VLBW infants, 21.1% for LBW infants, and 7.8%for NBW infants. The overall prevalence rate of ex-posure in this cohort is 10.7%.
Conditional ProbabilitiesTo better understand the utility of GC/MS confir-
mation for cocaine in this study, conditional proba-bilities were computed comparing the GC/MS re-sults with the EMIT screen and with maternal reportfrom the hospital interview. The probability ofGC/MS confirmation for cocaine given a positiveEMIT screen was .755 (n 5 787). The probability ofGC/MS confirmation for cocaine given that themother reported that she used cocaine and meco-nium was available was .662 (n 5 458). The proba-bility of GC/MS confirmation for cocaine given thatthe mother denied use of cocaine on the interviewwas .024 (n 5 7893).
Polydrug UsePolydrug use findings are shown in Table 7. The
table shows the rates of marijuana, alcohol, and to-bacco use from the maternal hospital interview forthe 4 centers by birth weight group. Marijuana usewas reported by 8% of the mothers, alcohol use by35%, and tobacco use by 26%. Of the 619 motherswho reported using cocaine, only 16 (2%) reported
TABLE 4. Number and Percent Positive Meconium Screenand Confirmation Results for Cocaine by Birth Weight Group
Birth Weight GroupGrams (n)
PositiveScreen
GC/MSConfirmation
No. (%) No. (%)
500–1000 (191) 19 (9.9) 12 (6.3)1001–1500 (292) 48 (16.4) 27 (9.2)1501–2000 (475) 86 (18.1) 64 (13.5)2001–2500 (1040) 209 (20.1) 179 (17.2)2501–3000 (1574) 206 (13.1) 173 (11.0)3001–3500 (2676) 164 (6.1) 109 (4.1)3501–4000 (1673) 64 (3.8) 28 (1.7).4000 (608) 13 (2.1) 2 (.3)Total (8529) 809 (9.4) 594 (7.0)
TABLE 5. Number and Percent Positive Maternal Report of Cocaine/Opiate Use by Center and Birth Weight Group
Center Birth Weight Cocaine Opiate Cocaine/Opiate
No. (%)
Wayne State University 501–1500 g 32 (18.2) 10 (5.7) 35 (19.9)1501–2500 g 117 (20.6) 23 (4.1) 125 (22.0).2500 g 121 (7.4) 28 (1.7) 131 (8.1)Total 270 (11.3) 61 (2.6) 291 (12.3)
University of Tennessee 501–1500 g 23 (14.6) 0 23 (14.6)1501–2500 g 68 (15.3) 1 (.2) 69 (15.5).2500 g 86 (7.7) 1 (.1) 86 (7.7)Total 177 (10.3) 2 (.1) 178 (10.3)
University of Miami 501–1500 g 6 (7.2) 0 6 (7.2)1501–2500 g 23 (9.1) 1 (.4) 23 (9.1).2500 g 71 (4.2) 4 (.2) 72 (4.2)Total 100 (4.9) 5 (.2) 101 (4.9)
Brown University 501–1500 g 2 (3.0) 1 (1.5) 3 (4.5)1501–2500 g 27 (10.8) 11 (4.4) 32 (12.8).2500 g 43 (2.1) 20 (1.0) 56 (2.7)Total 72 (3.0) 32 (1.4) 91 (3.8)
Total 501–1500 g 63 (13.0) 11 (2.3) 67 (13.9)1501–2500 g 235 (15.5) 36 (2.4) 249 (16.4).2500 g 321 (4.9) 53 (.8) 345 (5.3)Total 619 (7.3) 100 (1.2) 661 (7.8)
ARTICLES 313 at Indonesia:AAP Sponsored on May 31, 2013pediatrics.aappublications.orgDownloaded from

use of no other drugs (opiates, marijuana, alcohol, ortobacco). One hundred eighteen mothers (19%) re-ported the use of cocaine and one other drug. Twohundred sixty-two mothers (42%) reported using co-caine and 2 other drugs, 72% of which were alcoholand tobacco. Two hundred eleven mothers (35%)reported using cocaine and 3 other drugs, 86% ofwhich were marijuana, alcohol and tobacco. Only 3of 100 opiate users (3%) did not use at least 1 of theother 4 drugs; 12 used 4 other drugs.
Odds ratios (ORs) and 95% confidence intervals(CIs) were computed comparing cocaine use withother drug use during the pregnancy. Mothers whoused cocaine were more likely to use cigarettes (OR:23.1; CI: 19.5–27.4), alcohol (OR: 6.2; CI: 5.2–7.3) andmarijuana (OR: 14.2; CI: 12.2–16.5), than motherswho did not use cocaine. In addition, mothers who
used cigarettes were more likely to use alcohol (OR:3.3; CI: 3.0–3.6) and marijuana (OR: 10.6; CI: 9.1–12.3)than mothers who did not use cigarettes, and moth-ers who used alcohol were more likely to use mari-juana (OR: 4.0; CI: 3.5–4.7) than mothers who did notuse alcohol. The odds of using at least 1 of the other4 drugs if the mother admitted to using cocaine was37.7:1, while the odds for a mother who did notadmit to using cocaine was .77:1. This results in anOR of 49, indicating that a mother who admits tousing cocaine is 49 times more likely to also useopiates, alcohol, marijuana, or tobacco than a motherwho did not admit to using cocaine.
DISCUSSIONThis is the first large-scale report of cocaine and
other drug use during pregnancy using a meconium
TABLE 6. Number and Percent Positive Exposure Status by Maternal Self-Report or Meconium Confirmation by Center and BirthWeight Group
Center Birth Weight Cocaine Opiate Cocaine/Opiate
No. (%)
Wayne State University 501–1500 g 37 (21.0) 13 (7.4) 43 (24.4)1501–2500 g 150 (26.5) 30 (5.3) 158 (27.9).2500 g 174 (10.7) 57 (3.5) 209 (12.8)Total 361 (15.2) 100 (4.2) 410 (17.3)
University of Tennessee 501–1500 g 27 (17.2) 3 (1.9) 29 (18.5)1501–2500 g 83 (18.7) 5 (1.1) 86 (19.3).2500 g 107 (9.6) 12 (1.1) 115 (10.4)Total 217 (12.6) 20 (1.2) 230 (13.5)
University of Miami 501–1500 g 8 (9.6) 2 (2.4) 9 (10.8)1501–2500 g 31 (12.3) 1 (.4) 31 (12.3).2500 g 95 (5.6) 6 (.4) 97 (5.7)Total 134 (6.6) 9 (.5) 137 (6.7)
Brown University 501–1500 g 7 (10.4) 3 (4.5) 9 (13.4)1501–2500 g 33 (13.2) 18 (7.2) 44 (17.6).2500 g 57 (2.7) 36 (1.7) 85 (5.7)Total 97 (4.0) 57 (2.3) 138 (7.6)
Total 501–1500 g 79 (16.4) 21 (4.3) 90 (18.6)1501–2500 g 297 (19.6) 54 (3.6) 319 (21.1).2500 g 433 (6.6) 111 (1.7) 506 (7.8)Total 809 (9.5) 186 (2.2) 915 (10.7)
TABLE 7. Number and Percent Positive Maternal Report of Marijuana, Alcohol, and Tobacco Use by Center and Birth Weight Group
Center Birth Weight Alcohol Tobacco Marijuana
No. (%)
Wayne State University 501–1500 g 68 (38.6) 73 (41.5) 30 (17.0)1501–2500 g 265 (46.7) 291 (51.3) 119 (21).2500 g 575 (35.3) 566 (34.8) 242 (14.9)Total 908 (38.3) 930 (39.3) 391 (16.5)
University of Tennessee 501–1500 g 35 (22.3) 39 (24.8) 16 (10.2)1501–2500 g 149 (33.5) 153 (34.4) 55 (12.4).2500 g 333 (30.0) 306 (27.6) 106 (9.5)Total 517 (30.2) 498 (29.1) 177 (10.3)
University of Miami 501–1500 g 17 (20.5) 13 (15.7) 4 (4.8)1501–2500 g 79 (31.2) 44 (17.4) 13 (5.1).2500 g 577 (34.0) 203 (12.0) 35 (2.1)Total 673 (33.1) 260 (12.8) 52 (2.6)
Brown University 501–1500 g 22 (32.8) 24 (35.8) 4 (6.0)1501–2500 g 91 (36.4) 106 (42.4) 19 (7.6).2500 g 742 (35.5) 431 (20.6) 64 (3.1)Total 855 (35.5) 561 (23.3) 87 (3.7)
Total 501–1500 g 142 (29.4) 149 (30.8) 54 (11.2)1501–2500 g 584 (38.5) 594 (39.2) 206 (13.6).2500 g 2227 (34.1) 1506 (23.1) 447 (6.8)Total 2953 (34.6) 2249 (26.4) 707 (8.3)
314 MATERNAL LIFESTYLE STUDY OF DRUG USE BY MECONIUM AND MATERNAL SELF-REPORT at Indonesia:AAP Sponsored on May 31, 2013pediatrics.aappublications.orgDownloaded from

assay with confirmation and maternal history. In thissample of over 8500 dyads from 4 different sites, wefound an overall prevalence of cocaine/opiate expo-sure of 10.7% with the majority (9.5%) exposed tococaine, based on the combination of maternal self-report and meconium analysis. However, exposurestatus varied by site and birth weight; higher atWayne State and Tennessee than at Miami or Brownand higher in the 2 lower birth weight groups at eachsite. The higher prevalence of cocaine or opiate useamong women delivering prematurely has been pre-viously reported.29,31,32
The meconium assay that we used includedGC/MS confirmation. Historically, immunochemicalor thin-layer chromatographic screening methodswere thought to be sufficient for clinical and emer-gency toxicology use, whereas forensic applicationsrequire confirmation of positive screening results byGC/MS.33 However, in clinical settings, the accuratedetection of prenatal drug exposure may be compro-mised when presumptive positive screens are notconfirmed. Moore et al34 found up to a 43% false-positive rate for cocaine when drug screens wereused without confirmation. In our study, 75.5% ofthe positive screens were confirmed. Therefore, hadwe relied on screening alone, we could have incor-rectly included an additional 25% of mothers in thecocaine group. In our study, mothers who screenedpositive but were not confirmed with GC/MS werenot included in either group. Therefore, we probablyhave a more conservative estimate of cocaine expo-sure than some other studies. Other studies mayhave included positive screens that are not con-firmed in the control group. Lack of confirmationcould also help explain some of the variability acrossstudies in prevalence rates. For example, Ostrea et al1reported 30.7% of infants positive for cocaine in alarge-scale epidemiologic study based on a meco-nium screen without confirmation and a fourfoldincrease when the meconium screen was comparedwith self-report. It is difficult to evaluate these find-ings without knowing the false-positive rate of themeconium screen.
The addition of the HBE metabolite of cocaine, firstreported by Steele et al8 was important for our study.In one study,12 HBE was the only metabolite foundin 23% of the meconium specimens. In our study, theaddition of HBE resulted in a 10% increase inGC/MS confirmation to 85% when all 4 cocaine me-tabolites were used. Additional metabolites of co-caine may help reduce false-negative results and per-haps explain some of the variability in cocaineexposure by birth weight. For example, urine assayspredominantly test for BE, the major urinary metab-olite of cocaine. This method can only detect cocaineif it is present in high concentration. In a VLBWsample Browne et al10 found 7.5% positive for co-caine metabolites in the urine, compared with 19.8%in the meconium. However, BE was not detected inany of the meconium samples. We did find BE in ourVLBW infants and it is interesting that BE identifica-tion was lowest for VLBW at Wayne State (Table 3),although BE alone would have identified the major-ity of exposed infants in all 3 birth weight groups. It
is also interesting that the rate of cocaine exposureincreased through 2500 g (Table 4). It is possible, assuggested by Browne et al,10 that the chemical break-down and fetal metabolism of cocaine are a functionof gestational age and birth weight.
Some investigators have advocated the use ofquantitative analysis of drugs in meconium as ameans of estimating the degree of drug exposureduring gestation. Ostrea et al35 reported that theconcentrations of nicotine metabolites in meconiumwere directly related to the degree of active smokingby the mother. In a similar manner, Stolk et al36
observed a correlation between the maternal metha-done dose and the concentrations of methadone andEDDP, its primary metabolite, detected in meco-nium. It has even been suggested that serial analysisof meconium specimens may reflect both the chro-nology and degree of drug exposure. Ostrea et al37
proposed that meconium collected 0 to 10 hours afterbirth reflects gestational exposure up to 20 weeks, 11to 20 hours 21 to 30 weeks of gestation, and 21 to 36hours .30 weeks of gestation. The analysis of drugsin meconium and interpretation of test results arecomplex processes. Overinterpretation of meconiumdata are a dangerous practice, especially at the cur-rent stage of development of this new and usefultechnology. It is clear that there are matrix effectsassociated with the analysis of meconium, as thereare with each biological fluid or tissue. It is essentialthat standards and controls be prepared in meco-nium to prevent false-positive and false-negative testresults especially when using a urine- or differentmatrix-based immunoassay. The importance of a sec-ond confirmation test that is based on a differentanalytical method to improve the accuracy of testresults has been stressed, as well as the importance ofthe analytical cutoff or sensitivity of the method.However, there are other factors that contribute tothe difficulty of interpreting quantitative meconiumresults.
Many questions remain to be answered about thedisposition of drugs in meconium. It is not yetknown which are the most appropriate drug analytesto measure in meconium. It is clear that measure-ment of HBE is important for cocaine analysis andElSohly et al38 have recently described the impor-tance of 11-hydroxy-d9-tetrahydrocannabinol and8,11,dihydroxy-d9-tetrahydrocannabinol for detec-tion of marijuana exposure. Meconium from 11 neo-nates born to cocaine-abusing mothers were found tobe positive for cocaine, benzoylecgonine, norcocaine,and/or benzoylnorecgonine.39 Qualitative and quan-titative differences in the compounds detected wereobserved in the different infants. If a correlation be-tween the concentration of drug in meconium andmaternal drug exposure is attempted, should it bebased on the total concentration of all drug analytes,the parent drug, or a specific metabolite? The fetusmay metabolize drugs differently at specific gesta-tional ages. Could the presence of a particular ana-lyte be a marker for drug exposure at a certain ges-tational age? How important is enzymatic or acid/base hydrolysis of the meconium sample to accurateand sensitive drug measurement? Fetal maturity also
ARTICLES 315 at Indonesia:AAP Sponsored on May 31, 2013pediatrics.aappublications.orgDownloaded from

affects the efficiency of phase II metabolism and theproduction of glucuronide and other metabolites.False-negative results may occur if the immunoassaydoes not cross-react with the appropriate analytes orif the analyte is not free to react with the antibody, ie,if it is the glucuronidated metabolite. Moore et al40
found that the concentration of hydrocodone, hydro-morphone, and codeine increased markedly afteracid hydrolysis with a more moderate increase notedin the morphine concentration. This is in contrast toa report by Becker et al41 in which hydrolysis ofmeconium was not found to significantly increasethe morphine concentration. Also, fetal maturity wasfound to be a factor in the detection of methamphet-amine in meconium from guinea pigs after intraperi-toneal injection of the drug at different gestationalages.42 Furthermore, gestational age was determinedto be an important consideration in interpretingquantitative methamphetamine results.
There also is uncertainty about possible reabsorp-tion of drug from the fetal gastrointestinal track dur-ing gestation. Meconium is not a homogeneous spec-imen but a series of layers formed in the intestineduring gestation. It is possible that drugs may diffusethrough the meconium over time. Most analyticalmethods advise a thorough mixing of the specimenbefore analysis because the distribution of drugsthroughout a sample may not be uniform. Anotherimportant confounding factor is the possible contam-ination of the meconium specimen by urine. Differ-ent analytes may be present in urine at differentconcentrations. Contamination of meconium byurine could complicate the interpretation of quanti-tative results. It is clear that additional research isnecessary to address these important issues and toimprove our understanding of the disposition ofdrugs in meconium.
Exposure status in this study was based on analgorithm that used the results of meconium assaysand maternal self-report from an in-hospital inter-view. The advantage of using both drug toxicologyand maternal self-report has been shown in severalstudies.1,3,27,28 It is also important to distinguish be-tween maternal report based on a structured ques-tionnaire as we used and information collected aboutthe mother from medical record review. The latter isless reliable19 and may not be appropriate to com-pare with toxicology results.1 The importance of us-ing both meconium and maternal self-report is toidentify mothers who deny use but who did use asevidenced by positive meconium confirmation. It isgenerally assumed that mothers are less likely to saythey used illegal drugs when they did not. In ourstudy, 661 mothers admitted to cocaine/opiate use(619 to cocaine). An additional 254 mothers denieduse but their infant had a positive meconium confir-mation for cocaine/opiates (190 for cocaine). There-fore, we identified an additional 38% of the cocaine/opiate exposed infants (31% of the cocaine-exposed)based on the meconium assay alone. More impor-tantly, had we relied only on maternal self-report,these 254 infants would have been eligible for inclu-sion in the unexposed group.
From a public health perspective one could argue
that these 254 infants only represent 3.2% of the 7866of the total number of mothers in our sample whodenied cocaine/opiate use (190 of 7908 or 2.4% ofmothers who denied cocaine use) and that the effortand expense involved in collecting and conductingthe meconium assay (including GC/MS confirma-tion) may not be effective. In contrast, these 254infants represent a substantial (28%) proportion ofthe sample of the 915 cocaine/opiate users (or 190 of809), or 23% of the sample of cocaine users. There-fore, the use of the meconium assay in the forensicgold standard way in which it was used in this studymay have different implications for research than forpublic policy. Confirmation of presumptive positivesis essential for the accurate identification of womenwhose infants may be removed by State authorities.Also, in the research environment our use of theCertificate of Confidentiality could have influencedinformed consent and maternal report of drug use,an option not available in the public health arena.Therefore, under public health guidelines the under-reporting of maternal drug use could be substan-tially higher than that found in this study.
The probability that the mother reported that sheused cocaine given a positive GC/MS confirmationfor cocaine in this study was .66. Casanova et al13
also found a 66% agreement between positive toxi-cology results and positive maternal report. This isnot surprising because the meconium assay, at best,can only provide a record of drug use during thesecond half of pregnancy. Infants of mothers whoreport that they used cocaine but not in the secondhalf of pregnancy will have a negative meconium forappropriate reasons. Therefore, it would not be ad-visable to rely on the meconium assay exclusivelyand not include a structured interview.
We also addressed the issue of polydrug use in thisstudy. It is becoming increasingly clear that womenwho use cocaine during pregnancy are also likely touse other licit and illicit drugs. In our database ofpublished studies on cocaine and child outcome,only 13% of the studies reported that cocaine was theonly drug used.43 Chasnoff19 found that 32% of thepositive meconium specimens were positive for atleast 2 drugs. In our study, only 2% of the mothersreported that they used cocaine and no other drugs,and mothers were found to be 49 times more likely touse another drug if they used cocaine. The cocaineproblem has truly become a problem of polydruguse. This has implications for drug toxicology todevelop improved methods to identify drug-exposedinfants, especially those exposed to multiple drugs.There are also implications for developmental fol-low-up studies because little is known about theeffects of drug interactions on child behavior anddevelopment.
CONCLUSIONIn this large, prospective multisite study, we found
that the prevalence and observed metabolites of co-caine showed considerable variation among the 4sites and according to birth weight. Accurate identi-fication of prenatal drug exposure is likely to beimproved with GC/MS confirmation and when the
316 MATERNAL LIFESTYLE STUDY OF DRUG USE BY MECONIUM AND MATERNAL SELF-REPORT at Indonesia:AAP Sponsored on May 31, 2013pediatrics.aappublications.orgDownloaded from

meconium assay is used in conjunction with a ma-ternal hospital interview. However, the use ofGC/MS may have different implications for researchthan for public policy. Finally, the problem of cocaineuse has been redefined as one of polydrug use, whichhas implications for the fields of drug toxicology,pediatrics, and child development.
ACKNOWLEDGMENTSThis study was supported by the National Institute on Child
Health and Human Development through Cooperative Agree-ments U10 HD 27904, U10 HD 21397, U10 HD 21385, U10 HD27856, U10 HD 19897, NICHD Contract 5-U10-HD27904-02, andintraagency agreements with the National Institute on DrugAbuse, Administration on Children, Youth and Families, and theCenter for Substance Abuse Treatment.
REFERENCES1. Ostrea EM, Brady M, Gause S, et al. Drug screening of newborns by
meconium analysis: a large scale, prospective, epidemiologic study.Pediatrics. 1992;89:107–113
2. Schutzman DL, Frankenfield-Chernicoff M, Clatterbaugh HE, SingerJ. Incidence of intrauterine cocaine exposure in a suburban setting.Pediatrics. 1991;88:825–827
3. Frank DA, Zuckerman BS, Amaro H, et al. Cocaine use duringpregnancy: prevalence and correlates. Pediatrics. 1988;82:888–895
4. Ostrea EM, Parks P, Brady M. Rapid isolation and detection of drugs inmeconium of infants of drug dependent mothers. Clin Chem. 1988;34:2372–2373
5. Ostrea EM, Brady MJ, Parks PM, Asenio DC, Naluz A. Drug screeningof meconium in infants of drug dependent mothers: an alternative tourine screening. J Pediatr. 1989;115:474–477
6. Wingert WE, Feldman MS, Kim MH, et al. A comparison of meconium,maternal urine and neonatal urine for detection of maternal drug useduring pregnancy. J Forensic Sci. 1994;39:150–158
7. Clark GD, Rosenzweig IB, Raisys V, et al. The analysis of cocaine andbenzoylecgonine in meconium. J Anal Toxicol. 1992;16:261–263
8. Steele BW, Bandstra ES, Niou-Ching Wu, Hime GW, Hearne WL.m-Hydroxybenzoylecgonine: an important contributor to the immuno-reactivity in assays for benzoylecgonine in meconium. J Anal Toxicol.1993;17:348–352
9. Angus J, Greenglass E, Bermes E, Kahn S. Benzoylecgonine in themeconium of neonatal infants: an analysis by three methods. Clin Chem.1992;38:1016
10. Browne S, Moore C, Negrusz A, et al. Detection of cocaine, norcocaine,and cocaethylene in the meconium of premature neonates. J Forensic Sci.1994;39:1515–1519
11. Ryan RM, Wagner CL, Schultz JM, et al. Meconium analysis for im-proved identification of infants exposed to cocaine in utero. J Pediatr.1994;125:435–440
12. Lewis DE, Moore CM, Leikin JB, Koller A. Meconium analysis forcocaine: a validation study and comparison with paired urine analysis.J Anal Toxicol. 1995;19:148–150
13. Casanova OQ, Lombardero N, Behnke M, et al. Detection of cocaineexposure in the neonate: analyses of urine, meconium, and amnioticfluid from mothers and infants exposed to cocaine. Arch Pathol Lab Med.1994;118:988–993
14. Madden JD, Payne TF, Miller S. Maternal cocaine abuse and effect onthe newborn. Pediatrics. 1986;77:209–211
15. Bingol N, Fuchs M, Diaz V, Stone RK, Gromisch DS. Teratogenicity ofcocaine in humans. J Pediatr. 1987;110:93–96
16. Oro AS, Dixon SD. Perinatal cocaine and methamphetamine exposure:maternal and neonatal correlates. J Pediatr. 1987;111:571–578
17. Davis M. NMIS Fact Sheet. Hyattsville, MD: National Center for HealthStatistics; 1988
18. National Institute on Drug Abuse. National Pregnancy, Health Survey.
Rockville, MD: National Institutes of Health; 199619. Chasnoff IJ. Drug use and women: establishing a standard of care. Ann
N Y Acad Sci. 1989;562:208–21020. US General Accounting Office. Drug-Exposed Infants: A Generation at
Risk. Washington, DC: US General Accounting Office; 199021. Vega WA, Kolody B, Hwang J, Noble A. Prevalence and magnitude of
prenatal substance exposures in California. N Engl J Med. 1993;29:850–854
22. Nalty D. 1991 South Carolina Prevalence Study of Drug Use Among WomenGiving Birth. Columbia, SC: South Carolina Commission on Alcohol andDrug Abuse; 1991
23. Hollinshead WH, Griffin JS, Scott HD, Burke ME. Statewide prevalenceof illicit drug use by pregnant women—Rhode Island. MMWR MorbMortal Wkly Rep. 1990;39:225–227
24. George KD, Price J, Hauth JC, Barnette DM, Preston P. Drug abusescreening of childbearing-age women in Alabama public health clinics.Am J Obstet Gynecol. 1991;165:924–927
25. Madry K, Fredlund E, Wallisch, Spence R. 1990 Texas Survey of Postpar-tum Women and Drug-Exposed Infants. Austin TX: Texas Commission onAlcohol and Drug Abuse; 1991
26. DeVane D, Garite T, Hunt L, et al. Prevalence and Outcomes of PerinatalDrug and Alcohol Use by Women in Orange County, California. Costa Mesa,CA: March of Dimes Birth Defects Foundation; 1991
27. Chasnoff IJ, Landress H, Barrett M. The prevalence of illicit drug oralcohol use during pregnancy and discrepancies in Pinellas County,Florida. N Engl J Med. 1990;322:1202–1206
28. Zuckerman B, Frank DA, Hingson R, et al. Effects of maternal marijuanaand cocaine use on fetal growth. N Engl J Med. 1989;320:762–768
29. Chasnoff IJ, Burns WJ, Schnoll SH, et al. Cocaine use in pregnancy.N Engl J Med. 1985;313:666–669
30. ElSohly MA, Stanford DF, Murphy TP, et al. Immunoassay and GC-MSprocedures for the analysis of drugs of abuse in meconium. J AnalToxicol. 1999;23:436–445
31. Kliegman RM, Madura D, Kiwi R, et al. Relation of maternal cocaine useto the risks of prematurity and low birthweight. J Pediatr. 1994;124:751
32. Doberczak TT, Thornton JC, Bernstein J, et al. Impact of maternal drugdependency on birthweight and head circumference of offspring. Am JDis Child. 1987;141:1163
33. Lombardero N, Casanova O, Behnke M, Eyler FD, Bertholf RL. Mea-surement of cocaine and metabolites in urine, meconium and diapers bygas chromatography/mass spectrometry. Ann Clin Lab Sci. 1993;23:385–394
34. Moore C, Lewis D, Leikin J. False-positive and false-negative rates inmeconium drug testing. Clin Chem. 1995;41:1614–1616
35. Ostrea EM, Knapp D, Romero A, Montes M, Ostrea AR. Meconiumanalysis to assess fetal exposure to active and passive maternal smok-ing. J Pediatr. 1994;124:471–476
36. Stolk LM, Coenradie SM, Smit BJ, van As HL. Analysis of methadoneand its primary metabolite in meconium. J Anal Toxicol. 1997;21:154–159
37. Ostrea EM, Knapp DK, Tannenbaum L, et al. Serial meconium druganalysis can estimate the chronology and degree of the infant’s in uterodrug exposure. Pediatr Res. 1993;33:229A
38. ElSohly MA, Feng S. D9-THC metabolites in meconium: identification of11-OH-D9-THC, 8b, 11-diOH-D9-THC, and 11-nor-D9-THC-9-COOH asmajor metabolites of D9-THC. J Anal Toxicol. 1998;22:329–335
39. Murphey LJ, Olsen GD, Konkol RJ. Quantitation of benzoylnorecgonineand other cocaine metabolites in meconium by high-performance liquidchromatography. J Chromatogr. 1993;613:330–335
40. Moore CM, Deitermann D, Lewis D, Leikin J. The detection of hydro-codone in meconium: two case studies. J Anal Toxicol. 1995;6:514–518
41. Becker J, Moore C, Lewis D, Leikin J. Morphine detection in meconium:Hydrolyzed v. nonhydrolyzed specimens. Clin Chem. 1995;41:S114
42. Nakamura KT, Ayau EL, Uyehara CJ, et al. Methamphetamine detec-tion from meconium and amniotic fluid in guinea pigs depends ongestational age and metabolism. Dev Pharmacol Ther. 1992;19:183–190
43. Lester BM, LaGasse LL, Brunner SM. Data base of studies on prenatalcocaine exposure and child outcome. J Drug Issues. 1997;27:487
ARTICLES 317 at Indonesia:AAP Sponsored on May 31, 2013pediatrics.aappublications.orgDownloaded from

DOI: 10.1542/peds.107.2.309 2001;107;309Pediatrics
Marilyn A. Huestis, Loretta P. Finnegan and Penelope L. MazaVerter, Charles R. Bauer, Seetha Shankaran, Henrietta S. Bada, H. Chip Walls,
Barry M. Lester, Mahmoud ElSohly, Linda L. Wright, Vincent L. Smeriglio, JoelSelf-Report
The Maternal Lifestyle Study: Drug Use by Meconium Toxicology and Maternal
ServicesUpdated Information &
mlhttp://pediatrics.aappublications.org/content/107/2/309.full.htincluding high resolution figures, can be found at:
References
ml#ref-list-1http://pediatrics.aappublications.org/content/107/2/309.full.htat:This article cites 37 articles, 13 of which can be accessed free
Citations
ml#related-urlshttp://pediatrics.aappublications.org/content/107/2/309.full.htThis article has been cited by 26 HighWire-hosted articles:
Subspecialty Collections
and_newbornhttp://pediatrics.aappublications.org/cgi/collection/premature_Premature & Newbornfollowing collection(s):This article, along with others on similar topics, appears in the
Permissions & Licensing
mlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhttables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2001 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Indonesia:AAP Sponsored on May 31, 2013pediatrics.aappublications.orgDownloaded from